Session #1015 Surgical Pathology of Sinonasal Tract TumorsSurgical Pathology of Sinonasal Tract...
60
Session #1015 Surgical Pathology of Sinonasal Tract Tumors Lester D. R. Thompson Southern California Permanente Medical Group www.lester-thompson.com LDR Thompson, M.D. Used by Permission from: Diagnostic Pathology: Head & Neck LWW-Amirsys ASCP Annual Meeting Surgical Pathology of Sinonasal Tract Tumors Session # 1015 on September 21, 2013 Page 1 of 60
Transcript of Session #1015 Surgical Pathology of Sinonasal Tract TumorsSurgical Pathology of Sinonasal Tract...

Session #1015Surgical Pathology of
Sinonasal Tract Tumors
Lester D. R. ThompsonSouthern California Permanente
Medical Groupwww.lester-thompson.com
LDR Thompson, M.D. Used by Permission from: Diagnostic Pathology: Head & Neck LWW-Amirsys
ASCP Annual Meeting Surgical Pathology of Sinonasal Tract Tumors Session # 1015 on September 21, 2013
Page 1 of 60

Speaker DisclosureIn the past 12 months, I have not had a significant financial interest or other relationship with the manufacturer(s) of the product(s) or provider(s) of the service(s) that will be discussed in my presentation.
This presentation will (not) include discussion of pharmaceuticals or devices that have not been approved by the FDA or unapproved or “off-label” uses of pharmaceuticals or devices.
LDR Thompson, M.D. Used by Permission from: Diagnostic Pathology: Head & Neck LWW-Amirsys
ASCP Annual Meeting Surgical Pathology of Sinonasal Tract Tumors Session # 1015 on September 21, 2013
Page 2 of 60

NASOPHARYNGEAL CARCINOMA, NONKERATINIZING TYPES
Nonkeratinizing undifferentiated nasopharyngealcarcinoma is characterized by tumor nests demarcated from surrounding stroma, the latter lacking adesmoplastic reaction.
The intimate relationship of the neoplastic epithelial cells with the surrounding lymphocytes can make the
diagnosis very challenging.
TERMINOLOGY
Abbreviations• Nasopharyngeal carcinoma (NPC)
Synonyms• Lymphoepithelioma, Rigaud and Schmincke types of
lymphoepithelioma; transitional carcinomao Lymphoepithelioma is a misnomer
▪ Tumor entirely of epithelial origin with secondaryassociated benign lymphoid component
o Designations Rigaud and Schmincke refer tosyncytial vs. individual cell growth patterns,respectively, with no biologic import
Definitions• Type of squamous cell carcinoma originating from
nasopharyngeal mucosa with evidence of squamousdifferentiation
• World Health Organization classification of NPCo I. Nonkeratinizing carcinomao II. Keratinizing squamous cell carcinomao III. Basaloid squamous cell carcinoma
ETIOLOGY/PATHOGENESIS
Infectious Agents• Very strong association with Epstein-Barr virus (EBV)o Strong association indicates oncogenic role of EBV
in development of NPCo EBV early initiating event in development of NPC
▪ EBV found in preinvasive (precursor)nasopharyngeal lesions
▪ Clonal episomal EBV-DNA identified, suggestingviral entry into the nucleus before clonalexpansion
Environmental Exposure• Purported risk factors include
o High dietary levels of volatile nitrosamines in salt-preserved or fermented foods in high incidenceregions implicated as carcinogen
o Conversely, high consumption of fresh fruits andvegetables lowers risk of NPC in endemic regions
o Cigarette smokingo Occupational exposure to chemical fumes, smoke,
formaldehydeo Prior radiation exposure
Genetic and Geographic Factors• Familial clustering yields a familial RR of 10 fold
(highest genetic association for all types of cancer)• Incidence among Chinese people decreases after
emigration to low-incidence areas but still remainshigher than in non-Chinese populations
CLINICAL ISSUES
Epidemiology• Incidenceo In China, NPC accounts for 18% of all cancers, and
1 in 40 men develop NPC before age 72 yearso NPC, nonkeratinizing undifferentiated: ~60%o NPC, nonkeratinizing differentiated: ~15%o NPC, keratinizing: ~25%
• Ageo Most common in 4th-6th decadeso Nonkeratinizing undifferentiated may occur in
pediatric patients
▪ Less than 20% occur in pediatric age groups
▪ Pediatric NPC most common in northern and
central Africa, accounting for 10–20% of all cases
▪ Approximately 2% of NPC in China occurs inchildren
• Gendero Male > Female (3:1)
• Ethnicity
LDR Thompson, M.D. Used by Permission from: Diagnostic Pathology: Head & Neck LWW-Amirsys
ASCP Annual Meeting Surgical Pathology of Sinonasal Tract Tumors Session # 1015 on September 21, 2013
Page 3 of 60

NASOPHARYNGEAL CARCINOMA, NONKERATINIZING TYPES
Key Facts
o Endemic populations include southern China(including Hong Kong), southeast Asia, Malaysia,northern Africa, middle east, arctic
Site• Lateral wall (fossa of Rosenmüller) > superior posterior
wall
Presentation• Presence of asymptomatic cervical neck mass typically
localized to posterior cervical triangle or superiorjugular nodal chain commonly present
• Additional signs and symptoms includeo Nasal obstruction, nasal discharge, epistaxis, pain,
serous otitis media, otalgia, hearing loss, headache• Signs and symptoms in early stages often subtle and
nonspecific resulting in delay in diagnosiso Presentation often at more advanced clinical stage
• Up to 25% of patients may experience cranial nerveinvolvemento Considered adverse prognostic findingo Cranial nerves involved may include
▪ III, IV, ophthalmic branch of V, 3rd division of V(through parapharyngeal space in proximity tolateral nasopharyngeal wall), VI, IX-XII
Laboratory Tests• Positive serology against EBV in >90% of patients
reportedo Elevated titers of IgA antibodies (vs. viral capsid
antigen [VCA]) and IgG antibodies (vs. early antigen[EA])
▪ Detection rates range up to 93%
▪ Elevated titers used as marker to screenpopulations in high-risk areas and as potentialindicator of disease relapse
o Quantitative PCR testing for elevated circulatingEBV-DNA in plasma and serum reported sensitivityrates of up to 96%
o Newer antibody tests based on recombinant EBVantigens (e.g., EBV nuclear antigens [EBNA],
membrane antigen [MA], others) utilized indiagnosis
o Expression of EBV nuclear antigen-1 (EBNA-1),latent membrane protein-1 (LMP-1), EBV encodedRNA (EBER)
o EBV encoded miRNAs in circulation aid in earlydetection (biomarkers) and potential therapeuticagents in future
Treatment• Surgical approacheso Surgical intervention reserved for patients who fail
radiation therapy• Adjuvant therapyo Chemotherapy integrated with radiation (RT) in
advanced stage disease• Radiationo Supervoltage radiotherapy (6,500–7,000+ rads)
considered treatment of choice for all NPChistologic subtypes
▪ Given to nasopharynx and neck usingmegavoltage radiation with median dose of 70 Gy
Prognosis• Overall 5-year survival (approximately 75%)• Clinical stage at presentation represents most
important prognostic factoro 5-year disease-specific survival (DSS) for
▪ Stage I (98%)
▪ Stage IIA-B (95%)
▪ Stage III (86%)
▪ Stage IVA-B (73%)• Long-term outcomes in patients treated with
induction chemotherapy and radiotherapy (CRT) vs.radiotherapy alone (RT) showo Modest but significant decrease in relapse and
improvement in disease-specific survival inadvanced stage NPC
▪ Includes addition of cisplatin-based inductionchemotherapy (cisplatin, bleomycin, fluorouracilor cisplatin, and epirubicin) to RT
Terminology• Squamous cell carcinoma originating from
nasopharyngeal mucosa with evidence of squamousdifferentiation
Etiology/Pathogenesis• Strong association with Epstein-Barr virus (EBV)• Familial clustering and environmental exposures
Clinical Issues• Asymptomatic cervical neck mass typically localized
to posterior cervical triangle or superior jugular nodalchain
• Supervoltage radiotherapy treatment of choice• Overall 5-year survival approximately 65%
Microscopic Pathology• Nonkeratinizing differentiated type composed of
stratified cells with pleomorphic, hyperchromaticnuclei showing little to absent keratinization
• Nonkeratinizing undifferentiated type composedof cells with enlarged vesicular nuclei, prominenteosinophilic nucleoli
• Basaloid type with palisading, high N:C ratio,comedonecrosis, and abrupt keratinization
Ancillary Tests• CK-pan, CK5/6, and p63 strong and diffuse reaction• EBER ISH in up to 100% of NPC, nonkeratinizing
type
LDR Thompson, M.D. Used by Permission from: Diagnostic Pathology: Head & Neck LWW-Amirsys
ASCP Annual Meeting Surgical Pathology of Sinonasal Tract Tumors Session # 1015 on September 21, 2013
Page 4 of 60

NASOPHARYNGEAL CARCINOMA, NONKERATINIZING TYPES
o No substantive improvement in overall survivalreported
• Factors affecting prognosis may includeo Better prognosis associated with lower clinical stage,
younger patient age, female gendero Worse prognosis with higher stage tumors, older
patients, male gendero Undifferentiated (~75%) vs. keratinizing (~30%) 5-yr
survivalo Frequently metastasizes to regional lymph nodes
▪ Presence of lymph node metastasis decreases
survival by approximately 10–20%o Large percentage of NPCs, particularly
undifferentiated type, metastasize to sites belowclavicle, including lungs, bone (ribs and spine), liver
▪ Associated with worse prognosiso Poorer prognosis seen in patients with HLA-Aw33-
C3-B58/DR3 haplotype, while patients with A2-Cw11-Bw46/DR9 haplotype have longer survival
• Risk of developing synchronous or metachronous 2ndprimary malignancy approximately 4%
IMAGE FINDINGS
Radiographic Findings• Important diagnostic aid in assessing extent of disease
and presence of metastatic disease• Positron emission tomography and computed
tomography (PET/CT) is used in detection oflocoregional and distant spread of tumor
MR Findings• Preferred study for detection of invasion into soft
tissues, intracranial extension, and invasion into bone
MACROSCOPIC FEATURES
General Features• Varies to includeo No visible masso Mucosal bulge with overlying intact epitheliumo Demonstrable mass with extensive involvement of
surface epitheliumo Frankly infiltrative mass
MICROSCOPIC PATHOLOGY
Histologic Features• Nonkeratinizing differentiatedo Growth includes presence of interconnecting cords
or trabeculae
▪ Cystic change with associated necrosis commonlypresent
▪ Often metastases to lymph nodes include cysticchange with central necrosis
o Stratified cells with pleomorphic, hyperchromaticnuclei showing little to absent keratinization
▪ Well-defined cell borders and vague intercellularbridges may be present
▪ Keratinized cells may be identified
o Sharp delineation from surrounding stromao Increased mitotic activity, including atypical mitoseso Typically, absence of desmoplastic stromal response
to invasive growth• Nonkeratinizing undifferentiatedo Variable growth including cohesive or nested cell
nests (syncytial pattern) to diffuse cellular infiltratecomposed of dyscohesive cells
o Neoplastic cells characterized by
▪ Enlarged round nuclei with vesicular chromatin,prominent eosinophilic nucleoli, scanteosinophilic to amphophilic cytoplasm, indistinctborders
▪ Keratinization is typically absent but in any casemay be focally present
o Mitoses can be seen but typically not prominentlypresent
o Prominent nonneoplastic lymphoid componentcomposed of
▪ Mature lymphocytes and plasma cells
▪ May overrun and obscure invasive carcinomao Infiltrative growth generally does not produce host
desmoplastic response
▪ Absence of desmoplasia in conjunction withprominent benign lymphocytic infiltrateobscuring lesional cells may make diagnosisproblematic
▪ Absence of desmoplastic response may also bepresent in association with nodal metastasis
• Keratinizing typeo Infiltrative carcinoma characterized by presence of
keratinization and intercellular bridges
▪ Graded as well-, moderately, or poorlydifferentiated
o Desmoplastic stroma present in response to invasivecarcinoma
o Relative absence of associated lymphoid cellinfiltrate
• Basaloid squamous cell carcinomao Invasive neoplasm predominantly composed of
basaloid cells with associated squamous componento Varied growth patterns, including solid, lobular,
cribriform, cords, trabeculae, and gland-like or cystic
▪ Peripheral nuclear palisading and comedonecrosiso Squamous areas are typical focal areas of abrupt
keratinizationo Intercellular deposition of hyalin or mucohyalin
material can be seeno Infrequently, true neural-type rosettes may be
present• Uncommon to identify precursor lesion (i.e.,
intraepithelial dysplasia &/or carcinoma in situ)• Approximately 25% of NPCs show more than 1
histologic type
ANCILLARY TESTS
Immunohistochemistry• Strong immunoreactivity for cytokeratinso Pan-cytokeratins and high molecular weight
cytokeratins strongly positive
LDR Thompson, M.D. Used by Permission from: Diagnostic Pathology: Head & Neck LWW-Amirsys
ASCP Annual Meeting Surgical Pathology of Sinonasal Tract Tumors Session # 1015 on September 21, 2013
Page 5 of 60

NASOPHARYNGEAL CARCINOMA, NONKERATINIZING TYPES
o Weak immunoreactivity is present for low molecularweight cytokeratins
o Typically negative for cytokeratin 7, cytokeratin 20• Positive for EBVo Immunoreactivity for EBVo In situ hybridization for Epstein-Barr encoded RNA
(EBER)• Negative for p16
Molecular Genetics• Detection of EBV by polymerase chain reaction (PCR)
or in situ hybridization (ISH) found in 75-100% ofNPCs, nonkeratinizing typeso Not true in keratinizing subtype, in which detection
of EBV genomes is variableo Presence of EBV in keratinizing subtype generally
limited to scattered dysplastic intraepithelial cells• Development of NPC likely involves cumulative
genetic and epigenetic changes in background ofpredisposed genetic and environmental factors
DIFFERENTIAL DIAGNOSIS
Oropharyngeal Nonkeratinizing Carcinoma• Tonsillar and base of tongue carcinomas may share
histomorphologic features with NPC, differentiatedand undifferentiated typeso Such tumors are p16(+) and EBER(-)o Nodal metastatic p16(+), EBER(-) carcinomas may
originate from occult primary oropharyngealcarcinomas
o Work-up for nodal metastatic carcinomas withfeatures of NPC, differentiated and undifferentiated,should include staining for EBER and p16
Diffuse Large B-cell Lymphoma• Positive for hematolymphoid markers including CD45
(leucocyte common antigen) and B-cell markers• Negative for cytokeratins and EBV
Mucosal Malignant Melanoma• Positive for S100 protein, melanoma markers
(HMB-45, Melan-A, tyrosinase)
• Negative for cytokeratins and EBV
Rhabdomyosarcoma• Positive for myogenic markers (desmin, myoglobin,
myogenin)• Negative for cytokeratins and EBV
SELECTED REFERENCES1. He ML et al: MicroRNAs: potential diagnostic markers and
therapeutic targets for EBV-associated nasopharyngealcarcinoma. Biochim Biophys Acta. 1825(1):1-10, 2012
2. Caponigro F et al: Treatment approaches tonasopharyngeal carcinoma: a review. Anticancer Drugs.21(5):471-7, 2010
3. Singhi AD et al: Lymphoepithelial-like carcinoma of theoropharynx: a morphologic variant of HPV-related headand neck carcinoma. Am J Surg Pathol. 34(6):800-5, 2010
4. Afqir S et al: Nasopharyngeal carcinoma in adolescents:a retrospective review of 42 patients. Eur ArchOtorhinolaryngol. 266(11):1767-73, 2009
5. Liu T et al: FDG-PET, CT, MRI for diagnosis of local residualor recurrent nasopharyngeal carcinoma, which one is thebest? A systematic review. Radiother Oncol. 85(3):327-35,2007
6. Tao Q et al: Nasopharyngeal carcinoma: molecularpathogenesis and therapeutic developments. Expert RevMol Med. 9(12):1-24, 2007
7. Thompson LD: Update on nasopharyngeal carcinoma.Head Neck Pathol. 1(1):81-6, 2007
8. Brennan B: Nasopharyngeal carcinoma. Orphanet J RareDis. 1:23, 2006
9. Mirzamani N et al: Detection of EBV and HPV innasopharyngeal carcinoma by in situ hybridization. ExpMol Pathol. 81(3):231-4, 2006
10. Wei WI et al: Nasopharyngeal carcinoma. Lancet.365(9476):2041-54, 2005
11. Licitra L et al: Cancer of the nasopharynx. Crit Rev OncolHematol. 45(2):199-213, 2003
12. Ensley JF et al: Locally advanced nasopharyngeal cancer.Curr Treat Options Oncol. 2(1):15-23, 2001
13. Erkal HS et al: Nasopharyngeal carcinomas: analysis ofpatient, tumor and treatment characteristics determiningoutcome. Radiother Oncol. 61(3):247-56, 2001
14. Wenig BM: Nasopharyngeal carcinoma. Ann Diagn Pathol.3(6):374-85, 1999
Immunohistochemistry
Antibody Reactivity Staining Pattern CommentEBER Positive Nuclear All neoplastic cells (nonkeratinizing type)
CK5/6 Positive Cell membrane Nearly all tumor cells
p63 Positive Nuclear Nearly all neoplastic cells
CK-PAN Positive Cytoplasmic Nearly all neoplastic cells
34bE12 Positive Cytoplasmic Nearly all neoplastic cells
CK8/18/CAM5.2 Positive Cytoplasmic Patchy reaction
p53 Positive Nuclear Nearly all neoplastic cells
CK13 Positive Cytoplasmic
HLA-DR Positive Cytoplasmic Seldom used diagnostically
CK7 Negative
p16 Negative
S100 Negative
LDR Thompson, M.D. Used by Permission from: Diagnostic Pathology: Head & Neck LWW-Amirsys
ASCP Annual Meeting Surgical Pathology of Sinonasal Tract Tumors Session # 1015 on September 21, 2013
Page 6 of 60

NASOPHARYNGEAL CARCINOMA, NONKERATINIZING TYPES
Imaging Findings
(Left) This graphicdemonstrates a large massin the nasopharynx that hasexpanded into the base of theskull. (Right) Sagittal imageshows mass extending fromthe nasopharynx into the skullbase .
(Left) Coronal T1 C+ MR in apatient with NPC reveals bulkybilateral cervical adenopathy
. Notice that a smaller,right lateral tetropharyngealnode can also be seen nearthe skull base . (Right)This PET image demonstratesa very high signal in thearea of the nasopharyngealcarcinoma. This is shown witha superimposed computedtomography scan.
(Left) NPC, nonkeratinizingdifferentiated, may originatein the crypt epithelium
within the depth ofthe submucosa while thesurface epithelium isuninvolved by dysplasia &/or carcinoma. The carcinomashows cystic change andassociated necrosis. (Right)The neoplastic cells areexceedingly difficult to detect
in this NPC. There is nohost desmoplastic response.These findings give theimpression of a mixed reactiveinflammatory cell proliferation.
LDR Thompson, M.D. Used by Permission from: Diagnostic Pathology: Head & Neck LWW-Amirsys
ASCP Annual Meeting Surgical Pathology of Sinonasal Tract Tumors Session # 1015 on September 21, 2013
Page 7 of 60

NASOPHARYNGEAL CARCINOMA, NONKERATINIZING TYPES
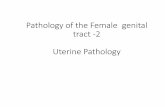
Microscopic Features
(Left) Sometimes, NPCmay grow in a sheet ofsyncytial cells that havea spindled morphology.There is an associatedlymphoid aggregate in thistumor, although not asheavy as in some lesions.(Right) NPC, nonkeratinizingundifferentiated type, showsa diffuse pattern of growthcomposed of dyscohesivecells with enlarged vesicularchromatin and prominentnucleoli. These overallfeatures raise concern fora possible misdiagnosis oflarge B-cell lymphoma.
(Left) A benign lymphocyticcell infiltrate is oftenpresent in associationwith the neoplastic cellsof NPC, nonkeratinizingundifferentiated type.In spite of the invasivegrowth, there is an absenceof desmoplasia. (Right)Amyloid may be presentin up to 5% of cases. Theextracellular, acellular,eosinophilic matrix materialseems to be identified only inendemic patients with NPC.
(Left) Nasopharyngealcarcinoma, nonkeratinizingdifferentiated type, ischaracterized by broadinterconnecting cords andtrabeculae of infiltrativecarcinoma. This patternof growth is indicative ofan infiltrative neoplasm.(Right) NPC, nonkeratinizingdifferentiated type, showsnuclear stratification withnuclear pleomorphism,increased mitotic figures ,absent keratinization, andabsent intercellular bridges.
LDR Thompson, M.D. Used by Permission from: Diagnostic Pathology: Head & Neck LWW-Amirsys
ASCP Annual Meeting Surgical Pathology of Sinonasal Tract Tumors Session # 1015 on September 21, 2013
Page 8 of 60

NASOPHARYNGEAL CARCINOMA, NONKERATINIZING TYPES
Subtypes of Nasopharyngeal Carcinoma
(Left) Nasopharyngealcarcinoma, nonkeratinizingdifferentiated type showslimited cytologic atypia, butmitoses, including atypicalforms are easily identified
. (Right) Nodal metastasisfrom a NPC, nonkeratinizingundifferentiated type, showscystic degeneration and anabsent desmoplastic reaction.The evaluation of such ametastasis may includeimmunohistochemistry toexclude another primarysource.
(Left) Nasopharyngeal invasivekeratinizing squamous cellcarcinoma invades into thesubmucosa with associateddesmoplastic stromal reactionand invasion into skeletalmuscle . (Right) Well-differentiated keratinizingsquamous cell carcinomais characterized by thepresence of limited (mild)cytologic atypia, cells withidentifiable keratinization ,and intercellular bridges .
(Left) Basaloid squamous cellcarcinoma is an infiltrativebasaloid cell neoplasm withvaried growth, includinglobular and trabecular patterns; abrupt squamousdifferentiation is present .(Right) Infiltrative nest orlobule with comedo-typenecrosis and adjacentarea show reduplicatedbasement membrane-likematerial reminiscent of salivarygland tumors . Basaloidcells predominate withoutsquamous differentiation.
LDR Thompson, M.D. Used by Permission from: Diagnostic Pathology: Head & Neck LWW-Amirsys
ASCP Annual Meeting Surgical Pathology of Sinonasal Tract Tumors Session # 1015 on September 21, 2013
Page 9 of 60

