Serge Rozenberg CHU St Pierre VUB-ULB Belgium serge...
81
In the center of the city, in the center of life, with passion for care Serge Rozenberg CHU St Pierre VUB-ULB Belgium [email protected] Clinical overview of conjugated estrogens/bazedoxifene (CE/BZA) BMS 14.11.2015
Transcript of Serge Rozenberg CHU St Pierre VUB-ULB Belgium serge...
In the center of the city in the center of life with passion for care
Serge Rozenberg CHU St Pierre VUB-ULB Belgium
serge_rozenbergstpierre-brube
Clinical overview of conjugated
estrogensbazedoxifene (CEBZA)
BMS 14112015
Conflict of interest amp Disclosure
Conflicts of interest nil
Disclosure SR
Research funding IRIS- King Baudouin Fondation Vesale research Foundation Amgen MSD
Speakers bureau ampor Advisory Boards
Abbot Pfizer Will Gedeon Richter MSD Amgen
1 Kagan R J Womenrsquos Health (Larchmt) 2012
the OPTIMAL Menopausal Therapy
should demonstrate1
ndash Favorable safety and tolerability profile
ndash Relief of menopausal symptoms
ndash Prevention of osteoporosis CVD Cognitive function
ndash No stimulation of the endometrium breast and ovary
1 Kagan R J Womenrsquos Health (Larchmt) 2012
the OPTIMAL Menopausal Therapy
should demonstrate1
ndash Favorable safety and tolerability profile
ndash Relief of menopausal symptoms
ndash Prevention of osteoporosis CVD Cognitive function
ndash No stimulation of the endometrium breast and ovary
Variations in Associated Breast Cancer Risk Between CE alone and
CEMPA
Cumulative hazards
adjusted for age and
raceethnicity for
invasive breast cancer
by randomization
assignment in the WHI
CE-alone and CEMPA
trials
Anderson GL et al Lancet
Oncol 2012
0 0
1 2 3 4 5 6 7 8 9 10 11 12 13
001
002
003
004
005
Cu
mu
lati
ve
ha
za
rd
Time since randomization (years)
CEMPA
Placebo (in CEMPA arm)
HR 125 (95 CI 107ndash146)
CE alone
Placebo (in CE-alone arm)
HR 077 (95 CI 062ndash095)
CEMPA
CE alone
Placebo (CE-alone)
Placebo (CEMPA)
Estrogen only therapy
Endometrial cancer
Hysterectomy specimen showing cancer invading myometrium
following unopposed estrogen therapy for 15 years
Courtesy Dr David Sturdee
Bazedoxifene (BZA) specifically selected in
combination with conjugated estrogens
1 Crabtree J et al Mol Cell Endocrinol 2008
2 Kharode Y et al Endocrinolology 2008
3 Duavive SmPC
Estrogen Receptor activity is dimmed
Estrogen Receptor activity is turned on
CEs are agonists BZA is an antagonist
In the uterus
bull The BZA component reduces the risk of endometrial hyperplasia that can occur with the conjugated estrogens component alone1-3
bull This means that progestins are not needed
From the Womenrsquos Health Initiative to the combination
of estrogen and selective estrogen receptor
modulators to avoid progestin addition
bull Marie-Ceacutecile Valera Pierre Gourdy Florence Treacutemolliegraveres Jean-Franccedilois Arnal
bull Maturitas Volume 82 Issue 3 November 2015 Pages 274ndash277
bull
Other combinations of an estrogen (E2) + a SERM studied have
not produced favorable results
bull Objective To compare effects of 52 weeksrsquo treatment with either raloxifene 60 mgday alone (RLX) or in combination with 17B-estradiol 1 mgday (RLX + E2) on vasomotor symptoms (n = 83) and endometrial safety (n = 123) in postmenopausal women who transitioned from estrogen-progestin therapy Endometrial effect Women in the RLX + E2 group had significantly increased endometrial thickness at 52 weeks from baseline and RLX alone had no increase Two women (328) in the RLX + E2 group had endometrial hyperplasia (one with atypia) on the exit biopsy No one in RLX alone did
bull 1 Stovall D et al Menopause The Journal of The North American Menopause Society 2007
bull For the safety analyses data from women randomized before and after the protocol amendment were pooled which included 62 women in the raloxifene group and 61 women in the raloxifene + estrogen group
EFFICACY
VASOMOTOR
SYMPTOMS
SMART-2
DUAVIVE Efficacy for the Treatment of Moderate to
Severe VMS Associated With Menopause
14
1 Pinkerton JV et al Menopause 2009
Postmenopausal women
with a uterus
Age 42-64 year
(avg 53 yr)
(N=318)
DUAVIVE (CE 045BZA 20)
(n=127)
Placebo
(n=63)
bull 12-week randomized double-blind placebo-controlled study1
bull Inclusion criteria
‒ Postmenopausal women with an intact uterus
‒ Minimum of 7 moderate to severe hot flushes per day or at least 50 per week at screening
Change from baseline to
Weeks 4 and 12 in
bull Average daily number of
moderate to severe hot
flushes
bull Average daily severity
score of hot flushes
Primary End Points
Safety population (took at least one dose)
Significant Reduction vs Placebo in
Average Daily Number of Hot Flushes
DUAVEE [package insert] New York NY Pfizer Inc 2013
ANCOVA=analysis of covariance
Reduction in average daily number of
moderate to severe hot flushes ndash primary end point
Ad
jus
ted
mean
ch
an
ge
fro
m b
aselin
edagger
Week 4 Week 12
ndash31
ndash27
Treatment
differencedagger ndash59
ndash28
ndash76
ndash49
Treatment
differencedagger
22
Plt001 vs placebo daggerBased on data analysis using ANCOVA model Change from baseline = Treatment + Baseline + Site
DUAVIV
E
Reduction in the Observed Average Daily Number
of Moderate to Severe Hot Flushes
Data on file CSR-67461 Protocol 3115A1-305 Table 1511 Pfizer Inc New York NY
change from baseline to week 12
74 for DUAVIVE
51 for placebo
Observed Average Daily Number of Hot Flushes
Ob
serv
ed a
vera
ge d
aily
nu
mb
er o
f m
od
erat
e to
sev
ere
ho
t fl
ush
es
0 1 2 3 4 5 6 7 8 9 10 12 0 1
11
2
4 3
6 5
7 8 9
10
28
54
DUAVIVE (n=122) Placebo (n=62)
Weeks
Primary analysis showed statistically significant separation at weeks 4 and 12
Average daily number of hot flushes from baseline to week 12
103 to 28 for DUAVIVE
105 to 54 for placebo
Based on mathematical means
not statistically analyzed
105 103
Pinkerton JV et al Menopause 2009
Significant Reduction vs Placebo in
Average Daily Severity Score of Hot Flushes
17
Week 4 Week 12
ndash05
ndash06
Treatment
differencedagger
Treatment
differencedagger
DUAVEE [package insert] New York NY Pfizer Inc 2013
Reduction in average daily severity score of hot flushes ndash primary end point
Ad
jus
ted
me
an
ch
an
ge
fro
m b
aselin
edagger
Plt001 vs placebo daggerBased on data analysis using ANCOVA model Change from baseline = Treatment + Baseline + Site
DUAVIV
E
Reduction in the Observed Average
Daily Severity Score of Hot Flushes
Observed Average Daily Severity Score of Hot Flushes
19
DUAVIVE (n=122) Placebo (n=62)
Weeks
Ob
serv
ed a
vera
ge d
aily
sev
erit
y sc
ore
of
ho
t fl
ush
es
0
05
10
15
25
20
0 1 2 3 4 5 6 7 8 9 10 12 11 0 1 2 3 4 5 6 7 8 9 10 12 11
14
Data on file CSR-67461 Protocol 3115A1-305 Table 1511 Pfizer Inc New York NY
Primary analysis at weeks 4 and 12 prespecified secondary end points at all other weeks
change from baseline to week 12
39 for DUAVIVE
14 for placebo
Average daily severity score of hot flashes from baseline to week 12
23 to 14 for DUAVIVE
23 to 19 for Placebo
Based on mathematical means
not statistically analyzed
23
23
Pinkerton JV et al Menopause 2009
Effects on bone mineral density (BMD)
SMART 512
20
bull 12-month double-blind randomized placebo- and active-controlled study
bull Primary end point endometrial hyperplasia at 1 year
bull Secondary BMD changes at 1 year
1 DUAVEE [package insert] New York NY Pfizer Inc 2013 2 Pinkerton J Clin Endocrin Metab 2014
This study included a different dose of CEBZA and comparators The schematic shown here depicts only the patients who received the approved dose of DUAVIVE or placebo
Change from baseline in
bull Lumbar Spine BMD (Primary ndash BMD Substudy)
bull Total Hip BMD (Secondary ndash BMD Substudy)
BMD Analysis
DUAVIVE
(CE 045BZA 20)
(n=119)
Placebo
(n=139)
BMD Analysis
Postmenopausal women with a uterus
Less than 5 years since LMP
(N=590)
DUAVIVE Significantly Increased Lumbar Spine and Total
Hip BMD vs Placebo at 12 Months ndash Study 2
M
ean
ch
an
ge f
rom
baselin
e
Lumbar Spine Total Hip
121 151 Treatment
difference Treatment
difference
Data on file CSR-81040 Protocol 3115A1-3307 Pfizer Inc New York NY Pinkerton J Clin Endocrin Metab 2014 30
Plt001 vs placebo
Adjusted mean changes and P-values based on an ANCOVA model with treatment and region (US or non-US) as factors and baseline BMD value and years since menopause as covariates using the modified intention to treat population with last observation carried forward
DUAVIV
E
TOLERABILITY
AND SAFETY
Rates of BleedingSpotting and Amenorrhea
Similar to Rates with Placebo
bull High and similar cumulative rates of amenorrhea at year 1 among women treated with CE 045BZA 20 and placebo and was higher than seen in women treated with CE 045MPA 151
bull Noncumulative rates of spotting and bleedingspotting were similar among women treated with CEBZA or placebo and consistently higher in women treated with CE 045MPA 152
0
90
Cycle
100
Pe
rce
nta
ge
of
Su
bje
cts
80
70
60
50
40
30
20
10
88
54
Placebo
CE 045BZA 20 CE 045MPA 15
Percentage of subjects with cumulative amenorrhea during consecutive 4-week periods (cycles) in SMART-5
MPA medroxyprogesterone acetate Plt0001 vs all other treatment groups 1 Pinkerton JV et al J Clin Endocrinol Metab 2014 2 Data on file CSR-81040 Protocol 3115A1-3307 Pfizer Inc New York NY
Adverse Reactions in Placebo-
Controlled Trials Safety analyses have been conducted in 6210 postmenopausal women aged 40 to 75 years (mean age 55 years) following up to 2 years of treatment in SMART-1 -2 -3 and -5
Adverse reactions (incidence ge5) that were more common with DUAVIVE
Incidence of serious adverse reactions
35 with DUAVIVE 48 with placebo
DUAVEE [package insert] New York NY Pfizer Inc 2013
CE 045 BZA 20 (N=1224)
n ()
Placebo (N=1069)
n ()
Gastrointestinal disorders
Nausea 100 (8) 58 (5)
Diarrhea 96 (8) 57 (5)
Dyspepsia 84 (7) 59 (6)
Abdominal pain upper 81 (7) 58 (5)
Musculoskeletal and connective tissue disorders
Muscle spasms 110 (9) 63 (6)
Neck pain 62 (5) 46 (4)
Nervous system disorders
Dizziness 65 (5) 37 (3)
Respiratory thoracic and mediastinal disorders
Oropharyngeal pain 80 (7) 61 (6)
Venous Thromboembolism (VTE) in
DUAVIVE Clinical Studies
bull Estrogen agonistantagonists (including BZA a component of DUAVIVE) and estrogens individually are known to increase the risk of VTE
bull In the clinical studies with DUAVIVE the reporting rates for VTE were low in all treatment groups
bull Adverse reactions of VTE reported by patients
bull Should VTE event occur or be suspected DUAVIVE should be discontinued immediately
bull Due to the low rates of events in both groups it is not possible to conclude that the risk of VTE with DUAVIVE is different from that seen with other estrogen therapies
DUAVEE [package insert] New York NY Pfizer Inc 2013
00 for DUAVIVE (n=1224)
01 for placebo (n=1069)
26
Effects of conjugated estrogensbazedoxifene on
lipid and coagulation variables a randomized
placebo- and active-controlled trial
bull postmenopausal women (N = 1843) with menopausal
symptoms
bull Lipid (N = 1843) and coagulation (N = 590) variables were assessed in women receiving daily CE 045 mgBZA 20 mg CE 0625 mgBZA 20 mg BZA 20 mg CE 045 mgmedroxyprogesterone acetate (MPA) 15 mg or placebo for 12 months
bull Skouby SO et al Menopause 2015 Jun22(6)640-9
Effects of conjugated estrogensbazedoxifene on
lipid and coagulation variables a randomized
placebo- and active-controlled trial
bull At 12 months
bull CE 045 mgBZA 20 mg
bull CE 0625 mgBZA 20 mg
bull BZA 20 mg
bull and CE 045 mgMPA 15 mg decreased total cholesterol and LDL- cholesterol vs placebo (P lt 001 for all)
bull Both CEBZA doses and CEMPA increased high-density lipoprotein cholesterol compared with placebo (P lt 005 for all)
bull CE 045 mgBZA 20 mg had a neutral effect on triglycerides
bull CE 0625 mgBZA 20 mg and CEMPA increased triglycerides compared with placebo (P lt 005)
bull Skouby SO et al Menopause 2015 Jun22(6)640-9
Effects of conjugated estrogensbazedoxifene on
lipid and coagulation variables a randomized
placebo- and active-controlled trial
bull At 12 months
bull Both CEBZA doses were associated with small but significant effects on hemostasis variables including reductions in antithrombin plasminogen activator inhibitor-1 and fibrinogen activity and an increase in plasminogen activity relative to placebo at 12 months Incidences of cardiovascular and venous thromboembolic events were similar among treatment groups
Skouby SO et al Menopause 2015
Jun22(6)640-9
Endometrial hyperplasia or malignancy occurred in lt1 of women
following up to 1 year of treatment with CEBZA12
Study Cumulative Incidence at month 12 (nN)
CE 045BZA 20 Placebo
SMART-11 000 (0336) 000 (0313)
SMART-52 030 (1335) 028 (1354)
Effects on the Endometrium
1 Pickar JH et al Fertil Steril 2009 2 Pinkerton at al J Clin Endocrinol Metab 2014
Through the eyes of an amazone
Marie Mandy
Breast tolerability profile similar to placebo following up to 2 years of treatment with CEBZA12
Pooled analysis of SMART clinical trials
CE 045BZA 20 (n=1585)
Placebo (n=1241)
Breast cancer incidence up to 2 years
(per 1000 woman-years)
100 (CI 000-321)
140 (CI 000-417)
Incidence of reported breast paintenderness up to 12 weeks
98-115 81-112
Incidence of abnormal mammogram at month 12
258 316
Mean change in breast density at month 12 (SMART-5)
ndash038 (n=186)
ndash032 (n=182)
Effects on the Breast
1 Pickar JH et al Menopause 2013 2 Pinkerton JV et al Obstet Gynecol 2013
CEBZA clinical overview - summary
bull In clinical trials CEBZA has demonstrated safety and efficacy in postmenopausal women with a uterus including the following
bull Significant reduction in number and severity of moderate to severe hot flushes1
bull Incidence of cumulative amenorrhea rate similar to placebo and significantly better than CEMPA2
bull Incidence of endometrial hyperplasia and breast tendernessdensity similar to that with placebo345
bull Incidence of adverse events and discontinuation rates similar to that with placebo6
1 Pinkerton JV et al Menopause 2009 2 Pinkerton JV et al J Clin Endocrinol Metab2014 3 Pickar JH et al
Fertil Steril 2009 4 Pinkerton at al J Clin Endocrinol Metab 2014 5 Pickar JH et al Menopause 2013 6 DUAVEE [package insert] New York NY Pfizer Inc 2013
CEBZA clinical overview - summary
Now women with a uterus who choose hormone therapy for management of menopausal symptoms have a choice
bull conventional estrogen-progestogen therapy or
bull a new combinationhellipconjugated estrogens paired with the SERM bazedoxifene
1 Pinkerton JV et al Menopause 2009 2 Pinkerton JV et al J Clin Endocrinol Metab2014 3 Pickar JH et al Fertil Steril 2009 4 Pinkerton at al J Clin Endocrinol Metab 2014 5 Pickar JH et al Menopause 2013 6 DUAVEE [package insert] New York NY Pfizer Inc 2013
Conjugated EstrogensBazedoxifene (CEBZA)
US indication
bull DUAVEE is indicated in women with a uterus for
bull 11 Treatment of Moderate to Severe Vasomotor Symptoms Associated with Menopause
bull 12 Prevention of Postmenopausal Osteoporosis
bull 13 Important Limitations of Use
bull Use DUAVEE for the shortest duration consistent with treatment goals and risks for the individual woman Postmenopausal women should be re-evaluated periodically as clinically appropriate to determine if treatment is still necessary
bull When prescribing solely for the prevention of postmenopausal osteoporosis therapy should only be considered for women at significant risk of osteoporosis and non-estrogen medication should be carefully considered
Conjugated EstrogensBazedoxifene (CEBZA)
EU indication
CEBZA is indicated for
bull Treatment of oestrogen deficiency symptoms in postmenopausal women with a uterus (with at least 12 months since the last menses) for whom treatment with progestin-containing therapy is not appropriate
bull The experience treating women older than 65 years is limited
bull Dose CE (045mg)Bazedoxifene (20mg)
Duavive SmPC
Which women with a uterus
could benefit from estrogens
without the need for a
progestin
Progestin intolerance is one of the main
factors for reduced compliance
bull About 20 of women receiving progestin-containing HT have significant progestin intolerance and half of these experience serious effects that prevent treatment continuation1
1 Panay N amp Studd J Human Reprod Update 1997
2 Panay N et al on behalf of the British Menopause Society and Womenrsquos Health Concern Menopause Int 2013
bull The 2013 British Menopause Society amp Womenrsquos Health
Concern recommendations on hormone replacement
therapy do recognise progestin intolerance as one of the
main factors for reduced compliance with HT 2
Proportion of patients () with at least one bleeding episode in relation to time and to the
used HT
Serge Rozenberg et al Hum Reprod 2009241739-1747
copy The Author 2009 Published by Oxford University Press on behalf of the European Society of
Human Reproduction and Embryology All rights reserved For Permissions please email
journalspermissionsoxfordjournalsorg
Breast tenderness after initiation of CEE
CEE + MPA (WHI)
and mammographic density change
bullCrandall et al Breast Cancer Res Treat DOI 101007s10549-011-1803-9
Breast density
Conclusion
bull CEEBAZO is an additional regimen for menopausal symptoms it provides also a prevention for osteoporosis
bull It is suitable for women with a uterus who are unsatisfied with an EPT regimen or who you are unwilling to treat with an EPT regimen
Adapted use of MHT
bull Lower dosage of estrogens
bull Other progestins
bull Better safety profile
bull Vaginal estrogen or SERMS
bull Non-hormonal therapy
bull Development of new products
bull SERMS + estrogens
Most common adverse events leading to
discontinuation are related to progestins12
bull breakthrough bleeding
bull Low compliance
bull Increase in the number of US
bull Stress
bull Cost
bull uterine procedures
bull Unnecessary endometrial biopsies Hysteroscopies DampC Hysterectomies
bull Morbidity
Proportion of patients who completed or discontinued treatment in relation to the used HT
Serge Rozenberg et al Hum Reprod 2009241739-1747
copy The Author 2009 Published by Oxford University Press on behalf of the European Society of
Human Reproduction and Embryology All rights reserved For Permissions please email
journalspermissionsoxfordjournalsorg
Most common adverse events leading to discontinuation
are related to progestins
bull breast paintenderness
Breast tenderness after initiation of CEE
CEE + MPA (WHI)
and mammographic density change
bullCrandall et al Breast Cancer Res Treat DOI 101007s10549-011-1803-9
Breast density
Hormone therapy use and mammographic
density in postmenopausal Norwegian women
bull Results differed when considering the combined effect of age and BMI
bull The effect of EPT on mammographic density was modified by age and BMI with no apparent association among the youngest women (aged 50-55) with the highest BMI (BMI ge 26)
bull A higher mammographic density was found in EPT users compared to never HT users particularly in women using high-dose NETA regimens Age and BMI modified the association between EPT use and mammographic density
bull Couto E et al Breast Cancer Res Treat 2011 Nov 4 [Epub ahead of print]
Breast Cancer Risk by Breast Density
Menopause and Postmenopausal Hormone
Therapy Use
Birads age HT Duration Risk
1 55-59 None 5 year risk 08 (95 CI 06- 09)
1 55-59
ET EPT 5 year risk 09 (95 CI 07 -11)
4 55-59
None 5 year risk 24 (95 CI 20 -28)
4 55-59
ET 5 year risk
30 (95 CI 26 -35)
4 55-59
EPT 5 year risk
42 (95 CI 37 -46)
Adapted from Kerlikowske et al JOURNAL OF CLINICAL ONCOLOGY 2010
Breast Cancer Risk by Breast Density
Menopause and Postmenopausal Hormone
Therapy Use
Adapted from Kerlikowske et al JOURNAL OF CLINICAL ONCOLOGY 2010
bull Postmenopausal women with high breast density are at increased risk of breast cancer and should be aware of the added risk of taking HT especially estrogen plus progestin
Medical condition which may be exacerbated by treatment
with progestins
Diabetes and metabolic syndrome
bull progestin-containing HT may be associated with increases in insulin resistance and deterioration in glucose tolerance123
bull Postmenopausal women with diabetes could be inappropriate for treatment with progestin-containing HT due to the potential risk of exacerbation of their condition
1) Panay N amp Studd JWW Human Reprod Update 1997
2) Godsland I et al Metabolism 1993
3) Sites CK et al J Clin Endocrinol Metab 2005
A Nath and R Sitruk-Ware CLIMACTERIC 200912(Suppl 1)96ndash101
A Nath and R Sitruk-Ware CLIMACTERIC 200912(Suppl 1)96ndash101
Diabetes an epidemy
bull UK 1996 14 million of diabetics
bull UK 2015 32 million (6 of the population)
bull UK 2025 5 million
bull httpwwwdiabetescoukdiabetes-prevalencehtml
Other progestin-related intolerance issues
bull Nausea
bull Depressive mood
bull Poor concentration
bull Hirsutism
bull Headache
bull Dizziness
bull Fluid retention
bull Weight gain Panay N amp Studd JWW Human Reprod Update 1997
Medical condition which may be exacerbated by treatment with progestins
PMSPMDDdepression
bull Progesterone-induced PMD can be exacerbated by exogenous progestin administration and can occur in association with HT or OC administration1
bull Significantly higher negative mood scores have been observed during the addition of a progestin to an estrogen in a sequential HT regimen in postmenopausal women with a history of PMS compared to those without2
bull Women with a history of PMS or PMD exacerbation of depression using progestins may therefore benefit from a progestin free treatment for menopausal symptoms
1) Nevatte T et al Arch Womens Ment Health 2013 2) Bjoumlrn I et al Climacteric 2006 PMS premenstrual syndrome
PMDD premenstrual dysphoric disorder
Conclusion
bull CEEBAZO is an additional regimen for menopausal symptoms it provides also a prevention for osteoporosis
bull It is suitable for women with a uterus who are unsatisfied with an EPT regimen or who you are unwilling to treat with an EPT regimen
For some postmenopausal women with a uterus there is a
need for progestin free treatment options
bull with demonstrated clinical efficacy
bull which protects the endometrium
bull improved tolerabilitysafety profile
In clinical practice this translates to women who are
intolerant of progestin-containing HT or have conditions
which may be exacerbated by treatment with progestins
Conclusion Medical need for alternative treatment option
Medical condition which may be exacerbated by treatment with progestins
Depression
bull Progestin-containing HT has been associated with increases in depressive symptoms in some individuals1
bull There is a biochemicalphysiological plausibility for the association of progestins with depression234
bull Therefore postmenopausal women who also have a medical history of depressive disorders or depression could be inappropriate for treatment with progestin-containing HT
Pfizer Confidential
65
1) Girdler SS et al J Womens Health Gend Based Med 1999 2) Traish AM et al Korean J Urol 2014 3) Stroumlhle A et al Biol Psychiatry 1999 4) Romeo E et
al Am J Psychiatry 1998
History of the following conditions may make progestin inappropriate
bull Depression
bull PMSPMDD
PMS premenstrual syndrome
PMD premenstrual dysphoric disorder
Medical conditions that may be exacerbated by treatment with progestins
Women for whom progestin-containing HT
would not be considered appropriate
minus Women who are intolerant of progestin-containing hormone therapy
minus Women with pre-existing medical conditions that may be exacerbated by progestins
Most common adverse events leading to discontinuation are related to progestins12
breakthrough bleeding
bull Increase in the number of uterine procedures (ie unnecessary endometrial biopsies)
breast paintenderness
bull Increase in the number of breast interventions
1 Steel SA et al Climacteric 2003 2 Ettinger B and Pressman A Am J Manag Care 1999 3 Komm BS Mirkin S
Pharmaceuticals 2012
4 Panay N amp Studd JWW Human Reprod Update 1997
bull Nausea bull Depressive mood bull Poor concentration bull Hirsutism bull Headache bull Dizziness bull Fluid retention bull Weight gain
Other progestin-related intolerance issues4
Unmet need with the treatment of postmenopausal symptoms
bull Alternatives to progestin are needed that will protect the endometrium while avoiding other progestin-associated effects and preserving the desired effects of estrogens in postmenopausal women3
Which women with a uterus could benefit from
estrogens without the need for a progestin
bull Women who are intolerant of progestin-containing hormone therapy
bull Women with pre-existing medical conditions that may be exacerbated by progestins (eg women with a history of depression PMSPMDD increased breast density diabetes and metabolic syndrome)
History of the following conditions may make progestin inappropriate
bull Depression
bull PMSPMDD
bull High breast density
bull Diabetes and metabolic syndrome
PMS premenstrual syndrome
PMD premenstrual dysphoric disorder
Medical conditions that may be exacerbated by treatment with progestins
Learning from WHI data
bull Hormone therapy (HT) is the conventional and established therapy option to effectively treat postmenopausal symptoms however it has been associated with some safety and tolerability concerns1 2
bull A review of WHI data suggests that many of the concerns with menopausal HT more often associated with EPT (CE+MPA) such as CHD risk increased breast density breast pain and breast cancer risk than with ET (CEE alone)2
1 Rolnick SJ Kopher RA DeFor TA et al Menopause 2005
2 Komm BS Mirkin S Pharmaceuticals 2012
WHI Womenrsquos Health Initiative trial
CHD coronary heart disease
CEE conjugated equine estrogens
Efficacy and Safety of Constant Oestrogen
Pulsed Progestogen vs
Continuous Combined HRT
Adverse Events
17b-oestradiol 17b-oestradiol norgestimate NETA (n = 150) (n = 172) Breast discomfort 14 27 Abdominal discomfort 14 22 Uterine bleeding 15 12 Dysmenorrhea 3 8 Oedema 5 8
Adapted from S Rozenberg et al Human Reproduction 2000
Medical condition which may be exacerbated by treatment
with progestins
Increased breast density
bull Increases in breast density are associated with progestin-containing HT which may adversely affect radiological detection of breast cancer1 and may be independently associated with an increased risk for the development of breast cancer2
bull The Postmenopausal EstrogenProgestin Interventions (PEPI) trial demonstrated that an increased mammographic breast density was associated with the use of E+P but not with the use of estrogen alone3
bull Women who already have high breast density may therefore be considered inappropriate for treatment with a progestin-containing HT
1) EU Core SPC for Hormone Replacement Therapy Products (CMDh1312003 Rev 4 June
2012)
2) De Villiers TJ et al on behalf of the International Menopause Society Climacteric 2013 16
3) Greendale GA et al J Natl Cancer Inst 2003
Stroke
0 25 5 75 10 125
Fractures
Diabetes
Breast cancer
Cholecystitis
Venothrombotic episodes
Endometrial cancer
Lung cancer
Coronary heart disease
Colorectal cancer
Overall mortality
15 125 10 75 5 25
Benefits Risks
CE
CE MPA
Santen RJ et al J Clin Endocrinol Metab 2010
The basis of the Endocrine Society scientific statement for postmenopausal hormone replacement therapy (HRT) excess risks and benefits of HRT for 5 years in women aged 50ndash59 years or within 10 years of the start of menopause E=estrogen P=progestin
bull Younger women (aged 50ndash59 years) had more favorable results bull There are differences between CE alone and CEMPA arms bull Overall benefitrisk ratio of CE-alone appears to be more favourable than CEMPA
Reevaluation of WHI data (stratified by age) Risks and
Benefits of HRT Cases per 1000 Women per 5 Years of
Use
Medical condition which may be exacerbated by treatment
with progestins
Diabetes and metabolic syndrome
bull Treatment of oestrogen deficiency symptoms with progestin-containing HT (unlike oestrogen alone) may be associated with increases in insulin resistance and deterioration in glucose tolerance123
bull Postmenopausal women with diabetes could be inappropriate for treatment with progestin-containing HT due to the potential risk of exacerbation of their condition
1) Panay N amp Studd JWW Human Reprod Update 1997
2) Godsland I et al Metabolism 1993
3) Sites CK et al J Clin Endocrinol Metab 2005
Variations in Associated Breast Cancer
Risks Between CE alone and CEMPA
bull Use of CE alone for a median of 59 years was associated with a lower incidence of invasive breast cancer (151 cases 027 per year) compared with placebo (199 cases 035 per year HR 077 95 CI 062ndash095 P=002)
bull In the CE alone group fewer women died from invasive breast cancer (6 deaths 0009 per year) compared with controls (16 deaths 0024 per year HR 037 95 CI 013ndash091 P=003)
Anderson GL et al Lancet
Oncol 2012
Bazedoxifene (BZA) specifically selected in
combination with conjugated estrogens
bull BZA has been specifically selected for its unique pharmacologic profile and effects on VMS and uterine tissue in particular123
1 Crabtree J et al Mol Cell Endocrinol 2008
2 Kharode Y et al Endocrinolology 2008
3 Duavive SmPC
Estrogen Receptor activity is dimmed
Estrogen Receptor activity is turned on
CEs are agonists BZA is an antagonist
In the uterus
bull The BZA component reduces the risk of endometrial hyperplasia that can occur with the conjugated estrogens component alone3 This means that progestins are not needed
Extensive global clinical development program for
CEBZA
aIncludes additional pilot dose-finding study 203 1 Lobo RA et al Fertil Steril 2009 2 Pinkerton JV et al Menopause 2009 3 Kagan R et al Menopause 2010 4 Mirkin S et al Climacteric 2013 5 Pinkerton JV et al Obstet Gynecol 2013
Effects of conjugated estrogensbazedoxifene on
lipid and coagulation variables a randomized
placebo- and active-controlled trial
bull At 12 months
bull Both CEBZA doses were associated with small but significant effects on hemostasis variables including reductions in antithrombin plasminogen activator inhibitor-1 and fibrinogen activity and an increase in plasminogen activity relative to placebo at 12 months Incidences of cardiovascular and venous thromboembolic events were similar among treatment groups
bull CONCLUSIONS
bull This study provides reassurance that CEBZA does not adversely affect lipid metabolism or hemostatic balance In accordance the incidences of venous thromboembolic events and cardiovascular events in postmenopausal women are similar to those observed with placebo

Conflict of interest amp Disclosure
Conflicts of interest nil
Disclosure SR
Research funding IRIS- King Baudouin Fondation Vesale research Foundation Amgen MSD
Speakers bureau ampor Advisory Boards
Abbot Pfizer Will Gedeon Richter MSD Amgen
1 Kagan R J Womenrsquos Health (Larchmt) 2012
the OPTIMAL Menopausal Therapy
should demonstrate1
ndash Favorable safety and tolerability profile
ndash Relief of menopausal symptoms
ndash Prevention of osteoporosis CVD Cognitive function
ndash No stimulation of the endometrium breast and ovary
1 Kagan R J Womenrsquos Health (Larchmt) 2012
the OPTIMAL Menopausal Therapy
should demonstrate1
ndash Favorable safety and tolerability profile
ndash Relief of menopausal symptoms
ndash Prevention of osteoporosis CVD Cognitive function
ndash No stimulation of the endometrium breast and ovary
Variations in Associated Breast Cancer Risk Between CE alone and
CEMPA
Cumulative hazards
adjusted for age and
raceethnicity for
invasive breast cancer
by randomization
assignment in the WHI
CE-alone and CEMPA
trials
Anderson GL et al Lancet
Oncol 2012
0 0
1 2 3 4 5 6 7 8 9 10 11 12 13
001
002
003
004
005
Cu
mu
lati
ve
ha
za
rd
Time since randomization (years)
CEMPA
Placebo (in CEMPA arm)
HR 125 (95 CI 107ndash146)
CE alone
Placebo (in CE-alone arm)
HR 077 (95 CI 062ndash095)
CEMPA
CE alone
Placebo (CE-alone)
Placebo (CEMPA)
Estrogen only therapy
Endometrial cancer
Hysterectomy specimen showing cancer invading myometrium
following unopposed estrogen therapy for 15 years
Courtesy Dr David Sturdee
Bazedoxifene (BZA) specifically selected in
combination with conjugated estrogens
1 Crabtree J et al Mol Cell Endocrinol 2008
2 Kharode Y et al Endocrinolology 2008
3 Duavive SmPC
Estrogen Receptor activity is dimmed
Estrogen Receptor activity is turned on
CEs are agonists BZA is an antagonist
In the uterus
bull The BZA component reduces the risk of endometrial hyperplasia that can occur with the conjugated estrogens component alone1-3
bull This means that progestins are not needed
From the Womenrsquos Health Initiative to the combination
of estrogen and selective estrogen receptor
modulators to avoid progestin addition
bull Marie-Ceacutecile Valera Pierre Gourdy Florence Treacutemolliegraveres Jean-Franccedilois Arnal
bull Maturitas Volume 82 Issue 3 November 2015 Pages 274ndash277
bull
Other combinations of an estrogen (E2) + a SERM studied have
not produced favorable results
bull Objective To compare effects of 52 weeksrsquo treatment with either raloxifene 60 mgday alone (RLX) or in combination with 17B-estradiol 1 mgday (RLX + E2) on vasomotor symptoms (n = 83) and endometrial safety (n = 123) in postmenopausal women who transitioned from estrogen-progestin therapy Endometrial effect Women in the RLX + E2 group had significantly increased endometrial thickness at 52 weeks from baseline and RLX alone had no increase Two women (328) in the RLX + E2 group had endometrial hyperplasia (one with atypia) on the exit biopsy No one in RLX alone did
bull 1 Stovall D et al Menopause The Journal of The North American Menopause Society 2007
bull For the safety analyses data from women randomized before and after the protocol amendment were pooled which included 62 women in the raloxifene group and 61 women in the raloxifene + estrogen group
EFFICACY
VASOMOTOR
SYMPTOMS
SMART-2
DUAVIVE Efficacy for the Treatment of Moderate to
Severe VMS Associated With Menopause
14
1 Pinkerton JV et al Menopause 2009
Postmenopausal women
with a uterus
Age 42-64 year
(avg 53 yr)
(N=318)
DUAVIVE (CE 045BZA 20)
(n=127)
Placebo
(n=63)
bull 12-week randomized double-blind placebo-controlled study1
bull Inclusion criteria
‒ Postmenopausal women with an intact uterus
‒ Minimum of 7 moderate to severe hot flushes per day or at least 50 per week at screening
Change from baseline to
Weeks 4 and 12 in
bull Average daily number of
moderate to severe hot
flushes
bull Average daily severity
score of hot flushes
Primary End Points
Safety population (took at least one dose)
Significant Reduction vs Placebo in
Average Daily Number of Hot Flushes
DUAVEE [package insert] New York NY Pfizer Inc 2013
ANCOVA=analysis of covariance
Reduction in average daily number of
moderate to severe hot flushes ndash primary end point
Ad
jus
ted
mean
ch
an
ge
fro
m b
aselin
edagger
Week 4 Week 12
ndash31
ndash27
Treatment
differencedagger ndash59
ndash28
ndash76
ndash49
Treatment
differencedagger
22
Plt001 vs placebo daggerBased on data analysis using ANCOVA model Change from baseline = Treatment + Baseline + Site
DUAVIV
E
Reduction in the Observed Average Daily Number
of Moderate to Severe Hot Flushes
Data on file CSR-67461 Protocol 3115A1-305 Table 1511 Pfizer Inc New York NY
change from baseline to week 12
74 for DUAVIVE
51 for placebo
Observed Average Daily Number of Hot Flushes
Ob
serv
ed a
vera
ge d
aily
nu
mb
er o
f m
od
erat
e to
sev
ere
ho
t fl
ush
es
0 1 2 3 4 5 6 7 8 9 10 12 0 1
11
2
4 3
6 5
7 8 9
10
28
54
DUAVIVE (n=122) Placebo (n=62)
Weeks
Primary analysis showed statistically significant separation at weeks 4 and 12
Average daily number of hot flushes from baseline to week 12
103 to 28 for DUAVIVE
105 to 54 for placebo
Based on mathematical means
not statistically analyzed
105 103
Pinkerton JV et al Menopause 2009
Significant Reduction vs Placebo in
Average Daily Severity Score of Hot Flushes
17
Week 4 Week 12
ndash05
ndash06
Treatment
differencedagger
Treatment
differencedagger
DUAVEE [package insert] New York NY Pfizer Inc 2013
Reduction in average daily severity score of hot flushes ndash primary end point
Ad
jus
ted
me
an
ch
an
ge
fro
m b
aselin
edagger
Plt001 vs placebo daggerBased on data analysis using ANCOVA model Change from baseline = Treatment + Baseline + Site
DUAVIV
E
Reduction in the Observed Average
Daily Severity Score of Hot Flushes
Observed Average Daily Severity Score of Hot Flushes
19
DUAVIVE (n=122) Placebo (n=62)
Weeks
Ob
serv
ed a
vera
ge d
aily
sev
erit
y sc
ore
of
ho
t fl
ush
es
0
05
10
15
25
20
0 1 2 3 4 5 6 7 8 9 10 12 11 0 1 2 3 4 5 6 7 8 9 10 12 11
14
Data on file CSR-67461 Protocol 3115A1-305 Table 1511 Pfizer Inc New York NY
Primary analysis at weeks 4 and 12 prespecified secondary end points at all other weeks
change from baseline to week 12
39 for DUAVIVE
14 for placebo
Average daily severity score of hot flashes from baseline to week 12
23 to 14 for DUAVIVE
23 to 19 for Placebo
Based on mathematical means
not statistically analyzed
23
23
Pinkerton JV et al Menopause 2009
Effects on bone mineral density (BMD)
SMART 512
20
bull 12-month double-blind randomized placebo- and active-controlled study
bull Primary end point endometrial hyperplasia at 1 year
bull Secondary BMD changes at 1 year
1 DUAVEE [package insert] New York NY Pfizer Inc 2013 2 Pinkerton J Clin Endocrin Metab 2014
This study included a different dose of CEBZA and comparators The schematic shown here depicts only the patients who received the approved dose of DUAVIVE or placebo
Change from baseline in
bull Lumbar Spine BMD (Primary ndash BMD Substudy)
bull Total Hip BMD (Secondary ndash BMD Substudy)
BMD Analysis
DUAVIVE
(CE 045BZA 20)
(n=119)
Placebo
(n=139)
BMD Analysis
Postmenopausal women with a uterus
Less than 5 years since LMP
(N=590)
DUAVIVE Significantly Increased Lumbar Spine and Total
Hip BMD vs Placebo at 12 Months ndash Study 2
M
ean
ch
an
ge f
rom
baselin
e
Lumbar Spine Total Hip
121 151 Treatment
difference Treatment
difference
Data on file CSR-81040 Protocol 3115A1-3307 Pfizer Inc New York NY Pinkerton J Clin Endocrin Metab 2014 30
Plt001 vs placebo
Adjusted mean changes and P-values based on an ANCOVA model with treatment and region (US or non-US) as factors and baseline BMD value and years since menopause as covariates using the modified intention to treat population with last observation carried forward
DUAVIV
E
TOLERABILITY
AND SAFETY
Rates of BleedingSpotting and Amenorrhea
Similar to Rates with Placebo
bull High and similar cumulative rates of amenorrhea at year 1 among women treated with CE 045BZA 20 and placebo and was higher than seen in women treated with CE 045MPA 151
bull Noncumulative rates of spotting and bleedingspotting were similar among women treated with CEBZA or placebo and consistently higher in women treated with CE 045MPA 152
0
90
Cycle
100
Pe
rce
nta
ge
of
Su
bje
cts
80
70
60
50
40
30
20
10
88
54
Placebo
CE 045BZA 20 CE 045MPA 15
Percentage of subjects with cumulative amenorrhea during consecutive 4-week periods (cycles) in SMART-5
MPA medroxyprogesterone acetate Plt0001 vs all other treatment groups 1 Pinkerton JV et al J Clin Endocrinol Metab 2014 2 Data on file CSR-81040 Protocol 3115A1-3307 Pfizer Inc New York NY
Adverse Reactions in Placebo-
Controlled Trials Safety analyses have been conducted in 6210 postmenopausal women aged 40 to 75 years (mean age 55 years) following up to 2 years of treatment in SMART-1 -2 -3 and -5
Adverse reactions (incidence ge5) that were more common with DUAVIVE
Incidence of serious adverse reactions
35 with DUAVIVE 48 with placebo
DUAVEE [package insert] New York NY Pfizer Inc 2013
CE 045 BZA 20 (N=1224)
n ()
Placebo (N=1069)
n ()
Gastrointestinal disorders
Nausea 100 (8) 58 (5)
Diarrhea 96 (8) 57 (5)
Dyspepsia 84 (7) 59 (6)
Abdominal pain upper 81 (7) 58 (5)
Musculoskeletal and connective tissue disorders
Muscle spasms 110 (9) 63 (6)
Neck pain 62 (5) 46 (4)
Nervous system disorders
Dizziness 65 (5) 37 (3)
Respiratory thoracic and mediastinal disorders
Oropharyngeal pain 80 (7) 61 (6)
Venous Thromboembolism (VTE) in
DUAVIVE Clinical Studies
bull Estrogen agonistantagonists (including BZA a component of DUAVIVE) and estrogens individually are known to increase the risk of VTE
bull In the clinical studies with DUAVIVE the reporting rates for VTE were low in all treatment groups
bull Adverse reactions of VTE reported by patients
bull Should VTE event occur or be suspected DUAVIVE should be discontinued immediately
bull Due to the low rates of events in both groups it is not possible to conclude that the risk of VTE with DUAVIVE is different from that seen with other estrogen therapies
DUAVEE [package insert] New York NY Pfizer Inc 2013
00 for DUAVIVE (n=1224)
01 for placebo (n=1069)
26
Effects of conjugated estrogensbazedoxifene on
lipid and coagulation variables a randomized
placebo- and active-controlled trial
bull postmenopausal women (N = 1843) with menopausal
symptoms
bull Lipid (N = 1843) and coagulation (N = 590) variables were assessed in women receiving daily CE 045 mgBZA 20 mg CE 0625 mgBZA 20 mg BZA 20 mg CE 045 mgmedroxyprogesterone acetate (MPA) 15 mg or placebo for 12 months
bull Skouby SO et al Menopause 2015 Jun22(6)640-9
Effects of conjugated estrogensbazedoxifene on
lipid and coagulation variables a randomized
placebo- and active-controlled trial
bull At 12 months
bull CE 045 mgBZA 20 mg
bull CE 0625 mgBZA 20 mg
bull BZA 20 mg
bull and CE 045 mgMPA 15 mg decreased total cholesterol and LDL- cholesterol vs placebo (P lt 001 for all)
bull Both CEBZA doses and CEMPA increased high-density lipoprotein cholesterol compared with placebo (P lt 005 for all)
bull CE 045 mgBZA 20 mg had a neutral effect on triglycerides
bull CE 0625 mgBZA 20 mg and CEMPA increased triglycerides compared with placebo (P lt 005)
bull Skouby SO et al Menopause 2015 Jun22(6)640-9
Effects of conjugated estrogensbazedoxifene on
lipid and coagulation variables a randomized
placebo- and active-controlled trial
bull At 12 months
bull Both CEBZA doses were associated with small but significant effects on hemostasis variables including reductions in antithrombin plasminogen activator inhibitor-1 and fibrinogen activity and an increase in plasminogen activity relative to placebo at 12 months Incidences of cardiovascular and venous thromboembolic events were similar among treatment groups
Skouby SO et al Menopause 2015
Jun22(6)640-9
Endometrial hyperplasia or malignancy occurred in lt1 of women
following up to 1 year of treatment with CEBZA12
Study Cumulative Incidence at month 12 (nN)
CE 045BZA 20 Placebo
SMART-11 000 (0336) 000 (0313)
SMART-52 030 (1335) 028 (1354)
Effects on the Endometrium
1 Pickar JH et al Fertil Steril 2009 2 Pinkerton at al J Clin Endocrinol Metab 2014
Through the eyes of an amazone
Marie Mandy
Breast tolerability profile similar to placebo following up to 2 years of treatment with CEBZA12
Pooled analysis of SMART clinical trials
CE 045BZA 20 (n=1585)
Placebo (n=1241)
Breast cancer incidence up to 2 years
(per 1000 woman-years)
100 (CI 000-321)
140 (CI 000-417)
Incidence of reported breast paintenderness up to 12 weeks
98-115 81-112
Incidence of abnormal mammogram at month 12
258 316
Mean change in breast density at month 12 (SMART-5)
ndash038 (n=186)
ndash032 (n=182)
Effects on the Breast
1 Pickar JH et al Menopause 2013 2 Pinkerton JV et al Obstet Gynecol 2013
CEBZA clinical overview - summary
bull In clinical trials CEBZA has demonstrated safety and efficacy in postmenopausal women with a uterus including the following
bull Significant reduction in number and severity of moderate to severe hot flushes1
bull Incidence of cumulative amenorrhea rate similar to placebo and significantly better than CEMPA2
bull Incidence of endometrial hyperplasia and breast tendernessdensity similar to that with placebo345
bull Incidence of adverse events and discontinuation rates similar to that with placebo6
1 Pinkerton JV et al Menopause 2009 2 Pinkerton JV et al J Clin Endocrinol Metab2014 3 Pickar JH et al
Fertil Steril 2009 4 Pinkerton at al J Clin Endocrinol Metab 2014 5 Pickar JH et al Menopause 2013 6 DUAVEE [package insert] New York NY Pfizer Inc 2013
CEBZA clinical overview - summary
Now women with a uterus who choose hormone therapy for management of menopausal symptoms have a choice
bull conventional estrogen-progestogen therapy or
bull a new combinationhellipconjugated estrogens paired with the SERM bazedoxifene
1 Pinkerton JV et al Menopause 2009 2 Pinkerton JV et al J Clin Endocrinol Metab2014 3 Pickar JH et al Fertil Steril 2009 4 Pinkerton at al J Clin Endocrinol Metab 2014 5 Pickar JH et al Menopause 2013 6 DUAVEE [package insert] New York NY Pfizer Inc 2013
Conjugated EstrogensBazedoxifene (CEBZA)
US indication
bull DUAVEE is indicated in women with a uterus for
bull 11 Treatment of Moderate to Severe Vasomotor Symptoms Associated with Menopause
bull 12 Prevention of Postmenopausal Osteoporosis
bull 13 Important Limitations of Use
bull Use DUAVEE for the shortest duration consistent with treatment goals and risks for the individual woman Postmenopausal women should be re-evaluated periodically as clinically appropriate to determine if treatment is still necessary
bull When prescribing solely for the prevention of postmenopausal osteoporosis therapy should only be considered for women at significant risk of osteoporosis and non-estrogen medication should be carefully considered
Conjugated EstrogensBazedoxifene (CEBZA)
EU indication
CEBZA is indicated for
bull Treatment of oestrogen deficiency symptoms in postmenopausal women with a uterus (with at least 12 months since the last menses) for whom treatment with progestin-containing therapy is not appropriate
bull The experience treating women older than 65 years is limited
bull Dose CE (045mg)Bazedoxifene (20mg)
Duavive SmPC
Which women with a uterus
could benefit from estrogens
without the need for a
progestin
Progestin intolerance is one of the main
factors for reduced compliance
bull About 20 of women receiving progestin-containing HT have significant progestin intolerance and half of these experience serious effects that prevent treatment continuation1
1 Panay N amp Studd J Human Reprod Update 1997
2 Panay N et al on behalf of the British Menopause Society and Womenrsquos Health Concern Menopause Int 2013
bull The 2013 British Menopause Society amp Womenrsquos Health
Concern recommendations on hormone replacement
therapy do recognise progestin intolerance as one of the
main factors for reduced compliance with HT 2
Proportion of patients () with at least one bleeding episode in relation to time and to the
used HT
Serge Rozenberg et al Hum Reprod 2009241739-1747
copy The Author 2009 Published by Oxford University Press on behalf of the European Society of
Human Reproduction and Embryology All rights reserved For Permissions please email
journalspermissionsoxfordjournalsorg
Breast tenderness after initiation of CEE
CEE + MPA (WHI)
and mammographic density change
bullCrandall et al Breast Cancer Res Treat DOI 101007s10549-011-1803-9
Breast density
Conclusion
bull CEEBAZO is an additional regimen for menopausal symptoms it provides also a prevention for osteoporosis
bull It is suitable for women with a uterus who are unsatisfied with an EPT regimen or who you are unwilling to treat with an EPT regimen
Adapted use of MHT
bull Lower dosage of estrogens
bull Other progestins
bull Better safety profile
bull Vaginal estrogen or SERMS
bull Non-hormonal therapy
bull Development of new products
bull SERMS + estrogens
Most common adverse events leading to
discontinuation are related to progestins12
bull breakthrough bleeding
bull Low compliance
bull Increase in the number of US
bull Stress
bull Cost
bull uterine procedures
bull Unnecessary endometrial biopsies Hysteroscopies DampC Hysterectomies
bull Morbidity
Proportion of patients who completed or discontinued treatment in relation to the used HT
Serge Rozenberg et al Hum Reprod 2009241739-1747
copy The Author 2009 Published by Oxford University Press on behalf of the European Society of
Human Reproduction and Embryology All rights reserved For Permissions please email
journalspermissionsoxfordjournalsorg
Most common adverse events leading to discontinuation
are related to progestins
bull breast paintenderness
Breast tenderness after initiation of CEE
CEE + MPA (WHI)
and mammographic density change
bullCrandall et al Breast Cancer Res Treat DOI 101007s10549-011-1803-9
Breast density
Hormone therapy use and mammographic
density in postmenopausal Norwegian women
bull Results differed when considering the combined effect of age and BMI
bull The effect of EPT on mammographic density was modified by age and BMI with no apparent association among the youngest women (aged 50-55) with the highest BMI (BMI ge 26)
bull A higher mammographic density was found in EPT users compared to never HT users particularly in women using high-dose NETA regimens Age and BMI modified the association between EPT use and mammographic density
bull Couto E et al Breast Cancer Res Treat 2011 Nov 4 [Epub ahead of print]
Breast Cancer Risk by Breast Density
Menopause and Postmenopausal Hormone
Therapy Use
Birads age HT Duration Risk
1 55-59 None 5 year risk 08 (95 CI 06- 09)
1 55-59
ET EPT 5 year risk 09 (95 CI 07 -11)
4 55-59
None 5 year risk 24 (95 CI 20 -28)
4 55-59
ET 5 year risk
30 (95 CI 26 -35)
4 55-59
EPT 5 year risk
42 (95 CI 37 -46)
Adapted from Kerlikowske et al JOURNAL OF CLINICAL ONCOLOGY 2010
Breast Cancer Risk by Breast Density
Menopause and Postmenopausal Hormone
Therapy Use
Adapted from Kerlikowske et al JOURNAL OF CLINICAL ONCOLOGY 2010
bull Postmenopausal women with high breast density are at increased risk of breast cancer and should be aware of the added risk of taking HT especially estrogen plus progestin
Medical condition which may be exacerbated by treatment
with progestins
Diabetes and metabolic syndrome
bull progestin-containing HT may be associated with increases in insulin resistance and deterioration in glucose tolerance123
bull Postmenopausal women with diabetes could be inappropriate for treatment with progestin-containing HT due to the potential risk of exacerbation of their condition
1) Panay N amp Studd JWW Human Reprod Update 1997
2) Godsland I et al Metabolism 1993
3) Sites CK et al J Clin Endocrinol Metab 2005
A Nath and R Sitruk-Ware CLIMACTERIC 200912(Suppl 1)96ndash101
A Nath and R Sitruk-Ware CLIMACTERIC 200912(Suppl 1)96ndash101
Diabetes an epidemy
bull UK 1996 14 million of diabetics
bull UK 2015 32 million (6 of the population)
bull UK 2025 5 million
bull httpwwwdiabetescoukdiabetes-prevalencehtml
Other progestin-related intolerance issues
bull Nausea
bull Depressive mood
bull Poor concentration
bull Hirsutism
bull Headache
bull Dizziness
bull Fluid retention
bull Weight gain Panay N amp Studd JWW Human Reprod Update 1997
Medical condition which may be exacerbated by treatment with progestins
PMSPMDDdepression
bull Progesterone-induced PMD can be exacerbated by exogenous progestin administration and can occur in association with HT or OC administration1
bull Significantly higher negative mood scores have been observed during the addition of a progestin to an estrogen in a sequential HT regimen in postmenopausal women with a history of PMS compared to those without2
bull Women with a history of PMS or PMD exacerbation of depression using progestins may therefore benefit from a progestin free treatment for menopausal symptoms
1) Nevatte T et al Arch Womens Ment Health 2013 2) Bjoumlrn I et al Climacteric 2006 PMS premenstrual syndrome
PMDD premenstrual dysphoric disorder
Conclusion
bull CEEBAZO is an additional regimen for menopausal symptoms it provides also a prevention for osteoporosis
bull It is suitable for women with a uterus who are unsatisfied with an EPT regimen or who you are unwilling to treat with an EPT regimen
For some postmenopausal women with a uterus there is a
need for progestin free treatment options
bull with demonstrated clinical efficacy
bull which protects the endometrium
bull improved tolerabilitysafety profile
In clinical practice this translates to women who are
intolerant of progestin-containing HT or have conditions
which may be exacerbated by treatment with progestins
Conclusion Medical need for alternative treatment option
Medical condition which may be exacerbated by treatment with progestins
Depression
bull Progestin-containing HT has been associated with increases in depressive symptoms in some individuals1
bull There is a biochemicalphysiological plausibility for the association of progestins with depression234
bull Therefore postmenopausal women who also have a medical history of depressive disorders or depression could be inappropriate for treatment with progestin-containing HT
Pfizer Confidential
65
1) Girdler SS et al J Womens Health Gend Based Med 1999 2) Traish AM et al Korean J Urol 2014 3) Stroumlhle A et al Biol Psychiatry 1999 4) Romeo E et
al Am J Psychiatry 1998
History of the following conditions may make progestin inappropriate
bull Depression
bull PMSPMDD
PMS premenstrual syndrome
PMD premenstrual dysphoric disorder
Medical conditions that may be exacerbated by treatment with progestins
Women for whom progestin-containing HT
would not be considered appropriate
minus Women who are intolerant of progestin-containing hormone therapy
minus Women with pre-existing medical conditions that may be exacerbated by progestins
Most common adverse events leading to discontinuation are related to progestins12
breakthrough bleeding
bull Increase in the number of uterine procedures (ie unnecessary endometrial biopsies)
breast paintenderness
bull Increase in the number of breast interventions
1 Steel SA et al Climacteric 2003 2 Ettinger B and Pressman A Am J Manag Care 1999 3 Komm BS Mirkin S
Pharmaceuticals 2012
4 Panay N amp Studd JWW Human Reprod Update 1997
bull Nausea bull Depressive mood bull Poor concentration bull Hirsutism bull Headache bull Dizziness bull Fluid retention bull Weight gain
Other progestin-related intolerance issues4
Unmet need with the treatment of postmenopausal symptoms
bull Alternatives to progestin are needed that will protect the endometrium while avoiding other progestin-associated effects and preserving the desired effects of estrogens in postmenopausal women3
Which women with a uterus could benefit from
estrogens without the need for a progestin
bull Women who are intolerant of progestin-containing hormone therapy
bull Women with pre-existing medical conditions that may be exacerbated by progestins (eg women with a history of depression PMSPMDD increased breast density diabetes and metabolic syndrome)
History of the following conditions may make progestin inappropriate
bull Depression
bull PMSPMDD
bull High breast density
bull Diabetes and metabolic syndrome
PMS premenstrual syndrome
PMD premenstrual dysphoric disorder
Medical conditions that may be exacerbated by treatment with progestins
Learning from WHI data
bull Hormone therapy (HT) is the conventional and established therapy option to effectively treat postmenopausal symptoms however it has been associated with some safety and tolerability concerns1 2
bull A review of WHI data suggests that many of the concerns with menopausal HT more often associated with EPT (CE+MPA) such as CHD risk increased breast density breast pain and breast cancer risk than with ET (CEE alone)2
1 Rolnick SJ Kopher RA DeFor TA et al Menopause 2005
2 Komm BS Mirkin S Pharmaceuticals 2012
WHI Womenrsquos Health Initiative trial
CHD coronary heart disease
CEE conjugated equine estrogens
Efficacy and Safety of Constant Oestrogen
Pulsed Progestogen vs
Continuous Combined HRT
Adverse Events
17b-oestradiol 17b-oestradiol norgestimate NETA (n = 150) (n = 172) Breast discomfort 14 27 Abdominal discomfort 14 22 Uterine bleeding 15 12 Dysmenorrhea 3 8 Oedema 5 8
Adapted from S Rozenberg et al Human Reproduction 2000
Medical condition which may be exacerbated by treatment
with progestins
Increased breast density
bull Increases in breast density are associated with progestin-containing HT which may adversely affect radiological detection of breast cancer1 and may be independently associated with an increased risk for the development of breast cancer2
bull The Postmenopausal EstrogenProgestin Interventions (PEPI) trial demonstrated that an increased mammographic breast density was associated with the use of E+P but not with the use of estrogen alone3
bull Women who already have high breast density may therefore be considered inappropriate for treatment with a progestin-containing HT
1) EU Core SPC for Hormone Replacement Therapy Products (CMDh1312003 Rev 4 June
2012)
2) De Villiers TJ et al on behalf of the International Menopause Society Climacteric 2013 16
3) Greendale GA et al J Natl Cancer Inst 2003
Stroke
0 25 5 75 10 125
Fractures
Diabetes
Breast cancer
Cholecystitis
Venothrombotic episodes
Endometrial cancer
Lung cancer
Coronary heart disease
Colorectal cancer
Overall mortality
15 125 10 75 5 25
Benefits Risks
CE
CE MPA
Santen RJ et al J Clin Endocrinol Metab 2010
The basis of the Endocrine Society scientific statement for postmenopausal hormone replacement therapy (HRT) excess risks and benefits of HRT for 5 years in women aged 50ndash59 years or within 10 years of the start of menopause E=estrogen P=progestin
bull Younger women (aged 50ndash59 years) had more favorable results bull There are differences between CE alone and CEMPA arms bull Overall benefitrisk ratio of CE-alone appears to be more favourable than CEMPA
Reevaluation of WHI data (stratified by age) Risks and
Benefits of HRT Cases per 1000 Women per 5 Years of
Use
Medical condition which may be exacerbated by treatment
with progestins
Diabetes and metabolic syndrome
bull Treatment of oestrogen deficiency symptoms with progestin-containing HT (unlike oestrogen alone) may be associated with increases in insulin resistance and deterioration in glucose tolerance123
bull Postmenopausal women with diabetes could be inappropriate for treatment with progestin-containing HT due to the potential risk of exacerbation of their condition
1) Panay N amp Studd JWW Human Reprod Update 1997
2) Godsland I et al Metabolism 1993
3) Sites CK et al J Clin Endocrinol Metab 2005
Variations in Associated Breast Cancer
Risks Between CE alone and CEMPA
bull Use of CE alone for a median of 59 years was associated with a lower incidence of invasive breast cancer (151 cases 027 per year) compared with placebo (199 cases 035 per year HR 077 95 CI 062ndash095 P=002)
bull In the CE alone group fewer women died from invasive breast cancer (6 deaths 0009 per year) compared with controls (16 deaths 0024 per year HR 037 95 CI 013ndash091 P=003)
Anderson GL et al Lancet
Oncol 2012
Bazedoxifene (BZA) specifically selected in
combination with conjugated estrogens
bull BZA has been specifically selected for its unique pharmacologic profile and effects on VMS and uterine tissue in particular123
1 Crabtree J et al Mol Cell Endocrinol 2008
2 Kharode Y et al Endocrinolology 2008
3 Duavive SmPC
Estrogen Receptor activity is dimmed
Estrogen Receptor activity is turned on
CEs are agonists BZA is an antagonist
In the uterus
bull The BZA component reduces the risk of endometrial hyperplasia that can occur with the conjugated estrogens component alone3 This means that progestins are not needed
Extensive global clinical development program for
CEBZA
aIncludes additional pilot dose-finding study 203 1 Lobo RA et al Fertil Steril 2009 2 Pinkerton JV et al Menopause 2009 3 Kagan R et al Menopause 2010 4 Mirkin S et al Climacteric 2013 5 Pinkerton JV et al Obstet Gynecol 2013
Effects of conjugated estrogensbazedoxifene on
lipid and coagulation variables a randomized
placebo- and active-controlled trial
bull At 12 months
bull Both CEBZA doses were associated with small but significant effects on hemostasis variables including reductions in antithrombin plasminogen activator inhibitor-1 and fibrinogen activity and an increase in plasminogen activity relative to placebo at 12 months Incidences of cardiovascular and venous thromboembolic events were similar among treatment groups
bull CONCLUSIONS
bull This study provides reassurance that CEBZA does not adversely affect lipid metabolism or hemostatic balance In accordance the incidences of venous thromboembolic events and cardiovascular events in postmenopausal women are similar to those observed with placebo
1 Kagan R J Womenrsquos Health (Larchmt) 2012
the OPTIMAL Menopausal Therapy
should demonstrate1
ndash Favorable safety and tolerability profile
ndash Relief of menopausal symptoms
ndash Prevention of osteoporosis CVD Cognitive function
ndash No stimulation of the endometrium breast and ovary
1 Kagan R J Womenrsquos Health (Larchmt) 2012
the OPTIMAL Menopausal Therapy
should demonstrate1
ndash Favorable safety and tolerability profile
ndash Relief of menopausal symptoms
ndash Prevention of osteoporosis CVD Cognitive function
ndash No stimulation of the endometrium breast and ovary
Variations in Associated Breast Cancer Risk Between CE alone and
CEMPA
Cumulative hazards
adjusted for age and
raceethnicity for
invasive breast cancer
by randomization
assignment in the WHI
CE-alone and CEMPA
trials
Anderson GL et al Lancet
Oncol 2012
0 0
1 2 3 4 5 6 7 8 9 10 11 12 13
001
002
003
004
005
Cu
mu
lati
ve
ha
za
rd
Time since randomization (years)
CEMPA
Placebo (in CEMPA arm)
HR 125 (95 CI 107ndash146)
CE alone
Placebo (in CE-alone arm)
HR 077 (95 CI 062ndash095)
CEMPA
CE alone
Placebo (CE-alone)
Placebo (CEMPA)
Estrogen only therapy
Endometrial cancer
Hysterectomy specimen showing cancer invading myometrium
following unopposed estrogen therapy for 15 years
Courtesy Dr David Sturdee
Bazedoxifene (BZA) specifically selected in
combination with conjugated estrogens
1 Crabtree J et al Mol Cell Endocrinol 2008
2 Kharode Y et al Endocrinolology 2008
3 Duavive SmPC
Estrogen Receptor activity is dimmed
Estrogen Receptor activity is turned on
CEs are agonists BZA is an antagonist
In the uterus
bull The BZA component reduces the risk of endometrial hyperplasia that can occur with the conjugated estrogens component alone1-3
bull This means that progestins are not needed
From the Womenrsquos Health Initiative to the combination
of estrogen and selective estrogen receptor
modulators to avoid progestin addition
bull Marie-Ceacutecile Valera Pierre Gourdy Florence Treacutemolliegraveres Jean-Franccedilois Arnal
bull Maturitas Volume 82 Issue 3 November 2015 Pages 274ndash277
bull
Other combinations of an estrogen (E2) + a SERM studied have
not produced favorable results
bull Objective To compare effects of 52 weeksrsquo treatment with either raloxifene 60 mgday alone (RLX) or in combination with 17B-estradiol 1 mgday (RLX + E2) on vasomotor symptoms (n = 83) and endometrial safety (n = 123) in postmenopausal women who transitioned from estrogen-progestin therapy Endometrial effect Women in the RLX + E2 group had significantly increased endometrial thickness at 52 weeks from baseline and RLX alone had no increase Two women (328) in the RLX + E2 group had endometrial hyperplasia (one with atypia) on the exit biopsy No one in RLX alone did
bull 1 Stovall D et al Menopause The Journal of The North American Menopause Society 2007
bull For the safety analyses data from women randomized before and after the protocol amendment were pooled which included 62 women in the raloxifene group and 61 women in the raloxifene + estrogen group
EFFICACY
VASOMOTOR
SYMPTOMS
SMART-2
DUAVIVE Efficacy for the Treatment of Moderate to
Severe VMS Associated With Menopause
14
1 Pinkerton JV et al Menopause 2009
Postmenopausal women
with a uterus
Age 42-64 year
(avg 53 yr)
(N=318)
DUAVIVE (CE 045BZA 20)
(n=127)
Placebo
(n=63)
bull 12-week randomized double-blind placebo-controlled study1
bull Inclusion criteria
‒ Postmenopausal women with an intact uterus
‒ Minimum of 7 moderate to severe hot flushes per day or at least 50 per week at screening
Change from baseline to
Weeks 4 and 12 in
bull Average daily number of
moderate to severe hot
flushes
bull Average daily severity
score of hot flushes
Primary End Points
Safety population (took at least one dose)
Significant Reduction vs Placebo in
Average Daily Number of Hot Flushes
DUAVEE [package insert] New York NY Pfizer Inc 2013
ANCOVA=analysis of covariance
Reduction in average daily number of
moderate to severe hot flushes ndash primary end point
Ad
jus
ted
mean
ch
an
ge
fro
m b
aselin
edagger
Week 4 Week 12
ndash31
ndash27
Treatment
differencedagger ndash59
ndash28
ndash76
ndash49
Treatment
differencedagger
22
Plt001 vs placebo daggerBased on data analysis using ANCOVA model Change from baseline = Treatment + Baseline + Site
DUAVIV
E
Reduction in the Observed Average Daily Number
of Moderate to Severe Hot Flushes
Data on file CSR-67461 Protocol 3115A1-305 Table 1511 Pfizer Inc New York NY
change from baseline to week 12
74 for DUAVIVE
51 for placebo
Observed Average Daily Number of Hot Flushes
Ob
serv
ed a
vera
ge d
aily
nu
mb
er o
f m
od
erat
e to
sev
ere
ho
t fl
ush
es
0 1 2 3 4 5 6 7 8 9 10 12 0 1
11
2
4 3
6 5
7 8 9
10
28
54
DUAVIVE (n=122) Placebo (n=62)
Weeks
Primary analysis showed statistically significant separation at weeks 4 and 12
Average daily number of hot flushes from baseline to week 12
103 to 28 for DUAVIVE
105 to 54 for placebo
Based on mathematical means
not statistically analyzed
105 103
Pinkerton JV et al Menopause 2009
Significant Reduction vs Placebo in
Average Daily Severity Score of Hot Flushes
17
Week 4 Week 12
ndash05
ndash06
Treatment
differencedagger
Treatment
differencedagger
DUAVEE [package insert] New York NY Pfizer Inc 2013
Reduction in average daily severity score of hot flushes ndash primary end point
Ad
jus
ted
me
an
ch
an
ge
fro
m b
aselin
edagger
Plt001 vs placebo daggerBased on data analysis using ANCOVA model Change from baseline = Treatment + Baseline + Site
DUAVIV
E
Reduction in the Observed Average
Daily Severity Score of Hot Flushes
Observed Average Daily Severity Score of Hot Flushes
19
DUAVIVE (n=122) Placebo (n=62)
Weeks
Ob
serv
ed a
vera
ge d
aily
sev
erit
y sc
ore
of
ho
t fl
ush
es
0
05
10
15
25
20
0 1 2 3 4 5 6 7 8 9 10 12 11 0 1 2 3 4 5 6 7 8 9 10 12 11
14
Data on file CSR-67461 Protocol 3115A1-305 Table 1511 Pfizer Inc New York NY
Primary analysis at weeks 4 and 12 prespecified secondary end points at all other weeks
change from baseline to week 12
39 for DUAVIVE
14 for placebo
Average daily severity score of hot flashes from baseline to week 12
23 to 14 for DUAVIVE
23 to 19 for Placebo
Based on mathematical means
not statistically analyzed
23
23
Pinkerton JV et al Menopause 2009
Effects on bone mineral density (BMD)
SMART 512
20
bull 12-month double-blind randomized placebo- and active-controlled study
bull Primary end point endometrial hyperplasia at 1 year
bull Secondary BMD changes at 1 year
1 DUAVEE [package insert] New York NY Pfizer Inc 2013 2 Pinkerton J Clin Endocrin Metab 2014
This study included a different dose of CEBZA and comparators The schematic shown here depicts only the patients who received the approved dose of DUAVIVE or placebo
Change from baseline in
bull Lumbar Spine BMD (Primary ndash BMD Substudy)
bull Total Hip BMD (Secondary ndash BMD Substudy)
BMD Analysis
DUAVIVE
(CE 045BZA 20)
(n=119)
Placebo
(n=139)
BMD Analysis
Postmenopausal women with a uterus
Less than 5 years since LMP
(N=590)
DUAVIVE Significantly Increased Lumbar Spine and Total
Hip BMD vs Placebo at 12 Months ndash Study 2
M
ean
ch
an
ge f
rom
baselin
e
Lumbar Spine Total Hip
121 151 Treatment
difference Treatment
difference
Data on file CSR-81040 Protocol 3115A1-3307 Pfizer Inc New York NY Pinkerton J Clin Endocrin Metab 2014 30
Plt001 vs placebo
Adjusted mean changes and P-values based on an ANCOVA model with treatment and region (US or non-US) as factors and baseline BMD value and years since menopause as covariates using the modified intention to treat population with last observation carried forward
DUAVIV
E
TOLERABILITY
AND SAFETY
Rates of BleedingSpotting and Amenorrhea
Similar to Rates with Placebo
bull High and similar cumulative rates of amenorrhea at year 1 among women treated with CE 045BZA 20 and placebo and was higher than seen in women treated with CE 045MPA 151
bull Noncumulative rates of spotting and bleedingspotting were similar among women treated with CEBZA or placebo and consistently higher in women treated with CE 045MPA 152
0
90
Cycle
100
Pe
rce
nta
ge
of
Su
bje
cts
80
70
60
50
40
30
20
10
88
54
Placebo
CE 045BZA 20 CE 045MPA 15
Percentage of subjects with cumulative amenorrhea during consecutive 4-week periods (cycles) in SMART-5
MPA medroxyprogesterone acetate Plt0001 vs all other treatment groups 1 Pinkerton JV et al J Clin Endocrinol Metab 2014 2 Data on file CSR-81040 Protocol 3115A1-3307 Pfizer Inc New York NY
Adverse Reactions in Placebo-
Controlled Trials Safety analyses have been conducted in 6210 postmenopausal women aged 40 to 75 years (mean age 55 years) following up to 2 years of treatment in SMART-1 -2 -3 and -5
Adverse reactions (incidence ge5) that were more common with DUAVIVE
Incidence of serious adverse reactions
35 with DUAVIVE 48 with placebo
DUAVEE [package insert] New York NY Pfizer Inc 2013
CE 045 BZA 20 (N=1224)
n ()
Placebo (N=1069)
n ()
Gastrointestinal disorders
Nausea 100 (8) 58 (5)
Diarrhea 96 (8) 57 (5)
Dyspepsia 84 (7) 59 (6)
Abdominal pain upper 81 (7) 58 (5)
Musculoskeletal and connective tissue disorders
Muscle spasms 110 (9) 63 (6)
Neck pain 62 (5) 46 (4)
Nervous system disorders
Dizziness 65 (5) 37 (3)
Respiratory thoracic and mediastinal disorders
Oropharyngeal pain 80 (7) 61 (6)
Venous Thromboembolism (VTE) in
DUAVIVE Clinical Studies
bull Estrogen agonistantagonists (including BZA a component of DUAVIVE) and estrogens individually are known to increase the risk of VTE
bull In the clinical studies with DUAVIVE the reporting rates for VTE were low in all treatment groups
bull Adverse reactions of VTE reported by patients
bull Should VTE event occur or be suspected DUAVIVE should be discontinued immediately
bull Due to the low rates of events in both groups it is not possible to conclude that the risk of VTE with DUAVIVE is different from that seen with other estrogen therapies
DUAVEE [package insert] New York NY Pfizer Inc 2013
00 for DUAVIVE (n=1224)
01 for placebo (n=1069)
26
Effects of conjugated estrogensbazedoxifene on
lipid and coagulation variables a randomized
placebo- and active-controlled trial
bull postmenopausal women (N = 1843) with menopausal
symptoms
bull Lipid (N = 1843) and coagulation (N = 590) variables were assessed in women receiving daily CE 045 mgBZA 20 mg CE 0625 mgBZA 20 mg BZA 20 mg CE 045 mgmedroxyprogesterone acetate (MPA) 15 mg or placebo for 12 months
bull Skouby SO et al Menopause 2015 Jun22(6)640-9
Effects of conjugated estrogensbazedoxifene on
lipid and coagulation variables a randomized
placebo- and active-controlled trial
bull At 12 months
bull CE 045 mgBZA 20 mg
bull CE 0625 mgBZA 20 mg
bull BZA 20 mg
bull and CE 045 mgMPA 15 mg decreased total cholesterol and LDL- cholesterol vs placebo (P lt 001 for all)
bull Both CEBZA doses and CEMPA increased high-density lipoprotein cholesterol compared with placebo (P lt 005 for all)
bull CE 045 mgBZA 20 mg had a neutral effect on triglycerides
bull CE 0625 mgBZA 20 mg and CEMPA increased triglycerides compared with placebo (P lt 005)
bull Skouby SO et al Menopause 2015 Jun22(6)640-9
Effects of conjugated estrogensbazedoxifene on
lipid and coagulation variables a randomized
placebo- and active-controlled trial
bull At 12 months
bull Both CEBZA doses were associated with small but significant effects on hemostasis variables including reductions in antithrombin plasminogen activator inhibitor-1 and fibrinogen activity and an increase in plasminogen activity relative to placebo at 12 months Incidences of cardiovascular and venous thromboembolic events were similar among treatment groups
Skouby SO et al Menopause 2015
Jun22(6)640-9
Endometrial hyperplasia or malignancy occurred in lt1 of women
following up to 1 year of treatment with CEBZA12
Study Cumulative Incidence at month 12 (nN)
CE 045BZA 20 Placebo
SMART-11 000 (0336) 000 (0313)
SMART-52 030 (1335) 028 (1354)
Effects on the Endometrium
1 Pickar JH et al Fertil Steril 2009 2 Pinkerton at al J Clin Endocrinol Metab 2014
Through the eyes of an amazone
Marie Mandy
Breast tolerability profile similar to placebo following up to 2 years of treatment with CEBZA12
Pooled analysis of SMART clinical trials
CE 045BZA 20 (n=1585)
Placebo (n=1241)
Breast cancer incidence up to 2 years
(per 1000 woman-years)
100 (CI 000-321)
140 (CI 000-417)
Incidence of reported breast paintenderness up to 12 weeks
98-115 81-112
Incidence of abnormal mammogram at month 12
258 316
Mean change in breast density at month 12 (SMART-5)
ndash038 (n=186)
ndash032 (n=182)
Effects on the Breast
1 Pickar JH et al Menopause 2013 2 Pinkerton JV et al Obstet Gynecol 2013
CEBZA clinical overview - summary
bull In clinical trials CEBZA has demonstrated safety and efficacy in postmenopausal women with a uterus including the following
bull Significant reduction in number and severity of moderate to severe hot flushes1
bull Incidence of cumulative amenorrhea rate similar to placebo and significantly better than CEMPA2
bull Incidence of endometrial hyperplasia and breast tendernessdensity similar to that with placebo345
bull Incidence of adverse events and discontinuation rates similar to that with placebo6
1 Pinkerton JV et al Menopause 2009 2 Pinkerton JV et al J Clin Endocrinol Metab2014 3 Pickar JH et al
Fertil Steril 2009 4 Pinkerton at al J Clin Endocrinol Metab 2014 5 Pickar JH et al Menopause 2013 6 DUAVEE [package insert] New York NY Pfizer Inc 2013
CEBZA clinical overview - summary
Now women with a uterus who choose hormone therapy for management of menopausal symptoms have a choice
bull conventional estrogen-progestogen therapy or
bull a new combinationhellipconjugated estrogens paired with the SERM bazedoxifene
1 Pinkerton JV et al Menopause 2009 2 Pinkerton JV et al J Clin Endocrinol Metab2014 3 Pickar JH et al Fertil Steril 2009 4 Pinkerton at al J Clin Endocrinol Metab 2014 5 Pickar JH et al Menopause 2013 6 DUAVEE [package insert] New York NY Pfizer Inc 2013
Conjugated EstrogensBazedoxifene (CEBZA)
US indication
bull DUAVEE is indicated in women with a uterus for
bull 11 Treatment of Moderate to Severe Vasomotor Symptoms Associated with Menopause
bull 12 Prevention of Postmenopausal Osteoporosis
bull 13 Important Limitations of Use
bull Use DUAVEE for the shortest duration consistent with treatment goals and risks for the individual woman Postmenopausal women should be re-evaluated periodically as clinically appropriate to determine if treatment is still necessary
bull When prescribing solely for the prevention of postmenopausal osteoporosis therapy should only be considered for women at significant risk of osteoporosis and non-estrogen medication should be carefully considered
Conjugated EstrogensBazedoxifene (CEBZA)
EU indication
CEBZA is indicated for
bull Treatment of oestrogen deficiency symptoms in postmenopausal women with a uterus (with at least 12 months since the last menses) for whom treatment with progestin-containing therapy is not appropriate
bull The experience treating women older than 65 years is limited
bull Dose CE (045mg)Bazedoxifene (20mg)
Duavive SmPC
Which women with a uterus
could benefit from estrogens
without the need for a
progestin
Progestin intolerance is one of the main
factors for reduced compliance
bull About 20 of women receiving progestin-containing HT have significant progestin intolerance and half of these experience serious effects that prevent treatment continuation1
1 Panay N amp Studd J Human Reprod Update 1997
2 Panay N et al on behalf of the British Menopause Society and Womenrsquos Health Concern Menopause Int 2013
bull The 2013 British Menopause Society amp Womenrsquos Health
Concern recommendations on hormone replacement
therapy do recognise progestin intolerance as one of the
main factors for reduced compliance with HT 2
Proportion of patients () with at least one bleeding episode in relation to time and to the
used HT
Serge Rozenberg et al Hum Reprod 2009241739-1747
copy The Author 2009 Published by Oxford University Press on behalf of the European Society of
Human Reproduction and Embryology All rights reserved For Permissions please email
journalspermissionsoxfordjournalsorg
Breast tenderness after initiation of CEE
CEE + MPA (WHI)
and mammographic density change
bullCrandall et al Breast Cancer Res Treat DOI 101007s10549-011-1803-9
Breast density
Conclusion
bull CEEBAZO is an additional regimen for menopausal symptoms it provides also a prevention for osteoporosis
bull It is suitable for women with a uterus who are unsatisfied with an EPT regimen or who you are unwilling to treat with an EPT regimen
Adapted use of MHT
bull Lower dosage of estrogens
bull Other progestins
bull Better safety profile
bull Vaginal estrogen or SERMS
bull Non-hormonal therapy
bull Development of new products
bull SERMS + estrogens
Most common adverse events leading to
discontinuation are related to progestins12
bull breakthrough bleeding
bull Low compliance
bull Increase in the number of US
bull Stress
bull Cost
bull uterine procedures
bull Unnecessary endometrial biopsies Hysteroscopies DampC Hysterectomies
bull Morbidity
Proportion of patients who completed or discontinued treatment in relation to the used HT
Serge Rozenberg et al Hum Reprod 2009241739-1747
copy The Author 2009 Published by Oxford University Press on behalf of the European Society of
Human Reproduction and Embryology All rights reserved For Permissions please email
journalspermissionsoxfordjournalsorg
Most common adverse events leading to discontinuation
are related to progestins
bull breast paintenderness
Breast tenderness after initiation of CEE
CEE + MPA (WHI)
and mammographic density change
bullCrandall et al Breast Cancer Res Treat DOI 101007s10549-011-1803-9
Breast density
Hormone therapy use and mammographic
density in postmenopausal Norwegian women
bull Results differed when considering the combined effect of age and BMI
bull The effect of EPT on mammographic density was modified by age and BMI with no apparent association among the youngest women (aged 50-55) with the highest BMI (BMI ge 26)
bull A higher mammographic density was found in EPT users compared to never HT users particularly in women using high-dose NETA regimens Age and BMI modified the association between EPT use and mammographic density
bull Couto E et al Breast Cancer Res Treat 2011 Nov 4 [Epub ahead of print]
Breast Cancer Risk by Breast Density
Menopause and Postmenopausal Hormone
Therapy Use
Birads age HT Duration Risk
1 55-59 None 5 year risk 08 (95 CI 06- 09)
1 55-59
ET EPT 5 year risk 09 (95 CI 07 -11)
4 55-59
None 5 year risk 24 (95 CI 20 -28)
4 55-59
ET 5 year risk
30 (95 CI 26 -35)
4 55-59
EPT 5 year risk
42 (95 CI 37 -46)
Adapted from Kerlikowske et al JOURNAL OF CLINICAL ONCOLOGY 2010
Breast Cancer Risk by Breast Density
Menopause and Postmenopausal Hormone
Therapy Use
Adapted from Kerlikowske et al JOURNAL OF CLINICAL ONCOLOGY 2010
bull Postmenopausal women with high breast density are at increased risk of breast cancer and should be aware of the added risk of taking HT especially estrogen plus progestin
Medical condition which may be exacerbated by treatment
with progestins
Diabetes and metabolic syndrome
bull progestin-containing HT may be associated with increases in insulin resistance and deterioration in glucose tolerance123
bull Postmenopausal women with diabetes could be inappropriate for treatment with progestin-containing HT due to the potential risk of exacerbation of their condition
1) Panay N amp Studd JWW Human Reprod Update 1997
2) Godsland I et al Metabolism 1993
3) Sites CK et al J Clin Endocrinol Metab 2005
A Nath and R Sitruk-Ware CLIMACTERIC 200912(Suppl 1)96ndash101
A Nath and R Sitruk-Ware CLIMACTERIC 200912(Suppl 1)96ndash101
Diabetes an epidemy
bull UK 1996 14 million of diabetics
bull UK 2015 32 million (6 of the population)
bull UK 2025 5 million
bull httpwwwdiabetescoukdiabetes-prevalencehtml
Other progestin-related intolerance issues
bull Nausea
bull Depressive mood
bull Poor concentration
bull Hirsutism
bull Headache
bull Dizziness
bull Fluid retention
bull Weight gain Panay N amp Studd JWW Human Reprod Update 1997
Medical condition which may be exacerbated by treatment with progestins
PMSPMDDdepression
bull Progesterone-induced PMD can be exacerbated by exogenous progestin administration and can occur in association with HT or OC administration1
bull Significantly higher negative mood scores have been observed during the addition of a progestin to an estrogen in a sequential HT regimen in postmenopausal women with a history of PMS compared to those without2
bull Women with a history of PMS or PMD exacerbation of depression using progestins may therefore benefit from a progestin free treatment for menopausal symptoms
1) Nevatte T et al Arch Womens Ment Health 2013 2) Bjoumlrn I et al Climacteric 2006 PMS premenstrual syndrome
PMDD premenstrual dysphoric disorder
Conclusion
bull CEEBAZO is an additional regimen for menopausal symptoms it provides also a prevention for osteoporosis
bull It is suitable for women with a uterus who are unsatisfied with an EPT regimen or who you are unwilling to treat with an EPT regimen
For some postmenopausal women with a uterus there is a
need for progestin free treatment options
bull with demonstrated clinical efficacy
bull which protects the endometrium
bull improved tolerabilitysafety profile
In clinical practice this translates to women who are
intolerant of progestin-containing HT or have conditions
which may be exacerbated by treatment with progestins
Conclusion Medical need for alternative treatment option
Medical condition which may be exacerbated by treatment with progestins
Depression
bull Progestin-containing HT has been associated with increases in depressive symptoms in some individuals1
bull There is a biochemicalphysiological plausibility for the association of progestins with depression234
bull Therefore postmenopausal women who also have a medical history of depressive disorders or depression could be inappropriate for treatment with progestin-containing HT
Pfizer Confidential
65
1) Girdler SS et al J Womens Health Gend Based Med 1999 2) Traish AM et al Korean J Urol 2014 3) Stroumlhle A et al Biol Psychiatry 1999 4) Romeo E et
al Am J Psychiatry 1998
History of the following conditions may make progestin inappropriate
bull Depression
bull PMSPMDD
PMS premenstrual syndrome
PMD premenstrual dysphoric disorder
Medical conditions that may be exacerbated by treatment with progestins
Women for whom progestin-containing HT
would not be considered appropriate
minus Women who are intolerant of progestin-containing hormone therapy
minus Women with pre-existing medical conditions that may be exacerbated by progestins
Most common adverse events leading to discontinuation are related to progestins12
breakthrough bleeding
bull Increase in the number of uterine procedures (ie unnecessary endometrial biopsies)
breast paintenderness
bull Increase in the number of breast interventions
1 Steel SA et al Climacteric 2003 2 Ettinger B and Pressman A Am J Manag Care 1999 3 Komm BS Mirkin S
Pharmaceuticals 2012
4 Panay N amp Studd JWW Human Reprod Update 1997
bull Nausea bull Depressive mood bull Poor concentration bull Hirsutism bull Headache bull Dizziness bull Fluid retention bull Weight gain
Other progestin-related intolerance issues4
Unmet need with the treatment of postmenopausal symptoms
bull Alternatives to progestin are needed that will protect the endometrium while avoiding other progestin-associated effects and preserving the desired effects of estrogens in postmenopausal women3
Which women with a uterus could benefit from
estrogens without the need for a progestin
bull Women who are intolerant of progestin-containing hormone therapy
bull Women with pre-existing medical conditions that may be exacerbated by progestins (eg women with a history of depression PMSPMDD increased breast density diabetes and metabolic syndrome)
History of the following conditions may make progestin inappropriate
bull Depression
bull PMSPMDD
bull High breast density
bull Diabetes and metabolic syndrome
PMS premenstrual syndrome
PMD premenstrual dysphoric disorder
Medical conditions that may be exacerbated by treatment with progestins
Learning from WHI data
bull Hormone therapy (HT) is the conventional and established therapy option to effectively treat postmenopausal symptoms however it has been associated with some safety and tolerability concerns1 2
bull A review of WHI data suggests that many of the concerns with menopausal HT more often associated with EPT (CE+MPA) such as CHD risk increased breast density breast pain and breast cancer risk than with ET (CEE alone)2
1 Rolnick SJ Kopher RA DeFor TA et al Menopause 2005
2 Komm BS Mirkin S Pharmaceuticals 2012
WHI Womenrsquos Health Initiative trial
CHD coronary heart disease
CEE conjugated equine estrogens
Efficacy and Safety of Constant Oestrogen
Pulsed Progestogen vs
Continuous Combined HRT
Adverse Events
17b-oestradiol 17b-oestradiol norgestimate NETA (n = 150) (n = 172) Breast discomfort 14 27 Abdominal discomfort 14 22 Uterine bleeding 15 12 Dysmenorrhea 3 8 Oedema 5 8
Adapted from S Rozenberg et al Human Reproduction 2000
Medical condition which may be exacerbated by treatment
with progestins
Increased breast density
bull Increases in breast density are associated with progestin-containing HT which may adversely affect radiological detection of breast cancer1 and may be independently associated with an increased risk for the development of breast cancer2
bull The Postmenopausal EstrogenProgestin Interventions (PEPI) trial demonstrated that an increased mammographic breast density was associated with the use of E+P but not with the use of estrogen alone3
bull Women who already have high breast density may therefore be considered inappropriate for treatment with a progestin-containing HT
1) EU Core SPC for Hormone Replacement Therapy Products (CMDh1312003 Rev 4 June
2012)
2) De Villiers TJ et al on behalf of the International Menopause Society Climacteric 2013 16
3) Greendale GA et al J Natl Cancer Inst 2003
Stroke
0 25 5 75 10 125
Fractures
Diabetes
Breast cancer
Cholecystitis
Venothrombotic episodes
Endometrial cancer
Lung cancer
Coronary heart disease
Colorectal cancer
Overall mortality
15 125 10 75 5 25
Benefits Risks
CE
CE MPA
Santen RJ et al J Clin Endocrinol Metab 2010
The basis of the Endocrine Society scientific statement for postmenopausal hormone replacement therapy (HRT) excess risks and benefits of HRT for 5 years in women aged 50ndash59 years or within 10 years of the start of menopause E=estrogen P=progestin
bull Younger women (aged 50ndash59 years) had more favorable results bull There are differences between CE alone and CEMPA arms bull Overall benefitrisk ratio of CE-alone appears to be more favourable than CEMPA
Reevaluation of WHI data (stratified by age) Risks and
Benefits of HRT Cases per 1000 Women per 5 Years of
Use
Medical condition which may be exacerbated by treatment
with progestins
Diabetes and metabolic syndrome
bull Treatment of oestrogen deficiency symptoms with progestin-containing HT (unlike oestrogen alone) may be associated with increases in insulin resistance and deterioration in glucose tolerance123
bull Postmenopausal women with diabetes could be inappropriate for treatment with progestin-containing HT due to the potential risk of exacerbation of their condition
1) Panay N amp Studd JWW Human Reprod Update 1997
2) Godsland I et al Metabolism 1993
3) Sites CK et al J Clin Endocrinol Metab 2005
Variations in Associated Breast Cancer
Risks Between CE alone and CEMPA
bull Use of CE alone for a median of 59 years was associated with a lower incidence of invasive breast cancer (151 cases 027 per year) compared with placebo (199 cases 035 per year HR 077 95 CI 062ndash095 P=002)
bull In the CE alone group fewer women died from invasive breast cancer (6 deaths 0009 per year) compared with controls (16 deaths 0024 per year HR 037 95 CI 013ndash091 P=003)
Anderson GL et al Lancet
Oncol 2012
Bazedoxifene (BZA) specifically selected in
combination with conjugated estrogens
bull BZA has been specifically selected for its unique pharmacologic profile and effects on VMS and uterine tissue in particular123
1 Crabtree J et al Mol Cell Endocrinol 2008
2 Kharode Y et al Endocrinolology 2008
3 Duavive SmPC
Estrogen Receptor activity is dimmed
Estrogen Receptor activity is turned on
CEs are agonists BZA is an antagonist
In the uterus
bull The BZA component reduces the risk of endometrial hyperplasia that can occur with the conjugated estrogens component alone3 This means that progestins are not needed
Extensive global clinical development program for
CEBZA
aIncludes additional pilot dose-finding study 203 1 Lobo RA et al Fertil Steril 2009 2 Pinkerton JV et al Menopause 2009 3 Kagan R et al Menopause 2010 4 Mirkin S et al Climacteric 2013 5 Pinkerton JV et al Obstet Gynecol 2013
Effects of conjugated estrogensbazedoxifene on
lipid and coagulation variables a randomized
placebo- and active-controlled trial
bull At 12 months
bull Both CEBZA doses were associated with small but significant effects on hemostasis variables including reductions in antithrombin plasminogen activator inhibitor-1 and fibrinogen activity and an increase in plasminogen activity relative to placebo at 12 months Incidences of cardiovascular and venous thromboembolic events were similar among treatment groups
bull CONCLUSIONS
bull This study provides reassurance that CEBZA does not adversely affect lipid metabolism or hemostatic balance In accordance the incidences of venous thromboembolic events and cardiovascular events in postmenopausal women are similar to those observed with placebo
1 Kagan R J Womenrsquos Health (Larchmt) 2012
the OPTIMAL Menopausal Therapy
should demonstrate1
ndash Favorable safety and tolerability profile
ndash Relief of menopausal symptoms
ndash Prevention of osteoporosis CVD Cognitive function
ndash No stimulation of the endometrium breast and ovary
Variations in Associated Breast Cancer Risk Between CE alone and
CEMPA
Cumulative hazards
adjusted for age and
raceethnicity for
invasive breast cancer
by randomization
assignment in the WHI
CE-alone and CEMPA
trials
Anderson GL et al Lancet
Oncol 2012
0 0
1 2 3 4 5 6 7 8 9 10 11 12 13
001
002
003
004
005
Cu
mu
lati
ve
ha
za
rd
Time since randomization (years)
CEMPA
Placebo (in CEMPA arm)
HR 125 (95 CI 107ndash146)
CE alone
Placebo (in CE-alone arm)
HR 077 (95 CI 062ndash095)
CEMPA
CE alone
Placebo (CE-alone)
Placebo (CEMPA)
Estrogen only therapy
Endometrial cancer
Hysterectomy specimen showing cancer invading myometrium
following unopposed estrogen therapy for 15 years
Courtesy Dr David Sturdee
Bazedoxifene (BZA) specifically selected in
combination with conjugated estrogens
1 Crabtree J et al Mol Cell Endocrinol 2008
2 Kharode Y et al Endocrinolology 2008
3 Duavive SmPC
Estrogen Receptor activity is dimmed
Estrogen Receptor activity is turned on
CEs are agonists BZA is an antagonist
In the uterus
bull The BZA component reduces the risk of endometrial hyperplasia that can occur with the conjugated estrogens component alone1-3
bull This means that progestins are not needed
From the Womenrsquos Health Initiative to the combination
of estrogen and selective estrogen receptor
modulators to avoid progestin addition
bull Marie-Ceacutecile Valera Pierre Gourdy Florence Treacutemolliegraveres Jean-Franccedilois Arnal
bull Maturitas Volume 82 Issue 3 November 2015 Pages 274ndash277
bull
Other combinations of an estrogen (E2) + a SERM studied have
not produced favorable results
bull Objective To compare effects of 52 weeksrsquo treatment with either raloxifene 60 mgday alone (RLX) or in combination with 17B-estradiol 1 mgday (RLX + E2) on vasomotor symptoms (n = 83) and endometrial safety (n = 123) in postmenopausal women who transitioned from estrogen-progestin therapy Endometrial effect Women in the RLX + E2 group had significantly increased endometrial thickness at 52 weeks from baseline and RLX alone had no increase Two women (328) in the RLX + E2 group had endometrial hyperplasia (one with atypia) on the exit biopsy No one in RLX alone did
bull 1 Stovall D et al Menopause The Journal of The North American Menopause Society 2007
bull For the safety analyses data from women randomized before and after the protocol amendment were pooled which included 62 women in the raloxifene group and 61 women in the raloxifene + estrogen group
EFFICACY
VASOMOTOR
SYMPTOMS
SMART-2
DUAVIVE Efficacy for the Treatment of Moderate to
Severe VMS Associated With Menopause
14
1 Pinkerton JV et al Menopause 2009
Postmenopausal women
with a uterus
Age 42-64 year
(avg 53 yr)
(N=318)
DUAVIVE (CE 045BZA 20)
(n=127)
Placebo
(n=63)
bull 12-week randomized double-blind placebo-controlled study1
bull Inclusion criteria
‒ Postmenopausal women with an intact uterus
‒ Minimum of 7 moderate to severe hot flushes per day or at least 50 per week at screening
Change from baseline to
Weeks 4 and 12 in
bull Average daily number of
moderate to severe hot
flushes
bull Average daily severity
score of hot flushes
Primary End Points
Safety population (took at least one dose)
Significant Reduction vs Placebo in
Average Daily Number of Hot Flushes
DUAVEE [package insert] New York NY Pfizer Inc 2013
ANCOVA=analysis of covariance
Reduction in average daily number of
moderate to severe hot flushes ndash primary end point
Ad
jus
ted
mean
ch
an
ge
fro
m b
aselin
edagger
Week 4 Week 12
ndash31
ndash27
Treatment
differencedagger ndash59
ndash28
ndash76
ndash49
Treatment
differencedagger
22
Plt001 vs placebo daggerBased on data analysis using ANCOVA model Change from baseline = Treatment + Baseline + Site
DUAVIV
E
Reduction in the Observed Average Daily Number
of Moderate to Severe Hot Flushes
Data on file CSR-67461 Protocol 3115A1-305 Table 1511 Pfizer Inc New York NY
change from baseline to week 12
74 for DUAVIVE
51 for placebo
Observed Average Daily Number of Hot Flushes
Ob
serv
ed a
vera
ge d
aily
nu
mb
er o
f m
od
erat
e to
sev
ere
ho
t fl
ush
es
0 1 2 3 4 5 6 7 8 9 10 12 0 1
11
2
4 3
6 5
7 8 9
10
28
54
DUAVIVE (n=122) Placebo (n=62)
Weeks
Primary analysis showed statistically significant separation at weeks 4 and 12
Average daily number of hot flushes from baseline to week 12
103 to 28 for DUAVIVE
105 to 54 for placebo
Based on mathematical means
not statistically analyzed
105 103
Pinkerton JV et al Menopause 2009
Significant Reduction vs Placebo in
Average Daily Severity Score of Hot Flushes
17
Week 4 Week 12
ndash05
ndash06
Treatment
differencedagger
Treatment
differencedagger
DUAVEE [package insert] New York NY Pfizer Inc 2013
Reduction in average daily severity score of hot flushes ndash primary end point
Ad
jus
ted
me
an
ch
an
ge
fro
m b
aselin
edagger
Plt001 vs placebo daggerBased on data analysis using ANCOVA model Change from baseline = Treatment + Baseline + Site
DUAVIV
E
Reduction in the Observed Average
Daily Severity Score of Hot Flushes
Observed Average Daily Severity Score of Hot Flushes
19
DUAVIVE (n=122) Placebo (n=62)
Weeks
Ob
serv
ed a
vera
ge d
aily
sev
erit
y sc
ore
of
ho
t fl
ush
es
0
05
10
15
25
20
0 1 2 3 4 5 6 7 8 9 10 12 11 0 1 2 3 4 5 6 7 8 9 10 12 11
14
Data on file CSR-67461 Protocol 3115A1-305 Table 1511 Pfizer Inc New York NY
Primary analysis at weeks 4 and 12 prespecified secondary end points at all other weeks
change from baseline to week 12
39 for DUAVIVE
14 for placebo
Average daily severity score of hot flashes from baseline to week 12
23 to 14 for DUAVIVE
23 to 19 for Placebo
Based on mathematical means
not statistically analyzed
23
23
Pinkerton JV et al Menopause 2009
Effects on bone mineral density (BMD)
SMART 512
20
bull 12-month double-blind randomized placebo- and active-controlled study
bull Primary end point endometrial hyperplasia at 1 year
bull Secondary BMD changes at 1 year
1 DUAVEE [package insert] New York NY Pfizer Inc 2013 2 Pinkerton J Clin Endocrin Metab 2014
This study included a different dose of CEBZA and comparators The schematic shown here depicts only the patients who received the approved dose of DUAVIVE or placebo
Change from baseline in
bull Lumbar Spine BMD (Primary ndash BMD Substudy)
bull Total Hip BMD (Secondary ndash BMD Substudy)
BMD Analysis
DUAVIVE
(CE 045BZA 20)
(n=119)
Placebo
(n=139)
BMD Analysis
Postmenopausal women with a uterus
Less than 5 years since LMP
(N=590)
DUAVIVE Significantly Increased Lumbar Spine and Total
Hip BMD vs Placebo at 12 Months ndash Study 2
M
ean
ch
an
ge f
rom
baselin
e
Lumbar Spine Total Hip
121 151 Treatment
difference Treatment
difference
Data on file CSR-81040 Protocol 3115A1-3307 Pfizer Inc New York NY Pinkerton J Clin Endocrin Metab 2014 30
Plt001 vs placebo
Adjusted mean changes and P-values based on an ANCOVA model with treatment and region (US or non-US) as factors and baseline BMD value and years since menopause as covariates using the modified intention to treat population with last observation carried forward
DUAVIV
E
TOLERABILITY
AND SAFETY
Rates of BleedingSpotting and Amenorrhea
Similar to Rates with Placebo
bull High and similar cumulative rates of amenorrhea at year 1 among women treated with CE 045BZA 20 and placebo and was higher than seen in women treated with CE 045MPA 151
bull Noncumulative rates of spotting and bleedingspotting were similar among women treated with CEBZA or placebo and consistently higher in women treated with CE 045MPA 152
0
90
Cycle
100
Pe
rce
nta
ge
of
Su
bje
cts
80
70
60
50
40
30
20
10
88
54
Placebo
CE 045BZA 20 CE 045MPA 15
Percentage of subjects with cumulative amenorrhea during consecutive 4-week periods (cycles) in SMART-5
MPA medroxyprogesterone acetate Plt0001 vs all other treatment groups 1 Pinkerton JV et al J Clin Endocrinol Metab 2014 2 Data on file CSR-81040 Protocol 3115A1-3307 Pfizer Inc New York NY
Adverse Reactions in Placebo-
Controlled Trials Safety analyses have been conducted in 6210 postmenopausal women aged 40 to 75 years (mean age 55 years) following up to 2 years of treatment in SMART-1 -2 -3 and -5
Adverse reactions (incidence ge5) that were more common with DUAVIVE
Incidence of serious adverse reactions
35 with DUAVIVE 48 with placebo
DUAVEE [package insert] New York NY Pfizer Inc 2013
CE 045 BZA 20 (N=1224)
n ()
Placebo (N=1069)
n ()
Gastrointestinal disorders
Nausea 100 (8) 58 (5)
Diarrhea 96 (8) 57 (5)
Dyspepsia 84 (7) 59 (6)
Abdominal pain upper 81 (7) 58 (5)
Musculoskeletal and connective tissue disorders
Muscle spasms 110 (9) 63 (6)
Neck pain 62 (5) 46 (4)
Nervous system disorders
Dizziness 65 (5) 37 (3)
Respiratory thoracic and mediastinal disorders
Oropharyngeal pain 80 (7) 61 (6)
Venous Thromboembolism (VTE) in
DUAVIVE Clinical Studies
bull Estrogen agonistantagonists (including BZA a component of DUAVIVE) and estrogens individually are known to increase the risk of VTE
bull In the clinical studies with DUAVIVE the reporting rates for VTE were low in all treatment groups
bull Adverse reactions of VTE reported by patients
bull Should VTE event occur or be suspected DUAVIVE should be discontinued immediately
bull Due to the low rates of events in both groups it is not possible to conclude that the risk of VTE with DUAVIVE is different from that seen with other estrogen therapies
DUAVEE [package insert] New York NY Pfizer Inc 2013
00 for DUAVIVE (n=1224)
01 for placebo (n=1069)
26
Effects of conjugated estrogensbazedoxifene on
lipid and coagulation variables a randomized
placebo- and active-controlled trial
bull postmenopausal women (N = 1843) with menopausal
symptoms
bull Lipid (N = 1843) and coagulation (N = 590) variables were assessed in women receiving daily CE 045 mgBZA 20 mg CE 0625 mgBZA 20 mg BZA 20 mg CE 045 mgmedroxyprogesterone acetate (MPA) 15 mg or placebo for 12 months
bull Skouby SO et al Menopause 2015 Jun22(6)640-9
Effects of conjugated estrogensbazedoxifene on
lipid and coagulation variables a randomized
placebo- and active-controlled trial
bull At 12 months
bull CE 045 mgBZA 20 mg
bull CE 0625 mgBZA 20 mg
bull BZA 20 mg
bull and CE 045 mgMPA 15 mg decreased total cholesterol and LDL- cholesterol vs placebo (P lt 001 for all)
bull Both CEBZA doses and CEMPA increased high-density lipoprotein cholesterol compared with placebo (P lt 005 for all)
bull CE 045 mgBZA 20 mg had a neutral effect on triglycerides
bull CE 0625 mgBZA 20 mg and CEMPA increased triglycerides compared with placebo (P lt 005)
bull Skouby SO et al Menopause 2015 Jun22(6)640-9
Effects of conjugated estrogensbazedoxifene on
lipid and coagulation variables a randomized
placebo- and active-controlled trial
bull At 12 months
bull Both CEBZA doses were associated with small but significant effects on hemostasis variables including reductions in antithrombin plasminogen activator inhibitor-1 and fibrinogen activity and an increase in plasminogen activity relative to placebo at 12 months Incidences of cardiovascular and venous thromboembolic events were similar among treatment groups
Skouby SO et al Menopause 2015
Jun22(6)640-9
Endometrial hyperplasia or malignancy occurred in lt1 of women
following up to 1 year of treatment with CEBZA12
Study Cumulative Incidence at month 12 (nN)
CE 045BZA 20 Placebo
SMART-11 000 (0336) 000 (0313)
SMART-52 030 (1335) 028 (1354)
Effects on the Endometrium
1 Pickar JH et al Fertil Steril 2009 2 Pinkerton at al J Clin Endocrinol Metab 2014
Through the eyes of an amazone
Marie Mandy
Breast tolerability profile similar to placebo following up to 2 years of treatment with CEBZA12
Pooled analysis of SMART clinical trials
CE 045BZA 20 (n=1585)
Placebo (n=1241)
Breast cancer incidence up to 2 years
(per 1000 woman-years)
100 (CI 000-321)
140 (CI 000-417)
Incidence of reported breast paintenderness up to 12 weeks
98-115 81-112
Incidence of abnormal mammogram at month 12
258 316
Mean change in breast density at month 12 (SMART-5)
ndash038 (n=186)
ndash032 (n=182)
Effects on the Breast
1 Pickar JH et al Menopause 2013 2 Pinkerton JV et al Obstet Gynecol 2013
CEBZA clinical overview - summary
bull In clinical trials CEBZA has demonstrated safety and efficacy in postmenopausal women with a uterus including the following
bull Significant reduction in number and severity of moderate to severe hot flushes1
bull Incidence of cumulative amenorrhea rate similar to placebo and significantly better than CEMPA2
bull Incidence of endometrial hyperplasia and breast tendernessdensity similar to that with placebo345
bull Incidence of adverse events and discontinuation rates similar to that with placebo6
1 Pinkerton JV et al Menopause 2009 2 Pinkerton JV et al J Clin Endocrinol Metab2014 3 Pickar JH et al
Fertil Steril 2009 4 Pinkerton at al J Clin Endocrinol Metab 2014 5 Pickar JH et al Menopause 2013 6 DUAVEE [package insert] New York NY Pfizer Inc 2013
CEBZA clinical overview - summary
Now women with a uterus who choose hormone therapy for management of menopausal symptoms have a choice
bull conventional estrogen-progestogen therapy or
bull a new combinationhellipconjugated estrogens paired with the SERM bazedoxifene
1 Pinkerton JV et al Menopause 2009 2 Pinkerton JV et al J Clin Endocrinol Metab2014 3 Pickar JH et al Fertil Steril 2009 4 Pinkerton at al J Clin Endocrinol Metab 2014 5 Pickar JH et al Menopause 2013 6 DUAVEE [package insert] New York NY Pfizer Inc 2013
Conjugated EstrogensBazedoxifene (CEBZA)
US indication
bull DUAVEE is indicated in women with a uterus for
bull 11 Treatment of Moderate to Severe Vasomotor Symptoms Associated with Menopause
bull 12 Prevention of Postmenopausal Osteoporosis
bull 13 Important Limitations of Use
bull Use DUAVEE for the shortest duration consistent with treatment goals and risks for the individual woman Postmenopausal women should be re-evaluated periodically as clinically appropriate to determine if treatment is still necessary
bull When prescribing solely for the prevention of postmenopausal osteoporosis therapy should only be considered for women at significant risk of osteoporosis and non-estrogen medication should be carefully considered
Conjugated EstrogensBazedoxifene (CEBZA)
EU indication
CEBZA is indicated for
bull Treatment of oestrogen deficiency symptoms in postmenopausal women with a uterus (with at least 12 months since the last menses) for whom treatment with progestin-containing therapy is not appropriate
bull The experience treating women older than 65 years is limited
bull Dose CE (045mg)Bazedoxifene (20mg)
Duavive SmPC
Which women with a uterus
could benefit from estrogens
without the need for a
progestin
Progestin intolerance is one of the main
factors for reduced compliance
bull About 20 of women receiving progestin-containing HT have significant progestin intolerance and half of these experience serious effects that prevent treatment continuation1
1 Panay N amp Studd J Human Reprod Update 1997
2 Panay N et al on behalf of the British Menopause Society and Womenrsquos Health Concern Menopause Int 2013
bull The 2013 British Menopause Society amp Womenrsquos Health
Concern recommendations on hormone replacement
therapy do recognise progestin intolerance as one of the
main factors for reduced compliance with HT 2
Proportion of patients () with at least one bleeding episode in relation to time and to the
used HT
Serge Rozenberg et al Hum Reprod 2009241739-1747
copy The Author 2009 Published by Oxford University Press on behalf of the European Society of
Human Reproduction and Embryology All rights reserved For Permissions please email
journalspermissionsoxfordjournalsorg
Breast tenderness after initiation of CEE
CEE + MPA (WHI)
and mammographic density change
bullCrandall et al Breast Cancer Res Treat DOI 101007s10549-011-1803-9
Breast density
Conclusion
bull CEEBAZO is an additional regimen for menopausal symptoms it provides also a prevention for osteoporosis
bull It is suitable for women with a uterus who are unsatisfied with an EPT regimen or who you are unwilling to treat with an EPT regimen
Adapted use of MHT
bull Lower dosage of estrogens
bull Other progestins
bull Better safety profile
bull Vaginal estrogen or SERMS
bull Non-hormonal therapy
bull Development of new products
bull SERMS + estrogens
Most common adverse events leading to
discontinuation are related to progestins12
bull breakthrough bleeding
bull Low compliance
bull Increase in the number of US
bull Stress
bull Cost
bull uterine procedures
bull Unnecessary endometrial biopsies Hysteroscopies DampC Hysterectomies
bull Morbidity
Proportion of patients who completed or discontinued treatment in relation to the used HT
Serge Rozenberg et al Hum Reprod 2009241739-1747
copy The Author 2009 Published by Oxford University Press on behalf of the European Society of
Human Reproduction and Embryology All rights reserved For Permissions please email
journalspermissionsoxfordjournalsorg
Most common adverse events leading to discontinuation
are related to progestins
bull breast paintenderness
Breast tenderness after initiation of CEE
CEE + MPA (WHI)
and mammographic density change
bullCrandall et al Breast Cancer Res Treat DOI 101007s10549-011-1803-9
Breast density
Hormone therapy use and mammographic
density in postmenopausal Norwegian women
bull Results differed when considering the combined effect of age and BMI
bull The effect of EPT on mammographic density was modified by age and BMI with no apparent association among the youngest women (aged 50-55) with the highest BMI (BMI ge 26)
bull A higher mammographic density was found in EPT users compared to never HT users particularly in women using high-dose NETA regimens Age and BMI modified the association between EPT use and mammographic density
bull Couto E et al Breast Cancer Res Treat 2011 Nov 4 [Epub ahead of print]
Breast Cancer Risk by Breast Density
Menopause and Postmenopausal Hormone
Therapy Use
Birads age HT Duration Risk
1 55-59 None 5 year risk 08 (95 CI 06- 09)
1 55-59
ET EPT 5 year risk 09 (95 CI 07 -11)
4 55-59
None 5 year risk 24 (95 CI 20 -28)
4 55-59
ET 5 year risk
30 (95 CI 26 -35)
4 55-59
EPT 5 year risk
42 (95 CI 37 -46)
Adapted from Kerlikowske et al JOURNAL OF CLINICAL ONCOLOGY 2010
Breast Cancer Risk by Breast Density
Menopause and Postmenopausal Hormone
Therapy Use
Adapted from Kerlikowske et al JOURNAL OF CLINICAL ONCOLOGY 2010
bull Postmenopausal women with high breast density are at increased risk of breast cancer and should be aware of the added risk of taking HT especially estrogen plus progestin
Medical condition which may be exacerbated by treatment
with progestins
Diabetes and metabolic syndrome
bull progestin-containing HT may be associated with increases in insulin resistance and deterioration in glucose tolerance123
bull Postmenopausal women with diabetes could be inappropriate for treatment with progestin-containing HT due to the potential risk of exacerbation of their condition
1) Panay N amp Studd JWW Human Reprod Update 1997
2) Godsland I et al Metabolism 1993
3) Sites CK et al J Clin Endocrinol Metab 2005
A Nath and R Sitruk-Ware CLIMACTERIC 200912(Suppl 1)96ndash101
A Nath and R Sitruk-Ware CLIMACTERIC 200912(Suppl 1)96ndash101
Diabetes an epidemy
bull UK 1996 14 million of diabetics
bull UK 2015 32 million (6 of the population)
bull UK 2025 5 million
bull httpwwwdiabetescoukdiabetes-prevalencehtml
Other progestin-related intolerance issues
bull Nausea
bull Depressive mood
bull Poor concentration
bull Hirsutism
bull Headache
bull Dizziness
bull Fluid retention
bull Weight gain Panay N amp Studd JWW Human Reprod Update 1997
Medical condition which may be exacerbated by treatment with progestins
PMSPMDDdepression
bull Progesterone-induced PMD can be exacerbated by exogenous progestin administration and can occur in association with HT or OC administration1
bull Significantly higher negative mood scores have been observed during the addition of a progestin to an estrogen in a sequential HT regimen in postmenopausal women with a history of PMS compared to those without2
bull Women with a history of PMS or PMD exacerbation of depression using progestins may therefore benefit from a progestin free treatment for menopausal symptoms
1) Nevatte T et al Arch Womens Ment Health 2013 2) Bjoumlrn I et al Climacteric 2006 PMS premenstrual syndrome
PMDD premenstrual dysphoric disorder
Conclusion
bull CEEBAZO is an additional regimen for menopausal symptoms it provides also a prevention for osteoporosis
bull It is suitable for women with a uterus who are unsatisfied with an EPT regimen or who you are unwilling to treat with an EPT regimen
For some postmenopausal women with a uterus there is a
need for progestin free treatment options
bull with demonstrated clinical efficacy
bull which protects the endometrium
bull improved tolerabilitysafety profile
In clinical practice this translates to women who are
intolerant of progestin-containing HT or have conditions
which may be exacerbated by treatment with progestins
Conclusion Medical need for alternative treatment option
Medical condition which may be exacerbated by treatment with progestins
Depression
bull Progestin-containing HT has been associated with increases in depressive symptoms in some individuals1
bull There is a biochemicalphysiological plausibility for the association of progestins with depression234
bull Therefore postmenopausal women who also have a medical history of depressive disorders or depression could be inappropriate for treatment with progestin-containing HT
Pfizer Confidential
65
1) Girdler SS et al J Womens Health Gend Based Med 1999 2) Traish AM et al Korean J Urol 2014 3) Stroumlhle A et al Biol Psychiatry 1999 4) Romeo E et
al Am J Psychiatry 1998
History of the following conditions may make progestin inappropriate
bull Depression
bull PMSPMDD
PMS premenstrual syndrome
PMD premenstrual dysphoric disorder
Medical conditions that may be exacerbated by treatment with progestins
Women for whom progestin-containing HT
would not be considered appropriate
minus Women who are intolerant of progestin-containing hormone therapy
minus Women with pre-existing medical conditions that may be exacerbated by progestins
Most common adverse events leading to discontinuation are related to progestins12
breakthrough bleeding
bull Increase in the number of uterine procedures (ie unnecessary endometrial biopsies)
breast paintenderness
bull Increase in the number of breast interventions
1 Steel SA et al Climacteric 2003 2 Ettinger B and Pressman A Am J Manag Care 1999 3 Komm BS Mirkin S
Pharmaceuticals 2012
4 Panay N amp Studd JWW Human Reprod Update 1997
bull Nausea bull Depressive mood bull Poor concentration bull Hirsutism bull Headache bull Dizziness bull Fluid retention bull Weight gain
Other progestin-related intolerance issues4
Unmet need with the treatment of postmenopausal symptoms
bull Alternatives to progestin are needed that will protect the endometrium while avoiding other progestin-associated effects and preserving the desired effects of estrogens in postmenopausal women3
Which women with a uterus could benefit from
estrogens without the need for a progestin
bull Women who are intolerant of progestin-containing hormone therapy
bull Women with pre-existing medical conditions that may be exacerbated by progestins (eg women with a history of depression PMSPMDD increased breast density diabetes and metabolic syndrome)
History of the following conditions may make progestin inappropriate
bull Depression
bull PMSPMDD
bull High breast density
bull Diabetes and metabolic syndrome
PMS premenstrual syndrome
PMD premenstrual dysphoric disorder
Medical conditions that may be exacerbated by treatment with progestins
Learning from WHI data
bull Hormone therapy (HT) is the conventional and established therapy option to effectively treat postmenopausal symptoms however it has been associated with some safety and tolerability concerns1 2
bull A review of WHI data suggests that many of the concerns with menopausal HT more often associated with EPT (CE+MPA) such as CHD risk increased breast density breast pain and breast cancer risk than with ET (CEE alone)2
1 Rolnick SJ Kopher RA DeFor TA et al Menopause 2005
2 Komm BS Mirkin S Pharmaceuticals 2012
WHI Womenrsquos Health Initiative trial
CHD coronary heart disease
CEE conjugated equine estrogens
Efficacy and Safety of Constant Oestrogen
Pulsed Progestogen vs
Continuous Combined HRT
Adverse Events
17b-oestradiol 17b-oestradiol norgestimate NETA (n = 150) (n = 172) Breast discomfort 14 27 Abdominal discomfort 14 22 Uterine bleeding 15 12 Dysmenorrhea 3 8 Oedema 5 8
Adapted from S Rozenberg et al Human Reproduction 2000
Medical condition which may be exacerbated by treatment
with progestins
Increased breast density
bull Increases in breast density are associated with progestin-containing HT which may adversely affect radiological detection of breast cancer1 and may be independently associated with an increased risk for the development of breast cancer2
bull The Postmenopausal EstrogenProgestin Interventions (PEPI) trial demonstrated that an increased mammographic breast density was associated with the use of E+P but not with the use of estrogen alone3
bull Women who already have high breast density may therefore be considered inappropriate for treatment with a progestin-containing HT
1) EU Core SPC for Hormone Replacement Therapy Products (CMDh1312003 Rev 4 June
2012)
2) De Villiers TJ et al on behalf of the International Menopause Society Climacteric 2013 16
3) Greendale GA et al J Natl Cancer Inst 2003
Stroke
0 25 5 75 10 125
Fractures
Diabetes
Breast cancer
Cholecystitis
Venothrombotic episodes
Endometrial cancer
Lung cancer
Coronary heart disease
Colorectal cancer
Overall mortality
15 125 10 75 5 25
Benefits Risks
CE
CE MPA
Santen RJ et al J Clin Endocrinol Metab 2010
The basis of the Endocrine Society scientific statement for postmenopausal hormone replacement therapy (HRT) excess risks and benefits of HRT for 5 years in women aged 50ndash59 years or within 10 years of the start of menopause E=estrogen P=progestin
bull Younger women (aged 50ndash59 years) had more favorable results bull There are differences between CE alone and CEMPA arms bull Overall benefitrisk ratio of CE-alone appears to be more favourable than CEMPA
Reevaluation of WHI data (stratified by age) Risks and
Benefits of HRT Cases per 1000 Women per 5 Years of
Use
Medical condition which may be exacerbated by treatment
with progestins
Diabetes and metabolic syndrome
bull Treatment of oestrogen deficiency symptoms with progestin-containing HT (unlike oestrogen alone) may be associated with increases in insulin resistance and deterioration in glucose tolerance123
bull Postmenopausal women with diabetes could be inappropriate for treatment with progestin-containing HT due to the potential risk of exacerbation of their condition
1) Panay N amp Studd JWW Human Reprod Update 1997
2) Godsland I et al Metabolism 1993
3) Sites CK et al J Clin Endocrinol Metab 2005
Variations in Associated Breast Cancer
Risks Between CE alone and CEMPA
bull Use of CE alone for a median of 59 years was associated with a lower incidence of invasive breast cancer (151 cases 027 per year) compared with placebo (199 cases 035 per year HR 077 95 CI 062ndash095 P=002)
bull In the CE alone group fewer women died from invasive breast cancer (6 deaths 0009 per year) compared with controls (16 deaths 0024 per year HR 037 95 CI 013ndash091 P=003)
Anderson GL et al Lancet
Oncol 2012
Bazedoxifene (BZA) specifically selected in
combination with conjugated estrogens
bull BZA has been specifically selected for its unique pharmacologic profile and effects on VMS and uterine tissue in particular123
1 Crabtree J et al Mol Cell Endocrinol 2008
2 Kharode Y et al Endocrinolology 2008
3 Duavive SmPC
Estrogen Receptor activity is dimmed
Estrogen Receptor activity is turned on
CEs are agonists BZA is an antagonist
In the uterus
bull The BZA component reduces the risk of endometrial hyperplasia that can occur with the conjugated estrogens component alone3 This means that progestins are not needed
Extensive global clinical development program for
CEBZA
aIncludes additional pilot dose-finding study 203 1 Lobo RA et al Fertil Steril 2009 2 Pinkerton JV et al Menopause 2009 3 Kagan R et al Menopause 2010 4 Mirkin S et al Climacteric 2013 5 Pinkerton JV et al Obstet Gynecol 2013
Effects of conjugated estrogensbazedoxifene on
lipid and coagulation variables a randomized
placebo- and active-controlled trial
bull At 12 months
bull Both CEBZA doses were associated with small but significant effects on hemostasis variables including reductions in antithrombin plasminogen activator inhibitor-1 and fibrinogen activity and an increase in plasminogen activity relative to placebo at 12 months Incidences of cardiovascular and venous thromboembolic events were similar among treatment groups
bull CONCLUSIONS
bull This study provides reassurance that CEBZA does not adversely affect lipid metabolism or hemostatic balance In accordance the incidences of venous thromboembolic events and cardiovascular events in postmenopausal women are similar to those observed with placebo
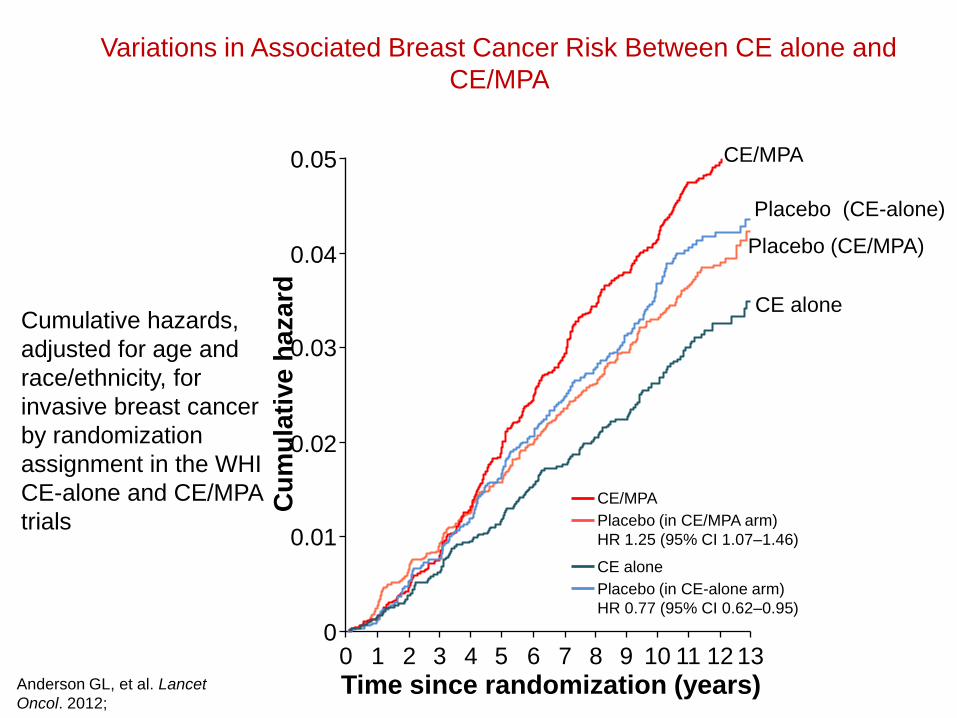
Variations in Associated Breast Cancer Risk Between CE alone and
CEMPA
Cumulative hazards
adjusted for age and
raceethnicity for
invasive breast cancer
by randomization
assignment in the WHI
CE-alone and CEMPA
trials
Anderson GL et al Lancet
Oncol 2012
0 0
1 2 3 4 5 6 7 8 9 10 11 12 13
001
002
003
004
005
Cu
mu
lati
ve
ha
za
rd
Time since randomization (years)
CEMPA
Placebo (in CEMPA arm)
HR 125 (95 CI 107ndash146)
CE alone
Placebo (in CE-alone arm)
HR 077 (95 CI 062ndash095)
CEMPA
CE alone
Placebo (CE-alone)
Placebo (CEMPA)
Estrogen only therapy
Endometrial cancer
Hysterectomy specimen showing cancer invading myometrium
following unopposed estrogen therapy for 15 years
Courtesy Dr David Sturdee
Bazedoxifene (BZA) specifically selected in
combination with conjugated estrogens
1 Crabtree J et al Mol Cell Endocrinol 2008
2 Kharode Y et al Endocrinolology 2008
3 Duavive SmPC
Estrogen Receptor activity is dimmed
Estrogen Receptor activity is turned on
CEs are agonists BZA is an antagonist
In the uterus
bull The BZA component reduces the risk of endometrial hyperplasia that can occur with the conjugated estrogens component alone1-3
bull This means that progestins are not needed
From the Womenrsquos Health Initiative to the combination
of estrogen and selective estrogen receptor
modulators to avoid progestin addition
bull Marie-Ceacutecile Valera Pierre Gourdy Florence Treacutemolliegraveres Jean-Franccedilois Arnal
bull Maturitas Volume 82 Issue 3 November 2015 Pages 274ndash277
bull
Other combinations of an estrogen (E2) + a SERM studied have
not produced favorable results
bull Objective To compare effects of 52 weeksrsquo treatment with either raloxifene 60 mgday alone (RLX) or in combination with 17B-estradiol 1 mgday (RLX + E2) on vasomotor symptoms (n = 83) and endometrial safety (n = 123) in postmenopausal women who transitioned from estrogen-progestin therapy Endometrial effect Women in the RLX + E2 group had significantly increased endometrial thickness at 52 weeks from baseline and RLX alone had no increase Two women (328) in the RLX + E2 group had endometrial hyperplasia (one with atypia) on the exit biopsy No one in RLX alone did
bull 1 Stovall D et al Menopause The Journal of The North American Menopause Society 2007
bull For the safety analyses data from women randomized before and after the protocol amendment were pooled which included 62 women in the raloxifene group and 61 women in the raloxifene + estrogen group
EFFICACY
VASOMOTOR
SYMPTOMS
SMART-2
DUAVIVE Efficacy for the Treatment of Moderate to
Severe VMS Associated With Menopause
14
1 Pinkerton JV et al Menopause 2009
Postmenopausal women
with a uterus
Age 42-64 year
(avg 53 yr)
(N=318)
DUAVIVE (CE 045BZA 20)
(n=127)
Placebo
(n=63)
bull 12-week randomized double-blind placebo-controlled study1
bull Inclusion criteria
‒ Postmenopausal women with an intact uterus
‒ Minimum of 7 moderate to severe hot flushes per day or at least 50 per week at screening
Change from baseline to
Weeks 4 and 12 in
bull Average daily number of
moderate to severe hot
flushes
bull Average daily severity
score of hot flushes
Primary End Points
Safety population (took at least one dose)
Significant Reduction vs Placebo in
Average Daily Number of Hot Flushes
DUAVEE [package insert] New York NY Pfizer Inc 2013
ANCOVA=analysis of covariance
Reduction in average daily number of
moderate to severe hot flushes ndash primary end point
Ad
jus
ted
mean
ch
an
ge
fro
m b
aselin
edagger
Week 4 Week 12
ndash31
ndash27
Treatment
differencedagger ndash59
ndash28
ndash76
ndash49
Treatment
differencedagger
22
Plt001 vs placebo daggerBased on data analysis using ANCOVA model Change from baseline = Treatment + Baseline + Site
DUAVIV
E
Reduction in the Observed Average Daily Number
of Moderate to Severe Hot Flushes
Data on file CSR-67461 Protocol 3115A1-305 Table 1511 Pfizer Inc New York NY
change from baseline to week 12
74 for DUAVIVE
51 for placebo
Observed Average Daily Number of Hot Flushes
Ob
serv
ed a
vera
ge d
aily
nu
mb
er o
f m
od
erat
e to
sev
ere
ho
t fl
ush
es
0 1 2 3 4 5 6 7 8 9 10 12 0 1
11
2
4 3
6 5
7 8 9
10
28
54
DUAVIVE (n=122) Placebo (n=62)
Weeks
Primary analysis showed statistically significant separation at weeks 4 and 12
Average daily number of hot flushes from baseline to week 12
103 to 28 for DUAVIVE
105 to 54 for placebo
Based on mathematical means
not statistically analyzed
105 103
Pinkerton JV et al Menopause 2009
Significant Reduction vs Placebo in
Average Daily Severity Score of Hot Flushes
17
Week 4 Week 12
ndash05
ndash06
Treatment
differencedagger
Treatment
differencedagger
DUAVEE [package insert] New York NY Pfizer Inc 2013
Reduction in average daily severity score of hot flushes ndash primary end point
Ad
jus
ted
me
an
ch
an
ge
fro
m b
aselin
edagger
Plt001 vs placebo daggerBased on data analysis using ANCOVA model Change from baseline = Treatment + Baseline + Site
DUAVIV
E
Reduction in the Observed Average
Daily Severity Score of Hot Flushes
Observed Average Daily Severity Score of Hot Flushes
19
DUAVIVE (n=122) Placebo (n=62)
Weeks
Ob
serv
ed a
vera
ge d
aily
sev
erit
y sc
ore
of
ho
t fl
ush
es
0
05
10
15
25
20
0 1 2 3 4 5 6 7 8 9 10 12 11 0 1 2 3 4 5 6 7 8 9 10 12 11
14
Data on file CSR-67461 Protocol 3115A1-305 Table 1511 Pfizer Inc New York NY
Primary analysis at weeks 4 and 12 prespecified secondary end points at all other weeks
change from baseline to week 12
39 for DUAVIVE
14 for placebo
Average daily severity score of hot flashes from baseline to week 12
23 to 14 for DUAVIVE
23 to 19 for Placebo
Based on mathematical means
not statistically analyzed
23
23
Pinkerton JV et al Menopause 2009
Effects on bone mineral density (BMD)
SMART 512
20
bull 12-month double-blind randomized placebo- and active-controlled study
bull Primary end point endometrial hyperplasia at 1 year
bull Secondary BMD changes at 1 year
1 DUAVEE [package insert] New York NY Pfizer Inc 2013 2 Pinkerton J Clin Endocrin Metab 2014
This study included a different dose of CEBZA and comparators The schematic shown here depicts only the patients who received the approved dose of DUAVIVE or placebo
Change from baseline in
bull Lumbar Spine BMD (Primary ndash BMD Substudy)
bull Total Hip BMD (Secondary ndash BMD Substudy)
BMD Analysis
DUAVIVE
(CE 045BZA 20)
(n=119)
Placebo
(n=139)
BMD Analysis
Postmenopausal women with a uterus
Less than 5 years since LMP
(N=590)
DUAVIVE Significantly Increased Lumbar Spine and Total
Hip BMD vs Placebo at 12 Months ndash Study 2
M
ean
ch
an
ge f
rom
baselin
e
Lumbar Spine Total Hip
121 151 Treatment
difference Treatment
difference
Data on file CSR-81040 Protocol 3115A1-3307 Pfizer Inc New York NY Pinkerton J Clin Endocrin Metab 2014 30
Plt001 vs placebo
Adjusted mean changes and P-values based on an ANCOVA model with treatment and region (US or non-US) as factors and baseline BMD value and years since menopause as covariates using the modified intention to treat population with last observation carried forward
DUAVIV
E
TOLERABILITY
AND SAFETY
Rates of BleedingSpotting and Amenorrhea
Similar to Rates with Placebo
bull High and similar cumulative rates of amenorrhea at year 1 among women treated with CE 045BZA 20 and placebo and was higher than seen in women treated with CE 045MPA 151
bull Noncumulative rates of spotting and bleedingspotting were similar among women treated with CEBZA or placebo and consistently higher in women treated with CE 045MPA 152
0
90
Cycle
100
Pe
rce
nta
ge
of
Su
bje
cts
80
70
60
50
40
30
20
10
88
54
Placebo
CE 045BZA 20 CE 045MPA 15
Percentage of subjects with cumulative amenorrhea during consecutive 4-week periods (cycles) in SMART-5
MPA medroxyprogesterone acetate Plt0001 vs all other treatment groups 1 Pinkerton JV et al J Clin Endocrinol Metab 2014 2 Data on file CSR-81040 Protocol 3115A1-3307 Pfizer Inc New York NY
Adverse Reactions in Placebo-
Controlled Trials Safety analyses have been conducted in 6210 postmenopausal women aged 40 to 75 years (mean age 55 years) following up to 2 years of treatment in SMART-1 -2 -3 and -5
Adverse reactions (incidence ge5) that were more common with DUAVIVE
Incidence of serious adverse reactions
35 with DUAVIVE 48 with placebo
DUAVEE [package insert] New York NY Pfizer Inc 2013
CE 045 BZA 20 (N=1224)
n ()
Placebo (N=1069)
n ()
Gastrointestinal disorders
Nausea 100 (8) 58 (5)
Diarrhea 96 (8) 57 (5)
Dyspepsia 84 (7) 59 (6)
Abdominal pain upper 81 (7) 58 (5)
Musculoskeletal and connective tissue disorders
Muscle spasms 110 (9) 63 (6)
Neck pain 62 (5) 46 (4)
Nervous system disorders
Dizziness 65 (5) 37 (3)
Respiratory thoracic and mediastinal disorders
Oropharyngeal pain 80 (7) 61 (6)
Venous Thromboembolism (VTE) in
DUAVIVE Clinical Studies
bull Estrogen agonistantagonists (including BZA a component of DUAVIVE) and estrogens individually are known to increase the risk of VTE
bull In the clinical studies with DUAVIVE the reporting rates for VTE were low in all treatment groups
bull Adverse reactions of VTE reported by patients
bull Should VTE event occur or be suspected DUAVIVE should be discontinued immediately
bull Due to the low rates of events in both groups it is not possible to conclude that the risk of VTE with DUAVIVE is different from that seen with other estrogen therapies
DUAVEE [package insert] New York NY Pfizer Inc 2013
00 for DUAVIVE (n=1224)
01 for placebo (n=1069)
26
Effects of conjugated estrogensbazedoxifene on
lipid and coagulation variables a randomized
placebo- and active-controlled trial
bull postmenopausal women (N = 1843) with menopausal
symptoms
bull Lipid (N = 1843) and coagulation (N = 590) variables were assessed in women receiving daily CE 045 mgBZA 20 mg CE 0625 mgBZA 20 mg BZA 20 mg CE 045 mgmedroxyprogesterone acetate (MPA) 15 mg or placebo for 12 months
bull Skouby SO et al Menopause 2015 Jun22(6)640-9
Effects of conjugated estrogensbazedoxifene on
lipid and coagulation variables a randomized
placebo- and active-controlled trial
bull At 12 months
bull CE 045 mgBZA 20 mg
bull CE 0625 mgBZA 20 mg
bull BZA 20 mg
bull and CE 045 mgMPA 15 mg decreased total cholesterol and LDL- cholesterol vs placebo (P lt 001 for all)
bull Both CEBZA doses and CEMPA increased high-density lipoprotein cholesterol compared with placebo (P lt 005 for all)
bull CE 045 mgBZA 20 mg had a neutral effect on triglycerides
bull CE 0625 mgBZA 20 mg and CEMPA increased triglycerides compared with placebo (P lt 005)
bull Skouby SO et al Menopause 2015 Jun22(6)640-9
Effects of conjugated estrogensbazedoxifene on
lipid and coagulation variables a randomized
placebo- and active-controlled trial
bull At 12 months
bull Both CEBZA doses were associated with small but significant effects on hemostasis variables including reductions in antithrombin plasminogen activator inhibitor-1 and fibrinogen activity and an increase in plasminogen activity relative to placebo at 12 months Incidences of cardiovascular and venous thromboembolic events were similar among treatment groups
Skouby SO et al Menopause 2015
Jun22(6)640-9
Endometrial hyperplasia or malignancy occurred in lt1 of women
following up to 1 year of treatment with CEBZA12
Study Cumulative Incidence at month 12 (nN)
CE 045BZA 20 Placebo
SMART-11 000 (0336) 000 (0313)
SMART-52 030 (1335) 028 (1354)
Effects on the Endometrium
1 Pickar JH et al Fertil Steril 2009 2 Pinkerton at al J Clin Endocrinol Metab 2014
Through the eyes of an amazone
Marie Mandy
Breast tolerability profile similar to placebo following up to 2 years of treatment with CEBZA12
Pooled analysis of SMART clinical trials
CE 045BZA 20 (n=1585)
Placebo (n=1241)
Breast cancer incidence up to 2 years
(per 1000 woman-years)
100 (CI 000-321)
140 (CI 000-417)
Incidence of reported breast paintenderness up to 12 weeks
98-115 81-112
Incidence of abnormal mammogram at month 12
258 316
Mean change in breast density at month 12 (SMART-5)
ndash038 (n=186)
ndash032 (n=182)
Effects on the Breast
1 Pickar JH et al Menopause 2013 2 Pinkerton JV et al Obstet Gynecol 2013
CEBZA clinical overview - summary
bull In clinical trials CEBZA has demonstrated safety and efficacy in postmenopausal women with a uterus including the following
bull Significant reduction in number and severity of moderate to severe hot flushes1
bull Incidence of cumulative amenorrhea rate similar to placebo and significantly better than CEMPA2
bull Incidence of endometrial hyperplasia and breast tendernessdensity similar to that with placebo345
bull Incidence of adverse events and discontinuation rates similar to that with placebo6
1 Pinkerton JV et al Menopause 2009 2 Pinkerton JV et al J Clin Endocrinol Metab2014 3 Pickar JH et al
Fertil Steril 2009 4 Pinkerton at al J Clin Endocrinol Metab 2014 5 Pickar JH et al Menopause 2013 6 DUAVEE [package insert] New York NY Pfizer Inc 2013
CEBZA clinical overview - summary
Now women with a uterus who choose hormone therapy for management of menopausal symptoms have a choice
bull conventional estrogen-progestogen therapy or
bull a new combinationhellipconjugated estrogens paired with the SERM bazedoxifene
1 Pinkerton JV et al Menopause 2009 2 Pinkerton JV et al J Clin Endocrinol Metab2014 3 Pickar JH et al Fertil Steril 2009 4 Pinkerton at al J Clin Endocrinol Metab 2014 5 Pickar JH et al Menopause 2013 6 DUAVEE [package insert] New York NY Pfizer Inc 2013
Conjugated EstrogensBazedoxifene (CEBZA)
US indication
bull DUAVEE is indicated in women with a uterus for
bull 11 Treatment of Moderate to Severe Vasomotor Symptoms Associated with Menopause
bull 12 Prevention of Postmenopausal Osteoporosis
bull 13 Important Limitations of Use
bull Use DUAVEE for the shortest duration consistent with treatment goals and risks for the individual woman Postmenopausal women should be re-evaluated periodically as clinically appropriate to determine if treatment is still necessary
bull When prescribing solely for the prevention of postmenopausal osteoporosis therapy should only be considered for women at significant risk of osteoporosis and non-estrogen medication should be carefully considered
Conjugated EstrogensBazedoxifene (CEBZA)
EU indication
CEBZA is indicated for
bull Treatment of oestrogen deficiency symptoms in postmenopausal women with a uterus (with at least 12 months since the last menses) for whom treatment with progestin-containing therapy is not appropriate
bull The experience treating women older than 65 years is limited
bull Dose CE (045mg)Bazedoxifene (20mg)
Duavive SmPC
Which women with a uterus
could benefit from estrogens
without the need for a
progestin
Progestin intolerance is one of the main
factors for reduced compliance
bull About 20 of women receiving progestin-containing HT have significant progestin intolerance and half of these experience serious effects that prevent treatment continuation1
1 Panay N amp Studd J Human Reprod Update 1997
2 Panay N et al on behalf of the British Menopause Society and Womenrsquos Health Concern Menopause Int 2013
bull The 2013 British Menopause Society amp Womenrsquos Health
Concern recommendations on hormone replacement
therapy do recognise progestin intolerance as one of the
main factors for reduced compliance with HT 2
Proportion of patients () with at least one bleeding episode in relation to time and to the
used HT
Serge Rozenberg et al Hum Reprod 2009241739-1747
copy The Author 2009 Published by Oxford University Press on behalf of the European Society of
Human Reproduction and Embryology All rights reserved For Permissions please email
journalspermissionsoxfordjournalsorg
Breast tenderness after initiation of CEE
CEE + MPA (WHI)
and mammographic density change
bullCrandall et al Breast Cancer Res Treat DOI 101007s10549-011-1803-9
Breast density
Conclusion
bull CEEBAZO is an additional regimen for menopausal symptoms it provides also a prevention for osteoporosis
bull It is suitable for women with a uterus who are unsatisfied with an EPT regimen or who you are unwilling to treat with an EPT regimen
Adapted use of MHT
bull Lower dosage of estrogens
bull Other progestins
bull Better safety profile
bull Vaginal estrogen or SERMS
bull Non-hormonal therapy
bull Development of new products
bull SERMS + estrogens
Most common adverse events leading to
discontinuation are related to progestins12
bull breakthrough bleeding
bull Low compliance
bull Increase in the number of US
bull Stress
bull Cost
bull uterine procedures
bull Unnecessary endometrial biopsies Hysteroscopies DampC Hysterectomies
bull Morbidity
Proportion of patients who completed or discontinued treatment in relation to the used HT
Serge Rozenberg et al Hum Reprod 2009241739-1747
copy The Author 2009 Published by Oxford University Press on behalf of the European Society of
Human Reproduction and Embryology All rights reserved For Permissions please email
journalspermissionsoxfordjournalsorg
Most common adverse events leading to discontinuation
are related to progestins
bull breast paintenderness
Breast tenderness after initiation of CEE
CEE + MPA (WHI)
and mammographic density change
bullCrandall et al Breast Cancer Res Treat DOI 101007s10549-011-1803-9
Breast density
Hormone therapy use and mammographic
density in postmenopausal Norwegian women
bull Results differed when considering the combined effect of age and BMI
bull The effect of EPT on mammographic density was modified by age and BMI with no apparent association among the youngest women (aged 50-55) with the highest BMI (BMI ge 26)
bull A higher mammographic density was found in EPT users compared to never HT users particularly in women using high-dose NETA regimens Age and BMI modified the association between EPT use and mammographic density
bull Couto E et al Breast Cancer Res Treat 2011 Nov 4 [Epub ahead of print]
Breast Cancer Risk by Breast Density
Menopause and Postmenopausal Hormone
Therapy Use
Birads age HT Duration Risk
1 55-59 None 5 year risk 08 (95 CI 06- 09)
1 55-59
ET EPT 5 year risk 09 (95 CI 07 -11)
4 55-59
None 5 year risk 24 (95 CI 20 -28)
4 55-59
ET 5 year risk
30 (95 CI 26 -35)
4 55-59
EPT 5 year risk
42 (95 CI 37 -46)
Adapted from Kerlikowske et al JOURNAL OF CLINICAL ONCOLOGY 2010
Breast Cancer Risk by Breast Density
Menopause and Postmenopausal Hormone
Therapy Use
Adapted from Kerlikowske et al JOURNAL OF CLINICAL ONCOLOGY 2010
bull Postmenopausal women with high breast density are at increased risk of breast cancer and should be aware of the added risk of taking HT especially estrogen plus progestin
Medical condition which may be exacerbated by treatment
with progestins
Diabetes and metabolic syndrome
bull progestin-containing HT may be associated with increases in insulin resistance and deterioration in glucose tolerance123
bull Postmenopausal women with diabetes could be inappropriate for treatment with progestin-containing HT due to the potential risk of exacerbation of their condition
1) Panay N amp Studd JWW Human Reprod Update 1997
2) Godsland I et al Metabolism 1993
3) Sites CK et al J Clin Endocrinol Metab 2005
A Nath and R Sitruk-Ware CLIMACTERIC 200912(Suppl 1)96ndash101
A Nath and R Sitruk-Ware CLIMACTERIC 200912(Suppl 1)96ndash101
Diabetes an epidemy
bull UK 1996 14 million of diabetics
bull UK 2015 32 million (6 of the population)
bull UK 2025 5 million
bull httpwwwdiabetescoukdiabetes-prevalencehtml
Other progestin-related intolerance issues
bull Nausea
bull Depressive mood
bull Poor concentration
bull Hirsutism
bull Headache
bull Dizziness
bull Fluid retention
bull Weight gain Panay N amp Studd JWW Human Reprod Update 1997
Medical condition which may be exacerbated by treatment with progestins
PMSPMDDdepression
bull Progesterone-induced PMD can be exacerbated by exogenous progestin administration and can occur in association with HT or OC administration1
bull Significantly higher negative mood scores have been observed during the addition of a progestin to an estrogen in a sequential HT regimen in postmenopausal women with a history of PMS compared to those without2
bull Women with a history of PMS or PMD exacerbation of depression using progestins may therefore benefit from a progestin free treatment for menopausal symptoms
1) Nevatte T et al Arch Womens Ment Health 2013 2) Bjoumlrn I et al Climacteric 2006 PMS premenstrual syndrome
PMDD premenstrual dysphoric disorder
Conclusion
bull CEEBAZO is an additional regimen for menopausal symptoms it provides also a prevention for osteoporosis
bull It is suitable for women with a uterus who are unsatisfied with an EPT regimen or who you are unwilling to treat with an EPT regimen
For some postmenopausal women with a uterus there is a
need for progestin free treatment options
bull with demonstrated clinical efficacy
bull which protects the endometrium
bull improved tolerabilitysafety profile
In clinical practice this translates to women who are
intolerant of progestin-containing HT or have conditions
which may be exacerbated by treatment with progestins
Conclusion Medical need for alternative treatment option
Medical condition which may be exacerbated by treatment with progestins
Depression
bull Progestin-containing HT has been associated with increases in depressive symptoms in some individuals1
bull There is a biochemicalphysiological plausibility for the association of progestins with depression234
bull Therefore postmenopausal women who also have a medical history of depressive disorders or depression could be inappropriate for treatment with progestin-containing HT
Pfizer Confidential
65
1) Girdler SS et al J Womens Health Gend Based Med 1999 2) Traish AM et al Korean J Urol 2014 3) Stroumlhle A et al Biol Psychiatry 1999 4) Romeo E et
al Am J Psychiatry 1998
History of the following conditions may make progestin inappropriate
bull Depression
bull PMSPMDD
PMS premenstrual syndrome
PMD premenstrual dysphoric disorder
Medical conditions that may be exacerbated by treatment with progestins
Women for whom progestin-containing HT
would not be considered appropriate
minus Women who are intolerant of progestin-containing hormone therapy
minus Women with pre-existing medical conditions that may be exacerbated by progestins
Most common adverse events leading to discontinuation are related to progestins12
breakthrough bleeding
bull Increase in the number of uterine procedures (ie unnecessary endometrial biopsies)
breast paintenderness
bull Increase in the number of breast interventions
1 Steel SA et al Climacteric 2003 2 Ettinger B and Pressman A Am J Manag Care 1999 3 Komm BS Mirkin S
Pharmaceuticals 2012
4 Panay N amp Studd JWW Human Reprod Update 1997
bull Nausea bull Depressive mood bull Poor concentration bull Hirsutism bull Headache bull Dizziness bull Fluid retention bull Weight gain
Other progestin-related intolerance issues4
Unmet need with the treatment of postmenopausal symptoms
bull Alternatives to progestin are needed that will protect the endometrium while avoiding other progestin-associated effects and preserving the desired effects of estrogens in postmenopausal women3
Which women with a uterus could benefit from
estrogens without the need for a progestin
bull Women who are intolerant of progestin-containing hormone therapy
bull Women with pre-existing medical conditions that may be exacerbated by progestins (eg women with a history of depression PMSPMDD increased breast density diabetes and metabolic syndrome)
History of the following conditions may make progestin inappropriate
bull Depression
bull PMSPMDD
bull High breast density
bull Diabetes and metabolic syndrome
PMS premenstrual syndrome
PMD premenstrual dysphoric disorder
Medical conditions that may be exacerbated by treatment with progestins
Learning from WHI data
bull Hormone therapy (HT) is the conventional and established therapy option to effectively treat postmenopausal symptoms however it has been associated with some safety and tolerability concerns1 2
bull A review of WHI data suggests that many of the concerns with menopausal HT more often associated with EPT (CE+MPA) such as CHD risk increased breast density breast pain and breast cancer risk than with ET (CEE alone)2
1 Rolnick SJ Kopher RA DeFor TA et al Menopause 2005
2 Komm BS Mirkin S Pharmaceuticals 2012
WHI Womenrsquos Health Initiative trial
CHD coronary heart disease
CEE conjugated equine estrogens
Efficacy and Safety of Constant Oestrogen
Pulsed Progestogen vs
Continuous Combined HRT
Adverse Events
17b-oestradiol 17b-oestradiol norgestimate NETA (n = 150) (n = 172) Breast discomfort 14 27 Abdominal discomfort 14 22 Uterine bleeding 15 12 Dysmenorrhea 3 8 Oedema 5 8
Adapted from S Rozenberg et al Human Reproduction 2000
Medical condition which may be exacerbated by treatment
with progestins
Increased breast density
bull Increases in breast density are associated with progestin-containing HT which may adversely affect radiological detection of breast cancer1 and may be independently associated with an increased risk for the development of breast cancer2
bull The Postmenopausal EstrogenProgestin Interventions (PEPI) trial demonstrated that an increased mammographic breast density was associated with the use of E+P but not with the use of estrogen alone3
bull Women who already have high breast density may therefore be considered inappropriate for treatment with a progestin-containing HT
1) EU Core SPC for Hormone Replacement Therapy Products (CMDh1312003 Rev 4 June
2012)
2) De Villiers TJ et al on behalf of the International Menopause Society Climacteric 2013 16
3) Greendale GA et al J Natl Cancer Inst 2003
Stroke
0 25 5 75 10 125
Fractures
Diabetes
Breast cancer
Cholecystitis
Venothrombotic episodes
Endometrial cancer
Lung cancer
Coronary heart disease
Colorectal cancer
Overall mortality
15 125 10 75 5 25
Benefits Risks
CE
CE MPA
Santen RJ et al J Clin Endocrinol Metab 2010
The basis of the Endocrine Society scientific statement for postmenopausal hormone replacement therapy (HRT) excess risks and benefits of HRT for 5 years in women aged 50ndash59 years or within 10 years of the start of menopause E=estrogen P=progestin
bull Younger women (aged 50ndash59 years) had more favorable results bull There are differences between CE alone and CEMPA arms bull Overall benefitrisk ratio of CE-alone appears to be more favourable than CEMPA
Reevaluation of WHI data (stratified by age) Risks and
Benefits of HRT Cases per 1000 Women per 5 Years of
Use
Medical condition which may be exacerbated by treatment
with progestins
Diabetes and metabolic syndrome
bull Treatment of oestrogen deficiency symptoms with progestin-containing HT (unlike oestrogen alone) may be associated with increases in insulin resistance and deterioration in glucose tolerance123
bull Postmenopausal women with diabetes could be inappropriate for treatment with progestin-containing HT due to the potential risk of exacerbation of their condition
1) Panay N amp Studd JWW Human Reprod Update 1997
2) Godsland I et al Metabolism 1993
3) Sites CK et al J Clin Endocrinol Metab 2005
Variations in Associated Breast Cancer
Risks Between CE alone and CEMPA
bull Use of CE alone for a median of 59 years was associated with a lower incidence of invasive breast cancer (151 cases 027 per year) compared with placebo (199 cases 035 per year HR 077 95 CI 062ndash095 P=002)
bull In the CE alone group fewer women died from invasive breast cancer (6 deaths 0009 per year) compared with controls (16 deaths 0024 per year HR 037 95 CI 013ndash091 P=003)
Anderson GL et al Lancet
Oncol 2012
Bazedoxifene (BZA) specifically selected in
combination with conjugated estrogens
bull BZA has been specifically selected for its unique pharmacologic profile and effects on VMS and uterine tissue in particular123
1 Crabtree J et al Mol Cell Endocrinol 2008
2 Kharode Y et al Endocrinolology 2008
3 Duavive SmPC
Estrogen Receptor activity is dimmed
Estrogen Receptor activity is turned on
CEs are agonists BZA is an antagonist
In the uterus
bull The BZA component reduces the risk of endometrial hyperplasia that can occur with the conjugated estrogens component alone3 This means that progestins are not needed
Extensive global clinical development program for
CEBZA
aIncludes additional pilot dose-finding study 203 1 Lobo RA et al Fertil Steril 2009 2 Pinkerton JV et al Menopause 2009 3 Kagan R et al Menopause 2010 4 Mirkin S et al Climacteric 2013 5 Pinkerton JV et al Obstet Gynecol 2013
Effects of conjugated estrogensbazedoxifene on
lipid and coagulation variables a randomized
placebo- and active-controlled trial
bull At 12 months
bull Both CEBZA doses were associated with small but significant effects on hemostasis variables including reductions in antithrombin plasminogen activator inhibitor-1 and fibrinogen activity and an increase in plasminogen activity relative to placebo at 12 months Incidences of cardiovascular and venous thromboembolic events were similar among treatment groups
bull CONCLUSIONS
bull This study provides reassurance that CEBZA does not adversely affect lipid metabolism or hemostatic balance In accordance the incidences of venous thromboembolic events and cardiovascular events in postmenopausal women are similar to those observed with placebo
Estrogen only therapy
Endometrial cancer
Hysterectomy specimen showing cancer invading myometrium
following unopposed estrogen therapy for 15 years
Courtesy Dr David Sturdee
Bazedoxifene (BZA) specifically selected in
combination with conjugated estrogens
1 Crabtree J et al Mol Cell Endocrinol 2008
2 Kharode Y et al Endocrinolology 2008
3 Duavive SmPC
Estrogen Receptor activity is dimmed
Estrogen Receptor activity is turned on
CEs are agonists BZA is an antagonist
In the uterus
bull The BZA component reduces the risk of endometrial hyperplasia that can occur with the conjugated estrogens component alone1-3
bull This means that progestins are not needed
From the Womenrsquos Health Initiative to the combination
of estrogen and selective estrogen receptor
modulators to avoid progestin addition
bull Marie-Ceacutecile Valera Pierre Gourdy Florence Treacutemolliegraveres Jean-Franccedilois Arnal
bull Maturitas Volume 82 Issue 3 November 2015 Pages 274ndash277
bull
Other combinations of an estrogen (E2) + a SERM studied have
not produced favorable results
bull Objective To compare effects of 52 weeksrsquo treatment with either raloxifene 60 mgday alone (RLX) or in combination with 17B-estradiol 1 mgday (RLX + E2) on vasomotor symptoms (n = 83) and endometrial safety (n = 123) in postmenopausal women who transitioned from estrogen-progestin therapy Endometrial effect Women in the RLX + E2 group had significantly increased endometrial thickness at 52 weeks from baseline and RLX alone had no increase Two women (328) in the RLX + E2 group had endometrial hyperplasia (one with atypia) on the exit biopsy No one in RLX alone did
bull 1 Stovall D et al Menopause The Journal of The North American Menopause Society 2007
bull For the safety analyses data from women randomized before and after the protocol amendment were pooled which included 62 women in the raloxifene group and 61 women in the raloxifene + estrogen group
EFFICACY
VASOMOTOR
SYMPTOMS
SMART-2
DUAVIVE Efficacy for the Treatment of Moderate to
Severe VMS Associated With Menopause
14
1 Pinkerton JV et al Menopause 2009
Postmenopausal women
with a uterus
Age 42-64 year
(avg 53 yr)
(N=318)
DUAVIVE (CE 045BZA 20)
(n=127)
Placebo
(n=63)
bull 12-week randomized double-blind placebo-controlled study1
bull Inclusion criteria
‒ Postmenopausal women with an intact uterus
‒ Minimum of 7 moderate to severe hot flushes per day or at least 50 per week at screening
Change from baseline to
Weeks 4 and 12 in
bull Average daily number of
moderate to severe hot
flushes
bull Average daily severity
score of hot flushes
Primary End Points
Safety population (took at least one dose)
Significant Reduction vs Placebo in
Average Daily Number of Hot Flushes
DUAVEE [package insert] New York NY Pfizer Inc 2013
ANCOVA=analysis of covariance
Reduction in average daily number of
moderate to severe hot flushes ndash primary end point
Ad
jus
ted
mean
ch
an
ge
fro
m b
aselin
edagger
Week 4 Week 12
ndash31
ndash27
Treatment
differencedagger ndash59
ndash28
ndash76
ndash49
Treatment
differencedagger
22
Plt001 vs placebo daggerBased on data analysis using ANCOVA model Change from baseline = Treatment + Baseline + Site
DUAVIV
E
Reduction in the Observed Average Daily Number
of Moderate to Severe Hot Flushes
Data on file CSR-67461 Protocol 3115A1-305 Table 1511 Pfizer Inc New York NY
change from baseline to week 12
74 for DUAVIVE
51 for placebo
Observed Average Daily Number of Hot Flushes
Ob
serv
ed a
vera
ge d
aily
nu
mb
er o
f m
od
erat
e to
sev
ere
ho
t fl
ush
es
0 1 2 3 4 5 6 7 8 9 10 12 0 1
11
2
4 3
6 5
7 8 9
10
28
54
DUAVIVE (n=122) Placebo (n=62)
Weeks
Primary analysis showed statistically significant separation at weeks 4 and 12
Average daily number of hot flushes from baseline to week 12
103 to 28 for DUAVIVE
105 to 54 for placebo
Based on mathematical means
not statistically analyzed
105 103
Pinkerton JV et al Menopause 2009
Significant Reduction vs Placebo in
Average Daily Severity Score of Hot Flushes
17
Week 4 Week 12
ndash05
ndash06
Treatment
differencedagger
Treatment
differencedagger
DUAVEE [package insert] New York NY Pfizer Inc 2013
Reduction in average daily severity score of hot flushes ndash primary end point
Ad
jus
ted
me
an
ch
an
ge
fro
m b
aselin
edagger
Plt001 vs placebo daggerBased on data analysis using ANCOVA model Change from baseline = Treatment + Baseline + Site
DUAVIV
E
Reduction in the Observed Average
Daily Severity Score of Hot Flushes
Observed Average Daily Severity Score of Hot Flushes
19
DUAVIVE (n=122) Placebo (n=62)
Weeks
Ob
serv
ed a
vera
ge d
aily
sev
erit
y sc
ore
of
ho
t fl
ush
es
0
05
10
15
25
20
0 1 2 3 4 5 6 7 8 9 10 12 11 0 1 2 3 4 5 6 7 8 9 10 12 11
14
Data on file CSR-67461 Protocol 3115A1-305 Table 1511 Pfizer Inc New York NY
Primary analysis at weeks 4 and 12 prespecified secondary end points at all other weeks
change from baseline to week 12
39 for DUAVIVE
14 for placebo
Average daily severity score of hot flashes from baseline to week 12
23 to 14 for DUAVIVE
23 to 19 for Placebo
Based on mathematical means
not statistically analyzed
23
23
Pinkerton JV et al Menopause 2009
Effects on bone mineral density (BMD)
SMART 512
20
bull 12-month double-blind randomized placebo- and active-controlled study
bull Primary end point endometrial hyperplasia at 1 year
bull Secondary BMD changes at 1 year
1 DUAVEE [package insert] New York NY Pfizer Inc 2013 2 Pinkerton J Clin Endocrin Metab 2014
This study included a different dose of CEBZA and comparators The schematic shown here depicts only the patients who received the approved dose of DUAVIVE or placebo
Change from baseline in
bull Lumbar Spine BMD (Primary ndash BMD Substudy)
bull Total Hip BMD (Secondary ndash BMD Substudy)
BMD Analysis
DUAVIVE
(CE 045BZA 20)
(n=119)
Placebo
(n=139)
BMD Analysis
Postmenopausal women with a uterus
Less than 5 years since LMP
(N=590)
DUAVIVE Significantly Increased Lumbar Spine and Total
Hip BMD vs Placebo at 12 Months ndash Study 2
M
ean
ch
an
ge f
rom
baselin
e
Lumbar Spine Total Hip
121 151 Treatment
difference Treatment
difference
Data on file CSR-81040 Protocol 3115A1-3307 Pfizer Inc New York NY Pinkerton J Clin Endocrin Metab 2014 30
Plt001 vs placebo
Adjusted mean changes and P-values based on an ANCOVA model with treatment and region (US or non-US) as factors and baseline BMD value and years since menopause as covariates using the modified intention to treat population with last observation carried forward
DUAVIV
E
TOLERABILITY
AND SAFETY
Rates of BleedingSpotting and Amenorrhea
Similar to Rates with Placebo
bull High and similar cumulative rates of amenorrhea at year 1 among women treated with CE 045BZA 20 and placebo and was higher than seen in women treated with CE 045MPA 151
bull Noncumulative rates of spotting and bleedingspotting were similar among women treated with CEBZA or placebo and consistently higher in women treated with CE 045MPA 152
0
90
Cycle
100
Pe
rce
nta
ge
of
Su
bje
cts
80
70
60
50
40
30
20
10
88
54
Placebo
CE 045BZA 20 CE 045MPA 15
Percentage of subjects with cumulative amenorrhea during consecutive 4-week periods (cycles) in SMART-5
MPA medroxyprogesterone acetate Plt0001 vs all other treatment groups 1 Pinkerton JV et al J Clin Endocrinol Metab 2014 2 Data on file CSR-81040 Protocol 3115A1-3307 Pfizer Inc New York NY
Adverse Reactions in Placebo-
Controlled Trials Safety analyses have been conducted in 6210 postmenopausal women aged 40 to 75 years (mean age 55 years) following up to 2 years of treatment in SMART-1 -2 -3 and -5
Adverse reactions (incidence ge5) that were more common with DUAVIVE
Incidence of serious adverse reactions
35 with DUAVIVE 48 with placebo
DUAVEE [package insert] New York NY Pfizer Inc 2013
CE 045 BZA 20 (N=1224)
n ()
Placebo (N=1069)
n ()
Gastrointestinal disorders
Nausea 100 (8) 58 (5)
Diarrhea 96 (8) 57 (5)
Dyspepsia 84 (7) 59 (6)
Abdominal pain upper 81 (7) 58 (5)
Musculoskeletal and connective tissue disorders
Muscle spasms 110 (9) 63 (6)
Neck pain 62 (5) 46 (4)
Nervous system disorders
Dizziness 65 (5) 37 (3)
Respiratory thoracic and mediastinal disorders
Oropharyngeal pain 80 (7) 61 (6)
Venous Thromboembolism (VTE) in
DUAVIVE Clinical Studies
bull Estrogen agonistantagonists (including BZA a component of DUAVIVE) and estrogens individually are known to increase the risk of VTE
bull In the clinical studies with DUAVIVE the reporting rates for VTE were low in all treatment groups
bull Adverse reactions of VTE reported by patients
bull Should VTE event occur or be suspected DUAVIVE should be discontinued immediately
bull Due to the low rates of events in both groups it is not possible to conclude that the risk of VTE with DUAVIVE is different from that seen with other estrogen therapies
DUAVEE [package insert] New York NY Pfizer Inc 2013
00 for DUAVIVE (n=1224)
01 for placebo (n=1069)
26
Effects of conjugated estrogensbazedoxifene on
lipid and coagulation variables a randomized
placebo- and active-controlled trial
bull postmenopausal women (N = 1843) with menopausal
symptoms
bull Lipid (N = 1843) and coagulation (N = 590) variables were assessed in women receiving daily CE 045 mgBZA 20 mg CE 0625 mgBZA 20 mg BZA 20 mg CE 045 mgmedroxyprogesterone acetate (MPA) 15 mg or placebo for 12 months
bull Skouby SO et al Menopause 2015 Jun22(6)640-9
Effects of conjugated estrogensbazedoxifene on
lipid and coagulation variables a randomized
placebo- and active-controlled trial
bull At 12 months
bull CE 045 mgBZA 20 mg
bull CE 0625 mgBZA 20 mg
bull BZA 20 mg
bull and CE 045 mgMPA 15 mg decreased total cholesterol and LDL- cholesterol vs placebo (P lt 001 for all)
bull Both CEBZA doses and CEMPA increased high-density lipoprotein cholesterol compared with placebo (P lt 005 for all)
bull CE 045 mgBZA 20 mg had a neutral effect on triglycerides
bull CE 0625 mgBZA 20 mg and CEMPA increased triglycerides compared with placebo (P lt 005)
bull Skouby SO et al Menopause 2015 Jun22(6)640-9
Effects of conjugated estrogensbazedoxifene on
lipid and coagulation variables a randomized
placebo- and active-controlled trial
bull At 12 months
bull Both CEBZA doses were associated with small but significant effects on hemostasis variables including reductions in antithrombin plasminogen activator inhibitor-1 and fibrinogen activity and an increase in plasminogen activity relative to placebo at 12 months Incidences of cardiovascular and venous thromboembolic events were similar among treatment groups
Skouby SO et al Menopause 2015
Jun22(6)640-9
Endometrial hyperplasia or malignancy occurred in lt1 of women
following up to 1 year of treatment with CEBZA12
Study Cumulative Incidence at month 12 (nN)
CE 045BZA 20 Placebo
SMART-11 000 (0336) 000 (0313)
SMART-52 030 (1335) 028 (1354)
Effects on the Endometrium
1 Pickar JH et al Fertil Steril 2009 2 Pinkerton at al J Clin Endocrinol Metab 2014
Through the eyes of an amazone
Marie Mandy
Breast tolerability profile similar to placebo following up to 2 years of treatment with CEBZA12
Pooled analysis of SMART clinical trials
CE 045BZA 20 (n=1585)
Placebo (n=1241)
Breast cancer incidence up to 2 years
(per 1000 woman-years)
100 (CI 000-321)
140 (CI 000-417)
Incidence of reported breast paintenderness up to 12 weeks
98-115 81-112
Incidence of abnormal mammogram at month 12
258 316
Mean change in breast density at month 12 (SMART-5)
ndash038 (n=186)
ndash032 (n=182)
Effects on the Breast
1 Pickar JH et al Menopause 2013 2 Pinkerton JV et al Obstet Gynecol 2013
CEBZA clinical overview - summary
bull In clinical trials CEBZA has demonstrated safety and efficacy in postmenopausal women with a uterus including the following
bull Significant reduction in number and severity of moderate to severe hot flushes1
bull Incidence of cumulative amenorrhea rate similar to placebo and significantly better than CEMPA2
bull Incidence of endometrial hyperplasia and breast tendernessdensity similar to that with placebo345
bull Incidence of adverse events and discontinuation rates similar to that with placebo6
1 Pinkerton JV et al Menopause 2009 2 Pinkerton JV et al J Clin Endocrinol Metab2014 3 Pickar JH et al
Fertil Steril 2009 4 Pinkerton at al J Clin Endocrinol Metab 2014 5 Pickar JH et al Menopause 2013 6 DUAVEE [package insert] New York NY Pfizer Inc 2013
CEBZA clinical overview - summary
Now women with a uterus who choose hormone therapy for management of menopausal symptoms have a choice
bull conventional estrogen-progestogen therapy or
bull a new combinationhellipconjugated estrogens paired with the SERM bazedoxifene
1 Pinkerton JV et al Menopause 2009 2 Pinkerton JV et al J Clin Endocrinol Metab2014 3 Pickar JH et al Fertil Steril 2009 4 Pinkerton at al J Clin Endocrinol Metab 2014 5 Pickar JH et al Menopause 2013 6 DUAVEE [package insert] New York NY Pfizer Inc 2013
Conjugated EstrogensBazedoxifene (CEBZA)
US indication
bull DUAVEE is indicated in women with a uterus for
bull 11 Treatment of Moderate to Severe Vasomotor Symptoms Associated with Menopause
bull 12 Prevention of Postmenopausal Osteoporosis
bull 13 Important Limitations of Use
bull Use DUAVEE for the shortest duration consistent with treatment goals and risks for the individual woman Postmenopausal women should be re-evaluated periodically as clinically appropriate to determine if treatment is still necessary
bull When prescribing solely for the prevention of postmenopausal osteoporosis therapy should only be considered for women at significant risk of osteoporosis and non-estrogen medication should be carefully considered
Conjugated EstrogensBazedoxifene (CEBZA)
EU indication
CEBZA is indicated for
bull Treatment of oestrogen deficiency symptoms in postmenopausal women with a uterus (with at least 12 months since the last menses) for whom treatment with progestin-containing therapy is not appropriate
bull The experience treating women older than 65 years is limited
bull Dose CE (045mg)Bazedoxifene (20mg)
Duavive SmPC
Which women with a uterus
could benefit from estrogens
without the need for a
progestin
Progestin intolerance is one of the main
factors for reduced compliance
bull About 20 of women receiving progestin-containing HT have significant progestin intolerance and half of these experience serious effects that prevent treatment continuation1
1 Panay N amp Studd J Human Reprod Update 1997
2 Panay N et al on behalf of the British Menopause Society and Womenrsquos Health Concern Menopause Int 2013
bull The 2013 British Menopause Society amp Womenrsquos Health
Concern recommendations on hormone replacement
therapy do recognise progestin intolerance as one of the
main factors for reduced compliance with HT 2
Proportion of patients () with at least one bleeding episode in relation to time and to the
used HT
Serge Rozenberg et al Hum Reprod 2009241739-1747
copy The Author 2009 Published by Oxford University Press on behalf of the European Society of
Human Reproduction and Embryology All rights reserved For Permissions please email
journalspermissionsoxfordjournalsorg
Breast tenderness after initiation of CEE
CEE + MPA (WHI)
and mammographic density change
bullCrandall et al Breast Cancer Res Treat DOI 101007s10549-011-1803-9
Breast density
Conclusion
bull CEEBAZO is an additional regimen for menopausal symptoms it provides also a prevention for osteoporosis
bull It is suitable for women with a uterus who are unsatisfied with an EPT regimen or who you are unwilling to treat with an EPT regimen
Adapted use of MHT
bull Lower dosage of estrogens
bull Other progestins
bull Better safety profile
bull Vaginal estrogen or SERMS
bull Non-hormonal therapy
bull Development of new products
bull SERMS + estrogens
Most common adverse events leading to
discontinuation are related to progestins12
bull breakthrough bleeding
bull Low compliance
bull Increase in the number of US
bull Stress
bull Cost
bull uterine procedures
bull Unnecessary endometrial biopsies Hysteroscopies DampC Hysterectomies
bull Morbidity
Proportion of patients who completed or discontinued treatment in relation to the used HT
Serge Rozenberg et al Hum Reprod 2009241739-1747
copy The Author 2009 Published by Oxford University Press on behalf of the European Society of
Human Reproduction and Embryology All rights reserved For Permissions please email
journalspermissionsoxfordjournalsorg
Most common adverse events leading to discontinuation
are related to progestins
bull breast paintenderness
Breast tenderness after initiation of CEE
CEE + MPA (WHI)
and mammographic density change
bullCrandall et al Breast Cancer Res Treat DOI 101007s10549-011-1803-9
Breast density
Hormone therapy use and mammographic
density in postmenopausal Norwegian women
bull Results differed when considering the combined effect of age and BMI
bull The effect of EPT on mammographic density was modified by age and BMI with no apparent association among the youngest women (aged 50-55) with the highest BMI (BMI ge 26)
bull A higher mammographic density was found in EPT users compared to never HT users particularly in women using high-dose NETA regimens Age and BMI modified the association between EPT use and mammographic density
bull Couto E et al Breast Cancer Res Treat 2011 Nov 4 [Epub ahead of print]
Breast Cancer Risk by Breast Density
Menopause and Postmenopausal Hormone
Therapy Use
Birads age HT Duration Risk
1 55-59 None 5 year risk 08 (95 CI 06- 09)
1 55-59
ET EPT 5 year risk 09 (95 CI 07 -11)
4 55-59
None 5 year risk 24 (95 CI 20 -28)
4 55-59
ET 5 year risk
30 (95 CI 26 -35)
4 55-59
EPT 5 year risk
42 (95 CI 37 -46)
Adapted from Kerlikowske et al JOURNAL OF CLINICAL ONCOLOGY 2010
Breast Cancer Risk by Breast Density
Menopause and Postmenopausal Hormone
Therapy Use
Adapted from Kerlikowske et al JOURNAL OF CLINICAL ONCOLOGY 2010
bull Postmenopausal women with high breast density are at increased risk of breast cancer and should be aware of the added risk of taking HT especially estrogen plus progestin
Medical condition which may be exacerbated by treatment
with progestins
Diabetes and metabolic syndrome
bull progestin-containing HT may be associated with increases in insulin resistance and deterioration in glucose tolerance123
bull Postmenopausal women with diabetes could be inappropriate for treatment with progestin-containing HT due to the potential risk of exacerbation of their condition
1) Panay N amp Studd JWW Human Reprod Update 1997
2) Godsland I et al Metabolism 1993
3) Sites CK et al J Clin Endocrinol Metab 2005
A Nath and R Sitruk-Ware CLIMACTERIC 200912(Suppl 1)96ndash101
A Nath and R Sitruk-Ware CLIMACTERIC 200912(Suppl 1)96ndash101
Diabetes an epidemy
bull UK 1996 14 million of diabetics
bull UK 2015 32 million (6 of the population)
bull UK 2025 5 million
bull httpwwwdiabetescoukdiabetes-prevalencehtml
Other progestin-related intolerance issues
bull Nausea
bull Depressive mood
bull Poor concentration
bull Hirsutism
bull Headache
bull Dizziness
bull Fluid retention
bull Weight gain Panay N amp Studd JWW Human Reprod Update 1997
Medical condition which may be exacerbated by treatment with progestins
PMSPMDDdepression
bull Progesterone-induced PMD can be exacerbated by exogenous progestin administration and can occur in association with HT or OC administration1
bull Significantly higher negative mood scores have been observed during the addition of a progestin to an estrogen in a sequential HT regimen in postmenopausal women with a history of PMS compared to those without2
bull Women with a history of PMS or PMD exacerbation of depression using progestins may therefore benefit from a progestin free treatment for menopausal symptoms
1) Nevatte T et al Arch Womens Ment Health 2013 2) Bjoumlrn I et al Climacteric 2006 PMS premenstrual syndrome
PMDD premenstrual dysphoric disorder
Conclusion
bull CEEBAZO is an additional regimen for menopausal symptoms it provides also a prevention for osteoporosis
bull It is suitable for women with a uterus who are unsatisfied with an EPT regimen or who you are unwilling to treat with an EPT regimen
For some postmenopausal women with a uterus there is a
need for progestin free treatment options
bull with demonstrated clinical efficacy
bull which protects the endometrium
bull improved tolerabilitysafety profile
In clinical practice this translates to women who are
intolerant of progestin-containing HT or have conditions
which may be exacerbated by treatment with progestins
Conclusion Medical need for alternative treatment option
Medical condition which may be exacerbated by treatment with progestins
Depression
bull Progestin-containing HT has been associated with increases in depressive symptoms in some individuals1
bull There is a biochemicalphysiological plausibility for the association of progestins with depression234
bull Therefore postmenopausal women who also have a medical history of depressive disorders or depression could be inappropriate for treatment with progestin-containing HT
Pfizer Confidential
65
1) Girdler SS et al J Womens Health Gend Based Med 1999 2) Traish AM et al Korean J Urol 2014 3) Stroumlhle A et al Biol Psychiatry 1999 4) Romeo E et
al Am J Psychiatry 1998
History of the following conditions may make progestin inappropriate
bull Depression
bull PMSPMDD
PMS premenstrual syndrome
PMD premenstrual dysphoric disorder
Medical conditions that may be exacerbated by treatment with progestins
Women for whom progestin-containing HT
would not be considered appropriate
minus Women who are intolerant of progestin-containing hormone therapy
minus Women with pre-existing medical conditions that may be exacerbated by progestins
Most common adverse events leading to discontinuation are related to progestins12
breakthrough bleeding
bull Increase in the number of uterine procedures (ie unnecessary endometrial biopsies)
breast paintenderness
bull Increase in the number of breast interventions
1 Steel SA et al Climacteric 2003 2 Ettinger B and Pressman A Am J Manag Care 1999 3 Komm BS Mirkin S
Pharmaceuticals 2012
4 Panay N amp Studd JWW Human Reprod Update 1997
bull Nausea bull Depressive mood bull Poor concentration bull Hirsutism bull Headache bull Dizziness bull Fluid retention bull Weight gain
Other progestin-related intolerance issues4
Unmet need with the treatment of postmenopausal symptoms
bull Alternatives to progestin are needed that will protect the endometrium while avoiding other progestin-associated effects and preserving the desired effects of estrogens in postmenopausal women3
Which women with a uterus could benefit from
estrogens without the need for a progestin
bull Women who are intolerant of progestin-containing hormone therapy
bull Women with pre-existing medical conditions that may be exacerbated by progestins (eg women with a history of depression PMSPMDD increased breast density diabetes and metabolic syndrome)
History of the following conditions may make progestin inappropriate
bull Depression
bull PMSPMDD
bull High breast density
bull Diabetes and metabolic syndrome
PMS premenstrual syndrome
PMD premenstrual dysphoric disorder
Medical conditions that may be exacerbated by treatment with progestins
Learning from WHI data
bull Hormone therapy (HT) is the conventional and established therapy option to effectively treat postmenopausal symptoms however it has been associated with some safety and tolerability concerns1 2
bull A review of WHI data suggests that many of the concerns with menopausal HT more often associated with EPT (CE+MPA) such as CHD risk increased breast density breast pain and breast cancer risk than with ET (CEE alone)2
1 Rolnick SJ Kopher RA DeFor TA et al Menopause 2005
2 Komm BS Mirkin S Pharmaceuticals 2012
WHI Womenrsquos Health Initiative trial
CHD coronary heart disease
CEE conjugated equine estrogens
Efficacy and Safety of Constant Oestrogen
Pulsed Progestogen vs
Continuous Combined HRT
Adverse Events
17b-oestradiol 17b-oestradiol norgestimate NETA (n = 150) (n = 172) Breast discomfort 14 27 Abdominal discomfort 14 22 Uterine bleeding 15 12 Dysmenorrhea 3 8 Oedema 5 8
Adapted from S Rozenberg et al Human Reproduction 2000
Medical condition which may be exacerbated by treatment
with progestins
Increased breast density
bull Increases in breast density are associated with progestin-containing HT which may adversely affect radiological detection of breast cancer1 and may be independently associated with an increased risk for the development of breast cancer2
bull The Postmenopausal EstrogenProgestin Interventions (PEPI) trial demonstrated that an increased mammographic breast density was associated with the use of E+P but not with the use of estrogen alone3
bull Women who already have high breast density may therefore be considered inappropriate for treatment with a progestin-containing HT
1) EU Core SPC for Hormone Replacement Therapy Products (CMDh1312003 Rev 4 June
2012)
2) De Villiers TJ et al on behalf of the International Menopause Society Climacteric 2013 16
3) Greendale GA et al J Natl Cancer Inst 2003
Stroke
0 25 5 75 10 125
Fractures
Diabetes
Breast cancer
Cholecystitis
Venothrombotic episodes
Endometrial cancer
Lung cancer
Coronary heart disease
Colorectal cancer
Overall mortality
15 125 10 75 5 25
Benefits Risks
CE
CE MPA
Santen RJ et al J Clin Endocrinol Metab 2010
The basis of the Endocrine Society scientific statement for postmenopausal hormone replacement therapy (HRT) excess risks and benefits of HRT for 5 years in women aged 50ndash59 years or within 10 years of the start of menopause E=estrogen P=progestin
bull Younger women (aged 50ndash59 years) had more favorable results bull There are differences between CE alone and CEMPA arms bull Overall benefitrisk ratio of CE-alone appears to be more favourable than CEMPA
Reevaluation of WHI data (stratified by age) Risks and
Benefits of HRT Cases per 1000 Women per 5 Years of
Use
Medical condition which may be exacerbated by treatment
with progestins
Diabetes and metabolic syndrome
bull Treatment of oestrogen deficiency symptoms with progestin-containing HT (unlike oestrogen alone) may be associated with increases in insulin resistance and deterioration in glucose tolerance123
bull Postmenopausal women with diabetes could be inappropriate for treatment with progestin-containing HT due to the potential risk of exacerbation of their condition
1) Panay N amp Studd JWW Human Reprod Update 1997
2) Godsland I et al Metabolism 1993
3) Sites CK et al J Clin Endocrinol Metab 2005
Variations in Associated Breast Cancer
Risks Between CE alone and CEMPA
bull Use of CE alone for a median of 59 years was associated with a lower incidence of invasive breast cancer (151 cases 027 per year) compared with placebo (199 cases 035 per year HR 077 95 CI 062ndash095 P=002)
bull In the CE alone group fewer women died from invasive breast cancer (6 deaths 0009 per year) compared with controls (16 deaths 0024 per year HR 037 95 CI 013ndash091 P=003)
Anderson GL et al Lancet
Oncol 2012
Bazedoxifene (BZA) specifically selected in
combination with conjugated estrogens
bull BZA has been specifically selected for its unique pharmacologic profile and effects on VMS and uterine tissue in particular123
1 Crabtree J et al Mol Cell Endocrinol 2008
2 Kharode Y et al Endocrinolology 2008
3 Duavive SmPC
Estrogen Receptor activity is dimmed
Estrogen Receptor activity is turned on
CEs are agonists BZA is an antagonist
In the uterus
bull The BZA component reduces the risk of endometrial hyperplasia that can occur with the conjugated estrogens component alone3 This means that progestins are not needed
Extensive global clinical development program for
CEBZA
aIncludes additional pilot dose-finding study 203 1 Lobo RA et al Fertil Steril 2009 2 Pinkerton JV et al Menopause 2009 3 Kagan R et al Menopause 2010 4 Mirkin S et al Climacteric 2013 5 Pinkerton JV et al Obstet Gynecol 2013
Effects of conjugated estrogensbazedoxifene on
lipid and coagulation variables a randomized
placebo- and active-controlled trial
bull At 12 months
bull Both CEBZA doses were associated with small but significant effects on hemostasis variables including reductions in antithrombin plasminogen activator inhibitor-1 and fibrinogen activity and an increase in plasminogen activity relative to placebo at 12 months Incidences of cardiovascular and venous thromboembolic events were similar among treatment groups
bull CONCLUSIONS
bull This study provides reassurance that CEBZA does not adversely affect lipid metabolism or hemostatic balance In accordance the incidences of venous thromboembolic events and cardiovascular events in postmenopausal women are similar to those observed with placebo
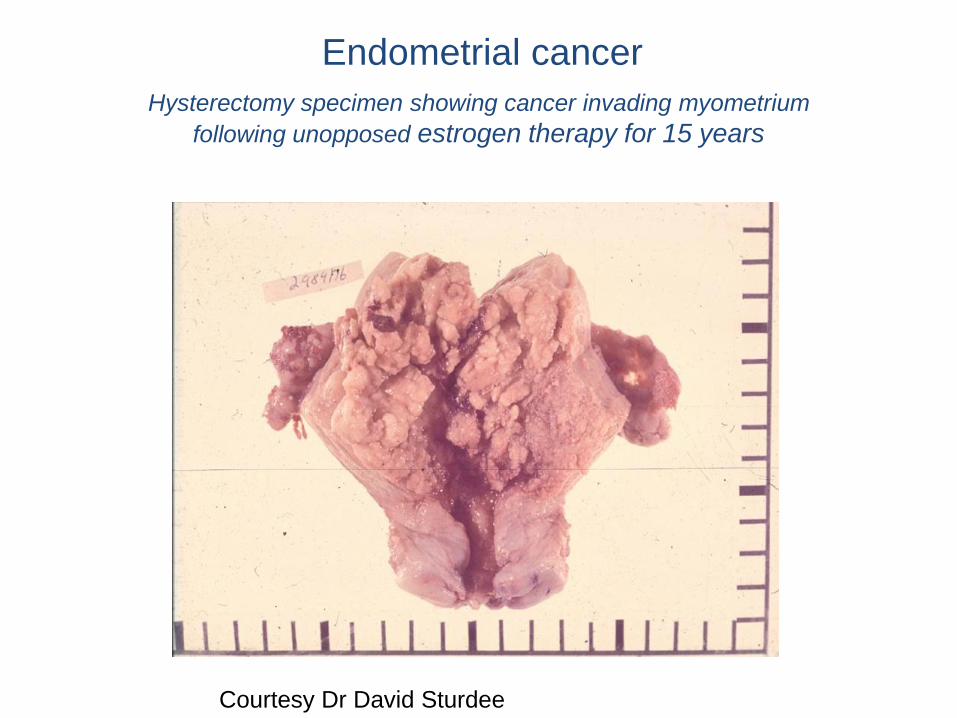
Endometrial cancer
Hysterectomy specimen showing cancer invading myometrium
following unopposed estrogen therapy for 15 years
Courtesy Dr David Sturdee
Bazedoxifene (BZA) specifically selected in
combination with conjugated estrogens
1 Crabtree J et al Mol Cell Endocrinol 2008
2 Kharode Y et al Endocrinolology 2008
3 Duavive SmPC
Estrogen Receptor activity is dimmed
Estrogen Receptor activity is turned on
CEs are agonists BZA is an antagonist
In the uterus
bull The BZA component reduces the risk of endometrial hyperplasia that can occur with the conjugated estrogens component alone1-3
bull This means that progestins are not needed
From the Womenrsquos Health Initiative to the combination
of estrogen and selective estrogen receptor
modulators to avoid progestin addition
bull Marie-Ceacutecile Valera Pierre Gourdy Florence Treacutemolliegraveres Jean-Franccedilois Arnal
bull Maturitas Volume 82 Issue 3 November 2015 Pages 274ndash277
bull
Other combinations of an estrogen (E2) + a SERM studied have
not produced favorable results
bull Objective To compare effects of 52 weeksrsquo treatment with either raloxifene 60 mgday alone (RLX) or in combination with 17B-estradiol 1 mgday (RLX + E2) on vasomotor symptoms (n = 83) and endometrial safety (n = 123) in postmenopausal women who transitioned from estrogen-progestin therapy Endometrial effect Women in the RLX + E2 group had significantly increased endometrial thickness at 52 weeks from baseline and RLX alone had no increase Two women (328) in the RLX + E2 group had endometrial hyperplasia (one with atypia) on the exit biopsy No one in RLX alone did
bull 1 Stovall D et al Menopause The Journal of The North American Menopause Society 2007
bull For the safety analyses data from women randomized before and after the protocol amendment were pooled which included 62 women in the raloxifene group and 61 women in the raloxifene + estrogen group
EFFICACY
VASOMOTOR
SYMPTOMS
SMART-2
DUAVIVE Efficacy for the Treatment of Moderate to
Severe VMS Associated With Menopause
14
1 Pinkerton JV et al Menopause 2009
Postmenopausal women
with a uterus
Age 42-64 year
(avg 53 yr)
(N=318)
DUAVIVE (CE 045BZA 20)
(n=127)
Placebo
(n=63)
bull 12-week randomized double-blind placebo-controlled study1
bull Inclusion criteria
‒ Postmenopausal women with an intact uterus
‒ Minimum of 7 moderate to severe hot flushes per day or at least 50 per week at screening
Change from baseline to
Weeks 4 and 12 in
bull Average daily number of
moderate to severe hot
flushes
bull Average daily severity
score of hot flushes
Primary End Points
Safety population (took at least one dose)
Significant Reduction vs Placebo in
Average Daily Number of Hot Flushes
DUAVEE [package insert] New York NY Pfizer Inc 2013
ANCOVA=analysis of covariance
Reduction in average daily number of
moderate to severe hot flushes ndash primary end point
Ad
jus
ted
mean
ch
an
ge
fro
m b
aselin
edagger
Week 4 Week 12
ndash31
ndash27
Treatment
differencedagger ndash59
ndash28
ndash76
ndash49
Treatment
differencedagger
22
Plt001 vs placebo daggerBased on data analysis using ANCOVA model Change from baseline = Treatment + Baseline + Site
DUAVIV
E
Reduction in the Observed Average Daily Number
of Moderate to Severe Hot Flushes
Data on file CSR-67461 Protocol 3115A1-305 Table 1511 Pfizer Inc New York NY
change from baseline to week 12
74 for DUAVIVE
51 for placebo
Observed Average Daily Number of Hot Flushes
Ob
serv
ed a
vera
ge d
aily
nu
mb
er o
f m
od
erat
e to
sev
ere
ho
t fl
ush
es
0 1 2 3 4 5 6 7 8 9 10 12 0 1
11
2
4 3
6 5
7 8 9
10
28
54
DUAVIVE (n=122) Placebo (n=62)
Weeks
Primary analysis showed statistically significant separation at weeks 4 and 12
Average daily number of hot flushes from baseline to week 12
103 to 28 for DUAVIVE
105 to 54 for placebo
Based on mathematical means
not statistically analyzed
105 103
Pinkerton JV et al Menopause 2009
Significant Reduction vs Placebo in
Average Daily Severity Score of Hot Flushes
17
Week 4 Week 12
ndash05
ndash06
Treatment
differencedagger
Treatment
differencedagger
DUAVEE [package insert] New York NY Pfizer Inc 2013
Reduction in average daily severity score of hot flushes ndash primary end point
Ad
jus
ted
me
an
ch
an
ge
fro
m b
aselin
edagger
Plt001 vs placebo daggerBased on data analysis using ANCOVA model Change from baseline = Treatment + Baseline + Site
DUAVIV
E
Reduction in the Observed Average
Daily Severity Score of Hot Flushes
Observed Average Daily Severity Score of Hot Flushes
19
DUAVIVE (n=122) Placebo (n=62)
Weeks
Ob
serv
ed a
vera
ge d
aily
sev
erit
y sc
ore
of
ho
t fl
ush
es
0
05
10
15
25
20
0 1 2 3 4 5 6 7 8 9 10 12 11 0 1 2 3 4 5 6 7 8 9 10 12 11
14
Data on file CSR-67461 Protocol 3115A1-305 Table 1511 Pfizer Inc New York NY
Primary analysis at weeks 4 and 12 prespecified secondary end points at all other weeks
change from baseline to week 12
39 for DUAVIVE
14 for placebo
Average daily severity score of hot flashes from baseline to week 12
23 to 14 for DUAVIVE
23 to 19 for Placebo
Based on mathematical means
not statistically analyzed
23
23
Pinkerton JV et al Menopause 2009
Effects on bone mineral density (BMD)
SMART 512
20
bull 12-month double-blind randomized placebo- and active-controlled study
bull Primary end point endometrial hyperplasia at 1 year
bull Secondary BMD changes at 1 year
1 DUAVEE [package insert] New York NY Pfizer Inc 2013 2 Pinkerton J Clin Endocrin Metab 2014
This study included a different dose of CEBZA and comparators The schematic shown here depicts only the patients who received the approved dose of DUAVIVE or placebo
Change from baseline in
bull Lumbar Spine BMD (Primary ndash BMD Substudy)
bull Total Hip BMD (Secondary ndash BMD Substudy)
BMD Analysis
DUAVIVE
(CE 045BZA 20)
(n=119)
Placebo
(n=139)
BMD Analysis
Postmenopausal women with a uterus
Less than 5 years since LMP
(N=590)
DUAVIVE Significantly Increased Lumbar Spine and Total
Hip BMD vs Placebo at 12 Months ndash Study 2
M
ean
ch
an
ge f
rom
baselin
e
Lumbar Spine Total Hip
121 151 Treatment
difference Treatment
difference
Data on file CSR-81040 Protocol 3115A1-3307 Pfizer Inc New York NY Pinkerton J Clin Endocrin Metab 2014 30
Plt001 vs placebo
Adjusted mean changes and P-values based on an ANCOVA model with treatment and region (US or non-US) as factors and baseline BMD value and years since menopause as covariates using the modified intention to treat population with last observation carried forward
DUAVIV
E
TOLERABILITY
AND SAFETY
Rates of BleedingSpotting and Amenorrhea
Similar to Rates with Placebo
bull High and similar cumulative rates of amenorrhea at year 1 among women treated with CE 045BZA 20 and placebo and was higher than seen in women treated with CE 045MPA 151
bull Noncumulative rates of spotting and bleedingspotting were similar among women treated with CEBZA or placebo and consistently higher in women treated with CE 045MPA 152
0
90
Cycle
100
Pe
rce
nta
ge
of
Su
bje
cts
80
70
60
50
40
30
20
10
88
54
Placebo
CE 045BZA 20 CE 045MPA 15
Percentage of subjects with cumulative amenorrhea during consecutive 4-week periods (cycles) in SMART-5
MPA medroxyprogesterone acetate Plt0001 vs all other treatment groups 1 Pinkerton JV et al J Clin Endocrinol Metab 2014 2 Data on file CSR-81040 Protocol 3115A1-3307 Pfizer Inc New York NY
Adverse Reactions in Placebo-
Controlled Trials Safety analyses have been conducted in 6210 postmenopausal women aged 40 to 75 years (mean age 55 years) following up to 2 years of treatment in SMART-1 -2 -3 and -5
Adverse reactions (incidence ge5) that were more common with DUAVIVE
Incidence of serious adverse reactions
35 with DUAVIVE 48 with placebo
DUAVEE [package insert] New York NY Pfizer Inc 2013
CE 045 BZA 20 (N=1224)
n ()
Placebo (N=1069)
n ()
Gastrointestinal disorders
Nausea 100 (8) 58 (5)
Diarrhea 96 (8) 57 (5)
Dyspepsia 84 (7) 59 (6)
Abdominal pain upper 81 (7) 58 (5)
Musculoskeletal and connective tissue disorders
Muscle spasms 110 (9) 63 (6)
Neck pain 62 (5) 46 (4)
Nervous system disorders
Dizziness 65 (5) 37 (3)
Respiratory thoracic and mediastinal disorders
Oropharyngeal pain 80 (7) 61 (6)
Venous Thromboembolism (VTE) in
DUAVIVE Clinical Studies
bull Estrogen agonistantagonists (including BZA a component of DUAVIVE) and estrogens individually are known to increase the risk of VTE
bull In the clinical studies with DUAVIVE the reporting rates for VTE were low in all treatment groups
bull Adverse reactions of VTE reported by patients
bull Should VTE event occur or be suspected DUAVIVE should be discontinued immediately
bull Due to the low rates of events in both groups it is not possible to conclude that the risk of VTE with DUAVIVE is different from that seen with other estrogen therapies
DUAVEE [package insert] New York NY Pfizer Inc 2013
00 for DUAVIVE (n=1224)
01 for placebo (n=1069)
26
Effects of conjugated estrogensbazedoxifene on
lipid and coagulation variables a randomized
placebo- and active-controlled trial
bull postmenopausal women (N = 1843) with menopausal
symptoms
bull Lipid (N = 1843) and coagulation (N = 590) variables were assessed in women receiving daily CE 045 mgBZA 20 mg CE 0625 mgBZA 20 mg BZA 20 mg CE 045 mgmedroxyprogesterone acetate (MPA) 15 mg or placebo for 12 months
bull Skouby SO et al Menopause 2015 Jun22(6)640-9
Effects of conjugated estrogensbazedoxifene on
lipid and coagulation variables a randomized
placebo- and active-controlled trial
bull At 12 months
bull CE 045 mgBZA 20 mg
bull CE 0625 mgBZA 20 mg
bull BZA 20 mg
bull and CE 045 mgMPA 15 mg decreased total cholesterol and LDL- cholesterol vs placebo (P lt 001 for all)
bull Both CEBZA doses and CEMPA increased high-density lipoprotein cholesterol compared with placebo (P lt 005 for all)
bull CE 045 mgBZA 20 mg had a neutral effect on triglycerides
bull CE 0625 mgBZA 20 mg and CEMPA increased triglycerides compared with placebo (P lt 005)
bull Skouby SO et al Menopause 2015 Jun22(6)640-9
Effects of conjugated estrogensbazedoxifene on
lipid and coagulation variables a randomized
placebo- and active-controlled trial
bull At 12 months
bull Both CEBZA doses were associated with small but significant effects on hemostasis variables including reductions in antithrombin plasminogen activator inhibitor-1 and fibrinogen activity and an increase in plasminogen activity relative to placebo at 12 months Incidences of cardiovascular and venous thromboembolic events were similar among treatment groups
Skouby SO et al Menopause 2015
Jun22(6)640-9
Endometrial hyperplasia or malignancy occurred in lt1 of women
following up to 1 year of treatment with CEBZA12
Study Cumulative Incidence at month 12 (nN)
CE 045BZA 20 Placebo
SMART-11 000 (0336) 000 (0313)
SMART-52 030 (1335) 028 (1354)
Effects on the Endometrium
1 Pickar JH et al Fertil Steril 2009 2 Pinkerton at al J Clin Endocrinol Metab 2014
Through the eyes of an amazone
Marie Mandy
Breast tolerability profile similar to placebo following up to 2 years of treatment with CEBZA12
Pooled analysis of SMART clinical trials
CE 045BZA 20 (n=1585)
Placebo (n=1241)
Breast cancer incidence up to 2 years
(per 1000 woman-years)
100 (CI 000-321)
140 (CI 000-417)
Incidence of reported breast paintenderness up to 12 weeks
98-115 81-112
Incidence of abnormal mammogram at month 12
258 316
Mean change in breast density at month 12 (SMART-5)
ndash038 (n=186)
ndash032 (n=182)
Effects on the Breast
1 Pickar JH et al Menopause 2013 2 Pinkerton JV et al Obstet Gynecol 2013
CEBZA clinical overview - summary
bull In clinical trials CEBZA has demonstrated safety and efficacy in postmenopausal women with a uterus including the following
bull Significant reduction in number and severity of moderate to severe hot flushes1
bull Incidence of cumulative amenorrhea rate similar to placebo and significantly better than CEMPA2
bull Incidence of endometrial hyperplasia and breast tendernessdensity similar to that with placebo345
bull Incidence of adverse events and discontinuation rates similar to that with placebo6
1 Pinkerton JV et al Menopause 2009 2 Pinkerton JV et al J Clin Endocrinol Metab2014 3 Pickar JH et al
Fertil Steril 2009 4 Pinkerton at al J Clin Endocrinol Metab 2014 5 Pickar JH et al Menopause 2013 6 DUAVEE [package insert] New York NY Pfizer Inc 2013
CEBZA clinical overview - summary
Now women with a uterus who choose hormone therapy for management of menopausal symptoms have a choice
bull conventional estrogen-progestogen therapy or
bull a new combinationhellipconjugated estrogens paired with the SERM bazedoxifene
1 Pinkerton JV et al Menopause 2009 2 Pinkerton JV et al J Clin Endocrinol Metab2014 3 Pickar JH et al Fertil Steril 2009 4 Pinkerton at al J Clin Endocrinol Metab 2014 5 Pickar JH et al Menopause 2013 6 DUAVEE [package insert] New York NY Pfizer Inc 2013
Conjugated EstrogensBazedoxifene (CEBZA)
US indication
bull DUAVEE is indicated in women with a uterus for
bull 11 Treatment of Moderate to Severe Vasomotor Symptoms Associated with Menopause
bull 12 Prevention of Postmenopausal Osteoporosis
bull 13 Important Limitations of Use
bull Use DUAVEE for the shortest duration consistent with treatment goals and risks for the individual woman Postmenopausal women should be re-evaluated periodically as clinically appropriate to determine if treatment is still necessary
bull When prescribing solely for the prevention of postmenopausal osteoporosis therapy should only be considered for women at significant risk of osteoporosis and non-estrogen medication should be carefully considered
Conjugated EstrogensBazedoxifene (CEBZA)
EU indication
CEBZA is indicated for
bull Treatment of oestrogen deficiency symptoms in postmenopausal women with a uterus (with at least 12 months since the last menses) for whom treatment with progestin-containing therapy is not appropriate
bull The experience treating women older than 65 years is limited
bull Dose CE (045mg)Bazedoxifene (20mg)
Duavive SmPC
Which women with a uterus
could benefit from estrogens
without the need for a
progestin
Progestin intolerance is one of the main
factors for reduced compliance
bull About 20 of women receiving progestin-containing HT have significant progestin intolerance and half of these experience serious effects that prevent treatment continuation1
1 Panay N amp Studd J Human Reprod Update 1997
2 Panay N et al on behalf of the British Menopause Society and Womenrsquos Health Concern Menopause Int 2013
bull The 2013 British Menopause Society amp Womenrsquos Health
Concern recommendations on hormone replacement
therapy do recognise progestin intolerance as one of the
main factors for reduced compliance with HT 2
Proportion of patients () with at least one bleeding episode in relation to time and to the
used HT
Serge Rozenberg et al Hum Reprod 2009241739-1747
copy The Author 2009 Published by Oxford University Press on behalf of the European Society of
Human Reproduction and Embryology All rights reserved For Permissions please email
journalspermissionsoxfordjournalsorg
Breast tenderness after initiation of CEE
CEE + MPA (WHI)
and mammographic density change
bullCrandall et al Breast Cancer Res Treat DOI 101007s10549-011-1803-9
Breast density
Conclusion
bull CEEBAZO is an additional regimen for menopausal symptoms it provides also a prevention for osteoporosis
bull It is suitable for women with a uterus who are unsatisfied with an EPT regimen or who you are unwilling to treat with an EPT regimen
Adapted use of MHT
bull Lower dosage of estrogens
bull Other progestins
bull Better safety profile
bull Vaginal estrogen or SERMS
bull Non-hormonal therapy
bull Development of new products
bull SERMS + estrogens
Most common adverse events leading to
discontinuation are related to progestins12
bull breakthrough bleeding
bull Low compliance
bull Increase in the number of US
bull Stress
bull Cost
bull uterine procedures
bull Unnecessary endometrial biopsies Hysteroscopies DampC Hysterectomies
bull Morbidity
Proportion of patients who completed or discontinued treatment in relation to the used HT
Serge Rozenberg et al Hum Reprod 2009241739-1747
copy The Author 2009 Published by Oxford University Press on behalf of the European Society of
Human Reproduction and Embryology All rights reserved For Permissions please email
journalspermissionsoxfordjournalsorg
Most common adverse events leading to discontinuation
are related to progestins
bull breast paintenderness
Breast tenderness after initiation of CEE
CEE + MPA (WHI)
and mammographic density change
bullCrandall et al Breast Cancer Res Treat DOI 101007s10549-011-1803-9
Breast density
Hormone therapy use and mammographic
density in postmenopausal Norwegian women
bull Results differed when considering the combined effect of age and BMI
bull The effect of EPT on mammographic density was modified by age and BMI with no apparent association among the youngest women (aged 50-55) with the highest BMI (BMI ge 26)
bull A higher mammographic density was found in EPT users compared to never HT users particularly in women using high-dose NETA regimens Age and BMI modified the association between EPT use and mammographic density
bull Couto E et al Breast Cancer Res Treat 2011 Nov 4 [Epub ahead of print]
Breast Cancer Risk by Breast Density
Menopause and Postmenopausal Hormone
Therapy Use
Birads age HT Duration Risk
1 55-59 None 5 year risk 08 (95 CI 06- 09)
1 55-59
ET EPT 5 year risk 09 (95 CI 07 -11)
4 55-59
None 5 year risk 24 (95 CI 20 -28)
4 55-59
ET 5 year risk
30 (95 CI 26 -35)
4 55-59
EPT 5 year risk
42 (95 CI 37 -46)
Adapted from Kerlikowske et al JOURNAL OF CLINICAL ONCOLOGY 2010
Breast Cancer Risk by Breast Density
Menopause and Postmenopausal Hormone
Therapy Use
Adapted from Kerlikowske et al JOURNAL OF CLINICAL ONCOLOGY 2010
bull Postmenopausal women with high breast density are at increased risk of breast cancer and should be aware of the added risk of taking HT especially estrogen plus progestin
Medical condition which may be exacerbated by treatment
with progestins
Diabetes and metabolic syndrome
bull progestin-containing HT may be associated with increases in insulin resistance and deterioration in glucose tolerance123
bull Postmenopausal women with diabetes could be inappropriate for treatment with progestin-containing HT due to the potential risk of exacerbation of their condition
1) Panay N amp Studd JWW Human Reprod Update 1997
2) Godsland I et al Metabolism 1993
3) Sites CK et al J Clin Endocrinol Metab 2005
A Nath and R Sitruk-Ware CLIMACTERIC 200912(Suppl 1)96ndash101
A Nath and R Sitruk-Ware CLIMACTERIC 200912(Suppl 1)96ndash101
Diabetes an epidemy
bull UK 1996 14 million of diabetics
bull UK 2015 32 million (6 of the population)
bull UK 2025 5 million
bull httpwwwdiabetescoukdiabetes-prevalencehtml
Other progestin-related intolerance issues
bull Nausea
bull Depressive mood
bull Poor concentration
bull Hirsutism
bull Headache
bull Dizziness
bull Fluid retention
bull Weight gain Panay N amp Studd JWW Human Reprod Update 1997
Medical condition which may be exacerbated by treatment with progestins
PMSPMDDdepression
bull Progesterone-induced PMD can be exacerbated by exogenous progestin administration and can occur in association with HT or OC administration1
bull Significantly higher negative mood scores have been observed during the addition of a progestin to an estrogen in a sequential HT regimen in postmenopausal women with a history of PMS compared to those without2
bull Women with a history of PMS or PMD exacerbation of depression using progestins may therefore benefit from a progestin free treatment for menopausal symptoms
1) Nevatte T et al Arch Womens Ment Health 2013 2) Bjoumlrn I et al Climacteric 2006 PMS premenstrual syndrome
PMDD premenstrual dysphoric disorder
Conclusion
bull CEEBAZO is an additional regimen for menopausal symptoms it provides also a prevention for osteoporosis
bull It is suitable for women with a uterus who are unsatisfied with an EPT regimen or who you are unwilling to treat with an EPT regimen
For some postmenopausal women with a uterus there is a
need for progestin free treatment options
bull with demonstrated clinical efficacy
bull which protects the endometrium
bull improved tolerabilitysafety profile
In clinical practice this translates to women who are
intolerant of progestin-containing HT or have conditions
which may be exacerbated by treatment with progestins
Conclusion Medical need for alternative treatment option
Medical condition which may be exacerbated by treatment with progestins
Depression
bull Progestin-containing HT has been associated with increases in depressive symptoms in some individuals1
bull There is a biochemicalphysiological plausibility for the association of progestins with depression234
bull Therefore postmenopausal women who also have a medical history of depressive disorders or depression could be inappropriate for treatment with progestin-containing HT
Pfizer Confidential
65
1) Girdler SS et al J Womens Health Gend Based Med 1999 2) Traish AM et al Korean J Urol 2014 3) Stroumlhle A et al Biol Psychiatry 1999 4) Romeo E et
al Am J Psychiatry 1998
History of the following conditions may make progestin inappropriate
bull Depression
bull PMSPMDD
PMS premenstrual syndrome
PMD premenstrual dysphoric disorder
Medical conditions that may be exacerbated by treatment with progestins
Women for whom progestin-containing HT
would not be considered appropriate
minus Women who are intolerant of progestin-containing hormone therapy
minus Women with pre-existing medical conditions that may be exacerbated by progestins
Most common adverse events leading to discontinuation are related to progestins12
breakthrough bleeding
bull Increase in the number of uterine procedures (ie unnecessary endometrial biopsies)
breast paintenderness
bull Increase in the number of breast interventions
1 Steel SA et al Climacteric 2003 2 Ettinger B and Pressman A Am J Manag Care 1999 3 Komm BS Mirkin S
Pharmaceuticals 2012
4 Panay N amp Studd JWW Human Reprod Update 1997
bull Nausea bull Depressive mood bull Poor concentration bull Hirsutism bull Headache bull Dizziness bull Fluid retention bull Weight gain
Other progestin-related intolerance issues4
Unmet need with the treatment of postmenopausal symptoms
bull Alternatives to progestin are needed that will protect the endometrium while avoiding other progestin-associated effects and preserving the desired effects of estrogens in postmenopausal women3
Which women with a uterus could benefit from
estrogens without the need for a progestin
bull Women who are intolerant of progestin-containing hormone therapy
bull Women with pre-existing medical conditions that may be exacerbated by progestins (eg women with a history of depression PMSPMDD increased breast density diabetes and metabolic syndrome)
History of the following conditions may make progestin inappropriate
bull Depression
bull PMSPMDD
bull High breast density
bull Diabetes and metabolic syndrome
PMS premenstrual syndrome
PMD premenstrual dysphoric disorder
Medical conditions that may be exacerbated by treatment with progestins
Learning from WHI data
bull Hormone therapy (HT) is the conventional and established therapy option to effectively treat postmenopausal symptoms however it has been associated with some safety and tolerability concerns1 2
bull A review of WHI data suggests that many of the concerns with menopausal HT more often associated with EPT (CE+MPA) such as CHD risk increased breast density breast pain and breast cancer risk than with ET (CEE alone)2
1 Rolnick SJ Kopher RA DeFor TA et al Menopause 2005
2 Komm BS Mirkin S Pharmaceuticals 2012
WHI Womenrsquos Health Initiative trial
CHD coronary heart disease
CEE conjugated equine estrogens
Efficacy and Safety of Constant Oestrogen
Pulsed Progestogen vs
Continuous Combined HRT
Adverse Events
17b-oestradiol 17b-oestradiol norgestimate NETA (n = 150) (n = 172) Breast discomfort 14 27 Abdominal discomfort 14 22 Uterine bleeding 15 12 Dysmenorrhea 3 8 Oedema 5 8
Adapted from S Rozenberg et al Human Reproduction 2000
Medical condition which may be exacerbated by treatment
with progestins
Increased breast density
bull Increases in breast density are associated with progestin-containing HT which may adversely affect radiological detection of breast cancer1 and may be independently associated with an increased risk for the development of breast cancer2
bull The Postmenopausal EstrogenProgestin Interventions (PEPI) trial demonstrated that an increased mammographic breast density was associated with the use of E+P but not with the use of estrogen alone3
bull Women who already have high breast density may therefore be considered inappropriate for treatment with a progestin-containing HT
1) EU Core SPC for Hormone Replacement Therapy Products (CMDh1312003 Rev 4 June
2012)
2) De Villiers TJ et al on behalf of the International Menopause Society Climacteric 2013 16
3) Greendale GA et al J Natl Cancer Inst 2003
Stroke
0 25 5 75 10 125
Fractures
Diabetes
Breast cancer
Cholecystitis
Venothrombotic episodes
Endometrial cancer
Lung cancer
Coronary heart disease
Colorectal cancer
Overall mortality
15 125 10 75 5 25
Benefits Risks
CE
CE MPA
Santen RJ et al J Clin Endocrinol Metab 2010
The basis of the Endocrine Society scientific statement for postmenopausal hormone replacement therapy (HRT) excess risks and benefits of HRT for 5 years in women aged 50ndash59 years or within 10 years of the start of menopause E=estrogen P=progestin
bull Younger women (aged 50ndash59 years) had more favorable results bull There are differences between CE alone and CEMPA arms bull Overall benefitrisk ratio of CE-alone appears to be more favourable than CEMPA
Reevaluation of WHI data (stratified by age) Risks and
Benefits of HRT Cases per 1000 Women per 5 Years of
Use
Medical condition which may be exacerbated by treatment
with progestins
Diabetes and metabolic syndrome
bull Treatment of oestrogen deficiency symptoms with progestin-containing HT (unlike oestrogen alone) may be associated with increases in insulin resistance and deterioration in glucose tolerance123
bull Postmenopausal women with diabetes could be inappropriate for treatment with progestin-containing HT due to the potential risk of exacerbation of their condition
1) Panay N amp Studd JWW Human Reprod Update 1997
2) Godsland I et al Metabolism 1993
3) Sites CK et al J Clin Endocrinol Metab 2005
Variations in Associated Breast Cancer
Risks Between CE alone and CEMPA
bull Use of CE alone for a median of 59 years was associated with a lower incidence of invasive breast cancer (151 cases 027 per year) compared with placebo (199 cases 035 per year HR 077 95 CI 062ndash095 P=002)
bull In the CE alone group fewer women died from invasive breast cancer (6 deaths 0009 per year) compared with controls (16 deaths 0024 per year HR 037 95 CI 013ndash091 P=003)
Anderson GL et al Lancet
Oncol 2012
Bazedoxifene (BZA) specifically selected in
combination with conjugated estrogens
bull BZA has been specifically selected for its unique pharmacologic profile and effects on VMS and uterine tissue in particular123
1 Crabtree J et al Mol Cell Endocrinol 2008
2 Kharode Y et al Endocrinolology 2008
3 Duavive SmPC
Estrogen Receptor activity is dimmed
Estrogen Receptor activity is turned on
CEs are agonists BZA is an antagonist
In the uterus
bull The BZA component reduces the risk of endometrial hyperplasia that can occur with the conjugated estrogens component alone3 This means that progestins are not needed
Extensive global clinical development program for
CEBZA
aIncludes additional pilot dose-finding study 203 1 Lobo RA et al Fertil Steril 2009 2 Pinkerton JV et al Menopause 2009 3 Kagan R et al Menopause 2010 4 Mirkin S et al Climacteric 2013 5 Pinkerton JV et al Obstet Gynecol 2013
Effects of conjugated estrogensbazedoxifene on
lipid and coagulation variables a randomized
placebo- and active-controlled trial
bull At 12 months
bull Both CEBZA doses were associated with small but significant effects on hemostasis variables including reductions in antithrombin plasminogen activator inhibitor-1 and fibrinogen activity and an increase in plasminogen activity relative to placebo at 12 months Incidences of cardiovascular and venous thromboembolic events were similar among treatment groups
bull CONCLUSIONS
bull This study provides reassurance that CEBZA does not adversely affect lipid metabolism or hemostatic balance In accordance the incidences of venous thromboembolic events and cardiovascular events in postmenopausal women are similar to those observed with placebo

