Self-care components of lifestyles: The importance of gender, attitudes and the social situation
16
Sot. Sci. Med. Vol. 29, No. 2, pp. 137-152, 1989 Printed in Great Britain. All rights reserved 0277-9536/89 S3.W + 0.00 Copyright c 1989 Pcrgamon Press plc SELF-CARE COMPONENTS OF LIFESTYLES: THE IMPORTANCE OF GENDER, ATTITUDES AND THE SOCIAL SITUATION KATHRYN DEAN Institute of Social Medicine, University of Copenhagen, Panum Institute, Blegdamsvej 3, DK-2200 Copenhagen, Denmark Abstract-Self-care practices of individuals are health related elements of lifestyles. In order to understand the influences that shape and maintain the self-care patterns of behaviour that determine health and functional ability, research frameworks for study of the social situations in which people live and the levels of influence among variables are needed. This paper reports on findings from an investigation of self-care practices in a population sample of persons over 45 yr of age in an attempt to study self-care in a lifestyle framework. The findings show the importance of examining patterns of behaviour rather than exclusive focus on the magnitude of differences in discrete behaviours. Gender was the major independent influence on patterns of health maintenance behaviour while social network variables assumed major importance for self-care responses to illness. Key words-self-cam, lifestyle, gender, social network, situational influence INTRODUCTION Focus on the bchaviour of individuals as a determi- nant of health status and functional capacity has been one of the major recent developments within the health sectors of industrialized nations. Increasing numbers of programmes developed under the rubric of lifestyle attempt to influence or change the health related behaviour of individuals. An impetus influ- encing these developments in Europe is the central focus placed on lifestyle programmes and research in the policy document adopted by Member States of the European Region of the World Health Organi- zation [l]. The concept of lifestyle in the growing number of projects, however, often differs signifi- cantly from that developed in WHO. Many lifestyle programmes focus on specific behavioural practices. Tobacco and alcohol con- sumption, eating habits and exercise are behaviours often singled out in lifestyle projects. This tendency arises from research studies where these behaviours handled as discrete behavioural risk factors have been associated with morbidity and mortality. However, discrete health behaviours are insufficient predictors of health outcomes [2,3]. Furthermore, a focus on specific behaviours does not consider the importance of the social and economic environment both as discrete influences on health and as factors influ- encing the behaviour of individuals [4]. Lifestyle-a sociocultural concept In the WHO conceptualization lifestyle is a way of life, a sociocultural phenomenon arising from inter- actions between patterns of behaviour and specific life situations rather than individual decisions to *“A way of life or style of living that reflects the attitudes and values of an individual or culture” (American Heritage Dictionary of the English language). avoid or accept certain health risks. Considered in this way behavioural practices are shaped by values and beliefs learned in specific cultures, and by oppor- tunities and constraints defined by specific social and economic situations [ 11. Reductionistic conceptual- izations of lifestyle are not compatible with this holistic notion. Individual practices are only elements of culturally and socially determined behavioural patterns. Correlations between specific behaviours and negative health outcomes can only be a starting point in the search for understanding the complex ways discrete habits affect health [5]. In operational terms discrete practices of individ- uals are more appropriately defined as self-care behaviours, while behaviours which cluster together and their interactions with cultural, social and psychosocial factors may more meaningfully be con- sidered lifestyles [6]. Lifestyles in this conceptualiza- tion are patterns of social interactions and attitudes with behavioural components. The holistic integra- tive aspects of the term* and the traditional meaning ascribed the concept in the social sciences [7] are thus maintained. Behaviours may then be distinguished and studied in the context of specific life situations with the various health related practices of an individ- ual constituting that person’s self-care behaviour. The term self-care has sometimes been reduced to mean lay illness care dichotomized from professional care, but this is a false dichotomy because it implies both that people only take care of themselves when they are ill, and that seeking professional care is something separate from the continuum of lay behaviour in illness. A holistic conceptualization of self-care recognizes that it is lay individuals interact- ing in specific social situations that perform health related behaviours, including decisions to seek and comply with professional care [8,9]. This is the implicit assumption behind all health education and promotion programmes directed toward influencing 137
-
Upload
kathryn-dean -
Category
Documents
-
view
212 -
download
0
Transcript of Self-care components of lifestyles: The importance of gender, attitudes and the social situation

Sot. Sci. Med. Vol. 29, No. 2, pp. 137-152, 1989 Printed in Great Britain. All rights reserved
0277-9536/89 S3.W + 0.00 Copyright c 1989 Pcrgamon Press plc
SELF-CARE COMPONENTS OF LIFESTYLES: THE IMPORTANCE OF GENDER, ATTITUDES
AND THE SOCIAL SITUATION
KATHRYN DEAN
Institute of Social Medicine, University of Copenhagen, Panum Institute, Blegdamsvej 3, DK-2200 Copenhagen, Denmark
Abstract-Self-care practices of individuals are health related elements of lifestyles. In order to understand the influences that shape and maintain the self-care patterns of behaviour that determine health and functional ability, research frameworks for study of the social situations in which people live and the levels of influence among variables are needed. This paper reports on findings from an investigation of self-care practices in a population sample of persons over 45 yr of age in an attempt to study self-care in a lifestyle framework. The findings show the importance of examining patterns of behaviour rather than exclusive focus on the magnitude of differences in discrete behaviours. Gender was the major independent influence on patterns of health maintenance behaviour while social network variables assumed major importance for self-care responses to illness.
Key words-self-cam, lifestyle, gender, social network, situational influence
INTRODUCTION
Focus on the bchaviour of individuals as a determi- nant of health status and functional capacity has been one of the major recent developments within the health sectors of industrialized nations. Increasing numbers of programmes developed under the rubric of lifestyle attempt to influence or change the health related behaviour of individuals. An impetus influ- encing these developments in Europe is the central focus placed on lifestyle programmes and research in the policy document adopted by Member States of the European Region of the World Health Organi- zation [l]. The concept of lifestyle in the growing number of projects, however, often differs signifi- cantly from that developed in WHO.
Many lifestyle programmes focus on specific behavioural practices. Tobacco and alcohol con- sumption, eating habits and exercise are behaviours often singled out in lifestyle projects. This tendency arises from research studies where these behaviours handled as discrete behavioural risk factors have been associated with morbidity and mortality. However, discrete health behaviours are insufficient predictors of health outcomes [2,3]. Furthermore, a focus on specific behaviours does not consider the importance of the social and economic environment both as discrete influences on health and as factors influ- encing the behaviour of individuals [4].
Lifestyle-a sociocultural concept
In the WHO conceptualization lifestyle is a way of life, a sociocultural phenomenon arising from inter- actions between patterns of behaviour and specific life situations rather than individual decisions to
*“A way of life or style of living that reflects the attitudes and values of an individual or culture” (American Heritage Dictionary of the English language).
avoid or accept certain health risks. Considered in this way behavioural practices are shaped by values and beliefs learned in specific cultures, and by oppor- tunities and constraints defined by specific social and economic situations [ 11. Reductionistic conceptual- izations of lifestyle are not compatible with this holistic notion. Individual practices are only elements of culturally and socially determined behavioural patterns. Correlations between specific behaviours and negative health outcomes can only be a starting point in the search for understanding the complex ways discrete habits affect health [5].
In operational terms discrete practices of individ- uals are more appropriately defined as self-care behaviours, while behaviours which cluster together and their interactions with cultural, social and psychosocial factors may more meaningfully be con- sidered lifestyles [6]. Lifestyles in this conceptualiza- tion are patterns of social interactions and attitudes with behavioural components. The holistic integra- tive aspects of the term* and the traditional meaning ascribed the concept in the social sciences [7] are thus maintained. Behaviours may then be distinguished and studied in the context of specific life situations with the various health related practices of an individ- ual constituting that person’s self-care behaviour. The term self-care has sometimes been reduced to mean lay illness care dichotomized from professional care, but this is a false dichotomy because it implies both that people only take care of themselves when they are ill, and that seeking professional care is something separate from the continuum of lay behaviour in illness. A holistic conceptualization of self-care recognizes that it is lay individuals interact- ing in specific social situations that perform health related behaviours, including decisions to seek and comply with professional care [8,9]. This is the implicit assumption behind all health education and promotion programmes directed toward influencing
137

138 KATHRYN DEAN
or changing personal habits and/or utilization of professional services.
Self-care components of lifestyle assume at least three major forms: (1) routine daily habits of living which affect health, e.g. smoking, drinking, sedentary routines, etc.; (2) conscious health maintenance behaviour; and (3) behavioural responses to symp- toms of illness. In order to understand the health damaging effects of behavioural elements of lifestyles it is necessary to understand the interactions among components of caring for the self and their interplay with sociocultural influences. The theoretical frame- work for the analysis presented in this paper builds on a situational perspective in which cultural and social situational variables are the major determi- nants of individual behaviour.
Gender--a fundamental sociocultural influence
Gender is perhaps the single characteristic which most fundamentally determines perceptions, behav- iour and position in most societies. No other charac- teristic of individuals may be subject to the same degree of cultural and social learning. Therefore, it may be that one of the most fruitful approaches to more meaningful knowledge regarding the health impact of lifestyle is to focus on gender differences in behavioural and attitudinal variables. Health related sex differences which have been consistently docu- mented lend support to this notion.
