
Religious Mobilizations for Development and Social Change: A

10/22/2015
AAOMPT Conference Louisville 2015, Rett Nicolai, DPT FAAOMPT 1
SELF-MOBILIZATIONS OF THE HIP WITH
BELTING TECHNIQUES
Everett Nicolai, DPT, FAAOMPT
AAOMPT Conference Louisville 2015 Rett Nicolai, DPT FAAOMPT, Ola Grimsby Institute
SELF-MOBILIZATIONS OF THE HIP WITH BELTING TECHNIQUES
Objectives
Description
Anatomy & Physiology
Arthrokinematics vs Osteokinematics
Mobilization Overview
Regional Interdependencies
Techniques
AAOMPT Conference Louisville 2015 Rett Nicolai, DPT FAAOMPT, Ola Grimsby Institute
SELF-MOBILIZATIONS OF THE HIP WITH BELTING TECHNIQUES
Objectives
Quick review of anatomy and biomechanics
Understand regional interdependencies
Instruct patients to perform home techniques
AAOMPT Conference Louisville 2015 Rett Nicolai, DPT FAAOMPT, Ola Grimsby Institute
SELF-MOBILIZATIONS OF THE HIP WITH BELTING TECHNIQUES
Description of LectureThe hip is of central importance for regional interdependencies for the lumbar spine, SIJ, knee and ankle. Self-mobilizations are brilliant ways to prepare the patient for discharge.
AAOMPT Conference Louisville 2015 Rett Nicolai, DPT FAAOMPT, Ola Grimsby Institute

10/22/2015
AAOMPT Conference Louisville 2015, Rett Nicolai, DPT FAAOMPT 2
ANATOMY & PHYSIOLOGY
AAOMPT Conference Louisville 2015 Rett Nicolai, DPT FAAOMPT, Ola Grimsby Institute
RANGE of MOTION (MaGee, 2008)
Flexion 120˚
Extension 10˚-20˚
Adduction 30˚
Abduction 30˚-50˚
External Rotation 40˚-60˚
Internal Rotation 30˚-40˚
ANATOMY & PHYSIOLOGYFunctional ROM Tie shoes (120˚ flexion)
Sit (112˚ flexion)
Squat (115˚ flexion, 20˚ abduction, 20˚ ER)
AAOMPT Conference Louisville 2015 Rett Nicolai, DPT FAAOMPT, Ola Grimsby Institute
ANATOMY & PHYSIOLOGY
BonesFemur sits in a
socket formed
by the innominate
AAOMPT Conference Louisville 2015 Rett Nicolai, DPT FAAOMPT, Ola Grimsby Institute
ANATOMY & PHYSIOLOGYFemoral AnglesColumn & Angle Anterior Antetorsion Angle Acetabular Angle
AAOMPT Conference Louisville 2015 Rett Nicolai, DPT FAAOMPT, Ola Grimsby Institute
10/22/2015
AAOMPT Conference Louisville 2015, Rett Nicolai, DPT FAAOMPT 3
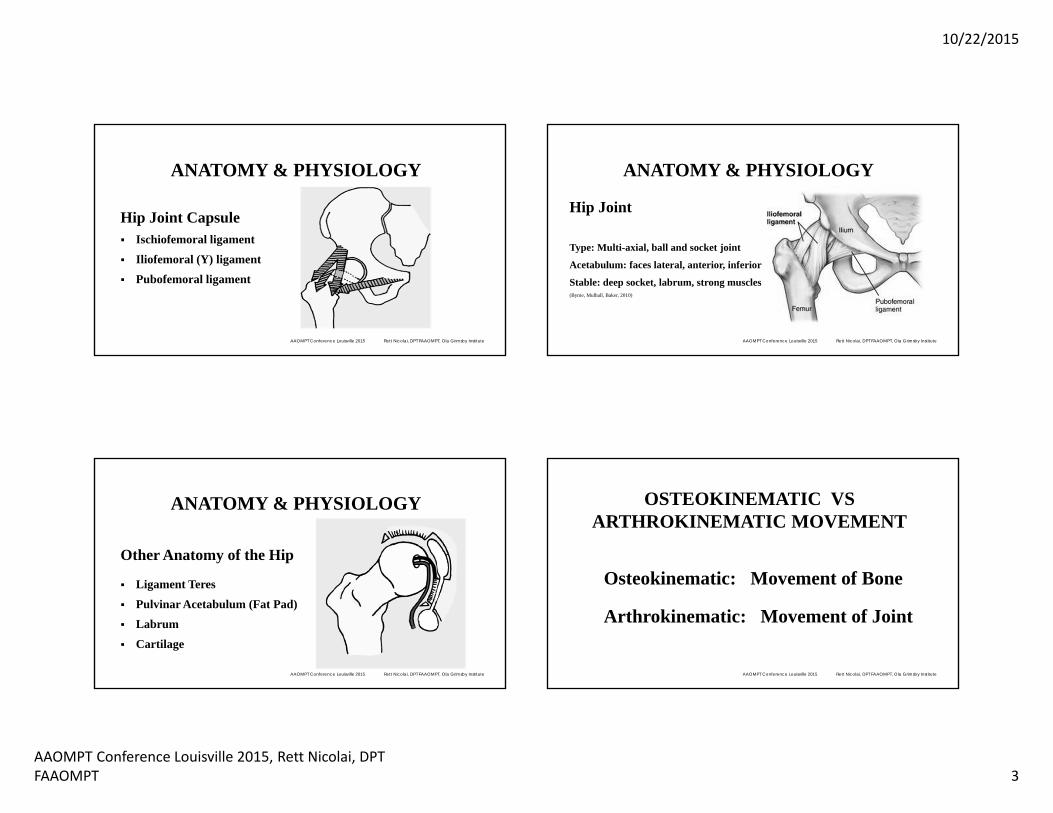
ANATOMY & PHYSIOLOGY
Hip Joint Capsule Ischiofemoral ligament
Iliofemoral (Y) ligament
Pubofemoral ligament
AAOMPT Conference Louisville 2015 Rett Nicolai, DPT FAAOMPT, Ola Grimsby Institute
ANATOMY & PHYSIOLOGY
Hip Joint
Type: Multi-axial, ball and socket joint
Acetabulum: faces lateral, anterior, inferior
Stable: deep socket, labrum, strong muscles(Byrne, Mulhall, Baker, 2010)
AAOMPT Conference Louisville 2015 Rett Nicolai, DPT FAAOMPT, Ola Grimsby Institute
ANATOMY & PHYSIOLOGY
Other Anatomy of the Hip
Ligament Teres
Pulvinar Acetabulum (Fat Pad)
Labrum
Cartilage
AAOMPT Conference Louisville 2015 Rett Nicolai, DPT FAAOMPT, Ola Grimsby Institute
OSTEOKINEMATIC VS ARTHROKINEMATIC MOVEMENT
Osteokinematic: Movement of Bone
Arthrokinematic: Movement of Joint
AAOMPT Conference Louisville 2015 Rett Nicolai, DPT FAAOMPT, Ola Grimsby Institute

10/22/2015
AAOMPT Conference Louisville 2015, Rett Nicolai, DPT FAAOMPT 4
OSTEOKINEMATIC VS ARTHROKINEMATIC MOVEMENT
AAOMPT Conference Louisville 2015 Rett Nicolai, DPT FAAOMPT, Ola Grimsby Institute
OSTEOKINEMATIC VS ARTHROKINEMATIC MOVEMENT
AAOMPT Conference Louisville 2015 Rett Nicolai, DPT FAAOMPT, Ola Grimsby Institute
To mobilize a CONCAVE surface:
A concave joint surface always moves in the same direction as the bone.
example: finger flexion
Push
BoneJoint Surface
X
X
Joint SurfaceBone
OSTEOKINEMATIC VS ARTHROKINEMATIC MOVEMENT
AAOMPT Conference Louisville 2015 Rett Nicolai, DPT FAAOMPT, Ola Grimsby Institute
To mobilize a CONVEX surface:
A convex joint surface always moves in the opposite direction as the bone.
example: shoulder abduction.