Bazedoxifene (BZA) specifically selected in
combination with conjugated estrogens
1 Crabtree J et al Mol Cell Endocrinol 2008
2 Kharode Y et al Endocrinolology 2008
3 Duavive SmPC
Estrogen Receptor activity is dimmed
Estrogen Receptor activity is turned on
CEs are agonists BZA is an antagonist
In the uterus
bull The BZA component reduces the risk of endometrial hyperplasia that can occur with the conjugated estrogens component alone1-3
bull This means that progestins are not needed
From the Womenrsquos Health Initiative to the combination
of estrogen and selective estrogen receptor
modulators to avoid progestin addition
bull Marie-Ceacutecile Valera Pierre Gourdy Florence Treacutemolliegraveres Jean-Franccedilois Arnal
bull Maturitas Volume 82 Issue 3 November 2015 Pages 274ndash277
bull
Other combinations of an estrogen (E2) + a SERM studied have
not produced favorable results
bull Objective To compare effects of 52 weeksrsquo treatment with either raloxifene 60 mgday alone (RLX) or in combination with 17B-estradiol 1 mgday (RLX + E2) on vasomotor symptoms (n = 83) and endometrial safety (n = 123) in postmenopausal women who transitioned from estrogen-progestin therapy Endometrial effect Women in the RLX + E2 group had significantly increased endometrial thickness at 52 weeks from baseline and RLX alone had no increase Two women (328) in the RLX + E2 group had endometrial hyperplasia (one with atypia) on the exit biopsy No one in RLX alone did
bull 1 Stovall D et al Menopause The Journal of The North American Menopause Society 2007
bull For the safety analyses data from women randomized before and after the protocol amendment were pooled which included 62 women in the raloxifene group and 61 women in the raloxifene + estrogen group
EFFICACY
VASOMOTOR
SYMPTOMS
SMART-2
DUAVIVE Efficacy for the Treatment of Moderate to
Severe VMS Associated With Menopause
14
1 Pinkerton JV et al Menopause 2009
Postmenopausal women
with a uterus
Age 42-64 year
(avg 53 yr)
(N=318)
DUAVIVE (CE 045BZA 20)
(n=127)
Placebo
(n=63)
bull 12-week randomized double-blind placebo-controlled study1
bull Inclusion criteria
‒ Postmenopausal women with an intact uterus
‒ Minimum of 7 moderate to severe hot flushes per day or at least 50 per week at screening
Change from baseline to
Weeks 4 and 12 in
bull Average daily number of
moderate to severe hot
flushes
bull Average daily severity
score of hot flushes
Primary End Points
Safety population (took at least one dose)
Significant Reduction vs Placebo in
Average Daily Number of Hot Flushes
DUAVEE [package insert] New York NY Pfizer Inc 2013
ANCOVA=analysis of covariance
Reduction in average daily number of
moderate to severe hot flushes ndash primary end point
Ad
jus
ted
mean
ch
an
ge
fro
m b
aselin
edagger
Week 4 Week 12
ndash31
ndash27
Treatment
differencedagger ndash59
ndash28
ndash76
ndash49
Treatment
differencedagger
22
Plt001 vs placebo daggerBased on data analysis using ANCOVA model Change from baseline = Treatment + Baseline + Site
DUAVIV
E
Reduction in the Observed Average Daily Number
of Moderate to Severe Hot Flushes
Data on file CSR-67461 Protocol 3115A1-305 Table 1511 Pfizer Inc New York NY
change from baseline to week 12
74 for DUAVIVE
51 for placebo
Observed Average Daily Number of Hot Flushes
Ob
serv
ed a
vera
ge d
aily
nu
mb
er o
f m
od
erat
e to
sev
ere
ho
t fl
ush
es
0 1 2 3 4 5 6 7 8 9 10 12 0 1
11
2
4 3
6 5
7 8 9
10
28
54
DUAVIVE (n=122) Placebo (n=62)
Weeks
Primary analysis showed statistically significant separation at weeks 4 and 12
Average daily number of hot flushes from baseline to week 12
103 to 28 for DUAVIVE
105 to 54 for placebo
Based on mathematical means
not statistically analyzed
105 103
Pinkerton JV et al Menopause 2009
Significant Reduction vs Placebo in
Average Daily Severity Score of Hot Flushes
17
Week 4 Week 12
ndash05
ndash06
Treatment
differencedagger
Treatment
differencedagger
DUAVEE [package insert] New York NY Pfizer Inc 2013
Reduction in average daily severity score of hot flushes ndash primary end point
Ad
jus
ted
me
an
ch
an
ge
fro
m b
aselin
edagger
Plt001 vs placebo daggerBased on data analysis using ANCOVA model Change from baseline = Treatment + Baseline + Site
DUAVIV
E
Reduction in the Observed Average
Daily Severity Score of Hot Flushes
Observed Average Daily Severity Score of Hot Flushes
19
DUAVIVE (n=122) Placebo (n=62)
Weeks
Ob
serv
ed a
vera
ge d
aily
sev
erit
y sc
ore
of
ho
t fl
ush
es
0
05
10
15
25
20
0 1 2 3 4 5 6 7 8 9 10 12 11 0 1 2 3 4 5 6 7 8 9 10 12 11
14
Data on file CSR-67461 Protocol 3115A1-305 Table 1511 Pfizer Inc New York NY
Primary analysis at weeks 4 and 12 prespecified secondary end points at all other weeks
change from baseline to week 12
39 for DUAVIVE
14 for placebo
Average daily severity score of hot flashes from baseline to week 12
23 to 14 for DUAVIVE
23 to 19 for Placebo
Based on mathematical means
not statistically analyzed
23
23
Pinkerton JV et al Menopause 2009
Effects on bone mineral density (BMD)
SMART 512
20
bull 12-month double-blind randomized placebo- and active-controlled study
bull Primary end point endometrial hyperplasia at 1 year
bull Secondary BMD changes at 1 year
1 DUAVEE [package insert] New York NY Pfizer Inc 2013 2 Pinkerton J Clin Endocrin Metab 2014
This study included a different dose of CEBZA and comparators The schematic shown here depicts only the patients who received the approved dose of DUAVIVE or placebo
Change from baseline in
bull Lumbar Spine BMD (Primary ndash BMD Substudy)
bull Total Hip BMD (Secondary ndash BMD Substudy)
BMD Analysis
DUAVIVE
(CE 045BZA 20)
(n=119)
Placebo
(n=139)
BMD Analysis
Postmenopausal women with a uterus
Less than 5 years since LMP
(N=590)
DUAVIVE Significantly Increased Lumbar Spine and Total
Hip BMD vs Placebo at 12 Months ndash Study 2
M
ean
ch
an
ge f
rom
baselin
e
Lumbar Spine Total Hip
121 151 Treatment
difference Treatment
difference
Data on file CSR-81040 Protocol 3115A1-3307 Pfizer Inc New York NY Pinkerton J Clin Endocrin Metab 2014 30
Plt001 vs placebo
Adjusted mean changes and P-values based on an ANCOVA model with treatment and region (US or non-US) as factors and baseline BMD value and years since menopause as covariates using the modified intention to treat population with last observation carried forward
DUAVIV
E
TOLERABILITY
AND SAFETY
Rates of BleedingSpotting and Amenorrhea
Similar to Rates with Placebo
bull High and similar cumulative rates of amenorrhea at year 1 among women treated with CE 045BZA 20 and placebo and was higher than seen in women treated with CE 045MPA 151
bull Noncumulative rates of spotting and bleedingspotting were similar among women treated with CEBZA or placebo and consistently higher in women treated with CE 045MPA 152
0
90
Cycle
100
Pe
rce
nta
ge
of
Su
bje
cts
80
70
60
50
40
30
20
10
88
54
Placebo
CE 045BZA 20 CE 045MPA 15
Percentage of subjects with cumulative amenorrhea during consecutive 4-week periods (cycles) in SMART-5
MPA medroxyprogesterone acetate Plt0001 vs all other treatment groups 1 Pinkerton JV et al J Clin Endocrinol Metab 2014 2 Data on file CSR-81040 Protocol 3115A1-3307 Pfizer Inc New York NY
Adverse Reactions in Placebo-
Controlled Trials Safety analyses have been conducted in 6210 postmenopausal women aged 40 to 75 years (mean age 55 years) following up to 2 years of treatment in SMART-1 -2 -3 and -5
Adverse reactions (incidence ge5) that were more common with DUAVIVE
Incidence of serious adverse reactions
35 with DUAVIVE 48 with placebo
DUAVEE [package insert] New York NY Pfizer Inc 2013
CE 045 BZA 20 (N=1224)
n ()
Placebo (N=1069)
n ()
Gastrointestinal disorders
Nausea 100 (8) 58 (5)
Diarrhea 96 (8) 57 (5)
Dyspepsia 84 (7) 59 (6)
Abdominal pain upper 81 (7) 58 (5)
Musculoskeletal and connective tissue disorders
Muscle spasms 110 (9) 63 (6)
Neck pain 62 (5) 46 (4)
Nervous system disorders
Dizziness 65 (5) 37 (3)
Respiratory thoracic and mediastinal disorders
Oropharyngeal pain 80 (7) 61 (6)
Venous Thromboembolism (VTE) in
DUAVIVE Clinical Studies
bull Estrogen agonistantagonists (including BZA a component of DUAVIVE) and estrogens individually are known to increase the risk of VTE
bull In the clinical studies with DUAVIVE the reporting rates for VTE were low in all treatment groups
bull Adverse reactions of VTE reported by patients
bull Should VTE event occur or be suspected DUAVIVE should be discontinued immediately
bull Due to the low rates of events in both groups it is not possible to conclude that the risk of VTE with DUAVIVE is different from that seen with other estrogen therapies
DUAVEE [package insert] New York NY Pfizer Inc 2013
00 for DUAVIVE (n=1224)
01 for placebo (n=1069)
26
Effects of conjugated estrogensbazedoxifene on
lipid and coagulation variables a randomized
placebo- and active-controlled trial
bull postmenopausal women (N = 1843) with menopausal
symptoms
bull Lipid (N = 1843) and coagulation (N = 590) variables were assessed in women receiving daily CE 045 mgBZA 20 mg CE 0625 mgBZA 20 mg BZA 20 mg CE 045 mgmedroxyprogesterone acetate (MPA) 15 mg or placebo for 12 months
bull Skouby SO et al Menopause 2015 Jun22(6)640-9
Effects of conjugated estrogensbazedoxifene on
lipid and coagulation variables a randomized
placebo- and active-controlled trial
bull At 12 months
bull CE 045 mgBZA 20 mg
bull CE 0625 mgBZA 20 mg
bull BZA 20 mg
bull and CE 045 mgMPA 15 mg decreased total cholesterol and LDL- cholesterol vs placebo (P lt 001 for all)
bull Both CEBZA doses and CEMPA increased high-density lipoprotein cholesterol compared with placebo (P lt 005 for all)
bull CE 045 mgBZA 20 mg had a neutral effect on triglycerides
bull CE 0625 mgBZA 20 mg and CEMPA increased triglycerides compared with placebo (P lt 005)
bull Skouby SO et al Menopause 2015 Jun22(6)640-9
Effects of conjugated estrogensbazedoxifene on
lipid and coagulation variables a randomized
placebo- and active-controlled trial
bull At 12 months
bull Both CEBZA doses were associated with small but significant effects on hemostasis variables including reductions in antithrombin plasminogen activator inhibitor-1 and fibrinogen activity and an increase in plasminogen activity relative to placebo at 12 months Incidences of cardiovascular and venous thromboembolic events were similar among treatment groups
Skouby SO et al Menopause 2015
Jun22(6)640-9
Endometrial hyperplasia or malignancy occurred in lt1 of women
following up to 1 year of treatment with CEBZA12
Study Cumulative Incidence at month 12 (nN)
CE 045BZA 20 Placebo
SMART-11 000 (0336) 000 (0313)
SMART-52 030 (1335) 028 (1354)
Effects on the Endometrium
1 Pickar JH et al Fertil Steril 2009 2 Pinkerton at al J Clin Endocrinol Metab 2014
Through the eyes of an amazone
Marie Mandy
Breast tolerability profile similar to placebo following up to 2 years of treatment with CEBZA12
Pooled analysis of SMART clinical trials
CE 045BZA 20 (n=1585)
Placebo (n=1241)
Breast cancer incidence up to 2 years
(per 1000 woman-years)
100 (CI 000-321)
140 (CI 000-417)
Incidence of reported breast paintenderness up to 12 weeks
98-115 81-112
Incidence of abnormal mammogram at month 12
258 316
Mean change in breast density at month 12 (SMART-5)
ndash038 (n=186)
ndash032 (n=182)
Effects on the Breast
1 Pickar JH et al Menopause 2013 2 Pinkerton JV et al Obstet Gynecol 2013
CEBZA clinical overview - summary
bull In clinical trials CEBZA has demonstrated safety and efficacy in postmenopausal women with a uterus including the following
bull Significant reduction in number and severity of moderate to severe hot flushes1
bull Incidence of cumulative amenorrhea rate similar to placebo and significantly better than CEMPA2
bull Incidence of endometrial hyperplasia and breast tendernessdensity similar to that with placebo345
bull Incidence of adverse events and discontinuation rates similar to that with placebo6
1 Pinkerton JV et al Menopause 2009 2 Pinkerton JV et al J Clin Endocrinol Metab2014 3 Pickar JH et al
Fertil Steril 2009 4 Pinkerton at al J Clin Endocrinol Metab 2014 5 Pickar JH et al Menopause 2013 6 DUAVEE [package insert] New York NY Pfizer Inc 2013
CEBZA clinical overview - summary
Now women with a uterus who choose hormone therapy for management of menopausal symptoms have a choice
bull conventional estrogen-progestogen therapy or
bull a new combinationhellipconjugated estrogens paired with the SERM bazedoxifene
1 Pinkerton JV et al Menopause 2009 2 Pinkerton JV et al J Clin Endocrinol Metab2014 3 Pickar JH et al Fertil Steril 2009 4 Pinkerton at al J Clin Endocrinol Metab 2014 5 Pickar JH et al Menopause 2013 6 DUAVEE [package insert] New York NY Pfizer Inc 2013
Conjugated EstrogensBazedoxifene (CEBZA)
US indication
bull DUAVEE is indicated in women with a uterus for
bull 11 Treatment of Moderate to Severe Vasomotor Symptoms Associated with Menopause
bull 12 Prevention of Postmenopausal Osteoporosis
bull 13 Important Limitations of Use
bull Use DUAVEE for the shortest duration consistent with treatment goals and risks for the individual woman Postmenopausal women should be re-evaluated periodically as clinically appropriate to determine if treatment is still necessary
bull When prescribing solely for the prevention of postmenopausal osteoporosis therapy should only be considered for women at significant risk of osteoporosis and non-estrogen medication should be carefully considered
Conjugated EstrogensBazedoxifene (CEBZA)
EU indication
CEBZA is indicated for
bull Treatment of oestrogen deficiency symptoms in postmenopausal women with a uterus (with at least 12 months since the last menses) for whom treatment with progestin-containing therapy is not appropriate
bull The experience treating women older than 65 years is limited
bull Dose CE (045mg)Bazedoxifene (20mg)
Duavive SmPC
Which women with a uterus
could benefit from estrogens
without the need for a
progestin
Progestin intolerance is one of the main
factors for reduced compliance
bull About 20 of women receiving progestin-containing HT have significant progestin intolerance and half of these experience serious effects that prevent treatment continuation1
1 Panay N amp Studd J Human Reprod Update 1997
2 Panay N et al on behalf of the British Menopause Society and Womenrsquos Health Concern Menopause Int 2013
bull The 2013 British Menopause Society amp Womenrsquos Health
Concern recommendations on hormone replacement
therapy do recognise progestin intolerance as one of the
main factors for reduced compliance with HT 2
Proportion of patients () with at least one bleeding episode in relation to time and to the
used HT
Serge Rozenberg et al Hum Reprod 2009241739-1747
copy The Author 2009 Published by Oxford University Press on behalf of the European Society of
Human Reproduction and Embryology All rights reserved For Permissions please email
journalspermissionsoxfordjournalsorg
Breast tenderness after initiation of CEE
CEE + MPA (WHI)
and mammographic density change
bullCrandall et al Breast Cancer Res Treat DOI 101007s10549-011-1803-9
Breast density
Conclusion
bull CEEBAZO is an additional regimen for menopausal symptoms it provides also a prevention for osteoporosis
bull It is suitable for women with a uterus who are unsatisfied with an EPT regimen or who you are unwilling to treat with an EPT regimen
Adapted use of MHT
bull Lower dosage of estrogens
bull Other progestins
bull Better safety profile
bull Vaginal estrogen or SERMS
bull Non-hormonal therapy
bull Development of new products
bull SERMS + estrogens
Most common adverse events leading to
discontinuation are related to progestins12
bull breakthrough bleeding
bull Low compliance
bull Increase in the number of US
bull Stress
bull Cost
bull uterine procedures
bull Unnecessary endometrial biopsies Hysteroscopies DampC Hysterectomies
bull Morbidity
Proportion of patients who completed or discontinued treatment in relation to the used HT
Serge Rozenberg et al Hum Reprod 2009241739-1747
copy The Author 2009 Published by Oxford University Press on behalf of the European Society of
Human Reproduction and Embryology All rights reserved For Permissions please email
journalspermissionsoxfordjournalsorg
Most common adverse events leading to discontinuation
are related to progestins
bull breast paintenderness
Breast tenderness after initiation of CEE
CEE + MPA (WHI)
and mammographic density change
bullCrandall et al Breast Cancer Res Treat DOI 101007s10549-011-1803-9
Breast density
Hormone therapy use and mammographic
density in postmenopausal Norwegian women
bull Results differed when considering the combined effect of age and BMI
bull The effect of EPT on mammographic density was modified by age and BMI with no apparent association among the youngest women (aged 50-55) with the highest BMI (BMI ge 26)
bull A higher mammographic density was found in EPT users compared to never HT users particularly in women using high-dose NETA regimens Age and BMI modified the association between EPT use and mammographic density
bull Couto E et al Breast Cancer Res Treat 2011 Nov 4 [Epub ahead of print]
Breast Cancer Risk by Breast Density
Menopause and Postmenopausal Hormone
Therapy Use
Birads age HT Duration Risk
1 55-59 None 5 year risk 08 (95 CI 06- 09)
1 55-59
ET EPT 5 year risk 09 (95 CI 07 -11)
4 55-59
None 5 year risk 24 (95 CI 20 -28)
4 55-59
ET 5 year risk
30 (95 CI 26 -35)
4 55-59
EPT 5 year risk
42 (95 CI 37 -46)
Adapted from Kerlikowske et al JOURNAL OF CLINICAL ONCOLOGY 2010
Breast Cancer Risk by Breast Density
Menopause and Postmenopausal Hormone
Therapy Use
Adapted from Kerlikowske et al JOURNAL OF CLINICAL ONCOLOGY 2010
bull Postmenopausal women with high breast density are at increased risk of breast cancer and should be aware of the added risk of taking HT especially estrogen plus progestin
Medical condition which may be exacerbated by treatment
with progestins
Diabetes and metabolic syndrome
bull progestin-containing HT may be associated with increases in insulin resistance and deterioration in glucose tolerance123
bull Postmenopausal women with diabetes could be inappropriate for treatment with progestin-containing HT due to the potential risk of exacerbation of their condition
1) Panay N amp Studd JWW Human Reprod Update 1997
2) Godsland I et al Metabolism 1993
3) Sites CK et al J Clin Endocrinol Metab 2005
A Nath and R Sitruk-Ware CLIMACTERIC 200912(Suppl 1)96ndash101
A Nath and R Sitruk-Ware CLIMACTERIC 200912(Suppl 1)96ndash101
Diabetes an epidemy
bull UK 1996 14 million of diabetics
bull UK 2015 32 million (6 of the population)
bull UK 2025 5 million
bull httpwwwdiabetescoukdiabetes-prevalencehtml
Other progestin-related intolerance issues
bull Nausea
bull Depressive mood
bull Poor concentration
bull Hirsutism
bull Headache
bull Dizziness
bull Fluid retention
bull Weight gain Panay N amp Studd JWW Human Reprod Update 1997
Medical condition which may be exacerbated by treatment with progestins
PMSPMDDdepression
bull Progesterone-induced PMD can be exacerbated by exogenous progestin administration and can occur in association with HT or OC administration1
bull Significantly higher negative mood scores have been observed during the addition of a progestin to an estrogen in a sequential HT regimen in postmenopausal women with a history of PMS compared to those without2
bull Women with a history of PMS or PMD exacerbation of depression using progestins may therefore benefit from a progestin free treatment for menopausal symptoms
1) Nevatte T et al Arch Womens Ment Health 2013 2) Bjoumlrn I et al Climacteric 2006 PMS premenstrual syndrome
PMDD premenstrual dysphoric disorder
Conclusion
bull CEEBAZO is an additional regimen for menopausal symptoms it provides also a prevention for osteoporosis
bull It is suitable for women with a uterus who are unsatisfied with an EPT regimen or who you are unwilling to treat with an EPT regimen
For some postmenopausal women with a uterus there is a
need for progestin free treatment options
bull with demonstrated clinical efficacy
bull which protects the endometrium
bull improved tolerabilitysafety profile
In clinical practice this translates to women who are
intolerant of progestin-containing HT or have conditions
which may be exacerbated by treatment with progestins
Conclusion Medical need for alternative treatment option
Medical condition which may be exacerbated by treatment with progestins
Depression
bull Progestin-containing HT has been associated with increases in depressive symptoms in some individuals1
bull There is a biochemicalphysiological plausibility for the association of progestins with depression234
bull Therefore postmenopausal women who also have a medical history of depressive disorders or depression could be inappropriate for treatment with progestin-containing HT
Pfizer Confidential
65
1) Girdler SS et al J Womens Health Gend Based Med 1999 2) Traish AM et al Korean J Urol 2014 3) Stroumlhle A et al Biol Psychiatry 1999 4) Romeo E et
al Am J Psychiatry 1998
History of the following conditions may make progestin inappropriate
bull Depression
bull PMSPMDD
PMS premenstrual syndrome
PMD premenstrual dysphoric disorder
Medical conditions that may be exacerbated by treatment with progestins
Women for whom progestin-containing HT
would not be considered appropriate
minus Women who are intolerant of progestin-containing hormone therapy
minus Women with pre-existing medical conditions that may be exacerbated by progestins
Most common adverse events leading to discontinuation are related to progestins12
breakthrough bleeding
bull Increase in the number of uterine procedures (ie unnecessary endometrial biopsies)
breast paintenderness
bull Increase in the number of breast interventions
1 Steel SA et al Climacteric 2003 2 Ettinger B and Pressman A Am J Manag Care 1999 3 Komm BS Mirkin S
Pharmaceuticals 2012
4 Panay N amp Studd JWW Human Reprod Update 1997
bull Nausea bull Depressive mood bull Poor concentration bull Hirsutism bull Headache bull Dizziness bull Fluid retention bull Weight gain
Other progestin-related intolerance issues4
Unmet need with the treatment of postmenopausal symptoms
bull Alternatives to progestin are needed that will protect the endometrium while avoiding other progestin-associated effects and preserving the desired effects of estrogens in postmenopausal women3
Which women with a uterus could benefit from
estrogens without the need for a progestin
bull Women who are intolerant of progestin-containing hormone therapy
bull Women with pre-existing medical conditions that may be exacerbated by progestins (eg women with a history of depression PMSPMDD increased breast density diabetes and metabolic syndrome)
History of the following conditions may make progestin inappropriate
bull Depression
bull PMSPMDD
bull High breast density
bull Diabetes and metabolic syndrome
PMS premenstrual syndrome
PMD premenstrual dysphoric disorder
Medical conditions that may be exacerbated by treatment with progestins
Learning from WHI data
bull Hormone therapy (HT) is the conventional and established therapy option to effectively treat postmenopausal symptoms however it has been associated with some safety and tolerability concerns1 2
bull A review of WHI data suggests that many of the concerns with menopausal HT more often associated with EPT (CE+MPA) such as CHD risk increased breast density breast pain and breast cancer risk than with ET (CEE alone)2
1 Rolnick SJ Kopher RA DeFor TA et al Menopause 2005
2 Komm BS Mirkin S Pharmaceuticals 2012
WHI Womenrsquos Health Initiative trial
CHD coronary heart disease
CEE conjugated equine estrogens
Efficacy and Safety of Constant Oestrogen
Pulsed Progestogen vs
Continuous Combined HRT
Adverse Events
17b-oestradiol 17b-oestradiol norgestimate NETA (n = 150) (n = 172) Breast discomfort 14 27 Abdominal discomfort 14 22 Uterine bleeding 15 12 Dysmenorrhea 3 8 Oedema 5 8
Adapted from S Rozenberg et al Human Reproduction 2000
Medical condition which may be exacerbated by treatment
with progestins
Increased breast density
bull Increases in breast density are associated with progestin-containing HT which may adversely affect radiological detection of breast cancer1 and may be independently associated with an increased risk for the development of breast cancer2
bull The Postmenopausal EstrogenProgestin Interventions (PEPI) trial demonstrated that an increased mammographic breast density was associated with the use of E+P but not with the use of estrogen alone3
bull Women who already have high breast density may therefore be considered inappropriate for treatment with a progestin-containing HT
1) EU Core SPC for Hormone Replacement Therapy Products (CMDh1312003 Rev 4 June
2012)
2) De Villiers TJ et al on behalf of the International Menopause Society Climacteric 2013 16
3) Greendale GA et al J Natl Cancer Inst 2003
Stroke
0 25 5 75 10 125
Fractures
Diabetes
Breast cancer
Cholecystitis
Venothrombotic episodes
Endometrial cancer
Lung cancer
Coronary heart disease
Colorectal cancer
Overall mortality
15 125 10 75 5 25
Benefits Risks
CE
CE MPA
Santen RJ et al J Clin Endocrinol Metab 2010
The basis of the Endocrine Society scientific statement for postmenopausal hormone replacement therapy (HRT) excess risks and benefits of HRT for 5 years in women aged 50ndash59 years or within 10 years of the start of menopause E=estrogen P=progestin
bull Younger women (aged 50ndash59 years) had more favorable results bull There are differences between CE alone and CEMPA arms bull Overall benefitrisk ratio of CE-alone appears to be more favourable than CEMPA
Reevaluation of WHI data (stratified by age) Risks and
Benefits of HRT Cases per 1000 Women per 5 Years of
Use
Medical condition which may be exacerbated by treatment
with progestins
Diabetes and metabolic syndrome
bull Treatment of oestrogen deficiency symptoms with progestin-containing HT (unlike oestrogen alone) may be associated with increases in insulin resistance and deterioration in glucose tolerance123
bull Postmenopausal women with diabetes could be inappropriate for treatment with progestin-containing HT due to the potential risk of exacerbation of their condition
1) Panay N amp Studd JWW Human Reprod Update 1997
2) Godsland I et al Metabolism 1993
3) Sites CK et al J Clin Endocrinol Metab 2005
Variations in Associated Breast Cancer
Risks Between CE alone and CEMPA
bull Use of CE alone for a median of 59 years was associated with a lower incidence of invasive breast cancer (151 cases 027 per year) compared with placebo (199 cases 035 per year HR 077 95 CI 062ndash095 P=002)
bull In the CE alone group fewer women died from invasive breast cancer (6 deaths 0009 per year) compared with controls (16 deaths 0024 per year HR 037 95 CI 013ndash091 P=003)
Anderson GL et al Lancet
Oncol 2012
Bazedoxifene (BZA) specifically selected in
combination with conjugated estrogens
bull BZA has been specifically selected for its unique pharmacologic profile and effects on VMS and uterine tissue in particular123
1 Crabtree J et al Mol Cell Endocrinol 2008
2 Kharode Y et al Endocrinolology 2008
3 Duavive SmPC
Estrogen Receptor activity is dimmed
Estrogen Receptor activity is turned on
CEs are agonists BZA is an antagonist
In the uterus
bull The BZA component reduces the risk of endometrial hyperplasia that can occur with the conjugated estrogens component alone3 This means that progestins are not needed
Extensive global clinical development program for
CEBZA
aIncludes additional pilot dose-finding study 203 1 Lobo RA et al Fertil Steril 2009 2 Pinkerton JV et al Menopause 2009 3 Kagan R et al Menopause 2010 4 Mirkin S et al Climacteric 2013 5 Pinkerton JV et al Obstet Gynecol 2013
Effects of conjugated estrogensbazedoxifene on
lipid and coagulation variables a randomized
placebo- and active-controlled trial
bull At 12 months
bull Both CEBZA doses were associated with small but significant effects on hemostasis variables including reductions in antithrombin plasminogen activator inhibitor-1 and fibrinogen activity and an increase in plasminogen activity relative to placebo at 12 months Incidences of cardiovascular and venous thromboembolic events were similar among treatment groups
bull CONCLUSIONS
bull This study provides reassurance that CEBZA does not adversely affect lipid metabolism or hemostatic balance In accordance the incidences of venous thromboembolic events and cardiovascular events in postmenopausal women are similar to those observed with placebo

From the Womenrsquos Health Initiative to the combination
of estrogen and selective estrogen receptor
modulators to avoid progestin addition
bull Marie-Ceacutecile Valera Pierre Gourdy Florence Treacutemolliegraveres Jean-Franccedilois Arnal
bull Maturitas Volume 82 Issue 3 November 2015 Pages 274ndash277
bull
Other combinations of an estrogen (E2) + a SERM studied have
not produced favorable results
bull Objective To compare effects of 52 weeksrsquo treatment with either raloxifene 60 mgday alone (RLX) or in combination with 17B-estradiol 1 mgday (RLX + E2) on vasomotor symptoms (n = 83) and endometrial safety (n = 123) in postmenopausal women who transitioned from estrogen-progestin therapy Endometrial effect Women in the RLX + E2 group had significantly increased endometrial thickness at 52 weeks from baseline and RLX alone had no increase Two women (328) in the RLX + E2 group had endometrial hyperplasia (one with atypia) on the exit biopsy No one in RLX alone did
bull 1 Stovall D et al Menopause The Journal of The North American Menopause Society 2007
bull For the safety analyses data from women randomized before and after the protocol amendment were pooled which included 62 women in the raloxifene group and 61 women in the raloxifene + estrogen group
EFFICACY
VASOMOTOR
SYMPTOMS
SMART-2
DUAVIVE Efficacy for the Treatment of Moderate to
Severe VMS Associated With Menopause
14
1 Pinkerton JV et al Menopause 2009
Postmenopausal women
with a uterus
Age 42-64 year
(avg 53 yr)
(N=318)
DUAVIVE (CE 045BZA 20)
(n=127)
Placebo
(n=63)
bull 12-week randomized double-blind placebo-controlled study1
bull Inclusion criteria
‒ Postmenopausal women with an intact uterus
‒ Minimum of 7 moderate to severe hot flushes per day or at least 50 per week at screening
Change from baseline to
Weeks 4 and 12 in
bull Average daily number of
moderate to severe hot
flushes
bull Average daily severity
score of hot flushes
Primary End Points
Safety population (took at least one dose)
Significant Reduction vs Placebo in
Average Daily Number of Hot Flushes
DUAVEE [package insert] New York NY Pfizer Inc 2013
ANCOVA=analysis of covariance
Reduction in average daily number of
moderate to severe hot flushes ndash primary end point
Ad
jus
ted
mean
ch
an
ge
fro
m b
aselin
edagger
Week 4 Week 12
ndash31
ndash27
Treatment
differencedagger ndash59
ndash28
ndash76
ndash49
Treatment
differencedagger
22
Plt001 vs placebo daggerBased on data analysis using ANCOVA model Change from baseline = Treatment + Baseline + Site
DUAVIV
E
Reduction in the Observed Average Daily Number
of Moderate to Severe Hot Flushes
Data on file CSR-67461 Protocol 3115A1-305 Table 1511 Pfizer Inc New York NY
change from baseline to week 12
74 for DUAVIVE
51 for placebo
Observed Average Daily Number of Hot Flushes
Ob
serv
ed a
vera
ge d
aily
nu
mb
er o
f m
od
erat
e to
sev
ere
ho
t fl
ush
es
0 1 2 3 4 5 6 7 8 9 10 12 0 1
11
2
4 3
6 5
7 8 9
10
28
54
DUAVIVE (n=122) Placebo (n=62)
Weeks
Primary analysis showed statistically significant separation at weeks 4 and 12
Average daily number of hot flushes from baseline to week 12
103 to 28 for DUAVIVE
105 to 54 for placebo
Based on mathematical means
not statistically analyzed
105 103
Pinkerton JV et al Menopause 2009
Significant Reduction vs Placebo in
Average Daily Severity Score of Hot Flushes
17
Week 4 Week 12
ndash05
ndash06
Treatment
differencedagger
Treatment
differencedagger
DUAVEE [package insert] New York NY Pfizer Inc 2013
Reduction in average daily severity score of hot flushes ndash primary end point
Ad
jus
ted
me
an
ch
an
ge
fro
m b
aselin
edagger
Plt001 vs placebo daggerBased on data analysis using ANCOVA model Change from baseline = Treatment + Baseline + Site
DUAVIV
E
Reduction in the Observed Average
Daily Severity Score of Hot Flushes
Observed Average Daily Severity Score of Hot Flushes
19
DUAVIVE (n=122) Placebo (n=62)
Weeks
Ob
serv
ed a
vera
ge d
aily
sev
erit
y sc
ore
of
ho
t fl
ush
es
0
05
10
15
25
20
0 1 2 3 4 5 6 7 8 9 10 12 11 0 1 2 3 4 5 6 7 8 9 10 12 11
14
Data on file CSR-67461 Protocol 3115A1-305 Table 1511 Pfizer Inc New York NY
Primary analysis at weeks 4 and 12 prespecified secondary end points at all other weeks
change from baseline to week 12
39 for DUAVIVE
14 for placebo
Average daily severity score of hot flashes from baseline to week 12
23 to 14 for DUAVIVE
23 to 19 for Placebo
Based on mathematical means
not statistically analyzed
23
23
Pinkerton JV et al Menopause 2009
Effects on bone mineral density (BMD)
SMART 512
20
bull 12-month double-blind randomized placebo- and active-controlled study
bull Primary end point endometrial hyperplasia at 1 year
bull Secondary BMD changes at 1 year
1 DUAVEE [package insert] New York NY Pfizer Inc 2013 2 Pinkerton J Clin Endocrin Metab 2014
This study included a different dose of CEBZA and comparators The schematic shown here depicts only the patients who received the approved dose of DUAVIVE or placebo
Change from baseline in
bull Lumbar Spine BMD (Primary ndash BMD Substudy)
bull Total Hip BMD (Secondary ndash BMD Substudy)
BMD Analysis
DUAVIVE
(CE 045BZA 20)
(n=119)
Placebo
(n=139)
BMD Analysis
Postmenopausal women with a uterus
Less than 5 years since LMP
(N=590)
DUAVIVE Significantly Increased Lumbar Spine and Total
Hip BMD vs Placebo at 12 Months ndash Study 2
M
ean
ch
an
ge f
rom
baselin
e
Lumbar Spine Total Hip
121 151 Treatment
difference Treatment
difference
Data on file CSR-81040 Protocol 3115A1-3307 Pfizer Inc New York NY Pinkerton J Clin Endocrin Metab 2014 30
Plt001 vs placebo
Adjusted mean changes and P-values based on an ANCOVA model with treatment and region (US or non-US) as factors and baseline BMD value and years since menopause as covariates using the modified intention to treat population with last observation carried forward
DUAVIV
E
TOLERABILITY
AND SAFETY
Rates of BleedingSpotting and Amenorrhea
Similar to Rates with Placebo
bull High and similar cumulative rates of amenorrhea at year 1 among women treated with CE 045BZA 20 and placebo and was higher than seen in women treated with CE 045MPA 151
bull Noncumulative rates of spotting and bleedingspotting were similar among women treated with CEBZA or placebo and consistently higher in women treated with CE 045MPA 152
0
90
Cycle
100
Pe
rce
nta
ge
of
Su
bje
cts
80
70
60
50
40
30
20
10
88
54
Placebo
CE 045BZA 20 CE 045MPA 15
Percentage of subjects with cumulative amenorrhea during consecutive 4-week periods (cycles) in SMART-5
MPA medroxyprogesterone acetate Plt0001 vs all other treatment groups 1 Pinkerton JV et al J Clin Endocrinol Metab 2014 2 Data on file CSR-81040 Protocol 3115A1-3307 Pfizer Inc New York NY
Adverse Reactions in Placebo-
Controlled Trials Safety analyses have been conducted in 6210 postmenopausal women aged 40 to 75 years (mean age 55 years) following up to 2 years of treatment in SMART-1 -2 -3 and -5
Adverse reactions (incidence ge5) that were more common with DUAVIVE
Incidence of serious adverse reactions
35 with DUAVIVE 48 with placebo
DUAVEE [package insert] New York NY Pfizer Inc 2013
CE 045 BZA 20 (N=1224)
n ()
Placebo (N=1069)
n ()
Gastrointestinal disorders
Nausea 100 (8) 58 (5)
Diarrhea 96 (8) 57 (5)
Dyspepsia 84 (7) 59 (6)
Abdominal pain upper 81 (7) 58 (5)
Musculoskeletal and connective tissue disorders
Muscle spasms 110 (9) 63 (6)
Neck pain 62 (5) 46 (4)
Nervous system disorders
Dizziness 65 (5) 37 (3)
Respiratory thoracic and mediastinal disorders
Oropharyngeal pain 80 (7) 61 (6)
Venous Thromboembolism (VTE) in
DUAVIVE Clinical Studies
bull Estrogen agonistantagonists (including BZA a component of DUAVIVE) and estrogens individually are known to increase the risk of VTE
bull In the clinical studies with DUAVIVE the reporting rates for VTE were low in all treatment groups
bull Adverse reactions of VTE reported by patients
bull Should VTE event occur or be suspected DUAVIVE should be discontinued immediately
bull Due to the low rates of events in both groups it is not possible to conclude that the risk of VTE with DUAVIVE is different from that seen with other estrogen therapies
DUAVEE [package insert] New York NY Pfizer Inc 2013
00 for DUAVIVE (n=1224)
01 for placebo (n=1069)
26
Effects of conjugated estrogensbazedoxifene on
lipid and coagulation variables a randomized
placebo- and active-controlled trial
bull postmenopausal women (N = 1843) with menopausal
symptoms
bull Lipid (N = 1843) and coagulation (N = 590) variables were assessed in women receiving daily CE 045 mgBZA 20 mg CE 0625 mgBZA 20 mg BZA 20 mg CE 045 mgmedroxyprogesterone acetate (MPA) 15 mg or placebo for 12 months
bull Skouby SO et al Menopause 2015 Jun22(6)640-9
Effects of conjugated estrogensbazedoxifene on
lipid and coagulation variables a randomized
placebo- and active-controlled trial
bull At 12 months
bull CE 045 mgBZA 20 mg
bull CE 0625 mgBZA 20 mg
bull BZA 20 mg
bull and CE 045 mgMPA 15 mg decreased total cholesterol and LDL- cholesterol vs placebo (P lt 001 for all)
bull Both CEBZA doses and CEMPA increased high-density lipoprotein cholesterol compared with placebo (P lt 005 for all)
bull CE 045 mgBZA 20 mg had a neutral effect on triglycerides
bull CE 0625 mgBZA 20 mg and CEMPA increased triglycerides compared with placebo (P lt 005)
bull Skouby SO et al Menopause 2015 Jun22(6)640-9
Effects of conjugated estrogensbazedoxifene on
lipid and coagulation variables a randomized
placebo- and active-controlled trial
bull At 12 months
bull Both CEBZA doses were associated with small but significant effects on hemostasis variables including reductions in antithrombin plasminogen activator inhibitor-1 and fibrinogen activity and an increase in plasminogen activity relative to placebo at 12 months Incidences of cardiovascular and venous thromboembolic events were similar among treatment groups
Skouby SO et al Menopause 2015
Jun22(6)640-9
Endometrial hyperplasia or malignancy occurred in lt1 of women
following up to 1 year of treatment with CEBZA12
Study Cumulative Incidence at month 12 (nN)
CE 045BZA 20 Placebo
SMART-11 000 (0336) 000 (0313)
SMART-52 030 (1335) 028 (1354)
Effects on the Endometrium
1 Pickar JH et al Fertil Steril 2009 2 Pinkerton at al J Clin Endocrinol Metab 2014
Through the eyes of an amazone
Marie Mandy
Breast tolerability profile similar to placebo following up to 2 years of treatment with CEBZA12
Pooled analysis of SMART clinical trials
CE 045BZA 20 (n=1585)
Placebo (n=1241)
Breast cancer incidence up to 2 years
(per 1000 woman-years)
100 (CI 000-321)
140 (CI 000-417)
Incidence of reported breast paintenderness up to 12 weeks
98-115 81-112
Incidence of abnormal mammogram at month 12
258 316
Mean change in breast density at month 12 (SMART-5)
ndash038 (n=186)
ndash032 (n=182)
Effects on the Breast
1 Pickar JH et al Menopause 2013 2 Pinkerton JV et al Obstet Gynecol 2013
CEBZA clinical overview - summary
bull In clinical trials CEBZA has demonstrated safety and efficacy in postmenopausal women with a uterus including the following
bull Significant reduction in number and severity of moderate to severe hot flushes1
bull Incidence of cumulative amenorrhea rate similar to placebo and significantly better than CEMPA2
bull Incidence of endometrial hyperplasia and breast tendernessdensity similar to that with placebo345
bull Incidence of adverse events and discontinuation rates similar to that with placebo6
1 Pinkerton JV et al Menopause 2009 2 Pinkerton JV et al J Clin Endocrinol Metab2014 3 Pickar JH et al
Fertil Steril 2009 4 Pinkerton at al J Clin Endocrinol Metab 2014 5 Pickar JH et al Menopause 2013 6 DUAVEE [package insert] New York NY Pfizer Inc 2013
CEBZA clinical overview - summary
Now women with a uterus who choose hormone therapy for management of menopausal symptoms have a choice
bull conventional estrogen-progestogen therapy or
bull a new combinationhellipconjugated estrogens paired with the SERM bazedoxifene
1 Pinkerton JV et al Menopause 2009 2 Pinkerton JV et al J Clin Endocrinol Metab2014 3 Pickar JH et al Fertil Steril 2009 4 Pinkerton at al J Clin Endocrinol Metab 2014 5 Pickar JH et al Menopause 2013 6 DUAVEE [package insert] New York NY Pfizer Inc 2013
Conjugated EstrogensBazedoxifene (CEBZA)
US indication
bull DUAVEE is indicated in women with a uterus for
bull 11 Treatment of Moderate to Severe Vasomotor Symptoms Associated with Menopause
bull 12 Prevention of Postmenopausal Osteoporosis
bull 13 Important Limitations of Use
bull Use DUAVEE for the shortest duration consistent with treatment goals and risks for the individual woman Postmenopausal women should be re-evaluated periodically as clinically appropriate to determine if treatment is still necessary
bull When prescribing solely for the prevention of postmenopausal osteoporosis therapy should only be considered for women at significant risk of osteoporosis and non-estrogen medication should be carefully considered
Conjugated EstrogensBazedoxifene (CEBZA)
EU indication
CEBZA is indicated for
bull Treatment of oestrogen deficiency symptoms in postmenopausal women with a uterus (with at least 12 months since the last menses) for whom treatment with progestin-containing therapy is not appropriate
bull The experience treating women older than 65 years is limited
bull Dose CE (045mg)Bazedoxifene (20mg)
Duavive SmPC
Which women with a uterus
could benefit from estrogens
without the need for a
progestin
Progestin intolerance is one of the main
factors for reduced compliance
bull About 20 of women receiving progestin-containing HT have significant progestin intolerance and half of these experience serious effects that prevent treatment continuation1
1 Panay N amp Studd J Human Reprod Update 1997
2 Panay N et al on behalf of the British Menopause Society and Womenrsquos Health Concern Menopause Int 2013
bull The 2013 British Menopause Society amp Womenrsquos Health
Concern recommendations on hormone replacement
therapy do recognise progestin intolerance as one of the
main factors for reduced compliance with HT 2
Proportion of patients () with at least one bleeding episode in relation to time and to the
used HT
Serge Rozenberg et al Hum Reprod 2009241739-1747
copy The Author 2009 Published by Oxford University Press on behalf of the European Society of
Human Reproduction and Embryology All rights reserved For Permissions please email
journalspermissionsoxfordjournalsorg
Breast tenderness after initiation of CEE
CEE + MPA (WHI)
and mammographic density change
bullCrandall et al Breast Cancer Res Treat DOI 101007s10549-011-1803-9
Breast density
Conclusion
bull CEEBAZO is an additional regimen for menopausal symptoms it provides also a prevention for osteoporosis
bull It is suitable for women with a uterus who are unsatisfied with an EPT regimen or who you are unwilling to treat with an EPT regimen
Adapted use of MHT
bull Lower dosage of estrogens
bull Other progestins
bull Better safety profile
bull Vaginal estrogen or SERMS
bull Non-hormonal therapy
bull Development of new products
bull SERMS + estrogens
Most common adverse events leading to
discontinuation are related to progestins12
bull breakthrough bleeding
bull Low compliance
bull Increase in the number of US
bull Stress
bull Cost
bull uterine procedures
bull Unnecessary endometrial biopsies Hysteroscopies DampC Hysterectomies
bull Morbidity
Proportion of patients who completed or discontinued treatment in relation to the used HT
Serge Rozenberg et al Hum Reprod 2009241739-1747
copy The Author 2009 Published by Oxford University Press on behalf of the European Society of
Human Reproduction and Embryology All rights reserved For Permissions please email
journalspermissionsoxfordjournalsorg
Most common adverse events leading to discontinuation
are related to progestins
bull breast paintenderness
Breast tenderness after initiation of CEE
CEE + MPA (WHI)
and mammographic density change
bullCrandall et al Breast Cancer Res Treat DOI 101007s10549-011-1803-9
Breast density
Hormone therapy use and mammographic
density in postmenopausal Norwegian women
bull Results differed when considering the combined effect of age and BMI
bull The effect of EPT on mammographic density was modified by age and BMI with no apparent association among the youngest women (aged 50-55) with the highest BMI (BMI ge 26)
bull A higher mammographic density was found in EPT users compared to never HT users particularly in women using high-dose NETA regimens Age and BMI modified the association between EPT use and mammographic density
bull Couto E et al Breast Cancer Res Treat 2011 Nov 4 [Epub ahead of print]
Breast Cancer Risk by Breast Density
Menopause and Postmenopausal Hormone
Therapy Use
Birads age HT Duration Risk
1 55-59 None 5 year risk 08 (95 CI 06- 09)
1 55-59
ET EPT 5 year risk 09 (95 CI 07 -11)
4 55-59
None 5 year risk 24 (95 CI 20 -28)
4 55-59
ET 5 year risk
30 (95 CI 26 -35)
4 55-59
EPT 5 year risk
42 (95 CI 37 -46)
Adapted from Kerlikowske et al JOURNAL OF CLINICAL ONCOLOGY 2010
Breast Cancer Risk by Breast Density
Menopause and Postmenopausal Hormone
Therapy Use
Adapted from Kerlikowske et al JOURNAL OF CLINICAL ONCOLOGY 2010
bull Postmenopausal women with high breast density are at increased risk of breast cancer and should be aware of the added risk of taking HT especially estrogen plus progestin
Medical condition which may be exacerbated by treatment
with progestins
Diabetes and metabolic syndrome
bull progestin-containing HT may be associated with increases in insulin resistance and deterioration in glucose tolerance123
bull Postmenopausal women with diabetes could be inappropriate for treatment with progestin-containing HT due to the potential risk of exacerbation of their condition
1) Panay N amp Studd JWW Human Reprod Update 1997
2) Godsland I et al Metabolism 1993
3) Sites CK et al J Clin Endocrinol Metab 2005
A Nath and R Sitruk-Ware CLIMACTERIC 200912(Suppl 1)96ndash101
A Nath and R Sitruk-Ware CLIMACTERIC 200912(Suppl 1)96ndash101
Diabetes an epidemy
bull UK 1996 14 million of diabetics
bull UK 2015 32 million (6 of the population)
bull UK 2025 5 million
bull httpwwwdiabetescoukdiabetes-prevalencehtml
Other progestin-related intolerance issues
bull Nausea
bull Depressive mood
bull Poor concentration
bull Hirsutism
bull Headache
bull Dizziness
bull Fluid retention
bull Weight gain Panay N amp Studd JWW Human Reprod Update 1997
Medical condition which may be exacerbated by treatment with progestins
PMSPMDDdepression
bull Progesterone-induced PMD can be exacerbated by exogenous progestin administration and can occur in association with HT or OC administration1
bull Significantly higher negative mood scores have been observed during the addition of a progestin to an estrogen in a sequential HT regimen in postmenopausal women with a history of PMS compared to those without2
bull Women with a history of PMS or PMD exacerbation of depression using progestins may therefore benefit from a progestin free treatment for menopausal symptoms
1) Nevatte T et al Arch Womens Ment Health 2013 2) Bjoumlrn I et al Climacteric 2006 PMS premenstrual syndrome
PMDD premenstrual dysphoric disorder
Conclusion
bull CEEBAZO is an additional regimen for menopausal symptoms it provides also a prevention for osteoporosis
bull It is suitable for women with a uterus who are unsatisfied with an EPT regimen or who you are unwilling to treat with an EPT regimen
For some postmenopausal women with a uterus there is a
need for progestin free treatment options
bull with demonstrated clinical efficacy
bull which protects the endometrium
bull improved tolerabilitysafety profile
In clinical practice this translates to women who are
intolerant of progestin-containing HT or have conditions
which may be exacerbated by treatment with progestins
Conclusion Medical need for alternative treatment option
Medical condition which may be exacerbated by treatment with progestins
Depression
bull Progestin-containing HT has been associated with increases in depressive symptoms in some individuals1
bull There is a biochemicalphysiological plausibility for the association of progestins with depression234
bull Therefore postmenopausal women who also have a medical history of depressive disorders or depression could be inappropriate for treatment with progestin-containing HT
Pfizer Confidential
65
1) Girdler SS et al J Womens Health Gend Based Med 1999 2) Traish AM et al Korean J Urol 2014 3) Stroumlhle A et al Biol Psychiatry 1999 4) Romeo E et
al Am J Psychiatry 1998
History of the following conditions may make progestin inappropriate
bull Depression
bull PMSPMDD
PMS premenstrual syndrome
PMD premenstrual dysphoric disorder
Medical conditions that may be exacerbated by treatment with progestins
Women for whom progestin-containing HT
would not be considered appropriate
minus Women who are intolerant of progestin-containing hormone therapy
minus Women with pre-existing medical conditions that may be exacerbated by progestins
Most common adverse events leading to discontinuation are related to progestins12
breakthrough bleeding
bull Increase in the number of uterine procedures (ie unnecessary endometrial biopsies)
breast paintenderness
bull Increase in the number of breast interventions
1 Steel SA et al Climacteric 2003 2 Ettinger B and Pressman A Am J Manag Care 1999 3 Komm BS Mirkin S
Pharmaceuticals 2012
4 Panay N amp Studd JWW Human Reprod Update 1997
bull Nausea bull Depressive mood bull Poor concentration bull Hirsutism bull Headache bull Dizziness bull Fluid retention bull Weight gain
Other progestin-related intolerance issues4
Unmet need with the treatment of postmenopausal symptoms
bull Alternatives to progestin are needed that will protect the endometrium while avoiding other progestin-associated effects and preserving the desired effects of estrogens in postmenopausal women3
Which women with a uterus could benefit from
estrogens without the need for a progestin
bull Women who are intolerant of progestin-containing hormone therapy
bull Women with pre-existing medical conditions that may be exacerbated by progestins (eg women with a history of depression PMSPMDD increased breast density diabetes and metabolic syndrome)
History of the following conditions may make progestin inappropriate
bull Depression
bull PMSPMDD
bull High breast density
bull Diabetes and metabolic syndrome
PMS premenstrual syndrome
PMD premenstrual dysphoric disorder
Medical conditions that may be exacerbated by treatment with progestins
Learning from WHI data
bull Hormone therapy (HT) is the conventional and established therapy option to effectively treat postmenopausal symptoms however it has been associated with some safety and tolerability concerns1 2
bull A review of WHI data suggests that many of the concerns with menopausal HT more often associated with EPT (CE+MPA) such as CHD risk increased breast density breast pain and breast cancer risk than with ET (CEE alone)2
1 Rolnick SJ Kopher RA DeFor TA et al Menopause 2005
2 Komm BS Mirkin S Pharmaceuticals 2012
WHI Womenrsquos Health Initiative trial
CHD coronary heart disease
CEE conjugated equine estrogens
Efficacy and Safety of Constant Oestrogen
Pulsed Progestogen vs
Continuous Combined HRT
Adverse Events
17b-oestradiol 17b-oestradiol norgestimate NETA (n = 150) (n = 172) Breast discomfort 14 27 Abdominal discomfort 14 22 Uterine bleeding 15 12 Dysmenorrhea 3 8 Oedema 5 8
Adapted from S Rozenberg et al Human Reproduction 2000
Medical condition which may be exacerbated by treatment
with progestins
Increased breast density
bull Increases in breast density are associated with progestin-containing HT which may adversely affect radiological detection of breast cancer1 and may be independently associated with an increased risk for the development of breast cancer2
bull The Postmenopausal EstrogenProgestin Interventions (PEPI) trial demonstrated that an increased mammographic breast density was associated with the use of E+P but not with the use of estrogen alone3
bull Women who already have high breast density may therefore be considered inappropriate for treatment with a progestin-containing HT
1) EU Core SPC for Hormone Replacement Therapy Products (CMDh1312003 Rev 4 June
2012)
2) De Villiers TJ et al on behalf of the International Menopause Society Climacteric 2013 16
3) Greendale GA et al J Natl Cancer Inst 2003
Stroke
0 25 5 75 10 125
Fractures
Diabetes
Breast cancer
Cholecystitis
Venothrombotic episodes
Endometrial cancer
Lung cancer
Coronary heart disease
Colorectal cancer
Overall mortality
15 125 10 75 5 25
Benefits Risks
CE
CE MPA
Santen RJ et al J Clin Endocrinol Metab 2010
The basis of the Endocrine Society scientific statement for postmenopausal hormone replacement therapy (HRT) excess risks and benefits of HRT for 5 years in women aged 50ndash59 years or within 10 years of the start of menopause E=estrogen P=progestin
bull Younger women (aged 50ndash59 years) had more favorable results bull There are differences between CE alone and CEMPA arms bull Overall benefitrisk ratio of CE-alone appears to be more favourable than CEMPA
Reevaluation of WHI data (stratified by age) Risks and
Benefits of HRT Cases per 1000 Women per 5 Years of
Use
Medical condition which may be exacerbated by treatment
with progestins
Diabetes and metabolic syndrome
bull Treatment of oestrogen deficiency symptoms with progestin-containing HT (unlike oestrogen alone) may be associated with increases in insulin resistance and deterioration in glucose tolerance123
bull Postmenopausal women with diabetes could be inappropriate for treatment with progestin-containing HT due to the potential risk of exacerbation of their condition
1) Panay N amp Studd JWW Human Reprod Update 1997
2) Godsland I et al Metabolism 1993
3) Sites CK et al J Clin Endocrinol Metab 2005
Variations in Associated Breast Cancer
Risks Between CE alone and CEMPA
bull Use of CE alone for a median of 59 years was associated with a lower incidence of invasive breast cancer (151 cases 027 per year) compared with placebo (199 cases 035 per year HR 077 95 CI 062ndash095 P=002)
bull In the CE alone group fewer women died from invasive breast cancer (6 deaths 0009 per year) compared with controls (16 deaths 0024 per year HR 037 95 CI 013ndash091 P=003)
Anderson GL et al Lancet
Oncol 2012
Bazedoxifene (BZA) specifically selected in
combination with conjugated estrogens
bull BZA has been specifically selected for its unique pharmacologic profile and effects on VMS and uterine tissue in particular123
1 Crabtree J et al Mol Cell Endocrinol 2008
2 Kharode Y et al Endocrinolology 2008
3 Duavive SmPC
Estrogen Receptor activity is dimmed
Estrogen Receptor activity is turned on
CEs are agonists BZA is an antagonist
In the uterus
bull The BZA component reduces the risk of endometrial hyperplasia that can occur with the conjugated estrogens component alone3 This means that progestins are not needed
Extensive global clinical development program for
CEBZA
aIncludes additional pilot dose-finding study 203 1 Lobo RA et al Fertil Steril 2009 2 Pinkerton JV et al Menopause 2009 3 Kagan R et al Menopause 2010 4 Mirkin S et al Climacteric 2013 5 Pinkerton JV et al Obstet Gynecol 2013
Effects of conjugated estrogensbazedoxifene on
lipid and coagulation variables a randomized
placebo- and active-controlled trial
bull At 12 months
bull Both CEBZA doses were associated with small but significant effects on hemostasis variables including reductions in antithrombin plasminogen activator inhibitor-1 and fibrinogen activity and an increase in plasminogen activity relative to placebo at 12 months Incidences of cardiovascular and venous thromboembolic events were similar among treatment groups
bull CONCLUSIONS
bull This study provides reassurance that CEBZA does not adversely affect lipid metabolism or hemostatic balance In accordance the incidences of venous thromboembolic events and cardiovascular events in postmenopausal women are similar to those observed with placebo

