sacral and hemi lumbar spine of low grade pelvic878 C. Zoccali et al. Figure 6 Postoperative X-ray...
5
Orthopaedics & Traumatology: Surgery & Research (2013) 99, 875—879 Available online at www.sciencedirect.com CASE REPORT Pelvic sacral and hemi lumbar spine resection of low grade pelvic chondrosarcoma: A multistage procedure involving vascular bypass, spine fixation and vascular exclusion C. Zoccali a,b,∗ , G. Marolda c , A. Di Francesco c , L. Favale d , N. Salducca d , R. Biagini d a Oncological Orthopaedics Department, Muscular-skeletal Tissue Bank, IFO-Regina Elena National Cancer Institute, Via Elio Chianesi 53, 00144 Rome, Italy b Department of Surgical Science, University of L’Aquila, L’Aquila, Italy c Orthopaedics Department, ‘‘San Salvatore Regional Hospital’’, via Vetoio 1, 67100 L’Aquila, Italy d Oncological Orthopaedics Department, IFO-Regina Elena National Cancer Institute, Via Elio Chianesi 53, 00144 Rome, Italy Accepted: 15 May 2013 KEYWORDS Pelvic chondrosarcoma; Pelvic tumor; Pelvic resection; Lumbar resection; Extra-anatomical vascular bypass Summary Peripheral chondrosarcoma is a rare tumor particularly insidious when arising from the pelvis, becoming symptomatic later in time when surgery may be too difficult and dangerous due to this complex area. In the present case, the tumor arose from an exostosis located on the medial surface of the left iliac wing. Its diameter was 25 cm × 20 cm × 15 cm, adhering to the last three vertebrae, involving the left iliac vein and artery, displacing the left ureter. In a similar case, a hindquarter amputation is indicated but, if the patient refuses, a resection remains possible. In this paper, we describe a multistage technique consisting of an extra- anatomic vascular bypass, a lumbar stabilization, a neurovascular bundles anterior isolation and a postero-lateral resection of this mass. After a five-year follow-up, the patient is alive and able to stand and walk with support, after undergoing twice lung metastasis removal. © 2013 Elsevier Masson SAS. All rights reserved. ∗ Corresponding author. IFO-Regina Elena National Cancer Institute, Via Elio Chianesi 53, Rome, Italy. Fax: +39 6 526 627 78; Mobile phone: +39 3 3863 550 40. E-mail address: [email protected] (C. Zoccali). 1877-0568/$ – see front matter © 2013 Elsevier Masson SAS. All rights reserved. http://dx.doi.org/10.1016/j.otsr.2013.05.007 CORE Metadata, citation and similar papers at core.ac.uk Provided by Elsevier - Publisher Connector
Transcript of sacral and hemi lumbar spine of low grade pelvic878 C. Zoccali et al. Figure 6 Postoperative X-ray...

CORE at core.ac.uk
Provided by Els
Orthopaedics & Traumatology: Surgery & Research (2013) 99, 875—879
Available online at
www.sciencedirect.com
CASE REPORT
Pelvic sacral and hemi lumbar spineresection of low grade pelvicchondrosarcoma: A multistage procedureinvolving vascular bypass, spine fixationand vascular exclusion
C. Zoccali a,b,∗, G. Maroldac, A. Di Francescoc, L. Favaled,N. Salduccad, R. Biaginid
a Oncological Orthopaedics Department, Muscular-skeletal Tissue Bank, IFO-Regina Elena National CancerInstitute, Via Elio Chianesi 53, 00144 Rome, Italyb Department of Surgical Science, University of L’Aquila, L’Aquila, Italyc Orthopaedics Department, ‘‘San Salvatore Regional Hospital’’, via Vetoio 1, 67100 L’Aquila, Italyd Oncological Orthopaedics Department, IFO-Regina Elena National Cancer Institute, Via Elio Chianesi 53,00144 Rome, Italy
Accepted: 15 May 2013
KEYWORDSPelvicchondrosarcoma;Pelvic tumor;Pelvic resection;Lumbar resection;
Summary Peripheral chondrosarcoma is a rare tumor particularly insidious when arising fromthe pelvis, becoming symptomatic later in time when surgery may be too difficult and dangerousdue to this complex area. In the present case, the tumor arose from an exostosis located onthe medial surface of the left iliac wing. Its diameter was 25 cm × 20 cm × 15 cm, adhering tothe last three vertebrae, involving the left iliac vein and artery, displacing the left ureter. Ina similar case, a hindquarter amputation is indicated but, if the patient refuses, a resection
Metadata, citation and similar papers
evier - Publisher Connector
Extra-anatomicalvascular bypass
remains possible. In this paper, we describe a multistage technique consisting of an extra-anatomic vascular bypass, a lumbar stabilization, a neurovascular bundles anterior isolationand a postero-lateral resection of this mass. After a five-year follow-up, the patient is alive and
able to stand and walk with support, after undergoing twice lung metastasis removal. © 2013 Elsevier Masson SAS. All∗ Corresponding author. IFO-Regina Elena National Cancer Institute, ViaMobile phone: +39 3 3863 550 40.
