SCVMC NURSING SERVICES: BRN 27.1 VOLUME II Page 1 of 13
14
SCVMC NURSING SERVICES: BRN 27.1 VOLUME II Page 1 of 13 *”FOR THE PURPOSES OF THIS DOCUMENT, ‘PROTOCOL’ IS A STANDARDIZED PROCEDURE” Applies to: √ Inpatient RNs only √ Ambulatory Care RNs only √ Psych Service RNs only TITLE: Influenza (Flu) / Pneumococcal Vaccine Administration PURPOSE: To outline the nursing responsibilities in the management of patients assessed or requesting annual Influenza (Flu) / Pneumoccocal vaccine immunization. LEVEL: Independent. This protocol is a Board of Registered Nursing Standardized Procedure and may be initiated without a physician order. SUPPORTIVE DATA: This protocol is performed by Registered Nurses (RNs) working in, but not limited to, the Ambulatory and Community Health Clinics (ACHS), and acute care settings in Santa Clara Valley Medical Center (SCVMC), who have been authorized through evaluation and approved in writing to initiate/ perform this protocol. No direct supervision of the RN is required. The Standard of Care in our community is to offer the influenza vaccine to whomever requests vaccination (subject to vaccine availability). Optimal timing for vaccination is October- November. The vaccine should not be given too early in the season because antibody titers may begin to decline before the flu season. The 2012 - 2013 vaccine is a combination to provide protection against H1N1, H3N2, and influenza B viruses, This years vaccine virus used for H1N1 was not changed, and it was recommended the H3N2 and B vaccine viruses be changed from those in the 2011 – 2012 vaccine. Influenza vaccine may be given to both children and adults when available and throughout the flu season: typically between October 1 st – March 31 st , and may be given early when available from the manufacture. The American Academy of Pediatrics states that influenza vaccine can be administered simultaneously (but at a different site and with a different syringe) with other routine, vaccinations in children. Children aged 6 months--8 years who did not receive 2 or more doses of seasonal vaccine since July 1, 2010 or uncertain if ever received seasonal influenza vaccine, should receive 2 doses of the 2012 – 2013 seasonal influenza vaccine. These 2 doses should be given at least 4 weeks apart. . (see Attachment A). A new intradermal vaccine Fluzone Intradermal, TIV preparation, was licensed in May 2011 as an alternative for persons 18 – 64 years of age. It contains less antigen than the intramuscular TIV preparation and the deltoid is the preferred site for injection. Common adverse reactions include: injection site erythema, induration, swelling, pain and Pruritus Fluzone High-Dose (Sanofi Pasteur) is available for persons 65 years of age and older. This contains a higher level of antigen than other preparations. LAIV (live attenuated influenza vaccine), FluMist is indicated for healthy, nonpregnant persons aged 2 through 49 years of age specified in the package insert. There is no preference in administering LAIV versus TIV in this age group. NOTE: The influenza vaccine is considered safe in pregnant patients. Vaccinations should not be postponed, regardless of stage of pregnancy, in patients who have high risk conditions and who will be in the first trimester of pregnancy when flu season begins.
Transcript of SCVMC NURSING SERVICES: BRN 27.1 VOLUME II Page 1 of 13

SCVMC NURSING SERVICES: BRN 27.1 VOLUME II Page 1 of 13
*”FOR THE PURPOSES OF THIS DOCUMENT, ‘PROTOCOL’ IS A STANDARDIZED PROCEDURE”
Applies to:
√ Inpatient RNs only
√ Ambulatory Care RNs only
√ Psych Service RNs only
TITLE: Influenza (Flu) / Pneumococcal Vaccine Administration PURPOSE: To outline the nursing responsibilities in the management of patients assessed or
requesting annual Influenza (Flu) / Pneumoccocal vaccine immunization. LEVEL: Independent. This protocol is a Board of Registered Nursing Standardized Procedure and
may be initiated without a physician order. SUPPORTIVE DATA: This protocol is performed by Registered Nurses (RNs) working in, but not limited to, the
Ambulatory and Community Health Clinics (ACHS), and acute care settings in Santa Clara Valley Medical Center (SCVMC), who have been authorized through evaluation and approved in writing to initiate/ perform this protocol. No direct supervision of the RN is required.