Other combinations of an estrogen (E2) + a SERM studied have
not produced favorable results
bull Objective To compare effects of 52 weeksrsquo treatment with either raloxifene 60 mgday alone (RLX) or in combination with 17B-estradiol 1 mgday (RLX + E2) on vasomotor symptoms (n = 83) and endometrial safety (n = 123) in postmenopausal women who transitioned from estrogen-progestin therapy Endometrial effect Women in the RLX + E2 group had significantly increased endometrial thickness at 52 weeks from baseline and RLX alone had no increase Two women (328) in the RLX + E2 group had endometrial hyperplasia (one with atypia) on the exit biopsy No one in RLX alone did
bull 1 Stovall D et al Menopause The Journal of The North American Menopause Society 2007
bull For the safety analyses data from women randomized before and after the protocol amendment were pooled which included 62 women in the raloxifene group and 61 women in the raloxifene + estrogen group
EFFICACY
VASOMOTOR
SYMPTOMS
SMART-2
DUAVIVE Efficacy for the Treatment of Moderate to
Severe VMS Associated With Menopause
14
1 Pinkerton JV et al Menopause 2009
Postmenopausal women
with a uterus
Age 42-64 year
(avg 53 yr)
(N=318)
DUAVIVE (CE 045BZA 20)
(n=127)
Placebo
(n=63)
bull 12-week randomized double-blind placebo-controlled study1
bull Inclusion criteria
‒ Postmenopausal women with an intact uterus
‒ Minimum of 7 moderate to severe hot flushes per day or at least 50 per week at screening
Change from baseline to
Weeks 4 and 12 in
bull Average daily number of
moderate to severe hot
flushes
bull Average daily severity
score of hot flushes
Primary End Points
Safety population (took at least one dose)
Significant Reduction vs Placebo in
Average Daily Number of Hot Flushes
DUAVEE [package insert] New York NY Pfizer Inc 2013
ANCOVA=analysis of covariance
Reduction in average daily number of
moderate to severe hot flushes ndash primary end point
Ad
jus
ted
mean
ch
an
ge
fro
m b
aselin
edagger
Week 4 Week 12
ndash31
ndash27
Treatment
differencedagger ndash59
ndash28
ndash76
ndash49
Treatment
differencedagger
22
Plt001 vs placebo daggerBased on data analysis using ANCOVA model Change from baseline = Treatment + Baseline + Site
DUAVIV
E
Reduction in the Observed Average Daily Number
of Moderate to Severe Hot Flushes
Data on file CSR-67461 Protocol 3115A1-305 Table 1511 Pfizer Inc New York NY
change from baseline to week 12
74 for DUAVIVE
51 for placebo
Observed Average Daily Number of Hot Flushes
Ob
serv
ed a
vera
ge d
aily
nu
mb
er o
f m
od
erat
e to
sev
ere
ho
t fl
ush
es
0 1 2 3 4 5 6 7 8 9 10 12 0 1
11
2
4 3
6 5
7 8 9
10
28
54
DUAVIVE (n=122) Placebo (n=62)
Weeks
Primary analysis showed statistically significant separation at weeks 4 and 12
Average daily number of hot flushes from baseline to week 12
103 to 28 for DUAVIVE
105 to 54 for placebo
Based on mathematical means
not statistically analyzed
105 103
Pinkerton JV et al Menopause 2009
Significant Reduction vs Placebo in
Average Daily Severity Score of Hot Flushes
17
Week 4 Week 12
ndash05
ndash06
Treatment
differencedagger
Treatment
differencedagger
DUAVEE [package insert] New York NY Pfizer Inc 2013
Reduction in average daily severity score of hot flushes ndash primary end point
Ad
jus
ted
me
an
ch
an
ge
fro
m b
aselin
edagger
Plt001 vs placebo daggerBased on data analysis using ANCOVA model Change from baseline = Treatment + Baseline + Site
DUAVIV
E
Reduction in the Observed Average
Daily Severity Score of Hot Flushes
Observed Average Daily Severity Score of Hot Flushes
19
DUAVIVE (n=122) Placebo (n=62)
Weeks
Ob
serv
ed a
vera
ge d
aily
sev
erit
y sc
ore
of
ho
t fl
ush
es
0
05
10
15
25
20
0 1 2 3 4 5 6 7 8 9 10 12 11 0 1 2 3 4 5 6 7 8 9 10 12 11
14
Data on file CSR-67461 Protocol 3115A1-305 Table 1511 Pfizer Inc New York NY
Primary analysis at weeks 4 and 12 prespecified secondary end points at all other weeks
change from baseline to week 12
39 for DUAVIVE
14 for placebo
Average daily severity score of hot flashes from baseline to week 12
23 to 14 for DUAVIVE
23 to 19 for Placebo
Based on mathematical means
not statistically analyzed
23
23
Pinkerton JV et al Menopause 2009
Effects on bone mineral density (BMD)
SMART 512
20
bull 12-month double-blind randomized placebo- and active-controlled study
bull Primary end point endometrial hyperplasia at 1 year
bull Secondary BMD changes at 1 year
1 DUAVEE [package insert] New York NY Pfizer Inc 2013 2 Pinkerton J Clin Endocrin Metab 2014
This study included a different dose of CEBZA and comparators The schematic shown here depicts only the patients who received the approved dose of DUAVIVE or placebo
Change from baseline in
bull Lumbar Spine BMD (Primary ndash BMD Substudy)
bull Total Hip BMD (Secondary ndash BMD Substudy)
BMD Analysis
DUAVIVE
(CE 045BZA 20)
(n=119)
Placebo
(n=139)
BMD Analysis
Postmenopausal women with a uterus
Less than 5 years since LMP
(N=590)
DUAVIVE Significantly Increased Lumbar Spine and Total
Hip BMD vs Placebo at 12 Months ndash Study 2
M
ean
ch
an
ge f
rom
baselin
e
Lumbar Spine Total Hip
121 151 Treatment
difference Treatment
difference
Data on file CSR-81040 Protocol 3115A1-3307 Pfizer Inc New York NY Pinkerton J Clin Endocrin Metab 2014 30
Plt001 vs placebo
Adjusted mean changes and P-values based on an ANCOVA model with treatment and region (US or non-US) as factors and baseline BMD value and years since menopause as covariates using the modified intention to treat population with last observation carried forward
DUAVIV
E
TOLERABILITY
AND SAFETY
Rates of BleedingSpotting and Amenorrhea
Similar to Rates with Placebo
bull High and similar cumulative rates of amenorrhea at year 1 among women treated with CE 045BZA 20 and placebo and was higher than seen in women treated with CE 045MPA 151
bull Noncumulative rates of spotting and bleedingspotting were similar among women treated with CEBZA or placebo and consistently higher in women treated with CE 045MPA 152
0
90
Cycle
100
Pe
rce
nta
ge
of
Su
bje
cts
80
70
60
50
40
30
20
10
88
54
Placebo
CE 045BZA 20 CE 045MPA 15
Percentage of subjects with cumulative amenorrhea during consecutive 4-week periods (cycles) in SMART-5
MPA medroxyprogesterone acetate Plt0001 vs all other treatment groups 1 Pinkerton JV et al J Clin Endocrinol Metab 2014 2 Data on file CSR-81040 Protocol 3115A1-3307 Pfizer Inc New York NY
Adverse Reactions in Placebo-
Controlled Trials Safety analyses have been conducted in 6210 postmenopausal women aged 40 to 75 years (mean age 55 years) following up to 2 years of treatment in SMART-1 -2 -3 and -5
Adverse reactions (incidence ge5) that were more common with DUAVIVE
Incidence of serious adverse reactions
35 with DUAVIVE 48 with placebo
DUAVEE [package insert] New York NY Pfizer Inc 2013
CE 045 BZA 20 (N=1224)
n ()
Placebo (N=1069)
n ()
Gastrointestinal disorders
Nausea 100 (8) 58 (5)
Diarrhea 96 (8) 57 (5)
Dyspepsia 84 (7) 59 (6)
Abdominal pain upper 81 (7) 58 (5)
Musculoskeletal and connective tissue disorders
Muscle spasms 110 (9) 63 (6)
Neck pain 62 (5) 46 (4)
Nervous system disorders
Dizziness 65 (5) 37 (3)
Respiratory thoracic and mediastinal disorders
Oropharyngeal pain 80 (7) 61 (6)
Venous Thromboembolism (VTE) in
DUAVIVE Clinical Studies
bull Estrogen agonistantagonists (including BZA a component of DUAVIVE) and estrogens individually are known to increase the risk of VTE
bull In the clinical studies with DUAVIVE the reporting rates for VTE were low in all treatment groups
bull Adverse reactions of VTE reported by patients
bull Should VTE event occur or be suspected DUAVIVE should be discontinued immediately
bull Due to the low rates of events in both groups it is not possible to conclude that the risk of VTE with DUAVIVE is different from that seen with other estrogen therapies
DUAVEE [package insert] New York NY Pfizer Inc 2013
00 for DUAVIVE (n=1224)
01 for placebo (n=1069)
26
Effects of conjugated estrogensbazedoxifene on
lipid and coagulation variables a randomized
placebo- and active-controlled trial
bull postmenopausal women (N = 1843) with menopausal
symptoms
bull Lipid (N = 1843) and coagulation (N = 590) variables were assessed in women receiving daily CE 045 mgBZA 20 mg CE 0625 mgBZA 20 mg BZA 20 mg CE 045 mgmedroxyprogesterone acetate (MPA) 15 mg or placebo for 12 months
bull Skouby SO et al Menopause 2015 Jun22(6)640-9
Effects of conjugated estrogensbazedoxifene on
lipid and coagulation variables a randomized
placebo- and active-controlled trial
bull At 12 months
bull CE 045 mgBZA 20 mg
bull CE 0625 mgBZA 20 mg
bull BZA 20 mg
bull and CE 045 mgMPA 15 mg decreased total cholesterol and LDL- cholesterol vs placebo (P lt 001 for all)
bull Both CEBZA doses and CEMPA increased high-density lipoprotein cholesterol compared with placebo (P lt 005 for all)
bull CE 045 mgBZA 20 mg had a neutral effect on triglycerides
bull CE 0625 mgBZA 20 mg and CEMPA increased triglycerides compared with placebo (P lt 005)
bull Skouby SO et al Menopause 2015 Jun22(6)640-9
Effects of conjugated estrogensbazedoxifene on
lipid and coagulation variables a randomized
placebo- and active-controlled trial
bull At 12 months
bull Both CEBZA doses were associated with small but significant effects on hemostasis variables including reductions in antithrombin plasminogen activator inhibitor-1 and fibrinogen activity and an increase in plasminogen activity relative to placebo at 12 months Incidences of cardiovascular and venous thromboembolic events were similar among treatment groups
Skouby SO et al Menopause 2015
Jun22(6)640-9
Endometrial hyperplasia or malignancy occurred in lt1 of women
following up to 1 year of treatment with CEBZA12
Study Cumulative Incidence at month 12 (nN)
CE 045BZA 20 Placebo
SMART-11 000 (0336) 000 (0313)
SMART-52 030 (1335) 028 (1354)
Effects on the Endometrium
1 Pickar JH et al Fertil Steril 2009 2 Pinkerton at al J Clin Endocrinol Metab 2014
Through the eyes of an amazone
Marie Mandy
Breast tolerability profile similar to placebo following up to 2 years of treatment with CEBZA12
Pooled analysis of SMART clinical trials
CE 045BZA 20 (n=1585)
Placebo (n=1241)
Breast cancer incidence up to 2 years
(per 1000 woman-years)
100 (CI 000-321)
140 (CI 000-417)
Incidence of reported breast paintenderness up to 12 weeks
98-115 81-112
Incidence of abnormal mammogram at month 12
258 316
Mean change in breast density at month 12 (SMART-5)
ndash038 (n=186)
ndash032 (n=182)
Effects on the Breast
1 Pickar JH et al Menopause 2013 2 Pinkerton JV et al Obstet Gynecol 2013
CEBZA clinical overview - summary
bull In clinical trials CEBZA has demonstrated safety and efficacy in postmenopausal women with a uterus including the following
bull Significant reduction in number and severity of moderate to severe hot flushes1
bull Incidence of cumulative amenorrhea rate similar to placebo and significantly better than CEMPA2
bull Incidence of endometrial hyperplasia and breast tendernessdensity similar to that with placebo345
bull Incidence of adverse events and discontinuation rates similar to that with placebo6
1 Pinkerton JV et al Menopause 2009 2 Pinkerton JV et al J Clin Endocrinol Metab2014 3 Pickar JH et al
Fertil Steril 2009 4 Pinkerton at al J Clin Endocrinol Metab 2014 5 Pickar JH et al Menopause 2013 6 DUAVEE [package insert] New York NY Pfizer Inc 2013
CEBZA clinical overview - summary
Now women with a uterus who choose hormone therapy for management of menopausal symptoms have a choice
bull conventional estrogen-progestogen therapy or
bull a new combinationhellipconjugated estrogens paired with the SERM bazedoxifene
1 Pinkerton JV et al Menopause 2009 2 Pinkerton JV et al J Clin Endocrinol Metab2014 3 Pickar JH et al Fertil Steril 2009 4 Pinkerton at al J Clin Endocrinol Metab 2014 5 Pickar JH et al Menopause 2013 6 DUAVEE [package insert] New York NY Pfizer Inc 2013
Conjugated EstrogensBazedoxifene (CEBZA)
US indication
bull DUAVEE is indicated in women with a uterus for
bull 11 Treatment of Moderate to Severe Vasomotor Symptoms Associated with Menopause
bull 12 Prevention of Postmenopausal Osteoporosis
bull 13 Important Limitations of Use
bull Use DUAVEE for the shortest duration consistent with treatment goals and risks for the individual woman Postmenopausal women should be re-evaluated periodically as clinically appropriate to determine if treatment is still necessary
bull When prescribing solely for the prevention of postmenopausal osteoporosis therapy should only be considered for women at significant risk of osteoporosis and non-estrogen medication should be carefully considered
Conjugated EstrogensBazedoxifene (CEBZA)
EU indication
CEBZA is indicated for
bull Treatment of oestrogen deficiency symptoms in postmenopausal women with a uterus (with at least 12 months since the last menses) for whom treatment with progestin-containing therapy is not appropriate
bull The experience treating women older than 65 years is limited
bull Dose CE (045mg)Bazedoxifene (20mg)
Duavive SmPC
Which women with a uterus
could benefit from estrogens
without the need for a
progestin
Progestin intolerance is one of the main
factors for reduced compliance
bull About 20 of women receiving progestin-containing HT have significant progestin intolerance and half of these experience serious effects that prevent treatment continuation1
1 Panay N amp Studd J Human Reprod Update 1997
2 Panay N et al on behalf of the British Menopause Society and Womenrsquos Health Concern Menopause Int 2013
bull The 2013 British Menopause Society amp Womenrsquos Health
Concern recommendations on hormone replacement
therapy do recognise progestin intolerance as one of the
main factors for reduced compliance with HT 2
Proportion of patients () with at least one bleeding episode in relation to time and to the
used HT
Serge Rozenberg et al Hum Reprod 2009241739-1747
copy The Author 2009 Published by Oxford University Press on behalf of the European Society of
Human Reproduction and Embryology All rights reserved For Permissions please email
journalspermissionsoxfordjournalsorg
Breast tenderness after initiation of CEE
CEE + MPA (WHI)
and mammographic density change
bullCrandall et al Breast Cancer Res Treat DOI 101007s10549-011-1803-9
Breast density
Conclusion
bull CEEBAZO is an additional regimen for menopausal symptoms it provides also a prevention for osteoporosis
bull It is suitable for women with a uterus who are unsatisfied with an EPT regimen or who you are unwilling to treat with an EPT regimen
Adapted use of MHT
bull Lower dosage of estrogens
bull Other progestins
bull Better safety profile
bull Vaginal estrogen or SERMS
bull Non-hormonal therapy
bull Development of new products
bull SERMS + estrogens
Most common adverse events leading to
discontinuation are related to progestins12
bull breakthrough bleeding
bull Low compliance
bull Increase in the number of US
bull Stress
bull Cost
bull uterine procedures
bull Unnecessary endometrial biopsies Hysteroscopies DampC Hysterectomies
bull Morbidity
Proportion of patients who completed or discontinued treatment in relation to the used HT
Serge Rozenberg et al Hum Reprod 2009241739-1747
copy The Author 2009 Published by Oxford University Press on behalf of the European Society of
Human Reproduction and Embryology All rights reserved For Permissions please email
journalspermissionsoxfordjournalsorg
Most common adverse events leading to discontinuation
are related to progestins
bull breast paintenderness
Breast tenderness after initiation of CEE
CEE + MPA (WHI)
and mammographic density change
bullCrandall et al Breast Cancer Res Treat DOI 101007s10549-011-1803-9
Breast density
Hormone therapy use and mammographic
density in postmenopausal Norwegian women
bull Results differed when considering the combined effect of age and BMI
bull The effect of EPT on mammographic density was modified by age and BMI with no apparent association among the youngest women (aged 50-55) with the highest BMI (BMI ge 26)
bull A higher mammographic density was found in EPT users compared to never HT users particularly in women using high-dose NETA regimens Age and BMI modified the association between EPT use and mammographic density
bull Couto E et al Breast Cancer Res Treat 2011 Nov 4 [Epub ahead of print]
Breast Cancer Risk by Breast Density
Menopause and Postmenopausal Hormone
Therapy Use
Birads age HT Duration Risk
1 55-59 None 5 year risk 08 (95 CI 06- 09)
1 55-59
ET EPT 5 year risk 09 (95 CI 07 -11)
4 55-59
None 5 year risk 24 (95 CI 20 -28)
4 55-59
ET 5 year risk
30 (95 CI 26 -35)
4 55-59
EPT 5 year risk
42 (95 CI 37 -46)
Adapted from Kerlikowske et al JOURNAL OF CLINICAL ONCOLOGY 2010
Breast Cancer Risk by Breast Density
Menopause and Postmenopausal Hormone
Therapy Use
Adapted from Kerlikowske et al JOURNAL OF CLINICAL ONCOLOGY 2010
bull Postmenopausal women with high breast density are at increased risk of breast cancer and should be aware of the added risk of taking HT especially estrogen plus progestin
Medical condition which may be exacerbated by treatment
with progestins
Diabetes and metabolic syndrome
bull progestin-containing HT may be associated with increases in insulin resistance and deterioration in glucose tolerance123
bull Postmenopausal women with diabetes could be inappropriate for treatment with progestin-containing HT due to the potential risk of exacerbation of their condition
1) Panay N amp Studd JWW Human Reprod Update 1997
2) Godsland I et al Metabolism 1993
3) Sites CK et al J Clin Endocrinol Metab 2005
A Nath and R Sitruk-Ware CLIMACTERIC 200912(Suppl 1)96ndash101
A Nath and R Sitruk-Ware CLIMACTERIC 200912(Suppl 1)96ndash101
Diabetes an epidemy
bull UK 1996 14 million of diabetics
bull UK 2015 32 million (6 of the population)
bull UK 2025 5 million
bull httpwwwdiabetescoukdiabetes-prevalencehtml
Other progestin-related intolerance issues
bull Nausea
bull Depressive mood
bull Poor concentration
bull Hirsutism
bull Headache
bull Dizziness
bull Fluid retention
bull Weight gain Panay N amp Studd JWW Human Reprod Update 1997
Medical condition which may be exacerbated by treatment with progestins
PMSPMDDdepression
bull Progesterone-induced PMD can be exacerbated by exogenous progestin administration and can occur in association with HT or OC administration1
bull Significantly higher negative mood scores have been observed during the addition of a progestin to an estrogen in a sequential HT regimen in postmenopausal women with a history of PMS compared to those without2
bull Women with a history of PMS or PMD exacerbation of depression using progestins may therefore benefit from a progestin free treatment for menopausal symptoms
1) Nevatte T et al Arch Womens Ment Health 2013 2) Bjoumlrn I et al Climacteric 2006 PMS premenstrual syndrome
PMDD premenstrual dysphoric disorder
Conclusion
bull CEEBAZO is an additional regimen for menopausal symptoms it provides also a prevention for osteoporosis
bull It is suitable for women with a uterus who are unsatisfied with an EPT regimen or who you are unwilling to treat with an EPT regimen
For some postmenopausal women with a uterus there is a
need for progestin free treatment options
bull with demonstrated clinical efficacy
bull which protects the endometrium
bull improved tolerabilitysafety profile
In clinical practice this translates to women who are
intolerant of progestin-containing HT or have conditions
which may be exacerbated by treatment with progestins
Conclusion Medical need for alternative treatment option
Medical condition which may be exacerbated by treatment with progestins
Depression
bull Progestin-containing HT has been associated with increases in depressive symptoms in some individuals1
bull There is a biochemicalphysiological plausibility for the association of progestins with depression234
bull Therefore postmenopausal women who also have a medical history of depressive disorders or depression could be inappropriate for treatment with progestin-containing HT
Pfizer Confidential
65
1) Girdler SS et al J Womens Health Gend Based Med 1999 2) Traish AM et al Korean J Urol 2014 3) Stroumlhle A et al Biol Psychiatry 1999 4) Romeo E et
al Am J Psychiatry 1998
History of the following conditions may make progestin inappropriate
bull Depression
bull PMSPMDD
PMS premenstrual syndrome
PMD premenstrual dysphoric disorder
Medical conditions that may be exacerbated by treatment with progestins
Women for whom progestin-containing HT
would not be considered appropriate
minus Women who are intolerant of progestin-containing hormone therapy
minus Women with pre-existing medical conditions that may be exacerbated by progestins
Most common adverse events leading to discontinuation are related to progestins12
breakthrough bleeding
bull Increase in the number of uterine procedures (ie unnecessary endometrial biopsies)
breast paintenderness
bull Increase in the number of breast interventions
1 Steel SA et al Climacteric 2003 2 Ettinger B and Pressman A Am J Manag Care 1999 3 Komm BS Mirkin S
Pharmaceuticals 2012
4 Panay N amp Studd JWW Human Reprod Update 1997
bull Nausea bull Depressive mood bull Poor concentration bull Hirsutism bull Headache bull Dizziness bull Fluid retention bull Weight gain
Other progestin-related intolerance issues4
Unmet need with the treatment of postmenopausal symptoms
bull Alternatives to progestin are needed that will protect the endometrium while avoiding other progestin-associated effects and preserving the desired effects of estrogens in postmenopausal women3
Which women with a uterus could benefit from
estrogens without the need for a progestin
bull Women who are intolerant of progestin-containing hormone therapy
bull Women with pre-existing medical conditions that may be exacerbated by progestins (eg women with a history of depression PMSPMDD increased breast density diabetes and metabolic syndrome)
History of the following conditions may make progestin inappropriate
bull Depression
bull PMSPMDD
bull High breast density
bull Diabetes and metabolic syndrome
PMS premenstrual syndrome
PMD premenstrual dysphoric disorder
Medical conditions that may be exacerbated by treatment with progestins
Learning from WHI data
bull Hormone therapy (HT) is the conventional and established therapy option to effectively treat postmenopausal symptoms however it has been associated with some safety and tolerability concerns1 2
bull A review of WHI data suggests that many of the concerns with menopausal HT more often associated with EPT (CE+MPA) such as CHD risk increased breast density breast pain and breast cancer risk than with ET (CEE alone)2
1 Rolnick SJ Kopher RA DeFor TA et al Menopause 2005
2 Komm BS Mirkin S Pharmaceuticals 2012
WHI Womenrsquos Health Initiative trial
CHD coronary heart disease
CEE conjugated equine estrogens
Efficacy and Safety of Constant Oestrogen
Pulsed Progestogen vs
Continuous Combined HRT
Adverse Events
17b-oestradiol 17b-oestradiol norgestimate NETA (n = 150) (n = 172) Breast discomfort 14 27 Abdominal discomfort 14 22 Uterine bleeding 15 12 Dysmenorrhea 3 8 Oedema 5 8
Adapted from S Rozenberg et al Human Reproduction 2000
Medical condition which may be exacerbated by treatment
with progestins
Increased breast density
bull Increases in breast density are associated with progestin-containing HT which may adversely affect radiological detection of breast cancer1 and may be independently associated with an increased risk for the development of breast cancer2
bull The Postmenopausal EstrogenProgestin Interventions (PEPI) trial demonstrated that an increased mammographic breast density was associated with the use of E+P but not with the use of estrogen alone3
bull Women who already have high breast density may therefore be considered inappropriate for treatment with a progestin-containing HT
1) EU Core SPC for Hormone Replacement Therapy Products (CMDh1312003 Rev 4 June
2012)
2) De Villiers TJ et al on behalf of the International Menopause Society Climacteric 2013 16
3) Greendale GA et al J Natl Cancer Inst 2003
Stroke
0 25 5 75 10 125
Fractures
Diabetes
Breast cancer
Cholecystitis
Venothrombotic episodes
Endometrial cancer
Lung cancer
Coronary heart disease
Colorectal cancer
Overall mortality
15 125 10 75 5 25
Benefits Risks
CE
CE MPA
Santen RJ et al J Clin Endocrinol Metab 2010
The basis of the Endocrine Society scientific statement for postmenopausal hormone replacement therapy (HRT) excess risks and benefits of HRT for 5 years in women aged 50ndash59 years or within 10 years of the start of menopause E=estrogen P=progestin
bull Younger women (aged 50ndash59 years) had more favorable results bull There are differences between CE alone and CEMPA arms bull Overall benefitrisk ratio of CE-alone appears to be more favourable than CEMPA
Reevaluation of WHI data (stratified by age) Risks and
Benefits of HRT Cases per 1000 Women per 5 Years of
Use
Medical condition which may be exacerbated by treatment
with progestins
Diabetes and metabolic syndrome
bull Treatment of oestrogen deficiency symptoms with progestin-containing HT (unlike oestrogen alone) may be associated with increases in insulin resistance and deterioration in glucose tolerance123
bull Postmenopausal women with diabetes could be inappropriate for treatment with progestin-containing HT due to the potential risk of exacerbation of their condition
1) Panay N amp Studd JWW Human Reprod Update 1997
2) Godsland I et al Metabolism 1993
3) Sites CK et al J Clin Endocrinol Metab 2005
Variations in Associated Breast Cancer
Risks Between CE alone and CEMPA
bull Use of CE alone for a median of 59 years was associated with a lower incidence of invasive breast cancer (151 cases 027 per year) compared with placebo (199 cases 035 per year HR 077 95 CI 062ndash095 P=002)
bull In the CE alone group fewer women died from invasive breast cancer (6 deaths 0009 per year) compared with controls (16 deaths 0024 per year HR 037 95 CI 013ndash091 P=003)
Anderson GL et al Lancet
Oncol 2012
Bazedoxifene (BZA) specifically selected in
combination with conjugated estrogens
bull BZA has been specifically selected for its unique pharmacologic profile and effects on VMS and uterine tissue in particular123
1 Crabtree J et al Mol Cell Endocrinol 2008
2 Kharode Y et al Endocrinolology 2008
3 Duavive SmPC
Estrogen Receptor activity is dimmed
Estrogen Receptor activity is turned on
CEs are agonists BZA is an antagonist
In the uterus
bull The BZA component reduces the risk of endometrial hyperplasia that can occur with the conjugated estrogens component alone3 This means that progestins are not needed
Extensive global clinical development program for
CEBZA
aIncludes additional pilot dose-finding study 203 1 Lobo RA et al Fertil Steril 2009 2 Pinkerton JV et al Menopause 2009 3 Kagan R et al Menopause 2010 4 Mirkin S et al Climacteric 2013 5 Pinkerton JV et al Obstet Gynecol 2013
Effects of conjugated estrogensbazedoxifene on
lipid and coagulation variables a randomized
placebo- and active-controlled trial
bull At 12 months
bull Both CEBZA doses were associated with small but significant effects on hemostasis variables including reductions in antithrombin plasminogen activator inhibitor-1 and fibrinogen activity and an increase in plasminogen activity relative to placebo at 12 months Incidences of cardiovascular and venous thromboembolic events were similar among treatment groups
bull CONCLUSIONS
bull This study provides reassurance that CEBZA does not adversely affect lipid metabolism or hemostatic balance In accordance the incidences of venous thromboembolic events and cardiovascular events in postmenopausal women are similar to those observed with placebo

EFFICACY
VASOMOTOR
SYMPTOMS
SMART-2
DUAVIVE Efficacy for the Treatment of Moderate to
Severe VMS Associated With Menopause
14
1 Pinkerton JV et al Menopause 2009
Postmenopausal women
with a uterus
Age 42-64 year
(avg 53 yr)
(N=318)
DUAVIVE (CE 045BZA 20)
(n=127)
Placebo
(n=63)
bull 12-week randomized double-blind placebo-controlled study1
bull Inclusion criteria
‒ Postmenopausal women with an intact uterus
‒ Minimum of 7 moderate to severe hot flushes per day or at least 50 per week at screening
Change from baseline to
Weeks 4 and 12 in
bull Average daily number of
moderate to severe hot
flushes
bull Average daily severity
score of hot flushes
Primary End Points
Safety population (took at least one dose)
Significant Reduction vs Placebo in
Average Daily Number of Hot Flushes
DUAVEE [package insert] New York NY Pfizer Inc 2013
ANCOVA=analysis of covariance
Reduction in average daily number of
moderate to severe hot flushes ndash primary end point
Ad
jus
ted
mean
ch
an
ge
fro
m b
aselin
edagger
Week 4 Week 12
ndash31
ndash27
Treatment
differencedagger ndash59
ndash28
ndash76
ndash49
Treatment
differencedagger
22
Plt001 vs placebo daggerBased on data analysis using ANCOVA model Change from baseline = Treatment + Baseline + Site
DUAVIV
E
Reduction in the Observed Average Daily Number
of Moderate to Severe Hot Flushes
Data on file CSR-67461 Protocol 3115A1-305 Table 1511 Pfizer Inc New York NY
change from baseline to week 12
74 for DUAVIVE
51 for placebo
Observed Average Daily Number of Hot Flushes
Ob
serv
ed a
vera
ge d
aily
nu
mb
er o
f m
od
erat
e to
sev
ere
ho
t fl
ush
es
0 1 2 3 4 5 6 7 8 9 10 12 0 1
11
2
4 3
6 5
7 8 9
10
28
54
DUAVIVE (n=122) Placebo (n=62)
Weeks
Primary analysis showed statistically significant separation at weeks 4 and 12
Average daily number of hot flushes from baseline to week 12
103 to 28 for DUAVIVE
105 to 54 for placebo
Based on mathematical means
not statistically analyzed
105 103
Pinkerton JV et al Menopause 2009
Significant Reduction vs Placebo in
Average Daily Severity Score of Hot Flushes
17
Week 4 Week 12
ndash05
ndash06
Treatment
differencedagger
Treatment
differencedagger
DUAVEE [package insert] New York NY Pfizer Inc 2013
Reduction in average daily severity score of hot flushes ndash primary end point
Ad
jus
ted
me
an
ch
an
ge
fro
m b
aselin
edagger
Plt001 vs placebo daggerBased on data analysis using ANCOVA model Change from baseline = Treatment + Baseline + Site
DUAVIV
E
Reduction in the Observed Average
Daily Severity Score of Hot Flushes
Observed Average Daily Severity Score of Hot Flushes
19
DUAVIVE (n=122) Placebo (n=62)
Weeks
Ob
serv
ed a
vera
ge d
aily
sev
erit
y sc
ore
of
ho
t fl
ush
es
0
05
10
15
25
20
0 1 2 3 4 5 6 7 8 9 10 12 11 0 1 2 3 4 5 6 7 8 9 10 12 11
14
Data on file CSR-67461 Protocol 3115A1-305 Table 1511 Pfizer Inc New York NY
Primary analysis at weeks 4 and 12 prespecified secondary end points at all other weeks
change from baseline to week 12
39 for DUAVIVE
14 for placebo
Average daily severity score of hot flashes from baseline to week 12
23 to 14 for DUAVIVE
23 to 19 for Placebo
Based on mathematical means
not statistically analyzed
23
23
Pinkerton JV et al Menopause 2009
Effects on bone mineral density (BMD)
SMART 512
20
bull 12-month double-blind randomized placebo- and active-controlled study
bull Primary end point endometrial hyperplasia at 1 year
bull Secondary BMD changes at 1 year
1 DUAVEE [package insert] New York NY Pfizer Inc 2013 2 Pinkerton J Clin Endocrin Metab 2014
This study included a different dose of CEBZA and comparators The schematic shown here depicts only the patients who received the approved dose of DUAVIVE or placebo
Change from baseline in
bull Lumbar Spine BMD (Primary ndash BMD Substudy)
bull Total Hip BMD (Secondary ndash BMD Substudy)
BMD Analysis
DUAVIVE
(CE 045BZA 20)
(n=119)
Placebo
(n=139)
BMD Analysis
Postmenopausal women with a uterus
Less than 5 years since LMP
(N=590)
DUAVIVE Significantly Increased Lumbar Spine and Total
Hip BMD vs Placebo at 12 Months ndash Study 2
M
ean
ch
an
ge f
rom
baselin
e
Lumbar Spine Total Hip
121 151 Treatment
difference Treatment
difference
Data on file CSR-81040 Protocol 3115A1-3307 Pfizer Inc New York NY Pinkerton J Clin Endocrin Metab 2014 30
Plt001 vs placebo
Adjusted mean changes and P-values based on an ANCOVA model with treatment and region (US or non-US) as factors and baseline BMD value and years since menopause as covariates using the modified intention to treat population with last observation carried forward
DUAVIV
E
TOLERABILITY
AND SAFETY
Rates of BleedingSpotting and Amenorrhea
Similar to Rates with Placebo
bull High and similar cumulative rates of amenorrhea at year 1 among women treated with CE 045BZA 20 and placebo and was higher than seen in women treated with CE 045MPA 151
bull Noncumulative rates of spotting and bleedingspotting were similar among women treated with CEBZA or placebo and consistently higher in women treated with CE 045MPA 152
0
90
Cycle
100
Pe
rce
nta
ge
of
Su
bje
cts
80
70
60
50
40
30
20
10
88
54
Placebo
CE 045BZA 20 CE 045MPA 15
Percentage of subjects with cumulative amenorrhea during consecutive 4-week periods (cycles) in SMART-5
MPA medroxyprogesterone acetate Plt0001 vs all other treatment groups 1 Pinkerton JV et al J Clin Endocrinol Metab 2014 2 Data on file CSR-81040 Protocol 3115A1-3307 Pfizer Inc New York NY
Adverse Reactions in Placebo-
Controlled Trials Safety analyses have been conducted in 6210 postmenopausal women aged 40 to 75 years (mean age 55 years) following up to 2 years of treatment in SMART-1 -2 -3 and -5
Adverse reactions (incidence ge5) that were more common with DUAVIVE
Incidence of serious adverse reactions
35 with DUAVIVE 48 with placebo
DUAVEE [package insert] New York NY Pfizer Inc 2013
CE 045 BZA 20 (N=1224)
n ()
Placebo (N=1069)
n ()
Gastrointestinal disorders
Nausea 100 (8) 58 (5)
Diarrhea 96 (8) 57 (5)
Dyspepsia 84 (7) 59 (6)
Abdominal pain upper 81 (7) 58 (5)
Musculoskeletal and connective tissue disorders
Muscle spasms 110 (9) 63 (6)
Neck pain 62 (5) 46 (4)
Nervous system disorders
Dizziness 65 (5) 37 (3)
Respiratory thoracic and mediastinal disorders
Oropharyngeal pain 80 (7) 61 (6)
Venous Thromboembolism (VTE) in
DUAVIVE Clinical Studies
bull Estrogen agonistantagonists (including BZA a component of DUAVIVE) and estrogens individually are known to increase the risk of VTE
bull In the clinical studies with DUAVIVE the reporting rates for VTE were low in all treatment groups
bull Adverse reactions of VTE reported by patients
bull Should VTE event occur or be suspected DUAVIVE should be discontinued immediately
bull Due to the low rates of events in both groups it is not possible to conclude that the risk of VTE with DUAVIVE is different from that seen with other estrogen therapies
DUAVEE [package insert] New York NY Pfizer Inc 2013
00 for DUAVIVE (n=1224)
01 for placebo (n=1069)
26
Effects of conjugated estrogensbazedoxifene on
lipid and coagulation variables a randomized
placebo- and active-controlled trial
bull postmenopausal women (N = 1843) with menopausal
symptoms
bull Lipid (N = 1843) and coagulation (N = 590) variables were assessed in women receiving daily CE 045 mgBZA 20 mg CE 0625 mgBZA 20 mg BZA 20 mg CE 045 mgmedroxyprogesterone acetate (MPA) 15 mg or placebo for 12 months
bull Skouby SO et al Menopause 2015 Jun22(6)640-9
Effects of conjugated estrogensbazedoxifene on
lipid and coagulation variables a randomized
placebo- and active-controlled trial
bull At 12 months
bull CE 045 mgBZA 20 mg
bull CE 0625 mgBZA 20 mg
bull BZA 20 mg
bull and CE 045 mgMPA 15 mg decreased total cholesterol and LDL- cholesterol vs placebo (P lt 001 for all)
bull Both CEBZA doses and CEMPA increased high-density lipoprotein cholesterol compared with placebo (P lt 005 for all)
bull CE 045 mgBZA 20 mg had a neutral effect on triglycerides
bull CE 0625 mgBZA 20 mg and CEMPA increased triglycerides compared with placebo (P lt 005)
bull Skouby SO et al Menopause 2015 Jun22(6)640-9
Effects of conjugated estrogensbazedoxifene on
lipid and coagulation variables a randomized
placebo- and active-controlled trial
bull At 12 months
bull Both CEBZA doses were associated with small but significant effects on hemostasis variables including reductions in antithrombin plasminogen activator inhibitor-1 and fibrinogen activity and an increase in plasminogen activity relative to placebo at 12 months Incidences of cardiovascular and venous thromboembolic events were similar among treatment groups
Skouby SO et al Menopause 2015
Jun22(6)640-9
Endometrial hyperplasia or malignancy occurred in lt1 of women
following up to 1 year of treatment with CEBZA12
Study Cumulative Incidence at month 12 (nN)
CE 045BZA 20 Placebo
SMART-11 000 (0336) 000 (0313)
SMART-52 030 (1335) 028 (1354)
Effects on the Endometrium
1 Pickar JH et al Fertil Steril 2009 2 Pinkerton at al J Clin Endocrinol Metab 2014
Through the eyes of an amazone
Marie Mandy
Breast tolerability profile similar to placebo following up to 2 years of treatment with CEBZA12
Pooled analysis of SMART clinical trials
CE 045BZA 20 (n=1585)
Placebo (n=1241)
Breast cancer incidence up to 2 years
(per 1000 woman-years)
100 (CI 000-321)
140 (CI 000-417)
Incidence of reported breast paintenderness up to 12 weeks
98-115 81-112
Incidence of abnormal mammogram at month 12
258 316
Mean change in breast density at month 12 (SMART-5)
ndash038 (n=186)
ndash032 (n=182)
Effects on the Breast
1 Pickar JH et al Menopause 2013 2 Pinkerton JV et al Obstet Gynecol 2013
CEBZA clinical overview - summary
bull In clinical trials CEBZA has demonstrated safety and efficacy in postmenopausal women with a uterus including the following
bull Significant reduction in number and severity of moderate to severe hot flushes1
bull Incidence of cumulative amenorrhea rate similar to placebo and significantly better than CEMPA2
bull Incidence of endometrial hyperplasia and breast tendernessdensity similar to that with placebo345
bull Incidence of adverse events and discontinuation rates similar to that with placebo6
1 Pinkerton JV et al Menopause 2009 2 Pinkerton JV et al J Clin Endocrinol Metab2014 3 Pickar JH et al
Fertil Steril 2009 4 Pinkerton at al J Clin Endocrinol Metab 2014 5 Pickar JH et al Menopause 2013 6 DUAVEE [package insert] New York NY Pfizer Inc 2013
CEBZA clinical overview - summary
Now women with a uterus who choose hormone therapy for management of menopausal symptoms have a choice
bull conventional estrogen-progestogen therapy or
bull a new combinationhellipconjugated estrogens paired with the SERM bazedoxifene
1 Pinkerton JV et al Menopause 2009 2 Pinkerton JV et al J Clin Endocrinol Metab2014 3 Pickar JH et al Fertil Steril 2009 4 Pinkerton at al J Clin Endocrinol Metab 2014 5 Pickar JH et al Menopause 2013 6 DUAVEE [package insert] New York NY Pfizer Inc 2013
Conjugated EstrogensBazedoxifene (CEBZA)
US indication
bull DUAVEE is indicated in women with a uterus for
bull 11 Treatment of Moderate to Severe Vasomotor Symptoms Associated with Menopause
bull 12 Prevention of Postmenopausal Osteoporosis
bull 13 Important Limitations of Use
bull Use DUAVEE for the shortest duration consistent with treatment goals and risks for the individual woman Postmenopausal women should be re-evaluated periodically as clinically appropriate to determine if treatment is still necessary
bull When prescribing solely for the prevention of postmenopausal osteoporosis therapy should only be considered for women at significant risk of osteoporosis and non-estrogen medication should be carefully considered
Conjugated EstrogensBazedoxifene (CEBZA)
EU indication
CEBZA is indicated for
bull Treatment of oestrogen deficiency symptoms in postmenopausal women with a uterus (with at least 12 months since the last menses) for whom treatment with progestin-containing therapy is not appropriate
bull The experience treating women older than 65 years is limited
bull Dose CE (045mg)Bazedoxifene (20mg)
Duavive SmPC
Which women with a uterus
could benefit from estrogens
without the need for a
progestin
Progestin intolerance is one of the main
factors for reduced compliance
bull About 20 of women receiving progestin-containing HT have significant progestin intolerance and half of these experience serious effects that prevent treatment continuation1
1 Panay N amp Studd J Human Reprod Update 1997
2 Panay N et al on behalf of the British Menopause Society and Womenrsquos Health Concern Menopause Int 2013
bull The 2013 British Menopause Society amp Womenrsquos Health
Concern recommendations on hormone replacement
therapy do recognise progestin intolerance as one of the
main factors for reduced compliance with HT 2
Proportion of patients () with at least one bleeding episode in relation to time and to the
used HT
Serge Rozenberg et al Hum Reprod 2009241739-1747
copy The Author 2009 Published by Oxford University Press on behalf of the European Society of
Human Reproduction and Embryology All rights reserved For Permissions please email
journalspermissionsoxfordjournalsorg
Breast tenderness after initiation of CEE
CEE + MPA (WHI)
and mammographic density change
bullCrandall et al Breast Cancer Res Treat DOI 101007s10549-011-1803-9
Breast density
Conclusion
bull CEEBAZO is an additional regimen for menopausal symptoms it provides also a prevention for osteoporosis
bull It is suitable for women with a uterus who are unsatisfied with an EPT regimen or who you are unwilling to treat with an EPT regimen
Adapted use of MHT
bull Lower dosage of estrogens
bull Other progestins
bull Better safety profile
bull Vaginal estrogen or SERMS
bull Non-hormonal therapy
bull Development of new products
bull SERMS + estrogens
Most common adverse events leading to
discontinuation are related to progestins12
bull breakthrough bleeding
bull Low compliance
bull Increase in the number of US
bull Stress
bull Cost
bull uterine procedures
bull Unnecessary endometrial biopsies Hysteroscopies DampC Hysterectomies
bull Morbidity
Proportion of patients who completed or discontinued treatment in relation to the used HT
Serge Rozenberg et al Hum Reprod 2009241739-1747
copy The Author 2009 Published by Oxford University Press on behalf of the European Society of
Human Reproduction and Embryology All rights reserved For Permissions please email
journalspermissionsoxfordjournalsorg
Most common adverse events leading to discontinuation
are related to progestins
bull breast paintenderness
Breast tenderness after initiation of CEE
CEE + MPA (WHI)
and mammographic density change
bullCrandall et al Breast Cancer Res Treat DOI 101007s10549-011-1803-9
Breast density
Hormone therapy use and mammographic
density in postmenopausal Norwegian women
bull Results differed when considering the combined effect of age and BMI
bull The effect of EPT on mammographic density was modified by age and BMI with no apparent association among the youngest women (aged 50-55) with the highest BMI (BMI ge 26)
bull A higher mammographic density was found in EPT users compared to never HT users particularly in women using high-dose NETA regimens Age and BMI modified the association between EPT use and mammographic density
bull Couto E et al Breast Cancer Res Treat 2011 Nov 4 [Epub ahead of print]
Breast Cancer Risk by Breast Density
Menopause and Postmenopausal Hormone
Therapy Use
Birads age HT Duration Risk
1 55-59 None 5 year risk 08 (95 CI 06- 09)
1 55-59
ET EPT 5 year risk 09 (95 CI 07 -11)
4 55-59
None 5 year risk 24 (95 CI 20 -28)
4 55-59
ET 5 year risk
30 (95 CI 26 -35)
4 55-59
EPT 5 year risk
42 (95 CI 37 -46)
Adapted from Kerlikowske et al JOURNAL OF CLINICAL ONCOLOGY 2010
Breast Cancer Risk by Breast Density
Menopause and Postmenopausal Hormone
Therapy Use
Adapted from Kerlikowske et al JOURNAL OF CLINICAL ONCOLOGY 2010
bull Postmenopausal women with high breast density are at increased risk of breast cancer and should be aware of the added risk of taking HT especially estrogen plus progestin
Medical condition which may be exacerbated by treatment
with progestins
Diabetes and metabolic syndrome
bull progestin-containing HT may be associated with increases in insulin resistance and deterioration in glucose tolerance123
bull Postmenopausal women with diabetes could be inappropriate for treatment with progestin-containing HT due to the potential risk of exacerbation of their condition
1) Panay N amp Studd JWW Human Reprod Update 1997
2) Godsland I et al Metabolism 1993
3) Sites CK et al J Clin Endocrinol Metab 2005
A Nath and R Sitruk-Ware CLIMACTERIC 200912(Suppl 1)96ndash101
A Nath and R Sitruk-Ware CLIMACTERIC 200912(Suppl 1)96ndash101
Diabetes an epidemy
bull UK 1996 14 million of diabetics
bull UK 2015 32 million (6 of the population)
bull UK 2025 5 million
bull httpwwwdiabetescoukdiabetes-prevalencehtml
Other progestin-related intolerance issues
bull Nausea
bull Depressive mood
bull Poor concentration
bull Hirsutism
bull Headache
bull Dizziness
bull Fluid retention
bull Weight gain Panay N amp Studd JWW Human Reprod Update 1997
Medical condition which may be exacerbated by treatment with progestins
PMSPMDDdepression
bull Progesterone-induced PMD can be exacerbated by exogenous progestin administration and can occur in association with HT or OC administration1
bull Significantly higher negative mood scores have been observed during the addition of a progestin to an estrogen in a sequential HT regimen in postmenopausal women with a history of PMS compared to those without2
bull Women with a history of PMS or PMD exacerbation of depression using progestins may therefore benefit from a progestin free treatment for menopausal symptoms
1) Nevatte T et al Arch Womens Ment Health 2013 2) Bjoumlrn I et al Climacteric 2006 PMS premenstrual syndrome
PMDD premenstrual dysphoric disorder
Conclusion
bull CEEBAZO is an additional regimen for menopausal symptoms it provides also a prevention for osteoporosis
bull It is suitable for women with a uterus who are unsatisfied with an EPT regimen or who you are unwilling to treat with an EPT regimen
For some postmenopausal women with a uterus there is a
need for progestin free treatment options
bull with demonstrated clinical efficacy
bull which protects the endometrium
bull improved tolerabilitysafety profile
In clinical practice this translates to women who are
intolerant of progestin-containing HT or have conditions
which may be exacerbated by treatment with progestins
Conclusion Medical need for alternative treatment option
Medical condition which may be exacerbated by treatment with progestins
Depression
bull Progestin-containing HT has been associated with increases in depressive symptoms in some individuals1
bull There is a biochemicalphysiological plausibility for the association of progestins with depression234
bull Therefore postmenopausal women who also have a medical history of depressive disorders or depression could be inappropriate for treatment with progestin-containing HT
Pfizer Confidential
65
1) Girdler SS et al J Womens Health Gend Based Med 1999 2) Traish AM et al Korean J Urol 2014 3) Stroumlhle A et al Biol Psychiatry 1999 4) Romeo E et
al Am J Psychiatry 1998
History of the following conditions may make progestin inappropriate
bull Depression
bull PMSPMDD
PMS premenstrual syndrome
PMD premenstrual dysphoric disorder
Medical conditions that may be exacerbated by treatment with progestins
Women for whom progestin-containing HT
would not be considered appropriate
minus Women who are intolerant of progestin-containing hormone therapy
minus Women with pre-existing medical conditions that may be exacerbated by progestins
Most common adverse events leading to discontinuation are related to progestins12
breakthrough bleeding
bull Increase in the number of uterine procedures (ie unnecessary endometrial biopsies)
breast paintenderness
bull Increase in the number of breast interventions
1 Steel SA et al Climacteric 2003 2 Ettinger B and Pressman A Am J Manag Care 1999 3 Komm BS Mirkin S
Pharmaceuticals 2012
4 Panay N amp Studd JWW Human Reprod Update 1997
bull Nausea bull Depressive mood bull Poor concentration bull Hirsutism bull Headache bull Dizziness bull Fluid retention bull Weight gain
Other progestin-related intolerance issues4
Unmet need with the treatment of postmenopausal symptoms
bull Alternatives to progestin are needed that will protect the endometrium while avoiding other progestin-associated effects and preserving the desired effects of estrogens in postmenopausal women3
Which women with a uterus could benefit from
estrogens without the need for a progestin
bull Women who are intolerant of progestin-containing hormone therapy
bull Women with pre-existing medical conditions that may be exacerbated by progestins (eg women with a history of depression PMSPMDD increased breast density diabetes and metabolic syndrome)
History of the following conditions may make progestin inappropriate
bull Depression
bull PMSPMDD
bull High breast density
bull Diabetes and metabolic syndrome
PMS premenstrual syndrome
PMD premenstrual dysphoric disorder
Medical conditions that may be exacerbated by treatment with progestins
Learning from WHI data
bull Hormone therapy (HT) is the conventional and established therapy option to effectively treat postmenopausal symptoms however it has been associated with some safety and tolerability concerns1 2
bull A review of WHI data suggests that many of the concerns with menopausal HT more often associated with EPT (CE+MPA) such as CHD risk increased breast density breast pain and breast cancer risk than with ET (CEE alone)2
1 Rolnick SJ Kopher RA DeFor TA et al Menopause 2005
2 Komm BS Mirkin S Pharmaceuticals 2012
WHI Womenrsquos Health Initiative trial
CHD coronary heart disease
CEE conjugated equine estrogens
Efficacy and Safety of Constant Oestrogen
Pulsed Progestogen vs
Continuous Combined HRT
Adverse Events
17b-oestradiol 17b-oestradiol norgestimate NETA (n = 150) (n = 172) Breast discomfort 14 27 Abdominal discomfort 14 22 Uterine bleeding 15 12 Dysmenorrhea 3 8 Oedema 5 8
Adapted from S Rozenberg et al Human Reproduction 2000
Medical condition which may be exacerbated by treatment
with progestins
Increased breast density
bull Increases in breast density are associated with progestin-containing HT which may adversely affect radiological detection of breast cancer1 and may be independently associated with an increased risk for the development of breast cancer2
bull The Postmenopausal EstrogenProgestin Interventions (PEPI) trial demonstrated that an increased mammographic breast density was associated with the use of E+P but not with the use of estrogen alone3
bull Women who already have high breast density may therefore be considered inappropriate for treatment with a progestin-containing HT
1) EU Core SPC for Hormone Replacement Therapy Products (CMDh1312003 Rev 4 June
2012)
2) De Villiers TJ et al on behalf of the International Menopause Society Climacteric 2013 16
3) Greendale GA et al J Natl Cancer Inst 2003
Stroke
0 25 5 75 10 125
Fractures
Diabetes
Breast cancer
Cholecystitis
Venothrombotic episodes
Endometrial cancer
Lung cancer
Coronary heart disease
Colorectal cancer
Overall mortality
15 125 10 75 5 25
Benefits Risks
CE
CE MPA
Santen RJ et al J Clin Endocrinol Metab 2010
The basis of the Endocrine Society scientific statement for postmenopausal hormone replacement therapy (HRT) excess risks and benefits of HRT for 5 years in women aged 50ndash59 years or within 10 years of the start of menopause E=estrogen P=progestin
bull Younger women (aged 50ndash59 years) had more favorable results bull There are differences between CE alone and CEMPA arms bull Overall benefitrisk ratio of CE-alone appears to be more favourable than CEMPA
Reevaluation of WHI data (stratified by age) Risks and
Benefits of HRT Cases per 1000 Women per 5 Years of
Use
Medical condition which may be exacerbated by treatment
with progestins
Diabetes and metabolic syndrome
bull Treatment of oestrogen deficiency symptoms with progestin-containing HT (unlike oestrogen alone) may be associated with increases in insulin resistance and deterioration in glucose tolerance123
bull Postmenopausal women with diabetes could be inappropriate for treatment with progestin-containing HT due to the potential risk of exacerbation of their condition
1) Panay N amp Studd JWW Human Reprod Update 1997
2) Godsland I et al Metabolism 1993
3) Sites CK et al J Clin Endocrinol Metab 2005
Variations in Associated Breast Cancer
Risks Between CE alone and CEMPA
bull Use of CE alone for a median of 59 years was associated with a lower incidence of invasive breast cancer (151 cases 027 per year) compared with placebo (199 cases 035 per year HR 077 95 CI 062ndash095 P=002)
bull In the CE alone group fewer women died from invasive breast cancer (6 deaths 0009 per year) compared with controls (16 deaths 0024 per year HR 037 95 CI 013ndash091 P=003)
Anderson GL et al Lancet
Oncol 2012
Bazedoxifene (BZA) specifically selected in
combination with conjugated estrogens
bull BZA has been specifically selected for its unique pharmacologic profile and effects on VMS and uterine tissue in particular123
1 Crabtree J et al Mol Cell Endocrinol 2008
2 Kharode Y et al Endocrinolology 2008
3 Duavive SmPC
Estrogen Receptor activity is dimmed
Estrogen Receptor activity is turned on
CEs are agonists BZA is an antagonist
In the uterus
bull The BZA component reduces the risk of endometrial hyperplasia that can occur with the conjugated estrogens component alone3 This means that progestins are not needed
Extensive global clinical development program for
CEBZA
aIncludes additional pilot dose-finding study 203 1 Lobo RA et al Fertil Steril 2009 2 Pinkerton JV et al Menopause 2009 3 Kagan R et al Menopause 2010 4 Mirkin S et al Climacteric 2013 5 Pinkerton JV et al Obstet Gynecol 2013
Effects of conjugated estrogensbazedoxifene on
lipid and coagulation variables a randomized
placebo- and active-controlled trial
bull At 12 months
bull Both CEBZA doses were associated with small but significant effects on hemostasis variables including reductions in antithrombin plasminogen activator inhibitor-1 and fibrinogen activity and an increase in plasminogen activity relative to placebo at 12 months Incidences of cardiovascular and venous thromboembolic events were similar among treatment groups
bull CONCLUSIONS
bull This study provides reassurance that CEBZA does not adversely affect lipid metabolism or hemostatic balance In accordance the incidences of venous thromboembolic events and cardiovascular events in postmenopausal women are similar to those observed with placebo

DUAVIVE Efficacy for the Treatment of Moderate to
Severe VMS Associated With Menopause
14
1 Pinkerton JV et al Menopause 2009
Postmenopausal women
with a uterus
Age 42-64 year
(avg 53 yr)
(N=318)
DUAVIVE (CE 045BZA 20)
(n=127)
Placebo
(n=63)
bull 12-week randomized double-blind placebo-controlled study1
bull Inclusion criteria
‒ Postmenopausal women with an intact uterus
‒ Minimum of 7 moderate to severe hot flushes per day or at least 50 per week at screening
Change from baseline to
Weeks 4 and 12 in
bull Average daily number of
moderate to severe hot
flushes
bull Average daily severity
score of hot flushes
Primary End Points
Safety population (took at least one dose)
Significant Reduction vs Placebo in
Average Daily Number of Hot Flushes
DUAVEE [package insert] New York NY Pfizer Inc 2013
ANCOVA=analysis of covariance
Reduction in average daily number of
moderate to severe hot flushes ndash primary end point
Ad
jus
ted
mean
ch
an
ge
fro
m b
aselin
edagger
Week 4 Week 12
ndash31
ndash27
Treatment
differencedagger ndash59
ndash28
ndash76
ndash49
Treatment
differencedagger
22
Plt001 vs placebo daggerBased on data analysis using ANCOVA model Change from baseline = Treatment + Baseline + Site
DUAVIV
E
Reduction in the Observed Average Daily Number
of Moderate to Severe Hot Flushes
Data on file CSR-67461 Protocol 3115A1-305 Table 1511 Pfizer Inc New York NY
change from baseline to week 12
74 for DUAVIVE
51 for placebo
Observed Average Daily Number of Hot Flushes
Ob
serv
ed a
vera
ge d
aily
nu
mb
er o
f m
od
erat
e to
sev
ere
ho
t fl
ush
es
0 1 2 3 4 5 6 7 8 9 10 12 0 1
11
2
4 3
6 5
7 8 9
10
28
54
DUAVIVE (n=122) Placebo (n=62)
Weeks
Primary analysis showed statistically significant separation at weeks 4 and 12
Average daily number of hot flushes from baseline to week 12
103 to 28 for DUAVIVE
105 to 54 for placebo
Based on mathematical means
not statistically analyzed
105 103
Pinkerton JV et al Menopause 2009
Significant Reduction vs Placebo in
Average Daily Severity Score of Hot Flushes
17
Week 4 Week 12
ndash05
ndash06
Treatment
differencedagger
Treatment
differencedagger
DUAVEE [package insert] New York NY Pfizer Inc 2013
Reduction in average daily severity score of hot flushes ndash primary end point
Ad
jus
ted
me
an
ch
an
ge
fro
m b
aselin
edagger
Plt001 vs placebo daggerBased on data analysis using ANCOVA model Change from baseline = Treatment + Baseline + Site
DUAVIV
E
Reduction in the Observed Average
Daily Severity Score of Hot Flushes
Observed Average Daily Severity Score of Hot Flushes
19
DUAVIVE (n=122) Placebo (n=62)
Weeks
Ob
serv
ed a
vera
ge d
aily
sev
erit
y sc
ore
of
ho
t fl
ush
es
0
05
10
15
25
20
0 1 2 3 4 5 6 7 8 9 10 12 11 0 1 2 3 4 5 6 7 8 9 10 12 11
14
Data on file CSR-67461 Protocol 3115A1-305 Table 1511 Pfizer Inc New York NY
Primary analysis at weeks 4 and 12 prespecified secondary end points at all other weeks
change from baseline to week 12
39 for DUAVIVE
14 for placebo
Average daily severity score of hot flashes from baseline to week 12
23 to 14 for DUAVIVE
23 to 19 for Placebo
Based on mathematical means
not statistically analyzed
23
23
Pinkerton JV et al Menopause 2009
Effects on bone mineral density (BMD)
SMART 512
20
bull 12-month double-blind randomized placebo- and active-controlled study
bull Primary end point endometrial hyperplasia at 1 year
bull Secondary BMD changes at 1 year
1 DUAVEE [package insert] New York NY Pfizer Inc 2013 2 Pinkerton J Clin Endocrin Metab 2014
This study included a different dose of CEBZA and comparators The schematic shown here depicts only the patients who received the approved dose of DUAVIVE or placebo
Change from baseline in
bull Lumbar Spine BMD (Primary ndash BMD Substudy)
bull Total Hip BMD (Secondary ndash BMD Substudy)
BMD Analysis
DUAVIVE
(CE 045BZA 20)
(n=119)
Placebo
(n=139)
BMD Analysis
Postmenopausal women with a uterus
Less than 5 years since LMP
(N=590)
DUAVIVE Significantly Increased Lumbar Spine and Total
Hip BMD vs Placebo at 12 Months ndash Study 2
M
ean
ch
an
ge f
rom
baselin
e
Lumbar Spine Total Hip
121 151 Treatment
difference Treatment
difference
Data on file CSR-81040 Protocol 3115A1-3307 Pfizer Inc New York NY Pinkerton J Clin Endocrin Metab 2014 30
Plt001 vs placebo
Adjusted mean changes and P-values based on an ANCOVA model with treatment and region (US or non-US) as factors and baseline BMD value and years since menopause as covariates using the modified intention to treat population with last observation carried forward
DUAVIV
E
TOLERABILITY
AND SAFETY
Rates of BleedingSpotting and Amenorrhea
Similar to Rates with Placebo
bull High and similar cumulative rates of amenorrhea at year 1 among women treated with CE 045BZA 20 and placebo and was higher than seen in women treated with CE 045MPA 151
bull Noncumulative rates of spotting and bleedingspotting were similar among women treated with CEBZA or placebo and consistently higher in women treated with CE 045MPA 152
0
90
Cycle
100
Pe
rce
nta
ge
of
Su
bje
cts
80
70
60
50
40
30
20
10
88
54
Placebo
CE 045BZA 20 CE 045MPA 15
Percentage of subjects with cumulative amenorrhea during consecutive 4-week periods (cycles) in SMART-5
MPA medroxyprogesterone acetate Plt0001 vs all other treatment groups 1 Pinkerton JV et al J Clin Endocrinol Metab 2014 2 Data on file CSR-81040 Protocol 3115A1-3307 Pfizer Inc New York NY
Adverse Reactions in Placebo-
Controlled Trials Safety analyses have been conducted in 6210 postmenopausal women aged 40 to 75 years (mean age 55 years) following up to 2 years of treatment in SMART-1 -2 -3 and -5
Adverse reactions (incidence ge5) that were more common with DUAVIVE
Incidence of serious adverse reactions
35 with DUAVIVE 48 with placebo
DUAVEE [package insert] New York NY Pfizer Inc 2013
CE 045 BZA 20 (N=1224)
n ()
Placebo (N=1069)
n ()
Gastrointestinal disorders
Nausea 100 (8) 58 (5)
Diarrhea 96 (8) 57 (5)
Dyspepsia 84 (7) 59 (6)
Abdominal pain upper 81 (7) 58 (5)
Musculoskeletal and connective tissue disorders
Muscle spasms 110 (9) 63 (6)
Neck pain 62 (5) 46 (4)
Nervous system disorders
Dizziness 65 (5) 37 (3)
Respiratory thoracic and mediastinal disorders
Oropharyngeal pain 80 (7) 61 (6)
Venous Thromboembolism (VTE) in
DUAVIVE Clinical Studies
bull Estrogen agonistantagonists (including BZA a component of DUAVIVE) and estrogens individually are known to increase the risk of VTE
bull In the clinical studies with DUAVIVE the reporting rates for VTE were low in all treatment groups
bull Adverse reactions of VTE reported by patients
bull Should VTE event occur or be suspected DUAVIVE should be discontinued immediately
bull Due to the low rates of events in both groups it is not possible to conclude that the risk of VTE with DUAVIVE is different from that seen with other estrogen therapies
DUAVEE [package insert] New York NY Pfizer Inc 2013
00 for DUAVIVE (n=1224)
01 for placebo (n=1069)
26
Effects of conjugated estrogensbazedoxifene on
lipid and coagulation variables a randomized
placebo- and active-controlled trial
bull postmenopausal women (N = 1843) with menopausal
symptoms
bull Lipid (N = 1843) and coagulation (N = 590) variables were assessed in women receiving daily CE 045 mgBZA 20 mg CE 0625 mgBZA 20 mg BZA 20 mg CE 045 mgmedroxyprogesterone acetate (MPA) 15 mg or placebo for 12 months
bull Skouby SO et al Menopause 2015 Jun22(6)640-9
Effects of conjugated estrogensbazedoxifene on
lipid and coagulation variables a randomized
placebo- and active-controlled trial
bull At 12 months
bull CE 045 mgBZA 20 mg
bull CE 0625 mgBZA 20 mg
bull BZA 20 mg
bull and CE 045 mgMPA 15 mg decreased total cholesterol and LDL- cholesterol vs placebo (P lt 001 for all)
bull Both CEBZA doses and CEMPA increased high-density lipoprotein cholesterol compared with placebo (P lt 005 for all)
bull CE 045 mgBZA 20 mg had a neutral effect on triglycerides
bull CE 0625 mgBZA 20 mg and CEMPA increased triglycerides compared with placebo (P lt 005)
bull Skouby SO et al Menopause 2015 Jun22(6)640-9
Effects of conjugated estrogensbazedoxifene on
lipid and coagulation variables a randomized
placebo- and active-controlled trial
bull At 12 months
bull Both CEBZA doses were associated with small but significant effects on hemostasis variables including reductions in antithrombin plasminogen activator inhibitor-1 and fibrinogen activity and an increase in plasminogen activity relative to placebo at 12 months Incidences of cardiovascular and venous thromboembolic events were similar among treatment groups
Skouby SO et al Menopause 2015
Jun22(6)640-9
Endometrial hyperplasia or malignancy occurred in lt1 of women
following up to 1 year of treatment with CEBZA12
Study Cumulative Incidence at month 12 (nN)
CE 045BZA 20 Placebo
SMART-11 000 (0336) 000 (0313)
SMART-52 030 (1335) 028 (1354)
Effects on the Endometrium
1 Pickar JH et al Fertil Steril 2009 2 Pinkerton at al J Clin Endocrinol Metab 2014
Through the eyes of an amazone
Marie Mandy
Breast tolerability profile similar to placebo following up to 2 years of treatment with CEBZA12
Pooled analysis of SMART clinical trials
CE 045BZA 20 (n=1585)
Placebo (n=1241)
Breast cancer incidence up to 2 years
(per 1000 woman-years)
100 (CI 000-321)
140 (CI 000-417)
Incidence of reported breast paintenderness up to 12 weeks
98-115 81-112
Incidence of abnormal mammogram at month 12
258 316
Mean change in breast density at month 12 (SMART-5)
ndash038 (n=186)
ndash032 (n=182)
Effects on the Breast
1 Pickar JH et al Menopause 2013 2 Pinkerton JV et al Obstet Gynecol 2013
CEBZA clinical overview - summary
bull In clinical trials CEBZA has demonstrated safety and efficacy in postmenopausal women with a uterus including the following
bull Significant reduction in number and severity of moderate to severe hot flushes1
bull Incidence of cumulative amenorrhea rate similar to placebo and significantly better than CEMPA2
bull Incidence of endometrial hyperplasia and breast tendernessdensity similar to that with placebo345
bull Incidence of adverse events and discontinuation rates similar to that with placebo6
1 Pinkerton JV et al Menopause 2009 2 Pinkerton JV et al J Clin Endocrinol Metab2014 3 Pickar JH et al
Fertil Steril 2009 4 Pinkerton at al J Clin Endocrinol Metab 2014 5 Pickar JH et al Menopause 2013 6 DUAVEE [package insert] New York NY Pfizer Inc 2013
CEBZA clinical overview - summary
Now women with a uterus who choose hormone therapy for management of menopausal symptoms have a choice
bull conventional estrogen-progestogen therapy or
bull a new combinationhellipconjugated estrogens paired with the SERM bazedoxifene
1 Pinkerton JV et al Menopause 2009 2 Pinkerton JV et al J Clin Endocrinol Metab2014 3 Pickar JH et al Fertil Steril 2009 4 Pinkerton at al J Clin Endocrinol Metab 2014 5 Pickar JH et al Menopause 2013 6 DUAVEE [package insert] New York NY Pfizer Inc 2013
Conjugated EstrogensBazedoxifene (CEBZA)
US indication
bull DUAVEE is indicated in women with a uterus for
bull 11 Treatment of Moderate to Severe Vasomotor Symptoms Associated with Menopause
bull 12 Prevention of Postmenopausal Osteoporosis
bull 13 Important Limitations of Use
bull Use DUAVEE for the shortest duration consistent with treatment goals and risks for the individual woman Postmenopausal women should be re-evaluated periodically as clinically appropriate to determine if treatment is still necessary
bull When prescribing solely for the prevention of postmenopausal osteoporosis therapy should only be considered for women at significant risk of osteoporosis and non-estrogen medication should be carefully considered
Conjugated EstrogensBazedoxifene (CEBZA)
EU indication
CEBZA is indicated for
bull Treatment of oestrogen deficiency symptoms in postmenopausal women with a uterus (with at least 12 months since the last menses) for whom treatment with progestin-containing therapy is not appropriate
bull The experience treating women older than 65 years is limited
bull Dose CE (045mg)Bazedoxifene (20mg)
Duavive SmPC
Which women with a uterus
could benefit from estrogens
without the need for a
progestin
Progestin intolerance is one of the main
factors for reduced compliance
bull About 20 of women receiving progestin-containing HT have significant progestin intolerance and half of these experience serious effects that prevent treatment continuation1
1 Panay N amp Studd J Human Reprod Update 1997
2 Panay N et al on behalf of the British Menopause Society and Womenrsquos Health Concern Menopause Int 2013
bull The 2013 British Menopause Society amp Womenrsquos Health
Concern recommendations on hormone replacement
therapy do recognise progestin intolerance as one of the
main factors for reduced compliance with HT 2
Proportion of patients () with at least one bleeding episode in relation to time and to the
used HT
Serge Rozenberg et al Hum Reprod 2009241739-1747
copy The Author 2009 Published by Oxford University Press on behalf of the European Society of
Human Reproduction and Embryology All rights reserved For Permissions please email
journalspermissionsoxfordjournalsorg
Breast tenderness after initiation of CEE
CEE + MPA (WHI)
and mammographic density change
bullCrandall et al Breast Cancer Res Treat DOI 101007s10549-011-1803-9
Breast density
Conclusion
bull CEEBAZO is an additional regimen for menopausal symptoms it provides also a prevention for osteoporosis
bull It is suitable for women with a uterus who are unsatisfied with an EPT regimen or who you are unwilling to treat with an EPT regimen
Adapted use of MHT
bull Lower dosage of estrogens
bull Other progestins
bull Better safety profile
bull Vaginal estrogen or SERMS
bull Non-hormonal therapy
bull Development of new products
bull SERMS + estrogens
Most common adverse events leading to
discontinuation are related to progestins12
bull breakthrough bleeding
bull Low compliance
bull Increase in the number of US
bull Stress
bull Cost
bull uterine procedures
bull Unnecessary endometrial biopsies Hysteroscopies DampC Hysterectomies
bull Morbidity
Proportion of patients who completed or discontinued treatment in relation to the used HT
Serge Rozenberg et al Hum Reprod 2009241739-1747
copy The Author 2009 Published by Oxford University Press on behalf of the European Society of
Human Reproduction and Embryology All rights reserved For Permissions please email
journalspermissionsoxfordjournalsorg
Most common adverse events leading to discontinuation
are related to progestins
bull breast paintenderness
Breast tenderness after initiation of CEE
CEE + MPA (WHI)
and mammographic density change
bullCrandall et al Breast Cancer Res Treat DOI 101007s10549-011-1803-9
Breast density
Hormone therapy use and mammographic
density in postmenopausal Norwegian women
bull Results differed when considering the combined effect of age and BMI
bull The effect of EPT on mammographic density was modified by age and BMI with no apparent association among the youngest women (aged 50-55) with the highest BMI (BMI ge 26)
bull A higher mammographic density was found in EPT users compared to never HT users particularly in women using high-dose NETA regimens Age and BMI modified the association between EPT use and mammographic density
bull Couto E et al Breast Cancer Res Treat 2011 Nov 4 [Epub ahead of print]
Breast Cancer Risk by Breast Density
Menopause and Postmenopausal Hormone
Therapy Use
Birads age HT Duration Risk
1 55-59 None 5 year risk 08 (95 CI 06- 09)
1 55-59
ET EPT 5 year risk 09 (95 CI 07 -11)
4 55-59
None 5 year risk 24 (95 CI 20 -28)
4 55-59
ET 5 year risk
30 (95 CI 26 -35)
4 55-59
EPT 5 year risk
42 (95 CI 37 -46)
Adapted from Kerlikowske et al JOURNAL OF CLINICAL ONCOLOGY 2010
Breast Cancer Risk by Breast Density
Menopause and Postmenopausal Hormone
Therapy Use
Adapted from Kerlikowske et al JOURNAL OF CLINICAL ONCOLOGY 2010
bull Postmenopausal women with high breast density are at increased risk of breast cancer and should be aware of the added risk of taking HT especially estrogen plus progestin
Medical condition which may be exacerbated by treatment
with progestins
Diabetes and metabolic syndrome
bull progestin-containing HT may be associated with increases in insulin resistance and deterioration in glucose tolerance123
bull Postmenopausal women with diabetes could be inappropriate for treatment with progestin-containing HT due to the potential risk of exacerbation of their condition
1) Panay N amp Studd JWW Human Reprod Update 1997
2) Godsland I et al Metabolism 1993
3) Sites CK et al J Clin Endocrinol Metab 2005
A Nath and R Sitruk-Ware CLIMACTERIC 200912(Suppl 1)96ndash101
A Nath and R Sitruk-Ware CLIMACTERIC 200912(Suppl 1)96ndash101
Diabetes an epidemy
bull UK 1996 14 million of diabetics
bull UK 2015 32 million (6 of the population)
bull UK 2025 5 million
bull httpwwwdiabetescoukdiabetes-prevalencehtml
Other progestin-related intolerance issues
bull Nausea
bull Depressive mood
bull Poor concentration
bull Hirsutism
bull Headache
bull Dizziness
bull Fluid retention
bull Weight gain Panay N amp Studd JWW Human Reprod Update 1997
Medical condition which may be exacerbated by treatment with progestins
PMSPMDDdepression
bull Progesterone-induced PMD can be exacerbated by exogenous progestin administration and can occur in association with HT or OC administration1
bull Significantly higher negative mood scores have been observed during the addition of a progestin to an estrogen in a sequential HT regimen in postmenopausal women with a history of PMS compared to those without2
bull Women with a history of PMS or PMD exacerbation of depression using progestins may therefore benefit from a progestin free treatment for menopausal symptoms
1) Nevatte T et al Arch Womens Ment Health 2013 2) Bjoumlrn I et al Climacteric 2006 PMS premenstrual syndrome
PMDD premenstrual dysphoric disorder
Conclusion
bull CEEBAZO is an additional regimen for menopausal symptoms it provides also a prevention for osteoporosis
bull It is suitable for women with a uterus who are unsatisfied with an EPT regimen or who you are unwilling to treat with an EPT regimen
For some postmenopausal women with a uterus there is a
need for progestin free treatment options
bull with demonstrated clinical efficacy
bull which protects the endometrium
bull improved tolerabilitysafety profile
In clinical practice this translates to women who are
intolerant of progestin-containing HT or have conditions
which may be exacerbated by treatment with progestins
Conclusion Medical need for alternative treatment option
Medical condition which may be exacerbated by treatment with progestins
Depression
bull Progestin-containing HT has been associated with increases in depressive symptoms in some individuals1
bull There is a biochemicalphysiological plausibility for the association of progestins with depression234
bull Therefore postmenopausal women who also have a medical history of depressive disorders or depression could be inappropriate for treatment with progestin-containing HT
Pfizer Confidential
65
1) Girdler SS et al J Womens Health Gend Based Med 1999 2) Traish AM et al Korean J Urol 2014 3) Stroumlhle A et al Biol Psychiatry 1999 4) Romeo E et
al Am J Psychiatry 1998
History of the following conditions may make progestin inappropriate
bull Depression
bull PMSPMDD
PMS premenstrual syndrome
PMD premenstrual dysphoric disorder
Medical conditions that may be exacerbated by treatment with progestins
Women for whom progestin-containing HT
would not be considered appropriate
minus Women who are intolerant of progestin-containing hormone therapy
minus Women with pre-existing medical conditions that may be exacerbated by progestins
Most common adverse events leading to discontinuation are related to progestins12
breakthrough bleeding
bull Increase in the number of uterine procedures (ie unnecessary endometrial biopsies)
breast paintenderness
bull Increase in the number of breast interventions
1 Steel SA et al Climacteric 2003 2 Ettinger B and Pressman A Am J Manag Care 1999 3 Komm BS Mirkin S
Pharmaceuticals 2012
4 Panay N amp Studd JWW Human Reprod Update 1997
bull Nausea bull Depressive mood bull Poor concentration bull Hirsutism bull Headache bull Dizziness bull Fluid retention bull Weight gain
Other progestin-related intolerance issues4
Unmet need with the treatment of postmenopausal symptoms
bull Alternatives to progestin are needed that will protect the endometrium while avoiding other progestin-associated effects and preserving the desired effects of estrogens in postmenopausal women3
Which women with a uterus could benefit from
estrogens without the need for a progestin
bull Women who are intolerant of progestin-containing hormone therapy
bull Women with pre-existing medical conditions that may be exacerbated by progestins (eg women with a history of depression PMSPMDD increased breast density diabetes and metabolic syndrome)
History of the following conditions may make progestin inappropriate
bull Depression
bull PMSPMDD
bull High breast density
bull Diabetes and metabolic syndrome
PMS premenstrual syndrome
PMD premenstrual dysphoric disorder
Medical conditions that may be exacerbated by treatment with progestins
Learning from WHI data
bull Hormone therapy (HT) is the conventional and established therapy option to effectively treat postmenopausal symptoms however it has been associated with some safety and tolerability concerns1 2
bull A review of WHI data suggests that many of the concerns with menopausal HT more often associated with EPT (CE+MPA) such as CHD risk increased breast density breast pain and breast cancer risk than with ET (CEE alone)2
1 Rolnick SJ Kopher RA DeFor TA et al Menopause 2005
2 Komm BS Mirkin S Pharmaceuticals 2012
WHI Womenrsquos Health Initiative trial
CHD coronary heart disease
CEE conjugated equine estrogens
Efficacy and Safety of Constant Oestrogen
Pulsed Progestogen vs
Continuous Combined HRT
Adverse Events
17b-oestradiol 17b-oestradiol norgestimate NETA (n = 150) (n = 172) Breast discomfort 14 27 Abdominal discomfort 14 22 Uterine bleeding 15 12 Dysmenorrhea 3 8 Oedema 5 8
Adapted from S Rozenberg et al Human Reproduction 2000
Medical condition which may be exacerbated by treatment
with progestins
Increased breast density
bull Increases in breast density are associated with progestin-containing HT which may adversely affect radiological detection of breast cancer1 and may be independently associated with an increased risk for the development of breast cancer2
bull The Postmenopausal EstrogenProgestin Interventions (PEPI) trial demonstrated that an increased mammographic breast density was associated with the use of E+P but not with the use of estrogen alone3
bull Women who already have high breast density may therefore be considered inappropriate for treatment with a progestin-containing HT
1) EU Core SPC for Hormone Replacement Therapy Products (CMDh1312003 Rev 4 June
2012)
2) De Villiers TJ et al on behalf of the International Menopause Society Climacteric 2013 16
3) Greendale GA et al J Natl Cancer Inst 2003
Stroke
0 25 5 75 10 125
Fractures
Diabetes
Breast cancer
Cholecystitis
Venothrombotic episodes
Endometrial cancer
Lung cancer
Coronary heart disease
Colorectal cancer
Overall mortality
15 125 10 75 5 25
Benefits Risks
CE
CE MPA
Santen RJ et al J Clin Endocrinol Metab 2010
The basis of the Endocrine Society scientific statement for postmenopausal hormone replacement therapy (HRT) excess risks and benefits of HRT for 5 years in women aged 50ndash59 years or within 10 years of the start of menopause E=estrogen P=progestin
bull Younger women (aged 50ndash59 years) had more favorable results bull There are differences between CE alone and CEMPA arms bull Overall benefitrisk ratio of CE-alone appears to be more favourable than CEMPA
Reevaluation of WHI data (stratified by age) Risks and
Benefits of HRT Cases per 1000 Women per 5 Years of
Use
Medical condition which may be exacerbated by treatment
with progestins
Diabetes and metabolic syndrome
bull Treatment of oestrogen deficiency symptoms with progestin-containing HT (unlike oestrogen alone) may be associated with increases in insulin resistance and deterioration in glucose tolerance123
bull Postmenopausal women with diabetes could be inappropriate for treatment with progestin-containing HT due to the potential risk of exacerbation of their condition
1) Panay N amp Studd JWW Human Reprod Update 1997
2) Godsland I et al Metabolism 1993
3) Sites CK et al J Clin Endocrinol Metab 2005
Variations in Associated Breast Cancer
Risks Between CE alone and CEMPA
bull Use of CE alone for a median of 59 years was associated with a lower incidence of invasive breast cancer (151 cases 027 per year) compared with placebo (199 cases 035 per year HR 077 95 CI 062ndash095 P=002)
bull In the CE alone group fewer women died from invasive breast cancer (6 deaths 0009 per year) compared with controls (16 deaths 0024 per year HR 037 95 CI 013ndash091 P=003)
Anderson GL et al Lancet
Oncol 2012
Bazedoxifene (BZA) specifically selected in
combination with conjugated estrogens
bull BZA has been specifically selected for its unique pharmacologic profile and effects on VMS and uterine tissue in particular123
1 Crabtree J et al Mol Cell Endocrinol 2008
2 Kharode Y et al Endocrinolology 2008
3 Duavive SmPC
Estrogen Receptor activity is dimmed
Estrogen Receptor activity is turned on
CEs are agonists BZA is an antagonist
In the uterus
bull The BZA component reduces the risk of endometrial hyperplasia that can occur with the conjugated estrogens component alone3 This means that progestins are not needed
Extensive global clinical development program for
CEBZA
aIncludes additional pilot dose-finding study 203 1 Lobo RA et al Fertil Steril 2009 2 Pinkerton JV et al Menopause 2009 3 Kagan R et al Menopause 2010 4 Mirkin S et al Climacteric 2013 5 Pinkerton JV et al Obstet Gynecol 2013
Effects of conjugated estrogensbazedoxifene on
lipid and coagulation variables a randomized
placebo- and active-controlled trial
bull At 12 months
bull Both CEBZA doses were associated with small but significant effects on hemostasis variables including reductions in antithrombin plasminogen activator inhibitor-1 and fibrinogen activity and an increase in plasminogen activity relative to placebo at 12 months Incidences of cardiovascular and venous thromboembolic events were similar among treatment groups
bull CONCLUSIONS
bull This study provides reassurance that CEBZA does not adversely affect lipid metabolism or hemostatic balance In accordance the incidences of venous thromboembolic events and cardiovascular events in postmenopausal women are similar to those observed with placebo

Significant Reduction vs Placebo in
Average Daily Number of Hot Flushes
DUAVEE [package insert] New York NY Pfizer Inc 2013
ANCOVA=analysis of covariance
Reduction in average daily number of
moderate to severe hot flushes ndash primary end point
Ad
jus
ted
mean
ch
an
ge
fro
m b
aselin
edagger
Week 4 Week 12
ndash31
ndash27
Treatment
differencedagger ndash59
ndash28
ndash76
ndash49
Treatment
differencedagger
22
Plt001 vs placebo daggerBased on data analysis using ANCOVA model Change from baseline = Treatment + Baseline + Site
DUAVIV
E
Reduction in the Observed Average Daily Number
of Moderate to Severe Hot Flushes
Data on file CSR-67461 Protocol 3115A1-305 Table 1511 Pfizer Inc New York NY
change from baseline to week 12
74 for DUAVIVE
51 for placebo
Observed Average Daily Number of Hot Flushes
Ob
serv
ed a
vera
ge d
aily
nu
mb
er o
f m
od
erat
e to
sev
ere
ho
t fl
ush
es
0 1 2 3 4 5 6 7 8 9 10 12 0 1
11
2
4 3
6 5
7 8 9
10
28
54
DUAVIVE (n=122) Placebo (n=62)
Weeks
Primary analysis showed statistically significant separation at weeks 4 and 12
Average daily number of hot flushes from baseline to week 12
103 to 28 for DUAVIVE
105 to 54 for placebo
Based on mathematical means
not statistically analyzed
105 103
Pinkerton JV et al Menopause 2009
Significant Reduction vs Placebo in
Average Daily Severity Score of Hot Flushes
17
Week 4 Week 12
ndash05
ndash06
Treatment
differencedagger
Treatment
differencedagger
DUAVEE [package insert] New York NY Pfizer Inc 2013
Reduction in average daily severity score of hot flushes ndash primary end point
Ad
jus
ted
me
an
ch
an
ge
fro
m b
aselin
edagger
Plt001 vs placebo daggerBased on data analysis using ANCOVA model Change from baseline = Treatment + Baseline + Site
DUAVIV
E
Reduction in the Observed Average
Daily Severity Score of Hot Flushes
Observed Average Daily Severity Score of Hot Flushes
19
DUAVIVE (n=122) Placebo (n=62)
Weeks
Ob
serv
ed a
vera
ge d
aily
sev
erit
y sc
ore
of
ho
t fl
ush
es
0
05
10
15
25
20
0 1 2 3 4 5 6 7 8 9 10 12 11 0 1 2 3 4 5 6 7 8 9 10 12 11
14
Data on file CSR-67461 Protocol 3115A1-305 Table 1511 Pfizer Inc New York NY
Primary analysis at weeks 4 and 12 prespecified secondary end points at all other weeks
change from baseline to week 12
39 for DUAVIVE
14 for placebo
Average daily severity score of hot flashes from baseline to week 12
23 to 14 for DUAVIVE
23 to 19 for Placebo
Based on mathematical means
not statistically analyzed
23
23
Pinkerton JV et al Menopause 2009
Effects on bone mineral density (BMD)
SMART 512
20
bull 12-month double-blind randomized placebo- and active-controlled study
bull Primary end point endometrial hyperplasia at 1 year
bull Secondary BMD changes at 1 year
1 DUAVEE [package insert] New York NY Pfizer Inc 2013 2 Pinkerton J Clin Endocrin Metab 2014
This study included a different dose of CEBZA and comparators The schematic shown here depicts only the patients who received the approved dose of DUAVIVE or placebo
Change from baseline in
bull Lumbar Spine BMD (Primary ndash BMD Substudy)
bull Total Hip BMD (Secondary ndash BMD Substudy)
BMD Analysis
DUAVIVE
(CE 045BZA 20)
(n=119)
Placebo
(n=139)
BMD Analysis
Postmenopausal women with a uterus
Less than 5 years since LMP
(N=590)
DUAVIVE Significantly Increased Lumbar Spine and Total
Hip BMD vs Placebo at 12 Months ndash Study 2
M
ean
ch
an
ge f
rom
baselin
e
Lumbar Spine Total Hip
121 151 Treatment
difference Treatment
difference
Data on file CSR-81040 Protocol 3115A1-3307 Pfizer Inc New York NY Pinkerton J Clin Endocrin Metab 2014 30
Plt001 vs placebo
Adjusted mean changes and P-values based on an ANCOVA model with treatment and region (US or non-US) as factors and baseline BMD value and years since menopause as covariates using the modified intention to treat population with last observation carried forward
DUAVIV
E
TOLERABILITY
AND SAFETY
Rates of BleedingSpotting and Amenorrhea
Similar to Rates with Placebo
bull High and similar cumulative rates of amenorrhea at year 1 among women treated with CE 045BZA 20 and placebo and was higher than seen in women treated with CE 045MPA 151
bull Noncumulative rates of spotting and bleedingspotting were similar among women treated with CEBZA or placebo and consistently higher in women treated with CE 045MPA 152
0
90
Cycle
100
Pe
rce
nta
ge
of
Su
bje
cts
80
70
60
50
40
30
20
10
88
54
Placebo
CE 045BZA 20 CE 045MPA 15
Percentage of subjects with cumulative amenorrhea during consecutive 4-week periods (cycles) in SMART-5
MPA medroxyprogesterone acetate Plt0001 vs all other treatment groups 1 Pinkerton JV et al J Clin Endocrinol Metab 2014 2 Data on file CSR-81040 Protocol 3115A1-3307 Pfizer Inc New York NY
Adverse Reactions in Placebo-
Controlled Trials Safety analyses have been conducted in 6210 postmenopausal women aged 40 to 75 years (mean age 55 years) following up to 2 years of treatment in SMART-1 -2 -3 and -5
Adverse reactions (incidence ge5) that were more common with DUAVIVE
Incidence of serious adverse reactions
35 with DUAVIVE 48 with placebo
DUAVEE [package insert] New York NY Pfizer Inc 2013
CE 045 BZA 20 (N=1224)
n ()
Placebo (N=1069)
n ()
Gastrointestinal disorders
Nausea 100 (8) 58 (5)
Diarrhea 96 (8) 57 (5)
Dyspepsia 84 (7) 59 (6)
Abdominal pain upper 81 (7) 58 (5)
Musculoskeletal and connective tissue disorders
Muscle spasms 110 (9) 63 (6)
Neck pain 62 (5) 46 (4)
Nervous system disorders
Dizziness 65 (5) 37 (3)
Respiratory thoracic and mediastinal disorders
Oropharyngeal pain 80 (7) 61 (6)
Venous Thromboembolism (VTE) in
DUAVIVE Clinical Studies
bull Estrogen agonistantagonists (including BZA a component of DUAVIVE) and estrogens individually are known to increase the risk of VTE
bull In the clinical studies with DUAVIVE the reporting rates for VTE were low in all treatment groups
bull Adverse reactions of VTE reported by patients
bull Should VTE event occur or be suspected DUAVIVE should be discontinued immediately
bull Due to the low rates of events in both groups it is not possible to conclude that the risk of VTE with DUAVIVE is different from that seen with other estrogen therapies
DUAVEE [package insert] New York NY Pfizer Inc 2013
00 for DUAVIVE (n=1224)
01 for placebo (n=1069)
26
Effects of conjugated estrogensbazedoxifene on
lipid and coagulation variables a randomized
placebo- and active-controlled trial
bull postmenopausal women (N = 1843) with menopausal
symptoms
bull Lipid (N = 1843) and coagulation (N = 590) variables were assessed in women receiving daily CE 045 mgBZA 20 mg CE 0625 mgBZA 20 mg BZA 20 mg CE 045 mgmedroxyprogesterone acetate (MPA) 15 mg or placebo for 12 months
bull Skouby SO et al Menopause 2015 Jun22(6)640-9
Effects of conjugated estrogensbazedoxifene on
lipid and coagulation variables a randomized
placebo- and active-controlled trial
bull At 12 months
bull CE 045 mgBZA 20 mg
bull CE 0625 mgBZA 20 mg
bull BZA 20 mg
bull and CE 045 mgMPA 15 mg decreased total cholesterol and LDL- cholesterol vs placebo (P lt 001 for all)
bull Both CEBZA doses and CEMPA increased high-density lipoprotein cholesterol compared with placebo (P lt 005 for all)
bull CE 045 mgBZA 20 mg had a neutral effect on triglycerides
bull CE 0625 mgBZA 20 mg and CEMPA increased triglycerides compared with placebo (P lt 005)
bull Skouby SO et al Menopause 2015 Jun22(6)640-9
Effects of conjugated estrogensbazedoxifene on
lipid and coagulation variables a randomized
placebo- and active-controlled trial
bull At 12 months
bull Both CEBZA doses were associated with small but significant effects on hemostasis variables including reductions in antithrombin plasminogen activator inhibitor-1 and fibrinogen activity and an increase in plasminogen activity relative to placebo at 12 months Incidences of cardiovascular and venous thromboembolic events were similar among treatment groups
Skouby SO et al Menopause 2015
Jun22(6)640-9
Endometrial hyperplasia or malignancy occurred in lt1 of women
following up to 1 year of treatment with CEBZA12
Study Cumulative Incidence at month 12 (nN)
CE 045BZA 20 Placebo
SMART-11 000 (0336) 000 (0313)
SMART-52 030 (1335) 028 (1354)
Effects on the Endometrium
1 Pickar JH et al Fertil Steril 2009 2 Pinkerton at al J Clin Endocrinol Metab 2014
Through the eyes of an amazone
Marie Mandy
Breast tolerability profile similar to placebo following up to 2 years of treatment with CEBZA12
Pooled analysis of SMART clinical trials
CE 045BZA 20 (n=1585)
Placebo (n=1241)
Breast cancer incidence up to 2 years
(per 1000 woman-years)
100 (CI 000-321)
140 (CI 000-417)
Incidence of reported breast paintenderness up to 12 weeks
98-115 81-112
Incidence of abnormal mammogram at month 12
258 316
Mean change in breast density at month 12 (SMART-5)
ndash038 (n=186)
ndash032 (n=182)
Effects on the Breast
1 Pickar JH et al Menopause 2013 2 Pinkerton JV et al Obstet Gynecol 2013
CEBZA clinical overview - summary
bull In clinical trials CEBZA has demonstrated safety and efficacy in postmenopausal women with a uterus including the following
bull Significant reduction in number and severity of moderate to severe hot flushes1
bull Incidence of cumulative amenorrhea rate similar to placebo and significantly better than CEMPA2
bull Incidence of endometrial hyperplasia and breast tendernessdensity similar to that with placebo345
bull Incidence of adverse events and discontinuation rates similar to that with placebo6
1 Pinkerton JV et al Menopause 2009 2 Pinkerton JV et al J Clin Endocrinol Metab2014 3 Pickar JH et al
Fertil Steril 2009 4 Pinkerton at al J Clin Endocrinol Metab 2014 5 Pickar JH et al Menopause 2013 6 DUAVEE [package insert] New York NY Pfizer Inc 2013
CEBZA clinical overview - summary
Now women with a uterus who choose hormone therapy for management of menopausal symptoms have a choice
bull conventional estrogen-progestogen therapy or
bull a new combinationhellipconjugated estrogens paired with the SERM bazedoxifene
1 Pinkerton JV et al Menopause 2009 2 Pinkerton JV et al J Clin Endocrinol Metab2014 3 Pickar JH et al Fertil Steril 2009 4 Pinkerton at al J Clin Endocrinol Metab 2014 5 Pickar JH et al Menopause 2013 6 DUAVEE [package insert] New York NY Pfizer Inc 2013
Conjugated EstrogensBazedoxifene (CEBZA)
US indication
bull DUAVEE is indicated in women with a uterus for
bull 11 Treatment of Moderate to Severe Vasomotor Symptoms Associated with Menopause
bull 12 Prevention of Postmenopausal Osteoporosis
bull 13 Important Limitations of Use
bull Use DUAVEE for the shortest duration consistent with treatment goals and risks for the individual woman Postmenopausal women should be re-evaluated periodically as clinically appropriate to determine if treatment is still necessary
bull When prescribing solely for the prevention of postmenopausal osteoporosis therapy should only be considered for women at significant risk of osteoporosis and non-estrogen medication should be carefully considered
Conjugated EstrogensBazedoxifene (CEBZA)
EU indication
CEBZA is indicated for
bull Treatment of oestrogen deficiency symptoms in postmenopausal women with a uterus (with at least 12 months since the last menses) for whom treatment with progestin-containing therapy is not appropriate
bull The experience treating women older than 65 years is limited
bull Dose CE (045mg)Bazedoxifene (20mg)
Duavive SmPC
Which women with a uterus
could benefit from estrogens
without the need for a
progestin
Progestin intolerance is one of the main
factors for reduced compliance
bull About 20 of women receiving progestin-containing HT have significant progestin intolerance and half of these experience serious effects that prevent treatment continuation1
1 Panay N amp Studd J Human Reprod Update 1997
2 Panay N et al on behalf of the British Menopause Society and Womenrsquos Health Concern Menopause Int 2013
bull The 2013 British Menopause Society amp Womenrsquos Health
Concern recommendations on hormone replacement
therapy do recognise progestin intolerance as one of the
main factors for reduced compliance with HT 2
Proportion of patients () with at least one bleeding episode in relation to time and to the
used HT
Serge Rozenberg et al Hum Reprod 2009241739-1747
copy The Author 2009 Published by Oxford University Press on behalf of the European Society of
Human Reproduction and Embryology All rights reserved For Permissions please email
journalspermissionsoxfordjournalsorg
Breast tenderness after initiation of CEE
CEE + MPA (WHI)
and mammographic density change
bullCrandall et al Breast Cancer Res Treat DOI 101007s10549-011-1803-9
Breast density
Conclusion
bull CEEBAZO is an additional regimen for menopausal symptoms it provides also a prevention for osteoporosis
bull It is suitable for women with a uterus who are unsatisfied with an EPT regimen or who you are unwilling to treat with an EPT regimen
Adapted use of MHT
bull Lower dosage of estrogens
bull Other progestins
bull Better safety profile
bull Vaginal estrogen or SERMS
bull Non-hormonal therapy
bull Development of new products
bull SERMS + estrogens
Most common adverse events leading to
discontinuation are related to progestins12
bull breakthrough bleeding
bull Low compliance
bull Increase in the number of US
bull Stress
bull Cost
bull uterine procedures
bull Unnecessary endometrial biopsies Hysteroscopies DampC Hysterectomies
bull Morbidity
Proportion of patients who completed or discontinued treatment in relation to the used HT
Serge Rozenberg et al Hum Reprod 2009241739-1747
copy The Author 2009 Published by Oxford University Press on behalf of the European Society of
Human Reproduction and Embryology All rights reserved For Permissions please email
journalspermissionsoxfordjournalsorg
Most common adverse events leading to discontinuation
are related to progestins
bull breast paintenderness
Breast tenderness after initiation of CEE
CEE + MPA (WHI)
and mammographic density change
bullCrandall et al Breast Cancer Res Treat DOI 101007s10549-011-1803-9
Breast density
Hormone therapy use and mammographic
density in postmenopausal Norwegian women
bull Results differed when considering the combined effect of age and BMI
bull The effect of EPT on mammographic density was modified by age and BMI with no apparent association among the youngest women (aged 50-55) with the highest BMI (BMI ge 26)
bull A higher mammographic density was found in EPT users compared to never HT users particularly in women using high-dose NETA regimens Age and BMI modified the association between EPT use and mammographic density
bull Couto E et al Breast Cancer Res Treat 2011 Nov 4 [Epub ahead of print]
Breast Cancer Risk by Breast Density
Menopause and Postmenopausal Hormone
Therapy Use
Birads age HT Duration Risk
1 55-59 None 5 year risk 08 (95 CI 06- 09)
1 55-59
ET EPT 5 year risk 09 (95 CI 07 -11)
4 55-59
None 5 year risk 24 (95 CI 20 -28)
4 55-59
ET 5 year risk
30 (95 CI 26 -35)
4 55-59
EPT 5 year risk
42 (95 CI 37 -46)
Adapted from Kerlikowske et al JOURNAL OF CLINICAL ONCOLOGY 2010
Breast Cancer Risk by Breast Density
Menopause and Postmenopausal Hormone
Therapy Use
Adapted from Kerlikowske et al JOURNAL OF CLINICAL ONCOLOGY 2010
bull Postmenopausal women with high breast density are at increased risk of breast cancer and should be aware of the added risk of taking HT especially estrogen plus progestin
Medical condition which may be exacerbated by treatment
with progestins
Diabetes and metabolic syndrome
bull progestin-containing HT may be associated with increases in insulin resistance and deterioration in glucose tolerance123
bull Postmenopausal women with diabetes could be inappropriate for treatment with progestin-containing HT due to the potential risk of exacerbation of their condition
1) Panay N amp Studd JWW Human Reprod Update 1997
2) Godsland I et al Metabolism 1993
3) Sites CK et al J Clin Endocrinol Metab 2005
A Nath and R Sitruk-Ware CLIMACTERIC 200912(Suppl 1)96ndash101
A Nath and R Sitruk-Ware CLIMACTERIC 200912(Suppl 1)96ndash101
Diabetes an epidemy
bull UK 1996 14 million of diabetics
bull UK 2015 32 million (6 of the population)
bull UK 2025 5 million
bull httpwwwdiabetescoukdiabetes-prevalencehtml
Other progestin-related intolerance issues
bull Nausea
bull Depressive mood
bull Poor concentration
bull Hirsutism
bull Headache
bull Dizziness
bull Fluid retention
bull Weight gain Panay N amp Studd JWW Human Reprod Update 1997
Medical condition which may be exacerbated by treatment with progestins
PMSPMDDdepression
bull Progesterone-induced PMD can be exacerbated by exogenous progestin administration and can occur in association with HT or OC administration1
bull Significantly higher negative mood scores have been observed during the addition of a progestin to an estrogen in a sequential HT regimen in postmenopausal women with a history of PMS compared to those without2
bull Women with a history of PMS or PMD exacerbation of depression using progestins may therefore benefit from a progestin free treatment for menopausal symptoms
1) Nevatte T et al Arch Womens Ment Health 2013 2) Bjoumlrn I et al Climacteric 2006 PMS premenstrual syndrome
PMDD premenstrual dysphoric disorder
Conclusion
bull CEEBAZO is an additional regimen for menopausal symptoms it provides also a prevention for osteoporosis
bull It is suitable for women with a uterus who are unsatisfied with an EPT regimen or who you are unwilling to treat with an EPT regimen
For some postmenopausal women with a uterus there is a
need for progestin free treatment options
bull with demonstrated clinical efficacy
bull which protects the endometrium
bull improved tolerabilitysafety profile
In clinical practice this translates to women who are
intolerant of progestin-containing HT or have conditions
which may be exacerbated by treatment with progestins
Conclusion Medical need for alternative treatment option
Medical condition which may be exacerbated by treatment with progestins
Depression
bull Progestin-containing HT has been associated with increases in depressive symptoms in some individuals1
bull There is a biochemicalphysiological plausibility for the association of progestins with depression234
bull Therefore postmenopausal women who also have a medical history of depressive disorders or depression could be inappropriate for treatment with progestin-containing HT
Pfizer Confidential
65
1) Girdler SS et al J Womens Health Gend Based Med 1999 2) Traish AM et al Korean J Urol 2014 3) Stroumlhle A et al Biol Psychiatry 1999 4) Romeo E et
al Am J Psychiatry 1998
History of the following conditions may make progestin inappropriate
bull Depression
bull PMSPMDD
PMS premenstrual syndrome
PMD premenstrual dysphoric disorder
Medical conditions that may be exacerbated by treatment with progestins
Women for whom progestin-containing HT
would not be considered appropriate
minus Women who are intolerant of progestin-containing hormone therapy
minus Women with pre-existing medical conditions that may be exacerbated by progestins
Most common adverse events leading to discontinuation are related to progestins12
breakthrough bleeding
bull Increase in the number of uterine procedures (ie unnecessary endometrial biopsies)
breast paintenderness
bull Increase in the number of breast interventions
1 Steel SA et al Climacteric 2003 2 Ettinger B and Pressman A Am J Manag Care 1999 3 Komm BS Mirkin S
Pharmaceuticals 2012
4 Panay N amp Studd JWW Human Reprod Update 1997
bull Nausea bull Depressive mood bull Poor concentration bull Hirsutism bull Headache bull Dizziness bull Fluid retention bull Weight gain
Other progestin-related intolerance issues4
Unmet need with the treatment of postmenopausal symptoms
bull Alternatives to progestin are needed that will protect the endometrium while avoiding other progestin-associated effects and preserving the desired effects of estrogens in postmenopausal women3
Which women with a uterus could benefit from
estrogens without the need for a progestin
bull Women who are intolerant of progestin-containing hormone therapy
bull Women with pre-existing medical conditions that may be exacerbated by progestins (eg women with a history of depression PMSPMDD increased breast density diabetes and metabolic syndrome)
History of the following conditions may make progestin inappropriate
bull Depression
bull PMSPMDD
bull High breast density
bull Diabetes and metabolic syndrome
PMS premenstrual syndrome
PMD premenstrual dysphoric disorder
Medical conditions that may be exacerbated by treatment with progestins
Learning from WHI data
bull Hormone therapy (HT) is the conventional and established therapy option to effectively treat postmenopausal symptoms however it has been associated with some safety and tolerability concerns1 2
bull A review of WHI data suggests that many of the concerns with menopausal HT more often associated with EPT (CE+MPA) such as CHD risk increased breast density breast pain and breast cancer risk than with ET (CEE alone)2
1 Rolnick SJ Kopher RA DeFor TA et al Menopause 2005
2 Komm BS Mirkin S Pharmaceuticals 2012
WHI Womenrsquos Health Initiative trial
CHD coronary heart disease
CEE conjugated equine estrogens
Efficacy and Safety of Constant Oestrogen
Pulsed Progestogen vs
Continuous Combined HRT
Adverse Events
17b-oestradiol 17b-oestradiol norgestimate NETA (n = 150) (n = 172) Breast discomfort 14 27 Abdominal discomfort 14 22 Uterine bleeding 15 12 Dysmenorrhea 3 8 Oedema 5 8
Adapted from S Rozenberg et al Human Reproduction 2000
Medical condition which may be exacerbated by treatment
with progestins
Increased breast density
bull Increases in breast density are associated with progestin-containing HT which may adversely affect radiological detection of breast cancer1 and may be independently associated with an increased risk for the development of breast cancer2
bull The Postmenopausal EstrogenProgestin Interventions (PEPI) trial demonstrated that an increased mammographic breast density was associated with the use of E+P but not with the use of estrogen alone3
bull Women who already have high breast density may therefore be considered inappropriate for treatment with a progestin-containing HT
1) EU Core SPC for Hormone Replacement Therapy Products (CMDh1312003 Rev 4 June
2012)
2) De Villiers TJ et al on behalf of the International Menopause Society Climacteric 2013 16
3) Greendale GA et al J Natl Cancer Inst 2003
Stroke
0 25 5 75 10 125
Fractures
Diabetes
Breast cancer
Cholecystitis
Venothrombotic episodes
Endometrial cancer
Lung cancer
Coronary heart disease
Colorectal cancer
Overall mortality
15 125 10 75 5 25
Benefits Risks
CE
CE MPA
Santen RJ et al J Clin Endocrinol Metab 2010
The basis of the Endocrine Society scientific statement for postmenopausal hormone replacement therapy (HRT) excess risks and benefits of HRT for 5 years in women aged 50ndash59 years or within 10 years of the start of menopause E=estrogen P=progestin
bull Younger women (aged 50ndash59 years) had more favorable results bull There are differences between CE alone and CEMPA arms bull Overall benefitrisk ratio of CE-alone appears to be more favourable than CEMPA
Reevaluation of WHI data (stratified by age) Risks and
Benefits of HRT Cases per 1000 Women per 5 Years of
Use
Medical condition which may be exacerbated by treatment
with progestins
Diabetes and metabolic syndrome
bull Treatment of oestrogen deficiency symptoms with progestin-containing HT (unlike oestrogen alone) may be associated with increases in insulin resistance and deterioration in glucose tolerance123
bull Postmenopausal women with diabetes could be inappropriate for treatment with progestin-containing HT due to the potential risk of exacerbation of their condition
1) Panay N amp Studd JWW Human Reprod Update 1997
2) Godsland I et al Metabolism 1993
3) Sites CK et al J Clin Endocrinol Metab 2005
Variations in Associated Breast Cancer
Risks Between CE alone and CEMPA
bull Use of CE alone for a median of 59 years was associated with a lower incidence of invasive breast cancer (151 cases 027 per year) compared with placebo (199 cases 035 per year HR 077 95 CI 062ndash095 P=002)
bull In the CE alone group fewer women died from invasive breast cancer (6 deaths 0009 per year) compared with controls (16 deaths 0024 per year HR 037 95 CI 013ndash091 P=003)
Anderson GL et al Lancet
Oncol 2012
Bazedoxifene (BZA) specifically selected in
combination with conjugated estrogens
bull BZA has been specifically selected for its unique pharmacologic profile and effects on VMS and uterine tissue in particular123
1 Crabtree J et al Mol Cell Endocrinol 2008
2 Kharode Y et al Endocrinolology 2008
3 Duavive SmPC
Estrogen Receptor activity is dimmed
Estrogen Receptor activity is turned on
CEs are agonists BZA is an antagonist
In the uterus
bull The BZA component reduces the risk of endometrial hyperplasia that can occur with the conjugated estrogens component alone3 This means that progestins are not needed
Extensive global clinical development program for
CEBZA
aIncludes additional pilot dose-finding study 203 1 Lobo RA et al Fertil Steril 2009 2 Pinkerton JV et al Menopause 2009 3 Kagan R et al Menopause 2010 4 Mirkin S et al Climacteric 2013 5 Pinkerton JV et al Obstet Gynecol 2013
Effects of conjugated estrogensbazedoxifene on
lipid and coagulation variables a randomized
placebo- and active-controlled trial
bull At 12 months
bull Both CEBZA doses were associated with small but significant effects on hemostasis variables including reductions in antithrombin plasminogen activator inhibitor-1 and fibrinogen activity and an increase in plasminogen activity relative to placebo at 12 months Incidences of cardiovascular and venous thromboembolic events were similar among treatment groups
bull CONCLUSIONS
bull This study provides reassurance that CEBZA does not adversely affect lipid metabolism or hemostatic balance In accordance the incidences of venous thromboembolic events and cardiovascular events in postmenopausal women are similar to those observed with placebo

Reduction in the Observed Average Daily Number
of Moderate to Severe Hot Flushes
Data on file CSR-67461 Protocol 3115A1-305 Table 1511 Pfizer Inc New York NY
change from baseline to week 12
74 for DUAVIVE
51 for placebo
Observed Average Daily Number of Hot Flushes
Ob
serv
ed a
vera
ge d
aily
nu
mb
er o
f m
od
erat
e to
sev
ere
ho
t fl
ush
es
0 1 2 3 4 5 6 7 8 9 10 12 0 1
11
2
4 3
6 5
7 8 9
10
28
54
DUAVIVE (n=122) Placebo (n=62)
Weeks
Primary analysis showed statistically significant separation at weeks 4 and 12
Average daily number of hot flushes from baseline to week 12
103 to 28 for DUAVIVE
105 to 54 for placebo
Based on mathematical means
not statistically analyzed
105 103
Pinkerton JV et al Menopause 2009
Significant Reduction vs Placebo in
Average Daily Severity Score of Hot Flushes
17
Week 4 Week 12
ndash05
ndash06
Treatment
differencedagger
Treatment
differencedagger
DUAVEE [package insert] New York NY Pfizer Inc 2013
Reduction in average daily severity score of hot flushes ndash primary end point
Ad
jus
ted
me
an
ch
an
ge
fro
m b
aselin
edagger
Plt001 vs placebo daggerBased on data analysis using ANCOVA model Change from baseline = Treatment + Baseline + Site
DUAVIV
E
Reduction in the Observed Average
Daily Severity Score of Hot Flushes
Observed Average Daily Severity Score of Hot Flushes
19
DUAVIVE (n=122) Placebo (n=62)
Weeks
Ob
serv
ed a
vera
ge d
aily
sev
erit
y sc
ore
of
ho
t fl
ush
es
0
05
10
15
25
20
0 1 2 3 4 5 6 7 8 9 10 12 11 0 1 2 3 4 5 6 7 8 9 10 12 11
14
Data on file CSR-67461 Protocol 3115A1-305 Table 1511 Pfizer Inc New York NY
Primary analysis at weeks 4 and 12 prespecified secondary end points at all other weeks
change from baseline to week 12
39 for DUAVIVE
14 for placebo
Average daily severity score of hot flashes from baseline to week 12
23 to 14 for DUAVIVE
23 to 19 for Placebo
Based on mathematical means
not statistically analyzed
23
23
Pinkerton JV et al Menopause 2009
Effects on bone mineral density (BMD)
SMART 512
20
bull 12-month double-blind randomized placebo- and active-controlled study
bull Primary end point endometrial hyperplasia at 1 year
bull Secondary BMD changes at 1 year
1 DUAVEE [package insert] New York NY Pfizer Inc 2013 2 Pinkerton J Clin Endocrin Metab 2014
This study included a different dose of CEBZA and comparators The schematic shown here depicts only the patients who received the approved dose of DUAVIVE or placebo
Change from baseline in
bull Lumbar Spine BMD (Primary ndash BMD Substudy)
bull Total Hip BMD (Secondary ndash BMD Substudy)
BMD Analysis
DUAVIVE
(CE 045BZA 20)
(n=119)
Placebo
(n=139)
BMD Analysis
Postmenopausal women with a uterus
Less than 5 years since LMP
(N=590)
DUAVIVE Significantly Increased Lumbar Spine and Total
Hip BMD vs Placebo at 12 Months ndash Study 2
M
ean
ch
an
ge f
rom
baselin
e
Lumbar Spine Total Hip
121 151 Treatment
difference Treatment
difference
Data on file CSR-81040 Protocol 3115A1-3307 Pfizer Inc New York NY Pinkerton J Clin Endocrin Metab 2014 30
Plt001 vs placebo
Adjusted mean changes and P-values based on an ANCOVA model with treatment and region (US or non-US) as factors and baseline BMD value and years since menopause as covariates using the modified intention to treat population with last observation carried forward
DUAVIV
E
TOLERABILITY
AND SAFETY
Rates of BleedingSpotting and Amenorrhea
Similar to Rates with Placebo
bull High and similar cumulative rates of amenorrhea at year 1 among women treated with CE 045BZA 20 and placebo and was higher than seen in women treated with CE 045MPA 151
bull Noncumulative rates of spotting and bleedingspotting were similar among women treated with CEBZA or placebo and consistently higher in women treated with CE 045MPA 152
0
90
Cycle
100
Pe
rce
nta
ge
of
Su
bje
cts
80
70
60
50
40
30
20
10
88
54
Placebo
CE 045BZA 20 CE 045MPA 15
Percentage of subjects with cumulative amenorrhea during consecutive 4-week periods (cycles) in SMART-5
MPA medroxyprogesterone acetate Plt0001 vs all other treatment groups 1 Pinkerton JV et al J Clin Endocrinol Metab 2014 2 Data on file CSR-81040 Protocol 3115A1-3307 Pfizer Inc New York NY
Adverse Reactions in Placebo-
Controlled Trials Safety analyses have been conducted in 6210 postmenopausal women aged 40 to 75 years (mean age 55 years) following up to 2 years of treatment in SMART-1 -2 -3 and -5
Adverse reactions (incidence ge5) that were more common with DUAVIVE
Incidence of serious adverse reactions
35 with DUAVIVE 48 with placebo
DUAVEE [package insert] New York NY Pfizer Inc 2013
CE 045 BZA 20 (N=1224)
n ()
Placebo (N=1069)
n ()
Gastrointestinal disorders
Nausea 100 (8) 58 (5)
Diarrhea 96 (8) 57 (5)
Dyspepsia 84 (7) 59 (6)
Abdominal pain upper 81 (7) 58 (5)
Musculoskeletal and connective tissue disorders
Muscle spasms 110 (9) 63 (6)
Neck pain 62 (5) 46 (4)
Nervous system disorders
Dizziness 65 (5) 37 (3)
Respiratory thoracic and mediastinal disorders
Oropharyngeal pain 80 (7) 61 (6)
Venous Thromboembolism (VTE) in
DUAVIVE Clinical Studies
bull Estrogen agonistantagonists (including BZA a component of DUAVIVE) and estrogens individually are known to increase the risk of VTE
bull In the clinical studies with DUAVIVE the reporting rates for VTE were low in all treatment groups
bull Adverse reactions of VTE reported by patients
bull Should VTE event occur or be suspected DUAVIVE should be discontinued immediately
bull Due to the low rates of events in both groups it is not possible to conclude that the risk of VTE with DUAVIVE is different from that seen with other estrogen therapies
DUAVEE [package insert] New York NY Pfizer Inc 2013
00 for DUAVIVE (n=1224)
01 for placebo (n=1069)
26
Effects of conjugated estrogensbazedoxifene on
lipid and coagulation variables a randomized
placebo- and active-controlled trial
bull postmenopausal women (N = 1843) with menopausal
symptoms
bull Lipid (N = 1843) and coagulation (N = 590) variables were assessed in women receiving daily CE 045 mgBZA 20 mg CE 0625 mgBZA 20 mg BZA 20 mg CE 045 mgmedroxyprogesterone acetate (MPA) 15 mg or placebo for 12 months
bull Skouby SO et al Menopause 2015 Jun22(6)640-9
Effects of conjugated estrogensbazedoxifene on
lipid and coagulation variables a randomized
placebo- and active-controlled trial
bull At 12 months
bull CE 045 mgBZA 20 mg
bull CE 0625 mgBZA 20 mg
bull BZA 20 mg
bull and CE 045 mgMPA 15 mg decreased total cholesterol and LDL- cholesterol vs placebo (P lt 001 for all)
bull Both CEBZA doses and CEMPA increased high-density lipoprotein cholesterol compared with placebo (P lt 005 for all)
bull CE 045 mgBZA 20 mg had a neutral effect on triglycerides
bull CE 0625 mgBZA 20 mg and CEMPA increased triglycerides compared with placebo (P lt 005)
bull Skouby SO et al Menopause 2015 Jun22(6)640-9
Effects of conjugated estrogensbazedoxifene on
lipid and coagulation variables a randomized
placebo- and active-controlled trial
bull At 12 months
bull Both CEBZA doses were associated with small but significant effects on hemostasis variables including reductions in antithrombin plasminogen activator inhibitor-1 and fibrinogen activity and an increase in plasminogen activity relative to placebo at 12 months Incidences of cardiovascular and venous thromboembolic events were similar among treatment groups
Skouby SO et al Menopause 2015
Jun22(6)640-9
Endometrial hyperplasia or malignancy occurred in lt1 of women
following up to 1 year of treatment with CEBZA12
Study Cumulative Incidence at month 12 (nN)
CE 045BZA 20 Placebo
SMART-11 000 (0336) 000 (0313)
SMART-52 030 (1335) 028 (1354)
Effects on the Endometrium
1 Pickar JH et al Fertil Steril 2009 2 Pinkerton at al J Clin Endocrinol Metab 2014
Through the eyes of an amazone
Marie Mandy
Breast tolerability profile similar to placebo following up to 2 years of treatment with CEBZA12
Pooled analysis of SMART clinical trials
CE 045BZA 20 (n=1585)
Placebo (n=1241)
Breast cancer incidence up to 2 years
(per 1000 woman-years)
100 (CI 000-321)
140 (CI 000-417)
Incidence of reported breast paintenderness up to 12 weeks
98-115 81-112
Incidence of abnormal mammogram at month 12
258 316
Mean change in breast density at month 12 (SMART-5)
ndash038 (n=186)
ndash032 (n=182)
Effects on the Breast
1 Pickar JH et al Menopause 2013 2 Pinkerton JV et al Obstet Gynecol 2013
CEBZA clinical overview - summary
bull In clinical trials CEBZA has demonstrated safety and efficacy in postmenopausal women with a uterus including the following
bull Significant reduction in number and severity of moderate to severe hot flushes1
bull Incidence of cumulative amenorrhea rate similar to placebo and significantly better than CEMPA2
bull Incidence of endometrial hyperplasia and breast tendernessdensity similar to that with placebo345
bull Incidence of adverse events and discontinuation rates similar to that with placebo6
1 Pinkerton JV et al Menopause 2009 2 Pinkerton JV et al J Clin Endocrinol Metab2014 3 Pickar JH et al
Fertil Steril 2009 4 Pinkerton at al J Clin Endocrinol Metab 2014 5 Pickar JH et al Menopause 2013 6 DUAVEE [package insert] New York NY Pfizer Inc 2013
CEBZA clinical overview - summary
Now women with a uterus who choose hormone therapy for management of menopausal symptoms have a choice
bull conventional estrogen-progestogen therapy or
bull a new combinationhellipconjugated estrogens paired with the SERM bazedoxifene
1 Pinkerton JV et al Menopause 2009 2 Pinkerton JV et al J Clin Endocrinol Metab2014 3 Pickar JH et al Fertil Steril 2009 4 Pinkerton at al J Clin Endocrinol Metab 2014 5 Pickar JH et al Menopause 2013 6 DUAVEE [package insert] New York NY Pfizer Inc 2013
Conjugated EstrogensBazedoxifene (CEBZA)
US indication
bull DUAVEE is indicated in women with a uterus for
bull 11 Treatment of Moderate to Severe Vasomotor Symptoms Associated with Menopause
bull 12 Prevention of Postmenopausal Osteoporosis
bull 13 Important Limitations of Use
bull Use DUAVEE for the shortest duration consistent with treatment goals and risks for the individual woman Postmenopausal women should be re-evaluated periodically as clinically appropriate to determine if treatment is still necessary
bull When prescribing solely for the prevention of postmenopausal osteoporosis therapy should only be considered for women at significant risk of osteoporosis and non-estrogen medication should be carefully considered
Conjugated EstrogensBazedoxifene (CEBZA)
EU indication
CEBZA is indicated for
bull Treatment of oestrogen deficiency symptoms in postmenopausal women with a uterus (with at least 12 months since the last menses) for whom treatment with progestin-containing therapy is not appropriate
bull The experience treating women older than 65 years is limited
bull Dose CE (045mg)Bazedoxifene (20mg)
Duavive SmPC
Which women with a uterus
could benefit from estrogens
without the need for a
progestin
Progestin intolerance is one of the main
factors for reduced compliance
bull About 20 of women receiving progestin-containing HT have significant progestin intolerance and half of these experience serious effects that prevent treatment continuation1
1 Panay N amp Studd J Human Reprod Update 1997
2 Panay N et al on behalf of the British Menopause Society and Womenrsquos Health Concern Menopause Int 2013
bull The 2013 British Menopause Society amp Womenrsquos Health
Concern recommendations on hormone replacement
therapy do recognise progestin intolerance as one of the
main factors for reduced compliance with HT 2
Proportion of patients () with at least one bleeding episode in relation to time and to the
used HT
Serge Rozenberg et al Hum Reprod 2009241739-1747
copy The Author 2009 Published by Oxford University Press on behalf of the European Society of
Human Reproduction and Embryology All rights reserved For Permissions please email
journalspermissionsoxfordjournalsorg
Breast tenderness after initiation of CEE
CEE + MPA (WHI)
and mammographic density change
bullCrandall et al Breast Cancer Res Treat DOI 101007s10549-011-1803-9
Breast density
Conclusion
bull CEEBAZO is an additional regimen for menopausal symptoms it provides also a prevention for osteoporosis
bull It is suitable for women with a uterus who are unsatisfied with an EPT regimen or who you are unwilling to treat with an EPT regimen
Adapted use of MHT
bull Lower dosage of estrogens
bull Other progestins
bull Better safety profile
bull Vaginal estrogen or SERMS
bull Non-hormonal therapy
bull Development of new products
bull SERMS + estrogens
Most common adverse events leading to
discontinuation are related to progestins12
bull breakthrough bleeding
bull Low compliance
bull Increase in the number of US
bull Stress
bull Cost
bull uterine procedures
bull Unnecessary endometrial biopsies Hysteroscopies DampC Hysterectomies
bull Morbidity
Proportion of patients who completed or discontinued treatment in relation to the used HT
Serge Rozenberg et al Hum Reprod 2009241739-1747
copy The Author 2009 Published by Oxford University Press on behalf of the European Society of
Human Reproduction and Embryology All rights reserved For Permissions please email
journalspermissionsoxfordjournalsorg
Most common adverse events leading to discontinuation
are related to progestins
bull breast paintenderness
Breast tenderness after initiation of CEE
CEE + MPA (WHI)
and mammographic density change
bullCrandall et al Breast Cancer Res Treat DOI 101007s10549-011-1803-9
Breast density
Hormone therapy use and mammographic
density in postmenopausal Norwegian women
bull Results differed when considering the combined effect of age and BMI
bull The effect of EPT on mammographic density was modified by age and BMI with no apparent association among the youngest women (aged 50-55) with the highest BMI (BMI ge 26)
bull A higher mammographic density was found in EPT users compared to never HT users particularly in women using high-dose NETA regimens Age and BMI modified the association between EPT use and mammographic density
bull Couto E et al Breast Cancer Res Treat 2011 Nov 4 [Epub ahead of print]
Breast Cancer Risk by Breast Density
Menopause and Postmenopausal Hormone
Therapy Use
Birads age HT Duration Risk
1 55-59 None 5 year risk 08 (95 CI 06- 09)
1 55-59
ET EPT 5 year risk 09 (95 CI 07 -11)
4 55-59
None 5 year risk 24 (95 CI 20 -28)
4 55-59
ET 5 year risk
30 (95 CI 26 -35)
4 55-59
EPT 5 year risk
42 (95 CI 37 -46)
Adapted from Kerlikowske et al JOURNAL OF CLINICAL ONCOLOGY 2010
Breast Cancer Risk by Breast Density
Menopause and Postmenopausal Hormone
Therapy Use
Adapted from Kerlikowske et al JOURNAL OF CLINICAL ONCOLOGY 2010
bull Postmenopausal women with high breast density are at increased risk of breast cancer and should be aware of the added risk of taking HT especially estrogen plus progestin
Medical condition which may be exacerbated by treatment
with progestins
Diabetes and metabolic syndrome
bull progestin-containing HT may be associated with increases in insulin resistance and deterioration in glucose tolerance123
bull Postmenopausal women with diabetes could be inappropriate for treatment with progestin-containing HT due to the potential risk of exacerbation of their condition
1) Panay N amp Studd JWW Human Reprod Update 1997
2) Godsland I et al Metabolism 1993
3) Sites CK et al J Clin Endocrinol Metab 2005
A Nath and R Sitruk-Ware CLIMACTERIC 200912(Suppl 1)96ndash101
A Nath and R Sitruk-Ware CLIMACTERIC 200912(Suppl 1)96ndash101
Diabetes an epidemy
bull UK 1996 14 million of diabetics
bull UK 2015 32 million (6 of the population)
bull UK 2025 5 million
bull httpwwwdiabetescoukdiabetes-prevalencehtml
Other progestin-related intolerance issues
bull Nausea
bull Depressive mood
bull Poor concentration
bull Hirsutism
bull Headache
bull Dizziness
bull Fluid retention
bull Weight gain Panay N amp Studd JWW Human Reprod Update 1997
Medical condition which may be exacerbated by treatment with progestins
PMSPMDDdepression
bull Progesterone-induced PMD can be exacerbated by exogenous progestin administration and can occur in association with HT or OC administration1
bull Significantly higher negative mood scores have been observed during the addition of a progestin to an estrogen in a sequential HT regimen in postmenopausal women with a history of PMS compared to those without2
bull Women with a history of PMS or PMD exacerbation of depression using progestins may therefore benefit from a progestin free treatment for menopausal symptoms
1) Nevatte T et al Arch Womens Ment Health 2013 2) Bjoumlrn I et al Climacteric 2006 PMS premenstrual syndrome
PMDD premenstrual dysphoric disorder
Conclusion
bull CEEBAZO is an additional regimen for menopausal symptoms it provides also a prevention for osteoporosis
bull It is suitable for women with a uterus who are unsatisfied with an EPT regimen or who you are unwilling to treat with an EPT regimen
For some postmenopausal women with a uterus there is a
need for progestin free treatment options
bull with demonstrated clinical efficacy
bull which protects the endometrium
bull improved tolerabilitysafety profile
In clinical practice this translates to women who are
intolerant of progestin-containing HT or have conditions
which may be exacerbated by treatment with progestins
Conclusion Medical need for alternative treatment option
Medical condition which may be exacerbated by treatment with progestins
Depression
bull Progestin-containing HT has been associated with increases in depressive symptoms in some individuals1
bull There is a biochemicalphysiological plausibility for the association of progestins with depression234
bull Therefore postmenopausal women who also have a medical history of depressive disorders or depression could be inappropriate for treatment with progestin-containing HT
Pfizer Confidential
65
1) Girdler SS et al J Womens Health Gend Based Med 1999 2) Traish AM et al Korean J Urol 2014 3) Stroumlhle A et al Biol Psychiatry 1999 4) Romeo E et
al Am J Psychiatry 1998
History of the following conditions may make progestin inappropriate
bull Depression
bull PMSPMDD
PMS premenstrual syndrome
PMD premenstrual dysphoric disorder
Medical conditions that may be exacerbated by treatment with progestins
Women for whom progestin-containing HT
would not be considered appropriate
minus Women who are intolerant of progestin-containing hormone therapy
minus Women with pre-existing medical conditions that may be exacerbated by progestins
Most common adverse events leading to discontinuation are related to progestins12
breakthrough bleeding
bull Increase in the number of uterine procedures (ie unnecessary endometrial biopsies)
breast paintenderness
bull Increase in the number of breast interventions
1 Steel SA et al Climacteric 2003 2 Ettinger B and Pressman A Am J Manag Care 1999 3 Komm BS Mirkin S
Pharmaceuticals 2012
4 Panay N amp Studd JWW Human Reprod Update 1997
bull Nausea bull Depressive mood bull Poor concentration bull Hirsutism bull Headache bull Dizziness bull Fluid retention bull Weight gain
Other progestin-related intolerance issues4
Unmet need with the treatment of postmenopausal symptoms
bull Alternatives to progestin are needed that will protect the endometrium while avoiding other progestin-associated effects and preserving the desired effects of estrogens in postmenopausal women3
Which women with a uterus could benefit from
estrogens without the need for a progestin
bull Women who are intolerant of progestin-containing hormone therapy
bull Women with pre-existing medical conditions that may be exacerbated by progestins (eg women with a history of depression PMSPMDD increased breast density diabetes and metabolic syndrome)
History of the following conditions may make progestin inappropriate
bull Depression
bull PMSPMDD
bull High breast density
bull Diabetes and metabolic syndrome
PMS premenstrual syndrome
PMD premenstrual dysphoric disorder
Medical conditions that may be exacerbated by treatment with progestins
Learning from WHI data
bull Hormone therapy (HT) is the conventional and established therapy option to effectively treat postmenopausal symptoms however it has been associated with some safety and tolerability concerns1 2
bull A review of WHI data suggests that many of the concerns with menopausal HT more often associated with EPT (CE+MPA) such as CHD risk increased breast density breast pain and breast cancer risk than with ET (CEE alone)2
1 Rolnick SJ Kopher RA DeFor TA et al Menopause 2005
2 Komm BS Mirkin S Pharmaceuticals 2012
WHI Womenrsquos Health Initiative trial
CHD coronary heart disease
CEE conjugated equine estrogens
Efficacy and Safety of Constant Oestrogen
Pulsed Progestogen vs
Continuous Combined HRT
Adverse Events
17b-oestradiol 17b-oestradiol norgestimate NETA (n = 150) (n = 172) Breast discomfort 14 27 Abdominal discomfort 14 22 Uterine bleeding 15 12 Dysmenorrhea 3 8 Oedema 5 8
Adapted from S Rozenberg et al Human Reproduction 2000
Medical condition which may be exacerbated by treatment
with progestins
Increased breast density
bull Increases in breast density are associated with progestin-containing HT which may adversely affect radiological detection of breast cancer1 and may be independently associated with an increased risk for the development of breast cancer2
bull The Postmenopausal EstrogenProgestin Interventions (PEPI) trial demonstrated that an increased mammographic breast density was associated with the use of E+P but not with the use of estrogen alone3
bull Women who already have high breast density may therefore be considered inappropriate for treatment with a progestin-containing HT
1) EU Core SPC for Hormone Replacement Therapy Products (CMDh1312003 Rev 4 June
2012)
2) De Villiers TJ et al on behalf of the International Menopause Society Climacteric 2013 16
3) Greendale GA et al J Natl Cancer Inst 2003
Stroke
0 25 5 75 10 125
Fractures
Diabetes
Breast cancer
Cholecystitis
Venothrombotic episodes
Endometrial cancer
Lung cancer
Coronary heart disease
Colorectal cancer
Overall mortality
15 125 10 75 5 25
Benefits Risks
CE
CE MPA
Santen RJ et al J Clin Endocrinol Metab 2010
The basis of the Endocrine Society scientific statement for postmenopausal hormone replacement therapy (HRT) excess risks and benefits of HRT for 5 years in women aged 50ndash59 years or within 10 years of the start of menopause E=estrogen P=progestin
bull Younger women (aged 50ndash59 years) had more favorable results bull There are differences between CE alone and CEMPA arms bull Overall benefitrisk ratio of CE-alone appears to be more favourable than CEMPA
Reevaluation of WHI data (stratified by age) Risks and
Benefits of HRT Cases per 1000 Women per 5 Years of
Use
Medical condition which may be exacerbated by treatment
with progestins
Diabetes and metabolic syndrome
bull Treatment of oestrogen deficiency symptoms with progestin-containing HT (unlike oestrogen alone) may be associated with increases in insulin resistance and deterioration in glucose tolerance123
bull Postmenopausal women with diabetes could be inappropriate for treatment with progestin-containing HT due to the potential risk of exacerbation of their condition
1) Panay N amp Studd JWW Human Reprod Update 1997
2) Godsland I et al Metabolism 1993
3) Sites CK et al J Clin Endocrinol Metab 2005
Variations in Associated Breast Cancer
Risks Between CE alone and CEMPA
bull Use of CE alone for a median of 59 years was associated with a lower incidence of invasive breast cancer (151 cases 027 per year) compared with placebo (199 cases 035 per year HR 077 95 CI 062ndash095 P=002)
bull In the CE alone group fewer women died from invasive breast cancer (6 deaths 0009 per year) compared with controls (16 deaths 0024 per year HR 037 95 CI 013ndash091 P=003)
Anderson GL et al Lancet
Oncol 2012
Bazedoxifene (BZA) specifically selected in
combination with conjugated estrogens
bull BZA has been specifically selected for its unique pharmacologic profile and effects on VMS and uterine tissue in particular123
1 Crabtree J et al Mol Cell Endocrinol 2008
2 Kharode Y et al Endocrinolology 2008
3 Duavive SmPC
Estrogen Receptor activity is dimmed
Estrogen Receptor activity is turned on
CEs are agonists BZA is an antagonist
In the uterus
bull The BZA component reduces the risk of endometrial hyperplasia that can occur with the conjugated estrogens component alone3 This means that progestins are not needed
Extensive global clinical development program for
CEBZA
aIncludes additional pilot dose-finding study 203 1 Lobo RA et al Fertil Steril 2009 2 Pinkerton JV et al Menopause 2009 3 Kagan R et al Menopause 2010 4 Mirkin S et al Climacteric 2013 5 Pinkerton JV et al Obstet Gynecol 2013
Effects of conjugated estrogensbazedoxifene on
lipid and coagulation variables a randomized
placebo- and active-controlled trial
bull At 12 months
bull Both CEBZA doses were associated with small but significant effects on hemostasis variables including reductions in antithrombin plasminogen activator inhibitor-1 and fibrinogen activity and an increase in plasminogen activity relative to placebo at 12 months Incidences of cardiovascular and venous thromboembolic events were similar among treatment groups
bull CONCLUSIONS
bull This study provides reassurance that CEBZA does not adversely affect lipid metabolism or hemostatic balance In accordance the incidences of venous thromboembolic events and cardiovascular events in postmenopausal women are similar to those observed with placebo
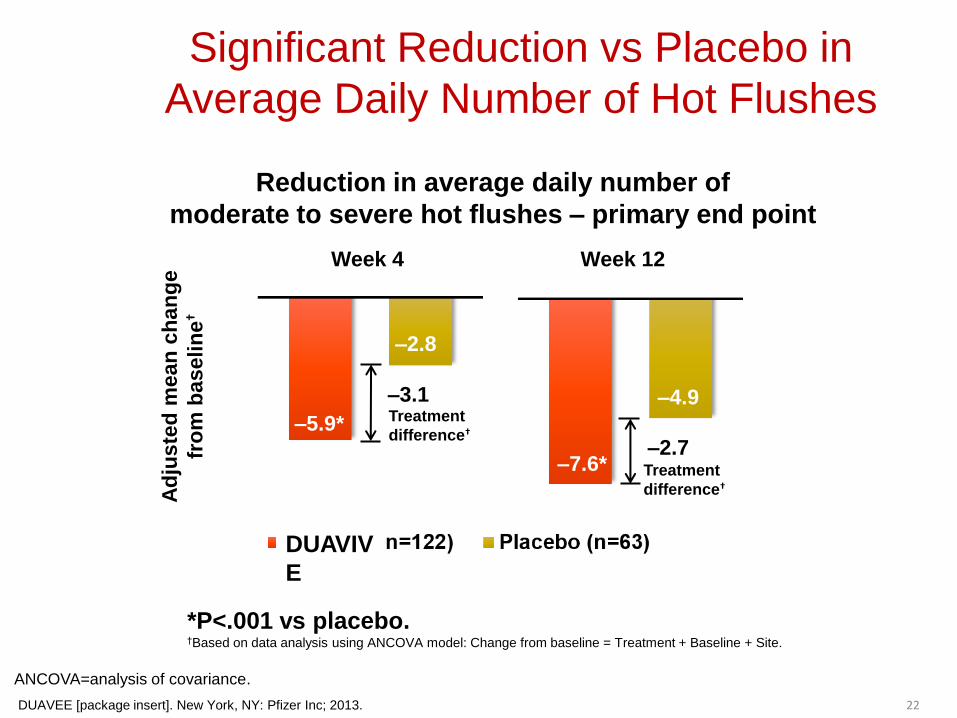
Significant Reduction vs Placebo in
Average Daily Severity Score of Hot Flushes
17
Week 4 Week 12
ndash05
ndash06
Treatment
differencedagger
Treatment
differencedagger
DUAVEE [package insert] New York NY Pfizer Inc 2013
Reduction in average daily severity score of hot flushes ndash primary end point
Ad
jus
ted
me
an
ch
an
ge
fro
m b
aselin
edagger
Plt001 vs placebo daggerBased on data analysis using ANCOVA model Change from baseline = Treatment + Baseline + Site
DUAVIV
E
Reduction in the Observed Average
Daily Severity Score of Hot Flushes
Observed Average Daily Severity Score of Hot Flushes
19
DUAVIVE (n=122) Placebo (n=62)
Weeks
Ob
serv
ed a
vera
ge d
aily
sev
erit
y sc
ore
of
ho
t fl
ush
es
0
05
10
15
25
20
0 1 2 3 4 5 6 7 8 9 10 12 11 0 1 2 3 4 5 6 7 8 9 10 12 11
14
Data on file CSR-67461 Protocol 3115A1-305 Table 1511 Pfizer Inc New York NY
Primary analysis at weeks 4 and 12 prespecified secondary end points at all other weeks
change from baseline to week 12
39 for DUAVIVE
14 for placebo
Average daily severity score of hot flashes from baseline to week 12
23 to 14 for DUAVIVE
23 to 19 for Placebo
Based on mathematical means
not statistically analyzed
23
23
Pinkerton JV et al Menopause 2009
Effects on bone mineral density (BMD)
SMART 512
20
bull 12-month double-blind randomized placebo- and active-controlled study
bull Primary end point endometrial hyperplasia at 1 year
bull Secondary BMD changes at 1 year
1 DUAVEE [package insert] New York NY Pfizer Inc 2013 2 Pinkerton J Clin Endocrin Metab 2014
This study included a different dose of CEBZA and comparators The schematic shown here depicts only the patients who received the approved dose of DUAVIVE or placebo
Change from baseline in
bull Lumbar Spine BMD (Primary ndash BMD Substudy)
bull Total Hip BMD (Secondary ndash BMD Substudy)
BMD Analysis
DUAVIVE
(CE 045BZA 20)
(n=119)
Placebo
(n=139)
BMD Analysis
Postmenopausal women with a uterus
Less than 5 years since LMP
(N=590)
DUAVIVE Significantly Increased Lumbar Spine and Total
Hip BMD vs Placebo at 12 Months ndash Study 2
M
ean
ch
an
ge f
rom
baselin
e
Lumbar Spine Total Hip
121 151 Treatment
difference Treatment
difference
Data on file CSR-81040 Protocol 3115A1-3307 Pfizer Inc New York NY Pinkerton J Clin Endocrin Metab 2014 30
Plt001 vs placebo
Adjusted mean changes and P-values based on an ANCOVA model with treatment and region (US or non-US) as factors and baseline BMD value and years since menopause as covariates using the modified intention to treat population with last observation carried forward
DUAVIV
E
TOLERABILITY
AND SAFETY
Rates of BleedingSpotting and Amenorrhea
Similar to Rates with Placebo
bull High and similar cumulative rates of amenorrhea at year 1 among women treated with CE 045BZA 20 and placebo and was higher than seen in women treated with CE 045MPA 151
bull Noncumulative rates of spotting and bleedingspotting were similar among women treated with CEBZA or placebo and consistently higher in women treated with CE 045MPA 152
0
90
Cycle
100
Pe
rce
nta
ge
of
Su
bje
cts
80
70
60
50
40
30
20
10
88
54
Placebo
CE 045BZA 20 CE 045MPA 15
Percentage of subjects with cumulative amenorrhea during consecutive 4-week periods (cycles) in SMART-5
MPA medroxyprogesterone acetate Plt0001 vs all other treatment groups 1 Pinkerton JV et al J Clin Endocrinol Metab 2014 2 Data on file CSR-81040 Protocol 3115A1-3307 Pfizer Inc New York NY
Adverse Reactions in Placebo-
Controlled Trials Safety analyses have been conducted in 6210 postmenopausal women aged 40 to 75 years (mean age 55 years) following up to 2 years of treatment in SMART-1 -2 -3 and -5
Adverse reactions (incidence ge5) that were more common with DUAVIVE
Incidence of serious adverse reactions
35 with DUAVIVE 48 with placebo
DUAVEE [package insert] New York NY Pfizer Inc 2013
CE 045 BZA 20 (N=1224)
n ()
Placebo (N=1069)
n ()
Gastrointestinal disorders
Nausea 100 (8) 58 (5)
Diarrhea 96 (8) 57 (5)
Dyspepsia 84 (7) 59 (6)
Abdominal pain upper 81 (7) 58 (5)
Musculoskeletal and connective tissue disorders
Muscle spasms 110 (9) 63 (6)
Neck pain 62 (5) 46 (4)
Nervous system disorders
Dizziness 65 (5) 37 (3)
Respiratory thoracic and mediastinal disorders
Oropharyngeal pain 80 (7) 61 (6)
Venous Thromboembolism (VTE) in
DUAVIVE Clinical Studies
bull Estrogen agonistantagonists (including BZA a component of DUAVIVE) and estrogens individually are known to increase the risk of VTE
bull In the clinical studies with DUAVIVE the reporting rates for VTE were low in all treatment groups
bull Adverse reactions of VTE reported by patients
bull Should VTE event occur or be suspected DUAVIVE should be discontinued immediately
bull Due to the low rates of events in both groups it is not possible to conclude that the risk of VTE with DUAVIVE is different from that seen with other estrogen therapies
DUAVEE [package insert] New York NY Pfizer Inc 2013
00 for DUAVIVE (n=1224)
01 for placebo (n=1069)
26
Effects of conjugated estrogensbazedoxifene on
lipid and coagulation variables a randomized
placebo- and active-controlled trial
bull postmenopausal women (N = 1843) with menopausal
symptoms
bull Lipid (N = 1843) and coagulation (N = 590) variables were assessed in women receiving daily CE 045 mgBZA 20 mg CE 0625 mgBZA 20 mg BZA 20 mg CE 045 mgmedroxyprogesterone acetate (MPA) 15 mg or placebo for 12 months
bull Skouby SO et al Menopause 2015 Jun22(6)640-9
Effects of conjugated estrogensbazedoxifene on
lipid and coagulation variables a randomized
placebo- and active-controlled trial
bull At 12 months
bull CE 045 mgBZA 20 mg
bull CE 0625 mgBZA 20 mg
bull BZA 20 mg
bull and CE 045 mgMPA 15 mg decreased total cholesterol and LDL- cholesterol vs placebo (P lt 001 for all)
bull Both CEBZA doses and CEMPA increased high-density lipoprotein cholesterol compared with placebo (P lt 005 for all)
bull CE 045 mgBZA 20 mg had a neutral effect on triglycerides
bull CE 0625 mgBZA 20 mg and CEMPA increased triglycerides compared with placebo (P lt 005)
bull Skouby SO et al Menopause 2015 Jun22(6)640-9
Effects of conjugated estrogensbazedoxifene on
lipid and coagulation variables a randomized
placebo- and active-controlled trial
bull At 12 months
bull Both CEBZA doses were associated with small but significant effects on hemostasis variables including reductions in antithrombin plasminogen activator inhibitor-1 and fibrinogen activity and an increase in plasminogen activity relative to placebo at 12 months Incidences of cardiovascular and venous thromboembolic events were similar among treatment groups
Skouby SO et al Menopause 2015
Jun22(6)640-9
Endometrial hyperplasia or malignancy occurred in lt1 of women
following up to 1 year of treatment with CEBZA12
Study Cumulative Incidence at month 12 (nN)
CE 045BZA 20 Placebo
SMART-11 000 (0336) 000 (0313)
SMART-52 030 (1335) 028 (1354)
Effects on the Endometrium
1 Pickar JH et al Fertil Steril 2009 2 Pinkerton at al J Clin Endocrinol Metab 2014
Through the eyes of an amazone
Marie Mandy
Breast tolerability profile similar to placebo following up to 2 years of treatment with CEBZA12
Pooled analysis of SMART clinical trials
CE 045BZA 20 (n=1585)
Placebo (n=1241)
Breast cancer incidence up to 2 years
(per 1000 woman-years)
100 (CI 000-321)
140 (CI 000-417)
Incidence of reported breast paintenderness up to 12 weeks
98-115 81-112
Incidence of abnormal mammogram at month 12
258 316
Mean change in breast density at month 12 (SMART-5)
ndash038 (n=186)
ndash032 (n=182)
Effects on the Breast
1 Pickar JH et al Menopause 2013 2 Pinkerton JV et al Obstet Gynecol 2013
CEBZA clinical overview - summary
bull In clinical trials CEBZA has demonstrated safety and efficacy in postmenopausal women with a uterus including the following
bull Significant reduction in number and severity of moderate to severe hot flushes1
bull Incidence of cumulative amenorrhea rate similar to placebo and significantly better than CEMPA2
bull Incidence of endometrial hyperplasia and breast tendernessdensity similar to that with placebo345
bull Incidence of adverse events and discontinuation rates similar to that with placebo6
1 Pinkerton JV et al Menopause 2009 2 Pinkerton JV et al J Clin Endocrinol Metab2014 3 Pickar JH et al
Fertil Steril 2009 4 Pinkerton at al J Clin Endocrinol Metab 2014 5 Pickar JH et al Menopause 2013 6 DUAVEE [package insert] New York NY Pfizer Inc 2013
CEBZA clinical overview - summary
Now women with a uterus who choose hormone therapy for management of menopausal symptoms have a choice
bull conventional estrogen-progestogen therapy or
bull a new combinationhellipconjugated estrogens paired with the SERM bazedoxifene
1 Pinkerton JV et al Menopause 2009 2 Pinkerton JV et al J Clin Endocrinol Metab2014 3 Pickar JH et al Fertil Steril 2009 4 Pinkerton at al J Clin Endocrinol Metab 2014 5 Pickar JH et al Menopause 2013 6 DUAVEE [package insert] New York NY Pfizer Inc 2013
Conjugated EstrogensBazedoxifene (CEBZA)
US indication
bull DUAVEE is indicated in women with a uterus for
bull 11 Treatment of Moderate to Severe Vasomotor Symptoms Associated with Menopause
bull 12 Prevention of Postmenopausal Osteoporosis
bull 13 Important Limitations of Use
bull Use DUAVEE for the shortest duration consistent with treatment goals and risks for the individual woman Postmenopausal women should be re-evaluated periodically as clinically appropriate to determine if treatment is still necessary
bull When prescribing solely for the prevention of postmenopausal osteoporosis therapy should only be considered for women at significant risk of osteoporosis and non-estrogen medication should be carefully considered
Conjugated EstrogensBazedoxifene (CEBZA)
EU indication
CEBZA is indicated for
bull Treatment of oestrogen deficiency symptoms in postmenopausal women with a uterus (with at least 12 months since the last menses) for whom treatment with progestin-containing therapy is not appropriate
bull The experience treating women older than 65 years is limited
bull Dose CE (045mg)Bazedoxifene (20mg)
Duavive SmPC
Which women with a uterus
could benefit from estrogens
without the need for a
progestin
Progestin intolerance is one of the main
factors for reduced compliance
bull About 20 of women receiving progestin-containing HT have significant progestin intolerance and half of these experience serious effects that prevent treatment continuation1
1 Panay N amp Studd J Human Reprod Update 1997
2 Panay N et al on behalf of the British Menopause Society and Womenrsquos Health Concern Menopause Int 2013
bull The 2013 British Menopause Society amp Womenrsquos Health
Concern recommendations on hormone replacement
therapy do recognise progestin intolerance as one of the
main factors for reduced compliance with HT 2
Proportion of patients () with at least one bleeding episode in relation to time and to the
used HT
Serge Rozenberg et al Hum Reprod 2009241739-1747
copy The Author 2009 Published by Oxford University Press on behalf of the European Society of
Human Reproduction and Embryology All rights reserved For Permissions please email
journalspermissionsoxfordjournalsorg
Breast tenderness after initiation of CEE
CEE + MPA (WHI)
and mammographic density change
bullCrandall et al Breast Cancer Res Treat DOI 101007s10549-011-1803-9
Breast density
Conclusion
bull CEEBAZO is an additional regimen for menopausal symptoms it provides also a prevention for osteoporosis
bull It is suitable for women with a uterus who are unsatisfied with an EPT regimen or who you are unwilling to treat with an EPT regimen
Adapted use of MHT
bull Lower dosage of estrogens
bull Other progestins
bull Better safety profile
bull Vaginal estrogen or SERMS
bull Non-hormonal therapy
bull Development of new products
bull SERMS + estrogens
Most common adverse events leading to
discontinuation are related to progestins12
bull breakthrough bleeding
bull Low compliance
bull Increase in the number of US
bull Stress
bull Cost
bull uterine procedures
bull Unnecessary endometrial biopsies Hysteroscopies DampC Hysterectomies
bull Morbidity
Proportion of patients who completed or discontinued treatment in relation to the used HT
Serge Rozenberg et al Hum Reprod 2009241739-1747
copy The Author 2009 Published by Oxford University Press on behalf of the European Society of
Human Reproduction and Embryology All rights reserved For Permissions please email
journalspermissionsoxfordjournalsorg
Most common adverse events leading to discontinuation
are related to progestins
bull breast paintenderness
Breast tenderness after initiation of CEE
CEE + MPA (WHI)
and mammographic density change
bullCrandall et al Breast Cancer Res Treat DOI 101007s10549-011-1803-9
Breast density
Hormone therapy use and mammographic
density in postmenopausal Norwegian women
bull Results differed when considering the combined effect of age and BMI
bull The effect of EPT on mammographic density was modified by age and BMI with no apparent association among the youngest women (aged 50-55) with the highest BMI (BMI ge 26)
bull A higher mammographic density was found in EPT users compared to never HT users particularly in women using high-dose NETA regimens Age and BMI modified the association between EPT use and mammographic density
bull Couto E et al Breast Cancer Res Treat 2011 Nov 4 [Epub ahead of print]
Breast Cancer Risk by Breast Density
Menopause and Postmenopausal Hormone
Therapy Use
Birads age HT Duration Risk
1 55-59 None 5 year risk 08 (95 CI 06- 09)
1 55-59
ET EPT 5 year risk 09 (95 CI 07 -11)
4 55-59
None 5 year risk 24 (95 CI 20 -28)
4 55-59
ET 5 year risk
30 (95 CI 26 -35)
4 55-59
EPT 5 year risk
42 (95 CI 37 -46)
Adapted from Kerlikowske et al JOURNAL OF CLINICAL ONCOLOGY 2010
Breast Cancer Risk by Breast Density
Menopause and Postmenopausal Hormone
Therapy Use
Adapted from Kerlikowske et al JOURNAL OF CLINICAL ONCOLOGY 2010
bull Postmenopausal women with high breast density are at increased risk of breast cancer and should be aware of the added risk of taking HT especially estrogen plus progestin
Medical condition which may be exacerbated by treatment
with progestins
Diabetes and metabolic syndrome
bull progestin-containing HT may be associated with increases in insulin resistance and deterioration in glucose tolerance123
bull Postmenopausal women with diabetes could be inappropriate for treatment with progestin-containing HT due to the potential risk of exacerbation of their condition
1) Panay N amp Studd JWW Human Reprod Update 1997
2) Godsland I et al Metabolism 1993
3) Sites CK et al J Clin Endocrinol Metab 2005
A Nath and R Sitruk-Ware CLIMACTERIC 200912(Suppl 1)96ndash101
A Nath and R Sitruk-Ware CLIMACTERIC 200912(Suppl 1)96ndash101
Diabetes an epidemy
bull UK 1996 14 million of diabetics
bull UK 2015 32 million (6 of the population)
bull UK 2025 5 million
bull httpwwwdiabetescoukdiabetes-prevalencehtml
Other progestin-related intolerance issues
bull Nausea
bull Depressive mood
bull Poor concentration
bull Hirsutism
bull Headache
bull Dizziness
bull Fluid retention
bull Weight gain Panay N amp Studd JWW Human Reprod Update 1997
Medical condition which may be exacerbated by treatment with progestins
PMSPMDDdepression
bull Progesterone-induced PMD can be exacerbated by exogenous progestin administration and can occur in association with HT or OC administration1
bull Significantly higher negative mood scores have been observed during the addition of a progestin to an estrogen in a sequential HT regimen in postmenopausal women with a history of PMS compared to those without2
bull Women with a history of PMS or PMD exacerbation of depression using progestins may therefore benefit from a progestin free treatment for menopausal symptoms
1) Nevatte T et al Arch Womens Ment Health 2013 2) Bjoumlrn I et al Climacteric 2006 PMS premenstrual syndrome
PMDD premenstrual dysphoric disorder
Conclusion
bull CEEBAZO is an additional regimen for menopausal symptoms it provides also a prevention for osteoporosis
bull It is suitable for women with a uterus who are unsatisfied with an EPT regimen or who you are unwilling to treat with an EPT regimen
For some postmenopausal women with a uterus there is a
need for progestin free treatment options
bull with demonstrated clinical efficacy
bull which protects the endometrium
bull improved tolerabilitysafety profile
In clinical practice this translates to women who are
intolerant of progestin-containing HT or have conditions
which may be exacerbated by treatment with progestins
Conclusion Medical need for alternative treatment option
Medical condition which may be exacerbated by treatment with progestins
Depression
bull Progestin-containing HT has been associated with increases in depressive symptoms in some individuals1
bull There is a biochemicalphysiological plausibility for the association of progestins with depression234
bull Therefore postmenopausal women who also have a medical history of depressive disorders or depression could be inappropriate for treatment with progestin-containing HT
Pfizer Confidential
65
1) Girdler SS et al J Womens Health Gend Based Med 1999 2) Traish AM et al Korean J Urol 2014 3) Stroumlhle A et al Biol Psychiatry 1999 4) Romeo E et
al Am J Psychiatry 1998
History of the following conditions may make progestin inappropriate
bull Depression
bull PMSPMDD
PMS premenstrual syndrome
PMD premenstrual dysphoric disorder
Medical conditions that may be exacerbated by treatment with progestins
Women for whom progestin-containing HT
would not be considered appropriate
minus Women who are intolerant of progestin-containing hormone therapy
minus Women with pre-existing medical conditions that may be exacerbated by progestins
Most common adverse events leading to discontinuation are related to progestins12
breakthrough bleeding
bull Increase in the number of uterine procedures (ie unnecessary endometrial biopsies)
breast paintenderness
bull Increase in the number of breast interventions
1 Steel SA et al Climacteric 2003 2 Ettinger B and Pressman A Am J Manag Care 1999 3 Komm BS Mirkin S
Pharmaceuticals 2012
4 Panay N amp Studd JWW Human Reprod Update 1997
bull Nausea bull Depressive mood bull Poor concentration bull Hirsutism bull Headache bull Dizziness bull Fluid retention bull Weight gain
Other progestin-related intolerance issues4
Unmet need with the treatment of postmenopausal symptoms
bull Alternatives to progestin are needed that will protect the endometrium while avoiding other progestin-associated effects and preserving the desired effects of estrogens in postmenopausal women3
Which women with a uterus could benefit from
estrogens without the need for a progestin
bull Women who are intolerant of progestin-containing hormone therapy
bull Women with pre-existing medical conditions that may be exacerbated by progestins (eg women with a history of depression PMSPMDD increased breast density diabetes and metabolic syndrome)
History of the following conditions may make progestin inappropriate
bull Depression
bull PMSPMDD
bull High breast density
bull Diabetes and metabolic syndrome
PMS premenstrual syndrome
PMD premenstrual dysphoric disorder
Medical conditions that may be exacerbated by treatment with progestins
Learning from WHI data
bull Hormone therapy (HT) is the conventional and established therapy option to effectively treat postmenopausal symptoms however it has been associated with some safety and tolerability concerns1 2
bull A review of WHI data suggests that many of the concerns with menopausal HT more often associated with EPT (CE+MPA) such as CHD risk increased breast density breast pain and breast cancer risk than with ET (CEE alone)2
1 Rolnick SJ Kopher RA DeFor TA et al Menopause 2005
2 Komm BS Mirkin S Pharmaceuticals 2012
WHI Womenrsquos Health Initiative trial
CHD coronary heart disease
CEE conjugated equine estrogens
Efficacy and Safety of Constant Oestrogen
Pulsed Progestogen vs
Continuous Combined HRT
Adverse Events
17b-oestradiol 17b-oestradiol norgestimate NETA (n = 150) (n = 172) Breast discomfort 14 27 Abdominal discomfort 14 22 Uterine bleeding 15 12 Dysmenorrhea 3 8 Oedema 5 8
Adapted from S Rozenberg et al Human Reproduction 2000
Medical condition which may be exacerbated by treatment
with progestins
Increased breast density
bull Increases in breast density are associated with progestin-containing HT which may adversely affect radiological detection of breast cancer1 and may be independently associated with an increased risk for the development of breast cancer2
bull The Postmenopausal EstrogenProgestin Interventions (PEPI) trial demonstrated that an increased mammographic breast density was associated with the use of E+P but not with the use of estrogen alone3
bull Women who already have high breast density may therefore be considered inappropriate for treatment with a progestin-containing HT
1) EU Core SPC for Hormone Replacement Therapy Products (CMDh1312003 Rev 4 June
2012)
2) De Villiers TJ et al on behalf of the International Menopause Society Climacteric 2013 16
3) Greendale GA et al J Natl Cancer Inst 2003
Stroke
0 25 5 75 10 125
Fractures
Diabetes
Breast cancer
Cholecystitis
Venothrombotic episodes
Endometrial cancer
Lung cancer
Coronary heart disease
Colorectal cancer
Overall mortality
15 125 10 75 5 25
Benefits Risks
CE
CE MPA
Santen RJ et al J Clin Endocrinol Metab 2010
The basis of the Endocrine Society scientific statement for postmenopausal hormone replacement therapy (HRT) excess risks and benefits of HRT for 5 years in women aged 50ndash59 years or within 10 years of the start of menopause E=estrogen P=progestin
bull Younger women (aged 50ndash59 years) had more favorable results bull There are differences between CE alone and CEMPA arms bull Overall benefitrisk ratio of CE-alone appears to be more favourable than CEMPA
Reevaluation of WHI data (stratified by age) Risks and
Benefits of HRT Cases per 1000 Women per 5 Years of
Use
Medical condition which may be exacerbated by treatment
with progestins
Diabetes and metabolic syndrome
bull Treatment of oestrogen deficiency symptoms with progestin-containing HT (unlike oestrogen alone) may be associated with increases in insulin resistance and deterioration in glucose tolerance123
bull Postmenopausal women with diabetes could be inappropriate for treatment with progestin-containing HT due to the potential risk of exacerbation of their condition
1) Panay N amp Studd JWW Human Reprod Update 1997
2) Godsland I et al Metabolism 1993
3) Sites CK et al J Clin Endocrinol Metab 2005
Variations in Associated Breast Cancer
Risks Between CE alone and CEMPA
bull Use of CE alone for a median of 59 years was associated with a lower incidence of invasive breast cancer (151 cases 027 per year) compared with placebo (199 cases 035 per year HR 077 95 CI 062ndash095 P=002)
bull In the CE alone group fewer women died from invasive breast cancer (6 deaths 0009 per year) compared with controls (16 deaths 0024 per year HR 037 95 CI 013ndash091 P=003)
Anderson GL et al Lancet
Oncol 2012
Bazedoxifene (BZA) specifically selected in
combination with conjugated estrogens
bull BZA has been specifically selected for its unique pharmacologic profile and effects on VMS and uterine tissue in particular123
1 Crabtree J et al Mol Cell Endocrinol 2008
2 Kharode Y et al Endocrinolology 2008
3 Duavive SmPC
Estrogen Receptor activity is dimmed
Estrogen Receptor activity is turned on
CEs are agonists BZA is an antagonist
In the uterus
bull The BZA component reduces the risk of endometrial hyperplasia that can occur with the conjugated estrogens component alone3 This means that progestins are not needed
Extensive global clinical development program for
CEBZA
aIncludes additional pilot dose-finding study 203 1 Lobo RA et al Fertil Steril 2009 2 Pinkerton JV et al Menopause 2009 3 Kagan R et al Menopause 2010 4 Mirkin S et al Climacteric 2013 5 Pinkerton JV et al Obstet Gynecol 2013
Effects of conjugated estrogensbazedoxifene on
lipid and coagulation variables a randomized
placebo- and active-controlled trial
bull At 12 months
bull Both CEBZA doses were associated with small but significant effects on hemostasis variables including reductions in antithrombin plasminogen activator inhibitor-1 and fibrinogen activity and an increase in plasminogen activity relative to placebo at 12 months Incidences of cardiovascular and venous thromboembolic events were similar among treatment groups
bull CONCLUSIONS
bull This study provides reassurance that CEBZA does not adversely affect lipid metabolism or hemostatic balance In accordance the incidences of venous thromboembolic events and cardiovascular events in postmenopausal women are similar to those observed with placebo