NASOPHARYNGEAL CARCINOMA, NONKERATINIZING TYPES
Immunohistochemistry Findings
(Left) Neural-type rosettescan be seen in BSCCraising concern for apossible diagnosis ofsmall cell undifferentiatedneuroendocrine carcinoma.BSCC typically lacksimmunostaining forneuroendocrine markers.(Right) The squamousdifferentiated componentof BSCC represents theminor component andmay be represented bypresence of focal areas ofabrupt keratinization to larger confluent foci ofkeratinization or invasiveSCC (not shown).
(Left) Cytokeratin staininghighlights the irregularclusters of carcinoma cells,as well as the extent ofthe invasive carcinoma.The extent of the invasivecarcinoma as demonstratedby the cytokeratin stainingmay not be appreciated bylight microscopic evaluation.(Right) There is a strong,diffuse, cytoplasmic andmembrane reactivity withCK5/6 in nasopharyngealcarcinoma, highlighting theepithelial cells within thebackground of lymphoidelements.
(Left) NPC, nonkeratinizingundifferentiated type isstrongly associated withEBV, as indicated by thepresence of nuclear labelingof tumor cells (in nests and individual cells )by in situ hybridizationfor EBER. (Right) Nearlyevery one of the neoplasticepithelial cells is stronglyand diffusely positive withEBER, evaluated by in situhybridization. This is a veryhelpful study to confirm thediagnosis of NPC.
LDR Thompson, M.D. Used by Permission from: Diagnostic Pathology: Head & Neck LWW-Amirsys
ASCP Annual Meeting Surgical Pathology of Sinonasal Tract Tumors Session # 1015 on September 21, 2013
Page 10 of 60

NASOPHARYNGEAL CARCINOMA, BASALOID SQUAMOUS CELL CARCINOMA
Basaloid squamous cell carcinoma is an infiltrativebasaloid cell neoplasm with varied growth, includinglobular and trabecular patterns; abrupt squamousdifferentiation is present .
The basaloid cells show marked nuclear pleomorphism,hyperchromasia, and increased mitotic activity .Peripheral nuclear palisading is present , but retractionartifact is not identified.
TERMINOLOGY
Abbreviations• Basaloid squamous cell carcinoma (BSCC)
Definitions• High-grade variant of squamous cell carcinoma
histologically characterized by invasive neoplasmcomposed predominantly of basaloid pleomorphiccells and variable squamous component
ETIOLOGY/PATHOGENESIS
Alcohol and Tobacco• Etiologic factors of BSCC occurring in more common
sites include excessive alcohol &/or tobacco use
Infectious Agents• Confusion in literature relative to association with
Epstein-Barr virus (EBV)o Asian patients reported EBV(+) while non-Asians
reported EBV(-)
▪ Likely not EBV associated; presence of EBVendemic to Asian population
o BSCC are typically not associated with humanpapillomavirus (HPV)
CLINICAL ISSUES
Epidemiology• Incidenceo Uncommon type of primary nasopharyngeal
carcinomao May occur in any mucosal site of upper
aerodigestive tract, but majority predilect tohypopharynx (piriform sinus), larynx (supraglottis),and palatine tonsil
• Age
o Occurs over wide age range from 3rd to 8th decadesof life (mean: 55 years)
• Gendero Male > Female
Presentation• Symptoms depend on site of occurrence and relative
to laryngeal tumors includeo Hoarseness, dysphagia, pain, or neck mass
Treatment• Options, risks, complicationso Radical surgical excisiono Due to early regional lymph node as well as distant
visceral metastases, radical neck dissection, andsupplemental radio- and chemotherapy may beincluded in initial management protocol
Prognosis• Nasopharyngeal BSCCs appear to have lower clinical
aggressiveness compared to BSCC of other head andneck siteso Of 6 cases reported
▪ 4 clinical stage T3 or T4
▪ 2 with nodal metastasis
▪ None with distant metastasis
▪ 3 with no evidence of disease at 34-52 months
▪ 3 alive with disease from 19-46 months• BSCCs of more common head and neck sites are
aggressive, high-grade tumors with increased tendencyto be multifocal, deeply invasive, and metastatico Metastases occur via lymphatics and blood vessels
with sites of predilection, including regional anddistant lymph nodes, lung, bone, skin, and brain
o Metastases include both basaloid and squamous cellcomponents
o Rapidly fatal associated with high mortality rateswithin 1st year following diagnosis
LDR Thompson, M.D. Used by Permission from: Diagnostic Pathology: Head & Neck LWW-Amirsys
ASCP Annual Meeting Surgical Pathology of Sinonasal Tract Tumors Session # 1015 on September 21, 2013
Page 11 of 60

NASOPHARYNGEAL CARCINOMA, BASALOID SQUAMOUS CELL CARCINOMA
Key Facts
MACROSCOPIC FEATURES
General Features• Firm to hard, tan-white mass often with associated
central necrosis• Infrequently may be exophytic in appearance
Size• May reach large size, measuring up to 6 cm in greatest
dimension
MICROSCOPIC PATHOLOGY
Histologic Features• Invasive neoplasm predominantly composed of
basaloid cells with associated squamous componento Varied growth patterns, including solid, lobular,
cribriform, cords, trabeculae, and gland-like or cystico Tends to be deeply invasive at presentation,
including neurotropism and lymph-vascularinvasion
▪ Shallow biopsies may belie depth and extent ofinvasion
• Basaloid cell componento Predominant cell typeo May be seen in direct continuity with surface
epitheliumo Pleomorphic, hyperchromatic nuclei, scanty
cytoplasm and variably sized but identifiablenucleoli
o Peripheral nuclear palisading may be presento Increased mitotic activity, including atypical mitoseso Necrosis commonly seen, including
▪ Comedonecrosis seen in center of neoplasticlobules
▪ Individual cell necrosiso Intercellular deposition of hyalin or mucohyalin
material can be seen
▪ Similar in appearance to reduplicated basementmembrane material seen in some salivary glandtumors
o Additional findings may include
▪ Cells with clear appearing cytoplasm may be seeneither focally or more extensively
▪ Spindle cell component may be identified butusually very focal, not predominate cell type
▪ Infrequently, true neural-type rosettes may bepresent
▪ Calcifications may be present• Squamous cell componento Typically, represents minor component
▪ May only be focally present
▪ In biopsies, squamous cell component may beabsent
o Includes intraepithelial dysplasia (moderateto severe dysplasia) &/or invasive squamouscell carcinoma with or without foci of abruptkeratinization
o Continuity with surface epithelium may be present
ANCILLARY TESTS
Histochemistry• Diastase-sensitive, periodic acid-Schiff(+)
intracytoplasmic material indicative of glycogen maybe present especially in cells with clear cytoplasm
Immunohistochemistry• Immunoreactivity consistently present for epithelial
markers, including cytokeratins (AE1/3, CAM5.2,others), EMA, and CEA
• Neuroendocrine markers, including chromogranin,synaptophysin, CD56 usually negative butoccasionally may be positive (synaptophysin >chromogranin)
• Likely EBV(-) although discrepant results reported• p16(-)o Oropharyngeal (tonsil, base of tongue) BSCC may be
p16(+)o Nonoropharyngeal BSCCs mostly p16(-)
• Variable expression seen for vimentin, NSE, S100protein, actin
Terminology• High-grade variant of squamous cell carcinoma
histologically characterized by invasive neoplasmcomposed predominantly of basaloid pleomorphiccells and variable squamous component
Clinical Issues• Uncommon type of primary nasopharyngeal
carcinoma• Nasopharyngeal BSCCs appear to have lower clinical
aggressiveness compared to BSCC of other head andneck sites
Microscopic Pathology• Invasive neoplasm predominantly composed of
basaloid cells with associated squamous component
• Varied growth patterns, including lobular (with orwithout comedonecrosis), solid, trabecular
• Basaloid cell component is predominant cell typecharacterized by pleomorphic, hyperchromatic nucleiwith increased mitotic activity
• Squamous cell component typically represents minorcomponent and may include keratinization, invasivesquamous cell carcinoma
• Intraepithelial dysplasia and carcinoma in situ maybe present
Ancillary Tests• Immunoreactivity consistently present for
cytokeratins• Neuroendocrine markers usually negative but
occasionally may be positive
LDR Thompson, M.D. Used by Permission from: Diagnostic Pathology: Head & Neck LWW-Amirsys
ASCP Annual Meeting Surgical Pathology of Sinonasal Tract Tumors Session # 1015 on September 21, 2013
Page 12 of 60

NASOPHARYNGEAL CARCINOMA, BASALOID SQUAMOUS CELL CARCINOMA
• Melanocytic markers (HMB-45, Melan-A, tyrosinase)and hematolymphoid markers negative
Electron Microscopy• Cell groups with numerous and prominent
tonofilament bundles, increased desmosomes,epithelial pearls, loose stellate granules, or replicatedbasal lamina within cystic spaces
• Absence of glandular differentiation
DIFFERENTIAL DIAGNOSIS
Oropharyngeal Nonkeratinizing Carcinoma• HPV-associated carcinoma distinct from BSCC• In situ and invasive carcinoma characterized by broad
interconnecting cords of tumor often with cysticchange and central necrosis
• Cells are nonkeratinizing characterized bypleomorphic basaloid-appearing nuclei with increasedmitotic activity
• Limited foci of squamous cell differentiation(keratinization) may be seen
• Immunoreactivity for p16
Adenoid Cystic Carcinoma• Characterized by isomorphic hyperchromatic basaloid
cells lacking pleomorphism, mitotic activity, andnecrosis
• Squamous differentiation not feature of AdCC• Immunohistochemical staining not helpful in
differential diagnosis
Small Cell Undifferentiated NeuroendocrineCarcinoma• Consistent immunoreactivity for neuroendocrine
markers (chromogranin, synaptophysin, CD56, CD57,TTF-1)
SELECTED REFERENCES1. Begum S et al: Basaloid squamous cell carcinoma of the
head and neck is a mixed variant that can be furtherresolved by HPV status. Am J Surg Pathol. 32(7):1044-50,2008
2. Muller E et al: The basaloid squamous cell carcinoma of thenasopharynx. Rhinology. 38(4):208-11, 2000
3. Paulino AF et al: Basaloid squamous cell carcinoma of thehead and neck. Laryngoscope. 110(9):1479-82, 2000
4. Barnes L et al: Basaloid squamous cell carcinoma of thehead and neck: clinicopathological features and differentialdiagnosis. Ann Otol Rhinol Laryngol. 105(1):75-82, 1996
5. Wan SK et al: Basaloid-squamous carcinoma of thenasopharynx. An Epstein-Barr virus-associated neoplasmcompared with morphologically identical tumors occurringin other sites. Cancer. 76(10):1689-93, 1995
6. Raslan WF et al: Basaloid squamous cell carcinoma of thehead and neck: a clinicopathologic and flow cytometricstudy of 10 new cases with review of the English literature.Am J Otolaryngol. 15(3):204-11, 1994
7. Klijanienko J et al: Basaloid squamous carcinoma of thehead and neck. Immunohistochemical comparison withadenoid cystic carcinoma and squamous cell carcinoma.Arch Otolaryngol Head Neck Surg. 119(8):887-90, 1993
8. Banks ER et al: Basaloid squamous cell carcinomaof the head and neck. A clinicopathologic andimmunohistochemical study of 40 cases. Am J Surg Pathol.16(10):939-46, 1992
Differential Diagnosis of Basaloid Squamous Cell Carcinoma
BSCC AdCC SCUNCAge/gender 6th-7th decades; M > F 5th-7th decades; equal
gender distribution except forsubmandibular tumors, whichpredilect to females
6th-7th decades; M > F
Location Predilects to hypopharynx (piriformsinus), larynx (supraglottis), andoropharynx (palatine tonsil)
Major and minor salivary glands Uncommon in head and neck;supraglottic larynx most commonsite
Surface involvement Present in the form of intraepithelialdysplasia
Absent Absent
Squamous component Present but is the minor componentand may only be found focally
Absent May be present; limited in extentwhen found
Neurotropism Present Present Present
Immunohistochemistry Immunoreactive for cytokeratins;neuroendocrine markers(chromogranin, synaptophysin,others) usually negative butoccasionally may be positive
Immunoreactivity for cytokeratins,p63, S100 protein, calponin,actins, and vimentin; negative forneuroendocrine markers
Positive for cytokeratins;immunoreactive for neuroendocrinemarkers (chromogranin,synaptophysin, CD56, CD57, TTF-1);calcitonin rarely is positive
HPV association No No No
Treatment Surgery, radiotherapy, chemotherapy Surgery, radiotherapy Systemic chemotherapy andtherapeutic irradiation
Prognosis Dependent on clinical stage butoverall considered to be poor;nasopharyngeal-based BSCC appearsto be less biologically aggressive thanother head and neck BSCCs
Short-term prognosis is good butlong-term prognosis is poor; survivalrates include 5-year (71-89%), 10-year(29-71%), 15-year (29-55%)
Poor: 2-year survival (16%), 5-yearsurvival (5%)
BSCC = basaloid squamous cell carcinoma of all head and neck sites; AdCC = adenoid cystic carcinoma; SCUNC = small cell undifferentiated neuroendocrine carcinoma.
LDR Thompson, M.D. Used by Permission from: Diagnostic Pathology: Head & Neck LWW-Amirsys
ASCP Annual Meeting Surgical Pathology of Sinonasal Tract Tumors Session # 1015 on September 21, 2013
Page 13 of 60

NASOPHARYNGEAL CARCINOMA, BASALOID SQUAMOUS CELL CARCINOMA
Microscopic Features
(Left) Infiltrative nests orlobules show a jigsaw-puzzle-like configurationpredominantly composedof malignant basaloid cellsshowing marked nuclearpleomorphism; squamousdifferentiated foci arenot identified. (Right)Infiltrative nest or lobulewith comedo-type necrosis
and adjacent area showreduplicated basementmembrane-like materialreminiscent of salivarygland tumors . Basaloidcells predominate withoutsquamous differentiation.
(Left) The squamousdifferentiated componentof BSCC represents theminor component andmay be represented bypresence of focal areasof abrupt keratinization
to larger confluentfoci of keratinizationor invasive keratinizingsquamous cell carcinoma(not shown). (Right) Inaddition to keratinizationor invasive squamous cellcarcinoma, there may beintraepithelial dysplasia orcarcinoma in situ, a featuresupporting origin fromsurface epithelium.
(Left) Additional cell typesthat can be seen in BSCC areclear cells that by specialstain contain glycogen (notshown). Note the prominentmalignant basaloid cells aswell as a focus of abruptkeratinization . (Right)Neural-type rosettes can beseen in BSCC raising concernfor a possible diagnosis ofsmall cell undifferentiatedneuroendocrine carcinoma(SCUNC). BSCC typicallylacks immunostaining forneuroendocrine markers,assisting in differentiating itfrom SCUNC.
LDR Thompson, M.D. Used by Permission from: Diagnostic Pathology: Head & Neck LWW-Amirsys
ASCP Annual Meeting Surgical Pathology of Sinonasal Tract Tumors Session # 1015 on September 21, 2013
Page 14 of 60

SINONASAL ADENOCARCINOMA, INTESTINAL TYPE
In this sinonasal tract intestinal-type adenocarcinoma,colonic type, a prevalence of tubuloglandulararchitecture, virtually identical to primary colonicadenocarcinoma, is shown.
The colonic type shows complex glandular growth withback to back glands . The histologic, histochemical,and immunohistochemical findings are identical tocolonic adenocarcinoma.
TERMINOLOGY
Abbreviations• Intestinal-type adenocarcinoma (ITAC)
Synonyms• Colonic-type adenocarcinoma• Enteric-type adenocarcinoma
Definitions• Malignant epithelial glandular tumors of sinonasal
tract (SNT) that histologically resemble intestinaladenocarcinoma
ETIOLOGY/PATHOGENESIS
Environmental Exposure• Exposure to hardwood dust, leather, and softwoodo Increased incidences in
▪ Woodworkers
▪ Workers in shoe and furniture industrieso May occur sporadically without environmental
exposure
CLINICAL ISSUES
Epidemiology• Incidenceo Adenocarcinomas (all types) comprise 10-20% of
sinonasal tract malignant neoplasms
▪ ITACs are rare• Ageo Occurs over wide range
▪ Most common in 5th to 7th decades of life• Gendero ITAC associated with environmental exposure
▪ Male > Femaleo ITAC not associated with environmental exposure
▪ Female > Male
Site• May arise anywhere in SNT but in decreasing order of
frequencyo Ethmoid sinus > nasal cavity (inferior and middle
turbinates) > maxillary sinus
Presentation• Early symptomso Nonspecific, varying from nasal stuffiness to
obstructiono May be associated with epistaxis
• Due to delay in diagnosis, tumors may reach large sizewith extensive invasion at time of presentationo Advanced tumors present with pain, cranial nerve
deficits, visual disturbances, and exophthalmos
Treatment• Surgical approacheso Complete surgical resection with radiation
▪ Depending on extent of neoplasm, surgery variesfrom local excision to more radical procedures(maxillectomy, ethmoidectomy, and additionalexenterations)
o Neck dissection not indicated• Radiationo Radiotherapy may be utilized for extensive disease
&/or for higher grade neoplasms
Prognosis• All ITACs considered as potentially aggressive, lethal
tumors• 5-year cumulative survival rate is around 40%, with
most deaths occurring within 3 years• Generally are locally aggressive tumors with frequent
local failure (approximately 50%)• Metastasis to cervical lymph nodes and spread
to distant sites are infrequent, occurring inapproximately 10% and 20%, respectively
LDR Thompson, M.D. Used by Permission from: Diagnostic Pathology: Head & Neck LWW-Amirsys
ASCP Annual Meeting Surgical Pathology of Sinonasal Tract Tumors Session # 1015 on September 21, 2013
Page 15 of 60

SINONASAL ADENOCARCINOMA, INTESTINAL TYPE
Key Facts
• Death results from uncontrollable local or regionaldisease with extension and invasion of vital structures&/or metastatic disease
• Most patients present with advanced local disease, soclinical staging generally has no relevant prognosticsignificance
• Histologic subtype identified as indicative of clinicalbehavioro Papillary type (grade I) behave more indolently than
other histologic variants• No difference in behavior between ITAC occurring in
occupational exposed individuals and sporadicallyoccurring ITACs
IMAGE FINDINGS
Radiographic Findings• Essential in determining extent of disease and
planning surgery• Early lesionso Soft tissue masso Absent to minimal bone destruction
• More advance lesions associated witho Osteodestructiono Invasion of contiguous anatomic structures/
compartments
▪ e.g., orbit, cranial cavity
MICROSCOPIC PATHOLOGY
Histologic Features• 2 histologic classifications proposedo Barnes vs. Kleinsasser and Schroeder
▪ Either classification is acceptable, but forsimplicity Barnes classification is preferred
o Barnes classification
▪ Papillary
▪ Colonic
▪ Solid
▪ Mucinous
▪ Mixed
o Kleinsasser and Schroeder classification
▪ Papillary tubular cylinder (PTCC) types I-III (I =well differentiated, II = moderately differentiated,III = poorly differentiated)
▪ Alveolar goblet type
▪ Signet ring type
▪ Transitional type• Papillary typeo Represents approximately 18% of caseso Shows predominance of papillary architecture with
occasional tubular glands, minimal cytologic atypia,rare mitotic figures
• Colonic typeo Represents approximately 40% of caseso Prevalence of tubuloglandular architecture, rare
papillae, with increased nuclear pleomorphism andmitotic activity
• Solid typeo Represents approximately 20% of caseso Loss of differentiation characterized by solid and
trabecular growth with isolated tubule formationo Marked increase in smaller cuboidal cells with
nuclear pleomorphism, round vesicular nuclei,prominent nucleoli, and increased mitotic figures
• Mucinous typeo Uncommon typeo One pattern shows
▪ Solid clusters of cells, individual glands, signetring cells, short papillary fronds with or withoutfibrovascular cores
▪ Mucin predominantly intracellular, andmucomyxoid matrix may be present
o Another pattern shows
▪ Presence of large, well-formed glands distended bymucus and extracellular mucin pools
▪ Pools of extracellular mucin separated by thinconnective tissue septa creating alveolar-typepattern
▪ Predominantly cuboidal or goblet tumor cellspresent in single layers at periphery of mucuslakes
Terminology• Malignant epithelial glandular tumors of sinonasal
tract that histologically resemble intestinaladenocarcinoma
Etiology/Pathogenesis• Exposure to hardwood dust, leather, and softwoodo Increased incidences in woodworkers, workers in
shoe and furniture industrieso May occur sporadically without environmental
exposure
Clinical Issues• May arise anywhere in SNT but in decreasing order of
frequencyo Ethmoid sinus > nasal cavity (inferior and middle
turbinates) > maxillary sinus
• Complete surgical resection with radiation• All ITACs considered potentially aggressive, lethal• 5-year cumulative survival rate is around 40%, with
most deaths occurring within 3 years
Microscopic Pathology• Barnes classificationo Papillaryo Colonico Solido Mucinouso Mixed
Ancillary Tests• Reactive for gastrointestinal type markerso CK20, CDX-2, villin, mucin-related antigens
(MUCs)
LDR Thompson, M.D. Used by Permission from: Diagnostic Pathology: Head & Neck LWW-Amirsys
ASCP Annual Meeting Surgical Pathology of Sinonasal Tract Tumors Session # 1015 on September 21, 2013
Page 16 of 60