The Standard of Care in our community is to offer the influenza vaccine to whomever requests vaccination (subject to vaccine availability). Optimal timing for vaccination is October- November. The vaccine should not be given too early in the season because antibody titers may begin to decline before the flu season. The 2012 - 2013 vaccine is a combination to provide protection against H1N1, H3N2, and influenza B viruses, This years vaccine virus used for H1N1 was not changed, and it was recommended the H3N2 and B vaccine viruses be changed from those in the 2011 – 2012 vaccine.
Influenza vaccine may be given to both children and adults when available and throughout the flu season: typically between October 1
st – March 31
st, and may be given early when
available from the manufacture.
The American Academy of Pediatrics states that influenza vaccine can be administered simultaneously (but at a different site and with a different syringe) with other routine, vaccinations in children.
Children aged 6 months--8 years who did not receive 2 or more doses of seasonal vaccine
since July 1, 2010 or uncertain if ever received seasonal influenza vaccine, should receive 2 doses of the 2012 – 2013 seasonal influenza vaccine. These 2 doses should be given at least 4 weeks apart. . (see Attachment A).
A new intradermal vaccine Fluzone Intradermal, TIV preparation, was licensed in May 2011 as an alternative for persons 18 – 64 years of age. It contains less antigen than the intramuscular TIV preparation and the deltoid is the preferred site for injection. Common adverse reactions include: injection site erythema, induration, swelling, pain and Pruritus Fluzone High-Dose (Sanofi Pasteur) is available for persons 65 years of age and older. This contains a higher level of antigen than other preparations. LAIV (live attenuated influenza vaccine), FluMist is indicated for healthy, nonpregnant persons aged 2 through 49 years of age specified in the package insert. There is no preference in administering LAIV versus TIV in this age group.
NOTE: The influenza vaccine is considered safe in pregnant patients. Vaccinations should not be postponed, regardless of stage of pregnancy, in patients who have high risk conditions and who will be in the first trimester of pregnancy when flu season begins.

SCVMC NURSING SERVICES: BRN 27.1 VOLUME II Page 2 of 13
*”FOR THE PURPOSES OF THIS DOCUMENT, ‘PROTOCOL’ IS A STANDARDIZED PROCEDURE”
Pneumoccocal vaccine should be given at least once in a lifetime. Re-vaccinations may be given based on criteria outlined below.
CONTENT: A. TARGET GROUPS: 1. INFLUENZA IMMUNIZATION; inclusion criteria:
a. Adults AND children 6 months - 99+ years old. b. High Risk patients may include: i. Adults and children with chronic cardiac and/or pulmonary disease.
ii. Adults and children (ages 2 - 64 years) with underlying chronic medical conditions iii. Adults and children in chronic care medical facilities. iv. Children 6 months – 18 years on chronic aspirin therapy v. American Indians/Alaska Natives vi. Morbidly obese (body mass index 40 or greater vii. All women who will be pregnant during the influenza season. viii. Immunocompromised adults and children. ix. Household contacts and care providers persons in the above mentioned groups
with emphasis on contacts with children under 6 months. x. Health care workers xi. Students/individual in institutional settings.
2. PNEUMOCCOCAL VACCINATION: Inclusion Criteria
a. All patients greater than or equal to 65 years old b. Patients between 2 and 64 years of age who have chronic heart, lung, renal, metabolic
(i.e., diabetes), or liver disease, anemia, alcoholism c. Patients with compromised or absent spleen (including sickle cell anemia) d. Immunocompromised patients: Congenital or acquired immunodeficiencies; HIV
infection/ AIDS; Chronic renal failure; Nephrotic syndrome; Leukemias; Lymphomas; Hodgkin’s disease; Generalized malignancy; Diseases requiring treatment with immunosuppressive drugs, including long-term systemic corticosteroids or radiation therapy; Solid organ transplantation; Multiple myeloma
e. Revaccinate if (1) the last dose was given greater than five years ago AND (2) the patient was less than 65 years old.
f. If patient is greater than or equal to 65 years old and vaccination history is unknown, administer the vaccine. (Pneumococcal Vaccine does NOT require a separate consent)
g. Patients 2 – 64 living in special environments or social settings (e.g. Alaska Native and certain American Indians)
B. ASSESSMENT:
1. For Outpatient Clinics, review Outpatient Immunization Questionnaire (attachment D) with patient; obtain patient/parent/guardian consent. a. For inpatient units review order form and notify provider if any exclusion criteria.
