Rigid probl/cosmetic dentistry course
143
INDIAN DENTAL ACADEMY Leader in continuing dental education www.indiandentalacademy.com www.indiandentalacademy.com
-
Upload
indian-dental-academy -
Category
Education
-
view
135 -
download
0
Transcript of Rigid probl/cosmetic dentistry course

INDIAN DENTAL ACADEMY
Leader in continuing dental education
www.indiandentalacademy.com
www.indiandentalacademy.com

Part I
• Introduction
• Keys to bone grafting
Bone grafting materials
Socket grafting
Part II
Maxillary sinus lift & sinus graft surgery
Intraoral autogenous donor bone grafts
Extraoral autogenous donor bone graftswww.indiandentalacademy.com

www.indiandentalacademy.com

Absence of infection
Soft tissue closure
Space maintenance
Graft immobilization
Regional acceleratory phenomenon (RAP)
Host bone vascularization
Growth factors
BMPs
Healing time
Defect size & topography
Transitional prosthesis
www.indiandentalacademy.com

Rapid solution mediated resorption in conditions of
low PH
www.indiandentalacademy.com

Causes of graft material infection
Endogenous bacteria
Lack of aseptic surgical technique
Failure of primary soft tissue closure
Lack of blood supply in early stages of
grafting
www.indiandentalacademy.com
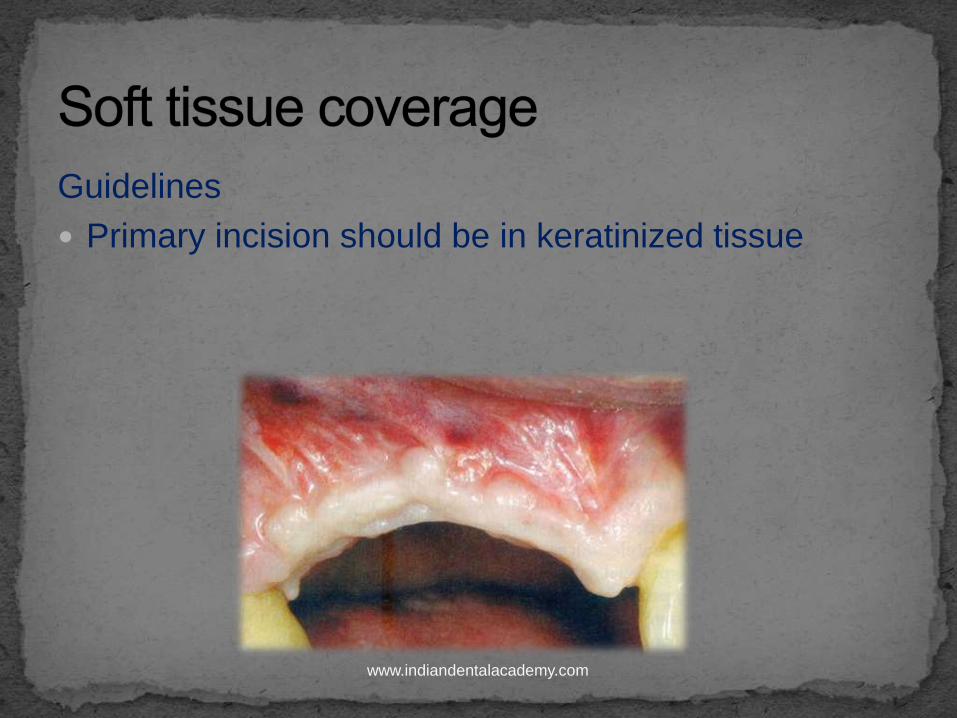
Guidelines
Primary incision should be in keratinized tissue
www.indiandentalacademy.com

Crestal incisionis designed more lingual
www.indiandentalacademy.com

Vertical incisions
www.indiandentalacademy.com

Vertical incisions are made to the height of MGJ &
flap is retracted only 5 mm above the height of MGJ.
This maintains more blood supply to the facial flap
Incision is not extended to mobile mucosa
www.indiandentalacademy.com

Soft tissue reflection distal to graft
Site is split thickness
Maintains some of the periosteum around incision
line
Early vascularization of incision line
Adhesion of the margins to reduce retraction during
initial healing
www.indiandentalacademy.com
2 techniques depending on
If less than 5 mm of advancement is necessary
To expand tissue over larger graft sites (15 x 10 mm)
-- submucosal space technique
www.indiandentalacademy.com
For a small graft site
More apical tissue reflection
Horizontal scoring of the periosteum parallel to
primary incision
www.indiandentalacademy.com
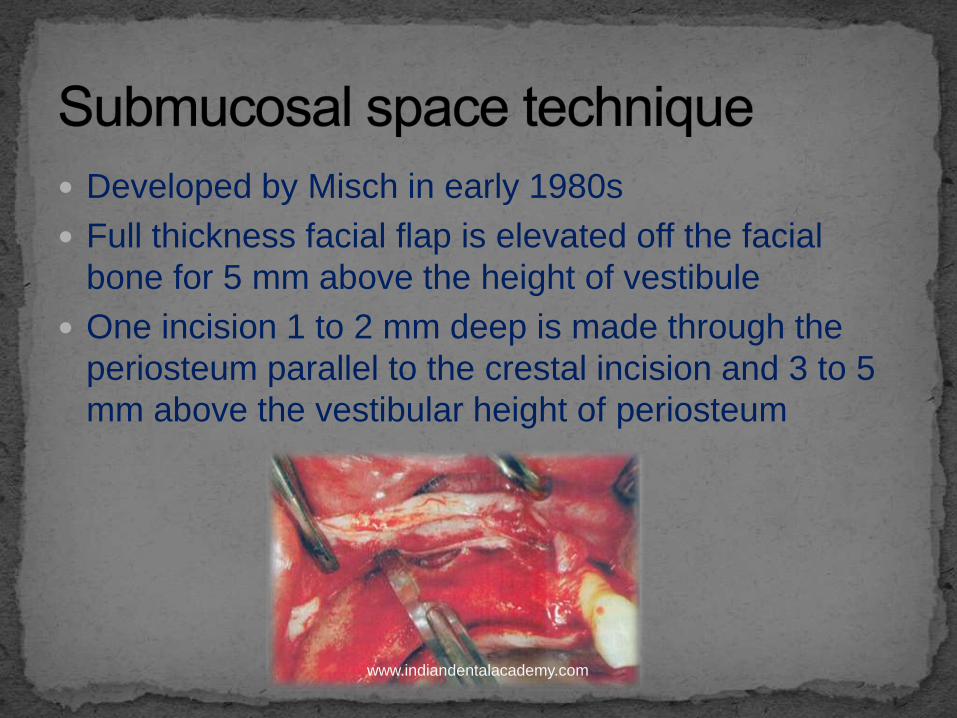
Developed by Misch in early 1980s
Full thickness facial flap is elevated off the facial
bone for 5 mm above the height of vestibule
One incision 1 to 2 mm deep is made through the
periosteum parallel to the crestal incision and 3 to 5
mm above the vestibular height of periosteum
www.indiandentalacademy.com

