
RIOGLOULINEMIA MISTA E LINFOMI NELL’ERA DEI … MISTA E LINFOMI NELL’ERA DEI DAAs ... Curaneous=...
60
CRIOGLOBULINEMIA MISTA E LINFOMI NELL’ERA DEI DAAs DI II GENERAZIONE Anna Linda Zignego
Transcript of RIOGLOULINEMIA MISTA E LINFOMI NELL’ERA DEI … MISTA E LINFOMI NELL’ERA DEI DAAs ... Curaneous=...

CRIOGLOBULINEMIA MISTA E LINFOMI NELLrsquoERA DEI DAAsDI II GENERAZIONE
Anna Linda Zignego
Eur J Gastroenterol Hepatol 2017
MC in the setting of HCV-related pathologies a typically female disease
Direct medical costs of extrahepatic manifestations of HCV in USA
Younossi et al
Evaluation of the annual costs (inpatientoutpatient and pharmacy) associated withextrahepatic manifestations of HCV
Total direct medical costs of extrahepaticmanifestations of HCV in 2014 US dollars were
estimated to be $1506 million (range $922 millionndash$2208 million in sensitivity analysis)
These estimates should be added to the liver-related burden of disease to obtain a more
accurate assessment of the total burden of HCVinfection
Direct medical costs of extrahepatic manifestations of HCV in EUROPE
ISG-EHCV
Ferri C Ramos-Casals M Zignego AL et al Autoimmun Rev 2016
1465
496717
Total Piter cohort no 8005 subjects the presence of MC was never tested in 80 ofcases in spite of its clinical and therapeutical importance Among the centres thatconsidered MC=-64 evaluated cryoglobulinemia only following a clinical suspicion-58 evaluated routinely cryoglobulinemia at admission with Complement RF levels-42 only in case of RF positivity-Cryo testing was not adequate in 39 of centres
252
These results for the first time showed the real-life variability of the MC diagnosticapproach suggesting that MC prevalence in HCV+ is generally underestimated
Kondili et al Liver Intern2017
CLASSIFICATION OF HCV EHDS ACCORDING TO THE STRENGTH OF SPECIFIC DATA SUPPORTING THE CURATIVE EFFECT OF AVT
Mixed Cryoglobulinemia Effectiveness of both IFN-based and IFN-free AVT
Marginal Zone NHL Effectiveness of both IFN- and DAA-based
AVT
Other low-grade B-cell NHL
HRQOL Available data also in DAA-based AVT
High-grade NHL= DLBCL Insufficient but positive data
CKD Sufficient specific data only for MC-CKD
Neuropsychiatric disorders Problematic IFN-based AVT Insufficient
data with DAAs
Curaneous= PCT and LP (OLP) Problematic IFNRBV-based AVT
Insufficient data with DAAs
Endocrinologic Thyroid and DM 2 Insufficient specific data with DAAs
Arthritis Insufficient specific data with DAAs
Zignego et al 2017
Landau DA et al Arthritis Rheum 2008 Montalbano M et al J Clin Gastroenterol 2007 Cacoub P et al Arthritis Rheum 2002
Mazzaro C et alJ Rheumatol 2003 Zignego AL et al Hepatology 2016 Gragnani L et al Hepatology 2015 Pietrogrande M
et al Autoimmun Rev 2011
Antiviral Treatment (AVT) of MC in the IFN Era
AVT of MC followed the evolution of hepatitis C AVT with frequent adjustments
essentially due to the possible side-effects of IFN andor RBV therapy (ie IFN
neurotoxicity and myelo-inhibitory action and RBV hemolytic effects)
Virological and clinical results progressively improved in spite of frequent side-effects
IFN-based AVT was recommended as the first-line option in mild to moderate MC
Clinical remission was generally correlated with virological response
Long follow-up showed that the majority (57) of SVR pts cleared all MC stigmata
Antiviral Treatment (AVT) of MC IFN-free regimensLimited data so-far concordant are available regarding IFN-free AVT in MC patients
Available data suggest that IFN-free AVT is safe generally well tolerated and effective in MC patients high rate of
clinical response (87) and low rates of serious adverse events was reported
Zignego AL Ramos-Casals M Ferri C et al AutoimmunReviews 2017
Antiviral Treatment (AVT) of MC IFN-free regimens
22 MCS treated with DAAs including 2 HCC and 2 NHL 100 SVR12 Clinical R in 100 (64 CR and 36 PR)
Progression of the small lymphocytic lymphoma
Lauletta et al 2017
Emery CS et al 2017
Retrospective analysis 17 MCS (10 with severelife-threatening vasculitis) and 65 asymptomatic MC treated with
DAAs SVR 889 MCS and 908 asymptomatic pts In MCS clinical R in 1117 (CR in 711) Lower clinical R inseverelife-threatening ndashespecial renal and neurological- vasculitis
Saadoun D et al 2017
Open-label prospective multi-center study on sofosbuvir plus daclatasvir treatment of 41 HCV MCS SVR in 100 and
clinical CR in 902 Disappearance of CGs in 50 of pts No serious adverse event or relapse of vasculitis
A case of rapid amelioration of HCV-associated cryoglobulinemic MPGN treated by
IFN-free DAAs for HCV in the absence of immunosuppressant
Fumiaki et al 2017
Zignego et al 2017
TIME POINTS
baseline EOT and week 12 and 24 of post-treatment f-up (SVR12 and SVR24 respectively)
HRQoL EVALUATION THROUGH PROs
the Short Form (36) Health Survey (SF-36)
the Functional Assessment of Chronic Illness Therapy-Fatigue (FACIT-F) from which we computed the Trial
Outcome Index (TOI)
Evaluation of The Impact on HRQol of IFN-free AVT In HCV CM
1 Physical Component Summary Score (PCS)
MC (54)
HCV (43) CV (85)
deg
A B C
degdegdeg
2 Mental Component Summary Score (MCS)
MCHCV CVD E F
degdegdegdegdeg
HCV
=plt001 vs baseline scores
degdeg=plt001 and degdegdeg=plt0001 vs EOT scores
Gragnani et al AASLD 2017
HCV Eradicationwith DAAs
To be preceded or combined with non-etiological pathogenetic therapy in severecatastrophic MCS
MCS Therapy in the IFN and DAAs Era from the complex to the simplified flow-chart
Dammacco F Sansonno D NEJM 2013
Zignego AL Pawlotsky JM Cacoub P Antiviral Ther in press Cacoub P et al Am J Med 2015
Mechanisms of HCV-related lymphomagenesis
DLBC HCV- induced
direct transformation
MCindolent NHL
accumulation of B RF
following BCR activation
and BC apoptosisinhibition
Zignego AL Ramos-Casals M Ferri C et al Autoimmun Rev 2017
Wang et al Hepatology 2016 Canioni et al Plos one 2016
Observational study on in situ expression of the oncogenic HCV NS3 protein on 116 HCV patients with B-NHL (DLBCL 36 and MZL 34)
NS3 immunostaining positive in 1214 DLBCL vs only 414 MZL (p = 0006) moreover 24 NS3+ MZL
were enriched in large cells
This study supports a new mechanism of transformation with a direct oncogenic role of
HCV proteins in the occurrence of high-grade B lymphomas
IN SITU HEPATITIS C NS3 PROTEIN DETECTION IS ASSOCIATED WITH HIGH GRADE
FEATURES IN HCV-ASSOCIATED B-CELL NON-HODGKIN LYMPHOMAS Danielle
Canioni et al 2016
In addition to the role of chronic antigenic stimulation in HCV related
lymphomagenesis this study supports a second mechanism of transformation due to a
direct oncogenic role of HCV infection of B-cells promoting the occurrence of high-grade Bcell lymphomas
Cohort study of 704 consecutive HIV-negative HCV-positive patients with indolent NHL from 1993 to
2009 in 39 centers of the FIL
Arcaini et al 2016
DLBC HCV- induced
direct transformation
No place of AVT as
1st line
Need of immediate delivery of
chemotherapy or concomitant (NHL
+ HCV targets)
THERAPY OF HCV+ DLBCL
ANTIVIRAL THERAPY IS ASSOCIATED WITH A BETTERSURVIVAL IN PATIENTS WITH HCV AND B-CELL NON-HODGKIN LYMPHOMAS ANRS HC-13 LYMPHO-CSTUDY Michot JM et al
Outcomes of HCV-associated B-NHL according to HCV AVT in prospective patients only (n 5 64)
Concurrent Systemic Chemoimmunotherapy and Sofosbuvir-Based Antiviral Treatment in a Hepatitis C Virus-Infected Patient With Diffuse Large B-Cell Lymphoma Evan C Ewers et al 2016
absolute neutrophil count and Hgb ALT and HCV viral load
Both complete response and SVR of HCV-associated DLBCL after concurrent chemoimmunotherapy and antiviral therapy using a sofosbuvir-based regimen
DAA-treatment in concomitance with chemotherapy showed to be safe and effective in influencing the remission of aggressive lymphomas in HCV patients
Persico M et al 2017
DFS in DAA treated and historical not-treated ptsAntiviral response rates in DAA treated patients
ANTIVIRAL THERAPY IN HCV+ B CELL NHL
IFN-based AVT induced hematological response along with SVR in patients with HCV-related indolent NHLs (especially
MZL)
Recent data with IFN-free regimens in HCV-associated LPDs suggest their anti-lymphoma activity too
AVT should be considered the first-line approach in HCV low grade lymphomas if there is no urgency of a conventional
treatment (ie systemic symptoms bulky disease or symptomatic splenomegaly) (ESMO NCCN EASL guidelines)
In aggressive lymphomas antiviral therapy after induction treatment is to be considered the standard at the moment but
in the next years (months) the association of immunochemotherapy and antiviral therapy will be considered the standard
Zignego AL Ramos-Casals M Ferri C et al Autoimmun Rev 2017
The Masve group
BASIC RESEARCH
Laura Gragnani
Patrizio Caini
Serena Lorini
Antonella Simone
CLINICAL RESEARCH
Monica Monti
Luisa Petraccia
Sinan Sadalla
Guia Cerretelli
Cristina Stasi
Adela Xheka
Universitagrave degli Studi di FirenzeDipartimento di Medicina Sperimentale e Clinica
Centro Manifestazioni Sistemiche da Virus EpatiticildquoMASVErdquo
Anna Linda Zignego
MASVE
UNDERGRADUATE STUDENTS Andrea Genovese Adrian Piscopo
ANTIVIRAL THERAPY IN HCV+ B CELL NHL
IFN-based AVT induced hematological response along with SVR in patients with HCV-related indolent
NHLs (especially MZL)
Recent data with IFN-free regimens in HCV-associated LPDs suggest their anti-lymphoma activity too
AVT should be considered the first-line approach in HCV low grade lymphomas if there is no urgency
of a conventional treatment (ie systemic symptoms bulky disease or symptomatic splenomegaly)
(ESMO NCCN EASL guidelines)
Main drugs for HCV-related MCS according to the target
HCV= DAAsB-cell Expansion= (a) B cell-depleting Mabs
-First-generation Rituximab (anti-CD20)-Second-generation Ofatumumab (anti-CD20) Veltuzumab (humanized
anti-CD20)-Third-generation Obinutuzumab (GA101) Oceratuzumab (humanized
anti-CD20)
(b) Alkylating agents
-Cyclophosfamide
Inflammation= Antiinflammatory agents
- Corticosteroids
Altered regulatory T-cell activity=
- IL-2
The impact on HRQoL of IFN-free AVT was prospectively evaluated in a cohort of HCV CV patients with limited
influencing variables linked to therapeutic schedulesviral GT
44 HCV GT2 CV patients mostly F0-F2 (29) and naiumlve (30) treated with SOFRBV for 1224wks
TIME POINTS
baseline EOT and week 12 and 24 of post-treatment f-up (SVR12 and SVR24 respectively)
HRQoL EVALUATION THROUGH PROs
the Short Form (36) Health Survey (SF-36)
the Functional Assessment of Chronic Illness Therapy-Fatigue (FACIT-F) from which we computed the Trial
Outcome Index (TOI)
Observational study on in situ expression of the oncogenic HCV NS3 protein on 116 HCV
patients with B-NHL (DLBCL 36 and MZL 34)
NS3 immunostaining positive in 1214 DLBCL vs only 414 MZL (p = 0006) moreover 24 NS3+
MZL were enriched in large cells
This study supports a new mechanism of transformation with a direct oncogenic role of
HCV proteins in the occurrence of high-grade B lymphomas
IN SITU HEPATITIS C NS3 PROTEIN DETECTION IS ASSOCIATED WITH HIGH GRADEFEATURES IN HCV-ASSOCIATED B-CELL NON-HODGKIN LYMPHOMAS Danielle
Canioni et al 2016
In addition to the role of chronic antigenic stimulation in HCV related
lymphomagenesis this study supports a second mechanism of transformation due toa direct oncogenic role of HCV infection of B-cells promoting the occurrence of high-grade Bcell lymphomas
ANTIVIRAL THERAPY IS ASSOCIATED WITH A BETTERSURVIVAL IN PATIENTS WITH HCV AND B-CELL NON-HODGKIN LYMPHOMAS ANRS HC-13 LYMPHO-CSTUDYMichot JM et al
Outcomes of HCV-associated B-NHL according to HCV AVT in prospective patients only (n 5 64)
(A) absolute neutrophil count and Hgb
(B) ALT and HCV viral load
This patient had HCV-associated DLBCL achieving both complete response and SVR after concurrent chemoimmunotherapy and antiviral therapy using a sofosbuvir-basedregimen
Concurrent Systemic Chemoimmunotherapy and Sofosbuvir-Based Antiviral Treatment in a Hepatitis C Virus-Infected Patient With Diffuse Large B-Cell LymphomaEvan C Ewers et al 2016
HCV-EHDs are responsible for increasing morbidity and mortality with important
consequences in terms of social costs
The analysis of mortality rates in large cohorts confirmed the association of HCV with
several EHDs including cardiovascular neurologic metabolic or renal diseases and tumors
Viral eradication significantly reduced the rate of extra-hepatic deaths
Cacoub P et al DLD 2014 Lee MH et al J Infect Dis 2012 Backus LI et al Clin Gastroenterol Hepatol 2011 El-Kamary S et al
Clin Infect Dis 2011 Hsu YC et al Hepatology 2014 Kawamura Y et al Am J Med 2007 Adinolfi LE et al WJG 2014
Extrahepatic Manifestations of HCV
Con il contributo di
Lee M-H et al J Infect Dis 2012206469-477
Follow-Up
(Years)
20
18
16
14
12
10
2
00 2 4 6 8 10 12 14 16 18 20
8
6
4
Follow-Up
(Years)
12
10
8
6
4
2
00 2 4 6 8 10 12 14 16 18 20
All Causes(n=2394)
Liver Cancer(n=115)
Extrahepatic Diseases(n=2199)
Cum
ula
tive M
ort
ali
ty (
)
Anti-HCV+ HCV RNA detectable Anti-HCV+ HCV RNA undetectable Anti-HCVndash
Follow-Up
(Years)
35
30
25
20
15
10
5
00 2 4 6 8 10 12 14 16 18 20
301
128124
104
16
03
198
122
110
MC is clinically benign but sometimes severe HCV EHD invalidating symptoms occur and
it may evolve into lymphoma
Cacoub P et al DLD 2014 Zignego AL et al DLD 2007 Zignego AL et al Intern Emerg Med 2012 Zignego AL et al Clin Dev
Immunol 2012 Zignego AL et al Expert Rev Clin Immunol 2015 Sene D et al J Rheumatol 2004
Mixed Cryoglobulinemia-MC
CGs reversibly precipitate when the temperature is lower than 37degC and
comprise IgMs with RF activity [mono- or oligo-clonal in type II MC or
polyclonal in type III MC] and polyclonal IgGs
MC pathological substrate is an HCV-driven B-cell
proliferation with consequent production of cryo- and non-
cryoprecipitable CICs in turn responsible for vasculitic
manifestations
Most (70ndash90) MC patients are HCV+ and HCV-patients are CGs+ (40ndash60) while 5ndash30 of
CGs+ have symptomatic MC since HCV infects about 170 million individuals worldwide the
number of patients at risk for developing MC is substantial
Type II
CGs
Type III
CGs
Zignego AL et al Autoimmun Rev 2017 Ferri C et al Autoimmunity rev 2016 Zignego AL et al DLD 2007 Cacoub P et al DLD
2014 Zignego AL et al DLD 2007 Zignego AL et al Intern Emerg Med 2012 Zignego AL et al Clin Dev Immunol 2012 Zignego
AL et al Expert Rev Clin Immunol 2015
MC clinical aspects MC Syndrome
MCS is characterized by the clinical triad -purpura weakness and
arthralgias- low complement C4 and various organsystem
involvement including cutaneous articular renal neurological
cardiac or digestive
It ranges from mild disease to severe even life-threatening
conditions
More serious lesions are generally characterized by neurologic and
renal involvement
Prognosis is highly dependent on renal involvement or on the extent
of vasculitis lesions
1 HCV is the main etiopathological agent as concordantly demonstrated by epidemiological clinico-pathological virological and laboratory investigations2 the association between HCV and disease is demonstrated in a significant proportion of patients and supported by in depth clinico-pathogeneticstudies3 the association is suggested by cohort studies a possible causative role may be limited to a small number of patients andor possibly more relevant in specific geographical areas 4 a number of anecdotal observations suggested a possible role of HCV further investigations are required
From P Cacoub 2015
HCV infection is closely related to LPDs mostly MC
40 to 60 of HCV patients show circulating CGs among this latter population 5-30
develop a symptomatic CV
AVT has been considered the first-line option in HCV-CV patients in fact in the majority
of cases viral eradication leads to CV clinical remission
Data about IFN-free regimens for the treatment of CV patients are still limited
HCV and MC
HCV and MC
Zignego 2015Ferri 2016Pozzato 2016 Sise 2016Saadoun 2015Gragnani 2016Gragnani 2016
Bonacci 2016Hegazy 2016Kondili 2016Emery 2017
Younossi et al
The annual costs (inpatient outpatient andpharmacy) associated with extrahepatic
manifestations of HCV were evaluated
Total direct medical costs of extrahepatic
manifestations of HCV in 2014 US dollars wereestimated to be $1506 million (range $922 millionndash
$2208 million in sensitivity analysis)
These estimates should be added to the liver-related
burden of disease to obtain a more accurateassessment of the total burden of HCV infection
The OBJECTIVE of the study was to estimate the annual direct medical costsassociated with HCV related EHM in the EU5 (France Germany Italy United Kingdom
Spain)
Extrahepatic Manifestations of HCV
Extrahepatic Manifestations of HCV
HCV may cause extrahepatic disorders (HCV-EHDs) classified according to the number and
strength of supporting scientific data
HCV-EHDs are responsible for increasing morbidity and mortality with important
consequences in terms of social costs
The analysis of mortality rates in large cohorts confirmed the association of HCV with
several EHDs including cardiovascular neurologic metabolic or renal diseases and tumors
Viral eradication significantly reduced the rate of extra-hepatic deaths
Cacoub P et al DLD 2014 Lee MH et al J Infect Dis 2012 Backus LI et al Clin Gastroenterol Hepatol 2011 El-Kamary S et al
Clin Infect Dis 2011 Hsu YC et al Hepatology 2014 Kawamura Y et al Am J Med 2007 Adinolfi LE et al WJG 2014
Con il contributo di
Lee M-H et al J Infect Dis 2012206469-477
Follow-Up
(Years)
20
18
16
14
12
10
2
00 2 4 6 8 10 12 14 16 18 20
8
6
4
Follow-Up
(Years)
12
10
8
6
4
2
00 2 4 6 8 10 12 14 16 18 20
All Causes(n=2394)
Liver Cancer(n=115)
Extrahepatic Diseases(n=2199)
Cum
ula
tive M
ort
ali
ty (
)
Anti-HCV+ HCV RNA detectable Anti-HCV+ HCV RNA undetectable Anti-HCVndash
Follow-Up
(Years)
35
30
25
20
15
10
5
00 2 4 6 8 10 12 14 16 18 20
301
128124
104
16
03
198
122
110
Extrahepatic Manifestations of HCV
The annual costs (inpatient outpatient andpharmacy) associated with extrahepatic
manifestations of HCV were evaluated
Total direct medical costs of extrahepatic
manifestations of HCV in 2014 US dollars wereestimated to be $1506 million (range $922 millionndash
$2208 million in sensitivity analysis)
These estimates should be added to the liver-related
burden of disease to obtain a more accurateassessment of the total burden of HCV infection
Younossi et al
Younossi et al
Costs up to $71000 per patient per year (ESRD) Among the most frequent EHM depression (245 in HCV vs 172 in non-HCV) had estimated annual cost of
$4307 million DM (15 vs 10 in non- HCV) had an annual cost of $4434 million in the USA= given the importance of DM and
its association with CVDs and mortality the clinical and economic impacts of HCV-related DM are substantial
The OBJECTIVE of the study was to estimate the annual direct medical costsassociated with HCV related EHM in the EU5 (France Germany Italy United Kingdom
Spain)
The OBJECTIVE of the study was to estimate the annual direct medicalcosts associated with HCV related EHM in the EU5 (France Germany
Italy United Kingdom Spain)
1 HCV is the main etiopathological agent as concordantly demonstrated by epidemiological clinico-pathological virological and laboratory investigations2 the association between HCV and disease is demonstrated in a significant proportion of patients and supported by in depth clinico-pathogeneticstudies3 the association is suggested by cohort studies a possible causative role may be limited to a small number of patients andor possibly more relevant in specific geographical areas 4 a number of anecdotal observations suggested a possible role of HCV further investigations are required
The most studied and frequent HCV-EHDs are B-LPDs andor autoimmune disorders
Their prototype is Mixed Cryoglobulinemia (MC) from researches on MC derived most of the
available information
MC as a precious model for all the HCV-EHDs and to evaluate the effects of viral eradication
Anti-HCV Treatment Evolution
IFN
6 mos
PegIFN RBV 12
mos
IFN
12 mos
IFNRBV
12 mos
PegIFN
12 mos
2001
1998
2011
Standardinterferon
Ribavirin
Peginterferon
1991
Direct-actingantivirals
PegIFN
RBV
DAA
IFNRBV
6 mos
6
16
34
4239
55
70+
0
20
40
60
80
100
DAAs
826
weeks
gt90
2015
Few side effects absence major
contraindications
Younossi et al
The annual costs (inpatient outpatient and pharmacy) associatedwith extrahepatic manifestations of HCV were evaluated
Total direct medical costs of extrahepatic manifestations of HCV in 2014US dollars were estimated to be $1506 million (range $922 millionndash
$2208 million in sensitivity analysis)
These estimates should be added to the liver-related burden of diseaseto obtain a more accurate assessment of the total burden of HCV
infection
The OBJECTIVE of the study was to estimate the annual direct medical costs associated with HCV related EHM in the EU5 (France Germany Italy United Kingdom Spain)
22 MCS treated with DAAs including 2 HCC and 2 NHL 100 SVR12 Clinical CR in 64 and PR in remaining 36 The small lymphocytic lymphoma progressed despite viral clearance
Lauletta et al 2017
Emery CS et al 2017
Retrospective analysis 17 MCS (10 with severelife-threatening vasculitis) and 65 asymptomatic CGs+ pts treated with DAAs SVR 889 MCS and 908 asymptomatic pts In MCS clinical response in 1117 (complete in 717) In severelife-threatening vasculitis lower clinical response especially in renal and neurological symptoms
Saadoun D et al 2017
Open-label prospective multi-center study on sofosbuvir plus daclatasvir treatment of 41 HCV MCS SVR in100 and clinical CR in 902 Disappearance of CGs in 50 of pts No serious adverse event or relapse ofvasculitis
Antiviral Treatment (AVT) of MCIFN-free regimens
MC is clinically benign but sometimes severe HCV EHD invalidating symptoms occur and
it may evolve into lymphoma
Cacoub P et al DLD 2014 Zignego AL et al DLD 2007 Zignego AL et al Intern Emerg Med 2012 Zignego AL et al Clin Dev
Immunol 2012 Zignego AL et al Expert Rev Clin Immunol 2015 Sene D et al J Rheumatol 2004
Mixed Cryoglobulinemia-MC
MC pathological substrate is an HCV-driven B-cell
proliferation with consequent production of cryo- and non-
cryoprecipitable CICs in turn responsible for vasculitic
manifestations
Most (70ndash90) MC patients are HCV+ and HCV-patients are CGs+ (40ndash60) while 5ndash30 of
CGs+ have symptomatic MC or cryoglobulinemic vasculitis since HCV infects about 170
million individuals worldwide the number of patients at risk for developing MC is
substantial
Type II CGs
monoclonal
RF+policlonal IgG
Type III CGs both
RF and IgG
polyclonal

Eur J Gastroenterol Hepatol 2017
MC in the setting of HCV-related pathologies a typically female disease
Direct medical costs of extrahepatic manifestations of HCV in USA
Younossi et al
Evaluation of the annual costs (inpatientoutpatient and pharmacy) associated withextrahepatic manifestations of HCV
Total direct medical costs of extrahepaticmanifestations of HCV in 2014 US dollars were
estimated to be $1506 million (range $922 millionndash$2208 million in sensitivity analysis)
These estimates should be added to the liver-related burden of disease to obtain a more
accurate assessment of the total burden of HCVinfection
Direct medical costs of extrahepatic manifestations of HCV in EUROPE
ISG-EHCV
Ferri C Ramos-Casals M Zignego AL et al Autoimmun Rev 2016
1465
496717
Total Piter cohort no 8005 subjects the presence of MC was never tested in 80 ofcases in spite of its clinical and therapeutical importance Among the centres thatconsidered MC=-64 evaluated cryoglobulinemia only following a clinical suspicion-58 evaluated routinely cryoglobulinemia at admission with Complement RF levels-42 only in case of RF positivity-Cryo testing was not adequate in 39 of centres
252
These results for the first time showed the real-life variability of the MC diagnosticapproach suggesting that MC prevalence in HCV+ is generally underestimated
Kondili et al Liver Intern2017
CLASSIFICATION OF HCV EHDS ACCORDING TO THE STRENGTH OF SPECIFIC DATA SUPPORTING THE CURATIVE EFFECT OF AVT
Mixed Cryoglobulinemia Effectiveness of both IFN-based and IFN-free AVT
Marginal Zone NHL Effectiveness of both IFN- and DAA-based
AVT
Other low-grade B-cell NHL
HRQOL Available data also in DAA-based AVT
High-grade NHL= DLBCL Insufficient but positive data
CKD Sufficient specific data only for MC-CKD
Neuropsychiatric disorders Problematic IFN-based AVT Insufficient
data with DAAs
Curaneous= PCT and LP (OLP) Problematic IFNRBV-based AVT
Insufficient data with DAAs
Endocrinologic Thyroid and DM 2 Insufficient specific data with DAAs
Arthritis Insufficient specific data with DAAs
Zignego et al 2017
Landau DA et al Arthritis Rheum 2008 Montalbano M et al J Clin Gastroenterol 2007 Cacoub P et al Arthritis Rheum 2002
Mazzaro C et alJ Rheumatol 2003 Zignego AL et al Hepatology 2016 Gragnani L et al Hepatology 2015 Pietrogrande M
et al Autoimmun Rev 2011
Antiviral Treatment (AVT) of MC in the IFN Era
AVT of MC followed the evolution of hepatitis C AVT with frequent adjustments
essentially due to the possible side-effects of IFN andor RBV therapy (ie IFN
neurotoxicity and myelo-inhibitory action and RBV hemolytic effects)
Virological and clinical results progressively improved in spite of frequent side-effects
IFN-based AVT was recommended as the first-line option in mild to moderate MC
Clinical remission was generally correlated with virological response
Long follow-up showed that the majority (57) of SVR pts cleared all MC stigmata
Antiviral Treatment (AVT) of MC IFN-free regimensLimited data so-far concordant are available regarding IFN-free AVT in MC patients
Available data suggest that IFN-free AVT is safe generally well tolerated and effective in MC patients high rate of
clinical response (87) and low rates of serious adverse events was reported
Zignego AL Ramos-Casals M Ferri C et al AutoimmunReviews 2017
Antiviral Treatment (AVT) of MC IFN-free regimens
22 MCS treated with DAAs including 2 HCC and 2 NHL 100 SVR12 Clinical R in 100 (64 CR and 36 PR)
Progression of the small lymphocytic lymphoma
Lauletta et al 2017
Emery CS et al 2017
Retrospective analysis 17 MCS (10 with severelife-threatening vasculitis) and 65 asymptomatic MC treated with
DAAs SVR 889 MCS and 908 asymptomatic pts In MCS clinical R in 1117 (CR in 711) Lower clinical R inseverelife-threatening ndashespecial renal and neurological- vasculitis
Saadoun D et al 2017
Open-label prospective multi-center study on sofosbuvir plus daclatasvir treatment of 41 HCV MCS SVR in 100 and
clinical CR in 902 Disappearance of CGs in 50 of pts No serious adverse event or relapse of vasculitis
A case of rapid amelioration of HCV-associated cryoglobulinemic MPGN treated by
IFN-free DAAs for HCV in the absence of immunosuppressant
Fumiaki et al 2017
Zignego et al 2017
TIME POINTS
baseline EOT and week 12 and 24 of post-treatment f-up (SVR12 and SVR24 respectively)
HRQoL EVALUATION THROUGH PROs
the Short Form (36) Health Survey (SF-36)
the Functional Assessment of Chronic Illness Therapy-Fatigue (FACIT-F) from which we computed the Trial
Outcome Index (TOI)
Evaluation of The Impact on HRQol of IFN-free AVT In HCV CM
1 Physical Component Summary Score (PCS)
MC (54)
HCV (43) CV (85)
deg
A B C
degdegdeg
2 Mental Component Summary Score (MCS)
MCHCV CVD E F
degdegdegdegdeg
HCV
=plt001 vs baseline scores
degdeg=plt001 and degdegdeg=plt0001 vs EOT scores
Gragnani et al AASLD 2017
HCV Eradicationwith DAAs
To be preceded or combined with non-etiological pathogenetic therapy in severecatastrophic MCS
MCS Therapy in the IFN and DAAs Era from the complex to the simplified flow-chart
Dammacco F Sansonno D NEJM 2013
Zignego AL Pawlotsky JM Cacoub P Antiviral Ther in press Cacoub P et al Am J Med 2015
Mechanisms of HCV-related lymphomagenesis
DLBC HCV- induced
direct transformation
MCindolent NHL
accumulation of B RF
following BCR activation
and BC apoptosisinhibition
Zignego AL Ramos-Casals M Ferri C et al Autoimmun Rev 2017
Wang et al Hepatology 2016 Canioni et al Plos one 2016
Observational study on in situ expression of the oncogenic HCV NS3 protein on 116 HCV patients with B-NHL (DLBCL 36 and MZL 34)
NS3 immunostaining positive in 1214 DLBCL vs only 414 MZL (p = 0006) moreover 24 NS3+ MZL
were enriched in large cells
This study supports a new mechanism of transformation with a direct oncogenic role of
HCV proteins in the occurrence of high-grade B lymphomas
IN SITU HEPATITIS C NS3 PROTEIN DETECTION IS ASSOCIATED WITH HIGH GRADE
FEATURES IN HCV-ASSOCIATED B-CELL NON-HODGKIN LYMPHOMAS Danielle
Canioni et al 2016
In addition to the role of chronic antigenic stimulation in HCV related
lymphomagenesis this study supports a second mechanism of transformation due to a
direct oncogenic role of HCV infection of B-cells promoting the occurrence of high-grade Bcell lymphomas
Cohort study of 704 consecutive HIV-negative HCV-positive patients with indolent NHL from 1993 to
2009 in 39 centers of the FIL
Arcaini et al 2016
DLBC HCV- induced
direct transformation
No place of AVT as
1st line
Need of immediate delivery of
chemotherapy or concomitant (NHL
+ HCV targets)
THERAPY OF HCV+ DLBCL
ANTIVIRAL THERAPY IS ASSOCIATED WITH A BETTERSURVIVAL IN PATIENTS WITH HCV AND B-CELL NON-HODGKIN LYMPHOMAS ANRS HC-13 LYMPHO-CSTUDY Michot JM et al
Outcomes of HCV-associated B-NHL according to HCV AVT in prospective patients only (n 5 64)
Concurrent Systemic Chemoimmunotherapy and Sofosbuvir-Based Antiviral Treatment in a Hepatitis C Virus-Infected Patient With Diffuse Large B-Cell Lymphoma Evan C Ewers et al 2016
absolute neutrophil count and Hgb ALT and HCV viral load
Both complete response and SVR of HCV-associated DLBCL after concurrent chemoimmunotherapy and antiviral therapy using a sofosbuvir-based regimen
DAA-treatment in concomitance with chemotherapy showed to be safe and effective in influencing the remission of aggressive lymphomas in HCV patients
Persico M et al 2017
DFS in DAA treated and historical not-treated ptsAntiviral response rates in DAA treated patients
ANTIVIRAL THERAPY IN HCV+ B CELL NHL
IFN-based AVT induced hematological response along with SVR in patients with HCV-related indolent NHLs (especially
MZL)
Recent data with IFN-free regimens in HCV-associated LPDs suggest their anti-lymphoma activity too
AVT should be considered the first-line approach in HCV low grade lymphomas if there is no urgency of a conventional
treatment (ie systemic symptoms bulky disease or symptomatic splenomegaly) (ESMO NCCN EASL guidelines)
In aggressive lymphomas antiviral therapy after induction treatment is to be considered the standard at the moment but
in the next years (months) the association of immunochemotherapy and antiviral therapy will be considered the standard
Zignego AL Ramos-Casals M Ferri C et al Autoimmun Rev 2017
The Masve group
BASIC RESEARCH
Laura Gragnani
Patrizio Caini
Serena Lorini
Antonella Simone
CLINICAL RESEARCH
Monica Monti
Luisa Petraccia
Sinan Sadalla
Guia Cerretelli
Cristina Stasi
Adela Xheka
Universitagrave degli Studi di FirenzeDipartimento di Medicina Sperimentale e Clinica
Centro Manifestazioni Sistemiche da Virus EpatiticildquoMASVErdquo
Anna Linda Zignego
MASVE
UNDERGRADUATE STUDENTS Andrea Genovese Adrian Piscopo
ANTIVIRAL THERAPY IN HCV+ B CELL NHL
IFN-based AVT induced hematological response along with SVR in patients with HCV-related indolent
NHLs (especially MZL)
Recent data with IFN-free regimens in HCV-associated LPDs suggest their anti-lymphoma activity too
AVT should be considered the first-line approach in HCV low grade lymphomas if there is no urgency
of a conventional treatment (ie systemic symptoms bulky disease or symptomatic splenomegaly)
(ESMO NCCN EASL guidelines)
Main drugs for HCV-related MCS according to the target
HCV= DAAsB-cell Expansion= (a) B cell-depleting Mabs
-First-generation Rituximab (anti-CD20)-Second-generation Ofatumumab (anti-CD20) Veltuzumab (humanized
anti-CD20)-Third-generation Obinutuzumab (GA101) Oceratuzumab (humanized
anti-CD20)
(b) Alkylating agents
-Cyclophosfamide
Inflammation= Antiinflammatory agents
- Corticosteroids
Altered regulatory T-cell activity=
- IL-2
The impact on HRQoL of IFN-free AVT was prospectively evaluated in a cohort of HCV CV patients with limited
influencing variables linked to therapeutic schedulesviral GT
44 HCV GT2 CV patients mostly F0-F2 (29) and naiumlve (30) treated with SOFRBV for 1224wks
TIME POINTS
baseline EOT and week 12 and 24 of post-treatment f-up (SVR12 and SVR24 respectively)
HRQoL EVALUATION THROUGH PROs
the Short Form (36) Health Survey (SF-36)
the Functional Assessment of Chronic Illness Therapy-Fatigue (FACIT-F) from which we computed the Trial
Outcome Index (TOI)
Observational study on in situ expression of the oncogenic HCV NS3 protein on 116 HCV
patients with B-NHL (DLBCL 36 and MZL 34)
NS3 immunostaining positive in 1214 DLBCL vs only 414 MZL (p = 0006) moreover 24 NS3+
MZL were enriched in large cells
This study supports a new mechanism of transformation with a direct oncogenic role of
HCV proteins in the occurrence of high-grade B lymphomas
IN SITU HEPATITIS C NS3 PROTEIN DETECTION IS ASSOCIATED WITH HIGH GRADEFEATURES IN HCV-ASSOCIATED B-CELL NON-HODGKIN LYMPHOMAS Danielle
Canioni et al 2016
In addition to the role of chronic antigenic stimulation in HCV related
lymphomagenesis this study supports a second mechanism of transformation due toa direct oncogenic role of HCV infection of B-cells promoting the occurrence of high-grade Bcell lymphomas
ANTIVIRAL THERAPY IS ASSOCIATED WITH A BETTERSURVIVAL IN PATIENTS WITH HCV AND B-CELL NON-HODGKIN LYMPHOMAS ANRS HC-13 LYMPHO-CSTUDYMichot JM et al
Outcomes of HCV-associated B-NHL according to HCV AVT in prospective patients only (n 5 64)
(A) absolute neutrophil count and Hgb
(B) ALT and HCV viral load
This patient had HCV-associated DLBCL achieving both complete response and SVR after concurrent chemoimmunotherapy and antiviral therapy using a sofosbuvir-basedregimen
Concurrent Systemic Chemoimmunotherapy and Sofosbuvir-Based Antiviral Treatment in a Hepatitis C Virus-Infected Patient With Diffuse Large B-Cell LymphomaEvan C Ewers et al 2016
HCV-EHDs are responsible for increasing morbidity and mortality with important
consequences in terms of social costs
The analysis of mortality rates in large cohorts confirmed the association of HCV with
several EHDs including cardiovascular neurologic metabolic or renal diseases and tumors
Viral eradication significantly reduced the rate of extra-hepatic deaths
Cacoub P et al DLD 2014 Lee MH et al J Infect Dis 2012 Backus LI et al Clin Gastroenterol Hepatol 2011 El-Kamary S et al
Clin Infect Dis 2011 Hsu YC et al Hepatology 2014 Kawamura Y et al Am J Med 2007 Adinolfi LE et al WJG 2014
Extrahepatic Manifestations of HCV
Con il contributo di
Lee M-H et al J Infect Dis 2012206469-477
Follow-Up
(Years)
20
18
16
14
12
10
2
00 2 4 6 8 10 12 14 16 18 20
8
6
4
Follow-Up
(Years)
12
10
8
6
4
2
00 2 4 6 8 10 12 14 16 18 20
All Causes(n=2394)
Liver Cancer(n=115)
Extrahepatic Diseases(n=2199)
Cum
ula
tive M
ort
ali
ty (
)
Anti-HCV+ HCV RNA detectable Anti-HCV+ HCV RNA undetectable Anti-HCVndash
Follow-Up
(Years)
35
30
25
20
15
10
5
00 2 4 6 8 10 12 14 16 18 20
301
128124
104
16
03
198
122
110
MC is clinically benign but sometimes severe HCV EHD invalidating symptoms occur and
it may evolve into lymphoma
Cacoub P et al DLD 2014 Zignego AL et al DLD 2007 Zignego AL et al Intern Emerg Med 2012 Zignego AL et al Clin Dev
Immunol 2012 Zignego AL et al Expert Rev Clin Immunol 2015 Sene D et al J Rheumatol 2004
Mixed Cryoglobulinemia-MC
CGs reversibly precipitate when the temperature is lower than 37degC and
comprise IgMs with RF activity [mono- or oligo-clonal in type II MC or
polyclonal in type III MC] and polyclonal IgGs
MC pathological substrate is an HCV-driven B-cell
proliferation with consequent production of cryo- and non-
cryoprecipitable CICs in turn responsible for vasculitic
manifestations
Most (70ndash90) MC patients are HCV+ and HCV-patients are CGs+ (40ndash60) while 5ndash30 of
CGs+ have symptomatic MC since HCV infects about 170 million individuals worldwide the
number of patients at risk for developing MC is substantial
Type II
CGs
Type III
CGs
Zignego AL et al Autoimmun Rev 2017 Ferri C et al Autoimmunity rev 2016 Zignego AL et al DLD 2007 Cacoub P et al DLD
2014 Zignego AL et al DLD 2007 Zignego AL et al Intern Emerg Med 2012 Zignego AL et al Clin Dev Immunol 2012 Zignego
AL et al Expert Rev Clin Immunol 2015
MC clinical aspects MC Syndrome
MCS is characterized by the clinical triad -purpura weakness and
arthralgias- low complement C4 and various organsystem
involvement including cutaneous articular renal neurological
cardiac or digestive
It ranges from mild disease to severe even life-threatening
conditions
More serious lesions are generally characterized by neurologic and
renal involvement
Prognosis is highly dependent on renal involvement or on the extent
of vasculitis lesions
1 HCV is the main etiopathological agent as concordantly demonstrated by epidemiological clinico-pathological virological and laboratory investigations2 the association between HCV and disease is demonstrated in a significant proportion of patients and supported by in depth clinico-pathogeneticstudies3 the association is suggested by cohort studies a possible causative role may be limited to a small number of patients andor possibly more relevant in specific geographical areas 4 a number of anecdotal observations suggested a possible role of HCV further investigations are required
From P Cacoub 2015
HCV infection is closely related to LPDs mostly MC
40 to 60 of HCV patients show circulating CGs among this latter population 5-30
develop a symptomatic CV
AVT has been considered the first-line option in HCV-CV patients in fact in the majority
of cases viral eradication leads to CV clinical remission
Data about IFN-free regimens for the treatment of CV patients are still limited
HCV and MC
HCV and MC
Zignego 2015Ferri 2016Pozzato 2016 Sise 2016Saadoun 2015Gragnani 2016Gragnani 2016
Bonacci 2016Hegazy 2016Kondili 2016Emery 2017
Younossi et al
The annual costs (inpatient outpatient andpharmacy) associated with extrahepatic
manifestations of HCV were evaluated
Total direct medical costs of extrahepatic
manifestations of HCV in 2014 US dollars wereestimated to be $1506 million (range $922 millionndash
$2208 million in sensitivity analysis)
These estimates should be added to the liver-related
burden of disease to obtain a more accurateassessment of the total burden of HCV infection
The OBJECTIVE of the study was to estimate the annual direct medical costsassociated with HCV related EHM in the EU5 (France Germany Italy United Kingdom
Spain)
Extrahepatic Manifestations of HCV
Extrahepatic Manifestations of HCV
HCV may cause extrahepatic disorders (HCV-EHDs) classified according to the number and
strength of supporting scientific data
HCV-EHDs are responsible for increasing morbidity and mortality with important
consequences in terms of social costs
The analysis of mortality rates in large cohorts confirmed the association of HCV with
several EHDs including cardiovascular neurologic metabolic or renal diseases and tumors
Viral eradication significantly reduced the rate of extra-hepatic deaths
Cacoub P et al DLD 2014 Lee MH et al J Infect Dis 2012 Backus LI et al Clin Gastroenterol Hepatol 2011 El-Kamary S et al
Clin Infect Dis 2011 Hsu YC et al Hepatology 2014 Kawamura Y et al Am J Med 2007 Adinolfi LE et al WJG 2014
Con il contributo di
Lee M-H et al J Infect Dis 2012206469-477
Follow-Up
(Years)
20
18
16
14
12
10
2
00 2 4 6 8 10 12 14 16 18 20
8
6
4
Follow-Up
(Years)
12
10
8
6
4
2
00 2 4 6 8 10 12 14 16 18 20
All Causes(n=2394)
Liver Cancer(n=115)
Extrahepatic Diseases(n=2199)
Cum
ula
tive M
ort
ali
ty (
)
Anti-HCV+ HCV RNA detectable Anti-HCV+ HCV RNA undetectable Anti-HCVndash
Follow-Up
(Years)
35
30
25
20
15
10
5
00 2 4 6 8 10 12 14 16 18 20
301
128124
104
16
03
198
122
110
Extrahepatic Manifestations of HCV
The annual costs (inpatient outpatient andpharmacy) associated with extrahepatic
manifestations of HCV were evaluated
Total direct medical costs of extrahepatic
manifestations of HCV in 2014 US dollars wereestimated to be $1506 million (range $922 millionndash
$2208 million in sensitivity analysis)
These estimates should be added to the liver-related
burden of disease to obtain a more accurateassessment of the total burden of HCV infection
Younossi et al
Younossi et al
Costs up to $71000 per patient per year (ESRD) Among the most frequent EHM depression (245 in HCV vs 172 in non-HCV) had estimated annual cost of
$4307 million DM (15 vs 10 in non- HCV) had an annual cost of $4434 million in the USA= given the importance of DM and
its association with CVDs and mortality the clinical and economic impacts of HCV-related DM are substantial
The OBJECTIVE of the study was to estimate the annual direct medical costsassociated with HCV related EHM in the EU5 (France Germany Italy United Kingdom
Spain)
The OBJECTIVE of the study was to estimate the annual direct medicalcosts associated with HCV related EHM in the EU5 (France Germany
Italy United Kingdom Spain)
1 HCV is the main etiopathological agent as concordantly demonstrated by epidemiological clinico-pathological virological and laboratory investigations2 the association between HCV and disease is demonstrated in a significant proportion of patients and supported by in depth clinico-pathogeneticstudies3 the association is suggested by cohort studies a possible causative role may be limited to a small number of patients andor possibly more relevant in specific geographical areas 4 a number of anecdotal observations suggested a possible role of HCV further investigations are required
The most studied and frequent HCV-EHDs are B-LPDs andor autoimmune disorders
Their prototype is Mixed Cryoglobulinemia (MC) from researches on MC derived most of the
available information
MC as a precious model for all the HCV-EHDs and to evaluate the effects of viral eradication
Anti-HCV Treatment Evolution
IFN
6 mos
PegIFN RBV 12
mos
IFN
12 mos
IFNRBV
12 mos
PegIFN
12 mos
2001
1998
2011
Standardinterferon
Ribavirin
Peginterferon
1991
Direct-actingantivirals
PegIFN
RBV
DAA
IFNRBV
6 mos
6
16
34
4239
55
70+
0
20
40
60
80
100
DAAs
826
weeks
gt90
2015
Few side effects absence major
contraindications
Younossi et al
The annual costs (inpatient outpatient and pharmacy) associatedwith extrahepatic manifestations of HCV were evaluated
Total direct medical costs of extrahepatic manifestations of HCV in 2014US dollars were estimated to be $1506 million (range $922 millionndash
$2208 million in sensitivity analysis)
These estimates should be added to the liver-related burden of diseaseto obtain a more accurate assessment of the total burden of HCV
infection
The OBJECTIVE of the study was to estimate the annual direct medical costs associated with HCV related EHM in the EU5 (France Germany Italy United Kingdom Spain)
22 MCS treated with DAAs including 2 HCC and 2 NHL 100 SVR12 Clinical CR in 64 and PR in remaining 36 The small lymphocytic lymphoma progressed despite viral clearance
Lauletta et al 2017
Emery CS et al 2017
Retrospective analysis 17 MCS (10 with severelife-threatening vasculitis) and 65 asymptomatic CGs+ pts treated with DAAs SVR 889 MCS and 908 asymptomatic pts In MCS clinical response in 1117 (complete in 717) In severelife-threatening vasculitis lower clinical response especially in renal and neurological symptoms
Saadoun D et al 2017
Open-label prospective multi-center study on sofosbuvir plus daclatasvir treatment of 41 HCV MCS SVR in100 and clinical CR in 902 Disappearance of CGs in 50 of pts No serious adverse event or relapse ofvasculitis
Antiviral Treatment (AVT) of MCIFN-free regimens
MC is clinically benign but sometimes severe HCV EHD invalidating symptoms occur and
it may evolve into lymphoma
Cacoub P et al DLD 2014 Zignego AL et al DLD 2007 Zignego AL et al Intern Emerg Med 2012 Zignego AL et al Clin Dev
Immunol 2012 Zignego AL et al Expert Rev Clin Immunol 2015 Sene D et al J Rheumatol 2004
Mixed Cryoglobulinemia-MC
MC pathological substrate is an HCV-driven B-cell
proliferation with consequent production of cryo- and non-
cryoprecipitable CICs in turn responsible for vasculitic
manifestations
Most (70ndash90) MC patients are HCV+ and HCV-patients are CGs+ (40ndash60) while 5ndash30 of
CGs+ have symptomatic MC or cryoglobulinemic vasculitis since HCV infects about 170
million individuals worldwide the number of patients at risk for developing MC is
substantial
Type II CGs
monoclonal
RF+policlonal IgG
Type III CGs both
RF and IgG
polyclonal

MC in the setting of HCV-related pathologies a typically female disease
Direct medical costs of extrahepatic manifestations of HCV in USA
Younossi et al
Evaluation of the annual costs (inpatientoutpatient and pharmacy) associated withextrahepatic manifestations of HCV
Total direct medical costs of extrahepaticmanifestations of HCV in 2014 US dollars were
estimated to be $1506 million (range $922 millionndash$2208 million in sensitivity analysis)
These estimates should be added to the liver-related burden of disease to obtain a more
accurate assessment of the total burden of HCVinfection
Direct medical costs of extrahepatic manifestations of HCV in EUROPE
ISG-EHCV
Ferri C Ramos-Casals M Zignego AL et al Autoimmun Rev 2016
1465
496717
Total Piter cohort no 8005 subjects the presence of MC was never tested in 80 ofcases in spite of its clinical and therapeutical importance Among the centres thatconsidered MC=-64 evaluated cryoglobulinemia only following a clinical suspicion-58 evaluated routinely cryoglobulinemia at admission with Complement RF levels-42 only in case of RF positivity-Cryo testing was not adequate in 39 of centres
252
These results for the first time showed the real-life variability of the MC diagnosticapproach suggesting that MC prevalence in HCV+ is generally underestimated
Kondili et al Liver Intern2017
CLASSIFICATION OF HCV EHDS ACCORDING TO THE STRENGTH OF SPECIFIC DATA SUPPORTING THE CURATIVE EFFECT OF AVT
Mixed Cryoglobulinemia Effectiveness of both IFN-based and IFN-free AVT
Marginal Zone NHL Effectiveness of both IFN- and DAA-based
AVT
Other low-grade B-cell NHL
HRQOL Available data also in DAA-based AVT
High-grade NHL= DLBCL Insufficient but positive data
CKD Sufficient specific data only for MC-CKD
Neuropsychiatric disorders Problematic IFN-based AVT Insufficient
data with DAAs
Curaneous= PCT and LP (OLP) Problematic IFNRBV-based AVT
Insufficient data with DAAs
Endocrinologic Thyroid and DM 2 Insufficient specific data with DAAs
Arthritis Insufficient specific data with DAAs
Zignego et al 2017
Landau DA et al Arthritis Rheum 2008 Montalbano M et al J Clin Gastroenterol 2007 Cacoub P et al Arthritis Rheum 2002
Mazzaro C et alJ Rheumatol 2003 Zignego AL et al Hepatology 2016 Gragnani L et al Hepatology 2015 Pietrogrande M
et al Autoimmun Rev 2011
Antiviral Treatment (AVT) of MC in the IFN Era
AVT of MC followed the evolution of hepatitis C AVT with frequent adjustments
essentially due to the possible side-effects of IFN andor RBV therapy (ie IFN
neurotoxicity and myelo-inhibitory action and RBV hemolytic effects)
Virological and clinical results progressively improved in spite of frequent side-effects
IFN-based AVT was recommended as the first-line option in mild to moderate MC
Clinical remission was generally correlated with virological response
Long follow-up showed that the majority (57) of SVR pts cleared all MC stigmata
Antiviral Treatment (AVT) of MC IFN-free regimensLimited data so-far concordant are available regarding IFN-free AVT in MC patients
Available data suggest that IFN-free AVT is safe generally well tolerated and effective in MC patients high rate of
clinical response (87) and low rates of serious adverse events was reported
Zignego AL Ramos-Casals M Ferri C et al AutoimmunReviews 2017
Antiviral Treatment (AVT) of MC IFN-free regimens
22 MCS treated with DAAs including 2 HCC and 2 NHL 100 SVR12 Clinical R in 100 (64 CR and 36 PR)
Progression of the small lymphocytic lymphoma
Lauletta et al 2017
Emery CS et al 2017
Retrospective analysis 17 MCS (10 with severelife-threatening vasculitis) and 65 asymptomatic MC treated with
DAAs SVR 889 MCS and 908 asymptomatic pts In MCS clinical R in 1117 (CR in 711) Lower clinical R inseverelife-threatening ndashespecial renal and neurological- vasculitis
Saadoun D et al 2017
Open-label prospective multi-center study on sofosbuvir plus daclatasvir treatment of 41 HCV MCS SVR in 100 and
clinical CR in 902 Disappearance of CGs in 50 of pts No serious adverse event or relapse of vasculitis
A case of rapid amelioration of HCV-associated cryoglobulinemic MPGN treated by
IFN-free DAAs for HCV in the absence of immunosuppressant
Fumiaki et al 2017
Zignego et al 2017
TIME POINTS
baseline EOT and week 12 and 24 of post-treatment f-up (SVR12 and SVR24 respectively)
HRQoL EVALUATION THROUGH PROs
the Short Form (36) Health Survey (SF-36)
the Functional Assessment of Chronic Illness Therapy-Fatigue (FACIT-F) from which we computed the Trial
Outcome Index (TOI)
Evaluation of The Impact on HRQol of IFN-free AVT In HCV CM
1 Physical Component Summary Score (PCS)
MC (54)
HCV (43) CV (85)
deg
A B C
degdegdeg
2 Mental Component Summary Score (MCS)
MCHCV CVD E F
degdegdegdegdeg
HCV
=plt001 vs baseline scores
degdeg=plt001 and degdegdeg=plt0001 vs EOT scores
Gragnani et al AASLD 2017
HCV Eradicationwith DAAs
To be preceded or combined with non-etiological pathogenetic therapy in severecatastrophic MCS
MCS Therapy in the IFN and DAAs Era from the complex to the simplified flow-chart
Dammacco F Sansonno D NEJM 2013
Zignego AL Pawlotsky JM Cacoub P Antiviral Ther in press Cacoub P et al Am J Med 2015
Mechanisms of HCV-related lymphomagenesis
DLBC HCV- induced
direct transformation
MCindolent NHL
accumulation of B RF
following BCR activation
and BC apoptosisinhibition
Zignego AL Ramos-Casals M Ferri C et al Autoimmun Rev 2017
Wang et al Hepatology 2016 Canioni et al Plos one 2016
Observational study on in situ expression of the oncogenic HCV NS3 protein on 116 HCV patients with B-NHL (DLBCL 36 and MZL 34)
NS3 immunostaining positive in 1214 DLBCL vs only 414 MZL (p = 0006) moreover 24 NS3+ MZL
were enriched in large cells
This study supports a new mechanism of transformation with a direct oncogenic role of
HCV proteins in the occurrence of high-grade B lymphomas
IN SITU HEPATITIS C NS3 PROTEIN DETECTION IS ASSOCIATED WITH HIGH GRADE
FEATURES IN HCV-ASSOCIATED B-CELL NON-HODGKIN LYMPHOMAS Danielle
Canioni et al 2016
In addition to the role of chronic antigenic stimulation in HCV related
lymphomagenesis this study supports a second mechanism of transformation due to a
direct oncogenic role of HCV infection of B-cells promoting the occurrence of high-grade Bcell lymphomas
Cohort study of 704 consecutive HIV-negative HCV-positive patients with indolent NHL from 1993 to
2009 in 39 centers of the FIL
Arcaini et al 2016
DLBC HCV- induced
direct transformation
No place of AVT as
1st line
Need of immediate delivery of
chemotherapy or concomitant (NHL
+ HCV targets)
THERAPY OF HCV+ DLBCL
ANTIVIRAL THERAPY IS ASSOCIATED WITH A BETTERSURVIVAL IN PATIENTS WITH HCV AND B-CELL NON-HODGKIN LYMPHOMAS ANRS HC-13 LYMPHO-CSTUDY Michot JM et al
Outcomes of HCV-associated B-NHL according to HCV AVT in prospective patients only (n 5 64)
Concurrent Systemic Chemoimmunotherapy and Sofosbuvir-Based Antiviral Treatment in a Hepatitis C Virus-Infected Patient With Diffuse Large B-Cell Lymphoma Evan C Ewers et al 2016
absolute neutrophil count and Hgb ALT and HCV viral load
Both complete response and SVR of HCV-associated DLBCL after concurrent chemoimmunotherapy and antiviral therapy using a sofosbuvir-based regimen
DAA-treatment in concomitance with chemotherapy showed to be safe and effective in influencing the remission of aggressive lymphomas in HCV patients
Persico M et al 2017
DFS in DAA treated and historical not-treated ptsAntiviral response rates in DAA treated patients
ANTIVIRAL THERAPY IN HCV+ B CELL NHL
IFN-based AVT induced hematological response along with SVR in patients with HCV-related indolent NHLs (especially
MZL)
Recent data with IFN-free regimens in HCV-associated LPDs suggest their anti-lymphoma activity too
AVT should be considered the first-line approach in HCV low grade lymphomas if there is no urgency of a conventional
treatment (ie systemic symptoms bulky disease or symptomatic splenomegaly) (ESMO NCCN EASL guidelines)
In aggressive lymphomas antiviral therapy after induction treatment is to be considered the standard at the moment but
in the next years (months) the association of immunochemotherapy and antiviral therapy will be considered the standard
Zignego AL Ramos-Casals M Ferri C et al Autoimmun Rev 2017
The Masve group
BASIC RESEARCH
Laura Gragnani
Patrizio Caini
Serena Lorini
Antonella Simone
CLINICAL RESEARCH
Monica Monti
Luisa Petraccia
Sinan Sadalla
Guia Cerretelli
Cristina Stasi
Adela Xheka
Universitagrave degli Studi di FirenzeDipartimento di Medicina Sperimentale e Clinica
Centro Manifestazioni Sistemiche da Virus EpatiticildquoMASVErdquo
Anna Linda Zignego
MASVE
UNDERGRADUATE STUDENTS Andrea Genovese Adrian Piscopo
ANTIVIRAL THERAPY IN HCV+ B CELL NHL
IFN-based AVT induced hematological response along with SVR in patients with HCV-related indolent
NHLs (especially MZL)
Recent data with IFN-free regimens in HCV-associated LPDs suggest their anti-lymphoma activity too
AVT should be considered the first-line approach in HCV low grade lymphomas if there is no urgency
of a conventional treatment (ie systemic symptoms bulky disease or symptomatic splenomegaly)
(ESMO NCCN EASL guidelines)
Main drugs for HCV-related MCS according to the target
HCV= DAAsB-cell Expansion= (a) B cell-depleting Mabs
-First-generation Rituximab (anti-CD20)-Second-generation Ofatumumab (anti-CD20) Veltuzumab (humanized
anti-CD20)-Third-generation Obinutuzumab (GA101) Oceratuzumab (humanized
anti-CD20)
(b) Alkylating agents
-Cyclophosfamide
Inflammation= Antiinflammatory agents
- Corticosteroids
Altered regulatory T-cell activity=
- IL-2
The impact on HRQoL of IFN-free AVT was prospectively evaluated in a cohort of HCV CV patients with limited
influencing variables linked to therapeutic schedulesviral GT
44 HCV GT2 CV patients mostly F0-F2 (29) and naiumlve (30) treated with SOFRBV for 1224wks
TIME POINTS
baseline EOT and week 12 and 24 of post-treatment f-up (SVR12 and SVR24 respectively)
HRQoL EVALUATION THROUGH PROs
the Short Form (36) Health Survey (SF-36)
the Functional Assessment of Chronic Illness Therapy-Fatigue (FACIT-F) from which we computed the Trial
Outcome Index (TOI)
Observational study on in situ expression of the oncogenic HCV NS3 protein on 116 HCV
patients with B-NHL (DLBCL 36 and MZL 34)
NS3 immunostaining positive in 1214 DLBCL vs only 414 MZL (p = 0006) moreover 24 NS3+
MZL were enriched in large cells
This study supports a new mechanism of transformation with a direct oncogenic role of
HCV proteins in the occurrence of high-grade B lymphomas
IN SITU HEPATITIS C NS3 PROTEIN DETECTION IS ASSOCIATED WITH HIGH GRADEFEATURES IN HCV-ASSOCIATED B-CELL NON-HODGKIN LYMPHOMAS Danielle
Canioni et al 2016
In addition to the role of chronic antigenic stimulation in HCV related
lymphomagenesis this study supports a second mechanism of transformation due toa direct oncogenic role of HCV infection of B-cells promoting the occurrence of high-grade Bcell lymphomas
ANTIVIRAL THERAPY IS ASSOCIATED WITH A BETTERSURVIVAL IN PATIENTS WITH HCV AND B-CELL NON-HODGKIN LYMPHOMAS ANRS HC-13 LYMPHO-CSTUDYMichot JM et al
Outcomes of HCV-associated B-NHL according to HCV AVT in prospective patients only (n 5 64)
(A) absolute neutrophil count and Hgb
(B) ALT and HCV viral load
This patient had HCV-associated DLBCL achieving both complete response and SVR after concurrent chemoimmunotherapy and antiviral therapy using a sofosbuvir-basedregimen
Concurrent Systemic Chemoimmunotherapy and Sofosbuvir-Based Antiviral Treatment in a Hepatitis C Virus-Infected Patient With Diffuse Large B-Cell LymphomaEvan C Ewers et al 2016
HCV-EHDs are responsible for increasing morbidity and mortality with important
consequences in terms of social costs
The analysis of mortality rates in large cohorts confirmed the association of HCV with
several EHDs including cardiovascular neurologic metabolic or renal diseases and tumors
Viral eradication significantly reduced the rate of extra-hepatic deaths
Cacoub P et al DLD 2014 Lee MH et al J Infect Dis 2012 Backus LI et al Clin Gastroenterol Hepatol 2011 El-Kamary S et al
Clin Infect Dis 2011 Hsu YC et al Hepatology 2014 Kawamura Y et al Am J Med 2007 Adinolfi LE et al WJG 2014
Extrahepatic Manifestations of HCV
Con il contributo di
Lee M-H et al J Infect Dis 2012206469-477
Follow-Up
(Years)
20
18
16
14
12
10
2
00 2 4 6 8 10 12 14 16 18 20
8
6
4
Follow-Up
(Years)
12
10
8
6
4
2
00 2 4 6 8 10 12 14 16 18 20
All Causes(n=2394)
Liver Cancer(n=115)
Extrahepatic Diseases(n=2199)
Cum
ula
tive M
ort
ali
ty (
)
Anti-HCV+ HCV RNA detectable Anti-HCV+ HCV RNA undetectable Anti-HCVndash
Follow-Up
(Years)
35
30
25
20
15
10
5
00 2 4 6 8 10 12 14 16 18 20
301
128124
104
16
03
198
122
110
MC is clinically benign but sometimes severe HCV EHD invalidating symptoms occur and
it may evolve into lymphoma
Cacoub P et al DLD 2014 Zignego AL et al DLD 2007 Zignego AL et al Intern Emerg Med 2012 Zignego AL et al Clin Dev
Immunol 2012 Zignego AL et al Expert Rev Clin Immunol 2015 Sene D et al J Rheumatol 2004
Mixed Cryoglobulinemia-MC
CGs reversibly precipitate when the temperature is lower than 37degC and
comprise IgMs with RF activity [mono- or oligo-clonal in type II MC or
polyclonal in type III MC] and polyclonal IgGs
MC pathological substrate is an HCV-driven B-cell
proliferation with consequent production of cryo- and non-
cryoprecipitable CICs in turn responsible for vasculitic
manifestations
Most (70ndash90) MC patients are HCV+ and HCV-patients are CGs+ (40ndash60) while 5ndash30 of
CGs+ have symptomatic MC since HCV infects about 170 million individuals worldwide the
number of patients at risk for developing MC is substantial
Type II
CGs
Type III
CGs
Zignego AL et al Autoimmun Rev 2017 Ferri C et al Autoimmunity rev 2016 Zignego AL et al DLD 2007 Cacoub P et al DLD
2014 Zignego AL et al DLD 2007 Zignego AL et al Intern Emerg Med 2012 Zignego AL et al Clin Dev Immunol 2012 Zignego
AL et al Expert Rev Clin Immunol 2015
MC clinical aspects MC Syndrome
MCS is characterized by the clinical triad -purpura weakness and
arthralgias- low complement C4 and various organsystem
involvement including cutaneous articular renal neurological
cardiac or digestive
It ranges from mild disease to severe even life-threatening
conditions
More serious lesions are generally characterized by neurologic and
renal involvement
Prognosis is highly dependent on renal involvement or on the extent
of vasculitis lesions
1 HCV is the main etiopathological agent as concordantly demonstrated by epidemiological clinico-pathological virological and laboratory investigations2 the association between HCV and disease is demonstrated in a significant proportion of patients and supported by in depth clinico-pathogeneticstudies3 the association is suggested by cohort studies a possible causative role may be limited to a small number of patients andor possibly more relevant in specific geographical areas 4 a number of anecdotal observations suggested a possible role of HCV further investigations are required
From P Cacoub 2015
HCV infection is closely related to LPDs mostly MC
40 to 60 of HCV patients show circulating CGs among this latter population 5-30
develop a symptomatic CV
AVT has been considered the first-line option in HCV-CV patients in fact in the majority
of cases viral eradication leads to CV clinical remission
Data about IFN-free regimens for the treatment of CV patients are still limited
HCV and MC
HCV and MC
Zignego 2015Ferri 2016Pozzato 2016 Sise 2016Saadoun 2015Gragnani 2016Gragnani 2016
Bonacci 2016Hegazy 2016Kondili 2016Emery 2017
Younossi et al
The annual costs (inpatient outpatient andpharmacy) associated with extrahepatic
manifestations of HCV were evaluated
Total direct medical costs of extrahepatic
manifestations of HCV in 2014 US dollars wereestimated to be $1506 million (range $922 millionndash
$2208 million in sensitivity analysis)
These estimates should be added to the liver-related
burden of disease to obtain a more accurateassessment of the total burden of HCV infection
The OBJECTIVE of the study was to estimate the annual direct medical costsassociated with HCV related EHM in the EU5 (France Germany Italy United Kingdom
Spain)
Extrahepatic Manifestations of HCV
Extrahepatic Manifestations of HCV
HCV may cause extrahepatic disorders (HCV-EHDs) classified according to the number and
strength of supporting scientific data
HCV-EHDs are responsible for increasing morbidity and mortality with important
consequences in terms of social costs
The analysis of mortality rates in large cohorts confirmed the association of HCV with
several EHDs including cardiovascular neurologic metabolic or renal diseases and tumors
Viral eradication significantly reduced the rate of extra-hepatic deaths
Cacoub P et al DLD 2014 Lee MH et al J Infect Dis 2012 Backus LI et al Clin Gastroenterol Hepatol 2011 El-Kamary S et al
Clin Infect Dis 2011 Hsu YC et al Hepatology 2014 Kawamura Y et al Am J Med 2007 Adinolfi LE et al WJG 2014
Con il contributo di
Lee M-H et al J Infect Dis 2012206469-477
Follow-Up
(Years)
20
18
16
14
12
10
2
00 2 4 6 8 10 12 14 16 18 20
8
6
4
Follow-Up
(Years)
12
10
8
6
4
2
00 2 4 6 8 10 12 14 16 18 20
All Causes(n=2394)
Liver Cancer(n=115)
Extrahepatic Diseases(n=2199)
Cum
ula
tive M
ort
ali
ty (
)
Anti-HCV+ HCV RNA detectable Anti-HCV+ HCV RNA undetectable Anti-HCVndash
Follow-Up
(Years)
35
30
25
20
15
10
5
00 2 4 6 8 10 12 14 16 18 20
301
128124
104
16
03
198
122
110
Extrahepatic Manifestations of HCV
The annual costs (inpatient outpatient andpharmacy) associated with extrahepatic
manifestations of HCV were evaluated
Total direct medical costs of extrahepatic
manifestations of HCV in 2014 US dollars wereestimated to be $1506 million (range $922 millionndash
$2208 million in sensitivity analysis)
These estimates should be added to the liver-related
burden of disease to obtain a more accurateassessment of the total burden of HCV infection
Younossi et al
Younossi et al
Costs up to $71000 per patient per year (ESRD) Among the most frequent EHM depression (245 in HCV vs 172 in non-HCV) had estimated annual cost of
$4307 million DM (15 vs 10 in non- HCV) had an annual cost of $4434 million in the USA= given the importance of DM and
its association with CVDs and mortality the clinical and economic impacts of HCV-related DM are substantial
The OBJECTIVE of the study was to estimate the annual direct medical costsassociated with HCV related EHM in the EU5 (France Germany Italy United Kingdom
Spain)
The OBJECTIVE of the study was to estimate the annual direct medicalcosts associated with HCV related EHM in the EU5 (France Germany
Italy United Kingdom Spain)
1 HCV is the main etiopathological agent as concordantly demonstrated by epidemiological clinico-pathological virological and laboratory investigations2 the association between HCV and disease is demonstrated in a significant proportion of patients and supported by in depth clinico-pathogeneticstudies3 the association is suggested by cohort studies a possible causative role may be limited to a small number of patients andor possibly more relevant in specific geographical areas 4 a number of anecdotal observations suggested a possible role of HCV further investigations are required
The most studied and frequent HCV-EHDs are B-LPDs andor autoimmune disorders
Their prototype is Mixed Cryoglobulinemia (MC) from researches on MC derived most of the
available information
MC as a precious model for all the HCV-EHDs and to evaluate the effects of viral eradication
Anti-HCV Treatment Evolution
IFN
6 mos
PegIFN RBV 12
mos
IFN
12 mos
IFNRBV
12 mos
PegIFN
12 mos
2001
1998
2011
Standardinterferon
Ribavirin
Peginterferon
1991
Direct-actingantivirals
PegIFN
RBV
DAA
IFNRBV
6 mos
6
16
34
4239
55
70+
0
20
40
60
80
100
DAAs
826
weeks
gt90
2015
Few side effects absence major
contraindications
Younossi et al
The annual costs (inpatient outpatient and pharmacy) associatedwith extrahepatic manifestations of HCV were evaluated
Total direct medical costs of extrahepatic manifestations of HCV in 2014US dollars were estimated to be $1506 million (range $922 millionndash
$2208 million in sensitivity analysis)
These estimates should be added to the liver-related burden of diseaseto obtain a more accurate assessment of the total burden of HCV
infection
The OBJECTIVE of the study was to estimate the annual direct medical costs associated with HCV related EHM in the EU5 (France Germany Italy United Kingdom Spain)
22 MCS treated with DAAs including 2 HCC and 2 NHL 100 SVR12 Clinical CR in 64 and PR in remaining 36 The small lymphocytic lymphoma progressed despite viral clearance
Lauletta et al 2017
Emery CS et al 2017
Retrospective analysis 17 MCS (10 with severelife-threatening vasculitis) and 65 asymptomatic CGs+ pts treated with DAAs SVR 889 MCS and 908 asymptomatic pts In MCS clinical response in 1117 (complete in 717) In severelife-threatening vasculitis lower clinical response especially in renal and neurological symptoms
Saadoun D et al 2017
Open-label prospective multi-center study on sofosbuvir plus daclatasvir treatment of 41 HCV MCS SVR in100 and clinical CR in 902 Disappearance of CGs in 50 of pts No serious adverse event or relapse ofvasculitis
Antiviral Treatment (AVT) of MCIFN-free regimens
MC is clinically benign but sometimes severe HCV EHD invalidating symptoms occur and
it may evolve into lymphoma
Cacoub P et al DLD 2014 Zignego AL et al DLD 2007 Zignego AL et al Intern Emerg Med 2012 Zignego AL et al Clin Dev
Immunol 2012 Zignego AL et al Expert Rev Clin Immunol 2015 Sene D et al J Rheumatol 2004
Mixed Cryoglobulinemia-MC
MC pathological substrate is an HCV-driven B-cell
proliferation with consequent production of cryo- and non-
cryoprecipitable CICs in turn responsible for vasculitic
manifestations
Most (70ndash90) MC patients are HCV+ and HCV-patients are CGs+ (40ndash60) while 5ndash30 of
CGs+ have symptomatic MC or cryoglobulinemic vasculitis since HCV infects about 170
million individuals worldwide the number of patients at risk for developing MC is
substantial
Type II CGs
monoclonal
RF+policlonal IgG
Type III CGs both
RF and IgG
polyclonal

