
Rome, 11 april 2008 Progress in treatment of pancreatic cancer Mariacristina Di Marco S.S.D....
91
Rome, 11 april 2008 Progress in treatment of pancreatic cancer Mariacristina Di Marco S.S.D. Oncologia Medica Prof.G.Biasco Istituto di Ematologia ed Oncologia Medica L. & A. Seragnoli Alma Mater Studiorum, Università di Bologna
-
Upload
priscila-kerridge -
Category
Documents
-
view
215 -
download
0
Transcript of Rome, 11 april 2008 Progress in treatment of pancreatic cancer Mariacristina Di Marco S.S.D....

Rome, 11 april 2008
Progress in treatment of pancreatic cancer
Mariacristina Di Marco
S.S.D. Oncologia Medica Prof.G.Biasco
Istituto di Ematologia ed Oncologia Medica L. & A. Seragnoli
Alma Mater Studiorum, Università di Bologna

Ten Leading Cancer Types for the Estimated New Cancer Cases and Deaths, by Sex, United States, 2008

• 15-20% of patients present resectable disease at the time of diagnosis;
• median life expectancy is 3 to 6 months for metastatic disease and 6 to 10 months for non metastatic disease;
•1-4% will be alive at 5 years.
Pancreatic cancer
Sultana A et al.: J Clin Oncol. 2007 Jun 20;25(18):2607-15


Pancreatic cancer: a majortherapeutic challenge
Most patients are not able to have surgery
Gemcitabine has been the standard of care for patients with advanced disease1
Little progress in improving clinical outcomes over the last decade
Treatment options remain limited
1Burris H, et al. J Clin Oncol 1997;15:2403–13
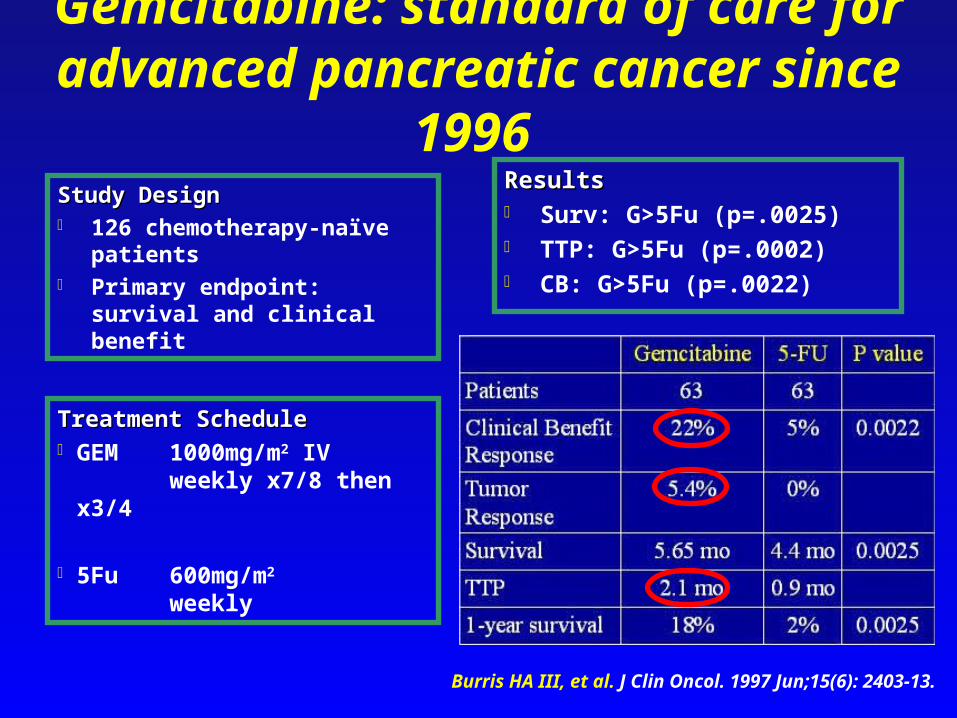
Gemcitabine: standard of care for advanced pancreatic cancer since 1996
Study DesignStudy Design 126 chemotherapy-naïve
patients Primary endpoint: survival and
clinical benefit
ResultsResults Surv: G>5Fu (p=.0025) TTP: G>5Fu (p=.0002) CB: G>5Fu (p=.0022)
Treatment ScheduleTreatment Schedule GEM 1000mg/m2 IV
weekly x7/8 then x3/4
5Fu 600mg/m2 weekly
Burris HA III, et al. J Clin Oncol. 1997 Jun;15(6): 2403-13.



Head-to-head studiesHead-to-head studies
Phase III trials

GEM vs. Marimastat: Bramhall SR, et al. – JCO 2001
Study DesignStudy Design 414 chemotherapy-naïve
patients Primary endpoint: survival
ResultsResults Surv: G>5Fu (p=.0025) TTP: G>5Fu (p=.0002) CB: G>5Fu (p=.0022)
Treatment ScheduleTreatment Schedule GEM 1000mg/m2 IV
weekly x7/8 then x3/4
MAR 5 mg, 10 mg, or 25 mgbid orally
J Clin Oncol. 2001 Aug 1;19(15):3447-55
G Mar5 Mar10 Mar25
# Pts. 103 104 105 102
RR (%) 26 3
PFS (wk) 16,4 8 8,4 8,1
MS (mo) 5,5 3,6 3,5 4,1
1YrS (%) 19 14 14 20

GEM combinations vs. GEM aloneGEM combinations vs. GEM alone
Phase III trials
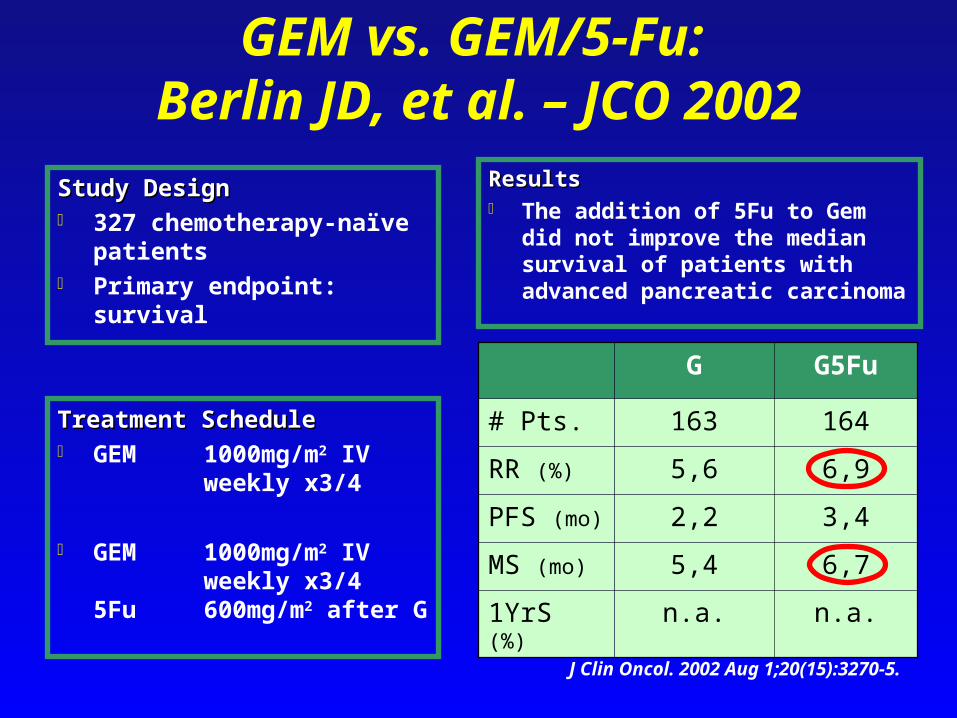
GEM vs. GEM/5-Fu: Berlin JD, et al. – JCO 2002
Study DesignStudy Design 327 chemotherapy-naïve
patients Primary endpoint: survival
ResultsResults The addition of 5Fu to Gem did not
improve the median survival of patients with advanced pancreatic carcinoma
J Clin Oncol. 2002 Aug 1;20(15):3270-5.
Treatment ScheduleTreatment Schedule GEM 1000mg/m2 IV
weekly x3/4
GEM 1000mg/m2 IV weekly x3/4
5Fu 600mg/m2 after G
G G5Fu
# Pts. 163 164
RR (%) 5,6 6,9
PFS (mo) 2,2 3,4
MS (mo) 5,4 6,7
1YrS (%) n.a. n.a.

GEM vs. GEM/Cis: Colucci G, et al. – Cancer 2002
Study DesignStudy Design 107 chemotherapy-naïve
patients Primary endpoint: TTP, clinical
benefit
ResultsResults Surv: GP=G (p=n.s.) TTP: GP>G (p=.048) CBR: GP=G (p=n.s.)
Cancer. 2002 Feb 15;94(4):902-10.
Treatment ScheduleTreatment Schedule GEM 1000mg/m2 IV
weekly x7/8 then x3/4
GEM 1000mg/m2 IV weekly x7/8 then x3/4
CIS 25mg/m2 1h before G
G GP
# Pts. 54 53
RR (%) 9,2 26,4
TTP (mo) 1,8 4,6
MS (mo) 4,6 6,9
1YrS (%) 11 11
CBR (%) 49 53

GEM vs. GEM/Irinotecan: Rocha-Lima CMS, et al. – ASCO 2003
Study DesignStudy Design 360 chemotherapy-naïve
patients Primary endpoint: overall
survival
ResultsResults RR: GIrino>G (p<.001) Based on this study, single agent
GEM remains the standard of care for 1st line therapy.
Treatment ScheduleTreatment Schedule GEM 1000mg/m2 IV
weekly x7/8 then x3/4
GEM 1000mg/m2 IV Irino 100mg/m2 after G
D1,8 Q21
G GIrino
# Pts. 180 180
RR (%) 4,4 16,1
TTP (mo) 3,0 3,5
MS (mo) 6,6 6,3
1YrS (%) 22 21
Proc Am Soc Clin Oncol. 2003:abstr 1005.

