Role of Osteopathic Manipulative Treatment in the ... di 9 aprile/Pediatria/6-Accorsi.pdf · Role...
28
Role of Osteopathic Manipulative Treatment in the management of children with ADHD Accorsi Alessandro D.O. M.R.O.I. Accademia Italiana Osteopatia Tradizionale Pescara - Italy [email protected]
Transcript of Role of Osteopathic Manipulative Treatment in the ... di 9 aprile/Pediatria/6-Accorsi.pdf · Role...

Role of Osteopathic Manipulative
Treatment in the management of
children with ADHD
Accorsi Alessandro D.O. M.R.O.I.
Accademia Italiana Osteopatia Tradizionale
Pescara - Italy
BACKGROUND (1)
• ATTENTION DEFICIT HYPERACTIVITY DISORDER
is a neuropsychological development disorder
affecting children and adolescents
• It is characterized by:
1. INATTENTION
2. IMPULSIVITY/IPERACTIVITY

BACKGROUND (2)
• DSM-IV defines three clinical forms of ADHD:
1) Inattentive
2) Hyperactive
3) Combined American Psychiatric Association. Diagnostic and statistical manual of mental health
disorders, 4th ed. Washington DC; 1994.
BACKGROUND (3)
EPIDEMIOLOGY
• USA
8% aged 4 – 17 years Centers for Disease Control (CDC). Prevalence of Diagnosis and Medication Treatment for Attention-Deficit/Hyperactivity Disorder - United States, 2003. MMWR 2005;54(34):841-47.)
• UK (age 5-15 years) 3,62% male
0,85% female National Institute for Clinical Excellence (NICE). Attention deficit hyperactivity disorder: Diagnosis and management of ADHD in children, young people and adults. September 2008. Disponibile all’indirizzo: http://www.nice.org.uk/guidance/cg72; ultima consultazione 4/11/2008.
• ITALY 3,6% Gallucci F, Bird HR, Berardi C, Gallai V, Pfanner P, Weinberg A. Symptoms of attention-deficit hyperactivity disorder in an Italian school sample: findings of a pilot study. J Am Acad Child Adolesc Psychiatry 1993;32:1051-8.
2% of the pedriatic population (ISS National institute of health)
• FRANCE (age 6-14 years)
2% Inserm, 2004.

BACKGROUND (4)
Not a rare health issue:
ONE OF THE MAJOR HEALTH PROBLEMS IN
TERMS OF HEALTH COSTS
ONE OF THE MOST FREQUENT INFANT EXTRA-
HOSPITAL PSYCHIATRIC DIAGNOSIS
ONE OF THE MOST COMMON CHILDHOOD
BEHAVIORAL PROBLEMS
BACKGROUND (5)
Multifactorial etiology:
Heritability based on genetic. Zhou et all. Meta-analysis of genome-wide linkage scans of attention deficit hyperactivity disorder. Am J Med Genet B Neuropsychiatr Genet. 2008 Dec; 1392-8.
Factors associated with brain morphology and the deficit in the modulation of neurotrasmitters.
Quantitative brain magnetic resonance imaging in girls with attention-deficit/hyperactivity disorder, Castellanos FX, Giedd JN, Berquin PC, Walter JM, Sharp W, Tran T, Vaituzis AC, Blumenthal JD, Nelson J, Bastain TM, Zijdenbos A, Evans AC, Rapoport JL.; Developmental trajectories of brain volume abnormalities in children and adolescents with attention-deficit/hyperactivity disorder, Castellanos FX, Lee PP, Sharp W, Jeffries NO, Greenstein DK, Clasen LS, Blumenthal JD, James RS, Ebens CL, Walter JM, Zijdenbos A, Evans AC, Giedd JN, Rapoport JL.JAMA. 2002 Oct 9;288(14):1740-8.
Prenatal , perinatal and/or traumatic factors during pregnancy and childbirth
Barkley, Russell A. Treating Children and Adolescents with ADHD: An Overview of Empirically Based Treatments. URL consultato il 01-08-2008.

