Scissor. telescope. brodie. bite
137
SCISSOR, TELESCOPE, BRODIE – BITE WHAT IS IT AND HOW TO MANAGE?? Prof. Dr. Maher Fouda Yasmine M. Hammad
-
Upload
yasmine-hammad -
Category
Health & Medicine
-
view
861 -
download
8
Transcript of Scissor. telescope. brodie. bite
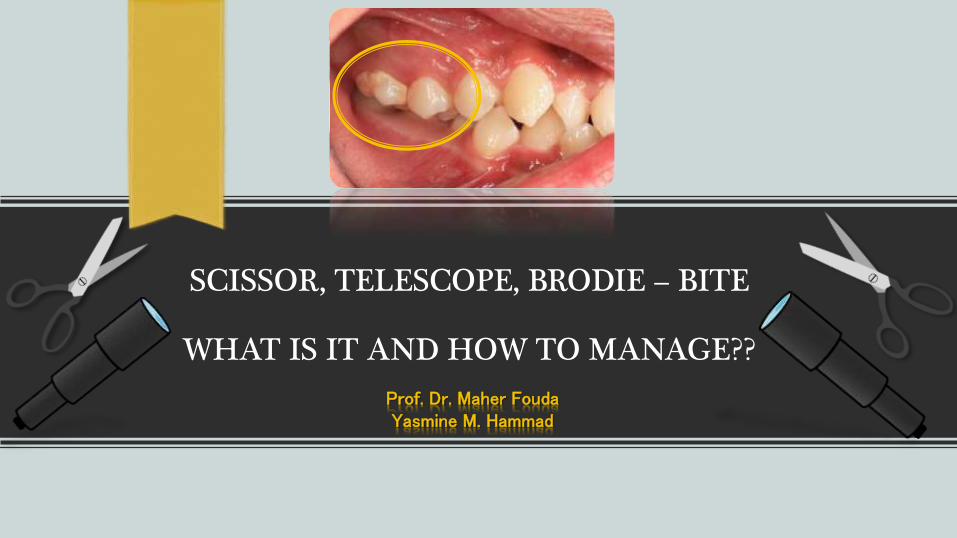
SCISSOR, TELESCOPE, BRODIE – BITE
WHAT IS IT AND HOW TO MANAGE??
Prof. Dr. Maher FoudaYasmine M. Hammad
Definition
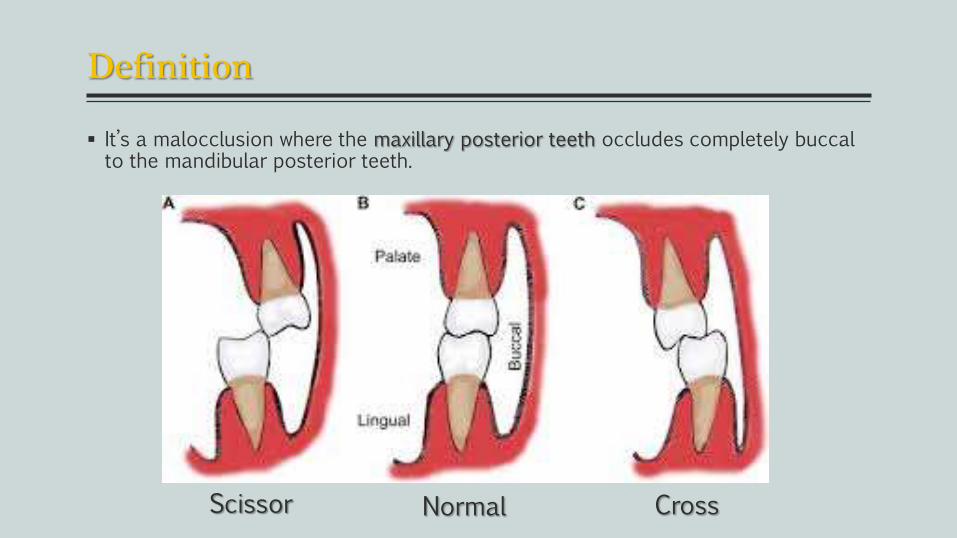
It’s a malocclusion where the maxillary posterior teeth occludes completely buccalto the mandibular posterior teeth.
Scissor Normal Cross
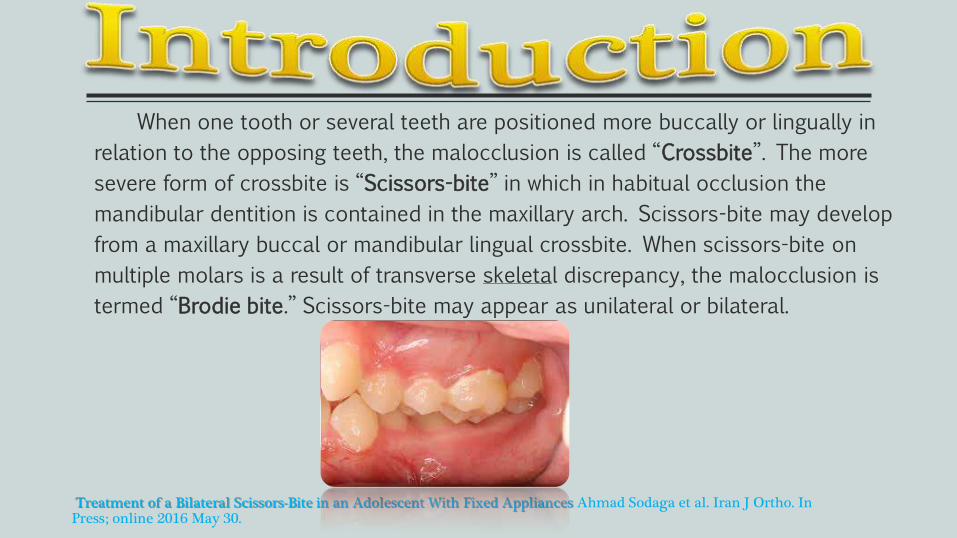
When one tooth or several teeth are positioned more buccally or lingually in
relation to the opposing teeth, the malocclusion is called “Crossbite”. The more
severe form of crossbite is “Scissors-bite” in which in habitual occlusion the
mandibular dentition is contained in the maxillary arch. Scissors-bite may develop
from a maxillary buccal or mandibular lingual crossbite. When scissors-bite on
multiple molars is a result of transverse skeletal discrepancy, the malocclusion is
termed “Brodie bite.” Scissors-bite may appear as unilateral or bilateral.
Treatment of a Bilateral Scissors-Bite in an Adolescent With Fixed Appliances Ahmad Sodaga et al. Iran J Ortho. In Press; online 2016 May 30.
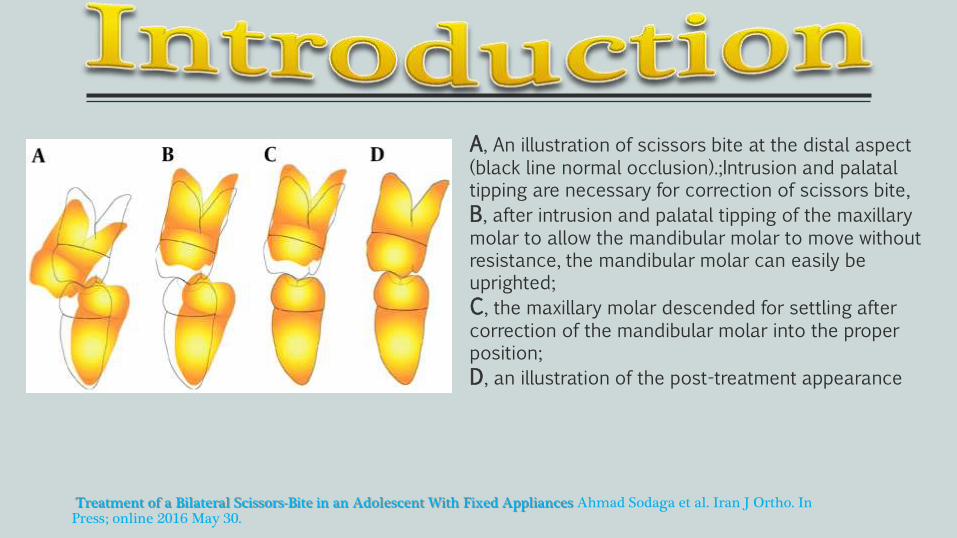
Treatment of a Bilateral Scissors-Bite in an Adolescent With Fixed Appliances Ahmad Sodaga et al. Iran J Ortho. In Press; online 2016 May 30.
A, An illustration of scissors bite at the distal aspect (black line normal occlusion).;Intrusion and palatal tipping are necessary for correction of scissors bite,
B, after intrusion and palatal tipping of the maxillary molar to allow the mandibular molar to move without resistance, the mandibular molar can easily be uprighted;
C, the maxillary molar descended for settling after correction of the mandibular molar into the proper position;
D, an illustration of the post-treatment appearance
CLASSIFICATION
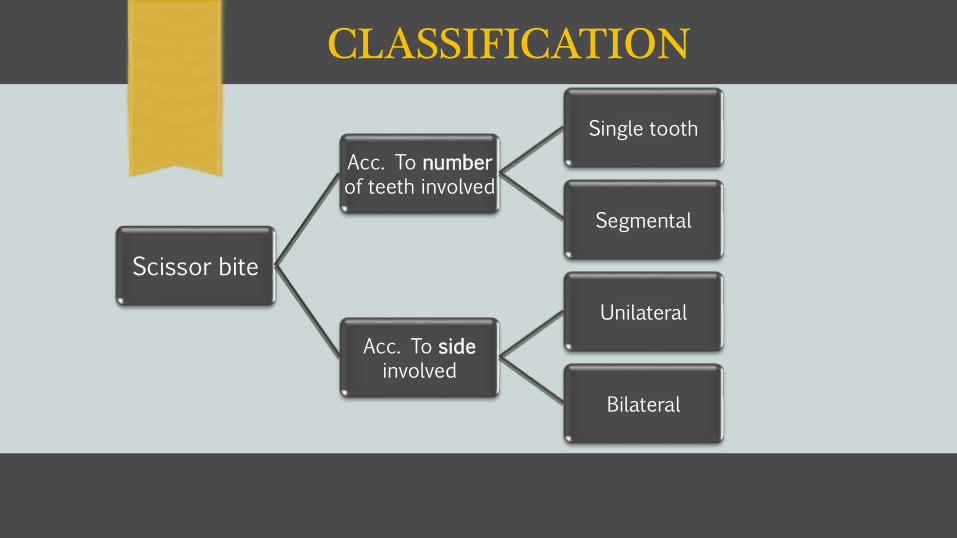
Scissor bite
Acc. To numberof teeth involved
Single tooth
Segmental
Acc. To sideinvolved
Unilateral
Bilateral
Severe forms of scissor bite or Brodie syndrome is rareorthodontic malocclusion that occurs with a frequency of 0.01% in general population. Several methods have been described to obtain a correction from a dental, skeletal and soft tissue points
of view.
In the literature various approaches were described: from jawsosteotomies, surgery first approach, to the use of orthopedic-
functional devices and extractions along with the fixed multibrackets orthodontics combined with miniscrews for the
skeletal anchorage.
Fantasia E, D'Emidio M, Padalino G, Rodi G. Comparison of Orthodontic Techniques used for treating patients with severe form of scissor bite: a systematic review. WebmedCentral ORTHODONTICS 2016
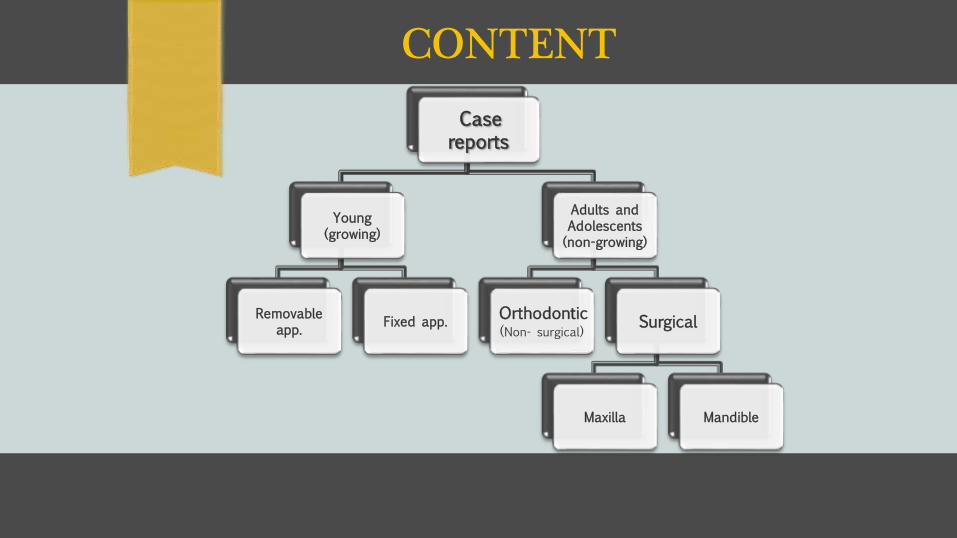
CONTENT
Case reports
Young(growing)
Removable app.
Fixed app.
Adults and Adolescents(non-growing)
Orthodontic (Non- surgical)
Surgical
Maxilla Mandible
Treatment options of Brodie-bite in children
4 case reports.
1. - Bilateral Brodie Bite in Early Mixed Dentition Using Bonded Constriction Quad-helix Appliance.
2. - Occlusal gujdance for unilateral scissors bite in primary dentition.
3. - Scissor bite in a young patient treated with an orthodontic-orthopedic device.
4. - Treatment and retention of a mandibular archtelescoped within the maxillary arch
Brodie bite, adversely affects chewing and muscle functions, but also impairs normal growth and development of the mandible.
This syndrome is rare occuring in 1-2% of the mixed dentition population. As it does not affect the aesthetics, parents are not aware of its presence amounting to the few case reports of this condition in the literature.
Like posterior crossbite (transverse discrepancy) it does not self corrected.
Problems of Brodie Bite:1. Affect chewing function
2. Muscle function
3. Impairs normal growth and development of the mandible.
This makes the early correction of this condition rather essential.
Possible causes of Brodie bite include: microglossia, hypoglossia, neurological and muscular mechanisms causing oral habits, skeletal Class II factors, and abnormal tooth germ position or eruption direction.
A Case report Bilateral Brodie Bite in Early Mixed Dentition Using Bonded Constriction Quad-helix Appliance..Nojima K. et al Bull Tokyo Dent Coll 2011 52: 39 - 46
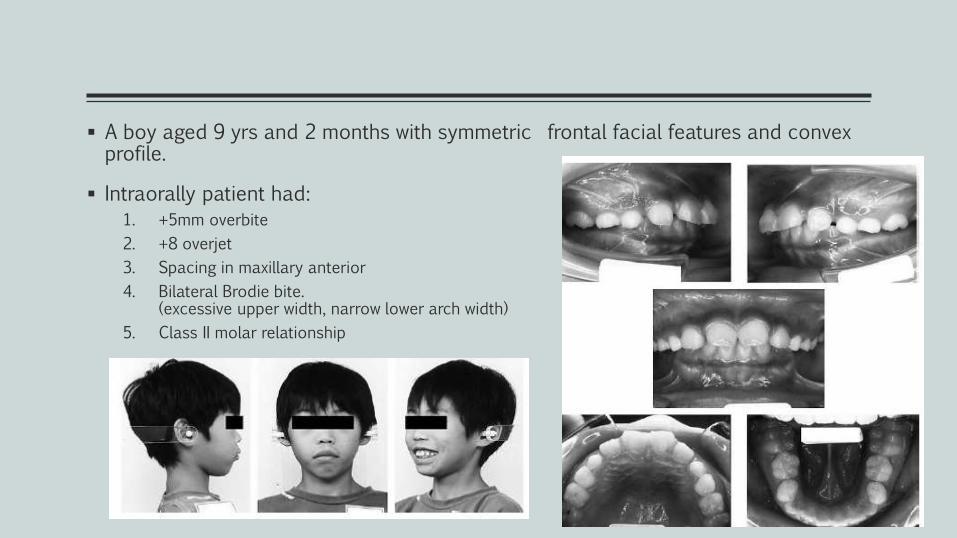
A boy aged 9 yrs and 2 months with symmetric frontal facial features and convex profile.
Intraorally patient had:
1. +5mm overbite
2. +8 overjet
3. Spacing in maxillary anterior
4. Bilateral Brodie bite. (excessive upper width, narrow lower arch width)
5. Class II molar relationship
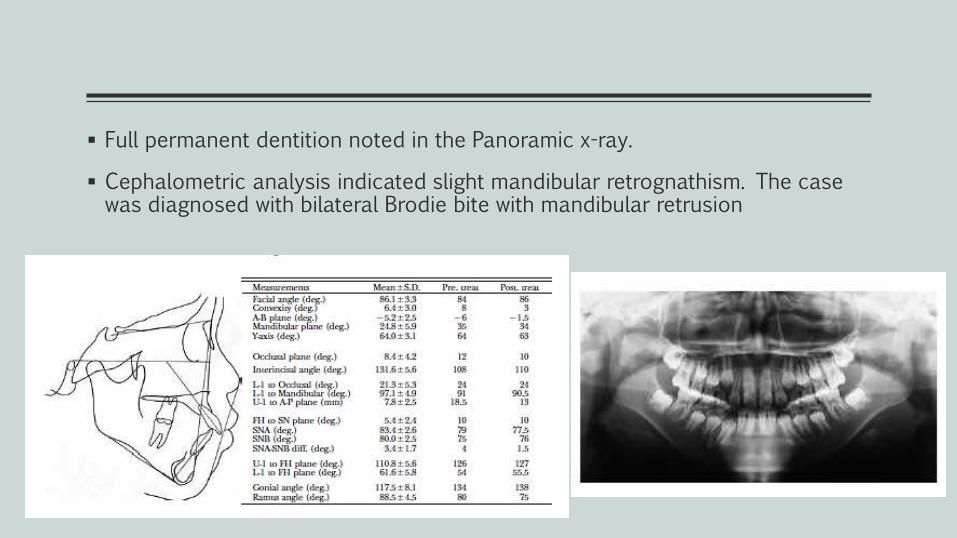
Full permanent dentition noted in the Panoramic x-ray.
Cephalometric analysis indicated slight mandibular retrognathism. The case was diagnosed with bilateral Brodie bite with mandibular retrusion
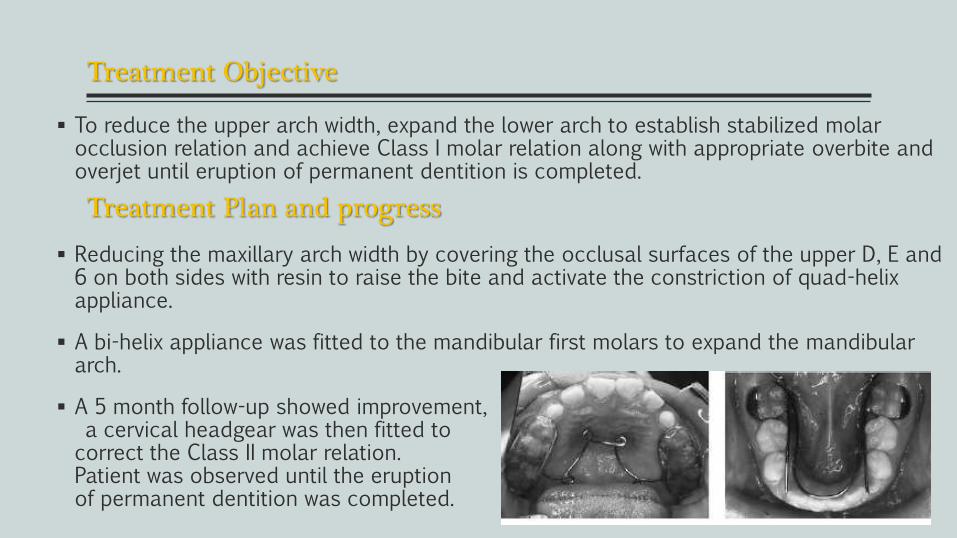
Treatment Objective
To reduce the upper arch width, expand the lower arch to establish stabilized molar occlusion relation and achieve Class I molar relation along with appropriate overbite and overjet until eruption of permanent dentition is completed.
Reducing the maxillary arch width by covering the occlusal surfaces of the upper D, E and 6 on both sides with resin to raise the bite and activate the constriction of quad-helix appliance.
A bi-helix appliance was fitted to the mandibular first molars to expand the mandibular arch.
A 5 month follow-up showed improvement,a cervical headgear was then fitted to
correct the Class II molar relation. Patient was observed until the eruption of permanent dentition was completed.
Treatment Plan and progress
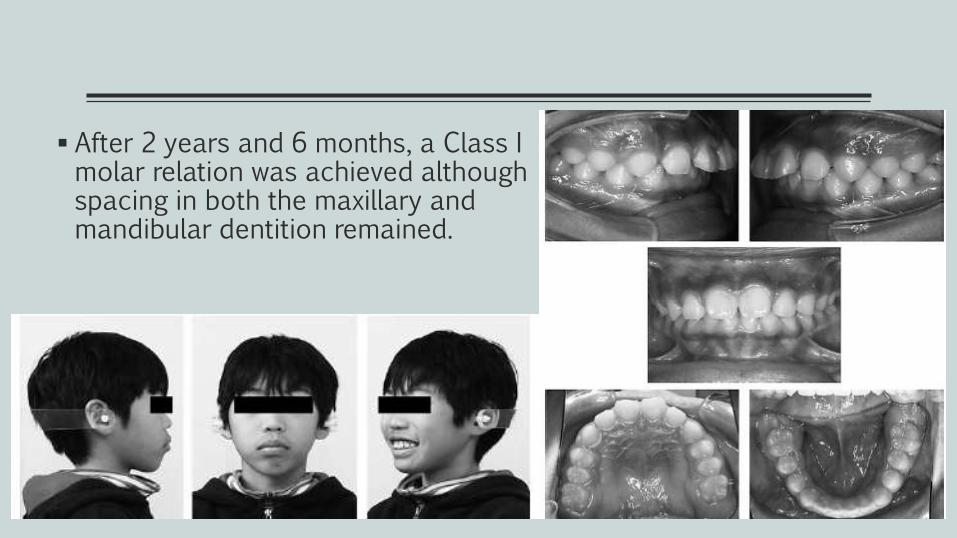
After 2 years and 6 months, a Class I molar relation was achieved although spacing in both the maxillary and mandibular dentition remained.
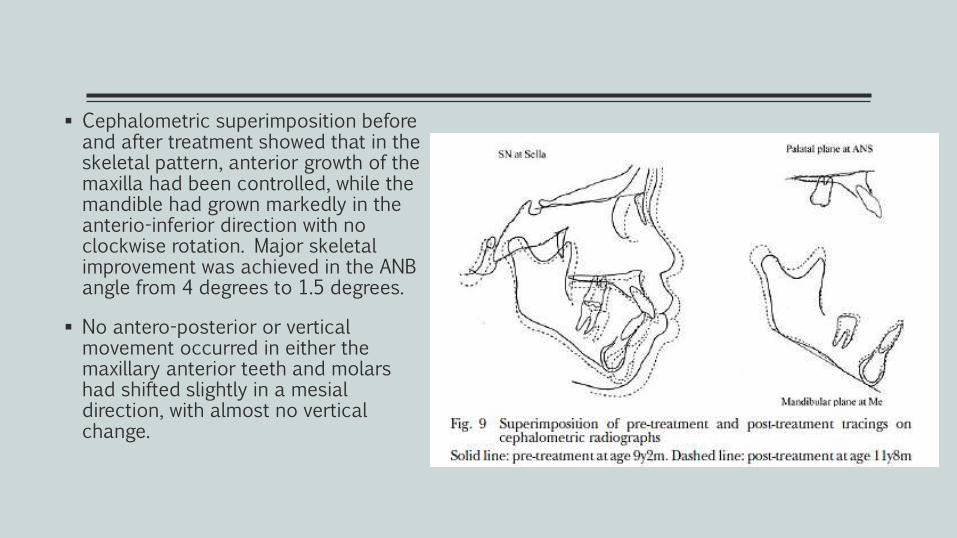
Cephalometric superimposition before and after treatment showed that in the skeletal pattern, anterior growth of the maxilla had been controlled, while the mandible had grown markedly in the anterio-inferior direction with no clockwise rotation. Major skeletal improvement was achieved in the ANB angle from 4 degrees to 1.5 degrees.
No antero-posterior or vertical movement occurred in either the maxillary anterior teeth and molars had shifted slightly in a mesial direction, with almost no vertical change.
