SD Modelling Case Studies
9
Dynamic Modelling to Support Collaborative Planning and Decision Making Case Studies October 2012 David Rees Founding Partner Synergia Ltd
description
Transcript of SD Modelling Case Studies

Dynamic Modelling to Support Collaborative Planning and Decision Making
Case Studies October 2012
David Rees Founding Partner Synergia Ltd

Long-Term Planning in Local Government (2011/12) (Work Conducted for District Council)
David Rees, Synergia, Auckland, New Zealand
While they had detailed and robust financial planning underpinning their Long Term Plan, a District Council found it difficult to respond quickly to requests for alteraIon to the plan. What would be the consequences, for example, of shiLing a major capital project back by two years? What would be the consequences of adding or deleIng any of the projects currently in the plan? While their financial models were detailed and robust, they were unable to answer quesIons such as these in an easy, flexible and speedy way. The development of a dynamic simulaIon model,
calibrated with their own financial model, provided them with a tool that enabled them to conduct mulIple ‘what-‐if’ scenarios. The model ‘dashboard’ allows them to quickly modify assumpIons in their LTP and see the consequences for revenues, expenditures and their overall financial posiIon over the lifeIme of the LTP.

Using Systems Modelling to Integrate Multiple Workstreams within Energy Sustainability Research (2011) (Work Conducted for University of Otago Energy Research Centre)
David Rees, Synergia, Auckland, New Zealand
Faced with data coming from mulIple research streams within the mulI-‐disciplinary research team, the research centre wanted ways of integraIng their findings. The purpose of the modelling was to disIll the key findings from the different research streams and any uncover issues that may have emerged during the research process. Phase II of that research project is now underway and over the next four years we will be working with the research team, using dynamic modelling to integrate the research workstreams, and use the simulaIon capabilites to explore future scenario arising out of the research.
Phase II (2012 – 2016) Energy Culture II Energy sustainability in households, transport and SMEs Renewable Energy & the Smart Grid Exploring the supply and demand dynamics in a future based on extensive use of renewable energy sources

Regional Transport in Canterbury: Health Impact Analysis (2010) (Work Conducted for Environment Canterbury)
David Rees, Synergia, Auckland, New Zealand Dr. Adrian Field, Synergia, Auckland, New Zealand
In October 2009 Environment Canterbury iniIated a Health Impact Assessment (HIA) of its Regional Land Transport Strategy. The aim of the HIA was to assess the links between transport planning, health determinants, and health outcomes for the Canterbury RLTS. This simulaIon model supported the HIA by exploring the links between transport planning and health outcomes that were idenIfied in the iniIal scoping workshop. The HIA idenIfied some of the linkages, such as those between safety and cycle use and focused its analysis on three key areas; safety, mode choice and healthier environments. The aim of the simulaIon model was to help inform policy by quanIfying some of the key linkages and the size and Iming of potenIal health impacts resulIng from policy opIons being considered in the RLTS.

Op$ons for Demen$a Care (2010/11) (Work Conducted for Health Workforce New Zealand)
David Rees, Synergia, Auckland, New Zealand Geoff McDonnell, AdapIve Care Systems, University of NSW Dr. Ray Naden, Clinical Director, Synergia
In work we undertook for Health Workforce New Zealand, Synergia explored the opportuniIes for improving care for people with moderate demenIa in the home and community secngs, and the potenIal impact this may have upon admissions to aged residenIal care (ARC). The report provided an overview of the modelling used to explore the dynamics of home-‐based care – specifically carer stress – and its impact upon reducing admissions to ARC. The report then provided a descripIon of the models of care required to bring that reducIon about. Because demenIa is an area in which there is a paucity of data, our modelling had to bring together informaIon from a number of sources. Furthermore, it had to allow a range of scenarios to be run under a range of different assumpIons. The model allows stakeholders to obtain a richer understanding of what the future possibiliIes are, the constraints upon those possibiliIes, and the variables that have an impact upon determining which scenario is more likely to come to pass.

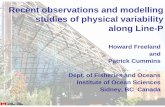
A Population-Based Approach to Planning Mental Health Services in Primary Care (2010) ((Work Conducted for Health Research Council)
David Rees, Synergia, Auckland, New Zealand Philip Gandar, Synergia, Auckland, New Zealand
MildSymptoms
ModerateSymptoms
SevereSymptomsbecoming
moderatebecoming
severe
need for MHservices
PMHCinterventions
SMHCinterventions
recoveringmoderate
recoveringsevere
recoveringmild
adequacy ofprovider resources
quality ofcare
prevention &management of risk
factors
investing inservice
improvement capability ofresources
amount ofresources
investing in riskmanagement
fundsavailable
investing in socialdeterminants
SocialStrength
change insocial strength
model of carerequirements
servicedemand
accesslevels
serviceprovision
<fundsavailable>
model ofcare
average level offunctioning
NoSignificantSymptoms developing
symptoms
developing moderatesymptoms
developing severesymptoms
individualattributes
RequiringSecondary
Careenteringsecondary care
discharging fromsecondary care
The issues that any region faces in planning Primary Mental Health Care (PMHC) are varied and complex. There is no one soluIon that can be applied across the country, and because of this it is important that planners in each region know their own populaIon and its needs, and the characterisIcs of the people and resources who can respond to them.
This model is designed to help facilitate conversaIons about PMHC in local regions, so that they can design soluIons that best fit their parIcular circumstances. It takes a systems approach because we know that any soluIon that does help improve mental health services will be required to address many issues. IsolaIng a single issue simply will not work. To facilitate the conversaIons we have designed a model of the key elements within PMHC and how those elements link together. The model is based on our conversaIons with planners and providers within each DHB and focuses on key themes that are common across all.

