Risk Stratification and Treatment for Sudden Cardiac...
11
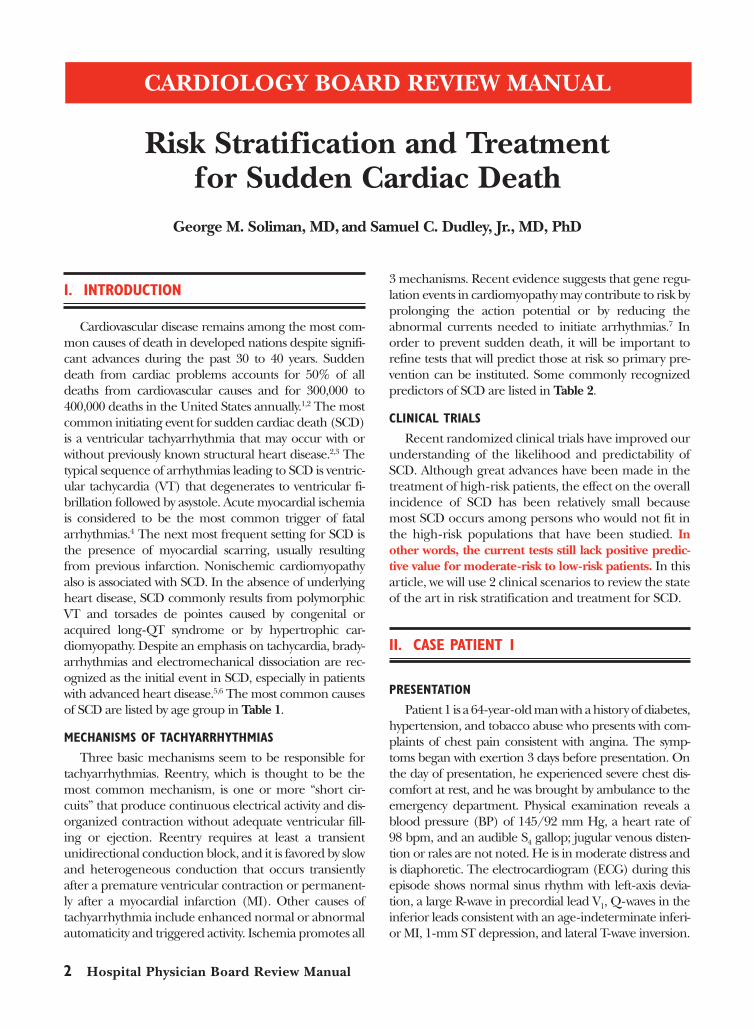
2 Hospital Physician Board Review Manual I. INTRODUCTION Cardiovascular disease remains among the most com- mon causes of death in developed nations despite signifi- cant advances during the past 30 to 40 years. Sudden death from cardiac problems accounts for 50% of all deaths from cardiovascular causes and for 300,000 to 400,000 deaths in the United States annually. 1,2 The most common initiating event for sudden cardiac death (SCD) is a ventricular tachyarrhythmia that may occur with or without previously known structural heart disease. 2,3 The typical sequence of arrhythmias leading to SCD is ventric- ular tachycardia (VT) that degenerates to ventricular fi- brillation followed by asystole. Acute myocardial ischemia is considered to be the most common trigger of fatal arrhythmias. 4 The next most frequent setting for SCD is the presence of myocardial scarring, usually resulting from previous infarction. Nonischemic cardiomyopathy also is associated with SCD. In the absence of underlying heart disease, SCD commonly results from polymorphic VT and torsades de pointes caused by congenital or acquired long-QT syndrome or by hypertrophic car- diomyopathy. Despite an emphasis on tachycardia, brady- arrhythmias and electromechanical dissociation are rec- ognized as the initial event in SCD, especially in patients with advanced heart disease. 5,6 The most common causes of SCD are listed by age group in Table 1. MECHANISMS OF TACHYARRHYTHMIAS Three basic mechanisms seem to be responsible for tachyarrhythmias. Reentry, which is thought to be the most common mechanism, is one or more “short cir- cuits” that produce continuous electrical activity and dis- organized contraction without adequate ventricular fill- ing or ejection. Reentry requires at least a transient unidirectional conduction block, and it is favored by slow and heterogeneous conduction that occurs transiently after a premature ventricular contraction or permanent- ly after a myocardial infarction (MI). Other causes of tachyarrhythmia include enhanced normal or abnormal automaticity and triggered activity. Ischemia promotes all 3 mechanisms. Recent evidence suggests that gene regu- lation events in cardiomyopathy may contribute to risk by prolonging the action potential or by reducing the abnormal currents needed to initiate arrhythmias. 7 In order to prevent sudden death, it will be important to refine tests that will predict those at risk so primary pre- vention can be instituted. Some commonly recognized predictors of SCD are listed in Table 2. CLINICAL TRIALS Recent randomized clinical trials have improved our understanding of the likelihood and predictability of SCD. Although great advances have been made in the treatment of high-risk patients, the effect on the overall incidence of SCD has been relatively small because most SCD occurs among persons who would not fit in the high-risk populations that have been studied. In other words, the current tests still lack positive predic- tive value for moderate-risk to low-risk patients. In this article, we will use 2 clinical scenarios to review the state of the art in risk stratification and treatment for SCD. II. CASE PATIENT 1 PRESENTATION Patient 1 is a 64-year-old man with a history of diabetes, hypertension, and tobacco abuse who presents with com- plaints of chest pain consistent with angina. The symp- toms began with exertion 3 days before presentation. On the day of presentation, he experienced severe chest dis- comfort at rest, and he was brought by ambulance to the emergency department. Physical examination reveals a blood pressure (BP) of 145/92 mm Hg, a heart rate of 98 bpm, and an audible S 4 gallop; jugular venous disten- tion or rales are not noted. He is in moderate distress and is diaphoretic. The electrocardiogram (ECG) during this episode shows normal sinus rhythm with left-axis devia- tion, a large R-wave in precordial lead V 1 , Q-waves in the inferior leads consistent with an age-indeterminate inferi- or MI, 1-mm ST depression, and lateral T-wave inversion. CARDIOLOGY BOARD REVIEW MANUAL Risk Stratification and Treatment for Sudden Cardiac Death George M. Soliman, MD,and Samuel C. Dudley, Jr., MD, PhD
Transcript of Risk Stratification and Treatment for Sudden Cardiac...