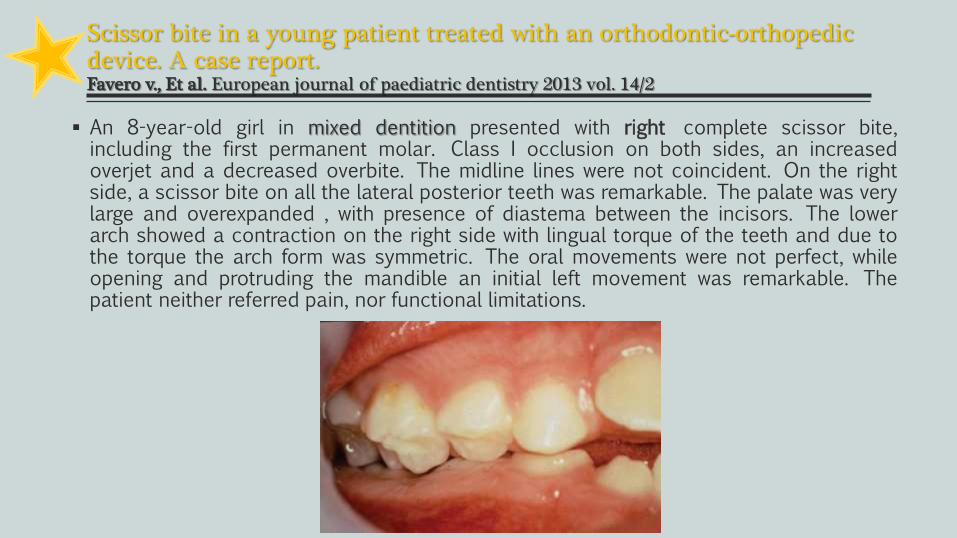
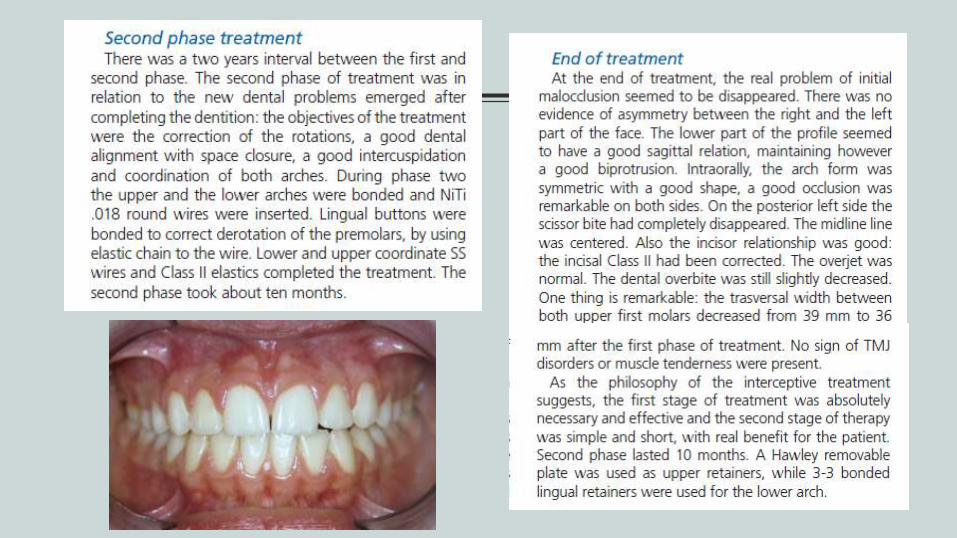
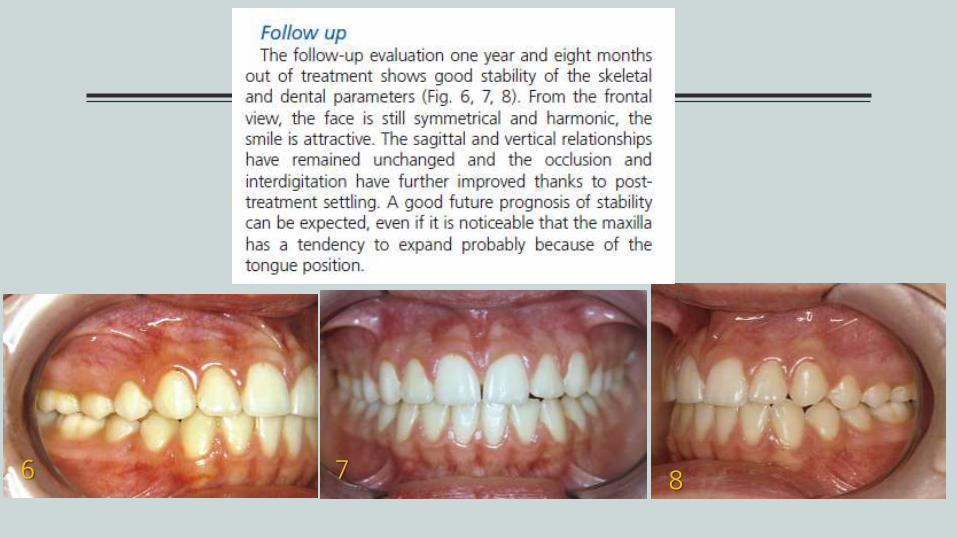
Scissor bite in a young patient treated with an orthodontic-orthopedic device. A case report.Favero v., Et al. European journal of paediatric dentistry 2013 vol. 14/2
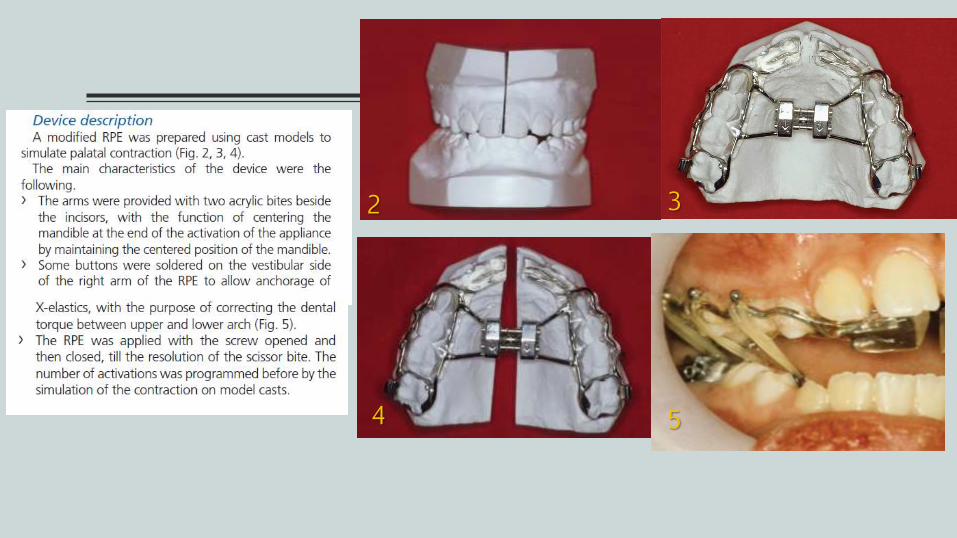
An 8-year-old girl in mixed dentition presented with right complete scissor bite,including the first permanent molar. Class I occlusion on both sides, an increasedoverjet and a decreased overbite. The midline lines were not coincident. On the rightside, a scissor bite on all the lateral posterior teeth was remarkable. The palate was verylarge and overexpanded , with presence of diastema between the incisors. The lowerarch showed a contraction on the right side with lingual torque of the teeth and due tothe torque the arch form was symmetric. The oral movements were not perfect, whileopening and protruding the mandible an initial left movement was remarkable. Thepatient neither referred pain, nor functional limitations.
2 3
4 5
7 86
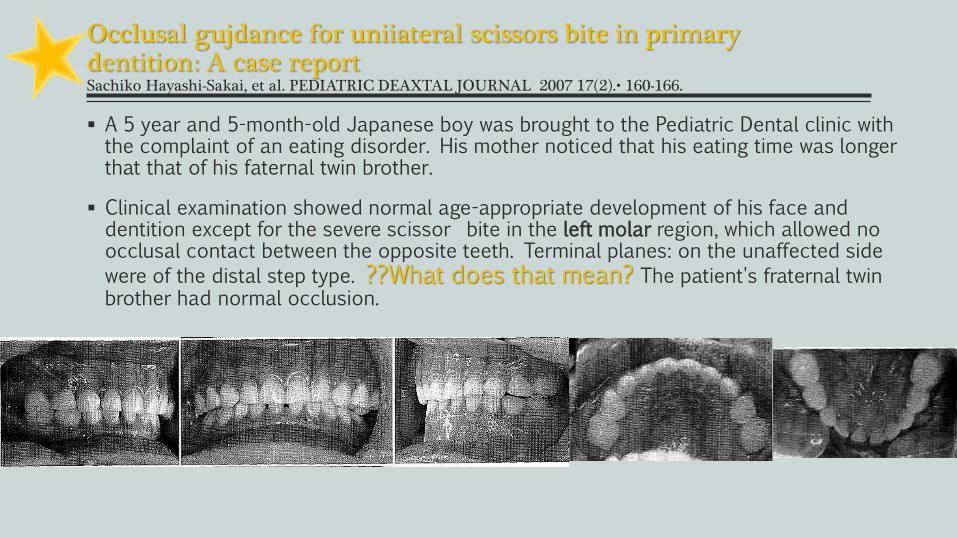
Occlusal gujdance for uniiateral scissors bite in primarydentition: A case reportSachiko Hayashi-Sakai, et al. PEDIATRIC DEAXTAL JOURNAL 2007 17(2).• 160-166.
A 5 year and 5-month-old Japanese boy was brought to the Pediatric Dental clinic with the complaint of an eating disorder. His mother noticed that his eating time was longer that that of his faternal twin brother.
Clinical examination showed normal age-appropriate development of his face and dentition except for the severe scissor bite in the left molar region, which allowed no occlusal contact between the opposite teeth. Terminal planes: on the unaffected side
were of the distal step type. ??What does that mean? The patient's fraternal twin brother had normal occlusion.
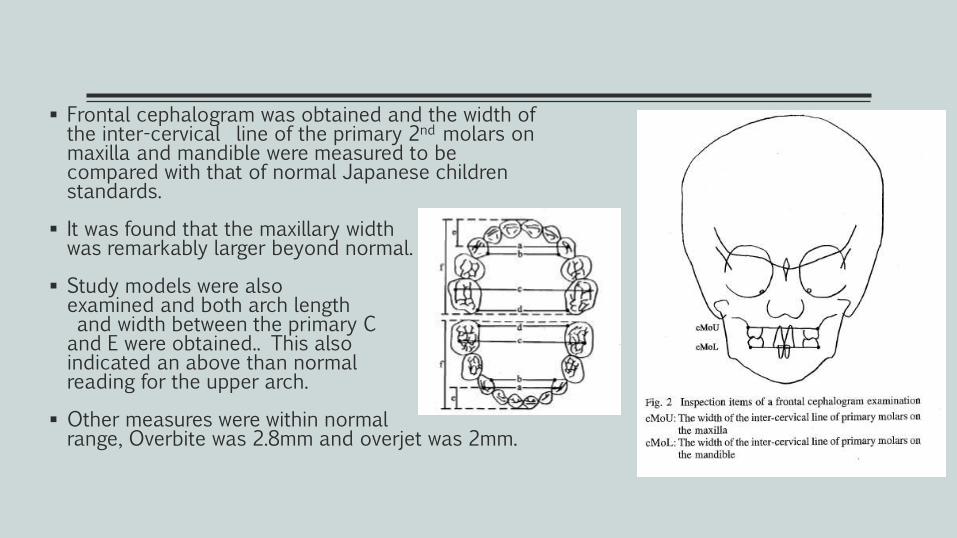
Frontal cephalogram was obtained and the width of the inter-cervical line of the primary 2nd molars on maxilla and mandible were measured to be compared with that of normal Japanese children standards.
It was found that the maxillary width was remarkably larger beyond normal.
Study models were also examined and both arch lengthand width between the primary C and E were obtained.. This also indicated an above than normal reading for the upper arch.
Other measures were within normal range, Overbite was 2.8mm and overjet was 2mm.
Treatment Plan
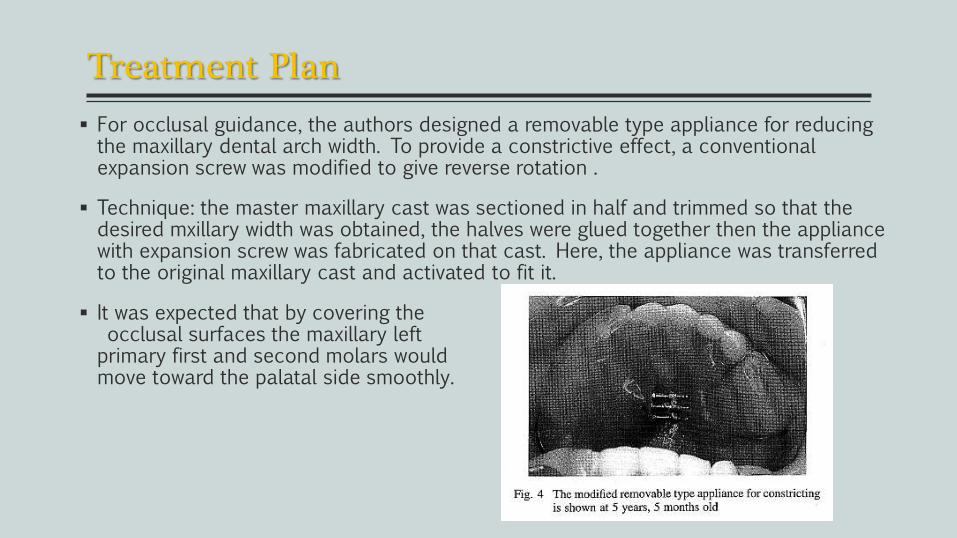
For occlusal guidance, the authors designed a removable type appliance for reducing the maxillary dental arch width. To provide a constrictive effect, a conventional expansion screw was modified to give reverse rotation .
Technique: the master maxillary cast was sectioned in half and trimmed so that the desired mxillary width was obtained, the halves were glued together then the appliance with expansion screw was fabricated on that cast. Here, the appliance was transferred to the original maxillary cast and activated to fit it.
It was expected that by covering theocclusal surfaces the maxillary left primary first and second molars would move toward the palatal side smoothly.
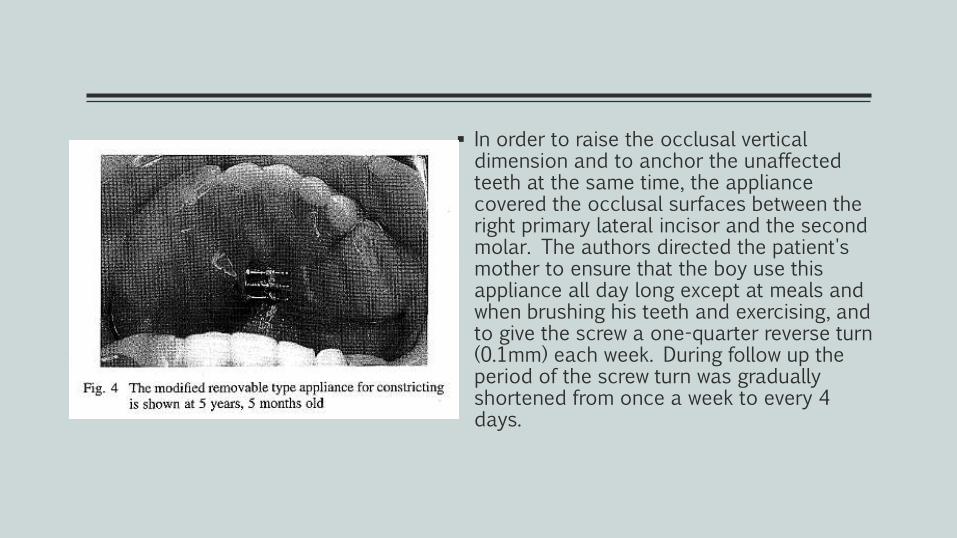
In order to raise the occlusal vertical dimension and to anchor the unaffected teeth at the same time, the appliance covered the occlusal surfaces between the right primary lateral incisor and the second molar. The authors directed the patient's mother to ensure that the boy use this appliance all day long except at meals and when brushing his teeth and exercising, and to give the screw a one-quarter reverse turn (0.1mm) each week. During follow up the period of the screw turn was gradually shortened from once a week to every 4 days.
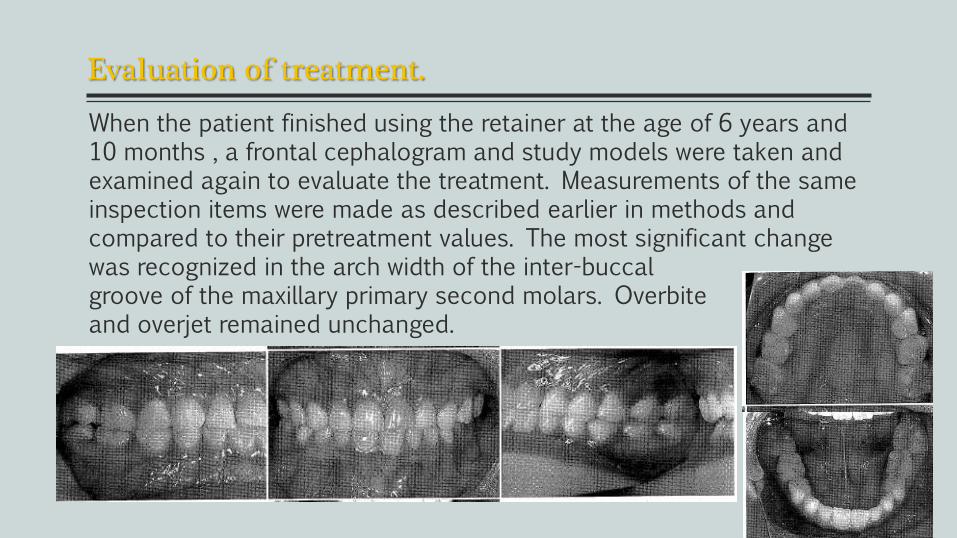
Evaluation of treatment.
When the patient finished using the retainer at the age of 6 years and 10 months , a frontal cephalogram and study models were taken and examined again to evaluate the treatment. Measurements of the same inspection items were made as described earlier in methods and compared to their pretreatment values. The most significant change was recognized in the arch width of the inter-buccalgroove of the maxillary primary second molars. Overbite and overjet remained unchanged.
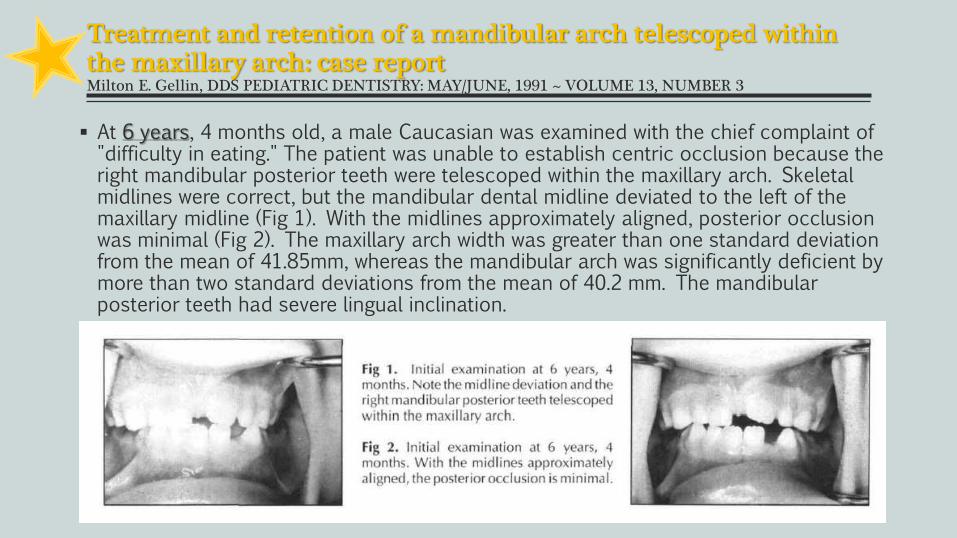
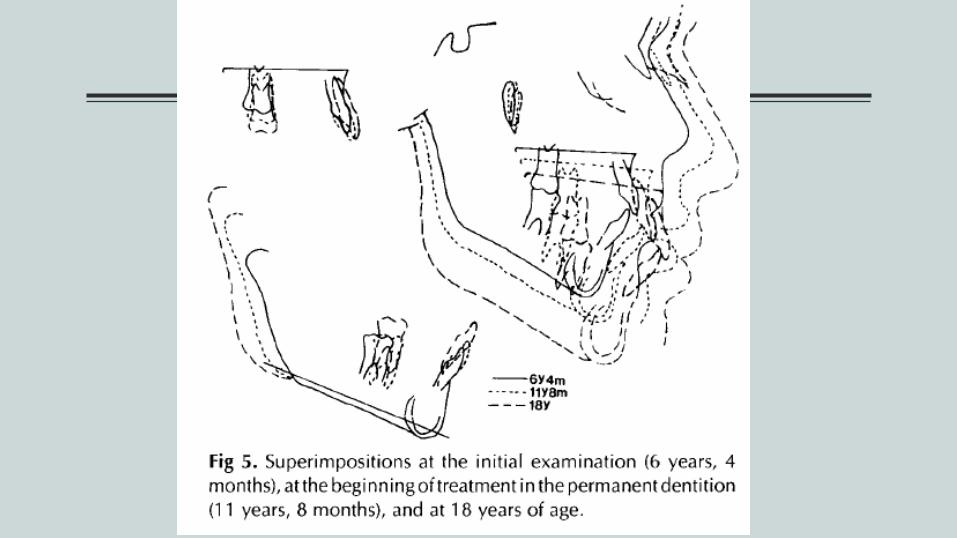
Treatment and retention of a mandibular arch telescoped within the maxillary arch: case reportMilton E. Gellin, DDS PEDIATRIC DENTISTRY: MAY/JUNE, 1991 ~ VOLUME 13, NUMBER 3
At 6 years, 4 months old, a male Caucasian was examined with the chief complaint of "difficulty in eating." The patient was unable to establish centric occlusion because the right mandibular posterior teeth were telescoped within the maxillary arch. Skeletal midlines were correct, but the mandibular dental midline deviated to the left of the maxillary midline (Fig 1). With the midlines approximately aligned, posterior occlusion was minimal (Fig 2). The maxillary arch width was greater than one standard deviation from the mean of 41.85mm, whereas the mandibular arch was significantly deficient by more than two standard deviations from the mean of 40.2 mm. The mandibular posterior teeth had severe lingual inclination.
Treatment objective
Was to expand the mandibular arch bilaterally, so that the posterior teethwould have an acceptable interdigitation. After expansion, the mandibular archwould be retained with a lingual arch until the late mixed dentition; then the patientwould be placed on periodic recalls to evaluate the stability of expansion in thepermanent dentition.
When the patient was 7 years, 9 months old, the mandibular permanentincisors were erupted fully. A lingual arch was selected to accomplish theexpansion, along with a maxillary bite plane to disengage the posterior occlusion.
The lingual arch was expanded to one half of the buccolingual width of thefirst permanent molars. Three additional activations followed at approximately onemonth intervals. When the lingual cusps of the mandibular posterior teeth began toocclude with the maxillary posterior teeth, the maxillary bite plane wasdiscontinued. The lingual arch served as a retainer for 15 months.
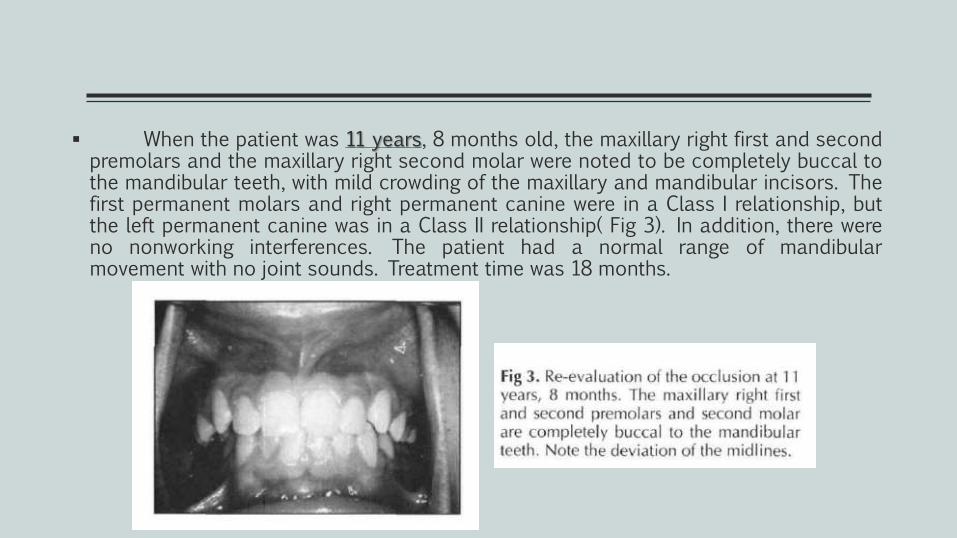
When the patient was 11 years, 8 months old, the maxillary right first and secondpremolars and the maxillary right second molar were noted to be completely buccal tothe mandibular teeth, with mild crowding of the maxillary and mandibular incisors. Thefirst permanent molars and right permanent canine were in a Class I relationship, butthe left permanent canine was in a Class II relationship( Fig 3). In addition, there wereno nonworking interferences. The patient had a normal range of mandibularmovement with no joint sounds. Treatment time was 18 months.
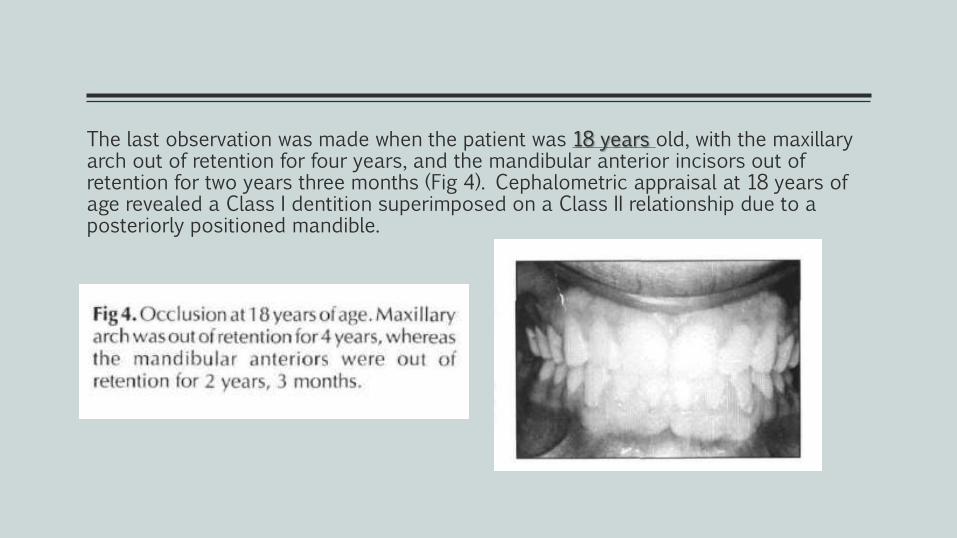
The last observation was made when the patient was 18 years old, with the maxillary arch out of retention for four years, and the mandibular anterior incisors out of retention for two years three months (Fig 4). Cephalometric appraisal at 18 years of age revealed a Class I dentition superimposed on a Class II relationship due to a posteriorly positioned mandible.

CONTENT
Case reports
Young(growing)
Removable app.
Fixed app.
Adults and Adolescents(non-growing)
Orthodontic (Non- surgical)
Surgical
Maxilla Mandible
Treatment options of Scissor-bite in Adolescents
3 case reports.
1. Scissor Bite Correction by Bite Plane2. Crowding, Protrusion and Scissors Bite: Extractions and Extra-
Alveolar Bone Screws3. Treatment of a Bilateral Scissors-Bite in an Adolescent With
Fixed Appliances
Features in scissor bite:
1. Facial profile-The scissor bite has no significant influence on the facial profile.
2. Airway-The scissor bite is not known to reduced airway.
3. Chewing function-The chewing function is bad since the molars make no contact with each other.
4. Jaw joints-Patients may experience a clicking or pain in the jaw joints since the jaw is usually forced to function in a deviated position during the chewing process.
5. Teeth wear-Molar wear is unlikely since the molars do not come in contact with each other.

Scissor Bite Correction by Bite PlaneAmit Prakash et al Indian J Dent Adv 2013; 5(4): 1425-1427
A female patient, 16 years and 3 months of age, consultedwith a chief complaint of improper occlusion and irregular teeth.She had a convex profile and a symmetric frontal view. She giveshistory of surgical treatment for the cleft lip (Figure1). On clinicalexamination, both canine and molar relationships were Class I onboth sides, but a scissors-bite of the posterior arch on the right sidewas observed. Overbite was 6.5 mm and overjet was1.1 mm. Thedental midline was deviated to right by 3 mm. On cast analysis, thearch-length discrepancy was 2.2 mm in the maxilla and 8.3 mm inthe mandible.
Treatment objectives
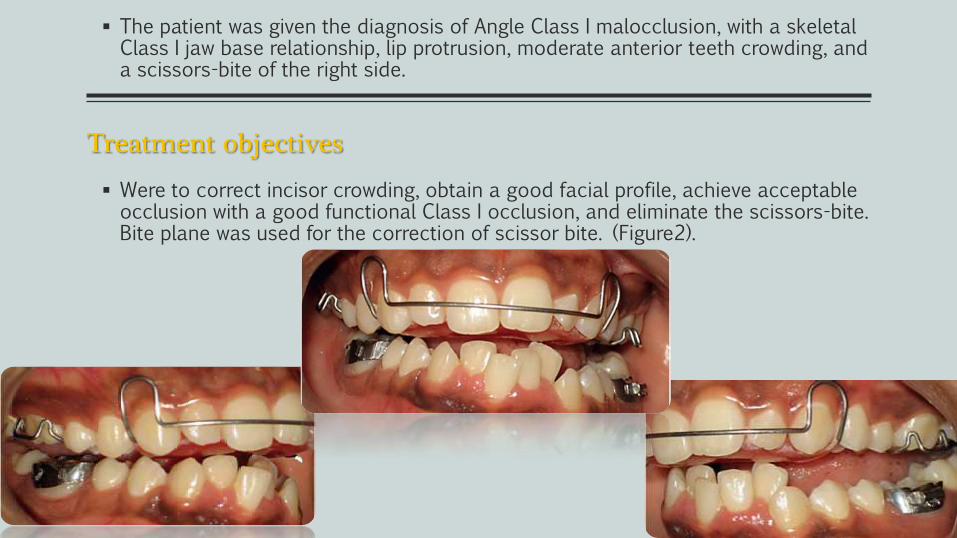
The patient was given the diagnosis of Angle Class I malocclusion, with a skeletal Class I jaw base relationship, lip protrusion, moderate anterior teeth crowding, and a scissors-bite of the right side.
