Seminar on Ameloblastoma
19
Good Morning
-
Upload
dr-abdul-qahar-qureshi -
Category
Health & Medicine
-
view
341 -
download
5
Transcript of Seminar on Ameloblastoma

Good Morning

Ameloblastoma ???Ameloblastoma ???
Presented by:
Dr. Abdul Qahar Qureshi
(PG Student)

IntroductionIntroduction
Ameloblastoma –Ameloblastoma – Ivey and ChurchhilIvey and Churchhil (1934) (1934)
Adamantinoma - Adamantinoma - Malassez Malassez (1885)(1885)
An odontogenic tumor reported since 1826An odontogenic tumor reported since 1826

Definition: Ameloblastoma as“ a odontogenic epithelial tumor that is usually unicentric, nonfunctional, intermittent in growth, anatomically benign and clinically persistent”.
– Robinson-1937
The Ameloblastoma is a true neoplasm of The Ameloblastoma is a true neoplasm of the enamel organ type tissue which does the enamel organ type tissue which does
not undergo differentiation to the point of not undergo differentiation to the point of enamel formation. enamel formation.
-WHO -WHO

• Clinical ClassificationClinical Classification
Multicystic or conventional solid ameloblastoma – 86%
Unicystic ameloblastoma – 13%
Peripheral or extraosseous ameloblastoma - 1%
Malignant ameloblastoma
Ameloblastic carcinoma
Pituitary ameloblastoma

Radiological ClassificationRadiological Classification
Lagundoye et al (1975) classified as
Multiloculated – multicystic
Unilocular
Septate- trabeculated Solid.

Histological classification:Histological classification: Plexiform type Plexiform type
Follicular type Follicular type
AcanthamatousAcanthamatous
GranularGranular
DesmoplasticDesmoplastic
Basal cell typeBasal cell type
Unicystic Unicystic
Plexiform unicysticPlexiform unicystic

Multicystic AmeloblastomaMulticystic Ameloblastoma
Clinical Features•Recur multiple times & can metastasize
•Older group of patients
•Average age presentation: 32.7 - 44 yr.
•Majority of cases involve the mandible
•Kameyama et al: 23:1 ratio of mandibular to maxillary ameloblastomas

Unicystic AmeloblastomaUnicystic AmeloblastomaClinical features
•Robinson & Martinez 1977
•May be associated with an unerupted tooth
Age & Location
Average age: 19.4 yr. To 27.7 yr.
•Almost exclusively in the mandible (few cases in the maxilla)
•More than 2/3 of the lesion occur in the molar-ramus region of the mandible
•Molar ramus area: 78% - 75%
•Symphysis area: 13%
•Cuspid-premolar area: 9.7% - 25%

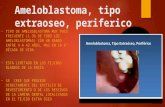
Peripheral AmeloblastomaPeripheral Ameloblastoma
Clinical Features
•Uncommon lesion
•More frequent in the mandible than in the maxilla (2:1)
•Male to female ratio of 1.6:1
•Mean age of diagnosis: 53 yr
•Painless, sessile, firm, exophytic lesion
•Occurs in the soft tissue overlying the alveolar bone
•There is not direct bone involvement, but signs of erosion or cupping may appear in response to the tumor growth

Malignant AmeloblastomaMalignant Ameloblastoma
Clinical Features
•Rare lesion
•Almost exclusively in the mandible
•Male to female ratio of 1.8:1
•Mean age of diagnosis: 28-32 yr.
•Common sites for metastasis : lungs (75%) spleen, kidney & ileum

Biological behaviourBiological behaviour
Benign, Benign, Locally aggressive, Locally aggressive, Infiltrative odontogenic neoplasm ,Infiltrative odontogenic neoplasm , Rare capacity to metastasize,Rare capacity to metastasize, Notorious tendency to recur. Notorious tendency to recur.

Low grade malignant.Low grade malignant.
Asymptomatic . Asymptomatic .
Tooth eruption and dental occlusion disturbance, Tooth eruption and dental occlusion disturbance,
tooth mobility and root resorption.tooth mobility and root resorption.
Either jaw - posterior maxilla or molar ramus area.Either jaw - posterior maxilla or molar ramus area.
Growth Pattern:- Bucco linguallyGrowth Pattern:- Bucco lingually

The medullary extension with intact cortex is The medullary extension with intact cortex is not an uncommon findingnot an uncommon finding
Grows by bone expansion rather than bone Grows by bone expansion rather than bone destruction. destruction.
Aggressively invade adjacent and regional Aggressively invade adjacent and regional tissues. tissues.
Metastasize to the bronchopulmonary system, Metastasize to the bronchopulmonary system, local and distant lymph nodes, and distant local and distant lymph nodes, and distant organs.organs.

Surgical optionsSurgical options
Curettage Curettage
Enucleation and CauterizationEnucleation and Cauterization
Wide excisionWide excision
Resection (segmental or en bloc) and Resection (segmental or en bloc) and
reconstructionreconstruction

Carlson and MarxCarlson and Marx ( JOMS 64: 2006) have ( JOMS 64: 2006) have rekindled the clinical controversy in the surgical rekindled the clinical controversy in the surgical management of ameloblastoma.management of ameloblastoma.
i.i. Assessing anatomic barrierAssessing anatomic barrierii.ii. Resection with 1 to 1.5 cm linear bone marginsResection with 1 to 1.5 cm linear bone marginsiii.iii. The use of specimen radiographsThe use of specimen radiographsiv.iv. The use of frozen section of medullary portion of the stumpThe use of frozen section of medullary portion of the stump
Their Their recommended protocolrecommended protocol for surgical for surgical
managemant of multicystic ameloblastom was;managemant of multicystic ameloblastom was;

Multilocular ameloblastomaMultilocular ameloblastoma - -Segmental Segmental resection and reconstructionresection and reconstruction
Desmoplastic ameloblastomaDesmoplastic ameloblastoma - - Wide excision Wide excision
and partial maxillectomy.and partial maxillectomy.
Unilocular ameloblastomaUnilocular ameloblastoma - - Enucleation and Enucleation and Cauterization.Cauterization.

ReferrencesReferrences Unisystic Ameloblastoma of Mandible(1997)Unisystic Ameloblastoma of Mandible(1997) Peripheral Ameloblastoma(1994,1995)Peripheral Ameloblastoma(1994,1995) Marsupialization of cystic ameloblastoma(1995)Marsupialization of cystic ameloblastoma(1995) The Ameloblastoma:Primary, Curative Surgical The Ameloblastoma:Primary, Curative Surgical
Management.Management.Eric R. Carlson and Robert E. MarxEric R. Carlson and Robert E. Marx Oral Pathology- NavilleOral Pathology- Naville Wood and GoazWood and Goaz Daniel M LaskinDaniel M Laskin Shafer’s Oral PathologyShafer’s Oral Pathology ArcherArcher