Push
BoneJoint Surface
X
X
Joint Surface
Bone
Fix
Fix
OSTEOKINEMATIC VS ARTHROKINEMATIC MOVEMENT
Accessory motions (Glide)Translational glide is inversely
Proportional to congruence and
depth of concavity:
Hip has ~180˚, therefore glide .8 - 4.2 mm
(posterior glide) (Loubert et al, 2013)
AAOMPT Conference Louisville 2015 Rett Nicolai, DPT FAAOMPT, Ola Grimsby Institute
Fix
Fix
Glide
Glide
X
X
10/22/2015
AAOMPT Conference Louisville 2015, Rett Nicolai, DPT FAAOMPT 5
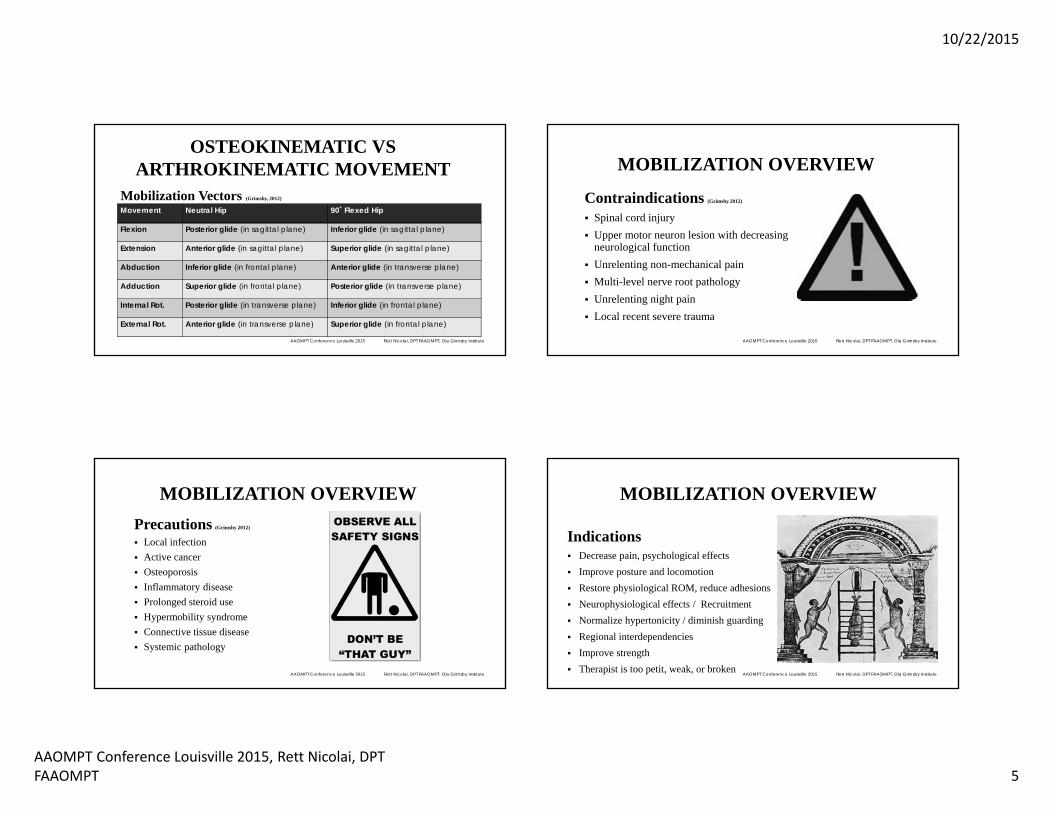
OSTEOKINEMATIC VS ARTHROKINEMATIC MOVEMENT
Mobilization Vectors (Grimsby, 2012)
AAOMPT Conference Louisville 2015 Rett Nicolai, DPT FAAOMPT, Ola Grimsby Institute
Movement Neutral Hip 90˚ Flexed Hip
Flexion Posterior glide (in sagittal plane) Inferior glide (in sagittal plane)
Extension Anterior glide (in sagittal plane) Superior glide (in sagittal plane)
Abduction Inferior glide (in frontal plane) Anterior glide (in transverse plane)
Adduction Superior glide (in frontal plane) Posterior glide (in transverse plane)
Internal Rot. Posterior glide (in transverse plane) Inferior glide (in frontal plane)
External Rot. Anterior glide (in transverse plane) Superior glide (in frontal plane)
MOBILIZATION OVERVIEW
Contraindications (Grimsby 2012)
Spinal cord injury Upper motor neuron lesion with decreasing
neurological function Unrelenting non-mechanical pain Multi-level nerve root pathology Unrelenting night pain Local recent severe trauma
AAOMPT Conference Louisville 2015 Rett Nicolai, DPT FAAOMPT, Ola Grimsby Institute
MOBILIZATION OVERVIEWPrecautions (Grimsby 2012)
Local infection Active cancer Osteoporosis Inflammatory disease Prolonged steroid use Hypermobility syndrome Connective tissue disease Systemic pathology
AAOMPT Conference Louisville 2015 Rett Nicolai, DPT FAAOMPT, Ola Grimsby Institute
MOBILIZATION OVERVIEW
Indications Decrease pain, psychological effects Improve posture and locomotion Restore physiological ROM, reduce adhesions Neurophysiological effects / Recruitment Normalize hypertonicity / diminish guarding Regional interdependencies Improve strength Therapist is too petit, weak, or broken
AAOMPT Conference Louisville 2015 Rett Nicolai, DPT FAAOMPT, Ola Grimsby Institute
10/22/2015
AAOMPT Conference Louisville 2015, Rett Nicolai, DPT FAAOMPT 6
