RSBY Revised Process Guidelinesrsby.gov.in/Docs/Revamp of RSBY Phase II- Process...RSBY Revised...
201
Transcript of RSBY Revised Process Guidelinesrsby.gov.in/Docs/Revamp of RSBY Phase II- Process...RSBY Revised...


RSBY Revised Process Guidelines
2 | P a g e
Document version and revision details
Sr. No.
Document version
Submission date
Reviewer Revision by Sign off by Date of sign off
Comments / remarks
1. Version 1.0 9th May 2014 Draft approved in-principle by Sub-groups
9th May 2014 Document will undergo continuous revisions over time for changes in policy/ field inputs
2. Version 2.0 13th May 2014 Approved at the Empowered Committee Meeting
15th May 2014
Document will undergo continuous revisions over time for changes in policy/ field inputs
3. Version 3.0 On-going

RSBY Revised Process Guidelines
3 | P a g e
Table of contents
S. No. Section Page number
1 Introduction …………………………………………………………. 1
2 Data preparation and pre-enrolment …………………………………………………………. 4
3 Enrolment …………………………………………………………. 19
4 Smart card and key management system …………………………………………………………. 35
5 Wellness check and payment of premium …………………………………………………………. 48
6 Hospital management …………………………………………………………. 60
7 Claim management …………………………………………………………. 75
8 Public grievance management …………………………………………………………. 84
9 Kiosk management …………………………………………………………. 106
10 MIS for RSBY …………………………………………………………. 122
11 Third party Audit of RSBY Scheme …………………………………………………………. 132
11 Annexures …………………………………………………………. 140

RSBY Revised Process Guidelines
1 | P a g e
Introduction
Social security and healthcare for all has been the motto of Government of India, and it has taken various steps in this regard.
One of the important policy milestones is the Unorganized Workers Social Security Act (2008) enacted by the Central Government to provide for the
social security and welfare of the unorganized workers. This act recommends that the central government provide social security schemes to mitigate
risks due to disability, health shocks, maternity, and old age, which all unorganized workers get exposed to, and are likely to suffer from. A number of
Central schemes are in operation and have provided protection to the beneficiaries from the unorganized worker segment. Additionally, a large number of
labour welfare funds set up by both central and state governments on non-contributory basis provide social security as well as financial assistance in some
cases to the unorganized workers in certain occupations.
One such policy initiatives in the health insurance space is RSBY that was launched in early 2008. RSBY was initially designed to target only the Below
Poverty Line (BPL) households, but has recently been expanded to cover a number of non-BPL categories of informal sector workers, including street
vendors, domestic workers, beedi workers, building and construction workers, and most importantly the workers who have worked for more than 15 days
under MGNREGS. Government of India and the State Governments are co-financing the premium cost for enrolled beneficiaries. Till date, more than 32
million eligible households are covered by RSBY. The program has the target to cover 70 million households by the end of the Twelfth Five Year Plan
(2012-17). Its service delivery model – demand financing, freedom of choice among accredited government and private hospitals, and cashless service
reimbursable to provider on a pre-determined package price basis, could become a strong pillar for the universal health care system laid down by
Government of India.
The scheme has faced various challenges in the implementation at the field level, and lack of complete and accurate information/data visibility on RSBY
services has been observed.
To address these challenges and to incorporate learnings of last 6 years, Ministry of Labour and Employment (MoLE) has decided for a major revamp of
complete system. These guidelines are first step in this direction. These guidelines have been prepared in consultation with sub-groups formed at Ministry
of Labour and Employment, Government of India, comprising of MoLE officers, State RSBY SNA teams, GIZ, and consulting partner support provided by
the World Bank.
The guideline document is a live document and needs to be re-visited / edited periodically based on learnings from field operations, policy changes
and technology modifications. The guideline highlights the current processes and modifications to these processes based on discussions with the sub-
groups at MoLE. The suggested changes shall be implemented by NIC in the stipulated time mentioned by MoLE to smoothen the existing RSBY phase.
The revised process guidelines for phase II for RSBY have been prepared for 8 sub-processes as depicted in the diagram below:

RSBY Revised Process Guidelines
2 | P a g e
Figure 1: RSBY Sub-processes

RSBY Revised Process Guidelines
3 | P a g e
Each sub-process has been assigned a process code and process objective, along with other placeholders within the guidelines template defined for every
sub-process. The placeholders that have been used in the template are depicted in Figure 2 below. The template captures the existing activities in RSBY,
and provides the revised set of activities, which will be taken up for implementation in the proposed phase II of revamped RSBY. The content in the
following sections of this document is subject to changes / modifications based on field experience, changes in the policy environment, and inputs from
various stakeholders and updates to the technology systems/applications.
Figure 2: Process template placeholders

RSBY Revised Process Guidelines
4 | P a g e
Pro
ce
ss
Co
de
I –DPENR Process Name
Data Preparation and pre-enrolment
Process Objective Current Status 1. Collection of beneficiary data from departments, deduplication of
data and creation of enrolment list for RSBY 2. Ensuring accuracy and consistency of data collected, both from a
structural and template perspective
1. Guidelines on 11 eligible beneficiary categories being used to solicit data from departments in the state
2. Different data formats (hard copy lists/excel/MS access/PDF) being used by departments to hand over pre-enrolment data to State Nodal Agencies (SNA’s). The formats vary across states and departments. It is expected that in future also, departments would continue to hand over data in their own format.
3. Data Collection template and enrolment/validation software is being changed to add attributes, such as NPR/Aadhaar number, which will make it easier to de-duplicate the data
Key Stakeholders Key Performance Indices (KPIs) 1. MoLE 2. State Departments responsible for pre-enrolment data collection
across 11 eligible categories Rural Development Department: BPL, NREGS (>15 days) and IGNOAPS Urban Local Bodies: BPL (U), Domestic worker, Rag pickers, sanitation workers and Rickshaw pullers Labor Welfare Commissioner: Beedi Workers State Board for Building and other construction workers: Construction worker State Transport department: Taxi/Auto drivers
Ministry of Mines/State department of Mines: Mine Workers Railways: porters Ministry of textiles. for textile worker data ( for using RSBY
Measures1: MoLE, SNA, Departments (relevant reports to be available, depending on role) 1. Data collected and processed from different department
Filters: User Category (Departments, SNA), Beneficiary category, Geography (State, District, Block, Village, Town, City (VTC), Processing status
2. Number of beneficiaries under multiple categories Filters: Geography
Key performance indicator2: (relevant KPI’s to be measured, depending on role) 1. Quality of deduplication as per audit report 2. Accuracy & completion of data shared by departments with SNA as per audit
report. (Accuracy to be measured as % of records which are de-duplicated at
1 All measures to be available as a report on a web portal in real-time/near-real-time. The data should be available in a warehouse, such that any extraction is possible to create ad-hoc reports
2 MIS on all KPIs to be available on a web portal in real-time/near-real-time, with authorised access

RSBY Revised Process Guidelines
5 | P a g e
platform) DFS – LIC data of AABY
3. SNA
source, and which follow data structure and template) 3. Total number and % of invalid records identified. Invalid records are those
with: - Missing mandatory information - Incorrect structure - Interchanged data, based on location (block, etc.)
4. Total number of records validated, de-duplicated and uploaded on MoLE servers for URN generation
5. Average time3 taken by MoLE to generate URN’s for all records after receipt of clean and de-duplicated pre-enrolment data from SNA’s
6. Average time taken by MoLE to hand over pre-enrolment data (URN generated) to Insurance company (IC)
7. Expected wait time to generate URN number for a reference data-set (for a district) when it is uploaded by the SNA - This will be computed and published every day based on current records
awaiting URN generation 8. Time taken by IC to acknowledge the validity of data received by MoLE
- This would be computed based on time difference between MoLE sending data, and IC notifying validity in the proposed web application
Current Challenges Summary of key suggestions 1. Pre-enrolment data shared by state departments in multiple
formats and data structures 2. Guidelines for validation /background check at field level of pre-
enrolment data not always followed by SNA 3. Lack of standard and practical guidelines and automated process
for de-duplication 4. In some states, data preparation for enrolment always starts
afresh and the data prepared for the previous year is not used, resulting in duplication of efforts. (Fresh pre-enrolment data uploaded by SNA does not include URN generated in the prior cycle)
5. Category prioritization guidelines for beneficiaries is not defined 6. Insurance company (IC) sometimes not provided with pre-
1. Standard template and data-structure to be used by departments for sharing data with SNA’s (eventually to do this using proposed web application). The proposed format is MS Access. (.mdb files)
2. Validation and deduplication of pre-enrolment data during entry by SNA’s (or eventually departments) in the proposed web application
3. Guidelines on prioritization of categories of beneficiaries (Annexure 1.1) to be defined and followed at the de-duplication stage for creating pre-enrolment data with URN
4. Standard deduplication and validation techniques to be followed by all departments and SNA’s (Annexure 1.2)
5. MoLE to provide URN generated pre-enrolment data to IC, 15 days prior to commencement of enrolment process, SNA should ensure to make available data to MoLE well in advance, taking into consideration expected waiting time
3 Average time to be calculated on the basis of time stamp associated with the activity available in data base

RSBY Revised Process Guidelines
6 | P a g e
enrolment data (with URN generated) in a timely manner by MoLE
7. Insurance company (IC) does not acknowledge the validity of data received by MoLE
indicated by MoLE 6. Robust process and system to be defined to check whether beneficiary
already has an RSBY card at the time of pre-enrolment. Departments to be encouraged to use a tablet/mobile based application for this purpose
7. Prior URN to be used at the time of pre-enrolment data preparation 8. Align the master data of geography (district, block) with that of census
Pre-requisites for the pre-enrolment and data preparation process 1. Availability of data capture templates (Annexure 1.3)with the state departments (till such time they start using the proposed web application) 2. Access of the proposed web application to SNA’s and MoLE users. (and eventually to departments) 3. Mandatory capture of atleast 1 key field for de-duplication (NPR number / Aadhaar number / Mobile number / NREGS ID / BPL card number) 4. On-boarding and training of MoLE technical team, SNA officials and state department officials on the pre-enrolment process.
Inputs to the revised process Output from the revised process 1. Pre-enrolment data from state departments 1. Pre-enrolment URN generated data for enrolment process
Processes and Responsibilities:
Sr. No
Current Process Responsibility Proposed Process Corresponding Responsibilities
Remarks
1 Preparation of data of eligible beneficiaries
1.1 Respective departments to collect pre-enrollment data
Respective state departments
1. Robust check at the time of pre-enrolment by State departments to ensure that the beneficiary does not have an RSBY card already. (can be done at the time of data collection by state department for respective scheme/program)
2. The format and template for capture of pre-enrolment data would be standard in the web application. The data capture
Respective state departments
1. In order to empower the departments for deduplication check at the time of pre-enrolment, electronic tools should be made available, through which they may search from the list of existing RSBY beneficiaries.
2. List of fields to be captured in the form:
S.No., Name of Beneficiary*, Father’s/Husband’s name, Date of birth / Age*, Gender*, Address*, VTC*

RSBY Revised Process Guidelines
7 | P a g e
Sr. No
Current Process Responsibility Proposed Process Corresponding Responsibilities
Remarks
template has been defined in Annexure 1.3 of the guidelines
(Village/Town/City), District*, State*, Pin-code, Caste Category* (SC/ST/OBC/General), BPL category (out of 11)*, Number of dependents to be covered*, Local language, minority status, Mobile number*, Aadhaar number, NPR number, NREGS Job Card number, BPL Card Number, Ration Card number, Category Identifier number (for any of the 11 categories), Existing RSBY Card Number, Flag to indicate whether any family member has an RSBY card* (Y/N). Demographic of all family members/dependents to be covered.
The fields marked * are mandatory fields.
The final list of data fields should be as per the latest “RSBY Data Format” as per Annexure 1.3 of this document
3. The location/geographic data to be referred should be the latest census data
4. For future reporting on RSBY beneficiaries for political constituencies mapping the same to census data of villages/towns in the constituency can be done.

RSBY Revised Process Guidelines
8 | P a g e
Sr. No
Current Process Responsibility Proposed Process Corresponding Responsibilities
Remarks
1.2 Previous year/cycle data not being used by SNA’s for fresh pre-enrolment resulting into duplication of efforts and potential duplication of beneficiary records
SNA Pre-enrolment data of previous year from MoLE to be used at the time of data validation and de-duplication.
SNA 1. At the time of data deduplication, the pre-enrolments records from previous year (with URN) should also be searched for.
2. Web-application for data collation, validation and de-duplication is proposed to be developed by NIC.
1.3 1. Merging the data received from various departments,
2. Deduplication of data by SNA
3. Transfer of final list to EDVASP software for format validation
SNA (The same is sometimes outsourced to an external agency or data management operators).
1. Merging of data received from various state departments should happen automatically in the proposed web-based system.
2. The system should prompt for invalid (format/structure) and duplicate records, which can be acted upon by an SNA official for processing the list.
SNA 1. The de-duplication would be a combination of automated duplicate alerts by the system (based on identifiers and demographic information) and simple manual confirmation to select appropriate records.
1.4 De-duplication of data being done
1. manually by SNA officials
2. not done at all
3. through locally developed application
SNA De-duplication of data, to be done through proposed web application using common identifiers like NPR number/ Aadhaar number/NREGS ID/ BPL card number/Mobile Number and other demographic parameters like name, fathers’ name, etc.
SNA 1. For de-duplication SNA to follow guideline provided by MoLE. For details refer Annexure 1.2
2. The de-duplication process should be allowed in an offline mode also, even though the prompting process will be done in a connected mode.
3. In case of duplicate records identified at MoLE level, the notification would go from MoLE to

RSBY Revised Process Guidelines
9 | P a g e
Sr. No
Current Process Responsibility Proposed Process Corresponding Responsibilities
Remarks
the states.
1.5 1. Preference of category is being selected manually by SNA at the time of processing of pre-enrolment data received from respective state departments
SNA The rule for selection of appropriate category should be selected at the time of de-duplication. The system should prompt for selection of high priority category at the time of de-duplication.
SNA 1. Selection of category (based on prioritization guidelines) should happen in tandem with the de-duplication check.
2. This is not being done currently and needs to be incorporated in the guideline. Detailed rules of category prioritization have been provided in Annexure 1.1
2 Making pre-enrolment data available to MoLE
2.1 Validate data for format correctness using the EDVASP software provided by MoLE
SNA 1. The data is automatically validated at the time of first entry into the proposed web application. The validation is built into the web application.
2. A notification would be prompted by the web application on the number or records requested, number of records accepted/loaded, and number of records rejected.
3. Any invalid records would be sent back to the state departments
SNA 1. This would be possible once the proposed web application is rolled out. (Phase II). The SNA user will submit the pre-enrolment data on the web application, which will then be available to MoLE.
2. The user will be allowed to search the data by multiple demographic /geographic parameters.
3. In the database table, the code/reason for rejection would also be available. This may be indicated in summary at the

RSBY Revised Process Guidelines
10 | P a g e
Sr. No
Current Process Responsibility Proposed Process Corresponding Responsibilities
Remarks
time of upload request.
2.2 SNA uses an FTP portal to upload all data in an MS Access file (.mdb) for MoLE consumption.
SNA Once the data is validated, de-duplicated and confirmed at the SNA level in the previous process, the data would be available to MoLE user on the web application for URN generation.
SNA This feature would be available once the proposed web application is rolled out. (Phase II)
3 URN generation for de-duplicated and valid records by MoLE
3.1 Validation of uploaded data using EDVASP and BDCS software
MoLE 1. Not required, as the web based application would already have valid and de-duplicated data available for URN generation
2. Since all records are already valid, MoLE may decide to do a de-duplication check again
3. MoLE may take a decision on priority category based on duplicate records found
4. The duplicate records pertaining to two different states would be made available to the respective states for resolution
MoLE 1. The de-duplication process and algorithm at the MoLE level would be the same as at the SNA level, i.e. a two stage process and well-defined rules for deduplication. These rules have been prescribed in Annexure 1.2
2. There is a possibility that the duplicate records may come from different states, and in that case, duplicate records which were missed during the SNA stage can be identified at MoLE.
3.2 17-digit URN generation at family record level
MoLE 1. URN generation to be done by the proposed web application after being prompted by MoLE
MoLE 1. This feature would be available once the proposed web application is

RSBY Revised Process Guidelines
11 | P a g e
Sr. No
Current Process Responsibility Proposed Process Corresponding Responsibilities
Remarks
done in EDVASP
URN structure
1, 2 – State Code 3, 4 – District Code 5, 6 – Block sequence number 7, 8, 9 – Village sequence number 10,11 – Year of generation 12, 13, 14, 15, 16 – Five digit serial number of family prefixed by zeroes. 17 – Check sum digit
official.
2. Fresh URN should be generated only for new families
3. Data source: Departments will be allowed to enter data on the web application, but MoLE can use data for URN generation only after flagging of data by SNA as “ready for URN generation”
4. Data entry in web application will be either by web application based data entry or upload of MS Access, i.e. .mdb file)
5. SNA will flag a batch of data, only after receiving data from all the departments, preferably after receiving the data for the categories with higher priority
rolled out.
2. The revised format of URN number is as below:
Proposed revised URN structure
1, 2, 3, 4, 5,6 – Census village code
7, 8 – Year of generation
9, 10, 11, 12, 13 – Five digit serial number of family prefixed by zeroes.
14 – Check sum digit
3. The URN number for the family will remain the same
4. In case of family split, a new URN number would be generated for the new family
5. In case of migrants, URN number would still remain the same. The address would change, and the reporting would happen on the address fields.
6. Referential integrity of records with previously allocated URN (associated with new URN) should

RSBY Revised Process Guidelines
12 | P a g e
Sr. No
Current Process Responsibility Proposed Process Corresponding Responsibilities
Remarks
be maintained.
7. The families which are not available now would be tagged as ‘inactive’. ‘Active’ families imply those families which exist on ground, but not subscribed (i.e. not under RSBY yet). ‘Inactive’ implies that families reported do not exist on ground. Audit will be conducted on sample basis for reported “active” & “inactive” family to verify the accuracy.
8. The current server capacity is 10 lakh URN generation per week, and the same would have to be enhanced to meet the KPI
9. The URN generation will happen in a pre-defined scheduled format (FIFO)
10. Exception to FIFO, if required, will be allowed only after approval of Project Director at MoLE
4 Providing data (URN generated) to Smart Card Service Provider (SCSP) for enrolment
4.1 1. Encryption of pre-enrolment data, with a hash key provided for each record to
MoLE 1. MoLE will select the SCSP from the Consortium of Public Sector Undertakings (CPSU), which will conduct the
1. MoLE
2. SNA
1. MoLE administrator will provide username and password for empaneled SCSP’s with restricted access only for their district data.

RSBY Revised Process Guidelines
13 | P a g e
Sr. No
Current Process Responsibility Proposed Process Corresponding Responsibilities
Remarks
detect tampering
2. Encryption of data file with public key of respective IC/SCSP
3. Upload on RSBY portal for download by IC/SCSP
enrolment process for RSBY.
2. SNA will select IC through an open tendering process at state level. It will tag district(s) to the IC. An IC master would be maintained in the web application.
3. The SCSP will be assigned districts based on the time of initiation of enrolment process. The approval and monitoring committee (A&M) will conduct the sequencing of enrolment process by the SCSP.
4. SCSP will upload the public key after logging into the web application. The enrolment data will
5. The MoLE official who has generated URN would indicate on the proposed web application that the data may now be made available to the SCSP. The SNA would then notify that the data (district wise sets) may now be made available to SCSP.
6. The data made available to the SCSP would only be for ‘active’
3. IC
4. SCSP
2. This feature would be available with the proposed web-based application.
3. The SCSP would not be able to delete any data from the web application.
4. Subscribed means families which are enrolled under RSBY. Unsubscribed families would imply those which have been covered under pre-enrolment, and for which URN was generated, but actual RSBY enrolment did not take place. The families which have not been pre-enrolled would also fall under the ‘unsubscribed category’.
5. The SCSP would have access to all data, depending on the districts where it has been assigned enrolment work.

RSBY Revised Process Guidelines
14 | P a g e
Sr. No
Current Process Responsibility Proposed Process Corresponding Responsibilities
Remarks
families who do not have an existing policy (families with existing policies would last for 3 years under normal circumstances. In case of change in IC before the 3 year tenure, there will be policy portability to the next IC with a provision for new policy number)
7. The SCSP will be provided secure access to proposed web application, from where it may download the data (for which URN has been generated). The data would be encrypted with the public key of smart card service provider (SCSP) for data security.
5. Updation of beneficiary data by respective state departments
5.1 Currently, the process of updation of data does not take place
SNA 1. The data of beneficiary can be received from various sources at the field such as in kiosk (where the beneficiary can submit a request for inclusion).
2. Such requests are to be logged into the web application and sent to the respective state
1. Respective state departments
2. SNA
1. The beneficiary data is to be updated every 6 months. The cycle of updation in the months of February and August to be continued.
2. The Welfare Commissioners of the States would be responsible for the respective departments to provide the updated data to SNA, every 6

RSBY Revised Process Guidelines
15 | P a g e
Sr. No
Current Process Responsibility Proposed Process Corresponding Responsibilities
Remarks
departments.
3. The state departments shall verify the data of the beneficiary, which shall then be sent to the SNA for inclusion in the beneficiary list.
months.
Policy decisions taken Meeting reference
Sr. No.
Decisions Date/Location/Chaired by:
1 Guidelines and process for selection of category based on prioritization (in case of duplicate record coming from different category) to be finalized as provided in Annexure 1.1)
Meeting held under Chairpersonship of Secretary (L&E) on 6th May 2014, minutes yet to be processed in file
2
Process of de-duplication finalized (as provided in Annexure 1.2). The process should have a 2-stage de-duplication (Alert/Confirmation) and the identifiers on which exact/partial/fuzzy match would happen would be defined. In case of duplicate records identified at the MoLE level, the notification would go from MoLE to the states
Meeting held under Chairpersonship of Secretary (L&E) on 6th May 2014, minutes yet to be processed in file
3 No RSBY record would be deleted, and the records which are not under the RSBY ambit anymore would become ‘Inactive’. This facility should be available by categories
Meeting held under Chairpersonship of Secretary (L&E) on 6th May 2014, minutes yet to be processed in file
4. Data of beneficiaries to be updated every six months by the respective state departments. The role of State Welfare Commissioners will be crucial in the process of updating the data of beneficiaries.
EC Meeting held under the Chairpersonship of Secretary (L&E) on 15th May 2014, minutes yet to be processed on file

RSBY Revised Process Guidelines
16 | P a g e
Policy Decision to be taken
Sr. No Decisions
1 De-duplication of beneficiary data to be done in two stages - by the data source departments and SNA
2 Category prioritization to be done at the time of de-duplication of data by the SNA
Incentive mechanism
1 NA
Training Needs Training to be provided to
Training to be provided by
1 Training on process of two-stage de-duplication in the proposed web application SNA and departments MoLE
2 Training on selection of beneficiary category prioritization in the proposed web application SNA MoLE
3 Training on pre-enrolment data capture with collection of mandatory fields in the prescribed format
Departments SNA
Human resource requirement Agency / department
1 Team to develop and roll-out the web based application for pre-enrolment and data preparation for enrolment
NIC
2 To add capacity to the SNA as per minutes of the empowered committee meeting held on 15th April 2014 SNA

RSBY Revised Process Guidelines
17 | P a g e
Input for RFP/FRS RFP/FRS for:
1 Category Prioritization (Annexure 1.1) / De-duplication guidelines (Annexure 2) to be made a part of RFP/FRS for the proposed web application by MoLE
FRS for Web Application Development Agency (NIC)
2 List of users and roles for the proposed web application FRS for Web Application Development Agency (NIC)
IEC Activities
1 To create awareness among the beneficiaries of different categories to get themselves registered for RSBY (Except BPL, in every category number of beneficiary can be increased at pre-enrolment stage also)
Other considerations
1 Inter-department meeting at a state level to be conducted once every month (1st week of every month) to present and discuss
(i) status, and (ii) plan for pre-enrolment and enrolment. The meeting has to be called upon, and hosted by SNA. The meetings should be used by SNA
to educate the departments of provisions under RSBY.

RSBY Revised Process Guidelines
18 | P a g e
Pro
ce
ss
Co
de
II – ENR Process Name
Enrolment
Process Objective Current Status 1. To increase the enrolment numbers for RSBY so that all intended beneficiaries
are covered 2. To educate & empower beneficiaries through IEC activities to utilize the RSBY
services using the RSBY card 3. To strengthen the process to ensure only intended people are getting enrolled 4. To ensure that data arising out of this process is accurate, clean and re-usable
1. ~3.6 Crore active RSBY smart cards
2. All Insurance companies (IC) / Smart card service provider (SCSP) using ECIS software as well as STQC certified Enrolment software for enrolment and card issuance
Key Stakeholders Measures and Key Performance Indices (KPIs) 1. Smart Card Service Provider (SCSP)
2. Field key officer (FKO) for verification for beneficiary and card issuance
3. State Nodal Agency (SNA)
4. District Key Manager (DKM) for creation of FKO’s in the system
5. District Information Officer (DIO)
Measures4: MoLE, SNA, IC/SCSP, DKM, FKO (relevant reports to be available, depending on role) 1. Number of beneficiary cards issued
Filters: Time Duration (from-to), Geography (district/ block/ village), SCSP, FKO, beneficiary category
2. Number of cards wasted Filters: Time Duration (from-to), Geography (district/ block/ village), SCSP, FKO,
KPI5: SNA, SCSP, DKM, FKO (relevant KPI’s to be measured, depending on role) 1. Number and % of enrolment completed at village, district and
state level (the baseline would be the number of pre-enrolment data records)
2. Average family size enrolled (with geography filters) 3. Number of active enrolment kits deployed (with geography
4 All measures to be available as a report on a web portal in real-time/near-real-time. The data should be available in a warehouse, such that any extraction is possible to create ad-hoc reports
5 All KPI’s to be available as a report on a web portal in real-time/near-real-time. The data should be available in a warehouse, such that any extraction is possible to create ad-hoc reports.

RSBY Revised Process Guidelines
19 | P a g e
filters) 4. Average time taken to create/issue an RSBY card – this should
be computed by computing the difference between timestamp on initiation and completion
5. Average time spent on field – computed by the difference between the last enrolment for the day, and first enrolment for the day
6. Number of villages covered by the SCSP 7. Time taken to get the FKO data uploaded on server 8. Number of villages with ‘ZERO’ enrolment 9. Number of FKO’s deployed 10. Number of ‘active’ FKO’s – defined as number of FKO’s who
have done atleast 1 enrolment 11. Number of active enrolment kits deployed
Summary of current challenges Summary of key suggestions 1. Low percentage of enrolment w.r.t. pre-enrolment data 2. Enrolments happening in the latter part of the enrolment time window,
resulting in reduction in effective policy period 3. Non delivery of card to enrolled families 4. Cases of unintended people getting the cards are reported – this is due to
unauthorized use of DKM and FKO cards 5. Non availability of MIS on a near real-time basis to MoLE or SNA for making key
policy decisions 6. Some of the villages completely getting skipped from enrolment process 7. Data coming from different channels are inconsistent, resulting in requirement
of continuous reconciliation
1. Close monitoring of enrolment activity through enhanced reporting across the enrolment lifecycle
2. Concurrent third party audit for ~0.1% - 0.5% cases to be executed by SNA (within one month after completion of enrolment process). The range is valid for every district. The third party audit for enrolment station/kits should happen concurrently, for at least 1% of the enrolment kits deployed. The third party for audit may be the same. The empanelment of hiring of agencies should happen at MoLE.
3. Performance evaluation of SCSP 4. High penalty for villages with “Zero” coverage
Pre-requisites for the process of enrolment 1. Finalization of specifications and procurement of enrolment kit 2. Pre-enrolment data availability with the SCSP 3. On-boarding of IC’s – legal contract between SNA and IC 4. On-boarding of SCSP – legal contract between SCSP and MoLE 5. Hospital empanelment should be completed, and district kiosks should be set up 6. Identification and appointment of FKO & DKM by SNA 7. Procurement and distribution of IEC material by the SCSP 8. A detailed checklist for the enrolment station, attached in Annexure 2.1

RSBY Revised Process Guidelines
20 | P a g e
Inputs to the revised process Output from the revised process 1. Pre-enrolment data
1. Issuance of RSBY cards to the intended beneficiaries 2. Collection of fixed fee from the beneficiary by the SCSP (issued
card to act as receipt for INR 30 paid by beneficiary) 3. FKO undertaking form, indicating the number of enrolments
4. Post-enrolment data by SCSP using a web-sync or batch upload to the central server
Processes and Responsibilities:
Sr. No
Current Process Responsibility Proposed Process Responsibilities Remarks
1 Pre-enrolment data availability with SCSP
1.1 1. Downloading the data from MoLE and sharing the data with SCSP for enrolment and card issuance
2. The data is split by
the SCSP as per geographical unit, and the data-sets is copied into the respective enrolment kits
IC 1. MoLE user would create the SCSP in the system. At the time of SCSP creation, the scanned copy of the agreement between MoLE and SCSP would be uploaded for records. An SCSP master would be created at MoLE
2. The selection of SCSP from the SCSP master will be done in the web application and assignment of the district(s) to the SCSP will take place based on enrolment initiation process at state/district.
3. SCSP will upload the public key after logging into the web application
4. SCSP should be a user in the
1. MoLE 2. SNA 3. SCSP
The flow of pre-enrolment data thus follows the following process. State Departments SNA MoLE SCSP in the same web application 1. At every stage, the data will flow to
next stage only after authorization of user
2. In most of the cases the data will move in batches

RSBY Revised Process Guidelines
21 | P a g e
Processes and Responsibilities:
Sr. No
Current Process Responsibility Proposed Process Responsibilities Remarks
proposed web application. The data is made available seamlessly to the SCSP which has been tagged MoLE/SNA for a given geography (district). This is done in the web application.
5. SCSP can download the data for any geographic unit and copy it to respective enrolment kit
2 Verification of beneficiaries at the time of enrolment
2.1 Quality check on the data downloaded from RSBY portal to ensure completeness, sanctity, etc.
SCSP 1. No change to the process of verification
2. Any errors would be reported by the SCSP through the web application to the SNA
SCSP
3 Master Personnel and Card Management
3.1 Identification of DKM SNA No change SNA 1. By default, district level officer of nodal department in state (Labour/Health) will act as DKM
2. DKM will identify one additional person to work as ADKM to support him in routine activities. They may be hired on deputation from government or on contract

RSBY Revised Process Guidelines
22 | P a g e
Processes and Responsibilities:
Sr. No
Current Process Responsibility Proposed Process Responsibilities Remarks
3.2 Identification of FKO DKM No change DKM 1. FKO has to be a person with good knowledge of local area
2. He/She, preferably be working with government department, or may be a member of Panchayati Raj Institution (PRI)
3.3 1. MoLE issues a DKM card (with security PIN) for each DKM after receiving requisition from SNA
2. Card is send to SNA by post, or through authorized person by MoLE officials.
3. SNA handover the cards to respective DKM
1. MoLE 2. SNA 3. DKM
1. MoLE issues the card to SNA, which is handed over to DKM
2. DKM goes to DIO for card personalization
3. DIO has the card personalization kit, including a biometric capture device
4. DIO will personalize the DKM card by capturing the biometrics of DKM
5. After issue of card to DKM, the information would be updated in the web application. This should have details of DIO issuing the card to DKM along with timestamp etc.
1. MoLE 2. SNA 3. DKM 4. DIO
1. This would prevent misuse of card 2. Under no circumstances, the card
should be issued to SCSP or its representatives
3. If in exceptional circumstances the card is sent through a person authorized by SNA, the card box should be properly sealed
4. Details of dispatch and receipt should be updated on web portal both by MoLE and SNA.
3.4 1. Issue of FKO Card (with security PIN) by MoLE on the basis of requisition sent by SNA
2. Cards are sent to SNA, who in turn will send the card to DKM, who will personalize it with fingerprint of FKO
DKM 1. DKM would issue the card to FKO only after his/her own biometric authentication. DIO may also issue cards with same access privileges to ADKM, who are notified by DKM as equivalent officers for issuing FKO cards.
2. DKM/ADKM will personalize the FKO card by capturing the biometrics of FKO and associating it with the card
3. After issue of card to FKO, the
1. DKM (Primary responsibility)
2. Additional DKM (ADKM)
3. DIO
1. This would prevent misuse of card 2. Under no circumstances, the card
should be issued to SCSP or its representatives.
3. If in exceptional circumstances the card is sent through a person authorized by SNA, the card box should be properly sealed.
4. Details of dispatch and receipt should be update on web portal both by MoLE and SNA.