E-mail address: [email protected] (C. Zoccali).
1877-0568/$ – see front matter © 2013 Elsevier Masson SAS. All rights rehttp://dx.doi.org/10.1016/j.otsr.2013.05.007
rights reserved.
Elio Chianesi 53, Rome, Italy. Fax: +39 6 526 627 78;
served.

8 C. Zoccali et al.
I
PtT(wltntmtftoitmcwda
C
ApStloejsh
sfEcbtsu
thwficstoltfcuru
Figure 1 A CT-scan showing the tumor mass arising from themedial aspect of the iliac bone from a preexisting exostosis,adhering to the last three vertebrae and dislocating the leftvascular bundle. In the square, it is possible to see the left iliacvessels in complete adherence to the mass. In addition, the rightiliac vessels are hidden by the right ilio-psoas muscle and themass.
Fa
‘Abt
76
ntroduction
eripheral chondrosarcoma (PCS) is a rare tumor arising fromhe peripheral bone usually from a pre-existing exostosis [1].he bones of the pelvis are the common sites of involvement39% in the Rizzoli Institute series), particularly insidioushen arising from the inner side, becoming symptomatic
ater in time when surgery is difficult and dangerous dueo the complex anatomy of the area and the presence ofeurovascular bundles [1]. Moreover, surgical resection ishe only available treatment since the usual adjuvant treat-ents are ineffective [1—3]. The precocious involvement of
he iliac vessels is the main problem. When to separate themrom the mass is not possible, vascular bypass is manda-ory in performing a wide resection, even when from anncological perspective amputation is the safer option. Thenvolvement of the acetabular roof, the sacroiliac joint andhe lumbar spine renders resection more complicated anday lead to spine, pelvis and hip instability. The aim of the
urrent study was to present a multistep strategy to allow aide resection of an enormous PCS 25 cm × 20 cm × 15 cm iniameter, adhering to the left iliac vessels, to the left ureternd to the last three vertebrae.
ase report
47-year-old male was referred to our department com-laining of the presence of a large mass in his abdomen.ix months before, because of the worsening of the symp-oms and the onset of an irradiated pain to his left leg, aumbar CT scan was performed. It highlighted the presencef a significant mass that developed from a suspected pre-xisting exostosis located in the medial area of the left wingust above the acetabular roof, involving the left iliac ves-els and adhering to the left ureter and to the last threeemibodies of the last three lumbar vertebrae (Fig. 1).
The imaging and symptoms suggested a primitivearcoma; consequently, a CT-guided trocar biopsy was per-ormed using an 8G needle through the lateral part ofnneking incision. The following histology exam confirmedlinical suspicion of a low-grade chondrosarcoma. An openiopsy was excluded in order to reduce the risk of con-amination even if a cartilagineous tumor was clinicallyuspected. The urography showed the dislocation of the leftreter.
Based on the low-grade histology and the absence of dis-ant metastases, a hindquarter amputation was proposed,owever, the patient refused, therefore, a wide resectionas scheduled to be carried out over several operations. Therst operation consisted in performing an extra-anatomicross line ilio-femoral arterial bypass using Dacron prosthe-is to guarantee blood supply to the left inferior limb fromhe right. The venous return was reconstructed with the endf distal controlateral saphena vein and anastomosed to theeft femoral vein. Both bypasses were placed anteriorly tohe superior part of the symphysis pubis to separate themrom the main access. After two weeks, a second surgery was
arried out, consisting of a L1 to S1 posterior transpedicularnilateral right stabilization as showed in a postoperative X-ay (Fig. 2). Two weeks later the third operation was done bysing the trans-peritoneal anterior approach, carrying out aitbs
igure 2 Posterior L1 to S1 hemistabilization, surgical aspectsnd postoperative X-ray.
