
SAISI WEBSITE: Newsletter Vol...2 Volume 24 | No 1 | 2014 SAISI WEBSITE: Views contained in articles...
30
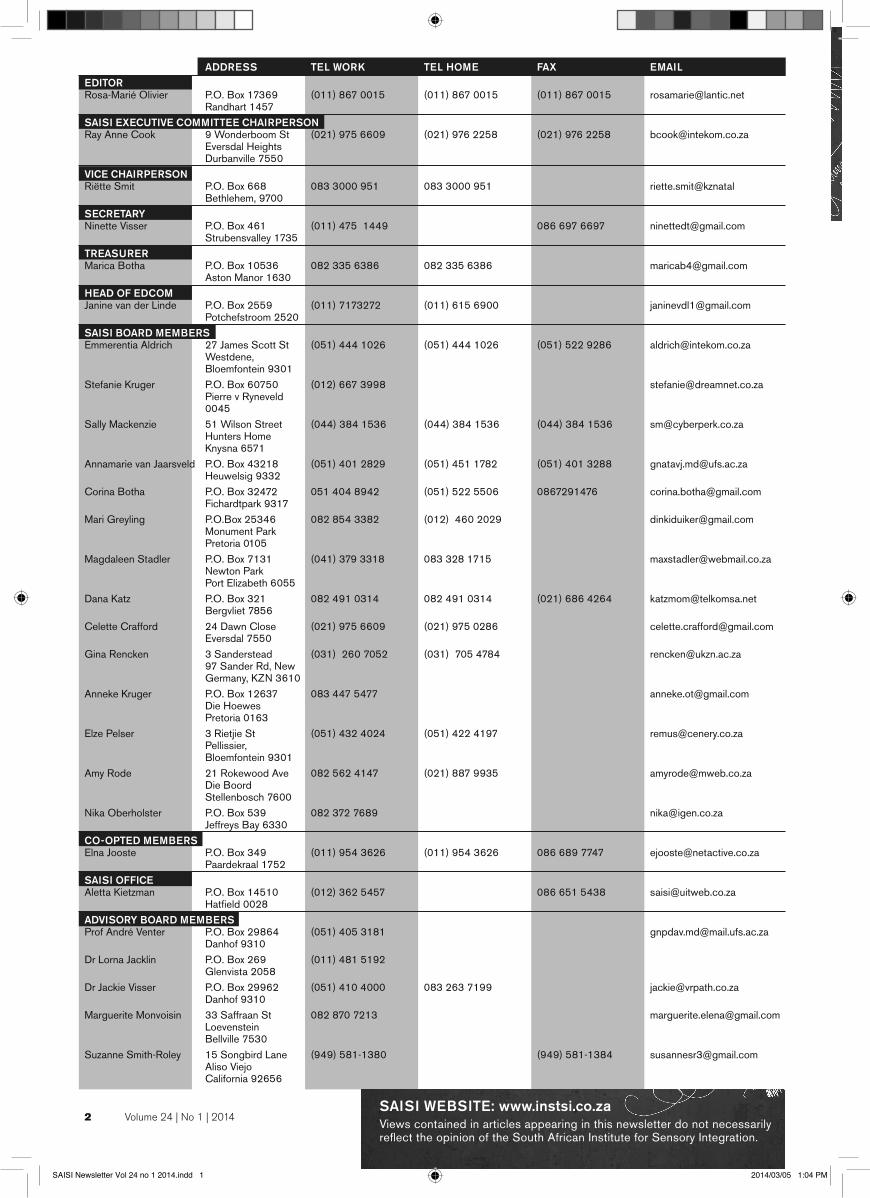
2 Volume 24 | No 1 | 2014 SAISI WEBSITE: www.instsi.co.za Views contained in articles appearing in this newsletter do not necessarily reflect the opinion of the South African Institute for Sensory Integration. ADDRESS TEL WORK TEL HOME FAX EMAIL EDITOR Rosa-Marié Olivier P.O. Box 17369 (011) 867 0015 (011) 867 0015 (011) 867 0015 [email protected] Randhart 1457 SAISI EXECUTIVE COMMITTEE CHAIRPERSON Ray Anne Cook 9 Wonderboom St (021) 975 6609 (021) 976 2258 (021) 976 2258 [email protected] Eversdal Heights Durbanville 7550 VICE CHAIRPERSON Riëtte Smit P.O. Box 668 083 3000 951 083 3000 951 riette.smit@kznatal Bethlehem, 9700 SECRETARY Ninette Visser P.O. Box 461 (011) 475 1449 086 697 6697 [email protected] Strubensvalley 1735 TREASURER Marica Botha P.O. Box 10536 082 335 6386 082 335 6386 [email protected] Aston Manor 1630 HEAD OF EDCOM Janine van der Linde P.O. Box 2559 (011) 7173272 (011) 615 6900 [email protected] Potchefstroom 2520 SAISI BOARD MEMBERS Emmerentia Aldrich 27 James Scott St (051) 444 1026 (051) 444 1026 (051) 522 9286 [email protected] Westdene, Bloemfontein 9301 Stefanie Kruger P.O. Box 60750 (012) 667 3998 [email protected] Pierre v Ryneveld 0045 Sally Mackenzie 51 Wilson Street (044) 384 1536 (044) 384 1536 (044) 384 1536 [email protected] Hunters Home Knysna 6571 Annamarie van Jaarsveld P.O. Box 43218 (051) 401 2829 (051) 451 1782 (051) 401 3288 [email protected] Heuwelsig 9332 Corina Botha P.O. Box 32472 051 404 8942 (051) 522 5506 0867291476 [email protected] Fichardtpark 9317 Mari Greyling P.O.Box 25346 082 854 3382 (012) 460 2029 [email protected] Monument Park Pretoria 0105 Magdaleen Stadler P.O. Box 7131 (041) 379 3318 083 328 1715 [email protected] Newton Park Port Elizabeth 6055 Dana Katz P.O. Box 321 082 491 0314 082 491 0314 (021) 686 4264 [email protected] Bergvliet 7856 Celette Crafford 24 Dawn Close (021) 975 6609 (021) 975 0286 [email protected] Eversdal 7550 Gina Rencken 3 Sanderstead (031) 260 7052 (031) 705 4784 [email protected] 97 Sander Rd, New Germany, KZN 3610 Anneke Kruger P.O. Box 12637 083 447 5477 [email protected] Die Hoewes Pretoria 0163 Elze Pelser 3 Rietjie St (051) 432 4024 (051) 422 4197 [email protected] Pellissier, Bloemfontein 9301 Amy Rode 21 Rokewood Ave 082 562 4147 (021) 887 9935 [email protected] Die Boord Stellenbosch 7600 Nika Oberholster P.O. Box 539 082 372 7689 [email protected] Jeffreys Bay 6330 CO-OPTED MEMBERS Elna Jooste P.O. Box 349 (011) 954 3626 (011) 954 3626 086 689 7747 [email protected] Paardekraal 1752 SAISI OFFICE Aletta Kietzman P.O. Box 14510 (012) 362 5457 086 651 5438 [email protected] Hatfield 0028 ADVISORY BOARD MEMBERS Prof André Venter P.O. Box 29864 (051) 405 3181 [email protected] Danhof 9310 Dr Lorna Jacklin P.O. Box 269 (011) 481 5192 Glenvista 2058 Dr Jackie Visser P.O. Box 29962 (051) 410 4000 083 263 7199 [email protected] Danhof 9310 Marguerite Monvoisin 33 Saffraan St 082 870 7213 [email protected] Loevenstein Bellville 7530 Suzanne Smith-Roley 15 Songbird Lane (949) 581-1380 (949) 581-1384 [email protected] Aliso Viejo California 92656 SAISI Newsletter Vol 24 no 1 2014.indd 1 2014/03/05 1:04 PM
Transcript of SAISI WEBSITE: Newsletter Vol...2 Volume 24 | No 1 | 2014 SAISI WEBSITE: Views contained in articles...
2 Volume 24 | No 1 | 2014SAISI WEBSITE: www.instsi.co.za Views contained in articles appearing in this newsletter do not necessarily reflect the opinion of the South African Institute for Sensory Integration.
ADDRESS TEL WORK TEL HOME FAX EMAIL EDITOR Rosa-Marié Olivier P.O. Box 17369 (011) 867 0015 (011) 867 0015 (011) 867 0015 [email protected] Randhart 1457SAISI EXECUTIVE COMMITTEE CHAIRPERSON Ray Anne Cook 9 Wonderboom St (021) 975 6609 (021) 976 2258 (021) 976 2258 [email protected] Eversdal Heights Durbanville 7550 VICE CHAIRPERSON Riëtte Smit P.O. Box 668 083 3000 951 083 3000 951 riette.smit@kznatal Bethlehem, 9700 SECRETARY Ninette Visser P.O. Box 461 (011) 475 1449 086 697 6697 [email protected] Strubensvalley 1735 TREASURER Marica Botha P.O. Box 10536 082 335 6386 082 335 6386 [email protected] Aston Manor 1630 HEAD OF EDCOM Janine van der Linde P.O. Box 2559 (011) 7173272 (011) 615 6900 [email protected] Potchefstroom 2520 SAISI BOARD MEMBERS Emmerentia Aldrich 27 James Scott St (051) 444 1026 (051) 444 1026 (051) 522 9286 [email protected] Westdene, Bloemfontein 9301 Stefanie Kruger P.O. Box 60750 (012) 667 3998 [email protected] Pierre v Ryneveld 0045 Sally Mackenzie 51 Wilson Street (044) 384 1536 (044) 384 1536 (044) 384 1536 [email protected] Hunters Home Knysna 6571 Annamarie van Jaarsveld P.O. Box 43218 (051) 401 2829 (051) 451 1782 (051) 401 3288 [email protected] Heuwelsig 9332 Corina Botha P.O. Box 32472 051 404 8942 (051) 522 5506 0867291476 [email protected] Fichardtpark 9317 Mari Greyling P.O.Box 25346 082 854 3382 (012) 460 2029 [email protected] Monument Park Pretoria 0105 Magdaleen Stadler P.O. Box 7131 (041) 379 3318 083 328 1715 [email protected] Newton Park Port Elizabeth 6055 Dana Katz P.O. Box 321 082 491 0314 082 491 0314 (021) 686 4264 [email protected] Bergvliet 7856 Celette Crafford 24 Dawn Close (021) 975 6609 (021) 975 0286 [email protected] Eversdal 7550Gina Rencken 3 Sanderstead (031) 260 7052 (031) 705 4784 [email protected] 97 Sander Rd, New Germany, KZN 3610Anneke Kruger P.O. Box 12637 083 447 5477 [email protected] Die Hoewes Pretoria 0163 Elze Pelser 3 Rietjie St (051) 432 4024 (051) 422 4197 [email protected] Pellissier, Bloemfontein 9301Amy Rode 21 Rokewood Ave 082 562 4147 (021) 887 9935 [email protected] Die Boord Stellenbosch 7600Nika Oberholster P.O. Box 539 082 372 7689 [email protected] Jeffreys Bay 6330 CO-OPTED MEMBERS Elna Jooste P.O. Box 349 (011) 954 3626 (011) 954 3626 086 689 7747 [email protected] Paardekraal 1752 SAISI OFFICE Aletta Kietzman P.O. Box 14510 (012) 362 5457 086 651 5438 [email protected] Hatfield 0028 ADVISORY BOARD MEMBERS Prof André Venter P.O. Box 29864 (051) 405 3181 [email protected] Danhof 9310 Dr Lorna Jacklin P.O. Box 269 (011) 481 5192 Glenvista 2058 Dr Jackie Visser P.O. Box 29962 (051) 410 4000 083 263 7199 [email protected] Danhof 9310 Marguerite Monvoisin 33 Saffraan St 082 870 7213 [email protected] Loevenstein Bellville 7530 Suzanne Smith-Roley 15 Songbird Lane (949) 581-1380 (949) 581-1384 [email protected] Aliso Viejo California 92656
SAISI Newsletter Vol 24 no 1 2014.indd 1 2014/03/05 1:04 PM