2. Assess patient’s allergy status, medication/food (i.e., egg allergy), latex and inclusion/exclusion criteria information.
3. Question patient regarding thimerosal sensitivity.
4. Take patient’s temperature, as applicable.
5. Ascertain history of problems following previous immunization with flu vaccine.
6. Question patient regarding symptoms of acute respiratory or other active infections.

SCVMC NURSING SERVICES: BRN 27.1 VOLUME II Page 3 of 13
*”FOR THE PURPOSES OF THIS DOCUMENT, ‘PROTOCOL’ IS A STANDARDIZED PROCEDURE”
D. CONTRAINDICATIONS:
1. INFLUENZA a. Anaphylactic hypersensitivity to eggs, latex or other vaccine components. b. Contraindicated for those individuals known to be sensitive to thimerosal. c. Use cautiously in patients with history of sulfite allergy. d. Per FDA approved information for Influenza Vaccine: “Persons with acute febrile illnesses
should not be vaccinated until their symptoms have abated. However, minor illnesses with or without fever should not contraindicate the use of influenza vaccine, particularly in children with a mild upper respiratory tract infection or allergic rhinitis.”
e. If have history of Guillain-Barré Syndrome (GBS), will need to discuss with the provider to determine if the influenza vaccine is contraindicated.
2. PNEUMOCCOCAL
a. Medically contraindicated because of bone marrow transplant within the past 12 months b. Patient is pregnant c. Previous allergic and/or neurologic reaction to this vaccine d. Currently receiving a scheduled course of chemotherapy or radiation therapy e. Platelets less than 25,000 mm3 f. Documented vaccination within 5 years g. Patient claims to have been vaccinated in the last 5 years h. Patient declines vaccine i. Patient does NOT meet any inclusion criteria j. Patient in the ICU
3. Provider order excluding patient from receiving specified vaccine. E. CONDITIONS TO REPORT AND CONSULT WITH PHYSICIAN:
1. Consult with physician if patient gives a history of problems after receiving previous flu vaccine. 2. Consult with physician if patient received bone marrow or organ transplant within the last six (6)
months
3. Notify physician immediately of allergic reaction (which usually occurs immediately). Complete and forward Adverse Drug Reaction Form (refer to SCVMC Formulary for current requirements).
4. Consult with physician if immunnodeficient/Immuno compromised patient requests booster vaccine. 5. WARNING: Platelet count: Do not administer pneumococcal vaccine without MD order if Platelets
< 25,000mm³. 6. If a history of Guillain-Barré Syndrome (GBS). 7. Consult with physician if patient has not vaccine history or unable to answer for self or family
member present to address medical history. F. PLAN/TREATMENT: (Initiated when no exclusion criteria is noted and patient meets one or more of the
inclusion criteria)
1. Influenza Vaccine should be administered intramuscularly (IM). a. Flumist administered nasally, comes in 0.2 mL pre-filled single-administration intranasal
sprayer containing 10 FFU (fluorescent focus units) of vaccine. i. Patient should stand upright when receiving the vaccine. Half the contents of
sprayer are sprayed into the first nostril. The dose-divider clip on the device is then removed, and the second half of the dose is sprayed into the second nostril.
ii. If the patient sneezes after administration, the spray should not be repeated.

SCVMC NURSING SERVICES: BRN 27.1 VOLUME II Page 4 of 13
*”FOR THE PURPOSES OF THIS DOCUMENT, ‘PROTOCOL’ IS A STANDARDIZED PROCEDURE”
b. Fluzone administered intradermally comes in 0.1 mL pre-filled single administration intradermal over the deltoid muscle, preferred.
