Risk of Breast Implant Bacterial Contamination From Endogenous ...
8
Breast Surgery Aesthetic Surgery Journal 32(8) 956–963 © 2012 The American Society for Aesthetic Plastic Surgery, Inc. Reprints and permission: http://www.sagepub.com/ journalsPermissions.nav DOI: 10.1177/1090820X12456841 www.aestheticsurgeryjournal.com Capsular contracture (CC) is one of the most frequent com- plications following breast augmentation and a leading cause for reoperation. 1–5 Clinical observations over the past 5 dec- ades have suggested a number of potential risk factors for CC, including gel bleed, propensity for hypertrophic scarring, postoperative hematomas, infection, surgical placement, and surgical incision site. 6 The etiology of contracture appears to be multifactorial, as no single factor can account for the full range of clinical observations. However, among the various proposed risk factors, the current body of evidence points most strongly to the role of subclinical infection and the underlying role of bacterial biofilms. 7–16 Risk of Breast Implant Bacterial Contamination From Endogenous Breast Flora, Prevention With Nipple Shields, and Implications for Biofilm Formation Roger N. Wixtrom, PhD, DABT; Ross L. Stutman, MD; Renee M. Burke, MD; Amy K. Mahoney, BS; and Mark A. Codner, MD Abstract Background: Capsular contracture (CC) is a common complication of breast augmentation that is thought to arise from bacterial contamination and subsequent biofilm formation on the implant. Endogenous breast flora expressed through the nipple may contaminate the sterile field during breast augmentation, acting as a possible source for initiation of biofilm formation. Objectives: The authors investigate the incidence of nipple bacterial contamination with endogenous breast flora after standard chest wall sterilization during breast augmentation. Methods: Bacterial contamination of nipples and nipple shields was assessed in a series of 32 consecutive patients presenting for breast augmentation (63 breasts: 31 bilateral procedures and 1 unilateral procedure). After standard sterilization of the chest wall, occlusive nipple shields were applied and breast augmentation was performed. At the conclusion of breast augmentation, the nipple shields were removed and, using the same swab, both the nipple/areolar area and occlusive dressings were cultured. Results: Data from 63 cultured nipples and nipple shields revealed that 22 nipples/nipple shields (34.9%) were positive for bacterial contamination. Three patients, all of whom had negative cultures, developed CC after augmentation. Conclusions: The exposed nipple is a potential source of implant contamination during breast augmentation. An improved understanding of biofilms and related risk factors for CC can provide surgeons with insights for addressing this common complication. Meticulous hemostasis, use of nipple shields, and submuscular device placement may contribute to a lower incidence of CC. Level of Evidence: 4 Keywords breast augmentation, biofilm, capsular contracture, nipple shields Accepted for publication May 10, 2012. Dr Wixtrom is a toxicologist and president of LSCI Inc, Springfield, Virginia. Dr Stutman and Dr Burke were oculoplastic and aesthetic surgery fellows at the private practice of Dr Codner in Atlanta, Georgia; Dr Stutman is now a plastic surgeon in private practice in Mesa, Arizona, and Dr Burke is a plastic surgeon in private practice in Hoffman Estates, Illinois. Ms Mahoney is a research assistant in the private practice of Dr Codner in Atlanta, Georgia. Dr Codner is a plastic surgeon in private practice in Atlanta, Georgia. Corresponding Author: Dr Mark A. Codner, 1800 Howell Mill Road, Suite 140, Atlanta, GA 30318, USA. E-mail: [email protected] Downloaded from https://academic.oup.com/asj/article-abstract/32/8/956/318056 by guest on 30 March 2018
Transcript of Risk of Breast Implant Bacterial Contamination From Endogenous ...