Blunt dissection is done using soft tissue scissors
(metzenbaum ) to create a tunnel apical to the
vestibule & above the unreflected periosteum
www.indiandentalacademy.com
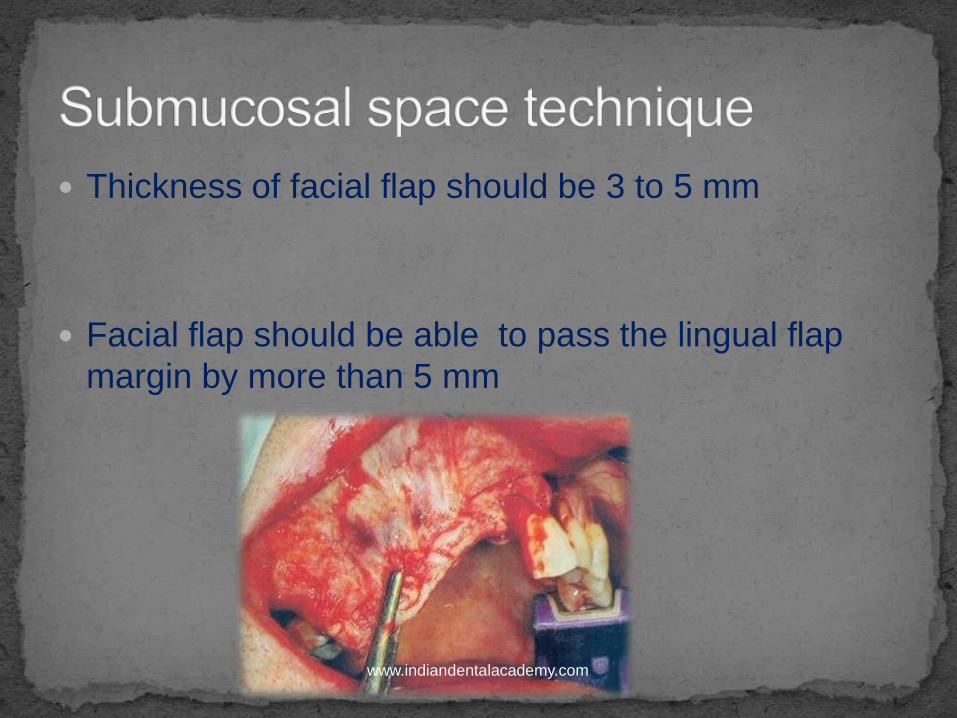
Thickness of facial flap should be 3 to 5 mm
Facial flap should be able to pass the lingual flap
margin by more than 5 mm
www.indiandentalacademy.com

Disadvantages
Loss of vestibular depth
Lack of keratinized tissue on facial region of grafted
site
www.indiandentalacademy.com

Methods
Tent screws
Barrier membrane
Ti reinforced membranes
Graft material beneath the membrane
www.indiandentalacademy.com

Barrier by bulk
Concept given by Misch
www.indiandentalacademy.com

Methods
Bone tacks
Tent screw
Bone screws work better with block bone grafts
than particulate
www.indiandentalacademy.com

Fixed transitional prosthesis
Indicated with barrier by bulk tech. using particulate
material
Prosthesis should have rest seats & clasps to
prevent loading soft tissues
www.indiandentalacademy.com

Local response to a noxious stimulus by which tissue
forms faster than the normal regional regeneration
rate
Healing is 2 to 10 times faster than normal
physiologic healing
Begins within a few days after injury , peaks at 1 to 2
months usually lasts 4 months in bone & may take
upto 6 to 24 months to subside
www.indiandentalacademy.com

www.indiandentalacademy.com

Source of blood vesels
Host cortical bone (few arterioles
Cancellous bone (intensely vascular network
Blood vessels are needed to
Help the autograftmaintain vitality
To repopulate the area with osteoblasts www.indiandentalacademy.com

Host site is decorticated with a rotary drill to increase
amount of host blood vessels at the graft site
There should be spaces available between graft
particles for blood vessels to enter
www.indiandentalacademy.com

Methods to increase tissue growth factors at graft site-
Use of autologous bone in graft
PRP
Use of allografts
RAP
www.indiandentalacademy.com

Gerald D , Carlson ER , Gotcher JE et al
J of Oral Maxillofacial Surg 2006 : 64 (443 – 451)
PDGF mixed with autologous bone can accelerate
mineralization by as much as 40 % during the first
year
www.indiandentalacademy.com

Factors affecting healing time
Local
Number of remaining walls of bone
Amount of autogenous bone in the graft
Size of the defect
Systemic
Diabetes
Hyperparathyroidism
Thyrotoxicosis
Osteomalacia
Osteoporosis
Paget’s diseasewww.indiandentalacademy.com
4 to 6 months -- graft volume is less than
5 mm
6 to 10 months -- graft volume is more
than 5 mm
www.indiandentalacademy.com

Defect size effect following aspects of augmentation
Healing time
Vascularization
Transitional prosthesis
Graft material selection
www.indiandentalacademy.com
Augmentation will be faster in an
extraction socket surrounded by 5
walls than for a onlay graft on div
D bone
www.indiandentalacademy.com

Transitional resto. effects
Soft tissue closure
Maintenance of space
Immobilization of graft during healing
Restores esthetics & function
Contours the soft tissue
www.indiandentalacademy.com

Transitional acrylic FPD
Metal reinforced acrylic FPD
Resin bonded prosthesis
Fixed temporary - eg temporaray implants
Removable restoration
www.indiandentalacademy.com

www.indiandentalacademy.com

Bone graft materials
collagen
Osteogenic
Eg autologousbone
Osteoinductive
Eg DFDB
osteoconductive
www.indiandentalacademy.com

Sources
Bovine collagen from achilles tendon in the
leg
DFDB
Collagen barrier membranes used for GBR
Resorption rates vary from a few months
to 1 year
www.indiandentalacademy.com

Autogenous trabecular bone
• Contains more osteoblasts
• More osteogenic
Autogenous cortical bone
• Contains more bone growth factors
• More osteoinductive
www.indiandentalacademy.com

Should remain vital to be able to produce osteoid
Recipient site is prepared first
Should be placed immediately after harvesting or stored
in
Sterile saline
lactated ringers solution
www.indiandentalacademy.com