2. Influenza vaccine dosage as applicable for patient’s age group: (Attachment B)
a. Adults & Children 9 years and over: 0.5 mL IM Inactivated Trivalent Influenza vaccine
Only one (1) dose required. b. Pregnant women 0.5mL IM Inactivated Trivalent Influenza vaccine
Thimerosal free only c. Children 3 to 9 years: 0.5 mL IM Inactivated Trivalent Influenza vaccine.
Repeat in 4 weeks unless child has been previously vaccinated. (see attachment A - Algorithm)
d. Children 6 months to 35 months:
0.25 mL IM. Inactivated Trivalent Influenza vaccine
Repeat in 4 weeks unless child has been previously vaccinated. Thimerosal free only (see Attachment A algorithm)
e. Healthy non-pregnant persons 2 years
to 49 years 0.2mL Flumist-Single dose intranasalsprayer-Live,
attenuated influenza vaccine (Thimerosal free) Restricted to patients with contraindications to Fluzone
2. Adult inpatient Hospital units will:
a. give the influenza vaccine if temperature <38˚ C/ 100.4˚ F b. Fax order form to the inpatient pharmacy
3. Age/weight appropriate acetaminophen dose for fever. 4. Pneumoccocal Vaccine
a. Pneumococcal Polysaccharide Vaccine 0.5 mL SQ single dose.
H. PATIENT EDUCATION/FOLLOW-UP:
1. Advise patient about risks of vaccination as compared with risk of influenza and its complications.
2. Ensure that patient understands that annual vaccination with the latest vaccine is necessary, because immunity to influenza decreases in the year after injection, and vaccination against the current yearly strain is required.
3. Inform patient that the vaccine cannot cause influenza, but that fever, malaise, and myalgia may
begin 6-12 hours after vaccination and last 1 to 2 days. Such systemic reactions are not common. 4. Instruct patient to take acetaminophen, as appropriate for age, for fever and apply ice compresses
to injection site to minimize discomfort. I. DOCUMENTATION:
1. Complete Nursing Documentation Section on the Outpatient Immunization Questionnaire (#6658-G) or Vaccine Orders section of the Hospital Order Form #8281PNM- Pneumoccal Vaccine and/or Inactivated Influenza Vaccine a. Date/Time b. Temperature/route, as applicable c. Vaccine name, Dosage; Lot #; Mfr. name; Expiration date d. Vaccine Information Sheet (VIS) edition date given e. Body site injection where injection given (preference right or left deltoid)

SCVMC NURSING SERVICES: BRN 27.1 VOLUME II Page 5 of 13
*”FOR THE PURPOSES OF THIS DOCUMENT, ‘PROTOCOL’ IS A STANDARDIZED PROCEDURE”
f. Document patient’s decision to not receive or refuses vaccination on the designated documentation tool.
g. Document the exclusion criteria g. Signature and title
J. REQUIREMENTS OF RN:
1. Education/Training: In-service/orientation and competency validation to the protocol.
2. Experience: Minimum of three (3) months experience as an RN in the Ambulatory Care Clinical setting or SCVMC acute care unit.
3. Initial Evaluation: Completion of in-service/orientation/competency validation to the protocol.
A list of RNs authorized to perform this protocol is maintained in the Unit Quality Improvement Manual, TAB: Mandatory Information, in the Manager’s Office, and entered into ‘One Staff’. (See attached “BRN Standardized Procedure Authorization Listing” Form).
