
RMNCH+A GAP ANALYSIS REPORTnrhmarunachal.gov.in/Field Visit Report/RMNCH A Lohit.pdfMale Population...
20
REGIONAL RESOURCE CENTRE FOR NE STATES KHANAPARA, GUWAHATI DATE – 17 Feb to 19 th Feb 2014 RMNCH+A GAP ANALYSIS REPORT District – Lohit, Arunachal Pradesh
Transcript of RMNCH+A GAP ANALYSIS REPORTnrhmarunachal.gov.in/Field Visit Report/RMNCH A Lohit.pdfMale Population...

REGIONAL RESOURCE CENTRE FOR NE STATES
KHANAPARA, GUWAHATI DATE – 17 Feb to 19th Feb 2014
RMNCH+A GAP ANALYSIS REPORT District – Lohit, Arunachal Pradesh
2
TEAM MEMBERS
Mr.Manash Mohan State Facilitator ,AP
Mr. Devajit Bora Consultant, Community Mobilization, AP
Mr.Narendra Jangra Consultant, UNICEF
District Visited
1. Lohit
Executive summary
Lohit is an administrative district in the state of Arunachal Pradesh in India. The district
headquarters are located at Tezu. As of 2011 it is the third most populous district of Arunachal
Pradesh (out of 16), after Papum Pare and Changlang. This area was one of the last territories to be
brought under British control after the punitive Abor and Mishmi Expedition in the first decade of
the 20th century.
Gaps and findings of sub center assessment- All visited Health Sub centers were functioning in
government buildings. The condition of buildings were good. only one third of the visited SCs were
having 24 x7 Water supply and electricity backups. Half of the visited SCs were having habitable
staff quarters for ANMs and at 33% of the sub centers having ANMs residing in their quarters.
Availability of RMNCH A essential commodities i.e IFA tabs, IFA syrup, Vit. A soln, etc. was major
matter of concern. Huge training gap was existing among the available HR for the provision of
RMNCH+A services in the district.
Gaps and findings of Non FRU institutions- Most of the non FRU facilities visited were having
govt building in good condition. Most of the specialist positions at CHC level were vacant as
compared to IPHS standard while at PHC level staff was adequate except SNs & LTs. While the
training gap was wide for various types of training at all level. Radiant warmer was available at all
NBCC without any training as how to operate radiant warmer. Availability of essential RMNCH A
commodities was poor which needs immediate attention for strengthening of supply chain
management system. Implementation of referral transportation under JSSK was very poor.
Gaps and Findings of FRU/ DH- most of the specialist positions at DH was filled except General
surgeon, C-sections are being conducted at the facility. SNCU was under construction. Blood
storage unit was not functional due non availability of license. PNC ward was un-clean. Cold chain
was not maintained properly.
ASHA Payment: Irregular payment of ASHA incentives was found during the visit.

3
JSSK, JSY & community level assessment- In community, awareness was good regarding JSY
scheme and its incentives while knowledge & awareness was very poor about various
entitlements under JSSK scheme though JSSK entitlements were displayed at most of the
PHC/CHCs visited. Late payments of JSY incentive was reported. Pickups and drop back of delivery
cases was reported very poor as they have to arrange for transportation with Out of Pocket
expenditure. Poor implementation of JSSK. CHC Namsai is taking user fees for laboratory testing
from pregnant lady.
One Maternal Death is reported by District during Year 2012-13.
Pregnancy Care:
The performance of the district in the area of pregnancy care is poor as compared to other
districts in State. Overall, Chongkham & Namsai are good performing block and Legank is
worst performing block.
The total registered pregnancies are 167% against the estimated, duplication of reporting can
be the reason.
Only 27.7% of the registered pregnancies have been registered early
One-third of PWs having 3 ANC checkups
Line listing of high risk pregnancies was not available at any of the health facility visited.
Child Birth:
The performance in the ‘Child birth’ domain is also poor as compared to other districts in State
yet the district has improved slightly in 2013-14 up to 3rd quarter as compared to the previous
year performance.
Overall, block Chongkham is the worst performing of the five blocks.
Post Natal Care:
Much improvement is needed in the area of postnatal care. Only11% of the reported deliveries
are seen within 48 hours.
99.2 % of mothers are discharged before 48 hrs after institutional delivery.
HBNC reports are not available
Child Health:
While the coverage of BCG vaccine and DPT1 are more than 100 %.
Awareness and practice of early breast feeding is good. Awareness of community for ORS+ Zinc,
Pneumonia and JSSK is very poor
Inadequate supply of IFA syrup, Albendazole Susp, Vit.A solution, etc.
Reproductive Health:
The performance of the district in RH is dismal uniformly across all blocks.
PPIUCD services are not provided at DH
Met need for FP is low as compared to the estimated no. of eligible couples in the district.