Were to correct incisor crowding, obtain a good facial profile, achieve acceptable occlusion with a good functional Class I occlusion, and eliminate the scissors-bite. Bite plane was used for the correction of scissor bite. (Figure2).
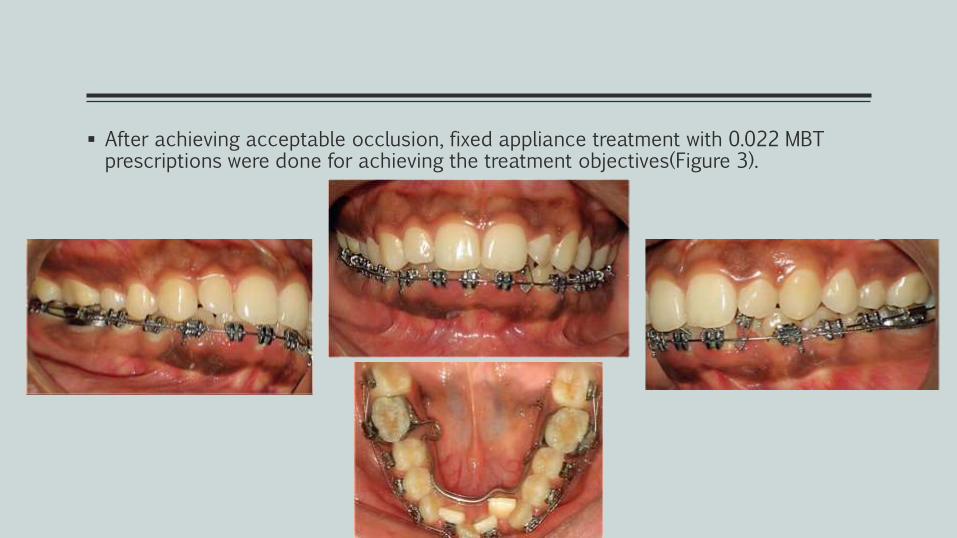
After achieving acceptable occlusion, fixed appliance treatment with 0.022 MBT prescriptions were done for achieving the treatment objectives(Figure 3).

Post treatment results were good and stable As a result, complete treatment of a scissors-bite in the present case was achieved in 5 months.(Figure 4)..
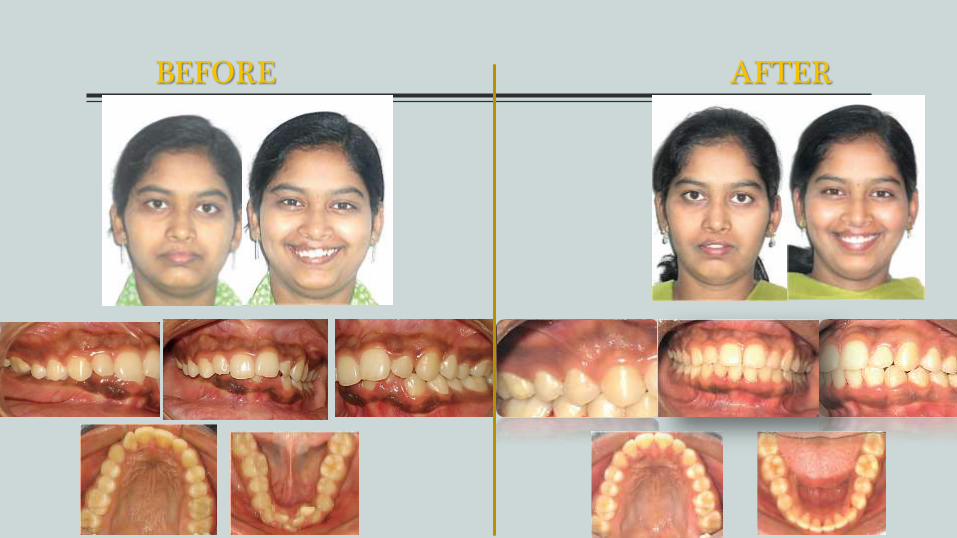
BEFORE AFTER
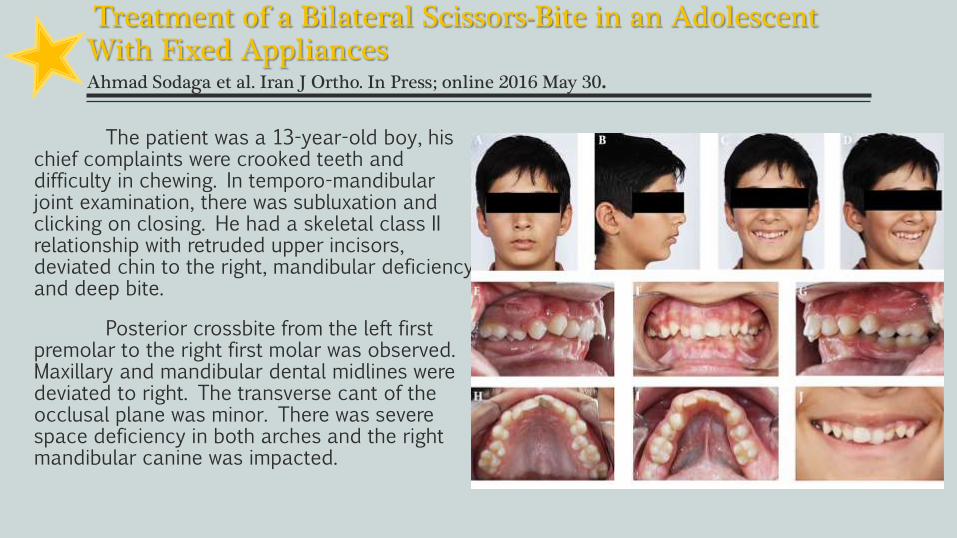
Treatment of a Bilateral Scissors-Bite in an Adolescent With Fixed AppliancesAhmad Sodaga et al. Iran J Ortho. In Press; online 2016 May 30.
The patient was a 13-year-old boy, his chief complaints were crooked teeth and difficulty in chewing. In temporo-mandibular joint examination, there was subluxation and clicking on closing. He had a skeletal class II relationship with retruded upper incisors, deviated chin to the right, mandibular deficiency and deep bite.
Posterior crossbite from the left first premolar to the right first molar was observed. Maxillary and mandibular dental midlines were deviated to right. The transverse cant of the occlusal plane was minor. There was severe space deficiency in both arches and the right mandibular canine was impacted.
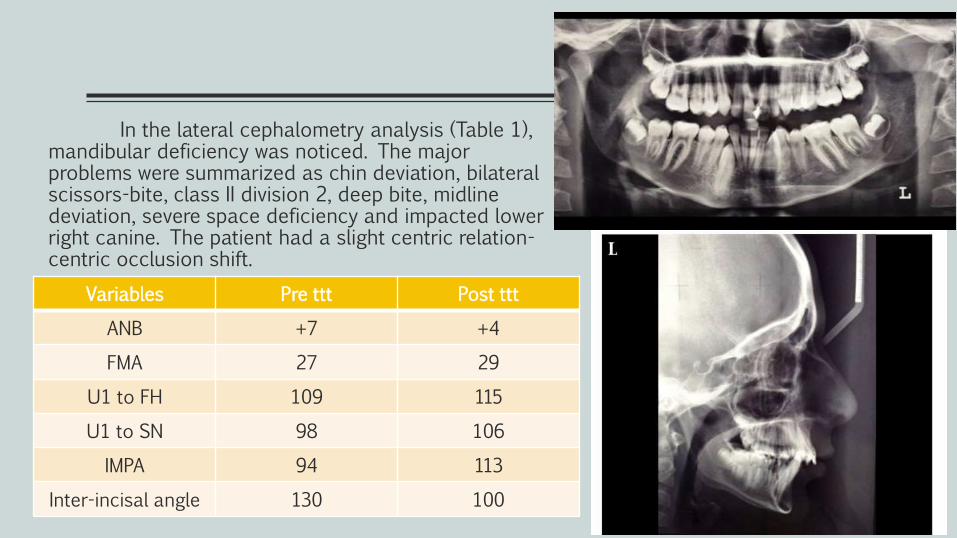
In the lateral cephalometry analysis (Table 1), mandibular deficiency was noticed. The major problems were summarized as chin deviation, bilateral scissors-bite, class II division 2, deep bite, midline deviation, severe space deficiency and impacted lower right canine. The patient had a slight centric relation-centric occlusion shift.
Variables Pre ttt Post ttt
ANB +7 +4
FMA 27 29
U1 to FH 109 115
U1 to SN 98 106
IMPA 94 113
Inter-incisal angle 130 100
Treatment Objectives
Treatment objectives were correcting dental crowding, traction of impacted canine to the arch, create normal overjet and overbite relationships with good functional occlusion, and eliminate scissors-bite. We planned to constrict maxillary arch with transpalatal arch and expand the mandibular arch with an active lingual arch, with aid of criss-cross elastics.
Treatment Alternatives
According to patient chief complaint, correction of scissors-bite was the first priority. However, in our view, correction of dental and skeletal class II relation was another major issue. Because of deep bite and reduced overjet, there was no option for growth modification at the first step. Therefore, we started the treatment with fixed appliance at the upper arch. Moreover, right mandibular canine was unerupted. As the lower dental arch was crowded and severely constricted, for traction of impacted tooth we could not extract any teeth. Therefore, we decide to expand the arch orthodontically and postpone growth modification; because it usually increases IMPA too.
Treatment Progress
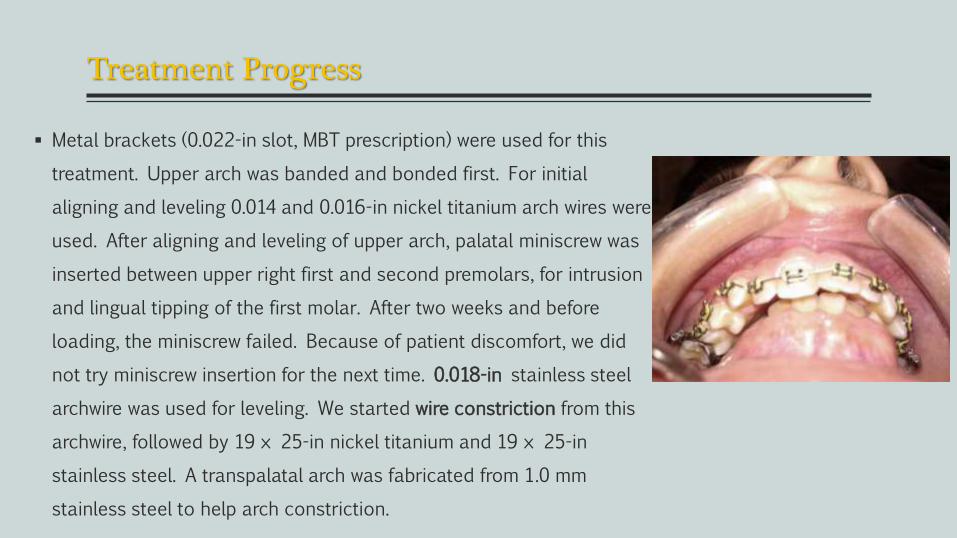
Metal brackets (0.022-in slot, MBT prescription) were used for this
treatment. Upper arch was banded and bonded first. For initial
aligning and leveling 0.014 and 0.016-in nickel titanium arch wires were
used. After aligning and leveling of upper arch, palatal miniscrew was
inserted between upper right first and second premolars, for intrusion
and lingual tipping of the first molar. After two weeks and before
loading, the miniscrew failed. Because of patient discomfort, we did
not try miniscrew insertion for the next time. 0.018-in stainless steel
archwire was used for leveling. We started wire constriction from this
archwire, followed by 19 × 25-in nickel titanium and 19 × 25-in
stainless steel. A transpalatal arch was fabricated from 1.0 mm
stainless steel to help arch constriction.
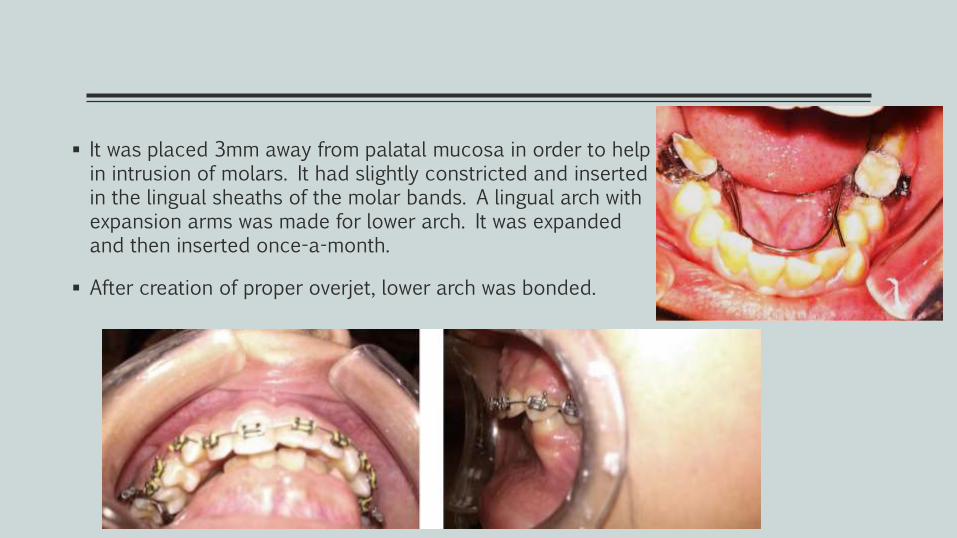
It was placed 3mm away from palatal mucosa in order to help in intrusion of molars. It had slightly constricted and inserted in the lingual sheaths of the molar bands. A lingual arch with expansion arms was made for lower arch. It was expanded and then inserted once-a-month.
After creation of proper overjet, lower arch was bonded.
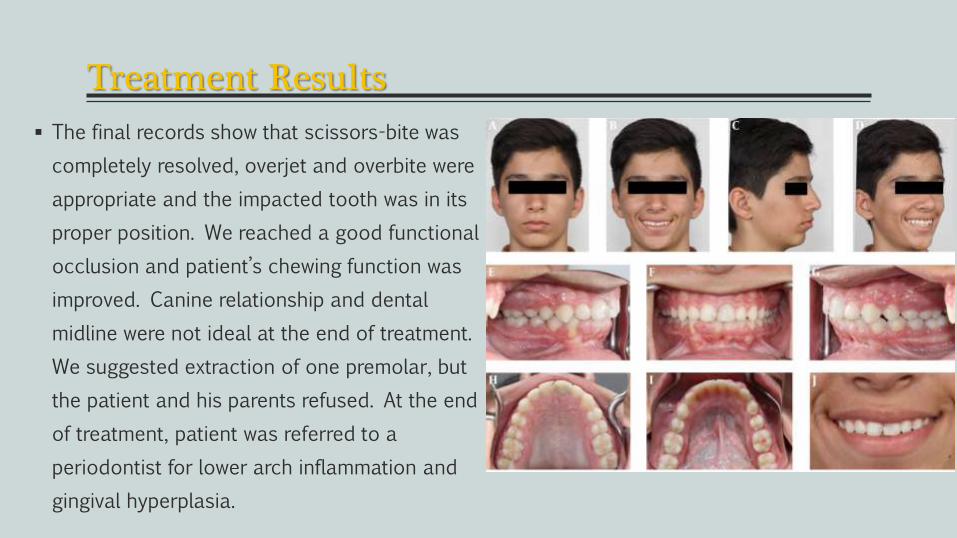
Treatment Results
The final records show that scissors-bite was
completely resolved, overjet and overbite were
appropriate and the impacted tooth was in its
proper position. We reached a good functional
occlusion and patient’s chewing function was
improved. Canine relationship and dental
midline were not ideal at the end of treatment.
We suggested extraction of one premolar, but
the patient and his parents refused. At the end
of treatment, patient was referred to a
periodontist for lower arch inflammation and
gingival hyperplasia.
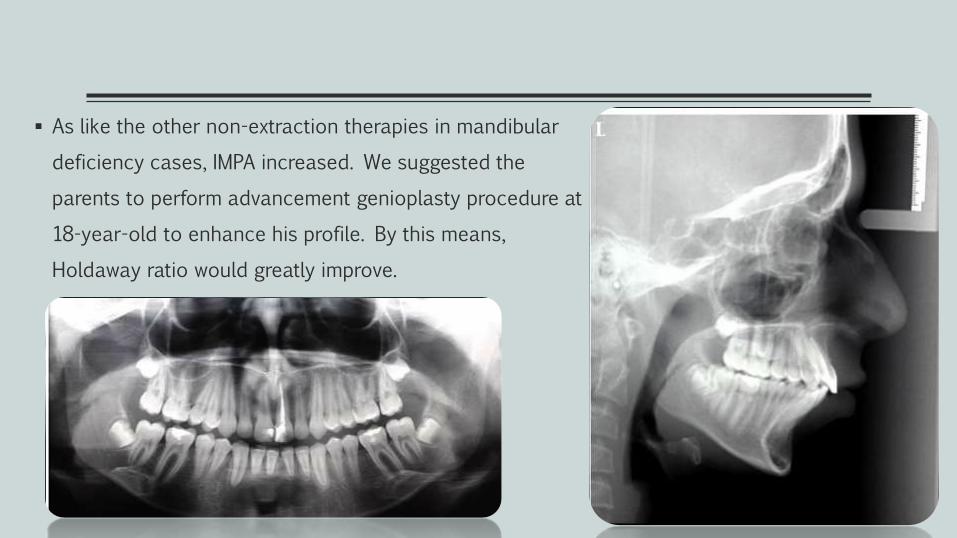
As like the other non-extraction therapies in mandibular
deficiency cases, IMPA increased. We suggested the
parents to perform advancement genioplasty procedure at
18-year-old to enhance his profile. By this means,
Holdaway ratio would greatly improve.
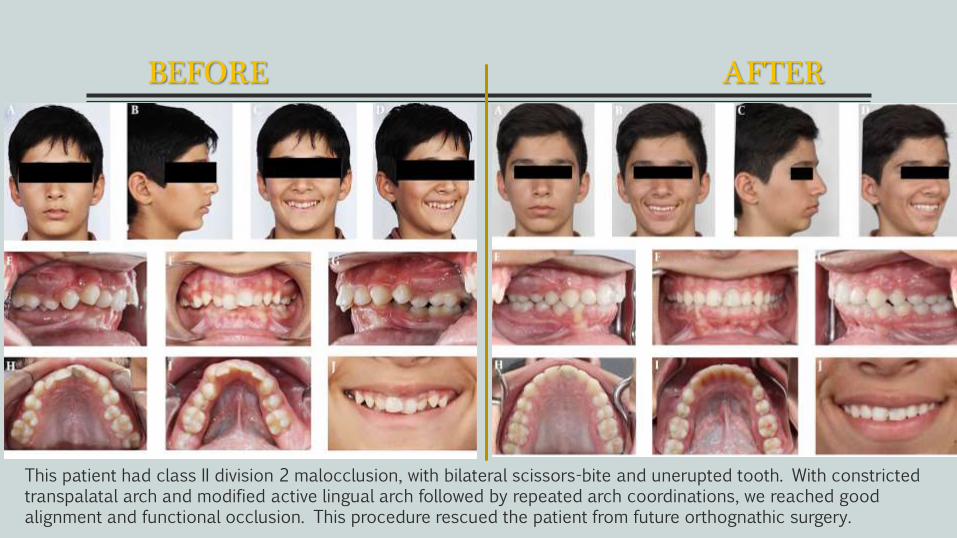
BEFORE AFTER
This patient had class II division 2 malocclusion, with bilateral scissors-bite and unerupted tooth. With constricted transpalatal arch and modified active lingual arch followed by repeated arch coordinations, we reached good alignment and functional occlusion. This procedure rescued the patient from future orthognathic surgery.
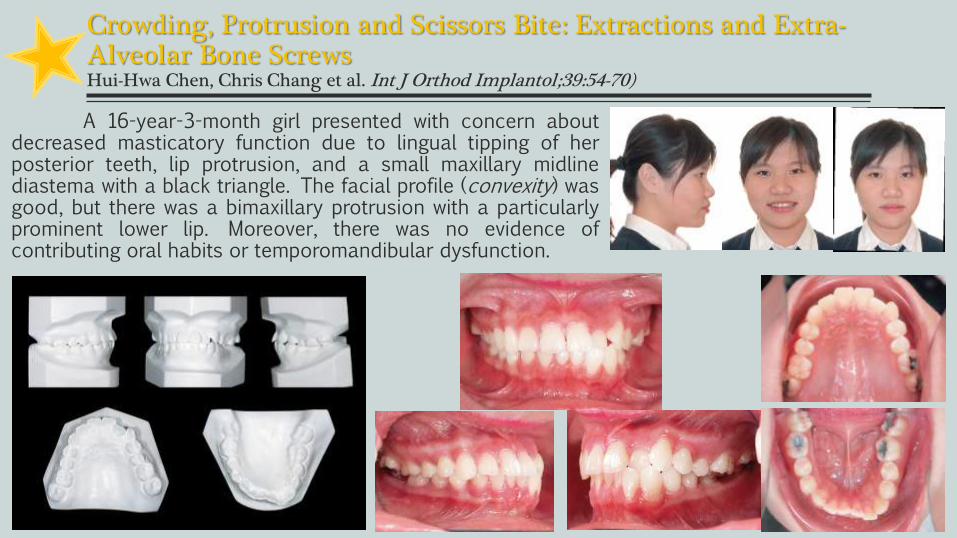
Crowding, Protrusion and Scissors Bite: Extractions and Extra-Alveolar Bone ScrewsHui-Hwa Chen, Chris Chang et al. Int J Orthod Implantol;39:54-70)
A 16-year-3-month girl presented with concern aboutdecreased masticatory function due to lingual tipping of herposterior teeth, lip protrusion, and a small maxillary midlinediastema with a black triangle. The facial profile (convexity) wasgood, but there was a bimaxillary protrusion with a particularlyprominent lower lip. Moreover, there was no evidence ofcontributing oral habits or temporomandibular dysfunction.
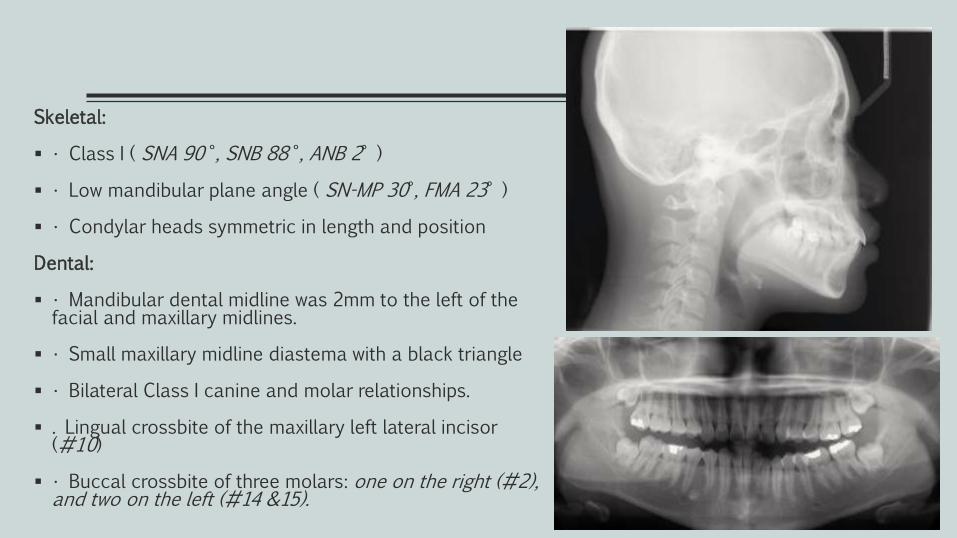
Skeletal:
• Class I ( SNA 90 °, SNB 88 °, ANB 2° )
• Low mandibular plane angle ( SN-MP 30°, FMA 23° )
• Condylar heads symmetric in length and position
Dental:
• Mandibular dental midline was 2mm to the left of the facial and maxillary midlines.
• Small maxillary midline diastema with a black triangle
• Bilateral Class I canine and molar relationships.
. Lingual crossbite of the maxillary left lateral incisor (#10)
• Buccal crossbite of three molars: one on the right (#2), and two on the left (#14 &15).
Objectives of Treatment
1. Resolve maxillary and mandibular crowding.
2. Correct bilateral buccal crossbites.
3. Achieve an ideal overjet and overbite relationship
Maintain the maxillary and mandibular skeletal bases in all planes of space
Maxillary Dentition: Retract incisors, intrude incisors, maintain inter-molar/inter-canine width
Mandibular Dentition: Retract incisors and decrease their axial inclination.
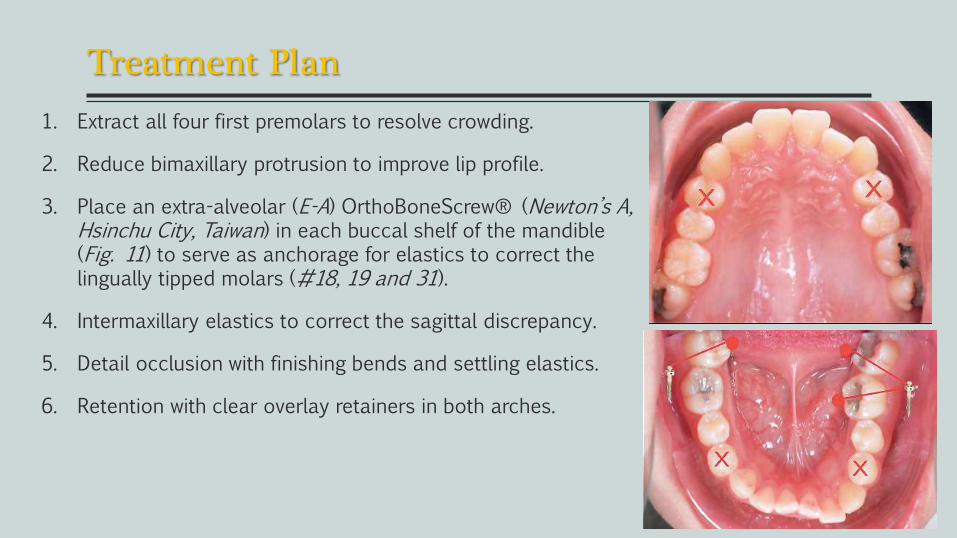
Treatment Plan
1. Extract all four first premolars to resolve crowding.
2. Reduce bimaxillary protrusion to improve lip profile.
3. Place an extra-alveolar (E-A) OrthoBoneScrew® (Newton’s A, Hsinchu City, Taiwan) in each buccal shelf of the mandible (Fig. 11) to serve as anchorage for elastics to correct the lingually tipped molars (#18, 19 and 31).
