Seizures in Neonates - دانشگاه علوم پزشکی اصفهان in... · PPT file · Web...
84
-
Upload
trankhuong -
Category
Documents
-
view
222 -
download
0
Transcript of Seizures in Neonates - دانشگاه علوم پزشکی اصفهان in... · PPT file · Web...


Seizures in
Neonates
Neonatal seizures are one of the few
neonatal neurologic conditions that require
immediate medical attention.
Medical personnel vary significantly in
their ability to recognize suspect behaviors,
contributing to both overdiagnosis
and underdiagnosis.

However,
abnormal motor or autonomic behaviors may represent
age- and state-specific behaviors in healthy infants, or nonepileptic paroxysmal conditions in symptomatic infants.

For these reasons, confirmation of suspect
clinical events with coincident EEG recordings is now more widely recommended.

because in patients with few seizures, these may be missed as brief random events on
routine EEG studies,
synchronized video/EEG/polygraphic
recordings potentially establish more reliable startpoints and endpoints for electrically confirmed seizures that require consideration for treatment
intervention.
• The clinical criteria for neonatal seizure diagnosis were historically
subdivided into five clinical categories:• focal clonic• multifocal or migratory clonic• tonic• myoclonic • subtle seizures
Clinical Categories
• This is the most frequently observed category of neonatal seizures, which include
repetitive buccolingual movements, orbital-ocular movements, unusual bicycling or peddling, and autonomic findings.
• alterations in cardiorespiratory regularity, body movements, and other behaviors during active (rapid eye movement) sleep, quiet (non-
rapid eye movement) sleep, or waking segments must be recognized before proceeding to a seizure evaluation.
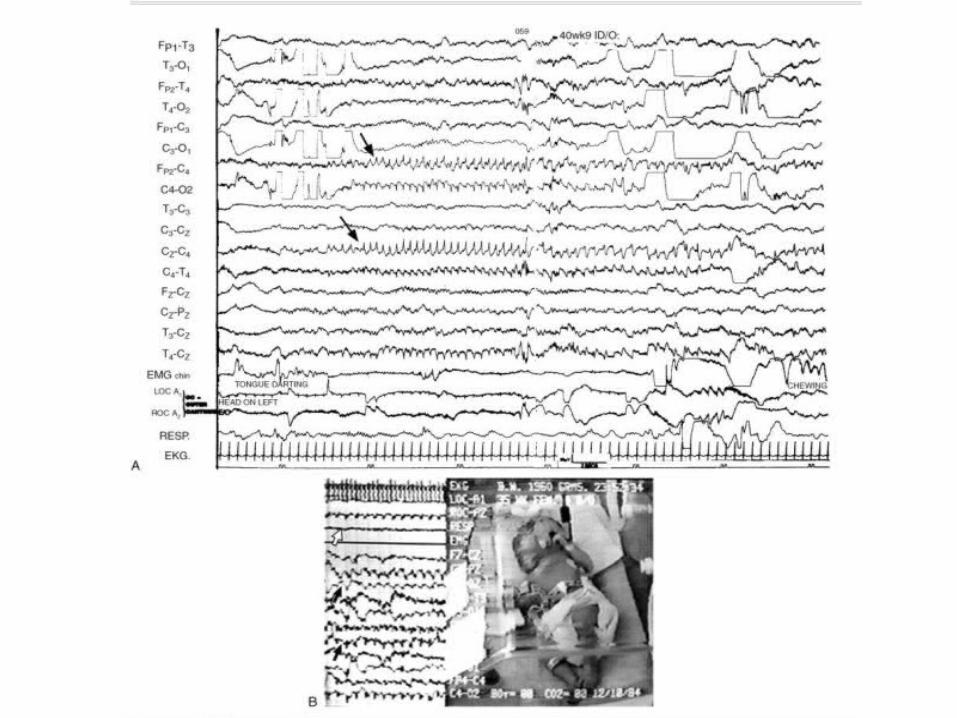
• Within the subtle category of neonatal seizures are stereotypical changes in heart rate, blood pressure, oxygenation, or other autonomic signs, particularly during pharmacologic paralysis for ventilatory care.
SUBTLE SEIZURE
• Because subtle seizures are clinically difficult to detect and only variably coincident with EEG seizures,
synchronized video/EEG/polygraphic recordings are recommended to document temporal relationships between clinical behaviors and coincident electrographic events.
SUBTLE SEIZURE
• Rhythmic movements of muscle groups in a focal distribution that consist of a rapid phase followed by a slow return movement are clonic seizures.
