
Septic arthritis &post arthroplasty infections Presenter R N MBUVA Moderator Mr MWANGI.
63
Septic Septic arthritis arthritis &post &post arthroplasty arthroplasty infections infections Presenter R N MBUVA Moderator Mr MWANGI
-
Upload
dominic-barker -
Category
Documents
-
view
214 -
download
0
Transcript of Septic arthritis &post arthroplasty infections Presenter R N MBUVA Moderator Mr MWANGI.

Septic arthritis Septic arthritis &post &post
arthroplasty arthroplasty infectionsinfections
Presenter R N MBUVAModerator Mr MWANGI

scopescope• Septic arthritis• Prosthetic infections

•Part 1

•Septic arthritis

DefinitionDefinition• Inflammation of a synovial membrane with
purulent effusion into the joint capsule, often due to bacterial infection

SynonymsSynonyms• Bacterial, suppurative, purulent or infectious
arthritis, gonococcal or nongonococcal

septic arthritisseptic arthritis• 0.2%-0.7% of hospital admissions• Peak incidence in the first years of 1st decade and
>50 years• Males>Females

Risk Factors for Septic Risk Factors for Septic ArthritisArthritis
• Previous arthritis• Trauma• Diabetes Mellitus• Immunosupression• Bacteremia• Sickle cell anemia• Prosthetic joint

Infection SourcesInfection Sources• Trauma: direct• Hematogenous: IV drug injection• Osteomyelitis adjacent to joint capsule• Soft tissue infections: cellulitis, abscess, bursitis,
tenosynovitis

PathogenesisPathogenesis• Systemic bacteremia-invades synovial cartilage• Postulation-collagen receptors in staph aureus -lack of basement membrane in capillaries of synovium -synovial fibroblasts inhibit
phagocytosis

pathogenesispathogenesis• Features of acute Infiltration• Lymphocytes 3/52• Destruction of cartilage after ground substance
degradation4-6/7• Depletion of ground substance-activation of
bacteria enzymes and T lymphocytes• Ground substance degradation-collagen exposed
Up-to-Date 2004

clinical presentationclinical presentation
• Painful ROM, swelling, erythema, not bearing weight, recent illnesses
• Children:o pseudoparalysis or disuse of limb, not septico antalgic limpo Fevers not consistento Have parent examine the child

LabsLabs• Leukocyte count not reliable early stages
o 25% of children had elevated counts and 65% the diff was abnormal
• ESR o Nonspecific test of inflammationo Affected by cell size, shape and protein content
• i.e. sickle cell, anemia, steroidso Not reliable in neonateso Elevated in 48-72 hrs returns to baseline 2-4 weeks
Mayo series, Morey et al:only 5 of 76 had ESR below 20mm/hr,elevated in 90% of patients w/ septic arthritis

ESRESR• No change w/ antibiotic therapy• Continues to rise 3-5 days – after this may
consider change in tx• Not good for early evaluation of tx

CRPCRP• Rises within 6 hrs and peaks 30-50hrs• Half life 47hrs• Makes this marker of greater value for early
diagnosis and resolution of inflammation• CRP is elevated in trauma, in otitis
media(22%bacterial 65% viral)

CulturesCultures• Blood cultures
o yield organisms 30-50% of caseso Decreases w/ previous antibiotic therapy
• Aspiration of joint fluido Gram stain, leukocyte cell count, PMNs
• Cell counts 80,000 – 100,000/ml likely septic arthritiso Frank and Nelson: 126 positive culture
• Counts of 50,000/ml or less in 55%, 34% had <25,000/ml, only 44% had >=100,000/ml
• Other inflammatory processes can give you >80,000/ml
• Gram stain can give you a presumptive early diagnosiso 1/3 are positive


ImagingImaging• Plain x rays• Ultrasound
o Used frequently in pediatrics assessing the hip for effusion/dislocations
o Cannot differentiate between TSH and septic arthritis by positive effusion alone
o If extracapsular effusion may distinguish between osteomyelitis around hip/pelvis
• CT,MRI&Bone scans not necessary• Bone scan – Tc99-good osteoblastic activity
indium111 and gallium citrate more sensitive and specific for infection
i
• CT scans-good anat,distinguishes soft tissue and bone infection
• MRI sensitivity 97% and specificity 92%

