Sadaf T. Bhutta M.B.,B.S. University of Arkansas for ... - Imaging of Pediatric... · University of...
56
Sadaf T. Bhutta M.B.,B.S. University of Arkansas for Medical Sciences Arkansas Children’s Hospital
Transcript of Sadaf T. Bhutta M.B.,B.S. University of Arkansas for ... - Imaging of Pediatric... · University of...

Sadaf T. Bhutta M.B.,B.S.
University of Arkansas for Medical Sciences
Arkansas Children’s Hospital

No financial disclosures
Gadolinium chelates for contrast enhanced MRA

Pediatric Hypertension Definition Hypertension is defined as average systolic blood
pressure (SBP) and/or diastolic blood pressure (DBP) that is ≥ 95th percentile for gender, age and height on ≥ 3 occasions
Pre-hypertension is defined when the child’s average BP is between 90th and 95th percentile.
Adolescent with BP > 120/80 is considered hypertensive, even if it is below 90th percentile for that child
[Guideline] NHLBI. National High Blood Pressure Education Program Working Group on High Blood Pressure in Children and Adolescents. The fourth report on the diagnosis, evaluation, and treatment of high blood pressure in children and adolescents.
Pediatrics. Aug 2004;114(2 Suppl 4th Report):555-76.

Epidemiology True incidence of pediatric hypertension is unknown
in this country.
No race predilection
No gender difference under 6 yrs of age, higher in girls from 6yrs till puberty and higher in boys after puberty
Height and weight affect BP

Factors affecting BP include Cardiac output Baroreceptors Extracellular volume Effective circulating volume
Atrial natriuretic hormones Mineral corticoids Angiotensin
Sympathetic nervous syndrome Vascular resistance Pressors
Angiotensin II Calcium (intracellular) Catecholamines Sympathetic nervous system Vasopressin
Depressors Atrial natriuretic hormones Endothelial relaxing factors Kinins Prostaglandin E 2 Prostaglandin I 2

Causes Primary
Generally found after puberty
Secondary Renal parenchymal disease (>70%)
Coarctation of Aorta (CoA)
Renal Artery Stenosis
Pheochromocytoma
Vasculitides
Other tumors and endocrine causes

Coarctation of Aorta
Edwards J.E.: Aortic arch system. In: Gould S.E., ed. Pathology of the Heart and Blood Vessels, 3rd ed. Springfield, IL: Charles C Thomas; 1968:416-454.
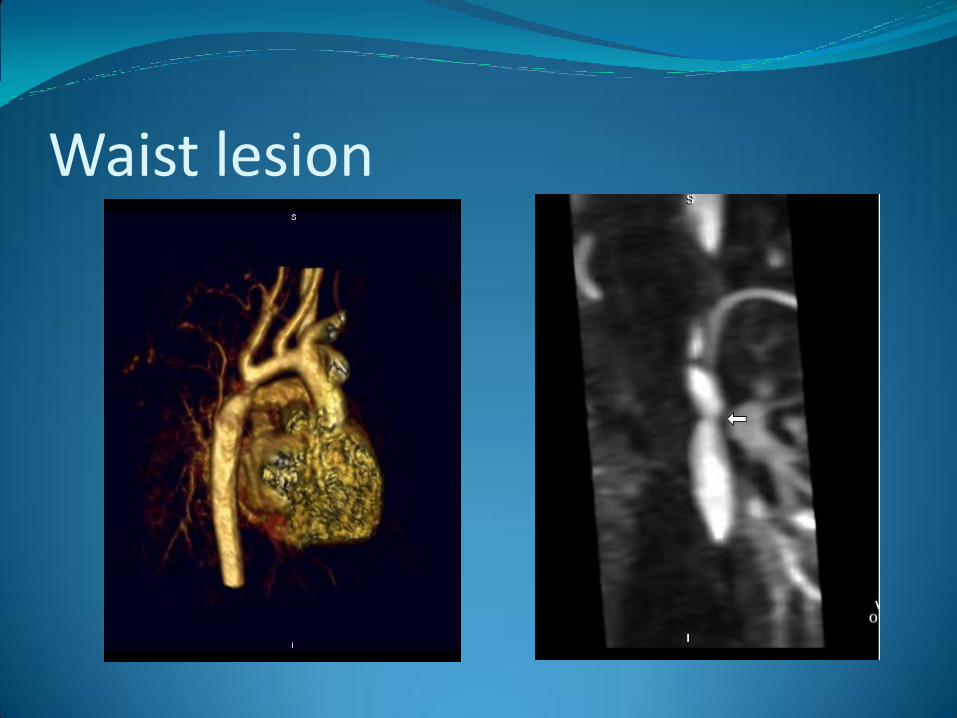
Waist lesion
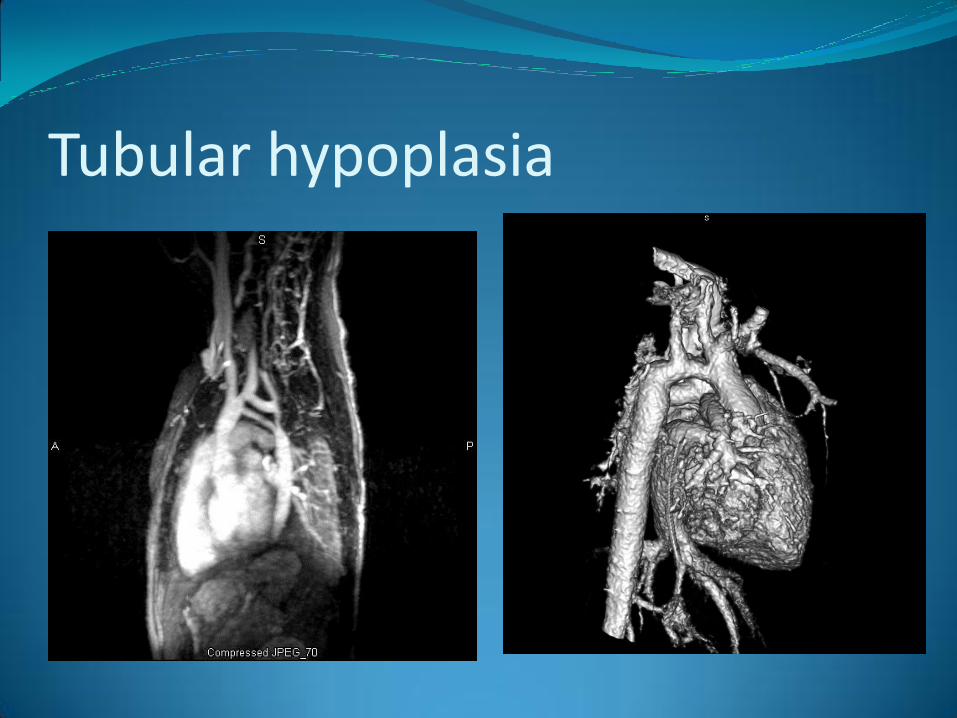
Tubular hypoplasia

