Sanjay kr. chaudhary..M.B.B.S. Student
29
TREATMENT OF HIV TREATMENT OF HIV INFECTION INFECTION BY…..SANJAY KR. CHAUDHARY. BY…..SANJAY KR. CHAUDHARY. Final year student (M.B.B.S.) Final year student (M.B.B.S.) UPRIMS&R UPRIMS&R
-
Upload
sanjay-kumar-chaudhary -
Category
Health & Medicine
-
view
75 -
download
2
Transcript of Sanjay kr. chaudhary..M.B.B.S. Student

TREATMENT OF HIV TREATMENT OF HIV INFECTIONINFECTION
BY…..SANJAY KR. CHAUDHARY.BY…..SANJAY KR. CHAUDHARY. Final year student (M.B.B.S.) UPRIMS&RFinal year student (M.B.B.S.) UPRIMS&R

GENERAL MEASURES-GENERAL MEASURES- Balanced dietBalanced diet
Quit smoking and intake of alcohalQuit smoking and intake of alcohal
Adequate restAdequate rest
Practice of safer sex to avoid infection Practice of safer sex to avoid infection of partnerof partner

ANTIRETROVIRAL DRUGSANTIRETROVIRAL DRUGS1.NUCLEOSIDE REVERSE TRANSCRIPTASE 1.NUCLEOSIDE REVERSE TRANSCRIPTASE
INHIBITOR(NRTI)INHIBITOR(NRTI) MECHANISMMECHANISM-- these active nucleoside incorporate into viral these active nucleoside incorporate into viral
DNA and cause premature chain terminationDNA and cause premature chain termination Eg- side effect Eg- side effect Zidovudine anemia, Zidovudine anemia,
hyperglycemia,nausea .hyperglycemia,nausea . Lamivudine Lamivudine
Emtricitabine hepatotoxicity .Emtricitabine hepatotoxicity . Abacavir hypersensitivity reaction, Abacavir hypersensitivity reaction,
fever etc.fever etc. Tenofovir osteomalacia. Tenofovir osteomalacia.

Mechanism-Mechanism-it bind directly to reverse it bind directly to reverse transcriptase enzyme and inhibit its functiontranscriptase enzyme and inhibit its function
Highly active against HIV-1 but not against Highly active against HIV-1 but not against HIV-2HIV-2
Eg- Side effectEg- Side effect Nevirapine skin rash, hepatotoxicity.Nevirapine skin rash, hepatotoxicity. Efavirenz rash, dysphoria, Efavirenz rash, dysphoria,
drowsiness.drowsiness. Etravirine rash, nausea. Etravirine rash, nausea. Rilpivirine nausea, dizziness.Rilpivirine nausea, dizziness.

4.PROTEASE INHIBITOR4.PROTEASE INHIBITORMECHANISMMECHANISM--inhibit protease enzyme, inhibit protease enzyme, so inhibit assembly of virus before its so inhibit assembly of virus before its release release Eg-Eg-•IndinavirIndinavir•RitonavirRitonavir•LopinavirLopinavir•SaquinavirSaquinavir•NelfinavirNelfinavir•S\E-S\E-•hyperglycemiahyperglycemia•raised cholesterolraised cholesterol

5.CCR5 INHIBITORS5.CCR5 INHIBITORSMechanismMechanism--bind to host cell through bind to host cell through CCR5 receptorsCCR5 receptors Eg-Eg-MaravirocMaravirocFUSION INHIBITORSFUSION INHIBITORSMechanism-Mechanism- block initial fusion of block initial fusion of HIV with cell surface receptorsHIV with cell surface receptorsEg-Eg-EnfuvirtideEnfuvirtideDrawback-Drawback- not active against HIV-2 not active against HIV-2

6. INTEGRASE INHIBITOR6. INTEGRASE INHIBITOR Mechanism of action-Mechanism of action- act by blocking act by blocking
the action of the HIV integrase enzyme.the action of the HIV integrase enzyme. Eg. ToxicityEg. Toxicity
Raltegravir Raltegravir Nausea,headache,diarrheaNausea,headache,diarrhea
Elvitegravir Diarrhea,nausea etc.Elvitegravir Diarrhea,nausea etc. Dolutegravir Insomnia,headache.Dolutegravir Insomnia,headache.

WHAT IS ART WHAT IS ART

Antiretroviral Therapy (ART)Antiretroviral Therapy (ART) ART is the combination of different ART is the combination of different
classes of ARV drugs.classes of ARV drugs. - to achieve maximal & most durable - to achieve maximal & most durable
suppression of viral replication.suppression of viral replication. - to prevent emergence of drug - to prevent emergence of drug
resistant mutants.resistant mutants. - to improve survival & quality of life.- to improve survival & quality of life.

