
Sequestration Erythrocytes Clearance Function ...iai.asm.org/content/36/1/96.full.pdf ·...
7
Vol. 36, No. 1 INFECTION AND IMMUNITY, Apr. 1982, p. 96-102 0019-9567/82/040096-07$02.00/0 Effect of Splenic Sequestration of Erythrocytes on Splenic Clearance Function and Susceptibility to Septic Peritonitis GARY J. GROVER AND DANIEL J. LOEGERING* Department of Physiology, Albany Medical College of Union University, Albany, New York 12208 Received 14 August 1981/Accepted 7 December 1981 The effect of splenic sequestration of erythrocytes (RBC) on splenic clearance function and susceptibility to septic peritonitis was studied. Homologous RBC were treated with 20 mM phenylhydrazine hydrochloride in vitro and injected into rats at doses of 5, 15, 75, and 150 mg of hemoglobin per 100 g. Splenic sequestration of these phenylhydrazine-treated RBC at 24 h after injection was 87, 93, 23, and 13% of the injected dose, respectively, whereas less than 2.1% of the same doses of washed RBC were localized in the spleen. The total quantity of phenylhydrazine-treated RBC sequestered by the spleen was similar for the three larger doses (40 to 45 mg of hemoglobin per g of tissue), indicating that this is the capacity of the spleen to take up this type of RBC in 24 h. The phenylhydrazine- treated RBC in doses of 15, 75, and 150 mg of hemoglobin per 100 g depressed the clearance rate and splenic localization of a test dose of phenylhydrazine-treated RBC, whereas splenic clearance function was unchanged after a dose of 5 mg of hemoglobin per 100 g. Splenectomy or injection of doses of phenylhydrazine- treated RBC which depressed splenic clearance function increased the suscepti- bility to septic peritonitis induced by cecal ligation and puncture. After thermal injury, splenic clearance function was found to be depressed. Also, splenic localization of RBC 24 h after thermal injury was found to be approximately equal to that after injection of the doses of phenylhydrazine-treated RBC which depressed splenic clearance function. It is concluded that splenic sequestration of RBC can depress splenic clearance function and increase susceptibility to peritonitis, and that this may be one mechanism for the increased susceptibility to infection seen after thermal injury. Thermal injury is well known to be associated with increased susceptibility to infection (1, 26, 29). Thermal injury is also often associated with increased splenic sequestration of erythrocytes (RBC) and anemia which may progress for sev- eral days postinjury (5, 15, 23, 32). Several studies have reported that patients with various types of anemias show an increased susceptibil- ity to infections (2, 4, 17, 27, 28). Apparently, splenic sequestration of a large number of RBC results in an enlarged spleen with very little functional capacity (28). This condition may be analogous to the increased susceptibility of sple- nectomized children to infection (3). Animal studies have also shown that splenectomy in- creases susceptibility to certain forms of infec- tion (12, 13, 22). Thus, it is possible that the splenic sequestration of RBC may impair splenic function and thereby contribute to the increased susceptibility to infection after thermal injury. The purpose of the present study was to: (i) characterize a form of altered RBC, phenylhy- drazine-treated RBC, which is sequestered pri- marily by the spleen; (ii) determine whether depression of splenic clearance function due to RBC sequestration is associated with increased susceptibility to experimental septic peritonitis; (iii) determine whether splenic RBC sequestra- tion after thermal injury is comparable to the extent of splenic sequestration required to in- duce increased susceptibility to infection. MATERIALS AND METHODS Preparation of washed RBC. Male, inbred Sprague- Dawley rats weighing 250 to 300 g were used for all experiments. Blood was collected in anticoagulant citrate dextrose from animals under ether anesthesia. The RBC were washed twice with phosphate-buffered saline (PBS; 0.9%o NaCl in 5 mM phosphate buffer, pH 7.4), and the buffy coat was removed. After the last wash the packed RBC were resuspended in an equal volume of PBS, and the hemoglobin (Hb) concentra- tion was determined by the cyanmethemoglobin meth- od. Preparation of phenylhydrazine-treated RBC. An equal volume of 20 mM phenylhydrazine hydrochlo- ride in 0.9% NaCl (pH 7.4) was added to a suspension of washed RBC in PBS. This RBC suspension was incubated at 37°C with gentle agitation for 45 min. The RBC were washed 3 times in PBS, the packed RBC were resuspended in an equal volume of PBS, and the Hb concentration was determined. Phenylhydrazine- 96 on November 5, 2018 by guest http://iai.asm.org/ Downloaded from
Transcript of Sequestration Erythrocytes Clearance Function ...iai.asm.org/content/36/1/96.full.pdf ·...
Vol. 36, No. 1INFECTION AND IMMUNITY, Apr. 1982, p. 96-1020019-9567/82/040096-07$02.00/0
Effect of Splenic Sequestration of Erythrocytes on SplenicClearance Function and Susceptibility to Septic Peritonitis
GARY J. GROVER AND DANIEL J. LOEGERING*Department of Physiology, Albany Medical College of Union University, Albany, New York 12208
Received 14 August 1981/Accepted 7 December 1981
The effect of splenic sequestration of erythrocytes (RBC) on splenic clearancefunction and susceptibility to septic peritonitis was studied. Homologous RBCwere treated with 20 mM phenylhydrazine hydrochloride in vitro and injected intorats at doses of 5, 15, 75, and 150 mg of hemoglobin per 100 g. Splenicsequestration of these phenylhydrazine-treated RBC at 24 h after injection was 87,93, 23, and 13% of the injected dose, respectively, whereas less than 2.1% of thesame doses of washed RBC were localized in the spleen. The total quantity ofphenylhydrazine-treated RBC sequestered by the spleen was similar for the threelarger doses (40 to 45 mg of hemoglobin per g of tissue), indicating that this is thecapacity of the spleen to take up this type of RBC in 24 h. The phenylhydrazine-treated RBC in doses of 15, 75, and 150 mg of hemoglobin per 100 g depressed theclearance rate and splenic localization of a test dose of phenylhydrazine-treatedRBC, whereas splenic clearance function was unchanged after a dose of 5 mg ofhemoglobin per 100 g. Splenectomy or injection of doses of phenylhydrazine-treated RBC which depressed splenic clearance function increased the suscepti-bility to septic peritonitis induced by cecal ligation and puncture. After thermalinjury, splenic clearance function was found to be depressed. Also, spleniclocalization of RBC 24 h after thermal injury was found to be approximately equalto that after injection of the doses of phenylhydrazine-treated RBC whichdepressed splenic clearance function. It is concluded that splenic sequestration ofRBC can depress splenic clearance function and increase susceptibility toperitonitis, and that this may be one mechanism for the increased susceptibility toinfection seen after thermal injury.