Associated Disorders High association with Turner’s syndrome and other
structural anomalies of X chromosome, bicuspid aortic valve and abnormal mitral valve
Coarctation complex in neonates
Coexisting vascular disorders: abnormal proximal and distal para-coarctation aortic media, aneurysms of circle of Willis, aneurysms of left subclavian and intercostal arteries, tortuous retinal arterioles, vascular rings and interruption of aortic arch

Retinal arterial tortuosity in a young adult with coarctation of aorta
Eye London 1996;10 (pp4):525-27
Berry aneurysm at circle of Willis

Double Outlet LV with CoA

Pathophysiology “Despite successful surgical repair, aortic coarctation is
associated with unfavourable prognosis mainly due to cardiovascular disease. Late timing of repair and arterial hypertension represent adverse prognostic factors. Arterial hypertension can recur after coarctation repair, despite the absence of residual obstruction, with a prevalence of up to 45%.”
Arterial hypertension and cardiovascular prognosis after successful
repair of aortic coarctation: a clinical model for the study of vascular function. deDivitiis M, Rubba P, Calabro R. Nutr Metab Cardiovasc Dis. 2005 Oct;15(5):382-94


Role of Imaging Echocardiography
CT Angiography
MR Angiography

Algorithm
Echocardiography
CTA MRA

Echocardiography Trans-thoracic vs. Trans-esophageal echocardiography
Suprasternal notch window with color flow
Localized zone of accelerated flow
Peak systolic velocity gives estimation of systolic gradient
Diastolic run-off with decreasing high-velocity forward flow during elastic recoil of ascending aorta suggests hemodynamic significance

Echocardiography

Echocardiography Post repair evaluation determines residual or recurrent
obstruction or para-coarctation aneurysm formation
Post-op exercise echo-Doppler is useful for gradients and ventricular function
Doppler peak systolic velocity has a better correlation with residual narrowing than the SBP gradient between the upper and lower extremities

CT Angiography (CTA) Pros
High spatial resolution….important for assessing collaterals
Easier technique with a shorter scan time
Decreases anesthesia/sedation use and time
Cons Radiation risk
Limited functional analysis

CTA protocol Peripheral IV line large enough to sustain a contrast
flow rate of at least 1 ml/sec, given by power injector
Except for infants, our usual flow rate is 3-4 ml/sec
Saline chaser at same rate
80 kVp uptil 50 kg. weight, increase to 100 kVp for higher weight patient
MAs modulated