Breast Surgery
Aesthetic Surgery Journal32(8) 956 –963© 2012 The American Society for Aesthetic Plastic Surgery, Inc.Reprints and permission: http://www .sagepub.com/journalsPermissions.navDOI: 10.1177/1090820X12456841www.aestheticsurgeryjournal.com
Capsular contracture (CC) is one of the most frequent com-plications following breast augmentation and a leading cause for reoperation.1–5 Clinical observations over the past 5 dec-ades have suggested a number of potential risk factors for CC, including gel bleed, propensity for hypertrophic scarring, postoperative hematomas, infection, surgical placement, and surgical incision site.6 The etiology of contracture appears to be multifactorial, as no single factor can account for the full range of clinical observations. However, among the various proposed risk factors, the current body of evidence points most strongly to the role of subclinical infection and the underlying role of bacterial biofilms.7–16
Risk of Breast Implant Bacterial Contamination From Endogenous Breast Flora, Prevention With Nipple Shields, and Implications for Biofilm Formation
Roger N. Wixtrom, PhD, DABT; Ross L. Stutman, MD; Renee M. Burke, MD; Amy K. Mahoney, BS; and Mark A. Codner, MD
AbstractBackground: Capsular contracture (CC) is a common complication of breast augmentation that is thought to arise from bacterial contamination and subsequent biofilm formation on the implant. Endogenous breast flora expressed through the nipple may contaminate the sterile field during breast augmentation, acting as a possible source for initiation of biofilm formation.Objectives: The authors investigate the incidence of nipple bacterial contamination with endogenous breast flora after standard chest wall sterilization during breast augmentation.Methods: Bacterial contamination of nipples and nipple shields was assessed in a series of 32 consecutive patients presenting for breast augmentation (63 breasts: 31 bilateral procedures and 1 unilateral procedure). After standard sterilization of the chest wall, occlusive nipple shields were applied and breast augmentation was performed. At the conclusion of breast augmentation, the nipple shields were removed and, using the same swab, both the nipple/areolar area and occlusive dressings were cultured.Results: Data from 63 cultured nipples and nipple shields revealed that 22 nipples/nipple shields (34.9%) were positive for bacterial contamination. Three patients, all of whom had negative cultures, developed CC after augmentation.Conclusions: The exposed nipple is a potential source of implant contamination during breast augmentation. An improved understanding of biofilms and related risk factors for CC can provide surgeons with insights for addressing this common complication. Meticulous hemostasis, use of nipple shields, and submuscular device placement may contribute to a lower incidence of CC.
Level of Evidence: 4
Keywordsbreast augmentation, biofilm, capsular contracture, nipple shields
Accepted for publication May 10, 2012.
Dr Wixtrom is a toxicologist and president of LSCI Inc, Springfield, Virginia. Dr Stutman and Dr Burke were oculoplastic and aesthetic surgery fellows at the private practice of Dr Codner in Atlanta, Georgia; Dr Stutman is now a plastic surgeon in private practice in Mesa, Arizona, and Dr Burke is a plastic surgeon in private practice in Hoffman Estates, Illinois. Ms Mahoney is a research assistant in the private practice of Dr Codner in Atlanta, Georgia. Dr Codner is a plastic surgeon in private practice in Atlanta, Georgia.
Corresponding Author:Dr Mark A. Codner, 1800 Howell Mill Road, Suite 140, Atlanta, GA 30318, USA. E-mail: [email protected]
Downloaded from https://academic.oup.com/asj/article-abstract/32/8/956/318056by gueston 30 March 2018

Wixtrom et al 957
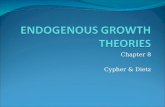
Biofilms have been defined most recently as “a coherent cluster of bacterial cells (one or several species) embedded in a matrix, which are more tolerant to most antimicrobials and the host defense than planktonic (i.e. single, free-floating) bacterial cells.”17 Figure 1 illustrates the current understand-ing of the biofilm life cycle: attachment of individual cells to the implant surface, replication and growth from a micro-colony to a mature biofilm, and then dispersion of cells from the colony. Biofilms are now believed to be responsible for approximately 80% or more of all human infections,18 includ-ing dental caries, otitis media, recurrent urinary tract infec-tions, chronic rhinosinusitis, chronic wounds, and—of particular significance to breast implants—a range of medical device infections.17,19–21 This is compounded by the fact that, in the presence of a foreign body, the number of bacteria required to initiate an infection may be reduced by as much as a millionfold.22 There is increasing recognition that most biofilms are multispecies and that interspecies interactions may play a crucial role in their clinical impact.17,19,21
In addition to skin bacteria that might contact the breast implant during surgical insertion, bacteria are also found within normal human breast tissue and breast nipple aspi-rates, representing additional potential sources for coloniza-tion of the implant surface.23–25 In 1999, Collis and colleagues first described the use of occlusive nipple coverings (nipple shields) during surgery to prevent expression of bacteria-containing secretions from the nipple ducts and thereby theo-retically reduce the incidence of CC.26 However, only recently
have surgeons begun advocating the routine use of nipple shields during breast augmentation, and data to support this recommendation are still scarce. In our practice, we have begun to cover the nipples with Tegaderm (3M, St. Paul, Minnesota) during augmentation mammoplasty and culture the nipples and nipple shields after the implant is placed in the pocket to better understand the potential risk of bacterial contamination from the nipple during placement of breast prostheses.