2 Hospital Physician Board Review Manual
I. INTRODUCTION
Cardiovascular disease remains among the most com-mon causes of death in developed nations despite signifi-cant advances during the past 30 to 40 years. Suddendeath from cardiac problems accounts for 50% of alldeaths from cardiovascular causes and for 300,000 to400,000 deaths in the United States annually.1,2 The mostcommon initiating event for sudden cardiac death (SCD)is a ventricular tachyarrhythmia that may occur with orwithout previously known structural heart disease.2,3 Thetypical sequence of arrhythmias leading to SCD is ventric-ular tachycardia (VT) that degenerates to ventricular fi-brillation followed by asystole. Acute myocardial ischemiais considered to be the most common trigger of fatalarrhythmias.4 The next most frequent setting for SCD isthe presence of myocardial scarring, usually resultingfrom previous infarction. Nonischemic cardiomyopathyalso is associated with SCD. In the absence of underlyingheart disease, SCD commonly results from polymorphicVT and torsades de pointes caused by congenital oracquired long-QT syndrome or by hypertrophic car-diomyopathy. Despite an emphasis on tachycardia, brady-arrhythmias and electromechanical dissociation are rec-ognized as the initial event in SCD, especially in patientswith advanced heart disease.5,6 The most common causesof SCD are listed by age group in Table 1.
MECHANISMS OF TACHYARRHYTHMIAS
Three basic mechanisms seem to be responsible fortachyarrhythmias. Reentry, which is thought to be themost common mechanism, is one or more “short cir-cuits” that produce continuous electrical activity and dis-organized contraction without adequate ventricular fill-ing or ejection. Reentry requires at least a transientunidirectional conduction block, and it is favored by slowand heterogeneous conduction that occurs transientlyafter a premature ventricular contraction or permanent-ly after a myocardial infarction (MI). Other causes oftachyarrhythmia include enhanced normal or abnormalautomaticity and triggered activity. Ischemia promotes all
3 mechanisms. Recent evidence suggests that gene regu-lation events in cardiomyopathy may contribute to risk byprolonging the action potential or by reducing theabnormal currents needed to initiate arrhythmias.7 Inorder to prevent sudden death, it will be important torefine tests that will predict those at risk so primary pre-vention can be instituted. Some commonly recognizedpredictors of SCD are listed in Table 2.
CLINICAL TRIALS
Recent randomized clinical trials have improved ourunderstanding of the likelihood and predictability ofSCD. Although great advances have been made in thetreatment of high-risk patients, the effect on the overallincidence of SCD has been relatively small becausemost SCD occurs among persons who would not fit inthe high-risk populations that have been studied. Inother words, the current tests still lack positive predic-tive value for moderate-risk to low-risk patients. In thisarticle, we will use 2 clinical scenarios to review the stateof the art in risk stratification and treatment for SCD.
II. CASE PATIENT 1
PRESENTATION
Patient 1 is a 64-year-old man with a history of diabetes,hypertension, and tobacco abuse who presents with com-plaints of chest pain consistent with angina. The symp-toms began with exertion 3 days before presentation. Onthe day of presentation, he experienced severe chest dis-comfort at rest, and he was brought by ambulance to theemergency department. Physical examination reveals ablood pressure (BP) of 145/92 mm Hg, a heart rate of98 bpm, and an audible S4 gallop; jugular venous disten-tion or rales are not noted. He is in moderate distress andis diaphoretic. The electrocardiogram (ECG) during thisepisode shows normal sinus rhythm with left-axis devia-tion, a large R-wave in precordial lead V1, Q-waves in theinferior leads consistent with an age-indeterminate inferi-or MI, 1-mm ST depression, and lateral T-wave inversion.
CARDIOLOGY BOARD REVIEW MANUAL
Risk Stratification and Treatment for Sudden Cardiac Death
George M. Soliman, MD, and Samuel C. Dudley, Jr., MD, PhD

His cardiac enzymes are positive for MI. During initial eval-uation, the patient develops pulseless VT and receives car-dioversion, which is successful.
After stabilization, the patient undergoes cardiaccatheterization that reveals a total occlusion of the mid-left circumflex coronary artery, a 50% stenosis of thedistal right coronary artery, and a 40% stenosis of thedistal left anterior descending artery. He undergoessuccessful angioplasty with stent placement at the cir-cumflex occlusion.
• Which classes of drugs have been shown to decreasethe risk of SCD in post-MI patients?
A) β-BlockersB) Class IC antiarrhythmicsC) Angiotensin-converting enzyme (ACE) inhibitorsD) A and C
DISCUSSION
The correct answer is D. Commonly identifiable car-diovascular risk factors (such as cigarette smoking, hyper-tension, elevated cholesterol, older age, and diabetes)confer an increased risk of SCD. The relationship be-tween these risk factors and SCD most likely is mediatedthrough myocardial ischemia that creates the substratefor arrhythmia propagation. Supporting this idea, occlu-sive coronary thrombus is found in 15% to 64% of pa-tients who die of SCD.8
Pharmacologic Therapy
The link between ischemia and SCD is strengthenedby the finding that drugs that can prevent future coro-nary events also can significantly reduce SCD. The ear-liest primary prevention trials examined the effect of β-blocker therapy in patients who had had an MI.Although these trials were not intended to specificallyexamine the effects on SCD, they identified a reductionin SCD in post-MI patients receiving therapy, which wasparticularly significant in those with depressed systolicfunction. The β-Blocker Heart Attack Trial (BHAT)showed a 25% reduction in all-cause mortality in post-MIpatients treated with propranolol.9,10 Despite a clear indi-cation for β-blocker use, however, only a fraction ofpatients (especially elderly persons, diabetics, andwomen) receive therapy. Other drugs that halt or delaythe progression of the underlying coronary disease (suchas aspirin and statins) have an overall mortality benefit,some of which is most likely the result of preventing SCD.
