
Ten-Year Incidence of Myocardial Infarction and Prognosis After ...
Upload
apollo-hospitalsCategory
view
63download
5
R
Role of li
inf
ipid prof
farction i
file in themy
in a rura
e short tyocardialal hospita
erm progl al in Sou
gnosis o
uth India
of acute
a
Apollo Medicine 2012 SeptemberVolume 9, Number 3; pp. 263e267 Research Article
Role of lipid profile in the short term prognosis of acute myocardialinfarction in a rural hospital in South India
M.G. Binua,*, P. Manojb, C. Vinodinic
aAssocGokula*CorreReceivCopyrihttp://d
ABSTRACT
Background: Acute myocardial infarction is a major cause of morbidity and mortality, more so in Indians.
Aim: To establish the hypothesis that cholesterol level affects the short term prognosis of acute myocardial infarction.
Method: One hundred patients with acute myocardial infarction attending a rural tertiary care hospital were selectedrandomly and assessed for complications their lipid profiles were measured and mean values calculated andcompared for complicated and uncomplicated groups.
Results: In the group without complications 79.1% had total cholesterol <250 mg/dl and 85.58% had non-HDLcholesterol <160 mg/dl. In the group with complications 69.7% had total cholesterol >250 mg/dl and 75.76% hadnon-HDL cholesterol >160 mg/dl. The mean non-HDLC values for the two groups were 124� 10 and 189� 8respectively (p¼ 0.08373).
Conclusions: The study shows strong relation between the short term prognosis of acute myocardial infarction andbaseline cholesterol values, especially non-HDL cholesterol.
Copyright © 2012, Indraprastha Medical Corporation Ltd. All rights reserved.
Keywords: Myocardial infarction, Total cholesterol, LDL cholesterol, Non-HDL cholesterol
INTRODUCTION
Increased levels of total cholesterol (TC), non-HDL choles-terol and LDL cholesterol (LDL-C) disturbs the endothelialfunction, while normalization of lipid profile improves itsactivity.1e4 Thus it can be expected, that hypercholesterol-emia found in some patients at the onset of acute myocardialinfarction (AMI) may unfavorably influence the course of thedisease and consequently the patients who display normallipid levels in AMI should have a more benign clinicaloutcome. To the best of our knowledge this matter has notyet been investigated in South Indian population. If the abovehypothesis proves to be correct, itwould be a further argumentin favor of early administration of statins in AMI. Suchpatients should then be also considered as high-risk and sub-jected to more intensive management. This may also bea strong indication for primary prophylaxis with statin.
iate Professor of Medicine, Fatima Institute of Medical Sciences, Kadam Institute of Medical Sciences, Venjarammoodu, Kerala, cSenior Assponding author. email: [email protected]: 30.4.2012; Accepted: 30.6.2012; Available online: 8.7.2012ght � 2012, Indraprastha Medical Corporation Ltd. All rights reservedx.doi.org/10.1016/j.apme.2012.06.012
AIM OF THE STUDY
The aim of our study was to test the hypothesis, whichstates that patients in whom lipid levels are found to beabove normal during the first hours of AMI have an unfa-vorable short term clinical outcome.
STUDY PATIENTS, METHODS
We included 100 consecutive patients (66 males) aged66.2 � 12 years (from 34 to 85), with confirmed AMI,who were admitted to hospital up to 24 h after the onsetof clinical symptoms (from 0.5 to 20 h; average6.5 � 5.5). The exclusion criteria were: lipid loweringtreatment in the month prior to AMI, lung, liver, kidneyand thyroid diseases as well as cancer. Myocardial
pa 516003, Andhra Pradesh, bAssociate Professor of Medicine, Sreesistant Surgeon, GH, Kuzhithurai, India.
.