Should not be mixed with other synthetic graft
materials
www.indiandentalacademy.com

Decortication of host bone
Directly placed on host bone
www.indiandentalacademy.com
Phase I
Osteogenesis
Bone regeneration by
surviving cells (osteoid)
4 weeks
Phase II
Osteoinduction
BMP release
2 wks to 6 months , peak at
6 wks
Phase III
Osteoconduction
Inorganic matrix
replaced by creeping
substitution
Phase IV
Cortical plate acts as a
barrier membrane
www.indiandentalacademy.com

The only osteogenic graft material
Osteoinductive property
Osteoconduction
Space maintenance- maintains contour of desired
augmentation
www.indiandentalacademy.com

Bone autografts
Allograftsosseous transplanted tissues from the same species as the recepientbut of different genotype
• Frozen bone
• Freeze dried bone
• Demineralized freeze dried bonewww.indiandentalacademy.com

Bone can be harvested , frozen & stored to be used
in the same patient at a later date
Allograft frozen bone is rarely used because of risk
of rejection & disease transmission
www.indiandentalacademy.com

Cortical & trabecular bone is harvested in a sterile
fashion from a disease free donor
Washed in distilled water & ground to a particle size of
500 micron to 5 mm
Immersed in 100 % ethanol to remove fat
Frozen in nitrogen
Freeze dried & ground to smaller particle size of 250 to
1500 micron
www.indiandentalacademy.com

Marx RE , Wong ME
J of Oral & maxillofacial surg 1987 : 45 ( page 988)
Solvent prserved products have been developed
instead of freeze drying to reduce antigenicity &
assure a minimal risk of contamination
www.indiandentalacademy.com

Ground bone powder is demineralized in 0.6 N HCl
or nitric acid for 6 to 16 hrs.
After acid bath it is washed & dehydrated
www.indiandentalacademy.com

Irradiation
• Doses greater than 2.5 Mrad are destructive to BMPs
Ethylene oxide sterilization
• 5 hr sterilization at 29 degree celsiusto maintain osteoinductive properties
www.indiandentalacademy.com

Age of cadaver
Type of bone
Cortical bone contains higher conc. Of BMPs than trabecularbone
Membranous cortical bone exhibits greater conc. Of BMPs than endochondral cortical bone
Particle size
Particles smaller than 150 micron are less effective than 250 micron or larger
Fibres of cortical bone (eg grafton ) are more effective than particles.
www.indiandentalacademy.com

Putty consistency products
Fillers do not participate in bone formation
www.indiandentalacademy.com

Allografts
• Freeze dried bone
Alloplasts
• Ceramics
• Polymers
• composites
Xenografts
• Fabricated from inorganic portion of bone from animals other than humans
www.indiandentalacademy.com

• Aluminium oxide
• Ti oxideBioinert
• Ca Phosphate
• Synthetic HA
• Bovine derived bone matrix
• Tricalcium phosphates
• Calcium carbonates
Bioactive
www.indiandentalacademy.com
• Non resorbable
• resorbable
• Dense
• porous
• Crysstalline
• amorphous
www.indiandentalacademy.com

www.indiandentalacademy.com

Atraumatic tooth extraction
Socket grafting
www.indiandentalacademy.com

Periosteum should not be reflected if bone volume is
ideal as it helps bone remodellimg or repair
Soft tissue drape around the tooth is also affected by
reflection of periosteum
www.indiandentalacademy.com
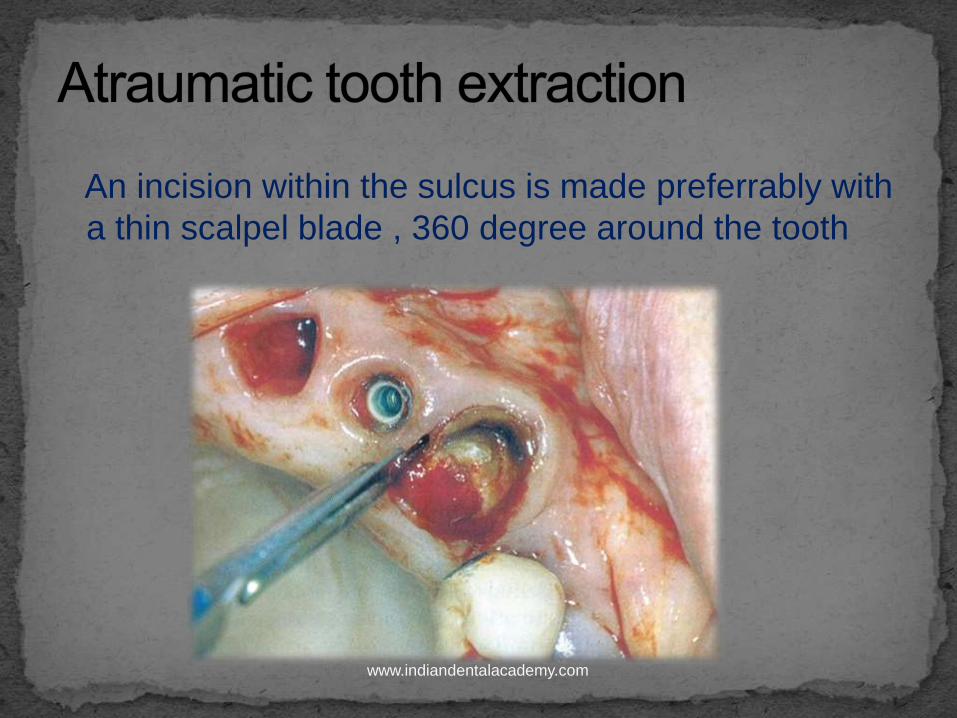
An incision within the sulcus is made preferrably with
a thin scalpel blade , 360 degree around the tooth
www.indiandentalacademy.com

Tooth to be extracted should be reduced mesio
distally if the path of removal is obstructed by
adjacent teeth
www.indiandentalacademy.com

Time period for socket regeneration is usually 3 to 6
months depending on
Tooth size
Root no.
No. of bony walls around the socket
Size of alveolus
Trauma of extraction
www.indiandentalacademy.com

In 1993 Miesch & Dietsh suggested different graft
materials & techniques based on the no. of bony
walls remaining after tooth is removed-
5 bony wall defect
4-5 wall defect
2-3 wall defect
1 wall defect
www.indiandentalacademy.com

Any resorbable graft material such as alloplast ,
allograft or autograft
www.indiandentalacademy.com

Socket grafting is indicated if
Labial plate of bone is missing
One of the lateral plates is thinner than 1.5 mm
Height is desired
2 techniques
BM with a mineralized alloplast or freeze dried bone
Modified socket seal surgery
www.indiandentalacademy.com