Direct medical costs of extrahepatic manifestations of HCV in USA
Younossi et al
Evaluation of the annual costs (inpatientoutpatient and pharmacy) associated withextrahepatic manifestations of HCV
Total direct medical costs of extrahepaticmanifestations of HCV in 2014 US dollars were
estimated to be $1506 million (range $922 millionndash$2208 million in sensitivity analysis)
These estimates should be added to the liver-related burden of disease to obtain a more
accurate assessment of the total burden of HCVinfection
Direct medical costs of extrahepatic manifestations of HCV in EUROPE
ISG-EHCV
Ferri C Ramos-Casals M Zignego AL et al Autoimmun Rev 2016
1465
496717
Total Piter cohort no 8005 subjects the presence of MC was never tested in 80 ofcases in spite of its clinical and therapeutical importance Among the centres thatconsidered MC=-64 evaluated cryoglobulinemia only following a clinical suspicion-58 evaluated routinely cryoglobulinemia at admission with Complement RF levels-42 only in case of RF positivity-Cryo testing was not adequate in 39 of centres
252
These results for the first time showed the real-life variability of the MC diagnosticapproach suggesting that MC prevalence in HCV+ is generally underestimated
Kondili et al Liver Intern2017
CLASSIFICATION OF HCV EHDS ACCORDING TO THE STRENGTH OF SPECIFIC DATA SUPPORTING THE CURATIVE EFFECT OF AVT
Mixed Cryoglobulinemia Effectiveness of both IFN-based and IFN-free AVT
Marginal Zone NHL Effectiveness of both IFN- and DAA-based
AVT
Other low-grade B-cell NHL
HRQOL Available data also in DAA-based AVT
High-grade NHL= DLBCL Insufficient but positive data
CKD Sufficient specific data only for MC-CKD
Neuropsychiatric disorders Problematic IFN-based AVT Insufficient
data with DAAs
Curaneous= PCT and LP (OLP) Problematic IFNRBV-based AVT
Insufficient data with DAAs
Endocrinologic Thyroid and DM 2 Insufficient specific data with DAAs
Arthritis Insufficient specific data with DAAs
Zignego et al 2017
Landau DA et al Arthritis Rheum 2008 Montalbano M et al J Clin Gastroenterol 2007 Cacoub P et al Arthritis Rheum 2002
Mazzaro C et alJ Rheumatol 2003 Zignego AL et al Hepatology 2016 Gragnani L et al Hepatology 2015 Pietrogrande M
et al Autoimmun Rev 2011
Antiviral Treatment (AVT) of MC in the IFN Era
AVT of MC followed the evolution of hepatitis C AVT with frequent adjustments
essentially due to the possible side-effects of IFN andor RBV therapy (ie IFN
neurotoxicity and myelo-inhibitory action and RBV hemolytic effects)
Virological and clinical results progressively improved in spite of frequent side-effects
IFN-based AVT was recommended as the first-line option in mild to moderate MC
Clinical remission was generally correlated with virological response
Long follow-up showed that the majority (57) of SVR pts cleared all MC stigmata
Antiviral Treatment (AVT) of MC IFN-free regimensLimited data so-far concordant are available regarding IFN-free AVT in MC patients
Available data suggest that IFN-free AVT is safe generally well tolerated and effective in MC patients high rate of
clinical response (87) and low rates of serious adverse events was reported
Zignego AL Ramos-Casals M Ferri C et al AutoimmunReviews 2017
Antiviral Treatment (AVT) of MC IFN-free regimens
22 MCS treated with DAAs including 2 HCC and 2 NHL 100 SVR12 Clinical R in 100 (64 CR and 36 PR)
Progression of the small lymphocytic lymphoma
Lauletta et al 2017
Emery CS et al 2017
Retrospective analysis 17 MCS (10 with severelife-threatening vasculitis) and 65 asymptomatic MC treated with
DAAs SVR 889 MCS and 908 asymptomatic pts In MCS clinical R in 1117 (CR in 711) Lower clinical R inseverelife-threatening ndashespecial renal and neurological- vasculitis
Saadoun D et al 2017
Open-label prospective multi-center study on sofosbuvir plus daclatasvir treatment of 41 HCV MCS SVR in 100 and
clinical CR in 902 Disappearance of CGs in 50 of pts No serious adverse event or relapse of vasculitis
A case of rapid amelioration of HCV-associated cryoglobulinemic MPGN treated by
IFN-free DAAs for HCV in the absence of immunosuppressant
Fumiaki et al 2017
Zignego et al 2017
TIME POINTS
baseline EOT and week 12 and 24 of post-treatment f-up (SVR12 and SVR24 respectively)
HRQoL EVALUATION THROUGH PROs
the Short Form (36) Health Survey (SF-36)
the Functional Assessment of Chronic Illness Therapy-Fatigue (FACIT-F) from which we computed the Trial
Outcome Index (TOI)
Evaluation of The Impact on HRQol of IFN-free AVT In HCV CM
1 Physical Component Summary Score (PCS)
MC (54)
HCV (43) CV (85)
deg
A B C
degdegdeg
2 Mental Component Summary Score (MCS)
MCHCV CVD E F
degdegdegdegdeg
HCV
=plt001 vs baseline scores
degdeg=plt001 and degdegdeg=plt0001 vs EOT scores
Gragnani et al AASLD 2017
HCV Eradicationwith DAAs
To be preceded or combined with non-etiological pathogenetic therapy in severecatastrophic MCS
MCS Therapy in the IFN and DAAs Era from the complex to the simplified flow-chart
Dammacco F Sansonno D NEJM 2013
Zignego AL Pawlotsky JM Cacoub P Antiviral Ther in press Cacoub P et al Am J Med 2015
Mechanisms of HCV-related lymphomagenesis
DLBC HCV- induced
direct transformation
MCindolent NHL
accumulation of B RF
following BCR activation
and BC apoptosisinhibition
Zignego AL Ramos-Casals M Ferri C et al Autoimmun Rev 2017
Wang et al Hepatology 2016 Canioni et al Plos one 2016
Observational study on in situ expression of the oncogenic HCV NS3 protein on 116 HCV patients with B-NHL (DLBCL 36 and MZL 34)
NS3 immunostaining positive in 1214 DLBCL vs only 414 MZL (p = 0006) moreover 24 NS3+ MZL
were enriched in large cells
This study supports a new mechanism of transformation with a direct oncogenic role of
HCV proteins in the occurrence of high-grade B lymphomas
IN SITU HEPATITIS C NS3 PROTEIN DETECTION IS ASSOCIATED WITH HIGH GRADE
FEATURES IN HCV-ASSOCIATED B-CELL NON-HODGKIN LYMPHOMAS Danielle
Canioni et al 2016
In addition to the role of chronic antigenic stimulation in HCV related
lymphomagenesis this study supports a second mechanism of transformation due to a
direct oncogenic role of HCV infection of B-cells promoting the occurrence of high-grade Bcell lymphomas
Cohort study of 704 consecutive HIV-negative HCV-positive patients with indolent NHL from 1993 to
2009 in 39 centers of the FIL
Arcaini et al 2016
DLBC HCV- induced
direct transformation
No place of AVT as
1st line
Need of immediate delivery of
chemotherapy or concomitant (NHL
+ HCV targets)
THERAPY OF HCV+ DLBCL
ANTIVIRAL THERAPY IS ASSOCIATED WITH A BETTERSURVIVAL IN PATIENTS WITH HCV AND B-CELL NON-HODGKIN LYMPHOMAS ANRS HC-13 LYMPHO-CSTUDY Michot JM et al
Outcomes of HCV-associated B-NHL according to HCV AVT in prospective patients only (n 5 64)
Concurrent Systemic Chemoimmunotherapy and Sofosbuvir-Based Antiviral Treatment in a Hepatitis C Virus-Infected Patient With Diffuse Large B-Cell Lymphoma Evan C Ewers et al 2016
absolute neutrophil count and Hgb ALT and HCV viral load
Both complete response and SVR of HCV-associated DLBCL after concurrent chemoimmunotherapy and antiviral therapy using a sofosbuvir-based regimen
DAA-treatment in concomitance with chemotherapy showed to be safe and effective in influencing the remission of aggressive lymphomas in HCV patients
Persico M et al 2017
DFS in DAA treated and historical not-treated ptsAntiviral response rates in DAA treated patients
ANTIVIRAL THERAPY IN HCV+ B CELL NHL
IFN-based AVT induced hematological response along with SVR in patients with HCV-related indolent NHLs (especially
MZL)
Recent data with IFN-free regimens in HCV-associated LPDs suggest their anti-lymphoma activity too
AVT should be considered the first-line approach in HCV low grade lymphomas if there is no urgency of a conventional
treatment (ie systemic symptoms bulky disease or symptomatic splenomegaly) (ESMO NCCN EASL guidelines)
In aggressive lymphomas antiviral therapy after induction treatment is to be considered the standard at the moment but
in the next years (months) the association of immunochemotherapy and antiviral therapy will be considered the standard
Zignego AL Ramos-Casals M Ferri C et al Autoimmun Rev 2017
The Masve group
BASIC RESEARCH
Laura Gragnani
Patrizio Caini
Serena Lorini
Antonella Simone
CLINICAL RESEARCH
Monica Monti
Luisa Petraccia
Sinan Sadalla
Guia Cerretelli
Cristina Stasi
Adela Xheka
Universitagrave degli Studi di FirenzeDipartimento di Medicina Sperimentale e Clinica
Centro Manifestazioni Sistemiche da Virus EpatiticildquoMASVErdquo
Anna Linda Zignego
MASVE
UNDERGRADUATE STUDENTS Andrea Genovese Adrian Piscopo
ANTIVIRAL THERAPY IN HCV+ B CELL NHL
IFN-based AVT induced hematological response along with SVR in patients with HCV-related indolent
NHLs (especially MZL)
Recent data with IFN-free regimens in HCV-associated LPDs suggest their anti-lymphoma activity too
AVT should be considered the first-line approach in HCV low grade lymphomas if there is no urgency
of a conventional treatment (ie systemic symptoms bulky disease or symptomatic splenomegaly)
(ESMO NCCN EASL guidelines)
Main drugs for HCV-related MCS according to the target
HCV= DAAsB-cell Expansion= (a) B cell-depleting Mabs
-First-generation Rituximab (anti-CD20)-Second-generation Ofatumumab (anti-CD20) Veltuzumab (humanized
anti-CD20)-Third-generation Obinutuzumab (GA101) Oceratuzumab (humanized
anti-CD20)
(b) Alkylating agents
-Cyclophosfamide
Inflammation= Antiinflammatory agents
- Corticosteroids
Altered regulatory T-cell activity=
- IL-2
The impact on HRQoL of IFN-free AVT was prospectively evaluated in a cohort of HCV CV patients with limited
influencing variables linked to therapeutic schedulesviral GT
44 HCV GT2 CV patients mostly F0-F2 (29) and naiumlve (30) treated with SOFRBV for 1224wks
TIME POINTS
baseline EOT and week 12 and 24 of post-treatment f-up (SVR12 and SVR24 respectively)
HRQoL EVALUATION THROUGH PROs
the Short Form (36) Health Survey (SF-36)
the Functional Assessment of Chronic Illness Therapy-Fatigue (FACIT-F) from which we computed the Trial
Outcome Index (TOI)
Observational study on in situ expression of the oncogenic HCV NS3 protein on 116 HCV
patients with B-NHL (DLBCL 36 and MZL 34)
NS3 immunostaining positive in 1214 DLBCL vs only 414 MZL (p = 0006) moreover 24 NS3+
MZL were enriched in large cells
This study supports a new mechanism of transformation with a direct oncogenic role of
HCV proteins in the occurrence of high-grade B lymphomas
IN SITU HEPATITIS C NS3 PROTEIN DETECTION IS ASSOCIATED WITH HIGH GRADEFEATURES IN HCV-ASSOCIATED B-CELL NON-HODGKIN LYMPHOMAS Danielle
Canioni et al 2016
In addition to the role of chronic antigenic stimulation in HCV related
lymphomagenesis this study supports a second mechanism of transformation due toa direct oncogenic role of HCV infection of B-cells promoting the occurrence of high-grade Bcell lymphomas
ANTIVIRAL THERAPY IS ASSOCIATED WITH A BETTERSURVIVAL IN PATIENTS WITH HCV AND B-CELL NON-HODGKIN LYMPHOMAS ANRS HC-13 LYMPHO-CSTUDYMichot JM et al
Outcomes of HCV-associated B-NHL according to HCV AVT in prospective patients only (n 5 64)
(A) absolute neutrophil count and Hgb
(B) ALT and HCV viral load
This patient had HCV-associated DLBCL achieving both complete response and SVR after concurrent chemoimmunotherapy and antiviral therapy using a sofosbuvir-basedregimen
Concurrent Systemic Chemoimmunotherapy and Sofosbuvir-Based Antiviral Treatment in a Hepatitis C Virus-Infected Patient With Diffuse Large B-Cell LymphomaEvan C Ewers et al 2016
HCV-EHDs are responsible for increasing morbidity and mortality with important
consequences in terms of social costs
The analysis of mortality rates in large cohorts confirmed the association of HCV with
several EHDs including cardiovascular neurologic metabolic or renal diseases and tumors
Viral eradication significantly reduced the rate of extra-hepatic deaths
Cacoub P et al DLD 2014 Lee MH et al J Infect Dis 2012 Backus LI et al Clin Gastroenterol Hepatol 2011 El-Kamary S et al
Clin Infect Dis 2011 Hsu YC et al Hepatology 2014 Kawamura Y et al Am J Med 2007 Adinolfi LE et al WJG 2014
Extrahepatic Manifestations of HCV
Con il contributo di
Lee M-H et al J Infect Dis 2012206469-477
Follow-Up
(Years)
20
18
16
14
12
10
2
00 2 4 6 8 10 12 14 16 18 20
8
6
4
Follow-Up
(Years)
12
10
8
6
4
2
00 2 4 6 8 10 12 14 16 18 20
All Causes(n=2394)
Liver Cancer(n=115)
Extrahepatic Diseases(n=2199)
Cum
ula
tive M
ort
ali
ty (
)
Anti-HCV+ HCV RNA detectable Anti-HCV+ HCV RNA undetectable Anti-HCVndash
Follow-Up
(Years)
35
30
25
20
15
10
5
00 2 4 6 8 10 12 14 16 18 20
301
128124
104
16
03
198
122
110
MC is clinically benign but sometimes severe HCV EHD invalidating symptoms occur and
it may evolve into lymphoma
Cacoub P et al DLD 2014 Zignego AL et al DLD 2007 Zignego AL et al Intern Emerg Med 2012 Zignego AL et al Clin Dev
Immunol 2012 Zignego AL et al Expert Rev Clin Immunol 2015 Sene D et al J Rheumatol 2004
Mixed Cryoglobulinemia-MC
CGs reversibly precipitate when the temperature is lower than 37degC and
comprise IgMs with RF activity [mono- or oligo-clonal in type II MC or
polyclonal in type III MC] and polyclonal IgGs
MC pathological substrate is an HCV-driven B-cell
proliferation with consequent production of cryo- and non-
cryoprecipitable CICs in turn responsible for vasculitic
manifestations
Most (70ndash90) MC patients are HCV+ and HCV-patients are CGs+ (40ndash60) while 5ndash30 of
CGs+ have symptomatic MC since HCV infects about 170 million individuals worldwide the
number of patients at risk for developing MC is substantial
Type II
CGs
Type III
CGs
Zignego AL et al Autoimmun Rev 2017 Ferri C et al Autoimmunity rev 2016 Zignego AL et al DLD 2007 Cacoub P et al DLD
2014 Zignego AL et al DLD 2007 Zignego AL et al Intern Emerg Med 2012 Zignego AL et al Clin Dev Immunol 2012 Zignego
AL et al Expert Rev Clin Immunol 2015
MC clinical aspects MC Syndrome
MCS is characterized by the clinical triad -purpura weakness and
arthralgias- low complement C4 and various organsystem
involvement including cutaneous articular renal neurological
cardiac or digestive
It ranges from mild disease to severe even life-threatening
conditions
More serious lesions are generally characterized by neurologic and
renal involvement
Prognosis is highly dependent on renal involvement or on the extent
of vasculitis lesions
1 HCV is the main etiopathological agent as concordantly demonstrated by epidemiological clinico-pathological virological and laboratory investigations2 the association between HCV and disease is demonstrated in a significant proportion of patients and supported by in depth clinico-pathogeneticstudies3 the association is suggested by cohort studies a possible causative role may be limited to a small number of patients andor possibly more relevant in specific geographical areas 4 a number of anecdotal observations suggested a possible role of HCV further investigations are required
From P Cacoub 2015
HCV infection is closely related to LPDs mostly MC
40 to 60 of HCV patients show circulating CGs among this latter population 5-30
develop a symptomatic CV
AVT has been considered the first-line option in HCV-CV patients in fact in the majority
of cases viral eradication leads to CV clinical remission
Data about IFN-free regimens for the treatment of CV patients are still limited
HCV and MC
HCV and MC
Zignego 2015Ferri 2016Pozzato 2016 Sise 2016Saadoun 2015Gragnani 2016Gragnani 2016
Bonacci 2016Hegazy 2016Kondili 2016Emery 2017
Younossi et al
The annual costs (inpatient outpatient andpharmacy) associated with extrahepatic
manifestations of HCV were evaluated
Total direct medical costs of extrahepatic
manifestations of HCV in 2014 US dollars wereestimated to be $1506 million (range $922 millionndash
$2208 million in sensitivity analysis)
These estimates should be added to the liver-related
burden of disease to obtain a more accurateassessment of the total burden of HCV infection
The OBJECTIVE of the study was to estimate the annual direct medical costsassociated with HCV related EHM in the EU5 (France Germany Italy United Kingdom
Spain)
Extrahepatic Manifestations of HCV
Extrahepatic Manifestations of HCV
HCV may cause extrahepatic disorders (HCV-EHDs) classified according to the number and
strength of supporting scientific data
HCV-EHDs are responsible for increasing morbidity and mortality with important
consequences in terms of social costs
The analysis of mortality rates in large cohorts confirmed the association of HCV with
several EHDs including cardiovascular neurologic metabolic or renal diseases and tumors
Viral eradication significantly reduced the rate of extra-hepatic deaths
Cacoub P et al DLD 2014 Lee MH et al J Infect Dis 2012 Backus LI et al Clin Gastroenterol Hepatol 2011 El-Kamary S et al
Clin Infect Dis 2011 Hsu YC et al Hepatology 2014 Kawamura Y et al Am J Med 2007 Adinolfi LE et al WJG 2014
Con il contributo di
Lee M-H et al J Infect Dis 2012206469-477
Follow-Up
(Years)
20
18
16
14
12
10
2
00 2 4 6 8 10 12 14 16 18 20
8
6
4
Follow-Up
(Years)
12
10
8
6
4
2
00 2 4 6 8 10 12 14 16 18 20
All Causes(n=2394)
Liver Cancer(n=115)
Extrahepatic Diseases(n=2199)
Cum
ula
tive M
ort
ali
ty (
)
Anti-HCV+ HCV RNA detectable Anti-HCV+ HCV RNA undetectable Anti-HCVndash
Follow-Up
(Years)
35
30
25
20
15
10
5
00 2 4 6 8 10 12 14 16 18 20
301
128124
104
16
03
198
122
110
Extrahepatic Manifestations of HCV
The annual costs (inpatient outpatient andpharmacy) associated with extrahepatic
manifestations of HCV were evaluated
Total direct medical costs of extrahepatic
manifestations of HCV in 2014 US dollars wereestimated to be $1506 million (range $922 millionndash
$2208 million in sensitivity analysis)
These estimates should be added to the liver-related
burden of disease to obtain a more accurateassessment of the total burden of HCV infection
Younossi et al
Younossi et al
Costs up to $71000 per patient per year (ESRD) Among the most frequent EHM depression (245 in HCV vs 172 in non-HCV) had estimated annual cost of
$4307 million DM (15 vs 10 in non- HCV) had an annual cost of $4434 million in the USA= given the importance of DM and
its association with CVDs and mortality the clinical and economic impacts of HCV-related DM are substantial
The OBJECTIVE of the study was to estimate the annual direct medical costsassociated with HCV related EHM in the EU5 (France Germany Italy United Kingdom
Spain)
The OBJECTIVE of the study was to estimate the annual direct medicalcosts associated with HCV related EHM in the EU5 (France Germany
Italy United Kingdom Spain)
1 HCV is the main etiopathological agent as concordantly demonstrated by epidemiological clinico-pathological virological and laboratory investigations2 the association between HCV and disease is demonstrated in a significant proportion of patients and supported by in depth clinico-pathogeneticstudies3 the association is suggested by cohort studies a possible causative role may be limited to a small number of patients andor possibly more relevant in specific geographical areas 4 a number of anecdotal observations suggested a possible role of HCV further investigations are required
The most studied and frequent HCV-EHDs are B-LPDs andor autoimmune disorders
Their prototype is Mixed Cryoglobulinemia (MC) from researches on MC derived most of the
available information
MC as a precious model for all the HCV-EHDs and to evaluate the effects of viral eradication
Anti-HCV Treatment Evolution
IFN
6 mos
PegIFN RBV 12
mos
IFN
12 mos
IFNRBV
12 mos
PegIFN
12 mos
2001
1998
2011
Standardinterferon
Ribavirin
Peginterferon
1991
Direct-actingantivirals
PegIFN
RBV
DAA
IFNRBV
6 mos
6
16
34
4239
55
70+
0
20
40
60
80
100
DAAs
826
weeks
gt90
2015
Few side effects absence major
contraindications
Younossi et al
The annual costs (inpatient outpatient and pharmacy) associatedwith extrahepatic manifestations of HCV were evaluated
Total direct medical costs of extrahepatic manifestations of HCV in 2014US dollars were estimated to be $1506 million (range $922 millionndash
$2208 million in sensitivity analysis)
These estimates should be added to the liver-related burden of diseaseto obtain a more accurate assessment of the total burden of HCV
infection
The OBJECTIVE of the study was to estimate the annual direct medical costs associated with HCV related EHM in the EU5 (France Germany Italy United Kingdom Spain)
22 MCS treated with DAAs including 2 HCC and 2 NHL 100 SVR12 Clinical CR in 64 and PR in remaining 36 The small lymphocytic lymphoma progressed despite viral clearance
Lauletta et al 2017
Emery CS et al 2017
Retrospective analysis 17 MCS (10 with severelife-threatening vasculitis) and 65 asymptomatic CGs+ pts treated with DAAs SVR 889 MCS and 908 asymptomatic pts In MCS clinical response in 1117 (complete in 717) In severelife-threatening vasculitis lower clinical response especially in renal and neurological symptoms
Saadoun D et al 2017
Open-label prospective multi-center study on sofosbuvir plus daclatasvir treatment of 41 HCV MCS SVR in100 and clinical CR in 902 Disappearance of CGs in 50 of pts No serious adverse event or relapse ofvasculitis
Antiviral Treatment (AVT) of MCIFN-free regimens
MC is clinically benign but sometimes severe HCV EHD invalidating symptoms occur and
it may evolve into lymphoma
Cacoub P et al DLD 2014 Zignego AL et al DLD 2007 Zignego AL et al Intern Emerg Med 2012 Zignego AL et al Clin Dev
Immunol 2012 Zignego AL et al Expert Rev Clin Immunol 2015 Sene D et al J Rheumatol 2004
Mixed Cryoglobulinemia-MC
MC pathological substrate is an HCV-driven B-cell
proliferation with consequent production of cryo- and non-
cryoprecipitable CICs in turn responsible for vasculitic
manifestations
Most (70ndash90) MC patients are HCV+ and HCV-patients are CGs+ (40ndash60) while 5ndash30 of
CGs+ have symptomatic MC or cryoglobulinemic vasculitis since HCV infects about 170
million individuals worldwide the number of patients at risk for developing MC is
substantial
Type II CGs
monoclonal
RF+policlonal IgG
Type III CGs both
RF and IgG
polyclonal

Direct medical costs of extrahepatic manifestations of HCV in EUROPE
ISG-EHCV
Ferri C Ramos-Casals M Zignego AL et al Autoimmun Rev 2016
1465
496717
Total Piter cohort no 8005 subjects the presence of MC was never tested in 80 ofcases in spite of its clinical and therapeutical importance Among the centres thatconsidered MC=-64 evaluated cryoglobulinemia only following a clinical suspicion-58 evaluated routinely cryoglobulinemia at admission with Complement RF levels-42 only in case of RF positivity-Cryo testing was not adequate in 39 of centres
252
These results for the first time showed the real-life variability of the MC diagnosticapproach suggesting that MC prevalence in HCV+ is generally underestimated
Kondili et al Liver Intern2017
CLASSIFICATION OF HCV EHDS ACCORDING TO THE STRENGTH OF SPECIFIC DATA SUPPORTING THE CURATIVE EFFECT OF AVT
Mixed Cryoglobulinemia Effectiveness of both IFN-based and IFN-free AVT
Marginal Zone NHL Effectiveness of both IFN- and DAA-based
AVT
Other low-grade B-cell NHL
HRQOL Available data also in DAA-based AVT
High-grade NHL= DLBCL Insufficient but positive data
CKD Sufficient specific data only for MC-CKD
Neuropsychiatric disorders Problematic IFN-based AVT Insufficient
data with DAAs
Curaneous= PCT and LP (OLP) Problematic IFNRBV-based AVT
Insufficient data with DAAs
Endocrinologic Thyroid and DM 2 Insufficient specific data with DAAs
Arthritis Insufficient specific data with DAAs
Zignego et al 2017
Landau DA et al Arthritis Rheum 2008 Montalbano M et al J Clin Gastroenterol 2007 Cacoub P et al Arthritis Rheum 2002
Mazzaro C et alJ Rheumatol 2003 Zignego AL et al Hepatology 2016 Gragnani L et al Hepatology 2015 Pietrogrande M
et al Autoimmun Rev 2011
Antiviral Treatment (AVT) of MC in the IFN Era
AVT of MC followed the evolution of hepatitis C AVT with frequent adjustments
essentially due to the possible side-effects of IFN andor RBV therapy (ie IFN
neurotoxicity and myelo-inhibitory action and RBV hemolytic effects)
Virological and clinical results progressively improved in spite of frequent side-effects
IFN-based AVT was recommended as the first-line option in mild to moderate MC
Clinical remission was generally correlated with virological response
Long follow-up showed that the majority (57) of SVR pts cleared all MC stigmata
Antiviral Treatment (AVT) of MC IFN-free regimensLimited data so-far concordant are available regarding IFN-free AVT in MC patients
Available data suggest that IFN-free AVT is safe generally well tolerated and effective in MC patients high rate of
clinical response (87) and low rates of serious adverse events was reported
Zignego AL Ramos-Casals M Ferri C et al AutoimmunReviews 2017
Antiviral Treatment (AVT) of MC IFN-free regimens
22 MCS treated with DAAs including 2 HCC and 2 NHL 100 SVR12 Clinical R in 100 (64 CR and 36 PR)
Progression of the small lymphocytic lymphoma
Lauletta et al 2017
Emery CS et al 2017
Retrospective analysis 17 MCS (10 with severelife-threatening vasculitis) and 65 asymptomatic MC treated with
DAAs SVR 889 MCS and 908 asymptomatic pts In MCS clinical R in 1117 (CR in 711) Lower clinical R inseverelife-threatening ndashespecial renal and neurological- vasculitis
Saadoun D et al 2017
Open-label prospective multi-center study on sofosbuvir plus daclatasvir treatment of 41 HCV MCS SVR in 100 and
clinical CR in 902 Disappearance of CGs in 50 of pts No serious adverse event or relapse of vasculitis
A case of rapid amelioration of HCV-associated cryoglobulinemic MPGN treated by
IFN-free DAAs for HCV in the absence of immunosuppressant
Fumiaki et al 2017
Zignego et al 2017
TIME POINTS
baseline EOT and week 12 and 24 of post-treatment f-up (SVR12 and SVR24 respectively)
HRQoL EVALUATION THROUGH PROs
the Short Form (36) Health Survey (SF-36)
the Functional Assessment of Chronic Illness Therapy-Fatigue (FACIT-F) from which we computed the Trial
Outcome Index (TOI)
Evaluation of The Impact on HRQol of IFN-free AVT In HCV CM
1 Physical Component Summary Score (PCS)
MC (54)
HCV (43) CV (85)
deg
A B C
degdegdeg
2 Mental Component Summary Score (MCS)
MCHCV CVD E F
degdegdegdegdeg
HCV
=plt001 vs baseline scores
degdeg=plt001 and degdegdeg=plt0001 vs EOT scores
Gragnani et al AASLD 2017
HCV Eradicationwith DAAs
To be preceded or combined with non-etiological pathogenetic therapy in severecatastrophic MCS
MCS Therapy in the IFN and DAAs Era from the complex to the simplified flow-chart
Dammacco F Sansonno D NEJM 2013
Zignego AL Pawlotsky JM Cacoub P Antiviral Ther in press Cacoub P et al Am J Med 2015
Mechanisms of HCV-related lymphomagenesis
DLBC HCV- induced
direct transformation
MCindolent NHL
accumulation of B RF
following BCR activation
and BC apoptosisinhibition
Zignego AL Ramos-Casals M Ferri C et al Autoimmun Rev 2017
Wang et al Hepatology 2016 Canioni et al Plos one 2016
Observational study on in situ expression of the oncogenic HCV NS3 protein on 116 HCV patients with B-NHL (DLBCL 36 and MZL 34)
NS3 immunostaining positive in 1214 DLBCL vs only 414 MZL (p = 0006) moreover 24 NS3+ MZL
were enriched in large cells
This study supports a new mechanism of transformation with a direct oncogenic role of
HCV proteins in the occurrence of high-grade B lymphomas
IN SITU HEPATITIS C NS3 PROTEIN DETECTION IS ASSOCIATED WITH HIGH GRADE
FEATURES IN HCV-ASSOCIATED B-CELL NON-HODGKIN LYMPHOMAS Danielle
Canioni et al 2016
In addition to the role of chronic antigenic stimulation in HCV related
lymphomagenesis this study supports a second mechanism of transformation due to a
direct oncogenic role of HCV infection of B-cells promoting the occurrence of high-grade Bcell lymphomas
Cohort study of 704 consecutive HIV-negative HCV-positive patients with indolent NHL from 1993 to
2009 in 39 centers of the FIL
Arcaini et al 2016
DLBC HCV- induced
direct transformation
No place of AVT as
1st line
Need of immediate delivery of
chemotherapy or concomitant (NHL
+ HCV targets)
THERAPY OF HCV+ DLBCL
ANTIVIRAL THERAPY IS ASSOCIATED WITH A BETTERSURVIVAL IN PATIENTS WITH HCV AND B-CELL NON-HODGKIN LYMPHOMAS ANRS HC-13 LYMPHO-CSTUDY Michot JM et al
Outcomes of HCV-associated B-NHL according to HCV AVT in prospective patients only (n 5 64)
Concurrent Systemic Chemoimmunotherapy and Sofosbuvir-Based Antiviral Treatment in a Hepatitis C Virus-Infected Patient With Diffuse Large B-Cell Lymphoma Evan C Ewers et al 2016
absolute neutrophil count and Hgb ALT and HCV viral load
Both complete response and SVR of HCV-associated DLBCL after concurrent chemoimmunotherapy and antiviral therapy using a sofosbuvir-based regimen
DAA-treatment in concomitance with chemotherapy showed to be safe and effective in influencing the remission of aggressive lymphomas in HCV patients
Persico M et al 2017
DFS in DAA treated and historical not-treated ptsAntiviral response rates in DAA treated patients
ANTIVIRAL THERAPY IN HCV+ B CELL NHL
IFN-based AVT induced hematological response along with SVR in patients with HCV-related indolent NHLs (especially
MZL)
Recent data with IFN-free regimens in HCV-associated LPDs suggest their anti-lymphoma activity too
AVT should be considered the first-line approach in HCV low grade lymphomas if there is no urgency of a conventional
treatment (ie systemic symptoms bulky disease or symptomatic splenomegaly) (ESMO NCCN EASL guidelines)
In aggressive lymphomas antiviral therapy after induction treatment is to be considered the standard at the moment but
in the next years (months) the association of immunochemotherapy and antiviral therapy will be considered the standard
Zignego AL Ramos-Casals M Ferri C et al Autoimmun Rev 2017
The Masve group
BASIC RESEARCH
Laura Gragnani
Patrizio Caini
Serena Lorini
Antonella Simone
CLINICAL RESEARCH
Monica Monti
Luisa Petraccia
Sinan Sadalla
Guia Cerretelli
Cristina Stasi
Adela Xheka
Universitagrave degli Studi di FirenzeDipartimento di Medicina Sperimentale e Clinica
Centro Manifestazioni Sistemiche da Virus EpatiticildquoMASVErdquo
Anna Linda Zignego
MASVE
UNDERGRADUATE STUDENTS Andrea Genovese Adrian Piscopo
ANTIVIRAL THERAPY IN HCV+ B CELL NHL
IFN-based AVT induced hematological response along with SVR in patients with HCV-related indolent
NHLs (especially MZL)
Recent data with IFN-free regimens in HCV-associated LPDs suggest their anti-lymphoma activity too
AVT should be considered the first-line approach in HCV low grade lymphomas if there is no urgency
of a conventional treatment (ie systemic symptoms bulky disease or symptomatic splenomegaly)
(ESMO NCCN EASL guidelines)
Main drugs for HCV-related MCS according to the target
HCV= DAAsB-cell Expansion= (a) B cell-depleting Mabs
-First-generation Rituximab (anti-CD20)-Second-generation Ofatumumab (anti-CD20) Veltuzumab (humanized
anti-CD20)-Third-generation Obinutuzumab (GA101) Oceratuzumab (humanized
anti-CD20)
(b) Alkylating agents
-Cyclophosfamide
Inflammation= Antiinflammatory agents
- Corticosteroids
Altered regulatory T-cell activity=
- IL-2
The impact on HRQoL of IFN-free AVT was prospectively evaluated in a cohort of HCV CV patients with limited
influencing variables linked to therapeutic schedulesviral GT
44 HCV GT2 CV patients mostly F0-F2 (29) and naiumlve (30) treated with SOFRBV for 1224wks
TIME POINTS
baseline EOT and week 12 and 24 of post-treatment f-up (SVR12 and SVR24 respectively)
HRQoL EVALUATION THROUGH PROs
the Short Form (36) Health Survey (SF-36)
the Functional Assessment of Chronic Illness Therapy-Fatigue (FACIT-F) from which we computed the Trial
Outcome Index (TOI)
Observational study on in situ expression of the oncogenic HCV NS3 protein on 116 HCV
patients with B-NHL (DLBCL 36 and MZL 34)
NS3 immunostaining positive in 1214 DLBCL vs only 414 MZL (p = 0006) moreover 24 NS3+
MZL were enriched in large cells
This study supports a new mechanism of transformation with a direct oncogenic role of
HCV proteins in the occurrence of high-grade B lymphomas
IN SITU HEPATITIS C NS3 PROTEIN DETECTION IS ASSOCIATED WITH HIGH GRADEFEATURES IN HCV-ASSOCIATED B-CELL NON-HODGKIN LYMPHOMAS Danielle
Canioni et al 2016
In addition to the role of chronic antigenic stimulation in HCV related
lymphomagenesis this study supports a second mechanism of transformation due toa direct oncogenic role of HCV infection of B-cells promoting the occurrence of high-grade Bcell lymphomas
ANTIVIRAL THERAPY IS ASSOCIATED WITH A BETTERSURVIVAL IN PATIENTS WITH HCV AND B-CELL NON-HODGKIN LYMPHOMAS ANRS HC-13 LYMPHO-CSTUDYMichot JM et al
Outcomes of HCV-associated B-NHL according to HCV AVT in prospective patients only (n 5 64)
(A) absolute neutrophil count and Hgb
(B) ALT and HCV viral load
This patient had HCV-associated DLBCL achieving both complete response and SVR after concurrent chemoimmunotherapy and antiviral therapy using a sofosbuvir-basedregimen
Concurrent Systemic Chemoimmunotherapy and Sofosbuvir-Based Antiviral Treatment in a Hepatitis C Virus-Infected Patient With Diffuse Large B-Cell LymphomaEvan C Ewers et al 2016
HCV-EHDs are responsible for increasing morbidity and mortality with important
consequences in terms of social costs
The analysis of mortality rates in large cohorts confirmed the association of HCV with
several EHDs including cardiovascular neurologic metabolic or renal diseases and tumors
Viral eradication significantly reduced the rate of extra-hepatic deaths
Cacoub P et al DLD 2014 Lee MH et al J Infect Dis 2012 Backus LI et al Clin Gastroenterol Hepatol 2011 El-Kamary S et al
Clin Infect Dis 2011 Hsu YC et al Hepatology 2014 Kawamura Y et al Am J Med 2007 Adinolfi LE et al WJG 2014
Extrahepatic Manifestations of HCV
Con il contributo di
Lee M-H et al J Infect Dis 2012206469-477
Follow-Up
(Years)
20
18
16
14
12
10
2
00 2 4 6 8 10 12 14 16 18 20
8
6
4
Follow-Up
(Years)
12
10
8
6
4
2
00 2 4 6 8 10 12 14 16 18 20
All Causes(n=2394)
Liver Cancer(n=115)
Extrahepatic Diseases(n=2199)
Cum
ula
tive M
ort
ali
ty (
)
Anti-HCV+ HCV RNA detectable Anti-HCV+ HCV RNA undetectable Anti-HCVndash
Follow-Up
(Years)
35
30
25
20
15
10
5
00 2 4 6 8 10 12 14 16 18 20
301
128124
104
16
03
198
122
110
MC is clinically benign but sometimes severe HCV EHD invalidating symptoms occur and
it may evolve into lymphoma
Cacoub P et al DLD 2014 Zignego AL et al DLD 2007 Zignego AL et al Intern Emerg Med 2012 Zignego AL et al Clin Dev
Immunol 2012 Zignego AL et al Expert Rev Clin Immunol 2015 Sene D et al J Rheumatol 2004
Mixed Cryoglobulinemia-MC
CGs reversibly precipitate when the temperature is lower than 37degC and
comprise IgMs with RF activity [mono- or oligo-clonal in type II MC or
polyclonal in type III MC] and polyclonal IgGs
MC pathological substrate is an HCV-driven B-cell
proliferation with consequent production of cryo- and non-
cryoprecipitable CICs in turn responsible for vasculitic
manifestations
Most (70ndash90) MC patients are HCV+ and HCV-patients are CGs+ (40ndash60) while 5ndash30 of
CGs+ have symptomatic MC since HCV infects about 170 million individuals worldwide the
number of patients at risk for developing MC is substantial
Type II
CGs
Type III
CGs
Zignego AL et al Autoimmun Rev 2017 Ferri C et al Autoimmunity rev 2016 Zignego AL et al DLD 2007 Cacoub P et al DLD
2014 Zignego AL et al DLD 2007 Zignego AL et al Intern Emerg Med 2012 Zignego AL et al Clin Dev Immunol 2012 Zignego
AL et al Expert Rev Clin Immunol 2015
MC clinical aspects MC Syndrome
MCS is characterized by the clinical triad -purpura weakness and
arthralgias- low complement C4 and various organsystem
involvement including cutaneous articular renal neurological
cardiac or digestive
It ranges from mild disease to severe even life-threatening
conditions
More serious lesions are generally characterized by neurologic and
renal involvement
Prognosis is highly dependent on renal involvement or on the extent
of vasculitis lesions
1 HCV is the main etiopathological agent as concordantly demonstrated by epidemiological clinico-pathological virological and laboratory investigations2 the association between HCV and disease is demonstrated in a significant proportion of patients and supported by in depth clinico-pathogeneticstudies3 the association is suggested by cohort studies a possible causative role may be limited to a small number of patients andor possibly more relevant in specific geographical areas 4 a number of anecdotal observations suggested a possible role of HCV further investigations are required
From P Cacoub 2015
HCV infection is closely related to LPDs mostly MC
40 to 60 of HCV patients show circulating CGs among this latter population 5-30
develop a symptomatic CV
AVT has been considered the first-line option in HCV-CV patients in fact in the majority
of cases viral eradication leads to CV clinical remission
Data about IFN-free regimens for the treatment of CV patients are still limited
HCV and MC
HCV and MC
Zignego 2015Ferri 2016Pozzato 2016 Sise 2016Saadoun 2015Gragnani 2016Gragnani 2016
Bonacci 2016Hegazy 2016Kondili 2016Emery 2017
Younossi et al
The annual costs (inpatient outpatient andpharmacy) associated with extrahepatic
manifestations of HCV were evaluated
Total direct medical costs of extrahepatic
manifestations of HCV in 2014 US dollars wereestimated to be $1506 million (range $922 millionndash
$2208 million in sensitivity analysis)
These estimates should be added to the liver-related
burden of disease to obtain a more accurateassessment of the total burden of HCV infection
The OBJECTIVE of the study was to estimate the annual direct medical costsassociated with HCV related EHM in the EU5 (France Germany Italy United Kingdom
Spain)
Extrahepatic Manifestations of HCV
Extrahepatic Manifestations of HCV
HCV may cause extrahepatic disorders (HCV-EHDs) classified according to the number and
strength of supporting scientific data
HCV-EHDs are responsible for increasing morbidity and mortality with important
consequences in terms of social costs
The analysis of mortality rates in large cohorts confirmed the association of HCV with
several EHDs including cardiovascular neurologic metabolic or renal diseases and tumors
Viral eradication significantly reduced the rate of extra-hepatic deaths
Cacoub P et al DLD 2014 Lee MH et al J Infect Dis 2012 Backus LI et al Clin Gastroenterol Hepatol 2011 El-Kamary S et al
Clin Infect Dis 2011 Hsu YC et al Hepatology 2014 Kawamura Y et al Am J Med 2007 Adinolfi LE et al WJG 2014
Con il contributo di
Lee M-H et al J Infect Dis 2012206469-477
Follow-Up
(Years)
20
18
16
14
12
10
2
00 2 4 6 8 10 12 14 16 18 20
8
6
4
Follow-Up
(Years)
12
10
8
6
4
2
00 2 4 6 8 10 12 14 16 18 20
All Causes(n=2394)
Liver Cancer(n=115)
Extrahepatic Diseases(n=2199)
Cum
ula
tive M
ort
ali
ty (
)
Anti-HCV+ HCV RNA detectable Anti-HCV+ HCV RNA undetectable Anti-HCVndash
Follow-Up
(Years)
35
30
25
20
15
10
5
00 2 4 6 8 10 12 14 16 18 20
301
128124
104
16
03
198
122
110
Extrahepatic Manifestations of HCV
The annual costs (inpatient outpatient andpharmacy) associated with extrahepatic
manifestations of HCV were evaluated
Total direct medical costs of extrahepatic
manifestations of HCV in 2014 US dollars wereestimated to be $1506 million (range $922 millionndash
$2208 million in sensitivity analysis)
These estimates should be added to the liver-related
burden of disease to obtain a more accurateassessment of the total burden of HCV infection
Younossi et al
Younossi et al
Costs up to $71000 per patient per year (ESRD) Among the most frequent EHM depression (245 in HCV vs 172 in non-HCV) had estimated annual cost of
$4307 million DM (15 vs 10 in non- HCV) had an annual cost of $4434 million in the USA= given the importance of DM and
its association with CVDs and mortality the clinical and economic impacts of HCV-related DM are substantial
The OBJECTIVE of the study was to estimate the annual direct medical costsassociated with HCV related EHM in the EU5 (France Germany Italy United Kingdom
Spain)
The OBJECTIVE of the study was to estimate the annual direct medicalcosts associated with HCV related EHM in the EU5 (France Germany
Italy United Kingdom Spain)
1 HCV is the main etiopathological agent as concordantly demonstrated by epidemiological clinico-pathological virological and laboratory investigations2 the association between HCV and disease is demonstrated in a significant proportion of patients and supported by in depth clinico-pathogeneticstudies3 the association is suggested by cohort studies a possible causative role may be limited to a small number of patients andor possibly more relevant in specific geographical areas 4 a number of anecdotal observations suggested a possible role of HCV further investigations are required
The most studied and frequent HCV-EHDs are B-LPDs andor autoimmune disorders
Their prototype is Mixed Cryoglobulinemia (MC) from researches on MC derived most of the
available information
MC as a precious model for all the HCV-EHDs and to evaluate the effects of viral eradication
Anti-HCV Treatment Evolution
IFN
6 mos
PegIFN RBV 12
mos
IFN
12 mos
IFNRBV
12 mos
PegIFN
12 mos
2001
1998
2011
Standardinterferon
Ribavirin
Peginterferon
1991
Direct-actingantivirals
PegIFN
RBV
DAA
IFNRBV
6 mos
6
16
34
4239
55
70+
0
20
40
60
80
100
DAAs
826
weeks
gt90
2015
Few side effects absence major
contraindications
Younossi et al
The annual costs (inpatient outpatient and pharmacy) associatedwith extrahepatic manifestations of HCV were evaluated
Total direct medical costs of extrahepatic manifestations of HCV in 2014US dollars were estimated to be $1506 million (range $922 millionndash
$2208 million in sensitivity analysis)
These estimates should be added to the liver-related burden of diseaseto obtain a more accurate assessment of the total burden of HCV
infection
The OBJECTIVE of the study was to estimate the annual direct medical costs associated with HCV related EHM in the EU5 (France Germany Italy United Kingdom Spain)
22 MCS treated with DAAs including 2 HCC and 2 NHL 100 SVR12 Clinical CR in 64 and PR in remaining 36 The small lymphocytic lymphoma progressed despite viral clearance
Lauletta et al 2017
Emery CS et al 2017
Retrospective analysis 17 MCS (10 with severelife-threatening vasculitis) and 65 asymptomatic CGs+ pts treated with DAAs SVR 889 MCS and 908 asymptomatic pts In MCS clinical response in 1117 (complete in 717) In severelife-threatening vasculitis lower clinical response especially in renal and neurological symptoms
Saadoun D et al 2017
Open-label prospective multi-center study on sofosbuvir plus daclatasvir treatment of 41 HCV MCS SVR in100 and clinical CR in 902 Disappearance of CGs in 50 of pts No serious adverse event or relapse ofvasculitis
Antiviral Treatment (AVT) of MCIFN-free regimens
MC is clinically benign but sometimes severe HCV EHD invalidating symptoms occur and
it may evolve into lymphoma
Cacoub P et al DLD 2014 Zignego AL et al DLD 2007 Zignego AL et al Intern Emerg Med 2012 Zignego AL et al Clin Dev
Immunol 2012 Zignego AL et al Expert Rev Clin Immunol 2015 Sene D et al J Rheumatol 2004
Mixed Cryoglobulinemia-MC
MC pathological substrate is an HCV-driven B-cell
proliferation with consequent production of cryo- and non-
cryoprecipitable CICs in turn responsible for vasculitic
manifestations
Most (70ndash90) MC patients are HCV+ and HCV-patients are CGs+ (40ndash60) while 5ndash30 of
CGs+ have symptomatic MC or cryoglobulinemic vasculitis since HCV infects about 170
million individuals worldwide the number of patients at risk for developing MC is
substantial
Type II CGs
monoclonal
RF+policlonal IgG
Type III CGs both
RF and IgG
polyclonal

ISG-EHCV
Ferri C Ramos-Casals M Zignego AL et al Autoimmun Rev 2016
1465
496717
Total Piter cohort no 8005 subjects the presence of MC was never tested in 80 ofcases in spite of its clinical and therapeutical importance Among the centres thatconsidered MC=-64 evaluated cryoglobulinemia only following a clinical suspicion-58 evaluated routinely cryoglobulinemia at admission with Complement RF levels-42 only in case of RF positivity-Cryo testing was not adequate in 39 of centres
252
These results for the first time showed the real-life variability of the MC diagnosticapproach suggesting that MC prevalence in HCV+ is generally underestimated
Kondili et al Liver Intern2017
CLASSIFICATION OF HCV EHDS ACCORDING TO THE STRENGTH OF SPECIFIC DATA SUPPORTING THE CURATIVE EFFECT OF AVT
Mixed Cryoglobulinemia Effectiveness of both IFN-based and IFN-free AVT
Marginal Zone NHL Effectiveness of both IFN- and DAA-based
AVT
Other low-grade B-cell NHL
HRQOL Available data also in DAA-based AVT
High-grade NHL= DLBCL Insufficient but positive data
CKD Sufficient specific data only for MC-CKD
Neuropsychiatric disorders Problematic IFN-based AVT Insufficient
data with DAAs
Curaneous= PCT and LP (OLP) Problematic IFNRBV-based AVT
Insufficient data with DAAs
Endocrinologic Thyroid and DM 2 Insufficient specific data with DAAs
Arthritis Insufficient specific data with DAAs
Zignego et al 2017
Landau DA et al Arthritis Rheum 2008 Montalbano M et al J Clin Gastroenterol 2007 Cacoub P et al Arthritis Rheum 2002
Mazzaro C et alJ Rheumatol 2003 Zignego AL et al Hepatology 2016 Gragnani L et al Hepatology 2015 Pietrogrande M
et al Autoimmun Rev 2011
Antiviral Treatment (AVT) of MC in the IFN Era
AVT of MC followed the evolution of hepatitis C AVT with frequent adjustments
essentially due to the possible side-effects of IFN andor RBV therapy (ie IFN
neurotoxicity and myelo-inhibitory action and RBV hemolytic effects)
Virological and clinical results progressively improved in spite of frequent side-effects
IFN-based AVT was recommended as the first-line option in mild to moderate MC
Clinical remission was generally correlated with virological response
Long follow-up showed that the majority (57) of SVR pts cleared all MC stigmata
Antiviral Treatment (AVT) of MC IFN-free regimensLimited data so-far concordant are available regarding IFN-free AVT in MC patients
Available data suggest that IFN-free AVT is safe generally well tolerated and effective in MC patients high rate of
clinical response (87) and low rates of serious adverse events was reported
Zignego AL Ramos-Casals M Ferri C et al AutoimmunReviews 2017
Antiviral Treatment (AVT) of MC IFN-free regimens
22 MCS treated with DAAs including 2 HCC and 2 NHL 100 SVR12 Clinical R in 100 (64 CR and 36 PR)
Progression of the small lymphocytic lymphoma
Lauletta et al 2017
Emery CS et al 2017
Retrospective analysis 17 MCS (10 with severelife-threatening vasculitis) and 65 asymptomatic MC treated with
DAAs SVR 889 MCS and 908 asymptomatic pts In MCS clinical R in 1117 (CR in 711) Lower clinical R inseverelife-threatening ndashespecial renal and neurological- vasculitis
Saadoun D et al 2017
Open-label prospective multi-center study on sofosbuvir plus daclatasvir treatment of 41 HCV MCS SVR in 100 and
clinical CR in 902 Disappearance of CGs in 50 of pts No serious adverse event or relapse of vasculitis
A case of rapid amelioration of HCV-associated cryoglobulinemic MPGN treated by
IFN-free DAAs for HCV in the absence of immunosuppressant
Fumiaki et al 2017
Zignego et al 2017
TIME POINTS
baseline EOT and week 12 and 24 of post-treatment f-up (SVR12 and SVR24 respectively)
HRQoL EVALUATION THROUGH PROs
the Short Form (36) Health Survey (SF-36)
the Functional Assessment of Chronic Illness Therapy-Fatigue (FACIT-F) from which we computed the Trial
Outcome Index (TOI)
Evaluation of The Impact on HRQol of IFN-free AVT In HCV CM
1 Physical Component Summary Score (PCS)
MC (54)
HCV (43) CV (85)
deg
A B C
degdegdeg
2 Mental Component Summary Score (MCS)
MCHCV CVD E F
degdegdegdegdeg
HCV
=plt001 vs baseline scores
degdeg=plt001 and degdegdeg=plt0001 vs EOT scores
Gragnani et al AASLD 2017
HCV Eradicationwith DAAs
To be preceded or combined with non-etiological pathogenetic therapy in severecatastrophic MCS
MCS Therapy in the IFN and DAAs Era from the complex to the simplified flow-chart
Dammacco F Sansonno D NEJM 2013
Zignego AL Pawlotsky JM Cacoub P Antiviral Ther in press Cacoub P et al Am J Med 2015
Mechanisms of HCV-related lymphomagenesis
DLBC HCV- induced
direct transformation
MCindolent NHL
accumulation of B RF
following BCR activation
and BC apoptosisinhibition
Zignego AL Ramos-Casals M Ferri C et al Autoimmun Rev 2017
Wang et al Hepatology 2016 Canioni et al Plos one 2016
Observational study on in situ expression of the oncogenic HCV NS3 protein on 116 HCV patients with B-NHL (DLBCL 36 and MZL 34)
NS3 immunostaining positive in 1214 DLBCL vs only 414 MZL (p = 0006) moreover 24 NS3+ MZL
were enriched in large cells
This study supports a new mechanism of transformation with a direct oncogenic role of
HCV proteins in the occurrence of high-grade B lymphomas
IN SITU HEPATITIS C NS3 PROTEIN DETECTION IS ASSOCIATED WITH HIGH GRADE
FEATURES IN HCV-ASSOCIATED B-CELL NON-HODGKIN LYMPHOMAS Danielle
Canioni et al 2016
In addition to the role of chronic antigenic stimulation in HCV related
lymphomagenesis this study supports a second mechanism of transformation due to a
direct oncogenic role of HCV infection of B-cells promoting the occurrence of high-grade Bcell lymphomas
Cohort study of 704 consecutive HIV-negative HCV-positive patients with indolent NHL from 1993 to
2009 in 39 centers of the FIL
Arcaini et al 2016
DLBC HCV- induced
direct transformation
No place of AVT as
1st line
Need of immediate delivery of
chemotherapy or concomitant (NHL
+ HCV targets)
THERAPY OF HCV+ DLBCL
ANTIVIRAL THERAPY IS ASSOCIATED WITH A BETTERSURVIVAL IN PATIENTS WITH HCV AND B-CELL NON-HODGKIN LYMPHOMAS ANRS HC-13 LYMPHO-CSTUDY Michot JM et al
Outcomes of HCV-associated B-NHL according to HCV AVT in prospective patients only (n 5 64)
Concurrent Systemic Chemoimmunotherapy and Sofosbuvir-Based Antiviral Treatment in a Hepatitis C Virus-Infected Patient With Diffuse Large B-Cell Lymphoma Evan C Ewers et al 2016
absolute neutrophil count and Hgb ALT and HCV viral load
Both complete response and SVR of HCV-associated DLBCL after concurrent chemoimmunotherapy and antiviral therapy using a sofosbuvir-based regimen
DAA-treatment in concomitance with chemotherapy showed to be safe and effective in influencing the remission of aggressive lymphomas in HCV patients
Persico M et al 2017
DFS in DAA treated and historical not-treated ptsAntiviral response rates in DAA treated patients
ANTIVIRAL THERAPY IN HCV+ B CELL NHL
IFN-based AVT induced hematological response along with SVR in patients with HCV-related indolent NHLs (especially
MZL)
Recent data with IFN-free regimens in HCV-associated LPDs suggest their anti-lymphoma activity too
AVT should be considered the first-line approach in HCV low grade lymphomas if there is no urgency of a conventional
treatment (ie systemic symptoms bulky disease or symptomatic splenomegaly) (ESMO NCCN EASL guidelines)
In aggressive lymphomas antiviral therapy after induction treatment is to be considered the standard at the moment but
in the next years (months) the association of immunochemotherapy and antiviral therapy will be considered the standard
Zignego AL Ramos-Casals M Ferri C et al Autoimmun Rev 2017
The Masve group
BASIC RESEARCH
Laura Gragnani
Patrizio Caini
Serena Lorini
Antonella Simone
CLINICAL RESEARCH
Monica Monti
Luisa Petraccia
Sinan Sadalla
Guia Cerretelli
Cristina Stasi
Adela Xheka
Universitagrave degli Studi di FirenzeDipartimento di Medicina Sperimentale e Clinica
Centro Manifestazioni Sistemiche da Virus EpatiticildquoMASVErdquo
Anna Linda Zignego
MASVE
UNDERGRADUATE STUDENTS Andrea Genovese Adrian Piscopo
ANTIVIRAL THERAPY IN HCV+ B CELL NHL
IFN-based AVT induced hematological response along with SVR in patients with HCV-related indolent
NHLs (especially MZL)
Recent data with IFN-free regimens in HCV-associated LPDs suggest their anti-lymphoma activity too
AVT should be considered the first-line approach in HCV low grade lymphomas if there is no urgency
of a conventional treatment (ie systemic symptoms bulky disease or symptomatic splenomegaly)
(ESMO NCCN EASL guidelines)
Main drugs for HCV-related MCS according to the target
HCV= DAAsB-cell Expansion= (a) B cell-depleting Mabs
-First-generation Rituximab (anti-CD20)-Second-generation Ofatumumab (anti-CD20) Veltuzumab (humanized
anti-CD20)-Third-generation Obinutuzumab (GA101) Oceratuzumab (humanized
anti-CD20)
(b) Alkylating agents
-Cyclophosfamide
Inflammation= Antiinflammatory agents
- Corticosteroids
Altered regulatory T-cell activity=
- IL-2
The impact on HRQoL of IFN-free AVT was prospectively evaluated in a cohort of HCV CV patients with limited
influencing variables linked to therapeutic schedulesviral GT
44 HCV GT2 CV patients mostly F0-F2 (29) and naiumlve (30) treated with SOFRBV for 1224wks
TIME POINTS
baseline EOT and week 12 and 24 of post-treatment f-up (SVR12 and SVR24 respectively)
HRQoL EVALUATION THROUGH PROs
the Short Form (36) Health Survey (SF-36)
the Functional Assessment of Chronic Illness Therapy-Fatigue (FACIT-F) from which we computed the Trial
Outcome Index (TOI)
Observational study on in situ expression of the oncogenic HCV NS3 protein on 116 HCV
patients with B-NHL (DLBCL 36 and MZL 34)
NS3 immunostaining positive in 1214 DLBCL vs only 414 MZL (p = 0006) moreover 24 NS3+
MZL were enriched in large cells
This study supports a new mechanism of transformation with a direct oncogenic role of
HCV proteins in the occurrence of high-grade B lymphomas
IN SITU HEPATITIS C NS3 PROTEIN DETECTION IS ASSOCIATED WITH HIGH GRADEFEATURES IN HCV-ASSOCIATED B-CELL NON-HODGKIN LYMPHOMAS Danielle
Canioni et al 2016
In addition to the role of chronic antigenic stimulation in HCV related
lymphomagenesis this study supports a second mechanism of transformation due toa direct oncogenic role of HCV infection of B-cells promoting the occurrence of high-grade Bcell lymphomas
ANTIVIRAL THERAPY IS ASSOCIATED WITH A BETTERSURVIVAL IN PATIENTS WITH HCV AND B-CELL NON-HODGKIN LYMPHOMAS ANRS HC-13 LYMPHO-CSTUDYMichot JM et al
Outcomes of HCV-associated B-NHL according to HCV AVT in prospective patients only (n 5 64)
(A) absolute neutrophil count and Hgb
(B) ALT and HCV viral load
This patient had HCV-associated DLBCL achieving both complete response and SVR after concurrent chemoimmunotherapy and antiviral therapy using a sofosbuvir-basedregimen
Concurrent Systemic Chemoimmunotherapy and Sofosbuvir-Based Antiviral Treatment in a Hepatitis C Virus-Infected Patient With Diffuse Large B-Cell LymphomaEvan C Ewers et al 2016
HCV-EHDs are responsible for increasing morbidity and mortality with important
consequences in terms of social costs
The analysis of mortality rates in large cohorts confirmed the association of HCV with
several EHDs including cardiovascular neurologic metabolic or renal diseases and tumors
Viral eradication significantly reduced the rate of extra-hepatic deaths
Cacoub P et al DLD 2014 Lee MH et al J Infect Dis 2012 Backus LI et al Clin Gastroenterol Hepatol 2011 El-Kamary S et al
Clin Infect Dis 2011 Hsu YC et al Hepatology 2014 Kawamura Y et al Am J Med 2007 Adinolfi LE et al WJG 2014
Extrahepatic Manifestations of HCV
Con il contributo di
Lee M-H et al J Infect Dis 2012206469-477
Follow-Up
(Years)
20
18
16
14
12
10
2
00 2 4 6 8 10 12 14 16 18 20
8
6
4
Follow-Up
(Years)
12
10
8
6
4
2
00 2 4 6 8 10 12 14 16 18 20
All Causes(n=2394)
Liver Cancer(n=115)
Extrahepatic Diseases(n=2199)
Cum
ula
tive M
ort
ali
ty (
)
Anti-HCV+ HCV RNA detectable Anti-HCV+ HCV RNA undetectable Anti-HCVndash
Follow-Up
(Years)
35
30
25
20
15
10
5
00 2 4 6 8 10 12 14 16 18 20
301
128124
104
16
03
198
122
110
MC is clinically benign but sometimes severe HCV EHD invalidating symptoms occur and
it may evolve into lymphoma
Cacoub P et al DLD 2014 Zignego AL et al DLD 2007 Zignego AL et al Intern Emerg Med 2012 Zignego AL et al Clin Dev
Immunol 2012 Zignego AL et al Expert Rev Clin Immunol 2015 Sene D et al J Rheumatol 2004
Mixed Cryoglobulinemia-MC
CGs reversibly precipitate when the temperature is lower than 37degC and
comprise IgMs with RF activity [mono- or oligo-clonal in type II MC or
polyclonal in type III MC] and polyclonal IgGs
MC pathological substrate is an HCV-driven B-cell
proliferation with consequent production of cryo- and non-
cryoprecipitable CICs in turn responsible for vasculitic
manifestations
Most (70ndash90) MC patients are HCV+ and HCV-patients are CGs+ (40ndash60) while 5ndash30 of
CGs+ have symptomatic MC since HCV infects about 170 million individuals worldwide the
number of patients at risk for developing MC is substantial
Type II
CGs
Type III
CGs
Zignego AL et al Autoimmun Rev 2017 Ferri C et al Autoimmunity rev 2016 Zignego AL et al DLD 2007 Cacoub P et al DLD
2014 Zignego AL et al DLD 2007 Zignego AL et al Intern Emerg Med 2012 Zignego AL et al Clin Dev Immunol 2012 Zignego
AL et al Expert Rev Clin Immunol 2015
MC clinical aspects MC Syndrome
MCS is characterized by the clinical triad -purpura weakness and
arthralgias- low complement C4 and various organsystem
involvement including cutaneous articular renal neurological
cardiac or digestive
It ranges from mild disease to severe even life-threatening
conditions
More serious lesions are generally characterized by neurologic and
renal involvement
Prognosis is highly dependent on renal involvement or on the extent
of vasculitis lesions
1 HCV is the main etiopathological agent as concordantly demonstrated by epidemiological clinico-pathological virological and laboratory investigations2 the association between HCV and disease is demonstrated in a significant proportion of patients and supported by in depth clinico-pathogeneticstudies3 the association is suggested by cohort studies a possible causative role may be limited to a small number of patients andor possibly more relevant in specific geographical areas 4 a number of anecdotal observations suggested a possible role of HCV further investigations are required
From P Cacoub 2015
HCV infection is closely related to LPDs mostly MC
40 to 60 of HCV patients show circulating CGs among this latter population 5-30
develop a symptomatic CV
AVT has been considered the first-line option in HCV-CV patients in fact in the majority
of cases viral eradication leads to CV clinical remission
Data about IFN-free regimens for the treatment of CV patients are still limited
HCV and MC
HCV and MC
Zignego 2015Ferri 2016Pozzato 2016 Sise 2016Saadoun 2015Gragnani 2016Gragnani 2016
Bonacci 2016Hegazy 2016Kondili 2016Emery 2017
Younossi et al
The annual costs (inpatient outpatient andpharmacy) associated with extrahepatic
manifestations of HCV were evaluated
Total direct medical costs of extrahepatic
manifestations of HCV in 2014 US dollars wereestimated to be $1506 million (range $922 millionndash
$2208 million in sensitivity analysis)
These estimates should be added to the liver-related
burden of disease to obtain a more accurateassessment of the total burden of HCV infection
The OBJECTIVE of the study was to estimate the annual direct medical costsassociated with HCV related EHM in the EU5 (France Germany Italy United Kingdom
Spain)
Extrahepatic Manifestations of HCV
Extrahepatic Manifestations of HCV
HCV may cause extrahepatic disorders (HCV-EHDs) classified according to the number and
strength of supporting scientific data
HCV-EHDs are responsible for increasing morbidity and mortality with important
consequences in terms of social costs
The analysis of mortality rates in large cohorts confirmed the association of HCV with
several EHDs including cardiovascular neurologic metabolic or renal diseases and tumors
Viral eradication significantly reduced the rate of extra-hepatic deaths
Cacoub P et al DLD 2014 Lee MH et al J Infect Dis 2012 Backus LI et al Clin Gastroenterol Hepatol 2011 El-Kamary S et al
Clin Infect Dis 2011 Hsu YC et al Hepatology 2014 Kawamura Y et al Am J Med 2007 Adinolfi LE et al WJG 2014
Con il contributo di
Lee M-H et al J Infect Dis 2012206469-477
Follow-Up
(Years)
20
18
16
14
12
10
2
00 2 4 6 8 10 12 14 16 18 20
8
6
4
Follow-Up
(Years)
12
10
8
6
4
2
00 2 4 6 8 10 12 14 16 18 20
All Causes(n=2394)
Liver Cancer(n=115)
Extrahepatic Diseases(n=2199)
Cum
ula
tive M
ort
ali
ty (
)
Anti-HCV+ HCV RNA detectable Anti-HCV+ HCV RNA undetectable Anti-HCVndash
Follow-Up
(Years)
35
30
25
20
15
10
5
00 2 4 6 8 10 12 14 16 18 20
301
128124
104
16
03
198
122
110
Extrahepatic Manifestations of HCV
The annual costs (inpatient outpatient andpharmacy) associated with extrahepatic
manifestations of HCV were evaluated
Total direct medical costs of extrahepatic
manifestations of HCV in 2014 US dollars wereestimated to be $1506 million (range $922 millionndash
$2208 million in sensitivity analysis)
These estimates should be added to the liver-related
burden of disease to obtain a more accurateassessment of the total burden of HCV infection
Younossi et al
Younossi et al
Costs up to $71000 per patient per year (ESRD) Among the most frequent EHM depression (245 in HCV vs 172 in non-HCV) had estimated annual cost of
$4307 million DM (15 vs 10 in non- HCV) had an annual cost of $4434 million in the USA= given the importance of DM and
its association with CVDs and mortality the clinical and economic impacts of HCV-related DM are substantial
The OBJECTIVE of the study was to estimate the annual direct medical costsassociated with HCV related EHM in the EU5 (France Germany Italy United Kingdom
Spain)
The OBJECTIVE of the study was to estimate the annual direct medicalcosts associated with HCV related EHM in the EU5 (France Germany
Italy United Kingdom Spain)
1 HCV is the main etiopathological agent as concordantly demonstrated by epidemiological clinico-pathological virological and laboratory investigations2 the association between HCV and disease is demonstrated in a significant proportion of patients and supported by in depth clinico-pathogeneticstudies3 the association is suggested by cohort studies a possible causative role may be limited to a small number of patients andor possibly more relevant in specific geographical areas 4 a number of anecdotal observations suggested a possible role of HCV further investigations are required
The most studied and frequent HCV-EHDs are B-LPDs andor autoimmune disorders
Their prototype is Mixed Cryoglobulinemia (MC) from researches on MC derived most of the
available information
MC as a precious model for all the HCV-EHDs and to evaluate the effects of viral eradication
Anti-HCV Treatment Evolution
IFN
6 mos
PegIFN RBV 12
mos
IFN
12 mos
IFNRBV
12 mos
PegIFN
12 mos
2001
1998
2011
Standardinterferon
Ribavirin
Peginterferon
1991
Direct-actingantivirals
PegIFN
RBV
DAA
IFNRBV
6 mos
6
16
34
4239
55
70+
0
20
40
60
80
100
DAAs
826
weeks
gt90
2015
Few side effects absence major
contraindications
Younossi et al
The annual costs (inpatient outpatient and pharmacy) associatedwith extrahepatic manifestations of HCV were evaluated
Total direct medical costs of extrahepatic manifestations of HCV in 2014US dollars were estimated to be $1506 million (range $922 millionndash
$2208 million in sensitivity analysis)
These estimates should be added to the liver-related burden of diseaseto obtain a more accurate assessment of the total burden of HCV
infection
The OBJECTIVE of the study was to estimate the annual direct medical costs associated with HCV related EHM in the EU5 (France Germany Italy United Kingdom Spain)
22 MCS treated with DAAs including 2 HCC and 2 NHL 100 SVR12 Clinical CR in 64 and PR in remaining 36 The small lymphocytic lymphoma progressed despite viral clearance
Lauletta et al 2017
Emery CS et al 2017
Retrospective analysis 17 MCS (10 with severelife-threatening vasculitis) and 65 asymptomatic CGs+ pts treated with DAAs SVR 889 MCS and 908 asymptomatic pts In MCS clinical response in 1117 (complete in 717) In severelife-threatening vasculitis lower clinical response especially in renal and neurological symptoms
Saadoun D et al 2017
Open-label prospective multi-center study on sofosbuvir plus daclatasvir treatment of 41 HCV MCS SVR in100 and clinical CR in 902 Disappearance of CGs in 50 of pts No serious adverse event or relapse ofvasculitis
Antiviral Treatment (AVT) of MCIFN-free regimens
MC is clinically benign but sometimes severe HCV EHD invalidating symptoms occur and
it may evolve into lymphoma
Cacoub P et al DLD 2014 Zignego AL et al DLD 2007 Zignego AL et al Intern Emerg Med 2012 Zignego AL et al Clin Dev
Immunol 2012 Zignego AL et al Expert Rev Clin Immunol 2015 Sene D et al J Rheumatol 2004
Mixed Cryoglobulinemia-MC
MC pathological substrate is an HCV-driven B-cell
proliferation with consequent production of cryo- and non-
cryoprecipitable CICs in turn responsible for vasculitic
manifestations
Most (70ndash90) MC patients are HCV+ and HCV-patients are CGs+ (40ndash60) while 5ndash30 of
CGs+ have symptomatic MC or cryoglobulinemic vasculitis since HCV infects about 170
million individuals worldwide the number of patients at risk for developing MC is
substantial
Type II CGs
monoclonal
RF+policlonal IgG
Type III CGs both
RF and IgG
polyclonal

1465
496717
Total Piter cohort no 8005 subjects the presence of MC was never tested in 80 ofcases in spite of its clinical and therapeutical importance Among the centres thatconsidered MC=-64 evaluated cryoglobulinemia only following a clinical suspicion-58 evaluated routinely cryoglobulinemia at admission with Complement RF levels-42 only in case of RF positivity-Cryo testing was not adequate in 39 of centres
252
These results for the first time showed the real-life variability of the MC diagnosticapproach suggesting that MC prevalence in HCV+ is generally underestimated
Kondili et al Liver Intern2017
CLASSIFICATION OF HCV EHDS ACCORDING TO THE STRENGTH OF SPECIFIC DATA SUPPORTING THE CURATIVE EFFECT OF AVT
Mixed Cryoglobulinemia Effectiveness of both IFN-based and IFN-free AVT
Marginal Zone NHL Effectiveness of both IFN- and DAA-based
AVT
Other low-grade B-cell NHL
HRQOL Available data also in DAA-based AVT
High-grade NHL= DLBCL Insufficient but positive data
CKD Sufficient specific data only for MC-CKD
Neuropsychiatric disorders Problematic IFN-based AVT Insufficient
data with DAAs
Curaneous= PCT and LP (OLP) Problematic IFNRBV-based AVT
Insufficient data with DAAs
Endocrinologic Thyroid and DM 2 Insufficient specific data with DAAs
Arthritis Insufficient specific data with DAAs
Zignego et al 2017
Landau DA et al Arthritis Rheum 2008 Montalbano M et al J Clin Gastroenterol 2007 Cacoub P et al Arthritis Rheum 2002
Mazzaro C et alJ Rheumatol 2003 Zignego AL et al Hepatology 2016 Gragnani L et al Hepatology 2015 Pietrogrande M
et al Autoimmun Rev 2011
Antiviral Treatment (AVT) of MC in the IFN Era
AVT of MC followed the evolution of hepatitis C AVT with frequent adjustments
essentially due to the possible side-effects of IFN andor RBV therapy (ie IFN
neurotoxicity and myelo-inhibitory action and RBV hemolytic effects)
Virological and clinical results progressively improved in spite of frequent side-effects
IFN-based AVT was recommended as the first-line option in mild to moderate MC
Clinical remission was generally correlated with virological response
Long follow-up showed that the majority (57) of SVR pts cleared all MC stigmata
Antiviral Treatment (AVT) of MC IFN-free regimensLimited data so-far concordant are available regarding IFN-free AVT in MC patients
Available data suggest that IFN-free AVT is safe generally well tolerated and effective in MC patients high rate of
clinical response (87) and low rates of serious adverse events was reported
Zignego AL Ramos-Casals M Ferri C et al AutoimmunReviews 2017
Antiviral Treatment (AVT) of MC IFN-free regimens
22 MCS treated with DAAs including 2 HCC and 2 NHL 100 SVR12 Clinical R in 100 (64 CR and 36 PR)
Progression of the small lymphocytic lymphoma
Lauletta et al 2017
Emery CS et al 2017
Retrospective analysis 17 MCS (10 with severelife-threatening vasculitis) and 65 asymptomatic MC treated with
DAAs SVR 889 MCS and 908 asymptomatic pts In MCS clinical R in 1117 (CR in 711) Lower clinical R inseverelife-threatening ndashespecial renal and neurological- vasculitis
Saadoun D et al 2017
Open-label prospective multi-center study on sofosbuvir plus daclatasvir treatment of 41 HCV MCS SVR in 100 and
clinical CR in 902 Disappearance of CGs in 50 of pts No serious adverse event or relapse of vasculitis
A case of rapid amelioration of HCV-associated cryoglobulinemic MPGN treated by
IFN-free DAAs for HCV in the absence of immunosuppressant
Fumiaki et al 2017
Zignego et al 2017
TIME POINTS
baseline EOT and week 12 and 24 of post-treatment f-up (SVR12 and SVR24 respectively)
HRQoL EVALUATION THROUGH PROs
the Short Form (36) Health Survey (SF-36)
the Functional Assessment of Chronic Illness Therapy-Fatigue (FACIT-F) from which we computed the Trial
Outcome Index (TOI)
Evaluation of The Impact on HRQol of IFN-free AVT In HCV CM
1 Physical Component Summary Score (PCS)
MC (54)
HCV (43) CV (85)
deg
A B C
degdegdeg
2 Mental Component Summary Score (MCS)
MCHCV CVD E F
degdegdegdegdeg
HCV
=plt001 vs baseline scores
degdeg=plt001 and degdegdeg=plt0001 vs EOT scores
Gragnani et al AASLD 2017
HCV Eradicationwith DAAs
To be preceded or combined with non-etiological pathogenetic therapy in severecatastrophic MCS
MCS Therapy in the IFN and DAAs Era from the complex to the simplified flow-chart
Dammacco F Sansonno D NEJM 2013
Zignego AL Pawlotsky JM Cacoub P Antiviral Ther in press Cacoub P et al Am J Med 2015
Mechanisms of HCV-related lymphomagenesis
DLBC HCV- induced
direct transformation
MCindolent NHL
accumulation of B RF
following BCR activation
and BC apoptosisinhibition
Zignego AL Ramos-Casals M Ferri C et al Autoimmun Rev 2017
Wang et al Hepatology 2016 Canioni et al Plos one 2016
Observational study on in situ expression of the oncogenic HCV NS3 protein on 116 HCV patients with B-NHL (DLBCL 36 and MZL 34)
NS3 immunostaining positive in 1214 DLBCL vs only 414 MZL (p = 0006) moreover 24 NS3+ MZL
were enriched in large cells
This study supports a new mechanism of transformation with a direct oncogenic role of
HCV proteins in the occurrence of high-grade B lymphomas
IN SITU HEPATITIS C NS3 PROTEIN DETECTION IS ASSOCIATED WITH HIGH GRADE
FEATURES IN HCV-ASSOCIATED B-CELL NON-HODGKIN LYMPHOMAS Danielle
Canioni et al 2016
In addition to the role of chronic antigenic stimulation in HCV related
lymphomagenesis this study supports a second mechanism of transformation due to a
direct oncogenic role of HCV infection of B-cells promoting the occurrence of high-grade Bcell lymphomas
Cohort study of 704 consecutive HIV-negative HCV-positive patients with indolent NHL from 1993 to
2009 in 39 centers of the FIL
Arcaini et al 2016
DLBC HCV- induced
direct transformation
No place of AVT as
1st line
Need of immediate delivery of
chemotherapy or concomitant (NHL
+ HCV targets)
THERAPY OF HCV+ DLBCL
ANTIVIRAL THERAPY IS ASSOCIATED WITH A BETTERSURVIVAL IN PATIENTS WITH HCV AND B-CELL NON-HODGKIN LYMPHOMAS ANRS HC-13 LYMPHO-CSTUDY Michot JM et al
Outcomes of HCV-associated B-NHL according to HCV AVT in prospective patients only (n 5 64)
Concurrent Systemic Chemoimmunotherapy and Sofosbuvir-Based Antiviral Treatment in a Hepatitis C Virus-Infected Patient With Diffuse Large B-Cell Lymphoma Evan C Ewers et al 2016
absolute neutrophil count and Hgb ALT and HCV viral load
Both complete response and SVR of HCV-associated DLBCL after concurrent chemoimmunotherapy and antiviral therapy using a sofosbuvir-based regimen
DAA-treatment in concomitance with chemotherapy showed to be safe and effective in influencing the remission of aggressive lymphomas in HCV patients
Persico M et al 2017
DFS in DAA treated and historical not-treated ptsAntiviral response rates in DAA treated patients
ANTIVIRAL THERAPY IN HCV+ B CELL NHL
IFN-based AVT induced hematological response along with SVR in patients with HCV-related indolent NHLs (especially
MZL)
Recent data with IFN-free regimens in HCV-associated LPDs suggest their anti-lymphoma activity too
AVT should be considered the first-line approach in HCV low grade lymphomas if there is no urgency of a conventional
treatment (ie systemic symptoms bulky disease or symptomatic splenomegaly) (ESMO NCCN EASL guidelines)
In aggressive lymphomas antiviral therapy after induction treatment is to be considered the standard at the moment but
in the next years (months) the association of immunochemotherapy and antiviral therapy will be considered the standard
Zignego AL Ramos-Casals M Ferri C et al Autoimmun Rev 2017
The Masve group
BASIC RESEARCH
Laura Gragnani
Patrizio Caini
Serena Lorini
Antonella Simone
CLINICAL RESEARCH
Monica Monti
Luisa Petraccia
Sinan Sadalla
Guia Cerretelli
Cristina Stasi
Adela Xheka
Universitagrave degli Studi di FirenzeDipartimento di Medicina Sperimentale e Clinica
Centro Manifestazioni Sistemiche da Virus EpatiticildquoMASVErdquo
Anna Linda Zignego
MASVE
UNDERGRADUATE STUDENTS Andrea Genovese Adrian Piscopo
ANTIVIRAL THERAPY IN HCV+ B CELL NHL
IFN-based AVT induced hematological response along with SVR in patients with HCV-related indolent
NHLs (especially MZL)
Recent data with IFN-free regimens in HCV-associated LPDs suggest their anti-lymphoma activity too
AVT should be considered the first-line approach in HCV low grade lymphomas if there is no urgency
of a conventional treatment (ie systemic symptoms bulky disease or symptomatic splenomegaly)
(ESMO NCCN EASL guidelines)
Main drugs for HCV-related MCS according to the target
HCV= DAAsB-cell Expansion= (a) B cell-depleting Mabs
-First-generation Rituximab (anti-CD20)-Second-generation Ofatumumab (anti-CD20) Veltuzumab (humanized
anti-CD20)-Third-generation Obinutuzumab (GA101) Oceratuzumab (humanized
anti-CD20)
(b) Alkylating agents
-Cyclophosfamide
Inflammation= Antiinflammatory agents
- Corticosteroids
Altered regulatory T-cell activity=
- IL-2
The impact on HRQoL of IFN-free AVT was prospectively evaluated in a cohort of HCV CV patients with limited
influencing variables linked to therapeutic schedulesviral GT
44 HCV GT2 CV patients mostly F0-F2 (29) and naiumlve (30) treated with SOFRBV for 1224wks
TIME POINTS
baseline EOT and week 12 and 24 of post-treatment f-up (SVR12 and SVR24 respectively)
HRQoL EVALUATION THROUGH PROs
the Short Form (36) Health Survey (SF-36)
the Functional Assessment of Chronic Illness Therapy-Fatigue (FACIT-F) from which we computed the Trial
Outcome Index (TOI)
Observational study on in situ expression of the oncogenic HCV NS3 protein on 116 HCV
patients with B-NHL (DLBCL 36 and MZL 34)
NS3 immunostaining positive in 1214 DLBCL vs only 414 MZL (p = 0006) moreover 24 NS3+
MZL were enriched in large cells
This study supports a new mechanism of transformation with a direct oncogenic role of
HCV proteins in the occurrence of high-grade B lymphomas
IN SITU HEPATITIS C NS3 PROTEIN DETECTION IS ASSOCIATED WITH HIGH GRADEFEATURES IN HCV-ASSOCIATED B-CELL NON-HODGKIN LYMPHOMAS Danielle
Canioni et al 2016
In addition to the role of chronic antigenic stimulation in HCV related
lymphomagenesis this study supports a second mechanism of transformation due toa direct oncogenic role of HCV infection of B-cells promoting the occurrence of high-grade Bcell lymphomas
ANTIVIRAL THERAPY IS ASSOCIATED WITH A BETTERSURVIVAL IN PATIENTS WITH HCV AND B-CELL NON-HODGKIN LYMPHOMAS ANRS HC-13 LYMPHO-CSTUDYMichot JM et al
Outcomes of HCV-associated B-NHL according to HCV AVT in prospective patients only (n 5 64)
(A) absolute neutrophil count and Hgb
(B) ALT and HCV viral load
This patient had HCV-associated DLBCL achieving both complete response and SVR after concurrent chemoimmunotherapy and antiviral therapy using a sofosbuvir-basedregimen
Concurrent Systemic Chemoimmunotherapy and Sofosbuvir-Based Antiviral Treatment in a Hepatitis C Virus-Infected Patient With Diffuse Large B-Cell LymphomaEvan C Ewers et al 2016
HCV-EHDs are responsible for increasing morbidity and mortality with important
consequences in terms of social costs
The analysis of mortality rates in large cohorts confirmed the association of HCV with
several EHDs including cardiovascular neurologic metabolic or renal diseases and tumors
Viral eradication significantly reduced the rate of extra-hepatic deaths
Cacoub P et al DLD 2014 Lee MH et al J Infect Dis 2012 Backus LI et al Clin Gastroenterol Hepatol 2011 El-Kamary S et al
Clin Infect Dis 2011 Hsu YC et al Hepatology 2014 Kawamura Y et al Am J Med 2007 Adinolfi LE et al WJG 2014
Extrahepatic Manifestations of HCV
Con il contributo di
Lee M-H et al J Infect Dis 2012206469-477
Follow-Up
(Years)
20
18
16
14
12
10
2
00 2 4 6 8 10 12 14 16 18 20
8
6
4
Follow-Up
(Years)
12
10
8
6
4
2
00 2 4 6 8 10 12 14 16 18 20
All Causes(n=2394)
Liver Cancer(n=115)
Extrahepatic Diseases(n=2199)
Cum
ula
tive M
ort
ali
ty (
)
Anti-HCV+ HCV RNA detectable Anti-HCV+ HCV RNA undetectable Anti-HCVndash
Follow-Up
(Years)
35
30
25
20
15
10
5
00 2 4 6 8 10 12 14 16 18 20
301
128124
104
16
03
198
122
110
MC is clinically benign but sometimes severe HCV EHD invalidating symptoms occur and
it may evolve into lymphoma
Cacoub P et al DLD 2014 Zignego AL et al DLD 2007 Zignego AL et al Intern Emerg Med 2012 Zignego AL et al Clin Dev
Immunol 2012 Zignego AL et al Expert Rev Clin Immunol 2015 Sene D et al J Rheumatol 2004
Mixed Cryoglobulinemia-MC
CGs reversibly precipitate when the temperature is lower than 37degC and
comprise IgMs with RF activity [mono- or oligo-clonal in type II MC or
polyclonal in type III MC] and polyclonal IgGs
MC pathological substrate is an HCV-driven B-cell
proliferation with consequent production of cryo- and non-
cryoprecipitable CICs in turn responsible for vasculitic
manifestations
Most (70ndash90) MC patients are HCV+ and HCV-patients are CGs+ (40ndash60) while 5ndash30 of
CGs+ have symptomatic MC since HCV infects about 170 million individuals worldwide the
number of patients at risk for developing MC is substantial
Type II
CGs
Type III
CGs
Zignego AL et al Autoimmun Rev 2017 Ferri C et al Autoimmunity rev 2016 Zignego AL et al DLD 2007 Cacoub P et al DLD
2014 Zignego AL et al DLD 2007 Zignego AL et al Intern Emerg Med 2012 Zignego AL et al Clin Dev Immunol 2012 Zignego
AL et al Expert Rev Clin Immunol 2015
MC clinical aspects MC Syndrome
MCS is characterized by the clinical triad -purpura weakness and
arthralgias- low complement C4 and various organsystem
involvement including cutaneous articular renal neurological
cardiac or digestive
It ranges from mild disease to severe even life-threatening
conditions
More serious lesions are generally characterized by neurologic and
renal involvement
Prognosis is highly dependent on renal involvement or on the extent
of vasculitis lesions
1 HCV is the main etiopathological agent as concordantly demonstrated by epidemiological clinico-pathological virological and laboratory investigations2 the association between HCV and disease is demonstrated in a significant proportion of patients and supported by in depth clinico-pathogeneticstudies3 the association is suggested by cohort studies a possible causative role may be limited to a small number of patients andor possibly more relevant in specific geographical areas 4 a number of anecdotal observations suggested a possible role of HCV further investigations are required
From P Cacoub 2015
HCV infection is closely related to LPDs mostly MC
40 to 60 of HCV patients show circulating CGs among this latter population 5-30
develop a symptomatic CV
AVT has been considered the first-line option in HCV-CV patients in fact in the majority
of cases viral eradication leads to CV clinical remission
Data about IFN-free regimens for the treatment of CV patients are still limited
HCV and MC
HCV and MC
Zignego 2015Ferri 2016Pozzato 2016 Sise 2016Saadoun 2015Gragnani 2016Gragnani 2016
Bonacci 2016Hegazy 2016Kondili 2016Emery 2017
Younossi et al
The annual costs (inpatient outpatient andpharmacy) associated with extrahepatic
manifestations of HCV were evaluated
Total direct medical costs of extrahepatic
manifestations of HCV in 2014 US dollars wereestimated to be $1506 million (range $922 millionndash
$2208 million in sensitivity analysis)
These estimates should be added to the liver-related
burden of disease to obtain a more accurateassessment of the total burden of HCV infection
The OBJECTIVE of the study was to estimate the annual direct medical costsassociated with HCV related EHM in the EU5 (France Germany Italy United Kingdom
Spain)
Extrahepatic Manifestations of HCV
Extrahepatic Manifestations of HCV
HCV may cause extrahepatic disorders (HCV-EHDs) classified according to the number and
strength of supporting scientific data
HCV-EHDs are responsible for increasing morbidity and mortality with important
consequences in terms of social costs
The analysis of mortality rates in large cohorts confirmed the association of HCV with
several EHDs including cardiovascular neurologic metabolic or renal diseases and tumors
Viral eradication significantly reduced the rate of extra-hepatic deaths
Cacoub P et al DLD 2014 Lee MH et al J Infect Dis 2012 Backus LI et al Clin Gastroenterol Hepatol 2011 El-Kamary S et al
Clin Infect Dis 2011 Hsu YC et al Hepatology 2014 Kawamura Y et al Am J Med 2007 Adinolfi LE et al WJG 2014
Con il contributo di
Lee M-H et al J Infect Dis 2012206469-477
Follow-Up
(Years)
20
18
16
14
12
10
2
00 2 4 6 8 10 12 14 16 18 20
8
6
4
Follow-Up
(Years)
12
10
8
6
4
2
00 2 4 6 8 10 12 14 16 18 20
All Causes(n=2394)
Liver Cancer(n=115)
Extrahepatic Diseases(n=2199)
Cum
ula
tive M
ort
ali
ty (
)
Anti-HCV+ HCV RNA detectable Anti-HCV+ HCV RNA undetectable Anti-HCVndash
Follow-Up
(Years)
35
30
25
20
15
10
5
00 2 4 6 8 10 12 14 16 18 20
301
128124
104
16
03
198
122
110
Extrahepatic Manifestations of HCV
The annual costs (inpatient outpatient andpharmacy) associated with extrahepatic
manifestations of HCV were evaluated
Total direct medical costs of extrahepatic
manifestations of HCV in 2014 US dollars wereestimated to be $1506 million (range $922 millionndash
$2208 million in sensitivity analysis)
These estimates should be added to the liver-related
burden of disease to obtain a more accurateassessment of the total burden of HCV infection
Younossi et al
Younossi et al
Costs up to $71000 per patient per year (ESRD) Among the most frequent EHM depression (245 in HCV vs 172 in non-HCV) had estimated annual cost of
$4307 million DM (15 vs 10 in non- HCV) had an annual cost of $4434 million in the USA= given the importance of DM and
its association with CVDs and mortality the clinical and economic impacts of HCV-related DM are substantial
The OBJECTIVE of the study was to estimate the annual direct medical costsassociated with HCV related EHM in the EU5 (France Germany Italy United Kingdom
Spain)
The OBJECTIVE of the study was to estimate the annual direct medicalcosts associated with HCV related EHM in the EU5 (France Germany
Italy United Kingdom Spain)
1 HCV is the main etiopathological agent as concordantly demonstrated by epidemiological clinico-pathological virological and laboratory investigations2 the association between HCV and disease is demonstrated in a significant proportion of patients and supported by in depth clinico-pathogeneticstudies3 the association is suggested by cohort studies a possible causative role may be limited to a small number of patients andor possibly more relevant in specific geographical areas 4 a number of anecdotal observations suggested a possible role of HCV further investigations are required
The most studied and frequent HCV-EHDs are B-LPDs andor autoimmune disorders
Their prototype is Mixed Cryoglobulinemia (MC) from researches on MC derived most of the
available information
MC as a precious model for all the HCV-EHDs and to evaluate the effects of viral eradication
Anti-HCV Treatment Evolution
IFN
6 mos
PegIFN RBV 12
mos
IFN
12 mos
IFNRBV
12 mos
PegIFN
12 mos
2001
1998
2011
Standardinterferon
Ribavirin
Peginterferon
1991
Direct-actingantivirals
PegIFN
RBV
DAA
IFNRBV
6 mos
6
16
34
4239
55
70+
0
20
40
60
80
100
DAAs
826
weeks
gt90
2015
Few side effects absence major
contraindications
Younossi et al
The annual costs (inpatient outpatient and pharmacy) associatedwith extrahepatic manifestations of HCV were evaluated
Total direct medical costs of extrahepatic manifestations of HCV in 2014US dollars were estimated to be $1506 million (range $922 millionndash
$2208 million in sensitivity analysis)
These estimates should be added to the liver-related burden of diseaseto obtain a more accurate assessment of the total burden of HCV
infection
The OBJECTIVE of the study was to estimate the annual direct medical costs associated with HCV related EHM in the EU5 (France Germany Italy United Kingdom Spain)
22 MCS treated with DAAs including 2 HCC and 2 NHL 100 SVR12 Clinical CR in 64 and PR in remaining 36 The small lymphocytic lymphoma progressed despite viral clearance
Lauletta et al 2017
Emery CS et al 2017
Retrospective analysis 17 MCS (10 with severelife-threatening vasculitis) and 65 asymptomatic CGs+ pts treated with DAAs SVR 889 MCS and 908 asymptomatic pts In MCS clinical response in 1117 (complete in 717) In severelife-threatening vasculitis lower clinical response especially in renal and neurological symptoms
Saadoun D et al 2017
Open-label prospective multi-center study on sofosbuvir plus daclatasvir treatment of 41 HCV MCS SVR in100 and clinical CR in 902 Disappearance of CGs in 50 of pts No serious adverse event or relapse ofvasculitis
Antiviral Treatment (AVT) of MCIFN-free regimens
MC is clinically benign but sometimes severe HCV EHD invalidating symptoms occur and
it may evolve into lymphoma
Cacoub P et al DLD 2014 Zignego AL et al DLD 2007 Zignego AL et al Intern Emerg Med 2012 Zignego AL et al Clin Dev
Immunol 2012 Zignego AL et al Expert Rev Clin Immunol 2015 Sene D et al J Rheumatol 2004
Mixed Cryoglobulinemia-MC
MC pathological substrate is an HCV-driven B-cell
proliferation with consequent production of cryo- and non-
cryoprecipitable CICs in turn responsible for vasculitic
manifestations
Most (70ndash90) MC patients are HCV+ and HCV-patients are CGs+ (40ndash60) while 5ndash30 of
CGs+ have symptomatic MC or cryoglobulinemic vasculitis since HCV infects about 170
million individuals worldwide the number of patients at risk for developing MC is
substantial
Type II CGs
monoclonal
RF+policlonal IgG
Type III CGs both
RF and IgG
polyclonal