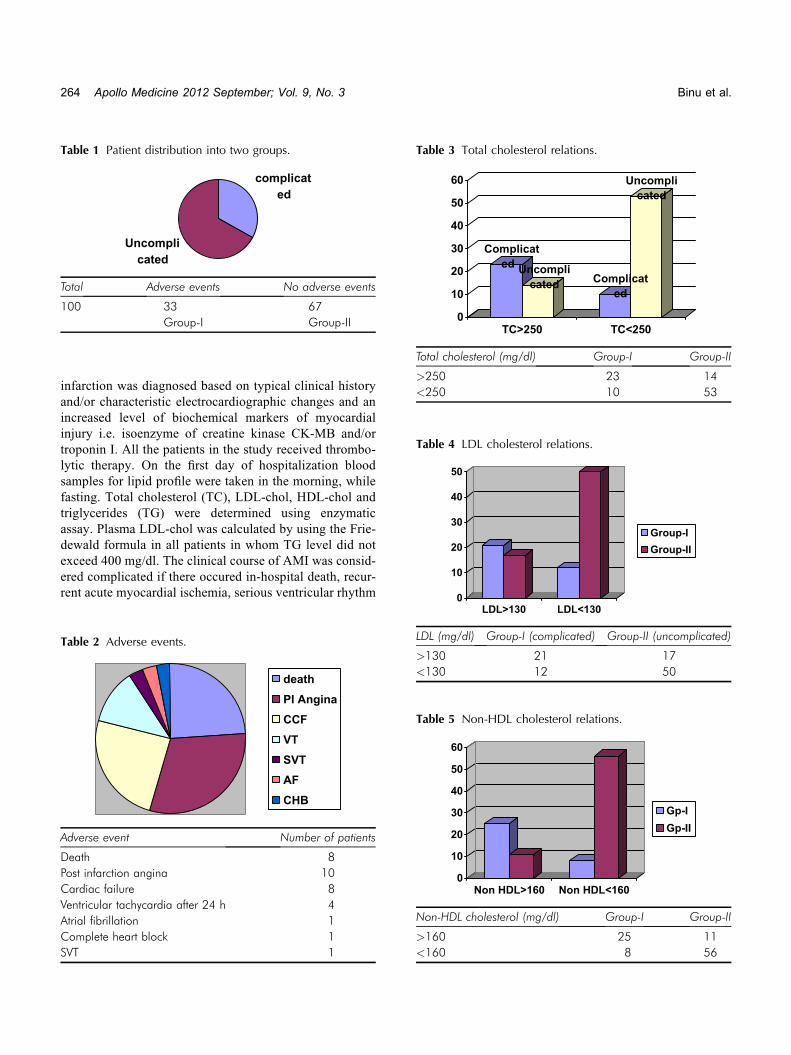
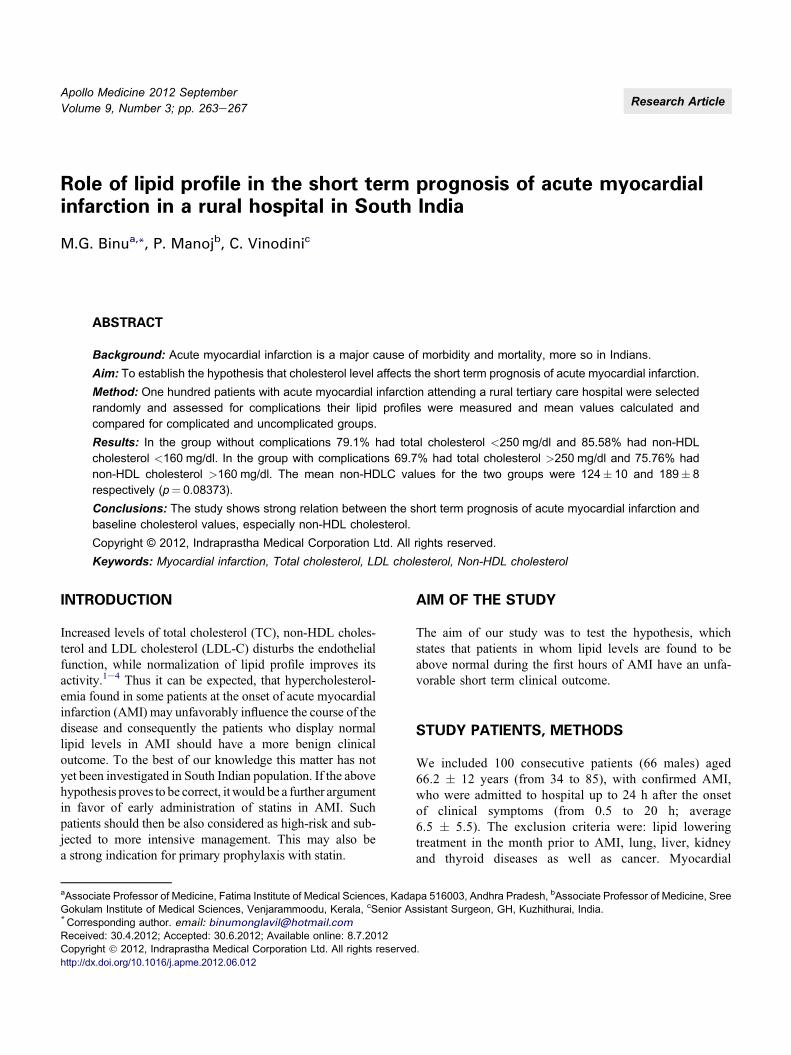
Table 1 Patient distribution into two groups.
complicat
ed
Uncompli
cated
Total Adverse events No adverse events
100 33 67Group-I Group-II
Table 3 Total cholesterol relations.
Complicat
edUncompli
catedComplicat
ed
Uncompli
cated
0
10
20
30
40
50
60
TC>250 TC<250
Total cholesterol (mg/dl) Group-I Group-II
>250 23 14<250 10 53
Table 4 LDL cholesterol relations.
0
10
20
30
40
50
Group-I
Group-II
264 Apollo Medicine 2012 September; Vol. 9, No. 3 Binu et al.