A periotome or thin periosteal elevator is used to
tunnel under the bone periosteum
www.indiandentalacademy.com

barrier membrane is then slid into the pocket created
under the tissue & it extends apical , mesial & distal
beyond the extraction site
Approx 6-8 mm of BM should extend above the
marginal tissue
www.indiandentalacademy.com

Bone graft material is placed & BM covers the top of
the socket & is tucked in below the palatal tissue
www.indiandentalacademy.com

Developed by Misch et al
It’s a composite graft consisting of connective tissue
, periosteum & trabecular bone used to seal a fresh
extraction socket
J of Oral Implantology 1999 ; 25 (pages 244 – 250 )
www.indiandentalacademy.com

Advantages
CT graft blends into the surrounding attached
gingiva , offering similar colour & texture of the
epitheliumcontains autogenous bone
Blood supply is established from the surrounding soft
tissue
Rapid healing (4 – 5 months )
www.indiandentalacademy.com

• Treated similar to 4 wall defect
Defect size is larger so more bone is
reqd.
www.indiandentalacademy.com

Block graft or cortical autogenous
bone
www.indiandentalacademy.com

Misch in 1990, Implant Dent 1993 ;2 (pages 158- 167)
Layers in GBR include the following
host bone -: decorticated to enhance blood supply , growth factors & RAP
An autograft-: results in more predictable & rapid bone growth by osteogenesis & osteoinduction
Mixture of DFDB (30%) , FDB (70%) , & PRP --: Provides growth factors & space maintenance
BM & Tent screw -:
BM prevents fibroblasts from invading the graft site for at least 6 wks.
Tent screw decreases mobility
Primary closure without tension -: prevents contamination & loss of graft materialwww.indiandentalacademy.com

www.indiandentalacademy.com

www.indiandentalacademy.com
Sinus grafting was introduced by Tatum in 1970s
In early 1970s Tatum began to augment post. Maxilla
with autogenous rib bone to produce adequate vertical
bone for implant support
In 1974 he developed modified caldwell luc procedure
In 1975 he developed a lateral approach surgical
technique toelevate sinus membrane & place implant
simultaneously
From 1974 to 1979 primary material for sinus grafting
was autologous bone. In 1980 , Tatum introduced the use
of synthetic bonewww.indiandentalacademy.com

Initial publication on sinus grafting was by Boyne &
James in 1980s
In 1983 Misch observed that the most predictable
intraoral region to grow boneis the max. sinus floor
once the mucosa has been elevated
www.indiandentalacademy.com

Root tips in the antrum
Pseudocysts
Oral antral opening
Extraction of hopeless teeth
Unerupted teeth
www.indiandentalacademy.com

Narrowing of osteomeatal complex
Enlargement of an air cell in the roof of sinus ( haller
cell )
Smoking
Smokers have a 7 % greater failure rate than non
smokers
Pt. should refrain from smoking at least 15 days
before surgery & 4-6 weeks after surgery
Chronic maxillary rhinosinusitiswww.indiandentalacademy.com

Active sinus infection on the day of surgery
Significant recurrent history of chronic
sinusitis
Significant recurrent history of fungal
sinusitis
Uncontrolled late stage diabetes
Cystic fibrosis
maxillary sinus hypoplasia
Neoplasms
Inferior turbinate or meatus pneumatizationwww.indiandentalacademy.com

Antimicrobial medication
Administered at least 1 full day before surgery &
extended for 5 days after surgery
Local antibiotic medications
To ensure adequate antibiotic levels in a sinus graft ,
it is recommended to add antibiotic to the graft
mixture
Mabry TW , Yukna RA J Periodontology 1985 ; 56 (74
– 81)www.indiandentalacademy.com

Oral antimicrobial rinse
Gentle oral rinses of chlorhexidine gluconate 0.12 % should be used twice daily for 2 weeks after surgery
Glucocorticoids
Initiated 1 day before surgery & continued foe 2 days after surgery to control oedeme
Decongestant medications
Oxymetazoline (0.05%)
Phenylephrine (1% )
www.indiandentalacademy.com
Analgesics
Codeine containing drugs such as tylenol 3 are the
drug of choice as they have a potent antitussive
effect
Cryotherapy
Cold dressings for the first 24 – 48 hrs ,elevation of
head & limited activity for 2-3 days helps reduce
swelling
After 2-3 days heat may be applied to increase blood
flow & lymph flowwww.indiandentalacademy.com

In 1984 Misch organised a treatment approach for
posterior maxilla based upon the amount of bone
below the antrum
www.indiandentalacademy.com

in 1995 , Misch modified his classificationto include
the lateral dimension of sinus cavity to modify the
healing period protocol
Smaller width sinnus (0-10 mm) -: less healing time
Larger width(> 15 mm) -: more time
www.indiandentalacademy.com
SA1 conventional implant placement
SA2 sinus lift & simultaneous implant placement
SA3 sinus graft with immediate or delayed
endosteal implant placement
SA4 sinus graft healing & extended delay of implant
insertion
www.indiandentalacademy.com

Indicated when sufficient bone height is present
for the placement of endosteal implants
Evaluation of sinus is less critical
Implants left to heal for 4-8 months
Progressive loading suggested in d3 & d4 bone
www.indiandentalacademy.com

Root form implants are used
At least a 12 mm in height implant for a 4
mm threaded implant
www.indiandentalacademy.com

Osteoplasty or augmentation is suggested to
increase width of bone
Augmentation may be done by
Bone spreading
Autogenous onlay
Appositional grafts
www.indiandentalacademy.com
Onlay autogenous bone grafts are
indicated
www.indiandentalacademy.com