Health System Assessment:

4
Supply Chain Management: Availability of essential RMNCH+A commodities was very poor at
the visited health facilities including at community level i.e. SC levels. Supply at Sub Health
Centers and ASHAs are replenished at PHC level while PHCs were also with stock out of
essential drugs supplies. So, procurement system and supply chain needs to be strengthened on
priority basis to ensure regular supply. Online stock position monitoring system can be devised
and implemented in the state.
Human Resource Management: all delivery points should be equipped with trained
manpower with necessary skills.
Emergency transportation: Facility ambulance were used for emergency transportation
purpose. But its utilization was poor due to poor road and network connectivity.
Implementation of entitlements under JSSK: Under JSSK Drugs and consumables were
procured at district level and supplied to the facilities while other entitlements under JSSK
were poorly implemented in the districts. Beneficiaries has to bear out of pockets for referral
transport & necessary lab tests.
Capacity building roll out of trainings: Major training gap was found for various types of
trainings among HR deployed at all levels. If capacity building of available HR is improved
through provision of appropriate training, quality services can be provided with efficient
utilization of available resources.
Lohit : District Profile:
Administration
The district headquarters are located at Tezu. Lohit District is situated in the foot hills of eastern part
of the Himalaya with a geographical area of 5212 sq. km, surrounded by Anjaw District in the East,
Changlang District and Assam in the South, Part of Lower Dibang Valley District in the North, Assam
State and part of Lower Dibang Valley District to the West.
The district is divided into 2 sub-divisions (Teju & Namsai) and 8 administrative circles, namely, Teju,
Sunpara, Namsai, Chongham, Wakro, Lekang, Piyong & Lathao. There are four Arunachal Pradesh
Legislative Assembly constituencies located in this district: Tezu, Chowkham, Namsai, and Lekang. All
of these are part of Arunachal East Lok Sabha constituency.
HIGHLIGHTS OF LOHIT DISTRICT
I T E M S P A R T I C U L A R S
Blocks 5
Villages 225
Town(Census Town) 2 (Tezu & Namsai)

5
Number of Household
I) Total 41,793
ii) Rural 32,494
iii)Urban 9,299
Lohit district experiences vast topographical and altitudinal variations that range from 140 to 686
meters above Mean Sea Level. The District is named after its principal river LOHIT, which flows
through Eastern Tibet and enters India in Kibithoo area, and enters Lohit district at PARASHURAM
KUND, a famous place of pilgrimage for the Hindus. Demographic Profile
According to the 2011 census Lohit district has a population of 145,538, roughly equal to the nation of
Saint Lucia. This gives it a ranking of 601st in India (out of a total of 640). The district has a population