CLASSIFICATION OF HCV EHDS ACCORDING TO THE STRENGTH OF SPECIFIC DATA SUPPORTING THE CURATIVE EFFECT OF AVT
Mixed Cryoglobulinemia Effectiveness of both IFN-based and IFN-free AVT
Marginal Zone NHL Effectiveness of both IFN- and DAA-based
AVT
Other low-grade B-cell NHL
HRQOL Available data also in DAA-based AVT
High-grade NHL= DLBCL Insufficient but positive data
CKD Sufficient specific data only for MC-CKD
Neuropsychiatric disorders Problematic IFN-based AVT Insufficient
data with DAAs
Curaneous= PCT and LP (OLP) Problematic IFNRBV-based AVT
Insufficient data with DAAs
Endocrinologic Thyroid and DM 2 Insufficient specific data with DAAs
Arthritis Insufficient specific data with DAAs
Zignego et al 2017
Landau DA et al Arthritis Rheum 2008 Montalbano M et al J Clin Gastroenterol 2007 Cacoub P et al Arthritis Rheum 2002
Mazzaro C et alJ Rheumatol 2003 Zignego AL et al Hepatology 2016 Gragnani L et al Hepatology 2015 Pietrogrande M
et al Autoimmun Rev 2011
Antiviral Treatment (AVT) of MC in the IFN Era
AVT of MC followed the evolution of hepatitis C AVT with frequent adjustments
essentially due to the possible side-effects of IFN andor RBV therapy (ie IFN
neurotoxicity and myelo-inhibitory action and RBV hemolytic effects)
Virological and clinical results progressively improved in spite of frequent side-effects
IFN-based AVT was recommended as the first-line option in mild to moderate MC
Clinical remission was generally correlated with virological response
Long follow-up showed that the majority (57) of SVR pts cleared all MC stigmata
Antiviral Treatment (AVT) of MC IFN-free regimensLimited data so-far concordant are available regarding IFN-free AVT in MC patients
Available data suggest that IFN-free AVT is safe generally well tolerated and effective in MC patients high rate of
clinical response (87) and low rates of serious adverse events was reported
Zignego AL Ramos-Casals M Ferri C et al AutoimmunReviews 2017
Antiviral Treatment (AVT) of MC IFN-free regimens
22 MCS treated with DAAs including 2 HCC and 2 NHL 100 SVR12 Clinical R in 100 (64 CR and 36 PR)
Progression of the small lymphocytic lymphoma
Lauletta et al 2017
Emery CS et al 2017
Retrospective analysis 17 MCS (10 with severelife-threatening vasculitis) and 65 asymptomatic MC treated with
DAAs SVR 889 MCS and 908 asymptomatic pts In MCS clinical R in 1117 (CR in 711) Lower clinical R inseverelife-threatening ndashespecial renal and neurological- vasculitis
Saadoun D et al 2017
Open-label prospective multi-center study on sofosbuvir plus daclatasvir treatment of 41 HCV MCS SVR in 100 and
clinical CR in 902 Disappearance of CGs in 50 of pts No serious adverse event or relapse of vasculitis
A case of rapid amelioration of HCV-associated cryoglobulinemic MPGN treated by
IFN-free DAAs for HCV in the absence of immunosuppressant
Fumiaki et al 2017
Zignego et al 2017
TIME POINTS
baseline EOT and week 12 and 24 of post-treatment f-up (SVR12 and SVR24 respectively)
HRQoL EVALUATION THROUGH PROs
the Short Form (36) Health Survey (SF-36)
the Functional Assessment of Chronic Illness Therapy-Fatigue (FACIT-F) from which we computed the Trial
Outcome Index (TOI)
Evaluation of The Impact on HRQol of IFN-free AVT In HCV CM
1 Physical Component Summary Score (PCS)
MC (54)
HCV (43) CV (85)
deg
A B C
degdegdeg
2 Mental Component Summary Score (MCS)
MCHCV CVD E F
degdegdegdegdeg
HCV
=plt001 vs baseline scores
degdeg=plt001 and degdegdeg=plt0001 vs EOT scores
Gragnani et al AASLD 2017
HCV Eradicationwith DAAs
To be preceded or combined with non-etiological pathogenetic therapy in severecatastrophic MCS
MCS Therapy in the IFN and DAAs Era from the complex to the simplified flow-chart
Dammacco F Sansonno D NEJM 2013
Zignego AL Pawlotsky JM Cacoub P Antiviral Ther in press Cacoub P et al Am J Med 2015
Mechanisms of HCV-related lymphomagenesis
DLBC HCV- induced
direct transformation
MCindolent NHL
accumulation of B RF
following BCR activation
and BC apoptosisinhibition
Zignego AL Ramos-Casals M Ferri C et al Autoimmun Rev 2017
Wang et al Hepatology 2016 Canioni et al Plos one 2016
Observational study on in situ expression of the oncogenic HCV NS3 protein on 116 HCV patients with B-NHL (DLBCL 36 and MZL 34)
NS3 immunostaining positive in 1214 DLBCL vs only 414 MZL (p = 0006) moreover 24 NS3+ MZL
were enriched in large cells
This study supports a new mechanism of transformation with a direct oncogenic role of
HCV proteins in the occurrence of high-grade B lymphomas
IN SITU HEPATITIS C NS3 PROTEIN DETECTION IS ASSOCIATED WITH HIGH GRADE
FEATURES IN HCV-ASSOCIATED B-CELL NON-HODGKIN LYMPHOMAS Danielle
Canioni et al 2016
In addition to the role of chronic antigenic stimulation in HCV related
lymphomagenesis this study supports a second mechanism of transformation due to a
direct oncogenic role of HCV infection of B-cells promoting the occurrence of high-grade Bcell lymphomas
Cohort study of 704 consecutive HIV-negative HCV-positive patients with indolent NHL from 1993 to
2009 in 39 centers of the FIL
Arcaini et al 2016
DLBC HCV- induced
direct transformation
No place of AVT as
1st line
Need of immediate delivery of
chemotherapy or concomitant (NHL
+ HCV targets)
THERAPY OF HCV+ DLBCL
ANTIVIRAL THERAPY IS ASSOCIATED WITH A BETTERSURVIVAL IN PATIENTS WITH HCV AND B-CELL NON-HODGKIN LYMPHOMAS ANRS HC-13 LYMPHO-CSTUDY Michot JM et al
Outcomes of HCV-associated B-NHL according to HCV AVT in prospective patients only (n 5 64)
Concurrent Systemic Chemoimmunotherapy and Sofosbuvir-Based Antiviral Treatment in a Hepatitis C Virus-Infected Patient With Diffuse Large B-Cell Lymphoma Evan C Ewers et al 2016
absolute neutrophil count and Hgb ALT and HCV viral load
Both complete response and SVR of HCV-associated DLBCL after concurrent chemoimmunotherapy and antiviral therapy using a sofosbuvir-based regimen
DAA-treatment in concomitance with chemotherapy showed to be safe and effective in influencing the remission of aggressive lymphomas in HCV patients
Persico M et al 2017
DFS in DAA treated and historical not-treated ptsAntiviral response rates in DAA treated patients
ANTIVIRAL THERAPY IN HCV+ B CELL NHL
IFN-based AVT induced hematological response along with SVR in patients with HCV-related indolent NHLs (especially
MZL)
Recent data with IFN-free regimens in HCV-associated LPDs suggest their anti-lymphoma activity too
AVT should be considered the first-line approach in HCV low grade lymphomas if there is no urgency of a conventional
treatment (ie systemic symptoms bulky disease or symptomatic splenomegaly) (ESMO NCCN EASL guidelines)
In aggressive lymphomas antiviral therapy after induction treatment is to be considered the standard at the moment but
in the next years (months) the association of immunochemotherapy and antiviral therapy will be considered the standard
Zignego AL Ramos-Casals M Ferri C et al Autoimmun Rev 2017
The Masve group
BASIC RESEARCH
Laura Gragnani
Patrizio Caini
Serena Lorini
Antonella Simone
CLINICAL RESEARCH
Monica Monti
Luisa Petraccia
Sinan Sadalla
Guia Cerretelli
Cristina Stasi
Adela Xheka
Universitagrave degli Studi di FirenzeDipartimento di Medicina Sperimentale e Clinica
Centro Manifestazioni Sistemiche da Virus EpatiticildquoMASVErdquo
Anna Linda Zignego
MASVE
UNDERGRADUATE STUDENTS Andrea Genovese Adrian Piscopo
ANTIVIRAL THERAPY IN HCV+ B CELL NHL
IFN-based AVT induced hematological response along with SVR in patients with HCV-related indolent
NHLs (especially MZL)
Recent data with IFN-free regimens in HCV-associated LPDs suggest their anti-lymphoma activity too
AVT should be considered the first-line approach in HCV low grade lymphomas if there is no urgency
of a conventional treatment (ie systemic symptoms bulky disease or symptomatic splenomegaly)
(ESMO NCCN EASL guidelines)
Main drugs for HCV-related MCS according to the target
HCV= DAAsB-cell Expansion= (a) B cell-depleting Mabs
-First-generation Rituximab (anti-CD20)-Second-generation Ofatumumab (anti-CD20) Veltuzumab (humanized
anti-CD20)-Third-generation Obinutuzumab (GA101) Oceratuzumab (humanized
anti-CD20)
(b) Alkylating agents
-Cyclophosfamide
Inflammation= Antiinflammatory agents
- Corticosteroids
Altered regulatory T-cell activity=
- IL-2
The impact on HRQoL of IFN-free AVT was prospectively evaluated in a cohort of HCV CV patients with limited
influencing variables linked to therapeutic schedulesviral GT
44 HCV GT2 CV patients mostly F0-F2 (29) and naiumlve (30) treated with SOFRBV for 1224wks
TIME POINTS
baseline EOT and week 12 and 24 of post-treatment f-up (SVR12 and SVR24 respectively)
HRQoL EVALUATION THROUGH PROs
the Short Form (36) Health Survey (SF-36)
the Functional Assessment of Chronic Illness Therapy-Fatigue (FACIT-F) from which we computed the Trial
Outcome Index (TOI)
Observational study on in situ expression of the oncogenic HCV NS3 protein on 116 HCV
patients with B-NHL (DLBCL 36 and MZL 34)
NS3 immunostaining positive in 1214 DLBCL vs only 414 MZL (p = 0006) moreover 24 NS3+
MZL were enriched in large cells
This study supports a new mechanism of transformation with a direct oncogenic role of
HCV proteins in the occurrence of high-grade B lymphomas
IN SITU HEPATITIS C NS3 PROTEIN DETECTION IS ASSOCIATED WITH HIGH GRADEFEATURES IN HCV-ASSOCIATED B-CELL NON-HODGKIN LYMPHOMAS Danielle
Canioni et al 2016
In addition to the role of chronic antigenic stimulation in HCV related
lymphomagenesis this study supports a second mechanism of transformation due toa direct oncogenic role of HCV infection of B-cells promoting the occurrence of high-grade Bcell lymphomas
ANTIVIRAL THERAPY IS ASSOCIATED WITH A BETTERSURVIVAL IN PATIENTS WITH HCV AND B-CELL NON-HODGKIN LYMPHOMAS ANRS HC-13 LYMPHO-CSTUDYMichot JM et al
Outcomes of HCV-associated B-NHL according to HCV AVT in prospective patients only (n 5 64)
(A) absolute neutrophil count and Hgb
(B) ALT and HCV viral load
This patient had HCV-associated DLBCL achieving both complete response and SVR after concurrent chemoimmunotherapy and antiviral therapy using a sofosbuvir-basedregimen
Concurrent Systemic Chemoimmunotherapy and Sofosbuvir-Based Antiviral Treatment in a Hepatitis C Virus-Infected Patient With Diffuse Large B-Cell LymphomaEvan C Ewers et al 2016
HCV-EHDs are responsible for increasing morbidity and mortality with important
consequences in terms of social costs
The analysis of mortality rates in large cohorts confirmed the association of HCV with
several EHDs including cardiovascular neurologic metabolic or renal diseases and tumors
Viral eradication significantly reduced the rate of extra-hepatic deaths
Cacoub P et al DLD 2014 Lee MH et al J Infect Dis 2012 Backus LI et al Clin Gastroenterol Hepatol 2011 El-Kamary S et al
Clin Infect Dis 2011 Hsu YC et al Hepatology 2014 Kawamura Y et al Am J Med 2007 Adinolfi LE et al WJG 2014
Extrahepatic Manifestations of HCV
Con il contributo di
Lee M-H et al J Infect Dis 2012206469-477
Follow-Up
(Years)
20
18
16
14
12
10
2
00 2 4 6 8 10 12 14 16 18 20
8
6
4
Follow-Up
(Years)
12
10
8
6
4
2
00 2 4 6 8 10 12 14 16 18 20
All Causes(n=2394)
Liver Cancer(n=115)
Extrahepatic Diseases(n=2199)
Cum
ula
tive M
ort
ali
ty (
)
Anti-HCV+ HCV RNA detectable Anti-HCV+ HCV RNA undetectable Anti-HCVndash
Follow-Up
(Years)
35
30
25
20
15
10
5
00 2 4 6 8 10 12 14 16 18 20
301
128124
104
16
03
198
122
110
MC is clinically benign but sometimes severe HCV EHD invalidating symptoms occur and
it may evolve into lymphoma
Cacoub P et al DLD 2014 Zignego AL et al DLD 2007 Zignego AL et al Intern Emerg Med 2012 Zignego AL et al Clin Dev
Immunol 2012 Zignego AL et al Expert Rev Clin Immunol 2015 Sene D et al J Rheumatol 2004
Mixed Cryoglobulinemia-MC
CGs reversibly precipitate when the temperature is lower than 37degC and
comprise IgMs with RF activity [mono- or oligo-clonal in type II MC or
polyclonal in type III MC] and polyclonal IgGs
MC pathological substrate is an HCV-driven B-cell
proliferation with consequent production of cryo- and non-
cryoprecipitable CICs in turn responsible for vasculitic
manifestations
Most (70ndash90) MC patients are HCV+ and HCV-patients are CGs+ (40ndash60) while 5ndash30 of
CGs+ have symptomatic MC since HCV infects about 170 million individuals worldwide the
number of patients at risk for developing MC is substantial
Type II
CGs
Type III
CGs
Zignego AL et al Autoimmun Rev 2017 Ferri C et al Autoimmunity rev 2016 Zignego AL et al DLD 2007 Cacoub P et al DLD
2014 Zignego AL et al DLD 2007 Zignego AL et al Intern Emerg Med 2012 Zignego AL et al Clin Dev Immunol 2012 Zignego
AL et al Expert Rev Clin Immunol 2015
MC clinical aspects MC Syndrome
MCS is characterized by the clinical triad -purpura weakness and
arthralgias- low complement C4 and various organsystem
involvement including cutaneous articular renal neurological
cardiac or digestive
It ranges from mild disease to severe even life-threatening
conditions
More serious lesions are generally characterized by neurologic and
renal involvement
Prognosis is highly dependent on renal involvement or on the extent
of vasculitis lesions
1 HCV is the main etiopathological agent as concordantly demonstrated by epidemiological clinico-pathological virological and laboratory investigations2 the association between HCV and disease is demonstrated in a significant proportion of patients and supported by in depth clinico-pathogeneticstudies3 the association is suggested by cohort studies a possible causative role may be limited to a small number of patients andor possibly more relevant in specific geographical areas 4 a number of anecdotal observations suggested a possible role of HCV further investigations are required
From P Cacoub 2015
HCV infection is closely related to LPDs mostly MC
40 to 60 of HCV patients show circulating CGs among this latter population 5-30
develop a symptomatic CV
AVT has been considered the first-line option in HCV-CV patients in fact in the majority
of cases viral eradication leads to CV clinical remission
Data about IFN-free regimens for the treatment of CV patients are still limited
HCV and MC
HCV and MC
Zignego 2015Ferri 2016Pozzato 2016 Sise 2016Saadoun 2015Gragnani 2016Gragnani 2016
Bonacci 2016Hegazy 2016Kondili 2016Emery 2017
Younossi et al
The annual costs (inpatient outpatient andpharmacy) associated with extrahepatic
manifestations of HCV were evaluated
Total direct medical costs of extrahepatic
manifestations of HCV in 2014 US dollars wereestimated to be $1506 million (range $922 millionndash
$2208 million in sensitivity analysis)
These estimates should be added to the liver-related
burden of disease to obtain a more accurateassessment of the total burden of HCV infection
The OBJECTIVE of the study was to estimate the annual direct medical costsassociated with HCV related EHM in the EU5 (France Germany Italy United Kingdom
Spain)
Extrahepatic Manifestations of HCV
Extrahepatic Manifestations of HCV
HCV may cause extrahepatic disorders (HCV-EHDs) classified according to the number and
strength of supporting scientific data
HCV-EHDs are responsible for increasing morbidity and mortality with important
consequences in terms of social costs
The analysis of mortality rates in large cohorts confirmed the association of HCV with
several EHDs including cardiovascular neurologic metabolic or renal diseases and tumors
Viral eradication significantly reduced the rate of extra-hepatic deaths
Cacoub P et al DLD 2014 Lee MH et al J Infect Dis 2012 Backus LI et al Clin Gastroenterol Hepatol 2011 El-Kamary S et al
Clin Infect Dis 2011 Hsu YC et al Hepatology 2014 Kawamura Y et al Am J Med 2007 Adinolfi LE et al WJG 2014
Con il contributo di
Lee M-H et al J Infect Dis 2012206469-477
Follow-Up
(Years)
20
18
16
14
12
10
2
00 2 4 6 8 10 12 14 16 18 20
8
6
4
Follow-Up
(Years)
12
10
8
6
4
2
00 2 4 6 8 10 12 14 16 18 20
All Causes(n=2394)
Liver Cancer(n=115)
Extrahepatic Diseases(n=2199)
Cum
ula
tive M
ort
ali
ty (
)
Anti-HCV+ HCV RNA detectable Anti-HCV+ HCV RNA undetectable Anti-HCVndash
Follow-Up
(Years)
35
30
25
20
15
10
5
00 2 4 6 8 10 12 14 16 18 20
301
128124
104
16
03
198
122
110
Extrahepatic Manifestations of HCV
The annual costs (inpatient outpatient andpharmacy) associated with extrahepatic
manifestations of HCV were evaluated
Total direct medical costs of extrahepatic
manifestations of HCV in 2014 US dollars wereestimated to be $1506 million (range $922 millionndash
$2208 million in sensitivity analysis)
These estimates should be added to the liver-related
burden of disease to obtain a more accurateassessment of the total burden of HCV infection
Younossi et al
Younossi et al
Costs up to $71000 per patient per year (ESRD) Among the most frequent EHM depression (245 in HCV vs 172 in non-HCV) had estimated annual cost of
$4307 million DM (15 vs 10 in non- HCV) had an annual cost of $4434 million in the USA= given the importance of DM and
its association with CVDs and mortality the clinical and economic impacts of HCV-related DM are substantial
The OBJECTIVE of the study was to estimate the annual direct medical costsassociated with HCV related EHM in the EU5 (France Germany Italy United Kingdom
Spain)
The OBJECTIVE of the study was to estimate the annual direct medicalcosts associated with HCV related EHM in the EU5 (France Germany
Italy United Kingdom Spain)
1 HCV is the main etiopathological agent as concordantly demonstrated by epidemiological clinico-pathological virological and laboratory investigations2 the association between HCV and disease is demonstrated in a significant proportion of patients and supported by in depth clinico-pathogeneticstudies3 the association is suggested by cohort studies a possible causative role may be limited to a small number of patients andor possibly more relevant in specific geographical areas 4 a number of anecdotal observations suggested a possible role of HCV further investigations are required
The most studied and frequent HCV-EHDs are B-LPDs andor autoimmune disorders
Their prototype is Mixed Cryoglobulinemia (MC) from researches on MC derived most of the
available information
MC as a precious model for all the HCV-EHDs and to evaluate the effects of viral eradication
Anti-HCV Treatment Evolution
IFN
6 mos
PegIFN RBV 12
mos
IFN
12 mos
IFNRBV
12 mos
PegIFN
12 mos
2001
1998
2011
Standardinterferon
Ribavirin
Peginterferon
1991
Direct-actingantivirals
PegIFN
RBV
DAA
IFNRBV
6 mos
6
16
34
4239
55
70+
0
20
40
60
80
100
DAAs
826
weeks
gt90
2015
Few side effects absence major
contraindications
Younossi et al
The annual costs (inpatient outpatient and pharmacy) associatedwith extrahepatic manifestations of HCV were evaluated
Total direct medical costs of extrahepatic manifestations of HCV in 2014US dollars were estimated to be $1506 million (range $922 millionndash
$2208 million in sensitivity analysis)
These estimates should be added to the liver-related burden of diseaseto obtain a more accurate assessment of the total burden of HCV
infection
The OBJECTIVE of the study was to estimate the annual direct medical costs associated with HCV related EHM in the EU5 (France Germany Italy United Kingdom Spain)
22 MCS treated with DAAs including 2 HCC and 2 NHL 100 SVR12 Clinical CR in 64 and PR in remaining 36 The small lymphocytic lymphoma progressed despite viral clearance
Lauletta et al 2017
Emery CS et al 2017
Retrospective analysis 17 MCS (10 with severelife-threatening vasculitis) and 65 asymptomatic CGs+ pts treated with DAAs SVR 889 MCS and 908 asymptomatic pts In MCS clinical response in 1117 (complete in 717) In severelife-threatening vasculitis lower clinical response especially in renal and neurological symptoms
Saadoun D et al 2017
Open-label prospective multi-center study on sofosbuvir plus daclatasvir treatment of 41 HCV MCS SVR in100 and clinical CR in 902 Disappearance of CGs in 50 of pts No serious adverse event or relapse ofvasculitis
Antiviral Treatment (AVT) of MCIFN-free regimens
MC is clinically benign but sometimes severe HCV EHD invalidating symptoms occur and
it may evolve into lymphoma
Cacoub P et al DLD 2014 Zignego AL et al DLD 2007 Zignego AL et al Intern Emerg Med 2012 Zignego AL et al Clin Dev
Immunol 2012 Zignego AL et al Expert Rev Clin Immunol 2015 Sene D et al J Rheumatol 2004
Mixed Cryoglobulinemia-MC
MC pathological substrate is an HCV-driven B-cell
proliferation with consequent production of cryo- and non-
cryoprecipitable CICs in turn responsible for vasculitic
manifestations
Most (70ndash90) MC patients are HCV+ and HCV-patients are CGs+ (40ndash60) while 5ndash30 of
CGs+ have symptomatic MC or cryoglobulinemic vasculitis since HCV infects about 170
million individuals worldwide the number of patients at risk for developing MC is
substantial
Type II CGs
monoclonal
RF+policlonal IgG
Type III CGs both
RF and IgG
polyclonal

Landau DA et al Arthritis Rheum 2008 Montalbano M et al J Clin Gastroenterol 2007 Cacoub P et al Arthritis Rheum 2002
Mazzaro C et alJ Rheumatol 2003 Zignego AL et al Hepatology 2016 Gragnani L et al Hepatology 2015 Pietrogrande M
et al Autoimmun Rev 2011
Antiviral Treatment (AVT) of MC in the IFN Era
AVT of MC followed the evolution of hepatitis C AVT with frequent adjustments
essentially due to the possible side-effects of IFN andor RBV therapy (ie IFN
neurotoxicity and myelo-inhibitory action and RBV hemolytic effects)
Virological and clinical results progressively improved in spite of frequent side-effects
IFN-based AVT was recommended as the first-line option in mild to moderate MC
Clinical remission was generally correlated with virological response
Long follow-up showed that the majority (57) of SVR pts cleared all MC stigmata
Antiviral Treatment (AVT) of MC IFN-free regimensLimited data so-far concordant are available regarding IFN-free AVT in MC patients
Available data suggest that IFN-free AVT is safe generally well tolerated and effective in MC patients high rate of
clinical response (87) and low rates of serious adverse events was reported
Zignego AL Ramos-Casals M Ferri C et al AutoimmunReviews 2017
Antiviral Treatment (AVT) of MC IFN-free regimens
22 MCS treated with DAAs including 2 HCC and 2 NHL 100 SVR12 Clinical R in 100 (64 CR and 36 PR)
Progression of the small lymphocytic lymphoma
Lauletta et al 2017
Emery CS et al 2017
Retrospective analysis 17 MCS (10 with severelife-threatening vasculitis) and 65 asymptomatic MC treated with
DAAs SVR 889 MCS and 908 asymptomatic pts In MCS clinical R in 1117 (CR in 711) Lower clinical R inseverelife-threatening ndashespecial renal and neurological- vasculitis
Saadoun D et al 2017
Open-label prospective multi-center study on sofosbuvir plus daclatasvir treatment of 41 HCV MCS SVR in 100 and
clinical CR in 902 Disappearance of CGs in 50 of pts No serious adverse event or relapse of vasculitis
A case of rapid amelioration of HCV-associated cryoglobulinemic MPGN treated by
IFN-free DAAs for HCV in the absence of immunosuppressant
Fumiaki et al 2017
Zignego et al 2017
TIME POINTS
baseline EOT and week 12 and 24 of post-treatment f-up (SVR12 and SVR24 respectively)
HRQoL EVALUATION THROUGH PROs
the Short Form (36) Health Survey (SF-36)
the Functional Assessment of Chronic Illness Therapy-Fatigue (FACIT-F) from which we computed the Trial
Outcome Index (TOI)
Evaluation of The Impact on HRQol of IFN-free AVT In HCV CM
1 Physical Component Summary Score (PCS)
MC (54)
HCV (43) CV (85)
deg
A B C
degdegdeg
2 Mental Component Summary Score (MCS)
MCHCV CVD E F
degdegdegdegdeg
HCV
=plt001 vs baseline scores
degdeg=plt001 and degdegdeg=plt0001 vs EOT scores
Gragnani et al AASLD 2017
HCV Eradicationwith DAAs
To be preceded or combined with non-etiological pathogenetic therapy in severecatastrophic MCS
MCS Therapy in the IFN and DAAs Era from the complex to the simplified flow-chart
Dammacco F Sansonno D NEJM 2013
Zignego AL Pawlotsky JM Cacoub P Antiviral Ther in press Cacoub P et al Am J Med 2015
Mechanisms of HCV-related lymphomagenesis
DLBC HCV- induced
direct transformation
MCindolent NHL
accumulation of B RF
following BCR activation
and BC apoptosisinhibition
Zignego AL Ramos-Casals M Ferri C et al Autoimmun Rev 2017
Wang et al Hepatology 2016 Canioni et al Plos one 2016
Observational study on in situ expression of the oncogenic HCV NS3 protein on 116 HCV patients with B-NHL (DLBCL 36 and MZL 34)
NS3 immunostaining positive in 1214 DLBCL vs only 414 MZL (p = 0006) moreover 24 NS3+ MZL
were enriched in large cells
This study supports a new mechanism of transformation with a direct oncogenic role of
HCV proteins in the occurrence of high-grade B lymphomas
IN SITU HEPATITIS C NS3 PROTEIN DETECTION IS ASSOCIATED WITH HIGH GRADE
FEATURES IN HCV-ASSOCIATED B-CELL NON-HODGKIN LYMPHOMAS Danielle
Canioni et al 2016
In addition to the role of chronic antigenic stimulation in HCV related
lymphomagenesis this study supports a second mechanism of transformation due to a
direct oncogenic role of HCV infection of B-cells promoting the occurrence of high-grade Bcell lymphomas
Cohort study of 704 consecutive HIV-negative HCV-positive patients with indolent NHL from 1993 to
2009 in 39 centers of the FIL
Arcaini et al 2016
DLBC HCV- induced
direct transformation
No place of AVT as
1st line
Need of immediate delivery of
chemotherapy or concomitant (NHL
+ HCV targets)
THERAPY OF HCV+ DLBCL
ANTIVIRAL THERAPY IS ASSOCIATED WITH A BETTERSURVIVAL IN PATIENTS WITH HCV AND B-CELL NON-HODGKIN LYMPHOMAS ANRS HC-13 LYMPHO-CSTUDY Michot JM et al
Outcomes of HCV-associated B-NHL according to HCV AVT in prospective patients only (n 5 64)
Concurrent Systemic Chemoimmunotherapy and Sofosbuvir-Based Antiviral Treatment in a Hepatitis C Virus-Infected Patient With Diffuse Large B-Cell Lymphoma Evan C Ewers et al 2016
absolute neutrophil count and Hgb ALT and HCV viral load
Both complete response and SVR of HCV-associated DLBCL after concurrent chemoimmunotherapy and antiviral therapy using a sofosbuvir-based regimen
DAA-treatment in concomitance with chemotherapy showed to be safe and effective in influencing the remission of aggressive lymphomas in HCV patients
Persico M et al 2017
DFS in DAA treated and historical not-treated ptsAntiviral response rates in DAA treated patients
ANTIVIRAL THERAPY IN HCV+ B CELL NHL
IFN-based AVT induced hematological response along with SVR in patients with HCV-related indolent NHLs (especially
MZL)
Recent data with IFN-free regimens in HCV-associated LPDs suggest their anti-lymphoma activity too
AVT should be considered the first-line approach in HCV low grade lymphomas if there is no urgency of a conventional
treatment (ie systemic symptoms bulky disease or symptomatic splenomegaly) (ESMO NCCN EASL guidelines)
In aggressive lymphomas antiviral therapy after induction treatment is to be considered the standard at the moment but
in the next years (months) the association of immunochemotherapy and antiviral therapy will be considered the standard
Zignego AL Ramos-Casals M Ferri C et al Autoimmun Rev 2017
The Masve group
BASIC RESEARCH
Laura Gragnani
Patrizio Caini
Serena Lorini
Antonella Simone
CLINICAL RESEARCH
Monica Monti
Luisa Petraccia
Sinan Sadalla
Guia Cerretelli
Cristina Stasi
Adela Xheka
Universitagrave degli Studi di FirenzeDipartimento di Medicina Sperimentale e Clinica
Centro Manifestazioni Sistemiche da Virus EpatiticildquoMASVErdquo
Anna Linda Zignego
MASVE
UNDERGRADUATE STUDENTS Andrea Genovese Adrian Piscopo
ANTIVIRAL THERAPY IN HCV+ B CELL NHL
IFN-based AVT induced hematological response along with SVR in patients with HCV-related indolent
NHLs (especially MZL)
Recent data with IFN-free regimens in HCV-associated LPDs suggest their anti-lymphoma activity too
AVT should be considered the first-line approach in HCV low grade lymphomas if there is no urgency
of a conventional treatment (ie systemic symptoms bulky disease or symptomatic splenomegaly)
(ESMO NCCN EASL guidelines)
Main drugs for HCV-related MCS according to the target
HCV= DAAsB-cell Expansion= (a) B cell-depleting Mabs
-First-generation Rituximab (anti-CD20)-Second-generation Ofatumumab (anti-CD20) Veltuzumab (humanized
anti-CD20)-Third-generation Obinutuzumab (GA101) Oceratuzumab (humanized
anti-CD20)
(b) Alkylating agents
-Cyclophosfamide
Inflammation= Antiinflammatory agents
- Corticosteroids
Altered regulatory T-cell activity=
- IL-2
The impact on HRQoL of IFN-free AVT was prospectively evaluated in a cohort of HCV CV patients with limited
influencing variables linked to therapeutic schedulesviral GT
44 HCV GT2 CV patients mostly F0-F2 (29) and naiumlve (30) treated with SOFRBV for 1224wks
TIME POINTS
baseline EOT and week 12 and 24 of post-treatment f-up (SVR12 and SVR24 respectively)
HRQoL EVALUATION THROUGH PROs
the Short Form (36) Health Survey (SF-36)
the Functional Assessment of Chronic Illness Therapy-Fatigue (FACIT-F) from which we computed the Trial
Outcome Index (TOI)
Observational study on in situ expression of the oncogenic HCV NS3 protein on 116 HCV
patients with B-NHL (DLBCL 36 and MZL 34)
NS3 immunostaining positive in 1214 DLBCL vs only 414 MZL (p = 0006) moreover 24 NS3+
MZL were enriched in large cells
This study supports a new mechanism of transformation with a direct oncogenic role of
HCV proteins in the occurrence of high-grade B lymphomas
IN SITU HEPATITIS C NS3 PROTEIN DETECTION IS ASSOCIATED WITH HIGH GRADEFEATURES IN HCV-ASSOCIATED B-CELL NON-HODGKIN LYMPHOMAS Danielle
Canioni et al 2016
In addition to the role of chronic antigenic stimulation in HCV related
lymphomagenesis this study supports a second mechanism of transformation due toa direct oncogenic role of HCV infection of B-cells promoting the occurrence of high-grade Bcell lymphomas
ANTIVIRAL THERAPY IS ASSOCIATED WITH A BETTERSURVIVAL IN PATIENTS WITH HCV AND B-CELL NON-HODGKIN LYMPHOMAS ANRS HC-13 LYMPHO-CSTUDYMichot JM et al
Outcomes of HCV-associated B-NHL according to HCV AVT in prospective patients only (n 5 64)
(A) absolute neutrophil count and Hgb
(B) ALT and HCV viral load
This patient had HCV-associated DLBCL achieving both complete response and SVR after concurrent chemoimmunotherapy and antiviral therapy using a sofosbuvir-basedregimen
Concurrent Systemic Chemoimmunotherapy and Sofosbuvir-Based Antiviral Treatment in a Hepatitis C Virus-Infected Patient With Diffuse Large B-Cell LymphomaEvan C Ewers et al 2016
HCV-EHDs are responsible for increasing morbidity and mortality with important
consequences in terms of social costs
The analysis of mortality rates in large cohorts confirmed the association of HCV with
several EHDs including cardiovascular neurologic metabolic or renal diseases and tumors
Viral eradication significantly reduced the rate of extra-hepatic deaths
Cacoub P et al DLD 2014 Lee MH et al J Infect Dis 2012 Backus LI et al Clin Gastroenterol Hepatol 2011 El-Kamary S et al
Clin Infect Dis 2011 Hsu YC et al Hepatology 2014 Kawamura Y et al Am J Med 2007 Adinolfi LE et al WJG 2014
Extrahepatic Manifestations of HCV
Con il contributo di
Lee M-H et al J Infect Dis 2012206469-477
Follow-Up
(Years)
20
18
16
14
12
10
2
00 2 4 6 8 10 12 14 16 18 20
8
6
4
Follow-Up
(Years)
12
10
8
6
4
2
00 2 4 6 8 10 12 14 16 18 20
All Causes(n=2394)
Liver Cancer(n=115)
Extrahepatic Diseases(n=2199)
Cum
ula
tive M
ort
ali
ty (
)
Anti-HCV+ HCV RNA detectable Anti-HCV+ HCV RNA undetectable Anti-HCVndash
Follow-Up
(Years)
35
30
25
20
15
10
5
00 2 4 6 8 10 12 14 16 18 20
301
128124
104
16
03
198
122
110
MC is clinically benign but sometimes severe HCV EHD invalidating symptoms occur and
it may evolve into lymphoma
Cacoub P et al DLD 2014 Zignego AL et al DLD 2007 Zignego AL et al Intern Emerg Med 2012 Zignego AL et al Clin Dev
Immunol 2012 Zignego AL et al Expert Rev Clin Immunol 2015 Sene D et al J Rheumatol 2004
Mixed Cryoglobulinemia-MC
CGs reversibly precipitate when the temperature is lower than 37degC and
comprise IgMs with RF activity [mono- or oligo-clonal in type II MC or
polyclonal in type III MC] and polyclonal IgGs
MC pathological substrate is an HCV-driven B-cell
proliferation with consequent production of cryo- and non-
cryoprecipitable CICs in turn responsible for vasculitic
manifestations
Most (70ndash90) MC patients are HCV+ and HCV-patients are CGs+ (40ndash60) while 5ndash30 of
CGs+ have symptomatic MC since HCV infects about 170 million individuals worldwide the
number of patients at risk for developing MC is substantial
Type II
CGs
Type III
CGs
Zignego AL et al Autoimmun Rev 2017 Ferri C et al Autoimmunity rev 2016 Zignego AL et al DLD 2007 Cacoub P et al DLD
2014 Zignego AL et al DLD 2007 Zignego AL et al Intern Emerg Med 2012 Zignego AL et al Clin Dev Immunol 2012 Zignego
AL et al Expert Rev Clin Immunol 2015
MC clinical aspects MC Syndrome
MCS is characterized by the clinical triad -purpura weakness and
arthralgias- low complement C4 and various organsystem
involvement including cutaneous articular renal neurological
cardiac or digestive
It ranges from mild disease to severe even life-threatening
conditions
More serious lesions are generally characterized by neurologic and
renal involvement
Prognosis is highly dependent on renal involvement or on the extent
of vasculitis lesions
1 HCV is the main etiopathological agent as concordantly demonstrated by epidemiological clinico-pathological virological and laboratory investigations2 the association between HCV and disease is demonstrated in a significant proportion of patients and supported by in depth clinico-pathogeneticstudies3 the association is suggested by cohort studies a possible causative role may be limited to a small number of patients andor possibly more relevant in specific geographical areas 4 a number of anecdotal observations suggested a possible role of HCV further investigations are required
From P Cacoub 2015
HCV infection is closely related to LPDs mostly MC
40 to 60 of HCV patients show circulating CGs among this latter population 5-30
develop a symptomatic CV
AVT has been considered the first-line option in HCV-CV patients in fact in the majority
of cases viral eradication leads to CV clinical remission
Data about IFN-free regimens for the treatment of CV patients are still limited
HCV and MC
HCV and MC
Zignego 2015Ferri 2016Pozzato 2016 Sise 2016Saadoun 2015Gragnani 2016Gragnani 2016
Bonacci 2016Hegazy 2016Kondili 2016Emery 2017
Younossi et al
The annual costs (inpatient outpatient andpharmacy) associated with extrahepatic
manifestations of HCV were evaluated
Total direct medical costs of extrahepatic
manifestations of HCV in 2014 US dollars wereestimated to be $1506 million (range $922 millionndash
$2208 million in sensitivity analysis)
These estimates should be added to the liver-related
burden of disease to obtain a more accurateassessment of the total burden of HCV infection
The OBJECTIVE of the study was to estimate the annual direct medical costsassociated with HCV related EHM in the EU5 (France Germany Italy United Kingdom
Spain)
Extrahepatic Manifestations of HCV
Extrahepatic Manifestations of HCV
HCV may cause extrahepatic disorders (HCV-EHDs) classified according to the number and
strength of supporting scientific data
HCV-EHDs are responsible for increasing morbidity and mortality with important
consequences in terms of social costs
The analysis of mortality rates in large cohorts confirmed the association of HCV with
several EHDs including cardiovascular neurologic metabolic or renal diseases and tumors
Viral eradication significantly reduced the rate of extra-hepatic deaths
Cacoub P et al DLD 2014 Lee MH et al J Infect Dis 2012 Backus LI et al Clin Gastroenterol Hepatol 2011 El-Kamary S et al
Clin Infect Dis 2011 Hsu YC et al Hepatology 2014 Kawamura Y et al Am J Med 2007 Adinolfi LE et al WJG 2014
Con il contributo di
Lee M-H et al J Infect Dis 2012206469-477
Follow-Up
(Years)
20
18
16
14
12
10
2
00 2 4 6 8 10 12 14 16 18 20
8
6
4
Follow-Up
(Years)
12
10
8
6
4
2
00 2 4 6 8 10 12 14 16 18 20
All Causes(n=2394)
Liver Cancer(n=115)
Extrahepatic Diseases(n=2199)
Cum
ula
tive M
ort
ali
ty (
)
Anti-HCV+ HCV RNA detectable Anti-HCV+ HCV RNA undetectable Anti-HCVndash
Follow-Up
(Years)
35
30
25
20
15
10
5
00 2 4 6 8 10 12 14 16 18 20
301
128124
104
16
03
198
122
110
Extrahepatic Manifestations of HCV
The annual costs (inpatient outpatient andpharmacy) associated with extrahepatic
manifestations of HCV were evaluated
Total direct medical costs of extrahepatic
manifestations of HCV in 2014 US dollars wereestimated to be $1506 million (range $922 millionndash
$2208 million in sensitivity analysis)
These estimates should be added to the liver-related
burden of disease to obtain a more accurateassessment of the total burden of HCV infection
Younossi et al
Younossi et al
Costs up to $71000 per patient per year (ESRD) Among the most frequent EHM depression (245 in HCV vs 172 in non-HCV) had estimated annual cost of
$4307 million DM (15 vs 10 in non- HCV) had an annual cost of $4434 million in the USA= given the importance of DM and
its association with CVDs and mortality the clinical and economic impacts of HCV-related DM are substantial
The OBJECTIVE of the study was to estimate the annual direct medical costsassociated with HCV related EHM in the EU5 (France Germany Italy United Kingdom
Spain)
The OBJECTIVE of the study was to estimate the annual direct medicalcosts associated with HCV related EHM in the EU5 (France Germany
Italy United Kingdom Spain)
1 HCV is the main etiopathological agent as concordantly demonstrated by epidemiological clinico-pathological virological and laboratory investigations2 the association between HCV and disease is demonstrated in a significant proportion of patients and supported by in depth clinico-pathogeneticstudies3 the association is suggested by cohort studies a possible causative role may be limited to a small number of patients andor possibly more relevant in specific geographical areas 4 a number of anecdotal observations suggested a possible role of HCV further investigations are required
The most studied and frequent HCV-EHDs are B-LPDs andor autoimmune disorders
Their prototype is Mixed Cryoglobulinemia (MC) from researches on MC derived most of the
available information
MC as a precious model for all the HCV-EHDs and to evaluate the effects of viral eradication
Anti-HCV Treatment Evolution
IFN
6 mos
PegIFN RBV 12
mos
IFN
12 mos
IFNRBV
12 mos
PegIFN
12 mos
2001
1998
2011
Standardinterferon
Ribavirin
Peginterferon
1991
Direct-actingantivirals
PegIFN
RBV
DAA
IFNRBV
6 mos
6
16
34
4239
55
70+
0
20
40
60
80
100
DAAs
826
weeks
gt90
2015
Few side effects absence major
contraindications
Younossi et al
The annual costs (inpatient outpatient and pharmacy) associatedwith extrahepatic manifestations of HCV were evaluated
Total direct medical costs of extrahepatic manifestations of HCV in 2014US dollars were estimated to be $1506 million (range $922 millionndash
$2208 million in sensitivity analysis)
These estimates should be added to the liver-related burden of diseaseto obtain a more accurate assessment of the total burden of HCV
infection
The OBJECTIVE of the study was to estimate the annual direct medical costs associated with HCV related EHM in the EU5 (France Germany Italy United Kingdom Spain)
22 MCS treated with DAAs including 2 HCC and 2 NHL 100 SVR12 Clinical CR in 64 and PR in remaining 36 The small lymphocytic lymphoma progressed despite viral clearance
Lauletta et al 2017
Emery CS et al 2017
Retrospective analysis 17 MCS (10 with severelife-threatening vasculitis) and 65 asymptomatic CGs+ pts treated with DAAs SVR 889 MCS and 908 asymptomatic pts In MCS clinical response in 1117 (complete in 717) In severelife-threatening vasculitis lower clinical response especially in renal and neurological symptoms
Saadoun D et al 2017
Open-label prospective multi-center study on sofosbuvir plus daclatasvir treatment of 41 HCV MCS SVR in100 and clinical CR in 902 Disappearance of CGs in 50 of pts No serious adverse event or relapse ofvasculitis
Antiviral Treatment (AVT) of MCIFN-free regimens
MC is clinically benign but sometimes severe HCV EHD invalidating symptoms occur and
it may evolve into lymphoma
Cacoub P et al DLD 2014 Zignego AL et al DLD 2007 Zignego AL et al Intern Emerg Med 2012 Zignego AL et al Clin Dev
Immunol 2012 Zignego AL et al Expert Rev Clin Immunol 2015 Sene D et al J Rheumatol 2004
Mixed Cryoglobulinemia-MC
MC pathological substrate is an HCV-driven B-cell
proliferation with consequent production of cryo- and non-
cryoprecipitable CICs in turn responsible for vasculitic
manifestations
Most (70ndash90) MC patients are HCV+ and HCV-patients are CGs+ (40ndash60) while 5ndash30 of
CGs+ have symptomatic MC or cryoglobulinemic vasculitis since HCV infects about 170
million individuals worldwide the number of patients at risk for developing MC is
substantial
Type II CGs
monoclonal
RF+policlonal IgG
Type III CGs both
RF and IgG
polyclonal

Antiviral Treatment (AVT) of MC IFN-free regimensLimited data so-far concordant are available regarding IFN-free AVT in MC patients
Available data suggest that IFN-free AVT is safe generally well tolerated and effective in MC patients high rate of
clinical response (87) and low rates of serious adverse events was reported
Zignego AL Ramos-Casals M Ferri C et al AutoimmunReviews 2017
Antiviral Treatment (AVT) of MC IFN-free regimens
22 MCS treated with DAAs including 2 HCC and 2 NHL 100 SVR12 Clinical R in 100 (64 CR and 36 PR)
Progression of the small lymphocytic lymphoma
Lauletta et al 2017
Emery CS et al 2017
Retrospective analysis 17 MCS (10 with severelife-threatening vasculitis) and 65 asymptomatic MC treated with
DAAs SVR 889 MCS and 908 asymptomatic pts In MCS clinical R in 1117 (CR in 711) Lower clinical R inseverelife-threatening ndashespecial renal and neurological- vasculitis
Saadoun D et al 2017
Open-label prospective multi-center study on sofosbuvir plus daclatasvir treatment of 41 HCV MCS SVR in 100 and
clinical CR in 902 Disappearance of CGs in 50 of pts No serious adverse event or relapse of vasculitis
A case of rapid amelioration of HCV-associated cryoglobulinemic MPGN treated by
IFN-free DAAs for HCV in the absence of immunosuppressant
Fumiaki et al 2017
Zignego et al 2017
TIME POINTS
baseline EOT and week 12 and 24 of post-treatment f-up (SVR12 and SVR24 respectively)
HRQoL EVALUATION THROUGH PROs
the Short Form (36) Health Survey (SF-36)
the Functional Assessment of Chronic Illness Therapy-Fatigue (FACIT-F) from which we computed the Trial
Outcome Index (TOI)
Evaluation of The Impact on HRQol of IFN-free AVT In HCV CM
1 Physical Component Summary Score (PCS)
MC (54)
HCV (43) CV (85)
deg
A B C
degdegdeg
2 Mental Component Summary Score (MCS)
MCHCV CVD E F
degdegdegdegdeg
HCV
=plt001 vs baseline scores
degdeg=plt001 and degdegdeg=plt0001 vs EOT scores
Gragnani et al AASLD 2017
HCV Eradicationwith DAAs
To be preceded or combined with non-etiological pathogenetic therapy in severecatastrophic MCS
MCS Therapy in the IFN and DAAs Era from the complex to the simplified flow-chart
Dammacco F Sansonno D NEJM 2013
Zignego AL Pawlotsky JM Cacoub P Antiviral Ther in press Cacoub P et al Am J Med 2015
Mechanisms of HCV-related lymphomagenesis
DLBC HCV- induced
direct transformation
MCindolent NHL
accumulation of B RF
following BCR activation
and BC apoptosisinhibition
Zignego AL Ramos-Casals M Ferri C et al Autoimmun Rev 2017
Wang et al Hepatology 2016 Canioni et al Plos one 2016
Observational study on in situ expression of the oncogenic HCV NS3 protein on 116 HCV patients with B-NHL (DLBCL 36 and MZL 34)
NS3 immunostaining positive in 1214 DLBCL vs only 414 MZL (p = 0006) moreover 24 NS3+ MZL
were enriched in large cells
This study supports a new mechanism of transformation with a direct oncogenic role of
HCV proteins in the occurrence of high-grade B lymphomas
IN SITU HEPATITIS C NS3 PROTEIN DETECTION IS ASSOCIATED WITH HIGH GRADE
FEATURES IN HCV-ASSOCIATED B-CELL NON-HODGKIN LYMPHOMAS Danielle
Canioni et al 2016
In addition to the role of chronic antigenic stimulation in HCV related
lymphomagenesis this study supports a second mechanism of transformation due to a
direct oncogenic role of HCV infection of B-cells promoting the occurrence of high-grade Bcell lymphomas
Cohort study of 704 consecutive HIV-negative HCV-positive patients with indolent NHL from 1993 to
2009 in 39 centers of the FIL
Arcaini et al 2016
DLBC HCV- induced
direct transformation
No place of AVT as
1st line
Need of immediate delivery of
chemotherapy or concomitant (NHL
+ HCV targets)
THERAPY OF HCV+ DLBCL
ANTIVIRAL THERAPY IS ASSOCIATED WITH A BETTERSURVIVAL IN PATIENTS WITH HCV AND B-CELL NON-HODGKIN LYMPHOMAS ANRS HC-13 LYMPHO-CSTUDY Michot JM et al
Outcomes of HCV-associated B-NHL according to HCV AVT in prospective patients only (n 5 64)
Concurrent Systemic Chemoimmunotherapy and Sofosbuvir-Based Antiviral Treatment in a Hepatitis C Virus-Infected Patient With Diffuse Large B-Cell Lymphoma Evan C Ewers et al 2016
absolute neutrophil count and Hgb ALT and HCV viral load
Both complete response and SVR of HCV-associated DLBCL after concurrent chemoimmunotherapy and antiviral therapy using a sofosbuvir-based regimen
DAA-treatment in concomitance with chemotherapy showed to be safe and effective in influencing the remission of aggressive lymphomas in HCV patients
Persico M et al 2017
DFS in DAA treated and historical not-treated ptsAntiviral response rates in DAA treated patients
ANTIVIRAL THERAPY IN HCV+ B CELL NHL
IFN-based AVT induced hematological response along with SVR in patients with HCV-related indolent NHLs (especially
MZL)
Recent data with IFN-free regimens in HCV-associated LPDs suggest their anti-lymphoma activity too
AVT should be considered the first-line approach in HCV low grade lymphomas if there is no urgency of a conventional
treatment (ie systemic symptoms bulky disease or symptomatic splenomegaly) (ESMO NCCN EASL guidelines)
In aggressive lymphomas antiviral therapy after induction treatment is to be considered the standard at the moment but
in the next years (months) the association of immunochemotherapy and antiviral therapy will be considered the standard
Zignego AL Ramos-Casals M Ferri C et al Autoimmun Rev 2017
The Masve group
BASIC RESEARCH
Laura Gragnani
Patrizio Caini
Serena Lorini
Antonella Simone
CLINICAL RESEARCH
Monica Monti
Luisa Petraccia
Sinan Sadalla
Guia Cerretelli
Cristina Stasi
Adela Xheka
Universitagrave degli Studi di FirenzeDipartimento di Medicina Sperimentale e Clinica
Centro Manifestazioni Sistemiche da Virus EpatiticildquoMASVErdquo
Anna Linda Zignego
MASVE
UNDERGRADUATE STUDENTS Andrea Genovese Adrian Piscopo
ANTIVIRAL THERAPY IN HCV+ B CELL NHL
IFN-based AVT induced hematological response along with SVR in patients with HCV-related indolent
NHLs (especially MZL)
Recent data with IFN-free regimens in HCV-associated LPDs suggest their anti-lymphoma activity too
AVT should be considered the first-line approach in HCV low grade lymphomas if there is no urgency
of a conventional treatment (ie systemic symptoms bulky disease or symptomatic splenomegaly)
(ESMO NCCN EASL guidelines)
Main drugs for HCV-related MCS according to the target
HCV= DAAsB-cell Expansion= (a) B cell-depleting Mabs
-First-generation Rituximab (anti-CD20)-Second-generation Ofatumumab (anti-CD20) Veltuzumab (humanized
anti-CD20)-Third-generation Obinutuzumab (GA101) Oceratuzumab (humanized
anti-CD20)
(b) Alkylating agents
-Cyclophosfamide
Inflammation= Antiinflammatory agents
- Corticosteroids
Altered regulatory T-cell activity=
- IL-2
The impact on HRQoL of IFN-free AVT was prospectively evaluated in a cohort of HCV CV patients with limited
influencing variables linked to therapeutic schedulesviral GT
44 HCV GT2 CV patients mostly F0-F2 (29) and naiumlve (30) treated with SOFRBV for 1224wks
TIME POINTS
baseline EOT and week 12 and 24 of post-treatment f-up (SVR12 and SVR24 respectively)
HRQoL EVALUATION THROUGH PROs
the Short Form (36) Health Survey (SF-36)
the Functional Assessment of Chronic Illness Therapy-Fatigue (FACIT-F) from which we computed the Trial
Outcome Index (TOI)
Observational study on in situ expression of the oncogenic HCV NS3 protein on 116 HCV
patients with B-NHL (DLBCL 36 and MZL 34)
NS3 immunostaining positive in 1214 DLBCL vs only 414 MZL (p = 0006) moreover 24 NS3+
MZL were enriched in large cells
This study supports a new mechanism of transformation with a direct oncogenic role of
HCV proteins in the occurrence of high-grade B lymphomas
IN SITU HEPATITIS C NS3 PROTEIN DETECTION IS ASSOCIATED WITH HIGH GRADEFEATURES IN HCV-ASSOCIATED B-CELL NON-HODGKIN LYMPHOMAS Danielle
Canioni et al 2016
In addition to the role of chronic antigenic stimulation in HCV related
lymphomagenesis this study supports a second mechanism of transformation due toa direct oncogenic role of HCV infection of B-cells promoting the occurrence of high-grade Bcell lymphomas
ANTIVIRAL THERAPY IS ASSOCIATED WITH A BETTERSURVIVAL IN PATIENTS WITH HCV AND B-CELL NON-HODGKIN LYMPHOMAS ANRS HC-13 LYMPHO-CSTUDYMichot JM et al
Outcomes of HCV-associated B-NHL according to HCV AVT in prospective patients only (n 5 64)
(A) absolute neutrophil count and Hgb
(B) ALT and HCV viral load
This patient had HCV-associated DLBCL achieving both complete response and SVR after concurrent chemoimmunotherapy and antiviral therapy using a sofosbuvir-basedregimen
Concurrent Systemic Chemoimmunotherapy and Sofosbuvir-Based Antiviral Treatment in a Hepatitis C Virus-Infected Patient With Diffuse Large B-Cell LymphomaEvan C Ewers et al 2016
HCV-EHDs are responsible for increasing morbidity and mortality with important
consequences in terms of social costs
The analysis of mortality rates in large cohorts confirmed the association of HCV with
several EHDs including cardiovascular neurologic metabolic or renal diseases and tumors
Viral eradication significantly reduced the rate of extra-hepatic deaths
Cacoub P et al DLD 2014 Lee MH et al J Infect Dis 2012 Backus LI et al Clin Gastroenterol Hepatol 2011 El-Kamary S et al
Clin Infect Dis 2011 Hsu YC et al Hepatology 2014 Kawamura Y et al Am J Med 2007 Adinolfi LE et al WJG 2014
Extrahepatic Manifestations of HCV
Con il contributo di
Lee M-H et al J Infect Dis 2012206469-477
Follow-Up
(Years)
20
18
16
14
12
10
2
00 2 4 6 8 10 12 14 16 18 20
8
6
4
Follow-Up
(Years)
12
10
8
6
4
2
00 2 4 6 8 10 12 14 16 18 20
All Causes(n=2394)
Liver Cancer(n=115)
Extrahepatic Diseases(n=2199)
Cum
ula
tive M
ort
ali
ty (
)
Anti-HCV+ HCV RNA detectable Anti-HCV+ HCV RNA undetectable Anti-HCVndash
Follow-Up
(Years)
35
30
25
20
15
10
5
00 2 4 6 8 10 12 14 16 18 20
301
128124
104
16
03
198
122
110
MC is clinically benign but sometimes severe HCV EHD invalidating symptoms occur and
it may evolve into lymphoma
Cacoub P et al DLD 2014 Zignego AL et al DLD 2007 Zignego AL et al Intern Emerg Med 2012 Zignego AL et al Clin Dev
Immunol 2012 Zignego AL et al Expert Rev Clin Immunol 2015 Sene D et al J Rheumatol 2004
Mixed Cryoglobulinemia-MC
CGs reversibly precipitate when the temperature is lower than 37degC and
comprise IgMs with RF activity [mono- or oligo-clonal in type II MC or
polyclonal in type III MC] and polyclonal IgGs
MC pathological substrate is an HCV-driven B-cell
proliferation with consequent production of cryo- and non-
cryoprecipitable CICs in turn responsible for vasculitic
manifestations
Most (70ndash90) MC patients are HCV+ and HCV-patients are CGs+ (40ndash60) while 5ndash30 of
CGs+ have symptomatic MC since HCV infects about 170 million individuals worldwide the
number of patients at risk for developing MC is substantial
Type II
CGs
Type III
CGs
Zignego AL et al Autoimmun Rev 2017 Ferri C et al Autoimmunity rev 2016 Zignego AL et al DLD 2007 Cacoub P et al DLD
2014 Zignego AL et al DLD 2007 Zignego AL et al Intern Emerg Med 2012 Zignego AL et al Clin Dev Immunol 2012 Zignego
AL et al Expert Rev Clin Immunol 2015
MC clinical aspects MC Syndrome
MCS is characterized by the clinical triad -purpura weakness and
arthralgias- low complement C4 and various organsystem
involvement including cutaneous articular renal neurological
cardiac or digestive
It ranges from mild disease to severe even life-threatening
conditions
More serious lesions are generally characterized by neurologic and
renal involvement
Prognosis is highly dependent on renal involvement or on the extent
of vasculitis lesions
1 HCV is the main etiopathological agent as concordantly demonstrated by epidemiological clinico-pathological virological and laboratory investigations2 the association between HCV and disease is demonstrated in a significant proportion of patients and supported by in depth clinico-pathogeneticstudies3 the association is suggested by cohort studies a possible causative role may be limited to a small number of patients andor possibly more relevant in specific geographical areas 4 a number of anecdotal observations suggested a possible role of HCV further investigations are required
From P Cacoub 2015
HCV infection is closely related to LPDs mostly MC
40 to 60 of HCV patients show circulating CGs among this latter population 5-30
develop a symptomatic CV
AVT has been considered the first-line option in HCV-CV patients in fact in the majority
of cases viral eradication leads to CV clinical remission
Data about IFN-free regimens for the treatment of CV patients are still limited
HCV and MC
HCV and MC
Zignego 2015Ferri 2016Pozzato 2016 Sise 2016Saadoun 2015Gragnani 2016Gragnani 2016
Bonacci 2016Hegazy 2016Kondili 2016Emery 2017
Younossi et al
The annual costs (inpatient outpatient andpharmacy) associated with extrahepatic
manifestations of HCV were evaluated
Total direct medical costs of extrahepatic
manifestations of HCV in 2014 US dollars wereestimated to be $1506 million (range $922 millionndash
$2208 million in sensitivity analysis)
These estimates should be added to the liver-related
burden of disease to obtain a more accurateassessment of the total burden of HCV infection
The OBJECTIVE of the study was to estimate the annual direct medical costsassociated with HCV related EHM in the EU5 (France Germany Italy United Kingdom
Spain)
Extrahepatic Manifestations of HCV
Extrahepatic Manifestations of HCV
HCV may cause extrahepatic disorders (HCV-EHDs) classified according to the number and
strength of supporting scientific data
HCV-EHDs are responsible for increasing morbidity and mortality with important
consequences in terms of social costs
The analysis of mortality rates in large cohorts confirmed the association of HCV with
several EHDs including cardiovascular neurologic metabolic or renal diseases and tumors
Viral eradication significantly reduced the rate of extra-hepatic deaths
Cacoub P et al DLD 2014 Lee MH et al J Infect Dis 2012 Backus LI et al Clin Gastroenterol Hepatol 2011 El-Kamary S et al
Clin Infect Dis 2011 Hsu YC et al Hepatology 2014 Kawamura Y et al Am J Med 2007 Adinolfi LE et al WJG 2014
Con il contributo di
Lee M-H et al J Infect Dis 2012206469-477
Follow-Up
(Years)
20
18
16
14
12
10
2
00 2 4 6 8 10 12 14 16 18 20
8
6
4
Follow-Up
(Years)
12
10
8
6
4
2
00 2 4 6 8 10 12 14 16 18 20
All Causes(n=2394)
Liver Cancer(n=115)
Extrahepatic Diseases(n=2199)
Cum
ula
tive M
ort
ali
ty (
)
Anti-HCV+ HCV RNA detectable Anti-HCV+ HCV RNA undetectable Anti-HCVndash
Follow-Up
(Years)
35
30
25
20
15
10
5
00 2 4 6 8 10 12 14 16 18 20
301
128124
104
16
03
198
122
110
Extrahepatic Manifestations of HCV
The annual costs (inpatient outpatient andpharmacy) associated with extrahepatic
manifestations of HCV were evaluated
Total direct medical costs of extrahepatic
manifestations of HCV in 2014 US dollars wereestimated to be $1506 million (range $922 millionndash
$2208 million in sensitivity analysis)
These estimates should be added to the liver-related
burden of disease to obtain a more accurateassessment of the total burden of HCV infection
Younossi et al
Younossi et al
Costs up to $71000 per patient per year (ESRD) Among the most frequent EHM depression (245 in HCV vs 172 in non-HCV) had estimated annual cost of
$4307 million DM (15 vs 10 in non- HCV) had an annual cost of $4434 million in the USA= given the importance of DM and
its association with CVDs and mortality the clinical and economic impacts of HCV-related DM are substantial
The OBJECTIVE of the study was to estimate the annual direct medical costsassociated with HCV related EHM in the EU5 (France Germany Italy United Kingdom
Spain)
The OBJECTIVE of the study was to estimate the annual direct medicalcosts associated with HCV related EHM in the EU5 (France Germany
Italy United Kingdom Spain)
1 HCV is the main etiopathological agent as concordantly demonstrated by epidemiological clinico-pathological virological and laboratory investigations2 the association between HCV and disease is demonstrated in a significant proportion of patients and supported by in depth clinico-pathogeneticstudies3 the association is suggested by cohort studies a possible causative role may be limited to a small number of patients andor possibly more relevant in specific geographical areas 4 a number of anecdotal observations suggested a possible role of HCV further investigations are required
The most studied and frequent HCV-EHDs are B-LPDs andor autoimmune disorders
Their prototype is Mixed Cryoglobulinemia (MC) from researches on MC derived most of the
available information
MC as a precious model for all the HCV-EHDs and to evaluate the effects of viral eradication
Anti-HCV Treatment Evolution
IFN
6 mos
PegIFN RBV 12
mos
IFN
12 mos
IFNRBV
12 mos
PegIFN
12 mos
2001
1998
2011
Standardinterferon
Ribavirin
Peginterferon
1991
Direct-actingantivirals
PegIFN
RBV
DAA
IFNRBV
6 mos
6
16
34
4239
55
70+
0
20
40
60
80
100
DAAs
826
weeks
gt90
2015
Few side effects absence major
contraindications
Younossi et al
The annual costs (inpatient outpatient and pharmacy) associatedwith extrahepatic manifestations of HCV were evaluated
Total direct medical costs of extrahepatic manifestations of HCV in 2014US dollars were estimated to be $1506 million (range $922 millionndash
$2208 million in sensitivity analysis)
These estimates should be added to the liver-related burden of diseaseto obtain a more accurate assessment of the total burden of HCV
infection
The OBJECTIVE of the study was to estimate the annual direct medical costs associated with HCV related EHM in the EU5 (France Germany Italy United Kingdom Spain)
22 MCS treated with DAAs including 2 HCC and 2 NHL 100 SVR12 Clinical CR in 64 and PR in remaining 36 The small lymphocytic lymphoma progressed despite viral clearance
Lauletta et al 2017
Emery CS et al 2017
Retrospective analysis 17 MCS (10 with severelife-threatening vasculitis) and 65 asymptomatic CGs+ pts treated with DAAs SVR 889 MCS and 908 asymptomatic pts In MCS clinical response in 1117 (complete in 717) In severelife-threatening vasculitis lower clinical response especially in renal and neurological symptoms
Saadoun D et al 2017
Open-label prospective multi-center study on sofosbuvir plus daclatasvir treatment of 41 HCV MCS SVR in100 and clinical CR in 902 Disappearance of CGs in 50 of pts No serious adverse event or relapse ofvasculitis
Antiviral Treatment (AVT) of MCIFN-free regimens
MC is clinically benign but sometimes severe HCV EHD invalidating symptoms occur and
it may evolve into lymphoma
Cacoub P et al DLD 2014 Zignego AL et al DLD 2007 Zignego AL et al Intern Emerg Med 2012 Zignego AL et al Clin Dev
Immunol 2012 Zignego AL et al Expert Rev Clin Immunol 2015 Sene D et al J Rheumatol 2004
Mixed Cryoglobulinemia-MC
MC pathological substrate is an HCV-driven B-cell
proliferation with consequent production of cryo- and non-
cryoprecipitable CICs in turn responsible for vasculitic
manifestations
Most (70ndash90) MC patients are HCV+ and HCV-patients are CGs+ (40ndash60) while 5ndash30 of
CGs+ have symptomatic MC or cryoglobulinemic vasculitis since HCV infects about 170
million individuals worldwide the number of patients at risk for developing MC is
substantial
Type II CGs
monoclonal
RF+policlonal IgG
Type III CGs both
RF and IgG
polyclonal

Antiviral Treatment (AVT) of MC IFN-free regimens
22 MCS treated with DAAs including 2 HCC and 2 NHL 100 SVR12 Clinical R in 100 (64 CR and 36 PR)
Progression of the small lymphocytic lymphoma
Lauletta et al 2017
Emery CS et al 2017
Retrospective analysis 17 MCS (10 with severelife-threatening vasculitis) and 65 asymptomatic MC treated with
DAAs SVR 889 MCS and 908 asymptomatic pts In MCS clinical R in 1117 (CR in 711) Lower clinical R inseverelife-threatening ndashespecial renal and neurological- vasculitis
Saadoun D et al 2017
Open-label prospective multi-center study on sofosbuvir plus daclatasvir treatment of 41 HCV MCS SVR in 100 and
clinical CR in 902 Disappearance of CGs in 50 of pts No serious adverse event or relapse of vasculitis
A case of rapid amelioration of HCV-associated cryoglobulinemic MPGN treated by
IFN-free DAAs for HCV in the absence of immunosuppressant
Fumiaki et al 2017
Zignego et al 2017
TIME POINTS
baseline EOT and week 12 and 24 of post-treatment f-up (SVR12 and SVR24 respectively)
HRQoL EVALUATION THROUGH PROs
the Short Form (36) Health Survey (SF-36)
the Functional Assessment of Chronic Illness Therapy-Fatigue (FACIT-F) from which we computed the Trial
Outcome Index (TOI)
Evaluation of The Impact on HRQol of IFN-free AVT In HCV CM
1 Physical Component Summary Score (PCS)
MC (54)
HCV (43) CV (85)
deg
A B C
degdegdeg
2 Mental Component Summary Score (MCS)
MCHCV CVD E F
degdegdegdegdeg
HCV
=plt001 vs baseline scores
degdeg=plt001 and degdegdeg=plt0001 vs EOT scores
Gragnani et al AASLD 2017
HCV Eradicationwith DAAs
To be preceded or combined with non-etiological pathogenetic therapy in severecatastrophic MCS
MCS Therapy in the IFN and DAAs Era from the complex to the simplified flow-chart
Dammacco F Sansonno D NEJM 2013
Zignego AL Pawlotsky JM Cacoub P Antiviral Ther in press Cacoub P et al Am J Med 2015
Mechanisms of HCV-related lymphomagenesis
DLBC HCV- induced
direct transformation
MCindolent NHL
accumulation of B RF
following BCR activation
and BC apoptosisinhibition
Zignego AL Ramos-Casals M Ferri C et al Autoimmun Rev 2017
Wang et al Hepatology 2016 Canioni et al Plos one 2016
Observational study on in situ expression of the oncogenic HCV NS3 protein on 116 HCV patients with B-NHL (DLBCL 36 and MZL 34)
NS3 immunostaining positive in 1214 DLBCL vs only 414 MZL (p = 0006) moreover 24 NS3+ MZL
were enriched in large cells
This study supports a new mechanism of transformation with a direct oncogenic role of
HCV proteins in the occurrence of high-grade B lymphomas
IN SITU HEPATITIS C NS3 PROTEIN DETECTION IS ASSOCIATED WITH HIGH GRADE
FEATURES IN HCV-ASSOCIATED B-CELL NON-HODGKIN LYMPHOMAS Danielle
Canioni et al 2016
In addition to the role of chronic antigenic stimulation in HCV related
lymphomagenesis this study supports a second mechanism of transformation due to a
direct oncogenic role of HCV infection of B-cells promoting the occurrence of high-grade Bcell lymphomas
Cohort study of 704 consecutive HIV-negative HCV-positive patients with indolent NHL from 1993 to
2009 in 39 centers of the FIL
Arcaini et al 2016
DLBC HCV- induced
direct transformation
No place of AVT as
1st line
Need of immediate delivery of
chemotherapy or concomitant (NHL
+ HCV targets)
THERAPY OF HCV+ DLBCL
ANTIVIRAL THERAPY IS ASSOCIATED WITH A BETTERSURVIVAL IN PATIENTS WITH HCV AND B-CELL NON-HODGKIN LYMPHOMAS ANRS HC-13 LYMPHO-CSTUDY Michot JM et al
Outcomes of HCV-associated B-NHL according to HCV AVT in prospective patients only (n 5 64)
Concurrent Systemic Chemoimmunotherapy and Sofosbuvir-Based Antiviral Treatment in a Hepatitis C Virus-Infected Patient With Diffuse Large B-Cell Lymphoma Evan C Ewers et al 2016
absolute neutrophil count and Hgb ALT and HCV viral load
Both complete response and SVR of HCV-associated DLBCL after concurrent chemoimmunotherapy and antiviral therapy using a sofosbuvir-based regimen
DAA-treatment in concomitance with chemotherapy showed to be safe and effective in influencing the remission of aggressive lymphomas in HCV patients
Persico M et al 2017
DFS in DAA treated and historical not-treated ptsAntiviral response rates in DAA treated patients
ANTIVIRAL THERAPY IN HCV+ B CELL NHL
IFN-based AVT induced hematological response along with SVR in patients with HCV-related indolent NHLs (especially
MZL)
Recent data with IFN-free regimens in HCV-associated LPDs suggest their anti-lymphoma activity too
AVT should be considered the first-line approach in HCV low grade lymphomas if there is no urgency of a conventional
treatment (ie systemic symptoms bulky disease or symptomatic splenomegaly) (ESMO NCCN EASL guidelines)
In aggressive lymphomas antiviral therapy after induction treatment is to be considered the standard at the moment but
in the next years (months) the association of immunochemotherapy and antiviral therapy will be considered the standard
Zignego AL Ramos-Casals M Ferri C et al Autoimmun Rev 2017
The Masve group
BASIC RESEARCH
Laura Gragnani
Patrizio Caini
Serena Lorini
Antonella Simone
CLINICAL RESEARCH
Monica Monti
Luisa Petraccia
Sinan Sadalla
Guia Cerretelli
Cristina Stasi
Adela Xheka
Universitagrave degli Studi di FirenzeDipartimento di Medicina Sperimentale e Clinica
Centro Manifestazioni Sistemiche da Virus EpatiticildquoMASVErdquo
Anna Linda Zignego
MASVE
UNDERGRADUATE STUDENTS Andrea Genovese Adrian Piscopo
ANTIVIRAL THERAPY IN HCV+ B CELL NHL
IFN-based AVT induced hematological response along with SVR in patients with HCV-related indolent
NHLs (especially MZL)
Recent data with IFN-free regimens in HCV-associated LPDs suggest their anti-lymphoma activity too
AVT should be considered the first-line approach in HCV low grade lymphomas if there is no urgency
of a conventional treatment (ie systemic symptoms bulky disease or symptomatic splenomegaly)
(ESMO NCCN EASL guidelines)
Main drugs for HCV-related MCS according to the target
HCV= DAAsB-cell Expansion= (a) B cell-depleting Mabs
-First-generation Rituximab (anti-CD20)-Second-generation Ofatumumab (anti-CD20) Veltuzumab (humanized
anti-CD20)-Third-generation Obinutuzumab (GA101) Oceratuzumab (humanized
anti-CD20)
(b) Alkylating agents
-Cyclophosfamide
Inflammation= Antiinflammatory agents
- Corticosteroids
Altered regulatory T-cell activity=
- IL-2
The impact on HRQoL of IFN-free AVT was prospectively evaluated in a cohort of HCV CV patients with limited
influencing variables linked to therapeutic schedulesviral GT
44 HCV GT2 CV patients mostly F0-F2 (29) and naiumlve (30) treated with SOFRBV for 1224wks
TIME POINTS
baseline EOT and week 12 and 24 of post-treatment f-up (SVR12 and SVR24 respectively)
HRQoL EVALUATION THROUGH PROs
the Short Form (36) Health Survey (SF-36)
the Functional Assessment of Chronic Illness Therapy-Fatigue (FACIT-F) from which we computed the Trial
Outcome Index (TOI)
Observational study on in situ expression of the oncogenic HCV NS3 protein on 116 HCV
patients with B-NHL (DLBCL 36 and MZL 34)
NS3 immunostaining positive in 1214 DLBCL vs only 414 MZL (p = 0006) moreover 24 NS3+
MZL were enriched in large cells
This study supports a new mechanism of transformation with a direct oncogenic role of
HCV proteins in the occurrence of high-grade B lymphomas
IN SITU HEPATITIS C NS3 PROTEIN DETECTION IS ASSOCIATED WITH HIGH GRADEFEATURES IN HCV-ASSOCIATED B-CELL NON-HODGKIN LYMPHOMAS Danielle
Canioni et al 2016
In addition to the role of chronic antigenic stimulation in HCV related
lymphomagenesis this study supports a second mechanism of transformation due toa direct oncogenic role of HCV infection of B-cells promoting the occurrence of high-grade Bcell lymphomas
ANTIVIRAL THERAPY IS ASSOCIATED WITH A BETTERSURVIVAL IN PATIENTS WITH HCV AND B-CELL NON-HODGKIN LYMPHOMAS ANRS HC-13 LYMPHO-CSTUDYMichot JM et al
Outcomes of HCV-associated B-NHL according to HCV AVT in prospective patients only (n 5 64)
(A) absolute neutrophil count and Hgb
(B) ALT and HCV viral load
This patient had HCV-associated DLBCL achieving both complete response and SVR after concurrent chemoimmunotherapy and antiviral therapy using a sofosbuvir-basedregimen
Concurrent Systemic Chemoimmunotherapy and Sofosbuvir-Based Antiviral Treatment in a Hepatitis C Virus-Infected Patient With Diffuse Large B-Cell LymphomaEvan C Ewers et al 2016
HCV-EHDs are responsible for increasing morbidity and mortality with important
consequences in terms of social costs
The analysis of mortality rates in large cohorts confirmed the association of HCV with
several EHDs including cardiovascular neurologic metabolic or renal diseases and tumors
Viral eradication significantly reduced the rate of extra-hepatic deaths
Cacoub P et al DLD 2014 Lee MH et al J Infect Dis 2012 Backus LI et al Clin Gastroenterol Hepatol 2011 El-Kamary S et al
Clin Infect Dis 2011 Hsu YC et al Hepatology 2014 Kawamura Y et al Am J Med 2007 Adinolfi LE et al WJG 2014
Extrahepatic Manifestations of HCV
Con il contributo di
Lee M-H et al J Infect Dis 2012206469-477
Follow-Up
(Years)
20
18
16
14
12
10
2
00 2 4 6 8 10 12 14 16 18 20
8
6
4
Follow-Up
(Years)
12
10
8
6
4
2
00 2 4 6 8 10 12 14 16 18 20
All Causes(n=2394)
Liver Cancer(n=115)
Extrahepatic Diseases(n=2199)
Cum
ula
tive M
ort
ali
ty (
)
Anti-HCV+ HCV RNA detectable Anti-HCV+ HCV RNA undetectable Anti-HCVndash
Follow-Up
(Years)
35
30
25
20
15
10
5
00 2 4 6 8 10 12 14 16 18 20
301
128124
104
16
03
198
122
110
MC is clinically benign but sometimes severe HCV EHD invalidating symptoms occur and
it may evolve into lymphoma
Cacoub P et al DLD 2014 Zignego AL et al DLD 2007 Zignego AL et al Intern Emerg Med 2012 Zignego AL et al Clin Dev
Immunol 2012 Zignego AL et al Expert Rev Clin Immunol 2015 Sene D et al J Rheumatol 2004
Mixed Cryoglobulinemia-MC
CGs reversibly precipitate when the temperature is lower than 37degC and
comprise IgMs with RF activity [mono- or oligo-clonal in type II MC or
polyclonal in type III MC] and polyclonal IgGs
MC pathological substrate is an HCV-driven B-cell
proliferation with consequent production of cryo- and non-
cryoprecipitable CICs in turn responsible for vasculitic
manifestations
Most (70ndash90) MC patients are HCV+ and HCV-patients are CGs+ (40ndash60) while 5ndash30 of
CGs+ have symptomatic MC since HCV infects about 170 million individuals worldwide the
number of patients at risk for developing MC is substantial
Type II
CGs
Type III
CGs
Zignego AL et al Autoimmun Rev 2017 Ferri C et al Autoimmunity rev 2016 Zignego AL et al DLD 2007 Cacoub P et al DLD
2014 Zignego AL et al DLD 2007 Zignego AL et al Intern Emerg Med 2012 Zignego AL et al Clin Dev Immunol 2012 Zignego
AL et al Expert Rev Clin Immunol 2015
MC clinical aspects MC Syndrome
MCS is characterized by the clinical triad -purpura weakness and
arthralgias- low complement C4 and various organsystem
involvement including cutaneous articular renal neurological
cardiac or digestive
It ranges from mild disease to severe even life-threatening
conditions
More serious lesions are generally characterized by neurologic and
renal involvement
Prognosis is highly dependent on renal involvement or on the extent
of vasculitis lesions
1 HCV is the main etiopathological agent as concordantly demonstrated by epidemiological clinico-pathological virological and laboratory investigations2 the association between HCV and disease is demonstrated in a significant proportion of patients and supported by in depth clinico-pathogeneticstudies3 the association is suggested by cohort studies a possible causative role may be limited to a small number of patients andor possibly more relevant in specific geographical areas 4 a number of anecdotal observations suggested a possible role of HCV further investigations are required
From P Cacoub 2015
HCV infection is closely related to LPDs mostly MC
40 to 60 of HCV patients show circulating CGs among this latter population 5-30
develop a symptomatic CV
AVT has been considered the first-line option in HCV-CV patients in fact in the majority
of cases viral eradication leads to CV clinical remission
Data about IFN-free regimens for the treatment of CV patients are still limited
HCV and MC
HCV and MC
Zignego 2015Ferri 2016Pozzato 2016 Sise 2016Saadoun 2015Gragnani 2016Gragnani 2016
Bonacci 2016Hegazy 2016Kondili 2016Emery 2017
Younossi et al
The annual costs (inpatient outpatient andpharmacy) associated with extrahepatic
manifestations of HCV were evaluated
Total direct medical costs of extrahepatic
manifestations of HCV in 2014 US dollars wereestimated to be $1506 million (range $922 millionndash
$2208 million in sensitivity analysis)
These estimates should be added to the liver-related
burden of disease to obtain a more accurateassessment of the total burden of HCV infection
The OBJECTIVE of the study was to estimate the annual direct medical costsassociated with HCV related EHM in the EU5 (France Germany Italy United Kingdom
Spain)
Extrahepatic Manifestations of HCV
Extrahepatic Manifestations of HCV
HCV may cause extrahepatic disorders (HCV-EHDs) classified according to the number and
strength of supporting scientific data
HCV-EHDs are responsible for increasing morbidity and mortality with important
consequences in terms of social costs
The analysis of mortality rates in large cohorts confirmed the association of HCV with
several EHDs including cardiovascular neurologic metabolic or renal diseases and tumors
Viral eradication significantly reduced the rate of extra-hepatic deaths
Cacoub P et al DLD 2014 Lee MH et al J Infect Dis 2012 Backus LI et al Clin Gastroenterol Hepatol 2011 El-Kamary S et al
Clin Infect Dis 2011 Hsu YC et al Hepatology 2014 Kawamura Y et al Am J Med 2007 Adinolfi LE et al WJG 2014
Con il contributo di
Lee M-H et al J Infect Dis 2012206469-477
Follow-Up
(Years)
20
18
16
14
12
10
2
00 2 4 6 8 10 12 14 16 18 20
8
6
4
Follow-Up
(Years)
12
10
8
6
4
2
00 2 4 6 8 10 12 14 16 18 20
All Causes(n=2394)
Liver Cancer(n=115)
Extrahepatic Diseases(n=2199)
Cum
ula
tive M
ort
ali
ty (
)
Anti-HCV+ HCV RNA detectable Anti-HCV+ HCV RNA undetectable Anti-HCVndash
Follow-Up
(Years)
35
30
25
20
15
10
5
00 2 4 6 8 10 12 14 16 18 20
301
128124
104
16
03
198
122
110
Extrahepatic Manifestations of HCV
The annual costs (inpatient outpatient andpharmacy) associated with extrahepatic
manifestations of HCV were evaluated
Total direct medical costs of extrahepatic
manifestations of HCV in 2014 US dollars wereestimated to be $1506 million (range $922 millionndash
$2208 million in sensitivity analysis)
These estimates should be added to the liver-related
burden of disease to obtain a more accurateassessment of the total burden of HCV infection
Younossi et al
Younossi et al
Costs up to $71000 per patient per year (ESRD) Among the most frequent EHM depression (245 in HCV vs 172 in non-HCV) had estimated annual cost of
$4307 million DM (15 vs 10 in non- HCV) had an annual cost of $4434 million in the USA= given the importance of DM and
its association with CVDs and mortality the clinical and economic impacts of HCV-related DM are substantial
The OBJECTIVE of the study was to estimate the annual direct medical costsassociated with HCV related EHM in the EU5 (France Germany Italy United Kingdom
Spain)
The OBJECTIVE of the study was to estimate the annual direct medicalcosts associated with HCV related EHM in the EU5 (France Germany
Italy United Kingdom Spain)
1 HCV is the main etiopathological agent as concordantly demonstrated by epidemiological clinico-pathological virological and laboratory investigations2 the association between HCV and disease is demonstrated in a significant proportion of patients and supported by in depth clinico-pathogeneticstudies3 the association is suggested by cohort studies a possible causative role may be limited to a small number of patients andor possibly more relevant in specific geographical areas 4 a number of anecdotal observations suggested a possible role of HCV further investigations are required
The most studied and frequent HCV-EHDs are B-LPDs andor autoimmune disorders
Their prototype is Mixed Cryoglobulinemia (MC) from researches on MC derived most of the
available information
MC as a precious model for all the HCV-EHDs and to evaluate the effects of viral eradication
Anti-HCV Treatment Evolution
IFN
6 mos
PegIFN RBV 12
mos
IFN
12 mos
IFNRBV
12 mos
PegIFN
12 mos
2001
1998
2011
Standardinterferon
Ribavirin
Peginterferon
1991
Direct-actingantivirals
PegIFN
RBV
DAA
IFNRBV
6 mos
6
16
34
4239
55
70+
0
20
40
60
80
100
DAAs
826
weeks
gt90
2015
Few side effects absence major
contraindications
Younossi et al
The annual costs (inpatient outpatient and pharmacy) associatedwith extrahepatic manifestations of HCV were evaluated
Total direct medical costs of extrahepatic manifestations of HCV in 2014US dollars were estimated to be $1506 million (range $922 millionndash
$2208 million in sensitivity analysis)
These estimates should be added to the liver-related burden of diseaseto obtain a more accurate assessment of the total burden of HCV
infection
The OBJECTIVE of the study was to estimate the annual direct medical costs associated with HCV related EHM in the EU5 (France Germany Italy United Kingdom Spain)
22 MCS treated with DAAs including 2 HCC and 2 NHL 100 SVR12 Clinical CR in 64 and PR in remaining 36 The small lymphocytic lymphoma progressed despite viral clearance
Lauletta et al 2017
Emery CS et al 2017
Retrospective analysis 17 MCS (10 with severelife-threatening vasculitis) and 65 asymptomatic CGs+ pts treated with DAAs SVR 889 MCS and 908 asymptomatic pts In MCS clinical response in 1117 (complete in 717) In severelife-threatening vasculitis lower clinical response especially in renal and neurological symptoms
Saadoun D et al 2017
Open-label prospective multi-center study on sofosbuvir plus daclatasvir treatment of 41 HCV MCS SVR in100 and clinical CR in 902 Disappearance of CGs in 50 of pts No serious adverse event or relapse ofvasculitis
Antiviral Treatment (AVT) of MCIFN-free regimens
MC is clinically benign but sometimes severe HCV EHD invalidating symptoms occur and
it may evolve into lymphoma
Cacoub P et al DLD 2014 Zignego AL et al DLD 2007 Zignego AL et al Intern Emerg Med 2012 Zignego AL et al Clin Dev
Immunol 2012 Zignego AL et al Expert Rev Clin Immunol 2015 Sene D et al J Rheumatol 2004
Mixed Cryoglobulinemia-MC
MC pathological substrate is an HCV-driven B-cell
proliferation with consequent production of cryo- and non-
cryoprecipitable CICs in turn responsible for vasculitic
manifestations
Most (70ndash90) MC patients are HCV+ and HCV-patients are CGs+ (40ndash60) while 5ndash30 of
CGs+ have symptomatic MC or cryoglobulinemic vasculitis since HCV infects about 170
million individuals worldwide the number of patients at risk for developing MC is
substantial
Type II CGs
monoclonal
RF+policlonal IgG
Type III CGs both
RF and IgG
polyclonal