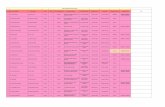
Before ART & after 1 year Before ART & after 1 year ART ART

GOALS OF ARTGOALS OF ARTGOALS
PRINCIPLE
Clinical
To prolong life & improve quality of life.
Virological Greatest possible reduction in viral load, as long as possible to halt disease progression & to prevent or delay resistance.
Immunological Immune reconstitution is both : 1. Quantitative(CD4 within normal range) 2. Qualitative (Pathogen specific immune response)
Therapeutic Rational sequencing of drugs to achieve previous three goals while : 1. Maintaining future therapeutic options. 2. Minimising drug toxicities & side effects. 3. Maximising treatment adherence.
Epidemiological To reduce HIV transmission.

Use of highly active antiretroviral therapy is Use of highly active antiretroviral therapy is successful in reducing morbidity in HIV patients successful in reducing morbidity in HIV patients and improving quality of lifeand improving quality of life
HAART indicates combination of drugs so as to HAART indicates combination of drugs so as to achieve the goalsachieve the goals
Suppresion of viral loadSuppresion of viral load
Restoration and preservation of immune functionRestoration and preservation of immune function
Reduction of HIV related mortality and morbidityReduction of HIV related mortality and morbidity

Indications for the Initiation of Antiretroviral Therapy in Patients with HIV Infection
I. Acute infection syndromeII. Chronic infectionA. Symptomatic disease (including HIV-associated nephropathy) B. Asymptomatic disease 1. CD4+ T cell count <500/La 2. PregnancyIII. Postexposure prophylaxis








COMBINATION FORMULA OF COMBINATION FORMULA OF ANTIRETROVIRAL DRUGSANTIRETROVIRAL DRUGS

MANAGEMENT DURING MANAGEMENT DURING PREGNANCYPREGNANCY Efavirenz Efavirenz - avoided in 1- avoided in 1stst trimester trimester
Standard recommendation to prevent MCTC Standard recommendation to prevent MCTC of HIV is use of oral ZDV throughout antenatal of HIV is use of oral ZDV throughout antenatal period ( atleast from 28 weeks onwards)period ( atleast from 28 weeks onwards)
Single dose Single dose nevirapine nevirapine regimen administered regimen administered intrapartum to mother & withing 72 hrs of intrapartum to mother & withing 72 hrs of delivery to baby is not recommemded as it delivery to baby is not recommemded as it reduces MCTC by only abt 50%reduces MCTC by only abt 50%
Anteretroviral prophylaxis should be offered Anteretroviral prophylaxis should be offered to reduce the chances of perinatal to reduce the chances of perinatal transmission.transmission.

MANAGEMENT DURING MANAGEMENT DURING PREGNANCYPREGNANCY
Time of Administration Zidovudine RegimenAntepartum 100 mg orally five times daily,
initiated at 14 to 34 weeks and continued throughout the pregnancy.a
Intrapartum During labor, intravenous zidovudine in a 1-hour initial dose of 2 mg/kg, followed by a continuous infusion of 1 mg/kg/hr until delivery.b
Neonate Begin at 8 to 12 hours after birth, and give syrup at 2 mg/kg every 6 hours for 6 weeks.c

PROPHYLAXIS IN AIDSPROPHYLAXIS IN AIDS
Tetanus/diphtheria vaccine Tetanus/diphtheria vaccine Human papillomavirus vaccine for HIV-infected Human papillomavirus vaccine for HIV-infected
women age 26 years or less. women age 26 years or less. Haemophilus influenzae type b vaccination Haemophilus influenzae type b vaccination Papanicolaou smears every 6 months for Papanicolaou smears every 6 months for
women women Pneumocystis jiroveci prophylaxis Pneumocystis jiroveci prophylaxis Mycobacterium avium complex prophylaxis Mycobacterium avium complex prophylaxis CMV prophylaxisCMV prophylaxis For all cases of HIV NEUROPATHY- For all cases of HIV NEUROPATHY- START ARTSTART ART


GUIDELINES FOR PEPGUIDELINES FOR PEP A combination of two nucleoside analogue A combination of two nucleoside analogue reverse transcriptase inhibitorreverse transcriptase inhibitor
Given for 4 weeks for Given for 4 weeks for LESS SEVERELESS SEVERE EXPOSURES.EXPOSURES.
A combination of two NRTI + a third drugA combination of two NRTI + a third drug
Given for 4 weeks for Given for 4 weeks for MORE SEVERE MORE SEVERE EXPOSURES. EXPOSURES.



THANK
YOU