infarction was diagnosed based on typical clinical historyand/or characteristic electrocardiographic changes and anincreased level of biochemical markers of myocardialinjury i.e. isoenzyme of creatine kinase CK-MB and/ortroponin I. All the patients in the study received thrombo-lytic therapy. On the first day of hospitalization bloodsamples for lipid profile were taken in the morning, whilefasting. Total cholesterol (TC), LDL-chol, HDL-chol andtriglycerides (TG) were determined using enzymaticassay. Plasma LDL-chol was calculated by using the Frie-dewald formula in all patients in whom TG level did notexceed 400 mg/dl. The clinical course of AMI was consid-ered complicated if there occured in-hospital death, recur-rent acute myocardial ischemia, serious ventricular rhythm
Table 2 Adverse events.
death
PI Angina
CCF
VT
SVT
AF
CHB
Adverse event Number of patients
Death 8Post infarction angina 10Cardiac failure 8Ventricular tachycardia after 24 h 4Atrial fibrillation 1Complete heart block 1SVT 1
LDL>130 LDL<130
LDL (mg/dl) Group-I (complicated) Group-II (uncomplicated)
>130 21 17<130 12 50
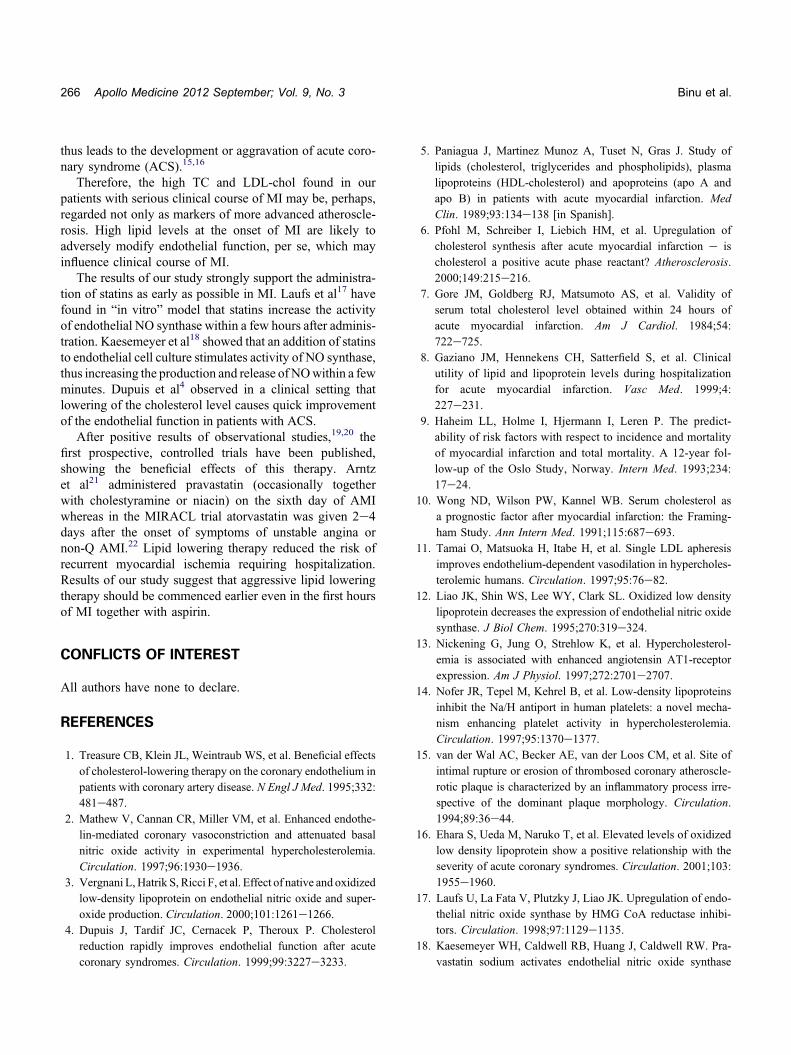
Table 5 Non-HDL cholesterol relations.
0
10
20
30
40
50
60
Non HDL>160 Non HDL<160
Gp-I
Gp-II
Non-HDL cholesterol (mg/dl) Group-I Group-II
>160 25 11<160 8 56
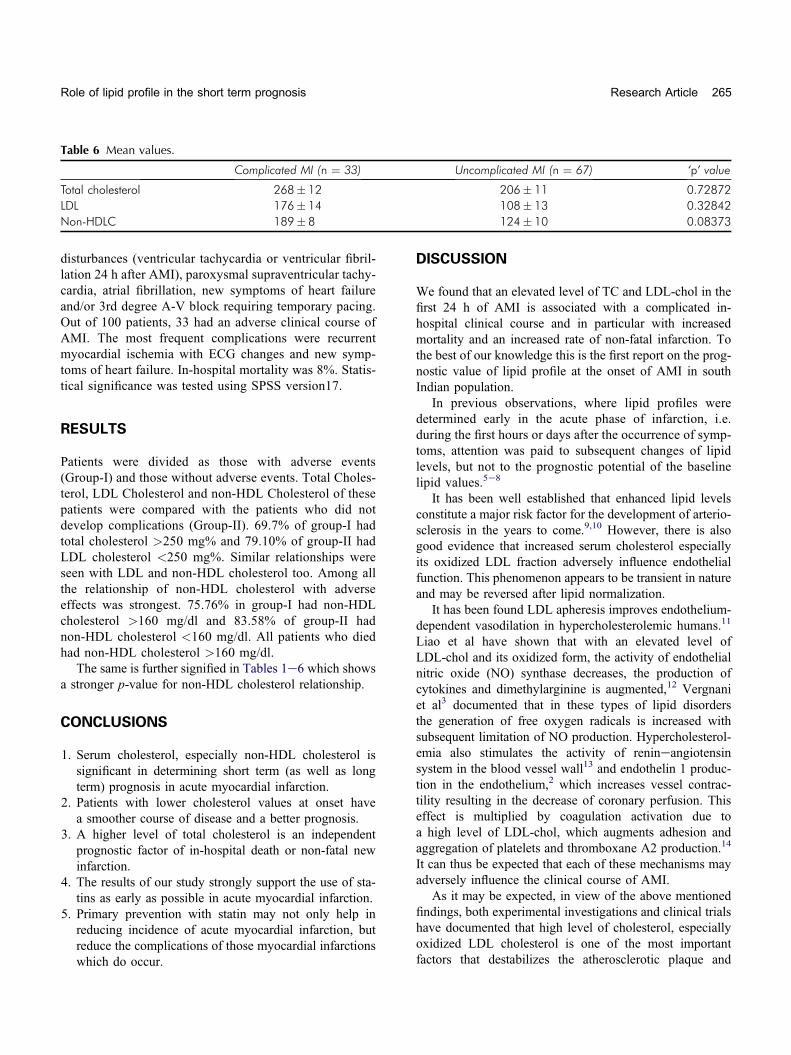
Table 6 Mean values.