Zignego et al 2017
TIME POINTS
baseline EOT and week 12 and 24 of post-treatment f-up (SVR12 and SVR24 respectively)
HRQoL EVALUATION THROUGH PROs
the Short Form (36) Health Survey (SF-36)
the Functional Assessment of Chronic Illness Therapy-Fatigue (FACIT-F) from which we computed the Trial
Outcome Index (TOI)
Evaluation of The Impact on HRQol of IFN-free AVT In HCV CM
1 Physical Component Summary Score (PCS)
MC (54)
HCV (43) CV (85)
deg
A B C
degdegdeg
2 Mental Component Summary Score (MCS)
MCHCV CVD E F
degdegdegdegdeg
HCV
=plt001 vs baseline scores
degdeg=plt001 and degdegdeg=plt0001 vs EOT scores
Gragnani et al AASLD 2017
HCV Eradicationwith DAAs
To be preceded or combined with non-etiological pathogenetic therapy in severecatastrophic MCS
MCS Therapy in the IFN and DAAs Era from the complex to the simplified flow-chart
Dammacco F Sansonno D NEJM 2013
Zignego AL Pawlotsky JM Cacoub P Antiviral Ther in press Cacoub P et al Am J Med 2015
Mechanisms of HCV-related lymphomagenesis
DLBC HCV- induced
direct transformation
MCindolent NHL
accumulation of B RF
following BCR activation
and BC apoptosisinhibition
Zignego AL Ramos-Casals M Ferri C et al Autoimmun Rev 2017
Wang et al Hepatology 2016 Canioni et al Plos one 2016
Observational study on in situ expression of the oncogenic HCV NS3 protein on 116 HCV patients with B-NHL (DLBCL 36 and MZL 34)
NS3 immunostaining positive in 1214 DLBCL vs only 414 MZL (p = 0006) moreover 24 NS3+ MZL
were enriched in large cells
This study supports a new mechanism of transformation with a direct oncogenic role of
HCV proteins in the occurrence of high-grade B lymphomas
IN SITU HEPATITIS C NS3 PROTEIN DETECTION IS ASSOCIATED WITH HIGH GRADE
FEATURES IN HCV-ASSOCIATED B-CELL NON-HODGKIN LYMPHOMAS Danielle
Canioni et al 2016
In addition to the role of chronic antigenic stimulation in HCV related
lymphomagenesis this study supports a second mechanism of transformation due to a
direct oncogenic role of HCV infection of B-cells promoting the occurrence of high-grade Bcell lymphomas
Cohort study of 704 consecutive HIV-negative HCV-positive patients with indolent NHL from 1993 to
2009 in 39 centers of the FIL
Arcaini et al 2016
DLBC HCV- induced
direct transformation
No place of AVT as
1st line
Need of immediate delivery of
chemotherapy or concomitant (NHL
+ HCV targets)
THERAPY OF HCV+ DLBCL
ANTIVIRAL THERAPY IS ASSOCIATED WITH A BETTERSURVIVAL IN PATIENTS WITH HCV AND B-CELL NON-HODGKIN LYMPHOMAS ANRS HC-13 LYMPHO-CSTUDY Michot JM et al
Outcomes of HCV-associated B-NHL according to HCV AVT in prospective patients only (n 5 64)
Concurrent Systemic Chemoimmunotherapy and Sofosbuvir-Based Antiviral Treatment in a Hepatitis C Virus-Infected Patient With Diffuse Large B-Cell Lymphoma Evan C Ewers et al 2016
absolute neutrophil count and Hgb ALT and HCV viral load
Both complete response and SVR of HCV-associated DLBCL after concurrent chemoimmunotherapy and antiviral therapy using a sofosbuvir-based regimen
DAA-treatment in concomitance with chemotherapy showed to be safe and effective in influencing the remission of aggressive lymphomas in HCV patients
Persico M et al 2017
DFS in DAA treated and historical not-treated ptsAntiviral response rates in DAA treated patients
ANTIVIRAL THERAPY IN HCV+ B CELL NHL
IFN-based AVT induced hematological response along with SVR in patients with HCV-related indolent NHLs (especially
MZL)
Recent data with IFN-free regimens in HCV-associated LPDs suggest their anti-lymphoma activity too
AVT should be considered the first-line approach in HCV low grade lymphomas if there is no urgency of a conventional
treatment (ie systemic symptoms bulky disease or symptomatic splenomegaly) (ESMO NCCN EASL guidelines)
In aggressive lymphomas antiviral therapy after induction treatment is to be considered the standard at the moment but
in the next years (months) the association of immunochemotherapy and antiviral therapy will be considered the standard
Zignego AL Ramos-Casals M Ferri C et al Autoimmun Rev 2017
The Masve group
BASIC RESEARCH
Laura Gragnani
Patrizio Caini
Serena Lorini
Antonella Simone
CLINICAL RESEARCH
Monica Monti
Luisa Petraccia
Sinan Sadalla
Guia Cerretelli
Cristina Stasi
Adela Xheka
Universitagrave degli Studi di FirenzeDipartimento di Medicina Sperimentale e Clinica
Centro Manifestazioni Sistemiche da Virus EpatiticildquoMASVErdquo
Anna Linda Zignego
MASVE
UNDERGRADUATE STUDENTS Andrea Genovese Adrian Piscopo
ANTIVIRAL THERAPY IN HCV+ B CELL NHL
IFN-based AVT induced hematological response along with SVR in patients with HCV-related indolent
NHLs (especially MZL)
Recent data with IFN-free regimens in HCV-associated LPDs suggest their anti-lymphoma activity too
AVT should be considered the first-line approach in HCV low grade lymphomas if there is no urgency
of a conventional treatment (ie systemic symptoms bulky disease or symptomatic splenomegaly)
(ESMO NCCN EASL guidelines)
Main drugs for HCV-related MCS according to the target
HCV= DAAsB-cell Expansion= (a) B cell-depleting Mabs
-First-generation Rituximab (anti-CD20)-Second-generation Ofatumumab (anti-CD20) Veltuzumab (humanized
anti-CD20)-Third-generation Obinutuzumab (GA101) Oceratuzumab (humanized
anti-CD20)
(b) Alkylating agents
-Cyclophosfamide
Inflammation= Antiinflammatory agents
- Corticosteroids
Altered regulatory T-cell activity=
- IL-2
The impact on HRQoL of IFN-free AVT was prospectively evaluated in a cohort of HCV CV patients with limited
influencing variables linked to therapeutic schedulesviral GT
44 HCV GT2 CV patients mostly F0-F2 (29) and naiumlve (30) treated with SOFRBV for 1224wks
TIME POINTS
baseline EOT and week 12 and 24 of post-treatment f-up (SVR12 and SVR24 respectively)
HRQoL EVALUATION THROUGH PROs
the Short Form (36) Health Survey (SF-36)
the Functional Assessment of Chronic Illness Therapy-Fatigue (FACIT-F) from which we computed the Trial
Outcome Index (TOI)
Observational study on in situ expression of the oncogenic HCV NS3 protein on 116 HCV
patients with B-NHL (DLBCL 36 and MZL 34)
NS3 immunostaining positive in 1214 DLBCL vs only 414 MZL (p = 0006) moreover 24 NS3+
MZL were enriched in large cells
This study supports a new mechanism of transformation with a direct oncogenic role of
HCV proteins in the occurrence of high-grade B lymphomas
IN SITU HEPATITIS C NS3 PROTEIN DETECTION IS ASSOCIATED WITH HIGH GRADEFEATURES IN HCV-ASSOCIATED B-CELL NON-HODGKIN LYMPHOMAS Danielle
Canioni et al 2016
In addition to the role of chronic antigenic stimulation in HCV related
lymphomagenesis this study supports a second mechanism of transformation due toa direct oncogenic role of HCV infection of B-cells promoting the occurrence of high-grade Bcell lymphomas
ANTIVIRAL THERAPY IS ASSOCIATED WITH A BETTERSURVIVAL IN PATIENTS WITH HCV AND B-CELL NON-HODGKIN LYMPHOMAS ANRS HC-13 LYMPHO-CSTUDYMichot JM et al
Outcomes of HCV-associated B-NHL according to HCV AVT in prospective patients only (n 5 64)
(A) absolute neutrophil count and Hgb
(B) ALT and HCV viral load
This patient had HCV-associated DLBCL achieving both complete response and SVR after concurrent chemoimmunotherapy and antiviral therapy using a sofosbuvir-basedregimen
Concurrent Systemic Chemoimmunotherapy and Sofosbuvir-Based Antiviral Treatment in a Hepatitis C Virus-Infected Patient With Diffuse Large B-Cell LymphomaEvan C Ewers et al 2016
HCV-EHDs are responsible for increasing morbidity and mortality with important
consequences in terms of social costs
The analysis of mortality rates in large cohorts confirmed the association of HCV with
several EHDs including cardiovascular neurologic metabolic or renal diseases and tumors
Viral eradication significantly reduced the rate of extra-hepatic deaths
Cacoub P et al DLD 2014 Lee MH et al J Infect Dis 2012 Backus LI et al Clin Gastroenterol Hepatol 2011 El-Kamary S et al
Clin Infect Dis 2011 Hsu YC et al Hepatology 2014 Kawamura Y et al Am J Med 2007 Adinolfi LE et al WJG 2014
Extrahepatic Manifestations of HCV
Con il contributo di
Lee M-H et al J Infect Dis 2012206469-477
Follow-Up
(Years)
20
18
16
14
12
10
2
00 2 4 6 8 10 12 14 16 18 20
8
6
4
Follow-Up
(Years)
12
10
8
6
4
2
00 2 4 6 8 10 12 14 16 18 20
All Causes(n=2394)
Liver Cancer(n=115)
Extrahepatic Diseases(n=2199)
Cum
ula
tive M
ort
ali
ty (
)
Anti-HCV+ HCV RNA detectable Anti-HCV+ HCV RNA undetectable Anti-HCVndash
Follow-Up
(Years)
35
30
25
20
15
10
5
00 2 4 6 8 10 12 14 16 18 20
301
128124
104
16
03
198
122
110
MC is clinically benign but sometimes severe HCV EHD invalidating symptoms occur and
it may evolve into lymphoma
Cacoub P et al DLD 2014 Zignego AL et al DLD 2007 Zignego AL et al Intern Emerg Med 2012 Zignego AL et al Clin Dev
Immunol 2012 Zignego AL et al Expert Rev Clin Immunol 2015 Sene D et al J Rheumatol 2004
Mixed Cryoglobulinemia-MC
CGs reversibly precipitate when the temperature is lower than 37degC and
comprise IgMs with RF activity [mono- or oligo-clonal in type II MC or
polyclonal in type III MC] and polyclonal IgGs
MC pathological substrate is an HCV-driven B-cell
proliferation with consequent production of cryo- and non-
cryoprecipitable CICs in turn responsible for vasculitic
manifestations
Most (70ndash90) MC patients are HCV+ and HCV-patients are CGs+ (40ndash60) while 5ndash30 of
CGs+ have symptomatic MC since HCV infects about 170 million individuals worldwide the
number of patients at risk for developing MC is substantial
Type II
CGs
Type III
CGs
Zignego AL et al Autoimmun Rev 2017 Ferri C et al Autoimmunity rev 2016 Zignego AL et al DLD 2007 Cacoub P et al DLD
2014 Zignego AL et al DLD 2007 Zignego AL et al Intern Emerg Med 2012 Zignego AL et al Clin Dev Immunol 2012 Zignego
AL et al Expert Rev Clin Immunol 2015
MC clinical aspects MC Syndrome
MCS is characterized by the clinical triad -purpura weakness and
arthralgias- low complement C4 and various organsystem
involvement including cutaneous articular renal neurological
cardiac or digestive
It ranges from mild disease to severe even life-threatening
conditions
More serious lesions are generally characterized by neurologic and
renal involvement
Prognosis is highly dependent on renal involvement or on the extent
of vasculitis lesions
1 HCV is the main etiopathological agent as concordantly demonstrated by epidemiological clinico-pathological virological and laboratory investigations2 the association between HCV and disease is demonstrated in a significant proportion of patients and supported by in depth clinico-pathogeneticstudies3 the association is suggested by cohort studies a possible causative role may be limited to a small number of patients andor possibly more relevant in specific geographical areas 4 a number of anecdotal observations suggested a possible role of HCV further investigations are required
From P Cacoub 2015
HCV infection is closely related to LPDs mostly MC
40 to 60 of HCV patients show circulating CGs among this latter population 5-30
develop a symptomatic CV
AVT has been considered the first-line option in HCV-CV patients in fact in the majority
of cases viral eradication leads to CV clinical remission
Data about IFN-free regimens for the treatment of CV patients are still limited
HCV and MC
HCV and MC
Zignego 2015Ferri 2016Pozzato 2016 Sise 2016Saadoun 2015Gragnani 2016Gragnani 2016
Bonacci 2016Hegazy 2016Kondili 2016Emery 2017
Younossi et al
The annual costs (inpatient outpatient andpharmacy) associated with extrahepatic
manifestations of HCV were evaluated
Total direct medical costs of extrahepatic
manifestations of HCV in 2014 US dollars wereestimated to be $1506 million (range $922 millionndash
$2208 million in sensitivity analysis)
These estimates should be added to the liver-related
burden of disease to obtain a more accurateassessment of the total burden of HCV infection
The OBJECTIVE of the study was to estimate the annual direct medical costsassociated with HCV related EHM in the EU5 (France Germany Italy United Kingdom
Spain)
Extrahepatic Manifestations of HCV
Extrahepatic Manifestations of HCV
HCV may cause extrahepatic disorders (HCV-EHDs) classified according to the number and
strength of supporting scientific data
HCV-EHDs are responsible for increasing morbidity and mortality with important
consequences in terms of social costs
The analysis of mortality rates in large cohorts confirmed the association of HCV with
several EHDs including cardiovascular neurologic metabolic or renal diseases and tumors
Viral eradication significantly reduced the rate of extra-hepatic deaths
Cacoub P et al DLD 2014 Lee MH et al J Infect Dis 2012 Backus LI et al Clin Gastroenterol Hepatol 2011 El-Kamary S et al
Clin Infect Dis 2011 Hsu YC et al Hepatology 2014 Kawamura Y et al Am J Med 2007 Adinolfi LE et al WJG 2014
Con il contributo di
Lee M-H et al J Infect Dis 2012206469-477
Follow-Up
(Years)
20
18
16
14
12
10
2
00 2 4 6 8 10 12 14 16 18 20
8
6
4
Follow-Up
(Years)
12
10
8
6
4
2
00 2 4 6 8 10 12 14 16 18 20
All Causes(n=2394)
Liver Cancer(n=115)
Extrahepatic Diseases(n=2199)
Cum
ula
tive M
ort
ali
ty (
)
Anti-HCV+ HCV RNA detectable Anti-HCV+ HCV RNA undetectable Anti-HCVndash
Follow-Up
(Years)
35
30
25
20
15
10
5
00 2 4 6 8 10 12 14 16 18 20
301
128124
104
16
03
198
122
110
Extrahepatic Manifestations of HCV
The annual costs (inpatient outpatient andpharmacy) associated with extrahepatic
manifestations of HCV were evaluated
Total direct medical costs of extrahepatic
manifestations of HCV in 2014 US dollars wereestimated to be $1506 million (range $922 millionndash
$2208 million in sensitivity analysis)
These estimates should be added to the liver-related
burden of disease to obtain a more accurateassessment of the total burden of HCV infection
Younossi et al
Younossi et al
Costs up to $71000 per patient per year (ESRD) Among the most frequent EHM depression (245 in HCV vs 172 in non-HCV) had estimated annual cost of
$4307 million DM (15 vs 10 in non- HCV) had an annual cost of $4434 million in the USA= given the importance of DM and
its association with CVDs and mortality the clinical and economic impacts of HCV-related DM are substantial
The OBJECTIVE of the study was to estimate the annual direct medical costsassociated with HCV related EHM in the EU5 (France Germany Italy United Kingdom
Spain)
The OBJECTIVE of the study was to estimate the annual direct medicalcosts associated with HCV related EHM in the EU5 (France Germany
Italy United Kingdom Spain)
1 HCV is the main etiopathological agent as concordantly demonstrated by epidemiological clinico-pathological virological and laboratory investigations2 the association between HCV and disease is demonstrated in a significant proportion of patients and supported by in depth clinico-pathogeneticstudies3 the association is suggested by cohort studies a possible causative role may be limited to a small number of patients andor possibly more relevant in specific geographical areas 4 a number of anecdotal observations suggested a possible role of HCV further investigations are required
The most studied and frequent HCV-EHDs are B-LPDs andor autoimmune disorders
Their prototype is Mixed Cryoglobulinemia (MC) from researches on MC derived most of the
available information
MC as a precious model for all the HCV-EHDs and to evaluate the effects of viral eradication
Anti-HCV Treatment Evolution
IFN
6 mos
PegIFN RBV 12
mos
IFN
12 mos
IFNRBV
12 mos
PegIFN
12 mos
2001
1998
2011
Standardinterferon
Ribavirin
Peginterferon
1991
Direct-actingantivirals
PegIFN
RBV
DAA
IFNRBV
6 mos
6
16
34
4239
55
70+
0
20
40
60
80
100
DAAs
826
weeks
gt90
2015
Few side effects absence major
contraindications
Younossi et al
The annual costs (inpatient outpatient and pharmacy) associatedwith extrahepatic manifestations of HCV were evaluated
Total direct medical costs of extrahepatic manifestations of HCV in 2014US dollars were estimated to be $1506 million (range $922 millionndash
$2208 million in sensitivity analysis)
These estimates should be added to the liver-related burden of diseaseto obtain a more accurate assessment of the total burden of HCV
infection
The OBJECTIVE of the study was to estimate the annual direct medical costs associated with HCV related EHM in the EU5 (France Germany Italy United Kingdom Spain)
22 MCS treated with DAAs including 2 HCC and 2 NHL 100 SVR12 Clinical CR in 64 and PR in remaining 36 The small lymphocytic lymphoma progressed despite viral clearance
Lauletta et al 2017
Emery CS et al 2017
Retrospective analysis 17 MCS (10 with severelife-threatening vasculitis) and 65 asymptomatic CGs+ pts treated with DAAs SVR 889 MCS and 908 asymptomatic pts In MCS clinical response in 1117 (complete in 717) In severelife-threatening vasculitis lower clinical response especially in renal and neurological symptoms
Saadoun D et al 2017
Open-label prospective multi-center study on sofosbuvir plus daclatasvir treatment of 41 HCV MCS SVR in100 and clinical CR in 902 Disappearance of CGs in 50 of pts No serious adverse event or relapse ofvasculitis
Antiviral Treatment (AVT) of MCIFN-free regimens
MC is clinically benign but sometimes severe HCV EHD invalidating symptoms occur and
it may evolve into lymphoma
Cacoub P et al DLD 2014 Zignego AL et al DLD 2007 Zignego AL et al Intern Emerg Med 2012 Zignego AL et al Clin Dev
Immunol 2012 Zignego AL et al Expert Rev Clin Immunol 2015 Sene D et al J Rheumatol 2004
Mixed Cryoglobulinemia-MC
MC pathological substrate is an HCV-driven B-cell
proliferation with consequent production of cryo- and non-
cryoprecipitable CICs in turn responsible for vasculitic
manifestations
Most (70ndash90) MC patients are HCV+ and HCV-patients are CGs+ (40ndash60) while 5ndash30 of
CGs+ have symptomatic MC or cryoglobulinemic vasculitis since HCV infects about 170
million individuals worldwide the number of patients at risk for developing MC is
substantial
Type II CGs
monoclonal
RF+policlonal IgG
Type III CGs both
RF and IgG
polyclonal

TIME POINTS
baseline EOT and week 12 and 24 of post-treatment f-up (SVR12 and SVR24 respectively)
HRQoL EVALUATION THROUGH PROs
the Short Form (36) Health Survey (SF-36)
the Functional Assessment of Chronic Illness Therapy-Fatigue (FACIT-F) from which we computed the Trial
Outcome Index (TOI)
Evaluation of The Impact on HRQol of IFN-free AVT In HCV CM
1 Physical Component Summary Score (PCS)
MC (54)
HCV (43) CV (85)
deg
A B C
degdegdeg
2 Mental Component Summary Score (MCS)
MCHCV CVD E F
degdegdegdegdeg
HCV
=plt001 vs baseline scores
degdeg=plt001 and degdegdeg=plt0001 vs EOT scores
Gragnani et al AASLD 2017
HCV Eradicationwith DAAs
To be preceded or combined with non-etiological pathogenetic therapy in severecatastrophic MCS
MCS Therapy in the IFN and DAAs Era from the complex to the simplified flow-chart
Dammacco F Sansonno D NEJM 2013
Zignego AL Pawlotsky JM Cacoub P Antiviral Ther in press Cacoub P et al Am J Med 2015
Mechanisms of HCV-related lymphomagenesis
DLBC HCV- induced
direct transformation
MCindolent NHL
accumulation of B RF
following BCR activation
and BC apoptosisinhibition
Zignego AL Ramos-Casals M Ferri C et al Autoimmun Rev 2017
Wang et al Hepatology 2016 Canioni et al Plos one 2016
Observational study on in situ expression of the oncogenic HCV NS3 protein on 116 HCV patients with B-NHL (DLBCL 36 and MZL 34)
NS3 immunostaining positive in 1214 DLBCL vs only 414 MZL (p = 0006) moreover 24 NS3+ MZL
were enriched in large cells
This study supports a new mechanism of transformation with a direct oncogenic role of
HCV proteins in the occurrence of high-grade B lymphomas
IN SITU HEPATITIS C NS3 PROTEIN DETECTION IS ASSOCIATED WITH HIGH GRADE
FEATURES IN HCV-ASSOCIATED B-CELL NON-HODGKIN LYMPHOMAS Danielle
Canioni et al 2016
In addition to the role of chronic antigenic stimulation in HCV related
lymphomagenesis this study supports a second mechanism of transformation due to a
direct oncogenic role of HCV infection of B-cells promoting the occurrence of high-grade Bcell lymphomas
Cohort study of 704 consecutive HIV-negative HCV-positive patients with indolent NHL from 1993 to
2009 in 39 centers of the FIL
Arcaini et al 2016
DLBC HCV- induced
direct transformation
No place of AVT as
1st line
Need of immediate delivery of
chemotherapy or concomitant (NHL
+ HCV targets)
THERAPY OF HCV+ DLBCL
ANTIVIRAL THERAPY IS ASSOCIATED WITH A BETTERSURVIVAL IN PATIENTS WITH HCV AND B-CELL NON-HODGKIN LYMPHOMAS ANRS HC-13 LYMPHO-CSTUDY Michot JM et al
Outcomes of HCV-associated B-NHL according to HCV AVT in prospective patients only (n 5 64)
Concurrent Systemic Chemoimmunotherapy and Sofosbuvir-Based Antiviral Treatment in a Hepatitis C Virus-Infected Patient With Diffuse Large B-Cell Lymphoma Evan C Ewers et al 2016
absolute neutrophil count and Hgb ALT and HCV viral load
Both complete response and SVR of HCV-associated DLBCL after concurrent chemoimmunotherapy and antiviral therapy using a sofosbuvir-based regimen
DAA-treatment in concomitance with chemotherapy showed to be safe and effective in influencing the remission of aggressive lymphomas in HCV patients
Persico M et al 2017
DFS in DAA treated and historical not-treated ptsAntiviral response rates in DAA treated patients
ANTIVIRAL THERAPY IN HCV+ B CELL NHL
IFN-based AVT induced hematological response along with SVR in patients with HCV-related indolent NHLs (especially
MZL)
Recent data with IFN-free regimens in HCV-associated LPDs suggest their anti-lymphoma activity too
AVT should be considered the first-line approach in HCV low grade lymphomas if there is no urgency of a conventional
treatment (ie systemic symptoms bulky disease or symptomatic splenomegaly) (ESMO NCCN EASL guidelines)
In aggressive lymphomas antiviral therapy after induction treatment is to be considered the standard at the moment but
in the next years (months) the association of immunochemotherapy and antiviral therapy will be considered the standard
Zignego AL Ramos-Casals M Ferri C et al Autoimmun Rev 2017
The Masve group
BASIC RESEARCH
Laura Gragnani
Patrizio Caini
Serena Lorini
Antonella Simone
CLINICAL RESEARCH
Monica Monti
Luisa Petraccia
Sinan Sadalla
Guia Cerretelli
Cristina Stasi
Adela Xheka
Universitagrave degli Studi di FirenzeDipartimento di Medicina Sperimentale e Clinica
Centro Manifestazioni Sistemiche da Virus EpatiticildquoMASVErdquo
Anna Linda Zignego
MASVE
UNDERGRADUATE STUDENTS Andrea Genovese Adrian Piscopo
ANTIVIRAL THERAPY IN HCV+ B CELL NHL
IFN-based AVT induced hematological response along with SVR in patients with HCV-related indolent
NHLs (especially MZL)
Recent data with IFN-free regimens in HCV-associated LPDs suggest their anti-lymphoma activity too
AVT should be considered the first-line approach in HCV low grade lymphomas if there is no urgency
of a conventional treatment (ie systemic symptoms bulky disease or symptomatic splenomegaly)
(ESMO NCCN EASL guidelines)
Main drugs for HCV-related MCS according to the target
HCV= DAAsB-cell Expansion= (a) B cell-depleting Mabs
-First-generation Rituximab (anti-CD20)-Second-generation Ofatumumab (anti-CD20) Veltuzumab (humanized
anti-CD20)-Third-generation Obinutuzumab (GA101) Oceratuzumab (humanized
anti-CD20)
(b) Alkylating agents
-Cyclophosfamide
Inflammation= Antiinflammatory agents
- Corticosteroids
Altered regulatory T-cell activity=
- IL-2
The impact on HRQoL of IFN-free AVT was prospectively evaluated in a cohort of HCV CV patients with limited
influencing variables linked to therapeutic schedulesviral GT
44 HCV GT2 CV patients mostly F0-F2 (29) and naiumlve (30) treated with SOFRBV for 1224wks
TIME POINTS
baseline EOT and week 12 and 24 of post-treatment f-up (SVR12 and SVR24 respectively)
HRQoL EVALUATION THROUGH PROs
the Short Form (36) Health Survey (SF-36)
the Functional Assessment of Chronic Illness Therapy-Fatigue (FACIT-F) from which we computed the Trial
Outcome Index (TOI)
Observational study on in situ expression of the oncogenic HCV NS3 protein on 116 HCV
patients with B-NHL (DLBCL 36 and MZL 34)
NS3 immunostaining positive in 1214 DLBCL vs only 414 MZL (p = 0006) moreover 24 NS3+
MZL were enriched in large cells
This study supports a new mechanism of transformation with a direct oncogenic role of
HCV proteins in the occurrence of high-grade B lymphomas
IN SITU HEPATITIS C NS3 PROTEIN DETECTION IS ASSOCIATED WITH HIGH GRADEFEATURES IN HCV-ASSOCIATED B-CELL NON-HODGKIN LYMPHOMAS Danielle
Canioni et al 2016
In addition to the role of chronic antigenic stimulation in HCV related
lymphomagenesis this study supports a second mechanism of transformation due toa direct oncogenic role of HCV infection of B-cells promoting the occurrence of high-grade Bcell lymphomas
ANTIVIRAL THERAPY IS ASSOCIATED WITH A BETTERSURVIVAL IN PATIENTS WITH HCV AND B-CELL NON-HODGKIN LYMPHOMAS ANRS HC-13 LYMPHO-CSTUDYMichot JM et al
Outcomes of HCV-associated B-NHL according to HCV AVT in prospective patients only (n 5 64)
(A) absolute neutrophil count and Hgb
(B) ALT and HCV viral load
This patient had HCV-associated DLBCL achieving both complete response and SVR after concurrent chemoimmunotherapy and antiviral therapy using a sofosbuvir-basedregimen
Concurrent Systemic Chemoimmunotherapy and Sofosbuvir-Based Antiviral Treatment in a Hepatitis C Virus-Infected Patient With Diffuse Large B-Cell LymphomaEvan C Ewers et al 2016
HCV-EHDs are responsible for increasing morbidity and mortality with important
consequences in terms of social costs
The analysis of mortality rates in large cohorts confirmed the association of HCV with
several EHDs including cardiovascular neurologic metabolic or renal diseases and tumors
Viral eradication significantly reduced the rate of extra-hepatic deaths
Cacoub P et al DLD 2014 Lee MH et al J Infect Dis 2012 Backus LI et al Clin Gastroenterol Hepatol 2011 El-Kamary S et al
Clin Infect Dis 2011 Hsu YC et al Hepatology 2014 Kawamura Y et al Am J Med 2007 Adinolfi LE et al WJG 2014
Extrahepatic Manifestations of HCV
Con il contributo di
Lee M-H et al J Infect Dis 2012206469-477
Follow-Up
(Years)
20
18
16
14
12
10
2
00 2 4 6 8 10 12 14 16 18 20
8
6
4
Follow-Up
(Years)
12
10
8
6
4
2
00 2 4 6 8 10 12 14 16 18 20
All Causes(n=2394)
Liver Cancer(n=115)
Extrahepatic Diseases(n=2199)
Cum
ula
tive M
ort
ali
ty (
)
Anti-HCV+ HCV RNA detectable Anti-HCV+ HCV RNA undetectable Anti-HCVndash
Follow-Up
(Years)
35
30
25
20
15
10
5
00 2 4 6 8 10 12 14 16 18 20
301
128124
104
16
03
198
122
110
MC is clinically benign but sometimes severe HCV EHD invalidating symptoms occur and
it may evolve into lymphoma
Cacoub P et al DLD 2014 Zignego AL et al DLD 2007 Zignego AL et al Intern Emerg Med 2012 Zignego AL et al Clin Dev
Immunol 2012 Zignego AL et al Expert Rev Clin Immunol 2015 Sene D et al J Rheumatol 2004
Mixed Cryoglobulinemia-MC
CGs reversibly precipitate when the temperature is lower than 37degC and
comprise IgMs with RF activity [mono- or oligo-clonal in type II MC or
polyclonal in type III MC] and polyclonal IgGs
MC pathological substrate is an HCV-driven B-cell
proliferation with consequent production of cryo- and non-
cryoprecipitable CICs in turn responsible for vasculitic
manifestations
Most (70ndash90) MC patients are HCV+ and HCV-patients are CGs+ (40ndash60) while 5ndash30 of
CGs+ have symptomatic MC since HCV infects about 170 million individuals worldwide the
number of patients at risk for developing MC is substantial
Type II
CGs
Type III
CGs
Zignego AL et al Autoimmun Rev 2017 Ferri C et al Autoimmunity rev 2016 Zignego AL et al DLD 2007 Cacoub P et al DLD
2014 Zignego AL et al DLD 2007 Zignego AL et al Intern Emerg Med 2012 Zignego AL et al Clin Dev Immunol 2012 Zignego
AL et al Expert Rev Clin Immunol 2015
MC clinical aspects MC Syndrome
MCS is characterized by the clinical triad -purpura weakness and
arthralgias- low complement C4 and various organsystem
involvement including cutaneous articular renal neurological
cardiac or digestive
It ranges from mild disease to severe even life-threatening
conditions
More serious lesions are generally characterized by neurologic and
renal involvement
Prognosis is highly dependent on renal involvement or on the extent
of vasculitis lesions
1 HCV is the main etiopathological agent as concordantly demonstrated by epidemiological clinico-pathological virological and laboratory investigations2 the association between HCV and disease is demonstrated in a significant proportion of patients and supported by in depth clinico-pathogeneticstudies3 the association is suggested by cohort studies a possible causative role may be limited to a small number of patients andor possibly more relevant in specific geographical areas 4 a number of anecdotal observations suggested a possible role of HCV further investigations are required
From P Cacoub 2015
HCV infection is closely related to LPDs mostly MC
40 to 60 of HCV patients show circulating CGs among this latter population 5-30
develop a symptomatic CV
AVT has been considered the first-line option in HCV-CV patients in fact in the majority
of cases viral eradication leads to CV clinical remission
Data about IFN-free regimens for the treatment of CV patients are still limited
HCV and MC
HCV and MC
Zignego 2015Ferri 2016Pozzato 2016 Sise 2016Saadoun 2015Gragnani 2016Gragnani 2016
Bonacci 2016Hegazy 2016Kondili 2016Emery 2017
Younossi et al
The annual costs (inpatient outpatient andpharmacy) associated with extrahepatic
manifestations of HCV were evaluated
Total direct medical costs of extrahepatic
manifestations of HCV in 2014 US dollars wereestimated to be $1506 million (range $922 millionndash
$2208 million in sensitivity analysis)
These estimates should be added to the liver-related
burden of disease to obtain a more accurateassessment of the total burden of HCV infection
The OBJECTIVE of the study was to estimate the annual direct medical costsassociated with HCV related EHM in the EU5 (France Germany Italy United Kingdom
Spain)
Extrahepatic Manifestations of HCV
Extrahepatic Manifestations of HCV
HCV may cause extrahepatic disorders (HCV-EHDs) classified according to the number and
strength of supporting scientific data
HCV-EHDs are responsible for increasing morbidity and mortality with important
consequences in terms of social costs
The analysis of mortality rates in large cohorts confirmed the association of HCV with
several EHDs including cardiovascular neurologic metabolic or renal diseases and tumors
Viral eradication significantly reduced the rate of extra-hepatic deaths
Cacoub P et al DLD 2014 Lee MH et al J Infect Dis 2012 Backus LI et al Clin Gastroenterol Hepatol 2011 El-Kamary S et al
Clin Infect Dis 2011 Hsu YC et al Hepatology 2014 Kawamura Y et al Am J Med 2007 Adinolfi LE et al WJG 2014
Con il contributo di
Lee M-H et al J Infect Dis 2012206469-477
Follow-Up
(Years)
20
18
16
14
12
10
2
00 2 4 6 8 10 12 14 16 18 20
8
6
4
Follow-Up
(Years)
12
10
8
6
4
2
00 2 4 6 8 10 12 14 16 18 20
All Causes(n=2394)
Liver Cancer(n=115)
Extrahepatic Diseases(n=2199)
Cum
ula
tive M
ort
ali
ty (
)
Anti-HCV+ HCV RNA detectable Anti-HCV+ HCV RNA undetectable Anti-HCVndash
Follow-Up
(Years)
35
30
25
20
15
10
5
00 2 4 6 8 10 12 14 16 18 20
301
128124
104
16
03
198
122
110
Extrahepatic Manifestations of HCV
The annual costs (inpatient outpatient andpharmacy) associated with extrahepatic
manifestations of HCV were evaluated
Total direct medical costs of extrahepatic
manifestations of HCV in 2014 US dollars wereestimated to be $1506 million (range $922 millionndash
$2208 million in sensitivity analysis)
These estimates should be added to the liver-related
burden of disease to obtain a more accurateassessment of the total burden of HCV infection
Younossi et al
Younossi et al
Costs up to $71000 per patient per year (ESRD) Among the most frequent EHM depression (245 in HCV vs 172 in non-HCV) had estimated annual cost of
$4307 million DM (15 vs 10 in non- HCV) had an annual cost of $4434 million in the USA= given the importance of DM and
its association with CVDs and mortality the clinical and economic impacts of HCV-related DM are substantial
The OBJECTIVE of the study was to estimate the annual direct medical costsassociated with HCV related EHM in the EU5 (France Germany Italy United Kingdom
Spain)
The OBJECTIVE of the study was to estimate the annual direct medicalcosts associated with HCV related EHM in the EU5 (France Germany
Italy United Kingdom Spain)
1 HCV is the main etiopathological agent as concordantly demonstrated by epidemiological clinico-pathological virological and laboratory investigations2 the association between HCV and disease is demonstrated in a significant proportion of patients and supported by in depth clinico-pathogeneticstudies3 the association is suggested by cohort studies a possible causative role may be limited to a small number of patients andor possibly more relevant in specific geographical areas 4 a number of anecdotal observations suggested a possible role of HCV further investigations are required
The most studied and frequent HCV-EHDs are B-LPDs andor autoimmune disorders
Their prototype is Mixed Cryoglobulinemia (MC) from researches on MC derived most of the
available information
MC as a precious model for all the HCV-EHDs and to evaluate the effects of viral eradication
Anti-HCV Treatment Evolution
IFN
6 mos
PegIFN RBV 12
mos
IFN
12 mos
IFNRBV
12 mos
PegIFN
12 mos
2001
1998
2011
Standardinterferon
Ribavirin
Peginterferon
1991
Direct-actingantivirals
PegIFN
RBV
DAA
IFNRBV
6 mos
6
16
34
4239
55
70+
0
20
40
60
80
100
DAAs
826
weeks
gt90
2015
Few side effects absence major
contraindications
Younossi et al
The annual costs (inpatient outpatient and pharmacy) associatedwith extrahepatic manifestations of HCV were evaluated
Total direct medical costs of extrahepatic manifestations of HCV in 2014US dollars were estimated to be $1506 million (range $922 millionndash
$2208 million in sensitivity analysis)
These estimates should be added to the liver-related burden of diseaseto obtain a more accurate assessment of the total burden of HCV
infection
The OBJECTIVE of the study was to estimate the annual direct medical costs associated with HCV related EHM in the EU5 (France Germany Italy United Kingdom Spain)
22 MCS treated with DAAs including 2 HCC and 2 NHL 100 SVR12 Clinical CR in 64 and PR in remaining 36 The small lymphocytic lymphoma progressed despite viral clearance
Lauletta et al 2017
Emery CS et al 2017
Retrospective analysis 17 MCS (10 with severelife-threatening vasculitis) and 65 asymptomatic CGs+ pts treated with DAAs SVR 889 MCS and 908 asymptomatic pts In MCS clinical response in 1117 (complete in 717) In severelife-threatening vasculitis lower clinical response especially in renal and neurological symptoms
Saadoun D et al 2017
Open-label prospective multi-center study on sofosbuvir plus daclatasvir treatment of 41 HCV MCS SVR in100 and clinical CR in 902 Disappearance of CGs in 50 of pts No serious adverse event or relapse ofvasculitis
Antiviral Treatment (AVT) of MCIFN-free regimens
MC is clinically benign but sometimes severe HCV EHD invalidating symptoms occur and
it may evolve into lymphoma
Cacoub P et al DLD 2014 Zignego AL et al DLD 2007 Zignego AL et al Intern Emerg Med 2012 Zignego AL et al Clin Dev
Immunol 2012 Zignego AL et al Expert Rev Clin Immunol 2015 Sene D et al J Rheumatol 2004
Mixed Cryoglobulinemia-MC
MC pathological substrate is an HCV-driven B-cell
proliferation with consequent production of cryo- and non-
cryoprecipitable CICs in turn responsible for vasculitic
manifestations
Most (70ndash90) MC patients are HCV+ and HCV-patients are CGs+ (40ndash60) while 5ndash30 of
CGs+ have symptomatic MC or cryoglobulinemic vasculitis since HCV infects about 170
million individuals worldwide the number of patients at risk for developing MC is
substantial
Type II CGs
monoclonal
RF+policlonal IgG
Type III CGs both
RF and IgG
polyclonal

HCV Eradicationwith DAAs
To be preceded or combined with non-etiological pathogenetic therapy in severecatastrophic MCS
MCS Therapy in the IFN and DAAs Era from the complex to the simplified flow-chart
Dammacco F Sansonno D NEJM 2013
Zignego AL Pawlotsky JM Cacoub P Antiviral Ther in press Cacoub P et al Am J Med 2015
Mechanisms of HCV-related lymphomagenesis
DLBC HCV- induced
direct transformation
MCindolent NHL
accumulation of B RF
following BCR activation
and BC apoptosisinhibition
Zignego AL Ramos-Casals M Ferri C et al Autoimmun Rev 2017
Wang et al Hepatology 2016 Canioni et al Plos one 2016
Observational study on in situ expression of the oncogenic HCV NS3 protein on 116 HCV patients with B-NHL (DLBCL 36 and MZL 34)
NS3 immunostaining positive in 1214 DLBCL vs only 414 MZL (p = 0006) moreover 24 NS3+ MZL
were enriched in large cells
This study supports a new mechanism of transformation with a direct oncogenic role of
HCV proteins in the occurrence of high-grade B lymphomas
IN SITU HEPATITIS C NS3 PROTEIN DETECTION IS ASSOCIATED WITH HIGH GRADE
FEATURES IN HCV-ASSOCIATED B-CELL NON-HODGKIN LYMPHOMAS Danielle
Canioni et al 2016
In addition to the role of chronic antigenic stimulation in HCV related
lymphomagenesis this study supports a second mechanism of transformation due to a
direct oncogenic role of HCV infection of B-cells promoting the occurrence of high-grade Bcell lymphomas
Cohort study of 704 consecutive HIV-negative HCV-positive patients with indolent NHL from 1993 to
2009 in 39 centers of the FIL
Arcaini et al 2016
DLBC HCV- induced
direct transformation
No place of AVT as
1st line
Need of immediate delivery of
chemotherapy or concomitant (NHL
+ HCV targets)
THERAPY OF HCV+ DLBCL
ANTIVIRAL THERAPY IS ASSOCIATED WITH A BETTERSURVIVAL IN PATIENTS WITH HCV AND B-CELL NON-HODGKIN LYMPHOMAS ANRS HC-13 LYMPHO-CSTUDY Michot JM et al
Outcomes of HCV-associated B-NHL according to HCV AVT in prospective patients only (n 5 64)
Concurrent Systemic Chemoimmunotherapy and Sofosbuvir-Based Antiviral Treatment in a Hepatitis C Virus-Infected Patient With Diffuse Large B-Cell Lymphoma Evan C Ewers et al 2016
absolute neutrophil count and Hgb ALT and HCV viral load
Both complete response and SVR of HCV-associated DLBCL after concurrent chemoimmunotherapy and antiviral therapy using a sofosbuvir-based regimen
DAA-treatment in concomitance with chemotherapy showed to be safe and effective in influencing the remission of aggressive lymphomas in HCV patients
Persico M et al 2017
DFS in DAA treated and historical not-treated ptsAntiviral response rates in DAA treated patients
ANTIVIRAL THERAPY IN HCV+ B CELL NHL
IFN-based AVT induced hematological response along with SVR in patients with HCV-related indolent NHLs (especially
MZL)
Recent data with IFN-free regimens in HCV-associated LPDs suggest their anti-lymphoma activity too
AVT should be considered the first-line approach in HCV low grade lymphomas if there is no urgency of a conventional
treatment (ie systemic symptoms bulky disease or symptomatic splenomegaly) (ESMO NCCN EASL guidelines)
In aggressive lymphomas antiviral therapy after induction treatment is to be considered the standard at the moment but
in the next years (months) the association of immunochemotherapy and antiviral therapy will be considered the standard
Zignego AL Ramos-Casals M Ferri C et al Autoimmun Rev 2017
The Masve group
BASIC RESEARCH
Laura Gragnani
Patrizio Caini
Serena Lorini
Antonella Simone
CLINICAL RESEARCH
Monica Monti
Luisa Petraccia
Sinan Sadalla
Guia Cerretelli
Cristina Stasi
Adela Xheka
Universitagrave degli Studi di FirenzeDipartimento di Medicina Sperimentale e Clinica
Centro Manifestazioni Sistemiche da Virus EpatiticildquoMASVErdquo
Anna Linda Zignego
MASVE
UNDERGRADUATE STUDENTS Andrea Genovese Adrian Piscopo
ANTIVIRAL THERAPY IN HCV+ B CELL NHL
IFN-based AVT induced hematological response along with SVR in patients with HCV-related indolent
NHLs (especially MZL)
Recent data with IFN-free regimens in HCV-associated LPDs suggest their anti-lymphoma activity too
AVT should be considered the first-line approach in HCV low grade lymphomas if there is no urgency
of a conventional treatment (ie systemic symptoms bulky disease or symptomatic splenomegaly)
(ESMO NCCN EASL guidelines)
Main drugs for HCV-related MCS according to the target
HCV= DAAsB-cell Expansion= (a) B cell-depleting Mabs
-First-generation Rituximab (anti-CD20)-Second-generation Ofatumumab (anti-CD20) Veltuzumab (humanized
anti-CD20)-Third-generation Obinutuzumab (GA101) Oceratuzumab (humanized
anti-CD20)
(b) Alkylating agents
-Cyclophosfamide
Inflammation= Antiinflammatory agents
- Corticosteroids
Altered regulatory T-cell activity=
- IL-2
The impact on HRQoL of IFN-free AVT was prospectively evaluated in a cohort of HCV CV patients with limited
influencing variables linked to therapeutic schedulesviral GT
44 HCV GT2 CV patients mostly F0-F2 (29) and naiumlve (30) treated with SOFRBV for 1224wks
TIME POINTS
baseline EOT and week 12 and 24 of post-treatment f-up (SVR12 and SVR24 respectively)
HRQoL EVALUATION THROUGH PROs
the Short Form (36) Health Survey (SF-36)
the Functional Assessment of Chronic Illness Therapy-Fatigue (FACIT-F) from which we computed the Trial
Outcome Index (TOI)
Observational study on in situ expression of the oncogenic HCV NS3 protein on 116 HCV
patients with B-NHL (DLBCL 36 and MZL 34)
NS3 immunostaining positive in 1214 DLBCL vs only 414 MZL (p = 0006) moreover 24 NS3+
MZL were enriched in large cells
This study supports a new mechanism of transformation with a direct oncogenic role of
HCV proteins in the occurrence of high-grade B lymphomas
IN SITU HEPATITIS C NS3 PROTEIN DETECTION IS ASSOCIATED WITH HIGH GRADEFEATURES IN HCV-ASSOCIATED B-CELL NON-HODGKIN LYMPHOMAS Danielle
Canioni et al 2016
In addition to the role of chronic antigenic stimulation in HCV related
lymphomagenesis this study supports a second mechanism of transformation due toa direct oncogenic role of HCV infection of B-cells promoting the occurrence of high-grade Bcell lymphomas
ANTIVIRAL THERAPY IS ASSOCIATED WITH A BETTERSURVIVAL IN PATIENTS WITH HCV AND B-CELL NON-HODGKIN LYMPHOMAS ANRS HC-13 LYMPHO-CSTUDYMichot JM et al
Outcomes of HCV-associated B-NHL according to HCV AVT in prospective patients only (n 5 64)
(A) absolute neutrophil count and Hgb
(B) ALT and HCV viral load
This patient had HCV-associated DLBCL achieving both complete response and SVR after concurrent chemoimmunotherapy and antiviral therapy using a sofosbuvir-basedregimen
Concurrent Systemic Chemoimmunotherapy and Sofosbuvir-Based Antiviral Treatment in a Hepatitis C Virus-Infected Patient With Diffuse Large B-Cell LymphomaEvan C Ewers et al 2016
HCV-EHDs are responsible for increasing morbidity and mortality with important
consequences in terms of social costs
The analysis of mortality rates in large cohorts confirmed the association of HCV with
several EHDs including cardiovascular neurologic metabolic or renal diseases and tumors
Viral eradication significantly reduced the rate of extra-hepatic deaths
Cacoub P et al DLD 2014 Lee MH et al J Infect Dis 2012 Backus LI et al Clin Gastroenterol Hepatol 2011 El-Kamary S et al
Clin Infect Dis 2011 Hsu YC et al Hepatology 2014 Kawamura Y et al Am J Med 2007 Adinolfi LE et al WJG 2014
Extrahepatic Manifestations of HCV
Con il contributo di
Lee M-H et al J Infect Dis 2012206469-477
Follow-Up
(Years)
20
18
16
14
12
10
2
00 2 4 6 8 10 12 14 16 18 20
8
6
4
Follow-Up
(Years)
12
10
8
6
4
2
00 2 4 6 8 10 12 14 16 18 20
All Causes(n=2394)
Liver Cancer(n=115)
Extrahepatic Diseases(n=2199)
Cum
ula
tive M
ort
ali
ty (
)
Anti-HCV+ HCV RNA detectable Anti-HCV+ HCV RNA undetectable Anti-HCVndash
Follow-Up
(Years)
35
30
25
20
15
10
5
00 2 4 6 8 10 12 14 16 18 20
301
128124
104
16
03
198
122
110
MC is clinically benign but sometimes severe HCV EHD invalidating symptoms occur and
it may evolve into lymphoma
Cacoub P et al DLD 2014 Zignego AL et al DLD 2007 Zignego AL et al Intern Emerg Med 2012 Zignego AL et al Clin Dev
Immunol 2012 Zignego AL et al Expert Rev Clin Immunol 2015 Sene D et al J Rheumatol 2004
Mixed Cryoglobulinemia-MC
CGs reversibly precipitate when the temperature is lower than 37degC and
comprise IgMs with RF activity [mono- or oligo-clonal in type II MC or
polyclonal in type III MC] and polyclonal IgGs
MC pathological substrate is an HCV-driven B-cell
proliferation with consequent production of cryo- and non-
cryoprecipitable CICs in turn responsible for vasculitic
manifestations
Most (70ndash90) MC patients are HCV+ and HCV-patients are CGs+ (40ndash60) while 5ndash30 of
CGs+ have symptomatic MC since HCV infects about 170 million individuals worldwide the
number of patients at risk for developing MC is substantial
Type II
CGs
Type III
CGs
Zignego AL et al Autoimmun Rev 2017 Ferri C et al Autoimmunity rev 2016 Zignego AL et al DLD 2007 Cacoub P et al DLD
2014 Zignego AL et al DLD 2007 Zignego AL et al Intern Emerg Med 2012 Zignego AL et al Clin Dev Immunol 2012 Zignego
AL et al Expert Rev Clin Immunol 2015
MC clinical aspects MC Syndrome
MCS is characterized by the clinical triad -purpura weakness and
arthralgias- low complement C4 and various organsystem
involvement including cutaneous articular renal neurological
cardiac or digestive
It ranges from mild disease to severe even life-threatening
conditions
More serious lesions are generally characterized by neurologic and
renal involvement
Prognosis is highly dependent on renal involvement or on the extent
of vasculitis lesions
1 HCV is the main etiopathological agent as concordantly demonstrated by epidemiological clinico-pathological virological and laboratory investigations2 the association between HCV and disease is demonstrated in a significant proportion of patients and supported by in depth clinico-pathogeneticstudies3 the association is suggested by cohort studies a possible causative role may be limited to a small number of patients andor possibly more relevant in specific geographical areas 4 a number of anecdotal observations suggested a possible role of HCV further investigations are required
From P Cacoub 2015
HCV infection is closely related to LPDs mostly MC
40 to 60 of HCV patients show circulating CGs among this latter population 5-30
develop a symptomatic CV
AVT has been considered the first-line option in HCV-CV patients in fact in the majority
of cases viral eradication leads to CV clinical remission
Data about IFN-free regimens for the treatment of CV patients are still limited
HCV and MC
HCV and MC
Zignego 2015Ferri 2016Pozzato 2016 Sise 2016Saadoun 2015Gragnani 2016Gragnani 2016
Bonacci 2016Hegazy 2016Kondili 2016Emery 2017
Younossi et al
The annual costs (inpatient outpatient andpharmacy) associated with extrahepatic
manifestations of HCV were evaluated
Total direct medical costs of extrahepatic
manifestations of HCV in 2014 US dollars wereestimated to be $1506 million (range $922 millionndash
$2208 million in sensitivity analysis)
These estimates should be added to the liver-related
burden of disease to obtain a more accurateassessment of the total burden of HCV infection
The OBJECTIVE of the study was to estimate the annual direct medical costsassociated with HCV related EHM in the EU5 (France Germany Italy United Kingdom
Spain)
Extrahepatic Manifestations of HCV
Extrahepatic Manifestations of HCV
HCV may cause extrahepatic disorders (HCV-EHDs) classified according to the number and
strength of supporting scientific data
HCV-EHDs are responsible for increasing morbidity and mortality with important
consequences in terms of social costs
The analysis of mortality rates in large cohorts confirmed the association of HCV with
several EHDs including cardiovascular neurologic metabolic or renal diseases and tumors
Viral eradication significantly reduced the rate of extra-hepatic deaths
Cacoub P et al DLD 2014 Lee MH et al J Infect Dis 2012 Backus LI et al Clin Gastroenterol Hepatol 2011 El-Kamary S et al
Clin Infect Dis 2011 Hsu YC et al Hepatology 2014 Kawamura Y et al Am J Med 2007 Adinolfi LE et al WJG 2014
Con il contributo di
Lee M-H et al J Infect Dis 2012206469-477
Follow-Up
(Years)
20
18
16
14
12
10
2
00 2 4 6 8 10 12 14 16 18 20
8
6
4
Follow-Up
(Years)
12
10
8
6
4
2
00 2 4 6 8 10 12 14 16 18 20
All Causes(n=2394)
Liver Cancer(n=115)
Extrahepatic Diseases(n=2199)
Cum
ula
tive M
ort
ali
ty (
)
Anti-HCV+ HCV RNA detectable Anti-HCV+ HCV RNA undetectable Anti-HCVndash
Follow-Up
(Years)
35
30
25
20
15
10
5
00 2 4 6 8 10 12 14 16 18 20
301
128124
104
16
03
198
122
110
Extrahepatic Manifestations of HCV
The annual costs (inpatient outpatient andpharmacy) associated with extrahepatic
manifestations of HCV were evaluated
Total direct medical costs of extrahepatic
manifestations of HCV in 2014 US dollars wereestimated to be $1506 million (range $922 millionndash
$2208 million in sensitivity analysis)
These estimates should be added to the liver-related
burden of disease to obtain a more accurateassessment of the total burden of HCV infection
Younossi et al
Younossi et al
Costs up to $71000 per patient per year (ESRD) Among the most frequent EHM depression (245 in HCV vs 172 in non-HCV) had estimated annual cost of
$4307 million DM (15 vs 10 in non- HCV) had an annual cost of $4434 million in the USA= given the importance of DM and
its association with CVDs and mortality the clinical and economic impacts of HCV-related DM are substantial
The OBJECTIVE of the study was to estimate the annual direct medical costsassociated with HCV related EHM in the EU5 (France Germany Italy United Kingdom
Spain)
The OBJECTIVE of the study was to estimate the annual direct medicalcosts associated with HCV related EHM in the EU5 (France Germany
Italy United Kingdom Spain)
1 HCV is the main etiopathological agent as concordantly demonstrated by epidemiological clinico-pathological virological and laboratory investigations2 the association between HCV and disease is demonstrated in a significant proportion of patients and supported by in depth clinico-pathogeneticstudies3 the association is suggested by cohort studies a possible causative role may be limited to a small number of patients andor possibly more relevant in specific geographical areas 4 a number of anecdotal observations suggested a possible role of HCV further investigations are required
The most studied and frequent HCV-EHDs are B-LPDs andor autoimmune disorders
Their prototype is Mixed Cryoglobulinemia (MC) from researches on MC derived most of the
available information
MC as a precious model for all the HCV-EHDs and to evaluate the effects of viral eradication
Anti-HCV Treatment Evolution
IFN
6 mos
PegIFN RBV 12
mos
IFN
12 mos
IFNRBV
12 mos
PegIFN
12 mos
2001
1998
2011
Standardinterferon
Ribavirin
Peginterferon
1991
Direct-actingantivirals
PegIFN
RBV
DAA
IFNRBV
6 mos
6
16
34
4239
55
70+
0
20
40
60
80
100
DAAs
826
weeks
gt90
2015
Few side effects absence major
contraindications
Younossi et al
The annual costs (inpatient outpatient and pharmacy) associatedwith extrahepatic manifestations of HCV were evaluated
Total direct medical costs of extrahepatic manifestations of HCV in 2014US dollars were estimated to be $1506 million (range $922 millionndash
$2208 million in sensitivity analysis)
These estimates should be added to the liver-related burden of diseaseto obtain a more accurate assessment of the total burden of HCV
infection
The OBJECTIVE of the study was to estimate the annual direct medical costs associated with HCV related EHM in the EU5 (France Germany Italy United Kingdom Spain)
22 MCS treated with DAAs including 2 HCC and 2 NHL 100 SVR12 Clinical CR in 64 and PR in remaining 36 The small lymphocytic lymphoma progressed despite viral clearance
Lauletta et al 2017
Emery CS et al 2017
Retrospective analysis 17 MCS (10 with severelife-threatening vasculitis) and 65 asymptomatic CGs+ pts treated with DAAs SVR 889 MCS and 908 asymptomatic pts In MCS clinical response in 1117 (complete in 717) In severelife-threatening vasculitis lower clinical response especially in renal and neurological symptoms
Saadoun D et al 2017
Open-label prospective multi-center study on sofosbuvir plus daclatasvir treatment of 41 HCV MCS SVR in100 and clinical CR in 902 Disappearance of CGs in 50 of pts No serious adverse event or relapse ofvasculitis
Antiviral Treatment (AVT) of MCIFN-free regimens
MC is clinically benign but sometimes severe HCV EHD invalidating symptoms occur and
it may evolve into lymphoma
Cacoub P et al DLD 2014 Zignego AL et al DLD 2007 Zignego AL et al Intern Emerg Med 2012 Zignego AL et al Clin Dev
Immunol 2012 Zignego AL et al Expert Rev Clin Immunol 2015 Sene D et al J Rheumatol 2004
Mixed Cryoglobulinemia-MC
MC pathological substrate is an HCV-driven B-cell
proliferation with consequent production of cryo- and non-
cryoprecipitable CICs in turn responsible for vasculitic
manifestations
Most (70ndash90) MC patients are HCV+ and HCV-patients are CGs+ (40ndash60) while 5ndash30 of
CGs+ have symptomatic MC or cryoglobulinemic vasculitis since HCV infects about 170
million individuals worldwide the number of patients at risk for developing MC is
substantial
Type II CGs
monoclonal
RF+policlonal IgG
Type III CGs both
RF and IgG
polyclonal

Mechanisms of HCV-related lymphomagenesis
DLBC HCV- induced
direct transformation
MCindolent NHL
accumulation of B RF
following BCR activation
and BC apoptosisinhibition
Zignego AL Ramos-Casals M Ferri C et al Autoimmun Rev 2017
Wang et al Hepatology 2016 Canioni et al Plos one 2016
Observational study on in situ expression of the oncogenic HCV NS3 protein on 116 HCV patients with B-NHL (DLBCL 36 and MZL 34)
NS3 immunostaining positive in 1214 DLBCL vs only 414 MZL (p = 0006) moreover 24 NS3+ MZL
were enriched in large cells
This study supports a new mechanism of transformation with a direct oncogenic role of
HCV proteins in the occurrence of high-grade B lymphomas
IN SITU HEPATITIS C NS3 PROTEIN DETECTION IS ASSOCIATED WITH HIGH GRADE
FEATURES IN HCV-ASSOCIATED B-CELL NON-HODGKIN LYMPHOMAS Danielle
Canioni et al 2016
In addition to the role of chronic antigenic stimulation in HCV related
lymphomagenesis this study supports a second mechanism of transformation due to a
direct oncogenic role of HCV infection of B-cells promoting the occurrence of high-grade Bcell lymphomas
Cohort study of 704 consecutive HIV-negative HCV-positive patients with indolent NHL from 1993 to
2009 in 39 centers of the FIL
Arcaini et al 2016
DLBC HCV- induced
direct transformation
No place of AVT as
1st line
Need of immediate delivery of
chemotherapy or concomitant (NHL
+ HCV targets)
THERAPY OF HCV+ DLBCL
ANTIVIRAL THERAPY IS ASSOCIATED WITH A BETTERSURVIVAL IN PATIENTS WITH HCV AND B-CELL NON-HODGKIN LYMPHOMAS ANRS HC-13 LYMPHO-CSTUDY Michot JM et al
Outcomes of HCV-associated B-NHL according to HCV AVT in prospective patients only (n 5 64)
Concurrent Systemic Chemoimmunotherapy and Sofosbuvir-Based Antiviral Treatment in a Hepatitis C Virus-Infected Patient With Diffuse Large B-Cell Lymphoma Evan C Ewers et al 2016
absolute neutrophil count and Hgb ALT and HCV viral load
Both complete response and SVR of HCV-associated DLBCL after concurrent chemoimmunotherapy and antiviral therapy using a sofosbuvir-based regimen
DAA-treatment in concomitance with chemotherapy showed to be safe and effective in influencing the remission of aggressive lymphomas in HCV patients
Persico M et al 2017
DFS in DAA treated and historical not-treated ptsAntiviral response rates in DAA treated patients
ANTIVIRAL THERAPY IN HCV+ B CELL NHL
IFN-based AVT induced hematological response along with SVR in patients with HCV-related indolent NHLs (especially
MZL)
Recent data with IFN-free regimens in HCV-associated LPDs suggest their anti-lymphoma activity too
AVT should be considered the first-line approach in HCV low grade lymphomas if there is no urgency of a conventional
treatment (ie systemic symptoms bulky disease or symptomatic splenomegaly) (ESMO NCCN EASL guidelines)
In aggressive lymphomas antiviral therapy after induction treatment is to be considered the standard at the moment but
in the next years (months) the association of immunochemotherapy and antiviral therapy will be considered the standard
Zignego AL Ramos-Casals M Ferri C et al Autoimmun Rev 2017
The Masve group
BASIC RESEARCH
Laura Gragnani
Patrizio Caini
Serena Lorini
Antonella Simone
CLINICAL RESEARCH
Monica Monti
Luisa Petraccia
Sinan Sadalla
Guia Cerretelli
Cristina Stasi
Adela Xheka
Universitagrave degli Studi di FirenzeDipartimento di Medicina Sperimentale e Clinica
Centro Manifestazioni Sistemiche da Virus EpatiticildquoMASVErdquo
Anna Linda Zignego
MASVE
UNDERGRADUATE STUDENTS Andrea Genovese Adrian Piscopo
ANTIVIRAL THERAPY IN HCV+ B CELL NHL
IFN-based AVT induced hematological response along with SVR in patients with HCV-related indolent
NHLs (especially MZL)
Recent data with IFN-free regimens in HCV-associated LPDs suggest their anti-lymphoma activity too
AVT should be considered the first-line approach in HCV low grade lymphomas if there is no urgency
of a conventional treatment (ie systemic symptoms bulky disease or symptomatic splenomegaly)
(ESMO NCCN EASL guidelines)
Main drugs for HCV-related MCS according to the target
HCV= DAAsB-cell Expansion= (a) B cell-depleting Mabs
-First-generation Rituximab (anti-CD20)-Second-generation Ofatumumab (anti-CD20) Veltuzumab (humanized
anti-CD20)-Third-generation Obinutuzumab (GA101) Oceratuzumab (humanized
anti-CD20)
(b) Alkylating agents
-Cyclophosfamide
Inflammation= Antiinflammatory agents
- Corticosteroids
Altered regulatory T-cell activity=
- IL-2
The impact on HRQoL of IFN-free AVT was prospectively evaluated in a cohort of HCV CV patients with limited
influencing variables linked to therapeutic schedulesviral GT
44 HCV GT2 CV patients mostly F0-F2 (29) and naiumlve (30) treated with SOFRBV for 1224wks
TIME POINTS
baseline EOT and week 12 and 24 of post-treatment f-up (SVR12 and SVR24 respectively)
HRQoL EVALUATION THROUGH PROs
the Short Form (36) Health Survey (SF-36)
the Functional Assessment of Chronic Illness Therapy-Fatigue (FACIT-F) from which we computed the Trial
Outcome Index (TOI)
Observational study on in situ expression of the oncogenic HCV NS3 protein on 116 HCV
patients with B-NHL (DLBCL 36 and MZL 34)
NS3 immunostaining positive in 1214 DLBCL vs only 414 MZL (p = 0006) moreover 24 NS3+
MZL were enriched in large cells
This study supports a new mechanism of transformation with a direct oncogenic role of
HCV proteins in the occurrence of high-grade B lymphomas
IN SITU HEPATITIS C NS3 PROTEIN DETECTION IS ASSOCIATED WITH HIGH GRADEFEATURES IN HCV-ASSOCIATED B-CELL NON-HODGKIN LYMPHOMAS Danielle
Canioni et al 2016
In addition to the role of chronic antigenic stimulation in HCV related
lymphomagenesis this study supports a second mechanism of transformation due toa direct oncogenic role of HCV infection of B-cells promoting the occurrence of high-grade Bcell lymphomas
ANTIVIRAL THERAPY IS ASSOCIATED WITH A BETTERSURVIVAL IN PATIENTS WITH HCV AND B-CELL NON-HODGKIN LYMPHOMAS ANRS HC-13 LYMPHO-CSTUDYMichot JM et al
Outcomes of HCV-associated B-NHL according to HCV AVT in prospective patients only (n 5 64)
(A) absolute neutrophil count and Hgb
(B) ALT and HCV viral load
This patient had HCV-associated DLBCL achieving both complete response and SVR after concurrent chemoimmunotherapy and antiviral therapy using a sofosbuvir-basedregimen
Concurrent Systemic Chemoimmunotherapy and Sofosbuvir-Based Antiviral Treatment in a Hepatitis C Virus-Infected Patient With Diffuse Large B-Cell LymphomaEvan C Ewers et al 2016
HCV-EHDs are responsible for increasing morbidity and mortality with important
consequences in terms of social costs
The analysis of mortality rates in large cohorts confirmed the association of HCV with
several EHDs including cardiovascular neurologic metabolic or renal diseases and tumors
Viral eradication significantly reduced the rate of extra-hepatic deaths
Cacoub P et al DLD 2014 Lee MH et al J Infect Dis 2012 Backus LI et al Clin Gastroenterol Hepatol 2011 El-Kamary S et al
Clin Infect Dis 2011 Hsu YC et al Hepatology 2014 Kawamura Y et al Am J Med 2007 Adinolfi LE et al WJG 2014
Extrahepatic Manifestations of HCV
Con il contributo di
Lee M-H et al J Infect Dis 2012206469-477
Follow-Up
(Years)
20
18
16
14
12
10
2
00 2 4 6 8 10 12 14 16 18 20
8
6
4
Follow-Up
(Years)
12
10
8
6
4
2
00 2 4 6 8 10 12 14 16 18 20
All Causes(n=2394)
Liver Cancer(n=115)
Extrahepatic Diseases(n=2199)
Cum
ula
tive M
ort
ali
ty (
)
Anti-HCV+ HCV RNA detectable Anti-HCV+ HCV RNA undetectable Anti-HCVndash
Follow-Up
(Years)
35
30
25
20
15
10
5
00 2 4 6 8 10 12 14 16 18 20
301
128124
104
16
03
198
122
110
MC is clinically benign but sometimes severe HCV EHD invalidating symptoms occur and
it may evolve into lymphoma
Cacoub P et al DLD 2014 Zignego AL et al DLD 2007 Zignego AL et al Intern Emerg Med 2012 Zignego AL et al Clin Dev
Immunol 2012 Zignego AL et al Expert Rev Clin Immunol 2015 Sene D et al J Rheumatol 2004
Mixed Cryoglobulinemia-MC
CGs reversibly precipitate when the temperature is lower than 37degC and
comprise IgMs with RF activity [mono- or oligo-clonal in type II MC or
polyclonal in type III MC] and polyclonal IgGs
MC pathological substrate is an HCV-driven B-cell
proliferation with consequent production of cryo- and non-
cryoprecipitable CICs in turn responsible for vasculitic
manifestations
Most (70ndash90) MC patients are HCV+ and HCV-patients are CGs+ (40ndash60) while 5ndash30 of
CGs+ have symptomatic MC since HCV infects about 170 million individuals worldwide the
number of patients at risk for developing MC is substantial
Type II
CGs
Type III
CGs
Zignego AL et al Autoimmun Rev 2017 Ferri C et al Autoimmunity rev 2016 Zignego AL et al DLD 2007 Cacoub P et al DLD
2014 Zignego AL et al DLD 2007 Zignego AL et al Intern Emerg Med 2012 Zignego AL et al Clin Dev Immunol 2012 Zignego
AL et al Expert Rev Clin Immunol 2015
MC clinical aspects MC Syndrome
MCS is characterized by the clinical triad -purpura weakness and
arthralgias- low complement C4 and various organsystem
involvement including cutaneous articular renal neurological
cardiac or digestive
It ranges from mild disease to severe even life-threatening
conditions
More serious lesions are generally characterized by neurologic and
renal involvement
Prognosis is highly dependent on renal involvement or on the extent
of vasculitis lesions
1 HCV is the main etiopathological agent as concordantly demonstrated by epidemiological clinico-pathological virological and laboratory investigations2 the association between HCV and disease is demonstrated in a significant proportion of patients and supported by in depth clinico-pathogeneticstudies3 the association is suggested by cohort studies a possible causative role may be limited to a small number of patients andor possibly more relevant in specific geographical areas 4 a number of anecdotal observations suggested a possible role of HCV further investigations are required
From P Cacoub 2015
HCV infection is closely related to LPDs mostly MC
40 to 60 of HCV patients show circulating CGs among this latter population 5-30
develop a symptomatic CV
AVT has been considered the first-line option in HCV-CV patients in fact in the majority
of cases viral eradication leads to CV clinical remission
Data about IFN-free regimens for the treatment of CV patients are still limited
HCV and MC
HCV and MC
Zignego 2015Ferri 2016Pozzato 2016 Sise 2016Saadoun 2015Gragnani 2016Gragnani 2016
Bonacci 2016Hegazy 2016Kondili 2016Emery 2017
Younossi et al
The annual costs (inpatient outpatient andpharmacy) associated with extrahepatic
manifestations of HCV were evaluated
Total direct medical costs of extrahepatic
manifestations of HCV in 2014 US dollars wereestimated to be $1506 million (range $922 millionndash
$2208 million in sensitivity analysis)
These estimates should be added to the liver-related
burden of disease to obtain a more accurateassessment of the total burden of HCV infection
The OBJECTIVE of the study was to estimate the annual direct medical costsassociated with HCV related EHM in the EU5 (France Germany Italy United Kingdom
Spain)
Extrahepatic Manifestations of HCV
Extrahepatic Manifestations of HCV
HCV may cause extrahepatic disorders (HCV-EHDs) classified according to the number and
strength of supporting scientific data
HCV-EHDs are responsible for increasing morbidity and mortality with important
consequences in terms of social costs
The analysis of mortality rates in large cohorts confirmed the association of HCV with
several EHDs including cardiovascular neurologic metabolic or renal diseases and tumors
Viral eradication significantly reduced the rate of extra-hepatic deaths
Cacoub P et al DLD 2014 Lee MH et al J Infect Dis 2012 Backus LI et al Clin Gastroenterol Hepatol 2011 El-Kamary S et al
Clin Infect Dis 2011 Hsu YC et al Hepatology 2014 Kawamura Y et al Am J Med 2007 Adinolfi LE et al WJG 2014
Con il contributo di
Lee M-H et al J Infect Dis 2012206469-477
Follow-Up
(Years)
20
18
16
14
12
10
2
00 2 4 6 8 10 12 14 16 18 20
8
6
4
Follow-Up
(Years)
12
10
8
6
4
2
00 2 4 6 8 10 12 14 16 18 20
All Causes(n=2394)
Liver Cancer(n=115)
Extrahepatic Diseases(n=2199)
Cum
ula
tive M
ort
ali
ty (
)
Anti-HCV+ HCV RNA detectable Anti-HCV+ HCV RNA undetectable Anti-HCVndash
Follow-Up
(Years)
35
30
25
20
15
10
5
00 2 4 6 8 10 12 14 16 18 20
301
128124
104
16
03
198
122
110
Extrahepatic Manifestations of HCV
The annual costs (inpatient outpatient andpharmacy) associated with extrahepatic
manifestations of HCV were evaluated
Total direct medical costs of extrahepatic
manifestations of HCV in 2014 US dollars wereestimated to be $1506 million (range $922 millionndash
$2208 million in sensitivity analysis)
These estimates should be added to the liver-related
burden of disease to obtain a more accurateassessment of the total burden of HCV infection
Younossi et al
Younossi et al
Costs up to $71000 per patient per year (ESRD) Among the most frequent EHM depression (245 in HCV vs 172 in non-HCV) had estimated annual cost of
$4307 million DM (15 vs 10 in non- HCV) had an annual cost of $4434 million in the USA= given the importance of DM and
its association with CVDs and mortality the clinical and economic impacts of HCV-related DM are substantial
The OBJECTIVE of the study was to estimate the annual direct medical costsassociated with HCV related EHM in the EU5 (France Germany Italy United Kingdom
Spain)
The OBJECTIVE of the study was to estimate the annual direct medicalcosts associated with HCV related EHM in the EU5 (France Germany
Italy United Kingdom Spain)
1 HCV is the main etiopathological agent as concordantly demonstrated by epidemiological clinico-pathological virological and laboratory investigations2 the association between HCV and disease is demonstrated in a significant proportion of patients and supported by in depth clinico-pathogeneticstudies3 the association is suggested by cohort studies a possible causative role may be limited to a small number of patients andor possibly more relevant in specific geographical areas 4 a number of anecdotal observations suggested a possible role of HCV further investigations are required
The most studied and frequent HCV-EHDs are B-LPDs andor autoimmune disorders
Their prototype is Mixed Cryoglobulinemia (MC) from researches on MC derived most of the
available information
MC as a precious model for all the HCV-EHDs and to evaluate the effects of viral eradication
Anti-HCV Treatment Evolution
IFN
6 mos
PegIFN RBV 12
mos
IFN
12 mos
IFNRBV
12 mos
PegIFN
12 mos
2001
1998
2011
Standardinterferon
Ribavirin
Peginterferon
1991
Direct-actingantivirals
PegIFN
RBV
DAA
IFNRBV
6 mos
6
16
34
4239
55
70+
0
20
40
60
80
100
DAAs
826
weeks
gt90
2015
Few side effects absence major
contraindications
Younossi et al
The annual costs (inpatient outpatient and pharmacy) associatedwith extrahepatic manifestations of HCV were evaluated
Total direct medical costs of extrahepatic manifestations of HCV in 2014US dollars were estimated to be $1506 million (range $922 millionndash
$2208 million in sensitivity analysis)
These estimates should be added to the liver-related burden of diseaseto obtain a more accurate assessment of the total burden of HCV
infection
The OBJECTIVE of the study was to estimate the annual direct medical costs associated with HCV related EHM in the EU5 (France Germany Italy United Kingdom Spain)
22 MCS treated with DAAs including 2 HCC and 2 NHL 100 SVR12 Clinical CR in 64 and PR in remaining 36 The small lymphocytic lymphoma progressed despite viral clearance
Lauletta et al 2017
Emery CS et al 2017
Retrospective analysis 17 MCS (10 with severelife-threatening vasculitis) and 65 asymptomatic CGs+ pts treated with DAAs SVR 889 MCS and 908 asymptomatic pts In MCS clinical response in 1117 (complete in 717) In severelife-threatening vasculitis lower clinical response especially in renal and neurological symptoms
Saadoun D et al 2017
Open-label prospective multi-center study on sofosbuvir plus daclatasvir treatment of 41 HCV MCS SVR in100 and clinical CR in 902 Disappearance of CGs in 50 of pts No serious adverse event or relapse ofvasculitis
Antiviral Treatment (AVT) of MCIFN-free regimens
MC is clinically benign but sometimes severe HCV EHD invalidating symptoms occur and
it may evolve into lymphoma
Cacoub P et al DLD 2014 Zignego AL et al DLD 2007 Zignego AL et al Intern Emerg Med 2012 Zignego AL et al Clin Dev
Immunol 2012 Zignego AL et al Expert Rev Clin Immunol 2015 Sene D et al J Rheumatol 2004
Mixed Cryoglobulinemia-MC
MC pathological substrate is an HCV-driven B-cell
proliferation with consequent production of cryo- and non-
cryoprecipitable CICs in turn responsible for vasculitic
manifestations
Most (70ndash90) MC patients are HCV+ and HCV-patients are CGs+ (40ndash60) while 5ndash30 of
CGs+ have symptomatic MC or cryoglobulinemic vasculitis since HCV infects about 170
million individuals worldwide the number of patients at risk for developing MC is
substantial
Type II CGs
monoclonal
RF+policlonal IgG
Type III CGs both
RF and IgG
polyclonal

