Scleritis and episcleritis - British Journal of Ophthalmology(30I eyes) with episcleritis and 159...
29
Brit. J. Ophthal. (I 976) 6o, I 63 Scleritis and episcleritis PETER G. WATSON* AND SOHAN SINGH HAYREHt From Moorfields Eye Hospital, City Road, London*, and Addenbrooke's Hospital, Cambridge*, and the Department of Ophthalmology, University of Iowa Hospitals and Clinics, Iowa City, USAt From the earliest available descriptions of episcleritis (Slade, 1838; Rognetta, i844; Desmarres, 1847) a confusion has existed between scleritis and episcleritis. This has led to contradictory views on the relative severity and prognosis of these conditions, and the erroneous belief that episcleritis is accompanied by serious complications (Viswaling- ham, 1936; Wood, 1936; Mann and Markson, I950; Clavel and Teulieres, 1958). While Slade (I838), Rognetta (i844), and Desmarres (I847), thought that episcleritis was both common and severe, Mackenzie (i 830) considered it to be neither and gave at the same time a vivid and accurate description of scleritis. This confusion still persists today. In an attempt to clarify the position we have been studying patients with scleritis and episcleritis in a special clinic at Moorfields Eye Hospital during the past io years. Of these, 207 patients (30I eyes) with episcleritis and 159 patients (2I7 eyes) with scleritis were analysed in depth.§ The results reported below have led us to conclude that scleritis and episcleritis are clinically distinct, with a different symptomatology and prognosis and requiring different management. The incidence of these conditions is not known, but Williamson (1974) suggested that it was about o-o8 per cent of hospital new patient referrals. Our series is from highly selected patients, all being referred from elsewhere, often where there was difficulty in diagnosis, and with unusual problems. This is reflected in the fact that go per cent of the patients who had rheumatoid arthritis were seen within a year of the start of the special clinic. Classification EPISCLERITIS Episcleritis has been recognized for over a century, although-,called by many different names, such as subconj4ctivitis by von Graefe (Duke-Elder and §Mr B. Augier and Mrs B. Phillips of the Institute of Ophthal- mology. London, used the University of London computer to analyse the findings Address for reprints: 22 Parkside, Cambridge, England*, or University of Iowa, Iowa City, Iowa 52242, USAt Leigh, I965), subconjunctival phlegma or simple or phlegmatous conjunctivitis by Mackenzie (I830), and episcleritis periodica fugax by Fuchs (I895). Duke-Elder and Leigh (I965) distinguished be- tween nodular episcleritis and rheumatic episcleritis, but such a differentiation appears to be unjustified as rheumatoid arthritis can be associated with either condition. We have classified episcleritis into two types: i. Simple episcleritis 2. Nodular episcleritis. SCLERITIS Many classifications of scleral disease have been proposed (Holthouse, I893; van der Hoeve, 1934; Franceschetti and Bischler, I950; Duke- Elder and Leigh, I965; Sevel, I967) which have been based on a mixture of clinical and pathological observations. Although we tried to adopt these, from the clinical point of view they have all been unsatisfactory. We eventually adopted the following classification because, although there is some slight overlap between the groups, clinically we have observed several distinct patterns. This classifica- tion has proved to be satisfactory and has enabled us to assign almost all the patients to a particular category at the initial examination. (a) Anterior scleritis i. Diffuse scleritis 2. Nodular scleritis 3. Necrotizing scleritis a. with inflammation b. without inflammation (scleromalacia per- forans) (b) Posterior scleritis. Material Using the above classification, patients were distributed as in Table I. Normal anatomy Before considering the criteria by which the differential diagnosis is reached it is necessary to. on February 1, 2020 by guest. Protected by copyright. http://bjo.bmj.com/ Br J Ophthalmol: first published as 10.1136/bjo.60.3.163 on 1 March 1976. Downloaded from
Transcript of Scleritis and episcleritis - British Journal of Ophthalmology(30I eyes) with episcleritis and 159...

Brit. J. Ophthal. (I 976) 6o, I 63
Scleritis and episcleritis
PETER G. WATSON* AND SOHAN SINGH HAYREHtFrom Moorfields Eye Hospital, City Road, London*, and Addenbrooke's Hospital, Cambridge*,and the Department of Ophthalmology, University of Iowa Hospitals and Clinics, Iowa City, USAt
From the earliest available descriptions of episcleritis(Slade, 1838; Rognetta, i844; Desmarres, 1847)a confusion has existed between scleritis andepiscleritis. This has led to contradictory viewson the relative severity and prognosis of theseconditions, and the erroneous belief that episcleritisis accompanied by serious complications (Viswaling-ham, 1936; Wood, 1936; Mann and Markson, I950;Clavel and Teulieres, 1958). While Slade (I838),Rognetta (i844), and Desmarres (I847), thoughtthat episcleritis was both common and severe,Mackenzie (i 830) considered it to be neither and gaveat the same time a vivid and accurate descriptionof scleritis. This confusion still persists today.
In an attempt to clarify the position we havebeen studying patients with scleritis and episcleritisin a special clinic at Moorfields Eye Hospitalduring the past io years. Of these, 207 patients(30I eyes) with episcleritis and 159 patients (2I7eyes) with scleritis were analysed in depth.§ Theresults reported below have led us to concludethat scleritis and episcleritis are clinically distinct,with a different symptomatology and prognosisand requiring different management.The incidence of these conditions is not known,
but Williamson (1974) suggested that it was abouto-o8 per cent of hospital new patient referrals. Ourseries is from highly selected patients, all beingreferred from elsewhere, often where there wasdifficulty in diagnosis, and with unusual problems.This is reflected in the fact that go per cent of thepatients who had rheumatoid arthritis were seenwithin a year of the start of the special clinic.
Classification
EPISCLERITIS
Episcleritis has been recognized for over a century,although-,called by many different names, such assubconj4ctivitis by von Graefe (Duke-Elder and§Mr B. Augier and Mrs B. Phillips of the Institute of Ophthal-mology. London, used the University of London computer toanalyse the findings
Address for reprints: 22 Parkside, Cambridge, England*, orUniversity of Iowa, Iowa City, Iowa 52242, USAt
Leigh, I965), subconjunctival phlegma or simpleor phlegmatous conjunctivitis by Mackenzie (I830),and episcleritis periodica fugax by Fuchs (I895).Duke-Elder and Leigh (I965) distinguished be-tween nodular episcleritis and rheumatic episcleritis,but such a differentiation appears to be unjustifiedas rheumatoid arthritis can be associated witheither condition. We have classified episcleritisinto two types:
i. Simple episcleritis2. Nodular episcleritis.
SCLERITIS
Many classifications of scleral disease have beenproposed (Holthouse, I893; van der Hoeve,1934; Franceschetti and Bischler, I950; Duke-Elder and Leigh, I965; Sevel, I967) which havebeen based on a mixture of clinical and pathologicalobservations. Although we tried to adopt these,from the clinical point of view they have all beenunsatisfactory. We eventually adopted the followingclassification because, although there is some slightoverlap between the groups, clinically we haveobserved several distinct patterns. This classifica-tion has proved to be satisfactory and has enabledus to assign almost all the patients to a particularcategory at the initial examination.(a) Anterior scleritis
i. Diffuse scleritis2. Nodular scleritis3. Necrotizing scleritis
a. with inflammationb. without inflammation (scleromalacia per-
forans)(b) Posterior scleritis.
Material
Using the above classification, patients weredistributed as in Table I.
Normal anatomy
Before considering the criteria by which thedifferential diagnosis is reached it is necessary to.
on February 1, 2020 by guest. P
rotected by copyright.http://bjo.bm
j.com/
Br J O
phthalmol: first published as 10.1136/bjo.60.3.163 on 1 M
arch 1976. Dow
nloaded from

164 British Journal of Ophthalmology
understand the normal vascular anatomy of theouter coats of the eye. The blood vessels of theepisclera are not easily seen in the uninflamed eye,but as soon as the eye becomes congested threequite separate vascular plexuses become readilyvisible.
i. Bulbar conjunctival plexus (Fig. i)This is the most superficial plexus of fine hair-likeinterlacing vessels freely moveable over the under-lying structures. Overlying the episclera theconjunctival arteries are derived from two sourcesthe anterior ciliary arteries at the limbus, and thepalpebral branches of the ophthalmic and lacrimalarteries. When they are inflamed the colour isbright red.
2. Episcleral plexus (Fig. i)
The vessels, which are straight and radiallyarranged, lie in the superficial episclera (parietallayer of Tenon's capsule) at a depth of about one-quarter to one-third of the distance between thesurface of the conjunctiva and sclera (Graves,1937). The visible vessels are mainly veins, accept-ing the aqueous veins at intervals around the globe.These vessels are moveable over the deep layers,although not so easily as the conjunctival vessels.In the anterior episcleral plexus (anterior to theequator and over the muscle) the vessels belong tothe anterior ciliary system; while in the posteriorepiscleral arterial plexus (posterior to the equator)they are derived from the arteries of the obliquemuscles, the posterior ciliary arteries, and the vesselsof the optic nerve sheaths (Hayreh and Baines,1972). When inflamed, these radially arranged vesselscan easily be seen, giving the eye a salmon pinkcolour.
3. Scleral (deep episcleral) plexus (Fig. I)This plexus consists of a rete (criss-cross) ofvessels lying within the visceral layer of Tenon'scapsule, closely applied to the sclera. At the limbusthe superficial and deep episcleral plexuses mergeinto one another and terminate in the superficialmarginal plexuses of the cornea. When congestedthis layer looks bluish-red in colour and is immobile.
Clinical examinationCareful examination will determine the depth ofthe inflammation, so that it is almost always possibleto decide when the patient is first seen whetherscleritis or episcleritis is present. This depends onaccurate observation of the relationship of onelayer of vessels to the other and to the underlyingsclera.
HISTORY
A detailed clinical history is taken of the patient'socular and systemic disorders, including familyhistory. Any contact with chemical irritants andsolvents is noted, as is any history of allergicconditions, rheumatic, connective-tissue or skindisease, gout, venereal disease, tuberculosis, orsarcoidosis. The site, distribution, and nature ofany ocular pain and disturbances of vision areimportant in deciding the type of inflammationpresent.
EXAMINATION OF THE EYE
After the visual acuity has been recorded, thefollowing routine of examination is used:
I. External examination of the eye in daylightIt is essential to examine a case of episcleritis indaylight as this is often the only way of distin-
FIG. i Normal vascular networks ofepisclera. There are three layers-the-deepest is almost invisible in theuninflamed eye
on February 1, 2020 by guest. P
rotected by copyright.http://bjo.bm
j.com/
Br J O
phthalmol: first published as 10.1136/bjo.60.3.163 on 1 M
arch 1976. Dow
nloaded from