SINONASAL ADENOCARCINOMA, INTESTINAL TYPE
▪ Mucus extravasation elicits inflammatory responsethat may include multinucleated giant cells
▪ Tumors where mucus component predominates(> 50%) are similar to their gastrointestinalcounterparts and may be classified as mucinousadenocarcinomas
• Papillary and colonic types are most commonhistologic types, whether occurring in association withenvironmental exposure or sporadically
• Irrespective of histologic type, ITACs histologicallysimulate normal intestinal mucosa and may includeo Villi, Paneth cells, enterochromaffin cells, and
muscularis mucosa• In rare instances, lesion is composed of well-formed
villi lined by columnar cells resembling resorptive cellso In such cases, bundles of smooth muscle cells
resembling muscularis mucosae may also beidentified under villi
• Mixed typeo Rare typeo Composed of admixture of 2 or more of the
previously defined patterns
ANCILLARY TESTS
Histochemistry• Mucicarmineo Intracytoplasmic and intraluminal positive
• PAS with diastaseo Diastase-resistant, PAS-positive intracytoplasmic and
intraluminal material
Immunohistochemistry• Reactive for gastrointestinal type markerso CK20 positivity (up to 86% of cases)o CDX-2 is nuclear transcription factor involved in
differentiation of intestinal epithelial cells anddiffusely expressed in intestinal adenocarcinomasreactive in ITACs
o Expression of villin also presento Mucin-related antigens (MUCs) include MUC2(+),
MUC5(+)• Strongly reactive with pancytokeratins• Variable CK7 reactivity (43-93% of cases)• Variably positive for other epithelial markers includingo Epithelial membrane antigen, B72.3, Ber-EP4,
BRST-1, Leu-M1, and human milk fat globule(HMFG-2)
o Variable CEA staining• Neoplastic cells may express variety of hormone
peptides includingo Serotonin, cholecystokinin, gastrin, somatostatin,
leu-enkephalin• Chromogranin, synaptophysin, CD56 positivity can
be identifiedo Rare examples of mixed ITAC-small cell
neuroendocrine carcinoma reported• Epidermal growth factor receptor (EGFR) protein
expression and EGFR gene copy gains reportedo Frequency of EGFR overexpression significantly
higher in woodworkers than in leatherworkers orthose with no known occupational history
o High levels of EGFR often associated with eithergene amplification or chromosome 7 polysomy
• p53 immunoreactivity can be identified• Increased proliferation rate by Ki-67 (MIB-1) staining
Cytogenetics• Chromosomal gains and losses identified by
comparative genomic hybridization (CGH)o Gains at 5p15, 20q13, and 8q24o Losses at 4q31-qter, 18q12-22, 8p12-pter, and 5q11-
qtero Microsatellite instability (MSI) not detected
Molecular Genetics• Discrepant molecular findings includingo K-ras mutations from 0-20%o H-ras mutations from 0-25%o P53 mutations from 14-44%
DIFFERENTIAL DIAGNOSIS
Metastatic Adenocarcinoma ofGastrointestinal Origin• Rare occurrence to sinonasal tract• Clinical history critical and mandatory in excluding
a metastasis to sinonasal tract from primarygastrointestinal tract (GIT) neoplasm
• Histology, histochemistry, and immunohistochemistryof ITAC essentially identical to GIT adenocarcinomas
Sinonasal Nonintestinal-NonsalivaryAdenocarcinoma• Morphologic features differ from ITACs• Lack immunoreactivity for gastrointestinal-type
markerso e.g., CK20, CDX-2, villin, mucins
Salivary Gland Adenocarcinomas• Most common type in SNT is adenoid cystic
carcinoma• Less common types includeo Acinic cell adenocarcinomao Mucoepidermoid carcinoma
• Overall histology of salivary gland carcinomas differfrom SNT ITACs
Nasopharyngeal Low-Grade PapillaryAdenocarcinoma• Localization to nasopharynx most often along lateral
wall• Immunoreactive for thyroid transcription factor 1
(TTF-1)• Lack immunoreactivity for gastrointestinal-type
markers
Papillary Sinusitis• Comprised of ciliated respiratory epithelium with
simple papillae lacking complex growth• Absence of dysplastic epithelial changes• Absence of infiltrative growth
LDR Thompson, M.D. Used by Permission from: Diagnostic Pathology: Head & Neck LWW-Amirsys
ASCP Annual Meeting Surgical Pathology of Sinonasal Tract Tumors Session # 1015 on September 21, 2013
Page 17 of 60

SINONASAL ADENOCARCINOMA, INTESTINAL TYPE
SELECTED REFERENCES1. Mayr SI et al: Characterization of initial clinical symptoms
and risk factors for sinonasal adenocarcinomas: resultsof a case-control study. Int Arch Occup Environ Health.83(6):631-8, 2010
2. Stelow EB et al: Adenocarcinoma of the upper aerodigestivetract. Adv Anat Pathol. 17(4):262-9, 2010
3. Thompson LD: Intestinal-type sinonasal adenocarcinoma.Ear Nose Throat J. 89(1):16-8, 2010
4. Hermsen MA et al: Genome-wide analysis of geneticchanges in intestinal-type sinonasal adenocarcinoma. HeadNeck. 31(3):290-7, 2009
5. Jain R et al: Composite intestinal-type adenocarcinomaand small cell carcinoma of sinonasal tract. J Clin Pathol.62(7):634-7, 2009
6. Llorente JL et al: Genetic and clinical aspects of wood dustrelated intestinal-type sinonasal adenocarcinoma: a review.Eur Arch Otorhinolaryngol. 266(1):1-7, 2009
7. Martínez JG et al: Microsatellite instability analysis ofsinonasal carcinomas. Otolaryngol Head Neck Surg.140(1):55-60, 2009
8. Perez-Ordoñez B: Hamartomas, papillomas andadenocarcinomas of the sinonasal tract and nasopharynx. JClin Pathol. 62(12):1085-95, 2009
9. Castillo C et al: Signet-ring cell adenocarcinoma ofsinonasal tract: an immunohistochemical study of themucins profile. Arch Pathol Lab Med. 131(6):961-4, 2007
10. Ozolek JA et al: Basal/myoepithelial cells in chronicsinusitis, respiratory epithelial adenomatoid hamartoma,inverted papilloma, and intestinal-type and nonintestinal-type sinonasal adenocarcinoma: an immunohistochemicalstudy. Arch Pathol Lab Med. 131(4):530-7, 2007
11. Luna MA: Sinonasal tubulopapillary low-gradeadenocarcinoma: a specific diagnosis or just anotherseromucous adenocarcinoma? Adv Anat Pathol.12(3):109-15, 2005
12. Yom SS et al: Genetic analysis of sinonasal adenocarcinomaphenotypes: distinct alterations of histogeneticsignificance. Mod Pathol. 18(3):315-9, 2005
13. Ariza M et al: Comparative genomic hybridizationin primary sinonasal adenocarcinomas. Cancer.100(2):335-41, 2004
14. Cathro HP et al: Immunophenotypic differences betweenintestinal-type and low-grade papillary sinonasaladenocarcinomas: an immunohistochemical study of22 cases utilizing CDX2 and MUC2. Am J Surg Pathol.28(8):1026-32, 2004
15. Franchi A et al: CDX-2, cytokeratin 7 and cytokeratin20 immunohistochemical expression in the differentialdiagnosis of primary adenocarcinomas of the sinonasaltract. Virchows Arch. 445(1):63-7, 2004
16. Kennedy MT et al: Expression pattern of CK7,CK20, CDX-2, and villin in intestinal-type sinonasaladenocarcinoma. J Clin Pathol. 57(9):932-7, 2004
17. Perez-Ordonez B et al: Expression of mismatch repairproteins, beta catenin, and E cadherin in intestinal-typesinonasal adenocarcinoma. J Clin Pathol. 57(10):1080-3,2004
18. Bashir AA et al: Sinonasal adenocarcinoma:immunohistochemical marking and expression ofoncoproteins. Head Neck. 25(9):763-71, 2003
19. Sklar EM et al: Sinonasal intestinal-type adenocarcinomainvolvement of the paranasal sinuses. AJNR Am JNeuroradiol. 24(6):1152-5, 2003
20. Franchi A et al: Clinical relevance of the histologicalclassification of sinonasal intestinal-type adenocarcinomas.Hum Pathol. 30(10):1140-5, 1999
21. Gallo O et al: Prognostic significance of c-erbB-2oncoprotein expression in intestinal-type adenocarcinomaof the sinonasal tract. Head Neck. 20(3):224-31, 1998
22. Saber AT et al: K-ras mutations in sinonasaladenocarcinomas in patients occupationally exposed towood or leather dust. Cancer Lett. 126(1):59-65, 1998
23. Franchi A et al: Prognostic implications of Sialosyl-Tn antigen expression in sinonasal intestinal-typeadenocarcinoma. Eur J Cancer B Oral Oncol. 32B(2):123-7,1996
24. Van den Oever R: Occupational exposure to dust andsinonasal cancer. An analysis of 386 cases reported to theN.C.C.S.F. Cancer Registry. Acta Otorhinolaryngol Belg.50(1):19-24, 1996
25. Leung SY et al: Epstein-Barr virus is present in a widehistological spectrum of sinonasal carcinomas. Am J SurgPathol. 19(9):994-1001, 1995
26. McKinney CD et al: Sinonasal intestinal-typeadenocarcinoma: immunohistochemical profile andcomparison with colonic adenocarcinoma. Mod Pathol.8(4):421-6, 1995
27. Urso C et al: Intestinal-type adenocarcinoma of thesinonasal tract: a clinicopathologic study of 18 cases.Tumori. 79(3):205-10, 1993
28. Franquemont DW et al: Histologic classification ofsinonasal intestinal-type adenocarcinoma. Am J SurgPathol. 15(4):368-75, 1991
29. López JI et al: Intestinal-type adenocarcinoma of the nasalcavity and paranasal sinuses. A clinicopathologic study of 6cases. Tumori. 76(3):250-4, 1990
30. Alessi DM et al: Nonsalivary sinonasal adenocarcinoma.Arch Otolaryngol Head Neck Surg. 114(9):996-9, 1988
31. Hayes RB et al: Wood-related occupations, wood dustexposure, and sinonasal cancer. Am J Epidemiol.124(4):569-77, 1986
32. Mills SE et al: Aggressive sinonasal lesion resemblingnormal intestinal mucosa. Am J Surg Pathol. 6(8):803-9,1982
Sinonasal Tract ITACs Classification
Barnes Kleinsasser & Schroeder Percentage of Cases 3-Year Cumulative SurvivalPapillary type Papillary tubular cylinder cell I 18% 82%
Colonic type Papillary tubular cylinder cell II 40% 54%
Solid type Papillary tubular cylinder cell III 20% 36%
Mucinous type Alveolar goblet Uncommon 48%
Signet ring Uncommon 0%
Mixed type Transitional Rare 71%
LDR Thompson, M.D. Used by Permission from: Diagnostic Pathology: Head & Neck LWW-Amirsys
ASCP Annual Meeting Surgical Pathology of Sinonasal Tract Tumors Session # 1015 on September 21, 2013
Page 18 of 60

SINONASAL ADENOCARCINOMA, INTESTINAL TYPE
Imaging and Microscopic Features
(Left) Axial CECT shows aheterogeneous mass withcystic foci, which arises in theanterior ethmoid sinuses, afrequent location for sinonasaladenocarcinomas associatedwith environmental exposures.The mass shows extensivelocal invasion, including intothe nasal soft tissues .(Right) Axial CT demonstratesa destructive lesion in theright sinonasal cavities witherosion of the medial antralwall and spread into thepterygopalatine fossa .
(Left) Sinonasal intestinal-typeadenocarcinoma, papillarytype, arises in the submucosaand is characterized bythe presence of papillaryarchitecture as well asglandular and cystic growthpatterns. (Right) Prominentpapillary architecture is seen with fibrovascularcores . These findingsrecapitulate the histologicfeatures of primary intestinaladenocarcinoma.
(Left) Sinonasaladenocarcinoma, mucinoustype, shows abundantextracellular mucin pools as well as scattered glandularepithelial structures . (Right)Scattered malignant neoplasticcells , including cells withintracellular mucin , liewithin copious extracellularmucinous pools . The extentof the extracellular mucinousmaterial defines the extent ofthe tumor even if epithelialstructures are not uniformlyseen.
LDR Thompson, M.D. Used by Permission from: Diagnostic Pathology: Head & Neck LWW-Amirsys
ASCP Annual Meeting Surgical Pathology of Sinonasal Tract Tumors Session # 1015 on September 21, 2013
Page 19 of 60

SINONASAL ADENOCARCINOMA, INTESTINAL TYPE
Microscopic and Immunohistochemical Features
(Left) All types ofsinonasal intestinal-type adenocarcinomas,irrespective of their histology,including mucinous type, arecapable of aggressive growthwith extensive invasion ofbone . (Right) The solidtype of sinonasal intestinaladenocarcinoma showsa loss of differentiationcharacterized by solidgrowth with attemptsat tubule formation ,scattered goblet cells ,and nuclear pleomorphism.
(Left) Immunohistochemicalstaining of sinonasalintestinal-typeadenocarcinoma is similarto that of primary colonicadenocarcinomas, includingthe presence of diffuseCK20 immunoreactivity.(Right) Diffuse and strong(nuclear) immunoreactivityis present for CDX-2, whichis a nuclear transcriptionfactor involved in thedifferentiation of intestinalepithelial cells and diffuselyexpressed in primaryintestinal adenocarcinomas.
(Left) In addition toCK20 and CDX-2, theimmunoreactivity ofsinonasal ITACs may alsoinclude villin. (Right) Mucin-related antigens (MUCs),including MUC2, arealso present in sinonasalITACs. On the basis of lightmicroscopy, histochemicaland immunohistochemicalstaining, there is nodifference between primarycolonic adenocarcinomaand ITACs. Clinical historyis important in trying todifferentiate between ITACand a metastasis.
LDR Thompson, M.D. Used by Permission from: Diagnostic Pathology: Head & Neck LWW-Amirsys
ASCP Annual Meeting Surgical Pathology of Sinonasal Tract Tumors Session # 1015 on September 21, 2013
Page 20 of 60

NASOPHARYNGEAL ANGIOFIBROMA
Hematoxylin & eosin shows an intact surface with a widevariety of vessels set within a fibrous stroma. Some of thevessels have smooth muscle and others do not. Patulousand compressed vessels are noted.
Hematoxylin & eosin shows smooth-muscle-walledvessels adjacent to vessels without smooth muscle ,along with numerous capillaries within a fibrous stroma.
TERMINOLOGY
Abbreviations• Juvenile angiofibroma (JNA)• Angiofibroma (AF)
Synonyms• Angiomyofibroblastoma-like tumor• Angiofibroma• Fibroangioma• Fibroma
Definitions• Benign, highly cellular and richly vascularized
mesenchymal neoplasm arising in nasopharynx inmales
ETIOLOGY/PATHOGENESIS
Hormonal• Testosterone-dependent puberty-induced growth can
be blocked with estrogen &/or progesterone therapy
Genetic• Reported association with familial adenomatous
polyposis
CLINICAL ISSUES
Epidemiology• Incidenceo < 1% of all nasopharyngeal tumorso < 0.1% of all head and neck neoplasms
• Ageo < 20 years old
▪ Adolescents to young men
▪ Peak in 2nd decade of life• Gendero Males exclusively
o If diagnosed in female, studies of sex chromosomesrequired to confirm gender
• Ethnicityo Higher frequency in fair-skinned, red-haired patients
▪ Develops throughout the world
Site• Nasopharynx usually affected• Pterygoid region usually affected• May expand to involve surrounding structures (30% of
cases)o Anterior: Nasal cavity and maxillary sinus via roof of
nasopharynxo Lateral: Temporal and infratemporal fossae via
pterygomaxillary fissure, resulting in cheek orintraoral buccal mass
o Posterior: Middle cranial fossao Superior: Pterygopalatine fossa and orbit via inferior
and superior orbital fissures resulting in proptosiso Medial: Contralateral side
Presentation• Nasal obstruction• Recurrent, spontaneous epistaxis• Nasal discharge• Facial deformity (proptosis), exophthalmia, diplopia• Rhinolalia, sinusitis• Otitis media, tinnitus, deafness• Headaches• Rarely, anosmia or pain• Increased frequency in red-haired, fair-skinned boyso Predicated on Caucasian population
• Symptoms present for 12-24 months (nonspecificpresentation)
Treatment• Options, risks, complicationso Benign tumor can show aggressive local growtho Biopsy is contraindicated due to potential
exsanguinationo Potential for facial deformity if allowed to grow
LDR Thompson, M.D. Used by Permission from: Diagnostic Pathology: Head & Neck LWW-Amirsys
ASCP Annual Meeting Surgical Pathology of Sinonasal Tract Tumors Session # 1015 on September 21, 2013
Page 21 of 60

NASOPHARYNGEAL ANGIOFIBROMA
Key Facts
• Surgical approacheso Surgery is treatment of choiceo Definitive resection is frequently associated with
significant morbidity• Drugso Preoperative hormone therapy
▪ Not as popular as other modalities
▪ Giving estrogens to pubertal males is undesirable• Radiationo Used to manage large, intracranial, or recurrent
tumors• Angiographyo Selective angiography allows embolization with
sclerosing agent or cryotherapy
Prognosis• Good• May have fatal exsanguination if incorrectly managed• Recurrences in ~ 20% of patientso Usually develop within 2 years of diagnosiso Commonly extends intracranially
IMAGE FINDINGS
General Features• Best diagnostic clueo Anterior bowing of posterior wall of maxillary sinus
with posterior displacement of pterygoid plates(Holman-Miller sign)
• Locationo Nasopharynx with extension into surrounding
structures• Angiography identifies feeding vessel(s) and allows for
presurgical embolizationo Tumor blush is characteristic
CT Findings• Allows for accurate determination of size and extent• Enhancement is different from adjacent muscle,
accentuated with contrast• Bony margins may be eroded
MACROSCOPIC FEATURES
General Features• Polypoid mass with multinodular contour• Red, gray-tan cut surface
Size• Mean: 4 cm• Range: Up to 22 cm
MICROSCOPIC PATHOLOGY
Histologic Features• Submucosal proliferation of vascular component
within fibrous stroma• Many variably sized disorganized vesselso Varying thickness of vessel wall with patchy muscle
contento Vessels are mostly thin-walled, slit-like ("staghorn")o Range from capillary size to large, dilated, patulous
vessels• Focal, pad-like, smooth muscle thickenings within
vessel walls• Endothelial cells may be plump but are usually
attenuated• Fibrous stroma consists of plump spindle, angular, or
stellate-shaped cells• Variable amounts of fine and coarse collagen fibers• Myxoid degeneration is common (especially in
embolized specimens)o May see foreign material within vessels in embolized
cases• As stroma increases, vascular compression results in
virtually nonexistent lumina• Elastic tissue is not identified within stroma• Stromal cells may be angulated, multinucleated, and
pleomorphic• Mitotic figures are sparse• Mast cells may be seen• Hormone treated cases show increased collagenization
of stroma with fewer, but thicker-walled vessels
Terminology• Benign, highly cellular and richly vascularized
mesenchymal neoplasm arising in nasopharynx inmales
Clinical Issues• Recurrent, spontaneous epistaxis• Nasopharynx is nearly always affected• Patients < 20 years old• Males exclusively• Recurrences in ~ 20% of patients• Range up to 22 cm in size
Image Findings• Anterior bowing of posterior wall of maxillary sinus
with posterior displacement of pterygoid plates(Holman-Miller sign)
• Angiography identifies feeding vessel(s) and allowsfor presurgical embolization
• Tumor blush is characteristic
Microscopic Pathology• Submucosal proliferation of vascular component
within fibrous stroma• Many variably sized, disorganized vessels• Fibrous stroma consists of plump spindle, angular, or
stellate-shaped cells• Variable amounts of fine and coarse collagen fibers• Elastic tissue is not identified within stroma
Top Differential Diagnoses• Lobular capillary hemangioma• Inflammatory polyp• Antrochoanal polyp
LDR Thompson, M.D. Used by Permission from: Diagnostic Pathology: Head & Neck LWW-Amirsys
ASCP Annual Meeting Surgical Pathology of Sinonasal Tract Tumors Session # 1015 on September 21, 2013
Page 22 of 60

