Separation of cough and reflex bronchoconstriction by ... · separately by local anaesthetics....
5
Eur Respir J 1990, 3, 579-583 Separation of cough and reflex bronchoconstriction by inhaled local anaesthetics N.B. Choudry*, R.W. Fuller*, N. Anderson**, J-A. Karlsson*** Separation of cough and reflex bronchoconstriction by i11hal ed local anaesthetics. N.B. Choudry, R.W. Fuller, N. Arull!rson, 1-A. Karlsson. ABSTRACT: Cough and airway constriction are common features of r es piratory diseases. Both can be caused by stimulation of alrway nerves. We bave st udied the effects of alrway anaesthesia on these reflexes, stimulated by inl1aled capsaicin, In order to determine whether tl1ey are controlled by the same sensory nerves. Ten vol unteers had capsaicin cough dose responses performed before and at 10 mln after Inhaling placebo (ascorbic acid In sa line), and the topical anaesthetics li gnocain e 40 mg, and dyclonlne 8 and 4 mg. Tbe effect of the drugs on respiratory resistance (Rrs), mea sured using a forced oscillation te chnique, was measured both before and after the Inhalation of a dose of capsaicin which caused less than two coughs. Lignocaine (40 mg) and dyclonine (8 mg) caused significant reports of oral anaesthesia but only li gnocain e r ed uced tlte cough response to Inhaled capsaicin, Increasing the log dose of capsaicin causing thr ee or more coughs by 162%. None of the treatments altered basal Rrs or Its Increase after ln.baled capsalcln . the cough and reflex bronchoconstrlction caused by Inhaled capsaicin have different sensitivities to inhaled local anaesthesia, suggestl.ng that tbe effect may be mediated by different sensory pathways. Eur Respir J., 1990, 3, 579-583. • Dept of Clinical Phumacology, Royal Postgraduate Medical School, London, UK. • • Dept of Clinical Pharmacology and Pharmacological Laboratory, AB, Draco, S- 221 Lwtd, Sweden. Correspondence: Dr R.W. Fuller, Dept of Oinical Pharmacology, Royal Postgraduate Medical School, Ducane Road, London W12 ONN, UK. Keywords: Cough; local anaesthetics; reflex bronchoconstriction. Accepted after revision February 8, 1990. Cough and wheezing due to bronchoconstriction are common symptoms of lung disease. Cough can also be an early manifestation of asthma [1, 2), point.ir!g to an apparent relationship between cough and bronchoconstriction in obstructive airways disease. Topically administered local anaesthetics (>200 mg of lignocaine) are used in bronchoscopy to block reflexes, including cough, produced by mechanical irritation of the larynx and tracheobronchial tree. Lignocaine has also been reported to suppress chronic cough in a few pa- tients [3, 4). The local anaesthetic bupivacaine inhibits citric acid induced cough and reflex bronchoconslriction in healthy subjects [5]. Despite the extensive use of local anaesthetics for endoscopy, very little is known about the sensitivity of airway reflexes to these drugs and whether different compounds separately affect different reflexes. studies [7-9] coughing is inhibited at lower doses of local anaesthetics than the Hering-Breuer reflex, which regulates the rate and depth of breathing [10]. Although afferent pathways in both reflexes are in the vagus nerves, cough is preswnably mediated by nerves with endings close to the airway epithelium, affording easier access for the local anaesthetic than the nerves controlling the Hering-Breuer reflex, which originate within the smooth muscle [ 11 ). Local anaesthetics may have different effects on nerve conduction, depending upon the type and size of nerve fibres. The physicochemical properties of the anaesthetic may also depend on the Hpophilicity of the anaesthetic drug and the surface membrane to which it is applied [6]. It can therefore be presumed that airway reflexes if conducted via different nerves or originating in different sites of the airway would be affected separately by local anaesthetics. Indeed, in animal The aim of the present study was to examine the effect of low doses of inhaled local anaesthetics on buccal anaesthesia, cough and reflex bronchoconstriction produced by nebulized capsaicin [12, 13] in healthy subjects. Lignocaine was compared to dyclonine (an ester-type local anaesthetic) which is reported to be about ten times more potent than lignocaine on the mucosal tissue [14]. Methods Subjects Ten healthy, nonsmoking volunteers (aged 23-34 yrs, 6 female) gave informed consent to take part in the study which had the approval of the local hospital Research
Transcript of Separation of cough and reflex bronchoconstriction by ... · separately by local anaesthetics....