density of 28 inhabitants per square kilometer (73 /sq mi). Its population growth rate over the decade
2001–2011 was 16.44%. Lohit has a sex ratio of 912 females for every 1000 males, and a literacy rate
of 68.18%.Lohit is the home of the Adi, Zekhring, Khampti, Deori, Ahom, Singpho, Chakma and Mishmi
tribes. A small group of Tibetan refugees have settled in Lohit since the 1960s. The Zekhring are
Tibetan Buddhists; the Khampti,Chakmas and Singpho are Theravada Buddhists, and the Mishmi are
mainly Animists.The Chakmas inhabit a land which is surrounded in all side by two mighty rivers, the
Kamlang to the north and Guri Kamlang to the south
Demographic Profile–
Background characteristics
Lohit Arunachal Pradesh
Census 2011
Census 2001
Census 2011
Census 2001
Geographic Area (in Sq. Kms)
5,212 5,212 83,743 83,743
Total population 1,45,538 1,24,991 13,82,611 1097968
Male Population 76,559 67,105 7,20,232 579941
Female Population 68,979 57,886 6,62,379 518027
Population density per Sq.Km
28 24 17 13
Population (0-6 yrs) – Total
23,901 25,026 202759 205871
Population (0-6 yrs) – Male
12,159 12,947 103430 104833

6
Source- Census-2011
Map of Lohit District
Health Facilities:
Health Facilities in District: The District has 1 District Hospital, 3 Community Health Centers, 6 PHCs
and 19 Sub Centers spread over 5 blocks
Details of Public Health facilities in the district
Type of the Health Facility Total No. of the functional
Health facilities
Sub Centre 19
Primary Health center 6
Population (0-6 yrs) – Female
11,742 12,079 99,329 101038
Literacy rate Average 68.18 58.73 66.95 54.74
Sex Ratio 912 863 920 901
7
Community Health center 3
District Hospital 1
Source- State Profile Report
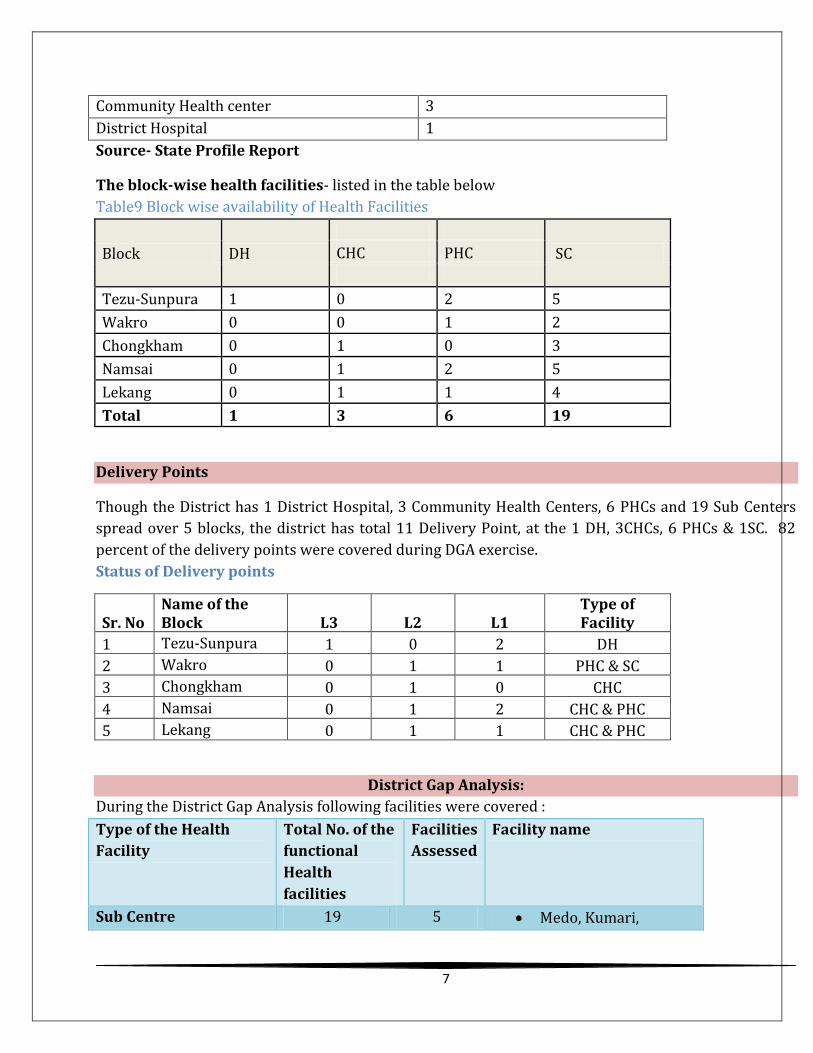
The block-wise health facilities- listed in the table below
Table9 Block wise availability of Health Facilities
Block DH
SC CHC PHC
Tezu-Sunpura 1 0 2 5
Wakro 0 0 1 2
Chongkham 0 1 0 3
Namsai 0 1 2 5
Lekang 0 1 1 4
Total 1 3 6 19
Delivery Points
Though the District has 1 District Hospital, 3 Community Health Centers, 6 PHCs and 19 Sub Centers
spread over 5 blocks, the district has total 11 Delivery Point, at the 1 DH, 3CHCs, 6 PHCs & 1SC. 82
percent of the delivery points were covered during DGA exercise.
Status of Delivery points
Sr. No Name of the Block L3 L2 L1
Type of Facility
1 Tezu-Sunpura 1 0 2 DH
2 Wakro 0 1 1 PHC & SC
3 Chongkham 0 1 0 CHC
4 Namsai 0 1 2 CHC & PHC
5 Lekang 0 1 1 CHC & PHC
District Gap Analysis:
During the District Gap Analysis following facilities were covered :
Type of the Health
Facility
Total No. of the
functional
Health
facilities
Facilities
Assessed
Facility name
Sub Centre 19 5 Medo, Kumari,
8
Sitapani, Monmow
Primary Health centre 6 4 Wakro, Loiliang,
Lathao & New Mohong
Community Health
centre
3 3 Chowkham, Namsai &
Mahadevpur
District Hospital 1 1 DH-Teju
In addition to the facilities, ASHAs and Beneficiaries were also covered during the DGA.