Kocher et al. Kocher et al. 19991999• Hx of fever• Nonweightbearing• ESR >40mm/hr• WBC >12,000/mm3
Kochers criteriaKochers criteria• The likelihood of septic arthritis was • 0.2% if no criteria were present,• 3% if one• 40% if two• 93% if three• 99% if four
• Unfortunately not reproducible• Caird et al-crp&esr –more likely• Luhmann-visit another facility more likely

Management Management • Nade • Principles-1joint adequately drained 2ABX given to diminish effects of sepsis 3joint rested in a stable position

Indications for Indications for SurgerySurgery• Aspiration vs. debridement• Joint does not respond to serial aspirations• No improvement in 48hrs of tx• Frank pus is aspirated• Loculations noted on MRI or U/S• Documented Hip and SI septic arthritis
should be debrided surgically• No change in morbidity between
arthroscopic vs. arthrotomy of knee

Abx TreatmentAbx Treatment• IV abx 4-7 days• Check CRP,WBC every 2 days• Once labs normalize and clinically improving
consider discharge• Continue tx 2-3 weeks with oral or IV abx (PICC
line)• No true standardization of tx• Get ID involved

RehabilitationRehabilitation• Splinting for 48 hrs• Salter 1981
o Rabbit knees septic S. aureuso Had arthrotomy and abx txo Casting vs. ROM w/ CPM vs. cage activityo CPM fared sig. better on pathology of cartilage w/ decreased ground
substance
• WBAT once rom and pain subsided

Prognosis and Prognosis and complicationscomplications
• Poor prognosis factorso Immunodeficiency, RA, prematurity,
osteomyelitis, hip, prosthetic infections, + blood cultures, symptoms >1 week, >4 joints, + cultures after aspiration after 7 days of abx tx
• Complications:o Mortality 8%-15% in three serieso arthritis stiffness, dislocation, subluxation,
AVN, local growth distrubance, osteomyelitis, postinfection synovitis
• Favorable outcome in 50%-80% of cases

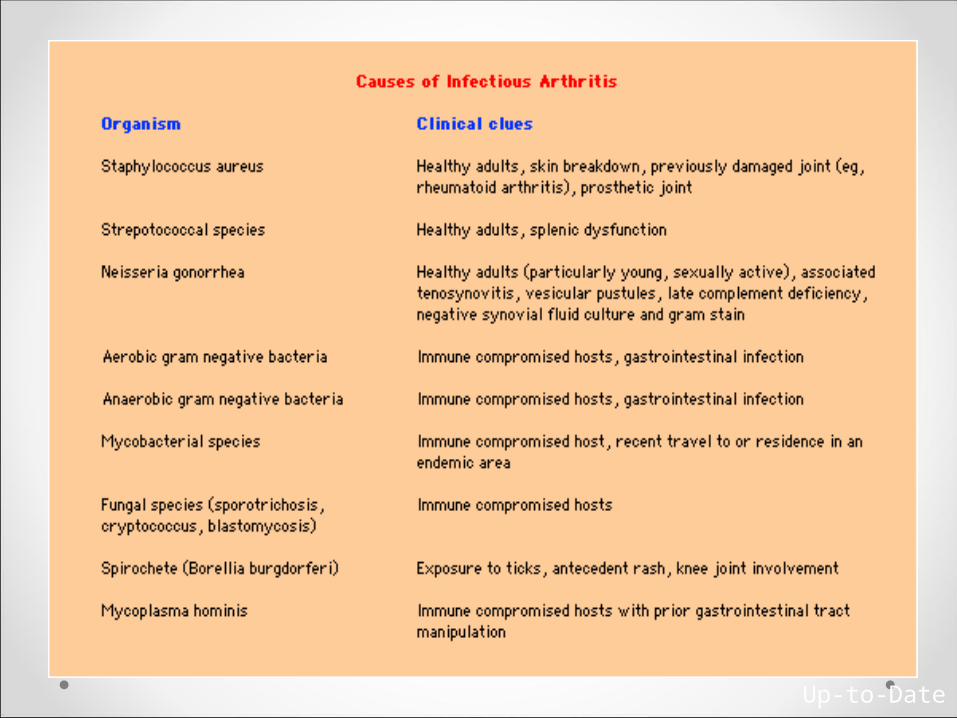
Lyme ArthritisLyme Arthritis• Caused by infection with the spirochete Borrelia
Burgdorferi• Early stage disease
o Localized - Erythema chronicum migrans, fever, arthralgia and myalgia, sore throat,
o Disseminated- disseminated skin lesions, facial palsy, meningitis, radiculoneuropathy, and rarely heart block
o Early disease may remit spontaneouslyo 50% of untreated cases develop late features
• Late o Arthritis is a manifestation of late disease-months or
years after exposureo Intermittent migratory asymmetric mono- or oligo-
arthritiso 10% develop chronic large joint inflammatory arthritis

