Rheumatoid Arthritis: New and Emerging Agents and … · Rheumatoid Arthritis: New and Emerging...
17
Rheumatoid Arthritis: New and Emerging Agents and Trends Arthur Kavanaugh, MD Director, Center for Innovative Therapy Professor of Medicine Division of Rheumatology, Allergy, and Immunology University of California San Diego La Jolla, CA Rheumatoid Arthritis: New and Emerging Agents and Trends Arthur Kavanaugh, MD Director, Center for Innovative Therapy Professor of Medicine Division of Rheumatology, Allergy, and Immunology University of California San Diego San Diego, CA
Transcript of Rheumatoid Arthritis: New and Emerging Agents and … · Rheumatoid Arthritis: New and Emerging...

Rheumatoid Arthritis: New and
Emerging Agents and Trends
Arthur Kavanaugh, MD
Director, Center for Innovative Therapy
Professor of Medicine
Division of Rheumatology, Allergy, and
Immunology
University of California San Diego
La Jolla, CA
Rheumatoid Arthritis: New and
Emerging Agents and Trends
Arthur Kavanaugh, MD
Director, Center for Innovative Therapy
Professor of Medicine
Division of Rheumatology, Allergy, and Immunology
University of California San Diego
San Diego, CA

Arthur Kavanaugh: Disclosures
Abbott
Amgen
Astra-Zeneca
Biogen-Idec
BMS
Celgene
Centocor
Genentech
TREG Consultants LLC
ITN
LCTC
MedImmune
NIH
Roche
Sanofi-Aventis
Teva
UCB
RA: Therapeutic Interventions Adjunctive (NSAIDs / COX-2 / Corticosteroids ), analgesics, PT/OT, etc
DMARDs
– MTX, LEF, SSZ, HCQ >> CsA, Min, IM gold, etc
– Tofacitinib (Jak3/1 inhibitor)
Biologics
– TNF-Inhibitors: etanercept, infliximab, adalimumab, certolizumab pegol, golimumab
– IL-1 Inhibitors: anakinra (IL-1ra); rilonacept (IL-1-TRAP), canakinumab
– Abatacept (CTLA-4-Ig)
– Rituximab (-CD20 mAb)
– Tocilizumab (-IL-6R mAb)
Experimental / Emerging
– other B cell (-CD22 [epratuzumab]: -BAFF/BLyS,TACI, APRIL)
– other IL-6 inhibitors (sirukimab, sarilumab etc)
– kinase inhibitors (Syk [fostamatinib], Jak, MEK, etc)
– -IL-12/23 mAb (ustekinumab, briakinumabetc)
– -IL-17 (secukinumab, ixekizumab, brodalumab)
– biosimilars
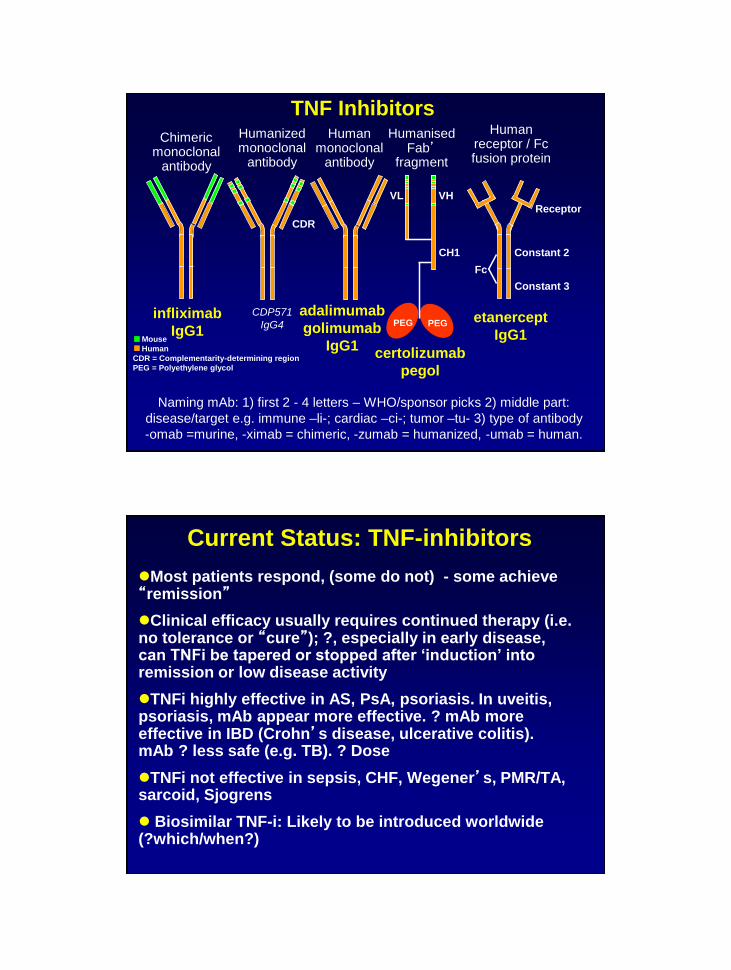
PEG PEG
Human receptor / Fc fusion protein
Humanised Fab’
fragment
Human monoclonal
antibody
Humanized monoclonal
antibody
Chimeric monoclonal
antibody
CDR
VL VH
CH1
Fc
Receptor
Constant 2
Constant 3
Mouse
Human
CDR = Complementarity-determining region
PEG = Polyethylene glycol
infliximab
IgG1
adalimumab
golimumab
IgG1
etanercept
IgG1
certolizumab
pegol
CDP571
IgG4
Naming mAb: 1) first 2 - 4 letters – WHO/sponsor picks 2) middle part:
disease/target e.g. immune –li-; cardiac –ci-; tumor –tu- 3) type of antibody
-omab =murine, -ximab = chimeric, -zumab = humanized, -umab = human.