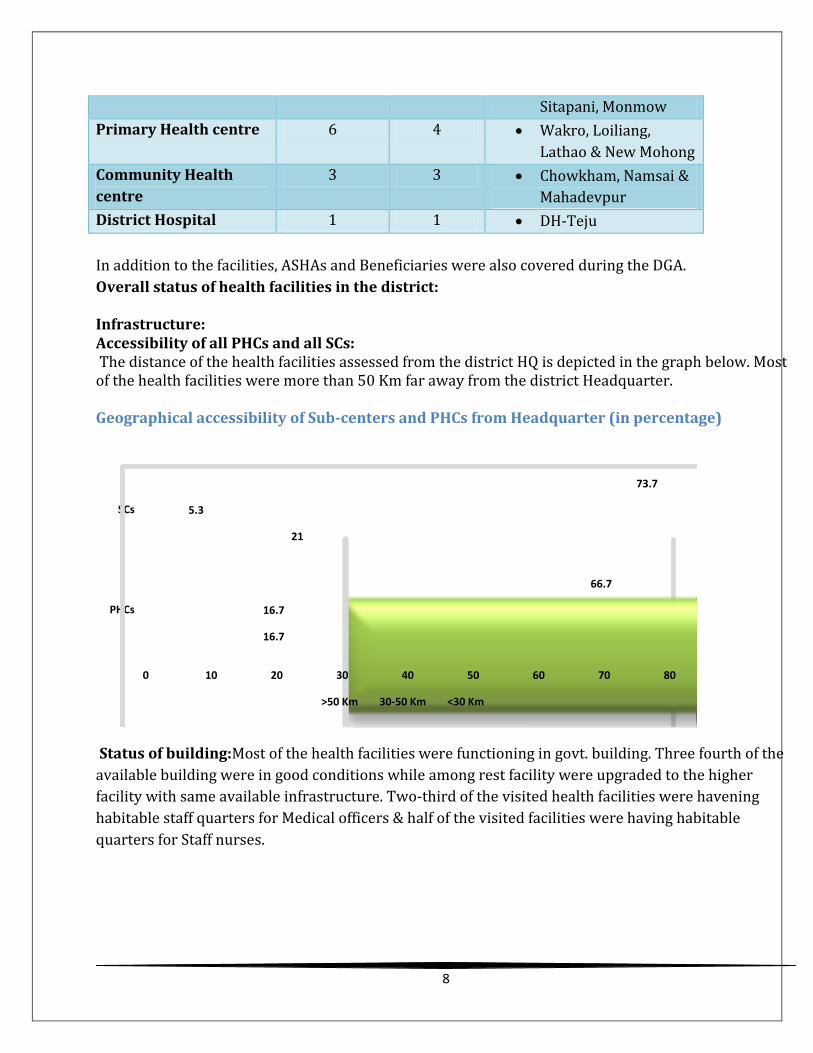
Overall status of health facilities in the district: Infrastructure: Accessibility of all PHCs and all SCs: The distance of the health facilities assessed from the district HQ is depicted in the graph below. Most of the health facilities were more than 50 Km far away from the district Headquarter. Geographical accessibility of Sub-centers and PHCs from Headquarter (in percentage)
16.7
21
16.7
5.3
66.7
73.7
0 10 20 30 40 50 60 70 80
PHCs
SCs
>50 Km 30-50 Km <30 Km
Status of building:Most of the health facilities were functioning in govt. building. Three fourth of the
available building were in good conditions while among rest facility were upgraded to the higher
facility with same available infrastructure. Two-third of the visited health facilities were havening
habitable staff quarters for Medical officers & half of the visited facilities were having habitable
quarters for Staff nurses.

9
Availability of residential quarter at DH, PHC, and CHC Level
87.5
75
62.5
50
0
10
20
30
40
50
60
70
80
90
100
Govt building Building in good condition Habitable Staff Quarters MOs
Habitable Staff Quarters SNs
All visited Health Sub centers were functioning in government buildings. The condition of buildings
were good. While, only one third of the visited SCs were having 24 x7 Water supply and electricity
backups. Half of the visited SCs were having habitable staff quarters for ANMs and at 33% of the sub
centers having ANMs residing in their quarters.
Only 40 percent of the ANMs at visited SCs were trained in Skill Birth Attendant (SBA) & cold chain
maintenance during immunization. Only one-fifth of the ANMs were trained in NSSK.
Availability of running water and electricity:
Graph 3 Sub-Health Centers (L1-Facilities) –Physical Infrastructure

10
District Hospital and CHC Chongham were having 24 x7 electricity and water supply as well as
functional toilets in the Labour room while CHCs in block Namsai & Lekang were facing problems for
24 x7 water supply and 24 x7 electricity power back.
Availability of running water and electricity
Block DH/ CHC Availability
24*7 Water Supply
24*7 Electricity Supply
Functional Toilets in LR
Tezu-Sunpura
1 1 1 1
Wakro 0 NA NA NA
Chongkham 1 1 1 1
Namsai 1 1 0 0
Lekang 1 0 0 1
All of the PHCs assessed were equipped with 24 x7 water supplies and functional toilets in Labor room
(LR)
Block Total PHCs Availability
24*7 Water Supply in LR
Functional Toilets in LR
Tezu-Sunpura
1 1 1
Wakro 1 1 1
Chongkham NA NA NA
Namsai 1 1 1
Lekang 1 1 1
Human Resource -
HR Position-As per revised Indian Public Health Standard (IPHS) norms for DH, 1-O&G specialist, 1-
Pediatrician & 1- Anesthetist were posted at DH. C-sections were also conducted at DH with well-
equipped OT.