ACE inhibitors have been extensively studied inpatients with left ventricular (LV) dysfunction. Large, ran-domized clinical trials have shown that ACE inhibitorsimprove patients’ survival after an MI.11–14 Post-MIpatients are at significantly increased risk for cardiovascu-lar death and nonfatal reinfarction, which are thought tobe related to LV dysfunction, LV remodeling, or progres-sion of atherosclerosis. SCD accounts for approximately50% of these deaths in post-MI patients. Although nostudy of ACE inhibitor therapy has had sufficient power todemonstrate the exact mechanism of reduction in cardio-vascular mortality, a meta-analysis suggests that reductionin SCD is an important component in the overall mortal-ity reduction in post-MI patients. Possible mechanisms ofthis effect include attenuation of LV dilation post-MI, pre-vention of recurrent ischemic events, sympatholytic activi-ty, and preservation of plasma potassium levels.15
Cardiology Volume 8, Part 5 3
R i s k S t r a t i f i c a t i o n a n d T r e a t m e n t f o r S u d d e n C a r d i a c D e a t h
Table 1. Common Causes of Sudden Cardiac Death
Causes of SCD in Order ofAge Group Decreasing Frequency
35 years or younger Hypertrophic cardiomyopathy (50%)
Idiopathic LVH
Coronary anomalies
Coronary artery disease
Primary electrophysiologic ab-normalities (long QT syndrome, RV dysplasia, Wolff-Parkinson-White syndrome, idiopathic)
Older than 35 years Coronary artery disease (80%)
Nonischemic cardiomyopathy
Hypertrophic cardiomyopathy
Valvular heart disease
Idiopathic
LVH = left ventricular hypertrophy; RV = right ventricular; SCD = sud-den cardiac death.
Table 2. Factors Associated with a High Risk ofSudden Cardiac Death
Left ventricular dysfunction
Frequent premature ventricular contractions
Nonsustained ventricular tachycardia
Inducible ventricular tachycardia on programmed electricalstimulation
Abnormal signal-averaged ECG (presence of late potentials)
Reduced heart rate variability
Presence of T-wave alternans
Increased QT-segment dispersion
ECG = electrocardiogram.

Aside from possibly amiodarone, no antiarrhythmicdrug has shown survival advantage in acute or post-MIpatients. In the Cardiac Arrhythmia Suppression Trial(CAST) I and II studies, patients with ischemic car-diomyopathy did worse when treated with a class ICagent.16,17 Mortality differences occurred soon after start-ing the drug, perhaps suggesting proarrhythmia fromdrug-induced Brugada syndrome. Therefore, theseagents are no longer used in patients with ischemia orstructurally abnormal hearts.
Other Therapy
Aborted SCD in the setting of an acute MI, occurringwithin the first 24 to 48 hours, is not considered to por-tend the same high risk as SCD in the absence of an MI.Arrhythmias during the acute event are thought to arisefrom transient abnormalities that will resolve as myo-cytes either die or are revascularized. In these cases, thepatient’s chronic risk is assessed best after these transientfactors have stabilized.
Aside from drug management of atherosclerosis, re-vascularization is the first-line therapy for arrhythmia inischemic cardiomyopathy. The Coronary Artery BypassGraft (CABG) Patch trial (a multicenter trial) enrolledpatients who were scheduled for elective coronary bypasssurgery, had depressed LV systolic function, and had anabnormal signal-averaged ECG. Then, the CABG Patchtrialists randomly assigned patients either to prophylacticplacement of an implanted cardioverter defibrillator(ICD) or to the control group. No survival benefit wasobserved in the ICD group. The most commonly accept-ed explanation for this result is that revascularizationdecreased the incidence of ischemia-triggered lethalarrhythmias and, therefore, decreased the rate of SCD inboth groups below predicted rates.18
FURTHER PRESENTATION OF PATIENT 1
The patient is monitored in the coronary care unitfor 2 days post-MI and subsequently is transferred to the
telemetry-monitoring ward. Two days later, he is foundto have several asymptomatic runs of nonsustained ven-tricular tachycardia (NSVT; Figure 1), some as long as20 beats and at rates up to 180 bpm. His medicationsinclude metoprolol, enalapril, aspirin, clopidogrel, andsimvastatin. An echocardiogram reveals an ejection frac-tion (EF) of 35%, with severe posterolateral hypokinesis.
• Which is the best test to risk stratify the patient withregard to future risk of SCD?
A) Signal-averaged ECGB) 24-Hour ambulatory (Holter) monitoringC) Electrophysiologic (EP) testingD) No risk stratification is indicated at this point.
DISCUSSION
The correct answer is C. The patient’s recent MI,NSVT, and extent of LV dysfunction place him in a high-risk group for SCD. In patients who are discharged fromthe hospital after MI with significant LV dysfunction, the6- to 12-month mortality is 10% or higher.19 Therefore,some form of risk stratification would be advisable.
Risk Stratification Testing
Signal-averaged ECG is a simple test that averages alarge number of QRS complexes in order to enhancedetection of late potentials at the end of ventriculardepolarization. These late potentials are constantly pres-ent, small voltage fluctuations of unknown etiology,which perhaps are partially completed reentrant cir-cuits or triggered activity. Late potentials prolong theQRS (> 114 ms), are of small root-mean-square volt-age (< 20 µV), and last more than 38 ms (using a40 Hz high-pass bidirectional filter). A positive signal-averaged ECG is shown in Figure 2. Although the neg-ative predictive value for the signal-averaged ECG isestimated to be 95% to 99%, the positive predictivevalue is thought to be as low as 14% to 29%.20 In otherwords, a negative signal-averaged ECG is reassuring,
4 Hospital Physician Board Review Manual
R i s k S t r a t i f i c a t i o n a n d T r e a t m e n t f o r S u d d e n C a r d i a c D e a t h
Figure 1. Electrocardiogram showing aburst of nonsustained ventricular tachy-cardia. V = ventricular beat.

but a positive one is not as helpful. In a large random-ized controlled trial, signal-averaged ECG was not ableto predict which patients undergoing bypass surgerywould benefit from an ICD.18
Holter monitoring would help document frequentpremature ventricular contractions (PVCs) and theirrelative, NSVT. Data have suggested that frequent PVCsand NSVT increase the risk of SCD in patients with con-gestive heart failure (CHF) and previous MI, but morerecent studies suggest that these extrasystoles may be asign of failing myocardium rather than a cause of ar-rhythmia.21 Although other interpretations have beenadvanced for the results, this idea is consistent with thelack of improvement seen in patients receiving class ICantiarrhythmic drugs that were highly effective at sup-pression of PVCs.22 Finally, patient 1 had demonstratedfrequent PVCs and NSVT on telemetry, so ambulatorymonitoring would not have provided any further infor-mation for risk stratification.