Scleritis and episcleritis I65
guishing episcleritis from the much more seriousscleral disease. In episcleritis the colour is salmonpink; in deep scleral disease the colour has amuch deeper purple hue. These colour changesare difficult to distinguish in tungsten or fluorescentlight. After recurrent attacks of scleral inflammationthe sclera may become more transparent and issometimes thinner, and as a consequence the greychoroid may be seen through the sclera. Some-times these areas are black and well defined, butmore often they give a faint grey tinge to the sclera.This is a particularly important observation inscleromalacia perforans, in which there is no sur-rounding inflammation. Time and again it ispossible to see areas of scleral thinning in daylightwhich were invisible with the slit-lamp or byillumination with tungsten or fluorescent light.
2. Slit-lamp microscopic examination
Of the greatest assistance in distinguishing epi-scleritis from scleritis is the relationship of onevascular network with another and the changeswithin them. The object of this examination is toconfirm the macroscopic findings. In scleritis, theexamination is directed to detecting scleral oedemaand the involvement of scleral vessels, ignoringthe fact that the overlying episclera will be con-gested and oedematous. In episcleritis there willbe no oedema of the sclera. In addition avascularpatches must be diligently searched for, as theseindicate a vasculitis and carry a poor prognosis.
Diffuse illumination confirms the macroscopicimpression that only episcleral tissue is involved,and in addition reveals any corneal changes.
Slit-lamp examination detects the depth of maxi-mum vascular involvement, infiltration, and oedemaof the episclera. Any corneal changes can becategorized and the anterior segment and vitreousscrutinized for evidence of uveitis.
Red-free light examination should never be omitted;it is the ideal method of examining the vascularchanges because the vessels become more easilyvisible. Infiltration of the episclera also showsup as a yellow patch. Adrenaline i: IOOO or io percent phenylephrine can be instilled into the con-junctival sac. This constricts the conjunctival andsuperficial episcleral vessels more than the deepscleral plexus, thus revealing any underlyingscleral disease.
3. General eye examination
It is essential to exclude complications such asglaucoma, uveitis, pars planitis, choroiditis, secon-
dary retinal detachment, and optic neuritis. Prop-tosis and limitation of movement of the extraocularmuscles are also looked for as evidence of aninvolvement of posterior sclera.
SYSTEMIC EXAMINATION
As scleritis is frequently a manifestation, andsometimes the first manifestation, of systemicdisease, a thorough physical examination is impera-tive, special attention being paid to the joints andthe cardiovascular system to eliminate a vasculitis.*
Special investigationsROUTINE STUDIES CARRIED OUT IN ALL PATIENTS
i. Full blood countThis included haemoglobin estimation, white bloodcell count and differential white cell count, anderythrocyte sedimentation rate.
2. Rheumatoid arthritis latex agglutination testThe Rose-Waaler sheep-cell agglutination test wasused as a confirmatory test for rheumatoid factor.
3. Serum uric acid estimation
4. Serological tests for syphilisA patient who had a positive Wassermann reactionalso had the fluorescent treponemal antibodyabsorption (FTA (ABS)) test, Reiter's comple-ment-fixation test, the Venereal Disease Refer-ence Laboratory (VDRL) test, and the Treponemapallidum immobilization (TPI) test to confirm thediagnosis of syphilis. It was recognized that somecases of syphilis might have been missed as only theWassermann and Kahn tests were performed as aroutine. In the case of any abnormal result thetest was repeated.
5. X-rays of the chest and sacro-iliac joints
These were taken whether the patient had anyrelevant complaints or not.
ADDITIONAL STUDIES CARRIED OUT IN CERTAINPATIENTS
i. A full immunological survey for tissue anti-bodies, soluble immune complexes, complement,lupus erythematosus cells, and antinuclear factor(ANF) were undertaken.2. Mantoux test.3. Electroretinograms and electro-oculograms were*r his was carried out in our clinic by the rheumatologists DrFawler, Dr Hazleman, and Dr Lachmann
on February 1, 2020 by guest. P
rotected by copyright.http://bjo.bm
j.com/
Br J O
phthalmol: first published as 10.1136/bjo.60.3.163 on 1 M
arch 1976. Dow
nloaded from
I66 British Journal of Ophthalmology
performed initially in all patients but later in theseries these were confined to patients with severedisease and to all those with posterior scleritis.
ResultsPATIENTS
The data were derived from 207 patients (30I eyes)with scleritis and 159 patients (2I7 eyes) withepiscleritis (Table I).
FAMILY HISTORY
A family history was elicited in 14 patients (fourof these patients had simple episcleritis, threenodular episcleritis, six nodular scleritis, andone diffuse anterior scleritis). In the case of thethree patients with nodular scleritis the conditionwas very similar to that seen in close relatives, butin all others the history was indefinite. Thisindicates that neither episcleritis nor scleritis is afamilial condition.
TIME BETWEEN ONSET AND FIRST ATTENDANCE
In contrast to episcleritis, patients with scleritisattended much sooner after the onset of the disease,but even so (presumably because the onset wasoften insidious) many patients did not seek adviceuntil the pain had become severe, which mightnot have been for several weeks. Of the patientswith episcleritis I3 per cent reported in the firstmonth and 64 per cent within two months. Ofthose with scleritis the results were very similar,37 per cent being seen within the first month and68 per cent before the end of the second month.
Table I Patients with episcleritis and scleritis whoserecords were analysed by computer
FurtherDiagnosis Patients Eyes subdivisions Eyes
Episcleritis I 59 217 Simple 170Nodular 47
Scleritis 207 30I Diffuse anterior II9Nodular anterior I34*Necrotizing
withinflammation 29
without 42inflammation I3 J
Posterior 6
*The incidence of necrotizing anterior scleritis is open to questionbecause, although sometimes obvious when the patient first presents,the disease more often starts as a diffuse or nodular anterior scleritis.Active treatment has certainly prevented some patients from de-veloping necrotic lesions. Only those patients whose diagnosis wasabsolutely certain have been included in this category
Within one year of the onset of this condition 92per cent had sought advice.
AGE AND SEX DISTRIBUTION
Scleritis was more than I times as common inwomen as in men. This contrasted with episcleritis,which was equally common in both sexes.
i. ScieritisAnalysis of the age and sex distribution for thedifferent types of scleritis revealed distinct pat-terns for each type of scleritis. The diffuse andnodular varieties were most prevalent. In menthe peak incidence occurred in the fourth decade(P= < o05); women showed two separate peakincidences, one in the third decade and anotherin the sixth decade (P= <o0o5).
Scleritis-diffuse anterior scleritisIn women the disease was commonest in thefourth to seventh decades, with no predilectionfor any age group. In men it was more prevalentin the third to sixth decades, with a distinct peakduring the fourth. The condition was rare in theyoung and the old.
Scleritis-nodular anterior scleritisThe nodular disease in both sexes was most pre-valent from the fourth to sixth decades, but inwomen there was a very marked peak during thesixth decade.
Scleritis-necrotizing type with inflammationOf the patients who presented with this severevariety of scleritis the majority were women, butof those who presented during the fourth decadeall but one were men.
Scleritis-necrotizing type without inflammation(scleromalacia perforans)All these patients were women. The age rangewas 35 to 75 years, most cases occurring in thefifth decade.
Scleritis-posterior scleritisPosterior scleritis was usually associated with adiffuse anterior scleritis, occurring most frequentlyin women in their sixth decade, but one woman of35 years was seen with this condition.
2. EpiscleritisAltogether 88 men and 71 women suffered fromepiscleritis. There was a significant variation in the
on February 1, 2020 by guest. P
rotected by copyright.http://bjo.bm
j.com/
Br J O
phthalmol: first published as 10.1136/bjo.60.3.163 on 1 M
arch 1976. Dow
nloaded from

Scleritis and episcleritis i67
sex distribution at different ages. The conditionwas not seen in childhood. Episcleritis in menoccurred maximally from the third to the sixthdecade, with a peak in the fourth decade. Inwomen, however, although there was a peakincidence in the fourth and fifth decades, the distri-bution did not show a predilection for any parti-cular age group. The difference between thepeak incidence in the different series was highlysignificant (P= < o005). There was no significantdifference in the sexes between the time of onset ofsimple and nodular episcleritis, but nodular epi-scleritis had a peak incidence in the fifth decadewhereas simple episcleritis was most common inthe fourth decade (P= <o0o5).
INVOLVEMENT OF ONE OR BOTH EYES
I. ScleritisIn 45 per cent of the patients the disease wasbilateral, but in cases in which the disease involvedonly one eye, one side was not involved more thanthe other. When each type of scleritis was furtheranalysed it showed that diffuse anterior scleritiswas more often bilateral (P= <o oo5) and thatnodular anterior scleritis was more often unilateral(P= < 0o005). In necrotizing scleritis with inflam-mation both eyes were more often affected than inpatients with scleromalacia perforans. These dif-ferences were not, however, significant.
Posterior scleritis was usually unilateral.In 35 per cent of those patients in whom the
condition became bilateral, the other eye wasaffected between one and three months after theonset of the condition in the first eye. In the restthe disease did not occur in the other eye in lessthan six years.
2. EpiscleritisOf patients with episcleritis, 36-5 per cent developedthe condition in both eyes. When only one eyewas affected there was no significant difference inthe distribution between right and left eyes.Nodular disease occurred more commonly uni-laterally than bilaterally. The fellow eye was affectedeither between one and three months or after sixyears. There were no exceptions to this in thisseries.
Symptoms
REDNESS
Almost all patients naturally presented withredness of the eyes. In simple episcleritis theonset was often extremely rapid, the eye becomingflushed within a few minutes of the onset of
symptoms; in nodular episcleritis, scleritis, anddiffuse anterior scleritis the onset was much moregradual, the intensity of the inflammation increasingover a period of several days. The redness wassectorial, ranging in intensity from the barelynoticeable to the fiery red; the degree of inflam-mation bearing no relationship with the seriousnessof the condition. Indeed, in scleromalacia perforans(necrotizing scleritis without surrounding inflam-mation) there might be no redness of the eye at all.
LACRIMATION, PHOTOPHOBIA, AND CONJUNCTIVALDISCHARGE
Conjunctival discharge was not a feature of scleritisor episcleritis. Indeed, if the discharge is anythingbut watery in consistency an incorrect diagnosis hasprobably been made. Photophobia and lacrimationdid not universally accompany episcleritis orscleritis, but where these symptoms were severethey often indicated the presence of a necrotizingprocess.
In scleritis these complaints were not universal;of the patients with diffuse anterior and nodularscleritis 27 per cent complained of some degree ofwatering. However, 70 per cent of the patientswith necrotizing scleritis complained of photo-phobia and in 50 per cent the eye watered. Photo-phobia was unusual in posterior scleritis butabout half the patients complained of some lacri-mation. No correlation with the presence or typeof keratitis could be demonstrated. The incidenceof keratitis in each type of scleritis was much lessthan suggested by the symptoms of photophobia orlacrimation. In episcleritis when these symptomsoccurred they were rarely, if ever, severe. Photo-phobia occurred in io per cent of the patients andlacrimation was complained of in 25 per cent.Patients with nodular disease did not have moresevere symptoms than those with simple episcleritis.Photophobia and lacrimation showed some cor-relation with corneal changes, but these symptomswere not always due to changes within the cornea.
PAIN
Scleritis
This is one of the very few severely painful eyeconditions and severe pain was complained of in6o per cent of these patients (Table II). The pain,which was boring in character, was either localizedto the eye or generalized, in which case it radiatedfrom the orbital margin to the temple or the jawin the distribution of the trigeminal nerve. Somepatients had been erroneously diagnosed as havingmigraine or sinusitis, and one patient was thoughtto have a cerebral tumour. Many other patients
on February 1, 2020 by guest. P
rotected by copyright.http://bjo.bm
j.com/
Br J O
phthalmol: first published as 10.1136/bjo.60.3.163 on 1 M
arch 1976. Dow
nloaded from

I68 British Journal of Ophthalmology
Table II Types of pain experienced in different types of scleritis (percentage)
Localized Generalized Both localized Total no.Type of scleritis only only and generalized of eyes
Diffuse anterior 14 I5 30 II9Nodular anterior 25 I6 20 134Necrotizing anteriorWith inflammation 0 I5 46 29Without inflarnmation
(scleromalacia perforans) 0 13 I9 I3Posterior 0 5 33 6
suffered mild discomfort, but as this did notconstitute one of their complaints these patientsare not included in the table. Pain is rarely com-plained of in scleromalacia perforans, in whichthere is no surrounding inflammation; this is inmarked contrast to the pain of necrotizing scleritis,which is the severest of all, often preventing sleepand causing severe loss of weight, and described byMackenzie (I830) more than I40 years ago['the pain . . . is pulsative and deep seated, the chiefpain, however, is not so much in the eyeball, as roundthe orbit, under the eyebrow, and in the temple, cheekand side of the nose, and is severely aggravated fromsunset to sunrise'].The pain could indeed be so severe that the eyehad to be removed.
EpiscleritisSevere pain is not a feature of episcleral involve-ment. Discomfort, rarely described as pain, oc-curred in 51 per cent of patients and was almostequally common in simple and nodular types. Thesensation in the eye was described as hot, sharp,a slight ache, or irritable. Equally the pain aroundthe eye was described as an ache and, although itsometimes radiated to the temple or jaw, it wasnever described as boring. However, very occa-sionally a patient will present with severe swellingof the lids, extreme discomfort, and even miosisand temporary myopia.The pain or discomfort was localized to the eye
in 25 per cent of those patients with simple epi-scleritis and 33 per cent of those with nodularepiscleritis, and was felt around the eye but notin the eye itself in only 9 per cent of those withsimple episcleritis and 14 per cent with nodularepiscleritis. Both localized and generalized painwas experienced in i9 per cent in simple episcleritisand in io per cent in the nodular variety.
Physical signsSCLERITIS
In the classification of scleritis which we haveadopted it has been possible to distinguish each of
the various types from their typical clinical appear-ances although, as already stated, while necrotizingscleral disease sometimes started as a nodularscleritis, its presence could usually be suspectedbecause of the severity of the symptoms.The essential diagnostic feature in scleritis was
the involvement of scleral tissue in the inflam-matory process. This usually took the form ofscleral oedema which could be detected by observ-ing the outward displacement of the deep vascularnetwork of the episclera (Fig. 2).
Because the episclera was always swollen andcongested in scleritis, scleral oedema was the signwhich had to be looked for. The deep episcleralvascular plexus was more congested than thesuperficial network, giving rise to the typicalbluish-red colour. The conjunctival vessels wererarely involved.
SCLERITIS-NODULAR ANTERIOR SCLERITIS (Fig. 3)
Although these patients resembled those withnodular episcleritis on cursory examination, de-tailed examination revealed marked differencesand rarely presented any difficulty in diagnosis.The nodule was deep red in colour, totally immo-bile and quite separate from the overlying con-gested episcleral tissues. All the vessels were liftedby the nodule. There was, of course, some secon-dary overlying episcleritis and conjunctival con-gestion which involved the whole anterior episclerain 20 per cent (Fig. 3). Multiple nodules were seenin 42 per cent, sometimes reaching an enormoussize; in 50 per cent they were tender.
SCLERITIS-DIFFUSE ANTERIOR SCLERITIS (Fig. 4)This was the most benign form of scleritis and itwas associated with the least severe of the associatedgeneral conditions. The patients might presentwith an eye in which the sclera was obscured bya diffuse redness and swollen episclera, whichmight be accompanied in severe cases by conjunc-tival oedema so severe as to obscure the corneaand protrude from between the eyelids. In thesepatients adrenaline i :iooo had to be applied to
on February 1, 2020 by guest. P
rotected by copyright.http://bjo.bm
j.com/
Br J O
phthalmol: first published as 10.1136/bjo.60.3.163 on 1 M
arch 1976. Dow
nloaded from