The primary objective of this study was to investigate the incidence of bacterial contamination of the nipples and nipple shields with endogenous breast flora during breast augmentation.
MEthOds
Between July 2010 and May 2011, a series of 32 consecutive patients who presented for bilateral (n = 31) or unilateral (n = 1) breast augmentation at the private practice of the senior author (MAC) gave informed consent and were included in the study. Patient characteristics are presented in Table 1.
Perioperative antibiosis consisted of 1 gm of first genera-tion cephalosporin administered intravenously (IV) at least 30 minutes prior to incision. For patients with penicillin allergy, clindamycin 600 gm IV was administered instead of a cephalosporin. After routine skin preparation of the chest wall and nipple/areolar area with povodine-iodine soap, the
Figure 1. The biofilm life cycle: initial adherence (left), biofilm production and growth (center), and bacterial dispersal (right), leading to potential creation of new biofilm colonies.
Downloaded from https://academic.oup.com/asj/article-abstract/32/8/956/318056by gueston 30 March 2018

958 Aesthetic Surgery Journal 32(8)
nipples were covered with Tegaderm transparent dressings as nipple shields (Figure 2), and the augmentations were per-formed. During augmentation, the breast pocket was irri-gated with triple antibiotic solution followed by dilute betadine before placement of implant. After completion of the procedure, the nipple shields were removed and each nipple and the breast-facing side of the respective nipple shield was swabbed with a single, sterile, cotton-tipped appli-cator. The swabs were then placed into designated containers per routine procedure and sent to a private laboratory for Gram stain and culture (Figure 3). Patients were evaluated at 2 weeks, 4 weeks, 2 months, and 6 months postoperatively. All complications, including infection, hematoma, hyper-trophic scarring, and CC, were recorded.
REsuLts
Based on culture results, the bacterial contamination rate was 34.9%, with 22 of 63 nipples/nipple shields testing positive for the presence of bacteria. The most common organisms identified were species considered to be normal skin flora including coagulase-negative Staphylococcus spe-cies and Staphylococcus epidermidis (Table 2). None of the
patients with culture-positive nipple shields or nipple swabs developed CC or infection.
Three patients with negative cultures developed CC: 1 patient who underwent primary breast augmentation with a submuscular pocket, 1 patient who underwent tertiary breast augmentation for Baker Grade IV CC with capsulectomy and neosubmuscular pocket location, and 1 patient who under-went a 7th breast augmentation procedure for recurrent CC with placement of Spectrum implant expanders (Mentor Worldwide LLC, Santa Barbara, California) and acellular der-mal matrix. The last patient did acquire a clinical infection, with cultures positive for methicillin-resistant Staphylococcus aureus (MRSA). No other patients developed clinical infec-tions and no change in postoperative antibiosis was made based on cultures, with the exception of the patient who developed a MRSA infection. No hematomas or hypertrophic scars were identified in any patients (Table 3).
disCussiOn
Numerous recent studies have reported the potential asso-ciation of infection, overt or subclinical, with the develop-ment of capsular thickening and contracture.5–16,27–32 The
Table 1. Patient Characteristics (N = 32)
Characteristic No. %
Mean age: 41.5 y (range, <30–50+)
Age at time of surgery, y
<30 3 9.4
30–34 8 25.0
35–39 6 18.8
40–44 5 15.6
45–49 4 12.5
50+ 6 18.8
Average fill volume: 319.5 cc (range, 150–550 cc)
Implant fill
Saline 1 3.1
Silicone gel 31 96.9
Type of breast augmentation
Primary breast augmentation 14 43.8
Primary augmentation/mastopexy 3 9.1
Secondary breast augmentation 5 15.6
Secondary augmentation/mastopexy 1 3.1
>3 breast surgeries 9 28.1
Figure 2. Tegaderm skin barrier (3M, St. Paul, Minnesota) covering the nipple to reduce contamination of the implant with endogenous breast flora.