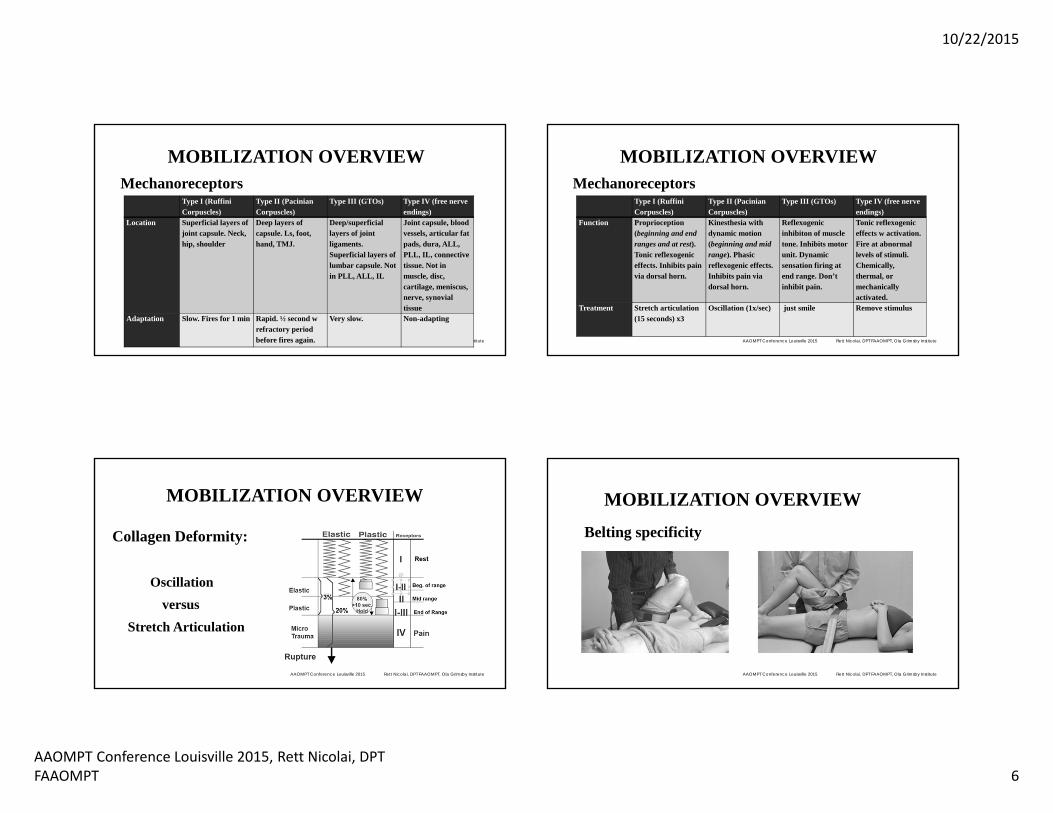
MOBILIZATION OVERVIEWMechanoreceptors
AAOMPT Conference Louisville 2015 Rett Nicolai, DPT FAAOMPT, Ola Grimsby Institute
Type I (Ruffini Corpuscles)
Type II (Pacinian Corpuscles)
Type III (GTOs) Type IV (free nerve endings)
Location Superficial layers of joint capsule. Neck, hip, shoulder
Deep layers of capsule. Ls, foot, hand, TMJ.
Deep/superficial layers of joint ligaments. Superficial layers of lumbar capsule. Not in PLL, ALL, IL
Joint capsule, blood vessels, articular fat pads, dura, ALL, PLL, IL, connective tissue. Not in muscle, disc, cartilage, meniscus, nerve, synovial tissue
Adaptation Slow. Fires for 1 min Rapid. ½ second w refractory period before fires again.
Very slow. Non-adapting
MOBILIZATION OVERVIEWMechanoreceptors
AAOMPT Conference Louisville 2015 Rett Nicolai, DPT FAAOMPT, Ola Grimsby Institute
Type I (RuffiniCorpuscles)
Type II (Pacinian Corpuscles)
Type III (GTOs) Type IV (free nerve endings)
Function Proprioception (beginning and end ranges and at rest). Tonic reflexogeniceffects. Inhibits pain via dorsal horn.
Kinesthesia with dynamic motion (beginning and mid range). Phasic reflexogenic effects. Inhibits pain via dorsal horn.
Reflexogenicinhibiton of muscle tone. Inhibits motor unit. Dynamic sensation firing at end range. Don’t inhibit pain.
Tonic reflexogeniceffects w activation. Fire at abnormal levels of stimuli. Chemically, thermal, or mechanically activated.
Treatment Stretch articulation (15 seconds) x3
Oscillation (1x/sec) just smile Remove stimulus
MOBILIZATION OVERVIEW
Collagen Deformity:
Oscillationversus
Stretch Articulation
AAOMPT Conference Louisville 2015 Rett Nicolai, DPT FAAOMPT, Ola Grimsby Institute
MOBILIZATION OVERVIEW
Belting specificity
AAOMPT Conference Louisville 2015 Rett Nicolai, DPT FAAOMPT, Ola Grimsby Institute

10/22/2015
AAOMPT Conference Louisville 2015, Rett Nicolai, DPT FAAOMPT 7
MOBILIZATION #1:OSCILLATORY
TECHNIQUE video here
AAOMPT Conference Louisville 2015 Rett Nicolai, DPT FAAOMPT, Ola Grimsby Institute
MOBILIZATION #2:STRETCH
ARTICULATION TECHNIQUE
video here
AAOMPT Conference Louisville 2015 Rett Nicolai, DPT FAAOMPT, Ola Grimsby Institute
PRACTICAL APPLICATIONS
You know the science.
Let’s apply it.