EP testing is a procedure in which extra stimuli areadded, generally in 2 sites of the right ventricle. The abil-ity to induce sustained, monomorphic VT is considereda positive result and signifies an increased risk of ven-tricular tachyarrhythmias and SCD.23 In patients withprevious MI and reduced LV function who have a posi-tive EP test result, several large studies have shown thatprophylactic ICD placement reduces overall mortality.The Multicenter Automatic Defibrillator ImplantationTrial (MADIT)24 and the Multicenter UnsustainedTachycardia Trial (MUSTT)25 used EP testing to riskstratify patients with depressed LV function, previous MI,and NSVT; results showed that this technique coulddefine a high-risk population.
CASE PATIENT 1 CONTINUED
The patient undergoes EP testing. He is found tohave inducible, monomorphic, sustained VT at a rate of210 bpm (Figure 3).
Cardiology Volume 8, Part 5 5
R i s k S t r a t i f i c a t i o n a n d T r e a t m e n t f o r S u d d e n C a r d i a c D e a t h
Figure 2. A signal-averaged electrocardiogram that shows the presence of late potentials (arrow), signifying increased risk for suddencardiac death. Late potentials are shaded (red) in the vector magnitude graph. LAS = low-amplitude signal; RMS = root-mean-squareamplitude; QRSD = QRS duration.
X Y Z VectorNumber of beats.........................................628 QRSD (ms) 132.00 132.00 144.50 144.50Final Noise....................................................0.305 µV RMS (µV) 62.52 22.04 32.29 71.12High pass frequency ...................................40 Hz RMS 40 (µV) 3.19 4.24 4.13 6.15Sampling frequency .....................................2000 Hz LAS (ms) 58.00 71.00 77.00 70.50
mV µV µV
Unfiltered leads Filtered leads Vector magnitudeScale: 204 µV/mm Scale: 800 nV/mm Scale: 1 µV/mm

• Which therapeutic option is the most effective atimproving long-term outcome in this patient?A) ICD placement B) EP-directed D,L-sotalolC) Empiric amiodaroneD) Holter monitor–guided therapy with a class IC
agent
DISCUSSION
The correct answer is A. All of these modalities havebeen used to reduce arrhythmic death in post-MI pa-tients. In general, trials with antiarrhythmic agents havebeen disappointing because of low therapeutic indicesand proarrhythmic properties. In CAST I, for example,
antiarrhythmic therapy guided by Holter monitoring wasused to suppress PVCs in post-MI patients.26 Althoughtreatment was efficacious in the suppression of PVCs, thepatients treated with the class IC agents had an increasedrisk of death.
Antiarrhythmic Drug Therapy
The Electrophysiology Study Versus Electrocardio-graphic Monitoring (ESVEM)26 trial randomly assigned486 patients with documented VT or resuscitated SCD toeither EP testing or Holter monitor–guided antiarrhyth-mic therapy. Among the objectives of this trial was a com-parison of the efficacy of 7 antiarrhythmic agents includ-ing sotalol, quinidine, propafenone, and procainamide
6 Hospital Physician Board Review Manual
R i s k S t r a t i f i c a t i o n a n d T r e a t m e n t f o r S u d d e n C a r d i a c D e a t h
Figure 3. A positive electrophysiologicstudy. Tracings from a programmed electri-cal stimulation test showing surface electro-cardiogram (ECG) as well as intracardiacrecordings. Panel (A) shows induction ofthe ventricular tachycardia (VT) by an extrastimulus (arrow). The first few beats arepaced (S1), and the last pacing stimulus (S2)is introduced early, which triggers mono-morphic VT. Panel (B) shows a 12-lead sur-face ECG of the VT.
A
B
III
II
I
V
V3
V2
V1 V4
V5
V6aVF
aVL
aVR
S1 S1 S2

among others. Of the agents used in the study to suppressPVCs, only D,L-sotalol was associated with a significantreduction of mortality. On the other hand, the Survivalwith Oral D-Sotalol (SWORD) Trial using the channelblocking rather than the β-blocking isomer of this class IIIagent demonstrated increased adverse outcome.27
Amiodarone, another class III antiarrhythmic, wasstudied in 2 large trials in the 1990s: the European Myo-cardial Infarct Amiodarone Trial (EMIAT)28 and theCanadian Amiodarone Myocardial Infarction ArrhythmiaTrial (CAMIAT).29 No overall survival benefit was noted inthese trials despite a reduction in sudden deaths that pre-sumably were caused by arrhythmias. Importantly, mortal-ity did not increase when compared with placebo. Two tri-als have examined the use of amiodarone in patients withheart failure, GESICA (Grupo de Estudio de la Sobrevidaen la Insuficiencia Cardiaca en Argentina) trial30 andCHF-STAT (Congestive Heart Failure Survival Trial ofAntiarrhythmic Therapy).31 In GESICA, the authors com-pared low-dose amiodarone with placebo in combina-tion with standard medical therapy including ACE inhib-itors. Interestingly, a 28% reduction in overall mortalitywas noted at 2 years; however, this result was not con-firmed in CHF-STAT. In GESICA, a larger proportion ofnonischemic cardiomyopathy (61% versus 30%) was ob-served. It is possible that amiodarone may exert a moreprotective role in those patients without a previous histo-ry of MI. Substudy analysis from GESICA suggests thatamiodarone may be more effective in patients with high(> 90 bpm) resting heart rate as well as when combinedwith β-blocker therapy.32 Further studies are needed toverify these observations. In summary, antiarrhythmicdrugs tend to be less effective and show a higher inci-dence of proarrhythmia as the EF decreases. Only amio-darone has been shown to be safe in those patients withlow EF or recent MI.
Implanted Cardioverter Defibrillator Use
Several large randomized clinical trials support theuse of prophylactic ICD placement instead of drugtherapy to reduce mortality in patients at high risk forSCD. As previously discussed, the MADIT study24
enrolled 196 patients with prior MI and EF of 35% orless who had episodes of documented, asymptomaticNSVT. The patients in this trial underwent EP testing.If inducible VT was not suppressed by procainamide,they were randomly assigned to ICD placement or con-ventional therapy, which in most patients (74/93)included amiodarone. There were 15 deaths in theICD group and 39 deaths in the conventional therapygroup (hazard ratio [HR], 0.46; 95% confidence inter-val, 0.26–0.82; P = 0.009) during the average follow-up
period of 27 months. This finding was highly signifi-cant and consistent with the findings in the MUSTTstudy.25 In this trial, 704 patients with coronary arterydisease, an EF of 40% or less, asymptomatic NSVT, andinducible VT on EP testing were randomly assigned totherapy, which included antiarrhythmic medicationsor ICD, or no antiarrhythmic therapy. When comparedwith patients assigned to antiarrhythmic therapy butwithout ICD, those receiving ICD had an adjusted rel-ative risk of arrhythmic events of 0.24 and an adjustedrelative risk of overall mortality of 0.40. No differenceswere noted in rates of arrhythmic death or overall mor-tality between patients receiving antiarrhythmic agentsand the group receiving conventional therapy.
