
ROLE OF LOCOREGIONAL TREATMENT IN THE MANAGEMENT...
124
ROLE OF LOCOREGIONAL TREATMENT IN THE MANAGEMENT OF METASTATIC BREAST CANCER Dr.Sivagnanam Balaji, MD RT, Cancer Institute (WIA),Adyar AIM OF THE STUDY: Aim of this retrospective study is to evaluate the role of loco regional treatment such as local radiotherapy and surgery in the management of patient with metastatic breast cancer. MATERIALS AND METHODS: One hundred and Ninety five patients with metastatic breast cancer between the years 2003 to 2008 were taken for this retrospective study. Among these, seventy five patients did not receive locoregional treatment, and the remaining one hundred and twenty patients received locoregional treatment to the primary. Locoregional treatment included radiotherapy and surgery. RESULTS: Patients survival was analyzed at the end of 1 year, 3 years, 5 years, and at the end of 10 years. It was found that, in patients receiving concurrent chemoradiation, survival at the end of 1, 3, 5 and 10 years were 89%, 58%, 46% and 42% respectively. Similarly, in patients receiving concurrent chemoradiation followed by surgery, survival was 97%, 80%, 71% and 70% respectively. Further,
Transcript of ROLE OF LOCOREGIONAL TREATMENT IN THE MANAGEMENT...
ROLE OF LOCOREGIONAL TREATMENT IN THE MANAGEMENT OF
METASTATIC BREAST CANCER
Dr.Sivagnanam Balaji, MD RT, Cancer Institute (WIA),Adyar
AIM OF THE STUDY:
Aim of this retrospective study is to evaluate the role of loco regional
treatment such as local radiotherapy and surgery in the management of patient with
metastatic breast cancer.
MATERIALS AND METHODS:
One hundred and Ninety five patients with metastatic breast cancer between
the years 2003 to 2008 were taken for this retrospective study. Among these,
seventy five patients did not receive locoregional treatment, and the remaining one
hundred and twenty patients received locoregional treatment to the primary.
Locoregional treatment included radiotherapy and surgery.
RESULTS:
Patients survival was analyzed at the end of 1 year, 3 years, 5 years, and at
the end of 10 years. It was found that, in patients receiving concurrent
chemoradiation, survival at the end of 1, 3, 5 and 10 years were 89%, 58%, 46%
and 42% respectively. Similarly, in patients receiving concurrent chemoradiation
followed by surgery, survival was 97%, 80%, 71% and 70% respectively. Further,

survival for chemotherapy was 60%, 5%, 2% and 0% respectively. Again, for the
arm including only radiotherapy, survival was around 67%, 33%, 33% and 33%
respectively. Those patients who receive only hormonal therapy had 50%, 13%,
13% and 13% overall survival at the end of 1, 3,5 and 10 years.
CONCLUSION:
The data reported in this retrospective study confirmed that chemo-radiation
improved overall survival and symptomatic local control, demonstrated in loco-
regionally treated patients with metastatic breast cancer.

1
INTRODUCTION
Evolution of breast cancer
As carcinoma of breast has no clear cause hence gained much
attention throughout the ages all over the world. The story of breast
cancer is complex as there is no happy ending unlike other diseases. The
development and milestones of breast cancer started from the ancient
civilization of the Chinese, Egyptian, Babylonian, Greek, Greeco-
Roman, middle ages Christian, Jewish, Arabic.
The Chinese form of medicine describes five forms of therapy for
tumors.
1. Spiritual care
2. Pharmacology
3. Diet
4. Acupuncture
5. Treatment of specific diseases

2
Egyptian form of medicine was described by IMHOTEP who used
cautery for cancer. Edwin Smith during his period obtained information
from Papyrous roll described that breast cancer that are cold on touch
has no treatment.
During Greek period, Hippocrates described diseases in three
groups.
Curable when medicine
1. Curable by knife
2. Curable by fire
Hippocrates also described that breast cancer was the cessation of
menstruation.
Greeco-Roman period – Aurelius Celsus described breast cancer
as a fixed irregular swelling with dilated veins and ulcers and divided
into four staged

3
1. Early cancer
2. Cancer without ulcer
3. Cancer with ulceration
4. Cancer with cauliflower like growth, and advised no treatment
for last three stages.
The first physician who operated breast cancer in the first century
was LEONIDES. His method of surgery was by using incision from the
uninvolved part of the breast and applied cautery to stop bleeding, the
same method was repeated until the whole breast is removed and the
underlying tissue was covered with eschar. Galen described breast
cancer was due to black bile and said breast cancer looks like a crabs leg
and suggested patient to be purged and bleed and to let out the tumor in
early stages.
From Middle Ages – downfall of Romans – beginning of
Renaissance - Christian
During this period the patron of breast disease was Saint Agatha in
the third century whose breast was cut off using sheets

4
Arabic Rhazes advised excision of breast cancer only if it was
completely operable. Hay ben Abbas advised compete excision of the
disease and allowed bleeding to evacuate the bad disease.
Renaissance – from medieval to modern Era
Andreas Vesalius recommended mastectomy for breast cancer and
used sutures instead of cautery. Ambrose Pare described lymph node
metastases of breast cancer. Serventus described the method of removal
of pectoralis muscle with axillary glands. Wilhelm Fabry, father of
German surgery compressed and fixed the base of breast and used knife
to amputate the breast. Johan Schultles, German surgeon, inventor of
surgical instruments .18th Century
Henri Le Dran of France described carcinoma of breast as a
localized disease in early stages and lymph nodal spread as bas disease
with bad prognosis. Jean Petit, friend of Le dran advised surgery of
breast cancer involves removal of breast, pectoral muscles and axillary
nodes. German surgeons, Lorez and Heister advised Guillotine machine
for breast tumor.

5
Heister described the relationship between surgeon and patient and
said that surgeons should be stead fast and not to be disconnected by the
cries of the patient.
19th Century- period of invention of aneasthesia and antisepsis
hence breast cancer surgery improved.
European surgery –
Nooth an English surgeon sprayed carbolic acid over the breast
instead of cautery. Syme described the need for axillary lymph node
dissection in breast cancer patients. Charles Moore believed in extensive
surgery for breast cancer and said that tumor should not be cut as it may
disperse the tumor and allow recurrence of the disease. He also advised
the entire removal of breast with skin and not to remove pectoralis
muscle. Richard Van Volkman advised extensive surgery even for small
tumors. Theodor Billorth also advised the same. Ernst Kuster advised
removal of axillary fat with axillary nodes. Lothar Heidenhain advised
removal of superficial pectoralis major muscle. Everard Home showed
appearance of cancer cells under microscope. Henrich Van
WaldeyerHantz described carcinoma arising from epithelial tissue and

6
sarcoma from mesodermal tissue. Victor Cornil described malignant
transformation of acinar epithelium of breast. David Van Hansemann
described diffentiation of cancer cells (ANAPLASIA)
American Surgery
Joseph Pancoast described the pre-anesthetic era of mastectomy
with axillary lymphatic drainage. Samuel.D.Gross described breast
conservation surgery. William Halsted advised removal of breast cancer
with pectoralis muscle. William Meyer modification of Halsted’s
procedure advocated removal of pectoralis minor muscle along with
pectoralis major. Cullen and William Welch was the first to do the
frozen session of the breast in the diagnosis of breast cancer.
20th century it became evident that cure can be achieved by
surgery. Halsted and Meyer surgery didn’t include supra clavicular and
internal mammary nodes and its removal did not show any improvement
in survival. William Handley showed the involvement of internal
mammary node when axillary node was involved in breast cancer
patients. Jerome and Owen Wangsteen advised supra radicle
Mastectomy which involved dissection of mediastinum and neck.

7
Cushman Haagensen classified breast cancer according to size and nodal
status . He was the first person to advise breast self-examination. In 1948
the first concept of modified radical mastectomy was done by Patey and
Dyson. Donald Morton and Giuliano developed sentinel node biopsy
technique. In 1937 London surgeon, Geoffrey Keynes described minimal
surgery for breast cancer and advised radiotherapy which had equally
good result . In 1948 simple Mastectomy followed by radiotherapy was
introduced by R. McWhirter.

8
Radiotherapy
Emile Grubbe medical graduate studying 2nd
year from Chicago
was the 1st person to irradiate breast cancer patients, he used tin foil to
protect the normal skin to protect the normal skin
In 1896 Hermann Gocht of Germany treated breast cancer patients
with radiation and used flexible led to protect normal tissue
In 1903 1st department of radiotherapy was founded by J.Pollock
in London George Perthes a surgeon from Germany described curative
effect of X- rays
Post op radiotherapy was used in America and Europe before
world war I. before world war I energy used was 150kv X-rays, after
world war II 170-200kv X-rays was used
In 1929 S. Harrington of the mayo clinic studied 1859 breast
cancer patients irradiated between 1910-1923. He expressed doubts
about ancillary RT George Pfahler from Philadelphia adviced post op RT

9
for all cases of breast cancer after 2 weeks of surgery. In his review of
102 patients there is no significant benefit in survival in stage I patients
but showed a improved 5 year survival in stage II patients.
Radiotherapy as a single modality for breast cancer was used in in
operable cases during the beginning of 20th century until 1922.
William Stone from New York showed the benefit of RT over
surgery in inoperable breast cancer based on his experience on 10000
patients.
Geoffrey Keynes from London in 1932 used radium for
therapeutic use irradiation and showed 5 years survival rate of 77% in
node negative patients and 36% with node positive patients.
1930 super voltage X-rays were available .Francois Baclesse of
Paris did local excision of breast cancer followed by RT from 1937-
1953, and said that results were equal for stage I and stage II breast
cancer , between post op RT vs only surgery.

10
In 1948 Robert McWhirter proposed simple mastectomy followed
by RT He said radical mastectiomy was over kill for stage I breast
cancer, but inadequate for stage II breast cancer.
1960 cobalt emerged
1970 linear accelerator emerged

11
Chemotherapy
Paul Ehrlich was the father of chemotherapy.Arsenic was used in
ancient times for breast cancer treatment.
1898 1st alkylating agent was used.
World war II nitrogen mustard came into use .
1957 C. Heidel Berger used 5FU in breast cancer.
In 1958 thiotriethylenephospharamide alkylating agent.
1963 E.Greens Span used multi drug trials using methotrexate
with thiotepa.
Gianni Bonodona was the 1st person to start CMF regimen in
breast cancer.

12
Hormone therapy
Hormone therapy in breast cancer patients was started even before
20th century in 1889- Schinzinger of Germany proposed oophorectomy
before mastectomy .
In 1896-1901 George Beatson advised oophorectomy for breast
cancer patients .
In 1900 Boyd was the 1st person to combine oophorectomy with
mastectomy.
In 1953 Charles Higgnes combined oophorectomy and
adrenalectomy .
In 1950s hypophysectomy was done for advanced breast cancer.
1939 P.Ulrich used testosterone for breast cancer .
In 1944 Alexander Haddow used synthetic oestrogen .
In 1938 Edward Dodds synthesized stilbesterol.
I.Naphasyn also synthesized stilbesterol .
In 1950-1960 oestrogen and androgens was used much.

13
In 1973 W.McGuire demonstrated oestrogen receptors in breast
cancer patients .
In 1975 K.Horowitz demonstrated progesterone receptors.
In 1980 tamoxifen and SERM was used

14
History of staging
Has a long history surgeons divided into two groups to decide on
surgery either inoperable or operable, on the basis of certain observations
staging was initiated .
Steinthall’s grouping
Group1
Group 2
Group3
In 1940 manchester classification consists of
stageI
stage II
stage III
stage IV
Portmann classification
In 1943 CCC(cloumbia clinical classification )evolved from
Haagensen and Stout’s
Stage A-D

15
In 1954 UICC emerged started TNM classification developed by
Pierre Denoix of France
In 1962 AJCC emerged .Carcinoma breast is the most commonly
diagnosed cancer in women all over the world, affecting nearly 21% of
all cancer diagnosed in females a with high ratios in North America,
Western Europe, intermediate rates in South America and Eastern
Europe and low rates in Asia. 10 percent of newly diagnosed breast
cancer patients have metastatic breast cancer. After all treatments nearly
one third of patients will have progressive disease . metastatic breast
cancer median survival for the 3 yrs.
The range is very wide with some patients having more indolent
disease that they can live upto 10 – 15 years, while for others with
disseminated metastatic disease, the prognosis will be in the range of
months from the time of diagnosis. This will represent the disease extent
and distribution of metastatic disease, and reflects the biological
behaviuor of carcinoma of breast, while some women have disease
which shows good response to hormonal treatments, while others
with triple negative breast cancer can show increased resistance to all
systemic therapies.