GEM vs. GEM/Cisplatin: Heinemann, et al. – ASCO 2003
Study DesignStudy Design 198 chemotherapy-naïve
patients Primary endpoint: survival
ResultsResults PFS: GP>G (p<.01) RR+SD: GP>G (p<.001)
Treatment ScheduleTreatment Schedule GEM 1000mg/m2
weekly x3/4
GEM 1000mg/m2 IV CIS 50mg/m2 after G
once every 2 weeks
G GP
# Pts. 100 98
RR (%) 8 10.2
PFS (mo) 2,8 5,4
MS (mo) 6 7.6
1YrS (%) n.a. n.a.
Proc Am Soc Clin Oncol. 2003:abstr 1003.
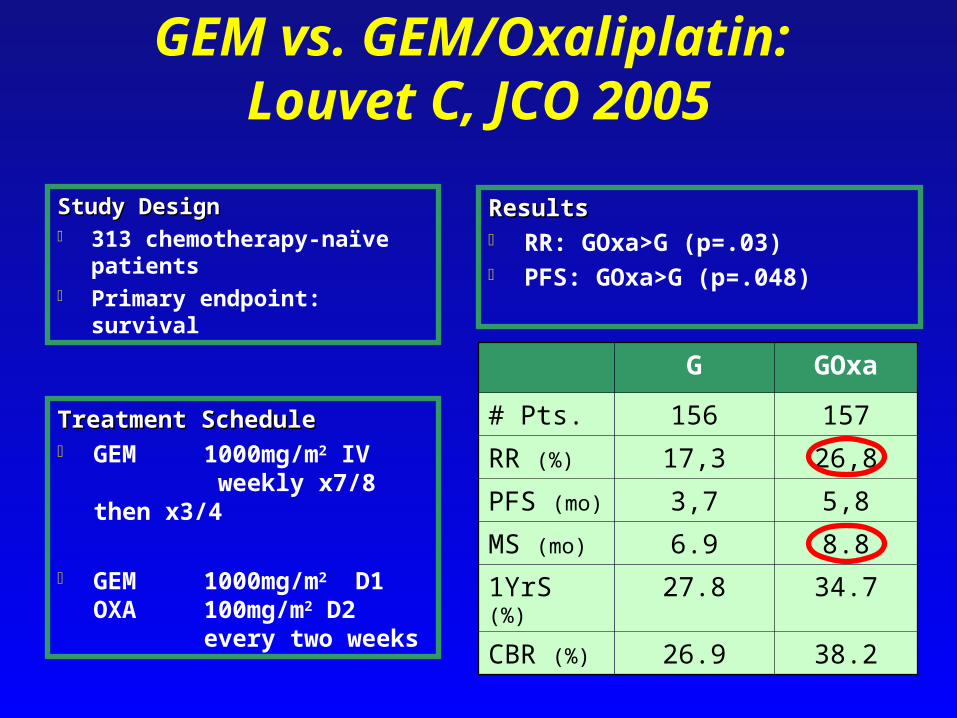
GEM vs. GEM/Oxaliplatin: Louvet C, JCO 2005
Study DesignStudy Design 313 chemotherapy-naïve
patients Primary endpoint: survival
ResultsResults RR: GOxa>G (p=.03) PFS: GOxa>G (p=.048)
Treatment ScheduleTreatment Schedule GEM 1000mg/m2 IV
weekly x7/8 then x3/4
GEM 1000mg/m2 D1 OXA 100mg/m2 D2
every two weeks
G GOxa
# Pts. 156 157
RR (%) 17,3 26,8
PFS (mo) 3,7 5,8
MS (mo) 6.9 8.8
1YrS (%) 27.8 34.7
CBR (%) 26.9 38.2



21
Xeloda: a new treatment option for pancreatic cancer
Ian Chau
Royal Marsden Hospital, London and Surrey, UK

Xeloda active in advanced pancreatic cancer
Single agent Xeloda1
objective response rate: 7.3%
clinical benefit: 24%
median survival: 6 months
Two phase I studies evaluated the combination of gemcitabine and Xeloda2,3
DLTs myelosuppression and mucositis1Cartwright TH et al. J Clin Oncol 2002;20:160–4
2Hess V et al. J Clin Oncol 2003;21:66–83Schilsky RL et al. J Clin Oncol 2002;20:582–7

UK NCRI GEMCAP versus gemcitabine phase III study in advanced pancreatic
cancer
Cunningham D et al. Eur J Cancer Suppl 2005;3:4 (Abst PS11)
Gemcitabine1 000mg/m2 weekly x7 q8w, thereafter weekly x3 q4w
GEMCAPGemcitabine 1 000mg/m2 weekly x3 q4wXeloda 830mg/m2 twice daily days 1–21 q4w
n=266
n=267
RANDOMIZATION 1º endpoint: overall survival

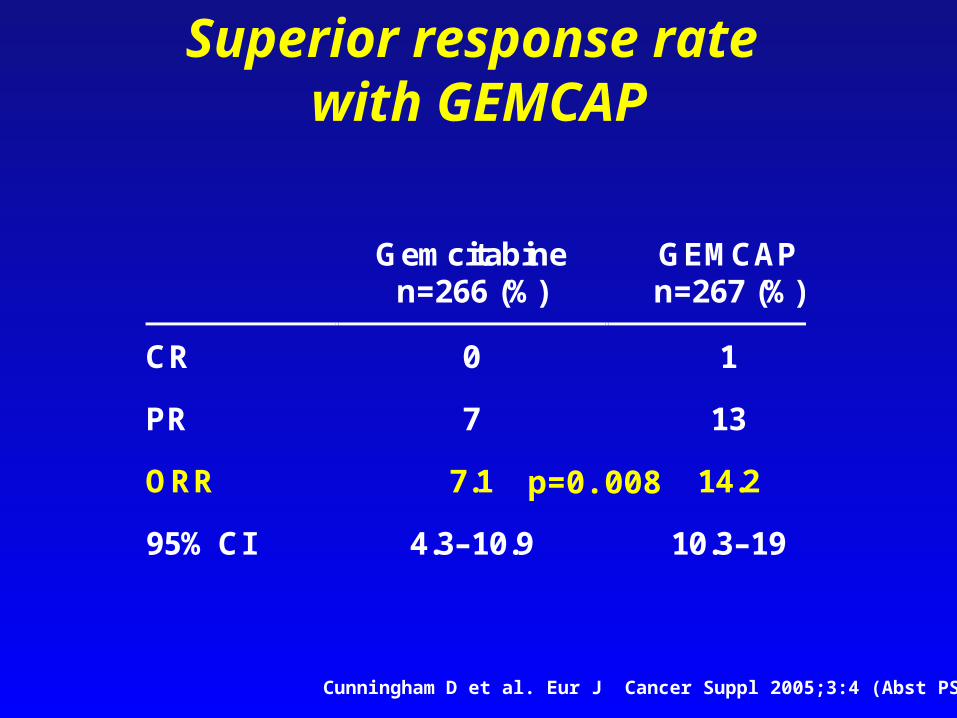
Gemcitabine n=266 (%)
GEMCAP n=267 (%)
CR 0 1
PR 7 13
ORR 7.1 14.2
95% CI 4.3–10.9 10.3–19
Superior response rate with GEMCAP
p=0.008
Cunningham D et al. Eur J Cancer Suppl 2005;3:4 (Abst PS11)

Significantly improved overallsurvival with GEMCAP
Hazard ratio: 0.8095% CI: 0.65–0.98Log-rank p=0.026
0 3 6 9 12 15 18 21 24 27
100
75
50
25
0
Patients surviving (%)
Months
12-month
survivalGEMCAP (n=267) 26%Gemcitabine (n=266) 19%
7.46.0
Cunningham D et al. Eur J Cancer Suppl 2005;3:4 (Abst PS11)


