Sensors and Actuators B: Chemical - ERNETweb.iitd.ernet.in/~sandeepjha/files/2018 Soni Sens...
8
Sensors and Actuators B 269 (2018) 346–353 Contents lists available at ScienceDirect Sensors and Actuators B: Chemical jo u r nal homep age: www.elsevier.com/locate/snb Smartphone based optical biosensor for the detection of urea in saliva Anuradha Soni a , Rajat Kumar Surana c , Sandeep Kumar Jha a,b,∗ a Centre for Biomedical Engineering, Indian Institute of Technology Delhi, Hauz Khas, New Delhi, 110016, India b Department of Biomedical Engineering, All India Institute of Medical Sciences, New Delhi, 110029 India c Department of Textile Technology, Indian Institute of Technology Delhi, Hauz Khas, New Delhi, 110016, India a r t i c l e i n f o Article history: Received 14 September 2017 Received in revised form 16 April 2018 Accepted 21 April 2018 Available online 22 April 2018 Keywords: Smartphone based biosensor Non-invasive biosensor Salivary urea Optical biosensor a b s t r a c t In the present study, we have developed a smartphone based handheld optical biosensor for determina- tion of urea in saliva. A simple strategy was adopted by immobilization of urease enzyme along with a pH indicator on a filter paper based strip. The strip changed color upon the reaction with urea present in saliva and the color change can be estimated using our smartphone based application based on RGB profiling. Calibration of the biosensor was carried out using spiked saliva samples and an exponentially decreas- ing calibration curve has been obtained for green pixel intensity in the broad range (10–1000 mgdL −1 ) with a linear detection range of 10–260 mgdL −1 and a response time of 20 s. The sensitivity reported for the biosensor in the clinically significant range was −0.005 average pixels sec −1 /mgdL −1 with a LOD of 10.4 mgdL −1 . Studies carried out on spiked saliva samples showed a good correlation between sali- vary urea estimated using our biosensor against phenol-hypochlorite based spectroscopic procedure. Development of a smartphone based biosensor for urea estimation eliminates the need for procuring a dedicated instrument as well as trained technician for daily monitoring and saves time as compared to traditional laboratory methods of analysis. © 2018 Elsevier B.V. All rights reserved. 1. Introduction Urea is the major end product of nitrogen metabolism in humans and is eliminated from the body mainly by the kidneys through urine but is also secreted in body fluids such as blood and saliva. Its level in urine ranges from 7 to 20 mgdL −1 which drastically rises under pathophysiological conditions thus providing key informa- tion of renal function and in the diagnosis of various kidney and liver disorders [1]. Increase in urea levels in blood, also referred to as azotemia or uremia is referred to as Chronic Kidney Disease (CKD) or End Stage Renal Disease (ESRD) and is generally caused due to the progressive loss of kidney function. Normal glomerular filtration rate (GFR) lies between 100–120 mL/min. which begins to fall below 70 mL/min with the onset of azotemia or uremia. For subjects with kidney failure, GFR reaches around or even less than 15 mL/minute [2]. Apart from CKD, several other conditions such as heart failure, hypovolemic shock, gastrointestinal bleeding, severe infections also leads to a rise in urea levels beyond normal [1]. Dia- betes and hypertension has been reported as the major risk factors for CKD in both developing as well as developed countries followed ∗ Corresponding author at: Centre for Biomedical Engineering, Indian Institute of Technology Delhi, Hauz Khas, New Delhi, 110016, India. E-mail address: [email protected] (S.K. Jha). by glomerulonephritis and cardiovascular disease [3,4].According to National Kidney Foundation, CKD affects around 10% of world’s population [5] and was ranked 18th among the various causes of deaths worldwide in 2010 with an annual death rate of 16.3 per 100000 [6] or over 1 million in total [3]. Therefore, diagnosis of kidney disease at an early stage is important in order to prevent the development of drastic consequences. Kidney Function tests play an important role in the diagnosis of renal disorders at early stages. Several tests such as urinalysis, urine protein, creatinine clearance, serum creatinine, Blood Urea Nitrogen (BUN), Glomerular Filtration Rate (GFR) etc. involving either urine or blood samples are commonly grouped under Kid- ney Function tests [7]. Most important of these tests are Blood Urea Nitrogen (BUN) and serum creatinine which are frequently used in every diagnostic laboratory for estimation of renal function. These tests also form an essential part of radiological screening proce- dures such as Magnetic Resonance Imaging (MRI) and Computed Tomography (CT) prior to the administration of radiological con- trast agents such as iodinated contrast or gadolinium based contrast agents so as to prevent complications such as contrast medium induced nephropathy and nephrogenic systemic fibrosis [8]. Amongst several methods for the estimation of urea in body flu- ids, most are based on colorimetric procedures. Some of these are nesslerization [9], phenol-hypochlorite or Berthelot method [10] https://doi.org/10.1016/j.snb.2018.04.108 0925-4005/© 2018 Elsevier B.V. All rights reserved.
Transcript of Sensors and Actuators B: Chemical - ERNETweb.iitd.ernet.in/~sandeepjha/files/2018 Soni Sens...