Complicated MI (n ¼ 33) Uncomplicated MI (n ¼ 67) ‘p’ value
Total cholesterol 268� 12 206� 11 0.72872LDL 176� 14 108� 13 0.32842Non-HDLC 189� 8 124� 10 0.08373
Role of lipid profile in the short term prognosis Research Article 265
disturbances (ventricular tachycardia or ventricular fibril-lation 24 h after AMI), paroxysmal supraventricular tachy-cardia, atrial fibrillation, new symptoms of heart failureand/or 3rd degree A-V block requiring temporary pacing.Out of 100 patients, 33 had an adverse clinical course ofAMI. The most frequent complications were recurrentmyocardial ischemia with ECG changes and new symp-toms of heart failure. In-hospital mortality was 8%. Statis-tical significance was tested using SPSS version17.
RESULTS
Patients were divided as those with adverse events(Group-I) and those without adverse events. Total Choles-terol, LDL Cholesterol and non-HDL Cholesterol of thesepatients were compared with the patients who did notdevelop complications (Group-II). 69.7% of group-I hadtotal cholesterol >250 mg% and 79.10% of group-II hadLDL cholesterol <250 mg%. Similar relationships wereseen with LDL and non-HDL cholesterol too. Among allthe relationship of non-HDL cholesterol with adverseeffects was strongest. 75.76% in group-I had non-HDLcholesterol >160 mg/dl and 83.58% of group-II hadnon-HDL cholesterol <160 mg/dl. All patients who diedhad non-HDL cholesterol >160 mg/dl.
The same is further signified in Tables 1e6 which showsa stronger p-value for non-HDL cholesterol relationship.
CONCLUSIONS
1. Serum cholesterol, especially non-HDL cholesterol issignificant in determining short term (as well as longterm) prognosis in acute myocardial infarction.
2. Patients with lower cholesterol values at onset havea smoother course of disease and a better prognosis.
3. A higher level of total cholesterol is an independentprognostic factor of in-hospital death or non-fatal newinfarction.
4. The results of our study strongly support the use of sta-tins as early as possible in acute myocardial infarction.
5. Primary prevention with statin may not only help inreducing incidence of acute myocardial infarction, butreduce the complications of those myocardial infarctionswhich do occur.
DISCUSSION
We found that an elevated level of TC and LDL-chol in thefirst 24 h of AMI is associated with a complicated in-hospital clinical course and in particular with increasedmortality and an increased rate of non-fatal infarction. Tothe best of our knowledge this is the first report on the prog-nostic value of lipid profile at the onset of AMI in southIndian population.
In previous observations, where lipid profiles weredetermined early in the acute phase of infarction, i.e.during the first hours or days after the occurrence of symp-toms, attention was paid to subsequent changes of lipidlevels, but not to the prognostic potential of the baselinelipid values.5e8
It has been well established that enhanced lipid levelsconstitute a major risk factor for the development of arterio-sclerosis in the years to come.9,10 However, there is alsogood evidence that increased serum cholesterol especiallyits oxidized LDL fraction adversely influence endothelialfunction. This phenomenon appears to be transient in natureand may be reversed after lipid normalization.