• Clonic movements can involve any body part such as the face, arm, leg, and even diaphragmatic or pharyngeal muscles.
• must be distinguished from the symmetric “to-and-fro” movements of
tremulousness or jitteriness. • Gentle flexion of the affected body part
easily suppresses the tremor, whereas clonic seizures
persist.
CLONIC SEIZURES
• Generalized clonic activities can occur in the newborn but rarely consist of a classic tonic followed by clonic phase, characteristic of the generalized motor seizure noted in older children and adults.
• Focal clonic and hemiclonic seizures have been described with localized brain injury, usually from cerebrovascular lesions,but can also be seen with generalized brain abnormalities.
• Clonic movements without EEG-confirmed seizures have been
described in neonates with normal EEG backgrounds, and their
neurodevelopmental outcome can be normal.
CLONIC SEIZURES
• Multifocal or migratory clonic activities spread over body parts either in a random or anatomically appropriate fashion. Such seizure movements may alternate from side to side and appear asynchronously between the two halves of the child’s body.
• Neonates with this seizure description suffer death or significant neurologic morbidity.
MULTIFOCAL CLONIC SEIZURES
• Tonic seizures refer to a sustained flexion or extension of axial or appendicular muscle groups.
• Tonic movements of a limb or sustained head or eye turning may also be noted.
• Tonic activity with coincident EEG needs to be carefully documented because 30% of such movements lack a correlation with electrographic seizures.
TONIC SEIZURES
• “Brainstem release” resulting from
functional decortication after severe neocortical dysfunction or damage.
• Extensive neocortical damage or dysfunction permits the
emergence of uninhibited subcortical expressions of extensor movements.
TONIC SEIZURES
• Myoclonic movements are rapid, isolated jerks that can be
generalized, multifocal, or focal in an axial or appendicular distribution.
• Myoclonus lacks the slow return phase of the clonic movement complex described.
• Healthy preterm infants commonly exhibit myoclonic movements without seizures or a brain disorder.• EEG, therefore, is recommended to confirm the
coincident appearance of electrographic discharges with these movements.
MYOCLONIC SEIZURES