‘T’’ incision (xypho-pubic plus a right transverse incision).fter positioning a catheter in the left ureter, the vascularundles were identified and isolated as far as possible fromhe tumor. The left iliac artery was ligated. Unfortunately,t was not possible to ligate the left iliac vein because it was
otally hidden by the tumor. A Gore-Tex spacer was insertedetween vascular bundles and the tumor to prevent con-equent adhesions. An arteriography performed after one
Multistep procedure to resect a giant lumbar-pelvic chondrosarcoma 877
F
dvpGdwtptrv
Figure 3 Arteriography performed one month after extra-anatomic cross line ilio-femoral bypass showed revasculariza-tion of the left inferior limb.
week showed the bypass to be functioning well and the leftiliac artery completely excluded (Fig. 3). A fourth surgeryhad to be carried out two weeks later: two balloons werepositioned, one in the inferior cave vein and the second onein the right iliac vein to immediately stop blood flow, incase of massive hemorrhage. The patient was positioned ina lateral right position; the Enneking incision was made plusa second one starting from the belly area, heading later-ally towards the superior-anterior iliac spine. The tumor wasremoved together with part of the left iliac bone, the left
sacroiliac joint and the last three left hemi-vertebrae, theleft iliac artery and vein. The nerve roots from L2 to S1 weresacrificed as planned and the femoral and sciatic nervescut (Fig. 4). During removal, the inferior cava vein wasFigure 4 The mass was isolated before removal; on the right,there is the head of the patient. It is possible to see the posterioraspect of the left iliac wing and the tumor arising from this site.In the left square, the operative field after tumor removal isshown and in the right square, the X-ray of the removed mass.
Ta
rorpaoafitt4
eiafiudwtifts
igure 5 Postoperative X-ray showing left hip dislocation.
amaged, the balloons inflated and the vein repaired by aascular surgeon without significant blood loss. The histologyerformed on the entire specimen revealed the presence of2 areas in the mass. The postoperative X-ray evidenced aislocation of the femoral head because the acetabular roofas partially resected during osteotomy (Fig. 5). This was
aken care of with an extra skeletal traction consequentlyostponing the related therapy. The following postopera-ive days were characterized by wound infection and severalevisions, so, after carefully examining the poor results, aacuum assisted closure therapy was applied for six months.he wound healed completely by performing a skin graftingt seven months from surgery.
At 18 and 24 months follow-up, the patient had surgery toesect a lung metastasis. At 32 months follow-up, a furtherperation was carried out to stabilize the lumbar spine byight lumbar access, positioning the patient in a left lateralosition. A mixed stabilization was performed by inserting
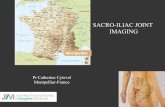
screw in the L2 vertebral body and in the medial partf the iliac wing that were linked by a rod and a fibularutograft with the morcellized homograft bone (Fig. 6). Thebular should have been vascularized nevertheless the anas-omosis was impossible to perform. After having verifiedhe arthrodesis, the patient was finally allowed to stand at0 months of follow-up.
After a five-year follow-up, the patient is alive withoutvidence of local relapse but with other lung metastases;t is able to stand and walk with a support without baringny weight on his left inferior limb. The X-ray, performed atve years of follow-up, highlighted damage to the acetab-lar roof but no evidence of the left femoral head beingisplaced (Fig. 7). The Musculoskeletal Tumor Society scoreas 26.7%, however, the patient was particularly satisfied
o be able to stand on his own and to have maintained his
nferior left limb. It was advisable for the patient to undergourther surgery to stabilize the left hip dislocation; however,he quality of the tissues and the presence of several inci-ions and lung metastasis discouraged a possible arthrodesis.
878
Figure 6 Postoperative X-ray showing the two screws in L1and in iliac right wing linked by a rod and the fibular autograft.
Fd
Twtftvb
D
Wc
idtttl
crmcEgtttiasfrt
rtstsp[iobrcngfitir
wbctaattt
onstss
igure 7 X-ray performed at 5 years of follow-up showing theamaged left acetabular roof not suitable to bearing weight.
he study was authorized by the local ethical committee andas performed in accordance with the Ethical standards of
he 1964 Declaration of Helsinki as revised in 2000. The needor an informed consent was waived by the ethical commit-ee since rights and interests of the patients would not beiolated and their privacy and anonymity would be assuredy this study design.
iscussion
hen PCS is located in the pelvic medial surface as in theurrent case, it can become large in size, growing indolent
em
p
C. Zoccali et al.
n the abdomino-pelvic cavity [1]. The surgical approach isifficult presenting two main problems: the resection andhe reconstruction; considering surgical margin as impor-ant prognostic factor, the primary surgical aim is completeumor resection and secondary preservation of stability andower limb function.