RSBY Revised Process Guidelines
23 | P a g e
Processes and Responsibilities:
Sr. No
Current Process Responsibility Proposed Process Responsibilities Remarks
information would be updated in the web application automatically. This should have details of DKM/ADKM issuing the card, FKO receiving the card, timestamp, etc.
4 Planning for field operations
4.1 1. IC, SCSP and DKM prepare the route plan
2. FKO’s are informed about the route plan
1. IC/SCSP 2. DKM
1. The format of the route plan would be available in the web application. The fields in the route plan would have date, village name, block name, number of kit to be deployed, SCSP personnel name and mobile number, supervisor name and contact details, FKO name and contact details. Additionally mobile number of village key persons (such as Sarpanch, teacher, ASHA, ANM, etc.) should also be captured in the route plan.
2. SCSP should prepare the route plan and digitize it into the proposed web application for access by SNA & DKM.
3. Immediately after submission of route plan, FKO’s have access to the route plan (An SMS/email may be sent to FKO’s) from the proposed web application)
4. Once the route plan is finalized, the system should be pinged for village
1. SCSP (Primary responsibility) 2. DKM
1. For preparing “route plan” , SCSP would take inputs from local functionaries
2. Once approved by DKM, “route plan” should not be changed without DKM’s permission. This will always be managed through the proposed web application
3. Route plan should include a. Schedule of enrolment b. Number of kits to be
deployed c. Every plan upto village level
should be tagged to a DKM and FKO, along with their registered mobile numbers and email addresses. Mobile number would be mandatory.
4. The route plan management would mean access of the proposed web application to one more users, i.e. DKM, This makes the total user set as state departments, SNA, MoLE, SCSP and DKM

RSBY Revised Process Guidelines
24 | P a g e
Processes and Responsibilities:
Sr. No
Current Process Responsibility Proposed Process Responsibilities Remarks
residents in the pre-enrolment data-set, and an SMS should go to the residents of the villagers with registered, mobile number indicating the date of the visit, as well as indicating the number of the FKO who would be the point of contact.
5. SMS/mobile number for notification is mandatory. Email is optional.
4.2 Workshop at block and district Headquarters with identified FKOs and local officials
1. IC 2. SCSP
1. SCSP shall organize the workshop 2. Workshop structure defined by
MoLE should be reinforced, with checklist of hand-outs to be provided during the workshop.
3. In the structure of the workshop, provision of lunch to be included.
4. Route plan may be tweaked in this workshop on the basis of feedback from FKOs
1. SCSP (primary responsibility)
2. Representative of DKM (may be a block level official)
1. In this workshop, FKOs should be made aware of the following: (i) Benefits of scheme (ii) Route Plan (iii) Roles and responsibility of SCSP and FKO during enrolment
2. Beneficiary list is made available to FKO for his/her area
3. FKO’s, while being created by DKM’s in the system, should be tagged to villages so that they can access pre-enrolment data of village beneficiaries
4.3 Route plan is published in the local media
IC 1. Route plan is published in local media
2. The final route plan should be published in local media (newspaper), along with details of supervisors and FKOs. In case of any major change, it should be re-published
SCSP Route plan should be published preferably in a daily newspaper in local language with maximum circulation in that area
4.3 1. Awareness and sensitization
1. IC/TPA 2. SCSP
1. The IEC material preparation should happen in consultation with
1. SCSP (Primary responsibility)
1. SCSP should ensure that beneficiaries are informed well in

RSBY Revised Process Guidelines
25 | P a g e
Processes and Responsibilities:
Sr. No
Current Process Responsibility Proposed Process Responsibilities Remarks
exercise using IEC material at the field level
Primary target: Beneficiaries Objective: 1. To mobilize the
beneficiary for enrolment
2. To make beneficiary aware of benefits available under scheme
3. DKM district/DKM
2. DKM (only signs off on IEC completion)
advance about schedule of enrolment in their villages and wards, through: i. print and electronic media (with focus in districts during the enrolment time window) ii. SMS
2. SCSP should also ensure that beneficiaries are made aware of benefits of scheme through village level meetings, wall paintings, and display of IEC material at village/ward offices or buildings, house-to-house slip distribution with local language content, loudspeaker announcement (munadi)
3. DKM should monitor the awareness and sensitization activity
4.4 Preparation of enrolment kits (EK) with pre-enrolment data, as per route plan. The data is provided in the form of encrypted access (.mdb) files from the central server (RSBY portal)
1. IC 2. SCSP
1. Once the web application is ready, the data splits (based on geography parameters) should happen at the web application level, and copy of data into enrolment kits may also happen from the web application
2. Authorized and secure data modification is permitted through the proposed web application only.
3. The enrolment application should flag for ‘potential duplicate’, depending on the pre-enrolment data copied on the enrolment kit. In case of a potential duplicate, the
1. SCSP
1. Data of a geographic area should be copied in the enrolment kits identified for that area only.
2. ‘Inactive’ records would be based on the guideline that the family does not reside in the village/ward at all. However, if the family is not available temporarily, the record should not be marked as ‘Inactive’. This feature should be made available in the enrolment software.

RSBY Revised Process Guidelines
26 | P a g e
Processes and Responsibilities:
Sr. No
Current Process Responsibility Proposed Process Responsibilities Remarks
SCSP should carefully identify the appropriate record from the list. This investigation should happen by looking at the family members details. A similar pop up should be made available in the enrolment software.
4. At the time of enrolment, a field could be added which would flag a record as ‘active’ or ‘inactive’.
5 Enrolment
5.1 Setting up enrollment station(s) at village enrolment center by SCSP and FKO on the day of enrolment as per route plan
1. IC/SCSP 2. FKO
The SCSP will setup the enrolment stations at the respective villages/ districts.
1. SCSP (primary responsibility)
2. FKO
1. Enrollment station to be set up as per approved route plan.
2. FKO should be available on time 3. All equipment of enrolment kit
should be in working condition, and should be tested before the commencement of enrolment and certified by the DKM. The DKM should also certify that 10% extra/backup kits are available, and the spares available with SCSP are of good quality. The backup 10% of the kits should be in custody of DKM, and should be used by DKM to address complaints from village residents where enrolment does not happen due to any reason. DKM can decide to keep these extra/backup kits at a location near to area where enrolment is going on

RSBY Revised Process Guidelines
27 | P a g e
Processes and Responsibilities:
Sr. No
Current Process Responsibility Proposed Process Responsibilities Remarks
4. FKO should use an enrolment station checklist (Annexure 2.1) to ensure all the required steps have been completed, before allowing commencement of enrolment.
5. In case of malfunctioning of any of the equipment, enrollment should be stopped, until it is replaced. Under no circumstances, partial enrolment should be allowed, it should be considered complete, only if beneficiary has received card after re-verification
5.2 Distribution of “Intimation slip” to beneficiaries
1. IC/SCSP
The SCSP shall distribute the “Intimation Slip” to the beneficiaries.
1. SCSP (Primary responsibility)
IC/SCSP should distribute “Intimation Slips” printed in local language containing URN number, name of family head, names of family members, date of enrolment atleast 48 hours before enrolment
5.3 Enrolment of Family (Family head, spouse and three other members identified by Family head)
1. IC/SCSP 2. FKO
1. Enrolment of family (Family head, spouse and three other members identified by family head), if available, should mandatorily be completed. In all cases, if male head of family is not available, female should be the head of family (HoF)
2. If family head or spouse is not available, then four other members other than family head/spouse can be covered under this scheme.
3. Demographic details all of other members should also be updated in
1. SCSP 2. FKO
1. Once family head presents his/her “Intimation slip”, the operator searches the details of family in database, and captures biometric data (fingerprint & photograph) of every member of family
2. DoB/Age/Gender can be changed at the time of enrolment for all members
3. Name and relationship of all members can be changed, except for head of family
4. Father’s name should be allowed to

RSBY Revised Process Guidelines
28 | P a g e
Processes and Responsibilities:
Sr. No
Current Process Responsibility Proposed Process Responsibilities Remarks
the database 4. If both family head and spouse are
deceased, then based on proof (such as death certificate), the next eldest member of family, preferably female, if available, should be treated as family head. If the name of member selected as HoF is available in database, the card can be issued without any additional verification. If the name is not available in database, matter can be referred to higher authority.
be added or updated 5. There should be an emphasis on
capture of mobile number and Aadhaar number. In case they are not available, ‘0000000000’ and ‘000000000000’ should be captured respectively.
6. The details in the FKO card should include: (i) URN Number (ii) CHIP serial number (iii) Names of all family
members who have been enrolled including HoF
(iv) Enrollment time stamp (v) Age and gender of family
members.
5.4 Printing and Personalization of card
1. IC/SCSP 2. FKO
The SCSP will personalize the card of the beneficiary based on authentication from the FKO
1. SCSP 2. FKO
FKO will authenticate printing & personalization of every card using his biometrics.
5.5 Re-verification of card SCSP 1. Re-verification of card is done with biometric authentication of both FKO and beneficiary.
2. The re-verification information should also go into the FKO card, and signed data in the SCSP kit.
3. Re-verification should be done for all 5 members of the family.
1. SCSP 2. FKO 3. Beneficiary
1. The purpose of re-verification is to ascertain that the finger print captured is of good quality. Currently it does not require authentication by FKO, resulting in by-passing of this important step.
2. Re-verification should be done for all 5 members of the family
3. In case fingerprint of any member is not verified, then his finger print should be recaptured and updated

RSBY Revised Process Guidelines
29 | P a g e
Processes and Responsibilities:
Sr. No
Current Process Responsibility Proposed Process Responsibilities Remarks
on card
5.6 Handing over the card to beneficiary after collecting Rs. 30
1. IC/SCSP 2. FKO
After authentication by FKO, the RSBY card shall be handed over to the beneficiary by SCSP in the presence of FKO. The FKO shall provide for a slip which serves as a receipt of payment of Rs. 30 and the RSBY card.
1. IC/SCSP 2. FKO
1. Once re-verification has been done successfully, card can be handed over to the head of family.
2. Enrollment Software should print a receipt, with receipt number, showing the URN number, names of head of family & other family members and the toll-free number. The receipt should also acknowledge the receipt of Rs. 30 for issuance of the card.
3. The FKO shall provide for the receipt number for each beneficiary in the FKO undertaking form which is to be submitted by him to the DKM office post enrolment. The data from the FKO undertaking shall be entered by the DKM office into the web based software for future reference purposes.
4. The beneficiary shall receive a call from the call center to confirm receipt of card and the receipt from the FKO during enrolment.
5. This is to ensure that the complaints regarding non receipt of cards can be investigated.
6 Post-enrolment activity and premium calculation

RSBY Revised Process Guidelines
30 | P a g e
Processes and Responsibilities:
Sr. No
Current Process Responsibility Proposed Process Responsibilities Remarks
6.1 1. Data upload from FKO card to DKM server at the district (DKMA office)
2. Encrypted signed data of enrollments (text files generated per kit per day) are uploaded by IC at the DKM server (at district/DKMA office)
3. Post enrolment data (csv files) are submitted by the IC/SCSP to the SNA. The process is to submit the data by uploading it on the state /central server. This contains the biometric data as well
4. The photographs and SQL back-up of the beneficiary data is created as SQL files and uploaded by the
1. FKO 2. IC/SCSP
1. Data upload directly from FKO card to MoLE server at the district (DKMA office) using a modified DKM application (instead of first downloading the data at local system) within 5 days from completion of enrolment limit. The member names should be included in the FKO card. From the DKM server, the data should flow back into the central web application server.
2. Encrypted signed data of enrollments (text files generated per kit per day) should be uploaded by SCSP within 5 days on the central RSBY server. This should include biometrics/photograph. Both MoLE and states (including DKM) should have data access from the central server.
1. FKO 2. DKM 3. SCSP
1. This feature will be available after development of web application
2. The provision of capturing time delay in uploading of encrypted data from SCSP in the web application will also be made available.
3. In order to accommodate data for up to 500 beneficiaries at a time, the FKO’s should be given 5 cards each per kit. This will ensure that the enrolment process is not stopped due to limitations of storage on the FKO card.

RSBY Revised Process Guidelines
31 | P a g e
Processes and Responsibilities:
Sr. No
Current Process Responsibility Proposed Process Responsibilities Remarks
IC/SCSP to the state/central server.
6.2 Handover of FKO card by FKO to DKM
FKO At the time of FKO card surrender by FKO to DKM, a system printed MIS report will be provided with the following information (i) URN numbers (ii) Head of family Name (iii) Date of card issuance. The report heading should have the following information (i) FKO information – name, address, mobile number (ii) village name.
FKO This is also to ensure that the complaints regarding non receipt of cards can be investigated.
6.3 No provision of audit post enrolment
Concurrent audit on randomly selected villages for up to 1% villages. - Audit to capture whether
beneficiaries received the card - Quality of card and chip
SNA 1. Audit agencies selected by MoLE /NGO or Pensioners can be employed to conduct random audits on enrolment activities
2. Checklist for post enrolment audit to be prepared as a guideline for audit agencies.
6.4 Wellness check is not included as a process for premium payment to the insurance company
Wellness check at nearest public health facility should be mandatory for the beneficiary and it will be the responsibility of the insurance company to ensure that all the beneficiaries have got their wellness check done within 60 days of start of policy.
IC (Primary responsibility)
Wellness check will be an optional activity for states which are prepared now (1st July 2014). From FY 2015-16 it will be a mandatory requirement for as well as existing cards.
6.5 Premium calculation 1. On the basis of
number of cards, as claimed by IC
2. Premium to be paid for full year
IC 1. If card is issued before policy start date, full payment will be payable to IC
2. IC, however, can claim premium for only those cards, for which wellness check has been completed
SNA The details of data flow and management during, wellness check, and premium payment are discussed in “Wellness Check and Premium Payment” process document.

RSBY Revised Process Guidelines
32 | P a g e
Processes and Responsibilities:
Sr. No
Current Process Responsibility Proposed Process Responsibilities Remarks
even if the card is issued late
3. Wellness check has to be completed within 60 days from start of policy
4. Responsibility of getting the wellness check done lies with IC. If it is getting delayed, penalty will be levied at following rate:
a. Wellness check is conducted after 2 months; penalty levied is 50% of premium for those beneficiaries whose wellness check is remaining.
b. Wellness check is conducted after 6 months; penalty levied is 100% of premium for those beneficiaries whose wellness check is remaining
5. The payment of premium should be done quarterly to the IC.

RSBY Revised Process Guidelines
33 | P a g e
Policy Decision taken Meeting reference
Sr. No Decisions
1 Wellness check to be made mandatory for activation of cards EC meeting dated 23.01.2014
2
Incentive to FKO: As of now some of states are paying incentive to FKO for managing the enrolment exercise. It is proposed that the incentive should be higher if the conversion is high. An indicative slab-wise rate is given here for SNAs.
for first 50% @ INR X per data, for next 20% @INR 1.5X per data and above 70% @ INR 2X per data and so on.
SNA can decide about exact rate and slab and appropriately reward the FKO’s post the enrolment process.
Meeting held on 06th May 2014, chaired by Secretary (L&E), minutes yet to be processed in file
3 In case of absence of both spouses, card should be issued with next eldest female member (younger than original HoF) as HoF, provided her/his name appears in the database.
Meeting held on 06th May 2014, chaired by Secretary (L&E), minutes yet to be processed in file
4
Mobile number for all beneficiaries to be collected so that 2 SMS (one in English, one in local language) are sent to RSBY beneficiaries at every transaction. Depending on the transaction, dynamic SMS templates in English and local language should be prepared and approved by MoLE. While mobile number should not be mandatory for the head of family, the data capture should ensure that ‘0000000000’ should be captured so that the data entry operator is not incentivized to leave the field blank. The same should be followed for Aadhaar number.
Meeting held on 06th May 2014, chaired by Secretary (L&E), minutes yet to be processed in file
5
Concurrent third party audit for ~0.1% - 0.5% cases to be executed by SNA (the audit should start within one month after start of enrolment process). The range is valid for every district. The third party audit for enrolment station/kits should happen concurrently, for at least 1% of the enrolment kits deployed. The third party for audit may be the same. The empanelment of hiring of agencies should happen at MoLE.
Meeting held on 06th May 2014, chaired by Secretary (L&E), minutes yet to be processed in file

RSBY Revised Process Guidelines
34 | P a g e
Decision to be taken
Sr. No Decisions
3 Use of MMS for monitoring the IEC at Enrolment center. IC can capture place, time and date stamped pictures of FKO in front of IEC material used and upload it.
4 Use of Audio Visual Clip for IEC at the time of enrolment
Incentive Mechanism
1 FKO incentive should be slab-wise. An indicative slab-wise rate is given here for SNAs. 1. for first 50% @ INR X per data, for next 20% @INR 1.5X per data and above 70% @ INR 2X per data and so on. SNA can decide about exact rate and slab
2 SCSP: Performance matrix should include all the KPIs listed above, an objective assessment of performance will give an edge to the performing SCSP
Training Needs Training to be provided to Training to be provided by
1 Roles and responsibilities of FKOs at Enrolment Centre
FKOs IC/SCSP under supervision of SNA/DKM
2 Using Enrolment Software Enrolment Operators / Supervisor SCSP
3 Post enrolment FKO and DKM procedures to be adopted
DKM, FKO and SCSP SNA

RSBY Revised Process Guidelines
35 | P a g e
Human Resource Requirement Where
1 Monitoring and Evaluation team, to closely monitor the progress of enrolment, ensure data accuracy and resolve any data conflict issues.
SNA
Input for RFP/FRS
1 Specifications for enrolment kit For empanelment of SCSP
2 Complete process flow of enrolment till premium payment For RFP to empanel IC
3 Content of Brochure to be distributed among beneficiary For empanelment of SCSP
4 IEC activity to be carried out For empanelment of SCSP
5
Various Incentive / penalty mechanism
1. Incentive for FKO
2. Penalty for delay in wellness check
For RFP to empanel IC
6 Performance Matrix
For RFP to empanel IC
Separate performance matrix for SCSP pertaining to its role in enrolment
IEC Activities
1 Publicize the dates of enrolment in the district / block
2 Benefits of Scheme to increase awareness among the target beneficiaries

RSBY Revised Process Guidelines
36 | P a g e
P
roce
ss
Co
de
III – SKMS
Process Name Smart Card and Key Management System
Process Objective Current Status 1. To create a secure and convenient environment for beneficiary transactions
using RSBY smart card 2. To ensure security of transaction data from unauthorized read or write access 3. To ensure that all beneficiary cards are personalized through authorized and
authentic personnel, master cards and equipment 4. To track all master smart cards throughout their life cycle to ensure that there
is no unauthorized usage or wastage of cards
1. Centralised procurement of master key cards by MoLE (CKGA)
from vendor identified by NIC, and empaneled by NICSI
2. Procurement of beneficiary smart cards by Smart Card Service Provider (SCSP), embedded with certified SCOSTA OS, and delivered to beneficiaries by Smart Card Service Provider (SCSP) in presence of Field Key Officer (FKO)
Key Stakeholders Measures and Key Performance Indices (KPIs) 1. National Informatics Centre (NIC)
2. Ministry of Labor and Employment (MoLE)
3. Central Key Generation Authority (CKGA)
4. District Informatics Officer (DIO)
5. District Key Management Agency (DKMA)
6. Field Key Officer (FKO)
7. Kiosk User(s)
8. Hospital
9. Public Health Facility (PHF)
10. Other departments collaborating with MoLE on similar beneficiary programs
Measures6: MoLE, SNA, DKM, FKO (relevant reports to be available, depending on role) 1. Number of master key cards issued
Filters: User Category (CKGA, DIO, DKM, Kiosk, Hospital, FKO etc.), Time Duration, Card Validity, Geography
2. Number of master cards surrendered, new cards personalized Filters: User Category, Time Duration. Geography
3. Total number of beneficiary cards issued Filters: User Category, Geography, Time Duration, Card Status (Active, Inactive)
4. Number of beneficiary card transactions Filters: Transaction type, Geography, Time Duration, Hospital/PHF, Block/District Kiosk
6 All measures to be available as a report on a web portal in real-time/near-real-time. The data should be available in a warehouse, such that any extraction is possible to create ad-hoc reports

RSBY Revised Process Guidelines
37 | P a g e
KPI7: SNA, DIO, DKM, ADKM, FKO (relevant KPI’s to be measured, depending on role) 1. Average master card utilization (depending on master card,
beneficiary cards issued, other cards personalized)
2. Number of reported cases of lost cards, card tampering in CGRMS
3. Number of corrupt/non-functional cards reported in CGRMS 4. Quality score of beneficiary cards (identified during the third
party audit) 5. Time delay in delivery/receipt of card after card request
(timestamp to be managed in card issuance systems, i.e. KMS and enrolment kit)
Summary of current challenges Summary of key suggestions 1. Sub-standard beneficiary cards are being procured and issued by IC/SCSP
resulting in high number of manual override 2. Master cards / beneficiary cards are not tracked throughout their lifecycle,
leading to poor/no information visibility at MoLE and SNA, making it difficult to know about the issues prevailing in field
3. DKMA cards are being misused due to lack of biometric authentication in DKMA cards, resulting in creation and handover of FKO cards to unauthorized personnel
4. Significant cases of cards being transferred from MoLE to states/districts by IC personnel
5. Wastage on beneficiary and FKO cards 6. Inconvenience to SNA and other users (Hospital, etc) to travel to MoLE, Delhi
for collection of master cards 7. Non-functioning of cards on field
1. Empanelment of beneficiary card vendors / SCSP centrally by MoLE
2. Use of key management system, to ensure use of Smart cards manufactured by empaneled vendor only
3. Use of Web-based KMS application for master card requisition, master card issuance and real-time report generation to ensure that without electronic requisition and approval, no master card is issued. Detailed SRS for online KMS application needs to be prepared by the IT agency.
4. Card personalisation to be decentralised, DKM/ADKM card to be personalised at districts by DIO. DKM / ADKM card can be used only with biometric authentication.
5. More data fields (mobile, Aadhaar number, NPR number ) to be captured in FKO card at the time of beneficiary enrolment and card issuance
7 All KPI’s to be available as a report on a web portal in real-time/near-real-time. The data should be available in a warehouse, such that any extraction is possible to create ad-hoc reports.

RSBY Revised Process Guidelines
38 | P a g e
6. FAQ’s on non-functioning of cards and devices to be made available on RSBY website, with details of ICs, SCSPs, and technical support team
7. Immediate deployment of Centralized technical support team (with availability of email, web and phone numbers) across entire IT solution portfolio, including central web application, KMS, TMS, CGRMS, card/biometric issues. To be integrated, eventually, with call centre, which will act as front-end for technical support, as well
8. A guideline to limit wastage and handle waste cards is to be prepared and enforced
9. Introduction of system audit, at least once per annum and on major changes in the system, to ensure that the key management and master card management processes are being followed
Pre-requisites for the process of enrolment 1. Card specifications 2. Pre-enrolment data
Inputs to the revised process Output from the revised process 2. Identification of prime CKGA user
1. Real-time inventory of all master and beneficiary cards on field, and relevant usage reports
Processes and Responsibilities:
Sr. No
Current Process Responsibility Proposed Process Responsibilities Remarks
1 Creation of Key Authority Card
1.1 Procurement of card by MoLE through a vendor identified by NICSI with OS prepared by NIC
MoLE No Change MoLE Since this card will be used for carrying and deriving keys, the OS has to be internal to NIC, hence it should always be procured internally through an identified vendor only

RSBY Revised Process Guidelines
39 | P a g e
Sr. No
Current Process Responsibility Proposed Process Responsibilities Remarks
1.2 Creation of Seed card of CKGA and 5 more members (Seed Members) Any 3 members, plus CKGA required for generation of master card Verification mode: PIN (6-8 characters alphanumeric)
MoLE 1. For any master card issuance authentication of 3 seed members out of 5 along with CKGA will be required
2. For all 5 seed members (excluding CKGA), mode of authentication will be biometric. For CKGA, however, authentication will be through PIN only
3. Card creation will continue to be in batch mode, authorization will be required only to start the session for a batch. A session can be initiated by CKGA and any 3 seed members out of 5.
4. The session should be active till all approved requisition cards are printed. In case of session break, it can be reinitiated only by CKGA along with 3 seed members
5. In case of any officer from the seed team leaving, the CKGA should be allowed to update the card with new member details, as well as biometrics of new member. The trail of previous member will have to be maintained in the web based KMS system.
MoLE At the time of requisition, the requestor (DIODKM/SNA etc.) would indicate the address where the card shipment is to be delivered. He/she can also indicate that the delivery/collection is to be done manually (by hand). 1. The approver can approve all requested
cards, or less, as deemed fit. The requisition and approval will both happen using the web based KMS system.
2. The web based KMS system should continue to capture issuance of all master cards automatically for information visibility. It would also update the inventory system.
3. The card personalization activity should be carried out in a physically secured environment.
4. As MSK Cards are the root of nationwide KMS, there should be disaster recovery backup sets of the MSK Cards to be used in case of damage/disaster. These disaster recovery locations shall be decided by MoLE.

RSBY Revised Process Guidelines
40 | P a g e
Sr. No
Current Process Responsibility Proposed Process Responsibilities Remarks
1.3 Estimation of number of DKM cards required in state
SNA 1. Users will estimate the client requirements, and make the requisition through the web based KMS system. The DKM users would make a requisition, and SNA would approve the request in the online requisition module of web-based KMS.
2. The SNA, before approval,
may increase/decrease the number of requested cards in the system.
3. The request, approval and
actual printing would happen on FIFO basis. CKGA, however, will have authority to change the priority through KMS web application
4. Once approved, MoLE would
be able to see the requisition. An email/SMS would go to the CKGA. This email should also indicate the expected date of dispatch.
5. At the time of master card
generation, during peak period, the number of kits for master card issuance should be increased. The base
SNA/DKM and system based
All state and district users (One each at state and district level) would have access to web based KMS system for online requisition. General requisition guidelines are: 1. 1 DIO card will be issued for every district 2. 1 DKM card will be issued for every district 3. 1 ADKM card will be issued for every
district 4. 2 Kiosk card will be issued for every kiosk 5. 5 FKO card may be issued for each kit. The
actual number however will be decided on the basis of number of kits to be deployed at any given point of time.
6. 1 Hospital cards for each hospital 7. 1 PHF cards (for wellness check) for each
PHF 8. Application creation card (APCC), as
required by other departments, after approval from SNA
9. DKM will be custodian for all the cards available at district. It will include
a. Additional ADKM, MHC, MKC &FKO kept at district
b. FKO card returned after field operation
10. DKM should be provided with a fire-proof secured vault to keep the card safely and securely.
11. ADKM should be a gazetted officer

RSBY Revised Process Guidelines
41 | P a g e
Sr. No
Current Process Responsibility Proposed Process Responsibilities Remarks
capacity should be 1.5 lakh cards printing in 200 days, i.e. 750 per day. Current capacity is 250 cards per day per kit.
1.4 Send request for DKM, Master Hospital Card (MHC), Master Kiosk Card (MKC), FKO Card, PHF Card to MoLE
SNA Requisition to be done through web-based KMS as described above
SNA Requisition for cards should be sent well in advance. Indicative deadline for sending different category of cards is given below 1. DIO/DKM/FKO Cards: 6 months before
start of enrolment 2. MHC/MKC: one month after onboarding of
IC 3. PHF Card: Before start of enrolment
1.5 Creation of DKMA Card Verification Mode: PIN Using Any of the 3 seed cards along with CKGA card
MoLE 1. Creation of DIO Card and DKM/ADKM cards using any of the 3 seed cards (with biometrics of seed members) along with CKGA card Verification Mode: Biometrics for seed members, PIN for CKGA
2. The DIO card would be personalized with PIN at CKGA. The DKM/ADKM cards will not be personalized, but district names would be written in chip and printed on card
3. DIO card will be sent by MoLE to DIO.
4. The DKM and ADKM cards will be sent to either SNA or DKM, as per address provided at the time of requisition.
5. Once the DKM and ADKM have
1. MoLE 2. DIO 3. SNA 4. DKM /
ADKM
1. Mode of transfer of DIO cards directly to DIO should be registered/speed post, or by hand through authorized government official. The officer responsible for the transfer should be CKGA.
2. Mode of transfer of master cards from
Delhi to SNA/DKM should be registered/speed post, or by hand through authorized government official. The delivery address would be as per address mentioned in requisition.
3. All DIO’s, DKM’s and ADKM’s should have
access to web-based KMS, and should also have personalization equipment (laptop, biometric device, 2 card readers, paper printer, camera). The issuance of cards should always happen using the web-enabled KMS in a connected mode.
4. Whenever a DKM or ADKM go to DIO with a

RSBY Revised Process Guidelines
42 | P a g e
Sr. No
Current Process Responsibility Proposed Process Responsibilities Remarks
received their cards, it should be indicated on the web portal. DKM and ADKM would carry their card and go to DIO for biometric personalization. The DIO will personalize the cards for ADKM and DKM by capturing biometrics and other details. The authentication of DIO card would be through PIN.
6. In case of transfer/change of DKM/ADKM, the new DKM/ADKM would go to DIO with the card and get the personalization details and biometrics updated. The same would take place using the web-based KMS so that the latest information is available to MoLE.
7. After biometric personalization, DKM/ADKM would take the card from DIO.
card for personalization, they would carry an authority letter.
5. The registered mobile number of all DIO’s,
DKM’s, ADKM’s, FKO’s would be captured during user creation and made available in the master table.
6. In case of change in mobile number, its
responsibility of concerned user to get it updated in the system
1.6 1. Master Hospital Card (MHC), Master Kiosk Card (MKC) are issued from MoLE (with hospital/kiosk unique code) to SNA
2. SNA sends it to DKM, 3. DKM sends it to
hospital/kiosk
MoLE SNA DKM
1. No change in issuance. 2. MHC,MKC cards would be
issued at MoLE, with code and name of entity printed on it and sent to DKM
3. 10% additional blank cards will be prepared and sent to DKM
4. DKM would personalize the cards and distribute it to Hospitals/Kiosks.
5. In case of loss/damage of
1. DIO 2. DKM/ADKM
1. PIN and PUC of the respective cards will be printed and dispatched by DKM/ADKM/MoLE only.

RSBY Revised Process Guidelines
43 | P a g e
Sr. No
Current Process Responsibility Proposed Process Responsibilities Remarks
cards, DKM will provide duplicate/replacement cards from inventory of Blank cards.
6. Name and code of entity can be printed using card printer at Kiosk
1.7 1. FKO card is printed and dispatched to SNA by CKGA at MoLE. The card has district and state codes in the chip and printed on face
2. SNA send the cards to respective DKM
3. DKM handovers the cards to FKO after personalizing it using DKM card and PIN.
DKM 1. FKO Card would be printed and dispatched to DKMA by CKGA at MoLE
2. DKM/ADKM would hand-over the card to FKO after personalization. Each personalization would require biometric details of FKO.
DKM/ADKM 1. SNA would monitor the card movement through web based KMS system.
2. Under no circumstances DKM/ADKM/FKO cards should be shared with IC/SCSP.
2 Procurement, personalization and issue of Beneficiary card
2.1 Specifications of beneficiary Cards
1. 64 KB card 2. SCOSTA certified
MoLE No Change MoLE 1. Since the card will be used for 3 years, quality of the card should not be compromised.
2. Choice of material and certification for cards should be done on the basis of available capacity in the market.
2.2 IC Procures the cards as per specifications decided by MoLE and provided in RFP
IC 1. MoLE to empanel vendors (SCSP) for procurement of cards
2. Vendor to manufacture special lot of cards, specifically for RSBY
3. SCSP to procure cards from
SCSP 1. MoLE to provide a key (transport key) to all empaneled vendors.
2. Vendor to inject transport key in all Smart Cards, manufactured for RSBY
3. ECIS /Kiosk application would be modified accordingly to allow, personalisation of cards with transport Key, only.

RSBY Revised Process Guidelines
44 | P a g e
Sr. No
Current Process Responsibility Proposed Process Responsibilities Remarks
empaneled vendors only
2.3 1. SCSP personalizes the beneficiary card after biometric authentication of FKO along with FKO card
2. Details (URN, Card Chip number) of all the cards issued is captured in FKO Card
3. At the end of enrolment session, signed data is generated for uploading to DKM server.
1. IC/SCSP 2. FKO
1. No Change in personalization process.
2. All the cards wasted at the time of personalization should be hot-listed in the chip as well as in the database.
3. Details of cards hot-listed should be captured in FKO cards.
4. At the end of enrolment session, signed data is generated for uploading it through web application
5. FKO Card data to be uploaded by DKM through the web application
1. IC/SCSP 2. FKO
1. FKO card would capture following additional details
a. Name of head of family b. Date with time stamp c. Number of family members
enrolled d. Name of family member
enrolled e. NPR Number f. Aadhar Number g. Mobile number
2. Increase in number of fields to be written in FKO card will warrant issuance of more number of FKO cards for each kit.
2.4 1. IC/SCSP updates its database with all the cards issued
IC/SCSP 1. Signed data will be uploaded through web application
2. Card chip number, time stamp and other demographic details, if updated during enrolment will be updated in central database.
3. Data from FKO card would also be updated in central database
SCSP 1. The data received from two independent secured sources (FKO Card and signed data) would be used to update the database.
2. MIS of cards issued will be available on near-real-time basis.
3 Other activities
2.6 Issuing duplicate card 1. Hot-lists old card 2. Data updated in
database at IC
Kiosks 1. Hot-list the old card using web based application
2. Update the data of hot-listed cards in local database of all
Kiosk A duplicate smart card with exactly same details and balance is issued in following conditions:

RSBY Revised Process Guidelines
45 | P a g e
Sr. No
Current Process Responsibility Proposed Process Responsibilities Remarks
server 3. IC informs
hospitals about hot-listed cards
empaneled hospital, when they are connected to central / state data base servers.
3. Personalize the card with data available at central server
4. Update the card chip number in the data base,
5. Keep the old card chip number in database
1. In case original RSBY card is lost or
damaged
2. Original card has stopped functioning
2.7 Issue of split card 1. Take the request from
HoF for issue of smart card
2. Check the available limit in card
3. Reduce the existing limit of primary card by amount (X) for which split card is to be made
4. Personalize the split card with a limit X
Kiosks 1. No Change 2. Update the Card chip number
in the central data base through web application,
Kiosks 1. Central database will have details of all the cards issued against a particular URN number.
2. Against a particular URN only one card will be active at a particular time, except in case of split cards, when two cards can be in active state against a particular URN
2.8 Validity of card 1. Card is valid for five
years, policy is valid for 1 year
2. Every year a new card is issued with fresh limit in case the beneficiary data provided by SNA was changed or SNA could not provide old URN
IC/SCSP 1. Card is valid for 5 years and policy can be extended maximum upto 3 years
2. After one year beneficiary will visit the kiosk to reset the limit to 30K, else
3. If beneficiary visits hospital, TMS will check at central data base and update the details of the limit on the beneficiary card.
1. IC 2. SCSP 3. Kiosks
Insurance policy will be valid for one year, and needs to be renewed every year upto a maximum of 3 years based on performance. To renew the policy, beneficiary will have to visit either kiosk or hospital.