Eur Respir J 1990, 3, 579-583
Separation of cough and reflex bronchoconstriction by inhaled local anaesthetics
N.B. Choudry*, R.W. Fuller*, N. Anderson**, J-A. Karlsson***
Separation of cough and reflex bronchoconstriction by i11haled local anaesthetics. N.B. Choudry, R.W. Fuller, N. Arull!rson, 1-A. Karlsson. ABSTRACT: Cough and airway constriction are common features of respiratory diseases. Both can be caused by stimulation of alrway nerves. We bave studied the effects of alrway anaesthesia on these reflexes, stimulated by inl1aled capsaicin, In order to determine whether tl1ey are controlled by the same sensory nerves. Ten volunteers had capsaicin cough dose responses performed before and at 10 mln after Inhaling placebo (ascorbic acid In saline), and the topical anaesthetics lignocaine 40 mg, and dyclonlne 8 and 4 mg. Tbe effect of the drugs on respiratory resistance (Rrs), meas ured using a forced oscillation technique, was measured both before and after the Inhalation of a dose of capsaicin which caused less than two coughs. Lignocaine (40 mg) and dyclonine (8 mg) caused significant reports of oral anaesthesia but only lignocaine reduced tlte cough response to Inhaled capsaicin, Increasing the log dose of capsaicin causing three or more coughs by 162%. None of the treatments altered basal Rrs or Its Increase after ln.baled capsalcln. Thu.~, the cough and reflex bronchoconstrlction caused by Inhaled capsaicin have different sensitivities to inhaled local anaesthesia, suggestl.ng that tbe effect may be mediated by different sensory pathways. Eur Respir J., 1990, 3, 579-583.
• Dept of Clinical Phumacology, Royal Postgraduate Medical School, London, UK.
• • Dept of Clinical Pharmacology and Pharmacological Laboratory, AB, Draco, S-221 Lwtd, Sweden.
Correspondence: Dr R.W. Fuller, Dept of Oinical Pharmacology, Royal Postgraduate Medical School, Ducane Road, London W12 ONN, UK.
Keywords: Cough; local anaesthetics; reflex bronchoconstriction.
Accepted after revision February 8, 1990.
Cough and wheezing due to bronchoconstriction are common symptoms of lung disease. Cough can also be an early manifestation of asthma [1, 2), point.ir!g to an apparent relationship between cough and bronchoconstriction in obstructive airways disease.
Topically administered local anaesthetics (>200 mg of lignocaine) are used in bronchoscopy to block reflexes, including cough, produced by mechanical irritation of the larynx and tracheobronchial tree. Lignocaine has also been reported to suppress chronic cough in a few patients [3, 4). The local anaesthetic bupivacaine inhibits citric acid induced cough and reflex bronchoconslriction in healthy subjects [5]. Despite the extensive use of local anaesthetics for endoscopy, very little is known about the sensitivity of airway reflexes to these drugs and whether different compounds separately affect different reflexes.
studies [7-9] coughing is inhibited at lower doses of local anaesthetics than the Hering-Breuer reflex, which regulates the rate and depth of breathing [10]. Although afferent pathways in both reflexes are in the vagus nerves, cough is preswnably mediated by nerves with endings close to the airway epithelium, affording easier access for the local anaesthetic than the nerves controlling the Hering-Breuer reflex, which originate within the smooth muscle [11).
Local anaesthetics may have different effects on nerve conduction, depending upon the type and size of nerve fibres. The physicochemical properties of the anaesthetic may also depend on the Hpophilicity of the anaesthetic drug and the surface membrane to which it is applied [6]. It can therefore be presumed that airway reflexes if conducted via different nerves or originating in different sites of the airway would be affected separately by local anaesthetics. Indeed, in animal
The aim of the present study was to examine the effect of low doses of inhaled local anaesthetics on buccal anaesthesia, cough and reflex bronchoconstriction produced by nebulized capsaicin [12, 13] in healthy subjects. Lignocaine was compared to dyclonine (an ester-type local anaesthetic) which is reported to be about ten times more potent than lignocaine on the mucosal tissue [14].