16
The aim of treatmentic breast cancer is to increase the symptom
free survival and increase quality of life . at the same time the side effect
of the treatment to be minimised. The treatment for metastatic breast
cancer is depends on the individual patient and receptor status, general
condition of the patient. Even with newer systemic and locoregional
treatment mestatic breast cancer cannot be cured at present.In few
pateints with good prognostic factor these treatment modalities increases
the progression free survival which inturn may significantly affects the
overall survival. Many patients with metastases may live several years
with modern locoregional treatment and systemic chemotherapy.
Regions No.of Cases CIR ASR
World 1676633 47.9 43.3
More Developed
Region
793684 124.1 74.1
Less Developed
Region
882949 30.9 31.3
India 144937 23.8 25.8
Chenai (09-10) 1568 34.2 35.7
Breast Cancer Statistics
Source: Globocan 2012,IARC Publications & MMTR Report
CIR: Crude Incidence Rate per 100000 Populations
TOTAL NO OF BREAST CASES IN CHENNAI IN THE YEAR OF
2012 - 1568

17
NATURAL HISTORY AND ORIGINS
Concepts regarding the natural history of breast cancer have
undergone great evolution over the past 100 years, with a profound
impact on the management of these patients. The Halstedmodel was
based on an orderly progression to the regional lymph nodes and from
there to distant metastatic sites. Later another hypothesis was fully
demonstrated in both laboratory and clinical studies by Fisher,who
advanced the concept that breast cancer, as a systemic process involving

18
host–tumor interactions, would not show substantial effects on survival
with variations in locoregional treatment.
A third hypothesis putforward by Hellmanconsiders breast cancer
as a heterogeneous disease with aspectrum extending from a tumor that
remains localized throughout its course to one that disseminates
systemically, even when detected as a small lesion, suggesting that
metastases are a function of tumor growth and progression factors.
BREAST CANCER RISK FACTORS
Established Risk factors,
1. Age of the patient
Early Menarche, late menopause, Age at first child birth( related
to estrogen exposure)
1. Duration of Breast feeding
Decreasing the breast cancer risk by delaying ovulation and
decreasing the hormone exposure
2. Height weight and body mass index

19
3. Physical activity
4. Alcohol consumption
5. High dose estrogen containing oral contraceptive pills
And hormone replacement therapy in postmenopausal women
6. Inonizing Radiation
7. Family history and genetic susceptibility
Possible risk factor
1. Fat and future
2. Dietary phytooestrogen
Hereditary breast cancer
5-10% of the breast cancer is due to familial risk factor.
The breast cancer susceptibility genes divided into three types.
1. High penetrance
2. Intermediate penetrance
3. Low penetrance
Low penetrance are the most common variety BRCA1 and
BRCA2 genes Fifty percent of the familial breast cancers are mainly due
to BRCA1 and BRCA2 genes.

20
This increases the relative risk of the cancer breast to 10 to 30
times of the normal population.
The prevalence is more common in jewish population. BRCA1
mutations characteristically has a basal – like phenotype, inactivating
germiline mutation. The similarity between hereditary BRCA1-related
sporadic BLBC sporadic basal like breast cancers may also harbor an
underlying defect in BRCA1, which has been termed “BRCAness”.
BRCA2 – related cancers do not have an association with TNBC or the
basal – like phenotype. Other rare breast cancer susceptibility genes
related to the breast cancer are CHEK2,TP53,PTEN,STK11

21
DISTIBUTION
Upper outer quadrant is the most common site of carcinoma breast
which contributes about 38% of the total incidence. The second common
site is the central area of the breast followed by upper inner quadrant and
then the lower inner quadrant.
The distribution correlates with the difference in density of breast
tissue in various quadrants.
LOCAL SPREAD
During the development and progression of the breast carcinoma,
it starts from the ducts and then breaches the basement membrane enters
into the surrounding breast parenchymal structure. The tumor can grow
through the wall of blood vessels, spread into the deep lymphatics of the
dermis, and eventually produce edema of the skin (peaud’orange), which
usually indicates that the superficial as well as the deep lymphatics are
involved. Skin dimpling can be caused by involvement of Cooper’s
ligament. Ulceration and infiltration of overlying skin, which may

22
develop late in the course of the disease, are usually preceded by fixation
and localized redness of the skin over the tumour.
Axillary Spread
Majority of the breast carcinoma spread through axillary nodes
and the percentage of the nodal involvement increases with tumour size.
The percentage varies from between 10% and 40% depending on the size
of the tumour.
Supraclavicular Spread
Spread to supraclavicular lymph nodes usually follows
involvement in the high axillary lymph nodes or IMNs. Clinical failure
in the supraclavicular fossa is relatively rare in patients with early-stage
breast cancer and is dependent on the degree of axillary involvement.
For patients with no or minimal nodal involvement (less than three
involved axillary nodes), supraclavicular failure is extremely rare.
23
Internal Mammary Spread
Metastases to the internal mammary nodes (IMNs) are correlated
with tumour size, are more frequent from medial half and central lesions,
and occur more frequently when there is axillary node involvement
Systemic Spread
Of the systemic metastasis,
Approximately 60% are in bone,
10% in lungs,5% in liver,
5%in central nervous system
15 to20% in multiple sites.
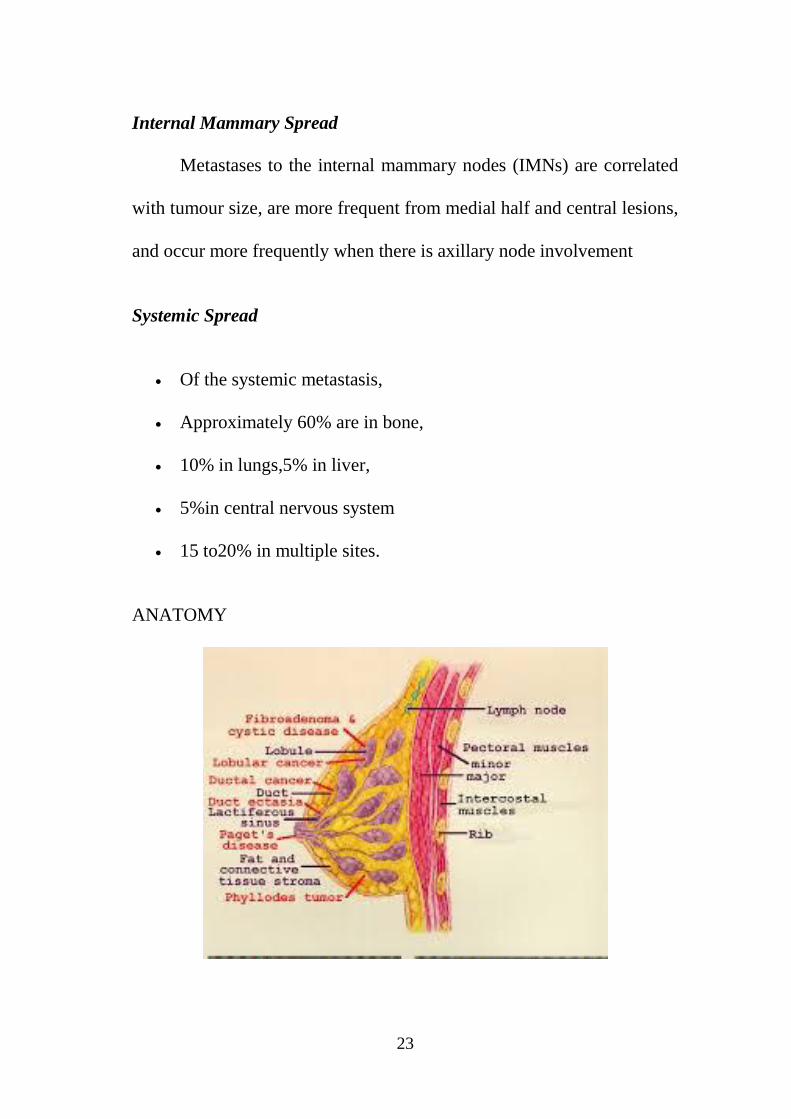
ANATOMY
24
The female breasts are modified eccrine glands on the anterior
chest wall, superiorly frim the second rib to inferiorly upto the 6th
rib,
medially to the sternal edge and laterally upto the mid axillary line. The
breast parenchyma is composed of lobules and ducts. The function of the
lobules is to produce milk and the function of the ducts is to transport
lactation products to the nipple The breast parenchyma is intermixed
with connective tissue, which has a richvascular and lymphatic network.
Mammary gland lymphatics begin in the interlobular or prelobular
spaces, follow the ducts, and end in the sub areolar network of
lymphatics of the skin.
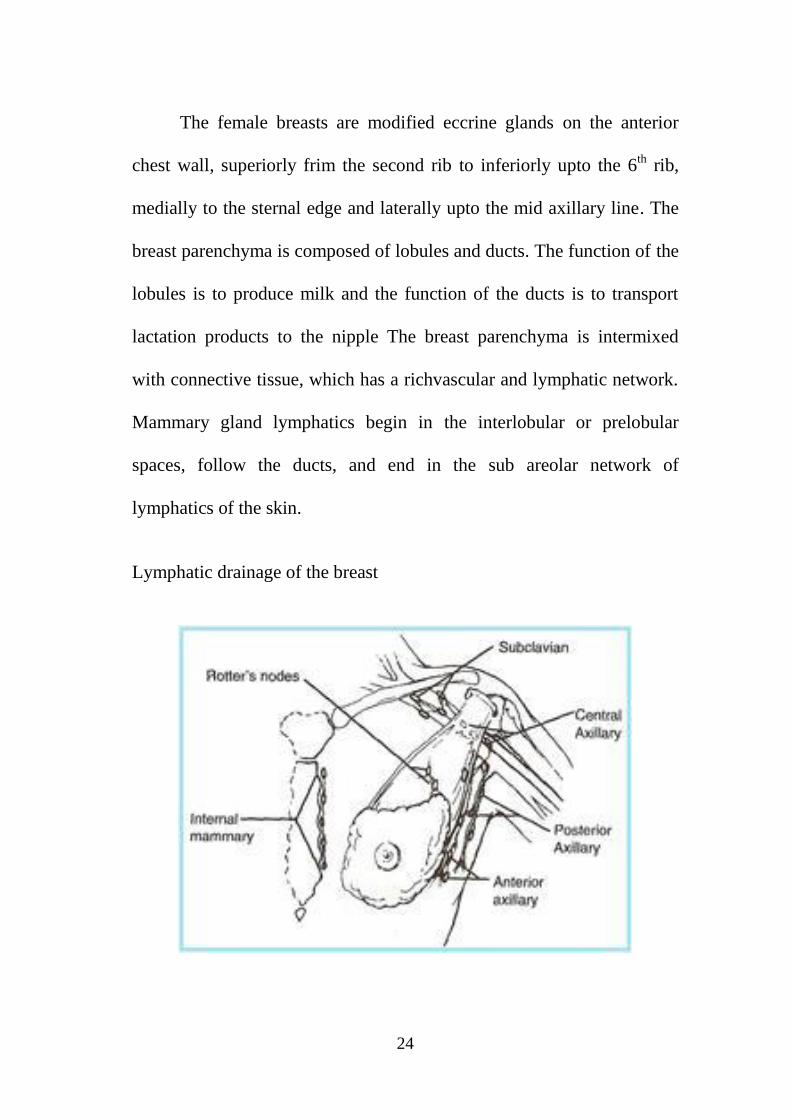
Lymphatic drainage of the breast
25
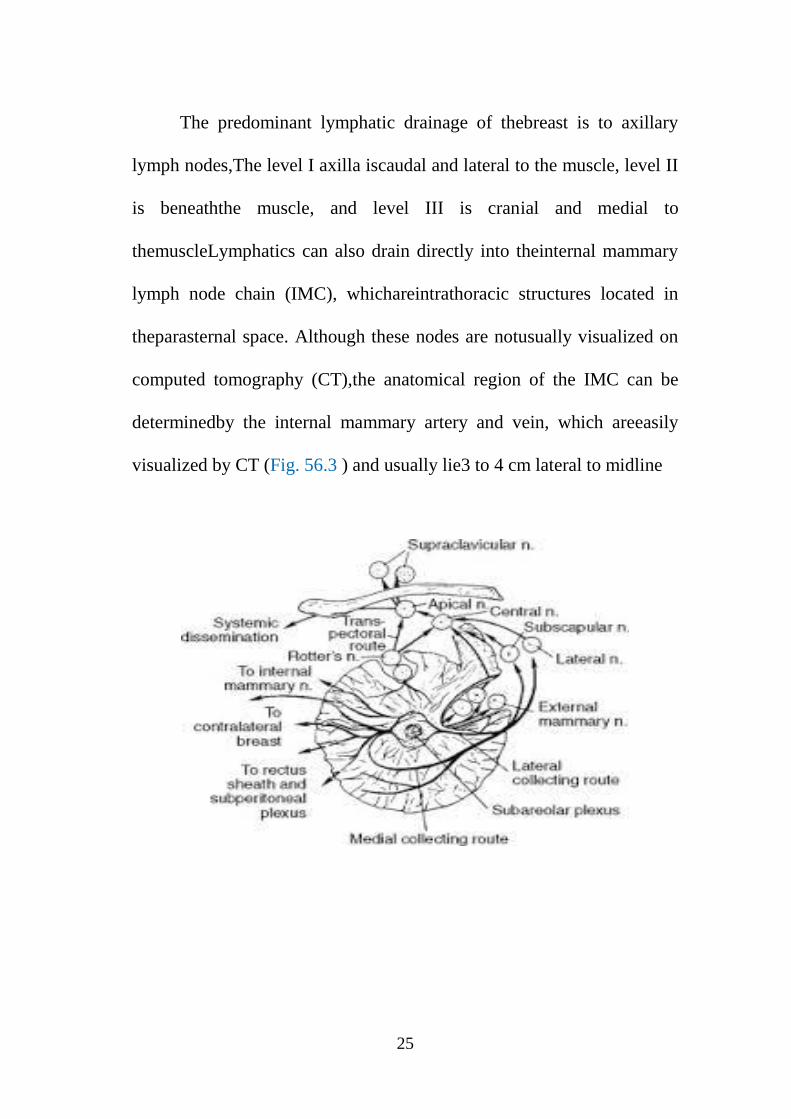
The predominant lymphatic drainage of thebreast is to axillary
lymph nodes,The level I axilla iscaudal and lateral to the muscle, level II
is beneaththe muscle, and level III is cranial and medial to
themuscleLymphatics can also drain directly into theinternal mammary
lymph node chain (IMC), whichareintrathoracic structures located in
theparasternal space. Although these nodes are notusually visualized on
computed tomography (CT),the anatomical region of the IMC can be
determinedby the internal mammary artery and vein, which areeasily
visualized by CT (Fig. 56.3 ) and usually lie3 to 4 cm lateral to midline

