Sacrospinous ligament vs: Uterosacral Ligament...
23
Sacrospinous ligament vs: Uterosacral Ligament suspension Magnus Murphy FRCSC Clinical Assistant Professor Department of Obstetrics and Gynecology University of Calgary Division of Urogynecology www.pelvicfloor.com
Transcript of Sacrospinous ligament vs: Uterosacral Ligament...

Sacrospinous ligament vs: Uterosacral Ligament suspension
Magnus Murphy FRCSC Clinical Assistant Professor Department of Obstetrics and Gynecology University of Calgary Division of Urogynecology www.pelvicfloor.com

Apical Prolapse
Vagina is a continuum Apex is always involved in higher stage prolapse Symptoms could be:
— Bulge (anterior/posterior/global) — Urinary — Defecatory — Sexual dysfunction
Apex is key
Apex correlation — anterior prolapse: High — Posterior prolapse: Moderate
Key message: — Apical fixation should almost always be done
Rooney, Kristin, Kimberly Kenton, Elizabeth R. Mueller, Mary Pat FitzGerald, and Linda Brubaker. “Advanced Anterior Vaginal Wall Prolapse Is Highly Correlated with Apical Prolapse.” American Journal of Obstetrics and Gynecology 195, no. 6 (December 2006): 1837–40.
Which Procedure
What are you trying to achieve? — Objective success — Patient’s subjective improvement — Expectation management — Avoidance of complications — Avoiding unnecessary difficulty — Avoiding extra dissection — Precision, consistency — Efficiency
What Is Success?
Your opinion is not that important Patient satisfaction, goal achievement
Is all that counts
Elkadry, Eman A., Kimberly S. Kenton, Mary P. FitzGerald, Susan Shott, and Linda Brubaker. “Patient-Selected Goals: A New Perspective on Surgical Outcome.” American Journal of Obstetrics and Gynecology 189, no. 6 (December 2003): 1551-1557-1558.
Vaginal Apical Suspensions: Not much new
McCall Culdeplasty SSLS Iliococcygeus suspension Prespinous fixation/suspension
The honest truth: It doesn’t matter – it’s a wash

McCall vs SSLS
Landmark study 1998 — Retrospective case control — 62 patients per arm — Results were reported as objective impressions
Results — No difference in Apical support failure (15%) — Significant difference in anterior failures McCAll: 6% SSLS: 21%
Latest Literature Review
No difference in outcome Both SSLS and USLS have less than 5% serious complications USLS: mostly ureteric obstruction SSLS: mostly buttock pain After 2 years: Equivalent
Siff, Lauren N., and Matthew D. Barber. “Native Tissue Prolapse Repairs: Comparative Effectiveness Trials.” Obstetrics and Gynecology Clinics of North America 43, no. 1 (March 2016): 69–81 Barber, Matthew D., Linda Brubaker, Kathryn L. Burgio, Holly E. Richter, Ingrid Nygaard, Alison C. Weidner, Shawn A. Menefee, et al. “Comparison of 2 Transvaginal Surgical Approaches and Perioperative Behavioral Therapy for Apical Vaginal Prolapse: The OPTIMAL Randomized Trial.” JAMA 311, no. 10 (March 12, 2014): 1023–34
‘Optimal’ Outcomes
Apical failure: Average study finding 15% — Success defined as both objective and subjective success
at 2 years postop — USLS/McCall: 59.2% (N=154) — SSLS: 60.5% (152) — Recurrent objective prolapse beyond hymen: 15.5% (no
difference) — Subjective outcomes: no difference
Barber, Matthew D., Linda Brubaker, Kathryn L. Burgio, Holly E. Richter, Ingrid Nygaard, Alison C. Weidner, Shawn A. Menefee, et al. “Comparison of 2 Transvaginal Surgical Approaches and Perioperative Behavioral Therapy for Apical Vaginal Prolapse: The OPTIMAL Randomized Trial.” JAMA 311, no. 10 (March 12, 2014): 1023–34
Perceived Success
Depends on definitions, choices of measurement and completely arbitrary decisions
There does seem to be higher risk of anterior recurrence with SSLS vs USLS and McCall
Morgan, Daniel M., Mary A. M. Rogers, Markus Huebner, John T. Wei, and John O. Delancey. “Heterogeneity in Anatomic Outcome of Sacrospinous Ligament Fixation for Prolapse: A Systematic Review.” Obstetrics and Gynecology 109, no. 6 (June 2007): 1424–33