Observational study on in situ expression of the oncogenic HCV NS3 protein on 116 HCV patients with B-NHL (DLBCL 36 and MZL 34)
NS3 immunostaining positive in 1214 DLBCL vs only 414 MZL (p = 0006) moreover 24 NS3+ MZL
were enriched in large cells
This study supports a new mechanism of transformation with a direct oncogenic role of
HCV proteins in the occurrence of high-grade B lymphomas
IN SITU HEPATITIS C NS3 PROTEIN DETECTION IS ASSOCIATED WITH HIGH GRADE
FEATURES IN HCV-ASSOCIATED B-CELL NON-HODGKIN LYMPHOMAS Danielle
Canioni et al 2016
In addition to the role of chronic antigenic stimulation in HCV related
lymphomagenesis this study supports a second mechanism of transformation due to a
direct oncogenic role of HCV infection of B-cells promoting the occurrence of high-grade Bcell lymphomas
Cohort study of 704 consecutive HIV-negative HCV-positive patients with indolent NHL from 1993 to
2009 in 39 centers of the FIL
Arcaini et al 2016
DLBC HCV- induced
direct transformation
No place of AVT as
1st line
Need of immediate delivery of
chemotherapy or concomitant (NHL
+ HCV targets)
THERAPY OF HCV+ DLBCL
ANTIVIRAL THERAPY IS ASSOCIATED WITH A BETTERSURVIVAL IN PATIENTS WITH HCV AND B-CELL NON-HODGKIN LYMPHOMAS ANRS HC-13 LYMPHO-CSTUDY Michot JM et al
Outcomes of HCV-associated B-NHL according to HCV AVT in prospective patients only (n 5 64)
Concurrent Systemic Chemoimmunotherapy and Sofosbuvir-Based Antiviral Treatment in a Hepatitis C Virus-Infected Patient With Diffuse Large B-Cell Lymphoma Evan C Ewers et al 2016
absolute neutrophil count and Hgb ALT and HCV viral load
Both complete response and SVR of HCV-associated DLBCL after concurrent chemoimmunotherapy and antiviral therapy using a sofosbuvir-based regimen
DAA-treatment in concomitance with chemotherapy showed to be safe and effective in influencing the remission of aggressive lymphomas in HCV patients
Persico M et al 2017
DFS in DAA treated and historical not-treated ptsAntiviral response rates in DAA treated patients
ANTIVIRAL THERAPY IN HCV+ B CELL NHL
IFN-based AVT induced hematological response along with SVR in patients with HCV-related indolent NHLs (especially
MZL)
Recent data with IFN-free regimens in HCV-associated LPDs suggest their anti-lymphoma activity too
AVT should be considered the first-line approach in HCV low grade lymphomas if there is no urgency of a conventional
treatment (ie systemic symptoms bulky disease or symptomatic splenomegaly) (ESMO NCCN EASL guidelines)
In aggressive lymphomas antiviral therapy after induction treatment is to be considered the standard at the moment but
in the next years (months) the association of immunochemotherapy and antiviral therapy will be considered the standard
Zignego AL Ramos-Casals M Ferri C et al Autoimmun Rev 2017
The Masve group
BASIC RESEARCH
Laura Gragnani
Patrizio Caini
Serena Lorini
Antonella Simone
CLINICAL RESEARCH
Monica Monti
Luisa Petraccia
Sinan Sadalla
Guia Cerretelli
Cristina Stasi
Adela Xheka
Universitagrave degli Studi di FirenzeDipartimento di Medicina Sperimentale e Clinica
Centro Manifestazioni Sistemiche da Virus EpatiticildquoMASVErdquo
Anna Linda Zignego
MASVE
UNDERGRADUATE STUDENTS Andrea Genovese Adrian Piscopo
ANTIVIRAL THERAPY IN HCV+ B CELL NHL
IFN-based AVT induced hematological response along with SVR in patients with HCV-related indolent
NHLs (especially MZL)
Recent data with IFN-free regimens in HCV-associated LPDs suggest their anti-lymphoma activity too
AVT should be considered the first-line approach in HCV low grade lymphomas if there is no urgency
of a conventional treatment (ie systemic symptoms bulky disease or symptomatic splenomegaly)
(ESMO NCCN EASL guidelines)
Main drugs for HCV-related MCS according to the target
HCV= DAAsB-cell Expansion= (a) B cell-depleting Mabs
-First-generation Rituximab (anti-CD20)-Second-generation Ofatumumab (anti-CD20) Veltuzumab (humanized
anti-CD20)-Third-generation Obinutuzumab (GA101) Oceratuzumab (humanized
anti-CD20)
(b) Alkylating agents
-Cyclophosfamide
Inflammation= Antiinflammatory agents
- Corticosteroids
Altered regulatory T-cell activity=
- IL-2
The impact on HRQoL of IFN-free AVT was prospectively evaluated in a cohort of HCV CV patients with limited
influencing variables linked to therapeutic schedulesviral GT
44 HCV GT2 CV patients mostly F0-F2 (29) and naiumlve (30) treated with SOFRBV for 1224wks
TIME POINTS
baseline EOT and week 12 and 24 of post-treatment f-up (SVR12 and SVR24 respectively)
HRQoL EVALUATION THROUGH PROs
the Short Form (36) Health Survey (SF-36)
the Functional Assessment of Chronic Illness Therapy-Fatigue (FACIT-F) from which we computed the Trial
Outcome Index (TOI)
Observational study on in situ expression of the oncogenic HCV NS3 protein on 116 HCV
patients with B-NHL (DLBCL 36 and MZL 34)
NS3 immunostaining positive in 1214 DLBCL vs only 414 MZL (p = 0006) moreover 24 NS3+
MZL were enriched in large cells
This study supports a new mechanism of transformation with a direct oncogenic role of
HCV proteins in the occurrence of high-grade B lymphomas
IN SITU HEPATITIS C NS3 PROTEIN DETECTION IS ASSOCIATED WITH HIGH GRADEFEATURES IN HCV-ASSOCIATED B-CELL NON-HODGKIN LYMPHOMAS Danielle
Canioni et al 2016
In addition to the role of chronic antigenic stimulation in HCV related
lymphomagenesis this study supports a second mechanism of transformation due toa direct oncogenic role of HCV infection of B-cells promoting the occurrence of high-grade Bcell lymphomas
ANTIVIRAL THERAPY IS ASSOCIATED WITH A BETTERSURVIVAL IN PATIENTS WITH HCV AND B-CELL NON-HODGKIN LYMPHOMAS ANRS HC-13 LYMPHO-CSTUDYMichot JM et al
Outcomes of HCV-associated B-NHL according to HCV AVT in prospective patients only (n 5 64)
(A) absolute neutrophil count and Hgb
(B) ALT and HCV viral load
This patient had HCV-associated DLBCL achieving both complete response and SVR after concurrent chemoimmunotherapy and antiviral therapy using a sofosbuvir-basedregimen
Concurrent Systemic Chemoimmunotherapy and Sofosbuvir-Based Antiviral Treatment in a Hepatitis C Virus-Infected Patient With Diffuse Large B-Cell LymphomaEvan C Ewers et al 2016
HCV-EHDs are responsible for increasing morbidity and mortality with important
consequences in terms of social costs
The analysis of mortality rates in large cohorts confirmed the association of HCV with
several EHDs including cardiovascular neurologic metabolic or renal diseases and tumors
Viral eradication significantly reduced the rate of extra-hepatic deaths
Cacoub P et al DLD 2014 Lee MH et al J Infect Dis 2012 Backus LI et al Clin Gastroenterol Hepatol 2011 El-Kamary S et al
Clin Infect Dis 2011 Hsu YC et al Hepatology 2014 Kawamura Y et al Am J Med 2007 Adinolfi LE et al WJG 2014
Extrahepatic Manifestations of HCV
Con il contributo di
Lee M-H et al J Infect Dis 2012206469-477
Follow-Up
(Years)
20
18
16
14
12
10
2
00 2 4 6 8 10 12 14 16 18 20
8
6
4
Follow-Up
(Years)
12
10
8
6
4
2
00 2 4 6 8 10 12 14 16 18 20
All Causes(n=2394)
Liver Cancer(n=115)
Extrahepatic Diseases(n=2199)
Cum
ula
tive M
ort
ali
ty (
)
Anti-HCV+ HCV RNA detectable Anti-HCV+ HCV RNA undetectable Anti-HCVndash
Follow-Up
(Years)
35
30
25
20
15
10
5
00 2 4 6 8 10 12 14 16 18 20
301
128124
104
16
03
198
122
110
MC is clinically benign but sometimes severe HCV EHD invalidating symptoms occur and
it may evolve into lymphoma
Cacoub P et al DLD 2014 Zignego AL et al DLD 2007 Zignego AL et al Intern Emerg Med 2012 Zignego AL et al Clin Dev
Immunol 2012 Zignego AL et al Expert Rev Clin Immunol 2015 Sene D et al J Rheumatol 2004
Mixed Cryoglobulinemia-MC
CGs reversibly precipitate when the temperature is lower than 37degC and
comprise IgMs with RF activity [mono- or oligo-clonal in type II MC or
polyclonal in type III MC] and polyclonal IgGs
MC pathological substrate is an HCV-driven B-cell
proliferation with consequent production of cryo- and non-
cryoprecipitable CICs in turn responsible for vasculitic
manifestations
Most (70ndash90) MC patients are HCV+ and HCV-patients are CGs+ (40ndash60) while 5ndash30 of
CGs+ have symptomatic MC since HCV infects about 170 million individuals worldwide the
number of patients at risk for developing MC is substantial
Type II
CGs
Type III
CGs
Zignego AL et al Autoimmun Rev 2017 Ferri C et al Autoimmunity rev 2016 Zignego AL et al DLD 2007 Cacoub P et al DLD
2014 Zignego AL et al DLD 2007 Zignego AL et al Intern Emerg Med 2012 Zignego AL et al Clin Dev Immunol 2012 Zignego
AL et al Expert Rev Clin Immunol 2015
MC clinical aspects MC Syndrome
MCS is characterized by the clinical triad -purpura weakness and
arthralgias- low complement C4 and various organsystem
involvement including cutaneous articular renal neurological
cardiac or digestive
It ranges from mild disease to severe even life-threatening
conditions
More serious lesions are generally characterized by neurologic and
renal involvement
Prognosis is highly dependent on renal involvement or on the extent
of vasculitis lesions
1 HCV is the main etiopathological agent as concordantly demonstrated by epidemiological clinico-pathological virological and laboratory investigations2 the association between HCV and disease is demonstrated in a significant proportion of patients and supported by in depth clinico-pathogeneticstudies3 the association is suggested by cohort studies a possible causative role may be limited to a small number of patients andor possibly more relevant in specific geographical areas 4 a number of anecdotal observations suggested a possible role of HCV further investigations are required
From P Cacoub 2015
HCV infection is closely related to LPDs mostly MC
40 to 60 of HCV patients show circulating CGs among this latter population 5-30
develop a symptomatic CV
AVT has been considered the first-line option in HCV-CV patients in fact in the majority
of cases viral eradication leads to CV clinical remission
Data about IFN-free regimens for the treatment of CV patients are still limited
HCV and MC
HCV and MC
Zignego 2015Ferri 2016Pozzato 2016 Sise 2016Saadoun 2015Gragnani 2016Gragnani 2016
Bonacci 2016Hegazy 2016Kondili 2016Emery 2017
Younossi et al
The annual costs (inpatient outpatient andpharmacy) associated with extrahepatic
manifestations of HCV were evaluated
Total direct medical costs of extrahepatic
manifestations of HCV in 2014 US dollars wereestimated to be $1506 million (range $922 millionndash
$2208 million in sensitivity analysis)
These estimates should be added to the liver-related
burden of disease to obtain a more accurateassessment of the total burden of HCV infection
The OBJECTIVE of the study was to estimate the annual direct medical costsassociated with HCV related EHM in the EU5 (France Germany Italy United Kingdom
Spain)
Extrahepatic Manifestations of HCV
Extrahepatic Manifestations of HCV
HCV may cause extrahepatic disorders (HCV-EHDs) classified according to the number and
strength of supporting scientific data
HCV-EHDs are responsible for increasing morbidity and mortality with important
consequences in terms of social costs
The analysis of mortality rates in large cohorts confirmed the association of HCV with
several EHDs including cardiovascular neurologic metabolic or renal diseases and tumors
Viral eradication significantly reduced the rate of extra-hepatic deaths
Cacoub P et al DLD 2014 Lee MH et al J Infect Dis 2012 Backus LI et al Clin Gastroenterol Hepatol 2011 El-Kamary S et al
Clin Infect Dis 2011 Hsu YC et al Hepatology 2014 Kawamura Y et al Am J Med 2007 Adinolfi LE et al WJG 2014
Con il contributo di
Lee M-H et al J Infect Dis 2012206469-477
Follow-Up
(Years)
20
18
16
14
12
10
2
00 2 4 6 8 10 12 14 16 18 20
8
6
4
Follow-Up
(Years)
12
10
8
6
4
2
00 2 4 6 8 10 12 14 16 18 20
All Causes(n=2394)
Liver Cancer(n=115)
Extrahepatic Diseases(n=2199)
Cum
ula
tive M
ort
ali
ty (
)
Anti-HCV+ HCV RNA detectable Anti-HCV+ HCV RNA undetectable Anti-HCVndash
Follow-Up
(Years)
35
30
25
20
15
10
5
00 2 4 6 8 10 12 14 16 18 20
301
128124
104
16
03
198
122
110
Extrahepatic Manifestations of HCV
The annual costs (inpatient outpatient andpharmacy) associated with extrahepatic
manifestations of HCV were evaluated
Total direct medical costs of extrahepatic
manifestations of HCV in 2014 US dollars wereestimated to be $1506 million (range $922 millionndash
$2208 million in sensitivity analysis)
These estimates should be added to the liver-related
burden of disease to obtain a more accurateassessment of the total burden of HCV infection
Younossi et al
Younossi et al
Costs up to $71000 per patient per year (ESRD) Among the most frequent EHM depression (245 in HCV vs 172 in non-HCV) had estimated annual cost of
$4307 million DM (15 vs 10 in non- HCV) had an annual cost of $4434 million in the USA= given the importance of DM and
its association with CVDs and mortality the clinical and economic impacts of HCV-related DM are substantial
The OBJECTIVE of the study was to estimate the annual direct medical costsassociated with HCV related EHM in the EU5 (France Germany Italy United Kingdom
Spain)
The OBJECTIVE of the study was to estimate the annual direct medicalcosts associated with HCV related EHM in the EU5 (France Germany
Italy United Kingdom Spain)
1 HCV is the main etiopathological agent as concordantly demonstrated by epidemiological clinico-pathological virological and laboratory investigations2 the association between HCV and disease is demonstrated in a significant proportion of patients and supported by in depth clinico-pathogeneticstudies3 the association is suggested by cohort studies a possible causative role may be limited to a small number of patients andor possibly more relevant in specific geographical areas 4 a number of anecdotal observations suggested a possible role of HCV further investigations are required
The most studied and frequent HCV-EHDs are B-LPDs andor autoimmune disorders
Their prototype is Mixed Cryoglobulinemia (MC) from researches on MC derived most of the
available information
MC as a precious model for all the HCV-EHDs and to evaluate the effects of viral eradication
Anti-HCV Treatment Evolution
IFN
6 mos
PegIFN RBV 12
mos
IFN
12 mos
IFNRBV
12 mos
PegIFN
12 mos
2001
1998
2011
Standardinterferon
Ribavirin
Peginterferon
1991
Direct-actingantivirals
PegIFN
RBV
DAA
IFNRBV
6 mos
6
16
34
4239
55
70+
0
20
40
60
80
100
DAAs
826
weeks
gt90
2015
Few side effects absence major
contraindications
Younossi et al
The annual costs (inpatient outpatient and pharmacy) associatedwith extrahepatic manifestations of HCV were evaluated
Total direct medical costs of extrahepatic manifestations of HCV in 2014US dollars were estimated to be $1506 million (range $922 millionndash
$2208 million in sensitivity analysis)
These estimates should be added to the liver-related burden of diseaseto obtain a more accurate assessment of the total burden of HCV
infection
The OBJECTIVE of the study was to estimate the annual direct medical costs associated with HCV related EHM in the EU5 (France Germany Italy United Kingdom Spain)
22 MCS treated with DAAs including 2 HCC and 2 NHL 100 SVR12 Clinical CR in 64 and PR in remaining 36 The small lymphocytic lymphoma progressed despite viral clearance
Lauletta et al 2017
Emery CS et al 2017
Retrospective analysis 17 MCS (10 with severelife-threatening vasculitis) and 65 asymptomatic CGs+ pts treated with DAAs SVR 889 MCS and 908 asymptomatic pts In MCS clinical response in 1117 (complete in 717) In severelife-threatening vasculitis lower clinical response especially in renal and neurological symptoms
Saadoun D et al 2017
Open-label prospective multi-center study on sofosbuvir plus daclatasvir treatment of 41 HCV MCS SVR in100 and clinical CR in 902 Disappearance of CGs in 50 of pts No serious adverse event or relapse ofvasculitis
Antiviral Treatment (AVT) of MCIFN-free regimens
MC is clinically benign but sometimes severe HCV EHD invalidating symptoms occur and
it may evolve into lymphoma
Cacoub P et al DLD 2014 Zignego AL et al DLD 2007 Zignego AL et al Intern Emerg Med 2012 Zignego AL et al Clin Dev
Immunol 2012 Zignego AL et al Expert Rev Clin Immunol 2015 Sene D et al J Rheumatol 2004
Mixed Cryoglobulinemia-MC
MC pathological substrate is an HCV-driven B-cell
proliferation with consequent production of cryo- and non-
cryoprecipitable CICs in turn responsible for vasculitic
manifestations
Most (70ndash90) MC patients are HCV+ and HCV-patients are CGs+ (40ndash60) while 5ndash30 of
CGs+ have symptomatic MC or cryoglobulinemic vasculitis since HCV infects about 170
million individuals worldwide the number of patients at risk for developing MC is
substantial
Type II CGs
monoclonal
RF+policlonal IgG
Type III CGs both
RF and IgG
polyclonal

Cohort study of 704 consecutive HIV-negative HCV-positive patients with indolent NHL from 1993 to
2009 in 39 centers of the FIL
Arcaini et al 2016
DLBC HCV- induced
direct transformation
No place of AVT as
1st line
Need of immediate delivery of
chemotherapy or concomitant (NHL
+ HCV targets)
THERAPY OF HCV+ DLBCL
ANTIVIRAL THERAPY IS ASSOCIATED WITH A BETTERSURVIVAL IN PATIENTS WITH HCV AND B-CELL NON-HODGKIN LYMPHOMAS ANRS HC-13 LYMPHO-CSTUDY Michot JM et al
Outcomes of HCV-associated B-NHL according to HCV AVT in prospective patients only (n 5 64)
Concurrent Systemic Chemoimmunotherapy and Sofosbuvir-Based Antiviral Treatment in a Hepatitis C Virus-Infected Patient With Diffuse Large B-Cell Lymphoma Evan C Ewers et al 2016
absolute neutrophil count and Hgb ALT and HCV viral load
Both complete response and SVR of HCV-associated DLBCL after concurrent chemoimmunotherapy and antiviral therapy using a sofosbuvir-based regimen
DAA-treatment in concomitance with chemotherapy showed to be safe and effective in influencing the remission of aggressive lymphomas in HCV patients
Persico M et al 2017
DFS in DAA treated and historical not-treated ptsAntiviral response rates in DAA treated patients
ANTIVIRAL THERAPY IN HCV+ B CELL NHL
IFN-based AVT induced hematological response along with SVR in patients with HCV-related indolent NHLs (especially
MZL)
Recent data with IFN-free regimens in HCV-associated LPDs suggest their anti-lymphoma activity too
AVT should be considered the first-line approach in HCV low grade lymphomas if there is no urgency of a conventional
treatment (ie systemic symptoms bulky disease or symptomatic splenomegaly) (ESMO NCCN EASL guidelines)
In aggressive lymphomas antiviral therapy after induction treatment is to be considered the standard at the moment but
in the next years (months) the association of immunochemotherapy and antiviral therapy will be considered the standard
Zignego AL Ramos-Casals M Ferri C et al Autoimmun Rev 2017
The Masve group
BASIC RESEARCH
Laura Gragnani
Patrizio Caini
Serena Lorini
Antonella Simone
CLINICAL RESEARCH
Monica Monti
Luisa Petraccia
Sinan Sadalla
Guia Cerretelli
Cristina Stasi
Adela Xheka
Universitagrave degli Studi di FirenzeDipartimento di Medicina Sperimentale e Clinica
Centro Manifestazioni Sistemiche da Virus EpatiticildquoMASVErdquo
Anna Linda Zignego
MASVE
UNDERGRADUATE STUDENTS Andrea Genovese Adrian Piscopo
ANTIVIRAL THERAPY IN HCV+ B CELL NHL
IFN-based AVT induced hematological response along with SVR in patients with HCV-related indolent
NHLs (especially MZL)
Recent data with IFN-free regimens in HCV-associated LPDs suggest their anti-lymphoma activity too
AVT should be considered the first-line approach in HCV low grade lymphomas if there is no urgency
of a conventional treatment (ie systemic symptoms bulky disease or symptomatic splenomegaly)
(ESMO NCCN EASL guidelines)
Main drugs for HCV-related MCS according to the target
HCV= DAAsB-cell Expansion= (a) B cell-depleting Mabs
-First-generation Rituximab (anti-CD20)-Second-generation Ofatumumab (anti-CD20) Veltuzumab (humanized
anti-CD20)-Third-generation Obinutuzumab (GA101) Oceratuzumab (humanized
anti-CD20)
(b) Alkylating agents
-Cyclophosfamide
Inflammation= Antiinflammatory agents
- Corticosteroids
Altered regulatory T-cell activity=
- IL-2
The impact on HRQoL of IFN-free AVT was prospectively evaluated in a cohort of HCV CV patients with limited
influencing variables linked to therapeutic schedulesviral GT
44 HCV GT2 CV patients mostly F0-F2 (29) and naiumlve (30) treated with SOFRBV for 1224wks
TIME POINTS
baseline EOT and week 12 and 24 of post-treatment f-up (SVR12 and SVR24 respectively)
HRQoL EVALUATION THROUGH PROs
the Short Form (36) Health Survey (SF-36)
the Functional Assessment of Chronic Illness Therapy-Fatigue (FACIT-F) from which we computed the Trial
Outcome Index (TOI)
Observational study on in situ expression of the oncogenic HCV NS3 protein on 116 HCV
patients with B-NHL (DLBCL 36 and MZL 34)
NS3 immunostaining positive in 1214 DLBCL vs only 414 MZL (p = 0006) moreover 24 NS3+
MZL were enriched in large cells
This study supports a new mechanism of transformation with a direct oncogenic role of
HCV proteins in the occurrence of high-grade B lymphomas
IN SITU HEPATITIS C NS3 PROTEIN DETECTION IS ASSOCIATED WITH HIGH GRADEFEATURES IN HCV-ASSOCIATED B-CELL NON-HODGKIN LYMPHOMAS Danielle
Canioni et al 2016
In addition to the role of chronic antigenic stimulation in HCV related
lymphomagenesis this study supports a second mechanism of transformation due toa direct oncogenic role of HCV infection of B-cells promoting the occurrence of high-grade Bcell lymphomas
ANTIVIRAL THERAPY IS ASSOCIATED WITH A BETTERSURVIVAL IN PATIENTS WITH HCV AND B-CELL NON-HODGKIN LYMPHOMAS ANRS HC-13 LYMPHO-CSTUDYMichot JM et al
Outcomes of HCV-associated B-NHL according to HCV AVT in prospective patients only (n 5 64)
(A) absolute neutrophil count and Hgb
(B) ALT and HCV viral load
This patient had HCV-associated DLBCL achieving both complete response and SVR after concurrent chemoimmunotherapy and antiviral therapy using a sofosbuvir-basedregimen
Concurrent Systemic Chemoimmunotherapy and Sofosbuvir-Based Antiviral Treatment in a Hepatitis C Virus-Infected Patient With Diffuse Large B-Cell LymphomaEvan C Ewers et al 2016
HCV-EHDs are responsible for increasing morbidity and mortality with important
consequences in terms of social costs
The analysis of mortality rates in large cohorts confirmed the association of HCV with
several EHDs including cardiovascular neurologic metabolic or renal diseases and tumors
Viral eradication significantly reduced the rate of extra-hepatic deaths
Cacoub P et al DLD 2014 Lee MH et al J Infect Dis 2012 Backus LI et al Clin Gastroenterol Hepatol 2011 El-Kamary S et al
Clin Infect Dis 2011 Hsu YC et al Hepatology 2014 Kawamura Y et al Am J Med 2007 Adinolfi LE et al WJG 2014
Extrahepatic Manifestations of HCV
Con il contributo di
Lee M-H et al J Infect Dis 2012206469-477
Follow-Up
(Years)
20
18
16
14
12
10
2
00 2 4 6 8 10 12 14 16 18 20
8
6
4
Follow-Up
(Years)
12
10
8
6
4
2
00 2 4 6 8 10 12 14 16 18 20
All Causes(n=2394)
Liver Cancer(n=115)
Extrahepatic Diseases(n=2199)
Cum
ula
tive M
ort
ali
ty (
)
Anti-HCV+ HCV RNA detectable Anti-HCV+ HCV RNA undetectable Anti-HCVndash
Follow-Up
(Years)
35
30
25
20
15
10
5
00 2 4 6 8 10 12 14 16 18 20
301
128124
104
16
03
198
122
110
MC is clinically benign but sometimes severe HCV EHD invalidating symptoms occur and
it may evolve into lymphoma
Cacoub P et al DLD 2014 Zignego AL et al DLD 2007 Zignego AL et al Intern Emerg Med 2012 Zignego AL et al Clin Dev
Immunol 2012 Zignego AL et al Expert Rev Clin Immunol 2015 Sene D et al J Rheumatol 2004
Mixed Cryoglobulinemia-MC
CGs reversibly precipitate when the temperature is lower than 37degC and
comprise IgMs with RF activity [mono- or oligo-clonal in type II MC or
polyclonal in type III MC] and polyclonal IgGs
MC pathological substrate is an HCV-driven B-cell
proliferation with consequent production of cryo- and non-
cryoprecipitable CICs in turn responsible for vasculitic
manifestations
Most (70ndash90) MC patients are HCV+ and HCV-patients are CGs+ (40ndash60) while 5ndash30 of
CGs+ have symptomatic MC since HCV infects about 170 million individuals worldwide the
number of patients at risk for developing MC is substantial
Type II
CGs
Type III
CGs
Zignego AL et al Autoimmun Rev 2017 Ferri C et al Autoimmunity rev 2016 Zignego AL et al DLD 2007 Cacoub P et al DLD
2014 Zignego AL et al DLD 2007 Zignego AL et al Intern Emerg Med 2012 Zignego AL et al Clin Dev Immunol 2012 Zignego
AL et al Expert Rev Clin Immunol 2015
MC clinical aspects MC Syndrome
MCS is characterized by the clinical triad -purpura weakness and
arthralgias- low complement C4 and various organsystem
involvement including cutaneous articular renal neurological
cardiac or digestive
It ranges from mild disease to severe even life-threatening
conditions
More serious lesions are generally characterized by neurologic and
renal involvement
Prognosis is highly dependent on renal involvement or on the extent
of vasculitis lesions
1 HCV is the main etiopathological agent as concordantly demonstrated by epidemiological clinico-pathological virological and laboratory investigations2 the association between HCV and disease is demonstrated in a significant proportion of patients and supported by in depth clinico-pathogeneticstudies3 the association is suggested by cohort studies a possible causative role may be limited to a small number of patients andor possibly more relevant in specific geographical areas 4 a number of anecdotal observations suggested a possible role of HCV further investigations are required
From P Cacoub 2015
HCV infection is closely related to LPDs mostly MC
40 to 60 of HCV patients show circulating CGs among this latter population 5-30
develop a symptomatic CV
AVT has been considered the first-line option in HCV-CV patients in fact in the majority
of cases viral eradication leads to CV clinical remission
Data about IFN-free regimens for the treatment of CV patients are still limited
HCV and MC
HCV and MC
Zignego 2015Ferri 2016Pozzato 2016 Sise 2016Saadoun 2015Gragnani 2016Gragnani 2016
Bonacci 2016Hegazy 2016Kondili 2016Emery 2017
Younossi et al
The annual costs (inpatient outpatient andpharmacy) associated with extrahepatic
manifestations of HCV were evaluated
Total direct medical costs of extrahepatic
manifestations of HCV in 2014 US dollars wereestimated to be $1506 million (range $922 millionndash
$2208 million in sensitivity analysis)
These estimates should be added to the liver-related
burden of disease to obtain a more accurateassessment of the total burden of HCV infection
The OBJECTIVE of the study was to estimate the annual direct medical costsassociated with HCV related EHM in the EU5 (France Germany Italy United Kingdom
Spain)
Extrahepatic Manifestations of HCV
Extrahepatic Manifestations of HCV
HCV may cause extrahepatic disorders (HCV-EHDs) classified according to the number and
strength of supporting scientific data
HCV-EHDs are responsible for increasing morbidity and mortality with important
consequences in terms of social costs
The analysis of mortality rates in large cohorts confirmed the association of HCV with
several EHDs including cardiovascular neurologic metabolic or renal diseases and tumors
Viral eradication significantly reduced the rate of extra-hepatic deaths
Cacoub P et al DLD 2014 Lee MH et al J Infect Dis 2012 Backus LI et al Clin Gastroenterol Hepatol 2011 El-Kamary S et al
Clin Infect Dis 2011 Hsu YC et al Hepatology 2014 Kawamura Y et al Am J Med 2007 Adinolfi LE et al WJG 2014
Con il contributo di
Lee M-H et al J Infect Dis 2012206469-477
Follow-Up
(Years)
20
18
16
14
12
10
2
00 2 4 6 8 10 12 14 16 18 20
8
6
4
Follow-Up
(Years)
12
10
8
6
4
2
00 2 4 6 8 10 12 14 16 18 20
All Causes(n=2394)
Liver Cancer(n=115)
Extrahepatic Diseases(n=2199)
Cum
ula
tive M
ort
ali
ty (
)
Anti-HCV+ HCV RNA detectable Anti-HCV+ HCV RNA undetectable Anti-HCVndash
Follow-Up
(Years)
35
30
25
20
15
10
5
00 2 4 6 8 10 12 14 16 18 20
301
128124
104
16
03
198
122
110
Extrahepatic Manifestations of HCV
The annual costs (inpatient outpatient andpharmacy) associated with extrahepatic
manifestations of HCV were evaluated
Total direct medical costs of extrahepatic
manifestations of HCV in 2014 US dollars wereestimated to be $1506 million (range $922 millionndash
$2208 million in sensitivity analysis)
These estimates should be added to the liver-related
burden of disease to obtain a more accurateassessment of the total burden of HCV infection
Younossi et al
Younossi et al
Costs up to $71000 per patient per year (ESRD) Among the most frequent EHM depression (245 in HCV vs 172 in non-HCV) had estimated annual cost of
$4307 million DM (15 vs 10 in non- HCV) had an annual cost of $4434 million in the USA= given the importance of DM and
its association with CVDs and mortality the clinical and economic impacts of HCV-related DM are substantial
The OBJECTIVE of the study was to estimate the annual direct medical costsassociated with HCV related EHM in the EU5 (France Germany Italy United Kingdom
Spain)
The OBJECTIVE of the study was to estimate the annual direct medicalcosts associated with HCV related EHM in the EU5 (France Germany
Italy United Kingdom Spain)
1 HCV is the main etiopathological agent as concordantly demonstrated by epidemiological clinico-pathological virological and laboratory investigations2 the association between HCV and disease is demonstrated in a significant proportion of patients and supported by in depth clinico-pathogeneticstudies3 the association is suggested by cohort studies a possible causative role may be limited to a small number of patients andor possibly more relevant in specific geographical areas 4 a number of anecdotal observations suggested a possible role of HCV further investigations are required
The most studied and frequent HCV-EHDs are B-LPDs andor autoimmune disorders
Their prototype is Mixed Cryoglobulinemia (MC) from researches on MC derived most of the
available information
MC as a precious model for all the HCV-EHDs and to evaluate the effects of viral eradication
Anti-HCV Treatment Evolution
IFN
6 mos
PegIFN RBV 12
mos
IFN
12 mos
IFNRBV
12 mos
PegIFN
12 mos
2001
1998
2011
Standardinterferon
Ribavirin
Peginterferon
1991
Direct-actingantivirals
PegIFN
RBV
DAA
IFNRBV
6 mos
6
16
34
4239
55
70+
0
20
40
60
80
100
DAAs
826
weeks
gt90
2015
Few side effects absence major
contraindications
Younossi et al
The annual costs (inpatient outpatient and pharmacy) associatedwith extrahepatic manifestations of HCV were evaluated
Total direct medical costs of extrahepatic manifestations of HCV in 2014US dollars were estimated to be $1506 million (range $922 millionndash
$2208 million in sensitivity analysis)
These estimates should be added to the liver-related burden of diseaseto obtain a more accurate assessment of the total burden of HCV
infection
The OBJECTIVE of the study was to estimate the annual direct medical costs associated with HCV related EHM in the EU5 (France Germany Italy United Kingdom Spain)
22 MCS treated with DAAs including 2 HCC and 2 NHL 100 SVR12 Clinical CR in 64 and PR in remaining 36 The small lymphocytic lymphoma progressed despite viral clearance
Lauletta et al 2017
Emery CS et al 2017
Retrospective analysis 17 MCS (10 with severelife-threatening vasculitis) and 65 asymptomatic CGs+ pts treated with DAAs SVR 889 MCS and 908 asymptomatic pts In MCS clinical response in 1117 (complete in 717) In severelife-threatening vasculitis lower clinical response especially in renal and neurological symptoms
Saadoun D et al 2017
Open-label prospective multi-center study on sofosbuvir plus daclatasvir treatment of 41 HCV MCS SVR in100 and clinical CR in 902 Disappearance of CGs in 50 of pts No serious adverse event or relapse ofvasculitis
Antiviral Treatment (AVT) of MCIFN-free regimens
MC is clinically benign but sometimes severe HCV EHD invalidating symptoms occur and
it may evolve into lymphoma
Cacoub P et al DLD 2014 Zignego AL et al DLD 2007 Zignego AL et al Intern Emerg Med 2012 Zignego AL et al Clin Dev
Immunol 2012 Zignego AL et al Expert Rev Clin Immunol 2015 Sene D et al J Rheumatol 2004
Mixed Cryoglobulinemia-MC
MC pathological substrate is an HCV-driven B-cell
proliferation with consequent production of cryo- and non-
cryoprecipitable CICs in turn responsible for vasculitic
manifestations
Most (70ndash90) MC patients are HCV+ and HCV-patients are CGs+ (40ndash60) while 5ndash30 of
CGs+ have symptomatic MC or cryoglobulinemic vasculitis since HCV infects about 170
million individuals worldwide the number of patients at risk for developing MC is
substantial
Type II CGs
monoclonal
RF+policlonal IgG
Type III CGs both
RF and IgG
polyclonal

Arcaini et al 2016
DLBC HCV- induced
direct transformation
No place of AVT as
1st line
Need of immediate delivery of
chemotherapy or concomitant (NHL
+ HCV targets)
THERAPY OF HCV+ DLBCL
ANTIVIRAL THERAPY IS ASSOCIATED WITH A BETTERSURVIVAL IN PATIENTS WITH HCV AND B-CELL NON-HODGKIN LYMPHOMAS ANRS HC-13 LYMPHO-CSTUDY Michot JM et al
Outcomes of HCV-associated B-NHL according to HCV AVT in prospective patients only (n 5 64)
Concurrent Systemic Chemoimmunotherapy and Sofosbuvir-Based Antiviral Treatment in a Hepatitis C Virus-Infected Patient With Diffuse Large B-Cell Lymphoma Evan C Ewers et al 2016
absolute neutrophil count and Hgb ALT and HCV viral load
Both complete response and SVR of HCV-associated DLBCL after concurrent chemoimmunotherapy and antiviral therapy using a sofosbuvir-based regimen
DAA-treatment in concomitance with chemotherapy showed to be safe and effective in influencing the remission of aggressive lymphomas in HCV patients
Persico M et al 2017
DFS in DAA treated and historical not-treated ptsAntiviral response rates in DAA treated patients
ANTIVIRAL THERAPY IN HCV+ B CELL NHL
IFN-based AVT induced hematological response along with SVR in patients with HCV-related indolent NHLs (especially
MZL)
Recent data with IFN-free regimens in HCV-associated LPDs suggest their anti-lymphoma activity too
AVT should be considered the first-line approach in HCV low grade lymphomas if there is no urgency of a conventional
treatment (ie systemic symptoms bulky disease or symptomatic splenomegaly) (ESMO NCCN EASL guidelines)
In aggressive lymphomas antiviral therapy after induction treatment is to be considered the standard at the moment but
in the next years (months) the association of immunochemotherapy and antiviral therapy will be considered the standard
Zignego AL Ramos-Casals M Ferri C et al Autoimmun Rev 2017
The Masve group
BASIC RESEARCH
Laura Gragnani
Patrizio Caini
Serena Lorini
Antonella Simone
CLINICAL RESEARCH
Monica Monti
Luisa Petraccia
Sinan Sadalla
Guia Cerretelli
Cristina Stasi
Adela Xheka
Universitagrave degli Studi di FirenzeDipartimento di Medicina Sperimentale e Clinica
Centro Manifestazioni Sistemiche da Virus EpatiticildquoMASVErdquo
Anna Linda Zignego
MASVE
UNDERGRADUATE STUDENTS Andrea Genovese Adrian Piscopo
ANTIVIRAL THERAPY IN HCV+ B CELL NHL
IFN-based AVT induced hematological response along with SVR in patients with HCV-related indolent
NHLs (especially MZL)
Recent data with IFN-free regimens in HCV-associated LPDs suggest their anti-lymphoma activity too
AVT should be considered the first-line approach in HCV low grade lymphomas if there is no urgency
of a conventional treatment (ie systemic symptoms bulky disease or symptomatic splenomegaly)
(ESMO NCCN EASL guidelines)
Main drugs for HCV-related MCS according to the target
HCV= DAAsB-cell Expansion= (a) B cell-depleting Mabs
-First-generation Rituximab (anti-CD20)-Second-generation Ofatumumab (anti-CD20) Veltuzumab (humanized
anti-CD20)-Third-generation Obinutuzumab (GA101) Oceratuzumab (humanized
anti-CD20)
(b) Alkylating agents
-Cyclophosfamide
Inflammation= Antiinflammatory agents
- Corticosteroids
Altered regulatory T-cell activity=
- IL-2
The impact on HRQoL of IFN-free AVT was prospectively evaluated in a cohort of HCV CV patients with limited
influencing variables linked to therapeutic schedulesviral GT
44 HCV GT2 CV patients mostly F0-F2 (29) and naiumlve (30) treated with SOFRBV for 1224wks
TIME POINTS
baseline EOT and week 12 and 24 of post-treatment f-up (SVR12 and SVR24 respectively)
HRQoL EVALUATION THROUGH PROs
the Short Form (36) Health Survey (SF-36)
the Functional Assessment of Chronic Illness Therapy-Fatigue (FACIT-F) from which we computed the Trial
Outcome Index (TOI)
Observational study on in situ expression of the oncogenic HCV NS3 protein on 116 HCV
patients with B-NHL (DLBCL 36 and MZL 34)
NS3 immunostaining positive in 1214 DLBCL vs only 414 MZL (p = 0006) moreover 24 NS3+
MZL were enriched in large cells
This study supports a new mechanism of transformation with a direct oncogenic role of
HCV proteins in the occurrence of high-grade B lymphomas
IN SITU HEPATITIS C NS3 PROTEIN DETECTION IS ASSOCIATED WITH HIGH GRADEFEATURES IN HCV-ASSOCIATED B-CELL NON-HODGKIN LYMPHOMAS Danielle
Canioni et al 2016
In addition to the role of chronic antigenic stimulation in HCV related
lymphomagenesis this study supports a second mechanism of transformation due toa direct oncogenic role of HCV infection of B-cells promoting the occurrence of high-grade Bcell lymphomas
ANTIVIRAL THERAPY IS ASSOCIATED WITH A BETTERSURVIVAL IN PATIENTS WITH HCV AND B-CELL NON-HODGKIN LYMPHOMAS ANRS HC-13 LYMPHO-CSTUDYMichot JM et al
Outcomes of HCV-associated B-NHL according to HCV AVT in prospective patients only (n 5 64)
(A) absolute neutrophil count and Hgb
(B) ALT and HCV viral load
This patient had HCV-associated DLBCL achieving both complete response and SVR after concurrent chemoimmunotherapy and antiviral therapy using a sofosbuvir-basedregimen
Concurrent Systemic Chemoimmunotherapy and Sofosbuvir-Based Antiviral Treatment in a Hepatitis C Virus-Infected Patient With Diffuse Large B-Cell LymphomaEvan C Ewers et al 2016
HCV-EHDs are responsible for increasing morbidity and mortality with important
consequences in terms of social costs
The analysis of mortality rates in large cohorts confirmed the association of HCV with
several EHDs including cardiovascular neurologic metabolic or renal diseases and tumors
Viral eradication significantly reduced the rate of extra-hepatic deaths
Cacoub P et al DLD 2014 Lee MH et al J Infect Dis 2012 Backus LI et al Clin Gastroenterol Hepatol 2011 El-Kamary S et al
Clin Infect Dis 2011 Hsu YC et al Hepatology 2014 Kawamura Y et al Am J Med 2007 Adinolfi LE et al WJG 2014
Extrahepatic Manifestations of HCV
Con il contributo di
Lee M-H et al J Infect Dis 2012206469-477
Follow-Up
(Years)
20
18
16
14
12
10
2
00 2 4 6 8 10 12 14 16 18 20
8
6
4
Follow-Up
(Years)
12
10
8
6
4
2
00 2 4 6 8 10 12 14 16 18 20
All Causes(n=2394)
Liver Cancer(n=115)
Extrahepatic Diseases(n=2199)
Cum
ula
tive M
ort
ali
ty (
)
Anti-HCV+ HCV RNA detectable Anti-HCV+ HCV RNA undetectable Anti-HCVndash
Follow-Up
(Years)
35
30
25
20
15
10
5
00 2 4 6 8 10 12 14 16 18 20
301
128124
104
16
03
198
122
110
MC is clinically benign but sometimes severe HCV EHD invalidating symptoms occur and
it may evolve into lymphoma
Cacoub P et al DLD 2014 Zignego AL et al DLD 2007 Zignego AL et al Intern Emerg Med 2012 Zignego AL et al Clin Dev
Immunol 2012 Zignego AL et al Expert Rev Clin Immunol 2015 Sene D et al J Rheumatol 2004
Mixed Cryoglobulinemia-MC
CGs reversibly precipitate when the temperature is lower than 37degC and
comprise IgMs with RF activity [mono- or oligo-clonal in type II MC or
polyclonal in type III MC] and polyclonal IgGs
MC pathological substrate is an HCV-driven B-cell
proliferation with consequent production of cryo- and non-
cryoprecipitable CICs in turn responsible for vasculitic
manifestations
Most (70ndash90) MC patients are HCV+ and HCV-patients are CGs+ (40ndash60) while 5ndash30 of
CGs+ have symptomatic MC since HCV infects about 170 million individuals worldwide the
number of patients at risk for developing MC is substantial
Type II
CGs
Type III
CGs
Zignego AL et al Autoimmun Rev 2017 Ferri C et al Autoimmunity rev 2016 Zignego AL et al DLD 2007 Cacoub P et al DLD
2014 Zignego AL et al DLD 2007 Zignego AL et al Intern Emerg Med 2012 Zignego AL et al Clin Dev Immunol 2012 Zignego
AL et al Expert Rev Clin Immunol 2015
MC clinical aspects MC Syndrome
MCS is characterized by the clinical triad -purpura weakness and
arthralgias- low complement C4 and various organsystem
involvement including cutaneous articular renal neurological
cardiac or digestive
It ranges from mild disease to severe even life-threatening
conditions
More serious lesions are generally characterized by neurologic and
renal involvement
Prognosis is highly dependent on renal involvement or on the extent
of vasculitis lesions
1 HCV is the main etiopathological agent as concordantly demonstrated by epidemiological clinico-pathological virological and laboratory investigations2 the association between HCV and disease is demonstrated in a significant proportion of patients and supported by in depth clinico-pathogeneticstudies3 the association is suggested by cohort studies a possible causative role may be limited to a small number of patients andor possibly more relevant in specific geographical areas 4 a number of anecdotal observations suggested a possible role of HCV further investigations are required
From P Cacoub 2015
HCV infection is closely related to LPDs mostly MC
40 to 60 of HCV patients show circulating CGs among this latter population 5-30
develop a symptomatic CV
AVT has been considered the first-line option in HCV-CV patients in fact in the majority
of cases viral eradication leads to CV clinical remission
Data about IFN-free regimens for the treatment of CV patients are still limited
HCV and MC
HCV and MC
Zignego 2015Ferri 2016Pozzato 2016 Sise 2016Saadoun 2015Gragnani 2016Gragnani 2016
Bonacci 2016Hegazy 2016Kondili 2016Emery 2017
Younossi et al
The annual costs (inpatient outpatient andpharmacy) associated with extrahepatic
manifestations of HCV were evaluated
Total direct medical costs of extrahepatic
manifestations of HCV in 2014 US dollars wereestimated to be $1506 million (range $922 millionndash
$2208 million in sensitivity analysis)
These estimates should be added to the liver-related
burden of disease to obtain a more accurateassessment of the total burden of HCV infection
The OBJECTIVE of the study was to estimate the annual direct medical costsassociated with HCV related EHM in the EU5 (France Germany Italy United Kingdom
Spain)
Extrahepatic Manifestations of HCV
Extrahepatic Manifestations of HCV
HCV may cause extrahepatic disorders (HCV-EHDs) classified according to the number and
strength of supporting scientific data
HCV-EHDs are responsible for increasing morbidity and mortality with important
consequences in terms of social costs
The analysis of mortality rates in large cohorts confirmed the association of HCV with
several EHDs including cardiovascular neurologic metabolic or renal diseases and tumors
Viral eradication significantly reduced the rate of extra-hepatic deaths
Cacoub P et al DLD 2014 Lee MH et al J Infect Dis 2012 Backus LI et al Clin Gastroenterol Hepatol 2011 El-Kamary S et al
Clin Infect Dis 2011 Hsu YC et al Hepatology 2014 Kawamura Y et al Am J Med 2007 Adinolfi LE et al WJG 2014
Con il contributo di
Lee M-H et al J Infect Dis 2012206469-477
Follow-Up
(Years)
20
18
16
14
12
10
2
00 2 4 6 8 10 12 14 16 18 20
8
6
4
Follow-Up
(Years)
12
10
8
6
4
2
00 2 4 6 8 10 12 14 16 18 20
All Causes(n=2394)
Liver Cancer(n=115)
Extrahepatic Diseases(n=2199)
Cum
ula
tive M
ort
ali
ty (
)
Anti-HCV+ HCV RNA detectable Anti-HCV+ HCV RNA undetectable Anti-HCVndash
Follow-Up
(Years)
35
30
25
20
15
10
5
00 2 4 6 8 10 12 14 16 18 20
301
128124
104
16
03
198
122
110
Extrahepatic Manifestations of HCV
The annual costs (inpatient outpatient andpharmacy) associated with extrahepatic
manifestations of HCV were evaluated
Total direct medical costs of extrahepatic
manifestations of HCV in 2014 US dollars wereestimated to be $1506 million (range $922 millionndash
$2208 million in sensitivity analysis)
These estimates should be added to the liver-related
burden of disease to obtain a more accurateassessment of the total burden of HCV infection
Younossi et al
Younossi et al
Costs up to $71000 per patient per year (ESRD) Among the most frequent EHM depression (245 in HCV vs 172 in non-HCV) had estimated annual cost of
$4307 million DM (15 vs 10 in non- HCV) had an annual cost of $4434 million in the USA= given the importance of DM and
its association with CVDs and mortality the clinical and economic impacts of HCV-related DM are substantial
The OBJECTIVE of the study was to estimate the annual direct medical costsassociated with HCV related EHM in the EU5 (France Germany Italy United Kingdom
Spain)
The OBJECTIVE of the study was to estimate the annual direct medicalcosts associated with HCV related EHM in the EU5 (France Germany
Italy United Kingdom Spain)
1 HCV is the main etiopathological agent as concordantly demonstrated by epidemiological clinico-pathological virological and laboratory investigations2 the association between HCV and disease is demonstrated in a significant proportion of patients and supported by in depth clinico-pathogeneticstudies3 the association is suggested by cohort studies a possible causative role may be limited to a small number of patients andor possibly more relevant in specific geographical areas 4 a number of anecdotal observations suggested a possible role of HCV further investigations are required
The most studied and frequent HCV-EHDs are B-LPDs andor autoimmune disorders
Their prototype is Mixed Cryoglobulinemia (MC) from researches on MC derived most of the
available information
MC as a precious model for all the HCV-EHDs and to evaluate the effects of viral eradication
Anti-HCV Treatment Evolution
IFN
6 mos
PegIFN RBV 12
mos
IFN
12 mos
IFNRBV
12 mos
PegIFN
12 mos
2001
1998
2011
Standardinterferon
Ribavirin
Peginterferon
1991
Direct-actingantivirals
PegIFN
RBV
DAA
IFNRBV
6 mos
6
16
34
4239
55
70+
0
20
40
60
80
100
DAAs
826
weeks
gt90
2015
Few side effects absence major
contraindications
Younossi et al
The annual costs (inpatient outpatient and pharmacy) associatedwith extrahepatic manifestations of HCV were evaluated
Total direct medical costs of extrahepatic manifestations of HCV in 2014US dollars were estimated to be $1506 million (range $922 millionndash
$2208 million in sensitivity analysis)
These estimates should be added to the liver-related burden of diseaseto obtain a more accurate assessment of the total burden of HCV
infection
The OBJECTIVE of the study was to estimate the annual direct medical costs associated with HCV related EHM in the EU5 (France Germany Italy United Kingdom Spain)
22 MCS treated with DAAs including 2 HCC and 2 NHL 100 SVR12 Clinical CR in 64 and PR in remaining 36 The small lymphocytic lymphoma progressed despite viral clearance
Lauletta et al 2017
Emery CS et al 2017
Retrospective analysis 17 MCS (10 with severelife-threatening vasculitis) and 65 asymptomatic CGs+ pts treated with DAAs SVR 889 MCS and 908 asymptomatic pts In MCS clinical response in 1117 (complete in 717) In severelife-threatening vasculitis lower clinical response especially in renal and neurological symptoms
Saadoun D et al 2017
Open-label prospective multi-center study on sofosbuvir plus daclatasvir treatment of 41 HCV MCS SVR in100 and clinical CR in 902 Disappearance of CGs in 50 of pts No serious adverse event or relapse ofvasculitis
Antiviral Treatment (AVT) of MCIFN-free regimens
MC is clinically benign but sometimes severe HCV EHD invalidating symptoms occur and
it may evolve into lymphoma
Cacoub P et al DLD 2014 Zignego AL et al DLD 2007 Zignego AL et al Intern Emerg Med 2012 Zignego AL et al Clin Dev
Immunol 2012 Zignego AL et al Expert Rev Clin Immunol 2015 Sene D et al J Rheumatol 2004
Mixed Cryoglobulinemia-MC
MC pathological substrate is an HCV-driven B-cell
proliferation with consequent production of cryo- and non-
cryoprecipitable CICs in turn responsible for vasculitic
manifestations
Most (70ndash90) MC patients are HCV+ and HCV-patients are CGs+ (40ndash60) while 5ndash30 of
CGs+ have symptomatic MC or cryoglobulinemic vasculitis since HCV infects about 170
million individuals worldwide the number of patients at risk for developing MC is
substantial
Type II CGs
monoclonal
RF+policlonal IgG
Type III CGs both
RF and IgG
polyclonal

DLBC HCV- induced
direct transformation
No place of AVT as
1st line
Need of immediate delivery of
chemotherapy or concomitant (NHL
+ HCV targets)
THERAPY OF HCV+ DLBCL
ANTIVIRAL THERAPY IS ASSOCIATED WITH A BETTERSURVIVAL IN PATIENTS WITH HCV AND B-CELL NON-HODGKIN LYMPHOMAS ANRS HC-13 LYMPHO-CSTUDY Michot JM et al
Outcomes of HCV-associated B-NHL according to HCV AVT in prospective patients only (n 5 64)
Concurrent Systemic Chemoimmunotherapy and Sofosbuvir-Based Antiviral Treatment in a Hepatitis C Virus-Infected Patient With Diffuse Large B-Cell Lymphoma Evan C Ewers et al 2016
absolute neutrophil count and Hgb ALT and HCV viral load
Both complete response and SVR of HCV-associated DLBCL after concurrent chemoimmunotherapy and antiviral therapy using a sofosbuvir-based regimen
DAA-treatment in concomitance with chemotherapy showed to be safe and effective in influencing the remission of aggressive lymphomas in HCV patients
Persico M et al 2017
DFS in DAA treated and historical not-treated ptsAntiviral response rates in DAA treated patients
ANTIVIRAL THERAPY IN HCV+ B CELL NHL
IFN-based AVT induced hematological response along with SVR in patients with HCV-related indolent NHLs (especially
MZL)
Recent data with IFN-free regimens in HCV-associated LPDs suggest their anti-lymphoma activity too
AVT should be considered the first-line approach in HCV low grade lymphomas if there is no urgency of a conventional
treatment (ie systemic symptoms bulky disease or symptomatic splenomegaly) (ESMO NCCN EASL guidelines)
In aggressive lymphomas antiviral therapy after induction treatment is to be considered the standard at the moment but
in the next years (months) the association of immunochemotherapy and antiviral therapy will be considered the standard
Zignego AL Ramos-Casals M Ferri C et al Autoimmun Rev 2017
The Masve group
BASIC RESEARCH
Laura Gragnani
Patrizio Caini
Serena Lorini
Antonella Simone
CLINICAL RESEARCH
Monica Monti
Luisa Petraccia
Sinan Sadalla
Guia Cerretelli
Cristina Stasi
Adela Xheka
Universitagrave degli Studi di FirenzeDipartimento di Medicina Sperimentale e Clinica
Centro Manifestazioni Sistemiche da Virus EpatiticildquoMASVErdquo
Anna Linda Zignego
MASVE
UNDERGRADUATE STUDENTS Andrea Genovese Adrian Piscopo
ANTIVIRAL THERAPY IN HCV+ B CELL NHL
IFN-based AVT induced hematological response along with SVR in patients with HCV-related indolent
NHLs (especially MZL)
Recent data with IFN-free regimens in HCV-associated LPDs suggest their anti-lymphoma activity too
AVT should be considered the first-line approach in HCV low grade lymphomas if there is no urgency
of a conventional treatment (ie systemic symptoms bulky disease or symptomatic splenomegaly)
(ESMO NCCN EASL guidelines)
Main drugs for HCV-related MCS according to the target
HCV= DAAsB-cell Expansion= (a) B cell-depleting Mabs
-First-generation Rituximab (anti-CD20)-Second-generation Ofatumumab (anti-CD20) Veltuzumab (humanized
anti-CD20)-Third-generation Obinutuzumab (GA101) Oceratuzumab (humanized
anti-CD20)
(b) Alkylating agents
-Cyclophosfamide
Inflammation= Antiinflammatory agents
- Corticosteroids
Altered regulatory T-cell activity=
- IL-2
The impact on HRQoL of IFN-free AVT was prospectively evaluated in a cohort of HCV CV patients with limited
influencing variables linked to therapeutic schedulesviral GT
44 HCV GT2 CV patients mostly F0-F2 (29) and naiumlve (30) treated with SOFRBV for 1224wks
TIME POINTS
baseline EOT and week 12 and 24 of post-treatment f-up (SVR12 and SVR24 respectively)
HRQoL EVALUATION THROUGH PROs
the Short Form (36) Health Survey (SF-36)
the Functional Assessment of Chronic Illness Therapy-Fatigue (FACIT-F) from which we computed the Trial
Outcome Index (TOI)
Observational study on in situ expression of the oncogenic HCV NS3 protein on 116 HCV
patients with B-NHL (DLBCL 36 and MZL 34)
NS3 immunostaining positive in 1214 DLBCL vs only 414 MZL (p = 0006) moreover 24 NS3+
MZL were enriched in large cells
This study supports a new mechanism of transformation with a direct oncogenic role of
HCV proteins in the occurrence of high-grade B lymphomas
IN SITU HEPATITIS C NS3 PROTEIN DETECTION IS ASSOCIATED WITH HIGH GRADEFEATURES IN HCV-ASSOCIATED B-CELL NON-HODGKIN LYMPHOMAS Danielle
Canioni et al 2016
In addition to the role of chronic antigenic stimulation in HCV related
lymphomagenesis this study supports a second mechanism of transformation due toa direct oncogenic role of HCV infection of B-cells promoting the occurrence of high-grade Bcell lymphomas
ANTIVIRAL THERAPY IS ASSOCIATED WITH A BETTERSURVIVAL IN PATIENTS WITH HCV AND B-CELL NON-HODGKIN LYMPHOMAS ANRS HC-13 LYMPHO-CSTUDYMichot JM et al
Outcomes of HCV-associated B-NHL according to HCV AVT in prospective patients only (n 5 64)
(A) absolute neutrophil count and Hgb
(B) ALT and HCV viral load
This patient had HCV-associated DLBCL achieving both complete response and SVR after concurrent chemoimmunotherapy and antiviral therapy using a sofosbuvir-basedregimen
Concurrent Systemic Chemoimmunotherapy and Sofosbuvir-Based Antiviral Treatment in a Hepatitis C Virus-Infected Patient With Diffuse Large B-Cell LymphomaEvan C Ewers et al 2016
HCV-EHDs are responsible for increasing morbidity and mortality with important
consequences in terms of social costs
The analysis of mortality rates in large cohorts confirmed the association of HCV with
several EHDs including cardiovascular neurologic metabolic or renal diseases and tumors
Viral eradication significantly reduced the rate of extra-hepatic deaths
Cacoub P et al DLD 2014 Lee MH et al J Infect Dis 2012 Backus LI et al Clin Gastroenterol Hepatol 2011 El-Kamary S et al
Clin Infect Dis 2011 Hsu YC et al Hepatology 2014 Kawamura Y et al Am J Med 2007 Adinolfi LE et al WJG 2014
Extrahepatic Manifestations of HCV
Con il contributo di
Lee M-H et al J Infect Dis 2012206469-477
Follow-Up
(Years)
20
18
16
14
12
10
2
00 2 4 6 8 10 12 14 16 18 20
8
6
4
Follow-Up
(Years)
12
10
8
6
4
2
00 2 4 6 8 10 12 14 16 18 20
All Causes(n=2394)
Liver Cancer(n=115)
Extrahepatic Diseases(n=2199)
Cum
ula
tive M
ort
ali
ty (
)
Anti-HCV+ HCV RNA detectable Anti-HCV+ HCV RNA undetectable Anti-HCVndash
Follow-Up
(Years)
35
30
25
20
15
10
5
00 2 4 6 8 10 12 14 16 18 20
301
128124
104
16
03
198
122
110
MC is clinically benign but sometimes severe HCV EHD invalidating symptoms occur and
it may evolve into lymphoma
Cacoub P et al DLD 2014 Zignego AL et al DLD 2007 Zignego AL et al Intern Emerg Med 2012 Zignego AL et al Clin Dev
Immunol 2012 Zignego AL et al Expert Rev Clin Immunol 2015 Sene D et al J Rheumatol 2004
Mixed Cryoglobulinemia-MC
CGs reversibly precipitate when the temperature is lower than 37degC and
comprise IgMs with RF activity [mono- or oligo-clonal in type II MC or
polyclonal in type III MC] and polyclonal IgGs
MC pathological substrate is an HCV-driven B-cell
proliferation with consequent production of cryo- and non-
cryoprecipitable CICs in turn responsible for vasculitic
manifestations
Most (70ndash90) MC patients are HCV+ and HCV-patients are CGs+ (40ndash60) while 5ndash30 of
CGs+ have symptomatic MC since HCV infects about 170 million individuals worldwide the
number of patients at risk for developing MC is substantial
Type II
CGs
Type III
CGs
Zignego AL et al Autoimmun Rev 2017 Ferri C et al Autoimmunity rev 2016 Zignego AL et al DLD 2007 Cacoub P et al DLD
2014 Zignego AL et al DLD 2007 Zignego AL et al Intern Emerg Med 2012 Zignego AL et al Clin Dev Immunol 2012 Zignego
AL et al Expert Rev Clin Immunol 2015
MC clinical aspects MC Syndrome
MCS is characterized by the clinical triad -purpura weakness and
arthralgias- low complement C4 and various organsystem
involvement including cutaneous articular renal neurological
cardiac or digestive
It ranges from mild disease to severe even life-threatening
conditions
More serious lesions are generally characterized by neurologic and
renal involvement
Prognosis is highly dependent on renal involvement or on the extent
of vasculitis lesions
1 HCV is the main etiopathological agent as concordantly demonstrated by epidemiological clinico-pathological virological and laboratory investigations2 the association between HCV and disease is demonstrated in a significant proportion of patients and supported by in depth clinico-pathogeneticstudies3 the association is suggested by cohort studies a possible causative role may be limited to a small number of patients andor possibly more relevant in specific geographical areas 4 a number of anecdotal observations suggested a possible role of HCV further investigations are required
From P Cacoub 2015
HCV infection is closely related to LPDs mostly MC
40 to 60 of HCV patients show circulating CGs among this latter population 5-30
develop a symptomatic CV
AVT has been considered the first-line option in HCV-CV patients in fact in the majority
of cases viral eradication leads to CV clinical remission
Data about IFN-free regimens for the treatment of CV patients are still limited
HCV and MC
HCV and MC
Zignego 2015Ferri 2016Pozzato 2016 Sise 2016Saadoun 2015Gragnani 2016Gragnani 2016
Bonacci 2016Hegazy 2016Kondili 2016Emery 2017
Younossi et al
The annual costs (inpatient outpatient andpharmacy) associated with extrahepatic
manifestations of HCV were evaluated
Total direct medical costs of extrahepatic
manifestations of HCV in 2014 US dollars wereestimated to be $1506 million (range $922 millionndash
$2208 million in sensitivity analysis)
These estimates should be added to the liver-related
burden of disease to obtain a more accurateassessment of the total burden of HCV infection
The OBJECTIVE of the study was to estimate the annual direct medical costsassociated with HCV related EHM in the EU5 (France Germany Italy United Kingdom
Spain)
Extrahepatic Manifestations of HCV
Extrahepatic Manifestations of HCV
HCV may cause extrahepatic disorders (HCV-EHDs) classified according to the number and
strength of supporting scientific data
HCV-EHDs are responsible for increasing morbidity and mortality with important
consequences in terms of social costs
The analysis of mortality rates in large cohorts confirmed the association of HCV with
several EHDs including cardiovascular neurologic metabolic or renal diseases and tumors
Viral eradication significantly reduced the rate of extra-hepatic deaths
Cacoub P et al DLD 2014 Lee MH et al J Infect Dis 2012 Backus LI et al Clin Gastroenterol Hepatol 2011 El-Kamary S et al
Clin Infect Dis 2011 Hsu YC et al Hepatology 2014 Kawamura Y et al Am J Med 2007 Adinolfi LE et al WJG 2014
Con il contributo di
Lee M-H et al J Infect Dis 2012206469-477
Follow-Up
(Years)
20
18
16
14
12
10
2
00 2 4 6 8 10 12 14 16 18 20
8
6
4
Follow-Up
(Years)
12
10
8
6
4
2
00 2 4 6 8 10 12 14 16 18 20
All Causes(n=2394)
Liver Cancer(n=115)
Extrahepatic Diseases(n=2199)
Cum
ula
tive M
ort
ali
ty (
)
Anti-HCV+ HCV RNA detectable Anti-HCV+ HCV RNA undetectable Anti-HCVndash
Follow-Up
(Years)
35
30
25
20
15
10
5
00 2 4 6 8 10 12 14 16 18 20
301
128124
104
16
03
198
122
110
Extrahepatic Manifestations of HCV
The annual costs (inpatient outpatient andpharmacy) associated with extrahepatic
manifestations of HCV were evaluated
Total direct medical costs of extrahepatic
manifestations of HCV in 2014 US dollars wereestimated to be $1506 million (range $922 millionndash
$2208 million in sensitivity analysis)
These estimates should be added to the liver-related
burden of disease to obtain a more accurateassessment of the total burden of HCV infection
Younossi et al
Younossi et al
Costs up to $71000 per patient per year (ESRD) Among the most frequent EHM depression (245 in HCV vs 172 in non-HCV) had estimated annual cost of
$4307 million DM (15 vs 10 in non- HCV) had an annual cost of $4434 million in the USA= given the importance of DM and
its association with CVDs and mortality the clinical and economic impacts of HCV-related DM are substantial
The OBJECTIVE of the study was to estimate the annual direct medical costsassociated with HCV related EHM in the EU5 (France Germany Italy United Kingdom
Spain)
The OBJECTIVE of the study was to estimate the annual direct medicalcosts associated with HCV related EHM in the EU5 (France Germany
Italy United Kingdom Spain)
1 HCV is the main etiopathological agent as concordantly demonstrated by epidemiological clinico-pathological virological and laboratory investigations2 the association between HCV and disease is demonstrated in a significant proportion of patients and supported by in depth clinico-pathogeneticstudies3 the association is suggested by cohort studies a possible causative role may be limited to a small number of patients andor possibly more relevant in specific geographical areas 4 a number of anecdotal observations suggested a possible role of HCV further investigations are required
The most studied and frequent HCV-EHDs are B-LPDs andor autoimmune disorders
Their prototype is Mixed Cryoglobulinemia (MC) from researches on MC derived most of the
available information
MC as a precious model for all the HCV-EHDs and to evaluate the effects of viral eradication
Anti-HCV Treatment Evolution
IFN
6 mos
PegIFN RBV 12
mos
IFN
12 mos
IFNRBV
12 mos
PegIFN
12 mos
2001
1998
2011
Standardinterferon
Ribavirin
Peginterferon
1991
Direct-actingantivirals
PegIFN
RBV
DAA
IFNRBV
6 mos
6
16
34
4239
55
70+
0
20
40
60
80
100
DAAs
826
weeks
gt90
2015
Few side effects absence major
contraindications
Younossi et al
The annual costs (inpatient outpatient and pharmacy) associatedwith extrahepatic manifestations of HCV were evaluated
Total direct medical costs of extrahepatic manifestations of HCV in 2014US dollars were estimated to be $1506 million (range $922 millionndash
$2208 million in sensitivity analysis)
These estimates should be added to the liver-related burden of diseaseto obtain a more accurate assessment of the total burden of HCV
infection
The OBJECTIVE of the study was to estimate the annual direct medical costs associated with HCV related EHM in the EU5 (France Germany Italy United Kingdom Spain)
22 MCS treated with DAAs including 2 HCC and 2 NHL 100 SVR12 Clinical CR in 64 and PR in remaining 36 The small lymphocytic lymphoma progressed despite viral clearance
Lauletta et al 2017
Emery CS et al 2017
Retrospective analysis 17 MCS (10 with severelife-threatening vasculitis) and 65 asymptomatic CGs+ pts treated with DAAs SVR 889 MCS and 908 asymptomatic pts In MCS clinical response in 1117 (complete in 717) In severelife-threatening vasculitis lower clinical response especially in renal and neurological symptoms
Saadoun D et al 2017
Open-label prospective multi-center study on sofosbuvir plus daclatasvir treatment of 41 HCV MCS SVR in100 and clinical CR in 902 Disappearance of CGs in 50 of pts No serious adverse event or relapse ofvasculitis
Antiviral Treatment (AVT) of MCIFN-free regimens
MC is clinically benign but sometimes severe HCV EHD invalidating symptoms occur and
it may evolve into lymphoma
Cacoub P et al DLD 2014 Zignego AL et al DLD 2007 Zignego AL et al Intern Emerg Med 2012 Zignego AL et al Clin Dev
Immunol 2012 Zignego AL et al Expert Rev Clin Immunol 2015 Sene D et al J Rheumatol 2004
Mixed Cryoglobulinemia-MC
MC pathological substrate is an HCV-driven B-cell
proliferation with consequent production of cryo- and non-
cryoprecipitable CICs in turn responsible for vasculitic
manifestations
Most (70ndash90) MC patients are HCV+ and HCV-patients are CGs+ (40ndash60) while 5ndash30 of
CGs+ have symptomatic MC or cryoglobulinemic vasculitis since HCV infects about 170
million individuals worldwide the number of patients at risk for developing MC is
substantial
Type II CGs
monoclonal
RF+policlonal IgG
Type III CGs both
RF and IgG
polyclonal

ANTIVIRAL THERAPY IS ASSOCIATED WITH A BETTERSURVIVAL IN PATIENTS WITH HCV AND B-CELL NON-HODGKIN LYMPHOMAS ANRS HC-13 LYMPHO-CSTUDY Michot JM et al
Outcomes of HCV-associated B-NHL according to HCV AVT in prospective patients only (n 5 64)
Concurrent Systemic Chemoimmunotherapy and Sofosbuvir-Based Antiviral Treatment in a Hepatitis C Virus-Infected Patient With Diffuse Large B-Cell Lymphoma Evan C Ewers et al 2016
absolute neutrophil count and Hgb ALT and HCV viral load
Both complete response and SVR of HCV-associated DLBCL after concurrent chemoimmunotherapy and antiviral therapy using a sofosbuvir-based regimen
DAA-treatment in concomitance with chemotherapy showed to be safe and effective in influencing the remission of aggressive lymphomas in HCV patients
Persico M et al 2017
DFS in DAA treated and historical not-treated ptsAntiviral response rates in DAA treated patients
ANTIVIRAL THERAPY IN HCV+ B CELL NHL
IFN-based AVT induced hematological response along with SVR in patients with HCV-related indolent NHLs (especially
MZL)
Recent data with IFN-free regimens in HCV-associated LPDs suggest their anti-lymphoma activity too
AVT should be considered the first-line approach in HCV low grade lymphomas if there is no urgency of a conventional
treatment (ie systemic symptoms bulky disease or symptomatic splenomegaly) (ESMO NCCN EASL guidelines)
In aggressive lymphomas antiviral therapy after induction treatment is to be considered the standard at the moment but
in the next years (months) the association of immunochemotherapy and antiviral therapy will be considered the standard
Zignego AL Ramos-Casals M Ferri C et al Autoimmun Rev 2017
The Masve group
BASIC RESEARCH
Laura Gragnani
Patrizio Caini
Serena Lorini
Antonella Simone
CLINICAL RESEARCH
Monica Monti
Luisa Petraccia
Sinan Sadalla
Guia Cerretelli
Cristina Stasi
Adela Xheka
Universitagrave degli Studi di FirenzeDipartimento di Medicina Sperimentale e Clinica
Centro Manifestazioni Sistemiche da Virus EpatiticildquoMASVErdquo
Anna Linda Zignego
MASVE
UNDERGRADUATE STUDENTS Andrea Genovese Adrian Piscopo
ANTIVIRAL THERAPY IN HCV+ B CELL NHL
IFN-based AVT induced hematological response along with SVR in patients with HCV-related indolent
NHLs (especially MZL)
Recent data with IFN-free regimens in HCV-associated LPDs suggest their anti-lymphoma activity too
AVT should be considered the first-line approach in HCV low grade lymphomas if there is no urgency
of a conventional treatment (ie systemic symptoms bulky disease or symptomatic splenomegaly)
(ESMO NCCN EASL guidelines)
Main drugs for HCV-related MCS according to the target
HCV= DAAsB-cell Expansion= (a) B cell-depleting Mabs
-First-generation Rituximab (anti-CD20)-Second-generation Ofatumumab (anti-CD20) Veltuzumab (humanized
anti-CD20)-Third-generation Obinutuzumab (GA101) Oceratuzumab (humanized
anti-CD20)
(b) Alkylating agents
-Cyclophosfamide
Inflammation= Antiinflammatory agents
- Corticosteroids
Altered regulatory T-cell activity=
- IL-2
The impact on HRQoL of IFN-free AVT was prospectively evaluated in a cohort of HCV CV patients with limited
influencing variables linked to therapeutic schedulesviral GT
44 HCV GT2 CV patients mostly F0-F2 (29) and naiumlve (30) treated with SOFRBV for 1224wks
TIME POINTS
baseline EOT and week 12 and 24 of post-treatment f-up (SVR12 and SVR24 respectively)
HRQoL EVALUATION THROUGH PROs
the Short Form (36) Health Survey (SF-36)
the Functional Assessment of Chronic Illness Therapy-Fatigue (FACIT-F) from which we computed the Trial
Outcome Index (TOI)
Observational study on in situ expression of the oncogenic HCV NS3 protein on 116 HCV
patients with B-NHL (DLBCL 36 and MZL 34)
NS3 immunostaining positive in 1214 DLBCL vs only 414 MZL (p = 0006) moreover 24 NS3+
MZL were enriched in large cells
This study supports a new mechanism of transformation with a direct oncogenic role of
HCV proteins in the occurrence of high-grade B lymphomas
IN SITU HEPATITIS C NS3 PROTEIN DETECTION IS ASSOCIATED WITH HIGH GRADEFEATURES IN HCV-ASSOCIATED B-CELL NON-HODGKIN LYMPHOMAS Danielle
Canioni et al 2016
In addition to the role of chronic antigenic stimulation in HCV related
lymphomagenesis this study supports a second mechanism of transformation due toa direct oncogenic role of HCV infection of B-cells promoting the occurrence of high-grade Bcell lymphomas
ANTIVIRAL THERAPY IS ASSOCIATED WITH A BETTERSURVIVAL IN PATIENTS WITH HCV AND B-CELL NON-HODGKIN LYMPHOMAS ANRS HC-13 LYMPHO-CSTUDYMichot JM et al
Outcomes of HCV-associated B-NHL according to HCV AVT in prospective patients only (n 5 64)
(A) absolute neutrophil count and Hgb
(B) ALT and HCV viral load
This patient had HCV-associated DLBCL achieving both complete response and SVR after concurrent chemoimmunotherapy and antiviral therapy using a sofosbuvir-basedregimen
Concurrent Systemic Chemoimmunotherapy and Sofosbuvir-Based Antiviral Treatment in a Hepatitis C Virus-Infected Patient With Diffuse Large B-Cell LymphomaEvan C Ewers et al 2016
HCV-EHDs are responsible for increasing morbidity and mortality with important
consequences in terms of social costs
The analysis of mortality rates in large cohorts confirmed the association of HCV with
several EHDs including cardiovascular neurologic metabolic or renal diseases and tumors
Viral eradication significantly reduced the rate of extra-hepatic deaths
Cacoub P et al DLD 2014 Lee MH et al J Infect Dis 2012 Backus LI et al Clin Gastroenterol Hepatol 2011 El-Kamary S et al
Clin Infect Dis 2011 Hsu YC et al Hepatology 2014 Kawamura Y et al Am J Med 2007 Adinolfi LE et al WJG 2014
Extrahepatic Manifestations of HCV
Con il contributo di
Lee M-H et al J Infect Dis 2012206469-477
Follow-Up
(Years)
20
18
16
14
12
10
2
00 2 4 6 8 10 12 14 16 18 20
8
6
4
Follow-Up
(Years)
12
10
8
6
4
2
00 2 4 6 8 10 12 14 16 18 20
All Causes(n=2394)
Liver Cancer(n=115)
Extrahepatic Diseases(n=2199)
Cum
ula
tive M
ort
ali
ty (
)
Anti-HCV+ HCV RNA detectable Anti-HCV+ HCV RNA undetectable Anti-HCVndash
Follow-Up
(Years)
35
30
25
20
15
10
5
00 2 4 6 8 10 12 14 16 18 20
301
128124
104
16
03
198
122
110
MC is clinically benign but sometimes severe HCV EHD invalidating symptoms occur and
it may evolve into lymphoma
Cacoub P et al DLD 2014 Zignego AL et al DLD 2007 Zignego AL et al Intern Emerg Med 2012 Zignego AL et al Clin Dev
Immunol 2012 Zignego AL et al Expert Rev Clin Immunol 2015 Sene D et al J Rheumatol 2004
Mixed Cryoglobulinemia-MC
CGs reversibly precipitate when the temperature is lower than 37degC and
comprise IgMs with RF activity [mono- or oligo-clonal in type II MC or
polyclonal in type III MC] and polyclonal IgGs
MC pathological substrate is an HCV-driven B-cell
proliferation with consequent production of cryo- and non-
cryoprecipitable CICs in turn responsible for vasculitic
manifestations
Most (70ndash90) MC patients are HCV+ and HCV-patients are CGs+ (40ndash60) while 5ndash30 of
CGs+ have symptomatic MC since HCV infects about 170 million individuals worldwide the
number of patients at risk for developing MC is substantial
Type II
CGs
Type III
CGs
Zignego AL et al Autoimmun Rev 2017 Ferri C et al Autoimmunity rev 2016 Zignego AL et al DLD 2007 Cacoub P et al DLD
2014 Zignego AL et al DLD 2007 Zignego AL et al Intern Emerg Med 2012 Zignego AL et al Clin Dev Immunol 2012 Zignego
AL et al Expert Rev Clin Immunol 2015
MC clinical aspects MC Syndrome
MCS is characterized by the clinical triad -purpura weakness and
arthralgias- low complement C4 and various organsystem
involvement including cutaneous articular renal neurological
cardiac or digestive
It ranges from mild disease to severe even life-threatening
conditions
More serious lesions are generally characterized by neurologic and
renal involvement
Prognosis is highly dependent on renal involvement or on the extent
of vasculitis lesions
1 HCV is the main etiopathological agent as concordantly demonstrated by epidemiological clinico-pathological virological and laboratory investigations2 the association between HCV and disease is demonstrated in a significant proportion of patients and supported by in depth clinico-pathogeneticstudies3 the association is suggested by cohort studies a possible causative role may be limited to a small number of patients andor possibly more relevant in specific geographical areas 4 a number of anecdotal observations suggested a possible role of HCV further investigations are required
From P Cacoub 2015
HCV infection is closely related to LPDs mostly MC
40 to 60 of HCV patients show circulating CGs among this latter population 5-30
develop a symptomatic CV
AVT has been considered the first-line option in HCV-CV patients in fact in the majority
of cases viral eradication leads to CV clinical remission
Data about IFN-free regimens for the treatment of CV patients are still limited
HCV and MC
HCV and MC
Zignego 2015Ferri 2016Pozzato 2016 Sise 2016Saadoun 2015Gragnani 2016Gragnani 2016
Bonacci 2016Hegazy 2016Kondili 2016Emery 2017
Younossi et al
The annual costs (inpatient outpatient andpharmacy) associated with extrahepatic
manifestations of HCV were evaluated
Total direct medical costs of extrahepatic
manifestations of HCV in 2014 US dollars wereestimated to be $1506 million (range $922 millionndash
$2208 million in sensitivity analysis)
These estimates should be added to the liver-related
burden of disease to obtain a more accurateassessment of the total burden of HCV infection
The OBJECTIVE of the study was to estimate the annual direct medical costsassociated with HCV related EHM in the EU5 (France Germany Italy United Kingdom
Spain)
Extrahepatic Manifestations of HCV
Extrahepatic Manifestations of HCV
HCV may cause extrahepatic disorders (HCV-EHDs) classified according to the number and
strength of supporting scientific data
HCV-EHDs are responsible for increasing morbidity and mortality with important
consequences in terms of social costs
The analysis of mortality rates in large cohorts confirmed the association of HCV with
several EHDs including cardiovascular neurologic metabolic or renal diseases and tumors
Viral eradication significantly reduced the rate of extra-hepatic deaths
Cacoub P et al DLD 2014 Lee MH et al J Infect Dis 2012 Backus LI et al Clin Gastroenterol Hepatol 2011 El-Kamary S et al
Clin Infect Dis 2011 Hsu YC et al Hepatology 2014 Kawamura Y et al Am J Med 2007 Adinolfi LE et al WJG 2014
Con il contributo di
Lee M-H et al J Infect Dis 2012206469-477
Follow-Up
(Years)
20
18
16
14
12
10
2
00 2 4 6 8 10 12 14 16 18 20
8
6
4
Follow-Up
(Years)
12
10
8
6
4
2
00 2 4 6 8 10 12 14 16 18 20
All Causes(n=2394)
Liver Cancer(n=115)
Extrahepatic Diseases(n=2199)
Cum
ula
tive M
ort
ali
ty (
)
Anti-HCV+ HCV RNA detectable Anti-HCV+ HCV RNA undetectable Anti-HCVndash
Follow-Up
(Years)
35
30
25
20
15
10
5
00 2 4 6 8 10 12 14 16 18 20
301
128124
104
16
03
198
122
110
Extrahepatic Manifestations of HCV
The annual costs (inpatient outpatient andpharmacy) associated with extrahepatic
manifestations of HCV were evaluated
Total direct medical costs of extrahepatic
manifestations of HCV in 2014 US dollars wereestimated to be $1506 million (range $922 millionndash
$2208 million in sensitivity analysis)
These estimates should be added to the liver-related
burden of disease to obtain a more accurateassessment of the total burden of HCV infection
Younossi et al
Younossi et al
Costs up to $71000 per patient per year (ESRD) Among the most frequent EHM depression (245 in HCV vs 172 in non-HCV) had estimated annual cost of
$4307 million DM (15 vs 10 in non- HCV) had an annual cost of $4434 million in the USA= given the importance of DM and
its association with CVDs and mortality the clinical and economic impacts of HCV-related DM are substantial
The OBJECTIVE of the study was to estimate the annual direct medical costsassociated with HCV related EHM in the EU5 (France Germany Italy United Kingdom
Spain)
The OBJECTIVE of the study was to estimate the annual direct medicalcosts associated with HCV related EHM in the EU5 (France Germany
Italy United Kingdom Spain)
1 HCV is the main etiopathological agent as concordantly demonstrated by epidemiological clinico-pathological virological and laboratory investigations2 the association between HCV and disease is demonstrated in a significant proportion of patients and supported by in depth clinico-pathogeneticstudies3 the association is suggested by cohort studies a possible causative role may be limited to a small number of patients andor possibly more relevant in specific geographical areas 4 a number of anecdotal observations suggested a possible role of HCV further investigations are required
The most studied and frequent HCV-EHDs are B-LPDs andor autoimmune disorders
Their prototype is Mixed Cryoglobulinemia (MC) from researches on MC derived most of the
available information
MC as a precious model for all the HCV-EHDs and to evaluate the effects of viral eradication
Anti-HCV Treatment Evolution
IFN
6 mos
PegIFN RBV 12
mos
IFN
12 mos
IFNRBV
12 mos
PegIFN
12 mos
2001
1998
2011
Standardinterferon
Ribavirin
Peginterferon
1991
Direct-actingantivirals
PegIFN
RBV
DAA
IFNRBV
6 mos
6
16
34
4239
55
70+
0
20
40
60
80
100
DAAs
826
weeks
gt90
2015
Few side effects absence major
contraindications
Younossi et al
The annual costs (inpatient outpatient and pharmacy) associatedwith extrahepatic manifestations of HCV were evaluated
Total direct medical costs of extrahepatic manifestations of HCV in 2014US dollars were estimated to be $1506 million (range $922 millionndash
$2208 million in sensitivity analysis)
These estimates should be added to the liver-related burden of diseaseto obtain a more accurate assessment of the total burden of HCV
infection
The OBJECTIVE of the study was to estimate the annual direct medical costs associated with HCV related EHM in the EU5 (France Germany Italy United Kingdom Spain)
22 MCS treated with DAAs including 2 HCC and 2 NHL 100 SVR12 Clinical CR in 64 and PR in remaining 36 The small lymphocytic lymphoma progressed despite viral clearance
Lauletta et al 2017
Emery CS et al 2017
Retrospective analysis 17 MCS (10 with severelife-threatening vasculitis) and 65 asymptomatic CGs+ pts treated with DAAs SVR 889 MCS and 908 asymptomatic pts In MCS clinical response in 1117 (complete in 717) In severelife-threatening vasculitis lower clinical response especially in renal and neurological symptoms
Saadoun D et al 2017
Open-label prospective multi-center study on sofosbuvir plus daclatasvir treatment of 41 HCV MCS SVR in100 and clinical CR in 902 Disappearance of CGs in 50 of pts No serious adverse event or relapse ofvasculitis
Antiviral Treatment (AVT) of MCIFN-free regimens
MC is clinically benign but sometimes severe HCV EHD invalidating symptoms occur and
it may evolve into lymphoma
Cacoub P et al DLD 2014 Zignego AL et al DLD 2007 Zignego AL et al Intern Emerg Med 2012 Zignego AL et al Clin Dev
Immunol 2012 Zignego AL et al Expert Rev Clin Immunol 2015 Sene D et al J Rheumatol 2004
Mixed Cryoglobulinemia-MC
MC pathological substrate is an HCV-driven B-cell
proliferation with consequent production of cryo- and non-
cryoprecipitable CICs in turn responsible for vasculitic
manifestations
Most (70ndash90) MC patients are HCV+ and HCV-patients are CGs+ (40ndash60) while 5ndash30 of
CGs+ have symptomatic MC or cryoglobulinemic vasculitis since HCV infects about 170
million individuals worldwide the number of patients at risk for developing MC is
substantial
Type II CGs
monoclonal
RF+policlonal IgG
Type III CGs both
RF and IgG
polyclonal