In those areas of the world where lifestyle fac- tors are considered potent influences on disease patterns, males have consistently poorer health out- comes relative to females. Since the beginning of the twentieth century the age adjusted death rates for females have been lower than for males in all developed countries. Men have higher prevalence rates for many chronic conditions related to the leading causes of death, higher rates of heart disease before age 50, higher injury rates at all ages, longer hospital stays and higher risk of all leading causes of death [lo, 111. At the same time women have more days of illness and more often use health services and take medicine [1 l-131. Thus while women have generally higher rates of illness, dis- ability days and medical consultations, men have more serious conditions.
No single explanation has (nor probably could) accounted for these health related X.X differences. The sharp increases over the past 50 yr in the differ- ence in the age adjusted death rates of men and women cannot be explained by biological factors alone [14]. Analytic overviews of mortality and morbidity trend data point to the importance of behavioural factors. Waldrom [ 151 concludes from U.S. data that in addition to the effects of biological differences and exposure to occupational hazards, mens’ higher death rates are due mainly to be- havioural influences such as higher rates of cigarette smoking, type A behaviour patterns and alcohol consumption. These behavioural habits fall into the first component of lifestyle mentioned above routine daily habits of living. In Denmark, evidence in rela- tion to the most commonly studied health related habits indicates that men use more tobacco while women are less physically active [16]. Men also consume considerably more alcohol than women
[17, 181. In research conducted in Sweden evidence points to male smoking behaviour as a major cause of sex differences in health [19].
Consciously undertaken health protective behav- iour and illness care may also be gender dependent. Verbrugge [lo] discusses varying tendencies to pre- vent health problems as prevention orientations and differential attention to symptoms or curative actions as illness orientations. She points to the widespread belief, but limited evidence, that men and women differ in their health related orientations. At least two behaviours that are conscious health maintenance practices are known to be gender dependent. Males use seatbelts less often in care travel [20,21] and obtain fewer preventive health examinations [20]. The greater physical activity among males which is related to their participation in active sports and exercise [ 161 may be conscious health maintenance, or it could be simply learned behaviour related to feelings of group identity and acceptance.
Evidence that illness related self-care behaviour is gender dependent has accumulated in different countries. Women’s greater use of medicine and health care services may represent more conscious health protective self-care. Hollnagel and Kamper- Jorgensen [13], studying sex differences in utilization of health services in Denmark, cannot find a suffi- cient biological explanation for the differential use of services. They conclude that the sex variable must be considered a psychosocial variable reflecting differences in the accumulated experience of men and women.
The different experiences of men and women come directly from cultural values and social learning and indirectly from attitudes, values and behaviours pre- vading dominant social structures and institutions, e.g. health care services [22], schools sports pro- grammes, and advertising. It is possible that gender determined socialization shapes health beliefs to indirectly influence self-care in adult life or that gender linked perceptions and behaviours are directly learned and reinforced over the life course occurring irrespective of health beliefs and knowledge.
Accumulated gender linked experiences, while theoretically of fundamental importance for under- standing and influencing behaviour, represent only one major influence. The specific social situations in which people currently live may also exert major influence on behaviour.
Social situational influences
Personal networks and their functioning as well as socio-economic factors that represent opportunities and constraints in the life situation may be considered major situational influences on behaviour. The large body of evidence on social class differences in health status [23-251 suggests that socio-economic factors may act as either stress buffers or direct stressors for health outcomes. Many research investigations have produced findings suggesting that supportive social networks buffer the effects of stress and may be directly health enhancing as well [26,27]. While be- havioural patterns are one pathway through which the social situation influences health, little is known about how social environments function to shape behaviours or otherwise protect health [18,28].

Self-care components of lifestyles 139
Correlations between social status variables and use of alcohol and tobacco have been documented in many studies, but little attention has been focused on the elaboration of the associations in relation to other variables. Similarly, the effects of social support on components of health related behaviour are not understood. Gottlieb and Green [29] examined a scale of behavioural practices in relation to social variables known to affect health. Relationships among measures of social network, stress, health related behaviours and health status were explored in data collected in the 1979 U.S. National Survey of Personal Health Practices and Consequences. Social networks and life events were directly related to a scale of lifestyle practices for women, while for men the social network, but not life events were related to the lifestyle practices. Thus is appears that network variables and stress may exert differential influence on the behavioural practices of men and women.
All of these findings are consistent with a situa- tional perspective in which the social environment is related to behavioural practices in sex linked pro- cesses of influence. The fundamental role of gender in social learning and development means that social networks, social support and most probably socio- economic factors as well affect behaviour and thereby health differently among men and women. Social norms make it more appropriate for men to smoke and drink as well as encouraging more direct risk taking [ 111. Women, on the other hand, are socialized to non-competitive, low-risk behavioural patterns where illness and sick role behaviour are culturally accepted and encouraged in the network. One inves- tigation among patients in a general medical practice found that wives tend to provide care during their husbands illnesses, while men more often suggest that their wives consult a doctor when symptoms appear [30]. Social norms also influence stress behaviour. Men are considered more prone to respond to stress producing problems or situations by using more tobacco or alcohol, or by simply ignoring them, while women more often seek social support, take medicine or consult professionals [9, lo]. Smoking prevalence among women, especially young women, has been increasing, but it is unclear to what extent the change in smoking behaviour is accompanied by a general shift toward more health damaging routine and stress reduction behaviours among women.
Based on these considerations significantly differ- ent self-care behaviours would characterize the Iife- styles of men and women. We might expect to find more health enhancing self-care behaviours among women than among men. Furthermore, conscious health directed self-care might be related to healthier habits of daily living for women than for men. These gender linked patterns of behaviour would arise from different health related attitudes, knowledge and social situational influences among men and women. Gender specific influences, however, represent only one pathway through which social situational vari- ables operate. While the specific social variables and their chains of influence may be expected to differ between men and women the situational variables would exert their influence within the two sex groups as well.
THE STUDY
In a Danish self-care project, discrete health related practices have been studied as behavioural elements of lifestyles [6,9]. The focus of the analyses in these studies has been on interconnectedness both of behavioural practices and of the situational factors which influence them. The findings from our first two investigations found significant age and gender differences in self-care responses to illness. Of course, it is not age or sex per se that determine patterns of behaviour, but social and psychosocial factors that are characteristic of specific age and gender groups. Social network, social support, habits of coping with stress and employment status have been identified as situational variables affecting age and gender differences in behaviour [31].
In the most recent investigation a major focus of the analysis has been to study the inter-relationships among habits of daily living, deliberately under- taken health maintenance behaviour and behavioural responses to illness in a sample of persons already middle aged and older. In this paper independent gender effects on behaviour that may arise from social and cultural learning over the life course are examined along with direct and indirect effects of health beliefs, social network, social support and income variables in order to identify influences that may either intervene in or supplement relationships between gender and self-care variables. The following hypotheses regarding statistically independent effects of gender on the three types of self-care behaviours were tested:
1. Women consume less tobacco and alcohol than men.
2. Women more often than men consciously under- take self initiated practices for the purpose of health enhancement.
3. Women more often than men take concrete action in response to symptoms, especially with regard to the use of medication and physician consul- tation.
4. Self-care behaviours are more inter-related in female than in male groups.
It is widely believed that health related beliefs are important determinants of health practices. While the evidence on this subject is mixed [S] it may be that gender differences in health beliefs both partially explain gender differences in behaviour and mask influence of health beliefs in some multivariate ana- lyses of combined data when gender is examined only as a control variable. For example, it may be that women more readily than men consider themselves responsible for health problems or believe that medical care will cure their health problems [l 1). Nevertheless, if health beliefs influence behaviour then relationships between belief and behavioural variables should be found within the gender groups even when there are between group differences in beliefs. To examine these issues the following hy- potheses were tested:
5. Female gender will be related to significantly higher values on measures of internal health locus of control, faith in medical science, confidence in one’s
140 KATHRYN DEAN
own ability to make decisions regarding health and preventive health knowledge.
5a. Internal health locus of control will be posi- tively related to health protective behaviours within both the male and female groups.
5b. Beliefs in the capacity of medical science to cure disease will be negatively related to health protective behaviours within both the male and female groups.
SC. Confidence in one’s own ability to make deci- sions regarding health will be positively associated with personal health protective behaviours and nega- tively associated with seeking medical care for illness episodes within both the male and female groups.
5d. The health knowledge variable will be posi- tively related to personal health protective behaviours and to seeking medical care within both the male and female groups.
In the research literature on social network influences on health, a major unresolved issue is the extent to which it is network composition, participation or sup- port that accounts for statistical differences in health outcomes. In examining behaviour as a possible mechanism through which network variables affect health, it is important to determine which network variables exert influence. Our earlier work suggests that, at least in relation to morbidity, it is support from the network when needed rather than the composition of the network or the amount of social contact that is the more significant variable [18]. In this study we have tested the different network influ- ences to see if our earlier findings are replicated.
Based on the logic that women are socialized to greater health consciousness and less risk taking, social situational variables may be expected to have greater influence on male health protective behaviour which has been less affected by independent socializa- tion to health protection.
6. Social network/support variables will exert greater influence on male than on female self-care behaviours.
6a. Support from the social network will be in- versely related to male use of tobacco and alcohol, and unrelated to female use of the two substances while network composition will be unrelated to habits of tobacco and alcohol consumption.
6b. Support from the social network will be positively related to deliberately undertaken health protective behaviours while network composition will be unrelated to conscious health protective behaviours.
6c. Network support, but not network composi- tion, will be inversely related to use of medicines and seeking professional help for illness episodes.