Downloaded from https://academic.oup.com/asj/article-abstract/32/8/956/318056by gueston 30 March 2018

Wixtrom et al 959
goal of this study was to establish endogenous breast flora as a potential contamination source leading to subclinical infection and biofilm formation. Endogenous bacteria are the normal flora of the breast tissue. While not usually clinically evident or pathologic, the addition of local surgi-cal manipulation and contact with an inert foreign body (the breast implant) may produce a nidus for subclinical infection and biofilm formation on the implant (Figure 4). In this study, more than one-third of culture swabs of the
nipple and occlusive dressings after breast augmentation were positive for bacteria which, without shields, would likely be expressed onto the sterile surgical field.
The process by which free-floating, or planktonic, bac-teria establish biofilm communities is now understood to involve significant levels of communication, or quorum sensing, among the bacteria.33 The production, secretion, and recognition of quorum-sensing molecules allow the bacteria to synchronously direct gene expression.33 Following adherence of bacteria to a surface such as a breast implant, a biofilm state is established, allowing the expression of previously silent genes, including those responsible for producing the extracellular matrix in which the community of biofilm bacteria is embedded.34 This extracellular matrix, comprising polysaccharides, protein, and extracellular DNA, is thought to exclude immune cells and antimicrobial peptides.19 In addition, it creates a micro-environment in which the oxygen gradient decreases, mov-ing from the biofilm surface to the substratum of the community.35,36 This contributes to the presence of dor-mant bacteria20 that can exhibit markedly lower suscepti-bility to antibiotics36–38 and explains the difficulty of treating biofilm infections with conventional antibiotics.
As a result of these dormant bacteria, biofilms may grow over a prolonged period prior to producing symp-toms, thereby accounting for the “subclinical” nature of many biofilm infections, including those thought to be associated with CC.20,37 The most direct evidence demon-strating a causal link among subclinical infection, biofilm formation, and CC was shown in a porcine model using a clinical isolate of Staphylococcus epidermidis from a patient with recurrent CC.10
One of the greatest challenges posed by biofilms in the clinical setting is the difficulty of detection. Standard swab culture methods often miss biofilm infections, lead-ing to the frequent reports of negative culture find-ings.39,40 The use of capsule sonication prior to culturing has been employed in several studies involving breast
Figure 3. Intraoperative culture swab of nipple and nipple shield after placement of the implant and removal of the nipple shield.
Table 2. Culture Results
OrganismNumber of Positive
CulturesPercentage of
Cultures Taken (n = 63)a
Normal skin flora 13 20.6
Staphylococcus epidermidis 5 7.9
Coagulase-negative Staphylococcus species
4 6.3
Propionibacterium acnes 1 1.6
aOne culture was positive for two organisms: normal skin flora and coagulase-negative Staphylococcus species.
Table 3. Complications
Complication Number of Patients (N = 32)
Capsular contracture 3
Primary breast augmentation 1
Tertiary augmentation with capsulectomy 1
>5 revision procedures with capsulectomy and placement of acellular dermis
1
Infection 1
Hypertrophic scarring 0
Hematoma 0
One patient with capsular contracture also developed an infection with methicillin-resistant Staphylococcus aureus (MRSA) and is therefore included in both groups.
Downloaded from https://academic.oup.com/asj/article-abstract/32/8/956/318056by gueston 30 March 2018

960 Aesthetic Surgery Journal 32(8)
implants;12,15,30–32 however, this technique may also miss a number of microorganisms that are present. Technologies have recently been introduced that provide “culture-independent” molecular methods capable of species-level identification, thereby detecting a multitude of microorganisms likely missed by older methods.40 These new molecular methods are expected to provide a much more sensitive and complete picture of bacterial biofilms encountered in plastic surgery.32,40–43
Hematomas have long been suggested to be associated with increased risk of CC and have often been listed as a risk factor independent from biofilms.44–46 Yet, upon further inspection, these 2 risk factors appear to be directly related. Hematomas represent a rich source of iron, which is often an essential nutrient for bacterial growth. Heme, in particular, has been found to be a preferred source of iron for patho-genic bacteria including Staphylococcus aureus.47 A statisti-cally-significant, nearly 3-fold increase risk of CC among patients who experienced hematoma demonstrates a clear benefit of meticulous hemostasis, which should limit bacte-rial access to iron that would otherwise fuel their growth.48,49
Surgical approach and device placement have been dis-cussed as potential factors that might impact the magnitude of exposure to bacteria during or after implantation and thereby influence subsequent risk of contracture.4,6,50–55 A 2008 study by Wiener examined the relationship of CC to