Wide margin might be more important in non-hemotherapy responsive tumors. Court et al. [4] report aecurrence percentage of 7% and 70% for adequate (wide andarginal) and inadequate margins respectively after surgi-
al excision of bone sarcomas involving the sacroiliac joint.ven if some authors recommend marginal margins in lowrade CS, we suggest adopting wide margins when possibleo reduce the risk of local recurrence that are very difficulto treat in this location [5,6]. Wide margins are also difficulto achieve because of the presence of neurovascular bundlesn the pelvic cavity so that when dissection is not possiblend safe, a vascular bypass must be scheduled. Moreover,acral and ilio-sacral joint involvement is an important riskactor for the onset of local recurrence [7], justifying poste-ior access, laminectomy, nerve roots bounding, section andhen tumor removal.
When extensive resection is done, reconstruction isequired to avoid severe functional disabilities [8,9]. Severalechniques are described in literature, and are based on theites and the extent of the resection. Some authors suggesthe use of an allograft to restore lumbar-sacral and pelvictability [10,11] and vascularized autograft [12—14], othersropose the use of a complex prosthesis or bone cement15]. Nevertheless, reconstruction procedures increase thenfection rate so the choice whether to reconstruct or notr what kind of reconstruction to be carried out must beased on the following factors: the entity of resection, theisk of infection, the need of the patient to undergoing ahemotherapy, the quality of the skin and the risk of woundecrosis [7,8,16]. Some authors recommend the use of auto-raft to decrease the risk of infection [17]. The use ofxation devices is an important risk factor for postopera-ive wound infection. Court et al. [4] report a postoperativenfection rate of 40% in patients undergoing sacroiliac tumoresection.
An original sequential multistep procedure was scheduledith an additional unexpected step, before tumor resection,y positioning two endovascular balloons, one in the inferiorave vein and the other in the left iliac vein [18,19]. Duringhe fourth surgical step, that consisted in tumor removal,fter performing osteotomies, the cava vein was damagednd the inflation of the two balloons allowed a safe repair sohat the total amount of vascular bleeding was only 2700 mL,hat is almost low considering the operation lasted seven-een hours.
Considering the hip dislocation and the partial stabilityf the lumbar spine, two other operations would have beenecessary to complete the surgical program. A hip arthrode-is was decided to be avoided because of the poor quality ofhe left tissue and to the limitation in accessing the site. Theame access problem emerged when stabilizing the lumbarpine on the left side; therefore, in this case, the right lat-
ral approach was the only possible option, despite being aore biomechanical than contralateral disadvantage.The onset of two pulmonary metastases suggested post-oning the surgery after their removal when the biological

sarc
[
[
[
[
[
[
[
[
[
[
[
Multistep procedure to resect a giant lumbar-pelvic chondro
aggressiveness of the disease was clarified. Finally, at32 months of follow-up from the primary mass removal,spine stabilization was performed.
Only one former study reports a combined resection ofposterior pelvis and lumbar spine [20]. The authors describethe outcome of 18 patients with pelvic sarcoma (13 highgrade sarcomas) who had undergone hemipelvectomy, fromthose 11 had a hemivertebrectomy of L5 and 7 had anL4—L5 hemivertebrectomy [20]. At a mean follow-up of56 months, 12 out the 18 patients were alive without disease[20].
Although modern techniques permit several complexoperations to be performed, pelvic resection must only beundertaken once the surgeon can ascertain that the removalof the tumor will be as radical as in a hindquarter ampu-tation. To guarantee better results thorough planning ismandatory.
When resection of a pelvic tumor and reconstruction isdone in one step, the percentage of complications increasesconsiderably as demonstrated in literature. This is particu-larly the case with regards to infection versus surgical timeand blood lost. Thus, we suggest to divide complex oper-ations into diverse steps taking into account the patient’sconditions, the amount of anaesthesia needed and the sur-geon’s preferences and to be sure the wound of the previousaccess was completely healed before performing anotherone [7,21]. This extreme surgery is more indicated forlow-grade tumors where a wide resection can change theprognosis of the patient.
Disclosure of interest
The authors declare that they have no conflicts of interestconcerning this article.
Acknowledgement
We thank Ms. Paula Franke and Tania Merlino for reviewingthe English language.
References
[1] Campanacci M. Bone soft tissue tumors. 2nd ed. New York:Springer; 1999.