Based on findings from our earlier investigations, income rather than social class was included in the analyses of social situational influences on behaviour. In our earlier findings bivariate correlations between social class and self-care responses to illness were marginal relationships arising from the age and sex distribution of the social class variable [31]. This
*A drink equals 1 beer, one seventh of a litre of wine or one twenty-fourth of a litre of spirits.
suggests that the amount of education and type of occupation, while they undoubtedly affect many things, do not affect health related behaviour inde- pendent of the influences arising from gender and from age cohort effects. Preliminary analyses in this data substantiated the earlier findings that educa- tional level and type of occupation exerted little independent influence on the various self-care vari- ables. Based on the extensive research literature documenting socioeconomic effects on health, in- come was included in the multivariate analyses of social situational influences, testing for the following behavioural effects:
7a. Family income will be inversely related to tobacco and alcohol consumption.
7b. Family income will be positively related to conscious health protective behaviours.
7c. Family income will be unrelated to medical contacts.
STUDY VARIABLES
Self-care behatliour
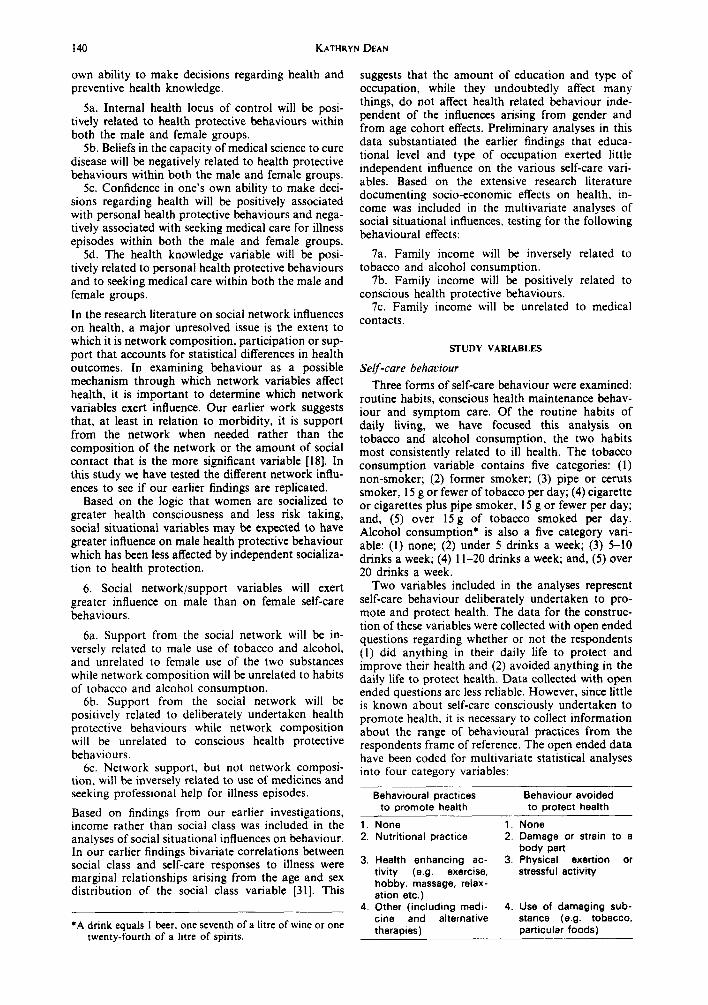
Three forms of self-care behaviour were examined: routine habits, conscious health maintenance behav- iour and symptom care. Of the routine habits of daily living, we have focused this analysis on tobacco and alcohol consumption, the two habits most consistently related to ill health. The tobacco consumption variable contains five categories: (1) non-smoker; (2) former smoker; (3) pipe or ceruts smoker, 15 g or fewer of tobacco per day; (4) cigarette or cigarettes plus pipe smoker, 15 g or fewer per day; and, (5) over 15 g of tobacco smoked per day. Alcohol consumption* is also a five category vari- able: (1) none; (2) under 5 drinks a week; (3) 5-10 drinks a week; (4) 1 l-20 drinks a week; and, (5) over 20 drinks a week.
Two variables included in the analyses represent self-care behaviour deliberately undertaken to pro- mote and protect health. The data for the construc- tion of these variables were collected with open ended questions regarding whether or not the respondents (1) did anything in their daily life to protect and improve their health and (2) avoided anything in the daily life to protect health. Data collected with open ended questions are less reliable. However, since little is known about self-care consciously undertaken to promote health, it is necessary to collect information about the range of behavioural practices from the respondents frame of reference. The open ended data have been coded for multivariate statistical analyses into four category variables:
Behavioural practices Behaviour avoided to promote health to protect health
1. None 1. None 2. Nutritional practice 2. Damage or strain to a
body part 3. Health enhancing ac- 3. Physical exertion or
tivity (e.g. exercise, stressful activity hobby, massage, relax- ation etc.)
4. Other (including medi- 4. Use of damaging sub- tine and alternative stance (e.g. tobacco, therapies) particular foods)

Self-care components of lifestyles 141
Data were also collected on routine physical activ- ity and use of preventive professional services: dental examination, blood pressure measurement, and breast examinations. Self-care responses to illness include: (1) nutritional treatment; (2) ‘home remedy’ (non-dietary); (3) medication; (4) bedrest; and, (5) decision to seek professional advice. The morbidity data were collected with a symptom list used in a procedure which combined symptoms experienced simultaneously into illness pisodes. For each illness episode a self-care response sheet was completed to collect information on whether or not one or more of the six types of behavioural responses occurred and the nature of the particular practice (i.e. which food or medicine was used or which type of professional was contacted).
Health related attitudes and knowledge
Three measures of attitudes toward health and medical care were examined in this study: faith in medical care; internal health locus of control; and, confidence in one’s own ability to make decisions regarding health.
The concept of locus of control is derived from social learning theory [32]. According to the theory, behaviour is a function of expectances developed from experience over time of positive or negative results of personal actions. Expectancy measures specific to health were developed into the Health Locus of Control Scale. In validation work, the scale was found to be multidimensional leading to the development of internal, powerful other and chance locus of control scales to tap the different dimensions [33]. Available evidence suggests that the internal locus of control scale may tap a more predictive dimension of health beliefs than other commonly used measures [5]. The powerful other locus of con- trol scale mixes concepts of professional care and personal network influence on health. Therefore, measures of faith in medical care and confidence in one’s own ability to make decisions regarding health were developed to study the influence of these con- cepts on self-care.
The health knowledge variable is a four category ordinal measure based on questions regarding pre- ventive action in relation to cancer, heart attack and high blood pressure.
Social situational variables
Measures of social network, social support and family income have been used to study the influence of social situational variables on the three compo- nents of self-care behaviour. The content of the social network and availability of its members were mea- sured with three variables: (1) Household composi- tion had the categories: living alone; living with a mate; and living with a mate and children or others. (2) The friendship network was measured as the number of friends the respondent could visit un- announced, which for analytic purposes was divided into two categories of 0-4 or limited network and a moderate to large network of 5 or more. (3) Distance to members of the extended family was measured in travel time as: under one half hour, one half to two hours, and, over two hours. A network contact variable included in our earlier work was unimpor-
tant for both health and behavioural variables. Pre- liminary analyses of the data in this investigation also suggested that it is not the amount of contact that is important with regard to behaviour.
A scale of psychosocial support was constructed from six items measuring available support from spouse, family friends and work colleagues, when needed. An instrumental support variable of low, medium and high scale values was developed from questions regarding practical help and care during illness or disability.
Stressful problems (‘objective’ stress) were scaled into a low, medium and high measure from a series of questions regarding death or illness of a close family member or friend, economic problems, loss of job, or change in household composition during the prior year to study possible invervening influences of stressful problems in social network relationships with other variables.
STATISTICAL METHODS
The first task in the analysis of the data involved the validation of the index scales. In social survey investigations the primary goal of scale validation should be to determine whether or not the proposed data reduction is admissible. That is, to determine if the raw scores (index values) constitute a sufficient statistic (341. The scales used in this investigation were validated in the framework of item response theory [35]. The procedures involved evaluating the suffi- ciency of the scales as measures of the underlying latent traits. Thereafter statistical control of the scales detected instances where item bias would lead to dis- tortions in the results of the multivariate analysis.
The goal of the multivariate analysis was to study the direct and indirect relationships among the behavioural, social and psychosocial variables. Statis- tical methods which could elaborate inter-relation- ships among many complex categorical variables and test for levels of influence among the variables were needed to achieve this goal. Many widely used statistical procedures have severe limitations for our purposes. The large number of quantitative and discrete variables in the analytic problem indicated that multivariate techniques for analysing contin- gency tables would be appropriate statistical methods for the analysis of the data. The statistical procedures used are based on mathematical graph models for the analysis of multiway contingency tables [36,37]. Of the available methods for analysing survey data, the graphical models are most appropriate both for addressing the research questions posed in the investi- gation, and for the nature of the data to be analysed. Since the variables were generally neither continuous nor normally distributed, but mostly categorical or ordinal and skewed in their distribution, the graphi- cal models could determine the structure of the data without building on assumptions which are generally violated with health and social survey data.
Variables were included in the investigation because of their known or theoretically hypothesized influence on health related behaviour. Our purpose was not only to determine if these variables are related to self-care behaviour, but to assess how they influence the behaviours. That is, we were interested

142 KATHRYN DEAN
in the joint and indirect influence of variables which may be hidden in other regression models due to problems of multicollinearity and inability to illumi- nate chains of influence. An u priori decision was made that important differences in the influence of the knowledge, attitudinal and situational variables on the male and female behaviour could not be detected in the multivariate analyses of the data set with sex examined only as a control variable. There- fore all analyses were conducted separately for males and females.