• Pathologic myoclonus in the absence of EEG seizures also
can occur in severely ill preterm or full-term infants after severe brain dysfunction or damage.
• myoclonus may reflect injury at multiple levels of the neuraxis from the spine, brainstem, to cortical regions.
• Rarely, healthy sleeping neonates exhibit abundant
myoclonus that subsides with arousal to the waking state, termed benign sleep myoclonus of the newborn.
MYOCLONIC SEIZURES
• Tremors are frequently misidentified as clonic activity. • Unlike the unequal phases of clonic movements described earlier,
the flexion and extension phases of tremor are equal in amplitude.
• Children are usually alert or hyperalert but may also appear somnolent.
• Passive flexion and repositioning of the affected tremulous body part diminishes or eliminates the movement.
Nonepileptic Behaviors of Neonates
TREMORS Or JITTERINESS

• Such movements are usually spontaneous but can be provoked by tactile stimulation. • Metabolic or toxin-induced
encephalopathies, including mild asphyxia, drug withdrawal, hypoglycemia, hypocalcemia, intracranial hemorrhage, hypothermia, and growth restriction, are common clinical scenarios when such movements occur.
Nonepileptic Behaviors of Neonates
TREMORS Or JITTERINESS

• Neonatal tremors usually decrease with age; for example, in 38 full-term infants, excessive tremulousness resolved spontaneously over a 6week period, with 92% neurologically normal at 3 years of age.
• Medications are rarely considered to treat this particular movement disorder.
Nonepileptic Behaviors of Neonates
TREMORS Or JITTERINESS
• NEONATAL MYOCLONUS WITHOUT ELECTROGRAPHIC SEIZURES
• NEONATAL DYSTONIA/DYSKINESIA WITHOUT ELECTROGRAPHIC SEIZURES
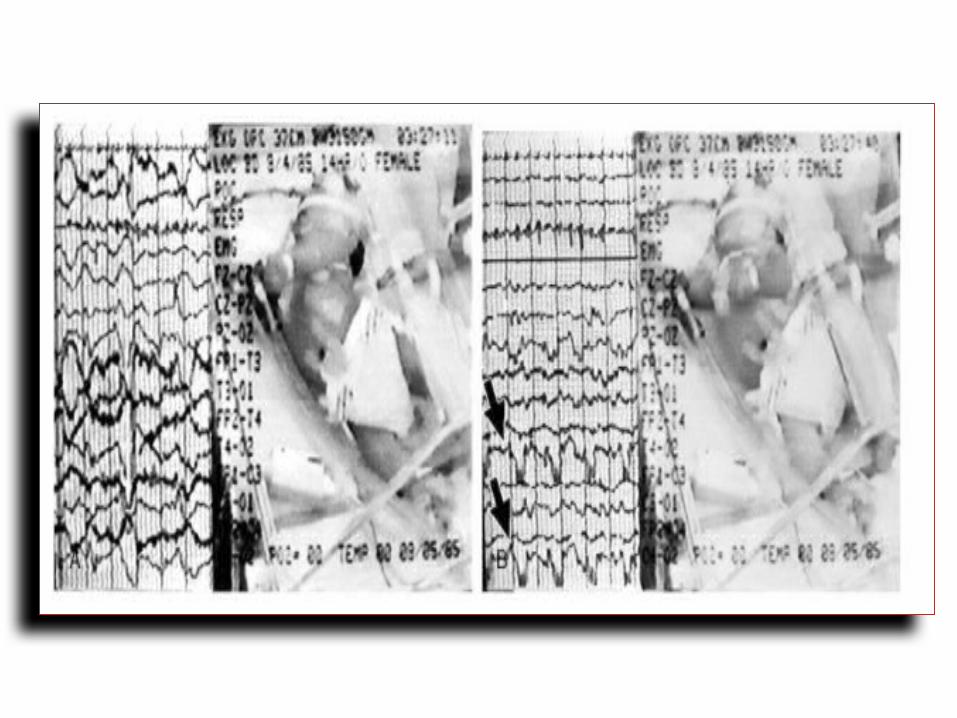
• Neonatal EEG seizure patterns commonly consist of a repetitive sequence of waveforms that evolve in frequency, amplitude, electrical field, and morphology.
• Four types of ictal patterns have been described:• focal ictal patterns with normal background• focal patterns with abnormal background• multifocal ictal patterns• focal monorhythmic periodic patterns of
various frequencies
ICTAL ELECTROENCEPHALOG
RAPHIC PATTERNS
• It is generally suggested that a minimal duration of 10 seconds with the evolution of discharges is required to distinguish electrographic seizures from repetitive but nonictal epileptiform discharges.
• The mean seizure duration was longer in the full-term infant (5 minutes) compared with the preterm infant (2.7 minutes).
ICTAL ELECTROENCEPHALOG
RAPHIC PATTERNS
• Uncoupling of the clinical and electrographic expressions of neonatal seizures after antiepileptic medication administration also contributes to an underestimation of the true seizure duration, including status epilepticus.
• Estimated that 25% of neonates expressed persistent EEG seizures despite resolution of their clinical seizure behaviors after receiving antiepileptic medications, termed electroclinical uncoupling.
ICTAL ELECTROENCEPHALOG
RAPHIC PATTERNS
• Using clinical criteria, seizure incidences ranged from 0.5% in term to 22.2% in preterm neonates
• Most neonatal electrographic seizures arise focally from one brain region.
• Generalized synchronous and symmetric repetitive discharges can also occur.
ICTAL ELECTROENCEPHALOG
RAPHIC PATTERNS