incision location.53 The results revealed a statistically-signifi-cant increased risk of CC in patients who underwent breast augmentation using a periareolar incision versus inframam-mary incision with subpectoral placement of saline-filled implants. Wiener hypothesized that the increased rate of CC observed with use of a periareloar incision may be due to increased bacterial contamination from contact with the endogenous bacteria within the glandular tissues of the breast. This hypothesis is supported by findings from Bartsich et al, who analyzed samples from reduction mammaplasty patients and found increasing quantitative bacterial cultures in periareolar breast tissue compared to either inframmamary or axillary areas.56 It is theorized that submuscular implants, when placed through an inframammary or transaxillary inci-sion, may have decreased contact with the glandular tissues of the breast, which subsequently reduces the risk of CC; this has caused some surgeons to question the safety of the peri-areolar approach.57 Decreased rates of CC have also been reported in patients with a submuscular pocket and use of textured implants.10,11,49,58,59
The bacterial culture findings from nipples and nipple shields in the current study update and extend the findings of Collis and colleagues26 to a US population more than a decade after that group’s original report. In the current study, we found the baseline risk of implant contamination from nipple bacteria to be present in approximately one-third of
Figure 4. Proposed mechanism for bacterial contamination contributing to capsular contracture. (A) Anatomic view of breast implant in subglandular pocket position. (B) Intraoperative risk of bacterial contamination from endogenous breast flora and potential seepage of bacteria through ductal glands in the nipple, contaminating the surgical field. (C) Bacterial contamination of breast implant with biofilm and early capsule formation. (D) Growth of bacterial biofilm colonization on breast implant shell causing host immune response and capsular contraction with effacement of desired implant contour.
Downloaded from https://academic.oup.com/asj/article-abstract/32/8/956/318056by gueston 30 March 2018

Wixtrom et al 961
patients undergoing breast augmentation. The use of nipple shields represents a rational approach to minimize the poten-tial for microbial seeding of the implant or breast pocket during surgery that would increase the potential for biofilm formation.4,6,11,55
This study involved 32 patients undergoing placement of breast prostheses. Three patients subsequently developed CC despite the use of nipple shields. Interestingly, only 1 of these patients underwent primary breast augmentation. The other 2 patients were undergoing capsulectomy for previous CC, and 1 of these patients had a culture-positive MRSA infection postoperatively. We postulate that these patients had previ-ously-established bacterial biofilms that were not completely removed or sterilized with standard capsulectomy and implant exchange.
Due to the relatively short length of follow-up in this study, it is possible that CC will develop in additional patients. However, the primary purpose of this study was to demonstrate the potential risk of bacterial seeding from endogenous breast glandular tissue onto the operative field through the mammary ducts and out of the nipple. A cause and effect relationship between bacterial contamination and CC was not the intent of this study and should not be concluded; rather, our findings should be interpreted in the context that the risk of contamination by endogenous breast flora may be a source for the initiation of biofilm formation. Further studies of a possible direct relationship to these bacteria and CC are needed, which could potentially be accomplished by evaluating cultures from tissue biopsy of contracted capsules and/or associated breast implants and comparing them with cultures from the initial postaugmen-tation nipple and swabs from adjacent breast skin. This may also help define which bacterial species are more likely to form biofilms in the setting of breast augmentation. An initial culture swab of adjacent breast tissue, away from the nipple shield, can also be helpful in identifying whether any additional sites of contamination exist.
All approaches aimed at reducing the risk of CC by preventing the formation of biofilms are potential impor-tant advancements. These approaches include minimizing the potential for microbial seeding of the implant and/or breast pocket and avoiding hematomas through meticu-lous hemostasis. Limitation of direct implant contact with glandular tissue may also be advantageous. Avoidance of incisions that cause manipulation of the glandular tissue and contact with the implant upon insertion may also be beneficial in reducing the frequency of biofilm formation. Finally, this study provides data supporting the use of low-cost occlusive nipple shields to reduce the risk of bacterial contamination of the surgical field during breast augmen-tation surgery, which may also help prevent biofilm forma-tion and the possibility of subsequent CC. We acknowledge the limitations of the culturing methodology used for assessment of the nipples and nipple shields, and that the results presented likely provide only a minimum estimate of contamination that would be higher if more advanced molecular methods were employed. Nevertheless, we believe the results directly support the increased use of nipple shields in breast augmentation surgery.