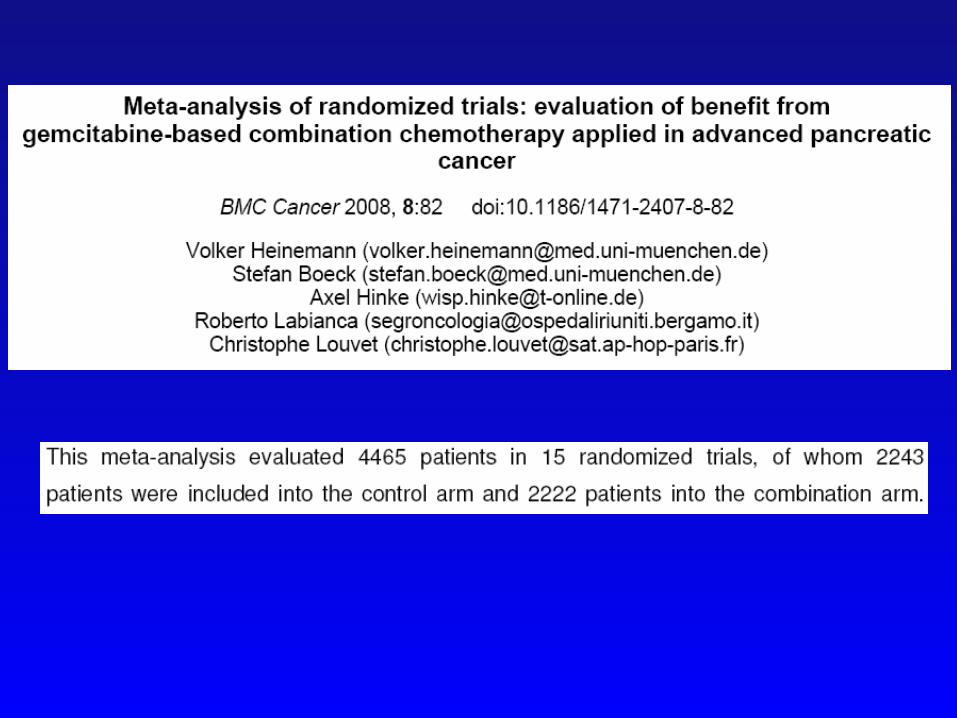
Of the 113 potentially relevant studies, 51 trials involving 9,970 patients met the inclusion criteria, and 33 of these trials involving 6,026 patients were included in the meta-analyses.


Targeted agents
Erlotinib Cetuximab Bevacizumab Sorafenib

Targeted agents
Erlotinib Cetuximab Bevacizumab Sorafenib

Erlotinib Plus Gemcitabine Compared to Gemcitabine Alone in Patients With
Advanced Pancreatic Cancer. A Phase III Trial of the National
Cancer Institute of Canada Clinical Trials Group [NCIC-CTG]
MJ Moore

Rationale for targeting HER1/EGFR in pancreatic cancer HER1/EGFR overexpression is common1,2
Elevated HER1/EGFR and EGF is associated with3–5 more aggressive disease
increased tumour size
late clinical stage
poor prognosis
reduced sensitivity to chemotherapy1Tobita K, et al. Int J Mol Med 2003;11:305–9
2Srivastava A, et al. Hum Pathol 2001;32:1184–893Ueda S, et al. Pancreas 2004;29:1–8
4Nicholson R, et al. Eur J Cancer 2001;37:S9–S15 5Xiong H, et al. Semin Oncol 2002;29:31–7
HER1/EGFR = human epidermal growth factor receptor

Rationale for Tarceva (erlotinib) in pancreatic cancer
In a preclinical study, Tarceva significantly inhibited cell growth and proliferation in pancreatic cancer cell lines in vitro1
Tarceva has been shown to enhance gemcitabine-induced apoptosis in pancreatic tumour cells2
1Durkin A, et al. Am J Surg 2003;186:431–62Ng SS, et al. Mol Cancer Ther 2002;1:777–83

*1:1 randomisationECOG = Eastern Cooperative Oncology GroupPS = performance status
PA.3: study schema
Stratified by:CentreECOG PS (0/1 vs 2)Stage of disease(locally advanced vsdistant metastases)(n=569)
RANDOM I SE
Gemcitabine 1,000mg/m2 i.v.+
Tarceva 100/150mg/day p.o.(n=285)
Gemcitabine 1,000mg/m2 i.v.+
placebo 100/150mg/day p.o.(n=284)
*
Moore M, et al. J Clin Oncol 2005;23(Suppl. 16 Pt I):1s (Abs. 1)Genentech: Tarceva® full prescribing information

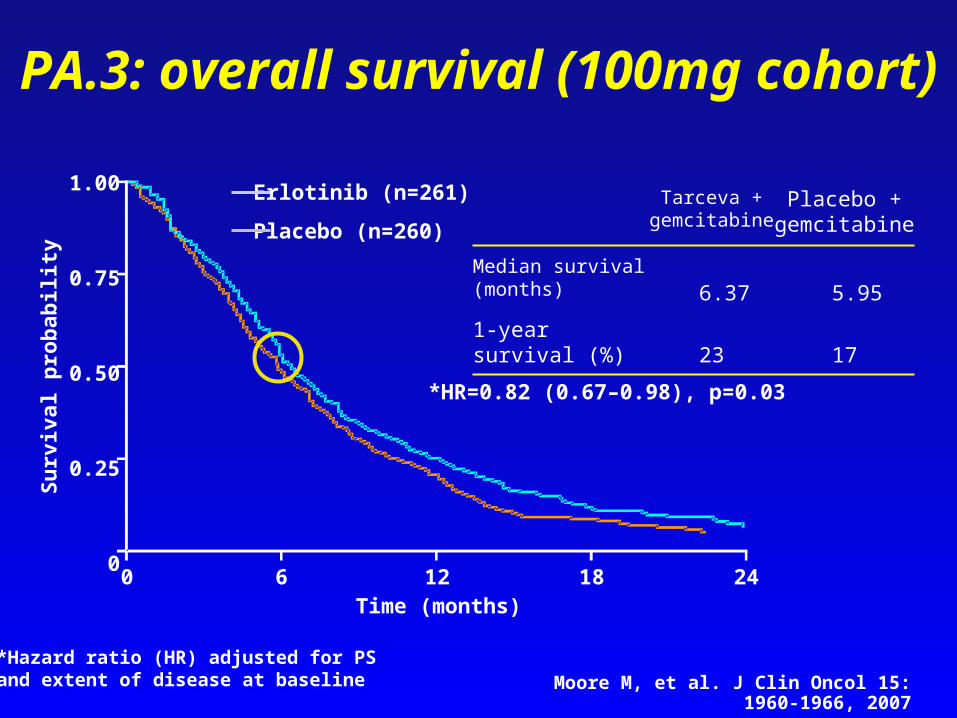
PA.3: overall survival (100mg cohort)
17231-year survival (%)
5.95 6.37Median survival (months)
Placebo + gemcitabine
Tarceva + gemcitabine
*HR=0.82 (0.67–0.98), p=0.03
1.00
0.75
0.50
0.25
0
Su
rviv
al p
rob
abil
ity
0 6 12 18 24Time (months)
Erlotinib (n=261)
Placebo (n=260)
*Hazard ratio (HR) adjusted for PS and extent of disease at baseline Moore M, et al. J Clin Oncol 15: 1960-1966, 2007

PA.3: survival by HER1/EGFR status (100mg cohort)
HER1/EGFR positive (n=70)HER1/EGFR negative (n=66)
1.00
0.75
0.50
0.25
00 6 12 18 24
Survival time (months)
Su
rviv
al p
rob
abil
ity
1.00
0.75
0.50
0.25
00 6 12 18 24
Survival time (months)
Su
rviv
al p
rob
abil
ity
Tarceva (n=34)
Placebo (n=32)
HR=0.75
95% CI: 0.46–1.23 (p=NS)
Tarceva (n=41)
Placebo (n=29)
HR=0.82
95% CI: 0.50–1.32 (p=NS)
NS = not significant Moore M, et al. J Clin Oncol 2005;23(Suppl.16 Pt I):1s (Abs. 1)


PA.3: overall survival according to grade of rash
HR (rash)=0.71, p<0.0001
Grade 0Grade 1Grade 2
1.0
0.8
0.6
0.4
0.2
0
Su
rviv
al p
rob
abil
ity
0 5 10 15 20Time (months)
439161-year survival (%)
10.55.85.3Median survival (months)
Grade 2(n=102)
Grade 1(n=101)
Grade 0(n=79)
Moore M, et al. J Clin Oncol 15: 1960-1966, 2007

Summary Gemcitabine has long been regarded as the
standard of care
PA.3 is the first randomised trial to show any drug to prolong survival in advanced pancreatic cancer versus single-agent gemcitabine
Provides ‘proof of principle’ for targeted cancer therapies
first demonstration of overall survival benefit with a HER1/EGFR inhibitor combined with chemotherapy
Tarceva was recently approved in the USA for treatment of advanced pancreatic cancer

molecular characterization of a subgroup of patients enrolled onto the Erlotinib trial showed mutations of K-ras in 79% (92 of 117) of the patients;
in non–small-cell lung cancer and in colorectal cancer patients have demonstrated that patients carrying K-ras mutations are resistant to epidermal growth factor receptor (EGFR) tyrosine kinase inhibitors;
the anti-EGFR agent produced a similar advantage in EGFR-positive and EGFR-negative patients;
no significant correlation were found between K-ras mutations and outcome in the patients enrolled on to Erlotinib trial.
J Clin Oncol. 2007 Dec 20;25(36):5836-7