The actual statistical procedure involved a strategy of step-wise analyses of the multidimensional contin- gency table [38], building on the over-riding demand that all marginal analyses move toward one unified model for the complete multidimensional research problem. The interactions between all marginal rela- tionships were examined to identify the sub-graphs or cliques to which all variables belong in an analysis of the structure of the data which resulted in a base model. The subsequent steps of the analysis involved testing the theoretically based hypotheses, recogniz- ing that valid conclusions drawn from the hypothesis testing must be consistent with the structure of the base model.
The sample
A sample of 465 persons over 45 years of age was obtained in this study, for a 7 1% response rate of 655 persons contacted in their homes.* All persons living in institutions and persons who were confused or otherwise unable to give information for themselves were excluded from the sample. Table 1 shows the age, sex and marital status, distributions of the population over 45 yr of age of the municipality studied and of the sample obtained.
It can be seen that the sample is representative of the study population on these sociodemographic characteristics. The sample members are slightly younger and more often married, but these deviations are small.
THE FINDINGS
Tables 2-7 present major findings of the analyses discussed in this paper. Tables 24 show the relative proportions of men and women reporting the different types of self care behaviour. Table 5 summa- rizes the gender differences in the behavioural belief and situational variables. Tables 6 and 7 present an overview of the results of the multivariate analyses. The gender specific correlation matrices identify
*An interviewing procedure was established to balance the need to assure the representiveness of the sample with funding constraints. An oversample was drawn based on a prior decision to conduct the interviews in the evenings and on weekends but not to return to residences where no one was at home. The non-respondents then are people who refused to participate in the study. This procedure is not technically correct since people who work irregular hours or are more frequently away from home may be under-represented in the sample. However, the sex, age and marital status distributions of the sample obtained in comparison to the study population suggest that this was not a problem.
Table I. Characteristics of the sample compared to those of the study population
sex Male Female
Age (Y) 45-54 55-64 65-74 75-84 85-94
Mariral smtw Single Married Separated/Divorced Widowed
Community Sample population
(N=465) (N = 10.138)
N oi. N %
212 (0.46) 4602 (0.45) 253 (0.54) 5536 (0.55)
154 (0.33) 3058 (0.30) 126 (0.27) 2934 (0.29) I21 (0.26) 2447 (0.24) 48 (0.10) 1356 (0.13) I6 (0.03) 343 (0.03)
32 (0.07) 766 (0.08) 326 (0.70) 667 1 (0.66)
28 (0.06) 732 (0.07) 79 (0.17) 1969 (0.19)
the statistically significant independent. indirect and marginal relationships among the behavioural, atti- tudinal and health knowledge variables. Indepen- dent relationships are direct statistical connections between variables which cannot be accounted for by any other variable in the contingency table. Indirect relationships are meaningful associations between variables which are conditional on one or more other variables. Statistical correlations between variables which are neither independent nor meaningful indi- rect relationships are accidental marginal relation- ships or ‘spurious’ connections between variables. All cases where two variables are directly dependent and the level of the statistical significance of the relationship are boxed. The indirect relationships are boxed with broken lines. The two summary tables (Tables 6 and 7) contain overviews of the results of the analysis of the structure of the data and the specific hypothesis testing. The direct and indirect relationships shown will be discussed below in the context of specific subject areas.
Routine tobacco and alcohol consumption
Table 2 shows that, as hypothesized, men and women over 45 yr of age in Denmark consume significantly different amounts of both tobacco and
Table 2. Tobacco and alcohol consumption among women and men over 45 yr of age in a Danish County
Tobacco
Non-smoker
Former smoker Pipe and/or cerut
(I 5 g of fewer g/day) Cigarettes or cigar and/or pipe
(I5 g or fewer/day) Cigarette or cigar and/or pipe
(over I5 g/day)
Women Men
% N % N
32 (74) I2 (24) 23 (53) 30 (62) 13 (29) 12 (25)
27 (62) 27 (55)
6 (13) I9 (40)
Alcoholic drinks’ per week
Non-drinker 44 (109) 20 (41) 1-l 29 (71) 20 (42) 5-10 20 (48) 26 (53)
II-20 7 (16) 20 (42) Over 20 I (.7) 14 (28)
*A drink equals one beer, one seventh of a litrc of wine or one twenty-fourth of a litrc of spirits.

Self-care components of lifestyles 143
Table 3. Health promotive and avoidance behaviours reported by men and women over 45 yr of age in a Danish county
Women MC”
% N % N
Behaeiour practiced IO promote health
NO”C 51 (129) 57 (119)
Nutritional practice 12 (31) 8 (16) Health enhancing actwines 32 (83) 28 (56)
(e.g. exercise, massage, relaxation practice etc.)
Other 4 (9) 7 (15)
Behooiour avoided 10 protect health
None 75 (186) 75 (155)
Damage or strain to a body part 7 (17) 2 (5) Physical exertion or stressful activity 12 (29) 9 (19) Use of damaging substance 7 (16) 14 (29)
(e.g. tobacco or particular food)
alcohol. Only 12% of the men compared to 32% of the women in this sample of persons over 45 yr of age have never smoked. The method of tobacco con- sumption and moderate use does not differ for the two sexes. However, heavy use (over 15 g of tobacco consumed each day) is found considerably more often among men than among women. At the same time, more men than women have stopped smoking.
Gender differences in alcohol consumption, also shown in Table 2, are far greater than differences in smoking behaviour. Indeed, the gender dependent use of alcohol is one of the largest statistically independent relationships found in the study (gamma = 0.53, P = 0.000). Forty-four percent of the women compared to 20% of men do not drink alcoholic beverages. Similarly, proportionately more women than men use only small amounts of alcohol on a regular basis. The proportional increase of male over female consumption from moderate to heavy use of alcohol is especially striking.
Sex differences in routine consumption of tobacco and alcohol are not limited to the amount of each of the substances used, but also apply to their joint consumption. There is a highly significant moderate relationship between the use of tobacco and alcohol by men (gamma = 0.24, P = 0.000). At the same time there is no relationship of any kind, neither partial nor marginal, between the use of the two substances by women.
The next question then becomes: do these clearly different patterns of routine use of potentially harmful substances parallel different patterns of consciously directed health maintenance and illness care for the two sexes?
Health maintenance behaviour .
A primary concern in relation to this component of self-care was to examine the responses to the
Table 4. Behavioural responses to illness episodes in a Danish population over 45 yr of age
Males Females (%) (%)
Illness episodes, N = 2297 0.40 0.60 No action 0.69 0.65 Dietary 0.03 0.05 Medicine 0.20 0.23 Bedrest 0.03 0.05 Professional contact 0.15 0.17 Home remedies 0.06 0.07
Table 5. Gamma correlations for gender differences in behavioural. health belief and social situational variables in a Danish community
sample of persons over 45 yr of age
Gamma
Use of tobacco 0.32 (M) Alcohol consumption 0.53 (M) Health promoting behaviour NSD Avoidance behaviour 11.0. (M) Routine physical exercise NSD Dental examination NSD Blood pressure examination NSD Home remedy treatments NSD Illness bed days NSD Use of medicine NSD Professional consultations NSD Health knowledge NSD Locus of health control NSD Confidence medical science NSD Confidence own judgement NSD Stressful problems NSD Phychosocial support 0.25 (M) Instrument support 0.30 (M) Household composition 0.25 (M) Available extended family NSD Income 0.18 (M)
l = chi square value. NSD = no significant difference. M = males have higher vahxs.
P
0.000 0.000
0.01
O.OW 0.000 0.001
0.002
open ended questions regarding behaviour deliber- ately undertaken for the purpose of protecting or promoting health. Therefore, the analysis was focused on the health enhancing and avoidance behaviour variables. However, to study different types and patterns of health protective behaviour, the interactions among these two variables, routine physical activity and use of preventive professional services were examined. Table 3 shows the propor- tions of men and women reporting behaviours con- sciously undertaken on a regular basis to promote health and behaviours avoided for the purpose of protecting health. Over half of the sample members did not report any deliberately undertaken health pro- tective behaviour. Proportionately more men than women reported no routine action to promote health. Women more often than men reported either some form of nutritional practice or special health enhanc- ing activity undertaken regularly for the express purpose of protecting health. Persons reporting such behaviour frequently named more than one practice. While in the hypothesized direction, the sex differences were small with only a slight tendency in the direction of more active health promotion among women.
Dietary practices to promote health were most often some type of fibre, protein or vitamin intake. Health directed activities frequently mentioned by both men and women were some form of exercise, often long walks or gardening. Sufficient or regular sleep, relaxing hobbies, relaxation techniques and massage were all reported more frequently by women than men. Consciously undertaken stress mainte- nance behaviours such as relaxation techniques or concerted efforts to reduce stress in daily life were only reported by women. Similarly, women more often reported the regular practice of an enjoyable hobby as health maintenance behaviour. On the other hand, slightly more men than women reported using some medication (usually a ‘natural’ medicine) or alcohol as a form of health protection.

I 2
Tabk 6. Independent and indirect
gamma nlationships between behaviouml, psychosocial and social variables for mm
over 45yr of age in a Danish community
3
4
5
6
7
8
9
IO
II
I2
I3
14
I5
I6
17
IS
19
20
21
22
23
24
25
I us
e or
toba
cco
. [
-0.0
6 10
.24’
1 -010
015
2
Alc
oh
ol
co
nsu
mp
tion
.