26
PATHOLOGY
Breast carcinomas are divided in to insitu carcinoma and invasive
carcinoma
Insitu carcinoma are divided into ductal carcinoma insitu and
lobular carcinoma insitu.
INVASIVE CARCINOMAS
The histological typing of breast cancer is made by exclusion
INVASIVE DUCTAL CARCINOMA (NOS) is an invasive carcinoma
that doesn’t fulfil definition of other categories.
Invasive lobular carcinoma, tubular carcinoma, mucinous
carcinoma, cribri form carcinoma, papillary carcinoma, scirrhous
carcinoma, comedo and medullary carcinomas are fuse specified types of
breast carcinoma. Histological used in the Brest cancer is proposed by
elston and ellis it is the modification of bloom rich at son in 1957 it has 3
factors

27
1. Tubule formation
2. Pleomorphism
3. Mitotic activity
Each factor scored on a scale of 1-3 tubule formation Histological
grade
3 – 5 - well differentiated tumours
6 – 7 - moderately differentiated
8 – 9 - poorly differentiated
Luminal A
100% ER positive,70% ER positive, good risk , 10 years relapse
free survival 70%, low risk on oncotype Dx and Mamma print and
hormone responsive tamoxifene responsive ,chemo insensitive ,Ki 67%
<14% primary tumor 62% T1 , 38% T2 , HER2 negative ,
Luminal B
ER positive less than 50%, PR positive bad prognosis , 10 years
relapse free survival 53% ,tamoxifene insensitive , aromatase inhibitor
sensitive , Ki 67% more than 14% ,younger age higher grade , 30% are

28
HER2 positive ,Intermediate to high risk on oncotype DX and Mamma
Basal type
Do not express ER,PR or HER2 negative 85% (triple negative) are
basal
Express myoepithelial cell membrane CK5 , C-Kit ,EGFR, HER2
tends to be high grade .
NG-III, present with large tumours T2 and above
chemoresponsive high relapse rate in CNS
BRCA1 tend to be basal line common in African Americans
Angiogenesis
Targeting angiogenesis in metastatic breast cancer Judah Folkman
in 1970 first described the concept of angiogenesis by targeting blood
vessel formation by preventing tumour growth and metastasis . he
defined anti angiogenesis therapy which causes regression of tumour by
altering tumour vasculature , normalization of surviving tumour
vasculature , inhibition of regrowth of vessel and neovascularisation in

29
tumours, eg. antiVEGF antibody-Bevacizumab dose:10mg /kg every
2weeks of 15mg /kg every 3weeks
Prognostic bio marker
Indicates the proabablity of specific clinical outcome such as
recurrence progression survival independent of treatment
Predictive bio marker
Indicates the chance of response to specific therapy
Response indicator
Monitors response and assist in stop vs continue treatement
Pharmacokinetic bio marker
It measures pharmacokinetic parameters of drug exposure
Pharmacodynamic bio marker
Measures end point of drug effect on target pathway and
downstream biological process
Prognostic multigenes signatures in carcinoma breast
Mamma print –microarray-70genes –freshfrozen tissue
Rotterdam signature-microarray-76 genes-freshfrozen tissue
Genomic grade index-microarray-97genes-freshfrozen tissue
Mammostrat IHC-5genes-Formaline embedded fixed paraffin

30
Oncotype DX –qRT-PCR-21 genes- Formaline embedded
fixed paraffin
DIAGNOSTIC EVALUATION
History
Complaints related to the breast cancer and history related to the
risk factors to be elicited history of any lump in the breast, nipple
discharge, skin changes, any axillary swellings to be asked.
Physical examination
It includes inspection and palpation of the breasts, axilla,
supraclavicular region,
The breast is examined by various positions including sitting with
arms either side, sitting positions with arms above the patient’s head,
patient’s hands pressed against her hips the following changes in the
breast to be noted
1. Any asymmetry of the breast
2. Inverted nipple
3. Skin changes

31
Palpation of breast.
It should be perform with the patients in supine position and also
in sitting position
Signs of breast cancer.
1. Palpable mass
2. Nipple discharge- unilateral bloody discharge
3. Nipple changes – any retraction, infiltration, pagets .
4. Skin changes – dimpling or skin retraction.

32
Biopsy
The following important factors to be identified in the specimen
which is needed for further management.
Hormone receptor status – ER,PR status
1. HER2 neu status
2. Histological type of cancer
3. Histological grading
Baseline investigations
1. Complete blood count
2. Blood biochemistry
3. Liver function test

33
4. Renal function test
5. X ray chest PA view
6. Ultrasound abdomen and pelvis
7. Ct chest
8. Bilateral mammogram.
MAMMOGRAM
Mammogram provides additional information
In the presence of palperable mass mammography is useful in
detecting occult lesion in same or opposite breast, it is classified as
screnning mammography of diagnostic mammography
Screening mammography to screen asymptomatic women
Diagnostic mammography is a definite imaging workup to locate a
mammographically visible lesion
IMPORTANCE OF MAMMOGRAPHY IN BREAST CANCER
Reduction in breast mortality
Swedish country trial 30% (40-74 years)
Malmo trial 36% (45-49 years)
Gottenberg trial 45% (39-49 years)
Metaanalysis of 5 swedish trials 29% (40-59 years)

34
TYPE OF VIEWS
In screening mammography –two views, mediolateral oblique
view and cranio caudal view
In diagnostic mammography – mediolateral view craniocaudal
view and exaggerated CCL –CCM
MAGNIFICATION VIEWS
BI-RADS ( british imaging reporting and data system) false
negative 75-80% due to dense breast in young women
Classification
Category 0 – assessment incomplete used in screening
Category 1 – normal
Category 2 – benign finding
Category 3 – benign probably
Category 4 – malignancy suspected
Category 5 – malignant
What is triple diagnosis?
Physical finding
FNAC
Mammogram

35
WHAT IS A MASS?
M –mobility T – tenderness
A –attachement L - location
S –shape C - consistency
S – size
DEFINED AS A PALPABLE ABNORMALITY DISTINCT FROM
SURROUNDING TISSUE
USG of breast
USG of breast is a useful complement to mammography for
evaluation of dense breast when results of physical examination and
mammography are equivocal useful in these group of patients
1. Those with dense breast and localized sysmptoms of with a
suspicious area detected in MMG
2. Those with non palpable abnormality discovered on MMG
3. Those with palpable masses considered intermediate on MMG
4. To guide aspiration of non palpable cystic structure
5. To do FNAC of small lumps

36
MRI of breast
Sensitivity 97-99%
Specificity 28-37%
Greatest strength of MRI to detect occult metastasis in dense
breast and recurrence after irridation
FDG PET scan
Sensitivity 93%
Specificity 73%
Accuracy 89%
Positive predictive value 92%
Negative predictive value 96%
False negative 20%
Bone scan: technetium 99, F18 – more specific recommended for
stage II and above cancers and T size >2cm
The mammographic findings for malignancy include ill definded
mass with spiculatlions, micro calcifications (100 to 300 um rod like,
tubular, branching or punctuate) and architectural distortion.
Magnetic Resonance Imaging

37
Indications
To assess the silicone implant integrity
To diagnose the malignancy in reconstructed breast
To rule out multifocal disease before doing Breast reconstructive
surgery
To assess the response to neoadjuvant chemotherapy
To diagnose the occult primary.
Positron Emission tomography The metabolism of the tumour
cells are mainly by glycolysis not by oxidative metabolism
This difference between tumor cells and normal cells is the basis
for the PET imaging.
Uses
1. To differentiatiate the recurrent breast cancer from postoperative
scar.
2. Have high accuracy in detecting presence or absence of lymph
node involvement

38
3. Able to screen the whole body in a single imaging method for
distant metastasis
4. Pet is very much useful in the quantitative response assessment
after neoadjuvant chemotherapy.
STAGING (TNM CLASSIFICATION) AJCC 2010
Tx Primary tumor cannot be assessed
T0 No evidence of primary tumor
Tis Carcinoma in situ
T1 mic Tumor</=1 in greates dimension
T1a Tumor>1<5 mm in greatest
dimension
T1b Tumor>5<10 mm in greatest
dimension
T1c Tumor>10>20 mm in greatest
dimension
T2 >2<5cm in greatest dimension

39
T3 >5cm in greatest dimension
T4a Extension to chest wall not including
pectoralis muscle
T4b Ulceration and/or ipsilateral satellite
nodules and/or edema (including
peau d’ orange) of the skin
T4c Both T4 a and T4b
T4d Inflammatory carcinoma
Nx Regional lymph nodes cannot be
assessed
No No regional lymph nodes
N1 Metastases to movable ipsilateral
axillary lymphnodes(s)
N2a Metastases in ipsilateral axillary
lymph nodes fixedto one another
(matted) or to other structures
N2b Metastases only in clinically detected
ipsilateral internal mammary nodes
and in the absence of clinically
evident axillary lymph node

40
metastases
N3a Metastases in
ipsilateralinfraclavicular lymph node
(s)
N3b Metastases in ipsilateral internal
mammary lymph nodes (s0 and
axillary lymph node (s)
N3c Metastases in ipsilaternal
supraclavicular lymph node(s)
M0 No distant metastasis
M1 Presence of distant metastasis
COMPOSITE STAGING
STAGE 0 Tis No Mo
STAGE1A T1 No Mo
STAGE1B To N1 mic Mo
STAGE2A T1 N1 mic Mo
STAGE2B T0 N1Mo, T1 N 1 Mo, T2 No Mo

41
STAGE3A T0N2Mo, T1 N2 M0, T2 N2 M0
T3 N1 M0, T3 N2 M0
STAGE3B T4 N0 Mo, T3 N1 M0 T4 N2 M0
STAGE3C Any T N3 M0
STAGE4 Any T Any NM1
Overall survival of breast cancer patients correlates with the stage
of diseae at presentation. The table depicts 5 years survival according to
stage of the disease”
Stage 5 Year Survival
0 100%
1 98%
2A 88%
2B 76%
3A 56%
3B/C 49%
4 16%

42
METASTASES:
The metastatic potency of cancer cells depends upon the intrinsic
properties of tumor and their interactions with tissue environment. The
steps of metastases include Proliferation of tumor cells by paracrine
growth (tissue environment), autocrine growth (from tumor itself)-
EGFR, c-erb /HER2neu, TGF- alpha, HRG, Neovascularisation due to
new vessel formation by factors released by the tumor and tumor cells
exhibit motility there by detachment and movement from the primary
site
Invasion is a process by which there is destruction of basement
membrane, connective tissues, adhesion and motility with response to
release of factors.Distant metastases is due to release of cancer cells in to
blood or lymphatic stream in to the body as single cell or emboli . These
emboli gets arrested in the draining sites like lymph nodes ,organs
,adhere to endothelial cells and capillary beds. Extravasation also
involves same steps of invasion 8) Growth in the deposited organ of
metastases depends upon the responses of paracrine and auto crine
factors of the tumor,once metastases establishes it becomes a source for
further metastases known as “ METASTASES OF METASTASES”.