• Neonates with brief discharges can suffer from hypoglycemia or PVL , which carries a higher risk for neurodevelopmental delay.
• Extremity movements were more significantly associated with synchronized electro-clinical seizures.
ICTAL ELECTROENCEPHALOG
RAPHIC PATTERNS

Interictal Electroencephalographic Pattern Abnormalities
• Interictal EEG abnormalities have important prognostic implications for both preterm and full-term infants.
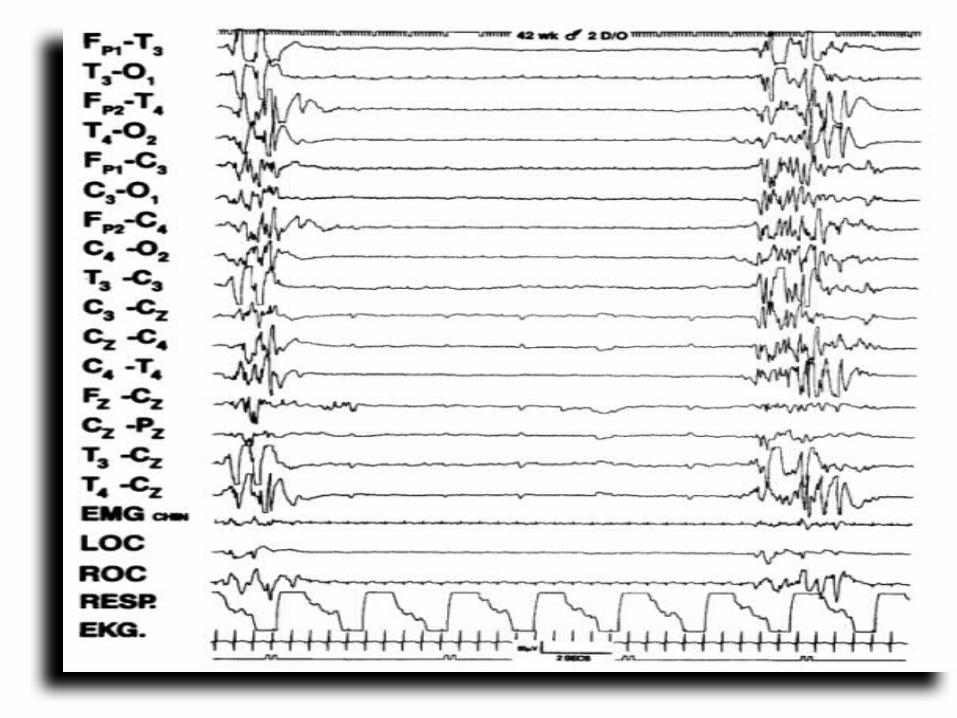
• Severely abnormal patterns include the
• burst suppression pattern,
• electrocerebral inactivity, • low-voltage invariant pattern,• persistently slow background pattern,• multifocal sharp waves, • and marked asynchrony.
• For infants with hypoxic-ischemic encephalopathy
(HIE), subclassifications of specific EEG patterns such
as burst suppression with or without reactivity may give a more accurate prediction of outcome.
• Dysmaturity of the EEG sleep background for child’s corrected age has also been an important feature to recognize; discordance between cerebral and noncerebral components of sleep state, or immaturity of EEG patterns for the given postconceptional age of the infant predict a higher risk for neurologic
sequelae.
Interictal Electroencephalographic Pattern Abnormalities
• Focal or regional patterns have prognostic significance, such as with preterm infants who express repetitive positive sharp waves at the midline or central regions often noted with IVH & PVL
• Screening infants at risk for neonatal seizures with a routine EEG soon after birth allows identification of more severe interictal EEG background abnormalities that more likely predict seizure occurrence on subsequent neonatal records.
Interictal Electroencephalographic Pattern Abnormalities
• Serial EEG studies better assist the clinician in diagnostic and prognostic interpretations.
• As with abnormal examination findings into the
second week of life, the persistence of EEG abnormalities also raises prognostic concerns.
• normal EEG features during the first few days after birth, may experience comparatively fewer neurologic sequelae.
Interictal Electroencephalographic Pattern Abnormalities
• Seizures may occur as part of an asphyxial brain disorder that is expressed after birth (termed HIE from intrapartum stress)
MAJOR ETIOLOGIES FOR SEIZURES
Hypoxia -Asphyxia
• Hypoxia-ischemia (i.e., asphyxia) is
traditionally considered the most common causal factor associated with neonatal seizures.
• Neonate suffer asphyxia either before or during parturition, and only 10% of cases of asphyxia
result from postnatal causes.• When asphyxia is suspected during the labor and delivery process,
biochemical confirmation can be attempted.
Hypoxia -Asphyxia