BACKGROUND (5)
Enviromental factors: exposure to alcohol, smoking, infections during pregnancy and at birth.
Braun JM, Kahn RS, Froehlich T, Auinger P, Lanphear BP (2006). Exposures to environmental toxicants and attention deficit hyperactivity disorder in U.S. children. Environ. Health Perspect. 114 (12): 1904–9. DOI:10.1289/ehp.10274
Inappropriate diet. Lidy M Pelsser, Klaas Frankena, Jan Toorman, Huub F Savelkoul, Anthony E Dubois, Rob Rodrigues Pereira, Ton A Haagen, Nanda N Rommelse, Jan K Buitelaar, Effects of a restricted elimination diet on the behaviour of children with attention-deficit hyperactivity disorder (INCA study): a randomised controlled trial, Lancet 2011; 377: 494–503
BACKGROUND (6)
THERAPY:
• Cognitive behavioral treatment
• Pharmaceutical treatment: methylphenidate
(Ritalin®) or Atomoxetine hydrochloride (Strattera®).
http://www.aifa.it/lineeguida.htm
Taylor et al. 1996; NICE 2000; AACAP 2002

BACKGROUND (7)
OMT AND ADHD
Significant tension of the dura mater and increased
density and hypomobility of cranial bones in
children with learning prolems. W.G.Sutherland, “La Sfera Craniale”, Futura 1998
Labor or delivery complications can interfere with
the physiological development of the nervous
system. Viola M. Frymann D.O.; I
edizione italiana Le opere di Viola M. Frymann, D.O. L’osteopatia rivolta ai bambini; Futura
Publishing Society 2009; pag.200.

BACKGROUND (8)
☞50% of children receiving OMT improved their clinical condition
Bierent-Vass A., Lang J., Neumann N., Osteopathic treatment of children with attention deficit disorders, with or without hyperactivity (ADD/ADHD) - is there any effect? A randomized controlled trial, October 2004, Germany,
http://www.osteopathic-research.com/cgi-bin/or/Search1.pl?show_one=30521.
☞An other clinical study in 2006 show that osteopathy has a positive influence on ADHD symptoms.
Birgit Hubmann, The Influence of Osteopathy on ADHD, Stainz, November 2006, http://www.osteopathic-research.com/paper_pdf/Hubmann_engl.pdf
AIM OF THE STUDY
TO ASSESS THE EFFECTIVENESS OF
OMT IN CHILDREN AFFECTED BY ADHD.

METHODS (1)
Pediatric Neuropsychology Unit (NPI) , Macerata Public
Hospital (Marche, Italy)
Non randomized trial
N=41 children entered in the study (Nov 08 – Sep 09)
N = 28 were enrolled according to exclusion criteria
N=14 Study group
N=14 Control group

METHODS (2)

METHODS (3)
Cognitive behavioral therapy included:
• Weekly individual and group
psychotherapy treatments
• BELLS TEST at T0 and T1

METHODS (4)
BELLS TEST
•A test for visual neglect which allows for an
approximation of the subject’s visual search strategy
•Visual neglect is defined as a lack of response or
attendance to visual stimuli presented to the left a or to the right of the median line of the body

METHODS (4)
BELLS TEST
• Test execution: the subject must circle all the bells encountered
• The performance of the subject is evaluated in terms of:
SPEED: number of bells found in 30 seconds
ACCURACY: number of bells found in 120 seconds

METHODS (5)
OMT was performed on the study group for the entire research
period at NPI.
The median number of treatments performed was 5 (4-10):
• One week between treatments 1 and 2
• Two weeks between treatments 2,3,4 and 5
The specific OMT techniques used were left to the
discretion of the treating osteopath and not based on a
predetermined protocol. Techniques included BLT, BMT,
myofascial release and osteopathy in the cranial field.
STATISTICAL ANALISIS (1)
• Descriptive analysis was performed using frequencies, arithmetic
mean, median and standard deviation.
• Univariate statistical test includes formal tests of difference between
study group and control group using the chi-square test for categorical
variables and t test "unparied" for continuous measurements.
• Primary outcomes were changes made from pre-post test of the bells.
• Multivariate linear regression analysis was used to evaluate the
independence of the effects of OMT on primary outcomes considered
simultaneously adjusting for all potential confounding factors.
• Statistical significance was based on a probability level (alpha)
equal to 0.05. All results were expressed in terms of point estimate and
95% confidence interval (CI).