Reduction in the Observed Average
Daily Severity Score of Hot Flushes
Observed Average Daily Severity Score of Hot Flushes
19
DUAVIVE (n=122) Placebo (n=62)
Weeks
Ob
serv
ed a
vera
ge d
aily
sev
erit
y sc
ore
of
ho
t fl
ush
es
0
05
10
15
25
20
0 1 2 3 4 5 6 7 8 9 10 12 11 0 1 2 3 4 5 6 7 8 9 10 12 11
14
Data on file CSR-67461 Protocol 3115A1-305 Table 1511 Pfizer Inc New York NY
Primary analysis at weeks 4 and 12 prespecified secondary end points at all other weeks
change from baseline to week 12
39 for DUAVIVE
14 for placebo
Average daily severity score of hot flashes from baseline to week 12
23 to 14 for DUAVIVE
23 to 19 for Placebo
Based on mathematical means
not statistically analyzed
23
23
Pinkerton JV et al Menopause 2009
Effects on bone mineral density (BMD)
SMART 512
20
bull 12-month double-blind randomized placebo- and active-controlled study
bull Primary end point endometrial hyperplasia at 1 year
bull Secondary BMD changes at 1 year
1 DUAVEE [package insert] New York NY Pfizer Inc 2013 2 Pinkerton J Clin Endocrin Metab 2014
This study included a different dose of CEBZA and comparators The schematic shown here depicts only the patients who received the approved dose of DUAVIVE or placebo
Change from baseline in
bull Lumbar Spine BMD (Primary ndash BMD Substudy)
bull Total Hip BMD (Secondary ndash BMD Substudy)
BMD Analysis
DUAVIVE
(CE 045BZA 20)
(n=119)
Placebo
(n=139)
BMD Analysis
Postmenopausal women with a uterus
Less than 5 years since LMP
(N=590)
DUAVIVE Significantly Increased Lumbar Spine and Total
Hip BMD vs Placebo at 12 Months ndash Study 2
M
ean
ch
an
ge f
rom
baselin
e
Lumbar Spine Total Hip
121 151 Treatment
difference Treatment
difference
Data on file CSR-81040 Protocol 3115A1-3307 Pfizer Inc New York NY Pinkerton J Clin Endocrin Metab 2014 30
Plt001 vs placebo
Adjusted mean changes and P-values based on an ANCOVA model with treatment and region (US or non-US) as factors and baseline BMD value and years since menopause as covariates using the modified intention to treat population with last observation carried forward
DUAVIV
E
TOLERABILITY
AND SAFETY
Rates of BleedingSpotting and Amenorrhea
Similar to Rates with Placebo
bull High and similar cumulative rates of amenorrhea at year 1 among women treated with CE 045BZA 20 and placebo and was higher than seen in women treated with CE 045MPA 151
bull Noncumulative rates of spotting and bleedingspotting were similar among women treated with CEBZA or placebo and consistently higher in women treated with CE 045MPA 152
0
90
Cycle
100
Pe
rce
nta
ge
of
Su
bje
cts
80
70
60
50
40
30
20
10
88
54
Placebo
CE 045BZA 20 CE 045MPA 15
Percentage of subjects with cumulative amenorrhea during consecutive 4-week periods (cycles) in SMART-5
MPA medroxyprogesterone acetate Plt0001 vs all other treatment groups 1 Pinkerton JV et al J Clin Endocrinol Metab 2014 2 Data on file CSR-81040 Protocol 3115A1-3307 Pfizer Inc New York NY
Adverse Reactions in Placebo-
Controlled Trials Safety analyses have been conducted in 6210 postmenopausal women aged 40 to 75 years (mean age 55 years) following up to 2 years of treatment in SMART-1 -2 -3 and -5
Adverse reactions (incidence ge5) that were more common with DUAVIVE
Incidence of serious adverse reactions
35 with DUAVIVE 48 with placebo
DUAVEE [package insert] New York NY Pfizer Inc 2013
CE 045 BZA 20 (N=1224)
n ()
Placebo (N=1069)
n ()
Gastrointestinal disorders
Nausea 100 (8) 58 (5)
Diarrhea 96 (8) 57 (5)
Dyspepsia 84 (7) 59 (6)
Abdominal pain upper 81 (7) 58 (5)
Musculoskeletal and connective tissue disorders
Muscle spasms 110 (9) 63 (6)
Neck pain 62 (5) 46 (4)
Nervous system disorders
Dizziness 65 (5) 37 (3)
Respiratory thoracic and mediastinal disorders
Oropharyngeal pain 80 (7) 61 (6)
Venous Thromboembolism (VTE) in
DUAVIVE Clinical Studies
bull Estrogen agonistantagonists (including BZA a component of DUAVIVE) and estrogens individually are known to increase the risk of VTE
bull In the clinical studies with DUAVIVE the reporting rates for VTE were low in all treatment groups
bull Adverse reactions of VTE reported by patients
bull Should VTE event occur or be suspected DUAVIVE should be discontinued immediately
bull Due to the low rates of events in both groups it is not possible to conclude that the risk of VTE with DUAVIVE is different from that seen with other estrogen therapies
DUAVEE [package insert] New York NY Pfizer Inc 2013
00 for DUAVIVE (n=1224)
01 for placebo (n=1069)
26
Effects of conjugated estrogensbazedoxifene on
lipid and coagulation variables a randomized
placebo- and active-controlled trial
bull postmenopausal women (N = 1843) with menopausal
symptoms
bull Lipid (N = 1843) and coagulation (N = 590) variables were assessed in women receiving daily CE 045 mgBZA 20 mg CE 0625 mgBZA 20 mg BZA 20 mg CE 045 mgmedroxyprogesterone acetate (MPA) 15 mg or placebo for 12 months
bull Skouby SO et al Menopause 2015 Jun22(6)640-9
Effects of conjugated estrogensbazedoxifene on
lipid and coagulation variables a randomized
placebo- and active-controlled trial
bull At 12 months
bull CE 045 mgBZA 20 mg
bull CE 0625 mgBZA 20 mg
bull BZA 20 mg
bull and CE 045 mgMPA 15 mg decreased total cholesterol and LDL- cholesterol vs placebo (P lt 001 for all)
bull Both CEBZA doses and CEMPA increased high-density lipoprotein cholesterol compared with placebo (P lt 005 for all)
bull CE 045 mgBZA 20 mg had a neutral effect on triglycerides
bull CE 0625 mgBZA 20 mg and CEMPA increased triglycerides compared with placebo (P lt 005)
bull Skouby SO et al Menopause 2015 Jun22(6)640-9
Effects of conjugated estrogensbazedoxifene on
lipid and coagulation variables a randomized
placebo- and active-controlled trial
bull At 12 months
bull Both CEBZA doses were associated with small but significant effects on hemostasis variables including reductions in antithrombin plasminogen activator inhibitor-1 and fibrinogen activity and an increase in plasminogen activity relative to placebo at 12 months Incidences of cardiovascular and venous thromboembolic events were similar among treatment groups
Skouby SO et al Menopause 2015
Jun22(6)640-9
Endometrial hyperplasia or malignancy occurred in lt1 of women
following up to 1 year of treatment with CEBZA12
Study Cumulative Incidence at month 12 (nN)
CE 045BZA 20 Placebo
SMART-11 000 (0336) 000 (0313)
SMART-52 030 (1335) 028 (1354)
Effects on the Endometrium
1 Pickar JH et al Fertil Steril 2009 2 Pinkerton at al J Clin Endocrinol Metab 2014
Through the eyes of an amazone
Marie Mandy
Breast tolerability profile similar to placebo following up to 2 years of treatment with CEBZA12
Pooled analysis of SMART clinical trials
CE 045BZA 20 (n=1585)
Placebo (n=1241)
Breast cancer incidence up to 2 years
(per 1000 woman-years)
100 (CI 000-321)
140 (CI 000-417)
Incidence of reported breast paintenderness up to 12 weeks
98-115 81-112
Incidence of abnormal mammogram at month 12
258 316
Mean change in breast density at month 12 (SMART-5)
ndash038 (n=186)
ndash032 (n=182)
Effects on the Breast
1 Pickar JH et al Menopause 2013 2 Pinkerton JV et al Obstet Gynecol 2013
CEBZA clinical overview - summary
bull In clinical trials CEBZA has demonstrated safety and efficacy in postmenopausal women with a uterus including the following
bull Significant reduction in number and severity of moderate to severe hot flushes1
bull Incidence of cumulative amenorrhea rate similar to placebo and significantly better than CEMPA2
bull Incidence of endometrial hyperplasia and breast tendernessdensity similar to that with placebo345
bull Incidence of adverse events and discontinuation rates similar to that with placebo6
1 Pinkerton JV et al Menopause 2009 2 Pinkerton JV et al J Clin Endocrinol Metab2014 3 Pickar JH et al
Fertil Steril 2009 4 Pinkerton at al J Clin Endocrinol Metab 2014 5 Pickar JH et al Menopause 2013 6 DUAVEE [package insert] New York NY Pfizer Inc 2013
CEBZA clinical overview - summary
Now women with a uterus who choose hormone therapy for management of menopausal symptoms have a choice
bull conventional estrogen-progestogen therapy or
bull a new combinationhellipconjugated estrogens paired with the SERM bazedoxifene
1 Pinkerton JV et al Menopause 2009 2 Pinkerton JV et al J Clin Endocrinol Metab2014 3 Pickar JH et al Fertil Steril 2009 4 Pinkerton at al J Clin Endocrinol Metab 2014 5 Pickar JH et al Menopause 2013 6 DUAVEE [package insert] New York NY Pfizer Inc 2013
Conjugated EstrogensBazedoxifene (CEBZA)
US indication
bull DUAVEE is indicated in women with a uterus for
bull 11 Treatment of Moderate to Severe Vasomotor Symptoms Associated with Menopause
bull 12 Prevention of Postmenopausal Osteoporosis
bull 13 Important Limitations of Use
bull Use DUAVEE for the shortest duration consistent with treatment goals and risks for the individual woman Postmenopausal women should be re-evaluated periodically as clinically appropriate to determine if treatment is still necessary
bull When prescribing solely for the prevention of postmenopausal osteoporosis therapy should only be considered for women at significant risk of osteoporosis and non-estrogen medication should be carefully considered
Conjugated EstrogensBazedoxifene (CEBZA)
EU indication
CEBZA is indicated for
bull Treatment of oestrogen deficiency symptoms in postmenopausal women with a uterus (with at least 12 months since the last menses) for whom treatment with progestin-containing therapy is not appropriate
bull The experience treating women older than 65 years is limited
bull Dose CE (045mg)Bazedoxifene (20mg)
Duavive SmPC
Which women with a uterus
could benefit from estrogens
without the need for a
progestin
Progestin intolerance is one of the main
factors for reduced compliance
bull About 20 of women receiving progestin-containing HT have significant progestin intolerance and half of these experience serious effects that prevent treatment continuation1
1 Panay N amp Studd J Human Reprod Update 1997
2 Panay N et al on behalf of the British Menopause Society and Womenrsquos Health Concern Menopause Int 2013
bull The 2013 British Menopause Society amp Womenrsquos Health
Concern recommendations on hormone replacement
therapy do recognise progestin intolerance as one of the
main factors for reduced compliance with HT 2
Proportion of patients () with at least one bleeding episode in relation to time and to the
used HT
Serge Rozenberg et al Hum Reprod 2009241739-1747
copy The Author 2009 Published by Oxford University Press on behalf of the European Society of
Human Reproduction and Embryology All rights reserved For Permissions please email
journalspermissionsoxfordjournalsorg
Breast tenderness after initiation of CEE
CEE + MPA (WHI)
and mammographic density change
bullCrandall et al Breast Cancer Res Treat DOI 101007s10549-011-1803-9
Breast density
Conclusion
bull CEEBAZO is an additional regimen for menopausal symptoms it provides also a prevention for osteoporosis
bull It is suitable for women with a uterus who are unsatisfied with an EPT regimen or who you are unwilling to treat with an EPT regimen
Adapted use of MHT
bull Lower dosage of estrogens
bull Other progestins
bull Better safety profile
bull Vaginal estrogen or SERMS
bull Non-hormonal therapy
bull Development of new products
bull SERMS + estrogens
Most common adverse events leading to
discontinuation are related to progestins12
bull breakthrough bleeding
bull Low compliance
bull Increase in the number of US
bull Stress
bull Cost
bull uterine procedures
bull Unnecessary endometrial biopsies Hysteroscopies DampC Hysterectomies
bull Morbidity
Proportion of patients who completed or discontinued treatment in relation to the used HT
Serge Rozenberg et al Hum Reprod 2009241739-1747
copy The Author 2009 Published by Oxford University Press on behalf of the European Society of
Human Reproduction and Embryology All rights reserved For Permissions please email
journalspermissionsoxfordjournalsorg
Most common adverse events leading to discontinuation
are related to progestins
bull breast paintenderness
Breast tenderness after initiation of CEE
CEE + MPA (WHI)
and mammographic density change
bullCrandall et al Breast Cancer Res Treat DOI 101007s10549-011-1803-9
Breast density
Hormone therapy use and mammographic
density in postmenopausal Norwegian women
bull Results differed when considering the combined effect of age and BMI
bull The effect of EPT on mammographic density was modified by age and BMI with no apparent association among the youngest women (aged 50-55) with the highest BMI (BMI ge 26)
bull A higher mammographic density was found in EPT users compared to never HT users particularly in women using high-dose NETA regimens Age and BMI modified the association between EPT use and mammographic density
bull Couto E et al Breast Cancer Res Treat 2011 Nov 4 [Epub ahead of print]
Breast Cancer Risk by Breast Density
Menopause and Postmenopausal Hormone
Therapy Use
Birads age HT Duration Risk
1 55-59 None 5 year risk 08 (95 CI 06- 09)
1 55-59
ET EPT 5 year risk 09 (95 CI 07 -11)
4 55-59
None 5 year risk 24 (95 CI 20 -28)
4 55-59
ET 5 year risk
30 (95 CI 26 -35)
4 55-59
EPT 5 year risk
42 (95 CI 37 -46)
Adapted from Kerlikowske et al JOURNAL OF CLINICAL ONCOLOGY 2010
Breast Cancer Risk by Breast Density
Menopause and Postmenopausal Hormone
Therapy Use
Adapted from Kerlikowske et al JOURNAL OF CLINICAL ONCOLOGY 2010
bull Postmenopausal women with high breast density are at increased risk of breast cancer and should be aware of the added risk of taking HT especially estrogen plus progestin
Medical condition which may be exacerbated by treatment
with progestins
Diabetes and metabolic syndrome
bull progestin-containing HT may be associated with increases in insulin resistance and deterioration in glucose tolerance123
bull Postmenopausal women with diabetes could be inappropriate for treatment with progestin-containing HT due to the potential risk of exacerbation of their condition
1) Panay N amp Studd JWW Human Reprod Update 1997
2) Godsland I et al Metabolism 1993
3) Sites CK et al J Clin Endocrinol Metab 2005
A Nath and R Sitruk-Ware CLIMACTERIC 200912(Suppl 1)96ndash101
A Nath and R Sitruk-Ware CLIMACTERIC 200912(Suppl 1)96ndash101
Diabetes an epidemy
bull UK 1996 14 million of diabetics
bull UK 2015 32 million (6 of the population)
bull UK 2025 5 million
bull httpwwwdiabetescoukdiabetes-prevalencehtml
Other progestin-related intolerance issues
bull Nausea
bull Depressive mood
bull Poor concentration
bull Hirsutism
bull Headache
bull Dizziness
bull Fluid retention
bull Weight gain Panay N amp Studd JWW Human Reprod Update 1997
Medical condition which may be exacerbated by treatment with progestins
PMSPMDDdepression
bull Progesterone-induced PMD can be exacerbated by exogenous progestin administration and can occur in association with HT or OC administration1
bull Significantly higher negative mood scores have been observed during the addition of a progestin to an estrogen in a sequential HT regimen in postmenopausal women with a history of PMS compared to those without2
bull Women with a history of PMS or PMD exacerbation of depression using progestins may therefore benefit from a progestin free treatment for menopausal symptoms
1) Nevatte T et al Arch Womens Ment Health 2013 2) Bjoumlrn I et al Climacteric 2006 PMS premenstrual syndrome
PMDD premenstrual dysphoric disorder
Conclusion
bull CEEBAZO is an additional regimen for menopausal symptoms it provides also a prevention for osteoporosis
bull It is suitable for women with a uterus who are unsatisfied with an EPT regimen or who you are unwilling to treat with an EPT regimen
For some postmenopausal women with a uterus there is a
need for progestin free treatment options
bull with demonstrated clinical efficacy
bull which protects the endometrium
bull improved tolerabilitysafety profile
In clinical practice this translates to women who are
intolerant of progestin-containing HT or have conditions
which may be exacerbated by treatment with progestins
Conclusion Medical need for alternative treatment option
Medical condition which may be exacerbated by treatment with progestins
Depression
bull Progestin-containing HT has been associated with increases in depressive symptoms in some individuals1
bull There is a biochemicalphysiological plausibility for the association of progestins with depression234
bull Therefore postmenopausal women who also have a medical history of depressive disorders or depression could be inappropriate for treatment with progestin-containing HT
Pfizer Confidential
65
1) Girdler SS et al J Womens Health Gend Based Med 1999 2) Traish AM et al Korean J Urol 2014 3) Stroumlhle A et al Biol Psychiatry 1999 4) Romeo E et
al Am J Psychiatry 1998
History of the following conditions may make progestin inappropriate
bull Depression
bull PMSPMDD
PMS premenstrual syndrome
PMD premenstrual dysphoric disorder
Medical conditions that may be exacerbated by treatment with progestins
Women for whom progestin-containing HT
would not be considered appropriate
minus Women who are intolerant of progestin-containing hormone therapy
minus Women with pre-existing medical conditions that may be exacerbated by progestins
Most common adverse events leading to discontinuation are related to progestins12
breakthrough bleeding
bull Increase in the number of uterine procedures (ie unnecessary endometrial biopsies)
breast paintenderness
bull Increase in the number of breast interventions
1 Steel SA et al Climacteric 2003 2 Ettinger B and Pressman A Am J Manag Care 1999 3 Komm BS Mirkin S
Pharmaceuticals 2012
4 Panay N amp Studd JWW Human Reprod Update 1997
bull Nausea bull Depressive mood bull Poor concentration bull Hirsutism bull Headache bull Dizziness bull Fluid retention bull Weight gain
Other progestin-related intolerance issues4
Unmet need with the treatment of postmenopausal symptoms
bull Alternatives to progestin are needed that will protect the endometrium while avoiding other progestin-associated effects and preserving the desired effects of estrogens in postmenopausal women3
Which women with a uterus could benefit from
estrogens without the need for a progestin
bull Women who are intolerant of progestin-containing hormone therapy
bull Women with pre-existing medical conditions that may be exacerbated by progestins (eg women with a history of depression PMSPMDD increased breast density diabetes and metabolic syndrome)
History of the following conditions may make progestin inappropriate
bull Depression
bull PMSPMDD
bull High breast density
bull Diabetes and metabolic syndrome
PMS premenstrual syndrome
PMD premenstrual dysphoric disorder
Medical conditions that may be exacerbated by treatment with progestins
Learning from WHI data
bull Hormone therapy (HT) is the conventional and established therapy option to effectively treat postmenopausal symptoms however it has been associated with some safety and tolerability concerns1 2
bull A review of WHI data suggests that many of the concerns with menopausal HT more often associated with EPT (CE+MPA) such as CHD risk increased breast density breast pain and breast cancer risk than with ET (CEE alone)2
1 Rolnick SJ Kopher RA DeFor TA et al Menopause 2005
2 Komm BS Mirkin S Pharmaceuticals 2012
WHI Womenrsquos Health Initiative trial
CHD coronary heart disease
CEE conjugated equine estrogens
Efficacy and Safety of Constant Oestrogen
Pulsed Progestogen vs
Continuous Combined HRT
Adverse Events
17b-oestradiol 17b-oestradiol norgestimate NETA (n = 150) (n = 172) Breast discomfort 14 27 Abdominal discomfort 14 22 Uterine bleeding 15 12 Dysmenorrhea 3 8 Oedema 5 8
Adapted from S Rozenberg et al Human Reproduction 2000
Medical condition which may be exacerbated by treatment
with progestins
Increased breast density
bull Increases in breast density are associated with progestin-containing HT which may adversely affect radiological detection of breast cancer1 and may be independently associated with an increased risk for the development of breast cancer2
bull The Postmenopausal EstrogenProgestin Interventions (PEPI) trial demonstrated that an increased mammographic breast density was associated with the use of E+P but not with the use of estrogen alone3
bull Women who already have high breast density may therefore be considered inappropriate for treatment with a progestin-containing HT
1) EU Core SPC for Hormone Replacement Therapy Products (CMDh1312003 Rev 4 June
2012)
2) De Villiers TJ et al on behalf of the International Menopause Society Climacteric 2013 16
3) Greendale GA et al J Natl Cancer Inst 2003
Stroke
0 25 5 75 10 125
Fractures
Diabetes
Breast cancer
Cholecystitis
Venothrombotic episodes
Endometrial cancer
Lung cancer
Coronary heart disease
Colorectal cancer
Overall mortality
15 125 10 75 5 25
Benefits Risks
CE
CE MPA
Santen RJ et al J Clin Endocrinol Metab 2010
The basis of the Endocrine Society scientific statement for postmenopausal hormone replacement therapy (HRT) excess risks and benefits of HRT for 5 years in women aged 50ndash59 years or within 10 years of the start of menopause E=estrogen P=progestin
bull Younger women (aged 50ndash59 years) had more favorable results bull There are differences between CE alone and CEMPA arms bull Overall benefitrisk ratio of CE-alone appears to be more favourable than CEMPA
Reevaluation of WHI data (stratified by age) Risks and
Benefits of HRT Cases per 1000 Women per 5 Years of
Use
Medical condition which may be exacerbated by treatment
with progestins
Diabetes and metabolic syndrome
bull Treatment of oestrogen deficiency symptoms with progestin-containing HT (unlike oestrogen alone) may be associated with increases in insulin resistance and deterioration in glucose tolerance123
bull Postmenopausal women with diabetes could be inappropriate for treatment with progestin-containing HT due to the potential risk of exacerbation of their condition
1) Panay N amp Studd JWW Human Reprod Update 1997
2) Godsland I et al Metabolism 1993
3) Sites CK et al J Clin Endocrinol Metab 2005
Variations in Associated Breast Cancer
Risks Between CE alone and CEMPA
bull Use of CE alone for a median of 59 years was associated with a lower incidence of invasive breast cancer (151 cases 027 per year) compared with placebo (199 cases 035 per year HR 077 95 CI 062ndash095 P=002)
bull In the CE alone group fewer women died from invasive breast cancer (6 deaths 0009 per year) compared with controls (16 deaths 0024 per year HR 037 95 CI 013ndash091 P=003)
Anderson GL et al Lancet
Oncol 2012
Bazedoxifene (BZA) specifically selected in
combination with conjugated estrogens
bull BZA has been specifically selected for its unique pharmacologic profile and effects on VMS and uterine tissue in particular123
1 Crabtree J et al Mol Cell Endocrinol 2008
2 Kharode Y et al Endocrinolology 2008
3 Duavive SmPC
Estrogen Receptor activity is dimmed
Estrogen Receptor activity is turned on
CEs are agonists BZA is an antagonist
In the uterus
bull The BZA component reduces the risk of endometrial hyperplasia that can occur with the conjugated estrogens component alone3 This means that progestins are not needed
Extensive global clinical development program for
CEBZA
aIncludes additional pilot dose-finding study 203 1 Lobo RA et al Fertil Steril 2009 2 Pinkerton JV et al Menopause 2009 3 Kagan R et al Menopause 2010 4 Mirkin S et al Climacteric 2013 5 Pinkerton JV et al Obstet Gynecol 2013
Effects of conjugated estrogensbazedoxifene on
lipid and coagulation variables a randomized
placebo- and active-controlled trial
bull At 12 months
bull Both CEBZA doses were associated with small but significant effects on hemostasis variables including reductions in antithrombin plasminogen activator inhibitor-1 and fibrinogen activity and an increase in plasminogen activity relative to placebo at 12 months Incidences of cardiovascular and venous thromboembolic events were similar among treatment groups
bull CONCLUSIONS
bull This study provides reassurance that CEBZA does not adversely affect lipid metabolism or hemostatic balance In accordance the incidences of venous thromboembolic events and cardiovascular events in postmenopausal women are similar to those observed with placebo

Effects on bone mineral density (BMD)
SMART 512
20
bull 12-month double-blind randomized placebo- and active-controlled study
bull Primary end point endometrial hyperplasia at 1 year
bull Secondary BMD changes at 1 year
1 DUAVEE [package insert] New York NY Pfizer Inc 2013 2 Pinkerton J Clin Endocrin Metab 2014
This study included a different dose of CEBZA and comparators The schematic shown here depicts only the patients who received the approved dose of DUAVIVE or placebo
Change from baseline in
bull Lumbar Spine BMD (Primary ndash BMD Substudy)
bull Total Hip BMD (Secondary ndash BMD Substudy)
BMD Analysis
DUAVIVE
(CE 045BZA 20)
(n=119)
Placebo
(n=139)
BMD Analysis
Postmenopausal women with a uterus
Less than 5 years since LMP
(N=590)
DUAVIVE Significantly Increased Lumbar Spine and Total
Hip BMD vs Placebo at 12 Months ndash Study 2
M
ean
ch
an
ge f
rom
baselin
e
Lumbar Spine Total Hip
121 151 Treatment
difference Treatment
difference
Data on file CSR-81040 Protocol 3115A1-3307 Pfizer Inc New York NY Pinkerton J Clin Endocrin Metab 2014 30
Plt001 vs placebo
Adjusted mean changes and P-values based on an ANCOVA model with treatment and region (US or non-US) as factors and baseline BMD value and years since menopause as covariates using the modified intention to treat population with last observation carried forward
DUAVIV
E
TOLERABILITY
AND SAFETY
Rates of BleedingSpotting and Amenorrhea
Similar to Rates with Placebo
bull High and similar cumulative rates of amenorrhea at year 1 among women treated with CE 045BZA 20 and placebo and was higher than seen in women treated with CE 045MPA 151
bull Noncumulative rates of spotting and bleedingspotting were similar among women treated with CEBZA or placebo and consistently higher in women treated with CE 045MPA 152
0
90
Cycle
100
Pe
rce
nta
ge
of
Su
bje
cts
80
70
60
50
40
30
20
10
88
54
Placebo
CE 045BZA 20 CE 045MPA 15
Percentage of subjects with cumulative amenorrhea during consecutive 4-week periods (cycles) in SMART-5
MPA medroxyprogesterone acetate Plt0001 vs all other treatment groups 1 Pinkerton JV et al J Clin Endocrinol Metab 2014 2 Data on file CSR-81040 Protocol 3115A1-3307 Pfizer Inc New York NY
Adverse Reactions in Placebo-
Controlled Trials Safety analyses have been conducted in 6210 postmenopausal women aged 40 to 75 years (mean age 55 years) following up to 2 years of treatment in SMART-1 -2 -3 and -5
Adverse reactions (incidence ge5) that were more common with DUAVIVE
Incidence of serious adverse reactions
35 with DUAVIVE 48 with placebo
DUAVEE [package insert] New York NY Pfizer Inc 2013
CE 045 BZA 20 (N=1224)
n ()
Placebo (N=1069)
n ()
Gastrointestinal disorders
Nausea 100 (8) 58 (5)
Diarrhea 96 (8) 57 (5)
Dyspepsia 84 (7) 59 (6)
Abdominal pain upper 81 (7) 58 (5)
Musculoskeletal and connective tissue disorders
Muscle spasms 110 (9) 63 (6)
Neck pain 62 (5) 46 (4)
Nervous system disorders
Dizziness 65 (5) 37 (3)
Respiratory thoracic and mediastinal disorders
Oropharyngeal pain 80 (7) 61 (6)
Venous Thromboembolism (VTE) in
DUAVIVE Clinical Studies
bull Estrogen agonistantagonists (including BZA a component of DUAVIVE) and estrogens individually are known to increase the risk of VTE
bull In the clinical studies with DUAVIVE the reporting rates for VTE were low in all treatment groups
bull Adverse reactions of VTE reported by patients
bull Should VTE event occur or be suspected DUAVIVE should be discontinued immediately
bull Due to the low rates of events in both groups it is not possible to conclude that the risk of VTE with DUAVIVE is different from that seen with other estrogen therapies
DUAVEE [package insert] New York NY Pfizer Inc 2013
00 for DUAVIVE (n=1224)
01 for placebo (n=1069)
26
Effects of conjugated estrogensbazedoxifene on
lipid and coagulation variables a randomized
placebo- and active-controlled trial
bull postmenopausal women (N = 1843) with menopausal
symptoms
bull Lipid (N = 1843) and coagulation (N = 590) variables were assessed in women receiving daily CE 045 mgBZA 20 mg CE 0625 mgBZA 20 mg BZA 20 mg CE 045 mgmedroxyprogesterone acetate (MPA) 15 mg or placebo for 12 months
bull Skouby SO et al Menopause 2015 Jun22(6)640-9
Effects of conjugated estrogensbazedoxifene on
lipid and coagulation variables a randomized
placebo- and active-controlled trial
bull At 12 months
bull CE 045 mgBZA 20 mg
bull CE 0625 mgBZA 20 mg
bull BZA 20 mg
bull and CE 045 mgMPA 15 mg decreased total cholesterol and LDL- cholesterol vs placebo (P lt 001 for all)
bull Both CEBZA doses and CEMPA increased high-density lipoprotein cholesterol compared with placebo (P lt 005 for all)
bull CE 045 mgBZA 20 mg had a neutral effect on triglycerides
bull CE 0625 mgBZA 20 mg and CEMPA increased triglycerides compared with placebo (P lt 005)
bull Skouby SO et al Menopause 2015 Jun22(6)640-9
Effects of conjugated estrogensbazedoxifene on
lipid and coagulation variables a randomized
placebo- and active-controlled trial
bull At 12 months
bull Both CEBZA doses were associated with small but significant effects on hemostasis variables including reductions in antithrombin plasminogen activator inhibitor-1 and fibrinogen activity and an increase in plasminogen activity relative to placebo at 12 months Incidences of cardiovascular and venous thromboembolic events were similar among treatment groups
Skouby SO et al Menopause 2015
Jun22(6)640-9
Endometrial hyperplasia or malignancy occurred in lt1 of women
following up to 1 year of treatment with CEBZA12
Study Cumulative Incidence at month 12 (nN)
CE 045BZA 20 Placebo
SMART-11 000 (0336) 000 (0313)
SMART-52 030 (1335) 028 (1354)
Effects on the Endometrium
1 Pickar JH et al Fertil Steril 2009 2 Pinkerton at al J Clin Endocrinol Metab 2014
Through the eyes of an amazone
Marie Mandy
Breast tolerability profile similar to placebo following up to 2 years of treatment with CEBZA12
Pooled analysis of SMART clinical trials
CE 045BZA 20 (n=1585)
Placebo (n=1241)
Breast cancer incidence up to 2 years
(per 1000 woman-years)
100 (CI 000-321)
140 (CI 000-417)
Incidence of reported breast paintenderness up to 12 weeks
98-115 81-112
Incidence of abnormal mammogram at month 12
258 316
Mean change in breast density at month 12 (SMART-5)
ndash038 (n=186)
ndash032 (n=182)
Effects on the Breast
1 Pickar JH et al Menopause 2013 2 Pinkerton JV et al Obstet Gynecol 2013
CEBZA clinical overview - summary
bull In clinical trials CEBZA has demonstrated safety and efficacy in postmenopausal women with a uterus including the following
bull Significant reduction in number and severity of moderate to severe hot flushes1
bull Incidence of cumulative amenorrhea rate similar to placebo and significantly better than CEMPA2
bull Incidence of endometrial hyperplasia and breast tendernessdensity similar to that with placebo345
bull Incidence of adverse events and discontinuation rates similar to that with placebo6
1 Pinkerton JV et al Menopause 2009 2 Pinkerton JV et al J Clin Endocrinol Metab2014 3 Pickar JH et al
Fertil Steril 2009 4 Pinkerton at al J Clin Endocrinol Metab 2014 5 Pickar JH et al Menopause 2013 6 DUAVEE [package insert] New York NY Pfizer Inc 2013
CEBZA clinical overview - summary
Now women with a uterus who choose hormone therapy for management of menopausal symptoms have a choice
bull conventional estrogen-progestogen therapy or
bull a new combinationhellipconjugated estrogens paired with the SERM bazedoxifene
1 Pinkerton JV et al Menopause 2009 2 Pinkerton JV et al J Clin Endocrinol Metab2014 3 Pickar JH et al Fertil Steril 2009 4 Pinkerton at al J Clin Endocrinol Metab 2014 5 Pickar JH et al Menopause 2013 6 DUAVEE [package insert] New York NY Pfizer Inc 2013
Conjugated EstrogensBazedoxifene (CEBZA)
US indication
bull DUAVEE is indicated in women with a uterus for
bull 11 Treatment of Moderate to Severe Vasomotor Symptoms Associated with Menopause
bull 12 Prevention of Postmenopausal Osteoporosis
bull 13 Important Limitations of Use
bull Use DUAVEE for the shortest duration consistent with treatment goals and risks for the individual woman Postmenopausal women should be re-evaluated periodically as clinically appropriate to determine if treatment is still necessary
bull When prescribing solely for the prevention of postmenopausal osteoporosis therapy should only be considered for women at significant risk of osteoporosis and non-estrogen medication should be carefully considered
Conjugated EstrogensBazedoxifene (CEBZA)
EU indication
CEBZA is indicated for
bull Treatment of oestrogen deficiency symptoms in postmenopausal women with a uterus (with at least 12 months since the last menses) for whom treatment with progestin-containing therapy is not appropriate
bull The experience treating women older than 65 years is limited
bull Dose CE (045mg)Bazedoxifene (20mg)
Duavive SmPC
Which women with a uterus
could benefit from estrogens
without the need for a
progestin
Progestin intolerance is one of the main
factors for reduced compliance
bull About 20 of women receiving progestin-containing HT have significant progestin intolerance and half of these experience serious effects that prevent treatment continuation1
1 Panay N amp Studd J Human Reprod Update 1997
2 Panay N et al on behalf of the British Menopause Society and Womenrsquos Health Concern Menopause Int 2013
bull The 2013 British Menopause Society amp Womenrsquos Health
Concern recommendations on hormone replacement
therapy do recognise progestin intolerance as one of the
main factors for reduced compliance with HT 2
Proportion of patients () with at least one bleeding episode in relation to time and to the
used HT
Serge Rozenberg et al Hum Reprod 2009241739-1747
copy The Author 2009 Published by Oxford University Press on behalf of the European Society of
Human Reproduction and Embryology All rights reserved For Permissions please email
journalspermissionsoxfordjournalsorg
Breast tenderness after initiation of CEE
CEE + MPA (WHI)
and mammographic density change
bullCrandall et al Breast Cancer Res Treat DOI 101007s10549-011-1803-9
Breast density
Conclusion
bull CEEBAZO is an additional regimen for menopausal symptoms it provides also a prevention for osteoporosis
bull It is suitable for women with a uterus who are unsatisfied with an EPT regimen or who you are unwilling to treat with an EPT regimen
Adapted use of MHT
bull Lower dosage of estrogens
bull Other progestins
bull Better safety profile
bull Vaginal estrogen or SERMS
bull Non-hormonal therapy
bull Development of new products
bull SERMS + estrogens
Most common adverse events leading to
discontinuation are related to progestins12
bull breakthrough bleeding
bull Low compliance
bull Increase in the number of US
bull Stress
bull Cost
bull uterine procedures
bull Unnecessary endometrial biopsies Hysteroscopies DampC Hysterectomies
bull Morbidity
Proportion of patients who completed or discontinued treatment in relation to the used HT
Serge Rozenberg et al Hum Reprod 2009241739-1747
copy The Author 2009 Published by Oxford University Press on behalf of the European Society of
Human Reproduction and Embryology All rights reserved For Permissions please email
journalspermissionsoxfordjournalsorg
Most common adverse events leading to discontinuation
are related to progestins
bull breast paintenderness
Breast tenderness after initiation of CEE
CEE + MPA (WHI)
and mammographic density change
bullCrandall et al Breast Cancer Res Treat DOI 101007s10549-011-1803-9
Breast density
Hormone therapy use and mammographic
density in postmenopausal Norwegian women
bull Results differed when considering the combined effect of age and BMI
bull The effect of EPT on mammographic density was modified by age and BMI with no apparent association among the youngest women (aged 50-55) with the highest BMI (BMI ge 26)
bull A higher mammographic density was found in EPT users compared to never HT users particularly in women using high-dose NETA regimens Age and BMI modified the association between EPT use and mammographic density
bull Couto E et al Breast Cancer Res Treat 2011 Nov 4 [Epub ahead of print]
Breast Cancer Risk by Breast Density
Menopause and Postmenopausal Hormone
Therapy Use
Birads age HT Duration Risk
1 55-59 None 5 year risk 08 (95 CI 06- 09)
1 55-59
ET EPT 5 year risk 09 (95 CI 07 -11)
4 55-59
None 5 year risk 24 (95 CI 20 -28)
4 55-59
ET 5 year risk
30 (95 CI 26 -35)
4 55-59
EPT 5 year risk
42 (95 CI 37 -46)
Adapted from Kerlikowske et al JOURNAL OF CLINICAL ONCOLOGY 2010
Breast Cancer Risk by Breast Density
Menopause and Postmenopausal Hormone
Therapy Use
Adapted from Kerlikowske et al JOURNAL OF CLINICAL ONCOLOGY 2010
bull Postmenopausal women with high breast density are at increased risk of breast cancer and should be aware of the added risk of taking HT especially estrogen plus progestin
Medical condition which may be exacerbated by treatment
with progestins
Diabetes and metabolic syndrome
bull progestin-containing HT may be associated with increases in insulin resistance and deterioration in glucose tolerance123
bull Postmenopausal women with diabetes could be inappropriate for treatment with progestin-containing HT due to the potential risk of exacerbation of their condition
1) Panay N amp Studd JWW Human Reprod Update 1997
2) Godsland I et al Metabolism 1993
3) Sites CK et al J Clin Endocrinol Metab 2005
A Nath and R Sitruk-Ware CLIMACTERIC 200912(Suppl 1)96ndash101
A Nath and R Sitruk-Ware CLIMACTERIC 200912(Suppl 1)96ndash101
Diabetes an epidemy
bull UK 1996 14 million of diabetics
bull UK 2015 32 million (6 of the population)
bull UK 2025 5 million
bull httpwwwdiabetescoukdiabetes-prevalencehtml
Other progestin-related intolerance issues
bull Nausea
bull Depressive mood
bull Poor concentration
bull Hirsutism
bull Headache
bull Dizziness
bull Fluid retention
bull Weight gain Panay N amp Studd JWW Human Reprod Update 1997
Medical condition which may be exacerbated by treatment with progestins
PMSPMDDdepression
bull Progesterone-induced PMD can be exacerbated by exogenous progestin administration and can occur in association with HT or OC administration1
bull Significantly higher negative mood scores have been observed during the addition of a progestin to an estrogen in a sequential HT regimen in postmenopausal women with a history of PMS compared to those without2
bull Women with a history of PMS or PMD exacerbation of depression using progestins may therefore benefit from a progestin free treatment for menopausal symptoms
1) Nevatte T et al Arch Womens Ment Health 2013 2) Bjoumlrn I et al Climacteric 2006 PMS premenstrual syndrome
PMDD premenstrual dysphoric disorder
Conclusion
bull CEEBAZO is an additional regimen for menopausal symptoms it provides also a prevention for osteoporosis
bull It is suitable for women with a uterus who are unsatisfied with an EPT regimen or who you are unwilling to treat with an EPT regimen
For some postmenopausal women with a uterus there is a
need for progestin free treatment options
bull with demonstrated clinical efficacy
bull which protects the endometrium
bull improved tolerabilitysafety profile
In clinical practice this translates to women who are
intolerant of progestin-containing HT or have conditions
which may be exacerbated by treatment with progestins
Conclusion Medical need for alternative treatment option
Medical condition which may be exacerbated by treatment with progestins
Depression
bull Progestin-containing HT has been associated with increases in depressive symptoms in some individuals1
bull There is a biochemicalphysiological plausibility for the association of progestins with depression234
bull Therefore postmenopausal women who also have a medical history of depressive disorders or depression could be inappropriate for treatment with progestin-containing HT
Pfizer Confidential
65
1) Girdler SS et al J Womens Health Gend Based Med 1999 2) Traish AM et al Korean J Urol 2014 3) Stroumlhle A et al Biol Psychiatry 1999 4) Romeo E et
al Am J Psychiatry 1998
History of the following conditions may make progestin inappropriate
bull Depression
bull PMSPMDD
PMS premenstrual syndrome
PMD premenstrual dysphoric disorder
Medical conditions that may be exacerbated by treatment with progestins
Women for whom progestin-containing HT
would not be considered appropriate
minus Women who are intolerant of progestin-containing hormone therapy
minus Women with pre-existing medical conditions that may be exacerbated by progestins
Most common adverse events leading to discontinuation are related to progestins12
breakthrough bleeding
bull Increase in the number of uterine procedures (ie unnecessary endometrial biopsies)
breast paintenderness
bull Increase in the number of breast interventions
1 Steel SA et al Climacteric 2003 2 Ettinger B and Pressman A Am J Manag Care 1999 3 Komm BS Mirkin S
Pharmaceuticals 2012
4 Panay N amp Studd JWW Human Reprod Update 1997
bull Nausea bull Depressive mood bull Poor concentration bull Hirsutism bull Headache bull Dizziness bull Fluid retention bull Weight gain
Other progestin-related intolerance issues4
Unmet need with the treatment of postmenopausal symptoms
bull Alternatives to progestin are needed that will protect the endometrium while avoiding other progestin-associated effects and preserving the desired effects of estrogens in postmenopausal women3
Which women with a uterus could benefit from
estrogens without the need for a progestin
bull Women who are intolerant of progestin-containing hormone therapy
bull Women with pre-existing medical conditions that may be exacerbated by progestins (eg women with a history of depression PMSPMDD increased breast density diabetes and metabolic syndrome)
History of the following conditions may make progestin inappropriate
bull Depression
bull PMSPMDD
bull High breast density
bull Diabetes and metabolic syndrome
PMS premenstrual syndrome
PMD premenstrual dysphoric disorder
Medical conditions that may be exacerbated by treatment with progestins
Learning from WHI data
bull Hormone therapy (HT) is the conventional and established therapy option to effectively treat postmenopausal symptoms however it has been associated with some safety and tolerability concerns1 2
bull A review of WHI data suggests that many of the concerns with menopausal HT more often associated with EPT (CE+MPA) such as CHD risk increased breast density breast pain and breast cancer risk than with ET (CEE alone)2
1 Rolnick SJ Kopher RA DeFor TA et al Menopause 2005
2 Komm BS Mirkin S Pharmaceuticals 2012
WHI Womenrsquos Health Initiative trial
CHD coronary heart disease
CEE conjugated equine estrogens
Efficacy and Safety of Constant Oestrogen
Pulsed Progestogen vs
Continuous Combined HRT
Adverse Events
17b-oestradiol 17b-oestradiol norgestimate NETA (n = 150) (n = 172) Breast discomfort 14 27 Abdominal discomfort 14 22 Uterine bleeding 15 12 Dysmenorrhea 3 8 Oedema 5 8
Adapted from S Rozenberg et al Human Reproduction 2000
Medical condition which may be exacerbated by treatment
with progestins
Increased breast density
bull Increases in breast density are associated with progestin-containing HT which may adversely affect radiological detection of breast cancer1 and may be independently associated with an increased risk for the development of breast cancer2
bull The Postmenopausal EstrogenProgestin Interventions (PEPI) trial demonstrated that an increased mammographic breast density was associated with the use of E+P but not with the use of estrogen alone3
bull Women who already have high breast density may therefore be considered inappropriate for treatment with a progestin-containing HT
1) EU Core SPC for Hormone Replacement Therapy Products (CMDh1312003 Rev 4 June
2012)
2) De Villiers TJ et al on behalf of the International Menopause Society Climacteric 2013 16
3) Greendale GA et al J Natl Cancer Inst 2003
Stroke
0 25 5 75 10 125
Fractures
Diabetes
Breast cancer
Cholecystitis
Venothrombotic episodes
Endometrial cancer
Lung cancer
Coronary heart disease
Colorectal cancer
Overall mortality
15 125 10 75 5 25
Benefits Risks
CE
CE MPA
Santen RJ et al J Clin Endocrinol Metab 2010
The basis of the Endocrine Society scientific statement for postmenopausal hormone replacement therapy (HRT) excess risks and benefits of HRT for 5 years in women aged 50ndash59 years or within 10 years of the start of menopause E=estrogen P=progestin
bull Younger women (aged 50ndash59 years) had more favorable results bull There are differences between CE alone and CEMPA arms bull Overall benefitrisk ratio of CE-alone appears to be more favourable than CEMPA
Reevaluation of WHI data (stratified by age) Risks and
Benefits of HRT Cases per 1000 Women per 5 Years of
Use
Medical condition which may be exacerbated by treatment
with progestins
Diabetes and metabolic syndrome
bull Treatment of oestrogen deficiency symptoms with progestin-containing HT (unlike oestrogen alone) may be associated with increases in insulin resistance and deterioration in glucose tolerance123
bull Postmenopausal women with diabetes could be inappropriate for treatment with progestin-containing HT due to the potential risk of exacerbation of their condition
1) Panay N amp Studd JWW Human Reprod Update 1997
2) Godsland I et al Metabolism 1993
3) Sites CK et al J Clin Endocrinol Metab 2005
Variations in Associated Breast Cancer
Risks Between CE alone and CEMPA
bull Use of CE alone for a median of 59 years was associated with a lower incidence of invasive breast cancer (151 cases 027 per year) compared with placebo (199 cases 035 per year HR 077 95 CI 062ndash095 P=002)
bull In the CE alone group fewer women died from invasive breast cancer (6 deaths 0009 per year) compared with controls (16 deaths 0024 per year HR 037 95 CI 013ndash091 P=003)
Anderson GL et al Lancet
Oncol 2012
Bazedoxifene (BZA) specifically selected in
combination with conjugated estrogens
bull BZA has been specifically selected for its unique pharmacologic profile and effects on VMS and uterine tissue in particular123
1 Crabtree J et al Mol Cell Endocrinol 2008
2 Kharode Y et al Endocrinolology 2008
3 Duavive SmPC
Estrogen Receptor activity is dimmed
Estrogen Receptor activity is turned on
CEs are agonists BZA is an antagonist
In the uterus
bull The BZA component reduces the risk of endometrial hyperplasia that can occur with the conjugated estrogens component alone3 This means that progestins are not needed
Extensive global clinical development program for
CEBZA
aIncludes additional pilot dose-finding study 203 1 Lobo RA et al Fertil Steril 2009 2 Pinkerton JV et al Menopause 2009 3 Kagan R et al Menopause 2010 4 Mirkin S et al Climacteric 2013 5 Pinkerton JV et al Obstet Gynecol 2013
Effects of conjugated estrogensbazedoxifene on
lipid and coagulation variables a randomized
placebo- and active-controlled trial
bull At 12 months
bull Both CEBZA doses were associated with small but significant effects on hemostasis variables including reductions in antithrombin plasminogen activator inhibitor-1 and fibrinogen activity and an increase in plasminogen activity relative to placebo at 12 months Incidences of cardiovascular and venous thromboembolic events were similar among treatment groups
bull CONCLUSIONS
bull This study provides reassurance that CEBZA does not adversely affect lipid metabolism or hemostatic balance In accordance the incidences of venous thromboembolic events and cardiovascular events in postmenopausal women are similar to those observed with placebo

DUAVIVE Significantly Increased Lumbar Spine and Total
Hip BMD vs Placebo at 12 Months ndash Study 2
M
ean
ch
an
ge f
rom
baselin
e
Lumbar Spine Total Hip
121 151 Treatment
difference Treatment
difference
Data on file CSR-81040 Protocol 3115A1-3307 Pfizer Inc New York NY Pinkerton J Clin Endocrin Metab 2014 30
Plt001 vs placebo
Adjusted mean changes and P-values based on an ANCOVA model with treatment and region (US or non-US) as factors and baseline BMD value and years since menopause as covariates using the modified intention to treat population with last observation carried forward
DUAVIV
E
TOLERABILITY
AND SAFETY
Rates of BleedingSpotting and Amenorrhea
Similar to Rates with Placebo
bull High and similar cumulative rates of amenorrhea at year 1 among women treated with CE 045BZA 20 and placebo and was higher than seen in women treated with CE 045MPA 151
bull Noncumulative rates of spotting and bleedingspotting were similar among women treated with CEBZA or placebo and consistently higher in women treated with CE 045MPA 152
0
90
Cycle
100
Pe
rce
nta
ge
of
Su
bje
cts
80
70
60
50
40
30
20
10
88
54
Placebo
CE 045BZA 20 CE 045MPA 15
Percentage of subjects with cumulative amenorrhea during consecutive 4-week periods (cycles) in SMART-5
MPA medroxyprogesterone acetate Plt0001 vs all other treatment groups 1 Pinkerton JV et al J Clin Endocrinol Metab 2014 2 Data on file CSR-81040 Protocol 3115A1-3307 Pfizer Inc New York NY
Adverse Reactions in Placebo-
Controlled Trials Safety analyses have been conducted in 6210 postmenopausal women aged 40 to 75 years (mean age 55 years) following up to 2 years of treatment in SMART-1 -2 -3 and -5
Adverse reactions (incidence ge5) that were more common with DUAVIVE
Incidence of serious adverse reactions
35 with DUAVIVE 48 with placebo
DUAVEE [package insert] New York NY Pfizer Inc 2013
CE 045 BZA 20 (N=1224)
n ()
Placebo (N=1069)
n ()
Gastrointestinal disorders
Nausea 100 (8) 58 (5)
Diarrhea 96 (8) 57 (5)
Dyspepsia 84 (7) 59 (6)
Abdominal pain upper 81 (7) 58 (5)
Musculoskeletal and connective tissue disorders
Muscle spasms 110 (9) 63 (6)
Neck pain 62 (5) 46 (4)
Nervous system disorders
Dizziness 65 (5) 37 (3)
Respiratory thoracic and mediastinal disorders
Oropharyngeal pain 80 (7) 61 (6)
Venous Thromboembolism (VTE) in
DUAVIVE Clinical Studies
bull Estrogen agonistantagonists (including BZA a component of DUAVIVE) and estrogens individually are known to increase the risk of VTE
bull In the clinical studies with DUAVIVE the reporting rates for VTE were low in all treatment groups
bull Adverse reactions of VTE reported by patients
bull Should VTE event occur or be suspected DUAVIVE should be discontinued immediately
bull Due to the low rates of events in both groups it is not possible to conclude that the risk of VTE with DUAVIVE is different from that seen with other estrogen therapies
DUAVEE [package insert] New York NY Pfizer Inc 2013
00 for DUAVIVE (n=1224)
01 for placebo (n=1069)
26
Effects of conjugated estrogensbazedoxifene on
lipid and coagulation variables a randomized
placebo- and active-controlled trial
bull postmenopausal women (N = 1843) with menopausal
symptoms
bull Lipid (N = 1843) and coagulation (N = 590) variables were assessed in women receiving daily CE 045 mgBZA 20 mg CE 0625 mgBZA 20 mg BZA 20 mg CE 045 mgmedroxyprogesterone acetate (MPA) 15 mg or placebo for 12 months
bull Skouby SO et al Menopause 2015 Jun22(6)640-9
Effects of conjugated estrogensbazedoxifene on
lipid and coagulation variables a randomized
placebo- and active-controlled trial
bull At 12 months
bull CE 045 mgBZA 20 mg
bull CE 0625 mgBZA 20 mg
bull BZA 20 mg
bull and CE 045 mgMPA 15 mg decreased total cholesterol and LDL- cholesterol vs placebo (P lt 001 for all)
bull Both CEBZA doses and CEMPA increased high-density lipoprotein cholesterol compared with placebo (P lt 005 for all)
bull CE 045 mgBZA 20 mg had a neutral effect on triglycerides
bull CE 0625 mgBZA 20 mg and CEMPA increased triglycerides compared with placebo (P lt 005)
bull Skouby SO et al Menopause 2015 Jun22(6)640-9
Effects of conjugated estrogensbazedoxifene on
lipid and coagulation variables a randomized
placebo- and active-controlled trial
bull At 12 months
bull Both CEBZA doses were associated with small but significant effects on hemostasis variables including reductions in antithrombin plasminogen activator inhibitor-1 and fibrinogen activity and an increase in plasminogen activity relative to placebo at 12 months Incidences of cardiovascular and venous thromboembolic events were similar among treatment groups
Skouby SO et al Menopause 2015
Jun22(6)640-9
Endometrial hyperplasia or malignancy occurred in lt1 of women
following up to 1 year of treatment with CEBZA12
Study Cumulative Incidence at month 12 (nN)
CE 045BZA 20 Placebo
SMART-11 000 (0336) 000 (0313)
SMART-52 030 (1335) 028 (1354)
Effects on the Endometrium
1 Pickar JH et al Fertil Steril 2009 2 Pinkerton at al J Clin Endocrinol Metab 2014
Through the eyes of an amazone
Marie Mandy
Breast tolerability profile similar to placebo following up to 2 years of treatment with CEBZA12
Pooled analysis of SMART clinical trials
CE 045BZA 20 (n=1585)
Placebo (n=1241)
Breast cancer incidence up to 2 years
(per 1000 woman-years)
100 (CI 000-321)
140 (CI 000-417)
Incidence of reported breast paintenderness up to 12 weeks
98-115 81-112
Incidence of abnormal mammogram at month 12
258 316
Mean change in breast density at month 12 (SMART-5)
ndash038 (n=186)
ndash032 (n=182)
Effects on the Breast
1 Pickar JH et al Menopause 2013 2 Pinkerton JV et al Obstet Gynecol 2013
CEBZA clinical overview - summary
bull In clinical trials CEBZA has demonstrated safety and efficacy in postmenopausal women with a uterus including the following
bull Significant reduction in number and severity of moderate to severe hot flushes1
bull Incidence of cumulative amenorrhea rate similar to placebo and significantly better than CEMPA2
bull Incidence of endometrial hyperplasia and breast tendernessdensity similar to that with placebo345
bull Incidence of adverse events and discontinuation rates similar to that with placebo6
1 Pinkerton JV et al Menopause 2009 2 Pinkerton JV et al J Clin Endocrinol Metab2014 3 Pickar JH et al
Fertil Steril 2009 4 Pinkerton at al J Clin Endocrinol Metab 2014 5 Pickar JH et al Menopause 2013 6 DUAVEE [package insert] New York NY Pfizer Inc 2013
CEBZA clinical overview - summary
Now women with a uterus who choose hormone therapy for management of menopausal symptoms have a choice
bull conventional estrogen-progestogen therapy or
bull a new combinationhellipconjugated estrogens paired with the SERM bazedoxifene
1 Pinkerton JV et al Menopause 2009 2 Pinkerton JV et al J Clin Endocrinol Metab2014 3 Pickar JH et al Fertil Steril 2009 4 Pinkerton at al J Clin Endocrinol Metab 2014 5 Pickar JH et al Menopause 2013 6 DUAVEE [package insert] New York NY Pfizer Inc 2013
Conjugated EstrogensBazedoxifene (CEBZA)
US indication
bull DUAVEE is indicated in women with a uterus for
bull 11 Treatment of Moderate to Severe Vasomotor Symptoms Associated with Menopause
bull 12 Prevention of Postmenopausal Osteoporosis
bull 13 Important Limitations of Use
bull Use DUAVEE for the shortest duration consistent with treatment goals and risks for the individual woman Postmenopausal women should be re-evaluated periodically as clinically appropriate to determine if treatment is still necessary
bull When prescribing solely for the prevention of postmenopausal osteoporosis therapy should only be considered for women at significant risk of osteoporosis and non-estrogen medication should be carefully considered
Conjugated EstrogensBazedoxifene (CEBZA)
EU indication
CEBZA is indicated for
bull Treatment of oestrogen deficiency symptoms in postmenopausal women with a uterus (with at least 12 months since the last menses) for whom treatment with progestin-containing therapy is not appropriate
bull The experience treating women older than 65 years is limited
bull Dose CE (045mg)Bazedoxifene (20mg)
Duavive SmPC
Which women with a uterus
could benefit from estrogens
without the need for a
progestin
Progestin intolerance is one of the main
factors for reduced compliance
bull About 20 of women receiving progestin-containing HT have significant progestin intolerance and half of these experience serious effects that prevent treatment continuation1
1 Panay N amp Studd J Human Reprod Update 1997
2 Panay N et al on behalf of the British Menopause Society and Womenrsquos Health Concern Menopause Int 2013
bull The 2013 British Menopause Society amp Womenrsquos Health
Concern recommendations on hormone replacement
therapy do recognise progestin intolerance as one of the
main factors for reduced compliance with HT 2
Proportion of patients () with at least one bleeding episode in relation to time and to the
used HT
Serge Rozenberg et al Hum Reprod 2009241739-1747
copy The Author 2009 Published by Oxford University Press on behalf of the European Society of
Human Reproduction and Embryology All rights reserved For Permissions please email
journalspermissionsoxfordjournalsorg
Breast tenderness after initiation of CEE
CEE + MPA (WHI)
and mammographic density change
bullCrandall et al Breast Cancer Res Treat DOI 101007s10549-011-1803-9
Breast density
Conclusion
bull CEEBAZO is an additional regimen for menopausal symptoms it provides also a prevention for osteoporosis
bull It is suitable for women with a uterus who are unsatisfied with an EPT regimen or who you are unwilling to treat with an EPT regimen
Adapted use of MHT
bull Lower dosage of estrogens
bull Other progestins
bull Better safety profile
bull Vaginal estrogen or SERMS
bull Non-hormonal therapy
bull Development of new products
bull SERMS + estrogens
Most common adverse events leading to
discontinuation are related to progestins12
bull breakthrough bleeding
bull Low compliance
bull Increase in the number of US
bull Stress
bull Cost
bull uterine procedures
bull Unnecessary endometrial biopsies Hysteroscopies DampC Hysterectomies
bull Morbidity
Proportion of patients who completed or discontinued treatment in relation to the used HT
Serge Rozenberg et al Hum Reprod 2009241739-1747
copy The Author 2009 Published by Oxford University Press on behalf of the European Society of
Human Reproduction and Embryology All rights reserved For Permissions please email
journalspermissionsoxfordjournalsorg
Most common adverse events leading to discontinuation
are related to progestins
bull breast paintenderness
Breast tenderness after initiation of CEE
CEE + MPA (WHI)
and mammographic density change
bullCrandall et al Breast Cancer Res Treat DOI 101007s10549-011-1803-9
Breast density
Hormone therapy use and mammographic
density in postmenopausal Norwegian women
bull Results differed when considering the combined effect of age and BMI
bull The effect of EPT on mammographic density was modified by age and BMI with no apparent association among the youngest women (aged 50-55) with the highest BMI (BMI ge 26)
bull A higher mammographic density was found in EPT users compared to never HT users particularly in women using high-dose NETA regimens Age and BMI modified the association between EPT use and mammographic density
bull Couto E et al Breast Cancer Res Treat 2011 Nov 4 [Epub ahead of print]
Breast Cancer Risk by Breast Density
Menopause and Postmenopausal Hormone
Therapy Use
Birads age HT Duration Risk
1 55-59 None 5 year risk 08 (95 CI 06- 09)
1 55-59
ET EPT 5 year risk 09 (95 CI 07 -11)
4 55-59
None 5 year risk 24 (95 CI 20 -28)
4 55-59
ET 5 year risk
30 (95 CI 26 -35)
4 55-59
EPT 5 year risk
42 (95 CI 37 -46)
Adapted from Kerlikowske et al JOURNAL OF CLINICAL ONCOLOGY 2010
Breast Cancer Risk by Breast Density
Menopause and Postmenopausal Hormone
Therapy Use
Adapted from Kerlikowske et al JOURNAL OF CLINICAL ONCOLOGY 2010
bull Postmenopausal women with high breast density are at increased risk of breast cancer and should be aware of the added risk of taking HT especially estrogen plus progestin
Medical condition which may be exacerbated by treatment
with progestins
Diabetes and metabolic syndrome
bull progestin-containing HT may be associated with increases in insulin resistance and deterioration in glucose tolerance123
bull Postmenopausal women with diabetes could be inappropriate for treatment with progestin-containing HT due to the potential risk of exacerbation of their condition
1) Panay N amp Studd JWW Human Reprod Update 1997
2) Godsland I et al Metabolism 1993
3) Sites CK et al J Clin Endocrinol Metab 2005
A Nath and R Sitruk-Ware CLIMACTERIC 200912(Suppl 1)96ndash101
A Nath and R Sitruk-Ware CLIMACTERIC 200912(Suppl 1)96ndash101
Diabetes an epidemy
bull UK 1996 14 million of diabetics
bull UK 2015 32 million (6 of the population)
bull UK 2025 5 million
bull httpwwwdiabetescoukdiabetes-prevalencehtml
Other progestin-related intolerance issues
bull Nausea
bull Depressive mood
bull Poor concentration
bull Hirsutism
bull Headache
bull Dizziness
bull Fluid retention
bull Weight gain Panay N amp Studd JWW Human Reprod Update 1997
Medical condition which may be exacerbated by treatment with progestins
PMSPMDDdepression
bull Progesterone-induced PMD can be exacerbated by exogenous progestin administration and can occur in association with HT or OC administration1
bull Significantly higher negative mood scores have been observed during the addition of a progestin to an estrogen in a sequential HT regimen in postmenopausal women with a history of PMS compared to those without2
bull Women with a history of PMS or PMD exacerbation of depression using progestins may therefore benefit from a progestin free treatment for menopausal symptoms
1) Nevatte T et al Arch Womens Ment Health 2013 2) Bjoumlrn I et al Climacteric 2006 PMS premenstrual syndrome
PMDD premenstrual dysphoric disorder
Conclusion
bull CEEBAZO is an additional regimen for menopausal symptoms it provides also a prevention for osteoporosis
bull It is suitable for women with a uterus who are unsatisfied with an EPT regimen or who you are unwilling to treat with an EPT regimen
For some postmenopausal women with a uterus there is a
need for progestin free treatment options
bull with demonstrated clinical efficacy
bull which protects the endometrium
bull improved tolerabilitysafety profile
In clinical practice this translates to women who are
intolerant of progestin-containing HT or have conditions
which may be exacerbated by treatment with progestins
Conclusion Medical need for alternative treatment option
Medical condition which may be exacerbated by treatment with progestins
Depression
bull Progestin-containing HT has been associated with increases in depressive symptoms in some individuals1
bull There is a biochemicalphysiological plausibility for the association of progestins with depression234
bull Therefore postmenopausal women who also have a medical history of depressive disorders or depression could be inappropriate for treatment with progestin-containing HT
Pfizer Confidential
65
1) Girdler SS et al J Womens Health Gend Based Med 1999 2) Traish AM et al Korean J Urol 2014 3) Stroumlhle A et al Biol Psychiatry 1999 4) Romeo E et
al Am J Psychiatry 1998
History of the following conditions may make progestin inappropriate
bull Depression
bull PMSPMDD
PMS premenstrual syndrome
PMD premenstrual dysphoric disorder
Medical conditions that may be exacerbated by treatment with progestins
Women for whom progestin-containing HT
would not be considered appropriate
minus Women who are intolerant of progestin-containing hormone therapy
minus Women with pre-existing medical conditions that may be exacerbated by progestins
Most common adverse events leading to discontinuation are related to progestins12
breakthrough bleeding
bull Increase in the number of uterine procedures (ie unnecessary endometrial biopsies)
breast paintenderness
bull Increase in the number of breast interventions
1 Steel SA et al Climacteric 2003 2 Ettinger B and Pressman A Am J Manag Care 1999 3 Komm BS Mirkin S
Pharmaceuticals 2012
4 Panay N amp Studd JWW Human Reprod Update 1997
bull Nausea bull Depressive mood bull Poor concentration bull Hirsutism bull Headache bull Dizziness bull Fluid retention bull Weight gain
Other progestin-related intolerance issues4
Unmet need with the treatment of postmenopausal symptoms
bull Alternatives to progestin are needed that will protect the endometrium while avoiding other progestin-associated effects and preserving the desired effects of estrogens in postmenopausal women3
Which women with a uterus could benefit from
estrogens without the need for a progestin
bull Women who are intolerant of progestin-containing hormone therapy
bull Women with pre-existing medical conditions that may be exacerbated by progestins (eg women with a history of depression PMSPMDD increased breast density diabetes and metabolic syndrome)
History of the following conditions may make progestin inappropriate
bull Depression
bull PMSPMDD
bull High breast density
bull Diabetes and metabolic syndrome
PMS premenstrual syndrome
PMD premenstrual dysphoric disorder
Medical conditions that may be exacerbated by treatment with progestins
Learning from WHI data
bull Hormone therapy (HT) is the conventional and established therapy option to effectively treat postmenopausal symptoms however it has been associated with some safety and tolerability concerns1 2
bull A review of WHI data suggests that many of the concerns with menopausal HT more often associated with EPT (CE+MPA) such as CHD risk increased breast density breast pain and breast cancer risk than with ET (CEE alone)2
1 Rolnick SJ Kopher RA DeFor TA et al Menopause 2005
2 Komm BS Mirkin S Pharmaceuticals 2012
WHI Womenrsquos Health Initiative trial
CHD coronary heart disease
CEE conjugated equine estrogens
Efficacy and Safety of Constant Oestrogen
Pulsed Progestogen vs
Continuous Combined HRT
Adverse Events
17b-oestradiol 17b-oestradiol norgestimate NETA (n = 150) (n = 172) Breast discomfort 14 27 Abdominal discomfort 14 22 Uterine bleeding 15 12 Dysmenorrhea 3 8 Oedema 5 8
Adapted from S Rozenberg et al Human Reproduction 2000
Medical condition which may be exacerbated by treatment
with progestins
Increased breast density
bull Increases in breast density are associated with progestin-containing HT which may adversely affect radiological detection of breast cancer1 and may be independently associated with an increased risk for the development of breast cancer2
bull The Postmenopausal EstrogenProgestin Interventions (PEPI) trial demonstrated that an increased mammographic breast density was associated with the use of E+P but not with the use of estrogen alone3
bull Women who already have high breast density may therefore be considered inappropriate for treatment with a progestin-containing HT
1) EU Core SPC for Hormone Replacement Therapy Products (CMDh1312003 Rev 4 June
2012)
2) De Villiers TJ et al on behalf of the International Menopause Society Climacteric 2013 16
3) Greendale GA et al J Natl Cancer Inst 2003
Stroke
0 25 5 75 10 125
Fractures
Diabetes
Breast cancer
Cholecystitis
Venothrombotic episodes
Endometrial cancer
Lung cancer
Coronary heart disease
Colorectal cancer
Overall mortality
15 125 10 75 5 25
Benefits Risks
CE
CE MPA
Santen RJ et al J Clin Endocrinol Metab 2010
The basis of the Endocrine Society scientific statement for postmenopausal hormone replacement therapy (HRT) excess risks and benefits of HRT for 5 years in women aged 50ndash59 years or within 10 years of the start of menopause E=estrogen P=progestin
bull Younger women (aged 50ndash59 years) had more favorable results bull There are differences between CE alone and CEMPA arms bull Overall benefitrisk ratio of CE-alone appears to be more favourable than CEMPA
Reevaluation of WHI data (stratified by age) Risks and
Benefits of HRT Cases per 1000 Women per 5 Years of
Use
Medical condition which may be exacerbated by treatment
with progestins
Diabetes and metabolic syndrome
bull Treatment of oestrogen deficiency symptoms with progestin-containing HT (unlike oestrogen alone) may be associated with increases in insulin resistance and deterioration in glucose tolerance123
bull Postmenopausal women with diabetes could be inappropriate for treatment with progestin-containing HT due to the potential risk of exacerbation of their condition
1) Panay N amp Studd JWW Human Reprod Update 1997
2) Godsland I et al Metabolism 1993
3) Sites CK et al J Clin Endocrinol Metab 2005
Variations in Associated Breast Cancer
Risks Between CE alone and CEMPA
bull Use of CE alone for a median of 59 years was associated with a lower incidence of invasive breast cancer (151 cases 027 per year) compared with placebo (199 cases 035 per year HR 077 95 CI 062ndash095 P=002)
bull In the CE alone group fewer women died from invasive breast cancer (6 deaths 0009 per year) compared with controls (16 deaths 0024 per year HR 037 95 CI 013ndash091 P=003)
Anderson GL et al Lancet
Oncol 2012
Bazedoxifene (BZA) specifically selected in
combination with conjugated estrogens
bull BZA has been specifically selected for its unique pharmacologic profile and effects on VMS and uterine tissue in particular123
1 Crabtree J et al Mol Cell Endocrinol 2008
2 Kharode Y et al Endocrinolology 2008
3 Duavive SmPC
Estrogen Receptor activity is dimmed
Estrogen Receptor activity is turned on
CEs are agonists BZA is an antagonist
In the uterus
bull The BZA component reduces the risk of endometrial hyperplasia that can occur with the conjugated estrogens component alone3 This means that progestins are not needed
Extensive global clinical development program for
CEBZA
aIncludes additional pilot dose-finding study 203 1 Lobo RA et al Fertil Steril 2009 2 Pinkerton JV et al Menopause 2009 3 Kagan R et al Menopause 2010 4 Mirkin S et al Climacteric 2013 5 Pinkerton JV et al Obstet Gynecol 2013
Effects of conjugated estrogensbazedoxifene on
lipid and coagulation variables a randomized
placebo- and active-controlled trial
bull At 12 months
bull Both CEBZA doses were associated with small but significant effects on hemostasis variables including reductions in antithrombin plasminogen activator inhibitor-1 and fibrinogen activity and an increase in plasminogen activity relative to placebo at 12 months Incidences of cardiovascular and venous thromboembolic events were similar among treatment groups
bull CONCLUSIONS
bull This study provides reassurance that CEBZA does not adversely affect lipid metabolism or hemostatic balance In accordance the incidences of venous thromboembolic events and cardiovascular events in postmenopausal women are similar to those observed with placebo

TOLERABILITY
AND SAFETY
Rates of BleedingSpotting and Amenorrhea
Similar to Rates with Placebo
bull High and similar cumulative rates of amenorrhea at year 1 among women treated with CE 045BZA 20 and placebo and was higher than seen in women treated with CE 045MPA 151
bull Noncumulative rates of spotting and bleedingspotting were similar among women treated with CEBZA or placebo and consistently higher in women treated with CE 045MPA 152
0
90
Cycle
100
Pe
rce
nta
ge
of
Su
bje
cts
80
70
60
50
40
30
20
10
88
54
Placebo
CE 045BZA 20 CE 045MPA 15
Percentage of subjects with cumulative amenorrhea during consecutive 4-week periods (cycles) in SMART-5
MPA medroxyprogesterone acetate Plt0001 vs all other treatment groups 1 Pinkerton JV et al J Clin Endocrinol Metab 2014 2 Data on file CSR-81040 Protocol 3115A1-3307 Pfizer Inc New York NY
Adverse Reactions in Placebo-
Controlled Trials Safety analyses have been conducted in 6210 postmenopausal women aged 40 to 75 years (mean age 55 years) following up to 2 years of treatment in SMART-1 -2 -3 and -5
Adverse reactions (incidence ge5) that were more common with DUAVIVE
Incidence of serious adverse reactions
35 with DUAVIVE 48 with placebo
DUAVEE [package insert] New York NY Pfizer Inc 2013
CE 045 BZA 20 (N=1224)
n ()
Placebo (N=1069)
n ()
Gastrointestinal disorders
Nausea 100 (8) 58 (5)
Diarrhea 96 (8) 57 (5)
Dyspepsia 84 (7) 59 (6)
Abdominal pain upper 81 (7) 58 (5)
Musculoskeletal and connective tissue disorders
Muscle spasms 110 (9) 63 (6)
Neck pain 62 (5) 46 (4)
Nervous system disorders
Dizziness 65 (5) 37 (3)
Respiratory thoracic and mediastinal disorders
Oropharyngeal pain 80 (7) 61 (6)
Venous Thromboembolism (VTE) in
DUAVIVE Clinical Studies
bull Estrogen agonistantagonists (including BZA a component of DUAVIVE) and estrogens individually are known to increase the risk of VTE
bull In the clinical studies with DUAVIVE the reporting rates for VTE were low in all treatment groups
bull Adverse reactions of VTE reported by patients
bull Should VTE event occur or be suspected DUAVIVE should be discontinued immediately
bull Due to the low rates of events in both groups it is not possible to conclude that the risk of VTE with DUAVIVE is different from that seen with other estrogen therapies
DUAVEE [package insert] New York NY Pfizer Inc 2013
00 for DUAVIVE (n=1224)
01 for placebo (n=1069)
26
Effects of conjugated estrogensbazedoxifene on
lipid and coagulation variables a randomized
placebo- and active-controlled trial
bull postmenopausal women (N = 1843) with menopausal
symptoms
bull Lipid (N = 1843) and coagulation (N = 590) variables were assessed in women receiving daily CE 045 mgBZA 20 mg CE 0625 mgBZA 20 mg BZA 20 mg CE 045 mgmedroxyprogesterone acetate (MPA) 15 mg or placebo for 12 months
bull Skouby SO et al Menopause 2015 Jun22(6)640-9
Effects of conjugated estrogensbazedoxifene on
lipid and coagulation variables a randomized
placebo- and active-controlled trial
bull At 12 months
bull CE 045 mgBZA 20 mg
bull CE 0625 mgBZA 20 mg
bull BZA 20 mg
bull and CE 045 mgMPA 15 mg decreased total cholesterol and LDL- cholesterol vs placebo (P lt 001 for all)
bull Both CEBZA doses and CEMPA increased high-density lipoprotein cholesterol compared with placebo (P lt 005 for all)
bull CE 045 mgBZA 20 mg had a neutral effect on triglycerides
bull CE 0625 mgBZA 20 mg and CEMPA increased triglycerides compared with placebo (P lt 005)
bull Skouby SO et al Menopause 2015 Jun22(6)640-9
Effects of conjugated estrogensbazedoxifene on
lipid and coagulation variables a randomized
placebo- and active-controlled trial
bull At 12 months
bull Both CEBZA doses were associated with small but significant effects on hemostasis variables including reductions in antithrombin plasminogen activator inhibitor-1 and fibrinogen activity and an increase in plasminogen activity relative to placebo at 12 months Incidences of cardiovascular and venous thromboembolic events were similar among treatment groups
Skouby SO et al Menopause 2015
Jun22(6)640-9
Endometrial hyperplasia or malignancy occurred in lt1 of women
following up to 1 year of treatment with CEBZA12
Study Cumulative Incidence at month 12 (nN)
CE 045BZA 20 Placebo
SMART-11 000 (0336) 000 (0313)
SMART-52 030 (1335) 028 (1354)
Effects on the Endometrium
1 Pickar JH et al Fertil Steril 2009 2 Pinkerton at al J Clin Endocrinol Metab 2014
Through the eyes of an amazone
Marie Mandy
Breast tolerability profile similar to placebo following up to 2 years of treatment with CEBZA12
Pooled analysis of SMART clinical trials
CE 045BZA 20 (n=1585)
Placebo (n=1241)
Breast cancer incidence up to 2 years
(per 1000 woman-years)
100 (CI 000-321)
140 (CI 000-417)
Incidence of reported breast paintenderness up to 12 weeks
98-115 81-112
Incidence of abnormal mammogram at month 12
258 316
Mean change in breast density at month 12 (SMART-5)
ndash038 (n=186)
ndash032 (n=182)
Effects on the Breast
1 Pickar JH et al Menopause 2013 2 Pinkerton JV et al Obstet Gynecol 2013
CEBZA clinical overview - summary
bull In clinical trials CEBZA has demonstrated safety and efficacy in postmenopausal women with a uterus including the following
bull Significant reduction in number and severity of moderate to severe hot flushes1
bull Incidence of cumulative amenorrhea rate similar to placebo and significantly better than CEMPA2
bull Incidence of endometrial hyperplasia and breast tendernessdensity similar to that with placebo345
bull Incidence of adverse events and discontinuation rates similar to that with placebo6
1 Pinkerton JV et al Menopause 2009 2 Pinkerton JV et al J Clin Endocrinol Metab2014 3 Pickar JH et al
Fertil Steril 2009 4 Pinkerton at al J Clin Endocrinol Metab 2014 5 Pickar JH et al Menopause 2013 6 DUAVEE [package insert] New York NY Pfizer Inc 2013
CEBZA clinical overview - summary
Now women with a uterus who choose hormone therapy for management of menopausal symptoms have a choice
bull conventional estrogen-progestogen therapy or
bull a new combinationhellipconjugated estrogens paired with the SERM bazedoxifene
1 Pinkerton JV et al Menopause 2009 2 Pinkerton JV et al J Clin Endocrinol Metab2014 3 Pickar JH et al Fertil Steril 2009 4 Pinkerton at al J Clin Endocrinol Metab 2014 5 Pickar JH et al Menopause 2013 6 DUAVEE [package insert] New York NY Pfizer Inc 2013
Conjugated EstrogensBazedoxifene (CEBZA)
US indication
bull DUAVEE is indicated in women with a uterus for
bull 11 Treatment of Moderate to Severe Vasomotor Symptoms Associated with Menopause
bull 12 Prevention of Postmenopausal Osteoporosis
bull 13 Important Limitations of Use
bull Use DUAVEE for the shortest duration consistent with treatment goals and risks for the individual woman Postmenopausal women should be re-evaluated periodically as clinically appropriate to determine if treatment is still necessary
bull When prescribing solely for the prevention of postmenopausal osteoporosis therapy should only be considered for women at significant risk of osteoporosis and non-estrogen medication should be carefully considered
Conjugated EstrogensBazedoxifene (CEBZA)
EU indication
CEBZA is indicated for
bull Treatment of oestrogen deficiency symptoms in postmenopausal women with a uterus (with at least 12 months since the last menses) for whom treatment with progestin-containing therapy is not appropriate
bull The experience treating women older than 65 years is limited
bull Dose CE (045mg)Bazedoxifene (20mg)
Duavive SmPC
Which women with a uterus
could benefit from estrogens
without the need for a
progestin
Progestin intolerance is one of the main
factors for reduced compliance
bull About 20 of women receiving progestin-containing HT have significant progestin intolerance and half of these experience serious effects that prevent treatment continuation1
1 Panay N amp Studd J Human Reprod Update 1997
2 Panay N et al on behalf of the British Menopause Society and Womenrsquos Health Concern Menopause Int 2013
bull The 2013 British Menopause Society amp Womenrsquos Health
Concern recommendations on hormone replacement
therapy do recognise progestin intolerance as one of the
main factors for reduced compliance with HT 2
Proportion of patients () with at least one bleeding episode in relation to time and to the
used HT
Serge Rozenberg et al Hum Reprod 2009241739-1747
copy The Author 2009 Published by Oxford University Press on behalf of the European Society of
Human Reproduction and Embryology All rights reserved For Permissions please email
journalspermissionsoxfordjournalsorg
Breast tenderness after initiation of CEE
CEE + MPA (WHI)
and mammographic density change
bullCrandall et al Breast Cancer Res Treat DOI 101007s10549-011-1803-9
Breast density
Conclusion
bull CEEBAZO is an additional regimen for menopausal symptoms it provides also a prevention for osteoporosis
bull It is suitable for women with a uterus who are unsatisfied with an EPT regimen or who you are unwilling to treat with an EPT regimen
Adapted use of MHT
bull Lower dosage of estrogens
bull Other progestins
bull Better safety profile
bull Vaginal estrogen or SERMS
bull Non-hormonal therapy
bull Development of new products
bull SERMS + estrogens
Most common adverse events leading to
discontinuation are related to progestins12
bull breakthrough bleeding
bull Low compliance
bull Increase in the number of US
bull Stress
bull Cost
bull uterine procedures
bull Unnecessary endometrial biopsies Hysteroscopies DampC Hysterectomies
bull Morbidity
Proportion of patients who completed or discontinued treatment in relation to the used HT
Serge Rozenberg et al Hum Reprod 2009241739-1747
copy The Author 2009 Published by Oxford University Press on behalf of the European Society of
Human Reproduction and Embryology All rights reserved For Permissions please email
journalspermissionsoxfordjournalsorg
Most common adverse events leading to discontinuation
are related to progestins
bull breast paintenderness
Breast tenderness after initiation of CEE
CEE + MPA (WHI)
and mammographic density change
bullCrandall et al Breast Cancer Res Treat DOI 101007s10549-011-1803-9
Breast density
Hormone therapy use and mammographic
density in postmenopausal Norwegian women
bull Results differed when considering the combined effect of age and BMI
bull The effect of EPT on mammographic density was modified by age and BMI with no apparent association among the youngest women (aged 50-55) with the highest BMI (BMI ge 26)
bull A higher mammographic density was found in EPT users compared to never HT users particularly in women using high-dose NETA regimens Age and BMI modified the association between EPT use and mammographic density
bull Couto E et al Breast Cancer Res Treat 2011 Nov 4 [Epub ahead of print]
Breast Cancer Risk by Breast Density
Menopause and Postmenopausal Hormone
Therapy Use
Birads age HT Duration Risk
1 55-59 None 5 year risk 08 (95 CI 06- 09)
1 55-59
ET EPT 5 year risk 09 (95 CI 07 -11)
4 55-59
None 5 year risk 24 (95 CI 20 -28)
4 55-59
ET 5 year risk
30 (95 CI 26 -35)
4 55-59
EPT 5 year risk
42 (95 CI 37 -46)
Adapted from Kerlikowske et al JOURNAL OF CLINICAL ONCOLOGY 2010
Breast Cancer Risk by Breast Density
Menopause and Postmenopausal Hormone
Therapy Use
Adapted from Kerlikowske et al JOURNAL OF CLINICAL ONCOLOGY 2010
bull Postmenopausal women with high breast density are at increased risk of breast cancer and should be aware of the added risk of taking HT especially estrogen plus progestin
Medical condition which may be exacerbated by treatment
with progestins
Diabetes and metabolic syndrome
bull progestin-containing HT may be associated with increases in insulin resistance and deterioration in glucose tolerance123
bull Postmenopausal women with diabetes could be inappropriate for treatment with progestin-containing HT due to the potential risk of exacerbation of their condition
1) Panay N amp Studd JWW Human Reprod Update 1997
2) Godsland I et al Metabolism 1993
3) Sites CK et al J Clin Endocrinol Metab 2005
A Nath and R Sitruk-Ware CLIMACTERIC 200912(Suppl 1)96ndash101
A Nath and R Sitruk-Ware CLIMACTERIC 200912(Suppl 1)96ndash101
Diabetes an epidemy
bull UK 1996 14 million of diabetics
bull UK 2015 32 million (6 of the population)
bull UK 2025 5 million
bull httpwwwdiabetescoukdiabetes-prevalencehtml
Other progestin-related intolerance issues
bull Nausea
bull Depressive mood
bull Poor concentration
bull Hirsutism
bull Headache
bull Dizziness
bull Fluid retention
bull Weight gain Panay N amp Studd JWW Human Reprod Update 1997
Medical condition which may be exacerbated by treatment with progestins
PMSPMDDdepression
bull Progesterone-induced PMD can be exacerbated by exogenous progestin administration and can occur in association with HT or OC administration1
bull Significantly higher negative mood scores have been observed during the addition of a progestin to an estrogen in a sequential HT regimen in postmenopausal women with a history of PMS compared to those without2
bull Women with a history of PMS or PMD exacerbation of depression using progestins may therefore benefit from a progestin free treatment for menopausal symptoms
1) Nevatte T et al Arch Womens Ment Health 2013 2) Bjoumlrn I et al Climacteric 2006 PMS premenstrual syndrome
PMDD premenstrual dysphoric disorder
Conclusion
bull CEEBAZO is an additional regimen for menopausal symptoms it provides also a prevention for osteoporosis
bull It is suitable for women with a uterus who are unsatisfied with an EPT regimen or who you are unwilling to treat with an EPT regimen
For some postmenopausal women with a uterus there is a
need for progestin free treatment options
bull with demonstrated clinical efficacy
bull which protects the endometrium
bull improved tolerabilitysafety profile
In clinical practice this translates to women who are
intolerant of progestin-containing HT or have conditions
which may be exacerbated by treatment with progestins
Conclusion Medical need for alternative treatment option
Medical condition which may be exacerbated by treatment with progestins
Depression
bull Progestin-containing HT has been associated with increases in depressive symptoms in some individuals1
bull There is a biochemicalphysiological plausibility for the association of progestins with depression234
bull Therefore postmenopausal women who also have a medical history of depressive disorders or depression could be inappropriate for treatment with progestin-containing HT
Pfizer Confidential
65
1) Girdler SS et al J Womens Health Gend Based Med 1999 2) Traish AM et al Korean J Urol 2014 3) Stroumlhle A et al Biol Psychiatry 1999 4) Romeo E et
al Am J Psychiatry 1998
History of the following conditions may make progestin inappropriate
bull Depression
bull PMSPMDD
PMS premenstrual syndrome
PMD premenstrual dysphoric disorder
Medical conditions that may be exacerbated by treatment with progestins
Women for whom progestin-containing HT
would not be considered appropriate
minus Women who are intolerant of progestin-containing hormone therapy
minus Women with pre-existing medical conditions that may be exacerbated by progestins
Most common adverse events leading to discontinuation are related to progestins12
breakthrough bleeding
bull Increase in the number of uterine procedures (ie unnecessary endometrial biopsies)
breast paintenderness
bull Increase in the number of breast interventions
1 Steel SA et al Climacteric 2003 2 Ettinger B and Pressman A Am J Manag Care 1999 3 Komm BS Mirkin S
Pharmaceuticals 2012
4 Panay N amp Studd JWW Human Reprod Update 1997
bull Nausea bull Depressive mood bull Poor concentration bull Hirsutism bull Headache bull Dizziness bull Fluid retention bull Weight gain
Other progestin-related intolerance issues4
Unmet need with the treatment of postmenopausal symptoms
bull Alternatives to progestin are needed that will protect the endometrium while avoiding other progestin-associated effects and preserving the desired effects of estrogens in postmenopausal women3
Which women with a uterus could benefit from
estrogens without the need for a progestin
bull Women who are intolerant of progestin-containing hormone therapy
bull Women with pre-existing medical conditions that may be exacerbated by progestins (eg women with a history of depression PMSPMDD increased breast density diabetes and metabolic syndrome)
History of the following conditions may make progestin inappropriate
bull Depression
bull PMSPMDD
bull High breast density
bull Diabetes and metabolic syndrome
PMS premenstrual syndrome
PMD premenstrual dysphoric disorder
Medical conditions that may be exacerbated by treatment with progestins
Learning from WHI data
bull Hormone therapy (HT) is the conventional and established therapy option to effectively treat postmenopausal symptoms however it has been associated with some safety and tolerability concerns1 2
bull A review of WHI data suggests that many of the concerns with menopausal HT more often associated with EPT (CE+MPA) such as CHD risk increased breast density breast pain and breast cancer risk than with ET (CEE alone)2
1 Rolnick SJ Kopher RA DeFor TA et al Menopause 2005
2 Komm BS Mirkin S Pharmaceuticals 2012
WHI Womenrsquos Health Initiative trial
CHD coronary heart disease
CEE conjugated equine estrogens
Efficacy and Safety of Constant Oestrogen
Pulsed Progestogen vs
Continuous Combined HRT
Adverse Events
17b-oestradiol 17b-oestradiol norgestimate NETA (n = 150) (n = 172) Breast discomfort 14 27 Abdominal discomfort 14 22 Uterine bleeding 15 12 Dysmenorrhea 3 8 Oedema 5 8
Adapted from S Rozenberg et al Human Reproduction 2000
Medical condition which may be exacerbated by treatment
with progestins
Increased breast density
bull Increases in breast density are associated with progestin-containing HT which may adversely affect radiological detection of breast cancer1 and may be independently associated with an increased risk for the development of breast cancer2
bull The Postmenopausal EstrogenProgestin Interventions (PEPI) trial demonstrated that an increased mammographic breast density was associated with the use of E+P but not with the use of estrogen alone3
bull Women who already have high breast density may therefore be considered inappropriate for treatment with a progestin-containing HT
1) EU Core SPC for Hormone Replacement Therapy Products (CMDh1312003 Rev 4 June
2012)
2) De Villiers TJ et al on behalf of the International Menopause Society Climacteric 2013 16
3) Greendale GA et al J Natl Cancer Inst 2003
Stroke
0 25 5 75 10 125
Fractures
Diabetes
Breast cancer
Cholecystitis
Venothrombotic episodes
Endometrial cancer
Lung cancer
Coronary heart disease
Colorectal cancer
Overall mortality
15 125 10 75 5 25
Benefits Risks
CE
CE MPA
Santen RJ et al J Clin Endocrinol Metab 2010
The basis of the Endocrine Society scientific statement for postmenopausal hormone replacement therapy (HRT) excess risks and benefits of HRT for 5 years in women aged 50ndash59 years or within 10 years of the start of menopause E=estrogen P=progestin
bull Younger women (aged 50ndash59 years) had more favorable results bull There are differences between CE alone and CEMPA arms bull Overall benefitrisk ratio of CE-alone appears to be more favourable than CEMPA
Reevaluation of WHI data (stratified by age) Risks and
Benefits of HRT Cases per 1000 Women per 5 Years of
Use
Medical condition which may be exacerbated by treatment
with progestins
Diabetes and metabolic syndrome
bull Treatment of oestrogen deficiency symptoms with progestin-containing HT (unlike oestrogen alone) may be associated with increases in insulin resistance and deterioration in glucose tolerance123
bull Postmenopausal women with diabetes could be inappropriate for treatment with progestin-containing HT due to the potential risk of exacerbation of their condition
1) Panay N amp Studd JWW Human Reprod Update 1997
2) Godsland I et al Metabolism 1993
3) Sites CK et al J Clin Endocrinol Metab 2005
Variations in Associated Breast Cancer
Risks Between CE alone and CEMPA
bull Use of CE alone for a median of 59 years was associated with a lower incidence of invasive breast cancer (151 cases 027 per year) compared with placebo (199 cases 035 per year HR 077 95 CI 062ndash095 P=002)
bull In the CE alone group fewer women died from invasive breast cancer (6 deaths 0009 per year) compared with controls (16 deaths 0024 per year HR 037 95 CI 013ndash091 P=003)
Anderson GL et al Lancet
Oncol 2012
Bazedoxifene (BZA) specifically selected in
combination with conjugated estrogens
bull BZA has been specifically selected for its unique pharmacologic profile and effects on VMS and uterine tissue in particular123
1 Crabtree J et al Mol Cell Endocrinol 2008
2 Kharode Y et al Endocrinolology 2008
3 Duavive SmPC
Estrogen Receptor activity is dimmed
Estrogen Receptor activity is turned on
CEs are agonists BZA is an antagonist
In the uterus
bull The BZA component reduces the risk of endometrial hyperplasia that can occur with the conjugated estrogens component alone3 This means that progestins are not needed
Extensive global clinical development program for
CEBZA
aIncludes additional pilot dose-finding study 203 1 Lobo RA et al Fertil Steril 2009 2 Pinkerton JV et al Menopause 2009 3 Kagan R et al Menopause 2010 4 Mirkin S et al Climacteric 2013 5 Pinkerton JV et al Obstet Gynecol 2013
Effects of conjugated estrogensbazedoxifene on
lipid and coagulation variables a randomized
placebo- and active-controlled trial
bull At 12 months
bull Both CEBZA doses were associated with small but significant effects on hemostasis variables including reductions in antithrombin plasminogen activator inhibitor-1 and fibrinogen activity and an increase in plasminogen activity relative to placebo at 12 months Incidences of cardiovascular and venous thromboembolic events were similar among treatment groups
bull CONCLUSIONS
bull This study provides reassurance that CEBZA does not adversely affect lipid metabolism or hemostatic balance In accordance the incidences of venous thromboembolic events and cardiovascular events in postmenopausal women are similar to those observed with placebo