• Intrauterine factors in the hours to days before labor can result
in antepartum fetal asphyxia without later documentation of acidosis at birth.
• Some maternal illnesses such as thrombophilia or preeclampsia, or specific uteroplacental abnormalities such as abruptio placentae or cord
compression may contribute to fetal asphyxial stress without providing the opportunity to document in utero acidosis at the end of parturition.
• Antepartum maternal trauma and chorioamnionitis are additional acquired conditions that cause or contribute to intrauterine asphyxia secondary to uteroplacental insufficiency.
Hypoxia -Asphyxia

• Placental weights < the 10th or > the 90th percentile
suggest chronic perfusion abnormalities to the fetus.
• Meconium passage into the amniotic fluid may also promote an inflammatory response in the placental membranes, causing vasoconstriction and additional asphyxia.
• Therefore, asphyxia-induced brain injuries may result
from in utero maternal-fetal-placental diseases that
later are expressed in part as neonatal seizures, independent of the biochemical marker of acidosis at birth, as well as the evolving HIE syndrome in the days after birth.
Hypoxia -Asphyxia
• Postnatal neonatal illnesses also cause or contribute
to asphyxia-induced brain injury and seizures without HIE, and after an uneventful delivery without fetal distress during labor or neonatal depression at birth.
Hypoxia -Asphyxia
• Post-asphyxial encephalopathy refers to an evolving clinical syndrome over days after birth depression during which neonatal seizures may occur, usually in children who also exhibit severe early metabolic acidosis, hypoglycemia or hypocalcemia, and multiorgan dysfunction.
• Postasphyxial seizures usually occur within the first 3 days of life, depending on the length and degree of asphyxial stress during the intrapartum period.
Hypoxia -Asphyxia
• An early occurrence of seizures, within several hours after delivery, sometimes suggests antepartum or peripartum occurrence of a fetal brain disorder when associated with specific fetal heart rate patterns.
• Earlier seizure onset, within 4 hours of birth, in
encephalopathic newborns may predict a particularly adverse outcome independent of etiology for asphyxia.
Hypoxia -Asphyxia
• The duration of asphyxia is difficult to assess based on either single or
even multiple PO2 values, but pH <7.2 are considered of greater clinical concern for predicting HIE, although the suggested guideline of a
pH <7.0 is one criterion by which the clinical entity of HIE might be predicted.
• A metabolic definition of asphyxia should also include a base
deficit of less than 12 mmol/L (BE > - 12) , although specific
researchers suggest BE > - 16 mmol/L because of its higher predictive power for the emergence of the HIE syndrome,
including clinical seizures.
Hypoxia -Asphyxia
• Low 1- and 5-minute Apgar scores indicate the
continued need for resuscitation, but only low scores at 10, 15, and particulary 20 minutes more accurately predict sequelae.
• Normal Apgar scores, however, do not eliminate the
possibility of severe brain injury, either from asphyxia or other causes.
• As many as 2/3 of neonates who exhibit CP at older ages had normal Apgar scores at birth without HIE.
Hypoxia -Asphyxia
• Hypertonicity, often with cortical fisting, in a previously depressed child who rapidly recovers after a resuscitative effort also commonly reflects longer-standing fetal neurologic dysfunction before labor or the mother’s admission to the hospital.
• Sustained hypotonia and unresponsiveness for
3 to 7 days are the expected signs of HIE after asphyxial stress during labor, with or without brain injury.
Hypoxia -Asphyxia