0.14 rm--p
"II_,
L
0.10
0.15
3 Health promoting
behaviour
.
1
001
~~0.12
4 Avoidypcbchaviour
.
-0.14
-0.02
5. Routine physical
cxcrcisc
.
0.20'
6. Dental examination
.
1. Breast examination
8. Blood prasure
examination
9.Dieury
IO. Home mmcdy/
~ylllplOllll
II. Bedrcst/symptoms
12. Uaiiition/symploms
13. Prokssional contact/
symptoms
14. Hcallh knowkdge
IS. Locus/health comrol
16. Conlidcncz/own
Jdgcmcnl
17 Con6dena/medical
care
IS. Stressful
problems
19. Psychoscal support
20 Instrumental
support
21 Frkndnhip network
22. Household composition
23. Availabk external
family
24. Income
25. Age
LG
Mcpmdent
statisticalnlationsbip.
L ___Ilndirm
stat
isti
cal re
latio
nshi
p.
"P do.001; ‘P
szo.
ol;c
P<o.
oS.
~
0.02
~0.06
0.01
0.05
-0.05
-0.04
0.09
-009
0.04
0.10
-0.03
-0.08
0 IO
009
(-o.zocI
008
0.03 10.17"1
E
0.09
021
m
-0.06
-0.02
0.05 m
-0.06
0 04
-0.l4C -0.13
-004
0.05
015
-0.07
013
Lo.;2_, -014'
r--a
~
~-
0.02
0.01
0.15
0.02
-0.11 '--a
&I.20
,[
-0.11
-002
-0.10
0.05
-0.02
005
[-j.34<
0.14
0.00
0.05
-0.11
0.M
-0.23
0.08
-0.06 i
-0.13
0.02 [
~0.11
-0.19 [-0.31c1 -0.06
0.02
0.13
0.00
0.02
0.14
-0.02
r--i
-0.02
-0.24c
0.18' -0.19
-0.14' -0.l4C
019'
-0.15=
0.09
0.00 ;j.?2q
0.17' ; j.lS:
0.19
0.08
-0 I3 rz+o.;2:,
r--i
~
(
0.13
-0.06
0.12
-0.20" -0.08
0.20'
0.00 m;-;;O;;1
-0.13'
0.04
0.10
027
L@O*,
0.30' 10.5;;;1:-;$
.
_
_
_
_
_
_
_
.
[j.gj
-0.07 r-Gq/-Gq
0.27' -0.06
0.12
0.03
0.07
0.10
0.16
-0.01 m
-0.10
-0.10
-0.06
0.15
.
m
0.71 ~0.78*11[-0.11
0.10
0.03
0.07
0.33' -0.08
-015
-0.04 ;-jj9f
0.32
-0.10
-005
.
~0.30 IXlrxq
-0.01
0.14 m
-0.20
-0.05
0.02
0.18
_0.28c. 3.29, -0.03
0.00
-0.07
r--
3
i
.
~]~I~[
-0.07
-0.24
0.12
-0.13
0.03
0.03
-0.27
-0.11
0.27
-007
0.13
.
rGqo.w"1:-;i4<
-0.06
0.03
0.06
0.w
-0.01 fzq-G3<~
0.10
-0 II'
0.15'
p
.
m
-0.06
0.00
-0.04
0.04 =[1-0.27*11[
-0.12
0.07
-0.06
0.15'
2
.
I-o.19c] -0.02 m
0.04
-0.04 1
0.36'
0.03
0.16 m;i.;Sz
.
-0.11 1-0.15
0.03
0.06
-0.10
-0.18
0.17
-0.13
-0.01
-0.06
$
g
.
mri.il<
0.16'
0.07
-0.15
-0 IO 1_0.32*11[
.
-0.08
002
0.01
0.15
001
0.06
-0.14
.
~~(03481(0.31*(
0 IO
-0.13c -0.03
.
-0.13 m
0.12 ~o.zaAl:-Zl~
r--i
.
027
0.13 m,mO.422,
.
[o.zo[0.3SAll_0.44AJ
.. -1
.
: 0 !.!_I -0 13
.1043"1 .

so’o- IO
‘O-
$1'0
II'O-
OI'O-
91'0
SI'O-
90'0-
91'0- 36Z'O-
ZWO-
SZ'O
$l'O-
zo'o- ,IZ'O-
So'0
IWO- 1.9E.O
Liz0 zo’o-
1.8z.o-_ l
J~OW
W
==FF~V
‘t
zo’o- zo‘o
co’o- 80’0-
$2.0 10'0
11'0
41'0
EO'O-
wo-
g.l.O-
Eo.0
$l.O-
91'0
10'0
01‘0
'"%wq
OU!l.nuoJd lll,=w 'C
coo- m
$1’0 E
O‘O
m
60‘0 zo’o-
LO’0 $l’O-
mo
11'0 m
wo-
90'0-
zo'o-
90'0-
wo-
co‘0
IJIZ.OaEt.0
zo'o
11'0 m
.
uo!lduansim ,oquqa(y 'Z
Y
I.oz.o_,,,.o
EO'O
,9,.o
Z,'o
Z@o
,9,'o
@'i;
$0'0
WO
,,'o
60'0
EO'O-
(0‘0
LO‘O- ~
0’0 91'0- $1'0
,IZ'O
SO'O-
W'O
OI'O-
80'0-
90'0
l
=-'qolJo WI
'I
fj
ST
PZ
cz
ZZ
IZ
OZ
61
81
LI 91
21
PI
Cl
ZI
II
01
6
8
L 9
S
v
C
Z
I
~l!,,W”JoJ
l,S!“Fza
B
U!
3%
JO
ll $p
13&O
“D
UlO
M
‘OJ
SS(C,E
!IS~ ,8f308
,B”B
,S!3O
%X
, d&
d ‘,““opB
yaq “aaw
q sdqruo!lapJ
swud
1m!p”!
pue luopwxbpul 'L o,q=x

146 KATHRYN DEAN
Examining the correlations between deliberate health behaviour (No. 3) routine physical exercise (No. 5) and use of preventive professional services (Nos 6 and 8) in Table 6, it is seen that, one statistically significant relationship is found. The moderately strong independent relationship between having seen a dentist and having had blood pressure checked, is the only relationship among these different health protective behaviours for men.
For women, however, a series of strong highly significant independent relationships are seen between: routine physical exercise and dental exami- nations (gamma = 0.41, P = 0.000); dental and blood pressure examinations (gamma = 0.42, P = 0.000); and breast and blood pressure examinations (gamma = 0.79, P = 0.000). The indirect significant relationship between dental and breast examinations (gamma = 0.35, P = 0.002) also holds in this context. Furthermore, while the small positive correlations between deliberate health promoting behaviours (No. 3) and routine physical exercise (No. 5), dental examination (No. 6) and blood pressure examination (No. 8) are not statistically significant, there is a consistent tendency for women who report deliber- ately undertaken behaviours to promote health to more often be physically active and to more often have seen a dentist and had blood pressure measured during the year prior to the interview. Furthermore, the chi square value between health promoting behaviours and routine physical exercise is a highly significant (see below) indirect relationship operating through the health knowledge and confidence in medical science variables.
Thus, a profile of healthy behaviour emerges among women. Those women who in their daily life consciously act to protect their health more often reported routine physical activities such as bicycling and swimming. While this relationship partially reflects the fact that health promoting behaviours reported by the sample members were sometimes forms of physical exercise, other health enhancing activities and nutritional practices also varied posi- tively with routine physical exercise. Sixty-six percent of women without regular physical exercise reported no behaviours undertaken to promote health, while only 35% of women falling in the high range of physical exercise did not report deliberately under- taken health protective behaviour. At the other extreme, 16 of the 17 women in the highest category of physical exercise did not report any behavioural practices undertaken specifically for the purpose of protecting health. (Women who are extremely physi- cally active apparently do not consider their routine physical exercise as health promotion thus explaining a chi square value of 3 1.2, df = 12, P = 0.002 between the health promoting behaviours and routine physical exercise variables even though the gamma was a NS 0.09.) At the same time the more physically active women more often visited the dentist, and dental, breast and blood pressure examinations were all positively inter-related.
Looking again at Table 3, fully three-quarters of the sample members did not report any health related acoidance behaviour. Equally high proportions of men and women failed to report any type of avoidance behaviour. Of those who did name some particular
behaviour avoided for health reasons, more men than women avoided a particular substance such as tobacco of fatty foods. Women more often said they avoid physical strain or stress. As seen in Tables 6 and 7, reporting avoidance behaviours was not inde- pendently related to routine physical activity or obtaining professional health checks for men, while avoidance behaviour and routine physical activity were negatively related for women. At the same time, the avoidance behaviour of women was positively related to blood pressure examinations.
The two measures of health protective behaviour, health promoting practices and avoidance behaviours were positively related for both sexes. That is, persons who more often did something in their daily life to protect health tended to practice health related avoid- ance behaviours (the chi square values for health protective and avoidance behaviours were 22.2, df = 9, P = 0.008 for women; and 29, df = 9, P = 0.001 for men when examined as yes, no responses gamma = 0.57, P = 0.000 for men and gamma = 0.53, P = 0.000 for women).
