
Session 3: Benefit package and the role of health … Observatory on Health Systems and Policies...
20
European Observatory on Health Systems and Policies Session 3: Benefit package and the role of health technology assessment (HTA) Health financing and efficiency gains workshop Ljubljana, 03 November 2015 Dr. med. Wilm Quentin, MSc HPPF Senior Research Fellow Technische Universität Berlin
-
Upload
nguyenkhanh -
Category
Documents
-
view
214 -
download
0
Transcript of Session 3: Benefit package and the role of health … Observatory on Health Systems and Policies...

European Observatory on Health Systems and Policies
Session 3: Benefit package and the role of health technology assessment (HTA)
Health financing and efficiency gains workshop
Ljubljana, 03 November 2015
Dr. med. Wilm Quentin, MSc HPPF
Senior Research Fellow
Technische Universität Berlin

European Observatory on Health Systems and Policies
The purchasing process
(Strategic) purchasing bridges the gap between
planning and budgetary allocations to promote
quality and efficiency in the use of health funds
– Which interventions should be purchased?
– How should these be purchased?
– What payment systems should be used?
2

European Observatory on Health Systems and Policies
A model for health care benefits
3
“All” possible health benefits
Covered benefit categories e.g. “inpatient curative care”, “pre-natal care”
Actually covered benefitse.g. cervical cancer screening with Papanicolau Test;
toxoplasma serology in the first trimester

European Observatory on Health Systems and Policies
Listing of benefits: process
4
“All” possiblehealth benefits
Covered benefit categories
Actual benefits
Representativeinstitutions, e.g.
Parliaments (Law)
Planning Bodies Coverage Commissions
using HTA
Third-party
Payers
Advisory bodies
(Social) Courts
Criteria

European Observatory on Health Systems and Policies
Why is HTA important?
5Kernick 2003
Demand/Need
Intervention options
Resources
1970s 1980s 1990s

European Observatory on Health Systems and Policies
Two alternatives for rationing ofbenefits
• Implicit rationing– Officially „no rationing“
– Decisions are made by providers
– Intransparent: effectively certain patients are not treated/certain services not provided (e.g. waiting lists)
• Explicit rationing– Official processes exist to make decisions about which
services to provide
– Improves transparency � allows making trade-offs explicit
– Political costs of negative coverage decisions but may leadto societal debate
6

European Observatory on Health Systems and Policies
HTA for decision making
7
“The goal of HTA is to provide input to decision making in policy and practice“(Henshall et al. 1997)
Industry claims
Providerpreferences
Patientwishes
Societal values
• Therapeutic value• Economic value• Social aspects
• Other aspects (ethical, legal…)

European Observatory on Health Systems and Policies
Challenges in Slovenia
• Explicit listing of covered services exists only for few areas, e.g. pharmaceuticals
• No systematic mechanism (based on HTA) that determines whether new services will be covered/existing removed/user charges changed
• No consensus about HTA body (institutional set-up, responsibilities)
• Resistance by stakeholders towards more explicit/evidence-based decision making
8