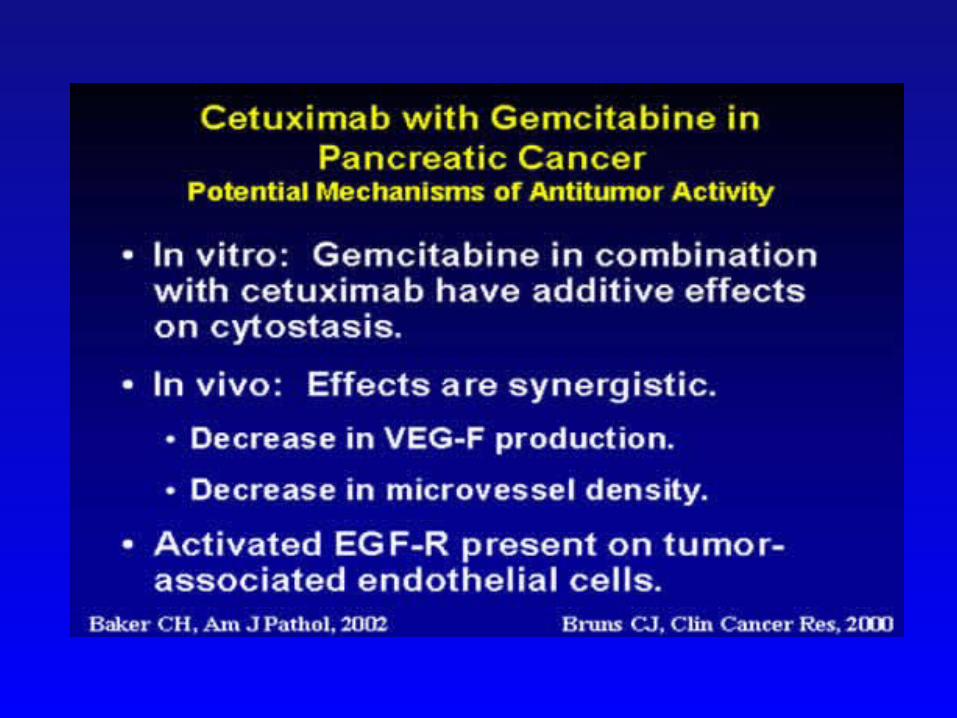
endothelial cells express the EGFR and its expression is correlated with the expression of EGFR ligands within the tumor;
treatment with anti-EGFR agents can induce apoptosis in endothelial cells of experimental tumors due to the ability of anti-EGFR agents to reduce the levels of secretion of VEGF in pancreatic cancer cells and directly to block the proliferation and the motility of endothelial cells, as evaluated in vitro;
these agents were found to produce significant levels of apoptosis only in tumor-associated endothelial cells that express activated EGFR;
Erlotinib in Pancreatic Cancer: Are Tumor Cells the (only) Target?
J Clin Oncol. 2007 Dec 20;25(36):5836-7

Conclusion: EGFR is expressed in different nontransformed cell types of the neoplastic environment that are involved in tumor growth and progression, including endothelial cells. Studying the effects of anti-EGFR agents in the different components of the tumor microenvironment might improve our knowledge of the mechanism of action of these drugs.
Erlotinib in Pancreatic Cancer: Are Tumor Cells the (only) Target?
J Clin Oncol. 2007 Dec 20;25(36):5836-7

Targeted agents
Erlotinib
Cetuximab Bevacizumab Sorafenib
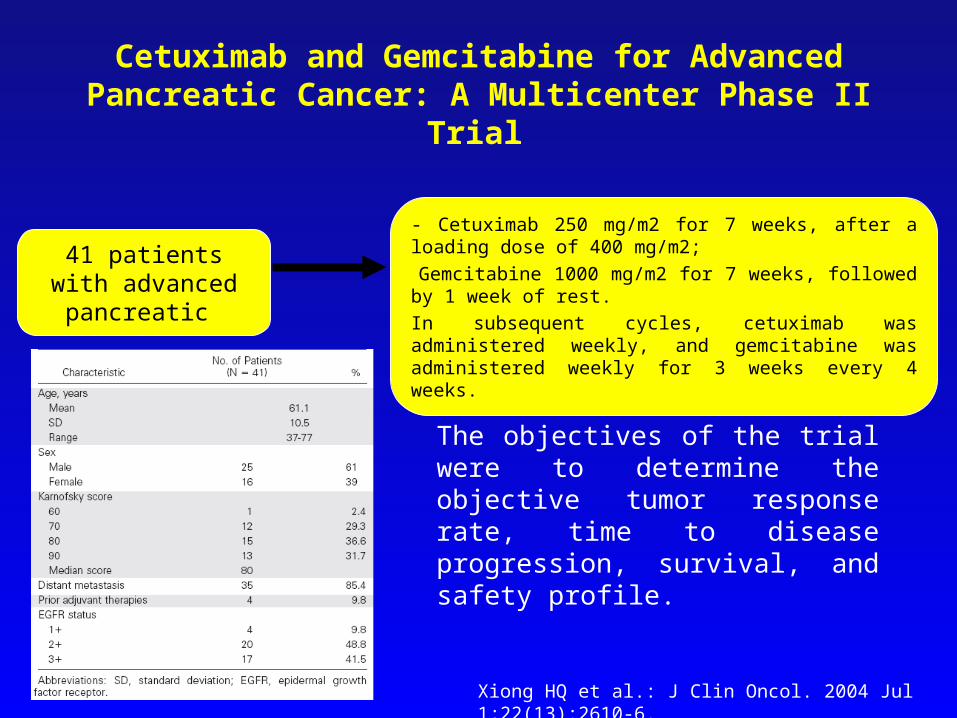
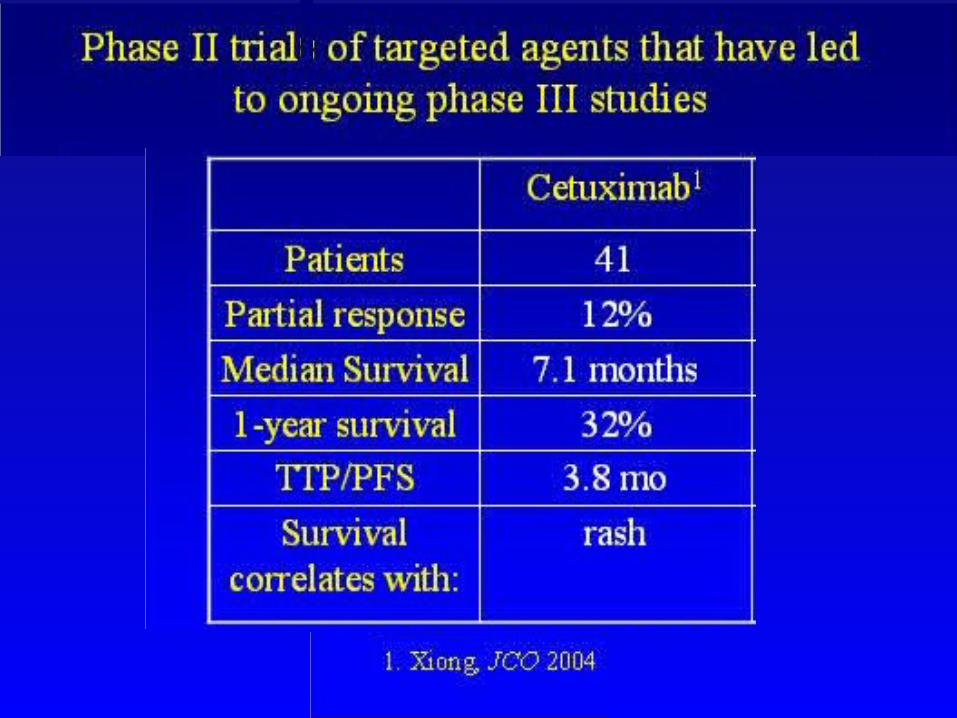
41 patients with advanced pancreatic
- Cetuximab 250 mg/m2 for 7 weeks, after a loading dose of 400 mg/m2;-Gemcitabine 1000 mg/m2 for 7 weeks, followed by 1 week of rest.
In subsequent cycles, cetuximab was administered weekly, and gemcitabine was administered weekly for 3 weeks every 4 weeks.
Cetuximab and Gemcitabine for Advanced Pancreatic Cancer: A Multicenter Phase II Trial
The objectives of the trial were to determine the objective tumor response rate, time to disease progression, survival, and safety profile.
Xiong HQ et al.: J Clin Oncol. 2004 Jul 1;22(13):2610-6.
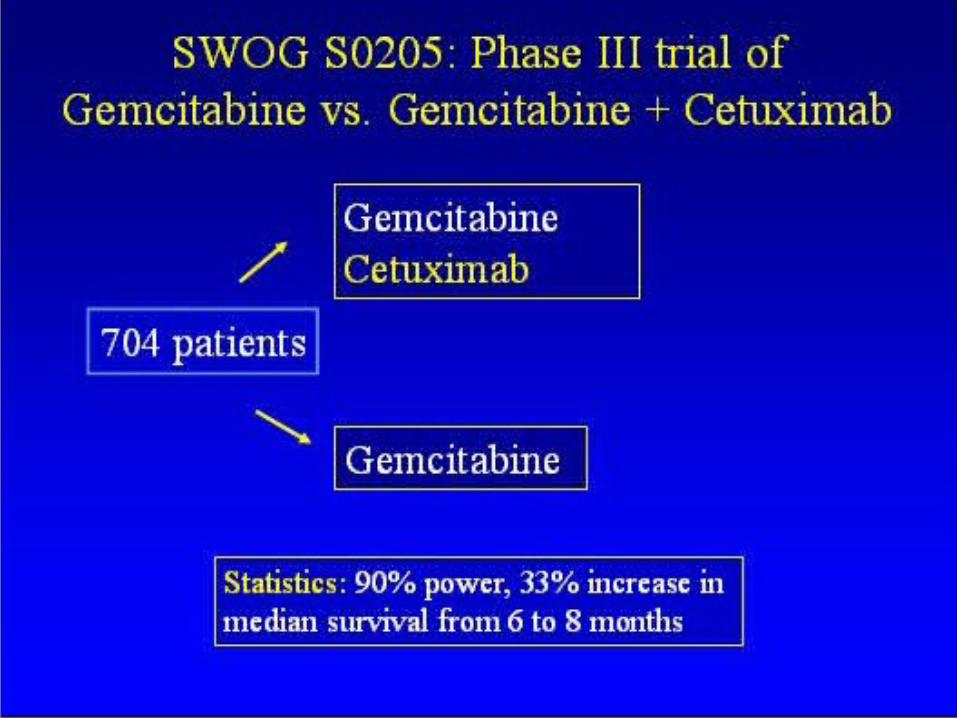