Methods
Subjects
Ten healthy, nonsmoking volunteers (aged 23-34 yrs, 6 female) gave informed consent to take part in the study which had the approval of the local hospital Research

580 N.B. CHOUDRY ET AL.
Ethics Committee. None of the subjects had a history of recent respiratory disease and none was taking any medication other than oral contraceptives.
Total respiratory resistance
Total respiratory resistance (Rrs) was measured using a forced oscillation technique [15]. The subject was seated, with cheeks and floor of the mouth supported by the palms of the hands, and breathed quietly on a mouthpiece connected to a screen pneumotachograph. A bias flow prevented changes in inspired 0 2 and C02•
Pseudo-random noise was applied at the mouth by means of a loudspeaker over the range 4-26 Hz for a 16 s period. Mouth pressure and flow across the pneumotachograph were recorded by two identical differential pressure transducers (Validyne PM 5%). Values for Rrs at 2Hz intervals between 4-26Hz were computed and represented the mean values for inspiration and expiration over the 16 s period of tidal breathing. Baseline measurements of Rrs were the mean of three consecutive 16 s periods of tidal breathing. To allow measurement of the airway constriction after inhaled capsaicin, the subjects inhaled a single breath of the highest concentration of capsaicin which caused fewer than two coughs (because coughing interferes with the measurement of Rrs); this dose was chosen from the baseline cough response on each day. The subject then immediately started to breathe on the mouthpiece and Rrs was measured over the next 16 s. The same dose of capsaicin was then used in the study for all subsequent measurements of the Rrs response to inhaled capsaicin.
Dose cough response
Capsaicin (Sigma Chemical, Poole, UK) was dissolved in absolute alcohol to make a stock 10·2 M solution and further diluted with 0.9% saline to 1.9x10's to 2.5xl0·3 for inhalation; 0.9% (w/v) saline was used as the control solution. Capsaicin dose cough responses (OCR) were performed by the subjects inhaling a single breath (0.02 ml particle size 3.5-4 J..Un) of saline or different doses of capsaicin (0.4-100 nmol) in 0.9% saline and 1% ethanol. The subject was unaware of the concentration of capsaicin in each inhalation. The doses were given from a compressed air nebulizer (Oevilbis) controlled by a breath-activated dosimeter (P. K. Morgan). The number of coughs was recorded by means of a microphone connected to a fast running chart recorder (Mingograph; Simons, Elema AB, Sweden). The doses were given in a random order at one minute intervals until a dose that caused more than five coughs was reached. From the OCR the largest dose that caused less than two coughs was taken for the measurements of the Rrs response to inhaled capsaicin and the lowest dose that caused three or more coughs (03) was taken for analysis of the sensitivity of the cough response.
10 a)
0 I
I •·• ~
o.e::• / I o e
J l i;.
0 '-----~-~~-
10 c)
0·· /I
-~· o·• "' i l
~~· 0 .___ ....... .....___...___ ....
.1 10 100
Cap .. lcln nmol
10 b)
10 d)
5 . .P/ · #,~.,·
!i/ :.:.• ~l ..•
0 .1 10 100
eapealcln nmol
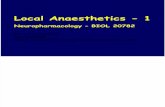
Fig. 1. - This shows the OCR capsaicin (a) before (open circles) and after (closed circles) placebo (ascorbic acid 4 mg), (b) lignocaine (40 mg), (c) dyclonine (4 mg) and (d) dyclonine (8 mg). OCR: dose cough response.
