Seminar 23-03-2016 mw. Dr. J. van den Bergh
59
Een 72jarige pa.ënte met een nieuwe fractuur na drie jaar bisfosfonaten, doorgaan of switchen? Prof. Dr. Joop van den Bergh, internist-endocrinoloog Maastricht UMC+ & VieCuri MC Noord-Limburg copyright Dr. J. van den Bergh
-
Upload
stichting-interdisciplinaire-werkgroep-osteoporose -
Category
Health & Medicine
-
view
150 -
download
1
Transcript of Seminar 23-03-2016 mw. Dr. J. van den Bergh

Een 72-‐jarige pa.ënte met een nieuwe fractuur na drie jaar bisfosfonaten,
doorgaan of switchen?
Prof. Dr. Joop van den Bergh, internist-endocrinoloog Maastricht UMC+ & VieCuri MC Noord-Limburg
copyright
Dr. J. van den Bergh

Rela.ons that could be relevant for the mee.ng Company name
• Research funds
• Speaker board / consultancy • Stakeholder • Stock or other…
• Amgen, MSD, Takeda, Eli Lilly, Novo Nordisk, Will Pharma
• Amgen, Eli Lilly, Will Pharma, MSD • -‐ • -‐
Disclosure of speaker’s interests
copyright
Dr. J. van den Bergh

Treatment failure?
copyright
Dr. J. van den Bergh

Treatment failure?
• What can be expected of treatment? • New fracture?
– Type of fracture – Dura.on of therapy
• BMD loss? • No effect on bone turnover markers? • Compliance / persistence?
• When to switch and when not?
copyright
Dr. J. van den Bergh

Treatment: expected efficacy
copyright
Dr. J. van den Bergh

Efficacy of treatments for the preven.on of fractures
Reid, I. R. Nat. Rev. Endocrinol. 2015;
copyright
Dr. J. van den Bergh

Efficacy of treatments for the preven.on of fractures
Reid, I. R. Nat. Rev. Endocrinol. 2015;
copyright
Dr. J. van den Bergh

Efficacy of treatments for the preven.on of fractures
Reid, I. R. Nat. Rev. Endocrinol. 2015;
copyright
Dr. J. van den Bergh

Efficacy of treatments for the preven.on of fractures
Reid, I. R. Nat. Rev. Endocrinol. 2015;
copyright
Dr. J. van den Bergh

six (hip, pelvis, leg, humerus, clavicle, and wrist) high trauma: sufficient to cause fracture in a person without osteoporosis or a young individual with normal bone mass
Mackey et al. JBMR 2011: 2411–2418
Effects of An.resorp.ve Treatment on Nonvertebral Fracture Outcomes
Five trials: 30,118 women were included in the analysis, follow-up > 36 months Alendronate, clodronate, zoledronate, denosumab, lasofoxifene
copyright
Dr. J. van den Bergh

Mackey et al. JBMR 2011: 2411–2418
copyright
Dr. J. van den Bergh

What is treatment failure?
• New fracture a^er xx months of treatment?
copyright
Dr. J. van den Bergh

Time to fracture reduc.on (months)
Vertebral Non-‐vertebral Hip Study
Alendronate 12 24 (12) 18 Post-‐hoc FIT (Fosit)
Risedronate 6 (6) 18 VERT (Meta-‐analysis 4 RCT’s)
Zoledronate 12 18 Horizon
Denosumab 12 24 18-‐24 (12)
Freedom (>75yr, FN T ≤ -‐2.5)
Teripara.de 12 18 Neer Study
Ø 12 months for vertebral fractures Ø At least 18 months for non-vertebral fractures
copyright
Dr. J. van den Bergh

Treatments do not eliminate fracture risk; they reduce it
• a^er > 12 months for vertebral fractures (50%) • a^er > 18-‐24 months for hip fractures (30-‐50%)
• a^er > 18-‐24 months for non-‐vertebral fractures (15-‐25%)
• Probably not for: chest, rib, hand, heel, toe, patella • ? for Elbow, finger
copyright
Dr. J. van den Bergh