Scieritis and episcleritis 169
FIG. zSlit-lamp appearances in scleritis.Sclera is swollen so that deep plexus of vessels isdisplaced forwards. Accompanying episcleritiscauses slight separation of superficial networks
~. complications other than scieral thinning and 40per cent suffered a deterioration of visual acuity.
P ~~~~~~~~~Thosepatients who were firstseen at the onset ofthe disease presented with a localized patch ofscleritis which was associated with acute congestion,sometimes so severe as to merit the term 'brawny'scleritis, but there was nothing in the physical
-~ appearances, the aetiology or prognosis, to justifyincluding them as a separate category.Another physical sign which must alert one to
the presence of severe necrotizing scleral diseaseis the avascularity of a patch of episcleral tissueoverlying or adjacent to an area of scleral oedema
FIG. 3 Nodular anterior scleritis. A discrete scleral (Fig. 6). This sign was found in 27-5 per cent ofnodule, displacement of deep vessels over nodule andsurrounding inflammation overlying unaffected scleraare characteristic of this condition
the conjunctival sac so that the deep scleral 4network and the scleral tissue itself could bevisualized, and any degree of scleral oedema deter-mined. In the less severe cases the area of rednessmight be confined to a small area of the globewith very little overlying congestion. The inflam-mation was more widespread than in the nodulardisease, and the extent of the involvement variedfrom a small area (61 per cent) to the whole anteriorsegment (39 per cent). The vascular pattern was I
occasionally grossly distorted and the normal radialpattern lost, with replacement of these vesselswith abnormal tortuous new channels (Fig. 5).The eye was tender in 54 per cent of patients.
SCLERITIS-NECROTIZING SCLERITIS WITH SIGNS OFADJACENTINFLAMMATION (Fig. 6) ~FIG. 4 Diffuse anterior scleritis. Underlying scleral
This was found to be the most destructive formn of oedema could be detected only by first blanchingthe disease. Of these patients 6o per cent developed swollen congested episclera with i :1000o adrenaline
on February 1, 2020 by guest. P
rotected by copyright.http://bjo.bm
j.com/
Br J O
phthalmol: first published as 10.1136/bjo.60.3.163 on 1 M
arch 1976. Dow
nloaded from

170 British Journal of Ophthalmology
FIG Abnormal, tortuous vascularN'iiU. ~~~~~~~~~~~~~~channelswhich develop after recurrent
attacks of diffuse anterior scieritis
had become involved (Fig.
mation subsided, or was suppressed by treatment,transparent sclera remained. Complications did not
-- ~~~~~~~~supervene until the inflammatory process had pro-gressed through almOst 360 degrees. Rarely thewhole anterior segment became inflamed at one andthe same time, and in some of these eyes areas ofnecrosis occurred which, if they had not been
l illtreatedurgently, would have become sequestrated,exposing the underlying uvea. It was not, however,our experience that staphyloma (bulging of the
FIG. 6 Necrotizingr anterior scleritis. Superficiallythis-patient appears to be similar to those shown in Figs4 and 5, but there is an avascular area adjacent tothe limbus. If this is not treated, ulceration rapidlyoccurs similar to that in Fig. 7
patients with necrotizing scleritis with inflammationvand in 23 per cent of those without inflammation(scleromalacia perforans).
Several types of response were noted. In some Keyes the inflammation remained localized to onesmall area, arid, if not checked by treatment, FIG. 7 Necrotizing anterior scleritis. Late stage ofresulted in almost total loss of scleral tissue from necrotizing scleritis. Inflammation is progressing aroundresultedrei aMosttoequentalls onfsleram tionssu tedf the globe, leaving an area of avascular necrotic sclerathat area. More frequently the inflammation started behind. Almost always these areas are crossed, as here,in one area and spread in both directions around by a large vein which drains the limbal area on a thinthe globe until the whole of the anterior segment bridge of normal sclera
on February 1, 2020 by guest. P
rotected by copyright.http://bjo.bm
j.com/
Br J O
phthalmol: first published as 10.1136/bjo.60.3.163 on 1 M
arch 1976. Dow
nloaded from

Scleritis and episcleritis I7I
uvea into the scleral defect) occurred unless theintraocular pressure became raised above 30 mmHgand had remained high for a prolonged period.
Avascularity of a patch of overlying sclera oc-curred in 27-5 per cent of the patients. These patchesoften occurred very early in the disease, and thecondition must be treated vigorously if furthernecrosis is to be prevented. The eye was tender in40 per cent of these patients.
SCLERITIS-NECROTIZING SCLERITIS WITHOUTADJACENT INFLAMMATION (SCLEROMALACIAPERFORANS) (Fig. 8)
This condition was associated with long-standingrheumatoid arthritis in 46 per cent of patients.They presented without any subjective symptoms,the doctor or the patient having noticed either agreyish or yellowish patch on the sclera or, inmore severe cases, areas of complete loss of tissue.Any inflammatory change was minimal. Therewas no reactive oedema because it appeared thatthe episcleral tissue overlying the defect had disap-peared, and elsewhere it was so thin as to be almostinvisible. The number of vessels in the remainingepiscleral tissue also appeared to be much dimin-ished, giving a porcelain-like appearance to thewhite of the eye when viewed from a distance.Altogether 40 per cent of the patients had morethan one necrotic patch. We had the opportunityof watching some of these develop and the patternseemed to be the same. The conjunctiva andremaining episclera might become suffused over awide area or might remain unaltered. A demar-cation line would develop in the sclera, like a
circular crack, and the area inside this would takeon a yellowish or greyish appearance and after avariable period would separate as a sequestrumtogether with the overlying episciera. Largeabnormal vessels surrounded and crossed the area,and where they crossed it near the limbus theyleft an area of about o 5 mm on either side of arelatively normal sclera. The resulting defect wascovered by a very thin layer of connective tissuewhich appeared to be derived from the conjunctiva.Unless the intraocular pressure rose, no staphy-loma was seen. In no case was the eve tender tothe touch.
SCLERITIS-POSTERIOR SCLERITIS
We were certain of the diagnosis in six cases(2z9 per cent), but it was suspected in severalcases, and it was likely that others escaped ournotice. Since there are no apparent external signsof posterior scleritis unless there is also an asso-ciated anterior scleritis, the presence of proptosis,exudative detachment and other fundus changes,including papilloedema, may mislead the ophthal-mologist to such an extent that the correct diag-nosis is never made. In view of this it is possiblethat the incidence of posterior scleritis may not beas low as indicated by the present series, as ourpatients were all referred from elsewhere. The con-dition was unilateral in four of the six cases.
PRESENTING FEATURES IN POSTERIOR SCLERITIS
Symptoms. In all the patients there was extremepain and tenderness.
FIG. 8 Necrotizing scleritis withoutinflammation (scleromalaciaperforans). Almost completedissolution of scleral collagen occurringwith little if any surroundinginflammation in woman of 6o yearswith long-standing rheumatoidarthritis
on February 1, 2020 by guest. P
rotected by copyright.http://bjo.bm
j.com/
Br J O
phthalmol: first published as 10.1136/bjo.60.3.163 on 1 M
arch 1976. Dow
nloaded from

172 British Journal of Ophthalmology
FIG. 9 Appearance offundus afterresolution of extensive serousdetachment in patient with posteriorscleritis who presented withdiminution of vision, anteriorscleritis, slight proptosis, and a
diffuse leak early in dye transit on
fluorescein angiography
Visual acuity. All eyes except one showed somereduction in visual acuity.
Fundus changes. In four of these patients therewas an exudative retinal detachment associatedwith swelling of the optic disc and an anteriordiffuse scleritis. The anterior scleral involvementwas minimal and had to be looked for carefully,but the retinal changes were typical. Areas ofexudation occurred beneath the retina, giving theappearance of pale greyish-white spots with asurrounding dark greyish line that could be seenthrough the overlying serous detachment (Fig. 9).
In the early stages there was a diffuse leak earlyin the dye transit on fluorescein angiography.
Proptosis. Two patients presented with proptosis,a diffuse anterior scleritis, limitation of ocularmovements, especially upwards, and retraction ofthe lower lid (Fig. io) when attempting to lookupwards. This physical sign seemed to be specificfor this condition and was presumably caused byinfiltration of both the tendons and the musclecone in the region of the posterior scleritis. Diplopiawas also a presenting feature of posterior scleritisbecause of involvement of the muscles and tissues
FIG. IO Posterior scleritis. Retractionof left lower lid in patient withposterior scleritis who also had severe
_ limitation of ocular movements. Ocular' movements became normal with- treatment but the lid sign remained
on February 1, 2020 by guest. P
rotected by copyright.http://bjo.bm
j.com/
Br J O
phthalmol: first published as 10.1136/bjo.60.3.163 on 1 M
arch 1976. Dow
nloaded from

Scleritis and episcleritis 173
within the muscle cone by the inflammatoryprocess. All these features returned to normalafter treatment. The exudative detachment in onepatient disappeared within five hours of startingtreatment. The site of inflammation remained paleand white after the inflammation had disappeared,leaving some areas of pigment migration at theedges, giving the appearance of a high-water mark.
EPISCLERITIS
Simple and nodular episcleritis differed in theirclinical signs, but in both, the oedema or infiltrationwere entirely within the episcleral tissue; the scleraitself was not involved. The episcleral vascularnetwork was maximally congested, with somecongestion of the conjunctival vessels and minimalcongestion of the scleral vessels (Fig. iI).
EPISCLERITIS-SIMPLE EPISCLERITIS
The redness of the episclera was often very intenseand was localized to one sector in 69 per cent ofpatients and generalized in 3I per cent. The epi-scleral vessels, although engorged, retained theirnormal radial position and architecture. Thecolour varied from fiery red to a mild red flushbut did not have the bluish hue so typically seen inscleritis.
In simple episcleritis there was a diffuse oedemaof the episcleral tissue which was sometimesinfiltrated by greyish deposits which appearedyellowish in red-free light. The depth of theoedema and its effect on the vascular plexus wasbest recognized by slit-lamp examination, using a
narrow beam. The eye was tender to the touch in33 per cent of cases.
FIG. 12 Nodular episcleritis. Swelling and oedemaconfined to episcleral tissue and vessels retain theirnormal architecture
EPISCLERITIS-NODULAR EPISCLERITIS
In contrast with simple episcleritis the oedema andinfiltration of nodular episcleritis were localized toone part of the globe, except in seven eyes inwhich the redness was widespread. A nodule fromwithin the episcleral tissue, which was surroundedby some congestion, was mobile on the underlyingsclera and there was no involvement of the sclerain the oedema. The scleral plexus of vessels couldbe distinguished deep to the nodule lying flat on thesclera, which retained its normal contour (Figs iIand I2). The nodules were usually single but weresometimes multiple, reaching the size of a large pea.The eye was tender to the touch in 40 per cent.
Vascular changes in the episcleraAlthough vascular changes were most unusual inepiscleritis, vessels that appeared to be abnormal
FIG. i iEpiscleritis. Although deep vascularnetwork is congested there is no scleral swelling,oedema and infiltration being confined to episclera
on February 1, 2020 by guest. P
rotected by copyright.http://bjo.bm
j.com/
Br J O
phthalmol: first published as 10.1136/bjo.60.3.163 on 1 M
arch 1976. Dow
nloaded from

