Richard E. Chaisson, MD Center for Tuberculosis Research Johns Hopkins University
25
Richard E. Chaisson, MD Center for Tuberculosis Research Johns Hopkins University TB/HIV Research Priorities and Recent Developments
description
TB/HIV Research Priorities and Recent Developments. Richard E. Chaisson, MD Center for Tuberculosis Research Johns Hopkins University. Examples of Research Needed. Basic –immunology, molecular biology, genomics, drug discovery Translational – pathogenesis - PowerPoint PPT Presentation
Transcript of Richard E. Chaisson, MD Center for Tuberculosis Research Johns Hopkins University

Richard E. Chaisson, MD
Center for Tuberculosis Research
Johns Hopkins University
TB/HIV Research Priorities and Recent Developments

Examples of Research Needed
• Basic –immunology, molecular biology, genomics, drug discovery
• Translational – pathogenesis • Clinical – observational, trials, outcomes• Public Health – intervention paradigms• Operational – functional strategies • Health Services – health system structure• Cost-effectiveness – impact on DALYs• Behavioral – health seeking behavior,
delays, clinician behavior

So many questions, so little time…
• Epidemiology of TB/HIV
• Diagnosis of latent and active TB
• TB/HIV clinical issues
• Treatment of TB in setting of HIV– ART, drug interactions and MDR– IRIS– New drugs
• Preventive therapy
• Public health interventions

So many questions, so little time…
• Epidemiology of TB/HIV• Diagnosis of latent and active TB• TB/HIV clinical issues• Treatment of TB in setting of HIV
– ART, drug interactions and MDR– IRIS– New drugs
• Preventive therapy• Public health interventions

Community TB Prevalence in Masipumelela, South Africa
Randomly Selected Community Sample
0
1
2
3
4
5
6
Prevalent Smear + Smear -/Cx+ Total
Per
cent
wit
h T
B
HIV+HIV-
Bekker et al., CROI 2006

So many questions, so little time…
• Epidemiology of TB/HIV
• Diagnosis of latent and active TB
• TB/HIV clinical issues
• Treatment of TB in setting of HIV– ART, drug interactions and MDR– IRIS– New drugs
• Preventive therapy
• Public health interventions

Current Approaches to Diagnosing TB in Resource Poor Settings
• Reliance on antiquated tools with poor sensitivity

Diagnosis of Latent and Active TBOpportunities for Research
• Latent TB– Interferon-gamma based assays– Proteomic-based antigen or antibody detection– Lateral flow and other platforms
• Active TB– MGIT based diagnostics– Novel culture systems– Antigen detection in sputum– Automated nucleic acid amplification

Clinical Markers for Confirming Smear Negative TB in HIV+ Patients in South Africa
• Follow up study in KZN• HIV+ and HIV- patients
with suspected SNTB• Response to therapy
monitored• Response to therapy at
week 8 = 96% for TB patients
0
10
20
30
40
50
60
70
80
90
100
Weight Haemoglobin C-ReactiveProtein
KarnofskyPerformance
Score
SymptomScore Ratio
Per
cen
tag
e o
f su
bje
cts
Week 2 Week 4 Week 8
D Wilson et al., Int J TB Lung Dis, 2006
D Wilson et al., WAC Toronto, Abstract MOPE0145
Cape Town Study, HIV+

Time to Positive Culture by MODS or L-J in 1639 Respiratory Specimens from TB
Suspects in Brazil and Honduras
0
10
20
30
40
50
60
70
80
90
100
0 5 10 15 20 25 30 35 40 45 50 55
Days to M. tuberculosis grow th
% p
ositi
ve fo
r gr
owth
LJ, smear negative
MODS, smear negative
LJ, smear positive
MODS, smear positive
Arias, Dorman et al., 2006
MODS – Sm+ LJ – Sm+

So many questions, so little time…
• Epidemiology of TB/HIV• Diagnosis of latent and active TB• TB/HIV clinical issues• Treatment of TB in setting of HIV
– ART, drug interactions and MDR– IRIS– New drugs
• Preventive therapy• Public health interventions

Impact of an Opt-Out vs. Opt-In Strategy for HIV Testing of TB Patients in the Eastern Cape, South Africa:
A Cluster Randomized Trial
Outcome Opt-Out Clinics Control
(Opt-In)
P-value*
# Range (%) # Range (%)
TB Patients Pre-test counseled
73 3-66 (23%) 31 1-6 (9%) 0.03**
TB Patients HIV tested 71 1-18 (22%) 26 0-6 (8%) 0.03
% counseled that tested 97% 79% 0.12
HIV test positive 31 0-10 (36%) 11 0-3 (43%) 0.75
Prescribed cotrimoxazole 6 0 - 2 (29%) 4 0-2 (33%) 0.89
Referred to ARV clinic 7 0 - 2 (4%) 2 0-1 (27%) 0.33
Pope et al., WAC Toronto, Abstract #THKC205

So many questions, so little time…
• Epidemiology of TB/HIV• Diagnosis of latent and active TB• TB/HIV clinical issues• Treatment of TB in setting of HIV
– ART, drug interactions and MDR– IRIS– New drugs
• Preventive therapy• Public health interventions