Treatment failure: BMD?
copyright
Dr. J. van den Bergh

Men
Women
80yr
70yr
60yr
50yr
Adapted from Johnell et al. 2005;20:1185–1194
copyright
Dr. J. van den Bergh

‘Normal’ BMD decline in .me
N Engl J Med 2012;366:225-33
-2.00 to -2.49
-1.50 to -1.99
-1.00 to -1.49 copyright
Dr. J. van den Bergh

Retes.ng BMD -‐ interval
N Engl J Med 2012;366:225-33
copyright
Dr. J. van den Bergh

Long-‐term effects of osteoporosis treatments on total hip BMD
Reid, I. R. Nat. Rev. Endocrinol. May 2015;
copyright
Dr. J. van den Bergh

1145 Hip BMD by DXA Can Reliably Es.mate Reduc.on in Hip Risk in Osteoporosis Trials: A Meta-‐Regression
ASBMR 2015
For 2 drugs with 2% vs 6% hip BMD effect, prediction of 10% vs. 59% reduction for hip fracture
copyright
Dr. J. van den Bergh

Chapurlat et al. Osteoporos Int (2005) 16: 842–848
Risk of fracture among women who lose bone density during treatment with alendronate
Hip BMD
copyright
Dr. J. van den Bergh

Chapurlat et al. Osteoporos Int (2005) 16: 842–848
Risk of fracture among women who lose bone density during treatment with alendronate
Spine BMD
copyright
Dr. J. van den Bergh

Measurement error Least significant change
• 2√2 maal meemout (CV)
copyright
Dr. J. van den Bergh

Treatment failure: BMD
• % BMD gain is related to % fracture risk reduc.on • Treatment (%RR) seems to be equally effec.ve irrespec.ve of decreased BMD (except loss > 4-‐5%?)
• The least significant change for BMD is 4.4% for FN-‐BMD and 5.5% for LS-‐BMD
Ø So a BMD loss of > 4% may be regarded as an insufficient effect of treatment
copyright
Dr. J. van den Bergh

Treatment failure: bone turnover markers?
copyright
Dr. J. van den Bergh

• Decrease in bone resorp.on accounts for a large propor.on of the reduc.on in fracture risk
• There may be a level of bone resorp.on reduc.on below which there is no further fracture benefit
Eastell et al. J Bone Miner Res 2003;18:1051–1056
copyright
Dr. J. van den Bergh

Least significant change
• 2√2 maal meemout (CV)
copyright
Dr. J. van den Bergh

Effect of Fx related to decrease in BTM
• Significant response a^er 6 months – 25% decline from baseline levels for an.-‐resorp.ve treatments
– 25 % increase for anabolic agents (PTH)
– For an.-‐resorp.ve treatments, if baseline levels are not known, a posi.ve response is a decrease below the average value of young healthy adults.
– It is assumed that the response is similar between men and women
copyright
Dr. J. van den Bergh

Role of Compliance and persistence
• Compliance – The extent to which a pa.ent acts in accordance with the prescribed interval
and dose of a dosing regimen
• Persistence – The dura.on of .me from ini.a.on to discon.nua.on of therapy
– The absence of a prescrip.on refill over a dura.on exceeding 30 days copyright
Dr. J. van den Bergh

Ross et al. V a l u e i n h e a l t h : 2 0 1 1 : 5 7 1 – 5 8 1
Hazard ratio for fracture: non-persistence versus persistence
copyright
Dr. J. van den Bergh

Meta-‐Analysis of Osteoporo.c Fracture Risk with Medica.on Nonadherence
Ross et al. V a l u e i n h e a l t h : 2 0 1 1 : 5 7 1 – 5 8 1
copyright
Dr. J. van den Bergh

copyright
Dr. J. van den Bergh

Hazard ratio for fracture: non versus compliance
copyright
Dr. J. van den Bergh

Risk Factors for Treatment Failure With An.-‐osteoporosis Medica.on: GLOW – 3 year follow-‐up
JBMR 2014, pp 260–267
copyright
Dr. J. van den Bergh

