Seminar of Endocarditis by Sudeep,(Pharm.D.)
26
-
Upload
sudeep -
Category
Healthcare
-
view
363 -
download
6
Transcript of Seminar of Endocarditis by Sudeep,(Pharm.D.)


Endocarditis: Definition:
“Endocarditis is an infection of the heart's valves or inner lining.
It occurs when germs get into the bloodstream and settle inside
the heart, often on a valve.”
The infection is usually caused by bacteria. In rare cases, it is
caused by fungi.
Other structures that may be involved include
the interventricular septum, the chordae tendineae, the mural
endocardium, or the surfaces of intracardiac devices.
“It causes an inflammation of the inner layer of the heart,
the endocardium. It usually involves the heart valves.”

Infective Endocarditis: It is a microbial infection of the
endocardial surface of the heart.
Common site:Heart valve, but may occur at septal defect,
on chordae tendinae or in the mural endocardium.
Classification: →Acute or Subacute-chronic on temporal basis, severity of presentation and progression.→By organism.→Native valve or prosthetic valve.

Characteristic pathological lesion: vegetation,
composed of platelets, fibrin, microorganisms
and inflammatory cells.
EPIDEMIOLOGY:
»Changing over the past
decade due to:
»Increased longevity
»New predisposing factors
»Nosocomial infections
In U.S and Western Europe
incidence of community –
»acquired endocarditis is 1.7-6.2
cases per 100,000 person-years.
»M:F ratio 1.7:1
»Mean age now 47-69 (30-40
previously).

»Incidence in IVDA group is estimated at 2000 per 100,000
person-years, even higher if there is known valvular heart
disease
»Increased longevitiy leads to more degenerative valvular
disease, placement of prosthetic valves and increased
exposure to nosocomial bacteremia.
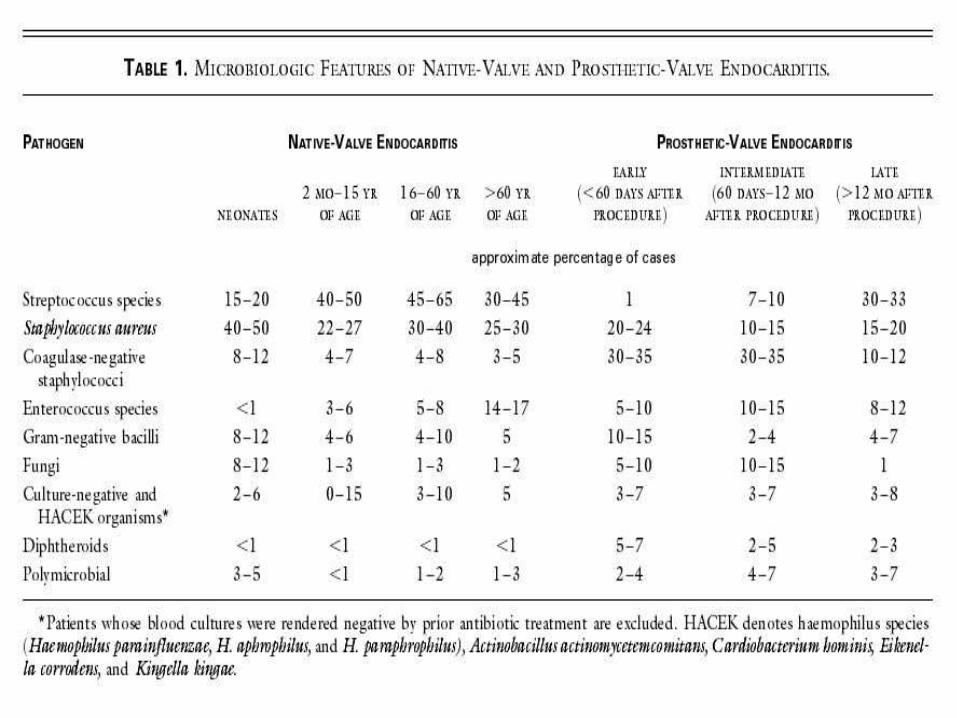
Aetiology:
1. Streptococci:Viridans streptococci/α-haemolytic streptococci
S. mitis, S. sanguis, S. oralisS. Bovis.
Associated with colonic carcinoma.2. Enterococci :
E. faecalis, E. faeciumAssociated with GU/GI tract proceduresApprox. 10% of patients with enterococcal bacteraemia.