AAOMPT Conference Louisville 2015 Rett Nicolai, DPT FAAOMPT, Ola Grimsby Institute
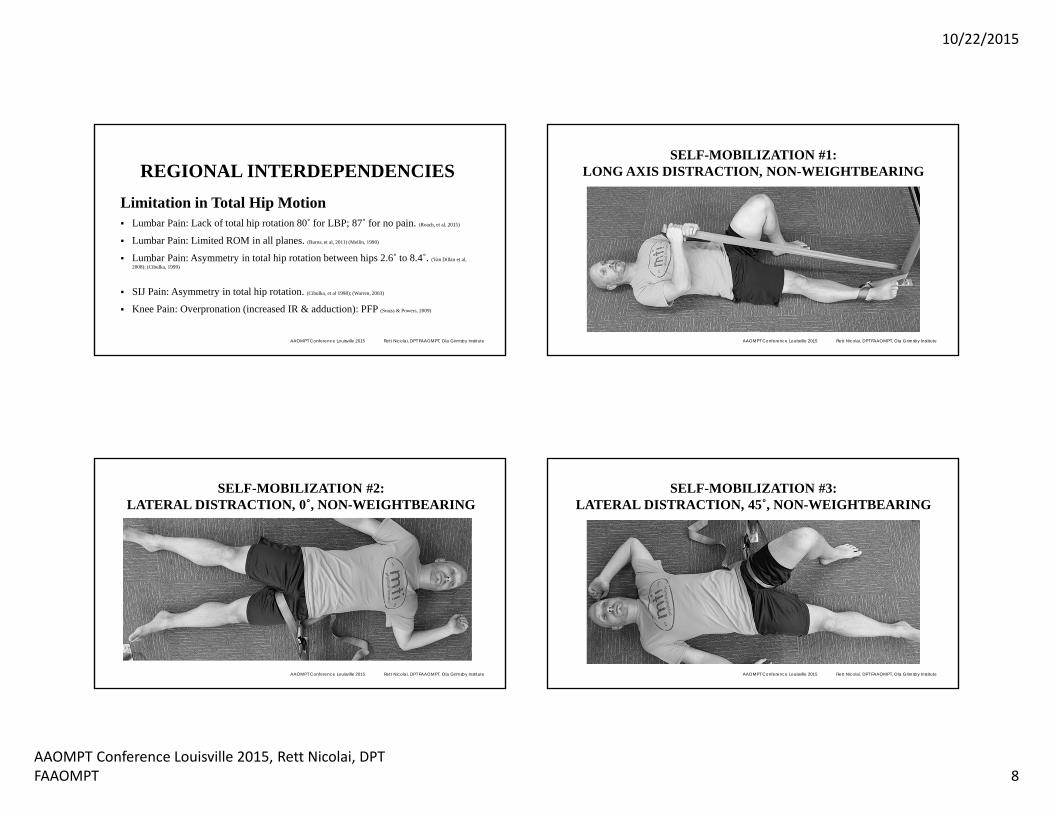
REGIONAL INTERDEPENDENCIES
Relationships between seemingly unrelated impairments in remote anatomical regions may contribute to the patient’s primary symptom. (Wainner, et al, 2007)
Biomedical model: musculoskeletal, neurophysiological, somatovisceral, biopsychosocial responses. (Sueki, Cleland, Wainner, 2013)
AAOMPT Conference Louisville 2015 Rett Nicolai, DPT FAAOMPT, Ola Grimsby Institute
10/22/2015
AAOMPT Conference Louisville 2015, Rett Nicolai, DPT FAAOMPT 8
REGIONAL INTERDEPENDENCIESLimitation in Total Hip Motion Lumbar Pain: Lack of total hip rotation 80˚ for LBP; 87˚ for no pain. (Roach, et al, 2015)
Lumbar Pain: Limited ROM in all planes. (Burns, et al, 2011) (Mellin, 1990)
Lumbar Pain: Asymmetry in total hip rotation between hips 2.6˚ to 8.4˚. (Van Dillan et al, 2008); (Cibulka, 1999)
SIJ Pain: Asymmetry in total hip rotation. (Cibulka, et al 1998); (Warren, 2003)
Knee Pain: Overpronation (increased IR & adduction): PFP (Souza & Powers, 2009)
AAOMPT Conference Louisville 2015 Rett Nicolai, DPT FAAOMPT, Ola Grimsby Institute
SELF-MOBILIZATION #1:LONG AXIS DISTRACTION, NON-WEIGHTBEARING
AAOMPT Conference Louisville 2015 Rett Nicolai, DPT FAAOMPT, Ola Grimsby Institute
SELF-MOBILIZATION #2:LATERAL DISTRACTION, 0˚, NON-WEIGHTBEARING
AAOMPT Conference Louisville 2015 Rett Nicolai, DPT FAAOMPT, Ola Grimsby Institute
SELF-MOBILIZATION #3:LATERAL DISTRACTION, 45˚, NON-WEIGHTBEARING
AAOMPT Conference Louisville 2015 Rett Nicolai, DPT FAAOMPT, Ola Grimsby Institute

10/22/2015
AAOMPT Conference Louisville 2015, Rett Nicolai, DPT FAAOMPT 9
SELF-MOBILIZATION #4:
LATERAL DISTRACTION, 0˚, WEIGHTBEARING
AAOMPT Conference Louisville 2015 Rett Nicolai, DPT FAAOMPT, Ola Grimsby Institute
REGIONAL INTERDEPENDENCIES
Limited Hip Flexion Lumbar Pain: Limited flexion. (Sjolie, 2004); (Mellin, 1988); (Zafereo, et al, 2015)
Knee Pain: Limited flexion: 34.8˚ for knee OA pain
37.4˚ was normal. (Cliborne, et al, 2004)
AAOMPT Conference Louisville 2015 Rett Nicolai, DPT FAAOMPT, Ola Grimsby Institute
OSTEOKINEMATIC VS ARTHROKINEMATIC MOVEMENT
Mobilization Vectors (Grimsby, 2012)
AAOMPT Conference Louisville 2015 Rett Nicolai, DPT FAAOMPT, Ola Grimsby Institute
Movement Neutral Hip 90˚ Flexed Hip
Flexion Posterior glide (in sagittal plane) Inferior glide (in sagittal plane)
Extension Anterior glide (in sagittal plane) Superior glide (in sagittal plane)
Abduction Inferior glide (in frontal plane) Anterior glide (in transverse plane)
Adduction Superior glide (in frontal plane) Posterior glide (in transverse plane)
Internal Rot. Posterior glide (in transverse plane) Inferior glide (in frontal plane)
External Rot. Anterior glide (in transverse plane) Superior glide (in frontal plane)
SELF-MOBILIZATION #6:INFERIOR GLIDE IN 90˚, (SAGITTAL PLANE), NWB
AAOMPT Conference Louisville 2015 Rett Nicolai, DPT FAAOMPT, Ola Grimsby Institute
10/22/2015
AAOMPT Conference Louisville 2015, Rett Nicolai, DPT FAAOMPT 10
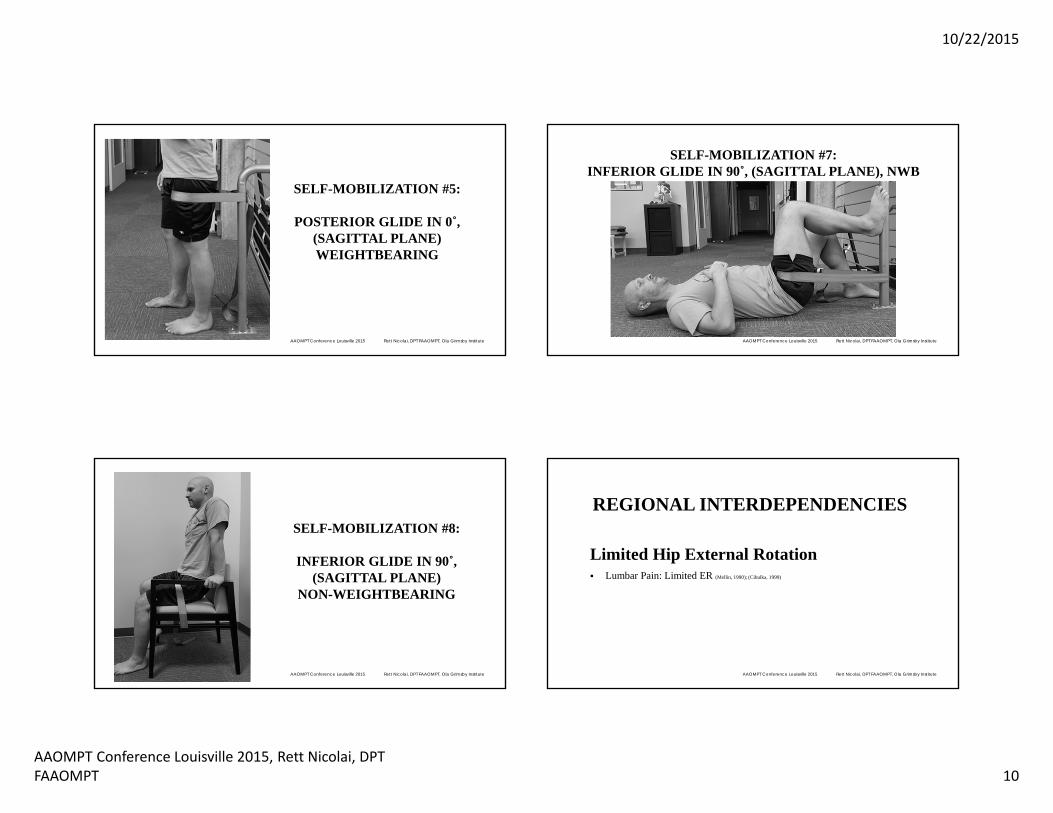
SELF-MOBILIZATION #5:
POSTERIOR GLIDE IN 0˚, (SAGITTAL PLANE) WEIGHTBEARING
AAOMPT Conference Louisville 2015 Rett Nicolai, DPT FAAOMPT, Ola Grimsby Institute
SELF-MOBILIZATION #7:INFERIOR GLIDE IN 90˚, (SAGITTAL PLANE), NWB
AAOMPT Conference Louisville 2015 Rett Nicolai, DPT FAAOMPT, Ola Grimsby Institute
SELF-MOBILIZATION #8:
INFERIOR GLIDE IN 90˚, (SAGITTAL PLANE)
NON-WEIGHTBEARING
AAOMPT Conference Louisville 2015 Rett Nicolai, DPT FAAOMPT, Ola Grimsby Institute
REGIONAL INTERDEPENDENCIES
Limited Hip External Rotation Lumbar Pain: Limited ER (Mellin, 1990); (Cibulka, 1999)
AAOMPT Conference Louisville 2015 Rett Nicolai, DPT FAAOMPT, Ola Grimsby Institute

10/22/2015
AAOMPT Conference Louisville 2015, Rett Nicolai, DPT FAAOMPT 11
OSTEOKINEMATIC VS ARTHROKINEMATIC MOVEMENT
Mobilization Vectors (Grimsby, 2012)
AAOMPT Conference Louisville 2015 Rett Nicolai, DPT FAAOMPT, Ola Grimsby Institute
Movement Neutral Hip 90˚ Flexed Hip
Flexion Posterior glide (in sagittal plane) Inferior glide (in sagittal plane)
Extension Anterior glide (in sagittal plane) Superior glide (in sagittal plane)
Abduction Inferior glide (in frontal plane) Anterior glide (in transverse plane)
Adduction Superior glide (in frontal plane) Posterior glide (in transverse plane)
Internal Rot. Posterior glide (in transverse plane) Inferior glide (in frontal plane)
External Rot. Anterior glide (in transverse plane) Superior glide (in frontal plane)
SELF-MOBILIZATION #11:SUPERIOR GLIDE IN 90˚, (FRONTAL PLANE)
NON-WEIGHTBEARING
AAOMPT Conference Louisville 2015 Rett Nicolai, DPT FAAOMPT, Ola Grimsby Institute
SELF-MOBILIZATION #9:
ANTERIOR GLIDE IN 0˚, (TRANSVERSE PLANE)
WEIGHTBEARING
AAOMPT Conference Louisville 2015 Rett Nicolai, DPT FAAOMPT, Ola Grimsby Institute
SELF-MOBILIZATION #10:
SUPERIOR GLIDE IN 90˚, (FRONTAL PLANE)
PARTIAL WEIGHTBEARING
AAOMPT Conference Louisville 2015 Rett Nicolai, DPT FAAOMPT, Ola Grimsby Institute
10/22/2015
AAOMPT Conference Louisville 2015, Rett Nicolai, DPT FAAOMPT 12
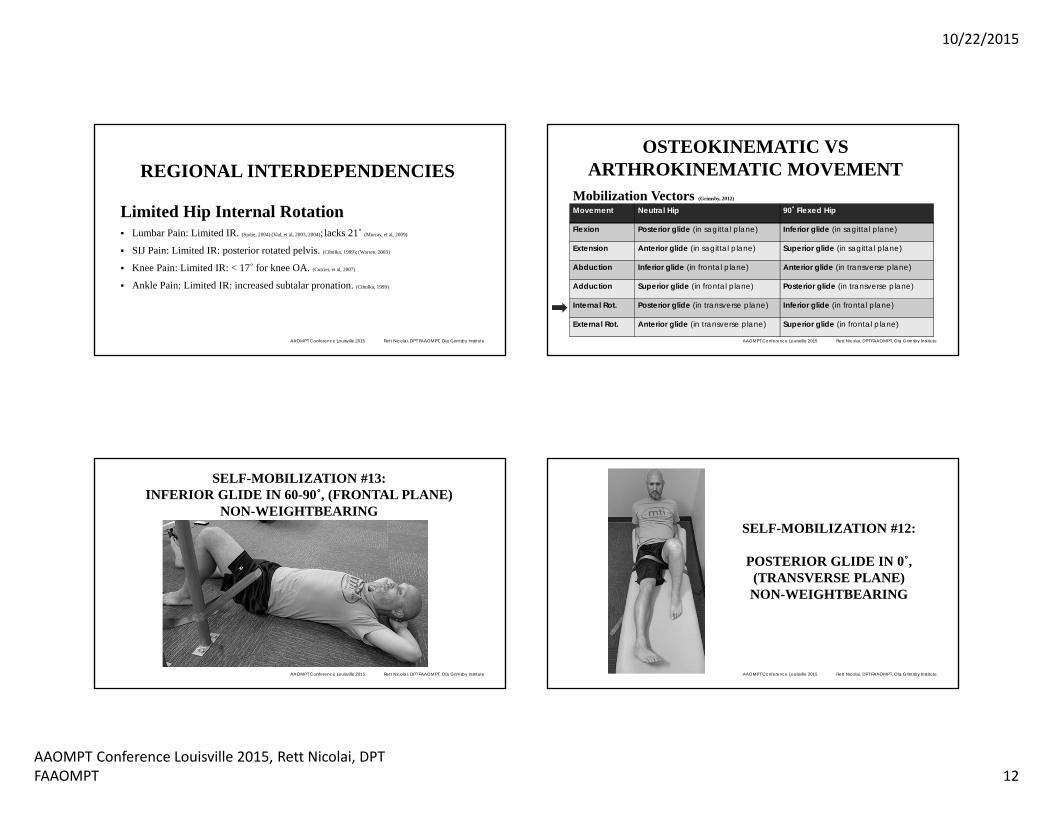
REGIONAL INTERDEPENDENCIES
Limited Hip Internal Rotation Lumbar Pain: Limited IR. (Sjolie, 2004) (Vad, et al, 2003, 2004); lacks 21˚ (Murray, et al, 2009)
SIJ Pain: Limited IR: posterior rotated pelvis. (Cibulka, 1999); (Warren, 2003)
Knee Pain: Limited IR: < 17˚ for knee OA. (Currier, et al, 2007)
Ankle Pain: Limited IR: increased subtalar pronation. (Cibulka, 1999)
AAOMPT Conference Louisville 2015 Rett Nicolai, DPT FAAOMPT, Ola Grimsby Institute
OSTEOKINEMATIC VS ARTHROKINEMATIC MOVEMENT
Mobilization Vectors (Grimsby, 2012)
AAOMPT Conference Louisville 2015 Rett Nicolai, DPT FAAOMPT, Ola Grimsby Institute
Movement Neutral Hip 90˚ Flexed Hip
Flexion Posterior glide (in sagittal plane) Inferior glide (in sagittal plane)
Extension Anterior glide (in sagittal plane) Superior glide (in sagittal plane)
Abduction Inferior glide (in frontal plane) Anterior glide (in transverse plane)
Adduction Superior glide (in frontal plane) Posterior glide (in transverse plane)
Internal Rot. Posterior glide (in transverse plane) Inferior glide (in frontal plane)