It appears that people actively concerned about their health engage in multiple health protective practices. Generally, however, the responses to these open ended questions suggest that, at least for the older segment of the population, active health pro- motion and protection have not become a conscious part of daily life for the majority of people. Those people that did report health promotion and/or avoidance behaviours have clearly been influenced by the bias toward cardiovascular risk factors in health information. Important health protective behaviours such as home and work safety. use of seat belts and other forms of driving or pedestrian traffic safety were generally not mentioned. Thus protective behaviours that may contribute the greatest numbers of well life years to the health of individuals and populations are apparently not recognized as health promotion.
An overview of the findings on this component of self-care behaviour suggests that active health protec- tive behaviours appear to be slightly more prevalent among women than men. However, the differences are not large. The more important findings are the inter-relationships among types of health protective behaviour among women in contrast to men. Deliber- ately undertaken health promoting practices are more frequently undertaken by women who exercise routinely and both of these forms of health enhance- ment are more frequent among women who obtain professional health maintenance services. The ten- dency for those women who obtain one professional service to also obtain others is especially strong.
Responses to symptoms of illness
The respondents reported having experienced 2297 illness episodes during the 6-month retrospec- tive study period. Sixty percent of the illnesses were reported by women who constituted 0.54% of the study sample. Table 5 shows that the self-care responses to illness generally did not differ for men and women. The hypothesis regarding gender differences in self-care responses to illness thus was not supported. Sixty-nine per cent of the male conditions compared to sixty-five per cent of the
Self-care components of lifestyles 147
conditions reported by women were not treated. The unusually high proportion* of symptom episodes which were not treated undoubtedly represent the large number of symptoms of chronic conditions present in this population group.
There was a very slight tendency for men to less often report sick role behaviour. The illness responses of women slightly more often involved staying in bed, taking medications and seeking professional help. However, the differences are too small to be con- sidered meaningful.
It can be seen in Tables 6 and 7 that the self- care responses to illness were strongly and similarly inter-related for both sexes. Symptom episodes that resulted in bedrest were very often medicated and the subject of professional consultations and frequently treated with some form of dietary response. At the same time home remedy responses were inversely related to the other types of self-care responses to illness for both men and women.
A wide range of home remedy treatments were reported including: herbal medicines; special clothing such as a corset, warm vest or neck scarf; use of a mechanical aid such as a heating pad or electrical massage machine; some form of exercise either gen- eral or of a particular body part; stress avoidance or reduction involving maintaining a balanced lifestyle or avoiding particular stressful situations, reducing smoking, providing a treatment such as gargling or rinsing a body part with a particular solution, etc.
Inter-relationships among types of self-care behaviours
The hypothesis that self-care behaviours are more inter-related among women than men was supported. As discussed above consciously undertaken behav- iour to promote health, routine physical exercise and professional examinations were inter-related for women in contrast to men. However, examining the relationships among the three types of self- care behaviour (routine use of potentially harmful substances, consciously undertaken health mainte- nance behaviour and behavioural responses to ill- ness), it is seen in Tables 6 and 7 that tobacco consumption generally is not related to other types of behaviour.
No statistically independent relationship between deliberately undertaken health promoting behaviour and use of tobacco was found for either men or women. Indeed, with the exception of a negative relationship among men between use of tobacco and health related avoidance behaviours (and the positive relationship between tobacco and alcohol consump- tion for men), smoking was not related to the other types of behaviour either in the male or female groups in this investigation.
Alcohol consumption was not related to the health promoting behaviours routine exercise or profes- sional health maintenance services among men. However, among women, alcohol consumption was related both to consciously undertaken health protec- tive behaviour, and also to preventive examinations.
*In a prior study of self-care responses to illness in the entire adult population, nothing was done about 37% of the reported conditions.
Somewhat surprisingly on first impression, the alco- hol consumption of women varied positively with health related behaviours. Regular behaviours under- taken to protect health were more often reported by women who drink alcohol. Moreover, proportion- ately more women who drink moderate amounts weekly had been to the dentist, had their blood pressure measured and been examined for breast cancer during the prior year. Likewise non-drinkers more frequently reported that they are either over or underweight. What emerges is a pattern in which women who totally abstain from alcohol less often undertake behaviours that are generally considered important for the protection of health. These findings in conjunction with the relatively moderate use of alcohol among women generally suggest that alcohol used as a discrete behaviour removed from the con- text of type and patterns of use is a poor indicator of health damaging behaviour [39].
The behavioural responses to illness were more often associated with health maintenance services among men than women. In addition to a moderate negative relationship between alcohol consump- tion and home remedies, avoidance behaviour was positively associated with taking action in response to symptoms and with taking medicine when ill. Additionally, blood pressure checks were positively related to active responses to illness, use of medicine and seeking professional help. The nature of these relationships suggests that for men the avoidance behaviour variable may represent responses to already existing disease, and thus secondary preven- tion and compliance with physician directives rather than general health promotion.
Among women the only independent relationships between health maintenance and illness behaviours were the negative associations between routine phys- ical excercise and both use of medicine and profes- sional consultation. The avoidance behaviours were not related to the illness behaviours, although they were related to less physical activity and having blood pressure checks. Thus for women the findings are more difficult to interpret with regard to the possi- bility that the avoidance behaviours may represent existing disease.
Influence of health related attitudes and knowledge on self -care behaviours
Contrary to expectations, the hypothesized gender differences were not found in the health belief vari- ables. The distributions of male and female values were similar for all three measures of health related beliefs. Likewise, contrary to expectations, there were no significant gender differences in knowledge regard- ing prevention of disease. The relationships between the attitudinal and self-care variables as seen in Tables 6 and 7 reveal that, also contrary to expecta- tions, health related attitudes as measured in this investigation generally exerted little influence on the various forms of self-care behaviour. The internal locus of health control variable was positively related to avoidance behaviours among men, but was not independently related to any of the female self-care behaviours.
Surprisingly, the confidence in the medical science variable was inversely related to having seen a dentist

148 KATHRYN DEAN
for both men and women with the relationship stronger and directly independent among women. Strong faith in medical cure also was inversely related to female physical exercise dependent on income. The influence of the attitudinal variable was seen among women with higher incomes, but was not related to the generally less prevalent routine physical exercise of lower income women. The measure of confidence in self-judgement regarding health, while generally unrelated to the different forms of self-care behav- iour, was negatively related to having seen a dentist and home remedy treatment for symptoms among both men and women. Additional findings regarding the confidence variable are seen in the relationships between this variable and social support variables. The self-confidence measure was positively related to psychosocial support for both sexes and to instru- mental support among women. This variable appears to represent some proxy measure of interpersonal relationships rather than being a simple health attitu- dinal variable.
Knowledge regarding behaviour that may help to prevent cancer and heart disease exerted more influence on the behaviours than did the measures of health beliefs. Additionally, while the expected gender differences in knowledge were not found, this variable did exert contrary to expectations, differ- ential influence on the self-care behaviours of men and women. The knowledge variable was positively related to health promoting behaviours among men, but not women; and to both routine exercise and dental checks among women, but not men.
Alcohol consumption was positively related to the knowledge variable for both sexes. At the same time, alcohol was generally absent from the open ended responses to the questions on the prevention of high blood pressure, heart disease and cancer. When sub- stances were named in response to these questions, avoidance of tobacco, fatty foods, salt and food additives were the most frequent replies. Alcohol was very seldom mentioned. It is also instructive to note that contrary to expectations the use of tobacco and blood pressure checks were unrelated to knowledge regarding disease prevention for both men and women.
With regard to illness related care, gender specific influence of health knowledge also was seen. The knowledge variable was positively related to home remedly treatments among women and unrelated to bedrest, professional consultation and use of medicine. Among men, the knowledge variable was negatively related to bedrest, professional consul- tation and indirectly through professional consulta- tion to use of medicines, but unrelated to home remedies.
Finally, it is relevant to examine the inter-relation- ships among the knowledge and attitude variables. While there were no significant gender differences in the distribution of the knowledge and attitude variables, unanticipated findings emerge in the inde- pendent inverse relationship between the health knowledge variable and both health locus of control and faith in medical science among men. Neither of the relationships applied to the women. However, for both sexes health locus of control was inversely related to faith in medical science, and confidence
in self judgement was positively related to faith in medical science.
Injuence of social situational variables on self-care behaciours
A number of gender differences in situational variables were found that may indirectly influence self-care behaviours to supplement the direct influ- ences discussed below. Men had significantly higher values on the measures of psychosocial and instru- mental support from the environment as well as on the measure of the number of friends that could be visited unannounced, while women more often lived alone. Thus women reported both smaller and less supportive networks. Travel time to members of the extended family did not differ significantly for men and women.
Examining the independent influence of the social network variables (Tables 6 and 7) it is seen that contrary to expectations the only significant relation- ship between a network variable and smoking was the inverse relationship between male smoking behaviour and household composition. Men who live alone smoke more than those who live in family situations. The indirect relationship between smoking and stress- ful problems among women is conditional on social support, suggesting that for women stress in the absence of supportive networks may increase smok- ing. The other correlations between smoking and situational variables were marginal associations due to the inverse relationship between smoking and age. For both men and women younger age was indepen- dently associated with smoking. Also contrary to expectations, the only social network variable inde- pendently related to alcohol consumption was the influence of larger friendship networks on female drinking behaviour.