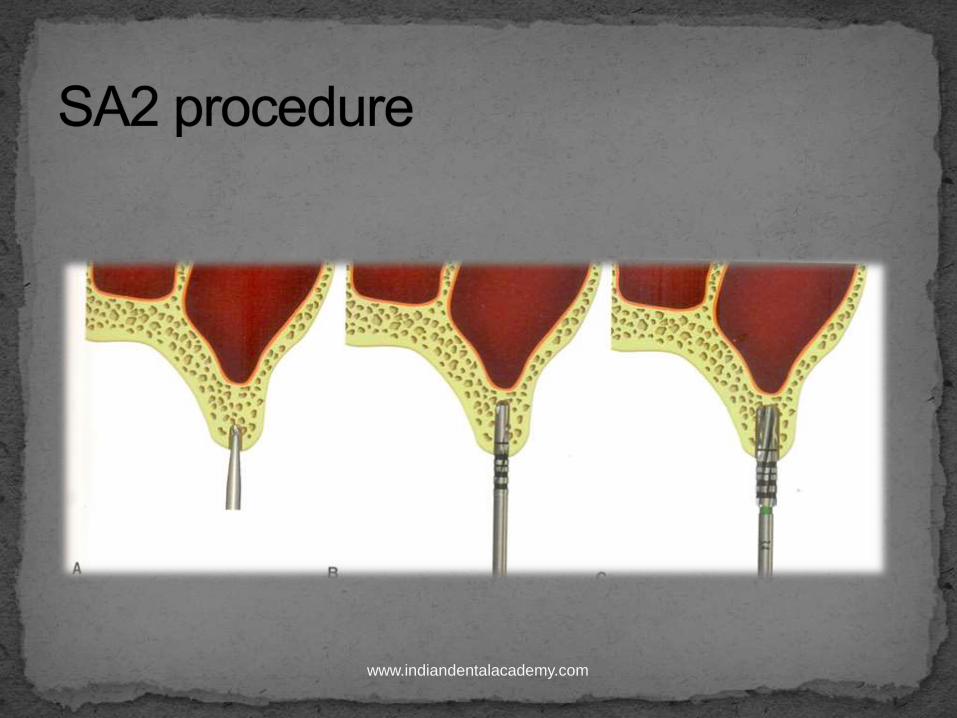
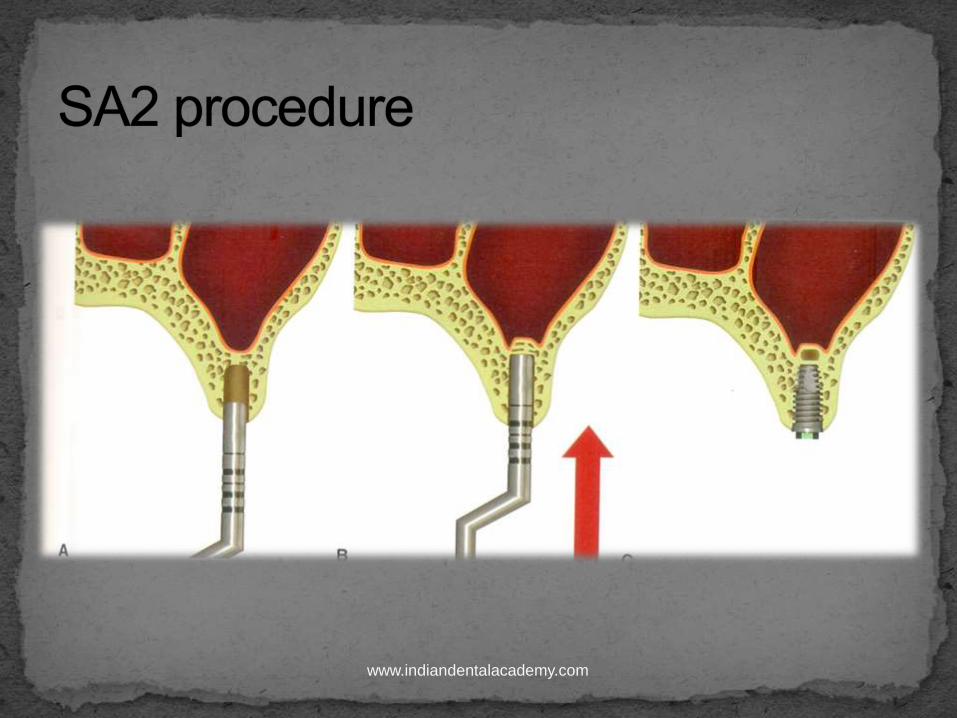
indicated when10-12 mm of vertical bone is present
Tatum originally developed the technique in 1970 &
Misch published it in 1987
Antral floor is elevated through implant osteotomy by
0-2mm
Compresses the bone below the antrum , causes a
greenstick fracture in the antral floor & slowly
elevates the unprepared bone & sinus membrane
over the broad based osteotome
Prosthetic treatment similar to SA1 after 4-6 months
www.indiandentalacademy.com
www.indiandentalacademy.com
www.indiandentalacademy.com

Indicated when at least 5 mm of vertical bone &
sufficient width are present between the anral floor &
crest of residual ridge
www.indiandentalacademy.com
Anesthesia
Maxillary branch of trigeminal nerve is blocked
Long acting anesthetic such as bupivacaine(0.5%) or etidocaine(1.5%) is preferred
Incision line & reflection
Crest incision is made on the palatal aspect of maxilla from tuberosity to one tooth anterior to the anterior wall of sinus
Vertical relief incision is made on the distal to enhance access to max. tuberosity
Anterior incision is made at least 10 mm ant to the ant wall of sinus
www.indiandentalacademy.com
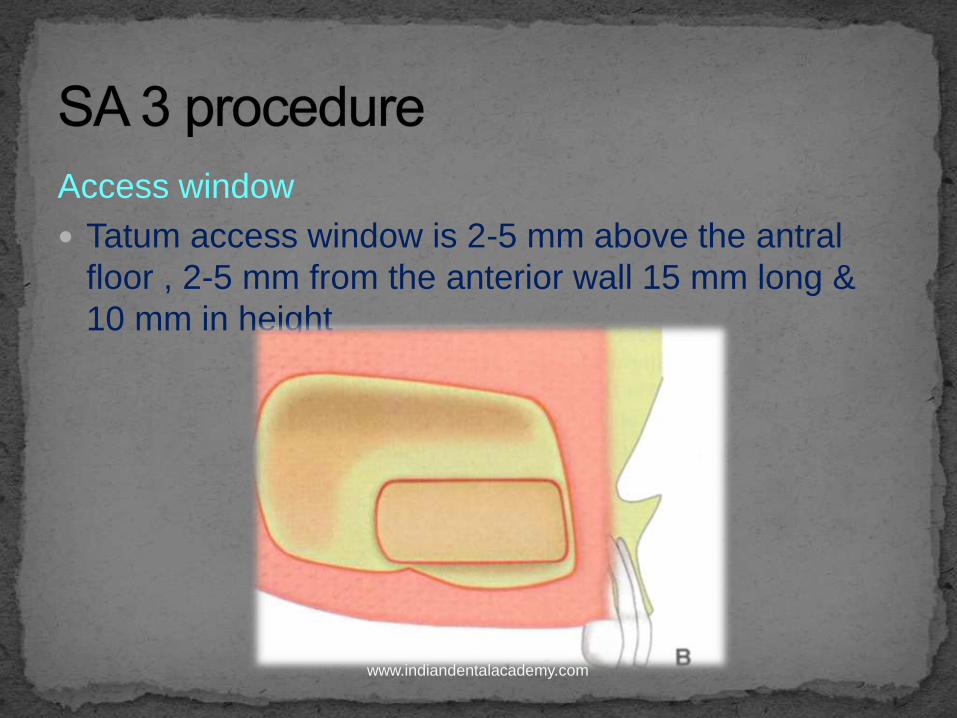
Access window
Tatum access window is 2-5 mm above the antral
floor , 2-5 mm from the anterior wall 15 mm long &
10 mm in height
www.indiandentalacademy.com