174 British Journal of Ophthalmology
either in course or type were noted in i 9 eyeswith simple episcleritis and iO eyes with nodularepiscieritis. All these patients had had recurrentattacks at the same site for many years. One patientshowed avascularity of the episcleral nodule whichwas thought to be due to the intensity of the oedema,as the vessels returned to normal as soon as treat-ment was given.
Complications
Complications of some sort were found in onlyI5 per cent of patients with episcleritis but ocularcomplications, other than simple increased scleraltransparency or thinning, occurred in 57 per centof all patients with scleritis. The complicationslooked for and analysed were:
i. Fall in visual acuity2. Keratitis3. Cataract4. Uveitis5. Glaucoma6. Scleral thinning (and scleral defects)
Fall in visual acuitySCLERITIS
A total of 42 eyes (14 per cent) in patients withscleritis lost a significant amount of vision afterthe disease had been present for one year. This fallin visual acuity was attributed to cataract (five eyes),anterior uveitis (two eyes), and posterior uveitis(two eyes). The commonest reason for the fall invisual acuity was the association with keratitis(Table IV), particularly if this was accompaniedby a uveitis.
EPISCLERITIS
No patient with episcleritis had a fall in visualacuity during the period of follow-up.
Table III Fall of visual acuity in scleritis
Fall in visual acuityTotal 2 lines or more during
Type of scleritis no. of period offollow-upeyes (per cent)
Diffuse anterior II9 15Nodular anterior I34 7Necrotizing anteriorWith inflammation 29 27Without inflammation
(scleromalaciaperforans) 1I3 31
Posterior 6 50
Table IV Fall of visual acuity in scleritis dueto keratitis
No. of eyes with fall in visual acuityKeratitis during follow-up
Superficial 2Midstromal 3Deep oGuttering 3Others 5
KeratitisSCLERITIS
Corneal changes of a type characteristically seenin scleritis were observed in 29 per cent of patients.This keratitis can be serious, leading to permanentchanges in the cornea; these are so characteristicthat when certain types of sclerosing keratitis andlipid changes are seen in an eye which is otherwisenormal, it can be inferred that the patient has hadscleritis at some time in the past.
Characteristic corneal changes were seen ineach type of anterior scleritis and could be classifiedas follows:
Nodular scleritis
i. Localized stromal keratitisii. Localized sclerosing keratitis
Diffuse scleritis
i. Acute stromal keratitisii. Sclerosing keratitis
iii. Corneal guttering
Necrotizing scleritis
i. Sclerosing keratitisii. Keratolysis
The incidence of keratitis in different types ofscleritis is given in Table V.
Acute stromal keratitis (Fig. I3)
In the severe necrotizing scleritis of acute onsetthe cornea became oedematous and dense whiteinfiltrates appeared within the stroma (Fig. I3).These were sometimes central and sometimesperipheral and might coalesce as the disease pro-gressed. If, in addition, there was anterior chamberactivity, keratic precipitates adhered to the pos-terior corneal surface. The opacity was sometimessurrounded by a 'precipitin' ring. If the scleritiswas treated vigorously with full doses of steroids
on February 1, 2020 by guest. P
rotected by copyright.http://bjo.bm
j.com/
Br J O
phthalmol: first published as 10.1136/bjo.60.3.163 on 1 M
arch 1976. Dow
nloaded from

Scleritis and episcleritis 175
Table V Keratitis and vascularization of the cornea in scleritis
Keratitis Corneal vascularizationTotal
Type of scleritis no. of Super- Mid- Gutter- Super- Mid-eyes ficial stromal Deep ing Other ficial stromal Deep Other
Diffuse anterior iI9 8 I0 2 4 4 3 2 3 2Nodular anterior 134 6 I4 4 5 6 5 0 I 0Necrotizing anteriorWith inflammation 29 4 4 2 4 3 2 I 3 0Without inflammation
(scleromalacia perforans) I3 0 3 I 3 0 I 3 2 IPosterior 6 0 0 I 0 0 0 0 0 0
Total 30I i8 3I Io i6 13 I I 6 9 3
these opacities could disappear without trace. Moreusually, however, linear opacities within thestroma remained and, if central, these impairedvision.
Sclerosing keratitis (Fig. 14)
The corneal opacities associated with scleral diseaseusually appeared less dramatically; the corneaadjacent to the swollen sclera became oedematousand vessels grew into this oedematous area. Vascu-larization never seemed to precede the oedema.Although these opacities usually occurred close tothe limbus they could appear in the superficial andmidstroma centrally in the cornea, having noobvious connexion with the site of the scleraldisease.Whatever the type or site of the corneal lesion,
treatment of the scleritis brought about resolution
of the keratitis which might be complete or, moreusually, the lamellae of the cornea were altered toleave thin linear opacities which looked exactlylike the sugar crystals of 'candy floss' (Fig. I4).Crystalline (candy-floss) opacities were seen in23 patients with diffuse and another 23 patientswith nodular scleritis, and five patients with necro-tizing scleral disease. This type of corneal changecould not be correlated with vascularization or anyparticular aetiological agent. Keratolysis was ob-served in four patients, all of whom had severenecrotizing anterior scleritis. These opacities, onceformed, never disappear. In very severe cases theopacification of the cornea progressed circum-ferentially until only a central clear area in thecornea remained, and even this area might disap-pear, resulting in a 'scleralized cornea'. Corneatgrafting was very successful in restoring the visualacuity in these patients.
'FIG. 13 Acute stromal keratitis inscleritis. Dene white infiltration incornea in same patient as in Fig. 9.Immune rings similar to those seen inFig. 14 appeared round these lesions.
AAll corneal signs, etc. disappearedafter treatment
on February 1, 2020 by guest. P
rotected by copyright.http://bjo.bm
j.com/
Br J O
phthalmol: first published as 10.1136/bjo.60.3.163 on 1 M
arch 1976. Dow
nloaded from

176 British Journal of Ophthalmology
FIG. 14 Sclerosing keratitis inscleritis. A 66-year-old woman with aI3-year history of recurrent bilateraldiffuse sclero-keratitis with crystalline(candy-floss)deposits in the deepstroma and a 'precipitin ring' aroundthe infiltration at 12.0 o'clock. Thevascularization is passive. Vesselsenter the cornea only at site ofadvancing edge of corneal change andat late stage in disease. Acutestromal keratitis will progress tothis if left untreated
Limbal guttering
Guttering of the peripheral cornea was not infre-quently seen, particularly in patients who hadsevere long-standing rheumatoid arthritis. Thesegutters never extend more than 2 mm from thelimbus, but may become circumferential and verythin, requiring grafting. Erosion of the deep stroma
resembling Terrien's disease may also occur, andin one case this led to an expansion of the eye to i8dioptres of astigmatism in that axis, necessitatingcorneo-scleral grafting over the affected region(Fig. I5).
KeratolysisThe most severe corneal disease of all is keratolysis.This was seen in only four patients, all of whomhad very severe necrotizing scleritis, usually, butnot invariably, accompanied by loss of scleraltissue. In this terrifying situation the wholestroma of the cornea disappeared with alarmingrapidity (Fig. i6). The progress could have beenstopped by full steroid therapy but only after veryprolonged treatment would any corneal tissue havebeen re-formed. It was usual therefore to graftthese eyes when the scleritis had become wellcontrolled or if rupture appeared imminent.
Lipid deposition occurred in areas where thecornea had been damaged and at the inner edge ofa long-standing corneal gutter. This was presum-ably because of interference with the usual flow of
these metabolites to the limbus and it was not aproduct of the corneal inflammation.
Posterior corneal changes
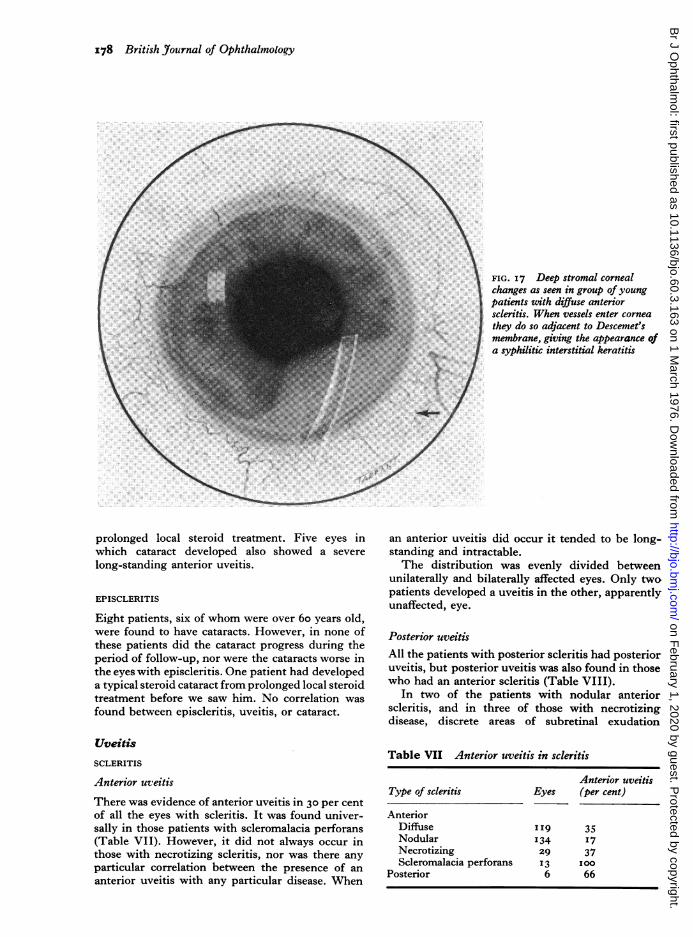
Although we have not analysed this series for it, wehave recently come to recognize another patternof corneal change in scleritis (Holt-Wilson andWatson, I974), which presented as an interstitialkeratitis indistinguishable from that seen in con-genital syphilis but which occurred in patientswho had a mild scleritis and inwhom the serologicalinvestigations were entirely negative (Fig. 17).
Keratitis could be considered the sole reason for asevere fall in visual acuity in I3 eyes (4 per cent).
EPISCLERITIS
Minimal corneal changes were seen in i5 per centof the patients with simple episcleritis and in 15per cent of those with nodular disease, but thesewere never severe. The oedema of the corneaoccurred when the episcleral inflammation wasclose to the limbus and seemed to be a consequenceof this adjacent inflammation. Keratitis was mostcommon in the superficial and midstromal layersof the cornea in both varieties. Some localizedcorneal guttering occurred in six eyes after recur-rent attacks in the same area for many months.Vascularization of the cornea occurred in six eyes,the vessels being deep in three, midstromal in one,
on February 1, 2020 by guest. P
rotected by copyright.http://bjo.bm
j.com/
Br J O
phthalmol: first published as 10.1136/bjo.60.3.163 on 1 M
arch 1976. Dow
nloaded from