• Significant Hypoglycemia is usually defined as glucose levels less of 35 to 40 mg/dL (BS < 50).
• No clear consensus exists concerning a direct cause-and-effect relationship of hypoglycemia with seizure occurrence.
• Associated disturbances may coexist, such as hypocalcemia, craniocerebral trauma, cerebrovascular lesions, and asphyxia,
which may also contribute to lowering the infant’s threshold for seizures.
MAJOR ETIOLOGIES FOR SEIZURES Hypoglycemia
• Total serum calcium levels below 7 (7.5) to 8 mg/dL generally define hypocalcemia.
• The ionized fraction is a more sensitive indicator of seizure vulnerability.
• The exact level of hypocalcemia at which seizures occur is debatable. An ionized fraction of 0.6 mg/dL or less may have a
more predictable association with the presence of seizures.
MAJOR ETIOLOGIES FOR SEIZURES
Hypocalcemia

• Hemorrhagic or ischemic cerebrovascular lesions are
associated with neonatal seizure.
• IVH or periventricular hemorrhage (PVH) is the most common intracranial hemorrhage (ICH) of the preterm infant, and
has been associated with seizures in as much as 45% of a preterm population with EEG-confirmed seizures.
MAJOR ETIOLOGIES FOR SEIZURES
Cerebrovascular Lesions
• Intracranial hemorrhage is usually expected in the first 72 hours of life of the preterm infant.
• the most frequent presentation is asymptomatic; (25% to 50% of infants with GMH-IVH have no obvious clinical signs) , the
neonate with a catastrophic deterioration of clinical status shows signs of apnea, bulging fontanelle, hypertonia, and seizures.
• Term infants present less commonly with intraventricular hemorrhage.
Cerebrovascular Lesions

• Other sites of intracranial hemorrhage include the
subarachnoid space (SAH) , which may cause seizures but is usually associated with a more favorable outcome.
• Subdural hematoma, whether
spontaneous or with craniocerebral trauma, should
always be considered particularly when focal trauma to the face, scalp, or head has occurred.
Cerebrovascular Lesions

• Cerebral infarction has been described in neonates with seizures and can result from events during the antepartum, intrapartum, or neonatal periods.
• Lateral or sagittal sinus thromboses after coagulopathy can occur secondary to systemic infection, polycythemia, or dehydration.
• Venous infarction in the deep white matter of the preterm brain also occurs in association with IVH.
Cerebrovascular Lesions

Cerebrovascular Lesions
a hemorrhagic infarction in the right posterior quadrant with surrounding edema

• CNS infections during the antepartum or postnatal periods can be associated with neonatal seizures.
• Congenital infections, commonly referred to by the
acronym TORCH can produce severe encephalopathic damage that results in seizures.
MAJOR ETIOLOGIES FOR SEIZURES Infectio
n
• Bacterial infections acquired in utero or postnatally from either gram-negative or gram-positive organisms are also associated with neonatal seizures.
• A high percentage of survivors has significant neurologic sequelae.
Infection

• Brain anomalies may occur as a result of either
genetic causes from conception or acquired defects during the first half of gestation.
• Specific dysgenesis syndromes, such as holoprosencephaly and lissencephaly, are often associated with characteristic facial or body anomalies.
MAJOR ETIOLOGIES FOR SEIZURES CNS
Malformations


• Focal or regional brain malformations are Rare causes of early-onset epilepsy in neonates and young infants.
CNS Malformations
• Intractable seizures associated with elevated lactate and pyruvate levels in blood and spinal fluid may reflect specific inborn errors of metabolism.
• The emergence of food intolerance as well as increasing lethargy, stupor, coma, and seizures is an early indication of an inborn metabolic disturbance during the first few days of life.
• The newborn with an inherited metabolic disorder may initially present as a neurologically depressed and hypotonic child with seizures.
MAJOR ETIOLOGIES FOR SEIZURES Inborn Errors
of Metabolism
•Vitamin B6 or pyridoxine deficiency is a rare cause of neonatal seizures.• Pyridoxine acts as a cofactor in GABA synthesis,
and its absence or paucity promotes seizures. • The mother occasionally reports paroxysmal fetal
movements.
Inborn Errors of Metabolism