Thermal injury is well known to be associatedwith increased susceptibility to infection (1, 26,29). Thermal injury is also often associated withincreased splenic sequestration of erythrocytes(RBC) and anemia which may progress for sev-eral days postinjury (5, 15, 23, 32). Severalstudies have reported that patients with varioustypes of anemias show an increased susceptibil-ity to infections (2, 4, 17, 27, 28). Apparently,splenic sequestration of a large number of RBCresults in an enlarged spleen with very littlefunctional capacity (28). This condition may beanalogous to the increased susceptibility of sple-nectomized children to infection (3). Animalstudies have also shown that splenectomy in-creases susceptibility to certain forms of infec-tion (12, 13, 22). Thus, it is possible that thesplenic sequestration ofRBC may impair splenicfunction and thereby contribute to the increasedsusceptibility to infection after thermal injury.The purpose of the present study was to: (i)
characterize a form of altered RBC, phenylhy-drazine-treated RBC, which is sequestered pri-marily by the spleen; (ii) determine whetherdepression of splenic clearance function due to
RBC sequestration is associated with increasedsusceptibility to experimental septic peritonitis;(iii) determine whether splenic RBC sequestra-tion after thermal injury is comparable to theextent of splenic sequestration required to in-duce increased susceptibility to infection.
MATERIALS AND METHODSPreparation of washed RBC. Male, inbred Sprague-
Dawley rats weighing 250 to 300 g were used for allexperiments. Blood was collected in anticoagulantcitrate dextrose from animals under ether anesthesia.The RBC were washed twice with phosphate-bufferedsaline (PBS; 0.9%o NaCl in 5 mM phosphate buffer, pH7.4), and the buffy coat was removed. After the lastwash the packed RBC were resuspended in an equalvolume of PBS, and the hemoglobin (Hb) concentra-tion was determined by the cyanmethemoglobin meth-od.
Preparation of phenylhydrazine-treated RBC. Anequal volume of 20 mM phenylhydrazine hydrochlo-ride in 0.9% NaCl (pH 7.4) was added to a suspensionof washed RBC in PBS. This RBC suspension wasincubated at 37°C with gentle agitation for 45 min. TheRBC were washed 3 times in PBS, the packed RBCwere resuspended in an equal volume of PBS, and theHb concentration was determined. Phenylhydrazine-
96
on Novem
ber 5, 2018 by guesthttp://iai.asm
.org/D
ownloaded from
SPLENIC RBC SEQUESTRATION AND HOST DEFENSE 97
treated RBC to be used for clearance and organlocalization studies were labeled with 5'Cr beforetreatment with phenylhydrazine.Blood clearance rate and organ localization of phenyl-
hydrazine-treated RBC. Clearance rate and organ lo-calization of phenylhydrazine-treated RBC were de-termined from the injection of four doses (5, 15, 75,and 150 mg of Hb per 100 g) of phenylhydrazine-treated RBC. Control animals received equal doses oflabeled washed RBC. The injections were made underether anesthesia, and small blood samples (0.1 ml)were taken from the tail at 24-min intervals for 2 h.Half-time was calculated from the slope of the linearregression equation of loglo of blood radioactivityversus time. Immediately after the last sample at 2 h,the animals were killed, and the radioactivity presentin the liver, spleen, and lungs was determined. In aseparate series of experiments, organ localization ofphenylhydrazine-treated RBC was determined 24 hafter injection. Organ localization data are expressedas the percentage of the injected dose per total organand as milligrams of Hb per gram of tissue.
Splenic dearance function. Splenic clearance func-tion was assessed from the clearance rate and organlocalization of labeled phenylhydrazine-treated RBCgiven at a dose of 15 mg ofHb per 100 g. The clearancerate was measured over 2 h and organ localization wasdetermined at 2 h after injection of the labeled phenyl-hydrazine-treated RBC as described above. Splenicclearance function was determined at 24 h after thephenylhydrazine-treated RBC doses of 5, 15, 75, and150 mg of Hb per 100 g as well as at 24 h after thermalinjury. Controls received injections of equal amountsof washed RBC.
Hepatic clearance function. Hepatic clearance func-tion was assessed from the clearance rate and organlocalization of formalinized sheep RBC (SRBC). He-patic clearance function was determined at 5 h afterinjection of the phenylhydrazine-treated RBC dose of150 mg of Hb per 100 g. Sheep blood (MA Bio-products, Walkersville, Md.) was washed in PBS threetimes, and the SRBC were labeled with 51Cr. TheSRBC were formalinized by the method of Czismas(14). Immediately before determination of hepaticclearance the animals were anesthetized with sodiumpentobarbital (30 mg/kg, intravenously), and a carotidartery was cannulated for taking blood samples. SRBCwere injected at a dose of 3 x 109/100 g; small bloodsamples (0.1 ml) were taken each minute for 5 min, andclearance half-time was calculated. Immediately afterthe last blood samples were taken, the animals werekilled, and the radioactivity present in the liver,spleen, and lungs was determined. Tissue radioactivitywas expressed as the percentage of the injected doseper organ.