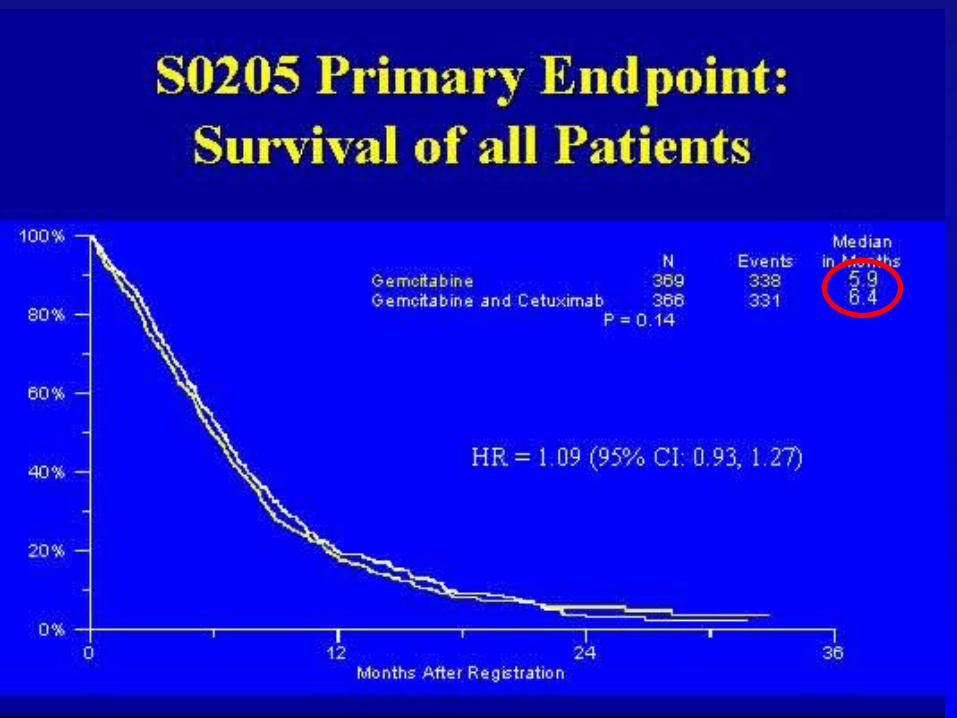
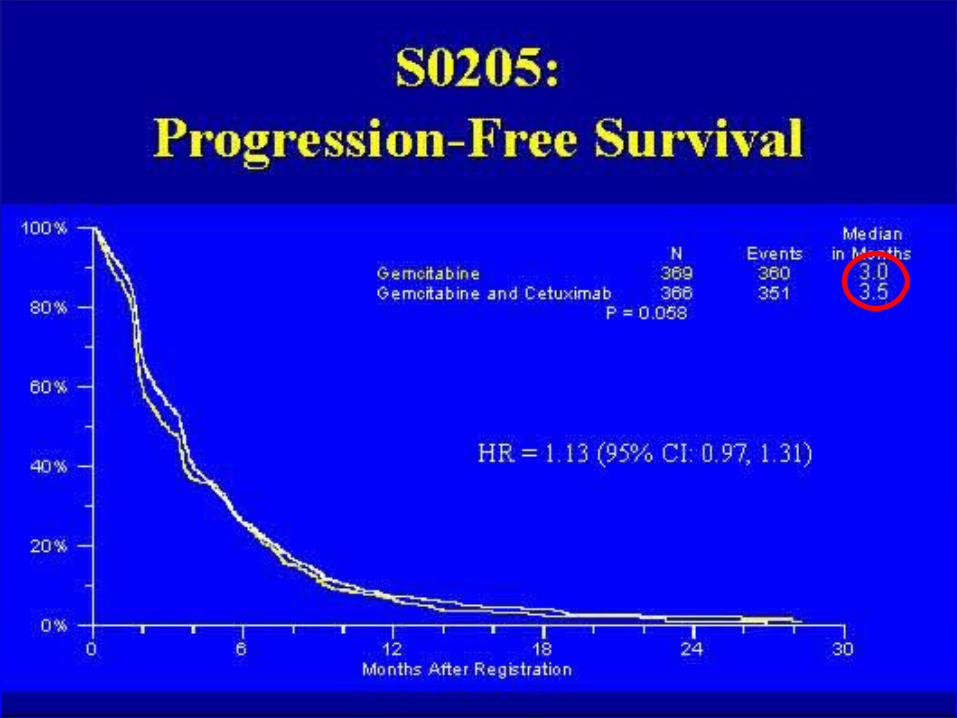

SWOG S0205 study
Conclusions: This study failed to demonstrate a clinically significant advantage of the addition of cetuximab to gemcitabine for overall survival, PFS and response in advanced pancreatic cancer.

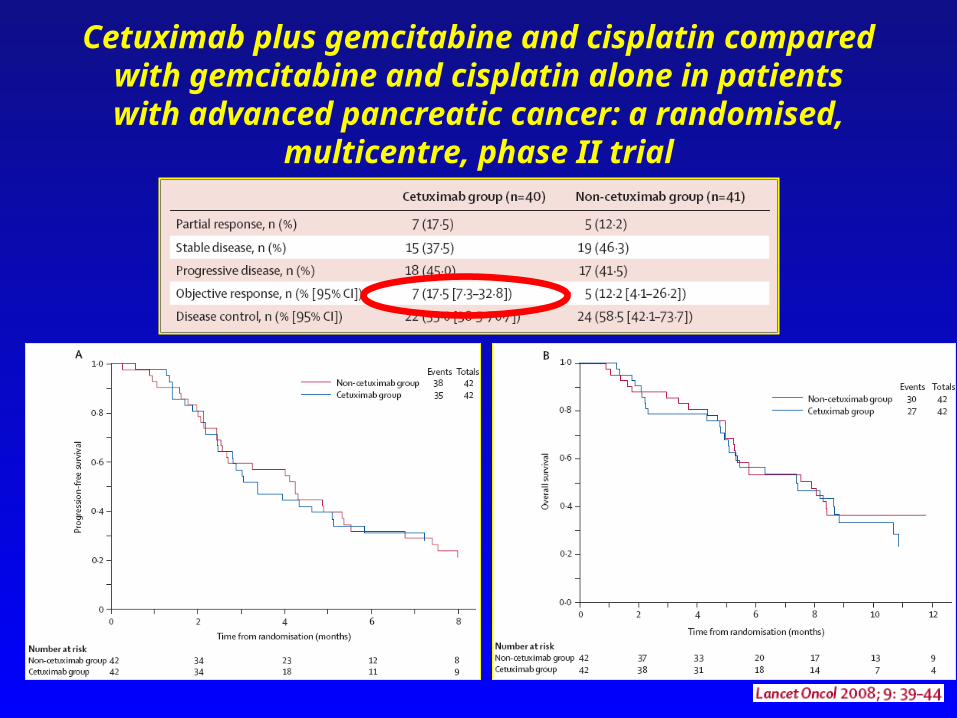
84 patients with advanced pancreatic
- Cetuximab 250 mg/m2 weekly, after a loading dose of 400 mg/m2;
- Gemcitabine 1000 mg/m2 on days 1 and 8 of a 21-day cycle;
- Cisplatin 35 mg/m2 on days 1 and 8 of a 21-day cycle.
- Gemcitabine 1000 mg/m2 on days 1 and 8 of a 21-day cycle;
- Cisplatin 35 mg/m2 on days 1 and 8 of a 21-day cycle.
Cetuximab plus gemcitabine and cisplatin compared with gemcitabine and cisplatin alone in
patients with advanced pancreatic cancer: a randomised, multicentre, phase II trial
The primary endpoint was objective response (OR), defined as the proportion of patients whose best response was either partial response (PR) or complete response (CR);Secondary endpoints included disease control (defined as the proportion of patients whose best response was PR, CR, or stable disease [SD]), progression-free survival (PFS), and overall survival (OS).
Cetuximab plus gemcitabine and cisplatin compared with gemcitabine and cisplatin alone in
patients with advanced pancreatic cancer: a randomised, multicentre, phase II trial

Targeted agents
Erlotinib Cetuximab
Bevacizumab Sorafenib
VEGF in pancreatic cancer
VEGF promotes pancreatic cancer growth via a paracrine angiogenic pathway and an autocrine mitogenic pathway1,2
Both VEGF and its receptors are overexpressed in pancreatic cancer3
High VEGF expression correlates with advanced stage, postoperative recurrence, lymph node and distant metastases, and decreased survival in patients with pancreatic cancer4
These observations provide a rationale for anti-VEGF therapy for the treatment of pancreatic cancer
1von Marschall Z, et al. Gastroenterology 2000;119:1358–722Buchler P, et al. Surgery 2003;134:772–82
3Seo Y, et al. Cancer 2000;88:2239–454Karayiannakis AJ, et al. Cancer Lett 2003;194:119–24VEGF = vascular endothelial growth factor