4. On-going Evaluation: Annual review of competency.
K. DEVELOPMENT & APPROVAL OF THE STANDARDIZED PROCEDURE:
1. Method: Developed and approved by authorized representatives of Administration, Medical Staff, and Nursing.
2. Review: Annual SIGNATURES OF AUTHORIZED REPRESENTATIVES:
Deputy Director, Ambulatory Care Date Interim Chief Nursing Officer, SCVMC Date Medical Director, SCVMC Pharmacy & Therapeutics Committee Date Chairperson, Interdisciplinary Practice Committee Date

SCVMC NURSING SERVICES: BRN 27.1 VOLUME II Page 6 of 13
BRN 27.1 INFLUENZA/ PNEUMOCOCCAL 082112 /S/ACHS STANDARDS
REFERENCE: MMWR August 17, 2012 / 61(32);613-618 CDC Website Prevention and Control of Influenza with Vaccines: Recommendations of the Advisory Committee on Immunization Practices (ACIP)-United States, 2012-13 Influenza Season
MMWR June 3, 2011 Update: 61 (21):394-395, CDC Website: CDC-Licensure of 13-Valent Pneumococcal Conjugate Vaccine for Adults Aged 50 years and Older
MMWR August 18, 2011, Prevention and Control of Influenza with Vaccines - Recommendations of the Advisory Committee on Immunization Practices (ACIP), 2011. CDC Website for Clinicians, Influenza Vaccination: A Summary for Clinicians, www.cdc.gov State of California DHS January 11, 2006 memo from Howard Baker MD, M.P.H., Chief CMS (Center for Medicare & Medicaid Services) requirements.
RESOURCES: Monica Cramer, BSN, RN, Nursing Clinical Standards Coordinator, Mosby Manager, Interim
Magnet Coordinator, Ambulatory and Community Health Services, Santa Clara Valley Medical Center (SCVMC).
Blaine Allen, RN, Critical Care Staff Developer, SCVMC Ambulatory and Community Health Services Pediatric Unit Council, SCVMC.
Ambulatory and Community Health Services “Patient Immunization Questionnaire” Form #6658-G. APPROVAL: 3/09, 10/10, 9/11, 9/11, 9/12 (Interdisciplinary Practice Committee) REVIEW: REVISION: 9/10, 5/11, 6/11, 8/11, 8/12

SCVMC NURSING SERVICES: BRN 27.1 VOLUME II Page 7 of 13
BRN 27.1 INFLUENZA/ PNEUMOCOCCAL 082112 /S/ACHS STANDARDS
ATTACHMENT A Recommendations for routine use of vaccines in children and adolescents are issued by CDC and are harmonized to the greatest extent possible with recommendations made by the American Academy of Pediatrics, the American Academy of Family Physicians (AAFP), and the American College of Obstetrics and Gynecology (ACOG). CDC recommendations for routine use of vaccines in adults are harmonized to the greatest extent possible with recommendations made by AAFP, ACOG, and the American College of Physicians. The Advisory Committee on Immunization Practices (ACIP) is chartered as a federal advisory committee to provide expert external advice and guidance to the Director of CDC on use of vaccines in the civilian population of the United States. ACIP members are named by the Secretary of the U.S. Department of Health and Human Services. ACIP recommendations become CDC policy once approved by the Director of CDC, on the date published by MMWR.
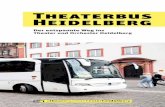
FIGURE 1. Influenza vaccine dosing algorithm for aged children 6 months through 8 years — Advisory Committee on Immunization Practices, United States, 2012–13 influenza season
* Doses should be administered at least 4 weeks apart.
† For simplicity, this algorithm takes into consideration only doses of seasonal influenza vaccine received since July 1, 2010. As an alternative approach in settings where vaccination history from before July 1, 2010, is available, if a child aged 6 months through 8 years is known to have received at least 2 seasonal influenza vaccines during any previous season, and at least 1 dose of a 2009(H1N1)-containing vaccine (i.e., either 2010–11 or 2011–12 seasonal vaccine or the monovalent 2009[H1N1] vaccine), then the child needs only 1 dose for 2012–13. Using this approach, children aged 6 months through 8 years need only 1 dose of vaccine in 2012–13 if they have received any of the following: 1) 2 or more doses of seasonal influenza vaccine since July 1, 2010; 2) 2 or more doses of seasonal influenza vaccine before July 1, 2010, and 1 or more doses of monovalent 2009(H1N1) vaccine; or 3) 1 or more doses of seasonal influenza vaccine before July 1, 2010, and 1 or more doses of seasonal influenza vaccine since July 1, 2010. Children for whom one of these conditions is not met require 2 doses in 2012–2013.