Splenic and hepatic erythrocyte sequestration afterthermal injury. To measure splenic and hepatic se-questration of normal RBC after thermal injury, ratswere injected with washed, 51Cr-labeled RBC (30 mgof Hb per 100 g) 30 min before injury. Thermal injuryconsisted of a 30-s scald in 90°C water on the dorsumwhich involved 26 to 28% of the body surface area(33). The rats were given intraperitoneal 0.9%o NaCl(10%o body weight) immediately before injury to re-duce mortality. Controls were given 51Cr-labeledwashed RBC 30 min before saline resuscitation with-out thermal injury. At 24 h after thermal injury, the
liver, spleen, and lungs were removed, and the per-centage of the injected dose of radioactivity per organwas determined. The amount of splenic RBC seques-tration after thermal injury was compared with theamount of splenic RBC sequestration observed withthe doses of phenylhydrazine-treated RBC which de-pressed splenic clearance function and increased sus-ceptibility to peritonitis.To estimate the amount of free Hb which would be
taken up by the liver and spleen after the intravascularhemolysis which accompanies thermal injury, the or-gan localization of labeled Hb was determined. Acrude preparation of rat Hb was prepared from 5tCr-labeled RBC as previously reported (25). The Hb wasdialyzed against PBS overnight to remove free 51Cr.Hepatic and splenic localization of the labeled Hbwere determined 24 h after injection of 50 mg of Hb per100 g. This dose was chosen because it producesplasma Hb levels similar to those seen after thermalinjury (25).
Experimental peritonitis. Peritonitis was induced byusing the cecal ligation method previously employed inthis laboratory which is based on the technique ofWichterman et al. (16, 35). Phenylhydrazine-treatedRBC were injected at doses of 5, 15, 75, or 150 mg ofHb per 100 g at 5 h before cecal ligation. This time waschosen because it is near the half-time for the threesmaller doses of phenylhydrazine-treated RBC. Con-trols received an injection of an equal dose of washedRBC. Sham-operated controls had the same abdomi-nal incision and cecal manipulation, but no cecalligation. In another series of experiments, splenecto-my or sham splenectomy was performed at the time ofcecal ligation.
For the induction of peritonitis, rats were anesthe-tized with ether, and the cecum was exposed through amidline incision and ligated just below the ileocecalvalve. The cecum was punctured twice with an 18-gauge needle, and a small amount (0.05 ml) of cecalcontents was squeezed out of each puncture. Mortalitywas recorded at 8-h intervals after surgery for 72 h,and time to death was ranked at these 8-hr intervals.
Statistical analysis. Data for half-times and organlocalization were expressed as the mean ± standarderror and statistically analyzed by using the Student t-test. Differences in death rates were analyzed usingthe Mann Whitney U test with tied ranks. The confi-dence level was placed at 95% for all experiments.
RESULTSClearance rate and organ localization of phen-
ylhydrazine-treated RBC. Preliminary studieswere done to establish the phenylhydrazinetreatment necessary to obtain RBC which werecleared primarily by the spleen. The data inTable 1 show that the treatment used resulted inRBC which were cleared with a half-time of 3 to5 h except for the largest dose (150 mg of Hb per100 g) which had a half-time of nearly 10 h.Splenic sequestration of these phenylhydrazine-treated RBC was always much higher than non-treated RBC. Splenic localization represented anearly constant fraction of the injected dose forthe three lowest doses at 2 h after injection. At24 h after injection virtually all of the smallest
VOL. 36, 1982
on Novem
ber 5, 2018 by guesthttp://iai.asm
.org/D
ownloaded from
98 GROVER AND LOEGERING
0C W - N" N 00 0
+1 tl +1 +1 +1 +1 +1 +100 - 0' o%00 oooCiNCA eq W)
o r"=
en000O-Q 0* . 0. . 0* .0.
0 0 N 000N oo-
+l +1 +1 +1 +1 +1 +1+l
0 oN e00
0 e0 -Q
.0. .0 .0 .0.00 11.0 C-I ~.0 V- It 00 110
000, 00+l +1 +1 +1 +1 +1+ +l
ON eo N o X
0n - 0\e' N r N\
. . 0* .0. *ON cOoN
V)00000000~~~o oooooo
+l +1 +1 +1 +1 +1 +1 +1r£NX N 0f £ o
N.-" 'N 00 " 0l 0\N
N-" .0 .
o HO o
00000
+l +l +1 +1 +1 +1 +1 +1VI)~ " en " 00
tN 0 o
*.0 .
.0 -0 .0
+1 + +1 +1 +1 +1+ +r - r- 'en
.0. .0 . 00.
Cl ClN 0 '0 0 "*. * . ~. -
+l +1 +1 +1 +1 +1+ +Im It 00 " " N 00
en
C
O I0
. *. >** >*
;N;I^ tt4) 4) 4)
._._ ._ ._
> e'0. '0. '0. '0.
U,#CX= 0'44)'44)'44)'4G);
= s: 0:===s-d NY
INFECT. IMMUN.
0
4)
'0'4-c00
+1
2
4)
.0
'40
4)
0
0
4)
'4
'4
0
0
'4
00
004)0.4)0_0'0o)4)
0n4)
I-
U'
'4
0._ 0
N C-
u0
O _S.g_ ,*=.
two doses were localized in the spleen, withprogressively lower fractions of the injecteddose present in the spleen for the two largerdoses. However, the total quantity of phenylhy-drazine-treated RBC sequestered by the spleenwas very similar for the highest 3 doses (40 to 45mg Hb per g of splenic tissue). With the lowestdose of phenylhydrazine-treated RBC the splen-ic localization was 13 mg of Hb per g. Hepaticlocalization demonstrated a nearly constantfraction of the injected dose present in the liverat each dose (Table 1). Hepatic localization ofthe phenylhydrazine-treated RBC was substan-tially less than the splenic localization, althoughat 24 h after injection of 150 mg of Hb per 100 g,the hepatic localization was 61.3% of the spleniclocalization. Lung localization of phenylhydra-zine-treated RBC never exceeded 2% of theinjected dose and did not vary with dose (Table1).