RSBY Revised Process Guidelines
46 | P a g e
Sr. No
Current Process Responsibility Proposed Process Responsibilities Remarks
3. In case the renewal data contained the old URN, the same card could be renewed by adding the next policy details
Policy decision taken
Sr. No Decisions Meeting reference
1 DIO to personalize DKM card Letter dated 22nd April 2014 from DDG NIC
2 DKM card to have biometrics for authentication at issuance of FKO card Meeting held on 6th May 2014, chaired by Secretary (L&E), MoM yet to be processed in file
3
All FKO, Hospital, and PHF cards to be personalized and issued by DKM. In absence of DKM, this can be electronically delegated to one or more ADKMs (upto 2) using the web based KMS. The responsibility of the inventory would be with DKM. In addition to delegation of DKM charge, ADKM can also be used for setting up additional DKMA in case of large districts
Meeting held on 6th May 2014, chaired by Secretary (L&E), MoM yet to be processed in file
4
Centralized technical support team across entire IT solution portfolio, including central web application, KMS, TMS, CGMS, card/biometric issues to be established at MoLE. The team can be reached through various channels viz. email, web and phone number. The team for this technical support should be outsourced. To start with the technical support agency will have separate resource and channel of communication (email, number and web channel). In future (at the start of next policy year i.e. FY 15-16), however, they may merge with CGMS.
Meeting held on 6th May 2014, chaired by Secretary (L&E), MoM yet to be processed in file
Policy decision to be taken

RSBY Revised Process Guidelines
47 | P a g e
Sr. No Decisions
1 FRS and SRS for web-based KMS application should be prepared at the earliest so that the same can be developed by NIC. FRS to be made by a third party agency. SRS to be made jointly by third party agency and NIC.
Incentive Mechanism
1 NA
Training Needs Training to be provided to Training to be provided by
1 Awareness and sensitization of master key card holders about criticality of KMS system and to use the new web based KMS system
CKGA, Seed members, DIO,DKM, ADKM, FKO
NIC
Human Resource Requirement Where
1 Additional DKMs to personalize FKO cards District
Input for RFP/FRS Input for RfP/FRS
1 The one time procurement and delivery of kits for DIO, DKM and 5 ADKM’s (laptop, biometric device, 2 card readers, paper printer, and camera) for card issuance and personalization. Once procured and delivered, the kit would become the property of the SNA.
RFP forSCSP
2 The specifications of card, issuance and personalization equipment and enrolment kit will be defined in the RFP. RFP for SCSP

RSBY Revised Process Guidelines
48 | P a g e
Input for RFP/FRS Input for RfP/FRS
3 Additional field to be captured on FKO cards FRS for KMS
IEC Activities
1 Not required

RSBY Revised Process Guidelines
49 | P a g e
Pro
ce
ss
Co
de
IV–WCPP Process Name
Public health wellness check and payment of premium
Process Objective Current Status 1. To inculcate the health seeking behaviour amongst
beneficiaries 2. To ensure that one member of the beneficiary family
undergoes timely and hassle free wellness check 3. To ensure accurate and timely calculation of
premium to the insurance company for activated RSBY cards
4. To ensure timely, accurate and hassle free payment of premium to the insurance company
1. Wellness check is a new feature being introduced for the beneficiary. This will ensure that at least one member of the family has undergone a wellness check at the public health facility (PHF / hospital).
2. The IC follows a manual process for raising an invoice to the SNA for payment of premium
Key Stakeholders Measures and Key Performance Indices (KPIs) 1. Beneficiary 2. Ministry of Labor and Employment (MoLE) 3. State Nodal Agency (SNA) 4. Insurance Company (IC) / Third Party Administrator
(TPA) 5. Public Health Facility (PHF) 6. Hospital
Measures8: MoLE, SNA, PHF, Hospital, IC/TPA (relevant reports to be available, depending on role)
1. Number of beneficiary wellness checks vs number of enrolments Filters: User Category (Beneficiary, PHF, Hospital, IC/ TPA), Geography, Time period of wellness check
2. Number of beneficiaries whose wellness checks have been conducted at PHF /
hospital Filters: User Category, Geography, Time period of activation
3. Number of cards for which timely payment of premium has been done to the insurance company by SNA Filters: User Category, Geography, Time of payment
4. Number of cards for which timely payment of premium has been done to the SNA by MoLE Filters: User Category, Geography, Time of payment
8 All measures to be available as a report on a web portal in real-time/near-real-time. The data should be available in a warehouse, such that any extraction is possible to create ad-hoc reports

RSBY Revised Process Guidelines
50 | P a g e
KPI9: MoLE, SNA, PHF, Hospital, IC/TPA (relevant KPI’s to be measured depending on role)
1. Number and % of beneficiaries that have visited the PHF / hospital for wellness checks by the due date (from date of commencement of policy, i.e. 60 days)
2. Number of beneficiaries whose biometrics have been recorded by the PHF /hospital during wellness checks
3. Average time taken by SNA to release payment to insurance company (SNA and
central share) 4. Average time taken by MoLE to release payment to SNA (central share)
Summary of current challenges Summary of key suggestions 1. Uncertainty on card actually being issued to
beneficiary 2. Poor health seeking behaviour of beneficiaries
having an RSBY card 3. Delayed payment to Insurances companies, and
coordination gaps between SNA and Insurance companies
1. Introduce wellness checks for beneficiary with predefined health parameters 2. Responsibility of mobilising beneficiaries for wellness check lies with IC 3. Full premium will be paid for all card issued, but only after completion of wellness check. 4. If wellness check is delayed by more than 60 days after commencement of policy, a
penalty will be levied on IC at following rate: a. If done after 60 days but before 90 days: Penalty will be 50% of the premium of
remaining beneficiaries whose wellness check is yet to be done b. If done after 90 days: penalty will be 100% of premium of remaining beneficiaries
whose wellness check is yet to be done 5. Wellness check being a new concept needs to be driven by IC with support of SNA/DKM/
FKO 6. Definition of health parameters within the wellness check activity needs to be updated
based on the health trends observed
Pre-requisites for wellness check and premium payment 1. Beneficiary to be issued the card during the enrolment process 2. PHF should have equipment, software and appropriate connectivity to update the database and card with wellness check data 3. Hospital has performed wellness check as per the wellness check activities laid out in Annexure 4.1
Inputs to the revised process Output from the revised process 1. Beneficiary card activation details
1. Wellness check of beneficiary 2. Confirmation of wellness checks performed by PHF / hospital 3. Payment of premium to insurance company
9 All KPI’s to be available as a report on a web portal in real-time/near-real-time. The data should be available in a warehouse, such that any extraction is possible to create ad-hoc reports.

RSBY Revised Process Guidelines
51 | P a g e
Process and responsibilities
Sr. No
Current Process Responsibility Proposed Process Responsibility Remarks
1 IEC activity by IC for wellness checks at PHF
1.1 NA (No current process exists)
NA IC and SCSP shall conduct IEC activities for making the beneficiaries aware of wellness checks at PHF.
Reminder SMS messages to be sent to beneficiaries to get their wellness check conducted after issue of card, 1 month before the due date, and 10 days before the due date
1. SCSP
2. IC
3. MoLE
1. SCSP should provide information brochures along with the RSBY card during the enrolment process. These information brochures shall be handed over to the SCSP by IC before the enrolment process commences. A section on the wellness check details should be included in the brochure. The card cover should have the due date for wellness check printed on it.
2. The SMS shall go from MoLE from the URN / enrolment data available at the central server.
2 Wellness check of the beneficiary
2.1 NA NA Beneficiary visits PHF / hospital for wellness check with RSBY card
Beneficiary / PHF 1. One member of the family visits the PHF / hospital for wellness check. This could even be the head of family or any other enrolled member of the family.
2. Responsibility of mobilising beneficiaries for wellness check lies with IC
3. Full premium will be paid for all cards
issued, but only after completion of

RSBY Revised Process Guidelines
52 | P a g e
Process and responsibilities
Sr. No
Current Process Responsibility Proposed Process Responsibility Remarks
wellness check.
4. Delayed wellness check will attract
penalty from the premium payable to
IC.
2.2 NA NA PHF / hospital performs wellness checks as laid out in Annexure-4.1
The components of the wellness check mentioned in Annexure 4.1 are basic level tests which can be performed by any PHF / hospital. The PHF / hospital must ensure that they are conducting all the tests and uploading the report on the central server. The PHF should also store minimum details of wellness check on the beneficiary card as laid out in Annexure 4.1(a). The larger details of wellness checks should be uploaded on the central server.
2.3 NA NA 1. After the wellness check is conducted, the PHF / hospital operator enters the details of the wellness check conducted into the new web based transaction management software (new TMS).
2. The status of wellness check should also be updated into the beneficiary card by the
PHF / hospital 1. The details of checks performed towards wellness check by PHF / hospital are entered into the proposed web based TMS, hosted on central server.
2. In the event of no connectivity at the PHF / hospital, the PHF/hospital would be responsible to transfer details of all the wellness checks completed by it at the central server

RSBY Revised Process Guidelines
53 | P a g e
Process and responsibilities
Sr. No
Current Process Responsibility Proposed Process Responsibility Remarks
PHF/hospital operator for keeping a medical record of the beneficiary.
3. Part of the medical details (listed in annexure 4.1.a) of beneficiary will be updated on card.
every 15 days. After 10 days the software would prompt for records which need to be updated in the central server.
3. 4 kb of space at card will be earmarked for Electronic Medical Record (EMR) of beneficiary
2.4 NA NA The beneficiary shall provide his biometrics at the PHF / hospital to confirm his visit for wellness check
1. Beneficiary,
2. PHF / hospital operator
1. The biometric of the beneficiary is taken post completion of the wellness check activity. This will confirm which member of the family has visited the PHF / hospital for a wellness check. This process will also help in creating a health history of the beneficiary for future references.
2. An SMS would go to the beneficiary from the central server, confirming the completion of wellness check and along with card balance details and a feedback shall also be sought from the beneficiary regarding the wellness check conducted.
2.5 NA NA 1. The beneficiary is provided with a print of the results of the wellness check.
2. There will be two prints, one
PHF/hospital 1. The PHF/hospital shall maintain pre-printed report forms, which can be downloaded from the RSBY website.
2. For test results, which are not

RSBY Revised Process Guidelines
54 | P a g e
Process and responsibilities
Sr. No
Current Process Responsibility Proposed Process Responsibility Remarks
which is instantly available, and one which is available after 1-2 days afterdetailed test results are available.
available instantly, the PHF / hospital would maintain a printed record and the beneficiary should be allowed to collect the test results within 30 days of the wellness check. The beneficiary would be notified by SMS on the availability of his/her wellness check test results.
3 Upload of wellness check report
3.1 NA NA The PHF / hospital should upload the wellness check report of beneficiary on the proposed web based application (new TMS), which is stored on the central server.
PHF/ hospital 1. Uploading of the report is mandatory after test results are available. If possible, the PHF/hospital operator should upload it immediately.
2. “Premium payable” flag should also be updated. In most cases, it should be TRUE, but if it is FALSE, the same information should be uploaded.
4 Premium payment to insurance company (IC)
4.1 Collection of INR 30 from beneficiary after handing over the RSBY card during enrolment process.
IC/SCSP The amount of INR 30 should be collected only after re-verification of cards at the enrolment station.
SCSP (Primary responsibility)
1. The verification of the receipt of cards by the beneficiary is done at the enrolment station. The beneficiary provides his biometric data towards confirmation of receipt of card.

RSBY Revised Process Guidelines
55 | P a g e
Process and responsibilities
Sr. No
Current Process Responsibility Proposed Process Responsibility Remarks
2. In the first year, the SCSP or its representative shall collect the first instalment of the premium for providing the insurance cover, i.e., a sum of Rs. 30 (Rupees Thirty Only) from each beneficiary family unit, at the time of enrolment and on delivery of the smart card.
4.2 1. IC manually raises an invoice to SNA for the remaining premium (i.e. state and center share) for all cards that are issued.
2. The IC needs to enter the
details of the premium bill raised on the RSBY portal. A Premium Claim Reference (PCR) number will be generated by the system.
3. This PCR number should
be mentioned on the bill submitted to the SNA. The SNA does not accept the bill without the PCR number.
IC 1. The web based application shall fetch data from the PHF / hospital for all the cards that have been where wellness check has been confirmed. The IC can generate an MIS for all such cards and raise an invoice accordingly to SNA for payment of premium from state and central government.
2. The IC will raise the invoice for all such cards through the proposed web based application itself so that there is an electronic invoice record. However, a printed invoice will also be sent to SNA.
3. The proposed web application would generate a unique PCR number for every invoice record which would act as
IC 1. The premium amount (state share + central share) is calculated by the proposed web based system depending on beneficiary category.
2. While calculating premium, following penalty provisions should be kept in mind
3. If wellness check is delayed by more than 60 days after commencement of policy, a penalty will be levied on IC at following rate:
a. If done after 60 days but before 90 days: Penalty will be 50% of the premium for remaining beneficiaries whose wellness check is yet to be conducted.
b. If done after 90 days: penalty will be 100% of premium for remaining beneficiaries whose

RSBY Revised Process Guidelines
56 | P a g e
Process and responsibilities
Sr. No
Current Process Responsibility Proposed Process Responsibility Remarks
reference, and would be mentioned on each invoice.
wellness check is yet to be conducted.
4.3 1. Assuming that A is the total premium cost bid by the IC, which includes the card cost of Rs. 60.
2. SNA calculates and pays the state share as per following formula 25% (A-60)-30. For NE states & JK, SNA uses 10% instead of 25%.
3. Rs. 30 is being retained by the SNA towards its administrative expenses.
SNA 1. The premium amount for the 1st year (state share) of premium is calculated by the proposed web based system with the same logic built into the system.
2. The state share to be paid
during 1st year would be 25% (A-60)-30. For NE states & JK, the central share would be 90% instead of 75%.
3. The SNA shall pay the
premium within 15 business days of receiving the invoice from IC. The payment must happen through the proposed web application. (Or atleast the payment record should be updated in the application as soon as the payment is made)
4. IC should get a notification SMS and email once the state share is paid.
SNA 1. This premium will only be paid for the beneficiary cards whose wellness check has been done and confirmed in the web based application.
2. A unique payment number would be used to update the payment data in the web based system.

RSBY Revised Process Guidelines
57 | P a g e
Process and responsibilities
Sr. No
Current Process Responsibility Proposed Process Responsibility Remarks
4.4 1. SNA calculates premium amount for payment of the central share of premium to IC as per following formula: 75% (A-60) +60
2. The SNA shall request
MoLE for its share of premium within 15 days of receipt of invoice from IC
3. The total amount that is
to be paid by MoLE towards the premium shall not exceed the amount that is calculated as [0.75 x (750 - 60) + 60]. Any portion of the premium in excess of such amount shall be borne by the SNA.
4. MoLE shall release
premium amount to SNA within 21 business days of receiving a request in the prescribed format.
5. SNA shall pay IC within 7
days of receiving the
1. SNA
2. MoLE
1. The premium amount for the central share of premium is calculated by the proposed web based system with the same logic built into the system, i.e.75% (A-60) + 60. For NE states and JK, the central share would be 90% instead of 75%
2. The SNA shall pay the
premium within 45 business days of receiving the invoice from IC. The process is as follows:
a. The SNA shall request MoLE for its contribution towards the invoiced amount within 5 business days from release of state share. The same would be done through the web application, with the same PCR number.
b. The total amount that is to be contributed by MoLE towards the premium payable on behalf of such RSBY beneficiary family unit shall not exceed the amount that is calculated as [0.75 x (750 - 60) + 60]. Any portion of the premium in excess of such
1. SNA
2. MoLE
1. The premium for the 2nd and 3rd installment will only be paid for the beneficiary cards whose wellness check has been done and confirmed in the web based application.
2. Once the state share is paid, IC is not
required to produce any additional documents/ information for the release of central share.
3. All payments must happen through the proposed web application. (Or atleast the payment record should be updated in the application as soon as the payment is made)
4. A unique payment number would be used to update the payment data in the web based application.

RSBY Revised Process Guidelines
58 | P a g e
Process and responsibilities
Sr. No
Current Process Responsibility Proposed Process Responsibility Remarks
amount from MoLE amount shall be borne by the SNA.
c. MoLE shall release this amount to the SNA within 15 business days of receiving a request in the web based application.
d. Upon receipt of such amount from MoLE, the SNA shall pay such amount to the Insurer within 10 business days.
4.5 There is no penalty on SNA for delay in payments, except for circumstances where delay is due to payments being withheld.
SNA Delay in premium payment by SNA to IC - SNA will pay IC an interest of 0.5% of premium amount for every 15 days delay if the premium payment is delayed beyond 6 months of the start of policy.
SNA The proposed web based application will calculate the time delay for payment of premium amount by SNA (both state and central share), and a report would be made available on the web application.
5 Premium refund
5.1 No premium refund / discount guidelines
MoLE In case an IC has not performed well in a year, and adjusted claim ratio (claim paid to hospitals + card issuance cost)/total premium received is less than 70%, it shall refund the differential amount to SNA/MoLE. The differential amount is calculated as (claim amount at a claim ratio of 70%) – actual total claims paid.
MoLE The objective of the scheme is not only to enroll beneficiaries but also to make sure that they get the benefit from the scheme. Therefore, keeping this in mind Insurance Company will have to refund a part of premium at the end of the first and second year if the “Claim Ratio” is lower than the threshold.

RSBY Revised Process Guidelines
59 | P a g e
Policy Decision taken Meeting reference
Sr. No Decisions
1 In case of delayed payment of premium, SNA will pay interest to IC @ 0.5% of amount for every 15 days delay, if the premium payment is delayed beyond 6 months of the start of policy
EC dated 23rd January 2014
2 Premium payment will be done based on data generated through the software system/application
EC dated 23rd January 2014
3
In case an IC has not performed well in a year, and adjusted claim ratio (claim paid to hospitals + card issuance cost)/total premium received is less than 70%, it shall refund the differential amount to SNA/MoLE. The differential amount is calculated as (claim amount at a claim ration of 70%) – actual total claims paid.
EC dated 23rd January 2014
Policy Decision to be taken
Sr. No Decisions
1
Issue related to card activation not happening due to lack of wellness check compliance
- What can be the estimated % of such cases? - Who does this estimation and takes the risk – IC? - What If majority of beneficiaries don’t turn up for wellness check? - Premium slab in the activation happens 60 days after the onset of policy? - Minimum amount of premium that should be paid to IC in case the beneficiary goes to hospital towards the last month of policy?
3 The wellness check has to be done within 60 days from the commencement of policy. The IEC messaging done by the IC should indicate a due date by which the beneficiary should get the wellness check completed. At the time of enrolment and card issuance also, the IC representatives should communicate to beneficiary the due date (and not 60 days).

RSBY Revised Process Guidelines
60 | P a g e
Policy Decision to be taken
Sr. No Decisions
4 If wellness check takes place after the due date, the policy would still be active for beneficiary. The coverage for the beneficiary for the remaining 10 months would be the same.
5 Checklist for wellness check needs to be approved by MoLE. The same is attached in Annexure 4.1, and is being used by Gujarat.
6 Delay in premium payment by SNA to IC - SNA will pay IC an interest of 0.5% of premium amount for every 15 days delay if the premium payment is delayed beyond 6 months of the start of policy. This will be applicable after MoLE has approved of the case
7 Whether premium discount needs to be applied for IC’s which have performed poorly, i.e. below the 70% claim ratio threshold. Whether this policy is required in addition to the already approved refund policy?
Training Needs Training to be provided to Training to be provided by
1 Training on usage of web based application for premium payment
Hospital Staff / IC / SNA MoLE / IT application agency
2 Training on usage of web application for management of wellness check information
PHF/Hospital Staff MoLE / IT application agency
Input for RFP/FRS RFP/FRS for:
1 Details on wellness check process, guidelines and data management IC Selection
2 Process, rules and method of payment of premium to IC on completion of wellness check and card activation till due date, and for the period beyond
IC Selection
IEC Activities
1 The insurance company shall have a strong focus on IEC activities due to payment of premium being linked to wellness checks. The RFP can include a list of tentative IEC activities that the IC must focus on.

RSBY Revised Process Guidelines
61 | P a g e
2 Wellness check due date information should be mentioned on RSBY card and cover
Incentive mechanism
1 Not applicable
S.No. Human Resource Requirement Where
1
Monitoring and evaluation personnel to closely monitor the progress of wellness checks being conducted, and subsequent card activation and premium payment process, including management of related audit processes
At SNA, i.e. one for every state

RSBY Revised Process Guidelines
62 | P a g e
-P
roce
ss
Co
de
V – HOSP Process Name Hospital Management
Process Objective Current Status 1. To ensure efficient and timely management of network hospitals 2. To increase the utilization and efficiency of RSBY healthcare
facilities offered to beneficiaries by network hospitals 3. To provide quality healthcare service delivery to beneficiaries at
hospitals in a convenient, easily accessible and affordable manner
1. The total number of hospitals currently empanelled under RSBY are 10,311 across 29 states and UT’s (data as per the issuance of MHC cards)
2. The distribution of private sector : public sector hospitals is 6093:4218 3. About 5400 hospitals have been verified by IC as active hospitals and only
about 1700 hospitals have been confirmed as active hospitals by the SNAs 4. The list of hospitals tagged upto district and block is published by MoLE
Key Stakeholders Key Performance Indices (KPIs) 1. Beneficiaries 2. SNA 3. IC/TPA 4. Hospitals 5. SCSP
Measures10: MoLE, SNA, PHF/Hospitals (relevant reports to be available, depending on role) 1. Number of hospitals empaneled and distribution across private and public
sector Filters: Geography (state, district, block), type of hospitals (public, private) Facilities available (Different surgeries etc.) Date of empanelment (from), date of de-empanelment (from)
2. Number of hospitals de-empaneled and distribution across private and public sector Filters: Geography (state, district, block), type of hospitals (public, private), Date of empanelment (from), date of de-empanelment(from)
Key performance indicator11: (relevant KPI’s to be measured, depending on role)
10 All measures to be available as a report on a web portal in real-time/near-real-time. The data should be available in a warehouse, such that any extraction is possible to create ad-hoc reports
11
MIS on all KPIs to be available on a web portal in real-time/near-real-time, with authorised access

RSBY Revised Process Guidelines
63 | P a g e
1. Number and % of district and blocks with empaneled hospitals 2. % of cases with authentication failures (manual override) 3. Number of patients treated, number and % of patients treated with
completely cashless hospitalization
4. Number of blocks with less than 2 hospitals empaneled
5. Number of complaints / grievances made against the hospital
6. Number of claims submitted by hospital
7. Number and % of total claims submitted within 1 week of discharge of
beneficiary
8. Average cash payment made by the beneficiary under RSBY – this should be
computed as total amount paid by beneficiaries at a hospital, and the total
number of beneficiaries treated by the hospital. The hospital is expected to
maintain this data (This data would be made available to audit teams and
the call center)
9. Average hospital equipment uptime in a month 10. Average in-patient time
11. Number and % of hospitals that have meet the NABH revised criteria 12. Number and % of hospitals not reporting claims for more than 3 months 13. Number and % of hospitals adhering to RSBY clinical protocols and STGs
14. Number of hospitals empaneled by IC in lieu of de-empaneled hospitals 15. Number of hospitals de-empaneled
All KPI’s would be measured with filters on public as well as private hospitals Summary of current challenges Summary of key suggestions 1. Beneficiaries are denied cashless medical services by hospitals/IC
on several grounds: - Requirement of additional ID proof (in few cases) - Equipment not functional - Amount charged for initiating treatment - Certain services not covered, and/or unavailability of
providers 2. Beneficiaries not aware of the empanelled hospital list, the
requirement to carry RSBY card to empanelled hospitals, and the procedure to be followed at the hospitals
1. Empanelment and de-empanelment of hospitals will continue to be primary
responsibility of IC, under the close supervision of SNA through a web based
system. SNA will also supervise random audits (number of visits per hospital
per month should to be fixed) conducted by independent 3rd party auditor,
to check the facilities available, and services offered by the hospital, till the
entire RSBY system is made transparent. 2. Updation and revision of package rates for procedures to address the cost
escalation and rationality of procedures including additions of procedures
beyond Rs. 30,000.

RSBY Revised Process Guidelines
64 | P a g e
3. Claim settlement process is not transparent (with little information visibility on claim status), discouraging hospitals from participating in the scheme
4. Hospitals feel that the package rates are too low for them to offer the necessary treatment, and often opt out of the scheme
5. Hospitals often offer treatments only for procedures which are profitable for them
6. Hospitals often provide unauthorized/inappropriate treatment, either to charge more from the IC and/or beneficiary, or to discourage beneficiaries from availing services under RSBY
7. Hospitals, even if they are interested and eligible, may not come on board, if they are not in good books of IC/TPA
8. IC/TPA may not empanel good hospitals, due to high claims 9. The current TMS does not have the option to capture clinical
indicators for future verifications 10. Lack of transparency and ambiguity in suspension and de-
empanelment of hospitals. 11. Beneficiary has no flexibility to opt out of the hospital once a
procedure is blocked on his card, nor he can go to any other hospital for availing treatment.
3. Transaction software (TMS) at the hospital should have the facility to capture pre-defined clinical indicators and outputs for post facto evaluation.
4. Enhanced education and empowerment of beneficiaries to avail RSBY services, and to communicate complaints /grievances/malpractices to authorities through the call centre (covered under complaints and grievance redressal) or local district kiosk.
5. SMS communication to beneficiaries (within the geographic area such as block) about empanelment and de-empanelment of hospitals
6. SMS communication to beneficiaries in case they have visited the hospital and taken treatment/drugs (in order to prevent fraudulent transactions) at a hospital
7. Publication of procedures and specialities available at a hospital on the RSBY website, in the RSBY brochure, as well as in local media. The same information should also be available with the call center. The user of the web application should be able to search through hospitals, specialities, procedures and FAQs. This information should be made available to public. In addition to this, publication of the hospital performance should also be published on the RSBY portal.
8. Publication of performance of the hospital on the web with respect to RSBY including quality accreditation, adherence to clinical protocols , patient satisfaction etc.
9. Standardization of hardware equipment and software which is maintained at the hospital
10. Mandated minimum standard information to be maintained and provided to the beneficiary by the hospital.
11. In case, a beneficiary opting to discontinue treatment after the package is blocked, facility will be created at CGRMS or at Kiosk for unblocking his card, with intimation to hospital.
Pre-requisites for the process 1. Empanelment criteria, and empanelment of hospitals 2. Creating list of approved packages and package rates 3. List of ailments/treatment excluded from scheme
Inputs to the revised process Output from the revised process 1. List of empanelled hospitals 2. Pre-agreed procedure rates / package rates
1. Efficient and timely delivery of health services to the beneficiary at the PHF /hospital

RSBY Revised Process Guidelines
65 | P a g e
3. Premium information 4. SLA’s for the hospital as per contract with the hospital 5. Transparent and responsive de-empanelment / suspension process
for hospitals
Processes and Responsibilities
Sr. No
Current activities Responsibility Proposed Activities Responsibility Remarks
1 Empanelment
1.1 1. SNA provides a list of hospitals available in the area to IC
2. IC adds list of additional hospitals
3. IC/TPA empanels the hospital on the basis of guideline provided by MoLE Empanelment criteria is given in Annexure 5.1
IC/TPA 1. MoLE will publish the empanelment criteria and guidelines (both online and offline)
2. Hospital empanelment will be made self-service where each hospital can apply for empanelment through the RSBY portal (and by post)
3. The empanelment requests submitted online are examined by the district committee and the selected hospital list is sent to the IC. The IC will verify the details submitted by the hospital and empanel the hospital. In case verification does not happen, IC will use the web application to keep the hospital on hold and indicate a reason for
1. MoLE 2. IC/TPA
(Primary empanelment responsibility)
3. District Committee
4. SNA
1. Empanelment implies readiness of hospitals to accept RSBY beneficiaries for treatment, and conduct transactions online.
2. In every district, the district administration will set up a district RSBY committee. This district RSBY committee will be chaired by District Magistrate/ Deputy Commissioner and will have District Key Manager of RSBY as the convener. The Chief Medical Officer will be other member of the committee. This committee can be any existing committee too.
3. Hospitals may apply for empanelment through web-portal. Hospitals will make the entry of their details through an online entry form on the website www.rsby.gov.in. On successful submission of hospital empanelment form, a “Reference Number” will be generated and this can be used further to track the status of their empanelment under RSBY.
4. Based on the RSBY beneficiary population of the district, number of hospitals should be empanelled in each block. This will include both public and private hospitals. There should be at least two hospitals in each block in each of the project districts.
5. There should be at least 5 hospitals at the district headquarter.

RSBY Revised Process Guidelines
66 | P a g e
Processes and Responsibilities
Sr. No
Current activities Responsibility Proposed Activities Responsibility Remarks
hold. The District Committee, however, can override the hold status to approve/select.
4. The final responsibility of empanelment of hospitals would rest with the IC. IC would log into the web application, and create hospital record and details.
5. Any new hospital proposed by IC would be allowed, but the same should be approved by the district committee.
6. The empanelment process should be completed 15 days prior to commencement of policy.
6. There should be at least one hospital for every 8,000 eligible beneficiaries (~2000 families) in the scheme
7. The following specialties shall be available through empanelled hospitals in each district
a. General Medicine
b. General Surgery
c. Obstetrics and Gynecology
d. Pediatrics
e. Ophthalmology
f. ENT
g. Orthopedic
1.2 Bi-partite agreement between hospital and IC
1. IC 2. Hospital
No change 1. IC 2. Hospital
The overall responsibility of empanelment and de-empanelment of Health Care Providers under RSBY will be of that of the Insurance Company, but with support and under the supervision of SNAs and the district
committee. 2 Readiness of operations at hospital
2.1 Hardware installation at hospitals
1. IC 2. Hospital
The SCSP will provide hardware and its installations at the public and private hospitals.
1. SCSP (primary responsibility)
2. Hospital
Hardware must be installed 15 days before commencement of policy. The readiness of hardware is gauged by dummy/test transaction between the hospital and central server.

RSBY Revised Process Guidelines
67 | P a g e
Processes and Responsibilities
Sr. No
Current activities Responsibility Proposed Activities Responsibility Remarks
2.2 Maintenance of hardware
1. IC 2. Hospital
The SCSP will be responsible for the AMC of the hardware installed at the public and private hospitals. The hardware and software uptime KPI should be measured, and strictly adhered to.
1. SCSP (primary responsibility)
2. Hospital
1. SCSP should ensure that all reported hardware related issues are resolved within the stipulated time as per SLA.
2. SNA should work with NIC to include remote monitoring functionality of the status of hardware.
3. The AMC contract draft, rates and service provider for maintaining the equipment needs to be finalized by the SCSP.
2.3 Transaction Management software readiness. The FTP software for data transfer is developed by MoLE, and the installation is done by IC.
1. MoLE 2. IC
A new software will be prepared by NIC with additional functions: 1. A web based TMS
application hosted at central server
2. All transactions to be online
3. User authentication through login id and password
1. MoLE 2. NIC 3. SNA
The transaction software will capture all the transactions (Registration/admission of beneficiary, blocking and unblocking of package in the card, discharge, pre authorization for unspecified packages, entry of fingerprint override code, treatment given etc.) done using RSBY cards. Hospitals raise a claim using this application, which is shared with SNA, MoLE and IC. New functionality required: 1. Indication of amount in case the package rate shows
NULL 2. Validation of override code given by IC, in case the
beneficiary authentication has to happen through RSBY card
3. The claim number should be visible on the transaction software
4. Status of every claim (including inter IC claims) should be visible to the hospital through the login on the web application, and/or RSBY portal. The information on claims is updated by the IC. The claim information from all hospitals (TMS) should go on the central server, and the respective insurance companies will act on it.

RSBY Revised Process Guidelines
68 | P a g e
Processes and Responsibilities
Sr. No
Current activities Responsibility Proposed Activities Responsibility Remarks
5. Wellness check status should also be visible to the TMS software after the RSBY card is used for authentication
6. Transaction software at the hospital should have the facility to capture pre-defined clinical indicators and outputs for post facto evaluation. The central server claims module (available through the web application) would have read/write interfaces/APIs for the insurance company to process the claim
7. The central server should have a facility to allow for card balance query, both through web and SMS channel
8. Timestamp for every transaction should be designed in the system, and captured to monitor turn-around-time compliance for every transaction
2.4 Claim Settlement software access with the Insurance company
IC This process is not required, as the same would be handled through a web application as described above.
NA Claim settlement will be done by the IC based on the claim submitted by the hospital. Any dispute in claims will have to be investigated by the district investigation committee along with the IC. Each stage of investigation shall be recorded in the web based software. Approvals and non-approvals will also be done through the web based software. The IC shall be responsible for closing any claims related issues within 30 days of receiving the claim from the hospital.
2.5 Master Hospital card (MHC) issuance
MoLE 1. No change in the issuance process
2. Decentralized process, where SNA and DIO would have additional cards their disposal, which may be personalized for issuance
DKM

RSBY Revised Process Guidelines
69 | P a g e
Processes and Responsibilities
Sr. No
Current activities Responsibility Proposed Activities Responsibility Remarks
to the hospital.
3 De-empanelment
3.1 De-empanelment 1. If any activity
by the hospital appears suspicious, IC keeps the hospital under watch list, with a notification to SNA.
2. If situation does not improve in a month’s time, IC de-empanels the hospital by writing to DKM.
IC De-empanelment 1. If any activity appears
suspicious from data patterns observed by IC or SNA, IC keeps the hospital under the watch list. The name of the hospital and date should appear under ‘Watch List’ tab in the web based application. The same is visible to the SNA. MoLE would have pan–India access of all hospitals under watch list. The SNA should get an SMS also as soon as a hospital is put on watch list.
2. IC investigators would monitor the situation. If it does not improve in a month’s time, a show cause notice is sent to the hospital by IC. The status of show cause notice would be updated by IC on the web application. The web
1. IC 2. SNA
1. The guidelines and rules/triggers for suspending the hospital for actual de-empanelment will be defined and published by MoLE. Examples are: - More than the expected cases treated under a
specific procedure - High % of manual override cases at the time of
beneficiary registration - Any other fraudulent activity
Detailed lists of triggeres is given in Annexure 5.2. However, these triggers will invoke investigations prior to any suspension activity being undertaken by IC.
2. An SMS is sent to all beneficiaries in the geographic location (block beneficiaries where the hospital is situated) informing about the de-empanelment
3. Hospitals shall continue to provide treatment to the beneficiaries, even during the period when they are placed on the watch-list or during suspension. Alternatively, beneficiaries who are admitted on the day of de-empanelment would also continue to receive the services from the hospital, and the claims for them would be honored by the IC.
4. The IC would be responsible to empanel another hospital in the same geographic location within 1 month.

RSBY Revised Process Guidelines
70 | P a g e
Processes and Responsibilities
Sr. No
Current activities Responsibility Proposed Activities Responsibility Remarks
application would also provide a template for show cause notice. The show cause notice would be uploaded on the web application, and the hospital primary user would get an SMS on his mobile. The show cause notice would be visible to the SNA also on the web application. SNA would get also an SMS alert about this.
3. If the hospital does not respond in 7 days, the IC de-empanels the hospital, and an SMS goes to DKM and SNA. During the period of 7 days, the hospital would function regularly and all RSBY services, including admission, treatment and claims would be functional.
4. IC would also have special authority to de-empanel the hospital instantly in an extreme scenario. However, such a de-empanelment would

RSBY Revised Process Guidelines
71 | P a g e
Processes and Responsibilities
Sr. No
Current activities Responsibility Proposed Activities Responsibility Remarks
always be complimented with an FIR. The scanned FIR copy would need to be uploaded on the web application.
4 Hospitalization
4.1 Registration of patient happens with RSBY card authentication by the patient
Hospital 1. The process does not undergo any change.
2. Direct web based data entry through a client with an offline data entry provision. Only in case of connectivity at the hospital, the functionality for authentication of the hospital user should be provided. So that, on an experimental basis, the authentication using login and password based access to the web application hosted on the central server may be tried.
3. Synchronization with the central server will be done once there is connectivity.
4. An SMS would be sent to the beneficiary to confirm the registration.
Hospital 1. The beneficiary can be advised for hospitalization through hospital emergency or an OPD within or outside a hospital.
2. The beneficiary visits RSBY helpdesk and produces the RSBY card.
3. Helpdesk verifies the beneficiary details and registers him/ her (by swiping the card on the PoS machine and verifying the fingerprints).
4. In the event of beneficiary not carrying the card during an emergency, the hospital can admit the beneficiary on the following condition: - The beneficiary or the family members give an
undertaking that if they fail to produce the card at the time of discharge, the treatment by the hospital shall be chargeable to the beneficiary
5. As per current process, a slip is given at the time of registration. This would continue to be provided and is mandatory for the hospital. A compliance check shall be done by the audit agencies through a random audit.
6. If the hospital demands out of pocket expenses for some reason from the beneficiary, the details of such out of pocket expenses shall be entered in the TMS and a receipt be provided to the beneficiary. The same shall be validated by the call center and the

RSBY Revised Process Guidelines
72 | P a g e
Processes and Responsibilities
Sr. No
Current activities Responsibility Proposed Activities Responsibility Remarks
audit teams during a random audit. Any hospital found guilty of wrongly charging out of pocket expenses shall be de-empaneled and fined as decided by the SNA/ district committee.
7. In the event that the hospital refuses treatment to the beneficiary, the same will be logged on the TMS with authentication from the beneficiary along with reasons. The investigative committee shall look into the matter of refusal of treatment and will approve of the refusal if the reasons entered by the hospital are found valid. If the hospital is proved wrong post investigation, it shall be de-empaneled and a fine shall be invoked. The IC will de-empanel such a hospital on the report of the investigative committee.
8. On discharge, the beneficiary should be provided with a detailed discharge summary including all expenses charged to him by the hospital along with all claimed expenses. This shall be generated through TMS and shall also be available to MoLE/ SNA/ IC for every beneficiary that has been provided treatment at the hospital. It is mandatory for the hospital to maintain and provide such details, else the claims shall be rejected by the IC.
4.2 1. Blocking the package and amount in the card
2. Hospitalization and selection of package
Hospital 1. No change in process 2. Indication of amount in
case the package rate shows NULL. This will be modified in the new software (web application with offline module) so that amount can be inserted in case it shows
Hospital If advised admission, a second transaction is conducted 1. By swiping the card 2. Verifying the beneficiary through fingerprint
authentication 3. Treatment code is selected from the package list and
amount automatically blocked by the software 4. Insurance company/ TPA receives the intimation
when the day’s transactions are uploaded through the provided utility.