NASOPHARYNGEAL ANGIOFIBROMA
• Sarcomatous transformation is exceedinglyuncommon evento Develops following massive doses of radiation
ANCILLARY TESTS
Histochemistry• Reticulin shows positive black staining around stromal
cells and blood vessels• Elastic van Gieson highlights elastic tissue within
vessel walls
Immunohistochemistry• Vessels are highlighted within myofibroblastic stroma
DIFFERENTIAL DIAGNOSIS
Lobular Capillary Hemangioma• Lesion is ulcerated; arises from different anatomic site;
has granulation-type tissue and lots of inflammation;vessels are more organized
Inflammatory Polyp• Especially if there are atypical stromal cells; usually
more edematous; lacks rich vascular investment
Antrochoanal Polyp• Arises from different location; heavy stromal fibrosis,
but usually lacks characteristic vascular pattern of JNA
SELECTED REFERENCES1. Bleier BS et al: Current management of juvenile
nasopharyngeal angiofibroma: a tertiary center experience1999-2007. Am J Rhinol Allergy. 23(3):328-30, 2009
2. Carrillo JF et al: Juvenile nasopharyngeal angiofibroma:clinical factors associated with recurrence, and proposal ofa staging system. J Surg Oncol. 98(2):75-80, 2008
3. Coutinho-Camillo CM et al: Genetic alterations in juvenilenasopharyngeal angiofibromas. Head Neck. 30(3):390-400,2008
4. Glad H et al: Juvenile nasopharyngeal angiofibromas inDenmark 1981-2003: diagnosis, incidence, and treatment.Acta Otolaryngol. 127(3):292-9, 2007
5. Tyagi I et al: Staging and surgical approaches in largejuvenile angiofibroma--study of 95 cases. Int J PediatrOtorhinolaryngol. 70(9):1619-27, 2006
6. Thompson LDR et al: Tumours of the Nasopharynx:Nasopharyngeal angiofibroma. Barnes EL et al: Pathologyand Genetics of Head and Neck Tumours. World HealthOrganization Classification of Tumours. Lyon, France:IARC Press. 102-3, 2005
7. Fletcher CD: Distinctive soft tissue tumors of the head andneck. Mod Pathol. 15(3):324-30, 2002
8. Lee JT et al: The role of radiation in the treatment ofadvanced juvenile angiofibroma. Laryngoscope. 112(7 Pt1):1213-20, 2002
9. Coffin CM et al: Fibroblastic-myofibroblastic tumors inchildren and adolescents: a clinicopathologic study of 108examples in 103 patients. Pediatr Pathol. 11(4):569-88,1991
10. Makek MS et al: Malignant transformation of anasopharyngeal angiofibroma. Laryngoscope. 99(10 Pt1):1088-92, 1989
Immunohistochemistry
Antibody Reactivity Staining Pattern CommentVimentin Positive Cytoplasmic All elements of tumor
Actin-sm Positive Cytoplasmic Smooth muscle of vessel walls highlighted
Actin-HHF-35 Positive Cytoplasmic Smooth muscle of vessel walls highlighted
Desmin Positive Cytoplasmic Only within larger vessel walls
Androgen receptor Positive Nuclear Stromal cells and endothelial cell nuclei
ER Positive Nuclear Variably reactive, mostly in vascular nuclei
PR Positive Nuclear Variably reactive, mostly in vascular nuclei
FVIIIRAg Positive Cytoplasmic Endothelial cells only
CD34 Positive Cytoplasmic Endothelial cells only
CD31 Positive Cytoplasmic Endothelial cells only
PDGF-B Positive Cytoplasmic
IGF-2 Positive Cytoplasmic
S100 Positive Nuclear & cytoplasmic Highlights entrapped nerves but not tumor cells
Staging for Nasopharyngeal Angiofibroma
Stage Radiographic, Clinical, or Pathologic FindingI Tumor limited to nasopharynx with no bone destruction
II Tumor invading nasal cavity, maxillary, ethmoid, and sphenoid sinus with no bone destruction
III Tumor invading pterygo-palatine fossa, infratemporal fossa, orbit, and parasellar region
IV Tumor with massive invasion of cranial cavity, cavernous sinus, optic chiasm, or pituitary fossa
LDR Thompson, M.D. Used by Permission from: Diagnostic Pathology: Head & Neck LWW-Amirsys
ASCP Annual Meeting Surgical Pathology of Sinonasal Tract Tumors Session # 1015 on September 21, 2013
Page 23 of 60

NASOPHARYNGEAL ANGIOFIBROMA
Radiographic and Microscopic Features
(Left) MR shows intracranialextension of a large,destructive, hyperintensemass in the nasopharynx.The bone has beenremodeled and pushedaside. Note the fluidcollection in the sinusesas a postobstructivephenomenon. (Right)Hematoxylin & eosinshows numerous vesselsof various calibers, somewith smooth muscle setin a heavily collagenizedstroma. The stroma showshypocellularity.
(Left) Hematoxylin &eosin shows increasedcollagen deposition, oftenseen in lesions of a longduration. Note how thevessels are compressedand narrowed to a nearlyslit-like configuration.(Right) Hematoxylin &eosin shows a "pad" ofsmooth muscle within thevessel wall . The vesselcontains erythrocytes. Notethe increased number ofmast cells in the stroma,which has wavy collagendeposition.
(Left) Elastic von Giesonshows elastic tissue (blackdeposition as short towavy fragments) in thelarger vessel but notin the smaller vessels. Thisresults in profuse epistaxis,as the vessels are unableto contract and staunchbleeding. (Right) Musclespecific actin highlights themuscle walls around vessels
. The variable intensityof the reaction helps todemonstrate the variableamounts of smooth muscleassociated with the vessels.
LDR Thompson, M.D. Used by Permission from: Diagnostic Pathology: Head & Neck LWW-Amirsys
ASCP Annual Meeting Surgical Pathology of Sinonasal Tract Tumors Session # 1015 on September 21, 2013
Page 24 of 60

SINONASAL (SCHNEIDERIAN) PAPILLOMA
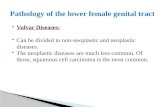
Endophytic or "inverted" growth pattern consists ofthickened epithelial nests arising from the surfacerespiratory epithelium with downward growth. The nestsmay not be very deep.
The epithelial proliferation is benign with an absenceof cytologic atypia. Intraepithelial inflammatory cells,cysts , and scattered mucocytes are features ofSchneiderian papillomas.
TERMINOLOGY
Synonyms• Sinonasal-type papillomas• 3 morphologic types identified includeo Invertedo Exophytic (fungiform, septal)o Oncocytic (cylindrical or columnar cell)
Definitions• Group of benign epithelial neoplasms arising from
sinonasal (Schneiderian) mucosa
ETIOLOGY/PATHOGENESIS
Infectious Agents• Human papillomavirus (HPV)o Found in septal and inverted papillomas by in situ
hybridization or polymerase chain reaction
▪ About 25% by ISH, consensus PCR, and type-specific PCR
o Types 6/11 > 16/18 (2.8:1 ratio); rarely other HPVtypes (e.g., HPV 57)
o HPV detection rates are higher in IP with high-gradedysplasia or carcinoma (~55%)
▪ Ratio of low risk to high risk HPV shifts frombenign to malignant (LR:HR 4.8:1 [benign] to1:2.4 [carcinoma])
o The presence of HPV is significantly associated witha likelihood of recurrence (OR: 10.2)
o Molecular biologic analysis to date on oncocyticpapillomas has not identified presence of HPV
• Discrepant reports on presence of Epstein-Barr virus inSchneiderian papillomas
CLINICAL ISSUES
Epidemiology• Incidenceo Represent less than 5% of all sinonasal tract tumors
▪ Literature supports septal type as most common,but in practical experience inverted type mostcommon
▪ Oncocytic type is least common• Ageo Occur over wide age range
▪ Rare in childreno Inverted type
▪ Most common in 5th to 8th decadeso Exophytic type
▪ Tend to occur in younger age groupo Oncocytic type
▪ Tend to occur in older age range (> 50 years)
▪ Uncommon under 4th decade of life
Site• Inverted typeo Occurs in maxillary sinus (42%) and ethmoid sinus/
recess (18%)
▪ Nasal cavity (15%) and turbinates (12%)frequently affected
▪ Less often extends/involves frontal (10%) andsphenoid (2%) sinuses
o May occur in paranasal sinus without involvementof nasal cavity
• Exophytic typeo Almost invariably limited to nasal septum
• Oncocytic typeo Most often occurs along lateral nasal wall
▪ May originate within paranasal sinus (maxillary orethmoid)
• Inverted and oncocytic types rarely occur on nasalseptum
• Typically, Schneiderian papillomas are unilateral
LDR Thompson, M.D. Used by Permission from: Diagnostic Pathology: Head & Neck LWW-Amirsys
ASCP Annual Meeting Surgical Pathology of Sinonasal Tract Tumors Session # 1015 on September 21, 2013
Page 25 of 60

SINONASAL (SCHNEIDERIAN) PAPILLOMA
Key Facts
o Bilateral papillomas, particularly inverted type, mayoccur in up to 10%
o In presence of bilateral disease
▪ Clinical evaluation indicated to exclude extensionfrom unilateral disease (i.e., septal perforation)
• Schneiderian-type papillomas may originate innasopharynx or ear without connection to sinonasaltracto Probably arise from misplaced ectodermal-derived
epithelial rests from sinonasal tract
Presentation• Symptoms vary according to site of occurrenceo Airway obstruction, epistaxis, asymptomatic mass,
pain
Treatment• Surgical approacheso Treatment for all sinonasal papillomas includes
complete surgical excision, including adjacentuninvolved mucosa
▪ Growth and extension along mucosa results frominduction of squamous metaplasia in adjacentsinonasal mucosa necessitating excision ofadjacent mucosa
▪ Adequate surgery includes lateral rhinotomy ormedial maxillectomy with en bloc excision
• Adjuvant therapyo Chemo- and radiotherapy have not been shown to
be of benefit
▪ Radiation may prove beneficial in selectpopulation of patients with unresectable tumorsdue to locally advanced disease
Prognosis• Good following complete surgical excision• Complicationso Tumors recur if incompletely resected
▪ Recurrence probably represents persistence ofdisease rather than multicentricity of neoplasm
o If left unchecked, capability of continued growthwith extension along mucosal surface with invasion/destruction of vital structures
IMAGE FINDINGS
General Features• Appearance varies with extent of diseaseo Soft tissue density seen early in diseaseo Opacification, mucosal thickening present with
more extensive diseaseo Evidence of pressure erosion of bone may be seen
MACROSCOPIC FEATURES
General Features• Inverted typeo Large, bulky, translucent masses with red to gray
color, varying from firm to friable in consistency• Exophytic typeo Papillary, exophytic, verrucoid lesion with pink to
tan appearance, firm to rubbery consistency; oftenattached to mucosa by narrow or broad-based stalk
• Oncocytic typeo Dark red to brown, papillary or polypoid lesions
MICROSCOPIC PATHOLOGY
Histologic Features• Inverted typeo Endophytic or "inverted" growth pattern consisting
of markedly thickened squamous epithelialproliferation growing downward
o Epithelium varies in cellularity composed ofsquamous, transitional, and columnar cells (all 3may be present in a given lesion) with admixedmucocytes (goblet cells) and intraepithelial mucouscysts
Terminology• Group of benign epithelial neoplasms arising from
sinonasal (Schneiderian) mucosa
Etiology/Pathogenesis• Human papillomavirus (HPV)o Cause and effect between presence of HPV and
development of Schneiderian papillomas remainsundetermined
Clinical Issues• Represent less than 5% of all sinonasal tract tumors• Treatment for all types includes complete surgical
excision, including adjacent uninvolved mucosao Tumors recur if incompletely resected
Microscopic Pathology• Inverted type
o Endophytic or "inverted" growth pattern consistingof markedly thickened squamous epithelialproliferation growing downward
o Thickened squamous epithelial proliferation withadmixed mucocytes, intraepithelial mucous cysts
• Exophytic typeo Exophytic (papillary) growtho Thickened squamous epithelial proliferation with
admixed mucocytes, intraepithelial mucous cysts• Oncocytic typeo Exophytic &/or endophytic growtho Multilayered epithelial proliferation composed of
columnar cells with abundant eosinophilic andgranular cytoplasm
o Admixed mucocytes (goblet cells) andintraepithelial mucous cysts
LDR Thompson, M.D. Used by Permission from: Diagnostic Pathology: Head & Neck LWW-Amirsys
ASCP Annual Meeting Surgical Pathology of Sinonasal Tract Tumors Session # 1015 on September 21, 2013
Page 26 of 60

SINONASAL (SCHNEIDERIAN) PAPILLOMA
▪ Cells generally bland in appearance with uniformnuclei, no piling up, but pleomorphism andcytologic atypia may be present
▪ Mitotic figures may be seen in basal and parabasallayers, but atypical mitotic figures are notidentified
▪ Epithelial cells may demonstrate extensive clearcell features indicative of abundant glycogencontent
o Mixed chronic inflammatory cell infiltratecharacteristically seen within all layers of surfaceepithelium
o Stromal component varies from myxoid to fibrouswith admixed chronic inflammatory cells andvariable vascularity
o May occur simultaneously with nasal inflammatorypolyps
o Surface keratinization may be present• Exophytic typeo Papillary fronds composed of thick epithelium,
which is predominantly squamous (epidermoid)and, less frequently, respiratory type
o Mucocytes (goblet cells) and intraepithelial mucouscysts are present
o Surface keratinization is uncommono Stromal component is composed of delicate
fibrovascular cores• Oncocytic typeo Exophytic &/or endophytic ("inverted") growtho Multilayered epithelial proliferation composed of
columnar cells with abundant eosinophilic andgranular cytoplasm
▪ Nuclei vary from vesicular to hyperchromatic;nucleoli are usually indistinct
▪ Outer surface of epithelial proliferation maydemonstrate cilia
o Intraepithelial mucin cysts, often containingpolymorphonuclear leukocytes, are seen; cysts arenot identified in submucosa
o Stromal component varies from myxoid to fibrouswith admixed chronic inflammatory cells andvariable vascularity
o May occur simultaneously with nasal inflammatorypolyps
• Malignant transformationo Incidence of malignant transformation varies per
subtype
▪ Inverted type ranges from 2-27%
▪ Oncocytic type ranges from 4-17%
▪ Exophytic type rarely, if evero Majority of malignancies are keratinizing
squamous cell carcinoma (SCC); less frequentlynonkeratinizing SCC
o Other carcinomas may rarely occur, including
▪ Verrucous carcinoma, mucoepidermoidcarcinoma, small cell carcinoma, adenocarcinoma,and undifferentiated carcinoma
o Carcinoma may occur synchronously ormetachronously with papilloma
o Carcinomatous foci may be limited or extensive,may show epithelial dysplasia/carcinoma in situ orinvasive carcinoma
o Evidence of preexisting papilloma
▪ May be present with obvious transition frombenign papilloma to overt carcinoma
▪ May include predominantly benign tumor(papilloma) with limited foci of carcinoma
▪ May predominantly include carcinoma withlimited residual papilloma
▪ May be no residual evidence of preexisting benigntumor; known to have prior papilloma only byhistory
o No reliable histologic features predict whichpapillomas likely to become malignant
▪ Moderate to severe epithelial dysplasia potentialindicator of malignant transformation
▪ Surface keratinization and dyskeratosisanecdotally considered possible predictors ofmalignant transformation
▪ Any sinonasal papilloma showing moderate tosevere dysplasia or surface keratinization shouldprompt histologic examination of all resectedtissue
▪ No correlation between number of recurrencesand development of carcinoma
▪ No correlation between presence of increasedcellularity, pleomorphism, and mitotic activityand transformation to carcinoma
o Treatment for malignant transformation includessurgery and radiotherapy
o Prognosis for patients with malignanttransformation varies
▪ Carcinoma only locally invasive associated withfavorable prognosis following treatment
▪ Carcinoma extensively invasive with involvementof vital structures &/or metastatic diseaseassociated with poor outcome
▪ Prognosis similar to de novo sinonasal squamouscarcinoma
ANCILLARY TESTS
Histochemistry• Mucicarmineo Intracytoplasmic mucin-positive material
• Periodic acid-Schiff with diastaseo Diastase-resistant, PAS-positive material
Immunohistochemistry• HPV DNA seen in IP• Strong positive: p16, p21, p27, pRb, cyclin D1• p53, p21 and p27 show increased intensity and altered
distribution in dysplasia and carcinoma• Ki-67 labeling index >20% and above the basal zone
usually seen in dysplasia and carcinoma
Molecular Genetics• Inverted papillomas shown to be monoclonal
proliferations, but unlike squamous epithelialdysplasia, do not harbor key genetic alterationsassociated with malignant transformation
• P53 gene mutation appears closely associated withmalignant transformation in sinonasal papillomas
LDR Thompson, M.D. Used by Permission from: Diagnostic Pathology: Head & Neck LWW-Amirsys
ASCP Annual Meeting Surgical Pathology of Sinonasal Tract Tumors Session # 1015 on September 21, 2013
Page 27 of 60

SINONASAL (SCHNEIDERIAN) PAPILLOMA
DIFFERENTIAL DIAGNOSIS
Sinonasal Inflammatory Polyps• Often coexist with Schneiderian papillomas but
lack epithelial proliferation with constituent cells ofSchneiderian papillomas
Squamous Papilloma of Nasal Vestibular Skin• Cutaneous lesion entirely comprised of squamous cells
without identifiable intraepithelial mucocytes• Staining for epithelial mucin (mucicarmine, DPAS)
helpful in differential diagnosis
Verruca Vulgaris of Nasal Vestibular Skin• Shows characteristic histopathologic findings
including presence of prominent keratinization withverrucoid or papillomatous growth, keratohyalinegranules, koilocytes and in turning of rete pegs, as wellas absence of intraepithelial mucocytes
Rhinosporidiosis• Specific differential diagnosis with oncocytic-type
papilloma• Intraepithelial and submucosal cysts containing
microorganisms
SELECTED REFERENCES1. Schneyer MS et al: Sites of attachment of Schneiderian
papilloma: a retrospective analysis. Int Forum AllergyRhinol. 1(4):324-8, 2011
2. Cheung FM et al: Schneiderian papillomas and carcinomas:a retrospective study with special reference to p53 and p16tumor suppressor gene expression and association withHPV. Ear Nose Throat J. 89(10):E5-E12, 2010
3. Giotakis E et al: Clinical outcomes of sinonasal invertedpapilloma surgery. A retrospective study of 67 cases. B-ENT.6(2):111-6, 2010
4. Shah AA et al: HPV DNA is associated with a subset ofSchneiderian papillomas but does not correlate withp16(INK4a) immunoreactivity. Head Neck Pathol.4(2):106-12, 2010
5. Tanvetyanon T et al: Survival outcomes of squamous cellcarcinoma arising from sinonasal inverted papilloma:report of 6 cases with systematic review and pooledanalysis. Am J Otolaryngol. 30(1):38-43, 2009
6. Wu HH et al: Fascin over expression is associated withdysplastic changes in sinonasal inverted papillomas: astudy of 47 cases. Head Neck Pathol. 3(3):212-6, 2009
7. Lawson W et al: The role of the human papillomavirusin the pathogenesis of Schneiderian inverted papillomas:an analytic overview of the evidence. Head Neck Pathol.2(2):49-59, 2008
8. Maitra A et al: Malignancies arising in oncocyticschneiderian papillomas: a report of 2 cases and review ofthe literature. Arch Pathol Lab Med. 125(10):1365-7, 2001
9. Califano J et al: Inverted sinonasal papilloma : a moleculargenetic appraisal of its putative status as a precursor tosquamous cell carcinoma. Am J Pathol. 156(1):333-7, 2000
10. Finkelstein SD et al: Malignant transformation in sinonasalpapillomas is closely associated with aberrant p53expression. Mol Diagn. 3(1):37-41, 1998
11. Mirza N et al: Identification of p53 and human papillomavirus in Schneiderian papillomas. Laryngoscope. 108(4 Pt1):497-501, 1998
12. Buchwald C et al: Human papillomavirus (HPV) insinonasal papillomas: a study of 78 cases using insitu hybridization and polymerase chain reaction.Laryngoscope. 105(1):66-71, 1995
13. Buchwald C et al: Sinonasal papillomas: a report of 82cases in Copenhagen County, including a longitudinalepidemiological and clinical study. Laryngoscope.105(1):72-9, 1995
14. Lawson W et al: Inverted papilloma: a report of 112 cases.Laryngoscope. 105(3 Pt 1):282-8, 1995
15. Kapadia SB et al: Carcinoma ex oncocytic Schneiderian(cylindrical cell) papilloma. Am J Otolaryngol. 14(5):332-8,1993
16. Barnes L et al: Oncocytic Schneiderian papilloma: areappraisal of cylindrical cell papilloma of the sinonasaltract. Hum Pathol. 15(4):344-51, 1984
Sinonasal (Schneiderian) Papillomas
Inverted Type Exophytic Type Oncocytic TypeIncidence 47-73% 20-50% 3-8%
Gender M > F M > F M = F
Age 40-70 years 20-50 years > 50 years
Location Lateral nasal wall in region of middleturbinates; may extend into sinuses(maxillary or ethmoid)
Nasal septum Lateral nasal wall and sinuses (maxillary orethmoid)
Focality Typically unilateral; rarely bilateral Unilateral Unilateral
Histology Endophytic or "inverted" growthcomposed predominantly ofsquamous (epidermoid) cells withscattered admixed mucocytes andintraepithelial mucous cysts; mixedchronic inflammatory cell infiltratecharacteristically seen within all layersof surface epithelium
Exophytic to papillary proliferationcomposed predominantly of squamous(epidermoid) epithelium with admixedmucocytes and intraepithelial mucouscysts; delicate fibrovascular cores
Multilayered epithelial proliferation composedof columnar cells with abundant eosinophilicand granular cytoplasm; outer surface ofepithelial proliferation may demonstrate cilia;intraepithelial mucous cysts, often containingpolymorphonuclear leukocytes
Association withHPV
~ 38% positive; HPV 6 and 11; lessfrequently HPV 16, 18; rarely HPV 57
~ 50% positive; HPV 6 and 11; lessfrequently HPV 16, 18; rarely HPV 57
Typically absent
Malignanttransformation
2-27%; most common type iskeratinizing SCC
Rare 4-17%; most common type is keratinizing SCC
HPV = human papillomavirus; SCC = squamous cell carcinoma.
LDR Thompson, M.D. Used by Permission from: Diagnostic Pathology: Head & Neck LWW-Amirsys
ASCP Annual Meeting Surgical Pathology of Sinonasal Tract Tumors Session # 1015 on September 21, 2013
Page 28 of 60