European Observatory on Health Systems and Policies
Listing of ALL covered services
9
HC.1 Services of curative care
HC.1.1 In-patient curative care HC.1.2 Day cases of curative care HC.1.3 Out-patient care HC.1.3.1 Basic medical and diagnostic services HC.1.3.2 Out-patient dental care HC.1.3.3 All other specialised health care HC.1.3.9 All other out-patient curative care HC.1.4 Services of curative home care HC.2 Services of rehabilitative care
HC.2.1 In-patient rehabilitative care HC.2.2 Day cases of rehabilitative care HC.2.3 Out-patient rehabilitative care HC.2.4 Services of rehabilitative home care HC.3 Services of long-term nursing care
HC.3.1 In-patient long-term nursing care HC.3.2 Day cases of long-term nursing care HC.3.3 Long-term nursing care: home care
HC.4 Ancillary services to health care
HC.4.1 Clinical laboratory HC.4.2 Diagnostic imaging HC.4.3 Patient transport and emergency rescue HC.4.9 All other miscellaneous services HC.5 Medical goods dispensed to out-patients
HC.5.1 Pharmaceuticals and other medical non-durables HC.5.1.1 Prescribed medicines HC.5.1.2 Over-the-counter medicines HC.5.2 Therapeutic appliances and other medical durables HC.5.2.1 Glasses and vision products HC.5.2.2 Orthopaedic appliances and other prosthetics HC.5.2.3 Hearing aids HC.5.2.4 Medico-technical devices, incl. wheelchairs HC.5.2.9 All other miscellaneous medical durables HC.6 Prevention and public health services
HC.6.1 Maternal and child health; family planning … HC.6.2 School health services HC.6.3 Prevention of communicable diseases HC.6.4 Prevention of non-communicable diseases HC.6.5 Occupational health care HC.6.9 All other miscellaneous public health services
OECD System of Health Accounts:
Health Care Functions
To be introduced
by 2017
Losely defined
by DRGs“All” possible health
benefits
European Observatory on Health Systems and Policies
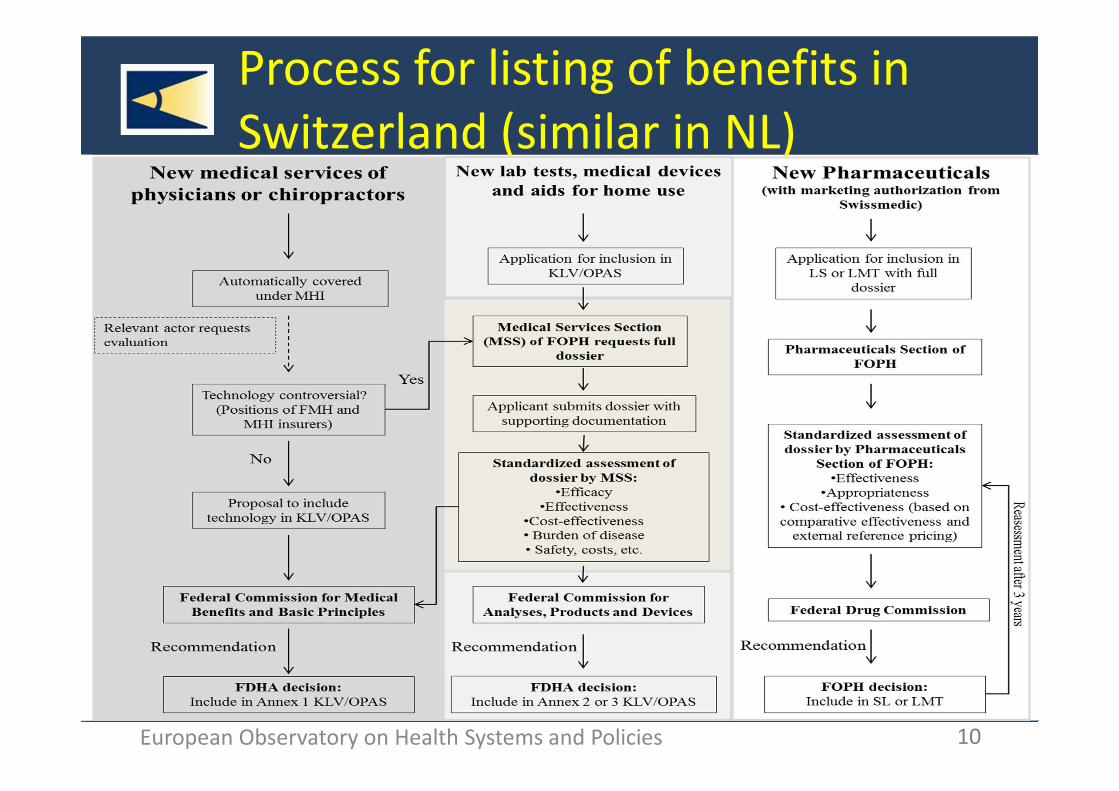
Process for listing of benefits in Switzerland (similar in NL)
10

European Observatory on Health Systems and Policies
HTA used for decision making
SK LV GR PL CZ HR LT RU EE SI BU HU
Pharmaceuticals
(include vaccines and
other biological
products)
X X X X X X X X X X X
Medical devices
(include diagnostic
products)
X X X X X X X
Medical procedures X X X X X
E-health technologies X
Public health
interventionsX X X X
Other X
11
Based on survey data, ADVANCE_HTA project, yet unpublished