PORTFOLIOMANAGERS
CONTENTSSAISI NEWSLETTER VOLUME 24 NO 1 2014
4 Editorial Letter
5 Notice Board
6 Liaison News
7 The Vestibular Bilateral Integration Pattern:
A Unique Contribution to Sensory
Integration Theory and Practice
13 Bilateral Integration and Sequencing
Dysfunction: Strategies for Clinical
Reasoning
25 Activity Ideas
30 Book Review
31 CPD Programme Questionnaire
Volume 24 | No 1 | 2014 3
SAISI BOARD
EXCORay Anne Cook Chairperson
Riëtte Smit Vice Chairperson
Ninette Visser Secretary
Marica Botha Treasurer
Janine van der Linde Head of Edcom
Magdaleen Stadler Head of Liaisons
LIAISONSAnneke Kruger Gauteng
Elze Pelser Free State & Northern Cape
Celette Crafford Western Cape
Magdaleen Stadler Eastern Cape
Sally Mackenzie Southern Cape
Gina Rencken KwaZulu Natal
Annamarie van Jaarsveld International Liaison
EDCOMEmmerentia Aldrich Course Facilitator
Stefanie Kruger Theory
Rosa-Marié Olivier SIPT & Clinical Observations
Riëtte Smit Interpretation
Janine van der Linde Protocols
Sally Mackenzie Treatment
Corina Botha Diverse Populations
Marié Greyling Additional Core Courses
OTHERDana Katz Marketing & Ethics
Corina Botha Website
Annamarie van Jaarsveld Universities & Research
Ninette Visser CPD
Rosa-Marié Olivier Newsletter
Amy Rode Website Public Domain
& Newsletter Support
Nika Oberholster Standing Orders, Job Descriptions
& Newsletter Support
Riëtte Smit Policies
Magdaleen Stander SAQA
CO-OPTED MEMBERElna Jooste
ADVERTISING COSTSPRIVATE
3-4 sentences R 360.00
A5 R 496.00
A4 R 870.00
SAISI MEMBERS
3-4 sentences R 225.00
A5 R 385.00
A4 R 605.00
CLOSING DATE
Closing date for contributions to
Newsletter vol 24 no 2 2014 is 23 June 2014.
bilateral integration & sequencing
SAISI Newsletter Vol 24 no 1 2014.indd 2 2014/03/05 1:04 PM

4 Volume 24 | No 1 | 2014
Editor’s Letter
2014 HAS STARTED WITH A “BANG”
... riding on the good momentum from last year. The promised electronic version of the Newsletter is imminent! The whole new face of SAISI in the form of an updated, interactive and cutting-edge website will be launched at the AGM in May this year.
This newsletter continues with the theme of “Back to Basics” and the SIPT diagnostic group of Bilateral Integration & Sequencing gets some well-deserved attention. The latest research, some still in print, is revealed! I trust you will find this letter informative and encouraging.
Thank you for the feedback on the SAISI Newsletter. We have taken your suggestions to heart and will co-ordinate as rhythmically and sequentially as we can.
“Nobody cares how much you know, until they know how much you care.”
– Theodore Roosevelt
AmyCo-editor
SAISI Newsletter Vol 24 no 1 2014.indd 3 2014/03/05 1:04 PM

Volume 24 | No 1 | 2014 5
Notice Board
WEBSITESAISI’s exciting new website will be launched at the AGM in the Western Cape in May!
PROTOCOLSRecord numbers of protocols have been received and SAISI is proud of its hard working members! Holding thumbs for great pass rates!
AGMSAISI is looking forward to another exciting AGM to be held in the Western Cape on 9 May. Venue and topics to be confirmed. Watch your emails for detailed information coming soon. Hope to see you there!
OT WhatsApp conversation:
Printed with permission from South East Rand OT’s.
“homework kills trees, stop this madness”
SAISI Newsletter Vol 24 no 1 2014.indd 4 2014/03/05 1:04 PM

6 Volume 24 | No 1 | 2014
Liaison News
We had a busy and exciting 2013. Our SAISI interest group was well attended by between 10 and 14 OTs. Our meetings were held mostly on Friday mornings from 8h30 to 11h30. We try to organize at least one meeting per term. 2013 was the year to find out more about other therapies
that OT’s use in conjunction with SI. The following topics
were covered that led to very interesting discussions.
Elrie Maree (Occupational Therapist) gave a very
informative talk about Cranio-Sacral therapy as well as
neurological processes involved. Madri Hammond (OT)
gave a presentation about the Tomatis So-Listen therapy.
Kath Megaw (paediatric dietician from Cape Town) gave
a talk about inborn errors of metabolism and later the
year on different diets ( GAPS, KETOGENIC, gluten free)
for different diagnosis e.g. , gut related, ADHD, Autism,
epilepsy, brain tumors, etc.)
Ray Anne Cook presented her talk on ADHD and SI as
well as the update of the SIPT. Unfortunately this was
poorly attended by the OT’s. The OT’s who attended,
enjoyed her presentation. One OT’s feedback was that Ray
Anne must move more! Competition for Ray Anne!
A parent/ teacher evening about the lifespan of ADHD that
Ray Anne presented, was also organized by the liason.
This was well attended (91 parent/teachers). Ray Anne did
a great job as usual and the feedback was that she must
come and do a follow-up in 2014.
Eastern Cape SAISI Interest Group 2013
SAISI Newsletter Vol 24 no 1 2014.indd 5 2014/03/05 1:04 PM

Volume 24 | No 1 | 2014 7
INTRODUCTIONDr. A. Jean Ayres first became interested in the role of the
vestibular system when she was completing post-doctoral
work at the Brain Research Institute at the University of
California at Los Angeles. Having worked with patients
who had frank neurological disorders such as cerebral
palsy and head injuries (Ayres, 1954, 1955a, 1955b,
1957), she was intrigued by the role that the tactile,
proprioceptive and vestibular sensory systems played
in learning, attention and behavior, as well as in social,
emotional, academic and skill development. During this
period in the 1960s, Ayres began to include a set of
measures in her early factor analytic studies that were
related to postural mechanisms, balance, ocular control
and laterality, as well as midline and bilateral integration
(Ayres, 1964, 1965, 1966a, 1966b, 1969). A grouping
of scores was consistently seen, which Ayres called
Disorders in Postural Bilateral Integration, and which she
described as:
“...poorly integrated primitive postural reflexes, immature equilibrium reactions, poor ocular control and deficits in a variety of subtle parameters that are related to the fact that man is a bilateral and symmetrical being. The lack of integration of function of the two sides of the body distinguishes this syndrome. “
(Ayres, 1972b, p.134)
During the 1970’s Ayres began to study the role of the
vestibular system more extensively and, in 1975 published
the Southern California Post Rotary Nystagmus Test
(Ayres, 1975) which allowed her to begin to include this
measure of central processing of vestibular input in her
research. She hypothesized that too little or “depressed”
post rotary nystagmus (PRN) reflected inefficient
processing of vestibular input in the vestibular nuclei of the
brainstem, while too much or “prolonged” PRN reflected
a problem in the typical inhibitory influences from other
neural centers, on this reflex.
In 1979, Ayres revised her description of Postural and
Bilateral Integration Deficit to Vestibular and Bilateral
Integration Deficit. She stated that,
“The symptoms of a vestibular-bilateral disorder are very subtle. These children are often considered completely normal until they enter school and have trouble with reading, arithmetic or other academic work...”
(Ayres, 1979, p. 79)
and she then proceeded to identify the following
Article
A Unique Contribution to Sensory Integration Theory & Practice
By Zoe Mailloux, OTD, OTR/L, FAOTA
THE VESTIBULAR BILATERAL INTEGRATION PATTERN:
SAISI Newsletter Vol 24 no 1 2014.indd 6 2014/03/05 1:04 PM