S
Aa
b
c
a
ARRAA
KSNSO
1
aulutlt(dfits1hibf
T
h0
Sensors and Actuators B 269 (2018) 346–353
Contents lists available at ScienceDirect
Sensors and Actuators B: Chemical
jo u r nal homep age: www.elsev ier .com/ locate /snb
martphone based optical biosensor for the detection of urea in saliva
nuradha Sonia, Rajat Kumar Suranac, Sandeep Kumar Jhaa,b,∗
Centre for Biomedical Engineering, Indian Institute of Technology Delhi, Hauz Khas, New Delhi, 110016, IndiaDepartment of Biomedical Engineering, All India Institute of Medical Sciences, New Delhi, 110029 IndiaDepartment of Textile Technology, Indian Institute of Technology Delhi, Hauz Khas, New Delhi, 110016, India
r t i c l e i n f o
rticle history:eceived 14 September 2017eceived in revised form 16 April 2018ccepted 21 April 2018vailable online 22 April 2018
eywords:martphone based biosensoron-invasive biosensor
a b s t r a c t
In the present study, we have developed a smartphone based handheld optical biosensor for determina-tion of urea in saliva. A simple strategy was adopted by immobilization of urease enzyme along with a pHindicator on a filter paper based strip. The strip changed color upon the reaction with urea present in salivaand the color change can be estimated using our smartphone based application based on RGB profiling.Calibration of the biosensor was carried out using spiked saliva samples and an exponentially decreas-ing calibration curve has been obtained for green pixel intensity in the broad range (10–1000 mgdL−1)with a linear detection range of 10–260 mgdL−1 and a response time of 20 s. The sensitivity reportedfor the biosensor in the clinically significant range was −0.005 average pixels sec−1/mgdL−1 with a LOD
−1
alivary ureaptical biosensorof 10.4 mgdL . Studies carried out on spiked saliva samples showed a good correlation between sali-vary urea estimated using our biosensor against phenol-hypochlorite based spectroscopic procedure.Development of a smartphone based biosensor for urea estimation eliminates the need for procuring adedicated instrument as well as trained technician for daily monitoring and saves time as compared totraditional laboratory methods of analysis.
© 2018 Elsevier B.V. All rights reserved.
. Introduction
Urea is the major end product of nitrogen metabolism in humansnd is eliminated from the body mainly by the kidneys throughrine but is also secreted in body fluids such as blood and saliva. Its
evel in urine ranges from 7 to 20 mgdL−1 which drastically risesnder pathophysiological conditions thus providing key informa-ion of renal function and in the diagnosis of various kidney andiver disorders [1]. Increase in urea levels in blood, also referredo as azotemia or uremia is referred to as Chronic Kidney DiseaseCKD) or End Stage Renal Disease (ESRD) and is generally causedue to the progressive loss of kidney function. Normal glomerularltration rate (GFR) lies between 100–120 mL/min. which beginso fall below 70 mL/min with the onset of azotemia or uremia. Forubjects with kidney failure, GFR reaches around or even less than5 mL/minute [2]. Apart from CKD, several other conditions such aseart failure, hypovolemic shock, gastrointestinal bleeding, severe
nfections also leads to a rise in urea levels beyond normal [1]. Dia-etes and hypertension has been reported as the major risk factorsor CKD in both developing as well as developed countries followed
∗ Corresponding author at: Centre for Biomedical Engineering, Indian Institute ofechnology Delhi, Hauz Khas, New Delhi, 110016, India.
E-mail address: [email protected] (S.K. Jha).
ttps://doi.org/10.1016/j.snb.2018.04.108925-4005/© 2018 Elsevier B.V. All rights reserved.
by glomerulonephritis and cardiovascular disease [3,4].Accordingto National Kidney Foundation, CKD affects around 10% of world’spopulation [5] and was ranked 18th among the various causes ofdeaths worldwide in 2010 with an annual death rate of 16.3 per100000 [6] or over 1 million in total [3]. Therefore, diagnosis ofkidney disease at an early stage is important in order to preventthe development of drastic consequences.
Kidney Function tests play an important role in the diagnosisof renal disorders at early stages. Several tests such as urinalysis,urine protein, creatinine clearance, serum creatinine, Blood UreaNitrogen (BUN), Glomerular Filtration Rate (GFR) etc. involvingeither urine or blood samples are commonly grouped under Kid-ney Function tests [7]. Most important of these tests are Blood UreaNitrogen (BUN) and serum creatinine which are frequently used inevery diagnostic laboratory for estimation of renal function. Thesetests also form an essential part of radiological screening proce-dures such as Magnetic Resonance Imaging (MRI) and ComputedTomography (CT) prior to the administration of radiological con-trast agents such as iodinated contrast or gadolinium based contrastagents so as to prevent complications such as contrast mediuminduced nephropathy and nephrogenic systemic fibrosis [8].
Amongst several methods for the estimation of urea in body flu-ids, most are based on colorimetric procedures. Some of these arenesslerization [9], phenol-hypochlorite or Berthelot method [10]

Actuat
a(lappiidgsdhuoi
bvoaasrAbuetoebnuwuAtu
scrcpmsbwpiddtc
rbswcasc
C
A. Soni et al. / Sensors and
nd diacetyl monoxime method [11,12]. Blood Urea Nitrogen testBUN) is most commonly used test for assessment of blood ureaevels and the test is frequently combined along with a serum cre-tinine test for the differential diagnosis of pre-renal, renal andost-renal hyperuremia. BUN measures the amount of nitrogenresent in a subject’s blood. The main drawback of this procedure
s that it is time-taking as well as involves blood extraction whichs painful and inconvenient to the subject undergoing the proce-ure; therefore use of alternate body fluids for urea estimation is ofreat importance. Among non-invasive body fluids such as urine,aliva, sweat and tears, saliva is most easily accessible to the userue to ease in collection and its availability. Several research groupsave also established a good correlation between salivary and bloodrea levels using conventional methods [13–17]. However, devel-pment of a biosensor for measuring urea levels in saliva sampless an immediate necessity.
The first urea biosensor was reported by Guilbault and Montalvoy using a potentiometric urease enzyme electrode [18]. Since thenarious biosensors have been reported till date for the estimationf urea in biological fluids employing both electrochemical [19–21]s well as optical methods [22–25] of detection. Various organics well as inorganic matrices have been used for immobilizationuch as latex polymers [26], conducting polymers such as polypyr-ole [27], metal nanoparticles [28], metal oxides [29] and so on.mong non-invasive category, several reverse iontophoresis basediosensors have been developed for the determination of bloodrea concentration using potentiometric techniques [30,31]. Chent al. developed a conductivity cell with 61 MHz surface acous-ic wave resonator based measurement circuit for determinationf urea in urine samples with a LOD of 30 ngml−1 [32].A piezo-lectric biosensor feasible for detecting urea in urine samples haseen developed by Yang et al. by immobilizing urease enzyme onanoporous alumina membrane [33]. Likewise, an amperometricrea biosensor capable of detecting urea in aqueous solutions asell as urine has been developed by covalent immobilization ofrease enzyme on N2 incorporated diamond nanowire film [34].nother voltammetric sensor based on single walled carbon nano-
ubes has been developed by Chen et al. which can sense urea inrine samples [35].