Behavioural practices undertaken deliberately to maintain health were inversely related to the size of the friendship network for men. The effect of the network variable is conditional on health knowledge. The positive effect of a large network was more important among men with lower values on the health knowledge variable. The correlation between health promoting behaviours and the size of the network for women was a spurious relationship due to correlations among other variables related to both health behaviours and the friendship network. The only situational influence on female health mainte- nance behaviour was the small independent inverse relationship between life problems and health pro- moting practices. On the other hand, stressful prob- lems affected the health related avoidance behaviour of men while being unrelated to the avoidance behaviour of women.
Routine physical activity was surprisingly unre- lated to the social network and support variables. Two conditional relationships were found. Living in family situations rather than alone was associated with routine physical activity among younger women. Another partial relationship found was that instru- mental support (help and care from the network during illness) was related to physical activity among low income men. Younger age and living in family settings were also associated with having a dental examination. Blood pressure checks were negatively

Self-care components of lifestyles 149
related to the size of the friendship network fat men.
The predominant influence of social support vat-i- ables on behavioural responses to illness, was that of network support on decisions to seek professional help. Support from the network was, as hypothesized, inversely related to seeking professional help in both the male and female groups. For men the size of the friendship network and instrumental support were also directly significant factors in seeking professional help. Besides social support only small negative relationships between household size and stressful problems exerted independent influence on female help seeking.
Living alone and less instrumental support from the network exerted independent influence on male use of medicine. Smaller friendship networks were indirectly associated with more medicine taken due to more frequent seeking of medical care resulting in greater use of medicines by men with smaller friend- ship networks. Social network variables generally as expected exerted less influence on the illness care of women than of men.
Family income, contrary to expectations, was un- related to use of tobacco and positively related to alcohol consumption. For men the relationship between income and alcohol consumption was con- ditional on the proximity of extended families (men living further from extended family members con- sume more regardless of income). Income was not, as expected, related to conscious health protective behaviour. It was, however, strongly related to visit- ing the dentist. Indeed, income was the most impor- tant independent statistical influence on obtaining dental care for both sexes. Routine physical exercise was also more prevalent among higher income people regardless of sex. Younger persons were more physi- cally active, but for men the age relationship held only among those with lower incomes. Among men regular physical activity was also affected by stressful problems among lower income persons. As expected, income was unrelated to illness related self-care in both the male and female groups.
Overview of injkence on self-care behaviours
The findings from this investigation partially sup- port the hypothesized influences of gender and social situational influences on components of self-care behaviour. As anticipated, gender exerted the most consistent influence on behaviour. Men more often consumed large amounts of alcohol and tobacco than women, and the joint use of the substances was positively related for men but not for women. Thus there were both quantitative and qualitative sex differences in the use of these two potentially damaging substances. With regard to the conscious health protective behaviours and illness responses, the influence of gender was found in sex differences in patterns of behaviour rather than in the magni- tude of the difference of specific male and female behaviours.
Contrary to expectations no evidence was found that more women than men practice deliberately undertaken behaviours to promote health or signifi- cantly more often treat symptoms of illness and seek professional care. Nor was evidence found that
consdiofis health directed self-care was related to healthier habits of tobacco and alcohol use. Indeed, tobacco consumption was unrelated to health pro- moting practices for both men and women, while avoidance behaviour was negatively related to the use of both substances among men and unrelated to female substance use. It appears that avoidance be- haviour as reported by the respondents in this study may represent attempts to prevent the deterioration of existing conditions rather than primary health promotion.
Examining patterns of behaviour, a profile of healthy behaviour emerged among women that was not found in the male group. Health promoting practices were more frequently reported by women who are regularly physically active. Furthermore, obtaining professional health maintenance services were highly inter-related and occurred more often among women who exercised regularly and reported health promoting practices. Thus with regard to gender differences in behaviour hypotheses 1 and 4 were confirmed, while hypotheses 2 and 3 were not substantiated.
Turning to the second set of hypotheses, antici- pated gender differences in health related beliefs and knowledge were not found. Generally, in relation to the variables examined, hypotheses 5 to 5c must be rejected. Only the moderate positive relation- ship between internal health locus of control and male avoidance behaviour, the inverse relationship between confidence in medical cure and female phys- ical exercise and perhaps the inverse relationship between confidence in self-judgement and dental visits lend some support to these hypotheses. On the other hand, hypothesis 5d, regarding health knowl- edge, was supported, although the effects were gender specific.
The generally greater importance of social network support variables for male self-care behaviour expected in hypothesis 6 was supported. However, the expected importance of network support in con- trast to network size for health protective behaviour was not substantiated. The findings from this study suggest that the effects of social network and support variables on health related behaviours are complex with loneliness and isolation perhaps playing a more important role in relation to health mainte- nance behaviour, while social support variables exert greater influence on behaviour responses to illness. Living alone was independently associated with greater tobacco consumption among men and less routine physical activity among women. Likewise, men with larger friendship networks more often reported behavioural practices to maintain health. Instrumental support from the network was associ- ated with regular male physical activity and available extended family with less male alcohol consumption regardless of income. On the other hand, seeking professional help for symptoms was more frequent for both men and women with less supportive net- works and among men who less often receive instru- mental help from the network when needed. The relationships between professional care seeking and support may reflect poorer health among persons with non-supportive networks, thus reflecting direct effects of social support on health.

150 KATHRYN DEAN
Hypotheses 7a-c were partially supported. Income was related to physical activity and was the most important variable included in this study for visiting the dentist. However, it was unrelated to tobacco consumption and to the variables which obtained open ended information on consciously undertaken health protective and avoidance behaviour. As expected, income was unrelated to illness related self-care in both the male and female groups. It is relevant to note that the effects of income and age on the network and support variables may have important implications for health and functional maintenance.
DISCUSSION
The purpose of this paper was to examine health related behaviours in a social situational framework. The theoretical logic in this framework builds on the perspective that individual behaviours are not simple measures of lifestyles nor by themselves meaningful representations of that construct. A conceptualiza- tion of lifestyles as ways of living shaped by social learning and socially and economically determined options means a shift in research focus to patterns of behaviour and the forces that shape them. Recogniz- ing that gender specific social learning and experi- ences are among the most fundamental processes influencing development, the analysis presented here concentrated on sex differences in behaviour. Exten- sive documentation of differences in both health related behaviour and health status from widely different national settings suggested that this would be a fruitful approach to more meaningful under- standing of the phrase ‘health related lifestyle’.
The findings do provide useful information regard- ing lifestyles and ways they may influence/contribute to health. At the same time, they illustrate how little is known about the subject. Some of the anticipated sex differences in individual self-care behaviour were found. With a few exceptions, however, the differ- ences were not large. Evidence of different patterns of routine use of potentially harmful substances and of health maintaining behaviour by men and women do, however, support behavioural explanations for sex differences in health status.
The relatively few sex differences in self-care responses to illness along with the finding that illness behaviour for the most part was unrelated to the other types of self-care suggest that the illness experience (discomfort and perceived severity) exerts greater influence on illness behaviour than sex differ- ences. at least in a population over 45 yr of age. Our results are consistent with other studies that find the major gender differences in illness behaviour occur among 17-44-yr-old people [1 I]. The findings prob- ably reflect both more comparable morbidity and more serious male conditions in samples of persons over 45 yr of age. The statistical correlation for the sex difference in smoking behaviour was moderate, but the bulk of the difference was found in the area of greatest danger-heavy tobacco consumption was much more prevalent among men. The generally greater use of alcohol among men follows the same pattern of striking differences at the low and high ends of the distributions. Yet more serious health
implications are seen in the tendency for heavy male smokers to also consume relatively more alcohol, whereas there is no relationslhip between smoking and drinking among women.
An important unanticipated finding was the gen- eral absence of relationships between the use of tobacco and both other forms of self-care and the knowledge and belief variables. The health related attitudes and knowledge variables included in this investigation have to do with perceptions regarding the influence of personal behaviour and medical care on the maintenance and restoration of health. Theories regarding health perceptions and beliefs would lead us to expect independent influence of the belief variables on self-care behaviours. The impor- tance of gender determined experiences on learning and behaviour would furthermore lead us to antici- pate significant differences in the health related beliefs and knowledge of men and women. In neither case were the anticipated findings produced in our ana- lyses. This suggests that generalized beliefs regarding the forces that shape health are less important for actual behaviour than social learning, group identifi- cation and network functioning.
The negative relationship between use of tobacco and avoidance behaviour among men examined in the light of the general pattern of relationships for the avoidance behaviour variables suggests smoking reductions due to existing diseases. If, as it appears, the avoidance behaviour variable represents behav- ioural responses to existing conditions for men, the findings are consistent with an interpretation that measures of locus of health control may be more influential in attempts to change health damaging practices that are well established than in habit formation. As suggested, situational determinants such as social learning in the family, peer group pressure and cultural values apparently exert more influence on the formation of habits [5]. Knowledge of social environmental influences on health damag- ing behaviour is an area in need of new approaches to investigation and analytical elaboration.
Large sex differences in alcohol consumption have been found in other investigations [ 17,401. Research findings suggest explanations for these sex differences which have important implications for health promo- tion programmes directed toward lifestyles. In a study of reasons for drinking, it was found that escape drinking (to relieve tension, cheer up or forget problems) in contrast to other reasons for drink- ing was considerably more prevalent among men. The ratio of male escape drinkers to female escape drinkers was 2 : 1, and for heavy-escape drinking, the male-female ratio was 3.5: 1 [40].
This investigation found less female alcohol consumption, but generally healthier patterns of behaviour among women who consume modest amounts of alcohol. It may be concluded that use of alcohol without reference to amount and nature of use is a poor indicator of health promotion. Indeed, the findings generally point to the need for more meaningful lifestyle and health promotion indicators.