Tumour characteristics and environment promote VEGF expression
EGF
Hypoxia PDGF
IL-8
bFGF
COX-2Nitric oxideOncogenes
VEGF releaseBinding and activation
of VEGF receptor
IGF-1
ProliferationSurvival Migration
ANGIOGENESISPermeability
Increased expression(MMP, tPA, uPA, uPAr,
eNOS, etc.)
– P
– P
P–
P–

Summary: mechanism of action of anti-VEGF therapy
Inhibition of VEGF may act against tumours in three ways regression of existing microvasculature normalisation of mature vasculature inhibition of production of new vasculature
EARLY BENEFIT CONTINUED BENEFIT
Regressionof existing microvasculature
Normalisationof surviving microvasculature
Inhibitionof vessel regrowth and neovascularisation
Avastin plus gemcitabine in patients with advanced pancreatic cancer: phase II
study design Uncontrolled phase II multicentre trial (NCI sponsored) at seven sites
Two-stage sequential design: trial to be stopped if 2 responses in first 21 patients
Treatment gemcitabine 1,000mg/m
2 i.v. on days 1, 8 and 15 of a 4-week cycle
Avastin 10mg/kg i.v. every 2 weeks initially six cycles of Avastin/gemcitabine planned
CT scans obtained every two cycles
Primary endpoint: objective tumour response
NCI = National Cancer InstituteCT = computed tomography
Kindler HL, et al. J Clin Oncol 2005;23:8033-8040
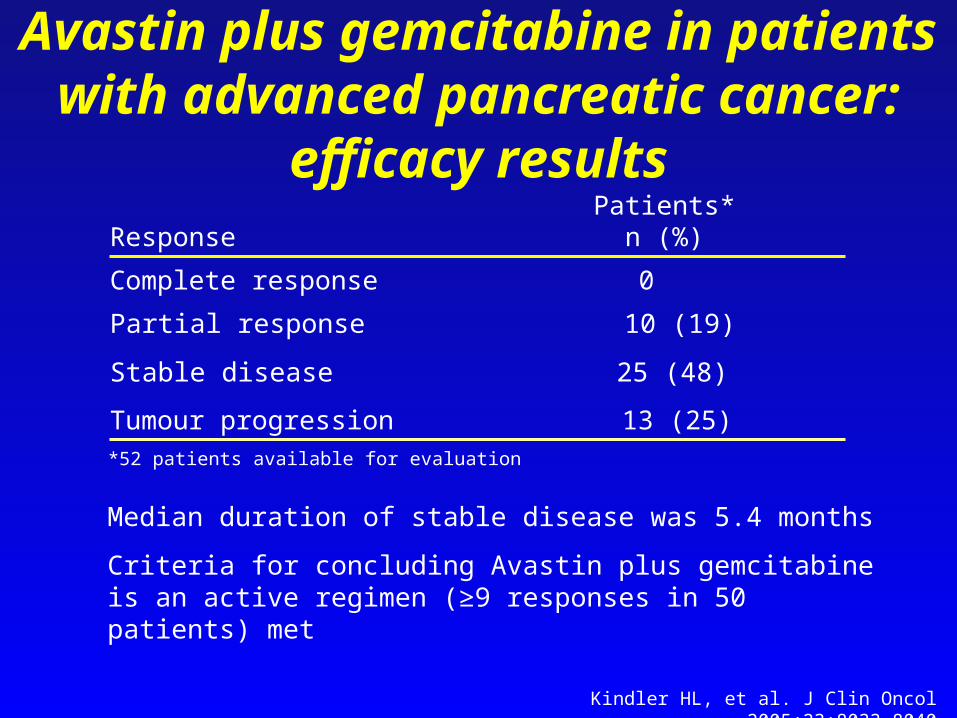
Avastin plus gemcitabine in patients with advanced pancreatic cancer: efficacy
results
13 (25)Tumour progression
10 (19)Partial response
25 (48)Stable disease
0Complete response
Patients*n (%)Response
*52 patients available for evaluation
Median duration of stable disease was 5.4 months
Criteria for concluding Avastin plus gemcitabine is an active regimen (≥9 responses in 50 patients) met
Kindler HL, et al. J Clin Oncol 2005;23:8033-8040

Avastin plus gemcitabine in patients with advanced pancreatic cancer: efficacy
results (cont’d)
75 (95% CI: 60–85)6-month survival (%)
8.7 (95% CI: 7.3–9.7)Median survival (months)
29 (95% CI: 16–44)1-year survival (%)
5.8 (95% CI: 4.8–7.1) Time to progression (months)
OutcomeResponse
52 patients available for evaluation
CI = confidence intervalKindler HL, et al. J Clin Oncol 2005;23:8033-8040
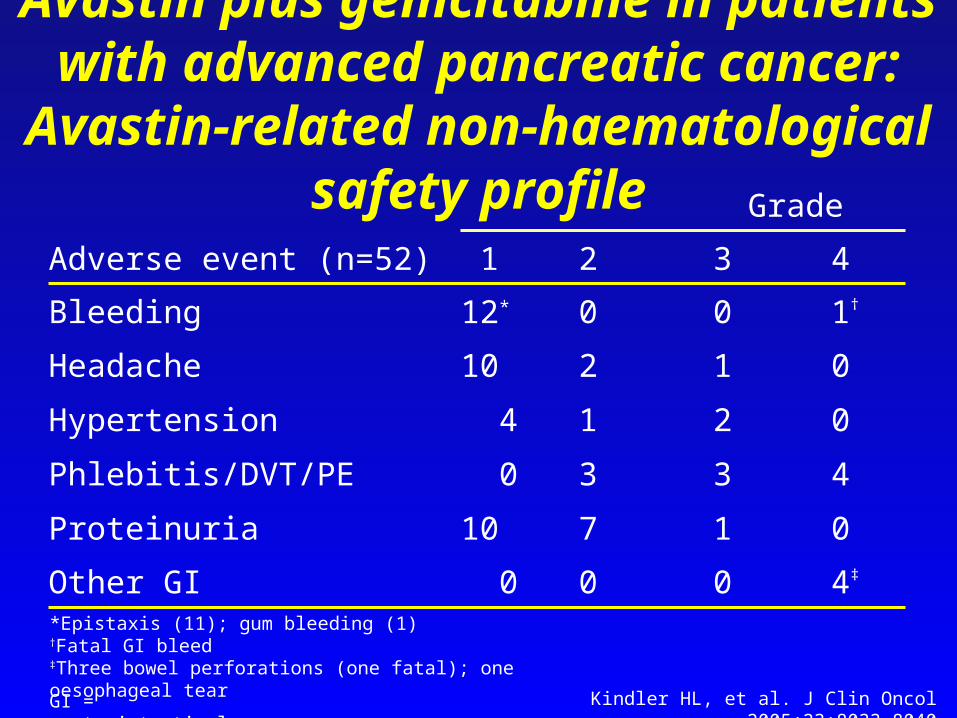
Avastin plus gemcitabine in patients with advanced pancreatic cancer: Avastin-
related non-haematological safety profile
4‡
0
4
0
0
1†
4
0
1
3
2
1
0
3
0
7
3
1
2
0
2
10Headache
12*Bleeding
0Phlebitis/DVT/PE
4Hypertension
0Other GI
10Proteinuria
1Adverse event (n=52)
Grade
*Epistaxis (11); gum bleeding (1)†Fatal GI bleed‡Three bowel perforations (one fatal); one oesophageal tear
GI = gastrointestinal Kindler HL, et al. J Clin Oncol 2005;23:8033-8040

Avastin plus gemcitabine in patients with advanced pancreatic cancer: conclusions
Addition of Avastin to gemcitabine resulted in improved response rate, time to progression and survival compared with that expected with gemcitabine alone in patients with advanced pancreatic cancer
The combination is well tolerated. Rates of thrombosis and significant bleeding are not higher than expected in this patient population
No correlation between pretreatment VEGF levels and response, progression-free or overall survival
Further study is warranted
Kindler HL, et al. J Clin Oncol 2005;23:8033-8040