4. Intermaxillary elastics to correct the sagittal discrepancy.
5. Detail occlusion with finishing bends and settling elastics.
6. Retention with clear overlay retainers in both arches.
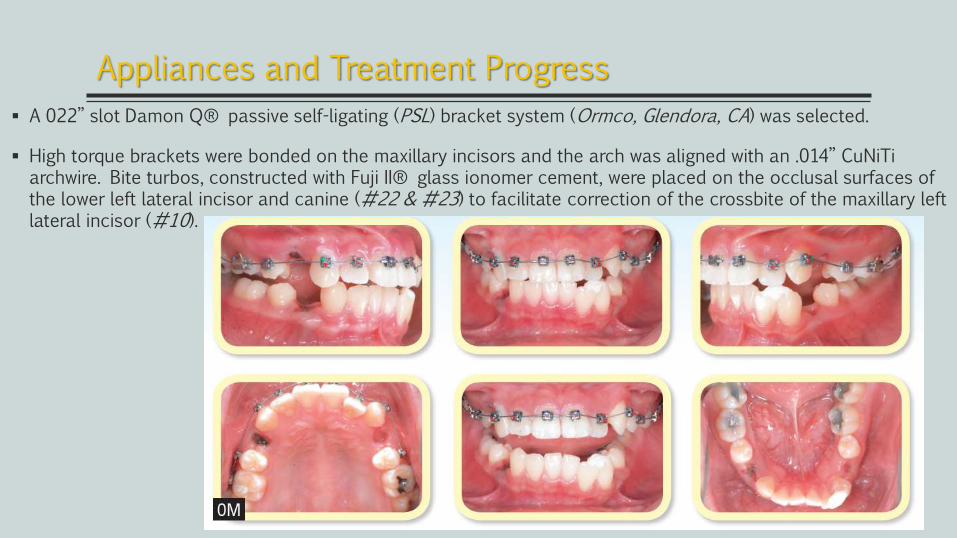
A 022” slot Damon Q® passive self-ligating (PSL) bracket system (Ormco, Glendora, CA) was selected.
High torque brackets were bonded on the maxillary incisors and the arch was aligned with an .014” CuNiTiarchwire. Bite turbos, constructed with Fuji II® glass ionomer cement, were placed on the occlusal surfaces of the lower left lateral incisor and canine (#22 & #23) to facilitate correction of the crossbite of the maxillary left lateral incisor (#10).
Appliances and Treatment Progress
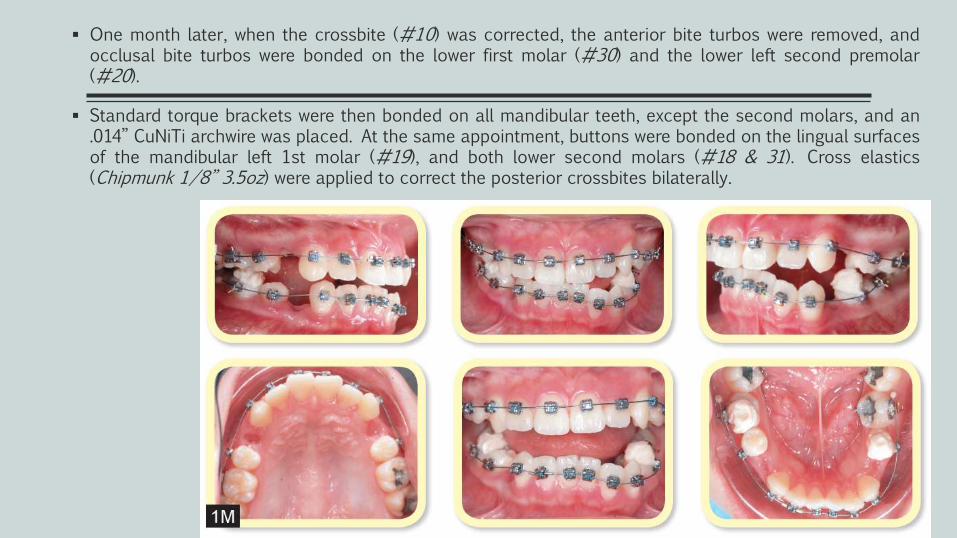
One month later, when the crossbite (#10) was corrected, the anterior bite turbos were removed, andocclusal bite turbos were bonded on the lower first molar (#30) and the lower left second premolar(#20).
Standard torque brackets were then bonded on all mandibular teeth, except the second molars, and an.014” CuNiTi archwire was placed. At the same appointment, buttons were bonded on the lingual surfacesof the mandibular left 1st molar (#19), and both lower second molars (#18 & 31). Cross elastics(Chipmunk 1/8” 3.5oz) were applied to correct the posterior crossbites bilaterally.
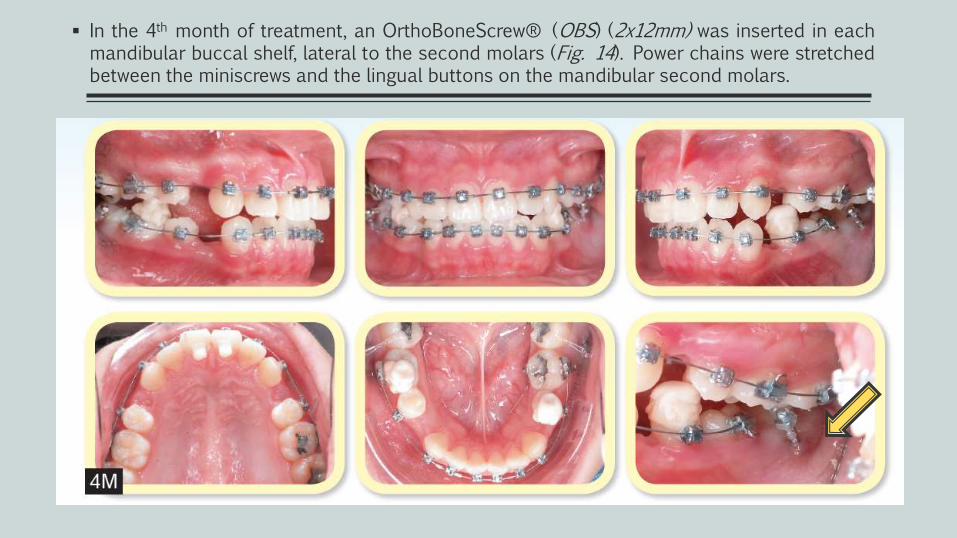
In the 4th month of treatment, an OrthoBoneScrew® (OBS) (2x12mm) was inserted in eachmandibular buccal shelf, lateral to the second molars (Fig. 14). Power chains were stretchedbetween the miniscrews and the lingual buttons on the mandibular second molars.
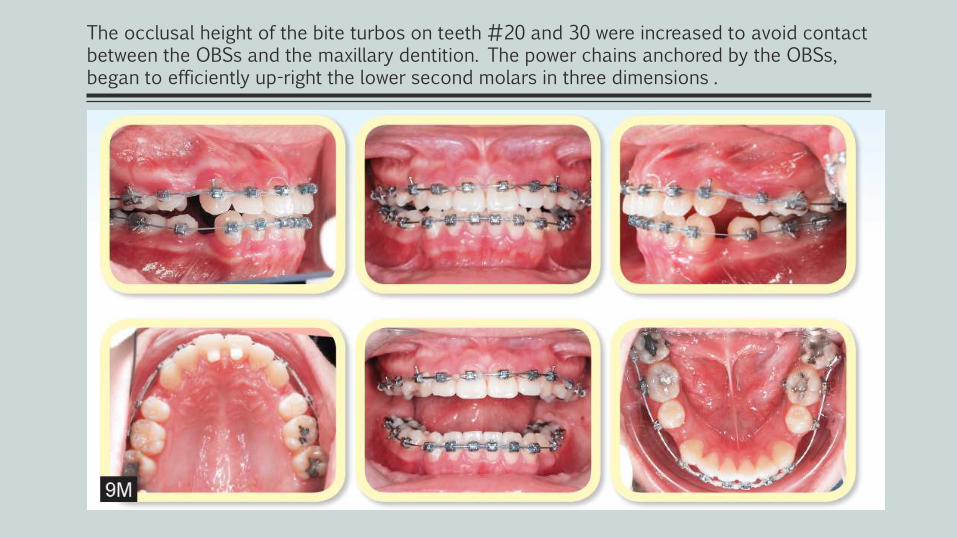
The occlusal height of the bite turbos on teeth #20 and 30 were increased to avoid contact between the OBSs and the maxillary dentition. The power chains anchored by the OBSs, began to efficiently up-right the lower second molars in three dimensions .
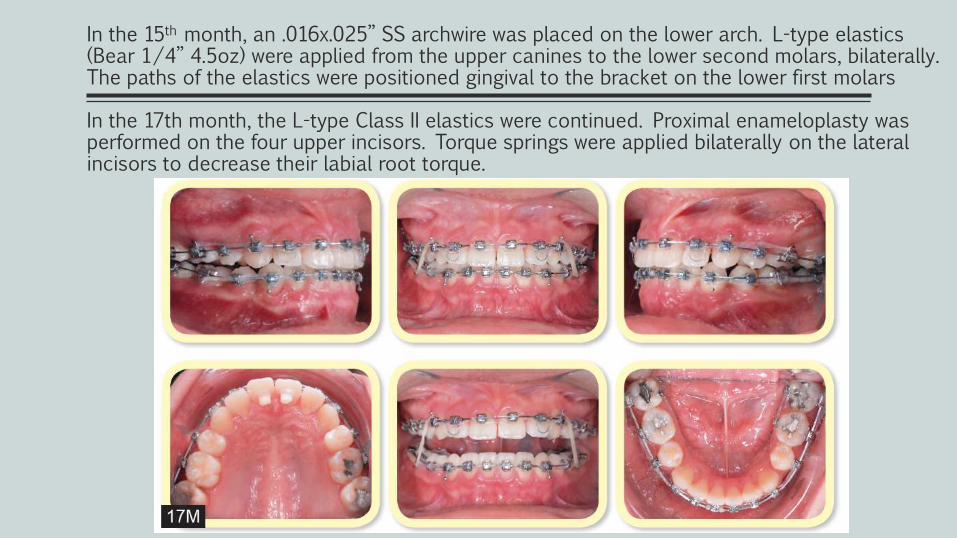
In the 15th month, an .016x.025” SS archwire was placed on the lower arch. L-type elastics (Bear 1/4” 4.5oz) were applied from the upper canines to the lower second molars, bilaterally. The paths of the elastics were positioned gingival to the bracket on the lower first molars
In the 17th month, the L-type Class II elastics were continued. Proximal enameloplasty was performed on the four upper incisors. Torque springs were applied bilaterally on the lateral incisors to decrease their labial root torque.

Maxillary Dentition
Antero-post: Retraction of incisors and protraction of the buccal segments. Vertical: Maintained. Inter-molar/Inter-canine Width: Crowding corrected with first premolar extraction
After 21 months of active treatment, the appliances were removed and retainers were delivered for both arches.
Mandibular Dentition
Antero-post: Retraction of incisors and protraction of the buccal segments. Vertical: Maintained. Inter-molar / Inter-canine Width: Crowding corrected with first premolar extraction
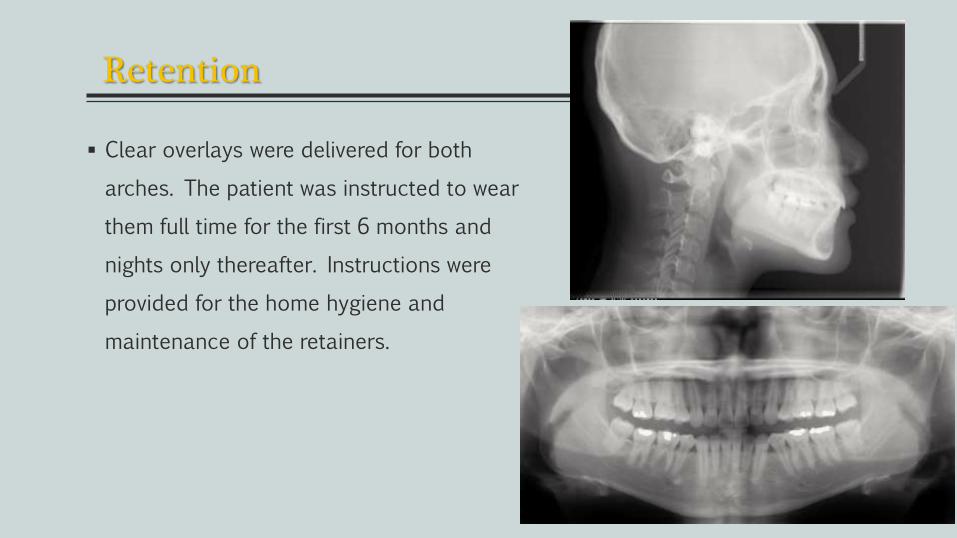
Retention
Clear overlays were delivered for both
arches. The patient was instructed to wear
them full time for the first 6 months and
nights only thereafter. Instructions were
provided for the home hygiene and
maintenance of the retainers.
Final Evaluation of the Treatment
T h e p a t i e n t w a s p l e a s e d w i t h t h e r e s u l t , particularly with regard to
masticatory function and facial harmony. Post-treatment intraoral photographs and study
casts show a Class I molar and canine on the right side, with Class II canine and Class I
molar relationships on the left side. The dental and facial midlines were coincident.
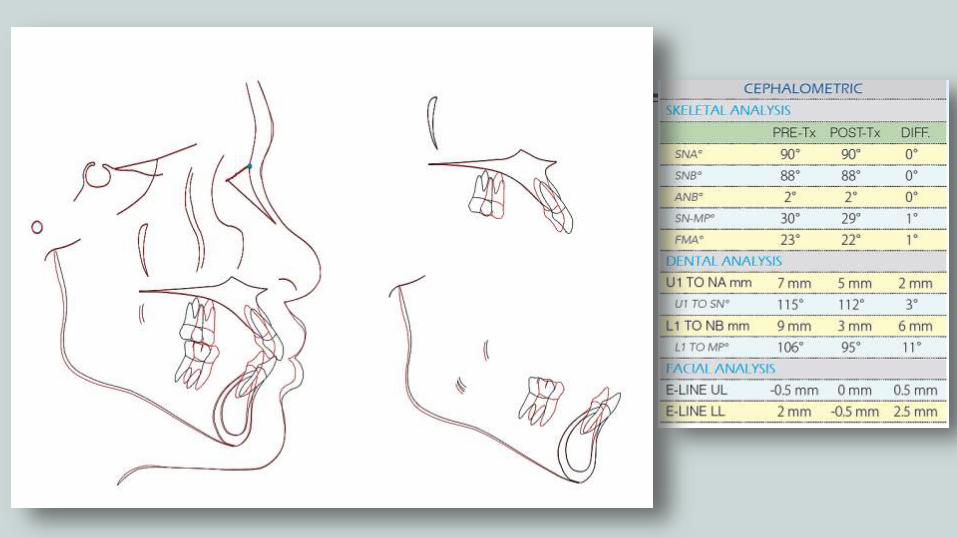
Superimpositions of tracings demonstrate the retraction of the incisors and protraction of
the buccal segments to close the first premolar extraction spaces. The lower lip was
retracted to relieve the lip protrusion and produce the lip balance that the patient
expected. The upper incisor to SN angle was decreased from 115 to 112°, and the lower
incisor to the mandibular plane angle was reduced from 106 to 95°.
Case report conclusions :)
Using extra-alveolar bone screws and bite turbos provided optimal
mechanics for correcting a bilateral scissors bite. This innovative method
was consistent with an overall excellent resolution of a challenging,
asymmetric malocclusion. Premolar extractions and space closure were an
efficient solution for resolving the bimaxillary protrusion in a timely manner.
Bimaxillary retraction with bone screws to correct bimaxillary protrusion
would have increased treatment time for the present patient, because they
could not be placed in an optimal location initially.
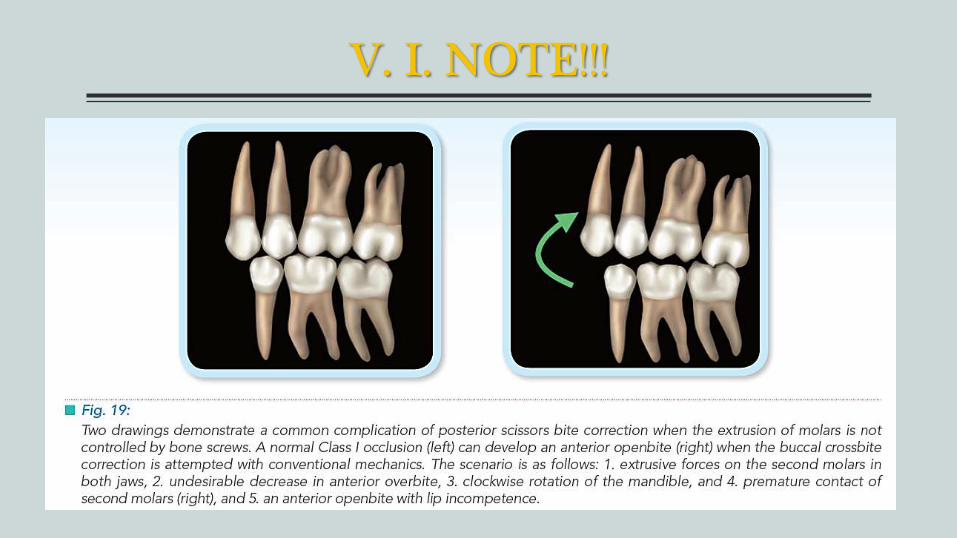
V. I. NOTE!!!

CONTENT
Case reports
Young(growing)
Removable app.
Fixed app.
Adolescents(non-growing)
Orthodontic (Non- surgical)
Surgical
Maxilla Mandible
Adults
Treatment options of Scissor-bite (Surgery)
6 case reports.
1. Mandibular Widening by Distraction Osteogenesis in the Treatment of a
Constricted Mandible and Telescopic Bite.
2. Unilateral Brodie bite treated with distraction Osteogenesis.
3. Treatment of unilateral buccal crossbite with mandibular symphyseal distraction
osteogenesis.
4. Orthognathic treatment for a patient with facial asymmetry associated with
unilateral scissors-bite and a collapsed mandibular arch.
5. Advantages of symphyseal distraction in the treatment of Brodie’s Syndrome.
To correct the Brodie –bite malocclusion, many treatment options were
proposed. They include dental extractions, interproximal reduction and
orthodontic compensation. The last option could damage the periodontium,
particularly if there is a vestibuloversion of the lower anterior teeth, because it
forces the teeth out of their alveolar bone.
Advantages of symphyseal distraction in the treatment of Brodie’s SyndromeChristine SAUVE, Thomas WOJCIK, Joe FERRI, J Dentofacial Anom Orthod 2013;16:405
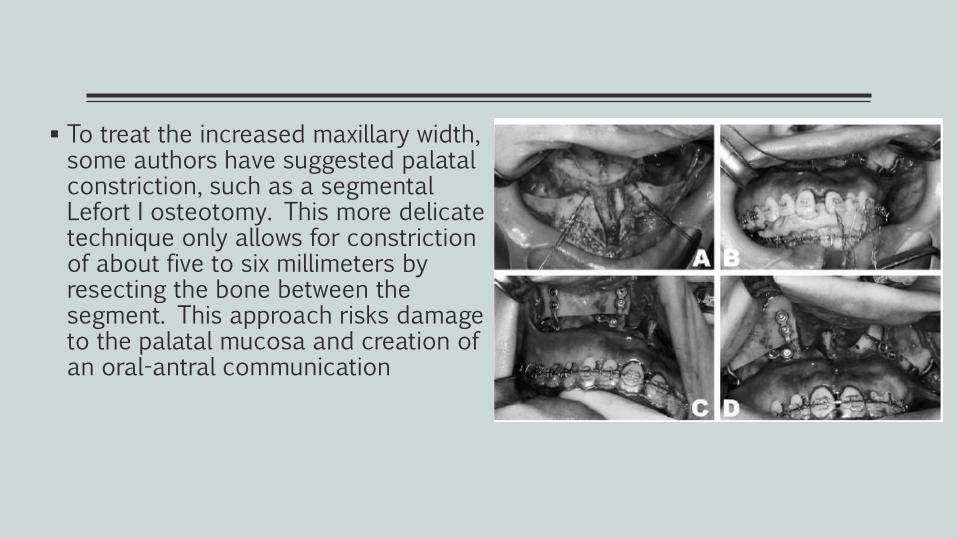
To treat the increased maxillary width, some authors have suggested palatal constriction, such as a segmental Lefort I osteotomy. This more delicate technique only allows for constriction of about five to six millimeters by resecting the bone between the segment. This approach risks damage to the palatal mucosa and creation of an oral-antral communication
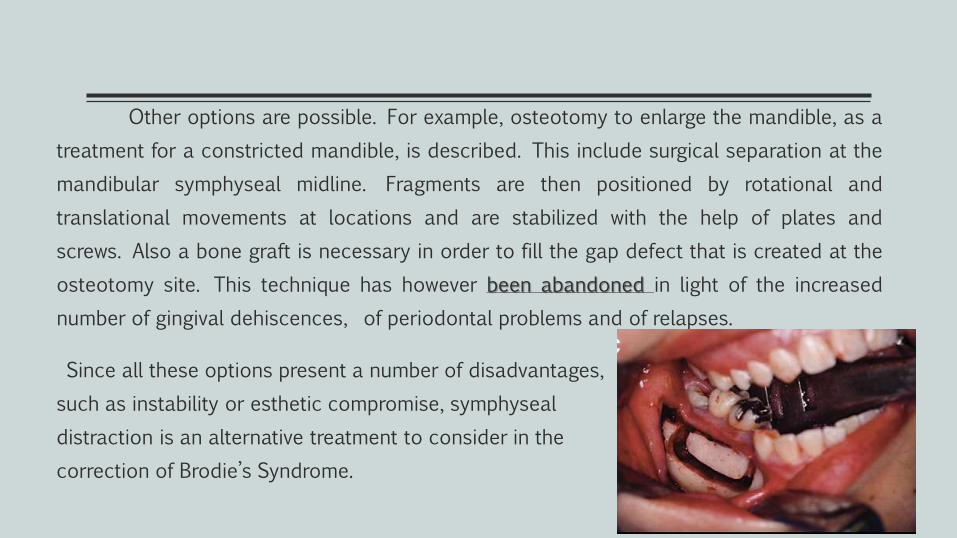
Other options are possible. For example, osteotomy to enlarge the mandible, as a
treatment for a constricted mandible, is described. This include surgical separation at the
mandibular symphyseal midline. Fragments are then positioned by rotational and
translational movements at locations and are stabilized with the help of plates and
screws. Also a bone graft is necessary in order to fill the gap defect that is created at the
osteotomy site. This technique has however been abandoned in light of the increased
number of gingival dehiscences, of periodontal problems and of relapses.
Since all these options present a number of disadvantages,
such as instability or esthetic compromise, symphyseal
distraction is an alternative treatment to consider in the
correction of Brodie’s Syndrome.
SYMPHYSEAL DISTRACTION
This distraction technique is utilized in order to increase the transverse
dimension of the symphysis. It presents a certain advantage when the dentoalveolar
or skeletal anomaly cannot be corrected by traditional orthodontic therapies. These
transverse deficits are found in an underdeveloped symphysis, in cases of significant
lower incisor overlapping, in syndromic malocclusions such as Pierre Robin,
Franceschetti and of course, Brodie’s Syndrome.
Osseous distraction is a procedure that allows the creation of new bone
between two osseous segments that are gradually separated by traction. which is
achieved progressively by daily activations of the distraction device. The
mineralization of the callus is initiated after the third week following the end of
activations (consolidation period).
Timing ??
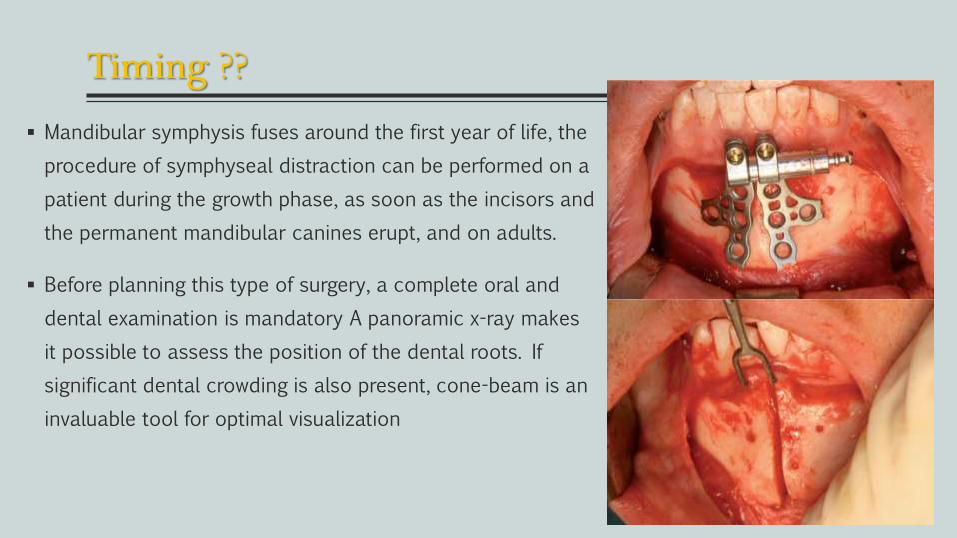
Mandibular symphysis fuses around the first year of life, the
procedure of symphyseal distraction can be performed on a
patient during the growth phase, as soon as the incisors and
the permanent mandibular canines erupt, and on adults.