However, all these biosensors developed for urea estimationuffers from several drawbacks such as use of complicated as well asostly methods in fabrication, requires trained personnel to gatheresults and most of them are not portable in nature, and hencean’t be used for in situ monitoring at hospitals or homes. One suchortable clinical analyzer has been developed by Abott with com-ercial name ‘iStat portable clinical analyzer’ which can measure
everal parameters such as urea and creatinine using few drops oflood through its disposable cartridges but the device is costly asell as invasive in nature, therefore is not preferred by commoneople for routine monitoring [36,37]. One recent breakthrough
n portable urea sensing was development of saliva urea nitrogenipstick test strips by Evans et al. which was used to detect kidneyisease in Malawi but had several limitations such as being qualita-ive and lacking accuracy, as the change in urease based pH strip’solor was compared using naked eye [38].
In this respect, for addressing all the drawbacks of theseeported sensors, we have developed a smartphone based opticaliosensor for the determination of urea in saliva samples using aimple methodology by immobilization of urease enzyme alongith pH responsive dye on a filter paper based strip. The strip
hanged color due to the increase in pH upon the formation ofmmonia as a result of urease enzyme reaction with urea present in
aliva sample. The enzymatic reaction of urea with urease enzymean be described as Eq. (1)O(NH2)2 + H2OUrease→ 2NH3 + CO2 (1)
ors B 269 (2018) 346–353 347
The higher the concentration of urea present in the sample,the more ammonia was liberated and hence color change wasmore profound. This color change in the paper strip was thenscreened through RGB profiling with the use of a smartphonebased application developed in-house. The urea concentration wasdeduced using calibration curve equation fed into the smartphoneapplication itself. In today’s digital era, smartphones have becomeubiquitous and contains several features such as high resolutioncamera, computational ability, and capability of integrating toseveral devices via in built Bluetooth and GPS systems, enablingresearchers to use smartphone as a diagnostic tool for the detec-tion of various diseases, metabolites, biomarkers, pathogens etc.[39–43]. Following this trend, we have also used smartphone basedplatform to make the device more user-friendly eliminating theneed for procuring a dedicated instrument for analysis. Moreover,slope based calculation of test results was followed to enhance thesensitivity of detection and reduce ambient light interferences. Inour previous studies, we had developed a smartphone based sali-vary glucose biosensor using a test strip and android app workingon slope based calculation method and validated it on real samplesfor mass diagnosis of diabetes [44]. The algorithm for detectionwas altered in this app for sensing salivary urea level. For exam-ple, instead of cumulative calculation of sensor response in termsof Slope (R + G + B), in the present work we employed slope of greenpixel intensity. The test strip preparation was also altered to suiturea detection.
Few other groups have also demonstrated smartphone baseddetection of biomolecules [45,46]. However their strategy involvesmore complex methods of fabrication of sensor or they haveused open source image processing softwares to deduce analyteconcentration in mostly offline mode compared to our online sens-ing method. In this respect, our present work involves a simplefabrication method where the strips are paper-based and hencebiodegradable. Moreover, the analysis is done onsite with the helpof developed smartphone app and hence can be used at such placeswhere healthcare facilities are not easily available.
2. Materials and methods
2.1. Materials
Smartphone (Samsung Galaxy SIII) was of Samsung India Lim-ited make; laminator (Model ECO 12) was from ExcelamTM. Filterpaper (Whatman number 1), polyvinyl alcohol (Cat. No.563900),urease enzyme (Cat. No. U4002-20 KU), sodium phosphate diba-sic (Cat. No.V800397), sodium phosphate monobasic (Cat. No.V800376), phenol (Cat. No. P4161), sodium hydroxide pellets (Cat.No. 221465) were procured from Sigma Aldrich India; urea (crys-talline, extrapure) was from Merck India Ltd.; phenol red indicator,sodium nitroprusside and sodium hypochlorite was procured fromFisher Scientific India. Lamination films, card stock sheets, doublesided tape, nylon mesh and ear buds were purchased from localmarket.
2.2. Methods
2.2.1. Preparation of test strips and immobilization of ureaseThe supporting material used for strip preparation was card
stock sheet (credit card size) with dimensions of 8.9 cm × 5 cm andthickness of about 0.35 �m. A 4.5 mm hole was created on the sup-porting layer at a distance of 1.5 cm from the top and the hole was
laminated using a thin lamination film. Circular filter paper with5 mm diameter was then placed on top of the lamination film cov-ering the hole and was again covered with another lamination filmcontaining a 4.5 mm hole such that the filter paper gets embed-
348 A. Soni et al. / Sensors and Actuators B 269 (2018) 346–353
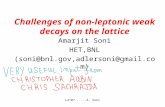
Fig. 1. (A) Reaction principle involved in the biosensor (B) Schematics of the biosensor showing steps for urea detection and (C) Color change in the strips with increase inu
detwdd
sa(iwpserm
2p
silp
vra
rea concentration (10–1000 mgdL−1).
ed between the two films leaving a 4.5 mm detection zone wherenzyme immobilization as well as detection takes place. The detec-ion zone was covered with 1.2 cm long and 0.8 cm wide nylon meshith a pore size of 500 �m held on both sides with the help of aouble sided adhesive tape. The layered structure of the strip isepicted in Supplement Fig. S1.
Immobilization of urease on the strips was carried out usingimple entrapment method where a solution of 13.5 mg ureaselong with 200 �L of dye (phenol red), 200 �L of phosphate buffer1 mM, pH 7.0) and 100 �L of 0.25% PVA was prepared for themmobilization of 100 test strips and 5 �L of the above solution
as immobilized per strip through the mesh with the help of aipette such that 10 U enzyme loading was obtained per strip. Thetrips were then dried and stored desiccated at 4 ◦C until use. Thenzyme activity of the strips was estimated using phenol hypochlo-ite method [10] and protein content was determined using Lowry’sethod [47].