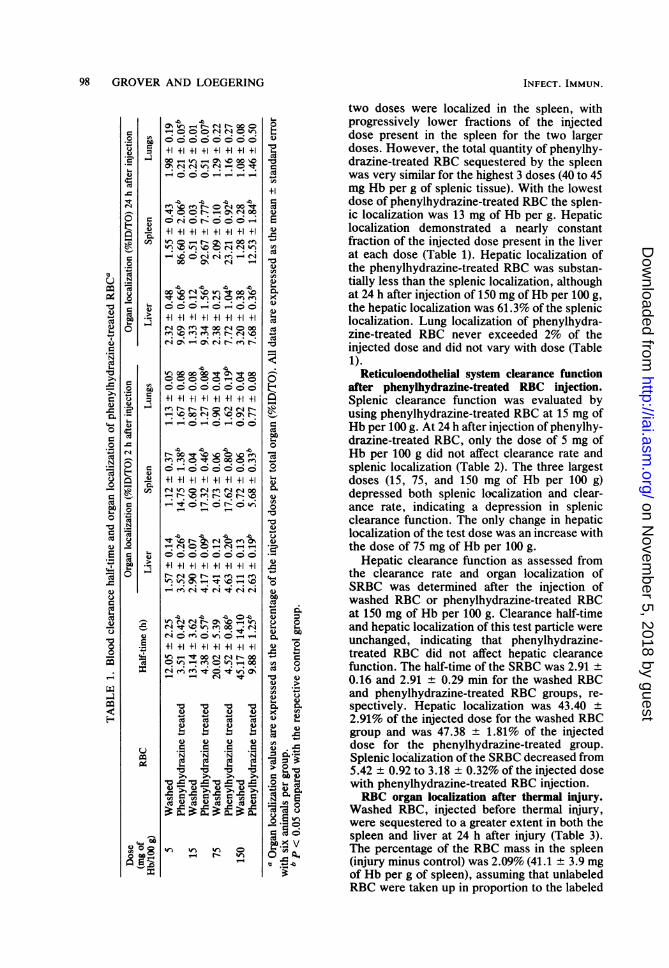
Reticuloendothelial system clearance functionafter phenylhydrazine-treated RBC inj,ection.Splenic clearance function was evaluated byusing phenylhydrazine-treated RBC at 15 mg ofHb per 100 g. At 24 h after injection of phenylhy-drazine-treated RBC, only the dose of 5 mg ofHb per 100 g did not affect clearance rate andsplenic localization (Table 2). The three largestdoses (15, 75, and 150 mg of Hb per 100 g)depressed both splenic localization and clear-ance rate, indicating a depression in splenicclearance function. The only change in hepaticlocalization of the test dose was an increase withthe dose of 75 mg of Hb per 100 g.
Hepatic clearance function as assessed fromthe clearance rate and organ localization ofSRBC was determined after the injection ofwashed RBC or phenylhydrazine-treated RBCat 150 mg of Hb per 100 g. Clearance half-timeand hepatic localization of this test particle wereunchanged, indicating that phenylhydrazine-treated RBC did not affect hepatic clearancefunction. The half-time of the SRBC was 2.91 ±0.16 and 2.91 ± 0.29 min for the washed RBCand phenylhydrazine-treated RBC groups, re-spectively. Hepatic localization was 43.40 +2.91% of the injected dose for the washed RBCgroup and was 47.38 ± 1.81% of the injecteddose for the phenylhydrazine-treated group.Splenic localization of the SRBC decreased from5.42 ± 0.92 to 3.18 + 0.32% of the injected dosewith phenylhydrazine-treated RBC injection.RBC organ localization after thermal inJury.
Washed RBC, injected before thermal injury,were sequestered to a greater extent in both thespleen and liver at 24 h after injury (Table 3).The percentage of the RBC mass in the spleen(injury minus control) was 2.09% (41.1 ± 3.9 mgof Hb per g of spleen), assuming that unlabeledRBC were taken up in proportion to the labeled
0r._E0
Ucu
4.)
01.(I)
t
'14N
00
fc
'4040
0.0
cdo9
00
I
4.)0:e
S.0
0
a'4elc
0
0
.No0u.2r.m
m4la'04-cd
0
'4-
0
r.
04)
*.0
0.0-
0
'4
N
0
0'4
40
I-
.
Ev
0
'00
'4
'.4
F4)
0
;.
4)4L)
c'
S.
Ci2
400
0
04
4)00
c)m
I--
0oco o
V'4
on Novem
ber 5, 2018 by guesthttp://iai.asm
.org/D
ownloaded from
SPLENIC RBC SEQUESTRATION AND HOST DEFENSE 99
TABLE 2. Splenic clearance function 24 h after injection of phenylhydrazine-treated RBC'
Dose Organ localization (%ID/TO)b(mg of RBC Half-time (h) Liver Spleen Lungs
Hb/100 g) Liver Spleen Lungs
5 Washed 5.96 t 1.92 3.82 t 0.22 12.33 ± 1.01 1.58 ± 0.14Phenylhydrazine 5.24 ± 0.94 4.22 t 0.47 12.85 ± 1.06 2.05 ± 0.28
treated15 Washed 4.41 ± 0.31 5.76 ± 0.44 20.07 ± 1.32 1.56 ± 0.14
Phenylhydrazine 5.89 + 0.51c 5.50 ± 0.59 15.07 ± 1.18c 1.74 ± 0.16treated
75 Washed 5.42 ± 1.22 4.70 ± 0.38 14.51 ± 1.81 1.58 ± 0.14Phenylhydrazine 14.89 ± 3.74c 6.21 ± 0.28c 7.44 ± 0.52c 2.77 ± 0.51c
treated150 Washed 6.24 ± 0.51 4.35 ± 0.03 17.59 ± 1.60 2.05 ± 0.07
Phenylhydrazine 12.34 ± 2.48c 4.18 + 0.26 10.25 + 1.24c 2.02 ± 0.22treated
a Splenic clearance function was assessed from the clearance rate and organ localization of phenylhydrazine-treated RBC (15 mg of Hb per 100 g) 24 h after injection of the indicated doses of phenylhydrazine-treated RBCor washed RBC. Half-times were measured over 2 h and organ localizations of the test dose were determined at 2h after injection.
b Organ localization is expressed as the percentage of the injected dose per total organ (%ID/TO). All data areexpressed as the mean + standard error with 6 to 12 animals per group.
c P < 0.05 compared with the respective control.