Lyme ArthritisLyme Arthritis• Treatment
o Early localized • Doxy 100 mg po BID or Amox 500 TID (kids) for 2-4 weeks
o Early disseminated or late disease• Oral or parenteral abx depending on the severity of the disease
o Neuro or cardiac disease usually treated with IV ceftriaxone 2 g daily for 3-4 weeks.
o Lyme arthritis may be treated with oral abx for 4 weeks.

Disseminated gonococcal Disseminated gonococcal
infectioninfection
• Occurs in 1-3% on patients infected with GC• Most patients have arthritis or arthralgia as a
principal manifestation• Common cause of acute non-traumatic mono- or
oligo-arthritis in the healthy host

Gonococcal arthritisGonococcal arthritis
Host factorsHost factors
• Women > men• Recent menstruation• Pregnancy or immediate postpartum state• Complement deficiency (C5-C9)• SLE

Gonococcal arthritis Gonococcal arthritis
• Consider screening/treating for chlamydia• HIV testing• Syphillis testing• Screen sexual partners

Gonococcal arthritisGonococcal arthritis• Ceftriaxone 1gm IV or IM q24 hours• Spectinomycin 2 gm IV or IM q12 hours for ceph
allergic patients • May use fluoroquinolones if susceptible

Parvovirus B19 Parvovirus B19 ArthritisArthritis
• Small non-enveloped DNA virus• Erythrovirus genus
o Replicates only in erythrocyte precursors
• Transmissiono Respiratory, parenteral, vertical
• 25-68% of infections are asymptomatic

Erythema InfectiosumErythema Infectiosum
• “5th disease”• 10% of children and
50% of adults have joint symptoms

Parvovirus B19 Parvovirus B19 ArthritisArthritis
• Begins about 2 weeks after infection• Symmetrical involvement of the small joints of
the hands and wrists and the knees• Usually resolves in about a month without joint
damage• 20% may have persistent disease**

Parvovirus B19Parvovirus B19• Clinical features may mimic an early autoimmune
disease• High prevalence of autoantibodies
o RF, ANA, ACA, ANCA, anti-ds DNAo May persist for some time after infection is cleared
• Has been implicated in the pathogenesis in both RA and SLE

Diagnosis and TherapyDiagnosis and Therapy• Parvovirus B19 IgM +
o Parvovirus B19 IgG indicates past infection.• highly prevalent in the general population since
asymptomatic infxn is very common.
• PCR can be usedo Immuncompromised people may not mount an
antibody response
• Therapy is supportiveo NSAIDso Steroids are rarely necessary

Tuberculous arthritisTuberculous arthritis
• History of exposure is helpful• PPD may be negative• Synovial fluid stain usually negative• Culture may take 6-8 weeks to grow• Best yield is probably synovial biopsy

•PART 2

•POST ARTHROPLASTY INFECTIONS

INCIDENCEINCIDENCE• For knee generally low 0.1-2%• For hip 1-2%

MECHANISMMECHANISM• Intraoperative seeding-low virulent• Blood spread• Fretting-micromotion between implants -DM -sepsis -steroid use -Long hospital stay -long theatre time>3hrs -blood loss > 1500cc -smoking

Methods of preventionMethods of prevention• Treatment of superficial and deep infection• I.V prophylactic antibiotics• Others-laminar flow -closed body exhaust suits -careful tissue handling -antibiotic cement -minimize theatre traffic

BIOFILMBIOFILM• There are five stages of biofilm development 1Initial attachment-van der waals forces 2Irreversible attachment-cell adhesion structures,
hydrophobicity,quorum sensing3Maturation I:4Maturation II:5Dispersion:

BIOFILMBIOFILM

Biofilm Biofilm • Pathophysiology has been greatly improved by
the biofilm model• Conditions for biofilm formation: necrotic tissue
and bone, which have a foreign-body effect and are colonized by bacteria.
• Pathogens 1st form surface colonies, multiply.