Alternate Text: The figure above shows influenza vaccine dosing algorithm for aged children 6 months through 8 years in the United States, during the 2012-13 influenza season. Children are recommended to receive 2 doses this season, even if 2 doses of seasonal influenza vaccine were received before the 2010-11 season. This is illustrated in two approaches for determining the number of doses required for children aged 6 months through 8 years, both of which are acceptable.

SCVMC NURSING SERVICES: BRN 27.1 VOLUME II Page 8 of 13
BRN 27.1 INFLUENZA/ PNEUMOCOCCAL 082112 /S/ACHS STANDARDS
ATTACHMENT B
TABLE. Influenza vaccine information, by age group — United States, 2012–13 influenza season*
Vaccine Trade name Manufacturer Presentation Mercury content (µg Hg per 0.5 mL dose)
Ovalbumin content (µg per 0.5mL dose)†
Age group
No. of doses
Route
TIV Fluzone Sanofi Pasteur 0.25 mL prefilled syringe
0.0 —§ 6–35 mos
1 or 2¶ IM**
0.5 mL prefilled syringe
0.0 —§ ≥36 mos
1 or 2¶ IM**
0.5 mL vial 0.0 —§ ≥36 mos
1 or 2¶ IM**
5.0 mL multidose vial
25.0 —§ ≥6 mos 1 or 2¶ IM**
TIV Agriflu Novartis Vaccines 0.5 mL prefilled syringe
0 <0.4 ≥18 yrs 1 IM**
TIV Fluvirin Novartis Vaccines 0.5 mL prefilled syringe
≤1 ≤1 ≥4 yrs 1 or 2¶ IM**
5.0 mL multidose vial
25.0 ≤1
TIV Fluarix GlaxoSmithKline 0.5 mL prefilled syringe
0 ≤0.05 ≥3 yrs 1 or 2¶ IM**
TIV FluLaval ID Biomedical Corporation of Quebec (distributed by GlaxoSmithKline)
5.0 mL multidose vial
<25.0 ≤0.3 ≥18 yrs 1 IM**
TIV Afluria CSL Biotherapies (distributed by Merck)
0.5 mL prefilled syringe
0.0 ≤1 ≥9 yrs††
1 IM**
5.0 mL multidose vial
24.5 ≤1
TIV high- dose§§
Fluzone High-Dose
Sanofi Pasteur 0.5 mL prefilled syringe
0.0 —§ ≥65 yrs 1 IM**
TIV intradermal¶¶
Fluzone Intradermal
Sanofi Pasteur 0.1 mL prefilled microinjection system
0.0 (per 0.1 mL)
—§ 18–64 yrs
1 ID

SCVMC NURSING SERVICES: BRN 27.1 VOLUME II Page 9 of 13
BRN 27.1 INFLUENZA/ PNEUMOCOCCAL 082112 /S/ACHS STANDARDS
LAIV FluMist*** MedImmune 0.2 mL prefilled intranasal sprayer
0.0 (per 0.2 mL)
<0.24 (per 0.2mL)†††
2–49 yrs§§§
1 or 2¶ IN
Abbreviations: TIV = trivalent inactivated vaccine; LAIV = live-attenuated influenza vaccine; IM = intramuscular; ID = intradermal; IN = intranasal.
* Vaccination providers should consult Food and Drug Administration–approved prescribing information for 2012–13 influenza vaccines for the most updated information, including indications, contraindications, and precautions.
† Data on maximum ovalbumin content is supplied in package inserts of certain vaccines. Persons with a history of mild allergy to egg (specifically, those who experience only hives) should receive TIV with additional precautions (Figure 2).
§ Information is not included in package insert but is available upon request from the manufacturer, Sanofi Pasteur, by contacting 1-800-822-2463 or [email protected].
¶ Figure 1 describes two approaches for determining the number of doses needed for children aged 6 months through 8 years.