• The infant who is unresponsive to conventional antiepileptic medications should promptly receive an IV injection of 50 to 500 mg of pyridoxine, preferably with concomitant EEG monitoring.
• Termination of the seizure within minutes to hours as well as resolution of EEG background disturbances suggests a pyridoxine-dependent seizure state.
• Prophylactic doses of pyridoxine may be needed to achieve and maintain seizure control.
Inborn Errors of Metabolism
• Exposure to barbiturates, alcohol, heroin, cocaine, or methadone commonly presents with
neurologic findings that include tremors and irritability. • Depending on the pattern of use and the timing of
last use, the onset of neonatal withdrawal from
narcotics generally begins in the first 2 to 3 days after birth but may occur as late as 4 weeks.
MAJOR ETIOLOGIES FOR SEIZURES Drug
Withdrawal

• Seizures may occur directly after substance withdrawal, or associated with longer-standing
uteroplacental insufficiency promoted by chronic substance use and poor prenatal health maintenance by the mother.
• Careful review of placental-cord specimens may reveal chronic or acute lesions that contribute to antepartum or intrauterine asphyxia.
Drug Withdrawal

• Inadvertent fetal injection with a local anesthetic agent during delivery may induce intoxication, which is a rare cause of seizures.
• Patients present during the first 6 to 8 hours of life with apnea, bradycardia, and hypotonia, and are comatose, without brainstem reflexes.
Drug Withdrawal
• If the obstetrical history indicates pudendal administration of an
anesthetic to the mother, a careful examination of the child’s scalp or body for puncture marks is indicated.
• Determination of plasma levels of the suspected anesthetic agent establishes the diagnosis.
• Treatment consists of ventilatory support and
removing the drug by therapeutic diuresis, acidification of the urine, or exchange transfusion.
• Antiepileptic medications are rarely indicated.
Drug Withdrawal

• Rapid infusion of glucose or other
supplemental electrolytes should be initiated before antiepileptic medications.
• Symptomatic hypoglycemia can be readily corrected by IV administration of 2 mL/kg of a 10% dextrose solution, beginning with an infusion of approximately 8 to 10 mg/kg per minute and increased as needed.
• Persistent hypoglycemia may require more hypertonic glucose solutions. Rarely, other pharmacologic measures (e.g., diazoxide) may be needed to establish a glucose level within the normal range .
TREATMENT
• Hypocalcemia-induced seizures should be treated with an IV infusion of 200 mg/kg of calcium gluconate.
• This dosage should be repeated every 5 to 6 hours over the first 24 hours.
• Serum magnesium concentrations should also be measured because hypomagnesemia may accompany hypocalcemia; 0.2 mg/kg of magnesium sulfate should be given by IM injection.
TREATMENT

• Pyridoxine dependency requires the injection of 50 to 500 mg of pyridoxine during a seizure with coincident EEG monitoring.
• A beneficial pyridoxine effect occurs either
immediately or over the first several hours.
• A daily dose of 50 to 100 mg of pyridoxine should then be administered.
TREATMENT

• If the decision to treat neonates with antiepileptic medications is reached,
important questions must be addressed with respect to who should be treated , when to begin treatment , which drug to use , and for how long should neonates be treated.
• Some authors suggest that only neonates with clinical seizures should receive medications; brief electrographic seizures need not be treated.
• Others suggest more aggressive treatment of EEG seizures because uncontrolled seizures potentially have an adverse effect on immature brain development.
TREATMENT
• Phenobarbital and phenytoin nonetheless remain
the most widely used antiepileptic medications• use of benzodiazepines, primidone, and valproic acid has been anecdotally
reported.
• The half-life of phenobarbital ranges from 45 to 173 hours ( 2 – 7 days) in the neonate.
• the initial loading dose is recommended at
20 mg/kg( 10 5 5 ), with a
maintenance dose of 3 to 4 mg/kg per day. • Therapeutic levels are usually suggested to range from 10 to 40 μg/mL,
although there is no consensus with respect to drug maintenance.
TREATMENT