Article
8 Volume 24 | No 1 | 2014
problems commonly associated with VBI disorder as:
poor eye muscle and postural responses; poor right-left
discrimination; delayed development of laterality and or
trouble crossing the midline, poor spatial orientation and
directionality, trouble with rhythm and bilateral actions and
a tendency to enjoy and seek movement activities without
typical signs of dizziness (Ayres, 1972d, 1979).
During this same period, in addition to conducting
research aimed at further clarification of patterns of
sensory integrative function and dysfunction, Ayres was
also examining the efficacy of the intervention methods
she had developed. In 1972, she published a paper
entitled Improving Academic Scores through Sensory
Integration in which she reported that a group of children
with learning disorders who received occupational therapy
using a sensory integration approach, five days a week
(25-40 minutes a day) for 5-6 months showed significantly
improved scores on the Wide Range Achievement Test
(WRAT) and on the Slosson Oral Reading Test (SORT) in
comparison to a matched group of children who received
equal time of classroom instruction (Ayres, 1972a).
While further studying the variables that would predict
positive educational outcomes, she published a paper
showing that duration of PRN was the best predictor of
change of reading and spelling scores with children who
had -1.1 SD or lower of PRN making greater gains that
those without shortened duration PRN (Ayres, 1978).
This study reflected her increasing understanding of the
role of the vestibular system and its role in academic
performance. In SI and the Child Ayres (1979) states,
“A number of studies in this country, in Australia, and in South America have shown that at least 50 percent of all children with learning or language problems have too short a duration of PRN. These findings suggest that some aspect of vestibular function is very important in meeting the demands of school-work, and this aspect is not functioning adequately in many school children today.” p. 72
This statement likely holds true even many decades later.
The Sensory Integration & Praxis TestsIn January 1989, the Sensory Integration and Praxis Tests
(SIPT) were published, one month after A. Jean Ayres
passed away following her battle with cancer. By the time
she was completing her work on the SIPT, her research
and clinical experience had reinforced that both depressed
and prolonged PRN were commonly seen in children with
learning and other developmental disorders. However, it
was also clear that these findings reflected different types
of sensory integrative problems. Because both high and
low PRN scores often existed in clinical populations, mean
PRN scores often “averaged” and appeared similar to the
mean scores of typically developing children. Therefore,
the SCPNT score did not load with other measures of
vestibular, postural and bilateral functions in the studies
through the 1970s and 1980s.
By the time Ayres had decided to revise the SCSIT
and SCPNT into the SIPT, she was keenly aware of
the increased standards in biostatistics. She hoped to
avoid the criticism of her work that would be likely should
she continue to include non-standardized measures of
vestibular-related postural and ocular mechanisms (e.g.
assumption of a prone extension position, eye tracking,
etc.) similar to the ones that she had previously used in
her studies. Instead, she relied solely on the carefully
designed tests of the SIPT, with their highly discriminative
items. The factor analyses that were conducted as part
of the development of the SIPT revealed a pattern that
was similar to the previously identified Vestibular Bilateral
Integration Disorder. However, without the presence of the
postural/ocular observation and with PRN not loading on
this pattern (most likely due to the issue of both low and
high PRN being present in the sample), she hesitated to
highlight the hypothesized vestibular nature of this pattern.
With several of the new tests loading on this pattern having
both a sequential element, as well as bilateral features,
(e.g. Sequencing Praxis, Oral Praxis and Manual Form
Perception), Ayres called this pattern Bilateral Integration
and Sequencing Deficit. In a discussion of bilateral
integration deficits in the SIPT manual, Ayres notes that
her clinical experience had suggested that short duration
of PRN was often associated with the BIS pattern
(Ayres, 1989).
SAISI Newsletter Vol 24 no 1 2014.indd 7 2014/03/05 1:04 PM

Volume 24 | No 1 | 2014 9
For the factor analyses that Ayres conducted with data
from the SIPT, she examined the loadings in a variety
of samples in order to select patterns that were seen
consistently. Some patterns, such as Visuopraxis and
Somatorpraxis emerged in both samples of typically
developing children, as well as in mixed samples and
samples of only children with identified difficulties.
This finding led Ayres to hypothesize that visual and visual
practic functions, as well as tactile and somatopractic
functions were associated in typical development as well
as in patterns of dysfunction. She also noted, however, that
the linking of tests measuring bilateral integration, balance
and sequencing formed a pattern that was only evident in
a sample of children with identified difficulties. Therefore,
she did not believe that vestibular based inefficiencies
that were hypothesized to underlie the PBI, VBI and
BIS pattern would be present in any stage of typical
development.
The presentation of the BIS pattern in Sensory Integration
Theory and Practice (Fisher, & Murray, 1991; Bundy &
Murray, Lane 2002) as a milder form of dyspraxia led to
some debate among experts in sensory integration, as
well as some confusion for clinicians. Ayres considered
the various iteration of the bilateral integration pattern
(first Postural Bilateral Integration (PBI), then Vestibular
Bilateral Integration (VBI) and finally Bilateral Integration
and Sequencing (BIS) reflective of a pattern of sensory
integrative dysfunction that was characterized by the
discreet vestibular based signs with the absence of more
significant tactile or praxis deficits seen in patterns such
as Somatodyspraxia. Mulligan found similar loadings of
bilateral and sequencing tests, without associations with
the core tactile and praxis tests in her subsequent research
(1998; 2000).
Current ResearchWith many decades of research demonstrating consistent
patterns of sensory integrative function and dysfunction,
the need for continued study of these groupings was not
evident. However, Davies and Tucker (2010), in a review
of types of sensory integrative problems chose to restrict
their analysis to papers published in 1998 or later.
This choice led to exclusion of all of Ayres’ research on
sensory integrative patterns. At the same time, there was
continued interest in managing the issue of the existence
of both depressed and prolonged PRN in samples.
In 2011, we published a study involving retrospective
chart review and analysis of 273 children, aged 4 to 9
years (Mailloux, et al., 2011). The sample in this study
consisted mostly of children who came for evaluation at
private practices and had not been identified through usual
medical or educational diagnostic routes. In fact, most
subjects in the sample (N=214, 78.4%) had no diagnosis
on file. While methods for statistically managing both high
and low PRN were being explored, it was noted that very
few subjects in this sample had high or prolonged PRN
(23 subjects or 8.4%). The lack of many children with
prolonged PRN resulted in a range of scores on this test
that was more similar to the other tests (i.e. average or
low scores but few high scores in a sample of children
with probable sensory integrative concerns). The patterns
that were found in this study did, in fact, include a similar
pattern to the BIS pattern found by Ayres (1989) and
Mulligan (1998) but with the added loading of the PRN
test. In addition, the Motor Accuracy Test also had a
significant loading on this pattern, hypothesized to reflect
the coordination of eye-head and hand movements, as
well as the ability to cross the body midline. We called this
pattern Vestibular Bilateral Integration and Sequencing
(VBIS). Thus, these findings reinforced a long-held view of
the significance of low PRN scores and validated Ayres’
(1989) theoretical assumption that bilateral integration
problems and other signs of vestibular inefficiencies are
associated with a shortened duration of PRN.
More recently, other studies have examined the use of
the PRN test, as well as further consideration of the
Vestibular Bilateral Integration and Sequencing pattern.
Consideration of the possibility that the PRN test might
be applied with children younger than the current norms
which start at four years, was spurred by the observation
that the age trend on this test (reported in the SIPT
manual) was flat from age 4years 0 months to 8 years 11
months. That is, in comparison to all the other tests of the
SIPT, the mean score for PRN did not change over this
age range. In order to test this, an adapted administration
was developed in which children were held in place in
an adult’s lap, while sitting on the nystagmus board for
The Vestibular Bilateral Integration Pattern: A Unique Contribution to Sensory Integration Theory & Practice
SAISI Newsletter Vol 24 no 1 2014.indd 8 2014/03/05 1:04 PM

Article
10 Volume 24 | No 1 | 2014
testing. Since there were no significant differences in the
PRN reflex in the standard versus held administrations, it
was determined that this method of testing would be valid.
Then, children aged 2 to 47 months were tested with
the adapted procedures. Since the mean scores for the
children under age 4 was not significantly different from
the mean scores published for 5 year olds in the SCPNT
manual, it was determined that this test can be used for
infants and toddlers with comparison to the SIPT 4 year
old norms (Mailloux, et al., in press).
Additional consideration of the Vestibular Bilateral and
Sequencing pattern also continues. Mulligan (2010)
reported that, “children with low-duration PRN scored
more poorly than children with average or prolonged
PRN on other SIPT tests measuring aspects of vestibular
function...” and she suggested that her results contribute
to “evidence supporting the PRN test’s valid¬ity as a
measure of some aspects of vestibular functioning” p 97).
In addition, Koester, et al. (in press) examined performance
on the SIPT in a sample of children with cochlear implants
and found a significant presence of the Vestibular Bilateral
Integration and Sequencing pattern in their sample.
Clinical Implications An understanding of the Vestibular Bilateral Integration and
Sequencing pattern is essential for occupational therapists
who work with children. This constellation of difficulties
is common among children referred for assessment of
sensory integrative concerns. For example, in our 2011
study, 98 children (over 38%) had shortened duration
PRN. The fact that most of these children did not have
any other diagnosis (nearly 80%) suggests that they were
not likely to have been identified for receiving services,
prior to their occupational therapy assessment of sensory
integration.
Characteristics of the Vestibular Bilateral Integration PatternThe research on constellations of sensory integration
function and dysfunction, as well as clinical experience,
suggests the following common signs that a vestibular
bilateral integration problem may be present:
• Shortened duration PRN
• Low muscle tone
• Difficulties in positions requiring extension, such as
assuming and maintaining a prone extension posture,
holding the head and upper body upright while sitting
for extended periods (such as at school).
• Poor ocular control
• Difficulty with righting or equilibrium reactions
• Inadequate balance or over dependence and on vision
for assuming and maintaining balance
• Delayed or lack of well-established laterality
• Difficulty or hesitancy in tasks involving crossing the
body midline
• Trouble with directionality or spatial orientation
• Poor bilateral integration, noted in observations and/or
test scores
• Difficulty with regulating state of arousal that seems
especially related to opportunities for movement
• A tendency to seek and enjoy large amounts of motion
without typical signs of dizziness
• The above signs are present in the absence of broader
signs of dyspraxia and somatosensory dysfunction.
If the above signs exist alongside other signs of
somatosensory and practic dysfunction, then these
vestibular bilateral signs are considered part of a
broader somatodyspraxia pattern.
Assessment of Vestibular Bilateral Integration FunctionsThe SIPT provide strong ability to identify the Vestibular
Bilateral Integration pattern and to discriminate this
pattern from other common patterns of sensory
integrative dysfunction. Structured and unstructured
observations of the child, as well as caregiver interviews
and questionnaires also help to identify this pattern. The
strongest indicators of the presence of the Vestibular
Bilateral Integration pattern include:
Below average scores on the following standardized tests
of the SIPT:
SAISI Newsletter Vol 24 no 1 2014.indd 9 2014/03/05 1:04 PM