Before planning this type of surgery, a complete oral and
dental examination is mandatory A panoramic x-ray makes
it possible to assess the position of the dental roots. If
significant dental crowding is also present, cone-beam is an
invaluable tool for optimal visualization
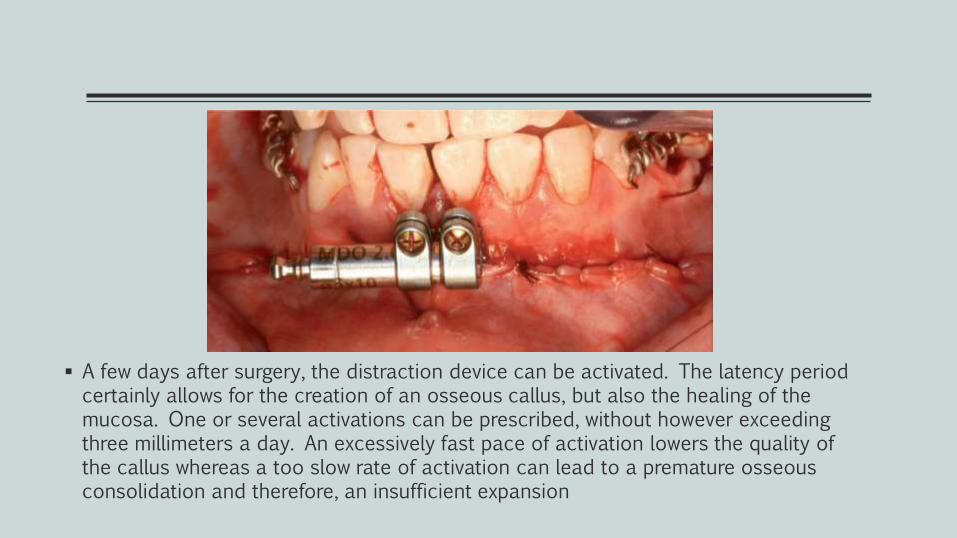
A few days after surgery, the distraction device can be activated. The latency period certainly allows for the creation of an osseous callus, but also the healing of the mucosa. One or several activations can be prescribed, without however exceeding three millimeters a day. An excessively fast pace of activation lowers the quality of the callus whereas a too slow rate of activation can lead to a premature osseous consolidation and therefore, an insufficient expansion
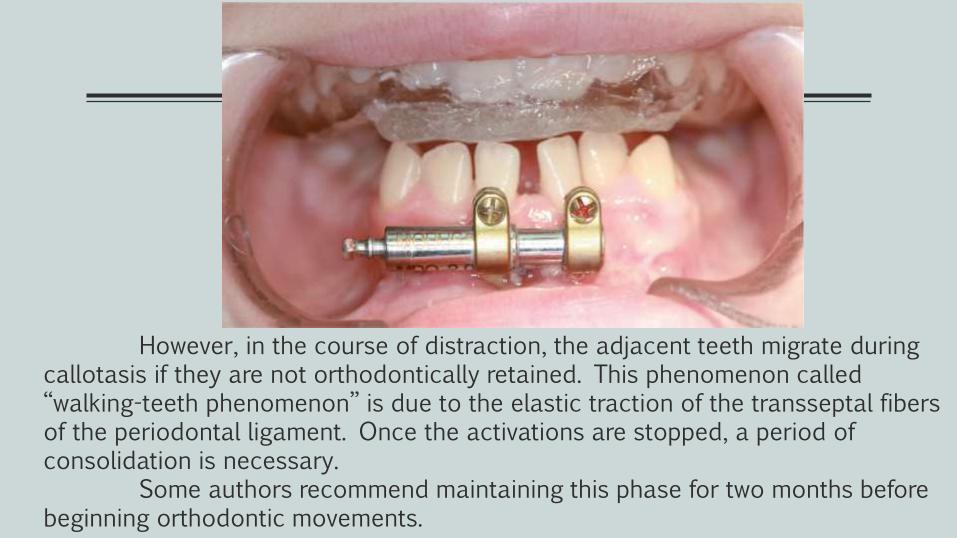
However, in the course of distraction, the adjacent teeth migrate during callotasis if they are not orthodontically retained. This phenomenon called ‘‘walking-teeth phenomenon’’ is due to the elastic traction of the transseptal fibers of the periodontal ligament. Once the activations are stopped, a period of consolidation is necessary.
Some authors recommend maintaining this phase for two months before beginning orthodontic movements.
In Conclusion
Even if Brodie’s Syndrome is not a common malocclusion, it is
important to know all the available therapeutic options to improve
patient’s occlusion, function and esthetics.. Symphyseal distraction
has proven to be a highly recommended treatment solution given its
many advantages, particularly concerning osseous growth and
periodontal preservation
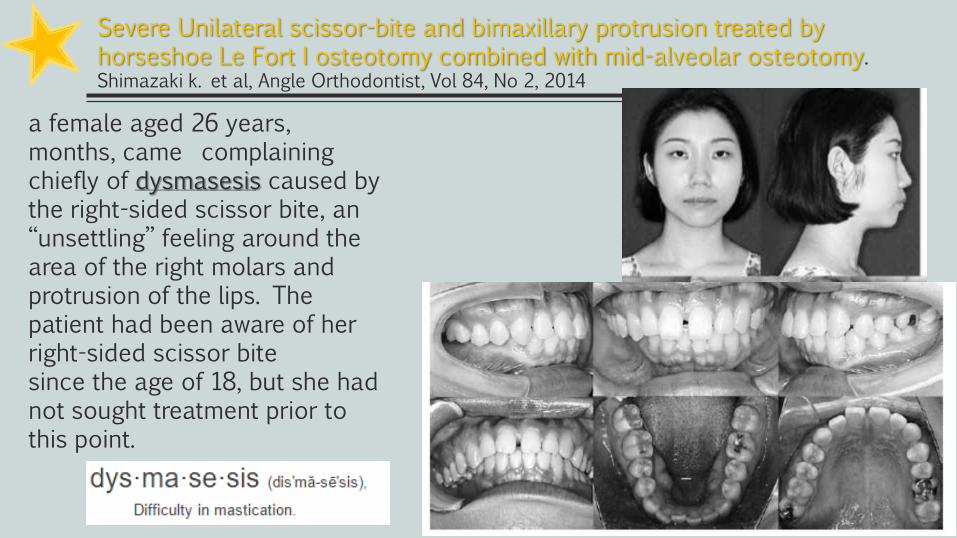
Severe Unilateral scissor-bite and bimaxillary protrusion treated by horseshoe Le Fort I osteotomy combined with mid-alveolar osteotomy.Shimazaki k. et al, Angle Orthodontist, Vol 84, No 2, 2014
a female aged 26 years, months, came complainingchiefly of dysmasesis caused by the right-sided scissor bite, an ‘‘unsettling’’ feeling around the area of the right molars and protrusion of the lips. Thepatient had been aware of her right-sided scissor bitesince the age of 18, but she had not sought treatment prior to this point.
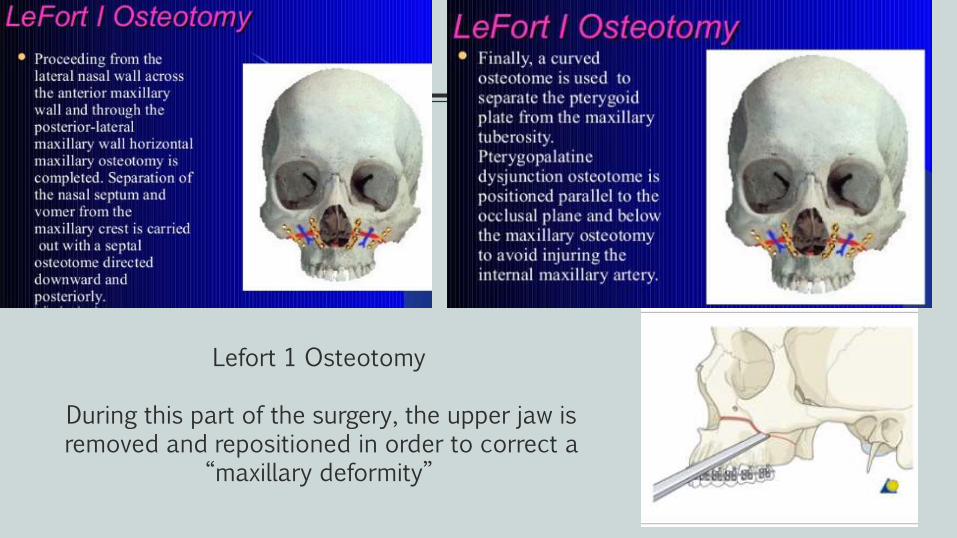
Lefort 1 Osteotomy
During this part of the surgery, the upper jaw is removed and repositioned in order to correct a
“maxillary deformity”
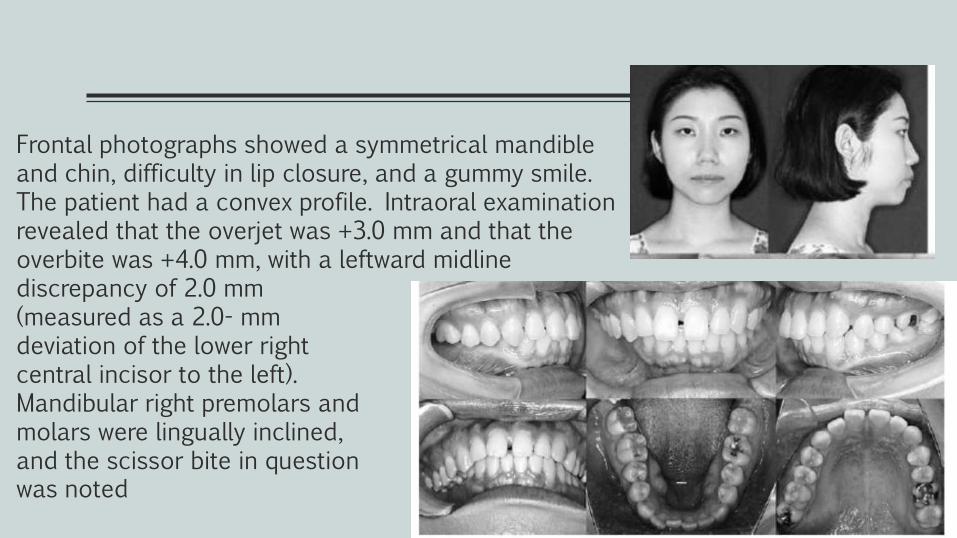
Frontal photographs showed a symmetrical mandible and chin, difficulty in lip closure, and a gummy smile. The patient had a convex profile. Intraoral examination revealed that the overjet was +3.0 mm and that the overbite was +4.0 mm, with a leftward midline discrepancy of 2.0 mm (measured as a 2.0- mm deviation of the lower right central incisor to the left). Mandibular right premolars and molars were lingually inclined, and the scissor bite in question was noted
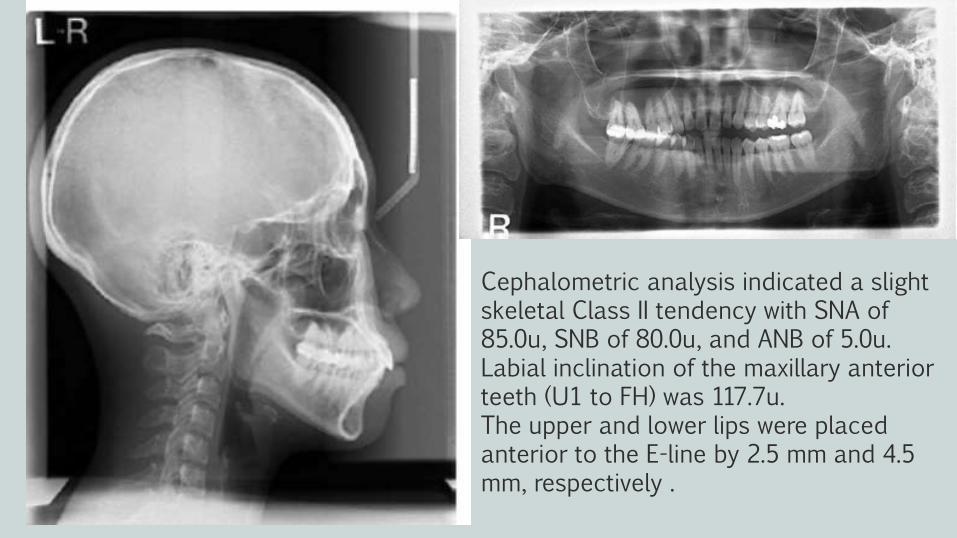
Cephalometric analysis indicated a slight skeletal Class II tendency with SNA of 85.0u, SNB of 80.0u, and ANB of 5.0u. Labial inclination of the maxillary anterior teeth (U1 to FH) was 117.7u.The upper and lower lips were placed anterior to the E-line by 2.5 mm and 4.5 mm, respectively .
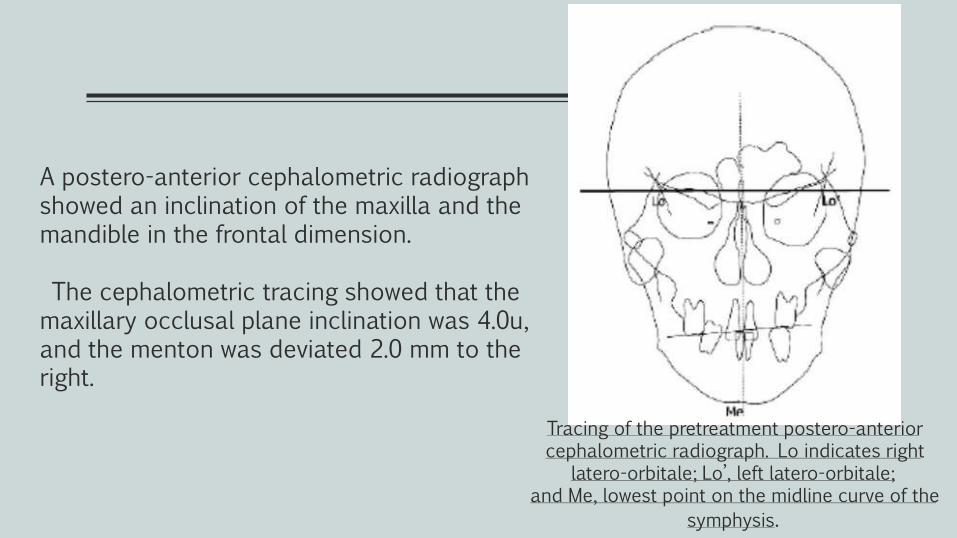
A postero-anterior cephalometric radiograph showed an inclination of the maxilla and the mandible in the frontal dimension.
The cephalometric tracing showed that the maxillary occlusal plane inclination was 4.0u, and the menton was deviated 2.0 mm to the right.
Tracing of the pretreatment postero-anterior cephalometric radiograph. Lo indicates right
latero-orbitale; Lo’, left latero-orbitale;and Me, lowest point on the midline curve of the
symphysis.
Treatment objectives
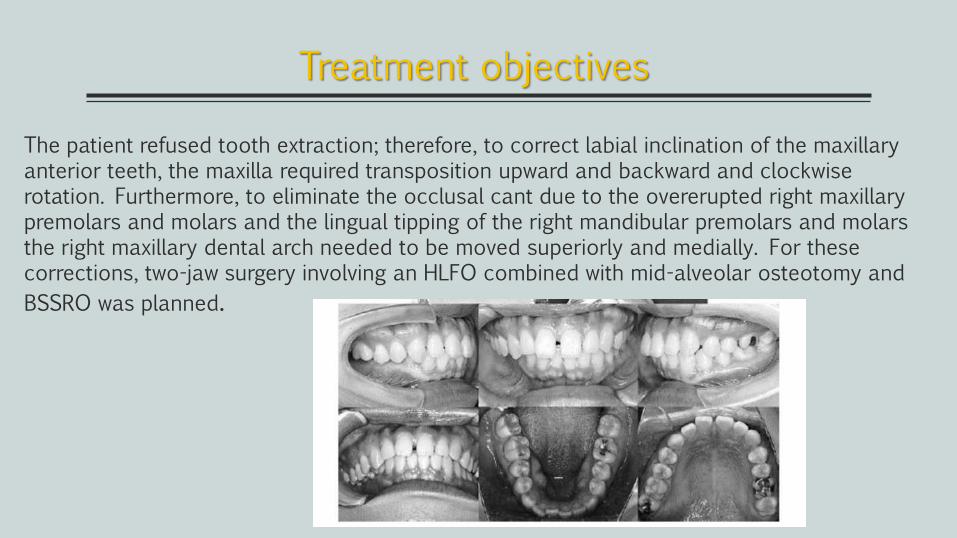
The patient refused tooth extraction; therefore, to correct labial inclination of the maxillary anterior teeth, the maxilla required transposition upward and backward and clockwise rotation. Furthermore, to eliminate the occlusal cant due to the overerupted right maxillary premolars and molars and the lingual tipping of the right mandibular premolars and molars the right maxillary dental arch needed to be moved superiorly and medially. For these corrections, two-jaw surgery involving an HLFO combined with mid-alveolar osteotomy and
BSSRO was planned.
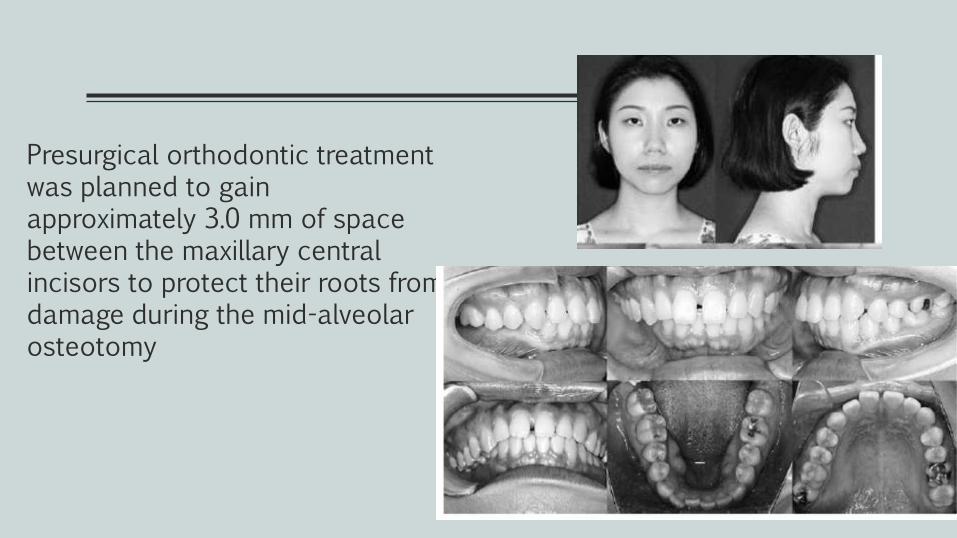
Presurgical orthodontic treatment was planned to gain approximately 3.0 mm of space between the maxillary central incisors to protect their roots from damage during the mid-alveolar osteotomy
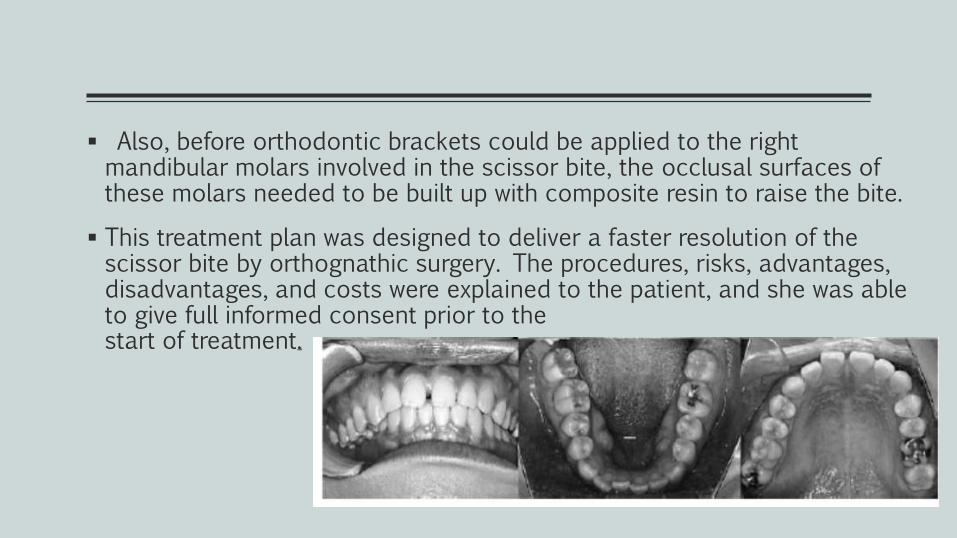
Also, before orthodontic brackets could be applied to the right mandibular molars involved in the scissor bite, the occlusal surfaces of these molars needed to be built up with composite resin to raise the bite.
This treatment plan was designed to deliver a faster resolution of the scissor bite by orthognathic surgery. The procedures, risks, advantages, disadvantages, and costs were explained to the patient, and she was able to give full informed consent prior to thestart of treatment.

The treatment alternative was orthodontic treatmentonly. The critical procedures for scissor bite
correctionare intrusion and palatal or buccal tipping of the
involved teeth when they are both extruded and tilted.After the scissor bite is corrected, additional premolar
extractions are needed to resolve bimaxillaryprotrusion.
However, the orthodontic procedure was deemedto be severe, and the patient was informed that thetreatment would be complicated and prolonged if
orthodontic procedures alone were used. The patientwas given the option (together with the advantagesand disadvantages) of having orthognathic surgery
combined with orthodontic treatment as an alternative.
The patient chose to accept this option .
Treatment Alternatives
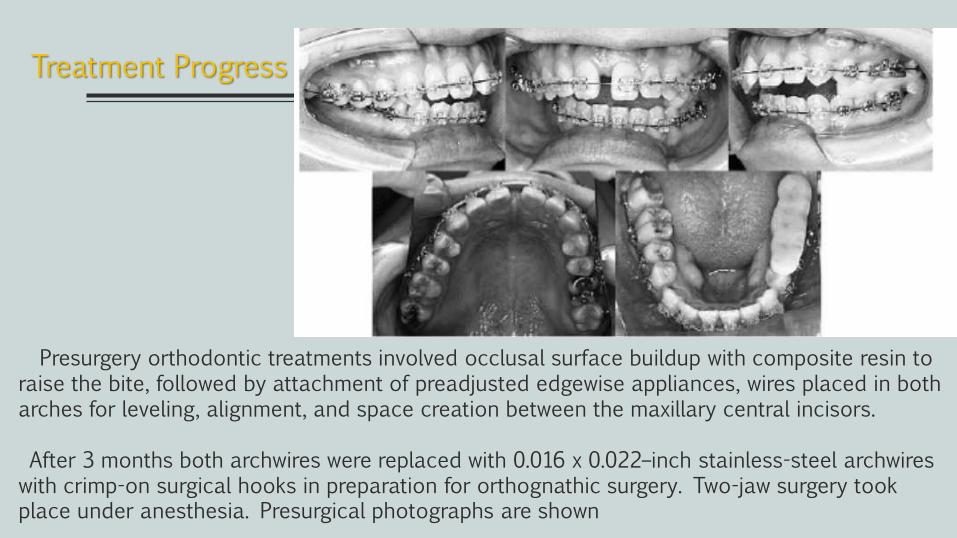
Presurgery orthodontic treatments involved occlusal surface buildup with composite resin to raise the bite, followed by attachment of preadjusted edgewise appliances, wires placed in both arches for leveling, alignment, and space creation between the maxillary central incisors.
After 3 months both archwires were replaced with 0.016 x 0.022–inch stainless-steel archwireswith crimp-on surgical hooks in preparation for orthognathic surgery. Two-jaw surgery took place under anesthesia. Presurgical photographs are shown
Treatment Progress
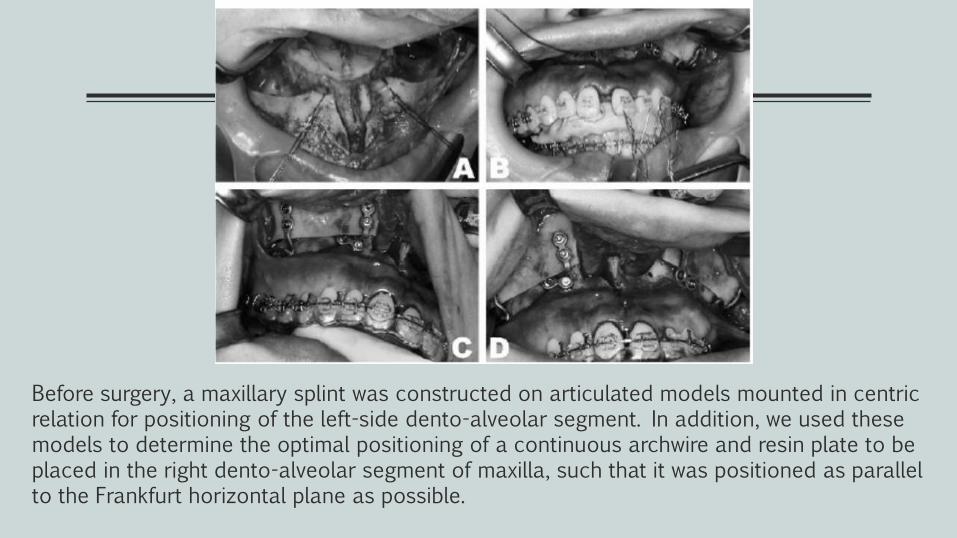
Before surgery, a maxillary splint was constructed on articulated models mounted in centric relation for positioning of the left-side dento-alveolar segment. In addition, we used these models to determine the optimal positioning of a continuous archwire and resin plate to be placed in the right dento-alveolar segment of maxilla, such that it was positioned as parallel to the Frankfurt horizontal plane as possible.
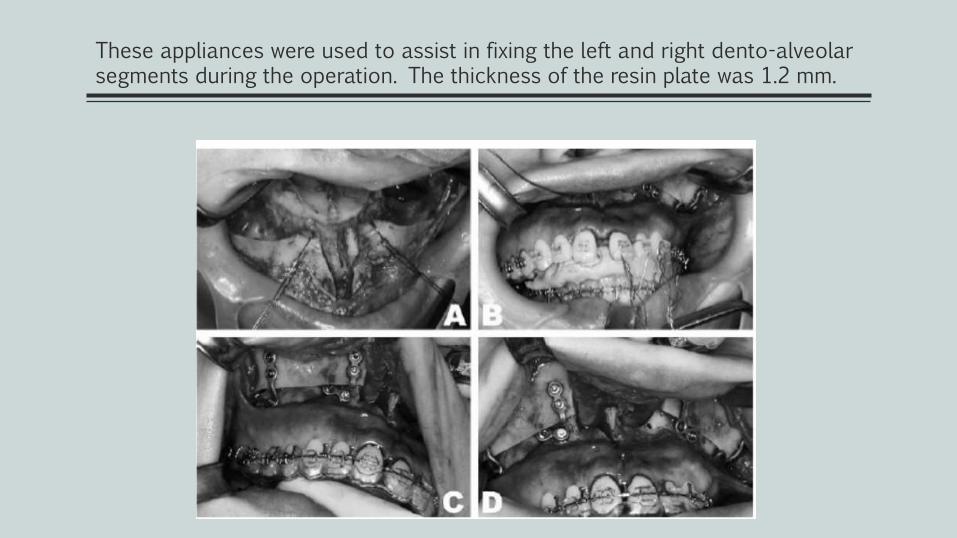
These appliances were used to assist in fixing the left and right dento-alveolar segments during the operation. The thickness of the resin plate was 1.2 mm.
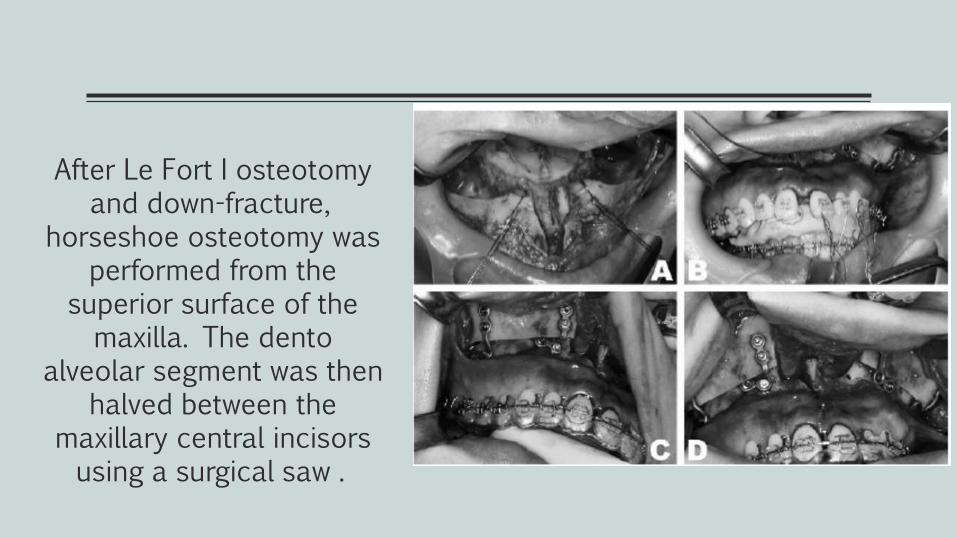
After Le Fort I osteotomy and down-fracture,
horseshoe osteotomy was performed from the
superior surface of the maxilla. The dento
alveolar segment was then halved between the
maxillary central incisors using a surgical saw .
