Sepsis Updates
43
1 Jacob Scott Spectrum Health Medical Group Sepsis Updates
-
Upload
spectrum-health-system -
Category
Healthcare
-
view
66 -
download
0
Transcript of Sepsis Updates
1
Jacob Scott
Spectrum Health Medical Group
Sepsis Updates
Disclosures
• No financial disclosures

Objectives
• Understand the new definitions of sepsis
• Understand current best practice for initial care of patients
with *severe* sepsis/septic shock
• Brief review of novel therapy with promise

Clinical Definition

New Definition-Why?
• Last definition update was in 2001-prior to landmark
research and extensive education efforts at standardizing
treatment
• Previous definitions were based on expert opinion—
professional societies felt it important to use more concrete
research to confirm best definition
• Cohorts were obtained from 5 large data sets encompassing
177 hospitals--~5,000,000 patient records were assess

New definition
• Infections were defined in a patient when cultures were
obtained and antibiotics were initiated in a 24 hours time
interval
• 4 separate candidate criteria for determining sepsis where
applied in cases of infection
• SIRS
• Sequential organ failure assessment (SOFA)
• Logistic organ dysfunction system (LODS)
• Quick sequential organ failure assessment (qSOFA)



New Definition
• Sepsis should be defined as life-threatening
organ dysfunction caused by a dysregulated host
response to infection
• Organ dysfunction defined by an increase in
SOFA score of 2 • These patient’s have a 10% increased risk of mortality
• Septic shock-sepsis requiring a vasopressor to
maintain MAP > 65, or sepsis with serum lactate
of 2 after adequate volume resuscitation• These patient have a 40% increased risk of mortality


New Rapid assessment for Sepsis in non-ICU Patients
• Non-ICU patients with a qSOFA score of
at least 2 much better discriminating
those with infections who at risk of
decompensation
• Criteria include RR > 22, SBP < 100,
and altered mental status
• Severe sepsis no longer exists—all
sepsis should be considered SEVERE

Treatment of Sepsis


Rivers Trial 2001

Questions About EGDT
• The Good-Sepsis mortality has fallen
nation wide since standardization efforts
have taken place (20-30%)
• Questions about what elements most
important

Rivers Trial 2001

What We Think We are Measuring

Is CVP a Good Measure of Volume Status?

What Else Did We Think in 1984?

How Bad is CVP?

What Is a Useful tool for Volume Status?
Am J Respir Crit
Care Med Vol 162.
pp 134–138, 2000

Rivers Trial 2001


Testing Rivers and EGDT
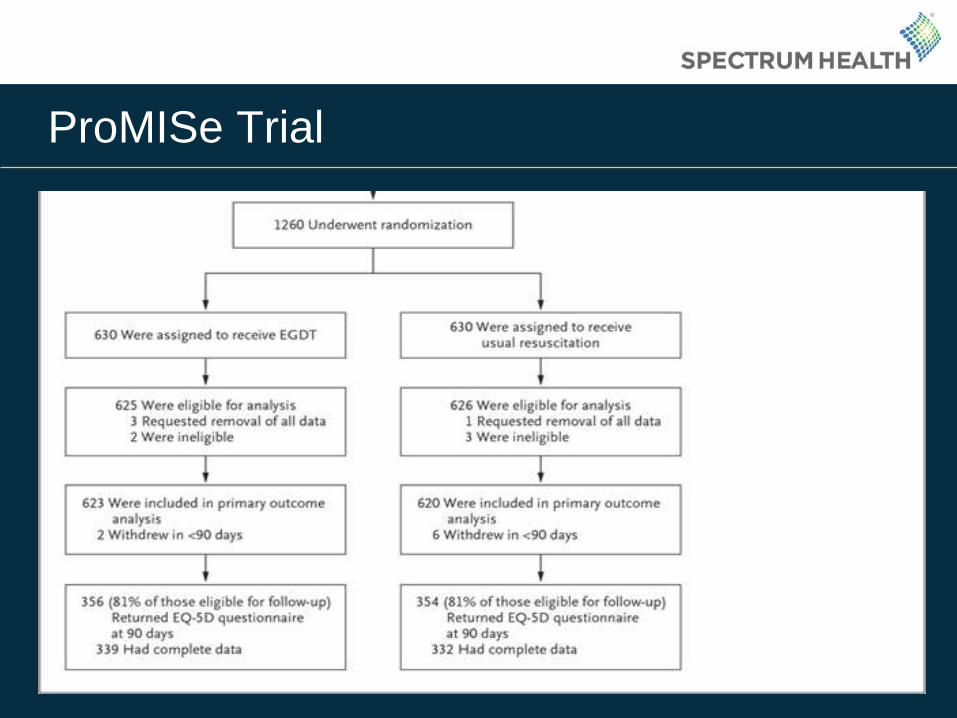
ProMISe Trial

ProMISe Trial

ProCESS Trial

ProCESS Trial

ARISE

ARISE


What Do I Make of These Studies?
• Understand “usual care” has been informed for
the last 20 years by EGDT and the surviving
sepsis guidelines
• Not all septic patients need lines
• Can probably get away from so much IVF, but
need to monitor something
• No longer strong evidence to follow SvO2 in
severe sepsis/septic shock, although it is not
wrong to do so

Take Home Points
• Early and appropriate antibiotics are super important

Effect of Abx Timing on Survival
Crit Care Med 2006;34:1589-96
Time from hypotension onset (hours)
Fra
cti
on
of
tota
l p
ati
en
ts
Take Home Points
• Early and appropriate antibiotics are super important
• The new definitions for sepsis are helpful for identifying
sicker patient that likely need our help in the ICU, but I don’t
know when they will be adopted
• Remember, it took 20 years for CMS guidelines to be
implemented based largely on EGDT
• Septic patients still need fluids, and dynamic measurements
of hemodynamic parameters are better than static
measurements (interpreting doc needs to know what they
are doing with dynamic measurements)

Surviving Sepsis 2017

Vitamin C
Marik PE, Khangoora V, Rivera R, Hooper MH, Catravas J, Hydrocortisone,
Vitamin C and Thiamine for the Treatment of Severe Sepsis and Septic Shock: A Retrospective
BeforeAfter
Study, CHEST (2017), doi: 10.1016/j.chest.2016.11.036.

• Patients with severe sepsis and septic shock and
with a procalcitonin > 2 admitted between January
2016-July 2016 were treated with study protocol
• Medications included 1.5 grams of vitamin C Q6H,
Thiamine 200 mg IV Q12H, and hydrocortisone 50
mg IV Q6H
• Control group was same patient population from
June 2015-December 2015


Questions???