Carbide bur in paint brush stroke is used to outline the
access window
www.indiandentalacademy.com

Flat ended metal punch & mallet is used to lightly
tap & green stick fracture the access window from
the lateral wall of maxilla
www.indiandentalacademy.com

Sharp blade of the curette is placed against the inner
wall of bone & is used to scrape off the sinus
membrane from the bone
www.indiandentalacademy.com

Layered approach to grafting
www.indiandentalacademy.com
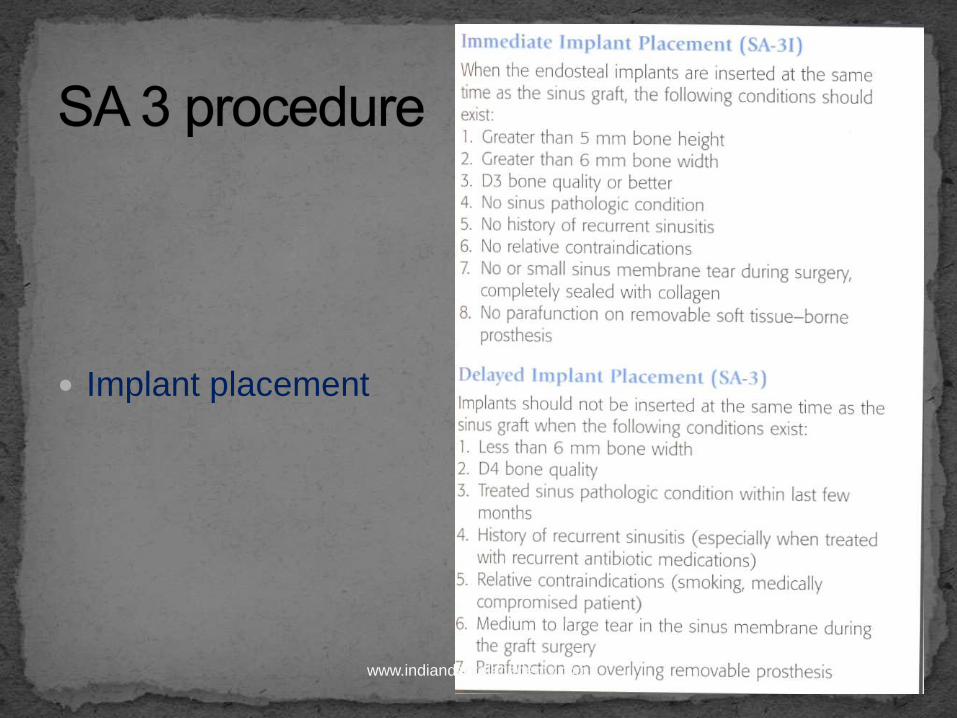
Implant placement
www.indiandentalacademy.com

Soft tissue closure
Soft tissues & periosteum must be approximated for
closure without tension
www.indiandentalacademy.com

Indicated when less than 5 mm bone exists between
sinus floor & crest of residual ridge
www.indiandentalacademy.com

Lateral wall approach is performed for sinus graft as
in SA 3 procedure
Medial wall of sinus membrane is elevated at least
16 mm fron the crest so that adequate height is
available for implant placement
If bone from max tuberosity is not enough ,
additional bone may be harvested from above the
roots of maxillary premolars or mandibular
ascending ramus www.indiandentalacademy.com

Intra operative
Membrane perforation
Antral septa
Bleeding
Short term
Incision line opening
Paresthesia
Acute maxillary rhinosinusitis
Long term
Oroantral fistula
Maxillary surgical cysts
www.indiandentalacademy.com
www.indiandentalacademy.com

Mandible
Symphysis
Body
Ramus
Maxillary tuberosity
Extraosseous tori
Ridge osteoplasty
Extraction sites
Implant osteotomy
www.indiandentalacademy.com

Convenient surgical access
No cutaneous scar
Patients report minimal donor site discomfort
Inherent biological benefits attributable to the
embryologic origin of donor bone
Experimental evidence shows that grafts from
membranous bone show less resorption than
endochondral bone. Maxilla & body of mandible are
membranous bones
J Oral Maxillofacial surgery 1996 : 54 (15-
20)www.indiandentalacademy.com

Early revascularization of membranous bone grafts
helps in improved maintenance of graft volume
Bone from the maxillofacial skeleton contains
increased concentration of growth factors & BMPs
Plastic reconstructive surgery 1994 : 93 ( 732 –
738)
Improved survival of craniofacial bone grafts is
caused by their 3-D structure
J oral maxillofacial surg 1996 :54 (15 –
20 )
Mand. Cortical bone grafts show little volume loss &
show good incorporation at short healing timeswww.indiandentalacademy.com
In 1992 Misch et al used mandibular symphysis &
ramus bone grafts for endosteal dental implants
J of oral maxillofacial implants 1992 : 7 ( 360 –
366 )
www.indiandentalacademy.com

Symphysis
Ramus
www.indiandentalacademy.com

Easier graft harvest
Less post – op discomfort
Less neurosensory complications
Less incision line opening
Less anesthesia reqd.
More profound LA with fewer drugs
Less concern of changes in facial
morphology
www.indiandentalacademy.com