It has been found LDL apheresis improves endothelium-dependent vasodilation in hypercholesterolemic humans.11
Liao et al have shown that with an elevated level ofLDL-chol and its oxidized form, the activity of endothelialnitric oxide (NO) synthase decreases, the production ofcytokines and dimethylarginine is augmented,12 Vergnaniet al3 documented that in these types of lipid disordersthe generation of free oxygen radicals is increased withsubsequent limitation of NO production. Hypercholesterol-emia also stimulates the activity of renineangiotensinsystem in the blood vessel wall13 and endothelin 1 produc-tion in the endothelium,2 which increases vessel contrac-tility resulting in the decrease of coronary perfusion. Thiseffect is multiplied by coagulation activation due toa high level of LDL-chol, which augments adhesion andaggregation of platelets and thromboxane A2 production.14
It can thus be expected that each of these mechanisms mayadversely influence the clinical course of AMI.
As it may be expected, in view of the above mentionedfindings, both experimental investigations and clinical trialshave documented that high level of cholesterol, especiallyoxidized LDL cholesterol is one of the most importantfactors that destabilizes the atherosclerotic plaque and
266 Apollo Medicine 2012 September; Vol. 9, No. 3 Binu et al.
thus leads to the development or aggravation of acute coro-nary syndrome (ACS).15,16
Therefore, the high TC and LDL-chol found in ourpatients with serious clinical course of MI may be, perhaps,regarded not only as markers of more advanced atheroscle-rosis. High lipid levels at the onset of MI are likely toadversely modify endothelial function, per se, which mayinfluence clinical course of MI.
The results of our study strongly support the administra-tion of statins as early as possible in MI. Laufs et al17 havefound in “in vitro” model that statins increase the activityof endothelial NO synthase within a few hours after adminis-tration. Kaesemeyer et al18 showed that an addition of statinsto endothelial cell culture stimulates activity of NO synthase,thus increasing the production and release of NOwithin a fewminutes. Dupuis et al4 observed in a clinical setting thatlowering of the cholesterol level causes quick improvementof the endothelial function in patients with ACS.
After positive results of observational studies,19,20 thefirst prospective, controlled trials have been published,showing the beneficial effects of this therapy. Arntzet al21 administered pravastatin (occasionally togetherwith cholestyramine or niacin) on the sixth day of AMIwhereas in the MIRACL trial atorvastatin was given 2e4days after the onset of symptoms of unstable angina ornon-Q AMI.22 Lipid lowering therapy reduced the risk ofrecurrent myocardial ischemia requiring hospitalization.Results of our study suggest that aggressive lipid loweringtherapy should be commenced earlier even in the first hoursof MI together with aspirin.
CONFLICTS OF INTEREST
All authors have none to declare.
REFERENCES
1. Treasure CB, Klein JL, Weintraub WS, et al. Beneficial effectsof cholesterol-lowering therapy on the coronary endothelium inpatients with coronary artery disease. N Engl J Med. 1995;332:481e487.
2. Mathew V, Cannan CR, Miller VM, et al. Enhanced endothe-lin-mediated coronary vasoconstriction and attenuated basalnitric oxide activity in experimental hypercholesterolemia.Circulation. 1997;96:1930e1936.
3. Vergnani L, Hatrik S, Ricci F, et al. Effect of native and oxidizedlow-density lipoprotein on endothelial nitric oxide and super-oxide production. Circulation. 2000;101:1261e1266.
4. Dupuis J, Tardif JC, Cernacek P, Theroux P. Cholesterolreduction rapidly improves endothelial function after acutecoronary syndromes. Circulation. 1999;99:3227e3233.
5. Paniagua J, Martinez Munoz A, Tuset N, Gras J. Study oflipids (cholesterol, triglycerides and phospholipids), plasmalipoproteins (HDL-cholesterol) and apoproteins (apo A andapo B) in patients with acute myocardial infarction. MedClin. 1989;93:134e138 [in Spanish].
6. Pfohl M, Schreiber I, Liebich HM, et al. Upregulation ofcholesterol synthesis after acute myocardial infarction e ischolesterol a positive acute phase reactant? Atherosclerosis.2000;149:215e216.