RSBY Revised Process Guidelines
73 | P a g e
Processes and Responsibilities
Sr. No
Current activities Responsibility Proposed Activities Responsibility Remarks
NULL or it gets displayed once the IC provides the pre-authorization code to the hospital.
3. SMS would be sent to the beneficiary
5. As per current process, a slip is given at the time of
package blocking. This would continue to be provides
and is mandatory for the hospital. A compliance
check shall be done by the audit agencies through a
random audit.
If transaction system is not working or the card cannot be authenticated, the insurer’s district representative should be called immediately and informed of the same.
4.3 Pre-authorization request for treatment which is not a part of approved package list (email / fax approval by IC)
1. Hospital 2. IC
1. If the treatment required is not part of approved package list, request for pre-authorization will be sent to IC using the new web-enabled TMS software. IC will respond to the request within 6 hours. In the event of no response from IC for 6 hours, the request will be considered as approved. The same web application will be used by the IC/TPA for approval.
2. In case connectivity is not available at that time, pre-authorization can be requested through phone/fax also. This shall be followed by an email/ fax confirmation to the requesting hospital for
1. Hospital 2. IC
1. The same process would be valid for inter- district claims too.
2. SMS will be sent to the hospital user, as well as to the beneficiary as soon as the pre-authorization request is approved.

RSBY Revised Process Guidelines
74 | P a g e
Processes and Responsibilities
Sr. No
Current activities Responsibility Proposed Activities Responsibility Remarks
recording on the TMS.
4.4 Entry of treatment details in the transaction management software
Hospital 1. No change in process 2. The entry would take
place in the new web enabled hospital software with an offline module (for business continuity plan)
Hospital Hospital will enter the details of treatment given to patient on the new transaction management software. The key new fields are:
- Signs and symptoms - Diagnosis - Diagnostics - Medications given to beneficiary (Gender of new
born in case of delivery The hospital shall be liable to enter accurate details of treatment suggested and provided to the beneficiary in the web based TMS. This will be helpful during processing of claims and any disputes arising out of it.
4.5 Transportation allowance to beneficiary at the time of discharge
Hospital 1. No change in process 2. Third party audit of 1%
sample of beneficiaries treated at hospital
3. Automated IVR call to beneficiary to validate receipt of Rs. 200 post treatment
4. In case of non-payment of Rs. 200, an SMS/email would be sent to the hospital user, based on the non-authentication by beneficiary at the hospital, confirming receipt of transport allowance.
Hospital At the time of dis-charge, hospital will pay transportation allowance to beneficiary. Also post-hospitalization medication is provided to the beneficiary for upto 5 days (as needed). The transport charges shall be part of the coverage amount of Rs. 30,000 and the beneficiary can avail a maximum of Rs. 2000 of transport allowance during a year of policy. The transport allowance shall be provided to the beneficiary in cash. The same shall be verified / audited by the 3rd party audit agency empaneled by MoLE. The beneficiary shall also validate with his finger prints at the hospital to confirm receipt of transport allowance of Rs. 200. Alternatively, he will also be given a call from the call center to confirm the same.

RSBY Revised Process Guidelines
75 | P a g e
Processes and Responsibilities
Sr. No
Current activities Responsibility Proposed Activities Responsibility Remarks
4.6 Discharge of beneficiary from hospital
Hospital 1. No change in process 2. The discharge slip would
continue to be given along with SMS to the patient
3. SMS and dis-charge slip, both should clearly mention the balance card value, apart from other details of diagnostics provided and the amount charged / claimed for the same.
Hospital The beneficiary is discharged from hospital and the claim transaction is conducted by swiping the card again and authenticating the fingerprint of the patient. The hospital will not be able to send the claim to the IC unless it does not have the fingerprint authentication from the beneficiary. It is mandatory for the hospital to provide a discharge summary to the beneficiary at the time of discharge. The same shall be validated with the fingerprint of the beneficiary, call center and audit teams. The hospital must also ensure that the beneficiary RSBY card is returned to the beneficiary at the time of discharge, Any hospital found retaining the beneficiary RSBY card shall be liable for de-empanelment and fine for non-compliance.
4.7 A claim is raised by the hospital post beneficiary discharge. Currently, the hospitals do not follow a stipulated time frame for raising claims.
Hospital 1. Swiping of beneficiary card and finger print authentication of beneficiary at the time of discharge should automatically trigger the claim activity within the web based software.
2. The hospital shall complete the activity, and upload the transaction activity on the same day using the new hospital software.
Hospital In case the discharge entry is not electronically created, only the admission (blocking) entry shall not automatically raise a claim and the hospital would have to confirm treatment through any other means (Fax, email) before admitting the claim. It is also mandatory to provide the fingerprint authentication of the beneficiary to raise a claim. The hospital shall have a maximum of 7 days to raise a claim post discharge of the beneficiary.

RSBY Revised Process Guidelines
76 | P a g e
Processes and Responsibilities
Sr. No
Current activities Responsibility Proposed Activities Responsibility Remarks
4.8 Maintenance of records of treatment for each beneficiary
Hospital 1. No change in process 2. The requirement to
maintain paper or electronic records needs to be reinforced. This shall be required at the time of random audits that will be initiated by the SNA / district authorities.
Hospital All diagnostic and in-patient records to be maintained by the hospital. These do not have to be submitted to the Insurance Company, but the Insurance Company or a TPA can always review and/ or ask for the copy of same at its own cost. Mole/ SNA/ District authorities will also ask for these documents through the audit agencies. Random audits shall be conducted without notice.
Policy decision taken Meeting reference
Sr. No Decisions
1 Hospitals attaining NABH entry level accreditation will automatically be empaneled as RSBY network hospitals based on their willingness
Empowered Committee Meeting of 23rd January 2014
2 IC will have to empanel at least 2 hospitals in each block of the district and one hospital per 8000 enrolled beneficiary families
Empowered Committee Meeting of 23rd January 2014
3 The empanelment of hospitals will take place with the consent of SNA only. If the SNA does not respond within 5 days of the intimation from IC, approval would have been deemed to be issued.
Empowered Committee Meeting of 23rd January 2014
Policy decision to be taken

RSBY Revised Process Guidelines
77 | P a g e
Sr. No Decisions
1 Transportation charges to be increased from Rs. 100 to Rs. 200 with a limit of 10 visits in a year. The decision to take this for approval of the Cabinet will be taken in the EC meeting on 15th May 2014.
2 Initiation of new web-based hospital management software (with offline module), which would connect with the central server
3 Capturing of mobile number of every beneficiary even at the time of registration at hospital, so that an SMS can be sent to beneficiary for every transaction (registration, pre-authorization, procedure and amount blocking, discharge)
4 Updation and revision of package rates for procedures to address the cost inflation and rationality of procedures. This should also include addition of procedures beyond INR 30,000. The decision to adopt package rates (i.e. CGHS or any other) will be taken in the EC meeting on 15th May 2014.
Incentive Mechanism
1 Not applicable
Training Needs Training to be provided to Training to be provided by
1 Training on handling hospital transaction management software and general hardware troubleshooting
Hospital Staff IC under supervision of SNA / DKM / ADKM
2
Training of hospital staff on procedures such as return of beneficiary card, biometric authentication at the time of registration, discharge, discharge slip provision to the beneficiary and return of RSBY card post discharge
Hospital staff IC under the supervision of SNA/ DKM / ADKM

RSBY Revised Process Guidelines
78 | P a g e

RSBY Revised Process Guidelines
79 | P a g e
Human Resource Requirement Where
1 Monitoring and evaluation personnel to closely monitor the progress of wellness checks being conducted, and premium payment process, including management of related audit processes
At SNA, i.e. one for every state
Input for RFP/FRS RFP/FRS
1 Guideline for empanelment of hospitals RFP for empanelment of IC
2 Package lists for hospitals (this needs to be consulted and prepared by a doctor) RFP for empanelment of IC
3 Pensioners can be engaged at hospitals to support the hospital operations and assist the beneficiaries in the wellness checks conducted at PHFs / hospitals
RFP for empanelment of IC
IEC Activities
1 Display the benefits of RSBY scheme at every hospital through a display board along with basic information on procedures available at hospital.
2 Helpdesk at every hospital to facilitate the beneficiaries.

RSBY Revised Process Guidelines
80 | P a g e
P
roce
ss
Co
de
VI – CLM Process Name Claims Settlement (including inter-district claims)
Process Objective Current Status 1. To ensure settlement of claims within mutually agreed timelines with least
number of disputes 2. To ensure that resident is not denied service or has to face inconvenience due
to delays in claim settlement 3. To ensure a system to reduce number of fraud claims
1. Hospitals send claim requests to IC/TPA electronically through
Transaction Management Software at the hospitals
Key Stakeholders Measures and Key Performance Indices (KPIs) 1. IC/TPA
2. Hospitals
3. SNA
4. MoLE
5. Grievance Committees (DGRC, SGRC and NGRC)
Measures12: MoLE, SNA, DKM, IC/TPA, Hospital (relevant reports to be available, depending on role) 1. Number and amount of claims raised by hospitals, and
number/amount/% settled by IC Filters: Hospital type (Private, Public), Time Duration (from-to)
2. Number and amount of claims settled by, and rejected by IC Filters: Hospital type (Private, Public), Time Duration (from-to)
3. List of outstanding claim as on date Filters: Hospital type (Private, Public), Date of claim request
KPI13: MoLE, SNA, DKM, IC/TPA, Hospital (relevant KPI’s to be measured, depending on role) 1. % of claims settled, % of claims rejected –these are w.r.t. total
12 All measures to be available as a report on a web portal in real-time/near-real-time. The data should be available in a warehouse, such that any extraction is possible to create ad-hoc reports
13
All KPI’s to be available as a report on a web portal in real-time/near-real-time. The data should be available in a warehouse, such that any extraction is possible to create ad-hoc reports.

RSBY Revised Process Guidelines
81 | P a g e
claim requests made 2. Average time taken to settle a claim from the time of claim
request 3. Average time taken to pre-authorize a transaction for undefined
packages 4. Average time taken to give finger-print override code for
business continuity 5. % of cases where fingerprint override was needed 6. % of cases audited by IC 7. Average time taken to submit the claims from the time of
discharge of beneficiary
Current Challenges Summary of key suggestions 1. Claim settlement is delayed by the IC, resulting in demotivation of the hospital
to serve beneficiaries 2. Fraudulent claims settled, resulting in loss to MoLE, dissatisfaction to
beneficiary and a bad reputation of the RSBY scheme 3. Claims are being rejected on flimsy grounds such as:
- Delay in claim request by hospital - Paper requirements from hospital by IC - URN number not found in IC database - Chip serial number not matching
Indicative claim rejection reasons are provided in Annexure 6.1 4. Claims are not reconciled - claims appearing in hospital books as outstanding
are appearing as settled in IC books 5. Lack of information visibility on claim settlement and claim status has resulted
in many un-reconciled claims, discouraging hospitals to join RSBY scheme 6. Lack of adherence to claim settlement SLA of 30 days by IC’s
1. Claim settlement, including claim request, payment and payment detail management, should be completely online
2. Medical audit to check fraudulent claims in a systematic manner with random sampling and in case of exception triggers from data
3. Well defined claim rejection guideline with rejection codes to be used in the application. Indicative list of rejection codes are given in Annexure 6.1
4. Upfront alerts related to ‘not covered condition’ at package blocking to minimize claim rejections due to exclusion/administrative reasons
5. In case rejected claims are invoked, it should be through reason codes selected from a drop down of pre-defined reason codes. Indicative list of rejection codes are given in Annexure 6.2
Pre-requisites for the process 1. RSBY services have been availed by beneficiary and the beneficiary has been discharged with his RSBY card
Inputs to the revised process Output from the revised process 1. RSBY beneficiaries avails cashless medical services at empaneled hospital
1. Hospitals receive timely payment from IC and system is updated
with the payment record

RSBY Revised Process Guidelines
82 | P a g e
Processes and Responsibilities
Sr. No
Current activities Responsibility Proposed Activities Responsibilities Remarks
1 Pre-authorization for undefined packages
1.1 Pre-authorization request for treatment which is not a part of approved package list (email / fax approval by IC)
1. Hospital 2. IC
1. If the treatment required is not part of approved package list, request for pre-authorization will be sent to IC using the new web-enabled TMS software/fax/email with auto-sync.
2. IC will respond to the request within 6 hours of pre-authorization request. In the event of no response from IC for 6 hours, the request will be deemed approved.
3. The same web application will be used by the IC/TPA for approval with auto-sync feature.
3. Hospital 4. IC
1. The same process would be valid for inter- district claims too.
2. SMS will be sent to IC/TPA and to the beneficiary as soon as pre-authorization request is made.
3. SMS will be sent to the hospital user, as well as to the beneficiary as soon as the pre-authorization request is approved.
4. The new web TMS software would also have a field to capture the pre-authorization approval amount.
2 Claim Request and Settlement
2.1 Hospital raises claims using TMS
Hospital 1. The new web TMS application would be accessible by the hospital, IC, SNA/State and central user.
2. Hospital raises claims using new web TMS (with auto-sync) automatically on patient discharge (single process of discharge and claim request), which would be connected to the central server.
Hospital 1. In case they are unable to raise the claims due to HW/SW related issues, it should be intimated to IC/SNA through phone/email.
2. The electronic claim request should be triggered as soon as connectivity is available.
3. The claim request files, which the IC’s can download, should have standard format which should be well communicated with insurance

RSBY Revised Process Guidelines
83 | P a g e
Processes and Responsibilities
Sr. No
Current activities Responsibility Proposed Activities Responsibilities Remarks
3. Hospital should raise claims, preferably on the day of discharge itself, and latest within 7 days of discharge, in case the two processes are done separately.
companies.
2.2 Verification/validation of claims
IC/TPA 1. No change of process 2. Data should go from the new
web TMS.
IC/TPA The hospital will upload all files/ documentation while raising claims.
2.3 Field verification/audit of case, if required
IC 1. No Change. The medical audit would continue to be done by IC.
2. The IC would ensure that all the cases which are medically audited by them are flagged, and the electronic details are available with the claim record.
IC 1. Field verification, if required should be done by a qualified person (at least an MBBS degree)
2. The audit data fields should be a part of RFP floated by RSBY for IC selection.
2.4 Approval of claim IC 1. The IC would download the claim request data from the new web-enabled TMS.
2. Claim should be approved on respective claim software of IC.
IC
2.6 Payment to hospital IC 1. Payment should be made electronically, directly into the accounts of hospital(s)
2. After every payment a report giving details of payment should be generated and made available on web application. The report shall be emailed to
IC 1. SMS/email alert is sent to hospital for accepting/rejecting the part payment
2. The bank details of all hospitals should be available with all IC’s on the new web-enabled TMS. It should be captured at the time of registering the hospital.

RSBY Revised Process Guidelines
84 | P a g e
Processes and Responsibilities
Sr. No
Current activities Responsibility Proposed Activities Responsibilities Remarks
hospital also 3. The TDS should be a separate
‘head’ in the claim payment file
2.7 Update of claim payment in claim management application
IC 1. Every claim payment should be updated in new web-based TMS by the IC. Hospital will access the details in new web based TMS, and electronically acknowledge that the payment is made.
2. Hospitals will have to acknowledge that the claim payment has been made within 5 working days after receipt of payment in their account. The record would also indicate the details of claim approval data/time.
IC Hospital
1. An SMS would go to the hospital user on his/her mobile number indicating that “Payment of XXX.00 has been made with reference number YYYY has been made to the bank account xxxx1845. Please acknowledge receipt on the web application”.
2. A reminder SMS would go to the hospital user after 3 working days for payment acknowledgement.
2.8 No provision for claims on hold for want of further information
1. IC can put a claim under hold, after asking for more information if required, instead of rejecting it altogether, this is particularly required for public hospitals.
As of now insurance company are directly rejecting a claim on technical ground, and government hospitals are not following up even if the rejection is on technical ground. Keeping a claim on hold will provide a status to hospital and health department for close monitoring and follow up with IC.
The SNA and district committees will monitor such claims that have been put on hold by the IC.

RSBY Revised Process Guidelines
85 | P a g e
Processes and Responsibilities
Sr. No
Current activities Responsibility Proposed Activities Responsibilities Remarks
2.9 Appeal against claim rejected/partly paid
Hospital 1. There should be no case of part payment
2. The hospital would complain using one of the existing grievance redressal channels
Hospital 1. All grievances will be tracked in CGRMS
2. Please refer to process document on grievance redressal
2.10 No penalty for delayed settlement of claims
A Penalty of 1% of claimed amount per 15 days of delay in settlement to be paid by IC to hospital.
IC
Policy Decision taken Meeting reference
Sr. No Decisions
1 In case claim ratio (Claim Settled + Card issuance cost)/Total premium receipt is less than 70%, IC will refund the balance amount to SNA, SNA in turn will refund the central share to MoLE
EC meeting dated 23rd January 2014
2 In case of delayed claim settlement a Penalty of 1% of claimed amount per 15 days of delay in settlement to be paid by IC to hospital
EC meeting dated 23rd January 2014
2 A clear guideline for processing of claims specifying admissible and non-admissible charges and minimizing scope of discretion shall be developed
Meeting of state sub committees with Secretary (L&E) on 9th April 2014
3 Set of agencies will be empaneled by MoLE, and SNA will hire one of them to conduct medical audit
Meeting of state sub committees with Secretary (L&E) on 9th April 2014
4 Part payment of claims should not be allowed, as it increases the chances of misuse by hospital/IC
Agreed in meeting with states under Secretary (L&E) on 06.05.2014, MoM yet to be processed in file
5 Performance levels of IC w.r.t. pending claims and rejected claims, if they fall below a certain threshold, should automatically go to the SNA as well as to the MD or senior business official of
Agreed in meeting with states under Secretary (L&E) on 06.05.2014, MoM yet to

RSBY Revised Process Guidelines
86 | P a g e
Policy Decision taken Meeting reference
Sr. No Decisions
the IC (preferably the representative of IC in NGRC and/or SGRC) be processed in file
6 Rejection codes to be applied in the new TMS so that all rejected claims can be analyzed systematically for root cause. No claim should be rejected without a rejection code and a remark in the system. List of codes are listed in Annexure ??
Agreed in meeting with states under Secretary (L&E) on 06.05.2014, MoM yet to be processed in file
Policy Decision to be taken
Sr. No Decisions
1 Development of the new web-based TMS (along with other components in the web based RSBY IT architecture) for the revised RSBY regime should be initiated by July 15. The identification of agency for development, deployment and maintenance should happen by June 30.
Incentive Mechanism
1 Not applicable
Training Needs Training to be provided to Training to be provided by
1 Facilities available under RSBY scheme and training of the proposed application (new web enabled TMS)
Hospitals (Help Desk Staff) IC
2 Training to IC on new TMS file format for claim data files so that they can integrate with their systems accordingly. This should include file structure details with additional fields on ‘medical audit’,
IC’s IT team RSBY central team for new web TMS development / IT application agency

RSBY Revised Process Guidelines
87 | P a g e
Training Needs Training to be provided to Training to be provided by
‘rejection codes’ and ‘TDS heads’
3 Claim rejection code training Hospital users RSBY central team for new web TMS
development / IT application agency
Human Resource Requirement Where
1 Not applicable Not applicable
Input for RFP/FRS RFP/FRS for:
1 Guideline for processing of claims specifying admissible and non-admissible charges and minimizing scope of discretion shall be developed
RFP for empanelment of IC
2 Provision of medical audit with random sampling using the new web based TMS system
1. RFP for empanelment of IC
2. FRS for selection of IT agency developing the new web-based TMS
3
(i) Audit fields for electronic claim record
(ii) Claim rejection codes
(iii) The requirement to have a separate TDS head in the claim settlement/payment data file
(iv) Calculation of penalty in case of delayed settlement of claim
1. RFP for empanelment of IC
2. FRS for selection of IT agency developing the new web-based TMS

RSBY Revised Process Guidelines
88 | P a g e
IEC Activities
1 Facilities available under RSBY activities and formalities to be completed to avail these services should be displayed in every empaneled hospital
2 Toll free number for making complaints should be available in every hospital in English and local language. The IEC material templates (for posters, etc.) should be designed centrally at MoLE, and should be provided to SNA for customization and further sharing with IC and hospitals
3 Poster at hospital to include that the RSBY beneficiary should insist on getting a statement in writing citing reasons as to why he/she is denied service at a hospital

RSBY Revised Process Guidelines
89 | P a g e
Pro
ce
ss
Co
de
VII–CGRMS
Process Name Complaint and Grievance Redressal Management System
Process Objective Current Status 1. To ensure a strong mechanism for redressal of complaints /
grievances for indirectly making the RSBY service delivery to beneficiaries more efficient
2. To provide adequate channels through which complaints / grievances can be registered, acknowledged, monitored and resolved at various levels
1. An online Central Grievance Redressal and Management System (CGRMS) is available for capturing grievances online as well as through fax/ email / phone
2. The complaint can be tracked through the online CGRMS portal using the Unique Complaint Number (UCN)
3. CGRMS does not have a provision for complaint / grievance registration through the call center and acknowledgement by SMS throughout the lifecycle till closure.
4. Grievance redressal committees have been set up at three levels: - District Grievance Redressal Committee (DGRC) - State Grievance Redressal Committee (SGRC) - National Grievance Redressal Committee (NGRC)
5. Very low usage of the CGRMS is observed (e.g. 39 grievances captured in Karnataka in 1 year)
Key Stakeholders Measures and Key Performance Indices (KPIs) 1. Beneficiary 2. Ministry of Labor and Employment (MoLE) 3. State Nodal Agency (SNA) 4. District Key Manager (DKM) 5. Field Key Officer (FKO) 6. Call Center managing GMS, inbound/outbound-calls, email, web,
SMS, post channels 7. District Grievance Redressal Committee (DGRC) 8. State Grievance Redressal Committee (SGRC) 9. National Grievance Redressal Committee (NGRC) 10. Insurance Company (IC) / Third Party Administrator (TPA) 11. Public Health Facility (PHF) 12. Hospital
Measures14: MoLE, SNA, DKM, FKO, PHF, Hospital, IC/TPA (relevant reports to be available, depending on role)
1. Number of complaints received Filters: User Category (Beneficiary, SNA, DKM, FKO, PHF, Hospital, IC/ TPA), Geography, Mode (Phone/ Call center, Email, Fax, Kiosk, post), Type, Estimated Resolution date
2. Number of complaints resolved
Filters: User Category, Mode, Geography, Time taken for Resolution, Mode of Acknowledgement (phone/call center, email, fax, Kiosk, post), Acknowledgement of Closure by Complainant (mode of closure – phone/call center, email, fax, SMS, Kiosk, post)
14
All measures to be available as a report on a web portal in real-time/near-real-time. The data should be available in a warehouse, such that any extraction is possible to create ad-hoc reports

RSBY Revised Process Guidelines
90 | P a g e
13. Smart Card Service Provider (SCSP) 14. Civil society
3. Number of complaints converted to grievances
Filters: User Category, Time Duration, Geography, Type, Referred to (DGRC/SGRC/NGRC),
4. Number of grievances closed Filters: User Category, Time Duration, Geography, Closed By (DGRC/SGRC/NGRC), Variance from Estimated Time, Mode Adopted for taking acknowledgement (phone/call center, email, fax, Kiosk, post), Acknowledgement of Closure by Complainant (mode of closure – phone/call center, email, fax, SMS, Kiosk, post)
KPI15: MoLE, SNA, FKO, DGRC, SGRC, NGRC, PHF, Hospital, IC/TPA (relevant KPI’s to be measured depending on role)
1. Number of complaints received against each user category
2. Number of complaints where user has acknowledged closure 3. Number of complaints resolved at District/ State/ National level
within stipulated time 4. Number of complaints converted to grievances 5. Number of complaints where appeal has been made to Committees 6. Number of complaints/ grievances with non-compliance to decisions 7. Number of complaints / grievances with compliance to decisions
within the stipulated time
Summary of current challenges Summary of key suggestions 1. Lack of awareness of grievance redressal system amongst
beneficiaries and other stakeholders leading to low usage of 1. Integration of Complaint and Grievance Management System (CGMS) with
national call center and SMS gateway; pre-printing of toll-free call center
15
All KPI’s to be available as a report on a web portal in real-time/near-real-time. The data should be available in a warehouse, such that any extraction is possible to create ad-hoc reports.

RSBY Revised Process Guidelines
91 | P a g e
CGRMS 2. Maturity of the grievance system (e.g. appropriateness of
channel, time mapping of open grievances, SLA’s for grievance redressal etc.) is low
3. Lack of adequate training to grievance committee members on addressing and streamlining the closure of grievances
4. Lack of adequate channels for registering complaints / grievances into the CGRMS – no integration with the call center which should be the most common channel
5. No acknowledgement/feedback to/from beneficiaries - no integration with SMS gateway
6. Non-compliance by IC, hospitals etc. to decisions made by grievance committees
7. No mechanism for district and state level grievance committee proceedings to be made available to NGRC
number on the beneficiary RSBY card /cover for registering grievances 2. Call centre support would be in all local language (Asamiya, Bangla, Gujarati,
Kannada, Kashmiri, Konkani, Malayalam, Marathi, Nepali, Oriya, Panjabi, Sanskrit, Tamil, Telugu, Urdu)
3. State initiatives related to call center to continue till such time national call center is in place. However the general guidelines are valid for any interim state call center also.
4. The confirmation to close the compliant will be done by the complainant. The call center would contact the beneficiary / aggrieved party to confirm closure (through any channel)
5. Open complaints will turn into grievances after a stipulated time period depending on the type of complaint
6. Automated grievance registration, notification (SMS/email) to concerned authority/organization once grievance has been entered for redressal by his office
7. Induce SLA’s to monitor grievances and redressal mechanism 8. Grievance redressal trainings for members of grievance committee at state
and district 9. Grievance Redressal training to kiosk operators at district / block for
registering grievances of beneficiaries on CGRMS 10. Conduct training of hospital staff and insurance company to register
grievances on CGRMS, and update status of resolved grievances which were registered against them
11. Incorporate MIS reporting for monitoring SLA for complaint / grievance resolution
12. Penalty for non- compliance by IC, hospitals etc. to decisions made by grievance committees
Pre-requisites for the grievance management process 1. Integration of CGRMS with SMS gateway and call center 2. MIS reports built into the CGMS for reporting 3. Training of DGRC/ SGRC/NGRC officials on grievance redressal 4. Training of hospital staff, IC and kiosk operator on CGRMS for grievance entry and complaint/ grievance resolution process
Inputs to the revised process Output from the revised process 1. Complaint / grievance Registration
1. Resolution of complaint grievance within the stipulated time 2. Feedback on closure from beneficiary

RSBY Revised Process Guidelines
92 | P a g e
Processes and Responsibilities:
Sr. No
Current Process Responsibility Proposed Process Responsibility Remarks
1 Constitution of Grievance Committees at District / State / Centre
1.1 A National Grievance Redressal Committee (NGRC) is constituted at the national Level.
MoLE 1. No change to NGRC structure
1. MoLE
2. IC
1. Annexure 7.1 provides details on the composition of NGRC
1.2 A State Grievance Redressal Committee (SGRC) is constituted at the state level within 15 days of signing of MoU with the central government.
SNA 1. No change to SGRC structure
2. MD / CEO of IC or his representative who is a decision making authority on behalf of IC should be included in SGRC.
3. MD/ CEO of IC or his representative who is included in SGRC should be included on a rotational basis.
1. SNA
2. IC
1. Annexure 7.1 provides details on the composition of SGRC.
2. The State Grievance Redressal Nodal Officer (SGRO) should be trained on CGRMS for electronic monitoring and closure of grievances.
3. The field audit reports with comments of SGRC should reach the NGRC within 3 days of conducting the audit. This shall be uploaded on the CGRMS for access by NGRC.
1.3 A District Grievance Redressal Committee is constituted at District level within 15 days of signing of MoU with IC.
SNA 1. No change to DGRC structure
2. A decision making authority from IC is to be made part of DGRC. IC should also ensure that the TPA does not represent the IC in the DGRC meetings.
SNA 1. Annexure 7.1 provides details on the composition of DGRC
2. District Grievance Redressal Nodal Officer (DGRO) should be trained on CGRMS for electronic monitoring and

RSBY Revised Process Guidelines
93 | P a g e
Sr. No
Current Process Responsibility Proposed Process Responsibility Remarks
closure of grievances.
2 Set up of investigative teams
2.1 Investigative teams set up at national level are to be nominated by MoLE along with NGRC.
The investigative teams will submit their report within 15 days of the grievance / complaint being handed over to them for investigation.
MoLE No change in process MoLE 1. Annexure 7.2 provides details on the composition of investigation teams at national level.
2. Depending on the nature of grievance, NGRC can nominate any other person of technical, legal, actuarial and any other experience on a case by case basis. This person shall have atleast 10 years of relevant experience.
2.2 No investigative teams set up at state level.
Set up investigative teams at State level as indicated in Annexure 7.2.
SNA Investigative teams to be set up / nominated by SGRC.
3 Allotment of National Toll-free number
3.1 State call centers exist in some states.
IC MoLE to apply for National Toll-free number to Department of Telecom (DoT).
MoLE has applied to DoT for allotment of four digit National Toll-free number.

RSBY Revised Process Guidelines
94 | P a g e
Sr. No
Current Process Responsibility Proposed Process Responsibility Remarks
4 Set up Call Centre for Grievance Redressal
4.1 Set up state level call centers for complaint / grievance registration on the CGRMS.
IC 1. The states should continue using their respective call centers in parallel to initiatives to set up the national call center. Eventually, depending on state convenience and readiness of national call center, they may phase out the state call centers.
2. The national call center for FY 14-15 should be made functional 15 days prior to commencement of enrolment process.
1. SNA (for state call center)
2. MoLE (for national call center)
1. Calls from national call center will be diverted to corresponding operator based on the selection of language done by the beneficiary.
2. The minimum number of call center seats (in every shift) for every state should be 5. This may be increased as the scheme progresses and there is better visibility on call volumes.
4.2 Set up national level call center and integrate with CGRMS.
MoLE 1. Selection of 3rd party for setting up call center at MoLE.
2. Define processes for call triaging in the call center as the call center will be run by a 3rd Party agency.
3. The services should be available 24/7 in three shifts (8 am – 4 pm, 4 pm to 12 midnight, and 12 midnight to 8m). The all night shift may have lesser number of operators depending on demand.
MoLE 1. Create list of support representatives, with contact information, for all the stakeholders so that calls can be easily triaged.
2. The minimum number of call center employees at national level should be minimum 5 for every state. This may be increased as the scheme progresses and there is better visibility on call volumes.

RSBY Revised Process Guidelines
95 | P a g e
Sr. No
Current Process Responsibility Proposed Process Responsibility Remarks
4. The services offered from call center operators operating CGMS would include CGRMS data updates, auto SMS triggers, inbound calls, outbound calls, email management. All call center operators would have login into CGRMS.
5. There would be two levels of agents at the call center – operators and supervisors. The call would be diverted to a supervisor in case the request is made by the caller.
6. All calls will be recorded, and audio files will be available for audit and quality check.
- The national call center would provide the following other services besides complaint and grievance redressal:
- Information/Advice/FAQ - Directory Services
4.3 The state call centers are not integrated with CGRMS.
IC NIC can outsource the call center function to a selected third party and this call center will have to be integrated with the CGRMS. While the national call center would be integrated with CGRMS, the API’s would be made available for integration with state call centers (for interim operations at state).
1. NIC
2. Call Center Agency
CGRMS needs to be integrated with state and national call centers for complaint / grievance redressal.

RSBY Revised Process Guidelines
96 | P a g e
Sr. No
Current Process Responsibility Proposed Process Responsibility Remarks
4.4 Conduct training of employees at national and state call center on the RSBY domain, applications and resolution processes.
3. MoLE
4. Call Center Agency
5. SNA
Employees of the national call center shall be trained on the process of handling, triaging calls and addressing complaints / grievances over the phone.
5 Conduct awareness to beneficiaries and training activities on call center and CGMS to DGRC / SGRC / NGRC / Hospital Officials / IC/ SCSP
5.1 Awareness activities on call center, email, post and CGRMS to the beneficiaries
1. Educate the beneficiary on call center, email, post and other complaint channels through print media/ audio media / electronic media / television / FKO / SNA / IC and other government communication channels such as broadcast media.
2. Printing of National Toll Free number on the RSBY card and card cover, and RSBY brochure.
3. Village walls to be painted with toll-free number
4. National call center number to be
1. MoLE/SNA / FKO / IC
2. SCSP
3. SNA / DKM
1. The beneficiary needs to be made aware of the call center facilities and the kind of complaints he/she can register or get resolutions for.
2. A probable/ indicative list of complaints / grievances exhibited in Annexure 7.3. This list can be elaborated based on the nature of complaints that are received over the period of RSBY operations.

RSBY Revised Process Guidelines
97 | P a g e
Sr. No
Current Process Responsibility Proposed Process Responsibility Remarks
printed on every IEC material
6 Complaint registration mechanism for beneficiary, and resolution at Hospital/IC/FKO level
6.1 Beneficiary registers his grievance using one of the limited existing channels
- Post - Email - Web - kiosk
Beneficiary 1. Register complaint through one of the following: national toll-free call center, email, post, SMS, web (CGRMS) and kiosk
2. Once the complaint is received, a detailed log is entered into the CGRMS system by the operator of the call center agency
3. An SMS/email would be sent to the beneficiary with the service request number and time for resolution of the complaint. The SMS would go in two languages (English and local).
4. If the complaint is against a specific hospital/IC/FKO, the record will be made available to the relevant stakeholder.
5. The beneficiary can reach out to the call center or any other channels again, to check the status of service request by indicating the request number.
Beneficiary The beneficiary can check the status of the complaint through the web, email and kiosk by providing the service request number.