Volume 24 | No 1 | 2014 11
• Postrotary Nsytagmus (PRN)
• Standing and Walking Balance (SWB)
• Bilateral Motor Coordination (BMC)
• Sequencing Praxis (SPr)
• Oral Praxis (OPr)
• Graphesthesia (GRA) and/or Manual Form
Perception (MFP)
• Motor Accuracy (MAc)
Other standardized tests of balance (such as on
developmental tests) or bilateral coordination (such as on
the Bruininks-Oseretsky (BOT)-2, Bruininks & Bruininks,
2005) may also assist in identifying this pattern.
The following observed or reported behaviors may also be
indicators:
• Poor ability to assume or maintain a prone extension
posture for age
• Difficulty with co-ordination of head and eye movements
• Tendency to lose balance or to lack age appropriate
righting and equilibrium reactions
• Trouble learning or performing upper extremity bilateral
tasks such as cutting, folding or tying or with full body
bilateral actions such as pedaling and steering a bicycle,
swimming or completing jumping jacks
• Right-left confusion; delayed or inconsistent
development of handedness; trouble with directionality
in forming letters or in navigating through space
• Lack of dizziness after activities that involve rotary or
orbital motion
Intervention for Problems in Vestibular Bilateral Integration
Children who have been identified with vestibular bilateral
integration problems will benefit from individually tailored
intervention which provides opportunities for active, self-
directed engagement movement activities. Specialized,
suspended equipment that provides motion in all planes
and that can be self-propelled is essential. For example,
net or Spandex swings in which a children can lie
prone and propel themselves with their hands on a mat;
“helicopter” or stirrup type swings in which children can
sit and run to launch themselves into orbital motion; or
tire swings on which children can sit or lie and activate
both linear and rotary movement are all excellent ways
for a child to participate in vestibular based therapeutic
activities. As with all forms of ASI intervention, it is critical
that the core principles of this approach are present,
including employing a purposeful, playful and self-directed
atmosphere where equipment is arranged in a safe way
that provides a just-right challenge with opportunities for
adaptive responses.
ConclusionAs noted by Ayres and others, the presence of vestibular
based problems in children with learning difficulties may be
as high as 50%. Given the likely prevalence of vestibular
based difficulties in children who are struggling in school
or in other aspects of childhood occupation, awareness
and understanding of the vestibular bilateral integration
pattern are important considerations for occupational
therapists assessing and treating sensory integration
concerns.
REFERENCES:
Ayres, A. J. (1954). Ontogenetic principles in the development
of arm and hand functions. American Journal of Occupational
Therapy, 8, 95-99.
Ayres, A. J. (1955a). Proprioceptive facilitation elicited through
the upper extremities. American Journal of Occupational Therapy,
9, 1-9, 57-58, 121-126.
Ayres, A. J. (1955b). A pilot study on the relationship between
work habits and workshop production. American Journal of
Occupational Therapy, 9, 264-276.
Ayres, A. J. (1957). A study of the manual dexterity and workshop
wages of thirty-nine cerebral palsied trainees. American Journal of
Physical Medicine, 36, 6-10.
Ayres, A.J. (1964). Tactile functions: Their relation to hyperactive
and perceptual motor behavior. American Journal of Occupational
Therapy, 18 (1), 6-11.
Ayres, A.J. (1965). Patterns of perceptual-motor dysfunction in
children: A factor analytic study. Perceptual and Motor Skills, 20,
335-368.
Ayres, A.J. (1966a). Interrelations among perceptual-motor
The Vestibular Bilateral Integration Pattern: A Unique Contribution to Sensory Integration Theory & Practice
SAISI Newsletter Vol 24 no 1 2014.indd 10 2014/03/05 1:04 PM

12 Volume 24 | No 1 | 2014
The Vestibular Bilateral Integration Pattern: A Unique Contribution to Sensory Integration Theory & Practice
abilities in a group of normal children. American Journal of
Occupational Therapy, 20 (6), 288-292.
Ayres, A.J. (1966b). Interrelationships among perceptual-motor
functions in children. American Journal of Occupational Therapy,
20 (2), 68-71.
Ayres, A.J. (1969). Deficits in sensory integration in educationally
handicapped children. Journal of Learning Disabilities, 2 (3), 44-
52.
Ayres, A.J. (1971). Characteristics of types of sensory integrative
dysfunction. American Journal of Occupational Therapy, 25 (7),
329-334.
Ayres, A.J. (1972a). Improving academic scores through sensory
integration. Journal of Learning Disabilities, 5, 338-343.
Ayres, A.J. (1972b). Sensory Integration and Learning Disorders.
Los Angeles: Western
Psychological Services.
Ayres, A.J. (1972c). Southern California Sensory Integration Test
Manual. Los Angeles: Western Psychological Services.
Ayres, A.J. (1972d). Types of sensory integrative dysfunction
among disabled learners. American Journal of Occupational
Therapy, 26 (1), 13-18.
Ayres, A.J. (1975). Southern California Post Rotary Nystagmus
Test Manual. Los Angeles: Western Psychological Services.
Ayres, A.J. (1977). Cluster analyses of measures of sensory
integration. American Journal of Occupational Therapy, 31 (6),
362-366.
Ayres, A.J. (1978). Learning disabilities and the vestibular system.
American Journal of Occupational Therapy, 11 (1), 150-161.
Ayres, A.J. (1979). Sensory Integration and the Child. Los
Angeles: Western
Psychological Services.
Ayres, A.J. (1989). Sensory Integration and Praxis Tests manual.
Los Angeles: Western
Psychological Services.
Bruininks, R.H. & Bruininks, B. D. (2005). Bruininks-Oseretsky
Test of Motor Proficiency, Second Edition (BOT™-2). San
Antonio, TX: Pearson
Bundy, A.C. & Murray, B. (2002). Sensory integration: A. Jean
Ayres theory revisited. In A. C. Bundy, S. J. Lane & E. A. Murray
(Eds). Sensory Integration Theory and Practice. Philadelphia, PA:
F.A. Davis
Carrasco Koester, A., Mailloux, Z., Baltazar Mori, A., Geppert
Coleman, G., Muhs, J., Blanche, E.I., ... & Cermak, S. (in press).
Sensory integration considerations for children with cochlear
implants. American Journal of Occupational Therapy.
Davies, P. L., & Tucker, R. (2010). Evidence review to investigate
the support for subtypes of children with difficulty processing and
integrating sensory information. American Journal of Occupational
Therapy, 64, 391–402.
Fisher, A. G. & Murray, E. A. (1991). Introduction to sensory
integration theory. In In A. G. Fisher, E. A. Murray & A. C. Bundy
(Eds). Sensory Integration Theory and Practice. Philadelphia, PA:
F.A. Davis
Mailloux, Z. Leao, M, Sochting, E., Baltazar Mori, A., Smith
Roley, S., Becera, T..., & Cermak, S, (in press) Modification of
the Postrotary Nystagmus Test for Evaluating Young Children.
American Journal of Occupational Therapy.
Mailloux, Z., Mulligan, S., Smith Roley, S., Blanche, E., Cermak, S.,
Coleman, G., ...& Lane, C. (2011) Verification and Clarification of
Patterns of Sensory Integrative Dysfunction. American Journal of
Occupational Therapy.65 (2). 143-151
Mulligan, S. (1998). Patterns of sensory integration dysfunction:
A confirmatory factor analysis. American Journal of Occupational
Therapy, 52, 819-828.
Mulligan, S. (2000). Cluster analysis of scores of children on
the Sensory Integration and Praxis Tests. Occupational Therapy
Journal of Research, 20(4), 256-270.
Mulligan, S. (2010). Validity of the Postrotary Nystagmus Test for
measuring vestibular function. OTJR: Occupation, participation,
and health, 31(2), 97-104.
SAISI Newsletter Vol 24 no 1 2014.indd 11 2014/03/05 1:04 PM

Volume 24 | No 1 | 2014 13
Spandex swings in which a child can lie prone and propel themselves with their hands on a mat; “helicopter” or stirrup type swings in which children can sit and run to launch themselves into orbital motion; or tire swings on which children can sit or lie and activate both linear and rotary movement are all excellent ways for a child to participate in vestibular based therapeutic activities.
SAISI Newsletter Vol 24 no 1 2014.indd 12 2014/03/05 1:04 PM

INTRODUCTION TO CASE
A little girl G is 6 years 11 months and was referred to the
Occupational therapist with the following difficulties:
STRENGTHS
Loving and helpful
Tells stories to others
Developmental milestones within norm
ADL TASKS
She is finding it difficult to eat with a knife and fork
Experience difficulties with fasteners
SCHOOL TASKS
She still confuses left and right
During writing tasks she swaps hands
Poor cutting skills
Rushes work
PLAY ACTIVITIES
Clumsy on the playground
Bump into things
BEHAVIOUR
Seeks attention and easily frustrated
Language skills good, but maths weaker
Poor task endurance and concentration
Emotional
Strategies for Clinical Reasoning
By Janine van der Linde, M.Sc. OT (Wits)
BILATERAL INTEGRATION AND SEQUENCING DYSFUNCTION:
Article
14 Volume 24 | No 1 | 2014
SAISI Newsletter Vol 24 no 1 2014.indd 13 2014/03/05 1:04 PM

Volume 24 | No 1 | 2014 15
Bilateral Integration and Sequencing Dysfunction:Strategies for Clinical Reasoning
Results of the SIPT test
CLINICAL OBSERVATIONS: Observations only include those that obtained a score of 2 or less.
Slow movements: Sec: 8 2 Coordination and rhythm poor, better out, then drop arms and fast back.
Diadokokinesia Movements stiff loses sequence.
Right (_7_times) 2
Left (_6_times) 1 Floppy.
Both (_3_times) 1 Deliberate, moves feet with hands, loose sequence ++
Thumb-Finger touching
Right 2 Finger opposition fair, effort ++ deliberate touching, looks.
Left 2
Both 1 Separate left and right, loses place of fingers.
Co-contraction
Upper limbs 2 Uses whole body, fixes shoulders, holds onto table very strong.
Neck 2
Prone extension: sec: 8 1 Effort to hold. Assumes well.
Supine flexion posture sec: 18 2 Neck tired a bit.
Schilder’s arm extension test
Involuntary movements 1 Can’t stand still with eyes closed, body sways ++++
Postural changes 1 Arms and feet move. Fixes shoulder girdle, difficult to keep arms up.
Trunk rotation 1 Arms move with head.
Hyperactivity 1
Tactile defensiveness 2 Slight and orally sensitive also.
Postural background movements 2 Slightly excessive.
left ... or right?
SAISI Newsletter Vol 24 no 1 2014.indd 14 2014/03/05 1:04 PM