7. Gore JM, Goldberg RJ, Matsumoto AS, et al. Validity ofserum total cholesterol level obtained within 24 hours ofacute myocardial infarction. Am J Cardiol. 1984;54:722e725.
8. Gaziano JM, Hennekens CH, Satterfield S, et al. Clinicalutility of lipid and lipoprotein levels during hospitalizationfor acute myocardial infarction. Vasc Med. 1999;4:227e231.
9. Haheim LL, Holme I, Hjermann I, Leren P. The predict-ability of risk factors with respect to incidence and mortalityof myocardial infarction and total mortality. A 12-year fol-low-up of the Oslo Study, Norway. Intern Med. 1993;234:17e24.
10. Wong ND, Wilson PW, Kannel WB. Serum cholesterol asa prognostic factor after myocardial infarction: the Framing-ham Study. Ann Intern Med. 1991;115:687e693.
11. Tamai O, Matsuoka H, Itabe H, et al. Single LDL apheresisimproves endothelium-dependent vasodilation in hypercholes-terolemic humans. Circulation. 1997;95:76e82.
12. Liao JK, Shin WS, Lee WY, Clark SL. Oxidized low densitylipoprotein decreases the expression of endothelial nitric oxidesynthase. J Biol Chem. 1995;270:319e324.
13. Nickening G, Jung O, Strehlow K, et al. Hypercholesterol-emia is associated with enhanced angiotensin AT1-receptorexpression. Am J Physiol. 1997;272:2701e2707.
14. Nofer JR, Tepel M, Kehrel B, et al. Low-density lipoproteinsinhibit the Na/H antiport in human platelets: a novel mecha-nism enhancing platelet activity in hypercholesterolemia.Circulation. 1997;95:1370e1377.
15. van der Wal AC, Becker AE, van der Loos CM, et al. Site ofintimal rupture or erosion of thrombosed coronary atheroscle-rotic plaque is characterized by an inflammatory process irre-spective of the dominant plaque morphology. Circulation.1994;89:36e44.
16. Ehara S, Ueda M, Naruko T, et al. Elevated levels of oxidizedlow density lipoprotein show a positive relationship with theseverity of acute coronary syndromes. Circulation. 2001;103:1955e1960.
17. Laufs U, La Fata V, Plutzky J, Liao JK. Upregulation of endo-thelial nitric oxide synthase by HMG CoA reductase inhibi-tors. Circulation. 1998;97:1129e1135.
18. Kaesemeyer WH, Caldwell RB, Huang J, Caldwell RW. Pra-vastatin sodium activates endothelial nitric oxide synthase

Role of lipid profile in the short term prognosis Research Article 267
independent of its cholesterol-lowering actions. J Am CollCardiol. 1999;33:234e241.
19. Aronow HD. Effect of lipid lowering therapy on earlymortality after acute coronary syndromes: an observationalstudy. Lancet. 2001;357:1063e1068.
20. Stenestrand U, Wallentin LW. Early statin treatmentfollowing acute myocardial infarction and 1-year survival.JAMA. 2001;285:430e436.
21. ArntzHR,AgrawalR,WunderlichW, et al. Beneficial effects ofpravastatin (� Cholestyramine/Niacin) initiated immediatelyafter a coronary event (The Randomized Lipid-CoronaryArteryDisease [L-CAD] Study). Am J Cardiol. 2000;86:1293e1298.
22. Schwartz GC, Olsson AG, Ezekowitz MD, et al. Effects ofAtorvastatin on early recurrent ischemic events in acute coro-nary syndromes. The MIRACL Study: a randomizedcontrolled trial. JAMA. 2001;285:1711e1718.

Apollo hospitals: http://www.apollohospitals.com/Twitter: https://twitter.com/HospitalsApolloYoutube: http://www.youtube.com/apollohospitalsindiaFacebook: http://www.facebook.com/TheApolloHospitalsSlideshare: http://www.slideshare.net/Apollo_HospitalsLinkedin: http://www.linkedin.com/company/apollo-hospitalsBlog:Blog: http://www.letstalkhealth.in/
