Scleritis and episcleritis I77
FIG. I6 Keratolysis. Severe necrotizing changes inboth cornea and sclera which occurred in a period offive weeks in a 74-year-old woman. Systemic steroidssuppressed inflammation and both cornea and sclerawere grafted successfullv
and superficial in two. No serious complicationswere found in any of the patients studied.
Cataract
SCLERITIS
Cataracts were detected in only 22 eyes, 7 per cent.These were bilateral and senile in type in 15 eyes.In 12 eyes the cataract was noted to have become
FIG. 15 Limbal guttering inscleritis. A 24-year-old man with a
\10\Vio-yearhistory of unilateral scleritis
localized to area of sclera between12.0 and 2.0 o'clock. Cornea in areahas become guttered and produced a
c..>f.'Terrien'-like change. This area
required grafting (Fig. I9) becauseX. of rapidly increasing expansion of
globe in this axis
worse during the course of the disease. All thesepatients were between the ages of 55 and 8o yearsand all had serious scleral disease. In only threepatients (five eyes) with an associated long-standing anterior uveitis was it felt certain that thesclero-uveitis was responsible for the cataracts.In two of these patients it was particularly notice-able that the cataract had developed rapidly oncethe scleritis had involved the sclera through 360°.Three of these cataracts have required extraction.The sclero-corneal wound has healed normallyafter cataract extraction in spite of continuingactive scleritis in the area of the wound. Oneeye developed a steroid-induced cataract after
Table VI Keratitis in episcleritis
EpiscleritisType of keratitis
Mid-Superficial stromal Deep Guttering
Simple 7 14 3 5Nodular 2 4 I IComeal
vascularization 2 I 3 o
NB Some eyes showed more than one type of keratitis
..........
on February 1, 2020 by guest. P
rotected by copyright.http://bjo.bm
j.com/
Br J O
phthalmol: first published as 10.1136/bjo.60.3.163 on 1 M
arch 1976. Dow
nloaded from
I78 British Journal of Ophthalmology
FIG. 17 Deep stromal cornealchanges as seen in group of youngpatients with diffuse anteriorscleritis. When vessels enter corneathey do so adjacent to Descemet'smembrane, giving the appearance ofa syphilitic interstitial keratitis
prolonged local steroid treatment. Five eyes inwhich cataract developed also showed a severe
long-standing anterior uveitis.
EPISCLERITIS
Eight patients, six of whom were over 6o years old,were found to have cataracts. However, in none ofthese patients did the cataract progress during theperiod of follow-up, nor were the cataracts worse inthe eyes with episcleritis. One patient had developeda typical steroid cataract from prolonged local steroidtreatment before we saw him. No correlation was
found between episcleritis, uveitis, or cataract.
Uveitis
SCLERITIS
Anterior uveitis
There was evidence of anterior uveitis in 30 per centof all the eyes with scleritis. It was found univer-sally in those patients with scleromalacia perforans(Table VII). However, it did not always occur inthose with necrotizing scleritis, nor was there anyparticular correlation between the presence of an
anterior uveitis with any particular disease. When
an anterior uveitis did occur it tended to be long-standing and intractable.The distribution was evenly divided between
unilaterally and bilaterally affected eyes. Only twopatients developed a uveitis in the other, apparentlyunaffected, eye.
Posterior uveitisAll the patients with posterior scleritis had posterioruveitis, but posterior uveitis was also found in thosewho had an anterior scleritis (Table VIII).
In two of the patients with nodular anteriorscleritis, and in three of those with necrotizingdisease, discrete areas of subretinal exudation
Table VII Anterior uveitis in scleritis
Anterior uveitisType of scleritis Eyes (per cent)
AnteriorDiffuse II9 35Nodular '34 17Necrotizing 29 37Scleromalacia perforans 13 100
Posterior 6 66
on February 1, 2020 by guest. P
rotected by copyright.http://bjo.bm
j.com/
Br J O
phthalmol: first published as 10.1136/bjo.60.3.163 on 1 M
arch 1976. Dow
nloaded from

Scleritis and episcleritis I79
Table VIII Posterior uveitis in scleritis
Posterior uveitisType of scleritis Eyes (per cent)
AnteriorDiffuse II9 13Nodular I34 3Necrotizing 29 17Scleromalacia perforans 13 23
Posterior 6 100
could be seen at the periphery of the fundus with a
'high-water mark' of retinal and subretinal oedemaaround the patches of exudation. One patientdeveloped an annular choroidal detachment atthe height of the scleritis.
EPISCLERITIS
No severe uveitis occurred in this series. Milduveitis, detectable on the slit-lamp by an increasein the number of cells in the anterior chamber anda mild aqueous flare, was found in I2 eyes. Intwo unilateral cases, flare and cells were noted inthe unaffected eye. No correlation between comealinvolvement and uveitis was detected.
Glaucoma
SCLERITIS
Glaucoma was present in 35 eyes (iI 6 per cent),of which 20 per cent showed associated keratitis.Of the patients with secondary glaucoma nine
had no abnormality other than scleritis, seven alsohad keratitis, and six uveitis.
Secondary glaucoma often accompanies severe
anterior scleritis, the cause apparently being dueto obstruction of the outflow channels by oedemabecause the intraocular pressure falls and the out-flow of aqueous rises as soon as the scleritis comes
under control with systemic treatment. Six patients,who had anterior synechiae and a long-standing
uveitis with secondary glaucoma, required othermedication for control of the intraocular pressure.
None of these patients has yet required surgery.No patient with posterior scleritis had glaucoma.One patient developed a steroid glaucoma which
has required continuous medication for its control.
EPISCLERITIS
Glaucoma was detected in nine eyes (4 per cent).Two patients were known to have chronic open-
angle glaucoma before the onset of the episcleritis.Five eyes had developed a steroid glaucoma fromprolonged administration of local steroids. In no
instance could the glaucoma be attributed to theepiscleral inflammation, although there was cornealinvolvement in one eye.
Scleral thinning
When the sclera looked blue in the daylight whencontrasted with surrounding white sclera this was
regarded in our analysis as scleral thinning. Thesclera in many of these patients had becometransparent rather than thin; however, the bluepatch appeared only in cases in which there hadbeen active disease. The change in transparencywas usually not apparent during the active stage ofthe disease but it was observed at the site of recur-
rent simple or nodular episcleritis in I 9 eyes
(8 per cent), and in 36-5 per cent of eyes affectedwith scleritis, during the period of follow-up.
After repeated attacks of episcleritis, particularlyif these occurred at the same site, the sclera mightbecome transparent but not thin. Similarly indiffuse and nodular scleritis the sclera mightbecome transparent with the blue choroid showingthrough. This was easily seen in daylight andcould be used as an indication of previous scleralinflammation. Ectasia and destruction of scleraltissue occurred only in necrotizing scleritis. Thiscould take the form of an avascular area appearingin the centre of an area of scleritis, which thenbroke down to form a slough and eventually toleave an area of thinning.
Table IX Glaucoma in scleritis
Total with Primary Primary Steroid-Type of scleritis Total glaucoma open-angle closed-angle Secondary induced
Diffuse anterior II9 12 6 0 6 0Nodular anterior I34 I I 6 0 5 0Necrotizing anterior 29 8 2 0 5 IScleromalacia perforans 13 4 0 0 4 0Posterior 6 0 0 0 0 0
30I 35 14 0 20 I
on February 1, 2020 by guest. P
rotected by copyright.http://bjo.bm
j.com/
Br J O
phthalmol: first published as 10.1136/bjo.60.3.163 on 1 M
arch 1976. Dow
nloaded from

I8o British _ournal of Ophthalmology
Table X Scleral thinning or transparency in scleritis
Eyes with thinning
Type of inflammation Total no. Total incidenceof eyes Localized Generalized (per cent)
EpiscleritisSimple 170 I2 3 9Nodular 47 4 0 9
ScleritisDiffuse anterior II9 23 15 32Nodular anterior 134 35 2 28Necrotizing anterior 29 II I0 69Scleromalacia perforans 13 7 6 I00Posterior 6 I 0 I6
In the type of necrotizing scleritis which pro-
gressed around the globe, the area behind theadvancing edge could become extremely thin,and sometimes melted away altogether. In thevariety of necrotizing scleritis without inflammation(scleromalacia perforans), the episclera was usuallyextremely thin (Fig. 8), and the underlying sclerawould become white, develop a demarcated margin,and then become sequestrated. The conjunctiva andthin episclera overlying this process might beslightly congested but this was by no means alwaysthe case. A combination of A- and B-scan ultrasoundcould be used to distinguish between thinning andincreased transparency-A-scan being used to esti-mate the thickness and B to locate the lesion.
Scleral defects (Fig. i8)
Scleral defects, as opposed to scleral thinning or
increased scleral transparency, were seen only inthe severest forms of necrotizing disease. When the
FIG. I8 Scleral defect. Scleral defect occurring inpatient with severe necrotizing scleritis. Ciliary body isexposed but no staphyloma occurs unless intraocularpressure rises above 40 mmHg
necrotizing disease was associated with inflamma-tion, the episclera became avascular, overlying thearea which would eventually become sequestrated.Treatment at this stage would prevent sequestration.In scleromalacia perforans sequestration might takeplace without any warning. The loss of tissue ineither condition might involve only a part of thescleral thickness.
Sequestration occurred in 22 eyes (7 per cent).Loss of tissue took place in 41 per cent of eyes withnecrotizing disease associated with inflammation,and in 77 per cent of those without inflammation.The rest of these eyes developed severe thinningwithout sequestration. Of eyes with scleral defects59 per cent also had keratitis, although this wasaccompanied by a loss of corneal tissue (keratolysis)in only three eyes (Fig. i6). No scleral defectsdeveloped in patients who had episcleritis or any ofthe less severe forms of scleritis.
Associated systemic diseases
The incidence of the various systemic conditionsdetected in this series is summarized in Table XI.
In eyes where scleritis and episcleritis co-existed, the area of severe damage occurred wherethe sclera was involved, and not where the episclerawas inflamed without deep involvement.We have observed, however, that the patients
with herpes zoster ophthalmicus developed anepiscleritis at the time of the vesicular eruption.The episcleritis disappeared as the skin conditionsubsided. Three patients developed a severenodular scleritis two or three months later at thesite of the original lesion. This does not implythat the episcleritis progressed to the scleritis,because there was a distinct interval between thetwo episodes during which the eye was apparentlynormal. Since making this observation we havestudied a further 20 patients who were not includedin this series presenting with herpes zoster ophthal-
on February 1, 2020 by guest. P
rotected by copyright.http://bjo.bm
j.com/
Br J O
phthalmol: first published as 10.1136/bjo.60.3.163 on 1 M
arch 1976. Dow
nloaded from

Scleritis and episcleritis I8r
Table XI Incidence of associated systemic diseases in episcleritis and scleritis
Disease
Rheumatoid arthritisAnkylosing spondylitisPsoriatic arthritisSystemic lupus
erythematosusPeriarteritis nodosaSystemic vasculitisWegener's granulomatosisRelapsing polychondritisRheumatic heart diseasePalindromic rheumatoid
Associated with hypersensitivitydisordersErythema nodosumSevere asthma or hay feverErythema multiformeHenoch-Schonlein purpuraPenicillin sensitivityContact dermatitisAfter desensitization
vaccinationRosacea
Associated with granulomatousconditions
TuberculosisActiveInactive
Syphilis
Associated with virus infectionHerpes zosterHerpes simplex
Episcleritis
Simple Nodular
5 2o oo o
o 0o 0o 0o 0o o2 Io o
0
0
I
2
2
0
0
0
0
0
I
Scleritis
Diffuseanterior
8I0
0
0
I0
0
I
0
0
2
0
0
0
0
Nodularanterior
40
3
I
0
0
0
0
I
0
2
0
0
0
0
0
Necrotizinganterior
300
2
2I
I
20
2
0
00
0
0
0
Scleromalaciaperforans
60
0
0
0
0
0
0
0
0
00
0
0
0
0
Posterior
0
00
0
0
00
0
00
000
0
0
0
2 0 0 0 0 0 0I 2 0 2 0 0 0
I 0I 2O I
2 Io 0
I
0I
0
0
3
30
2
2 14 00 2 0
0
00
0
0
0
00
0
0
Associated with metabolicdisordersGoutOther associated conditions*
6 5I 0
2 3 0IO 7 I
*In simple episcleritis one patient had regional ileitisIn diffuse anterior scleritis Io patients had other diseases-orbital granuloma (I), essential hypertension (3), postirradiation to other eye (I),fragilitas osseum (I), thyrotoxicosis (I), degenerative osteoarthritis (2), ankylosing spondylitis (I)In nodular anterior scleritis seven patients had other diseases-for example, Cogan's syndrome (3), thyrotoxicosis (2), ophthalmia nodosa (I),.hypertension (I)One patient with necrotizing scleritis had hypertension as the only other systemic disease. There was no other evidence of a generalizedsystemic vasculitis
micus and episcleral disease. This phenomenon oflate appearance of scleral disease was observed inseven of the 20 patients (35 per cent).
Laboratory investigations
The various laboratory investigations carried out inthese patients are mentioned on page i65.
In the latter part of the series plasma proteinestimations and electrophoresis were performedroutinely in all patients with scleritis, and an im-munological survey performed by the ImmunologyDepartment of the University of Glasgow. Althoughthese results apply only to those patients who wereseen during the last nine months of the analysis,they are shown in Table XIII because they showed
0
00
0
on February 1, 2020 by guest. P
rotected by copyright.http://bjo.bm
j.com/
Br J O
phthalmol: first published as 10.1136/bjo.60.3.163 on 1 M
arch 1976. Dow
nloaded from