SINONASAL (SCHNEIDERIAN) PAPILLOMA
Imaging, Endoscopic, and Microscopic Features
(Left) A graphic of aSchneiderian papillomainvolving the lateral nasalwall with expansion intothe maxillary sinus. There isaccumulation of secretions
within the sinus. (Right)Coronal bone CT shows alobular inverted papillomacentered at the middle meatus
. The lesion enters themaxillary sinus via an enlargedinfundibulum and is partiallycalcified .
(Left) Endoscopic photographduring nasal endoscopyof an inverted papillomashows a pale, lobular mass
at the middle meatus.The lesion abuts the nasalseptum medially. (Right)An example of an invertedpapilloma, but highlighting themultiple papillary projectionswhich can be seen by thesurgeon macroscopically.This is a frequent cause ofconfusion when the tumor isexophytic macroscopically butendophytic microscopically.
(Left) Endophytic or "inverted"growth pattern of thickenedepithelial nests arisingfrom surface epithelium ischaracteristic of inverted-type papilloma. Stroma showsalterations similar to thoseseen in inflammatory polyps
. (Right) Multiple invertedprojections are seen deepwithin the stroma below anintact surface epithelium.The nests all show a welldefined border, helping toexclude an invasive neoplasm.
LDR Thompson, M.D. Used by Permission from: Diagnostic Pathology: Head & Neck LWW-Amirsys
ASCP Annual Meeting Surgical Pathology of Sinonasal Tract Tumors Session # 1015 on September 21, 2013
Page 29 of 60

SINONASAL (SCHNEIDERIAN) PAPILLOMA
Microscopic Features
(Left) Multiple papillaryprojections are seen inthis tumor, which is anexample of an inverted typeSchneiderian papilloma.There is an inverted growthof the proliferation intothe stroma, even thoughthere is an exophyticoverall projection. (Right)Multiple inverted projectionsare noted. There is ageneral complexity to thisproliferation as it shows abroad, pushing border withthe surrounding stroma.
(Left) Endophytic or"inverted" growth patternconsists of thickenedepithelial nests arising fromthe surface respiratoryepithelium withdownward growth. Surfacesquamous metaplasia ispresent . (Right) Thistumor shows multiplemucocytes at the surfaceand within the proliferation.There are also microabscessof inflammatory cells within the epithelium,another feature seen inSchneiderian papilloma.
(Left) At higher magnificationthe nonkeratinizingsquamous epitheliumshows cytomorphologicuniformity with cellularmaturation, retentionof cellular polarity, andabsence of cytologic atypia.Focally, scattered mucocytesare present . This isan exophytic papilloma.(Right) Exophytic papillomais the most superficialaspect retaining respiratoryepithelial mucocytes butis otherwise replaced bybenign-appearing squamous(epidermoid) epithelium.
LDR Thompson, M.D. Used by Permission from: Diagnostic Pathology: Head & Neck LWW-Amirsys
ASCP Annual Meeting Surgical Pathology of Sinonasal Tract Tumors Session # 1015 on September 21, 2013
Page 30 of 60

SINONASAL (SCHNEIDERIAN) PAPILLOMA
Oncocytic Papilloma
(Left) Schneiderian papilloma,oncocytic type, shows anepithelial proliferation withexophytic/papillary and focally endophytic growth. The stroma showsedematous changes similarto that of sinonasal polyps.(Right) There is a very richoncocytic appearance to theepithelium in this oncocyticSchneiderian papilloma. Thereis a uniformity to the cells asthe columnar epithelial cellsare expanded to the surface.Cilia are easily noted.
(Left) The epithelium ismultilayered, characterized bycells with prominent granulareosinophilic cytoplasmas well as the presence ofintraepithelial mucin cystscontaining amorphous pinkmaterial &/or neutrophils
. (Right) Histochemicalstaining shows the presenceof intraluminal andintracytoplasmic diastase-resistant, PAS-positive material.
(Left) Sinonasal papillomastypically lack keratinization,and the presence ofkeratinization raisesconcern for the possibilityof SCC (coexisting ordevelopment into a squamouscell carcinoma). With thisoccurrence, all of the tissueshould be processed forhistologic evaluation. (Right)There is expansion of thistumor into the bone withdestructive growth into thedeep stroma. This is a tumorthat has undergone malignanttransformation into carcinoma.
LDR Thompson, M.D. Used by Permission from: Diagnostic Pathology: Head & Neck LWW-Amirsys
ASCP Annual Meeting Surgical Pathology of Sinonasal Tract Tumors Session # 1015 on September 21, 2013
Page 31 of 60

SINONASAL (SCHNEIDERIAN) PAPILLOMA
Malignant Transformation
(Left) This exophyticpapilloma shows increasedkeratinization whilethe left side of the imageshows a transformation intoa carcinoma. In this case it isa squamous cell carcinoma,but any tumor type can beseen. (Right) Bone invasion
by the neoplastic cells isnot a feature that would beseen in a benign papilloma.Fragments of turbinatebone may sometimes bepresent, but they are notdestroyed by the neoplasticproliferation.
(Left) Genuine, comedo-typenecrosis is a feature seenin malignant transformationof Schneiderian papilloma.This is not a degenerativetype necrosis, but a truetumor necrosis. (Right)While mitoses can be seenin papilloma, the remarkablenumber seen in this tumor
, along with atypicalforms , are beyond whatwould be seen in a benignlesion, and is a tip-off to thediagnosis of carcinoma. Thisis an example of squamouscell carcinoma.
(Left) A haphazardgrowth and loss of normalmaturation towards thesurface is clue to malignanttransformation within aSchneiderian papilloma.There are also atypicalmitoses present in thislesion. (Right) The p63is identified only at thebasal zone in a benignSchneiderian papilloma,but expands to fill the entireproliferation when thereis malignant transformation.This is also true of p53 (notillustrated).
LDR Thompson, M.D. Used by Permission from: Diagnostic Pathology: Head & Neck LWW-Amirsys
ASCP Annual Meeting Surgical Pathology of Sinonasal Tract Tumors Session # 1015 on September 21, 2013
Page 32 of 60

MALIGNANT MUCOSAL MELANOMA
Atypical junctional melanocytes are noted within therespiratory epithelium, arranged in a pagetoid spread .The tumor cells are also present within the stroma.
Hematoxylin & eosin shows a spindled to polygonalpopulation of highly atypical, pigmented neoplasticcells. These changes are characteristic for a pigmentedmelanoma.
TERMINOLOGY
Abbreviations• Malignant mucosal melanoma (MMM)• Sinonasal tract and nasopharynx mucosal malignant
melanoma (STMMM)
Definitions• Neural crest-derived neoplasms originating from
melanocytes and demonstrating melanocyticdifferentiation
ETIOLOGY/PATHOGENESIS
Environmental Exposure• Formalin• Possibly radiation• UV exposure
CLINICAL ISSUES
Epidemiology• Incidenceo Rare
▪ Represents < 1% of all melanomas
▪ < 5% of all sinonasal tract neoplasms
▪ 15-20% of all skin melanomas occur in head andneck
▪ STMMM represent < 4% of all head and neckmelanomas
• Ageo Wide range, usually in 5th to 8th decades
• Gendero Equal gender distribution
• Ethnicityo Increased incidence in Japanese patients
Site• About 15-20% of melanomas arise in head and neck
o 80% are cutaneous in origino Ocular origin account for majority of remaining
MMMo Sinonasal tract is next most common site
• Anterior nasal septum > maxillary sinus
Presentation• Nasal obstruction• Epistaxis or nasal dischargeo Melanorrhea: Black-flecked (melanin) discharge
• Polyp• Pain is uncommon
Treatment• Options, risks, complicationso Metastatic melanoma to sinonasal tract can develop
but is vanishingly rareo Breslow thickness and Clark level are not used in
sinonasal tract• Surgical approacheso Wide local excision is treatment of choice
• Radiationo Can be used after surgery
▪ In most cases, it is palliative
Prognosis• Poor overall• 5-year survival (17-47%)• Recurrences are common• Poor prognosis associated witho Obstruction as presenting symptomo Nasopharynx or "mixed site" of involvemento Tumor ≥ 3 cmo Undifferentiated histologyo High mitotic counto Recurrenceo Stage of tumor
• Matrix metalloproteinases (MMPs) (proteolyticenzymes required for extracellular matrix degradation)expression may be associated with patient outcome
LDR Thompson, M.D. Used by Permission from: Diagnostic Pathology: Head & Neck LWW-Amirsys
ASCP Annual Meeting Surgical Pathology of Sinonasal Tract Tumors Session # 1015 on September 21, 2013
Page 33 of 60

MALIGNANT MUCOSAL MELANOMA
Key Facts
o Decreased MMP2 expression associated with greateroverall survival
o Positive MMP14 expression associated with poorsurvival
IMAGE FINDINGS
Radiographic Findings• Usually identifies extent of tumor and bone invasion• Positron emission tomography (PET) tends to show
posterior nasal cavity and sinus tumors better thananterior nasal tumors
• Locoregional and metastatic disease can be detected
MACROSCOPIC FEATURES
General Features• Most are polypoid• White to gray, brown, or black• Surface ulceration/erosion is common
Size• Range up to 6 cm• Mean: 2-3 cm
MICROSCOPIC PATHOLOGY
Histologic Features• Protean histology, mimic of many other primary
tumor types• Junctional activity and epidermal migration (Pagetoid
spread) help to confirm primary tumor• Surface ulceration is common, obscuring "in situ"
component• Bone or soft tissue invasion is common• Many patterns of growtho Peritheliomatous: Distinctive and unique for
STMMMo Epithelioido Solid
o Organoido Sheetso Nestso Fascicles and interlacing bundleso Storiformo Meningothelialo Hemangiopericytoma-likeo Papillary
• Variety of cell types can be seeno Undifferentiatedo Epithelioid, polygonalo Small cello Plasmacytoido Rhabdoido Giant cell
• Vesicular nuclei although sometimes hyperchromatic• Prominent, irregular, brightly eosinophilic, enlarged
nucleoli• Intranuclear cytoplasmic inclusions usually present• Melanin-containing tumor cells can be seen• Tumor cell necrosis is common• Mitotic figures, including atypical forms, usually easily
found and increased• Inflammation may be present but not of consequence• Desmoplastic type fibrosis can be seen, but is not
common• Perineural invasion, when present, is poor prognostic
indicator• Tumor depth of invasion (Clark) impossible to
accurately assess• Tumor thickness (Breslow) not meaningful in
sinonasal tract
Lymphatic/Vascular Invasion• Usually present but difficult to assess
Margins• Difficult to assess, as samples are frequently
fragmented and removed piecemeal
Terminology• Neural crest-derived neoplasms originating from
melanocytes and demonstrating melanocyticdifferentiation
Clinical Issues• Anterior nasal septum > maxillary sinus• Overall prognosis is poor
Macroscopic Features• Most are polypoid
Microscopic Pathology• Protean histology, mimic of many other primary
tumor types• Junctional activity and epidermal migration (Pagetoid
spread) help to confirm primary tumor• Many patterns of growth
• Variety of cell types can be seen• Prominent, irregular, brightly eosinophilic, enlarged
nucleoli• Intranuclear cytoplasmic inclusions usually present• Melanin-containing tumor cells can be seen
Ancillary Tests• Positive: S100 protein, HMB-45, Melan-A,
microphthalmia transcription factor, tyrosinase,vimentin
Top Differential Diagnoses• Olfactory neuroblastoma• Sinonasal undifferentiated carcinoma• Melanotic neuroectodermal tumor of infancy• Rhabdomyosarcoma• Lymphoma
LDR Thompson, M.D. Used by Permission from: Diagnostic Pathology: Head & Neck LWW-Amirsys
ASCP Annual Meeting Surgical Pathology of Sinonasal Tract Tumors Session # 1015 on September 21, 2013
Page 34 of 60

MALIGNANT MUCOSAL MELANOMA
ANCILLARY TESTS
Histochemistry• Fontana-Massono Reactivity: Positiveo Staining pattern
▪ Melanin bleach will confirm melanin incytoplasm
Immunohistochemistry• Positive: S100 protein, HMB-45, Melan-A,
microphthalmia transcription factor, tyrosinase,vimentin
• p16 expression is lost in most MMM (74%)
Cytogenetics• Comparative genomic hybridization (CGH) shows
chromosome arm 1q is gained in nearly all tumorsstudied
• Gains of 6p (93%) and 8q (57%) are also identified
Electron Microscopy• Premelanosomes and melanosomes confirms
melanocytic origin
DIFFERENTIAL DIAGNOSIS
Olfactory Neuroblastoma• Lobular architecture• Fibrillary matrix material associated with rosettes and
pseudorosettes• CD56, chromogranin, synaptophysin, and
sustentacular S100 protein reaction
Sinonasal Undifferentiated Carcinoma• Small cells with high nuclear to cytoplasmic ratio• Necrosis, destructive growth, and vascular invasion• Strong, diffuse keratin immunoreactivity
Melanotic Neuroectodermal Tumor ofInfancy• Tumor of neonatal period, affecting gnathic bones• Biphasic tumor with small and large cells, with
pigment easily identified
Rhabdomyosarcoma• Tends to develop in younger patients (although not
alveolar type)• Nests, alveolar patterns are similar• Strap and rhabdoid patterns are helpful• Cross striations can confirm diagnosis• Immunoreactive with desmin, MYOD1, myogenin,
SMA, MSA, CD56
Leiomyosarcoma• Fascicular architecture, frequently associated with
necrosis and high mitotic index• Perinuclear vacuoles and cigar-shaped nuclei are rare
in melanoma• Muscle markers positive, while nonreactive with
melanoma markers
Plasmacytoma• Hematologic neoplasm giving sheet-like pattern of
plasmacytoid cells• "Hof" zone, paranuclear clearing, and rounded nuclei
with clock face-like chromatin distribution• CD138, CD79a, κ or λ, and other hematologic markers
will be positive
Metastatic Melanoma• While theoretic consideration, junctional/Pagetoid
spread helps to exclude this possibility• Clinical and radiographic examinations are the only
way to make definitive separation
Mesenchymal Chondrosarcoma• Small, undifferentiated cell appearance, but if enough
sections are taken, cartilaginous features can be seen• S100 protein will be positive (chondrocytic tumors are
positive), but HMB-45, tyrosinase, Melan-A will notreact
SELECTED REFERENCES1. Wenig BM: Undifferentiated malignant neoplasms of the
sinonasal tract. Arch Pathol Lab Med. 133(5):699-712, 20092. Bachar G et al: Mucosal melanomas of the head and neck:
experience of the Princess Margaret Hospital. Head Neck.30(10):1325-31, 2008
3. Dauer EH et al: Sinonasal melanoma: a clinicopathologicreview of 61 cases. Otolaryngol Head Neck Surg.138(3):347-52, 2008
4. Kim DK et al: Ki67 antigen as a predictive factor forprognosis of sinonasal mucosal melanoma. Clin ExpOtorhinolaryngol. 1(4):206-10, 2008
5. Kondratiev S et al: Expression and prognostic roleof MMP2, MMP9, MMP13, and MMP14 matrixmetalloproteinases in sinonasal and oral malignantmelanomas. Hum Pathol. 39(3):337-43, 2008
6. McLean N et al: Primary mucosal melanoma of thehead and neck. Comparison of clinical presentation andhistopathologic features of oral and sinonasal melanoma.Oral Oncol. 44(11):1039-46, 2008
7. Cheng YF et al: Toward a better understanding of sinonasalmucosal melanoma: clinical review of 23 cases. J Chin MedAssoc. 70(1):24-9, 2007
8. Martin JM et al: Outcomes in sinonasal mucosalmelanoma. ANZ J Surg. 74(10):838-42, 2004
9. Prasad ML et al: Clinicopathologic differences in malignantmelanoma arising in oral squamous and sinonasalrespiratory mucosa of the upper aerodigestive tract. ArchPathol Lab Med. 127(8):997-1002, 2003
10. Thompson LD et al: Sinonasal tract and nasopharyngealmelanomas: a clinicopathologic study of 115 cases with aproposed staging system. Am J Surg Pathol. 27(5):594-611,2003
11. van Dijk M et al: Distinct chromosomal aberrations insinonasal mucosal melanoma as detected by comparativegenomic hybridization. Genes Chromosomes Cancer.36(2):151-8, 2003
12. Patel SG et al: Primary mucosal malignant melanoma ofthe head and neck. Head Neck. 24(3):247-57, 2002
13. Kardon DE et al: Sinonasal mucosal malignant melanoma:report of an unusual case mimicking schwannoma. AnnDiagn Pathol. 4(5):303-7, 2000
14. Regauer S et al: Primary mucosal melanomas of the nasalcavity and paranasal sinuses. A clinicopathological analysisof 14 cases. APMIS. 106(3):403-10, 1998
LDR Thompson, M.D. Used by Permission from: Diagnostic Pathology: Head & Neck LWW-Amirsys
ASCP Annual Meeting Surgical Pathology of Sinonasal Tract Tumors Session # 1015 on September 21, 2013
Page 35 of 60

MALIGNANT MUCOSAL MELANOMA
Immunohistochemistry
Antibody Reactivity Staining Pattern CommentS100 Positive Nuclear & cytoplasmic Diffuse and strong stain usually; identified in about 90% of cases
HMB-45 Positive Cytoplasmic Variably reactive in most cases (~ 75%)
Tyrosinase Positive Cytoplasmic Variably reactive in most cases (~ 75%)
melan-A103 Positive Cytoplasmic Variably reactive in majority of cases (~ 66%)
MITF Positive Nuclear Positive in majority of cases (~ 55%)
NSE Positive Cytoplasmic Positive in < 50% of tumor cells, often focal
CD117 Positive Cytoplasmic Positive in ~ 33% of cases
CD99 Positive Cytoplasmic Positive in ~ 25% of cases
Vimentin Positive Cytoplasmic All tumor cells
CD56 Positive Cell membrane & cytoplasm ~ 7% of cases
Synaptophysin Positive Cytoplasmic Nonspecific, in ~ 10% of cases
EMA Positive Cytoplasmic < 5% of tumor cells
Chromogranin-A Negative
CD45RB Negative
CK-PAN Negative
GFAP Negative
CD45RB Negative
Actin-HHF-35 Negative
Actin-sm Negative
Desmin Negative
MYOD1 Negative
Proposed Staging for Sinonasal Tract Melanomas
Classification Description
Primary Tumor
T1 Single anatomic site
T2 2 or more anatomic sites
Regional Lymph Nodes
N0 No lymph node involvement
N1 Any lymph node metastases
Distant Metastasis
M0 No distant metastases
M1 Distant metastasis
Stage Grouping
I T1 N0 M0
II T2 N0 M0
III Any T, N1, M0
IV Any T, Any N, M1
LDR Thompson, M.D. Used by Permission from: Diagnostic Pathology: Head & Neck LWW-Amirsys
ASCP Annual Meeting Surgical Pathology of Sinonasal Tract Tumors Session # 1015 on September 21, 2013
Page 36 of 60

MALIGNANT MUCOSAL MELANOMA
Radiographic and Microscopic Features
(Left) This MR image (T2-weighted axial) demonstrateshigh signal within the maxillarysinus, focally associatedwith fluid in the posteriorportion . This lesion wasa maxillary sinus malignantmelanoma, without associatedinvolvement of the nasalcavity. (Right) The nasalseptum cartilage is beingdestroyed by the infiltrativeneoplasm. The tumor forms athick, sheet-like distribution.No pattern of growth can beseen at this magnification,although ulceration is present.
(Left) Isolated junctionalneoplastic cells are noted
in this MMM. Theneoplastic cells in thestroma show pleomorphismand a plasmacytoidappearance. Pigment iseasily identified. (Right)This "peritheliomatous" orperivascular distributionof the neoplastic cells is quitecharacteristic for a melanoma.It is thought to represent viabletumor cells remaining aroundvessels. This pattern can beseen in other tumors but not tothe same frequency as it is inmelanoma.
(Left) MMM can be arrangedin a number of differentarchitectures, with a fasciculararchitecture seen here. Thespindle cells are arranged inshort, intersecting fascicles.The cells are somewhatsyncytial in appearance.(Right) It is not uncommonto have an "undifferentiated"or "small round blue cell"appearance to MMM. Thereis a slightly plasmacytoidappearance to the cells. Notethe very prominent nucleoli.Mitotic figures are noted, butpigment is absent.
LDR Thompson, M.D. Used by Permission from: Diagnostic Pathology: Head & Neck LWW-Amirsys
ASCP Annual Meeting Surgical Pathology of Sinonasal Tract Tumors Session # 1015 on September 21, 2013
Page 37 of 60

MALIGNANT MUCOSAL MELANOMA
Microscopic and Immunohistochemical Features
(Left) This tumor showsa very pronouncedplasmacytoid appearance,including a "Hof zone"adjacent to the nucleus
. There are intranuclearcytoplasmic inclusions aswell as binucleation in thisMMM. (Right) Pleomorphicpolygonal cells comprisethis melanoma. Thereis remarkable variabilitybetween cells. Prominent,eosinophilic nucleoliare noted, along withintranuclear cytoplasmicinclusions . Mitotic figuresare also noted .
(Left) A rhabdoidappearance with darklyopacified, eosinophiliccytoplasm is the dominantpattern in this MMM.Nucleoli are not as enlarged.Mitotic figures, necrosis,and pigment are notappreciated. (Right) It isnot uncommon to havea variable architectureand cellular morphologyin a single tumor. Here apolygonal and spindled cellpopulation shows melaninpigment, prominent nucleoli,and intranuclear cytoplasmicinclusions .
(Left) Positive S100 proteinis immunoreactive in thisspindled cell melanoma.There is both cytoplasmicand nuclear reactivity withthis marker that highlightsnearly all of the cells. (Right)Positive HMB-45 in this"small round blue cell"pattern demonstrates someof the variability that can beseen both within a tumor aswell as between tumors. Theintensity of the staining aswell as the number of cells,which are positive, can bequite variable.
LDR Thompson, M.D. Used by Permission from: Diagnostic Pathology: Head & Neck LWW-Amirsys
ASCP Annual Meeting Surgical Pathology of Sinonasal Tract Tumors Session # 1015 on September 21, 2013
Page 38 of 60