Rates of BleedingSpotting and Amenorrhea
Similar to Rates with Placebo
bull High and similar cumulative rates of amenorrhea at year 1 among women treated with CE 045BZA 20 and placebo and was higher than seen in women treated with CE 045MPA 151
bull Noncumulative rates of spotting and bleedingspotting were similar among women treated with CEBZA or placebo and consistently higher in women treated with CE 045MPA 152
0
90
Cycle
100
Pe
rce
nta
ge
of
Su
bje
cts
80
70
60
50
40
30
20
10
88
54
Placebo
CE 045BZA 20 CE 045MPA 15
Percentage of subjects with cumulative amenorrhea during consecutive 4-week periods (cycles) in SMART-5
MPA medroxyprogesterone acetate Plt0001 vs all other treatment groups 1 Pinkerton JV et al J Clin Endocrinol Metab 2014 2 Data on file CSR-81040 Protocol 3115A1-3307 Pfizer Inc New York NY
Adverse Reactions in Placebo-
Controlled Trials Safety analyses have been conducted in 6210 postmenopausal women aged 40 to 75 years (mean age 55 years) following up to 2 years of treatment in SMART-1 -2 -3 and -5
Adverse reactions (incidence ge5) that were more common with DUAVIVE
Incidence of serious adverse reactions
35 with DUAVIVE 48 with placebo
DUAVEE [package insert] New York NY Pfizer Inc 2013
CE 045 BZA 20 (N=1224)
n ()
Placebo (N=1069)
n ()
Gastrointestinal disorders
Nausea 100 (8) 58 (5)
Diarrhea 96 (8) 57 (5)
Dyspepsia 84 (7) 59 (6)
Abdominal pain upper 81 (7) 58 (5)
Musculoskeletal and connective tissue disorders
Muscle spasms 110 (9) 63 (6)
Neck pain 62 (5) 46 (4)
Nervous system disorders
Dizziness 65 (5) 37 (3)
Respiratory thoracic and mediastinal disorders
Oropharyngeal pain 80 (7) 61 (6)
Venous Thromboembolism (VTE) in
DUAVIVE Clinical Studies
bull Estrogen agonistantagonists (including BZA a component of DUAVIVE) and estrogens individually are known to increase the risk of VTE
bull In the clinical studies with DUAVIVE the reporting rates for VTE were low in all treatment groups
bull Adverse reactions of VTE reported by patients
bull Should VTE event occur or be suspected DUAVIVE should be discontinued immediately
bull Due to the low rates of events in both groups it is not possible to conclude that the risk of VTE with DUAVIVE is different from that seen with other estrogen therapies
DUAVEE [package insert] New York NY Pfizer Inc 2013
00 for DUAVIVE (n=1224)
01 for placebo (n=1069)
26
Effects of conjugated estrogensbazedoxifene on
lipid and coagulation variables a randomized
placebo- and active-controlled trial
bull postmenopausal women (N = 1843) with menopausal
symptoms
bull Lipid (N = 1843) and coagulation (N = 590) variables were assessed in women receiving daily CE 045 mgBZA 20 mg CE 0625 mgBZA 20 mg BZA 20 mg CE 045 mgmedroxyprogesterone acetate (MPA) 15 mg or placebo for 12 months
bull Skouby SO et al Menopause 2015 Jun22(6)640-9
Effects of conjugated estrogensbazedoxifene on
lipid and coagulation variables a randomized
placebo- and active-controlled trial
bull At 12 months
bull CE 045 mgBZA 20 mg
bull CE 0625 mgBZA 20 mg
bull BZA 20 mg
bull and CE 045 mgMPA 15 mg decreased total cholesterol and LDL- cholesterol vs placebo (P lt 001 for all)
bull Both CEBZA doses and CEMPA increased high-density lipoprotein cholesterol compared with placebo (P lt 005 for all)
bull CE 045 mgBZA 20 mg had a neutral effect on triglycerides
bull CE 0625 mgBZA 20 mg and CEMPA increased triglycerides compared with placebo (P lt 005)
bull Skouby SO et al Menopause 2015 Jun22(6)640-9
Effects of conjugated estrogensbazedoxifene on
lipid and coagulation variables a randomized
placebo- and active-controlled trial
bull At 12 months
bull Both CEBZA doses were associated with small but significant effects on hemostasis variables including reductions in antithrombin plasminogen activator inhibitor-1 and fibrinogen activity and an increase in plasminogen activity relative to placebo at 12 months Incidences of cardiovascular and venous thromboembolic events were similar among treatment groups
Skouby SO et al Menopause 2015
Jun22(6)640-9
Endometrial hyperplasia or malignancy occurred in lt1 of women
following up to 1 year of treatment with CEBZA12
Study Cumulative Incidence at month 12 (nN)
CE 045BZA 20 Placebo
SMART-11 000 (0336) 000 (0313)
SMART-52 030 (1335) 028 (1354)
Effects on the Endometrium
1 Pickar JH et al Fertil Steril 2009 2 Pinkerton at al J Clin Endocrinol Metab 2014
Through the eyes of an amazone
Marie Mandy
Breast tolerability profile similar to placebo following up to 2 years of treatment with CEBZA12
Pooled analysis of SMART clinical trials
CE 045BZA 20 (n=1585)
Placebo (n=1241)
Breast cancer incidence up to 2 years
(per 1000 woman-years)
100 (CI 000-321)
140 (CI 000-417)
Incidence of reported breast paintenderness up to 12 weeks
98-115 81-112
Incidence of abnormal mammogram at month 12
258 316
Mean change in breast density at month 12 (SMART-5)
ndash038 (n=186)
ndash032 (n=182)
Effects on the Breast
1 Pickar JH et al Menopause 2013 2 Pinkerton JV et al Obstet Gynecol 2013
CEBZA clinical overview - summary
bull In clinical trials CEBZA has demonstrated safety and efficacy in postmenopausal women with a uterus including the following
bull Significant reduction in number and severity of moderate to severe hot flushes1
bull Incidence of cumulative amenorrhea rate similar to placebo and significantly better than CEMPA2
bull Incidence of endometrial hyperplasia and breast tendernessdensity similar to that with placebo345
bull Incidence of adverse events and discontinuation rates similar to that with placebo6
1 Pinkerton JV et al Menopause 2009 2 Pinkerton JV et al J Clin Endocrinol Metab2014 3 Pickar JH et al
Fertil Steril 2009 4 Pinkerton at al J Clin Endocrinol Metab 2014 5 Pickar JH et al Menopause 2013 6 DUAVEE [package insert] New York NY Pfizer Inc 2013
CEBZA clinical overview - summary
Now women with a uterus who choose hormone therapy for management of menopausal symptoms have a choice
bull conventional estrogen-progestogen therapy or
bull a new combinationhellipconjugated estrogens paired with the SERM bazedoxifene
1 Pinkerton JV et al Menopause 2009 2 Pinkerton JV et al J Clin Endocrinol Metab2014 3 Pickar JH et al Fertil Steril 2009 4 Pinkerton at al J Clin Endocrinol Metab 2014 5 Pickar JH et al Menopause 2013 6 DUAVEE [package insert] New York NY Pfizer Inc 2013
Conjugated EstrogensBazedoxifene (CEBZA)
US indication
bull DUAVEE is indicated in women with a uterus for
bull 11 Treatment of Moderate to Severe Vasomotor Symptoms Associated with Menopause
bull 12 Prevention of Postmenopausal Osteoporosis
bull 13 Important Limitations of Use
bull Use DUAVEE for the shortest duration consistent with treatment goals and risks for the individual woman Postmenopausal women should be re-evaluated periodically as clinically appropriate to determine if treatment is still necessary
bull When prescribing solely for the prevention of postmenopausal osteoporosis therapy should only be considered for women at significant risk of osteoporosis and non-estrogen medication should be carefully considered
Conjugated EstrogensBazedoxifene (CEBZA)
EU indication
CEBZA is indicated for
bull Treatment of oestrogen deficiency symptoms in postmenopausal women with a uterus (with at least 12 months since the last menses) for whom treatment with progestin-containing therapy is not appropriate
bull The experience treating women older than 65 years is limited
bull Dose CE (045mg)Bazedoxifene (20mg)
Duavive SmPC
Which women with a uterus
could benefit from estrogens
without the need for a
progestin
Progestin intolerance is one of the main
factors for reduced compliance
bull About 20 of women receiving progestin-containing HT have significant progestin intolerance and half of these experience serious effects that prevent treatment continuation1
1 Panay N amp Studd J Human Reprod Update 1997
2 Panay N et al on behalf of the British Menopause Society and Womenrsquos Health Concern Menopause Int 2013
bull The 2013 British Menopause Society amp Womenrsquos Health
Concern recommendations on hormone replacement
therapy do recognise progestin intolerance as one of the
main factors for reduced compliance with HT 2
Proportion of patients () with at least one bleeding episode in relation to time and to the
used HT
Serge Rozenberg et al Hum Reprod 2009241739-1747
copy The Author 2009 Published by Oxford University Press on behalf of the European Society of
Human Reproduction and Embryology All rights reserved For Permissions please email
journalspermissionsoxfordjournalsorg
Breast tenderness after initiation of CEE
CEE + MPA (WHI)
and mammographic density change
bullCrandall et al Breast Cancer Res Treat DOI 101007s10549-011-1803-9
Breast density
Conclusion
bull CEEBAZO is an additional regimen for menopausal symptoms it provides also a prevention for osteoporosis
bull It is suitable for women with a uterus who are unsatisfied with an EPT regimen or who you are unwilling to treat with an EPT regimen
Adapted use of MHT
bull Lower dosage of estrogens
bull Other progestins
bull Better safety profile
bull Vaginal estrogen or SERMS
bull Non-hormonal therapy
bull Development of new products
bull SERMS + estrogens
Most common adverse events leading to
discontinuation are related to progestins12
bull breakthrough bleeding
bull Low compliance
bull Increase in the number of US
bull Stress
bull Cost
bull uterine procedures
bull Unnecessary endometrial biopsies Hysteroscopies DampC Hysterectomies
bull Morbidity
Proportion of patients who completed or discontinued treatment in relation to the used HT
Serge Rozenberg et al Hum Reprod 2009241739-1747
copy The Author 2009 Published by Oxford University Press on behalf of the European Society of
Human Reproduction and Embryology All rights reserved For Permissions please email
journalspermissionsoxfordjournalsorg
Most common adverse events leading to discontinuation
are related to progestins
bull breast paintenderness
Breast tenderness after initiation of CEE
CEE + MPA (WHI)
and mammographic density change
bullCrandall et al Breast Cancer Res Treat DOI 101007s10549-011-1803-9
Breast density
Hormone therapy use and mammographic
density in postmenopausal Norwegian women
bull Results differed when considering the combined effect of age and BMI
bull The effect of EPT on mammographic density was modified by age and BMI with no apparent association among the youngest women (aged 50-55) with the highest BMI (BMI ge 26)
bull A higher mammographic density was found in EPT users compared to never HT users particularly in women using high-dose NETA regimens Age and BMI modified the association between EPT use and mammographic density
bull Couto E et al Breast Cancer Res Treat 2011 Nov 4 [Epub ahead of print]
Breast Cancer Risk by Breast Density
Menopause and Postmenopausal Hormone
Therapy Use
Birads age HT Duration Risk
1 55-59 None 5 year risk 08 (95 CI 06- 09)
1 55-59
ET EPT 5 year risk 09 (95 CI 07 -11)
4 55-59
None 5 year risk 24 (95 CI 20 -28)
4 55-59
ET 5 year risk
30 (95 CI 26 -35)
4 55-59
EPT 5 year risk
42 (95 CI 37 -46)
Adapted from Kerlikowske et al JOURNAL OF CLINICAL ONCOLOGY 2010
Breast Cancer Risk by Breast Density
Menopause and Postmenopausal Hormone
Therapy Use
Adapted from Kerlikowske et al JOURNAL OF CLINICAL ONCOLOGY 2010
bull Postmenopausal women with high breast density are at increased risk of breast cancer and should be aware of the added risk of taking HT especially estrogen plus progestin
Medical condition which may be exacerbated by treatment
with progestins
Diabetes and metabolic syndrome
bull progestin-containing HT may be associated with increases in insulin resistance and deterioration in glucose tolerance123
bull Postmenopausal women with diabetes could be inappropriate for treatment with progestin-containing HT due to the potential risk of exacerbation of their condition
1) Panay N amp Studd JWW Human Reprod Update 1997
2) Godsland I et al Metabolism 1993
3) Sites CK et al J Clin Endocrinol Metab 2005
A Nath and R Sitruk-Ware CLIMACTERIC 200912(Suppl 1)96ndash101
A Nath and R Sitruk-Ware CLIMACTERIC 200912(Suppl 1)96ndash101
Diabetes an epidemy
bull UK 1996 14 million of diabetics
bull UK 2015 32 million (6 of the population)
bull UK 2025 5 million
bull httpwwwdiabetescoukdiabetes-prevalencehtml
Other progestin-related intolerance issues
bull Nausea
bull Depressive mood
bull Poor concentration
bull Hirsutism
bull Headache
bull Dizziness
bull Fluid retention
bull Weight gain Panay N amp Studd JWW Human Reprod Update 1997
Medical condition which may be exacerbated by treatment with progestins
PMSPMDDdepression
bull Progesterone-induced PMD can be exacerbated by exogenous progestin administration and can occur in association with HT or OC administration1
bull Significantly higher negative mood scores have been observed during the addition of a progestin to an estrogen in a sequential HT regimen in postmenopausal women with a history of PMS compared to those without2
bull Women with a history of PMS or PMD exacerbation of depression using progestins may therefore benefit from a progestin free treatment for menopausal symptoms
1) Nevatte T et al Arch Womens Ment Health 2013 2) Bjoumlrn I et al Climacteric 2006 PMS premenstrual syndrome
PMDD premenstrual dysphoric disorder
Conclusion
bull CEEBAZO is an additional regimen for menopausal symptoms it provides also a prevention for osteoporosis
bull It is suitable for women with a uterus who are unsatisfied with an EPT regimen or who you are unwilling to treat with an EPT regimen
For some postmenopausal women with a uterus there is a
need for progestin free treatment options
bull with demonstrated clinical efficacy
bull which protects the endometrium
bull improved tolerabilitysafety profile
In clinical practice this translates to women who are
intolerant of progestin-containing HT or have conditions
which may be exacerbated by treatment with progestins
Conclusion Medical need for alternative treatment option
Medical condition which may be exacerbated by treatment with progestins
Depression
bull Progestin-containing HT has been associated with increases in depressive symptoms in some individuals1
bull There is a biochemicalphysiological plausibility for the association of progestins with depression234
bull Therefore postmenopausal women who also have a medical history of depressive disorders or depression could be inappropriate for treatment with progestin-containing HT
Pfizer Confidential
65
1) Girdler SS et al J Womens Health Gend Based Med 1999 2) Traish AM et al Korean J Urol 2014 3) Stroumlhle A et al Biol Psychiatry 1999 4) Romeo E et
al Am J Psychiatry 1998
History of the following conditions may make progestin inappropriate
bull Depression
bull PMSPMDD
PMS premenstrual syndrome
PMD premenstrual dysphoric disorder
Medical conditions that may be exacerbated by treatment with progestins
Women for whom progestin-containing HT
would not be considered appropriate
minus Women who are intolerant of progestin-containing hormone therapy
minus Women with pre-existing medical conditions that may be exacerbated by progestins
Most common adverse events leading to discontinuation are related to progestins12
breakthrough bleeding
bull Increase in the number of uterine procedures (ie unnecessary endometrial biopsies)
breast paintenderness
bull Increase in the number of breast interventions
1 Steel SA et al Climacteric 2003 2 Ettinger B and Pressman A Am J Manag Care 1999 3 Komm BS Mirkin S
Pharmaceuticals 2012
4 Panay N amp Studd JWW Human Reprod Update 1997
bull Nausea bull Depressive mood bull Poor concentration bull Hirsutism bull Headache bull Dizziness bull Fluid retention bull Weight gain
Other progestin-related intolerance issues4
Unmet need with the treatment of postmenopausal symptoms
bull Alternatives to progestin are needed that will protect the endometrium while avoiding other progestin-associated effects and preserving the desired effects of estrogens in postmenopausal women3
Which women with a uterus could benefit from
estrogens without the need for a progestin
bull Women who are intolerant of progestin-containing hormone therapy
bull Women with pre-existing medical conditions that may be exacerbated by progestins (eg women with a history of depression PMSPMDD increased breast density diabetes and metabolic syndrome)
History of the following conditions may make progestin inappropriate
bull Depression
bull PMSPMDD
bull High breast density
bull Diabetes and metabolic syndrome
PMS premenstrual syndrome
PMD premenstrual dysphoric disorder
Medical conditions that may be exacerbated by treatment with progestins
Learning from WHI data
bull Hormone therapy (HT) is the conventional and established therapy option to effectively treat postmenopausal symptoms however it has been associated with some safety and tolerability concerns1 2
bull A review of WHI data suggests that many of the concerns with menopausal HT more often associated with EPT (CE+MPA) such as CHD risk increased breast density breast pain and breast cancer risk than with ET (CEE alone)2
1 Rolnick SJ Kopher RA DeFor TA et al Menopause 2005
2 Komm BS Mirkin S Pharmaceuticals 2012
WHI Womenrsquos Health Initiative trial
CHD coronary heart disease
CEE conjugated equine estrogens
Efficacy and Safety of Constant Oestrogen
Pulsed Progestogen vs
Continuous Combined HRT
Adverse Events
17b-oestradiol 17b-oestradiol norgestimate NETA (n = 150) (n = 172) Breast discomfort 14 27 Abdominal discomfort 14 22 Uterine bleeding 15 12 Dysmenorrhea 3 8 Oedema 5 8
Adapted from S Rozenberg et al Human Reproduction 2000
Medical condition which may be exacerbated by treatment
with progestins
Increased breast density
bull Increases in breast density are associated with progestin-containing HT which may adversely affect radiological detection of breast cancer1 and may be independently associated with an increased risk for the development of breast cancer2
bull The Postmenopausal EstrogenProgestin Interventions (PEPI) trial demonstrated that an increased mammographic breast density was associated with the use of E+P but not with the use of estrogen alone3
bull Women who already have high breast density may therefore be considered inappropriate for treatment with a progestin-containing HT
1) EU Core SPC for Hormone Replacement Therapy Products (CMDh1312003 Rev 4 June
2012)
2) De Villiers TJ et al on behalf of the International Menopause Society Climacteric 2013 16
3) Greendale GA et al J Natl Cancer Inst 2003
Stroke
0 25 5 75 10 125
Fractures
Diabetes
Breast cancer
Cholecystitis
Venothrombotic episodes
Endometrial cancer
Lung cancer
Coronary heart disease
Colorectal cancer
Overall mortality
15 125 10 75 5 25
Benefits Risks
CE
CE MPA
Santen RJ et al J Clin Endocrinol Metab 2010
The basis of the Endocrine Society scientific statement for postmenopausal hormone replacement therapy (HRT) excess risks and benefits of HRT for 5 years in women aged 50ndash59 years or within 10 years of the start of menopause E=estrogen P=progestin
bull Younger women (aged 50ndash59 years) had more favorable results bull There are differences between CE alone and CEMPA arms bull Overall benefitrisk ratio of CE-alone appears to be more favourable than CEMPA
Reevaluation of WHI data (stratified by age) Risks and
Benefits of HRT Cases per 1000 Women per 5 Years of
Use
Medical condition which may be exacerbated by treatment
with progestins
Diabetes and metabolic syndrome
bull Treatment of oestrogen deficiency symptoms with progestin-containing HT (unlike oestrogen alone) may be associated with increases in insulin resistance and deterioration in glucose tolerance123
bull Postmenopausal women with diabetes could be inappropriate for treatment with progestin-containing HT due to the potential risk of exacerbation of their condition
1) Panay N amp Studd JWW Human Reprod Update 1997
2) Godsland I et al Metabolism 1993
3) Sites CK et al J Clin Endocrinol Metab 2005
Variations in Associated Breast Cancer
Risks Between CE alone and CEMPA
bull Use of CE alone for a median of 59 years was associated with a lower incidence of invasive breast cancer (151 cases 027 per year) compared with placebo (199 cases 035 per year HR 077 95 CI 062ndash095 P=002)
bull In the CE alone group fewer women died from invasive breast cancer (6 deaths 0009 per year) compared with controls (16 deaths 0024 per year HR 037 95 CI 013ndash091 P=003)
Anderson GL et al Lancet
Oncol 2012
Bazedoxifene (BZA) specifically selected in
combination with conjugated estrogens
bull BZA has been specifically selected for its unique pharmacologic profile and effects on VMS and uterine tissue in particular123
1 Crabtree J et al Mol Cell Endocrinol 2008
2 Kharode Y et al Endocrinolology 2008
3 Duavive SmPC
Estrogen Receptor activity is dimmed
Estrogen Receptor activity is turned on
CEs are agonists BZA is an antagonist
In the uterus
bull The BZA component reduces the risk of endometrial hyperplasia that can occur with the conjugated estrogens component alone3 This means that progestins are not needed
Extensive global clinical development program for
CEBZA
aIncludes additional pilot dose-finding study 203 1 Lobo RA et al Fertil Steril 2009 2 Pinkerton JV et al Menopause 2009 3 Kagan R et al Menopause 2010 4 Mirkin S et al Climacteric 2013 5 Pinkerton JV et al Obstet Gynecol 2013
Effects of conjugated estrogensbazedoxifene on
lipid and coagulation variables a randomized
placebo- and active-controlled trial
bull At 12 months
bull Both CEBZA doses were associated with small but significant effects on hemostasis variables including reductions in antithrombin plasminogen activator inhibitor-1 and fibrinogen activity and an increase in plasminogen activity relative to placebo at 12 months Incidences of cardiovascular and venous thromboembolic events were similar among treatment groups
bull CONCLUSIONS
bull This study provides reassurance that CEBZA does not adversely affect lipid metabolism or hemostatic balance In accordance the incidences of venous thromboembolic events and cardiovascular events in postmenopausal women are similar to those observed with placebo
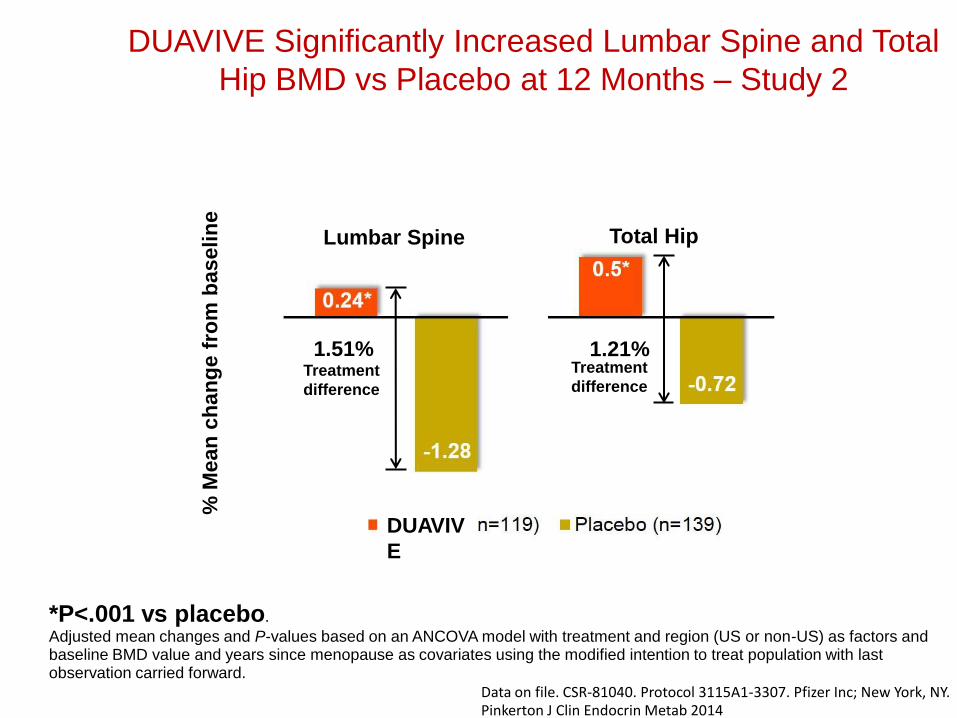
Adverse Reactions in Placebo-
Controlled Trials Safety analyses have been conducted in 6210 postmenopausal women aged 40 to 75 years (mean age 55 years) following up to 2 years of treatment in SMART-1 -2 -3 and -5
Adverse reactions (incidence ge5) that were more common with DUAVIVE
Incidence of serious adverse reactions
35 with DUAVIVE 48 with placebo
DUAVEE [package insert] New York NY Pfizer Inc 2013
CE 045 BZA 20 (N=1224)
n ()
Placebo (N=1069)
n ()
Gastrointestinal disorders
Nausea 100 (8) 58 (5)
Diarrhea 96 (8) 57 (5)
Dyspepsia 84 (7) 59 (6)
Abdominal pain upper 81 (7) 58 (5)
Musculoskeletal and connective tissue disorders
Muscle spasms 110 (9) 63 (6)
Neck pain 62 (5) 46 (4)
Nervous system disorders
Dizziness 65 (5) 37 (3)
Respiratory thoracic and mediastinal disorders
Oropharyngeal pain 80 (7) 61 (6)
Venous Thromboembolism (VTE) in
DUAVIVE Clinical Studies
bull Estrogen agonistantagonists (including BZA a component of DUAVIVE) and estrogens individually are known to increase the risk of VTE
bull In the clinical studies with DUAVIVE the reporting rates for VTE were low in all treatment groups
bull Adverse reactions of VTE reported by patients
bull Should VTE event occur or be suspected DUAVIVE should be discontinued immediately
bull Due to the low rates of events in both groups it is not possible to conclude that the risk of VTE with DUAVIVE is different from that seen with other estrogen therapies
DUAVEE [package insert] New York NY Pfizer Inc 2013
00 for DUAVIVE (n=1224)
01 for placebo (n=1069)
26
Effects of conjugated estrogensbazedoxifene on
lipid and coagulation variables a randomized
placebo- and active-controlled trial
bull postmenopausal women (N = 1843) with menopausal
symptoms
bull Lipid (N = 1843) and coagulation (N = 590) variables were assessed in women receiving daily CE 045 mgBZA 20 mg CE 0625 mgBZA 20 mg BZA 20 mg CE 045 mgmedroxyprogesterone acetate (MPA) 15 mg or placebo for 12 months
bull Skouby SO et al Menopause 2015 Jun22(6)640-9
Effects of conjugated estrogensbazedoxifene on
lipid and coagulation variables a randomized
placebo- and active-controlled trial
bull At 12 months
bull CE 045 mgBZA 20 mg
bull CE 0625 mgBZA 20 mg
bull BZA 20 mg
bull and CE 045 mgMPA 15 mg decreased total cholesterol and LDL- cholesterol vs placebo (P lt 001 for all)
bull Both CEBZA doses and CEMPA increased high-density lipoprotein cholesterol compared with placebo (P lt 005 for all)
bull CE 045 mgBZA 20 mg had a neutral effect on triglycerides
bull CE 0625 mgBZA 20 mg and CEMPA increased triglycerides compared with placebo (P lt 005)
bull Skouby SO et al Menopause 2015 Jun22(6)640-9
Effects of conjugated estrogensbazedoxifene on
lipid and coagulation variables a randomized
placebo- and active-controlled trial
bull At 12 months
bull Both CEBZA doses were associated with small but significant effects on hemostasis variables including reductions in antithrombin plasminogen activator inhibitor-1 and fibrinogen activity and an increase in plasminogen activity relative to placebo at 12 months Incidences of cardiovascular and venous thromboembolic events were similar among treatment groups
Skouby SO et al Menopause 2015
Jun22(6)640-9
Endometrial hyperplasia or malignancy occurred in lt1 of women
following up to 1 year of treatment with CEBZA12
Study Cumulative Incidence at month 12 (nN)
CE 045BZA 20 Placebo
SMART-11 000 (0336) 000 (0313)
SMART-52 030 (1335) 028 (1354)
Effects on the Endometrium
1 Pickar JH et al Fertil Steril 2009 2 Pinkerton at al J Clin Endocrinol Metab 2014
Through the eyes of an amazone
Marie Mandy
Breast tolerability profile similar to placebo following up to 2 years of treatment with CEBZA12
Pooled analysis of SMART clinical trials
CE 045BZA 20 (n=1585)
Placebo (n=1241)
Breast cancer incidence up to 2 years
(per 1000 woman-years)
100 (CI 000-321)
140 (CI 000-417)
Incidence of reported breast paintenderness up to 12 weeks
98-115 81-112
Incidence of abnormal mammogram at month 12
258 316
Mean change in breast density at month 12 (SMART-5)
ndash038 (n=186)
ndash032 (n=182)
Effects on the Breast
1 Pickar JH et al Menopause 2013 2 Pinkerton JV et al Obstet Gynecol 2013
CEBZA clinical overview - summary
bull In clinical trials CEBZA has demonstrated safety and efficacy in postmenopausal women with a uterus including the following
bull Significant reduction in number and severity of moderate to severe hot flushes1
bull Incidence of cumulative amenorrhea rate similar to placebo and significantly better than CEMPA2
bull Incidence of endometrial hyperplasia and breast tendernessdensity similar to that with placebo345
bull Incidence of adverse events and discontinuation rates similar to that with placebo6
1 Pinkerton JV et al Menopause 2009 2 Pinkerton JV et al J Clin Endocrinol Metab2014 3 Pickar JH et al
Fertil Steril 2009 4 Pinkerton at al J Clin Endocrinol Metab 2014 5 Pickar JH et al Menopause 2013 6 DUAVEE [package insert] New York NY Pfizer Inc 2013
CEBZA clinical overview - summary
Now women with a uterus who choose hormone therapy for management of menopausal symptoms have a choice
bull conventional estrogen-progestogen therapy or
bull a new combinationhellipconjugated estrogens paired with the SERM bazedoxifene
1 Pinkerton JV et al Menopause 2009 2 Pinkerton JV et al J Clin Endocrinol Metab2014 3 Pickar JH et al Fertil Steril 2009 4 Pinkerton at al J Clin Endocrinol Metab 2014 5 Pickar JH et al Menopause 2013 6 DUAVEE [package insert] New York NY Pfizer Inc 2013
Conjugated EstrogensBazedoxifene (CEBZA)
US indication
bull DUAVEE is indicated in women with a uterus for
bull 11 Treatment of Moderate to Severe Vasomotor Symptoms Associated with Menopause
bull 12 Prevention of Postmenopausal Osteoporosis
bull 13 Important Limitations of Use
bull Use DUAVEE for the shortest duration consistent with treatment goals and risks for the individual woman Postmenopausal women should be re-evaluated periodically as clinically appropriate to determine if treatment is still necessary
bull When prescribing solely for the prevention of postmenopausal osteoporosis therapy should only be considered for women at significant risk of osteoporosis and non-estrogen medication should be carefully considered
Conjugated EstrogensBazedoxifene (CEBZA)
EU indication
CEBZA is indicated for
bull Treatment of oestrogen deficiency symptoms in postmenopausal women with a uterus (with at least 12 months since the last menses) for whom treatment with progestin-containing therapy is not appropriate
bull The experience treating women older than 65 years is limited
bull Dose CE (045mg)Bazedoxifene (20mg)
Duavive SmPC
Which women with a uterus
could benefit from estrogens
without the need for a
progestin
Progestin intolerance is one of the main
factors for reduced compliance
bull About 20 of women receiving progestin-containing HT have significant progestin intolerance and half of these experience serious effects that prevent treatment continuation1
1 Panay N amp Studd J Human Reprod Update 1997
2 Panay N et al on behalf of the British Menopause Society and Womenrsquos Health Concern Menopause Int 2013
bull The 2013 British Menopause Society amp Womenrsquos Health
Concern recommendations on hormone replacement
therapy do recognise progestin intolerance as one of the
main factors for reduced compliance with HT 2
Proportion of patients () with at least one bleeding episode in relation to time and to the
used HT
Serge Rozenberg et al Hum Reprod 2009241739-1747
copy The Author 2009 Published by Oxford University Press on behalf of the European Society of
Human Reproduction and Embryology All rights reserved For Permissions please email
journalspermissionsoxfordjournalsorg
Breast tenderness after initiation of CEE
CEE + MPA (WHI)
and mammographic density change
bullCrandall et al Breast Cancer Res Treat DOI 101007s10549-011-1803-9
Breast density
Conclusion
bull CEEBAZO is an additional regimen for menopausal symptoms it provides also a prevention for osteoporosis
bull It is suitable for women with a uterus who are unsatisfied with an EPT regimen or who you are unwilling to treat with an EPT regimen
Adapted use of MHT
bull Lower dosage of estrogens
bull Other progestins
bull Better safety profile
bull Vaginal estrogen or SERMS
bull Non-hormonal therapy
bull Development of new products
bull SERMS + estrogens
Most common adverse events leading to
discontinuation are related to progestins12
bull breakthrough bleeding
bull Low compliance
bull Increase in the number of US
bull Stress
bull Cost
bull uterine procedures
bull Unnecessary endometrial biopsies Hysteroscopies DampC Hysterectomies
bull Morbidity
Proportion of patients who completed or discontinued treatment in relation to the used HT
Serge Rozenberg et al Hum Reprod 2009241739-1747
copy The Author 2009 Published by Oxford University Press on behalf of the European Society of
Human Reproduction and Embryology All rights reserved For Permissions please email
journalspermissionsoxfordjournalsorg
Most common adverse events leading to discontinuation
are related to progestins
bull breast paintenderness
Breast tenderness after initiation of CEE
CEE + MPA (WHI)
and mammographic density change
bullCrandall et al Breast Cancer Res Treat DOI 101007s10549-011-1803-9
Breast density
Hormone therapy use and mammographic
density in postmenopausal Norwegian women
bull Results differed when considering the combined effect of age and BMI
bull The effect of EPT on mammographic density was modified by age and BMI with no apparent association among the youngest women (aged 50-55) with the highest BMI (BMI ge 26)
bull A higher mammographic density was found in EPT users compared to never HT users particularly in women using high-dose NETA regimens Age and BMI modified the association between EPT use and mammographic density
bull Couto E et al Breast Cancer Res Treat 2011 Nov 4 [Epub ahead of print]
Breast Cancer Risk by Breast Density
Menopause and Postmenopausal Hormone
Therapy Use
Birads age HT Duration Risk
1 55-59 None 5 year risk 08 (95 CI 06- 09)
1 55-59
ET EPT 5 year risk 09 (95 CI 07 -11)
4 55-59
None 5 year risk 24 (95 CI 20 -28)
4 55-59
ET 5 year risk
30 (95 CI 26 -35)
4 55-59
EPT 5 year risk
42 (95 CI 37 -46)
Adapted from Kerlikowske et al JOURNAL OF CLINICAL ONCOLOGY 2010
Breast Cancer Risk by Breast Density
Menopause and Postmenopausal Hormone
Therapy Use
Adapted from Kerlikowske et al JOURNAL OF CLINICAL ONCOLOGY 2010
bull Postmenopausal women with high breast density are at increased risk of breast cancer and should be aware of the added risk of taking HT especially estrogen plus progestin
Medical condition which may be exacerbated by treatment
with progestins
Diabetes and metabolic syndrome
bull progestin-containing HT may be associated with increases in insulin resistance and deterioration in glucose tolerance123
bull Postmenopausal women with diabetes could be inappropriate for treatment with progestin-containing HT due to the potential risk of exacerbation of their condition
1) Panay N amp Studd JWW Human Reprod Update 1997
2) Godsland I et al Metabolism 1993
3) Sites CK et al J Clin Endocrinol Metab 2005
A Nath and R Sitruk-Ware CLIMACTERIC 200912(Suppl 1)96ndash101
A Nath and R Sitruk-Ware CLIMACTERIC 200912(Suppl 1)96ndash101
Diabetes an epidemy
bull UK 1996 14 million of diabetics
bull UK 2015 32 million (6 of the population)
bull UK 2025 5 million
bull httpwwwdiabetescoukdiabetes-prevalencehtml
Other progestin-related intolerance issues
bull Nausea
bull Depressive mood
bull Poor concentration
bull Hirsutism
bull Headache
bull Dizziness
bull Fluid retention
bull Weight gain Panay N amp Studd JWW Human Reprod Update 1997
Medical condition which may be exacerbated by treatment with progestins
PMSPMDDdepression
bull Progesterone-induced PMD can be exacerbated by exogenous progestin administration and can occur in association with HT or OC administration1
bull Significantly higher negative mood scores have been observed during the addition of a progestin to an estrogen in a sequential HT regimen in postmenopausal women with a history of PMS compared to those without2
bull Women with a history of PMS or PMD exacerbation of depression using progestins may therefore benefit from a progestin free treatment for menopausal symptoms
1) Nevatte T et al Arch Womens Ment Health 2013 2) Bjoumlrn I et al Climacteric 2006 PMS premenstrual syndrome
PMDD premenstrual dysphoric disorder
Conclusion
bull CEEBAZO is an additional regimen for menopausal symptoms it provides also a prevention for osteoporosis
bull It is suitable for women with a uterus who are unsatisfied with an EPT regimen or who you are unwilling to treat with an EPT regimen
For some postmenopausal women with a uterus there is a
need for progestin free treatment options
bull with demonstrated clinical efficacy
bull which protects the endometrium
bull improved tolerabilitysafety profile
In clinical practice this translates to women who are
intolerant of progestin-containing HT or have conditions
which may be exacerbated by treatment with progestins
Conclusion Medical need for alternative treatment option
Medical condition which may be exacerbated by treatment with progestins
Depression
bull Progestin-containing HT has been associated with increases in depressive symptoms in some individuals1
bull There is a biochemicalphysiological plausibility for the association of progestins with depression234
bull Therefore postmenopausal women who also have a medical history of depressive disorders or depression could be inappropriate for treatment with progestin-containing HT
Pfizer Confidential
65
1) Girdler SS et al J Womens Health Gend Based Med 1999 2) Traish AM et al Korean J Urol 2014 3) Stroumlhle A et al Biol Psychiatry 1999 4) Romeo E et
al Am J Psychiatry 1998
History of the following conditions may make progestin inappropriate
bull Depression
bull PMSPMDD
PMS premenstrual syndrome
PMD premenstrual dysphoric disorder
Medical conditions that may be exacerbated by treatment with progestins
Women for whom progestin-containing HT
would not be considered appropriate
minus Women who are intolerant of progestin-containing hormone therapy
minus Women with pre-existing medical conditions that may be exacerbated by progestins
Most common adverse events leading to discontinuation are related to progestins12
breakthrough bleeding
bull Increase in the number of uterine procedures (ie unnecessary endometrial biopsies)
breast paintenderness
bull Increase in the number of breast interventions
1 Steel SA et al Climacteric 2003 2 Ettinger B and Pressman A Am J Manag Care 1999 3 Komm BS Mirkin S
Pharmaceuticals 2012
4 Panay N amp Studd JWW Human Reprod Update 1997
bull Nausea bull Depressive mood bull Poor concentration bull Hirsutism bull Headache bull Dizziness bull Fluid retention bull Weight gain
Other progestin-related intolerance issues4
Unmet need with the treatment of postmenopausal symptoms
bull Alternatives to progestin are needed that will protect the endometrium while avoiding other progestin-associated effects and preserving the desired effects of estrogens in postmenopausal women3
Which women with a uterus could benefit from
estrogens without the need for a progestin
bull Women who are intolerant of progestin-containing hormone therapy
bull Women with pre-existing medical conditions that may be exacerbated by progestins (eg women with a history of depression PMSPMDD increased breast density diabetes and metabolic syndrome)
History of the following conditions may make progestin inappropriate
bull Depression
bull PMSPMDD
bull High breast density
bull Diabetes and metabolic syndrome
PMS premenstrual syndrome
PMD premenstrual dysphoric disorder
Medical conditions that may be exacerbated by treatment with progestins
Learning from WHI data
bull Hormone therapy (HT) is the conventional and established therapy option to effectively treat postmenopausal symptoms however it has been associated with some safety and tolerability concerns1 2
bull A review of WHI data suggests that many of the concerns with menopausal HT more often associated with EPT (CE+MPA) such as CHD risk increased breast density breast pain and breast cancer risk than with ET (CEE alone)2
1 Rolnick SJ Kopher RA DeFor TA et al Menopause 2005
2 Komm BS Mirkin S Pharmaceuticals 2012
WHI Womenrsquos Health Initiative trial
CHD coronary heart disease
CEE conjugated equine estrogens
Efficacy and Safety of Constant Oestrogen
Pulsed Progestogen vs
Continuous Combined HRT
Adverse Events
17b-oestradiol 17b-oestradiol norgestimate NETA (n = 150) (n = 172) Breast discomfort 14 27 Abdominal discomfort 14 22 Uterine bleeding 15 12 Dysmenorrhea 3 8 Oedema 5 8
Adapted from S Rozenberg et al Human Reproduction 2000
Medical condition which may be exacerbated by treatment
with progestins
Increased breast density
bull Increases in breast density are associated with progestin-containing HT which may adversely affect radiological detection of breast cancer1 and may be independently associated with an increased risk for the development of breast cancer2
bull The Postmenopausal EstrogenProgestin Interventions (PEPI) trial demonstrated that an increased mammographic breast density was associated with the use of E+P but not with the use of estrogen alone3
bull Women who already have high breast density may therefore be considered inappropriate for treatment with a progestin-containing HT
1) EU Core SPC for Hormone Replacement Therapy Products (CMDh1312003 Rev 4 June
2012)
2) De Villiers TJ et al on behalf of the International Menopause Society Climacteric 2013 16
3) Greendale GA et al J Natl Cancer Inst 2003
Stroke
0 25 5 75 10 125
Fractures
Diabetes
Breast cancer
Cholecystitis
Venothrombotic episodes
Endometrial cancer
Lung cancer
Coronary heart disease
Colorectal cancer
Overall mortality
15 125 10 75 5 25
Benefits Risks
CE
CE MPA
Santen RJ et al J Clin Endocrinol Metab 2010
The basis of the Endocrine Society scientific statement for postmenopausal hormone replacement therapy (HRT) excess risks and benefits of HRT for 5 years in women aged 50ndash59 years or within 10 years of the start of menopause E=estrogen P=progestin
bull Younger women (aged 50ndash59 years) had more favorable results bull There are differences between CE alone and CEMPA arms bull Overall benefitrisk ratio of CE-alone appears to be more favourable than CEMPA
Reevaluation of WHI data (stratified by age) Risks and
Benefits of HRT Cases per 1000 Women per 5 Years of
Use
Medical condition which may be exacerbated by treatment
with progestins
Diabetes and metabolic syndrome
bull Treatment of oestrogen deficiency symptoms with progestin-containing HT (unlike oestrogen alone) may be associated with increases in insulin resistance and deterioration in glucose tolerance123
bull Postmenopausal women with diabetes could be inappropriate for treatment with progestin-containing HT due to the potential risk of exacerbation of their condition
1) Panay N amp Studd JWW Human Reprod Update 1997
2) Godsland I et al Metabolism 1993
3) Sites CK et al J Clin Endocrinol Metab 2005
Variations in Associated Breast Cancer
Risks Between CE alone and CEMPA
bull Use of CE alone for a median of 59 years was associated with a lower incidence of invasive breast cancer (151 cases 027 per year) compared with placebo (199 cases 035 per year HR 077 95 CI 062ndash095 P=002)
bull In the CE alone group fewer women died from invasive breast cancer (6 deaths 0009 per year) compared with controls (16 deaths 0024 per year HR 037 95 CI 013ndash091 P=003)
Anderson GL et al Lancet
Oncol 2012
Bazedoxifene (BZA) specifically selected in
combination with conjugated estrogens
bull BZA has been specifically selected for its unique pharmacologic profile and effects on VMS and uterine tissue in particular123
1 Crabtree J et al Mol Cell Endocrinol 2008
2 Kharode Y et al Endocrinolology 2008
3 Duavive SmPC
Estrogen Receptor activity is dimmed
Estrogen Receptor activity is turned on
CEs are agonists BZA is an antagonist
In the uterus
bull The BZA component reduces the risk of endometrial hyperplasia that can occur with the conjugated estrogens component alone3 This means that progestins are not needed
Extensive global clinical development program for
CEBZA
aIncludes additional pilot dose-finding study 203 1 Lobo RA et al Fertil Steril 2009 2 Pinkerton JV et al Menopause 2009 3 Kagan R et al Menopause 2010 4 Mirkin S et al Climacteric 2013 5 Pinkerton JV et al Obstet Gynecol 2013
Effects of conjugated estrogensbazedoxifene on
lipid and coagulation variables a randomized
placebo- and active-controlled trial
bull At 12 months
bull Both CEBZA doses were associated with small but significant effects on hemostasis variables including reductions in antithrombin plasminogen activator inhibitor-1 and fibrinogen activity and an increase in plasminogen activity relative to placebo at 12 months Incidences of cardiovascular and venous thromboembolic events were similar among treatment groups
bull CONCLUSIONS
bull This study provides reassurance that CEBZA does not adversely affect lipid metabolism or hemostatic balance In accordance the incidences of venous thromboembolic events and cardiovascular events in postmenopausal women are similar to those observed with placebo
Venous Thromboembolism (VTE) in
DUAVIVE Clinical Studies
bull Estrogen agonistantagonists (including BZA a component of DUAVIVE) and estrogens individually are known to increase the risk of VTE
bull In the clinical studies with DUAVIVE the reporting rates for VTE were low in all treatment groups
bull Adverse reactions of VTE reported by patients
bull Should VTE event occur or be suspected DUAVIVE should be discontinued immediately
bull Due to the low rates of events in both groups it is not possible to conclude that the risk of VTE with DUAVIVE is different from that seen with other estrogen therapies
DUAVEE [package insert] New York NY Pfizer Inc 2013
00 for DUAVIVE (n=1224)
01 for placebo (n=1069)
26
Effects of conjugated estrogensbazedoxifene on
lipid and coagulation variables a randomized
placebo- and active-controlled trial
bull postmenopausal women (N = 1843) with menopausal
symptoms
bull Lipid (N = 1843) and coagulation (N = 590) variables were assessed in women receiving daily CE 045 mgBZA 20 mg CE 0625 mgBZA 20 mg BZA 20 mg CE 045 mgmedroxyprogesterone acetate (MPA) 15 mg or placebo for 12 months
bull Skouby SO et al Menopause 2015 Jun22(6)640-9
Effects of conjugated estrogensbazedoxifene on
lipid and coagulation variables a randomized
placebo- and active-controlled trial
bull At 12 months
bull CE 045 mgBZA 20 mg
bull CE 0625 mgBZA 20 mg
bull BZA 20 mg
bull and CE 045 mgMPA 15 mg decreased total cholesterol and LDL- cholesterol vs placebo (P lt 001 for all)
bull Both CEBZA doses and CEMPA increased high-density lipoprotein cholesterol compared with placebo (P lt 005 for all)
bull CE 045 mgBZA 20 mg had a neutral effect on triglycerides
bull CE 0625 mgBZA 20 mg and CEMPA increased triglycerides compared with placebo (P lt 005)
bull Skouby SO et al Menopause 2015 Jun22(6)640-9
Effects of conjugated estrogensbazedoxifene on
lipid and coagulation variables a randomized
placebo- and active-controlled trial
bull At 12 months
bull Both CEBZA doses were associated with small but significant effects on hemostasis variables including reductions in antithrombin plasminogen activator inhibitor-1 and fibrinogen activity and an increase in plasminogen activity relative to placebo at 12 months Incidences of cardiovascular and venous thromboembolic events were similar among treatment groups
Skouby SO et al Menopause 2015
Jun22(6)640-9
Endometrial hyperplasia or malignancy occurred in lt1 of women
following up to 1 year of treatment with CEBZA12
Study Cumulative Incidence at month 12 (nN)
CE 045BZA 20 Placebo
SMART-11 000 (0336) 000 (0313)
SMART-52 030 (1335) 028 (1354)
Effects on the Endometrium
1 Pickar JH et al Fertil Steril 2009 2 Pinkerton at al J Clin Endocrinol Metab 2014
Through the eyes of an amazone
Marie Mandy
Breast tolerability profile similar to placebo following up to 2 years of treatment with CEBZA12
Pooled analysis of SMART clinical trials
CE 045BZA 20 (n=1585)
Placebo (n=1241)
Breast cancer incidence up to 2 years
(per 1000 woman-years)
100 (CI 000-321)
140 (CI 000-417)
Incidence of reported breast paintenderness up to 12 weeks
98-115 81-112
Incidence of abnormal mammogram at month 12
258 316
Mean change in breast density at month 12 (SMART-5)
ndash038 (n=186)
ndash032 (n=182)
Effects on the Breast
1 Pickar JH et al Menopause 2013 2 Pinkerton JV et al Obstet Gynecol 2013
CEBZA clinical overview - summary
bull In clinical trials CEBZA has demonstrated safety and efficacy in postmenopausal women with a uterus including the following
bull Significant reduction in number and severity of moderate to severe hot flushes1
bull Incidence of cumulative amenorrhea rate similar to placebo and significantly better than CEMPA2
bull Incidence of endometrial hyperplasia and breast tendernessdensity similar to that with placebo345
bull Incidence of adverse events and discontinuation rates similar to that with placebo6
1 Pinkerton JV et al Menopause 2009 2 Pinkerton JV et al J Clin Endocrinol Metab2014 3 Pickar JH et al
Fertil Steril 2009 4 Pinkerton at al J Clin Endocrinol Metab 2014 5 Pickar JH et al Menopause 2013 6 DUAVEE [package insert] New York NY Pfizer Inc 2013
CEBZA clinical overview - summary
Now women with a uterus who choose hormone therapy for management of menopausal symptoms have a choice
bull conventional estrogen-progestogen therapy or
bull a new combinationhellipconjugated estrogens paired with the SERM bazedoxifene
1 Pinkerton JV et al Menopause 2009 2 Pinkerton JV et al J Clin Endocrinol Metab2014 3 Pickar JH et al Fertil Steril 2009 4 Pinkerton at al J Clin Endocrinol Metab 2014 5 Pickar JH et al Menopause 2013 6 DUAVEE [package insert] New York NY Pfizer Inc 2013
Conjugated EstrogensBazedoxifene (CEBZA)
US indication
bull DUAVEE is indicated in women with a uterus for
bull 11 Treatment of Moderate to Severe Vasomotor Symptoms Associated with Menopause
bull 12 Prevention of Postmenopausal Osteoporosis
bull 13 Important Limitations of Use
bull Use DUAVEE for the shortest duration consistent with treatment goals and risks for the individual woman Postmenopausal women should be re-evaluated periodically as clinically appropriate to determine if treatment is still necessary
bull When prescribing solely for the prevention of postmenopausal osteoporosis therapy should only be considered for women at significant risk of osteoporosis and non-estrogen medication should be carefully considered
Conjugated EstrogensBazedoxifene (CEBZA)
EU indication
CEBZA is indicated for
bull Treatment of oestrogen deficiency symptoms in postmenopausal women with a uterus (with at least 12 months since the last menses) for whom treatment with progestin-containing therapy is not appropriate
bull The experience treating women older than 65 years is limited
bull Dose CE (045mg)Bazedoxifene (20mg)
Duavive SmPC
Which women with a uterus
could benefit from estrogens
without the need for a
progestin
Progestin intolerance is one of the main
factors for reduced compliance
bull About 20 of women receiving progestin-containing HT have significant progestin intolerance and half of these experience serious effects that prevent treatment continuation1
1 Panay N amp Studd J Human Reprod Update 1997
2 Panay N et al on behalf of the British Menopause Society and Womenrsquos Health Concern Menopause Int 2013
bull The 2013 British Menopause Society amp Womenrsquos Health
Concern recommendations on hormone replacement
therapy do recognise progestin intolerance as one of the
main factors for reduced compliance with HT 2
Proportion of patients () with at least one bleeding episode in relation to time and to the
used HT
Serge Rozenberg et al Hum Reprod 2009241739-1747
copy The Author 2009 Published by Oxford University Press on behalf of the European Society of
Human Reproduction and Embryology All rights reserved For Permissions please email
journalspermissionsoxfordjournalsorg
Breast tenderness after initiation of CEE
CEE + MPA (WHI)
and mammographic density change
bullCrandall et al Breast Cancer Res Treat DOI 101007s10549-011-1803-9
Breast density
Conclusion
bull CEEBAZO is an additional regimen for menopausal symptoms it provides also a prevention for osteoporosis
bull It is suitable for women with a uterus who are unsatisfied with an EPT regimen or who you are unwilling to treat with an EPT regimen
Adapted use of MHT
bull Lower dosage of estrogens
bull Other progestins
bull Better safety profile
bull Vaginal estrogen or SERMS
bull Non-hormonal therapy
bull Development of new products
bull SERMS + estrogens
Most common adverse events leading to
discontinuation are related to progestins12
bull breakthrough bleeding
bull Low compliance
bull Increase in the number of US
bull Stress
bull Cost
bull uterine procedures
bull Unnecessary endometrial biopsies Hysteroscopies DampC Hysterectomies
bull Morbidity
Proportion of patients who completed or discontinued treatment in relation to the used HT
Serge Rozenberg et al Hum Reprod 2009241739-1747
copy The Author 2009 Published by Oxford University Press on behalf of the European Society of
Human Reproduction and Embryology All rights reserved For Permissions please email
journalspermissionsoxfordjournalsorg
Most common adverse events leading to discontinuation
are related to progestins
bull breast paintenderness
Breast tenderness after initiation of CEE
CEE + MPA (WHI)
and mammographic density change
bullCrandall et al Breast Cancer Res Treat DOI 101007s10549-011-1803-9
Breast density
Hormone therapy use and mammographic
density in postmenopausal Norwegian women
bull Results differed when considering the combined effect of age and BMI
bull The effect of EPT on mammographic density was modified by age and BMI with no apparent association among the youngest women (aged 50-55) with the highest BMI (BMI ge 26)
bull A higher mammographic density was found in EPT users compared to never HT users particularly in women using high-dose NETA regimens Age and BMI modified the association between EPT use and mammographic density
bull Couto E et al Breast Cancer Res Treat 2011 Nov 4 [Epub ahead of print]
Breast Cancer Risk by Breast Density
Menopause and Postmenopausal Hormone
Therapy Use
Birads age HT Duration Risk
1 55-59 None 5 year risk 08 (95 CI 06- 09)
1 55-59
ET EPT 5 year risk 09 (95 CI 07 -11)
4 55-59
None 5 year risk 24 (95 CI 20 -28)
4 55-59
ET 5 year risk
30 (95 CI 26 -35)
4 55-59
EPT 5 year risk
42 (95 CI 37 -46)
Adapted from Kerlikowske et al JOURNAL OF CLINICAL ONCOLOGY 2010
Breast Cancer Risk by Breast Density
Menopause and Postmenopausal Hormone
Therapy Use
Adapted from Kerlikowske et al JOURNAL OF CLINICAL ONCOLOGY 2010
bull Postmenopausal women with high breast density are at increased risk of breast cancer and should be aware of the added risk of taking HT especially estrogen plus progestin
Medical condition which may be exacerbated by treatment
with progestins
Diabetes and metabolic syndrome
bull progestin-containing HT may be associated with increases in insulin resistance and deterioration in glucose tolerance123
bull Postmenopausal women with diabetes could be inappropriate for treatment with progestin-containing HT due to the potential risk of exacerbation of their condition
1) Panay N amp Studd JWW Human Reprod Update 1997
2) Godsland I et al Metabolism 1993
3) Sites CK et al J Clin Endocrinol Metab 2005
A Nath and R Sitruk-Ware CLIMACTERIC 200912(Suppl 1)96ndash101
A Nath and R Sitruk-Ware CLIMACTERIC 200912(Suppl 1)96ndash101
Diabetes an epidemy
bull UK 1996 14 million of diabetics
bull UK 2015 32 million (6 of the population)
bull UK 2025 5 million
bull httpwwwdiabetescoukdiabetes-prevalencehtml
Other progestin-related intolerance issues
bull Nausea
bull Depressive mood
bull Poor concentration
bull Hirsutism
bull Headache
bull Dizziness
bull Fluid retention
bull Weight gain Panay N amp Studd JWW Human Reprod Update 1997
Medical condition which may be exacerbated by treatment with progestins
PMSPMDDdepression
bull Progesterone-induced PMD can be exacerbated by exogenous progestin administration and can occur in association with HT or OC administration1
bull Significantly higher negative mood scores have been observed during the addition of a progestin to an estrogen in a sequential HT regimen in postmenopausal women with a history of PMS compared to those without2
bull Women with a history of PMS or PMD exacerbation of depression using progestins may therefore benefit from a progestin free treatment for menopausal symptoms
1) Nevatte T et al Arch Womens Ment Health 2013 2) Bjoumlrn I et al Climacteric 2006 PMS premenstrual syndrome
PMDD premenstrual dysphoric disorder
Conclusion
bull CEEBAZO is an additional regimen for menopausal symptoms it provides also a prevention for osteoporosis
bull It is suitable for women with a uterus who are unsatisfied with an EPT regimen or who you are unwilling to treat with an EPT regimen
For some postmenopausal women with a uterus there is a
need for progestin free treatment options
bull with demonstrated clinical efficacy
bull which protects the endometrium
bull improved tolerabilitysafety profile
In clinical practice this translates to women who are
intolerant of progestin-containing HT or have conditions
which may be exacerbated by treatment with progestins
Conclusion Medical need for alternative treatment option
Medical condition which may be exacerbated by treatment with progestins
Depression
bull Progestin-containing HT has been associated with increases in depressive symptoms in some individuals1
bull There is a biochemicalphysiological plausibility for the association of progestins with depression234
bull Therefore postmenopausal women who also have a medical history of depressive disorders or depression could be inappropriate for treatment with progestin-containing HT
Pfizer Confidential
65
1) Girdler SS et al J Womens Health Gend Based Med 1999 2) Traish AM et al Korean J Urol 2014 3) Stroumlhle A et al Biol Psychiatry 1999 4) Romeo E et
al Am J Psychiatry 1998
History of the following conditions may make progestin inappropriate
bull Depression
bull PMSPMDD
PMS premenstrual syndrome
PMD premenstrual dysphoric disorder
Medical conditions that may be exacerbated by treatment with progestins
Women for whom progestin-containing HT
would not be considered appropriate
minus Women who are intolerant of progestin-containing hormone therapy
minus Women with pre-existing medical conditions that may be exacerbated by progestins
Most common adverse events leading to discontinuation are related to progestins12
breakthrough bleeding
bull Increase in the number of uterine procedures (ie unnecessary endometrial biopsies)
breast paintenderness
bull Increase in the number of breast interventions
1 Steel SA et al Climacteric 2003 2 Ettinger B and Pressman A Am J Manag Care 1999 3 Komm BS Mirkin S
Pharmaceuticals 2012
4 Panay N amp Studd JWW Human Reprod Update 1997
bull Nausea bull Depressive mood bull Poor concentration bull Hirsutism bull Headache bull Dizziness bull Fluid retention bull Weight gain
Other progestin-related intolerance issues4
Unmet need with the treatment of postmenopausal symptoms
bull Alternatives to progestin are needed that will protect the endometrium while avoiding other progestin-associated effects and preserving the desired effects of estrogens in postmenopausal women3
Which women with a uterus could benefit from
estrogens without the need for a progestin
bull Women who are intolerant of progestin-containing hormone therapy
bull Women with pre-existing medical conditions that may be exacerbated by progestins (eg women with a history of depression PMSPMDD increased breast density diabetes and metabolic syndrome)
History of the following conditions may make progestin inappropriate
bull Depression
bull PMSPMDD
bull High breast density
bull Diabetes and metabolic syndrome
PMS premenstrual syndrome
PMD premenstrual dysphoric disorder
Medical conditions that may be exacerbated by treatment with progestins
Learning from WHI data
bull Hormone therapy (HT) is the conventional and established therapy option to effectively treat postmenopausal symptoms however it has been associated with some safety and tolerability concerns1 2
bull A review of WHI data suggests that many of the concerns with menopausal HT more often associated with EPT (CE+MPA) such as CHD risk increased breast density breast pain and breast cancer risk than with ET (CEE alone)2
1 Rolnick SJ Kopher RA DeFor TA et al Menopause 2005
2 Komm BS Mirkin S Pharmaceuticals 2012
WHI Womenrsquos Health Initiative trial
CHD coronary heart disease
CEE conjugated equine estrogens
Efficacy and Safety of Constant Oestrogen
Pulsed Progestogen vs
Continuous Combined HRT
Adverse Events
17b-oestradiol 17b-oestradiol norgestimate NETA (n = 150) (n = 172) Breast discomfort 14 27 Abdominal discomfort 14 22 Uterine bleeding 15 12 Dysmenorrhea 3 8 Oedema 5 8
Adapted from S Rozenberg et al Human Reproduction 2000
Medical condition which may be exacerbated by treatment
with progestins
Increased breast density
bull Increases in breast density are associated with progestin-containing HT which may adversely affect radiological detection of breast cancer1 and may be independently associated with an increased risk for the development of breast cancer2
bull The Postmenopausal EstrogenProgestin Interventions (PEPI) trial demonstrated that an increased mammographic breast density was associated with the use of E+P but not with the use of estrogen alone3
bull Women who already have high breast density may therefore be considered inappropriate for treatment with a progestin-containing HT
1) EU Core SPC for Hormone Replacement Therapy Products (CMDh1312003 Rev 4 June
2012)
2) De Villiers TJ et al on behalf of the International Menopause Society Climacteric 2013 16
3) Greendale GA et al J Natl Cancer Inst 2003
Stroke
0 25 5 75 10 125
Fractures
Diabetes
Breast cancer
Cholecystitis
Venothrombotic episodes
Endometrial cancer
Lung cancer
Coronary heart disease
Colorectal cancer
Overall mortality
15 125 10 75 5 25
Benefits Risks
CE
CE MPA
Santen RJ et al J Clin Endocrinol Metab 2010
The basis of the Endocrine Society scientific statement for postmenopausal hormone replacement therapy (HRT) excess risks and benefits of HRT for 5 years in women aged 50ndash59 years or within 10 years of the start of menopause E=estrogen P=progestin
bull Younger women (aged 50ndash59 years) had more favorable results bull There are differences between CE alone and CEMPA arms bull Overall benefitrisk ratio of CE-alone appears to be more favourable than CEMPA
Reevaluation of WHI data (stratified by age) Risks and
Benefits of HRT Cases per 1000 Women per 5 Years of
Use
Medical condition which may be exacerbated by treatment
with progestins
Diabetes and metabolic syndrome
bull Treatment of oestrogen deficiency symptoms with progestin-containing HT (unlike oestrogen alone) may be associated with increases in insulin resistance and deterioration in glucose tolerance123
bull Postmenopausal women with diabetes could be inappropriate for treatment with progestin-containing HT due to the potential risk of exacerbation of their condition
1) Panay N amp Studd JWW Human Reprod Update 1997
2) Godsland I et al Metabolism 1993
3) Sites CK et al J Clin Endocrinol Metab 2005
Variations in Associated Breast Cancer
Risks Between CE alone and CEMPA
bull Use of CE alone for a median of 59 years was associated with a lower incidence of invasive breast cancer (151 cases 027 per year) compared with placebo (199 cases 035 per year HR 077 95 CI 062ndash095 P=002)
bull In the CE alone group fewer women died from invasive breast cancer (6 deaths 0009 per year) compared with controls (16 deaths 0024 per year HR 037 95 CI 013ndash091 P=003)
Anderson GL et al Lancet
Oncol 2012
Bazedoxifene (BZA) specifically selected in
combination with conjugated estrogens
bull BZA has been specifically selected for its unique pharmacologic profile and effects on VMS and uterine tissue in particular123
1 Crabtree J et al Mol Cell Endocrinol 2008
2 Kharode Y et al Endocrinolology 2008
3 Duavive SmPC
Estrogen Receptor activity is dimmed
Estrogen Receptor activity is turned on
CEs are agonists BZA is an antagonist
In the uterus
bull The BZA component reduces the risk of endometrial hyperplasia that can occur with the conjugated estrogens component alone3 This means that progestins are not needed
Extensive global clinical development program for
CEBZA
aIncludes additional pilot dose-finding study 203 1 Lobo RA et al Fertil Steril 2009 2 Pinkerton JV et al Menopause 2009 3 Kagan R et al Menopause 2010 4 Mirkin S et al Climacteric 2013 5 Pinkerton JV et al Obstet Gynecol 2013
Effects of conjugated estrogensbazedoxifene on
lipid and coagulation variables a randomized
placebo- and active-controlled trial
bull At 12 months
bull Both CEBZA doses were associated with small but significant effects on hemostasis variables including reductions in antithrombin plasminogen activator inhibitor-1 and fibrinogen activity and an increase in plasminogen activity relative to placebo at 12 months Incidences of cardiovascular and venous thromboembolic events were similar among treatment groups
bull CONCLUSIONS
bull This study provides reassurance that CEBZA does not adversely affect lipid metabolism or hemostatic balance In accordance the incidences of venous thromboembolic events and cardiovascular events in postmenopausal women are similar to those observed with placebo

Effects of conjugated estrogensbazedoxifene on
lipid and coagulation variables a randomized
placebo- and active-controlled trial
bull postmenopausal women (N = 1843) with menopausal
symptoms
bull Lipid (N = 1843) and coagulation (N = 590) variables were assessed in women receiving daily CE 045 mgBZA 20 mg CE 0625 mgBZA 20 mg BZA 20 mg CE 045 mgmedroxyprogesterone acetate (MPA) 15 mg or placebo for 12 months
bull Skouby SO et al Menopause 2015 Jun22(6)640-9
Effects of conjugated estrogensbazedoxifene on
lipid and coagulation variables a randomized
placebo- and active-controlled trial
bull At 12 months
bull CE 045 mgBZA 20 mg
bull CE 0625 mgBZA 20 mg
bull BZA 20 mg
bull and CE 045 mgMPA 15 mg decreased total cholesterol and LDL- cholesterol vs placebo (P lt 001 for all)
bull Both CEBZA doses and CEMPA increased high-density lipoprotein cholesterol compared with placebo (P lt 005 for all)
bull CE 045 mgBZA 20 mg had a neutral effect on triglycerides
bull CE 0625 mgBZA 20 mg and CEMPA increased triglycerides compared with placebo (P lt 005)
bull Skouby SO et al Menopause 2015 Jun22(6)640-9
Effects of conjugated estrogensbazedoxifene on
lipid and coagulation variables a randomized
placebo- and active-controlled trial
bull At 12 months
bull Both CEBZA doses were associated with small but significant effects on hemostasis variables including reductions in antithrombin plasminogen activator inhibitor-1 and fibrinogen activity and an increase in plasminogen activity relative to placebo at 12 months Incidences of cardiovascular and venous thromboembolic events were similar among treatment groups
Skouby SO et al Menopause 2015
Jun22(6)640-9
Endometrial hyperplasia or malignancy occurred in lt1 of women
following up to 1 year of treatment with CEBZA12
Study Cumulative Incidence at month 12 (nN)
CE 045BZA 20 Placebo
SMART-11 000 (0336) 000 (0313)
SMART-52 030 (1335) 028 (1354)
Effects on the Endometrium
1 Pickar JH et al Fertil Steril 2009 2 Pinkerton at al J Clin Endocrinol Metab 2014
Through the eyes of an amazone
Marie Mandy
Breast tolerability profile similar to placebo following up to 2 years of treatment with CEBZA12
Pooled analysis of SMART clinical trials
CE 045BZA 20 (n=1585)
Placebo (n=1241)
Breast cancer incidence up to 2 years
(per 1000 woman-years)
100 (CI 000-321)
140 (CI 000-417)
Incidence of reported breast paintenderness up to 12 weeks
98-115 81-112
Incidence of abnormal mammogram at month 12
258 316
Mean change in breast density at month 12 (SMART-5)
ndash038 (n=186)
ndash032 (n=182)
Effects on the Breast
1 Pickar JH et al Menopause 2013 2 Pinkerton JV et al Obstet Gynecol 2013
CEBZA clinical overview - summary
bull In clinical trials CEBZA has demonstrated safety and efficacy in postmenopausal women with a uterus including the following
bull Significant reduction in number and severity of moderate to severe hot flushes1
bull Incidence of cumulative amenorrhea rate similar to placebo and significantly better than CEMPA2
bull Incidence of endometrial hyperplasia and breast tendernessdensity similar to that with placebo345
bull Incidence of adverse events and discontinuation rates similar to that with placebo6
1 Pinkerton JV et al Menopause 2009 2 Pinkerton JV et al J Clin Endocrinol Metab2014 3 Pickar JH et al
Fertil Steril 2009 4 Pinkerton at al J Clin Endocrinol Metab 2014 5 Pickar JH et al Menopause 2013 6 DUAVEE [package insert] New York NY Pfizer Inc 2013
CEBZA clinical overview - summary
Now women with a uterus who choose hormone therapy for management of menopausal symptoms have a choice
bull conventional estrogen-progestogen therapy or
bull a new combinationhellipconjugated estrogens paired with the SERM bazedoxifene
1 Pinkerton JV et al Menopause 2009 2 Pinkerton JV et al J Clin Endocrinol Metab2014 3 Pickar JH et al Fertil Steril 2009 4 Pinkerton at al J Clin Endocrinol Metab 2014 5 Pickar JH et al Menopause 2013 6 DUAVEE [package insert] New York NY Pfizer Inc 2013
Conjugated EstrogensBazedoxifene (CEBZA)
US indication
bull DUAVEE is indicated in women with a uterus for
bull 11 Treatment of Moderate to Severe Vasomotor Symptoms Associated with Menopause
bull 12 Prevention of Postmenopausal Osteoporosis
bull 13 Important Limitations of Use
bull Use DUAVEE for the shortest duration consistent with treatment goals and risks for the individual woman Postmenopausal women should be re-evaluated periodically as clinically appropriate to determine if treatment is still necessary
bull When prescribing solely for the prevention of postmenopausal osteoporosis therapy should only be considered for women at significant risk of osteoporosis and non-estrogen medication should be carefully considered
Conjugated EstrogensBazedoxifene (CEBZA)
EU indication
CEBZA is indicated for
bull Treatment of oestrogen deficiency symptoms in postmenopausal women with a uterus (with at least 12 months since the last menses) for whom treatment with progestin-containing therapy is not appropriate
bull The experience treating women older than 65 years is limited
bull Dose CE (045mg)Bazedoxifene (20mg)
Duavive SmPC
Which women with a uterus
could benefit from estrogens
without the need for a
progestin
Progestin intolerance is one of the main
factors for reduced compliance
bull About 20 of women receiving progestin-containing HT have significant progestin intolerance and half of these experience serious effects that prevent treatment continuation1
1 Panay N amp Studd J Human Reprod Update 1997
2 Panay N et al on behalf of the British Menopause Society and Womenrsquos Health Concern Menopause Int 2013
bull The 2013 British Menopause Society amp Womenrsquos Health
Concern recommendations on hormone replacement
therapy do recognise progestin intolerance as one of the
main factors for reduced compliance with HT 2
Proportion of patients () with at least one bleeding episode in relation to time and to the
used HT
Serge Rozenberg et al Hum Reprod 2009241739-1747
copy The Author 2009 Published by Oxford University Press on behalf of the European Society of
Human Reproduction and Embryology All rights reserved For Permissions please email
journalspermissionsoxfordjournalsorg
Breast tenderness after initiation of CEE
CEE + MPA (WHI)
and mammographic density change
bullCrandall et al Breast Cancer Res Treat DOI 101007s10549-011-1803-9
Breast density
Conclusion
bull CEEBAZO is an additional regimen for menopausal symptoms it provides also a prevention for osteoporosis
bull It is suitable for women with a uterus who are unsatisfied with an EPT regimen or who you are unwilling to treat with an EPT regimen
Adapted use of MHT
bull Lower dosage of estrogens
bull Other progestins
bull Better safety profile
bull Vaginal estrogen or SERMS
bull Non-hormonal therapy
bull Development of new products
bull SERMS + estrogens
Most common adverse events leading to
discontinuation are related to progestins12
bull breakthrough bleeding
bull Low compliance
bull Increase in the number of US
bull Stress
bull Cost
bull uterine procedures
bull Unnecessary endometrial biopsies Hysteroscopies DampC Hysterectomies
bull Morbidity
Proportion of patients who completed or discontinued treatment in relation to the used HT
Serge Rozenberg et al Hum Reprod 2009241739-1747
copy The Author 2009 Published by Oxford University Press on behalf of the European Society of
Human Reproduction and Embryology All rights reserved For Permissions please email
journalspermissionsoxfordjournalsorg
Most common adverse events leading to discontinuation
are related to progestins
bull breast paintenderness
Breast tenderness after initiation of CEE
CEE + MPA (WHI)
and mammographic density change
bullCrandall et al Breast Cancer Res Treat DOI 101007s10549-011-1803-9
Breast density
Hormone therapy use and mammographic
density in postmenopausal Norwegian women
bull Results differed when considering the combined effect of age and BMI
bull The effect of EPT on mammographic density was modified by age and BMI with no apparent association among the youngest women (aged 50-55) with the highest BMI (BMI ge 26)
bull A higher mammographic density was found in EPT users compared to never HT users particularly in women using high-dose NETA regimens Age and BMI modified the association between EPT use and mammographic density
bull Couto E et al Breast Cancer Res Treat 2011 Nov 4 [Epub ahead of print]
Breast Cancer Risk by Breast Density
Menopause and Postmenopausal Hormone
Therapy Use
Birads age HT Duration Risk
1 55-59 None 5 year risk 08 (95 CI 06- 09)
1 55-59
ET EPT 5 year risk 09 (95 CI 07 -11)
4 55-59
None 5 year risk 24 (95 CI 20 -28)
4 55-59
ET 5 year risk
30 (95 CI 26 -35)
4 55-59
EPT 5 year risk
42 (95 CI 37 -46)
Adapted from Kerlikowske et al JOURNAL OF CLINICAL ONCOLOGY 2010
Breast Cancer Risk by Breast Density
Menopause and Postmenopausal Hormone
Therapy Use
Adapted from Kerlikowske et al JOURNAL OF CLINICAL ONCOLOGY 2010
bull Postmenopausal women with high breast density are at increased risk of breast cancer and should be aware of the added risk of taking HT especially estrogen plus progestin
Medical condition which may be exacerbated by treatment
with progestins
Diabetes and metabolic syndrome
bull progestin-containing HT may be associated with increases in insulin resistance and deterioration in glucose tolerance123
bull Postmenopausal women with diabetes could be inappropriate for treatment with progestin-containing HT due to the potential risk of exacerbation of their condition
1) Panay N amp Studd JWW Human Reprod Update 1997
2) Godsland I et al Metabolism 1993
3) Sites CK et al J Clin Endocrinol Metab 2005
A Nath and R Sitruk-Ware CLIMACTERIC 200912(Suppl 1)96ndash101
A Nath and R Sitruk-Ware CLIMACTERIC 200912(Suppl 1)96ndash101
Diabetes an epidemy
bull UK 1996 14 million of diabetics
bull UK 2015 32 million (6 of the population)
bull UK 2025 5 million
bull httpwwwdiabetescoukdiabetes-prevalencehtml
Other progestin-related intolerance issues
bull Nausea
bull Depressive mood
bull Poor concentration
bull Hirsutism
bull Headache
bull Dizziness
bull Fluid retention
bull Weight gain Panay N amp Studd JWW Human Reprod Update 1997
Medical condition which may be exacerbated by treatment with progestins
PMSPMDDdepression
bull Progesterone-induced PMD can be exacerbated by exogenous progestin administration and can occur in association with HT or OC administration1
bull Significantly higher negative mood scores have been observed during the addition of a progestin to an estrogen in a sequential HT regimen in postmenopausal women with a history of PMS compared to those without2
bull Women with a history of PMS or PMD exacerbation of depression using progestins may therefore benefit from a progestin free treatment for menopausal symptoms
1) Nevatte T et al Arch Womens Ment Health 2013 2) Bjoumlrn I et al Climacteric 2006 PMS premenstrual syndrome
PMDD premenstrual dysphoric disorder
Conclusion
bull CEEBAZO is an additional regimen for menopausal symptoms it provides also a prevention for osteoporosis
bull It is suitable for women with a uterus who are unsatisfied with an EPT regimen or who you are unwilling to treat with an EPT regimen
For some postmenopausal women with a uterus there is a
need for progestin free treatment options
bull with demonstrated clinical efficacy
bull which protects the endometrium
bull improved tolerabilitysafety profile
In clinical practice this translates to women who are
intolerant of progestin-containing HT or have conditions
which may be exacerbated by treatment with progestins
Conclusion Medical need for alternative treatment option
Medical condition which may be exacerbated by treatment with progestins
Depression
bull Progestin-containing HT has been associated with increases in depressive symptoms in some individuals1
bull There is a biochemicalphysiological plausibility for the association of progestins with depression234
bull Therefore postmenopausal women who also have a medical history of depressive disorders or depression could be inappropriate for treatment with progestin-containing HT
Pfizer Confidential
65
1) Girdler SS et al J Womens Health Gend Based Med 1999 2) Traish AM et al Korean J Urol 2014 3) Stroumlhle A et al Biol Psychiatry 1999 4) Romeo E et
al Am J Psychiatry 1998
History of the following conditions may make progestin inappropriate
bull Depression
bull PMSPMDD
PMS premenstrual syndrome
PMD premenstrual dysphoric disorder
Medical conditions that may be exacerbated by treatment with progestins
Women for whom progestin-containing HT
would not be considered appropriate
minus Women who are intolerant of progestin-containing hormone therapy
minus Women with pre-existing medical conditions that may be exacerbated by progestins
Most common adverse events leading to discontinuation are related to progestins12
breakthrough bleeding
bull Increase in the number of uterine procedures (ie unnecessary endometrial biopsies)
breast paintenderness
bull Increase in the number of breast interventions
1 Steel SA et al Climacteric 2003 2 Ettinger B and Pressman A Am J Manag Care 1999 3 Komm BS Mirkin S
Pharmaceuticals 2012
4 Panay N amp Studd JWW Human Reprod Update 1997
bull Nausea bull Depressive mood bull Poor concentration bull Hirsutism bull Headache bull Dizziness bull Fluid retention bull Weight gain
Other progestin-related intolerance issues4
Unmet need with the treatment of postmenopausal symptoms
bull Alternatives to progestin are needed that will protect the endometrium while avoiding other progestin-associated effects and preserving the desired effects of estrogens in postmenopausal women3
Which women with a uterus could benefit from
estrogens without the need for a progestin
bull Women who are intolerant of progestin-containing hormone therapy
bull Women with pre-existing medical conditions that may be exacerbated by progestins (eg women with a history of depression PMSPMDD increased breast density diabetes and metabolic syndrome)
History of the following conditions may make progestin inappropriate
bull Depression
bull PMSPMDD
bull High breast density
bull Diabetes and metabolic syndrome
PMS premenstrual syndrome
PMD premenstrual dysphoric disorder
Medical conditions that may be exacerbated by treatment with progestins
Learning from WHI data
bull Hormone therapy (HT) is the conventional and established therapy option to effectively treat postmenopausal symptoms however it has been associated with some safety and tolerability concerns1 2
bull A review of WHI data suggests that many of the concerns with menopausal HT more often associated with EPT (CE+MPA) such as CHD risk increased breast density breast pain and breast cancer risk than with ET (CEE alone)2
1 Rolnick SJ Kopher RA DeFor TA et al Menopause 2005
2 Komm BS Mirkin S Pharmaceuticals 2012
WHI Womenrsquos Health Initiative trial
CHD coronary heart disease
CEE conjugated equine estrogens
Efficacy and Safety of Constant Oestrogen
Pulsed Progestogen vs
Continuous Combined HRT
Adverse Events
17b-oestradiol 17b-oestradiol norgestimate NETA (n = 150) (n = 172) Breast discomfort 14 27 Abdominal discomfort 14 22 Uterine bleeding 15 12 Dysmenorrhea 3 8 Oedema 5 8
Adapted from S Rozenberg et al Human Reproduction 2000
Medical condition which may be exacerbated by treatment
with progestins
Increased breast density
bull Increases in breast density are associated with progestin-containing HT which may adversely affect radiological detection of breast cancer1 and may be independently associated with an increased risk for the development of breast cancer2
bull The Postmenopausal EstrogenProgestin Interventions (PEPI) trial demonstrated that an increased mammographic breast density was associated with the use of E+P but not with the use of estrogen alone3
bull Women who already have high breast density may therefore be considered inappropriate for treatment with a progestin-containing HT
1) EU Core SPC for Hormone Replacement Therapy Products (CMDh1312003 Rev 4 June
2012)
2) De Villiers TJ et al on behalf of the International Menopause Society Climacteric 2013 16
3) Greendale GA et al J Natl Cancer Inst 2003
Stroke
0 25 5 75 10 125
Fractures
Diabetes
Breast cancer
Cholecystitis
Venothrombotic episodes
Endometrial cancer
Lung cancer
Coronary heart disease
Colorectal cancer
Overall mortality
15 125 10 75 5 25
Benefits Risks
CE
CE MPA
Santen RJ et al J Clin Endocrinol Metab 2010
The basis of the Endocrine Society scientific statement for postmenopausal hormone replacement therapy (HRT) excess risks and benefits of HRT for 5 years in women aged 50ndash59 years or within 10 years of the start of menopause E=estrogen P=progestin
bull Younger women (aged 50ndash59 years) had more favorable results bull There are differences between CE alone and CEMPA arms bull Overall benefitrisk ratio of CE-alone appears to be more favourable than CEMPA
Reevaluation of WHI data (stratified by age) Risks and
Benefits of HRT Cases per 1000 Women per 5 Years of
Use
Medical condition which may be exacerbated by treatment
with progestins
Diabetes and metabolic syndrome
bull Treatment of oestrogen deficiency symptoms with progestin-containing HT (unlike oestrogen alone) may be associated with increases in insulin resistance and deterioration in glucose tolerance123
bull Postmenopausal women with diabetes could be inappropriate for treatment with progestin-containing HT due to the potential risk of exacerbation of their condition
1) Panay N amp Studd JWW Human Reprod Update 1997
2) Godsland I et al Metabolism 1993
3) Sites CK et al J Clin Endocrinol Metab 2005
Variations in Associated Breast Cancer
Risks Between CE alone and CEMPA
bull Use of CE alone for a median of 59 years was associated with a lower incidence of invasive breast cancer (151 cases 027 per year) compared with placebo (199 cases 035 per year HR 077 95 CI 062ndash095 P=002)
bull In the CE alone group fewer women died from invasive breast cancer (6 deaths 0009 per year) compared with controls (16 deaths 0024 per year HR 037 95 CI 013ndash091 P=003)
Anderson GL et al Lancet
Oncol 2012
Bazedoxifene (BZA) specifically selected in
combination with conjugated estrogens
bull BZA has been specifically selected for its unique pharmacologic profile and effects on VMS and uterine tissue in particular123
1 Crabtree J et al Mol Cell Endocrinol 2008
2 Kharode Y et al Endocrinolology 2008
3 Duavive SmPC
Estrogen Receptor activity is dimmed
Estrogen Receptor activity is turned on
CEs are agonists BZA is an antagonist
In the uterus
bull The BZA component reduces the risk of endometrial hyperplasia that can occur with the conjugated estrogens component alone3 This means that progestins are not needed
Extensive global clinical development program for
CEBZA
aIncludes additional pilot dose-finding study 203 1 Lobo RA et al Fertil Steril 2009 2 Pinkerton JV et al Menopause 2009 3 Kagan R et al Menopause 2010 4 Mirkin S et al Climacteric 2013 5 Pinkerton JV et al Obstet Gynecol 2013
Effects of conjugated estrogensbazedoxifene on
lipid and coagulation variables a randomized
placebo- and active-controlled trial
bull At 12 months
bull Both CEBZA doses were associated with small but significant effects on hemostasis variables including reductions in antithrombin plasminogen activator inhibitor-1 and fibrinogen activity and an increase in plasminogen activity relative to placebo at 12 months Incidences of cardiovascular and venous thromboembolic events were similar among treatment groups
bull CONCLUSIONS
bull This study provides reassurance that CEBZA does not adversely affect lipid metabolism or hemostatic balance In accordance the incidences of venous thromboembolic events and cardiovascular events in postmenopausal women are similar to those observed with placebo

Effects of conjugated estrogensbazedoxifene on
lipid and coagulation variables a randomized
placebo- and active-controlled trial
bull At 12 months
bull CE 045 mgBZA 20 mg
bull CE 0625 mgBZA 20 mg
bull BZA 20 mg
bull and CE 045 mgMPA 15 mg decreased total cholesterol and LDL- cholesterol vs placebo (P lt 001 for all)
bull Both CEBZA doses and CEMPA increased high-density lipoprotein cholesterol compared with placebo (P lt 005 for all)
bull CE 045 mgBZA 20 mg had a neutral effect on triglycerides
bull CE 0625 mgBZA 20 mg and CEMPA increased triglycerides compared with placebo (P lt 005)
bull Skouby SO et al Menopause 2015 Jun22(6)640-9
Effects of conjugated estrogensbazedoxifene on
lipid and coagulation variables a randomized
placebo- and active-controlled trial
bull At 12 months
bull Both CEBZA doses were associated with small but significant effects on hemostasis variables including reductions in antithrombin plasminogen activator inhibitor-1 and fibrinogen activity and an increase in plasminogen activity relative to placebo at 12 months Incidences of cardiovascular and venous thromboembolic events were similar among treatment groups
Skouby SO et al Menopause 2015
Jun22(6)640-9
Endometrial hyperplasia or malignancy occurred in lt1 of women
following up to 1 year of treatment with CEBZA12
Study Cumulative Incidence at month 12 (nN)
CE 045BZA 20 Placebo
SMART-11 000 (0336) 000 (0313)
SMART-52 030 (1335) 028 (1354)
Effects on the Endometrium
1 Pickar JH et al Fertil Steril 2009 2 Pinkerton at al J Clin Endocrinol Metab 2014
Through the eyes of an amazone
Marie Mandy
Breast tolerability profile similar to placebo following up to 2 years of treatment with CEBZA12
Pooled analysis of SMART clinical trials
CE 045BZA 20 (n=1585)
Placebo (n=1241)
Breast cancer incidence up to 2 years
(per 1000 woman-years)
100 (CI 000-321)
140 (CI 000-417)
Incidence of reported breast paintenderness up to 12 weeks
98-115 81-112
Incidence of abnormal mammogram at month 12
258 316
Mean change in breast density at month 12 (SMART-5)
ndash038 (n=186)
ndash032 (n=182)
Effects on the Breast
1 Pickar JH et al Menopause 2013 2 Pinkerton JV et al Obstet Gynecol 2013
CEBZA clinical overview - summary
bull In clinical trials CEBZA has demonstrated safety and efficacy in postmenopausal women with a uterus including the following
bull Significant reduction in number and severity of moderate to severe hot flushes1
bull Incidence of cumulative amenorrhea rate similar to placebo and significantly better than CEMPA2
bull Incidence of endometrial hyperplasia and breast tendernessdensity similar to that with placebo345
bull Incidence of adverse events and discontinuation rates similar to that with placebo6
1 Pinkerton JV et al Menopause 2009 2 Pinkerton JV et al J Clin Endocrinol Metab2014 3 Pickar JH et al
Fertil Steril 2009 4 Pinkerton at al J Clin Endocrinol Metab 2014 5 Pickar JH et al Menopause 2013 6 DUAVEE [package insert] New York NY Pfizer Inc 2013
CEBZA clinical overview - summary
Now women with a uterus who choose hormone therapy for management of menopausal symptoms have a choice
bull conventional estrogen-progestogen therapy or
bull a new combinationhellipconjugated estrogens paired with the SERM bazedoxifene
1 Pinkerton JV et al Menopause 2009 2 Pinkerton JV et al J Clin Endocrinol Metab2014 3 Pickar JH et al Fertil Steril 2009 4 Pinkerton at al J Clin Endocrinol Metab 2014 5 Pickar JH et al Menopause 2013 6 DUAVEE [package insert] New York NY Pfizer Inc 2013
Conjugated EstrogensBazedoxifene (CEBZA)
US indication
bull DUAVEE is indicated in women with a uterus for
bull 11 Treatment of Moderate to Severe Vasomotor Symptoms Associated with Menopause
bull 12 Prevention of Postmenopausal Osteoporosis
bull 13 Important Limitations of Use
bull Use DUAVEE for the shortest duration consistent with treatment goals and risks for the individual woman Postmenopausal women should be re-evaluated periodically as clinically appropriate to determine if treatment is still necessary
bull When prescribing solely for the prevention of postmenopausal osteoporosis therapy should only be considered for women at significant risk of osteoporosis and non-estrogen medication should be carefully considered
Conjugated EstrogensBazedoxifene (CEBZA)
EU indication
CEBZA is indicated for
bull Treatment of oestrogen deficiency symptoms in postmenopausal women with a uterus (with at least 12 months since the last menses) for whom treatment with progestin-containing therapy is not appropriate
bull The experience treating women older than 65 years is limited
bull Dose CE (045mg)Bazedoxifene (20mg)
Duavive SmPC
Which women with a uterus
could benefit from estrogens
without the need for a
progestin
Progestin intolerance is one of the main
factors for reduced compliance
bull About 20 of women receiving progestin-containing HT have significant progestin intolerance and half of these experience serious effects that prevent treatment continuation1
1 Panay N amp Studd J Human Reprod Update 1997
2 Panay N et al on behalf of the British Menopause Society and Womenrsquos Health Concern Menopause Int 2013
bull The 2013 British Menopause Society amp Womenrsquos Health
Concern recommendations on hormone replacement
therapy do recognise progestin intolerance as one of the
main factors for reduced compliance with HT 2
Proportion of patients () with at least one bleeding episode in relation to time and to the
used HT
Serge Rozenberg et al Hum Reprod 2009241739-1747
copy The Author 2009 Published by Oxford University Press on behalf of the European Society of
Human Reproduction and Embryology All rights reserved For Permissions please email
journalspermissionsoxfordjournalsorg
Breast tenderness after initiation of CEE
CEE + MPA (WHI)
and mammographic density change
bullCrandall et al Breast Cancer Res Treat DOI 101007s10549-011-1803-9
Breast density
Conclusion
bull CEEBAZO is an additional regimen for menopausal symptoms it provides also a prevention for osteoporosis
bull It is suitable for women with a uterus who are unsatisfied with an EPT regimen or who you are unwilling to treat with an EPT regimen
Adapted use of MHT
bull Lower dosage of estrogens
bull Other progestins
bull Better safety profile
bull Vaginal estrogen or SERMS
bull Non-hormonal therapy
bull Development of new products
bull SERMS + estrogens
Most common adverse events leading to
discontinuation are related to progestins12
bull breakthrough bleeding
bull Low compliance
bull Increase in the number of US
bull Stress
bull Cost
bull uterine procedures
bull Unnecessary endometrial biopsies Hysteroscopies DampC Hysterectomies
bull Morbidity
Proportion of patients who completed or discontinued treatment in relation to the used HT
Serge Rozenberg et al Hum Reprod 2009241739-1747
copy The Author 2009 Published by Oxford University Press on behalf of the European Society of
Human Reproduction and Embryology All rights reserved For Permissions please email
journalspermissionsoxfordjournalsorg
Most common adverse events leading to discontinuation
are related to progestins
bull breast paintenderness
Breast tenderness after initiation of CEE
CEE + MPA (WHI)
and mammographic density change
bullCrandall et al Breast Cancer Res Treat DOI 101007s10549-011-1803-9
Breast density
Hormone therapy use and mammographic
density in postmenopausal Norwegian women
bull Results differed when considering the combined effect of age and BMI
bull The effect of EPT on mammographic density was modified by age and BMI with no apparent association among the youngest women (aged 50-55) with the highest BMI (BMI ge 26)
bull A higher mammographic density was found in EPT users compared to never HT users particularly in women using high-dose NETA regimens Age and BMI modified the association between EPT use and mammographic density
bull Couto E et al Breast Cancer Res Treat 2011 Nov 4 [Epub ahead of print]
Breast Cancer Risk by Breast Density
Menopause and Postmenopausal Hormone
Therapy Use
Birads age HT Duration Risk
1 55-59 None 5 year risk 08 (95 CI 06- 09)
1 55-59
ET EPT 5 year risk 09 (95 CI 07 -11)
4 55-59
None 5 year risk 24 (95 CI 20 -28)
4 55-59
ET 5 year risk
30 (95 CI 26 -35)
4 55-59
EPT 5 year risk
42 (95 CI 37 -46)
Adapted from Kerlikowske et al JOURNAL OF CLINICAL ONCOLOGY 2010
Breast Cancer Risk by Breast Density
Menopause and Postmenopausal Hormone
Therapy Use
Adapted from Kerlikowske et al JOURNAL OF CLINICAL ONCOLOGY 2010
bull Postmenopausal women with high breast density are at increased risk of breast cancer and should be aware of the added risk of taking HT especially estrogen plus progestin
Medical condition which may be exacerbated by treatment
with progestins
Diabetes and metabolic syndrome
bull progestin-containing HT may be associated with increases in insulin resistance and deterioration in glucose tolerance123
bull Postmenopausal women with diabetes could be inappropriate for treatment with progestin-containing HT due to the potential risk of exacerbation of their condition
1) Panay N amp Studd JWW Human Reprod Update 1997
2) Godsland I et al Metabolism 1993
3) Sites CK et al J Clin Endocrinol Metab 2005
A Nath and R Sitruk-Ware CLIMACTERIC 200912(Suppl 1)96ndash101
A Nath and R Sitruk-Ware CLIMACTERIC 200912(Suppl 1)96ndash101
Diabetes an epidemy
bull UK 1996 14 million of diabetics
bull UK 2015 32 million (6 of the population)
bull UK 2025 5 million
bull httpwwwdiabetescoukdiabetes-prevalencehtml
Other progestin-related intolerance issues
bull Nausea
bull Depressive mood
bull Poor concentration
bull Hirsutism
bull Headache
bull Dizziness
bull Fluid retention
bull Weight gain Panay N amp Studd JWW Human Reprod Update 1997
Medical condition which may be exacerbated by treatment with progestins
PMSPMDDdepression
bull Progesterone-induced PMD can be exacerbated by exogenous progestin administration and can occur in association with HT or OC administration1
bull Significantly higher negative mood scores have been observed during the addition of a progestin to an estrogen in a sequential HT regimen in postmenopausal women with a history of PMS compared to those without2
bull Women with a history of PMS or PMD exacerbation of depression using progestins may therefore benefit from a progestin free treatment for menopausal symptoms
1) Nevatte T et al Arch Womens Ment Health 2013 2) Bjoumlrn I et al Climacteric 2006 PMS premenstrual syndrome
PMDD premenstrual dysphoric disorder
Conclusion
bull CEEBAZO is an additional regimen for menopausal symptoms it provides also a prevention for osteoporosis
bull It is suitable for women with a uterus who are unsatisfied with an EPT regimen or who you are unwilling to treat with an EPT regimen
For some postmenopausal women with a uterus there is a
need for progestin free treatment options
bull with demonstrated clinical efficacy
bull which protects the endometrium
bull improved tolerabilitysafety profile
In clinical practice this translates to women who are
intolerant of progestin-containing HT or have conditions
which may be exacerbated by treatment with progestins
Conclusion Medical need for alternative treatment option
Medical condition which may be exacerbated by treatment with progestins
Depression
bull Progestin-containing HT has been associated with increases in depressive symptoms in some individuals1
bull There is a biochemicalphysiological plausibility for the association of progestins with depression234
bull Therefore postmenopausal women who also have a medical history of depressive disorders or depression could be inappropriate for treatment with progestin-containing HT
Pfizer Confidential
65
1) Girdler SS et al J Womens Health Gend Based Med 1999 2) Traish AM et al Korean J Urol 2014 3) Stroumlhle A et al Biol Psychiatry 1999 4) Romeo E et
al Am J Psychiatry 1998
History of the following conditions may make progestin inappropriate
bull Depression
bull PMSPMDD
PMS premenstrual syndrome
PMD premenstrual dysphoric disorder
Medical conditions that may be exacerbated by treatment with progestins
Women for whom progestin-containing HT
would not be considered appropriate
minus Women who are intolerant of progestin-containing hormone therapy
minus Women with pre-existing medical conditions that may be exacerbated by progestins
Most common adverse events leading to discontinuation are related to progestins12
breakthrough bleeding
bull Increase in the number of uterine procedures (ie unnecessary endometrial biopsies)
breast paintenderness
bull Increase in the number of breast interventions
1 Steel SA et al Climacteric 2003 2 Ettinger B and Pressman A Am J Manag Care 1999 3 Komm BS Mirkin S
Pharmaceuticals 2012
4 Panay N amp Studd JWW Human Reprod Update 1997
bull Nausea bull Depressive mood bull Poor concentration bull Hirsutism bull Headache bull Dizziness bull Fluid retention bull Weight gain
Other progestin-related intolerance issues4
Unmet need with the treatment of postmenopausal symptoms
bull Alternatives to progestin are needed that will protect the endometrium while avoiding other progestin-associated effects and preserving the desired effects of estrogens in postmenopausal women3
Which women with a uterus could benefit from
estrogens without the need for a progestin
bull Women who are intolerant of progestin-containing hormone therapy
bull Women with pre-existing medical conditions that may be exacerbated by progestins (eg women with a history of depression PMSPMDD increased breast density diabetes and metabolic syndrome)
History of the following conditions may make progestin inappropriate
bull Depression
bull PMSPMDD
bull High breast density
bull Diabetes and metabolic syndrome
PMS premenstrual syndrome
PMD premenstrual dysphoric disorder
Medical conditions that may be exacerbated by treatment with progestins
Learning from WHI data
bull Hormone therapy (HT) is the conventional and established therapy option to effectively treat postmenopausal symptoms however it has been associated with some safety and tolerability concerns1 2
bull A review of WHI data suggests that many of the concerns with menopausal HT more often associated with EPT (CE+MPA) such as CHD risk increased breast density breast pain and breast cancer risk than with ET (CEE alone)2
1 Rolnick SJ Kopher RA DeFor TA et al Menopause 2005
2 Komm BS Mirkin S Pharmaceuticals 2012
WHI Womenrsquos Health Initiative trial
CHD coronary heart disease
CEE conjugated equine estrogens
Efficacy and Safety of Constant Oestrogen
Pulsed Progestogen vs
Continuous Combined HRT
Adverse Events
17b-oestradiol 17b-oestradiol norgestimate NETA (n = 150) (n = 172) Breast discomfort 14 27 Abdominal discomfort 14 22 Uterine bleeding 15 12 Dysmenorrhea 3 8 Oedema 5 8
Adapted from S Rozenberg et al Human Reproduction 2000
Medical condition which may be exacerbated by treatment
with progestins
Increased breast density
bull Increases in breast density are associated with progestin-containing HT which may adversely affect radiological detection of breast cancer1 and may be independently associated with an increased risk for the development of breast cancer2
bull The Postmenopausal EstrogenProgestin Interventions (PEPI) trial demonstrated that an increased mammographic breast density was associated with the use of E+P but not with the use of estrogen alone3
bull Women who already have high breast density may therefore be considered inappropriate for treatment with a progestin-containing HT
1) EU Core SPC for Hormone Replacement Therapy Products (CMDh1312003 Rev 4 June
2012)
2) De Villiers TJ et al on behalf of the International Menopause Society Climacteric 2013 16
3) Greendale GA et al J Natl Cancer Inst 2003
Stroke
0 25 5 75 10 125
Fractures
Diabetes
Breast cancer
Cholecystitis
Venothrombotic episodes
Endometrial cancer
Lung cancer
Coronary heart disease
Colorectal cancer
Overall mortality
15 125 10 75 5 25
Benefits Risks
CE
CE MPA
Santen RJ et al J Clin Endocrinol Metab 2010
The basis of the Endocrine Society scientific statement for postmenopausal hormone replacement therapy (HRT) excess risks and benefits of HRT for 5 years in women aged 50ndash59 years or within 10 years of the start of menopause E=estrogen P=progestin
bull Younger women (aged 50ndash59 years) had more favorable results bull There are differences between CE alone and CEMPA arms bull Overall benefitrisk ratio of CE-alone appears to be more favourable than CEMPA
Reevaluation of WHI data (stratified by age) Risks and
Benefits of HRT Cases per 1000 Women per 5 Years of
Use
Medical condition which may be exacerbated by treatment
with progestins
Diabetes and metabolic syndrome
bull Treatment of oestrogen deficiency symptoms with progestin-containing HT (unlike oestrogen alone) may be associated with increases in insulin resistance and deterioration in glucose tolerance123
bull Postmenopausal women with diabetes could be inappropriate for treatment with progestin-containing HT due to the potential risk of exacerbation of their condition
1) Panay N amp Studd JWW Human Reprod Update 1997
2) Godsland I et al Metabolism 1993
3) Sites CK et al J Clin Endocrinol Metab 2005
Variations in Associated Breast Cancer
Risks Between CE alone and CEMPA
bull Use of CE alone for a median of 59 years was associated with a lower incidence of invasive breast cancer (151 cases 027 per year) compared with placebo (199 cases 035 per year HR 077 95 CI 062ndash095 P=002)
bull In the CE alone group fewer women died from invasive breast cancer (6 deaths 0009 per year) compared with controls (16 deaths 0024 per year HR 037 95 CI 013ndash091 P=003)
Anderson GL et al Lancet
Oncol 2012
Bazedoxifene (BZA) specifically selected in
combination with conjugated estrogens
bull BZA has been specifically selected for its unique pharmacologic profile and effects on VMS and uterine tissue in particular123
1 Crabtree J et al Mol Cell Endocrinol 2008
2 Kharode Y et al Endocrinolology 2008
3 Duavive SmPC
Estrogen Receptor activity is dimmed
Estrogen Receptor activity is turned on
CEs are agonists BZA is an antagonist
In the uterus
bull The BZA component reduces the risk of endometrial hyperplasia that can occur with the conjugated estrogens component alone3 This means that progestins are not needed
Extensive global clinical development program for
CEBZA
aIncludes additional pilot dose-finding study 203 1 Lobo RA et al Fertil Steril 2009 2 Pinkerton JV et al Menopause 2009 3 Kagan R et al Menopause 2010 4 Mirkin S et al Climacteric 2013 5 Pinkerton JV et al Obstet Gynecol 2013
Effects of conjugated estrogensbazedoxifene on
lipid and coagulation variables a randomized
placebo- and active-controlled trial
bull At 12 months
bull Both CEBZA doses were associated with small but significant effects on hemostasis variables including reductions in antithrombin plasminogen activator inhibitor-1 and fibrinogen activity and an increase in plasminogen activity relative to placebo at 12 months Incidences of cardiovascular and venous thromboembolic events were similar among treatment groups
bull CONCLUSIONS
bull This study provides reassurance that CEBZA does not adversely affect lipid metabolism or hemostatic balance In accordance the incidences of venous thromboembolic events and cardiovascular events in postmenopausal women are similar to those observed with placebo
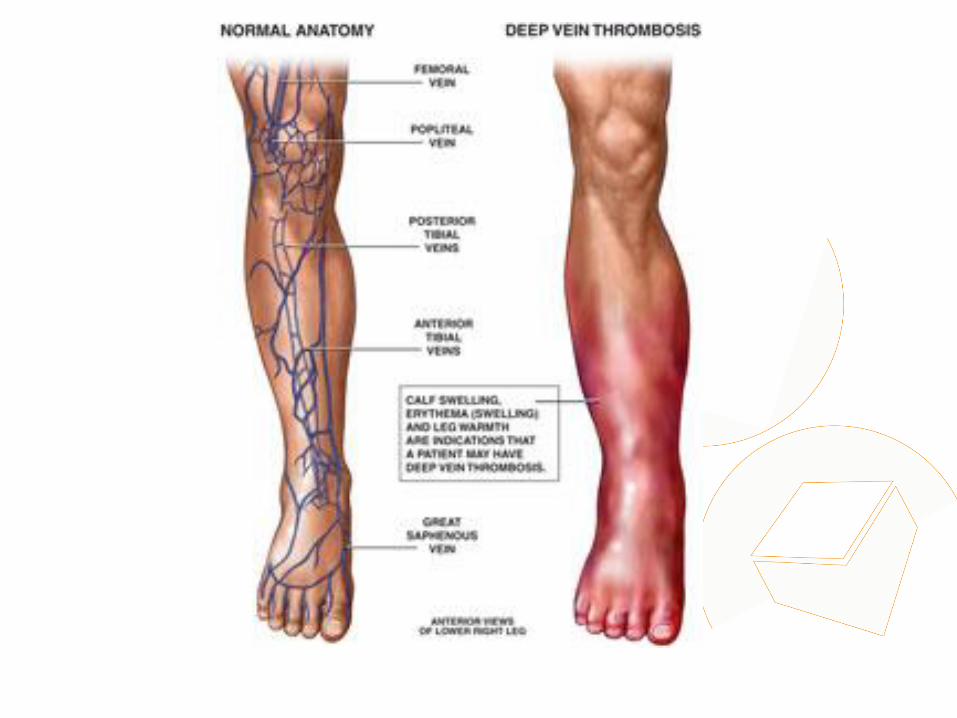
Effects of conjugated estrogensbazedoxifene on
lipid and coagulation variables a randomized
placebo- and active-controlled trial
bull At 12 months
bull Both CEBZA doses were associated with small but significant effects on hemostasis variables including reductions in antithrombin plasminogen activator inhibitor-1 and fibrinogen activity and an increase in plasminogen activity relative to placebo at 12 months Incidences of cardiovascular and venous thromboembolic events were similar among treatment groups
Skouby SO et al Menopause 2015
Jun22(6)640-9
Endometrial hyperplasia or malignancy occurred in lt1 of women
following up to 1 year of treatment with CEBZA12
Study Cumulative Incidence at month 12 (nN)
CE 045BZA 20 Placebo
SMART-11 000 (0336) 000 (0313)
SMART-52 030 (1335) 028 (1354)
Effects on the Endometrium
1 Pickar JH et al Fertil Steril 2009 2 Pinkerton at al J Clin Endocrinol Metab 2014
Through the eyes of an amazone
Marie Mandy
Breast tolerability profile similar to placebo following up to 2 years of treatment with CEBZA12
Pooled analysis of SMART clinical trials
CE 045BZA 20 (n=1585)
Placebo (n=1241)
Breast cancer incidence up to 2 years
(per 1000 woman-years)
100 (CI 000-321)
140 (CI 000-417)
Incidence of reported breast paintenderness up to 12 weeks
98-115 81-112
Incidence of abnormal mammogram at month 12
258 316
Mean change in breast density at month 12 (SMART-5)
ndash038 (n=186)
ndash032 (n=182)
Effects on the Breast
1 Pickar JH et al Menopause 2013 2 Pinkerton JV et al Obstet Gynecol 2013
CEBZA clinical overview - summary
bull In clinical trials CEBZA has demonstrated safety and efficacy in postmenopausal women with a uterus including the following
bull Significant reduction in number and severity of moderate to severe hot flushes1
bull Incidence of cumulative amenorrhea rate similar to placebo and significantly better than CEMPA2
bull Incidence of endometrial hyperplasia and breast tendernessdensity similar to that with placebo345
bull Incidence of adverse events and discontinuation rates similar to that with placebo6
1 Pinkerton JV et al Menopause 2009 2 Pinkerton JV et al J Clin Endocrinol Metab2014 3 Pickar JH et al
Fertil Steril 2009 4 Pinkerton at al J Clin Endocrinol Metab 2014 5 Pickar JH et al Menopause 2013 6 DUAVEE [package insert] New York NY Pfizer Inc 2013
CEBZA clinical overview - summary
Now women with a uterus who choose hormone therapy for management of menopausal symptoms have a choice
bull conventional estrogen-progestogen therapy or
bull a new combinationhellipconjugated estrogens paired with the SERM bazedoxifene
1 Pinkerton JV et al Menopause 2009 2 Pinkerton JV et al J Clin Endocrinol Metab2014 3 Pickar JH et al Fertil Steril 2009 4 Pinkerton at al J Clin Endocrinol Metab 2014 5 Pickar JH et al Menopause 2013 6 DUAVEE [package insert] New York NY Pfizer Inc 2013
Conjugated EstrogensBazedoxifene (CEBZA)
US indication
bull DUAVEE is indicated in women with a uterus for
bull 11 Treatment of Moderate to Severe Vasomotor Symptoms Associated with Menopause
bull 12 Prevention of Postmenopausal Osteoporosis
bull 13 Important Limitations of Use
bull Use DUAVEE for the shortest duration consistent with treatment goals and risks for the individual woman Postmenopausal women should be re-evaluated periodically as clinically appropriate to determine if treatment is still necessary
bull When prescribing solely for the prevention of postmenopausal osteoporosis therapy should only be considered for women at significant risk of osteoporosis and non-estrogen medication should be carefully considered
Conjugated EstrogensBazedoxifene (CEBZA)
EU indication
CEBZA is indicated for
bull Treatment of oestrogen deficiency symptoms in postmenopausal women with a uterus (with at least 12 months since the last menses) for whom treatment with progestin-containing therapy is not appropriate
bull The experience treating women older than 65 years is limited
bull Dose CE (045mg)Bazedoxifene (20mg)
Duavive SmPC
Which women with a uterus
could benefit from estrogens
without the need for a
progestin
Progestin intolerance is one of the main
factors for reduced compliance
bull About 20 of women receiving progestin-containing HT have significant progestin intolerance and half of these experience serious effects that prevent treatment continuation1
1 Panay N amp Studd J Human Reprod Update 1997
2 Panay N et al on behalf of the British Menopause Society and Womenrsquos Health Concern Menopause Int 2013
bull The 2013 British Menopause Society amp Womenrsquos Health
Concern recommendations on hormone replacement
therapy do recognise progestin intolerance as one of the
main factors for reduced compliance with HT 2
Proportion of patients () with at least one bleeding episode in relation to time and to the
used HT
Serge Rozenberg et al Hum Reprod 2009241739-1747
copy The Author 2009 Published by Oxford University Press on behalf of the European Society of
Human Reproduction and Embryology All rights reserved For Permissions please email
journalspermissionsoxfordjournalsorg
Breast tenderness after initiation of CEE
CEE + MPA (WHI)
and mammographic density change
bullCrandall et al Breast Cancer Res Treat DOI 101007s10549-011-1803-9
Breast density
Conclusion
bull CEEBAZO is an additional regimen for menopausal symptoms it provides also a prevention for osteoporosis
bull It is suitable for women with a uterus who are unsatisfied with an EPT regimen or who you are unwilling to treat with an EPT regimen
Adapted use of MHT
bull Lower dosage of estrogens
bull Other progestins
bull Better safety profile
bull Vaginal estrogen or SERMS
bull Non-hormonal therapy
bull Development of new products
bull SERMS + estrogens
Most common adverse events leading to
discontinuation are related to progestins12
bull breakthrough bleeding
bull Low compliance
bull Increase in the number of US
bull Stress
bull Cost
bull uterine procedures
bull Unnecessary endometrial biopsies Hysteroscopies DampC Hysterectomies
bull Morbidity
Proportion of patients who completed or discontinued treatment in relation to the used HT
Serge Rozenberg et al Hum Reprod 2009241739-1747
copy The Author 2009 Published by Oxford University Press on behalf of the European Society of
Human Reproduction and Embryology All rights reserved For Permissions please email
journalspermissionsoxfordjournalsorg
Most common adverse events leading to discontinuation
are related to progestins
bull breast paintenderness
Breast tenderness after initiation of CEE
CEE + MPA (WHI)
and mammographic density change
bullCrandall et al Breast Cancer Res Treat DOI 101007s10549-011-1803-9
Breast density
Hormone therapy use and mammographic
density in postmenopausal Norwegian women
bull Results differed when considering the combined effect of age and BMI
bull The effect of EPT on mammographic density was modified by age and BMI with no apparent association among the youngest women (aged 50-55) with the highest BMI (BMI ge 26)
bull A higher mammographic density was found in EPT users compared to never HT users particularly in women using high-dose NETA regimens Age and BMI modified the association between EPT use and mammographic density
bull Couto E et al Breast Cancer Res Treat 2011 Nov 4 [Epub ahead of print]
Breast Cancer Risk by Breast Density
Menopause and Postmenopausal Hormone
Therapy Use
Birads age HT Duration Risk
1 55-59 None 5 year risk 08 (95 CI 06- 09)
1 55-59
ET EPT 5 year risk 09 (95 CI 07 -11)
4 55-59
None 5 year risk 24 (95 CI 20 -28)
4 55-59
ET 5 year risk
30 (95 CI 26 -35)
4 55-59
EPT 5 year risk
42 (95 CI 37 -46)
Adapted from Kerlikowske et al JOURNAL OF CLINICAL ONCOLOGY 2010
Breast Cancer Risk by Breast Density
Menopause and Postmenopausal Hormone
Therapy Use
Adapted from Kerlikowske et al JOURNAL OF CLINICAL ONCOLOGY 2010
bull Postmenopausal women with high breast density are at increased risk of breast cancer and should be aware of the added risk of taking HT especially estrogen plus progestin
Medical condition which may be exacerbated by treatment
with progestins
Diabetes and metabolic syndrome
bull progestin-containing HT may be associated with increases in insulin resistance and deterioration in glucose tolerance123
bull Postmenopausal women with diabetes could be inappropriate for treatment with progestin-containing HT due to the potential risk of exacerbation of their condition
1) Panay N amp Studd JWW Human Reprod Update 1997
2) Godsland I et al Metabolism 1993
3) Sites CK et al J Clin Endocrinol Metab 2005
A Nath and R Sitruk-Ware CLIMACTERIC 200912(Suppl 1)96ndash101
A Nath and R Sitruk-Ware CLIMACTERIC 200912(Suppl 1)96ndash101
Diabetes an epidemy
bull UK 1996 14 million of diabetics
bull UK 2015 32 million (6 of the population)
bull UK 2025 5 million
bull httpwwwdiabetescoukdiabetes-prevalencehtml
Other progestin-related intolerance issues
bull Nausea
bull Depressive mood
bull Poor concentration
bull Hirsutism
bull Headache
bull Dizziness
bull Fluid retention
bull Weight gain Panay N amp Studd JWW Human Reprod Update 1997
Medical condition which may be exacerbated by treatment with progestins
PMSPMDDdepression
bull Progesterone-induced PMD can be exacerbated by exogenous progestin administration and can occur in association with HT or OC administration1
bull Significantly higher negative mood scores have been observed during the addition of a progestin to an estrogen in a sequential HT regimen in postmenopausal women with a history of PMS compared to those without2
bull Women with a history of PMS or PMD exacerbation of depression using progestins may therefore benefit from a progestin free treatment for menopausal symptoms
1) Nevatte T et al Arch Womens Ment Health 2013 2) Bjoumlrn I et al Climacteric 2006 PMS premenstrual syndrome
PMDD premenstrual dysphoric disorder
Conclusion
bull CEEBAZO is an additional regimen for menopausal symptoms it provides also a prevention for osteoporosis
bull It is suitable for women with a uterus who are unsatisfied with an EPT regimen or who you are unwilling to treat with an EPT regimen
For some postmenopausal women with a uterus there is a
need for progestin free treatment options
bull with demonstrated clinical efficacy
bull which protects the endometrium
bull improved tolerabilitysafety profile
In clinical practice this translates to women who are
intolerant of progestin-containing HT or have conditions
which may be exacerbated by treatment with progestins
Conclusion Medical need for alternative treatment option
Medical condition which may be exacerbated by treatment with progestins
Depression
bull Progestin-containing HT has been associated with increases in depressive symptoms in some individuals1
bull There is a biochemicalphysiological plausibility for the association of progestins with depression234
bull Therefore postmenopausal women who also have a medical history of depressive disorders or depression could be inappropriate for treatment with progestin-containing HT
Pfizer Confidential
65
1) Girdler SS et al J Womens Health Gend Based Med 1999 2) Traish AM et al Korean J Urol 2014 3) Stroumlhle A et al Biol Psychiatry 1999 4) Romeo E et
al Am J Psychiatry 1998
History of the following conditions may make progestin inappropriate
bull Depression
bull PMSPMDD
PMS premenstrual syndrome
PMD premenstrual dysphoric disorder
Medical conditions that may be exacerbated by treatment with progestins
Women for whom progestin-containing HT
would not be considered appropriate
minus Women who are intolerant of progestin-containing hormone therapy
minus Women with pre-existing medical conditions that may be exacerbated by progestins
Most common adverse events leading to discontinuation are related to progestins12
breakthrough bleeding
bull Increase in the number of uterine procedures (ie unnecessary endometrial biopsies)
breast paintenderness
bull Increase in the number of breast interventions
1 Steel SA et al Climacteric 2003 2 Ettinger B and Pressman A Am J Manag Care 1999 3 Komm BS Mirkin S
Pharmaceuticals 2012
4 Panay N amp Studd JWW Human Reprod Update 1997
bull Nausea bull Depressive mood bull Poor concentration bull Hirsutism bull Headache bull Dizziness bull Fluid retention bull Weight gain
Other progestin-related intolerance issues4
Unmet need with the treatment of postmenopausal symptoms
bull Alternatives to progestin are needed that will protect the endometrium while avoiding other progestin-associated effects and preserving the desired effects of estrogens in postmenopausal women3
Which women with a uterus could benefit from
estrogens without the need for a progestin
bull Women who are intolerant of progestin-containing hormone therapy
bull Women with pre-existing medical conditions that may be exacerbated by progestins (eg women with a history of depression PMSPMDD increased breast density diabetes and metabolic syndrome)
History of the following conditions may make progestin inappropriate
bull Depression
bull PMSPMDD
bull High breast density
bull Diabetes and metabolic syndrome
PMS premenstrual syndrome
PMD premenstrual dysphoric disorder
Medical conditions that may be exacerbated by treatment with progestins
Learning from WHI data
bull Hormone therapy (HT) is the conventional and established therapy option to effectively treat postmenopausal symptoms however it has been associated with some safety and tolerability concerns1 2
bull A review of WHI data suggests that many of the concerns with menopausal HT more often associated with EPT (CE+MPA) such as CHD risk increased breast density breast pain and breast cancer risk than with ET (CEE alone)2
1 Rolnick SJ Kopher RA DeFor TA et al Menopause 2005
2 Komm BS Mirkin S Pharmaceuticals 2012
WHI Womenrsquos Health Initiative trial
CHD coronary heart disease
CEE conjugated equine estrogens
Efficacy and Safety of Constant Oestrogen
Pulsed Progestogen vs
Continuous Combined HRT
Adverse Events
17b-oestradiol 17b-oestradiol norgestimate NETA (n = 150) (n = 172) Breast discomfort 14 27 Abdominal discomfort 14 22 Uterine bleeding 15 12 Dysmenorrhea 3 8 Oedema 5 8
Adapted from S Rozenberg et al Human Reproduction 2000
Medical condition which may be exacerbated by treatment
with progestins
Increased breast density
bull Increases in breast density are associated with progestin-containing HT which may adversely affect radiological detection of breast cancer1 and may be independently associated with an increased risk for the development of breast cancer2
bull The Postmenopausal EstrogenProgestin Interventions (PEPI) trial demonstrated that an increased mammographic breast density was associated with the use of E+P but not with the use of estrogen alone3
bull Women who already have high breast density may therefore be considered inappropriate for treatment with a progestin-containing HT
1) EU Core SPC for Hormone Replacement Therapy Products (CMDh1312003 Rev 4 June
2012)
2) De Villiers TJ et al on behalf of the International Menopause Society Climacteric 2013 16
3) Greendale GA et al J Natl Cancer Inst 2003
Stroke
0 25 5 75 10 125
Fractures
Diabetes
Breast cancer
Cholecystitis
Venothrombotic episodes
Endometrial cancer
Lung cancer
Coronary heart disease
Colorectal cancer
Overall mortality
15 125 10 75 5 25
Benefits Risks
CE
CE MPA
Santen RJ et al J Clin Endocrinol Metab 2010
The basis of the Endocrine Society scientific statement for postmenopausal hormone replacement therapy (HRT) excess risks and benefits of HRT for 5 years in women aged 50ndash59 years or within 10 years of the start of menopause E=estrogen P=progestin
bull Younger women (aged 50ndash59 years) had more favorable results bull There are differences between CE alone and CEMPA arms bull Overall benefitrisk ratio of CE-alone appears to be more favourable than CEMPA
Reevaluation of WHI data (stratified by age) Risks and
Benefits of HRT Cases per 1000 Women per 5 Years of
Use
Medical condition which may be exacerbated by treatment
with progestins
Diabetes and metabolic syndrome
bull Treatment of oestrogen deficiency symptoms with progestin-containing HT (unlike oestrogen alone) may be associated with increases in insulin resistance and deterioration in glucose tolerance123
bull Postmenopausal women with diabetes could be inappropriate for treatment with progestin-containing HT due to the potential risk of exacerbation of their condition
1) Panay N amp Studd JWW Human Reprod Update 1997
2) Godsland I et al Metabolism 1993
3) Sites CK et al J Clin Endocrinol Metab 2005
Variations in Associated Breast Cancer
Risks Between CE alone and CEMPA
bull Use of CE alone for a median of 59 years was associated with a lower incidence of invasive breast cancer (151 cases 027 per year) compared with placebo (199 cases 035 per year HR 077 95 CI 062ndash095 P=002)
bull In the CE alone group fewer women died from invasive breast cancer (6 deaths 0009 per year) compared with controls (16 deaths 0024 per year HR 037 95 CI 013ndash091 P=003)
Anderson GL et al Lancet
Oncol 2012
Bazedoxifene (BZA) specifically selected in
combination with conjugated estrogens
bull BZA has been specifically selected for its unique pharmacologic profile and effects on VMS and uterine tissue in particular123
1 Crabtree J et al Mol Cell Endocrinol 2008
2 Kharode Y et al Endocrinolology 2008
3 Duavive SmPC
Estrogen Receptor activity is dimmed
Estrogen Receptor activity is turned on
CEs are agonists BZA is an antagonist
In the uterus
bull The BZA component reduces the risk of endometrial hyperplasia that can occur with the conjugated estrogens component alone3 This means that progestins are not needed
Extensive global clinical development program for
CEBZA
aIncludes additional pilot dose-finding study 203 1 Lobo RA et al Fertil Steril 2009 2 Pinkerton JV et al Menopause 2009 3 Kagan R et al Menopause 2010 4 Mirkin S et al Climacteric 2013 5 Pinkerton JV et al Obstet Gynecol 2013
Effects of conjugated estrogensbazedoxifene on
lipid and coagulation variables a randomized
placebo- and active-controlled trial
bull At 12 months
bull Both CEBZA doses were associated with small but significant effects on hemostasis variables including reductions in antithrombin plasminogen activator inhibitor-1 and fibrinogen activity and an increase in plasminogen activity relative to placebo at 12 months Incidences of cardiovascular and venous thromboembolic events were similar among treatment groups
bull CONCLUSIONS
bull This study provides reassurance that CEBZA does not adversely affect lipid metabolism or hemostatic balance In accordance the incidences of venous thromboembolic events and cardiovascular events in postmenopausal women are similar to those observed with placebo

Endometrial hyperplasia or malignancy occurred in lt1 of women
following up to 1 year of treatment with CEBZA12
Study Cumulative Incidence at month 12 (nN)
CE 045BZA 20 Placebo
SMART-11 000 (0336) 000 (0313)
SMART-52 030 (1335) 028 (1354)
Effects on the Endometrium
1 Pickar JH et al Fertil Steril 2009 2 Pinkerton at al J Clin Endocrinol Metab 2014
Through the eyes of an amazone
Marie Mandy
Breast tolerability profile similar to placebo following up to 2 years of treatment with CEBZA12
Pooled analysis of SMART clinical trials
CE 045BZA 20 (n=1585)
Placebo (n=1241)
Breast cancer incidence up to 2 years
(per 1000 woman-years)
100 (CI 000-321)
140 (CI 000-417)
Incidence of reported breast paintenderness up to 12 weeks
98-115 81-112
Incidence of abnormal mammogram at month 12
258 316
Mean change in breast density at month 12 (SMART-5)
ndash038 (n=186)
ndash032 (n=182)
Effects on the Breast
1 Pickar JH et al Menopause 2013 2 Pinkerton JV et al Obstet Gynecol 2013
CEBZA clinical overview - summary
bull In clinical trials CEBZA has demonstrated safety and efficacy in postmenopausal women with a uterus including the following
bull Significant reduction in number and severity of moderate to severe hot flushes1
bull Incidence of cumulative amenorrhea rate similar to placebo and significantly better than CEMPA2
bull Incidence of endometrial hyperplasia and breast tendernessdensity similar to that with placebo345
bull Incidence of adverse events and discontinuation rates similar to that with placebo6
1 Pinkerton JV et al Menopause 2009 2 Pinkerton JV et al J Clin Endocrinol Metab2014 3 Pickar JH et al
Fertil Steril 2009 4 Pinkerton at al J Clin Endocrinol Metab 2014 5 Pickar JH et al Menopause 2013 6 DUAVEE [package insert] New York NY Pfizer Inc 2013
CEBZA clinical overview - summary
Now women with a uterus who choose hormone therapy for management of menopausal symptoms have a choice
bull conventional estrogen-progestogen therapy or
bull a new combinationhellipconjugated estrogens paired with the SERM bazedoxifene
1 Pinkerton JV et al Menopause 2009 2 Pinkerton JV et al J Clin Endocrinol Metab2014 3 Pickar JH et al Fertil Steril 2009 4 Pinkerton at al J Clin Endocrinol Metab 2014 5 Pickar JH et al Menopause 2013 6 DUAVEE [package insert] New York NY Pfizer Inc 2013
Conjugated EstrogensBazedoxifene (CEBZA)
US indication
bull DUAVEE is indicated in women with a uterus for
bull 11 Treatment of Moderate to Severe Vasomotor Symptoms Associated with Menopause
bull 12 Prevention of Postmenopausal Osteoporosis
bull 13 Important Limitations of Use
bull Use DUAVEE for the shortest duration consistent with treatment goals and risks for the individual woman Postmenopausal women should be re-evaluated periodically as clinically appropriate to determine if treatment is still necessary
bull When prescribing solely for the prevention of postmenopausal osteoporosis therapy should only be considered for women at significant risk of osteoporosis and non-estrogen medication should be carefully considered
Conjugated EstrogensBazedoxifene (CEBZA)
EU indication
CEBZA is indicated for
bull Treatment of oestrogen deficiency symptoms in postmenopausal women with a uterus (with at least 12 months since the last menses) for whom treatment with progestin-containing therapy is not appropriate
bull The experience treating women older than 65 years is limited
bull Dose CE (045mg)Bazedoxifene (20mg)
Duavive SmPC
Which women with a uterus
could benefit from estrogens
without the need for a
progestin
Progestin intolerance is one of the main
factors for reduced compliance
bull About 20 of women receiving progestin-containing HT have significant progestin intolerance and half of these experience serious effects that prevent treatment continuation1
1 Panay N amp Studd J Human Reprod Update 1997
2 Panay N et al on behalf of the British Menopause Society and Womenrsquos Health Concern Menopause Int 2013
bull The 2013 British Menopause Society amp Womenrsquos Health
Concern recommendations on hormone replacement
therapy do recognise progestin intolerance as one of the
main factors for reduced compliance with HT 2
Proportion of patients () with at least one bleeding episode in relation to time and to the
used HT
Serge Rozenberg et al Hum Reprod 2009241739-1747
copy The Author 2009 Published by Oxford University Press on behalf of the European Society of
Human Reproduction and Embryology All rights reserved For Permissions please email
journalspermissionsoxfordjournalsorg
Breast tenderness after initiation of CEE
CEE + MPA (WHI)
and mammographic density change
bullCrandall et al Breast Cancer Res Treat DOI 101007s10549-011-1803-9
Breast density
Conclusion
bull CEEBAZO is an additional regimen for menopausal symptoms it provides also a prevention for osteoporosis
bull It is suitable for women with a uterus who are unsatisfied with an EPT regimen or who you are unwilling to treat with an EPT regimen
Adapted use of MHT
bull Lower dosage of estrogens
bull Other progestins
bull Better safety profile
bull Vaginal estrogen or SERMS
bull Non-hormonal therapy
bull Development of new products
bull SERMS + estrogens
Most common adverse events leading to
discontinuation are related to progestins12
bull breakthrough bleeding
bull Low compliance
bull Increase in the number of US
bull Stress
bull Cost
bull uterine procedures
bull Unnecessary endometrial biopsies Hysteroscopies DampC Hysterectomies
bull Morbidity
Proportion of patients who completed or discontinued treatment in relation to the used HT
Serge Rozenberg et al Hum Reprod 2009241739-1747
copy The Author 2009 Published by Oxford University Press on behalf of the European Society of
Human Reproduction and Embryology All rights reserved For Permissions please email
journalspermissionsoxfordjournalsorg
Most common adverse events leading to discontinuation
are related to progestins
bull breast paintenderness
Breast tenderness after initiation of CEE
CEE + MPA (WHI)
and mammographic density change
bullCrandall et al Breast Cancer Res Treat DOI 101007s10549-011-1803-9
Breast density
Hormone therapy use and mammographic
density in postmenopausal Norwegian women
bull Results differed when considering the combined effect of age and BMI
bull The effect of EPT on mammographic density was modified by age and BMI with no apparent association among the youngest women (aged 50-55) with the highest BMI (BMI ge 26)
bull A higher mammographic density was found in EPT users compared to never HT users particularly in women using high-dose NETA regimens Age and BMI modified the association between EPT use and mammographic density
bull Couto E et al Breast Cancer Res Treat 2011 Nov 4 [Epub ahead of print]
Breast Cancer Risk by Breast Density
Menopause and Postmenopausal Hormone
Therapy Use
Birads age HT Duration Risk
1 55-59 None 5 year risk 08 (95 CI 06- 09)
1 55-59
ET EPT 5 year risk 09 (95 CI 07 -11)
4 55-59
None 5 year risk 24 (95 CI 20 -28)
4 55-59
ET 5 year risk
30 (95 CI 26 -35)
4 55-59
EPT 5 year risk
42 (95 CI 37 -46)
Adapted from Kerlikowske et al JOURNAL OF CLINICAL ONCOLOGY 2010
Breast Cancer Risk by Breast Density
Menopause and Postmenopausal Hormone
Therapy Use
Adapted from Kerlikowske et al JOURNAL OF CLINICAL ONCOLOGY 2010
bull Postmenopausal women with high breast density are at increased risk of breast cancer and should be aware of the added risk of taking HT especially estrogen plus progestin
Medical condition which may be exacerbated by treatment
with progestins
Diabetes and metabolic syndrome
bull progestin-containing HT may be associated with increases in insulin resistance and deterioration in glucose tolerance123
bull Postmenopausal women with diabetes could be inappropriate for treatment with progestin-containing HT due to the potential risk of exacerbation of their condition
1) Panay N amp Studd JWW Human Reprod Update 1997
2) Godsland I et al Metabolism 1993
3) Sites CK et al J Clin Endocrinol Metab 2005
A Nath and R Sitruk-Ware CLIMACTERIC 200912(Suppl 1)96ndash101
A Nath and R Sitruk-Ware CLIMACTERIC 200912(Suppl 1)96ndash101
Diabetes an epidemy
bull UK 1996 14 million of diabetics
bull UK 2015 32 million (6 of the population)
bull UK 2025 5 million
bull httpwwwdiabetescoukdiabetes-prevalencehtml
Other progestin-related intolerance issues
bull Nausea
bull Depressive mood
bull Poor concentration
bull Hirsutism
bull Headache
bull Dizziness
bull Fluid retention
bull Weight gain Panay N amp Studd JWW Human Reprod Update 1997
Medical condition which may be exacerbated by treatment with progestins
PMSPMDDdepression
bull Progesterone-induced PMD can be exacerbated by exogenous progestin administration and can occur in association with HT or OC administration1
bull Significantly higher negative mood scores have been observed during the addition of a progestin to an estrogen in a sequential HT regimen in postmenopausal women with a history of PMS compared to those without2
bull Women with a history of PMS or PMD exacerbation of depression using progestins may therefore benefit from a progestin free treatment for menopausal symptoms
1) Nevatte T et al Arch Womens Ment Health 2013 2) Bjoumlrn I et al Climacteric 2006 PMS premenstrual syndrome
PMDD premenstrual dysphoric disorder
Conclusion
bull CEEBAZO is an additional regimen for menopausal symptoms it provides also a prevention for osteoporosis
bull It is suitable for women with a uterus who are unsatisfied with an EPT regimen or who you are unwilling to treat with an EPT regimen
For some postmenopausal women with a uterus there is a
need for progestin free treatment options
bull with demonstrated clinical efficacy
bull which protects the endometrium
bull improved tolerabilitysafety profile
In clinical practice this translates to women who are
intolerant of progestin-containing HT or have conditions
which may be exacerbated by treatment with progestins
Conclusion Medical need for alternative treatment option
Medical condition which may be exacerbated by treatment with progestins
Depression
bull Progestin-containing HT has been associated with increases in depressive symptoms in some individuals1
bull There is a biochemicalphysiological plausibility for the association of progestins with depression234
bull Therefore postmenopausal women who also have a medical history of depressive disorders or depression could be inappropriate for treatment with progestin-containing HT
Pfizer Confidential
65
1) Girdler SS et al J Womens Health Gend Based Med 1999 2) Traish AM et al Korean J Urol 2014 3) Stroumlhle A et al Biol Psychiatry 1999 4) Romeo E et
al Am J Psychiatry 1998
History of the following conditions may make progestin inappropriate
bull Depression
bull PMSPMDD
PMS premenstrual syndrome
PMD premenstrual dysphoric disorder
Medical conditions that may be exacerbated by treatment with progestins
Women for whom progestin-containing HT
would not be considered appropriate
minus Women who are intolerant of progestin-containing hormone therapy
minus Women with pre-existing medical conditions that may be exacerbated by progestins
Most common adverse events leading to discontinuation are related to progestins12
breakthrough bleeding
bull Increase in the number of uterine procedures (ie unnecessary endometrial biopsies)
breast paintenderness
bull Increase in the number of breast interventions
1 Steel SA et al Climacteric 2003 2 Ettinger B and Pressman A Am J Manag Care 1999 3 Komm BS Mirkin S
Pharmaceuticals 2012
4 Panay N amp Studd JWW Human Reprod Update 1997
bull Nausea bull Depressive mood bull Poor concentration bull Hirsutism bull Headache bull Dizziness bull Fluid retention bull Weight gain
Other progestin-related intolerance issues4
Unmet need with the treatment of postmenopausal symptoms
bull Alternatives to progestin are needed that will protect the endometrium while avoiding other progestin-associated effects and preserving the desired effects of estrogens in postmenopausal women3
Which women with a uterus could benefit from
estrogens without the need for a progestin
bull Women who are intolerant of progestin-containing hormone therapy
bull Women with pre-existing medical conditions that may be exacerbated by progestins (eg women with a history of depression PMSPMDD increased breast density diabetes and metabolic syndrome)
History of the following conditions may make progestin inappropriate
bull Depression
bull PMSPMDD
bull High breast density
bull Diabetes and metabolic syndrome
PMS premenstrual syndrome
PMD premenstrual dysphoric disorder
Medical conditions that may be exacerbated by treatment with progestins
Learning from WHI data
bull Hormone therapy (HT) is the conventional and established therapy option to effectively treat postmenopausal symptoms however it has been associated with some safety and tolerability concerns1 2
bull A review of WHI data suggests that many of the concerns with menopausal HT more often associated with EPT (CE+MPA) such as CHD risk increased breast density breast pain and breast cancer risk than with ET (CEE alone)2
1 Rolnick SJ Kopher RA DeFor TA et al Menopause 2005
2 Komm BS Mirkin S Pharmaceuticals 2012
WHI Womenrsquos Health Initiative trial
CHD coronary heart disease
CEE conjugated equine estrogens
Efficacy and Safety of Constant Oestrogen
Pulsed Progestogen vs
Continuous Combined HRT
Adverse Events
17b-oestradiol 17b-oestradiol norgestimate NETA (n = 150) (n = 172) Breast discomfort 14 27 Abdominal discomfort 14 22 Uterine bleeding 15 12 Dysmenorrhea 3 8 Oedema 5 8
Adapted from S Rozenberg et al Human Reproduction 2000
Medical condition which may be exacerbated by treatment
with progestins
Increased breast density
bull Increases in breast density are associated with progestin-containing HT which may adversely affect radiological detection of breast cancer1 and may be independently associated with an increased risk for the development of breast cancer2
bull The Postmenopausal EstrogenProgestin Interventions (PEPI) trial demonstrated that an increased mammographic breast density was associated with the use of E+P but not with the use of estrogen alone3
bull Women who already have high breast density may therefore be considered inappropriate for treatment with a progestin-containing HT
1) EU Core SPC for Hormone Replacement Therapy Products (CMDh1312003 Rev 4 June
2012)
2) De Villiers TJ et al on behalf of the International Menopause Society Climacteric 2013 16
3) Greendale GA et al J Natl Cancer Inst 2003
Stroke
0 25 5 75 10 125
Fractures
Diabetes
Breast cancer
Cholecystitis
Venothrombotic episodes
Endometrial cancer
Lung cancer
Coronary heart disease
Colorectal cancer
Overall mortality
15 125 10 75 5 25
Benefits Risks
CE
CE MPA
Santen RJ et al J Clin Endocrinol Metab 2010
The basis of the Endocrine Society scientific statement for postmenopausal hormone replacement therapy (HRT) excess risks and benefits of HRT for 5 years in women aged 50ndash59 years or within 10 years of the start of menopause E=estrogen P=progestin
bull Younger women (aged 50ndash59 years) had more favorable results bull There are differences between CE alone and CEMPA arms bull Overall benefitrisk ratio of CE-alone appears to be more favourable than CEMPA
Reevaluation of WHI data (stratified by age) Risks and
Benefits of HRT Cases per 1000 Women per 5 Years of
Use
Medical condition which may be exacerbated by treatment
with progestins
Diabetes and metabolic syndrome
bull Treatment of oestrogen deficiency symptoms with progestin-containing HT (unlike oestrogen alone) may be associated with increases in insulin resistance and deterioration in glucose tolerance123
bull Postmenopausal women with diabetes could be inappropriate for treatment with progestin-containing HT due to the potential risk of exacerbation of their condition
1) Panay N amp Studd JWW Human Reprod Update 1997
2) Godsland I et al Metabolism 1993
3) Sites CK et al J Clin Endocrinol Metab 2005
Variations in Associated Breast Cancer
Risks Between CE alone and CEMPA
bull Use of CE alone for a median of 59 years was associated with a lower incidence of invasive breast cancer (151 cases 027 per year) compared with placebo (199 cases 035 per year HR 077 95 CI 062ndash095 P=002)
bull In the CE alone group fewer women died from invasive breast cancer (6 deaths 0009 per year) compared with controls (16 deaths 0024 per year HR 037 95 CI 013ndash091 P=003)
Anderson GL et al Lancet
Oncol 2012
Bazedoxifene (BZA) specifically selected in
combination with conjugated estrogens
bull BZA has been specifically selected for its unique pharmacologic profile and effects on VMS and uterine tissue in particular123
1 Crabtree J et al Mol Cell Endocrinol 2008
2 Kharode Y et al Endocrinolology 2008
3 Duavive SmPC
Estrogen Receptor activity is dimmed
Estrogen Receptor activity is turned on
CEs are agonists BZA is an antagonist
In the uterus
bull The BZA component reduces the risk of endometrial hyperplasia that can occur with the conjugated estrogens component alone3 This means that progestins are not needed
Extensive global clinical development program for
CEBZA
aIncludes additional pilot dose-finding study 203 1 Lobo RA et al Fertil Steril 2009 2 Pinkerton JV et al Menopause 2009 3 Kagan R et al Menopause 2010 4 Mirkin S et al Climacteric 2013 5 Pinkerton JV et al Obstet Gynecol 2013
Effects of conjugated estrogensbazedoxifene on
lipid and coagulation variables a randomized
placebo- and active-controlled trial
bull At 12 months
bull Both CEBZA doses were associated with small but significant effects on hemostasis variables including reductions in antithrombin plasminogen activator inhibitor-1 and fibrinogen activity and an increase in plasminogen activity relative to placebo at 12 months Incidences of cardiovascular and venous thromboembolic events were similar among treatment groups
bull CONCLUSIONS
bull This study provides reassurance that CEBZA does not adversely affect lipid metabolism or hemostatic balance In accordance the incidences of venous thromboembolic events and cardiovascular events in postmenopausal women are similar to those observed with placebo