Concurrent Systemic Chemoimmunotherapy and Sofosbuvir-Based Antiviral Treatment in a Hepatitis C Virus-Infected Patient With Diffuse Large B-Cell Lymphoma Evan C Ewers et al 2016
absolute neutrophil count and Hgb ALT and HCV viral load
Both complete response and SVR of HCV-associated DLBCL after concurrent chemoimmunotherapy and antiviral therapy using a sofosbuvir-based regimen
DAA-treatment in concomitance with chemotherapy showed to be safe and effective in influencing the remission of aggressive lymphomas in HCV patients
Persico M et al 2017
DFS in DAA treated and historical not-treated ptsAntiviral response rates in DAA treated patients
ANTIVIRAL THERAPY IN HCV+ B CELL NHL
IFN-based AVT induced hematological response along with SVR in patients with HCV-related indolent NHLs (especially
MZL)
Recent data with IFN-free regimens in HCV-associated LPDs suggest their anti-lymphoma activity too
AVT should be considered the first-line approach in HCV low grade lymphomas if there is no urgency of a conventional
treatment (ie systemic symptoms bulky disease or symptomatic splenomegaly) (ESMO NCCN EASL guidelines)
In aggressive lymphomas antiviral therapy after induction treatment is to be considered the standard at the moment but
in the next years (months) the association of immunochemotherapy and antiviral therapy will be considered the standard
Zignego AL Ramos-Casals M Ferri C et al Autoimmun Rev 2017
The Masve group
BASIC RESEARCH
Laura Gragnani
Patrizio Caini
Serena Lorini
Antonella Simone
CLINICAL RESEARCH
Monica Monti
Luisa Petraccia
Sinan Sadalla
Guia Cerretelli
Cristina Stasi
Adela Xheka
Universitagrave degli Studi di FirenzeDipartimento di Medicina Sperimentale e Clinica
Centro Manifestazioni Sistemiche da Virus EpatiticildquoMASVErdquo
Anna Linda Zignego
MASVE
UNDERGRADUATE STUDENTS Andrea Genovese Adrian Piscopo
ANTIVIRAL THERAPY IN HCV+ B CELL NHL
IFN-based AVT induced hematological response along with SVR in patients with HCV-related indolent
NHLs (especially MZL)
Recent data with IFN-free regimens in HCV-associated LPDs suggest their anti-lymphoma activity too
AVT should be considered the first-line approach in HCV low grade lymphomas if there is no urgency
of a conventional treatment (ie systemic symptoms bulky disease or symptomatic splenomegaly)
(ESMO NCCN EASL guidelines)
Main drugs for HCV-related MCS according to the target
HCV= DAAsB-cell Expansion= (a) B cell-depleting Mabs
-First-generation Rituximab (anti-CD20)-Second-generation Ofatumumab (anti-CD20) Veltuzumab (humanized
anti-CD20)-Third-generation Obinutuzumab (GA101) Oceratuzumab (humanized
anti-CD20)
(b) Alkylating agents
-Cyclophosfamide
Inflammation= Antiinflammatory agents
- Corticosteroids
Altered regulatory T-cell activity=
- IL-2
The impact on HRQoL of IFN-free AVT was prospectively evaluated in a cohort of HCV CV patients with limited
influencing variables linked to therapeutic schedulesviral GT
44 HCV GT2 CV patients mostly F0-F2 (29) and naiumlve (30) treated with SOFRBV for 1224wks
TIME POINTS
baseline EOT and week 12 and 24 of post-treatment f-up (SVR12 and SVR24 respectively)
HRQoL EVALUATION THROUGH PROs
the Short Form (36) Health Survey (SF-36)
the Functional Assessment of Chronic Illness Therapy-Fatigue (FACIT-F) from which we computed the Trial
Outcome Index (TOI)
Observational study on in situ expression of the oncogenic HCV NS3 protein on 116 HCV
patients with B-NHL (DLBCL 36 and MZL 34)
NS3 immunostaining positive in 1214 DLBCL vs only 414 MZL (p = 0006) moreover 24 NS3+
MZL were enriched in large cells
This study supports a new mechanism of transformation with a direct oncogenic role of
HCV proteins in the occurrence of high-grade B lymphomas
IN SITU HEPATITIS C NS3 PROTEIN DETECTION IS ASSOCIATED WITH HIGH GRADEFEATURES IN HCV-ASSOCIATED B-CELL NON-HODGKIN LYMPHOMAS Danielle
Canioni et al 2016
In addition to the role of chronic antigenic stimulation in HCV related
lymphomagenesis this study supports a second mechanism of transformation due toa direct oncogenic role of HCV infection of B-cells promoting the occurrence of high-grade Bcell lymphomas
ANTIVIRAL THERAPY IS ASSOCIATED WITH A BETTERSURVIVAL IN PATIENTS WITH HCV AND B-CELL NON-HODGKIN LYMPHOMAS ANRS HC-13 LYMPHO-CSTUDYMichot JM et al
Outcomes of HCV-associated B-NHL according to HCV AVT in prospective patients only (n 5 64)
(A) absolute neutrophil count and Hgb
(B) ALT and HCV viral load
This patient had HCV-associated DLBCL achieving both complete response and SVR after concurrent chemoimmunotherapy and antiviral therapy using a sofosbuvir-basedregimen
Concurrent Systemic Chemoimmunotherapy and Sofosbuvir-Based Antiviral Treatment in a Hepatitis C Virus-Infected Patient With Diffuse Large B-Cell LymphomaEvan C Ewers et al 2016
HCV-EHDs are responsible for increasing morbidity and mortality with important
consequences in terms of social costs
The analysis of mortality rates in large cohorts confirmed the association of HCV with
several EHDs including cardiovascular neurologic metabolic or renal diseases and tumors
Viral eradication significantly reduced the rate of extra-hepatic deaths
Cacoub P et al DLD 2014 Lee MH et al J Infect Dis 2012 Backus LI et al Clin Gastroenterol Hepatol 2011 El-Kamary S et al
Clin Infect Dis 2011 Hsu YC et al Hepatology 2014 Kawamura Y et al Am J Med 2007 Adinolfi LE et al WJG 2014
Extrahepatic Manifestations of HCV
Con il contributo di
Lee M-H et al J Infect Dis 2012206469-477
Follow-Up
(Years)
20
18
16
14
12
10
2
00 2 4 6 8 10 12 14 16 18 20
8
6
4
Follow-Up
(Years)
12
10
8
6
4
2
00 2 4 6 8 10 12 14 16 18 20
All Causes(n=2394)
Liver Cancer(n=115)
Extrahepatic Diseases(n=2199)
Cum
ula
tive M
ort
ali
ty (
)
Anti-HCV+ HCV RNA detectable Anti-HCV+ HCV RNA undetectable Anti-HCVndash
Follow-Up
(Years)
35
30
25
20
15
10
5
00 2 4 6 8 10 12 14 16 18 20
301
128124
104
16
03
198
122
110
MC is clinically benign but sometimes severe HCV EHD invalidating symptoms occur and
it may evolve into lymphoma
Cacoub P et al DLD 2014 Zignego AL et al DLD 2007 Zignego AL et al Intern Emerg Med 2012 Zignego AL et al Clin Dev
Immunol 2012 Zignego AL et al Expert Rev Clin Immunol 2015 Sene D et al J Rheumatol 2004
Mixed Cryoglobulinemia-MC
CGs reversibly precipitate when the temperature is lower than 37degC and
comprise IgMs with RF activity [mono- or oligo-clonal in type II MC or
polyclonal in type III MC] and polyclonal IgGs
MC pathological substrate is an HCV-driven B-cell
proliferation with consequent production of cryo- and non-
cryoprecipitable CICs in turn responsible for vasculitic
manifestations
Most (70ndash90) MC patients are HCV+ and HCV-patients are CGs+ (40ndash60) while 5ndash30 of
CGs+ have symptomatic MC since HCV infects about 170 million individuals worldwide the
number of patients at risk for developing MC is substantial
Type II
CGs
Type III
CGs
Zignego AL et al Autoimmun Rev 2017 Ferri C et al Autoimmunity rev 2016 Zignego AL et al DLD 2007 Cacoub P et al DLD
2014 Zignego AL et al DLD 2007 Zignego AL et al Intern Emerg Med 2012 Zignego AL et al Clin Dev Immunol 2012 Zignego
AL et al Expert Rev Clin Immunol 2015
MC clinical aspects MC Syndrome
MCS is characterized by the clinical triad -purpura weakness and
arthralgias- low complement C4 and various organsystem
involvement including cutaneous articular renal neurological
cardiac or digestive
It ranges from mild disease to severe even life-threatening
conditions
More serious lesions are generally characterized by neurologic and
renal involvement
Prognosis is highly dependent on renal involvement or on the extent
of vasculitis lesions
1 HCV is the main etiopathological agent as concordantly demonstrated by epidemiological clinico-pathological virological and laboratory investigations2 the association between HCV and disease is demonstrated in a significant proportion of patients and supported by in depth clinico-pathogeneticstudies3 the association is suggested by cohort studies a possible causative role may be limited to a small number of patients andor possibly more relevant in specific geographical areas 4 a number of anecdotal observations suggested a possible role of HCV further investigations are required
From P Cacoub 2015
HCV infection is closely related to LPDs mostly MC
40 to 60 of HCV patients show circulating CGs among this latter population 5-30
develop a symptomatic CV
AVT has been considered the first-line option in HCV-CV patients in fact in the majority
of cases viral eradication leads to CV clinical remission
Data about IFN-free regimens for the treatment of CV patients are still limited
HCV and MC
HCV and MC
Zignego 2015Ferri 2016Pozzato 2016 Sise 2016Saadoun 2015Gragnani 2016Gragnani 2016
Bonacci 2016Hegazy 2016Kondili 2016Emery 2017
Younossi et al
The annual costs (inpatient outpatient andpharmacy) associated with extrahepatic
manifestations of HCV were evaluated
Total direct medical costs of extrahepatic
manifestations of HCV in 2014 US dollars wereestimated to be $1506 million (range $922 millionndash
$2208 million in sensitivity analysis)
These estimates should be added to the liver-related
burden of disease to obtain a more accurateassessment of the total burden of HCV infection
The OBJECTIVE of the study was to estimate the annual direct medical costsassociated with HCV related EHM in the EU5 (France Germany Italy United Kingdom
Spain)
Extrahepatic Manifestations of HCV
Extrahepatic Manifestations of HCV
HCV may cause extrahepatic disorders (HCV-EHDs) classified according to the number and
strength of supporting scientific data
HCV-EHDs are responsible for increasing morbidity and mortality with important
consequences in terms of social costs
The analysis of mortality rates in large cohorts confirmed the association of HCV with
several EHDs including cardiovascular neurologic metabolic or renal diseases and tumors
Viral eradication significantly reduced the rate of extra-hepatic deaths
Cacoub P et al DLD 2014 Lee MH et al J Infect Dis 2012 Backus LI et al Clin Gastroenterol Hepatol 2011 El-Kamary S et al
Clin Infect Dis 2011 Hsu YC et al Hepatology 2014 Kawamura Y et al Am J Med 2007 Adinolfi LE et al WJG 2014
Con il contributo di
Lee M-H et al J Infect Dis 2012206469-477
Follow-Up
(Years)
20
18
16
14
12
10
2
00 2 4 6 8 10 12 14 16 18 20
8
6
4
Follow-Up
(Years)
12
10
8
6
4
2
00 2 4 6 8 10 12 14 16 18 20
All Causes(n=2394)
Liver Cancer(n=115)
Extrahepatic Diseases(n=2199)
Cum
ula
tive M
ort
ali
ty (
)
Anti-HCV+ HCV RNA detectable Anti-HCV+ HCV RNA undetectable Anti-HCVndash
Follow-Up
(Years)
35
30
25
20
15
10
5
00 2 4 6 8 10 12 14 16 18 20
301
128124
104
16
03
198
122
110
Extrahepatic Manifestations of HCV
The annual costs (inpatient outpatient andpharmacy) associated with extrahepatic
manifestations of HCV were evaluated
Total direct medical costs of extrahepatic
manifestations of HCV in 2014 US dollars wereestimated to be $1506 million (range $922 millionndash
$2208 million in sensitivity analysis)
These estimates should be added to the liver-related
burden of disease to obtain a more accurateassessment of the total burden of HCV infection
Younossi et al
Younossi et al
Costs up to $71000 per patient per year (ESRD) Among the most frequent EHM depression (245 in HCV vs 172 in non-HCV) had estimated annual cost of
$4307 million DM (15 vs 10 in non- HCV) had an annual cost of $4434 million in the USA= given the importance of DM and
its association with CVDs and mortality the clinical and economic impacts of HCV-related DM are substantial
The OBJECTIVE of the study was to estimate the annual direct medical costsassociated with HCV related EHM in the EU5 (France Germany Italy United Kingdom
Spain)
The OBJECTIVE of the study was to estimate the annual direct medicalcosts associated with HCV related EHM in the EU5 (France Germany
Italy United Kingdom Spain)
1 HCV is the main etiopathological agent as concordantly demonstrated by epidemiological clinico-pathological virological and laboratory investigations2 the association between HCV and disease is demonstrated in a significant proportion of patients and supported by in depth clinico-pathogeneticstudies3 the association is suggested by cohort studies a possible causative role may be limited to a small number of patients andor possibly more relevant in specific geographical areas 4 a number of anecdotal observations suggested a possible role of HCV further investigations are required
The most studied and frequent HCV-EHDs are B-LPDs andor autoimmune disorders
Their prototype is Mixed Cryoglobulinemia (MC) from researches on MC derived most of the
available information
MC as a precious model for all the HCV-EHDs and to evaluate the effects of viral eradication
Anti-HCV Treatment Evolution
IFN
6 mos
PegIFN RBV 12
mos
IFN
12 mos
IFNRBV
12 mos
PegIFN
12 mos
2001
1998
2011
Standardinterferon
Ribavirin
Peginterferon
1991
Direct-actingantivirals
PegIFN
RBV
DAA
IFNRBV
6 mos
6
16
34
4239
55
70+
0
20
40
60
80
100
DAAs
826
weeks
gt90
2015
Few side effects absence major
contraindications
Younossi et al
The annual costs (inpatient outpatient and pharmacy) associatedwith extrahepatic manifestations of HCV were evaluated
Total direct medical costs of extrahepatic manifestations of HCV in 2014US dollars were estimated to be $1506 million (range $922 millionndash
$2208 million in sensitivity analysis)
These estimates should be added to the liver-related burden of diseaseto obtain a more accurate assessment of the total burden of HCV
infection
The OBJECTIVE of the study was to estimate the annual direct medical costs associated with HCV related EHM in the EU5 (France Germany Italy United Kingdom Spain)
22 MCS treated with DAAs including 2 HCC and 2 NHL 100 SVR12 Clinical CR in 64 and PR in remaining 36 The small lymphocytic lymphoma progressed despite viral clearance
Lauletta et al 2017
Emery CS et al 2017
Retrospective analysis 17 MCS (10 with severelife-threatening vasculitis) and 65 asymptomatic CGs+ pts treated with DAAs SVR 889 MCS and 908 asymptomatic pts In MCS clinical response in 1117 (complete in 717) In severelife-threatening vasculitis lower clinical response especially in renal and neurological symptoms
Saadoun D et al 2017
Open-label prospective multi-center study on sofosbuvir plus daclatasvir treatment of 41 HCV MCS SVR in100 and clinical CR in 902 Disappearance of CGs in 50 of pts No serious adverse event or relapse ofvasculitis
Antiviral Treatment (AVT) of MCIFN-free regimens
MC is clinically benign but sometimes severe HCV EHD invalidating symptoms occur and
it may evolve into lymphoma
Cacoub P et al DLD 2014 Zignego AL et al DLD 2007 Zignego AL et al Intern Emerg Med 2012 Zignego AL et al Clin Dev
Immunol 2012 Zignego AL et al Expert Rev Clin Immunol 2015 Sene D et al J Rheumatol 2004
Mixed Cryoglobulinemia-MC
MC pathological substrate is an HCV-driven B-cell
proliferation with consequent production of cryo- and non-
cryoprecipitable CICs in turn responsible for vasculitic
manifestations
Most (70ndash90) MC patients are HCV+ and HCV-patients are CGs+ (40ndash60) while 5ndash30 of
CGs+ have symptomatic MC or cryoglobulinemic vasculitis since HCV infects about 170
million individuals worldwide the number of patients at risk for developing MC is
substantial
Type II CGs
monoclonal
RF+policlonal IgG
Type III CGs both
RF and IgG
polyclonal

DAA-treatment in concomitance with chemotherapy showed to be safe and effective in influencing the remission of aggressive lymphomas in HCV patients
Persico M et al 2017
DFS in DAA treated and historical not-treated ptsAntiviral response rates in DAA treated patients
ANTIVIRAL THERAPY IN HCV+ B CELL NHL
IFN-based AVT induced hematological response along with SVR in patients with HCV-related indolent NHLs (especially
MZL)
Recent data with IFN-free regimens in HCV-associated LPDs suggest their anti-lymphoma activity too
AVT should be considered the first-line approach in HCV low grade lymphomas if there is no urgency of a conventional
treatment (ie systemic symptoms bulky disease or symptomatic splenomegaly) (ESMO NCCN EASL guidelines)
In aggressive lymphomas antiviral therapy after induction treatment is to be considered the standard at the moment but
in the next years (months) the association of immunochemotherapy and antiviral therapy will be considered the standard
Zignego AL Ramos-Casals M Ferri C et al Autoimmun Rev 2017
The Masve group
BASIC RESEARCH
Laura Gragnani
Patrizio Caini
Serena Lorini
Antonella Simone
CLINICAL RESEARCH
Monica Monti
Luisa Petraccia
Sinan Sadalla
Guia Cerretelli
Cristina Stasi
Adela Xheka
Universitagrave degli Studi di FirenzeDipartimento di Medicina Sperimentale e Clinica
Centro Manifestazioni Sistemiche da Virus EpatiticildquoMASVErdquo
Anna Linda Zignego
MASVE
UNDERGRADUATE STUDENTS Andrea Genovese Adrian Piscopo
ANTIVIRAL THERAPY IN HCV+ B CELL NHL
IFN-based AVT induced hematological response along with SVR in patients with HCV-related indolent
NHLs (especially MZL)
Recent data with IFN-free regimens in HCV-associated LPDs suggest their anti-lymphoma activity too
AVT should be considered the first-line approach in HCV low grade lymphomas if there is no urgency
of a conventional treatment (ie systemic symptoms bulky disease or symptomatic splenomegaly)
(ESMO NCCN EASL guidelines)
Main drugs for HCV-related MCS according to the target
HCV= DAAsB-cell Expansion= (a) B cell-depleting Mabs
-First-generation Rituximab (anti-CD20)-Second-generation Ofatumumab (anti-CD20) Veltuzumab (humanized
anti-CD20)-Third-generation Obinutuzumab (GA101) Oceratuzumab (humanized
anti-CD20)
(b) Alkylating agents
-Cyclophosfamide
Inflammation= Antiinflammatory agents
- Corticosteroids
Altered regulatory T-cell activity=
- IL-2
The impact on HRQoL of IFN-free AVT was prospectively evaluated in a cohort of HCV CV patients with limited
influencing variables linked to therapeutic schedulesviral GT
44 HCV GT2 CV patients mostly F0-F2 (29) and naiumlve (30) treated with SOFRBV for 1224wks
TIME POINTS
baseline EOT and week 12 and 24 of post-treatment f-up (SVR12 and SVR24 respectively)
HRQoL EVALUATION THROUGH PROs
the Short Form (36) Health Survey (SF-36)
the Functional Assessment of Chronic Illness Therapy-Fatigue (FACIT-F) from which we computed the Trial
Outcome Index (TOI)
Observational study on in situ expression of the oncogenic HCV NS3 protein on 116 HCV
patients with B-NHL (DLBCL 36 and MZL 34)
NS3 immunostaining positive in 1214 DLBCL vs only 414 MZL (p = 0006) moreover 24 NS3+
MZL were enriched in large cells
This study supports a new mechanism of transformation with a direct oncogenic role of
HCV proteins in the occurrence of high-grade B lymphomas
IN SITU HEPATITIS C NS3 PROTEIN DETECTION IS ASSOCIATED WITH HIGH GRADEFEATURES IN HCV-ASSOCIATED B-CELL NON-HODGKIN LYMPHOMAS Danielle
Canioni et al 2016
In addition to the role of chronic antigenic stimulation in HCV related
lymphomagenesis this study supports a second mechanism of transformation due toa direct oncogenic role of HCV infection of B-cells promoting the occurrence of high-grade Bcell lymphomas
ANTIVIRAL THERAPY IS ASSOCIATED WITH A BETTERSURVIVAL IN PATIENTS WITH HCV AND B-CELL NON-HODGKIN LYMPHOMAS ANRS HC-13 LYMPHO-CSTUDYMichot JM et al
Outcomes of HCV-associated B-NHL according to HCV AVT in prospective patients only (n 5 64)
(A) absolute neutrophil count and Hgb
(B) ALT and HCV viral load
This patient had HCV-associated DLBCL achieving both complete response and SVR after concurrent chemoimmunotherapy and antiviral therapy using a sofosbuvir-basedregimen
Concurrent Systemic Chemoimmunotherapy and Sofosbuvir-Based Antiviral Treatment in a Hepatitis C Virus-Infected Patient With Diffuse Large B-Cell LymphomaEvan C Ewers et al 2016
HCV-EHDs are responsible for increasing morbidity and mortality with important
consequences in terms of social costs
The analysis of mortality rates in large cohorts confirmed the association of HCV with
several EHDs including cardiovascular neurologic metabolic or renal diseases and tumors
Viral eradication significantly reduced the rate of extra-hepatic deaths
Cacoub P et al DLD 2014 Lee MH et al J Infect Dis 2012 Backus LI et al Clin Gastroenterol Hepatol 2011 El-Kamary S et al
Clin Infect Dis 2011 Hsu YC et al Hepatology 2014 Kawamura Y et al Am J Med 2007 Adinolfi LE et al WJG 2014
Extrahepatic Manifestations of HCV
Con il contributo di
Lee M-H et al J Infect Dis 2012206469-477
Follow-Up
(Years)
20
18
16
14
12
10
2
00 2 4 6 8 10 12 14 16 18 20
8
6
4
Follow-Up
(Years)
12
10
8
6
4
2
00 2 4 6 8 10 12 14 16 18 20
All Causes(n=2394)
Liver Cancer(n=115)
Extrahepatic Diseases(n=2199)
Cum
ula
tive M
ort
ali
ty (
)
Anti-HCV+ HCV RNA detectable Anti-HCV+ HCV RNA undetectable Anti-HCVndash
Follow-Up
(Years)
35
30
25
20
15
10
5
00 2 4 6 8 10 12 14 16 18 20
301
128124
104
16
03
198
122
110
MC is clinically benign but sometimes severe HCV EHD invalidating symptoms occur and
it may evolve into lymphoma
Cacoub P et al DLD 2014 Zignego AL et al DLD 2007 Zignego AL et al Intern Emerg Med 2012 Zignego AL et al Clin Dev
Immunol 2012 Zignego AL et al Expert Rev Clin Immunol 2015 Sene D et al J Rheumatol 2004
Mixed Cryoglobulinemia-MC
CGs reversibly precipitate when the temperature is lower than 37degC and
comprise IgMs with RF activity [mono- or oligo-clonal in type II MC or
polyclonal in type III MC] and polyclonal IgGs
MC pathological substrate is an HCV-driven B-cell
proliferation with consequent production of cryo- and non-
cryoprecipitable CICs in turn responsible for vasculitic
manifestations
Most (70ndash90) MC patients are HCV+ and HCV-patients are CGs+ (40ndash60) while 5ndash30 of
CGs+ have symptomatic MC since HCV infects about 170 million individuals worldwide the
number of patients at risk for developing MC is substantial
Type II
CGs
Type III
CGs
Zignego AL et al Autoimmun Rev 2017 Ferri C et al Autoimmunity rev 2016 Zignego AL et al DLD 2007 Cacoub P et al DLD
2014 Zignego AL et al DLD 2007 Zignego AL et al Intern Emerg Med 2012 Zignego AL et al Clin Dev Immunol 2012 Zignego
AL et al Expert Rev Clin Immunol 2015
MC clinical aspects MC Syndrome
MCS is characterized by the clinical triad -purpura weakness and
arthralgias- low complement C4 and various organsystem
involvement including cutaneous articular renal neurological
cardiac or digestive
It ranges from mild disease to severe even life-threatening
conditions
More serious lesions are generally characterized by neurologic and
renal involvement
Prognosis is highly dependent on renal involvement or on the extent
of vasculitis lesions
1 HCV is the main etiopathological agent as concordantly demonstrated by epidemiological clinico-pathological virological and laboratory investigations2 the association between HCV and disease is demonstrated in a significant proportion of patients and supported by in depth clinico-pathogeneticstudies3 the association is suggested by cohort studies a possible causative role may be limited to a small number of patients andor possibly more relevant in specific geographical areas 4 a number of anecdotal observations suggested a possible role of HCV further investigations are required
From P Cacoub 2015
HCV infection is closely related to LPDs mostly MC
40 to 60 of HCV patients show circulating CGs among this latter population 5-30
develop a symptomatic CV
AVT has been considered the first-line option in HCV-CV patients in fact in the majority
of cases viral eradication leads to CV clinical remission
Data about IFN-free regimens for the treatment of CV patients are still limited
HCV and MC
HCV and MC
Zignego 2015Ferri 2016Pozzato 2016 Sise 2016Saadoun 2015Gragnani 2016Gragnani 2016
Bonacci 2016Hegazy 2016Kondili 2016Emery 2017
Younossi et al
The annual costs (inpatient outpatient andpharmacy) associated with extrahepatic
manifestations of HCV were evaluated
Total direct medical costs of extrahepatic
manifestations of HCV in 2014 US dollars wereestimated to be $1506 million (range $922 millionndash
$2208 million in sensitivity analysis)
These estimates should be added to the liver-related
burden of disease to obtain a more accurateassessment of the total burden of HCV infection
The OBJECTIVE of the study was to estimate the annual direct medical costsassociated with HCV related EHM in the EU5 (France Germany Italy United Kingdom
Spain)
Extrahepatic Manifestations of HCV
Extrahepatic Manifestations of HCV
HCV may cause extrahepatic disorders (HCV-EHDs) classified according to the number and
strength of supporting scientific data
HCV-EHDs are responsible for increasing morbidity and mortality with important
consequences in terms of social costs
The analysis of mortality rates in large cohorts confirmed the association of HCV with
several EHDs including cardiovascular neurologic metabolic or renal diseases and tumors
Viral eradication significantly reduced the rate of extra-hepatic deaths
Cacoub P et al DLD 2014 Lee MH et al J Infect Dis 2012 Backus LI et al Clin Gastroenterol Hepatol 2011 El-Kamary S et al
Clin Infect Dis 2011 Hsu YC et al Hepatology 2014 Kawamura Y et al Am J Med 2007 Adinolfi LE et al WJG 2014
Con il contributo di
Lee M-H et al J Infect Dis 2012206469-477
Follow-Up
(Years)
20
18
16
14
12
10
2
00 2 4 6 8 10 12 14 16 18 20
8
6
4
Follow-Up
(Years)
12
10
8
6
4
2
00 2 4 6 8 10 12 14 16 18 20
All Causes(n=2394)
Liver Cancer(n=115)
Extrahepatic Diseases(n=2199)
Cum
ula
tive M
ort
ali
ty (
)
Anti-HCV+ HCV RNA detectable Anti-HCV+ HCV RNA undetectable Anti-HCVndash
Follow-Up
(Years)
35
30
25
20
15
10
5
00 2 4 6 8 10 12 14 16 18 20
301
128124
104
16
03
198
122
110
Extrahepatic Manifestations of HCV
The annual costs (inpatient outpatient andpharmacy) associated with extrahepatic
manifestations of HCV were evaluated
Total direct medical costs of extrahepatic
manifestations of HCV in 2014 US dollars wereestimated to be $1506 million (range $922 millionndash
$2208 million in sensitivity analysis)
These estimates should be added to the liver-related
burden of disease to obtain a more accurateassessment of the total burden of HCV infection
Younossi et al
Younossi et al
Costs up to $71000 per patient per year (ESRD) Among the most frequent EHM depression (245 in HCV vs 172 in non-HCV) had estimated annual cost of
$4307 million DM (15 vs 10 in non- HCV) had an annual cost of $4434 million in the USA= given the importance of DM and
its association with CVDs and mortality the clinical and economic impacts of HCV-related DM are substantial
The OBJECTIVE of the study was to estimate the annual direct medical costsassociated with HCV related EHM in the EU5 (France Germany Italy United Kingdom
Spain)
The OBJECTIVE of the study was to estimate the annual direct medicalcosts associated with HCV related EHM in the EU5 (France Germany
Italy United Kingdom Spain)
1 HCV is the main etiopathological agent as concordantly demonstrated by epidemiological clinico-pathological virological and laboratory investigations2 the association between HCV and disease is demonstrated in a significant proportion of patients and supported by in depth clinico-pathogeneticstudies3 the association is suggested by cohort studies a possible causative role may be limited to a small number of patients andor possibly more relevant in specific geographical areas 4 a number of anecdotal observations suggested a possible role of HCV further investigations are required
The most studied and frequent HCV-EHDs are B-LPDs andor autoimmune disorders
Their prototype is Mixed Cryoglobulinemia (MC) from researches on MC derived most of the
available information
MC as a precious model for all the HCV-EHDs and to evaluate the effects of viral eradication
Anti-HCV Treatment Evolution
IFN
6 mos
PegIFN RBV 12
mos
IFN
12 mos
IFNRBV
12 mos
PegIFN
12 mos
2001
1998
2011
Standardinterferon
Ribavirin
Peginterferon
1991
Direct-actingantivirals
PegIFN
RBV
DAA
IFNRBV
6 mos
6
16
34
4239
55
70+
0
20
40
60
80
100
DAAs
826
weeks
gt90
2015
Few side effects absence major
contraindications
Younossi et al
The annual costs (inpatient outpatient and pharmacy) associatedwith extrahepatic manifestations of HCV were evaluated
Total direct medical costs of extrahepatic manifestations of HCV in 2014US dollars were estimated to be $1506 million (range $922 millionndash
$2208 million in sensitivity analysis)
These estimates should be added to the liver-related burden of diseaseto obtain a more accurate assessment of the total burden of HCV
infection
The OBJECTIVE of the study was to estimate the annual direct medical costs associated with HCV related EHM in the EU5 (France Germany Italy United Kingdom Spain)
22 MCS treated with DAAs including 2 HCC and 2 NHL 100 SVR12 Clinical CR in 64 and PR in remaining 36 The small lymphocytic lymphoma progressed despite viral clearance
Lauletta et al 2017
Emery CS et al 2017
Retrospective analysis 17 MCS (10 with severelife-threatening vasculitis) and 65 asymptomatic CGs+ pts treated with DAAs SVR 889 MCS and 908 asymptomatic pts In MCS clinical response in 1117 (complete in 717) In severelife-threatening vasculitis lower clinical response especially in renal and neurological symptoms
Saadoun D et al 2017
Open-label prospective multi-center study on sofosbuvir plus daclatasvir treatment of 41 HCV MCS SVR in100 and clinical CR in 902 Disappearance of CGs in 50 of pts No serious adverse event or relapse ofvasculitis
Antiviral Treatment (AVT) of MCIFN-free regimens
MC is clinically benign but sometimes severe HCV EHD invalidating symptoms occur and
it may evolve into lymphoma
Cacoub P et al DLD 2014 Zignego AL et al DLD 2007 Zignego AL et al Intern Emerg Med 2012 Zignego AL et al Clin Dev
Immunol 2012 Zignego AL et al Expert Rev Clin Immunol 2015 Sene D et al J Rheumatol 2004
Mixed Cryoglobulinemia-MC
MC pathological substrate is an HCV-driven B-cell
proliferation with consequent production of cryo- and non-
cryoprecipitable CICs in turn responsible for vasculitic
manifestations
Most (70ndash90) MC patients are HCV+ and HCV-patients are CGs+ (40ndash60) while 5ndash30 of
CGs+ have symptomatic MC or cryoglobulinemic vasculitis since HCV infects about 170
million individuals worldwide the number of patients at risk for developing MC is
substantial
Type II CGs
monoclonal
RF+policlonal IgG
Type III CGs both
RF and IgG
polyclonal

ANTIVIRAL THERAPY IN HCV+ B CELL NHL
IFN-based AVT induced hematological response along with SVR in patients with HCV-related indolent NHLs (especially
MZL)
Recent data with IFN-free regimens in HCV-associated LPDs suggest their anti-lymphoma activity too
AVT should be considered the first-line approach in HCV low grade lymphomas if there is no urgency of a conventional
treatment (ie systemic symptoms bulky disease or symptomatic splenomegaly) (ESMO NCCN EASL guidelines)
In aggressive lymphomas antiviral therapy after induction treatment is to be considered the standard at the moment but
in the next years (months) the association of immunochemotherapy and antiviral therapy will be considered the standard
Zignego AL Ramos-Casals M Ferri C et al Autoimmun Rev 2017
The Masve group
BASIC RESEARCH
Laura Gragnani
Patrizio Caini
Serena Lorini
Antonella Simone
CLINICAL RESEARCH
Monica Monti
Luisa Petraccia
Sinan Sadalla
Guia Cerretelli
Cristina Stasi
Adela Xheka
Universitagrave degli Studi di FirenzeDipartimento di Medicina Sperimentale e Clinica
Centro Manifestazioni Sistemiche da Virus EpatiticildquoMASVErdquo
Anna Linda Zignego
MASVE
UNDERGRADUATE STUDENTS Andrea Genovese Adrian Piscopo
ANTIVIRAL THERAPY IN HCV+ B CELL NHL
IFN-based AVT induced hematological response along with SVR in patients with HCV-related indolent
NHLs (especially MZL)
Recent data with IFN-free regimens in HCV-associated LPDs suggest their anti-lymphoma activity too
AVT should be considered the first-line approach in HCV low grade lymphomas if there is no urgency
of a conventional treatment (ie systemic symptoms bulky disease or symptomatic splenomegaly)
(ESMO NCCN EASL guidelines)
Main drugs for HCV-related MCS according to the target
HCV= DAAsB-cell Expansion= (a) B cell-depleting Mabs
-First-generation Rituximab (anti-CD20)-Second-generation Ofatumumab (anti-CD20) Veltuzumab (humanized
anti-CD20)-Third-generation Obinutuzumab (GA101) Oceratuzumab (humanized
anti-CD20)
(b) Alkylating agents
-Cyclophosfamide
Inflammation= Antiinflammatory agents
- Corticosteroids
Altered regulatory T-cell activity=
- IL-2
The impact on HRQoL of IFN-free AVT was prospectively evaluated in a cohort of HCV CV patients with limited
influencing variables linked to therapeutic schedulesviral GT
44 HCV GT2 CV patients mostly F0-F2 (29) and naiumlve (30) treated with SOFRBV for 1224wks
TIME POINTS
baseline EOT and week 12 and 24 of post-treatment f-up (SVR12 and SVR24 respectively)
HRQoL EVALUATION THROUGH PROs
the Short Form (36) Health Survey (SF-36)
the Functional Assessment of Chronic Illness Therapy-Fatigue (FACIT-F) from which we computed the Trial
Outcome Index (TOI)
Observational study on in situ expression of the oncogenic HCV NS3 protein on 116 HCV
patients with B-NHL (DLBCL 36 and MZL 34)
NS3 immunostaining positive in 1214 DLBCL vs only 414 MZL (p = 0006) moreover 24 NS3+
MZL were enriched in large cells
This study supports a new mechanism of transformation with a direct oncogenic role of
HCV proteins in the occurrence of high-grade B lymphomas
IN SITU HEPATITIS C NS3 PROTEIN DETECTION IS ASSOCIATED WITH HIGH GRADEFEATURES IN HCV-ASSOCIATED B-CELL NON-HODGKIN LYMPHOMAS Danielle
Canioni et al 2016
In addition to the role of chronic antigenic stimulation in HCV related
lymphomagenesis this study supports a second mechanism of transformation due toa direct oncogenic role of HCV infection of B-cells promoting the occurrence of high-grade Bcell lymphomas
ANTIVIRAL THERAPY IS ASSOCIATED WITH A BETTERSURVIVAL IN PATIENTS WITH HCV AND B-CELL NON-HODGKIN LYMPHOMAS ANRS HC-13 LYMPHO-CSTUDYMichot JM et al
Outcomes of HCV-associated B-NHL according to HCV AVT in prospective patients only (n 5 64)
(A) absolute neutrophil count and Hgb
(B) ALT and HCV viral load
This patient had HCV-associated DLBCL achieving both complete response and SVR after concurrent chemoimmunotherapy and antiviral therapy using a sofosbuvir-basedregimen
Concurrent Systemic Chemoimmunotherapy and Sofosbuvir-Based Antiviral Treatment in a Hepatitis C Virus-Infected Patient With Diffuse Large B-Cell LymphomaEvan C Ewers et al 2016
HCV-EHDs are responsible for increasing morbidity and mortality with important
consequences in terms of social costs
The analysis of mortality rates in large cohorts confirmed the association of HCV with
several EHDs including cardiovascular neurologic metabolic or renal diseases and tumors
Viral eradication significantly reduced the rate of extra-hepatic deaths
Cacoub P et al DLD 2014 Lee MH et al J Infect Dis 2012 Backus LI et al Clin Gastroenterol Hepatol 2011 El-Kamary S et al
Clin Infect Dis 2011 Hsu YC et al Hepatology 2014 Kawamura Y et al Am J Med 2007 Adinolfi LE et al WJG 2014
Extrahepatic Manifestations of HCV
Con il contributo di
Lee M-H et al J Infect Dis 2012206469-477
Follow-Up
(Years)
20
18
16
14
12
10
2
00 2 4 6 8 10 12 14 16 18 20
8
6
4
Follow-Up
(Years)
12
10
8
6
4
2
00 2 4 6 8 10 12 14 16 18 20
All Causes(n=2394)
Liver Cancer(n=115)
Extrahepatic Diseases(n=2199)
Cum
ula
tive M
ort
ali
ty (
)
Anti-HCV+ HCV RNA detectable Anti-HCV+ HCV RNA undetectable Anti-HCVndash
Follow-Up
(Years)
35
30
25
20
15
10
5
00 2 4 6 8 10 12 14 16 18 20
301
128124
104
16
03
198
122
110
MC is clinically benign but sometimes severe HCV EHD invalidating symptoms occur and
it may evolve into lymphoma
Cacoub P et al DLD 2014 Zignego AL et al DLD 2007 Zignego AL et al Intern Emerg Med 2012 Zignego AL et al Clin Dev
Immunol 2012 Zignego AL et al Expert Rev Clin Immunol 2015 Sene D et al J Rheumatol 2004
Mixed Cryoglobulinemia-MC
CGs reversibly precipitate when the temperature is lower than 37degC and
comprise IgMs with RF activity [mono- or oligo-clonal in type II MC or
polyclonal in type III MC] and polyclonal IgGs
MC pathological substrate is an HCV-driven B-cell
proliferation with consequent production of cryo- and non-
cryoprecipitable CICs in turn responsible for vasculitic
manifestations
Most (70ndash90) MC patients are HCV+ and HCV-patients are CGs+ (40ndash60) while 5ndash30 of
CGs+ have symptomatic MC since HCV infects about 170 million individuals worldwide the
number of patients at risk for developing MC is substantial
Type II
CGs
Type III
CGs
Zignego AL et al Autoimmun Rev 2017 Ferri C et al Autoimmunity rev 2016 Zignego AL et al DLD 2007 Cacoub P et al DLD
2014 Zignego AL et al DLD 2007 Zignego AL et al Intern Emerg Med 2012 Zignego AL et al Clin Dev Immunol 2012 Zignego
AL et al Expert Rev Clin Immunol 2015
MC clinical aspects MC Syndrome
MCS is characterized by the clinical triad -purpura weakness and
arthralgias- low complement C4 and various organsystem
involvement including cutaneous articular renal neurological
cardiac or digestive
It ranges from mild disease to severe even life-threatening
conditions
More serious lesions are generally characterized by neurologic and
renal involvement
Prognosis is highly dependent on renal involvement or on the extent
of vasculitis lesions
1 HCV is the main etiopathological agent as concordantly demonstrated by epidemiological clinico-pathological virological and laboratory investigations2 the association between HCV and disease is demonstrated in a significant proportion of patients and supported by in depth clinico-pathogeneticstudies3 the association is suggested by cohort studies a possible causative role may be limited to a small number of patients andor possibly more relevant in specific geographical areas 4 a number of anecdotal observations suggested a possible role of HCV further investigations are required
From P Cacoub 2015
HCV infection is closely related to LPDs mostly MC
40 to 60 of HCV patients show circulating CGs among this latter population 5-30
develop a symptomatic CV
AVT has been considered the first-line option in HCV-CV patients in fact in the majority
of cases viral eradication leads to CV clinical remission
Data about IFN-free regimens for the treatment of CV patients are still limited
HCV and MC
HCV and MC
Zignego 2015Ferri 2016Pozzato 2016 Sise 2016Saadoun 2015Gragnani 2016Gragnani 2016
Bonacci 2016Hegazy 2016Kondili 2016Emery 2017
Younossi et al
The annual costs (inpatient outpatient andpharmacy) associated with extrahepatic
manifestations of HCV were evaluated
Total direct medical costs of extrahepatic
manifestations of HCV in 2014 US dollars wereestimated to be $1506 million (range $922 millionndash
$2208 million in sensitivity analysis)
These estimates should be added to the liver-related
burden of disease to obtain a more accurateassessment of the total burden of HCV infection
The OBJECTIVE of the study was to estimate the annual direct medical costsassociated with HCV related EHM in the EU5 (France Germany Italy United Kingdom
Spain)
Extrahepatic Manifestations of HCV
Extrahepatic Manifestations of HCV
HCV may cause extrahepatic disorders (HCV-EHDs) classified according to the number and
strength of supporting scientific data
HCV-EHDs are responsible for increasing morbidity and mortality with important
consequences in terms of social costs
The analysis of mortality rates in large cohorts confirmed the association of HCV with
several EHDs including cardiovascular neurologic metabolic or renal diseases and tumors
Viral eradication significantly reduced the rate of extra-hepatic deaths
Cacoub P et al DLD 2014 Lee MH et al J Infect Dis 2012 Backus LI et al Clin Gastroenterol Hepatol 2011 El-Kamary S et al
Clin Infect Dis 2011 Hsu YC et al Hepatology 2014 Kawamura Y et al Am J Med 2007 Adinolfi LE et al WJG 2014
Con il contributo di
Lee M-H et al J Infect Dis 2012206469-477
Follow-Up
(Years)
20
18
16
14
12
10
2
00 2 4 6 8 10 12 14 16 18 20
8
6
4
Follow-Up
(Years)
12
10
8
6
4
2
00 2 4 6 8 10 12 14 16 18 20
All Causes(n=2394)
Liver Cancer(n=115)
Extrahepatic Diseases(n=2199)
Cum
ula
tive M
ort
ali
ty (
)
Anti-HCV+ HCV RNA detectable Anti-HCV+ HCV RNA undetectable Anti-HCVndash
Follow-Up
(Years)
35
30
25
20
15
10
5
00 2 4 6 8 10 12 14 16 18 20
301
128124
104
16
03
198
122
110
Extrahepatic Manifestations of HCV
The annual costs (inpatient outpatient andpharmacy) associated with extrahepatic
manifestations of HCV were evaluated
Total direct medical costs of extrahepatic
manifestations of HCV in 2014 US dollars wereestimated to be $1506 million (range $922 millionndash
$2208 million in sensitivity analysis)
These estimates should be added to the liver-related
burden of disease to obtain a more accurateassessment of the total burden of HCV infection
Younossi et al
Younossi et al
Costs up to $71000 per patient per year (ESRD) Among the most frequent EHM depression (245 in HCV vs 172 in non-HCV) had estimated annual cost of
$4307 million DM (15 vs 10 in non- HCV) had an annual cost of $4434 million in the USA= given the importance of DM and
its association with CVDs and mortality the clinical and economic impacts of HCV-related DM are substantial
The OBJECTIVE of the study was to estimate the annual direct medical costsassociated with HCV related EHM in the EU5 (France Germany Italy United Kingdom
Spain)
The OBJECTIVE of the study was to estimate the annual direct medicalcosts associated with HCV related EHM in the EU5 (France Germany
Italy United Kingdom Spain)
1 HCV is the main etiopathological agent as concordantly demonstrated by epidemiological clinico-pathological virological and laboratory investigations2 the association between HCV and disease is demonstrated in a significant proportion of patients and supported by in depth clinico-pathogeneticstudies3 the association is suggested by cohort studies a possible causative role may be limited to a small number of patients andor possibly more relevant in specific geographical areas 4 a number of anecdotal observations suggested a possible role of HCV further investigations are required
The most studied and frequent HCV-EHDs are B-LPDs andor autoimmune disorders
Their prototype is Mixed Cryoglobulinemia (MC) from researches on MC derived most of the
available information
MC as a precious model for all the HCV-EHDs and to evaluate the effects of viral eradication
Anti-HCV Treatment Evolution
IFN
6 mos
PegIFN RBV 12
mos
IFN
12 mos
IFNRBV
12 mos
PegIFN
12 mos
2001
1998
2011
Standardinterferon
Ribavirin
Peginterferon
1991
Direct-actingantivirals
PegIFN
RBV
DAA
IFNRBV
6 mos
6
16
34
4239
55
70+
0
20
40
60
80
100
DAAs
826
weeks
gt90
2015
Few side effects absence major
contraindications
Younossi et al
The annual costs (inpatient outpatient and pharmacy) associatedwith extrahepatic manifestations of HCV were evaluated
Total direct medical costs of extrahepatic manifestations of HCV in 2014US dollars were estimated to be $1506 million (range $922 millionndash
$2208 million in sensitivity analysis)
These estimates should be added to the liver-related burden of diseaseto obtain a more accurate assessment of the total burden of HCV
infection
The OBJECTIVE of the study was to estimate the annual direct medical costs associated with HCV related EHM in the EU5 (France Germany Italy United Kingdom Spain)
22 MCS treated with DAAs including 2 HCC and 2 NHL 100 SVR12 Clinical CR in 64 and PR in remaining 36 The small lymphocytic lymphoma progressed despite viral clearance
Lauletta et al 2017
Emery CS et al 2017
Retrospective analysis 17 MCS (10 with severelife-threatening vasculitis) and 65 asymptomatic CGs+ pts treated with DAAs SVR 889 MCS and 908 asymptomatic pts In MCS clinical response in 1117 (complete in 717) In severelife-threatening vasculitis lower clinical response especially in renal and neurological symptoms
Saadoun D et al 2017
Open-label prospective multi-center study on sofosbuvir plus daclatasvir treatment of 41 HCV MCS SVR in100 and clinical CR in 902 Disappearance of CGs in 50 of pts No serious adverse event or relapse ofvasculitis
Antiviral Treatment (AVT) of MCIFN-free regimens
MC is clinically benign but sometimes severe HCV EHD invalidating symptoms occur and
it may evolve into lymphoma
Cacoub P et al DLD 2014 Zignego AL et al DLD 2007 Zignego AL et al Intern Emerg Med 2012 Zignego AL et al Clin Dev
Immunol 2012 Zignego AL et al Expert Rev Clin Immunol 2015 Sene D et al J Rheumatol 2004
Mixed Cryoglobulinemia-MC
MC pathological substrate is an HCV-driven B-cell
proliferation with consequent production of cryo- and non-
cryoprecipitable CICs in turn responsible for vasculitic
manifestations
Most (70ndash90) MC patients are HCV+ and HCV-patients are CGs+ (40ndash60) while 5ndash30 of
CGs+ have symptomatic MC or cryoglobulinemic vasculitis since HCV infects about 170
million individuals worldwide the number of patients at risk for developing MC is
substantial
Type II CGs
monoclonal
RF+policlonal IgG
Type III CGs both
RF and IgG
polyclonal

The Masve group
BASIC RESEARCH
Laura Gragnani
Patrizio Caini
Serena Lorini
Antonella Simone
CLINICAL RESEARCH
Monica Monti
Luisa Petraccia
Sinan Sadalla
Guia Cerretelli
Cristina Stasi
Adela Xheka
Universitagrave degli Studi di FirenzeDipartimento di Medicina Sperimentale e Clinica
Centro Manifestazioni Sistemiche da Virus EpatiticildquoMASVErdquo
Anna Linda Zignego
MASVE
UNDERGRADUATE STUDENTS Andrea Genovese Adrian Piscopo
ANTIVIRAL THERAPY IN HCV+ B CELL NHL
IFN-based AVT induced hematological response along with SVR in patients with HCV-related indolent
NHLs (especially MZL)
Recent data with IFN-free regimens in HCV-associated LPDs suggest their anti-lymphoma activity too
AVT should be considered the first-line approach in HCV low grade lymphomas if there is no urgency
of a conventional treatment (ie systemic symptoms bulky disease or symptomatic splenomegaly)
(ESMO NCCN EASL guidelines)
Main drugs for HCV-related MCS according to the target
HCV= DAAsB-cell Expansion= (a) B cell-depleting Mabs
-First-generation Rituximab (anti-CD20)-Second-generation Ofatumumab (anti-CD20) Veltuzumab (humanized
anti-CD20)-Third-generation Obinutuzumab (GA101) Oceratuzumab (humanized
anti-CD20)
(b) Alkylating agents
-Cyclophosfamide
Inflammation= Antiinflammatory agents
- Corticosteroids
Altered regulatory T-cell activity=
- IL-2
The impact on HRQoL of IFN-free AVT was prospectively evaluated in a cohort of HCV CV patients with limited
influencing variables linked to therapeutic schedulesviral GT
44 HCV GT2 CV patients mostly F0-F2 (29) and naiumlve (30) treated with SOFRBV for 1224wks
TIME POINTS
baseline EOT and week 12 and 24 of post-treatment f-up (SVR12 and SVR24 respectively)
HRQoL EVALUATION THROUGH PROs
the Short Form (36) Health Survey (SF-36)
the Functional Assessment of Chronic Illness Therapy-Fatigue (FACIT-F) from which we computed the Trial
Outcome Index (TOI)
Observational study on in situ expression of the oncogenic HCV NS3 protein on 116 HCV
patients with B-NHL (DLBCL 36 and MZL 34)
NS3 immunostaining positive in 1214 DLBCL vs only 414 MZL (p = 0006) moreover 24 NS3+
MZL were enriched in large cells
This study supports a new mechanism of transformation with a direct oncogenic role of
HCV proteins in the occurrence of high-grade B lymphomas
IN SITU HEPATITIS C NS3 PROTEIN DETECTION IS ASSOCIATED WITH HIGH GRADEFEATURES IN HCV-ASSOCIATED B-CELL NON-HODGKIN LYMPHOMAS Danielle
Canioni et al 2016
In addition to the role of chronic antigenic stimulation in HCV related
lymphomagenesis this study supports a second mechanism of transformation due toa direct oncogenic role of HCV infection of B-cells promoting the occurrence of high-grade Bcell lymphomas
ANTIVIRAL THERAPY IS ASSOCIATED WITH A BETTERSURVIVAL IN PATIENTS WITH HCV AND B-CELL NON-HODGKIN LYMPHOMAS ANRS HC-13 LYMPHO-CSTUDYMichot JM et al
Outcomes of HCV-associated B-NHL according to HCV AVT in prospective patients only (n 5 64)
(A) absolute neutrophil count and Hgb
(B) ALT and HCV viral load
This patient had HCV-associated DLBCL achieving both complete response and SVR after concurrent chemoimmunotherapy and antiviral therapy using a sofosbuvir-basedregimen
Concurrent Systemic Chemoimmunotherapy and Sofosbuvir-Based Antiviral Treatment in a Hepatitis C Virus-Infected Patient With Diffuse Large B-Cell LymphomaEvan C Ewers et al 2016
HCV-EHDs are responsible for increasing morbidity and mortality with important
consequences in terms of social costs
The analysis of mortality rates in large cohorts confirmed the association of HCV with
several EHDs including cardiovascular neurologic metabolic or renal diseases and tumors
Viral eradication significantly reduced the rate of extra-hepatic deaths
Cacoub P et al DLD 2014 Lee MH et al J Infect Dis 2012 Backus LI et al Clin Gastroenterol Hepatol 2011 El-Kamary S et al
Clin Infect Dis 2011 Hsu YC et al Hepatology 2014 Kawamura Y et al Am J Med 2007 Adinolfi LE et al WJG 2014
Extrahepatic Manifestations of HCV
Con il contributo di
Lee M-H et al J Infect Dis 2012206469-477
Follow-Up
(Years)
20
18
16
14
12
10
2
00 2 4 6 8 10 12 14 16 18 20
8
6
4
Follow-Up
(Years)
12
10
8
6
4
2
00 2 4 6 8 10 12 14 16 18 20
All Causes(n=2394)
Liver Cancer(n=115)
Extrahepatic Diseases(n=2199)
Cum
ula
tive M
ort
ali
ty (
)
Anti-HCV+ HCV RNA detectable Anti-HCV+ HCV RNA undetectable Anti-HCVndash
Follow-Up
(Years)
35
30
25
20
15
10
5
00 2 4 6 8 10 12 14 16 18 20
301
128124
104
16
03
198
122
110
MC is clinically benign but sometimes severe HCV EHD invalidating symptoms occur and
it may evolve into lymphoma
Cacoub P et al DLD 2014 Zignego AL et al DLD 2007 Zignego AL et al Intern Emerg Med 2012 Zignego AL et al Clin Dev
Immunol 2012 Zignego AL et al Expert Rev Clin Immunol 2015 Sene D et al J Rheumatol 2004
Mixed Cryoglobulinemia-MC
CGs reversibly precipitate when the temperature is lower than 37degC and
comprise IgMs with RF activity [mono- or oligo-clonal in type II MC or
polyclonal in type III MC] and polyclonal IgGs
MC pathological substrate is an HCV-driven B-cell
proliferation with consequent production of cryo- and non-
cryoprecipitable CICs in turn responsible for vasculitic
manifestations
Most (70ndash90) MC patients are HCV+ and HCV-patients are CGs+ (40ndash60) while 5ndash30 of
CGs+ have symptomatic MC since HCV infects about 170 million individuals worldwide the
number of patients at risk for developing MC is substantial
Type II
CGs
Type III
CGs
Zignego AL et al Autoimmun Rev 2017 Ferri C et al Autoimmunity rev 2016 Zignego AL et al DLD 2007 Cacoub P et al DLD
2014 Zignego AL et al DLD 2007 Zignego AL et al Intern Emerg Med 2012 Zignego AL et al Clin Dev Immunol 2012 Zignego
AL et al Expert Rev Clin Immunol 2015
MC clinical aspects MC Syndrome
MCS is characterized by the clinical triad -purpura weakness and
arthralgias- low complement C4 and various organsystem
involvement including cutaneous articular renal neurological
cardiac or digestive
It ranges from mild disease to severe even life-threatening
conditions
More serious lesions are generally characterized by neurologic and
renal involvement
Prognosis is highly dependent on renal involvement or on the extent
of vasculitis lesions
1 HCV is the main etiopathological agent as concordantly demonstrated by epidemiological clinico-pathological virological and laboratory investigations2 the association between HCV and disease is demonstrated in a significant proportion of patients and supported by in depth clinico-pathogeneticstudies3 the association is suggested by cohort studies a possible causative role may be limited to a small number of patients andor possibly more relevant in specific geographical areas 4 a number of anecdotal observations suggested a possible role of HCV further investigations are required
From P Cacoub 2015
HCV infection is closely related to LPDs mostly MC
40 to 60 of HCV patients show circulating CGs among this latter population 5-30
develop a symptomatic CV
AVT has been considered the first-line option in HCV-CV patients in fact in the majority
of cases viral eradication leads to CV clinical remission
Data about IFN-free regimens for the treatment of CV patients are still limited
HCV and MC
HCV and MC
Zignego 2015Ferri 2016Pozzato 2016 Sise 2016Saadoun 2015Gragnani 2016Gragnani 2016
Bonacci 2016Hegazy 2016Kondili 2016Emery 2017
Younossi et al
The annual costs (inpatient outpatient andpharmacy) associated with extrahepatic
manifestations of HCV were evaluated
Total direct medical costs of extrahepatic
manifestations of HCV in 2014 US dollars wereestimated to be $1506 million (range $922 millionndash
$2208 million in sensitivity analysis)
These estimates should be added to the liver-related
burden of disease to obtain a more accurateassessment of the total burden of HCV infection
The OBJECTIVE of the study was to estimate the annual direct medical costsassociated with HCV related EHM in the EU5 (France Germany Italy United Kingdom
Spain)
Extrahepatic Manifestations of HCV
Extrahepatic Manifestations of HCV
HCV may cause extrahepatic disorders (HCV-EHDs) classified according to the number and
strength of supporting scientific data
HCV-EHDs are responsible for increasing morbidity and mortality with important
consequences in terms of social costs
The analysis of mortality rates in large cohorts confirmed the association of HCV with
several EHDs including cardiovascular neurologic metabolic or renal diseases and tumors
Viral eradication significantly reduced the rate of extra-hepatic deaths
Cacoub P et al DLD 2014 Lee MH et al J Infect Dis 2012 Backus LI et al Clin Gastroenterol Hepatol 2011 El-Kamary S et al
Clin Infect Dis 2011 Hsu YC et al Hepatology 2014 Kawamura Y et al Am J Med 2007 Adinolfi LE et al WJG 2014
Con il contributo di
Lee M-H et al J Infect Dis 2012206469-477
Follow-Up
(Years)
20
18
16
14
12
10
2
00 2 4 6 8 10 12 14 16 18 20
8
6
4
Follow-Up
(Years)
12
10
8
6
4
2
00 2 4 6 8 10 12 14 16 18 20
All Causes(n=2394)
Liver Cancer(n=115)
Extrahepatic Diseases(n=2199)
Cum
ula
tive M
ort
ali
ty (
)
Anti-HCV+ HCV RNA detectable Anti-HCV+ HCV RNA undetectable Anti-HCVndash
Follow-Up
(Years)
35
30
25
20
15
10
5
00 2 4 6 8 10 12 14 16 18 20
301
128124
104
16
03
198
122
110
Extrahepatic Manifestations of HCV
The annual costs (inpatient outpatient andpharmacy) associated with extrahepatic
manifestations of HCV were evaluated
Total direct medical costs of extrahepatic
manifestations of HCV in 2014 US dollars wereestimated to be $1506 million (range $922 millionndash
$2208 million in sensitivity analysis)
These estimates should be added to the liver-related
burden of disease to obtain a more accurateassessment of the total burden of HCV infection
Younossi et al
Younossi et al
Costs up to $71000 per patient per year (ESRD) Among the most frequent EHM depression (245 in HCV vs 172 in non-HCV) had estimated annual cost of
$4307 million DM (15 vs 10 in non- HCV) had an annual cost of $4434 million in the USA= given the importance of DM and
its association with CVDs and mortality the clinical and economic impacts of HCV-related DM are substantial
The OBJECTIVE of the study was to estimate the annual direct medical costsassociated with HCV related EHM in the EU5 (France Germany Italy United Kingdom
Spain)
The OBJECTIVE of the study was to estimate the annual direct medicalcosts associated with HCV related EHM in the EU5 (France Germany
Italy United Kingdom Spain)
1 HCV is the main etiopathological agent as concordantly demonstrated by epidemiological clinico-pathological virological and laboratory investigations2 the association between HCV and disease is demonstrated in a significant proportion of patients and supported by in depth clinico-pathogeneticstudies3 the association is suggested by cohort studies a possible causative role may be limited to a small number of patients andor possibly more relevant in specific geographical areas 4 a number of anecdotal observations suggested a possible role of HCV further investigations are required
The most studied and frequent HCV-EHDs are B-LPDs andor autoimmune disorders
Their prototype is Mixed Cryoglobulinemia (MC) from researches on MC derived most of the
available information
MC as a precious model for all the HCV-EHDs and to evaluate the effects of viral eradication
Anti-HCV Treatment Evolution
IFN
6 mos
PegIFN RBV 12
mos
IFN
12 mos
IFNRBV
12 mos
PegIFN
12 mos
2001
1998
2011
Standardinterferon
Ribavirin
Peginterferon
1991
Direct-actingantivirals
PegIFN
RBV
DAA
IFNRBV
6 mos
6
16
34
4239
55
70+
0
20
40
60
80
100
DAAs
826
weeks
gt90
2015
Few side effects absence major
contraindications
Younossi et al
The annual costs (inpatient outpatient and pharmacy) associatedwith extrahepatic manifestations of HCV were evaluated
Total direct medical costs of extrahepatic manifestations of HCV in 2014US dollars were estimated to be $1506 million (range $922 millionndash
$2208 million in sensitivity analysis)
These estimates should be added to the liver-related burden of diseaseto obtain a more accurate assessment of the total burden of HCV
infection
The OBJECTIVE of the study was to estimate the annual direct medical costs associated with HCV related EHM in the EU5 (France Germany Italy United Kingdom Spain)
22 MCS treated with DAAs including 2 HCC and 2 NHL 100 SVR12 Clinical CR in 64 and PR in remaining 36 The small lymphocytic lymphoma progressed despite viral clearance
Lauletta et al 2017
Emery CS et al 2017
Retrospective analysis 17 MCS (10 with severelife-threatening vasculitis) and 65 asymptomatic CGs+ pts treated with DAAs SVR 889 MCS and 908 asymptomatic pts In MCS clinical response in 1117 (complete in 717) In severelife-threatening vasculitis lower clinical response especially in renal and neurological symptoms
Saadoun D et al 2017
Open-label prospective multi-center study on sofosbuvir plus daclatasvir treatment of 41 HCV MCS SVR in100 and clinical CR in 902 Disappearance of CGs in 50 of pts No serious adverse event or relapse ofvasculitis
Antiviral Treatment (AVT) of MCIFN-free regimens
MC is clinically benign but sometimes severe HCV EHD invalidating symptoms occur and
it may evolve into lymphoma
Cacoub P et al DLD 2014 Zignego AL et al DLD 2007 Zignego AL et al Intern Emerg Med 2012 Zignego AL et al Clin Dev
Immunol 2012 Zignego AL et al Expert Rev Clin Immunol 2015 Sene D et al J Rheumatol 2004
Mixed Cryoglobulinemia-MC
MC pathological substrate is an HCV-driven B-cell
proliferation with consequent production of cryo- and non-
cryoprecipitable CICs in turn responsible for vasculitic
manifestations
Most (70ndash90) MC patients are HCV+ and HCV-patients are CGs+ (40ndash60) while 5ndash30 of
CGs+ have symptomatic MC or cryoglobulinemic vasculitis since HCV infects about 170
million individuals worldwide the number of patients at risk for developing MC is
substantial
Type II CGs
monoclonal
RF+policlonal IgG
Type III CGs both
RF and IgG
polyclonal

ANTIVIRAL THERAPY IN HCV+ B CELL NHL
IFN-based AVT induced hematological response along with SVR in patients with HCV-related indolent
NHLs (especially MZL)
Recent data with IFN-free regimens in HCV-associated LPDs suggest their anti-lymphoma activity too
AVT should be considered the first-line approach in HCV low grade lymphomas if there is no urgency
of a conventional treatment (ie systemic symptoms bulky disease or symptomatic splenomegaly)
(ESMO NCCN EASL guidelines)
Main drugs for HCV-related MCS according to the target
HCV= DAAsB-cell Expansion= (a) B cell-depleting Mabs
-First-generation Rituximab (anti-CD20)-Second-generation Ofatumumab (anti-CD20) Veltuzumab (humanized
anti-CD20)-Third-generation Obinutuzumab (GA101) Oceratuzumab (humanized
anti-CD20)
(b) Alkylating agents
-Cyclophosfamide
Inflammation= Antiinflammatory agents
- Corticosteroids
Altered regulatory T-cell activity=
- IL-2
The impact on HRQoL of IFN-free AVT was prospectively evaluated in a cohort of HCV CV patients with limited
influencing variables linked to therapeutic schedulesviral GT
44 HCV GT2 CV patients mostly F0-F2 (29) and naiumlve (30) treated with SOFRBV for 1224wks
TIME POINTS
baseline EOT and week 12 and 24 of post-treatment f-up (SVR12 and SVR24 respectively)
HRQoL EVALUATION THROUGH PROs
the Short Form (36) Health Survey (SF-36)
the Functional Assessment of Chronic Illness Therapy-Fatigue (FACIT-F) from which we computed the Trial
Outcome Index (TOI)
Observational study on in situ expression of the oncogenic HCV NS3 protein on 116 HCV
patients with B-NHL (DLBCL 36 and MZL 34)
NS3 immunostaining positive in 1214 DLBCL vs only 414 MZL (p = 0006) moreover 24 NS3+
MZL were enriched in large cells
This study supports a new mechanism of transformation with a direct oncogenic role of
HCV proteins in the occurrence of high-grade B lymphomas
IN SITU HEPATITIS C NS3 PROTEIN DETECTION IS ASSOCIATED WITH HIGH GRADEFEATURES IN HCV-ASSOCIATED B-CELL NON-HODGKIN LYMPHOMAS Danielle
Canioni et al 2016
In addition to the role of chronic antigenic stimulation in HCV related
lymphomagenesis this study supports a second mechanism of transformation due toa direct oncogenic role of HCV infection of B-cells promoting the occurrence of high-grade Bcell lymphomas
ANTIVIRAL THERAPY IS ASSOCIATED WITH A BETTERSURVIVAL IN PATIENTS WITH HCV AND B-CELL NON-HODGKIN LYMPHOMAS ANRS HC-13 LYMPHO-CSTUDYMichot JM et al
Outcomes of HCV-associated B-NHL according to HCV AVT in prospective patients only (n 5 64)
(A) absolute neutrophil count and Hgb
(B) ALT and HCV viral load
This patient had HCV-associated DLBCL achieving both complete response and SVR after concurrent chemoimmunotherapy and antiviral therapy using a sofosbuvir-basedregimen
Concurrent Systemic Chemoimmunotherapy and Sofosbuvir-Based Antiviral Treatment in a Hepatitis C Virus-Infected Patient With Diffuse Large B-Cell LymphomaEvan C Ewers et al 2016
HCV-EHDs are responsible for increasing morbidity and mortality with important
consequences in terms of social costs
The analysis of mortality rates in large cohorts confirmed the association of HCV with
several EHDs including cardiovascular neurologic metabolic or renal diseases and tumors
Viral eradication significantly reduced the rate of extra-hepatic deaths
Cacoub P et al DLD 2014 Lee MH et al J Infect Dis 2012 Backus LI et al Clin Gastroenterol Hepatol 2011 El-Kamary S et al
Clin Infect Dis 2011 Hsu YC et al Hepatology 2014 Kawamura Y et al Am J Med 2007 Adinolfi LE et al WJG 2014
Extrahepatic Manifestations of HCV
Con il contributo di
Lee M-H et al J Infect Dis 2012206469-477
Follow-Up
(Years)
20
18
16
14
12
10
2
00 2 4 6 8 10 12 14 16 18 20
8
6
4
Follow-Up
(Years)
12
10
8
6
4
2
00 2 4 6 8 10 12 14 16 18 20
All Causes(n=2394)
Liver Cancer(n=115)
Extrahepatic Diseases(n=2199)
Cum
ula
tive M
ort
ali
ty (
)
Anti-HCV+ HCV RNA detectable Anti-HCV+ HCV RNA undetectable Anti-HCVndash
Follow-Up
(Years)
35
30
25
20
15
10
5
00 2 4 6 8 10 12 14 16 18 20
301
128124
104
16
03
198
122
110
MC is clinically benign but sometimes severe HCV EHD invalidating symptoms occur and
it may evolve into lymphoma
Cacoub P et al DLD 2014 Zignego AL et al DLD 2007 Zignego AL et al Intern Emerg Med 2012 Zignego AL et al Clin Dev
Immunol 2012 Zignego AL et al Expert Rev Clin Immunol 2015 Sene D et al J Rheumatol 2004
Mixed Cryoglobulinemia-MC
CGs reversibly precipitate when the temperature is lower than 37degC and
comprise IgMs with RF activity [mono- or oligo-clonal in type II MC or
polyclonal in type III MC] and polyclonal IgGs
MC pathological substrate is an HCV-driven B-cell
proliferation with consequent production of cryo- and non-
cryoprecipitable CICs in turn responsible for vasculitic
manifestations
Most (70ndash90) MC patients are HCV+ and HCV-patients are CGs+ (40ndash60) while 5ndash30 of
CGs+ have symptomatic MC since HCV infects about 170 million individuals worldwide the
number of patients at risk for developing MC is substantial
Type II
CGs
Type III
CGs
Zignego AL et al Autoimmun Rev 2017 Ferri C et al Autoimmunity rev 2016 Zignego AL et al DLD 2007 Cacoub P et al DLD
2014 Zignego AL et al DLD 2007 Zignego AL et al Intern Emerg Med 2012 Zignego AL et al Clin Dev Immunol 2012 Zignego
AL et al Expert Rev Clin Immunol 2015
MC clinical aspects MC Syndrome
MCS is characterized by the clinical triad -purpura weakness and
arthralgias- low complement C4 and various organsystem
involvement including cutaneous articular renal neurological
cardiac or digestive
It ranges from mild disease to severe even life-threatening
conditions
More serious lesions are generally characterized by neurologic and
renal involvement
Prognosis is highly dependent on renal involvement or on the extent
of vasculitis lesions
1 HCV is the main etiopathological agent as concordantly demonstrated by epidemiological clinico-pathological virological and laboratory investigations2 the association between HCV and disease is demonstrated in a significant proportion of patients and supported by in depth clinico-pathogeneticstudies3 the association is suggested by cohort studies a possible causative role may be limited to a small number of patients andor possibly more relevant in specific geographical areas 4 a number of anecdotal observations suggested a possible role of HCV further investigations are required
From P Cacoub 2015
HCV infection is closely related to LPDs mostly MC
40 to 60 of HCV patients show circulating CGs among this latter population 5-30
develop a symptomatic CV
AVT has been considered the first-line option in HCV-CV patients in fact in the majority
of cases viral eradication leads to CV clinical remission
Data about IFN-free regimens for the treatment of CV patients are still limited
HCV and MC
HCV and MC
Zignego 2015Ferri 2016Pozzato 2016 Sise 2016Saadoun 2015Gragnani 2016Gragnani 2016
Bonacci 2016Hegazy 2016Kondili 2016Emery 2017
Younossi et al
The annual costs (inpatient outpatient andpharmacy) associated with extrahepatic
manifestations of HCV were evaluated
Total direct medical costs of extrahepatic
manifestations of HCV in 2014 US dollars wereestimated to be $1506 million (range $922 millionndash
$2208 million in sensitivity analysis)
These estimates should be added to the liver-related
burden of disease to obtain a more accurateassessment of the total burden of HCV infection
The OBJECTIVE of the study was to estimate the annual direct medical costsassociated with HCV related EHM in the EU5 (France Germany Italy United Kingdom
Spain)
Extrahepatic Manifestations of HCV
Extrahepatic Manifestations of HCV
HCV may cause extrahepatic disorders (HCV-EHDs) classified according to the number and
strength of supporting scientific data
HCV-EHDs are responsible for increasing morbidity and mortality with important
consequences in terms of social costs
The analysis of mortality rates in large cohorts confirmed the association of HCV with
several EHDs including cardiovascular neurologic metabolic or renal diseases and tumors
Viral eradication significantly reduced the rate of extra-hepatic deaths
Cacoub P et al DLD 2014 Lee MH et al J Infect Dis 2012 Backus LI et al Clin Gastroenterol Hepatol 2011 El-Kamary S et al
Clin Infect Dis 2011 Hsu YC et al Hepatology 2014 Kawamura Y et al Am J Med 2007 Adinolfi LE et al WJG 2014
Con il contributo di
Lee M-H et al J Infect Dis 2012206469-477
Follow-Up
(Years)
20
18
16
14
12
10
2
00 2 4 6 8 10 12 14 16 18 20
8
6
4
Follow-Up
(Years)
12
10
8
6
4
2
00 2 4 6 8 10 12 14 16 18 20
All Causes(n=2394)
Liver Cancer(n=115)
Extrahepatic Diseases(n=2199)
Cum
ula
tive M
ort
ali
ty (
)
Anti-HCV+ HCV RNA detectable Anti-HCV+ HCV RNA undetectable Anti-HCVndash
Follow-Up
(Years)
35
30
25
20
15
10
5
00 2 4 6 8 10 12 14 16 18 20
301
128124
104
16
03
198
122
110
Extrahepatic Manifestations of HCV
The annual costs (inpatient outpatient andpharmacy) associated with extrahepatic
manifestations of HCV were evaluated
Total direct medical costs of extrahepatic
manifestations of HCV in 2014 US dollars wereestimated to be $1506 million (range $922 millionndash
$2208 million in sensitivity analysis)
These estimates should be added to the liver-related
burden of disease to obtain a more accurateassessment of the total burden of HCV infection
Younossi et al
Younossi et al
Costs up to $71000 per patient per year (ESRD) Among the most frequent EHM depression (245 in HCV vs 172 in non-HCV) had estimated annual cost of
$4307 million DM (15 vs 10 in non- HCV) had an annual cost of $4434 million in the USA= given the importance of DM and
its association with CVDs and mortality the clinical and economic impacts of HCV-related DM are substantial
The OBJECTIVE of the study was to estimate the annual direct medical costsassociated with HCV related EHM in the EU5 (France Germany Italy United Kingdom
Spain)
The OBJECTIVE of the study was to estimate the annual direct medicalcosts associated with HCV related EHM in the EU5 (France Germany
Italy United Kingdom Spain)
1 HCV is the main etiopathological agent as concordantly demonstrated by epidemiological clinico-pathological virological and laboratory investigations2 the association between HCV and disease is demonstrated in a significant proportion of patients and supported by in depth clinico-pathogeneticstudies3 the association is suggested by cohort studies a possible causative role may be limited to a small number of patients andor possibly more relevant in specific geographical areas 4 a number of anecdotal observations suggested a possible role of HCV further investigations are required
The most studied and frequent HCV-EHDs are B-LPDs andor autoimmune disorders
Their prototype is Mixed Cryoglobulinemia (MC) from researches on MC derived most of the
available information
MC as a precious model for all the HCV-EHDs and to evaluate the effects of viral eradication
Anti-HCV Treatment Evolution
IFN
6 mos
PegIFN RBV 12
mos
IFN
12 mos
IFNRBV
12 mos
PegIFN
12 mos
2001
1998
2011
Standardinterferon
Ribavirin
Peginterferon
1991
Direct-actingantivirals
PegIFN
RBV
DAA
IFNRBV
6 mos
6
16
34
4239
55
70+
0
20
40
60
80
100
DAAs
826
weeks
gt90
2015
Few side effects absence major
contraindications
Younossi et al
The annual costs (inpatient outpatient and pharmacy) associatedwith extrahepatic manifestations of HCV were evaluated
Total direct medical costs of extrahepatic manifestations of HCV in 2014US dollars were estimated to be $1506 million (range $922 millionndash
$2208 million in sensitivity analysis)
These estimates should be added to the liver-related burden of diseaseto obtain a more accurate assessment of the total burden of HCV
infection
The OBJECTIVE of the study was to estimate the annual direct medical costs associated with HCV related EHM in the EU5 (France Germany Italy United Kingdom Spain)
22 MCS treated with DAAs including 2 HCC and 2 NHL 100 SVR12 Clinical CR in 64 and PR in remaining 36 The small lymphocytic lymphoma progressed despite viral clearance
Lauletta et al 2017
Emery CS et al 2017
Retrospective analysis 17 MCS (10 with severelife-threatening vasculitis) and 65 asymptomatic CGs+ pts treated with DAAs SVR 889 MCS and 908 asymptomatic pts In MCS clinical response in 1117 (complete in 717) In severelife-threatening vasculitis lower clinical response especially in renal and neurological symptoms
Saadoun D et al 2017
Open-label prospective multi-center study on sofosbuvir plus daclatasvir treatment of 41 HCV MCS SVR in100 and clinical CR in 902 Disappearance of CGs in 50 of pts No serious adverse event or relapse ofvasculitis
Antiviral Treatment (AVT) of MCIFN-free regimens
MC is clinically benign but sometimes severe HCV EHD invalidating symptoms occur and
it may evolve into lymphoma
Cacoub P et al DLD 2014 Zignego AL et al DLD 2007 Zignego AL et al Intern Emerg Med 2012 Zignego AL et al Clin Dev
Immunol 2012 Zignego AL et al Expert Rev Clin Immunol 2015 Sene D et al J Rheumatol 2004
Mixed Cryoglobulinemia-MC
MC pathological substrate is an HCV-driven B-cell
proliferation with consequent production of cryo- and non-
cryoprecipitable CICs in turn responsible for vasculitic
manifestations
Most (70ndash90) MC patients are HCV+ and HCV-patients are CGs+ (40ndash60) while 5ndash30 of
CGs+ have symptomatic MC or cryoglobulinemic vasculitis since HCV infects about 170
million individuals worldwide the number of patients at risk for developing MC is
substantial
Type II CGs
monoclonal
RF+policlonal IgG
Type III CGs both
RF and IgG
polyclonal

Main drugs for HCV-related MCS according to the target
HCV= DAAsB-cell Expansion= (a) B cell-depleting Mabs
-First-generation Rituximab (anti-CD20)-Second-generation Ofatumumab (anti-CD20) Veltuzumab (humanized
anti-CD20)-Third-generation Obinutuzumab (GA101) Oceratuzumab (humanized
anti-CD20)
(b) Alkylating agents
-Cyclophosfamide
Inflammation= Antiinflammatory agents
- Corticosteroids
Altered regulatory T-cell activity=
- IL-2
The impact on HRQoL of IFN-free AVT was prospectively evaluated in a cohort of HCV CV patients with limited
influencing variables linked to therapeutic schedulesviral GT
44 HCV GT2 CV patients mostly F0-F2 (29) and naiumlve (30) treated with SOFRBV for 1224wks
TIME POINTS
baseline EOT and week 12 and 24 of post-treatment f-up (SVR12 and SVR24 respectively)
HRQoL EVALUATION THROUGH PROs
the Short Form (36) Health Survey (SF-36)
the Functional Assessment of Chronic Illness Therapy-Fatigue (FACIT-F) from which we computed the Trial
Outcome Index (TOI)
Observational study on in situ expression of the oncogenic HCV NS3 protein on 116 HCV
patients with B-NHL (DLBCL 36 and MZL 34)
NS3 immunostaining positive in 1214 DLBCL vs only 414 MZL (p = 0006) moreover 24 NS3+
MZL were enriched in large cells
This study supports a new mechanism of transformation with a direct oncogenic role of
HCV proteins in the occurrence of high-grade B lymphomas
IN SITU HEPATITIS C NS3 PROTEIN DETECTION IS ASSOCIATED WITH HIGH GRADEFEATURES IN HCV-ASSOCIATED B-CELL NON-HODGKIN LYMPHOMAS Danielle
Canioni et al 2016
In addition to the role of chronic antigenic stimulation in HCV related
lymphomagenesis this study supports a second mechanism of transformation due toa direct oncogenic role of HCV infection of B-cells promoting the occurrence of high-grade Bcell lymphomas
ANTIVIRAL THERAPY IS ASSOCIATED WITH A BETTERSURVIVAL IN PATIENTS WITH HCV AND B-CELL NON-HODGKIN LYMPHOMAS ANRS HC-13 LYMPHO-CSTUDYMichot JM et al
Outcomes of HCV-associated B-NHL according to HCV AVT in prospective patients only (n 5 64)
(A) absolute neutrophil count and Hgb
(B) ALT and HCV viral load
This patient had HCV-associated DLBCL achieving both complete response and SVR after concurrent chemoimmunotherapy and antiviral therapy using a sofosbuvir-basedregimen
Concurrent Systemic Chemoimmunotherapy and Sofosbuvir-Based Antiviral Treatment in a Hepatitis C Virus-Infected Patient With Diffuse Large B-Cell LymphomaEvan C Ewers et al 2016
HCV-EHDs are responsible for increasing morbidity and mortality with important
consequences in terms of social costs
The analysis of mortality rates in large cohorts confirmed the association of HCV with
several EHDs including cardiovascular neurologic metabolic or renal diseases and tumors
Viral eradication significantly reduced the rate of extra-hepatic deaths
Cacoub P et al DLD 2014 Lee MH et al J Infect Dis 2012 Backus LI et al Clin Gastroenterol Hepatol 2011 El-Kamary S et al
Clin Infect Dis 2011 Hsu YC et al Hepatology 2014 Kawamura Y et al Am J Med 2007 Adinolfi LE et al WJG 2014
Extrahepatic Manifestations of HCV
Con il contributo di
Lee M-H et al J Infect Dis 2012206469-477
Follow-Up
(Years)
20
18
16
14
12
10
2
00 2 4 6 8 10 12 14 16 18 20
8
6
4
Follow-Up
(Years)
12
10
8
6
4
2
00 2 4 6 8 10 12 14 16 18 20
All Causes(n=2394)
Liver Cancer(n=115)
Extrahepatic Diseases(n=2199)
Cum
ula
tive M
ort
ali
ty (
)
Anti-HCV+ HCV RNA detectable Anti-HCV+ HCV RNA undetectable Anti-HCVndash
Follow-Up
(Years)
35
30
25
20
15
10
5
00 2 4 6 8 10 12 14 16 18 20
301
128124
104
16
03
198
122
110
MC is clinically benign but sometimes severe HCV EHD invalidating symptoms occur and
it may evolve into lymphoma
Cacoub P et al DLD 2014 Zignego AL et al DLD 2007 Zignego AL et al Intern Emerg Med 2012 Zignego AL et al Clin Dev
Immunol 2012 Zignego AL et al Expert Rev Clin Immunol 2015 Sene D et al J Rheumatol 2004
Mixed Cryoglobulinemia-MC
CGs reversibly precipitate when the temperature is lower than 37degC and
comprise IgMs with RF activity [mono- or oligo-clonal in type II MC or
polyclonal in type III MC] and polyclonal IgGs
MC pathological substrate is an HCV-driven B-cell
proliferation with consequent production of cryo- and non-
cryoprecipitable CICs in turn responsible for vasculitic
manifestations
Most (70ndash90) MC patients are HCV+ and HCV-patients are CGs+ (40ndash60) while 5ndash30 of
CGs+ have symptomatic MC since HCV infects about 170 million individuals worldwide the
number of patients at risk for developing MC is substantial
Type II
CGs
Type III
CGs
Zignego AL et al Autoimmun Rev 2017 Ferri C et al Autoimmunity rev 2016 Zignego AL et al DLD 2007 Cacoub P et al DLD
2014 Zignego AL et al DLD 2007 Zignego AL et al Intern Emerg Med 2012 Zignego AL et al Clin Dev Immunol 2012 Zignego
AL et al Expert Rev Clin Immunol 2015
MC clinical aspects MC Syndrome
MCS is characterized by the clinical triad -purpura weakness and
arthralgias- low complement C4 and various organsystem
involvement including cutaneous articular renal neurological
cardiac or digestive
It ranges from mild disease to severe even life-threatening
conditions
More serious lesions are generally characterized by neurologic and
renal involvement
Prognosis is highly dependent on renal involvement or on the extent
of vasculitis lesions
1 HCV is the main etiopathological agent as concordantly demonstrated by epidemiological clinico-pathological virological and laboratory investigations2 the association between HCV and disease is demonstrated in a significant proportion of patients and supported by in depth clinico-pathogeneticstudies3 the association is suggested by cohort studies a possible causative role may be limited to a small number of patients andor possibly more relevant in specific geographical areas 4 a number of anecdotal observations suggested a possible role of HCV further investigations are required
From P Cacoub 2015
HCV infection is closely related to LPDs mostly MC
40 to 60 of HCV patients show circulating CGs among this latter population 5-30
develop a symptomatic CV
AVT has been considered the first-line option in HCV-CV patients in fact in the majority
of cases viral eradication leads to CV clinical remission
Data about IFN-free regimens for the treatment of CV patients are still limited
HCV and MC
HCV and MC
Zignego 2015Ferri 2016Pozzato 2016 Sise 2016Saadoun 2015Gragnani 2016Gragnani 2016
Bonacci 2016Hegazy 2016Kondili 2016Emery 2017
Younossi et al
The annual costs (inpatient outpatient andpharmacy) associated with extrahepatic
manifestations of HCV were evaluated
Total direct medical costs of extrahepatic
manifestations of HCV in 2014 US dollars wereestimated to be $1506 million (range $922 millionndash
$2208 million in sensitivity analysis)
These estimates should be added to the liver-related
burden of disease to obtain a more accurateassessment of the total burden of HCV infection
The OBJECTIVE of the study was to estimate the annual direct medical costsassociated with HCV related EHM in the EU5 (France Germany Italy United Kingdom
Spain)
Extrahepatic Manifestations of HCV
Extrahepatic Manifestations of HCV
HCV may cause extrahepatic disorders (HCV-EHDs) classified according to the number and
strength of supporting scientific data
HCV-EHDs are responsible for increasing morbidity and mortality with important
consequences in terms of social costs
The analysis of mortality rates in large cohorts confirmed the association of HCV with
several EHDs including cardiovascular neurologic metabolic or renal diseases and tumors
Viral eradication significantly reduced the rate of extra-hepatic deaths
Cacoub P et al DLD 2014 Lee MH et al J Infect Dis 2012 Backus LI et al Clin Gastroenterol Hepatol 2011 El-Kamary S et al
Clin Infect Dis 2011 Hsu YC et al Hepatology 2014 Kawamura Y et al Am J Med 2007 Adinolfi LE et al WJG 2014
Con il contributo di
Lee M-H et al J Infect Dis 2012206469-477
Follow-Up
(Years)
20
18
16
14
12
10
2
00 2 4 6 8 10 12 14 16 18 20
8
6
4
Follow-Up
(Years)
12
10
8
6
4
2
00 2 4 6 8 10 12 14 16 18 20
All Causes(n=2394)
Liver Cancer(n=115)
Extrahepatic Diseases(n=2199)
Cum
ula
tive M
ort
ali
ty (
)
Anti-HCV+ HCV RNA detectable Anti-HCV+ HCV RNA undetectable Anti-HCVndash
Follow-Up
(Years)
35
30
25
20
15
10
5
00 2 4 6 8 10 12 14 16 18 20
301
128124
104
16
03
198
122
110
Extrahepatic Manifestations of HCV
The annual costs (inpatient outpatient andpharmacy) associated with extrahepatic
manifestations of HCV were evaluated
Total direct medical costs of extrahepatic
manifestations of HCV in 2014 US dollars wereestimated to be $1506 million (range $922 millionndash
$2208 million in sensitivity analysis)
These estimates should be added to the liver-related
burden of disease to obtain a more accurateassessment of the total burden of HCV infection
Younossi et al
Younossi et al
Costs up to $71000 per patient per year (ESRD) Among the most frequent EHM depression (245 in HCV vs 172 in non-HCV) had estimated annual cost of
$4307 million DM (15 vs 10 in non- HCV) had an annual cost of $4434 million in the USA= given the importance of DM and
its association with CVDs and mortality the clinical and economic impacts of HCV-related DM are substantial
The OBJECTIVE of the study was to estimate the annual direct medical costsassociated with HCV related EHM in the EU5 (France Germany Italy United Kingdom
Spain)
The OBJECTIVE of the study was to estimate the annual direct medicalcosts associated with HCV related EHM in the EU5 (France Germany
Italy United Kingdom Spain)
1 HCV is the main etiopathological agent as concordantly demonstrated by epidemiological clinico-pathological virological and laboratory investigations2 the association between HCV and disease is demonstrated in a significant proportion of patients and supported by in depth clinico-pathogeneticstudies3 the association is suggested by cohort studies a possible causative role may be limited to a small number of patients andor possibly more relevant in specific geographical areas 4 a number of anecdotal observations suggested a possible role of HCV further investigations are required
The most studied and frequent HCV-EHDs are B-LPDs andor autoimmune disorders
Their prototype is Mixed Cryoglobulinemia (MC) from researches on MC derived most of the
available information
MC as a precious model for all the HCV-EHDs and to evaluate the effects of viral eradication
Anti-HCV Treatment Evolution
IFN
6 mos
PegIFN RBV 12
mos
IFN
12 mos
IFNRBV
12 mos
PegIFN
12 mos
2001
1998
2011
Standardinterferon
Ribavirin
Peginterferon
1991
Direct-actingantivirals
PegIFN
RBV
DAA
IFNRBV
6 mos
6
16
34
4239
55
70+
0
20
40
60
80
100
DAAs
826
weeks
gt90
2015
Few side effects absence major
contraindications
Younossi et al
The annual costs (inpatient outpatient and pharmacy) associatedwith extrahepatic manifestations of HCV were evaluated
Total direct medical costs of extrahepatic manifestations of HCV in 2014US dollars were estimated to be $1506 million (range $922 millionndash
$2208 million in sensitivity analysis)
These estimates should be added to the liver-related burden of diseaseto obtain a more accurate assessment of the total burden of HCV
infection
The OBJECTIVE of the study was to estimate the annual direct medical costs associated with HCV related EHM in the EU5 (France Germany Italy United Kingdom Spain)
22 MCS treated with DAAs including 2 HCC and 2 NHL 100 SVR12 Clinical CR in 64 and PR in remaining 36 The small lymphocytic lymphoma progressed despite viral clearance
Lauletta et al 2017
Emery CS et al 2017
Retrospective analysis 17 MCS (10 with severelife-threatening vasculitis) and 65 asymptomatic CGs+ pts treated with DAAs SVR 889 MCS and 908 asymptomatic pts In MCS clinical response in 1117 (complete in 717) In severelife-threatening vasculitis lower clinical response especially in renal and neurological symptoms
Saadoun D et al 2017
Open-label prospective multi-center study on sofosbuvir plus daclatasvir treatment of 41 HCV MCS SVR in100 and clinical CR in 902 Disappearance of CGs in 50 of pts No serious adverse event or relapse ofvasculitis
Antiviral Treatment (AVT) of MCIFN-free regimens
MC is clinically benign but sometimes severe HCV EHD invalidating symptoms occur and
it may evolve into lymphoma
Cacoub P et al DLD 2014 Zignego AL et al DLD 2007 Zignego AL et al Intern Emerg Med 2012 Zignego AL et al Clin Dev
Immunol 2012 Zignego AL et al Expert Rev Clin Immunol 2015 Sene D et al J Rheumatol 2004
Mixed Cryoglobulinemia-MC
MC pathological substrate is an HCV-driven B-cell
proliferation with consequent production of cryo- and non-
cryoprecipitable CICs in turn responsible for vasculitic
manifestations
Most (70ndash90) MC patients are HCV+ and HCV-patients are CGs+ (40ndash60) while 5ndash30 of
CGs+ have symptomatic MC or cryoglobulinemic vasculitis since HCV infects about 170
million individuals worldwide the number of patients at risk for developing MC is
substantial
Type II CGs
monoclonal
RF+policlonal IgG
Type III CGs both
RF and IgG
polyclonal