The Occupational therapist (OT) hypothesizes that the
child may have a Bilateral Integration and Sequencing
dysfunction (BIS).
In studying the SIPT results and looking at the clinical
observations the therapist will be able to gain more
information on the child’s functioning and will be able to
confirm or refute this diagnosis.
The SIPT was developed as a diagnostic and descriptive
tool to assess praxis and the sensory processing of the
different senses and how these difficulties manifest in
behavioural issues (Ayres, 2004, Asher et al., 2008).
It is currently the golden standard in the testing of sensory
integration function, as it was found to have the ability to
discriminate between children with learning disabilities and
the typical population and proved to be very reliable and
valid (Asher et al., 2008).
Using the SIPT requires specialist training and a
good understanding of sensory integration and
the neurobiological background, as well as a good
understanding of the tests and subtests.
In a study by Asher and Parham (2008) on the inter-rated
validity of the SIPT they emphasised that the ability to
make a reliable diagnosis was related to prior training in
using the assessment tool and in using specific strategies
in decision making for a final diagnosis (Asher et al., 2008).
This article will look at a step by step approach/strategies
in determining the final pattern of SI dysfunction taking into
account all the information from the assessments.
GROSS MOTOR: Scoring out of 5
Kneel, wal, forward / 4 Fast, but OK.
backward 2 Sways +++ poor hip extension. Fair.
Galloping 4 Rhythm and jerky, a bit poor. Taught.
Skipping 4 Rhythm and jerky, a bit poor. Taught.
Ipsilateral leg slap 3 Bilateral motor fair but co-ordination jerky.
Contralateral leg slap 1 Can’t, with teaching improved, but difficult to sustain.
Star jump 5 Taught.
Stride jump 1 Cant jump side to side.
Long jump 5 Good take off and land.
Hopping R 4 Left weaker. Effort to do it.
L 2
Jump hop sequence 2 2 seq. correct, can’t sustain movement pattern.
Bounce a ball 5 Good.
Throwing 4 Fair.
Catching 4 Fair.
Article
16 Volume 24 | No 1 | 2014
SAISI Newsletter Vol 24 no 1 2014.indd 15 2014/03/05 1:04 PM

STEP 1: LOOK AT THE SIPT BAR GRAPH TO DETERMINE THE PROBLEM AREASSee bar graph in case background
A study by van Jaarsveld (2012) investigated whether the SIPT is appropriate for use with the South African population.
This study showed that 12 of the 17 tests compare well against the normative US sample, but found that South African
children within the age band 6y 0m – 8y 11m performed significantly better on Design copying, Oral Praxis, Bilateral motor
co-ordination, Standing and walking balance and Motor co-ordination than the US sample. These five tests therefore needs
to be adapted with ½ a standard deviation unit to the negative side when interpreting the SIPT scores of local children (Van
Jaarsveld et al., 2012).
As G falls within this age band (6 years 11 months) the scores needs to be adapted according to the recommendations
made by van Jaarsveld.
STEP 2: ADAPT DC, OPr, BMC, SWB & MAC scores with 0.5 SD to the negative side
Bilateral Integration and Sequencing Dysfunction:Strategies for Clinical Reasoning
Volume 24 | No 1 | 2014 17
Space Visualization -1.63 Figure-Ground Perc 0.79 Man. Form Perception -1.42
Kinethesia N/A Finger Identification 0.45 Graphethesia -0.16 Loc. Tactile Stimuli 1.24 Praxis Verb. Command -0.25 Design Copying -1.92
Constructional Praxis -0.90 Postural Praxis 0.74 Oral Praxis -1.98 Sequencing Praxis -1.56 Bilateral Motor Co-ord -1.59
Stand & Walk Balance -1.93 Motor Accuracy -1.91 Postrotary Nystagmus -1.55
SD LOW AVERAGE HIGH-3 -2 -1 0 -1 -2 -3
Percentile
0.5 1 5 10 25 50 75 90 95 99 99.5
SAISI Newsletter Vol 24 no 1 2014.indd 16 2014/03/05 1:04 PM

STEP 3: FIND ALL THE TEST SCORES BELOW -1.0 SD
After adapting the scores look at all the subtests to determine the scores falling below -1.0SD.
In this specific case the following scores were found to be low:
SV -1.64 OPr -1.98 SWB -1.93 SVCU -1.37
MFP -1.42 SPr -1.56 MAC -1.91 PHU -2.84
DC -1.92 BMC -1.59 PRN -1.55
These results then lead to two questions: What does low scores in these subtests mean?
How do these scores fit in with the patterns of SI dysfunction?
STEP 4: DETERMINE IF THE SCORES FIT WITH PATTERN OF SI DYSFUNCTION
Over the years various factor analysis and cluster analysis were done to determine sensory integration patterns. It is of value
to understand how this evolved as this helps to understand the current patterns that are found.
The discussion will mostly focus on the bilateral integration and sequencing dysfunction patterns.
Various studies by Ayres, Fisher, Bundy, Mulligan and Mailloux et.al tried to determine and verify the different patterns of
sensory integration (Ayres, 2004, Fisher et al., 1991, Mulligan, 1998, Bundy et al., 2002, Mailloux and Parham, Mailloux et
al., 2011). Bilateral Integration and Sequencing deficits (BIS) were consistently identified as one of the patterns seen with
the results of the SIPT test.
Initially it was Ayres who found that BIS was linked to a postural ocular movement disorder (Ayres, 2004). Ayres described
bilateral integration and sequencing as a dysfunction that include poor postural abilities, decreased muscle tone and
decreased bilateral motor coordination. She considered it to be a type of motor coordination disorder and associated it
with vestibular functions although she did not necessarily consider it a dyspraxia. In a factor analyses by Ayres in 1989 the
following tests indicated a bilateral integration and sequencing pattern (Ayres, 2004).
The low scores on the following tests indicated a BIS dysfunction:
OPr SPr GRA BMC SWB MFP
Fisher (1991) then further investigated bilateral integration in terms of the influence of motor control and motor learning
theories on motor and cognitive components of movement (Fisher et al., 1991). She used motor learning theories to look
at the relationship between vestibular and proprioceptive systems in praxis. This discussion brought forward terms such as
feed-forward and feedback and hypothesized that postural control, ocular motor control and projected action sequences
accompanied by BIS can result in praxis deficits (Fisher et al., 1991).
Article
18 Volume 24 | No 1 | 2014
SAISI Newsletter Vol 24 no 1 2014.indd 17 2014/03/05 1:04 PM

In a large study by Mulligan (1998) factor and cluster analysis found similar patters namely: Bilateral Integration and
Sequencing, Somatosensory, Visuo-praxis and Dyspraxia (Mulligan, 1998). She found an overarching pattern of general
SI problems and recommended that these patterns should rather be seen as having a general practice dysfunction with a
weakness in a specific area e.g. bilateral integration. Further recommendations in this study also looked at the influence of
specific subtests that are weak in terms of retest reliability (Mulligan, 1998).
The following subtest were said to indicate a pattern of BIS (Mulligan, 1998)
OPr SPr GRA BMC SWB KIN
Bundy et.al (2002 p6) introduced the view of BIS as a practice disorder(Bundy et al., 2002). They still associated BIS
with difficulties in vestibular and proprioceptive input, but also viewed BIS as a practice disorder, but less severe than
somatodyspraxia.(Bundy et al., 2002).
In the latest research by Mailloux et al (2011) they found similar patterns, but described that a dysfunction of Vestibular and
Proprioceptive Bilateral Integration and Sequencing has emerged. No evidence of underlying practice difficulties was found
in this analysis for BIS. (Mailloux et al., 2011)
The factor and cluster analysis found a Vestibular and Proprioceptive Bilateral Integration and sequencing pattern that
showed high loadings on the following subtest:
- Oral Praxis (OPR)
- Standing walking balance (SWB)
- Post rotary Nystagmus (PRN)
- Bilateral motor coordination (BMC)
- Motor Accuracy (MAC)
OLD PATTERNS NEW PATTERN EMERGED (Mailloux et al., 2011)
↓ Opr score OPr score
↓ SPr score SPr score
↓ BMC score ↓ BMC score
↓ GRA score SWB score
↓ PPr may be low PRN score
MAC score
↓ KIN score
↓ SVCU score SVCU score
A new finding was the fact that MAC clusters with this group. This test reflects eye hand coordination in a variety of
postures and positions and integration of two sides of the body. Mailloux, et al., (2011, p. 148) found that it “reflect the
vestibular and bilateral functions needed for the coordination of eye, head, and hand movements; postural adjustments; and
crossing of body midline needed in this test.” (Mailloux et al., 2011). KIN only loaded modestly with this group, reflecting the
proprioceptive involvement in the BIS dysfunction. (Mailloux et al., 2011)
Bilateral Integration and Sequencing Dysfunction:Strategies for Clinical Reasoning
Volume 24 | No 1 | 2014 19
SAISI Newsletter Vol 24 no 1 2014.indd 18 2014/03/05 1:04 PM