** For adults and older children, the recommended site of vaccination is the deltoid muscle. The preferred site for infants and young children is the anterolateral aspect of the thigh.
†† Age indication per package insert is ≥5 years; however, the Advisory Committee on Immunization Practices recommends that Afluria not be used in children aged 6 months through 8 years because of increased risk for febrile reactions noted in this age group with CSL's 2010 Southern Hemisphere TIV. If no other age-appropriate, licensed inactivated seasonal influenza vaccine is available for a child aged 5 through 8 years who has a medical condition that increases the child's risk for influenza complications, Afluria can be used; however, vaccination providers should discuss with the parents or caregivers the benefits and risks of influenza vaccination with Afluria before administering this vaccine. Afluria may be used in persons aged ≥9 years.
§§ A 0.5-mL dose contains 60 µg of each vaccine antigen (180 µg total).
¶¶ A 0.1-mL dose contains 9 µg of each vaccine antigen (27 µg total).
*** A new quadrivalent formulation of FluMist was approved by the Food and Drug Administration in February 2012. It is anticipated that this formulation will replace the currently available seasonal trivalent LAIV formulation for the 2013–14 season. FluMist is shipped refrigerated and stored in the refrigerator at 35°F–46°F (2°C–8°C) after arrival in the vaccination clinic. The dose is 0.2 mL divided equally between each nostril. Health-care providers should consult the medical record, when available, to identify children aged 2 through 4 years with asthma or recurrent wheezing that might indicate asthma. In addition, to identify children who might be at greater risk for asthma and possibly at increased risk for wheezing after receiving LAIV, parents or caregivers of children aged 2 through 4 years should be asked, "In the past 12 months, has a health-care provider ever told you that your child had wheezing or asthma?" Children whose parents or caregivers answer "yes" to this question and children who have asthma or who had a wheezing episode noted in the medical record within the past 12 months should not receive FluMist.
††† Insufficient data available for use of LAIV in egg-allergic persons.
§§§ Flumist is indicated for healthy, nonpregnant persons aged 2 through 49 years. Persons who care for severely immunosuppressed persons who require a protective environment should not receive FluMist given the theoretical risk for transmission of the live-attenuated vaccine virus.

ATTACHMENT C
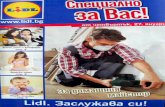
FIGURE 2. Recommendations regarding influenza vaccination for persons who report allergy to eggs — Advisory Committee on Immunization Practices, United States, 2012–13 influenza season
Abbreviation: TIV = trivalent inactivated vaccine.
* Persons with egg allergy might tolerate egg in baked products (e.g., bread or cake). Tolerance to egg-containing foods does not exclude the possibility of egg allergy.
Alternate Text: The figure above shows recommendations regarding influenza vaccination for persons who report a history of egg allergy, in the United States during the 2012-13 influenza season. Persons with a history of egg allergy who have experienced only hives after exposure to egg should receive influenza vaccine, with the use of additional safety measures
CDC-Prevention and Control of Influenza with Vaccines: Recommendations of the Advisory Committee on Immunization Practices (ACIP)-United States, 2012-13 Influenza Season

6658-G Rev 082712 DISPOSITION: ORIGINAL to Medical Record: Progress Notes
751 South Bascom Avenue San Jose, CA 95128
OUTPATIENT INFLUENZA
VACCINE PATIENT
QUESTIONNAIRE / CONSENT
Page 1 of 1
1) If you received a flu shot last year, did you have any problems after the injection? Yes ____ No _____ N/A _____
2) Do you have any infections now, such as a “cold”? Yes ____ No _____
4) Contraindications to the LAIV (Monovalent Vaccine Live, Intranasal) Child under 24 months or ≥ 50 yrs 2 -17 yrs receiving aspirin or aspirin containing therapy Asthma, child < 5 yrs, or chronic respiratory disease Currently Pregnant or breastfeeding (injectable [killed vaccine] acceptable) Close contact with severely immunocompromised individual(s) (includes HIV)
5) Guillain-Barré Syndrome (refer to PCP) I consent to the vaccine I decline receiving the vaccine
Patient Signature Date (FDA approved information for influenza Vaccine: “Persons with acute febrile illnesses should not be vaccinated until their symptoms have abated. However, minor illness, with or without fever, should not contraindicate the use of influenza vaccine, particularly in children with a mild upper respiratory tract infection or allergic rhinitis.)