.2.2. Development of android smartphone application for RGBrofiling
For the estimation of urea concentration using RGB profiling,martphone based android application (app) has been developedn-house incorporating the smartphone camera as well as flash-ight. The application could estimate urea levels with respect toixel intensity using slope method.
Slope method (change in sensor response divided by time inter-al) has been chosen against differential method (change in sensoresponse between two time intervals) to increase the sensitivitys well as reduction of interference from fluctuations in flashlight
intensity which can lead to errors in measurement. Moreover, nobaseline correction was required in case of slope method during cal-ibration, as slope of sensor response curve remains almost constantwithin the dynamic range. Whereas, in case of differential methodthe sensor response changes with time, requiring to deduct base-line value and in the event of a baseline shift the results are oftenerroneous. The developed app was different from its earlier version[44] in a sense that it calculated Slope[G] instead of Slope [R + G + B]pixels.
For urea estimation using the developed application, saliva sam-ple was applied on the strip which was placed inside a cardboardbox (3 cm height) containing a hole so that the flashlight of thecamera illuminates the detection zone when smartphone is placedover it. The requirement of a box was to minimize the problemassociated with variations in distance from camera with the detec-tion zone, if one was to hold the test strip in hand or against asurface. The effect of height wise variation on the strip under ambi-ent light condition has been checked for printed strips (red, greenand blue color) and slopes for red, blue and green pixel intensitywere obtained within a fixed time interval with varying height.Results are depicted in Supplement Fig. S2. After placing the teststrip inside the box, the app was initiated by adjusting the timeinterval for obtaining sensor response slope (between 10 and 20 s.in this case). The android app after initiation captures first image ofdetection zone at 0 s. Thereafter it calculates average G values for 20random pixels within the detection zone. Second image is captured
after 10th sec in similar manner. The difference of average G valuesat two intervals is subtracted and divided by 10 s to calculate slopeof response curve. Hence, the units of sensor response have been
A. Soni et al. / Sensors and Actuat
Fig. 2. (A) Calibration curve plotted against urea concentration v/s change in slopefor R (-�-), G (-©-) and B pixels (-�-) in the broad range (10–1000 mgdL−1). (B)CBb
twisdecPf
2
psc(1vmctsoss
alibration curve for urea concentration v/s change in Slope for R (-�-), G (-©-) and (-�-) pixels within the linear range of 10–260 mgdL−1. Maximum sensitivity haseen reported for Slope (G) within this range.
aken as average pixel/sec throughout the calculations. These soft-are based calculations are not visible to the user and continues
n background. If the test is successful, it’ll show the slope value oncreen, else, a prompt is shown stating that test was unsuccessfulue to improper saliva volume. The change in slope (�pixel/10 s forach color) is then used for urea concentration calculation usingalibration equation fed into the app (Supplement Fig. S3 and S4).rior to that, to obtain calibration equation, raw slope data obtainedrom app is plotted against known spiked urea concentrations.
.2.3. Biosensor measurementsIn order to minimize variation in viscosity and other salivary
arameters, calibration of the biosensor was carried out using salivaamples of healthy individual spiked with 5% volume of knownoncentrations of synthetic urea prepared in phosphate buffer1 mM, pH 7.0) so as to prepare concentration ranging from 0 to000 mgdL−1. Urea concentration already present in healthy indi-idual’s saliva sample was estimated using phenol-hypochloriteethod and the values obtained were added to the known con-
entration so as to obtain actual concentration of urea present inhe spiked sample. For biosensor measurements, 5 �L of the above
ample was applied on the strip through the mesh with the helpf a pipette and color changes on the opposite site of the strip wascreened using RGB profiling through our developed application ashown in Section 2.2.2. The reaction principle and schematics ofors B 269 (2018) 346–353 349
salivary urea detection using the developed biosensor and colorchanges in the strips with increasing glucose concentration aredepicted in Fig. 1(A–C).The response time was fixed as 20 s where10 s was the time required for sample application and placing thestrip inside the dark box and then the slope was taken for remain-ing 10 s, altogether giving a response time of 20 s. Change in slopefor R, G and B pixels was obtained and calibration curves wereplotted against urea concentration v/s Slope (average pixels/sec)using Originlab 2017 software. For calibration, all the readings wereobtained in triplicates and data plotted with standard deviation aserror bars. Shelf life study on the biosensor strips was also carriedout for a period of 30 days.
2.2.4. Effect of chemical interferents on sensor responseAscorbic acid, lactic acid and uric acid are the most common
interferents present in human saliva which can cause changes insensor response. The concentration of these acids in human mouthrange from 0 to 20 mgdL−1, which varies between individuals and atdifferent times of the day depending upon the food intake [48–50].Ascorbic acid levels in human saliva increases with the intake offoods rich in vitamin C whereas presence of lactate is mainly admin-istered with bacterial fermentation process occurring in humanmouth. To study the effects of these interferents on sensor response,5 �L of saliva sample was added onto the strip with or withoutspiking with synthetic urea. For carrying out these studies, salivasample was spiked using 15 mgdL−1 urea and lactic or ascorbic acidconcentrations in the range of 0–20 mgdL−1. The change in slopefor green pixel intensity was obtained within a response time of20 s for samples containing ascorbate/lactate alone and for sam-ples containing urea along with an interferent. pH changes on thestrips upon addition of these samples was also recorded to predictthe buffering action of saliva on addition of these acids. Interfer-ence studies with uric acid were also carried out in the range of0–20 mgdL−1 uric acid. All the studies were carried out in triplicatesand data plotted using standard deviation as error bars.
2.2.5. Clinical validation of the biosensor with real samplesFor validation of the biosensor on real samples, saliva samples
from few healthy donors was obtained after obtaining their writ-ten consent as per the ethical guidelines, some of these sampleswere spiked with synthetic urea samples prepared in phosphatebuffer so as to obtain higher concentrations as found in subjectswith impaired renal function. Fresh saliva was used for analysisand the sample was obtained after rinsing of mouth with drink-ing water so as to nullify the effect of all possible interferencescaused due to the presence of substances such as ascorbate, andlactate commonly found in human mouth. The samples obtainedwere tested using our developed sensor and also using the standardphenol-hypochlorite based spectrophotometric procedure and acorrelation was established between both these methods usingt-test performed using Microsoft Excel software.