The findings were similar when antiarrhythmicdrugs were tested against an ICD for secondary preven-tion of SCD. The Antiarrhythmic Versus ImplantableDefibrillators (AVID) trial33 compared use of antiar-rhythmic drugs with ICD. Greater survival was observedwith the use of ICD in this high-risk population, withthe adjusted HR for death from any cause being 0.67when compared with the antiarrhythmic drug therapygroup.
Data indicate that ICD placement is the most effectivetherapy for patients with characteristics similar to thoseseen in patient 1. Recently published data suggest thattherapy with ICD placement in certain high-risk patientscan reduce overall mortality without risk stratificationusing EP testing. The recently published MADIT II study34
enrolled 1232 patients with prior MI and EFs of 30% orless. Unlike previous trials, documentation of NSVT andinducible VT were not used as entry criteria. They founda reduction in all-cause mortality in the ICD group whencompared with conventional therapy group (HR, 0.69).Although these findings are highly significant and con-firm the efficacy of ICD placement, an important ques-tion still remains regarding which, if any, risk stratificationtechnique is most useful. The financial cost of imple-menting this approach in caring for this patient popula-tion would obviously be tremendous. Careful review ofthe results of the EP testing done on a significant portionof the patients in this trial may provide insight into how tointerpret the data.
III. CASE PATIENT 2
PRESENTATION
Patient 2 is a 48-year-old woman who has a historyof idiopathic dilated cardiomyopathy and has had asyncopal episode. Two years ago, she presented with
Cardiology Volume 8, Part 5 7
R i s k S t r a t i f i c a t i o n a n d T r e a t m e n t f o r S u d d e n C a r d i a c D e a t h

exertional dyspnea, fatigue, and symptoms of CHF. Herinitial evaluation included an echocardiogram that dem-onstrated 4-chamber dilation and severe global hypoki-nesis. The EF was estimated to be 25% at that time, andcardiac catheterization showed normal coronary arteries.Her medications included lisinopril (40 mg/day), digox-in (0.125 mg/day), furosemide (40 mg/day), and car-vedilol (25 mg twice daily). A cardiologist is asked to eval-uate her in the emergency department after she presentswith syncope.
During the past 2 weeks, she has had several episodesof palpitations that she describes as feeling as though her“heart is racing.” These episodes lasted several secondsafter which she felt “drained.” On the day of presentation,she experienced a prolonged episode similar to the pre-vious ones; however, she became lightheaded, diaphoret-ic, and lost consciousness during this episode. She wasobserved to slump in her chair, but she quickly regainedconsciousness. She had no loss of bladder or bowel con-trol and no post-event confusion. Evaluation in the emer-gency department reveals a BP of 104/60 mm Hg; heartrate of 68 bpm; and a physical examination without signsof volume overload, orthostasis, or carotid hypersensitivi-ty. The ECG showed normal sinus rhythm and a previ-ously documented left bundle branch block. Blood chem-istry results, including potassium and magnesium levels,are all normal. While on the cardiac monitor in the emer-gency department, the patient is noted to have frequentPVCs and occasional asymptomatic runs of NSVT.
• What is the appropriate next step in the managementof this patient?
A) Signal-averaged ECGB) Placement of an ICDC) Tilt-table testingD) EP study
DISCUSSION
The correct answer is B. Syncope in patients withidiopathic dilated cardiomyopathy is an ominous signthat identifies a subgroup of patients at higher risk forSCD. Depending on the severity of disease, the annualmortality in patients with idiopathic dilated cardiomy-opathy ranges from 10% to 50%. In a meta-analysis thatexamined 1432 patients from 14 studies, the mean mor-tality rate after a 4-year follow-up was 42%, with 28% ofdeaths resulting from SCD.35
The symptoms and risk profile of patient 2 make a car-diac cause of syncope most likely. Most signal-averagedECG analysis is done in the time domain where one ofthe criteria for a positive test is a prolonged QRS-intervalduration. Therefore, a traditional signal-averaged ECG
would be of little value because of the presence of a leftbundle branch block on the baseline ECG.20 Tilt-tabletesting is an examination for neurally mediated syncopeduring orthostatic stress.36 As the initial evaluation, thistest would be reserved for patients at low risk for tachy-arrhythmias (ie, in patients with structurally normalhearts or those in whom other risk predictors have beenpreviously evaluated).