Success
Studies bedeviled by additional procedures and lack of standardization
USLS and SSLS equivalent — Depends on definitions Strict anatomical success based on POPQ, is low (37-64%) Clinically relevant success (not below hymen) better
(82-94%)
Why I don’t like USLS/McCall
Ureter obstruction up to 11% (more common than studies will have you believe)
TEN fold increase risk if anterior colporrhaphe is done as well
This is difficult/impossible to prevent Not easy to do extra-peritoneally
Jackson, Elisha, Jorge A. Bilbao, Robert W. Vera, Zuber D. Mulla, Veronica T. Mallett, and T. Ignacio Montoya. “Risk Factors for Ureteral Occlusion during Transvaginal Uterosacral Ligament Suspension.” International Urogynecology Journal 26, no. 12 Margulies, Rebecca U., Mary A. M. Rogers, and Daniel M. Morgan. “Outcomes of Transvaginal Uterosacral Ligament Suspension: Systematic Review and Metaanalysis.” American Journal of Obstetrics and Gynecology 202, no. 2
I Don’t Like Ureter Complications!!
To me and my patients, the rate with USLS/McCall is unacceptable — Too much hassle, stress, waste of time, undoing of hard
work — I don’t want to have to call urologist
Procedure less ‘specific’ than SSLS
USLS/McCalls
Much more ‘vague’ More difficult to teach More difficult to be consistent More difficult than usually admitted
— Just watch someone struggle — Just watch them take ‘shortcuts’ Euphemistically called ‘modified’ procedure
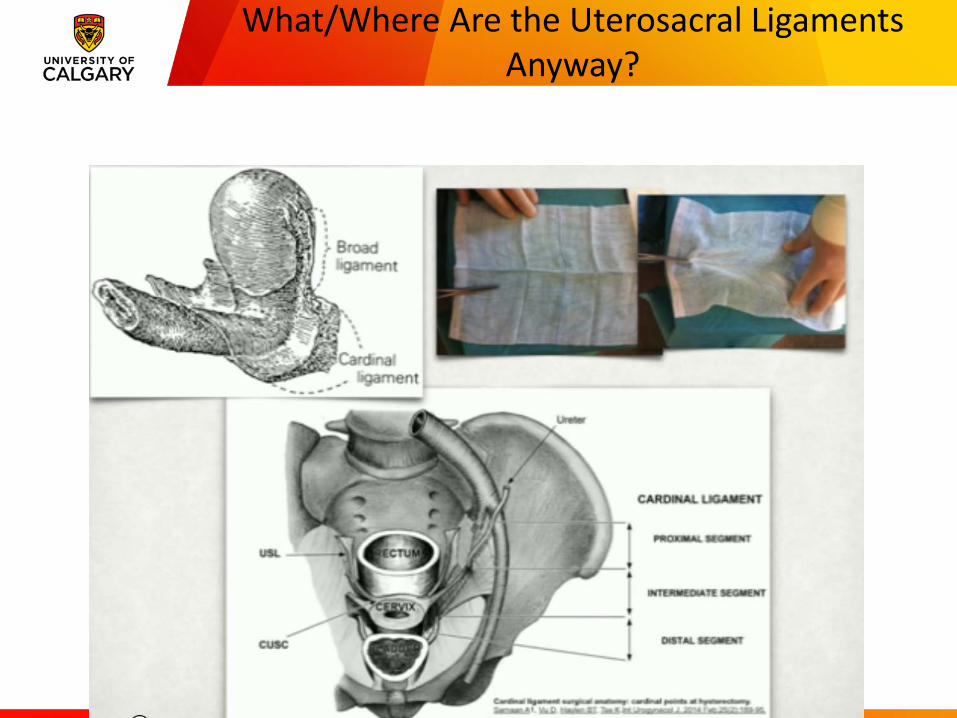
What/Where Are the Uterosacral Ligaments Anyway?
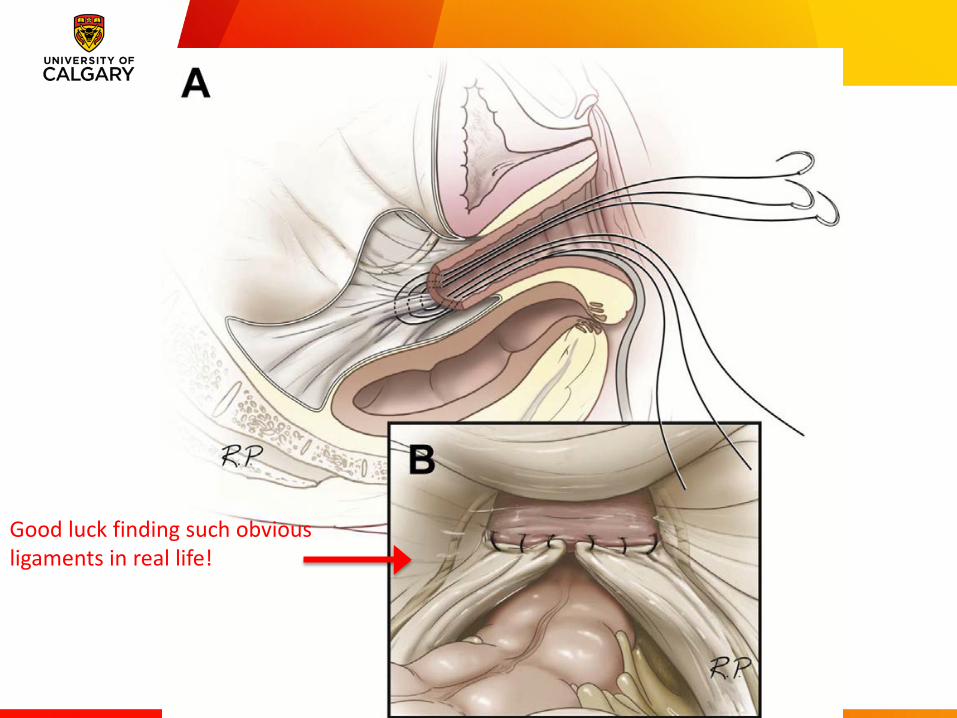
Good luck finding such obvious ligaments in real life!
Fooling Yourself
Let me make this perfectly clear
If you are simply tying the cut end of the USL to the vault (in a patient with prolapse)
– you are not doing a proper Level I support!
SSLS Benefits
More specific Easier to mitigate risk
— Direct palpation of landmarks — Use of device to prevent deep stitches
Possible ways to prevent anterior recurrence Easy intra-and extra-peritoneal approaches

