Screening Mammography: The Controversy, and … PC...• Screening mammography is the only modality...
44
Screening Mammography: The Controversy, Risk Assessment and Individualized Screening recommendations. Jonathan T. Sims MD, MBA
Transcript of Screening Mammography: The Controversy, and … PC...• Screening mammography is the only modality...

Screening Mammography: The Controversy, Risk Assessment and
Individualized Screening recommendations.
Jonathan T. Sims MD, MBA

I have no relevant Financial Disclosures

Agenda
• Discuss the recent studies calling into question the benefits of mammography.
• What are the facts and statistics we track
• Screening recommendations in the general public, special populations, and the importance of breast density

RECENT STUDIES CALLING INTO QUESTION THE BENEFITS OF MAMMOGRAPHY

• UK Independent Review
• Nordic Cochrane Institute Review
• US Preventive Services Task Force Review
• EUROSCREEN Review – All of the studies attempted to answer the question
“how many women need to undergo breast cancer screening, in order to save 1 woman’s life, from dying from breast cancer (during the observation time period)?”
– Results varied from 80-2,000

Why the large variance?
• Definition of undergo breast cancer screening – Nordic Cochrane Institute Review considered a women
being notified and instructed to undergo mammography as “being screened.” • 23% of women didn’t show up.
• During the observational time period – Studies ranged from 10 years to 20 years
• The longer the observational time period, the more efficaous screening mammography became.
• Which ages were included – 40-74 – 50-74

Nordic Cochrane Institute Review
• 2,000 women need to get “screened” to save 1 life. – Screening means- getting a reminder
– Time period- over 10 years
– Age- 40-74.
• Change the variables, changes the numbers: – 600:1- Screening=mammogram, time frame is 20
years, ages included 40-74
– 300:1 – restrict ages to 50-74

The controversy’s take home points
• Screening mammography works-
• Are the benefits immediate-
• The benefits can be concentrated-
• But they shouldn't be

FACTS
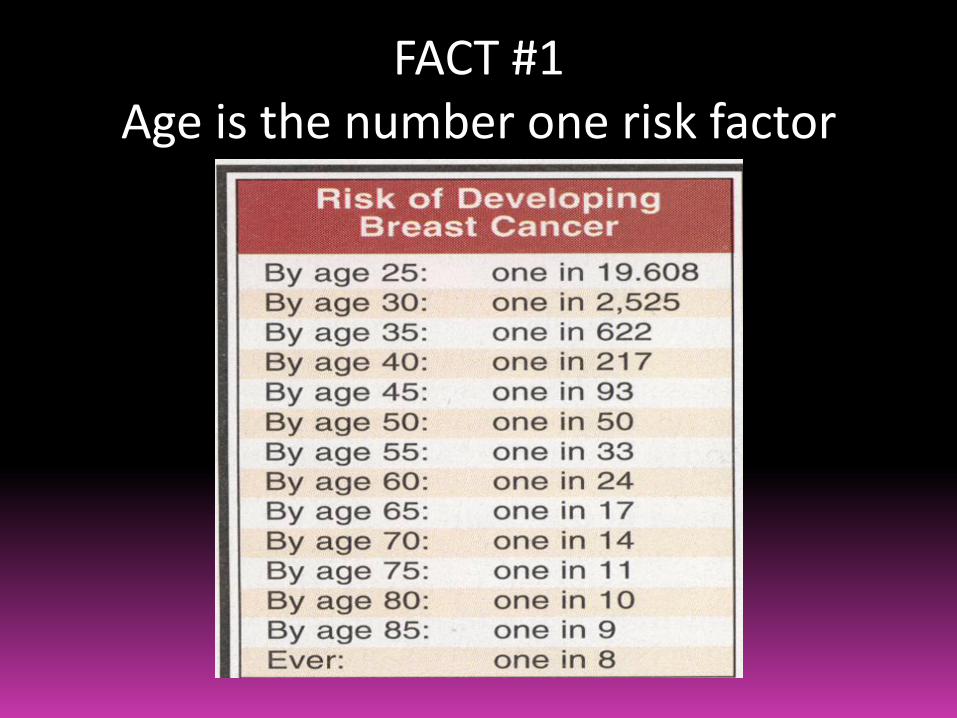
FACT #1 Age is the number one risk factor