Unfortunately, risk stratification for SCD in patientswith nonischemic cardiomyopathy is even more diffi-cult than it is in ischemic patients. Although EP testinghas significant utility in patients with a previous historyof MI, it is less predictive in patients without coronarydisease, which may result from significant differences inthe mechanisms of SCD in the 2 groups. In patientswith previous MI, reentry seems to account for a higherproportion of tachyarrhythmias, whereas triggeredactivity and automaticity might be more common inpatients with nonischemic causes of cardiomyopathy.Programmed electrical stimulation (PES), with its pre-mature extra stimuli, is predominately a test for latentreentrant circuits, which may account for the reducednegative predictive value of PES in patients with nonis-chemic cardiomyopathy.37 Therefore, it is appropriateto proceed with placement of an ICD in these patientswith advanced heart failure and syncope.38
OTHER RISK STRATIFICATION TECHNIQUESHeart Rate Variability
The shortcomings of EP testing have lead to thesearch for other risk stratification techniques. Patientswith CHF have autonomic dysfunction, which may play arole in the development of cardiac arrhythmias. Heartrate variability (HRV) has been studied as a measure ofboth sympathetic and parasympathetic signaling to theheart. Several studies have examined the utility of mea-suring HRV to predict those patients at increased risk forSCD. To assess this risk, an ambulatory ECG recording ofsufficient length is used and, after correction for extrasys-toles, measures of the variability between RR-intervals areassessed. Patients with reduced HRV are thought to be atincreased risk of death.39 Nolan and colleagues conclud-ed that a standard deviation of normal-to-normal beats(SDNN), which is a time domain measure of HRV, of lessthan 50 ms was a better risk predictor of all-cause mor-tality from progressive heart failure than other commonmeasures, such as the cardiothoracic ratio. SDNN waslargely independent of EF, suggesting SDNN may con-tain independent data on SCD risk.39 The first large scale,randomized clinical trial addressing the utility of HRV isunderway (Azimilide Post-Infarct Survival Evaluation[ALIVE] trial).40
8 Hospital Physician Board Review Manual
R i s k S t r a t i f i c a t i o n a n d T r e a t m e n t f o r S u d d e n C a r d i a c D e a t h

QT-Interval Dispersion
Another marker of SCD is QT-interval dispersion,which is the difference between the maximal and mini-mal QT-intervals as measured from different leads onthe ECG. The hypothesis is that heterogeneity of repo-larization will lead to the possibility of initiation andmaintenance of arrhythmia. Results from studies havebeen inconsistent; however, this inconsistency may stemfrom methodological difficulties in an accurate mea-surement of QT-interval dispersion.41
T-Wave Alternans
T-wave alternans is another noninvasive means ofassessing risk for SCD that is currently being evaluated. T-wave alternans is defined as beat-to-beat variations inthe T-wave amplitude. An extreme example of T-wavealternans is shown in Figure 4. Generally, the amplitudeof these fluctuations is within the microvolt range, requir-ing special recording techniques. Measurements areobtained during exercise, pacing, or dobutamine infu-sion when the heart rate is between 105 and 110 bpm.Measurements of microvolt T-wave alternans were per-formed prospectively in a high-risk group of patientsundergoing ICD placement and were compared with EPtesting and other noninvasive tests used to predict the riskfor SCD. T-wave alternans compared favorably with EPtesting in this high-risk population.42 Although most ofthe data available regarding the utility of T-wave alternanshave focused on patients with ischemic heart disease, evi-dence suggests it may be valuable in patients with nonis-chemic cardiomyopathy.43 These results may not be gen-eralizable, but this technique is promising. An approachusing a combination of noninvasive markers of increasedSCD risk may ultimately prove to be the most effective.The ongoing Alternans before Cardioverter Defibrillator(ABCD) trial will help define the clinical role of this test.
In summary, prediction of SCD is still difficult, espe-cially in patients with nonischemic cardiomyopathy.Traditional techniques have higher negative than posi-tive predictive values. Newer techniques show promise,but it is likely that combinations of several tests will benecessary to screen intermediate-risk patients. Advan-tages and limitations of these various techniques arereviewed in Table 3. Interestingly, SCD events appear tooccur in a nonrandom but nonlinear way. Fractal geo-metric analysis, a method of describing such behavior,may help predict patients at increased risk of SCD.44
Nevertheless, ICD placement has shown efficacy inischemic and nonischemic patients, becoming the stan-dard of care for high-risk patients.24,25,33,34
IV. FUTURE DIRECTIONS
In the near future, it is unlikely that we will have sufficient tools to predict who is at risk for SCD in a low-risk population. The 2 cases discussed in this review de-scribe patients in identifiable high-risk groups for whomevidence-based management strategies have been evaluat-ed. Although the percentage of patients in this group whohave had SCD annually is the highest, the actual overallincidence is low. Greater effect on overall public healthcould be made if SCD were reduced in patients withoutpreviously diagnosed structural heart disease but who pre-sent with SCD. In this group, perhaps wide availability ofautomated external defibrillators (AEDs) will help.
Two major studies have examined the effects of mak-ing AEDs available in public areas. One study assessedtheir use on commercial aircraft45 and the other evalu-ated their use by security guards in casinos.46 Both stud-ies demonstrate safety and efficacy of these devices with increased chance of survival to discharge from the
Cardiology Volume 8, Part 5 9
R i s k S t r a t i f i c a t i o n a n d T r e a t m e n t f o r S u d d e n C a r d i a c D e a t h
Figure 4. An extreme example of T-wavealternans (arrows) in a rhythm strip from apatient with an acute anterior myocardialinfarction.
V4
V5
V6

hospital. These results have led the American HeartAssociation to recommend wide public access to AEDs.47
The cost-benefit analysis of this type of therapy is still notquantified, but market forces are sure to play a significantrole in this determination. The results of the PublicAccess Defibrillation Trial, sponsored by the NationalInstitutes of Health, may provide valuable informationregarding the efficacy and the cost of such therapy.
V. SUMMARY POINTS
• The most common initiating event for sudden car-diac death (SCD) is a ventricular tachyarrhythmia
that may occur with or without previously knownstructural heart disease.
• Medical management of ischemia reduces SCD.Post–myocardial infarction (MI) patients treated withβ-blockers have a substantial reduction in all-causemortality. Despite a clear indication for β-blocker use,however, only a fraction of patients (especially elder-ly persons, diabetics, and women) receive therapy.
• Except for amiodarone, no antiarrhythmic drug hasshown survival advantage in acute or post-MI patients.Only amiodarone has been shown to be safe in thosepatients with low ejection fraction or recent MI.
• Although electrophysiologic testing has significantutility in patients with previous history of MI, it is less
10 Hospital Physician Board Review Manual
R i s k S t r a t i f i c a t i o n a n d T r e a t m e n t f o r S u d d e n C a r d i a c D e a t h
Table 3. Assessment of Tests for Risk Stratification of Sudden Cardiac Death
Test Mechanism Advantage Limitations
Ejection fraction
Frequent PVCs
NSVT
Signal-averaged ECG
T-wave alternans
QT-interval dispersion
Heart rate variability
EP testing with PES
ECG = electrocardiogram; EP = electrophysiologic; ICD = implanted cardioverter defibrillator; MADIT = Multicenter Automatic DefibrillatorImplantation Trial; NSVT = nonsustained ventricular tachycardia; PES = programmed electrical stimulation; PVC = premature ventricular con-traction; SCD = sudden cardiac death.