RSBY Revised Process Guidelines
98 | P a g e
Sr. No
Current Process Responsibility Proposed Process Responsibility Remarks
6.2 No well-defined process for complaint resolution
IC / hospital / FKO
1. The Hospital/IC/FKO acts upon the registered complaint for resolution at their end.
2. Once the complaint is resolved at their end, they will update the CGRMS through one of the channels, against the service request number. The tentative closure of the complaint would be available in CGRMS.
3. The call center operator would call the beneficiary to verify whether the complaint has been resolved. If the call is not taken, the call center operator would try two more times within 24 hours.
4. Once verified, the call center operator would ‘close’ the complaint. An SMS would go to the beneficiary and corresponding IC/Hospital/FKO about the closure. The complaint would be deemed closed if the beneficiary is not able to take any of the 3 calls.
5. If the beneficiary still has a complaint, the status would be reversed to ‘open’, and the hospital/IC/FKO would receive
1. IC
2. Hospital
3. Beneficiary
4. FKO
5. Call center Agency
After the stipulated period of 15 days, the complaint, if still unresolved, would turn into a grievance.

RSBY Revised Process Guidelines
99 | P a g e
Sr. No
Current Process Responsibility Proposed Process Responsibility Remarks
an SMS/email notification
6.3 Grievances once entered into the system are taken up for resolution by DGRC/ SGRC/NGRC / DGLW as per priority and escalation levels.
DGRC / SGRC / NGRC / MoLE
The CGRMS shall provide for auto assignment of grievances to respective grievance committees through automated CGRMS if the complaint is not resolved within the stipulated timeline.
6. DGRC / SGRC / NGRC / MoLE
1. A daily summary SMS/email notification will be sent to the respective grievance redressal committees for grievances that have been referred to their office.
2. DGRC shall receive a grievance if the complaint is not resolved within 15 days.
6.4 District and state level grievance committees do not update the decisions of their meetings / decisions to NGRC.
DGRC/SGRC DGRC / SGRC shall update the proceedings / decisions of their meetings on CGRMS for further reference by NGRC.
DGRC / SGRC This will serve as crucial information for MIS generation and history of a grievance in the event of escalation of a grievance at the central level (NGRC).
7 Complaint registration mechanism for hospitals, and resolution at IC level
7.1 Hospital submits its complaint in writing to DGRC.
Hospital/ PHF 1. Register complaint through one of the following: national toll-free call center, email, post, SMS, web (CGMS), kiosk.
2. Once the complaint is received, the call center operator updates the complaint log in CGRMS system.
3. An SMS/email would be sent to
1. Hospital / PHF
2. Call Center Agency
1. This would be possible after CGMS has been modified with a ticket based system. The hospital should be provided with a username and password to the CGRMS for entering its complaint or monitoring the status.
2. Awareness about CGRMS and

RSBY Revised Process Guidelines
100 | P a g e
Sr. No
Current Process Responsibility Proposed Process Responsibility Remarks
hospital user with the service request number. The SMS would go in two languages (English and local).
4. If the complaint is against a specific IC, the record will be made available to the IC, DGRO as well as to DKM and SNA.
5. The hospital can check the status of the service request through the call center or any other channels (web, kiosk).
the call center would need to be carried out round the year to encourage its usage.
7.2 No well-defined process for complaint resolution
1. The IC acts upon the registered complaint registered for resolution at their end.
2. Once they have resolved the complaint at their end, they shall update the CGRMS through one of the channels, against the service request number. The tentative closure of the complaint would be available in CGRMS.
3. The call center operator would call the hospital to verify whether the complaint has been resolved. If the call is not taken, the call center operator would try and additional two more times within 24 hours.
1. IC / SCSP
2. Hospital / PHF
3. Call Center Agency
The hospital / PHF can check the status of the complaint through the web, email and kiosk by providing the service request number.

RSBY Revised Process Guidelines
101 | P a g e
Sr. No
Current Process Responsibility Proposed Process Responsibility Remarks
4. Once verified, the call center operator would ‘close’ the complaint. An SMS would go to the hospital and IC about the closure. The complaint would be deemed closed if the hospital user is not able to take any of the 3 calls.
5. If the hospital still has the complaint, the status would be reversed to ‘open’, and the IC would receive an SMS/email notification.
8 Complaint registration mechanism for IC, and resolution at hospital level
8.1 IC submits its complaint in writing to DGRC.
IC / SCSP 1. Register complaint through one of the following: national toll-free call center, email, post, SMS, web (CGMS), kiosk.
2. Once the complaint is received, the call center operator updates the complaint log in CGRMS system.
3. An SMS/email would go the IC/SCSP user with the service request number. The SMS would go in two languages (English and local).
4. If the complaint is against a specific hospital and/or beneficiary, the
1. IC/ SCSP
2. Call Center Agency
1. This would be possible after CGRMS has been modified with a ticket based system and integrated with the proposed web based application.
2. The IC / SCSP should be provided with a username and password to the CGMS for entering its grievance.
3. SNA would create authorized IC users in CGRMS.
4. IC would create authorized SCSP users in CGRMS.

RSBY Revised Process Guidelines
102 | P a g e
Sr. No
Current Process Responsibility Proposed Process Responsibility Remarks
record will be made available to the hospital and/or beneficiary, DGRO as well as to DKM and SNA.
5. If the complaint is against SNA, the record will be made available to the SNA and to NGRO.
6. The IC / SCSP can check the status of the service request through the call center or any other channels (web, kiosk).
8.2 No well-defined process for complaint resolution
1. The hospital acts upon the complaint to resolve it at their end.
2. Once they have resolved the complaint at their end, they will update the CGRMS through one of the channels, against the service request number. The tentative closure of the complaint would be available in CGRMS.
3. The call center operator would call the IC to verify whether the complaint has been resolved. If the call is not taken, the call center operator would try two more times within 24 hours.
4. Once verified, the call center operator would ‘close’ the complaint. An SMS would be sent to
1. Hospital / PHF
2. IC/ SCSP
3. Call Center Agency
If the IC still has a complaint, the status would be reversed to ‘open’, and the hospital would receive an SMS/email notification.

RSBY Revised Process Guidelines
103 | P a g e
Sr. No
Current Process Responsibility Proposed Process Responsibility Remarks
the hospital and IC about the closure. The complaint would be deemed closed if the IC user is not able to take any of the 3 calls.
9 Grievance registration mechanism for SNA
9.1 SNA submits in writing to SGRC / NGRC.
SNA 1. SNA registers the complaint through web (CGRMS), post, call center.
2. Once the complaint is received, a complaint log is entered into the CGRMS system by the operator of the agency operating the call center.
3. If the complaint comes by post to NGRC, NGRO would digitize the complaint and upload the details on CGRMS.
4. An SMS/email would be sent to the SNA user with the service request number. The SMS would go in two languages (English and local)
5. If the complaint is against a specific hospital and/or IC, the record will be made available to the hospital and/or IC, with a notification to
SNA 1. This would be possible after CGRMS has been modified with a ticket based system and integrated with the proposed web based application.
2. The SNA should be provided with a username and password to the CGRMS for entering its grievance.

RSBY Revised Process Guidelines
104 | P a g e
Sr. No
Current Process Responsibility Proposed Process Responsibility Remarks
NGRO.
10 Grievance Redressal Mechanism – Beneficiary (once complaint turns into grievance)
10.1 1. The beneficiary approaches DGRC with a grievance against FKO, IC, hospital or their representatives.
2. DGRC should take a decision within 30 days of receiving the complaint.
1. Beneficiary
2. DGRC
1. In CGRMS, the complaint is visible as grievance after 15 days (stipulated timeline). This complaint will automatically be assigned to the DGRC office along with an SMS and email to the beneficiary and DGRO.
2. The grievance is shown in DGRO inbox for resolution. DGRC shall investigate and provide a resolution of the grievance / compliant on the CGMS after the DGRC meeting.
3. The beneficiary will get a registered mobile call verifying the resolution, once DGRC has updated the same on CGRMS. If the beneficiary does not provide a response after three tries the resolution is deemed accepted.
4. If the beneficiary does not verify on the registered mobile (indicating the resolution has not happened as per his satisfaction), he/she would be given an option on call to
1. Beneficiary
2. DGRO
3. SGRO
4. Call Center Agency
1. The escalation from DGRC to SGRC would happen automatically if the issue is not resolved within 30 days. However, if the issue is resolved at DGRC, and the beneficiary is not satisfied, the escalation can take place before 30 days after consent from beneficiary.
2. If DGRC decision is not complied by IC/Hospital or any other stakeholder, it is in the interest of DGRO to ensure compliance before closure of the request in CGRMS. Else, it would result in escalation to SGRC after consent from beneficiary.
3. The IC/hospital against which the original complaint was made by the beneficiary would indicate compliance in the system after DGRC decision. The DGRO would ensure

RSBY Revised Process Guidelines
105 | P a g e
Sr. No
Current Process Responsibility Proposed Process Responsibility Remarks
escalate to SGRC. In case the answer is yes, the same electronic grievance request would go to SGRC inbox and a same process of redressal would follow.
compliance through the system. The DGRO may go ahead and update the issue as closed, but the responsibility of ensuring compliance would be that of DGRO.
4. There would be an option to verify the closure of grievance using email also. The email would be sent by contact center operator.
11 Grievance Redressal Mechanism – Hospital (once complaint turns into grievance)
11.1 1. If the hospital has any grievance with respect to beneficiary, IC, or their representatives, state government officials etc. It will approach the respective redressal committee, and can go another level up in case the grievance is not redressed.
2. DGRC / SGRC / NGRC should take a decision within 30 days of receiving the complaint. Only one appeal is allowed.
1. Hospital
2. DGRC/ SGRC /
1. In CGRMS, the complaint is visible as a grievance after 15 days (stipulated timeline). This complaint will automatically be assigned to the DGRC office along with an SMS and email to the hospital user and DGRO.
2. The grievance is shown in DGRO inbox for resolution. DGRC shall investigate and provide a resolution of the grievance / compliant on the CGMS after the DGRC meeting.
3. The hospital will get a registered mobile call verifying the resolution, once DGRO has updated the same
1. Hospital
2. DGRO
3. SGRO
4. NGRO
5. Call Center Agency
1. The escalation from DGRC to SGRC (and subsequently to NGRC) would happen automatically if the issue is not resolved within 30 days. However, if the issue is resolved at DGRC end, and the hospital is not satisfied, the escalation can happen before 30 days after consent from hospital.
2. If DGRC decision is not complied by IC or any other stakeholder, it is in the interest of DGRO to ensure compliance before closure of the request in

RSBY Revised Process Guidelines
106 | P a g e
Sr. No
Current Process Responsibility Proposed Process Responsibility Remarks
NGRC
on CGMS. The resolution shall be deemed accepted if the hospital user does not respond to 3 calls.
4. If the hospital does not verify on registered mobile (indicating the resolution has not happened as per his satisfaction), he/she would be given an option on call to escalate to SGRC. In case the answer is yes, the same electronic grievance request would go to SGRC inbox and a same process of redressal would follow.
5. If the resolution does not happen even at SGRC level, the hospital would have the same choice to escalate to NGRC.
CGMS. Else, it would result in escalation to SGRC after consent from hospital.
3. The IC or any other stakeholder against whom the original complaint was made by the hospital would indicate compliance in the system after DGRC decision. The DGRO would ensure compliance through the system. The DGRO may go ahead and update the issue as closed, but the responsibility of ensuring compliance would be of DGRO.
4. The three points above are valid for further escalation from SGRC to NGRC as well.
5. There would be an option to verify the closure of grievance using email also. The email would be sent by call center operator.
12 Grievance Redressal Mechanism – Insurance Company (once complaint turns into grievance)
12.1 1. If the IC has any grievance with respect to beneficiary, hospital, state government
1. Hospital
2. DGRC/SG
1. In CGRMS, the complaint is visible as a grievance after 15 days (stipulated timeline). This complaint
1. IC 1. The escalation from DGRC to SGRC (and subsequently to NGRC) would happen

RSBY Revised Process Guidelines
107 | P a g e
Sr. No
Current Process Responsibility Proposed Process Responsibility Remarks
officials etc. It will approach the respective redressal committee, and can go a level up in case the grievance is not redressed.
2. DGRC / SGRC / NGRC should be able take a decision within 30 days of receiving the complaint. One appeal is allowed.
RC/NGRC
will automatically be assigned to the DGRC office along with an SMS and email to hospital user and DGRO.
2. The grievance is shown in DGRO inbox for resolution. DGRC shall investigate and provide a resolution of the grievance / compliant on the CGMS after the DGRC meeting.
3. The IC shall get a call verifying the resolution, once the DGRO has updated the same on CGMS. If the IC does not provide a response after three tries the resolution is deemed accepted.
4. If the IC does not verify on registered mobile (indicating the resolution has not happened as per his satisfaction), it would be given an option on call to escalate to SGRC. In case the answer is yes, the same electronic grievance request would go to SGRC inbox and the same process of redressal would follow. If the resolution does not happen even at SGRC level, the IC would have the same choice to escalate to NGRC.
2. DGRO
3. SGRO
4. NGRO
5. Call Center Agency
automatically if the issue is not resolved within 30 days. However, if the issue is resolved at DGRC end, and the IC is not satisfied, the escalation can happen before 30 days also after consent from IC.
2. If the DGRC decision is not complied by hospital or any other stakeholder, it is in the interest of DGRO to ensure compliance before closure of the request in CGRMS. Else, it would result in escalation to SGRC after consent from IC.
3. The hospital or any other stakeholder against which the original complaint was made by the IC would indicate compliance in the system after DGRC decision. The DGRO would ensure compliance through the system. The DGRO may go ahead and update the issue as closed, but the responsibility of ensuring compliance would be of DGRO.
4. The three points above are valid for further escalation

RSBY Revised Process Guidelines
108 | P a g e
Sr. No
Current Process Responsibility Proposed Process Responsibility Remarks
from SGRC to NGRC as well.
5. There would be an option to verify the closure of grievance using email which can be sent by the call center operator.
13 Complaint and Grievance Redressal Mechanism –for complaints/grievances to/against SNA / State Government

RSBY Revised Process Guidelines
109 | P a g e
Sr. No
Current Process Responsibility Proposed Process Responsibility Remarks
13.1 1. A grievance against the action or decision of the SNA / State Government can be referred to NGRC in writing.
2. The complaint can be made by beneficiary/IC/hospital/FKO or any other stakeholder.
1. Aggrieved party
2. NGRC
1. Depending on the nature of complaint, the contact center operator would decide whether it is a complaint against SNA/state. The SNA/state user would get an email/SMS indicating a complaint. The SNA/state may act upon it and close the complaint at their end.
2. The call center operator would give a call on registered mobile number of the aggrieved party to verify resolution. The call would be tried thrice in 24 hours. If the aggrieved agrees to resolution, the complaint would be closed. However, if the party does not indicate satisfaction, the complaint would turn into a grievance and would go to NGRC, and would appear in NGRC inbox with an email/SMS to NGRO.
3. NGRC would investigate and take a decision in this regard. The NGRO, before updating the CGMS, would ensure compliance.
1. Aggrieved party
2. SNA / state Government
3. Call Centre Agency
Policy decision taken Meeting reference
Sr. No Decisions Date
1 Manual for Grievance Redressal Mechanism 18th March 2014

RSBY Revised Process Guidelines
110 | P a g e
2 Integration with SMS gateway of DeitY 23rd January 2014
3 National Toll-free number for beneficiaries 9th April 2014
4 The current practice of transferring a grievance from SGRC to NGRC may be continued with a limit of one appeal per beneficiary
Meeting dated 6th May 2014, chaired by Secretary (L&E), MoM yet to be processed in file
5 The meeting of SGRC is to be held every month Meeting dated 6th May 2014, chaired by Secretary (L&E), MoM yet to be processed in file
6
Hiring of additional manpower (2-3 people) to manage grievances at SNA & NGRC. The hiring of this manpower shall be dependent on the number of grievances that have been escalated to SGRC & NGRC. The role of such manpower shall be to:
a. analyze the grievances received, b. investigate past action taken before getting converted to grievances, c. bring out appropriate measures to the SGRC / NGRC for resolving these grievances; and
Ensuring compliance to the decisions of SGRC/ NGRC within the stipulated time period by various stakeholders
Meeting dated 6th May 2014, chaired by Secretary (L&E), MoM yet to be processed in file
Policy Decision to be taken
Sr. No Decisions
1 Decision on whether to have a single location of national call center i.e. single physical location, or a distributed model where call center operators would sit out of different offices at state level
2 The end to end responsibility of development/enhancement of the overall RSBY IT platform portfolio including but not limited to (i) current GMS to a robust CGRMS with email/SMS/call-center integration (ii) central server, web application (iii) new TMS software at hospital can be outsourced to a renowned IT organization with guidance from NIC.
3 Hiring of RSBY field coordinator identified at every district level needs to be enforced, and the deadline for the same should be June 30
Training Needs Training to be provided to Training to be provided by
1 Training on handling the CGRMS application and handling complaints / grievance process
MoLE / NIC / SNA / DKM / district and state grievance committees / kiosk operators / e-entrepreneurs / e-pensioners / call center staff
IT application agency / call center agency
Input for RFP/FRS RFP / FRS
1 Setting up of Call Center to be run by 3rd Party Agency and integration of RFP / FRS

RSBY Revised Process Guidelines
111 | P a g e
Call Center with Grievance Management System
2 Empanelment of audit agency for CGRMS by MoLE RFP
IEC Activities
1 Awareness and education of beneficiaries / all stakeholders on CGRMS system and process for RSBY

RSBY Revised Process Guidelines
112 | P a g e
Pro
ce
ss
Co
de
VIII - KSK Process Name
Kiosk Management
Process Objective Current Status 1. Providing RSBY administrative services to the beneficiary upto
the block / taluka / mandal level for enhanced beneficiary access 2. Provide convenience of member addition / data updation / lost
card replacement to the RSBY beneficiary, as well as complaint or grievance registration
1. Kiosks exist only at district level 2. Centralized software for kiosks exits, which works in offline mode and
updates data once connected to the internet. The kiosk connects to the insurance company server in some cases or functions only when the post-enrolment data is available on the district server. This data is loaded on the kiosk computer, which usually is done after 2-3 months of enrolment process
3. Some of the kiosks at district level are non-functional due to lack of post enrolled data, manpower, internet connectivity or infrastructure
4. Multitasking of the kiosk operator (use of kiosk personnel for other RSBY related work in the district or by the DKMA)
Key Stakeholders Measures and Key Performance Indices (KPIs) 1. Beneficiary 2. Ministry of Labor and Employment (MoLE) 3. State Nodal Agency (SNA) 4. Insurance Company (IC) / Third Party Administrator (TPA) 5. Hospitals 6. District Key Manager (DKM) 7. Kiosk operator
Measures16: MoLE, SNA, DKM, IC/TPA, kiosk operator (relevant reports to be available, depending on role) 1. Number of kiosks made functional
Filters: User Category (SNA, DKM, SCSP, Kiosk operator), Geography (District, Taluka/ Block, Mandal etc.), Time period by which made functional17(15 days prior to enrolment process), Trained Kiosk operators
2. Number and type of transactions performed by kiosk
Filters: Transaction Type (add, update, card replacement, card splitting, complaint registration, status update to beneficiary, update of manual transactions by the hospitals), Kiosk Type (district / block), Geography, Time period of transactions, Average Time per Transaction
3. Uptime of the kiosk
16
All measures to be available as a report on a web portal in real-time/near-real-time. The data should be available in a warehouse, such that any extraction is possible to create ad-hoc reports 17
Functional kiosk means one that has functional software and hardware, trained kiosk operator and can conduct transactions, record complaints / grievances of the beneficiaries

RSBY Revised Process Guidelines
113 | P a g e
Filters: User Category, Geography, Start Time, End Time, Offline data upload time
4. Number of kiosks non-functional Filters: User Category (Kiosk operator), Geography, Start Time, End Time, Complaint registered (call center, Web/email), Complaint Type (hardware/ software / network failure)
5. Time to resolve non-functionality of kiosk Filters: User Category, Geography, Date of Complaint Registration, Date of Complaint Resolution, Uptime of Kiosk
KPI18: MoLE, SNA, SCSP, Kiosk Operator (relevant KPI’s to be measured depending on role) 1. Number and % of kiosks setup and made functional
2. Number and type of transactions performed by the kiosk (including
complaint and grievance registration and status update to beneficiary) 3. Average time taken per transaction type 4. Average uptime of the kiosk per day/ per month/per quarter/ per year 5. Average time taken to resolve hardware/ software/ connectivity issues at
kiosk
Summary of current challenges Summary of key suggestions 1. Non-accessibility of kiosks for the beneficiary (only at district)
leading to difficulty in accessing RSBY administrative services by beneficiary.
2. Non issuance of username and password to kiosk operator by IC. 3. District kiosks do not have timely access to post enrolment data
to provide services to RSBY beneficiaries 4. Lack of standard operating procedures at kiosks, with no SLA’s
1. Establishment of kiosks at the block level to expand reach of services for RSBY beneficiaries, which will be managed by the centrally empaneled SCSP
2. SNA shall provide the SCSP with civil and electrical work at the identified kiosk location
3. The SCSP shall provide the manpower, hardware, training and services to the beneficiaries through the kiosk
4. Additional stress on training and access of new web application as well as
18
All KPI’s to be available as a report on a web portal in real-time/near-real-time. The data should be available in a warehouse, such that any extraction is possible to create ad-hoc reports.

RSBY Revised Process Guidelines
114 | P a g e
for performance monitoring of kiosks 5. No synchronization of pre and post enrolment data and hospital
claim data for facilitating kiosk operations 6. Low level of awareness about the utility of kiosks for different
beneficiaries 7. Lack of training to kiosk operators for efficient service delivery
CGRMS interface for kiosk operators 5. Introduction of SLA’s for electronic performance monitoring of kiosks
through the web application; audit of kiosk operations 6. The SCSP can also choose to employ e-entrepreneurs /pensioners / self-help
groups at block / district level as kiosk operators
Pre-requisites for kiosk set-up and management 1. Identification of kiosk location at district and block level; hiring of kiosk operators 2. Access to central web application and CGRMS for the kiosk operator for transactions at district /block level for delivering services to RSBY
beneficiaries 3. Access to of URN generated data, transaction data of beneficiary for the kiosk operator through the central web application
Inputs to the revised process Output from the revised process 1. Beneficiary request for addition/updation/lost card replacement
of RSBY enrolment data, or for logging a complaint 1. Delivery of administrative services to the RSBY beneficiary 2. Updated / modified enrolment data in the central server
Processes and Responsibilities:
Sr. No
Current Process Responsibility Proposed Process Responsibility Remarks
1 Establishment of Kiosk
1.1 IC receives work order from SNA and it makes a request for availability of space at district and block to operationalize the kiosk.
SNA 1. The centrally empaneled SCSP makes a request to SCSP for availability of space at district and block to operationalize the kiosk.
2. SNA will ask DKM to provide options of space for kiosks at block and district at a public place which is frequented and easily accessible.
1. SNA
2. DKM
1. SNA will provide the confirmation of space for kiosks at block/ district level to SCSP with the help of DKM within 15 days of receiving the request from SCSP.
2. SCSP and DKM will confirm the requirement of civil / electric work at the space provided.
3. SNA & DKM shall ensure that

RSBY Revised Process Guidelines
115 | P a g e
Sr. No
Current Process Responsibility Proposed Process Responsibility Remarks
3. SCSP will establish kiosks at district and block level.
3. SCSP basic civil and electrical work is completed at the location of kiosk for smooth operations. The SNA will bear the cost of civil & electrical infrastructure work at the identified kiosk locations.
1.2 IC procures hardware and commences installation at district kiosk.
IC The SCSP will establish kiosk at block level too. It will be required to procure hardware for both district and block level kiosks.
SCSP 1. SCSP will provide for hardware and other related infrastructure at the kiosk. The details of the hardware to be provided by SCSP at the district/ block kiosk are provided at Annexure 8.1.
2. The software will be provided by MoLE, which would a centralized web application.
1.3 IC signs the Annual Maintenance Contract (AMC) agreement for kiosk hardware and kiosk management software.
IC SCSP signs Annual Maintenance Contract (AMC) agreement for kiosk hardware and application as part of the contract agreement with SNA.
SCSP 1. The SCSP shall own the AMC for the hardware, software and related infrastructure for smooth operations.
2. The software for RSBY kiosk operations shall be maintained by the SCSP operating the kiosk with the help of MoLE / SNA. It will be the responsibility of SCSP to communicate/update the offline-module upgrades of the kiosk application.

RSBY Revised Process Guidelines
116 | P a g e
Sr. No
Current Process Responsibility Proposed Process Responsibility Remarks
1.4 Installation of stand-alone (offline) module kiosk management software at kiosk.
IC No change SCSP MoLE shall provide SCSP with the stand-alone kiosk management software for installation at kiosk and provide a username and login for performing transactions.
1.5 IC performs testing of all equipment, software and connectivity at the kiosk.
IC The SCSP will perform testing of all equipment, software and connectivity at kiosk and certify the functioning of the kiosk.
SCSP The SCSP will ensure the functioning of the kiosk software and hardware and shall resolve any connectivity issues. It may obtain support of the SNA / DKM in case of major issues faced in obtaining connectivity for the kiosk.
1.6 No hoarding / information board outside the kiosk, displaying the key services provided.
IC 1. Hoarding / information board to be provided by the SCSP. Basic information to facilitate services to the beneficiary will be displayed on the hoarding/ board.
2. The guidelines and template for IEC material should be provided by MoLE, and customized by SCSP for kiosk setup. A tentative format of the display board is provided in Annexure 8.2
1. SCSP
2. MoLE
The kiosk shall display a hoarding / information board which will display the benefits of the scheme, services being provided at the kiosk along with their rates, national toll-free number, procedure for filing a complaint / grievance, updated brochures of empaneled hospitals / web list of empaneled hospitals for beneficiaries.
2 Recruitment and Training of manpower for kiosk

RSBY Revised Process Guidelines
117 | P a g e
Sr. No
Current Process Responsibility Proposed Process Responsibility Remarks
2.1 IC advertises and recruits manpower for kiosk operations at district level.
IC 1. The SCSP will recruit operators for block and district kiosks. It will also train these operators and ensure that these operators are ready to conduct transactions prior to the commencement of enrolment process.
2. The SCSP will provide a record of all hired operators 15 days prior to the enrolment process so that the operator details and mobile numbers are fed into the central system to create operator records.
SCSP 1. The SCSP may consider the hiring of e-entrepreneurs, pensioners and self-help workers for manning the kiosks. This exercise must be completed prior to commencement of enrolment process.
2. The kiosk personnel should not be engaged in other activities apart from RSBY related activities and should be available at kiosk during the agreed designated hours.

RSBY Revised Process Guidelines
118 | P a g e
Sr. No
Current Process Responsibility Proposed Process Responsibility Remarks
2.2 IC provides training to the kiosk operators at district level on kiosk operations and card management.
IC 1. The SCSP will provide training of kiosk operators at district / block level on kiosk operations, card management and handling the CGRMS application.
2. The training of kiosk operators to be done as per the structured training manual for RSBY kiosk operations prepared by MoLE.
3. The DKM shall closely monitor the training of kiosk operators. The successful completion of training shall be updated in the web based application by DKM.
4. The SCPSP updates the record/login for all operators in the central web application as well as in CGRMS and provides confirmation on training of operators.
1. SCSP
2. DKM
3. MoLE
Two day workshop to be conducted by SCSP with hands-on training for all operators prior to commencement of enrolment. The - training shall be provided on the following areas:
- General Kiosk operations and use of Master Kiosk Card (MKC)
- Management of card (updation / modification / card split / lost card replacement / invalid card replacement)
- CGRMS and managing complaints for entry into CGRMS
- Call center functions - Charges for each service
The SCSP can add additional areas of training as per the requirements.
2.3 No training provided to stakeholders at district level
IC 1. Training of other stakeholders from state, district and block shall be provided by the SCSP.
2. The SNA shall provide funds for training for all stakeholders.
3. DKM shall provide a sign-off on
1. SCSP
2. DKM
3. SNA
A two day workshop to be conducted by the SCSP with hands-on training for all stakeholders (SNA, DKM, FKO, DIO) prior to commencement of enrolment. The training shall be provided on:
- CGMS and managing

RSBY Revised Process Guidelines
119 | P a g e
Sr. No
Current Process Responsibility Proposed Process Responsibility Remarks
the completion of training to the SCSP. This shall be updated in the web based application.
complaints for entry into CGMS
- Call center functions - Kiosk operations and card
management (DIO card, DKM card, MKC card, MHC and PHC card, FKO card)
The SCSP can add additional areas of training as per the requirements.
2.4 The kiosk operators at district are issued the Master Kiosk Card (MKC) for conducting transactions at kiosk post completion of training. The MKC card is personalized by the DKM prior to issuance to kiosk operator.
DKM 1. The DKM will personalize the MKC card which will also include the biometrics of the kiosk operator which needs to be authenticated prior to accessing the kiosk management system.
2. The MKC would be issued to every operator at the block level as well.
3. The contact numbers of block level kiosk operators should be made available to the contact center agents, through the web based system, so that the callers may be referred to them.
DKM The details of all the MKC cards issued will be stored in the web based application, for further authentication during kiosk operations.
2.5 The IC will create user name and password for the kiosk operator.
IC The SCSP will issue the username and password to the kiosk operator for logging into the kiosk interface of the web application and the stand-alone module. This will be a pre-requisite for conducting valid
SCSP 1. The SCSP will create accounts for kiosk operators through the web application for access to the kiosk software / stand-alone application.

RSBY Revised Process Guidelines
120 | P a g e
Sr. No
Current Process Responsibility Proposed Process Responsibility Remarks
transactions at the kiosk. 2. The SCSP will be provided with a privilege to create kiosk operator accounts limited to the number of kiosks they will be setting up at district and block.
3. The SCSP will provide the SNA with the number and details of kiosks they will be setting up at district / block level.
3 Providing various services to RSBY beneficiary through the kiosk
3.1 The beneficiary goes to district kiosk for availing services such as updation / modification / card split / lost card replacement / invalid card replacement etc.
Kiosk operator The beneficiary will now be able to get services such as updation / modification / card split / lost card replacement / invalid card replacement from the district/ block kiosk.
Kiosk operator 1. Only existing enrolment data can be added to the replacement card. Enrolment of new family member can be done only if the slot is empty on the card.
2. Alternatively a kiosk portal can also be created, wherein the beneficiary can request for a service from his door step/PHF/hospital etc
3.2 Re-issuance of card at district
1. At the district kiosk, based on the URN, the current card serial number will be marked as hot-listed in the backend
District kiosk operator
Re-issuance of card at district / block kiosk using MKC card.
The following is process of card re-issuance:
District kiosk operator
Re-issuance of card can be done when the beneficiary card is reported lost or the card is invalid / damaged. The following is the process to be adopted by the district

RSBY Revised Process Guidelines
121 | P a g e
Sr. No
Current Process Responsibility Proposed Process Responsibility Remarks
to prevent misuse of the lost/ missing/ damaged card.
2. The existing data of the beneficiary including photograph, fingerprint and transaction details shall be pulled up from the state server, verified by the beneficiary and validated using the beneficiary fingerprints.
3. The beneficiary family shall be given a date (based on SLA with state government) for collection of the re-issued card.
4. It is the responsibility of the insurance company to collate transaction details of the beneficiary family from their central server (to ensure that any transactions done in some other district are also available).
5. The re-issued card is
personalized with details of beneficiary family, transaction details and insurance details within the defined time using the Master
1. At the district kiosk, based on the URN, the current card serial number will be marked as hot-listed in the backend to prevent misuse of the lost/ missing/ damaged card.
2. The existing data of the beneficiary including photograph, fingerprint and transaction details shall be pulled up from the central server, verified by the beneficiary and validated using the beneficiary fingerprints.
3. The beneficiary family shall be given a date (based on SLA with state government) for collection of the re-issued card.
4. The transaction details shall be updated at the central server.
5. The re-issued card is personalized with details of beneficiary family, transaction details and insurance details within the defined time using the Master Kiosk Card (MKC).
6. The beneficiary pays the cost of the smart card at the district
kiosk:
The beneficiary shall pay the cost of the smart card as decided by MoLE.

RSBY Revised Process Guidelines
122 | P a g e
Sr. No
Current Process Responsibility Proposed Process Responsibility Remarks
Kiosk Card (MKC).
6. The beneficiary pays the cost of the smart card at the district kiosk and collects his new card.
kiosk and collects his new card.
3.3 Card split service is offered at the district kiosk. The following is the process followed for card split:
- The fingerprints of any family member shall be verified against those available in card.
- The splitting ratio should be confirmed from the beneficiary. Only currently available amount (i.e. amount insured - amount utilized) can be split between the two cards. The insured amount currently available in the main card is modified.
- The cost of the additional smart card needs to be paid by the beneficiary at the district kiosk
- The beneficiary’s existing data, photograph, fingerprint and transaction details are fetched from the district server and a fresh card (add-on card) will be
District kiosk operator
1. No change in the process. The card split facility shall continue to be offered only from the district kiosk.
2. The beneficiary’s existing data, photograph, fingerprint and transaction details shall be fetched from the central server instead of the district server in the already existing process.
District kiosk operator
Card splitting is done at district (using MKC card) and kiosk to help the beneficiary to avail the facilities at two diverse locations i.e. when the beneficiary wishes to split the insurance amount available on the card between two cards
The points to be kept in mind while performing a card split are as follows:
1. The existing data including text details, images and transaction details shall be fetched from the central server.
2. Card split may be carried out only if there is no blocked transaction currently on the card
3. - In case a split card was issued in the interim, both cards would be required to be present at the time of modification.

RSBY Revised Process Guidelines
123 | P a g e
Sr. No
Current Process Responsibility Proposed Process Responsibility Remarks
issued immediately to the beneficiary family. Both cards would have details of all family members.
- The existing card will be modified and add on card issued using the MKC card.
- Fresh and modified data shall be uploaded to the central server as well.
3.4 Card modification service is provided at district kiosk is done using the MKC card. The following is the process for modification / updation in the beneficiary card:
1. During the time of enrolment if only the head of the family was present, the details of other family members can be updated in the RSBY card at the district kiosk.
2. In the event of death of any person in beneficiary family, enrolled on the card, another family member from the beneficiary family list associated with the URN is to
District kiosk operator
1. Card modification will now be available at district / block kiosk using MKC card.
2. A new photograph of the family may be taken (if all the members are present or the beneficiary family demands it).
3. Fingerprint of additional members needs to be captured.
4. Data of family members has to be updated on the chip of the card.
5. The existing details need to be modified in the database (central server).
District / block operator
It is to be ensured that only members listed on the original category list provided by the state are enrolled on the card. As in the case of enrolment, no modifications except to age and gender may be done.