Correlation between blood and salivary urea concentration wascarried out for 19 subjects enrolled at IIT Delhi hospital with writ-ten consent obtained from them. Salivary urea concentration wasobtained using our developed biosensor and blood urea nitrogenreadings were obtained from the pathology lab of IIT Delhi hos-pital where the blood urea concentration was estimated usingspectrophotometric method with the help of autoanalyzer (CobasIntegra). Correlation between blood and salivary urea concentra-tion was established by t-test using Microsoft Excel. Tests for
repeatability and reproducibility were carried out by obtaining ureaconcentration using the developed sensor for same sample multi-ple times and for three different samples at three different timeintervals.
350 A. Soni et al. / Sensors and Actuators B 269 (2018) 346–353
Fig. 3. Interference studies using lactic and ascorbic acid. (A) Effect of ascorbic acid concentration on sensor response. It has been observed that in the clinically relevantrange of ascorbic acid found in mouth, saliva was found to act as a buffer to some extent while with higher concentrations of ascorbic acid, sensor response increases withd id. (Cn fferingo
3
3
ctsaeobm0
ecrease in pH. (B) Study of buffering action of saliva upon addition of ascorbic acoted as in the case of ascorbic acid with increasing concentration. (D) Study of bun sensor response.
. Results and discussion
.1. Immobilization and characterization of urease on the strips
Schematic of strip preparation and immobilization along witholor change in the strips with respect to increasing urea concen-ration is depicted in Fig. 1(B&C respectively). The immobilizedtrips were stored desiccated at 4 ◦C until use. Enzyme activitynd protein content of the strips were estimated in triplicates. Thenzyme activity per strip calculated as per the phenol-hypochlorite
r Berthelot assay was about 4.6 U (indicating ∼46% yield of immo-ilization) whereas the protein content deduced from Lowry’sethod was found to be around 225 �g in a detection zone of.635 cm2 circular area. Specific activity was therefore calculated
) Effect of lactic acid concentration on sensor response. Similar behavior has been capacity of saliva upon addition of lactic acid. (E) Effect of uric acid concentration
as 20.5 U/mg protein. Shelf life studies carried out on the stripsshowed an exponential decay trend with around 50% loss of activ-ity after a period of 30 days (Supplement Fig. S5). This was obviousfor the reason urease is not that stable enzyme when comparedto glucose oxidase. However, in entrapped condition, its activitydecreases and saturates after few days of immobilization [51].
3.2. Biosensor measurements
Calibration curves for the biosensor were obtained after cal-
culating slope of response curves for Red, Blue and Green pixelintensity v/s urea concentration within a response time of 20 s (10 sfor sample handling + 10 s slope) using Originlab software. Withinthe broad range (10–1000 mgdL−1) an exponentially decreasing
Actuators B 269 (2018) 346–353 351
cGiwrrfpiGRmX
Y
1o
Y
bop1npws
3
fcistitselwttiscfffi(afccaawa
Fig. 4. (A) Correlation between salivary urea concentration obtained using phenol-hypochlorite method with salivary urea concentration deduced using our developedbiosensor (-�-). Studies were carried out by spiking saliva samples obtained from 3healthy subjects with synthetic urea solutions prepared in phosphate buffer (1 mM,
A. Soni et al. / Sensors and
alibration curve has been obtained for Green pixel intensity (Slope). For Blue (Slope B) and Red pixels (Slope R) an exponentially
ncreasing as well as linear curves were obtained respectively,hile showing negligible change in pixel intensity with respect to
ed pixels (Fig. 2A). The curves exhibit good linearity within theange of 10–260 mgdL−1 (Fig. 2B). Highest sensitivity was obtainedor Green pixel intensity (Slope G) as compared to Blue and Redixels within the clinically relevant range; therefore for clinical val-
dation and other studies, calibration curve for Green pixels (Slope) with respect to urea concentration was chosen against Blue anded pixels. The calibration curve within the broad range (10–1000gdL−1) for Green pixels (Slope G) can be depicted by Eq. (2) where
denotes unknown urea concentration and Y denotes Slope (G)
= 1.42 × e(−X/137.33)−1.464 (2)
The calibration curve for Slope (G) within the linear range of0–260 mgdL−1 can be depicted by Eq. (3) below with a sensitivityf −0.005 average pixels sec−1/mgdL−1.
= −0.005 × X−0.09 (3)
Limit of Detection (LOD) of a sensor can be practically calculatedy measuring the pixel intensity change (Slope G) in samples devoidf urea. For estimation of LOD of the developed sensor, saliva sam-le from a healthy donor was made to react with urease enzyme for
h till whole urea present in the sample gets consumed. The sensoroise level for this sample (n = 4) was found to be −0.0565 averageixels/second, which corresponded to 10.4 mgdL−1 as LOD. Thisas significant, as the clinically relevant range for urea in serum
tarts at about 20 mgdL−1 concentration.
.3. Interference studies carried out on the biosensor
To estimate the effect of chemicals on sensor response, inter-erence studies were carried out using ascorbic, lactic and uric acidoncentrations within the range of 0–20 mgdL−1, which is a rangen excess of what usually found in saliva. It was observed that whenaliva sample was spiked with ascorbic or lactic acid alone withouthe addition of urea, the slope of green pixel intensity showed anncreasing trend towards positive axis with increase in concentra-ions of these acids, which was due to the decrease in overall pH ofample. However, in samples containing urea along with interfer-nt (ascorbic or lactic acid), saliva was found to act as a buffer atower concentrations of these acids [52,53] and the pixel intensity
as found to be almost constant for lower concentrations whichhen slowly started to increase with the increase in acid content inhe saliva due to the decrease in pH. The trend has been depictedn Fig. 3(A–D). Fasting lactic acid concentration present in humanaliva sample is around 1.8 mgdL−1 [49] and values for ascorbateoncentration often ranges in between 0 and 20 mgdL−1 [48]. Thus,or such subjects the sensor was found to be free of these inter-erents within the clinically relevant range. The sensor was alsoound to be selective for urea, with no interferences with uric acidn the clinically relevant range of uric acid present in human mouth0–8 mgdL−1) (Fig. 3E). However, for subjects who have undertaken
vitamin C rich diet or suffering from dental caries, slight inter-erences may result due to the presence of these acids in higheroncentrations in mouth. Therefore, to obtain uniformity in sampleollection and eliminate all possible interferences, subjects were
dvised not to eat or drink anything especially vitamin C rich diett least 2–3 h before the test and were told to rinse their mouthith drinking water prior to sample collection. Only fresh salivaccumulated in mouth was to be collected for measurements.
pH 7.0) (B) Correlation between blood urea concentration obtained using an autoan-alyzer with salivary urea obtained using our developed biosensor (-©-) for healthysubjects.