This study confirmed Ayres view that a shortened PRN can be linked with bilateral integration problems and vestibular
difficulties; however, the recent study did not find an association between measures of directionality, crossing midline and
laterality with this pattern of dysfunction. (Ayres, 2004, Mailloux et al., 2011)
If you then compare all the scores found on the SIPT the case will look like this.
Visuopraxis Visual VBIS Somatopraxis Praxis Perception on Verbal difficulties command
SV -1.63 Form and Space BMC -1.59 High Loadings PrVC Low -0.25
MFP -1.42 SV -1.63 SPr -1.56 PPr 0.74 PRN - 1.55
DC -1.92 FG 0.79 Opr -1.98 OPr -1.98 (Need average to high)
CPr -0.90 SWB -1.93 SPr -1.56 Poor Sequence
FG 0.79 Visual Praxis PRN -1.55 BMC -1.59 Possible Low
DC -1.92 MAC -1.93 GRA -0.16 Scores
CPR -0.90 GRA -0.16 Strong Indicator BMC -1.59
MAC -1.92 Moderate Link SPr -1.56
KIN : Not tested Lower Loadings Opr -1.98
Haptic Form SVCU -1.37 PrVC -0.25 SWB -1.93
↓ and Space PHU -2.84 CPr -0.90 DC -1.92
MFP -1.42 SWB -1.93
GRA -0.16 FI 0.45
↓
The SIPT test scores indicate that the child has bilateral integration and sequencing dysfunction. These scores showed
the involvement of the vestibular in the low PRN score, but observations made in clinical observations can add further
confirmation.
STEP 5: CLINICAL OBSERVATIONS
Looking at the unstructured clinical observations it is necessary to look for evidence that support difficulties in vestibular
processing, proprioceptive processing and bilateral integration and sequencing difficulties.
Vestibular processing
Some vestibular processing difficulties can be seen in vestibular ocular responses and postural control. Vestibular ocular
responses include stabilization of eyes and head during movement, coordination of head and eye movements with neck
and body stabilization and gaze stabilization during movement (Smith Roley et al., 2001). Vestibular influences on postural
control include postural tone (especially extensor muscle tone) and balance reactions. It contributes to the child’s awareness
Article
20 Volume 24 | No 1 | 2014
SAISI Newsletter Vol 24 no 1 2014.indd 19 2014/03/05 1:04 PM

of his body position and movement through space, and to a child’s ability to stabilize the eyes when the head is moving
(Smith Roley et al., 2001).
Trunk stability is also associated with bilateral integration as the trunk needs to be stable to assist limbs to dissociate from
the trunk when moving.
It is also important to look at eye movements, postural tone, and equilibrium reactions, righting reactions, protective
extension and dissociation between head and body. The ability to assume and maintain a totally extended posture against
gravity is hypothesized to require adequate processing of gravity information via the vestibular nuclei (Fisher et al., 1991).
Flexing the neck in the supine flexion position the vestibular-proprioceptive system facilitates righting of the head and upper
trunk. Postural background movements can also be an indication of difficulties with vestibular processing and is closely
related to muscle tone, residual activity of primitive reflexes, equilibrium reactions and proximal stability.
Proprioceptive processing
The discriminative function of proprioception is the basis of body scheme and plays a role in the spatial orientation of our
bodies or body parts in space, the rate and timing of our movements, how much force our muscles are exerting, postural
control (including muscle tone) and produces co-ordinated movements.
Difficulties in proprioceptive can be seen in the following clinical observations: TFT (look at how hard the child presses, uses
excessive vision), Finger nose test (inaccuracy of movements, needs to use vision), Schilder’s Arm Extension (want to
open eyes, spoon or fix in hands). Decreased awareness of position of limbs) and Slow movements (unaware of position of
arms and grading of movement is poor (Blanche et al., 2012).
Other unstructured observations may include postural control mechanisms i.e. tone, grading of force, speed and timing of
movements e.g. during ball games or tension in the pencil grip, pressure exerted on the pencil when drawing (Blanche et al.,
2012).
Bilateral integration
Children with bilateral integration and sequencing difficulties may experience difficulties with crossing of the midline, left/
right discrimination, difficulty in sustaining the movement pattern sequence, cutting with scissors, eating with knife and
fork, shoelaces/buttons/fasteners. In the clinical observations test you can look at the DDK and TFT test and the difference
between left, right or when doing it with both hands together. Ayres proposed that the ability to cross the midline of the body
is an indication of how well both sides of the body have become integrated (Blanche et al., 2012).
Projected action sequences also plays a role in bilateral integration and sequencing as it requires the ability to plan
movements in response to changing events in the environment (Bundy et al., 2002). Catching a bounced ball and jumping
into a series of squares placed on the floor are examples of this as it requires the child to control their movements before
they can move in relation to the environment (Fisher et al., 1991). This movement is built on an internal model of the world
and dependent on previous experiences (feed-forward). Feed-forward is used to detect wrong patterns in movement
before the actual movement is started. It is therefore associated with the planning and execution of bilateral motor action
sequences (Fisher et al., 1991).
Bilateral Integration and Sequencing Dysfunction:Strategies for Clinical Reasoning
Volume 24 | No 1 | 2014 21
SAISI Newsletter Vol 24 no 1 2014.indd 20 2014/03/05 1:04 PM
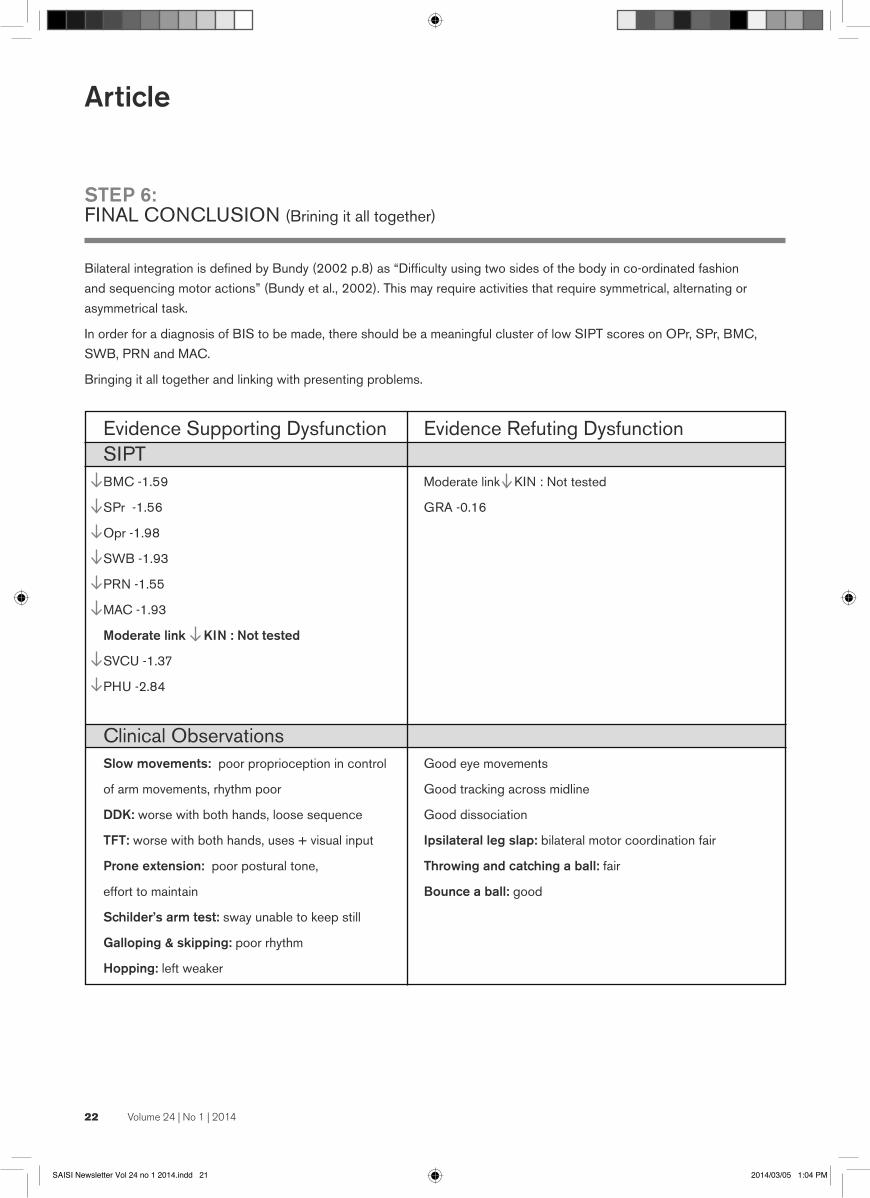
STEP 6: FINAL CONCLUSION (Brining it all together)
Bilateral integration is defined by Bundy (2002 p.8) as “Difficulty using two sides of the body in co-ordinated fashion
and sequencing motor actions” (Bundy et al., 2002). This may require activities that require symmetrical, alternating or
asymmetrical task.
In order for a diagnosis of BIS to be made, there should be a meaningful cluster of low SIPT scores on OPr, SPr, BMC,
SWB, PRN and MAC.
Bringing it all together and linking with presenting problems.
Evidence Supporting Dysfunction Evidence Refuting Dysfunction SIPT
↓ BMC -1.59 Moderate link KIN : Not tested
↓ SPr -1.56 GRA -0.16
↓ Opr -1.98
↓ SWB -1.93
↓ PRN -1.55
↓ MAC -1.93
Moderate link KIN : Not tested
SVCU -1.37
↓ PHU -2.84
Clinical Observations
Slow movements: poor proprioception in control Good eye movements
of arm movements, rhythm poor Good tracking across midline
DDK: worse with both hands, loose sequence Good dissociation
TFT: worse with both hands, uses + visual input Ipsilateral leg slap: bilateral motor coordination fair
Prone extension: poor postural tone, Throwing and catching a ball: fair
effort to maintain Bounce a ball: good
Schilder’s arm test: sway unable to keep still
Galloping & skipping: poor rhythm
Hopping: left weaker
Article
22 Volume 24 | No 1 | 2014
SAISI Newsletter Vol 24 no 1 2014.indd 21 2014/03/05 1:04 PM

Presenting problems
Difficulty to eat with a knife and form Loving and helpful
Difficulties with fasteners Language skills good but maths weaker ???
Confuses left and right.
Poor coordination with left and right
Poor cutting skills
Clumsy on playground
Bump into things
During writing tasks she swaps hands
Difficulties with vestibular processing can be seen in the scores obtained for PRN (-1.55) and SWB (-1.93), as well as in
observations made such as being clumsy and bumping into things.
SWB and PRN performance reflects vestibule-proprioceptive processing and the vestibular-proprioceptive system is linked
with BIS, it could thus have an influence on BIS (Ayres, 2004). Mailloux et.al 2011 indicated that a low PRN is indicative
of hypo responsiveness to vestibular input and proof that bilateral integration problems are associated with vestibular
insufficiencies (Mailloux et al., 2011). G is clumsy and bumps into things at school. The low scores on these items could
give an explanation for these observations as poor vestibular processing plays a role in postural control and balance (Smith
Roley et al., 2001).
G still confuses left and right and tends to swap hands when crossing the midline. Literature confirms that a child with
under-reactive vestibular responses often has poor integration of the two sides of the body. The child often fails to develop a
skilled hand dominance or preference and avoid crossing the midline of the body (Smith Roley et al., 2001).
Difficulties in eating with a knife and fork, dressing (doing fasteners) and organising her movements in space may be as a
result of poor body scheme and proprioception. G was also observed to experience difficulties with grading force and speed
of movements. These functional difficulties would thus support a hypothesis of dysfunction of the proprioceptive system.
G found some tasks that required bilateral projected action sequences such as star jumps, ipsilateral stride jump and
jumping sequences, hard to execute with good coordination. She was able to jump with both feet into consecutive squares
but was unable to perform it accurately and in a smooth and rhythmic manner, indicating a problem with projected action
sequences. She did however do well with timing the catching and throwing of a ball.
G had difficulty with both the pattern and rhythm when performing DDK and TFT and the execution of these tasks bilaterally
decreased. She also relied on her vision and used a lot of pressure to provide feedback during the activities.
A low score (-1.56) on the SPr test can be an indication of difficulties with sequencing, as the task requires the ability to
complete a series of hand and finger movements (Ayres, 2004). Other difficulties with sequencing could be observed in the
DDK and TFT tests and in the execution of the gross motor tasks.
Difficulty with BIS will have an influence on hopping, skipping, jumping, star jumps as well as symmetrical and reciprocal
stride jumping (Murray-Slutsky and Paris, 2000). G experienced difficulty in executing these tasks.
Further confirmation of the difficulties with BIS is in the low score (-1.59) obtained for BMC. This test measures the ability of
the hands and feet to move together in a smooth and rhythm way. The motor demands on this test includes the smoothness
of the movement, rhythm, sequencing and timing (Ayres, 2004).
Bilateral Integration and Sequencing Dysfunction:Strategies for Clinical Reasoning
Volume 24 | No 1 | 2014 23
SAISI Newsletter Vol 24 no 1 2014.indd 22 2014/03/05 1:04 PM