RSBY Revised Process Guidelines
124 | P a g e
Sr. No
Current Process Responsibility Proposed Process Responsibility Remarks
be added to the card.
3.5 District kiosk operator provides data to IC for all online and offline transactions. IC updates this data on its server.
1. Kiosk operator
2. IC
District / block kiosk operator provides data to central server for all online and offline transactions through the web application.
Kiosk operator The kiosk operator can conduct transactions using the stand- alone software provided to him and can synchronize the data once he has connectivity. The data shall be synchronized with the central server which can be accessed with the web based application.
3.6 Card split and duplicate card issuance requires visit to district kiosk
NA 1. Beneficiary will visit nearest block kiosks to request for a split card or duplicate card
2. In case of duplicate card block kiosk will hot-list the lost card, and initiate a request for duplicate card
3. For split card, he will capture the request along with required information such as split amount, members on split card and initiate a request on the web based software
4. Beneficiary can also give his preference of a district kiosk from where he can collect the new card
Block kiosk operator
1. Block kiosk will provide all the services, which do not require use of card printer. For services which require card printer he will only initiate the request, which can be completed at district kiosks. This will reduce the hassles for beneficiaries and will reduce the load on district kiosks
2. In the case of states with high migrant population, card printers can be provisioned at the block level as well

RSBY Revised Process Guidelines
125 | P a g e
Sr. No
Current Process Responsibility Proposed Process Responsibility Remarks
5. Beneficiary will be provided with a date on which he can collect his duplicate/split card from district kiosk
4 Re-issue of MKC card to the kiosk operator
4.1 In the event of loss of MKC card / card becoming invalid / broken card, the kiosk operator requests the DKM to provide him with a replacement card.
DKM 1. In the event of loss of MKC card / card becoming invalid / broken card, the kiosk operator requests for a new card either by calling the national toll-free call center number or calling the District coordinator.
2. The DKM / district coordinator will provide the kiosk operator with a replacement card within 3 days of receiving the request either through the web based application / direct request / call center request/ email.
DKM / District coordinator
1. The preferable mode for kiosk operator is to request through the call center as an SMS / email will be sent to the DKM to issue and personalize the MKC card.
2. The kiosk operator at the district/ block level is required to travel to the DKM for authentication and collection of new MKC card.
4.2 Master hospital card cannot be prepared at district level
1. MoLE will provide additional blank master hospital card to DKMA
2. In case of requirement of hospital cards, DKMA will personalize a new blank card
3. District kiosk will print name and code on the hospital card,
1. DKMA
2. Kiosk operator
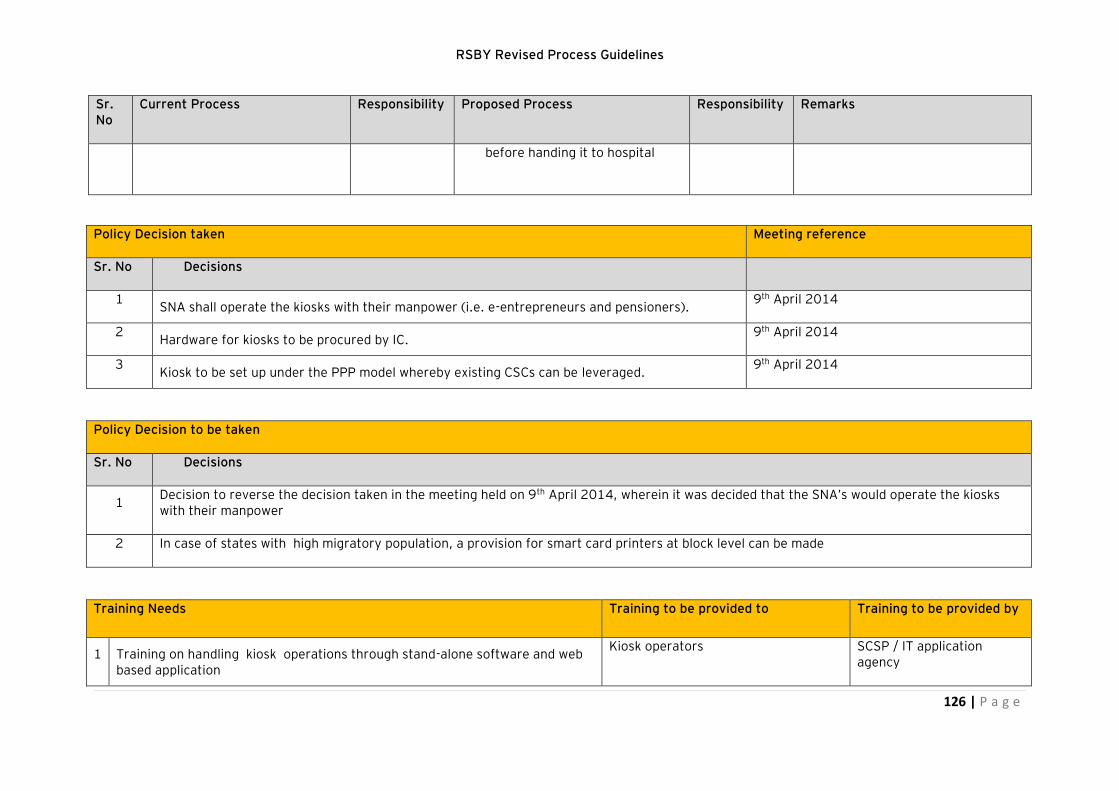
RSBY Revised Process Guidelines
126 | P a g e
Sr. No
Current Process Responsibility Proposed Process Responsibility Remarks
before handing it to hospital
Policy Decision taken Meeting reference
Sr. No Decisions
1 SNA shall operate the kiosks with their manpower (i.e. e-entrepreneurs and pensioners).
9th April 2014
2 Hardware for kiosks to be procured by IC.
9th April 2014
3 Kiosk to be set up under the PPP model whereby existing CSCs can be leveraged.
9th April 2014
Policy Decision to be taken
Sr. No Decisions
1 Decision to reverse the decision taken in the meeting held on 9th April 2014, wherein it was decided that the SNA’s would operate the kiosks with their manpower
2 In case of states with high migratory population, a provision for smart card printers at block level can be made
Training Needs Training to be provided to Training to be provided by
1 Training on handling kiosk operations through stand-alone software and web based application
Kiosk operators SCSP / IT application agency

RSBY Revised Process Guidelines
127 | P a g e
3 Training on handling the CGRMS and entering beneficiary grievances into the portal at kiosk.
Kiosk operators (e-entrepreneurs / pensioners)
SCSP / IT application agency
Input for RFP/FRS Inputs for:
1 Details on setting up of kiosk at district / block level
RFP for SCSP selection
2 Eligibility on minimum qualification and IT/communication skills to become a kiosk operator at district / block level
RFP for SCSP selection
3 Maintenance of kiosks, hardware, software and related equipment for smooth functioning of kiosks
RFP for SCSP selection
4 Central web application and CGRMS access to kiosk operators, with offline module for synchronization back with central server on all transactions (addition/update/lost-card-replacement) and complaints
FRS for IT agency
IEC Activities
1 Education of beneficiaries and hospitals and other stake holders on facilities available at kiosk
2 Continuous education / training of operators on any new functionality changes in the RSBY scheme
Incentive mechanism
1 States (SNA) can take a decision on the incentive to kiosk operator for excellent performance and service to beneficiaries
Human Resource Requirement Where
1 Hiring of kiosk operators by the SCSP. The SCSP can hire e-entrepreneurs, e-pensioners, self-help workers etc., to man the kiosks and provide services to RSBY beneficiaries
District / block

RSBY Revised Process Guidelines
128 | P a g e
Management Information System for proposed RSBY implementation
Management Information System (MIS) is one of the most important tools to track the progress and effectiveness of a program. A good MIS system
provides a robust decision support system to the management / executive(s).
In a scheme like RSBY, the importance of MIS increases manifold due to multiple stakeholders and the complexity involved. The complexity increases with
the spread of the scheme across 28 states and the large number of beneficiaries involved.
MIS for RSBY plays a very crucial role in providing an understanding of the way the project is functioning on a daily/ monthly/ quarterly/ half
yearly/yearly basis. The data reported in such MIS will be helpful in understanding the trends in healthcare amongst the un-organized sector, which can
further help the government in enhancing the health seeking behaviour within this sector through various policy and process mechanisms.
RSBY being an evolving scheme, with dynamic ground level complexities, a strong MIS will play a very crucial role in its success. The focus on designing
the MIS has been the beneficiary, wherein each stakeholder in RSBY will have access to relative information about how the beneficiary in benefitting from
the program, so as to make the RSBY service delivery much more efficient for the beneficiary.
The reports generated by MIS will be primarily of two types:
1. To measure the progress of scheme, MIS will primarily be used as a Decision Support System by the Executive Management Committee at Central
Government level, thereby facilitating policy decisions and understanding benefits being accrued by the targeted beneficiaries.
2. To measure the key performance indicators of each stakeholder and the regional progress, MIS will be available at State / District level. This will
allow close monitoring of the scheme within each State / District, as well as monitoring of hospital and insurance company performance to help
the stakeholders take remedial measures to make the scheme efficient.
The MIS reports should be designed on the basis of their periodicity which will be available through the web based platform and can be classified under
following categories:
1. Fixed periodic (Daily, weekly, Monthly, Quarterly & annual) report
2. Fixed periodic (Daily, weekly, Monthly, Quarterly & annual) exception report
3. Exception report on the basis of pre-defined triggers
4. Detailed report generated by business intelligence team
5. Reports to be made available in the public domain (it will be sub-set of the above four reports)

RSBY Revised Process Guidelines
129 | P a g e
While the periodicity has been defined for must-have analysis, the data that are generated through the system should be available for ad-hoc reporting in
real-time/near-real-time. The following reports have been identified and listed for each of the 8 processes within RSBY. The MIS list is not exhaustive and
will undergo changes over a period of time based on the information requirements or structural changes or policy changes within the scheme.
Process I – Data preparation and pre-enrolment
MIS Reports
Sr. No
Name of MIS Report Filters Fields Role based access to19:
Remarks
1
Pre-enrolment data fields (This is not necessarily a report, but a mode to allow authorized users to search for one or more fields in the database) to drill down to specific records
Geography, Category (11), Caste Category, Period (From, to)
S.No., Name of Beneficiary*, Father’s/Husband’s name, Date of birth / Age*, Gender*, Address*, VTC* (Village/Town/City), District*, State*, Pin-code, Caste Category (SC/ST/OBC/General), BPL category (out of 11)*, Date of pre-enrolment*, Number of dependents to be covered*, Mobile number, Aadhaar number, NPR number, NREGS Job Card number, BPL Card Number, Ration Card number, Category Identifier number (for any of the 11 categories), Existing RSBY Card Number, URN number, flag to indicate whether any family member has an RSBY card* (Y/N)
MoLE, Corresponding state department, SNA
1. State department data available to department for only those beneficiaries for which the data has been collected by that department
2. Mandatory fields have been marked as *
3. The refreshed data should be available daily for search
4. Data should be made available on the proposed web application for authorized users
2. Category wise pre-enrolment data report
Village, Block, District, State, Period((From/To), Caste Category, Only
Name of Category*, Number of pre-enrolment data records collected, Number and % of pre-
SNA 1. Mandatory fields have been marked as *
19
Not all information is available to everyone. Each stakeholder gets to see the information that is required for him / her to take necessary action

RSBY Revised Process Guidelines
130 | P a g e
MIS Reports
Sr. No
Name of MIS Report Filters Fields Role based access to19:
Remarks
The reports using an ad-hoc query builder would take into account multiple filters and one or more parameters.
records with valid NPR number /Aadhaar number / Mobile number/NREGS ID/BPL card number / Ration card number.
enrolment data records rejected due to duplication, Number and % of pre-enrolment data records rejected due to invalid structure/format
2. The refreshed data should be available daily for search
3. The report should be made available on the proposed web application.
Process II- Enrolment
MIS Reports
Sr. No Name of MIS report
Filters Field Role based access to20
Remarks
1 Area wise % enrolment
Village, Block, District, State, period (from-to)
S.No., area (Village/Town/City, District*), Number of pre-enrollments, number of URN generated, number of actual enrolments, % of enrolment from URN generated
MoLE, SNA, DKM, SCSP, IC
1. The reports should be made available through the proposed web application
2. List of areas with % coverage between
Village, Block, District, State, period (from-to)
S.No., area (Village/Town/City, District*), Number of pre-enrollments, number of URN generated, number of
MoLE, SNA, DKM,
1. This report would be used to identify slab-wisecompletion
20
Not all information is available to everyone. Each stakeholder gets to see the information that is required for him / her to take necessary action

RSBY Revised Process Guidelines
131 | P a g e
MIS Reports
Sr. No Name of MIS report
Filters Field Role based access to20
Remarks
x1 and x2
X1, x2 can have values of 0, 10, 20, 30…90, 100.
actual enrolments, % of enrolment from URN generated SCSP, IC of enrolment
2.
3 Number of villages with more than 5% variation between number of signed and FKO data
Village, Block, District, State, period (from-to)
S.No., area (Village/Town/City, District*), Number of FKO card Data, number of Signed data, , variation
MoLE, SNA, DKM, SCSP, IC
This is an exception report, should be monitored
4 Report of villages where enrolment could not start
Block, District, State
S.No., area (Village/Town/City, District*), Scheduled date of enrolment
MoLE, SNA, DKM, SCSP, IC
This is an exception report, should be monitored closely
5 Activation of cards
Village, Block, District, State, PHF, period (from-to)
S.No., area (Village/Town/City, District*), Number of enrollments, number of cards activated, % of activated cards
MoLE, SNA, DKM, SCSP, IC
The reports should be made available through the proposed web application to understand the extent of wellness check completed
6 Addition of family members
Village, Block, District, State, Kiosk Operator, period (from-to)
S.No., area (Village/Town/City, District*), Number of enrollments, number and % of cards for which additional family members have been added
MoLE, SNA, DKM, SCSP, IC
The reports should be made available through the proposed web application to understand the impact of kiosk in addition of family members to RSBY card

RSBY Revised Process Guidelines
132 | P a g e
MIS Reports
Sr. No Name of MIS report
Filters Field Role based access to20
Remarks
7 Area wise spilt of cards and issue of new cards
VTC, District, State, IC, Kiosk Operator, period (from-to)
S.No., area (Village/Town/City, District*), Number of enrollments, number and % of families for which additional cards have been issued, number and % of families for which additional cards have been issued due to family split, number and % of families for which additional cards have been issued due to lost card replacement,
MoLE, SNA, DKM, SCSP, IC
The reports should be made available through the proposed web application to understand the impact of kiosk in issuance of new card due to family split or lost card replacement
Process III – Smart card and key management system
MIS Reports
Sr. No Name of MIS report Filters Field Role based access to21
Remarks
1 Number of cards issued
State, District, Block, Village, master, beneficiary, Hospital, Kiosk, PHF, DIO, DKM, FKO, period (from-to)
S.N,, Number of cards issued, % of total cards issued
MoLE, SNA, DKMA, IC,SCSP
To be available in public domain
21
Not all information is available to everyone. Each stakeholder gets to see the information that is required for him / her to take necessary action. In some cases, depending on the filter, some new fields would appearin the report. For example, if State name is selected as filter, district name should appear as a field. If district is selected as filter, block/villages would appear in the fields. The user of the MIS should be allowed to select the filter(s) and the fileds that should appear in the report

RSBY Revised Process Guidelines
133 | P a g e
MIS Reports
Sr. No Name of MIS report Filters Field Role based access to21
Remarks
2. Number of cards hot-listed
State, District, Block, Village, master, beneficiary, Hospital, Kiosk, PHF, DIO, DKM, FKO , period (from-to)
S.N., Number of cards hot-listed, % of total cards hot-listed
MoLE, SNA, DKMA
To be monitored by MoLE, SNA, DKMA
3 Number of duplicate cards issued
State, District, Block, Village, master, beneficiary, Hospital, Kiosk, PHF, DIO, DKM, FKO, Period (from-to)
S.N., Number of duplicate cards issued, % of total duplicate cards issued
MoLE, SNA, DKMA
To be monitored by MoLE, SNA, DKMA
Process IV – Wellness check and payment of premium
MIS Reports
Sr. No Content of MIS Report
Filters Fields Role based access by22
Remarks
1 Wellness check completion
State, District, Block, Village period (from-to), PHF, flag on wellness data updated in the system, flag on wellness-check completed-within-first-two-months, flag on wellness-check-completed-between-second-and-third month
S.N., number of families (cards) with wellness check completed, number of families (cards) with wellness check pending, % of wellness check completion
MoLE, SNA, DKM, PHF, IC/ SCSCP
1. The MIS report aims to provide numbers and details on wellness check
2. The numbers may be computed on various parameters/filters which are available as a field
22
Not all information is available to everyone. Each stakeholder gets to see the information that is required for him / her to take necessary action

RSBY Revised Process Guidelines
134 | P a g e
MIS Reports
Sr. No Content of MIS Report
Filters Fields Role based access by22
Remarks
2
Time taken to pay the premium (by SNA or by MoLE)
State, District, 100% premium payment cases, 50% premium payment cases
S.N, Average time taken to make the payment to IC
MoLE, SNA, DKM
1. This MIS report will provide details on the timely payment to IC’s after wellness check
Process V – Hospital Management
MIS Reports
Sr. No Name of MIS report Filters Field Role based access by23
Remarks
1
Number of hospitals empaneled
State, district, block, IC, S.N., number of hospitals empaneled, type of hospital (public/private)
MoLE, SNA, DKMA, IC/TPA
The MIS report will provide number of hospitals empaneled in an area
23
Not all information is available to everyone. Each stakeholder gets to see the information that is required for him / her to take necessary action

RSBY Revised Process Guidelines
135 | P a g e
MIS Reports
Sr. No Name of MIS report Filters Field Role based access by23
Remarks
2.
% of hospitals reporting claims (empaneled and non-empaneled)
State, district, block, type of hospital (public/private), IC/TPA, period (from, to)
S.N., number of hospitals empaneled, number of hospitals reporting claim, % of hospital reporting claim,
MoLE, SNA, DKMA, IC/ TPA
The MIS report will provide the number and % of hospitals who have raised claims during a period
3
Number of blocks without empaneled hospital
State, district S.N. number of blocks without empaneled hospital, total number of block in the district
MoLE, SNA, DKMA, IC/ TPA
This is an exception report and need to be monitored closely
4
Report to track status of training provided to hospitals during a period
State, district, block, IC, hospital type (public/private), period (from, to)
S.N., number of hospitals empaneled, number of hospitals with training completed flag
MoLE, SNA, DKMA, IC/ TPA
1. The MIS report aims to provide the details on number of hospitals that have been provided training during a period
5 List of hospitals with high number of manual overrides
State, district, block, IC, hospital type (public/private), range of % manual override
S.N., number of hospitals empaneled, number of manual over rides, total number of claims, % of manual override with respect to total number of claims
MoLE, SNA, DKMA
The MIS report will provide the list of hospitals using manual override option more frequently
6
Number of hospitals with hardware and software issues
State, district, block, IC, hospital type (public/private), date
S. N., number of hospitals empaneled, number of hospitals with reported non-functional SW/HWs, % of hospitals with reported non-functional SW/HWs
MoLE, SNA, DKMA
1. The MIS report will provide the number and % of hospitals that are non-functional due to hardware and software issues

RSBY Revised Process Guidelines
136 | P a g e
Process VI – Claims Management
MIS Reports
Sr. No Name of MIS report
Filters24 Fields Role based access to
Remarks
1 % of Claim settled (number)
State, district, block, hospital, IC, period (from-to)
S.N., number of claims raised, number of claims settled, % of claimed settled in numbers, amount of claims raised, amount of claims settled, % of claimed settled in amount
MoLE, SNA, DKM, IC/TPA, Hospital
This report will provide status of claim settlement in a geography during a period
2 List of pending claims
State, district, block, hospital, IC, package code
S.N., claim id, amount of claim raised, claim date, pending for (days),
MoLE, SNA, DKM, IC/TPA, Hospital
This report will provide list of all pending claims, which can be prepared for a geography, for an IC, for a hospital or for a package code
4 % of claims partly paid
State, district, block, hospital, IC, period (from-to), package code
S.N. no of claims raised, number of claims partly paid, % of claims partly paid
MoLE, SNA, DKM, IC/TPA, Hospital
This report will provide % of claims which are partly paid by IC
5 Time taken to settle the claim
State, district, block, hospital, IC, time taken to settle the claim ( e.g. % of claims settled in 7 days, 15 days, 30 days), package code
S.N., total number of claims settled, number of claims settled during the period, % of claims settled during that period
MoLE, SNA, DKM, IC/TPA, Hospital
This report will provide information about time taken to settle a claim, by an IC for a hospital for a package
24
One or more filters may be applied to data table with fields to generate desired MIS report

RSBY Revised Process Guidelines
137 | P a g e
Process VII – Complaint and grievance redressal management system
MIS Reports
Sr. No
Content of MIS Report Filters Fields Role based access by25
Remarks
1 Status report of complaints
Medium of logging complaint (National call center, online through CGRMS, post etc), state, district, block, Complaint type,
S.N., number of complaints received, number of complaints resolved, average time taken for resolution, % of complaints turned in to grievance
MoLE / SNA/ NGRC / SGRC / DGRC / DKM
This report will provide an overview of status of complaints received through different channels
2 Status of grievances state, district, Grievance type
S.N., number of grievance received, number of grievances closed, % of grievances closed, % of decisions against which appeal was made
MoLE, SNA, NGRC, SGRC, DGRC
This report will provide summary of status of grievances on a particular day
Process VIII – Kiosk management
MIS Reports
Sr. No
Content of MIS Report Filters Fields Role based access by26
Remarks
1 Uptime of each kiosk at district and block level
State, district, block, Kiosk type (district / block),
S.N., number of kiosks, average uptime during the period, % of days when uptime was more than X%
MoLE / SNA / DKM/ IC/TPA
The MIS report will provide status of the kiosk in terms of uptime
2 Transactions carried out at kiosks
State, district, block, Transaction type (modify, update, card replacement, complaint registration, grievance registration, status update to beneficiary),
S.N., number of transactions, average Time per Transaction, % of offline transactions with stand-alone software, % of offline transactions synchronized with state / central server
MoLE / SNA / DKM/ IC/TPA
The MIS report will provide snapshot of transactions being carried out at kiosks
25
Not all information is available to everyone. Each stakeholder gets to see the information that is required for him / her to take necessary action 26
Not all information is available to everyone. Each stakeholder gets to see the information that is required for him / her to take necessary action

RSBY Revised Process Guidelines
138 | P a g e
Third party audit of RSBY processes
RSBY involves varied number of transactions being conducted at different places by different stakeholders. The existing processes and software leaves
scope for mal-practice at many places. It is imperative to track and monitor these transactions and activities through IT interventions. While not all the
activities can be tracked directly through IT interventions, some of these require field level visits to check conformity to the processes. The concept of
audit of RSBY processes and activities is being brought in for the first time. Various sub-groups have had consultations and
It is hence proposed to introduce various types of audits on the activities taking place in various processes of RSBY. In some cases audit will be
concurrent while for some it will be periodical. This section lists downs the activities which need to be audited. It also mentions the frequency and sample
size for which this audit is need to be conducted. Third party audit agencies will be selected for conducting such audits and these firms will be empaneled
centrally. An indicative list of audit types has been provided below:
Concurrent audit: This will happen in case of activities, where the number of transactions are of high value and regular, such as enrolment and card
issuance by SCSP, kiosk etc.. In these cases the frequency will be high but % of cases selected as sample will be low.
System audit: All application/software developed will undergo functionality testing before going live and IT security audit should be conducted during first
year of operations. A regular system audit may be done as and when changes to the system take place or a random system audit may be conducted.
Medical audit: a team of qualified doctors will conduct the audit of randomly selected cases to verify whether the treatment given provided was actually
required or whether the requisite treatment was actually given or not.
Field audit: This will comprise of field checks, such as for wellness checks, kiosk operations. This type of audit can be initiated at any time based on
exceptions from MIS/ field reports/ call center complaints.
For all the audits following points should be taken in to account:
1. Sample will be selected purely on random basis. System will have the provision to generate random samples for audit
2. In some cases system will generate random samples from select datasets on the basis of pre-defined triggers
3. Sample will be generated maximum 12 hours before the actual audit is scheduled.
4. Audit has to be conducted within 12 hours of sample generation
5. Audit report has to be uploaded to the system within 24 hours of audit
Who will conduct the audit: Audit will be conducted by firms that have been centrally empaneled by MoLE. These firms shall have prior experience of
conducting audits of similar nature. These firms can be chartered accountancy firms (based on the kind of audit) and other firms that have extensive field
level experience and specific expertise to suit the audit requirements of RSBY. These firms shall have multi-disciplinary expertise in-house or empaneled

RSBY Revised Process Guidelines
139 | P a g e
to conduct the requisite audit for RSBY procedures. The audit firms shall sign an undertaking that none of the partners / members of the team of auditors
of the firm face any disciplinary action on account of frauds or collusion or any act which can be construed as moral turpitude, during the empanelment
process and prior to executing an audit as desired by MoLE.
Selection of audit firms: The audit firms shall be selected on a zonal basis. The States and Union Territories shall be divided into five zones – North East
West South and Central. A minimum of two audit firms shall be selected and they would be allocated states and select districts for audit based on an RFQ
by the State Nodal Agency (SNA). The audit firm shall be selected on a zone wise basis. Once they have been selected on a zonal basis they can be
allocated work in any state in the zone for a period not exceeding one year in the state and a maximum of three years in the zone.
Disqualification of audit firms: In the process of bidding in case it is found that an audit firm tries in any way to approach or influence members who shall
select the firms there shall be automatic disqualification. In case the audit firm or any partner has any professional or any other interest in the activity of
any stakeholder, it shall have to be disclosed and in case not done and found later would attract disqualification. In case the conflict of interest is
substantial lie the auditor is also auditing a stakeholder or is on the board of an IC in the state concerned, there shall be automatic disqualification at the
selection stage.
Suggested audits in each process of RSBY: The list below provides for suggestive audits that can be conducted for each sub-process of RSBY. MoLE /
SNA can change/ add additional audit parameters based on the requirements and the status of the project/ issued observed in operations. It is envisaged
that the proposed web based application shall provide reports which MoLE / SNA can use for initiating audits apart from field reports, call center
complaints etc.
Process No- I: Data preparation and pre-enrolment
Audit required
Sr. No
Activity/systems to be audited Entity involved Audit agency Sample size Sample type Periodicity Triggers
1 De-duplication process
SNA 3rd party Audit Team
5% of suspicious cases
Randomly generated by system from pre-enrolment data submitted by
Once at the time of enrolment data preparation, before submitting the data to mole
High number of potential duplicate records found at MoLE

RSBY Revised Process Guidelines
140 | P a g e
Audit required
Sr. No
Activity/systems to be audited Entity involved Audit agency Sample size Sample type Periodicity Triggers
departments
2 Accuracy and completion of data shared by departments
Department Field Audit team
0.1% of complete data
Randomly generated by system from pre-enrolment data submitted by departments
Once at the time of enrolment data preparation, before submitting the data to mole
Sudden rise or fall in number of beneficiary from a particular category
3 Reporting of “Active” and “Inactive” family
SCSP Field audit team
5% of data Randomly generated by system from enrolment data submitted by IC
At least once during enrolment period
Process No – II: Enrolment
Audit required
Sr. No Activity/systems to be audited Entity involved
Audit agency Sample size Sample type
Periodicity Triggers
1 Setting up of enrolment stations
( time, quality of equipment, IEC activity,
SCSP 3rd party agency
5% Randomly selected system
At least once a week, during enrolment
Complaints against a particular SCSP

RSBY Revised Process Guidelines
141 | P a g e
Audit required
Sr. No Activity/systems to be audited Entity involved
Audit agency Sample size Sample type
Periodicity Triggers
quality of cards, re-verification of cards, presence of FKO, extent of family data updated)
generated records from the master set
window Continuous low coverage by an SCSP
2
Quality of fingerprint captured
Phase I: SCSP to provide biometric data of randomly selected URN to audit agency
Phase II : Audit agency to randomly fetch data from central database
SCSP 3rd Party agency
5% Randomly selected system generated records from the master set
Continuous basis,
High number of manual overrides from a particular district
Process No. – III: Smart card and Key management system
Audit required
Sr. No Activity/systems to be audited
Entity involved
Audit agency Sample size
Sample type Periodicity Triggers
1 FKO card personalization
DKM/ADKM Field Audit Team
5% System generated random sample
At least twice, during FKO card personalization period
Same FKO card is being used in more than one village
2 Beneficiary card issuance
FKO Field Audit team
0.1% System generated random sample
At least twice during enrolment period
Too high or too low coverage
3 KMS system audit CKGA/DIO/D System Audit NA System generated Before start of every Complaints of non-functioning of master

RSBY Revised Process Guidelines
142 | P a g e
KM/FKO team random sample enrolment cards
Process No. IV – Wellness check and payment of premium
Audit requirements
Sr. No
Activity/systems to be audited
Entity involved Audit agency
Sample size
Sample type Periodicity Triggers
1
Wellness check audit
MoLE / SNA 3rd party audit agency
1% Randomly selected system generated records from the master set
Once a year post enrolment process
Only for data sets for which wellness check has happened
2
Premium payment system audit
MoLE / SNA 3rd party audit agency
NA System generated records from master set
Once a year A complete system audit for functionality and information security
Process No. V – Hospital management
Audit required
Sr. No Activity/systems to be audited
Entity involved
Audit agency Sample size Sample Type Periodicity Triggers
1 Claims raised by hospital Insurance company
Insurance companies
1% of total cases
Randomly selected system generated records from the master
At least once a month
Too many claims of similar types from
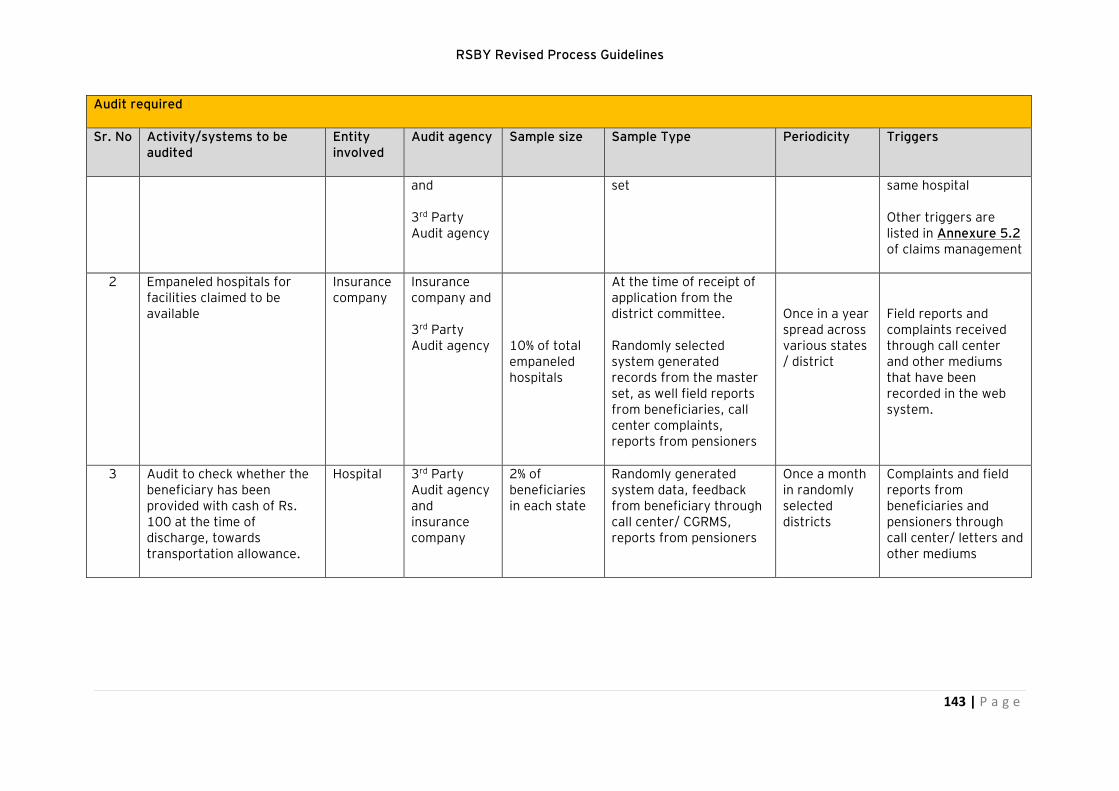
RSBY Revised Process Guidelines
143 | P a g e
Audit required
Sr. No Activity/systems to be audited
Entity involved
Audit agency Sample size Sample Type Periodicity Triggers
and
3rd Party Audit agency
set same hospital
Other triggers are listed in Annexure 5.2 of claims management
2 Empaneled hospitals for facilities claimed to be available
Insurance company
Insurance company and
3rd Party Audit agency
10% of total empaneled hospitals
At the time of receipt of application from the district committee.
Randomly selected system generated records from the master set, as well field reports from beneficiaries, call center complaints, reports from pensioners
Once in a year spread across various states / district
Field reports and complaints received through call center and other mediums that have been recorded in the web system.
3 Audit to check whether the beneficiary has been provided with cash of Rs. 100 at the time of discharge, towards transportation allowance.
Hospital 3rd Party Audit agency and insurance company
2% of beneficiaries in each state
Randomly generated system data, feedback from beneficiary through call center/ CGRMS, reports from pensioners
Once a month in randomly selected districts
Complaints and field reports from beneficiaries and pensioners through call center/ letters and other mediums

RSBY Revised Process Guidelines
144 | P a g e
Process No. VI – Claims management
Audit required
Sr. No Activity/systems to be audited
Entity involved
Audit agency
Sample size
Sample type Periodicity Triggers
1 Claims raised by hospital
Hospital 3rd party agency
1% System generated random sample from hospital claim data
Continuous process with audit at hospital or at beneficiary location happening at random
Unusually high number of claims raised by a hospital during a specific time duration
2 Claims rejected by IC IC or hospital
3rd party agency
10% System generated random sample from hospital claim data
Continuous process with audit at hospital
Very high claim reject percentage by a specific IC, or for a hospital
Process No. VII – Complaint and grievance redressal management system
Audit requirements
Sr. No
Activity/systems to be audited Entity involved Audit agency Sample size Sample type Periodicity Triggers
1 CGRMS system audit MoLE / SNA 3rd party audit agency
NA Complete system
Once a year before commencement of enrolment
New features / modules added
2 Complaint audit MoLE / SNA 3rd party audit agency
5% System generated random sample
At least twice a year
Type of complaint, pending complaints

RSBY Revised Process Guidelines
145 | P a g e
Audit requirements
Sr. No
Activity/systems to be audited Entity involved Audit agency Sample size Sample type Periodicity Triggers
3 Grievance audit MoLE 3rd party audit agency
5% System generated random sample
At least twice a year
Type of grievance, pending grievances, number of appeals
Process No. VIII – Kiosk Management
Audit requirements
Sr. No
Activity/systems to be audited
Entity involved
Audit agency Sample size
Periodicity Triggers
1 Kiosk audit
MoLE / SNA 3rd party audit agency
10% Twice a year Audit teams should conduct surprise audits to check the state of kiosks on parameters such as functioning hardware, designated kiosk operator presence, service delivery satisfaction by beneficiaries through a kiosk.
2 Fraudulent access to kiosk software
MoLE / SNA 3rd party audit agency
Based on exception reports
This can be conducted in case such events are reported in the MIS exception reports.
There may be instances when unauthorized access takes place in the kiosk software. This may be due to wrong entry of password by the kiosk operator, biometrics not matching due to faulty biometric reader; user apart from kiosk operator tries to access the software etc. Each such reported instance will have to be audited.