The impact on HRQoL of IFN-free AVT was prospectively evaluated in a cohort of HCV CV patients with limited
influencing variables linked to therapeutic schedulesviral GT
44 HCV GT2 CV patients mostly F0-F2 (29) and naiumlve (30) treated with SOFRBV for 1224wks
TIME POINTS
baseline EOT and week 12 and 24 of post-treatment f-up (SVR12 and SVR24 respectively)
HRQoL EVALUATION THROUGH PROs
the Short Form (36) Health Survey (SF-36)
the Functional Assessment of Chronic Illness Therapy-Fatigue (FACIT-F) from which we computed the Trial
Outcome Index (TOI)
Observational study on in situ expression of the oncogenic HCV NS3 protein on 116 HCV
patients with B-NHL (DLBCL 36 and MZL 34)
NS3 immunostaining positive in 1214 DLBCL vs only 414 MZL (p = 0006) moreover 24 NS3+
MZL were enriched in large cells
This study supports a new mechanism of transformation with a direct oncogenic role of
HCV proteins in the occurrence of high-grade B lymphomas
IN SITU HEPATITIS C NS3 PROTEIN DETECTION IS ASSOCIATED WITH HIGH GRADEFEATURES IN HCV-ASSOCIATED B-CELL NON-HODGKIN LYMPHOMAS Danielle
Canioni et al 2016
In addition to the role of chronic antigenic stimulation in HCV related
lymphomagenesis this study supports a second mechanism of transformation due toa direct oncogenic role of HCV infection of B-cells promoting the occurrence of high-grade Bcell lymphomas
ANTIVIRAL THERAPY IS ASSOCIATED WITH A BETTERSURVIVAL IN PATIENTS WITH HCV AND B-CELL NON-HODGKIN LYMPHOMAS ANRS HC-13 LYMPHO-CSTUDYMichot JM et al
Outcomes of HCV-associated B-NHL according to HCV AVT in prospective patients only (n 5 64)
(A) absolute neutrophil count and Hgb
(B) ALT and HCV viral load
This patient had HCV-associated DLBCL achieving both complete response and SVR after concurrent chemoimmunotherapy and antiviral therapy using a sofosbuvir-basedregimen
Concurrent Systemic Chemoimmunotherapy and Sofosbuvir-Based Antiviral Treatment in a Hepatitis C Virus-Infected Patient With Diffuse Large B-Cell LymphomaEvan C Ewers et al 2016
HCV-EHDs are responsible for increasing morbidity and mortality with important
consequences in terms of social costs
The analysis of mortality rates in large cohorts confirmed the association of HCV with
several EHDs including cardiovascular neurologic metabolic or renal diseases and tumors
Viral eradication significantly reduced the rate of extra-hepatic deaths
Cacoub P et al DLD 2014 Lee MH et al J Infect Dis 2012 Backus LI et al Clin Gastroenterol Hepatol 2011 El-Kamary S et al
Clin Infect Dis 2011 Hsu YC et al Hepatology 2014 Kawamura Y et al Am J Med 2007 Adinolfi LE et al WJG 2014
Extrahepatic Manifestations of HCV
Con il contributo di
Lee M-H et al J Infect Dis 2012206469-477
Follow-Up
(Years)
20
18
16
14
12
10
2
00 2 4 6 8 10 12 14 16 18 20
8
6
4
Follow-Up
(Years)
12
10
8
6
4
2
00 2 4 6 8 10 12 14 16 18 20
All Causes(n=2394)
Liver Cancer(n=115)
Extrahepatic Diseases(n=2199)
Cum
ula
tive M
ort
ali
ty (
)
Anti-HCV+ HCV RNA detectable Anti-HCV+ HCV RNA undetectable Anti-HCVndash
Follow-Up
(Years)
35
30
25
20
15
10
5
00 2 4 6 8 10 12 14 16 18 20
301
128124
104
16
03
198
122
110
MC is clinically benign but sometimes severe HCV EHD invalidating symptoms occur and
it may evolve into lymphoma
Cacoub P et al DLD 2014 Zignego AL et al DLD 2007 Zignego AL et al Intern Emerg Med 2012 Zignego AL et al Clin Dev
Immunol 2012 Zignego AL et al Expert Rev Clin Immunol 2015 Sene D et al J Rheumatol 2004
Mixed Cryoglobulinemia-MC
CGs reversibly precipitate when the temperature is lower than 37degC and
comprise IgMs with RF activity [mono- or oligo-clonal in type II MC or
polyclonal in type III MC] and polyclonal IgGs
MC pathological substrate is an HCV-driven B-cell
proliferation with consequent production of cryo- and non-
cryoprecipitable CICs in turn responsible for vasculitic
manifestations
Most (70ndash90) MC patients are HCV+ and HCV-patients are CGs+ (40ndash60) while 5ndash30 of
CGs+ have symptomatic MC since HCV infects about 170 million individuals worldwide the
number of patients at risk for developing MC is substantial
Type II
CGs
Type III
CGs
Zignego AL et al Autoimmun Rev 2017 Ferri C et al Autoimmunity rev 2016 Zignego AL et al DLD 2007 Cacoub P et al DLD
2014 Zignego AL et al DLD 2007 Zignego AL et al Intern Emerg Med 2012 Zignego AL et al Clin Dev Immunol 2012 Zignego
AL et al Expert Rev Clin Immunol 2015
MC clinical aspects MC Syndrome
MCS is characterized by the clinical triad -purpura weakness and
arthralgias- low complement C4 and various organsystem
involvement including cutaneous articular renal neurological
cardiac or digestive
It ranges from mild disease to severe even life-threatening
conditions
More serious lesions are generally characterized by neurologic and
renal involvement
Prognosis is highly dependent on renal involvement or on the extent
of vasculitis lesions
1 HCV is the main etiopathological agent as concordantly demonstrated by epidemiological clinico-pathological virological and laboratory investigations2 the association between HCV and disease is demonstrated in a significant proportion of patients and supported by in depth clinico-pathogeneticstudies3 the association is suggested by cohort studies a possible causative role may be limited to a small number of patients andor possibly more relevant in specific geographical areas 4 a number of anecdotal observations suggested a possible role of HCV further investigations are required
From P Cacoub 2015
HCV infection is closely related to LPDs mostly MC
40 to 60 of HCV patients show circulating CGs among this latter population 5-30
develop a symptomatic CV
AVT has been considered the first-line option in HCV-CV patients in fact in the majority
of cases viral eradication leads to CV clinical remission
Data about IFN-free regimens for the treatment of CV patients are still limited
HCV and MC
HCV and MC
Zignego 2015Ferri 2016Pozzato 2016 Sise 2016Saadoun 2015Gragnani 2016Gragnani 2016
Bonacci 2016Hegazy 2016Kondili 2016Emery 2017
Younossi et al
The annual costs (inpatient outpatient andpharmacy) associated with extrahepatic
manifestations of HCV were evaluated
Total direct medical costs of extrahepatic
manifestations of HCV in 2014 US dollars wereestimated to be $1506 million (range $922 millionndash
$2208 million in sensitivity analysis)
These estimates should be added to the liver-related
burden of disease to obtain a more accurateassessment of the total burden of HCV infection
The OBJECTIVE of the study was to estimate the annual direct medical costsassociated with HCV related EHM in the EU5 (France Germany Italy United Kingdom
Spain)
Extrahepatic Manifestations of HCV
Extrahepatic Manifestations of HCV
HCV may cause extrahepatic disorders (HCV-EHDs) classified according to the number and
strength of supporting scientific data
HCV-EHDs are responsible for increasing morbidity and mortality with important
consequences in terms of social costs
The analysis of mortality rates in large cohorts confirmed the association of HCV with
several EHDs including cardiovascular neurologic metabolic or renal diseases and tumors
Viral eradication significantly reduced the rate of extra-hepatic deaths
Cacoub P et al DLD 2014 Lee MH et al J Infect Dis 2012 Backus LI et al Clin Gastroenterol Hepatol 2011 El-Kamary S et al
Clin Infect Dis 2011 Hsu YC et al Hepatology 2014 Kawamura Y et al Am J Med 2007 Adinolfi LE et al WJG 2014
Con il contributo di
Lee M-H et al J Infect Dis 2012206469-477
Follow-Up
(Years)
20
18
16
14
12
10
2
00 2 4 6 8 10 12 14 16 18 20
8
6
4
Follow-Up
(Years)
12
10
8
6
4
2
00 2 4 6 8 10 12 14 16 18 20
All Causes(n=2394)
Liver Cancer(n=115)
Extrahepatic Diseases(n=2199)
Cum
ula
tive M
ort
ali
ty (
)
Anti-HCV+ HCV RNA detectable Anti-HCV+ HCV RNA undetectable Anti-HCVndash
Follow-Up
(Years)
35
30
25
20
15
10
5
00 2 4 6 8 10 12 14 16 18 20
301
128124
104
16
03
198
122
110
Extrahepatic Manifestations of HCV
The annual costs (inpatient outpatient andpharmacy) associated with extrahepatic
manifestations of HCV were evaluated
Total direct medical costs of extrahepatic
manifestations of HCV in 2014 US dollars wereestimated to be $1506 million (range $922 millionndash
$2208 million in sensitivity analysis)
These estimates should be added to the liver-related
burden of disease to obtain a more accurateassessment of the total burden of HCV infection
Younossi et al
Younossi et al
Costs up to $71000 per patient per year (ESRD) Among the most frequent EHM depression (245 in HCV vs 172 in non-HCV) had estimated annual cost of
$4307 million DM (15 vs 10 in non- HCV) had an annual cost of $4434 million in the USA= given the importance of DM and
its association with CVDs and mortality the clinical and economic impacts of HCV-related DM are substantial
The OBJECTIVE of the study was to estimate the annual direct medical costsassociated with HCV related EHM in the EU5 (France Germany Italy United Kingdom
Spain)
The OBJECTIVE of the study was to estimate the annual direct medicalcosts associated with HCV related EHM in the EU5 (France Germany
Italy United Kingdom Spain)
1 HCV is the main etiopathological agent as concordantly demonstrated by epidemiological clinico-pathological virological and laboratory investigations2 the association between HCV and disease is demonstrated in a significant proportion of patients and supported by in depth clinico-pathogeneticstudies3 the association is suggested by cohort studies a possible causative role may be limited to a small number of patients andor possibly more relevant in specific geographical areas 4 a number of anecdotal observations suggested a possible role of HCV further investigations are required
The most studied and frequent HCV-EHDs are B-LPDs andor autoimmune disorders
Their prototype is Mixed Cryoglobulinemia (MC) from researches on MC derived most of the
available information
MC as a precious model for all the HCV-EHDs and to evaluate the effects of viral eradication
Anti-HCV Treatment Evolution
IFN
6 mos
PegIFN RBV 12
mos
IFN
12 mos
IFNRBV
12 mos
PegIFN
12 mos
2001
1998
2011
Standardinterferon
Ribavirin
Peginterferon
1991
Direct-actingantivirals
PegIFN
RBV
DAA
IFNRBV
6 mos
6
16
34
4239
55
70+
0
20
40
60
80
100
DAAs
826
weeks
gt90
2015
Few side effects absence major
contraindications
Younossi et al
The annual costs (inpatient outpatient and pharmacy) associatedwith extrahepatic manifestations of HCV were evaluated
Total direct medical costs of extrahepatic manifestations of HCV in 2014US dollars were estimated to be $1506 million (range $922 millionndash
$2208 million in sensitivity analysis)
These estimates should be added to the liver-related burden of diseaseto obtain a more accurate assessment of the total burden of HCV
infection
The OBJECTIVE of the study was to estimate the annual direct medical costs associated with HCV related EHM in the EU5 (France Germany Italy United Kingdom Spain)
22 MCS treated with DAAs including 2 HCC and 2 NHL 100 SVR12 Clinical CR in 64 and PR in remaining 36 The small lymphocytic lymphoma progressed despite viral clearance
Lauletta et al 2017
Emery CS et al 2017
Retrospective analysis 17 MCS (10 with severelife-threatening vasculitis) and 65 asymptomatic CGs+ pts treated with DAAs SVR 889 MCS and 908 asymptomatic pts In MCS clinical response in 1117 (complete in 717) In severelife-threatening vasculitis lower clinical response especially in renal and neurological symptoms
Saadoun D et al 2017
Open-label prospective multi-center study on sofosbuvir plus daclatasvir treatment of 41 HCV MCS SVR in100 and clinical CR in 902 Disappearance of CGs in 50 of pts No serious adverse event or relapse ofvasculitis
Antiviral Treatment (AVT) of MCIFN-free regimens
MC is clinically benign but sometimes severe HCV EHD invalidating symptoms occur and
it may evolve into lymphoma
Cacoub P et al DLD 2014 Zignego AL et al DLD 2007 Zignego AL et al Intern Emerg Med 2012 Zignego AL et al Clin Dev
Immunol 2012 Zignego AL et al Expert Rev Clin Immunol 2015 Sene D et al J Rheumatol 2004
Mixed Cryoglobulinemia-MC
MC pathological substrate is an HCV-driven B-cell
proliferation with consequent production of cryo- and non-
cryoprecipitable CICs in turn responsible for vasculitic
manifestations
Most (70ndash90) MC patients are HCV+ and HCV-patients are CGs+ (40ndash60) while 5ndash30 of
CGs+ have symptomatic MC or cryoglobulinemic vasculitis since HCV infects about 170
million individuals worldwide the number of patients at risk for developing MC is
substantial
Type II CGs
monoclonal
RF+policlonal IgG
Type III CGs both
RF and IgG
polyclonal

Observational study on in situ expression of the oncogenic HCV NS3 protein on 116 HCV
patients with B-NHL (DLBCL 36 and MZL 34)
NS3 immunostaining positive in 1214 DLBCL vs only 414 MZL (p = 0006) moreover 24 NS3+
MZL were enriched in large cells
This study supports a new mechanism of transformation with a direct oncogenic role of
HCV proteins in the occurrence of high-grade B lymphomas
IN SITU HEPATITIS C NS3 PROTEIN DETECTION IS ASSOCIATED WITH HIGH GRADEFEATURES IN HCV-ASSOCIATED B-CELL NON-HODGKIN LYMPHOMAS Danielle
Canioni et al 2016
In addition to the role of chronic antigenic stimulation in HCV related
lymphomagenesis this study supports a second mechanism of transformation due toa direct oncogenic role of HCV infection of B-cells promoting the occurrence of high-grade Bcell lymphomas
ANTIVIRAL THERAPY IS ASSOCIATED WITH A BETTERSURVIVAL IN PATIENTS WITH HCV AND B-CELL NON-HODGKIN LYMPHOMAS ANRS HC-13 LYMPHO-CSTUDYMichot JM et al
Outcomes of HCV-associated B-NHL according to HCV AVT in prospective patients only (n 5 64)
(A) absolute neutrophil count and Hgb
(B) ALT and HCV viral load
This patient had HCV-associated DLBCL achieving both complete response and SVR after concurrent chemoimmunotherapy and antiviral therapy using a sofosbuvir-basedregimen
Concurrent Systemic Chemoimmunotherapy and Sofosbuvir-Based Antiviral Treatment in a Hepatitis C Virus-Infected Patient With Diffuse Large B-Cell LymphomaEvan C Ewers et al 2016
HCV-EHDs are responsible for increasing morbidity and mortality with important
consequences in terms of social costs
The analysis of mortality rates in large cohorts confirmed the association of HCV with
several EHDs including cardiovascular neurologic metabolic or renal diseases and tumors
Viral eradication significantly reduced the rate of extra-hepatic deaths
Cacoub P et al DLD 2014 Lee MH et al J Infect Dis 2012 Backus LI et al Clin Gastroenterol Hepatol 2011 El-Kamary S et al
Clin Infect Dis 2011 Hsu YC et al Hepatology 2014 Kawamura Y et al Am J Med 2007 Adinolfi LE et al WJG 2014
Extrahepatic Manifestations of HCV
Con il contributo di
Lee M-H et al J Infect Dis 2012206469-477
Follow-Up
(Years)
20
18
16
14
12
10
2
00 2 4 6 8 10 12 14 16 18 20
8
6
4
Follow-Up
(Years)
12
10
8
6
4
2
00 2 4 6 8 10 12 14 16 18 20
All Causes(n=2394)
Liver Cancer(n=115)
Extrahepatic Diseases(n=2199)
Cum
ula
tive M
ort
ali
ty (
)
Anti-HCV+ HCV RNA detectable Anti-HCV+ HCV RNA undetectable Anti-HCVndash
Follow-Up
(Years)
35
30
25
20
15
10
5
00 2 4 6 8 10 12 14 16 18 20
301
128124
104
16
03
198
122
110
MC is clinically benign but sometimes severe HCV EHD invalidating symptoms occur and
it may evolve into lymphoma
Cacoub P et al DLD 2014 Zignego AL et al DLD 2007 Zignego AL et al Intern Emerg Med 2012 Zignego AL et al Clin Dev
Immunol 2012 Zignego AL et al Expert Rev Clin Immunol 2015 Sene D et al J Rheumatol 2004
Mixed Cryoglobulinemia-MC
CGs reversibly precipitate when the temperature is lower than 37degC and
comprise IgMs with RF activity [mono- or oligo-clonal in type II MC or
polyclonal in type III MC] and polyclonal IgGs
MC pathological substrate is an HCV-driven B-cell
proliferation with consequent production of cryo- and non-
cryoprecipitable CICs in turn responsible for vasculitic
manifestations
Most (70ndash90) MC patients are HCV+ and HCV-patients are CGs+ (40ndash60) while 5ndash30 of
CGs+ have symptomatic MC since HCV infects about 170 million individuals worldwide the
number of patients at risk for developing MC is substantial
Type II
CGs
Type III
CGs
Zignego AL et al Autoimmun Rev 2017 Ferri C et al Autoimmunity rev 2016 Zignego AL et al DLD 2007 Cacoub P et al DLD
2014 Zignego AL et al DLD 2007 Zignego AL et al Intern Emerg Med 2012 Zignego AL et al Clin Dev Immunol 2012 Zignego
AL et al Expert Rev Clin Immunol 2015
MC clinical aspects MC Syndrome
MCS is characterized by the clinical triad -purpura weakness and
arthralgias- low complement C4 and various organsystem
involvement including cutaneous articular renal neurological
cardiac or digestive
It ranges from mild disease to severe even life-threatening
conditions
More serious lesions are generally characterized by neurologic and
renal involvement
Prognosis is highly dependent on renal involvement or on the extent
of vasculitis lesions
1 HCV is the main etiopathological agent as concordantly demonstrated by epidemiological clinico-pathological virological and laboratory investigations2 the association between HCV and disease is demonstrated in a significant proportion of patients and supported by in depth clinico-pathogeneticstudies3 the association is suggested by cohort studies a possible causative role may be limited to a small number of patients andor possibly more relevant in specific geographical areas 4 a number of anecdotal observations suggested a possible role of HCV further investigations are required
From P Cacoub 2015
HCV infection is closely related to LPDs mostly MC
40 to 60 of HCV patients show circulating CGs among this latter population 5-30
develop a symptomatic CV
AVT has been considered the first-line option in HCV-CV patients in fact in the majority
of cases viral eradication leads to CV clinical remission
Data about IFN-free regimens for the treatment of CV patients are still limited
HCV and MC
HCV and MC
Zignego 2015Ferri 2016Pozzato 2016 Sise 2016Saadoun 2015Gragnani 2016Gragnani 2016
Bonacci 2016Hegazy 2016Kondili 2016Emery 2017
Younossi et al
The annual costs (inpatient outpatient andpharmacy) associated with extrahepatic
manifestations of HCV were evaluated
Total direct medical costs of extrahepatic
manifestations of HCV in 2014 US dollars wereestimated to be $1506 million (range $922 millionndash
$2208 million in sensitivity analysis)
These estimates should be added to the liver-related
burden of disease to obtain a more accurateassessment of the total burden of HCV infection
The OBJECTIVE of the study was to estimate the annual direct medical costsassociated with HCV related EHM in the EU5 (France Germany Italy United Kingdom
Spain)
Extrahepatic Manifestations of HCV
Extrahepatic Manifestations of HCV
HCV may cause extrahepatic disorders (HCV-EHDs) classified according to the number and
strength of supporting scientific data
HCV-EHDs are responsible for increasing morbidity and mortality with important
consequences in terms of social costs
The analysis of mortality rates in large cohorts confirmed the association of HCV with
several EHDs including cardiovascular neurologic metabolic or renal diseases and tumors
Viral eradication significantly reduced the rate of extra-hepatic deaths
Cacoub P et al DLD 2014 Lee MH et al J Infect Dis 2012 Backus LI et al Clin Gastroenterol Hepatol 2011 El-Kamary S et al
Clin Infect Dis 2011 Hsu YC et al Hepatology 2014 Kawamura Y et al Am J Med 2007 Adinolfi LE et al WJG 2014
Con il contributo di
Lee M-H et al J Infect Dis 2012206469-477
Follow-Up
(Years)
20
18
16
14
12
10
2
00 2 4 6 8 10 12 14 16 18 20
8
6
4
Follow-Up
(Years)
12
10
8
6
4
2
00 2 4 6 8 10 12 14 16 18 20
All Causes(n=2394)
Liver Cancer(n=115)
Extrahepatic Diseases(n=2199)
Cum
ula
tive M
ort
ali
ty (
)
Anti-HCV+ HCV RNA detectable Anti-HCV+ HCV RNA undetectable Anti-HCVndash
Follow-Up
(Years)
35
30
25
20
15
10
5
00 2 4 6 8 10 12 14 16 18 20
301
128124
104
16
03
198
122
110
Extrahepatic Manifestations of HCV
The annual costs (inpatient outpatient andpharmacy) associated with extrahepatic
manifestations of HCV were evaluated
Total direct medical costs of extrahepatic
manifestations of HCV in 2014 US dollars wereestimated to be $1506 million (range $922 millionndash
$2208 million in sensitivity analysis)
These estimates should be added to the liver-related
burden of disease to obtain a more accurateassessment of the total burden of HCV infection
Younossi et al
Younossi et al
Costs up to $71000 per patient per year (ESRD) Among the most frequent EHM depression (245 in HCV vs 172 in non-HCV) had estimated annual cost of
$4307 million DM (15 vs 10 in non- HCV) had an annual cost of $4434 million in the USA= given the importance of DM and
its association with CVDs and mortality the clinical and economic impacts of HCV-related DM are substantial
The OBJECTIVE of the study was to estimate the annual direct medical costsassociated with HCV related EHM in the EU5 (France Germany Italy United Kingdom
Spain)
The OBJECTIVE of the study was to estimate the annual direct medicalcosts associated with HCV related EHM in the EU5 (France Germany
Italy United Kingdom Spain)
1 HCV is the main etiopathological agent as concordantly demonstrated by epidemiological clinico-pathological virological and laboratory investigations2 the association between HCV and disease is demonstrated in a significant proportion of patients and supported by in depth clinico-pathogeneticstudies3 the association is suggested by cohort studies a possible causative role may be limited to a small number of patients andor possibly more relevant in specific geographical areas 4 a number of anecdotal observations suggested a possible role of HCV further investigations are required
The most studied and frequent HCV-EHDs are B-LPDs andor autoimmune disorders
Their prototype is Mixed Cryoglobulinemia (MC) from researches on MC derived most of the
available information
MC as a precious model for all the HCV-EHDs and to evaluate the effects of viral eradication
Anti-HCV Treatment Evolution
IFN
6 mos
PegIFN RBV 12
mos
IFN
12 mos
IFNRBV
12 mos
PegIFN
12 mos
2001
1998
2011
Standardinterferon
Ribavirin
Peginterferon
1991
Direct-actingantivirals
PegIFN
RBV
DAA
IFNRBV
6 mos
6
16
34
4239
55
70+
0
20
40
60
80
100
DAAs
826
weeks
gt90
2015
Few side effects absence major
contraindications
Younossi et al
The annual costs (inpatient outpatient and pharmacy) associatedwith extrahepatic manifestations of HCV were evaluated
Total direct medical costs of extrahepatic manifestations of HCV in 2014US dollars were estimated to be $1506 million (range $922 millionndash
$2208 million in sensitivity analysis)
These estimates should be added to the liver-related burden of diseaseto obtain a more accurate assessment of the total burden of HCV
infection
The OBJECTIVE of the study was to estimate the annual direct medical costs associated with HCV related EHM in the EU5 (France Germany Italy United Kingdom Spain)
22 MCS treated with DAAs including 2 HCC and 2 NHL 100 SVR12 Clinical CR in 64 and PR in remaining 36 The small lymphocytic lymphoma progressed despite viral clearance
Lauletta et al 2017
Emery CS et al 2017
Retrospective analysis 17 MCS (10 with severelife-threatening vasculitis) and 65 asymptomatic CGs+ pts treated with DAAs SVR 889 MCS and 908 asymptomatic pts In MCS clinical response in 1117 (complete in 717) In severelife-threatening vasculitis lower clinical response especially in renal and neurological symptoms
Saadoun D et al 2017
Open-label prospective multi-center study on sofosbuvir plus daclatasvir treatment of 41 HCV MCS SVR in100 and clinical CR in 902 Disappearance of CGs in 50 of pts No serious adverse event or relapse ofvasculitis
Antiviral Treatment (AVT) of MCIFN-free regimens
MC is clinically benign but sometimes severe HCV EHD invalidating symptoms occur and
it may evolve into lymphoma
Cacoub P et al DLD 2014 Zignego AL et al DLD 2007 Zignego AL et al Intern Emerg Med 2012 Zignego AL et al Clin Dev
Immunol 2012 Zignego AL et al Expert Rev Clin Immunol 2015 Sene D et al J Rheumatol 2004
Mixed Cryoglobulinemia-MC
MC pathological substrate is an HCV-driven B-cell
proliferation with consequent production of cryo- and non-
cryoprecipitable CICs in turn responsible for vasculitic
manifestations
Most (70ndash90) MC patients are HCV+ and HCV-patients are CGs+ (40ndash60) while 5ndash30 of
CGs+ have symptomatic MC or cryoglobulinemic vasculitis since HCV infects about 170
million individuals worldwide the number of patients at risk for developing MC is
substantial
Type II CGs
monoclonal
RF+policlonal IgG
Type III CGs both
RF and IgG
polyclonal

ANTIVIRAL THERAPY IS ASSOCIATED WITH A BETTERSURVIVAL IN PATIENTS WITH HCV AND B-CELL NON-HODGKIN LYMPHOMAS ANRS HC-13 LYMPHO-CSTUDYMichot JM et al
Outcomes of HCV-associated B-NHL according to HCV AVT in prospective patients only (n 5 64)
(A) absolute neutrophil count and Hgb
(B) ALT and HCV viral load
This patient had HCV-associated DLBCL achieving both complete response and SVR after concurrent chemoimmunotherapy and antiviral therapy using a sofosbuvir-basedregimen
Concurrent Systemic Chemoimmunotherapy and Sofosbuvir-Based Antiviral Treatment in a Hepatitis C Virus-Infected Patient With Diffuse Large B-Cell LymphomaEvan C Ewers et al 2016
HCV-EHDs are responsible for increasing morbidity and mortality with important
consequences in terms of social costs
The analysis of mortality rates in large cohorts confirmed the association of HCV with
several EHDs including cardiovascular neurologic metabolic or renal diseases and tumors
Viral eradication significantly reduced the rate of extra-hepatic deaths
Cacoub P et al DLD 2014 Lee MH et al J Infect Dis 2012 Backus LI et al Clin Gastroenterol Hepatol 2011 El-Kamary S et al
Clin Infect Dis 2011 Hsu YC et al Hepatology 2014 Kawamura Y et al Am J Med 2007 Adinolfi LE et al WJG 2014
Extrahepatic Manifestations of HCV
Con il contributo di
Lee M-H et al J Infect Dis 2012206469-477
Follow-Up
(Years)
20
18
16
14
12
10
2
00 2 4 6 8 10 12 14 16 18 20
8
6
4
Follow-Up
(Years)
12
10
8
6
4
2
00 2 4 6 8 10 12 14 16 18 20
All Causes(n=2394)
Liver Cancer(n=115)
Extrahepatic Diseases(n=2199)
Cum
ula
tive M
ort
ali
ty (
)
Anti-HCV+ HCV RNA detectable Anti-HCV+ HCV RNA undetectable Anti-HCVndash
Follow-Up
(Years)
35
30
25
20
15
10
5
00 2 4 6 8 10 12 14 16 18 20
301
128124
104
16
03
198
122
110
MC is clinically benign but sometimes severe HCV EHD invalidating symptoms occur and
it may evolve into lymphoma
Cacoub P et al DLD 2014 Zignego AL et al DLD 2007 Zignego AL et al Intern Emerg Med 2012 Zignego AL et al Clin Dev
Immunol 2012 Zignego AL et al Expert Rev Clin Immunol 2015 Sene D et al J Rheumatol 2004
Mixed Cryoglobulinemia-MC
CGs reversibly precipitate when the temperature is lower than 37degC and
comprise IgMs with RF activity [mono- or oligo-clonal in type II MC or
polyclonal in type III MC] and polyclonal IgGs
MC pathological substrate is an HCV-driven B-cell
proliferation with consequent production of cryo- and non-
cryoprecipitable CICs in turn responsible for vasculitic
manifestations
Most (70ndash90) MC patients are HCV+ and HCV-patients are CGs+ (40ndash60) while 5ndash30 of
CGs+ have symptomatic MC since HCV infects about 170 million individuals worldwide the
number of patients at risk for developing MC is substantial
Type II
CGs
Type III
CGs
Zignego AL et al Autoimmun Rev 2017 Ferri C et al Autoimmunity rev 2016 Zignego AL et al DLD 2007 Cacoub P et al DLD
2014 Zignego AL et al DLD 2007 Zignego AL et al Intern Emerg Med 2012 Zignego AL et al Clin Dev Immunol 2012 Zignego
AL et al Expert Rev Clin Immunol 2015
MC clinical aspects MC Syndrome
MCS is characterized by the clinical triad -purpura weakness and
arthralgias- low complement C4 and various organsystem
involvement including cutaneous articular renal neurological
cardiac or digestive
It ranges from mild disease to severe even life-threatening
conditions
More serious lesions are generally characterized by neurologic and
renal involvement
Prognosis is highly dependent on renal involvement or on the extent
of vasculitis lesions
1 HCV is the main etiopathological agent as concordantly demonstrated by epidemiological clinico-pathological virological and laboratory investigations2 the association between HCV and disease is demonstrated in a significant proportion of patients and supported by in depth clinico-pathogeneticstudies3 the association is suggested by cohort studies a possible causative role may be limited to a small number of patients andor possibly more relevant in specific geographical areas 4 a number of anecdotal observations suggested a possible role of HCV further investigations are required
From P Cacoub 2015
HCV infection is closely related to LPDs mostly MC
40 to 60 of HCV patients show circulating CGs among this latter population 5-30
develop a symptomatic CV
AVT has been considered the first-line option in HCV-CV patients in fact in the majority
of cases viral eradication leads to CV clinical remission
Data about IFN-free regimens for the treatment of CV patients are still limited
HCV and MC
HCV and MC
Zignego 2015Ferri 2016Pozzato 2016 Sise 2016Saadoun 2015Gragnani 2016Gragnani 2016
Bonacci 2016Hegazy 2016Kondili 2016Emery 2017
Younossi et al
The annual costs (inpatient outpatient andpharmacy) associated with extrahepatic
manifestations of HCV were evaluated
Total direct medical costs of extrahepatic
manifestations of HCV in 2014 US dollars wereestimated to be $1506 million (range $922 millionndash
$2208 million in sensitivity analysis)
These estimates should be added to the liver-related
burden of disease to obtain a more accurateassessment of the total burden of HCV infection
The OBJECTIVE of the study was to estimate the annual direct medical costsassociated with HCV related EHM in the EU5 (France Germany Italy United Kingdom
Spain)
Extrahepatic Manifestations of HCV
Extrahepatic Manifestations of HCV
HCV may cause extrahepatic disorders (HCV-EHDs) classified according to the number and
strength of supporting scientific data
HCV-EHDs are responsible for increasing morbidity and mortality with important
consequences in terms of social costs
The analysis of mortality rates in large cohorts confirmed the association of HCV with
several EHDs including cardiovascular neurologic metabolic or renal diseases and tumors
Viral eradication significantly reduced the rate of extra-hepatic deaths
Cacoub P et al DLD 2014 Lee MH et al J Infect Dis 2012 Backus LI et al Clin Gastroenterol Hepatol 2011 El-Kamary S et al
Clin Infect Dis 2011 Hsu YC et al Hepatology 2014 Kawamura Y et al Am J Med 2007 Adinolfi LE et al WJG 2014
Con il contributo di
Lee M-H et al J Infect Dis 2012206469-477
Follow-Up
(Years)
20
18
16
14
12
10
2
00 2 4 6 8 10 12 14 16 18 20
8
6
4
Follow-Up
(Years)
12
10
8
6
4
2
00 2 4 6 8 10 12 14 16 18 20
All Causes(n=2394)
Liver Cancer(n=115)
Extrahepatic Diseases(n=2199)
Cum
ula
tive M
ort
ali
ty (
)
Anti-HCV+ HCV RNA detectable Anti-HCV+ HCV RNA undetectable Anti-HCVndash
Follow-Up
(Years)
35
30
25
20
15
10
5
00 2 4 6 8 10 12 14 16 18 20
301
128124
104
16
03
198
122
110
Extrahepatic Manifestations of HCV
The annual costs (inpatient outpatient andpharmacy) associated with extrahepatic
manifestations of HCV were evaluated
Total direct medical costs of extrahepatic
manifestations of HCV in 2014 US dollars wereestimated to be $1506 million (range $922 millionndash
$2208 million in sensitivity analysis)
These estimates should be added to the liver-related
burden of disease to obtain a more accurateassessment of the total burden of HCV infection
Younossi et al
Younossi et al
Costs up to $71000 per patient per year (ESRD) Among the most frequent EHM depression (245 in HCV vs 172 in non-HCV) had estimated annual cost of
$4307 million DM (15 vs 10 in non- HCV) had an annual cost of $4434 million in the USA= given the importance of DM and
its association with CVDs and mortality the clinical and economic impacts of HCV-related DM are substantial
The OBJECTIVE of the study was to estimate the annual direct medical costsassociated with HCV related EHM in the EU5 (France Germany Italy United Kingdom
Spain)
The OBJECTIVE of the study was to estimate the annual direct medicalcosts associated with HCV related EHM in the EU5 (France Germany
Italy United Kingdom Spain)
1 HCV is the main etiopathological agent as concordantly demonstrated by epidemiological clinico-pathological virological and laboratory investigations2 the association between HCV and disease is demonstrated in a significant proportion of patients and supported by in depth clinico-pathogeneticstudies3 the association is suggested by cohort studies a possible causative role may be limited to a small number of patients andor possibly more relevant in specific geographical areas 4 a number of anecdotal observations suggested a possible role of HCV further investigations are required
The most studied and frequent HCV-EHDs are B-LPDs andor autoimmune disorders
Their prototype is Mixed Cryoglobulinemia (MC) from researches on MC derived most of the
available information
MC as a precious model for all the HCV-EHDs and to evaluate the effects of viral eradication
Anti-HCV Treatment Evolution
IFN
6 mos
PegIFN RBV 12
mos
IFN
12 mos
IFNRBV
12 mos
PegIFN
12 mos
2001
1998
2011
Standardinterferon
Ribavirin
Peginterferon
1991
Direct-actingantivirals
PegIFN
RBV
DAA
IFNRBV
6 mos
6
16
34
4239
55
70+
0
20
40
60
80
100
DAAs
826
weeks
gt90
2015
Few side effects absence major
contraindications
Younossi et al
The annual costs (inpatient outpatient and pharmacy) associatedwith extrahepatic manifestations of HCV were evaluated
Total direct medical costs of extrahepatic manifestations of HCV in 2014US dollars were estimated to be $1506 million (range $922 millionndash
$2208 million in sensitivity analysis)
These estimates should be added to the liver-related burden of diseaseto obtain a more accurate assessment of the total burden of HCV
infection
The OBJECTIVE of the study was to estimate the annual direct medical costs associated with HCV related EHM in the EU5 (France Germany Italy United Kingdom Spain)
22 MCS treated with DAAs including 2 HCC and 2 NHL 100 SVR12 Clinical CR in 64 and PR in remaining 36 The small lymphocytic lymphoma progressed despite viral clearance
Lauletta et al 2017
Emery CS et al 2017
Retrospective analysis 17 MCS (10 with severelife-threatening vasculitis) and 65 asymptomatic CGs+ pts treated with DAAs SVR 889 MCS and 908 asymptomatic pts In MCS clinical response in 1117 (complete in 717) In severelife-threatening vasculitis lower clinical response especially in renal and neurological symptoms
Saadoun D et al 2017
Open-label prospective multi-center study on sofosbuvir plus daclatasvir treatment of 41 HCV MCS SVR in100 and clinical CR in 902 Disappearance of CGs in 50 of pts No serious adverse event or relapse ofvasculitis
Antiviral Treatment (AVT) of MCIFN-free regimens
MC is clinically benign but sometimes severe HCV EHD invalidating symptoms occur and
it may evolve into lymphoma
Cacoub P et al DLD 2014 Zignego AL et al DLD 2007 Zignego AL et al Intern Emerg Med 2012 Zignego AL et al Clin Dev
Immunol 2012 Zignego AL et al Expert Rev Clin Immunol 2015 Sene D et al J Rheumatol 2004
Mixed Cryoglobulinemia-MC
MC pathological substrate is an HCV-driven B-cell
proliferation with consequent production of cryo- and non-
cryoprecipitable CICs in turn responsible for vasculitic
manifestations
Most (70ndash90) MC patients are HCV+ and HCV-patients are CGs+ (40ndash60) while 5ndash30 of
CGs+ have symptomatic MC or cryoglobulinemic vasculitis since HCV infects about 170
million individuals worldwide the number of patients at risk for developing MC is
substantial
Type II CGs
monoclonal
RF+policlonal IgG
Type III CGs both
RF and IgG
polyclonal

(A) absolute neutrophil count and Hgb
(B) ALT and HCV viral load
This patient had HCV-associated DLBCL achieving both complete response and SVR after concurrent chemoimmunotherapy and antiviral therapy using a sofosbuvir-basedregimen
Concurrent Systemic Chemoimmunotherapy and Sofosbuvir-Based Antiviral Treatment in a Hepatitis C Virus-Infected Patient With Diffuse Large B-Cell LymphomaEvan C Ewers et al 2016
HCV-EHDs are responsible for increasing morbidity and mortality with important
consequences in terms of social costs
The analysis of mortality rates in large cohorts confirmed the association of HCV with
several EHDs including cardiovascular neurologic metabolic or renal diseases and tumors
Viral eradication significantly reduced the rate of extra-hepatic deaths
Cacoub P et al DLD 2014 Lee MH et al J Infect Dis 2012 Backus LI et al Clin Gastroenterol Hepatol 2011 El-Kamary S et al
Clin Infect Dis 2011 Hsu YC et al Hepatology 2014 Kawamura Y et al Am J Med 2007 Adinolfi LE et al WJG 2014
Extrahepatic Manifestations of HCV
Con il contributo di
Lee M-H et al J Infect Dis 2012206469-477
Follow-Up
(Years)
20
18
16
14
12
10
2
00 2 4 6 8 10 12 14 16 18 20
8
6
4
Follow-Up
(Years)
12
10
8
6
4
2
00 2 4 6 8 10 12 14 16 18 20
All Causes(n=2394)
Liver Cancer(n=115)
Extrahepatic Diseases(n=2199)
Cum
ula
tive M
ort
ali
ty (
)
Anti-HCV+ HCV RNA detectable Anti-HCV+ HCV RNA undetectable Anti-HCVndash
Follow-Up
(Years)
35
30
25
20
15
10
5
00 2 4 6 8 10 12 14 16 18 20
301
128124
104
16
03
198
122
110
MC is clinically benign but sometimes severe HCV EHD invalidating symptoms occur and
it may evolve into lymphoma
Cacoub P et al DLD 2014 Zignego AL et al DLD 2007 Zignego AL et al Intern Emerg Med 2012 Zignego AL et al Clin Dev
Immunol 2012 Zignego AL et al Expert Rev Clin Immunol 2015 Sene D et al J Rheumatol 2004
Mixed Cryoglobulinemia-MC
CGs reversibly precipitate when the temperature is lower than 37degC and
comprise IgMs with RF activity [mono- or oligo-clonal in type II MC or
polyclonal in type III MC] and polyclonal IgGs
MC pathological substrate is an HCV-driven B-cell
proliferation with consequent production of cryo- and non-
cryoprecipitable CICs in turn responsible for vasculitic
manifestations
Most (70ndash90) MC patients are HCV+ and HCV-patients are CGs+ (40ndash60) while 5ndash30 of
CGs+ have symptomatic MC since HCV infects about 170 million individuals worldwide the
number of patients at risk for developing MC is substantial
Type II
CGs
Type III
CGs
Zignego AL et al Autoimmun Rev 2017 Ferri C et al Autoimmunity rev 2016 Zignego AL et al DLD 2007 Cacoub P et al DLD
2014 Zignego AL et al DLD 2007 Zignego AL et al Intern Emerg Med 2012 Zignego AL et al Clin Dev Immunol 2012 Zignego
AL et al Expert Rev Clin Immunol 2015
MC clinical aspects MC Syndrome
MCS is characterized by the clinical triad -purpura weakness and
arthralgias- low complement C4 and various organsystem
involvement including cutaneous articular renal neurological
cardiac or digestive
It ranges from mild disease to severe even life-threatening
conditions
More serious lesions are generally characterized by neurologic and
renal involvement
Prognosis is highly dependent on renal involvement or on the extent
of vasculitis lesions
1 HCV is the main etiopathological agent as concordantly demonstrated by epidemiological clinico-pathological virological and laboratory investigations2 the association between HCV and disease is demonstrated in a significant proportion of patients and supported by in depth clinico-pathogeneticstudies3 the association is suggested by cohort studies a possible causative role may be limited to a small number of patients andor possibly more relevant in specific geographical areas 4 a number of anecdotal observations suggested a possible role of HCV further investigations are required
From P Cacoub 2015
HCV infection is closely related to LPDs mostly MC
40 to 60 of HCV patients show circulating CGs among this latter population 5-30
develop a symptomatic CV
AVT has been considered the first-line option in HCV-CV patients in fact in the majority
of cases viral eradication leads to CV clinical remission
Data about IFN-free regimens for the treatment of CV patients are still limited
HCV and MC
HCV and MC
Zignego 2015Ferri 2016Pozzato 2016 Sise 2016Saadoun 2015Gragnani 2016Gragnani 2016
Bonacci 2016Hegazy 2016Kondili 2016Emery 2017
Younossi et al
The annual costs (inpatient outpatient andpharmacy) associated with extrahepatic
manifestations of HCV were evaluated
Total direct medical costs of extrahepatic
manifestations of HCV in 2014 US dollars wereestimated to be $1506 million (range $922 millionndash
$2208 million in sensitivity analysis)
These estimates should be added to the liver-related
burden of disease to obtain a more accurateassessment of the total burden of HCV infection
The OBJECTIVE of the study was to estimate the annual direct medical costsassociated with HCV related EHM in the EU5 (France Germany Italy United Kingdom
Spain)
Extrahepatic Manifestations of HCV
Extrahepatic Manifestations of HCV
HCV may cause extrahepatic disorders (HCV-EHDs) classified according to the number and
strength of supporting scientific data
HCV-EHDs are responsible for increasing morbidity and mortality with important
consequences in terms of social costs
The analysis of mortality rates in large cohorts confirmed the association of HCV with
several EHDs including cardiovascular neurologic metabolic or renal diseases and tumors
Viral eradication significantly reduced the rate of extra-hepatic deaths
Cacoub P et al DLD 2014 Lee MH et al J Infect Dis 2012 Backus LI et al Clin Gastroenterol Hepatol 2011 El-Kamary S et al
Clin Infect Dis 2011 Hsu YC et al Hepatology 2014 Kawamura Y et al Am J Med 2007 Adinolfi LE et al WJG 2014
Con il contributo di
Lee M-H et al J Infect Dis 2012206469-477
Follow-Up
(Years)
20
18
16
14
12
10
2
00 2 4 6 8 10 12 14 16 18 20
8
6
4
Follow-Up
(Years)
12
10
8
6
4
2
00 2 4 6 8 10 12 14 16 18 20
All Causes(n=2394)
Liver Cancer(n=115)
Extrahepatic Diseases(n=2199)
Cum
ula
tive M
ort
ali
ty (
)
Anti-HCV+ HCV RNA detectable Anti-HCV+ HCV RNA undetectable Anti-HCVndash
Follow-Up
(Years)
35
30
25
20
15
10
5
00 2 4 6 8 10 12 14 16 18 20
301
128124
104
16
03
198
122
110
Extrahepatic Manifestations of HCV
The annual costs (inpatient outpatient andpharmacy) associated with extrahepatic
manifestations of HCV were evaluated
Total direct medical costs of extrahepatic
manifestations of HCV in 2014 US dollars wereestimated to be $1506 million (range $922 millionndash
$2208 million in sensitivity analysis)
These estimates should be added to the liver-related
burden of disease to obtain a more accurateassessment of the total burden of HCV infection
Younossi et al
Younossi et al
Costs up to $71000 per patient per year (ESRD) Among the most frequent EHM depression (245 in HCV vs 172 in non-HCV) had estimated annual cost of
$4307 million DM (15 vs 10 in non- HCV) had an annual cost of $4434 million in the USA= given the importance of DM and
its association with CVDs and mortality the clinical and economic impacts of HCV-related DM are substantial
The OBJECTIVE of the study was to estimate the annual direct medical costsassociated with HCV related EHM in the EU5 (France Germany Italy United Kingdom
Spain)
The OBJECTIVE of the study was to estimate the annual direct medicalcosts associated with HCV related EHM in the EU5 (France Germany
Italy United Kingdom Spain)
1 HCV is the main etiopathological agent as concordantly demonstrated by epidemiological clinico-pathological virological and laboratory investigations2 the association between HCV and disease is demonstrated in a significant proportion of patients and supported by in depth clinico-pathogeneticstudies3 the association is suggested by cohort studies a possible causative role may be limited to a small number of patients andor possibly more relevant in specific geographical areas 4 a number of anecdotal observations suggested a possible role of HCV further investigations are required
The most studied and frequent HCV-EHDs are B-LPDs andor autoimmune disorders
Their prototype is Mixed Cryoglobulinemia (MC) from researches on MC derived most of the
available information
MC as a precious model for all the HCV-EHDs and to evaluate the effects of viral eradication
Anti-HCV Treatment Evolution
IFN
6 mos
PegIFN RBV 12
mos
IFN
12 mos
IFNRBV
12 mos
PegIFN
12 mos
2001
1998
2011
Standardinterferon
Ribavirin
Peginterferon
1991
Direct-actingantivirals
PegIFN
RBV
DAA
IFNRBV
6 mos
6
16
34
4239
55
70+
0
20
40
60
80
100
DAAs
826
weeks
gt90
2015
Few side effects absence major
contraindications
Younossi et al
The annual costs (inpatient outpatient and pharmacy) associatedwith extrahepatic manifestations of HCV were evaluated
Total direct medical costs of extrahepatic manifestations of HCV in 2014US dollars were estimated to be $1506 million (range $922 millionndash
$2208 million in sensitivity analysis)
These estimates should be added to the liver-related burden of diseaseto obtain a more accurate assessment of the total burden of HCV
infection
The OBJECTIVE of the study was to estimate the annual direct medical costs associated with HCV related EHM in the EU5 (France Germany Italy United Kingdom Spain)
22 MCS treated with DAAs including 2 HCC and 2 NHL 100 SVR12 Clinical CR in 64 and PR in remaining 36 The small lymphocytic lymphoma progressed despite viral clearance
Lauletta et al 2017
Emery CS et al 2017
Retrospective analysis 17 MCS (10 with severelife-threatening vasculitis) and 65 asymptomatic CGs+ pts treated with DAAs SVR 889 MCS and 908 asymptomatic pts In MCS clinical response in 1117 (complete in 717) In severelife-threatening vasculitis lower clinical response especially in renal and neurological symptoms
Saadoun D et al 2017
Open-label prospective multi-center study on sofosbuvir plus daclatasvir treatment of 41 HCV MCS SVR in100 and clinical CR in 902 Disappearance of CGs in 50 of pts No serious adverse event or relapse ofvasculitis
Antiviral Treatment (AVT) of MCIFN-free regimens
MC is clinically benign but sometimes severe HCV EHD invalidating symptoms occur and
it may evolve into lymphoma
Cacoub P et al DLD 2014 Zignego AL et al DLD 2007 Zignego AL et al Intern Emerg Med 2012 Zignego AL et al Clin Dev
Immunol 2012 Zignego AL et al Expert Rev Clin Immunol 2015 Sene D et al J Rheumatol 2004
Mixed Cryoglobulinemia-MC
MC pathological substrate is an HCV-driven B-cell
proliferation with consequent production of cryo- and non-
cryoprecipitable CICs in turn responsible for vasculitic
manifestations
Most (70ndash90) MC patients are HCV+ and HCV-patients are CGs+ (40ndash60) while 5ndash30 of
CGs+ have symptomatic MC or cryoglobulinemic vasculitis since HCV infects about 170
million individuals worldwide the number of patients at risk for developing MC is
substantial
Type II CGs
monoclonal
RF+policlonal IgG
Type III CGs both
RF and IgG
polyclonal

HCV-EHDs are responsible for increasing morbidity and mortality with important
consequences in terms of social costs
The analysis of mortality rates in large cohorts confirmed the association of HCV with
several EHDs including cardiovascular neurologic metabolic or renal diseases and tumors
Viral eradication significantly reduced the rate of extra-hepatic deaths
Cacoub P et al DLD 2014 Lee MH et al J Infect Dis 2012 Backus LI et al Clin Gastroenterol Hepatol 2011 El-Kamary S et al
Clin Infect Dis 2011 Hsu YC et al Hepatology 2014 Kawamura Y et al Am J Med 2007 Adinolfi LE et al WJG 2014
Extrahepatic Manifestations of HCV
Con il contributo di
Lee M-H et al J Infect Dis 2012206469-477
Follow-Up
(Years)
20
18
16
14
12
10
2
00 2 4 6 8 10 12 14 16 18 20
8
6
4
Follow-Up
(Years)
12
10
8
6
4
2
00 2 4 6 8 10 12 14 16 18 20
All Causes(n=2394)
Liver Cancer(n=115)
Extrahepatic Diseases(n=2199)
Cum
ula
tive M
ort
ali
ty (
)
Anti-HCV+ HCV RNA detectable Anti-HCV+ HCV RNA undetectable Anti-HCVndash
Follow-Up
(Years)
35
30
25
20
15
10
5
00 2 4 6 8 10 12 14 16 18 20
301
128124
104
16
03
198
122
110
MC is clinically benign but sometimes severe HCV EHD invalidating symptoms occur and
it may evolve into lymphoma
Cacoub P et al DLD 2014 Zignego AL et al DLD 2007 Zignego AL et al Intern Emerg Med 2012 Zignego AL et al Clin Dev
Immunol 2012 Zignego AL et al Expert Rev Clin Immunol 2015 Sene D et al J Rheumatol 2004
Mixed Cryoglobulinemia-MC
CGs reversibly precipitate when the temperature is lower than 37degC and
comprise IgMs with RF activity [mono- or oligo-clonal in type II MC or
polyclonal in type III MC] and polyclonal IgGs
MC pathological substrate is an HCV-driven B-cell
proliferation with consequent production of cryo- and non-
cryoprecipitable CICs in turn responsible for vasculitic
manifestations
Most (70ndash90) MC patients are HCV+ and HCV-patients are CGs+ (40ndash60) while 5ndash30 of
CGs+ have symptomatic MC since HCV infects about 170 million individuals worldwide the
number of patients at risk for developing MC is substantial
Type II
CGs
Type III
CGs
Zignego AL et al Autoimmun Rev 2017 Ferri C et al Autoimmunity rev 2016 Zignego AL et al DLD 2007 Cacoub P et al DLD
2014 Zignego AL et al DLD 2007 Zignego AL et al Intern Emerg Med 2012 Zignego AL et al Clin Dev Immunol 2012 Zignego
AL et al Expert Rev Clin Immunol 2015
MC clinical aspects MC Syndrome
MCS is characterized by the clinical triad -purpura weakness and
arthralgias- low complement C4 and various organsystem
involvement including cutaneous articular renal neurological
cardiac or digestive
It ranges from mild disease to severe even life-threatening
conditions
More serious lesions are generally characterized by neurologic and
renal involvement
Prognosis is highly dependent on renal involvement or on the extent
of vasculitis lesions
1 HCV is the main etiopathological agent as concordantly demonstrated by epidemiological clinico-pathological virological and laboratory investigations2 the association between HCV and disease is demonstrated in a significant proportion of patients and supported by in depth clinico-pathogeneticstudies3 the association is suggested by cohort studies a possible causative role may be limited to a small number of patients andor possibly more relevant in specific geographical areas 4 a number of anecdotal observations suggested a possible role of HCV further investigations are required
From P Cacoub 2015
HCV infection is closely related to LPDs mostly MC
40 to 60 of HCV patients show circulating CGs among this latter population 5-30
develop a symptomatic CV
AVT has been considered the first-line option in HCV-CV patients in fact in the majority
of cases viral eradication leads to CV clinical remission
Data about IFN-free regimens for the treatment of CV patients are still limited
HCV and MC
HCV and MC
Zignego 2015Ferri 2016Pozzato 2016 Sise 2016Saadoun 2015Gragnani 2016Gragnani 2016
Bonacci 2016Hegazy 2016Kondili 2016Emery 2017
Younossi et al
The annual costs (inpatient outpatient andpharmacy) associated with extrahepatic
manifestations of HCV were evaluated
Total direct medical costs of extrahepatic
manifestations of HCV in 2014 US dollars wereestimated to be $1506 million (range $922 millionndash
$2208 million in sensitivity analysis)
These estimates should be added to the liver-related
burden of disease to obtain a more accurateassessment of the total burden of HCV infection
The OBJECTIVE of the study was to estimate the annual direct medical costsassociated with HCV related EHM in the EU5 (France Germany Italy United Kingdom
Spain)
Extrahepatic Manifestations of HCV
Extrahepatic Manifestations of HCV
HCV may cause extrahepatic disorders (HCV-EHDs) classified according to the number and
strength of supporting scientific data
HCV-EHDs are responsible for increasing morbidity and mortality with important
consequences in terms of social costs
The analysis of mortality rates in large cohorts confirmed the association of HCV with
several EHDs including cardiovascular neurologic metabolic or renal diseases and tumors
Viral eradication significantly reduced the rate of extra-hepatic deaths
Cacoub P et al DLD 2014 Lee MH et al J Infect Dis 2012 Backus LI et al Clin Gastroenterol Hepatol 2011 El-Kamary S et al
Clin Infect Dis 2011 Hsu YC et al Hepatology 2014 Kawamura Y et al Am J Med 2007 Adinolfi LE et al WJG 2014
Con il contributo di
Lee M-H et al J Infect Dis 2012206469-477
Follow-Up
(Years)
20
18
16
14
12
10
2
00 2 4 6 8 10 12 14 16 18 20
8
6
4
Follow-Up
(Years)
12
10
8
6
4
2
00 2 4 6 8 10 12 14 16 18 20
All Causes(n=2394)
Liver Cancer(n=115)
Extrahepatic Diseases(n=2199)
Cum
ula
tive M
ort
ali
ty (
)
Anti-HCV+ HCV RNA detectable Anti-HCV+ HCV RNA undetectable Anti-HCVndash
Follow-Up
(Years)
35
30
25
20
15
10
5
00 2 4 6 8 10 12 14 16 18 20
301
128124
104
16
03
198
122
110
Extrahepatic Manifestations of HCV
The annual costs (inpatient outpatient andpharmacy) associated with extrahepatic
manifestations of HCV were evaluated
Total direct medical costs of extrahepatic
manifestations of HCV in 2014 US dollars wereestimated to be $1506 million (range $922 millionndash
$2208 million in sensitivity analysis)
These estimates should be added to the liver-related
burden of disease to obtain a more accurateassessment of the total burden of HCV infection
Younossi et al
Younossi et al
Costs up to $71000 per patient per year (ESRD) Among the most frequent EHM depression (245 in HCV vs 172 in non-HCV) had estimated annual cost of
$4307 million DM (15 vs 10 in non- HCV) had an annual cost of $4434 million in the USA= given the importance of DM and
its association with CVDs and mortality the clinical and economic impacts of HCV-related DM are substantial
The OBJECTIVE of the study was to estimate the annual direct medical costsassociated with HCV related EHM in the EU5 (France Germany Italy United Kingdom
Spain)
The OBJECTIVE of the study was to estimate the annual direct medicalcosts associated with HCV related EHM in the EU5 (France Germany
Italy United Kingdom Spain)
1 HCV is the main etiopathological agent as concordantly demonstrated by epidemiological clinico-pathological virological and laboratory investigations2 the association between HCV and disease is demonstrated in a significant proportion of patients and supported by in depth clinico-pathogeneticstudies3 the association is suggested by cohort studies a possible causative role may be limited to a small number of patients andor possibly more relevant in specific geographical areas 4 a number of anecdotal observations suggested a possible role of HCV further investigations are required
The most studied and frequent HCV-EHDs are B-LPDs andor autoimmune disorders
Their prototype is Mixed Cryoglobulinemia (MC) from researches on MC derived most of the
available information
MC as a precious model for all the HCV-EHDs and to evaluate the effects of viral eradication
Anti-HCV Treatment Evolution
IFN
6 mos
PegIFN RBV 12
mos
IFN
12 mos
IFNRBV
12 mos
PegIFN
12 mos
2001
1998
2011
Standardinterferon
Ribavirin
Peginterferon
1991
Direct-actingantivirals
PegIFN
RBV
DAA
IFNRBV
6 mos
6
16
34
4239
55
70+
0
20
40
60
80
100
DAAs
826
weeks
gt90
2015
Few side effects absence major
contraindications
Younossi et al
The annual costs (inpatient outpatient and pharmacy) associatedwith extrahepatic manifestations of HCV were evaluated
Total direct medical costs of extrahepatic manifestations of HCV in 2014US dollars were estimated to be $1506 million (range $922 millionndash
$2208 million in sensitivity analysis)
These estimates should be added to the liver-related burden of diseaseto obtain a more accurate assessment of the total burden of HCV
infection
The OBJECTIVE of the study was to estimate the annual direct medical costs associated with HCV related EHM in the EU5 (France Germany Italy United Kingdom Spain)
22 MCS treated with DAAs including 2 HCC and 2 NHL 100 SVR12 Clinical CR in 64 and PR in remaining 36 The small lymphocytic lymphoma progressed despite viral clearance
Lauletta et al 2017
Emery CS et al 2017
Retrospective analysis 17 MCS (10 with severelife-threatening vasculitis) and 65 asymptomatic CGs+ pts treated with DAAs SVR 889 MCS and 908 asymptomatic pts In MCS clinical response in 1117 (complete in 717) In severelife-threatening vasculitis lower clinical response especially in renal and neurological symptoms
Saadoun D et al 2017
Open-label prospective multi-center study on sofosbuvir plus daclatasvir treatment of 41 HCV MCS SVR in100 and clinical CR in 902 Disappearance of CGs in 50 of pts No serious adverse event or relapse ofvasculitis
Antiviral Treatment (AVT) of MCIFN-free regimens
MC is clinically benign but sometimes severe HCV EHD invalidating symptoms occur and
it may evolve into lymphoma
Cacoub P et al DLD 2014 Zignego AL et al DLD 2007 Zignego AL et al Intern Emerg Med 2012 Zignego AL et al Clin Dev
Immunol 2012 Zignego AL et al Expert Rev Clin Immunol 2015 Sene D et al J Rheumatol 2004
Mixed Cryoglobulinemia-MC
MC pathological substrate is an HCV-driven B-cell
proliferation with consequent production of cryo- and non-
cryoprecipitable CICs in turn responsible for vasculitic
manifestations
Most (70ndash90) MC patients are HCV+ and HCV-patients are CGs+ (40ndash60) while 5ndash30 of
CGs+ have symptomatic MC or cryoglobulinemic vasculitis since HCV infects about 170
million individuals worldwide the number of patients at risk for developing MC is
substantial
Type II CGs
monoclonal
RF+policlonal IgG
Type III CGs both
RF and IgG
polyclonal

MC is clinically benign but sometimes severe HCV EHD invalidating symptoms occur and
it may evolve into lymphoma
Cacoub P et al DLD 2014 Zignego AL et al DLD 2007 Zignego AL et al Intern Emerg Med 2012 Zignego AL et al Clin Dev
Immunol 2012 Zignego AL et al Expert Rev Clin Immunol 2015 Sene D et al J Rheumatol 2004
Mixed Cryoglobulinemia-MC
CGs reversibly precipitate when the temperature is lower than 37degC and
comprise IgMs with RF activity [mono- or oligo-clonal in type II MC or
polyclonal in type III MC] and polyclonal IgGs
MC pathological substrate is an HCV-driven B-cell
proliferation with consequent production of cryo- and non-
cryoprecipitable CICs in turn responsible for vasculitic
manifestations
Most (70ndash90) MC patients are HCV+ and HCV-patients are CGs+ (40ndash60) while 5ndash30 of
CGs+ have symptomatic MC since HCV infects about 170 million individuals worldwide the
number of patients at risk for developing MC is substantial
Type II
CGs
Type III
CGs
Zignego AL et al Autoimmun Rev 2017 Ferri C et al Autoimmunity rev 2016 Zignego AL et al DLD 2007 Cacoub P et al DLD
2014 Zignego AL et al DLD 2007 Zignego AL et al Intern Emerg Med 2012 Zignego AL et al Clin Dev Immunol 2012 Zignego
AL et al Expert Rev Clin Immunol 2015
MC clinical aspects MC Syndrome
MCS is characterized by the clinical triad -purpura weakness and
arthralgias- low complement C4 and various organsystem
involvement including cutaneous articular renal neurological
cardiac or digestive
It ranges from mild disease to severe even life-threatening
conditions
More serious lesions are generally characterized by neurologic and
renal involvement
Prognosis is highly dependent on renal involvement or on the extent
of vasculitis lesions
1 HCV is the main etiopathological agent as concordantly demonstrated by epidemiological clinico-pathological virological and laboratory investigations2 the association between HCV and disease is demonstrated in a significant proportion of patients and supported by in depth clinico-pathogeneticstudies3 the association is suggested by cohort studies a possible causative role may be limited to a small number of patients andor possibly more relevant in specific geographical areas 4 a number of anecdotal observations suggested a possible role of HCV further investigations are required
From P Cacoub 2015
HCV infection is closely related to LPDs mostly MC
40 to 60 of HCV patients show circulating CGs among this latter population 5-30
develop a symptomatic CV
AVT has been considered the first-line option in HCV-CV patients in fact in the majority
of cases viral eradication leads to CV clinical remission
Data about IFN-free regimens for the treatment of CV patients are still limited
HCV and MC
HCV and MC
Zignego 2015Ferri 2016Pozzato 2016 Sise 2016Saadoun 2015Gragnani 2016Gragnani 2016
Bonacci 2016Hegazy 2016Kondili 2016Emery 2017
Younossi et al
The annual costs (inpatient outpatient andpharmacy) associated with extrahepatic
manifestations of HCV were evaluated
Total direct medical costs of extrahepatic
manifestations of HCV in 2014 US dollars wereestimated to be $1506 million (range $922 millionndash
$2208 million in sensitivity analysis)
These estimates should be added to the liver-related
burden of disease to obtain a more accurateassessment of the total burden of HCV infection
The OBJECTIVE of the study was to estimate the annual direct medical costsassociated with HCV related EHM in the EU5 (France Germany Italy United Kingdom
Spain)
Extrahepatic Manifestations of HCV
Extrahepatic Manifestations of HCV
HCV may cause extrahepatic disorders (HCV-EHDs) classified according to the number and
strength of supporting scientific data
HCV-EHDs are responsible for increasing morbidity and mortality with important
consequences in terms of social costs
The analysis of mortality rates in large cohorts confirmed the association of HCV with
several EHDs including cardiovascular neurologic metabolic or renal diseases and tumors
Viral eradication significantly reduced the rate of extra-hepatic deaths
Cacoub P et al DLD 2014 Lee MH et al J Infect Dis 2012 Backus LI et al Clin Gastroenterol Hepatol 2011 El-Kamary S et al
Clin Infect Dis 2011 Hsu YC et al Hepatology 2014 Kawamura Y et al Am J Med 2007 Adinolfi LE et al WJG 2014
Con il contributo di
Lee M-H et al J Infect Dis 2012206469-477
Follow-Up
(Years)
20
18
16
14
12
10
2
00 2 4 6 8 10 12 14 16 18 20
8
6
4
Follow-Up
(Years)
12
10
8
6
4
2
00 2 4 6 8 10 12 14 16 18 20
All Causes(n=2394)
Liver Cancer(n=115)
Extrahepatic Diseases(n=2199)
Cum
ula
tive M
ort
ali
ty (
)
Anti-HCV+ HCV RNA detectable Anti-HCV+ HCV RNA undetectable Anti-HCVndash
Follow-Up
(Years)
35
30
25
20
15
10
5
00 2 4 6 8 10 12 14 16 18 20
301
128124
104
16
03
198
122
110
Extrahepatic Manifestations of HCV
The annual costs (inpatient outpatient andpharmacy) associated with extrahepatic
manifestations of HCV were evaluated
Total direct medical costs of extrahepatic
manifestations of HCV in 2014 US dollars wereestimated to be $1506 million (range $922 millionndash
$2208 million in sensitivity analysis)
These estimates should be added to the liver-related
burden of disease to obtain a more accurateassessment of the total burden of HCV infection
Younossi et al
Younossi et al
Costs up to $71000 per patient per year (ESRD) Among the most frequent EHM depression (245 in HCV vs 172 in non-HCV) had estimated annual cost of
$4307 million DM (15 vs 10 in non- HCV) had an annual cost of $4434 million in the USA= given the importance of DM and
its association with CVDs and mortality the clinical and economic impacts of HCV-related DM are substantial
The OBJECTIVE of the study was to estimate the annual direct medical costsassociated with HCV related EHM in the EU5 (France Germany Italy United Kingdom
Spain)
The OBJECTIVE of the study was to estimate the annual direct medicalcosts associated with HCV related EHM in the EU5 (France Germany
Italy United Kingdom Spain)
1 HCV is the main etiopathological agent as concordantly demonstrated by epidemiological clinico-pathological virological and laboratory investigations2 the association between HCV and disease is demonstrated in a significant proportion of patients and supported by in depth clinico-pathogeneticstudies3 the association is suggested by cohort studies a possible causative role may be limited to a small number of patients andor possibly more relevant in specific geographical areas 4 a number of anecdotal observations suggested a possible role of HCV further investigations are required
The most studied and frequent HCV-EHDs are B-LPDs andor autoimmune disorders
Their prototype is Mixed Cryoglobulinemia (MC) from researches on MC derived most of the
available information
MC as a precious model for all the HCV-EHDs and to evaluate the effects of viral eradication
Anti-HCV Treatment Evolution
IFN
6 mos
PegIFN RBV 12
mos
IFN
12 mos
IFNRBV
12 mos
PegIFN
12 mos
2001
1998
2011
Standardinterferon
Ribavirin
Peginterferon
1991
Direct-actingantivirals
PegIFN
RBV
DAA
IFNRBV
6 mos
6
16
34
4239
55
70+
0
20
40
60
80
100
DAAs
826
weeks
gt90
2015
Few side effects absence major
contraindications
Younossi et al
The annual costs (inpatient outpatient and pharmacy) associatedwith extrahepatic manifestations of HCV were evaluated
Total direct medical costs of extrahepatic manifestations of HCV in 2014US dollars were estimated to be $1506 million (range $922 millionndash
$2208 million in sensitivity analysis)
These estimates should be added to the liver-related burden of diseaseto obtain a more accurate assessment of the total burden of HCV
infection
The OBJECTIVE of the study was to estimate the annual direct medical costs associated with HCV related EHM in the EU5 (France Germany Italy United Kingdom Spain)
22 MCS treated with DAAs including 2 HCC and 2 NHL 100 SVR12 Clinical CR in 64 and PR in remaining 36 The small lymphocytic lymphoma progressed despite viral clearance
Lauletta et al 2017
Emery CS et al 2017
Retrospective analysis 17 MCS (10 with severelife-threatening vasculitis) and 65 asymptomatic CGs+ pts treated with DAAs SVR 889 MCS and 908 asymptomatic pts In MCS clinical response in 1117 (complete in 717) In severelife-threatening vasculitis lower clinical response especially in renal and neurological symptoms
Saadoun D et al 2017
Open-label prospective multi-center study on sofosbuvir plus daclatasvir treatment of 41 HCV MCS SVR in100 and clinical CR in 902 Disappearance of CGs in 50 of pts No serious adverse event or relapse ofvasculitis
Antiviral Treatment (AVT) of MCIFN-free regimens
MC is clinically benign but sometimes severe HCV EHD invalidating symptoms occur and
it may evolve into lymphoma
Cacoub P et al DLD 2014 Zignego AL et al DLD 2007 Zignego AL et al Intern Emerg Med 2012 Zignego AL et al Clin Dev
Immunol 2012 Zignego AL et al Expert Rev Clin Immunol 2015 Sene D et al J Rheumatol 2004
Mixed Cryoglobulinemia-MC
MC pathological substrate is an HCV-driven B-cell
proliferation with consequent production of cryo- and non-
cryoprecipitable CICs in turn responsible for vasculitic
manifestations
Most (70ndash90) MC patients are HCV+ and HCV-patients are CGs+ (40ndash60) while 5ndash30 of
CGs+ have symptomatic MC or cryoglobulinemic vasculitis since HCV infects about 170
million individuals worldwide the number of patients at risk for developing MC is
substantial
Type II CGs
monoclonal
RF+policlonal IgG
Type III CGs both
RF and IgG
polyclonal
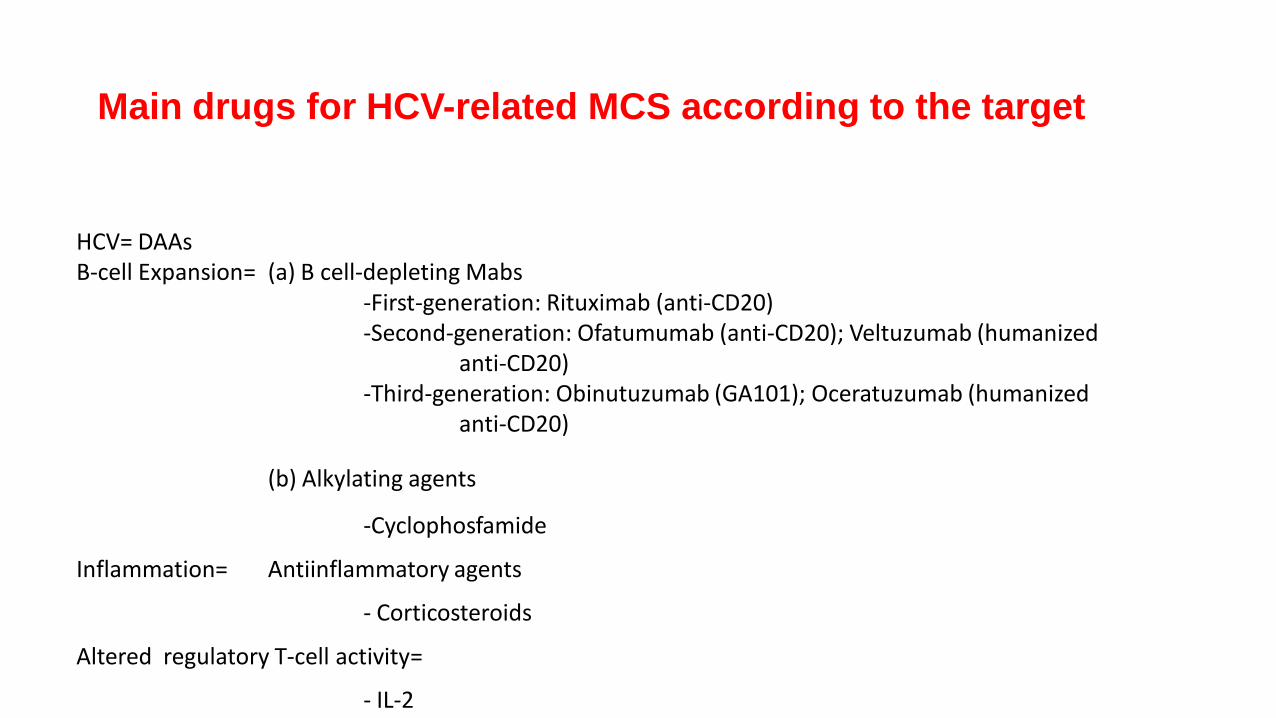
Zignego AL et al Autoimmun Rev 2017 Ferri C et al Autoimmunity rev 2016 Zignego AL et al DLD 2007 Cacoub P et al DLD
2014 Zignego AL et al DLD 2007 Zignego AL et al Intern Emerg Med 2012 Zignego AL et al Clin Dev Immunol 2012 Zignego
AL et al Expert Rev Clin Immunol 2015
MC clinical aspects MC Syndrome
MCS is characterized by the clinical triad -purpura weakness and
arthralgias- low complement C4 and various organsystem
involvement including cutaneous articular renal neurological
cardiac or digestive
It ranges from mild disease to severe even life-threatening
conditions
More serious lesions are generally characterized by neurologic and
renal involvement
Prognosis is highly dependent on renal involvement or on the extent
of vasculitis lesions
1 HCV is the main etiopathological agent as concordantly demonstrated by epidemiological clinico-pathological virological and laboratory investigations2 the association between HCV and disease is demonstrated in a significant proportion of patients and supported by in depth clinico-pathogeneticstudies3 the association is suggested by cohort studies a possible causative role may be limited to a small number of patients andor possibly more relevant in specific geographical areas 4 a number of anecdotal observations suggested a possible role of HCV further investigations are required
From P Cacoub 2015
HCV infection is closely related to LPDs mostly MC
40 to 60 of HCV patients show circulating CGs among this latter population 5-30
develop a symptomatic CV
AVT has been considered the first-line option in HCV-CV patients in fact in the majority
of cases viral eradication leads to CV clinical remission
Data about IFN-free regimens for the treatment of CV patients are still limited
HCV and MC
HCV and MC
Zignego 2015Ferri 2016Pozzato 2016 Sise 2016Saadoun 2015Gragnani 2016Gragnani 2016
Bonacci 2016Hegazy 2016Kondili 2016Emery 2017
Younossi et al
The annual costs (inpatient outpatient andpharmacy) associated with extrahepatic
manifestations of HCV were evaluated
Total direct medical costs of extrahepatic
manifestations of HCV in 2014 US dollars wereestimated to be $1506 million (range $922 millionndash
$2208 million in sensitivity analysis)
These estimates should be added to the liver-related
burden of disease to obtain a more accurateassessment of the total burden of HCV infection
The OBJECTIVE of the study was to estimate the annual direct medical costsassociated with HCV related EHM in the EU5 (France Germany Italy United Kingdom
Spain)
Extrahepatic Manifestations of HCV
Extrahepatic Manifestations of HCV
HCV may cause extrahepatic disorders (HCV-EHDs) classified according to the number and
strength of supporting scientific data
HCV-EHDs are responsible for increasing morbidity and mortality with important
consequences in terms of social costs
The analysis of mortality rates in large cohorts confirmed the association of HCV with
several EHDs including cardiovascular neurologic metabolic or renal diseases and tumors
Viral eradication significantly reduced the rate of extra-hepatic deaths
Cacoub P et al DLD 2014 Lee MH et al J Infect Dis 2012 Backus LI et al Clin Gastroenterol Hepatol 2011 El-Kamary S et al
Clin Infect Dis 2011 Hsu YC et al Hepatology 2014 Kawamura Y et al Am J Med 2007 Adinolfi LE et al WJG 2014
Con il contributo di
Lee M-H et al J Infect Dis 2012206469-477
Follow-Up
(Years)
20
18
16
14
12
10
2
00 2 4 6 8 10 12 14 16 18 20
8
6
4
Follow-Up
(Years)
12
10
8
6
4
2
00 2 4 6 8 10 12 14 16 18 20
All Causes(n=2394)
Liver Cancer(n=115)
Extrahepatic Diseases(n=2199)
Cum
ula
tive M
ort
ali
ty (
)
Anti-HCV+ HCV RNA detectable Anti-HCV+ HCV RNA undetectable Anti-HCVndash
Follow-Up
(Years)
35
30
25
20
15
10
5
00 2 4 6 8 10 12 14 16 18 20
301
128124
104
16
03
198
122
110
Extrahepatic Manifestations of HCV
The annual costs (inpatient outpatient andpharmacy) associated with extrahepatic
manifestations of HCV were evaluated
Total direct medical costs of extrahepatic
manifestations of HCV in 2014 US dollars wereestimated to be $1506 million (range $922 millionndash
$2208 million in sensitivity analysis)
These estimates should be added to the liver-related
burden of disease to obtain a more accurateassessment of the total burden of HCV infection
Younossi et al
Younossi et al
Costs up to $71000 per patient per year (ESRD) Among the most frequent EHM depression (245 in HCV vs 172 in non-HCV) had estimated annual cost of
$4307 million DM (15 vs 10 in non- HCV) had an annual cost of $4434 million in the USA= given the importance of DM and
its association with CVDs and mortality the clinical and economic impacts of HCV-related DM are substantial
The OBJECTIVE of the study was to estimate the annual direct medical costsassociated with HCV related EHM in the EU5 (France Germany Italy United Kingdom
Spain)
The OBJECTIVE of the study was to estimate the annual direct medicalcosts associated with HCV related EHM in the EU5 (France Germany
Italy United Kingdom Spain)
1 HCV is the main etiopathological agent as concordantly demonstrated by epidemiological clinico-pathological virological and laboratory investigations2 the association between HCV and disease is demonstrated in a significant proportion of patients and supported by in depth clinico-pathogeneticstudies3 the association is suggested by cohort studies a possible causative role may be limited to a small number of patients andor possibly more relevant in specific geographical areas 4 a number of anecdotal observations suggested a possible role of HCV further investigations are required
The most studied and frequent HCV-EHDs are B-LPDs andor autoimmune disorders
Their prototype is Mixed Cryoglobulinemia (MC) from researches on MC derived most of the
available information
MC as a precious model for all the HCV-EHDs and to evaluate the effects of viral eradication
Anti-HCV Treatment Evolution
IFN
6 mos
PegIFN RBV 12
mos
IFN
12 mos
IFNRBV
12 mos
PegIFN
12 mos
2001
1998
2011
Standardinterferon
Ribavirin
Peginterferon
1991
Direct-actingantivirals
PegIFN
RBV
DAA
IFNRBV
6 mos
6
16
34
4239
55
70+
0
20
40
60
80
100
DAAs
826
weeks
gt90
2015
Few side effects absence major
contraindications
Younossi et al
The annual costs (inpatient outpatient and pharmacy) associatedwith extrahepatic manifestations of HCV were evaluated
Total direct medical costs of extrahepatic manifestations of HCV in 2014US dollars were estimated to be $1506 million (range $922 millionndash
$2208 million in sensitivity analysis)
These estimates should be added to the liver-related burden of diseaseto obtain a more accurate assessment of the total burden of HCV
infection
The OBJECTIVE of the study was to estimate the annual direct medical costs associated with HCV related EHM in the EU5 (France Germany Italy United Kingdom Spain)
22 MCS treated with DAAs including 2 HCC and 2 NHL 100 SVR12 Clinical CR in 64 and PR in remaining 36 The small lymphocytic lymphoma progressed despite viral clearance
Lauletta et al 2017
Emery CS et al 2017
Retrospective analysis 17 MCS (10 with severelife-threatening vasculitis) and 65 asymptomatic CGs+ pts treated with DAAs SVR 889 MCS and 908 asymptomatic pts In MCS clinical response in 1117 (complete in 717) In severelife-threatening vasculitis lower clinical response especially in renal and neurological symptoms
Saadoun D et al 2017
Open-label prospective multi-center study on sofosbuvir plus daclatasvir treatment of 41 HCV MCS SVR in100 and clinical CR in 902 Disappearance of CGs in 50 of pts No serious adverse event or relapse ofvasculitis
Antiviral Treatment (AVT) of MCIFN-free regimens
MC is clinically benign but sometimes severe HCV EHD invalidating symptoms occur and
it may evolve into lymphoma
Cacoub P et al DLD 2014 Zignego AL et al DLD 2007 Zignego AL et al Intern Emerg Med 2012 Zignego AL et al Clin Dev
Immunol 2012 Zignego AL et al Expert Rev Clin Immunol 2015 Sene D et al J Rheumatol 2004
Mixed Cryoglobulinemia-MC
MC pathological substrate is an HCV-driven B-cell
proliferation with consequent production of cryo- and non-
cryoprecipitable CICs in turn responsible for vasculitic
manifestations
Most (70ndash90) MC patients are HCV+ and HCV-patients are CGs+ (40ndash60) while 5ndash30 of
CGs+ have symptomatic MC or cryoglobulinemic vasculitis since HCV infects about 170
million individuals worldwide the number of patients at risk for developing MC is
substantial
Type II CGs
monoclonal
RF+policlonal IgG
Type III CGs both
RF and IgG
polyclonal