NURSING DOCUMENTATION SECTION: Questionnaire Reviewed by: _____________________ See Electronic Health Record for Nursing Documentation
Provider notification: ______________________________________________
VIS Given: _ Yes_ No Publication Date _________________________
Lot #/Exp Date/Manufacture Intranasal IM SQ Right Left Deltoid Thigh
Vaccine(s) administered by:
_____________________________________________________________________________________ Signature/Title (RN/LVN/MA) Date/Time Verified by(RN/Provider ) ______________________________________________________________
3) Please check those items you are allergic to or History of:
Eggs Guillain-Barré Syndrome
Thimerosal Asthma or chronic respiratory disease
Latex Currently Pregnant or breastfeeding
Sulfite allergy (use cautiously) Exposure to individual with Flu
Close contact with severely immunocompromised individual(s) (includes HIV infection)
Other _________________________________________________

ATTACHMENT E


SCVMC BRN STANDARDIZED PROCEDURE AUTHORIZATION LISTING TITLE OF PROCEDURE: INFLUENZA (FLU) VACCINE ADMINISTRATION______________
The following registered nurses have been validated for competency for the above California BRN Standardized Procedure. Competency validation is performed annually.
NAME DATE VALIDATED BY: NAME/TITLE
1. 2. 3. 4. 5. 6. 7. 8. 9. 10.
THE ORIGINAL COMPLETED FORM IS TO BE PLACED IN THE CLINIC MANAGERS ORIENTATION/ANNUAL COMPETENCY VALIDATION MANUAL ACHS - TAB: BRN PROTOCOLSAND ENTERED INTO ‘ONE STAFF’.

6658-G Rev 082712 DISPOSITION: ORIGINAL to Medical Record: Progress Notes
751 South Bascom Avenue San Jose, CA 95128
OUTPATIENT INFLUENZA
VACCINE PATIENT
QUESTIONNAIRE / CONSENT
Page 1 of 1
1) If you received a flu shot last year, did you have any problems after the injection?
Yes ____ No _____ N/A _____
2) Do you have any infections now, such as a “cold”? Yes ____ No _____
4) Contraindications to the LAIV (Monovalent Vaccine Live, Intranasal)
Child under 24 months or ≥ 50 yrs
2 -17 yrs receiving aspirin or aspirin containing therapy
Asthma, child < 5 yrs, or chronic respiratory disease
Currently Pregnant or breastfeeding (injectable [killed vaccine] acceptable)
Close contact with severely immunocompromised individual(s) (includes HIV) 5) Guillain-Barré Syndrome (refer to PCP)
I consent to the vaccine I decline receiving the vaccine
Patient Signature Date (FDA approved information for influenza Vaccine: “Persons with acute febrile illnesses should not be vaccinated until their symptoms have abated. However, minor illness, with or without fever, should not contraindicate the use of influenza vaccine, particularly in children with a mild upper respiratory tract infection or allergic rhinitis.)
NURSING DOCUMENTATION SECTION: Questionnaire Reviewed by: _____________________ See Electronic Health Record for Nursing Documentation
Provider notification: ______________________________________________
VIS Given: _ Yes_ No Publication Date _________________________
Lot #/Exp Date/Manufacture Intranasal IM SQ Right Left Deltoid Thigh
Vaccine(s) administered by:
_____________________________________________________________________________________ Signature/Title (RN/LVN/MA) Date/Time
Verified by(RN/Provider ) ______________________________________________________________
3) Please check those items you are allergic to or History of:
Eggs Guillain-Barré Syndrome
Thimerosal Asthma or chronic respiratory disease
Latex Currently Pregnant or breastfeeding
Sulfite allergy (use cautiously) Exposure to individual with Flu
Close contact with severely immunocompromised individual(s) (includes HIV infection)
Other _________________________________________________