I82 British Journal of Ophthalmology
Table XII Laboratory investigations: abnormalfindings in patients
Episcleritis ScleritisTest
No. (percent) No. (percent)
Erythrocyte sedimen-tation rate 22 I4 76 37
White blood count 7 4 I4 7Latex test for
rheumatoid factor 12 7 28 I3 5Wassermann reaction I o-6 6 3Uric acid I8 II.3 14 7
that a more sophisticated survey would revealevidence of immunological abnormality not re-
vealed by routine laboratory testing.Of the 48 patients with scleritis, 27 (56 per cent)
had some positive result in the immunological test.Eight patients had more than one positive result.These are presented with a control series of 30
patients matched for age and sex, with eye diseasebut with no scleral or uveal involvement.Of the I2 patients with a positive result in the
rheumatoid arthritis latex agglutination test, onlytwo had clinical rheumatoid arthritis.
Skin tests
Intradermal or prick tests-inhalant, mould, fabric,dusts, and pollens-were performed in 30 patientswith episcleritis, particularly those who gave some
history of allergy. Mild reactions were detectedto several agents in eight patients, but no overallpattern of allergic response as judged by thisresponse could be detected. Two patients gave a
history of a flare-up of episcleritis when in contactwith printer's ink. The results of intradermal, patchand prick tests were negative, but vapour exposure
produced flushing of the episclera.
X-ray examination
X-ray examination of the chest and sacro-iliac jointswas carried out routinely in all patients withscleritis unless there was some contraindication.The seven-day rule with regard to ovulation was
applied. Other examinations were carried out ifindicated. Of patients in this series 42 per centwere intensively investigated by Fowler (1970),who found sacro-iliac abnormalities in seven, ofwhom three had definite ankylosing spondylitis.Only one patient had symptoms which wouldhave led to this diagnosis without specific examina-tion.
Electrodiagnostic investigations
Electro-oculograms (EOG) were performed initiallyin all patients; later in the series they were per-formed if the patient had severe disease or posteriorscleritis. In 71 consecutive patients with episcleritisand scleritis presenting in the scleritis clinic, I3had subnormal EOGs in the affected eye. All butone of these patients had scleritis but this was notsevere in every case. The other patients had re-
current episcleritis and glaucoma.
Tissue biopsy
Biopsy of scleral tissue is not recommended unlessthere is great difficulty in diagnosing the eyecondition or the underlying systemic disease.Episcleral biopsies were performed on threepatients to try to elucidate the underlying disease.Two showed infiltration of the tissue with chronicinflammatory cells including occasional plasmacells, but no changes specific to any other disease.One revealed a lvmphomatous infiltration of theepisclera.
Treatment (see pages i87 to I89)
The various medical treatments given for scleritisand episcleritis are summarized in Tables XIVand XV. Recently oxyphenbutazone (Tanderil)ophthalmic ointment has been used in episcleritisand has been the subject of a double-blind controlledtrial (Watson, McKay, Clemmett, and Wilkinson,1973), but it was not used in the patients in thisseries.
Surgical treatment
Three cataracts have required extraction in the
Table XIII Tissue antibody responses
RheumatoidAntinuclear factor Thyroid Tanned Smooth Gastric Raised
Patients factor (latex) R3 antibodv RBC muscle parietal y-globulin
Scleritis (48) 3 1I2 2 5 2 7 6 4Control (30) 0 0 0 2 0 I 2 0
on February 1, 2020 by guest. P
rotected by copyright.http://bjo.bm
j.com/
Br J O
phthalmol: first published as 10.1136/bjo.60.3.163 on 1 M
arch 1976. Dow
nloaded from

Scleritis and episcleritis I83
presence of active scleritis. No complicationsfollowed these operations.
Four patients have had corneo-scleral grafts fordescemetocele formation, expansion of the globe,increasing corneal guttering, and threatened per-foration (Fig. I9). All have done well.Two patients were given scleral grafts to cover
thin sclera. The graft remained in place in one;in the other patient the graft became involved byscleritis and eroded away, leaving the choroidcovered by a thin layer of conjunctiva. The courseof the scleral disease was not influenced by thegrafting.
Table XIV Treatments given in episcleritis
Simple Nodularepiscleritis episcleritisTreatment
Not knownPlaceboLocal prednisolone dropsSystemic prednisolone*Systemic sintisoneSystemic other steroidSystemic antibioticsSystemic oxyphenbutazoneSystemic indomethacinOther systemic treatment
for example, aspirinLocal steroid with
systemic steroidLocal steroid with systemic
oxyphenbutazoneLocal steroid with systemic
indomethacinOther antibiotics
26
8o2
300
222
30
17I
200
22
4
I0 4
917
517
06
Enucleation
Scleritis is a serious condition and even if fully andcarefully treated can lead to the loss of the eye, asindeed happened in three of the patients in thisseries. Only one of these patients was seen early inthe disease and she was not able to tolerate steroidtreatment; the eye was removed for intractablepain after the necrotizing disease had spreadinexorably around the globe. The vision was pre-served until the last area of undamaged sclerabecame involved, but then fell rapidly from 6/i8 tohand movements within a week. Another eye wasremoved because it was blind and extremely painful.The third patient had severe keratolysis andnecrotizing scleritis with loss of corneal and scleraltissue when first seen. Attempts at covering thesedefects by grafting failed and the eye was eventuallyremoved.
Follow-upOf the 159 patients with episcleritis and the 207patients with scleritis, 146 (9i per cent) and i86(go per cent), respectively, have been followed-upduring a period of between one and eight years(mean 5-8 years). All the patients who had notattended the clinic for six months and had had thedisease for at least one year were sent a question-naire in an attempt to determine the recurrencerate. Altogether 332 patients, of 366 who werecircularized (9I per cent), replied to the question-naire or returned to the clinic for follow-up.
In cases in which scleritis was seen in the initialstages and fully treated the recurrence rate wasonly 20 per cent. The recurrence rate was higher inthose patients with anterior diffuse scleritis than
Table XV Treatments given in scleritis
AnteriorTreatment
Diffuse Nodular Necrotizing Scleromalaciaperforans
Not knownPlaceboLocal steroidSystemic prednisoloneSystemic sintisoneSystemic antibioticsSystemic oxyphenbutazoneSystemic indomethacinOther systemic treatmentLocal steroid with systemic steroidOther systemic steroidLocal steroid with systemic oxyphenbutazoneLocal steroid with systemic indomethacinOther combinations
20
22
I0
70
74I
'90
'7426
70
34712
I5
I
I40
21
427
000
00200
70
50
'4
Posterior
0
0
0
0
0
0
0
0
2
0
2
0
I
00
20
0200
5000
3
on February 1, 2020 by guest. P
rotected by copyright.http://bjo.bm
j.com/
Br J O
phthalmol: first published as 10.1136/bjo.60.3.163 on 1 M
arch 1976. Dow
nloaded from

184 British Journal of Ophthalmology
FIG. I9 Overlay corneo-sclerallamellar graft on same patient as inFig. I5 whose astigmatism wasreducedfrom I5D to 6D by thisprocedure. Grafting only addssupporting tissue and does not affectunderlying pathology
with any other variety. The recurrences were alsomore severe in scleritis than episcleritis, 6o percent of them requiring further hospital treatment.
It is important to follow up those patients withnecrotizing disease because the disease can continueto progress when they are symptom-free, and theymay require continuous treatment even when thedisease is quiescent.
In episcleritis, however, each attack is self-limiting and usually clears without treatment. Thishas been confirmed in a double-blind controlledtrial (Watson and others, 1973) in which eachattack varied from a few hours to several days, theaverage being about seven days. Episcleritis wasmost common in the interpalpebral region, oftenchanging from one side to the other with each attack.However, some patients always developed theinflammation at the same site although recurrencesof both episcleritis and scleritis could occur up to30 years after the onset of the disease (Table XVII).
Two-thirds of the patients had recurrences up tosix years after the onset of the disease, but afterthis the recurrence rate fell. We found that therewas often a considerable interval between the onsetof the disease and the first attendance of thepatient, who often came only because of apprehen-sion caused by the recurrent attacks rather thanthe severity of the symptoms.
Deaths (Table XIX)
Of the I4 patients who were known to have diedduring the period of follow-up, only two hadepiscleritis. One died as a result of a road accident,and the other committed suicide. Of the remaining
patients, six (43 per cent) had had necrotizingscleral disease, one diffuse anterior scieritis, andfive nodular scleritis. None of the patients withscleromalacia perforans was known to have diedduring this period, although many of these patients
Table XVI Duration of disease
Months YearsDisease
6 i8 3 6 10 15 20 30
Episcleritis 6 35 24 I7 I I 29 0 4Scleritis 10 34 24 I9 6 I 0 6
Table XVII Percentage of recurrences
Recurrence Total Same Othereye eye
Both eyes
Simul- At differenttaneously times
Episcleritis 64 46 5 27 22Scleritis 69 48 4 31 15
Table XVIII Severity of recurrences (per cent)
Treatment needed
Disease Not At By own By self-severe hospital doctor medication
Episcleritis 3 IScleritis 27
38 26 46o 13 I
on February 1, 2020 by guest. P
rotected by copyright.http://bjo.bm
j.com/
Br J O
phthalmol: first published as 10.1136/bjo.60.3.163 on 1 M
arch 1976. Dow
nloaded from

Scleritis and episcleritis I85
Table XIX Cause of death in the I4 patients who died during the period offollow-up
Patient Sex
I1 Female
2 Female3 Male
45
6
789I0I I
I2
'3I4
FemaleFemale
Male
MaleMaleMaleMaleMaleMaleMaleMale
Type of scleritis
Necrotizing
NecrotizingNecrotizing
NecrotizingNecrotizing
Necrotizing
Diffuse anteriorNodularNodularNodularNodularNodularNodularSimple episcleritis
General conditions
Rheumatoid arthritisCardiovascular diseaseRheumatoid arthritisDiffuse connective-tissue diseaseChronic nephritisHypertensionHypertensionBronchitisEmphysemaPulmonary tuberculosisEmphysemaBronchiectasisPolyarteritis nodosaRheumatoid arthritis
Old herpes zoster ophthalmicusOld herpes zoster ophthalmriicus
Cause of death
Coronary thrombosis
BronchopneumoniaCerebral haemorrhage
Cerebral haemorrhageCongestive heart failure
Bronchopneumonia
Gastrointestinal haemorrhageCoronary thrombosisMyocardial infarctionMyocardial infarctionMyocardial infarctionStabbed to deathSuicideRoad accident
had long-standing rheumatoid arthritis and weregenerally unwell at the time of their initial exami-nation. Unfortunately three of these patientswere not found for follow-up and might well havedied in the interim. Of those who died of naturalcauses, 54 per cent had necrotizing disease, and27 per cent of the patients with severe necrotizingscleritis were dead within eight years of the onsetof the scleritis.
Five of the patients who died were known tohave had diffuse connective-tissue disease; 2I percent of all those with connective-tissue disease inthis series. Another had hypertension and, it wasthought, could have had a systemic vasculitis. As nonecropsy was performed this could not be confirmed.
Discussion
While scleritis is an uncommon disease, accountingfor only o-o8 per cent of new referrals to eyedepartments (Williamson, I974), of those with thenecrotizing disease 21 per cent died withineight years of the onset. The presence of scleritismay therefore portend serious systemic disease.Early diagnosis may lead to early treatment of thegeneral condition, prolonging and probably im-proving the quality of life for these patients.
In our present series 46 per cent of the patientswith scleritis had a known associated systemiccondition. Of these, I5 per cent had definiteconnective-tissue disease, confirmed by a rheuma-tologist (Table XI). This incidence has recentlybeen confirmed in an analysis of a further 88patients with scleritis, in whom the incidence of
associated systemic disease was 42 per cent, ofwhich I5 per cent consisted of connective-tissuediseases.
It has been suggested in the literature (Duke-Elder and Leigh, I965) that rheumatoid arthritisis the commonest single associated condition, but itwas found in only io per cent of our patients.Scleritis also occurs in association with otherconnective-tissue diseases-systemic lupus erythe-matosus, polyarteritis nodosa, relapsing polychon-dritis, Wegener's granulomatosis-thus reflectingthe collagenous nature of the tissue of which thesclera is composed. Altogether 31 patients (15 percent) were found to have manifest connective-tissuedisease; in seven of these the scleritis was thepresenting feature. In I9 other patients there wereconditions thought to have been immunologicallyinduced, including two who had erythema nodosum.A total of 40 had positive latex agglutination testsfor rheumatoid arthritis and a positive antinuclearfactor, and if all the immunological tests are in-cluded, 72 patients (35 per cent) in the series testedhad some abnormality of this type.
It seems that necrotizing scleral disease repre-sents a different phase of scleritis in certain patients.In some patients who have had recurrent scleraldisease for many years the scleritis has changed intype, coinciding with a change in the character ofthe systemic disease-for example, the onset ofvasculitis in rheumatoid arthritis and renal diseasein systemic lupus erythematosus. In otherpatients the onset of disease is 'malignant' witprogressive and inexorable destruction of scler..tissues if treatment is not adequate. The mortality
on February 1, 2020 by guest. P
rotected by copyright.http://bjo.bm
j.com/
Br J O
phthalmol: first published as 10.1136/bjo.60.3.163 on 1 M
arch 1976. Dow
nloaded from