3. Staphylococci:Staphylococcci have surpassed viridans streptococci as the most
common cause of infective endocarditis.
S. Aureus:Native valves,Acute endocarditis.
Coagulase-negative staphylococci,Prosthetic valve endocarditis.
4. Gram-negative rodsHACEK group
Haemophilus aphrophilus, Actinobacillusactinomycetemcomitans, Cardiobacterium hominis, Eikenella corrodens, Kingella kingae.
Fastidious oropharyngeal GNBs
E. coli, Klebsiella etcUncommon
Pseudomonas aeruginosaIVDA
Neisseria gonorrhoae:Rare since introduction of penicillin

5. Others:
Fungi
Candida species, Aspergillus species
Q fever
Chlamydia
Bartonella
Legionella

Risk factors:
Those at highest risk of endocarditis are those who have:
Artificial heart valves. Germs are more likely to attach to an
artificial (prosthetic) heart valve than to a normal heart valve.
Congenital heart defects. If you were born with certain types of heart
defects, your heart may be more susceptible to infection.
A history of endocarditis. An episode of endocarditis damages heart
tissue and valves, increasing the risk of a future heart infection.
Damaged heart valves. Certain medical conditions — such as
rheumatic fever or infection — can damage or scar one or more of
your heart valves, making them more prone to endocarditis.
History of intravenous (IV) illegal drug use. People who use illegal
drugs by injecting them are at a greater risk of endocarditis. The
needles used to inject drugs can be contaminated with the bacteria
that can cause endocarditis.

Pathogenesis:
Bacteraemia:
Transient bacteraemia occurs when a heavily colonised
mucosal surface is traumatised
Dental extraction
Periodontal surgery
Tooth brushing
Tonsillectomy
Operations involving the respiratory, GI or GU tract
mucosa
Oesophageal dilatation
Biliary tract surgery


Site of Infection:
Aortic valve more common than mitral.
Aortic:Vegetation usually on ventricular aspect, all 3 cusps usually affected.
Perforation or dysfunction of valve.
Root abscess.
Mitral:Dysfunction by rupture of chordaeTendanae.

Clinical Presentation:
Signs&Symptoms:
Fever, most common symptom, sign (but may be absent) Anorexia, weight-loss, malaise, night sweatsHeart murmurPetechiae on the skin, conjunctivae, oral mucosaSplenomegalyRight-sided endocarditis is not associated with peripheral emboli/phenomena but pulmonary findings
LAB TESTS: 1. Blood culture test.
2. Echo:
TTE
TOE
3. FBC/ESR/CRP.
4. Rheumatoid Factor.
5. MSU.

Janeway
lesions:
Nontender
erythematous,
haemorrhagic,
or pustular
lesions often
on palms or
soles.
Oslers’ nodes
Tender, s/c
nodules

Diagnosis: Duke Criteria:
In 1994 a group at Duke University standardised criteria
for assessing patients with suspected endocarditis
Include:
-Predisposing Factors.
-Blood culture isolates or persistence of bacteremia.
-Echocardiogram findings with other clinical, laboratory
findings
Duke Criteria: Definite:: 2 major criteria: 1 major and 3 minor criteria: 5 minor criteria: pathology/histology findings
Possible :1 major and 1 minor criteria: 3 minor criteria
Rejected :firm alternate diagnosis: resolution of manifestations of IE
with 4 days antimicrobial therapy or less

Echocardiography:
Trans Thoracic Echocardiograpy (TTE):
Rapid, non-invasive – excellent specificity (98%) but poor sensitivity.
Obesity, chronic obstructive pulmonary disease and chest wall deformities.
Transesophageal Echo (TOE) :
More invasive, sensitivity up to 95%, useful for prosthetic valves and to evaluate myocardial invasion.
Negative predictive valve of 92%.
TOE more cost effective in those with S. aureus catheter-associated bacteremia and bacteremia/fever and recent IVDA.