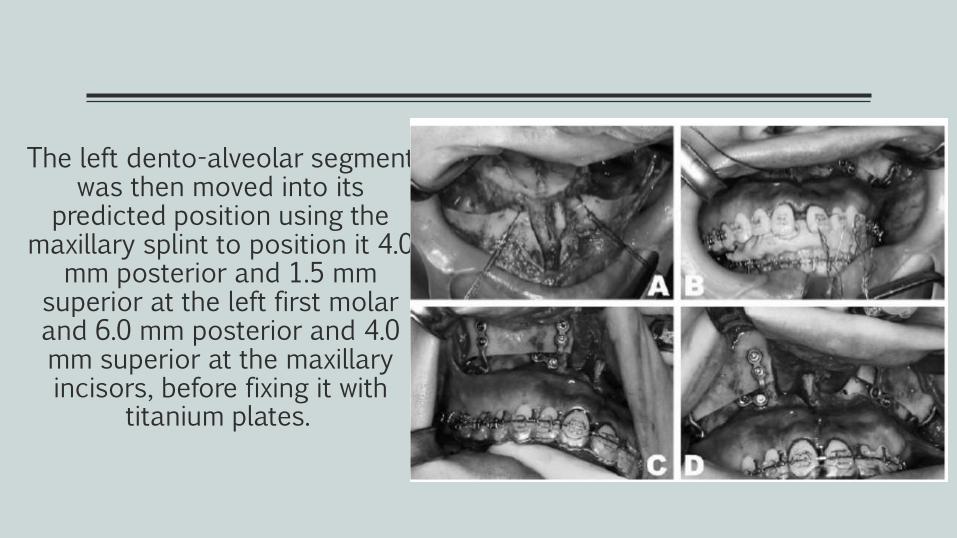
The left dento-alveolar segment was then moved into its
predicted position using the maxillary splint to position it 4.0
mm posterior and 1.5 mm superior at the left first molar and 6.0 mm posterior and 4.0 mm superior at the maxillary incisors, before fixing it with
titanium plates.
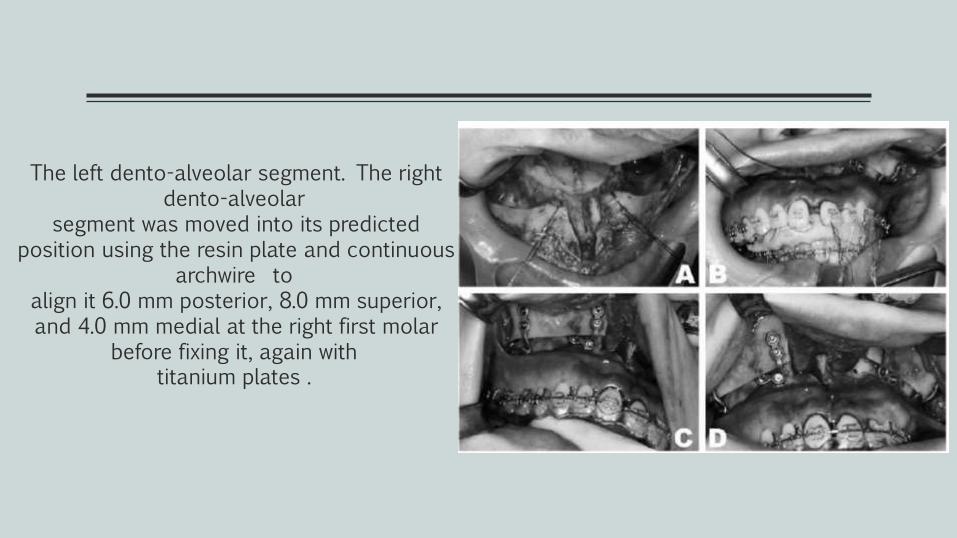
The left dento-alveolar segment. The right dento-alveolar
segment was moved into its predicted position using the resin plate and continuous
archwire toalign it 6.0 mm posterior, 8.0 mm superior, and 4.0 mm medial at the right first molar
before fixing it, again withtitanium plates .

Before After
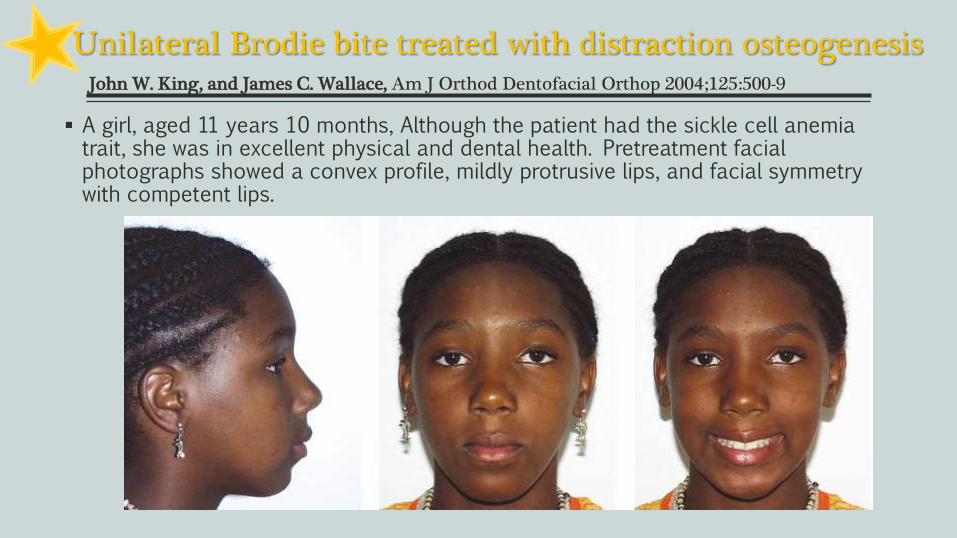
Unilateral Brodie bite treated with distraction osteogenesisJohn W. King, and James C. Wallace, Am J Orthod Dentofacial Orthop 2004;125:500-9
A girl, aged 11 years 10 months, Although the patient had the sickle cell anemia trait, she was in excellent physical and dental health. Pretreatment facial photographs showed a convex profile, mildly protrusive lips, and facial symmetry with competent lips.
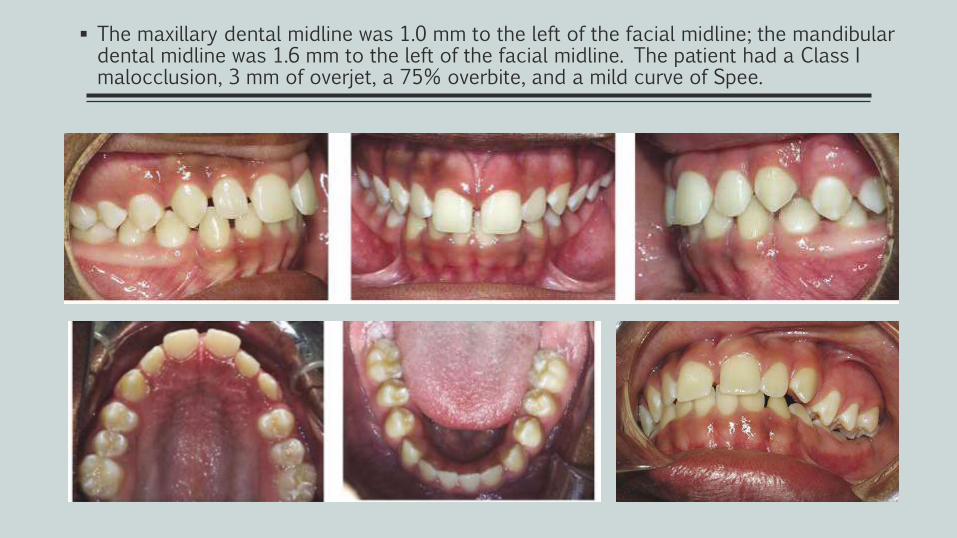
The maxillary dental midline was 1.0 mm to the left of the facial midline; the mandibular dental midline was 1.6 mm to the left of the facial midline. The patient had a Class I malocclusion, 3 mm of overjet, a 75% overbite, and a mild curve of Spee.
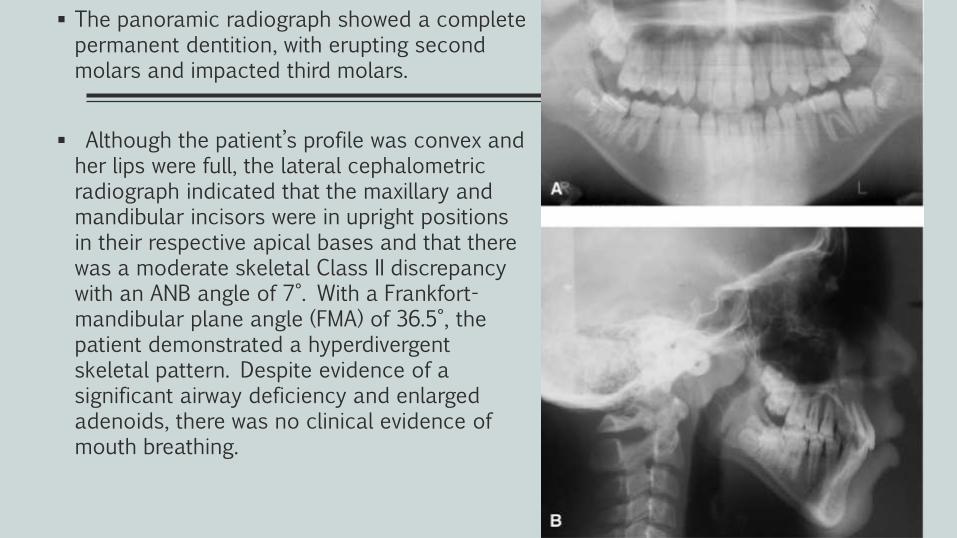
The panoramic radiograph showed a complete permanent dentition, with erupting second molars and impacted third molars.
Although the patient’s profile was convex and her lips were full, the lateral cephalometricradiograph indicated that the maxillary and mandibular incisors were in upright positions in their respective apical bases and that there was a moderate skeletal Class II discrepancy with an ANB angle of 7°. With a Frankfort-mandibular plane angle (FMA) of 36.5°, the patient demonstrated a hyperdivergentskeletal pattern. Despite evidence of a significant airway deficiency and enlarged adenoids, there was no clinical evidence of mouth breathing.
Treatment objectives
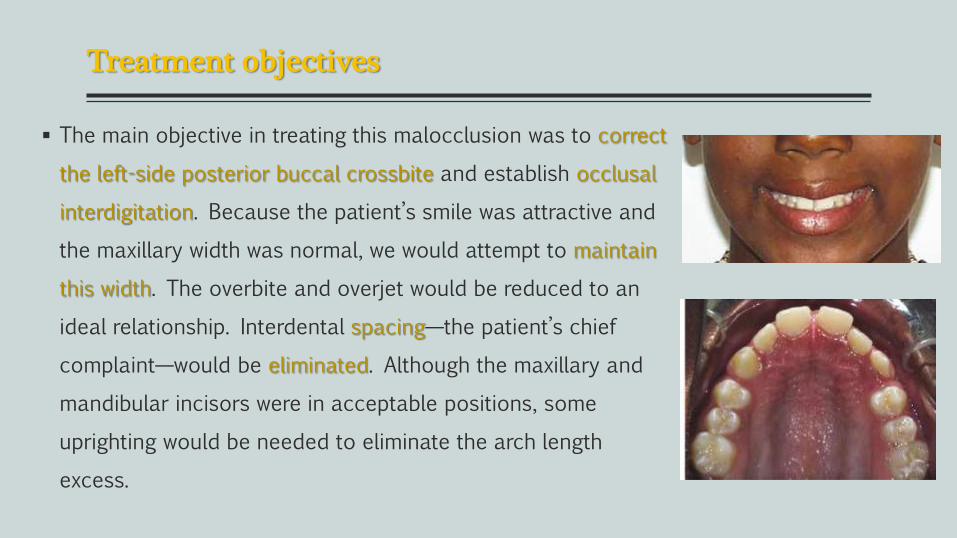
The main objective in treating this malocclusion was to correct
the left-side posterior buccal crossbite and establish occlusal
interdigitation. Because the patient’s smile was attractive and
the maxillary width was normal, we would attempt to maintain
this width. The overbite and overjet would be reduced to an
ideal relationship. Interdental spacing—the patient’s chief
complaint—would be eliminated. Although the maxillary and
mandibular incisors were in acceptable positions, some
uprighting would be needed to eliminate the arch length
excess.
Treatment Alternatives
The 1st treatment option: was to use intermaxillary crossbite elastics to tip the mandibular left posterior teeth labially and the maxillary left posterior teeth lingually. But because the diagnosis indicated the crossbite was primarily a skeletal problem, long-term stability was a concern. Also, lingual tipping of the maxillary left posterior teeth might alter the pleasing pretreatment smile.
The 2nd option: was to place a Hyrax expander in an “open” position, to produce palatal constriction and narrow the maxilla bilaterally. This technique would correct the left buccalcrossbite but might also create a right posterior crossbite. Also, there was some concern about changing the preexisting broad smile.
The 3rd option: involved closing the mandibular interdental spacing and maintaining the mandibular intercanine and intermolar widths. A maxillary segmental osteotomy could be used to correct the crossbite.
The 4th option : involved maintaining the maxillary width and closing the interdental spaces. The left posterior buccal crossbite would be corrected through mandibular widening by midsymphyseal distraction osteogenesis. Because the buccal crossbite was a true unilateral problem, the widening would have to be primarily on the left side while the right occlusion was maintained.
The patient and her mother selected the fourth option, which targeted the primary orthodontic problem (the mandibular transverse deficiency). If the right posterior occlusion could be maintained, this treatment option would provide the best combination of occlusal function, optimal esthetics, and long-term stability.
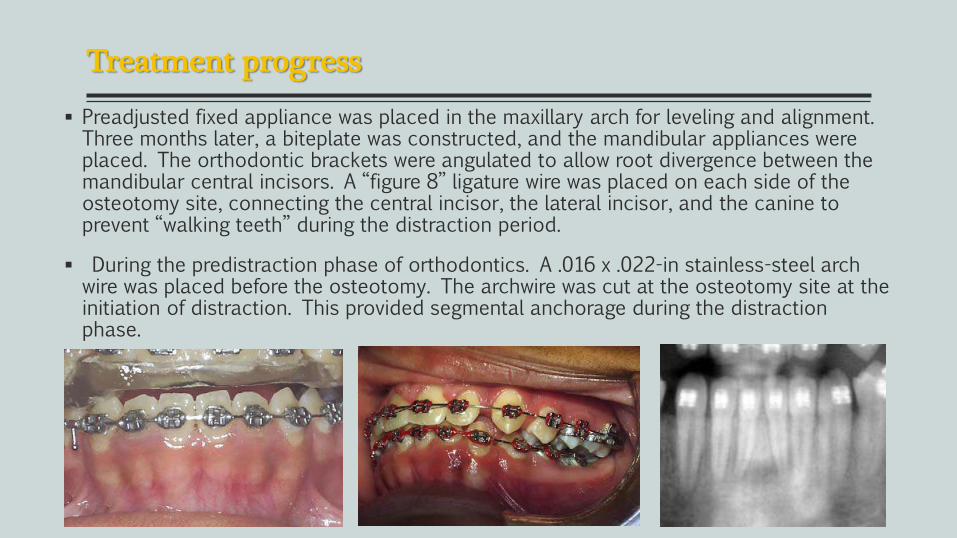
Treatment progress
Preadjusted fixed appliance was placed in the maxillary arch for leveling and alignment. Three months later, a biteplate was constructed, and the mandibular appliances were placed. The orthodontic brackets were angulated to allow root divergence between the mandibular central incisors. A “figure 8” ligature wire was placed on each side of the osteotomy site, connecting the central incisor, the lateral incisor, and the canine to prevent “walking teeth” during the distraction period.
During the predistraction phase of orthodontics. A .016 x .022-in stainless-steel arch wire was placed before the osteotomy. The archwire was cut at the osteotomy site at the initiation of distraction. This provided segmental anchorage during the distraction phase.
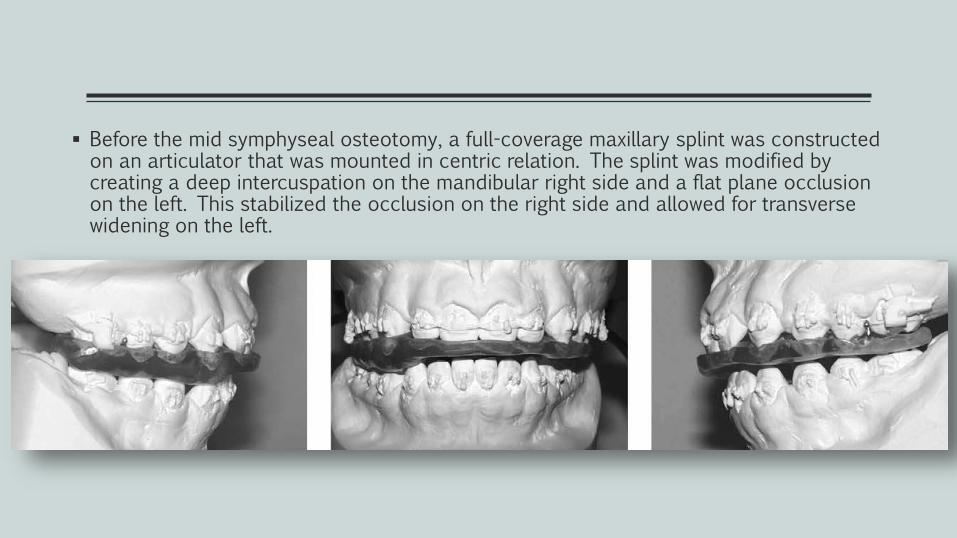
Before the mid symphyseal osteotomy, a full-coverage maxillary splint was constructed on an articulator that was mounted in centric relation. The splint was modified by creating a deep intercuspation on the mandibular right side and a flat plane occlusion on the left. This stabilized the occlusion on the right side and allowed for transverse widening on the left.
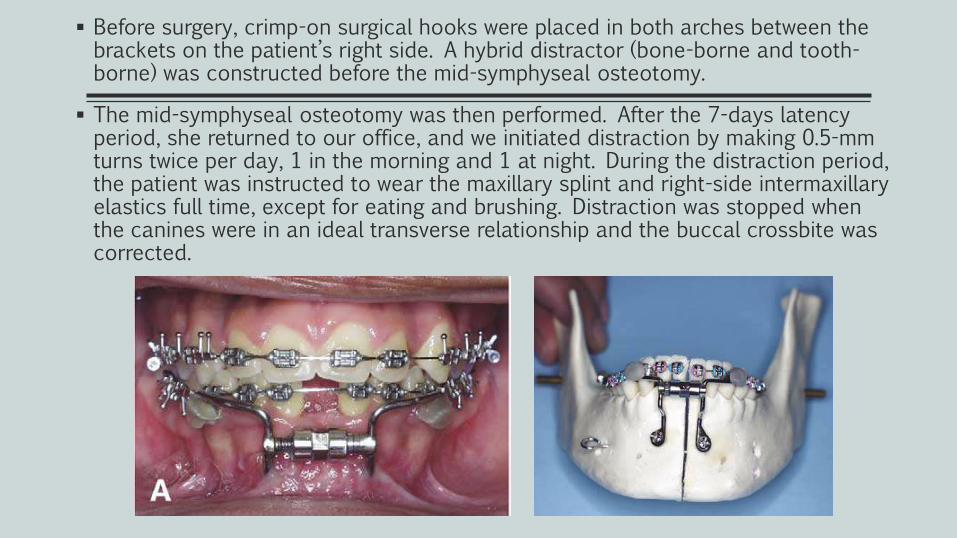
Before surgery, crimp-on surgical hooks were placed in both arches between the brackets on the patient’s right side. A hybrid distractor (bone-borne and tooth-borne) was constructed before the mid-symphyseal osteotomy.
The mid-symphyseal osteotomy was then performed. After the 7-days latency period, she returned to our office, and we initiated distraction by making 0.5-mm turns twice per day, 1 in the morning and 1 at night. During the distraction period, the patient was instructed to wear the maxillary splint and right-side intermaxillaryelastics full time, except for eating and brushing. Distraction was stopped when the canines were in an ideal transverse relationship and the buccal crossbite was corrected.
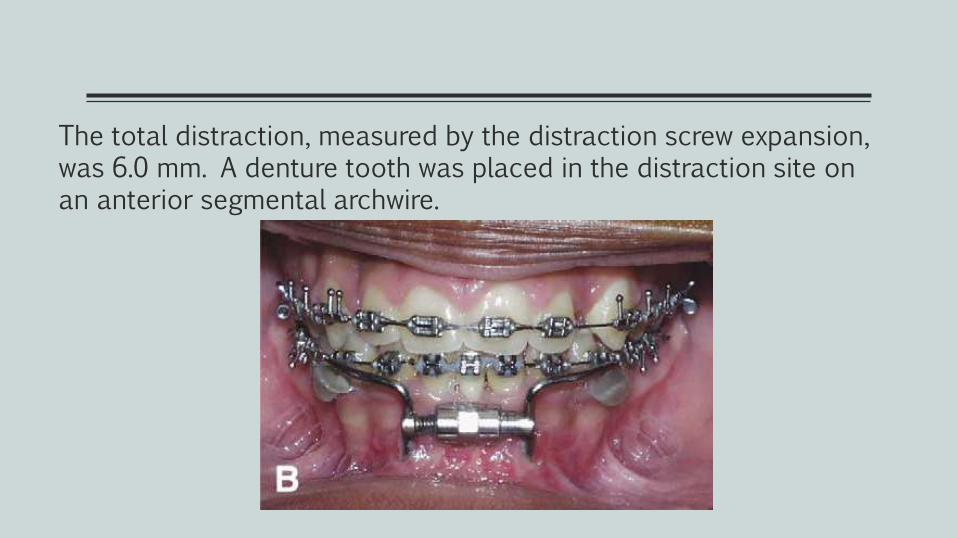
The total distraction, measured by the distraction screw expansion, was 6.0 mm. A denture tooth was placed in the distraction site on an anterior segmental archwire.
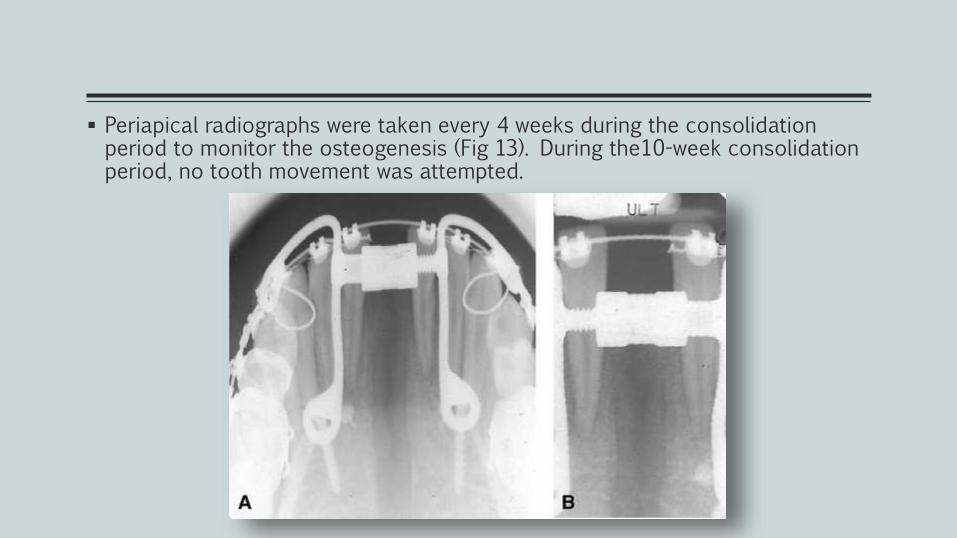
Periapical radiographs were taken every 4 weeks during the consolidation period to monitor the osteogenesis (Fig 13). During the10-week consolidation period, no tooth movement was attempted.
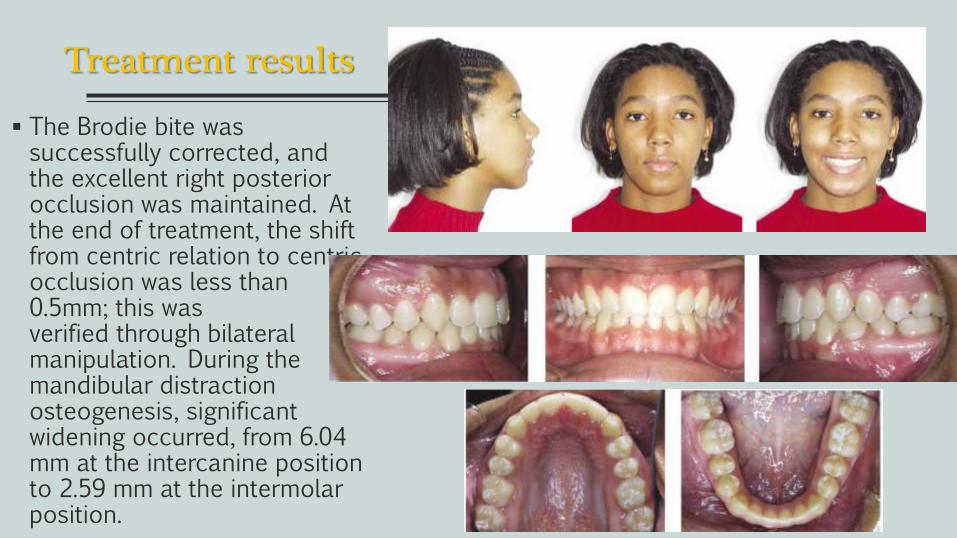
Treatment results
The Brodie bite was successfully corrected, and the excellent right posterior occlusion was maintained. At the end of treatment, the shift from centric relation to centric occlusion was less than 0.5mm; this was verified through bilateral manipulation. During the mandibular distraction osteogenesis, significant widening occurred, from 6.04 mm at the intercanine position to 2.59 mm at the intermolarposition.