Protocol
Each subject attended the Clinical Laboratory at the same time of day on four separate occasions. Following baseline measurements of Rrs, a capsaicin DCR was performed. After a further baseline measurement of Rrs, the subject inhaled the highest dose of capsaicin that caused less than two coughs and Rrs was immediately measured. Treatment was then administered with subjects inhaling tidally via the same nebulizer as used in the cough challenge driven by compressed air at 8 l·min·1 until all of the drug was inhaled. The drugs were dissolved in 0.9% saline immediately before use and administered in a randomized, double-blind manner. The subjects inhaled 1 ml of solution containing 40 mg lignocaine, 4 mg and 8 mg dyclonine or 4 mg ascorbic acid (control solution having a pH similar to that of the solutions of the active drugs) on the different study days. Two minutes after inhalation, Rrs was again measured followed by the Rrs response to the doses of inhaled capsaicin which caused less than two coughs. At 10 min subjects were asked to report their level of oropharyngeal anaesthesia on a scale 0, 1 slight, 2 mild, 3 moderate and 4 complete anaesthesia. A second capsaicin OCR was then performed.
Data analysis
Capsaicin OCR are shown graphically as the median number of coughs at each dose of capsaicin inhaled for the group of ten subjects. The results in the text for Rrs

SEPARATION OF COUGH AND REFLEX BRONCHOCONSTR!CTION 581
Table 1. -Ten healthy subjects inhaled placebo (ascorbic acid 4 mg), lignocaine 40 mg or dyclonine 4 and 8 mg from a nebulizer. The median (range) anaesthesia score, geometric mean (95% Cl) dose of capsaicin causing three more coughs (0
3), mean±95% Cl Rrs before and after treatment and the mean±95% Cl capsaicin induced
percentage increase in Rrs before and after treatment are shown
Treatment Anaesthesia 0 3 Baseline Rts % increase Rrs cmHp·t1·s after capsaicin
Pre Post Pre Post Pre Post
Placebo 0 (0-3) 4.5(3.4-5.9) 7.8(4.8-12.5) 1.7±0.2 1.8±0.2 25±7 20±4 Lignocaine 40 mg 3(1-4)" 4.8(3.5-6.6) 12.6(7.8-20.4). 1.9±0.3 2.2±0.3 22±6 18±4 Dyclonine 4 mg 1(0-2) 5.9(4.1-8.4) 8.9(5.1-15.7) 1.8±0.3 1.9±0.3 24±4 18±8 Dycloninc 8 mg 2.5(1-4)' 4.0(2.9-5.1) 6.8(3.0-12.0) 1.9±0.4 2.1±0.3 23±6 24±7
. : p<0.05, compared to post placebo; Rrs: respiratory resistance; Cl: confidence intervals.
are the mean (95% confidence intervals), for the 03
the geometric mean (95% confidence intervals), and for anaesthesia score median (range). Analysis of Rrs and 0
3 was by multiple analysis of variance and for the anaesthesia score and 0 3 was by Friedman's analysis of ranks.
Results
In agreement with the previous studies with inhaled capsaicin, DCR could be constructed by giving the doses in random order with no evidence of tachyphylaxis (fig. 1). Inhaled capsaicin, in doses that cause fewer than two coughs, consistently caused an increase in Rrs at all frequencies in the first 16 s with a mean increase of 23.4±1.5% in 40 pre-drug studies recorded at 6 Hz. There was no difference between the anaesthesia score for lignocaine (40 mg) and dyclonine (8 mg) and both were s ignificantly (p<O.Ol) hjgher than placebo or dyclonine (4 mg) (table 1). Only lignocaine (40 mg) significantly (p<0.05) shifted the capsaicin DCR to the right (fig. 1). There was no difference in the concentration of capsaicin causing three or more coughs (D:J before and after inhalation of dyclonine 4 and 8 mg and placebo (ascorbic acid, 4 mg) (table 1). Lignocaine (40 mg), on the other hand, produced a 2.6 fold inc rease in D 3 (p<0.05) (table l). None of the trentmems affected either the baseline or the increase in Rrs induced by inhaling a dose of capsaicin which caused <2 coughs (table 1).
Discussion
Cough and the increase in airways resis tance produced by inhaling capsaicin were reproducible in lhe present study, with no evidence of tachyphylaxis. This is in accordance with previous studies [16) and makes it a suitable method for the evaluation of antitussive and antibronchoconstrictor agents.