CULTURE TEST:
Negative Endocarditis:
5-7% of patients with endocarditis will have sterile blood cultures.
1 Year study from France . 44 of 88 cases of CNE, negative cultures were associated with prior administration of antibiotics.
Fasidious or non-culturable organism.
Non-infective endocarditis.
Withhold empirical therapy until cultures drawn.

COMPLICATIONS OF ENDOCARDITIS:
Cardiac : congestive cardiac failure-valvular damage, more common with aortic valve endocarditis, infection beyond valve→ CCF, higher mortality, need for surgery, A-V, fascicular or bundle branch block, pericarditis, tamponadeor fistulae.
Systemic emboli:
Risk depends on valve (mitral>aortic), size of vegetation, (high risk if >10 mm).
20-40% of patients with endocarditis,risk decreases once appropriate antimicrobial therapy started.

Prolonged Fever: usually fever associated with endocarditis resolves
in 2-3 days after commencing appropriate antimicrobial therapy
with less virulent organisms and 90% by the end ot the second
week.
Recurrent fever:
Infection beyond the valve.
Focal metastatic disease.
Drug hypersentivity.
Nosocomial infection or others e.g. Pulmonary embolus.

TREATMENT:
Antimicrobial therapyUse a bactericidal regimen.
Use a recommended regimen for the organism isolated.
E.g. American Heart Association JAMA 1995; 274: 1706-13., British Society for Antimicrobial Chemotherapy.
Repeat blood cultures until blood is demonstrated to be sterileSurgery.
Get cardiothoracic teams involved early

Streptococci/Enterococci:
Determine MIC of Penicillin
Penicillin +/- aminoglycoside
Ceftriaxone alone
Vancomycin +/- aminoglycoside
Cefotaxime/ceftriaxone
Staphylococci:
Native valve
Flucloxacillin +/- aminoglycoside
Vancomycin +/- aminoglycoside/ rifampicin
Prosthetic valve
Flucloxacillin + aminoglycoside + rifampicin
Vancomycin + aminoglycoside + rifampicin


Surgical Therapy:
Indications: Congestive cardiac failure,perivalvular invasive disease.
Uncontrolled infection despite maximal antimicrobial therapy.
Pseudomonas aeruginosa, Brucella species, Coxiella burnetti, Candida and fungi.
Presence of prosthetic valve endocarditis unless late infectionLarge vegetation.
Major embolus.Heart block.
The hemodynamic status at the time determines principally
operative mortality

Prevention:
Antimicrobial prophylaxis is given to at risk patients when bacteraemia-inducing procedures are performed.
The incidence of endocarditis following most procedures in patients
with underlying cardiac disease is low.
A reasonable approach for endocarditis prophylaxis should consider
the following:
the degree to which the patient’s underlying condition creates a risk of
endocarditis; the apparent risk of bacteremia with the procedure (as
defined in these recommendations); the potential adverse reactions of
the prophylactic antimicrobial agent to be used; and the cost-benefit
aspects of the recommended prophylactic regimen.
Failure to consider all of these factors may lead to overuse of
antimicrobial agents, excessive cost, and risk of adverse drug
reactions.
This statement provides guidelines for prevention of bacterial
endocarditis. It is not intended as the standard of care or as a
substitute for clinical judgment. The current recommendations
are an update of those made by the committee in 19901and
incorporate new data and include opinions voiced by national
and international experts at endocarditis meetings around the
world.
.
Failure to consider all of these factors may lead to
overuse of antimicrobial agents, excessive cost, and risk
of adverse drug reactions.
Kasper DL, Braunwald E, Fauci AS, Hauser S, Longo DL,
Jameson JL (May 2005).
Harrison's Principles of Internal Medicine. McGraw-Hill (
pp. 731–40.)
Robbins and Cotran pathologic basis of disease.
Cotran, Ramzi S.; Kumar, Vinay; Fausto, Nelson;
Robbins, Stanley L.; Abbas, Abul K. (2005).
www.medicinenet.com