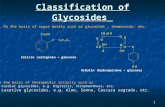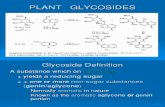
Natural glycosides & therapeutic potential Of Cardiac Glycosides
Upload
adrian-tisdelCategory
view
217download
2
Safe PrescribingWeek 3 – Amino
glycosides + electrolytes
Safe PrescribingWeek 3 – Amino
glycosides + electrolytes
Dr Ian Coombes,
Senior Clinical Lecturer University of Queensland Schools of Medicine and Pharmacy
Safe Medication Practice Unit, Queensland Health
Dr Ian Coombes,
Senior Clinical Lecturer University of Queensland Schools of Medicine and Pharmacy
Safe Medication Practice Unit, Queensland Health
The University of Queensland

Objectives
• Principles of once daily Aminoglycoside dosing and avoiding toxicity
• Key messages about analgesia use

Gentamicin Revision
• Gram negative bactericidal agent• Excellent anti-pseudomonal cover• Once daily dosing benefits vs tds or bd:
- high peak level – excellent distribution- post antibiotic effect (>24-36 hours) - reduced monitoring and administration- reduced nephro and ototoxicity- easier monitoring (10-12 hours post dose)

Severe risks of nephrotoxicity and ototoxicity
• Mrs HR• 78 years, wt 57kg• Admitted to outlying hospital acute exacerbation COPD• Baseline Cr 80mol/L• Charted gentamicin 160mg daily for 5/7• CrCl = 45ml/min

Date Gent Dose Level Cr Urea3/6 0.08 8.55/6 160mg6/6 160mg 0.11 15.57/6 160mg 6.2 0.138/6 160mg 9.0 0.17 21.99/6 160mg10/6 ceased 16.9 0.22 28.311/612/6 7.8 0.36 35.013/6 0.3914/6 0.41 33.615/6 0.5016/6 0.59 38.917/6 0.65 40.6


• 21/6 Gent level still 1.4!!!!
• 23/6 complaining of dizziness, unsteady feeling, vestibular symptoms, vomiting
• 1/7 Cr 0.21 recovering

Aminoglycoside dosing and Monitoring
Case continued…
Day 3:• Mr AD (67yrs) has now developed sever hospital acquired
pneumonia • Ward round decisions
- start gentamicin once a day dose as per levels each night at 20:00 recall patient weighs 70 kg creatinine has improved (now 140 micro mole/l)
- start Co-Amoxiclav 1.2g IV q8h


Creatinine Clearance• Do NOT use eGFR provided by AusLab(calculated using standard 70 kg patient can lead to over-dosing)
• Recall Cockcroft-Gault Formula:
CrCl (mL/min) = [140-age (years)] * ideal weight (kg) [0.814 * serum creatinine
(micromol/L)]
{♀ * 0.85 }If patient 70 kg, 67 y.o. with serum creat~140micromol/L:
CrCl ≈ 42 mL/min (140-67 X 70) / (0.814 x 140)

Calculating first dose gent

Gentamicin Dose Adjustment
Day 4: gentamicin level = 2.5
(taken 08:00, 12 hrs post dose)• The initial dose given in emergency department
was 280mg (4mg/kg x approx 70kg)
Prescribe new gentamicin dose based on level

2.5

Adjusting doses of gentamicin

Gentamicin Dose Adjustment
• Level at 12 hours = 2.5 (ideal = < 2)
• New Dose = Level Wanted (mg/L) x Dose Given (mg)Level Achieved (mg/L)
In this case: (1.5/2.5) x 280 = 168 mg• round down to 160 (nearest multiple of 40 mg)
- amps = 40 mg/mL

When NOT to take levels
• Do not take levels if:• Stat dose • Or• Patient has Normal renal function and is only
receiving 1 or 2 doses ie prophylactic

Variable Dose MedicationDrug Level and Time Taken
Dose Time and Actual Time Given

Use in moderate to sever renal function
• Where ever possible withhold other nephrotoxic drugs and ensure no other altenative
• Ie unavoidable use of gentamicin:• Requires extended dose intervals 36, 48 or 96
hours• Effectively daily levels wait til < 1.0mmol/l
then dose again

Gentamicin FAQs• Patient returns from OT, septic, at 4 p.m.?
- dose now - get level 8 a.m. (difficult to get bloods during night)
if level < 0.5, clearance satisfactory• Patient in ED at 4 a.m. with severe pneumonia?
- give standard dose now; dose again at 8 p.m.• Level low but adequate dose? (patient ok clinically)
- dose 4-5mg/kg has long post antibiotic effect- don’t increase
• If in doubt, CHECK!- Registrar; clinicial pharmacists; ID team

Gentamicin Ordering key messages
• If elderly (renal impaired) is there an alternative safer drug?• Do not write as a regular medication – prescribe dose for regular
dosing after levels available• Dose according to gentamicin level• Use aminoglycoside dosing guides
- these notes www.wiki.tox.org.2.17 safe prescribing• Try to prescribe in multiples of 40mg (ampoule contains
80mg/2mL = 40mg/mL)• Where possible, dose at a time that allows level to be taken on
next day’s blood round

Questions?