11
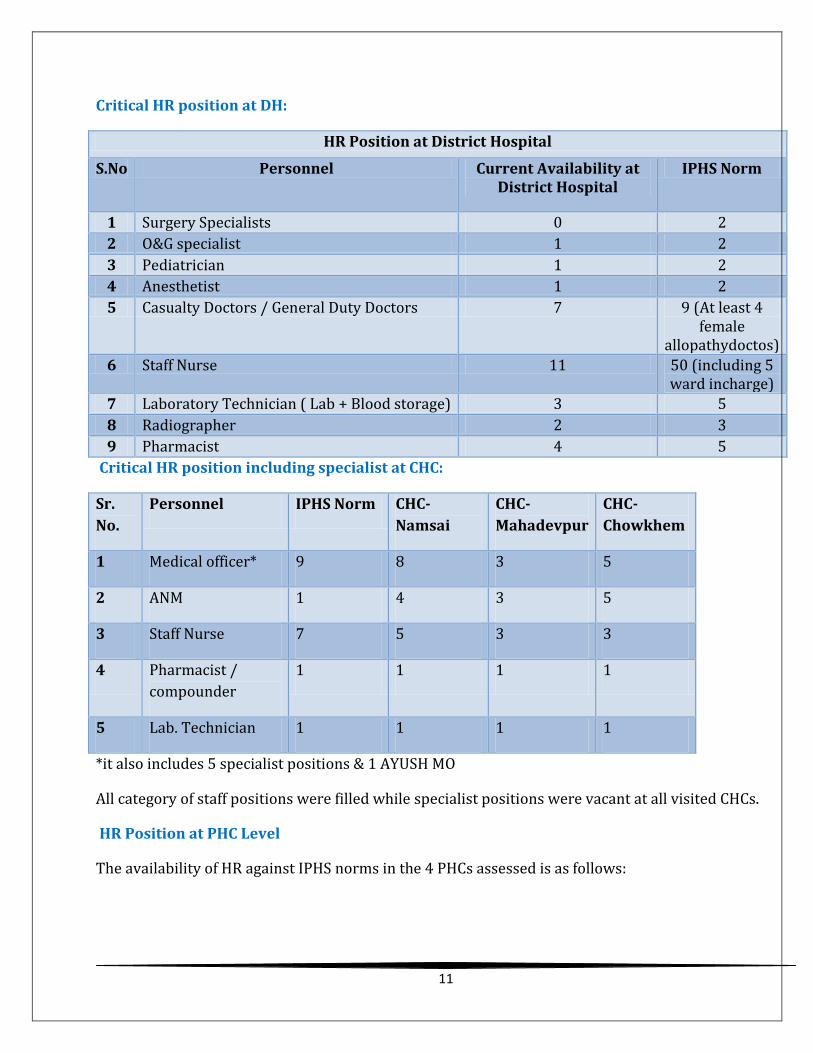
Critical HR position at DH:
HR Position at District Hospital
S.No Personnel Current Availability at District Hospital
IPHS Norm
1 Surgery Specialists 0 2
2 O&G specialist 1 2
3 Pediatrician 1 2
4 Anesthetist 1 2
5 Casualty Doctors / General Duty Doctors 7 9 (At least 4 female
allopathydoctos)
6 Staff Nurse 11 50 (including 5 ward incharge)
7 Laboratory Technician ( Lab + Blood storage) 3 5
8 Radiographer 2 3
9 Pharmacist 4 5
Critical HR position including specialist at CHC:
Sr.
No.
Personnel IPHS Norm CHC-
Namsai
CHC-
Mahadevpur
CHC-
Chowkhem
1 Medical officer* 9 8 3 5
2 ANM 1 4 3 5
3 Staff Nurse 7 5 3 3
4 Pharmacist /
compounder
1 1 1 1
5 Lab. Technician 1 1 1 1
*it also includes 5 specialist positions & 1 AYUSH MO
All category of staff positions were filled while specialist positions were vacant at all visited CHCs.
HR Position at PHC Level
The availability of HR against IPHS norms in the 4 PHCs assessed is as follows:

12
Sr. no.
Personnel IPHS Norms
PHC-Wakro
PHC-Loiliang
PHC-Lathao
PHC-New Mohong
1 Medical Officer 2 2 1 2 2
2 Pharmacist 1 0 1 1 1
3 Nurse - Midwife (Staff Nurse)
3 0 0 1 2
4 Health Worker (Female)
1 9 3 3 1
5 Laboratory Technician
1 1 1 1 0
6 Health Educator 1 0 0 0 0
MO positions were filled at most of the visited PHCs but 50% of Staff Nurse Positions were vacant at
the PHCs visited.
HR availability at Sub Health Center level: The SCs visited all had ANMs and two-thirds had MPWs.
In terms of NRHM’s Programme Management staff, the positions are fully filled and there is no net HR
deficitTraining Status of HR- The training status is reflected in the table below. Critical gap exists at
various levels and various categories of Health care providers, especially in the areas of FP, IMNCI, E-
IMNCI, RTI/STI, BEmOC, NSSK etc.