RBC. Hepatic localization of washed RBC was
also increased after thermal injury and repre-sented 1.71% of the RBC mass (injury minuscontrol). The measurement of labeled Hb organlocalization in noninjured animals showed thatwith a dose of 50 mg of Hb per 100 g 3.79 ± 0.29and 0.51 ± 0.03% of the injected dose was
localized in the liver and spleen, respectively (n= 6). This indicates that labeled Hb free in thecirculation as a result of intravascular hemolysiscontributed very little to the organ localizationsofwashed RBC after thermal injury, and that thesplenic localization of 51Cr was primarily due tosequestration of unlysed RBC. The dose of 50mg of Hb per 100 g was chosen to mimic theextent of intravascular hemolysis which accom-panies this degree of thermal injury (25).
Effect of thermal inijury on splenic clearancefunction. At 24 h after thermal injury, splenicclearance function was depressed as indicatedby a decrease in clearance rate and spleniclocalization of the phenylhydrazine-treated testRBC (Table 4). Hepatic and pulmonary localiza-tion of the test RBC were unchanged.
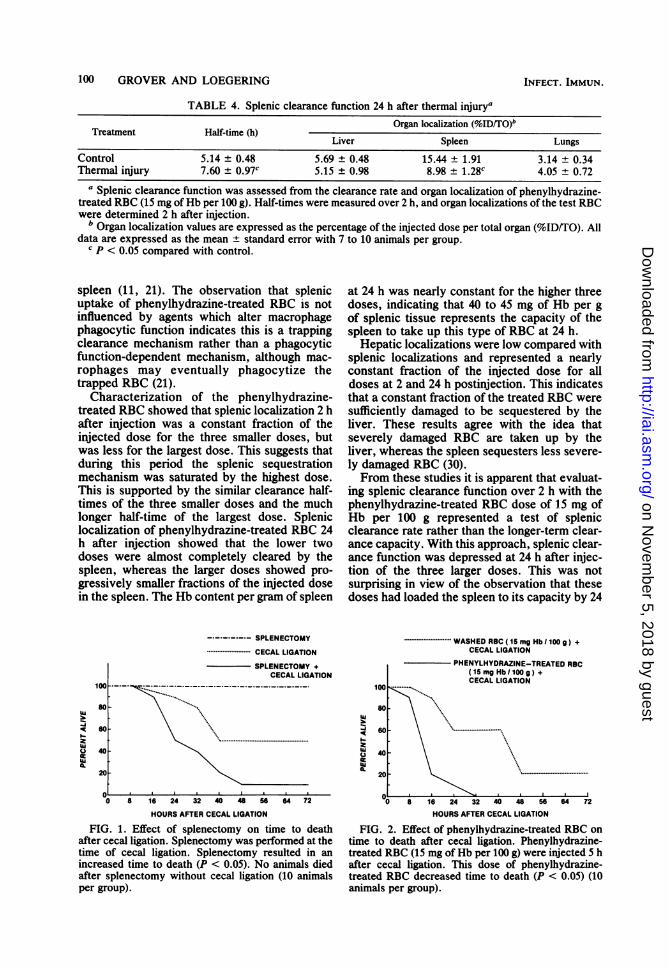
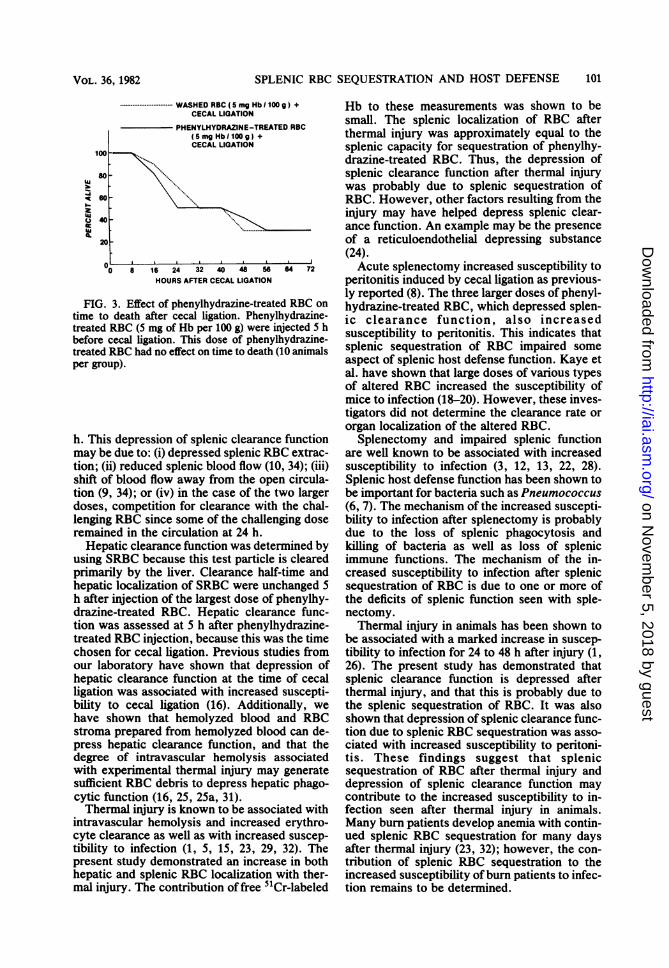
Effect of splenectomy and phenylhydrazine-treated RBC on susceptibility to infection. Sple-nectomy at the time of cecal ligation reducedsurvival time, indicating that the absence ofsplenic function decreases time to death withperitonitis (Fig. 1). Sham cecal ligation was notassociated with any mortality (Fig. 1). Injectionof phenylhydrazine-treated RBC at 15 mg of Hbper 100 g 5 h before cecal ligation decreased timeto death (Fig. 2), whereas the dose of 5 mg of Hbper 100 g had no effect on time to death (Fig. 3).The phenylhydrazine-treated RBC doses of 75and 150 mg of Hb per 100 g also decreased timeto death after cecal ligation. Control animalswith cecal ligation received injections of equaldoses of washed RBC.