In the present study, nebulized local anaesthetics caused moderate anaesthesia of the oropharynx, which could be sensed for up to 15 min and was dose-dependent (table I). Lignocaine (40 mg) suppressed the cough response to capsaicin significantly shifting the log DCR to the r:ighl by 162%, a greater change than that found in previous studies in normal humans using nebulized citric acid. CRoss et al. [5], for example, found that citric acid induced cough was abolished by 10 min inhalation of a strong aerosol of the potent local anaesthetic bupivacaine (50 mg·ml·'. yielding peak plasma concentrations of about 1 J.l.g·ml·1). However, it cannot be excluded that cough induced by capsaicin is more sensitive to lignocaine than that induced by citric acid. Another explanation is that li gnocaine is a more pote nt an titussive than bupivacaine.
The shift produced by thi s dose of nebulized lignocaine appears to be quite modest. However, a larger dose would probably have produced a larger degree of inhibition and, moreover, the presently used method (DCR) may show smaller changes than, for example, repeat 1 min inhalations of capsaicin [17]. Interestingly, the effect of inhaled lignocaine in the present study is of the same magnitude as that of systemic administration of a large dose of opiates [16). These data demonstrate that low dose anaesthesia could be used to reduce the sensitivity of the cough reflex. This reduction would be sufficient to return the abnormal sensitivity of the reflex to normal in patients in whom this is associated with cough [18].
The capsa ic in- induced tran s ient in crease in respiratory resistance is inhibited by an anticholinergic drug, indicating that it is a vagal cholinergic renex [13). In contrast to the cough response, lignocaine was without effect on the increase in respiratory resistance. With the exception of the study by C.wss et al. [5], in which a citric acid induced bronchial obstruction in one subject was attenuated by inhaled lignocaine, most studies have shown no topical effect of administered local anaesthetics on reflex bronchoconstriction in man [18-20]. Bronchoconstriction is mediated by rapidly adapting

582 N.B. CHOUDRY ET AL.
stretch receptors and c-fibres, whereas rapidly adapting stretch receptors are believed to constitute the afferent pathway in the cough reflex [11]. A role for afferent c-fibres in cough also seems possible [11, 19]. Although it is not clear in man which fibres are stimulated by inhaled capsaicin, animal studies suggest that it is a rather selective stimulant of c-fibre endings [21]. Cough can be induced in the absence of bronchoconstriction and vice versa, and the two reflexes have a separate sensitivity to drugs and, therefore, different afferent nerves are believed to mediate these reflexes. It seems probable that capsaicin may activate a number of different pathways. Alternatively, it could be argued that the two reflexes occur from different levels of stimulation of the same sensory nerves. However, the present findings that lignocaine inhibits only one of the components support the view that different groups of sensory nerves are involved. These data are in accordance with the observations of SHEPPARD et al. [19] that lignocaine inhibits cough but not bronchoconstriction produced by inhaled distilled water in asthmatics. Interestingly, the water induced bronchial obstruction, but not cough, is sensitive to cromoglycate [19, 22]. Together with the observation that the two reflexes can be induced separately by, for example, inhaled aqueous solutions of different ionic composition and osmolarity [23, 24] it seems likely that these reflexes have separate afferent neural pathways.
Aerosolized local anaesthetics are rapidly absorbed from the airways to yield substantial plasma concentrations [25, 26]. The possibility exists, therefore, that the antitussive effect of lignocaine was due to an interaction of absorbed drug with peripheral or central nervous pathways in the cough reflex. However, to attenuate the cough reflex, plasma levels of >3 j.1g·ml·1 of intravenous lignocaine [27] have to be achieved. Antitussive doses of inhaled lignocaine 20-80 mg, as used in this study, according to MmaEoN et al. [17) would produce low plasma levels of lignocaine. It is, therefore, likely that lignocaine acted locally in the airways to inhibit conduction in the afferent neurones mediating cough. Unexpectedly, neither dose of dyclonine had an effect on the cough response or the change in respiratory resistance produced by capsaicin. Earlier human studies of anaesthesia of the mucosa of the tongue have suggested dyclonine to be 5- 10 times more potent than lignocaine [14) and in the present study a similar degree of oropharyngeal anaesthesia was observed by 8 mg dyclonine and 40 mg lignocaine. This observation also rules out the possibility of a chemical inactivation of dyclonine in the nebulizer. The most likely explanation for the different effects on cough is a difference in the rate of penetration of the two local anaesthetics through the airway mucosa to the sensory nerve endings in the airway responsible for cough, al though other factors such as the local metabolism and clearance of the anaesthetics from their site of action cannot be excluded.