3.4. Measurements with clinical samples
Clinical validation of the biosensor was carried out using spikedsaliva samples. Fresh saliva was collected from 3 healthy donorsafter rinsing of mouth with drinking water without involvement ofany filtration or centrifugation step. Saliva samples from these threesubjects were then spiked with different concentrations of ureaprepared in phosphate buffer. Nineteen different samples werethus obtained (after simulated spiking). Salivary urea levels of allthese samples were then obtained using our developed sensor andat the same time phenol-hypochlorite method was also used tocalculate urea concentration in conventional manner. Correlationbetween salivary urea concentrations obtained using these twomethods was then established by t-test using Microsoft Excel soft-ware. Further, for establishing correlation between blood urea level(using an autoanalyzer) and salivary urea concentration (calculatedusing our biosensor), validation was carried out on 19 healthy sub-jects between the age group of 30–70 years and correlated was
obtained by t-test in similar manner.R2 value of 0.93 (n = 19, Slope = 1.01, Pearson’s R = 0.96) withP value of 0.16 was found between salivary urea concentrationin spiked samples obtained using our biosensor and spectropho-

3 Actuat
tigpemba(s(rvvcanubtst
ocu1cwt
4
sitslGaadmtiCfclsbtfursmp
A
vS
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
52 A. Soni et al. / Sensors and
ometric procedure (phenol hypochlorite method), thus showingnsignificant difference between the two methods (Fig. 4A). Thus aood correlation obtained with standard procedure in spiked sam-les suggests that the developed biosensor can be used for ureastimation in saliva samples obtained from healthy as well as ure-ic subjects for diagnosis of renal dysfunction. Similarly, when
lood urea concentrations in healthy volunteers obtained using anutoanalyzer was correlated with their salivary urea concentrationobtained using our developed sensor), R2 value of 0.68, with Pear-on’s R value of 0.83 (n = 19, Slope = 0.8, P = 1.33E−06) was obtainedFig. 4B). In these volunteers, the blood urea levels were within theange of 10–40 mgdL−1. Such correlation was similar to that pre-iously reported in literature (Pearson’s R2 ∼70) [54] and hencealidated our device performance. In continuation of our studies,orrelation tests with uremic subjects, particularly those with CKDnd other disorders shall be carried out in future after obtainingecessary ethical clearances for larger study samples. In the case ofremic subjects, significant correlation (R value >/ = 0.9) betweenlood and salivary urea concentration is expected. Higher correla-ion is also expected in case of subjects with hypertension or thoseuffering from diabetes, where more urea leaches out in saliva dueo the damage of epithelial lining of salivary gland.
Further, repeatability of sensor measurement was evaluated bybtaining urea concentration for a healthy donor’s saliva sampleoncurrently for five times (n = 5), the studies showed an averagerea concentration of 18.17 mgdL−1 with a standard deviation of.8. Test for assessing the reproducibility of the biosensor was alsoarried out. The sensor was found to be around 90% reproduciblehen readings were obtained for three different saliva samples at
hree different time intervals (Supplement Fig. S6).
. Conclusion
In the present study we have developed an optical urea biosen-or using saliva sample and a smartphone. The urease-pH indicatormmobilized strips changed color with respect to urea concentra-ion in saliva sample and the color changes were detected usingmartphone based app using RGB profiling and slope based calcu-ation method. Calibration curve with green pixel intensity (Slope) was found to be most sensitive with a sensitivity of −0.005 aver-ge pixels sec−1/mgdL−1 within the linear range of 10–260 mgdL−1
nd a LOD of 10.4 mgdL−1. Salivary urea determination using oureveloped biosensor shows good correlation with spectroscopicethod such as phenol-hypochlorite for spiked samples. Correla-
ion of 0.83 was obtained between blood and salivary concentrationn case of healthy subjects; however more studies are required onKD patients and those suffering from hypertension and diabetesor better standardization of the sensor. The developed biosensoran be used by a layman with limited training against commonaboratory methods that can be performed only by trained profes-ionals. Another benefit of the developed sensor is that results cane obtained in less time (just 20 s) against time consuming spec-rophotometric procedures where a patient has to wait for reportor a day or at least few hours. Our developed sensor is fabricatedsing simple technique just by immobilizing urease along with pHesponsive dye on a filter paper and is cost-effective. Moreover, thecreening is done through a smartphone which has become a com-on gadget nowadays among people, thus eliminating the need for
rocuring a dedicated instrument for analysis.
cknowledgements
The author is obliged for the intramural financial support pro-ided by Indian Institute of Technology Delhi. The author Anuradhaoni thanks Indian Council of Medical Research, New Delhi for
[
ors B 269 (2018) 346–353
research fellowship. A part of this work has been filed for IndianPatent (1587/DEL/2015 dated 1/6/2016).
Appendix A. Supplementary data
Supplementary data associated with this article can be found, inthe online version, at https://doi.org/10.1016/j.snb.2018.04.108.
References
[1] C. Higgins, Urea and the Clinical Value of Measuring Blood UreaConcentration, 2016.
[2] GFR (Glomerular Filtration rate) www.kidney.org.[3] W.G. Couser, G. Remuzzi, S. Mendis, M. Tonelli, The contribution of chronic
kidney disease to the global burden of major noncommunicable diseases,Kidney Int. 80368 (2011) 1258–1270.