Locally advanced (stage III) and
metastatic (stage IV) first-line pancreatic
cancer (n=530)
Gemcitabine + placebo
Gemcitabine + Avastin (10mg/kg) every
2 weeks
PD
PD
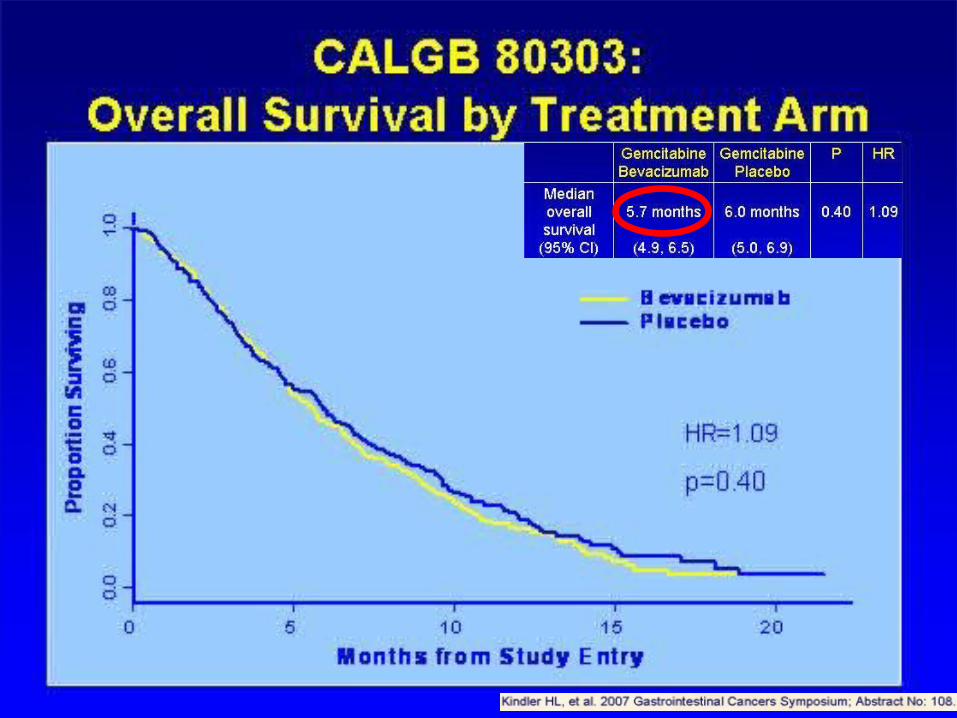
Phase III trial of first-line Avastin with gemcitabine in pancreatic cancer
(CALGB 80303)
Primary endpoint: overall survival (90% power to detect a 35% increase in survival from 6 to 8.1 months)
Treatment administration gemcitabine 1,000mg/m2 weekly for 3 weeks of each 4-week cycle Avastin 10mg/kg every 2 weeks
CALGB = Cancer and Leukemia Group B




Rationale for combining bevacizumab and erlotinib
Both HER1/EGFR and VEGF are overexpressed in many tumours1
VEGF has been implicated in resistance to anti-HER1/EGFR therapy
Treatment with two agents targeted against critical pathways may be more effective than a single pathway2
Preclinical studies have shown that anti-VEGF and anti-HER1/EGFR therapies have at least additive effects3
Clinical trials in various indications (renal cell cancer,4 non-small cell lung cancer,5 head and neck squamous cell carcinoma6) have shown that the combination of bevacizumab and erlotinib is active
1Viloria-Petit A, et al. Cancer Res 2001;61:5090–101; 2Herbst RS, et al. Eur J Cancer Suppl 2003;1:S293; 3Ciardiello F, et al. Clin Cancer Res 2000;6:3739–47; 4Spigel DR, et al. J Clin Oncol 2005;23(June 1 Suppl.):
Abstract 4540; 5Sandler AB, et al. J Clin Oncol 2004;22(July 15 Suppl.): Abstract 2000; 6Vokes EE, et al. J Clin Oncol 2005;23(June 1 Suppl.): Abstract 5504

Primary endpoint: overall survival (increase from 6.9 to 9.0 months)Secondary endpoints include progression-free survival and response rateAvastin 5mg/kg every 2 weeks until disease progression
Previously untreated metastatic pancreatic
cancer (n=600)
Gemcitabine + Tarceva + placebo
Gemcitabine + Tarceva + Avastin 5mg/kg every
2 weeks
PD*
PD
PD = progression of disease*No cross over will be permitted
Phase III trial of first-line gemcitabine plus Tarceva with or without Avastin in
pancreatic cancer (AVITA)

Targeted agents
Erlotinib Cetuximab Bevacizumab
Sorafenib
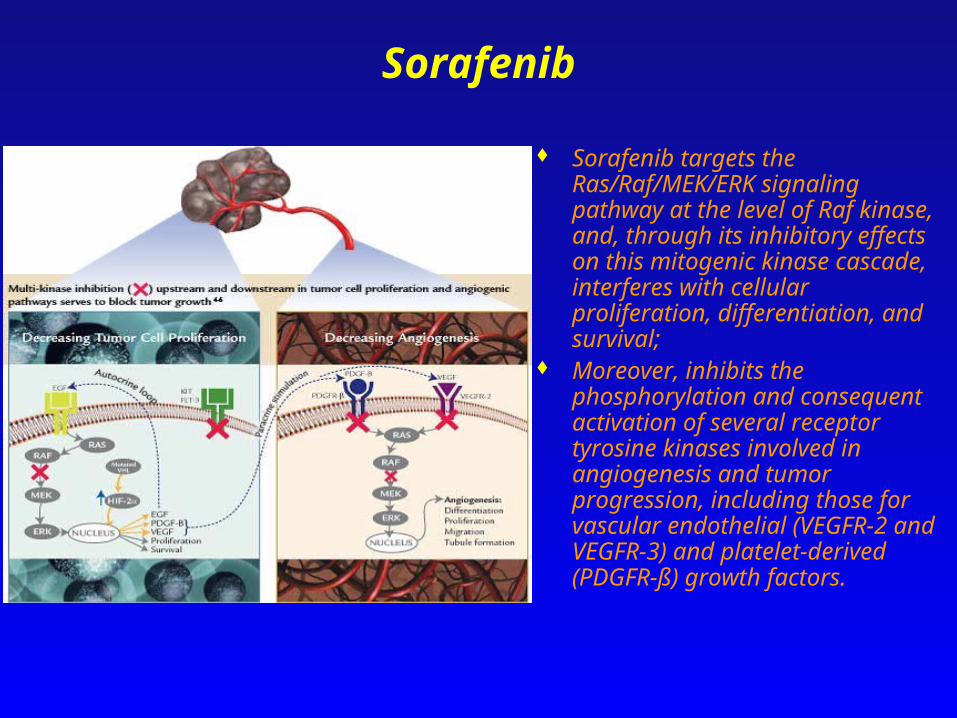
Sorafenib
Sorafenib targets the Ras/Raf/MEK/ERK signaling pathway at the level of Raf kinase, and, through its inhibitory effects on this mitogenic kinase cascade, interferes with cellular proliferation, differentiation, and survival;
Moreover, inhibits the phosphorylation and consequent activation of several receptor tyrosine kinases involved in angiogenesis and tumor progression, including those for vascular endothelial (VEGFR-2 and VEGFR-3) and platelet-derived (PDGFR-ß) growth factors.

Sorafenib and GemcitabineA phase II study

Sorafenib and GemcitabineA phase II study
17 patients enrolled

Gemcitabine is commonly used in patients with pancreatic cancer with the purpose of symptom palliation, there is no clear evidence of efficacy in terms of survival increase or progression control;
EGFR inhibitor (erlotinib) showed a small survival advantage when combined with gemcitabine;
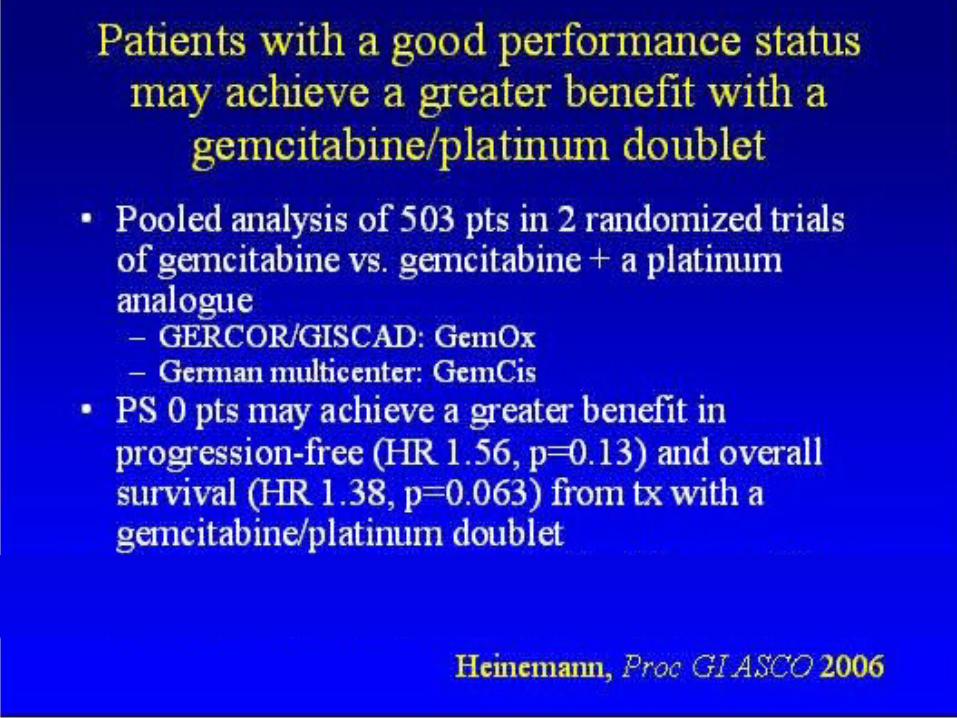
A meta-analysis of randomised trials comparing gemcitabine versus gemcitabine and platinum analogues showed a statistical significant survival advantage for the combination;
RAS and RAF mutations are quite common in pancreatic cancer; Sorafenib is an inhibitor of the RAS/RAF signalling pathway.
Furthermore, sorafenib is able to inhibit both VEGFR and PDGFR.
A RANDOMIZED PHASE II STUDY OF GEMCITABINE/CISPLATIN WITH OR WITHOUT SORAFENIB TO EVALUATE THE EFFICACY
AND SAFETY IN PATIENTS WITH LOCALLY ADVANCED OR METASTATIC PANCREATIC CANCER