MENINGIOMA
Hematoxylin & eosin shows an intact respiratory mucosasubtended by a syncytial neoplastic proliferation ofmeningothelial cells.
Hematoxylin & eosin shows a whorled pattern ofmeningothelial cells set adjacent to uninvolved surfacesquamous epithelium .
TERMINOLOGY
Definitions• Benign neoplasm of meningothelial cells within nasal
cavity, sinonasal tract, and nasopharynx
ETIOLOGY/PATHOGENESIS
Pathogenesis• Arachnoid cells from arachnoid granulations or
pacchionian bodies lining sheaths of nerves andvessels through skull foramina
CLINICAL ISSUES
Epidemiology• Incidenceo Approximately 0.2% of sinonasal tract and
nasopharynx tumors
▪ 20% of meningiomas have extracranial extension• Ageo Mean: 40-48 years oldo Women older than men by over a decade
• Gendero Female > Male (1.2:1)
Site• Mixed nasal cavity and paranasal sinuses (majority)• Nasal cavity alone (~ 25%)• Frontal sinus most commonly affected in isolation• Majority are left sided
Presentation• Mass, obstruction, discharge, and epistaxis• Sinusitis, pain, headache, seizure activity• Exophthalmos, periorbital edema, visual changes,
ptosis
Treatment• Surgical approacheso Excision (although difficult at times)
Prognosis• Good outcome: 10-year survival (80%)• Recurrences develop (usually < 5 years after primary)
IMAGE FINDINGS
Radiographic Findings• Must exclude direct CNS extension from en plaque
tumor• Bony sclerosis with focal destruction of bony tissues• Widening of suture lines and foramina at base of skull
MACROSCOPIC FEATURES
General Features• Intact surface mucosa but infiltrative into bone• Multiple fragments of grayish, white-tan, gritty, firm
to rubbery masses• Many are polypoid
Size• Range: 1-8 cm, mean: 3.5 cm
MICROSCOPIC PATHOLOGY
Histologic Features• Infiltrative growth of neoplastic cells, including soft
tissue and bone• Meningothelial (syncytial) lobules of neoplastic cells
without distinct borders• Whorled architecture• Psammoma bodies or "pre-psammoma" bodies• Epithelioid cells with round to regular nuclei and even
nuclear chromatin
LDR Thompson, M.D. Used by Permission from: Diagnostic Pathology: Head & Neck LWW-Amirsys
ASCP Annual Meeting Surgical Pathology of Sinonasal Tract Tumors Session # 1015 on September 21, 2013
Page 39 of 60

MENINGIOMA
Key Facts
IMAGE GALLERY
(Left) Hematoxylin & eosin shows multiple small nests of meningothelial cells showing a slightly whorled appearance. (Center) Hematoxylin &eosin demonstrates a nest of cells without cell borders, showing nuclear hyperchromasia. (Right) EMA shows modest cytoplasmic reactivity.
• Intranuclear cytoplasmic inclusions (invaginations)• Histologic subtypes can be seeno Transitional, metaplastic, atypical
ANCILLARY TESTS
Immunohistochemistry• Positive: EMA, keratin (pre-psammoma-body pattern),
CAM5.2• Weak positive: S100 protein• Negative: Chromogranin, synaptophysin
DIFFERENTIAL DIAGNOSIS
Angiofibroma• Males only; nasopharynx; collagenized stroma, stellate
stromal cells, haphazard vessels (staghorn)
Aggressive Psammomatoid OssifyingFibroma• Young patients; abundant psammoma bodies;
osteoclasts and osteoblasts; compact to storiformstroma
Olfactory Neuroblastoma• Cribriform plate; lobular growth; small cells with scant
cytoplasm; fibrillar background; rosette/pseudorosetteformations
Melanoma• Protean mimic; intranuclear cytoplasmic inclusions;
prominent nucleoli; melanoma markers positive
Paraganglioma• Rare in sinonasal tract; nested architecture,
basophilic cytoplasm; S100 protein sustentacular andchromogranin paraganglia reaction
SELECTED REFERENCES1. Dekker G et al: Meningioma presenting as an
oropharyngeal mass--an unusual presentation. S Afr Med J.97(5):342, 2007
2. Petrulionis M et al: Primary extracranial meningioma ofthe sinonasal tract. Acta Radiol. 46(4):415-8, 2005
3. Thompson LD et al: Extracranial sinonasal tractmeningiomas: a clinicopathologic study of 30 cases witha review of the literature. Am J Surg Pathol. 24(5):640-50,2000
4. Moulin G et al: Plaque-like meningioma involving thetemporal bone, sinonasal cavities and both parapharyngealspaces: CT and MRI. Neuroradiology. 36(8):629-31, 1994
5. Gabibov GA et al: Meningiomas of the anterior skull baseexpanding into the orbit, paranasal sinuses, nasopharynx,and oropharynx. J Craniofac Surg. 4(3):124-7; discussion134, 1993
6. Perzin KH et al: Nonepithelial tumors of the nasal cavity,paranasal sinuses, and nasopharynx. A clinicopathologicstudy. XIII: Meningiomas. Cancer. 54(9):1860-9, 1984
Terminology• Benign neoplasm of meningothelial cells
Clinical Issues• Approximately 0.2% of sinonasal tract and
nasopharynx tumors• Female > Male (1.2:1)o Women older by over a decade
• Good outcome: 10-year survival (80%)
Image Findings• Must exclude direct CNS extension
Microscopic Pathology• Infiltrative growth of neoplastic cells, including soft
tissue and bone• Meningothelial (syncytial) lobules of neoplastic cells
without distinct borders• Whorled architecture, psammoma bodies
LDR Thompson, M.D. Used by Permission from: Diagnostic Pathology: Head & Neck LWW-Amirsys
ASCP Annual Meeting Surgical Pathology of Sinonasal Tract Tumors Session # 1015 on September 21, 2013
Page 40 of 60

MUCOCELE OF PARANASAL SINUS
Axial NECT reveals a low-density, expansile, left ethmoidmucocele. The lamina papyracea is remodeled, and thereis mass effect on the medial rectus muscle .
Histologic features associated with an internal mucoceleinclude a respiratory epithelial-lined cyst lying near tothe bony wall of the sinus , as shown. The bone showsreactive changes.
TERMINOLOGY
Definitions• Distinct clinicopathologic entity characterized byo Expansion of sinus cavity due to obstruction of
outflow tract (ostium or duct) resulting in cysticlesion of paranasal sinus
o Diagnosis requires correlation between clinical,radiographic, and pathologic findings, ashistopathologic findings alone are nonspecific
o Expansion of bony walls of sinus is sine qua non forparanasal sinus mucocele
ETIOLOGY/PATHOGENESIS
Developmental Anomaly• Thought to occur as result of increase in pressure
within a given sinus secondary to blockage of sinusoutlet (ostium)o Most often result of inflammatory or allergic process
• Additional factors implicated include trauma, priorsurgery, or neoplasm
CLINICAL ISSUES
Epidemiology• Ageo Occurs in all age groups
• Gendero Equal gender distribution
Site• > 90% occur in frontal and ethmoid sinuseso Frontonasal duct relatively long and narrow, easily
obstructed especially following surgery to this region• Maxillary sinus uncommonly involved (5-10%)• Sphenoid sinus involvement considered rare
Presentation• Chronic process with signs and symptoms occurring
over time rather than acutely• Symptoms depend on site of involvement as well as
direction, extent of expansiono Paino Facial swelling or deformityo Proptosis, exophthalmos, diplopiao Rhinorrhea, nasal obstruction
Treatment• Surgical approacheso Complete surgical excision is treatment of choice
▪ Trend toward transnasal endoscopic management
Prognosis• Excellent with long-term controlo Near zero recurrence rates
• Complications may include superimposed infection(pyocele), meningitis, brain abscess
IMAGE FINDINGS
Radiographic Findings• Opacification of involved sinus• Erosion &/or destruction of sinus walls with loss of
typical scalloped outline along mucoperiosteum• Abnormal radiolucency due to loss of bone• Sclerosis of adjacent bone• Cavity manifests smoothly contoured, expanded wall
with reactive bony thickening• Radiographic picture can be highly characteristic based
ono Strikingly rounded appearance, presence of
homogeneous mucoid contents
LDR Thompson, M.D. Used by Permission from: Diagnostic Pathology: Head & Neck LWW-Amirsys
ASCP Annual Meeting Surgical Pathology of Sinonasal Tract Tumors Session # 1015 on September 21, 2013
Page 41 of 60

MUCOCELE OF PARANASAL SINUS
Key Facts
IMAGE GALLERY
(Left) Coronal graphic shows left anterior ethmoid mucocele extending into the left frontal sinus. (Center) Axial CT image demonstrates an airlessand grossly expanded sphenoid sinus with smooth expansion of the bony walls and areas of bone erosion, with extension into the medial andposterior orbit. (Right) External mucocele with herniation into the cranial cavity shows the respiratory epithelial-lined cyst overlying centralnervous system tissue .
MACROSCOPIC FEATURES
General Features• 2 types of mucoceles are identifiedo Internal
▪ Herniation of cyst into submucosal tissue adjacentto bony wall of sinus
o External
▪ Herniation of cyst through bony wall of sinuswith extension into subcutaneous tissue or intocranial cavity
MICROSCOPIC PATHOLOGY
Histologic Features• Cysts lined by flattened, pseudostratified, ciliated,
columnar epithelium• In longstanding cases, squamous metaplasia may be
presento Metaplastic changes uncommon
• Reactive bone formation lying in proximity to cystepithelium
• Variable chronic inflammatory cell infiltrate may bepresent
• Additional changes may includeo Fibrosis, granulation tissue, hemorrhage, cholesterol
granulomao Central nervous tissue can be seen if herniation into
cranial cavity
DIFFERENTIAL DIAGNOSIS
Mucus Retention Cyst• a.k.a. salivary mucocele• Cystic lesion of minor salivary glands characterized
by well-circumscribed, submucosal mucus-filled,epithelial-lined cyst
DIAGNOSTIC CHECKLIST
Pathologic Interpretation Pearls• Diagnosis requires correlation between clinical,
radiographic, and pathologic findings, ashistopathologic findings alone are nonspecific
SELECTED REFERENCES1. Socher JA et al: Diagnosis and treatment of isolated
sphenoid sinus disease: a review of 109 cases. ActaOtolaryngol. 128(9):1004-10, 2008
2. Serrano E et al: Surgical management of paranasal sinusmucoceles: a long-term study of 60 cases. OtolaryngolHead Neck Surg. 131(1):133-40, 2004
3. Har-El G: Endoscopic management of 108 sinus mucoceles.Laryngoscope. 111(12):2131-4, 2001
4. Evans C: Aetiology and treatment of fronto-ethmoidalmucocele. J Laryngol Otol. 95(4):361-75, 1981
5. van Nostrand AW et al: Pathologic aspects of mucosallesions of the maxillary sinus. Otolaryngol Clin North Am.9(1):21-34, 1976
Clinical Issues• Distinct clinicopathologic entity characterized byo Expansion of sinus cavity due to obstruction
resulting in cystic lesion of sinuso Expansion of sinus bony walls is sine qua non for
paranasal sinus mucocele• Thought to occur due to increase in sinus pressure
secondary to blockage of sinus outlet, often as resultof inflammatory or allergic process
• > 90% occur in frontal and ethmoid sinuses• Complete surgical excision is treatment of choice
Macroscopic Features• Internal: Herniation of cyst into submucosal tissue
adjacent to bony wall of sinus• External: Herniation of cyst through bony wall of
sinus with extension into subcutaneous tissue or intocranial cavity
LDR Thompson, M.D. Used by Permission from: Diagnostic Pathology: Head & Neck LWW-Amirsys
ASCP Annual Meeting Surgical Pathology of Sinonasal Tract Tumors Session # 1015 on September 21, 2013
Page 42 of 60

GLOMANGIOPERICYTOMA (SINONASAL-TYPE HEMANGIOPERICYTOMA)
Hematoxylin & eosin shows an intact, uninvolvedrespiratory epithelium subtended by a thick band offibrosis. Below this is a patternless, bland, cellularproliferation.
The strong, heavy, perivascular (peritheliomatous)hyalinization is quite characteristic for this tumor in thesetting of a monotonous proliferation. The neoplasm isbland and arranged in a syncytium.
TERMINOLOGY
Abbreviations• Sinonasal-type hemangiopericytoma (SNTHPC)
Synonyms• Sinonasal hemangiopericytoma-like tumor• Glomus tumor• Hemangiopericytoma• Solitary fibrous tumor (inaccurate in sinonasal site)• Intranasal myopericytoma
Definitions• Soft tissue tumor showing perivascular myoid
differentiation defined by glomus (myoid) andhemangiopericytoma (pericyte) features within samelesion
ETIOLOGY/PATHOGENESIS
Myopericyte• May arise from plentiful pericytes associated with
vessels of nasal cavity
CLINICAL ISSUES
Epidemiology• Incidenceo Rare, comprising < 0.5% of sinonasal primary
neoplasms• Ageo Broad range at presentation (5-90 years old)o Mean: 7th decadeo Age at presentation does not affect prognosis
• Gendero Female > Male (1.2:1)o No difference in outcome based on gender
Site• Nasal cavity is usually affected in isolationo Turbinate and septum are occasionally affected in
isolation• Maxillary and ethmoid sinuses may also be affected in
conjunction with nasal cavity• Bilateral tumors are uncommon (approximately 5%)
Presentation• Nasal obstruction• Epistaxis• Mass, polyps• Difficulty breathing• Sinusitis• Headache, congestion, pain• Discharge• Changes in smell• Symptoms usually present for < 1 year• Rare association with osteomalacia
Treatment• Options, risks, complicationso Surgery is treatment of choice, although radiation
has been used in nonsurgical candidates
▪ Endoscopic resection achieves similar outcome toopen resection
o Chemotherapy is not used• Surgical approacheso Polypectomy or wide surgical excisiono Complete surgical extirpation decreases risk of
recurrence (Odd ratio = 11.5)
Prognosis• Excellent long-term survival (5-year survival ~ 90%)• Recurrences may develop (~ 27%)o Multiple recurrences may be seen
• Recurrences are associated witho Long duration of symptomso Bone invasiono Severe nuclear pleomorphism
LDR Thompson, M.D. Used by Permission from: Diagnostic Pathology: Head & Neck LWW-Amirsys
ASCP Annual Meeting Surgical Pathology of Sinonasal Tract Tumors Session # 1015 on September 21, 2013
Page 43 of 60

GLOMANGIOPERICYTOMA (SINONASAL-TYPE HEMANGIOPERICYTOMA)
Key Facts
• Long-term clinical follow-up advocated as recurrencesmay develop late
IMAGE FINDINGS
CT Findings• Nasal cavity opacification by polypoid mass
accompanied by bone erosion or sclerosis• Destructive mass of nasal cavity and paranasal sinuses• No cribriform plate involvement• Angiograms show tumor blush• Nonspecific sinusitis frequently concurrent
MACROSCOPIC FEATURES
General Features• Tends to be polypoid• Beefy red to grayish pink• Soft, edematous, and fleshy• Frequently associated with hemorrhage
Size• Range: 0.8-8 cm• Mean: 3.1 cmo Tumors in females often larger than in males (mean:
3.3 cm vs. 2.8 cm)• Size does not correlate with recurrence
MICROSCOPIC PATHOLOGY
Histologic Features• Surface epithelium usually intact (respiratory type or
metaplastic squamous mucosa)• Subepithelial proliferation separated from surface
(Grenz zone)• Proliferation effaces normal architecture, although
entrapped minor mucoserous glands can be seen• Bone remodeling or compression may occur but not
direct invasion• Cellular, diffuse, syncytial arrangement
• Many patterns of growth, often within same tumoro May be be fascicular (short not long fascicles),
storiform, solid, whorled, meningothelial,reticulated, palisaded, peritheliomatous
• Spindled, epithelioid or rounded cells with indistinctcell borders
• Clear to amphophilic to slightly eosinophiliccytoplasm
• Absent to mild pleomorphism• Oval to spindle nuclei with coarse nuclear chromatin• Mitotic figures uncommon (< 1/10 HPFs)• Atypical mitotic figures absent• Ramifying, branching pattern of thin-walled vesselso "Staghorn" or antler-like vessels
• Peritheliomatous (perivascular) hyalinization ischaracteristic
• Extravasated erythrocytes• Mixture of inflammatory cells in backgroundo Eosinophils, mast cells, and lymphocytes, though
the first two predominate• Tumor giant cells can be seen but are uncommon• Fatty (lipomatous) change rare• Hematopoiesis very rare• Other tumors (solitary fibrous tumor, fibrosarcoma,
respiratory epithelial adenomatoid hamartoma) andreactive changes (sinonasal polyps) can be seen
• Rare cases may show profound pleomorphism,increased mitotic activity, and necrosiso These tumors are considered to be "malignant"
ANCILLARY TESTS
Histochemistry• May-Grünwald Giemsa highlights mast cells
Immunohistochemistry• Shows myoid phenotype (actins positive); β-catenin
and FXIIIa positive• Lacks vascular markers in neoplastic cells (only
background vessels will be positive)
Terminology• Soft tissue tumor showing perivascular myoid
differentiation
Clinical Issues• Nasal cavity is usually affected in isolation• Present with nasal obstruction and epistaxis• Excellent long-term outcome with surgery alone,
although recurrences develop
Macroscopic Features• Tends to be polypoid mass about 3 cm
Microscopic Pathology• Peritheliomatous (perivascular) hyalinization is
characteristic• Cellular, diffuse, syncytial arrangement
• Surface epithelium usually intact (respiratory type ormetaplastic squamous mucosa)
• Many patterns of growth, often within same tumor• Ramifying, branching pattern of vessels• Mixture of inflammatory cells in backgroundo Eosinophils, mast cells, and lymphocytes, although
first two predominate• Extravasated erythrocytes
Ancillary Tests• Shows myoid phenotype (actins positive)• Lacks vascular markers (CD34, CD31, FVIIIRAg)
Top Differential Diagnoses• Lobular capillary hemangioma• Solitary fibrous tumor• Nasopharyngeal angiofibroma
LDR Thompson, M.D. Used by Permission from: Diagnostic Pathology: Head & Neck LWW-Amirsys
ASCP Annual Meeting Surgical Pathology of Sinonasal Tract Tumors Session # 1015 on September 21, 2013
Page 44 of 60

GLOMANGIOPERICYTOMA (SINONASAL-TYPE HEMANGIOPERICYTOMA)
DIFFERENTIAL DIAGNOSIS
Lobular Capillary Hemangioma• Lobular growth around central vessel• Granulation tissue with ulcerated surface• Rich inflammatory infiltrate• Lacks perivascular hyalinization
Solitary Fibrous Tumor• Spindle cell tumor with thin-walled vascular
proliferation• Heavy ropy-keloid-like collagen deposition• Lacks inflammatory cells• Strong and diffuse CD34, bcl-2, and CD99
immunoreactivity
Nasopharyngeal Angiofibroma• Nasopharynx origin• Heavy stromal hyalinization around variably sized
vessels with possible smooth muscle walls• Lacks myoid phenotype
Fibrosarcoma• Cellular tumor with short, interlacing fascicles of
elongated spindle cells with tapered spindle nuclei• Lacks vascular background• Has increased mitoses• Vimentin positive only
Meningioma• Whorled pattern of growth comprised of
meningothelial or epithelioid cells• Intranuclear cytoplasmic inclusions• Psammoma bodies
Peripheral Nerve Sheath Tumor• Palisaded growth of spindle cells• Arranged in Antoni A and Antoni B areas• Perivascular hyalinization• Verocay bodies• Strong S100 protein immunoreactivity
SELECTED REFERENCES1. Duval M et al: Systematic review of treatment and
prognosis of sinonasal hemangiopericytoma. Head Neck.Epub ahead of print, 2012
2. Beech TJ et al: A haemangiopericytoma of the ethmoidsinus causing oncogenic osteomalacia: a case reportand review of the literature. Int J Oral Maxillofac Surg.36(10):956-8, 2007
3. Kuo FY et al: Sinonasal hemangiopericytoma-liketumor with true pericytic myoid differentiation: aclinicopathologic and immunohistochemical study of fivecases. Head Neck. 27(2):124-9, 2005
4. Folpe AL et al: Most osteomalacia-associated mesenchymaltumors are a single histopathologic entity: an analysis of32 cases and a comprehensive review of the literature. Am JSurg Pathol. 28(1):1-30, 2004
5. Thompson LD: Sinonasal tract glomangiopericytoma(hemangiopericytoma). Ear Nose Throat J. 83(12):807,2004
6. Thompson LD et al: Sinonasal-type hemangiopericytoma:a clinicopathologic and immunophenotypic analysis of104 cases showing perivascular myoid differentiation. Am JSurg Pathol. 27(6):737-49, 2003
7. Tse LL et al: Sinonasal haemangiopericytoma-like tumour:a sinonasal glomus tumour or a haemangiopericytoma?Histopathology. 40(6):510-7, 2002
8. Watanabe K et al: True hemangiopericytoma of the nasalcavity. Arch Pathol Lab Med. 125(5):686-90, 2001
9. Weber W et al: Haemangiopericytoma of the nasal cavity.Neuroradiology. 43(2):183-6, 2001
Immunohistochemistry
Antibody Reactivity Staining Pattern CommentVimentin Positive Cytoplasmic 100% of tumor cells
Actin-sm Positive Cytoplasmic Majority of tumor cells positive
Actin-HHF-35 Positive Cytoplasmic Majority of tumor cells positive
β-catenin Positive Nuclear & cytoplasmic Nearly all tumor cells
FXIIIA Positive Cytoplasmic Focal, granular immunoreactivity
Laminin Positive Stromal matrix Adjacent to neoplastic cells
CD34 Positive Cytoplasmic < 5% of cases
S100 Positive Nuclear & cytoplasmic < 3% of cases
CD68 Positive Cytoplasmic < 2% of cases
GFAP Positive Cytoplasmic < 1% of cases
Bcl-2 Positive Nuclear < 1% of cases
Ki-67 Positive Nuclear Usually < 5% of nuclei
CD31 Negative
FVIIIRAg Negative
CD117 Negative Only reactive in mast cells
Desmin Negative
CK-PAN Negative
EMA Negative
NSE Negative
LDR Thompson, M.D. Used by Permission from: Diagnostic Pathology: Head & Neck LWW-Amirsys
ASCP Annual Meeting Surgical Pathology of Sinonasal Tract Tumors Session # 1015 on September 21, 2013
Page 45 of 60