Identifies extent of structuralheart disease
Identifies presence of inter-mittent triggers
Identifies presence of inter-mittent triggers and corre-lates with extent of under-lying heart disease
Identifies the presence ofunderlying electrical abnor-malities that may predis-pose to SCD
Identifies presence of abnor-mal, fluctuating repolariza-tion, which may allow fordevelopment of ventriculararrhythmias
Identifies repolarization inho-mogeneity
Evaluates sympathetic andparasympathetic tone onthe heart
Identifies presence of reen-trant circuits, which are asubstrate for ventriculararrhythmias
Simple, easily obtained, non-invasive
Noninvasive, easily deter-mined
Easily assessed, noninvasive,positive predictive valueimproved when combinedwith PES
Noninvasive, high negativepredictive value
Noninvasive, high predictivevalue in high-risk patients
Measured on standard ECG
Simple to obtain and non-invasive
Highly specific in certainhigh-risk groups ofpatients, particularly thosewith ischemic heart disease
Low specificity in identifyingrisk of SCD
Low positive predictive valueif used alone
New data from MADIT IIstudy suggest that its pres-ence is not necessary toidentify high-risk groups whobenefit from ICD therapy
Low positive predictivevalue; use in patients withnonischemic disease needsfurther evaluation
Value in low-risk or moder-ately high-risk patientsunclear; use in nonischemicpatients needs to be betterdefined
Inconsistent results andmethodological problemsresult in limited accuracy
Predictive value yet to bedetermined in large trials
Invasive, necessity now inquestion with recentMADIT II data; lower nega-tive and positive predictivevalues in patients with non-ischemic cardiomyopathy

predictive in patients without coronary disease. • Implanted cardioverter defibrillators (ICDs) have
shown efficacy in preventing SCD in ischemic andnonischemic patients; therefore, ICDs are currentlythe standard of care for high-risk patients.
• Newer measures, such as heart rate variability and T-wave alternans, show promise for risk stratification.
REFERENCES
1. Myerburg RJ, Kessler KM, Castellanos A. Sudden cardiacdeath: epidemiology, transient risk, and intervention as-sessment. Ann Intern Med 1993;119:1187–97.
2. Zipes DP, Wellens HJ. Sudden cardiac death. Circulation1998;98:2334–51.
3. Myerburg RJ, Interian A Jr, Mitrani RM, et al. Frequencyof sudden cardiac death and profiles of risk. Am J Cardiol1997;80:10F–19F.
4. Davies MJ. Anatomic features in victims of sudden coro-nary death. Coronary artery pathology. Circulation 1992;85:I19–I24.
5. Luu M, Stevenson WG, Stevenson LW, et al. Diversemechanisms of unexpected cardiac arrest in advancedheart failure. Circulation 1989;80:1675–80.
6. Epstein AE, Carlson MD, Fogoros RN, et al. Classificationof death in antiarrhythmia trials. J Am Coll Cardiol 1996;27:433–42.
7. Pogwizd SM, Qi M, Yuan W, et al. Upregulation ofNa(+)/Ca(2+) exchanger expression and function in anarrhythmogenic rabbit model of heart failure. Circ Res1999;85:1009–19.
8. Roberts WC, Kragel AH, Gertz SD, Roberts CS. Coronaryarteries in unstable angina pectoris, acute myocardialinfarction, and sudden coronary death. Am Heart J 1994;127:1588–93.
9. Yusuf S, Peto R, Lewis J, et al. Beta blockade during andafter myocardial infarction: an overview of the random-ized trials. Prog Cardiovasc Dis 1985;27:335–71.
10. A randomized trial of propranolol in patients with acutemyocardial infarction. I. Mortality results. JAMA 1982;247:1707–14.
11. Pfeffer MA, Braunwald E, Moye LA, et al. Effect of cap-topril on mortality and morbidity in patients with leftventricular dysfunction after myocardial infarction.Results of the survival and ventricular enlargement trial.The SAVE Investigators. N Engl J Med 1992;327:669–77.
12. Pfeffer MA, Lamas GA, Vaughan DE, et al. Effect of cap-topril on progressive ventricular dilatation after anteriormyocardial infarction. N Engl J Med 1988;319:80–6.
13. Effect of enalapril on survival in patients with reducedleft ventricular EFs and congestive heart failure. TheSOLVD Investigators. N Engl J Med 1991;325:293–302.
14. Effect of enalapril on mortality and the development ofheart failure in asymptomatic patients with reduced leftventricular EFs. The SOLVD Investigators [published erra-tum appears in N Engl J Med 1992;327:1768]. N Engl JMed 1992;327:685–91.
15. Domanski MJ, Exner DV, Borkowf CB, et al. Effect ofangiotensin converting enzyme inhibition on suddencardiac death in patients following acute myocardialinfarction. A meta-analysis of randomized clinical trials.J Am Coll Cardiol 1999;33:598–604.
16. Preliminary report: effect of encainide and flecainide onmortality in a randomized trial of arrhythmia suppressionafter myocardial infarction. The Cardiac ArrhythmiaSuppression Trial (CAST) Investigators. N Engl J Med1989;321:406–12.
17. Effect of the antiarrhythmic agent moricizine on survivalafter myocardial infarction. The Cardiac Arrhythmia Sup-pression Trial II Investigators. N Engl J Med 1992;327:227–33.
18. Bigger JT Jr. Prophylactic use of implanted cardiac defi-brillators in patients at high risk for ventricular arrhyth-mias after coronary-artery bypass graft surgery. CoronaryArtery Bypass Graft (CABG) Patch Trial Investigators.N Engl J Med 1997;337:1569–75.
19. Tavazzi L, Volpi A. Remarks about postinfarction progno-sis in light of the experience with the Gruppo Italiano perlo Studio della Sopravvivenza nell’ Infarto Miocardico(GISSI) trials. Circulation 1997;95:1341–5.
20. Signal-averaged electrocardiography. J Am Coll Cardiol1996;27:238–49.
21. Singh SN, Fisher SG, Carson PE, Fletcher RD. Prevalenceand significance of nonsustained ventricular tachycardiain patients with premature ventricular contractions andheart failure treated with vasodilator therapy. Departmentof Veterans Affairs CHF STAT Investigators. J Am CollCardiol 1998;32:942–7.
22. Echt DS, Liebson PR, Mitchell LB, et al. Mortality and mor-bidity in patients receiving encainide, flecainide, or place-bo. The Cardiac Arrhythmia Suppression Trial. N Engl JMed 1991;324:781–8.
23. Brugada P, Green M, Abdollah H, Wellens HJ. Significanceof ventricular arrhythmias initiated by programmed ven-tricular stimulation: the importance of the type of ventric-ular arrhythmia induced and the number of prematurestimuli required. Circulation 1984;69:87–92.