Risk Factors for Treatment Failure With An.-‐osteoporosis Medica.on: GLOW – 3 year follow-‐up
JBMR 2014, pp 260–267
copyright
Dr. J. van den Bergh

Incident fractures by fracture type (GLOW study)
JBMR 2014, pp 260–267 6.5% 1.3%
copyright
Dr. J. van den Bergh

Incident fractures by fracture type (GLOW study)
JBMR 2014, pp 260–267 6.5% 1.3%
copyright
Dr. J. van den Bergh

Incident fractures by fracture type (GLOW study)
JBMR 2014, pp 260–267
×
×
×?
6.5% 1.3%
copyright
Dr. J. van den Bergh

Risk Factors for Treatment Failure With An.-‐osteoporosis Medica.on: GLOW – 3 year follow-‐up
JBMR 2014, pp 260–267
copyright
Dr. J. van den Bergh

Presence of Metabolic bone disorders
(Secondary osteoporosis)
copyright
Dr. J. van den Bergh

Onderliggende aandoeningen bij pa.ënten > 50 jaar met een recente fractuur
van den Bergh et al. Nature Reviews. Rheumatol. 2012; 163–172
copyright
Dr. J. van den Bergh

Subclinical contributors to low BMD and/or fragility fracture in more than 40% of the subjects with apparent primary osteoporosis.
European Journal of Endocrinology 2013:225–237
38,9%
copyright
Dr. J. van den Bergh

High prevalence of secondary factors for bone fragility in pa.ents with a recent fracture independently of BMD
• Laboratory inves.ga.ons iden.fied an underlying factor for bone fragility in:
– 18% of pa.ents with normal BMD
– 29 % of pa.ents with osteopenia – 35% of pa.ents with osteoporosis
Malgo et al. Arch Osteoporos (2016) 11:12
copyright
Dr. J. van den Bergh

Bours et al. Curr Opin Rheumatol 2014, 26:430–439
copyright
Dr. J. van den Bergh

Bours et al. Curr Opin Rheumatol 2014, 26:430–439 Bours et al. Curr Opin Rheumatol 2014, 26:430–439
2 3
2 2
3
2
1
3 2
3
2
1
2
copyright
Dr. J. van den Bergh

The importance of Vertebral fractures
copyright
Dr. J. van den Bergh

Vertebral Fractures
Osteoporos Int (2007) 18:761–770
copyright
Dr. J. van den Bergh

Vertebral Fractures
Osteoporos Int (2007) 18:761–770
copyright
Dr. J. van den Bergh

Approach to evaluate treatment failure
• Check ini.al indica.on • Discuss compliance and adherence • Clinical risk factor assessment
• Fall risk assessment • DEXA and VFA • Laboratory test for metabolic bone disorders
• Consider Bone turnover markers
copyright
Dr. J. van den Bergh

Treatment Failure -‐> change therapy 1. 2 or more incident fragility fractures*
– Fractures of the hand, skull, digits, feet and ankle are not considered as fragility fractures.
2. One incident fracture* – Elevated serum βCTX or PINP at baseline with no significant reduc.on
during treatment (>25%)
– A significant decrease in BMD (>5% LS and >4% hip) or both
3. No significant decrease in serum βCTX or PINP (>25%) and a significant decrease in BMD (>5% LS and 4% hip)
4. New / progression vertebral fractures*
Diez Perez Osteoporos Int 2012
*Adequate compliance / persistence during at least > 12 for vertebral and > 18 months for non vertebral fractures
copyright
Dr. J. van den Bergh

Switch medica.on: Three rules
1. A weaker an.-‐resorp.ve is reasonably replaced by a more potent drug of the same class
2. An oral drug is reasonably replaceable by an injected drug
3. A strong an.-‐resorp.ve is reasonably replaceable by an anabolic agent
• Vertebral fractures
• Glucocor.coid use
Based on the opinion of the IOF working group
Diez Perez Osteoporos Int 2012
copyright
Dr. J. van den Bergh