43
The risk of relapse in carcinoma breast patients is more during the
first 2 yrs after diagnosis and treatment, the time of events and survival
of cells vary in circulation within minutes to years.
Genes associated with metastases in carcinoma breast are
S100A4/MTA-1/ Osteopontin /bcl-2/maspin.Genes associated with
suppressing of carcinoma breast are nm23/ KAI1 /KiSS 1/BRMS1.
Metastases in breast cancer was described by Stephen Paget base on”
seed and soil “hypothesis .
Role of surgery in metastatic breast cancer
At present carcinoma of breast has replaced carcinoma of cervix in
Indian tumor registries. Survival of these patients has increased over the
years. Over the years systemic therapy is the treatment of chronic and
local therapy like Radiotherapy and Surgery.
Mechanism of Metastases in breast cancer
Halsted was the first person to state the therapy of metastases.
According to him breast cancer is a localized disease in the breast and it

44
spreads to axillary nodes and to the sanctuary site. Hence he advocated
extensive loco-regional treatment.
Bernard Fischer later defined that breast cancer was a systemic
disease, which has a capacity to spread to other sites even before
diagnosis. Later Spectrum theory emerged and stated that exact meaning
of metastases to distant sites was unclear. Hence advised both systemic
and local therapy.
STEPS IN METASTATIC PROCESS

45
Lang et al described three theories
1. Parallel evolution, which says that circulating tumor cells present
in the tumor is the cause for the metastases during tumorigenesis
even before the development of the intact primary tumor.
2. Gene expression profile theory says that potential for metastases is
an inherent property genetically present in breast cancer patients
during early stages
3. Stem cell model says that metastatic potential of breast cancer or a
specialized tumor initiating cancer cells.
Danna et al defined the concept of surgery in metastatic breast
cancer by the theory of immune-suppression, which is reversible by the
surgical removal of primary tumor. The first study in evaluating the
treatment of metastatic breast cancer was by Khan et al in 2002, which
was a retrospective study, which showed survival benefits.
Survival benefit?
Question to be answered before initiating the treatment.
At present survival for visceral metastases is 6 months, nodal
disease is 18 months, bone only disease is 3-4 years.

46
In Khan et al study which reviewed NCDB, 3 years survival was
24.9% for the whole group. Survival for total Mastectomy 31.9 months,
partial mastectomy 26.9 months, no surgery 19.3 months .
There are several studies which showed survival benefit like
Rapids et al, Gnerlich et al, Blanchard et al, McGuire et al , Babiere et al
, Neuman et al, reported trends towards increased survival. But it was not
statically significant.
Should lymph node dissection be done?
The exact details are not reported not so far in most of the reviews.
When the logic of improving the survival applies to removal of the
primary, the same can be applied to ALND. Hence patient under going
total Mastectomy can be given the benefit of ALND. NCDB conclude
that ALND can be a contributing factor for survival with total
mastectomy but it is an independent prognostic factor. Studies evaluating
the benefit of ALND are Rapids et al, McGuire et al and Neuman et al.
All these studies showed some survival benefit and advised ALND as a
part of treatment approach.
Negative margin be attempted?

47
Even though negative margin is the fundamental concept of
oncology, there is a lack of data towards the role of negative margin
resection in metastatic breast cancer. The studies evaluating this are
Rapids et al, McGuire et al and Khan et al. These studies supported the
need for negative margins based on the review, which showed five-year
survival of 27% for negative margin, 16 % for positive margin and 12 %
for unknown margin. Hence it will be better to give negative margin.
When to operate?
When the decision of loco-regional treatment is offered, then the
timing of the surgery is to be decided. Based on the review of articles
showed that surgery may be done after three months of initial
diagnosis/chemotherapy improved progression free survival. The time
gap between diagnosis/ chemotherapy makes the oncologist to study the
behavior of the disease. Studies favoring this are Babiere et al, Neuman
et al, and Rao et al.
Prospective Trials

48
The MF 07-01 9(NCT00557986) is phase 3 RCT that compares
metastatic breast cancers patients at presentation who receive loco
regional treatment Vs no treatment and to assess the overall survival
benefit, which was activated in 2007. Short interim remits in ASCO
2010 shows no evidence for surgery. Similar NCT 00193778 study from
India familiar to show such benefit.
The current evidence is not enough to use surgery for primary
MBC. However there is subset of patients who may be offered loco-
regional treatment such as surgery to maximize survival.
CONCURRENT CHEMOIRRADIATION
There is no enough dsatafavouring concurrent chemoirradiation in
locally advanced breast cancer and metastatic breast cancer ,but there are
studies favouring concurrent chemoirradiation in breast conservation
surgery even though not practiced much.Studies favouring concurrent
chemoirradiation are the following.
Study1: Argangelia et al did randomized study using concurrent
Vs sequential CMF chemotherapy.

49
Sample size 206 pts,TD 50Gy/20# over 4 wks followed by 10-15
Gy electron boost following BCS.there was no difference in breast
recurrence, metastasesfree ,diseasefree ,overall survival in the two
treatment. all patients completed the total dose of Rt and there was no
difference in toxicity profile between the two arms ,study showed that
RT can be delayed for 7 months if margins were negative and considered
concurrent CMF as a safe regimen and may be used in patients with
high risk of local recurrence.
Study2:Rousse et al study used FNC regimen consisting of Inj
5FU 500 mg/m2 / Mitoxantrone 12mg/m2/ Cyclophosphamide
500mg/m2 to sequential FEC regimen consisting of Inj2FU200mg/m2/
Epiribicin 60mg/m2/ Cyclophosphamide 500mg/m2.
Sample size 650 pts RT in node positive breast cancer
ptspts.There was no difference in DFS or overall survival(3% Vs 7%)
out these 6 had LRR in concurrent arm and 18 had LRR in sequential
arm.

50
Study3: Tolenado et al studied Arm –A sequential chemo +RT,
Arm B concurrent chemo irradiation using FNC regimen consisting Inj
5FU/Mitoxantrone/Cyclophosphamide. Sample size 214 pts,local control
was superior in concurrent arm but toxicity was more like subcutaneous
fibrosis/ telangiectasia /skin pigmentation /breastatrophy.but there was
no difference in Grade II skin reaction/breast pain/lymphedema
Study4: Calais et al similar to Rousse et al study .Toxicity was more, LC
was good/LRR was low.
Study5:Bellon et all: was prospective single arm study which
showed good local control in high risk group patients with
le received concurrent CTRT 109 ptsVs 426 pts received sequential RT,
local control and locoregional relapse was lesser in CTRT arm ,these
studies did not use Adriamycin and taxanes.
Study7:Goyal et al studied using Bevacizumab in
combinatconcurrentCMFand lesser dose of RT.
Study:Rerospective study from Yaion with whole breast RT Vs RT alone
there was no difference in grade III reactions/no fatigue of RT/RT
fibrosis/ pneumonitis / lymphedema between the two arms.

51
HYPOFRACTIONATED WHOLE BREAST IRRADIATION
It is growing trend at present which involves delivering higher
dose per fraction with in a short period of time to a biologically
equivalent dose .START Trial A -1-( pT1-3a pN0M0)-TD:50 Gy25#Vs
41.6Gy or 39Gy in 13# of 3.2Gy or 3.0Gy over 5weeks after surgery.
Over all treatment time was kept constant in all three arms including
SCL& Axilla. Primary end point was LRR .LRR at 5 yrs was 3.6% for
50 Gy/3.5% for 41.6Gy/5.2% for 39 Gy.START B Trial- (pT1-3a pNo-1
M0)-TD 50Gy25#/40Gy 15# of 2.67 Gy over 3 weeks .Here over all
treatment time was not consistent.LRR at 5 yrs was 2.2 % for 40
Gy/3.3% for 50 Gy. Whelan et al study after BCS randomized to TD:50
Gy @25# vs 42.5 Gy@ 16#.LRR at 10 yrs was 6.7% for 50 Gy 25
#/6.2% for 42.5 Gy 16 #.
ASTRO 2011 concluded that hypofractionated whole breast
irradiation is equivalent to conventional irradiation who meet the
following criteria 1)50 yrs and above 2)pathologicT1-T2 N0 treated with
lumpectomy 3)patient not receiving chemotherapy 4)minimum and
maximum dose along central axis not <93% and not >107%.heart should
be excluded from treatment fields during planning hypofractionated

52
RT.RTOG 1005 is phase III study on hypofractionated RT.Taking
age/comorbidities/distance of RT facility in to consideration
Hypofractionated RT may be offered to these patients. Accelerated
Partial Breast Irradiation :
Even though whole breast irradiation is the standard of treatment
for BCS patients APBI is an alternate approach which can shortern
treatment time ,there by more easier for patient,easier delivery of
radiation and chemotherapy ,also reduces the treatment cost.
The concept behind this approach is that much of recurrences
occur at near the operated site.
This modality includes multicatheter interstitial implants which is
placed around the operated site, Mammosite technology which uses
single ballon catheter in were in a radiation source is afterloaded at the
operated site ,external beam conformal partial breast irradiation and
intraoperative single dose irradiation.
This modality has not yet under a randomized study to prove it is
equivalent to whole breast irradiation . The current study under trail is
NSABP-39/RTOG-0413 which allows one of three APBI techniques.

53
Multicatheter Interstial Techniques: This modality includes tumors
< 3 cm after lumpectomy,negative margins,0-3 nodes positive,no
ECE.Dose LDR APBI-45 Gy in 3.5 t0 5 days or HDR APBI 34 Gy in 10
BD # with in 5 days.No significant adverse effects was noted,No
statistically significant ipsilateral breast recurrences, or
LRR,OS,DFS.Studies evaluating APBI are Kuske et al , Vicini et al
,Arhur et al ,Wazer et a ,
Mammosite:More extensively used in America,this contains a
catheter with a central ballon inflated at the lumpectomy site,the distance
between ballon and skin is > 5mm or ideally >7 mm,treatment is
delivered by HDR remote after loading system with 1 cm circumference
around the tumor.Dose 3.4 Gy at 1 cm twice daily to atotal dose of 34
Gy over 5 days.It was said that treatment benefit,cosmetic effect,toxicity
at 5yrs using Mammosite was similar to other forms of APBI.

54
APBI (Accelerated Partial Breast Irradiation)
External Beam Conformal Radiation.
At present over 70 percent of breast cancer patients being treated
with 3D-CRT which is totally non invasive with homogenous dose
delivery and distribution.Dose 38.5 Gy at 3.85 Gy/# delivered daily CTV
included operated site + 1-1.5 cm clearance and 5 mm within the skin
surface and chest – lung interface.
Intraoperative Accelerated Partial breast Irradiation:radiation dose
is delivered using single intraoperative dose to the operative site at the
time of surgery using intraoperative electrons or intra operative
photons.Dose-20 Gy.
ASTRO 2009 consensus for APBI-patients > 60 yrs/node
negative/invasive ductal tumors <2 cm/negative margins/ER+/no LVSI.

55
Bone metastasis
Bone is the most common site of metastatic disease in the breast
cancer and affects up to 70% of women with metastases. Matastasis
occurs mostly in the axial skeleton.
Aim of Of treatment in bone metastasis is avoid skeletal related
events.median survival after bone metastasis is 19-25 months. if a
pathological fracture occurs it is reduced to 12 months.
Sometimes survival may prolonged with good risk factors like low
grade tumours, bone disease at initial presentation, long disease free
survival, hormone receptor positive . Bone-only disease has a better
prognosis than disease associated with visceral involvement.
Treatment for metastatic breast cancer with bone metastasis is
mainly hormone therapy therapies and bisphosphonates Radiotherapy
plays a major role in the treatment of bone metastasis as a palliation. . It
is of particular benefit for those patients with painful bone disease or

56
spinal cord compression and even in the face of a large burned of
metastatic disease due to the high response rate and low toxicity.
EFFECTS OF RT ON BONE:
The majority of bone destruction is meditated by osteoclasts,
which are in turn influenced by humoral factors released by thetumor.
Malignant stimulation of the RANK signaling pathway increases the
osteoplastic activity . New bone formation is predominantly reactive ,but
may be exuberant, generating new bone that often lacks the strength of
normal lamellar bone.
Pain may be either nociceptive (mediated by prostaglandins,
substance P, and other cytosine’s) or neuropathic (as a result of bone
destruction and increased resorption, peri-osteal irritation and nerve
entrapment). The mechanism by which radiotherapy improves pain is not
clearly understood.
Progression
Either an increase in worst pain score of 2 or more at the treated
site without reduction in analgesic use or an increase of 25% or more in

57
daily oral morphine. Equivalent compared with baseline without a
reduction in baseline worst pain score.
Fraction in the treatment of localized bone metastases
The largest single randomized study – the Dutch bone metastasis
study (DBMS) (13) – randomized only 29% of eligible patients. All of
the randomized studies included multiple different tumor types, but in all
cases breast and/or prostate cancer formed the predominant patient
groups. In the DBMS, 49.7% of the 1157 patients had breast cancer.
A single fraction of 8Gy delivered for palliation achieves a 60%
response rate by intention-to-treat analysis. Approximately one-third of
patients treated have a complete pain response. Overall, mean time to
response is 3 weeks and mean duration of remission is 18 weeks. Single
fraction are clearly more convenient for the patient and increase
treatment capacity for the radiotherapy center. While single fractions are
commonly employed in the United Kingdom and Canada, fractionated
regimens such as 20gy in 5 fractions or 30Gy in 10 fractions are the
norm in the rest of the world.