Less width & length of bone
www.indiandentalacademy.com

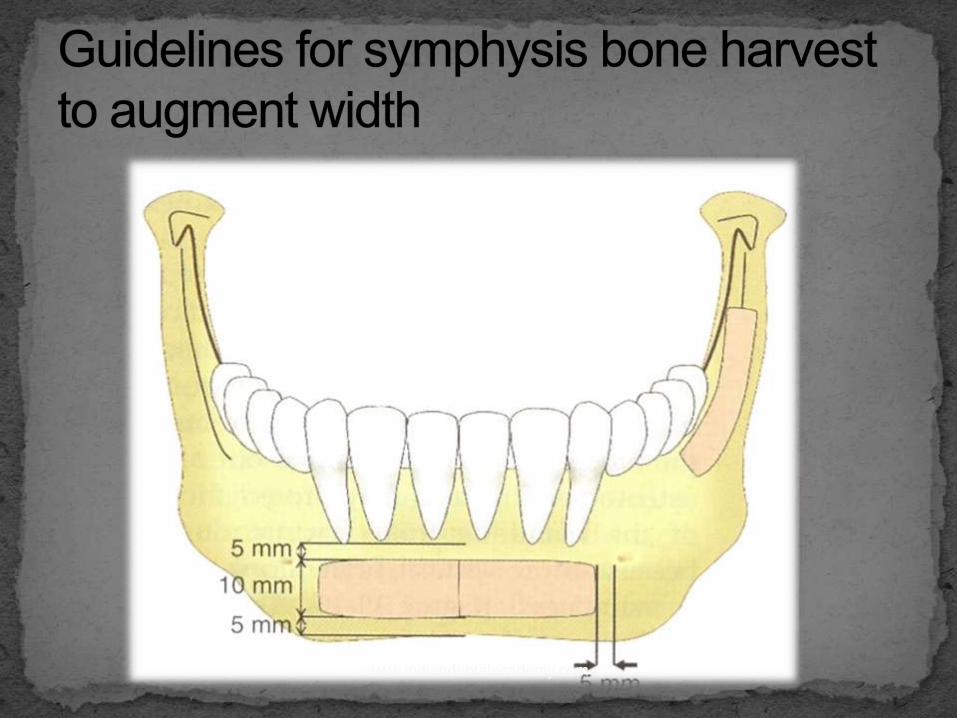
Slight curved triangular shape in the midlineis often
well suited for re-establishing the arch form in
maxillary anterior ridges
Average interforaminal distance is greater than 4 cm
, so more bone volume is available
www.indiandentalacademy.com
Width & height requirements for augmentation
Mandibular symphysis : when more than 4 cm of
bone is desired ( C-w bone volume )
Mandibular ramus :when graft width is less than 4
mm ( div. B to B-w bone volume )
Mandibular symphysis along with its cortical inferior
border : when an augmentation for height is required
www.indiandentalacademy.com
Location of the host or recepient site
Recepient site
• Anterior mandible
• Posterior mandible
• maxilla
Donor site
• Symphysis
• Ramus
• ramus
www.indiandentalacademy.com

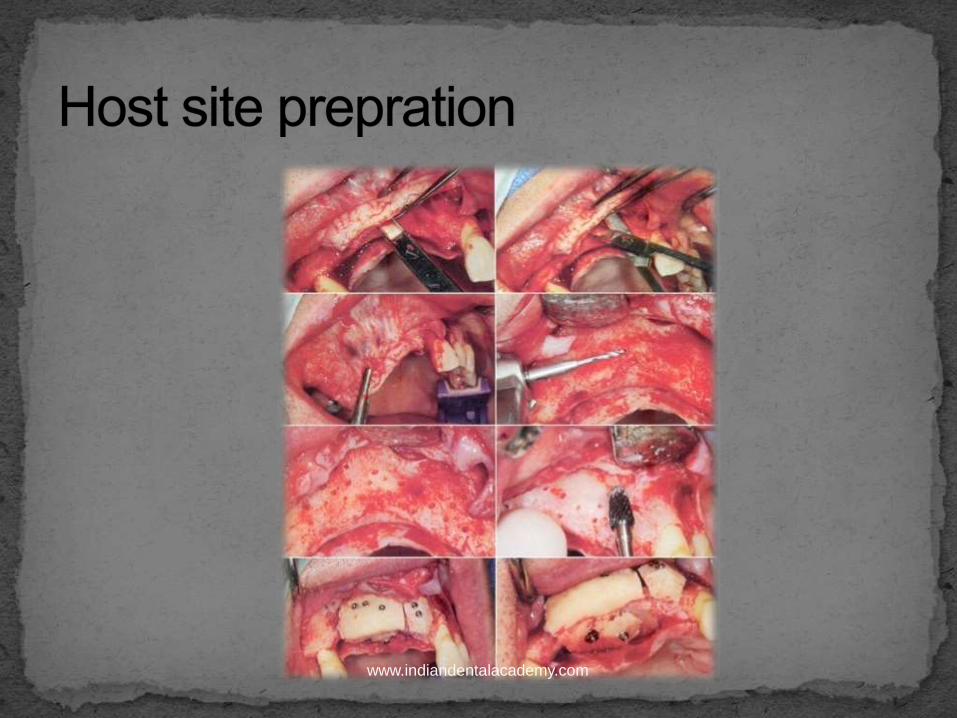
host site prepration
Bone harvest
Graft fixation
Post operative instructions
www.indiandentalacademy.com

www.indiandentalacademy.com
www.indiandentalacademy.com

www.indiandentalacademy.com

www.indiandentalacademy.com
www.indiandentalacademy.com

www.indiandentalacademy.com

Presence or absence of molars
Width & height of external oblique ridge in the body
of the mandible
Distance from the external oblique ridge & ramus to
the inferior alveolar nerve
Width of posterior ramus is evaluated using
reformatted CT image
www.indiandentalacademy.com
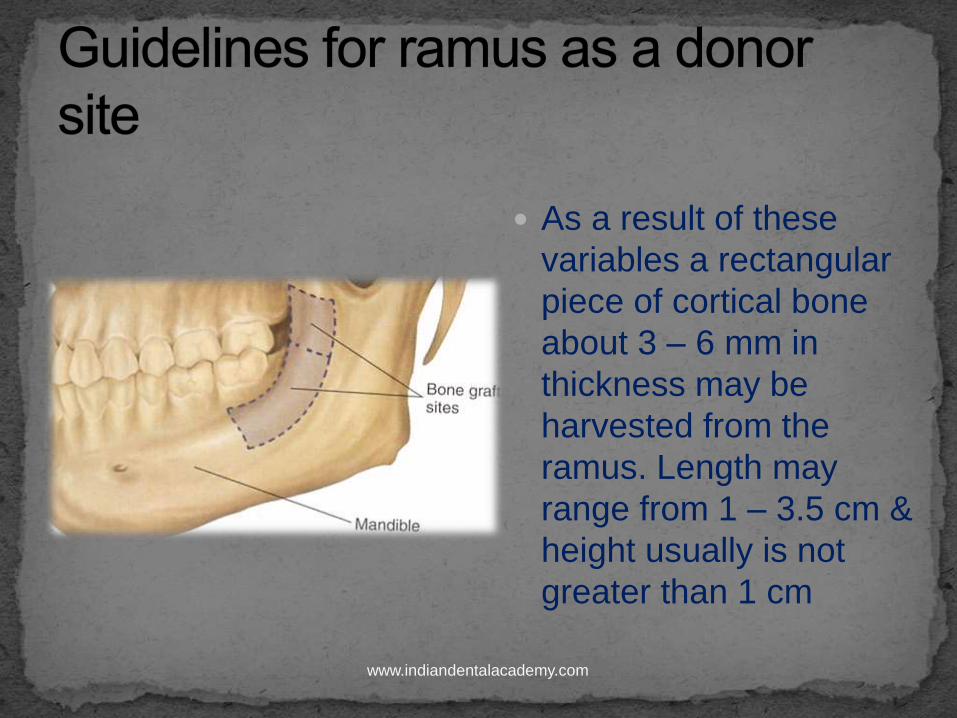
As a result of these
variables a rectangular
piece of cortical bone
about 3 – 6 mm in
thickness may be
harvested from the
ramus. Length may
range from 1 – 3.5 cm &
height usually is not
greater than 1 cm
www.indiandentalacademy.com