[2] Gelderblom H, Hogendoorn PC, Dijkstra SD, Van Rijswijk CS,Krol AD, Taminiau AH, et al. The clinical approach towardschondrosarcoma. Oncologist 2008;13:320—9.
[3] Riedel RF, Larrier N, Dodd L, Kirsch D, Martinez S, BrigmanBE. The clinical management of chondrosarcoma. Curr Treat
Options Oncol 2009;10:94—106.[4] Court C, Bosca L, Le Cesne A, Nordin JY, Missenard G. Surgicalexcision of bone sarcomas involving the sacroiliac joint. ClinOrthop Relat Res 2006;451:189—94.
[
oma 879
[5] Donati D, El Ghoneimy A, Bertoni F, Di Bella C, Mercuri M.Surgical treatment and outcome of conventional pelvic chon-drosarcoma. J Bone Joint Surg (Br) 2005;87:1527—30.
[6] Fiorenza F, Abudu A, Grimer RJ, et al. Risk factors for survivaland local control in chondrosarcoma of bone. J Bone Joint Surg(Br) 2002;84:93—9.
[7] O’Connor MI, Sim FH. Salvage of the limb in the treat-ment of malignant pelvic tumors. J Bone Joint Surg (Am)1989;71:481—94.
[8] Wirbel RJ, Schulte M, Mutschler WE. Surgical treatmentof pelvic sarcomas: oncologic and functional outcome. ClinOrthop Relat Res 2001;390:190—205.
[9] Zeifang F, Buchner M, Zahlten-Hinguranage A, Bernd L, SaboD. Complications following operative treatment of primarymalignant bone tumours in the pelvis. Eur J Surg Oncol2004;30:893—9.
10] Harrington KD. The use of hemipelvic allografts or autoclavedgrafts for reconstruction after wide resections of malignanttumors of the pelvis. J Bone Joint Surg (Am) 1992;74:331—41.
11] Delloye C, Banse X, Brichard B, Docquier PL, Cornu O.Pelvic reconstruction with a structural pelvic allograft afterresection of a malignant bone tumor. J Bone Joint Surg (Am)2007;89:579—87.
12] Hubert DM, Low DW, Serletti JM, Chang B, Dormans JP.Fibula free flap reconstruction of the pelvis in children afterlimb-sparing internal hemipelvectomy for bone sarcoma. PlastReconstr Surg 2010;125:195—200.
13] Mendel E, Mayerson JL, Nathoo N, Edgar RL, Schmidt C, MillerMJ. Reconstruction of the pelvis and lumbar-pelvic junctionusing 2 vascularized autologous bone grafts after en blocresection for an iliosacral chondrosarcoma. J Neurosurg Spine2011;15:168—73.
14] Laffosse JM, Pourcel A, Reina N, et al. Primary tumor of theperiacetabular region: resection and reconstruction using asegmental ipsilateral femur autograft. Orthop Traumatol SurgRes 2012;98:309—18.
15] Natarajan MV, Bose JC, Mazhavan V, Rajagopal TS, Selvam K.The saddle prosthesis in periacetabular tumours. Int Orthop2001;25:107—9.
16] Aydinli U, Ozturk C, Yalcinkaya U, Tirelioglu O, Ersozlu S. Limb-sparing surgery for primary malignant tumours of the pelvis.Acta Orthop Belg 2004;70:417—22.
17] Hillmann A, Hoffmann C, Gosheger G, Rödl R, Winkelmann W,Ozaki T. Tumors of the pelvis: complications after reconstruc-tion. Arch Orthop Trauma Surg 2003;123:340—4.
18] Yu H, Stavas JM, Dixon RG, Burke CT, Mauro MA. Temporaryballoon tamponade for managing subclavian arterial injury byinadvertent central venous catheter placement. J Vasc IntervRadiol 2011;22:654—9.
19] Taylor CL, Selman WR, Kiefer SP, Ratcheson RA. Temporary ves-sel occlusion during intracranial aneurysm repair. Neurosurgery1996;39:893—905.
20] Fuchs B, Yaszemski MJ, Sim FH. Combined posterior pelvisand lumbar spine resection for sarcoma. Clin Orthop Relat Res2002;397:12—8.
21] Abudu A, Grimer RJ, Cannon SR, Carter SR, Sneath RS. Recon-struction of the hemipelvis after the excision of malignanttumours. Complications and functional outcome of prostheses.J Bone Joint Surg (Br) 1997;79:773—9.