From the present study i£ can be concluded that cough and reflex bronchoconstriction have a separate sensitivity to inhaled local anaesthetics. Thus, separate afferent pathways are likely to be involved.
Furthermore, different types of local anaesthetics differentially affect these two airway reflexes despite producing the same sensation of oropharyngeal anaesthesia. Selective inhibition of airway reflexes can thus be achieved by using inhaled local anaesthetics.
This also implies that selecting local anaesthetics as putative antitussives has to be based upon experiments involving tussive challenge, rather than based on the potency as anaesthetics in other sites.
Ackrrowkdgemerrls: The authors would like to thank the Chest, Heart and Stroke Association and the Medical Research Council for their support of thls work.
References
1. McFadden ER Jr. - Exertional dyspnca and cough as preludes to acute attacks of bronchial asthma. N Engl J Med, 1975, 292, 555-559. 2. Corrao WM, Braman SS, hwin RS. - Chronic cough as the sole presenting manifestation of bronchial asthma. N Engl J Med, 1979, 300, 633-637. 3. Howard P, Cayton RM. Brennan SR, Anderson PB. -Lignocaine aerosol and persistent cough. Br J Dis Chest, 1977, 71, 19- 24. 4. Sanders RV , Kirkpatrick MB. Prolonged suppression of cough after inhalation of lidocaine in a patient with sarcoidosis . J Am Med Assoc, 1984, 252, 2456-2457. 5. Cross A, Guz A, Jain SK, Archer S, Stevens J, Reynolds F. - The effect of anaesthesia of the airway in dog and man: a study of respiratory reflexes, sensations and lung mechanics. Clin Sci Mol Med, 1976, 50, 439-454. 6. Strichartz GR, Ritchie JM. - Action of local anaesthetics on ion channels of excitable tissues. In: Local anaesthetics. Handbook of Experimental Pharmacology. G.R. Strichartz cd., Springer Verlag, Berlin. 1985. 7. Jain SK, Trenchard D, Reynolds F. Noble MIM, Guz A. - The effect of local anaesthesia of the airway on respiratory reflexes in the rabbit. Clin Sci, 1973, 44, 519-539. 8. Dain DS, Boushcy HA, Gold WM. - Inhibition of respiratory reflexes by local anaesthetic aerosols in dogs and rabbits. J Appl Physiol, 1975, 38, 1045-1050. 9. Fuller RW, Choudry NB. - Increased cough reflex associated with angiotensin converting enzyme inhibitor cough. Br Med J, 1987, 295, 1025-1026. 10. Sant'Ambrogio G. - Information arising from the tracheobronchial tree of mammals. Physiol Rev, 1982, 62, 531- 569. 11. Karlsson 1-A, Sant' Ambrogio G, Widdicombe J. -Afferent neural pathways in cough and reflex bronchoconstriction. J Appl Physio/, 1988, 65, 1007- 1023. 12. Collier JG, Fuller RW. - Capsaicin inhalation in man and the effects of sodium cromoglycate. Br J Pharmacol, 1984, 81, 113-117. 13. Fuller RW, Dixon CMS, Barnes PJ. Bronchoconstrictor response to inhaled capsaicin in humans. J Appl Physiol, 1985, 58, 1080-1084. 14. Adriani J, Zepemick R, Arens J. Authement E. - The comparative potency and effectiveness of topical anaesthetics in man. C/in PJw.rmacol Ther, 1964, 5, 49-62.