DISCUSSIONPhenylhydrazine-treated RBC are known to
be removed from the circulation primarily by thespleen (11, 21). This clearance is thought to bedue to Heinz body inclusions and altered mem-brane properties causing sequestration of theRBC by the unique vascular architecture of the
TABLE 3. Organ localization of washed RBC after thermal injuryaOrgan localization (%ID/TO)b
TreatmentLiver Spleen Lungs
Control 2.13 ± 0.10 1.47 ± 0.05 0.75 ± 0.03Thermal injury 3.84 ± 0.19c 3.56 ± 0.37c 0.68 ± 0.09
a Washed RBC (30 mg of Hb per 100 g, 51Cr labeled) were injected 0.5 h before thermal injury. Organs werecollected 24 h postinjury.
b Values are expressed as the percentage of injected dose per total or total organ (%ID/TO). All data areexpressed as the mean ± standard error with six animals per group.
c P < 0.05 compared with control group.
VOL. 36, 1982
on Novem
ber 5, 2018 by guesthttp://iai.asm
.org/D
ownloaded from
100 GROVER AND LOEGERING
TABLE 4. Splenic clearance function 24 h after thermal injuryaOrgan localization (%ID/TO)b
Treatment Half-time (h)Liver Spleen Lungs
Control 5.14 ± 0.48 5.69 ± 0.48 15.44 ± 1.91 3.14 ± 0.34Thermal injury 7.60 ± 0.97c 5.15 ± 0.98 8.98 ± 1.28c 4.05 ± 0.72
a Splenic clearance function was assessed from the clearance rate and organ localization of phenylhydrazine-treated RBC (15 mg of Hb per 100 g). Half-times were measured over 2 h, and organ localizations of the test RBCwere determined 2 h after injection.
b Organ localization values are expressed as the percentage of the injected dose per total organ (%ID/TO). Alldata are expressed as the mean ± standard error with 7 to 10 animals per group.
c P < 0.05 compared with control.
spleen (11, 21). The observation that splenicuptake of phenylhydrazine-treated RBC is notinfluenced by agents which alter macrophagephagocytic function indicates this is a trappingclearance mechanism rather than a phagocyticfunction-dependent mechanism, although mac-rophages may eventually phagocytize thetrapped RBC (21).
Characterization of the phenylhydrazine-treated RBC showed that splenic localization 2 hafter injection was a constant fraction of theinjected dose for the three smaller doses, butwas less for the largest dose. This suggests thatduring this period the splenic sequestrationmechanism was saturated by the highest dose.This is supported by the similar clearance half-times of the three smaller doses and the muchlonger half-time of the largest dose. Spleniclocalization of phenylhydrazine-treated RBC 24h after injection showed that the lower twodoses were almost completely cleared by thespleen, whereas the larger doses showed pro-gressively smaller fractions of the injected dosein the spleen. The Hb content per gram of spleen
-------- SPLENECTOMY
*-------------- ---- CECAL LIGATION
SPLENECTOMY +CECAL LIGATION
w\\so
.2~~~~~~~~~~~~~~~~~~~~~................
0 40 -
20
0 8 16 24 32 40 48 56 64 72
HOURS AFTER CECAL LIGATION
FIG. 1. Effect of splenectomy on time to deathafter cecal ligation. Splenectomy was performed at thetime of cecal ligation. Splenectomy resulted in anincreased time to death (P < 0.05). No animals diedafter splenectomy without cecal ligation (10 animalsper group).
at 24 h was nearly constant for the higher threedoses, indicating that 40 to 45 mg of Hb per gof splenic tissue represents the capacity of thespleen to take up this type of RBC at 24 h.
Hepatic localizations were low compared withsplenic localizations and represented a nearlyconstant fraction of the injected dose for alldoses at 2 and 24 h postinjection. This indicatesthat a constant fraction of the treated RBC weresufficiently damaged to be sequestered by theliver. These results agree with the idea thatseverely damaged RBC are taken up by theliver, whereas the spleen sequesters less severe-ly damaged RBC (30).From these studies it is apparent that evaluat-
ing splenic clearance function over 2 h with thephenylhydrazine-treated RBC dose of 15 mg ofHb per 100 g represented a test of splenicclearance rate rather than the longer-term clear-ance capacity. With this approach, splenic clear-ance function was depressed at 24 h after injec-tion of the three larger doses. This was notsurprising in view of the observation that thesedoses had loaded the spleen to its capacity by 24
*-------- WASHEDRBC(15mgHb/1009) +CECAL LIGATION
PHENYLHYDRAZINE-TREATED RBC(15mgHb/100g) +CECAL LIGATION
Q60 - -..............
40-
20 ....
J .0 8 16 24 32 40 48 56 64 72
HOURS AFTER CECAL LIGATION
FIG. 2. Effect of phenylhydrazine-treated RBC ontime to death after cecal ligation. Phenylhydrazine-treated RBC (15 mg of Hb per 100 g) were injected 5 hafter cecal ligation. This dose of phenylhydrazine-treated RBC decreased time to death (P < 0.05) (10animals per group).