In addi.on
• Op.mise compliance / adherence • Op.mise fall risk • Treatment of metabolic bone disorders
copyright
Dr. J. van den Bergh

copyright
Dr. J. van den Bergh

Brown et al. Osteoporos Int (2014) 25:1953–1961
copyright
Dr. J. van den Bergh
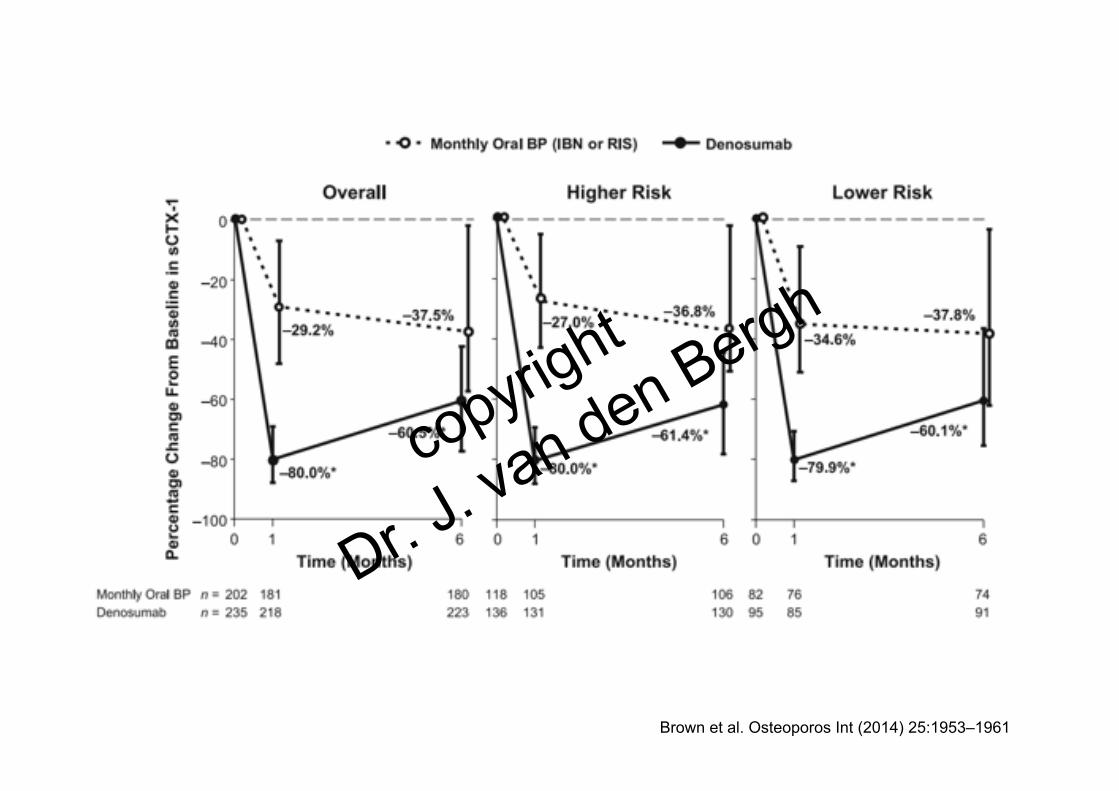
Brown et al. Osteoporos Int (2014) 25:1953–1961
copyright
Dr. J. van den Bergh

Saag KG et al. N Engl J Med 2007;357:2028-‐2039.
copyright
Dr. J. van den Bergh

Highlights ASBMR 2015 Lancet 2015; 386: 1147–55
copyright
Dr. J. van den Bergh

Highlights ASBMR 2015 58 Lancet 2015; 386: 1147–55
copyright
Dr. J. van den Bergh

Thank you!
copyright
Dr. J. van den Bergh