COnCLusiOns
A more in-depth understanding of bacterial biofilms and potentially related risk factors for CC will provide surgeons with important insights into addressing this common com-plication of breast augmentation surgery. Based on the cultures from nipples and nipple shields in this study of consecutive breast augmentation patients, the baseline risk of implant contamination from nipple bacteria was found to be 34.9%. These data are not intended to prove the bacte-rial theory of CC. However, given the most recent data on CC and biofilms, it can be concluded that the routine use of nipple shields may reduce the risk of bacterial contamina-tion of breast implants during breast augmentation.
disclosures
Drs Codner and Wixtrom have served as paid consultants to Mentor Worldwide LLC. Dr Codner has also received educa-tional grants from Mentor and Syneron Medical Ltd., and receives royalties for books published by Quality Medical Pub-lishing, Inc and Elsevier. He is also an investigator for the US Food and Drug Administration Premarket Approval Mentor Core Gel study and Allergan 410 study. The other authors declare that they have no conflicts of interest.
Funding
This study was funded by a grant from Mentor Worldwide LLC, including support for data collection, analysis, and authoring of the current manuscript. Mentor Worldwide LLC did not have a role in the design and conduct of the study, nor in the collection analysis or interpretation of data. The spon-sor did not have a role in the preparation of the manuscript, review of the manuscript, nor was editorial assistance provided.
REFEREnCEs
1. Cunningham B, McCue J. Safety and effectiveness of Mentor’s MemoryGel implants at 6 years. Aesthetic Plast Surg. 2009;33:440-444.
2. Spear SL, Murphy DK, Slicton A, Walker PS. Inamed Sili-cone Breast Implant U.S. Study Group. Inamed silicone breast implant core study results at 6 years. Plast Reconstr Surg. 2007;120:8S-16S, 17S-18S.
3. Cunningham B. The mentor study on contour profile gel silicone memory gel breast implants. Plast Reconstr Surg. 2007;120:33S-39S.
4. Bengston BP. Complications, reoperations, and revisions in breast augmentation. Clin Plast Surg. 2009;36:139-156.
5. Araco A, Gravante G, Araco F, et al. Capsular contracture: results of 3002 patients with aesthetic breast augmenta-tion. Plast Reconstr Surg. 2006;118(6):1499-1500.
6. Adams WP Jr. Capsular contracture: what is it? what causes it? how can it be prevented and managed? Clin Plast Surg. 2009;36:119-126.
7. Deva AK, Chang LC. Bacterial biofilms: a cause for accelerated capsular contracture? Aesth Surg J. 1999;19(2):130-133.
Downloaded from https://academic.oup.com/asj/article-abstract/32/8/956/318056by gueston 30 March 2018

962 Aesthetic Surgery Journal 32(8)
8. Prantl L, Schreml S, Fichtner-Feigl S, et al. Clinical and morphological conditions in capsular contracture formed around silicone breast implants. Plast Reconstr Surg. 2007;120(1):275-284.
9. Baker J, Chandler ML, LeVier RR. Occurrence and activity of myofibroblasts in human capsular tissue surrounding breast implants. Plast Reconstr Surg. 1981;68(6):905-1012.
10. McCurdy JA Jr. Capsular Contracture following aug-mentation mammaplasty: etiology and pathogenesis. In: Shiffman MA, ed. Breast Augmentation Principles and Practice. 1st ed. Berlin: Springer; 2009:525-540.
11. Araco A, Caruso R, Araco F, et al. Capsular contracture: a systematic review. Plast Reconstr Surg. 2009;124(6):1808-1819.
12. Pajkos A, Deva AK, Vickery K, Cope C, Chang L, Cossart YE. Detection of subclinical infection in significant breast implant capsules. Plast Reconstr Surg. 2003;111(5):1605-1611.
13. Tamboto H, Vickery K, Deva AK. Subclinical (biofilm) infection causes capsular contracture in a porcine model following augmentation mammaplasty. Plast Reconstr Surg. 2010;126(3):835-842.
14. Tran VT, Del Pozo JL, Petty PM, et al. Bacteria on breast implants are associated with capsular contracture. Plast Reconstr Surg. 2009;124(4S):38-39.
15. Del Pozo JL, Tran NV, Petty PM, et al. Pilot study of asso-ciation of bacteria on breast implants with capsular con-tracture. J. Clin. Microbiol. 2009;47(5):1333-1337.