Through the eyes of an amazone
Marie Mandy
Breast tolerability profile similar to placebo following up to 2 years of treatment with CEBZA12
Pooled analysis of SMART clinical trials
CE 045BZA 20 (n=1585)
Placebo (n=1241)
Breast cancer incidence up to 2 years
(per 1000 woman-years)
100 (CI 000-321)
140 (CI 000-417)
Incidence of reported breast paintenderness up to 12 weeks
98-115 81-112
Incidence of abnormal mammogram at month 12
258 316
Mean change in breast density at month 12 (SMART-5)
ndash038 (n=186)
ndash032 (n=182)
Effects on the Breast
1 Pickar JH et al Menopause 2013 2 Pinkerton JV et al Obstet Gynecol 2013
CEBZA clinical overview - summary
bull In clinical trials CEBZA has demonstrated safety and efficacy in postmenopausal women with a uterus including the following
bull Significant reduction in number and severity of moderate to severe hot flushes1
bull Incidence of cumulative amenorrhea rate similar to placebo and significantly better than CEMPA2
bull Incidence of endometrial hyperplasia and breast tendernessdensity similar to that with placebo345
bull Incidence of adverse events and discontinuation rates similar to that with placebo6
1 Pinkerton JV et al Menopause 2009 2 Pinkerton JV et al J Clin Endocrinol Metab2014 3 Pickar JH et al
Fertil Steril 2009 4 Pinkerton at al J Clin Endocrinol Metab 2014 5 Pickar JH et al Menopause 2013 6 DUAVEE [package insert] New York NY Pfizer Inc 2013
CEBZA clinical overview - summary
Now women with a uterus who choose hormone therapy for management of menopausal symptoms have a choice
bull conventional estrogen-progestogen therapy or
bull a new combinationhellipconjugated estrogens paired with the SERM bazedoxifene
1 Pinkerton JV et al Menopause 2009 2 Pinkerton JV et al J Clin Endocrinol Metab2014 3 Pickar JH et al Fertil Steril 2009 4 Pinkerton at al J Clin Endocrinol Metab 2014 5 Pickar JH et al Menopause 2013 6 DUAVEE [package insert] New York NY Pfizer Inc 2013
Conjugated EstrogensBazedoxifene (CEBZA)
US indication
bull DUAVEE is indicated in women with a uterus for
bull 11 Treatment of Moderate to Severe Vasomotor Symptoms Associated with Menopause
bull 12 Prevention of Postmenopausal Osteoporosis
bull 13 Important Limitations of Use
bull Use DUAVEE for the shortest duration consistent with treatment goals and risks for the individual woman Postmenopausal women should be re-evaluated periodically as clinically appropriate to determine if treatment is still necessary
bull When prescribing solely for the prevention of postmenopausal osteoporosis therapy should only be considered for women at significant risk of osteoporosis and non-estrogen medication should be carefully considered
Conjugated EstrogensBazedoxifene (CEBZA)
EU indication
CEBZA is indicated for
bull Treatment of oestrogen deficiency symptoms in postmenopausal women with a uterus (with at least 12 months since the last menses) for whom treatment with progestin-containing therapy is not appropriate
bull The experience treating women older than 65 years is limited
bull Dose CE (045mg)Bazedoxifene (20mg)
Duavive SmPC
Which women with a uterus
could benefit from estrogens
without the need for a
progestin
Progestin intolerance is one of the main
factors for reduced compliance
bull About 20 of women receiving progestin-containing HT have significant progestin intolerance and half of these experience serious effects that prevent treatment continuation1
1 Panay N amp Studd J Human Reprod Update 1997
2 Panay N et al on behalf of the British Menopause Society and Womenrsquos Health Concern Menopause Int 2013
bull The 2013 British Menopause Society amp Womenrsquos Health
Concern recommendations on hormone replacement
therapy do recognise progestin intolerance as one of the
main factors for reduced compliance with HT 2
Proportion of patients () with at least one bleeding episode in relation to time and to the
used HT
Serge Rozenberg et al Hum Reprod 2009241739-1747
copy The Author 2009 Published by Oxford University Press on behalf of the European Society of
Human Reproduction and Embryology All rights reserved For Permissions please email
journalspermissionsoxfordjournalsorg
Breast tenderness after initiation of CEE
CEE + MPA (WHI)
and mammographic density change
bullCrandall et al Breast Cancer Res Treat DOI 101007s10549-011-1803-9
Breast density
Conclusion
bull CEEBAZO is an additional regimen for menopausal symptoms it provides also a prevention for osteoporosis
bull It is suitable for women with a uterus who are unsatisfied with an EPT regimen or who you are unwilling to treat with an EPT regimen
Adapted use of MHT
bull Lower dosage of estrogens
bull Other progestins
bull Better safety profile
bull Vaginal estrogen or SERMS
bull Non-hormonal therapy
bull Development of new products
bull SERMS + estrogens
Most common adverse events leading to
discontinuation are related to progestins12
bull breakthrough bleeding
bull Low compliance
bull Increase in the number of US
bull Stress
bull Cost
bull uterine procedures
bull Unnecessary endometrial biopsies Hysteroscopies DampC Hysterectomies
bull Morbidity
Proportion of patients who completed or discontinued treatment in relation to the used HT
Serge Rozenberg et al Hum Reprod 2009241739-1747
copy The Author 2009 Published by Oxford University Press on behalf of the European Society of
Human Reproduction and Embryology All rights reserved For Permissions please email
journalspermissionsoxfordjournalsorg
Most common adverse events leading to discontinuation
are related to progestins
bull breast paintenderness
Breast tenderness after initiation of CEE
CEE + MPA (WHI)
and mammographic density change
bullCrandall et al Breast Cancer Res Treat DOI 101007s10549-011-1803-9
Breast density
Hormone therapy use and mammographic
density in postmenopausal Norwegian women
bull Results differed when considering the combined effect of age and BMI
bull The effect of EPT on mammographic density was modified by age and BMI with no apparent association among the youngest women (aged 50-55) with the highest BMI (BMI ge 26)
bull A higher mammographic density was found in EPT users compared to never HT users particularly in women using high-dose NETA regimens Age and BMI modified the association between EPT use and mammographic density
bull Couto E et al Breast Cancer Res Treat 2011 Nov 4 [Epub ahead of print]
Breast Cancer Risk by Breast Density
Menopause and Postmenopausal Hormone
Therapy Use
Birads age HT Duration Risk
1 55-59 None 5 year risk 08 (95 CI 06- 09)
1 55-59
ET EPT 5 year risk 09 (95 CI 07 -11)
4 55-59
None 5 year risk 24 (95 CI 20 -28)
4 55-59
ET 5 year risk
30 (95 CI 26 -35)
4 55-59
EPT 5 year risk
42 (95 CI 37 -46)
Adapted from Kerlikowske et al JOURNAL OF CLINICAL ONCOLOGY 2010
Breast Cancer Risk by Breast Density
Menopause and Postmenopausal Hormone
Therapy Use
Adapted from Kerlikowske et al JOURNAL OF CLINICAL ONCOLOGY 2010
bull Postmenopausal women with high breast density are at increased risk of breast cancer and should be aware of the added risk of taking HT especially estrogen plus progestin
Medical condition which may be exacerbated by treatment
with progestins
Diabetes and metabolic syndrome
bull progestin-containing HT may be associated with increases in insulin resistance and deterioration in glucose tolerance123
bull Postmenopausal women with diabetes could be inappropriate for treatment with progestin-containing HT due to the potential risk of exacerbation of their condition
1) Panay N amp Studd JWW Human Reprod Update 1997
2) Godsland I et al Metabolism 1993
3) Sites CK et al J Clin Endocrinol Metab 2005
A Nath and R Sitruk-Ware CLIMACTERIC 200912(Suppl 1)96ndash101
A Nath and R Sitruk-Ware CLIMACTERIC 200912(Suppl 1)96ndash101
Diabetes an epidemy
bull UK 1996 14 million of diabetics
bull UK 2015 32 million (6 of the population)
bull UK 2025 5 million
bull httpwwwdiabetescoukdiabetes-prevalencehtml
Other progestin-related intolerance issues
bull Nausea
bull Depressive mood
bull Poor concentration
bull Hirsutism
bull Headache
bull Dizziness
bull Fluid retention
bull Weight gain Panay N amp Studd JWW Human Reprod Update 1997
Medical condition which may be exacerbated by treatment with progestins
PMSPMDDdepression
bull Progesterone-induced PMD can be exacerbated by exogenous progestin administration and can occur in association with HT or OC administration1
bull Significantly higher negative mood scores have been observed during the addition of a progestin to an estrogen in a sequential HT regimen in postmenopausal women with a history of PMS compared to those without2
bull Women with a history of PMS or PMD exacerbation of depression using progestins may therefore benefit from a progestin free treatment for menopausal symptoms
1) Nevatte T et al Arch Womens Ment Health 2013 2) Bjoumlrn I et al Climacteric 2006 PMS premenstrual syndrome
PMDD premenstrual dysphoric disorder
Conclusion
bull CEEBAZO is an additional regimen for menopausal symptoms it provides also a prevention for osteoporosis
bull It is suitable for women with a uterus who are unsatisfied with an EPT regimen or who you are unwilling to treat with an EPT regimen
For some postmenopausal women with a uterus there is a
need for progestin free treatment options
bull with demonstrated clinical efficacy
bull which protects the endometrium
bull improved tolerabilitysafety profile
In clinical practice this translates to women who are
intolerant of progestin-containing HT or have conditions
which may be exacerbated by treatment with progestins
Conclusion Medical need for alternative treatment option
Medical condition which may be exacerbated by treatment with progestins
Depression
bull Progestin-containing HT has been associated with increases in depressive symptoms in some individuals1
bull There is a biochemicalphysiological plausibility for the association of progestins with depression234
bull Therefore postmenopausal women who also have a medical history of depressive disorders or depression could be inappropriate for treatment with progestin-containing HT
Pfizer Confidential
65
1) Girdler SS et al J Womens Health Gend Based Med 1999 2) Traish AM et al Korean J Urol 2014 3) Stroumlhle A et al Biol Psychiatry 1999 4) Romeo E et
al Am J Psychiatry 1998
History of the following conditions may make progestin inappropriate
bull Depression
bull PMSPMDD
PMS premenstrual syndrome
PMD premenstrual dysphoric disorder
Medical conditions that may be exacerbated by treatment with progestins
Women for whom progestin-containing HT
would not be considered appropriate
minus Women who are intolerant of progestin-containing hormone therapy
minus Women with pre-existing medical conditions that may be exacerbated by progestins
Most common adverse events leading to discontinuation are related to progestins12
breakthrough bleeding
bull Increase in the number of uterine procedures (ie unnecessary endometrial biopsies)
breast paintenderness
bull Increase in the number of breast interventions
1 Steel SA et al Climacteric 2003 2 Ettinger B and Pressman A Am J Manag Care 1999 3 Komm BS Mirkin S
Pharmaceuticals 2012
4 Panay N amp Studd JWW Human Reprod Update 1997
bull Nausea bull Depressive mood bull Poor concentration bull Hirsutism bull Headache bull Dizziness bull Fluid retention bull Weight gain
Other progestin-related intolerance issues4
Unmet need with the treatment of postmenopausal symptoms
bull Alternatives to progestin are needed that will protect the endometrium while avoiding other progestin-associated effects and preserving the desired effects of estrogens in postmenopausal women3
Which women with a uterus could benefit from
estrogens without the need for a progestin
bull Women who are intolerant of progestin-containing hormone therapy
bull Women with pre-existing medical conditions that may be exacerbated by progestins (eg women with a history of depression PMSPMDD increased breast density diabetes and metabolic syndrome)
History of the following conditions may make progestin inappropriate
bull Depression
bull PMSPMDD
bull High breast density
bull Diabetes and metabolic syndrome
PMS premenstrual syndrome
PMD premenstrual dysphoric disorder
Medical conditions that may be exacerbated by treatment with progestins
Learning from WHI data
bull Hormone therapy (HT) is the conventional and established therapy option to effectively treat postmenopausal symptoms however it has been associated with some safety and tolerability concerns1 2
bull A review of WHI data suggests that many of the concerns with menopausal HT more often associated with EPT (CE+MPA) such as CHD risk increased breast density breast pain and breast cancer risk than with ET (CEE alone)2
1 Rolnick SJ Kopher RA DeFor TA et al Menopause 2005
2 Komm BS Mirkin S Pharmaceuticals 2012
WHI Womenrsquos Health Initiative trial
CHD coronary heart disease
CEE conjugated equine estrogens
Efficacy and Safety of Constant Oestrogen
Pulsed Progestogen vs
Continuous Combined HRT
Adverse Events
17b-oestradiol 17b-oestradiol norgestimate NETA (n = 150) (n = 172) Breast discomfort 14 27 Abdominal discomfort 14 22 Uterine bleeding 15 12 Dysmenorrhea 3 8 Oedema 5 8
Adapted from S Rozenberg et al Human Reproduction 2000
Medical condition which may be exacerbated by treatment
with progestins
Increased breast density
bull Increases in breast density are associated with progestin-containing HT which may adversely affect radiological detection of breast cancer1 and may be independently associated with an increased risk for the development of breast cancer2
bull The Postmenopausal EstrogenProgestin Interventions (PEPI) trial demonstrated that an increased mammographic breast density was associated with the use of E+P but not with the use of estrogen alone3
bull Women who already have high breast density may therefore be considered inappropriate for treatment with a progestin-containing HT
1) EU Core SPC for Hormone Replacement Therapy Products (CMDh1312003 Rev 4 June
2012)
2) De Villiers TJ et al on behalf of the International Menopause Society Climacteric 2013 16
3) Greendale GA et al J Natl Cancer Inst 2003
Stroke
0 25 5 75 10 125
Fractures
Diabetes
Breast cancer
Cholecystitis
Venothrombotic episodes
Endometrial cancer
Lung cancer
Coronary heart disease
Colorectal cancer
Overall mortality
15 125 10 75 5 25
Benefits Risks
CE
CE MPA
Santen RJ et al J Clin Endocrinol Metab 2010
The basis of the Endocrine Society scientific statement for postmenopausal hormone replacement therapy (HRT) excess risks and benefits of HRT for 5 years in women aged 50ndash59 years or within 10 years of the start of menopause E=estrogen P=progestin
bull Younger women (aged 50ndash59 years) had more favorable results bull There are differences between CE alone and CEMPA arms bull Overall benefitrisk ratio of CE-alone appears to be more favourable than CEMPA
Reevaluation of WHI data (stratified by age) Risks and
Benefits of HRT Cases per 1000 Women per 5 Years of
Use
Medical condition which may be exacerbated by treatment
with progestins
Diabetes and metabolic syndrome
bull Treatment of oestrogen deficiency symptoms with progestin-containing HT (unlike oestrogen alone) may be associated with increases in insulin resistance and deterioration in glucose tolerance123
bull Postmenopausal women with diabetes could be inappropriate for treatment with progestin-containing HT due to the potential risk of exacerbation of their condition
1) Panay N amp Studd JWW Human Reprod Update 1997
2) Godsland I et al Metabolism 1993
3) Sites CK et al J Clin Endocrinol Metab 2005
Variations in Associated Breast Cancer
Risks Between CE alone and CEMPA
bull Use of CE alone for a median of 59 years was associated with a lower incidence of invasive breast cancer (151 cases 027 per year) compared with placebo (199 cases 035 per year HR 077 95 CI 062ndash095 P=002)
bull In the CE alone group fewer women died from invasive breast cancer (6 deaths 0009 per year) compared with controls (16 deaths 0024 per year HR 037 95 CI 013ndash091 P=003)
Anderson GL et al Lancet
Oncol 2012
Bazedoxifene (BZA) specifically selected in
combination with conjugated estrogens
bull BZA has been specifically selected for its unique pharmacologic profile and effects on VMS and uterine tissue in particular123
1 Crabtree J et al Mol Cell Endocrinol 2008
2 Kharode Y et al Endocrinolology 2008
3 Duavive SmPC
Estrogen Receptor activity is dimmed
Estrogen Receptor activity is turned on
CEs are agonists BZA is an antagonist
In the uterus
bull The BZA component reduces the risk of endometrial hyperplasia that can occur with the conjugated estrogens component alone3 This means that progestins are not needed
Extensive global clinical development program for
CEBZA
aIncludes additional pilot dose-finding study 203 1 Lobo RA et al Fertil Steril 2009 2 Pinkerton JV et al Menopause 2009 3 Kagan R et al Menopause 2010 4 Mirkin S et al Climacteric 2013 5 Pinkerton JV et al Obstet Gynecol 2013
Effects of conjugated estrogensbazedoxifene on
lipid and coagulation variables a randomized
placebo- and active-controlled trial
bull At 12 months
bull Both CEBZA doses were associated with small but significant effects on hemostasis variables including reductions in antithrombin plasminogen activator inhibitor-1 and fibrinogen activity and an increase in plasminogen activity relative to placebo at 12 months Incidences of cardiovascular and venous thromboembolic events were similar among treatment groups
bull CONCLUSIONS
bull This study provides reassurance that CEBZA does not adversely affect lipid metabolism or hemostatic balance In accordance the incidences of venous thromboembolic events and cardiovascular events in postmenopausal women are similar to those observed with placebo
Breast tolerability profile similar to placebo following up to 2 years of treatment with CEBZA12
Pooled analysis of SMART clinical trials
CE 045BZA 20 (n=1585)
Placebo (n=1241)
Breast cancer incidence up to 2 years
(per 1000 woman-years)
100 (CI 000-321)
140 (CI 000-417)
Incidence of reported breast paintenderness up to 12 weeks
98-115 81-112
Incidence of abnormal mammogram at month 12
258 316
Mean change in breast density at month 12 (SMART-5)
ndash038 (n=186)
ndash032 (n=182)
Effects on the Breast
1 Pickar JH et al Menopause 2013 2 Pinkerton JV et al Obstet Gynecol 2013
CEBZA clinical overview - summary
bull In clinical trials CEBZA has demonstrated safety and efficacy in postmenopausal women with a uterus including the following
bull Significant reduction in number and severity of moderate to severe hot flushes1
bull Incidence of cumulative amenorrhea rate similar to placebo and significantly better than CEMPA2
bull Incidence of endometrial hyperplasia and breast tendernessdensity similar to that with placebo345
bull Incidence of adverse events and discontinuation rates similar to that with placebo6
1 Pinkerton JV et al Menopause 2009 2 Pinkerton JV et al J Clin Endocrinol Metab2014 3 Pickar JH et al
Fertil Steril 2009 4 Pinkerton at al J Clin Endocrinol Metab 2014 5 Pickar JH et al Menopause 2013 6 DUAVEE [package insert] New York NY Pfizer Inc 2013
CEBZA clinical overview - summary
Now women with a uterus who choose hormone therapy for management of menopausal symptoms have a choice
bull conventional estrogen-progestogen therapy or
bull a new combinationhellipconjugated estrogens paired with the SERM bazedoxifene
1 Pinkerton JV et al Menopause 2009 2 Pinkerton JV et al J Clin Endocrinol Metab2014 3 Pickar JH et al Fertil Steril 2009 4 Pinkerton at al J Clin Endocrinol Metab 2014 5 Pickar JH et al Menopause 2013 6 DUAVEE [package insert] New York NY Pfizer Inc 2013
Conjugated EstrogensBazedoxifene (CEBZA)
US indication
bull DUAVEE is indicated in women with a uterus for
bull 11 Treatment of Moderate to Severe Vasomotor Symptoms Associated with Menopause
bull 12 Prevention of Postmenopausal Osteoporosis
bull 13 Important Limitations of Use
bull Use DUAVEE for the shortest duration consistent with treatment goals and risks for the individual woman Postmenopausal women should be re-evaluated periodically as clinically appropriate to determine if treatment is still necessary
bull When prescribing solely for the prevention of postmenopausal osteoporosis therapy should only be considered for women at significant risk of osteoporosis and non-estrogen medication should be carefully considered
Conjugated EstrogensBazedoxifene (CEBZA)
EU indication
CEBZA is indicated for
bull Treatment of oestrogen deficiency symptoms in postmenopausal women with a uterus (with at least 12 months since the last menses) for whom treatment with progestin-containing therapy is not appropriate
bull The experience treating women older than 65 years is limited
bull Dose CE (045mg)Bazedoxifene (20mg)
Duavive SmPC
Which women with a uterus
could benefit from estrogens
without the need for a
progestin
Progestin intolerance is one of the main
factors for reduced compliance
bull About 20 of women receiving progestin-containing HT have significant progestin intolerance and half of these experience serious effects that prevent treatment continuation1
1 Panay N amp Studd J Human Reprod Update 1997
2 Panay N et al on behalf of the British Menopause Society and Womenrsquos Health Concern Menopause Int 2013
bull The 2013 British Menopause Society amp Womenrsquos Health
Concern recommendations on hormone replacement
therapy do recognise progestin intolerance as one of the
main factors for reduced compliance with HT 2
Proportion of patients () with at least one bleeding episode in relation to time and to the
used HT
Serge Rozenberg et al Hum Reprod 2009241739-1747
copy The Author 2009 Published by Oxford University Press on behalf of the European Society of
Human Reproduction and Embryology All rights reserved For Permissions please email
journalspermissionsoxfordjournalsorg
Breast tenderness after initiation of CEE
CEE + MPA (WHI)
and mammographic density change
bullCrandall et al Breast Cancer Res Treat DOI 101007s10549-011-1803-9
Breast density
Conclusion
bull CEEBAZO is an additional regimen for menopausal symptoms it provides also a prevention for osteoporosis
bull It is suitable for women with a uterus who are unsatisfied with an EPT regimen or who you are unwilling to treat with an EPT regimen
Adapted use of MHT
bull Lower dosage of estrogens
bull Other progestins
bull Better safety profile
bull Vaginal estrogen or SERMS
bull Non-hormonal therapy
bull Development of new products
bull SERMS + estrogens
Most common adverse events leading to
discontinuation are related to progestins12
bull breakthrough bleeding
bull Low compliance
bull Increase in the number of US
bull Stress
bull Cost
bull uterine procedures
bull Unnecessary endometrial biopsies Hysteroscopies DampC Hysterectomies
bull Morbidity
Proportion of patients who completed or discontinued treatment in relation to the used HT
Serge Rozenberg et al Hum Reprod 2009241739-1747
copy The Author 2009 Published by Oxford University Press on behalf of the European Society of
Human Reproduction and Embryology All rights reserved For Permissions please email
journalspermissionsoxfordjournalsorg
Most common adverse events leading to discontinuation
are related to progestins
bull breast paintenderness
Breast tenderness after initiation of CEE
CEE + MPA (WHI)
and mammographic density change
bullCrandall et al Breast Cancer Res Treat DOI 101007s10549-011-1803-9
Breast density
Hormone therapy use and mammographic
density in postmenopausal Norwegian women
bull Results differed when considering the combined effect of age and BMI
bull The effect of EPT on mammographic density was modified by age and BMI with no apparent association among the youngest women (aged 50-55) with the highest BMI (BMI ge 26)
bull A higher mammographic density was found in EPT users compared to never HT users particularly in women using high-dose NETA regimens Age and BMI modified the association between EPT use and mammographic density
bull Couto E et al Breast Cancer Res Treat 2011 Nov 4 [Epub ahead of print]
Breast Cancer Risk by Breast Density
Menopause and Postmenopausal Hormone
Therapy Use
Birads age HT Duration Risk
1 55-59 None 5 year risk 08 (95 CI 06- 09)
1 55-59
ET EPT 5 year risk 09 (95 CI 07 -11)
4 55-59
None 5 year risk 24 (95 CI 20 -28)
4 55-59
ET 5 year risk
30 (95 CI 26 -35)
4 55-59
EPT 5 year risk
42 (95 CI 37 -46)
Adapted from Kerlikowske et al JOURNAL OF CLINICAL ONCOLOGY 2010
Breast Cancer Risk by Breast Density
Menopause and Postmenopausal Hormone
Therapy Use
Adapted from Kerlikowske et al JOURNAL OF CLINICAL ONCOLOGY 2010
bull Postmenopausal women with high breast density are at increased risk of breast cancer and should be aware of the added risk of taking HT especially estrogen plus progestin
Medical condition which may be exacerbated by treatment
with progestins
Diabetes and metabolic syndrome
bull progestin-containing HT may be associated with increases in insulin resistance and deterioration in glucose tolerance123
bull Postmenopausal women with diabetes could be inappropriate for treatment with progestin-containing HT due to the potential risk of exacerbation of their condition
1) Panay N amp Studd JWW Human Reprod Update 1997
2) Godsland I et al Metabolism 1993
3) Sites CK et al J Clin Endocrinol Metab 2005
A Nath and R Sitruk-Ware CLIMACTERIC 200912(Suppl 1)96ndash101
A Nath and R Sitruk-Ware CLIMACTERIC 200912(Suppl 1)96ndash101
Diabetes an epidemy
bull UK 1996 14 million of diabetics
bull UK 2015 32 million (6 of the population)
bull UK 2025 5 million
bull httpwwwdiabetescoukdiabetes-prevalencehtml
Other progestin-related intolerance issues
bull Nausea
bull Depressive mood
bull Poor concentration
bull Hirsutism
bull Headache
bull Dizziness
bull Fluid retention
bull Weight gain Panay N amp Studd JWW Human Reprod Update 1997
Medical condition which may be exacerbated by treatment with progestins
PMSPMDDdepression
bull Progesterone-induced PMD can be exacerbated by exogenous progestin administration and can occur in association with HT or OC administration1
bull Significantly higher negative mood scores have been observed during the addition of a progestin to an estrogen in a sequential HT regimen in postmenopausal women with a history of PMS compared to those without2
bull Women with a history of PMS or PMD exacerbation of depression using progestins may therefore benefit from a progestin free treatment for menopausal symptoms
1) Nevatte T et al Arch Womens Ment Health 2013 2) Bjoumlrn I et al Climacteric 2006 PMS premenstrual syndrome
PMDD premenstrual dysphoric disorder
Conclusion
bull CEEBAZO is an additional regimen for menopausal symptoms it provides also a prevention for osteoporosis
bull It is suitable for women with a uterus who are unsatisfied with an EPT regimen or who you are unwilling to treat with an EPT regimen
For some postmenopausal women with a uterus there is a
need for progestin free treatment options
bull with demonstrated clinical efficacy
bull which protects the endometrium
bull improved tolerabilitysafety profile
In clinical practice this translates to women who are
intolerant of progestin-containing HT or have conditions
which may be exacerbated by treatment with progestins
Conclusion Medical need for alternative treatment option
Medical condition which may be exacerbated by treatment with progestins
Depression
bull Progestin-containing HT has been associated with increases in depressive symptoms in some individuals1
bull There is a biochemicalphysiological plausibility for the association of progestins with depression234
bull Therefore postmenopausal women who also have a medical history of depressive disorders or depression could be inappropriate for treatment with progestin-containing HT
Pfizer Confidential
65
1) Girdler SS et al J Womens Health Gend Based Med 1999 2) Traish AM et al Korean J Urol 2014 3) Stroumlhle A et al Biol Psychiatry 1999 4) Romeo E et
al Am J Psychiatry 1998
History of the following conditions may make progestin inappropriate
bull Depression
bull PMSPMDD
PMS premenstrual syndrome
PMD premenstrual dysphoric disorder
Medical conditions that may be exacerbated by treatment with progestins
Women for whom progestin-containing HT
would not be considered appropriate
minus Women who are intolerant of progestin-containing hormone therapy
minus Women with pre-existing medical conditions that may be exacerbated by progestins
Most common adverse events leading to discontinuation are related to progestins12
breakthrough bleeding
bull Increase in the number of uterine procedures (ie unnecessary endometrial biopsies)
breast paintenderness
bull Increase in the number of breast interventions
1 Steel SA et al Climacteric 2003 2 Ettinger B and Pressman A Am J Manag Care 1999 3 Komm BS Mirkin S
Pharmaceuticals 2012
4 Panay N amp Studd JWW Human Reprod Update 1997
bull Nausea bull Depressive mood bull Poor concentration bull Hirsutism bull Headache bull Dizziness bull Fluid retention bull Weight gain
Other progestin-related intolerance issues4
Unmet need with the treatment of postmenopausal symptoms
bull Alternatives to progestin are needed that will protect the endometrium while avoiding other progestin-associated effects and preserving the desired effects of estrogens in postmenopausal women3
Which women with a uterus could benefit from
estrogens without the need for a progestin
bull Women who are intolerant of progestin-containing hormone therapy
bull Women with pre-existing medical conditions that may be exacerbated by progestins (eg women with a history of depression PMSPMDD increased breast density diabetes and metabolic syndrome)
History of the following conditions may make progestin inappropriate
bull Depression
bull PMSPMDD
bull High breast density
bull Diabetes and metabolic syndrome
PMS premenstrual syndrome
PMD premenstrual dysphoric disorder
Medical conditions that may be exacerbated by treatment with progestins
Learning from WHI data
bull Hormone therapy (HT) is the conventional and established therapy option to effectively treat postmenopausal symptoms however it has been associated with some safety and tolerability concerns1 2
bull A review of WHI data suggests that many of the concerns with menopausal HT more often associated with EPT (CE+MPA) such as CHD risk increased breast density breast pain and breast cancer risk than with ET (CEE alone)2
1 Rolnick SJ Kopher RA DeFor TA et al Menopause 2005
2 Komm BS Mirkin S Pharmaceuticals 2012
WHI Womenrsquos Health Initiative trial
CHD coronary heart disease
CEE conjugated equine estrogens
Efficacy and Safety of Constant Oestrogen
Pulsed Progestogen vs
Continuous Combined HRT
Adverse Events
17b-oestradiol 17b-oestradiol norgestimate NETA (n = 150) (n = 172) Breast discomfort 14 27 Abdominal discomfort 14 22 Uterine bleeding 15 12 Dysmenorrhea 3 8 Oedema 5 8
Adapted from S Rozenberg et al Human Reproduction 2000
Medical condition which may be exacerbated by treatment
with progestins
Increased breast density
bull Increases in breast density are associated with progestin-containing HT which may adversely affect radiological detection of breast cancer1 and may be independently associated with an increased risk for the development of breast cancer2
bull The Postmenopausal EstrogenProgestin Interventions (PEPI) trial demonstrated that an increased mammographic breast density was associated with the use of E+P but not with the use of estrogen alone3
bull Women who already have high breast density may therefore be considered inappropriate for treatment with a progestin-containing HT
1) EU Core SPC for Hormone Replacement Therapy Products (CMDh1312003 Rev 4 June
2012)
2) De Villiers TJ et al on behalf of the International Menopause Society Climacteric 2013 16
3) Greendale GA et al J Natl Cancer Inst 2003
Stroke
0 25 5 75 10 125
Fractures
Diabetes
Breast cancer
Cholecystitis
Venothrombotic episodes
Endometrial cancer
Lung cancer
Coronary heart disease
Colorectal cancer
Overall mortality
15 125 10 75 5 25
Benefits Risks
CE
CE MPA
Santen RJ et al J Clin Endocrinol Metab 2010
The basis of the Endocrine Society scientific statement for postmenopausal hormone replacement therapy (HRT) excess risks and benefits of HRT for 5 years in women aged 50ndash59 years or within 10 years of the start of menopause E=estrogen P=progestin
bull Younger women (aged 50ndash59 years) had more favorable results bull There are differences between CE alone and CEMPA arms bull Overall benefitrisk ratio of CE-alone appears to be more favourable than CEMPA
Reevaluation of WHI data (stratified by age) Risks and
Benefits of HRT Cases per 1000 Women per 5 Years of
Use
Medical condition which may be exacerbated by treatment
with progestins
Diabetes and metabolic syndrome
bull Treatment of oestrogen deficiency symptoms with progestin-containing HT (unlike oestrogen alone) may be associated with increases in insulin resistance and deterioration in glucose tolerance123
bull Postmenopausal women with diabetes could be inappropriate for treatment with progestin-containing HT due to the potential risk of exacerbation of their condition
1) Panay N amp Studd JWW Human Reprod Update 1997
2) Godsland I et al Metabolism 1993
3) Sites CK et al J Clin Endocrinol Metab 2005
Variations in Associated Breast Cancer
Risks Between CE alone and CEMPA
bull Use of CE alone for a median of 59 years was associated with a lower incidence of invasive breast cancer (151 cases 027 per year) compared with placebo (199 cases 035 per year HR 077 95 CI 062ndash095 P=002)
bull In the CE alone group fewer women died from invasive breast cancer (6 deaths 0009 per year) compared with controls (16 deaths 0024 per year HR 037 95 CI 013ndash091 P=003)
Anderson GL et al Lancet
Oncol 2012
Bazedoxifene (BZA) specifically selected in
combination with conjugated estrogens
bull BZA has been specifically selected for its unique pharmacologic profile and effects on VMS and uterine tissue in particular123
1 Crabtree J et al Mol Cell Endocrinol 2008
2 Kharode Y et al Endocrinolology 2008
3 Duavive SmPC
Estrogen Receptor activity is dimmed
Estrogen Receptor activity is turned on
CEs are agonists BZA is an antagonist
In the uterus
bull The BZA component reduces the risk of endometrial hyperplasia that can occur with the conjugated estrogens component alone3 This means that progestins are not needed
Extensive global clinical development program for
CEBZA
aIncludes additional pilot dose-finding study 203 1 Lobo RA et al Fertil Steril 2009 2 Pinkerton JV et al Menopause 2009 3 Kagan R et al Menopause 2010 4 Mirkin S et al Climacteric 2013 5 Pinkerton JV et al Obstet Gynecol 2013
Effects of conjugated estrogensbazedoxifene on
lipid and coagulation variables a randomized
placebo- and active-controlled trial
bull At 12 months
bull Both CEBZA doses were associated with small but significant effects on hemostasis variables including reductions in antithrombin plasminogen activator inhibitor-1 and fibrinogen activity and an increase in plasminogen activity relative to placebo at 12 months Incidences of cardiovascular and venous thromboembolic events were similar among treatment groups
bull CONCLUSIONS
bull This study provides reassurance that CEBZA does not adversely affect lipid metabolism or hemostatic balance In accordance the incidences of venous thromboembolic events and cardiovascular events in postmenopausal women are similar to those observed with placebo
CEBZA clinical overview - summary
bull In clinical trials CEBZA has demonstrated safety and efficacy in postmenopausal women with a uterus including the following
bull Significant reduction in number and severity of moderate to severe hot flushes1
bull Incidence of cumulative amenorrhea rate similar to placebo and significantly better than CEMPA2
bull Incidence of endometrial hyperplasia and breast tendernessdensity similar to that with placebo345
bull Incidence of adverse events and discontinuation rates similar to that with placebo6
1 Pinkerton JV et al Menopause 2009 2 Pinkerton JV et al J Clin Endocrinol Metab2014 3 Pickar JH et al
Fertil Steril 2009 4 Pinkerton at al J Clin Endocrinol Metab 2014 5 Pickar JH et al Menopause 2013 6 DUAVEE [package insert] New York NY Pfizer Inc 2013
CEBZA clinical overview - summary
Now women with a uterus who choose hormone therapy for management of menopausal symptoms have a choice
bull conventional estrogen-progestogen therapy or
bull a new combinationhellipconjugated estrogens paired with the SERM bazedoxifene
1 Pinkerton JV et al Menopause 2009 2 Pinkerton JV et al J Clin Endocrinol Metab2014 3 Pickar JH et al Fertil Steril 2009 4 Pinkerton at al J Clin Endocrinol Metab 2014 5 Pickar JH et al Menopause 2013 6 DUAVEE [package insert] New York NY Pfizer Inc 2013
Conjugated EstrogensBazedoxifene (CEBZA)
US indication
bull DUAVEE is indicated in women with a uterus for
bull 11 Treatment of Moderate to Severe Vasomotor Symptoms Associated with Menopause
bull 12 Prevention of Postmenopausal Osteoporosis
bull 13 Important Limitations of Use
bull Use DUAVEE for the shortest duration consistent with treatment goals and risks for the individual woman Postmenopausal women should be re-evaluated periodically as clinically appropriate to determine if treatment is still necessary
bull When prescribing solely for the prevention of postmenopausal osteoporosis therapy should only be considered for women at significant risk of osteoporosis and non-estrogen medication should be carefully considered
Conjugated EstrogensBazedoxifene (CEBZA)
EU indication
CEBZA is indicated for
bull Treatment of oestrogen deficiency symptoms in postmenopausal women with a uterus (with at least 12 months since the last menses) for whom treatment with progestin-containing therapy is not appropriate
bull The experience treating women older than 65 years is limited
bull Dose CE (045mg)Bazedoxifene (20mg)
Duavive SmPC
Which women with a uterus
could benefit from estrogens
without the need for a
progestin
Progestin intolerance is one of the main
factors for reduced compliance
bull About 20 of women receiving progestin-containing HT have significant progestin intolerance and half of these experience serious effects that prevent treatment continuation1
1 Panay N amp Studd J Human Reprod Update 1997
2 Panay N et al on behalf of the British Menopause Society and Womenrsquos Health Concern Menopause Int 2013
bull The 2013 British Menopause Society amp Womenrsquos Health
Concern recommendations on hormone replacement
therapy do recognise progestin intolerance as one of the
main factors for reduced compliance with HT 2
Proportion of patients () with at least one bleeding episode in relation to time and to the
used HT
Serge Rozenberg et al Hum Reprod 2009241739-1747
copy The Author 2009 Published by Oxford University Press on behalf of the European Society of
Human Reproduction and Embryology All rights reserved For Permissions please email
journalspermissionsoxfordjournalsorg
Breast tenderness after initiation of CEE
CEE + MPA (WHI)
and mammographic density change
bullCrandall et al Breast Cancer Res Treat DOI 101007s10549-011-1803-9
Breast density
Conclusion
bull CEEBAZO is an additional regimen for menopausal symptoms it provides also a prevention for osteoporosis
bull It is suitable for women with a uterus who are unsatisfied with an EPT regimen or who you are unwilling to treat with an EPT regimen
Adapted use of MHT
bull Lower dosage of estrogens
bull Other progestins
bull Better safety profile
bull Vaginal estrogen or SERMS
bull Non-hormonal therapy
bull Development of new products
bull SERMS + estrogens
Most common adverse events leading to
discontinuation are related to progestins12
bull breakthrough bleeding
bull Low compliance
bull Increase in the number of US
bull Stress
bull Cost
bull uterine procedures
bull Unnecessary endometrial biopsies Hysteroscopies DampC Hysterectomies
bull Morbidity
Proportion of patients who completed or discontinued treatment in relation to the used HT
Serge Rozenberg et al Hum Reprod 2009241739-1747
copy The Author 2009 Published by Oxford University Press on behalf of the European Society of
Human Reproduction and Embryology All rights reserved For Permissions please email
journalspermissionsoxfordjournalsorg
Most common adverse events leading to discontinuation
are related to progestins
bull breast paintenderness
Breast tenderness after initiation of CEE
CEE + MPA (WHI)
and mammographic density change
bullCrandall et al Breast Cancer Res Treat DOI 101007s10549-011-1803-9
Breast density
Hormone therapy use and mammographic
density in postmenopausal Norwegian women
bull Results differed when considering the combined effect of age and BMI
bull The effect of EPT on mammographic density was modified by age and BMI with no apparent association among the youngest women (aged 50-55) with the highest BMI (BMI ge 26)
bull A higher mammographic density was found in EPT users compared to never HT users particularly in women using high-dose NETA regimens Age and BMI modified the association between EPT use and mammographic density
bull Couto E et al Breast Cancer Res Treat 2011 Nov 4 [Epub ahead of print]
Breast Cancer Risk by Breast Density
Menopause and Postmenopausal Hormone
Therapy Use
Birads age HT Duration Risk
1 55-59 None 5 year risk 08 (95 CI 06- 09)
1 55-59
ET EPT 5 year risk 09 (95 CI 07 -11)
4 55-59
None 5 year risk 24 (95 CI 20 -28)
4 55-59
ET 5 year risk
30 (95 CI 26 -35)
4 55-59
EPT 5 year risk
42 (95 CI 37 -46)
Adapted from Kerlikowske et al JOURNAL OF CLINICAL ONCOLOGY 2010
Breast Cancer Risk by Breast Density
Menopause and Postmenopausal Hormone
Therapy Use
Adapted from Kerlikowske et al JOURNAL OF CLINICAL ONCOLOGY 2010
bull Postmenopausal women with high breast density are at increased risk of breast cancer and should be aware of the added risk of taking HT especially estrogen plus progestin
Medical condition which may be exacerbated by treatment
with progestins
Diabetes and metabolic syndrome
bull progestin-containing HT may be associated with increases in insulin resistance and deterioration in glucose tolerance123
bull Postmenopausal women with diabetes could be inappropriate for treatment with progestin-containing HT due to the potential risk of exacerbation of their condition
1) Panay N amp Studd JWW Human Reprod Update 1997
2) Godsland I et al Metabolism 1993
3) Sites CK et al J Clin Endocrinol Metab 2005
A Nath and R Sitruk-Ware CLIMACTERIC 200912(Suppl 1)96ndash101
A Nath and R Sitruk-Ware CLIMACTERIC 200912(Suppl 1)96ndash101
Diabetes an epidemy
bull UK 1996 14 million of diabetics
bull UK 2015 32 million (6 of the population)
bull UK 2025 5 million
bull httpwwwdiabetescoukdiabetes-prevalencehtml
Other progestin-related intolerance issues
bull Nausea
bull Depressive mood
bull Poor concentration
bull Hirsutism
bull Headache
bull Dizziness
bull Fluid retention
bull Weight gain Panay N amp Studd JWW Human Reprod Update 1997
Medical condition which may be exacerbated by treatment with progestins
PMSPMDDdepression
bull Progesterone-induced PMD can be exacerbated by exogenous progestin administration and can occur in association with HT or OC administration1
bull Significantly higher negative mood scores have been observed during the addition of a progestin to an estrogen in a sequential HT regimen in postmenopausal women with a history of PMS compared to those without2
bull Women with a history of PMS or PMD exacerbation of depression using progestins may therefore benefit from a progestin free treatment for menopausal symptoms
1) Nevatte T et al Arch Womens Ment Health 2013 2) Bjoumlrn I et al Climacteric 2006 PMS premenstrual syndrome
PMDD premenstrual dysphoric disorder
Conclusion
bull CEEBAZO is an additional regimen for menopausal symptoms it provides also a prevention for osteoporosis
bull It is suitable for women with a uterus who are unsatisfied with an EPT regimen or who you are unwilling to treat with an EPT regimen
For some postmenopausal women with a uterus there is a
need for progestin free treatment options
bull with demonstrated clinical efficacy
bull which protects the endometrium
bull improved tolerabilitysafety profile
In clinical practice this translates to women who are
intolerant of progestin-containing HT or have conditions
which may be exacerbated by treatment with progestins
Conclusion Medical need for alternative treatment option
Medical condition which may be exacerbated by treatment with progestins
Depression
bull Progestin-containing HT has been associated with increases in depressive symptoms in some individuals1
bull There is a biochemicalphysiological plausibility for the association of progestins with depression234
bull Therefore postmenopausal women who also have a medical history of depressive disorders or depression could be inappropriate for treatment with progestin-containing HT
Pfizer Confidential
65
1) Girdler SS et al J Womens Health Gend Based Med 1999 2) Traish AM et al Korean J Urol 2014 3) Stroumlhle A et al Biol Psychiatry 1999 4) Romeo E et
al Am J Psychiatry 1998
History of the following conditions may make progestin inappropriate
bull Depression
bull PMSPMDD
PMS premenstrual syndrome
PMD premenstrual dysphoric disorder
Medical conditions that may be exacerbated by treatment with progestins
Women for whom progestin-containing HT
would not be considered appropriate
minus Women who are intolerant of progestin-containing hormone therapy
minus Women with pre-existing medical conditions that may be exacerbated by progestins
Most common adverse events leading to discontinuation are related to progestins12
breakthrough bleeding
bull Increase in the number of uterine procedures (ie unnecessary endometrial biopsies)
breast paintenderness
bull Increase in the number of breast interventions
1 Steel SA et al Climacteric 2003 2 Ettinger B and Pressman A Am J Manag Care 1999 3 Komm BS Mirkin S
Pharmaceuticals 2012
4 Panay N amp Studd JWW Human Reprod Update 1997
bull Nausea bull Depressive mood bull Poor concentration bull Hirsutism bull Headache bull Dizziness bull Fluid retention bull Weight gain
Other progestin-related intolerance issues4
Unmet need with the treatment of postmenopausal symptoms
bull Alternatives to progestin are needed that will protect the endometrium while avoiding other progestin-associated effects and preserving the desired effects of estrogens in postmenopausal women3
Which women with a uterus could benefit from
estrogens without the need for a progestin
bull Women who are intolerant of progestin-containing hormone therapy
bull Women with pre-existing medical conditions that may be exacerbated by progestins (eg women with a history of depression PMSPMDD increased breast density diabetes and metabolic syndrome)
History of the following conditions may make progestin inappropriate
bull Depression
bull PMSPMDD
bull High breast density
bull Diabetes and metabolic syndrome
PMS premenstrual syndrome
PMD premenstrual dysphoric disorder
Medical conditions that may be exacerbated by treatment with progestins
Learning from WHI data
bull Hormone therapy (HT) is the conventional and established therapy option to effectively treat postmenopausal symptoms however it has been associated with some safety and tolerability concerns1 2
bull A review of WHI data suggests that many of the concerns with menopausal HT more often associated with EPT (CE+MPA) such as CHD risk increased breast density breast pain and breast cancer risk than with ET (CEE alone)2
1 Rolnick SJ Kopher RA DeFor TA et al Menopause 2005
2 Komm BS Mirkin S Pharmaceuticals 2012
WHI Womenrsquos Health Initiative trial
CHD coronary heart disease
CEE conjugated equine estrogens
Efficacy and Safety of Constant Oestrogen
Pulsed Progestogen vs
Continuous Combined HRT
Adverse Events
17b-oestradiol 17b-oestradiol norgestimate NETA (n = 150) (n = 172) Breast discomfort 14 27 Abdominal discomfort 14 22 Uterine bleeding 15 12 Dysmenorrhea 3 8 Oedema 5 8
Adapted from S Rozenberg et al Human Reproduction 2000
Medical condition which may be exacerbated by treatment
with progestins
Increased breast density
bull Increases in breast density are associated with progestin-containing HT which may adversely affect radiological detection of breast cancer1 and may be independently associated with an increased risk for the development of breast cancer2
bull The Postmenopausal EstrogenProgestin Interventions (PEPI) trial demonstrated that an increased mammographic breast density was associated with the use of E+P but not with the use of estrogen alone3
bull Women who already have high breast density may therefore be considered inappropriate for treatment with a progestin-containing HT
1) EU Core SPC for Hormone Replacement Therapy Products (CMDh1312003 Rev 4 June
2012)
2) De Villiers TJ et al on behalf of the International Menopause Society Climacteric 2013 16
3) Greendale GA et al J Natl Cancer Inst 2003
Stroke
0 25 5 75 10 125
Fractures
Diabetes
Breast cancer
Cholecystitis
Venothrombotic episodes
Endometrial cancer
Lung cancer
Coronary heart disease
Colorectal cancer
Overall mortality
15 125 10 75 5 25
Benefits Risks
CE
CE MPA
Santen RJ et al J Clin Endocrinol Metab 2010
The basis of the Endocrine Society scientific statement for postmenopausal hormone replacement therapy (HRT) excess risks and benefits of HRT for 5 years in women aged 50ndash59 years or within 10 years of the start of menopause E=estrogen P=progestin
bull Younger women (aged 50ndash59 years) had more favorable results bull There are differences between CE alone and CEMPA arms bull Overall benefitrisk ratio of CE-alone appears to be more favourable than CEMPA
Reevaluation of WHI data (stratified by age) Risks and
Benefits of HRT Cases per 1000 Women per 5 Years of
Use
Medical condition which may be exacerbated by treatment
with progestins
Diabetes and metabolic syndrome
bull Treatment of oestrogen deficiency symptoms with progestin-containing HT (unlike oestrogen alone) may be associated with increases in insulin resistance and deterioration in glucose tolerance123
bull Postmenopausal women with diabetes could be inappropriate for treatment with progestin-containing HT due to the potential risk of exacerbation of their condition
1) Panay N amp Studd JWW Human Reprod Update 1997
2) Godsland I et al Metabolism 1993
3) Sites CK et al J Clin Endocrinol Metab 2005
Variations in Associated Breast Cancer
Risks Between CE alone and CEMPA
bull Use of CE alone for a median of 59 years was associated with a lower incidence of invasive breast cancer (151 cases 027 per year) compared with placebo (199 cases 035 per year HR 077 95 CI 062ndash095 P=002)
bull In the CE alone group fewer women died from invasive breast cancer (6 deaths 0009 per year) compared with controls (16 deaths 0024 per year HR 037 95 CI 013ndash091 P=003)
Anderson GL et al Lancet
Oncol 2012
Bazedoxifene (BZA) specifically selected in
combination with conjugated estrogens
bull BZA has been specifically selected for its unique pharmacologic profile and effects on VMS and uterine tissue in particular123
1 Crabtree J et al Mol Cell Endocrinol 2008
2 Kharode Y et al Endocrinolology 2008
3 Duavive SmPC
Estrogen Receptor activity is dimmed
Estrogen Receptor activity is turned on
CEs are agonists BZA is an antagonist
In the uterus
bull The BZA component reduces the risk of endometrial hyperplasia that can occur with the conjugated estrogens component alone3 This means that progestins are not needed
Extensive global clinical development program for
CEBZA
aIncludes additional pilot dose-finding study 203 1 Lobo RA et al Fertil Steril 2009 2 Pinkerton JV et al Menopause 2009 3 Kagan R et al Menopause 2010 4 Mirkin S et al Climacteric 2013 5 Pinkerton JV et al Obstet Gynecol 2013
Effects of conjugated estrogensbazedoxifene on
lipid and coagulation variables a randomized
placebo- and active-controlled trial
bull At 12 months
bull Both CEBZA doses were associated with small but significant effects on hemostasis variables including reductions in antithrombin plasminogen activator inhibitor-1 and fibrinogen activity and an increase in plasminogen activity relative to placebo at 12 months Incidences of cardiovascular and venous thromboembolic events were similar among treatment groups
bull CONCLUSIONS
bull This study provides reassurance that CEBZA does not adversely affect lipid metabolism or hemostatic balance In accordance the incidences of venous thromboembolic events and cardiovascular events in postmenopausal women are similar to those observed with placebo

CEBZA clinical overview - summary
Now women with a uterus who choose hormone therapy for management of menopausal symptoms have a choice
bull conventional estrogen-progestogen therapy or
bull a new combinationhellipconjugated estrogens paired with the SERM bazedoxifene
1 Pinkerton JV et al Menopause 2009 2 Pinkerton JV et al J Clin Endocrinol Metab2014 3 Pickar JH et al Fertil Steril 2009 4 Pinkerton at al J Clin Endocrinol Metab 2014 5 Pickar JH et al Menopause 2013 6 DUAVEE [package insert] New York NY Pfizer Inc 2013
Conjugated EstrogensBazedoxifene (CEBZA)
US indication
bull DUAVEE is indicated in women with a uterus for
bull 11 Treatment of Moderate to Severe Vasomotor Symptoms Associated with Menopause
bull 12 Prevention of Postmenopausal Osteoporosis
bull 13 Important Limitations of Use
bull Use DUAVEE for the shortest duration consistent with treatment goals and risks for the individual woman Postmenopausal women should be re-evaluated periodically as clinically appropriate to determine if treatment is still necessary
bull When prescribing solely for the prevention of postmenopausal osteoporosis therapy should only be considered for women at significant risk of osteoporosis and non-estrogen medication should be carefully considered
Conjugated EstrogensBazedoxifene (CEBZA)
EU indication
CEBZA is indicated for
bull Treatment of oestrogen deficiency symptoms in postmenopausal women with a uterus (with at least 12 months since the last menses) for whom treatment with progestin-containing therapy is not appropriate
bull The experience treating women older than 65 years is limited
bull Dose CE (045mg)Bazedoxifene (20mg)
Duavive SmPC
Which women with a uterus
could benefit from estrogens
without the need for a
progestin
Progestin intolerance is one of the main
factors for reduced compliance
bull About 20 of women receiving progestin-containing HT have significant progestin intolerance and half of these experience serious effects that prevent treatment continuation1
1 Panay N amp Studd J Human Reprod Update 1997
2 Panay N et al on behalf of the British Menopause Society and Womenrsquos Health Concern Menopause Int 2013
bull The 2013 British Menopause Society amp Womenrsquos Health
Concern recommendations on hormone replacement
therapy do recognise progestin intolerance as one of the
main factors for reduced compliance with HT 2
Proportion of patients () with at least one bleeding episode in relation to time and to the
used HT
Serge Rozenberg et al Hum Reprod 2009241739-1747
copy The Author 2009 Published by Oxford University Press on behalf of the European Society of
Human Reproduction and Embryology All rights reserved For Permissions please email
journalspermissionsoxfordjournalsorg
Breast tenderness after initiation of CEE
CEE + MPA (WHI)
and mammographic density change
bullCrandall et al Breast Cancer Res Treat DOI 101007s10549-011-1803-9
Breast density
Conclusion
bull CEEBAZO is an additional regimen for menopausal symptoms it provides also a prevention for osteoporosis
bull It is suitable for women with a uterus who are unsatisfied with an EPT regimen or who you are unwilling to treat with an EPT regimen
Adapted use of MHT
bull Lower dosage of estrogens
bull Other progestins
bull Better safety profile
bull Vaginal estrogen or SERMS
bull Non-hormonal therapy
bull Development of new products
bull SERMS + estrogens
Most common adverse events leading to
discontinuation are related to progestins12
bull breakthrough bleeding
bull Low compliance
bull Increase in the number of US
bull Stress
bull Cost
bull uterine procedures
bull Unnecessary endometrial biopsies Hysteroscopies DampC Hysterectomies
bull Morbidity
Proportion of patients who completed or discontinued treatment in relation to the used HT
Serge Rozenberg et al Hum Reprod 2009241739-1747
copy The Author 2009 Published by Oxford University Press on behalf of the European Society of
Human Reproduction and Embryology All rights reserved For Permissions please email
journalspermissionsoxfordjournalsorg
Most common adverse events leading to discontinuation
are related to progestins
bull breast paintenderness
Breast tenderness after initiation of CEE
CEE + MPA (WHI)
and mammographic density change
bullCrandall et al Breast Cancer Res Treat DOI 101007s10549-011-1803-9
Breast density
Hormone therapy use and mammographic
density in postmenopausal Norwegian women
bull Results differed when considering the combined effect of age and BMI
bull The effect of EPT on mammographic density was modified by age and BMI with no apparent association among the youngest women (aged 50-55) with the highest BMI (BMI ge 26)
bull A higher mammographic density was found in EPT users compared to never HT users particularly in women using high-dose NETA regimens Age and BMI modified the association between EPT use and mammographic density
bull Couto E et al Breast Cancer Res Treat 2011 Nov 4 [Epub ahead of print]
Breast Cancer Risk by Breast Density
Menopause and Postmenopausal Hormone
Therapy Use
Birads age HT Duration Risk
1 55-59 None 5 year risk 08 (95 CI 06- 09)
1 55-59
ET EPT 5 year risk 09 (95 CI 07 -11)
4 55-59
None 5 year risk 24 (95 CI 20 -28)
4 55-59
ET 5 year risk
30 (95 CI 26 -35)
4 55-59
EPT 5 year risk
42 (95 CI 37 -46)
Adapted from Kerlikowske et al JOURNAL OF CLINICAL ONCOLOGY 2010
Breast Cancer Risk by Breast Density
Menopause and Postmenopausal Hormone
Therapy Use
Adapted from Kerlikowske et al JOURNAL OF CLINICAL ONCOLOGY 2010
bull Postmenopausal women with high breast density are at increased risk of breast cancer and should be aware of the added risk of taking HT especially estrogen plus progestin
Medical condition which may be exacerbated by treatment
with progestins
Diabetes and metabolic syndrome
bull progestin-containing HT may be associated with increases in insulin resistance and deterioration in glucose tolerance123
bull Postmenopausal women with diabetes could be inappropriate for treatment with progestin-containing HT due to the potential risk of exacerbation of their condition
1) Panay N amp Studd JWW Human Reprod Update 1997
2) Godsland I et al Metabolism 1993
3) Sites CK et al J Clin Endocrinol Metab 2005
A Nath and R Sitruk-Ware CLIMACTERIC 200912(Suppl 1)96ndash101
A Nath and R Sitruk-Ware CLIMACTERIC 200912(Suppl 1)96ndash101
Diabetes an epidemy
bull UK 1996 14 million of diabetics
bull UK 2015 32 million (6 of the population)
bull UK 2025 5 million
bull httpwwwdiabetescoukdiabetes-prevalencehtml
Other progestin-related intolerance issues
bull Nausea
bull Depressive mood
bull Poor concentration
bull Hirsutism
bull Headache
bull Dizziness
bull Fluid retention
bull Weight gain Panay N amp Studd JWW Human Reprod Update 1997
Medical condition which may be exacerbated by treatment with progestins
PMSPMDDdepression
bull Progesterone-induced PMD can be exacerbated by exogenous progestin administration and can occur in association with HT or OC administration1
bull Significantly higher negative mood scores have been observed during the addition of a progestin to an estrogen in a sequential HT regimen in postmenopausal women with a history of PMS compared to those without2
bull Women with a history of PMS or PMD exacerbation of depression using progestins may therefore benefit from a progestin free treatment for menopausal symptoms
1) Nevatte T et al Arch Womens Ment Health 2013 2) Bjoumlrn I et al Climacteric 2006 PMS premenstrual syndrome
PMDD premenstrual dysphoric disorder
Conclusion
bull CEEBAZO is an additional regimen for menopausal symptoms it provides also a prevention for osteoporosis
bull It is suitable for women with a uterus who are unsatisfied with an EPT regimen or who you are unwilling to treat with an EPT regimen
For some postmenopausal women with a uterus there is a
need for progestin free treatment options
bull with demonstrated clinical efficacy
bull which protects the endometrium
bull improved tolerabilitysafety profile
In clinical practice this translates to women who are
intolerant of progestin-containing HT or have conditions
which may be exacerbated by treatment with progestins
Conclusion Medical need for alternative treatment option
Medical condition which may be exacerbated by treatment with progestins
Depression
bull Progestin-containing HT has been associated with increases in depressive symptoms in some individuals1
bull There is a biochemicalphysiological plausibility for the association of progestins with depression234
bull Therefore postmenopausal women who also have a medical history of depressive disorders or depression could be inappropriate for treatment with progestin-containing HT
Pfizer Confidential
65
1) Girdler SS et al J Womens Health Gend Based Med 1999 2) Traish AM et al Korean J Urol 2014 3) Stroumlhle A et al Biol Psychiatry 1999 4) Romeo E et
al Am J Psychiatry 1998
History of the following conditions may make progestin inappropriate
bull Depression
bull PMSPMDD
PMS premenstrual syndrome
PMD premenstrual dysphoric disorder
Medical conditions that may be exacerbated by treatment with progestins
Women for whom progestin-containing HT
would not be considered appropriate
minus Women who are intolerant of progestin-containing hormone therapy
minus Women with pre-existing medical conditions that may be exacerbated by progestins
Most common adverse events leading to discontinuation are related to progestins12
breakthrough bleeding
bull Increase in the number of uterine procedures (ie unnecessary endometrial biopsies)
breast paintenderness
bull Increase in the number of breast interventions
1 Steel SA et al Climacteric 2003 2 Ettinger B and Pressman A Am J Manag Care 1999 3 Komm BS Mirkin S
Pharmaceuticals 2012
4 Panay N amp Studd JWW Human Reprod Update 1997
bull Nausea bull Depressive mood bull Poor concentration bull Hirsutism bull Headache bull Dizziness bull Fluid retention bull Weight gain
Other progestin-related intolerance issues4
Unmet need with the treatment of postmenopausal symptoms
bull Alternatives to progestin are needed that will protect the endometrium while avoiding other progestin-associated effects and preserving the desired effects of estrogens in postmenopausal women3
Which women with a uterus could benefit from
estrogens without the need for a progestin
bull Women who are intolerant of progestin-containing hormone therapy
bull Women with pre-existing medical conditions that may be exacerbated by progestins (eg women with a history of depression PMSPMDD increased breast density diabetes and metabolic syndrome)
History of the following conditions may make progestin inappropriate
bull Depression
bull PMSPMDD
bull High breast density
bull Diabetes and metabolic syndrome
PMS premenstrual syndrome
PMD premenstrual dysphoric disorder
Medical conditions that may be exacerbated by treatment with progestins
Learning from WHI data
bull Hormone therapy (HT) is the conventional and established therapy option to effectively treat postmenopausal symptoms however it has been associated with some safety and tolerability concerns1 2
bull A review of WHI data suggests that many of the concerns with menopausal HT more often associated with EPT (CE+MPA) such as CHD risk increased breast density breast pain and breast cancer risk than with ET (CEE alone)2
1 Rolnick SJ Kopher RA DeFor TA et al Menopause 2005
2 Komm BS Mirkin S Pharmaceuticals 2012
WHI Womenrsquos Health Initiative trial
CHD coronary heart disease
CEE conjugated equine estrogens
Efficacy and Safety of Constant Oestrogen
Pulsed Progestogen vs
Continuous Combined HRT
Adverse Events
17b-oestradiol 17b-oestradiol norgestimate NETA (n = 150) (n = 172) Breast discomfort 14 27 Abdominal discomfort 14 22 Uterine bleeding 15 12 Dysmenorrhea 3 8 Oedema 5 8
Adapted from S Rozenberg et al Human Reproduction 2000
Medical condition which may be exacerbated by treatment
with progestins
Increased breast density
bull Increases in breast density are associated with progestin-containing HT which may adversely affect radiological detection of breast cancer1 and may be independently associated with an increased risk for the development of breast cancer2
bull The Postmenopausal EstrogenProgestin Interventions (PEPI) trial demonstrated that an increased mammographic breast density was associated with the use of E+P but not with the use of estrogen alone3
bull Women who already have high breast density may therefore be considered inappropriate for treatment with a progestin-containing HT
1) EU Core SPC for Hormone Replacement Therapy Products (CMDh1312003 Rev 4 June
2012)
2) De Villiers TJ et al on behalf of the International Menopause Society Climacteric 2013 16
3) Greendale GA et al J Natl Cancer Inst 2003
Stroke
0 25 5 75 10 125
Fractures
Diabetes
Breast cancer
Cholecystitis
Venothrombotic episodes
Endometrial cancer
Lung cancer
Coronary heart disease
Colorectal cancer
Overall mortality
15 125 10 75 5 25
Benefits Risks
CE
CE MPA
Santen RJ et al J Clin Endocrinol Metab 2010
The basis of the Endocrine Society scientific statement for postmenopausal hormone replacement therapy (HRT) excess risks and benefits of HRT for 5 years in women aged 50ndash59 years or within 10 years of the start of menopause E=estrogen P=progestin
bull Younger women (aged 50ndash59 years) had more favorable results bull There are differences between CE alone and CEMPA arms bull Overall benefitrisk ratio of CE-alone appears to be more favourable than CEMPA
Reevaluation of WHI data (stratified by age) Risks and
Benefits of HRT Cases per 1000 Women per 5 Years of
Use
Medical condition which may be exacerbated by treatment
with progestins
Diabetes and metabolic syndrome
bull Treatment of oestrogen deficiency symptoms with progestin-containing HT (unlike oestrogen alone) may be associated with increases in insulin resistance and deterioration in glucose tolerance123
bull Postmenopausal women with diabetes could be inappropriate for treatment with progestin-containing HT due to the potential risk of exacerbation of their condition
1) Panay N amp Studd JWW Human Reprod Update 1997
2) Godsland I et al Metabolism 1993
3) Sites CK et al J Clin Endocrinol Metab 2005
Variations in Associated Breast Cancer
Risks Between CE alone and CEMPA
bull Use of CE alone for a median of 59 years was associated with a lower incidence of invasive breast cancer (151 cases 027 per year) compared with placebo (199 cases 035 per year HR 077 95 CI 062ndash095 P=002)
bull In the CE alone group fewer women died from invasive breast cancer (6 deaths 0009 per year) compared with controls (16 deaths 0024 per year HR 037 95 CI 013ndash091 P=003)
Anderson GL et al Lancet
Oncol 2012
Bazedoxifene (BZA) specifically selected in
combination with conjugated estrogens
bull BZA has been specifically selected for its unique pharmacologic profile and effects on VMS and uterine tissue in particular123
1 Crabtree J et al Mol Cell Endocrinol 2008
2 Kharode Y et al Endocrinolology 2008
3 Duavive SmPC
Estrogen Receptor activity is dimmed
Estrogen Receptor activity is turned on
CEs are agonists BZA is an antagonist
In the uterus
bull The BZA component reduces the risk of endometrial hyperplasia that can occur with the conjugated estrogens component alone3 This means that progestins are not needed
Extensive global clinical development program for
CEBZA
aIncludes additional pilot dose-finding study 203 1 Lobo RA et al Fertil Steril 2009 2 Pinkerton JV et al Menopause 2009 3 Kagan R et al Menopause 2010 4 Mirkin S et al Climacteric 2013 5 Pinkerton JV et al Obstet Gynecol 2013
Effects of conjugated estrogensbazedoxifene on
lipid and coagulation variables a randomized
placebo- and active-controlled trial
bull At 12 months
bull Both CEBZA doses were associated with small but significant effects on hemostasis variables including reductions in antithrombin plasminogen activator inhibitor-1 and fibrinogen activity and an increase in plasminogen activity relative to placebo at 12 months Incidences of cardiovascular and venous thromboembolic events were similar among treatment groups
bull CONCLUSIONS
bull This study provides reassurance that CEBZA does not adversely affect lipid metabolism or hemostatic balance In accordance the incidences of venous thromboembolic events and cardiovascular events in postmenopausal women are similar to those observed with placebo

Conjugated EstrogensBazedoxifene (CEBZA)
US indication
bull DUAVEE is indicated in women with a uterus for
bull 11 Treatment of Moderate to Severe Vasomotor Symptoms Associated with Menopause
bull 12 Prevention of Postmenopausal Osteoporosis
bull 13 Important Limitations of Use
bull Use DUAVEE for the shortest duration consistent with treatment goals and risks for the individual woman Postmenopausal women should be re-evaluated periodically as clinically appropriate to determine if treatment is still necessary
bull When prescribing solely for the prevention of postmenopausal osteoporosis therapy should only be considered for women at significant risk of osteoporosis and non-estrogen medication should be carefully considered
Conjugated EstrogensBazedoxifene (CEBZA)
EU indication
CEBZA is indicated for
bull Treatment of oestrogen deficiency symptoms in postmenopausal women with a uterus (with at least 12 months since the last menses) for whom treatment with progestin-containing therapy is not appropriate
bull The experience treating women older than 65 years is limited
bull Dose CE (045mg)Bazedoxifene (20mg)
Duavive SmPC
Which women with a uterus
could benefit from estrogens
without the need for a
progestin
Progestin intolerance is one of the main
factors for reduced compliance
bull About 20 of women receiving progestin-containing HT have significant progestin intolerance and half of these experience serious effects that prevent treatment continuation1
1 Panay N amp Studd J Human Reprod Update 1997
2 Panay N et al on behalf of the British Menopause Society and Womenrsquos Health Concern Menopause Int 2013
bull The 2013 British Menopause Society amp Womenrsquos Health
Concern recommendations on hormone replacement
therapy do recognise progestin intolerance as one of the
main factors for reduced compliance with HT 2
Proportion of patients () with at least one bleeding episode in relation to time and to the
used HT
Serge Rozenberg et al Hum Reprod 2009241739-1747
copy The Author 2009 Published by Oxford University Press on behalf of the European Society of
Human Reproduction and Embryology All rights reserved For Permissions please email
journalspermissionsoxfordjournalsorg
Breast tenderness after initiation of CEE
CEE + MPA (WHI)
and mammographic density change
bullCrandall et al Breast Cancer Res Treat DOI 101007s10549-011-1803-9
Breast density
Conclusion
bull CEEBAZO is an additional regimen for menopausal symptoms it provides also a prevention for osteoporosis
bull It is suitable for women with a uterus who are unsatisfied with an EPT regimen or who you are unwilling to treat with an EPT regimen
Adapted use of MHT
bull Lower dosage of estrogens
bull Other progestins
bull Better safety profile
bull Vaginal estrogen or SERMS
bull Non-hormonal therapy
bull Development of new products
bull SERMS + estrogens
Most common adverse events leading to
discontinuation are related to progestins12
bull breakthrough bleeding
bull Low compliance
bull Increase in the number of US
bull Stress
bull Cost
bull uterine procedures
bull Unnecessary endometrial biopsies Hysteroscopies DampC Hysterectomies
bull Morbidity
Proportion of patients who completed or discontinued treatment in relation to the used HT
Serge Rozenberg et al Hum Reprod 2009241739-1747
copy The Author 2009 Published by Oxford University Press on behalf of the European Society of
Human Reproduction and Embryology All rights reserved For Permissions please email
journalspermissionsoxfordjournalsorg
Most common adverse events leading to discontinuation
are related to progestins
bull breast paintenderness
Breast tenderness after initiation of CEE
CEE + MPA (WHI)
and mammographic density change
bullCrandall et al Breast Cancer Res Treat DOI 101007s10549-011-1803-9
Breast density
Hormone therapy use and mammographic
density in postmenopausal Norwegian women
bull Results differed when considering the combined effect of age and BMI
bull The effect of EPT on mammographic density was modified by age and BMI with no apparent association among the youngest women (aged 50-55) with the highest BMI (BMI ge 26)
bull A higher mammographic density was found in EPT users compared to never HT users particularly in women using high-dose NETA regimens Age and BMI modified the association between EPT use and mammographic density
bull Couto E et al Breast Cancer Res Treat 2011 Nov 4 [Epub ahead of print]
Breast Cancer Risk by Breast Density
Menopause and Postmenopausal Hormone
Therapy Use
Birads age HT Duration Risk
1 55-59 None 5 year risk 08 (95 CI 06- 09)
1 55-59
ET EPT 5 year risk 09 (95 CI 07 -11)
4 55-59
None 5 year risk 24 (95 CI 20 -28)
4 55-59
ET 5 year risk
30 (95 CI 26 -35)
4 55-59
EPT 5 year risk
42 (95 CI 37 -46)
Adapted from Kerlikowske et al JOURNAL OF CLINICAL ONCOLOGY 2010
Breast Cancer Risk by Breast Density
Menopause and Postmenopausal Hormone
Therapy Use
Adapted from Kerlikowske et al JOURNAL OF CLINICAL ONCOLOGY 2010
bull Postmenopausal women with high breast density are at increased risk of breast cancer and should be aware of the added risk of taking HT especially estrogen plus progestin
Medical condition which may be exacerbated by treatment
with progestins
Diabetes and metabolic syndrome
bull progestin-containing HT may be associated with increases in insulin resistance and deterioration in glucose tolerance123
bull Postmenopausal women with diabetes could be inappropriate for treatment with progestin-containing HT due to the potential risk of exacerbation of their condition
1) Panay N amp Studd JWW Human Reprod Update 1997
2) Godsland I et al Metabolism 1993
3) Sites CK et al J Clin Endocrinol Metab 2005
A Nath and R Sitruk-Ware CLIMACTERIC 200912(Suppl 1)96ndash101
A Nath and R Sitruk-Ware CLIMACTERIC 200912(Suppl 1)96ndash101
Diabetes an epidemy
bull UK 1996 14 million of diabetics
bull UK 2015 32 million (6 of the population)
bull UK 2025 5 million
bull httpwwwdiabetescoukdiabetes-prevalencehtml
Other progestin-related intolerance issues
bull Nausea
bull Depressive mood
bull Poor concentration
bull Hirsutism
bull Headache
bull Dizziness
bull Fluid retention
bull Weight gain Panay N amp Studd JWW Human Reprod Update 1997
Medical condition which may be exacerbated by treatment with progestins
PMSPMDDdepression
bull Progesterone-induced PMD can be exacerbated by exogenous progestin administration and can occur in association with HT or OC administration1
bull Significantly higher negative mood scores have been observed during the addition of a progestin to an estrogen in a sequential HT regimen in postmenopausal women with a history of PMS compared to those without2
bull Women with a history of PMS or PMD exacerbation of depression using progestins may therefore benefit from a progestin free treatment for menopausal symptoms
1) Nevatte T et al Arch Womens Ment Health 2013 2) Bjoumlrn I et al Climacteric 2006 PMS premenstrual syndrome
PMDD premenstrual dysphoric disorder
Conclusion
bull CEEBAZO is an additional regimen for menopausal symptoms it provides also a prevention for osteoporosis
bull It is suitable for women with a uterus who are unsatisfied with an EPT regimen or who you are unwilling to treat with an EPT regimen
For some postmenopausal women with a uterus there is a
need for progestin free treatment options
bull with demonstrated clinical efficacy
bull which protects the endometrium
bull improved tolerabilitysafety profile
In clinical practice this translates to women who are
intolerant of progestin-containing HT or have conditions
which may be exacerbated by treatment with progestins
Conclusion Medical need for alternative treatment option
Medical condition which may be exacerbated by treatment with progestins
Depression
bull Progestin-containing HT has been associated with increases in depressive symptoms in some individuals1
bull There is a biochemicalphysiological plausibility for the association of progestins with depression234
bull Therefore postmenopausal women who also have a medical history of depressive disorders or depression could be inappropriate for treatment with progestin-containing HT
Pfizer Confidential
65
1) Girdler SS et al J Womens Health Gend Based Med 1999 2) Traish AM et al Korean J Urol 2014 3) Stroumlhle A et al Biol Psychiatry 1999 4) Romeo E et
al Am J Psychiatry 1998
History of the following conditions may make progestin inappropriate
bull Depression
bull PMSPMDD
PMS premenstrual syndrome
PMD premenstrual dysphoric disorder
Medical conditions that may be exacerbated by treatment with progestins
Women for whom progestin-containing HT
would not be considered appropriate
minus Women who are intolerant of progestin-containing hormone therapy
minus Women with pre-existing medical conditions that may be exacerbated by progestins
Most common adverse events leading to discontinuation are related to progestins12
breakthrough bleeding
bull Increase in the number of uterine procedures (ie unnecessary endometrial biopsies)
breast paintenderness
bull Increase in the number of breast interventions
1 Steel SA et al Climacteric 2003 2 Ettinger B and Pressman A Am J Manag Care 1999 3 Komm BS Mirkin S
Pharmaceuticals 2012
4 Panay N amp Studd JWW Human Reprod Update 1997
bull Nausea bull Depressive mood bull Poor concentration bull Hirsutism bull Headache bull Dizziness bull Fluid retention bull Weight gain
Other progestin-related intolerance issues4
Unmet need with the treatment of postmenopausal symptoms
bull Alternatives to progestin are needed that will protect the endometrium while avoiding other progestin-associated effects and preserving the desired effects of estrogens in postmenopausal women3
Which women with a uterus could benefit from
estrogens without the need for a progestin
bull Women who are intolerant of progestin-containing hormone therapy
bull Women with pre-existing medical conditions that may be exacerbated by progestins (eg women with a history of depression PMSPMDD increased breast density diabetes and metabolic syndrome)
History of the following conditions may make progestin inappropriate
bull Depression
bull PMSPMDD
bull High breast density
bull Diabetes and metabolic syndrome
PMS premenstrual syndrome
PMD premenstrual dysphoric disorder
Medical conditions that may be exacerbated by treatment with progestins
Learning from WHI data
bull Hormone therapy (HT) is the conventional and established therapy option to effectively treat postmenopausal symptoms however it has been associated with some safety and tolerability concerns1 2
bull A review of WHI data suggests that many of the concerns with menopausal HT more often associated with EPT (CE+MPA) such as CHD risk increased breast density breast pain and breast cancer risk than with ET (CEE alone)2
1 Rolnick SJ Kopher RA DeFor TA et al Menopause 2005
2 Komm BS Mirkin S Pharmaceuticals 2012
WHI Womenrsquos Health Initiative trial
CHD coronary heart disease
CEE conjugated equine estrogens
Efficacy and Safety of Constant Oestrogen
Pulsed Progestogen vs
Continuous Combined HRT
Adverse Events
17b-oestradiol 17b-oestradiol norgestimate NETA (n = 150) (n = 172) Breast discomfort 14 27 Abdominal discomfort 14 22 Uterine bleeding 15 12 Dysmenorrhea 3 8 Oedema 5 8
Adapted from S Rozenberg et al Human Reproduction 2000
Medical condition which may be exacerbated by treatment
with progestins
Increased breast density
bull Increases in breast density are associated with progestin-containing HT which may adversely affect radiological detection of breast cancer1 and may be independently associated with an increased risk for the development of breast cancer2
bull The Postmenopausal EstrogenProgestin Interventions (PEPI) trial demonstrated that an increased mammographic breast density was associated with the use of E+P but not with the use of estrogen alone3
bull Women who already have high breast density may therefore be considered inappropriate for treatment with a progestin-containing HT
1) EU Core SPC for Hormone Replacement Therapy Products (CMDh1312003 Rev 4 June
2012)
2) De Villiers TJ et al on behalf of the International Menopause Society Climacteric 2013 16
3) Greendale GA et al J Natl Cancer Inst 2003
Stroke
0 25 5 75 10 125
Fractures
Diabetes
Breast cancer
Cholecystitis
Venothrombotic episodes
Endometrial cancer
Lung cancer
Coronary heart disease
Colorectal cancer
Overall mortality
15 125 10 75 5 25
Benefits Risks
CE
CE MPA
Santen RJ et al J Clin Endocrinol Metab 2010
The basis of the Endocrine Society scientific statement for postmenopausal hormone replacement therapy (HRT) excess risks and benefits of HRT for 5 years in women aged 50ndash59 years or within 10 years of the start of menopause E=estrogen P=progestin
bull Younger women (aged 50ndash59 years) had more favorable results bull There are differences between CE alone and CEMPA arms bull Overall benefitrisk ratio of CE-alone appears to be more favourable than CEMPA
Reevaluation of WHI data (stratified by age) Risks and
Benefits of HRT Cases per 1000 Women per 5 Years of
Use
Medical condition which may be exacerbated by treatment
with progestins
Diabetes and metabolic syndrome
bull Treatment of oestrogen deficiency symptoms with progestin-containing HT (unlike oestrogen alone) may be associated with increases in insulin resistance and deterioration in glucose tolerance123
bull Postmenopausal women with diabetes could be inappropriate for treatment with progestin-containing HT due to the potential risk of exacerbation of their condition
1) Panay N amp Studd JWW Human Reprod Update 1997
2) Godsland I et al Metabolism 1993
3) Sites CK et al J Clin Endocrinol Metab 2005
Variations in Associated Breast Cancer
Risks Between CE alone and CEMPA
bull Use of CE alone for a median of 59 years was associated with a lower incidence of invasive breast cancer (151 cases 027 per year) compared with placebo (199 cases 035 per year HR 077 95 CI 062ndash095 P=002)
bull In the CE alone group fewer women died from invasive breast cancer (6 deaths 0009 per year) compared with controls (16 deaths 0024 per year HR 037 95 CI 013ndash091 P=003)
Anderson GL et al Lancet
Oncol 2012
Bazedoxifene (BZA) specifically selected in
combination with conjugated estrogens
bull BZA has been specifically selected for its unique pharmacologic profile and effects on VMS and uterine tissue in particular123
1 Crabtree J et al Mol Cell Endocrinol 2008
2 Kharode Y et al Endocrinolology 2008
3 Duavive SmPC
Estrogen Receptor activity is dimmed
Estrogen Receptor activity is turned on
CEs are agonists BZA is an antagonist
In the uterus
bull The BZA component reduces the risk of endometrial hyperplasia that can occur with the conjugated estrogens component alone3 This means that progestins are not needed
Extensive global clinical development program for
CEBZA
aIncludes additional pilot dose-finding study 203 1 Lobo RA et al Fertil Steril 2009 2 Pinkerton JV et al Menopause 2009 3 Kagan R et al Menopause 2010 4 Mirkin S et al Climacteric 2013 5 Pinkerton JV et al Obstet Gynecol 2013
Effects of conjugated estrogensbazedoxifene on
lipid and coagulation variables a randomized
placebo- and active-controlled trial
bull At 12 months
bull Both CEBZA doses were associated with small but significant effects on hemostasis variables including reductions in antithrombin plasminogen activator inhibitor-1 and fibrinogen activity and an increase in plasminogen activity relative to placebo at 12 months Incidences of cardiovascular and venous thromboembolic events were similar among treatment groups
bull CONCLUSIONS
bull This study provides reassurance that CEBZA does not adversely affect lipid metabolism or hemostatic balance In accordance the incidences of venous thromboembolic events and cardiovascular events in postmenopausal women are similar to those observed with placebo

Conjugated EstrogensBazedoxifene (CEBZA)
EU indication
CEBZA is indicated for
bull Treatment of oestrogen deficiency symptoms in postmenopausal women with a uterus (with at least 12 months since the last menses) for whom treatment with progestin-containing therapy is not appropriate
bull The experience treating women older than 65 years is limited
bull Dose CE (045mg)Bazedoxifene (20mg)
Duavive SmPC
Which women with a uterus
could benefit from estrogens
without the need for a
progestin
Progestin intolerance is one of the main
factors for reduced compliance
bull About 20 of women receiving progestin-containing HT have significant progestin intolerance and half of these experience serious effects that prevent treatment continuation1
1 Panay N amp Studd J Human Reprod Update 1997
2 Panay N et al on behalf of the British Menopause Society and Womenrsquos Health Concern Menopause Int 2013
bull The 2013 British Menopause Society amp Womenrsquos Health
Concern recommendations on hormone replacement
therapy do recognise progestin intolerance as one of the
main factors for reduced compliance with HT 2
Proportion of patients () with at least one bleeding episode in relation to time and to the
used HT
Serge Rozenberg et al Hum Reprod 2009241739-1747
copy The Author 2009 Published by Oxford University Press on behalf of the European Society of
Human Reproduction and Embryology All rights reserved For Permissions please email
journalspermissionsoxfordjournalsorg
Breast tenderness after initiation of CEE
CEE + MPA (WHI)
and mammographic density change
bullCrandall et al Breast Cancer Res Treat DOI 101007s10549-011-1803-9
Breast density
Conclusion
bull CEEBAZO is an additional regimen for menopausal symptoms it provides also a prevention for osteoporosis
bull It is suitable for women with a uterus who are unsatisfied with an EPT regimen or who you are unwilling to treat with an EPT regimen
Adapted use of MHT
bull Lower dosage of estrogens
bull Other progestins
bull Better safety profile
bull Vaginal estrogen or SERMS
bull Non-hormonal therapy
bull Development of new products
bull SERMS + estrogens
Most common adverse events leading to
discontinuation are related to progestins12
bull breakthrough bleeding
bull Low compliance
bull Increase in the number of US
bull Stress
bull Cost
bull uterine procedures
bull Unnecessary endometrial biopsies Hysteroscopies DampC Hysterectomies
bull Morbidity
Proportion of patients who completed or discontinued treatment in relation to the used HT
Serge Rozenberg et al Hum Reprod 2009241739-1747
copy The Author 2009 Published by Oxford University Press on behalf of the European Society of
Human Reproduction and Embryology All rights reserved For Permissions please email
journalspermissionsoxfordjournalsorg
Most common adverse events leading to discontinuation
are related to progestins
bull breast paintenderness
Breast tenderness after initiation of CEE
CEE + MPA (WHI)
and mammographic density change
bullCrandall et al Breast Cancer Res Treat DOI 101007s10549-011-1803-9
Breast density
Hormone therapy use and mammographic
density in postmenopausal Norwegian women
bull Results differed when considering the combined effect of age and BMI
bull The effect of EPT on mammographic density was modified by age and BMI with no apparent association among the youngest women (aged 50-55) with the highest BMI (BMI ge 26)
bull A higher mammographic density was found in EPT users compared to never HT users particularly in women using high-dose NETA regimens Age and BMI modified the association between EPT use and mammographic density
bull Couto E et al Breast Cancer Res Treat 2011 Nov 4 [Epub ahead of print]
Breast Cancer Risk by Breast Density
Menopause and Postmenopausal Hormone
Therapy Use
Birads age HT Duration Risk
1 55-59 None 5 year risk 08 (95 CI 06- 09)
1 55-59
ET EPT 5 year risk 09 (95 CI 07 -11)
4 55-59
None 5 year risk 24 (95 CI 20 -28)
4 55-59
ET 5 year risk
30 (95 CI 26 -35)
4 55-59
EPT 5 year risk
42 (95 CI 37 -46)
Adapted from Kerlikowske et al JOURNAL OF CLINICAL ONCOLOGY 2010
Breast Cancer Risk by Breast Density
Menopause and Postmenopausal Hormone
Therapy Use
Adapted from Kerlikowske et al JOURNAL OF CLINICAL ONCOLOGY 2010
bull Postmenopausal women with high breast density are at increased risk of breast cancer and should be aware of the added risk of taking HT especially estrogen plus progestin
Medical condition which may be exacerbated by treatment
with progestins
Diabetes and metabolic syndrome
bull progestin-containing HT may be associated with increases in insulin resistance and deterioration in glucose tolerance123
bull Postmenopausal women with diabetes could be inappropriate for treatment with progestin-containing HT due to the potential risk of exacerbation of their condition
1) Panay N amp Studd JWW Human Reprod Update 1997
2) Godsland I et al Metabolism 1993
3) Sites CK et al J Clin Endocrinol Metab 2005
A Nath and R Sitruk-Ware CLIMACTERIC 200912(Suppl 1)96ndash101
A Nath and R Sitruk-Ware CLIMACTERIC 200912(Suppl 1)96ndash101
Diabetes an epidemy
bull UK 1996 14 million of diabetics
bull UK 2015 32 million (6 of the population)
bull UK 2025 5 million
bull httpwwwdiabetescoukdiabetes-prevalencehtml
Other progestin-related intolerance issues
bull Nausea
bull Depressive mood
bull Poor concentration
bull Hirsutism
bull Headache
bull Dizziness
bull Fluid retention
bull Weight gain Panay N amp Studd JWW Human Reprod Update 1997
Medical condition which may be exacerbated by treatment with progestins
PMSPMDDdepression
bull Progesterone-induced PMD can be exacerbated by exogenous progestin administration and can occur in association with HT or OC administration1
bull Significantly higher negative mood scores have been observed during the addition of a progestin to an estrogen in a sequential HT regimen in postmenopausal women with a history of PMS compared to those without2
bull Women with a history of PMS or PMD exacerbation of depression using progestins may therefore benefit from a progestin free treatment for menopausal symptoms
1) Nevatte T et al Arch Womens Ment Health 2013 2) Bjoumlrn I et al Climacteric 2006 PMS premenstrual syndrome
PMDD premenstrual dysphoric disorder
Conclusion
bull CEEBAZO is an additional regimen for menopausal symptoms it provides also a prevention for osteoporosis
bull It is suitable for women with a uterus who are unsatisfied with an EPT regimen or who you are unwilling to treat with an EPT regimen
For some postmenopausal women with a uterus there is a
need for progestin free treatment options
bull with demonstrated clinical efficacy
bull which protects the endometrium
bull improved tolerabilitysafety profile
In clinical practice this translates to women who are
intolerant of progestin-containing HT or have conditions
which may be exacerbated by treatment with progestins
Conclusion Medical need for alternative treatment option
Medical condition which may be exacerbated by treatment with progestins
Depression
bull Progestin-containing HT has been associated with increases in depressive symptoms in some individuals1
bull There is a biochemicalphysiological plausibility for the association of progestins with depression234
bull Therefore postmenopausal women who also have a medical history of depressive disorders or depression could be inappropriate for treatment with progestin-containing HT
Pfizer Confidential
65
1) Girdler SS et al J Womens Health Gend Based Med 1999 2) Traish AM et al Korean J Urol 2014 3) Stroumlhle A et al Biol Psychiatry 1999 4) Romeo E et
al Am J Psychiatry 1998
History of the following conditions may make progestin inappropriate
bull Depression
bull PMSPMDD
PMS premenstrual syndrome
PMD premenstrual dysphoric disorder
Medical conditions that may be exacerbated by treatment with progestins
Women for whom progestin-containing HT
would not be considered appropriate
minus Women who are intolerant of progestin-containing hormone therapy
minus Women with pre-existing medical conditions that may be exacerbated by progestins
Most common adverse events leading to discontinuation are related to progestins12
breakthrough bleeding
bull Increase in the number of uterine procedures (ie unnecessary endometrial biopsies)
breast paintenderness
bull Increase in the number of breast interventions
1 Steel SA et al Climacteric 2003 2 Ettinger B and Pressman A Am J Manag Care 1999 3 Komm BS Mirkin S
Pharmaceuticals 2012
4 Panay N amp Studd JWW Human Reprod Update 1997
bull Nausea bull Depressive mood bull Poor concentration bull Hirsutism bull Headache bull Dizziness bull Fluid retention bull Weight gain
Other progestin-related intolerance issues4
Unmet need with the treatment of postmenopausal symptoms
bull Alternatives to progestin are needed that will protect the endometrium while avoiding other progestin-associated effects and preserving the desired effects of estrogens in postmenopausal women3
Which women with a uterus could benefit from
estrogens without the need for a progestin
bull Women who are intolerant of progestin-containing hormone therapy
bull Women with pre-existing medical conditions that may be exacerbated by progestins (eg women with a history of depression PMSPMDD increased breast density diabetes and metabolic syndrome)
History of the following conditions may make progestin inappropriate
bull Depression
bull PMSPMDD
bull High breast density
bull Diabetes and metabolic syndrome
PMS premenstrual syndrome
PMD premenstrual dysphoric disorder
Medical conditions that may be exacerbated by treatment with progestins
Learning from WHI data
bull Hormone therapy (HT) is the conventional and established therapy option to effectively treat postmenopausal symptoms however it has been associated with some safety and tolerability concerns1 2
bull A review of WHI data suggests that many of the concerns with menopausal HT more often associated with EPT (CE+MPA) such as CHD risk increased breast density breast pain and breast cancer risk than with ET (CEE alone)2
1 Rolnick SJ Kopher RA DeFor TA et al Menopause 2005
2 Komm BS Mirkin S Pharmaceuticals 2012
WHI Womenrsquos Health Initiative trial
CHD coronary heart disease
CEE conjugated equine estrogens
Efficacy and Safety of Constant Oestrogen
Pulsed Progestogen vs
Continuous Combined HRT
Adverse Events
17b-oestradiol 17b-oestradiol norgestimate NETA (n = 150) (n = 172) Breast discomfort 14 27 Abdominal discomfort 14 22 Uterine bleeding 15 12 Dysmenorrhea 3 8 Oedema 5 8
Adapted from S Rozenberg et al Human Reproduction 2000
Medical condition which may be exacerbated by treatment
with progestins
Increased breast density
bull Increases in breast density are associated with progestin-containing HT which may adversely affect radiological detection of breast cancer1 and may be independently associated with an increased risk for the development of breast cancer2
bull The Postmenopausal EstrogenProgestin Interventions (PEPI) trial demonstrated that an increased mammographic breast density was associated with the use of E+P but not with the use of estrogen alone3
bull Women who already have high breast density may therefore be considered inappropriate for treatment with a progestin-containing HT
1) EU Core SPC for Hormone Replacement Therapy Products (CMDh1312003 Rev 4 June
2012)
2) De Villiers TJ et al on behalf of the International Menopause Society Climacteric 2013 16
3) Greendale GA et al J Natl Cancer Inst 2003
Stroke
0 25 5 75 10 125
Fractures
Diabetes
Breast cancer
Cholecystitis
Venothrombotic episodes
Endometrial cancer
Lung cancer
Coronary heart disease
Colorectal cancer
Overall mortality
15 125 10 75 5 25
Benefits Risks
CE
CE MPA
Santen RJ et al J Clin Endocrinol Metab 2010
The basis of the Endocrine Society scientific statement for postmenopausal hormone replacement therapy (HRT) excess risks and benefits of HRT for 5 years in women aged 50ndash59 years or within 10 years of the start of menopause E=estrogen P=progestin
bull Younger women (aged 50ndash59 years) had more favorable results bull There are differences between CE alone and CEMPA arms bull Overall benefitrisk ratio of CE-alone appears to be more favourable than CEMPA
Reevaluation of WHI data (stratified by age) Risks and
Benefits of HRT Cases per 1000 Women per 5 Years of
Use
Medical condition which may be exacerbated by treatment
with progestins
Diabetes and metabolic syndrome
bull Treatment of oestrogen deficiency symptoms with progestin-containing HT (unlike oestrogen alone) may be associated with increases in insulin resistance and deterioration in glucose tolerance123
bull Postmenopausal women with diabetes could be inappropriate for treatment with progestin-containing HT due to the potential risk of exacerbation of their condition
1) Panay N amp Studd JWW Human Reprod Update 1997
2) Godsland I et al Metabolism 1993
3) Sites CK et al J Clin Endocrinol Metab 2005
Variations in Associated Breast Cancer
Risks Between CE alone and CEMPA
bull Use of CE alone for a median of 59 years was associated with a lower incidence of invasive breast cancer (151 cases 027 per year) compared with placebo (199 cases 035 per year HR 077 95 CI 062ndash095 P=002)
bull In the CE alone group fewer women died from invasive breast cancer (6 deaths 0009 per year) compared with controls (16 deaths 0024 per year HR 037 95 CI 013ndash091 P=003)
Anderson GL et al Lancet
Oncol 2012
Bazedoxifene (BZA) specifically selected in
combination with conjugated estrogens
bull BZA has been specifically selected for its unique pharmacologic profile and effects on VMS and uterine tissue in particular123
1 Crabtree J et al Mol Cell Endocrinol 2008
2 Kharode Y et al Endocrinolology 2008
3 Duavive SmPC
Estrogen Receptor activity is dimmed
Estrogen Receptor activity is turned on
CEs are agonists BZA is an antagonist
In the uterus
bull The BZA component reduces the risk of endometrial hyperplasia that can occur with the conjugated estrogens component alone3 This means that progestins are not needed
Extensive global clinical development program for
CEBZA
aIncludes additional pilot dose-finding study 203 1 Lobo RA et al Fertil Steril 2009 2 Pinkerton JV et al Menopause 2009 3 Kagan R et al Menopause 2010 4 Mirkin S et al Climacteric 2013 5 Pinkerton JV et al Obstet Gynecol 2013
Effects of conjugated estrogensbazedoxifene on
lipid and coagulation variables a randomized
placebo- and active-controlled trial
bull At 12 months
bull Both CEBZA doses were associated with small but significant effects on hemostasis variables including reductions in antithrombin plasminogen activator inhibitor-1 and fibrinogen activity and an increase in plasminogen activity relative to placebo at 12 months Incidences of cardiovascular and venous thromboembolic events were similar among treatment groups
bull CONCLUSIONS
bull This study provides reassurance that CEBZA does not adversely affect lipid metabolism or hemostatic balance In accordance the incidences of venous thromboembolic events and cardiovascular events in postmenopausal women are similar to those observed with placebo

Which women with a uterus
could benefit from estrogens
without the need for a
progestin
Progestin intolerance is one of the main
factors for reduced compliance
bull About 20 of women receiving progestin-containing HT have significant progestin intolerance and half of these experience serious effects that prevent treatment continuation1
1 Panay N amp Studd J Human Reprod Update 1997
2 Panay N et al on behalf of the British Menopause Society and Womenrsquos Health Concern Menopause Int 2013
bull The 2013 British Menopause Society amp Womenrsquos Health
Concern recommendations on hormone replacement
therapy do recognise progestin intolerance as one of the
main factors for reduced compliance with HT 2
Proportion of patients () with at least one bleeding episode in relation to time and to the
used HT
Serge Rozenberg et al Hum Reprod 2009241739-1747
copy The Author 2009 Published by Oxford University Press on behalf of the European Society of
Human Reproduction and Embryology All rights reserved For Permissions please email
journalspermissionsoxfordjournalsorg
Breast tenderness after initiation of CEE
CEE + MPA (WHI)
and mammographic density change
bullCrandall et al Breast Cancer Res Treat DOI 101007s10549-011-1803-9
Breast density
Conclusion
bull CEEBAZO is an additional regimen for menopausal symptoms it provides also a prevention for osteoporosis
bull It is suitable for women with a uterus who are unsatisfied with an EPT regimen or who you are unwilling to treat with an EPT regimen
Adapted use of MHT
bull Lower dosage of estrogens
bull Other progestins
bull Better safety profile
bull Vaginal estrogen or SERMS
bull Non-hormonal therapy
bull Development of new products
bull SERMS + estrogens
Most common adverse events leading to
discontinuation are related to progestins12
bull breakthrough bleeding
bull Low compliance
bull Increase in the number of US
bull Stress
bull Cost
bull uterine procedures
bull Unnecessary endometrial biopsies Hysteroscopies DampC Hysterectomies
bull Morbidity
Proportion of patients who completed or discontinued treatment in relation to the used HT
Serge Rozenberg et al Hum Reprod 2009241739-1747
copy The Author 2009 Published by Oxford University Press on behalf of the European Society of
Human Reproduction and Embryology All rights reserved For Permissions please email
journalspermissionsoxfordjournalsorg
Most common adverse events leading to discontinuation
are related to progestins
bull breast paintenderness
Breast tenderness after initiation of CEE
CEE + MPA (WHI)
and mammographic density change
bullCrandall et al Breast Cancer Res Treat DOI 101007s10549-011-1803-9
Breast density
Hormone therapy use and mammographic
density in postmenopausal Norwegian women
bull Results differed when considering the combined effect of age and BMI
bull The effect of EPT on mammographic density was modified by age and BMI with no apparent association among the youngest women (aged 50-55) with the highest BMI (BMI ge 26)
bull A higher mammographic density was found in EPT users compared to never HT users particularly in women using high-dose NETA regimens Age and BMI modified the association between EPT use and mammographic density
bull Couto E et al Breast Cancer Res Treat 2011 Nov 4 [Epub ahead of print]
Breast Cancer Risk by Breast Density
Menopause and Postmenopausal Hormone
Therapy Use
Birads age HT Duration Risk
1 55-59 None 5 year risk 08 (95 CI 06- 09)
1 55-59
ET EPT 5 year risk 09 (95 CI 07 -11)
4 55-59
None 5 year risk 24 (95 CI 20 -28)
4 55-59
ET 5 year risk
30 (95 CI 26 -35)
4 55-59
EPT 5 year risk
42 (95 CI 37 -46)
Adapted from Kerlikowske et al JOURNAL OF CLINICAL ONCOLOGY 2010
Breast Cancer Risk by Breast Density
Menopause and Postmenopausal Hormone
Therapy Use
Adapted from Kerlikowske et al JOURNAL OF CLINICAL ONCOLOGY 2010
bull Postmenopausal women with high breast density are at increased risk of breast cancer and should be aware of the added risk of taking HT especially estrogen plus progestin
Medical condition which may be exacerbated by treatment
with progestins
Diabetes and metabolic syndrome
bull progestin-containing HT may be associated with increases in insulin resistance and deterioration in glucose tolerance123
bull Postmenopausal women with diabetes could be inappropriate for treatment with progestin-containing HT due to the potential risk of exacerbation of their condition
1) Panay N amp Studd JWW Human Reprod Update 1997
2) Godsland I et al Metabolism 1993
3) Sites CK et al J Clin Endocrinol Metab 2005
A Nath and R Sitruk-Ware CLIMACTERIC 200912(Suppl 1)96ndash101
A Nath and R Sitruk-Ware CLIMACTERIC 200912(Suppl 1)96ndash101
Diabetes an epidemy
bull UK 1996 14 million of diabetics
bull UK 2015 32 million (6 of the population)
bull UK 2025 5 million
bull httpwwwdiabetescoukdiabetes-prevalencehtml
Other progestin-related intolerance issues
bull Nausea
bull Depressive mood
bull Poor concentration
bull Hirsutism
bull Headache
bull Dizziness
bull Fluid retention
bull Weight gain Panay N amp Studd JWW Human Reprod Update 1997
Medical condition which may be exacerbated by treatment with progestins
PMSPMDDdepression
bull Progesterone-induced PMD can be exacerbated by exogenous progestin administration and can occur in association with HT or OC administration1
bull Significantly higher negative mood scores have been observed during the addition of a progestin to an estrogen in a sequential HT regimen in postmenopausal women with a history of PMS compared to those without2
bull Women with a history of PMS or PMD exacerbation of depression using progestins may therefore benefit from a progestin free treatment for menopausal symptoms
1) Nevatte T et al Arch Womens Ment Health 2013 2) Bjoumlrn I et al Climacteric 2006 PMS premenstrual syndrome
PMDD premenstrual dysphoric disorder
Conclusion
bull CEEBAZO is an additional regimen for menopausal symptoms it provides also a prevention for osteoporosis
bull It is suitable for women with a uterus who are unsatisfied with an EPT regimen or who you are unwilling to treat with an EPT regimen
For some postmenopausal women with a uterus there is a
need for progestin free treatment options
bull with demonstrated clinical efficacy
bull which protects the endometrium
bull improved tolerabilitysafety profile
In clinical practice this translates to women who are
intolerant of progestin-containing HT or have conditions
which may be exacerbated by treatment with progestins
Conclusion Medical need for alternative treatment option
Medical condition which may be exacerbated by treatment with progestins
Depression
bull Progestin-containing HT has been associated with increases in depressive symptoms in some individuals1
bull There is a biochemicalphysiological plausibility for the association of progestins with depression234
bull Therefore postmenopausal women who also have a medical history of depressive disorders or depression could be inappropriate for treatment with progestin-containing HT
Pfizer Confidential
65
1) Girdler SS et al J Womens Health Gend Based Med 1999 2) Traish AM et al Korean J Urol 2014 3) Stroumlhle A et al Biol Psychiatry 1999 4) Romeo E et
al Am J Psychiatry 1998
History of the following conditions may make progestin inappropriate
bull Depression
bull PMSPMDD
PMS premenstrual syndrome
PMD premenstrual dysphoric disorder
Medical conditions that may be exacerbated by treatment with progestins
Women for whom progestin-containing HT
would not be considered appropriate
minus Women who are intolerant of progestin-containing hormone therapy
minus Women with pre-existing medical conditions that may be exacerbated by progestins
Most common adverse events leading to discontinuation are related to progestins12
breakthrough bleeding
bull Increase in the number of uterine procedures (ie unnecessary endometrial biopsies)
breast paintenderness
bull Increase in the number of breast interventions
1 Steel SA et al Climacteric 2003 2 Ettinger B and Pressman A Am J Manag Care 1999 3 Komm BS Mirkin S
Pharmaceuticals 2012
4 Panay N amp Studd JWW Human Reprod Update 1997
bull Nausea bull Depressive mood bull Poor concentration bull Hirsutism bull Headache bull Dizziness bull Fluid retention bull Weight gain
Other progestin-related intolerance issues4
Unmet need with the treatment of postmenopausal symptoms
bull Alternatives to progestin are needed that will protect the endometrium while avoiding other progestin-associated effects and preserving the desired effects of estrogens in postmenopausal women3
Which women with a uterus could benefit from
estrogens without the need for a progestin
bull Women who are intolerant of progestin-containing hormone therapy
bull Women with pre-existing medical conditions that may be exacerbated by progestins (eg women with a history of depression PMSPMDD increased breast density diabetes and metabolic syndrome)
History of the following conditions may make progestin inappropriate
bull Depression
bull PMSPMDD
bull High breast density
bull Diabetes and metabolic syndrome
PMS premenstrual syndrome
PMD premenstrual dysphoric disorder
Medical conditions that may be exacerbated by treatment with progestins
Learning from WHI data
bull Hormone therapy (HT) is the conventional and established therapy option to effectively treat postmenopausal symptoms however it has been associated with some safety and tolerability concerns1 2
bull A review of WHI data suggests that many of the concerns with menopausal HT more often associated with EPT (CE+MPA) such as CHD risk increased breast density breast pain and breast cancer risk than with ET (CEE alone)2
1 Rolnick SJ Kopher RA DeFor TA et al Menopause 2005
2 Komm BS Mirkin S Pharmaceuticals 2012
WHI Womenrsquos Health Initiative trial
CHD coronary heart disease
CEE conjugated equine estrogens
Efficacy and Safety of Constant Oestrogen
Pulsed Progestogen vs
Continuous Combined HRT
Adverse Events
17b-oestradiol 17b-oestradiol norgestimate NETA (n = 150) (n = 172) Breast discomfort 14 27 Abdominal discomfort 14 22 Uterine bleeding 15 12 Dysmenorrhea 3 8 Oedema 5 8
Adapted from S Rozenberg et al Human Reproduction 2000
Medical condition which may be exacerbated by treatment
with progestins
Increased breast density
bull Increases in breast density are associated with progestin-containing HT which may adversely affect radiological detection of breast cancer1 and may be independently associated with an increased risk for the development of breast cancer2
bull The Postmenopausal EstrogenProgestin Interventions (PEPI) trial demonstrated that an increased mammographic breast density was associated with the use of E+P but not with the use of estrogen alone3
bull Women who already have high breast density may therefore be considered inappropriate for treatment with a progestin-containing HT
1) EU Core SPC for Hormone Replacement Therapy Products (CMDh1312003 Rev 4 June
2012)
2) De Villiers TJ et al on behalf of the International Menopause Society Climacteric 2013 16
3) Greendale GA et al J Natl Cancer Inst 2003
Stroke
0 25 5 75 10 125
Fractures
Diabetes
Breast cancer
Cholecystitis
Venothrombotic episodes
Endometrial cancer
Lung cancer
Coronary heart disease
Colorectal cancer
Overall mortality
15 125 10 75 5 25
Benefits Risks
CE
CE MPA
Santen RJ et al J Clin Endocrinol Metab 2010
The basis of the Endocrine Society scientific statement for postmenopausal hormone replacement therapy (HRT) excess risks and benefits of HRT for 5 years in women aged 50ndash59 years or within 10 years of the start of menopause E=estrogen P=progestin
bull Younger women (aged 50ndash59 years) had more favorable results bull There are differences between CE alone and CEMPA arms bull Overall benefitrisk ratio of CE-alone appears to be more favourable than CEMPA
Reevaluation of WHI data (stratified by age) Risks and
Benefits of HRT Cases per 1000 Women per 5 Years of
Use
Medical condition which may be exacerbated by treatment
with progestins
Diabetes and metabolic syndrome
bull Treatment of oestrogen deficiency symptoms with progestin-containing HT (unlike oestrogen alone) may be associated with increases in insulin resistance and deterioration in glucose tolerance123
bull Postmenopausal women with diabetes could be inappropriate for treatment with progestin-containing HT due to the potential risk of exacerbation of their condition
1) Panay N amp Studd JWW Human Reprod Update 1997
2) Godsland I et al Metabolism 1993
3) Sites CK et al J Clin Endocrinol Metab 2005
Variations in Associated Breast Cancer
Risks Between CE alone and CEMPA
bull Use of CE alone for a median of 59 years was associated with a lower incidence of invasive breast cancer (151 cases 027 per year) compared with placebo (199 cases 035 per year HR 077 95 CI 062ndash095 P=002)
bull In the CE alone group fewer women died from invasive breast cancer (6 deaths 0009 per year) compared with controls (16 deaths 0024 per year HR 037 95 CI 013ndash091 P=003)
Anderson GL et al Lancet
Oncol 2012
Bazedoxifene (BZA) specifically selected in
combination with conjugated estrogens
bull BZA has been specifically selected for its unique pharmacologic profile and effects on VMS and uterine tissue in particular123
1 Crabtree J et al Mol Cell Endocrinol 2008
2 Kharode Y et al Endocrinolology 2008
3 Duavive SmPC
Estrogen Receptor activity is dimmed
Estrogen Receptor activity is turned on
CEs are agonists BZA is an antagonist
In the uterus
bull The BZA component reduces the risk of endometrial hyperplasia that can occur with the conjugated estrogens component alone3 This means that progestins are not needed
Extensive global clinical development program for
CEBZA
aIncludes additional pilot dose-finding study 203 1 Lobo RA et al Fertil Steril 2009 2 Pinkerton JV et al Menopause 2009 3 Kagan R et al Menopause 2010 4 Mirkin S et al Climacteric 2013 5 Pinkerton JV et al Obstet Gynecol 2013
Effects of conjugated estrogensbazedoxifene on
lipid and coagulation variables a randomized
placebo- and active-controlled trial
bull At 12 months
bull Both CEBZA doses were associated with small but significant effects on hemostasis variables including reductions in antithrombin plasminogen activator inhibitor-1 and fibrinogen activity and an increase in plasminogen activity relative to placebo at 12 months Incidences of cardiovascular and venous thromboembolic events were similar among treatment groups
bull CONCLUSIONS
bull This study provides reassurance that CEBZA does not adversely affect lipid metabolism or hemostatic balance In accordance the incidences of venous thromboembolic events and cardiovascular events in postmenopausal women are similar to those observed with placebo

Progestin intolerance is one of the main
factors for reduced compliance
bull About 20 of women receiving progestin-containing HT have significant progestin intolerance and half of these experience serious effects that prevent treatment continuation1
1 Panay N amp Studd J Human Reprod Update 1997
2 Panay N et al on behalf of the British Menopause Society and Womenrsquos Health Concern Menopause Int 2013
bull The 2013 British Menopause Society amp Womenrsquos Health
Concern recommendations on hormone replacement
therapy do recognise progestin intolerance as one of the
main factors for reduced compliance with HT 2
Proportion of patients () with at least one bleeding episode in relation to time and to the
used HT
Serge Rozenberg et al Hum Reprod 2009241739-1747
copy The Author 2009 Published by Oxford University Press on behalf of the European Society of
Human Reproduction and Embryology All rights reserved For Permissions please email
journalspermissionsoxfordjournalsorg
Breast tenderness after initiation of CEE
CEE + MPA (WHI)
and mammographic density change
bullCrandall et al Breast Cancer Res Treat DOI 101007s10549-011-1803-9
Breast density
Conclusion
bull CEEBAZO is an additional regimen for menopausal symptoms it provides also a prevention for osteoporosis
bull It is suitable for women with a uterus who are unsatisfied with an EPT regimen or who you are unwilling to treat with an EPT regimen
Adapted use of MHT
bull Lower dosage of estrogens
bull Other progestins
bull Better safety profile
bull Vaginal estrogen or SERMS
bull Non-hormonal therapy
bull Development of new products
bull SERMS + estrogens
Most common adverse events leading to
discontinuation are related to progestins12
bull breakthrough bleeding
bull Low compliance
bull Increase in the number of US
bull Stress
bull Cost
bull uterine procedures
bull Unnecessary endometrial biopsies Hysteroscopies DampC Hysterectomies
bull Morbidity
Proportion of patients who completed or discontinued treatment in relation to the used HT
Serge Rozenberg et al Hum Reprod 2009241739-1747
copy The Author 2009 Published by Oxford University Press on behalf of the European Society of
Human Reproduction and Embryology All rights reserved For Permissions please email
journalspermissionsoxfordjournalsorg
Most common adverse events leading to discontinuation
are related to progestins
bull breast paintenderness
Breast tenderness after initiation of CEE
CEE + MPA (WHI)
and mammographic density change
bullCrandall et al Breast Cancer Res Treat DOI 101007s10549-011-1803-9
Breast density
Hormone therapy use and mammographic
density in postmenopausal Norwegian women
bull Results differed when considering the combined effect of age and BMI
bull The effect of EPT on mammographic density was modified by age and BMI with no apparent association among the youngest women (aged 50-55) with the highest BMI (BMI ge 26)
bull A higher mammographic density was found in EPT users compared to never HT users particularly in women using high-dose NETA regimens Age and BMI modified the association between EPT use and mammographic density
bull Couto E et al Breast Cancer Res Treat 2011 Nov 4 [Epub ahead of print]
Breast Cancer Risk by Breast Density
Menopause and Postmenopausal Hormone
Therapy Use
Birads age HT Duration Risk
1 55-59 None 5 year risk 08 (95 CI 06- 09)
1 55-59
ET EPT 5 year risk 09 (95 CI 07 -11)
4 55-59
None 5 year risk 24 (95 CI 20 -28)
4 55-59
ET 5 year risk
30 (95 CI 26 -35)
4 55-59
EPT 5 year risk
42 (95 CI 37 -46)
Adapted from Kerlikowske et al JOURNAL OF CLINICAL ONCOLOGY 2010
Breast Cancer Risk by Breast Density
Menopause and Postmenopausal Hormone
Therapy Use
Adapted from Kerlikowske et al JOURNAL OF CLINICAL ONCOLOGY 2010
bull Postmenopausal women with high breast density are at increased risk of breast cancer and should be aware of the added risk of taking HT especially estrogen plus progestin
Medical condition which may be exacerbated by treatment
with progestins
Diabetes and metabolic syndrome
bull progestin-containing HT may be associated with increases in insulin resistance and deterioration in glucose tolerance123
bull Postmenopausal women with diabetes could be inappropriate for treatment with progestin-containing HT due to the potential risk of exacerbation of their condition
1) Panay N amp Studd JWW Human Reprod Update 1997
2) Godsland I et al Metabolism 1993
3) Sites CK et al J Clin Endocrinol Metab 2005
A Nath and R Sitruk-Ware CLIMACTERIC 200912(Suppl 1)96ndash101
A Nath and R Sitruk-Ware CLIMACTERIC 200912(Suppl 1)96ndash101
Diabetes an epidemy
bull UK 1996 14 million of diabetics
bull UK 2015 32 million (6 of the population)
bull UK 2025 5 million
bull httpwwwdiabetescoukdiabetes-prevalencehtml
Other progestin-related intolerance issues
bull Nausea
bull Depressive mood
bull Poor concentration
bull Hirsutism
bull Headache
bull Dizziness
bull Fluid retention
bull Weight gain Panay N amp Studd JWW Human Reprod Update 1997
Medical condition which may be exacerbated by treatment with progestins
PMSPMDDdepression
bull Progesterone-induced PMD can be exacerbated by exogenous progestin administration and can occur in association with HT or OC administration1
bull Significantly higher negative mood scores have been observed during the addition of a progestin to an estrogen in a sequential HT regimen in postmenopausal women with a history of PMS compared to those without2
bull Women with a history of PMS or PMD exacerbation of depression using progestins may therefore benefit from a progestin free treatment for menopausal symptoms
1) Nevatte T et al Arch Womens Ment Health 2013 2) Bjoumlrn I et al Climacteric 2006 PMS premenstrual syndrome
PMDD premenstrual dysphoric disorder
Conclusion
bull CEEBAZO is an additional regimen for menopausal symptoms it provides also a prevention for osteoporosis
bull It is suitable for women with a uterus who are unsatisfied with an EPT regimen or who you are unwilling to treat with an EPT regimen
For some postmenopausal women with a uterus there is a
need for progestin free treatment options
bull with demonstrated clinical efficacy
bull which protects the endometrium
bull improved tolerabilitysafety profile
In clinical practice this translates to women who are
intolerant of progestin-containing HT or have conditions
which may be exacerbated by treatment with progestins
Conclusion Medical need for alternative treatment option
Medical condition which may be exacerbated by treatment with progestins
Depression
bull Progestin-containing HT has been associated with increases in depressive symptoms in some individuals1
bull There is a biochemicalphysiological plausibility for the association of progestins with depression234
bull Therefore postmenopausal women who also have a medical history of depressive disorders or depression could be inappropriate for treatment with progestin-containing HT
Pfizer Confidential
65
1) Girdler SS et al J Womens Health Gend Based Med 1999 2) Traish AM et al Korean J Urol 2014 3) Stroumlhle A et al Biol Psychiatry 1999 4) Romeo E et
al Am J Psychiatry 1998
History of the following conditions may make progestin inappropriate
bull Depression
bull PMSPMDD
PMS premenstrual syndrome
PMD premenstrual dysphoric disorder
Medical conditions that may be exacerbated by treatment with progestins
Women for whom progestin-containing HT
would not be considered appropriate
minus Women who are intolerant of progestin-containing hormone therapy
minus Women with pre-existing medical conditions that may be exacerbated by progestins
Most common adverse events leading to discontinuation are related to progestins12
breakthrough bleeding
bull Increase in the number of uterine procedures (ie unnecessary endometrial biopsies)
breast paintenderness
bull Increase in the number of breast interventions
1 Steel SA et al Climacteric 2003 2 Ettinger B and Pressman A Am J Manag Care 1999 3 Komm BS Mirkin S
Pharmaceuticals 2012
4 Panay N amp Studd JWW Human Reprod Update 1997
bull Nausea bull Depressive mood bull Poor concentration bull Hirsutism bull Headache bull Dizziness bull Fluid retention bull Weight gain
Other progestin-related intolerance issues4
Unmet need with the treatment of postmenopausal symptoms
bull Alternatives to progestin are needed that will protect the endometrium while avoiding other progestin-associated effects and preserving the desired effects of estrogens in postmenopausal women3
Which women with a uterus could benefit from
estrogens without the need for a progestin
bull Women who are intolerant of progestin-containing hormone therapy
bull Women with pre-existing medical conditions that may be exacerbated by progestins (eg women with a history of depression PMSPMDD increased breast density diabetes and metabolic syndrome)
History of the following conditions may make progestin inappropriate
bull Depression
bull PMSPMDD
bull High breast density
bull Diabetes and metabolic syndrome
PMS premenstrual syndrome
PMD premenstrual dysphoric disorder
Medical conditions that may be exacerbated by treatment with progestins
Learning from WHI data
bull Hormone therapy (HT) is the conventional and established therapy option to effectively treat postmenopausal symptoms however it has been associated with some safety and tolerability concerns1 2
bull A review of WHI data suggests that many of the concerns with menopausal HT more often associated with EPT (CE+MPA) such as CHD risk increased breast density breast pain and breast cancer risk than with ET (CEE alone)2
1 Rolnick SJ Kopher RA DeFor TA et al Menopause 2005
2 Komm BS Mirkin S Pharmaceuticals 2012
WHI Womenrsquos Health Initiative trial
CHD coronary heart disease
CEE conjugated equine estrogens
Efficacy and Safety of Constant Oestrogen
Pulsed Progestogen vs
Continuous Combined HRT
Adverse Events
17b-oestradiol 17b-oestradiol norgestimate NETA (n = 150) (n = 172) Breast discomfort 14 27 Abdominal discomfort 14 22 Uterine bleeding 15 12 Dysmenorrhea 3 8 Oedema 5 8
Adapted from S Rozenberg et al Human Reproduction 2000
Medical condition which may be exacerbated by treatment
with progestins
Increased breast density
bull Increases in breast density are associated with progestin-containing HT which may adversely affect radiological detection of breast cancer1 and may be independently associated with an increased risk for the development of breast cancer2
bull The Postmenopausal EstrogenProgestin Interventions (PEPI) trial demonstrated that an increased mammographic breast density was associated with the use of E+P but not with the use of estrogen alone3
bull Women who already have high breast density may therefore be considered inappropriate for treatment with a progestin-containing HT
1) EU Core SPC for Hormone Replacement Therapy Products (CMDh1312003 Rev 4 June
2012)
2) De Villiers TJ et al on behalf of the International Menopause Society Climacteric 2013 16
3) Greendale GA et al J Natl Cancer Inst 2003
Stroke
0 25 5 75 10 125
Fractures
Diabetes
Breast cancer
Cholecystitis
Venothrombotic episodes
Endometrial cancer
Lung cancer
Coronary heart disease
Colorectal cancer
Overall mortality
15 125 10 75 5 25
Benefits Risks
CE
CE MPA
Santen RJ et al J Clin Endocrinol Metab 2010
The basis of the Endocrine Society scientific statement for postmenopausal hormone replacement therapy (HRT) excess risks and benefits of HRT for 5 years in women aged 50ndash59 years or within 10 years of the start of menopause E=estrogen P=progestin
bull Younger women (aged 50ndash59 years) had more favorable results bull There are differences between CE alone and CEMPA arms bull Overall benefitrisk ratio of CE-alone appears to be more favourable than CEMPA
Reevaluation of WHI data (stratified by age) Risks and
Benefits of HRT Cases per 1000 Women per 5 Years of
Use
Medical condition which may be exacerbated by treatment
with progestins
Diabetes and metabolic syndrome
bull Treatment of oestrogen deficiency symptoms with progestin-containing HT (unlike oestrogen alone) may be associated with increases in insulin resistance and deterioration in glucose tolerance123
bull Postmenopausal women with diabetes could be inappropriate for treatment with progestin-containing HT due to the potential risk of exacerbation of their condition
1) Panay N amp Studd JWW Human Reprod Update 1997
2) Godsland I et al Metabolism 1993
3) Sites CK et al J Clin Endocrinol Metab 2005
Variations in Associated Breast Cancer
Risks Between CE alone and CEMPA
bull Use of CE alone for a median of 59 years was associated with a lower incidence of invasive breast cancer (151 cases 027 per year) compared with placebo (199 cases 035 per year HR 077 95 CI 062ndash095 P=002)
bull In the CE alone group fewer women died from invasive breast cancer (6 deaths 0009 per year) compared with controls (16 deaths 0024 per year HR 037 95 CI 013ndash091 P=003)
Anderson GL et al Lancet
Oncol 2012
Bazedoxifene (BZA) specifically selected in
combination with conjugated estrogens
bull BZA has been specifically selected for its unique pharmacologic profile and effects on VMS and uterine tissue in particular123
1 Crabtree J et al Mol Cell Endocrinol 2008
2 Kharode Y et al Endocrinolology 2008
3 Duavive SmPC
Estrogen Receptor activity is dimmed
Estrogen Receptor activity is turned on
CEs are agonists BZA is an antagonist
In the uterus
bull The BZA component reduces the risk of endometrial hyperplasia that can occur with the conjugated estrogens component alone3 This means that progestins are not needed
Extensive global clinical development program for
CEBZA
aIncludes additional pilot dose-finding study 203 1 Lobo RA et al Fertil Steril 2009 2 Pinkerton JV et al Menopause 2009 3 Kagan R et al Menopause 2010 4 Mirkin S et al Climacteric 2013 5 Pinkerton JV et al Obstet Gynecol 2013
Effects of conjugated estrogensbazedoxifene on
lipid and coagulation variables a randomized
placebo- and active-controlled trial
bull At 12 months
bull Both CEBZA doses were associated with small but significant effects on hemostasis variables including reductions in antithrombin plasminogen activator inhibitor-1 and fibrinogen activity and an increase in plasminogen activity relative to placebo at 12 months Incidences of cardiovascular and venous thromboembolic events were similar among treatment groups
bull CONCLUSIONS
bull This study provides reassurance that CEBZA does not adversely affect lipid metabolism or hemostatic balance In accordance the incidences of venous thromboembolic events and cardiovascular events in postmenopausal women are similar to those observed with placebo

Proportion of patients () with at least one bleeding episode in relation to time and to the
used HT
Serge Rozenberg et al Hum Reprod 2009241739-1747
copy The Author 2009 Published by Oxford University Press on behalf of the European Society of
Human Reproduction and Embryology All rights reserved For Permissions please email
journalspermissionsoxfordjournalsorg
Breast tenderness after initiation of CEE
CEE + MPA (WHI)
and mammographic density change
bullCrandall et al Breast Cancer Res Treat DOI 101007s10549-011-1803-9
Breast density
Conclusion
bull CEEBAZO is an additional regimen for menopausal symptoms it provides also a prevention for osteoporosis
bull It is suitable for women with a uterus who are unsatisfied with an EPT regimen or who you are unwilling to treat with an EPT regimen
Adapted use of MHT
bull Lower dosage of estrogens
bull Other progestins
bull Better safety profile
bull Vaginal estrogen or SERMS
bull Non-hormonal therapy
bull Development of new products
bull SERMS + estrogens
Most common adverse events leading to
discontinuation are related to progestins12
bull breakthrough bleeding
bull Low compliance
bull Increase in the number of US
bull Stress
bull Cost
bull uterine procedures
bull Unnecessary endometrial biopsies Hysteroscopies DampC Hysterectomies
bull Morbidity
Proportion of patients who completed or discontinued treatment in relation to the used HT
Serge Rozenberg et al Hum Reprod 2009241739-1747
copy The Author 2009 Published by Oxford University Press on behalf of the European Society of
Human Reproduction and Embryology All rights reserved For Permissions please email
journalspermissionsoxfordjournalsorg
Most common adverse events leading to discontinuation
are related to progestins
bull breast paintenderness
Breast tenderness after initiation of CEE
CEE + MPA (WHI)
and mammographic density change
bullCrandall et al Breast Cancer Res Treat DOI 101007s10549-011-1803-9
Breast density
Hormone therapy use and mammographic
density in postmenopausal Norwegian women
bull Results differed when considering the combined effect of age and BMI
bull The effect of EPT on mammographic density was modified by age and BMI with no apparent association among the youngest women (aged 50-55) with the highest BMI (BMI ge 26)
bull A higher mammographic density was found in EPT users compared to never HT users particularly in women using high-dose NETA regimens Age and BMI modified the association between EPT use and mammographic density
bull Couto E et al Breast Cancer Res Treat 2011 Nov 4 [Epub ahead of print]
Breast Cancer Risk by Breast Density
Menopause and Postmenopausal Hormone
Therapy Use
Birads age HT Duration Risk
1 55-59 None 5 year risk 08 (95 CI 06- 09)
1 55-59
ET EPT 5 year risk 09 (95 CI 07 -11)
4 55-59
None 5 year risk 24 (95 CI 20 -28)
4 55-59
ET 5 year risk
30 (95 CI 26 -35)
4 55-59
EPT 5 year risk
42 (95 CI 37 -46)
Adapted from Kerlikowske et al JOURNAL OF CLINICAL ONCOLOGY 2010
Breast Cancer Risk by Breast Density
Menopause and Postmenopausal Hormone
Therapy Use
Adapted from Kerlikowske et al JOURNAL OF CLINICAL ONCOLOGY 2010
bull Postmenopausal women with high breast density are at increased risk of breast cancer and should be aware of the added risk of taking HT especially estrogen plus progestin
Medical condition which may be exacerbated by treatment
with progestins
Diabetes and metabolic syndrome
bull progestin-containing HT may be associated with increases in insulin resistance and deterioration in glucose tolerance123
bull Postmenopausal women with diabetes could be inappropriate for treatment with progestin-containing HT due to the potential risk of exacerbation of their condition
1) Panay N amp Studd JWW Human Reprod Update 1997
2) Godsland I et al Metabolism 1993
3) Sites CK et al J Clin Endocrinol Metab 2005
A Nath and R Sitruk-Ware CLIMACTERIC 200912(Suppl 1)96ndash101
A Nath and R Sitruk-Ware CLIMACTERIC 200912(Suppl 1)96ndash101
Diabetes an epidemy
bull UK 1996 14 million of diabetics
bull UK 2015 32 million (6 of the population)
bull UK 2025 5 million
bull httpwwwdiabetescoukdiabetes-prevalencehtml
Other progestin-related intolerance issues
bull Nausea
bull Depressive mood
bull Poor concentration
bull Hirsutism
bull Headache
bull Dizziness
bull Fluid retention
bull Weight gain Panay N amp Studd JWW Human Reprod Update 1997
Medical condition which may be exacerbated by treatment with progestins
PMSPMDDdepression
bull Progesterone-induced PMD can be exacerbated by exogenous progestin administration and can occur in association with HT or OC administration1
bull Significantly higher negative mood scores have been observed during the addition of a progestin to an estrogen in a sequential HT regimen in postmenopausal women with a history of PMS compared to those without2
bull Women with a history of PMS or PMD exacerbation of depression using progestins may therefore benefit from a progestin free treatment for menopausal symptoms
1) Nevatte T et al Arch Womens Ment Health 2013 2) Bjoumlrn I et al Climacteric 2006 PMS premenstrual syndrome
PMDD premenstrual dysphoric disorder
Conclusion
bull CEEBAZO is an additional regimen for menopausal symptoms it provides also a prevention for osteoporosis
bull It is suitable for women with a uterus who are unsatisfied with an EPT regimen or who you are unwilling to treat with an EPT regimen
For some postmenopausal women with a uterus there is a
need for progestin free treatment options
bull with demonstrated clinical efficacy
bull which protects the endometrium
bull improved tolerabilitysafety profile
In clinical practice this translates to women who are
intolerant of progestin-containing HT or have conditions
which may be exacerbated by treatment with progestins
Conclusion Medical need for alternative treatment option
Medical condition which may be exacerbated by treatment with progestins
Depression
bull Progestin-containing HT has been associated with increases in depressive symptoms in some individuals1
bull There is a biochemicalphysiological plausibility for the association of progestins with depression234
bull Therefore postmenopausal women who also have a medical history of depressive disorders or depression could be inappropriate for treatment with progestin-containing HT
Pfizer Confidential
65
1) Girdler SS et al J Womens Health Gend Based Med 1999 2) Traish AM et al Korean J Urol 2014 3) Stroumlhle A et al Biol Psychiatry 1999 4) Romeo E et
al Am J Psychiatry 1998
History of the following conditions may make progestin inappropriate
bull Depression
bull PMSPMDD
PMS premenstrual syndrome
PMD premenstrual dysphoric disorder
Medical conditions that may be exacerbated by treatment with progestins
Women for whom progestin-containing HT
would not be considered appropriate
minus Women who are intolerant of progestin-containing hormone therapy
minus Women with pre-existing medical conditions that may be exacerbated by progestins
Most common adverse events leading to discontinuation are related to progestins12
breakthrough bleeding
bull Increase in the number of uterine procedures (ie unnecessary endometrial biopsies)
breast paintenderness
bull Increase in the number of breast interventions
1 Steel SA et al Climacteric 2003 2 Ettinger B and Pressman A Am J Manag Care 1999 3 Komm BS Mirkin S
Pharmaceuticals 2012
4 Panay N amp Studd JWW Human Reprod Update 1997
bull Nausea bull Depressive mood bull Poor concentration bull Hirsutism bull Headache bull Dizziness bull Fluid retention bull Weight gain
Other progestin-related intolerance issues4
Unmet need with the treatment of postmenopausal symptoms
bull Alternatives to progestin are needed that will protect the endometrium while avoiding other progestin-associated effects and preserving the desired effects of estrogens in postmenopausal women3
Which women with a uterus could benefit from
estrogens without the need for a progestin
bull Women who are intolerant of progestin-containing hormone therapy
bull Women with pre-existing medical conditions that may be exacerbated by progestins (eg women with a history of depression PMSPMDD increased breast density diabetes and metabolic syndrome)
History of the following conditions may make progestin inappropriate
bull Depression
bull PMSPMDD
bull High breast density
bull Diabetes and metabolic syndrome
PMS premenstrual syndrome
PMD premenstrual dysphoric disorder
Medical conditions that may be exacerbated by treatment with progestins
Learning from WHI data
bull Hormone therapy (HT) is the conventional and established therapy option to effectively treat postmenopausal symptoms however it has been associated with some safety and tolerability concerns1 2
bull A review of WHI data suggests that many of the concerns with menopausal HT more often associated with EPT (CE+MPA) such as CHD risk increased breast density breast pain and breast cancer risk than with ET (CEE alone)2
1 Rolnick SJ Kopher RA DeFor TA et al Menopause 2005
2 Komm BS Mirkin S Pharmaceuticals 2012
WHI Womenrsquos Health Initiative trial
CHD coronary heart disease
CEE conjugated equine estrogens
Efficacy and Safety of Constant Oestrogen
Pulsed Progestogen vs
Continuous Combined HRT
Adverse Events
17b-oestradiol 17b-oestradiol norgestimate NETA (n = 150) (n = 172) Breast discomfort 14 27 Abdominal discomfort 14 22 Uterine bleeding 15 12 Dysmenorrhea 3 8 Oedema 5 8
Adapted from S Rozenberg et al Human Reproduction 2000
Medical condition which may be exacerbated by treatment
with progestins
Increased breast density
bull Increases in breast density are associated with progestin-containing HT which may adversely affect radiological detection of breast cancer1 and may be independently associated with an increased risk for the development of breast cancer2
bull The Postmenopausal EstrogenProgestin Interventions (PEPI) trial demonstrated that an increased mammographic breast density was associated with the use of E+P but not with the use of estrogen alone3
bull Women who already have high breast density may therefore be considered inappropriate for treatment with a progestin-containing HT
1) EU Core SPC for Hormone Replacement Therapy Products (CMDh1312003 Rev 4 June
2012)
2) De Villiers TJ et al on behalf of the International Menopause Society Climacteric 2013 16
3) Greendale GA et al J Natl Cancer Inst 2003
Stroke
0 25 5 75 10 125
Fractures
Diabetes
Breast cancer
Cholecystitis
Venothrombotic episodes
Endometrial cancer
Lung cancer
Coronary heart disease
Colorectal cancer
Overall mortality
15 125 10 75 5 25
Benefits Risks
CE
CE MPA
Santen RJ et al J Clin Endocrinol Metab 2010
The basis of the Endocrine Society scientific statement for postmenopausal hormone replacement therapy (HRT) excess risks and benefits of HRT for 5 years in women aged 50ndash59 years or within 10 years of the start of menopause E=estrogen P=progestin
bull Younger women (aged 50ndash59 years) had more favorable results bull There are differences between CE alone and CEMPA arms bull Overall benefitrisk ratio of CE-alone appears to be more favourable than CEMPA
Reevaluation of WHI data (stratified by age) Risks and
Benefits of HRT Cases per 1000 Women per 5 Years of
Use
Medical condition which may be exacerbated by treatment
with progestins
Diabetes and metabolic syndrome
bull Treatment of oestrogen deficiency symptoms with progestin-containing HT (unlike oestrogen alone) may be associated with increases in insulin resistance and deterioration in glucose tolerance123
bull Postmenopausal women with diabetes could be inappropriate for treatment with progestin-containing HT due to the potential risk of exacerbation of their condition
1) Panay N amp Studd JWW Human Reprod Update 1997
2) Godsland I et al Metabolism 1993
3) Sites CK et al J Clin Endocrinol Metab 2005
Variations in Associated Breast Cancer
Risks Between CE alone and CEMPA
bull Use of CE alone for a median of 59 years was associated with a lower incidence of invasive breast cancer (151 cases 027 per year) compared with placebo (199 cases 035 per year HR 077 95 CI 062ndash095 P=002)
bull In the CE alone group fewer women died from invasive breast cancer (6 deaths 0009 per year) compared with controls (16 deaths 0024 per year HR 037 95 CI 013ndash091 P=003)
Anderson GL et al Lancet
Oncol 2012
Bazedoxifene (BZA) specifically selected in
combination with conjugated estrogens
bull BZA has been specifically selected for its unique pharmacologic profile and effects on VMS and uterine tissue in particular123
1 Crabtree J et al Mol Cell Endocrinol 2008
2 Kharode Y et al Endocrinolology 2008
3 Duavive SmPC
Estrogen Receptor activity is dimmed
Estrogen Receptor activity is turned on
CEs are agonists BZA is an antagonist
In the uterus
bull The BZA component reduces the risk of endometrial hyperplasia that can occur with the conjugated estrogens component alone3 This means that progestins are not needed
Extensive global clinical development program for
CEBZA
aIncludes additional pilot dose-finding study 203 1 Lobo RA et al Fertil Steril 2009 2 Pinkerton JV et al Menopause 2009 3 Kagan R et al Menopause 2010 4 Mirkin S et al Climacteric 2013 5 Pinkerton JV et al Obstet Gynecol 2013
Effects of conjugated estrogensbazedoxifene on
lipid and coagulation variables a randomized
placebo- and active-controlled trial
bull At 12 months
bull Both CEBZA doses were associated with small but significant effects on hemostasis variables including reductions in antithrombin plasminogen activator inhibitor-1 and fibrinogen activity and an increase in plasminogen activity relative to placebo at 12 months Incidences of cardiovascular and venous thromboembolic events were similar among treatment groups
bull CONCLUSIONS
bull This study provides reassurance that CEBZA does not adversely affect lipid metabolism or hemostatic balance In accordance the incidences of venous thromboembolic events and cardiovascular events in postmenopausal women are similar to those observed with placebo

Breast tenderness after initiation of CEE
CEE + MPA (WHI)
and mammographic density change
bullCrandall et al Breast Cancer Res Treat DOI 101007s10549-011-1803-9
Breast density
Conclusion
bull CEEBAZO is an additional regimen for menopausal symptoms it provides also a prevention for osteoporosis
bull It is suitable for women with a uterus who are unsatisfied with an EPT regimen or who you are unwilling to treat with an EPT regimen
Adapted use of MHT
bull Lower dosage of estrogens
bull Other progestins
bull Better safety profile
bull Vaginal estrogen or SERMS
bull Non-hormonal therapy
bull Development of new products
bull SERMS + estrogens
Most common adverse events leading to
discontinuation are related to progestins12
bull breakthrough bleeding
bull Low compliance
bull Increase in the number of US
bull Stress
bull Cost
bull uterine procedures
bull Unnecessary endometrial biopsies Hysteroscopies DampC Hysterectomies
bull Morbidity
Proportion of patients who completed or discontinued treatment in relation to the used HT
Serge Rozenberg et al Hum Reprod 2009241739-1747
copy The Author 2009 Published by Oxford University Press on behalf of the European Society of
Human Reproduction and Embryology All rights reserved For Permissions please email
journalspermissionsoxfordjournalsorg
Most common adverse events leading to discontinuation
are related to progestins
bull breast paintenderness
Breast tenderness after initiation of CEE
CEE + MPA (WHI)
and mammographic density change
bullCrandall et al Breast Cancer Res Treat DOI 101007s10549-011-1803-9
Breast density
Hormone therapy use and mammographic
density in postmenopausal Norwegian women
bull Results differed when considering the combined effect of age and BMI
bull The effect of EPT on mammographic density was modified by age and BMI with no apparent association among the youngest women (aged 50-55) with the highest BMI (BMI ge 26)
bull A higher mammographic density was found in EPT users compared to never HT users particularly in women using high-dose NETA regimens Age and BMI modified the association between EPT use and mammographic density
bull Couto E et al Breast Cancer Res Treat 2011 Nov 4 [Epub ahead of print]
Breast Cancer Risk by Breast Density
Menopause and Postmenopausal Hormone
Therapy Use
Birads age HT Duration Risk
1 55-59 None 5 year risk 08 (95 CI 06- 09)
1 55-59
ET EPT 5 year risk 09 (95 CI 07 -11)
4 55-59
None 5 year risk 24 (95 CI 20 -28)
4 55-59
ET 5 year risk
30 (95 CI 26 -35)
4 55-59
EPT 5 year risk
42 (95 CI 37 -46)
Adapted from Kerlikowske et al JOURNAL OF CLINICAL ONCOLOGY 2010
Breast Cancer Risk by Breast Density
Menopause and Postmenopausal Hormone
Therapy Use
Adapted from Kerlikowske et al JOURNAL OF CLINICAL ONCOLOGY 2010
bull Postmenopausal women with high breast density are at increased risk of breast cancer and should be aware of the added risk of taking HT especially estrogen plus progestin
Medical condition which may be exacerbated by treatment
with progestins
Diabetes and metabolic syndrome
bull progestin-containing HT may be associated with increases in insulin resistance and deterioration in glucose tolerance123
bull Postmenopausal women with diabetes could be inappropriate for treatment with progestin-containing HT due to the potential risk of exacerbation of their condition
1) Panay N amp Studd JWW Human Reprod Update 1997
2) Godsland I et al Metabolism 1993
3) Sites CK et al J Clin Endocrinol Metab 2005
A Nath and R Sitruk-Ware CLIMACTERIC 200912(Suppl 1)96ndash101
A Nath and R Sitruk-Ware CLIMACTERIC 200912(Suppl 1)96ndash101
Diabetes an epidemy
bull UK 1996 14 million of diabetics
bull UK 2015 32 million (6 of the population)
bull UK 2025 5 million
bull httpwwwdiabetescoukdiabetes-prevalencehtml
Other progestin-related intolerance issues
bull Nausea
bull Depressive mood
bull Poor concentration
bull Hirsutism
bull Headache
bull Dizziness
bull Fluid retention
bull Weight gain Panay N amp Studd JWW Human Reprod Update 1997
Medical condition which may be exacerbated by treatment with progestins
PMSPMDDdepression
bull Progesterone-induced PMD can be exacerbated by exogenous progestin administration and can occur in association with HT or OC administration1
bull Significantly higher negative mood scores have been observed during the addition of a progestin to an estrogen in a sequential HT regimen in postmenopausal women with a history of PMS compared to those without2
bull Women with a history of PMS or PMD exacerbation of depression using progestins may therefore benefit from a progestin free treatment for menopausal symptoms
1) Nevatte T et al Arch Womens Ment Health 2013 2) Bjoumlrn I et al Climacteric 2006 PMS premenstrual syndrome
PMDD premenstrual dysphoric disorder
Conclusion
bull CEEBAZO is an additional regimen for menopausal symptoms it provides also a prevention for osteoporosis
bull It is suitable for women with a uterus who are unsatisfied with an EPT regimen or who you are unwilling to treat with an EPT regimen
For some postmenopausal women with a uterus there is a
need for progestin free treatment options
bull with demonstrated clinical efficacy
bull which protects the endometrium
bull improved tolerabilitysafety profile
In clinical practice this translates to women who are
intolerant of progestin-containing HT or have conditions
which may be exacerbated by treatment with progestins
Conclusion Medical need for alternative treatment option
Medical condition which may be exacerbated by treatment with progestins
Depression
bull Progestin-containing HT has been associated with increases in depressive symptoms in some individuals1
bull There is a biochemicalphysiological plausibility for the association of progestins with depression234
bull Therefore postmenopausal women who also have a medical history of depressive disorders or depression could be inappropriate for treatment with progestin-containing HT
Pfizer Confidential
65
1) Girdler SS et al J Womens Health Gend Based Med 1999 2) Traish AM et al Korean J Urol 2014 3) Stroumlhle A et al Biol Psychiatry 1999 4) Romeo E et
al Am J Psychiatry 1998
History of the following conditions may make progestin inappropriate
bull Depression
bull PMSPMDD
PMS premenstrual syndrome
PMD premenstrual dysphoric disorder
Medical conditions that may be exacerbated by treatment with progestins
Women for whom progestin-containing HT
would not be considered appropriate
minus Women who are intolerant of progestin-containing hormone therapy
minus Women with pre-existing medical conditions that may be exacerbated by progestins
Most common adverse events leading to discontinuation are related to progestins12
breakthrough bleeding
bull Increase in the number of uterine procedures (ie unnecessary endometrial biopsies)
breast paintenderness
bull Increase in the number of breast interventions
1 Steel SA et al Climacteric 2003 2 Ettinger B and Pressman A Am J Manag Care 1999 3 Komm BS Mirkin S
Pharmaceuticals 2012
4 Panay N amp Studd JWW Human Reprod Update 1997
bull Nausea bull Depressive mood bull Poor concentration bull Hirsutism bull Headache bull Dizziness bull Fluid retention bull Weight gain
Other progestin-related intolerance issues4
Unmet need with the treatment of postmenopausal symptoms
bull Alternatives to progestin are needed that will protect the endometrium while avoiding other progestin-associated effects and preserving the desired effects of estrogens in postmenopausal women3
Which women with a uterus could benefit from
estrogens without the need for a progestin
bull Women who are intolerant of progestin-containing hormone therapy
bull Women with pre-existing medical conditions that may be exacerbated by progestins (eg women with a history of depression PMSPMDD increased breast density diabetes and metabolic syndrome)
History of the following conditions may make progestin inappropriate
bull Depression
bull PMSPMDD
bull High breast density
bull Diabetes and metabolic syndrome
PMS premenstrual syndrome
PMD premenstrual dysphoric disorder
Medical conditions that may be exacerbated by treatment with progestins
Learning from WHI data
bull Hormone therapy (HT) is the conventional and established therapy option to effectively treat postmenopausal symptoms however it has been associated with some safety and tolerability concerns1 2
bull A review of WHI data suggests that many of the concerns with menopausal HT more often associated with EPT (CE+MPA) such as CHD risk increased breast density breast pain and breast cancer risk than with ET (CEE alone)2
1 Rolnick SJ Kopher RA DeFor TA et al Menopause 2005
2 Komm BS Mirkin S Pharmaceuticals 2012
WHI Womenrsquos Health Initiative trial
CHD coronary heart disease
CEE conjugated equine estrogens
Efficacy and Safety of Constant Oestrogen
Pulsed Progestogen vs
Continuous Combined HRT
Adverse Events
17b-oestradiol 17b-oestradiol norgestimate NETA (n = 150) (n = 172) Breast discomfort 14 27 Abdominal discomfort 14 22 Uterine bleeding 15 12 Dysmenorrhea 3 8 Oedema 5 8
Adapted from S Rozenberg et al Human Reproduction 2000
Medical condition which may be exacerbated by treatment
with progestins
Increased breast density
bull Increases in breast density are associated with progestin-containing HT which may adversely affect radiological detection of breast cancer1 and may be independently associated with an increased risk for the development of breast cancer2
bull The Postmenopausal EstrogenProgestin Interventions (PEPI) trial demonstrated that an increased mammographic breast density was associated with the use of E+P but not with the use of estrogen alone3
bull Women who already have high breast density may therefore be considered inappropriate for treatment with a progestin-containing HT
1) EU Core SPC for Hormone Replacement Therapy Products (CMDh1312003 Rev 4 June
2012)
2) De Villiers TJ et al on behalf of the International Menopause Society Climacteric 2013 16
3) Greendale GA et al J Natl Cancer Inst 2003
Stroke
0 25 5 75 10 125
Fractures
Diabetes
Breast cancer
Cholecystitis
Venothrombotic episodes
Endometrial cancer
Lung cancer
Coronary heart disease
Colorectal cancer
Overall mortality
15 125 10 75 5 25
Benefits Risks
CE
CE MPA
Santen RJ et al J Clin Endocrinol Metab 2010
The basis of the Endocrine Society scientific statement for postmenopausal hormone replacement therapy (HRT) excess risks and benefits of HRT for 5 years in women aged 50ndash59 years or within 10 years of the start of menopause E=estrogen P=progestin
bull Younger women (aged 50ndash59 years) had more favorable results bull There are differences between CE alone and CEMPA arms bull Overall benefitrisk ratio of CE-alone appears to be more favourable than CEMPA
Reevaluation of WHI data (stratified by age) Risks and
Benefits of HRT Cases per 1000 Women per 5 Years of
Use
Medical condition which may be exacerbated by treatment
with progestins
Diabetes and metabolic syndrome
bull Treatment of oestrogen deficiency symptoms with progestin-containing HT (unlike oestrogen alone) may be associated with increases in insulin resistance and deterioration in glucose tolerance123
bull Postmenopausal women with diabetes could be inappropriate for treatment with progestin-containing HT due to the potential risk of exacerbation of their condition
1) Panay N amp Studd JWW Human Reprod Update 1997
2) Godsland I et al Metabolism 1993
3) Sites CK et al J Clin Endocrinol Metab 2005
Variations in Associated Breast Cancer
Risks Between CE alone and CEMPA
bull Use of CE alone for a median of 59 years was associated with a lower incidence of invasive breast cancer (151 cases 027 per year) compared with placebo (199 cases 035 per year HR 077 95 CI 062ndash095 P=002)
bull In the CE alone group fewer women died from invasive breast cancer (6 deaths 0009 per year) compared with controls (16 deaths 0024 per year HR 037 95 CI 013ndash091 P=003)
Anderson GL et al Lancet
Oncol 2012
Bazedoxifene (BZA) specifically selected in
combination with conjugated estrogens
bull BZA has been specifically selected for its unique pharmacologic profile and effects on VMS and uterine tissue in particular123
1 Crabtree J et al Mol Cell Endocrinol 2008
2 Kharode Y et al Endocrinolology 2008
3 Duavive SmPC
Estrogen Receptor activity is dimmed
Estrogen Receptor activity is turned on
CEs are agonists BZA is an antagonist
In the uterus
bull The BZA component reduces the risk of endometrial hyperplasia that can occur with the conjugated estrogens component alone3 This means that progestins are not needed
Extensive global clinical development program for
CEBZA
aIncludes additional pilot dose-finding study 203 1 Lobo RA et al Fertil Steril 2009 2 Pinkerton JV et al Menopause 2009 3 Kagan R et al Menopause 2010 4 Mirkin S et al Climacteric 2013 5 Pinkerton JV et al Obstet Gynecol 2013
Effects of conjugated estrogensbazedoxifene on
lipid and coagulation variables a randomized
placebo- and active-controlled trial
bull At 12 months
bull Both CEBZA doses were associated with small but significant effects on hemostasis variables including reductions in antithrombin plasminogen activator inhibitor-1 and fibrinogen activity and an increase in plasminogen activity relative to placebo at 12 months Incidences of cardiovascular and venous thromboembolic events were similar among treatment groups
bull CONCLUSIONS
bull This study provides reassurance that CEBZA does not adversely affect lipid metabolism or hemostatic balance In accordance the incidences of venous thromboembolic events and cardiovascular events in postmenopausal women are similar to those observed with placebo

Breast density
Conclusion
bull CEEBAZO is an additional regimen for menopausal symptoms it provides also a prevention for osteoporosis
bull It is suitable for women with a uterus who are unsatisfied with an EPT regimen or who you are unwilling to treat with an EPT regimen
Adapted use of MHT
bull Lower dosage of estrogens
bull Other progestins
bull Better safety profile
bull Vaginal estrogen or SERMS
bull Non-hormonal therapy
bull Development of new products
bull SERMS + estrogens
Most common adverse events leading to
discontinuation are related to progestins12
bull breakthrough bleeding
bull Low compliance
bull Increase in the number of US
bull Stress
bull Cost
bull uterine procedures
bull Unnecessary endometrial biopsies Hysteroscopies DampC Hysterectomies
bull Morbidity
Proportion of patients who completed or discontinued treatment in relation to the used HT
Serge Rozenberg et al Hum Reprod 2009241739-1747
copy The Author 2009 Published by Oxford University Press on behalf of the European Society of
Human Reproduction and Embryology All rights reserved For Permissions please email
journalspermissionsoxfordjournalsorg
Most common adverse events leading to discontinuation
are related to progestins
bull breast paintenderness
Breast tenderness after initiation of CEE
CEE + MPA (WHI)
and mammographic density change
bullCrandall et al Breast Cancer Res Treat DOI 101007s10549-011-1803-9
Breast density
Hormone therapy use and mammographic
density in postmenopausal Norwegian women
bull Results differed when considering the combined effect of age and BMI
bull The effect of EPT on mammographic density was modified by age and BMI with no apparent association among the youngest women (aged 50-55) with the highest BMI (BMI ge 26)
bull A higher mammographic density was found in EPT users compared to never HT users particularly in women using high-dose NETA regimens Age and BMI modified the association between EPT use and mammographic density
bull Couto E et al Breast Cancer Res Treat 2011 Nov 4 [Epub ahead of print]
Breast Cancer Risk by Breast Density
Menopause and Postmenopausal Hormone
Therapy Use
Birads age HT Duration Risk
1 55-59 None 5 year risk 08 (95 CI 06- 09)
1 55-59
ET EPT 5 year risk 09 (95 CI 07 -11)
4 55-59
None 5 year risk 24 (95 CI 20 -28)
4 55-59
ET 5 year risk
30 (95 CI 26 -35)
4 55-59
EPT 5 year risk
42 (95 CI 37 -46)
Adapted from Kerlikowske et al JOURNAL OF CLINICAL ONCOLOGY 2010
Breast Cancer Risk by Breast Density
Menopause and Postmenopausal Hormone
Therapy Use
Adapted from Kerlikowske et al JOURNAL OF CLINICAL ONCOLOGY 2010
bull Postmenopausal women with high breast density are at increased risk of breast cancer and should be aware of the added risk of taking HT especially estrogen plus progestin
Medical condition which may be exacerbated by treatment
with progestins
Diabetes and metabolic syndrome
bull progestin-containing HT may be associated with increases in insulin resistance and deterioration in glucose tolerance123
bull Postmenopausal women with diabetes could be inappropriate for treatment with progestin-containing HT due to the potential risk of exacerbation of their condition
1) Panay N amp Studd JWW Human Reprod Update 1997
2) Godsland I et al Metabolism 1993
3) Sites CK et al J Clin Endocrinol Metab 2005
A Nath and R Sitruk-Ware CLIMACTERIC 200912(Suppl 1)96ndash101
A Nath and R Sitruk-Ware CLIMACTERIC 200912(Suppl 1)96ndash101
Diabetes an epidemy
bull UK 1996 14 million of diabetics
bull UK 2015 32 million (6 of the population)
bull UK 2025 5 million
bull httpwwwdiabetescoukdiabetes-prevalencehtml
Other progestin-related intolerance issues
bull Nausea
bull Depressive mood
bull Poor concentration
bull Hirsutism
bull Headache
bull Dizziness
bull Fluid retention
bull Weight gain Panay N amp Studd JWW Human Reprod Update 1997
Medical condition which may be exacerbated by treatment with progestins
PMSPMDDdepression
bull Progesterone-induced PMD can be exacerbated by exogenous progestin administration and can occur in association with HT or OC administration1
bull Significantly higher negative mood scores have been observed during the addition of a progestin to an estrogen in a sequential HT regimen in postmenopausal women with a history of PMS compared to those without2
bull Women with a history of PMS or PMD exacerbation of depression using progestins may therefore benefit from a progestin free treatment for menopausal symptoms
1) Nevatte T et al Arch Womens Ment Health 2013 2) Bjoumlrn I et al Climacteric 2006 PMS premenstrual syndrome
PMDD premenstrual dysphoric disorder
Conclusion
bull CEEBAZO is an additional regimen for menopausal symptoms it provides also a prevention for osteoporosis
bull It is suitable for women with a uterus who are unsatisfied with an EPT regimen or who you are unwilling to treat with an EPT regimen
For some postmenopausal women with a uterus there is a
need for progestin free treatment options
bull with demonstrated clinical efficacy
bull which protects the endometrium
bull improved tolerabilitysafety profile
In clinical practice this translates to women who are
intolerant of progestin-containing HT or have conditions
which may be exacerbated by treatment with progestins
Conclusion Medical need for alternative treatment option
Medical condition which may be exacerbated by treatment with progestins
Depression
bull Progestin-containing HT has been associated with increases in depressive symptoms in some individuals1
bull There is a biochemicalphysiological plausibility for the association of progestins with depression234
bull Therefore postmenopausal women who also have a medical history of depressive disorders or depression could be inappropriate for treatment with progestin-containing HT
Pfizer Confidential
65
1) Girdler SS et al J Womens Health Gend Based Med 1999 2) Traish AM et al Korean J Urol 2014 3) Stroumlhle A et al Biol Psychiatry 1999 4) Romeo E et
al Am J Psychiatry 1998
History of the following conditions may make progestin inappropriate
bull Depression
bull PMSPMDD
PMS premenstrual syndrome
PMD premenstrual dysphoric disorder
Medical conditions that may be exacerbated by treatment with progestins
Women for whom progestin-containing HT
would not be considered appropriate
minus Women who are intolerant of progestin-containing hormone therapy
minus Women with pre-existing medical conditions that may be exacerbated by progestins
Most common adverse events leading to discontinuation are related to progestins12
breakthrough bleeding
bull Increase in the number of uterine procedures (ie unnecessary endometrial biopsies)
breast paintenderness
bull Increase in the number of breast interventions
1 Steel SA et al Climacteric 2003 2 Ettinger B and Pressman A Am J Manag Care 1999 3 Komm BS Mirkin S
Pharmaceuticals 2012
4 Panay N amp Studd JWW Human Reprod Update 1997
bull Nausea bull Depressive mood bull Poor concentration bull Hirsutism bull Headache bull Dizziness bull Fluid retention bull Weight gain
Other progestin-related intolerance issues4
Unmet need with the treatment of postmenopausal symptoms
bull Alternatives to progestin are needed that will protect the endometrium while avoiding other progestin-associated effects and preserving the desired effects of estrogens in postmenopausal women3
Which women with a uterus could benefit from
estrogens without the need for a progestin
bull Women who are intolerant of progestin-containing hormone therapy
bull Women with pre-existing medical conditions that may be exacerbated by progestins (eg women with a history of depression PMSPMDD increased breast density diabetes and metabolic syndrome)
History of the following conditions may make progestin inappropriate
bull Depression
bull PMSPMDD
bull High breast density
bull Diabetes and metabolic syndrome
PMS premenstrual syndrome
PMD premenstrual dysphoric disorder
Medical conditions that may be exacerbated by treatment with progestins
Learning from WHI data
bull Hormone therapy (HT) is the conventional and established therapy option to effectively treat postmenopausal symptoms however it has been associated with some safety and tolerability concerns1 2
bull A review of WHI data suggests that many of the concerns with menopausal HT more often associated with EPT (CE+MPA) such as CHD risk increased breast density breast pain and breast cancer risk than with ET (CEE alone)2
1 Rolnick SJ Kopher RA DeFor TA et al Menopause 2005
2 Komm BS Mirkin S Pharmaceuticals 2012
WHI Womenrsquos Health Initiative trial
CHD coronary heart disease
CEE conjugated equine estrogens
Efficacy and Safety of Constant Oestrogen
Pulsed Progestogen vs
Continuous Combined HRT
Adverse Events
17b-oestradiol 17b-oestradiol norgestimate NETA (n = 150) (n = 172) Breast discomfort 14 27 Abdominal discomfort 14 22 Uterine bleeding 15 12 Dysmenorrhea 3 8 Oedema 5 8
Adapted from S Rozenberg et al Human Reproduction 2000
Medical condition which may be exacerbated by treatment
with progestins
Increased breast density
bull Increases in breast density are associated with progestin-containing HT which may adversely affect radiological detection of breast cancer1 and may be independently associated with an increased risk for the development of breast cancer2
bull The Postmenopausal EstrogenProgestin Interventions (PEPI) trial demonstrated that an increased mammographic breast density was associated with the use of E+P but not with the use of estrogen alone3
bull Women who already have high breast density may therefore be considered inappropriate for treatment with a progestin-containing HT
1) EU Core SPC for Hormone Replacement Therapy Products (CMDh1312003 Rev 4 June
2012)
2) De Villiers TJ et al on behalf of the International Menopause Society Climacteric 2013 16
3) Greendale GA et al J Natl Cancer Inst 2003
Stroke
0 25 5 75 10 125
Fractures
Diabetes
Breast cancer
Cholecystitis
Venothrombotic episodes
Endometrial cancer
Lung cancer
Coronary heart disease
Colorectal cancer
Overall mortality
15 125 10 75 5 25
Benefits Risks
CE
CE MPA
Santen RJ et al J Clin Endocrinol Metab 2010
The basis of the Endocrine Society scientific statement for postmenopausal hormone replacement therapy (HRT) excess risks and benefits of HRT for 5 years in women aged 50ndash59 years or within 10 years of the start of menopause E=estrogen P=progestin
bull Younger women (aged 50ndash59 years) had more favorable results bull There are differences between CE alone and CEMPA arms bull Overall benefitrisk ratio of CE-alone appears to be more favourable than CEMPA
Reevaluation of WHI data (stratified by age) Risks and
Benefits of HRT Cases per 1000 Women per 5 Years of
Use
Medical condition which may be exacerbated by treatment
with progestins
Diabetes and metabolic syndrome
bull Treatment of oestrogen deficiency symptoms with progestin-containing HT (unlike oestrogen alone) may be associated with increases in insulin resistance and deterioration in glucose tolerance123
bull Postmenopausal women with diabetes could be inappropriate for treatment with progestin-containing HT due to the potential risk of exacerbation of their condition
1) Panay N amp Studd JWW Human Reprod Update 1997
2) Godsland I et al Metabolism 1993
3) Sites CK et al J Clin Endocrinol Metab 2005
Variations in Associated Breast Cancer
Risks Between CE alone and CEMPA
bull Use of CE alone for a median of 59 years was associated with a lower incidence of invasive breast cancer (151 cases 027 per year) compared with placebo (199 cases 035 per year HR 077 95 CI 062ndash095 P=002)
bull In the CE alone group fewer women died from invasive breast cancer (6 deaths 0009 per year) compared with controls (16 deaths 0024 per year HR 037 95 CI 013ndash091 P=003)
Anderson GL et al Lancet
Oncol 2012
Bazedoxifene (BZA) specifically selected in
combination with conjugated estrogens
bull BZA has been specifically selected for its unique pharmacologic profile and effects on VMS and uterine tissue in particular123
1 Crabtree J et al Mol Cell Endocrinol 2008
2 Kharode Y et al Endocrinolology 2008
3 Duavive SmPC
Estrogen Receptor activity is dimmed
Estrogen Receptor activity is turned on
CEs are agonists BZA is an antagonist
In the uterus
bull The BZA component reduces the risk of endometrial hyperplasia that can occur with the conjugated estrogens component alone3 This means that progestins are not needed
Extensive global clinical development program for
CEBZA
aIncludes additional pilot dose-finding study 203 1 Lobo RA et al Fertil Steril 2009 2 Pinkerton JV et al Menopause 2009 3 Kagan R et al Menopause 2010 4 Mirkin S et al Climacteric 2013 5 Pinkerton JV et al Obstet Gynecol 2013
Effects of conjugated estrogensbazedoxifene on
lipid and coagulation variables a randomized
placebo- and active-controlled trial
bull At 12 months
bull Both CEBZA doses were associated with small but significant effects on hemostasis variables including reductions in antithrombin plasminogen activator inhibitor-1 and fibrinogen activity and an increase in plasminogen activity relative to placebo at 12 months Incidences of cardiovascular and venous thromboembolic events were similar among treatment groups
bull CONCLUSIONS
bull This study provides reassurance that CEBZA does not adversely affect lipid metabolism or hemostatic balance In accordance the incidences of venous thromboembolic events and cardiovascular events in postmenopausal women are similar to those observed with placebo