Review of Aged-‐Care Workforce (2010) (Work Conducted for Health Workforce New Zealand)
David Rees, Synergia, Auckland, New Zealand Geoff McDonnell, AdapIve Care Systems, University of NSW Dr. Ray Naden, Clinical Director, Synergia
Trainees Workforce
Older People Receiving
Care
Service Configuration
A System Dynamics (SD) Model was designed to provide a framework for meeIng the challenge of developing and managing the future aged-‐care workforce. It did so by describing the dynamic relaIonships between older people in need of health care services, the services that have been established to respond to those needs and the workforce that exists within each service. Central to the model is the key quesIon; “What is the workload that the workforce has to undertake?” Furthermore, the model highlights that workload is a funcIon of those receiving care and the configuraIon of the services designed to provide that care. In addiIon, the configuraIon of the services is a funcIon of the work needed to be done and the workforce able to undertake it. As a consequence, discussions about future workforce requirements has to be based on an understanding of the dynamic interplay between each of the three elements. The need for care was modelled by using funcIonal impairment as the key modifiable factor. The data for calculaIng this was taken from the Department of StaIsIcs and from the Australian Bureau of StaIsIcs survey of disability, ageing and carers, which was calibrated for the New Zealand populaIon. This survey (which is a self assessment) provided the best available data on the likely levels of funcIonal impairment (disability) in the populaIon. FuncIonal impairment was defined as any limitaIon, restricIon or impairment, (physical or cogniIve) which has lasted or is likely to last for at least 6 months and restricts everyday acIviIes. Model projecIons indicate that those 65+ with severe funcIonal impairment will rise from 127,874 in 2010 to 207,409 by 2026. Research indicates that the rates at which people develop funcIonal impairment could be reduced by as much as 30%. If this did occur the numbers of people with severe funcIonal impairment would rise to 175,178, by 2026; a reducIon of 43,000 when compared with the baseline.

Exploring the Impact of Adherence to Asthma Medication on Healthcare Utilisation (2010) (Work Conducted for private healthcare provider)
David Rees, Synergia, Auckland, New Zealand
Recently a private healthcare provider completed a trial of a medicaIon adherence programme, which involved targeted text messaging designed to change percepIons and improve adherence to asthma preventer medicaIon. The results were impressive, showing a 39% increase in adherence, versus the baseline, aLer 6 months. The quesIon that this raised for the Company was whether or not this improvement could have significant enough impacts upon healthcare uIlisaIon to jusIfy further investments in the programme. Of special interest was whether or not the impact upon healthcare uIlisaIon could be significant enough to interest Pharmac in supporIng the programme. To help answer this Synergia was commissioned to develop a dynamic simulaIon model that could explore the impact of increased adherence, generated by programme, on healthcare uIlisaIon. This would then enable the Company to make a more rigorous assessment of its commercial viability in the New Zealand market.

A Whole of System Approach to Compare Op$ons for CVD Interven$ons in Coun$es Manukau, New Zealand (2009) (Australia New Zealand Journal Of Public Health. (2012) Volume 65, Issue 3.)
SmokingPrevalence
ObesityPrevalence
Secondhandsmoke
Poor dietfraction
Inadequatephysical activity
fraction
Stressedfraction
Diagnosisand control
First-time CVevent and death
rates
Use of smoking quitproducts and
services
Use of mental healthservices by stressed
Sources ofstress
Use of weight lossservices by obese
Use ofprimary care
Particulate airpollution
Use of qualityprimary care
Tobacco taxes andsales/marketing
regulations
Smoking bans atwork and public
places
Quality of primarycare provision
Anti-smokingsocial marketing
Highcholesterol
High bloodpressure
Diabetes
UncontrolledChronic Disorder
Prevalences
Non-CVDPopn
Post-CVDPopnFirst-time
events survived
Recurrent CVevent and death
rates
CV events anddeaths
Peopleturning 35
Non-CVD Popndeaths
Post-CVD Popndeaths
Timothy Kenealy, SecIon of Integrated Care, South Auckland Clinical School, University of Auckland, New Zealand David Rees, Synergia, Auckland, New Zealand Nicolese Sheridan, SecIon of Integrated Care, South Auckland Clinical School, University of Auckland, New Zealand Allan Moffis, Director of Primary Care, CounIes Manukau District Health Board, New Zealand Sarah Tibby, Programme Manager, Long term CondiIons, CounIes Manukau District Health Board, New Zealand Jack Homer, Homer ConsulIng, Voorhees, New Jersey, United States.
Objec$ve To assess the usefulness, to planning and funding decision makers, of a naIonal and a local System Dynamics model of cardiovascular disease. Methods In an iteraIve process, an exisIng naIonal model, based on earlier work by Jack Homer, was populated with local data and was presented to stakeholders, in CounIes Manukau, New Zealand. They explored the plausibility, usefulness and implicaIons of the model. Data were collected from 30 people using quesIonnaires, and from field notes and interviews, both of which were themaIcally analysed. Results PotenIal users readily understood the model and acIvely engaged in discussing it. None disputed the overall model structure, but most wanted extensions to the model to elaborate areas of specific interest to them. Local data made lisle qualitaIve difference to data interpretaIon but was nevertheless considered to be a necessary step to support confident local decisions. Conclusion Some limitaIons to the model and its use were recognised, but users could allow for these and sIll derive use from the model to qualitaIvely compare decision opIons. Implica$ons The System Dynamics modelling process is useful in complex systems and is likely to become established as part of the rouInely used suite of tools used to support complex decisions in CounIes Manukau District Health Board. Keywords Cardiovascular diseases, system dynamics, populaIon health, decision making, health care quality access and evaluaIon