1 HCV is the main etiopathological agent as concordantly demonstrated by epidemiological clinico-pathological virological and laboratory investigations2 the association between HCV and disease is demonstrated in a significant proportion of patients and supported by in depth clinico-pathogeneticstudies3 the association is suggested by cohort studies a possible causative role may be limited to a small number of patients andor possibly more relevant in specific geographical areas 4 a number of anecdotal observations suggested a possible role of HCV further investigations are required
From P Cacoub 2015
HCV infection is closely related to LPDs mostly MC
40 to 60 of HCV patients show circulating CGs among this latter population 5-30
develop a symptomatic CV
AVT has been considered the first-line option in HCV-CV patients in fact in the majority
of cases viral eradication leads to CV clinical remission
Data about IFN-free regimens for the treatment of CV patients are still limited
HCV and MC
HCV and MC
Zignego 2015Ferri 2016Pozzato 2016 Sise 2016Saadoun 2015Gragnani 2016Gragnani 2016
Bonacci 2016Hegazy 2016Kondili 2016Emery 2017
Younossi et al
The annual costs (inpatient outpatient andpharmacy) associated with extrahepatic
manifestations of HCV were evaluated
Total direct medical costs of extrahepatic
manifestations of HCV in 2014 US dollars wereestimated to be $1506 million (range $922 millionndash
$2208 million in sensitivity analysis)
These estimates should be added to the liver-related
burden of disease to obtain a more accurateassessment of the total burden of HCV infection
The OBJECTIVE of the study was to estimate the annual direct medical costsassociated with HCV related EHM in the EU5 (France Germany Italy United Kingdom
Spain)
Extrahepatic Manifestations of HCV
Extrahepatic Manifestations of HCV
HCV may cause extrahepatic disorders (HCV-EHDs) classified according to the number and
strength of supporting scientific data
HCV-EHDs are responsible for increasing morbidity and mortality with important
consequences in terms of social costs
The analysis of mortality rates in large cohorts confirmed the association of HCV with
several EHDs including cardiovascular neurologic metabolic or renal diseases and tumors
Viral eradication significantly reduced the rate of extra-hepatic deaths
Cacoub P et al DLD 2014 Lee MH et al J Infect Dis 2012 Backus LI et al Clin Gastroenterol Hepatol 2011 El-Kamary S et al
Clin Infect Dis 2011 Hsu YC et al Hepatology 2014 Kawamura Y et al Am J Med 2007 Adinolfi LE et al WJG 2014
Con il contributo di
Lee M-H et al J Infect Dis 2012206469-477
Follow-Up
(Years)
20
18
16
14
12
10
2
00 2 4 6 8 10 12 14 16 18 20
8
6
4
Follow-Up
(Years)
12
10
8
6
4
2
00 2 4 6 8 10 12 14 16 18 20
All Causes(n=2394)
Liver Cancer(n=115)
Extrahepatic Diseases(n=2199)
Cum
ula
tive M
ort
ali
ty (
)
Anti-HCV+ HCV RNA detectable Anti-HCV+ HCV RNA undetectable Anti-HCVndash
Follow-Up
(Years)
35
30
25
20
15
10
5
00 2 4 6 8 10 12 14 16 18 20
301
128124
104
16
03
198
122
110
Extrahepatic Manifestations of HCV
The annual costs (inpatient outpatient andpharmacy) associated with extrahepatic
manifestations of HCV were evaluated
Total direct medical costs of extrahepatic
manifestations of HCV in 2014 US dollars wereestimated to be $1506 million (range $922 millionndash
$2208 million in sensitivity analysis)
These estimates should be added to the liver-related
burden of disease to obtain a more accurateassessment of the total burden of HCV infection
Younossi et al
Younossi et al
Costs up to $71000 per patient per year (ESRD) Among the most frequent EHM depression (245 in HCV vs 172 in non-HCV) had estimated annual cost of
$4307 million DM (15 vs 10 in non- HCV) had an annual cost of $4434 million in the USA= given the importance of DM and
its association with CVDs and mortality the clinical and economic impacts of HCV-related DM are substantial
The OBJECTIVE of the study was to estimate the annual direct medical costsassociated with HCV related EHM in the EU5 (France Germany Italy United Kingdom
Spain)
The OBJECTIVE of the study was to estimate the annual direct medicalcosts associated with HCV related EHM in the EU5 (France Germany
Italy United Kingdom Spain)
1 HCV is the main etiopathological agent as concordantly demonstrated by epidemiological clinico-pathological virological and laboratory investigations2 the association between HCV and disease is demonstrated in a significant proportion of patients and supported by in depth clinico-pathogeneticstudies3 the association is suggested by cohort studies a possible causative role may be limited to a small number of patients andor possibly more relevant in specific geographical areas 4 a number of anecdotal observations suggested a possible role of HCV further investigations are required
The most studied and frequent HCV-EHDs are B-LPDs andor autoimmune disorders
Their prototype is Mixed Cryoglobulinemia (MC) from researches on MC derived most of the
available information
MC as a precious model for all the HCV-EHDs and to evaluate the effects of viral eradication
Anti-HCV Treatment Evolution
IFN
6 mos
PegIFN RBV 12
mos
IFN
12 mos
IFNRBV
12 mos
PegIFN
12 mos
2001
1998
2011
Standardinterferon
Ribavirin
Peginterferon
1991
Direct-actingantivirals
PegIFN
RBV
DAA
IFNRBV
6 mos
6
16
34
4239
55
70+
0
20
40
60
80
100
DAAs
826
weeks
gt90
2015
Few side effects absence major
contraindications
Younossi et al
The annual costs (inpatient outpatient and pharmacy) associatedwith extrahepatic manifestations of HCV were evaluated
Total direct medical costs of extrahepatic manifestations of HCV in 2014US dollars were estimated to be $1506 million (range $922 millionndash
$2208 million in sensitivity analysis)
These estimates should be added to the liver-related burden of diseaseto obtain a more accurate assessment of the total burden of HCV
infection
The OBJECTIVE of the study was to estimate the annual direct medical costs associated with HCV related EHM in the EU5 (France Germany Italy United Kingdom Spain)
22 MCS treated with DAAs including 2 HCC and 2 NHL 100 SVR12 Clinical CR in 64 and PR in remaining 36 The small lymphocytic lymphoma progressed despite viral clearance
Lauletta et al 2017
Emery CS et al 2017
Retrospective analysis 17 MCS (10 with severelife-threatening vasculitis) and 65 asymptomatic CGs+ pts treated with DAAs SVR 889 MCS and 908 asymptomatic pts In MCS clinical response in 1117 (complete in 717) In severelife-threatening vasculitis lower clinical response especially in renal and neurological symptoms
Saadoun D et al 2017
Open-label prospective multi-center study on sofosbuvir plus daclatasvir treatment of 41 HCV MCS SVR in100 and clinical CR in 902 Disappearance of CGs in 50 of pts No serious adverse event or relapse ofvasculitis
Antiviral Treatment (AVT) of MCIFN-free regimens
MC is clinically benign but sometimes severe HCV EHD invalidating symptoms occur and
it may evolve into lymphoma
Cacoub P et al DLD 2014 Zignego AL et al DLD 2007 Zignego AL et al Intern Emerg Med 2012 Zignego AL et al Clin Dev
Immunol 2012 Zignego AL et al Expert Rev Clin Immunol 2015 Sene D et al J Rheumatol 2004
Mixed Cryoglobulinemia-MC
MC pathological substrate is an HCV-driven B-cell
proliferation with consequent production of cryo- and non-
cryoprecipitable CICs in turn responsible for vasculitic
manifestations
Most (70ndash90) MC patients are HCV+ and HCV-patients are CGs+ (40ndash60) while 5ndash30 of
CGs+ have symptomatic MC or cryoglobulinemic vasculitis since HCV infects about 170
million individuals worldwide the number of patients at risk for developing MC is
substantial
Type II CGs
monoclonal
RF+policlonal IgG
Type III CGs both
RF and IgG
polyclonal

HCV infection is closely related to LPDs mostly MC
40 to 60 of HCV patients show circulating CGs among this latter population 5-30
develop a symptomatic CV
AVT has been considered the first-line option in HCV-CV patients in fact in the majority
of cases viral eradication leads to CV clinical remission
Data about IFN-free regimens for the treatment of CV patients are still limited
HCV and MC
HCV and MC
Zignego 2015Ferri 2016Pozzato 2016 Sise 2016Saadoun 2015Gragnani 2016Gragnani 2016
Bonacci 2016Hegazy 2016Kondili 2016Emery 2017
Younossi et al
The annual costs (inpatient outpatient andpharmacy) associated with extrahepatic
manifestations of HCV were evaluated
Total direct medical costs of extrahepatic
manifestations of HCV in 2014 US dollars wereestimated to be $1506 million (range $922 millionndash
$2208 million in sensitivity analysis)
These estimates should be added to the liver-related
burden of disease to obtain a more accurateassessment of the total burden of HCV infection
The OBJECTIVE of the study was to estimate the annual direct medical costsassociated with HCV related EHM in the EU5 (France Germany Italy United Kingdom
Spain)
Extrahepatic Manifestations of HCV
Extrahepatic Manifestations of HCV
HCV may cause extrahepatic disorders (HCV-EHDs) classified according to the number and
strength of supporting scientific data
HCV-EHDs are responsible for increasing morbidity and mortality with important
consequences in terms of social costs
The analysis of mortality rates in large cohorts confirmed the association of HCV with
several EHDs including cardiovascular neurologic metabolic or renal diseases and tumors
Viral eradication significantly reduced the rate of extra-hepatic deaths
Cacoub P et al DLD 2014 Lee MH et al J Infect Dis 2012 Backus LI et al Clin Gastroenterol Hepatol 2011 El-Kamary S et al
Clin Infect Dis 2011 Hsu YC et al Hepatology 2014 Kawamura Y et al Am J Med 2007 Adinolfi LE et al WJG 2014
Con il contributo di
Lee M-H et al J Infect Dis 2012206469-477
Follow-Up
(Years)
20
18
16
14
12
10
2
00 2 4 6 8 10 12 14 16 18 20
8
6
4
Follow-Up
(Years)
12
10
8
6
4
2
00 2 4 6 8 10 12 14 16 18 20
All Causes(n=2394)
Liver Cancer(n=115)
Extrahepatic Diseases(n=2199)
Cum
ula
tive M
ort
ali
ty (
)
Anti-HCV+ HCV RNA detectable Anti-HCV+ HCV RNA undetectable Anti-HCVndash
Follow-Up
(Years)
35
30
25
20
15
10
5
00 2 4 6 8 10 12 14 16 18 20
301
128124
104
16
03
198
122
110
Extrahepatic Manifestations of HCV
The annual costs (inpatient outpatient andpharmacy) associated with extrahepatic
manifestations of HCV were evaluated
Total direct medical costs of extrahepatic
manifestations of HCV in 2014 US dollars wereestimated to be $1506 million (range $922 millionndash
$2208 million in sensitivity analysis)
These estimates should be added to the liver-related
burden of disease to obtain a more accurateassessment of the total burden of HCV infection
Younossi et al
Younossi et al
Costs up to $71000 per patient per year (ESRD) Among the most frequent EHM depression (245 in HCV vs 172 in non-HCV) had estimated annual cost of
$4307 million DM (15 vs 10 in non- HCV) had an annual cost of $4434 million in the USA= given the importance of DM and
its association with CVDs and mortality the clinical and economic impacts of HCV-related DM are substantial
The OBJECTIVE of the study was to estimate the annual direct medical costsassociated with HCV related EHM in the EU5 (France Germany Italy United Kingdom
Spain)
The OBJECTIVE of the study was to estimate the annual direct medicalcosts associated with HCV related EHM in the EU5 (France Germany
Italy United Kingdom Spain)
1 HCV is the main etiopathological agent as concordantly demonstrated by epidemiological clinico-pathological virological and laboratory investigations2 the association between HCV and disease is demonstrated in a significant proportion of patients and supported by in depth clinico-pathogeneticstudies3 the association is suggested by cohort studies a possible causative role may be limited to a small number of patients andor possibly more relevant in specific geographical areas 4 a number of anecdotal observations suggested a possible role of HCV further investigations are required
The most studied and frequent HCV-EHDs are B-LPDs andor autoimmune disorders
Their prototype is Mixed Cryoglobulinemia (MC) from researches on MC derived most of the
available information
MC as a precious model for all the HCV-EHDs and to evaluate the effects of viral eradication
Anti-HCV Treatment Evolution
IFN
6 mos
PegIFN RBV 12
mos
IFN
12 mos
IFNRBV
12 mos
PegIFN
12 mos
2001
1998
2011
Standardinterferon
Ribavirin
Peginterferon
1991
Direct-actingantivirals
PegIFN
RBV
DAA
IFNRBV
6 mos
6
16
34
4239
55
70+
0
20
40
60
80
100
DAAs
826
weeks
gt90
2015
Few side effects absence major
contraindications
Younossi et al
The annual costs (inpatient outpatient and pharmacy) associatedwith extrahepatic manifestations of HCV were evaluated
Total direct medical costs of extrahepatic manifestations of HCV in 2014US dollars were estimated to be $1506 million (range $922 millionndash
$2208 million in sensitivity analysis)
These estimates should be added to the liver-related burden of diseaseto obtain a more accurate assessment of the total burden of HCV
infection
The OBJECTIVE of the study was to estimate the annual direct medical costs associated with HCV related EHM in the EU5 (France Germany Italy United Kingdom Spain)
22 MCS treated with DAAs including 2 HCC and 2 NHL 100 SVR12 Clinical CR in 64 and PR in remaining 36 The small lymphocytic lymphoma progressed despite viral clearance
Lauletta et al 2017
Emery CS et al 2017
Retrospective analysis 17 MCS (10 with severelife-threatening vasculitis) and 65 asymptomatic CGs+ pts treated with DAAs SVR 889 MCS and 908 asymptomatic pts In MCS clinical response in 1117 (complete in 717) In severelife-threatening vasculitis lower clinical response especially in renal and neurological symptoms
Saadoun D et al 2017
Open-label prospective multi-center study on sofosbuvir plus daclatasvir treatment of 41 HCV MCS SVR in100 and clinical CR in 902 Disappearance of CGs in 50 of pts No serious adverse event or relapse ofvasculitis
Antiviral Treatment (AVT) of MCIFN-free regimens
MC is clinically benign but sometimes severe HCV EHD invalidating symptoms occur and
it may evolve into lymphoma
Cacoub P et al DLD 2014 Zignego AL et al DLD 2007 Zignego AL et al Intern Emerg Med 2012 Zignego AL et al Clin Dev
Immunol 2012 Zignego AL et al Expert Rev Clin Immunol 2015 Sene D et al J Rheumatol 2004
Mixed Cryoglobulinemia-MC
MC pathological substrate is an HCV-driven B-cell
proliferation with consequent production of cryo- and non-
cryoprecipitable CICs in turn responsible for vasculitic
manifestations
Most (70ndash90) MC patients are HCV+ and HCV-patients are CGs+ (40ndash60) while 5ndash30 of
CGs+ have symptomatic MC or cryoglobulinemic vasculitis since HCV infects about 170
million individuals worldwide the number of patients at risk for developing MC is
substantial
Type II CGs
monoclonal
RF+policlonal IgG
Type III CGs both
RF and IgG
polyclonal
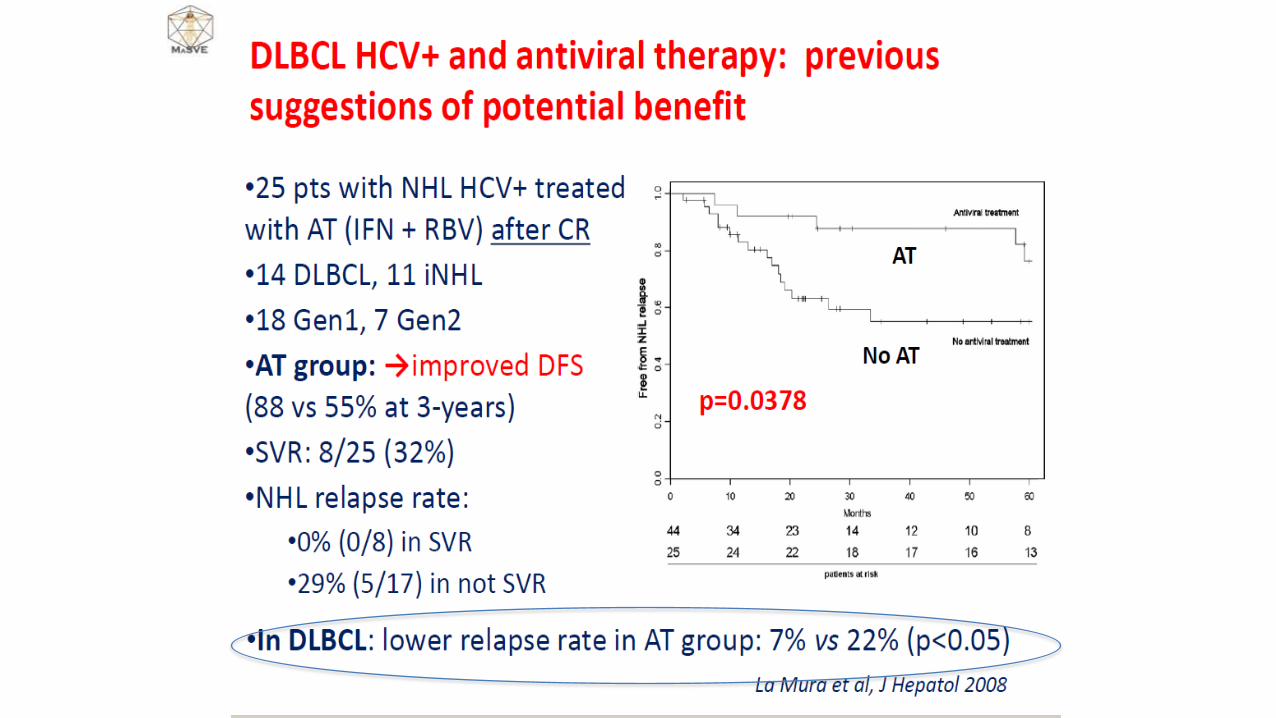
Younossi et al
The annual costs (inpatient outpatient andpharmacy) associated with extrahepatic
manifestations of HCV were evaluated
Total direct medical costs of extrahepatic
manifestations of HCV in 2014 US dollars wereestimated to be $1506 million (range $922 millionndash
$2208 million in sensitivity analysis)
These estimates should be added to the liver-related
burden of disease to obtain a more accurateassessment of the total burden of HCV infection
The OBJECTIVE of the study was to estimate the annual direct medical costsassociated with HCV related EHM in the EU5 (France Germany Italy United Kingdom
Spain)
Extrahepatic Manifestations of HCV
Extrahepatic Manifestations of HCV
HCV may cause extrahepatic disorders (HCV-EHDs) classified according to the number and
strength of supporting scientific data
HCV-EHDs are responsible for increasing morbidity and mortality with important
consequences in terms of social costs
The analysis of mortality rates in large cohorts confirmed the association of HCV with
several EHDs including cardiovascular neurologic metabolic or renal diseases and tumors
Viral eradication significantly reduced the rate of extra-hepatic deaths
Cacoub P et al DLD 2014 Lee MH et al J Infect Dis 2012 Backus LI et al Clin Gastroenterol Hepatol 2011 El-Kamary S et al
Clin Infect Dis 2011 Hsu YC et al Hepatology 2014 Kawamura Y et al Am J Med 2007 Adinolfi LE et al WJG 2014
Con il contributo di
Lee M-H et al J Infect Dis 2012206469-477
Follow-Up
(Years)
20
18
16
14
12
10
2
00 2 4 6 8 10 12 14 16 18 20
8
6
4
Follow-Up
(Years)
12
10
8
6
4
2
00 2 4 6 8 10 12 14 16 18 20
All Causes(n=2394)
Liver Cancer(n=115)
Extrahepatic Diseases(n=2199)
Cum
ula
tive M
ort
ali
ty (
)
Anti-HCV+ HCV RNA detectable Anti-HCV+ HCV RNA undetectable Anti-HCVndash
Follow-Up
(Years)
35
30
25
20
15
10
5
00 2 4 6 8 10 12 14 16 18 20
301
128124
104
16
03
198
122
110
Extrahepatic Manifestations of HCV
The annual costs (inpatient outpatient andpharmacy) associated with extrahepatic
manifestations of HCV were evaluated
Total direct medical costs of extrahepatic
manifestations of HCV in 2014 US dollars wereestimated to be $1506 million (range $922 millionndash
$2208 million in sensitivity analysis)
These estimates should be added to the liver-related
burden of disease to obtain a more accurateassessment of the total burden of HCV infection
Younossi et al
Younossi et al
Costs up to $71000 per patient per year (ESRD) Among the most frequent EHM depression (245 in HCV vs 172 in non-HCV) had estimated annual cost of
$4307 million DM (15 vs 10 in non- HCV) had an annual cost of $4434 million in the USA= given the importance of DM and
its association with CVDs and mortality the clinical and economic impacts of HCV-related DM are substantial
The OBJECTIVE of the study was to estimate the annual direct medical costsassociated with HCV related EHM in the EU5 (France Germany Italy United Kingdom
Spain)
The OBJECTIVE of the study was to estimate the annual direct medicalcosts associated with HCV related EHM in the EU5 (France Germany
Italy United Kingdom Spain)
1 HCV is the main etiopathological agent as concordantly demonstrated by epidemiological clinico-pathological virological and laboratory investigations2 the association between HCV and disease is demonstrated in a significant proportion of patients and supported by in depth clinico-pathogeneticstudies3 the association is suggested by cohort studies a possible causative role may be limited to a small number of patients andor possibly more relevant in specific geographical areas 4 a number of anecdotal observations suggested a possible role of HCV further investigations are required
The most studied and frequent HCV-EHDs are B-LPDs andor autoimmune disorders
Their prototype is Mixed Cryoglobulinemia (MC) from researches on MC derived most of the
available information
MC as a precious model for all the HCV-EHDs and to evaluate the effects of viral eradication
Anti-HCV Treatment Evolution
IFN
6 mos
PegIFN RBV 12
mos
IFN
12 mos
IFNRBV
12 mos
PegIFN
12 mos
2001
1998
2011
Standardinterferon
Ribavirin
Peginterferon
1991
Direct-actingantivirals
PegIFN
RBV
DAA
IFNRBV
6 mos
6
16
34
4239
55
70+
0
20
40
60
80
100
DAAs
826
weeks
gt90
2015
Few side effects absence major
contraindications
Younossi et al
The annual costs (inpatient outpatient and pharmacy) associatedwith extrahepatic manifestations of HCV were evaluated
Total direct medical costs of extrahepatic manifestations of HCV in 2014US dollars were estimated to be $1506 million (range $922 millionndash
$2208 million in sensitivity analysis)
These estimates should be added to the liver-related burden of diseaseto obtain a more accurate assessment of the total burden of HCV
infection
The OBJECTIVE of the study was to estimate the annual direct medical costs associated with HCV related EHM in the EU5 (France Germany Italy United Kingdom Spain)
22 MCS treated with DAAs including 2 HCC and 2 NHL 100 SVR12 Clinical CR in 64 and PR in remaining 36 The small lymphocytic lymphoma progressed despite viral clearance
Lauletta et al 2017
Emery CS et al 2017
Retrospective analysis 17 MCS (10 with severelife-threatening vasculitis) and 65 asymptomatic CGs+ pts treated with DAAs SVR 889 MCS and 908 asymptomatic pts In MCS clinical response in 1117 (complete in 717) In severelife-threatening vasculitis lower clinical response especially in renal and neurological symptoms
Saadoun D et al 2017
Open-label prospective multi-center study on sofosbuvir plus daclatasvir treatment of 41 HCV MCS SVR in100 and clinical CR in 902 Disappearance of CGs in 50 of pts No serious adverse event or relapse ofvasculitis
Antiviral Treatment (AVT) of MCIFN-free regimens
MC is clinically benign but sometimes severe HCV EHD invalidating symptoms occur and
it may evolve into lymphoma
Cacoub P et al DLD 2014 Zignego AL et al DLD 2007 Zignego AL et al Intern Emerg Med 2012 Zignego AL et al Clin Dev
Immunol 2012 Zignego AL et al Expert Rev Clin Immunol 2015 Sene D et al J Rheumatol 2004
Mixed Cryoglobulinemia-MC
MC pathological substrate is an HCV-driven B-cell
proliferation with consequent production of cryo- and non-
cryoprecipitable CICs in turn responsible for vasculitic
manifestations
Most (70ndash90) MC patients are HCV+ and HCV-patients are CGs+ (40ndash60) while 5ndash30 of
CGs+ have symptomatic MC or cryoglobulinemic vasculitis since HCV infects about 170
million individuals worldwide the number of patients at risk for developing MC is
substantial
Type II CGs
monoclonal
RF+policlonal IgG
Type III CGs both
RF and IgG
polyclonal

The OBJECTIVE of the study was to estimate the annual direct medical costsassociated with HCV related EHM in the EU5 (France Germany Italy United Kingdom
Spain)
Extrahepatic Manifestations of HCV
Extrahepatic Manifestations of HCV
HCV may cause extrahepatic disorders (HCV-EHDs) classified according to the number and
strength of supporting scientific data
HCV-EHDs are responsible for increasing morbidity and mortality with important
consequences in terms of social costs
The analysis of mortality rates in large cohorts confirmed the association of HCV with
several EHDs including cardiovascular neurologic metabolic or renal diseases and tumors
Viral eradication significantly reduced the rate of extra-hepatic deaths
Cacoub P et al DLD 2014 Lee MH et al J Infect Dis 2012 Backus LI et al Clin Gastroenterol Hepatol 2011 El-Kamary S et al
Clin Infect Dis 2011 Hsu YC et al Hepatology 2014 Kawamura Y et al Am J Med 2007 Adinolfi LE et al WJG 2014
Con il contributo di
Lee M-H et al J Infect Dis 2012206469-477
Follow-Up
(Years)
20
18
16
14
12
10
2
00 2 4 6 8 10 12 14 16 18 20
8
6
4
Follow-Up
(Years)
12
10
8
6
4
2
00 2 4 6 8 10 12 14 16 18 20
All Causes(n=2394)
Liver Cancer(n=115)
Extrahepatic Diseases(n=2199)
Cum
ula
tive M
ort
ali
ty (
)
Anti-HCV+ HCV RNA detectable Anti-HCV+ HCV RNA undetectable Anti-HCVndash
Follow-Up
(Years)
35
30
25
20
15
10
5
00 2 4 6 8 10 12 14 16 18 20
301
128124
104
16
03
198
122
110
Extrahepatic Manifestations of HCV
The annual costs (inpatient outpatient andpharmacy) associated with extrahepatic
manifestations of HCV were evaluated
Total direct medical costs of extrahepatic
manifestations of HCV in 2014 US dollars wereestimated to be $1506 million (range $922 millionndash
$2208 million in sensitivity analysis)
These estimates should be added to the liver-related
burden of disease to obtain a more accurateassessment of the total burden of HCV infection
Younossi et al
Younossi et al
Costs up to $71000 per patient per year (ESRD) Among the most frequent EHM depression (245 in HCV vs 172 in non-HCV) had estimated annual cost of
$4307 million DM (15 vs 10 in non- HCV) had an annual cost of $4434 million in the USA= given the importance of DM and
its association with CVDs and mortality the clinical and economic impacts of HCV-related DM are substantial
The OBJECTIVE of the study was to estimate the annual direct medical costsassociated with HCV related EHM in the EU5 (France Germany Italy United Kingdom
Spain)
The OBJECTIVE of the study was to estimate the annual direct medicalcosts associated with HCV related EHM in the EU5 (France Germany
Italy United Kingdom Spain)
1 HCV is the main etiopathological agent as concordantly demonstrated by epidemiological clinico-pathological virological and laboratory investigations2 the association between HCV and disease is demonstrated in a significant proportion of patients and supported by in depth clinico-pathogeneticstudies3 the association is suggested by cohort studies a possible causative role may be limited to a small number of patients andor possibly more relevant in specific geographical areas 4 a number of anecdotal observations suggested a possible role of HCV further investigations are required
The most studied and frequent HCV-EHDs are B-LPDs andor autoimmune disorders
Their prototype is Mixed Cryoglobulinemia (MC) from researches on MC derived most of the
available information
MC as a precious model for all the HCV-EHDs and to evaluate the effects of viral eradication
Anti-HCV Treatment Evolution
IFN
6 mos
PegIFN RBV 12
mos
IFN
12 mos
IFNRBV
12 mos
PegIFN
12 mos
2001
1998
2011
Standardinterferon
Ribavirin
Peginterferon
1991
Direct-actingantivirals
PegIFN
RBV
DAA
IFNRBV
6 mos
6
16
34
4239
55
70+
0
20
40
60
80
100
DAAs
826
weeks
gt90
2015
Few side effects absence major
contraindications
Younossi et al
The annual costs (inpatient outpatient and pharmacy) associatedwith extrahepatic manifestations of HCV were evaluated
Total direct medical costs of extrahepatic manifestations of HCV in 2014US dollars were estimated to be $1506 million (range $922 millionndash
$2208 million in sensitivity analysis)
These estimates should be added to the liver-related burden of diseaseto obtain a more accurate assessment of the total burden of HCV
infection
The OBJECTIVE of the study was to estimate the annual direct medical costs associated with HCV related EHM in the EU5 (France Germany Italy United Kingdom Spain)
22 MCS treated with DAAs including 2 HCC and 2 NHL 100 SVR12 Clinical CR in 64 and PR in remaining 36 The small lymphocytic lymphoma progressed despite viral clearance
Lauletta et al 2017
Emery CS et al 2017
Retrospective analysis 17 MCS (10 with severelife-threatening vasculitis) and 65 asymptomatic CGs+ pts treated with DAAs SVR 889 MCS and 908 asymptomatic pts In MCS clinical response in 1117 (complete in 717) In severelife-threatening vasculitis lower clinical response especially in renal and neurological symptoms
Saadoun D et al 2017
Open-label prospective multi-center study on sofosbuvir plus daclatasvir treatment of 41 HCV MCS SVR in100 and clinical CR in 902 Disappearance of CGs in 50 of pts No serious adverse event or relapse ofvasculitis
Antiviral Treatment (AVT) of MCIFN-free regimens
MC is clinically benign but sometimes severe HCV EHD invalidating symptoms occur and
it may evolve into lymphoma
Cacoub P et al DLD 2014 Zignego AL et al DLD 2007 Zignego AL et al Intern Emerg Med 2012 Zignego AL et al Clin Dev
Immunol 2012 Zignego AL et al Expert Rev Clin Immunol 2015 Sene D et al J Rheumatol 2004
Mixed Cryoglobulinemia-MC
MC pathological substrate is an HCV-driven B-cell
proliferation with consequent production of cryo- and non-
cryoprecipitable CICs in turn responsible for vasculitic
manifestations
Most (70ndash90) MC patients are HCV+ and HCV-patients are CGs+ (40ndash60) while 5ndash30 of
CGs+ have symptomatic MC or cryoglobulinemic vasculitis since HCV infects about 170
million individuals worldwide the number of patients at risk for developing MC is
substantial
Type II CGs
monoclonal
RF+policlonal IgG
Type III CGs both
RF and IgG
polyclonal

Extrahepatic Manifestations of HCV
Extrahepatic Manifestations of HCV
HCV may cause extrahepatic disorders (HCV-EHDs) classified according to the number and
strength of supporting scientific data
HCV-EHDs are responsible for increasing morbidity and mortality with important
consequences in terms of social costs
The analysis of mortality rates in large cohorts confirmed the association of HCV with
several EHDs including cardiovascular neurologic metabolic or renal diseases and tumors
Viral eradication significantly reduced the rate of extra-hepatic deaths
Cacoub P et al DLD 2014 Lee MH et al J Infect Dis 2012 Backus LI et al Clin Gastroenterol Hepatol 2011 El-Kamary S et al
Clin Infect Dis 2011 Hsu YC et al Hepatology 2014 Kawamura Y et al Am J Med 2007 Adinolfi LE et al WJG 2014
Con il contributo di
Lee M-H et al J Infect Dis 2012206469-477
Follow-Up
(Years)
20
18
16
14
12
10
2
00 2 4 6 8 10 12 14 16 18 20
8
6
4
Follow-Up
(Years)
12
10
8
6
4
2
00 2 4 6 8 10 12 14 16 18 20
All Causes(n=2394)
Liver Cancer(n=115)
Extrahepatic Diseases(n=2199)
Cum
ula
tive M
ort
ali
ty (
)
Anti-HCV+ HCV RNA detectable Anti-HCV+ HCV RNA undetectable Anti-HCVndash
Follow-Up
(Years)
35
30
25
20
15
10
5
00 2 4 6 8 10 12 14 16 18 20
301
128124
104
16
03
198
122
110
Extrahepatic Manifestations of HCV
The annual costs (inpatient outpatient andpharmacy) associated with extrahepatic
manifestations of HCV were evaluated
Total direct medical costs of extrahepatic
manifestations of HCV in 2014 US dollars wereestimated to be $1506 million (range $922 millionndash
$2208 million in sensitivity analysis)
These estimates should be added to the liver-related
burden of disease to obtain a more accurateassessment of the total burden of HCV infection
Younossi et al
Younossi et al
Costs up to $71000 per patient per year (ESRD) Among the most frequent EHM depression (245 in HCV vs 172 in non-HCV) had estimated annual cost of
$4307 million DM (15 vs 10 in non- HCV) had an annual cost of $4434 million in the USA= given the importance of DM and
its association with CVDs and mortality the clinical and economic impacts of HCV-related DM are substantial
The OBJECTIVE of the study was to estimate the annual direct medical costsassociated with HCV related EHM in the EU5 (France Germany Italy United Kingdom
Spain)
The OBJECTIVE of the study was to estimate the annual direct medicalcosts associated with HCV related EHM in the EU5 (France Germany
Italy United Kingdom Spain)
1 HCV is the main etiopathological agent as concordantly demonstrated by epidemiological clinico-pathological virological and laboratory investigations2 the association between HCV and disease is demonstrated in a significant proportion of patients and supported by in depth clinico-pathogeneticstudies3 the association is suggested by cohort studies a possible causative role may be limited to a small number of patients andor possibly more relevant in specific geographical areas 4 a number of anecdotal observations suggested a possible role of HCV further investigations are required
The most studied and frequent HCV-EHDs are B-LPDs andor autoimmune disorders
Their prototype is Mixed Cryoglobulinemia (MC) from researches on MC derived most of the
available information
MC as a precious model for all the HCV-EHDs and to evaluate the effects of viral eradication
Anti-HCV Treatment Evolution
IFN
6 mos
PegIFN RBV 12
mos
IFN
12 mos
IFNRBV
12 mos
PegIFN
12 mos
2001
1998
2011
Standardinterferon
Ribavirin
Peginterferon
1991
Direct-actingantivirals
PegIFN
RBV
DAA
IFNRBV
6 mos
6
16
34
4239
55
70+
0
20
40
60
80
100
DAAs
826
weeks
gt90
2015
Few side effects absence major
contraindications
Younossi et al
The annual costs (inpatient outpatient and pharmacy) associatedwith extrahepatic manifestations of HCV were evaluated
Total direct medical costs of extrahepatic manifestations of HCV in 2014US dollars were estimated to be $1506 million (range $922 millionndash
$2208 million in sensitivity analysis)
These estimates should be added to the liver-related burden of diseaseto obtain a more accurate assessment of the total burden of HCV
infection
The OBJECTIVE of the study was to estimate the annual direct medical costs associated with HCV related EHM in the EU5 (France Germany Italy United Kingdom Spain)
22 MCS treated with DAAs including 2 HCC and 2 NHL 100 SVR12 Clinical CR in 64 and PR in remaining 36 The small lymphocytic lymphoma progressed despite viral clearance
Lauletta et al 2017
Emery CS et al 2017
Retrospective analysis 17 MCS (10 with severelife-threatening vasculitis) and 65 asymptomatic CGs+ pts treated with DAAs SVR 889 MCS and 908 asymptomatic pts In MCS clinical response in 1117 (complete in 717) In severelife-threatening vasculitis lower clinical response especially in renal and neurological symptoms
Saadoun D et al 2017
Open-label prospective multi-center study on sofosbuvir plus daclatasvir treatment of 41 HCV MCS SVR in100 and clinical CR in 902 Disappearance of CGs in 50 of pts No serious adverse event or relapse ofvasculitis
Antiviral Treatment (AVT) of MCIFN-free regimens
MC is clinically benign but sometimes severe HCV EHD invalidating symptoms occur and
it may evolve into lymphoma
Cacoub P et al DLD 2014 Zignego AL et al DLD 2007 Zignego AL et al Intern Emerg Med 2012 Zignego AL et al Clin Dev
Immunol 2012 Zignego AL et al Expert Rev Clin Immunol 2015 Sene D et al J Rheumatol 2004
Mixed Cryoglobulinemia-MC
MC pathological substrate is an HCV-driven B-cell
proliferation with consequent production of cryo- and non-
cryoprecipitable CICs in turn responsible for vasculitic
manifestations
Most (70ndash90) MC patients are HCV+ and HCV-patients are CGs+ (40ndash60) while 5ndash30 of
CGs+ have symptomatic MC or cryoglobulinemic vasculitis since HCV infects about 170
million individuals worldwide the number of patients at risk for developing MC is
substantial
Type II CGs
monoclonal
RF+policlonal IgG
Type III CGs both
RF and IgG
polyclonal

Extrahepatic Manifestations of HCV
HCV may cause extrahepatic disorders (HCV-EHDs) classified according to the number and
strength of supporting scientific data
HCV-EHDs are responsible for increasing morbidity and mortality with important
consequences in terms of social costs
The analysis of mortality rates in large cohorts confirmed the association of HCV with
several EHDs including cardiovascular neurologic metabolic or renal diseases and tumors
Viral eradication significantly reduced the rate of extra-hepatic deaths
Cacoub P et al DLD 2014 Lee MH et al J Infect Dis 2012 Backus LI et al Clin Gastroenterol Hepatol 2011 El-Kamary S et al
Clin Infect Dis 2011 Hsu YC et al Hepatology 2014 Kawamura Y et al Am J Med 2007 Adinolfi LE et al WJG 2014
Con il contributo di
Lee M-H et al J Infect Dis 2012206469-477
Follow-Up
(Years)
20
18
16
14
12
10
2
00 2 4 6 8 10 12 14 16 18 20
8
6
4
Follow-Up
(Years)
12
10
8
6
4
2
00 2 4 6 8 10 12 14 16 18 20
All Causes(n=2394)
Liver Cancer(n=115)
Extrahepatic Diseases(n=2199)
Cum
ula
tive M
ort
ali
ty (
)
Anti-HCV+ HCV RNA detectable Anti-HCV+ HCV RNA undetectable Anti-HCVndash
Follow-Up
(Years)
35
30
25
20
15
10
5
00 2 4 6 8 10 12 14 16 18 20
301
128124
104
16
03
198
122
110
Extrahepatic Manifestations of HCV
The annual costs (inpatient outpatient andpharmacy) associated with extrahepatic
manifestations of HCV were evaluated
Total direct medical costs of extrahepatic
manifestations of HCV in 2014 US dollars wereestimated to be $1506 million (range $922 millionndash
$2208 million in sensitivity analysis)
These estimates should be added to the liver-related
burden of disease to obtain a more accurateassessment of the total burden of HCV infection
Younossi et al
Younossi et al
Costs up to $71000 per patient per year (ESRD) Among the most frequent EHM depression (245 in HCV vs 172 in non-HCV) had estimated annual cost of
$4307 million DM (15 vs 10 in non- HCV) had an annual cost of $4434 million in the USA= given the importance of DM and
its association with CVDs and mortality the clinical and economic impacts of HCV-related DM are substantial
The OBJECTIVE of the study was to estimate the annual direct medical costsassociated with HCV related EHM in the EU5 (France Germany Italy United Kingdom
Spain)
The OBJECTIVE of the study was to estimate the annual direct medicalcosts associated with HCV related EHM in the EU5 (France Germany
Italy United Kingdom Spain)
1 HCV is the main etiopathological agent as concordantly demonstrated by epidemiological clinico-pathological virological and laboratory investigations2 the association between HCV and disease is demonstrated in a significant proportion of patients and supported by in depth clinico-pathogeneticstudies3 the association is suggested by cohort studies a possible causative role may be limited to a small number of patients andor possibly more relevant in specific geographical areas 4 a number of anecdotal observations suggested a possible role of HCV further investigations are required
The most studied and frequent HCV-EHDs are B-LPDs andor autoimmune disorders
Their prototype is Mixed Cryoglobulinemia (MC) from researches on MC derived most of the
available information
MC as a precious model for all the HCV-EHDs and to evaluate the effects of viral eradication
Anti-HCV Treatment Evolution
IFN
6 mos
PegIFN RBV 12
mos
IFN
12 mos
IFNRBV
12 mos
PegIFN
12 mos
2001
1998
2011
Standardinterferon
Ribavirin
Peginterferon
1991
Direct-actingantivirals
PegIFN
RBV
DAA
IFNRBV
6 mos
6
16
34
4239
55
70+
0
20
40
60
80
100
DAAs
826
weeks
gt90
2015
Few side effects absence major
contraindications
Younossi et al
The annual costs (inpatient outpatient and pharmacy) associatedwith extrahepatic manifestations of HCV were evaluated
Total direct medical costs of extrahepatic manifestations of HCV in 2014US dollars were estimated to be $1506 million (range $922 millionndash
$2208 million in sensitivity analysis)
These estimates should be added to the liver-related burden of diseaseto obtain a more accurate assessment of the total burden of HCV
infection
The OBJECTIVE of the study was to estimate the annual direct medical costs associated with HCV related EHM in the EU5 (France Germany Italy United Kingdom Spain)
22 MCS treated with DAAs including 2 HCC and 2 NHL 100 SVR12 Clinical CR in 64 and PR in remaining 36 The small lymphocytic lymphoma progressed despite viral clearance
Lauletta et al 2017
Emery CS et al 2017
Retrospective analysis 17 MCS (10 with severelife-threatening vasculitis) and 65 asymptomatic CGs+ pts treated with DAAs SVR 889 MCS and 908 asymptomatic pts In MCS clinical response in 1117 (complete in 717) In severelife-threatening vasculitis lower clinical response especially in renal and neurological symptoms
Saadoun D et al 2017
Open-label prospective multi-center study on sofosbuvir plus daclatasvir treatment of 41 HCV MCS SVR in100 and clinical CR in 902 Disappearance of CGs in 50 of pts No serious adverse event or relapse ofvasculitis
Antiviral Treatment (AVT) of MCIFN-free regimens
MC is clinically benign but sometimes severe HCV EHD invalidating symptoms occur and
it may evolve into lymphoma
Cacoub P et al DLD 2014 Zignego AL et al DLD 2007 Zignego AL et al Intern Emerg Med 2012 Zignego AL et al Clin Dev
Immunol 2012 Zignego AL et al Expert Rev Clin Immunol 2015 Sene D et al J Rheumatol 2004
Mixed Cryoglobulinemia-MC
MC pathological substrate is an HCV-driven B-cell
proliferation with consequent production of cryo- and non-
cryoprecipitable CICs in turn responsible for vasculitic
manifestations
Most (70ndash90) MC patients are HCV+ and HCV-patients are CGs+ (40ndash60) while 5ndash30 of
CGs+ have symptomatic MC or cryoglobulinemic vasculitis since HCV infects about 170
million individuals worldwide the number of patients at risk for developing MC is
substantial
Type II CGs
monoclonal
RF+policlonal IgG
Type III CGs both
RF and IgG
polyclonal

HCV-EHDs are responsible for increasing morbidity and mortality with important
consequences in terms of social costs
The analysis of mortality rates in large cohorts confirmed the association of HCV with
several EHDs including cardiovascular neurologic metabolic or renal diseases and tumors
Viral eradication significantly reduced the rate of extra-hepatic deaths
Cacoub P et al DLD 2014 Lee MH et al J Infect Dis 2012 Backus LI et al Clin Gastroenterol Hepatol 2011 El-Kamary S et al
Clin Infect Dis 2011 Hsu YC et al Hepatology 2014 Kawamura Y et al Am J Med 2007 Adinolfi LE et al WJG 2014
Con il contributo di
Lee M-H et al J Infect Dis 2012206469-477
Follow-Up
(Years)
20
18
16
14
12
10
2
00 2 4 6 8 10 12 14 16 18 20
8
6
4
Follow-Up
(Years)
12
10
8
6
4
2
00 2 4 6 8 10 12 14 16 18 20
All Causes(n=2394)
Liver Cancer(n=115)
Extrahepatic Diseases(n=2199)
Cum
ula
tive M
ort
ali
ty (
)
Anti-HCV+ HCV RNA detectable Anti-HCV+ HCV RNA undetectable Anti-HCVndash
Follow-Up
(Years)
35
30
25
20
15
10
5
00 2 4 6 8 10 12 14 16 18 20
301
128124
104
16
03
198
122
110
Extrahepatic Manifestations of HCV
The annual costs (inpatient outpatient andpharmacy) associated with extrahepatic
manifestations of HCV were evaluated
Total direct medical costs of extrahepatic
manifestations of HCV in 2014 US dollars wereestimated to be $1506 million (range $922 millionndash
$2208 million in sensitivity analysis)
These estimates should be added to the liver-related
burden of disease to obtain a more accurateassessment of the total burden of HCV infection
Younossi et al
Younossi et al
Costs up to $71000 per patient per year (ESRD) Among the most frequent EHM depression (245 in HCV vs 172 in non-HCV) had estimated annual cost of
$4307 million DM (15 vs 10 in non- HCV) had an annual cost of $4434 million in the USA= given the importance of DM and
its association with CVDs and mortality the clinical and economic impacts of HCV-related DM are substantial
The OBJECTIVE of the study was to estimate the annual direct medical costsassociated with HCV related EHM in the EU5 (France Germany Italy United Kingdom
Spain)
The OBJECTIVE of the study was to estimate the annual direct medicalcosts associated with HCV related EHM in the EU5 (France Germany
Italy United Kingdom Spain)
1 HCV is the main etiopathological agent as concordantly demonstrated by epidemiological clinico-pathological virological and laboratory investigations2 the association between HCV and disease is demonstrated in a significant proportion of patients and supported by in depth clinico-pathogeneticstudies3 the association is suggested by cohort studies a possible causative role may be limited to a small number of patients andor possibly more relevant in specific geographical areas 4 a number of anecdotal observations suggested a possible role of HCV further investigations are required
The most studied and frequent HCV-EHDs are B-LPDs andor autoimmune disorders
Their prototype is Mixed Cryoglobulinemia (MC) from researches on MC derived most of the
available information
MC as a precious model for all the HCV-EHDs and to evaluate the effects of viral eradication
Anti-HCV Treatment Evolution
IFN
6 mos
PegIFN RBV 12
mos
IFN
12 mos
IFNRBV
12 mos
PegIFN
12 mos
2001
1998
2011
Standardinterferon
Ribavirin
Peginterferon
1991
Direct-actingantivirals
PegIFN
RBV
DAA
IFNRBV
6 mos
6
16
34
4239
55
70+
0
20
40
60
80
100
DAAs
826
weeks
gt90
2015
Few side effects absence major
contraindications
Younossi et al
The annual costs (inpatient outpatient and pharmacy) associatedwith extrahepatic manifestations of HCV were evaluated
Total direct medical costs of extrahepatic manifestations of HCV in 2014US dollars were estimated to be $1506 million (range $922 millionndash
$2208 million in sensitivity analysis)
These estimates should be added to the liver-related burden of diseaseto obtain a more accurate assessment of the total burden of HCV
infection
The OBJECTIVE of the study was to estimate the annual direct medical costs associated with HCV related EHM in the EU5 (France Germany Italy United Kingdom Spain)
22 MCS treated with DAAs including 2 HCC and 2 NHL 100 SVR12 Clinical CR in 64 and PR in remaining 36 The small lymphocytic lymphoma progressed despite viral clearance
Lauletta et al 2017
Emery CS et al 2017
Retrospective analysis 17 MCS (10 with severelife-threatening vasculitis) and 65 asymptomatic CGs+ pts treated with DAAs SVR 889 MCS and 908 asymptomatic pts In MCS clinical response in 1117 (complete in 717) In severelife-threatening vasculitis lower clinical response especially in renal and neurological symptoms
Saadoun D et al 2017
Open-label prospective multi-center study on sofosbuvir plus daclatasvir treatment of 41 HCV MCS SVR in100 and clinical CR in 902 Disappearance of CGs in 50 of pts No serious adverse event or relapse ofvasculitis
Antiviral Treatment (AVT) of MCIFN-free regimens
MC is clinically benign but sometimes severe HCV EHD invalidating symptoms occur and
it may evolve into lymphoma
Cacoub P et al DLD 2014 Zignego AL et al DLD 2007 Zignego AL et al Intern Emerg Med 2012 Zignego AL et al Clin Dev
Immunol 2012 Zignego AL et al Expert Rev Clin Immunol 2015 Sene D et al J Rheumatol 2004
Mixed Cryoglobulinemia-MC
MC pathological substrate is an HCV-driven B-cell
proliferation with consequent production of cryo- and non-
cryoprecipitable CICs in turn responsible for vasculitic
manifestations
Most (70ndash90) MC patients are HCV+ and HCV-patients are CGs+ (40ndash60) while 5ndash30 of
CGs+ have symptomatic MC or cryoglobulinemic vasculitis since HCV infects about 170
million individuals worldwide the number of patients at risk for developing MC is
substantial
Type II CGs
monoclonal
RF+policlonal IgG
Type III CGs both
RF and IgG
polyclonal

The annual costs (inpatient outpatient andpharmacy) associated with extrahepatic
manifestations of HCV were evaluated
Total direct medical costs of extrahepatic
manifestations of HCV in 2014 US dollars wereestimated to be $1506 million (range $922 millionndash
$2208 million in sensitivity analysis)
These estimates should be added to the liver-related
burden of disease to obtain a more accurateassessment of the total burden of HCV infection
Younossi et al
Younossi et al
Costs up to $71000 per patient per year (ESRD) Among the most frequent EHM depression (245 in HCV vs 172 in non-HCV) had estimated annual cost of
$4307 million DM (15 vs 10 in non- HCV) had an annual cost of $4434 million in the USA= given the importance of DM and
its association with CVDs and mortality the clinical and economic impacts of HCV-related DM are substantial
The OBJECTIVE of the study was to estimate the annual direct medical costsassociated with HCV related EHM in the EU5 (France Germany Italy United Kingdom
Spain)
The OBJECTIVE of the study was to estimate the annual direct medicalcosts associated with HCV related EHM in the EU5 (France Germany
Italy United Kingdom Spain)
1 HCV is the main etiopathological agent as concordantly demonstrated by epidemiological clinico-pathological virological and laboratory investigations2 the association between HCV and disease is demonstrated in a significant proportion of patients and supported by in depth clinico-pathogeneticstudies3 the association is suggested by cohort studies a possible causative role may be limited to a small number of patients andor possibly more relevant in specific geographical areas 4 a number of anecdotal observations suggested a possible role of HCV further investigations are required
The most studied and frequent HCV-EHDs are B-LPDs andor autoimmune disorders
Their prototype is Mixed Cryoglobulinemia (MC) from researches on MC derived most of the
available information
MC as a precious model for all the HCV-EHDs and to evaluate the effects of viral eradication
Anti-HCV Treatment Evolution
IFN
6 mos
PegIFN RBV 12
mos
IFN
12 mos
IFNRBV
12 mos
PegIFN
12 mos
2001
1998
2011
Standardinterferon
Ribavirin
Peginterferon
1991
Direct-actingantivirals
PegIFN
RBV
DAA
IFNRBV
6 mos
6
16
34
4239
55
70+
0
20
40
60
80
100
DAAs
826
weeks
gt90
2015
Few side effects absence major
contraindications
Younossi et al
The annual costs (inpatient outpatient and pharmacy) associatedwith extrahepatic manifestations of HCV were evaluated
Total direct medical costs of extrahepatic manifestations of HCV in 2014US dollars were estimated to be $1506 million (range $922 millionndash
$2208 million in sensitivity analysis)
These estimates should be added to the liver-related burden of diseaseto obtain a more accurate assessment of the total burden of HCV
infection
The OBJECTIVE of the study was to estimate the annual direct medical costs associated with HCV related EHM in the EU5 (France Germany Italy United Kingdom Spain)
22 MCS treated with DAAs including 2 HCC and 2 NHL 100 SVR12 Clinical CR in 64 and PR in remaining 36 The small lymphocytic lymphoma progressed despite viral clearance
Lauletta et al 2017
Emery CS et al 2017
Retrospective analysis 17 MCS (10 with severelife-threatening vasculitis) and 65 asymptomatic CGs+ pts treated with DAAs SVR 889 MCS and 908 asymptomatic pts In MCS clinical response in 1117 (complete in 717) In severelife-threatening vasculitis lower clinical response especially in renal and neurological symptoms
Saadoun D et al 2017
Open-label prospective multi-center study on sofosbuvir plus daclatasvir treatment of 41 HCV MCS SVR in100 and clinical CR in 902 Disappearance of CGs in 50 of pts No serious adverse event or relapse ofvasculitis
Antiviral Treatment (AVT) of MCIFN-free regimens
MC is clinically benign but sometimes severe HCV EHD invalidating symptoms occur and
it may evolve into lymphoma
Cacoub P et al DLD 2014 Zignego AL et al DLD 2007 Zignego AL et al Intern Emerg Med 2012 Zignego AL et al Clin Dev
Immunol 2012 Zignego AL et al Expert Rev Clin Immunol 2015 Sene D et al J Rheumatol 2004
Mixed Cryoglobulinemia-MC
MC pathological substrate is an HCV-driven B-cell
proliferation with consequent production of cryo- and non-
cryoprecipitable CICs in turn responsible for vasculitic
manifestations
Most (70ndash90) MC patients are HCV+ and HCV-patients are CGs+ (40ndash60) while 5ndash30 of
CGs+ have symptomatic MC or cryoglobulinemic vasculitis since HCV infects about 170
million individuals worldwide the number of patients at risk for developing MC is
substantial
Type II CGs
monoclonal
RF+policlonal IgG
Type III CGs both
RF and IgG
polyclonal

Younossi et al
Costs up to $71000 per patient per year (ESRD) Among the most frequent EHM depression (245 in HCV vs 172 in non-HCV) had estimated annual cost of
$4307 million DM (15 vs 10 in non- HCV) had an annual cost of $4434 million in the USA= given the importance of DM and
its association with CVDs and mortality the clinical and economic impacts of HCV-related DM are substantial
The OBJECTIVE of the study was to estimate the annual direct medical costsassociated with HCV related EHM in the EU5 (France Germany Italy United Kingdom
Spain)
The OBJECTIVE of the study was to estimate the annual direct medicalcosts associated with HCV related EHM in the EU5 (France Germany
Italy United Kingdom Spain)
1 HCV is the main etiopathological agent as concordantly demonstrated by epidemiological clinico-pathological virological and laboratory investigations2 the association between HCV and disease is demonstrated in a significant proportion of patients and supported by in depth clinico-pathogeneticstudies3 the association is suggested by cohort studies a possible causative role may be limited to a small number of patients andor possibly more relevant in specific geographical areas 4 a number of anecdotal observations suggested a possible role of HCV further investigations are required
The most studied and frequent HCV-EHDs are B-LPDs andor autoimmune disorders
Their prototype is Mixed Cryoglobulinemia (MC) from researches on MC derived most of the
available information
MC as a precious model for all the HCV-EHDs and to evaluate the effects of viral eradication
Anti-HCV Treatment Evolution
IFN
6 mos
PegIFN RBV 12
mos
IFN
12 mos
IFNRBV
12 mos
PegIFN
12 mos
2001
1998
2011
Standardinterferon
Ribavirin
Peginterferon
1991
Direct-actingantivirals
PegIFN
RBV
DAA
IFNRBV
6 mos
6
16
34
4239
55
70+
0
20
40
60
80
100
DAAs
826
weeks
gt90
2015
Few side effects absence major
contraindications
Younossi et al
The annual costs (inpatient outpatient and pharmacy) associatedwith extrahepatic manifestations of HCV were evaluated
Total direct medical costs of extrahepatic manifestations of HCV in 2014US dollars were estimated to be $1506 million (range $922 millionndash
$2208 million in sensitivity analysis)
These estimates should be added to the liver-related burden of diseaseto obtain a more accurate assessment of the total burden of HCV
infection
The OBJECTIVE of the study was to estimate the annual direct medical costs associated with HCV related EHM in the EU5 (France Germany Italy United Kingdom Spain)
22 MCS treated with DAAs including 2 HCC and 2 NHL 100 SVR12 Clinical CR in 64 and PR in remaining 36 The small lymphocytic lymphoma progressed despite viral clearance
Lauletta et al 2017
Emery CS et al 2017
Retrospective analysis 17 MCS (10 with severelife-threatening vasculitis) and 65 asymptomatic CGs+ pts treated with DAAs SVR 889 MCS and 908 asymptomatic pts In MCS clinical response in 1117 (complete in 717) In severelife-threatening vasculitis lower clinical response especially in renal and neurological symptoms
Saadoun D et al 2017
Open-label prospective multi-center study on sofosbuvir plus daclatasvir treatment of 41 HCV MCS SVR in100 and clinical CR in 902 Disappearance of CGs in 50 of pts No serious adverse event or relapse ofvasculitis
Antiviral Treatment (AVT) of MCIFN-free regimens
MC is clinically benign but sometimes severe HCV EHD invalidating symptoms occur and
it may evolve into lymphoma
Cacoub P et al DLD 2014 Zignego AL et al DLD 2007 Zignego AL et al Intern Emerg Med 2012 Zignego AL et al Clin Dev
Immunol 2012 Zignego AL et al Expert Rev Clin Immunol 2015 Sene D et al J Rheumatol 2004
Mixed Cryoglobulinemia-MC
MC pathological substrate is an HCV-driven B-cell
proliferation with consequent production of cryo- and non-
cryoprecipitable CICs in turn responsible for vasculitic
manifestations
Most (70ndash90) MC patients are HCV+ and HCV-patients are CGs+ (40ndash60) while 5ndash30 of
CGs+ have symptomatic MC or cryoglobulinemic vasculitis since HCV infects about 170
million individuals worldwide the number of patients at risk for developing MC is
substantial
Type II CGs
monoclonal
RF+policlonal IgG
Type III CGs both
RF and IgG
polyclonal

The OBJECTIVE of the study was to estimate the annual direct medical costsassociated with HCV related EHM in the EU5 (France Germany Italy United Kingdom
Spain)
The OBJECTIVE of the study was to estimate the annual direct medicalcosts associated with HCV related EHM in the EU5 (France Germany
Italy United Kingdom Spain)
1 HCV is the main etiopathological agent as concordantly demonstrated by epidemiological clinico-pathological virological and laboratory investigations2 the association between HCV and disease is demonstrated in a significant proportion of patients and supported by in depth clinico-pathogeneticstudies3 the association is suggested by cohort studies a possible causative role may be limited to a small number of patients andor possibly more relevant in specific geographical areas 4 a number of anecdotal observations suggested a possible role of HCV further investigations are required
The most studied and frequent HCV-EHDs are B-LPDs andor autoimmune disorders
Their prototype is Mixed Cryoglobulinemia (MC) from researches on MC derived most of the
available information
MC as a precious model for all the HCV-EHDs and to evaluate the effects of viral eradication
Anti-HCV Treatment Evolution
IFN
6 mos
PegIFN RBV 12
mos
IFN
12 mos
IFNRBV
12 mos
PegIFN
12 mos
2001
1998
2011
Standardinterferon
Ribavirin
Peginterferon
1991
Direct-actingantivirals
PegIFN
RBV
DAA
IFNRBV
6 mos
6
16
34
4239
55
70+
0
20
40
60
80
100
DAAs
826
weeks
gt90
2015
Few side effects absence major
contraindications
Younossi et al
The annual costs (inpatient outpatient and pharmacy) associatedwith extrahepatic manifestations of HCV were evaluated
Total direct medical costs of extrahepatic manifestations of HCV in 2014US dollars were estimated to be $1506 million (range $922 millionndash
$2208 million in sensitivity analysis)
These estimates should be added to the liver-related burden of diseaseto obtain a more accurate assessment of the total burden of HCV
infection
The OBJECTIVE of the study was to estimate the annual direct medical costs associated with HCV related EHM in the EU5 (France Germany Italy United Kingdom Spain)
22 MCS treated with DAAs including 2 HCC and 2 NHL 100 SVR12 Clinical CR in 64 and PR in remaining 36 The small lymphocytic lymphoma progressed despite viral clearance
Lauletta et al 2017
Emery CS et al 2017
Retrospective analysis 17 MCS (10 with severelife-threatening vasculitis) and 65 asymptomatic CGs+ pts treated with DAAs SVR 889 MCS and 908 asymptomatic pts In MCS clinical response in 1117 (complete in 717) In severelife-threatening vasculitis lower clinical response especially in renal and neurological symptoms
Saadoun D et al 2017
Open-label prospective multi-center study on sofosbuvir plus daclatasvir treatment of 41 HCV MCS SVR in100 and clinical CR in 902 Disappearance of CGs in 50 of pts No serious adverse event or relapse ofvasculitis
Antiviral Treatment (AVT) of MCIFN-free regimens
MC is clinically benign but sometimes severe HCV EHD invalidating symptoms occur and
it may evolve into lymphoma
Cacoub P et al DLD 2014 Zignego AL et al DLD 2007 Zignego AL et al Intern Emerg Med 2012 Zignego AL et al Clin Dev
Immunol 2012 Zignego AL et al Expert Rev Clin Immunol 2015 Sene D et al J Rheumatol 2004
Mixed Cryoglobulinemia-MC
MC pathological substrate is an HCV-driven B-cell
proliferation with consequent production of cryo- and non-
cryoprecipitable CICs in turn responsible for vasculitic
manifestations
Most (70ndash90) MC patients are HCV+ and HCV-patients are CGs+ (40ndash60) while 5ndash30 of
CGs+ have symptomatic MC or cryoglobulinemic vasculitis since HCV infects about 170
million individuals worldwide the number of patients at risk for developing MC is
substantial
Type II CGs
monoclonal
RF+policlonal IgG
Type III CGs both
RF and IgG
polyclonal

The OBJECTIVE of the study was to estimate the annual direct medicalcosts associated with HCV related EHM in the EU5 (France Germany
Italy United Kingdom Spain)
1 HCV is the main etiopathological agent as concordantly demonstrated by epidemiological clinico-pathological virological and laboratory investigations2 the association between HCV and disease is demonstrated in a significant proportion of patients and supported by in depth clinico-pathogeneticstudies3 the association is suggested by cohort studies a possible causative role may be limited to a small number of patients andor possibly more relevant in specific geographical areas 4 a number of anecdotal observations suggested a possible role of HCV further investigations are required
The most studied and frequent HCV-EHDs are B-LPDs andor autoimmune disorders
Their prototype is Mixed Cryoglobulinemia (MC) from researches on MC derived most of the
available information
MC as a precious model for all the HCV-EHDs and to evaluate the effects of viral eradication
Anti-HCV Treatment Evolution
IFN
6 mos
PegIFN RBV 12
mos
IFN
12 mos
IFNRBV
12 mos
PegIFN
12 mos
2001
1998
2011
Standardinterferon
Ribavirin
Peginterferon
1991
Direct-actingantivirals
PegIFN
RBV
DAA
IFNRBV
6 mos
6
16
34
4239
55
70+
0
20
40
60
80
100
DAAs
826
weeks
gt90
2015
Few side effects absence major
contraindications
Younossi et al
The annual costs (inpatient outpatient and pharmacy) associatedwith extrahepatic manifestations of HCV were evaluated
Total direct medical costs of extrahepatic manifestations of HCV in 2014US dollars were estimated to be $1506 million (range $922 millionndash
$2208 million in sensitivity analysis)
These estimates should be added to the liver-related burden of diseaseto obtain a more accurate assessment of the total burden of HCV
infection
The OBJECTIVE of the study was to estimate the annual direct medical costs associated with HCV related EHM in the EU5 (France Germany Italy United Kingdom Spain)
22 MCS treated with DAAs including 2 HCC and 2 NHL 100 SVR12 Clinical CR in 64 and PR in remaining 36 The small lymphocytic lymphoma progressed despite viral clearance
Lauletta et al 2017
Emery CS et al 2017
Retrospective analysis 17 MCS (10 with severelife-threatening vasculitis) and 65 asymptomatic CGs+ pts treated with DAAs SVR 889 MCS and 908 asymptomatic pts In MCS clinical response in 1117 (complete in 717) In severelife-threatening vasculitis lower clinical response especially in renal and neurological symptoms
Saadoun D et al 2017
Open-label prospective multi-center study on sofosbuvir plus daclatasvir treatment of 41 HCV MCS SVR in100 and clinical CR in 902 Disappearance of CGs in 50 of pts No serious adverse event or relapse ofvasculitis
Antiviral Treatment (AVT) of MCIFN-free regimens
MC is clinically benign but sometimes severe HCV EHD invalidating symptoms occur and
it may evolve into lymphoma
Cacoub P et al DLD 2014 Zignego AL et al DLD 2007 Zignego AL et al Intern Emerg Med 2012 Zignego AL et al Clin Dev
Immunol 2012 Zignego AL et al Expert Rev Clin Immunol 2015 Sene D et al J Rheumatol 2004
Mixed Cryoglobulinemia-MC
MC pathological substrate is an HCV-driven B-cell
proliferation with consequent production of cryo- and non-
cryoprecipitable CICs in turn responsible for vasculitic
manifestations
Most (70ndash90) MC patients are HCV+ and HCV-patients are CGs+ (40ndash60) while 5ndash30 of
CGs+ have symptomatic MC or cryoglobulinemic vasculitis since HCV infects about 170
million individuals worldwide the number of patients at risk for developing MC is
substantial
Type II CGs
monoclonal
RF+policlonal IgG
Type III CGs both
RF and IgG
polyclonal

1 HCV is the main etiopathological agent as concordantly demonstrated by epidemiological clinico-pathological virological and laboratory investigations2 the association between HCV and disease is demonstrated in a significant proportion of patients and supported by in depth clinico-pathogeneticstudies3 the association is suggested by cohort studies a possible causative role may be limited to a small number of patients andor possibly more relevant in specific geographical areas 4 a number of anecdotal observations suggested a possible role of HCV further investigations are required
The most studied and frequent HCV-EHDs are B-LPDs andor autoimmune disorders
Their prototype is Mixed Cryoglobulinemia (MC) from researches on MC derived most of the
available information
MC as a precious model for all the HCV-EHDs and to evaluate the effects of viral eradication
Anti-HCV Treatment Evolution
IFN
6 mos
PegIFN RBV 12
mos
IFN
12 mos
IFNRBV
12 mos
PegIFN
12 mos
2001
1998
2011
Standardinterferon
Ribavirin
Peginterferon
1991
Direct-actingantivirals
PegIFN
RBV
DAA
IFNRBV
6 mos
6
16
34
4239
55
70+
0
20
40
60
80
100
DAAs
826
weeks
gt90
2015
Few side effects absence major
contraindications
Younossi et al
The annual costs (inpatient outpatient and pharmacy) associatedwith extrahepatic manifestations of HCV were evaluated
Total direct medical costs of extrahepatic manifestations of HCV in 2014US dollars were estimated to be $1506 million (range $922 millionndash
$2208 million in sensitivity analysis)
These estimates should be added to the liver-related burden of diseaseto obtain a more accurate assessment of the total burden of HCV
infection
The OBJECTIVE of the study was to estimate the annual direct medical costs associated with HCV related EHM in the EU5 (France Germany Italy United Kingdom Spain)
22 MCS treated with DAAs including 2 HCC and 2 NHL 100 SVR12 Clinical CR in 64 and PR in remaining 36 The small lymphocytic lymphoma progressed despite viral clearance
Lauletta et al 2017
Emery CS et al 2017
Retrospective analysis 17 MCS (10 with severelife-threatening vasculitis) and 65 asymptomatic CGs+ pts treated with DAAs SVR 889 MCS and 908 asymptomatic pts In MCS clinical response in 1117 (complete in 717) In severelife-threatening vasculitis lower clinical response especially in renal and neurological symptoms
Saadoun D et al 2017
Open-label prospective multi-center study on sofosbuvir plus daclatasvir treatment of 41 HCV MCS SVR in100 and clinical CR in 902 Disappearance of CGs in 50 of pts No serious adverse event or relapse ofvasculitis
Antiviral Treatment (AVT) of MCIFN-free regimens
MC is clinically benign but sometimes severe HCV EHD invalidating symptoms occur and
it may evolve into lymphoma
Cacoub P et al DLD 2014 Zignego AL et al DLD 2007 Zignego AL et al Intern Emerg Med 2012 Zignego AL et al Clin Dev
Immunol 2012 Zignego AL et al Expert Rev Clin Immunol 2015 Sene D et al J Rheumatol 2004
Mixed Cryoglobulinemia-MC
MC pathological substrate is an HCV-driven B-cell
proliferation with consequent production of cryo- and non-
cryoprecipitable CICs in turn responsible for vasculitic
manifestations
Most (70ndash90) MC patients are HCV+ and HCV-patients are CGs+ (40ndash60) while 5ndash30 of
CGs+ have symptomatic MC or cryoglobulinemic vasculitis since HCV infects about 170
million individuals worldwide the number of patients at risk for developing MC is
substantial
Type II CGs
monoclonal
RF+policlonal IgG
Type III CGs both
RF and IgG
polyclonal

Anti-HCV Treatment Evolution
IFN
6 mos
PegIFN RBV 12
mos
IFN
12 mos
IFNRBV
12 mos
PegIFN
12 mos
2001
1998
2011
Standardinterferon
Ribavirin
Peginterferon
1991
Direct-actingantivirals
PegIFN
RBV
DAA
IFNRBV
6 mos
6
16
34
4239
55
70+
0
20
40
60
80
100
DAAs
826
weeks
gt90
2015
Few side effects absence major
contraindications
Younossi et al
The annual costs (inpatient outpatient and pharmacy) associatedwith extrahepatic manifestations of HCV were evaluated
Total direct medical costs of extrahepatic manifestations of HCV in 2014US dollars were estimated to be $1506 million (range $922 millionndash
$2208 million in sensitivity analysis)
These estimates should be added to the liver-related burden of diseaseto obtain a more accurate assessment of the total burden of HCV
infection
The OBJECTIVE of the study was to estimate the annual direct medical costs associated with HCV related EHM in the EU5 (France Germany Italy United Kingdom Spain)
22 MCS treated with DAAs including 2 HCC and 2 NHL 100 SVR12 Clinical CR in 64 and PR in remaining 36 The small lymphocytic lymphoma progressed despite viral clearance
Lauletta et al 2017
Emery CS et al 2017
Retrospective analysis 17 MCS (10 with severelife-threatening vasculitis) and 65 asymptomatic CGs+ pts treated with DAAs SVR 889 MCS and 908 asymptomatic pts In MCS clinical response in 1117 (complete in 717) In severelife-threatening vasculitis lower clinical response especially in renal and neurological symptoms
Saadoun D et al 2017
Open-label prospective multi-center study on sofosbuvir plus daclatasvir treatment of 41 HCV MCS SVR in100 and clinical CR in 902 Disappearance of CGs in 50 of pts No serious adverse event or relapse ofvasculitis
Antiviral Treatment (AVT) of MCIFN-free regimens
MC is clinically benign but sometimes severe HCV EHD invalidating symptoms occur and
it may evolve into lymphoma
Cacoub P et al DLD 2014 Zignego AL et al DLD 2007 Zignego AL et al Intern Emerg Med 2012 Zignego AL et al Clin Dev
Immunol 2012 Zignego AL et al Expert Rev Clin Immunol 2015 Sene D et al J Rheumatol 2004
Mixed Cryoglobulinemia-MC
MC pathological substrate is an HCV-driven B-cell
proliferation with consequent production of cryo- and non-
cryoprecipitable CICs in turn responsible for vasculitic
manifestations
Most (70ndash90) MC patients are HCV+ and HCV-patients are CGs+ (40ndash60) while 5ndash30 of
CGs+ have symptomatic MC or cryoglobulinemic vasculitis since HCV infects about 170
million individuals worldwide the number of patients at risk for developing MC is
substantial
Type II CGs
monoclonal
RF+policlonal IgG
Type III CGs both
RF and IgG
polyclonal

Younossi et al
The annual costs (inpatient outpatient and pharmacy) associatedwith extrahepatic manifestations of HCV were evaluated
Total direct medical costs of extrahepatic manifestations of HCV in 2014US dollars were estimated to be $1506 million (range $922 millionndash
$2208 million in sensitivity analysis)
These estimates should be added to the liver-related burden of diseaseto obtain a more accurate assessment of the total burden of HCV
infection
The OBJECTIVE of the study was to estimate the annual direct medical costs associated with HCV related EHM in the EU5 (France Germany Italy United Kingdom Spain)
22 MCS treated with DAAs including 2 HCC and 2 NHL 100 SVR12 Clinical CR in 64 and PR in remaining 36 The small lymphocytic lymphoma progressed despite viral clearance
Lauletta et al 2017
Emery CS et al 2017
Retrospective analysis 17 MCS (10 with severelife-threatening vasculitis) and 65 asymptomatic CGs+ pts treated with DAAs SVR 889 MCS and 908 asymptomatic pts In MCS clinical response in 1117 (complete in 717) In severelife-threatening vasculitis lower clinical response especially in renal and neurological symptoms
Saadoun D et al 2017
Open-label prospective multi-center study on sofosbuvir plus daclatasvir treatment of 41 HCV MCS SVR in100 and clinical CR in 902 Disappearance of CGs in 50 of pts No serious adverse event or relapse ofvasculitis
Antiviral Treatment (AVT) of MCIFN-free regimens
MC is clinically benign but sometimes severe HCV EHD invalidating symptoms occur and
it may evolve into lymphoma
Cacoub P et al DLD 2014 Zignego AL et al DLD 2007 Zignego AL et al Intern Emerg Med 2012 Zignego AL et al Clin Dev
Immunol 2012 Zignego AL et al Expert Rev Clin Immunol 2015 Sene D et al J Rheumatol 2004
Mixed Cryoglobulinemia-MC
MC pathological substrate is an HCV-driven B-cell
proliferation with consequent production of cryo- and non-
cryoprecipitable CICs in turn responsible for vasculitic
manifestations
Most (70ndash90) MC patients are HCV+ and HCV-patients are CGs+ (40ndash60) while 5ndash30 of
CGs+ have symptomatic MC or cryoglobulinemic vasculitis since HCV infects about 170
million individuals worldwide the number of patients at risk for developing MC is
substantial
Type II CGs
monoclonal
RF+policlonal IgG
Type III CGs both
RF and IgG
polyclonal
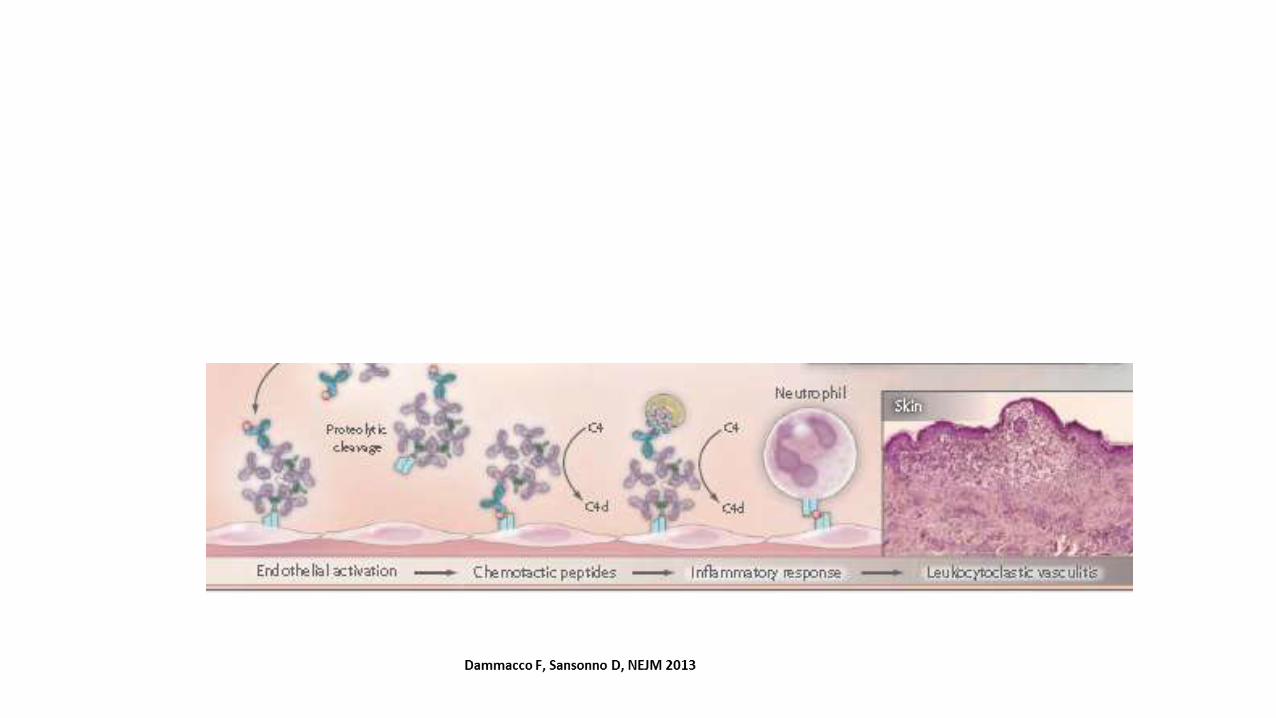
The OBJECTIVE of the study was to estimate the annual direct medical costs associated with HCV related EHM in the EU5 (France Germany Italy United Kingdom Spain)
22 MCS treated with DAAs including 2 HCC and 2 NHL 100 SVR12 Clinical CR in 64 and PR in remaining 36 The small lymphocytic lymphoma progressed despite viral clearance
Lauletta et al 2017
Emery CS et al 2017
Retrospective analysis 17 MCS (10 with severelife-threatening vasculitis) and 65 asymptomatic CGs+ pts treated with DAAs SVR 889 MCS and 908 asymptomatic pts In MCS clinical response in 1117 (complete in 717) In severelife-threatening vasculitis lower clinical response especially in renal and neurological symptoms
Saadoun D et al 2017
Open-label prospective multi-center study on sofosbuvir plus daclatasvir treatment of 41 HCV MCS SVR in100 and clinical CR in 902 Disappearance of CGs in 50 of pts No serious adverse event or relapse ofvasculitis
Antiviral Treatment (AVT) of MCIFN-free regimens
MC is clinically benign but sometimes severe HCV EHD invalidating symptoms occur and
it may evolve into lymphoma
Cacoub P et al DLD 2014 Zignego AL et al DLD 2007 Zignego AL et al Intern Emerg Med 2012 Zignego AL et al Clin Dev
Immunol 2012 Zignego AL et al Expert Rev Clin Immunol 2015 Sene D et al J Rheumatol 2004
Mixed Cryoglobulinemia-MC
MC pathological substrate is an HCV-driven B-cell
proliferation with consequent production of cryo- and non-
cryoprecipitable CICs in turn responsible for vasculitic
manifestations
Most (70ndash90) MC patients are HCV+ and HCV-patients are CGs+ (40ndash60) while 5ndash30 of
CGs+ have symptomatic MC or cryoglobulinemic vasculitis since HCV infects about 170
million individuals worldwide the number of patients at risk for developing MC is
substantial
Type II CGs
monoclonal
RF+policlonal IgG
Type III CGs both
RF and IgG
polyclonal

22 MCS treated with DAAs including 2 HCC and 2 NHL 100 SVR12 Clinical CR in 64 and PR in remaining 36 The small lymphocytic lymphoma progressed despite viral clearance
Lauletta et al 2017
Emery CS et al 2017
Retrospective analysis 17 MCS (10 with severelife-threatening vasculitis) and 65 asymptomatic CGs+ pts treated with DAAs SVR 889 MCS and 908 asymptomatic pts In MCS clinical response in 1117 (complete in 717) In severelife-threatening vasculitis lower clinical response especially in renal and neurological symptoms
Saadoun D et al 2017
Open-label prospective multi-center study on sofosbuvir plus daclatasvir treatment of 41 HCV MCS SVR in100 and clinical CR in 902 Disappearance of CGs in 50 of pts No serious adverse event or relapse ofvasculitis
Antiviral Treatment (AVT) of MCIFN-free regimens
MC is clinically benign but sometimes severe HCV EHD invalidating symptoms occur and
it may evolve into lymphoma
Cacoub P et al DLD 2014 Zignego AL et al DLD 2007 Zignego AL et al Intern Emerg Med 2012 Zignego AL et al Clin Dev
Immunol 2012 Zignego AL et al Expert Rev Clin Immunol 2015 Sene D et al J Rheumatol 2004
Mixed Cryoglobulinemia-MC
MC pathological substrate is an HCV-driven B-cell
proliferation with consequent production of cryo- and non-
cryoprecipitable CICs in turn responsible for vasculitic
manifestations
Most (70ndash90) MC patients are HCV+ and HCV-patients are CGs+ (40ndash60) while 5ndash30 of
CGs+ have symptomatic MC or cryoglobulinemic vasculitis since HCV infects about 170
million individuals worldwide the number of patients at risk for developing MC is
substantial
Type II CGs
monoclonal
RF+policlonal IgG
Type III CGs both
RF and IgG
polyclonal

MC is clinically benign but sometimes severe HCV EHD invalidating symptoms occur and
it may evolve into lymphoma
Cacoub P et al DLD 2014 Zignego AL et al DLD 2007 Zignego AL et al Intern Emerg Med 2012 Zignego AL et al Clin Dev
Immunol 2012 Zignego AL et al Expert Rev Clin Immunol 2015 Sene D et al J Rheumatol 2004
Mixed Cryoglobulinemia-MC
MC pathological substrate is an HCV-driven B-cell
proliferation with consequent production of cryo- and non-
cryoprecipitable CICs in turn responsible for vasculitic
manifestations
Most (70ndash90) MC patients are HCV+ and HCV-patients are CGs+ (40ndash60) while 5ndash30 of
CGs+ have symptomatic MC or cryoglobulinemic vasculitis since HCV infects about 170
million individuals worldwide the number of patients at risk for developing MC is
substantial
Type II CGs
monoclonal
RF+policlonal IgG
Type III CGs both
RF and IgG
polyclonal


