INFECT. IMMUN.
on Novem
ber 5, 2018 by guesthttp://iai.asm
.org/D
ownloaded from
SPLENIC RBC SEQUESTRATION AND HOST DEFENSE
Ii
'U
I.-
100
80
60
40
20
-. WASHED RBC (5 mg HbI 100 g) +CECAL LIGATION
PHENYLHYDRAZINE-TREATED RBC(5mgHbO100g) +CECAL LIGATION
0 8 16 24 32 40 48 56 64 72HOURS AFTER CECAL LIGATION
FIG. 3. Effect of phenylhydrazine-treated RBC ontime to death after cecal ligation. Phenylhydrazine-treated RBC (5 mg of Hb per 100 g) were injected 5 hbefore cecal ligation. This dose of phenylhydrazine-treated RBC had no effect on time to death (10 animalsper group).
h. This depression of splenic clearance functionmay be due to: (i) depressed splenic RBC extrac-tion; (ii) reduced splenic blood flow (10, 34); (iii)shift of blood flow away from the open circula-tion (9, 34); or (iv) in the case of the two largerdoses, competition for clearance with the chal-lenging RBC since some of the challenging doseremained in the circulation at 24 h.
Hepatic clearance function was determined byusing SRBC because this test particle is clearedprimarily by the liver. Clearance half-time andhepatic localization of SRBC were unchanged 5
h after injection of the largest dose of phenylhy-drazine-treated RBC. Hepatic clearance func-tion was assessed at 5 h after phenylhydrazine-treated RBC injection, because this was the timechosen for cecal ligation. Previous studies fromour laboratory have shown that depression ofhepatic clearance function at the time of cecalligation was associated with increased suscepti-bility to cecal ligation (16). Additionally, wehave shown that hemolyzed blood and RBCstroma prepared from hemolyzed blood can de-press hepatic clearance function, and that thedegree of intravascular hemolysis associatedwith experimental thermal injury may generatesufficient RBC debris to depress hepatic phago-cytic function (16, 25, 25a, 31).Thermal injury is known to be associated with
intravascular hemolysis and increased erythro-cyte clearance as well as with increased suscep-tibility to infection (1, 5, 15, 23, 29, 32). Thepresent study demonstrated an increase in bothhepatic and splenic RBC localization with ther-mal injury. The contribution of free 51Cr-labeled
Hb to these measurements was shown to besmall. The splenic localization of RBC afterthermal injury was approximately equal to thesplenic capacity for sequestration of phenylhy-drazine-treated RBC. Thus, the depression ofsplenic clearance function after thermal injurywas probably due to splenic sequestration ofRBC. However, other factors resulting from theinjury may have helped depress splenic clear-ance function. An example may be the presenceof a reticuloendothelial depressing substance(24).Acute splenectomy increased susceptibility to
peritonitis induced by cecal ligation as previous-ly reported (8). The three larger doses of phenyl-hydrazine-treated RBC, which depressed splen-ic clearance function, also increasedsusceptibility to peritonitis. This indicates thatsplenic sequestration of RBC impaired someaspect of splenic host defense function. Kaye etal. have shown that large doses of various typesof altered RBC increased the susceptibility ofmice to infection (18-20). However, these inves-tigators did not determine the clearance rate ororgan localization of the altered RBC.Splenectomy and impaired splenic function
are well known to be associated with increasedsusceptibility to infection (3, 12, 13, 22, 28).Splenic host defense function has been shown tobe important for bacteria such as Pneumococcus(6, 7). The mechanism of the increased suscepti-bility to infection after splenectomy is probablydue to the loss of splenic phagocytosis andkilling of bacteria as well as loss of splenicimmune functions. The mechanism of the in-creased susceptibility to infection after splenicsequestration of RBC is due to one or more ofthe deficits of splenic function seen with sple-nectomy.Thermal injury in animals has been shown to
be associated with a marked increase in suscep-tibility to infection for 24 to 48 h after injury (1,26). The present study has demonstrated thatsplenic clearance function is depressed afterthermal injury, and that this is probably due tothe splenic sequestration of RBC. It was alsoshown that depression of splenic clearance func-tion due to splenic RBC sequestration was asso-ciated with increased susceptibility to peritoni-tis. These findings suggest that splenicsequestration of RBC after thermal injury anddepression of splenic clearance function maycontribute to the increased susceptibility to in-fection seen after thermal injury in animals.Many burn patients develop anemia with contin-ued splenic RBC sequestration for many daysafter thermal injury (23, 32); however, the con-tribution of splenic RBC sequestration to theincreased susceptibility ofburn patients to infec-tion remains to be determined.
VOL. 36, 1982 101
on Novem
ber 5, 2018 by guesthttp://iai.asm
.org/D
ownloaded from
102 GROVER AND LOEGERING
ACKNOWLEDGMENTSWe acknowledge the fine technical assistance of Lisa Gary.This study was supported by Public Health Service grant
GM-26102 from the National Institutes of Health. G.J.G. is apredoctoral trainee supported by Public Health Service grantHL-07194 from the National Institutes of Health.
LITERATURE CITED1. Alexander, J. W. 1968. Effect of thermal injury upon the
early resistance to infection. J. Surg. Res. 8:128-137.2. Barrett-Connor, E. 1971. Bacterial infection and sickle
cell anemia. Medicine 50:97-112.3. Belfanz, J. R., M. E. Nesbit, Jr., C. Jarvis, and W. Krivit.
1976. Overwhelming sepsis following splenectomy fortrauma. J. Pediatr. 88:458-460.
4. Bennett, I. L., Jr., and E. W. Hood. 1959. Infectiousdiseases (some aspects of salmonellosis). Annu. Rev.Med. 10:1-20.
5. Bhargava, M., K. N. Agaswal, and S. Kumar. 1969. Sitesof red cell destruction in the anemia of experimentalburns. Br. J. Haematol. 17:179-185.
6. Brown, E. J., S. W. Hosea, and M. M. Frank. 1981. Therole of the spleen in experimental pneumococcal bacter-emia. J. Clin. Invest. 67:975-982.
7. Brown, E. J., S. W. Hosea, and M. M. Frank. 1981. Therole of complement in the localization of Pneumococci inthe splenic reticuloendothelial system during experimen-tal bacteremia. J. Immunol. 126:2230-2235.
8. Chaudry, I. H., Y. Tabata, B. A. Schleck and A. E. Baue.1980. Effect of splenectomy on reticuloendothelial func-tion and survival following sepsis. J. Trauma 20:649-655.