Based on the theoretical perspective of this study, it was postulated that social environmental variables exert major causal influence on self-care behaviours

Self-care components of lifestyles 151
supplementing the fundamental role of gender. Social support was less important for health maintenance forms of self-care than expected. It appears that loneliness and isolation may be a major factor increasing health damaging behaviour, especially for men. Even though women more often lived alone and reported non-supportive networks, they may take more active steps to reduce isolation. We will not be able to understand the influence of social support before we find out more about social functioning. At this time, it would appear that forces of socializa- tion and cultural values are the major factors shaping behaviour while social network variables assume importance when stress or social functioning intensify already existing patterns of behaviour or result in symptoms of illness.
While our expectations regarding gender influences on behaviour received considerable support, even among women, active health maintenance was not prevalent. Persons who reported one deliberate health promotive practice often reported others, but over half of the sample did not mention any. There may be some effect from this information having been collected with open ended questions, but the bulk of the evidence suggests a group of active health pro- moters, more often women, and a group of persons, more often men, that may live health damaging lifestyles.
Furthermore, in the responses of the sample mem- bers, health promotion behaviour was conceived quite narrowly, clearly biased toward individual behaviours statistically associated with cardiovascu- lar diseases and cancer. The health maintenance behaviour data were collected prior to the informa- tion on knowledge and attitudes to avoid contamina- tion of the behavioural responses. The findings thus indicate that the focus on cardiovascular diseases and cancer which permeates the health sector and the information it produces (also clearly reflected in the design of this study) has succeeded in shaping con- cepts of health protection in lay populations.
At least two major implications of these develop- ments may be considered priority issues for health promotion. First of all, the excessive focus on a few individual behaviours must be questioned. The atten- tion directed toward a narrow range of personal practices statistically associated with chronic diseases of late life neglects behaviours that may be equally or more important for promoting the health of popula- tions (e.g. work and traffic safety). Other factors that contribute to chronic diseases, but are less extensively studied in the health field are also neglected under this biased focus on individual practices (e.g. action to protect the quality of air, water and food, etc.).
A second major implication of the findings related to the behaviouristic focus on individuals in many programmes concerned with habit formation and behavioural change. Behaviouristic approaches to health promotion implicity, if not explicity, separate individuals from the social, physical and economic environments in which they live. Many health infor- mation programmes operate as though personal behaviour is a simple matter of informed choice rather than of complex processes involving opportu- nities for choosing healthy ways of living combined with personal strength and resources for making
health enhancing choices. The evidence from this investigation indicates that the socioeconomic situa- tion exerts more influence on self-care behaviours than health attitudes and knowledge. Income was clearly the most influential variable related to dental care and a major factor for regular physical exercise for both men and women. Social support variables appear to be more important factors shaping self- care responses to illness, while stressful situations apparently intervene in consciously undertaken health protective practices, especially avoiding health damaging behaviours and routine physical exercise among men.
Perhaps the most important implication of the findings relates to the limitations of focusing on differences in discrete behaviours rather than patterns of behaviour. Gender differences found in the discrete behaviours were fewer and smaller (with the excep- tion of alcohol consumption) than expected while gender differences in patterns of behaviour were striking. Possible cohort effects as well as cultural and structural influences specific to Denmark must be considered in the interpretation of these findings. Only longitudinal cross-cultural research investi- gations can successfully untangle the causal influences shaping self-care behaviours. In the mean- time, studies which focus on interactions among multiple influences and levels of influence among variables can increase our understanding of behav- ioural influences on health and improve the knowl- edge base for effective longitudinal and cross-cultural investigations.
Acknowledgemenrs-The author acknowledges with appre- ciation the helpful comments and useful criticisms provided by Signild Vallgarda and the Social Science & Medicine reviewers of an earlier version of this manuscript.
1.
2.
3.
4.
5.
6.
7.
8.
9.
10.
11.
REFERENCES
World Health Organization. Targets for He&h for AI/. WHO Regional Of& for Europe, Copenhagen, !985. Badura B. Social epidemiology in theory and practice. Eur. Monog. Hllh Educ. Res. 5, 1984. Kaplan R. The connection between clinical health promotion and health status, a critical overview. Am. Psychol. 39, 1984. Anderson R. Health promotion: an overview. Eur. Monogr. HIth Educ. Res. 6, 1, 1984. Dean K. Influence of health beliefs on lifestyles: what do we know? Eur. Monogr. Hlth Educ. Res. 6, 127. 1984. Dean K. Methodological issues in the study of health related behaviour. In Research on Health Behaviour: Its Application in Health Promotion (Edited by Anderson R., Davis J., Kickbusch I., McQueen D., Turner J.). Oxford University Press, 1988. Coreil J., Levin G. and Jaco G. Life style-an emerg- ing concept in the sociomedical sciences. Gulf. Med. Psychiat. 9, 423-437, 198. Levin L., Katz A. and Hoist E. Se/j-Cure. Prodist, New York, 1976. Dean K. Self care: implications for aging. In Self Cure and Health in Old Age (Edited by Dean K., Hickey T. and Holstein B.). Croom Helm, London, 1986. Verbrugge L. Sex differences in health. Prevention 97, 417, 1982. Verbrugge L. Gender and health: an update on hypo- theses and evidence. J. Hlth sot. Behav. 26, 156, 1985.

152 KATHRYN DEAN
12
13.
14.
15.
16.
17.
18.
19.
20.
21.
22.
23.
24.
Dunnell K. and Cartwright A. Medicine Takers, Prescribers and Hoarders. Routledge & Kegan Paul, London, 1972. Hollnagel H. and Kamper-Jorgensen F. Utilization of health services by 40-year-old men and women in the Glostrup area, Denmark. Dan. med. Bull. 27, 130, 1980. Nathanson C. Sex, illness and medical care: a review of data, theory and method. Sot. Sci. Med. 11, 13-25, 1977. Waldrom I. An analysis of causes of sex. Differences in mortality and morbidity. In The Fundamental Connection between Nature and Nurrure (Edited by Grove W. and Carpenter I.). Lexington Books, Lexing- ton, Mass., 1982. Holt P. and Jeune B. Fysisk Inaktivitet Blandt Yngre Voksne (Physical inactivity among young adults). Dan. med. J. 146, 42, 1984. Saelan H. Alkohol og Alkoholisme. Institute of Social Medicine, University of Copenhagen, Copenhagen, 1984. Dean K. Social support and health: pathways of influence. Hlth Promor. 1, 133, 1986. Mellstriim D. and Svanborg A. Tobacco smoking-a major cause of sex differences in health. Comprehens. Geront. A. 1, 34, 1987. Langlie J. Social networks, health beliefs and preventive health behavior. J. Hlth sot. Behao. 18, 244, 1977. Heidam L., Kaaber K., Pelle H., Poulstrup A. and Thomsen A. Sundhedraafard Bland! Yngre Voksne. Working Group Report, Vejle County, 1985. Kastrup M., Petersson B. and Helweg-Larsen K. Kuinden som Patient (The Women as a Palient). Lindhardt & Ringhop, Denmark, 1982. Department of Health and Social Security. Inequalities in Health. The Black Reoorr. Her Maiestv’s Stationerv Office, London, 1980. .
_ _
Townsend P. and Davidson N. Inequalities in Health. Penguin Books, London, 1982.
25.
26.
27.
28.
29.
30.
31.
32.
33.
34.
35.
36.
37.
38.
39.
40.
Syme S. and Berkman L. Social class, susceptibility and sickness. Am. J. Em&m. 104. l-8, 1976. Cohen S. and Syme L. Social Supporr and Health. Academic Press, New York, 1985. Turner R. Social support and psychological distress. In Psychosocial Srress (Edited by Kaplan H.). Academic Press, New York 1983. Berkman L. Social networks, support and health: taking the next step forward. J. Epidem. 123, 559-562, 1986. Gottlieb N. and Green L. Life-events, social networks. life-style and health. Hlth Educ. Q. 11, 91, 1984. Elliott Binns C. An analysis of lay medicine. J. R. Coil. Gen. Pratt. 23, 255, 1973. Dean K., Holst E. and Wagner M. Self-care of common illness in Denmark. Med. Care 21, 1012-1032, 1983. Rotter J. Generalized expectancies for internal versus external control of reinforcement. Psychol. Monogr. 80, 609, 1966. Wallston B., Wallston K. and DeVellis R. Develop- ment of the multidimensional health locus of control (MHLC) scales. Hlfh Educ. Monogr. 6, 160, 1978. Andersen E. B. Sulhcient statistics and latent trait models. Psychometrica 42, 69-82, 1977. Rasch C. Probabilistic Models for Inrelligence and Atrainmen! Tests. Nielsen & Lydicke, Copenhagen, 1960. Edwards D. and Kreiner S The analysis of contingency tables by graphical methods. Biomerrika 70, 553, 1983. Wennuth N. and Lam&en S. Graphical and recursive models for contingency tables. Biomerrika 70,537, 1983. Kreiner S. Analysis of multidimensional contingency tables by exact conditional tests: techniques and strate- gies. Stand. J. Statist. 14, 97-112, 1987. Dean K. Issues in the development of health promotion indicators. Hlth Promot. 3, 1988. Celentano D. and McQueen D. Comparison of alco- holism prevalance rates obtained by survey and indirect estimators. J. Stud. Alcohol. 39, 420, 1978.