[4] V. Jha, G. Garcia-Garcia, K. Iseki, Z. Li, S. Naicker, B. Plattner, et al., Chronickidney disease: global dimension and perspectives, Lancet 382 (2013)260–272.
[5] Global Facts About Kidney Disease, The National Kidney Foundation, 2018.[6] R. Lozano, M. Naghavi, S.S. Lim, S.Y. Ahn MPH, M.B. Alvarado, K.G. Andrews
MPH, et al., Global and regional mortality from 235 causes of death for 20 agegroups in 1990 and 2010: a systematic analysis for the Global Burden ofDisease Study 2010, Lancet 380 (2012) 2095–2128.
[7] Tests to Measure Kidney Function, Damage and Detect Abnormalities, TheNational Kidney Foundation, 2018.
[8] S. Haneder, A. Gutfleisch, C. Meier, J. Brade, D. Hannak, S.O. Schoenberg, et al.,Evaluation of a handheld creatinine measurement device for real-timedetermination of serum creatinine in radiology departments, World J. Radiol.4 (2012) 328–334.
[9] B. John Frederick Barrett, A Modified Nessler’s Reagent for themicro-determination of urea in tungstic acid blood filtrate, Biochem. J. 29(1935) 2442–2445.
10] M.W. Weatherburn, Phenol-hypochlorite reaction for determination ofammonia, Anal. Chem. 39 (1967) 971–974.
11] R.T. Evans, Manual and automated methods for measuring urea based on amodification of its reaction with diacetyl monoxime and thiosemicarbazide, J.Clin. Path. 21 (1968) 527–532.
12] W.H. Marsh, B. Fin, H. Miller, Automated and manual direct methods for thedetermination of blood urea, Clin. Chem. 11 (1965) 624–627.
13] N. Ahmed, A. Mehmood, N. Dawani, S. Roshan, Salivary Urea A marker forchronic renal disease, Pak. J. Med. Dent. 4 (2015) 3–7.
14] T. Akai, K. Naka, C. Yoshikawa, K. Okuda, T. Okamoto, S. Yamagami, et al.,Salivary urea nitrogen as an index to renal function: a test-strip method, Clin.Chem. 29 (1983).
15] T.J. Lasisi, Y.R. Raji, B.L. Salako, Salivary creatinine and urea analysis in patientswith chronic kidney disease: a case control study, BMC Nephrol. 17 (2016) 10.
16] D. Pandya, A.K. Nagarajappa, K.S. Ravi, Assessment and correlation of urea andcreatinine levels in saliva and serum of patients with chronic kidney disease,diabetes and hypertension–a research study, J. Clin. Diagn. Res. 10 (2016)58–62.
17] I. Tomás, J.S. Marinho, J. Limeres, M.J. Santos, L. Araújo, P. Diz, Changes insalivary composition in patients with renal failure, Arch. Oral Biol. 53 (2008)528–532.
18] G.G. Guilbault, J.G. Montalvo, Urea-specific enzyme electrode, J. Am. Chem.Soc. 91 (1969) 2164–2165.
19] J. Das, P. Sarkar, Enzymatic electrochemical biosensor for urea with apolyaniline grafted conducting hydrogel composite modified electrode, RSCAdv. 6 (2016) 92520–92533.
20] W.O. Ho, S. Krause, C.J. McNeil, J.A. Pritchard, R.D. Armstrong, D. Athey, et al.,Electrochemical sensor for measurement of urea and creatinine in serumbased on ac impedance measurement of enzyme-catalyzed polymertransformation, Anal. Chem. 71 (1999) 1940–1946.
21] S.K. Jha, A. Topkar, S.F.D. ‘souza, Development of potentiometric ureabiosensor based on urease immobilized in PVA–PAA composite matrix forestimation of blood urea nitrogen (BUN), J. Biochem. Biophys. Methods 70(2008) 1145–1150.
22] H. Chen, E. Wang, Optical urea biosensor based on ammonium ion selectivemembrane, Anal. Lett. 33 (2000) 997–1011.
23] C.-P. Huang, Y.-K. Li, T.-M. Chen, A highly sensitive system for urea detectionby using CdSe/ZnS core-shell quantum dots, Biosens. Bioelectron. 22 (2007)1835–1838.
24] M. Swati, N.K. Hase, R. Srivastava, Nanoengineered optical urea biosensor forestimating hemodialysis parameters in spent dialysate, Anal. Chim. Acta 676(2010) 68–74.
25] O.S. Wolfbeis, H. Li, Fluorescence optical urea biosensor with an ammoniumoptrode as transducer, Biosens. Bioelectron. 8 (1993) 161–166.
26] H. Barhoumi, A. Maaref, M. Rammah, C. Martelet, N. Jaffrezic-Renault, C.
Mousty, et al., Insulator semiconductor structures coated with biodegradablelatexes as encapsulation matrix for urease, Biosens. Bioelectron. 20 (2005)2318–2323.27] P.C. Pandey, A.P. Mishra, Conducting polymer-coated enzyme microsensor forurea, Analyst 213 (1988) 329–331.

Actuat
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
at Banasthali University, India; Korea University, South
A. Soni et al. / Sensors and
28] Y. Yang, Z. Wang, M. Yang, M. Guo, Z. Wu, G. Shen, et al., Inhibitivedetermination of mercury ion using a renewable urea biosensor based onself-assembled gold nanoparticles, Sens. Actuators, B 114 (2006) 1–8.
29] M. Tyagi, M. Tomar, V. Gupta, NiO nanoparticle-based urea biosensor, Biosens.Bioelectron. 41 (2013) 110–115.
30] E.K. Varadharaj, N. Jampana, Screen printed potentiometric sensor fornon-Invasive measurement of blood urea in human subjects using reverseiontophoresis, ECS Trans. 66 (2015) 1–22.
31] E.K. Varadharaj, N. Jampana, Non-Invasive potentiometric sensor formeasurement of blood urea in human subjects using reverse iontophoresis, J.Electrochem. Soc. 163 (2016) B340–B347.
32] K. Chen, D. Liu, L. Nie, S. Yao, Determination of urea in urine using aconductivity cell with surface acoustic wave resonator-based measurementcircuit, Talanta 41 (1994) 2195–2200.