FACT #2 Must catch it early
• Prognosis most influenced by axillary node status – No nodes- 5 year survival 82.8%
– 1-3 nodes- 5 year survival 73%
– 4-12 nodes- 5 year survival 46%
– >13 nodes- 5 year survival 28.4%
• Tumor size matters immediate and long term – size correlates with axillary node status And is an
independent prognostic indicator – <1cm- 99% five year survival (88% 20 year recurrence free
survival)
– 1-3 cm – 89% (72% 20 year recurrence free survival)
– >3 cm – 86% (59% 20 year recurrence-free survival

FACT #3 Screening mammography works
• Technological improvements have led to better detection

FACT #4 Detecting small tumors decreases
mortality

Take home facts:
• Screening mammography is the only modality that is proven to save lives
• Best chances of surviving breast cancer is catching it early • 1/8 women will have breast cancer sometime during their lifetime • Of women that undergo screening mammography, about 6-8% will
need additional evaluation, and 6-8% of those women will be diagnosised with breast cancer
• Of all the baseline screening exams, almost 1% will have breast cancer
• Non baseline screening exams, about 0.5% will have breast cancer • Over the last 4 months OIC has diagnosised 13 breast cancers in
asymptomatic women between 40-50 years of age. • All of our mammographers see every cancer that is diagnosised at
OIC

ACR target statistics

RECOMMENDATIONS: THEN, NOW, AND TOMORROW

THEN: Screening recommendations
Normal Risk
Yearly Mammograms- starting at 40 years of age and continuing for as long as the patient is in good health
Clinical breast exams, every three years from 20-40, yearly for patients >40
Monthly self breast exams

NOW: Screening recommendations
Normal Risk Moderate Risk High Risk
Yearly Mammograms- starting at 40 years of age and continuing for as long as the patient is in good health
Clinical breast exams, every three years from 20-40, yearly for patients >40
Monthly self breast exams
NOW: recommendations are influenced by breast density, and personal/familial risk factors.

Family history
• Family history risk:
– Strong family history – First degree w/ premenopausal
– Male relatives
– Known family history of BRCA genes
– Intermediate family history – First degree w/ postmenopausal
– Weak family history – Second degree relatives
– No family history

Family history of proven genetic cancer syndromes
• Li-fraumeni syndrome (p53 gene mutation) – Sarcoma, breast, leukemia and adrenal gland (SBLA) syndrome
• Bannayan-Riley-Ruvalcaba syndrome (PTEN mutation)
• Cowden syndrome – breast carcinoma, follicular carcinoma of the thyroid, and
endometrial carcinoma (hamartomas everywhere)

Personal medical history
• History of XRT of chest for lymphoma
• History of Breast Cancer (IDC or ILC)
• Previous breast biopsies
– Atypical anything
– LCIS (50% multi ipse, 30% bilateral)
• 5-20% will be diagnosised with breast cancer within the next 5 years.

Mammographic breast density
• Not perceived density on breast exam.
• Proportion of breast composed of glandular elements and stoma seen at mammography

Mammographic breast density • Senate bill 420
– Effective January 1, 2014 Oregon became the 11th state to pass breast density legislation requiring providers to inform women with dense breast tissue that they have dense breasts. • This increases their risk of developing breast cancer
• Decreases the sensitivity of screening mammography
• The patient may need additional screening
– Failed to require the additional screening be covered by insurances
– “intended to start a conversation between patients and their providers concerning if and what they need.”

Required notification

Required notification


Case report
• Patient presents with confusion-
– “I got a letter saying “no breast cancer.” But on the same letter, it says I have “dense breasts” so I might have cancer. And I was instructed to talk to you.”

Reassure and risk stratify
• Risk stratify
– Risk model (like the Gail model)
– Take a detailed history

Personal breast cancer risk assessment
• Gail model, the Claus model, and the Tyrer-Cuzick model
– Give approximate estimates of breast cancer risk based on different combination of risk factors and different data sets
• May give different risk estimates for the same women
• Take home- Gail model is the best one currently- used for determining adjuvant hormonal therapy

Gail model
• The tool calculates a woman's risk of developing breast cancer within the next five years and within her lifetime (up to age 90). It takes into account seven key risk factors for breast cancer.
– Age – Age at first period – Age at the time of the birth of her first child (or has not given birth) – Family history of breast cancer (mother, sister or daughter) – Number of past breast biopsies – Number of breast biopsies showing atypical hyperplasia – Race/ethnicity
• Women with a five-year risk of 1.67 percent or higher are classified as "high-risk." This score (a five-year risk of 1.67 percent or higher) is the cut-off for the FDA guidelines for taking tamoxifen or raloxifene to reduce breast cancer risk.
• Limitations- based on white women, no paternal history), doesn’t take into account personal history of DCIS, IDC, LCIS, or ILC

NOW: Screening recommendations Normal Risk (10-15%)
Moderate Risk (15-20%)
High Risk (>20%) High Risk and dense
Yearly Mammograms- starting at 40 years of age and continuing for as long as the patient is in good health
Clinical breast exams, every three years from 20-40, yearly for patients >40
Monthly self breast exams
NOW: recommendations are influenced by breast density, and personal/familial risk factors.