European Observatory on Health Systems and Policies
Criteria for benefit setting differ
across countries and benefits
12
Service Categories D DK E F H I NL PL UKCurative Care
In-patient services A; CE; Ex.; N
B; N C; E; N; S
N; E; S
C; E A; N; B C; E; N n.s. B; C; N
Out-patient services CE; Ex.; N
B; N C; E; N; S
N; E; S
C; E A; E; N; B
C; E n.s. C; E; N
Rehabilitative Care CE; Ex.; N
B; N N N n.s. A A n.s. E; N
Long-term nursing care C N N N n.s. A; E; N; B
n.s. n.s. E; N
Ancillary services A; Ex. N C; E; N N n.s. C; E n.s. n.s. E; NMedical goods for out-patients
Pharmaceuticals andnon-durables
E; N B; CE; N
B; N; U C; E; I; S
B; CE; E; N; S
C; E B; CE; I C B; E; N; S
Appliances and durables
E; U U CE; E; S E; U n.s. N; C C N; C E; N; S
a Denmark (DK), France (F) Germany (D), Hungary (H), Italy (I), Netherlands (NL), Poland (PL), Spain (E), England (UK);n.s.: not stated
A: Appropriateness, B: Budget, C: Costs, CE: Cost-effectiveness,E: Effectiveness, Ex.: Expedience, I: Innovation-degree,
N: Need, S: Safety, U: Utility
Velasco-Garrido 2006

European Observatory on Health Systems and Policies
HTA: institutional setup and tasks
13
Separate
entitiesIntegrated Regulatory
body
HTA institution
Coverage body
TV = Therapeuticvalue
EV = economicvalue
AP = appraisal
Allen 2013

European Observatory on Health Systems and Policies
HTA: responsible institutions
14
Bulgaria National Council on prices and reimbursement of medicinal products (NCPR) is responsible for assessment, appraisal and reimbursement.
Croatia
Agency for Quality and Accreditation in Health Care and Social Welfare is responsible for assessment. Croatian Institute for Health Insurance (CIHI) (“Drug Committee” and “Medical Devices Committee”) is responsible for appraisal.
Cyprus Drug committee is responsible for assessment, appraisal and decision of reimbursement of medical products.
Czech Repulbic Marketing authorization holder (MAH) is responsible to assessment State Institute of Drug Control (SÙKL) is responsible for appraisal
Estonia
Estonian Heath Insurance Fund is responsible for appraisal. The assessment is based on information submitted by applicant. [no formal process of HTA]
Greece
National Drug Organization (EOF) in collaboration with the National Organisation for the Provision of Healthcare Services of Greece (EOPYY) are responsible for assessment and appraisal process. [no formal process of HTA]
Hungary
Technology Appraisal Head Department (TAHD) in the National Institute for Quality and Organisational Development in Healthcare and medicines (THAD – GYEMSZI TEI-) is responsible for assessment and appraisal.
Kosovo [no formal process of HTA]
Latvia Centre of Health Economics (CHE) within the NHS is responsible for assessment and appraisal
State Health Care Accreditation Agency (VASPVT) perform assessment of medical device.

European Observatory on Health Systems and Policies
HTA schemes in five CEE countries
15
Gulacsi et al. 2014

European Observatory on Health Systems and Policies
HTA prinicples
16
Stephens et al. 2012
���� Stakeholder involvement
���� Include all relevant technologies
���� Clearly defined link to policy-making

European Observatory on Health Systems and Policies
HTA practices in Europe
17
Stephens et al. 2012
v
v

European Observatory on Health Systems and Policies
Summary: international experiences
• HTA can be a useful tool to determine which
(new) benefits are to be covered
– Should include all types of services and technologies
– HTA body should be independent of financial interests and not-for-profit
• Selecting topics, evaluation, and decision-
making requires involvement of several actors
– Needs a clear, explicit and regulated definition of roles and responsibilities
18

European Observatory on Health Systems and Policies
• Clear criteria are needed to guide evaluations
– Internationally, effectiveness, safety and costs (or cost-effectiveness) are most frequently employed
– Collaborate with more experienced countries
• An evidence-based explicit definition of benefits is likely to meet resistance
– If coverage decisions are taken transparently can lead to debate about societal preferences
– Stakeholder involvement is vital to counteract resistance on the provider side
19
Slovenia is a
member of
EUnetHTA
Summary: international experiences

European Observatory on Health Systems and Policies
Thank you!
For more information:
www.euro.who.int/observatory
www.mig.tu-berlin.de
20


