GLOMANGIOPERICYTOMA (SINONASAL-TYPE HEMANGIOPERICYTOMA)
Microscopic and Immunohistochemical Features
(Left) A variety of differentpatterns can be seen. Theleft side demonstratesa whorled appearancewith a richly vascularizedstroma. The right side showspatulous, open vessels withextravasated erythrocytes.(Right) There is no specificpattern to this proliferationalthough the vessels areeasily identified betweenthe lesional cells. Mastcells , eosinophils, andextravasated erythrocytes arequite characteristic for thetumor.
(Left) Occasionally, tumormultinucleated giant cells
will be seen withinthe proliferation. Thesecells have an identicalimmunohistochemistryto the rest of the tumorcells, confirming theirneoplastic nature. Notethe peritheliomatoushyalinization. (Right) Actinswill be strongly and diffuselyimmunoreactive in theneoplastic cells, althoughthere can be some variationto the intensity of thestaining. A smooth muscleactin (left) or a musclespecific actin (right).
(Left) Vascular markers arenot positive in the neoplasticcells, although CD31 (left)and CD34 are positive inthe endothelial cells. Note amitotic figure . β-catenin(right) shows a strongnuclear and cytoplasmicreaction in the neoplasticcells. (Right) Vimentin (left)is strongly and diffuselyimmunoreactive. CD117(right) is not required forthe diagnosis, but it is awell-known marker for mastcells, and so the mast cellswithin the tumor will beimmunoreactive.
LDR Thompson, M.D. Used by Permission from: Diagnostic Pathology: Head & Neck LWW-Amirsys
ASCP Annual Meeting Surgical Pathology of Sinonasal Tract Tumors Session # 1015 on September 21, 2013
Page 46 of 60

OLFACTORY NEUROBLASTOMA
This low-power H&E shows the well-developed lobulararchitecture of the primitive neuroblastoma cells that is socharacteristic for olfactory neuroblastoma (ONB). Thereare richly vascularized fibrovascular septa.
An intact respiratory epithelial surface overlies theneoplastic proliferation of "small round blue cells." Thereis an in-situ component to the neoplasm. Note numerousrosettes.
TERMINOLOGY
Abbreviations• Olfactory neuroblastoma (ONB)
Synonyms• Esthesioneuroblastoma (ENB)• Olfactory placode tumor• Esthesioneurocytoma• Esthesioneuroepithelioma• Esthesioneuroma
Definitions• Malignant neoplasm arising from specialized sensory
neuroepithelial (neuroectodermal) olfactory cellsnormally found in upper part of nasal cavity,specifically cribriform plate of ethmoid sinus
ETIOLOGY/PATHOGENESIS
Proposed Origin• Arise from specialized sensory neuroepithelial
olfactory cells (bipolar neurons) of olfactorymembrane
• Normally identified ino Jacobson organ (vomeronasal organ)o Sphenopalatine ganglion (pterygoid gland)o Ectodermal olfactory placodeo Ganglion of Loci (nervus terminalis)o Autonomic ganglia of nasal mucosao Olfactory neuroepithelium
▪ Cribriform plate
▪ Upper 1/3 to 1/2 of nasal septum
▪ Superomedial surface of superior turbinate(concha)
▪ Upper nasopharynx• Olfactory epithelium contains 3 cell types (also
present in tumor)
o Basal cells (stem cell compartment, thought to giverise to tumor)
o Olfactory neurosensory cellso Supporting sustentacular cells
CLINICAL ISSUES
Epidemiology• Incidenceo Represents ~ 2-3% of all sinonasal tract tumorso ~ 0.4/1,000,000 population/year
• Ageo Range: 2-94 yearso Bimodal peak: 2nd and 6th decades
• Gendero Male > Female (1.2:1)
Site• Nearly always involves cribriform plate of ethmoid
sinus• Much less common: Superior nasal concha, upper part
of septum, roof of nose
Presentation• Unilateral nasal obstruction (70%)• Epistaxis (50%)• Other symptoms includeo Headaches, pain, excessive lacrimation, rhinorrhea,
visual disturbanceso Anosmia: < 5% of patients, even though tumor
involves olfactory epithelium• Symptoms are nonspecific, so usually present for some
time• Rarely, may produce ectopic adrenocorticotrophic
hormone (ACTH) or antidiuretic hormone secretion(vasopressin)
Treatment• Options, risks, complications
LDR Thompson, M.D. Used by Permission from: Diagnostic Pathology: Head & Neck LWW-Amirsys
ASCP Annual Meeting Surgical Pathology of Sinonasal Tract Tumors Session # 1015 on September 21, 2013
Page 47 of 60

OLFACTORY NEUROBLASTOMA
Key Facts
o Due to tumor vascularity, biopsy is discouragedo Consider combination surgery and radiation for best
outcome
▪ However, surgery alone has same outcome assurgery + radiotherapy at 5 and 10 years
o Meningitis, CSF leak (liquorrhea), and dermatitis arepotential complications
• Surgical approacheso Complete craniofacial resection, including removal
of cribriform plate, is treatment of choice
▪ Endoscopic-assisted endonasal and anteriorcraniotomy resection (bi-cranial-facial approach;trephination)
▪ Endoscopic surgery vs. open techniques tend tohave better survival rate
▪ Larger tumors tend to be managed by opentechnique
▪ Patients with clear margins do better than thosewith positive margins
o Neck dissection recommended if clinicallysuspicious
• Drugso Chemotherapy is reserved for large, high-grade,
unresectable, disseminated, &/or salvage
▪ High-dose chemotherapy with cisplatin andetoposide (adjuvant did better)
• Radiationo Full-course radiotherapy post surgeryo Patients managed with radiation alone have worse
outcomeo Proton-beam therapy may yield better dose
distributiono Elective neck irradiation may be of value
• Autologous bone marrow transplantationo Limited cases have shown promise
Prognosis• Overall survival: 70% 5-year survival (stage and grade
dependent)o Low grade: 80% 5-year survivalo High grade: 25% 5-year survivalo Most patients present with Kadish stage C disease
o Best outcome with combination surgery andradiotherapy (~ 85% 5-year survival)
• Most tumors show local invasion (orbit, cranial cavity)• Local recurrence: Up to 30% (range: 15-70%)o Tend to develop within 1st 2 years after presentation
• 35% of patients develop metastatic diseaseo Cervical lymph nodes (up to 25%): Poor prognosis, <
30% 5-year survivalo Distant metastases (10%): Parotid glands, lung,
bone, liver, skin, and spinal cord• Negative prognostic indicators includeo High-grade tumor (Hyams grade 3 or 4)o Cervical or distant metastasiso Kadish Group Co Femaleo Age: < 20 or > 65 years at presentationo Extensive intracranial spreado Tumor recurrenceo High proliferation indexo Polyploidy/aneuploidy
IMAGE FINDINGS
General Features• Best diagnostic clueo Classic appearance: Dumbbell-shaped mass with
upper portion in intracranial fossa & lower portionin upper nasal cavity
▪ "Waist" at level of cribriform plateo Presence of peripheral tumor cysts at intracranial
tumor margin is highly suggestive of diagnosis ofONB
o Radiographic findings dependent on tumor size andsymptom duration
▪ Small: Unilateral nasal mass centered on superiornasal wall
▪ Large: Anterior cranial fossa, maxillary sinuses,orbit
MR Findings• T1WI
Terminology• Malignant neoplasm arising from specialized sensory
neuroepithelial (neuroectodermal) olfactory cells
Clinical Issues• Bimodal age peak: 2nd and 6th decades• Unilateral nasal obstruction (70%), epistaxis (50%)o Anosmia: < 5% of patients
• Involves cribriform plate of ethmoid sinus• Complete craniofacial resection with follow-up
radiation is standard treatment• Overall survival: 70% 5-year (stage and grade
dependent)
Microscopic Pathology• Lobular arrangement of primitive neuroblastoma cells
is characteristic
• Small round blue cellso Arranged in a syncytium, with a tangle of neuronal
processeso Pseudorosettes: Neoplastic cells palisaded around
finely fibrillary neural matrixo True rosettes: True tight annular formation by
neoplastic cells
Ancillary Tests• Positive: Neuroendocrine markers; S100 protein
sustentacular cells; rarely, keratin
Top Differential Diagnoses• Sinonasal undifferentiated carcinoma,
neuroendocrine carcinoma, NUT midline carcinoma,extranodal NK-/T-cell lymphoma nasal-type,rhabdomyosarcoma, PNET/Ewing sarcoma
LDR Thompson, M.D. Used by Permission from: Diagnostic Pathology: Head & Neck LWW-Amirsys
ASCP Annual Meeting Surgical Pathology of Sinonasal Tract Tumors Session # 1015 on September 21, 2013
Page 48 of 60

OLFACTORY NEUROBLASTOMA
o Hypointense to intermediate signal intensity masscompared to brain
o Areas of hemorrhage/necrosis are hypointense• T1WI with gadolinium contrasto Avid homogeneous tumor enhancemento Enhancement heterogeneous in areas of necrosis
• T2WIo Intermediate to hyperintense compared to braino Areas of cystic degeneration are hyperintense
CT Findings• Bone CT (no contrast)o Bone erosion/remodeling of lamina papyracea,
cribriform plate, &/or fovea ethmoidaliso Speckled calcifications within tumor matrix
frequently present• Contrast enhancedo Homogeneously enhancing masso Nonenhancing areas suggest necrosis
MACROSCOPIC FEATURES
General Features• Glistening, unilateral, mucosal-covered, soft, polypoid
mass• Red-gray, with gray-tan to pink cut surface• Mimics other sinonasal tract primary malignancies
Size• Range: < 1 cm to huge mass filling nasal cavity and
intracranial regionso Possible extension into adjacent paranasal sinuses
and nasopharynx
MICROSCOPIC PATHOLOGY
Histologic Features• Histologic appearance varies based on degree of
differentiation• Lobular arrangement of primitive neuroblastoma cells
is characteristic (irrespective of grade)o Lobule of cells surrounded by richly vascularized
stroma creating fibrovascular septao Sustentacular supporting cells line the lobule (S100
protein highlighted)• Surface epithelium is intacto "In situ" tumor within respiratory epithelium is
rarely identified• Neoplastic cells are classic "small round blue cells,"
slightly larger than mature lymphocyteso High nuclear to cytoplasmic ratioo Small, uniform nuclei with delicate, "salt and
pepper" chromatin distributiono Nucleoli are small to absent
• Cells arranged in syncytium, with a tangle of neuronalprocesseso Centrally located neurofibrillary material creates
pseudorosette (Homer Wright type)• Nuclear pleomorphism, mitoses, and necrosiso Absent or limited in low-grade lesions (grade 1 or 2)o Present in high-grade lesions (grade 3 or 4)
• 2 types of rosettes are recognizedo Pseudorosettes (Homer Wright type)
▪ Neoplastic cells palisading or cuffing aroundfinely fibrillary, delicate edematous neural matrixmaterial
▪ Up to 30% of cases
▪ Seen in grade 1 and 2 tumorso True rosettes (of Flexner-Wintersteiner)
▪ Gland-like, tight annular formation by neoplasticcells creating duct-like space with nonciliatedcolumnar cells
▪ About 5% of cases
▪ Seen in grade 3 and 4 tumorso Peritheliomatous "rosettes" are not considered of
diagnostic utility• Calcification (psammomatous or concretion) may be
seeno Decrease in frequency as grade increases
• Rarely presento Vascular invasiono Ganglion cellso Melanin-containing cellso Rhabdomyoblastic cells
• Tumors are separated into 4 gradeso Overall grade based on degree of differentiation,
presence of neural stroma, mitotic figures, andnecrosis
ANCILLARY TESTS
Histochemistry• Silver stains highlight neurosecretory granuleso Bodian, Churukian-Schenck, Grimelius
Immunohistochemistry• Positive: Neuroendocrine markers; S100 protein
sustentacular cellso Rare reaction with low molecular weight cytokeratin
(CAM5.2)• Negative: Desmin, myogenin, CD45RB, CD99
Flow Cytometry• High rate of polyploidy and aneuploidy, related to
adverse prognosis
Cytogenetics• Chromosomal alterations of 19, 8q, 15q, 22q, 4q• Deletion of chromosome 11 and gains of 1p associated
with increased risk of metastases and worse prognosis• RT-PCR of human achaete-scute homologue (hASH1)
expression may be specific marker of ONB• No EWS/FLI1 gene fusion
Electron Microscopy• Membrane-bound dense core neurosecretory
granules present in cytoplasm and nerve processeso Granule diameter: 50-250 μm
• Fibrillary stroma corresponds to immature nerveprocesseso Nerve processes may contain neurotubules and
neurofilaments▪ Occasionally, Schwann-like cells can be seen
LDR Thompson, M.D. Used by Permission from: Diagnostic Pathology: Head & Neck LWW-Amirsys
ASCP Annual Meeting Surgical Pathology of Sinonasal Tract Tumors Session # 1015 on September 21, 2013
Page 49 of 60

OLFACTORY NEUROBLASTOMA
• Flexner-Wintersteiner rosette lining cells may haveapical cilia or microvilli and olfactory vesicles
DIFFERENTIAL DIAGNOSIS
Sinonasal Undifferentiated Carcinoma(SNUC)• High-grade, usually widely destructive neoplasm• Extensive coagulative necrosis and vascular invasion• Strong and diffuse keratin immunoreactivity; may
show limited neuroendocrine markers
Neuroendocrine Carcinoma• High-grade tumors with extensive necrosis, high
mitoses, and apoptosis• Punctate paranuclear keratin immunoreactivity; may
show TTF-1 positive
NUT Midline Carcinoma• Poorly differentiated, high-grade carcinoma, often
with squamous differentiation, usually in youngpatients, vast majority in midline, with t(15;19)(q14;p13)
• Requires identification of nuclear protein in testis(NUT) gene on chromosome 15q14 (FISH or RT-PCRtechniques)o Balanced translocation: BRD4 (19p13.1) with NUT
(15q14), creating fusion gene BRD4-NUT• Frequently also show CD34 expression
Extranodal NK-/T-cell Lymphoma, NasalType• High-grade tumors with extensive vascular invasion
and coagulative necrosis• Positive: NK- or T-cell markers; negative with
neuroendocrine markers, S100 protein, keratin
Rhabdomyosarcoma• Often in same bimodal age distribution; similar
radiographic, gross, and clinical findings• Rhabdomyoblastic differentiation with strap cells and
eccentric, eosinophilic cytoplasm• Positive: Muscle markers; keratin and CD56 can be
positive in 5-10% of cases
Malignant Melanoma• Wide variety of architectural patterns and wide variety
of morphologic appearances• Polygonal cells, eosinophilic, plasmacytoid cytoplasm,
intranuclear cytoplasmic inclusions and pigment• Positive: S100 protein, HMB-45, Melan-A, MIFT;
negative: Neuroendocrine markers
PNET/Ewing Sarcoma• Characteristic "small round blue cell" tumor, showing
coagulative necrosis• Diffuse, sheet-like cells with indistinct cell borders,
uniform small cells with finely dispersed chromatindistribution and small nucleoli
• Positive: FLI-1, CD99, NSE; sometimes synaptophysin;negative: Chromogranin, GFAP
• FISH for t(11;22)(q24;q12)
Pituitary Adenoma• Sphenoid sinus mass, ribbons, festoons, lobular
architecture, polygonal cells, lacking pleomorphismand mitoses
• Positive: Neuroendocrine and peptide markers, keratin
Extramedullary Plasmacytoma• Plasmacytoid cells with "clockface" nuclear chromatin
distribution, Hof-zone in cytoplasm• Positive: CD138, CD79a, κ or λ restricted• Negative: Epithelial or neuroendocrine markers
Metastatic Neuroblastoma• Histologically identical, but has myc amplification
GRADING
Hyams Grading• Grade 1: Majority of tumors; lobular, syncytial,
neurofibrillary matrix, vesicular chromatin, no mitosesor necrosis
• Grade 2: Less neurofibrillary matrix, scattered mitoses• Grade 3: More pleomorphic cells, Flexner-
Wintersteiner rosettes, possible necrosis• Grade 4: Least number of tumors; anaplastic, high
mitoses, necrosis
STAGING
Kadish Staging• A: Tumor confined to nasal cavity (18%)• B: Tumor involves nasal cavity plus one or more
paranasal sinuses (32%)• C: Extension of tumor beyond sinonasal cavities (50%)
SELECTED REFERENCES1. Soler ZM et al: Endoscopic versus open craniofacial
resection of esthesioneuroblastoma: what is the evidence?Laryngoscope. 122(2):244-5, 2012
2. Kane AJ et al: Posttreatment prognosis of patients withesthesioneuroblastoma. J Neurosurg. 113(2):340-51, 2010
3. Ozsahin M et al: Outcome and prognostic factors inolfactory neuroblastoma: a rare cancer network study. Int JRadiat Oncol Biol Phys. 78(4):992-7, 2010
4. Bragg TM et al: Clinicopathological review:esthesioneuroblastoma. Neurosurgery. 64(4):764-70;discussion 770, 2009
5. Devaiah AK et al: Treatment of esthesioneuroblastoma:a 16-year meta-analysis of 361 patients. Laryngoscope.119(7):1412-6, 2009
6. Faragalla H et al: Olfactory neuroblastoma: a review andupdate. Adv Anat Pathol. 16(5):322-31, 2009
7. Folbe A et al: Endoscopic endonasal resection ofesthesioneuroblastoma: a multicenter study. Am J RhinolAllergy. 23(1):91-4, 2009
8. Thompson LD: Olfactory neuroblastoma. Head NeckPathol. 3(3):252-9, 2009
9. Wenig BM: Undifferentiated malignant neoplasms of thesinonasal tract. Arch Pathol Lab Med. 133(5):699-712, 2009
10. Bachar G et al: Esthesioneuroblastoma: The PrincessMargaret Hospital experience. Head Neck. 30(12):1607-14,2008
LDR Thompson, M.D. Used by Permission from: Diagnostic Pathology: Head & Neck LWW-Amirsys
ASCP Annual Meeting Surgical Pathology of Sinonasal Tract Tumors Session # 1015 on September 21, 2013
Page 50 of 60

OLFACTORY NEUROBLASTOMA
11. Wang SL et al: Absence of Epstein-Barr virus in olfactoryneuroblastoma. Pathology. 39(6):565-6, 2007
12. Sugita Y et al: Olfactory neuroepithelioma: animmunohistochemical and ultrastructural study.Neuropathology. 26(5):400-8, 2006
13. Iezzoni JC et al: "Undifferentiated" small round cell tumorsof the sinonasal tract: differential diagnosis update. Am JClin Pathol. 124 Suppl:S110-21, 2005
14. Klepin HD et al: Esthesioneuroblastoma. Curr TreatOptions Oncol. 6(6):509-18, 2005
15. Ferlito A et al: Contemporary clinical commentary:esthesioneuroblastoma: an update on management of theneck. Laryngoscope. 113(11):1935-8, 2003
16. Theilgaard SA et al: Esthesioneuroblastoma: a Danishdemographic study of 40 patients registered between 1978and 2000. Acta Otolaryngol. 123(3):433-9, 2003
17. Ingeholm P et al: Esthesioneuroblastoma: a Danishclinicopathological study of 40 consecutive cases. APMIS.110(9):639-45, 2002
18. Rinaldo A et al: Esthesioneuroblastoma and cervical lymphnode metastases: clinical and therapeutic implications.Acta Otolaryngol. 122(2):215-21, 2002
19. Dulguerov P et al: Esthesioneuroblastoma: a meta-analysisand review. Lancet Oncol. 2(11):683-90, 2001
20. Resto VA et al: Esthesioneuroblastoma: the Johns Hopkinsexperience. Head Neck. 22(6):550-8, 2000
Immunohistochemistry
Antibody Reactivity Staining Pattern CommentChromogranin-A Positive Cytoplasmic Majority of tumor cells
Synaptophysin Positive Cytoplasmic Majority of tumor cells
CD56 Positive Cell membrane & cytoplasm Nearly all neoplastic cells
NSE Positive Cytoplasmic Nearly all neoplastic cells
NFP Positive Cytoplasmic Accentuates neural matrix
β-tubulin Positive Cytoplasmic Most tumor cells
S100 Positive Nuclear & cytoplasmic Accentuates peripheral sustentacular cells
GFAP Positive Cytoplasmic Highlights peripheral sustentacular cells
CK8/18/CAM5.2 Positive Cytoplasmic Only about 5% of tumors
Ki-67 Positive Nuclear Proliferation index ranges from 5-50%
Calretinin Positive Nuclear & cytoplasmic Only about 5-10% of cells will be positive
EBER Negative
CD99 Negative
Desmin Negative
Myogenin Negative
CD45RB Negative
p63 Negative
Histologic Grading (Hyams's Criteria)
MicroscopicFeatures
Grade 1 Grade 2 Grade 3 Grade 4
Architecture Lobular Lobular ± lobular ± lobular
Pleomorphism Absent to slight Present Prominent Marked
Neurofibrillary matrix Prominent Present May be present Limited
Rosettes Homer Wright pseudorosettes Homer Wright pseudorosettes Flexner-Wintersteiner rosettes Flexner-Wintersteiner rosettes
Mitoses Absent Present Prominent Marked
Necrosis Absent Absent Present Prominent
Glands May be present May be present Usually limited Focally present
Calcifications Variable Variable Absent Absent
Hyams VJ et al. Tumors of the Upper Respiratory Tract and Ear. Armed Forces Institute of Pathology Fascicles. 2nd series. Washington: American Registry of Pathology Press, Armed ForcesInstitute of Pathology, 1988.
Kadish Staging System
Stage Criteria OutcomeStage A Tumor confined to nasal cavity 5-year survival: > 90%
Stage B Tumor involves nasal cavity plus one or more paranasal sinuses 5-year survival: ~ 70%
Stage C Extension of tumor beyond sinonasal cavities 5-year survival: < 50%
Kadish S et al: Olfactory neuroblastoma. A clinical analysis of 17 cases. Cancer. 37(3):1571-6, 1976.
LDR Thompson, M.D. Used by Permission from: Diagnostic Pathology: Head & Neck LWW-Amirsys
ASCP Annual Meeting Surgical Pathology of Sinonasal Tract Tumors Session # 1015 on September 21, 2013
Page 51 of 60