CTA protocol Bolus tracker in descending aorta
Slice thickness= 0.5 mm, reformatted at 1-2 mm
Non-gated, breath-hold vs. free breathing
Z-axis= thoracic inlet to diaphragm
Post-processing for 2-D multi-planar reformatted (MIP) and 3-D volume rendered images on a separate workstation

CTA

MR Angiography Pros
Less invasive than catheter angiography
No ionizing radiation
Morphology AND function
Cons
Contra-indications
Sedation/anesthesia risk
Longer acquisition and post-processing time

MRA protocol Primary Coarctation
Axial black blood sequence
3D SSFP (non gadolinium MRA)
Gadolinium enhanced MRA
Flow analysis
Pre-coarctation
Coarctation
Aorta at diaphragm

MRA Protocol Follow-up Coarctation
Axial black blood Cine imaging
Vertical long axis LV Outflow Short axis
3D SSFP (non gadolinium MRA with emphasis on heart) Gadolinium enhanced MRA Flow Analysis
Aorta Pulmonary artery Atrio-ventricular valves
Delayed enhancement (optional)

MRA
Non-Gd MRA Gd enhanced MRA


At coarctation

Post coarctation

At diaphragm
Renal Artery Stenosis Renovascular hypertension (RVHT) denotes secondary
hypertension in which a causal relationship exists between anatomically evident arterial occlusive disease and elevated blood pressure
Renal artery stenosis (RAS) is a major cause of RVHT

Pediatric causes Systemic disease (Arteritis or diffuse vasculitis)
Compression/mass effect (e.g. tumor)
Aneurysm/pseudoaneurysm
Thrombo-embolic disease
RAS of transplant kidney
Fibromuscular dysplasia

Pathophysiology Renin-angiotensin-aldosterone mechanism
Physiologic testing to assess R-A-A system
Plasma renin levels (stimulated or unstimulated)
Assess renal function (nuclear studies)
Perfusion studies to assess relative renal blood flow
Vascular studies to directly image renal arteries (DSA, CTA, MRA)
Imaging in RAS Digital Subtraction Angiography (DSA)
Ultrasonography
CTA
MRA
Nuclear Renogram/split function scans
DSA-Gold standard Hypertensive children without co-morbid conditions
who have RAS usually have single, focal branch artery stenosis. This distribution supports angiography in these patients because of its superior sensitivity in detecting branch vessel disease and its therapeutic role in percutaneous transluminal renal angioplasty.
Vo NJ, Hammelman BD, Racadio JM, Strife CF, Johnson ND,
Racadio JM. Anatomic distribution of renal artery stenosis in children:
implications for imaging. Pediatr Radiol 2006 Oct;36(10):1032-6. Epub
2006 Jul 4.

DSA Not a screening tool!!

Renal artery stenosis




Ultrasonography (USG) Safe, inexpensive, widely used (sens= 60-97%, spec=
85-99%)
Renal size assessment
Imaging of renal arteries and color flow
Measurement of blood flow velocity and pressure waveforms
Spectral sampling proximal to stenosis shows spectral widening and increased velocity

USG criteria Ratio of peak systolic velocity between main renal
artery and aorta is indicative of luminal narrowing
Magnitude of peak systolic velocity at the narrowed segment correlates with degree of luminal narrowing
Turbulent flow in post-stenotic segment
If renal arteries are visualized but no doppler signal, “total occlusion” should be suspected
USG criteria Tardus-Parvus phenomenon
Loss of early systolic peak
Acceleration rate <3 m/s²
Acceleration index >4
Acceleration time to systolic peak >0.07 s
Pulsatility index >0.12




CTA Protocol Similar protocol as Coarctation of aorta except scan
extends from diaphragm to below aortic bifurcation
2-D MIP images and 3-D volume rendered images
Size, shape of kidneys and accessory renal arteries
Degree and location of stenosis
Metal stents

Left ICA lat view Right ICA frontal view


MRI/MRA T-1 weighted contrast enhanced MRA acquisitions
have increased sensitivity (from 88-100%) and specificity (from 71-99%) for diagnosing RAS (caveat)
Fain SB, King BF et al. High spatial resolution contrast enhanced MR angiography of
the renal arteries: a prospective comparison with digital substraction angiography. Radiology.
2001;218(2):481-90
Volk M, Strotzer M et al. Time-resolved MR angiography of renal artery stenosis:
Diagnostic accuracy and interobserver variability. Am J Roentgenol. 2000;174(6):1583-88
Shorter acquisition times and higher spatial and temporal resolution

Williams syndrome



Conclusion Imaging in pediatric hypertension is useful for
vascular causes
Diagnostic (therapeutic) and follow-up
Look for associated findings