SSLS
Apical success equivalent to USLS — Objective failure 2.4-19%
Anterior failure more common — However mostly asymptomatic
No difference in subjective satisfaction with degree of support, as long as at or above hymen
Barber, Matthew D., and Christopher Maher. “Apical Prolapse.” International Urogynecology Journal 24, no. 11 (November 2013): 1815–33 Hill, Audra Jolyn, and Matthew D. Barber. “Apical Prolapse Repair: Weighing the Risks and Benefits.” Current Opinion in Obstetrics & Gynecology 27, no. 5 (October 2015): 373–79

SSLS Risks
Buttock pain Sacral/pudendal neurovascular injury
Review of 1,229 SSLS
— 0.2% severe hemorrhage — Transfusion rate 2% — Buttock pain 3% (resolved by six weeks)
Sze, E. H., and M. M. Karram. “Transvaginal Repair of Vault Prolapse: A Review.” Obstetrics and Gynecology 89, no. 3 (March 1997): 466–75

SSLF vs SCP
Studies are conflicting No hard evidence that one is superior Cost effectiveness studies conflicting and dependent
on input parameter modeling Seems to be consensus that SCP better long term
Ohno, Mika S., Monica L. Richardson, and Eric R. Sokol. “Abdominal Sacral Colpopexy versus Sacrospinous Ligament Fixation: A Cost-Effectiveness Analysis.” International Urogynecology Journal 27, no. 2 (February 2016): 233–37.

Summary: Why SSLS?
Strong anchor point Very low ureteral obstruction Easy to do with or without hysterectomy
— Trans-peritoneal or extra-peritoneal
Consistency, in contrast to USL — Can be more specific with exact position
Easier and quicker!
CUMMING SCHOOL OF MEDICINE
Thank You