58
Re-treatment of bone deposits
Re treatment after a single fraction is recorded for 21.5% of
patients as compared with 7.4% of those receiving multiple fraction.
Single-fraction treatment has also been tested against multiple fractions
in the treatment of neuropathic bone pain, where it has been argued that
multiple fractions are required to required to reduce tumour mass and
relive pressure on nerves .
Axial metastasis
Presentation in the descending order in carcinoma breast
1. Vertebra primarily thorocolumbar
2. Pelvis
3. Ribs
4. Femur
5. Humerus
6. Other sites eg.scapula,tibia,skull

59
Spinal metastasis
30-70% of patients with carcinoma breast has spinal metastasis at
the time of death
Pain in spinal metastasis is due to release of local chemical
mediators subatance P , bradykinin and histamine and due to enlarging
tumour mass, bone defect leading to pathological fracture /deformity
kyphosis /scoliosis or both ,nerve root compression due to tumour mass
,compression of spinal cord due to tumour mass because of tissue
reaction or fractured fragments
MANAGEMENT OF SPINAL METASTASIS
Class I –no nerve involvement –chemotherapy or local RT
Class II –involvement of bone no collapse – chemotherapy of local RT
Class III – neurological involvement –without body involvement –local
RT/steroids
Class VI – vertebral collapse with instability without nerve involvement
– surgery
Class V – vertebral collapse with nerve involvement – surgery

60
Goals of spinal surgery should include neural decompression,
spinal stability, correction of spinal deformity
However with the advent of minimally invasive spinal surgery it is
concentrating on three main areas , biopsy , replacing bone loss by
vertibroplasty and kyphoplasty , reconstruction and stabilization through
endoscopic procedures
MANAGEMENT OF ACETABULAR METASTASIS
Class I –lateral cortex - superior medial walls intact – cemented THR
Class II – deficient medial wall – protrusio cup cemented THR
Class III – deficient lateral and superior wall – protrusion cup with
fixation with cemented THR
Class IV – solitary metastasis resection of lesion – girdle stone saddle
prosthesis of custom made prosthesis
Mirel’s scoring system for appendicular metastasis
Location –peritrochantric (3) – lower extremity (2) – upper extremity(1)
Lesion type – lytic (3) -mixed: lytic & blastic (2)- blastic (1)

61
Amount of cortical loss ->2/3 (3) – 1/3 to 2/3 (2) - <1/3 (1)
Pain - functional (3) – functional, moderate(2) – moderate (1)
A score of 8 and above is indicative of surgery 30 -50 %of loss in bone
mineral density has to occur to be picked up on a plain X-ray film >50%
loss in thickness of cortical bone in plain X- ray signifies impending
fracture and osteolytic lesion >2.5cm is considered significant
CHARESTESTRICS OF METASTSTIC TNBC
TNBCs have a poor prognosis in the adjuvant setting,
characterised in particularly by early recurrence compared to other
subtypes of breast cancer. This occurs despite a high sensitivity to (neo)
adjuvant chemotherapy. Although cancers that have a pathologic
complete response (pathCR) to neoadjuvant chemotherapy have a good
prognosis, those cancers that donotachive a path CR have a marked poor
prognosis sith frequent and early relapse. Distance disease free survival
at 4 years was 87% for those who had a path CR compare to 69% in
those who didnot.

62
A vast majority relapses from TNBC occur in the first 5 years
following prognosis the reasons for poor prognosis in the metastatic
setting are multi factorial. This reflects the lack of targeted therapies for
TNBEC and the highly proliferative nature of TNBC this reflects the
pattern of metastasis seen in TNBCs characterised by less frequent bone
and liver metastasis and more frequent lung and brain metastasis.
Current evidence suggests that triple negative basal like and non basal
like breast cancers have similar pattern of metastasis
Molecular subtype is also predictive for risk of loco regional
recurrence after these breast conserving surgery and mastectomy with
contemporary trastuzumab containing adjuvant systemic therapy the
outcome of the HER2 enriched group is now likely to have improved
,leaving BLBC as the cancer subtype with highest risk of local relapse.

63
LEPTOMENINGEAL METASTASES:
It is commonly seen with lobular histology of carcinoma breast
,it arises mostly from the pia and archanoid space or subarachnoid space
,spread is due through blood ,direct extension through venous plexus
along nerves or perineural invasion .Once it reaches the meninges it
spreads through CSF. Symptoms will be due to raised ICT ,local
inflammatory responses like severe headache and vomiting ,focal
neurological deficits,seizures.Investigation of choice will be Gadalinium
enhanced MRI, prognosis is poor ,survival will be 5-7 months.
Radiotherapy to craniospinal axis is difficult due to bone marrow
toxicity. Intrathecal chemotherapy and systemic chemotherapy is
advised in these conditions.
INTRA MEDULLARY METASTASES:
One of the rare presentation in breast cancer 0.1-6%, overall
survival 13 months .commonly involves cervical spine. Clinical signs
depends upon the level of involvement. Investigation of choice is MRI
64
(iso intense and nodular on T1 images and pencil shaped hyper intense
on T2 images .Treatment involves steroids and radiotherapy.In patients
with stable disease and without leptomeningeal spread surgery can be
attempted.
EPIDURAL METASTASES:
The most vascular portion which is the posterior part vertebral
body is the site of metastases, commonly involves thoracic vertebra(50-
60%),lumbar (30-35%),cervical(10-115%)in proportion to the volume of
bone marrow . Back pain is the most common symptom ,myelopathy due
to spinal cord compression , sensory disturbances. Investigation of
choice will be MRI ,plain X-ray may be useful to see the stability of
spine .
Goal of treatment
1. preserve neurological function
2. relieve pain
3. preserve stability of spine.
65
Conservative treatment includes inj dexamethasone, radiotherapy
with one level above and one level below. Surgery involves
laminectomy and spinal stabilization followed by post op RT after 3
weeks. Surgery may involve anterior or posterior decompression .Recent
advances in treatment involves procedures like vertebroplasty or
kyphoplasty .
“To cure sometimes To relieve sometimes To comfort always .”
TREATMENT
Carcinoma Breast has been divided into Early stage, Locally
advanced and metastatic breast cancer. Treatment options vary
according to the stage of the disease. The surgical management of breast
cancer improved a lot for the past 30 years. Inially according to
Halsteadian principles aggressive surgical management was done by
Classical radical mastectomy.
Another hypothesis suggested that the extent of surgical resection
alone not sidnificantly affect patients outcome and this supported bt
trials also. As a result administration of poatoperative systemic

66
chemotherapy, hormonal therapy or both become standard practice for
the majority of the patients. It reduces the rate of recurrence and
metastasis ,so increases the overall survival. So surgery may be
modified radical mastectomy or breast conservative surgery.
Neoadjuvant chemotherapy plays a major role in locally advanced breast
cancer to make the inoperable tumors to operable one. Even in operable
tumorsneoadjuvant therapy is used before breast concervative surgery.
SURGERY:
The surgical management of patients is involves both the primary
tumor and regional lymphatics. The primary tumor may be managed by
modified radical mastectomy or Breast conservative surgery .Axilla is
treated by either axillary dissection or sentinallymphnode biopsy.
CHEMOTHERAPY
SCIENTIFIC RATIONALE for primary systemic chemotherapy
The role of is primary systemic chemotherapy or neoadjuvant
chemotherapy was justified by several hypothesis.it indicated that non

67
courative reduction of tumor cell burden increased the
proliferaticells.after surgery of the primary tumoue there is an increase in
the proliferation of remaining tumour cells in the metastatic sites. This
change occurs even after primary tumour irradiation. Removal of a
primary tumor exerts its affect over the metastatic sites and causes
stimulation of growth following surgical removal or reduction was due
to soluble growth factor..
The neoadjuvant chemotherapy helps to decreases the
micrometastases and prevent cancer growth cyclophosphamide,t
amoxifen and radiotherapy prior to surgery prevent kinetic alterations
suppresses tumor growth which inturn may increase the survival.
The Goldie – coldman hypothesis
As tumor cell population increases, an ever expanding number of
duly resistant phenotypic variants arise time to spontonous somatic
mutations that become more difficult to eradicate. The resistant cells
can be minimized by initiating combination of non cross resistant drugs
when the tumor cells are less in number. when the tumor grows not only
the number of resistant cases increases and so is the proportion of
resistants cells in the total cell population. Resistant phenotypes

68
multiply not only as a results of their own intrinsic growth rates and also
due to the addition of new mutation.
Increased proliferation of cells following surgery causes increase
in the number of resistant phenotypes in the metastasis. Neoadjuvant
therapy not only stop cell proliferation but also eliminate cells that would
have been made more sensitive by their kinetic alteration following
surgery.
Scientific rationale for adjuvant chemotherapy
Skipper and schabelconcept
They proposed that growth fraction and doubling times of tumors
differs in from those in micro metastasis. So later they may well respond
to adjuvant chemotherapy. After the primary surgery with decrease in
tumour burden may alter the growth charecteristics and increase the
chemosensitivity of the adjuvant treatment. It justifies the adjuvant
chemotherapy.

69
Adavantages of neoadjuvant chemotherapy
1. Chemotherpay response can be assessed in vivo
2. Downstaging of the primary tumour and nodes.
3. Feasibility of surgery is enhanced due to reduction in tumour
growth
4. Response to the chemotherapy act as a prognostic factor for long
term survival.
Disadvantages of neoadjuvant chemotherapy
1. It delays the effective primary therapy
2. Imprecise clinical and radiological staging
3. Loss of prognostic significance of axillary nodal statusUnknown
relevance of surgical margin
4. Large no of drug resistant cells may present
5. Response to the primary tumour may not correlate with the
response to the micrometastasis

70
Antracycline and Taxane based chemotherapy regimens are
currently the most effective agents for women with locally advanced and
operable breast cancer. The most recent Eastern Breast Cancer
TraialistsGroup(EBCTCG)results published in 2005 concluded that
treatment with approximately 6 months of anthracycline-based
chemotherapy with a regimen such as 5-fluorouracil, Adriamycin, and
Cyclophosphamide (FAC) reduces the annual breast cancer death rate by
about 38% for women younger than 50 years of age and by about 20%
for those of age 50 to 69.
71
This meta-analysis also confirmed a moderate but highly
significant advantage for anthracycline-based regimens (those including
Adriamycin or Epirubicin) to regimens consisting of Cyclophosphamide,
methotrexate, and 5-fluorouracil (CMF) in trials involving more than
14,000 patients. The Cancer and LeukaemiaGroup(CALGB) 9344 study
randomized 3121 women who had node-positive breast cancer to four
cycles of AC or four cycles of AC followed by four cycles of Paclitaxel
(AC-T) with dose-escalated doxorubicin. The addition of Paclitaxel was
associated with significant 5-year DFS (70% versus 65%) and OS (80%
versus 77%) benefits.
Pacitaxel 200mg/m2 IV over 3 hrs on day 1, repeat cycle every
21 days.
Docetaxel 75 mg/m2IV on day 1,reapeat cycle every 21 days.
Paclitaxel1 bevacicizumab - Paclitaxel:90 mg/m2IV on days
1,8,15.
Bevacizumab;(Monoclonal antibody) anti vegf –antibody 10
mg/m2 on days 1 and 15,repeat Cycle every 21 days.

72
CHEMOTHERAPY RESPONSE ASSESSMENT
Tumour response assessment usually occurs 8-12 weeks after the
starting of chemotherapy and comprises a summary of radiological and
clinical responses, symptomatic benefit (including any improvement in
performance status) balanced against toxicities of treatment.
Radiological response (determined by response evaluation criteria in
Solid Tumours (RECIST) criteria, is an improvement guide to the
clinician in deciding whether to continue or change therapies.
While objective tumour responses (i.e., tumour shrinkage by more
than 30%; Table @) set the standard user in clinical trials to judge the
efficacy of chemotherapy, stabilisation of disease by RECIST criteria
with a symptomatic benefit is an equally important endpoint. In patients
with non-measurable disease, (e.g., bone-only disease) treated with
chemotherapy, serial tumour markers together with symptomatic benefit
are important indications of response to treatment.