When is additional screening recommended?
• People at normal risk (10-15% lifetime risk)- No change
– CBE q3 years between ages 20-40
– CBE q1 year beginning at age 40
– Screening digital mammography starting at age 40
• Yearly, for as long as the patient is in moderately good health.

Patients at moderate risk 15-20% lifetime risk. Would additionally
screen with bilateral whole breast US with elastography
• Dense breasts
• Previous biopsy results of LCIS, atypical anything
• Intermediate family history and heterogeneously dense breasts

Additional Screening with Whole breast US
• Is elastography important- yes
• What screening interval?
• Is this covered by insurance?
• Is this done else where in the world?

Patients at high risk >20% lifetime risk. Strongly consider additional breast
MRI • Personal or family history of genetically
proven cancer syndrome (BRCA/p53/PTEN)
• Strong family history (1st degree w/ pre-menpasual disease, or male relatives)
• Previous mediastinal XRT (starting 10 years after cessation of mediastinal XRT)
• Previous breast cancer (IDC or ILC)

Additional screening with Breast MRI
• Best done at a facility that also does breast biopsies. Or the patient may ultimately get billed for an additional breast MRI.

Low Risk (10-15%)
Intermediate Risk (15-20%)
High Risk (>20%)
High risk and dense
Family History No family history, a few 2nd degrees
1st degree post Multi 2nd degrees
1st degree w/ pre male Carrier/possible carrier of proven cancer syn.
Personal history of:
Breast Bx Atypical anything LCIS
Mediastinal XRT Previous Breast CA (IDC or ILC)
Breast Density (if dense breasts shift column to right)
Extremely Dense or Heterogenously dense.
Yearly dig Mammo with US at least q2 yr
Yearly dig mammo And occ. MRI and occ. US
Yearly dig mammo AND yearly MRI

TOMORROW: Screening recommendations??????
Digital genonmics, tomosynthesis, automated US

My patient received the letter stating she has dense breasts. Now she is wondering whether she should continue to get mammograms
at all.
She should continue to get screening mammograms. The breat density law does not reflect any change in the current
mammography screening recommendations by professional medical societies. Mammograms have been shown to be effective in
lowering breast cancer mortality for all breast densities.

My patient received the new breast density letter. She is concerned because she now thinks she is at high risk for breast cancer.
Reassure the patient that breast density alone has only a small impact on breast cancer risk.
She wants to know specifically how it changes her risk.
Look up the mammogram report. Her density will be either heterogeneously dense (RR= 1.2), or extremely dense (RR= 2.0)
So a 50 y/o female with no other risk factors fatty or scattered Risk is 1/42
50 y/o female with no risk factors and hetero, risk is 1.2/42.
50 y/o female with no risk factors and extememly dense, risk is 1/21.

My patient received the letter stating she has dense breasts. Now she wants to be screened with another modality instead of
mammography.
THERE IS NO MODALITY RECOMMENDED TO REPLACE MAMMOGRAPHY. Certain findings of cancer are ONLY seen on
mammography. Other screening options referred to in the letter are in addition to, and not instead of, a routine screening mammogram.

My patient received the letter stating she has “heterogneeously dense” or “extremely dense” breasts. She has completed a risk assessment showing her overall risk to be high (>20% lifetime risk), or has a BRCA mutation or
history of mantle radiation.
Recommend annual breast MRI and annual memmogram for screening.
Screening breast MRI is typically covered by insurance for high-risk women.
If a woman is being screened annually with MRI and mammogram, no additional screening tests (such as ultrasound) are needed.

My patient received the letter stating she has “heterogneeously dense” or “extremely dense”
breasts. She has completed a risk assessment showing her overall risk to be high (>20% lifetime risk).
I recommended an annual MRI, but the patient has either claustrophobia, pacemaker, contrast allergy,
limited insurance coverage plan, or other reasons why she does not want to have an MRI
Recommend screening ultrasound as the second-best supplementary screening test for high risk women.
Studies have shown some utility for ultrasound in high risk women if screening MRI is not performed.