33] Z. Yang, S. Si, H. Dai, C. Zhang, Piezoelectric urea biosensor based onimmobilization of urease onto nanoporous alumina membranes, Biosens.Bioelectron. 22 (2007) 3283–3287.
34] J. Shalini, K.J. Sankaran, C.-Y. Lee, N.-H. Tai, I.-N. Lin, An amperometric ureabisosensor based on covalent immobilization of urease on N2 incorporateddiamond nanowire electrode, Biosens. Bioelectron. 56 (2014) 64–70.
35] Z. Xu, X. Chen, X. Qu, J. Jia, S. Dong, Single-wall carbon nanotube-basedvoltammetric sensor and biosensor, Biosens. Bioelectron. 20 (2004) 579–584.
36] K.A. Erickson, P. Wilding, Evaluation of a novel point-of-care system, thei-STAT portable clinical analyzer, Clin. Chem. 39 (1993).
37] T. Mock, D. Morrison, R. Yatscoff, Evaluation of the i-STAT ® system: a portablechemistry analyzer for the measurement of sodium, potassium, chloride,urea, glucose, and hematocrit, Clin. Biochem. 28 (1995) 187–192.
38] R. Evans, V. Calice-Silva, J.G. Raimann, U. Hemmila, A. Craik, M. Mtekateka,et al., Diagnostic performance of a saliva urea nitrogen dipstick to detectkidney disease in Malawi, Kidney Int. Rep. 2 (2017) 219–227.
39] D. Erickson, D. O’Dell, L. Jiang, V. Oncescu, A. Gumus, S. Lee, et al., Smartphonetechnology can be transformative to the deployment of lab-on-chipdiagnostics, Lab Chip 14 (2014) 3159.
40] V. Oncescu, D. O’Dell, D. Erickson, Smartphone based health accessory forcolorimetric detection of biomarkers in sweat and saliva, Lab Chip 13 (2013)3232–3238.
41] A. Roda, E. Michelini, M. Zangheri, M. Di Fusco, D. Calabria, P. Simoni,Smartphone-based biosensors: a critical review and perspectives, TrACTrends Anal. Chem. 79 (2016) 317–319.
42] S. Vashist, E. Schneider, J. Luong, Commercial smartphone-based devices andsmart applications for personalized healthcare monitoring and management,Diagnostics 4 (2014) 104–128.
43] D. Zhang, Q. Liu, Biosensors and bioelectronics on smartphone for portablebiochemical detection, Biosens. Bioelectron. 75 (2016) 273–284.
44] A. Soni, S.K. Jha, Smartphone based non-invasive salivary glucose biosensor,Anal. Chim. Acta 996 (2017) 54–63.
45] A. Roda, M. Guardigli, D. Calabria, M.M. Calabretta, L. Ceveninia, E.Micheliniab, A 3D-printed device for a smartphone-based chemiluminescencebiosensor for lactate in oral fluid and sweat, Analyst 139 (2014) 6494–6501.
46] R.D. Stedtfeld, D.M. Tourlousse, G. Seyrig, T.M. Stedtfeld, M. Kronlein, S. Price,et al., Gene-Z: a device for point of care genetic testing using a smartphone,Lab Chip 12 (2012) 1454–1462.
47] O.H. Lowry, N.J. Rosebrough, A.L. Farr, R.J. Randall, Protein measurement withthe folin phenol reagent, J. Biol. Chem. 193 (1951) 265–275.
48] E. Mäkilä, P. Kirveskari, A study of ascorbic acid in human saliva, Arch. OralBiol. 14 (1969) 1285–1292.
49] G. Palleschi, M.H. Faridnia, G.J. Lubrano, G.G. Guilbault, Determination oflactate in human saliva with an electrochemical enzyme probe, Anal. Chim.Acta 245 (1991) 151–157.
ors B 269 (2018) 346–353 353
50] R. Segura, C. Javierre, J.L.L. Ventura, M.A. Lizarraga, B. Campos, E. Garrido, Anew approach to the assessment of anaerobic metabolism: measurement oflactate in saliva, Br. J. Sports Med. 30 (1996) 305–309.
51] S.K. Jha, S.F. D’Souza, Preparation of polyvinyl alcohol-polyacrylamidecomposite polymer membrane by gamma-irradiation for entrapment ofurease, J. Biochem. Biophys. Methods 62 (2005) 215–218.
52] S. Dreizen, A.W. Mann, J.K. Cline, T.D. Spies, The buffer capacity of saliva as ameasure of dental caries activity, J. Dent. Res. 25 (1946) 213–222.
53] J.F. Helm, W.J. Dodds, W.J. Hogan, K.H. Soergel, M.S. Egide, C.M. Wood, Acidneutralizing capacity of human saliva, Gastroenterology 83 (1982) 69–74.
54] K.T. Sein, G. Arumainayagam, Correlation between serum urea and salivaryurea, Clin. Chem. 33 (1987) 2303–2304.
Biographies
Ms. Anuradha Soni Anuradha Soni is a Ph.D. researchscholar at Centre for Biomedical Engineering (CBME),Indian Institute of Technology Delhi and has been work-ing on development of clinical biosensors, especially thosewhich are non-invasive in nature. She has authored 2manuscripts and has developed a smartphone based non-invasive biosensor for salivary glucose detection.
Mr. Rajat Kumar Surana is former B.Tech. student atDepartment of Textile Technology at Indian Institute ofTechnology Delhi and has interest in Android program-ming.
Dr. Sandeep K.Jha is a joint faculty at the Centrefor Biomedical Engineering (CBME), Indian Instituteof Technology Delhi and All India Institute of Medi-cal Sciences New Delhi. His areas of interest includeLab-on-a-chip and Microfluidics devices for biomedicalapplications; electrochemical and optical chemical andbiosensors; bioinstrumentation & nanomaterials, con-ducting and synthetic polymers based immobilizationtechniques. Previously he served under various capacities
Korea; KIIT University, Bhubaneswar, India; Myongji Uni-versity, South Korea; Indian Institute of Technology,Mumbai, India and Bhabha Atomic Research Center, Mum-
bai, India.