13
Training status of key of District:
Training DH-Teju
CHC-Namsa
i
CHC-Chowkha
m
CHC-Mahadevpu
r
PHC-Wakr
o
PHC-Latha
o
PHC-Loilian
g
PHC-New
Mohong
EmONC 1 0 0 0 0 NA NA NA
LSAS 0 0 0 0 NA NA NA
BeMONC 0 3 0 1-MO 1 0 0 0
MTP/MVA 1-MO
0 1 2-MO 0 0 0 0
NSV 0 0 0 0 0 0 0 0
F-IMNCI 0 0 0 0 0 0 0 0
Mini Lap-Sterilizations
0 0 0 0 0 0 0 1-MO
Laparoscopy- Sterilizations
0 0 0 0 0 0 0 0
Blood storage 1-SN 0 0 0 0 NA NA NA
IMEP 0 0 0 0 0 0 0 0
PPIUCD 0 0 0 0 0 NA NA NA
SBA 0 0 2-MO, 1-SN, 1-ANM
2 SN 0 0 0 1-SN
IMNCI 0 0 0 1-MO 1 0 0 0
NSSK 0 0 2-MO, 1-SN, 1-ANM
1-MO, 1-SN 0 0 0 0
IUCD 1-MO, 1-ANM
0 1-MO 1-MO, 2 SN 1 2 1-MO, 3- ANM
0
Immunization & cold chain
1-HA
1-HA 0 1-HA 2 3 1-MO, 1- ANM
1-MO
RTI/STI 0 0 0 1-MO 1 1 1-MO 1-MO
Equipment: The availability of equipment at various levels is reflected in the following graphs

14
Status of equipment at SC
Status of equipment at PHC and CHC Level
Commodities:
The availability of RMNCH+A essential commodities is reflected in the graphs below. In terms of major
stock outs the following are the observations:
Essential Drug list (EDL) was not displayed at any health facilities visited
Stock outs of major RMNCH+A essential drugs i.e. IFA large tab, IFA Blue tab, IFA Syrup, Vit. A
solution, zinc Sulphate dispersible tablets etc. was observed at all health facility visited.
Tab. Misoprostol was not available at any of the SC visited.
15
Community level assessment:In community, awareness was good regarding JSY scheme and
its incentives while knowledge & awareness was very poor about various entitlements under
JSSK scheme though JSSK entitlements were displayed at most of the PHC/CHCs visited. Late
payments of JSY incentive was reported. Pickups and drop back of delivery cases was reported
very poor as they have to arrange for transportation with Out of Pocket expenditure.
Quality of care by ASHA:
Of the 225 ASHAs selected in the district, all were trained in module 6-7 first round. ASHAs
were aware of their roles and responsibilities i.e. community mobilization on VHNDs,
awareness generation, HBNC etc.
All ASHAs were provided with drug kits but supply of near to expire drugs were observed
during field visit.
Late payment of JSY incentive and non-payment of other ASHA incentives were reported during
the field visit. The district was responsible for delayed release of fund to all health facilities for
ASHA incentive.
Health System Management:
Supply Chain Management: Availability of essential RMNCH+A commodities was very poor at
the visited health facilities including at community level i.e. SC levels. Supply at Sub Health
Centers and ASHAs are replenished at PHC level while PHCs were also with stock out of
essential drugs supplies. So, procurement system and supply chain needs to be strengthened on
priority basis to ensure regular supply. Online stock position monitoring system can be devised
and implemented in the state.
Human Resource Management: all delivery points should be equipped with trained
manpower with necessary skills.
Emergency transportation: Facility ambulance were used for emergency transportation
purpose. But its utilization was poor due to poor road and network connectivity.
Implementation of entitlements under JSSK: Under JSSK Drugs and consumables were
procured at district level and supplied to the facilities while other entitlements under
JSSK were poorly implemented in the districts. Beneficiaries has to bear out of pockets for
referral transport & necessary lab tests.
Capacity building roll out of trainings: Major training gap was found for various types of
trainings among HR deployed at all levels. If capacity building of available HR is improved
through provision of appropriate training, quality services can be provided with efficient
utilization of available resources.
16
Pregnancy Care:
The performance of the district in the area of pregnancy care is poor as compared to other
districts in State. Overall, Chongkham & Namsai are good performing block and Legank is
worst performing block.
One-third of PWs having 3 ANC checkups
Line listing of high risk pregnancies was not available at any of the health facility visited.
Recommendations:
o Strengthening of regular outreach activities in coordination with ICDS deptt. At VHND
platform and supportive supervision to ensure improved service provision.
o Improving the skills of the ASHAs/ ANMs and ensuring early pregnancy testing,
including regular supply of PTKs so that ANC services can be started through early
registration.
o Listing of villages where ANC is low and ensuring adequate supportive supervision visits
o Strengthening of IEC and communication strategy and involvement of the Faith Based
Organizations in the effort
o Tracking High Risk pregnancies and inclusion of review of the high risk pregnancy list as
a standing agenda in all the district and sub-district reviews
Child Birth:
The performance in the ‘Child birth’ domain is also poor as compared to other districts in State
yet the district has improved slightly in 2013-14 up to 3rd quarter as compared to the previous
year performance.