Biofilm Biofilm • Matrix offers protection from mechanical
influences and makes it harder for AB, body’s own defense cells, and Ig to penetrate, functioning as a diffusion barrier.
• Pathogens pass from a high metabolic rate and rapid multiplication into greatly reduced metabolism and slowed biological Rx.
• This can reduce their sensitivity to antibiotics by a factor of 10(3)

Biofilm Biofilm • Neutrophilic granulocytes penetrate the biofilm
poorly and in the process lose their ability to phagocytose.
• Apoptosis occurs with excessive complement activation and release of radicals and proteases, resulting in a local immune deficiency.

Biofilm Biofilm • In lower layers of the biofilm, conditions are
anaerobic, reducing growth rate and metabolic activity of pathogens.
• Insensitive to antibiotics. • After Tx has ended, return --->active mode, show
resistance to the originally administered AB

Biofilm Biofilm • return from sessile to planktonic phase is
possible, and clinically triggers local or systemic recurrence of Ix.
• Biofilm population = permanent source of virulent pathogens
• Safest Tx= surgical removal of sequestrum bearing biofilm

Culprit bacteriaCulprit bacteria• Staph aureus,MRSA,epidermidis-65-70%• Gram –ve(biofilm forming pseudomonas)• Anaerobes• Polymicrobial-wound discharges• Others-gas gangrene

diagnosisdiagnosis• A combination –clinical -radiological -pathologicaln/b –biofilm shields the bacteria hence neg bone /WBC scans -bacteria at times in a semi dormant state –
neg cultures

clinicalclinical• Pain• Loss of ROM• Swelling• Local warmth• Signs-sinus,effusion,wound erythema

investigationsinvestigations• X rays-periosteal reaction,subchondral bone
resorption• Aspiration• Bone scan-Tc-not sensitive -indium WBC –more sensitive -others-marrow scans -monoclonal ab scans• Intraop frozen scans >5PMN/hpf –mirra• Synovial biopsy-last resort• pcr

classificationclassification• GUSTILLO• Early post op infection<4/52• Late chronic>4/52

Coventry Coventry • Stage I within 3 months of surgery
o Usually transmitted at the time of surgeryo Staph and other gram positives most commono Pain, wound drainage, erythema, induration
• Stage II 3-24 months• Stage III >2 years post-surgery
o Usually caused by hematogenous spread to abnormal joint surfaceso Joint pain predominates

Tsukayama and Tsukayama and colleagues-1996colleagues-1996
1.+ve intraop cultures-iv antibiotics2.Early post op infection -1/123.Late chronic infection4.Acute haematogenous infection

Periprosthetic joint Periprosthetic joint infection musculoskeletal infection musculoskeletal
infection society scoreinfection society scorecategory staging description
Infection type 1 Early post op infection <4/52
2 Haematogenous infection<4/52
3 Late chronic infection >4/52
Systemic host grade A UNCOMPROMISSED
B Compromised <2 compromissing factor
C Compromissed >2 compromissing factors
Local extremity grade 1 uncompromissed
2 Compromissed <2
3 Compromissed>2

Management Management • Debridement with prosthesis retention• Debridement with prosthesis removal -one stage -two stage

GOLD STANDARDGOLD STANDARD• 2 stage-removal of prosthesis -I.V antibiotics 6/52 -cement spacer or prostalac -use of cement in re implantation -stemmed component

Salvaging failed re Salvaging failed re implantationimplantation
• Options1 fusion-those who may ambulate2resection arthroplasty-fibrosis3.amputation

Prognosis Prognosis • Poor if• Delayed diagnosis• Virulent organisms• Poor debridement• ISS• Host bed scarred and poor

• end





![WELCOME [arthroplasty-conference.org]arthroplasty-conference.org/pdf/(IAC-2020)ARTHROPLASTY-PROGRA… · KEYNOTE LECTURERS: Wael Barsoum President of Cleveland Clinic, Florida, USA](https://static.fdocuments.net/doc/165x107/5edc4a09ad6a402d6666e51c/welcome-arthroplasty-arthroplasty-iac-2020arthroplasty-progra-keynote-lecturers.jpg)