External Rot. Anterior glide (in transverse plane) Superior glide (in frontal plane)
SELF-MOBILIZATION #13:INFERIOR GLIDE IN 60-90˚, (FRONTAL PLANE)
NON-WEIGHTBEARING
AAOMPT Conference Louisville 2015 Rett Nicolai, DPT FAAOMPT, Ola Grimsby Institute
SELF-MOBILIZATION #12:
POSTERIOR GLIDE IN 0˚, (TRANSVERSE PLANE) NON-WEIGHTBEARING
AAOMPT Conference Louisville 2015 Rett Nicolai, DPT FAAOMPT, Ola Grimsby Institute
10/22/2015
AAOMPT Conference Louisville 2015, Rett Nicolai, DPT FAAOMPT 13
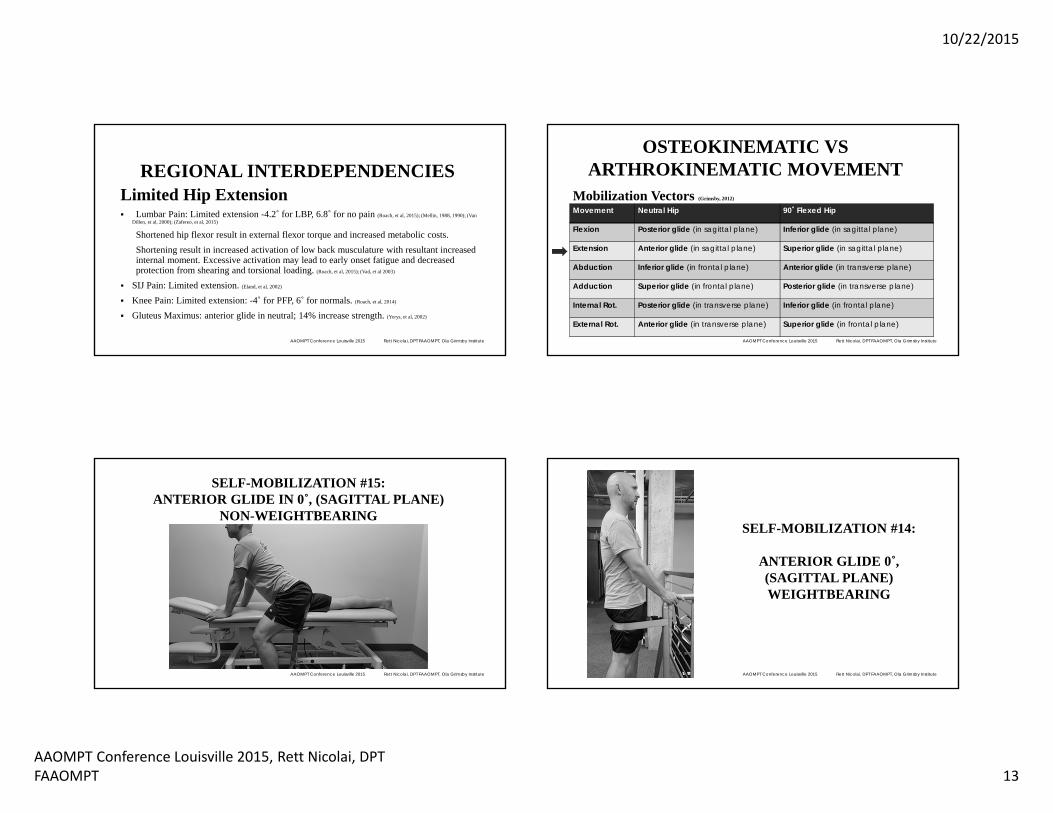
REGIONAL INTERDEPENDENCIESLimited Hip Extension Lumbar Pain: Limited extension -4.2˚ for LBP, 6.8˚ for no pain (Roach, et al, 2015); (Mellin, 1988, 1990); (Van
Dillen, et al, 2000); (Zafereo, et al, 2015)
Shortened hip flexor result in external flexor torque and increased metabolic costs. Shortening result in increased activation of low back musculature with resultant increased internal moment. Excessive activation may lead to early onset fatigue and decreased protection from shearing and torsional loading. (Roach, et al, 2015); (Vad, et al 2003)
SIJ Pain: Limited extension. (Eland, et al, 2002)
Knee Pain: Limited extension: -4˚ for PFP, 6˚ for normals. (Roach, et al, 2014)
Gluteus Maximus: anterior glide in neutral; 14% increase strength. (Yerys, et al, 2002)
AAOMPT Conference Louisville 2015 Rett Nicolai, DPT FAAOMPT, Ola Grimsby Institute
OSTEOKINEMATIC VS ARTHROKINEMATIC MOVEMENT
Mobilization Vectors (Grimsby, 2012)
AAOMPT Conference Louisville 2015 Rett Nicolai, DPT FAAOMPT, Ola Grimsby Institute
Movement Neutral Hip 90˚ Flexed Hip
Flexion Posterior glide (in sagittal plane) Inferior glide (in sagittal plane)
Extension Anterior glide (in sagittal plane) Superior glide (in sagittal plane)
Abduction Inferior glide (in frontal plane) Anterior glide (in transverse plane)
Adduction Superior glide (in frontal plane) Posterior glide (in transverse plane)
Internal Rot. Posterior glide (in transverse plane) Inferior glide (in frontal plane)
External Rot. Anterior glide (in transverse plane) Superior glide (in frontal plane)
SELF-MOBILIZATION #15:ANTERIOR GLIDE IN 0˚, (SAGITTAL PLANE)
NON-WEIGHTBEARING
AAOMPT Conference Louisville 2015 Rett Nicolai, DPT FAAOMPT, Ola Grimsby Institute
SELF-MOBILIZATION #14:
ANTERIOR GLIDE 0˚, (SAGITTAL PLANE) WEIGHTBEARING
AAOMPT Conference Louisville 2015 Rett Nicolai, DPT FAAOMPT, Ola Grimsby Institute
10/22/2015
AAOMPT Conference Louisville 2015, Rett Nicolai, DPT FAAOMPT 14
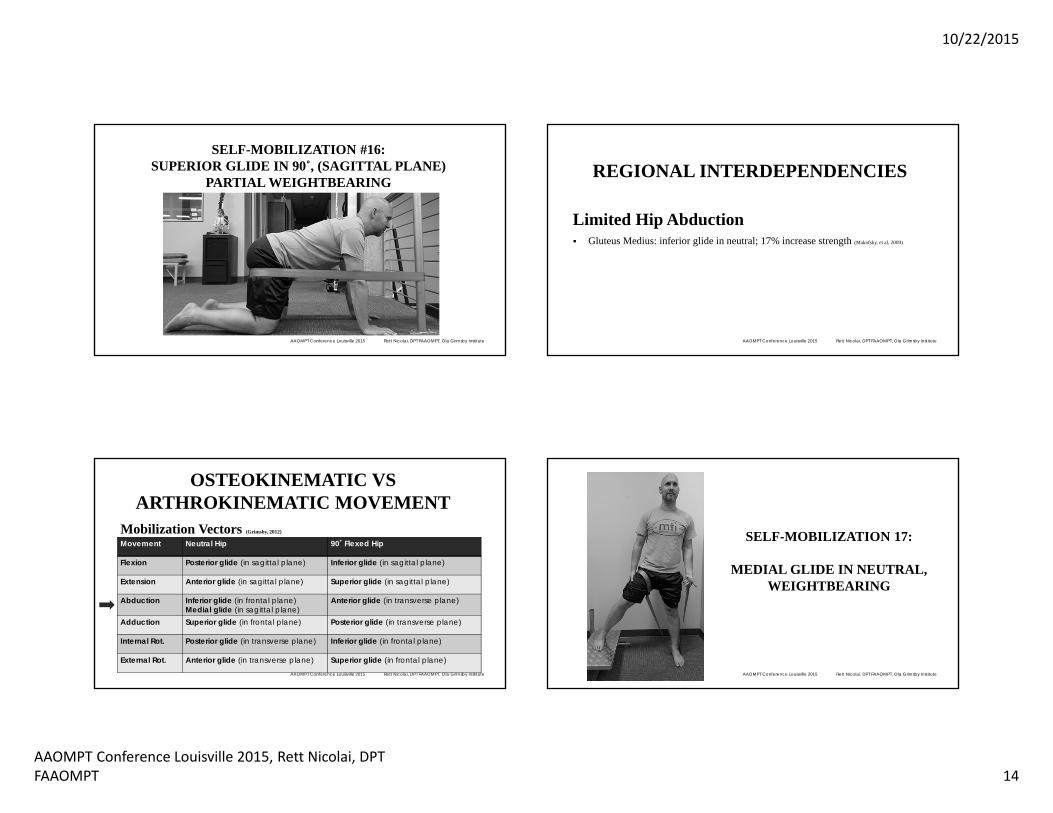
SELF-MOBILIZATION #16:SUPERIOR GLIDE IN 90˚, (SAGITTAL PLANE)
PARTIAL WEIGHTBEARING
AAOMPT Conference Louisville 2015 Rett Nicolai, DPT FAAOMPT, Ola Grimsby Institute
REGIONAL INTERDEPENDENCIES
Limited Hip Abduction Gluteus Medius: inferior glide in neutral; 17% increase strength (Makofsky, et al, 2009)
AAOMPT Conference Louisville 2015 Rett Nicolai, DPT FAAOMPT, Ola Grimsby Institute
OSTEOKINEMATIC VS ARTHROKINEMATIC MOVEMENT
Mobilization Vectors (Grimsby, 2012)
AAOMPT Conference Louisville 2015 Rett Nicolai, DPT FAAOMPT, Ola Grimsby Institute
Movement Neutral Hip 90˚ Flexed Hip
Flexion Posterior glide (in sagittal plane) Inferior glide (in sagittal plane)