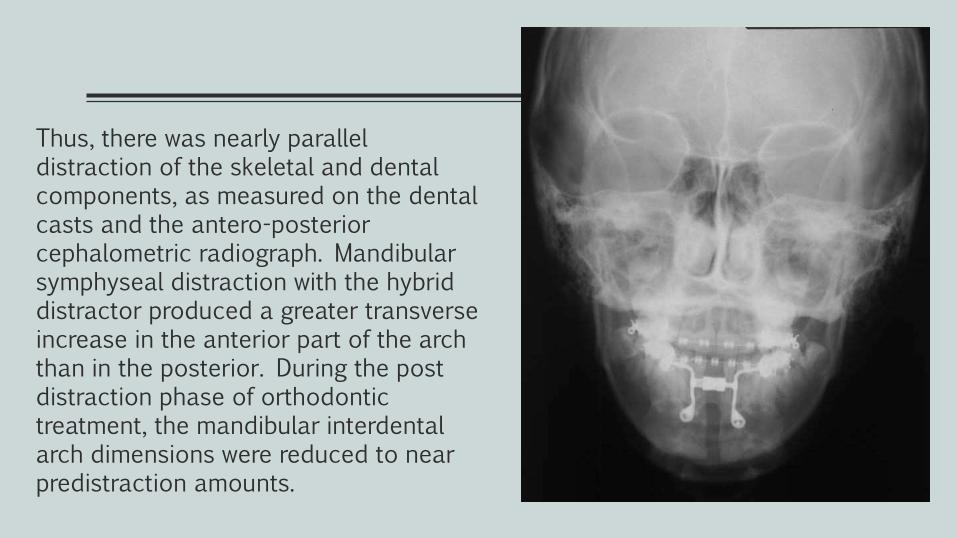
Thus, there was nearly parallel distraction of the skeletal and dental components, as measured on the dental casts and the antero-posterior cephalometric radiograph. Mandibular symphyseal distraction with the hybrid distractor produced a greater transverse increase in the anterior part of the arch than in the posterior. During the post distraction phase of orthodontic treatment, the mandibular interdental arch dimensions were reduced to near predistraction amounts.
Life is all about sharing ;)
CONTENT
Case reports
Young(growing)
Removable app.
Fixed app.
Adolescents(non-growing)
Orthodontic (Non- surgical)
Surgical
Maxilla Mandible
Adults
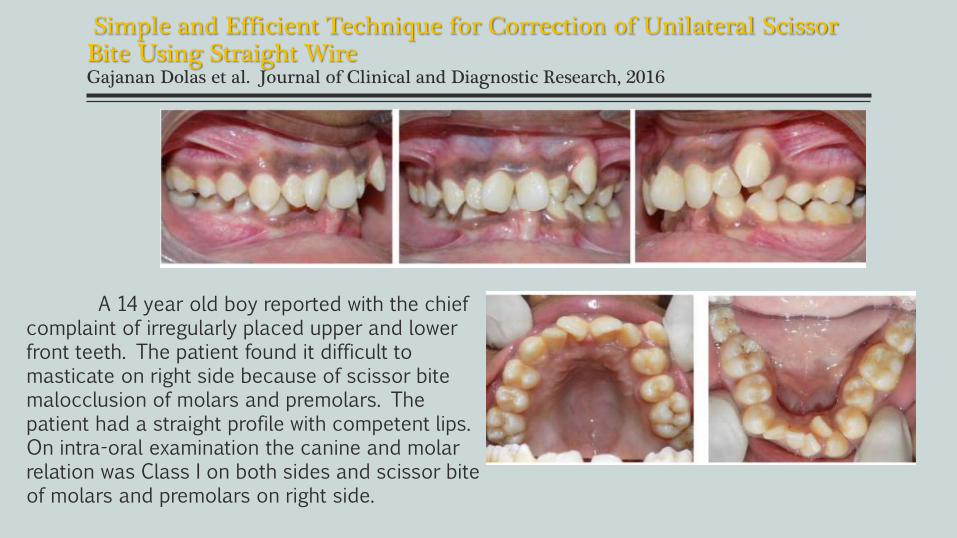
Simple and Efficient Technique for Correction of Unilateral Scissor Bite Using Straight WireGajanan Dolas et al. Journal of Clinical and Diagnostic Research, 2016
A 14 year old boy reported with the chief complaint of irregularly placed upper and lower front teeth. The patient found it difficult to masticate on right side because of scissor bite malocclusion of molars and premolars. The patient had a straight profile with competent lips. On intra-oral examination the canine and molar relation was Class I on both sides and scissor bite of molars and premolars on right side.
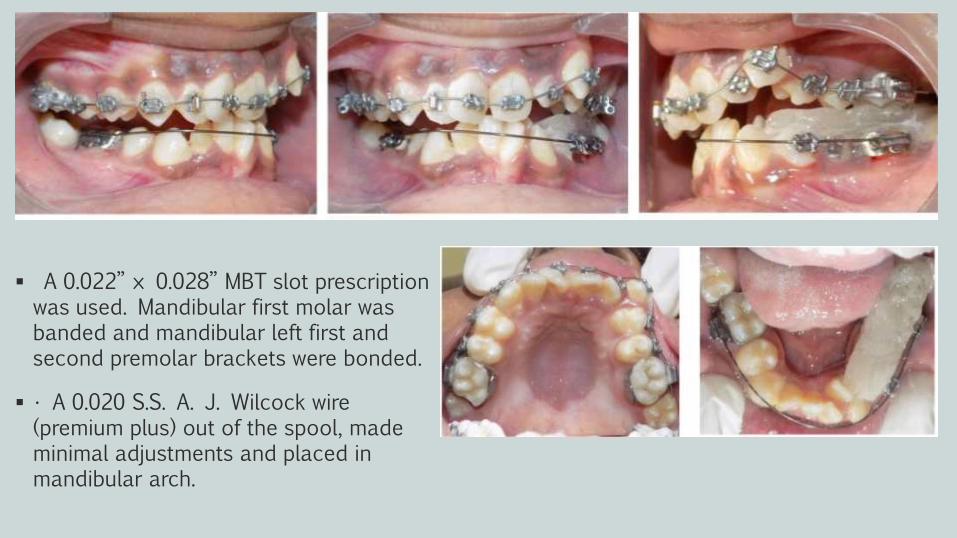
Treatment plan and progress
A 0.022” × 0.028” MBT slot prescription was used. Mandibular first molar was banded and mandibular left first and second premolar brackets were bonded.
• A 0.020 S.S. A. J. Wilcock wire (premium plus) out of the spool, made minimal adjustments and placed in mandibular arch.
Treatment plan and progress
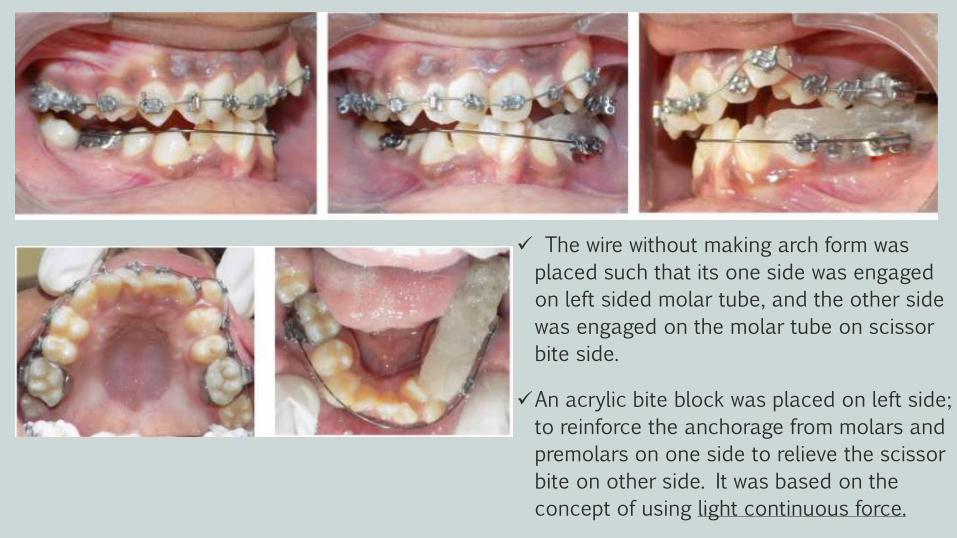
The wire without making arch form was
placed such that its one side was engaged
on left sided molar tube, and the other side
was engaged on the molar tube on scissor
bite side.
An acrylic bite block was placed on left side;
to reinforce the anchorage from molars and
premolars on one side to relieve the scissor
bite on other side. It was based on the
concept of using light continuous force.
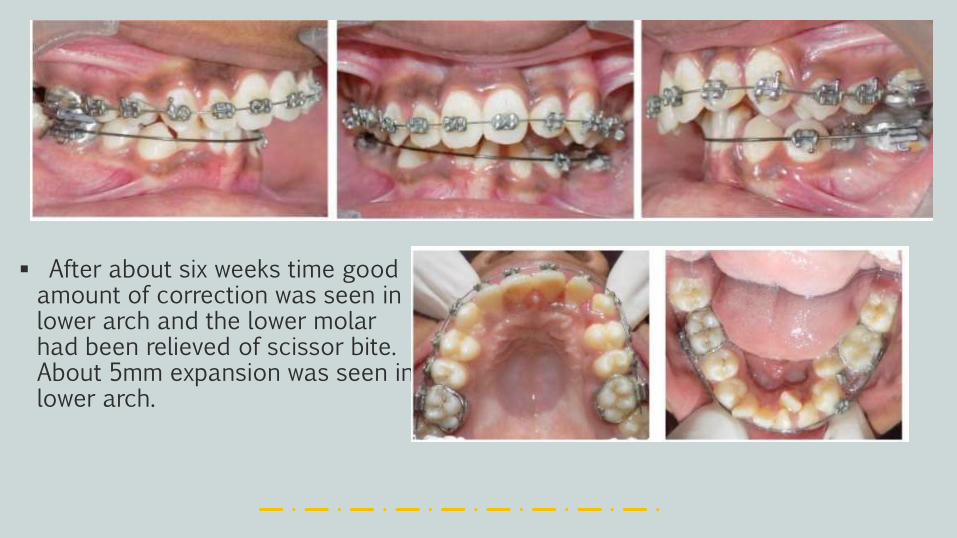
After about six weeks time good amount of correction was seen in lower arch and the lower molar had been relieved of scissor bite. About 5mm expansion was seen in lower arch.
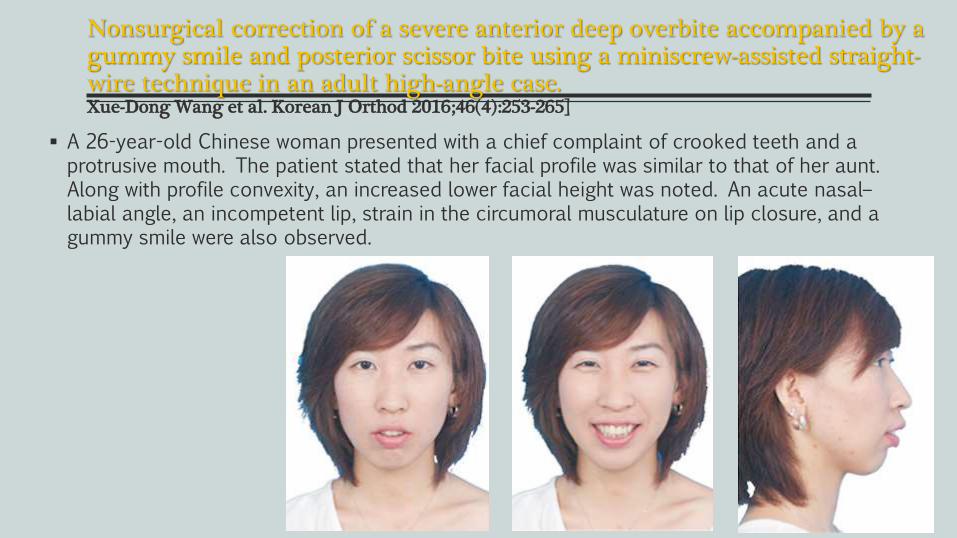
Nonsurgical correction of a severe anterior deep overbite accompanied by a gummy smile and posterior scissor bite using a miniscrew-assisted straight-wire technique in an adult high-angle case.Xue-Dong Wang et al. Korean J Orthod 2016;46(4):253-265]
A 26-year-old Chinese woman presented with a chief complaint of crooked teeth and a protrusive mouth. The patient stated that her facial profile was similar to that of her aunt. Along with profile convexity, an increased lower facial height was noted. An acute nasal–labial angle, an incompetent lip, strain in the circumoral musculature on lip closure, and a gummy smile were also observed.
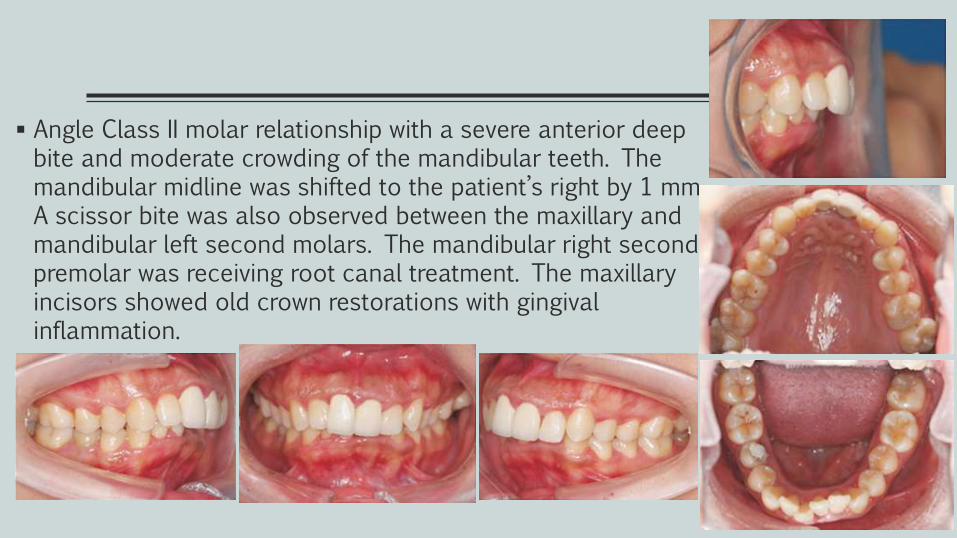
Angle Class II molar relationship with a severe anterior deep bite and moderate crowding of the mandibular teeth. The mandibular midline was shifted to the patient’s right by 1 mm. A scissor bite was also observed between the maxillary and mandibular left second molars. The mandibular right second premolar was receiving root canal treatment. The maxillary incisors showed old crown restorations with gingival inflammation.
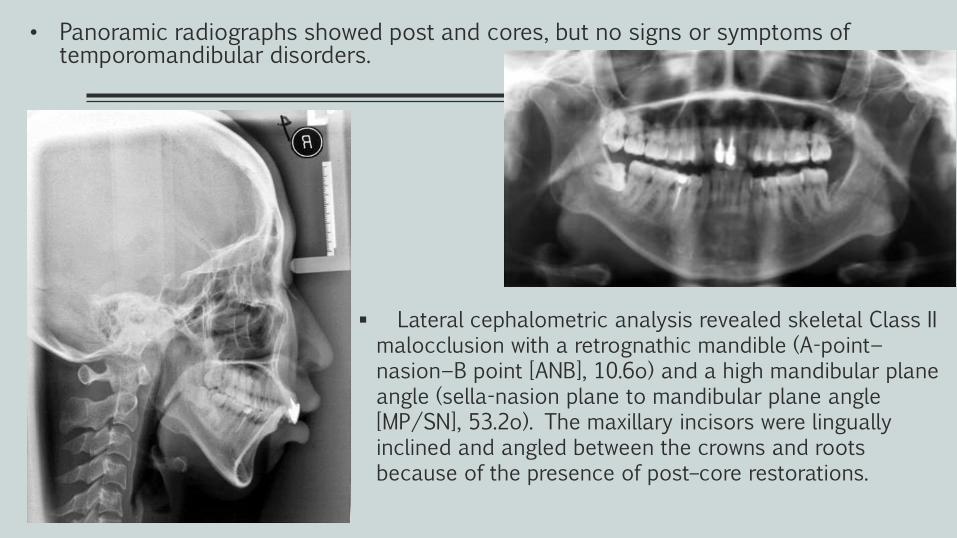
• Panoramic radiographs showed post and cores, but no signs or symptoms of temporomandibular disorders.
Lateral cephalometric analysis revealed skeletal Class II malocclusion with a retrognathic mandible (A-point− nasion−B point [ANB], 10.6o) and a high mandibular plane angle (sella-nasion plane to mandibular plane angle [MP/SN], 53.2o). The maxillary incisors were linguallyinclined and angled between the crowns and roots because of the presence of post–core restorations.
Treatment objectives
The principal treatment objectives including the following: tooth alignment, achievement of an optimal overjet and overbite. establishment of Class I canine and molar relationships, and correction of the gummy smile and facial profile.
Different treatment options were presented to the patient involving leForte I osteotomy, geneoplasty as well as fixed appliance ith extraction ot with miniscrew. The patient chose the last (miniscrew) option.
Treatment alternatives
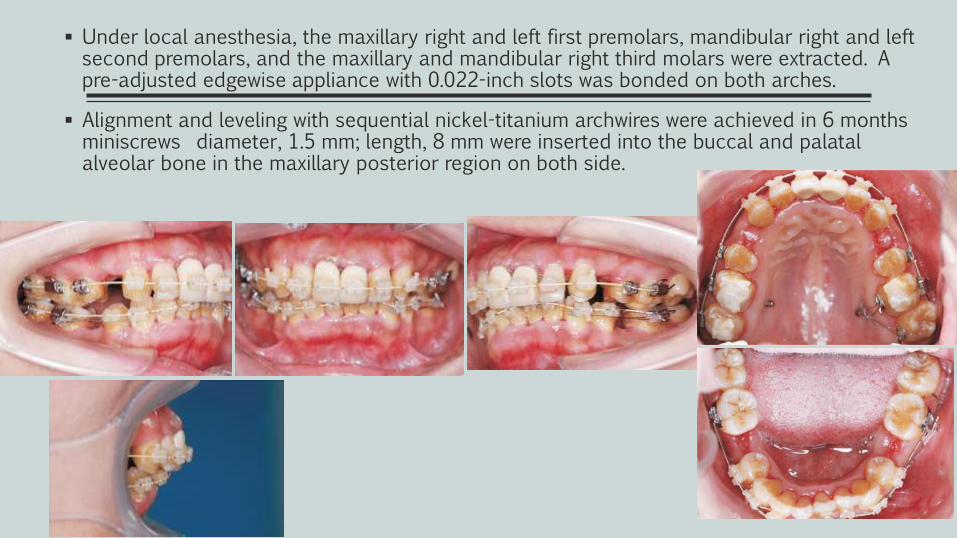
Under local anesthesia, the maxillary right and left first premolars, mandibular right and left second premolars, and the maxillary and mandibular right third molars were extracted. A pre-adjusted edgewise appliance with 0.022-inch slots was bonded on both arches.
Alignment and leveling with sequential nickel-titanium archwires were achieved in 6 months miniscrews diameter, 1.5 mm; length, 8 mm were inserted into the buccal and palatal alveolar bone in the maxillary posterior region on both side.
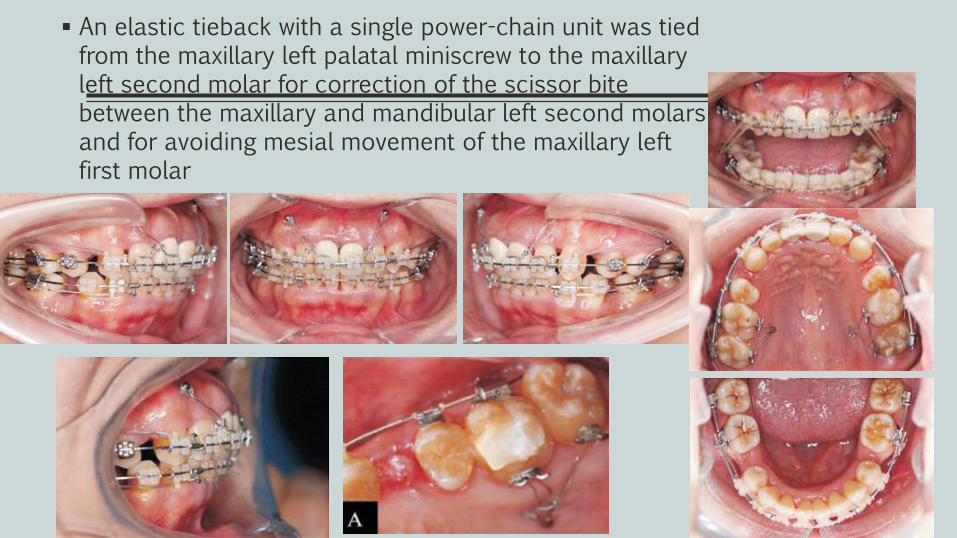
An elastic tieback with a single power-chain unit was tied from the maxillary left palatal miniscrew to the maxillary left second molar for correction of the scissor bite between the maxillary and mandibular left second molars and for avoiding mesial movement of the maxillary left first molar
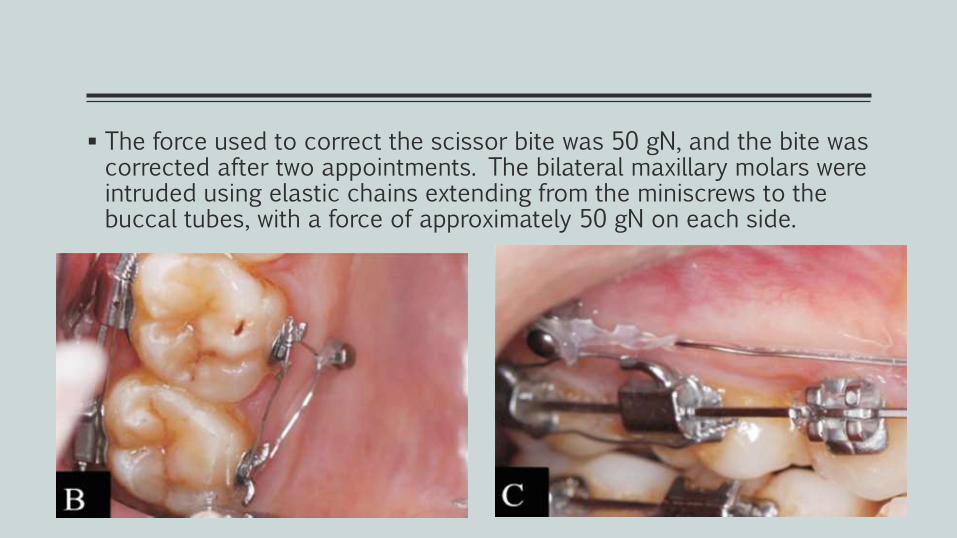
The force used to correct the scissor bite was 50 gN, and the bite was corrected after two appointments. The bilateral maxillary molars were intruded using elastic chains extending from the miniscrews to the buccal tubes, with a force of approximately 50 gN on each side.
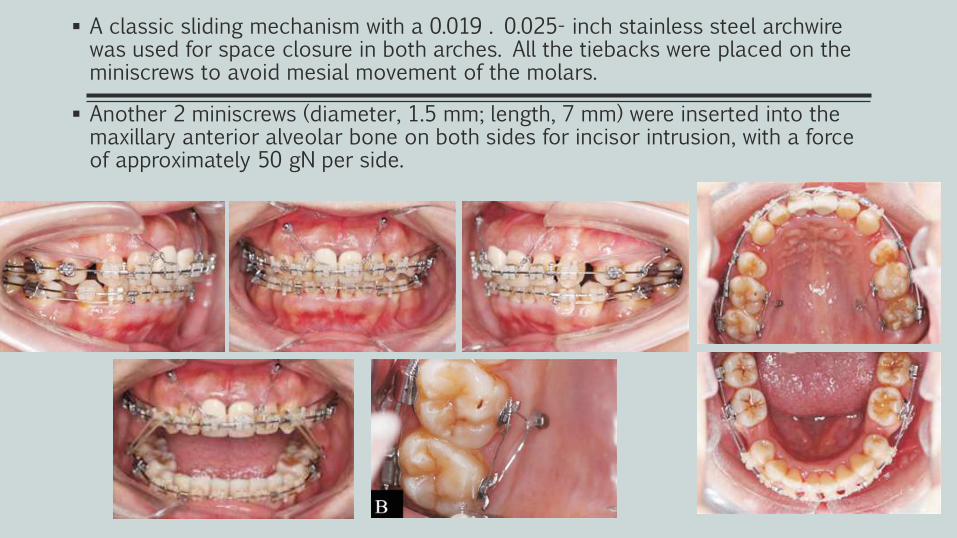
A classic sliding mechanism with a 0.019 . 0.025- inch stainless steel archwirewas used for space closure in both arches. All the tiebacks were placed on the miniscrews to avoid mesial movement of the molars.
Another 2 miniscrews (diameter, 1.5 mm; length, 7 mm) were inserted into the maxillary anterior alveolar bone on both sides for incisor intrusion, with a force of approximately 50 gN per side.
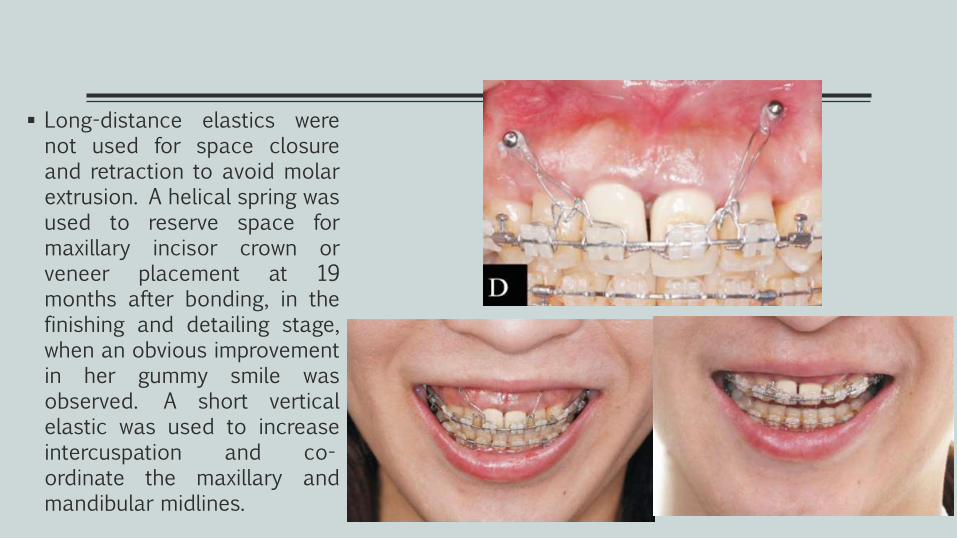
Long-distance elastics werenot used for space closureand retraction to avoid molarextrusion. A helical spring wasused to reserve space formaxillary incisor crown orveneer placement at 19months after bonding, in thefinishing and detailing stage,when an obvious improvementin her gummy smile wasobserved. A short verticalelastic was used to increaseintercuspation and co-ordinate the maxillary andmandibular midlines.
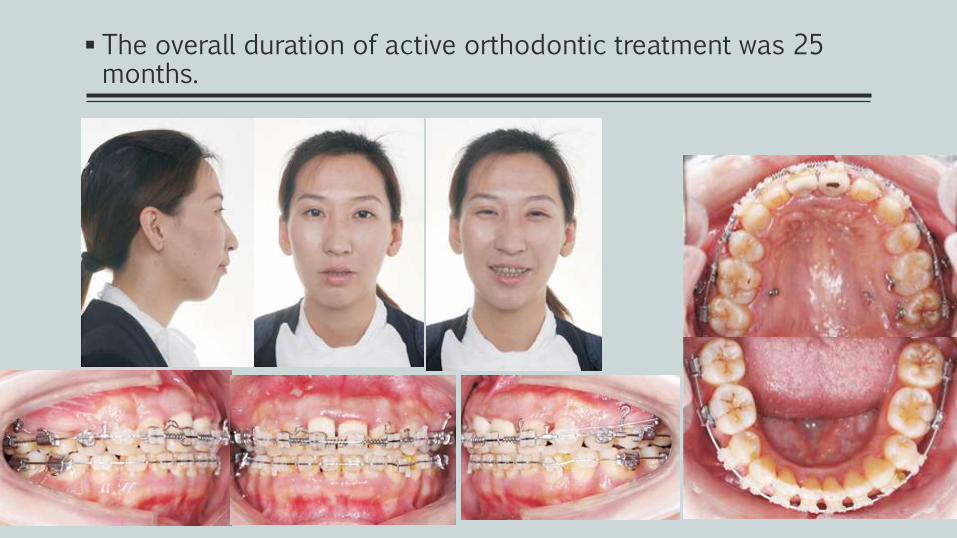
The overall duration of active orthodontic treatment was 25 months.