After harvesting graft may be stored in sterile saline
or immediately fixed to the recepient site
Trabecular surface of the graft should be in contact
with decorticated surface of the host bone
Donor block & recepient site contouring
2 or more fixation screw sites should be prepared for
each bone block
www.indiandentalacademy.com
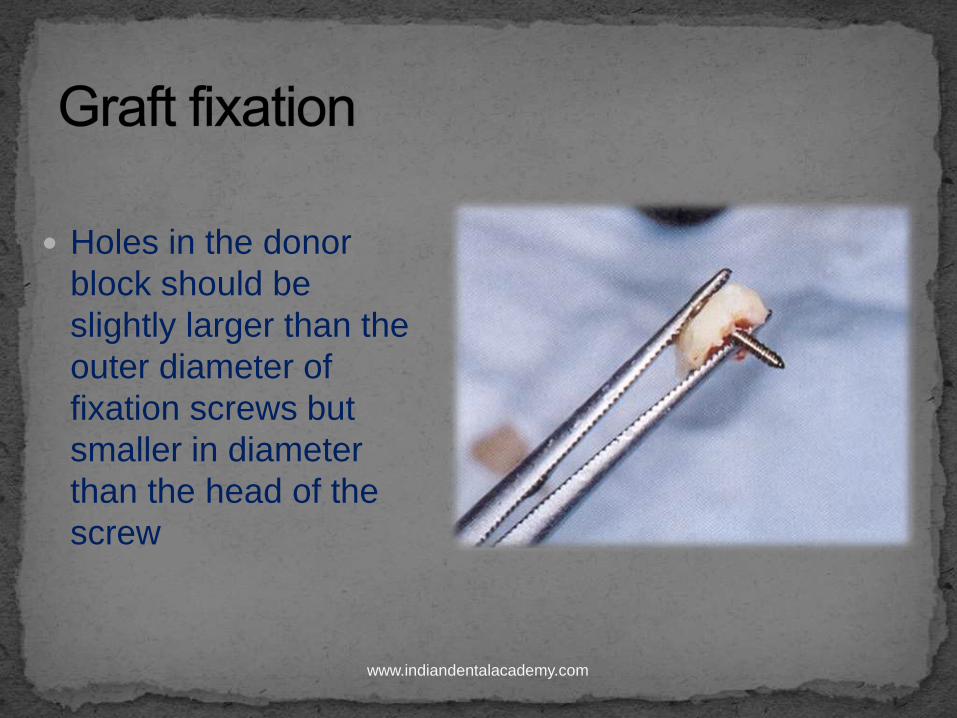
Holes in the donor
block should be
slightly larger than the
outer diameter of
fixation screws but
smaller in diameter
than the head of the
screw
www.indiandentalacademy.com

A high speed lindemann bur or carbides are then
used to recontour the block bone & smmothen any
sharp edges or corner after it is fixed
Barrier membrane
Not routinely used with cortical block bone grafts
Indicated if more particulate or trabecular bone is
used
Indicated if block graft is inadequate to fill the entire
space
www.indiandentalacademy.com
Flap should be approximated &
sutures placed such that there is no
incision line tension or tissue ischemia
www.indiandentalacademy.com

Stop smoking at least 3 days before surgery &
until incision line has healed
Removeble soft tissue prosthesis should not be
worn
Confirm to regular post operative follow up
www.indiandentalacademy.com

Intraoral block grafts
4 months for maxillary recepient
5 – 6 months for mandibular recepient sites
Particulate onlay grafts
6 -9 months
www.indiandentalacademy.com

Iliac crest
Tibia
Cranium
Rib
fibula
www.indiandentalacademy.com

Advantages
Large volumeouter portion of the graft may be
primarily cortical with major portion of trabecular
bone underneath
Volume of the bone harvested permits contouring of
2/3 of the mandible or maxilla or filling a large bony
defect
Relative ease of access & harvesting
www.indiandentalacademy.com

Disadvantages
Rapid bone resorption of 30 – 90 % has been
reported when conventional dentures are placed on
top of the reconstruction
Curtis et al JPD 1987 ; 57 (73-
78)
• post operative pain & gait disturbances
www.indiandentalacademy.com

Complications
Pain
Herniation of the abdominal contents
Fracture neuralgia
Hematoma seroma
Infection cosmetic deformity
www.indiandentalacademy.com
Proximal tibial metaphysis provides an excellent
source of trabecular bone
Primarily used with with BM & GBR procedure
because major part of the harvest is trabecular in
nature
www.indiandentalacademy.com

Disadvantages
Contraindicated in adolescents & children coz
disruption of epiphyseal growth centre my occur
Fat content of the marrow is sometimes greater than
that found in the ilium
www.indiandentalacademy.com

Complications
Hematoma
Post operative pain
Infection
Dhiscence ( incidence ranging from 1-4% )
www.indiandentalacademy.com

Sites
Iliac crest
Scapula
indications
Blood supplybto the graft site is severely
compromised
Recipient bed is scarred
Carcinoma patients who have undergone radiation
therapy
Div. E bone anatomy : discontinuity defects of the
jaw
www.indiandentalacademy.com

Advantages
Maintains normal physiologic function
Simultaneous placement of implants with
microvascular bone flap reconstruction has shown
an approximately 80% success rateusing Ti implants
with a short follow up
www.indiandentalacademy.com
Disadvantages
Attaing primary graft stability is often
difficult coz graft is often very
spongeous with a thin cortical layer
www.indiandentalacademy.com

Refers to the formation of new bone between
vascular bone surfaces created by an osteotomy &
separated by gradual distraction
Indications
Mucoskeletal conditions such as post traumatic
defects
Repair of continuity defects
Mandibular lengthening
Maxillary advancement
www.indiandentalacademy.com

www.indiandentalacademy.com

Contemporary implant dentistry by Carl E Misch ; 3
ed
Dental update 1997 ; 24 (332-337)
www.indiandentalacademy.com