16. Snell L, Brown M. Breast implant capsules and subclini-cal infection. Plast Reconstr Surg. 2009;124(4S): 38.
17. Bjarnsholt T. Introduction to biofilms. In: Bjarnsholt T, Moser C, Jensen PØ, Høiby N, eds. Biofilm Infections. New York, NY: Springer; 2011:1-9.
18. NIH, National Heart, Lung, and Blood Institute. Research on Microbial Biofilms (PA-03-047). http://grants.nih.gov/grants/guide/pa-files/PA-03-047.html. Published Decem-ber 20, 2002. Accessed August 5, 2012.
19. Costerton JW, Stewart PS, Greenberg EP. Bacterial bio-films: a common cause of persistent infections. Science. 1999;284(5418):1318-1322.
20. Fux CA, Stoodley P, Hall-Stoodley L, Costerton JW. Bac-terial biofilms: a diagnostic and therapeutic challenge. Expert Rev Anti Infect Ther. 2003;1(4):667-683.
21. Percival SL, Thomas JG, Williams D. An introduction to the world of microbiology and biofilmology. In: Percival S, Cutting K, eds. Microbiology of Wounds. Boca Raton, FL: CRC Press; 2010:1-58.
22. Zimmerli W, Waldvogel FA, Vaudaux P, Nydegger UE. Pathogenesis of foreign body infection: description and characteristics of an animal model. J Infect Dis. 1982;146(4):487-497.
23. Ransjö U, Asplund OA, Gylbert L, Jurell G. Bacteria in the female breast. Scand J Plast Reconstr Surg. 1985;19(1):87-89.
24. Thornton JW, Argenta LC, McClatchey KD, Marks MW. Studies on the endogenous flora of the human breast. Ann Plast Surg. 1988;20(1):39-42.
25. Mladick RA. Significance of Staphylococcus epidermi-dis causing subclinical infection. Plast Reconstr Surg. 2005;115(5):1426-1427.
26. Collis N, Mirza S, Stanley PR, Campbell L, Sharpe DT. Reduction of potential contamination of breast implants by the use of “nipple shields.” Br J Plast Surg. 1999;52(6):445-447.
27. Williams C, Aston S, Rees TD. The effect of hematoma on the thickness of pseudosheaths around silicone implants. Plast Reconstr Surg. 1975;56(2):194-198.
28. Burkhardt BR, Fried M, Schnur PL, Tofield JJ. Capsules, infection, and intraluminal antibiotics. Plast Reconstr Surg. 1981;68(1):43-49.
29. Shah Z, Lehman JA Jr, Tan J. Does infection play a role in breast capsular contracture? Plast Reconstr Surg. 1981;68(1):34-42.
30. Virden CP, Dobke MK, Stein P, Parsons CL, Frank DH. Subclinical infection of the silicone breast implant sur-face as a possible cause of capsular contracture. Aesthetic Plast Surg. 1992;16(2):173-179.
31. Dobke MK, Svahn JK, Vastine VL, et al. Characterization of microbial presence at the surface of silicone mammary implants. Ann Plast Surg. 1995;34(6):563-569.
32. Rieger UM, Pierer G, Lüscher NJ, Trampuz A. Sonication of removed breast implants for improved detection of subclini-cal infection. Aesthetic Plast Surg. 2009;33(3):404-408.
33. Ng WL, Bassler BL. Bacterial quorum-sensing network architectures. Annu Rev Genet. 2009;43:197-222.
34. Jensen PØ, Bjarnsholt T, Phipps R, et al. Rapid necrotic killing of polymorphonuclear leukocytes is caused by quorum-sensing-controlled production of rhamnolipid by Pseudomonas aeruginosa. Microbiology. 2007;153(pt 5):1329-1338.
35. Xu KD, Stewart PS, Xia F, Huang C-T, McFeters GA. Spa-tial physiological heterogeneity in Pseudomonas aerugi-nosa biofilm is determined by oxygen availability. Appl Environ Microbiol. 1998;64(10):4035-4039.
36. Chambless JD, Hunt SM, Stewart PS. A three-dimen-sional computer model of four hypothetical mechanisms protecting biofilms from antimicrobials. Appl Environ Microbiol. 2006;72:2005-2013.
37. Harrison JJ, Turner RJ, Marques LLR, Ceri H. Biofilms. Am Sci. 2005;93:508-515.
38. O’Connell HA, Kottkamp GS, Eppelbaum JL, et al. Influ-ences of biofilm structure and antibiotic resistance mechanisms on indirect pathogenicity in a model polymi-crobial biofilm. Appl Environ Microbiol. 2006;72(2):5013-5019.