73
Miller-Payne histological criteria for grading response to solid
tumours to chemotherapy in breast cancer.
Grade Description
1 No change
2 A minor loss up to 30% loss
3 Between 30% and 90% reduction in tumour cells
4
A marked disappearance of tumour cells
more than 90% loss of tumour cells
5
No malignant cells identifiable in sections from the
site of the tumour; only vascular fibroelastoticstroma
remains often containing macrophages. However,
ductal carcinoma in situ (DCIS) may be present
RADIOTHERAPY
The worldwide trend to be less radical treatment in the
management of Carcinoma Breast has led to increasing role of
radiotherapy in this disease. The first major use of radiotherapy in breast
cancer was adjuvant to radical mastectomy. As the risk of local
recurrence after mastectomy was 10 to 15% it was hoped that
prophylactic radiotherapy would decrease this. Fletcher has also stressed

74
the judicious use of postoperative radiotherapy since the probability of
control of gross local or regional recurrence from breast cancer is less
than 60%. Post operative radiotherapy helps to decrease chances of local
recurrence and increase local control & hence increase survival.
The technique of breast irradiation has evolved from use of
conventional two dimensional planning with and without using wedges
to 3 D conformal radiotherapy and intensity modulated radiotherapy
(IMRT). Standard opposed tangential fields with appropriate use of
wedges to optimize dose homogeneity remain the most commonly
employed method for delivery of whole breast irradiation. These
approaches include multicatheter interstitial implants placed around the
excision cavity, single balloon catheter that can be afterloaded with a
central radiation source (MammoSite) which is placed into the excision
cavity, external beam conformal partial breast irradiation, and
intraoperative single-dose irradiation.
Even after mastectomy and systemic therapy occult disease may
remain in the chest wall and or regional lymph nodes. The residual
disease may serve not only as a source of potentially morbid loco-

75
regional recurrence but also an important reservoir from which distant
metastases may be seeded after the initial elimination of distant disease
by systemic therapies. Therefor postmastectomy radiation therapy
(PMRT) is an essential part of the treatment. Postop RT decreases risk of
loco regional recurrence by treating residual microscopic disease that has
spread beyond margins of surgical resection. The term local recurrence
means the evidence of disease appearing in scar site or skin belonging to
breast anatomical area or nodal drainage areas after adequate primary
management.
Loco-regional failure can occur in the following sites
1. Ipsilateral chest wall/ Mastectomy Scar
2. Axillary Lymph nodes/Soft tissues
3. Supra/Infraclavicular Lymph nodes
4. Internal mammary Lymph nodes
Types
1. Skin 2. Scar 3. Nodal 4.Combined.
Local skin recurrence may be nodular or inflammatory. Nodular
may be solitary or multiple occurring most frequently in skin or

76
subcutaneous tissues in and around mastectomy scar. Small nodules are
usually asymptomatic while larger ones can cause pain, itching or
ulceration. In advanced situation confluent nodules may encircle chest to
form cancer encuirasse.
The inflammatory type also called as erypeseloid is less common.
The lesion appears as diffuse reddening of skin associated with slight
induration and increase in local temperature. Patients with this type of
recurrence have poor prognosis and usually die of widespread metastatic
disease within a short span of time. The scar recurrence is usually in the
form of nodules or ulcers. Lymph node recurrence takes the form of
nodules growing and getting fixed and ulcerating producing
lymphedema of arm and painful limitation of arm movements.
Principles Of Concurrent chemoradiation:
Concurrent chemoradiation has produced important improvements
in treatment outcome. Randomized clinic trials show improved local
control and survival through the use of concurrent chemotherapy and
radiation therapy for patients with high-grade gliomas and locally
advanced cancers of the head and neck, lung, esophagus, stomatch,
rectum, and anus.
77
The first is mechanism is radiosensitization.. The underlying
concept is that the observed effect of using chemotherapy and radiation
concurrently is greater than simply adding the two together synergy
cannot be determined simply by normalizing the radiation cell-survival
curve for drug-induced cytotoxicity
A second proposed reason to combine radiation and chemotherapy
is to realize the benefit of improved local control radiation along with the
systematic effect of chemotherapy; a concept called spatial additivity.
Although concurrent chemotherapy has improved survival and
organ conservation, further advances are limited by the toxicity of
treatment. For example, in the curative treatment of locally advanced
head and neck cancer with chemoirradiation. It is now standard toplace a
gastrostomy tube prophymucositis that they are unable to maintain
adequate nutrition orally. The toxicity of treatment resukts from the
relative lack of specificity of both radiation and chemotherapy for cancer
cells as opposed to rapidly dividing normal cells.

78
MECHANISMS OF LOCAL RECURRNECE
1. Extra mechanism is unknown Proposed theories include
2. Seedling from peripheral extensions of tumour
3. Implantation from vessels that ooze blood or lymph containing
tumour emboil.
4. Retrograde movement of tumour cells to edge of the wound
5. Immunological factors.
Chest wall is the most common site of recurrent disease,
accountiong for two-thirds to three-quarters of all local-regional
recurrences.
RISK CATEGORIES FOR LOCOREGIONAL RELAPSES
AFTER MATECTOMY AND AXILLARY CLEARANCE
RISK
CATEGORY
LOW INTERMEDIATE HIGH
RISK <10% 10-20% >20%
TUMOUR
STAGE
T1-T2 T1-T2 T3-T4

79
NO OF
AXILLARY
NODES
0 1-3 >3
GRADE 1-2 3
VASCULAR
INVASION
- +
HISTOLOGY DUCTAL LOBULAR
RISK OF AXILLARY RUCURRENCE
1-3 +VE LN (10YR-LRF)
2-5 LN dissected 7%
6-10 LN 5%
>11LN 1.5%
>4 +VE Ln (10yr-lrf)
4-5ln DISSECTED 12%
6-10 8%
>11 LN 6%

80
Early breast cancer Trialists’ collaborative group and 2002
Cochrance review have shown that postoperative radiotherapy decreases
recurrence rates by two their. Post operative RT decreases recurrences
rates in stage 1 by 5%, stage 2 by 10% and stage 3 by 10 to 15%.

81
REVIEW OF LITERATURE
ROLE OF SURGERY
Prospective Trials
The MF 07-01 9(NCT00557986) is phase 3 RCT that compares
metastatic breast cancers patients at presentation who receive loco
regional treatment Vs no treatment and to assess the overall survival
benefit, which was activated in 2007. Short interim remits in ASCO
2010 shows no evidence for surgery. Similar NCT 00193778 study from
India familiar to show such benefit.
The current evidence is not enough to use surgery for primary
MBC. However there is subset of patients who may be offered loco-
regional treatment such as surgery to maximize survival.

82
ROLE OF RADIOTHERAPY
Review of literature
.A study from the Centre René Huguenin (Paris, France), loco
regional radiotherapy was significantly associated with increased
survival on multivariable analysis. In this study they were rarely used
surgery as a primary treatment in metastatic breast cancer. They used
locoregional radiotherapy as a main modality. The conclusion in that
trial was locoregionalradiotherapy ,may be an alternate modality for
surgery in metastatic breast cancer with leess morbidity 11
Another study from the Institute Gustave-Rousse (Paris, France),
239 women with stage IV breast cancer received loco regional treatment,
either with radiotherapy alone or surgery with or without radiotherapy.
In this study there was no significant difference in overall survival was
observed, again it showed that radiotherapy, without surgery, was an
adequate loco regional treatment metastatic breast cancer of women.
Retrospective Studies
A trial from Tata Memorial Hospital (Mumbai, India) was
initiated in 2005.] In this trial, chemotherapy is given before any

83
locoregional treatment. Preliminary results reported that 72% of patients
in the locoregional treatment arm are free of disease progression
compared with 61% in the observation arm. On multivariable analysis,
locoregional treatment is a significant factor for progression-free
survival.

84
THEORETICAL ADVANTAGES OF LOCOREGIONAL
TREATMENT OFTHE PRIMARY DISEASE BY SURGERY
1. The removal of the intact primary tumor has been
hypothesized to potentially reduce hematogeneous seeding by
micrometastatic populations since local disease may serve as a
hub of tumor stem cells
2. Another theoretical advantage of loco regional treatment in the
setting of stage IV disease can reduce levels of circulating tumor
cells that improved disease response and survival, and longer time
to progression are associated with a lower number of circulating
tumor
3. .Some biologists contend that tumor dissemination can
compromise the immune system. The primary tumor can produce
immunosuppressive factors that may help cancer cells avoid
eradication by the immune system. In this context, surgical
resection can reduce tumor load and lessen harmful immuno-
suppression.

85
o A Theoretical Disadvantage of local therapy is based on the
hypothesis that the primary local tumor can secrete substances that
inhibit new blood vessels that support tumor growth.
o Removal of the primary disease can induce an angiogenic surge
and promote the progression of metastases.
o Some believe that trauma induced by surgical intervention and
general anesthesia can generate cytokines that stimulate neoplastic
proliferation and compromise the integrity of the immune system.
Advantages of radiotherapy
Radiotherapy is a scientific surgery
1. Non invasive
2. No risk of anaesthesia
3. No risk of comorbidities
4. Can be given in patients with disseminated disease.
5. Skin is the best dressing and protection of the tumor which is not
disturbed .
6. Cost effective , no need of hospital admission

86
AIM OF THE STUDY
Aim of this retrospective study is to evaluate the role of loco
regional treatment such as local radiotherapy and surgery in the
management of patient with metastatic breast cancer.
METHODS AND MATERIALS
Study design: This study is a retrospective study to evaluate the
role of 11 loco regional treatment such as radiotherapy and surgery in
Metastatic Breast Cancer.
Inclusion and exclusion criteria
Inclusion criteria
In our retrospective study we reviewed female patients with metastatic
breast cancer registered at cancer Institute were analyzed from the year
2003 to 2008.
Inclusion criteria for this study were the following
Study setting
All medical records of female patients with metastatic breast
cancer registered at cancer Institute from the year 2003 TO 2008 and

87
who fulfil the inclusion and exclusion criteria of the study were reviewed
and included in this study
Duration of the study
patients from the year 2003 to 2008
SAMPLE SIZE:
195 patients (120 patients underwent loco regional treatment 75
no treatment)
TREATMENT PROTOCOL
All patients were treated with chemotherapy with or without
concurrent radiotherapy. After six months of initial treatment response
was assessed and decision regarding surgery was taken. Radiotherapy
was given concurrently with chemotherapy.
Whole Breast Irradiation
Treatment volume
The areas treated generally include the whole breast with or
without supraclavicular, axillary regions. The entire breast and chest
wall are included in the irradiated volume. The upper margin of the

88
portals should be placed at the head of the clavicle to include the entire
breast. The medial margin should be at or 1cm over the midline. The
lateral posterior margin should be placed 2cm beyond all palpable breast
tissue. Which is usually near the mid-axillary line. The inferior margin is
drawn 2 to 3 cm below the inframammary fold. In patients treated with
6-MV or lower energy photons with side tangential fields.
The entire ipsilateral breast should be encompassed. Conventional
field borders are used. BREAST is treated using two tangential fields,
medial and lateral tangents. Superior border is kept at second intercostal
space. Medical border is at midline or matched with internal mammary

89
field when used. Lateral border is kept at midaxillary line. Inferior
border is at 2 cms below opposite inframammary fold.
SUPRACLAVICULAR FIELD
Supraclavicular nodes are ususlly encompassed, with a single
anterior oblique photon field angled slightly away from the spinal cord.
The medial border is placed at the insertion of the clavicular head. The
lateral border is placed to include approximately one-third of the
humeral head. The inferior border is the inferior border of the clavicle or
the superior border of the chest wall field. The superior border is set at
the thyrocricoid groove. A humeral head block is added to block the
humeral head and acromioclavicular join 54
To avoid the problem of hot spot whoile matching supraclavicular
and chest wall fields following methods are used. Angling the foot of the
treatment couch away from the radiation source to direct the tangential
fields inferiorly so that superior edge of these beams line up perfectly
with inferior border of supraclavicular field. We canalso used the three
field single isocentre technique or Hanging block technique. Half beam
block can also be used.

90
INTERNAL MAMMARY FIELD
The internal mammary chain lies beside the sternum, generally in
the first through the third intercostal space, althoiugh the depth may
vary. Various methods of encompassing the ionternbal mammary chain
have been described, including extended tangent fields, partially wide
tangent fields and matching electron and photon fields. But prophylactic
internal mammary nodal irradiation is not recommended even in medial
quadrant tumors.40
POSTERIOR AXILLARY BOOST
The dose provided to the axillary nodes through the
supraclavicular/axillary field can sometimes creat suboptimal dose
distributions to deeper lying level 3 axillary nodes. If coverage is
suboptimal, the dose can be supplemented with a posterior axillary field.
The field is set up opposed to the supraclavicular/axillary field. The
medial border of this field is drawn to allow 1.5 to 2 cm of lung. If the
inferior border is at the same level as the inferior border of the
supraclavicular field, the lateral border just blocks falloff across the
posterior axillary fold, the superior border splits the clavicle, and the
superolateral border shields or splits the humeral head. 54

91
DOSE
Most commonly employed dose schedule is 40-45Gy in 22- 25
fractions at conventional 180cGy daily for 5 weeks

92

93
DOSE VOLUME HISTOGRAM
FOLLOW UP
Subsequently patients were followed up monthly for the first year
and once in threemonths for a period of five years from date of
completion of radiotherapy after 5 years yearly follow-up was done
ASSESSMENT TOOLS
Medical records were reviewed for the following factors.
1. age at diagnosis
2. laterality