ART, Drug Interactions and MDR TB
• TB in patients on ART (Lawn et al., WAC Toronto, #MOPE 0175)
– 944 patients initiating ART in Western Cape– 25% prevalent TB, 10% with new TB– TB incidence after ART 10.4 cases per 100 PY
• MDR TB (Vargas et al., WAC Toronto, Abstract #WEPE0166)
– 209 HIV+/TB patients in Lima– 34% MDR, 10% INH-resistant, median CD4 = 44
• XDR TB (Gandhi et al., WAC Toronto,#THLB0210)
– Epidemic MDR and XDR TB in KZN, South Africa– All XDR TB patients HIV+, 51% with no prior treatment

DTH Responses Measured by Elispot in Patients with and without IRISDTH Responses Measured by Elispot in Patients with and without IRIS
22 HIV-TB co-infected patients prospectively followed after anti-mycobacterial (TBK) then ARV (M0) therapy initiation
IRS+ n=9 (41%) IRS- n=13
p =0.006
NS
T BK M 0 M1 M 3 M60
500
1000
1500
2000
2500
3000
3500
4000
SF
C/1
06 PB
MC
T BK M 0 T IRS M 3 M 60
500
1000
1500
2000
2500
3000
3500
4000 PPD CMV
SF
C/1
06 PB
MC
Bourgarit et al., AIDS. 2006;20:F1-7, CROI 2006

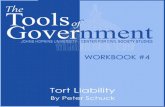
TBTC Study 27: Moxifloxacin vs. Ethambutol as 4th Drug in Initial Treatment of Smear+ TB
Proportion of Patients with Negative Culture
01020304050607080
2 4 6 8
Weeks of treatment
Spu
tum
cul
ture
co
nver
sion Moxifloxacin
Ethambutol
P=0.02 P=0.003
Median Time to Culture Conversion: Moxi 43 d vs. EMB 56 d (p=0.01)
Burman et al., AJRCCM 2006;174:331-8

TBTC Study 27Sputum culture conversion
among key sub-groups
CavitationNo cavitation
Age <31 yearsAge >31 years
AfricanNorth American
Culture conversion
66% (137/206)84% ( 60/71)
66% ( 89/134)76% (108/143)
63% (110/175)85% ( 87/102)
Adjusted P
0.03
0.003
<0.0001
Burman et al., AJRCCM 2006;174:331-8

CFU counts after 2 months treatment
0
1
2
3
4
5
6
7
8
Pre-Rx RMZ RMZPa PaMZ RPaZ RMPa
Regimen
Lo
g(1
0) C
FU
co
un
t
Lung
Spleen
R, rifampin; M, moxifloxacin; Z, pyrazinamide; Pa, PA-824.
Moxifloxacin and PA-824 in a Murine TB Model
Nuermberger et al., Antimicrob Agents Chemother 2006;50:2621

So many questions, so little time…
• Epidemiology of TB/HIV• Diagnosis of latent and active TB• TB/HIV clinical issues• Treatment of TB in setting of HIV
– ART, drug interactions and MDR– IRIS– New drugs
• Preventive therapy• Public health interventions

TB Incidence in Brazilian HIVPatients by Treatment Category
Treatment category
Person-Years
TB Cases
Incidence Rate(per 100 PYs)
Naïve 3,865 157 4.06 (3.45-4.75
HAART only 11,629 229 1.97 (1.72-2.24)
INH only 395 5 1.27 (0.41-2.95)
HAART and INH
1,253 13 1.04 (0.55-1.78)
Total 17,142 404 2.36 (2.13-2.60)
Golub et al., WAC Toronto, Abstract MOPE0395

Novel TB Preventive Regimens in HIV-Infected Adults in Soweto: PHRU/JHU Trial
• Open label, randomized trial• HIV+/PPD+ adults not on HAART at enrollment• Active TB excluded (23% screen failures TB+)• Regimens
– Rifapentine 900 mg/INH 900 weekly for 12 weeks
– Rifampin 600 mg/INH 600 mg twice weekly for 12 weeks
– INH 300 mg daily continuously
– INH 300 mg daily for 6 months
• Endpoint – TB-free survival

Probability of TB After Enrollment (All Treatment Groups)

So many questions, so little time…
• Epidemiology of TB/HIV• Diagnosis of latent and active TB• TB/HIV clinical issues• Treatment of TB in setting of HIV
– ART, drug interactions and MDR– IRIS– New drugs
• Preventive therapy• Public health interventions

Study/Site Intervention(s) Design (N)
Thibela TB
SA Gold Mines
Mass preventive therapy
Cluster randomized trial
(>40,000)
ZAMSTAR
Zambia/South Africa
Intensive case finding, household
interventions
Community randomized trial
(~2 million)
THRio
Rio de Janeiro
Preventive therapy and ARVs
Phased implementation
trial
(12,000)
C R E A E

Research in TB/HIVResearch in TB/HIV
• The need is enormous
• There are abundant opportunities to contribute
• Interdisciplinary and novel approaches are needed
• New paradigms must be developed• “The greatest obstacle to discovery is
not ignorance - it is the illusion of knowledge.” --Daniel Boorstein
• The need is enormous
• There are abundant opportunities to contribute
• Interdisciplinary and novel approaches are needed
• New paradigms must be developed• “The greatest obstacle to discovery is
not ignorance - it is the illusion of knowledge.” --Daniel Boorstein