39. Costerton JW, Montanaro L, Aricola CR. Biofilm in implant infections: its production and regulation. Int J Artif Organs. 2005;28(11):1062-1068.
40. Costerton JW, Post JC, et al. New methods for the detec-tion of orthopedic and other biofilm infections. FEMS Immunol Med Microbiol. 2011;61(2):133-140.
41. Stoodley P, Conti SF, Demeo PJ, et al. Characterization of a mixed MRSA/MRSE biofilm in an explanted total ankle arthroplasty. FEMS Immunol Med Microbiol. 2011;62:66-74.
42. Liao EC, Nyame T, Lemon KP, et al. High throughput assay for bacterial biofilm formation on biomaterials. Plast Reconstr Surg. 2009;124(4S):107.
43. Wolk DM, Blyn LB, Hall TA, et al. Pathogen profiling: rapid molecular characterization of Staphylococcus
Downloaded from https://academic.oup.com/asj/article-abstract/32/8/956/318056by gueston 30 March 2018

Wixtrom et al 963
aureus by PCR/electrospray ionization-mass spectrom-etry and correlation with phenotype. J Clin Microbiol. 2009;47(10):3129-3137.
44. Williams C, Aston S, Rees TD. The effect of hematoma on the thickness of pseudosheaths around silicone implants. Plast Reconstr Surg. 1975;56(2):194-198.
45. Handel N, Cordray T, Gutierrez J, Jensen JA. A long-term study of outcomes, complications, and patient satisfaction with breast implants. Plast Reconstr Surg. 2006;117(3):757-767.
46. Lewis V. Chronic expanding hematoma within a peripros-thetic breast capsule. Plast Reconstr Surg. 1996;97(7):1469-1472.
47. Rouault TA. Microbiology. Pathogenic bacteria prefer heme. Science. 2004;305(5690):1577-1578.
48. Adams WP Jr, Rios JL, Smith SJ. Enhancing patient out-comes in aesthetic and reconstructive breast surgery using triple antibiotic breast irrigation: six year prospec-tive clinical study. Plast Reconstr Surg. 2006;117(1):30-36.
49. Burkhardt BR, Eades E. The effect of Biocell texturing and povidone-iodine irrigation on capsular contracture around saline-inflatable breast implants. Plast Reconstr Surg. 1995;96(6):1317-1325.
50. Codner MA, Mejia JD, Locke MB, et al. A 15-year experi-ence with primary breast augmentation. Plast Reconstr Surg. 2011;127(3):1300-1310.
51. Courtiss EH, Goldwyn RM, Anastasi GW. The fate of breast implants with infections around them. Plast Recon-str Surg. 1979;63(6):812-816.
52. Wiener TC. The role of betadine irrigation in breast aug-mentation. Plast Reconstr Surg. 2007;119(1):11-15.
53. Wiener TC. Relationship of incision choice to capsular contracture. Aesthetic Plast Surg. 2008;32(2):303-306.
54. Wong C, Samuel M, Tan B, et al. Capsular contracture in subglandular breast augmentation with textured versus smooth breast implants: a systematic review. Plast Recon-str Surg. 2006;118(5):1224-1236.
55. Thorne C. An evidence-based approach to augmentation mammplasty. Plast Reconstr Surg. 2010;126(6):2184-2188.
56. Bartsich S, Ascherman JA, Whittier S, Yao CA, Rohde C. The breast: a clean-contaminated surgical site. Aesthetic Surg J. 2011;31(7):802-806.
57. Teitelbaum S. A fresh look at the periareolar incision: should it be abandoned? Paper presented at: 28th Annual Atlanta Breast Surgery Symposium; January 14, 2012; Atlanta, GA.
58. Puckett CL, Croll GH, Reichel CA, Concannon MJ. A criti-cal look at capsular contracture in subglandular versus subpectoral mammary augmentation. Aesth Plast Surg. 1987;11(1):23-28.
59. Biggs TM, Yarish RS. Augmentation mammaplasty: a com-parative analysis. Plast Reconstr Surg. 1990;85(3):368-372.
Downloaded from https://academic.oup.com/asj/article-abstract/32/8/956/318056by gueston 30 March 2018


