Introduction to PrescribingAnalgesia and Pain Relief
Presented by: [insert presenter name here]

You have been asked to write up a patient’s analgesia…
What patient factors do you need to consider?

Patient Assessment
Goal to individualise analgesic therapy
Assess patient characteristics:
- indication for analgesia- age, sex, weight- culture - vital signs - allergies/ADRs- opioid tolerance
- respiratory status - renal/hepatic function- other medical co-morbidities- mental state - other Rx - availability of oral/rectal routes

WHO Analgesic Ladder (ideally fro chronic pain)
Level 1: Non opioid/adjuvant(paracetamol; NSAIDs; amitriptyline; local anaesthetics)
Level 2: Weak opioid + non-opioid
Level 3: Strong opioid +/- non-opioid/adjuvant1 2 3
NOT ACCEPTED- Use Multimodal Analgesia

DRUGS
PAIN TYPE
Nociceptivee.g. fracture
Neuropathiceg neuralgia
Inflammatory e.g. rheumatoid arthritis
Paracetamol Effective when taken regularly at max. dose
Less effective Effective, but not anti-inflammatory
Opioids Effective May be effective(agent + dose)
May be effective (depends on dose)
NSAIDs Effective Not effective Effective
TCAs, parenteral, local anaesthetics antiepileptic
Rarely used (clonidine may be effective as adjunct)
May be effective
Rarely used (may be effective as adjunct)
Adapted from Table 3-1, Australian Medicines Handbook

NSAIDs- Adverse EffectsSide effects Cautions
• hypersensitivity/allergy
• GI (GORD/PUD)
• platelet inhibition
• sodium retention, oedema
• renal toxicity
• hepatic toxicity

NSAIDs- Adverse EffectsSide effects Cautions
• hypersensitivity/allergy - asthma
• GI (GORD/PUD) - GI bleeding/ulceration
• platelet inhibition - coagulation disorders- warfarin therapy
• sodium retention, oedema - hypertension- cardiac failure- ACEI/ARA/diuretics
• renal toxicity - renal impairment- gentamicin therapy
• hepatic toxicity - hepatic impairment

NSAIDs – Caution!
Major cause of ADEs and hospital admissions
use lowest effective dose for shortest possible time use paracetamol as alternative or to reduce NSAID dose COX-2 inhibitors
- similar adverse effects to non-selective- increase risk of thrombotic events (stroke; MI)!
little difference in efficacy between NSAIDs avoid aspirin < 18 yrs in viral illness (Reye’s syndrome) elderly - increased risk of adverse effects
Continue only if effective. Avoid if possible!

Potential Adverse Effects of Opioids?

respiratory depression sedation nausea and vomiting confusion hypotension; bradycardia pruritus constipation / ∆ gut motility urinary retention
Opioids – Adverse Effects

Opioids – Precautions
hypotension, shock concomitant CNS depression impaired respiration /↓ respiratory reserve elderly hepatic impairment renal impairment epilepsy/recognised seizure risk biliary colic or surgery phaeochromocytoma

Regular vs PRN Analgesia
regular analgesia is better in setting of continuous pain PRN only if pain intermittent and unpredictable in most settings, pain is predictable problems with using only PRN analgesia
- dose prescribed by Dr/administered by nurse- patients don’t ask for medication
inadequate or infrequent dosing → unrelieved pain keeping up with pain is easier than catching up with pain prn dose = 1/6 →1/12 total regular daily dose

Key Messages individualise analgesic therapy choose analgesics judiciously use multimodal analgesia regular pain monitoring is critical to outcomes regularly review and revise analgesic doses adjust regular dose according to breakthrough usage anticipate and manage analgesic-associated adverse
events avoid NSAIDs – major cause of morbidity/mortality! avoid tramadol, dextropropoxyphene, pethidine

Electrolyte Objectives
• Fluid requirements• Common error traps• Electrolyte requirements • Key messages for safe electrolyte
prescribing

Maintenance Fluid for “Standard” Patient
–70 kg–euvolaemic–no electrolyte derangements–not septic–normal cardiac and renal function–no additional ongoing fluid losses

Sodium Glucose Potassium
Daily Requirement 2 mmol/kg >100G 1 mmol/kg
0.9% NaCl 1L
(Normal Saline) +/- 20/40 mmol KCl/l
150 mmol 00, 20 or 40
mmol
4% glucose & 0.18% NaCl 1L
30 mmol 40G 0
3.3% glucose & 0.3% NaCl +/-
20/40 mmol KCl 1L50 mmol 33G
0, 20 or 40 mmol

Risks of Having IV Line
• Infection– Time and effort to re-site every 48 hours
• Immobility • Thrombophlebitis• Direct costs of consumables• Overdosing of fluids and electrolytes

Key Messages IV Fluid Ordering
• Supply orally if possible• Assess current fluid status-wet / dry / ‘just right’? -how do you tell?
• Review fluid balance chart• Assess ongoing requirements and losses• Reassess fluid status at least daily

Potassium
• What is normal?• Where do you lose it from?• How much do you need?• How can you replace it?• Routes of administration? • How fast can you replace it?• Quantities?• What goes wrong?