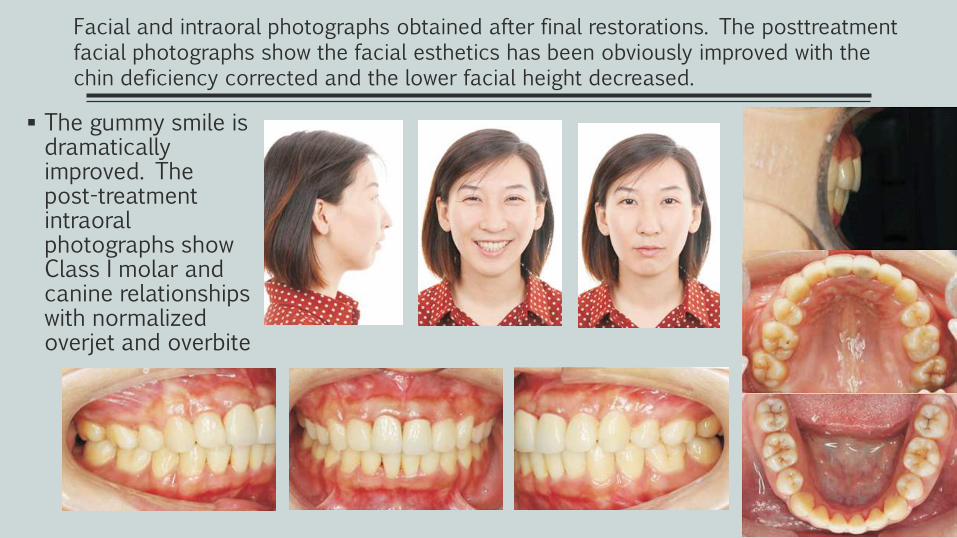
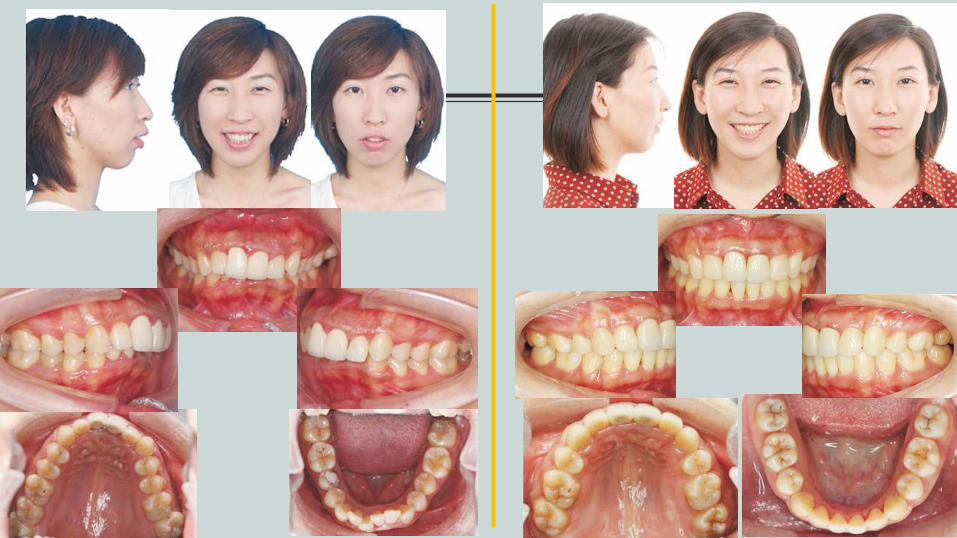
The gummy smile is dramatically improved. The post-treatment intraoral photographs show Class I molar and canine relationships with normalized overjet and overbite
Facial and intraoral photographs obtained after final restorations. The posttreatmentfacial photographs show the facial esthetics has been obviously improved with the chin deficiency corrected and the lower facial height decreased.
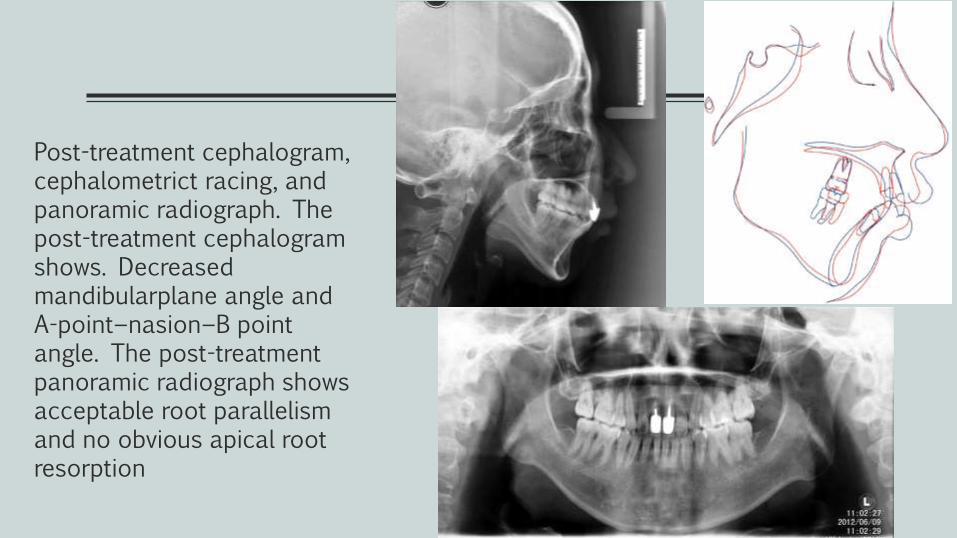
Post-treatment cephalogram, cephalometrict racing, and panoramic radiograph. The post-treatment cephalogramshows. Decreased mandibularplane angle and A-point−nasion−B point angle. The post-treatment panoramic radiograph shows acceptable root parallelism and no obvious apical root resorption
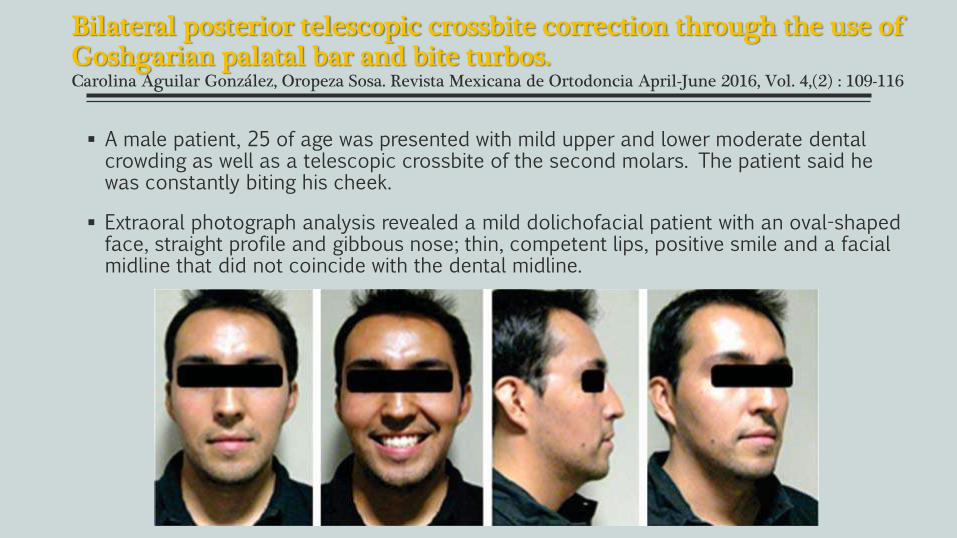
Bilateral posterior telescopic crossbite correction through the use of Goshgarian palatal bar and bite turbos.Carolina Aguilar González, Oropeza Sosa. Revista Mexicana de Ortodoncia April-June 2016, Vol. 4,(2) : 109-116
A male patient, 25 of age was presented with mild upper and lower moderate dental crowding as well as a telescopic crossbite of the second molars. The patient said he was constantly biting his cheek.
Extraoral photograph analysis revealed a mild dolichofacial patient with an oval-shaped face, straight profile and gibbous nose; thin, competent lips, positive smile and a facial midline that did not coincide with the dental midline.
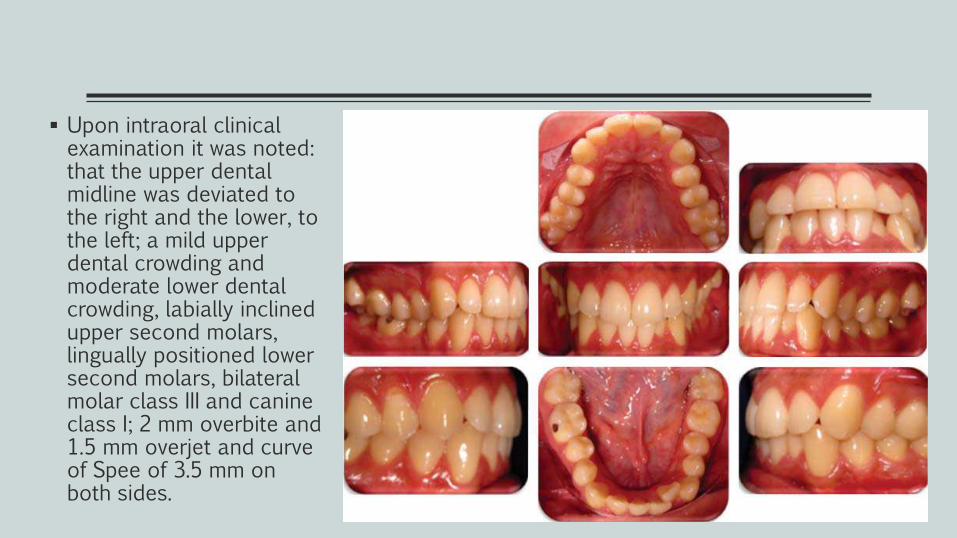
Upon intraoral clinical examination it was noted: that the upper dental midline was deviated to the right and the lower, to the left; a mild upper dental crowding and moderate lower dental crowding, labially inclined upper second molars, lingually positioned lower second molars, bilateral molar class III and canine class I; 2 mm overbite and 1.5 mm overjet and curve of Spee of 3.5 mm on both sides.
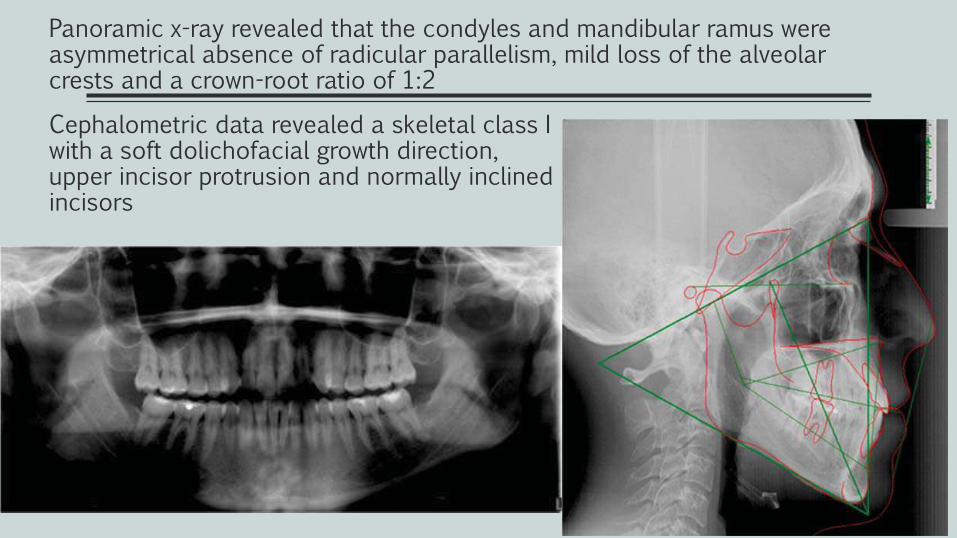
Panoramic x-ray revealed that the condyles and mandibular ramus were asymmetrical absence of radicular parallelism, mild loss of the alveolar crests and a crown-root ratio of 1:2
Cephalometric data revealed a skeletal class I with a soft dolichofacial growth direction, upper incisor protrusion and normally inclinedincisors
Treatment plan
Two treatment options were suggested to the patient. One of them involved using 0.022” x 0.025” Roth GAC In-Ovation®R self-ligating appliances and 2 mini-implants, either with or without corticotomies.
The second treatment option was 0.022” Roth GAC In-Ovation®R appliances and for the correction of the upper second molars, a 0.036” TMA removable palatal bar.
The patient did not accept the mini-implants or the corticotomies, so the second option was chosen.
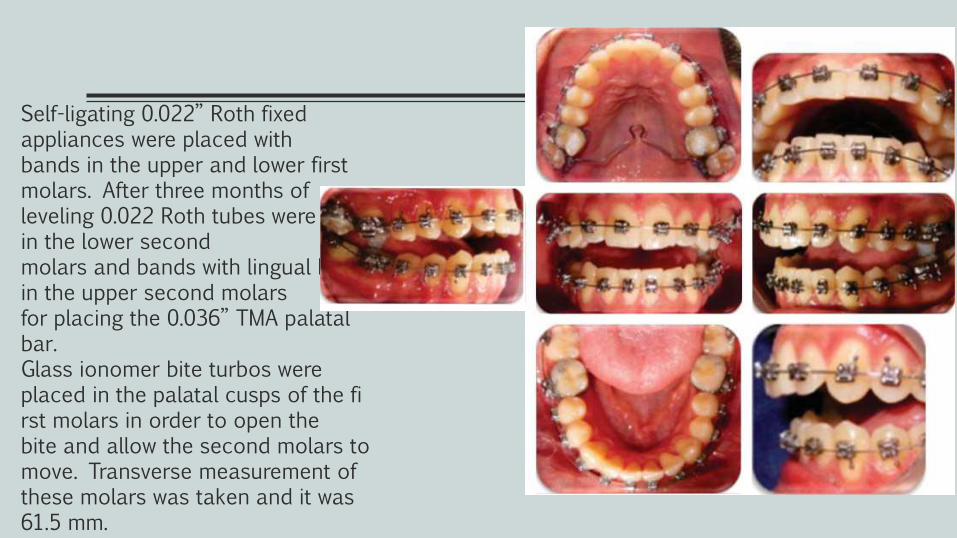
Self-ligating 0.022” Roth fixed appliances were placed withbands in the upper and lower first molars. After three months ofleveling 0.022 Roth tubes were placed in the lower second molars and bands with lingual boxes in the upper second molars for placing the 0.036” TMA palatal bar. Glass ionomer bite turbos were placed in the palatal cusps of the fi rst molars in order to open thebite and allow the second molars to move. Transverse measurement of these molars was taken and it was 61.5 mm.
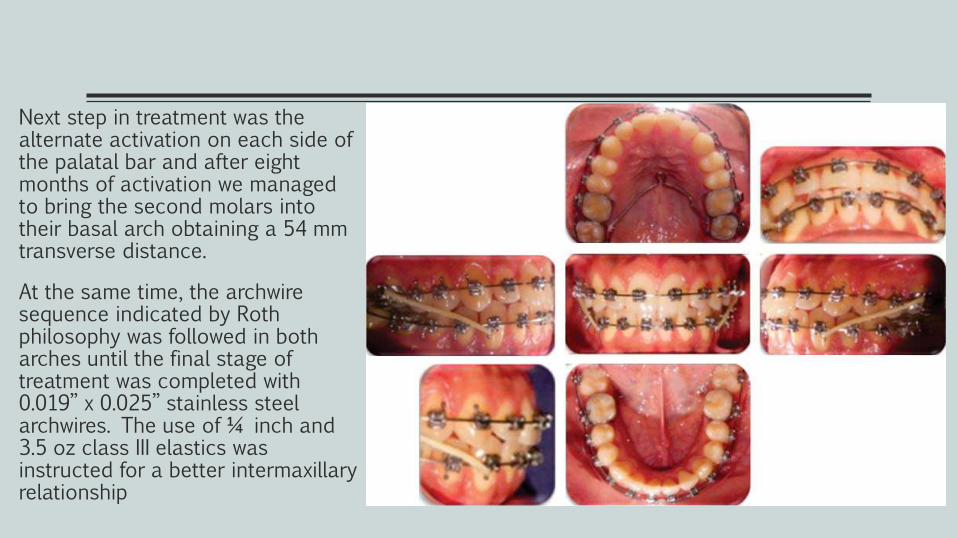
Next step in treatment was the alternate activation on each side of the palatal bar and after eight months of activation we managed to bring the second molars into their basal arch obtaining a 54 mm transverse distance.
At the same time, the archwiresequence indicated by Roth philosophy was followed in both arches until the final stage of treatment was completed with 0.019” x 0.025” stainless steel archwires. The use of ¼ inch and 3.5 oz class III elastics was instructed for a better intermaxillaryrelationship
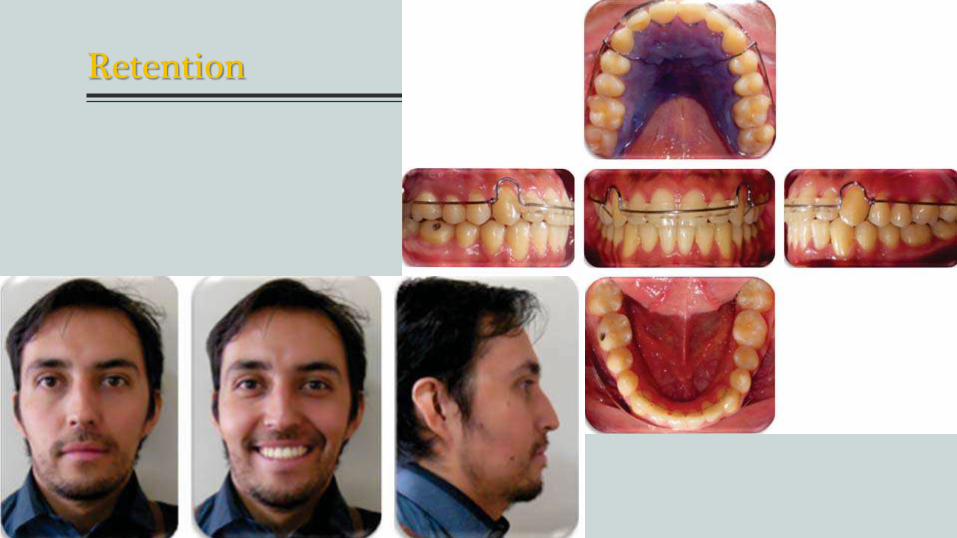
Retention
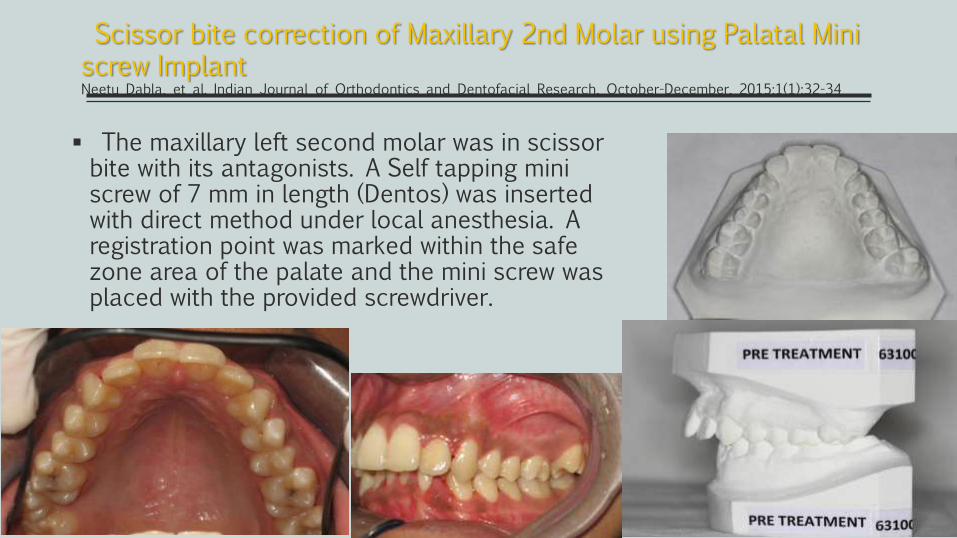
The maxillary left second molar was in scissor bite with its antagonists. A Self tapping mini screw of 7 mm in length (Dentos) was inserted with direct method under local anesthesia. A registration point was marked within the safe zone area of the palate and the mini screw was placed with the provided screwdriver.
Scissor bite correction of Maxillary 2nd Molar using Palatal Mini screw Implant Neetu Dabla, et al. Indian Journal of Orthodontics and Dentofacial Research, October-December, 2015;1(1):32-34
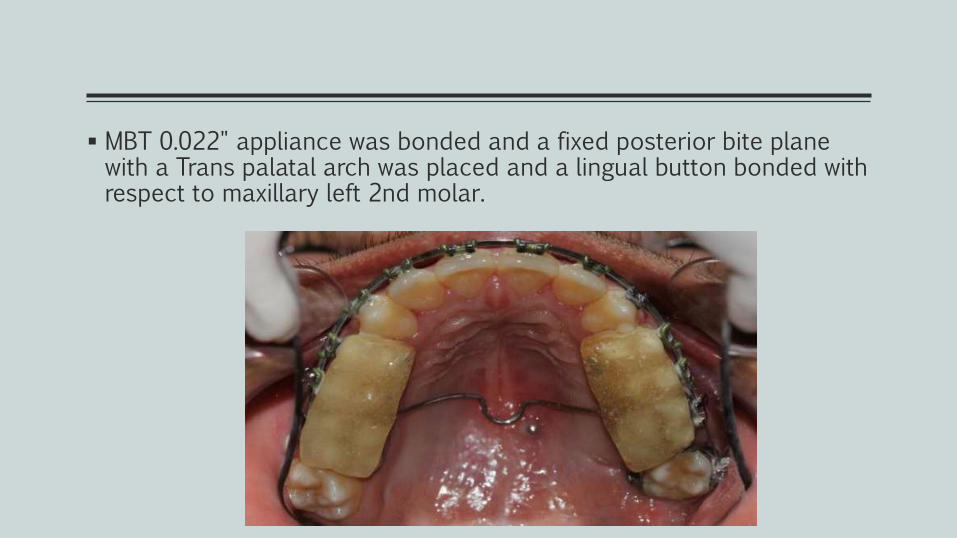
MBT 0.022" appliance was bonded and a fixed posterior bite plane with a Trans palatal arch was placed and a lingual button bonded with respect to maxillary left 2nd molar.
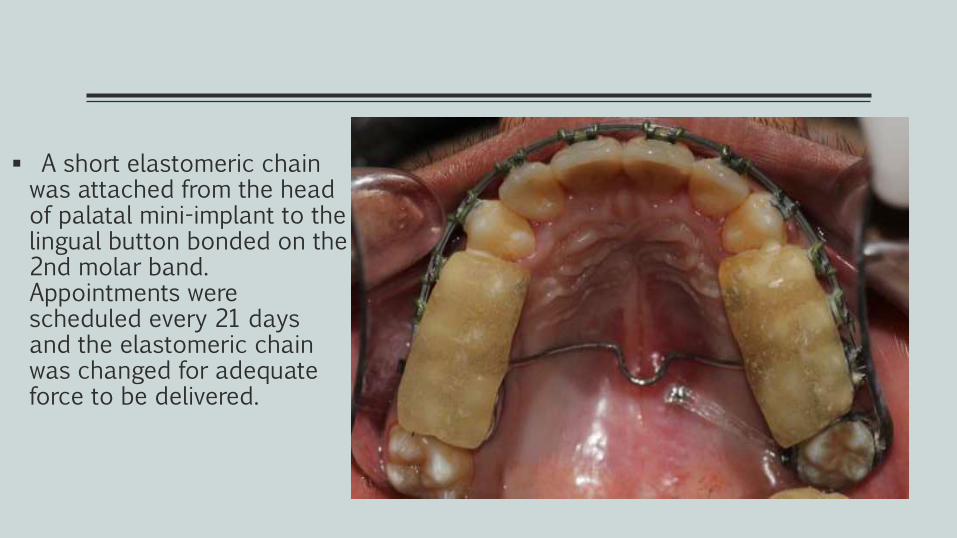
A short elastomeric chain was attached from the head of palatal mini-implant to the lingual button bonded on the 2nd molar band. Appointments were scheduled every 21 days and the elastomeric chain was changed for adequate force to be delivered.
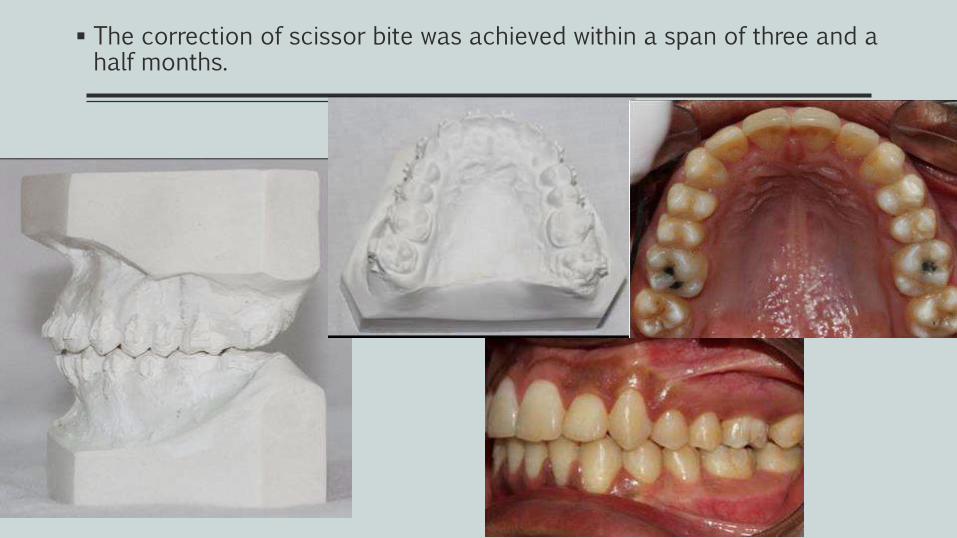
The correction of scissor bite was achieved within a span of three and a half months.
There isn’t a standard approach !!
Each form of clinical case requires a proper evaluation considering the age of
patient, the features of pathology as the presence of other complications.
The ortho-surgical correction remains the golden standard in severe
dentofacial deformities because of its more applicability, lower risks of failure and
rapidity, as it doesn’t need patient compliance.
However not all the patients accept to undergo surgery, so pure orthodontic
approach is need. So the combination of fixed orthodontics with skeletal anchorage
has proven the best effective and stable to 5 years from therapy.
Moreover in young patient with mild form of malocclusion when it was
intercepted early, a functional therapy should be attempted.
Fantasia E, D'Emidio M, Padalino G, Rodi G. Comparison of Orthodontic Techniques used for treating patients with severe form of scissor bite: a systematic review. WebmedCentral ORTHODONTICS 2016