24. Moss AJ, Hall WJ, Cannom DS, et al. Improved survivalwith an implanted defibrillator in patients with coronarydisease at high risk for ventricular arrhythmia. MulticenterAutomatic Defibrillator Implantation Trial Investigators.N Engl J Med 1996;335:1933–40.
25. Buxton AE, Lee KL, Fisher JD, et al. A randomized studyof the prevention of sudden death in patients with coro-nary artery disease. Multicenter Unsustained TachycardiaTrial Investigators [published erratum appears in N Engl
Cardiology Volume 8, Part 5 11
R i s k S t r a t i f i c a t i o n a n d T r e a t m e n t f o r S u d d e n C a r d i a c D e a t h
J Med 2000;342:1300]. N Engl J Med 1999;341:1882–90.
26. Klein RC. Comparative efficacy of sotalol and class Iantiarrhythmic agents in patients with ventricular tachy-cardia or fibrillation: results of the ElectrophysiologyStudy Versus Electrocardiographic Monitoring (ESVEM)Trial. Eur Heart J 1993;14 Suppl H:78–84.
27. Waldo AL, Camm AJ, deRuyter H. Effect of D-sotalol onmortality in patients with left ventricular dysfunctionafter recent and remote myocardial infarction. TheSWORD Investigators. Survival With Oral D-Sotalol [pub-lished erratum appears in Lancet 1996;348:416]. Lancet1996;348:7–12.
28. Julian DG, Camm AJ, Frangin G, et al. Randomised trialof effect of amiodarone on mortality in patients with left-ventricular dysfunction after recent myocardial infarc-tion: EMIAT. European Myocardial Infarct AmiodaroneTrial Investigators [published erratum appears in Lancet1997;349:1180]. Lancet 1997;349:667–74.
29. Cairns JA, Connolly SJ, Roberts R, et al. Randomised trialof outcome after myocardial infarction in patients with fre-quent or repetitive ventricular premature depolarisations:CAMIAT. Canadian Amiodarone Myocardial InfarctionArrhythmia Trial Investigators [published erratum appearsin Lancet 1997;349:1176]. Lancet 1997;349:675–82.
30. Doval HC, Nul DR, Grancelli HO, et al. Randomised trialof low-dose amiodarone in severe congestive heart failure.Grupo de Estudio de la Sobrevida en la InsuficienciaCardiaca en Argentina (GESICA). Lancet 1994;344:493–8.
31. Massie BM, Fisher SG, Radford M, et al. Effect of amio-darone on clinical status and left ventricular function inpatients with congestive heart failure. CHF-STAT In-vestigators [published erratum appears in Circulation1996;94:2668]. Circulation 1996;93:2128–34.
32. Nul DR, Doval HC, Grancelli HO, et al. Heart rate is amarker of amiodarone mortality reduction in severeheart failure. The GESICA-GEMA Investigators. Grupode Estudio de la Sobrevida en la Insuficiencia Cardiacaen Argentina-Grupo de Estudios Multicentricos enArgentina. J Am Coll Cardiol 1997;29:1199–205.
33. A comparison of antiarrhythmic-drug therapy withimplantable defibrillators in patients resuscitated fromnear-fatal ventricular arrhythmias. The Antiarrhythmicsversus Implantable Defibrillators (AVID) Investigators.N Engl J Med 1997;337:1576–83.
34. Moss AJ, Zareba W, Hall WJ, et al. Prophylactic implanta-tion of a defibrillator in patients with myocardial infarc-tion and reduced EF. N Engl J Med 2002;346:877–83.
35. Tamburro P, Wilber D. Sudden death in idiopathic dilat-ed cardiomyopathy. Am Heart J 1992;124:1035–45.
36. Benditt DG, Ferguson DW, Grubb BP, et al. Tilt table test-ing for assessing syncope. American College of Cardiology.J Am Coll Cardiol 1996;28:263–75.
37. Brachmann J, Hilbel T, Grunig E, et al. Ventricular arrhyth-mias in dilated cardiomyopathy. Pacing Clin Electrophysiol1997;20:2714–8.
38. Middlekauff HR, Stevenson WG, Stevenson LW, SaxonLA. Syncope in advanced heart failure: high risk of suddendeath regardless of origin of syncope. J Am Coll Cardiol1993;21:110–6.
39. Nolan J, Batin PD, Andrews R, et al. Prospective study ofheart rate variability and mortality in chronic heart fail-ure: results of the United Kingdom heart failure evalua-tion and assessment of risk trial (UK-heart). Circulation1998;98:1510–6.
40. Camm AJ, Karam R, Pratt CM. The azimilide post-infarctsurvival evaluation (ALIVE) trial. Am J Cardiol 1998;81:35D–39D.
41. Statters DJ, Malik M, Ward DE, Camm AJ. QT dispersion:problems of methodology and clinical significance.J Cardiovasc Electrophysiol 1994;5:672–85.
42. Hohnloser SH, Klingenheben T, Li YG. T wave alternansas a predictor of recurrent ventricular tachyarrhythmiasin ICD recipients: prospective comparison with conven-tional risk markers. J Cardiovasc Electrophysiol 1998;9:1258–68.
43. Adachi K, Ohnishi Y, Shima T, et al. Determinant ofmicrovolt-level T-wave alternans in patients with dilatedcardiomyopathy. J Am Coll Cardiol 1999;34:374–80.
44. Stein KM, Karagounis LA, Anderson JL, et al. Fractalclustering of ventricular ectopy correlates with sympa-thetic tone preceding ectopic beats. Circulation 1995;91:722–7.
45. Page RL, Joglar JA, Kowal RC, et al. Use of automatedexternal defibrillators by a U.S. airline. N Engl J Med2000;343:1210–6.
46. Valenzuela TD, Roe DJ, Nichol G, et al. Outcomes ofrapid defibrillation by security officers after cardiac arrestin casinos. N Engl J Med 2000;343:1206–9.
47. Weisfeldt ML, Kerber RE, McGoldrick RP, et al. AmericanHeart Association Report on the Public Access Defibril-lation Conference December 8–10, 1994. AutomaticExternal Defibrillation Task Force. Circulation 1995;92:2740–7.
12 Hospital Physician Board Review Manual
R i s k S t r a t i f i c a t i o n a n d T r e a t m e n t f o r S u d d e n C a r d i a c D e a t h