24 Volume 24 | No 1 | 2014
The SIPT scores indicate a cluster of low scores that fit with the pattern of
Vestibular Bilateral Integration and Sequencing dysfunction (Mailloux et al., 2011).
The presenting problems of having difficulty to eat with a knife and fork, experience
difficulties with fasteners, confusion of left and right, swapping hands during
writing tasks, poor cutting skills and being clumsy could be linked to an underlying
vestibular, proprioceptive processing difficulties that result in a bilateral integration
and sequencing dysfunction.
REFERENCES:
ASHER, A. V., PARHAM, L. D. & KNOX, S. 2008. Interrater reliability of Sensory Integration
and Praxis Tests (SIPT) score interpretation. Am J Occup Ther, 62, 308-19.
AYRES, A. J. 2004. Sensory Integration and Praxis test manual, Los Angeles, Western
Psychological services.
BLANCHE, E. I., BODISON, S., CHANG, M. C. & REINOSO, G. 2012. Development of the
comprehensive observations of proprioception (COP): validity, reliability, and factor analysis.
Am J Occup Ther, 66, 691-8.
BUNDY, A. C., LANE, S. J. & MURRAY, E. A. 2002. Sensory Integration: Theory and
Practice., Philadelphia, F.A. Davies Company.
FISHER, A. G., MURRAY, E. A. & BUNDY, A. C. 1991. Sensory Integration: Theory and
Practice, United states of America, Davis Company F.A.
MAILLOUX, Z., MULLIGAN, S., ROLEY, S. S., BLANCHE, E., CERMAK, S., COLEMAN, G.
G., BODISON, S. & LANE, C. J. 2011. Verification and clarification of patterns of sensory
integrative dysfunction. Am J Occup Ther, 65, 143-51.
MAILLOUX, Z. & PARHAM, L. D. Sensory Integration. In: CASE-SMITH, J. & O BRIEN, O.
(eds.) Occupational Therapy in Children. 6th Edition ed. Missouri: Mosby Elsevier.
MULLIGAN, S. 1998. Patterns of Sensory Integration Dysfunction: A Confirmatory factor
analysis. The American Journal of Occupational Therapy, 52, 819-825.
MURRAY-SLUTSKY, M. S. & PARIS, B. 2000. Exploring the Spectrum of Autism and
Pervasive developmental disorders, USA, Therapy Skill builders.
SMITH ROLEY, S., BLANCHE, E. I. & SCHAAF, R. C. 2001. Understanding the nature of
Sensory Integration with Diverse Populations, USA, Therapy Skills Builders.
VAN JAARSVELD, A., MAILLOUX, Z. & HERZBERG, D. S. 2012. The use of the Sensory
Integration and Praxis test with South African children. The South African Journal of
Occupational Therapy, 42.
Bilateral Integration and Sequencing Dysfunction:Strategies for Clinical Reasoning
A Special thank you to Ray Anne Cook for her assistance in providing a suitable case study for this article.
SAISI Newsletter Vol 24 no 1 2014.indd 23 2014/03/05 1:04 PM

The activities are divided into three groups:1. Activities to enhance symmetrical functioning
2. Activities to enhance alternating functioning
3. Activities to enhance midline crossing
(to be published in the next newsletter)
Grading:A. Symmetrical use of the whole body
B. Symmetrical use of lower extremities
C. Symmetrical use of upper extremities
Further grading according to positioning, namely from prone to
stand; from shoulder girdle to wrist; as well as from isometric
and isotonic movements.
Equipment:1. Bolster swing
2. Inner tubes
3. Scooter board
4. Hammock
5. Balance board
6. Trapeze swing
7. Flexion swing
Activity ideas
Suggested Activities for the Improvement of Bilateral IntegrationBy Esta Steenkamp
Volume 24 | No 1 | 2014 25
(This article was first published in the SAISI Newsletter of January 1986)
SAISI Newsletter Vol 24 no 1 2014.indd 24 2014/03/05 1:04 PM

26 Volume 24 | No 1 | 2014
1. ACTIVITIES TO ENHANCE SYMMETRICAL FUNCTIONING
A. ACTIVITIES TO ENHANCE SYMMETRICAL USE OF THE WHOLE BODY
A.1 Bolster SwingProne: Isotonic: Lie over bolster, kick away from wall and throw a ball in the “fish pond”
or over the wall. Lie over bolster, pull on stick or rope and move
backwards and forwards through symmetrical movements of extremities.
Sitting: Isotonic: Sit with legs across bolster and swing by pulling rope.
Sit, hold on with legs and row bilaterally.
Sit, hold on with legs and throw and catch balls; or throw balls through
hoopla hoop; or hold stick with both hands and hit balls.
Sit on edge of bolster, hold on with hands and kick a ball.
Sitting: Isometric: Two sit on bolster, hold on with legs and push against each other
with palms of hands.
Kneeling: Isometric: Kneel and hit ball with head.
Standing: Isotonic: Child swings bolster and pulls him/herself up and hang with legs flexed.
A.2 Inner Tube:Prone: Isotonic: Lie on tummy over vertically suspended tube.
Kick away from wall, or push away with hands
from wall.
Lie on tummy and pull with both hands on rope
or stick, or throw balls in a “dam”.
Swing forwards and push blocks over using
both hands.
Sitting: Isotonic: Sit in swinging tube and hold on to trapeze
with both hands.
Kick medicine ball using both feet.
Sit on vertically suspended tube and bunny hop
through tube while holding onto trapeze.
Sit in tube, holding on with legs and hit a ball
with a stick using both hands.
Put tube flat on floor and let child jump like a frog
with legs across the tube.
Kneeling: Isotonic: Hold tube in vertical position and roll forwards.
Child dives through.
Place tube flat on floor: child jumps up and down
on knees.
Squatting: Isometric: Child is in squat position on tube and therapist
pulls child over floor.
Standing: Isotonic: Run and jump into tube covered with thick material
like blankets and pillow in the middle.
Swing on trapeze and land inside tube.
Tube can be on different heights to use more isometric
flexion in elbow joints.
Build an obstacle course with varying sized tubes.
Child jumps from the one to the other, forwards,
backwards and sideways, clapping hands in between.
SAISI Newsletter Vol 24 no 1 2014.indd 25 2014/03/05 1:04 PM

Volume 24 | No 1 | 2014 27
Activity ideas
A.3 Scooter BoardProne: Isotonic: Lie with legs extended and use arms in symmetrical movements patterns:
ride and throw sponges into a container or towards a target; ride into a
crash mat with both arms pushing it away.
Lie on scooter board and push with both hands and feet.
Ride down ramp and hit shapes, sponges, road signs etc.
simultaneously on both sides.
Prone: Isometric: Lie and hold onto a friend’s legs while on scooter board.
Holding onto big bag or stick, go and “deliver” goods.
Pull child, turn and let him roll onto a mattress.
Sitting: Isotonic: Move with legs and pull on rope with hands bilaterally
to “cross the river”.
Sitting: Isometric: Sit and hold on while being pulled with a stick/rope.
A.4 HammockProne: Isometric: Use heavy additional equipment like big balls etc.
Prone: Isotonic: Kick away from wall and throw a ball through a
hoopla hoop.
Kick away with feet and if possible on the opposite
side, push away with the hands.
Sitting: Isotonic: Sit in hammock and shift forwards and backwards by
supporting with hands bilaterally and moving with feet.
Standing: Isometric: Swing to and fro in standing position.
A.5 Balance Board(Alternating isometric and isotonic contraction)
Prone: Lie while throwing and catching a ball.
Sitting and kneeling:
Sit and maintain balance whilst taking part in
eye-hand coordination activities, e.g. throwing
bean bags to a target etc.
A.6 TrapezeSitting: As combined in previously
mentioned activities.
SAISI Newsletter Vol 24 no 1 2014.indd 26 2014/03/05 1:04 PM