Conclusion
bull CEEBAZO is an additional regimen for menopausal symptoms it provides also a prevention for osteoporosis
bull It is suitable for women with a uterus who are unsatisfied with an EPT regimen or who you are unwilling to treat with an EPT regimen
Adapted use of MHT
bull Lower dosage of estrogens
bull Other progestins
bull Better safety profile
bull Vaginal estrogen or SERMS
bull Non-hormonal therapy
bull Development of new products
bull SERMS + estrogens
Most common adverse events leading to
discontinuation are related to progestins12
bull breakthrough bleeding
bull Low compliance
bull Increase in the number of US
bull Stress
bull Cost
bull uterine procedures
bull Unnecessary endometrial biopsies Hysteroscopies DampC Hysterectomies
bull Morbidity
Proportion of patients who completed or discontinued treatment in relation to the used HT
Serge Rozenberg et al Hum Reprod 2009241739-1747
copy The Author 2009 Published by Oxford University Press on behalf of the European Society of
Human Reproduction and Embryology All rights reserved For Permissions please email
journalspermissionsoxfordjournalsorg
Most common adverse events leading to discontinuation
are related to progestins
bull breast paintenderness
Breast tenderness after initiation of CEE
CEE + MPA (WHI)
and mammographic density change
bullCrandall et al Breast Cancer Res Treat DOI 101007s10549-011-1803-9
Breast density
Hormone therapy use and mammographic
density in postmenopausal Norwegian women
bull Results differed when considering the combined effect of age and BMI
bull The effect of EPT on mammographic density was modified by age and BMI with no apparent association among the youngest women (aged 50-55) with the highest BMI (BMI ge 26)
bull A higher mammographic density was found in EPT users compared to never HT users particularly in women using high-dose NETA regimens Age and BMI modified the association between EPT use and mammographic density
bull Couto E et al Breast Cancer Res Treat 2011 Nov 4 [Epub ahead of print]
Breast Cancer Risk by Breast Density
Menopause and Postmenopausal Hormone
Therapy Use
Birads age HT Duration Risk
1 55-59 None 5 year risk 08 (95 CI 06- 09)
1 55-59
ET EPT 5 year risk 09 (95 CI 07 -11)
4 55-59
None 5 year risk 24 (95 CI 20 -28)
4 55-59
ET 5 year risk
30 (95 CI 26 -35)
4 55-59
EPT 5 year risk
42 (95 CI 37 -46)
Adapted from Kerlikowske et al JOURNAL OF CLINICAL ONCOLOGY 2010
Breast Cancer Risk by Breast Density
Menopause and Postmenopausal Hormone
Therapy Use
Adapted from Kerlikowske et al JOURNAL OF CLINICAL ONCOLOGY 2010
bull Postmenopausal women with high breast density are at increased risk of breast cancer and should be aware of the added risk of taking HT especially estrogen plus progestin
Medical condition which may be exacerbated by treatment
with progestins
Diabetes and metabolic syndrome
bull progestin-containing HT may be associated with increases in insulin resistance and deterioration in glucose tolerance123
bull Postmenopausal women with diabetes could be inappropriate for treatment with progestin-containing HT due to the potential risk of exacerbation of their condition
1) Panay N amp Studd JWW Human Reprod Update 1997
2) Godsland I et al Metabolism 1993
3) Sites CK et al J Clin Endocrinol Metab 2005
A Nath and R Sitruk-Ware CLIMACTERIC 200912(Suppl 1)96ndash101
A Nath and R Sitruk-Ware CLIMACTERIC 200912(Suppl 1)96ndash101
Diabetes an epidemy
bull UK 1996 14 million of diabetics
bull UK 2015 32 million (6 of the population)
bull UK 2025 5 million
bull httpwwwdiabetescoukdiabetes-prevalencehtml
Other progestin-related intolerance issues
bull Nausea
bull Depressive mood
bull Poor concentration
bull Hirsutism
bull Headache
bull Dizziness
bull Fluid retention
bull Weight gain Panay N amp Studd JWW Human Reprod Update 1997
Medical condition which may be exacerbated by treatment with progestins
PMSPMDDdepression
bull Progesterone-induced PMD can be exacerbated by exogenous progestin administration and can occur in association with HT or OC administration1
bull Significantly higher negative mood scores have been observed during the addition of a progestin to an estrogen in a sequential HT regimen in postmenopausal women with a history of PMS compared to those without2
bull Women with a history of PMS or PMD exacerbation of depression using progestins may therefore benefit from a progestin free treatment for menopausal symptoms
1) Nevatte T et al Arch Womens Ment Health 2013 2) Bjoumlrn I et al Climacteric 2006 PMS premenstrual syndrome
PMDD premenstrual dysphoric disorder
Conclusion
bull CEEBAZO is an additional regimen for menopausal symptoms it provides also a prevention for osteoporosis
bull It is suitable for women with a uterus who are unsatisfied with an EPT regimen or who you are unwilling to treat with an EPT regimen
For some postmenopausal women with a uterus there is a
need for progestin free treatment options
bull with demonstrated clinical efficacy
bull which protects the endometrium
bull improved tolerabilitysafety profile
In clinical practice this translates to women who are
intolerant of progestin-containing HT or have conditions
which may be exacerbated by treatment with progestins
Conclusion Medical need for alternative treatment option
Medical condition which may be exacerbated by treatment with progestins
Depression
bull Progestin-containing HT has been associated with increases in depressive symptoms in some individuals1
bull There is a biochemicalphysiological plausibility for the association of progestins with depression234
bull Therefore postmenopausal women who also have a medical history of depressive disorders or depression could be inappropriate for treatment with progestin-containing HT
Pfizer Confidential
65
1) Girdler SS et al J Womens Health Gend Based Med 1999 2) Traish AM et al Korean J Urol 2014 3) Stroumlhle A et al Biol Psychiatry 1999 4) Romeo E et
al Am J Psychiatry 1998
History of the following conditions may make progestin inappropriate
bull Depression
bull PMSPMDD
PMS premenstrual syndrome
PMD premenstrual dysphoric disorder
Medical conditions that may be exacerbated by treatment with progestins
Women for whom progestin-containing HT
would not be considered appropriate
minus Women who are intolerant of progestin-containing hormone therapy
minus Women with pre-existing medical conditions that may be exacerbated by progestins
Most common adverse events leading to discontinuation are related to progestins12
breakthrough bleeding
bull Increase in the number of uterine procedures (ie unnecessary endometrial biopsies)
breast paintenderness
bull Increase in the number of breast interventions
1 Steel SA et al Climacteric 2003 2 Ettinger B and Pressman A Am J Manag Care 1999 3 Komm BS Mirkin S
Pharmaceuticals 2012
4 Panay N amp Studd JWW Human Reprod Update 1997
bull Nausea bull Depressive mood bull Poor concentration bull Hirsutism bull Headache bull Dizziness bull Fluid retention bull Weight gain
Other progestin-related intolerance issues4
Unmet need with the treatment of postmenopausal symptoms
bull Alternatives to progestin are needed that will protect the endometrium while avoiding other progestin-associated effects and preserving the desired effects of estrogens in postmenopausal women3
Which women with a uterus could benefit from
estrogens without the need for a progestin
bull Women who are intolerant of progestin-containing hormone therapy
bull Women with pre-existing medical conditions that may be exacerbated by progestins (eg women with a history of depression PMSPMDD increased breast density diabetes and metabolic syndrome)
History of the following conditions may make progestin inappropriate
bull Depression
bull PMSPMDD
bull High breast density
bull Diabetes and metabolic syndrome
PMS premenstrual syndrome
PMD premenstrual dysphoric disorder
Medical conditions that may be exacerbated by treatment with progestins
Learning from WHI data
bull Hormone therapy (HT) is the conventional and established therapy option to effectively treat postmenopausal symptoms however it has been associated with some safety and tolerability concerns1 2
bull A review of WHI data suggests that many of the concerns with menopausal HT more often associated with EPT (CE+MPA) such as CHD risk increased breast density breast pain and breast cancer risk than with ET (CEE alone)2
1 Rolnick SJ Kopher RA DeFor TA et al Menopause 2005
2 Komm BS Mirkin S Pharmaceuticals 2012
WHI Womenrsquos Health Initiative trial
CHD coronary heart disease
CEE conjugated equine estrogens
Efficacy and Safety of Constant Oestrogen
Pulsed Progestogen vs
Continuous Combined HRT
Adverse Events
17b-oestradiol 17b-oestradiol norgestimate NETA (n = 150) (n = 172) Breast discomfort 14 27 Abdominal discomfort 14 22 Uterine bleeding 15 12 Dysmenorrhea 3 8 Oedema 5 8
Adapted from S Rozenberg et al Human Reproduction 2000
Medical condition which may be exacerbated by treatment
with progestins
Increased breast density
bull Increases in breast density are associated with progestin-containing HT which may adversely affect radiological detection of breast cancer1 and may be independently associated with an increased risk for the development of breast cancer2
bull The Postmenopausal EstrogenProgestin Interventions (PEPI) trial demonstrated that an increased mammographic breast density was associated with the use of E+P but not with the use of estrogen alone3
bull Women who already have high breast density may therefore be considered inappropriate for treatment with a progestin-containing HT
1) EU Core SPC for Hormone Replacement Therapy Products (CMDh1312003 Rev 4 June
2012)
2) De Villiers TJ et al on behalf of the International Menopause Society Climacteric 2013 16
3) Greendale GA et al J Natl Cancer Inst 2003
Stroke
0 25 5 75 10 125
Fractures
Diabetes
Breast cancer
Cholecystitis
Venothrombotic episodes
Endometrial cancer
Lung cancer
Coronary heart disease
Colorectal cancer
Overall mortality
15 125 10 75 5 25
Benefits Risks
CE
CE MPA
Santen RJ et al J Clin Endocrinol Metab 2010
The basis of the Endocrine Society scientific statement for postmenopausal hormone replacement therapy (HRT) excess risks and benefits of HRT for 5 years in women aged 50ndash59 years or within 10 years of the start of menopause E=estrogen P=progestin
bull Younger women (aged 50ndash59 years) had more favorable results bull There are differences between CE alone and CEMPA arms bull Overall benefitrisk ratio of CE-alone appears to be more favourable than CEMPA
Reevaluation of WHI data (stratified by age) Risks and
Benefits of HRT Cases per 1000 Women per 5 Years of
Use
Medical condition which may be exacerbated by treatment
with progestins
Diabetes and metabolic syndrome
bull Treatment of oestrogen deficiency symptoms with progestin-containing HT (unlike oestrogen alone) may be associated with increases in insulin resistance and deterioration in glucose tolerance123
bull Postmenopausal women with diabetes could be inappropriate for treatment with progestin-containing HT due to the potential risk of exacerbation of their condition
1) Panay N amp Studd JWW Human Reprod Update 1997
2) Godsland I et al Metabolism 1993
3) Sites CK et al J Clin Endocrinol Metab 2005
Variations in Associated Breast Cancer
Risks Between CE alone and CEMPA
bull Use of CE alone for a median of 59 years was associated with a lower incidence of invasive breast cancer (151 cases 027 per year) compared with placebo (199 cases 035 per year HR 077 95 CI 062ndash095 P=002)
bull In the CE alone group fewer women died from invasive breast cancer (6 deaths 0009 per year) compared with controls (16 deaths 0024 per year HR 037 95 CI 013ndash091 P=003)
Anderson GL et al Lancet
Oncol 2012
Bazedoxifene (BZA) specifically selected in
combination with conjugated estrogens
bull BZA has been specifically selected for its unique pharmacologic profile and effects on VMS and uterine tissue in particular123
1 Crabtree J et al Mol Cell Endocrinol 2008
2 Kharode Y et al Endocrinolology 2008
3 Duavive SmPC
Estrogen Receptor activity is dimmed
Estrogen Receptor activity is turned on
CEs are agonists BZA is an antagonist
In the uterus
bull The BZA component reduces the risk of endometrial hyperplasia that can occur with the conjugated estrogens component alone3 This means that progestins are not needed
Extensive global clinical development program for
CEBZA
aIncludes additional pilot dose-finding study 203 1 Lobo RA et al Fertil Steril 2009 2 Pinkerton JV et al Menopause 2009 3 Kagan R et al Menopause 2010 4 Mirkin S et al Climacteric 2013 5 Pinkerton JV et al Obstet Gynecol 2013
Effects of conjugated estrogensbazedoxifene on
lipid and coagulation variables a randomized
placebo- and active-controlled trial
bull At 12 months
bull Both CEBZA doses were associated with small but significant effects on hemostasis variables including reductions in antithrombin plasminogen activator inhibitor-1 and fibrinogen activity and an increase in plasminogen activity relative to placebo at 12 months Incidences of cardiovascular and venous thromboembolic events were similar among treatment groups
bull CONCLUSIONS
bull This study provides reassurance that CEBZA does not adversely affect lipid metabolism or hemostatic balance In accordance the incidences of venous thromboembolic events and cardiovascular events in postmenopausal women are similar to those observed with placebo
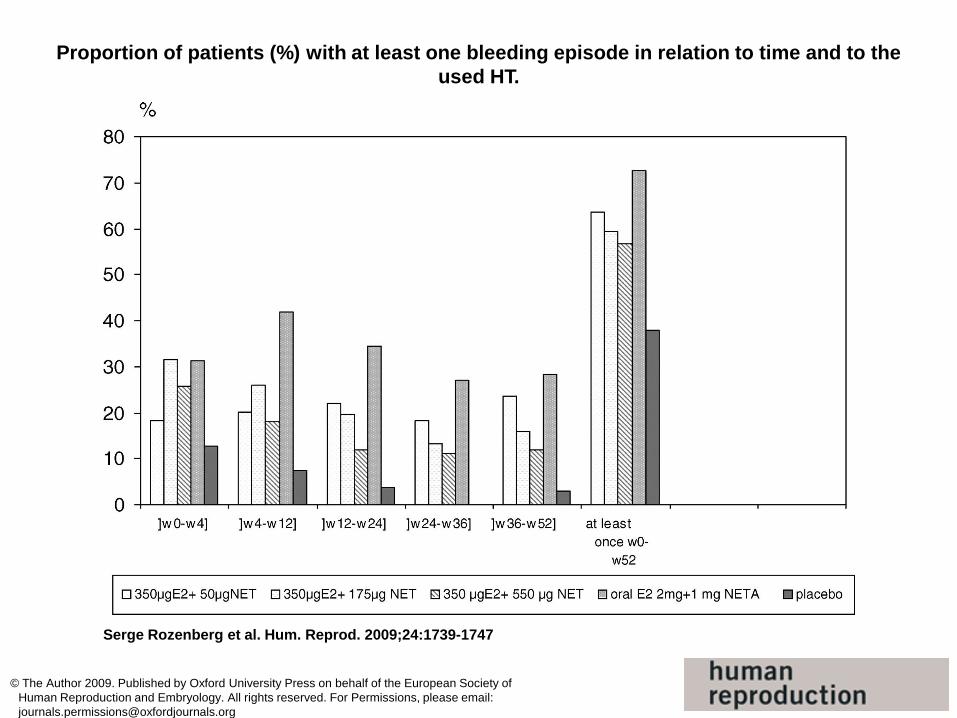
Adapted use of MHT
bull Lower dosage of estrogens
bull Other progestins
bull Better safety profile
bull Vaginal estrogen or SERMS
bull Non-hormonal therapy
bull Development of new products
bull SERMS + estrogens
Most common adverse events leading to
discontinuation are related to progestins12
bull breakthrough bleeding
bull Low compliance
bull Increase in the number of US
bull Stress
bull Cost
bull uterine procedures
bull Unnecessary endometrial biopsies Hysteroscopies DampC Hysterectomies
bull Morbidity
Proportion of patients who completed or discontinued treatment in relation to the used HT
Serge Rozenberg et al Hum Reprod 2009241739-1747
copy The Author 2009 Published by Oxford University Press on behalf of the European Society of
Human Reproduction and Embryology All rights reserved For Permissions please email
journalspermissionsoxfordjournalsorg
Most common adverse events leading to discontinuation
are related to progestins
bull breast paintenderness
Breast tenderness after initiation of CEE
CEE + MPA (WHI)
and mammographic density change
bullCrandall et al Breast Cancer Res Treat DOI 101007s10549-011-1803-9
Breast density
Hormone therapy use and mammographic
density in postmenopausal Norwegian women
bull Results differed when considering the combined effect of age and BMI
bull The effect of EPT on mammographic density was modified by age and BMI with no apparent association among the youngest women (aged 50-55) with the highest BMI (BMI ge 26)
bull A higher mammographic density was found in EPT users compared to never HT users particularly in women using high-dose NETA regimens Age and BMI modified the association between EPT use and mammographic density
bull Couto E et al Breast Cancer Res Treat 2011 Nov 4 [Epub ahead of print]
Breast Cancer Risk by Breast Density
Menopause and Postmenopausal Hormone
Therapy Use
Birads age HT Duration Risk
1 55-59 None 5 year risk 08 (95 CI 06- 09)
1 55-59
ET EPT 5 year risk 09 (95 CI 07 -11)
4 55-59
None 5 year risk 24 (95 CI 20 -28)
4 55-59
ET 5 year risk
30 (95 CI 26 -35)
4 55-59
EPT 5 year risk
42 (95 CI 37 -46)
Adapted from Kerlikowske et al JOURNAL OF CLINICAL ONCOLOGY 2010
Breast Cancer Risk by Breast Density
Menopause and Postmenopausal Hormone
Therapy Use
Adapted from Kerlikowske et al JOURNAL OF CLINICAL ONCOLOGY 2010
bull Postmenopausal women with high breast density are at increased risk of breast cancer and should be aware of the added risk of taking HT especially estrogen plus progestin
Medical condition which may be exacerbated by treatment
with progestins
Diabetes and metabolic syndrome
bull progestin-containing HT may be associated with increases in insulin resistance and deterioration in glucose tolerance123
bull Postmenopausal women with diabetes could be inappropriate for treatment with progestin-containing HT due to the potential risk of exacerbation of their condition
1) Panay N amp Studd JWW Human Reprod Update 1997
2) Godsland I et al Metabolism 1993
3) Sites CK et al J Clin Endocrinol Metab 2005
A Nath and R Sitruk-Ware CLIMACTERIC 200912(Suppl 1)96ndash101
A Nath and R Sitruk-Ware CLIMACTERIC 200912(Suppl 1)96ndash101
Diabetes an epidemy
bull UK 1996 14 million of diabetics
bull UK 2015 32 million (6 of the population)
bull UK 2025 5 million
bull httpwwwdiabetescoukdiabetes-prevalencehtml
Other progestin-related intolerance issues
bull Nausea
bull Depressive mood
bull Poor concentration
bull Hirsutism
bull Headache
bull Dizziness
bull Fluid retention
bull Weight gain Panay N amp Studd JWW Human Reprod Update 1997
Medical condition which may be exacerbated by treatment with progestins
PMSPMDDdepression
bull Progesterone-induced PMD can be exacerbated by exogenous progestin administration and can occur in association with HT or OC administration1
bull Significantly higher negative mood scores have been observed during the addition of a progestin to an estrogen in a sequential HT regimen in postmenopausal women with a history of PMS compared to those without2
bull Women with a history of PMS or PMD exacerbation of depression using progestins may therefore benefit from a progestin free treatment for menopausal symptoms
1) Nevatte T et al Arch Womens Ment Health 2013 2) Bjoumlrn I et al Climacteric 2006 PMS premenstrual syndrome
PMDD premenstrual dysphoric disorder
Conclusion
bull CEEBAZO is an additional regimen for menopausal symptoms it provides also a prevention for osteoporosis
bull It is suitable for women with a uterus who are unsatisfied with an EPT regimen or who you are unwilling to treat with an EPT regimen
For some postmenopausal women with a uterus there is a
need for progestin free treatment options
bull with demonstrated clinical efficacy
bull which protects the endometrium
bull improved tolerabilitysafety profile
In clinical practice this translates to women who are
intolerant of progestin-containing HT or have conditions
which may be exacerbated by treatment with progestins
Conclusion Medical need for alternative treatment option
Medical condition which may be exacerbated by treatment with progestins
Depression
bull Progestin-containing HT has been associated with increases in depressive symptoms in some individuals1
bull There is a biochemicalphysiological plausibility for the association of progestins with depression234
bull Therefore postmenopausal women who also have a medical history of depressive disorders or depression could be inappropriate for treatment with progestin-containing HT
Pfizer Confidential
65
1) Girdler SS et al J Womens Health Gend Based Med 1999 2) Traish AM et al Korean J Urol 2014 3) Stroumlhle A et al Biol Psychiatry 1999 4) Romeo E et
al Am J Psychiatry 1998
History of the following conditions may make progestin inappropriate
bull Depression
bull PMSPMDD
PMS premenstrual syndrome
PMD premenstrual dysphoric disorder
Medical conditions that may be exacerbated by treatment with progestins
Women for whom progestin-containing HT
would not be considered appropriate
minus Women who are intolerant of progestin-containing hormone therapy
minus Women with pre-existing medical conditions that may be exacerbated by progestins
Most common adverse events leading to discontinuation are related to progestins12
breakthrough bleeding
bull Increase in the number of uterine procedures (ie unnecessary endometrial biopsies)
breast paintenderness
bull Increase in the number of breast interventions
1 Steel SA et al Climacteric 2003 2 Ettinger B and Pressman A Am J Manag Care 1999 3 Komm BS Mirkin S
Pharmaceuticals 2012
4 Panay N amp Studd JWW Human Reprod Update 1997
bull Nausea bull Depressive mood bull Poor concentration bull Hirsutism bull Headache bull Dizziness bull Fluid retention bull Weight gain
Other progestin-related intolerance issues4
Unmet need with the treatment of postmenopausal symptoms
bull Alternatives to progestin are needed that will protect the endometrium while avoiding other progestin-associated effects and preserving the desired effects of estrogens in postmenopausal women3
Which women with a uterus could benefit from
estrogens without the need for a progestin
bull Women who are intolerant of progestin-containing hormone therapy
bull Women with pre-existing medical conditions that may be exacerbated by progestins (eg women with a history of depression PMSPMDD increased breast density diabetes and metabolic syndrome)
History of the following conditions may make progestin inappropriate
bull Depression
bull PMSPMDD
bull High breast density
bull Diabetes and metabolic syndrome
PMS premenstrual syndrome
PMD premenstrual dysphoric disorder
Medical conditions that may be exacerbated by treatment with progestins
Learning from WHI data
bull Hormone therapy (HT) is the conventional and established therapy option to effectively treat postmenopausal symptoms however it has been associated with some safety and tolerability concerns1 2
bull A review of WHI data suggests that many of the concerns with menopausal HT more often associated with EPT (CE+MPA) such as CHD risk increased breast density breast pain and breast cancer risk than with ET (CEE alone)2
1 Rolnick SJ Kopher RA DeFor TA et al Menopause 2005
2 Komm BS Mirkin S Pharmaceuticals 2012
WHI Womenrsquos Health Initiative trial
CHD coronary heart disease
CEE conjugated equine estrogens
Efficacy and Safety of Constant Oestrogen
Pulsed Progestogen vs
Continuous Combined HRT
Adverse Events
17b-oestradiol 17b-oestradiol norgestimate NETA (n = 150) (n = 172) Breast discomfort 14 27 Abdominal discomfort 14 22 Uterine bleeding 15 12 Dysmenorrhea 3 8 Oedema 5 8
Adapted from S Rozenberg et al Human Reproduction 2000
Medical condition which may be exacerbated by treatment
with progestins
Increased breast density
bull Increases in breast density are associated with progestin-containing HT which may adversely affect radiological detection of breast cancer1 and may be independently associated with an increased risk for the development of breast cancer2
bull The Postmenopausal EstrogenProgestin Interventions (PEPI) trial demonstrated that an increased mammographic breast density was associated with the use of E+P but not with the use of estrogen alone3
bull Women who already have high breast density may therefore be considered inappropriate for treatment with a progestin-containing HT
1) EU Core SPC for Hormone Replacement Therapy Products (CMDh1312003 Rev 4 June
2012)
2) De Villiers TJ et al on behalf of the International Menopause Society Climacteric 2013 16
3) Greendale GA et al J Natl Cancer Inst 2003
Stroke
0 25 5 75 10 125
Fractures
Diabetes
Breast cancer
Cholecystitis
Venothrombotic episodes
Endometrial cancer
Lung cancer
Coronary heart disease
Colorectal cancer
Overall mortality
15 125 10 75 5 25
Benefits Risks
CE
CE MPA
Santen RJ et al J Clin Endocrinol Metab 2010
The basis of the Endocrine Society scientific statement for postmenopausal hormone replacement therapy (HRT) excess risks and benefits of HRT for 5 years in women aged 50ndash59 years or within 10 years of the start of menopause E=estrogen P=progestin
bull Younger women (aged 50ndash59 years) had more favorable results bull There are differences between CE alone and CEMPA arms bull Overall benefitrisk ratio of CE-alone appears to be more favourable than CEMPA
Reevaluation of WHI data (stratified by age) Risks and
Benefits of HRT Cases per 1000 Women per 5 Years of
Use
Medical condition which may be exacerbated by treatment
with progestins
Diabetes and metabolic syndrome
bull Treatment of oestrogen deficiency symptoms with progestin-containing HT (unlike oestrogen alone) may be associated with increases in insulin resistance and deterioration in glucose tolerance123
bull Postmenopausal women with diabetes could be inappropriate for treatment with progestin-containing HT due to the potential risk of exacerbation of their condition
1) Panay N amp Studd JWW Human Reprod Update 1997
2) Godsland I et al Metabolism 1993
3) Sites CK et al J Clin Endocrinol Metab 2005
Variations in Associated Breast Cancer
Risks Between CE alone and CEMPA
bull Use of CE alone for a median of 59 years was associated with a lower incidence of invasive breast cancer (151 cases 027 per year) compared with placebo (199 cases 035 per year HR 077 95 CI 062ndash095 P=002)
bull In the CE alone group fewer women died from invasive breast cancer (6 deaths 0009 per year) compared with controls (16 deaths 0024 per year HR 037 95 CI 013ndash091 P=003)
Anderson GL et al Lancet
Oncol 2012
Bazedoxifene (BZA) specifically selected in
combination with conjugated estrogens
bull BZA has been specifically selected for its unique pharmacologic profile and effects on VMS and uterine tissue in particular123
1 Crabtree J et al Mol Cell Endocrinol 2008
2 Kharode Y et al Endocrinolology 2008
3 Duavive SmPC
Estrogen Receptor activity is dimmed
Estrogen Receptor activity is turned on
CEs are agonists BZA is an antagonist
In the uterus
bull The BZA component reduces the risk of endometrial hyperplasia that can occur with the conjugated estrogens component alone3 This means that progestins are not needed
Extensive global clinical development program for
CEBZA
aIncludes additional pilot dose-finding study 203 1 Lobo RA et al Fertil Steril 2009 2 Pinkerton JV et al Menopause 2009 3 Kagan R et al Menopause 2010 4 Mirkin S et al Climacteric 2013 5 Pinkerton JV et al Obstet Gynecol 2013
Effects of conjugated estrogensbazedoxifene on
lipid and coagulation variables a randomized
placebo- and active-controlled trial
bull At 12 months
bull Both CEBZA doses were associated with small but significant effects on hemostasis variables including reductions in antithrombin plasminogen activator inhibitor-1 and fibrinogen activity and an increase in plasminogen activity relative to placebo at 12 months Incidences of cardiovascular and venous thromboembolic events were similar among treatment groups
bull CONCLUSIONS
bull This study provides reassurance that CEBZA does not adversely affect lipid metabolism or hemostatic balance In accordance the incidences of venous thromboembolic events and cardiovascular events in postmenopausal women are similar to those observed with placebo
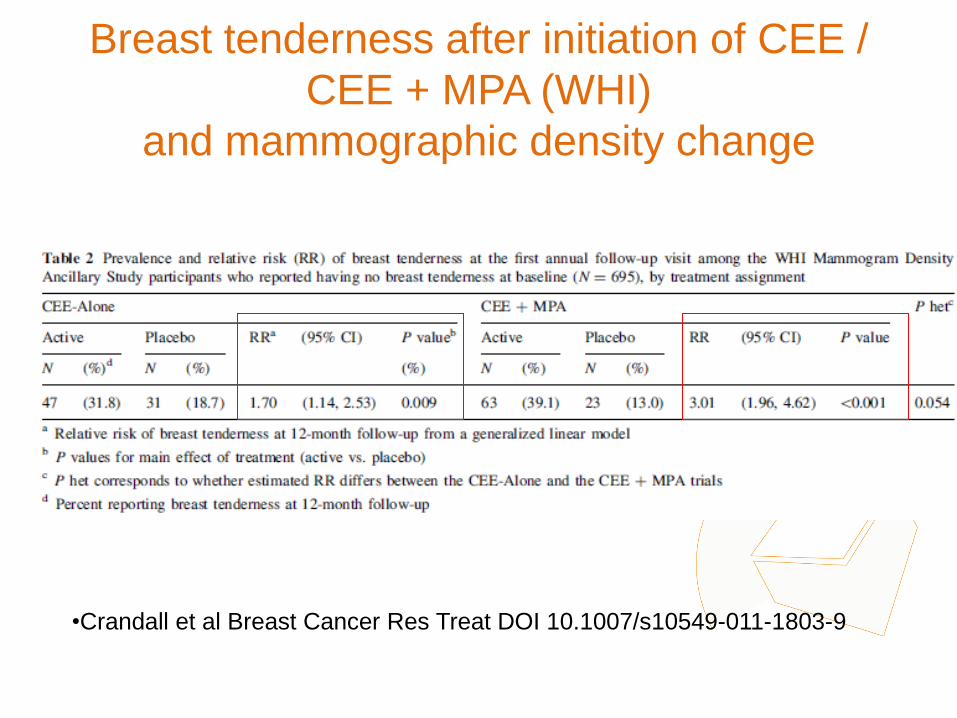
Most common adverse events leading to
discontinuation are related to progestins12
bull breakthrough bleeding
bull Low compliance
bull Increase in the number of US
bull Stress
bull Cost
bull uterine procedures
bull Unnecessary endometrial biopsies Hysteroscopies DampC Hysterectomies
bull Morbidity
Proportion of patients who completed or discontinued treatment in relation to the used HT
Serge Rozenberg et al Hum Reprod 2009241739-1747
copy The Author 2009 Published by Oxford University Press on behalf of the European Society of
Human Reproduction and Embryology All rights reserved For Permissions please email
journalspermissionsoxfordjournalsorg
Most common adverse events leading to discontinuation
are related to progestins
bull breast paintenderness
Breast tenderness after initiation of CEE
CEE + MPA (WHI)
and mammographic density change
bullCrandall et al Breast Cancer Res Treat DOI 101007s10549-011-1803-9
Breast density
Hormone therapy use and mammographic
density in postmenopausal Norwegian women
bull Results differed when considering the combined effect of age and BMI
bull The effect of EPT on mammographic density was modified by age and BMI with no apparent association among the youngest women (aged 50-55) with the highest BMI (BMI ge 26)
bull A higher mammographic density was found in EPT users compared to never HT users particularly in women using high-dose NETA regimens Age and BMI modified the association between EPT use and mammographic density
bull Couto E et al Breast Cancer Res Treat 2011 Nov 4 [Epub ahead of print]
Breast Cancer Risk by Breast Density
Menopause and Postmenopausal Hormone
Therapy Use
Birads age HT Duration Risk
1 55-59 None 5 year risk 08 (95 CI 06- 09)
1 55-59
ET EPT 5 year risk 09 (95 CI 07 -11)
4 55-59
None 5 year risk 24 (95 CI 20 -28)
4 55-59
ET 5 year risk
30 (95 CI 26 -35)
4 55-59
EPT 5 year risk
42 (95 CI 37 -46)
Adapted from Kerlikowske et al JOURNAL OF CLINICAL ONCOLOGY 2010
Breast Cancer Risk by Breast Density
Menopause and Postmenopausal Hormone
Therapy Use
Adapted from Kerlikowske et al JOURNAL OF CLINICAL ONCOLOGY 2010
bull Postmenopausal women with high breast density are at increased risk of breast cancer and should be aware of the added risk of taking HT especially estrogen plus progestin
Medical condition which may be exacerbated by treatment
with progestins
Diabetes and metabolic syndrome
bull progestin-containing HT may be associated with increases in insulin resistance and deterioration in glucose tolerance123
bull Postmenopausal women with diabetes could be inappropriate for treatment with progestin-containing HT due to the potential risk of exacerbation of their condition
1) Panay N amp Studd JWW Human Reprod Update 1997
2) Godsland I et al Metabolism 1993
3) Sites CK et al J Clin Endocrinol Metab 2005
A Nath and R Sitruk-Ware CLIMACTERIC 200912(Suppl 1)96ndash101
A Nath and R Sitruk-Ware CLIMACTERIC 200912(Suppl 1)96ndash101
Diabetes an epidemy
bull UK 1996 14 million of diabetics
bull UK 2015 32 million (6 of the population)
bull UK 2025 5 million
bull httpwwwdiabetescoukdiabetes-prevalencehtml
Other progestin-related intolerance issues
bull Nausea
bull Depressive mood
bull Poor concentration
bull Hirsutism
bull Headache
bull Dizziness
bull Fluid retention
bull Weight gain Panay N amp Studd JWW Human Reprod Update 1997
Medical condition which may be exacerbated by treatment with progestins
PMSPMDDdepression
bull Progesterone-induced PMD can be exacerbated by exogenous progestin administration and can occur in association with HT or OC administration1
bull Significantly higher negative mood scores have been observed during the addition of a progestin to an estrogen in a sequential HT regimen in postmenopausal women with a history of PMS compared to those without2
bull Women with a history of PMS or PMD exacerbation of depression using progestins may therefore benefit from a progestin free treatment for menopausal symptoms
1) Nevatte T et al Arch Womens Ment Health 2013 2) Bjoumlrn I et al Climacteric 2006 PMS premenstrual syndrome
PMDD premenstrual dysphoric disorder
Conclusion
bull CEEBAZO is an additional regimen for menopausal symptoms it provides also a prevention for osteoporosis
bull It is suitable for women with a uterus who are unsatisfied with an EPT regimen or who you are unwilling to treat with an EPT regimen
For some postmenopausal women with a uterus there is a
need for progestin free treatment options
bull with demonstrated clinical efficacy
bull which protects the endometrium
bull improved tolerabilitysafety profile
In clinical practice this translates to women who are
intolerant of progestin-containing HT or have conditions
which may be exacerbated by treatment with progestins
Conclusion Medical need for alternative treatment option
Medical condition which may be exacerbated by treatment with progestins
Depression
bull Progestin-containing HT has been associated with increases in depressive symptoms in some individuals1
bull There is a biochemicalphysiological plausibility for the association of progestins with depression234
bull Therefore postmenopausal women who also have a medical history of depressive disorders or depression could be inappropriate for treatment with progestin-containing HT
Pfizer Confidential
65
1) Girdler SS et al J Womens Health Gend Based Med 1999 2) Traish AM et al Korean J Urol 2014 3) Stroumlhle A et al Biol Psychiatry 1999 4) Romeo E et
al Am J Psychiatry 1998
History of the following conditions may make progestin inappropriate
bull Depression
bull PMSPMDD
PMS premenstrual syndrome
PMD premenstrual dysphoric disorder
Medical conditions that may be exacerbated by treatment with progestins
Women for whom progestin-containing HT
would not be considered appropriate
minus Women who are intolerant of progestin-containing hormone therapy
minus Women with pre-existing medical conditions that may be exacerbated by progestins
Most common adverse events leading to discontinuation are related to progestins12
breakthrough bleeding
bull Increase in the number of uterine procedures (ie unnecessary endometrial biopsies)
breast paintenderness
bull Increase in the number of breast interventions
1 Steel SA et al Climacteric 2003 2 Ettinger B and Pressman A Am J Manag Care 1999 3 Komm BS Mirkin S
Pharmaceuticals 2012
4 Panay N amp Studd JWW Human Reprod Update 1997
bull Nausea bull Depressive mood bull Poor concentration bull Hirsutism bull Headache bull Dizziness bull Fluid retention bull Weight gain
Other progestin-related intolerance issues4
Unmet need with the treatment of postmenopausal symptoms
bull Alternatives to progestin are needed that will protect the endometrium while avoiding other progestin-associated effects and preserving the desired effects of estrogens in postmenopausal women3
Which women with a uterus could benefit from
estrogens without the need for a progestin
bull Women who are intolerant of progestin-containing hormone therapy
bull Women with pre-existing medical conditions that may be exacerbated by progestins (eg women with a history of depression PMSPMDD increased breast density diabetes and metabolic syndrome)
History of the following conditions may make progestin inappropriate
bull Depression
bull PMSPMDD
bull High breast density
bull Diabetes and metabolic syndrome
PMS premenstrual syndrome
PMD premenstrual dysphoric disorder
Medical conditions that may be exacerbated by treatment with progestins
Learning from WHI data
bull Hormone therapy (HT) is the conventional and established therapy option to effectively treat postmenopausal symptoms however it has been associated with some safety and tolerability concerns1 2
bull A review of WHI data suggests that many of the concerns with menopausal HT more often associated with EPT (CE+MPA) such as CHD risk increased breast density breast pain and breast cancer risk than with ET (CEE alone)2
1 Rolnick SJ Kopher RA DeFor TA et al Menopause 2005
2 Komm BS Mirkin S Pharmaceuticals 2012
WHI Womenrsquos Health Initiative trial
CHD coronary heart disease
CEE conjugated equine estrogens
Efficacy and Safety of Constant Oestrogen
Pulsed Progestogen vs
Continuous Combined HRT
Adverse Events
17b-oestradiol 17b-oestradiol norgestimate NETA (n = 150) (n = 172) Breast discomfort 14 27 Abdominal discomfort 14 22 Uterine bleeding 15 12 Dysmenorrhea 3 8 Oedema 5 8
Adapted from S Rozenberg et al Human Reproduction 2000
Medical condition which may be exacerbated by treatment
with progestins
Increased breast density
bull Increases in breast density are associated with progestin-containing HT which may adversely affect radiological detection of breast cancer1 and may be independently associated with an increased risk for the development of breast cancer2
bull The Postmenopausal EstrogenProgestin Interventions (PEPI) trial demonstrated that an increased mammographic breast density was associated with the use of E+P but not with the use of estrogen alone3
bull Women who already have high breast density may therefore be considered inappropriate for treatment with a progestin-containing HT
1) EU Core SPC for Hormone Replacement Therapy Products (CMDh1312003 Rev 4 June
2012)
2) De Villiers TJ et al on behalf of the International Menopause Society Climacteric 2013 16
3) Greendale GA et al J Natl Cancer Inst 2003
Stroke
0 25 5 75 10 125
Fractures
Diabetes
Breast cancer
Cholecystitis
Venothrombotic episodes
Endometrial cancer
Lung cancer
Coronary heart disease
Colorectal cancer
Overall mortality
15 125 10 75 5 25
Benefits Risks
CE
CE MPA
Santen RJ et al J Clin Endocrinol Metab 2010
The basis of the Endocrine Society scientific statement for postmenopausal hormone replacement therapy (HRT) excess risks and benefits of HRT for 5 years in women aged 50ndash59 years or within 10 years of the start of menopause E=estrogen P=progestin
bull Younger women (aged 50ndash59 years) had more favorable results bull There are differences between CE alone and CEMPA arms bull Overall benefitrisk ratio of CE-alone appears to be more favourable than CEMPA
Reevaluation of WHI data (stratified by age) Risks and
Benefits of HRT Cases per 1000 Women per 5 Years of
Use
Medical condition which may be exacerbated by treatment
with progestins
Diabetes and metabolic syndrome
bull Treatment of oestrogen deficiency symptoms with progestin-containing HT (unlike oestrogen alone) may be associated with increases in insulin resistance and deterioration in glucose tolerance123
bull Postmenopausal women with diabetes could be inappropriate for treatment with progestin-containing HT due to the potential risk of exacerbation of their condition
1) Panay N amp Studd JWW Human Reprod Update 1997
2) Godsland I et al Metabolism 1993
3) Sites CK et al J Clin Endocrinol Metab 2005
Variations in Associated Breast Cancer
Risks Between CE alone and CEMPA
bull Use of CE alone for a median of 59 years was associated with a lower incidence of invasive breast cancer (151 cases 027 per year) compared with placebo (199 cases 035 per year HR 077 95 CI 062ndash095 P=002)
bull In the CE alone group fewer women died from invasive breast cancer (6 deaths 0009 per year) compared with controls (16 deaths 0024 per year HR 037 95 CI 013ndash091 P=003)
Anderson GL et al Lancet
Oncol 2012
Bazedoxifene (BZA) specifically selected in
combination with conjugated estrogens
bull BZA has been specifically selected for its unique pharmacologic profile and effects on VMS and uterine tissue in particular123
1 Crabtree J et al Mol Cell Endocrinol 2008
2 Kharode Y et al Endocrinolology 2008
3 Duavive SmPC
Estrogen Receptor activity is dimmed
Estrogen Receptor activity is turned on
CEs are agonists BZA is an antagonist
In the uterus
bull The BZA component reduces the risk of endometrial hyperplasia that can occur with the conjugated estrogens component alone3 This means that progestins are not needed
Extensive global clinical development program for
CEBZA
aIncludes additional pilot dose-finding study 203 1 Lobo RA et al Fertil Steril 2009 2 Pinkerton JV et al Menopause 2009 3 Kagan R et al Menopause 2010 4 Mirkin S et al Climacteric 2013 5 Pinkerton JV et al Obstet Gynecol 2013
Effects of conjugated estrogensbazedoxifene on
lipid and coagulation variables a randomized
placebo- and active-controlled trial
bull At 12 months
bull Both CEBZA doses were associated with small but significant effects on hemostasis variables including reductions in antithrombin plasminogen activator inhibitor-1 and fibrinogen activity and an increase in plasminogen activity relative to placebo at 12 months Incidences of cardiovascular and venous thromboembolic events were similar among treatment groups
bull CONCLUSIONS
bull This study provides reassurance that CEBZA does not adversely affect lipid metabolism or hemostatic balance In accordance the incidences of venous thromboembolic events and cardiovascular events in postmenopausal women are similar to those observed with placebo
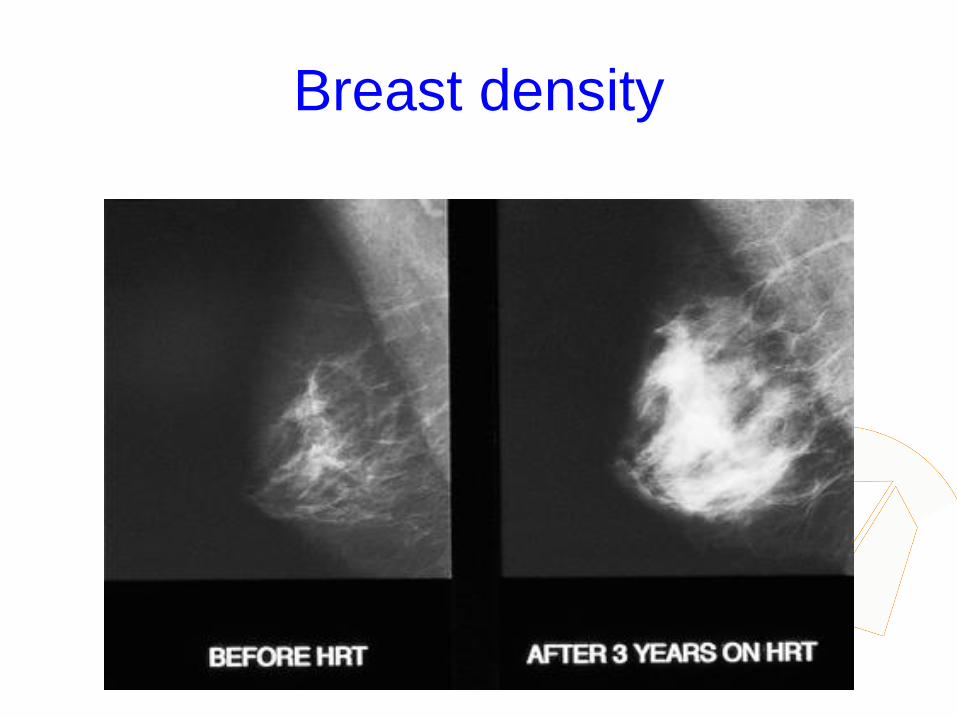
Proportion of patients who completed or discontinued treatment in relation to the used HT
Serge Rozenberg et al Hum Reprod 2009241739-1747
copy The Author 2009 Published by Oxford University Press on behalf of the European Society of
Human Reproduction and Embryology All rights reserved For Permissions please email
journalspermissionsoxfordjournalsorg
Most common adverse events leading to discontinuation
are related to progestins
bull breast paintenderness
Breast tenderness after initiation of CEE
CEE + MPA (WHI)
and mammographic density change
bullCrandall et al Breast Cancer Res Treat DOI 101007s10549-011-1803-9
Breast density
Hormone therapy use and mammographic
density in postmenopausal Norwegian women
bull Results differed when considering the combined effect of age and BMI
bull The effect of EPT on mammographic density was modified by age and BMI with no apparent association among the youngest women (aged 50-55) with the highest BMI (BMI ge 26)
bull A higher mammographic density was found in EPT users compared to never HT users particularly in women using high-dose NETA regimens Age and BMI modified the association between EPT use and mammographic density
bull Couto E et al Breast Cancer Res Treat 2011 Nov 4 [Epub ahead of print]
Breast Cancer Risk by Breast Density
Menopause and Postmenopausal Hormone
Therapy Use
Birads age HT Duration Risk
1 55-59 None 5 year risk 08 (95 CI 06- 09)
1 55-59
ET EPT 5 year risk 09 (95 CI 07 -11)
4 55-59
None 5 year risk 24 (95 CI 20 -28)
4 55-59
ET 5 year risk
30 (95 CI 26 -35)
4 55-59
EPT 5 year risk
42 (95 CI 37 -46)
Adapted from Kerlikowske et al JOURNAL OF CLINICAL ONCOLOGY 2010
Breast Cancer Risk by Breast Density
Menopause and Postmenopausal Hormone
Therapy Use
Adapted from Kerlikowske et al JOURNAL OF CLINICAL ONCOLOGY 2010
bull Postmenopausal women with high breast density are at increased risk of breast cancer and should be aware of the added risk of taking HT especially estrogen plus progestin
Medical condition which may be exacerbated by treatment
with progestins
Diabetes and metabolic syndrome
bull progestin-containing HT may be associated with increases in insulin resistance and deterioration in glucose tolerance123
bull Postmenopausal women with diabetes could be inappropriate for treatment with progestin-containing HT due to the potential risk of exacerbation of their condition
1) Panay N amp Studd JWW Human Reprod Update 1997
2) Godsland I et al Metabolism 1993
3) Sites CK et al J Clin Endocrinol Metab 2005
A Nath and R Sitruk-Ware CLIMACTERIC 200912(Suppl 1)96ndash101
A Nath and R Sitruk-Ware CLIMACTERIC 200912(Suppl 1)96ndash101
Diabetes an epidemy
bull UK 1996 14 million of diabetics
bull UK 2015 32 million (6 of the population)
bull UK 2025 5 million
bull httpwwwdiabetescoukdiabetes-prevalencehtml
Other progestin-related intolerance issues
bull Nausea
bull Depressive mood
bull Poor concentration
bull Hirsutism
bull Headache
bull Dizziness
bull Fluid retention
bull Weight gain Panay N amp Studd JWW Human Reprod Update 1997
Medical condition which may be exacerbated by treatment with progestins
PMSPMDDdepression
bull Progesterone-induced PMD can be exacerbated by exogenous progestin administration and can occur in association with HT or OC administration1
bull Significantly higher negative mood scores have been observed during the addition of a progestin to an estrogen in a sequential HT regimen in postmenopausal women with a history of PMS compared to those without2
bull Women with a history of PMS or PMD exacerbation of depression using progestins may therefore benefit from a progestin free treatment for menopausal symptoms
1) Nevatte T et al Arch Womens Ment Health 2013 2) Bjoumlrn I et al Climacteric 2006 PMS premenstrual syndrome
PMDD premenstrual dysphoric disorder
Conclusion
bull CEEBAZO is an additional regimen for menopausal symptoms it provides also a prevention for osteoporosis
bull It is suitable for women with a uterus who are unsatisfied with an EPT regimen or who you are unwilling to treat with an EPT regimen
For some postmenopausal women with a uterus there is a
need for progestin free treatment options
bull with demonstrated clinical efficacy
bull which protects the endometrium
bull improved tolerabilitysafety profile
In clinical practice this translates to women who are
intolerant of progestin-containing HT or have conditions
which may be exacerbated by treatment with progestins
Conclusion Medical need for alternative treatment option
Medical condition which may be exacerbated by treatment with progestins
Depression
bull Progestin-containing HT has been associated with increases in depressive symptoms in some individuals1
bull There is a biochemicalphysiological plausibility for the association of progestins with depression234
bull Therefore postmenopausal women who also have a medical history of depressive disorders or depression could be inappropriate for treatment with progestin-containing HT
Pfizer Confidential
65
1) Girdler SS et al J Womens Health Gend Based Med 1999 2) Traish AM et al Korean J Urol 2014 3) Stroumlhle A et al Biol Psychiatry 1999 4) Romeo E et
al Am J Psychiatry 1998
History of the following conditions may make progestin inappropriate
bull Depression
bull PMSPMDD
PMS premenstrual syndrome
PMD premenstrual dysphoric disorder
Medical conditions that may be exacerbated by treatment with progestins
Women for whom progestin-containing HT
would not be considered appropriate
minus Women who are intolerant of progestin-containing hormone therapy
minus Women with pre-existing medical conditions that may be exacerbated by progestins
Most common adverse events leading to discontinuation are related to progestins12
breakthrough bleeding
bull Increase in the number of uterine procedures (ie unnecessary endometrial biopsies)
breast paintenderness
bull Increase in the number of breast interventions
1 Steel SA et al Climacteric 2003 2 Ettinger B and Pressman A Am J Manag Care 1999 3 Komm BS Mirkin S
Pharmaceuticals 2012
4 Panay N amp Studd JWW Human Reprod Update 1997
bull Nausea bull Depressive mood bull Poor concentration bull Hirsutism bull Headache bull Dizziness bull Fluid retention bull Weight gain
Other progestin-related intolerance issues4
Unmet need with the treatment of postmenopausal symptoms
bull Alternatives to progestin are needed that will protect the endometrium while avoiding other progestin-associated effects and preserving the desired effects of estrogens in postmenopausal women3
Which women with a uterus could benefit from
estrogens without the need for a progestin
bull Women who are intolerant of progestin-containing hormone therapy
bull Women with pre-existing medical conditions that may be exacerbated by progestins (eg women with a history of depression PMSPMDD increased breast density diabetes and metabolic syndrome)
History of the following conditions may make progestin inappropriate
bull Depression
bull PMSPMDD
bull High breast density
bull Diabetes and metabolic syndrome
PMS premenstrual syndrome
PMD premenstrual dysphoric disorder
Medical conditions that may be exacerbated by treatment with progestins
Learning from WHI data
bull Hormone therapy (HT) is the conventional and established therapy option to effectively treat postmenopausal symptoms however it has been associated with some safety and tolerability concerns1 2
bull A review of WHI data suggests that many of the concerns with menopausal HT more often associated with EPT (CE+MPA) such as CHD risk increased breast density breast pain and breast cancer risk than with ET (CEE alone)2
1 Rolnick SJ Kopher RA DeFor TA et al Menopause 2005
2 Komm BS Mirkin S Pharmaceuticals 2012
WHI Womenrsquos Health Initiative trial
CHD coronary heart disease
CEE conjugated equine estrogens
Efficacy and Safety of Constant Oestrogen
Pulsed Progestogen vs
Continuous Combined HRT
Adverse Events
17b-oestradiol 17b-oestradiol norgestimate NETA (n = 150) (n = 172) Breast discomfort 14 27 Abdominal discomfort 14 22 Uterine bleeding 15 12 Dysmenorrhea 3 8 Oedema 5 8
Adapted from S Rozenberg et al Human Reproduction 2000
Medical condition which may be exacerbated by treatment
with progestins
Increased breast density
bull Increases in breast density are associated with progestin-containing HT which may adversely affect radiological detection of breast cancer1 and may be independently associated with an increased risk for the development of breast cancer2
bull The Postmenopausal EstrogenProgestin Interventions (PEPI) trial demonstrated that an increased mammographic breast density was associated with the use of E+P but not with the use of estrogen alone3
bull Women who already have high breast density may therefore be considered inappropriate for treatment with a progestin-containing HT
1) EU Core SPC for Hormone Replacement Therapy Products (CMDh1312003 Rev 4 June
2012)
2) De Villiers TJ et al on behalf of the International Menopause Society Climacteric 2013 16
3) Greendale GA et al J Natl Cancer Inst 2003
Stroke
0 25 5 75 10 125
Fractures
Diabetes
Breast cancer
Cholecystitis
Venothrombotic episodes
Endometrial cancer
Lung cancer
Coronary heart disease
Colorectal cancer
Overall mortality
15 125 10 75 5 25
Benefits Risks
CE
CE MPA
Santen RJ et al J Clin Endocrinol Metab 2010
The basis of the Endocrine Society scientific statement for postmenopausal hormone replacement therapy (HRT) excess risks and benefits of HRT for 5 years in women aged 50ndash59 years or within 10 years of the start of menopause E=estrogen P=progestin
bull Younger women (aged 50ndash59 years) had more favorable results bull There are differences between CE alone and CEMPA arms bull Overall benefitrisk ratio of CE-alone appears to be more favourable than CEMPA
Reevaluation of WHI data (stratified by age) Risks and
Benefits of HRT Cases per 1000 Women per 5 Years of
Use
Medical condition which may be exacerbated by treatment
with progestins
Diabetes and metabolic syndrome
bull Treatment of oestrogen deficiency symptoms with progestin-containing HT (unlike oestrogen alone) may be associated with increases in insulin resistance and deterioration in glucose tolerance123
bull Postmenopausal women with diabetes could be inappropriate for treatment with progestin-containing HT due to the potential risk of exacerbation of their condition
1) Panay N amp Studd JWW Human Reprod Update 1997
2) Godsland I et al Metabolism 1993
3) Sites CK et al J Clin Endocrinol Metab 2005
Variations in Associated Breast Cancer
Risks Between CE alone and CEMPA
bull Use of CE alone for a median of 59 years was associated with a lower incidence of invasive breast cancer (151 cases 027 per year) compared with placebo (199 cases 035 per year HR 077 95 CI 062ndash095 P=002)
bull In the CE alone group fewer women died from invasive breast cancer (6 deaths 0009 per year) compared with controls (16 deaths 0024 per year HR 037 95 CI 013ndash091 P=003)
Anderson GL et al Lancet
Oncol 2012
Bazedoxifene (BZA) specifically selected in
combination with conjugated estrogens
bull BZA has been specifically selected for its unique pharmacologic profile and effects on VMS and uterine tissue in particular123
1 Crabtree J et al Mol Cell Endocrinol 2008
2 Kharode Y et al Endocrinolology 2008
3 Duavive SmPC
Estrogen Receptor activity is dimmed
Estrogen Receptor activity is turned on
CEs are agonists BZA is an antagonist
In the uterus
bull The BZA component reduces the risk of endometrial hyperplasia that can occur with the conjugated estrogens component alone3 This means that progestins are not needed
Extensive global clinical development program for
CEBZA
aIncludes additional pilot dose-finding study 203 1 Lobo RA et al Fertil Steril 2009 2 Pinkerton JV et al Menopause 2009 3 Kagan R et al Menopause 2010 4 Mirkin S et al Climacteric 2013 5 Pinkerton JV et al Obstet Gynecol 2013
Effects of conjugated estrogensbazedoxifene on
lipid and coagulation variables a randomized
placebo- and active-controlled trial
bull At 12 months
bull Both CEBZA doses were associated with small but significant effects on hemostasis variables including reductions in antithrombin plasminogen activator inhibitor-1 and fibrinogen activity and an increase in plasminogen activity relative to placebo at 12 months Incidences of cardiovascular and venous thromboembolic events were similar among treatment groups
bull CONCLUSIONS
bull This study provides reassurance that CEBZA does not adversely affect lipid metabolism or hemostatic balance In accordance the incidences of venous thromboembolic events and cardiovascular events in postmenopausal women are similar to those observed with placebo

Most common adverse events leading to discontinuation
are related to progestins
bull breast paintenderness
Breast tenderness after initiation of CEE
CEE + MPA (WHI)
and mammographic density change
bullCrandall et al Breast Cancer Res Treat DOI 101007s10549-011-1803-9
Breast density
Hormone therapy use and mammographic
density in postmenopausal Norwegian women
bull Results differed when considering the combined effect of age and BMI
bull The effect of EPT on mammographic density was modified by age and BMI with no apparent association among the youngest women (aged 50-55) with the highest BMI (BMI ge 26)
bull A higher mammographic density was found in EPT users compared to never HT users particularly in women using high-dose NETA regimens Age and BMI modified the association between EPT use and mammographic density
bull Couto E et al Breast Cancer Res Treat 2011 Nov 4 [Epub ahead of print]
Breast Cancer Risk by Breast Density
Menopause and Postmenopausal Hormone
Therapy Use
Birads age HT Duration Risk
1 55-59 None 5 year risk 08 (95 CI 06- 09)
1 55-59
ET EPT 5 year risk 09 (95 CI 07 -11)
4 55-59
None 5 year risk 24 (95 CI 20 -28)
4 55-59
ET 5 year risk
30 (95 CI 26 -35)
4 55-59
EPT 5 year risk
42 (95 CI 37 -46)
Adapted from Kerlikowske et al JOURNAL OF CLINICAL ONCOLOGY 2010
Breast Cancer Risk by Breast Density
Menopause and Postmenopausal Hormone
Therapy Use
Adapted from Kerlikowske et al JOURNAL OF CLINICAL ONCOLOGY 2010
bull Postmenopausal women with high breast density are at increased risk of breast cancer and should be aware of the added risk of taking HT especially estrogen plus progestin
Medical condition which may be exacerbated by treatment
with progestins
Diabetes and metabolic syndrome
bull progestin-containing HT may be associated with increases in insulin resistance and deterioration in glucose tolerance123
bull Postmenopausal women with diabetes could be inappropriate for treatment with progestin-containing HT due to the potential risk of exacerbation of their condition
1) Panay N amp Studd JWW Human Reprod Update 1997
2) Godsland I et al Metabolism 1993
3) Sites CK et al J Clin Endocrinol Metab 2005
A Nath and R Sitruk-Ware CLIMACTERIC 200912(Suppl 1)96ndash101
A Nath and R Sitruk-Ware CLIMACTERIC 200912(Suppl 1)96ndash101
Diabetes an epidemy
bull UK 1996 14 million of diabetics
bull UK 2015 32 million (6 of the population)
bull UK 2025 5 million
bull httpwwwdiabetescoukdiabetes-prevalencehtml
Other progestin-related intolerance issues
bull Nausea
bull Depressive mood
bull Poor concentration
bull Hirsutism
bull Headache
bull Dizziness
bull Fluid retention
bull Weight gain Panay N amp Studd JWW Human Reprod Update 1997
Medical condition which may be exacerbated by treatment with progestins
PMSPMDDdepression
bull Progesterone-induced PMD can be exacerbated by exogenous progestin administration and can occur in association with HT or OC administration1
bull Significantly higher negative mood scores have been observed during the addition of a progestin to an estrogen in a sequential HT regimen in postmenopausal women with a history of PMS compared to those without2
bull Women with a history of PMS or PMD exacerbation of depression using progestins may therefore benefit from a progestin free treatment for menopausal symptoms
1) Nevatte T et al Arch Womens Ment Health 2013 2) Bjoumlrn I et al Climacteric 2006 PMS premenstrual syndrome
PMDD premenstrual dysphoric disorder
Conclusion
bull CEEBAZO is an additional regimen for menopausal symptoms it provides also a prevention for osteoporosis
bull It is suitable for women with a uterus who are unsatisfied with an EPT regimen or who you are unwilling to treat with an EPT regimen
For some postmenopausal women with a uterus there is a
need for progestin free treatment options
bull with demonstrated clinical efficacy
bull which protects the endometrium
bull improved tolerabilitysafety profile
In clinical practice this translates to women who are
intolerant of progestin-containing HT or have conditions
which may be exacerbated by treatment with progestins
Conclusion Medical need for alternative treatment option
Medical condition which may be exacerbated by treatment with progestins
Depression
bull Progestin-containing HT has been associated with increases in depressive symptoms in some individuals1
bull There is a biochemicalphysiological plausibility for the association of progestins with depression234
bull Therefore postmenopausal women who also have a medical history of depressive disorders or depression could be inappropriate for treatment with progestin-containing HT
Pfizer Confidential
65
1) Girdler SS et al J Womens Health Gend Based Med 1999 2) Traish AM et al Korean J Urol 2014 3) Stroumlhle A et al Biol Psychiatry 1999 4) Romeo E et
al Am J Psychiatry 1998
History of the following conditions may make progestin inappropriate
bull Depression
bull PMSPMDD
PMS premenstrual syndrome
PMD premenstrual dysphoric disorder
Medical conditions that may be exacerbated by treatment with progestins
Women for whom progestin-containing HT
would not be considered appropriate
minus Women who are intolerant of progestin-containing hormone therapy
minus Women with pre-existing medical conditions that may be exacerbated by progestins
Most common adverse events leading to discontinuation are related to progestins12
breakthrough bleeding
bull Increase in the number of uterine procedures (ie unnecessary endometrial biopsies)
breast paintenderness
bull Increase in the number of breast interventions
1 Steel SA et al Climacteric 2003 2 Ettinger B and Pressman A Am J Manag Care 1999 3 Komm BS Mirkin S
Pharmaceuticals 2012
4 Panay N amp Studd JWW Human Reprod Update 1997
bull Nausea bull Depressive mood bull Poor concentration bull Hirsutism bull Headache bull Dizziness bull Fluid retention bull Weight gain
Other progestin-related intolerance issues4
Unmet need with the treatment of postmenopausal symptoms
bull Alternatives to progestin are needed that will protect the endometrium while avoiding other progestin-associated effects and preserving the desired effects of estrogens in postmenopausal women3
Which women with a uterus could benefit from
estrogens without the need for a progestin
bull Women who are intolerant of progestin-containing hormone therapy
bull Women with pre-existing medical conditions that may be exacerbated by progestins (eg women with a history of depression PMSPMDD increased breast density diabetes and metabolic syndrome)
History of the following conditions may make progestin inappropriate
bull Depression
bull PMSPMDD
bull High breast density
bull Diabetes and metabolic syndrome
PMS premenstrual syndrome
PMD premenstrual dysphoric disorder
Medical conditions that may be exacerbated by treatment with progestins
Learning from WHI data
bull Hormone therapy (HT) is the conventional and established therapy option to effectively treat postmenopausal symptoms however it has been associated with some safety and tolerability concerns1 2
bull A review of WHI data suggests that many of the concerns with menopausal HT more often associated with EPT (CE+MPA) such as CHD risk increased breast density breast pain and breast cancer risk than with ET (CEE alone)2
1 Rolnick SJ Kopher RA DeFor TA et al Menopause 2005
2 Komm BS Mirkin S Pharmaceuticals 2012
WHI Womenrsquos Health Initiative trial
CHD coronary heart disease
CEE conjugated equine estrogens
Efficacy and Safety of Constant Oestrogen
Pulsed Progestogen vs
Continuous Combined HRT
Adverse Events
17b-oestradiol 17b-oestradiol norgestimate NETA (n = 150) (n = 172) Breast discomfort 14 27 Abdominal discomfort 14 22 Uterine bleeding 15 12 Dysmenorrhea 3 8 Oedema 5 8
Adapted from S Rozenberg et al Human Reproduction 2000
Medical condition which may be exacerbated by treatment
with progestins
Increased breast density
bull Increases in breast density are associated with progestin-containing HT which may adversely affect radiological detection of breast cancer1 and may be independently associated with an increased risk for the development of breast cancer2
bull The Postmenopausal EstrogenProgestin Interventions (PEPI) trial demonstrated that an increased mammographic breast density was associated with the use of E+P but not with the use of estrogen alone3
bull Women who already have high breast density may therefore be considered inappropriate for treatment with a progestin-containing HT
1) EU Core SPC for Hormone Replacement Therapy Products (CMDh1312003 Rev 4 June
2012)
2) De Villiers TJ et al on behalf of the International Menopause Society Climacteric 2013 16
3) Greendale GA et al J Natl Cancer Inst 2003
Stroke
0 25 5 75 10 125
Fractures
Diabetes
Breast cancer
Cholecystitis
Venothrombotic episodes
Endometrial cancer
Lung cancer
Coronary heart disease
Colorectal cancer
Overall mortality
15 125 10 75 5 25
Benefits Risks
CE
CE MPA
Santen RJ et al J Clin Endocrinol Metab 2010
The basis of the Endocrine Society scientific statement for postmenopausal hormone replacement therapy (HRT) excess risks and benefits of HRT for 5 years in women aged 50ndash59 years or within 10 years of the start of menopause E=estrogen P=progestin
bull Younger women (aged 50ndash59 years) had more favorable results bull There are differences between CE alone and CEMPA arms bull Overall benefitrisk ratio of CE-alone appears to be more favourable than CEMPA
Reevaluation of WHI data (stratified by age) Risks and
Benefits of HRT Cases per 1000 Women per 5 Years of
Use
Medical condition which may be exacerbated by treatment
with progestins
Diabetes and metabolic syndrome
bull Treatment of oestrogen deficiency symptoms with progestin-containing HT (unlike oestrogen alone) may be associated with increases in insulin resistance and deterioration in glucose tolerance123
bull Postmenopausal women with diabetes could be inappropriate for treatment with progestin-containing HT due to the potential risk of exacerbation of their condition
1) Panay N amp Studd JWW Human Reprod Update 1997
2) Godsland I et al Metabolism 1993
3) Sites CK et al J Clin Endocrinol Metab 2005
Variations in Associated Breast Cancer
Risks Between CE alone and CEMPA
bull Use of CE alone for a median of 59 years was associated with a lower incidence of invasive breast cancer (151 cases 027 per year) compared with placebo (199 cases 035 per year HR 077 95 CI 062ndash095 P=002)
bull In the CE alone group fewer women died from invasive breast cancer (6 deaths 0009 per year) compared with controls (16 deaths 0024 per year HR 037 95 CI 013ndash091 P=003)
Anderson GL et al Lancet
Oncol 2012
Bazedoxifene (BZA) specifically selected in
combination with conjugated estrogens
bull BZA has been specifically selected for its unique pharmacologic profile and effects on VMS and uterine tissue in particular123
1 Crabtree J et al Mol Cell Endocrinol 2008
2 Kharode Y et al Endocrinolology 2008
3 Duavive SmPC
Estrogen Receptor activity is dimmed
Estrogen Receptor activity is turned on
CEs are agonists BZA is an antagonist
In the uterus
bull The BZA component reduces the risk of endometrial hyperplasia that can occur with the conjugated estrogens component alone3 This means that progestins are not needed
Extensive global clinical development program for
CEBZA
aIncludes additional pilot dose-finding study 203 1 Lobo RA et al Fertil Steril 2009 2 Pinkerton JV et al Menopause 2009 3 Kagan R et al Menopause 2010 4 Mirkin S et al Climacteric 2013 5 Pinkerton JV et al Obstet Gynecol 2013
Effects of conjugated estrogensbazedoxifene on
lipid and coagulation variables a randomized
placebo- and active-controlled trial
bull At 12 months
bull Both CEBZA doses were associated with small but significant effects on hemostasis variables including reductions in antithrombin plasminogen activator inhibitor-1 and fibrinogen activity and an increase in plasminogen activity relative to placebo at 12 months Incidences of cardiovascular and venous thromboembolic events were similar among treatment groups
bull CONCLUSIONS
bull This study provides reassurance that CEBZA does not adversely affect lipid metabolism or hemostatic balance In accordance the incidences of venous thromboembolic events and cardiovascular events in postmenopausal women are similar to those observed with placebo

Breast tenderness after initiation of CEE
CEE + MPA (WHI)
and mammographic density change
bullCrandall et al Breast Cancer Res Treat DOI 101007s10549-011-1803-9
Breast density
Hormone therapy use and mammographic
density in postmenopausal Norwegian women
bull Results differed when considering the combined effect of age and BMI
bull The effect of EPT on mammographic density was modified by age and BMI with no apparent association among the youngest women (aged 50-55) with the highest BMI (BMI ge 26)
bull A higher mammographic density was found in EPT users compared to never HT users particularly in women using high-dose NETA regimens Age and BMI modified the association between EPT use and mammographic density
bull Couto E et al Breast Cancer Res Treat 2011 Nov 4 [Epub ahead of print]
Breast Cancer Risk by Breast Density
Menopause and Postmenopausal Hormone
Therapy Use
Birads age HT Duration Risk
1 55-59 None 5 year risk 08 (95 CI 06- 09)
1 55-59
ET EPT 5 year risk 09 (95 CI 07 -11)
4 55-59
None 5 year risk 24 (95 CI 20 -28)
4 55-59
ET 5 year risk
30 (95 CI 26 -35)
4 55-59
EPT 5 year risk
42 (95 CI 37 -46)
Adapted from Kerlikowske et al JOURNAL OF CLINICAL ONCOLOGY 2010
Breast Cancer Risk by Breast Density
Menopause and Postmenopausal Hormone
Therapy Use
Adapted from Kerlikowske et al JOURNAL OF CLINICAL ONCOLOGY 2010
bull Postmenopausal women with high breast density are at increased risk of breast cancer and should be aware of the added risk of taking HT especially estrogen plus progestin
Medical condition which may be exacerbated by treatment
with progestins
Diabetes and metabolic syndrome
bull progestin-containing HT may be associated with increases in insulin resistance and deterioration in glucose tolerance123
bull Postmenopausal women with diabetes could be inappropriate for treatment with progestin-containing HT due to the potential risk of exacerbation of their condition
1) Panay N amp Studd JWW Human Reprod Update 1997
2) Godsland I et al Metabolism 1993
3) Sites CK et al J Clin Endocrinol Metab 2005
A Nath and R Sitruk-Ware CLIMACTERIC 200912(Suppl 1)96ndash101
A Nath and R Sitruk-Ware CLIMACTERIC 200912(Suppl 1)96ndash101
Diabetes an epidemy
bull UK 1996 14 million of diabetics
bull UK 2015 32 million (6 of the population)
bull UK 2025 5 million
bull httpwwwdiabetescoukdiabetes-prevalencehtml
Other progestin-related intolerance issues
bull Nausea
bull Depressive mood
bull Poor concentration
bull Hirsutism
bull Headache
bull Dizziness
bull Fluid retention
bull Weight gain Panay N amp Studd JWW Human Reprod Update 1997
Medical condition which may be exacerbated by treatment with progestins
PMSPMDDdepression
bull Progesterone-induced PMD can be exacerbated by exogenous progestin administration and can occur in association with HT or OC administration1
bull Significantly higher negative mood scores have been observed during the addition of a progestin to an estrogen in a sequential HT regimen in postmenopausal women with a history of PMS compared to those without2
bull Women with a history of PMS or PMD exacerbation of depression using progestins may therefore benefit from a progestin free treatment for menopausal symptoms
1) Nevatte T et al Arch Womens Ment Health 2013 2) Bjoumlrn I et al Climacteric 2006 PMS premenstrual syndrome
PMDD premenstrual dysphoric disorder
Conclusion
bull CEEBAZO is an additional regimen for menopausal symptoms it provides also a prevention for osteoporosis
bull It is suitable for women with a uterus who are unsatisfied with an EPT regimen or who you are unwilling to treat with an EPT regimen
For some postmenopausal women with a uterus there is a
need for progestin free treatment options
bull with demonstrated clinical efficacy
bull which protects the endometrium
bull improved tolerabilitysafety profile
In clinical practice this translates to women who are
intolerant of progestin-containing HT or have conditions
which may be exacerbated by treatment with progestins
Conclusion Medical need for alternative treatment option
Medical condition which may be exacerbated by treatment with progestins
Depression
bull Progestin-containing HT has been associated with increases in depressive symptoms in some individuals1
bull There is a biochemicalphysiological plausibility for the association of progestins with depression234
bull Therefore postmenopausal women who also have a medical history of depressive disorders or depression could be inappropriate for treatment with progestin-containing HT
Pfizer Confidential
65
1) Girdler SS et al J Womens Health Gend Based Med 1999 2) Traish AM et al Korean J Urol 2014 3) Stroumlhle A et al Biol Psychiatry 1999 4) Romeo E et
al Am J Psychiatry 1998
History of the following conditions may make progestin inappropriate
bull Depression
bull PMSPMDD
PMS premenstrual syndrome
PMD premenstrual dysphoric disorder
Medical conditions that may be exacerbated by treatment with progestins
Women for whom progestin-containing HT
would not be considered appropriate
minus Women who are intolerant of progestin-containing hormone therapy
minus Women with pre-existing medical conditions that may be exacerbated by progestins
Most common adverse events leading to discontinuation are related to progestins12
breakthrough bleeding
bull Increase in the number of uterine procedures (ie unnecessary endometrial biopsies)
breast paintenderness
bull Increase in the number of breast interventions
1 Steel SA et al Climacteric 2003 2 Ettinger B and Pressman A Am J Manag Care 1999 3 Komm BS Mirkin S
Pharmaceuticals 2012
4 Panay N amp Studd JWW Human Reprod Update 1997
bull Nausea bull Depressive mood bull Poor concentration bull Hirsutism bull Headache bull Dizziness bull Fluid retention bull Weight gain
Other progestin-related intolerance issues4
Unmet need with the treatment of postmenopausal symptoms
bull Alternatives to progestin are needed that will protect the endometrium while avoiding other progestin-associated effects and preserving the desired effects of estrogens in postmenopausal women3
Which women with a uterus could benefit from
estrogens without the need for a progestin
bull Women who are intolerant of progestin-containing hormone therapy
bull Women with pre-existing medical conditions that may be exacerbated by progestins (eg women with a history of depression PMSPMDD increased breast density diabetes and metabolic syndrome)
History of the following conditions may make progestin inappropriate
bull Depression
bull PMSPMDD
bull High breast density
bull Diabetes and metabolic syndrome
PMS premenstrual syndrome
PMD premenstrual dysphoric disorder
Medical conditions that may be exacerbated by treatment with progestins
Learning from WHI data
bull Hormone therapy (HT) is the conventional and established therapy option to effectively treat postmenopausal symptoms however it has been associated with some safety and tolerability concerns1 2
bull A review of WHI data suggests that many of the concerns with menopausal HT more often associated with EPT (CE+MPA) such as CHD risk increased breast density breast pain and breast cancer risk than with ET (CEE alone)2
1 Rolnick SJ Kopher RA DeFor TA et al Menopause 2005
2 Komm BS Mirkin S Pharmaceuticals 2012
WHI Womenrsquos Health Initiative trial
CHD coronary heart disease
CEE conjugated equine estrogens
Efficacy and Safety of Constant Oestrogen
Pulsed Progestogen vs
Continuous Combined HRT
Adverse Events
17b-oestradiol 17b-oestradiol norgestimate NETA (n = 150) (n = 172) Breast discomfort 14 27 Abdominal discomfort 14 22 Uterine bleeding 15 12 Dysmenorrhea 3 8 Oedema 5 8
Adapted from S Rozenberg et al Human Reproduction 2000
Medical condition which may be exacerbated by treatment
with progestins
Increased breast density
bull Increases in breast density are associated with progestin-containing HT which may adversely affect radiological detection of breast cancer1 and may be independently associated with an increased risk for the development of breast cancer2
bull The Postmenopausal EstrogenProgestin Interventions (PEPI) trial demonstrated that an increased mammographic breast density was associated with the use of E+P but not with the use of estrogen alone3
bull Women who already have high breast density may therefore be considered inappropriate for treatment with a progestin-containing HT
1) EU Core SPC for Hormone Replacement Therapy Products (CMDh1312003 Rev 4 June
2012)
2) De Villiers TJ et al on behalf of the International Menopause Society Climacteric 2013 16
3) Greendale GA et al J Natl Cancer Inst 2003
Stroke
0 25 5 75 10 125
Fractures
Diabetes
Breast cancer
Cholecystitis
Venothrombotic episodes
Endometrial cancer
Lung cancer
Coronary heart disease
Colorectal cancer
Overall mortality
15 125 10 75 5 25
Benefits Risks
CE
CE MPA
Santen RJ et al J Clin Endocrinol Metab 2010
The basis of the Endocrine Society scientific statement for postmenopausal hormone replacement therapy (HRT) excess risks and benefits of HRT for 5 years in women aged 50ndash59 years or within 10 years of the start of menopause E=estrogen P=progestin
bull Younger women (aged 50ndash59 years) had more favorable results bull There are differences between CE alone and CEMPA arms bull Overall benefitrisk ratio of CE-alone appears to be more favourable than CEMPA
Reevaluation of WHI data (stratified by age) Risks and
Benefits of HRT Cases per 1000 Women per 5 Years of
Use
Medical condition which may be exacerbated by treatment
with progestins
Diabetes and metabolic syndrome
bull Treatment of oestrogen deficiency symptoms with progestin-containing HT (unlike oestrogen alone) may be associated with increases in insulin resistance and deterioration in glucose tolerance123
bull Postmenopausal women with diabetes could be inappropriate for treatment with progestin-containing HT due to the potential risk of exacerbation of their condition
1) Panay N amp Studd JWW Human Reprod Update 1997
2) Godsland I et al Metabolism 1993
3) Sites CK et al J Clin Endocrinol Metab 2005
Variations in Associated Breast Cancer
Risks Between CE alone and CEMPA
bull Use of CE alone for a median of 59 years was associated with a lower incidence of invasive breast cancer (151 cases 027 per year) compared with placebo (199 cases 035 per year HR 077 95 CI 062ndash095 P=002)
bull In the CE alone group fewer women died from invasive breast cancer (6 deaths 0009 per year) compared with controls (16 deaths 0024 per year HR 037 95 CI 013ndash091 P=003)
Anderson GL et al Lancet
Oncol 2012
Bazedoxifene (BZA) specifically selected in
combination with conjugated estrogens
bull BZA has been specifically selected for its unique pharmacologic profile and effects on VMS and uterine tissue in particular123
1 Crabtree J et al Mol Cell Endocrinol 2008
2 Kharode Y et al Endocrinolology 2008
3 Duavive SmPC
Estrogen Receptor activity is dimmed
Estrogen Receptor activity is turned on
CEs are agonists BZA is an antagonist
In the uterus
bull The BZA component reduces the risk of endometrial hyperplasia that can occur with the conjugated estrogens component alone3 This means that progestins are not needed
Extensive global clinical development program for
CEBZA
aIncludes additional pilot dose-finding study 203 1 Lobo RA et al Fertil Steril 2009 2 Pinkerton JV et al Menopause 2009 3 Kagan R et al Menopause 2010 4 Mirkin S et al Climacteric 2013 5 Pinkerton JV et al Obstet Gynecol 2013
Effects of conjugated estrogensbazedoxifene on
lipid and coagulation variables a randomized
placebo- and active-controlled trial
bull At 12 months
bull Both CEBZA doses were associated with small but significant effects on hemostasis variables including reductions in antithrombin plasminogen activator inhibitor-1 and fibrinogen activity and an increase in plasminogen activity relative to placebo at 12 months Incidences of cardiovascular and venous thromboembolic events were similar among treatment groups
bull CONCLUSIONS
bull This study provides reassurance that CEBZA does not adversely affect lipid metabolism or hemostatic balance In accordance the incidences of venous thromboembolic events and cardiovascular events in postmenopausal women are similar to those observed with placebo
Breast density
Hormone therapy use and mammographic
density in postmenopausal Norwegian women
bull Results differed when considering the combined effect of age and BMI
bull The effect of EPT on mammographic density was modified by age and BMI with no apparent association among the youngest women (aged 50-55) with the highest BMI (BMI ge 26)
bull A higher mammographic density was found in EPT users compared to never HT users particularly in women using high-dose NETA regimens Age and BMI modified the association between EPT use and mammographic density
bull Couto E et al Breast Cancer Res Treat 2011 Nov 4 [Epub ahead of print]
Breast Cancer Risk by Breast Density
Menopause and Postmenopausal Hormone
Therapy Use
Birads age HT Duration Risk
1 55-59 None 5 year risk 08 (95 CI 06- 09)
1 55-59
ET EPT 5 year risk 09 (95 CI 07 -11)
4 55-59
None 5 year risk 24 (95 CI 20 -28)
4 55-59
ET 5 year risk
30 (95 CI 26 -35)
4 55-59
EPT 5 year risk
42 (95 CI 37 -46)
Adapted from Kerlikowske et al JOURNAL OF CLINICAL ONCOLOGY 2010
Breast Cancer Risk by Breast Density
Menopause and Postmenopausal Hormone
Therapy Use
Adapted from Kerlikowske et al JOURNAL OF CLINICAL ONCOLOGY 2010
bull Postmenopausal women with high breast density are at increased risk of breast cancer and should be aware of the added risk of taking HT especially estrogen plus progestin
Medical condition which may be exacerbated by treatment
with progestins
Diabetes and metabolic syndrome
bull progestin-containing HT may be associated with increases in insulin resistance and deterioration in glucose tolerance123
bull Postmenopausal women with diabetes could be inappropriate for treatment with progestin-containing HT due to the potential risk of exacerbation of their condition
1) Panay N amp Studd JWW Human Reprod Update 1997
2) Godsland I et al Metabolism 1993
3) Sites CK et al J Clin Endocrinol Metab 2005
A Nath and R Sitruk-Ware CLIMACTERIC 200912(Suppl 1)96ndash101
A Nath and R Sitruk-Ware CLIMACTERIC 200912(Suppl 1)96ndash101
Diabetes an epidemy
bull UK 1996 14 million of diabetics
bull UK 2015 32 million (6 of the population)
bull UK 2025 5 million
bull httpwwwdiabetescoukdiabetes-prevalencehtml
Other progestin-related intolerance issues
bull Nausea
bull Depressive mood
bull Poor concentration
bull Hirsutism
bull Headache
bull Dizziness
bull Fluid retention
bull Weight gain Panay N amp Studd JWW Human Reprod Update 1997
Medical condition which may be exacerbated by treatment with progestins
PMSPMDDdepression
bull Progesterone-induced PMD can be exacerbated by exogenous progestin administration and can occur in association with HT or OC administration1
bull Significantly higher negative mood scores have been observed during the addition of a progestin to an estrogen in a sequential HT regimen in postmenopausal women with a history of PMS compared to those without2
bull Women with a history of PMS or PMD exacerbation of depression using progestins may therefore benefit from a progestin free treatment for menopausal symptoms
1) Nevatte T et al Arch Womens Ment Health 2013 2) Bjoumlrn I et al Climacteric 2006 PMS premenstrual syndrome
PMDD premenstrual dysphoric disorder
Conclusion
bull CEEBAZO is an additional regimen for menopausal symptoms it provides also a prevention for osteoporosis
bull It is suitable for women with a uterus who are unsatisfied with an EPT regimen or who you are unwilling to treat with an EPT regimen
For some postmenopausal women with a uterus there is a
need for progestin free treatment options
bull with demonstrated clinical efficacy
bull which protects the endometrium
bull improved tolerabilitysafety profile
In clinical practice this translates to women who are
intolerant of progestin-containing HT or have conditions
which may be exacerbated by treatment with progestins
Conclusion Medical need for alternative treatment option
Medical condition which may be exacerbated by treatment with progestins
Depression
bull Progestin-containing HT has been associated with increases in depressive symptoms in some individuals1
bull There is a biochemicalphysiological plausibility for the association of progestins with depression234
bull Therefore postmenopausal women who also have a medical history of depressive disorders or depression could be inappropriate for treatment with progestin-containing HT
Pfizer Confidential
65
1) Girdler SS et al J Womens Health Gend Based Med 1999 2) Traish AM et al Korean J Urol 2014 3) Stroumlhle A et al Biol Psychiatry 1999 4) Romeo E et
al Am J Psychiatry 1998
History of the following conditions may make progestin inappropriate
bull Depression
bull PMSPMDD
PMS premenstrual syndrome
PMD premenstrual dysphoric disorder
Medical conditions that may be exacerbated by treatment with progestins
Women for whom progestin-containing HT
would not be considered appropriate
minus Women who are intolerant of progestin-containing hormone therapy
minus Women with pre-existing medical conditions that may be exacerbated by progestins
Most common adverse events leading to discontinuation are related to progestins12
breakthrough bleeding
bull Increase in the number of uterine procedures (ie unnecessary endometrial biopsies)
breast paintenderness
bull Increase in the number of breast interventions
1 Steel SA et al Climacteric 2003 2 Ettinger B and Pressman A Am J Manag Care 1999 3 Komm BS Mirkin S
Pharmaceuticals 2012
4 Panay N amp Studd JWW Human Reprod Update 1997
bull Nausea bull Depressive mood bull Poor concentration bull Hirsutism bull Headache bull Dizziness bull Fluid retention bull Weight gain
Other progestin-related intolerance issues4
Unmet need with the treatment of postmenopausal symptoms
bull Alternatives to progestin are needed that will protect the endometrium while avoiding other progestin-associated effects and preserving the desired effects of estrogens in postmenopausal women3
Which women with a uterus could benefit from
estrogens without the need for a progestin
bull Women who are intolerant of progestin-containing hormone therapy
bull Women with pre-existing medical conditions that may be exacerbated by progestins (eg women with a history of depression PMSPMDD increased breast density diabetes and metabolic syndrome)
History of the following conditions may make progestin inappropriate
bull Depression
bull PMSPMDD
bull High breast density
bull Diabetes and metabolic syndrome
PMS premenstrual syndrome
PMD premenstrual dysphoric disorder
Medical conditions that may be exacerbated by treatment with progestins
Learning from WHI data
bull Hormone therapy (HT) is the conventional and established therapy option to effectively treat postmenopausal symptoms however it has been associated with some safety and tolerability concerns1 2
bull A review of WHI data suggests that many of the concerns with menopausal HT more often associated with EPT (CE+MPA) such as CHD risk increased breast density breast pain and breast cancer risk than with ET (CEE alone)2
1 Rolnick SJ Kopher RA DeFor TA et al Menopause 2005
2 Komm BS Mirkin S Pharmaceuticals 2012
WHI Womenrsquos Health Initiative trial
CHD coronary heart disease
CEE conjugated equine estrogens
Efficacy and Safety of Constant Oestrogen
Pulsed Progestogen vs
Continuous Combined HRT
Adverse Events
17b-oestradiol 17b-oestradiol norgestimate NETA (n = 150) (n = 172) Breast discomfort 14 27 Abdominal discomfort 14 22 Uterine bleeding 15 12 Dysmenorrhea 3 8 Oedema 5 8
Adapted from S Rozenberg et al Human Reproduction 2000
Medical condition which may be exacerbated by treatment
with progestins
Increased breast density
bull Increases in breast density are associated with progestin-containing HT which may adversely affect radiological detection of breast cancer1 and may be independently associated with an increased risk for the development of breast cancer2
bull The Postmenopausal EstrogenProgestin Interventions (PEPI) trial demonstrated that an increased mammographic breast density was associated with the use of E+P but not with the use of estrogen alone3
bull Women who already have high breast density may therefore be considered inappropriate for treatment with a progestin-containing HT
1) EU Core SPC for Hormone Replacement Therapy Products (CMDh1312003 Rev 4 June
2012)
2) De Villiers TJ et al on behalf of the International Menopause Society Climacteric 2013 16
3) Greendale GA et al J Natl Cancer Inst 2003
Stroke
0 25 5 75 10 125
Fractures
Diabetes
Breast cancer
Cholecystitis
Venothrombotic episodes
Endometrial cancer
Lung cancer
Coronary heart disease
Colorectal cancer
Overall mortality
15 125 10 75 5 25
Benefits Risks
CE
CE MPA
Santen RJ et al J Clin Endocrinol Metab 2010
The basis of the Endocrine Society scientific statement for postmenopausal hormone replacement therapy (HRT) excess risks and benefits of HRT for 5 years in women aged 50ndash59 years or within 10 years of the start of menopause E=estrogen P=progestin
bull Younger women (aged 50ndash59 years) had more favorable results bull There are differences between CE alone and CEMPA arms bull Overall benefitrisk ratio of CE-alone appears to be more favourable than CEMPA
Reevaluation of WHI data (stratified by age) Risks and
Benefits of HRT Cases per 1000 Women per 5 Years of
Use
Medical condition which may be exacerbated by treatment
with progestins
Diabetes and metabolic syndrome
bull Treatment of oestrogen deficiency symptoms with progestin-containing HT (unlike oestrogen alone) may be associated with increases in insulin resistance and deterioration in glucose tolerance123
bull Postmenopausal women with diabetes could be inappropriate for treatment with progestin-containing HT due to the potential risk of exacerbation of their condition
1) Panay N amp Studd JWW Human Reprod Update 1997
2) Godsland I et al Metabolism 1993
3) Sites CK et al J Clin Endocrinol Metab 2005
Variations in Associated Breast Cancer
Risks Between CE alone and CEMPA
bull Use of CE alone for a median of 59 years was associated with a lower incidence of invasive breast cancer (151 cases 027 per year) compared with placebo (199 cases 035 per year HR 077 95 CI 062ndash095 P=002)
bull In the CE alone group fewer women died from invasive breast cancer (6 deaths 0009 per year) compared with controls (16 deaths 0024 per year HR 037 95 CI 013ndash091 P=003)
Anderson GL et al Lancet
Oncol 2012
Bazedoxifene (BZA) specifically selected in
combination with conjugated estrogens
bull BZA has been specifically selected for its unique pharmacologic profile and effects on VMS and uterine tissue in particular123
1 Crabtree J et al Mol Cell Endocrinol 2008
2 Kharode Y et al Endocrinolology 2008
3 Duavive SmPC
Estrogen Receptor activity is dimmed
Estrogen Receptor activity is turned on
CEs are agonists BZA is an antagonist
In the uterus
bull The BZA component reduces the risk of endometrial hyperplasia that can occur with the conjugated estrogens component alone3 This means that progestins are not needed
Extensive global clinical development program for
CEBZA
aIncludes additional pilot dose-finding study 203 1 Lobo RA et al Fertil Steril 2009 2 Pinkerton JV et al Menopause 2009 3 Kagan R et al Menopause 2010 4 Mirkin S et al Climacteric 2013 5 Pinkerton JV et al Obstet Gynecol 2013
Effects of conjugated estrogensbazedoxifene on
lipid and coagulation variables a randomized
placebo- and active-controlled trial
bull At 12 months
bull Both CEBZA doses were associated with small but significant effects on hemostasis variables including reductions in antithrombin plasminogen activator inhibitor-1 and fibrinogen activity and an increase in plasminogen activity relative to placebo at 12 months Incidences of cardiovascular and venous thromboembolic events were similar among treatment groups
bull CONCLUSIONS
bull This study provides reassurance that CEBZA does not adversely affect lipid metabolism or hemostatic balance In accordance the incidences of venous thromboembolic events and cardiovascular events in postmenopausal women are similar to those observed with placebo

Hormone therapy use and mammographic
density in postmenopausal Norwegian women
bull Results differed when considering the combined effect of age and BMI
bull The effect of EPT on mammographic density was modified by age and BMI with no apparent association among the youngest women (aged 50-55) with the highest BMI (BMI ge 26)
bull A higher mammographic density was found in EPT users compared to never HT users particularly in women using high-dose NETA regimens Age and BMI modified the association between EPT use and mammographic density
bull Couto E et al Breast Cancer Res Treat 2011 Nov 4 [Epub ahead of print]
Breast Cancer Risk by Breast Density
Menopause and Postmenopausal Hormone
Therapy Use
Birads age HT Duration Risk
1 55-59 None 5 year risk 08 (95 CI 06- 09)
1 55-59
ET EPT 5 year risk 09 (95 CI 07 -11)
4 55-59
None 5 year risk 24 (95 CI 20 -28)
4 55-59
ET 5 year risk
30 (95 CI 26 -35)
4 55-59
EPT 5 year risk
42 (95 CI 37 -46)
Adapted from Kerlikowske et al JOURNAL OF CLINICAL ONCOLOGY 2010
Breast Cancer Risk by Breast Density
Menopause and Postmenopausal Hormone
Therapy Use
Adapted from Kerlikowske et al JOURNAL OF CLINICAL ONCOLOGY 2010
bull Postmenopausal women with high breast density are at increased risk of breast cancer and should be aware of the added risk of taking HT especially estrogen plus progestin
Medical condition which may be exacerbated by treatment
with progestins
Diabetes and metabolic syndrome
bull progestin-containing HT may be associated with increases in insulin resistance and deterioration in glucose tolerance123
bull Postmenopausal women with diabetes could be inappropriate for treatment with progestin-containing HT due to the potential risk of exacerbation of their condition
1) Panay N amp Studd JWW Human Reprod Update 1997
2) Godsland I et al Metabolism 1993
3) Sites CK et al J Clin Endocrinol Metab 2005
A Nath and R Sitruk-Ware CLIMACTERIC 200912(Suppl 1)96ndash101
A Nath and R Sitruk-Ware CLIMACTERIC 200912(Suppl 1)96ndash101
Diabetes an epidemy
bull UK 1996 14 million of diabetics
bull UK 2015 32 million (6 of the population)
bull UK 2025 5 million
bull httpwwwdiabetescoukdiabetes-prevalencehtml
Other progestin-related intolerance issues
bull Nausea
bull Depressive mood
bull Poor concentration
bull Hirsutism
bull Headache
bull Dizziness
bull Fluid retention
bull Weight gain Panay N amp Studd JWW Human Reprod Update 1997
Medical condition which may be exacerbated by treatment with progestins
PMSPMDDdepression
bull Progesterone-induced PMD can be exacerbated by exogenous progestin administration and can occur in association with HT or OC administration1
bull Significantly higher negative mood scores have been observed during the addition of a progestin to an estrogen in a sequential HT regimen in postmenopausal women with a history of PMS compared to those without2
bull Women with a history of PMS or PMD exacerbation of depression using progestins may therefore benefit from a progestin free treatment for menopausal symptoms
1) Nevatte T et al Arch Womens Ment Health 2013 2) Bjoumlrn I et al Climacteric 2006 PMS premenstrual syndrome
PMDD premenstrual dysphoric disorder
Conclusion
bull CEEBAZO is an additional regimen for menopausal symptoms it provides also a prevention for osteoporosis
bull It is suitable for women with a uterus who are unsatisfied with an EPT regimen or who you are unwilling to treat with an EPT regimen
For some postmenopausal women with a uterus there is a
need for progestin free treatment options
bull with demonstrated clinical efficacy
bull which protects the endometrium
bull improved tolerabilitysafety profile
In clinical practice this translates to women who are
intolerant of progestin-containing HT or have conditions
which may be exacerbated by treatment with progestins
Conclusion Medical need for alternative treatment option
Medical condition which may be exacerbated by treatment with progestins
Depression
bull Progestin-containing HT has been associated with increases in depressive symptoms in some individuals1
bull There is a biochemicalphysiological plausibility for the association of progestins with depression234
bull Therefore postmenopausal women who also have a medical history of depressive disorders or depression could be inappropriate for treatment with progestin-containing HT
Pfizer Confidential
65
1) Girdler SS et al J Womens Health Gend Based Med 1999 2) Traish AM et al Korean J Urol 2014 3) Stroumlhle A et al Biol Psychiatry 1999 4) Romeo E et
al Am J Psychiatry 1998
History of the following conditions may make progestin inappropriate
bull Depression
bull PMSPMDD
PMS premenstrual syndrome
PMD premenstrual dysphoric disorder
Medical conditions that may be exacerbated by treatment with progestins
Women for whom progestin-containing HT
would not be considered appropriate
minus Women who are intolerant of progestin-containing hormone therapy
minus Women with pre-existing medical conditions that may be exacerbated by progestins
Most common adverse events leading to discontinuation are related to progestins12
breakthrough bleeding
bull Increase in the number of uterine procedures (ie unnecessary endometrial biopsies)
breast paintenderness
bull Increase in the number of breast interventions
1 Steel SA et al Climacteric 2003 2 Ettinger B and Pressman A Am J Manag Care 1999 3 Komm BS Mirkin S
Pharmaceuticals 2012
4 Panay N amp Studd JWW Human Reprod Update 1997
bull Nausea bull Depressive mood bull Poor concentration bull Hirsutism bull Headache bull Dizziness bull Fluid retention bull Weight gain
Other progestin-related intolerance issues4
Unmet need with the treatment of postmenopausal symptoms
bull Alternatives to progestin are needed that will protect the endometrium while avoiding other progestin-associated effects and preserving the desired effects of estrogens in postmenopausal women3
Which women with a uterus could benefit from
estrogens without the need for a progestin
bull Women who are intolerant of progestin-containing hormone therapy
bull Women with pre-existing medical conditions that may be exacerbated by progestins (eg women with a history of depression PMSPMDD increased breast density diabetes and metabolic syndrome)
History of the following conditions may make progestin inappropriate
bull Depression
bull PMSPMDD
bull High breast density
bull Diabetes and metabolic syndrome
PMS premenstrual syndrome
PMD premenstrual dysphoric disorder
Medical conditions that may be exacerbated by treatment with progestins
Learning from WHI data
bull Hormone therapy (HT) is the conventional and established therapy option to effectively treat postmenopausal symptoms however it has been associated with some safety and tolerability concerns1 2
bull A review of WHI data suggests that many of the concerns with menopausal HT more often associated with EPT (CE+MPA) such as CHD risk increased breast density breast pain and breast cancer risk than with ET (CEE alone)2
1 Rolnick SJ Kopher RA DeFor TA et al Menopause 2005
2 Komm BS Mirkin S Pharmaceuticals 2012
WHI Womenrsquos Health Initiative trial
CHD coronary heart disease
CEE conjugated equine estrogens
Efficacy and Safety of Constant Oestrogen
Pulsed Progestogen vs
Continuous Combined HRT
Adverse Events
17b-oestradiol 17b-oestradiol norgestimate NETA (n = 150) (n = 172) Breast discomfort 14 27 Abdominal discomfort 14 22 Uterine bleeding 15 12 Dysmenorrhea 3 8 Oedema 5 8
Adapted from S Rozenberg et al Human Reproduction 2000
Medical condition which may be exacerbated by treatment
with progestins
Increased breast density
bull Increases in breast density are associated with progestin-containing HT which may adversely affect radiological detection of breast cancer1 and may be independently associated with an increased risk for the development of breast cancer2
bull The Postmenopausal EstrogenProgestin Interventions (PEPI) trial demonstrated that an increased mammographic breast density was associated with the use of E+P but not with the use of estrogen alone3
bull Women who already have high breast density may therefore be considered inappropriate for treatment with a progestin-containing HT
1) EU Core SPC for Hormone Replacement Therapy Products (CMDh1312003 Rev 4 June
2012)
2) De Villiers TJ et al on behalf of the International Menopause Society Climacteric 2013 16
3) Greendale GA et al J Natl Cancer Inst 2003
Stroke
0 25 5 75 10 125
Fractures
Diabetes
Breast cancer
Cholecystitis
Venothrombotic episodes
Endometrial cancer
Lung cancer
Coronary heart disease
Colorectal cancer
Overall mortality
15 125 10 75 5 25
Benefits Risks
CE
CE MPA
Santen RJ et al J Clin Endocrinol Metab 2010
The basis of the Endocrine Society scientific statement for postmenopausal hormone replacement therapy (HRT) excess risks and benefits of HRT for 5 years in women aged 50ndash59 years or within 10 years of the start of menopause E=estrogen P=progestin
bull Younger women (aged 50ndash59 years) had more favorable results bull There are differences between CE alone and CEMPA arms bull Overall benefitrisk ratio of CE-alone appears to be more favourable than CEMPA
Reevaluation of WHI data (stratified by age) Risks and
Benefits of HRT Cases per 1000 Women per 5 Years of
Use
Medical condition which may be exacerbated by treatment
with progestins
Diabetes and metabolic syndrome
bull Treatment of oestrogen deficiency symptoms with progestin-containing HT (unlike oestrogen alone) may be associated with increases in insulin resistance and deterioration in glucose tolerance123
bull Postmenopausal women with diabetes could be inappropriate for treatment with progestin-containing HT due to the potential risk of exacerbation of their condition
1) Panay N amp Studd JWW Human Reprod Update 1997
2) Godsland I et al Metabolism 1993
3) Sites CK et al J Clin Endocrinol Metab 2005
Variations in Associated Breast Cancer
Risks Between CE alone and CEMPA
bull Use of CE alone for a median of 59 years was associated with a lower incidence of invasive breast cancer (151 cases 027 per year) compared with placebo (199 cases 035 per year HR 077 95 CI 062ndash095 P=002)
bull In the CE alone group fewer women died from invasive breast cancer (6 deaths 0009 per year) compared with controls (16 deaths 0024 per year HR 037 95 CI 013ndash091 P=003)
Anderson GL et al Lancet
Oncol 2012
Bazedoxifene (BZA) specifically selected in
combination with conjugated estrogens
bull BZA has been specifically selected for its unique pharmacologic profile and effects on VMS and uterine tissue in particular123
1 Crabtree J et al Mol Cell Endocrinol 2008
2 Kharode Y et al Endocrinolology 2008
3 Duavive SmPC
Estrogen Receptor activity is dimmed
Estrogen Receptor activity is turned on
CEs are agonists BZA is an antagonist
In the uterus
bull The BZA component reduces the risk of endometrial hyperplasia that can occur with the conjugated estrogens component alone3 This means that progestins are not needed
Extensive global clinical development program for
CEBZA
aIncludes additional pilot dose-finding study 203 1 Lobo RA et al Fertil Steril 2009 2 Pinkerton JV et al Menopause 2009 3 Kagan R et al Menopause 2010 4 Mirkin S et al Climacteric 2013 5 Pinkerton JV et al Obstet Gynecol 2013
Effects of conjugated estrogensbazedoxifene on
lipid and coagulation variables a randomized
placebo- and active-controlled trial
bull At 12 months
bull Both CEBZA doses were associated with small but significant effects on hemostasis variables including reductions in antithrombin plasminogen activator inhibitor-1 and fibrinogen activity and an increase in plasminogen activity relative to placebo at 12 months Incidences of cardiovascular and venous thromboembolic events were similar among treatment groups
bull CONCLUSIONS
bull This study provides reassurance that CEBZA does not adversely affect lipid metabolism or hemostatic balance In accordance the incidences of venous thromboembolic events and cardiovascular events in postmenopausal women are similar to those observed with placebo
Breast Cancer Risk by Breast Density
Menopause and Postmenopausal Hormone
Therapy Use
Birads age HT Duration Risk
1 55-59 None 5 year risk 08 (95 CI 06- 09)
1 55-59
ET EPT 5 year risk 09 (95 CI 07 -11)
4 55-59
None 5 year risk 24 (95 CI 20 -28)
4 55-59
ET 5 year risk
30 (95 CI 26 -35)
4 55-59
EPT 5 year risk
42 (95 CI 37 -46)
Adapted from Kerlikowske et al JOURNAL OF CLINICAL ONCOLOGY 2010
Breast Cancer Risk by Breast Density
Menopause and Postmenopausal Hormone
Therapy Use
Adapted from Kerlikowske et al JOURNAL OF CLINICAL ONCOLOGY 2010
bull Postmenopausal women with high breast density are at increased risk of breast cancer and should be aware of the added risk of taking HT especially estrogen plus progestin
Medical condition which may be exacerbated by treatment
with progestins
Diabetes and metabolic syndrome
bull progestin-containing HT may be associated with increases in insulin resistance and deterioration in glucose tolerance123
bull Postmenopausal women with diabetes could be inappropriate for treatment with progestin-containing HT due to the potential risk of exacerbation of their condition
1) Panay N amp Studd JWW Human Reprod Update 1997
2) Godsland I et al Metabolism 1993
3) Sites CK et al J Clin Endocrinol Metab 2005
A Nath and R Sitruk-Ware CLIMACTERIC 200912(Suppl 1)96ndash101
A Nath and R Sitruk-Ware CLIMACTERIC 200912(Suppl 1)96ndash101
Diabetes an epidemy
bull UK 1996 14 million of diabetics
bull UK 2015 32 million (6 of the population)
bull UK 2025 5 million
bull httpwwwdiabetescoukdiabetes-prevalencehtml
Other progestin-related intolerance issues
bull Nausea
bull Depressive mood
bull Poor concentration
bull Hirsutism
bull Headache
bull Dizziness
bull Fluid retention
bull Weight gain Panay N amp Studd JWW Human Reprod Update 1997
Medical condition which may be exacerbated by treatment with progestins
PMSPMDDdepression
bull Progesterone-induced PMD can be exacerbated by exogenous progestin administration and can occur in association with HT or OC administration1
bull Significantly higher negative mood scores have been observed during the addition of a progestin to an estrogen in a sequential HT regimen in postmenopausal women with a history of PMS compared to those without2
bull Women with a history of PMS or PMD exacerbation of depression using progestins may therefore benefit from a progestin free treatment for menopausal symptoms
1) Nevatte T et al Arch Womens Ment Health 2013 2) Bjoumlrn I et al Climacteric 2006 PMS premenstrual syndrome
PMDD premenstrual dysphoric disorder
Conclusion
bull CEEBAZO is an additional regimen for menopausal symptoms it provides also a prevention for osteoporosis
bull It is suitable for women with a uterus who are unsatisfied with an EPT regimen or who you are unwilling to treat with an EPT regimen
For some postmenopausal women with a uterus there is a
need for progestin free treatment options
bull with demonstrated clinical efficacy
bull which protects the endometrium
bull improved tolerabilitysafety profile
In clinical practice this translates to women who are
intolerant of progestin-containing HT or have conditions
which may be exacerbated by treatment with progestins
Conclusion Medical need for alternative treatment option
Medical condition which may be exacerbated by treatment with progestins
Depression
bull Progestin-containing HT has been associated with increases in depressive symptoms in some individuals1
bull There is a biochemicalphysiological plausibility for the association of progestins with depression234
bull Therefore postmenopausal women who also have a medical history of depressive disorders or depression could be inappropriate for treatment with progestin-containing HT
Pfizer Confidential
65
1) Girdler SS et al J Womens Health Gend Based Med 1999 2) Traish AM et al Korean J Urol 2014 3) Stroumlhle A et al Biol Psychiatry 1999 4) Romeo E et
al Am J Psychiatry 1998
History of the following conditions may make progestin inappropriate
bull Depression
bull PMSPMDD
PMS premenstrual syndrome
PMD premenstrual dysphoric disorder
Medical conditions that may be exacerbated by treatment with progestins
Women for whom progestin-containing HT
would not be considered appropriate
minus Women who are intolerant of progestin-containing hormone therapy
minus Women with pre-existing medical conditions that may be exacerbated by progestins
Most common adverse events leading to discontinuation are related to progestins12
breakthrough bleeding
bull Increase in the number of uterine procedures (ie unnecessary endometrial biopsies)
breast paintenderness
bull Increase in the number of breast interventions
1 Steel SA et al Climacteric 2003 2 Ettinger B and Pressman A Am J Manag Care 1999 3 Komm BS Mirkin S
Pharmaceuticals 2012
4 Panay N amp Studd JWW Human Reprod Update 1997
bull Nausea bull Depressive mood bull Poor concentration bull Hirsutism bull Headache bull Dizziness bull Fluid retention bull Weight gain
Other progestin-related intolerance issues4
Unmet need with the treatment of postmenopausal symptoms
bull Alternatives to progestin are needed that will protect the endometrium while avoiding other progestin-associated effects and preserving the desired effects of estrogens in postmenopausal women3
Which women with a uterus could benefit from
estrogens without the need for a progestin
bull Women who are intolerant of progestin-containing hormone therapy
bull Women with pre-existing medical conditions that may be exacerbated by progestins (eg women with a history of depression PMSPMDD increased breast density diabetes and metabolic syndrome)
History of the following conditions may make progestin inappropriate
bull Depression
bull PMSPMDD
bull High breast density
bull Diabetes and metabolic syndrome
PMS premenstrual syndrome
PMD premenstrual dysphoric disorder
Medical conditions that may be exacerbated by treatment with progestins
Learning from WHI data
bull Hormone therapy (HT) is the conventional and established therapy option to effectively treat postmenopausal symptoms however it has been associated with some safety and tolerability concerns1 2
bull A review of WHI data suggests that many of the concerns with menopausal HT more often associated with EPT (CE+MPA) such as CHD risk increased breast density breast pain and breast cancer risk than with ET (CEE alone)2
1 Rolnick SJ Kopher RA DeFor TA et al Menopause 2005
2 Komm BS Mirkin S Pharmaceuticals 2012
WHI Womenrsquos Health Initiative trial
CHD coronary heart disease
CEE conjugated equine estrogens
Efficacy and Safety of Constant Oestrogen
Pulsed Progestogen vs
Continuous Combined HRT
Adverse Events
17b-oestradiol 17b-oestradiol norgestimate NETA (n = 150) (n = 172) Breast discomfort 14 27 Abdominal discomfort 14 22 Uterine bleeding 15 12 Dysmenorrhea 3 8 Oedema 5 8
Adapted from S Rozenberg et al Human Reproduction 2000
Medical condition which may be exacerbated by treatment
with progestins
Increased breast density
bull Increases in breast density are associated with progestin-containing HT which may adversely affect radiological detection of breast cancer1 and may be independently associated with an increased risk for the development of breast cancer2
bull The Postmenopausal EstrogenProgestin Interventions (PEPI) trial demonstrated that an increased mammographic breast density was associated with the use of E+P but not with the use of estrogen alone3
bull Women who already have high breast density may therefore be considered inappropriate for treatment with a progestin-containing HT
1) EU Core SPC for Hormone Replacement Therapy Products (CMDh1312003 Rev 4 June
2012)
2) De Villiers TJ et al on behalf of the International Menopause Society Climacteric 2013 16
3) Greendale GA et al J Natl Cancer Inst 2003
Stroke
0 25 5 75 10 125
Fractures
Diabetes
Breast cancer
Cholecystitis
Venothrombotic episodes
Endometrial cancer
Lung cancer
Coronary heart disease
Colorectal cancer
Overall mortality
15 125 10 75 5 25
Benefits Risks
CE
CE MPA
Santen RJ et al J Clin Endocrinol Metab 2010
The basis of the Endocrine Society scientific statement for postmenopausal hormone replacement therapy (HRT) excess risks and benefits of HRT for 5 years in women aged 50ndash59 years or within 10 years of the start of menopause E=estrogen P=progestin
bull Younger women (aged 50ndash59 years) had more favorable results bull There are differences between CE alone and CEMPA arms bull Overall benefitrisk ratio of CE-alone appears to be more favourable than CEMPA
Reevaluation of WHI data (stratified by age) Risks and
Benefits of HRT Cases per 1000 Women per 5 Years of
Use
Medical condition which may be exacerbated by treatment
with progestins
Diabetes and metabolic syndrome
bull Treatment of oestrogen deficiency symptoms with progestin-containing HT (unlike oestrogen alone) may be associated with increases in insulin resistance and deterioration in glucose tolerance123
bull Postmenopausal women with diabetes could be inappropriate for treatment with progestin-containing HT due to the potential risk of exacerbation of their condition
1) Panay N amp Studd JWW Human Reprod Update 1997
2) Godsland I et al Metabolism 1993
3) Sites CK et al J Clin Endocrinol Metab 2005
Variations in Associated Breast Cancer
Risks Between CE alone and CEMPA
bull Use of CE alone for a median of 59 years was associated with a lower incidence of invasive breast cancer (151 cases 027 per year) compared with placebo (199 cases 035 per year HR 077 95 CI 062ndash095 P=002)
bull In the CE alone group fewer women died from invasive breast cancer (6 deaths 0009 per year) compared with controls (16 deaths 0024 per year HR 037 95 CI 013ndash091 P=003)
Anderson GL et al Lancet
Oncol 2012
Bazedoxifene (BZA) specifically selected in
combination with conjugated estrogens
bull BZA has been specifically selected for its unique pharmacologic profile and effects on VMS and uterine tissue in particular123
1 Crabtree J et al Mol Cell Endocrinol 2008
2 Kharode Y et al Endocrinolology 2008
3 Duavive SmPC
Estrogen Receptor activity is dimmed
Estrogen Receptor activity is turned on
CEs are agonists BZA is an antagonist
In the uterus
bull The BZA component reduces the risk of endometrial hyperplasia that can occur with the conjugated estrogens component alone3 This means that progestins are not needed
Extensive global clinical development program for
CEBZA
aIncludes additional pilot dose-finding study 203 1 Lobo RA et al Fertil Steril 2009 2 Pinkerton JV et al Menopause 2009 3 Kagan R et al Menopause 2010 4 Mirkin S et al Climacteric 2013 5 Pinkerton JV et al Obstet Gynecol 2013
Effects of conjugated estrogensbazedoxifene on
lipid and coagulation variables a randomized
placebo- and active-controlled trial
bull At 12 months
bull Both CEBZA doses were associated with small but significant effects on hemostasis variables including reductions in antithrombin plasminogen activator inhibitor-1 and fibrinogen activity and an increase in plasminogen activity relative to placebo at 12 months Incidences of cardiovascular and venous thromboembolic events were similar among treatment groups
bull CONCLUSIONS
bull This study provides reassurance that CEBZA does not adversely affect lipid metabolism or hemostatic balance In accordance the incidences of venous thromboembolic events and cardiovascular events in postmenopausal women are similar to those observed with placebo

Breast Cancer Risk by Breast Density
Menopause and Postmenopausal Hormone
Therapy Use
Adapted from Kerlikowske et al JOURNAL OF CLINICAL ONCOLOGY 2010
bull Postmenopausal women with high breast density are at increased risk of breast cancer and should be aware of the added risk of taking HT especially estrogen plus progestin
Medical condition which may be exacerbated by treatment
with progestins
Diabetes and metabolic syndrome
bull progestin-containing HT may be associated with increases in insulin resistance and deterioration in glucose tolerance123
bull Postmenopausal women with diabetes could be inappropriate for treatment with progestin-containing HT due to the potential risk of exacerbation of their condition
1) Panay N amp Studd JWW Human Reprod Update 1997
2) Godsland I et al Metabolism 1993
3) Sites CK et al J Clin Endocrinol Metab 2005
A Nath and R Sitruk-Ware CLIMACTERIC 200912(Suppl 1)96ndash101
A Nath and R Sitruk-Ware CLIMACTERIC 200912(Suppl 1)96ndash101
Diabetes an epidemy
bull UK 1996 14 million of diabetics
bull UK 2015 32 million (6 of the population)
bull UK 2025 5 million
bull httpwwwdiabetescoukdiabetes-prevalencehtml
Other progestin-related intolerance issues
bull Nausea
bull Depressive mood
bull Poor concentration
bull Hirsutism
bull Headache
bull Dizziness
bull Fluid retention
bull Weight gain Panay N amp Studd JWW Human Reprod Update 1997
Medical condition which may be exacerbated by treatment with progestins
PMSPMDDdepression
bull Progesterone-induced PMD can be exacerbated by exogenous progestin administration and can occur in association with HT or OC administration1
bull Significantly higher negative mood scores have been observed during the addition of a progestin to an estrogen in a sequential HT regimen in postmenopausal women with a history of PMS compared to those without2
bull Women with a history of PMS or PMD exacerbation of depression using progestins may therefore benefit from a progestin free treatment for menopausal symptoms
1) Nevatte T et al Arch Womens Ment Health 2013 2) Bjoumlrn I et al Climacteric 2006 PMS premenstrual syndrome
PMDD premenstrual dysphoric disorder
Conclusion
bull CEEBAZO is an additional regimen for menopausal symptoms it provides also a prevention for osteoporosis
bull It is suitable for women with a uterus who are unsatisfied with an EPT regimen or who you are unwilling to treat with an EPT regimen
For some postmenopausal women with a uterus there is a
need for progestin free treatment options
bull with demonstrated clinical efficacy
bull which protects the endometrium
bull improved tolerabilitysafety profile
In clinical practice this translates to women who are
intolerant of progestin-containing HT or have conditions
which may be exacerbated by treatment with progestins
Conclusion Medical need for alternative treatment option
Medical condition which may be exacerbated by treatment with progestins
Depression
bull Progestin-containing HT has been associated with increases in depressive symptoms in some individuals1
bull There is a biochemicalphysiological plausibility for the association of progestins with depression234
bull Therefore postmenopausal women who also have a medical history of depressive disorders or depression could be inappropriate for treatment with progestin-containing HT
Pfizer Confidential
65
1) Girdler SS et al J Womens Health Gend Based Med 1999 2) Traish AM et al Korean J Urol 2014 3) Stroumlhle A et al Biol Psychiatry 1999 4) Romeo E et
al Am J Psychiatry 1998
History of the following conditions may make progestin inappropriate
bull Depression
bull PMSPMDD
PMS premenstrual syndrome
PMD premenstrual dysphoric disorder
Medical conditions that may be exacerbated by treatment with progestins
Women for whom progestin-containing HT
would not be considered appropriate
minus Women who are intolerant of progestin-containing hormone therapy
minus Women with pre-existing medical conditions that may be exacerbated by progestins
Most common adverse events leading to discontinuation are related to progestins12
breakthrough bleeding
bull Increase in the number of uterine procedures (ie unnecessary endometrial biopsies)
breast paintenderness
bull Increase in the number of breast interventions
1 Steel SA et al Climacteric 2003 2 Ettinger B and Pressman A Am J Manag Care 1999 3 Komm BS Mirkin S
Pharmaceuticals 2012
4 Panay N amp Studd JWW Human Reprod Update 1997
bull Nausea bull Depressive mood bull Poor concentration bull Hirsutism bull Headache bull Dizziness bull Fluid retention bull Weight gain
Other progestin-related intolerance issues4
Unmet need with the treatment of postmenopausal symptoms
bull Alternatives to progestin are needed that will protect the endometrium while avoiding other progestin-associated effects and preserving the desired effects of estrogens in postmenopausal women3
Which women with a uterus could benefit from
estrogens without the need for a progestin
bull Women who are intolerant of progestin-containing hormone therapy
bull Women with pre-existing medical conditions that may be exacerbated by progestins (eg women with a history of depression PMSPMDD increased breast density diabetes and metabolic syndrome)
History of the following conditions may make progestin inappropriate
bull Depression
bull PMSPMDD
bull High breast density
bull Diabetes and metabolic syndrome
PMS premenstrual syndrome
PMD premenstrual dysphoric disorder
Medical conditions that may be exacerbated by treatment with progestins
Learning from WHI data
bull Hormone therapy (HT) is the conventional and established therapy option to effectively treat postmenopausal symptoms however it has been associated with some safety and tolerability concerns1 2
bull A review of WHI data suggests that many of the concerns with menopausal HT more often associated with EPT (CE+MPA) such as CHD risk increased breast density breast pain and breast cancer risk than with ET (CEE alone)2
1 Rolnick SJ Kopher RA DeFor TA et al Menopause 2005
2 Komm BS Mirkin S Pharmaceuticals 2012
WHI Womenrsquos Health Initiative trial
CHD coronary heart disease
CEE conjugated equine estrogens
Efficacy and Safety of Constant Oestrogen
Pulsed Progestogen vs
Continuous Combined HRT
Adverse Events
17b-oestradiol 17b-oestradiol norgestimate NETA (n = 150) (n = 172) Breast discomfort 14 27 Abdominal discomfort 14 22 Uterine bleeding 15 12 Dysmenorrhea 3 8 Oedema 5 8
Adapted from S Rozenberg et al Human Reproduction 2000
Medical condition which may be exacerbated by treatment
with progestins
Increased breast density
bull Increases in breast density are associated with progestin-containing HT which may adversely affect radiological detection of breast cancer1 and may be independently associated with an increased risk for the development of breast cancer2
bull The Postmenopausal EstrogenProgestin Interventions (PEPI) trial demonstrated that an increased mammographic breast density was associated with the use of E+P but not with the use of estrogen alone3
bull Women who already have high breast density may therefore be considered inappropriate for treatment with a progestin-containing HT
1) EU Core SPC for Hormone Replacement Therapy Products (CMDh1312003 Rev 4 June
2012)
2) De Villiers TJ et al on behalf of the International Menopause Society Climacteric 2013 16
3) Greendale GA et al J Natl Cancer Inst 2003
Stroke
0 25 5 75 10 125
Fractures
Diabetes
Breast cancer
Cholecystitis
Venothrombotic episodes
Endometrial cancer
Lung cancer
Coronary heart disease
Colorectal cancer
Overall mortality
15 125 10 75 5 25
Benefits Risks
CE
CE MPA
Santen RJ et al J Clin Endocrinol Metab 2010
The basis of the Endocrine Society scientific statement for postmenopausal hormone replacement therapy (HRT) excess risks and benefits of HRT for 5 years in women aged 50ndash59 years or within 10 years of the start of menopause E=estrogen P=progestin
bull Younger women (aged 50ndash59 years) had more favorable results bull There are differences between CE alone and CEMPA arms bull Overall benefitrisk ratio of CE-alone appears to be more favourable than CEMPA
Reevaluation of WHI data (stratified by age) Risks and
Benefits of HRT Cases per 1000 Women per 5 Years of
Use
Medical condition which may be exacerbated by treatment
with progestins
Diabetes and metabolic syndrome
bull Treatment of oestrogen deficiency symptoms with progestin-containing HT (unlike oestrogen alone) may be associated with increases in insulin resistance and deterioration in glucose tolerance123
bull Postmenopausal women with diabetes could be inappropriate for treatment with progestin-containing HT due to the potential risk of exacerbation of their condition
1) Panay N amp Studd JWW Human Reprod Update 1997
2) Godsland I et al Metabolism 1993
3) Sites CK et al J Clin Endocrinol Metab 2005
Variations in Associated Breast Cancer
Risks Between CE alone and CEMPA
bull Use of CE alone for a median of 59 years was associated with a lower incidence of invasive breast cancer (151 cases 027 per year) compared with placebo (199 cases 035 per year HR 077 95 CI 062ndash095 P=002)
bull In the CE alone group fewer women died from invasive breast cancer (6 deaths 0009 per year) compared with controls (16 deaths 0024 per year HR 037 95 CI 013ndash091 P=003)
Anderson GL et al Lancet
Oncol 2012
Bazedoxifene (BZA) specifically selected in
combination with conjugated estrogens
bull BZA has been specifically selected for its unique pharmacologic profile and effects on VMS and uterine tissue in particular123
1 Crabtree J et al Mol Cell Endocrinol 2008
2 Kharode Y et al Endocrinolology 2008
3 Duavive SmPC
Estrogen Receptor activity is dimmed
Estrogen Receptor activity is turned on
CEs are agonists BZA is an antagonist
In the uterus
bull The BZA component reduces the risk of endometrial hyperplasia that can occur with the conjugated estrogens component alone3 This means that progestins are not needed
Extensive global clinical development program for
CEBZA
aIncludes additional pilot dose-finding study 203 1 Lobo RA et al Fertil Steril 2009 2 Pinkerton JV et al Menopause 2009 3 Kagan R et al Menopause 2010 4 Mirkin S et al Climacteric 2013 5 Pinkerton JV et al Obstet Gynecol 2013
Effects of conjugated estrogensbazedoxifene on
lipid and coagulation variables a randomized
placebo- and active-controlled trial
bull At 12 months
bull Both CEBZA doses were associated with small but significant effects on hemostasis variables including reductions in antithrombin plasminogen activator inhibitor-1 and fibrinogen activity and an increase in plasminogen activity relative to placebo at 12 months Incidences of cardiovascular and venous thromboembolic events were similar among treatment groups
bull CONCLUSIONS
bull This study provides reassurance that CEBZA does not adversely affect lipid metabolism or hemostatic balance In accordance the incidences of venous thromboembolic events and cardiovascular events in postmenopausal women are similar to those observed with placebo