• The preferred loading dose of phenytoin is 15 to 20 mg/kg. • maintenance dose of 4-5 (8) mg/kg per
day. • Serum levels of phenytoin are difficult to maintain
because this drug is rapidly redistributed to body tissues. Blood levels cannot be well maintained using an oral preparation.
• Benzodiazepines may also be used to control neonatal
seizures. The drug most widely used is diazepam & midazolam (0.05-0.15mg/kg --- 0.01-0.06 mg/kg/h ).
TREATMENT
• most studies apply only a clinical endpoint to seizure cessation.
• Coincident EEG studies are now suggested to verify the
resolution of electrographic seizures because 30% of neonates may have persistent
EEG seizures after suppression of clinical seizure behaviors even after drug administration.
Efficacy of Treatment
• With doses of phenobarbital as high as 40 mg/ kg, the rate of seizure control may be up to 85%
• The earlier administration of high-dose phenobarbital in a group of asphyxiated infants was associated with a 27% reduction in clinical seizures together with better outcome than in a group who did not receive high dosages.
Efficacy of Treatment
• The clinician’s decision to maintain or discontinue antiepileptic
drug use also depends on variable factors.
• Discontinuation of drugs before discharge from the neonatal unit is usually recommended so that clinical assessments of arousal, tone, and behavior will not be hampered by medication effect.
• Newborns with congenital or destructive brain lesions on
neuroimaging, or those with persistently abnormal neurologic examinations at the time of discharge, may suggest to the clinician that a slower tapering of medication is required over several weeks or months.
Discontinuation of Drug Use
• Neonatal seizures rarely reoccur during the first 2 years of life, and
prophylactic antiepileptic drug administration need not be maintained past 3 months of age, even in the child at risk.
• This “honeymoon period” without seizures
commonly persists for many years in most children, before isolated or recurrent seizures appear.
Discontinuation of Drug Use
• The potential damage to the developing CNS by antiepileptic drugs also
emphasizes the need to consider early discontinuation of these agents in the newborn period.
• Adverse effects on the morphology and metabolism of neuronal cells have been extensively reported from collective research performed over the last several decades
Discontinuation of Drug Use

• Repetitive or prolonged neonatal seizures increase the susceptibility of the developing brain to subsequent seizure-induced brain injury during adolescence or early adulthood from altered neuronal connectivity rather than increased cell death.
• Neonatal seizures therefore may initiate a cascade of diverse changes in brain development that become maladaptive at older ages, and increase the risk of damage after subsequent insults.
• Finally, antiepileptic drug use may have teratogenetic effects on brain development with exposure over long periods.
Discontinuation of Drug Use
• Even if major neurodevelopmental sequelae such as motor deficits and mental retardation were avoided in survivors after neonatal seizures,
Subtle neurodevelopmental vulnerability
may manifest in late teenage years as specific learning difficulties or poor social adjustment, underscoring experimental findings of long-term deficits in animal populations.
PROGNOSIS
• More accurate imaging procedures (MRI) have heightened awareness of destructive as well as congenital brain lesions with a higher risk for compromised outcome.
• Interictal EEG pattern abnormalities are extremely helpful in predicting neurologic outcome in the neonate with seizures.
PROGNOSIS
• Major background disturbances such as burst suppression are highly predictive of
poor outcome, particularly when persistently abnormal findings are still present on serial EEG studies into the second week of life.
• Ictal patterns alone may not be as accurate for predicting outcome.
• unless they occur in high numbers, long durations, and multifocal distribution.
PROGNOSIS
• Normal findings on interictal EEG were associated with an 86% chance of normal development at 4 years of age in 139 neonates with seizures.
PROGNOSIS