28 Volume 24 | No 1 | 2014
1. ACTIVITIES TO ENHANCE SYMMETRICAL FUNCTIONING
B. ACTIVITIES TO ENHANCE SYMMETRICAL USE OF LOWER EXTREMITIES
Prone or supine: Lie on back and kick a suspended ball.
Lie on back or tummy on scooter board and propel with legs.
Lie on back and kick away from wall, ride off the ramp and
kick down a heap of sponges.
Sitting: Sit on cardboard and move forwards/backwards using legs.
Sit and pick up bean bags with feet. Grade the weight of
these objects. Sit on scooter board and propel with legs in a
symmetrical movement pattern.
Standing: Bunny hops.
Jumping on trampoline: forwards, backwards, sideways, with eyes
opened/closed, to and fro over line, over different heights.
Shoulder Movements: Isotonic: Rhythmical exercises with music.
Obstacle courses with big apparatus.
Stick used in bilateral handling, to row, to hit etc.
Sit on bolster and pull on knotted rope or trapeze
Swimming breast stroke or butterfly in swimming pool.
Pillow fight.
Lie over ball, bolster, or in vertically suspended tube.
Pick up bean bags/sand bags and throw through
hoopla hoop/over wall/in pond.
Skipping rope activities.
Animal jumps, e.g. frog jumps.
Angels in the snow.
Bilateral blackboard patterns.
Hit cymbals, drums, other musical percussion
instruments.
Bounce a ball.
Put a ball in the middle of a blanket. Two children take
two corners of the blanket each and “bounce” the ball
up and down without touching the ball.
Shoulder movements: Isometric: “Push wall over” with two hands together.
Hang onto rope or net or trapeze.
Sit in a box, or on a scooter and therapist pulls child
whilst holding on to stick with both hands.
Pull someone else around.
Elbow movements: Isotonic: Sand with sandpaper.
Tearing pages from a magazine.
Arm movements on music.
Finger paint or paint with two big brushes.
Catching and throwing a ball.
Elbow movements: Isometric: Wheelbarrow walk.
Swing on trapeze with maintained elbow flexion.
Wrists and hands: Isotonic: Pronation/supination; finger adduction/abduction,
flexion/extension.
Paper collages.
C. ACTIVITIES TO ENHANCE SYMMETRICAL USE OF UPPER EXTREMITIES
SAISI Newsletter Vol 24 no 1 2014.indd 27 2014/03/05 1:04 PM

Volume 24 | No 1 | 2014 29
Grading:
1. From prone to standing positions where much
more balance and equilibrium skills are required.
2. Activities are more isotonic in nature.
2.1 Bolster SwingProne: Lie on tummy and row with alternating arms to propel
self forward. If swing is low enough, child can also
push him/herself forward with hands alternately
pushing on floor.
Sitting: Sit on bolster while objects are being thrown to the
child from different directions so that he/she has to
catch it with alternating hands.
2.2 Scooter BoardProne:
Child pulls him/herself across the “river” with
alternating hands.
Ride down ramp and catch a ball with left and right
hands alternately.
Ride down ramp and hit sponge blocks alternating
between hands used.
2.3 HammockProne:
Child swings forward and backward, hitting objects
with alternating hands.
Crawling:
Crawl through hammock filled with sponges.
2.4 Flexion SwingSitting:
Swing and throw balls into container with alternating
hands; or hit/push other suspended equipment away
using hands alternately.
2. ACTIVITIES TO ENHANCE ALTERNATING USE OF UPPER AND LOWER EXTREMITIES
Origami.
Knitting.
Fastening and loosening of screws.
Playing with finger puppets.
Knotting ropes with fingers.
Straw constructions.
Cutting and pasting.
Play dough activities.
Rolling and tearing paper.
Playing with pegs.
Hands
Isometric use is elicited through a variety of grips, e.g.
palmar grip, pinch grip etc. whenever the hands are
holding onto an object.
SAISI Newsletter Vol 24 no 1 2014.indd 28 2014/03/05 1:04 PM

30 Volume 23 | No 2 | 2013
Book Review
Below is a list of various books and articles that cover various aspects of bilateral integration and sequencing. May you find this inspiring and thought provocative.
1. Ayres, A.J. (2007). Sensory Integration and Praxis Tests
Manual. 9th Ed. Los Angeles: Western Psychological
Services.
2. Ayres, A.J. (2005). Sensory Integration and the Child.
2nd Ed. Los Angeles: Western Psychological Services.
3. Ayres, A.J. (1979). Sensory Integration and the Child.
1st Ed. Los Angeles: Western Psychological Services.
4. Bundy, A.C., Lane S.J. & Murray, E.A. (2002). Sensory
Integration Theory and Practice. 2nd Ed. Philadelphia: F.A.
Davis Company.
5. Case Smith, J. & O’Brien, J.C. (2010). Occupational
Therapy for Children. 6th Ed. Missouri: Mosby Elsevier.
6. Goddard, S. Reflexes, Learning and Behavior. (2005).
Eugene, Oregon: Fern Ridge Press.
7. Murray Slutsky, C. & Paris, B.A. (2000). Exploring
the Spectrum of Autism and Pervasive Developmental
Disorders: Intervention Strategies. Therapy Skill Builders.
8. SAISI Clinical Observations of Gross Motor Items.
(2004). SAISI.
9. Shumway-Cook, A & Woollacott, M.H. Motor Control.
Translating Research into Clinical Practice. 4th Ed.
Lippincott Williams & Wilkins.
10. Smith Roley, S, Blanche, E.I. & Schaaf, R.C. (2001).
Understanding the Nature of Sensory Integration with
Diverse Populations. Therapy Skill Builders.
Articles:
1. Mailloux, Z, Mulligan, S, Smith Roley, S, Blanche, E.I.,
Cermak, S, Coleman, G.G., Bodison, S & Lane, C.J.
(2011). Verification and Clarification of Patterns of Sensory
Integrative Dysfunction. American Journal of Occupational
Therapy, 65 (2), 143-151.
2. SAISI Newsletter Articles on Bilateral Integration and Midline Crossing:
• Sept – Dec 1986: Theoretical approaches to Manual
Crossing of the Midline of the body and Ways of
Assessment. Erica Jooste.
• VOL 5 NO.3 1994: The Meaning of Manual Midline
Crossing. Janet Stillwell.
• VOL 10 NO.1 1999: The Child with Low Postural Tone
and Minor Motor Dysfunction – Occupational Therapy
Considerations. Thea Coetzer.
• VOL 10 NO.2 1999: The Role of Sensory Systems in
the Development of Postural Control and Movement. Kate
Bailey.
• VOL 13 NO.2 2002: Occupational Therapy Intervention
with a Child with Half a Brain. A Case Study. Sally
Mackenzie.
• VOL 13 Nr 2 2003: Assessing Handedness –
Evaluating the Effectiveness of Three SIPT Tests to
Determine the Extent of Manual Specialization. Elke Kraus.
Recommended Resources for Bilateral Integration and SequencingCompiled by Rosa-Marié Olivier (Editor)
SAISI Newsletter Vol 24 no 1 2014.indd 29 2014/03/05 1:04 PM

If you have not used CPD Solutions before, go to www.cpdsolutions.co.za and click on ‘Help’ to download the CPD Solutions SMS guide for instructions on how to register with your cell phone and answer multiple choice tests with an SMS.
ANSWER ALL QUESTIONS TRUE (A) OR FALSE (B)
QUESTIONNAIRE 34.1 (a19547) The Vestibular Bilateral Integration Pattern: A Unique Contribution to Sensory Integration Theory & Practice, By Zoe Mailloux, OTD, OTR/L, FAOTA1 Jean Ayres became interested in the role of the vestibular system in the 1960’s when she started to work with children with learning difficulties.
2 The lack of integration of function of the two sides of the body distinguishes the Disorder in Postural Bilateral Integration as first described by Ayres.
3 Ayres started using the Southern California Post Rotary Nystagmus Test as a measure of central processing of vestibular input in 1975.
4 A “depressed” measure of the PRN reflected a problem in the typical inhibitory influences from other neural centers on this reflex, while a “prolonged” PRN reflected inefficient processing of vestibular input in the vestibular nuclei of the brainstem.
5 Ayres revised her description of the Postural and Bilateral Integration Deficit to a Vestibular and Bilateral Integration Deficit, stating that “The symptoms of a vestibular-bilateral disorder are very subtle. These children are often considered completely normal until they enter school and have trouble with reading, arithmetic or other academic work…”
6 Ayres later stated: “ A number of studies in this country, in Australia, and in South America have shown that at least 50 percent of all children with learning or language problems have too long a duration of PRN. These findings suggest that some aspect of vestibular function is very important in meeting the demands of school-work, and this aspect is not functioning adequately in many school children today.”
7 Ayres finally iterated Bilateral Integration and Sequencing (BIS) being reflective of a pattern of sensory integrative dysfunction that was characterized by the discreet vestibular based signs with the absence of more significant tactile or praxis deficits seen in patterns such as Somatodyspraxia.
8 Mailloux, et al. published research in 2011 where the findings reinforced a long-held view of the significance of low PRN scores and validated Ayres’ (1989) theoretical assumption that bilateral integration problems and other signs of vestibular inefficiencies are associated with a shortened duration of PRN.
9 Another research project by Mailloux, et al., currently in press, identified that the PRN test can be administered to infants and toddlers using the 4 year old SIPT norms.
10 The strongest indicators of the presence of the Vestibular Bilateral Integration pattern include: Below average scores on the following standardized tests of the SIPT: Postrotary Nsytagmus (PRN), Standing and Walking Balance (SWB), Bilateral Motor Coordination (BMC), Sequencing Praxis (SPr), Oral Praxis (OPr), Graphesthesia (GRA) and/or Manual Form Perception (MFP), Motor Accuracy (MAc).
QUESTIONNAIRE 34.2 (a85978) Bilateral Integration and Sequencing Dysfunction: Strategies for clinical reasoning by Janine van der Linde, M.Sc.OT (Wits)1 A study by van Jaarsveld (2012) investigated whether the SIPT is appropriate for use with the South African population. This study showed that 5 test items have to be adapted with ½ a standard deviation unit to the positive side.
2 This adaptation of scores is for ages 6 years 0 months to 8 years 11 months only.
3 Ayres described bilateral integration and sequencing as a dysfunction that include poor postural abilities, decreased muscle tone and decreased bilateral motor coordination. She considered it to be a type of motor coordination disorder and associated it with vestibular functions although she did not necessarily consider it a dyspraxia.
4 Fischer brought forward terms such as feed-forward and feedback and hypothesized that postural control, ocular motor control and projected action sequences accompanied by BIS can result in praxis deficits.
5 A new finding was the fact that MAC does not clusters with this group. This test reflects eye hand coordination in a variety of postures and positions and integration of two sides of the body.
6 The use of clinical observations can refute the test results of the SIPT.
7 The ability to assume and maintain a totally extended posture against gravity is hypothesized to require adequate processing of gravity information via the vestibular nuclei and thus indicative of vestibular processing.
8 Grading of force in movement is indicative of the processing of the proprioceptive system.
9 Projected action sequences also plays a role in bilateral integration and sequencing as it requires the ability to plan movements in response to stable events in the environment.
10 Feed-forward is used to detect wrong patterns in movement before the actual movement is started.
CPD Programme Questionnaire
Volume 23 | No 2 | 2013 31
SAISI Newsletter Vol 24 no 1 2014.indd 30 2014/03/05 1:04 PM


