94
3. histology of the tumor
4. clinical and pathologic size of the primary tumor
5. lymph node status
6. hormone receptor status
7. her 2 over expression
8. location and number of metastases mode
9. date of surgical treatmen
10. t, margin status,
11. use of radiotherapy
12. systemic therapy
13. The time of death
14. the time of last review among alive patients
15. Patients with metastatic Breast cancer excluding brain metastasis
at presentation were included.
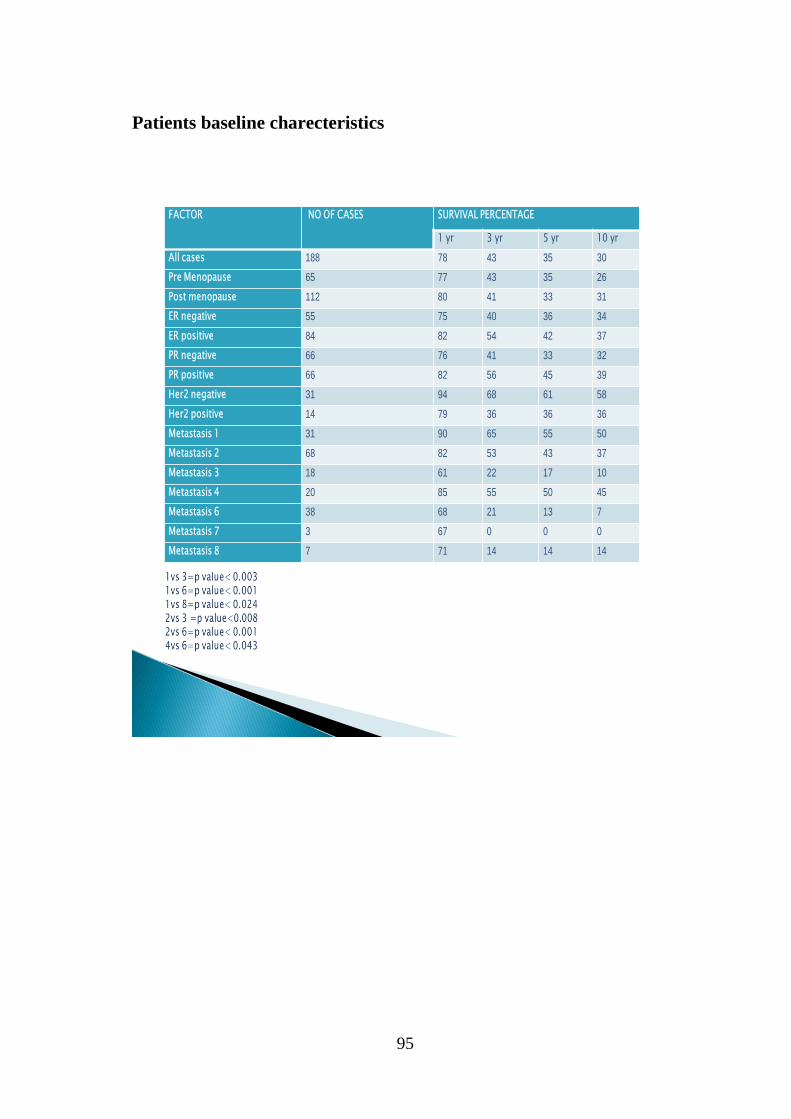
95
Patients baseline charecteristics
FACTOR NO OF CASES SURVIVAL PERCENTAGE
1 yr 3 yr 5 yr 10 yr
All cases 188 78 43 35 30
Pre Menopause 65 77 43 35 26
Post menopause 112 80 41 33 31
ER negative 55 75 40 36 34
ER positive 84 82 54 42 37
PR negative 66 76 41 33 32
PR positive 66 82 56 45 39
Her2 negative 31 94 68 61 58
Her2 positive 14 79 36 36 36
Metastasis 1 31 90 65 55 50
Metastasis 2 68 82 53 43 37
Metastasis 3 18 61 22 17 10
Metastasis 4 20 85 55 50 45
Metastasis 6 38 68 21 13 7
Metastasis 7 3 67 0 0 0
Metastasis 8 7 71 14 14 14

96
MENOPAUSAL STATUS
0
20
40
60
80
100
120
premopausal postmenopausal
NO OF PATIENTS
NO OF PATIENTS
Most of the patients in this study were premenopausal.
ESTROGEN RECEPTOR STATUS
0
10
20
30
40
50
60
70
80
90
Estrogen +ve Estrogen-ve
HR status
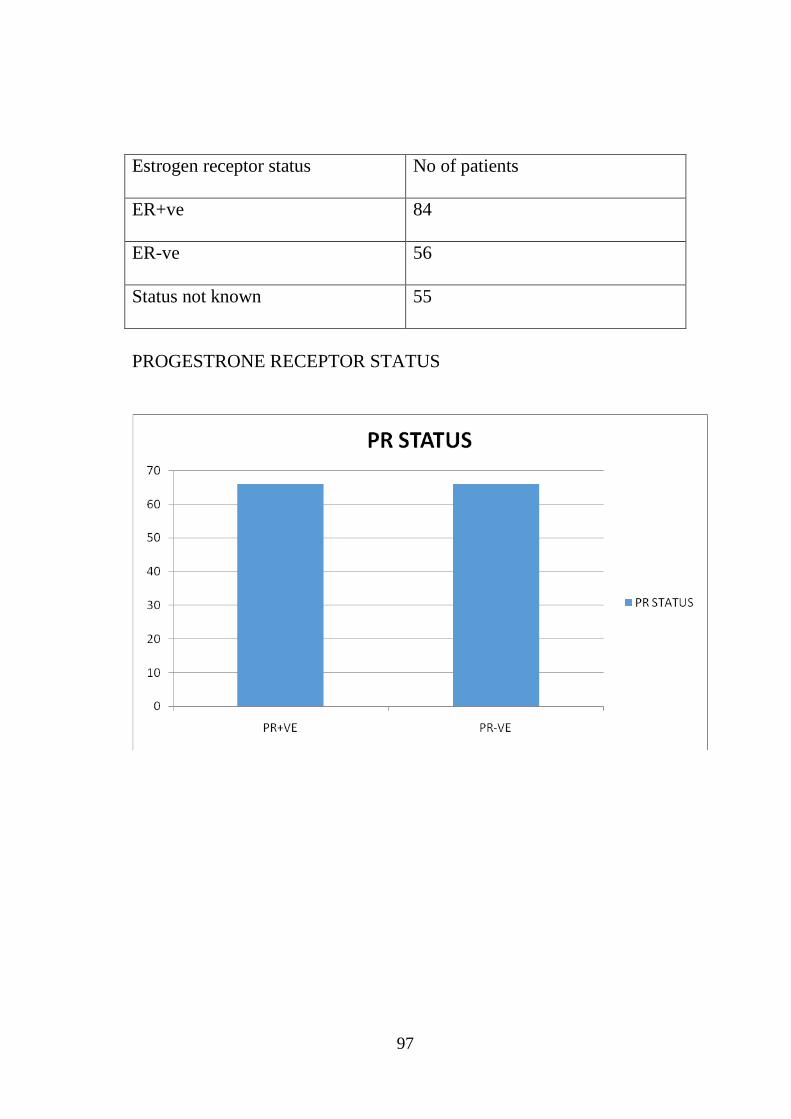
97
Estrogen receptor status No of patients
ER+ve 84
ER-ve 56
Status not known 55
PROGESTRONE RECEPTOR STATUS

98
PR STATUS NO OF PATIENTS
PR+VE 66
PR-VE 66
Results
Tumour stage of the patients
Out of 195 patients 118 had T3 tumor size and 37 pts had T4
disease ,remaining 36 patients comes under T1,T2,T0
Tumor size No of pts
T4 37
T3 118
T1,T2,T0 36

99
T 4 T 3 T 1 , T 2 , T 0
37
118
36
SERIES 1
Most common tumour stage was T3
NODAL STAGE OF THE PATIENTS
24% of the patients had N3 disease and 31 had N2 stage , 36% of
them had N1 and 9%
Had N0 disease
NODAL STAGE PERCENTAGE OF PATIENTS
N3 24
N2 31
N1 36
N0 9

100
24%
31%
36%
9%
NODAL STAGE
N3 N2 N1 N0
Most common nodal stage was N1
Out of 195 pts 86 pts are hormone receptor positive and in 109 pts
the details of Receptor status not known.

101
Receptor status No
HR positive 86
HR not known 109
Her2neu status of the patients
Graph:Precentage of patients with left and right sided tumours

102
54%
46%
0% 0%
Most common sides
In this study right sided tumours were found to be more common
than left side tumours.
Incidence of bone metastasis
Out of 195 patients 33 patients (32%) had single bone metastasis
and 70 patients (68%) had multiple bone metastasis
NO OF BONE METASTASIS NO OF PATIENTS
SINGLE METS 33
MULTIPLE METS 70

103
Graph : Percentage of pts with single and multiple bone metastasis
LIVER AND LUNG METASTASIS
out of 195 total patients 18 patients (9%) had liver metastasis and
21 patients (11%) had lung metastasis ,two patients (1%) had both liver
and lung metastasis.
Site of metastasis No of patients
Liver 18
Lung 21
Both liver and lung 2

104
Patients with multiple metastasis
40 patients (21%) had multple visceral and nonvisceral metastasis
excluding brain which is not included in the study.
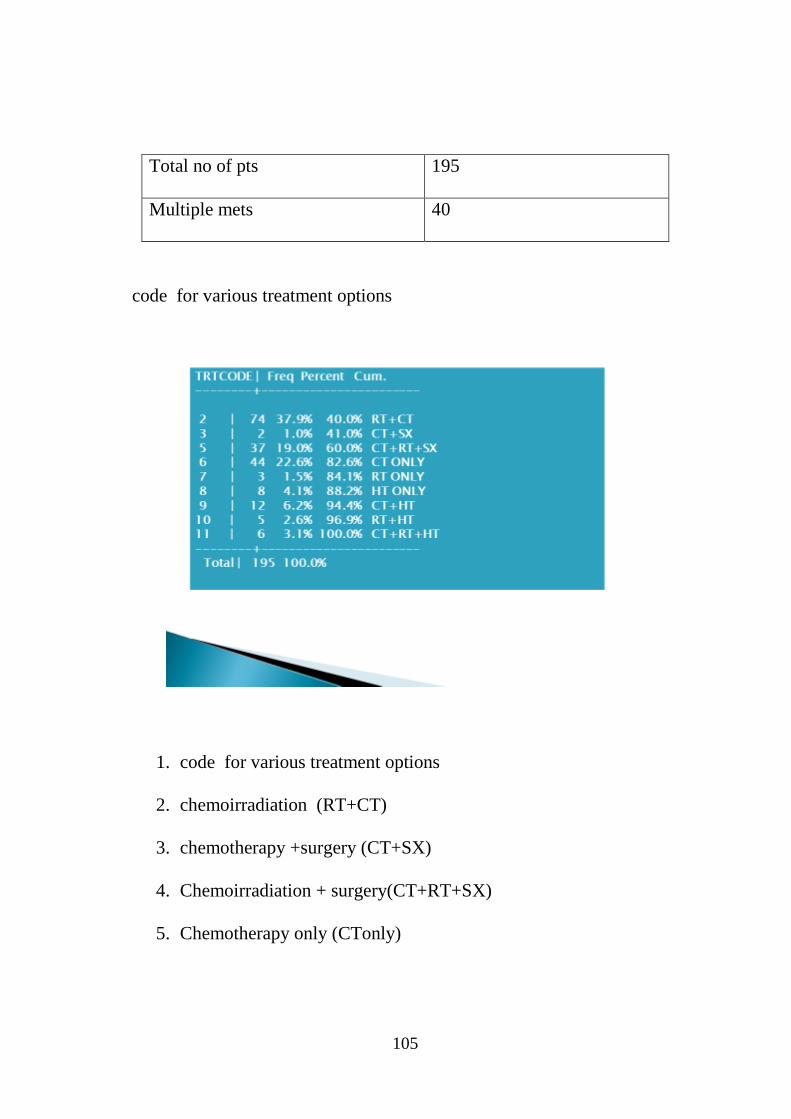
105
Total no of pts 195
Multiple mets 40
code for various treatment options
1. code for various treatment options
2. chemoirradiation (RT+CT)
3. chemotherapy +surgery (CT+SX)
4. Chemoirradiation + surgery(CT+RT+SX)
5. Chemotherapy only (CTonly)
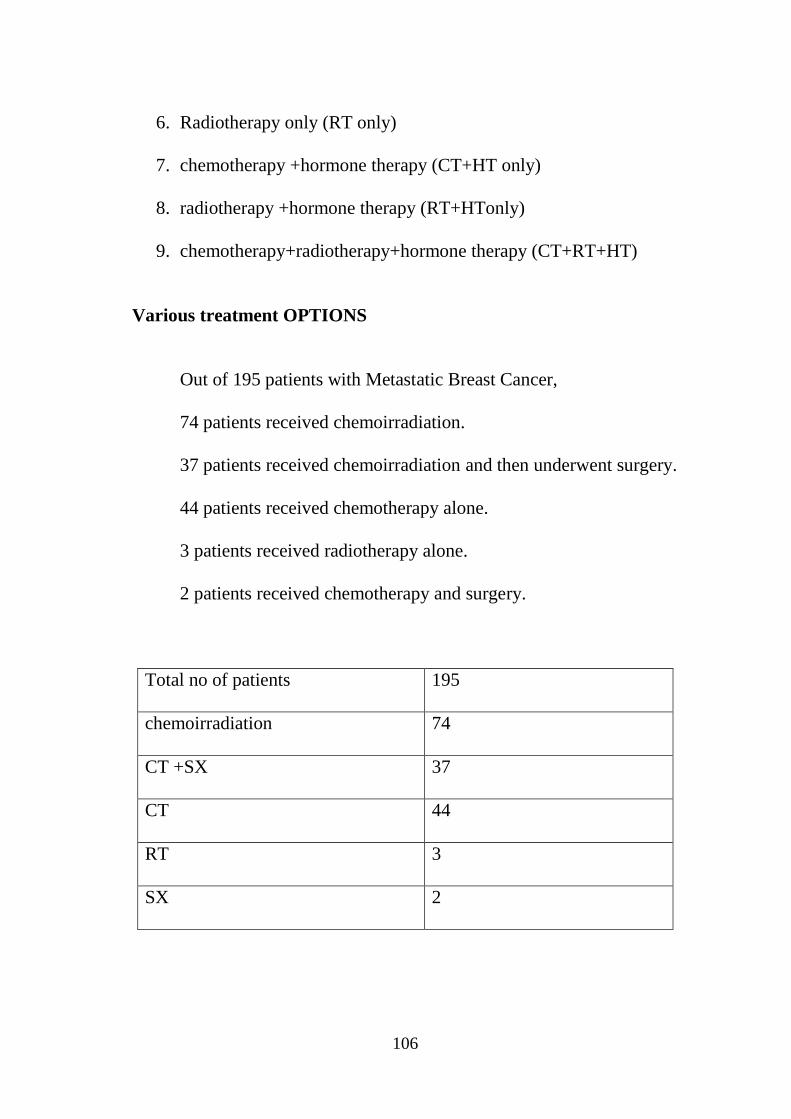
106
6. Radiotherapy only (RT only)
7. chemotherapy +hormone therapy (CT+HT only)
8. radiotherapy +hormone therapy (RT+HTonly)
9. chemotherapy+radiotherapy+hormone therapy (CT+RT+HT)
Various treatment OPTIONS
Out of 195 patients with Metastatic Breast Cancer,
74 patients received chemoirradiation.
37 patients received chemoirradiation and then underwent surgery.
44 patients received chemotherapy alone.
3 patients received radiotherapy alone.
2 patients received chemotherapy and surgery.
Total no of patients 195
chemoirradiation 74
CT +SX 37
CT 44
RT 3
SX 2

107

108
CHEMOIRRADIATION
Out of 195 patients 74 patients received chemoirradiation .
RESULTS
In patients receiving CT+RT survival at the end of 1 yr was
(89%) 3 yr (58%) 5 yr (46%) 10 yr,(42%).