i86 British Journal of Ophthalmology
in this group is very high. Finally, there appears tobe yet another type of scleral disease, scleromalaciaperforans, which is almost completely confined towomen, half of whom have long-standing rheu-matoid arthritis. In these sequestration of thesclera occurs without warning and little, if any,inflammation. This type of scleral reaction is neitherthe same as that found in other forms of scleritisnor does it necessarily have the same pathogenesis.A biopsy is contraindicated in scleral disease
because the sclera does not heal easily-a fact wellknown to surgeons performing detachment opera-tions a few years ago when scleral surgery was therule. Large scleral nodules often contain pultaceousmaterial which, if released, exposes the underlyingchoroid, but they may heal with fibrosis if left alone(Watson, I974). Much of our knowledge of theunderlying processes has therefore to be derivedfrom the few biopsy specimens which have becomeavailable, and from those eyes which have beenenucleated for severe disease (Sevel, I967; Verhoeffand King, 1958; Anderson and Margolis, 1952;Fransois, 1970; Henkind, I974). This unfortunatelymeans thatwe can find out little about the disease inmost of the patients other than what can be deducedfrom their clinical examination and serological in-vestigations. Biopsy of the episcleral lesions showedoedema, separation ofthe episcleral fibres, infiltrationwith lymphocytes, and some cuffing of the vessels.Henkind and Gold (I973) observed a rheumatoidnodule in the episcleral tissue but we have not seenthis. It is certain, however, that the changes typicalof rheumatoid nodules occur in the sclera in certainpatients with necrotizing scleritis and rheumatoidarthritis. More typical, however, is a granulomatousreaction in the sclera, similar to that found else-where in the body in connective-tissue disease, thepredominant feature being fibrinoid necrosis.Similar lesions can be produced in animals with theSchwartzmann reaction. It was probable thereforethat in many cases the altered immunity in thepatient was the underlying cause of this condition.The sclera is also involved in gout, in which theresponse is due to inflammation caused by pro-teolytic enzymes released from polymorphs whichhave ingested uric acid crystals.The chronic granulomatous diseases of bacterial
origin have also been quoted as a cause of scleritis(Duke-Elder and Leigh, I965). We saw only twopatients with active pulmonary tuberculosis andscleritis, although ancient photographs and histo-logical sections make it clear that this was a muchcommoner condition when tuberculosis was severeand less easily treatable. We have not knowinglyseen scleritis in association with sarcoidosis.
Syphilis, however, can present as a scleritis.Four patients have presented in this way with theeye changes as their only symptom. They were
found to have severe active syphilis with a positivecerebrospinal fluid serological result. The scleritisdisappeared when the syphilis was fully treated.Altogether 14 patients had a positive Wassermannreaction in this series, seven presented with simpleepiscleritis and the others with a diffuse anteriorand nodular scleritis. The scleritis associated withsyphilis and tuberculosis was in no way differentfrom the other forms.The aetiology of episcleritis is even more un-
certain. However, two patterns are apparent. Mostpatients have intermittent bouts of moderate orsevere inflammation at intervals of one to threemonths, lasting seven to ten days and occurringmuch more commonly during the spring andautumn than in the summer or winter. Only rarelycan any certain precipitating factor be found, theattacks usually being related to family upsets andworries at work. Occasionally, however, a clearhistory of exogenous sensitization is given-forexample, contact with printer's inks. In one instancethe patient had only to be inside the printing worksfor his eyes to flare up; exposure to the vapoursof the ink also produced an attack under hospitalconditions, but skin tests gave negative results. i i percent of patients with episcleritis had recurrently highserum uric acid values (more than 6 5 mg per cent onthree readings), and 7 per cent had clinical gout.12 per cent also had a history of asthma and hayfever; only one patient related the attacks tomenstruation. Two patients developed episcleritisafter a desensitization vaccination.The second group of patients gave no history of
periodicity but rather of mild, prolonged attacksof inflammation. Into this category came almost allthose patients who had some other intercurrentdisease. Seven patients had a positive Wassermannreaction (one with active syphilis), four had mildrheumatoid arthritis with a positive rheumatoidfactor but only a few joint symptoms, and two haderythema multiforme; the others had active tuber-culosis, Henoch-Schonlein purpura, or rosacea.Herpes simplex virus has been grown from onelesion. The appearances of the episcleritis didnot differ in these two groups, and in neitherdid the episcleritis progress to a scleritis exceptin those patients with herpes zoster who havealready been discussed. General physical examin-ation and chest x-ray failed to reveal any evidenceof focal sepsis.Herpes zoster involves both the cornea and
sclera. As already discussed, an episcleritis mayoccur in the early vesicular stage of the disease,disappearing completely and then presenting as adeep localized scleritis at the site of the originallesion some two to three months later. Alternativelythe sclera may be involved early in the disease, inwhich case a nodular scleritis is the rule.
on February 1, 2020 by guest. P
rotected by copyright.http://bjo.bm
j.com/
Br J O
phthalmol: first published as 10.1136/bjo.60.3.163 on 1 M
arch 1976. Dow
nloaded from

Scleritis and episcleritis I87
Clinical gout was found in five patients whopresented with episcleral and scleral disease, and32 had raised levels of uric acid on more than oneoccasion. The serum uric acid is a notoriously un-
reliable test and a single positive recording shouldnot be taken as indicative of underlying gout. It wasobserved that those patients with clinical gout andscleral and episcleral disease had deposits of uricacid beneath the conjunctiva around the anteriorciliary vessels at the plica. It was hoped that thiscould be used as a diagnostic sign, but depositswhich look almost identical are frequently seen inpatients whose serum uric acid is normal.
It could be suggested that this group of patientswith episcleritis may represent the earlier stages ofa benign form of scleritis. If this was so, one wouldexpect a significant number of cases to progressfrom episcleritis to scleritis, but during the eight-year period of follow-up we did not see this. Wedid see three patients who had episcleritis in one
part and scleritis in another part of the same
eye. However, it is an interesting and definiteobservation that the episcleritis did not progressto scleritis even during a prolonged follow-up.We feel that this suggests that episcleritis andscleritis are two different types of reaction to a
similar antigen within the different tissues. Thus thefact that the episclera is involved in the course ofthe disease does not mean that the underlyingsclera would become involved, even after a longperiod of time. We have, as yet, no definite evidencethat scleritis is an autoimmune disease, and theevidence presented in this paper is only circum-stantial. Equivalents of Koch's postulates whichneed to be satisfied for auto-immune disease are
as follows (Glynn, 1974):i. There must be a specific antigen. It may not
be from the tissue involved in order thatcomplexes may be formed elsewhere. Ingeneral, one would expect the antigen tobe found at the site of the lesion, for instancethe thyroid antigen in autoimmune thyroiditis.It should be possible to:
2. Extract the antigen.3. Reproduce the disease in some experimental
animal.4. Demonstrate specific antibodies to the antigen
or specifically sensitize cells reacting withantigen.
We were not able to fulfil these postulates partlybecause of the undesirability of obtaining biopsytissue in our patients, and because of uncertainty thatthe disease produced in animals was of the same
nature. However, the circumstantial evidence fromthe well-proven association with known connective-tissue disease is strongly suggestive that this is a
manifestation of immune complex disease in a
large number of cases. In herpes zoster ophthal-micus and gout the precipitating cause is known,but until more is known about the precipitatingfactors of the immune-complex disease we are notjustified in making any further conclusions.
Whatever the pathogenesis might be, we foundthat by careful differential diagnosis we were ableto treat the disease appropriately and adequatelyso as to prevent a serious destructive changetaking place in the eye. The differential diagnosisof scleritis and episcleritis is summarized inTable XX.
TREATMENT
Apart from the very few patients in whom a
specific bacterial or viral agent could be found to
Table XX Cardinal features in the differentiation of scleritis from episcleritis
Episcleritis Scleritis
Anterior
Onset
RednessPain
Photophobia andlacrimation
Vsacular changes
ChemosisScleral thinning ortransparencyVisual acuity
Simple
Sudden
Nodular
Usuallysudden
Bright red Red Dusky redSlight Slight Moderate,localized localized localized and
referredOccasionally Occasionally Occasionally
Bluish redModerate,localized andreferredOccasionally
Superficial Superficial Superficial and Superficial andepiscleral episcleral deep episcleral deep episcleral
Occasionally RareRare Rare
Rare CommonCommon Common
Bluish redSevere,localized andreferredCommon
Superficial anddeep episcleraland occasionallyavascular patchVariableCommon
Normal Normal Normal Occasional loss Common loss
Posterior
Gradual
Very slight VariableSlight, if any Severe,
localized andreferred
None Unusual
Avascular area Superficialand deepepiscleral
Absent CommonAlways Rare
Common loss Very common
loss
ScleromalaciaNodular Diffuse Necrotizing perforans
Gradual Gradual Gradual Insidious
on February 1, 2020 by guest. P
rotected by copyright.http://bjo.bm
j.com/
Br J O
phthalmol: first published as 10.1136/bjo.60.3.163 on 1 M
arch 1976. Dow
nloaded from

i88 British Journal of Ophthalmology
have caused episcleritis or scleritis, the treatmentis suppression of the inflammation in order torelieve the discomfort and prevent the destructivechanges which may accompany the inflammation.Treatment, which must be continued until thedisease has followed its natural course, has provedto be effective and many eyes are being saved orprevented from developing severe complications.Only three eyes (o.6 per cent) were lost-one thatof a patient who could not tolerate the treatmentrather than because of the severity of the eye disease.
EPISCLERITIS
As the condition is self-limiting, harmless, andfrequently symptomless, treatment may not benecessary. Double-blind controlled studies havebeen conducted to determine first whether anytreatment was necessary and secondly whichdrugs were most effective in suppressing theinflammation.
In this trial some patients received placebo,others local steroid ointment, and the remainderoxyphenbutazone ointment. All the patients re-covered within I0 days. Both oxyphenbutazoneeye ointment and betamethasone ointment ap-peared to hasten the recovery by about one day,but the differences were not significant (Watsonand others, 1973) (Fig. 20).
If it is felt necessary to treat the patient, eitherbecause of the symptomatology or because of
100.
90
80
70
E
t; 50
c0E 40
$ 30
20
0,
10
0
..'*.t
Betamethasone.........Oxyphenbutazone
Placebo
0
Days7 14 21
FIG. 20 Improvement of conjunctival and episcleralinjection in patients with episcleritis treated witheither placebo, oxyphenbutazone ointment or
betamethasone i per cent ointment. Although thosetreated with active substances improved slightly faster,8o per cent of those receiving placebo had recovered by2I days
multiple recurrences, we recommend the followingroutine:
Topical medication: Any one of the followingmedications may be used:
i. Prednisolone eye drops 0o5 per cent hourlyuntil 24 hours after the inflammation hassubsided, then reduced to three times a dayfor a further four days.
2. Betamethasone (Betnesol) eye ointment i percent four times a day during the attack, and fora further week after the attack has subsided.
3. Oxyphenbutazone (Tanderil) eye ointmentio per cent four times a day during theattack, and for a further week after the attackhas subsided.
Systemic therapy: Occasionally patients will not res-pond adequately to local therapy, in which casesystemic oxyphenbutazone, indomethacin (Indocid),or corticosteroid may be needed.
i. Oxyphenbutazone: 6oo mg daily in divideddoses is given until there is a response. Thedose is then reduced to 400 mg until the eye isquiet and then it is stopped. This treatmentis given in addition to local treatment.
2. Indomethacin: If the patient fails to make arapid recovery the drug may be changed toindomethacin I00 mg daily in divided doses,and then reduced to 75 mg as soon as there isa response. A double-blind controlled studyjust completed indicates that oxyphenbuta-zone and indomethacin are equally effectiveas anti-inflammatory agents, although somepatients respond better to one drug than theother.
3. Corticosteroids: In the rare case which doesnot respond to local treatment, or systemicoxyphenbutazone or indomethacin, it isjustifiable to give a short, intensive course ofprednisolone or its equivalent. A suppressivedose for this condition is 6o mg prednisolonedaily which, as soon as the inflammation startsto regress, can be reduced rapidly with a viewto withdrawing the drug entirely within onemonth.
A double-blind controlled study was carried outin these patients (Watson, Lobascher, Sabiston,Lewis-Faning, Fowler, and Jones, I966) whichrevealed that both oxyphenbutazone and predni-solone were effective, but that patients receivingsystemic prednisolone had a rebound of theirsymptoms, while those having oxyphenbutazoneremained symptom-free.
SCLERITIS
Because of the depth and severity of the inflam-mation local steroid treatment is ineffective. Drops
on February 1, 2020 by guest. P
rotected by copyright.http://bjo.bm
j.com/
Br J O
phthalmol: first published as 10.1136/bjo.60.3.163 on 1 M
arch 1976. Dow
nloaded from