9. Chen, L. T., 1980. Intrasplenic microcirculation in ratswith acute hemolytic anemia. Blood 56:737-740.
10. Chen, L. T., and U. Scheffel. 1977. Blood flow andphagocytic activity of the spleen of the rat with acutehemolytic anemia. RES J. Reticuloendothel. Soc. 22:507-521.
11. Chen, L. T., and L. Weiss. 1973. The role of the sinus wallin the passage of erythrocytes through the spleen. Blood41:529-537.
12. Cooney, D. R., J. C. Dearth, S. E. Swanson, M. K.Dewanjee, and R. L. Telander. 1979. Relative merits ofpartial splenectomy, splenic reimplantation and immuni-zation in preventing post-splenectomy infection. Surgery86:561-568.
13. Cooney, D. R., S. E. Swanson, J. C. Dearth, M. K.Dewanjee, and R. L. Telander. 1979. Heterotropic splenicautotransplantation in prevention of overwhelming post-splenectomy infection. J. Pediatr. Surg. 14:335-342.
14. Czlsmas, L. 1960. Preparation of formalinized erythro-cytes. Proc. Soc. Exp. Biol. Med. 103:157-160.
15. Davis, A. K., and E. L. Alpen. 1956. Mechanism oferythrocyte destruction in the burned rat. Am. J. Physiol.184:151-154.
16. Grover, G. J., and D. J. Loegering. 1981. Effect oferythrocyte debris on reticuloendothelial function andsusceptibility to experimental peritonitis. Proc. Soc. Exp.Biol. Med. 167:30-35.
17. Hook, E. W. 1969. Salmonellosis: certain factors influenc-ing the interaction of Salmonella and the human host.Bull. N.Y. Acad. Med. 37:499-512.
18. Kaye, D., F. A. Gill, and E. W. Hook. 1967. Factorsinfluencing host resistance to Salmonella infections: the
effects of hemolysis and erythrophagocytosis. Am. J.Med. Sci. 254:205-215.
19. Kaye, D., and E. W. Hook. 1963. The influence ofhemolysis or blood loss on susceptibility to infection. J.Immunol. 91:65-75.
20. Kaye, D., and E. W. Hook. 1963. The influence of hemoly-sis on susceptibility to Salmonella infection: additionalobservations. J. Immunol. 91:518-527.
21. Klausner, M. A., L. J. Hirsch, P. F. Leblond, J. R.Chamberlain, M. R. Klemperer, and G. B. Segal. 1975.Contrasting splenic mechanisms in the blood clearance ofred cells and colloidal particles. Blood 46:965-976.
22. Leung, L. E., G. J. Szal, and R. H. Drachman. 1972.Increased susceptibility of splenectomized rats to infec-tion with Diplococcus pneumoniae. J. Infect. Dis.126:507-513.
23. Loebl, E. C., C. R. Baxter, and P. W. Curreri. 1973. Themechanism of erythrocyte destruction in the early post-burn period. Ann. Surg. 178:681-686.
24. LoegerLng, D. J. 1981. Circulating reticuloendothelial de-pressing substance following thermal injury and intestinalischemia. Proc. Soc. Exp. Biol. Med. 166:515-521.
25. Loegering, D. J. 1981. Hemolysis following thermal injuryand depression of reticuloendothelial system phagocyticfunction. J. Trauma 21:130-134.
25a.Loegering, D. J., and L. J. Garrett. 1981. Reticuloendo-thelial system depression with hemolyzed blood and sus-ceptibility to endotoxin shock and thermal injury. Circ.Shock 8:473-482.
26. McRipley, R. J., and D. W. Garrison. 1965. Effect of burnsin rats on defense mechanisms against Pseudomonasaeruginosa. J. Infect. Dis. 115:159-170.
27. Pearson, H. A. 1977. Sickle cell anemia and severe infec-tions due to encapsulated bacteria. J. Infect. Dis.136:S25-S30.
28. Pearson, H. A., R. P. Spencer, and E. A. Cornelius. 1969.Functional asplenia in sickle cell anemia. N. Engl. J. Med.281:923-926.
29. Robson, M. C., T. J. Krizek, R. C. Wary, Jr. 1979. Care ofthe thermally injured patient, p. 676-678. In G. D. Zui-dema, R. B. Rutherford, and W. F. Ballanger (ed.), Themanagement of trauma. The W. B. Saunders Co., Phila-delphia.
30. Rifldnd, R. A. 1966. Destruction of injured red cells invivo. Am. J. Med. 41:711-723.
31. Schneidkraut, M. J., and D. J. Loegering. 1979. Effect ofhemolyzed blood on reticuloendothelial function and sus-ceptibility to hemorrhagic shock. Proc. Soc. Exp. Biol.Med. 159:418-423.
32. Shen, S. C., T. H. Ham, and E. M. Fleming. 1943. Studieson the destruction of red blood cells. III. Mechanisms andcomplications of hemoglobinuria in patients with thermalburns: spherocytosis and increased osmotic fragility ofred blood cells. N. Engl. J. Med. 229:701-713.
33. Turinsky, J., and S. A. Patterson. 1979. Proximity to aburn wound as a new factor in considerations of post-burninsulin resistance. J. Surg. Res. 26:171-174.
34. Vaupel, P., H. Ruppert, and H. Hutten. 1977. Splenicblood flow and intrasplenic flow distribution in rats.Pfluegers Arch. 369:193-201.
35. Wkhterman, K. A., A. E. Baue, and I. H. Chaudry. 1980.Sepsis and septic shock-a review of laboratory modelsand a proposal. J. Surg. Res. 29:189-201.
INFECT. IMMUN.
on Novem
ber 5, 2018 by guesthttp://iai.asm
.org/D
ownloaded from




![ERYTHROCYTES [RBCs]](https://static.fdocuments.net/doc/165x107/56813dc0550346895da78963/erythrocytes-rbcs-56ea22b2e2743.jpg)