Medical condition which may be exacerbated by treatment
with progestins
Diabetes and metabolic syndrome
bull progestin-containing HT may be associated with increases in insulin resistance and deterioration in glucose tolerance123
bull Postmenopausal women with diabetes could be inappropriate for treatment with progestin-containing HT due to the potential risk of exacerbation of their condition
1) Panay N amp Studd JWW Human Reprod Update 1997
2) Godsland I et al Metabolism 1993
3) Sites CK et al J Clin Endocrinol Metab 2005
A Nath and R Sitruk-Ware CLIMACTERIC 200912(Suppl 1)96ndash101
A Nath and R Sitruk-Ware CLIMACTERIC 200912(Suppl 1)96ndash101
Diabetes an epidemy
bull UK 1996 14 million of diabetics
bull UK 2015 32 million (6 of the population)
bull UK 2025 5 million
bull httpwwwdiabetescoukdiabetes-prevalencehtml
Other progestin-related intolerance issues
bull Nausea
bull Depressive mood
bull Poor concentration
bull Hirsutism
bull Headache
bull Dizziness
bull Fluid retention
bull Weight gain Panay N amp Studd JWW Human Reprod Update 1997
Medical condition which may be exacerbated by treatment with progestins
PMSPMDDdepression
bull Progesterone-induced PMD can be exacerbated by exogenous progestin administration and can occur in association with HT or OC administration1
bull Significantly higher negative mood scores have been observed during the addition of a progestin to an estrogen in a sequential HT regimen in postmenopausal women with a history of PMS compared to those without2
bull Women with a history of PMS or PMD exacerbation of depression using progestins may therefore benefit from a progestin free treatment for menopausal symptoms
1) Nevatte T et al Arch Womens Ment Health 2013 2) Bjoumlrn I et al Climacteric 2006 PMS premenstrual syndrome
PMDD premenstrual dysphoric disorder
Conclusion
bull CEEBAZO is an additional regimen for menopausal symptoms it provides also a prevention for osteoporosis
bull It is suitable for women with a uterus who are unsatisfied with an EPT regimen or who you are unwilling to treat with an EPT regimen
For some postmenopausal women with a uterus there is a
need for progestin free treatment options
bull with demonstrated clinical efficacy
bull which protects the endometrium
bull improved tolerabilitysafety profile
In clinical practice this translates to women who are
intolerant of progestin-containing HT or have conditions
which may be exacerbated by treatment with progestins
Conclusion Medical need for alternative treatment option
Medical condition which may be exacerbated by treatment with progestins
Depression
bull Progestin-containing HT has been associated with increases in depressive symptoms in some individuals1
bull There is a biochemicalphysiological plausibility for the association of progestins with depression234
bull Therefore postmenopausal women who also have a medical history of depressive disorders or depression could be inappropriate for treatment with progestin-containing HT
Pfizer Confidential
65
1) Girdler SS et al J Womens Health Gend Based Med 1999 2) Traish AM et al Korean J Urol 2014 3) Stroumlhle A et al Biol Psychiatry 1999 4) Romeo E et
al Am J Psychiatry 1998
History of the following conditions may make progestin inappropriate
bull Depression
bull PMSPMDD
PMS premenstrual syndrome
PMD premenstrual dysphoric disorder
Medical conditions that may be exacerbated by treatment with progestins
Women for whom progestin-containing HT
would not be considered appropriate
minus Women who are intolerant of progestin-containing hormone therapy
minus Women with pre-existing medical conditions that may be exacerbated by progestins
Most common adverse events leading to discontinuation are related to progestins12
breakthrough bleeding
bull Increase in the number of uterine procedures (ie unnecessary endometrial biopsies)
breast paintenderness
bull Increase in the number of breast interventions
1 Steel SA et al Climacteric 2003 2 Ettinger B and Pressman A Am J Manag Care 1999 3 Komm BS Mirkin S
Pharmaceuticals 2012
4 Panay N amp Studd JWW Human Reprod Update 1997
bull Nausea bull Depressive mood bull Poor concentration bull Hirsutism bull Headache bull Dizziness bull Fluid retention bull Weight gain
Other progestin-related intolerance issues4
Unmet need with the treatment of postmenopausal symptoms
bull Alternatives to progestin are needed that will protect the endometrium while avoiding other progestin-associated effects and preserving the desired effects of estrogens in postmenopausal women3
Which women with a uterus could benefit from
estrogens without the need for a progestin
bull Women who are intolerant of progestin-containing hormone therapy
bull Women with pre-existing medical conditions that may be exacerbated by progestins (eg women with a history of depression PMSPMDD increased breast density diabetes and metabolic syndrome)
History of the following conditions may make progestin inappropriate
bull Depression
bull PMSPMDD
bull High breast density
bull Diabetes and metabolic syndrome
PMS premenstrual syndrome
PMD premenstrual dysphoric disorder
Medical conditions that may be exacerbated by treatment with progestins
Learning from WHI data
bull Hormone therapy (HT) is the conventional and established therapy option to effectively treat postmenopausal symptoms however it has been associated with some safety and tolerability concerns1 2
bull A review of WHI data suggests that many of the concerns with menopausal HT more often associated with EPT (CE+MPA) such as CHD risk increased breast density breast pain and breast cancer risk than with ET (CEE alone)2
1 Rolnick SJ Kopher RA DeFor TA et al Menopause 2005
2 Komm BS Mirkin S Pharmaceuticals 2012
WHI Womenrsquos Health Initiative trial
CHD coronary heart disease
CEE conjugated equine estrogens
Efficacy and Safety of Constant Oestrogen
Pulsed Progestogen vs
Continuous Combined HRT
Adverse Events
17b-oestradiol 17b-oestradiol norgestimate NETA (n = 150) (n = 172) Breast discomfort 14 27 Abdominal discomfort 14 22 Uterine bleeding 15 12 Dysmenorrhea 3 8 Oedema 5 8
Adapted from S Rozenberg et al Human Reproduction 2000
Medical condition which may be exacerbated by treatment
with progestins
Increased breast density
bull Increases in breast density are associated with progestin-containing HT which may adversely affect radiological detection of breast cancer1 and may be independently associated with an increased risk for the development of breast cancer2
bull The Postmenopausal EstrogenProgestin Interventions (PEPI) trial demonstrated that an increased mammographic breast density was associated with the use of E+P but not with the use of estrogen alone3
bull Women who already have high breast density may therefore be considered inappropriate for treatment with a progestin-containing HT
1) EU Core SPC for Hormone Replacement Therapy Products (CMDh1312003 Rev 4 June
2012)
2) De Villiers TJ et al on behalf of the International Menopause Society Climacteric 2013 16
3) Greendale GA et al J Natl Cancer Inst 2003
Stroke
0 25 5 75 10 125
Fractures
Diabetes
Breast cancer
Cholecystitis
Venothrombotic episodes
Endometrial cancer
Lung cancer
Coronary heart disease
Colorectal cancer
Overall mortality
15 125 10 75 5 25
Benefits Risks
CE
CE MPA
Santen RJ et al J Clin Endocrinol Metab 2010
The basis of the Endocrine Society scientific statement for postmenopausal hormone replacement therapy (HRT) excess risks and benefits of HRT for 5 years in women aged 50ndash59 years or within 10 years of the start of menopause E=estrogen P=progestin
bull Younger women (aged 50ndash59 years) had more favorable results bull There are differences between CE alone and CEMPA arms bull Overall benefitrisk ratio of CE-alone appears to be more favourable than CEMPA
Reevaluation of WHI data (stratified by age) Risks and
Benefits of HRT Cases per 1000 Women per 5 Years of
Use
Medical condition which may be exacerbated by treatment
with progestins
Diabetes and metabolic syndrome
bull Treatment of oestrogen deficiency symptoms with progestin-containing HT (unlike oestrogen alone) may be associated with increases in insulin resistance and deterioration in glucose tolerance123
bull Postmenopausal women with diabetes could be inappropriate for treatment with progestin-containing HT due to the potential risk of exacerbation of their condition
1) Panay N amp Studd JWW Human Reprod Update 1997
2) Godsland I et al Metabolism 1993
3) Sites CK et al J Clin Endocrinol Metab 2005
Variations in Associated Breast Cancer
Risks Between CE alone and CEMPA
bull Use of CE alone for a median of 59 years was associated with a lower incidence of invasive breast cancer (151 cases 027 per year) compared with placebo (199 cases 035 per year HR 077 95 CI 062ndash095 P=002)
bull In the CE alone group fewer women died from invasive breast cancer (6 deaths 0009 per year) compared with controls (16 deaths 0024 per year HR 037 95 CI 013ndash091 P=003)
Anderson GL et al Lancet
Oncol 2012
Bazedoxifene (BZA) specifically selected in
combination with conjugated estrogens
bull BZA has been specifically selected for its unique pharmacologic profile and effects on VMS and uterine tissue in particular123
1 Crabtree J et al Mol Cell Endocrinol 2008
2 Kharode Y et al Endocrinolology 2008
3 Duavive SmPC
Estrogen Receptor activity is dimmed
Estrogen Receptor activity is turned on
CEs are agonists BZA is an antagonist
In the uterus
bull The BZA component reduces the risk of endometrial hyperplasia that can occur with the conjugated estrogens component alone3 This means that progestins are not needed
Extensive global clinical development program for
CEBZA
aIncludes additional pilot dose-finding study 203 1 Lobo RA et al Fertil Steril 2009 2 Pinkerton JV et al Menopause 2009 3 Kagan R et al Menopause 2010 4 Mirkin S et al Climacteric 2013 5 Pinkerton JV et al Obstet Gynecol 2013
Effects of conjugated estrogensbazedoxifene on
lipid and coagulation variables a randomized
placebo- and active-controlled trial
bull At 12 months
bull Both CEBZA doses were associated with small but significant effects on hemostasis variables including reductions in antithrombin plasminogen activator inhibitor-1 and fibrinogen activity and an increase in plasminogen activity relative to placebo at 12 months Incidences of cardiovascular and venous thromboembolic events were similar among treatment groups
bull CONCLUSIONS
bull This study provides reassurance that CEBZA does not adversely affect lipid metabolism or hemostatic balance In accordance the incidences of venous thromboembolic events and cardiovascular events in postmenopausal women are similar to those observed with placebo
A Nath and R Sitruk-Ware CLIMACTERIC 200912(Suppl 1)96ndash101
A Nath and R Sitruk-Ware CLIMACTERIC 200912(Suppl 1)96ndash101
Diabetes an epidemy
bull UK 1996 14 million of diabetics
bull UK 2015 32 million (6 of the population)
bull UK 2025 5 million
bull httpwwwdiabetescoukdiabetes-prevalencehtml
Other progestin-related intolerance issues
bull Nausea
bull Depressive mood
bull Poor concentration
bull Hirsutism
bull Headache
bull Dizziness
bull Fluid retention
bull Weight gain Panay N amp Studd JWW Human Reprod Update 1997
Medical condition which may be exacerbated by treatment with progestins
PMSPMDDdepression
bull Progesterone-induced PMD can be exacerbated by exogenous progestin administration and can occur in association with HT or OC administration1
bull Significantly higher negative mood scores have been observed during the addition of a progestin to an estrogen in a sequential HT regimen in postmenopausal women with a history of PMS compared to those without2
bull Women with a history of PMS or PMD exacerbation of depression using progestins may therefore benefit from a progestin free treatment for menopausal symptoms
1) Nevatte T et al Arch Womens Ment Health 2013 2) Bjoumlrn I et al Climacteric 2006 PMS premenstrual syndrome
PMDD premenstrual dysphoric disorder
Conclusion
bull CEEBAZO is an additional regimen for menopausal symptoms it provides also a prevention for osteoporosis
bull It is suitable for women with a uterus who are unsatisfied with an EPT regimen or who you are unwilling to treat with an EPT regimen
For some postmenopausal women with a uterus there is a
need for progestin free treatment options
bull with demonstrated clinical efficacy
bull which protects the endometrium
bull improved tolerabilitysafety profile
In clinical practice this translates to women who are
intolerant of progestin-containing HT or have conditions
which may be exacerbated by treatment with progestins
Conclusion Medical need for alternative treatment option
Medical condition which may be exacerbated by treatment with progestins
Depression
bull Progestin-containing HT has been associated with increases in depressive symptoms in some individuals1
bull There is a biochemicalphysiological plausibility for the association of progestins with depression234
bull Therefore postmenopausal women who also have a medical history of depressive disorders or depression could be inappropriate for treatment with progestin-containing HT
Pfizer Confidential
65
1) Girdler SS et al J Womens Health Gend Based Med 1999 2) Traish AM et al Korean J Urol 2014 3) Stroumlhle A et al Biol Psychiatry 1999 4) Romeo E et
al Am J Psychiatry 1998
History of the following conditions may make progestin inappropriate
bull Depression
bull PMSPMDD
PMS premenstrual syndrome
PMD premenstrual dysphoric disorder
Medical conditions that may be exacerbated by treatment with progestins
Women for whom progestin-containing HT
would not be considered appropriate
minus Women who are intolerant of progestin-containing hormone therapy
minus Women with pre-existing medical conditions that may be exacerbated by progestins
Most common adverse events leading to discontinuation are related to progestins12
breakthrough bleeding
bull Increase in the number of uterine procedures (ie unnecessary endometrial biopsies)
breast paintenderness
bull Increase in the number of breast interventions
1 Steel SA et al Climacteric 2003 2 Ettinger B and Pressman A Am J Manag Care 1999 3 Komm BS Mirkin S
Pharmaceuticals 2012
4 Panay N amp Studd JWW Human Reprod Update 1997
bull Nausea bull Depressive mood bull Poor concentration bull Hirsutism bull Headache bull Dizziness bull Fluid retention bull Weight gain
Other progestin-related intolerance issues4
Unmet need with the treatment of postmenopausal symptoms
bull Alternatives to progestin are needed that will protect the endometrium while avoiding other progestin-associated effects and preserving the desired effects of estrogens in postmenopausal women3
Which women with a uterus could benefit from
estrogens without the need for a progestin
bull Women who are intolerant of progestin-containing hormone therapy
bull Women with pre-existing medical conditions that may be exacerbated by progestins (eg women with a history of depression PMSPMDD increased breast density diabetes and metabolic syndrome)
History of the following conditions may make progestin inappropriate
bull Depression
bull PMSPMDD
bull High breast density
bull Diabetes and metabolic syndrome
PMS premenstrual syndrome
PMD premenstrual dysphoric disorder
Medical conditions that may be exacerbated by treatment with progestins
Learning from WHI data
bull Hormone therapy (HT) is the conventional and established therapy option to effectively treat postmenopausal symptoms however it has been associated with some safety and tolerability concerns1 2
bull A review of WHI data suggests that many of the concerns with menopausal HT more often associated with EPT (CE+MPA) such as CHD risk increased breast density breast pain and breast cancer risk than with ET (CEE alone)2
1 Rolnick SJ Kopher RA DeFor TA et al Menopause 2005
2 Komm BS Mirkin S Pharmaceuticals 2012
WHI Womenrsquos Health Initiative trial
CHD coronary heart disease
CEE conjugated equine estrogens
Efficacy and Safety of Constant Oestrogen
Pulsed Progestogen vs
Continuous Combined HRT
Adverse Events
17b-oestradiol 17b-oestradiol norgestimate NETA (n = 150) (n = 172) Breast discomfort 14 27 Abdominal discomfort 14 22 Uterine bleeding 15 12 Dysmenorrhea 3 8 Oedema 5 8
Adapted from S Rozenberg et al Human Reproduction 2000
Medical condition which may be exacerbated by treatment
with progestins
Increased breast density
bull Increases in breast density are associated with progestin-containing HT which may adversely affect radiological detection of breast cancer1 and may be independently associated with an increased risk for the development of breast cancer2
bull The Postmenopausal EstrogenProgestin Interventions (PEPI) trial demonstrated that an increased mammographic breast density was associated with the use of E+P but not with the use of estrogen alone3
bull Women who already have high breast density may therefore be considered inappropriate for treatment with a progestin-containing HT
1) EU Core SPC for Hormone Replacement Therapy Products (CMDh1312003 Rev 4 June
2012)
2) De Villiers TJ et al on behalf of the International Menopause Society Climacteric 2013 16
3) Greendale GA et al J Natl Cancer Inst 2003
Stroke
0 25 5 75 10 125
Fractures
Diabetes
Breast cancer
Cholecystitis
Venothrombotic episodes
Endometrial cancer
Lung cancer
Coronary heart disease
Colorectal cancer
Overall mortality
15 125 10 75 5 25
Benefits Risks
CE
CE MPA
Santen RJ et al J Clin Endocrinol Metab 2010
The basis of the Endocrine Society scientific statement for postmenopausal hormone replacement therapy (HRT) excess risks and benefits of HRT for 5 years in women aged 50ndash59 years or within 10 years of the start of menopause E=estrogen P=progestin
bull Younger women (aged 50ndash59 years) had more favorable results bull There are differences between CE alone and CEMPA arms bull Overall benefitrisk ratio of CE-alone appears to be more favourable than CEMPA
Reevaluation of WHI data (stratified by age) Risks and
Benefits of HRT Cases per 1000 Women per 5 Years of
Use
Medical condition which may be exacerbated by treatment
with progestins
Diabetes and metabolic syndrome
bull Treatment of oestrogen deficiency symptoms with progestin-containing HT (unlike oestrogen alone) may be associated with increases in insulin resistance and deterioration in glucose tolerance123
bull Postmenopausal women with diabetes could be inappropriate for treatment with progestin-containing HT due to the potential risk of exacerbation of their condition
1) Panay N amp Studd JWW Human Reprod Update 1997
2) Godsland I et al Metabolism 1993
3) Sites CK et al J Clin Endocrinol Metab 2005
Variations in Associated Breast Cancer
Risks Between CE alone and CEMPA
bull Use of CE alone for a median of 59 years was associated with a lower incidence of invasive breast cancer (151 cases 027 per year) compared with placebo (199 cases 035 per year HR 077 95 CI 062ndash095 P=002)
bull In the CE alone group fewer women died from invasive breast cancer (6 deaths 0009 per year) compared with controls (16 deaths 0024 per year HR 037 95 CI 013ndash091 P=003)
Anderson GL et al Lancet
Oncol 2012
Bazedoxifene (BZA) specifically selected in
combination with conjugated estrogens
bull BZA has been specifically selected for its unique pharmacologic profile and effects on VMS and uterine tissue in particular123
1 Crabtree J et al Mol Cell Endocrinol 2008
2 Kharode Y et al Endocrinolology 2008
3 Duavive SmPC
Estrogen Receptor activity is dimmed
Estrogen Receptor activity is turned on
CEs are agonists BZA is an antagonist
In the uterus
bull The BZA component reduces the risk of endometrial hyperplasia that can occur with the conjugated estrogens component alone3 This means that progestins are not needed
Extensive global clinical development program for
CEBZA
aIncludes additional pilot dose-finding study 203 1 Lobo RA et al Fertil Steril 2009 2 Pinkerton JV et al Menopause 2009 3 Kagan R et al Menopause 2010 4 Mirkin S et al Climacteric 2013 5 Pinkerton JV et al Obstet Gynecol 2013
Effects of conjugated estrogensbazedoxifene on
lipid and coagulation variables a randomized
placebo- and active-controlled trial
bull At 12 months
bull Both CEBZA doses were associated with small but significant effects on hemostasis variables including reductions in antithrombin plasminogen activator inhibitor-1 and fibrinogen activity and an increase in plasminogen activity relative to placebo at 12 months Incidences of cardiovascular and venous thromboembolic events were similar among treatment groups
bull CONCLUSIONS
bull This study provides reassurance that CEBZA does not adversely affect lipid metabolism or hemostatic balance In accordance the incidences of venous thromboembolic events and cardiovascular events in postmenopausal women are similar to those observed with placebo

A Nath and R Sitruk-Ware CLIMACTERIC 200912(Suppl 1)96ndash101
Diabetes an epidemy
bull UK 1996 14 million of diabetics
bull UK 2015 32 million (6 of the population)
bull UK 2025 5 million
bull httpwwwdiabetescoukdiabetes-prevalencehtml
Other progestin-related intolerance issues
bull Nausea
bull Depressive mood
bull Poor concentration
bull Hirsutism
bull Headache
bull Dizziness
bull Fluid retention
bull Weight gain Panay N amp Studd JWW Human Reprod Update 1997
Medical condition which may be exacerbated by treatment with progestins
PMSPMDDdepression
bull Progesterone-induced PMD can be exacerbated by exogenous progestin administration and can occur in association with HT or OC administration1
bull Significantly higher negative mood scores have been observed during the addition of a progestin to an estrogen in a sequential HT regimen in postmenopausal women with a history of PMS compared to those without2
bull Women with a history of PMS or PMD exacerbation of depression using progestins may therefore benefit from a progestin free treatment for menopausal symptoms
1) Nevatte T et al Arch Womens Ment Health 2013 2) Bjoumlrn I et al Climacteric 2006 PMS premenstrual syndrome
PMDD premenstrual dysphoric disorder
Conclusion
bull CEEBAZO is an additional regimen for menopausal symptoms it provides also a prevention for osteoporosis
bull It is suitable for women with a uterus who are unsatisfied with an EPT regimen or who you are unwilling to treat with an EPT regimen
For some postmenopausal women with a uterus there is a
need for progestin free treatment options
bull with demonstrated clinical efficacy
bull which protects the endometrium
bull improved tolerabilitysafety profile
In clinical practice this translates to women who are
intolerant of progestin-containing HT or have conditions
which may be exacerbated by treatment with progestins
Conclusion Medical need for alternative treatment option
Medical condition which may be exacerbated by treatment with progestins
Depression
bull Progestin-containing HT has been associated with increases in depressive symptoms in some individuals1
bull There is a biochemicalphysiological plausibility for the association of progestins with depression234
bull Therefore postmenopausal women who also have a medical history of depressive disorders or depression could be inappropriate for treatment with progestin-containing HT
Pfizer Confidential
65
1) Girdler SS et al J Womens Health Gend Based Med 1999 2) Traish AM et al Korean J Urol 2014 3) Stroumlhle A et al Biol Psychiatry 1999 4) Romeo E et
al Am J Psychiatry 1998
History of the following conditions may make progestin inappropriate
bull Depression
bull PMSPMDD
PMS premenstrual syndrome
PMD premenstrual dysphoric disorder
Medical conditions that may be exacerbated by treatment with progestins
Women for whom progestin-containing HT
would not be considered appropriate
minus Women who are intolerant of progestin-containing hormone therapy
minus Women with pre-existing medical conditions that may be exacerbated by progestins
Most common adverse events leading to discontinuation are related to progestins12
breakthrough bleeding
bull Increase in the number of uterine procedures (ie unnecessary endometrial biopsies)
breast paintenderness
bull Increase in the number of breast interventions
1 Steel SA et al Climacteric 2003 2 Ettinger B and Pressman A Am J Manag Care 1999 3 Komm BS Mirkin S
Pharmaceuticals 2012
4 Panay N amp Studd JWW Human Reprod Update 1997
bull Nausea bull Depressive mood bull Poor concentration bull Hirsutism bull Headache bull Dizziness bull Fluid retention bull Weight gain
Other progestin-related intolerance issues4
Unmet need with the treatment of postmenopausal symptoms
bull Alternatives to progestin are needed that will protect the endometrium while avoiding other progestin-associated effects and preserving the desired effects of estrogens in postmenopausal women3
Which women with a uterus could benefit from
estrogens without the need for a progestin
bull Women who are intolerant of progestin-containing hormone therapy
bull Women with pre-existing medical conditions that may be exacerbated by progestins (eg women with a history of depression PMSPMDD increased breast density diabetes and metabolic syndrome)
History of the following conditions may make progestin inappropriate
bull Depression
bull PMSPMDD
bull High breast density
bull Diabetes and metabolic syndrome
PMS premenstrual syndrome
PMD premenstrual dysphoric disorder
Medical conditions that may be exacerbated by treatment with progestins
Learning from WHI data
bull Hormone therapy (HT) is the conventional and established therapy option to effectively treat postmenopausal symptoms however it has been associated with some safety and tolerability concerns1 2
bull A review of WHI data suggests that many of the concerns with menopausal HT more often associated with EPT (CE+MPA) such as CHD risk increased breast density breast pain and breast cancer risk than with ET (CEE alone)2
1 Rolnick SJ Kopher RA DeFor TA et al Menopause 2005
2 Komm BS Mirkin S Pharmaceuticals 2012
WHI Womenrsquos Health Initiative trial
CHD coronary heart disease
CEE conjugated equine estrogens
Efficacy and Safety of Constant Oestrogen
Pulsed Progestogen vs
Continuous Combined HRT
Adverse Events
17b-oestradiol 17b-oestradiol norgestimate NETA (n = 150) (n = 172) Breast discomfort 14 27 Abdominal discomfort 14 22 Uterine bleeding 15 12 Dysmenorrhea 3 8 Oedema 5 8
Adapted from S Rozenberg et al Human Reproduction 2000
Medical condition which may be exacerbated by treatment
with progestins
Increased breast density
bull Increases in breast density are associated with progestin-containing HT which may adversely affect radiological detection of breast cancer1 and may be independently associated with an increased risk for the development of breast cancer2
bull The Postmenopausal EstrogenProgestin Interventions (PEPI) trial demonstrated that an increased mammographic breast density was associated with the use of E+P but not with the use of estrogen alone3
bull Women who already have high breast density may therefore be considered inappropriate for treatment with a progestin-containing HT
1) EU Core SPC for Hormone Replacement Therapy Products (CMDh1312003 Rev 4 June
2012)
2) De Villiers TJ et al on behalf of the International Menopause Society Climacteric 2013 16
3) Greendale GA et al J Natl Cancer Inst 2003
Stroke
0 25 5 75 10 125
Fractures
Diabetes
Breast cancer
Cholecystitis
Venothrombotic episodes
Endometrial cancer
Lung cancer
Coronary heart disease
Colorectal cancer
Overall mortality
15 125 10 75 5 25
Benefits Risks
CE
CE MPA
Santen RJ et al J Clin Endocrinol Metab 2010
The basis of the Endocrine Society scientific statement for postmenopausal hormone replacement therapy (HRT) excess risks and benefits of HRT for 5 years in women aged 50ndash59 years or within 10 years of the start of menopause E=estrogen P=progestin
bull Younger women (aged 50ndash59 years) had more favorable results bull There are differences between CE alone and CEMPA arms bull Overall benefitrisk ratio of CE-alone appears to be more favourable than CEMPA
Reevaluation of WHI data (stratified by age) Risks and
Benefits of HRT Cases per 1000 Women per 5 Years of
Use
Medical condition which may be exacerbated by treatment
with progestins
Diabetes and metabolic syndrome
bull Treatment of oestrogen deficiency symptoms with progestin-containing HT (unlike oestrogen alone) may be associated with increases in insulin resistance and deterioration in glucose tolerance123
bull Postmenopausal women with diabetes could be inappropriate for treatment with progestin-containing HT due to the potential risk of exacerbation of their condition
1) Panay N amp Studd JWW Human Reprod Update 1997
2) Godsland I et al Metabolism 1993
3) Sites CK et al J Clin Endocrinol Metab 2005
Variations in Associated Breast Cancer
Risks Between CE alone and CEMPA
bull Use of CE alone for a median of 59 years was associated with a lower incidence of invasive breast cancer (151 cases 027 per year) compared with placebo (199 cases 035 per year HR 077 95 CI 062ndash095 P=002)
bull In the CE alone group fewer women died from invasive breast cancer (6 deaths 0009 per year) compared with controls (16 deaths 0024 per year HR 037 95 CI 013ndash091 P=003)
Anderson GL et al Lancet
Oncol 2012
Bazedoxifene (BZA) specifically selected in
combination with conjugated estrogens
bull BZA has been specifically selected for its unique pharmacologic profile and effects on VMS and uterine tissue in particular123
1 Crabtree J et al Mol Cell Endocrinol 2008
2 Kharode Y et al Endocrinolology 2008
3 Duavive SmPC
Estrogen Receptor activity is dimmed
Estrogen Receptor activity is turned on
CEs are agonists BZA is an antagonist
In the uterus
bull The BZA component reduces the risk of endometrial hyperplasia that can occur with the conjugated estrogens component alone3 This means that progestins are not needed
Extensive global clinical development program for
CEBZA
aIncludes additional pilot dose-finding study 203 1 Lobo RA et al Fertil Steril 2009 2 Pinkerton JV et al Menopause 2009 3 Kagan R et al Menopause 2010 4 Mirkin S et al Climacteric 2013 5 Pinkerton JV et al Obstet Gynecol 2013
Effects of conjugated estrogensbazedoxifene on
lipid and coagulation variables a randomized
placebo- and active-controlled trial
bull At 12 months
bull Both CEBZA doses were associated with small but significant effects on hemostasis variables including reductions in antithrombin plasminogen activator inhibitor-1 and fibrinogen activity and an increase in plasminogen activity relative to placebo at 12 months Incidences of cardiovascular and venous thromboembolic events were similar among treatment groups
bull CONCLUSIONS
bull This study provides reassurance that CEBZA does not adversely affect lipid metabolism or hemostatic balance In accordance the incidences of venous thromboembolic events and cardiovascular events in postmenopausal women are similar to those observed with placebo

Diabetes an epidemy
bull UK 1996 14 million of diabetics
bull UK 2015 32 million (6 of the population)
bull UK 2025 5 million
bull httpwwwdiabetescoukdiabetes-prevalencehtml
Other progestin-related intolerance issues
bull Nausea
bull Depressive mood
bull Poor concentration
bull Hirsutism
bull Headache
bull Dizziness
bull Fluid retention
bull Weight gain Panay N amp Studd JWW Human Reprod Update 1997
Medical condition which may be exacerbated by treatment with progestins
PMSPMDDdepression
bull Progesterone-induced PMD can be exacerbated by exogenous progestin administration and can occur in association with HT or OC administration1
bull Significantly higher negative mood scores have been observed during the addition of a progestin to an estrogen in a sequential HT regimen in postmenopausal women with a history of PMS compared to those without2
bull Women with a history of PMS or PMD exacerbation of depression using progestins may therefore benefit from a progestin free treatment for menopausal symptoms
1) Nevatte T et al Arch Womens Ment Health 2013 2) Bjoumlrn I et al Climacteric 2006 PMS premenstrual syndrome
PMDD premenstrual dysphoric disorder
Conclusion
bull CEEBAZO is an additional regimen for menopausal symptoms it provides also a prevention for osteoporosis
bull It is suitable for women with a uterus who are unsatisfied with an EPT regimen or who you are unwilling to treat with an EPT regimen
For some postmenopausal women with a uterus there is a
need for progestin free treatment options
bull with demonstrated clinical efficacy
bull which protects the endometrium
bull improved tolerabilitysafety profile
In clinical practice this translates to women who are
intolerant of progestin-containing HT or have conditions
which may be exacerbated by treatment with progestins
Conclusion Medical need for alternative treatment option
Medical condition which may be exacerbated by treatment with progestins
Depression
bull Progestin-containing HT has been associated with increases in depressive symptoms in some individuals1
bull There is a biochemicalphysiological plausibility for the association of progestins with depression234
bull Therefore postmenopausal women who also have a medical history of depressive disorders or depression could be inappropriate for treatment with progestin-containing HT
Pfizer Confidential
65
1) Girdler SS et al J Womens Health Gend Based Med 1999 2) Traish AM et al Korean J Urol 2014 3) Stroumlhle A et al Biol Psychiatry 1999 4) Romeo E et
al Am J Psychiatry 1998
History of the following conditions may make progestin inappropriate
bull Depression
bull PMSPMDD
PMS premenstrual syndrome
PMD premenstrual dysphoric disorder
Medical conditions that may be exacerbated by treatment with progestins
Women for whom progestin-containing HT
would not be considered appropriate
minus Women who are intolerant of progestin-containing hormone therapy
minus Women with pre-existing medical conditions that may be exacerbated by progestins
Most common adverse events leading to discontinuation are related to progestins12
breakthrough bleeding
bull Increase in the number of uterine procedures (ie unnecessary endometrial biopsies)
breast paintenderness
bull Increase in the number of breast interventions
1 Steel SA et al Climacteric 2003 2 Ettinger B and Pressman A Am J Manag Care 1999 3 Komm BS Mirkin S
Pharmaceuticals 2012
4 Panay N amp Studd JWW Human Reprod Update 1997
bull Nausea bull Depressive mood bull Poor concentration bull Hirsutism bull Headache bull Dizziness bull Fluid retention bull Weight gain
Other progestin-related intolerance issues4
Unmet need with the treatment of postmenopausal symptoms
bull Alternatives to progestin are needed that will protect the endometrium while avoiding other progestin-associated effects and preserving the desired effects of estrogens in postmenopausal women3
Which women with a uterus could benefit from
estrogens without the need for a progestin
bull Women who are intolerant of progestin-containing hormone therapy
bull Women with pre-existing medical conditions that may be exacerbated by progestins (eg women with a history of depression PMSPMDD increased breast density diabetes and metabolic syndrome)
History of the following conditions may make progestin inappropriate
bull Depression
bull PMSPMDD
bull High breast density
bull Diabetes and metabolic syndrome
PMS premenstrual syndrome
PMD premenstrual dysphoric disorder
Medical conditions that may be exacerbated by treatment with progestins
Learning from WHI data
bull Hormone therapy (HT) is the conventional and established therapy option to effectively treat postmenopausal symptoms however it has been associated with some safety and tolerability concerns1 2
bull A review of WHI data suggests that many of the concerns with menopausal HT more often associated with EPT (CE+MPA) such as CHD risk increased breast density breast pain and breast cancer risk than with ET (CEE alone)2
1 Rolnick SJ Kopher RA DeFor TA et al Menopause 2005
2 Komm BS Mirkin S Pharmaceuticals 2012
WHI Womenrsquos Health Initiative trial
CHD coronary heart disease
CEE conjugated equine estrogens
Efficacy and Safety of Constant Oestrogen
Pulsed Progestogen vs
Continuous Combined HRT
Adverse Events
17b-oestradiol 17b-oestradiol norgestimate NETA (n = 150) (n = 172) Breast discomfort 14 27 Abdominal discomfort 14 22 Uterine bleeding 15 12 Dysmenorrhea 3 8 Oedema 5 8
Adapted from S Rozenberg et al Human Reproduction 2000
Medical condition which may be exacerbated by treatment
with progestins
Increased breast density
bull Increases in breast density are associated with progestin-containing HT which may adversely affect radiological detection of breast cancer1 and may be independently associated with an increased risk for the development of breast cancer2
bull The Postmenopausal EstrogenProgestin Interventions (PEPI) trial demonstrated that an increased mammographic breast density was associated with the use of E+P but not with the use of estrogen alone3
bull Women who already have high breast density may therefore be considered inappropriate for treatment with a progestin-containing HT
1) EU Core SPC for Hormone Replacement Therapy Products (CMDh1312003 Rev 4 June
2012)
2) De Villiers TJ et al on behalf of the International Menopause Society Climacteric 2013 16
3) Greendale GA et al J Natl Cancer Inst 2003
Stroke
0 25 5 75 10 125
Fractures
Diabetes
Breast cancer
Cholecystitis
Venothrombotic episodes
Endometrial cancer
Lung cancer
Coronary heart disease
Colorectal cancer
Overall mortality
15 125 10 75 5 25
Benefits Risks
CE
CE MPA
Santen RJ et al J Clin Endocrinol Metab 2010
The basis of the Endocrine Society scientific statement for postmenopausal hormone replacement therapy (HRT) excess risks and benefits of HRT for 5 years in women aged 50ndash59 years or within 10 years of the start of menopause E=estrogen P=progestin
bull Younger women (aged 50ndash59 years) had more favorable results bull There are differences between CE alone and CEMPA arms bull Overall benefitrisk ratio of CE-alone appears to be more favourable than CEMPA
Reevaluation of WHI data (stratified by age) Risks and
Benefits of HRT Cases per 1000 Women per 5 Years of
Use
Medical condition which may be exacerbated by treatment
with progestins
Diabetes and metabolic syndrome
bull Treatment of oestrogen deficiency symptoms with progestin-containing HT (unlike oestrogen alone) may be associated with increases in insulin resistance and deterioration in glucose tolerance123
bull Postmenopausal women with diabetes could be inappropriate for treatment with progestin-containing HT due to the potential risk of exacerbation of their condition
1) Panay N amp Studd JWW Human Reprod Update 1997
2) Godsland I et al Metabolism 1993
3) Sites CK et al J Clin Endocrinol Metab 2005
Variations in Associated Breast Cancer
Risks Between CE alone and CEMPA
bull Use of CE alone for a median of 59 years was associated with a lower incidence of invasive breast cancer (151 cases 027 per year) compared with placebo (199 cases 035 per year HR 077 95 CI 062ndash095 P=002)
bull In the CE alone group fewer women died from invasive breast cancer (6 deaths 0009 per year) compared with controls (16 deaths 0024 per year HR 037 95 CI 013ndash091 P=003)
Anderson GL et al Lancet
Oncol 2012
Bazedoxifene (BZA) specifically selected in
combination with conjugated estrogens
bull BZA has been specifically selected for its unique pharmacologic profile and effects on VMS and uterine tissue in particular123
1 Crabtree J et al Mol Cell Endocrinol 2008
2 Kharode Y et al Endocrinolology 2008
3 Duavive SmPC
Estrogen Receptor activity is dimmed
Estrogen Receptor activity is turned on
CEs are agonists BZA is an antagonist
In the uterus
bull The BZA component reduces the risk of endometrial hyperplasia that can occur with the conjugated estrogens component alone3 This means that progestins are not needed
Extensive global clinical development program for
CEBZA
aIncludes additional pilot dose-finding study 203 1 Lobo RA et al Fertil Steril 2009 2 Pinkerton JV et al Menopause 2009 3 Kagan R et al Menopause 2010 4 Mirkin S et al Climacteric 2013 5 Pinkerton JV et al Obstet Gynecol 2013
Effects of conjugated estrogensbazedoxifene on
lipid and coagulation variables a randomized
placebo- and active-controlled trial
bull At 12 months
bull Both CEBZA doses were associated with small but significant effects on hemostasis variables including reductions in antithrombin plasminogen activator inhibitor-1 and fibrinogen activity and an increase in plasminogen activity relative to placebo at 12 months Incidences of cardiovascular and venous thromboembolic events were similar among treatment groups
bull CONCLUSIONS
bull This study provides reassurance that CEBZA does not adversely affect lipid metabolism or hemostatic balance In accordance the incidences of venous thromboembolic events and cardiovascular events in postmenopausal women are similar to those observed with placebo

Other progestin-related intolerance issues
bull Nausea
bull Depressive mood
bull Poor concentration
bull Hirsutism
bull Headache
bull Dizziness
bull Fluid retention
bull Weight gain Panay N amp Studd JWW Human Reprod Update 1997
Medical condition which may be exacerbated by treatment with progestins
PMSPMDDdepression
bull Progesterone-induced PMD can be exacerbated by exogenous progestin administration and can occur in association with HT or OC administration1
bull Significantly higher negative mood scores have been observed during the addition of a progestin to an estrogen in a sequential HT regimen in postmenopausal women with a history of PMS compared to those without2
bull Women with a history of PMS or PMD exacerbation of depression using progestins may therefore benefit from a progestin free treatment for menopausal symptoms
1) Nevatte T et al Arch Womens Ment Health 2013 2) Bjoumlrn I et al Climacteric 2006 PMS premenstrual syndrome
PMDD premenstrual dysphoric disorder
Conclusion
bull CEEBAZO is an additional regimen for menopausal symptoms it provides also a prevention for osteoporosis
bull It is suitable for women with a uterus who are unsatisfied with an EPT regimen or who you are unwilling to treat with an EPT regimen
For some postmenopausal women with a uterus there is a
need for progestin free treatment options
bull with demonstrated clinical efficacy
bull which protects the endometrium
bull improved tolerabilitysafety profile
In clinical practice this translates to women who are
intolerant of progestin-containing HT or have conditions
which may be exacerbated by treatment with progestins
Conclusion Medical need for alternative treatment option
Medical condition which may be exacerbated by treatment with progestins
Depression
bull Progestin-containing HT has been associated with increases in depressive symptoms in some individuals1
bull There is a biochemicalphysiological plausibility for the association of progestins with depression234
bull Therefore postmenopausal women who also have a medical history of depressive disorders or depression could be inappropriate for treatment with progestin-containing HT
Pfizer Confidential
65
1) Girdler SS et al J Womens Health Gend Based Med 1999 2) Traish AM et al Korean J Urol 2014 3) Stroumlhle A et al Biol Psychiatry 1999 4) Romeo E et
al Am J Psychiatry 1998
History of the following conditions may make progestin inappropriate
bull Depression
bull PMSPMDD
PMS premenstrual syndrome
PMD premenstrual dysphoric disorder
Medical conditions that may be exacerbated by treatment with progestins
Women for whom progestin-containing HT
would not be considered appropriate
minus Women who are intolerant of progestin-containing hormone therapy
minus Women with pre-existing medical conditions that may be exacerbated by progestins
Most common adverse events leading to discontinuation are related to progestins12
breakthrough bleeding
bull Increase in the number of uterine procedures (ie unnecessary endometrial biopsies)
breast paintenderness
bull Increase in the number of breast interventions
1 Steel SA et al Climacteric 2003 2 Ettinger B and Pressman A Am J Manag Care 1999 3 Komm BS Mirkin S
Pharmaceuticals 2012
4 Panay N amp Studd JWW Human Reprod Update 1997
bull Nausea bull Depressive mood bull Poor concentration bull Hirsutism bull Headache bull Dizziness bull Fluid retention bull Weight gain
Other progestin-related intolerance issues4
Unmet need with the treatment of postmenopausal symptoms
bull Alternatives to progestin are needed that will protect the endometrium while avoiding other progestin-associated effects and preserving the desired effects of estrogens in postmenopausal women3
Which women with a uterus could benefit from
estrogens without the need for a progestin
bull Women who are intolerant of progestin-containing hormone therapy
bull Women with pre-existing medical conditions that may be exacerbated by progestins (eg women with a history of depression PMSPMDD increased breast density diabetes and metabolic syndrome)
History of the following conditions may make progestin inappropriate
bull Depression
bull PMSPMDD
bull High breast density
bull Diabetes and metabolic syndrome
PMS premenstrual syndrome
PMD premenstrual dysphoric disorder
Medical conditions that may be exacerbated by treatment with progestins
Learning from WHI data
bull Hormone therapy (HT) is the conventional and established therapy option to effectively treat postmenopausal symptoms however it has been associated with some safety and tolerability concerns1 2
bull A review of WHI data suggests that many of the concerns with menopausal HT more often associated with EPT (CE+MPA) such as CHD risk increased breast density breast pain and breast cancer risk than with ET (CEE alone)2
1 Rolnick SJ Kopher RA DeFor TA et al Menopause 2005
2 Komm BS Mirkin S Pharmaceuticals 2012
WHI Womenrsquos Health Initiative trial
CHD coronary heart disease
CEE conjugated equine estrogens
Efficacy and Safety of Constant Oestrogen
Pulsed Progestogen vs
Continuous Combined HRT
Adverse Events
17b-oestradiol 17b-oestradiol norgestimate NETA (n = 150) (n = 172) Breast discomfort 14 27 Abdominal discomfort 14 22 Uterine bleeding 15 12 Dysmenorrhea 3 8 Oedema 5 8
Adapted from S Rozenberg et al Human Reproduction 2000
Medical condition which may be exacerbated by treatment
with progestins
Increased breast density
bull Increases in breast density are associated with progestin-containing HT which may adversely affect radiological detection of breast cancer1 and may be independently associated with an increased risk for the development of breast cancer2
bull The Postmenopausal EstrogenProgestin Interventions (PEPI) trial demonstrated that an increased mammographic breast density was associated with the use of E+P but not with the use of estrogen alone3
bull Women who already have high breast density may therefore be considered inappropriate for treatment with a progestin-containing HT
1) EU Core SPC for Hormone Replacement Therapy Products (CMDh1312003 Rev 4 June
2012)
2) De Villiers TJ et al on behalf of the International Menopause Society Climacteric 2013 16
3) Greendale GA et al J Natl Cancer Inst 2003
Stroke
0 25 5 75 10 125
Fractures
Diabetes
Breast cancer
Cholecystitis
Venothrombotic episodes
Endometrial cancer
Lung cancer
Coronary heart disease
Colorectal cancer
Overall mortality
15 125 10 75 5 25
Benefits Risks
CE
CE MPA
Santen RJ et al J Clin Endocrinol Metab 2010
The basis of the Endocrine Society scientific statement for postmenopausal hormone replacement therapy (HRT) excess risks and benefits of HRT for 5 years in women aged 50ndash59 years or within 10 years of the start of menopause E=estrogen P=progestin
bull Younger women (aged 50ndash59 years) had more favorable results bull There are differences between CE alone and CEMPA arms bull Overall benefitrisk ratio of CE-alone appears to be more favourable than CEMPA
Reevaluation of WHI data (stratified by age) Risks and
Benefits of HRT Cases per 1000 Women per 5 Years of
Use
Medical condition which may be exacerbated by treatment
with progestins
Diabetes and metabolic syndrome
bull Treatment of oestrogen deficiency symptoms with progestin-containing HT (unlike oestrogen alone) may be associated with increases in insulin resistance and deterioration in glucose tolerance123
bull Postmenopausal women with diabetes could be inappropriate for treatment with progestin-containing HT due to the potential risk of exacerbation of their condition
1) Panay N amp Studd JWW Human Reprod Update 1997
2) Godsland I et al Metabolism 1993
3) Sites CK et al J Clin Endocrinol Metab 2005
Variations in Associated Breast Cancer
Risks Between CE alone and CEMPA
bull Use of CE alone for a median of 59 years was associated with a lower incidence of invasive breast cancer (151 cases 027 per year) compared with placebo (199 cases 035 per year HR 077 95 CI 062ndash095 P=002)
bull In the CE alone group fewer women died from invasive breast cancer (6 deaths 0009 per year) compared with controls (16 deaths 0024 per year HR 037 95 CI 013ndash091 P=003)
Anderson GL et al Lancet
Oncol 2012
Bazedoxifene (BZA) specifically selected in
combination with conjugated estrogens
bull BZA has been specifically selected for its unique pharmacologic profile and effects on VMS and uterine tissue in particular123
1 Crabtree J et al Mol Cell Endocrinol 2008
2 Kharode Y et al Endocrinolology 2008
3 Duavive SmPC
Estrogen Receptor activity is dimmed
Estrogen Receptor activity is turned on
CEs are agonists BZA is an antagonist
In the uterus
bull The BZA component reduces the risk of endometrial hyperplasia that can occur with the conjugated estrogens component alone3 This means that progestins are not needed
Extensive global clinical development program for
CEBZA
aIncludes additional pilot dose-finding study 203 1 Lobo RA et al Fertil Steril 2009 2 Pinkerton JV et al Menopause 2009 3 Kagan R et al Menopause 2010 4 Mirkin S et al Climacteric 2013 5 Pinkerton JV et al Obstet Gynecol 2013
Effects of conjugated estrogensbazedoxifene on
lipid and coagulation variables a randomized
placebo- and active-controlled trial
bull At 12 months
bull Both CEBZA doses were associated with small but significant effects on hemostasis variables including reductions in antithrombin plasminogen activator inhibitor-1 and fibrinogen activity and an increase in plasminogen activity relative to placebo at 12 months Incidences of cardiovascular and venous thromboembolic events were similar among treatment groups
bull CONCLUSIONS
bull This study provides reassurance that CEBZA does not adversely affect lipid metabolism or hemostatic balance In accordance the incidences of venous thromboembolic events and cardiovascular events in postmenopausal women are similar to those observed with placebo
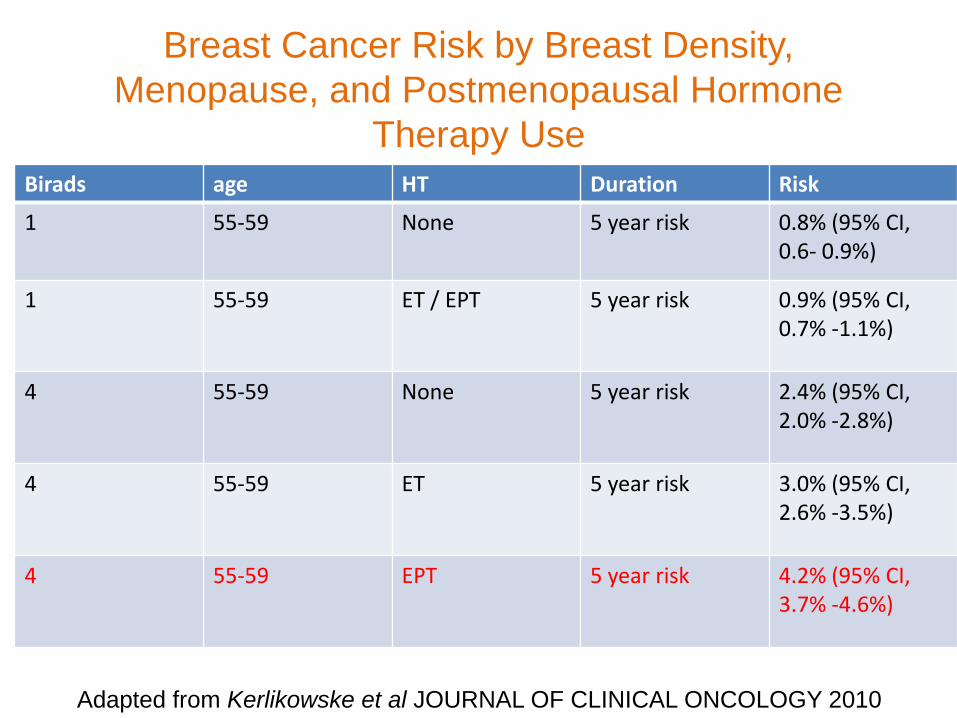
Medical condition which may be exacerbated by treatment with progestins
PMSPMDDdepression
bull Progesterone-induced PMD can be exacerbated by exogenous progestin administration and can occur in association with HT or OC administration1
bull Significantly higher negative mood scores have been observed during the addition of a progestin to an estrogen in a sequential HT regimen in postmenopausal women with a history of PMS compared to those without2
bull Women with a history of PMS or PMD exacerbation of depression using progestins may therefore benefit from a progestin free treatment for menopausal symptoms
1) Nevatte T et al Arch Womens Ment Health 2013 2) Bjoumlrn I et al Climacteric 2006 PMS premenstrual syndrome
PMDD premenstrual dysphoric disorder
Conclusion
bull CEEBAZO is an additional regimen for menopausal symptoms it provides also a prevention for osteoporosis
bull It is suitable for women with a uterus who are unsatisfied with an EPT regimen or who you are unwilling to treat with an EPT regimen
For some postmenopausal women with a uterus there is a
need for progestin free treatment options
bull with demonstrated clinical efficacy
bull which protects the endometrium
bull improved tolerabilitysafety profile
In clinical practice this translates to women who are
intolerant of progestin-containing HT or have conditions
which may be exacerbated by treatment with progestins
Conclusion Medical need for alternative treatment option
Medical condition which may be exacerbated by treatment with progestins
Depression
bull Progestin-containing HT has been associated with increases in depressive symptoms in some individuals1
bull There is a biochemicalphysiological plausibility for the association of progestins with depression234
bull Therefore postmenopausal women who also have a medical history of depressive disorders or depression could be inappropriate for treatment with progestin-containing HT
Pfizer Confidential
65
1) Girdler SS et al J Womens Health Gend Based Med 1999 2) Traish AM et al Korean J Urol 2014 3) Stroumlhle A et al Biol Psychiatry 1999 4) Romeo E et
al Am J Psychiatry 1998
History of the following conditions may make progestin inappropriate
bull Depression
bull PMSPMDD
PMS premenstrual syndrome
PMD premenstrual dysphoric disorder
Medical conditions that may be exacerbated by treatment with progestins
Women for whom progestin-containing HT
would not be considered appropriate
minus Women who are intolerant of progestin-containing hormone therapy
minus Women with pre-existing medical conditions that may be exacerbated by progestins
Most common adverse events leading to discontinuation are related to progestins12
breakthrough bleeding
bull Increase in the number of uterine procedures (ie unnecessary endometrial biopsies)
breast paintenderness
bull Increase in the number of breast interventions
1 Steel SA et al Climacteric 2003 2 Ettinger B and Pressman A Am J Manag Care 1999 3 Komm BS Mirkin S
Pharmaceuticals 2012
4 Panay N amp Studd JWW Human Reprod Update 1997
bull Nausea bull Depressive mood bull Poor concentration bull Hirsutism bull Headache bull Dizziness bull Fluid retention bull Weight gain
Other progestin-related intolerance issues4
Unmet need with the treatment of postmenopausal symptoms
bull Alternatives to progestin are needed that will protect the endometrium while avoiding other progestin-associated effects and preserving the desired effects of estrogens in postmenopausal women3
Which women with a uterus could benefit from
estrogens without the need for a progestin
bull Women who are intolerant of progestin-containing hormone therapy
bull Women with pre-existing medical conditions that may be exacerbated by progestins (eg women with a history of depression PMSPMDD increased breast density diabetes and metabolic syndrome)
History of the following conditions may make progestin inappropriate
bull Depression
bull PMSPMDD
bull High breast density
bull Diabetes and metabolic syndrome
PMS premenstrual syndrome
PMD premenstrual dysphoric disorder
Medical conditions that may be exacerbated by treatment with progestins
Learning from WHI data
bull Hormone therapy (HT) is the conventional and established therapy option to effectively treat postmenopausal symptoms however it has been associated with some safety and tolerability concerns1 2
bull A review of WHI data suggests that many of the concerns with menopausal HT more often associated with EPT (CE+MPA) such as CHD risk increased breast density breast pain and breast cancer risk than with ET (CEE alone)2
1 Rolnick SJ Kopher RA DeFor TA et al Menopause 2005
2 Komm BS Mirkin S Pharmaceuticals 2012
WHI Womenrsquos Health Initiative trial
CHD coronary heart disease
CEE conjugated equine estrogens
Efficacy and Safety of Constant Oestrogen
Pulsed Progestogen vs
Continuous Combined HRT
Adverse Events
17b-oestradiol 17b-oestradiol norgestimate NETA (n = 150) (n = 172) Breast discomfort 14 27 Abdominal discomfort 14 22 Uterine bleeding 15 12 Dysmenorrhea 3 8 Oedema 5 8
Adapted from S Rozenberg et al Human Reproduction 2000
Medical condition which may be exacerbated by treatment
with progestins
Increased breast density
bull Increases in breast density are associated with progestin-containing HT which may adversely affect radiological detection of breast cancer1 and may be independently associated with an increased risk for the development of breast cancer2
bull The Postmenopausal EstrogenProgestin Interventions (PEPI) trial demonstrated that an increased mammographic breast density was associated with the use of E+P but not with the use of estrogen alone3
bull Women who already have high breast density may therefore be considered inappropriate for treatment with a progestin-containing HT
1) EU Core SPC for Hormone Replacement Therapy Products (CMDh1312003 Rev 4 June
2012)
2) De Villiers TJ et al on behalf of the International Menopause Society Climacteric 2013 16
3) Greendale GA et al J Natl Cancer Inst 2003
Stroke
0 25 5 75 10 125
Fractures
Diabetes
Breast cancer
Cholecystitis
Venothrombotic episodes
Endometrial cancer
Lung cancer
Coronary heart disease
Colorectal cancer
Overall mortality
15 125 10 75 5 25
Benefits Risks
CE
CE MPA
Santen RJ et al J Clin Endocrinol Metab 2010
The basis of the Endocrine Society scientific statement for postmenopausal hormone replacement therapy (HRT) excess risks and benefits of HRT for 5 years in women aged 50ndash59 years or within 10 years of the start of menopause E=estrogen P=progestin
bull Younger women (aged 50ndash59 years) had more favorable results bull There are differences between CE alone and CEMPA arms bull Overall benefitrisk ratio of CE-alone appears to be more favourable than CEMPA
Reevaluation of WHI data (stratified by age) Risks and
Benefits of HRT Cases per 1000 Women per 5 Years of
Use
Medical condition which may be exacerbated by treatment
with progestins
Diabetes and metabolic syndrome
bull Treatment of oestrogen deficiency symptoms with progestin-containing HT (unlike oestrogen alone) may be associated with increases in insulin resistance and deterioration in glucose tolerance123
bull Postmenopausal women with diabetes could be inappropriate for treatment with progestin-containing HT due to the potential risk of exacerbation of their condition
1) Panay N amp Studd JWW Human Reprod Update 1997
2) Godsland I et al Metabolism 1993
3) Sites CK et al J Clin Endocrinol Metab 2005
Variations in Associated Breast Cancer
Risks Between CE alone and CEMPA
bull Use of CE alone for a median of 59 years was associated with a lower incidence of invasive breast cancer (151 cases 027 per year) compared with placebo (199 cases 035 per year HR 077 95 CI 062ndash095 P=002)
bull In the CE alone group fewer women died from invasive breast cancer (6 deaths 0009 per year) compared with controls (16 deaths 0024 per year HR 037 95 CI 013ndash091 P=003)
Anderson GL et al Lancet
Oncol 2012
Bazedoxifene (BZA) specifically selected in
combination with conjugated estrogens
bull BZA has been specifically selected for its unique pharmacologic profile and effects on VMS and uterine tissue in particular123
1 Crabtree J et al Mol Cell Endocrinol 2008
2 Kharode Y et al Endocrinolology 2008
3 Duavive SmPC
Estrogen Receptor activity is dimmed
Estrogen Receptor activity is turned on
CEs are agonists BZA is an antagonist
In the uterus
bull The BZA component reduces the risk of endometrial hyperplasia that can occur with the conjugated estrogens component alone3 This means that progestins are not needed
Extensive global clinical development program for
CEBZA
aIncludes additional pilot dose-finding study 203 1 Lobo RA et al Fertil Steril 2009 2 Pinkerton JV et al Menopause 2009 3 Kagan R et al Menopause 2010 4 Mirkin S et al Climacteric 2013 5 Pinkerton JV et al Obstet Gynecol 2013
Effects of conjugated estrogensbazedoxifene on
lipid and coagulation variables a randomized
placebo- and active-controlled trial
bull At 12 months
bull Both CEBZA doses were associated with small but significant effects on hemostasis variables including reductions in antithrombin plasminogen activator inhibitor-1 and fibrinogen activity and an increase in plasminogen activity relative to placebo at 12 months Incidences of cardiovascular and venous thromboembolic events were similar among treatment groups
bull CONCLUSIONS
bull This study provides reassurance that CEBZA does not adversely affect lipid metabolism or hemostatic balance In accordance the incidences of venous thromboembolic events and cardiovascular events in postmenopausal women are similar to those observed with placebo
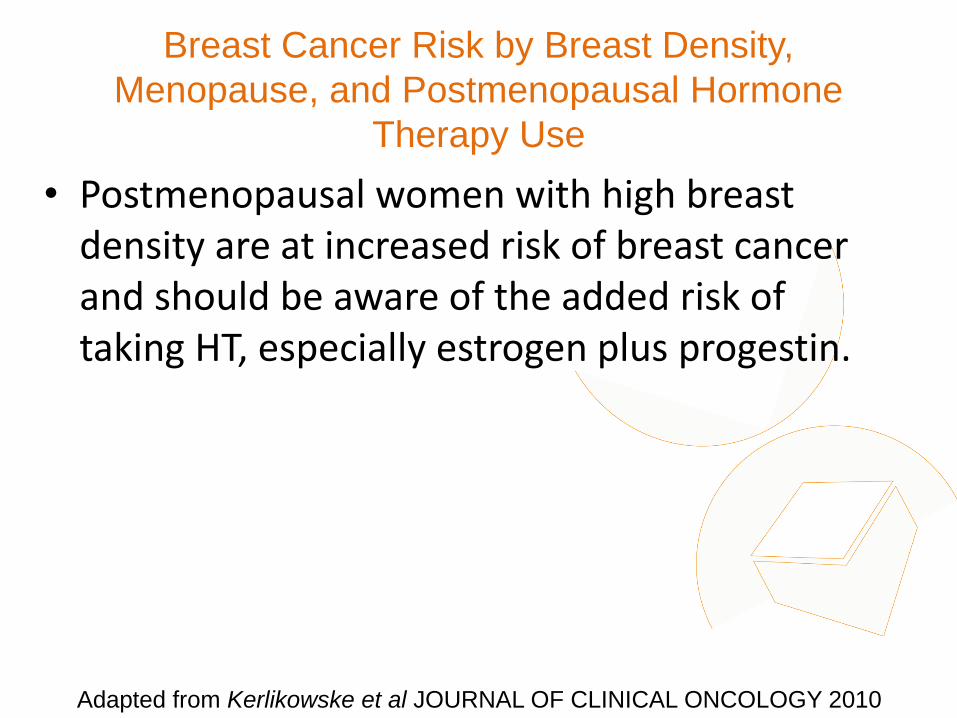
Conclusion
bull CEEBAZO is an additional regimen for menopausal symptoms it provides also a prevention for osteoporosis
bull It is suitable for women with a uterus who are unsatisfied with an EPT regimen or who you are unwilling to treat with an EPT regimen
For some postmenopausal women with a uterus there is a
need for progestin free treatment options
bull with demonstrated clinical efficacy
bull which protects the endometrium
bull improved tolerabilitysafety profile
In clinical practice this translates to women who are
intolerant of progestin-containing HT or have conditions
which may be exacerbated by treatment with progestins
Conclusion Medical need for alternative treatment option
Medical condition which may be exacerbated by treatment with progestins
Depression
bull Progestin-containing HT has been associated with increases in depressive symptoms in some individuals1
bull There is a biochemicalphysiological plausibility for the association of progestins with depression234
bull Therefore postmenopausal women who also have a medical history of depressive disorders or depression could be inappropriate for treatment with progestin-containing HT
Pfizer Confidential
65
1) Girdler SS et al J Womens Health Gend Based Med 1999 2) Traish AM et al Korean J Urol 2014 3) Stroumlhle A et al Biol Psychiatry 1999 4) Romeo E et
al Am J Psychiatry 1998
History of the following conditions may make progestin inappropriate
bull Depression
bull PMSPMDD
PMS premenstrual syndrome
PMD premenstrual dysphoric disorder
Medical conditions that may be exacerbated by treatment with progestins
Women for whom progestin-containing HT
would not be considered appropriate
minus Women who are intolerant of progestin-containing hormone therapy
minus Women with pre-existing medical conditions that may be exacerbated by progestins
Most common adverse events leading to discontinuation are related to progestins12
breakthrough bleeding
bull Increase in the number of uterine procedures (ie unnecessary endometrial biopsies)
breast paintenderness
bull Increase in the number of breast interventions
1 Steel SA et al Climacteric 2003 2 Ettinger B and Pressman A Am J Manag Care 1999 3 Komm BS Mirkin S
Pharmaceuticals 2012
4 Panay N amp Studd JWW Human Reprod Update 1997
bull Nausea bull Depressive mood bull Poor concentration bull Hirsutism bull Headache bull Dizziness bull Fluid retention bull Weight gain
Other progestin-related intolerance issues4
Unmet need with the treatment of postmenopausal symptoms
bull Alternatives to progestin are needed that will protect the endometrium while avoiding other progestin-associated effects and preserving the desired effects of estrogens in postmenopausal women3
Which women with a uterus could benefit from
estrogens without the need for a progestin
bull Women who are intolerant of progestin-containing hormone therapy
bull Women with pre-existing medical conditions that may be exacerbated by progestins (eg women with a history of depression PMSPMDD increased breast density diabetes and metabolic syndrome)
History of the following conditions may make progestin inappropriate
bull Depression
bull PMSPMDD
bull High breast density
bull Diabetes and metabolic syndrome
PMS premenstrual syndrome
PMD premenstrual dysphoric disorder
Medical conditions that may be exacerbated by treatment with progestins
Learning from WHI data
bull Hormone therapy (HT) is the conventional and established therapy option to effectively treat postmenopausal symptoms however it has been associated with some safety and tolerability concerns1 2
bull A review of WHI data suggests that many of the concerns with menopausal HT more often associated with EPT (CE+MPA) such as CHD risk increased breast density breast pain and breast cancer risk than with ET (CEE alone)2
1 Rolnick SJ Kopher RA DeFor TA et al Menopause 2005
2 Komm BS Mirkin S Pharmaceuticals 2012
WHI Womenrsquos Health Initiative trial
CHD coronary heart disease
CEE conjugated equine estrogens
Efficacy and Safety of Constant Oestrogen
Pulsed Progestogen vs
Continuous Combined HRT
Adverse Events
17b-oestradiol 17b-oestradiol norgestimate NETA (n = 150) (n = 172) Breast discomfort 14 27 Abdominal discomfort 14 22 Uterine bleeding 15 12 Dysmenorrhea 3 8 Oedema 5 8
Adapted from S Rozenberg et al Human Reproduction 2000
Medical condition which may be exacerbated by treatment
with progestins
Increased breast density
bull Increases in breast density are associated with progestin-containing HT which may adversely affect radiological detection of breast cancer1 and may be independently associated with an increased risk for the development of breast cancer2
bull The Postmenopausal EstrogenProgestin Interventions (PEPI) trial demonstrated that an increased mammographic breast density was associated with the use of E+P but not with the use of estrogen alone3
bull Women who already have high breast density may therefore be considered inappropriate for treatment with a progestin-containing HT
1) EU Core SPC for Hormone Replacement Therapy Products (CMDh1312003 Rev 4 June
2012)
2) De Villiers TJ et al on behalf of the International Menopause Society Climacteric 2013 16
3) Greendale GA et al J Natl Cancer Inst 2003
Stroke
0 25 5 75 10 125
Fractures
Diabetes
Breast cancer
Cholecystitis
Venothrombotic episodes
Endometrial cancer
Lung cancer
Coronary heart disease
Colorectal cancer
Overall mortality
15 125 10 75 5 25
Benefits Risks
CE
CE MPA
Santen RJ et al J Clin Endocrinol Metab 2010
The basis of the Endocrine Society scientific statement for postmenopausal hormone replacement therapy (HRT) excess risks and benefits of HRT for 5 years in women aged 50ndash59 years or within 10 years of the start of menopause E=estrogen P=progestin
bull Younger women (aged 50ndash59 years) had more favorable results bull There are differences between CE alone and CEMPA arms bull Overall benefitrisk ratio of CE-alone appears to be more favourable than CEMPA
Reevaluation of WHI data (stratified by age) Risks and
Benefits of HRT Cases per 1000 Women per 5 Years of
Use
Medical condition which may be exacerbated by treatment
with progestins
Diabetes and metabolic syndrome
bull Treatment of oestrogen deficiency symptoms with progestin-containing HT (unlike oestrogen alone) may be associated with increases in insulin resistance and deterioration in glucose tolerance123
bull Postmenopausal women with diabetes could be inappropriate for treatment with progestin-containing HT due to the potential risk of exacerbation of their condition
1) Panay N amp Studd JWW Human Reprod Update 1997
2) Godsland I et al Metabolism 1993
3) Sites CK et al J Clin Endocrinol Metab 2005
Variations in Associated Breast Cancer
Risks Between CE alone and CEMPA
bull Use of CE alone for a median of 59 years was associated with a lower incidence of invasive breast cancer (151 cases 027 per year) compared with placebo (199 cases 035 per year HR 077 95 CI 062ndash095 P=002)
bull In the CE alone group fewer women died from invasive breast cancer (6 deaths 0009 per year) compared with controls (16 deaths 0024 per year HR 037 95 CI 013ndash091 P=003)
Anderson GL et al Lancet
Oncol 2012
Bazedoxifene (BZA) specifically selected in
combination with conjugated estrogens
bull BZA has been specifically selected for its unique pharmacologic profile and effects on VMS and uterine tissue in particular123
1 Crabtree J et al Mol Cell Endocrinol 2008
2 Kharode Y et al Endocrinolology 2008
3 Duavive SmPC
Estrogen Receptor activity is dimmed
Estrogen Receptor activity is turned on
CEs are agonists BZA is an antagonist
In the uterus
bull The BZA component reduces the risk of endometrial hyperplasia that can occur with the conjugated estrogens component alone3 This means that progestins are not needed
Extensive global clinical development program for
CEBZA
aIncludes additional pilot dose-finding study 203 1 Lobo RA et al Fertil Steril 2009 2 Pinkerton JV et al Menopause 2009 3 Kagan R et al Menopause 2010 4 Mirkin S et al Climacteric 2013 5 Pinkerton JV et al Obstet Gynecol 2013
Effects of conjugated estrogensbazedoxifene on
lipid and coagulation variables a randomized
placebo- and active-controlled trial
bull At 12 months
bull Both CEBZA doses were associated with small but significant effects on hemostasis variables including reductions in antithrombin plasminogen activator inhibitor-1 and fibrinogen activity and an increase in plasminogen activity relative to placebo at 12 months Incidences of cardiovascular and venous thromboembolic events were similar among treatment groups
bull CONCLUSIONS
bull This study provides reassurance that CEBZA does not adversely affect lipid metabolism or hemostatic balance In accordance the incidences of venous thromboembolic events and cardiovascular events in postmenopausal women are similar to those observed with placebo

For some postmenopausal women with a uterus there is a
need for progestin free treatment options
bull with demonstrated clinical efficacy
bull which protects the endometrium
bull improved tolerabilitysafety profile
In clinical practice this translates to women who are
intolerant of progestin-containing HT or have conditions
which may be exacerbated by treatment with progestins
Conclusion Medical need for alternative treatment option
Medical condition which may be exacerbated by treatment with progestins
Depression
bull Progestin-containing HT has been associated with increases in depressive symptoms in some individuals1
bull There is a biochemicalphysiological plausibility for the association of progestins with depression234
bull Therefore postmenopausal women who also have a medical history of depressive disorders or depression could be inappropriate for treatment with progestin-containing HT
Pfizer Confidential
65
1) Girdler SS et al J Womens Health Gend Based Med 1999 2) Traish AM et al Korean J Urol 2014 3) Stroumlhle A et al Biol Psychiatry 1999 4) Romeo E et
al Am J Psychiatry 1998
History of the following conditions may make progestin inappropriate
bull Depression
bull PMSPMDD
PMS premenstrual syndrome
PMD premenstrual dysphoric disorder
Medical conditions that may be exacerbated by treatment with progestins
Women for whom progestin-containing HT
would not be considered appropriate
minus Women who are intolerant of progestin-containing hormone therapy
minus Women with pre-existing medical conditions that may be exacerbated by progestins
Most common adverse events leading to discontinuation are related to progestins12
breakthrough bleeding
bull Increase in the number of uterine procedures (ie unnecessary endometrial biopsies)
breast paintenderness
bull Increase in the number of breast interventions
1 Steel SA et al Climacteric 2003 2 Ettinger B and Pressman A Am J Manag Care 1999 3 Komm BS Mirkin S
Pharmaceuticals 2012
4 Panay N amp Studd JWW Human Reprod Update 1997
bull Nausea bull Depressive mood bull Poor concentration bull Hirsutism bull Headache bull Dizziness bull Fluid retention bull Weight gain
Other progestin-related intolerance issues4
Unmet need with the treatment of postmenopausal symptoms
bull Alternatives to progestin are needed that will protect the endometrium while avoiding other progestin-associated effects and preserving the desired effects of estrogens in postmenopausal women3
Which women with a uterus could benefit from
estrogens without the need for a progestin
bull Women who are intolerant of progestin-containing hormone therapy
bull Women with pre-existing medical conditions that may be exacerbated by progestins (eg women with a history of depression PMSPMDD increased breast density diabetes and metabolic syndrome)
History of the following conditions may make progestin inappropriate
bull Depression
bull PMSPMDD
bull High breast density
bull Diabetes and metabolic syndrome
PMS premenstrual syndrome
PMD premenstrual dysphoric disorder
Medical conditions that may be exacerbated by treatment with progestins
Learning from WHI data
bull Hormone therapy (HT) is the conventional and established therapy option to effectively treat postmenopausal symptoms however it has been associated with some safety and tolerability concerns1 2
bull A review of WHI data suggests that many of the concerns with menopausal HT more often associated with EPT (CE+MPA) such as CHD risk increased breast density breast pain and breast cancer risk than with ET (CEE alone)2
1 Rolnick SJ Kopher RA DeFor TA et al Menopause 2005
2 Komm BS Mirkin S Pharmaceuticals 2012
WHI Womenrsquos Health Initiative trial
CHD coronary heart disease
CEE conjugated equine estrogens
Efficacy and Safety of Constant Oestrogen
Pulsed Progestogen vs
Continuous Combined HRT
Adverse Events
17b-oestradiol 17b-oestradiol norgestimate NETA (n = 150) (n = 172) Breast discomfort 14 27 Abdominal discomfort 14 22 Uterine bleeding 15 12 Dysmenorrhea 3 8 Oedema 5 8
Adapted from S Rozenberg et al Human Reproduction 2000
Medical condition which may be exacerbated by treatment
with progestins
Increased breast density
bull Increases in breast density are associated with progestin-containing HT which may adversely affect radiological detection of breast cancer1 and may be independently associated with an increased risk for the development of breast cancer2
bull The Postmenopausal EstrogenProgestin Interventions (PEPI) trial demonstrated that an increased mammographic breast density was associated with the use of E+P but not with the use of estrogen alone3
bull Women who already have high breast density may therefore be considered inappropriate for treatment with a progestin-containing HT
1) EU Core SPC for Hormone Replacement Therapy Products (CMDh1312003 Rev 4 June
2012)
2) De Villiers TJ et al on behalf of the International Menopause Society Climacteric 2013 16
3) Greendale GA et al J Natl Cancer Inst 2003
Stroke
0 25 5 75 10 125
Fractures
Diabetes
Breast cancer
Cholecystitis
Venothrombotic episodes
Endometrial cancer
Lung cancer
Coronary heart disease
Colorectal cancer
Overall mortality
15 125 10 75 5 25
Benefits Risks
CE
CE MPA
Santen RJ et al J Clin Endocrinol Metab 2010
The basis of the Endocrine Society scientific statement for postmenopausal hormone replacement therapy (HRT) excess risks and benefits of HRT for 5 years in women aged 50ndash59 years or within 10 years of the start of menopause E=estrogen P=progestin
bull Younger women (aged 50ndash59 years) had more favorable results bull There are differences between CE alone and CEMPA arms bull Overall benefitrisk ratio of CE-alone appears to be more favourable than CEMPA
Reevaluation of WHI data (stratified by age) Risks and
Benefits of HRT Cases per 1000 Women per 5 Years of
Use
Medical condition which may be exacerbated by treatment
with progestins
Diabetes and metabolic syndrome
bull Treatment of oestrogen deficiency symptoms with progestin-containing HT (unlike oestrogen alone) may be associated with increases in insulin resistance and deterioration in glucose tolerance123
bull Postmenopausal women with diabetes could be inappropriate for treatment with progestin-containing HT due to the potential risk of exacerbation of their condition
1) Panay N amp Studd JWW Human Reprod Update 1997
2) Godsland I et al Metabolism 1993
3) Sites CK et al J Clin Endocrinol Metab 2005
Variations in Associated Breast Cancer
Risks Between CE alone and CEMPA
bull Use of CE alone for a median of 59 years was associated with a lower incidence of invasive breast cancer (151 cases 027 per year) compared with placebo (199 cases 035 per year HR 077 95 CI 062ndash095 P=002)
bull In the CE alone group fewer women died from invasive breast cancer (6 deaths 0009 per year) compared with controls (16 deaths 0024 per year HR 037 95 CI 013ndash091 P=003)
Anderson GL et al Lancet
Oncol 2012
Bazedoxifene (BZA) specifically selected in
combination with conjugated estrogens
bull BZA has been specifically selected for its unique pharmacologic profile and effects on VMS and uterine tissue in particular123
1 Crabtree J et al Mol Cell Endocrinol 2008
2 Kharode Y et al Endocrinolology 2008
3 Duavive SmPC
Estrogen Receptor activity is dimmed
Estrogen Receptor activity is turned on
CEs are agonists BZA is an antagonist
In the uterus
bull The BZA component reduces the risk of endometrial hyperplasia that can occur with the conjugated estrogens component alone3 This means that progestins are not needed
Extensive global clinical development program for
CEBZA
aIncludes additional pilot dose-finding study 203 1 Lobo RA et al Fertil Steril 2009 2 Pinkerton JV et al Menopause 2009 3 Kagan R et al Menopause 2010 4 Mirkin S et al Climacteric 2013 5 Pinkerton JV et al Obstet Gynecol 2013
Effects of conjugated estrogensbazedoxifene on
lipid and coagulation variables a randomized
placebo- and active-controlled trial
bull At 12 months
bull Both CEBZA doses were associated with small but significant effects on hemostasis variables including reductions in antithrombin plasminogen activator inhibitor-1 and fibrinogen activity and an increase in plasminogen activity relative to placebo at 12 months Incidences of cardiovascular and venous thromboembolic events were similar among treatment groups
bull CONCLUSIONS
bull This study provides reassurance that CEBZA does not adversely affect lipid metabolism or hemostatic balance In accordance the incidences of venous thromboembolic events and cardiovascular events in postmenopausal women are similar to those observed with placebo
Medical condition which may be exacerbated by treatment with progestins
Depression
bull Progestin-containing HT has been associated with increases in depressive symptoms in some individuals1
bull There is a biochemicalphysiological plausibility for the association of progestins with depression234
bull Therefore postmenopausal women who also have a medical history of depressive disorders or depression could be inappropriate for treatment with progestin-containing HT
Pfizer Confidential
65
1) Girdler SS et al J Womens Health Gend Based Med 1999 2) Traish AM et al Korean J Urol 2014 3) Stroumlhle A et al Biol Psychiatry 1999 4) Romeo E et
al Am J Psychiatry 1998
History of the following conditions may make progestin inappropriate
bull Depression
bull PMSPMDD
PMS premenstrual syndrome
PMD premenstrual dysphoric disorder
Medical conditions that may be exacerbated by treatment with progestins
Women for whom progestin-containing HT
would not be considered appropriate
minus Women who are intolerant of progestin-containing hormone therapy
minus Women with pre-existing medical conditions that may be exacerbated by progestins
Most common adverse events leading to discontinuation are related to progestins12
breakthrough bleeding
bull Increase in the number of uterine procedures (ie unnecessary endometrial biopsies)
breast paintenderness
bull Increase in the number of breast interventions
1 Steel SA et al Climacteric 2003 2 Ettinger B and Pressman A Am J Manag Care 1999 3 Komm BS Mirkin S
Pharmaceuticals 2012
4 Panay N amp Studd JWW Human Reprod Update 1997
bull Nausea bull Depressive mood bull Poor concentration bull Hirsutism bull Headache bull Dizziness bull Fluid retention bull Weight gain
Other progestin-related intolerance issues4
Unmet need with the treatment of postmenopausal symptoms
bull Alternatives to progestin are needed that will protect the endometrium while avoiding other progestin-associated effects and preserving the desired effects of estrogens in postmenopausal women3
Which women with a uterus could benefit from
estrogens without the need for a progestin
bull Women who are intolerant of progestin-containing hormone therapy
bull Women with pre-existing medical conditions that may be exacerbated by progestins (eg women with a history of depression PMSPMDD increased breast density diabetes and metabolic syndrome)
History of the following conditions may make progestin inappropriate
bull Depression
bull PMSPMDD
bull High breast density
bull Diabetes and metabolic syndrome
PMS premenstrual syndrome
PMD premenstrual dysphoric disorder
Medical conditions that may be exacerbated by treatment with progestins
Learning from WHI data
bull Hormone therapy (HT) is the conventional and established therapy option to effectively treat postmenopausal symptoms however it has been associated with some safety and tolerability concerns1 2
bull A review of WHI data suggests that many of the concerns with menopausal HT more often associated with EPT (CE+MPA) such as CHD risk increased breast density breast pain and breast cancer risk than with ET (CEE alone)2
1 Rolnick SJ Kopher RA DeFor TA et al Menopause 2005
2 Komm BS Mirkin S Pharmaceuticals 2012
WHI Womenrsquos Health Initiative trial
CHD coronary heart disease
CEE conjugated equine estrogens
Efficacy and Safety of Constant Oestrogen
Pulsed Progestogen vs
Continuous Combined HRT
Adverse Events
17b-oestradiol 17b-oestradiol norgestimate NETA (n = 150) (n = 172) Breast discomfort 14 27 Abdominal discomfort 14 22 Uterine bleeding 15 12 Dysmenorrhea 3 8 Oedema 5 8
Adapted from S Rozenberg et al Human Reproduction 2000
Medical condition which may be exacerbated by treatment
with progestins
Increased breast density
bull Increases in breast density are associated with progestin-containing HT which may adversely affect radiological detection of breast cancer1 and may be independently associated with an increased risk for the development of breast cancer2
bull The Postmenopausal EstrogenProgestin Interventions (PEPI) trial demonstrated that an increased mammographic breast density was associated with the use of E+P but not with the use of estrogen alone3
bull Women who already have high breast density may therefore be considered inappropriate for treatment with a progestin-containing HT
1) EU Core SPC for Hormone Replacement Therapy Products (CMDh1312003 Rev 4 June
2012)
2) De Villiers TJ et al on behalf of the International Menopause Society Climacteric 2013 16
3) Greendale GA et al J Natl Cancer Inst 2003
Stroke
0 25 5 75 10 125
Fractures
Diabetes
Breast cancer
Cholecystitis
Venothrombotic episodes
Endometrial cancer
Lung cancer
Coronary heart disease
Colorectal cancer
Overall mortality
15 125 10 75 5 25
Benefits Risks
CE
CE MPA
Santen RJ et al J Clin Endocrinol Metab 2010
The basis of the Endocrine Society scientific statement for postmenopausal hormone replacement therapy (HRT) excess risks and benefits of HRT for 5 years in women aged 50ndash59 years or within 10 years of the start of menopause E=estrogen P=progestin
bull Younger women (aged 50ndash59 years) had more favorable results bull There are differences between CE alone and CEMPA arms bull Overall benefitrisk ratio of CE-alone appears to be more favourable than CEMPA
Reevaluation of WHI data (stratified by age) Risks and
Benefits of HRT Cases per 1000 Women per 5 Years of
Use
Medical condition which may be exacerbated by treatment
with progestins
Diabetes and metabolic syndrome
bull Treatment of oestrogen deficiency symptoms with progestin-containing HT (unlike oestrogen alone) may be associated with increases in insulin resistance and deterioration in glucose tolerance123
bull Postmenopausal women with diabetes could be inappropriate for treatment with progestin-containing HT due to the potential risk of exacerbation of their condition
1) Panay N amp Studd JWW Human Reprod Update 1997
2) Godsland I et al Metabolism 1993
3) Sites CK et al J Clin Endocrinol Metab 2005
Variations in Associated Breast Cancer
Risks Between CE alone and CEMPA
bull Use of CE alone for a median of 59 years was associated with a lower incidence of invasive breast cancer (151 cases 027 per year) compared with placebo (199 cases 035 per year HR 077 95 CI 062ndash095 P=002)
bull In the CE alone group fewer women died from invasive breast cancer (6 deaths 0009 per year) compared with controls (16 deaths 0024 per year HR 037 95 CI 013ndash091 P=003)
Anderson GL et al Lancet
Oncol 2012
Bazedoxifene (BZA) specifically selected in
combination with conjugated estrogens
bull BZA has been specifically selected for its unique pharmacologic profile and effects on VMS and uterine tissue in particular123
1 Crabtree J et al Mol Cell Endocrinol 2008
2 Kharode Y et al Endocrinolology 2008
3 Duavive SmPC
Estrogen Receptor activity is dimmed
Estrogen Receptor activity is turned on
CEs are agonists BZA is an antagonist
In the uterus
bull The BZA component reduces the risk of endometrial hyperplasia that can occur with the conjugated estrogens component alone3 This means that progestins are not needed
Extensive global clinical development program for
CEBZA
aIncludes additional pilot dose-finding study 203 1 Lobo RA et al Fertil Steril 2009 2 Pinkerton JV et al Menopause 2009 3 Kagan R et al Menopause 2010 4 Mirkin S et al Climacteric 2013 5 Pinkerton JV et al Obstet Gynecol 2013
Effects of conjugated estrogensbazedoxifene on
lipid and coagulation variables a randomized
placebo- and active-controlled trial
bull At 12 months
bull Both CEBZA doses were associated with small but significant effects on hemostasis variables including reductions in antithrombin plasminogen activator inhibitor-1 and fibrinogen activity and an increase in plasminogen activity relative to placebo at 12 months Incidences of cardiovascular and venous thromboembolic events were similar among treatment groups
bull CONCLUSIONS
bull This study provides reassurance that CEBZA does not adversely affect lipid metabolism or hemostatic balance In accordance the incidences of venous thromboembolic events and cardiovascular events in postmenopausal women are similar to those observed with placebo

History of the following conditions may make progestin inappropriate
bull Depression
bull PMSPMDD
PMS premenstrual syndrome
PMD premenstrual dysphoric disorder
Medical conditions that may be exacerbated by treatment with progestins
Women for whom progestin-containing HT
would not be considered appropriate
minus Women who are intolerant of progestin-containing hormone therapy
minus Women with pre-existing medical conditions that may be exacerbated by progestins
Most common adverse events leading to discontinuation are related to progestins12
breakthrough bleeding
bull Increase in the number of uterine procedures (ie unnecessary endometrial biopsies)
breast paintenderness
bull Increase in the number of breast interventions
1 Steel SA et al Climacteric 2003 2 Ettinger B and Pressman A Am J Manag Care 1999 3 Komm BS Mirkin S
Pharmaceuticals 2012
4 Panay N amp Studd JWW Human Reprod Update 1997
bull Nausea bull Depressive mood bull Poor concentration bull Hirsutism bull Headache bull Dizziness bull Fluid retention bull Weight gain
Other progestin-related intolerance issues4
Unmet need with the treatment of postmenopausal symptoms
bull Alternatives to progestin are needed that will protect the endometrium while avoiding other progestin-associated effects and preserving the desired effects of estrogens in postmenopausal women3
Which women with a uterus could benefit from
estrogens without the need for a progestin
bull Women who are intolerant of progestin-containing hormone therapy
bull Women with pre-existing medical conditions that may be exacerbated by progestins (eg women with a history of depression PMSPMDD increased breast density diabetes and metabolic syndrome)
History of the following conditions may make progestin inappropriate
bull Depression
bull PMSPMDD
bull High breast density
bull Diabetes and metabolic syndrome
PMS premenstrual syndrome
PMD premenstrual dysphoric disorder
Medical conditions that may be exacerbated by treatment with progestins
Learning from WHI data
bull Hormone therapy (HT) is the conventional and established therapy option to effectively treat postmenopausal symptoms however it has been associated with some safety and tolerability concerns1 2
bull A review of WHI data suggests that many of the concerns with menopausal HT more often associated with EPT (CE+MPA) such as CHD risk increased breast density breast pain and breast cancer risk than with ET (CEE alone)2
1 Rolnick SJ Kopher RA DeFor TA et al Menopause 2005
2 Komm BS Mirkin S Pharmaceuticals 2012
WHI Womenrsquos Health Initiative trial
CHD coronary heart disease
CEE conjugated equine estrogens
Efficacy and Safety of Constant Oestrogen
Pulsed Progestogen vs
Continuous Combined HRT
Adverse Events
17b-oestradiol 17b-oestradiol norgestimate NETA (n = 150) (n = 172) Breast discomfort 14 27 Abdominal discomfort 14 22 Uterine bleeding 15 12 Dysmenorrhea 3 8 Oedema 5 8
Adapted from S Rozenberg et al Human Reproduction 2000
Medical condition which may be exacerbated by treatment
with progestins
Increased breast density
bull Increases in breast density are associated with progestin-containing HT which may adversely affect radiological detection of breast cancer1 and may be independently associated with an increased risk for the development of breast cancer2
bull The Postmenopausal EstrogenProgestin Interventions (PEPI) trial demonstrated that an increased mammographic breast density was associated with the use of E+P but not with the use of estrogen alone3
bull Women who already have high breast density may therefore be considered inappropriate for treatment with a progestin-containing HT
1) EU Core SPC for Hormone Replacement Therapy Products (CMDh1312003 Rev 4 June
2012)
2) De Villiers TJ et al on behalf of the International Menopause Society Climacteric 2013 16
3) Greendale GA et al J Natl Cancer Inst 2003
Stroke
0 25 5 75 10 125
Fractures
Diabetes
Breast cancer
Cholecystitis
Venothrombotic episodes
Endometrial cancer
Lung cancer
Coronary heart disease
Colorectal cancer
Overall mortality
15 125 10 75 5 25
Benefits Risks
CE
CE MPA
Santen RJ et al J Clin Endocrinol Metab 2010
The basis of the Endocrine Society scientific statement for postmenopausal hormone replacement therapy (HRT) excess risks and benefits of HRT for 5 years in women aged 50ndash59 years or within 10 years of the start of menopause E=estrogen P=progestin
bull Younger women (aged 50ndash59 years) had more favorable results bull There are differences between CE alone and CEMPA arms bull Overall benefitrisk ratio of CE-alone appears to be more favourable than CEMPA
Reevaluation of WHI data (stratified by age) Risks and
Benefits of HRT Cases per 1000 Women per 5 Years of
Use
Medical condition which may be exacerbated by treatment
with progestins
Diabetes and metabolic syndrome
bull Treatment of oestrogen deficiency symptoms with progestin-containing HT (unlike oestrogen alone) may be associated with increases in insulin resistance and deterioration in glucose tolerance123
bull Postmenopausal women with diabetes could be inappropriate for treatment with progestin-containing HT due to the potential risk of exacerbation of their condition
1) Panay N amp Studd JWW Human Reprod Update 1997
2) Godsland I et al Metabolism 1993
3) Sites CK et al J Clin Endocrinol Metab 2005
Variations in Associated Breast Cancer
Risks Between CE alone and CEMPA
bull Use of CE alone for a median of 59 years was associated with a lower incidence of invasive breast cancer (151 cases 027 per year) compared with placebo (199 cases 035 per year HR 077 95 CI 062ndash095 P=002)
bull In the CE alone group fewer women died from invasive breast cancer (6 deaths 0009 per year) compared with controls (16 deaths 0024 per year HR 037 95 CI 013ndash091 P=003)
Anderson GL et al Lancet
Oncol 2012
Bazedoxifene (BZA) specifically selected in
combination with conjugated estrogens
bull BZA has been specifically selected for its unique pharmacologic profile and effects on VMS and uterine tissue in particular123
1 Crabtree J et al Mol Cell Endocrinol 2008
2 Kharode Y et al Endocrinolology 2008
3 Duavive SmPC
Estrogen Receptor activity is dimmed
Estrogen Receptor activity is turned on
CEs are agonists BZA is an antagonist
In the uterus
bull The BZA component reduces the risk of endometrial hyperplasia that can occur with the conjugated estrogens component alone3 This means that progestins are not needed
Extensive global clinical development program for
CEBZA
aIncludes additional pilot dose-finding study 203 1 Lobo RA et al Fertil Steril 2009 2 Pinkerton JV et al Menopause 2009 3 Kagan R et al Menopause 2010 4 Mirkin S et al Climacteric 2013 5 Pinkerton JV et al Obstet Gynecol 2013
Effects of conjugated estrogensbazedoxifene on
lipid and coagulation variables a randomized
placebo- and active-controlled trial
bull At 12 months
bull Both CEBZA doses were associated with small but significant effects on hemostasis variables including reductions in antithrombin plasminogen activator inhibitor-1 and fibrinogen activity and an increase in plasminogen activity relative to placebo at 12 months Incidences of cardiovascular and venous thromboembolic events were similar among treatment groups
bull CONCLUSIONS
bull This study provides reassurance that CEBZA does not adversely affect lipid metabolism or hemostatic balance In accordance the incidences of venous thromboembolic events and cardiovascular events in postmenopausal women are similar to those observed with placebo
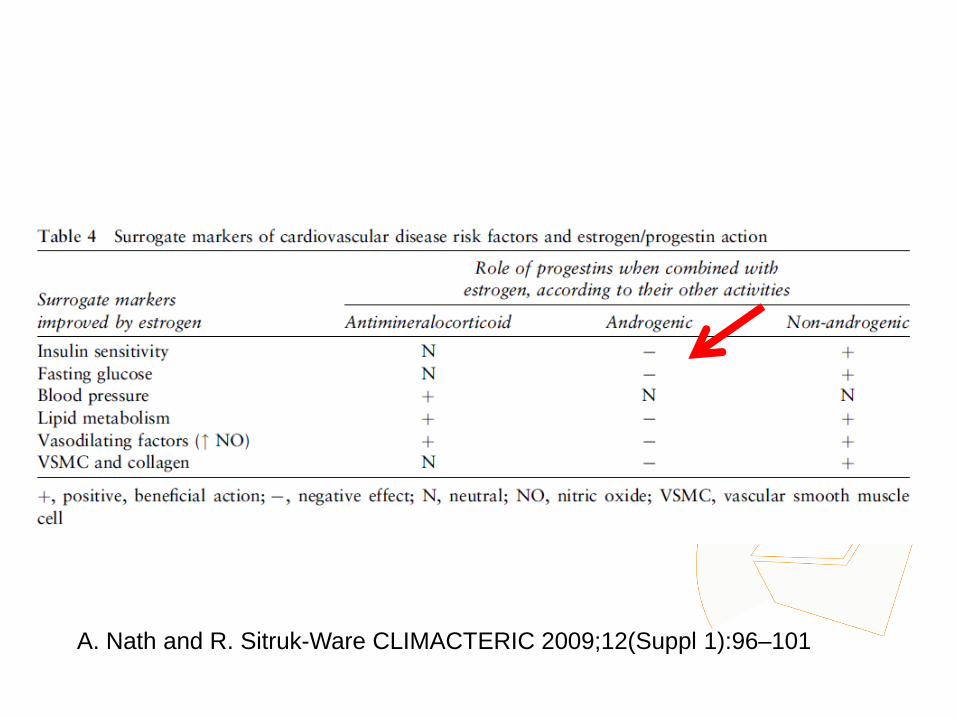
Women for whom progestin-containing HT
would not be considered appropriate
minus Women who are intolerant of progestin-containing hormone therapy
minus Women with pre-existing medical conditions that may be exacerbated by progestins
Most common adverse events leading to discontinuation are related to progestins12
breakthrough bleeding
bull Increase in the number of uterine procedures (ie unnecessary endometrial biopsies)
breast paintenderness
bull Increase in the number of breast interventions
1 Steel SA et al Climacteric 2003 2 Ettinger B and Pressman A Am J Manag Care 1999 3 Komm BS Mirkin S
Pharmaceuticals 2012
4 Panay N amp Studd JWW Human Reprod Update 1997
bull Nausea bull Depressive mood bull Poor concentration bull Hirsutism bull Headache bull Dizziness bull Fluid retention bull Weight gain
Other progestin-related intolerance issues4
Unmet need with the treatment of postmenopausal symptoms
bull Alternatives to progestin are needed that will protect the endometrium while avoiding other progestin-associated effects and preserving the desired effects of estrogens in postmenopausal women3
Which women with a uterus could benefit from
estrogens without the need for a progestin
bull Women who are intolerant of progestin-containing hormone therapy
bull Women with pre-existing medical conditions that may be exacerbated by progestins (eg women with a history of depression PMSPMDD increased breast density diabetes and metabolic syndrome)
History of the following conditions may make progestin inappropriate
bull Depression
bull PMSPMDD
bull High breast density
bull Diabetes and metabolic syndrome
PMS premenstrual syndrome
PMD premenstrual dysphoric disorder
Medical conditions that may be exacerbated by treatment with progestins
Learning from WHI data
bull Hormone therapy (HT) is the conventional and established therapy option to effectively treat postmenopausal symptoms however it has been associated with some safety and tolerability concerns1 2
bull A review of WHI data suggests that many of the concerns with menopausal HT more often associated with EPT (CE+MPA) such as CHD risk increased breast density breast pain and breast cancer risk than with ET (CEE alone)2
1 Rolnick SJ Kopher RA DeFor TA et al Menopause 2005
2 Komm BS Mirkin S Pharmaceuticals 2012
WHI Womenrsquos Health Initiative trial
CHD coronary heart disease
CEE conjugated equine estrogens
Efficacy and Safety of Constant Oestrogen
Pulsed Progestogen vs
Continuous Combined HRT
Adverse Events
17b-oestradiol 17b-oestradiol norgestimate NETA (n = 150) (n = 172) Breast discomfort 14 27 Abdominal discomfort 14 22 Uterine bleeding 15 12 Dysmenorrhea 3 8 Oedema 5 8
Adapted from S Rozenberg et al Human Reproduction 2000
Medical condition which may be exacerbated by treatment
with progestins
Increased breast density
bull Increases in breast density are associated with progestin-containing HT which may adversely affect radiological detection of breast cancer1 and may be independently associated with an increased risk for the development of breast cancer2
bull The Postmenopausal EstrogenProgestin Interventions (PEPI) trial demonstrated that an increased mammographic breast density was associated with the use of E+P but not with the use of estrogen alone3
bull Women who already have high breast density may therefore be considered inappropriate for treatment with a progestin-containing HT
1) EU Core SPC for Hormone Replacement Therapy Products (CMDh1312003 Rev 4 June
2012)
2) De Villiers TJ et al on behalf of the International Menopause Society Climacteric 2013 16
3) Greendale GA et al J Natl Cancer Inst 2003
Stroke
0 25 5 75 10 125
Fractures
Diabetes
Breast cancer
Cholecystitis
Venothrombotic episodes
Endometrial cancer
Lung cancer
Coronary heart disease
Colorectal cancer
Overall mortality
15 125 10 75 5 25
Benefits Risks
CE
CE MPA
Santen RJ et al J Clin Endocrinol Metab 2010
The basis of the Endocrine Society scientific statement for postmenopausal hormone replacement therapy (HRT) excess risks and benefits of HRT for 5 years in women aged 50ndash59 years or within 10 years of the start of menopause E=estrogen P=progestin
bull Younger women (aged 50ndash59 years) had more favorable results bull There are differences between CE alone and CEMPA arms bull Overall benefitrisk ratio of CE-alone appears to be more favourable than CEMPA
Reevaluation of WHI data (stratified by age) Risks and
Benefits of HRT Cases per 1000 Women per 5 Years of
Use
Medical condition which may be exacerbated by treatment
with progestins
Diabetes and metabolic syndrome
bull Treatment of oestrogen deficiency symptoms with progestin-containing HT (unlike oestrogen alone) may be associated with increases in insulin resistance and deterioration in glucose tolerance123
bull Postmenopausal women with diabetes could be inappropriate for treatment with progestin-containing HT due to the potential risk of exacerbation of their condition
1) Panay N amp Studd JWW Human Reprod Update 1997
2) Godsland I et al Metabolism 1993
3) Sites CK et al J Clin Endocrinol Metab 2005
Variations in Associated Breast Cancer
Risks Between CE alone and CEMPA
bull Use of CE alone for a median of 59 years was associated with a lower incidence of invasive breast cancer (151 cases 027 per year) compared with placebo (199 cases 035 per year HR 077 95 CI 062ndash095 P=002)
bull In the CE alone group fewer women died from invasive breast cancer (6 deaths 0009 per year) compared with controls (16 deaths 0024 per year HR 037 95 CI 013ndash091 P=003)
Anderson GL et al Lancet
Oncol 2012
Bazedoxifene (BZA) specifically selected in
combination with conjugated estrogens
bull BZA has been specifically selected for its unique pharmacologic profile and effects on VMS and uterine tissue in particular123
1 Crabtree J et al Mol Cell Endocrinol 2008
2 Kharode Y et al Endocrinolology 2008
3 Duavive SmPC
Estrogen Receptor activity is dimmed
Estrogen Receptor activity is turned on
CEs are agonists BZA is an antagonist
In the uterus
bull The BZA component reduces the risk of endometrial hyperplasia that can occur with the conjugated estrogens component alone3 This means that progestins are not needed
Extensive global clinical development program for
CEBZA
aIncludes additional pilot dose-finding study 203 1 Lobo RA et al Fertil Steril 2009 2 Pinkerton JV et al Menopause 2009 3 Kagan R et al Menopause 2010 4 Mirkin S et al Climacteric 2013 5 Pinkerton JV et al Obstet Gynecol 2013
Effects of conjugated estrogensbazedoxifene on
lipid and coagulation variables a randomized
placebo- and active-controlled trial
bull At 12 months
bull Both CEBZA doses were associated with small but significant effects on hemostasis variables including reductions in antithrombin plasminogen activator inhibitor-1 and fibrinogen activity and an increase in plasminogen activity relative to placebo at 12 months Incidences of cardiovascular and venous thromboembolic events were similar among treatment groups
bull CONCLUSIONS
bull This study provides reassurance that CEBZA does not adversely affect lipid metabolism or hemostatic balance In accordance the incidences of venous thromboembolic events and cardiovascular events in postmenopausal women are similar to those observed with placebo

Most common adverse events leading to discontinuation are related to progestins12
breakthrough bleeding
bull Increase in the number of uterine procedures (ie unnecessary endometrial biopsies)
breast paintenderness
bull Increase in the number of breast interventions
1 Steel SA et al Climacteric 2003 2 Ettinger B and Pressman A Am J Manag Care 1999 3 Komm BS Mirkin S
Pharmaceuticals 2012
4 Panay N amp Studd JWW Human Reprod Update 1997
bull Nausea bull Depressive mood bull Poor concentration bull Hirsutism bull Headache bull Dizziness bull Fluid retention bull Weight gain
Other progestin-related intolerance issues4
Unmet need with the treatment of postmenopausal symptoms
bull Alternatives to progestin are needed that will protect the endometrium while avoiding other progestin-associated effects and preserving the desired effects of estrogens in postmenopausal women3
Which women with a uterus could benefit from
estrogens without the need for a progestin
bull Women who are intolerant of progestin-containing hormone therapy
bull Women with pre-existing medical conditions that may be exacerbated by progestins (eg women with a history of depression PMSPMDD increased breast density diabetes and metabolic syndrome)
History of the following conditions may make progestin inappropriate
bull Depression
bull PMSPMDD
bull High breast density
bull Diabetes and metabolic syndrome
PMS premenstrual syndrome
PMD premenstrual dysphoric disorder
Medical conditions that may be exacerbated by treatment with progestins
Learning from WHI data
bull Hormone therapy (HT) is the conventional and established therapy option to effectively treat postmenopausal symptoms however it has been associated with some safety and tolerability concerns1 2
bull A review of WHI data suggests that many of the concerns with menopausal HT more often associated with EPT (CE+MPA) such as CHD risk increased breast density breast pain and breast cancer risk than with ET (CEE alone)2
1 Rolnick SJ Kopher RA DeFor TA et al Menopause 2005
2 Komm BS Mirkin S Pharmaceuticals 2012
WHI Womenrsquos Health Initiative trial
CHD coronary heart disease
CEE conjugated equine estrogens
Efficacy and Safety of Constant Oestrogen
Pulsed Progestogen vs
Continuous Combined HRT
Adverse Events
17b-oestradiol 17b-oestradiol norgestimate NETA (n = 150) (n = 172) Breast discomfort 14 27 Abdominal discomfort 14 22 Uterine bleeding 15 12 Dysmenorrhea 3 8 Oedema 5 8
Adapted from S Rozenberg et al Human Reproduction 2000
Medical condition which may be exacerbated by treatment
with progestins
Increased breast density
bull Increases in breast density are associated with progestin-containing HT which may adversely affect radiological detection of breast cancer1 and may be independently associated with an increased risk for the development of breast cancer2
bull The Postmenopausal EstrogenProgestin Interventions (PEPI) trial demonstrated that an increased mammographic breast density was associated with the use of E+P but not with the use of estrogen alone3
bull Women who already have high breast density may therefore be considered inappropriate for treatment with a progestin-containing HT
1) EU Core SPC for Hormone Replacement Therapy Products (CMDh1312003 Rev 4 June
2012)
2) De Villiers TJ et al on behalf of the International Menopause Society Climacteric 2013 16
3) Greendale GA et al J Natl Cancer Inst 2003
Stroke
0 25 5 75 10 125
Fractures
Diabetes
Breast cancer
Cholecystitis
Venothrombotic episodes
Endometrial cancer
Lung cancer
Coronary heart disease
Colorectal cancer
Overall mortality
15 125 10 75 5 25
Benefits Risks
CE
CE MPA
Santen RJ et al J Clin Endocrinol Metab 2010
The basis of the Endocrine Society scientific statement for postmenopausal hormone replacement therapy (HRT) excess risks and benefits of HRT for 5 years in women aged 50ndash59 years or within 10 years of the start of menopause E=estrogen P=progestin
bull Younger women (aged 50ndash59 years) had more favorable results bull There are differences between CE alone and CEMPA arms bull Overall benefitrisk ratio of CE-alone appears to be more favourable than CEMPA
Reevaluation of WHI data (stratified by age) Risks and
Benefits of HRT Cases per 1000 Women per 5 Years of
Use
Medical condition which may be exacerbated by treatment
with progestins
Diabetes and metabolic syndrome
bull Treatment of oestrogen deficiency symptoms with progestin-containing HT (unlike oestrogen alone) may be associated with increases in insulin resistance and deterioration in glucose tolerance123
bull Postmenopausal women with diabetes could be inappropriate for treatment with progestin-containing HT due to the potential risk of exacerbation of their condition
1) Panay N amp Studd JWW Human Reprod Update 1997
2) Godsland I et al Metabolism 1993
3) Sites CK et al J Clin Endocrinol Metab 2005
Variations in Associated Breast Cancer
Risks Between CE alone and CEMPA
bull Use of CE alone for a median of 59 years was associated with a lower incidence of invasive breast cancer (151 cases 027 per year) compared with placebo (199 cases 035 per year HR 077 95 CI 062ndash095 P=002)
bull In the CE alone group fewer women died from invasive breast cancer (6 deaths 0009 per year) compared with controls (16 deaths 0024 per year HR 037 95 CI 013ndash091 P=003)
Anderson GL et al Lancet
Oncol 2012
Bazedoxifene (BZA) specifically selected in
combination with conjugated estrogens
bull BZA has been specifically selected for its unique pharmacologic profile and effects on VMS and uterine tissue in particular123
1 Crabtree J et al Mol Cell Endocrinol 2008
2 Kharode Y et al Endocrinolology 2008
3 Duavive SmPC
Estrogen Receptor activity is dimmed
Estrogen Receptor activity is turned on
CEs are agonists BZA is an antagonist
In the uterus
bull The BZA component reduces the risk of endometrial hyperplasia that can occur with the conjugated estrogens component alone3 This means that progestins are not needed
Extensive global clinical development program for
CEBZA
aIncludes additional pilot dose-finding study 203 1 Lobo RA et al Fertil Steril 2009 2 Pinkerton JV et al Menopause 2009 3 Kagan R et al Menopause 2010 4 Mirkin S et al Climacteric 2013 5 Pinkerton JV et al Obstet Gynecol 2013
Effects of conjugated estrogensbazedoxifene on
lipid and coagulation variables a randomized
placebo- and active-controlled trial
bull At 12 months
bull Both CEBZA doses were associated with small but significant effects on hemostasis variables including reductions in antithrombin plasminogen activator inhibitor-1 and fibrinogen activity and an increase in plasminogen activity relative to placebo at 12 months Incidences of cardiovascular and venous thromboembolic events were similar among treatment groups
bull CONCLUSIONS
bull This study provides reassurance that CEBZA does not adversely affect lipid metabolism or hemostatic balance In accordance the incidences of venous thromboembolic events and cardiovascular events in postmenopausal women are similar to those observed with placebo

Which women with a uterus could benefit from
estrogens without the need for a progestin
bull Women who are intolerant of progestin-containing hormone therapy
bull Women with pre-existing medical conditions that may be exacerbated by progestins (eg women with a history of depression PMSPMDD increased breast density diabetes and metabolic syndrome)
History of the following conditions may make progestin inappropriate
bull Depression
bull PMSPMDD
bull High breast density
bull Diabetes and metabolic syndrome
PMS premenstrual syndrome
PMD premenstrual dysphoric disorder
Medical conditions that may be exacerbated by treatment with progestins
Learning from WHI data
bull Hormone therapy (HT) is the conventional and established therapy option to effectively treat postmenopausal symptoms however it has been associated with some safety and tolerability concerns1 2
bull A review of WHI data suggests that many of the concerns with menopausal HT more often associated with EPT (CE+MPA) such as CHD risk increased breast density breast pain and breast cancer risk than with ET (CEE alone)2
1 Rolnick SJ Kopher RA DeFor TA et al Menopause 2005
2 Komm BS Mirkin S Pharmaceuticals 2012
WHI Womenrsquos Health Initiative trial
CHD coronary heart disease
CEE conjugated equine estrogens
Efficacy and Safety of Constant Oestrogen
Pulsed Progestogen vs
Continuous Combined HRT
Adverse Events
17b-oestradiol 17b-oestradiol norgestimate NETA (n = 150) (n = 172) Breast discomfort 14 27 Abdominal discomfort 14 22 Uterine bleeding 15 12 Dysmenorrhea 3 8 Oedema 5 8
Adapted from S Rozenberg et al Human Reproduction 2000
Medical condition which may be exacerbated by treatment
with progestins
Increased breast density
bull Increases in breast density are associated with progestin-containing HT which may adversely affect radiological detection of breast cancer1 and may be independently associated with an increased risk for the development of breast cancer2
bull The Postmenopausal EstrogenProgestin Interventions (PEPI) trial demonstrated that an increased mammographic breast density was associated with the use of E+P but not with the use of estrogen alone3
bull Women who already have high breast density may therefore be considered inappropriate for treatment with a progestin-containing HT
1) EU Core SPC for Hormone Replacement Therapy Products (CMDh1312003 Rev 4 June
2012)
2) De Villiers TJ et al on behalf of the International Menopause Society Climacteric 2013 16
3) Greendale GA et al J Natl Cancer Inst 2003
Stroke
0 25 5 75 10 125
Fractures
Diabetes
Breast cancer
Cholecystitis
Venothrombotic episodes
Endometrial cancer
Lung cancer
Coronary heart disease
Colorectal cancer
Overall mortality
15 125 10 75 5 25
Benefits Risks
CE
CE MPA
Santen RJ et al J Clin Endocrinol Metab 2010
The basis of the Endocrine Society scientific statement for postmenopausal hormone replacement therapy (HRT) excess risks and benefits of HRT for 5 years in women aged 50ndash59 years or within 10 years of the start of menopause E=estrogen P=progestin
bull Younger women (aged 50ndash59 years) had more favorable results bull There are differences between CE alone and CEMPA arms bull Overall benefitrisk ratio of CE-alone appears to be more favourable than CEMPA
Reevaluation of WHI data (stratified by age) Risks and
Benefits of HRT Cases per 1000 Women per 5 Years of
Use
Medical condition which may be exacerbated by treatment
with progestins
Diabetes and metabolic syndrome
bull Treatment of oestrogen deficiency symptoms with progestin-containing HT (unlike oestrogen alone) may be associated with increases in insulin resistance and deterioration in glucose tolerance123
bull Postmenopausal women with diabetes could be inappropriate for treatment with progestin-containing HT due to the potential risk of exacerbation of their condition
1) Panay N amp Studd JWW Human Reprod Update 1997
2) Godsland I et al Metabolism 1993
3) Sites CK et al J Clin Endocrinol Metab 2005
Variations in Associated Breast Cancer
Risks Between CE alone and CEMPA
bull Use of CE alone for a median of 59 years was associated with a lower incidence of invasive breast cancer (151 cases 027 per year) compared with placebo (199 cases 035 per year HR 077 95 CI 062ndash095 P=002)
bull In the CE alone group fewer women died from invasive breast cancer (6 deaths 0009 per year) compared with controls (16 deaths 0024 per year HR 037 95 CI 013ndash091 P=003)
Anderson GL et al Lancet
Oncol 2012
Bazedoxifene (BZA) specifically selected in
combination with conjugated estrogens
bull BZA has been specifically selected for its unique pharmacologic profile and effects on VMS and uterine tissue in particular123
1 Crabtree J et al Mol Cell Endocrinol 2008
2 Kharode Y et al Endocrinolology 2008
3 Duavive SmPC
Estrogen Receptor activity is dimmed
Estrogen Receptor activity is turned on
CEs are agonists BZA is an antagonist
In the uterus
bull The BZA component reduces the risk of endometrial hyperplasia that can occur with the conjugated estrogens component alone3 This means that progestins are not needed
Extensive global clinical development program for
CEBZA
aIncludes additional pilot dose-finding study 203 1 Lobo RA et al Fertil Steril 2009 2 Pinkerton JV et al Menopause 2009 3 Kagan R et al Menopause 2010 4 Mirkin S et al Climacteric 2013 5 Pinkerton JV et al Obstet Gynecol 2013
Effects of conjugated estrogensbazedoxifene on
lipid and coagulation variables a randomized
placebo- and active-controlled trial
bull At 12 months
bull Both CEBZA doses were associated with small but significant effects on hemostasis variables including reductions in antithrombin plasminogen activator inhibitor-1 and fibrinogen activity and an increase in plasminogen activity relative to placebo at 12 months Incidences of cardiovascular and venous thromboembolic events were similar among treatment groups
bull CONCLUSIONS
bull This study provides reassurance that CEBZA does not adversely affect lipid metabolism or hemostatic balance In accordance the incidences of venous thromboembolic events and cardiovascular events in postmenopausal women are similar to those observed with placebo

History of the following conditions may make progestin inappropriate
bull Depression
bull PMSPMDD
bull High breast density
bull Diabetes and metabolic syndrome
PMS premenstrual syndrome
PMD premenstrual dysphoric disorder
Medical conditions that may be exacerbated by treatment with progestins
Learning from WHI data
bull Hormone therapy (HT) is the conventional and established therapy option to effectively treat postmenopausal symptoms however it has been associated with some safety and tolerability concerns1 2
bull A review of WHI data suggests that many of the concerns with menopausal HT more often associated with EPT (CE+MPA) such as CHD risk increased breast density breast pain and breast cancer risk than with ET (CEE alone)2
1 Rolnick SJ Kopher RA DeFor TA et al Menopause 2005
2 Komm BS Mirkin S Pharmaceuticals 2012
WHI Womenrsquos Health Initiative trial
CHD coronary heart disease
CEE conjugated equine estrogens
Efficacy and Safety of Constant Oestrogen
Pulsed Progestogen vs
Continuous Combined HRT
Adverse Events
17b-oestradiol 17b-oestradiol norgestimate NETA (n = 150) (n = 172) Breast discomfort 14 27 Abdominal discomfort 14 22 Uterine bleeding 15 12 Dysmenorrhea 3 8 Oedema 5 8
Adapted from S Rozenberg et al Human Reproduction 2000
Medical condition which may be exacerbated by treatment
with progestins
Increased breast density
bull Increases in breast density are associated with progestin-containing HT which may adversely affect radiological detection of breast cancer1 and may be independently associated with an increased risk for the development of breast cancer2
bull The Postmenopausal EstrogenProgestin Interventions (PEPI) trial demonstrated that an increased mammographic breast density was associated with the use of E+P but not with the use of estrogen alone3
bull Women who already have high breast density may therefore be considered inappropriate for treatment with a progestin-containing HT
1) EU Core SPC for Hormone Replacement Therapy Products (CMDh1312003 Rev 4 June
2012)
2) De Villiers TJ et al on behalf of the International Menopause Society Climacteric 2013 16
3) Greendale GA et al J Natl Cancer Inst 2003
Stroke
0 25 5 75 10 125
Fractures
Diabetes
Breast cancer
Cholecystitis
Venothrombotic episodes
Endometrial cancer
Lung cancer
Coronary heart disease
Colorectal cancer
Overall mortality
15 125 10 75 5 25
Benefits Risks
CE
CE MPA
Santen RJ et al J Clin Endocrinol Metab 2010
The basis of the Endocrine Society scientific statement for postmenopausal hormone replacement therapy (HRT) excess risks and benefits of HRT for 5 years in women aged 50ndash59 years or within 10 years of the start of menopause E=estrogen P=progestin
bull Younger women (aged 50ndash59 years) had more favorable results bull There are differences between CE alone and CEMPA arms bull Overall benefitrisk ratio of CE-alone appears to be more favourable than CEMPA
Reevaluation of WHI data (stratified by age) Risks and
Benefits of HRT Cases per 1000 Women per 5 Years of
Use
Medical condition which may be exacerbated by treatment
with progestins
Diabetes and metabolic syndrome
bull Treatment of oestrogen deficiency symptoms with progestin-containing HT (unlike oestrogen alone) may be associated with increases in insulin resistance and deterioration in glucose tolerance123
bull Postmenopausal women with diabetes could be inappropriate for treatment with progestin-containing HT due to the potential risk of exacerbation of their condition
1) Panay N amp Studd JWW Human Reprod Update 1997
2) Godsland I et al Metabolism 1993
3) Sites CK et al J Clin Endocrinol Metab 2005
Variations in Associated Breast Cancer
Risks Between CE alone and CEMPA
bull Use of CE alone for a median of 59 years was associated with a lower incidence of invasive breast cancer (151 cases 027 per year) compared with placebo (199 cases 035 per year HR 077 95 CI 062ndash095 P=002)
bull In the CE alone group fewer women died from invasive breast cancer (6 deaths 0009 per year) compared with controls (16 deaths 0024 per year HR 037 95 CI 013ndash091 P=003)
Anderson GL et al Lancet
Oncol 2012
Bazedoxifene (BZA) specifically selected in
combination with conjugated estrogens
bull BZA has been specifically selected for its unique pharmacologic profile and effects on VMS and uterine tissue in particular123
1 Crabtree J et al Mol Cell Endocrinol 2008
2 Kharode Y et al Endocrinolology 2008
3 Duavive SmPC
Estrogen Receptor activity is dimmed
Estrogen Receptor activity is turned on
CEs are agonists BZA is an antagonist
In the uterus
bull The BZA component reduces the risk of endometrial hyperplasia that can occur with the conjugated estrogens component alone3 This means that progestins are not needed
Extensive global clinical development program for
CEBZA
aIncludes additional pilot dose-finding study 203 1 Lobo RA et al Fertil Steril 2009 2 Pinkerton JV et al Menopause 2009 3 Kagan R et al Menopause 2010 4 Mirkin S et al Climacteric 2013 5 Pinkerton JV et al Obstet Gynecol 2013
Effects of conjugated estrogensbazedoxifene on
lipid and coagulation variables a randomized
placebo- and active-controlled trial
bull At 12 months
bull Both CEBZA doses were associated with small but significant effects on hemostasis variables including reductions in antithrombin plasminogen activator inhibitor-1 and fibrinogen activity and an increase in plasminogen activity relative to placebo at 12 months Incidences of cardiovascular and venous thromboembolic events were similar among treatment groups
bull CONCLUSIONS
bull This study provides reassurance that CEBZA does not adversely affect lipid metabolism or hemostatic balance In accordance the incidences of venous thromboembolic events and cardiovascular events in postmenopausal women are similar to those observed with placebo

Learning from WHI data
bull Hormone therapy (HT) is the conventional and established therapy option to effectively treat postmenopausal symptoms however it has been associated with some safety and tolerability concerns1 2
bull A review of WHI data suggests that many of the concerns with menopausal HT more often associated with EPT (CE+MPA) such as CHD risk increased breast density breast pain and breast cancer risk than with ET (CEE alone)2
1 Rolnick SJ Kopher RA DeFor TA et al Menopause 2005
2 Komm BS Mirkin S Pharmaceuticals 2012
WHI Womenrsquos Health Initiative trial
CHD coronary heart disease
CEE conjugated equine estrogens
Efficacy and Safety of Constant Oestrogen
Pulsed Progestogen vs
Continuous Combined HRT
Adverse Events
17b-oestradiol 17b-oestradiol norgestimate NETA (n = 150) (n = 172) Breast discomfort 14 27 Abdominal discomfort 14 22 Uterine bleeding 15 12 Dysmenorrhea 3 8 Oedema 5 8
Adapted from S Rozenberg et al Human Reproduction 2000
Medical condition which may be exacerbated by treatment
with progestins
Increased breast density
bull Increases in breast density are associated with progestin-containing HT which may adversely affect radiological detection of breast cancer1 and may be independently associated with an increased risk for the development of breast cancer2
bull The Postmenopausal EstrogenProgestin Interventions (PEPI) trial demonstrated that an increased mammographic breast density was associated with the use of E+P but not with the use of estrogen alone3
bull Women who already have high breast density may therefore be considered inappropriate for treatment with a progestin-containing HT
1) EU Core SPC for Hormone Replacement Therapy Products (CMDh1312003 Rev 4 June
2012)
2) De Villiers TJ et al on behalf of the International Menopause Society Climacteric 2013 16
3) Greendale GA et al J Natl Cancer Inst 2003
Stroke
0 25 5 75 10 125
Fractures
Diabetes
Breast cancer
Cholecystitis
Venothrombotic episodes
Endometrial cancer
Lung cancer
Coronary heart disease
Colorectal cancer
Overall mortality
15 125 10 75 5 25
Benefits Risks
CE
CE MPA
Santen RJ et al J Clin Endocrinol Metab 2010
The basis of the Endocrine Society scientific statement for postmenopausal hormone replacement therapy (HRT) excess risks and benefits of HRT for 5 years in women aged 50ndash59 years or within 10 years of the start of menopause E=estrogen P=progestin
bull Younger women (aged 50ndash59 years) had more favorable results bull There are differences between CE alone and CEMPA arms bull Overall benefitrisk ratio of CE-alone appears to be more favourable than CEMPA
Reevaluation of WHI data (stratified by age) Risks and
Benefits of HRT Cases per 1000 Women per 5 Years of
Use
Medical condition which may be exacerbated by treatment
with progestins
Diabetes and metabolic syndrome
bull Treatment of oestrogen deficiency symptoms with progestin-containing HT (unlike oestrogen alone) may be associated with increases in insulin resistance and deterioration in glucose tolerance123
bull Postmenopausal women with diabetes could be inappropriate for treatment with progestin-containing HT due to the potential risk of exacerbation of their condition
1) Panay N amp Studd JWW Human Reprod Update 1997
2) Godsland I et al Metabolism 1993
3) Sites CK et al J Clin Endocrinol Metab 2005
Variations in Associated Breast Cancer
Risks Between CE alone and CEMPA
bull Use of CE alone for a median of 59 years was associated with a lower incidence of invasive breast cancer (151 cases 027 per year) compared with placebo (199 cases 035 per year HR 077 95 CI 062ndash095 P=002)
bull In the CE alone group fewer women died from invasive breast cancer (6 deaths 0009 per year) compared with controls (16 deaths 0024 per year HR 037 95 CI 013ndash091 P=003)
Anderson GL et al Lancet
Oncol 2012
Bazedoxifene (BZA) specifically selected in
combination with conjugated estrogens
bull BZA has been specifically selected for its unique pharmacologic profile and effects on VMS and uterine tissue in particular123
1 Crabtree J et al Mol Cell Endocrinol 2008
2 Kharode Y et al Endocrinolology 2008
3 Duavive SmPC
Estrogen Receptor activity is dimmed
Estrogen Receptor activity is turned on
CEs are agonists BZA is an antagonist
In the uterus
bull The BZA component reduces the risk of endometrial hyperplasia that can occur with the conjugated estrogens component alone3 This means that progestins are not needed
Extensive global clinical development program for
CEBZA
aIncludes additional pilot dose-finding study 203 1 Lobo RA et al Fertil Steril 2009 2 Pinkerton JV et al Menopause 2009 3 Kagan R et al Menopause 2010 4 Mirkin S et al Climacteric 2013 5 Pinkerton JV et al Obstet Gynecol 2013
Effects of conjugated estrogensbazedoxifene on
lipid and coagulation variables a randomized
placebo- and active-controlled trial
bull At 12 months
bull Both CEBZA doses were associated with small but significant effects on hemostasis variables including reductions in antithrombin plasminogen activator inhibitor-1 and fibrinogen activity and an increase in plasminogen activity relative to placebo at 12 months Incidences of cardiovascular and venous thromboembolic events were similar among treatment groups
bull CONCLUSIONS
bull This study provides reassurance that CEBZA does not adversely affect lipid metabolism or hemostatic balance In accordance the incidences of venous thromboembolic events and cardiovascular events in postmenopausal women are similar to those observed with placebo

Efficacy and Safety of Constant Oestrogen
Pulsed Progestogen vs
Continuous Combined HRT
Adverse Events
17b-oestradiol 17b-oestradiol norgestimate NETA (n = 150) (n = 172) Breast discomfort 14 27 Abdominal discomfort 14 22 Uterine bleeding 15 12 Dysmenorrhea 3 8 Oedema 5 8
Adapted from S Rozenberg et al Human Reproduction 2000
Medical condition which may be exacerbated by treatment
with progestins
Increased breast density
bull Increases in breast density are associated with progestin-containing HT which may adversely affect radiological detection of breast cancer1 and may be independently associated with an increased risk for the development of breast cancer2
bull The Postmenopausal EstrogenProgestin Interventions (PEPI) trial demonstrated that an increased mammographic breast density was associated with the use of E+P but not with the use of estrogen alone3
bull Women who already have high breast density may therefore be considered inappropriate for treatment with a progestin-containing HT
1) EU Core SPC for Hormone Replacement Therapy Products (CMDh1312003 Rev 4 June
2012)
2) De Villiers TJ et al on behalf of the International Menopause Society Climacteric 2013 16
3) Greendale GA et al J Natl Cancer Inst 2003
Stroke
0 25 5 75 10 125
Fractures
Diabetes
Breast cancer
Cholecystitis
Venothrombotic episodes
Endometrial cancer
Lung cancer
Coronary heart disease
Colorectal cancer
Overall mortality
15 125 10 75 5 25
Benefits Risks
CE
CE MPA
Santen RJ et al J Clin Endocrinol Metab 2010
The basis of the Endocrine Society scientific statement for postmenopausal hormone replacement therapy (HRT) excess risks and benefits of HRT for 5 years in women aged 50ndash59 years or within 10 years of the start of menopause E=estrogen P=progestin
bull Younger women (aged 50ndash59 years) had more favorable results bull There are differences between CE alone and CEMPA arms bull Overall benefitrisk ratio of CE-alone appears to be more favourable than CEMPA
Reevaluation of WHI data (stratified by age) Risks and
Benefits of HRT Cases per 1000 Women per 5 Years of
Use
Medical condition which may be exacerbated by treatment
with progestins
Diabetes and metabolic syndrome
bull Treatment of oestrogen deficiency symptoms with progestin-containing HT (unlike oestrogen alone) may be associated with increases in insulin resistance and deterioration in glucose tolerance123
bull Postmenopausal women with diabetes could be inappropriate for treatment with progestin-containing HT due to the potential risk of exacerbation of their condition
1) Panay N amp Studd JWW Human Reprod Update 1997
2) Godsland I et al Metabolism 1993
3) Sites CK et al J Clin Endocrinol Metab 2005
Variations in Associated Breast Cancer
Risks Between CE alone and CEMPA
bull Use of CE alone for a median of 59 years was associated with a lower incidence of invasive breast cancer (151 cases 027 per year) compared with placebo (199 cases 035 per year HR 077 95 CI 062ndash095 P=002)
bull In the CE alone group fewer women died from invasive breast cancer (6 deaths 0009 per year) compared with controls (16 deaths 0024 per year HR 037 95 CI 013ndash091 P=003)
Anderson GL et al Lancet
Oncol 2012
Bazedoxifene (BZA) specifically selected in
combination with conjugated estrogens
bull BZA has been specifically selected for its unique pharmacologic profile and effects on VMS and uterine tissue in particular123
1 Crabtree J et al Mol Cell Endocrinol 2008
2 Kharode Y et al Endocrinolology 2008
3 Duavive SmPC
Estrogen Receptor activity is dimmed
Estrogen Receptor activity is turned on
CEs are agonists BZA is an antagonist
In the uterus
bull The BZA component reduces the risk of endometrial hyperplasia that can occur with the conjugated estrogens component alone3 This means that progestins are not needed
Extensive global clinical development program for
CEBZA
aIncludes additional pilot dose-finding study 203 1 Lobo RA et al Fertil Steril 2009 2 Pinkerton JV et al Menopause 2009 3 Kagan R et al Menopause 2010 4 Mirkin S et al Climacteric 2013 5 Pinkerton JV et al Obstet Gynecol 2013
Effects of conjugated estrogensbazedoxifene on
lipid and coagulation variables a randomized
placebo- and active-controlled trial
bull At 12 months
bull Both CEBZA doses were associated with small but significant effects on hemostasis variables including reductions in antithrombin plasminogen activator inhibitor-1 and fibrinogen activity and an increase in plasminogen activity relative to placebo at 12 months Incidences of cardiovascular and venous thromboembolic events were similar among treatment groups
bull CONCLUSIONS
bull This study provides reassurance that CEBZA does not adversely affect lipid metabolism or hemostatic balance In accordance the incidences of venous thromboembolic events and cardiovascular events in postmenopausal women are similar to those observed with placebo
Medical condition which may be exacerbated by treatment
with progestins
Increased breast density
bull Increases in breast density are associated with progestin-containing HT which may adversely affect radiological detection of breast cancer1 and may be independently associated with an increased risk for the development of breast cancer2
bull The Postmenopausal EstrogenProgestin Interventions (PEPI) trial demonstrated that an increased mammographic breast density was associated with the use of E+P but not with the use of estrogen alone3
bull Women who already have high breast density may therefore be considered inappropriate for treatment with a progestin-containing HT
1) EU Core SPC for Hormone Replacement Therapy Products (CMDh1312003 Rev 4 June
2012)
2) De Villiers TJ et al on behalf of the International Menopause Society Climacteric 2013 16
3) Greendale GA et al J Natl Cancer Inst 2003
Stroke
0 25 5 75 10 125
Fractures
Diabetes
Breast cancer
Cholecystitis
Venothrombotic episodes
Endometrial cancer
Lung cancer
Coronary heart disease
Colorectal cancer
Overall mortality
15 125 10 75 5 25
Benefits Risks
CE
CE MPA
Santen RJ et al J Clin Endocrinol Metab 2010
The basis of the Endocrine Society scientific statement for postmenopausal hormone replacement therapy (HRT) excess risks and benefits of HRT for 5 years in women aged 50ndash59 years or within 10 years of the start of menopause E=estrogen P=progestin
bull Younger women (aged 50ndash59 years) had more favorable results bull There are differences between CE alone and CEMPA arms bull Overall benefitrisk ratio of CE-alone appears to be more favourable than CEMPA
Reevaluation of WHI data (stratified by age) Risks and
Benefits of HRT Cases per 1000 Women per 5 Years of
Use
Medical condition which may be exacerbated by treatment
with progestins
Diabetes and metabolic syndrome
bull Treatment of oestrogen deficiency symptoms with progestin-containing HT (unlike oestrogen alone) may be associated with increases in insulin resistance and deterioration in glucose tolerance123
bull Postmenopausal women with diabetes could be inappropriate for treatment with progestin-containing HT due to the potential risk of exacerbation of their condition
1) Panay N amp Studd JWW Human Reprod Update 1997
2) Godsland I et al Metabolism 1993
3) Sites CK et al J Clin Endocrinol Metab 2005
Variations in Associated Breast Cancer
Risks Between CE alone and CEMPA
bull Use of CE alone for a median of 59 years was associated with a lower incidence of invasive breast cancer (151 cases 027 per year) compared with placebo (199 cases 035 per year HR 077 95 CI 062ndash095 P=002)
bull In the CE alone group fewer women died from invasive breast cancer (6 deaths 0009 per year) compared with controls (16 deaths 0024 per year HR 037 95 CI 013ndash091 P=003)
Anderson GL et al Lancet
Oncol 2012
Bazedoxifene (BZA) specifically selected in
combination with conjugated estrogens
bull BZA has been specifically selected for its unique pharmacologic profile and effects on VMS and uterine tissue in particular123
1 Crabtree J et al Mol Cell Endocrinol 2008
2 Kharode Y et al Endocrinolology 2008
3 Duavive SmPC
Estrogen Receptor activity is dimmed
Estrogen Receptor activity is turned on
CEs are agonists BZA is an antagonist
In the uterus
bull The BZA component reduces the risk of endometrial hyperplasia that can occur with the conjugated estrogens component alone3 This means that progestins are not needed
Extensive global clinical development program for
CEBZA
aIncludes additional pilot dose-finding study 203 1 Lobo RA et al Fertil Steril 2009 2 Pinkerton JV et al Menopause 2009 3 Kagan R et al Menopause 2010 4 Mirkin S et al Climacteric 2013 5 Pinkerton JV et al Obstet Gynecol 2013
Effects of conjugated estrogensbazedoxifene on
lipid and coagulation variables a randomized
placebo- and active-controlled trial
bull At 12 months
bull Both CEBZA doses were associated with small but significant effects on hemostasis variables including reductions in antithrombin plasminogen activator inhibitor-1 and fibrinogen activity and an increase in plasminogen activity relative to placebo at 12 months Incidences of cardiovascular and venous thromboembolic events were similar among treatment groups
bull CONCLUSIONS
bull This study provides reassurance that CEBZA does not adversely affect lipid metabolism or hemostatic balance In accordance the incidences of venous thromboembolic events and cardiovascular events in postmenopausal women are similar to those observed with placebo

Stroke
0 25 5 75 10 125
Fractures
Diabetes
Breast cancer
Cholecystitis
Venothrombotic episodes
Endometrial cancer
Lung cancer
Coronary heart disease
Colorectal cancer
Overall mortality
15 125 10 75 5 25
Benefits Risks
CE
CE MPA
Santen RJ et al J Clin Endocrinol Metab 2010
The basis of the Endocrine Society scientific statement for postmenopausal hormone replacement therapy (HRT) excess risks and benefits of HRT for 5 years in women aged 50ndash59 years or within 10 years of the start of menopause E=estrogen P=progestin
bull Younger women (aged 50ndash59 years) had more favorable results bull There are differences between CE alone and CEMPA arms bull Overall benefitrisk ratio of CE-alone appears to be more favourable than CEMPA
Reevaluation of WHI data (stratified by age) Risks and
Benefits of HRT Cases per 1000 Women per 5 Years of
Use
Medical condition which may be exacerbated by treatment
with progestins
Diabetes and metabolic syndrome
bull Treatment of oestrogen deficiency symptoms with progestin-containing HT (unlike oestrogen alone) may be associated with increases in insulin resistance and deterioration in glucose tolerance123
bull Postmenopausal women with diabetes could be inappropriate for treatment with progestin-containing HT due to the potential risk of exacerbation of their condition
1) Panay N amp Studd JWW Human Reprod Update 1997
2) Godsland I et al Metabolism 1993
3) Sites CK et al J Clin Endocrinol Metab 2005
Variations in Associated Breast Cancer
Risks Between CE alone and CEMPA
bull Use of CE alone for a median of 59 years was associated with a lower incidence of invasive breast cancer (151 cases 027 per year) compared with placebo (199 cases 035 per year HR 077 95 CI 062ndash095 P=002)
bull In the CE alone group fewer women died from invasive breast cancer (6 deaths 0009 per year) compared with controls (16 deaths 0024 per year HR 037 95 CI 013ndash091 P=003)
Anderson GL et al Lancet
Oncol 2012
Bazedoxifene (BZA) specifically selected in
combination with conjugated estrogens
bull BZA has been specifically selected for its unique pharmacologic profile and effects on VMS and uterine tissue in particular123
1 Crabtree J et al Mol Cell Endocrinol 2008
2 Kharode Y et al Endocrinolology 2008
3 Duavive SmPC
Estrogen Receptor activity is dimmed
Estrogen Receptor activity is turned on
CEs are agonists BZA is an antagonist
In the uterus
bull The BZA component reduces the risk of endometrial hyperplasia that can occur with the conjugated estrogens component alone3 This means that progestins are not needed
Extensive global clinical development program for
CEBZA
aIncludes additional pilot dose-finding study 203 1 Lobo RA et al Fertil Steril 2009 2 Pinkerton JV et al Menopause 2009 3 Kagan R et al Menopause 2010 4 Mirkin S et al Climacteric 2013 5 Pinkerton JV et al Obstet Gynecol 2013
Effects of conjugated estrogensbazedoxifene on
lipid and coagulation variables a randomized
placebo- and active-controlled trial
bull At 12 months
bull Both CEBZA doses were associated with small but significant effects on hemostasis variables including reductions in antithrombin plasminogen activator inhibitor-1 and fibrinogen activity and an increase in plasminogen activity relative to placebo at 12 months Incidences of cardiovascular and venous thromboembolic events were similar among treatment groups
bull CONCLUSIONS
bull This study provides reassurance that CEBZA does not adversely affect lipid metabolism or hemostatic balance In accordance the incidences of venous thromboembolic events and cardiovascular events in postmenopausal women are similar to those observed with placebo

Medical condition which may be exacerbated by treatment
with progestins
Diabetes and metabolic syndrome
bull Treatment of oestrogen deficiency symptoms with progestin-containing HT (unlike oestrogen alone) may be associated with increases in insulin resistance and deterioration in glucose tolerance123
bull Postmenopausal women with diabetes could be inappropriate for treatment with progestin-containing HT due to the potential risk of exacerbation of their condition
1) Panay N amp Studd JWW Human Reprod Update 1997
2) Godsland I et al Metabolism 1993
3) Sites CK et al J Clin Endocrinol Metab 2005
Variations in Associated Breast Cancer
Risks Between CE alone and CEMPA
bull Use of CE alone for a median of 59 years was associated with a lower incidence of invasive breast cancer (151 cases 027 per year) compared with placebo (199 cases 035 per year HR 077 95 CI 062ndash095 P=002)
bull In the CE alone group fewer women died from invasive breast cancer (6 deaths 0009 per year) compared with controls (16 deaths 0024 per year HR 037 95 CI 013ndash091 P=003)
Anderson GL et al Lancet
Oncol 2012
Bazedoxifene (BZA) specifically selected in
combination with conjugated estrogens
bull BZA has been specifically selected for its unique pharmacologic profile and effects on VMS and uterine tissue in particular123
1 Crabtree J et al Mol Cell Endocrinol 2008
2 Kharode Y et al Endocrinolology 2008
3 Duavive SmPC
Estrogen Receptor activity is dimmed
Estrogen Receptor activity is turned on
CEs are agonists BZA is an antagonist
In the uterus
bull The BZA component reduces the risk of endometrial hyperplasia that can occur with the conjugated estrogens component alone3 This means that progestins are not needed
Extensive global clinical development program for
CEBZA
aIncludes additional pilot dose-finding study 203 1 Lobo RA et al Fertil Steril 2009 2 Pinkerton JV et al Menopause 2009 3 Kagan R et al Menopause 2010 4 Mirkin S et al Climacteric 2013 5 Pinkerton JV et al Obstet Gynecol 2013
Effects of conjugated estrogensbazedoxifene on
lipid and coagulation variables a randomized
placebo- and active-controlled trial
bull At 12 months
bull Both CEBZA doses were associated with small but significant effects on hemostasis variables including reductions in antithrombin plasminogen activator inhibitor-1 and fibrinogen activity and an increase in plasminogen activity relative to placebo at 12 months Incidences of cardiovascular and venous thromboembolic events were similar among treatment groups
bull CONCLUSIONS
bull This study provides reassurance that CEBZA does not adversely affect lipid metabolism or hemostatic balance In accordance the incidences of venous thromboembolic events and cardiovascular events in postmenopausal women are similar to those observed with placebo

Variations in Associated Breast Cancer
Risks Between CE alone and CEMPA
bull Use of CE alone for a median of 59 years was associated with a lower incidence of invasive breast cancer (151 cases 027 per year) compared with placebo (199 cases 035 per year HR 077 95 CI 062ndash095 P=002)
bull In the CE alone group fewer women died from invasive breast cancer (6 deaths 0009 per year) compared with controls (16 deaths 0024 per year HR 037 95 CI 013ndash091 P=003)
Anderson GL et al Lancet
Oncol 2012
Bazedoxifene (BZA) specifically selected in
combination with conjugated estrogens
bull BZA has been specifically selected for its unique pharmacologic profile and effects on VMS and uterine tissue in particular123
1 Crabtree J et al Mol Cell Endocrinol 2008
2 Kharode Y et al Endocrinolology 2008
3 Duavive SmPC
Estrogen Receptor activity is dimmed
Estrogen Receptor activity is turned on
CEs are agonists BZA is an antagonist
In the uterus
bull The BZA component reduces the risk of endometrial hyperplasia that can occur with the conjugated estrogens component alone3 This means that progestins are not needed
Extensive global clinical development program for
CEBZA
aIncludes additional pilot dose-finding study 203 1 Lobo RA et al Fertil Steril 2009 2 Pinkerton JV et al Menopause 2009 3 Kagan R et al Menopause 2010 4 Mirkin S et al Climacteric 2013 5 Pinkerton JV et al Obstet Gynecol 2013
Effects of conjugated estrogensbazedoxifene on
lipid and coagulation variables a randomized
placebo- and active-controlled trial
bull At 12 months
bull Both CEBZA doses were associated with small but significant effects on hemostasis variables including reductions in antithrombin plasminogen activator inhibitor-1 and fibrinogen activity and an increase in plasminogen activity relative to placebo at 12 months Incidences of cardiovascular and venous thromboembolic events were similar among treatment groups
bull CONCLUSIONS
bull This study provides reassurance that CEBZA does not adversely affect lipid metabolism or hemostatic balance In accordance the incidences of venous thromboembolic events and cardiovascular events in postmenopausal women are similar to those observed with placebo

Bazedoxifene (BZA) specifically selected in
combination with conjugated estrogens
bull BZA has been specifically selected for its unique pharmacologic profile and effects on VMS and uterine tissue in particular123
1 Crabtree J et al Mol Cell Endocrinol 2008
2 Kharode Y et al Endocrinolology 2008
3 Duavive SmPC
Estrogen Receptor activity is dimmed
Estrogen Receptor activity is turned on
CEs are agonists BZA is an antagonist
In the uterus
bull The BZA component reduces the risk of endometrial hyperplasia that can occur with the conjugated estrogens component alone3 This means that progestins are not needed
Extensive global clinical development program for
CEBZA
aIncludes additional pilot dose-finding study 203 1 Lobo RA et al Fertil Steril 2009 2 Pinkerton JV et al Menopause 2009 3 Kagan R et al Menopause 2010 4 Mirkin S et al Climacteric 2013 5 Pinkerton JV et al Obstet Gynecol 2013
Effects of conjugated estrogensbazedoxifene on
lipid and coagulation variables a randomized
placebo- and active-controlled trial
bull At 12 months
bull Both CEBZA doses were associated with small but significant effects on hemostasis variables including reductions in antithrombin plasminogen activator inhibitor-1 and fibrinogen activity and an increase in plasminogen activity relative to placebo at 12 months Incidences of cardiovascular and venous thromboembolic events were similar among treatment groups
bull CONCLUSIONS
bull This study provides reassurance that CEBZA does not adversely affect lipid metabolism or hemostatic balance In accordance the incidences of venous thromboembolic events and cardiovascular events in postmenopausal women are similar to those observed with placebo

Extensive global clinical development program for
CEBZA
aIncludes additional pilot dose-finding study 203 1 Lobo RA et al Fertil Steril 2009 2 Pinkerton JV et al Menopause 2009 3 Kagan R et al Menopause 2010 4 Mirkin S et al Climacteric 2013 5 Pinkerton JV et al Obstet Gynecol 2013
Effects of conjugated estrogensbazedoxifene on
lipid and coagulation variables a randomized
placebo- and active-controlled trial
bull At 12 months
bull Both CEBZA doses were associated with small but significant effects on hemostasis variables including reductions in antithrombin plasminogen activator inhibitor-1 and fibrinogen activity and an increase in plasminogen activity relative to placebo at 12 months Incidences of cardiovascular and venous thromboembolic events were similar among treatment groups
bull CONCLUSIONS
bull This study provides reassurance that CEBZA does not adversely affect lipid metabolism or hemostatic balance In accordance the incidences of venous thromboembolic events and cardiovascular events in postmenopausal women are similar to those observed with placebo

Effects of conjugated estrogensbazedoxifene on
lipid and coagulation variables a randomized
placebo- and active-controlled trial
bull At 12 months
bull Both CEBZA doses were associated with small but significant effects on hemostasis variables including reductions in antithrombin plasminogen activator inhibitor-1 and fibrinogen activity and an increase in plasminogen activity relative to placebo at 12 months Incidences of cardiovascular and venous thromboembolic events were similar among treatment groups
bull CONCLUSIONS
bull This study provides reassurance that CEBZA does not adversely affect lipid metabolism or hemostatic balance In accordance the incidences of venous thromboembolic events and cardiovascular events in postmenopausal women are similar to those observed with placebo