Overall, block Chongkham is the worst performing of the five blocks.
While CEmOC services are available in the DH, there is a need to strengthen the BEmOC services
at CHC/PHC level and the SBA training to SNs/ANMs.
Recommendations:
o Capacity building of contractual staff in SBA/ BEmOC training of staff at CHC/PHC level
(L2).
o Listing of villages with large number of home deliveries and rapid training of ANMs
catering to these villages at the earliest
o Ensuring institutional delivery for the high risk pregnancies- many villages are
inaccessible and provision for maternity waiting homes may be included in the PIPs.
o Equip ASHAs with disposable delivery kits to assist home deliveries.
Post Natal Care:
Much improvement is needed in the area of postnatal care. Only11% of the reported deliveries
are seen within 48 hours.
99.2 % of mothers are discharged before 48 hrs after institutional delivery.
HBNC reports are not available
Recommendations:

17
o Though HBNC training to ASHAs has been given, though there is need for handholding
and mentoring of ASHAs for the roll out of HBNC.
o Strengthening of HBNC review at all level with strong reporting system.
o Motivation of ASHAs for regular HBNC visits through regular payment of incentives.
o Use of RMNCH A counselor at high case load facilities for counselling on PNC, Newborn
care, Immunization, FP etc.
o The district also does not have a SNCU nor any stabilization units and the NBCC non-
functional due to lack of training in use of radiant warmer in many of the visited
facilities.
Child Health:
While the coverage of BCG vaccine and DPT1 are more than 100 %.
Awareness and practice of early breast feeding is good. Awareness of community for ORS+ Zinc,
Pneumonia and JSSK is very poor
Inadequate supply of IFA syrup, Albendazole Susp, Vit.A solution, etc.
Recommendations:
o There is a need for regular monitoring and validation of data
o Given than the API in the district is >10, and the district is endemic for Pf, there is a need
to have a better understanding of the malaria cases and related deaths among children.
o Ensure proper implementation of RBSK through adequate & regular supply of RMNCH A
essential supplies.
o Focused IEC/ IPC plans to include component of ORS-Zn.
Reproductive Health:
The performance of the district in RH is dismal uniformly across all blocks.
PPIUCD services are not provided at DH
Met need for FP is low as compared to the estimated no. of eligible couples in the district.
Recommendations:
o PPIUCD can be started at DH
o Motivation to ASHAs for Inter-Personal Communication (IPC) for FP and social
marketing of OCPs, condoms, ECs etc.
o ASHAs should be paid regular incentives for mobilization of beneficiaries for
permanent sterilization.
o IEC/BCC needs to be strengthened to create awareness and generate demand for
FP services.
18
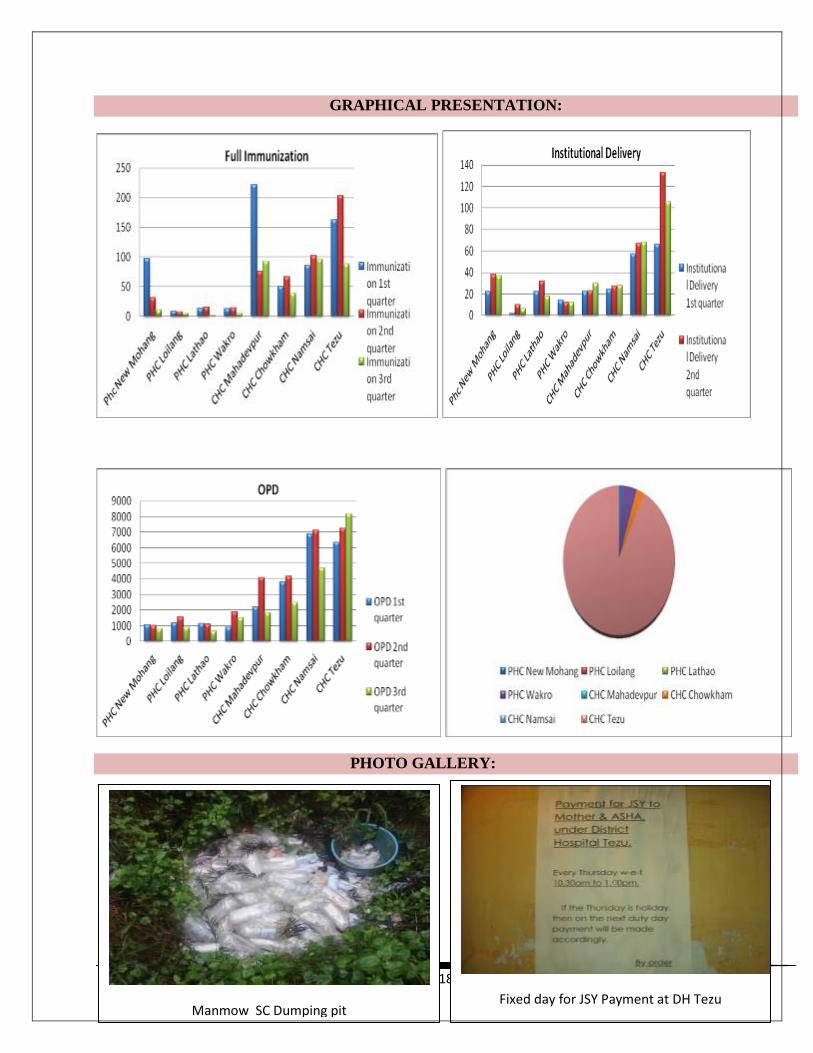
GRAPHICAL PRESENTATION:
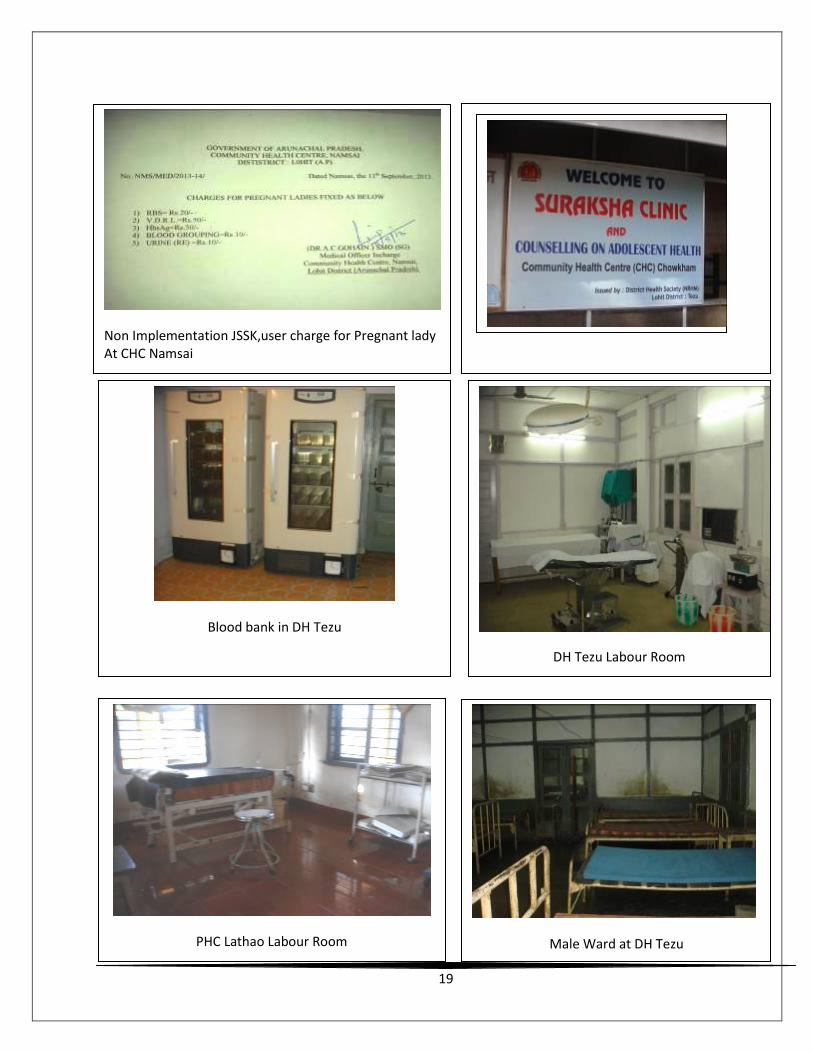
PHOTO GALLERY:
Manmow SC Dumping pit
Fixed day for JSY Payment at DH Tezu
19
Non Implementation JSSK,user charge for Pregnant lady At CHC Namsai
At
Blood bank in DH Tezu
DH Tezu Labour Room
PHC Lathao Labour Room
ARSH Clinic CHC Chowkham
Male Ward at DH Tezu

20
JSSK IEC at DH Tezu
New Building under construction PHC New
Mohong
Generator Room Constructed under RKS
fund PHC Lathao
JSY payment register PHC New Mohong













![Developing a country RMNCH scorecard - ALMA 2030 · evidence-based, country-led RMNCH strategy/planning dialogue INTRODUCTION Objectives of Country countdown “[Bring] old and new](https://static.fdocuments.net/doc/165x107/5e1c399a5bd17741ee6a423b/developing-a-country-rmnch-scorecard-alma-evidence-based-country-led-rmnch-strategyplanning.jpg)