Extension Anterior glide (in sagittal plane) Superior glide (in sagittal plane)
Abduction Inferior glide (in frontal plane)Medial glide (in sagittal plane)
Anterior glide (in transverse plane)
Adduction Superior glide (in frontal plane) Posterior glide (in transverse plane)
Internal Rot. Posterior glide (in transverse plane) Inferior glide (in frontal plane)
External Rot. Anterior glide (in transverse plane) Superior glide (in frontal plane)
SELF-MOBILIZATION 17:
MEDIAL GLIDE IN NEUTRAL, WEIGHTBEARING
AAOMPT Conference Louisville 2015 Rett Nicolai, DPT FAAOMPT, Ola Grimsby Institute
10/22/2015
AAOMPT Conference Louisville 2015, Rett Nicolai, DPT FAAOMPT 15
REGIONAL INTERDEPENDENCIES
Neurophysiological, Somatovisceral, Radicular Pain Joints’ mechancoreceptors influence motor unit activation, therefore muscle
function. It may increase strength by removing the reflexogenic inhibition from mechanoreceptors. (Makofsky, et al, 2009); (Warmerdam, 1985); (Wyke, 1985); (Yerys, et al, 2002); (Grimsby, 2012);
While simultaneously defacilitating through reciprocal innervation. (Yerys, et al, 2002)
Hypoalgesia effects after mobilization (Bialosky, Bishop, George, 2008)
AAOMPT Conference Louisville 2015 Rett Nicolai, DPT FAAOMPT, Ola Grimsby Institute
REGIONAL INTERDEPENDENCIES
These people may never have problems…
AAOMPT Conference Louisville 2015 Rett Nicolai, DPT FAAOMPT, Ola Grimsby Institute
MOBILIZATION TECHNIQUESProblem Solving for Self-Mobilization Techniques Safety, don’t articulate in close-packed position Lack equipment (belt or stable fixture) Poor set-up position (individual’s posture or where the belt is) Loss of contact point pressure, fix & support one bone Incorrect vector Incorrect force Incorrect amplitude Patient not relaxed, motor moron
AAOMPT Conference Louisville 2015 Rett Nicolai, DPT FAAOMPT, Ola Grimsby Institute
References:Grimsby O. Ola Grimsby Institute, Residency Program Curriculum 2006.Grimsby O. Ola Grimsby Institute, Fellowship Program Curriculum 2008.Grimsby O. Ola Grimsby Institute, PhD Program Curriculum 2012.
Rivard JR, Grimsby O. Science, Theory and Clinical Application in Orthopaedic Manual Physical Therapy: Vol 3: Scientific Therapeutic Exercise Progressions (STEP): The Back and Lower Extremity. Taylorsville, UT: Academy of Graduate Physical Therapy Inc.; 2008.
MaGee, D. Orthopedic Physical Assessment, 5th ed. St Louis, MO: Saunders Elsevier; 2008; 659-726.
Warmerdam A. Arthorkinematic Therapy: Improving Muscle Performance through Joint Manipulation. Wantagh, NY: Pine Publications, 1999; 32-44.
Wyke BD. Articular Neurology. In: Glasgow EF, Twoney LT, Scull ER, Kleynhans AM, eds. Aspects of Manipulative Therapy. New York: Churchill Livingstone, 1985; 72-77.
Sueki DG, Cleland JA, Wainner RS. A Regional Interdependence model of musculoskeletal dysfunction: Research, Mechanisms, and Clinical Implications. J Man Manip Ther. 2013; 21 (2): 90-102.
Wainner RS, Whitman JM, Cleland JA, Flynn TW. Regional Interdependence: A Musculoskeletal Examination Model Whose Time Has Come. J Orthop Sports PhysTher. 2007; 37(11): 658-660.