114 patients with pancreatic cancer
- Sorafenib 400 mg po bid, continuously;
- Gemcitabine 1000 mg/m2 on days 1 and 8 of a 21-day cycle;
- Cisplatin 25 mg/m2 on days 1 and 8 of a 21-day cycle.
- Gemcitabine 1000 mg/m2 on days 1 and 8 of a 21-day cycle;
- Cisplatin 25 mg/m2 on days 1 and 8 of a 21-day cycle.
A RANDOMIZED PHASE II STUDY OF GEMCITABINE/CISPLATIN WITH OR WITHOUT SORAFENIB TO EVALUATE THE EFFICACY
AND SAFETY IN PATIENTS WITH LOCALLY ADVANCED OR METASTATIC PANCREATIC CANCER
Proposed number of countries and centers ►21Primary endpoint: efficacy, in term of Progression Free Survival (PFS)Secondary endpoints include Overall Response Rate (RECIST Criteria), Duration of response, Time to treatment failure, Overall survival time and Safety of the combination.
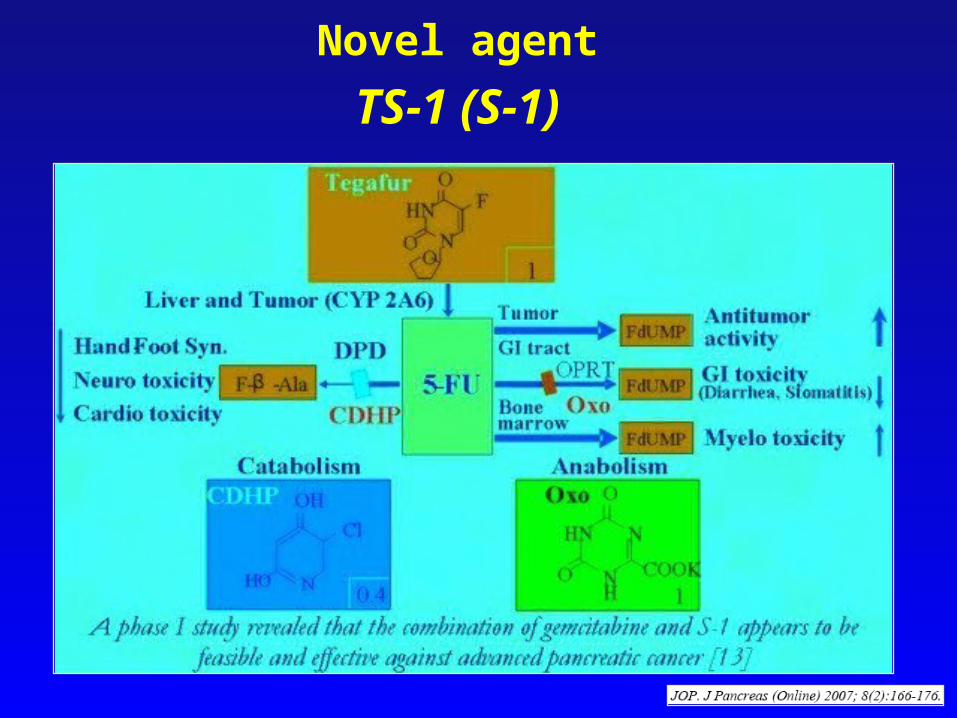
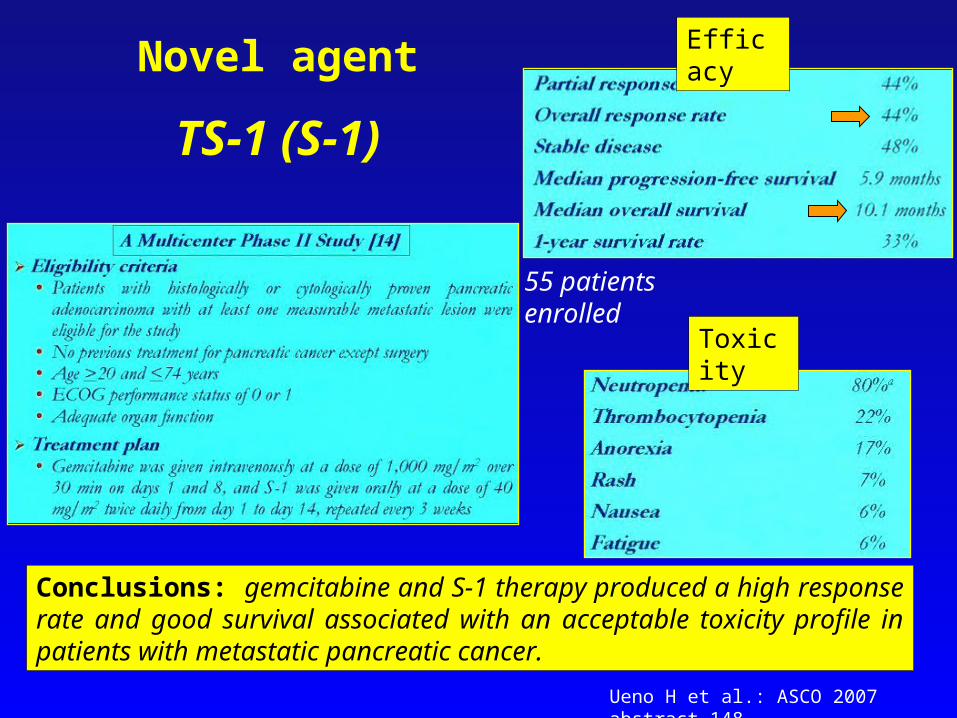
Novel agent
TS-1 (S-1)
Novel agent
TS-1 (S-1)
Efficacy
Toxicity
Conclusions: gemcitabine and S-1 therapy produced a high response rate and good survival associated with an acceptable toxicity profile in patients with metastatic pancreatic cancer.
55 patients enrolled
Ueno H et al.: ASCO 2007 abstract 148
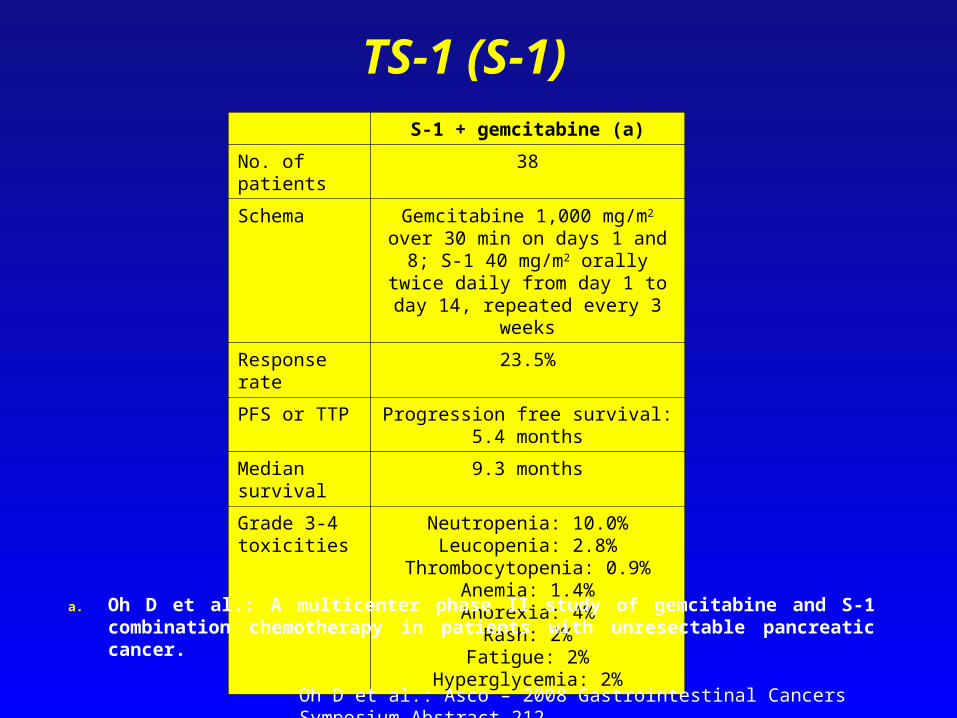
S-1 + gemcitabine (a)
No. of patients 38
Schema Gemcitabine 1,000 mg/m2 over 30 min on days 1 and 8; S-1 40 mg/m2 orally
twice daily from day 1 to day 14, repeated every 3 weeks
Response rate 23.5%
PFS or TTP Progression free survival: 5.4 months
Median survival 9.3 months
Grade 3-4 toxicities
Neutropenia: 10.0%Leucopenia: 2.8%
Thrombocytopenia: 0.9%Anemia: 1.4%Anorexia: 4%
Rash: 2%Fatigue: 2%
Hyperglycemia: 2%
a. Oh D et al.: A multicenter phase II study of gemcitabine and S-1 combination chemotherapy in patients with unresectable pancreatic cancer.
TS-1 (S-1)
Oh D et al.: Asco – 2008 Gastrointestinal Cancers Symposium Abstract 212


Progress made but more neededin pancreatic cancer
Gemcitabine monotherapy reference treatmentuntil 2005
Unprecedented survival benefits in 2005 GEM-Tarceva GEMCAP
Future combine Tarceva and Xeloda build in new agents
Avastin oxaliplatin?
optimal patient selection


