RSBY Revised Process Guidelines
146 | P a g e
Annexures
Annexure 1.1 – Guidelines on prioritization of beneficiary categories for de-duplication
1. Beneficiaries shall be prioritized based on the amount of premium to be paid by him. The categories for which the beneficiaries have to
pay the lowest premium will get highest priority. In case the premium to be paid by beneficiary is same for two categories, the
beneficiary will be considered under the category, where number of beneficiaries is higher. However if the premium for a particular
category is being paid by the respective agency then that category will have higher priority, even if the number of beneficiaries is lower
than any other category. At the de-duplication stage while selecting a record, the beneficiary with category in higher priority should be
given preference. E.g. a beneficiary from BOCW will be given highest preference as the premium paid by beneficiary is only Rs. 30.
2. The priority will be in this order
a. BOCW (100% premium to be paid by BOCW + 30 rupees fixed fee to be paid by beneficiary)
b. All other categories except those mentioned in (a), (c) & (d) the (beneficiary to pay 30 rupees fixed fee
c. Colie/porters (25% premium to be paid by beneficiary + 75% premium to be paid by Ministry of Railways)
d. Auto Rickshaw/Taxi Drivers (50% premium and Rs. 30 fixed fee to be paid by beneficiaries + 50% premium to be paid by central and
state departments)
Annexure 1.1 (a): Categories of beneficiaries
S.
No
Category National
Estimated
Numbers
Eligibility Criteria for getting RSBY benefits Nodal Department /
Agency
1 Below Poverty
Line (BPL)
Rural: 2209.24
Lakh lives or
441.84 Lakh
households
Urban: 807.96
Lakh lives or
161.59 Lakh
The definition of BPL would be the one prescribed by the Planning
Commission for the purposes of determining the eligible BPL population in
each State/district. It would be the responsibility of the respective State
Government to verify the eligibility of specific BPL workers
Rural Development
Department of the State
Government for Rural
BPL
Urban Local Bodies of
the State Government

RSBY Revised Process Guidelines
147 | P a g e
S.
No
Category National
Estimated
Numbers
Eligibility Criteria for getting RSBY benefits Nodal Department /
Agency
households
(as per NSSO 61st
Round 2004-05)
for Urban BPL
2. Building & Other
Construction
Workers
4.46 crore
(as per NSSO
2009-10)
Registered with the Building & Other Constriction Workers Welfare Boards
(Premium is paid by the Welfare Boards from the Cess collected)
State Labour
Department (BOCWW
Board)
3. Street Vendors 42.19 Lakhs
(as per census
2001)
Registered urban street vendors (as per the National Policy on Urban
Street Vendors 2009) with Town Vending Committee in the
Municipalities/Urban Local Bodies
State Government /
Urban Local Bodies
4. MGNREGA
Workers
350.00 Lakhs Workers having worked for at least 15 days in the preceding financial
year.
Rural Development
Department of the State
Government
5. Beedi Workers 49.80 Lakhs
(I-cards have been
issued to them)
Beedi Workers identified and registered by the State Governments State Labour
Department (Labour
Welfare Commissioners)
6. Domestic Workers 47.50 Lakhs
((NSSO 61st
Round 2004-5)
any two of the following criteria:
Certificate from RWA to the effect that a person is working as a domestic worker in the area
Employer Certificate
Certificate from a registered trade union that the concerned person
State Labour
Department/ Urban
Local Bodies

RSBY Revised Process Guidelines
148 | P a g e
S.
No
Category National
Estimated
Numbers
Eligibility Criteria for getting RSBY benefits Nodal Department /
Agency
is working as a domestic worker Police verification certificate which certifies that the person is
working as a domestic worker
7. Railway Porters Approx. 50
thousand. SO?
Licensed Porters, Licensed Vendors and Licensed Hawkers Railways
8. Sanitation
Workers
10.08 Lakhs
(as per census
2001)
Sanitation Worker’ means a person engaged in, or employed for, any
sanitation work, other than manual scavenging. This includes Sewage
Labourers and Sweepers. State Government will prepare Data
State Government /
Urban Local Bodies
9. Rickshaw
Drivers/Pullers
13.68 Lakhs
(as per census
2001)
Cycle Rickshaw driver driving cycle rickshaw on hire or as paid employee
to transport passengers. Rickshaw pullers pulls hand rickshaw on hire or
as a paid employee to transport one or two passengers/goods from one
place to another in urban areas or on hills assisted by one or more pullers.
State Government will prepare data
State Government /
Urban Local Bodies
10. Mine Workers 17.79 Lakhs
(NSSO 61st Round
2004-5)
Employment in hazardous mining and quarrying industry. List of
Hazardous Mines given in Cabinet Note
State Government (State
Department of Mines)
11. Rag Pickers 11.63 Lakhs
(as per census
2001)
More than 18 years of age, a self-declaration that he/she is rag picker and
any one of the following document:
Letter from Mohalla Committee/RWA/Area Sabha/Ward Committee/ Commercial Complex/ Hotel Management stating that picker is collecting waste from their premises.
Membership of an organisation for the benefit of rag pickers (like their trade unions)
Letter from scrap dealer
State Government /
Urban Local Bodies

RSBY Revised Process Guidelines
149 | P a g e
S.
No
Category National
Estimated
Numbers
Eligibility Criteria for getting RSBY benefits Nodal Department /
Agency
Any Identity card issued by the ULB or State Government or Government of India certifying that he is waste picker
12. Auto/Taxi Drivers 35.39 Lakhs Auto/Taxi Drivers registered with State Transport Authorities
State Government /
Transport Department
13 Weavers and
Textile workers
15 lakhs Use of RSBY platform for IPD and OP benefits. Ministry of textiles
Annexure 1.2 – Data De-Duplication Process
The de-duplication should be a two stage process,
Stage 1: In the first stage, the system would prompt for potential duplicate records, but no final decisions of accept/reject is taken.
Stage 2: In the second stage, the SNA official would accept/reject the record based on pre-defined guidelines.
The rules for deduplication checks using the web-application should be defined in the following manner.
a) Check Aadhaar number availability in both records. If there is an exact match, flag as duplicate. If no, move to next step.
b) Check NPR number availability in both records. If there is an exact match, flag as duplicate. If no, move to next step.
c) Check Mobile number availability in both records. If there is an exact match, flag as duplicate. If no, move to next step.
d) Follow similar steps for NREGS ID, BPL card number and Ration card number.
(v) Check on demographic data based on exact/partial/fuzzy match. The details would be defined in the system FRS. (utmost care to be taken while deciding whether the record is duplicate)

RSBY Revised Process Guidelines
150 | P a g e
Annexure 1.3 – Revised RSBY Data Format
A. Location Particulars 1 State
3 Sub-district
2 District
4 Village/Town
5 GP/Ward
B. Family Details C. Family Identifiers
1 Family Name (Surname)
S. No. Scheme Card Number
2 Address 1 BPL (Rural) Card Number
2 BPL (Urban) Card Number
3 Ration Card Card Number
3 Pin-code 4 RSBY Old URN
4 Local Language 5 RSBY Chip Number
5 Minority 6 NREGS Job card number
6 Caste category 7
8
7 Category to be covered

RSBY Revised Process Guidelines
151 | P a g e
D. Family Members
S. No.
Member Name in (a) English (b) Hindi and (c) Local Language
(a) DoB type (Verified, Declared, approximate) (b) DoB (c) Age
(a)Sex (b)Marital Status (c)Relationship with Head
Name of (a) Father, (b) Mother & (c) Spouse in full
(a) Phone, (b) Mobile & (c) Email
Category of Worker (11) (upto 3 category)
Corresponding Category Card No.
(a) NPR (b) Aadhar (c))Old URN
1 a
b
c
2
a
b
c
3
a
b
c
4
a
b
c
5
a
b
c
6
a
b
c

RSBY Revised Process Guidelines
152 | P a g e
Annexure 2.1: Checklist for enrolment station
S. No. Description Requirement
1 Number of enrolment kit As per population of village, to be calculated @ one kit for 100 family
2 Electricity backup 1 for every enrolment station
3 Operator 1 per kit
4 Supervisor 1 per 5 operator
5 Technician 1 per 10 kit
6 IEC coordinator 1 per 5 enrolment kit
7 Field manager 1 for every 5 supervisor
8 IEC material Brochure: 1 per family Flex Board: 2 per enrolment station One showing enrolment process, another showing benefits of RSBY scheme
Components of enrolment kit - An enrolment kit includes the following:
1. A smart card printer, 2. Laptop, 3. Two smart card readers, 4. One fingerprint scanner, 5. Web camera, 6. Certified enrolment software and other related software.
Specifications for hardware and software requirement at enrolment station
Hardware components Remarks District / block kiosk
Laptop
► This should be capable of supporting all other devices required.
► It should be loaded with standard software as per specifications provided by the MoLE
Configuration:
Desktop with dual core processor with 2 GHz, 80 GB hard drive, DVD r/w drive, 2 GB RAM, graphics
card, minimum of 4 USB ports etc.
District and block kiosk

RSBY Revised Process Guidelines
153 | P a g e
Hardware components Remarks District / block kiosk
Fingerprint Scanner /
Reader Module
(1 in number)
► Thin optical sensor
► 500 ppi optical fingerprint scanner (22 x 24mm)
► High quality computer based fingerprint capture (enrolment)
► Preferably have a proven capability to capture good quality fingerprints in the Indian rural
environment
► Capable of converting fingerprint image to RBI approved ISO 19794-2 template.
► Preferably Bio API version 1.1 compliant
District and block kiosk
Camera
(1 in number)
► Sensor: High quality VGA
► Still Image Capture: up to 1.3 megapixels (software enhanced)
► Native resolution is 640 x 480
► Automatic adjustment for low light conditions
District and block kiosk
Smartcard Readers (2 in
number)
► PC/SC and ISO 7816 compliant
► Read and write all microprocessor cards with T=0 and T=1 protocols
► USB 2.0 full speed interface to PC with simple command structure
► PC/SC compatible Drivers
District and block kiosk
Smart card printer
► Supports Color dye sublimation and monochrome thermal transfer
► Edge to edge printing standard
► Integrated ribbon saver for monochrome printing
► Minimum printing resolution of 300 dpi
► Prints at least 150 cards/ hour in full color and up to 1000 cards an hour in monochrome
► Minimum Printing resolution of 300 dpi
► Compatible with Windows / Linux
► Automatic or manual feeder for card loading
► Compatible to Microprocessor chip personalization
► USB connectivity
► Printer with hardware/software protection to disallow unauthorized usage of printer
► Inbuilt encoding unit (ISO7816 and PCSC compliant) to personalize microcontroller chip
based contact cards in a single pass
► Smart card printing ribbon as required
District kiosk
Fingerprint scanner ► The fingerprint capture device at enrolment as well as verification will be single finger type
► Compliance with “fingerprint_image_data_standard_ver.1.0” mentioned on
District and block kiosk

RSBY Revised Process Guidelines
154 | P a g e
Hardware components Remarks District / block kiosk
www.egovstandards.gov.in. All specifications confirming to ”Setting level 31” will be
applicable for RSBY related enrolment and verification
► The images should be stored in .png format
Power backup ► UPS of capacity 860VA or higher
► Minimum 8 hours of power backup for specified hardware set
District and block kiosk
Telephone Line (1 Nos.) ► This is required to provide support as a helpline District and block kiosk
Internet Connection ► This is required to upload/send data/ access the web based software for RSBY District and block kiosk
Master Kiosk card ► The card issuance system should be able to personalize a 64 KB NIC certified SCOSTA smart
card for the RSBY scheme as per the card layout.
District and block kiosk

RSBY Revised Process Guidelines
155 | P a g e
Annexure 2.2: Information to be provided in Brochure
1. Details of benefits available under RSBY Scheme
► Facilities available
► Exclusion list
2. How to avail the benefits
3. Do’s and Don’ts
4. FAQs
5. Details of empanelled Hospitals
6. Toll Free Number
Annexure 2.3: Format for reporting Awareness and Sensitization workshop conducted by IC at district/block
S No Description Response Remarks
1 Date of Workshop
2 Venue
3 Person present in the workshop (attach attendance sheet)
4 Route Plan discussed (Y/N)
5 Changes suggested in route plan
6 Route plan finalised (Y/N)

RSBY Revised Process Guidelines
156 | P a g e
Annexure 2.4: Suggestive guideline for Route Planning
1. Route plan should be an iterative process
2. At first stage SCSP along with DKM should create a broad route plan for district, it should be a macro level plan and should be in following format
S.No. Block Population Number of village Estimated number of days required Tentative Start date Number of Kits required
3. This plan should be discussed and finalised in workshop conducted at District along with block/taluka level functionaries
4. In second stage representatives of SCSP and Block functionaries should prepare a micro plan in following format
Sr No
Name of village
Population Number of days required
Tentative Start date
Number of kits to be deployed
Proposed enrolment centre (School/Panchayat Bhavan etc.)
Name of FKO
Name of Supervisor (SCSP)
5. This plan should be discussed and finalised in workshop conducted with FKOs at Block level in following format
Sr No
Name of village
Population Number of days required
Date Number of kits to be deployed
Proposed enrolment centre (School/Panchayat Bhavan etc)
Name of FKO
Name of Supervisor (SCSP)
6. While finalising the route plan following points to be considered:
► It should cover each and every village of the district/block
► Villager should not be made to travel more than a kilometre for enrolment
► It should preferably start from the area where number of hospitals are more

RSBY Revised Process Guidelines
157 | P a g e
Annexure 2.5: Daily report and undertaking by FKO
Rashtriya Swasthya Bima Yojna Daily Report by Field Key Officer
Name-
Date Gram Panchayat
Block Village
Sr. No Activity Response Remarks
1 Arrival time of team
2 Enrolment start time
3 Enrolment completion time
4 Number of kits required as per route plan
5 Number of kits available
6 Number of kits in working condition
7 Number of kits actually used
8 Number of beneficiary family as per route plan
9 Number of families enrolled today
8 Whether IEC material were used at enrolment station If yes give the details
9 Whether brochures were given to each beneficiary
10 Whether plastic cover were given along with card
11 Whether cards were given on the spot
12 How much money was collected from each family
13 Have you received any incentive for this work

RSBY Revised Process Guidelines
158 | P a g e
UNDERTAKING BY THE FIELD KEY OFFICER
I, _________________________________________ Designated as Field Key Officer for Rashtriya Swasthya Bima Yojna as per following:
Date and Duration:
Village (s) Name:
Block:
District:
State:
Hereby, declare that I was present at the RSBY enrolment station and have performed all the tasks assigned to me to the best of my ability.
Total number of RSBY families, which were enrolled and, verified by me are _________
SIGNATURE Name
Designation
Date:

RSBY Revised Process Guidelines
159 | P a g e
Annexure 3.1: Data fields on the beneficiary RSBY card
Balance on Card
Field Data
Issue date Card issue date
Validity Card validity date
Balance Available Balance
BalModDat Last Balance Modified date
AddOnBal Available Balance for add on packages.
AddOnBalModDate Last Add on Balance Modified date
Policy Extension file
Field Data
Policy No Policy Number
Policy validity Validity of policy
ExtBy Extension of Policy by card-ID (Authority ID)
ExtAt Extension of Policy at Kiosk (Kiosk Code)
ExtUpDate Extension Update Date
ExtBalance Balance
Mortality Information File
Field Data
Member-ID Member ID
Mortality Mortality (Y/N)

RSBY Revised Process Guidelines
160 | P a g e
Annexure 3.2: Beneficiary card specifications Card Specifications
► Microprocessor based Integrated Circuit(s) card with Contacts, with minimum 64 Kbytes available EEPROM for application data or enhanced available EEPROM as per guidelines issued by MoLE.
► Compliant with ISO/IEC 7816-1, 2, 3 ► Compliant to SCOSTA 1.2b Dt. 15 March 2002 with latest addendum and errata ► Supply Voltage: 3V nominal. ► Communication Protocol T=0 or T=1. ► Data Retention: minimum 10 years. ► Write cycles: minimum 300,000 numbers. ► Operating Temperature Range: –25 to +70 degree Celsius. ► Plastic Construction PVC or Composite with ABS with PVC overlay ► Quality Assurance: The compliance certificates will be provided for the quality test under taken with each lot of supply for the processes involved
such as gold plating, chip bonding etc. ► The chip module will be sourced from OEM or their authorized distributors / partners ► Surface: glossy
Card layout
The detailed visual & machine readable card layout including the background image to be used is available on the website www.rsby.gov.in. It is
mandatory to follow these guidelines for physical personalization of the RSBY beneficiary card.
For the chip personalization, detailed specification has been provided in the RSBY KMS document available on the website www.rsby.gov.in. Along with
these NIC has issued specific component for personalization. It is mandatory to follow these specifications and use the prescribed component provided by
NIC.
Chip operating system
► SCOSTA-CL (latest copy of SCOSTA from http://scosta.gov.in)
► Valid SCOSTA-CL compliance certificate from NIC
► Chips will be security certified to common criteria EAL+4 or more

RSBY Revised Process Guidelines
161 | P a g e
Chip security
► Chip module will be manufactured in EMV certified facility
► The derived key though the Key Management System (KMS) will be embedded into the chip during fabrication
Card Body
► The artwork of the design for the card body with all security features will be done through the National Institute of Design – Ahmedabad.
► The card body will be of glossy surface, PETG (50%) plastic construction sandwiched between PVC layers with overlay to allow colour dye
sublimation (dye diffused thermal transfer) printing.
► Operating ambient temperature range should be -25 degrees Celsius to +70 degree Celsius
Visual security
► Guilloche Pattern
► Micro text
► Card serial number will be printed on the card for traceability

RSBY Revised Process Guidelines
162 | P a g e
Annexure – 4.1: Components of wellness check
Components Elements
Establishment of the beneficiary’s medical/family history
At a minimum, collect and document the following:
1. Medical events in the beneficiary’s parents and any siblings and children, including diseases that may be hereditary or place the beneficiary at increased risk;
2. Past medical and surgical history, including experiences with illnesses, hospital stays, operations, allergies, injuries, and treatments; and
3. Use of or exposure to medications and supplements, including calcium and vitamins
An assessment can be undertaken by Medical or Para Medical staff posted at the Institution
Obtain the following measurements: (minimum)
1. Height, weight, body mass index (or waist circumference, if appropriate), and blood pressure; and
2. Other routine measurements like Urine Sugar/ Albumin, Hb% ,and PS for MP or any other investigations as deemed appropriate, and available at the intuition based on medical and family history
Treatment 1. Fever or general complaints.
2. Preventive Immunizations 3. Collection / utilization of Family welfare services
Counselling and advise For availing benefits under different schemes
1. Family welfare and immunization activities 2. Counselling for HIV/STD if available

RSBY Revised Process Guidelines
163 | P a g e
Annexure 4.1 (a): Health Check Template
1. Demographic Information: to be populated from the card.
2. Capture the mobile number and Aadhar number or NPR number if not captured at the time of enrolment or if they are not same.
The following information can be stored on the beneficiary card and this information can be seen and populated by use of TMS at any hospital and is useful
at the time of emergency when the patient is unconscious.
a. Patient History:
1. Habits: 1. Smoking 2. Alcohol 3. Drug abuse
2. History of pre-existing conditions: 1. Hypertension 2. Diabetes 3. Asthma, chronic bronchitis 4. Bleeding Disorders 5. Epilepsy
3. History of allergies 1. Penicillin 2. Sulpha 3. NSAIDs
3. History of immunisation. These details should again be recorded through a template (i.e. Providing selection in a check-box format) It shall be recorded for below mentioned categories:
a) children of up to 5 or 6 years: 1. Fully immunised as per national schedule 2. Partially immunised - if any of the vaccinations are not taken. 3. If No immunisation
b) Pregnant women: 1. TT 2. TT2
4. History of Previous surgery. (Major procedure only)
1. Head 2. Neck 3. Thorax 4. Abdomen 5. Bone 6. Ob & Gyn

RSBY Revised Process Guidelines
164 | P a g e
2. Patient parameters.
1. Height: ( in cms) 2. Weight: ( in kgs) 3. BMI – automatically calculated
4. Blood Pressure: 1. Normal range. 2. Border line 3. Abnormal
5. Blood Group.
1. A Positive 2. A- Negative 3. B- Positive 4. B- Negative 5. AB- Positive 6. AB – Negative
7. O- Positive 8. O- Negative
Along with the above information the following information can be stored on central web application.

RSBY Revised Process Guidelines
165 | P a g e
RASHTRIYA SWATHYA BIMA YOJANA
WELLNESS CHECK SCHEDULE:
Name of the PHF: District: State:
Date of wellness check: Time start: Time end:
Name of the beneficiary:
S/o , D/o ,W/o
Smart card URN number
Mobile number / Telephone number of the beneficiary
To be collected from the smart card
Name of the PHF personnel doing wellness check:
Date of wellness check: Time start:
Time end
1. Patient History
Web entry made and
uploaded on ------------------

RSBY Revised Process Guidelines
166 | P a g e
1. Habits: 1. Smoking Yes / No
2. Alcohol. Yes / No
3. Drug abuse Yes / No
2. H/O pre-existing conditions: 1. Hypertension Yes / No
2. Diabetes Yes / No
3. Asthma, chronic bronchitis Yes / No
4. Bleeding Disorders Yes / No
5. Epilepsy. Yes / No
3. H/o allergies
1. Penicillin Yes / No
2. Sulpha Yes / No
3. NSAIDs Yes / No
4. H/O of immunisation
children of up to 5 or 6 years:
1. Fully immunised as per national schedule Yes / No
2. Partially immunised,- if any of the vaccinations
are not taken.
Yes / No
3. if No immunisation Yes / No
Pregnant women 1. TT Yes / No
2 TT2 Yes / No

RSBY Revised Process Guidelines
167 | P a g e
5. H/O of Previous surgery. (Major
procedure only)
1. Head Yes / No
2. Neck Yes / No
3. Thorax Yes / No
4. Abdomen Yes / No
5. Bone Yes / No
6. Ob & Gyn Yes / No
6. Present complaints H/o of cough for more than 15 days. Yes / No
Sputum with blood. Yes / No
Chest pain with palpitation Yes/ No
Rapid weight loss during last 3 months Yes/ No
Pain and blood in urine Yes/ No
Any episodes of unconsciousness Yes/ No
Blood in stools during/ after defecation. Yes / No
Not able to see properly. Yes/ No
Fever Yes/ No
Is the women Pregnant Yes / No
For women Pain and bleeding during Menses. Yes/ No
Any mass or lump in the breast Yes/ No

RSBY Revised Process Guidelines
168 | P a g e
Any mass protruding out and down from below Yes / No
If the answer is Yes to any of the questions at 6, refer for treatment.
7. Patient parameters 1. Height ( in cms)
2. Weight: ( in kgs)
3. BMI – automatically calculated.
4. Blood Pressure
5. Blood Group
6. Haemoglobin
7. Urine Sugar
8. Urine Albumin
8. Treatment Provided Fever or general complaints. Yes/ No
Preventive Immunizations: Yes/ No
Collection / utilization of Family welfare services
Yes/ No
9. Counselling and advise 1. Family welfare and immunization activities
Yes/ No
2. Counselling for HIV/STD if available
Yes/ No
Signature or Signature of MO/ Para medic Thumb impression of beneficiary

RSBY Revised Process Guidelines
169 | P a g e
Annexure 5.1: Empanelment criteria for hospitals
Criteria for empanelment of Public Health Care Providers All Government hospitals as decided by the State Government (including Community Health Centres) and Employee State Insurance Scheme
hospitals shall be empanelled provided they possess the following minimum facilities
a. Telephone/Fax, b. An operational pharmacy and diagnostic test services, or should be able to link with the same in close vicinity so as to provide ‘cashless’
service to the patient. c. Maintaining of necessary records as required and providing necessary records of the RSBY patients to the Insurer or his representative/
Government/Nodal Agency as and when required. d. A Bank account which is operated by the health care provider through Rogi Kalyan Samiti or equivalent body.
Criteria for empanelment of Private Health Care Providers The criteria for empanelling private hospitals and health facilities would be as follows:
a. At least 10 functioning inpatient beds or as determined by State Nodal Agency. The facility should have an operational pharmacy and diagnostic test services, or should be able to link with the same in close vicinity so as to provide ‘cash less’ service to the patient.
b. Those facilities undertaking surgical operations should have a fully equipped Operating Theatre of their own. c. Fully qualified doctors and nursing staff under its employment round the clock. d. Maintaining of necessary records as required and providing necessary records of the insured patient to the Insurer or his representative/
Government/Nodal Agency as and when required. e. Registration with Income Tax Department. f. Telephone/Fax.
IT Infrastructure needed for empanelment in RSBY a. Both public and private health care providers which fulfil the criteria for empanelment and are selected for empanelment in RSBY by the
Insurance Company or their representatives will need to put in place infrastructure (hardware and software) as per requirement b. The Insurer shall be responsible for providing and installing the entire IT infrastructure (i.e., hardware and software) for each public
Empanelled Health Care Provider in a district before commencement of enrolment in that district. c. Each private Empanelled Health Care Provider will be responsible for providing and installing the entire IT infrastructure (i.e., hardware
and software) before commencement of enrolment in the district where such Empanelled Health Care Provider is located.
It is the responsibility of the hospitals to ensure that the system is running at all times and to inform the concerned SCSP/TPA which has installed the
system, in case there are any problems related to it’s proper use as required.

RSBY Revised Process Guidelines
170 | P a g e
Annexure 5.1 (a): Hardware specifications for hospital and PHC’s
The following are the hardware and software specifications for hospitals and PHC’s where wellness checks can also be carried out.
► Depending on RSBY turnaround sufficient number of desktops or laptop systems with dual core processor with 2 GHz, 80 GB hard disk drive, DVD
R/W drive, 2 GB RAM, graphics card, minimum 4 USB ports etc.
► Other software environment shall be as below:
a. Centralized TMS software b. Licensed MS windows 7 Operating System 32/ 64 bit or above
c. Microsoft.NET Framework 3.5 or above d. MySQL database, ODBC connectivity e. Microsoft crystal reports
f. Drivers for all the peripherals (printer, fingerprint scanner, smart card reader etc.)
► Printer (laser/dot matrix/inkjet etc.)
► Finger print scanner (one with each computer system) – One biometric fingerprint recognition device to be connected to desktop through USB port
with the following configuration:
a. 5v DC 500mA (supplied via USB port)
b. Operating temperature range: 0c to 50c
c. Operating humidity range: 10% to 90%
d. Compliance: FCC home or office use, CE and C-Tick
e. 500 dpi optical fingerprint scanner (22 x 24 mm)
f. USB 1.1 or above interface
g. Drivers for the device should be available on windows or Linux platform
h. Should provide PNG image as well as templates as per ISO 19794 and Minex format
i. Capable of converting fingerprint image to RBI approved ISO 19794 and Minex template
► Smart Card reader (two for each computer system) – two smart card readers with the following configuration:
a. PCSC and ISO 7816 compliant
b. Read and write all microprocessor cards with T=0 and T=1 protocols
c. USB 2.0 full speed interface to PC with simple command structure
► Internet connectivity for data transfer to SNA, central server etc.
► Externally powered USB hub with minimum 4 ports

RSBY Revised Process Guidelines
171 | P a g e
Annexure 5.1 (b): Hardware specifications for hospital and PHC’s
The following are the hardware and software specifications for tablets to be used in hospitals and PHC’s where wellness checks can also be carried
out in the event that desktop/laptop are not available.
S. No. Hardware description for tablet PC Specifications 1 Processor Cortex A8-1GHz 2 RAM 512 MB 3 Internal memory 4 GB 4 Memory (expandable) 32 GB 5 LCD screen 7 inch 6 LCD resolution 1024 x 600 7 Touch sensitivity Resistive/capacitive 8 Operating system Android 4.0 (ICS) 9 Video HD 720p 10 Battery Lithium polymer 4000 mAH 11 Battery life 4 hours 12 USB ports 2 Nos 13 Micro SD card slot 1 Nos
14 Wi-Fi connectivity Available 15 Bluetooth connectivity Available 16 3G dongle connectivity Available (external) 17 TV connectivity HDMI 18 Camera 3 MP 19 Audio jack 3.5 mm 20 MIC Inbuilt 21 Documents supported DOC, DOCX, XLS, XLSX, PPT, PPTX, Adobe flash 10.1 support 22 Audio format MP3, WMA, AAC, AMR, m4a, mp2, off, WAV, 3gp, 3gpp 23 Video format MPEG2, MPEG4, AVI, FLV, 3GP, MOV, DIVX, WMV
24 Multimedia display PNG, JPG, BMP, TIFF and GIF display 25 Adaptor 5V, 2A 26 Operating temperature 0 degrees Celsius to 50 degrees Celsius

RSBY Revised Process Guidelines
172 | P a g e
27 Storage temperature -20 degrees Celsius to +70 degrees Celsius 28 Weight 400 gms 29 Dimension 203 x 120 x 12 mm
Other specifications at PHC:
a. Other software environment will be as below:
i. PHC “wellness check” software
ii. Sqlite database
iii. Drivers for all peripherals (printer, fingerprint scanner, smartcard reader)
b. Printer (laser/inkjet etc.)
c. Finger print scanner (one in each desktop/laptop/tablet PC system)
d. One biometric fingerprint recognition device to be connected to desktop/laptop/tablet PC through USB port with the following
configuration:
i. 5V DC 500mA (supplied via USB port)
ii. Operating temperature range: 0 degrees Celsius to 50 degrees Celsius
iii. Compliance: FCC Home or Office use, CE and C-Tick
iv. 500 dpi optical fingerprint scanner (22 x 24 mm)
v. USB 1.1 or above interface
vi. Should provide PNG image as well as templates as per ISO 19794 and Minex format
vii. Capable of converting fingerprint image to RBI approved ISO 19794 and Minex template
e. Smart card reader (two for each desktop/laptop/ tablet PC system) – two smart card readers with the following configuration
i. PCSC and ISO 7816 compliant
ii. Read and write all microprocessor cards with T=0 and T=1 protocols
iii. USB 2.0 full speed interface to PC with simple command structure
f. Internet connectivity for data transfer to SNA, central server etc.
g. External powered USB hub with minimum 4 ports

RSBY Revised Process Guidelines
173 | P a g e
Annexure 5.2 Triggers for audit of hospitals
S. No. Triggers Remarks
1 RSBY admissions exceeding the registered bed strength of the hospital.
Refer the empanelled form/ information collected
2 Patient blocked/ transacted for discipline not available in the hospital.
Refer the empanelled form/ information collected
3 Same type of transactions happening / blocking of claims happening during fortnight.
The claim data to be analysed and flagged.
4 The claim transaction pattern different from the transaction pattern of the district.
The transactions of other hospitals with similar infrastructure to be matched.
5 Claim/ transactions with gender disparity Claims/ transactions which can only happen in females are blocked for male patients and vice versa
6 Claims/ transactions with age specificity Claims / Transactions are blocked for procedures which are unusual for a particular age.
7 All High value procedures above INR 15000 All high value transactions are high end procedures and require infrastructure and specialist services and needs to be investigated and verified.
8 Patient blocked for Hysterectomy - vaginal and abdominal
Commonly abused procedure
9 Patient blocked for Caesarean Section Commonly abused procedure
10 Patient blocked for Cholecystectomy and GB procedures.
Commonly abused procedure
11 Patient blocked for multiple procedures.
12 Use of frequent over ride codes for patient authentication.
This facility is commonly misused.
13 Any organ removal - cataract, appendix, GB etc.
To match the URN for past procedures if any.
14 Unusual increase in number of transaction Atleast more than 25 percent of average admissions per day for the hospital
15 Locality specific pattern of admissions To match the claims with area at backend.
16 Frequent Inter district claims / blocking To check the catchment of the hospital

RSBY Revised Process Guidelines
174 | P a g e
S. No. Triggers Remarks
17 Unusual increase in number inter district claims/ blocking
18 Blocking of Blood transfusion. To check whether the hospitals follows NBTC guidelines.
19 Frequent breakdown of software and hardware To check for tempering.
20 Transaction on hot listed card.
21 Similar pattern of admission and claim blocking
Say - blocking all medical admissions for 3 days
22 Patient blocked for ICU for more than 7 days
Annexure 6.1: Claim Rejection Reasons and codes under RSBY
The Insurance Companies receives the claims from hospitals through electronic data. The claims should be settled within 30 days of the receipt.
While rejecting claims, insurance company should select the reasons from the drop down. List of frequently used reasons along with reason codes are
listed down below:
S. No. Code Reject Reason
1 R0001 Data not uploaded within 7 days of transaction (transaction done within 24 hours of discharging patient).
2 R0002 Data not uploaded within 7 days of transaction and also Transaction not done within 24 hours of discharging patient.
3 R0003 Transaction not done within 24 hours after discharge
4 R0004 Patient stay in hospital is >24 hours (It is not a Day care package).

RSBY Revised Process Guidelines
175 | P a g e
S. No. Code Reject Reason
5 R0005
Normal pre and postsurgical expenses are included in package. Hence General ward/ICU shall not be payable in continuation and prior
to Package. Payment for this service is included in the payment of major package blocked on the same day/admission. (Extending
patient beyond of LOS of surgical package requires written intimation with the TPA/ Payment for this service is included in the
payment for a related service performed on the same day.)
6 R0006 No investigation brief, indications of admissions, disease description, and line of treatment mentioned with package blocked.
7 R0007
The surgery package blocked is already included in previous major surgery blocked. It is the utilization of multiple codes, require
additional information/ similar procedure done in same admission and this is not justified. Hence claim not admissible. (mention the
first major package)
8 R0008 Registering, Blocking, Discharging transactions in 0 LOS.
9 R0009 Registering, blocking, discharging transactions in ___ duration for Day Care procedures
10 R0010 During the course of investigation it reveals that the hospital involves in the practice of charging money to patient. (TPA will confirm
it).
11 R0011 Patient and hospital admission documents (medical documents, registration of patient in admission register etc.) not found in hospital
of URN and package blocked. (If patient is not present at the time of visit, check with case file).
12 R0012 Procedure done does not match the diagnosis.
13 R0013 Rejected as deficiency of medical documents (specify the kind medical documents required, basis also).
14 R0014 Duplicate claim – twice uploaded for same Hospitalization
15 R0015 Hospital was found to be involved in a major fraud.