Byrne DP, Mulhall KJ, Baker JF. Anatomy & Biomechanics of Hip. Open Sports Medicine J. 2010; 4: 51-57.
Roach SM, San Juan JG, Suprak DN, Lyda M, Boydston C. Patellofemoral Pain Subjects Exhibit Decreased Passive Hip Range of Motion Compared to Controls. Int J Sports Phys Ther. 2014; 9 (4): 468-175.
Cliborne AV, Wainner RS, Rhon DI, Judd CD, Fee TT, Matekel RL, Whitman JM. Clinical Hip Tests and a Functional Squat Test with Knee Osteoarthritis: Reliability, Prevalence of Positive Test Findings, and Short-Term Response to Hip Mobilization. J Orthop Sports Phys Ther. 2004; 34 (11): 676-85.
AAOMPT Conference Louisville 2015 Rett Nicolai, DPT FAAOMPT, Ola Grimsby Institute

10/22/2015
AAOMPT Conference Louisville 2015, Rett Nicolai, DPT FAAOMPT 16
References:Roach SM, San Juan JG, Suprak DN, Lyda M, Bies AJ, Boydstom CR. Passive Hip Range of Motion is Reduced in Active Subjects with Chronic Low Back Pain Compared to Controls. Int J Sports Phys Ther. 2015; 10 (1): 13-20.
Van Dillen LR, Bloom NJ, Gombatto SP, Susco TM. Hip Rotation Range of Motion in People with and without Low Back Pain Who Participate in Rotation-Related Sports. Phy Ther Sport. 2008; 9 (2). 72-81.
Burns SA, Mintken PE, Austin GP, Cleland J. Short-Term Response of Hip Mobilizations and Exercise in Individuals with Chronic Low Back Pain: A Case Series. J Man Manip Ther. 2011; 19 (2). 100-107.
Makofsky H, Panicker S, Abbruzzese J, Aridas C, Camp M, Drakes J, Franco C, Sileo R. Immediate Effect of Grade IV Inferior Hip Joint Mobilization on Hip Abduction Torque: a Pilot Study. J of Man Manip Ther. 2007; 15 (2): 103-111.
Yerys S, Makofsky H, Byrd C, Pennachio J, Cinkay J. Effect on Mobilization of the Anterior Hip Capsule on Gluteus Maximus Strength. J Man Manip Ther. 2002; 10 (4): 218-224.
Loubert PV, Zipple JT, Klobucher MJ, Marquardt ED, Opolka MJ. In Vivo Ultrasound Measurement of Posterior Femoral Glide during Hip Joint Mobilization in Healthy College Students. J Orthop Sports Phys Ther. 2013; 43 (8): 534-541.
Crow JB, Gelfand B, Su EP. Use of Joint Mobilization in a Patient with Severely Restricted Hip Motion Following Bilateral Hip Resurfacing Arthroplasty. Phys Ther. 2008; 88: 1591-1600.
Bialosky, JE, Bishop MD, George SZ. Regional Interdependence: A Musculoskeletal Examination Model Whose Time Has Come. Letter to the Editor. J Orthop Sports Phys Ther. 2008; 38 (3): 159-160.
Souza RB, Powers CM. Differences in Hip Kinematics, Muscle Strength, and Muscle Activation Between Subjects with and without Patellofemoral Pain. J OrthopSports Phys Ther. 2009; 39 (1): 12-19.
Powers CM. The Influence of Abnormal Hip Mechanics on Knee Injury: A Biomechanical Perspective. J Orthop Sports Phys Ther. 2010; 40 (2): 42-51.
AAOMPT Conference Louisville 2015 Rett Nicolai, DPT FAAOMPT, Ola Grimsby Institute
References:Warren PH. Management of a Patient with Sacroiliac Joint Dysfunction: A Correlation of Hip Range of Motion Asymmetry with Sitting and Standing Postural Habits. J Man Manip Ther. 2003; 11 (3): 153-159.
Cibulka MT, Sinacore DR, Cromer GS, Delitto A. Unilateral Hip Rotation Range of Motion Asymmetry in Patients with Sacroiliac Joint Regional Pain. Spine. 1998; 23 (9): 1009-1015.
Cibulka MT. Low Back Pain and Its Relation to the Hip and Foot. J Orthop Sports Phys Ther. 1999; 29 (10): 595-601.
Mellin G. Correlations of Hip Mobility with Degree of Back Pain and Lumbar Spinal Mobility in Chronic Low-Back Pain Patients. Spine. 1988; 13 (6): 668-670.
Mellin G. Decreased Joint and Spinal Mobility Associated with Low Back Pain in Young Adults. J Spinal Disord. 1990; 3 (3): 238-243.
Vad VB, Bhat AL, Basrai D, Gebeh A, Aspergren DD, Andrews JR. Low Back Pain in Professional Golfers: the Role of Associated Hip and Low Back Range of Motion Deficits. Am J Sports Med. 2004; 32 (2): 494-497.
Val VB, Gebeh A, Dines D, Altchek D, Norris B. Hip and Shoulder Internal Rotation Range of Motion Deficits in Professional Tennis Players. J Sci Med Sport. 2003; 6 (1): 71-75.
Reiman MP, Matheson JW. Restricted Hip Mobility: Clinical Suggestions for Self-Mobilization and Muscle Re-education. Int J Sports Phys Ther. 2013; 8 (5): 729-740.
Murray E, Birley E, Twycross-Lewis R, Morrissey D. The Relationship between Hip Rotation Range of Movement and Low Back Pain Prevalence in Amateur Golfers: an Observational Study. Phys Ther Sport. 2009; 10 (4): 131-135.
Sjolie AN. Low-Back Pain in Adolescents is Associated with Poor Hip Mobility and High Body Mass Index. Scan J Med Sci Sports. 2004; 14 (3): 168-175.
Eland DC, Singleton BS, Conaster MS, Howell JN, Pheley AM, Karlene MM, Robinson JM. The “Iliacus Test”: New Information for the evaluation of hip extension dysfunction. JAOA. 2002; 102 (3): 130-142.
AAOMPT Conference Louisville 2015 Rett Nicolai, DPT FAAOMPT, Ola Grimsby Institute
References:Van Dillen LR, McDonnell MK, Fleming DA, Sahrmann SA. Effect of Knee and Hip Position on Hip Extension Range of Motion in Individuals with and without Low Back Pain. J Orthop Sports Phys Ther. 2000; 30 (6): 307-316.
Currier LL, Froehlich PJ, Carow SD, McAndrew RK, Cliborne AV, Boyles RE, Mansfield LT, Wainner RS. Development of a Clinical Prediction Rule to Identify Patients with Knee Pain and Clinical Evidence of Knee Osteoarthritis Who Demonstrate a Favorable Short-Term Response to Hip Mobilization. Phys Ther. 2007; 87 (9): 1106-1119.
Zafereo J, Devanna R, Mulligan E, Wang-Price S. Hip Stiffness Patterns in Lumbar Flexion or Extension Based Movement. Arch Phys Med Rehabil. 2015; 96 (2): 292-297
AAOMPT Conference Louisville 2015 Rett Nicolai, DPT FAAOMPT, Ola Grimsby Institute


