Potassium
• Normal serum K+ = 3.8-4.9 mmol/L• Daily requirement = 1 mmol/kg• Dietary K+ < 25 mmol (1gram)/day leads to
hypokalaemia• Is magnesium low (< 0.5 mmol/L)?
(makes it difficult to correct potassium)

Causes of Hypokalaemia
• Potential sites for K+ loss- urine; faeces; drain sites; vomitus
• Intracellular shifts- insulin- β adrenoceptor agonists- caffeine- hyperthyroidism- correction of acidosis
• Increased external losses- Drugs that promote renal K+ excretion
loop diuretics (eg frusemide) aldosterone; thiazides; penicillins

Potassium Replacement• There is no single way to correct potassium• serum K+ of 0.3 mmol/L = overall deficiency
100 mmol K+ (but extremely variable)• Replace with oral supplements where possible• Ideally, correction of potassium should occur over a
period of days• Account for deficit + ongoing normal requirements

Case Study - Mr KCl
• 72 y.o. ♂• Med Hx: hypertension, heart failure• Rx: frusemide 80mg mane; lisinopril 10mg mane;
amlodipine 10mg mane• Admitted for elective TKR• Pre-op serum potassium: 2.9 mmol/L• Registrar:
- “Give him some IV KCl and fluids pre-op”- suggests 40 mmol in 100mL N Sal over 60 min
- What happened?

Potassium Administration
• In non critical care cases, Should NOT give KCL > 10 mmol/hour WITHOUT a pump
• With a pump max. rate = 20 mmol/hour• Concentrations > 40 mmol/L: risk causing
thrombophlebitis, pain and loss of IV site • If via central line, concentration NOT a concern,
but RATE is!

Causes of Hyperkalaemia
• ↓ K+ excretion (renal insufficiency)• ↑ K+ intake (but rapid K+ excretion 2o to ↑ intake) • K+ release from cells• Metabolic acidoses• Medications• Hypoaldosteronism/resistance to aldosterone

Managing Hyperkalaemia
– What are your aims?– What are the risks? – What do you do?– How do you do it?

Cardiovascular Protection
Calcium Gluconate by slow IV push
–decreases membrane excitability–10 mL of 10% calcium gluconate (2.2 mmol)–onset 2-5 minutes, lasts up to an hour–can repeat if no ∆ ECG after 5-10 minutes

Shift Intravascular → Intracellular
• Insulin- 10 units insulin in 50 mL of 50% glucose- via syringe or free running drip- onset 15-30 minutes, lasts 1-3 hours-↓ plasma K+ by 0.5-1.5 mmol/L
• Nebulised salbutamol- 5 mg- onset within 30 minutes, lasts 2-4 hours-↓ plasma K+ by 0.5-1.5 mmol/L

Removing Excess Potassium
• Resonium® A (sodium polystyrene sulfonate)- promotes exchange of Na+ for K+ in the GIT - 30g orally or 60g enema mixed with glucose- onset within 2 hours, peak effect at 6 hours- 1 gram binds 1 mmol K+ and releases 2-3 mmol Na+
- generally lowers plasma K+ by 0.5-1.0 mmol/L- can give up to 4 doses per day (as per levels)
• Haemodialysis- severe life-threatening hyperkalaemia unresponsive
to more conservative measures

Sodium Replacement
• Consider- ? over filling (heart, renal, liver failure) - ? over diuresis - ? SIADH – SSRIs; TCAs; carbamazepine
• Replace Na+ gradually (↑ plasma Na+ by ≤ 10 mmol/L/day)• Na+ required to ↑ plasma Na+ by 10 mmol/L:
[0.6 * total body weight (kg)] * 10 = x mmol/L Na+
NEVER attempt to replace sodium with hypertonic saline!- IRREVERSIBLE osmotic demyelination of CNS
(several cases in QLD in recent years)

Magnesium
• Indications- hypomagnesaemia - post MI- antiarrythmic- acute asthma- pre-eclampsia
• Oral - limited value (laxative)• Be aware of IV rate - vasodilator!

Key Messages
• Use oral route for electrolytes if possible• Significant patient harm 2° to rapid/concentrated KCl• K+ reduction - protect heart (short and long term)• NO place for hypertonic saline – demyelenitaion risk• Magnesium used for hypertension

Questions?