109
CHEMORADIATION AND SURGERY
Out of 195 patients 37 patients received chemoirradiation
and then underwent surgery.
37
158
CT +SX other patients 158
RESULTS;
In patients receiving CT+RT + surgery at the end of 1 yr was
(97%) 3 yr (80%) 5yr(70%) 10 yr,(71%).
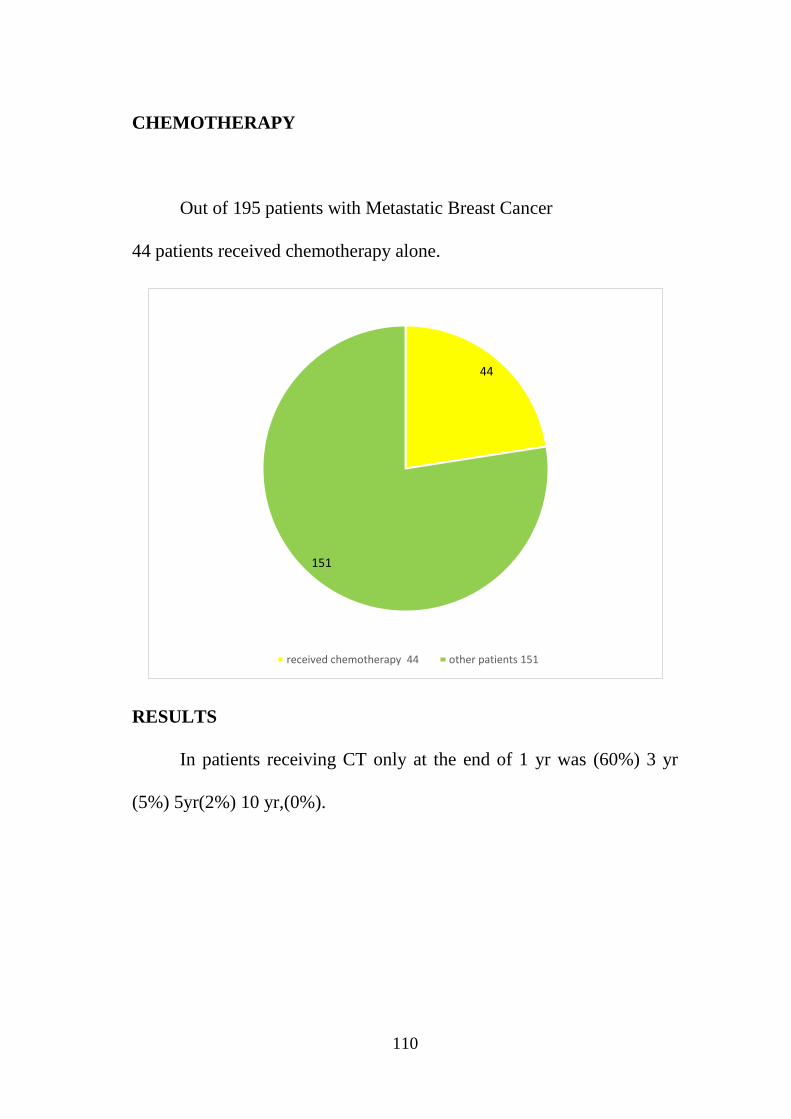
110
CHEMOTHERAPY
Out of 195 patients with Metastatic Breast Cancer
44 patients received chemotherapy alone.
44
151
received chemotherapy 44 other patients 151
RESULTS
In patients receiving CT only at the end of 1 yr was (60%) 3 yr
(5%) 5yr(2%) 10 yr,(0%).

111
RADIOTHERAPY
Out of 195 patients with Metastatic Breast Cancer 3
patients received radiotherapy alone.
RESULTS:
In patients receiving RT only at the end of 1 yr was (67%) 3 yr
(33%) 5yr(33%) 10 yr,(33%).

112
CHEMOTHERAPY AND SURGERY
OUT OF 195 PATIENTS RECEIVED chemotherapy and surgery
2
193
00
.
patients received chemotherapy and durgery other patients
Hormonal therapy
8 patients received hormonal therapy alone.
12 patients got chemotherapy and hormonal therapy
5 patients received radiotherapy and hormonal therapy.
6 patient srecivedhemoirradiation and hormonal therapy

113
NO OF PATIENTS 195
HT 8
CT+HT 12
RT+HT 5
CT+RT+HT 6
HORMONAL THERAPY
Out of 195 patients with Metastatic Breast Cancer
8 patients received hormonal therapy alone.
patients received hormonal therapy other patients
In patients receiving HT only at the end of 1 yr was (50%)
3 yr (13%) 5yr (13%) 10 yr,(13%).

114
Chemotherapy and hormonal therapy
Out of 195 patients with Metastatic Breast Cancer12 patients got
chemotherapy and
hormonal therapy
In patients receiving CT+HT at the end of 1 yr was (58%) 3yr (8%)
5yr(0%) 10 yr,(0%).

115
Radiotherapy and hormonal therapy
Out of 195 patients with Metastatic Breast Cancer
5 patients received radiotherapy and hormonal therapy
.
In patients receiving RT + HT at the end of 1 yrsurvival
was (50%) 3yr(0%) 5yr(0%) 10 yr,(0%).
Chemoirradiation and hormonal therapy. Out of 195 patients with
Metastatic Breast Cancer 6 patientsrecived Chemoirradiation and
hormonal therapy.

116
6
189
00
patients recived chemoirradiation and hormonal therapy. other patients
In patients receiving CT+RT + HT survival at the end of 1 yr was (67%)
3yr(50%) 5yr(0%) 10 yr,(0%).
VARIUOS TREATMENT MODALITIES
39%
23%
19%
2%1%
4%
6%3% 3%
CT+RT CT CT+RT+SX RT CT+SX HT CT+HT RT=HT CT+RT+HT

117
FACTOR NO OF CASES SURVIVAL PERCENTAGE
1 yr 3 yr 5 yr 10 yr
Treatment modality
0 4 50 25 25 0
2 72 89 58 46 42
3 1 100 100 100 100
5 35 97 80 77 71
6 43 60 5 2 0
7 3 67 33 33 33
8 8 50 13 13 13
9 12 58 8 0 0
10 4 50 0 0 0
11 6 67 50 0 0
V Out of 195 patients 74 patients received chemoirradiation and then
underwent surgery.

118
FACTOR NO OF CASES SURVIVAL PERCENTAGE
1 yr 3 yr 5 yr 10 yr
All cases 188 78 43 35 30
Pre Menopause 65 77 43 35 26
Post menopause 112 80 41 33 31
ER negative 55 75 40 36 34
ER positive 84 82 54 42 37
PR negative 66 76 41 33 32
PR positive 66 82 56 45 39
Her2 negative 31 94 68 61 58
Her2 positive 14 79 36 36 36
Metastasis 1 31 90 65 55 50
Metastasis 2 68 82 53 43 37
Metastasis 3 18 61 22 17 10
Metastasis 4 20 85 55 50 45
Metastasis 6 38 68 21 13 7
Metastasis 7 3 67 0 0 0
Metastasis 8 7 71 14 14 14
FACTOR NO OF CASES SURVIVAL PERCENTAGE
1 yr 3 yr 5 yr 10 yr
Treatment modality
0 4 50 25 25 0
2 72 89 58 46 42
3 1 100 100 100 100
5 35 97 80 77 71
6 43 60 5 2 0
7 3 67 33 33 33
8 8 50 13 13 13
9 12 58 8 0 0
10 4 50 0 0 0
11 6 67 50 0 0

119
Discussion
The purpose of the study was to evaluate the role of locoregional
treatment in metastatic breast cancer since this was a retrospective study
between the year of 2003 – 2008 all medical records of female metastatic
breast cancer patients excluding brain metastasis were revised and
analysed with a following factors such as menopausal status, hormone
receptor status, HER2 neu status, no of metastasis (including visceral
and non-visceral)
65 patients in this study were premenopausal and 112 patients
were belonged to postmenopausal group 55 patients were ER negative
and 84 patients were ER positive and out of 195 patients 14 patients
were HER2 positive and 31 patients were HER2 negative and in the
remaining cases status not known.
31 patients had single bone metastasis and 68 pts had multiple
bone metastasis 18 patients had liver metastasis and 21 patients had lung
metastasis 2 patients had metastasis liver and lung 3 patients with
supraclavicular metastasis 7 patients had axillary metastasis.

120
All patients underwent various treatment modalities according to
tumour board policy. 74 patients underwent chemo radiation 2 patients
had chemotherapy followed by surgery 37 patients got concurrent chemo
radiation followed by surgery. 44 patients received chemotherapy
alone.3 patients had only radiotherapy 12 patients received
chemotherapy and harmonic therapy 8 patients had harmonic therapy
only in 5 patients radiotherapy and harmonic therapy was given 6
patients had chemo radiation followed by hormonal therapy.
Patients survival was analysed at the end of 1 yr, 3 yr, 5 yr, and 10
years. In patients receiving CT+RT survival at the end of 1 yr was (89%)
3 yr (58%) 5 yr (46%) 10 yr,(42%). In patients receiving CT+RT +
surgery at the end of 1 yr was (97%) 3 yr (80%) 5yr(70%) 10 yr,(71%).
In patients receiving CT only at the end of 1 yr was (60%) 3 yr (5%)
5yr(2%) 10 yr,(0%). In patients receiving RT only at the end of 1 yr was
(67%) 3 yr (33%) 5yr(33%) 10 yr,(33%). In patients receiving HT only
at the end of 1 yr was (50%) 3 yr (13%) 5yr (13%) 10 yr,(13%).
In patients receiving CT+HT at the end of 1 yr was (58%) 3yr
(8%) 5yr(0%) 10 yr,(0%). In patients receiving RT + HT at the end of 1
121
yr was (50%) 3yr(0%) 5yr(0%) 10 yr,(0%). In patients receiving CT+RT
+ HTat the end of 1 yr was (67%) 3yr(50%) 5yr(0%) 10 yr,(0%).
Conclusion
The data reported in this retrospective study confirmed that
chemo-radiation improved overall survival and symptomatic local
control were demonstrated in locoregionally treated patients with
metastatic breast cancer. The optimal local management of patients with
metastatic breast cancer remains unknown. An ongoing phase III trial,
E2108, has been designed to assess the effect of locoregional
management in metastatic patients responding to first-line systemic
therapy.Loco regional radiation can be an integral part in metastatic
breast cancer treatment to improve the quality of life. If the patient did
not have any metastasis at the end of one year mastectomy can be added
to still more improve the local control according to this study as there is
a significant overall survival and better local control with concurrent
chemo radiation hence RT has a integral part in the management of
metastatic breast cancer.

122
BIBLIOGRAPHY:
1. Textbook of Breast diseases, Bland and Copeland
2. Handbook of metastatic breast cancer, 2nd
edition: Charles
Swanton, Stefan R.D Johnston
3. Textbook of Breast cancer-A clinical Guide to therapy, 3rd
edition:
Gianni Bonnodona, Gabriel N.Hortobagyi
4. Cancer Breast, 5th
edition: William L.Donegan, John.S.Pratt
5. Perez and Brady’s Principles of Radiation Oncology, 6th
edition
6. Devita, Principles of Oncology, 9th
edition
7. David H Nguyen – Metastatic breast cancer
8. nci.cu.edu.org – publication
9. Theodore Lawrence - publication
10. Gonzalez-Anguio
11. Manjeet Chadda – publication
12. www.ncbi.nim.nih.gov
13. Chow.E. publication
14. Ogston K.N.
15. Breast Cancer Research and Treatment,12/2006


