OLFACTORY NEUROBLASTOMA
Imaging, Gross, and Microscopic Features
(Left) Coronal graphic ofinvasive ONB shows thelesion centered high inthe nasal cavity, invadingthe anterior cranial fossathrough the cribriform plate
. Note characteristicintracranial cysts , ahelpful radiographic findingfor this tumor. (Right)Coronal CECT demonstratesright nasal cavity ONBwith destruction of thecribriform plate andlamina papyracea . Notelow-density obstructedmaxillary secretions .
(Left) Coronal T1-weightedcontrast-enhanced MR imageshows a heterogeneousenhancement throughoutthe large mass, destroyingthe cribriform plate andexpanding into the frontallobe. Note cysts withinthe mass. (Right) Multiplepolypoid fragments ofmucosal-covered soft tissueshow a red to red-tanappearance, suggesting therich vascularity of the tumor.
(Left) Many fibrovascularsepta dissect and surroundthe tumor lobules. Thelobular architecture ispresent to a variable degreein all ONB no matter whathistologic grade. (Right)There are multiple small,tight lobules of tumor setwithin an edematous torichly vascularized stroma.This lobular architecture isquite characteristic of ONBand is a histologic featureat low power that can bequite helpful in confirmingthe diagnosis.
LDR Thompson, M.D. Used by Permission from: Diagnostic Pathology: Head & Neck LWW-Amirsys
ASCP Annual Meeting Surgical Pathology of Sinonasal Tract Tumors Session # 1015 on September 21, 2013
Page 52 of 60

OLFACTORY NEUROBLASTOMA
Microscopic Features
(Left) The respiratoryepithelium is intact, separatedby fibrous connective tissuefrom the lobular neoplasticinfiltrate in the stroma. There islimited pleomorphism, with afibrillary matrix noted betweenthe syncytium of cells. (Right)The tumors are quite cellular,showing lobules of primitiveneuroblastoma-like cells thathave a very high nuclear tocytoplasmic ratio and arearranged in a syncytium. Afew vessels can be easilyidentified even at this lowmagnification.
(Left) This grade 1 tumorshows classic "salt andpepper" nuclear chromatinwithout any cellular variability.The fibrovascular septaseparate the neoplasticcells into lobules. Neuronalmatrix material is notedwithin the lobules. (Right)The neoplastic cells showthe "small round blue cell"pattern so characteristic ofneuroblastoma. The nucleiare monotonous, with evenlydistributed chromatin. Thevascularized stroma is noted.
(Left) The neoplastic cellsare arranged in a syncytium,lacking any well-definedcell borders. There is a highnuclear to cytoplasmic ratio.Nucleoli are focally identifiedin cells that show delicate,"salt and pepper" nuclearchromatin distribution. Notethe Homer Wright rosette ,a finding seen in up to 30% ofgrade 2 tumors. (Right) Thereis a greater degree of nuclearpleomorphism and variabilityin this grade 2 tumor, showingnuclear hyperchromasia.Mitoses and necrosis areabsent.
LDR Thompson, M.D. Used by Permission from: Diagnostic Pathology: Head & Neck LWW-Amirsys
ASCP Annual Meeting Surgical Pathology of Sinonasal Tract Tumors Session # 1015 on September 21, 2013
Page 53 of 60

OLFACTORY NEUROBLASTOMA
Microscopic Features
(Left) Within a lobule, theneoplastic cells have a highnuclear to cytoplasmic ratio,nuclear hyperchromasia,and a suggestion ofpseudorosettes. Thistumor shows a syncytialarchitecture. (Right) Thereis slightly more variabilityamong the nuclei of thistumor, with marked nuclearhyperchromasia. This is anexample of a grade 3 tumor.Other histologic featureswere present elsewhere inthe sample.
(Left) ONB are very vasculartumors, with a richlyvascularized fibrovascularstroma and septa .This tumor would bleedquite profusely if it werebiopsied; hence biopsiesare discouraged. (Right)Native, residual minormucoserous glands can be surrounded orinvaded by the neoplasticproliferation. It is importantto separate these structuresfrom true rosettes (Flexner-Wintersteiner), which areonly identified in high-gradetumors.
(Left) A grade 3 ONB willshow nuclear pleomorphism
and tumor necrosis, along with increased
mitoses. There is agreater degree of nuclearhyperchromasia. (Right)Coagulative-type necrosisis present in the center ofthis lobule of tumor. This is apattern of growth that wouldbe seen in a grade 3 or 4ONB.
LDR Thompson, M.D. Used by Permission from: Diagnostic Pathology: Head & Neck LWW-Amirsys
ASCP Annual Meeting Surgical Pathology of Sinonasal Tract Tumors Session # 1015 on September 21, 2013
Page 54 of 60

OLFACTORY NEUROBLASTOMA
Microscopic Features
(Left) It is not uncommon in asingle tumor to have a numberof different appearances,in which the cells becomeslightly larger (center) thanthe remaining cells, a findingseen more commonly inhigher grade tumors. (Right) Apseudorosette (Homer Wrighttype) shows a peripheralpalisade of neoplastic cellscuffing a finely fibrillary neuralmatrix material in the center
. This pseudorosette is seenin up to 30% of grade 1 and 2tumors.
(Left) True rosettes (of Flexner-Wintersteiner) have gland-like, tight annular formationswith concretions in the lumen.The cells lining these duct-like spaces are nonciliatedcolumnar cells. These rosettesare present in ~ 5% of grade 3or 4 tumors. (Right) This grade3 tumor shows a number ofgland-like structures, witha true lumen, while alsoshowing pseudorosettes.There is significant nuclearpleomorphism. Note thecalcification , present inselected cases.
(Left) Calcifications canbe seen in ONB, althoughthey tend to be seenmore frequently in lowergrade tumors. Multiplepsammomatoid calcificationsare seen in this grade 1tumor. (Right) Cervicallymph node metastasesare seen in up to 25% ofpatients. In this case, nearly7/8 of the lymph node isreplaced by the neoplasm. Themetastatic foci recapitulatethe primary, maintaining alobular architecture and arichly vascularized stroma.
LDR Thompson, M.D. Used by Permission from: Diagnostic Pathology: Head & Neck LWW-Amirsys
ASCP Annual Meeting Surgical Pathology of Sinonasal Tract Tumors Session # 1015 on September 21, 2013
Page 55 of 60

OLFACTORY NEUROBLASTOMA
Ancillary Techniques
(Left) The neurosecretorygranules can be highlightedin the neoplastic cellsby applying silver stains,with the Grimeliusstain illustrated. (Staincourtesy L. Grimelius,MD.) (Right) A widevariety of neuroendocrinemarkers can be appliedto highlight the neoplasticcells. Synaptophysin oftengives a very strong, heavychromogen depositionin the neoplastic cells, asillustrated here. There isa slight granularity to thestaining pattern.
(Left) Chromogranin yieldsa very strong, diffuse,cytoplasmic reaction inONB. While chromogranin-Aor -B can be used, A tends togive a more consistent result.(Right) The sustentacularcells at the periphery ofthe lobule are stronglyhighlighted with S100protein, yielding a nuclearand cytoplasmic reaction.This pattern of reactivitysupports the notion that thevarious cellular componentsof olfactory epithelium are allpresent in the tumor (basal,neurosensory, sustentacularcells).
(Left) CD56 yields avery strong and diffusemembranous andcytoplasmic reactionin the ONB cells. It isimportant to rememberthat CD56 is also reactivein rhabdomyosarcomaand NK-/T-cell lymphomanasal-type tumors that areincluded in the differentialdiagnosis. (Right) Thesurface epithelium actsas an internal control forthe CK-pan. Note the rare,isolated, and weak reactivitywithin the ONB cells withthe stroma and also withinthe surface epithelium.
LDR Thompson, M.D. Used by Permission from: Diagnostic Pathology: Head & Neck LWW-Amirsys
ASCP Annual Meeting Surgical Pathology of Sinonasal Tract Tumors Session # 1015 on September 21, 2013
Page 56 of 60

ALLERGIC FUNGAL SINUSITIS
Hematoxylin & eosin shows "tide lines," "tree rings,"or alternating bands of nuclear and cytoplasmic debris,findings characteristic for allergic fungal sinusitis.
Hematoxylin & eosin shows degenerated inflammatorycells and eosinophils with Charcot-Leyden crystals(breakdown products of eosinophils).
TERMINOLOGY
Abbreviations• Allergic fungal sinusitis (AFS)
Synonyms• Allergic mucin• Eosinophilic fungal rhinosinusitis (EFRS)• Eosinophilic mucin rhinosinusitis (EMRS)• Allergic fungal rhinosinusitis• Hypertrophic sinus disease (HSD)• Atopical fungal sinusitis
Definitions• Allergic response in sinonasal tract mucosa
to aerosolized fungal allergens, amplified andperpetuated by eosinophils
ETIOLOGY/PATHOGENESIS
Environmental Exposure• Allergic reaction to inhaled fungal elementso Class II genes in major histocompatibility complex
are involved in antigen presentation and immuneresponse/modulation
o Allergic reaction develops in immunocompetentpeople
o Aspergillus species most commono Dematiaceous (brown-pigmented) fungi
▪ Widespread in soil, wood, and decomposing plantmaterial
▪ Alternaria
▪ Bipolaris
▪ Curvularia
▪ Exserohilum
▪ Phialophora specieso Mucor is uncommon agent
Pathogenesis• Atopic host is exposed to finely dispersed fungi
• Inflammatory response is mediated byimmunoglobulin E (IgE)o Type 1 hypersensitivity reaction
• Tissue edema with sinus obstruction and stasis• Proliferation of fungus results in increased antigenic
exposure• Self-perpetuating cycle producing allergic mucin and
possibly polyps
CLINICAL ISSUES
Epidemiology• Incidenceo Common
▪ Approximately 10% of patients with chronicrhinosinusitis or nasal polyposis have AFSconcurrently
▪ Increased frequency in patients with asthma,allergies (atopic), and allergic bronchopulmonaryaspergillosis (ABPA)
o Increased in warmer climates• Ageo Usually in 3rd to 7th decadeso Not a disease seen in children
• Gendero Equal gender distribution
▪ Males more likely to present with bone erosionthan females
Site• Nasal cavity• Paranasal sinuseso Maxillary and ethmoid sinuses most common
Presentation• Atopy is common (allergy)• Chronic, unrelenting rhinosinusitis• Masso May result in facial dysmorphia and proptosis
LDR Thompson, M.D. Used by Permission from: Diagnostic Pathology: Head & Neck LWW-Amirsys
ASCP Annual Meeting Surgical Pathology of Sinonasal Tract Tumors Session # 1015 on September 21, 2013
Page 57 of 60

ALLERGIC FUNGAL SINUSITIS
Key Facts
▪ If proptosis is present, visual disturbances arereported
• Discharge• Rhinorrhea• Headache
Laboratory Tests• Peripheral eosinophilia• Elevated fungal-specific IgEo May also have elevated levels of fungal-specific IgG3
• Cultures performed to identify etiologic fungal agento Results used to conduct desensitization treatmentso Cultures are not used to provide antibiotic
sensitivities since there is no invasive fungalinfection
Treatment• Options, risks, complicationso Usually requires combination of surgery and
medical therapy to yield best long-term outcome• Surgical approacheso Extensive debridement and complete evacuation of
impacted mucin is mainstay of therapyo Polypectomy and marsupialization of involved
sinuses at minimumo Procedures may be endoscopic
▪ Functional endoscopic sinus surgery (FESS)• Drugso Postoperative anti-inflammatory therapy
▪ Oral corticosteroids usually yield best outcomeo Postoperative azoles (specifically, itraconazole) may
reduce recurrenceso Medical management of allergic inflammatory
disease• Allergic desensitization (immunotherapy)
Prognosis• Good with integrated medical and surgical approach• Recurrences develop with fair frequencyo Can be problematic to functional status of patient
IMAGE FINDINGS
CT Findings• Expansile, sometimes destructive mass within nasal
cavity and paranasal sinuses• Bone remodeling or destructiono Orbital expansion and bony erosion are prominent
features• Bone erosion can be seen in advanced cases
MACROSCOPIC FEATURES
General Features• Foul odor• Polypoid fragments• Putty or crunchy peanut butter-like consistency• Muddy consistency• Greasy to palpation
Size• Range: 0.1-0.4 cm fragments of tissueo Mean overall aggregate: Up to 8 cm
MICROSCOPIC PATHOLOGY
Histologic Features• Multiple polypoid fragments identified histologically• "Mucinous" material is free floating, unattached to
surrounding respiratory tissues• "Tide lines," "tree rings," waves, or rippleso Appearance due to mucin material alternating with
inflammatory debriso Yields overall "blue and pink" alternating appearance
• Degenerated material composed of neutrophils,eosinophils, and mucinous debriso Ghost outlines of cells commono Nuclear debris tends to aggregate
• Charcot-Leyden crystals (degenerated eosinophils)o Long, needle-shaped, or bipyramidal crystalso Dropped sub-stage condenser will yield refractile
appearance to crystals
Terminology• Eosinophilic fungal rhinosinusitis (EFRS)• Allergic response within sinonasal tract mucosa
to aerosolized fungal allergens, amplified andperpetuated by eosinophils
Etiology/Pathogenesis• Allergic reaction to inhaled fungal elements• Aspergillus species most common
Clinical Issues• Atopy is common (allergy)• Polyps with putty-like material• Peripheral eosinophilia• Elevated fungal-specific IgE• Extensive debridement and complete evacuation of
impacted mucin is mainstay of therapy
• Postoperative anti-inflammatory therapy, includingoral corticosteroids
Macroscopic Features• Foul odor• Putty or crunchy peanut butter-like consistency• Muddy or greasy consistency
Microscopic Pathology• "Tide lines," "tree rings," waves, or ripples of mucin
material alternating with inflammatory debris
Ancillary Tests• GMS (Gomori methenamine silver); PAS/light green
Top Differential Diagnoses• Invasive fungal sinusitis• Mycetoma
LDR Thompson, M.D. Used by Permission from: Diagnostic Pathology: Head & Neck LWW-Amirsys
ASCP Annual Meeting Surgical Pathology of Sinonasal Tract Tumors Session # 1015 on September 21, 2013
Page 58 of 60

ALLERGIC FUNGAL SINUSITIS
• Fungal elements often difficult to detect (even withspecial stains)o When fungal elements not identified, EMRS can be
used instead• Concurrent sinonasal pathologyo Sinonasal inflammatory polyps
▪ Polyps may show inflammation but not abscessesor necrotic material
o Chronic rhinosinusitis
ANCILLARY TESTS
Histochemistry• GMS (Gomori methenamine silver)o Highlights fungal hyphae (when present)
• PAS/light greeno Highlights fungal hyphae (when present)
DIFFERENTIAL DIAGNOSIS
Invasive Fungal Sinusitis• Fungal hyphae identified withino Vessel walls or vascular spaceso Tissue
• Significant host response within stromao Inflammatory cells are identified within tissue rather
than floating in lumen mucin as seen with AFS• No alternating pattern
Sinonasal Polyps• Polypoid structures with intact surface epithelium• Mucinous or edema material in background mixed
with inflammatory cellso Eosinophils may be seen but usually not
degenerated or associated with Charcot Leydencrystals
• Lacks alternating pattern• Generally contains minor mucoserous glands in
stroma
Mycetoma• Aggregation or ball of fungi (yeasts &/or hyphae)• Fruiting heads are common in this fungal disease• Usually no host responseo If present, can be lymphohistiocytic or eosinophilic
• Dematiaceous fungi most common
DIAGNOSTIC CHECKLIST
Pathologic Interpretation Pearls• Putty-like gross appearance• Alternating "tide lines" or "tree rings"• Eosinophils and their breakdown products• Do not need to prove fungal elements are present
SELECTED REFERENCES1. Wise SK et al: Antigen-specific IgE in sinus mucosa of
allergic fungal rhinosinusitis patients. Am J Rhinol.22(5):451-6, 2008
2. Aribandi M et al: Imaging features of invasive andnoninvasive fungal sinusitis: a review. Radiographics.27(5):1283-96, 2007
3. Driemel O et al: [Allergic fungal sinusitis, fungus ball andinvasive sinonasal mycosis - three fungal-related diseases]Mund Kiefer Gesichtschir. 11(3):153-9, 2007
4. Ghegan MD et al: Socioeconomic factors in allergic fungalrhinosinusitis with bone erosion. Am J Rhinol. 21(5):560-3,2007
5. Kimura M et al: Usefulness of Fungiflora Y to detectfungus in a frozen section of allergic mucin. Pathol Int.57(9):613-7, 2007
6. Mirante JP et al: Endoscopic view of allergic fungalsinusitis. Ear Nose Throat J. 86(2):74, 2007
7. Orlandi RR et al: Microarray analysis of allergic fungalsinusitis and eosinophilic mucin rhinosinusitis.Otolaryngol Head Neck Surg. 136(5):707-13, 2007
8. Revankar SG: Dematiaceous fungi. Mycoses. 50(2):91-101,2007
9. Ryan MW et al: Allergic fungal rhinosinusitis: diagnosisand management. Curr Opin Otolaryngol Head Neck Surg.15(1):18-22, 2007
10. Schubert MS: Allergic fungal sinusitis. Clin AllergyImmunol. 20:263-71, 2007
11. Schubert MS: Allergic fungal sinusitis. Clin Rev AllergyImmunol. 30(3):205-16, 2006
12. Heffner DK: Allergic fungal sinusitis is a histopathologicdiagnosis; paranasal mucocele is not. Ann Diagn Pathol.8(5):316-23, 2004
13. Huchton DM: Allergic fungal sinusitis: anotorhinolaryngologic perspective. Allergy Asthma Proc.24(5):307-11, 2003
14. Ferguson BJ: Definitions of fungal rhinosinusitis.Otolaryngol Clin North Am. 33(2):227-35, 2000
15. Kuhn FA et al: Allergic fungal rhinosinusitis: perioperativemanagement, prevention of recurrence, and role of steroidsand antifungal agents. Otolaryngol Clin North Am.33(2):419-33, 2000
16. Mabry RL et al: Allergic fungal sinusitis: the roleof immunotherapy. Otolaryngol Clin North Am.33(2):433-40, 2000
17. Marple BF: Allergic fungal rhinosinusitis: surgicalmanagement. Otolaryngol Clin North Am. 33(2):409-19,2000
LDR Thompson, M.D. Used by Permission from: Diagnostic Pathology: Head & Neck LWW-Amirsys
ASCP Annual Meeting Surgical Pathology of Sinonasal Tract Tumors Session # 1015 on September 21, 2013
Page 59 of 60

ALLERGIC FUNGAL SINUSITIS
Radiographic, Gross, and Microscopic Features
(Left) Radiologic imageshows opacification butno destruction of the nasalcavity and sinuses (left)by allergic fungal sinusitis
. Polyps are noted inthe contralateral maxillarysinus, a frequent concurrentfinding. (Right) Radiologicimage shows opacification ofthe sinuses and nasal cavityby a homogeneous density.Note polypoid tissue andmucosal thickening in theopposite maxillary sinus,frequently concurrentlyidentified.
(Left) Gross photographshows a polypoid fragmentof tissue with multipleprojections. The tissue wasgreasy with a putty-likeconsistency on cut section.(Right) Hematoxylin & eosinshows alternating ripples ofeosinophils and neutrophils.The mucinous to myxoiddegeneration creates these"light" and "dark" rings orbands. This feature alone isquite characteristic of thedisorder, seldom requiringany additional studies orevaluation.
(Left) Hematoxylin &eosin shows degeneratedinflammatory cells withmucinous material andneutrophilic and eosinophilicdebris. The cracking artifactswithin the tissue highlightthe tide-line appearance.(Right) Composite imageshows fungal organismsembedded within thedegenerated debris. Top:GMS highlights Aspergillusspecies with acute anglebranching and septations.Bottom: Hematoxylin &eosin stain highlights Mucorspecies with wide, ribbon-like, aseptate hyphae.
LDR Thompson, M.D. Used by Permission from: Diagnostic Pathology: Head & Neck LWW-Amirsys
ASCP Annual Meeting Surgical Pathology of Sinonasal Tract Tumors Session # 1015 on September 21, 2013
Page 60 of 60