RSBY Revised Process Guidelines
176 | P a g e
S. No. Code Reject Reason
16 R0016 Claims rejected in case of policy exclusions.
17 R0017 Member not enrolled.
18 R0018 Patient not required hospitalization.
19 R0019 OVERWRITING / MALPRACTICE
20 R0020 FP/BCP code Mismatch
21 R0021 Age/Gender Mismatch
22 R0022 Directly Discharge from ICU
23 R0023 Claim Rejected under Hotlist Card
24 R0024 Rejected as deficiency of medical documents (specify the kind medical documents required, basis also).
25 R0025 Rejected as the diagnostic package is blocked independently which is against RSBY guidelines
26 R0026 Rejected due to as per package list length of stay (LOS) is ------------- days but patient admitted & discharged in ------------- days
27 R0027 Rejected due to pre-Authorization was not taken prior to performing hysterectomy on patient below 40 yrs of age as per MOLE
guideline

RSBY Revised Process Guidelines
177 | P a g e
Apart from this a claim can be rejected on following grounds as well:
A. Fraud Related Reasons
1. During the course of investigation it is found that the hospital is involved in the practice of charging money from the patient even when the smart
card has balance left
2. Patient not found during hospitalization during a visit
3. The patient was not admitted & did not avail In-Patient treatment in the hospital
4. During Audit/Investigation Treatment not taken by patient proved and admitted
5. Unjustified blocking of higher-priced package(s) for the provided diagnosis
6. Connivance with beneficiaries for a claim without any ailment or treatment
7. Impersonation in connivance with cardholder
8. Procedure done does not match the diagnosis
9. Showing admission in ICU though treatment is being/was treated in general/ private wards.
10. The surgery package blocked is already included in previous major surgery blocked
11. Rejected due to patient directly discharged from ICU
12. Since minimum stay of 24 hours is required in the hospital by the patient, if the patient stay in hospital <24 hours (It is not a Day care package)
13. The disease/ailment is excluded in RSBY guideline
14. During investigation admission documents not found or incomplete in hospital
B. Policy Related Reasons 1. The pre-authorization was not taken prior to performing hysterectomy on patient below 40 years of age as per MOLE guidelines

RSBY Revised Process Guidelines
178 | P a g e
Annexure 7.1: Structure of Grievance Redressal Committee at district, state and national level
a. National Grievance Redressal Committee (NGRC):
The National Grievance Redressal Committee (NGRC) is formed by MoLE much before the commencement of the enrolment process with the following members:
1. Chairman - Additional Secretary (L&E), MoLE
2. Member – Joint Secretary & Chief Vigilance Officer, MoLE
3. Convener - Economic Advisor / Deputy Director in DGLW Office
4. NGRC may also invite other experts / officers for their inputs in specific areas.
5. NGRC may also take assistance of Director (Vigilance) and Director (RSBY)
6. The Additional Secretary or nominee, Department of Financial Services would be invitee to the NGRC meeting
b. State Grievance Redressal Committee (SGRC):
1. Chairman or his nominee (but not below the rank of Commissioner) - State Principal Secretary/Secretary of Department handling RSBY
2. Convener - State Nodal Officer for RSBY/ State Grievance Nodal Officer for RSBY
3. Member - State Representative of the Insurance Company (if more than one insurance company is active in the State, then one insurance
company may be selected for a fixed period on a rotation basis). IC should be represented by MD/CEO or their representative capable of making
financial decisions
4. Welfare Commissioner (in charge of the State), MoLE, GoI
5. The SGRC can also invite other experts / officers for their inputs in specific areas.

RSBY Revised Process Guidelines
179 | P a g e
c. District Grievance Redressal Committee (DGRC):
1. Chairman - District Magistrate or an officer of the rank of Addl. District Magistrate or his nominee or Chief Medical Officer ( if different than DKMA)
2. Convener - District Key Manager/ District Grievance Nodal Officer
3. Member - Representative of the Insurance Company, capable of making decisions
4. The DGRC can also invite other experts / officers for their inputs in specific areas
5. The DGRC shall meet once a month to resolve all grievances in the district
6. District Coordinator from insurance company to be included in the DGRC

RSBY Revised Process Guidelines
180 | P a g e
Annexure 7.2: Investigative Teams to support the grievance redressal committees at national and state level:
The investigative teams are to be set up at national and state level by MoLE to support the national and state grievance committees in resolving
grievances where extensive ground investigation activities are to be conducted before arising on a final decision.
a. National investigative team
The following is the composition of the national investigative team
1. Government Officer of atleast Under Secretary level
2. Medical Officer (from Government / private sector) with atleast 10 years of experience
3. The NGRC may nominate another member to provide inputs on technical matters such as technology, actuarial science, legal etc. He may be
nominated on a case by case basis
b. State investigative team
The state investigative team shall be nominated by the state grievance redressal committee (SGRC). The investigative teams will submit their report within 15 days of the grievance / complaint being given to them for investigation. The following is the composition of the state investigative team
1. Government Officer nominated by SGRC
2. Depending on the nature of grievance, SGRC can nominate any other person of technical, legal, actuarial and any other experience on a case by case basis. (from Government / private sector)

RSBY Revised Process Guidelines
181 | P a g e
Annexure 7.3: List of possible grievances / complaints for various categories
1. List of possible complaints / grievances pertaining to enrolment and action
S.
No.
Possible grievance / complaint Type
1 Smart Card not prepared despite name in the list Complaint
2 Registration money collected but enrolment not done , photographs taken but card not given on the spot Complaint
3 Additional money demanded apart from registration fees for issuance of card Complaint
4 Poor quality smart card given /Hospital List not provided with the Smart card Complaint
5 Card given to someone by enrolment team /and the person is demanding money to return card Complaint/ Grievance
6 Enrolment team returned back without doing enrolment, enrolment team did not turn up for enrolment Complaint/ Grievance
7 Kiosk not functional/ closed Complaint/ Grievance
8 Operator at Kiosk demanding money for addition and doing modification in card/ issuance of duplicate card or
splitting of card.
Complaint/ Grievance
9 FKO not present at the time of enrolment Complaint/ Grievance
10 DKMA demanding money for certifying enrolment Complaint/ Grievance
11 District and block level exercises for enrolment preparatory activities not done Complaint/ Grievance
12 Enrolment teams not reaching on time Complaint/ Grievance
13 Overpromise by the IA/ TPA regarding deployment of number of enrolment teams and kits/ enrolment kits not
Complaint/ Grievance

RSBY Revised Process Guidelines
182 | P a g e
S.
No.
Possible grievance / complaint Type
deployed as planned
14 Non deployment of District personnel /absence of District personnel of Insurer of Insurer Complaint/ Grievance
15 Villages not visited and left out by the enrolment team Complaint/ Grievance
16 Adequate publicity not done for mobilization of beneficiaries. Complaint/ Grievance
17 Signed data / FKO data or Post enrolled data not provided on time Complaint / Grievance
2. List of possible grievances / Complaints pertaining to empanelment of hospitals
S. No. Possible grievance / complaint Type
1 Hospital not empanelled Enquiry
2 Hospital has applied online, but not empanelled. Enquiry
3 Hospital applied online, recommended by District committee but still not empanelled
Possible reasons:
District committee list is not received at State Nodal Agency (SNA)
MHC cards are not received:
SNA has not sent request for MHC cards
Cards area not generated
Cards have been received at SNA but have not been given to the hospitals MOU between the hospital and Insurance company is not signed.
Hardware is not available
Transaction software is not installed
Grievance

RSBY Revised Process Guidelines
183 | P a g e
S. No. Possible grievance / complaint Type
4 Hospital was part of RSBY network but not empanelled for the current round Grievance
5 Hospital complaints about in appropriate practices for empanelment Grievance
6 Hospital suspended/ De-empanelled during last policy period but not empanelled despite District committee
recommendations
Grievance
7 Hospital kept on watch list for no obvious reasons Grievance
8 Hospital suspended citing unusual claim transactions Grievance
9 Hospital suspended citing non adherence of MOU clauses Grievance
10 Hospital suspended citing Fraud and malpractices hospital Grievance
11 Hospital suspended following Fraud and malpractices reported in a hospital by new paper Grievance
12 Hospital suspended without following process Grievance
13 Hospital suspension following unsatisfactory reply to show cause notice Grievance
14 Hospital suspended but suspension not revoked even after 30 days.
1. Investigations by insurance companies not conclusive
2. Investigation not completed by Insurance company
Grievance
15 Hospital De- empanelled Grievance
16 Hospital complaint - inappropriate practices by the Insurance company and harassment. Grievance

RSBY Revised Process Guidelines
184 | P a g e
3. List of possible grievances / Complaints pertaining to Claims settlement and action
S. No. Possible grievance / complaint Type
1 Claim details / payment details not received Complaint
2 Delayed payments Complaint
3 Claims rejected without giving reasons Complaint/Grievance
4 IA asking for Case/ patient records for claim settlement Complaint
5 Pending payments Grievance
6 Claims rejected on flimsy grounds. Grievance
7 IC/ TPA demanding money or incentive for claim settlement Grievance
8 Claims rejected by IC - URN not found, chip serial number mismatch Grievance

RSBY Revised Process Guidelines
185 | P a g e
Annexure 8.1: Basic infrastructure for kiosk to provide services to RSBY beneficiaries
The insurance company will setup and operationalize the district/ block kiosk in all the project districts within 15 days of signing the contract with the
state government.
1. Location of the district kiosk: The district/block kiosk is to be located at the district/block headquarters at a place frequented and easily
accessible. The state government will provide a place at the district/block headquarters to the insurance company to setup the district/block
kiosk. It should be located at a prominent place which is easily accessible and locatable by beneficiaries. Alternatively, the insurance company can
setup the district kiosk in their own district office. Sitting and waiting space, utilities, and water facilities for the beneficiaries to be ensured.
2. Specifications of the district kiosk: The district/block kiosk should be equipped with at least the following hardware and software (according to
the specifications provided by the Government of India),
Hardware components for district and block kiosk27:
Hardware components Remarks District / block kiosk
Computer / Desktop PC
(1 in number)
► This should be capable of supporting all other devices required.
► It should be loaded with standard software as per specifications provided by the MoLE.
Configuration:
Desktop with dual core processor with 2 GHz, 80 GB hard drive, DVD r/w drive, 2 GB RAM, graphics
card, minimum of 4 USB ports etc.
District and block kiosk
Fingerprint Scanner /
Reader Module
(1 in number)
► Thin optical sensor
► 500 ppi optical fingerprint scanner (22 x 24mm)
► High quality computer based fingerprint capture (enrolment)
► Preferably have a proven capability to capture good quality fingerprints in the Indian rural
environment
► Capable of converting fingerprint image to RBI approved ISO 19794-2 template.
District and block kiosk
27
The hardware specifications provided is an indicative list and are subject to change depending on the decisions taken

RSBY Revised Process Guidelines
186 | P a g e
Hardware components Remarks District / block kiosk
► Preferably Bio API version 1.1 compliant
Camera
(1 in number)
► Sensor: High quality VGA
► Still Image Capture: up to 1.3 megapixels (software enhanced)
► Native resolution is 640 x 480
► Automatic adjustment for low light conditions
District and block kiosk
Smartcard Readers (2 in
number)
► PC/SC and ISO 7816 compliant
► Read and write all microprocessor cards with T=0 and T=1 protocols
► USB 2.0 full speed interface to PC with simple command structure
► PC/SC compatible Drivers
District and block kiosk
Smart card printer
(1 in number)
► Supports Color dye sublimation and monochrome thermal transfer
► Edge to edge printing standard
► Integrated ribbon saver for monochrome printing
► Minimum printing resolution of 300 dpi
► Prints at least 150 cards/ hour in full color and up to 1000 cards an hour in monochrome
► Minimum Printing resolution of 300 dpi
► Compatible with Windows / Linux
► Automatic or manual feeder for card loading
► Compatible to Microprocessor chip personalization
► USB connectivity
► Printer with hardware/software protection to disallow unauthorized usage of printer
► Inbuilt encoding unit (ISO7816 and PCSC compliant) to personalize microcontroller chip
based contact cards in a single pass
► Smart card printing ribbon as required
District kiosk
Fingerprint scanner
► The fingerprint capture device at enrolment as well as verification will be single finger type
► Compliance with “fingerprint_image_data_standard_ver.1.0” mentioned on
www.egovstandards.gov.in. All specifications confirming to ”Setting level 31” will be
applicable for RSBY related enrolment and verification
► The images should be stored in .png format
District and block kiosk
Power backup ► UPS of capacity 860VA or higher
► Minimum 8 hours of power backup for specified hardware set
District and block kiosk
Telephone Line (1 Nos.) ► This is required to provide support as a helpline District and block kiosk

RSBY Revised Process Guidelines
187 | P a g e
Hardware components Remarks District / block kiosk
Internet Connection ► This is required to upload/send data/ access the web based software for RSBY District and block kiosk
Master Kiosk card ► The card issuance system should be able to personalize a 64 KB NIC certified SCOSTA smart
card for the RSBY scheme as per the card layout.
District and block kiosk
Software components:
Software components Remarks District / block kiosk
Operating System
Vendor can adapt any OS for their software as long as it is compatible with the software
Suggestive software is: MS Windows 7 operating System 32/64 bit or above
District and block kiosk
System Software
The software for RSBY shall be provided by MoLE. Any updates and modifications shall be done with
instructions from MoLE.
The SCSP must ensure that the updated stand-alone software is provided to the kiosk operator
within 5 business days of the update.
District and block kiosk

RSBY Revised Process Guidelines
188 | P a g e
Annexure 8.2: Format for information display on hoarding / information board at kiosk
a. Facilities available at kiosk
b. Benefits under RSBY
c. Process of hospitalisation
d. Beneficiary rights
e. Do and don’ts for beneficiaries

RSBY Revised Process Guidelines
189 | P a g e
Appendix – I:
a. Roles and responsibility: Each individual officer / designate or department/ agency at the Central / State / District teams will hold a specific set of
responsibilities. The following describes the roles and responsibilities for each department/ agency / individual at the Central / State / District:
i. Ministry of Labour and Employment (MoLE):
► Issuance and periodic revision of guidelines benefits thereof for the scheme.
► Develop and provide qualifying criteria for empanelment and selection of different agencies like Insurance Company (IC), Third Party
Administrator (TPA), and Smart Card service Providers (SCSP), Audit agencies, IT agencies for software development etc.
► Develop RFP template for different process under RSBY
► Provide and support development of IT applications and software’s for the programme implementation like enrolment software, transaction
software, kiosk software, DKMA software etc.
► Develop Memorandum of Association (templates) between different stakeholders which can be used by the State Government and Insurance
Companies.
► In consultation with the States, development of such protocols and common standards as may be necessary to ensure effective functioning of the
RSBY scheme on a national basis. This would include determination of the protocol for national unique identification numbers for beneficiary
families, specification of the minimal technical standards of the smart card, ensuring timely transfer of the Central financing share of insurance
premium, establishment of common reporting protocols for states as part of scheme monitoring and such other design and implementation issues
considered necessary for the functioning of a coherent national system.
► Organizing periodic inter-ministerial meeting for coordination and convergence.
► Receive the beneficiary data from the state nodal agency (SNA) and checking it for internal consistency and duplication, generate URN, and
upload and map the approved data on the website within 7 days of receiving such data to the selected IC / SCSP.
► Receive the proposal from the SNA after they have selected the Insurance Company and place it before the Approval and Monitoring Committee
within 7 days of receiving such proposals from the SNA.
► Provide DKM and FKO cards within 7 days of receiving the request from the SNA along with the format for maintaining the record of these cards.
► Facilitate the appointment of District Information Officers (all selected districts for RSBY implementation) for selected CKGA functions as well as
upload and flow of DKMA data.
► Provide central contribution towards the premium for both new and renewal policy (if any) districts. The premium may vary between districts
during the year but the contribution and commitment for the premium shall be as per the following formula in consonance with Insurance Act,
1938. i.e. calculated as 75% of (X-60) + 60 (X being the premium amount per family).
► For both new and renewal set of districts, contribute premium as per the formula mentioned above to the insurance company selected for that
district.

RSBY Revised Process Guidelines
190 | P a g e
► Develop indicative package rate list and quality improvement parameters for RSBY hospitals.
► Develop training modules for different process and conduct TOT programmer for different stake holders.
► Provide technical guidance and assistance to the State Government and State Nodal Agency from time to time.
► Set up and monitor the functioning of National RSBY Toll free help line/call centre.
► Setting up of Complaints and grievance redressal management system (CGRMS).
► Setting up and functioning of National Grievance Redressal Committee (NGRC).
► Setting up and functioning of Program/ Technical Management division for - which would provide expert inputs to Central and State Governments
on matters pertaining to the design, implementation and monitoring/evaluation of the scheme implementation including external assistance and
cooperation.
► Organize National level reviews and conferences.
Conduct periodic reviews for monitoring the progress made in the project.
Commissioning short term evaluations, as well as special investigations as and when required.
i. State Nodal Agency (SNA): ► Identification of Districts to be taken up in for implementation of RSBY.
► Prepare BPL / other RSBY category data in the prescribed format as provided on the RSBY website www.rsby.gov.in conforming to
specifications laid down by Planning Commission for each project district and send the same to MoLE for internal consistency checking.
This process should be completed for the district before the scheme is launched. MoLE will upload the data on the RSBY website
(www.rsby.gov.in) after verifying the data and generating Unique Relationship Number (URN) for each target family.
► Advertise/tender for selection of Insurance Company for each of the identified districts as per the RFP document available on
www.rsby.gov.in. Only MoLE empanelled Insurance companies will participate in the tender.
► Form a committee for technical and financial bid evaluation. Committee shall have a Government nominee and may include technical
experts. Both the technical and financial evaluation shall preferably be done on the same day.
► Send the proposal in the prescribed format to the MoLE where it will be placed before the Approval and Monitoring Committee (A&M).
Once the proposal is accepted and approved by the committee SNA shall commence the implementation process.
► Prepare a contract document (MCA) to be signed with the selected Insurance Company (ies) based on the draft contract document
provided on the RSBY website www.rsby.gov.in.
► Appoint a District Key Management Authority (DKMA) for each of the identified districts. The SNA shall convey the details of the DKM to
MoLE at the earliest for issue of DKM card by CKGA.
► Providing DKMA Server including Smart card readers and fingerprint scanners at district headquarter within 10 days of signing of the
agreement with the IC.

RSBY Revised Process Guidelines
191 | P a g e
► Install DKMA software for issue of FKO cards and for downloading of data subsequently from FKO cards and uploading on central web
application.
► Set-up and staff State Nodal Agency (SNA) to implement the scheme in the State. The Nodal agency shall be appropriately staffed as per
GOI communications to carry out its functions effectively in implementing the scheme. This should be a separate legal entity under the
control of the state government. Most of the responsibilities of the state government could be executed by the SNA.
► Set up and staff district level offices for effective implementation of RSBY in the district. The district level units in addition to the DKMA
will house additional staff for assistance and better coordination.
► Constituting and conducting of interdepartmental meetings on a periodic basis (monthly) consisting of representatives of at least Labour,
Health and Rural Development Ministries in the state.
► Organize a state-level workshop wherein the MoU between Central and State Government will be signed. Preferably the Contract between
State Government and Insurance Company (ies) shall also be signed in this workshop.
► Provide assistance to the SCSP in the registration of beneficiaries and issue of smart cards by:
Identifying and appointing District Key Managers (DKM) before signing of the agreement with the insurance company and convey
the details to the Central Government within 5 days of signing the agreement with the insurance company.
Providing DKMA Server at District Headquarter within 7 days of signing of the agreement with the insurance company. Install
DKMA software for issue of FKO cards and for downloading of data subsequently from FKO cards.
Nominating Field Key Officers (FKO) in the required prior to commencement of enrolment. The FKO numbers shall be identified at
the time of signing of the agreement with the insurance company. (FKOs will jointly visit each enrolment station along with the
SCSP representative for the enrolment of the beneficiaries)
Receive DKM and FKO cards from MoLE and maintain the records of it in the web based application as well as in the format
prescribed by the SNA.
► Assist the insurance companies and SCSP in organizing district-level Workshops and ensure that all related officials participate in the
workshop.
► Provide support and assistance to the SCSP through the district and block level officials in the issuance of smart cards in the village by:
o Finalizing village-wise schedule with the SCSP.
o Helping to publicise the visit of the enrolment team in advance.
o Support in identifying location for the enrolment inside the village
o Ensure presence of nominated official FKO for authenticating cards at the time of issue.
► Retain Rs. 30/- collected from the beneficiary as registration fees for meeting administrative expenses in implementing the scheme at the
state.
► Make available the public health care facilities, such as district hospital and Community Health Centres (CHCs), for being considered for
‘network’ hospitals by the insurance company.

RSBY Revised Process Guidelines
192 | P a g e
► Ensure that sufficient number of hospitals have been empanelled before start of the enrolment of beneficiaries in the concerned district.
This may be done with the help of the district level officials.
► Ensure that the district and block kiosks are set up in each of the project districts/ blocks and are operational before the commencement
of the enrolment process in the district. Request the district administration to provide space for the district / block kiosks in a government
designated place which is easily accessible and well recognised. The SCSP may be asked to pay rent for the space provided.
► To ensure that the public hospitals are equipped with necessary hardware and software to enable transactions in the hospital through the
smart card. (These should be PC based systems as defined in Annexure-5. Identify at least two personnel in each hospital who would be
trained by the insurance company representatives to man the RSBY help desk at the hospital and ensure that the insurance company or
their representative provides training to these personnel about RSBY, usage of hardware and software at the hospital and conduct
transactions.
► Commitment for 25% contribution of the premium and for incurring the administrative costs. Procure the necessary approvals from the
concerned state departments to ensure timely flow of state contribution towards the premium as per the defined formula in consonance
with Insurance Act, 1938.
► Ensure timely release of premium of state share to the insurance company.
► Request MoLE for the release of central share of premium within 5 days of releasing state share of premium to the insurance company,
through the web based application.
► Transfer the central share of the premium to the insurance company within 20 days of the receipt of the amount from MoLE.
► Provide financial and technical support to the district level RSBY offices.
► Take necessary steps for improving the awareness level by organising different activities like health camps etc. through Civil Society
organisations/ NGOs/ experts to improve awareness and to facilitate access to health services.
► Putting in place mechanisms for incentivizing staff at various levels like FKO, hospitals, etc. to improve both enrolment, wellness check
and utilization.
► Facilitate, monitor and evaluate the implementation of the scheme as per the guidelines issued from time to time by MoLE and any
additional guidelines the state government itself shall adopt from time to time in relation to the scheme.
► Organize periodic review meetings with the Insurance Company to review the implementation of the scheme.
► Access the data from central server at MoLE to analyse data and MIS reports for monitoring implementation of the scheme and
performance of various stakeholders.
► Conduct evaluation of RSBY performance in the State. The process of selection of agencies for doing this independent evaluation and
tools involved therein has been provided on the RSBY website www.rsby.gov.in.
► Provide timely information, either directly or through the web application / in prescribed format as desired by MoLE from time to time.
The required information and the reporting format shall be intimated by MoLE.

RSBY Revised Process Guidelines
193 | P a g e
► Ensure resolution of complaints at state level by involving the insurance company, hospital or any other stakeholder against whom the
complaint has been filed.
► Participate in grievance redressal and ensure that SGRC report is available to NGRC and MoLE for resolution of grievances escalated to
NGRC.
ii. District Key Manager (DKM):
► A person of class -1 rank is designated as the District Key Manager (DKM)
► DKM may delegate additional authority, of equivalent rank, to work on his behalf or during his absence. Such an official will be known as
the Additional DKM.
► DKMA will send request to CKGA through SNA in a prescribed format for number of required Field Key Officer (FKO) cards.
► DKMA will receive the required number of cards from the CKGA through SNA.
► DKMA will be responsible for the safe custody of the cards in a safe place under a vault (or lock and key arrangement), and shall keep an
account of these cards through manual procedures as well as on the web based application.
DKMA would personalize and issue the FKO card after obtaining proper receipt from FKOs according to the specified schedule. The
data of issuance of cards will be stored on the DKMA computer automatically by the software and can be tracked. FKO card
personalization is done by using data and fingerprint of the designated FKOs stored in the database on the DKMA computer. In
case of change of FKOs, the DKM should re-personalize the card for new FKOs.
► DKMA will ensure upload of data from the FKO cards and retain the FKO cards post completion of enrolment process.
► Facilitate and coordinate the working of district RSBY committee for empanelment of adequate number of hospitals as well as ensure that
reputed hospitals are also empanelled, besides organizing periodic reviews for monitoring the progress of scheme implementation.
► Personalize and issue key cards to the hospitals and authorize the hospitals for RSBY transactions.
► As Member convener of District level grievance redressal committee, ensure regular meetings and compliance of directions issued.
► Provide space or make arrangement for establishment of district/ block kiosks and monitor its operations.
► Personalize and issue key cards to the kiosk and authorize the kiosk for operations.
► Support the insurance companies for organizing district level workshops and FKO training.
► Carry out awareness activities for enrolment and utilization of services under the scheme.
iii. Field Key Officer (FKO): The responsibilities of FKO can be categorized under pre-enrolment, enrolment and post enrolment phases.
Pre-enrolment activities:
► Receive personalized Master Issuance Card (FKO card) from the DKM after providing the fingerprint.

RSBY Revised Process Guidelines
194 | P a g e
► Receive information about the name of the village (s) and the location of the enrolment station inside the village where the FKO will
perform the enrolment.
► Receive the contact details of the SCSP or their field agency representative for enrolment process.
► Keep track of the date on which enrolment has to take place.
► Reach the enrolment station at the given time and date (Inform the SCSP and DKM a day in advance in case the FKO is unable to come)
► Ensure that the FKO card is personalized with his/ her details and fingerprints and is not handed over to anyone else at any time during
enrolment and post enrolment.
► Should ensure that at least 1 card for every 300 beneficiaries, expected at the enrolment camp, is issued to him i.e., in case the BPL list
for a location is more than 300, they should get more than 1 FKO card personalized with their details & fingerprint and carry with them for
the enrolment.
Post enrolment activities:
► Ensure that the BPL list is displayed at the enrolment station
► Identify the beneficiary at the enrolment station either by face or with the help of identification document (Can also make use of the Gram
Pradhan or any other person to correctly identify the beneficiary).
► Make sure that the enrolment team inputs the correct name, gender and age data of dependents in the field in case of any mismatch with
the already provided data.
► Make sure that the enrolment team is not ‘willingly’ excluding any member of the identified and verified BPL households for RSBY
enrolment.
► Immediately after card is printed, the FKO should validate the card by inserting his/ her smart card and provide his/her fingerprint for
personalizing the beneficiary card.
► Make sure that the enrolment team is issuing the smart card on the spot to the beneficiary.
► Make sure that the enrolment team is collecting only Rs. 30 from the beneficiaries and also issuing the beneficiary a receipt of the same
along with the card.
► Ensure that the details of all eligible (within RSBY limits of Head of family + spouse + 3 dependents) family members as per BPL list and
available at the enrolment station entered on the card, their fingerprints & photograph taken and recorded on the beneficiary card.
► Ensure that the enrolment team is providing a brochure to each BPL family along with the smart card
► Ensure that the smart card is given inside a plastic cover and beneficiaries are explained not to laminate it. The FKO should also ensure
that the national toll-free number is printed on the card cover provided to the beneficiary along with the card.
► If a beneficiary complains that their name is missing from the BPL list then make sure that this information is collected in the specified
format and shared with the district administration.

RSBY Revised Process Guidelines
195 | P a g e
► If all dependents of a beneficiary, eligible for enrolment are not present at the camp, they should be informed that a request for addition
to the card can be made at the district/block kiosk.
Post enrolment activities:
► Return the FKO card(s) to the DKM after the enrolment is over at the location(s) for which the FKO is responsible.
► At the time of returning the card, ensure that the enrolment data is downloaded from the card and that the number of records
downloaded is the same as the number verified at the enrolment camp. In case of any discrepancy, the difference should be conveyed to
the DKM and the card be sent to CKGA for technical resolution.
► Furnish a brief report of the enrolment process to the DKM along with a signed undertaking.
► Hand over the list of left out people, collected at the enrolment camp to the DKM.
► Receive the incentive from the State Government (if any).
iv. Insurance Company (IC):
► Enter into agreement with other insurance companies working in RSBY regarding usability of the same smart card across India at any of
the networked hospital. This will ensure that beneficiary can use his/ her smart card across India to get treatment in any of the
empanelled health care providers.
► Set up state and district level offices for RSBY implementation and coordination.
► The insurance company will necessarily need to complete the following activities before the start of the enrolment in the district:
Empanelment of adequate number of hospitals in each district
Printing of the booklets which is to be given to the beneficiaries with the smart cards or requisite information for the booklet is
provide to the SCSP for printing these booklets.
Ensuring availability of policy number for the district prior to enrolment.
Ensuring that the correct addition of insurance policy details and policy dates, i.e., start and end dates, to the central server.
Ensuring that contact details of the nodal officer of the Insurer, the nodal officer of the TPA and the nodal officer of the service
provider are updated on the RSBY website.
► Ensuring that hospitals adhere to the agreements as per RSBY guidelines.
► Send data related to hospitalization, claims raised, settled and paid and other aspects of the scheme to the central and state government
at periodic intervals (on a monthly basis as well as when desired).
► Take immediate remedial action on beneficiary feedbacks/complaints and update the results on the web application for reference of state
government/nodal agency/MoLE.

RSBY Revised Process Guidelines
196 | P a g e
► The Insurer will be responsible for ensuring that the functions and standards outlined in the RFQ for empanelment are met, whether direct
implementation rests with the Insurer or one or more of its partners under service agreements. It shall be the responsibility of the Insurer
to ensure that any service agreements with the organizations outlined above provide for appropriate recourse and remedies for the
Insurer in the case of non- or partial performance by such other organizations.
► Ensure that the hospitals are raising claims within 7 days of the discharge of the beneficiary.
► Capture the facilities and treatments provided by the empaneled hospitals and publish the same on the RSBY website post this data has
been verified by MoLE.
► Update the packages as and when revisions take place in the procedures and convey the changes to SNA and MoLE within 3 days of
making the change.
► Manage and the empanelment and de-empanelment process for hospitals and monitor hospitals on a regular basis.
► Empanel another hospital within the area in the event of de-empanelment of hospital to maintain the number and spread of hospitals.
► Adhere to the SLA’s for claim settlement and payment to hospitals.
► Participate in periodic reviews and coordination meetings of SNA and Districts.
► Participate in state and district level grievance committees.
► Provide requisite training to SNA, DKM, SCSP and hospital staff pertaining to policy and system usage.
► Provide IEC activities post enrolment for beneficiaries, by ensuring detailed hoardings/ information boards at the empaneled hospitals.
v. Smart card service provider (SCSP): ► To provide a route map to the SNA, DKM and FKO prior to commencement of enrolment process
► To manage and drive the enrolment process by enrolling maximum beneficiaries
► To manage and operate the district/block kiosk
► To provide, install and maintain the smart card related infrastructure at the public hospitals. They would also be responsible for training all
empanelled hospitals on the RSBY policy as well as usage of the system along with the IC.
► Provide for Annual Maintenance Contract (AMC) of the equipment supplied at public hospitals and PHF’s.
► Facilitate field audit at enrolment stations and hospitals on a regular basis.
► Provide IEC and BCC activities, especially for the enrolment process (prior to commencement of enrolment).
vi. Hospitals or Health Care Providers:
► Private hospitals shall ensure that the requisite hardware is procured and functional prior to applying for empanelment under RSBY.
► Ensuring cashless treatment to the RSBY beneficiary.
► Display status of being an empanelled provider of RSBY in the prescribed format given by State Nodal Agency outside/ at their main gate.

RSBY Revised Process Guidelines
197 | P a g e
► Provide a functional help desk for giving necessary assistance to the RSBY beneficiaries. At least two persons in the hospital will be
nominated by the hospital that will be trained in different aspects of RSBY and related hardware and software by the insurance company
and SCSP.
► Display the RSBY information poster near the reception/admission desks along with the other materials supplied by the insurance
company for the access of beneficiaries. The template of empanelled status and poster for reception area will be provided by the SNA.
► Present claims on the insurer electronically through the web based application. The empanelled health care providers shall avoid making
manual claims.
► Update hospitalisation data of RSBY patients electronically on a daily basis such that it reflects in the central server.
► Maintain such records and documentation as are required for the insurance company to pre-authorise treatments and process claims.
► Cooperate with the insurance company and the SNA and provide access to all facilities, records and information for the conduct of audits
or any other performance evaluations of the performance by the empanelled health care provider.
► Comply with the provisions of all applicable laws, statutes, rules and regulations, as amended from time to time.
vii. Public health facilities / Center (PHF / PHC): ► Provide pre-designed basic wellness check for the enrolled RSBY beneficiaries as per the format mentioned in Annexure 4.1 (a).
► Ensure that basic wellness check data is stored on the card of the beneficiary before he leaves the PHC.
► Display and provide information about the facilities available free cost at the wellness check centre.
► Provide treatment to the common ailments to the beneficiaries.
► Provide counselling services about health conditions to the beneficiaries.
► Upload data on basic wellness check to central server.
viii. Welfare Commissioner:
► The data of the beneficiaries is to be updated once in six months. It is the responsibility of the welfare commissioner to coordinate with the
respective departments in the state for providing the MoLE/SNA with updated data of all beneficiaries.
► The welfare commissioner shall also extend his support to the SNA during the data collection process / pre-enrolment stage by ensuring
timely receipt of data from the state departments for the enrolment process.
ix. District Informatics Officer (DIO):
► The DIO shall be responsible to personalize the DKM card received from MoLE ensuring that all the details of the DKM have been stored
(including biometrics).

RSBY Revised Process Guidelines
198 | P a g e
x. District/ block kiosk:
► The kiosk shall provide RSBY services such as modification / updation, card split (at district), card replacement (at district) to the
beneficiary.
► Upload the transaction data on the central server if done through the stand-alone module.
► Submit request for enrolment in RSBY by a beneficiary to the SNA.
► Enter complaints/ grievances from the beneficiaries on the CGRMS.
xi. Role of Pensioners
Since RSBY is being implemented at grass root level i.e. Panchayats/block/ward level there are large number of retired civil and defence
pensioners at these locations. It is felt that their services can be utilized in various ways for benefit of the beneficiaries.
The Registered Associations for civil pensioners and pensioners who have retired from defence/para military forces at
district/panchayat/ward level could be engaged by the SNA for the services. The SNA would decide the qualification of pensioners to be
engaged as per their requirement. An honorarium could be paid to pensioners by SNAs out of administrative expenses through Registered
Associations of the Pensioners based on the criteria of payment of honorarium to the Block Level Officers (BLO) by the Election
Commission.
The pensioners could perform following functions:
► Awareness generation amongst the target groups about their eligibility, process of enrolment and guiding them at the
enrolment stations.
► During the enrolment, guide them to nearest PHC/ hospital for wellness checks.
► Ensure that the beneficiaries are informed by the stakeholders about any change in the enrolment schedule/extension in
policy end, if any.
► Assisting the beneficiaries at empanelled hospitals and educating them at the hospital to avail the benefits
► Facilitate the beneficiaries in the registration and discharge process in the hospital
► Surprise visits to hospitals/enrolment stations to collect feedback from the beneficiaries in the format designed by SNA






![RSBY Studies in Chhattisgarh - Planning Commissionplanningcommission.nic.in/data/ngo/csw/csw_rsby.pdf · Key findings from Final Report on Evaluation of RSBY in Chhattisgarh [CTRD]](https://static.fdocuments.net/doc/165x107/5b8c9d5b09d3f23b638d47a3/rsby-studies-in-chhattisgarh-planning-commissi-key-findings-from-final-report.jpg)