STUDY POPULATION
• Univariate analysis showed no statistically significant differences in
terms of the main characteristics measured at T0, including
medications and psychotherapy (Table 2).
Table 2. General features of the population at t0. n (%) p value from t test
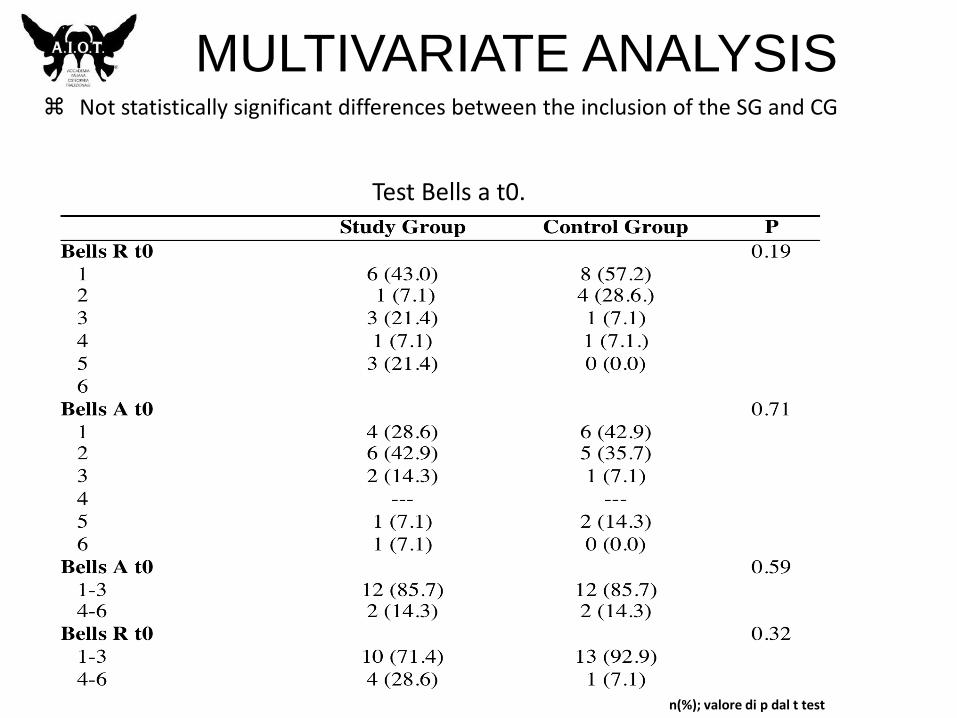
MULTIVARIATE ANALYSIS Not statistically significant differences between the inclusion of the SG and CG
n(%); valore di p dal t test
Test Bells a t0.

UNIVARIATE ANALYSIS
• Bells A:
• p<0.05 for OMT, sex, age> 8
years and no medication
• Bells R:
• No differences between SG and
CG

CONCLUSION
• Promising results in terms of attention
improvement
• OMT is associated with a significant
improvement in bells test

STUDY LIMITATIONS
• Non randomized patient allocation
• Sample size not based on power
estimation
• Additionally internationally validated
measures not included
CONCLUSION (1)
•Adolescent clinical outcomes for young people with attention-deficit hyperactivity disorder. Langley K, Fowler T, Ford T, Thapar AK, van den Bree M, Harold G, Owen MJ, O'Donovan MC, Thapar A ; Br J Psychiatry. 2010 Mar;196:235-40.
RESULTS: Most adolescents (69.8%) continued to meet full criteria for ADHD, were known to specialist services and exhibited high levels of antisocial behaviour, criminal activity and substance use problems. Maternal childhood conduct disorder predicted offspring ADHD continuity; maternal childhood conduct disorder, lower child IQ and social class predicted offspring conduct disorder symptoms.
CONCLUSIONS: The treatment and monitoring of ADHD need to be intensified as outcomes are poor.

CONCLUSION (2)
• Communication between pediatric
neurologists, psycotherapists and
osteopaths is needed to improve
children well-being

ACKNOWLEDGMENT
• CHIARA LUCCI D.O.
• CRISTINA GRANCHELLI D.O.
• LORENZO DI MATTIA D.O.
• FRANCESCO CERRITELLI D.O.
• GIANFRANCO PIZZOLORUSSO D.O.
• A.I.O.T