SEPARATION OF COUGH AND REFLEX BRONCHOCONSTRICTION 583
5. Landser FJ, Nagels J, Demedts M, Billiet L, van de /oestijne KP. - A new method to determine frequency
characteristics of the respiratory system. J Appl Physiol, 1976, 41, 101- 106. 16. Fuller RW, Karlsson J-A, Choudry NB, Pride NB. Effect of inhaled and systemic opiates on response to inhaled capsaicin in humans. J App/ Physiol, 1988, 65, 1125- 1130. 17. Midgren B, Simonsson BG, Per sson CGA . -Topical capsaicin and lidocaine in cough induction and suppression in man. Acta Pham uu:o/ Toxicol. 1986, (Suppl. V), 339. 18. Thomson NC. -The effect of different pharmacological agents on respiratory reflexes in normal and aslhmatic subjects. Clin Sci, 1979, 56, 235- 341. 19. Sheppard D, Riz.k NW, Boushey HA, Bethel RA. -Mechanism of cough and bronchoconstriction induced by distilled water aerosol. Am Rev Respir Dis, 1983, 127, 691-694. 20. Forsberg K, Karlsson J-A, Theodorsson E, Lundberg JM, Persson CGA. - Cough and bronchoconstriction mediated by capsaicin-sensitive sensory neurons in the guinea-pig. Pu/mono/ Pharrrw.col, 1988, 1, 33- 39. 21. Coleridge JCG, Coleridge HM. - Afferent vagal innervation of the lungs and airways and its functional significance. Rev Physiol BiochemPharmacol, 1984,99, 1- 110. 22. Fuller RW, Collier JG. - Sodium cromoglycate and atropine block the fall in FEV 1 but not the cough induced by hypotonic mist. Thorax, 1984, 39, 766-770. 23. Eschenbacher WL, Boushey HA, Sheppard D. -Alteration in osmolarity of inhaled aerosols causes bronchoconstriction and cough but absence of a permeant anion causes cough alone. Am Rev Respir Dis, 1984, 129, 211- 215. 24. Higenbottam T. - Ci>ugh induced by changes of ionic composilion of airway surface liquid. Bull Eur Physiopathol Respir, 1984, 20, 553- 563. 25. McBumey A, Jones DA, Stanley PJ, Ward JW. -Absorption of lignocaine and bupivacaine from the respiratory tract during fibreoptic bronchoscopy. Br J Clin Pharmacol, 1984, 17, 61- 66.
26. Efthimiou J, Higenbottam T, Holt D, Cochrane GM. - Plasma concentrations of lignocaine during fibrcoptic bronchoscopy. Thorax, 1982, 37, 68-71. 27. Yukioka H, Yoshirnoto N, Nishimura K, Fujirnorin M. Intravenous lidocaine as a suppressant of coughing during tracheal intubation. Anesth Analg, 1985, 64, 1189-1192.
Distinction de la toux et du reflexe de bronchoconstriction par /'inhalation d' anesthlsiques locaux. N.B. Choudry, R.W. Fuller, N. Anderson, J-A. Karlsson . RESUME: La ioux et la constriction des voies aeriennes sont des traits frequents dans les maladies respiratoires. Les deux peuvent i!tre provoqoes par la stimulation des nerfs des voies aerienncs. Nous avons etudie les effets de l'anestMsie des voies aeriennes sur ces reflexes, stimu]es par !'inhalation de capsaicin, afm de determiner s'ils etaient contrOles par les memes nerfs sensitifs. 10 volontaires ont ete soumis a une etude dose-reponse de la toux par capsaicin, avant et Dix minutes apres !"inhalation de placebo (acide ascorbique dans la solution saline isotonique), et d'ancsthesiques topiques (l ignocaine 40 mg, dyclonine 8 et 4 mg). L'effet des m&licaments sur la resistance respiratoire (Rrs), mesurec par la technique d'oscillotion forcCc, ache etudic avant et apres }'inhalation d'une dose de capsaicin qui causait moins de 2 secousses de toux. La lign.ocalne (40 mg) Cl la dyclonine (8 mg) ont provoque toutes deux une anesthesie buccale, mais seule la lignocaine a r&luit la repon.se tussigene a !'inhalation de capsaicin, en augmentant de 162% la dose log de capsaicin, provoquant 3 secousses de toux ou davantage. Aucun des traitements n'a modifie la Rrs basale ou son augmentation apres inhalation de capsaicin. Done, les reflexes de toux et les reflexes de bronchoconstriction causes par ]'inhalation de capsaicin ont une sensibilite differente a l'egard de l'anesthesie locale par inhalation, ce qui suggere que cet effet pourrait etre medie par des voies scnsitives differentes. Eur Respir J .• 1990, 3, 578-583.