Scleritis and episcleritis I89
or ointment are soothing and reduce the inflam-mation but are not sufficient to control the scleritis.As a result of our experience we have come to
the conclusion that the following regimen oftreatment is the most likely to be effective:As soon as scleritis is diagnosed:
Systemic oxyphenbutazone 6oo mg daily individed doses for four days, followed by 400 mgdaily until the condition is suppressed. This dosageis continued for one week after all symptoms havesubsided. Or
Systemic indomethacin I00 mg daily in divideddoses, reduced to 75 mg daily in divided doses as soonas there is a response. Treatment is continued untilthe condition has been quiescent for seven days.These two drugs appear to be more effective
than any of the other anti-inflammatory agents ingeneral use-for example aspirin, ibuprofen (Bru-fen), etc.
Local steroids
Usually prednisolone or betamethasone can begiven in addition.
Subconjunctival steroids are not recommended inscleritis
We have seen two patients in whom extremethinning has occurred at the site of a subconjunc-tival injection of steroid (Watson, I974; Fraun-felder and Watson, 1976). It is not certain whether itis the vehicle in which the steroid is contained orthe steroid itself which is the irritating factor. Wehave from time to time given intraorbital steroidinjections in patients unable to take steroid syste-mically. The effect is transient and the injectionshave to be repeated weekly to be effective. Mostpatients will not tolerate this regimen and so it isnot satisfactory for routine use.
Systemic corticosteroids
If the scleritis is very severe, and does not respondto the oxyphenbutazone or indomethacin within aweek, or if any avascular areas appear in theepisclera, systemic steroids must be given in heavysuppressive doses. The sclera is avascular and highconcentrations are required to produce a thera-peutic effect.
Systemic prednisolone8o mg a day in divided doses is usually sufficientas an initial dose. If it is effective the response isdramatic; although there is little change in 24hours or even 48 hours, the pain disappears. Theeye signs may not improve for a further 48 hours,
after which time they rapidly regress. As soon asthe condition is brought under control the dosagecan be dropped within a week to a maintenancelevel which is usually between io and 20 mgprednisolone daily. Cautious reduction from thislevel usually enables the patient to be taken off thedrug or to be maintained with another anti-inflam-matory agent within three to four weeks. In patientswho have been unable to tolerate, or have failed torespond to, prednisolone, occasionally a responsecan be obtained with Sintisone (prednisolone2I-stearoylglycolate), eight tablets (each tabletcontaining o-63 mg) daily in divided doses (Hayrehand Watson, I970). Why this preparation is soeffective is uncertain, but we have several patientswho have to be maintained on it rather than on theconventional steroids.
SurgerySurgery is very rarely necessary in scleral disease.Provided the condition is seen early and treatedvigorously, scleral necrosis can be largely prevented.Comeal grafting has had to be performed in fourpatients because of threatened perforation, anexpanding globe, for peripheral corneal guttering,and for descemetocele. The corneal grafts havetaken well and in all cases the scleritis has becomeless severe after this was done.Many reports appear in the literature of scleral
grafting for scleromalacia perforans (Holthouse,I893; Ashton and Hobbs, 1952; Torchia, Dunn,Pease, I968; Vancea, Vancea, Jalobceastii, Colev,and Calin, 1971; Sevel and Abramson, 1972; andothers). This has been necessary in only two patientsin this series-neither of whom could toleratesteroids. In both patients the graft took well.In one the whole necrotic area was removed andthe residual area of scleral inflammation could becontrolled with local steroids and oxyphenbutazonesystemically. In the other the necrotizing processcontinued from the edge of the scleral overlap andthe eye was eventually lost, no other medicaltreatment being tolerated.We consider scleritis to be a medically treatable
condition, and provided the dosages of the drugsare adequate to suppress the inflammatory change,the condition will be controlled. In this we disagreewith Sevel and Abramson (1972) and Aronson andElliott (I974). We feel our results justify our claim.
SummaryThe data from I59 patients (217 eyes) with epis-scleritis and 207 patients (30I eyes) with scleritishave been investigated in detail and the resultsanalysed with the help of a computer. Of thesepatients, 9I per cent were followed-up during a
on February 1, 2020 by guest. P
rotected by copyright.http://bjo.bm
j.com/
Br J O
phthalmol: first published as 10.1136/bjo.60.3.163 on 1 M
arch 1976. Dow
nloaded from
o90 British Journal of Ophthalmology
period of one to eight years. A new classificationis presented which is as follows:
Episcleritis (217 eyes)Simple episcleritis (170 eyes)Nodular episcleritis (47 eyes)Scleritis (30I eyes)Diffuse anterior scleritis (i I9 eyes)Nodular anterior scleritis (134 eyes)Necrotizing scleritis (42 eyes). Of these, 13 were
regarded as scleromalacia perforans.Posterior scleritis (6 eyes)
The diagnosis is based on an exact clinicalexamination which is fully described.
Episcleritis has been shown to be a benignrecurring condition, a mild keratitis being the onlyoccasional complication. Episcleritis does notprogress to scleritis, except in the case of herpeszoster which sometimes starts as an episcleritiswith the vesicular stage of the eruption, to reappearthree months later as a scleritis in the same site.No clear conclusions could be drawn as to the
aetiology of episcleritis.Scleritis is always accompanied by episcleral
inflammation which must be ignored in makingthe diagnosis. Scleritis is a much more severe diseasethan episcleritis, leading to loss of visual acuityfrom corneal changes, uveitis, cataract, or retinaldetachment if not treated. Necrotizing scleritis withinflammation is the severest form of the diseaseand 2I per cent of the patients with this conditiondied within the eight-year-period of follow-up.
Connective-tissue disease was the commonestassociated general condition; the incidence ofnecrotizing scleritis was higher in this group and
21 per cent of these patients were among those thatdied. It is probable that necrotizing scleritisrepresents the eye changes of the malignant phase ofsystemic connective-tissue disease.Treatment is unnecessary in episcleritis but in
scleritis systemic treatment with anti-inflammatoryagents or corticosteroids is obligatory. Using theseroutines of treatment only three patients (o-6per cent) have lost an eye.
Apart from ourselves, the following have worked inthe Scleritis Clinic during the past io years: A. Atkinson,P. Awdry, P. E. Cleary, R. S. Clemett, P. Fowler,A. Freedman, B. Hazleman, P. Henderson, A. D.Holt-Wilson, D. Jones, S. Lachmann, D. Lloyd-Jones,D. Lobascher, A. J. Lyne, and D. A. R. Mackay, andwe would like to thank them all for their help andideas. We are sure many of these ideas are incorporatedin this article but it is impossible to acknowledge themproperly because we have forgotten where they origi-nated. We should also like to thank all those surgeonswho have referred patients to us: without them therewould be no clinic.The computer analysis was completed at the Institute
of Ophthalmology and many of the illustrations werereproduced there; the rest were done in the MedicalIllustration Department of Addenbrooke's Hospital,Cambridge.
Figs 6 and I4 were reproduced from the Transactionsof the Ophthalmological Society of the United Kingdom;Fig. i6 from Connective-tissue disease in the eye, inRecent Advances in Ophthalmology, ed. P. Trevor-Roper,published by Blackwell; and Fig. 20 from the BritishJournal of Ophthalmology.
Last but not least we should like to thank all thosewho have at various times typed part or all of thismanuscript, in particular Mrs J. Field and Mrs J.McCombie.
References
ANDERSON, B., and MARGOLIS, G. (1952) Amer. Jt. Ophthal., 35, 9I7ARONSON, S. B., and ELLIOTT, J. H. (1974) Scleritis, in 'Ocular Inflammatory Disease', ed. Bruce Golden, p. 43.Thomas, Springfield, Ill.
ASHTON, N., and HOBBS, H. E. (1952) Brit. _r. Ophthal., 36, 373CLAVEL and TEULIERES, J. (1958) Bull. Soc. Ophtal. Fr., II, 749DESMARRES, L. A. (I847) 'Maladies des yeux', p. 360. Bailliere, ParisDUKE-ELDER, s., and LEIGH, A. G. (I965) In 'System of Ophthalmology', vol. VIII, chap. VIII. Kimpton, LondonFOWLER, P. D. (1970) Ann. rheum. Dis., 29, I95FRANCESCHETTI, A., and BISCHLER, V. (1950) Ann. Oculist. (Paris), 183, 737FRAN9OIS, J. (1970) Adv. Ophthal., 23, IFRAUNFELDER, F. T., and WATSON, P. G. (1976) Brit. J7. Ophthal., 6o, 227FUCHS, E. (I895) V. Graefes Arch. Ophthal., 41, 229GLYNN, L. E. (I974) Trans. ophthal. Soc. UK, 94, 783GRAVES, B. (1937) Brit. J7. Ophthal., 21, 534HAYREH, s. s., and BAINES, J. A. B. (1972) Ibid., 56, 7I9
, and WATSON, P. G. (I970) Ibid., 54, 394HENKIND, P. (I974) Trans. ophthal. Soc. UK, 94, 782
, and GOLD, D. H. (1973) Rheumatology, 4, 13HOLTHOUSE, E. H. (I893) Roy. Lond. ophthal. Hosp. Rep., 13, 415HOLT-WILSON, A. D., and WATSON, P. G. (1974) Trans. ophthal. Soc. UK, 94, 52MACKENZIE, W. (I830) 'Practical Treatise of the Diseases of the Eye', p. 406. London
on February 1, 2020 by guest. P
rotected by copyright.http://bjo.bm
j.com/
Br J O
phthalmol: first published as 10.1136/bjo.60.3.163 on 1 M
arch 1976. Dow
nloaded from

Scleritis and episcleritis I9i
MANN, W. A., and MARKSON, D. E. (1950) Amer. J7. Ophthal., 33, 459ROGNETTA, A. (I844) 'Traite philosophique et clinique d'ophtalmologie', p. 275. ParisSEVEL, D. (I967) Amer. J3. Ophthal., 64, 1125
, and ABRAMSON, A. (1972) Brit. J. Ophthal., 56, 791SLADE, j. (I838) 'Ophthalmia', p. 23. LondonTORCHIA, K. T., DUNN, R. E., and PEASE, P. J. (I968) Amer. J. Ophthal., 66, 705VANCEA, P., VANCEA, P.-P., JALOBCEASTII, L., COLEV, G., and CALIN, A. (197I) Arch. Ophtal. (Paris), 3I, 687VAN DER HOEVE, J. (I934) Arch. Ophthal. (Chicago), II, iiiVERHOEFF, F. H., and KING, R. J. (1938) Arch. Ophthal., 20, 10I3VISWALINGHAM, A. (1936) Brit. 7. Ophthal., 20. 449WATSON, P. G. (I974) Trans. ophthal. Soc. UK, 94, 773
, LOBASCHER, D. J., SABISTON, D. W., LEWIS-FANING, E., FOWLER, P. D., and JONES, B. R. (I966) Brit. Y.Ophthal., 50, 463
, MCKAY, D. A. R., CLEMETT, R. S., and WILKINSON, P. (1973) Ibid., 57, 866WILLIAMSON, J. (I974) Trans. ophthal. Soc. UK, 94, 742WOOD, D. J. (1936) Brit. Y. Ophthal., 20, 5IO
on February 1, 2020 by guest. P
rotected by copyright.http://bjo.bm
j.com/
Br J O
phthalmol: first published as 10.1136/bjo.60.3.163 on 1 M
arch 1976. Dow
nloaded from