TNF Inhibitors
Current Status: TNF-inhibitors
Most patients respond, (some do not) - some achieve “remission”
Clinical efficacy usually requires continued therapy (i.e. no tolerance or “cure”); ?, especially in early disease, can TNFi be tapered or stopped after ‘induction’ into remission or low disease activity
TNFi highly effective in AS, PsA, psoriasis. In uveitis, psoriasis, mAb appear more effective. ? mAb more effective in IBD (Crohn’s disease, ulcerative colitis). mAb ? less safe (e.g. TB). ? Dose
TNFi not effective in sepsis, CHF, Wegener’s, PMR/TA, sarcoid, Sjogrens
Biosimilar TNF-i: Likely to be introduced worldwide (?which/when?)
Personalized Medicine: Promise and Pitfalls
For individual patients, this could
Predict responses to individual drugs
Predict toxicities to individual drugs
Optimize benefits / risks of treatment
Achieve better outcomes
Reduce costs
Personalized Medicine: Promise and Pitfalls
For individual patients, this could
Predict responses to individual drugs
Predict toxicities to individual drugs
Optimize benefits / risks of treatment
Achieve better outcomes
Reduce costs
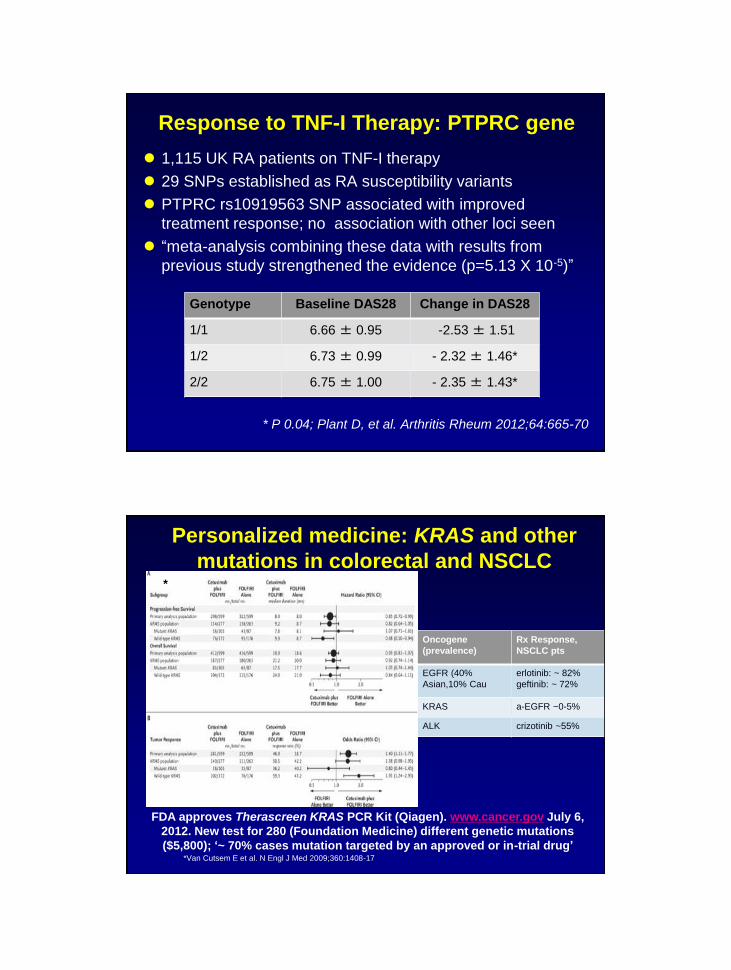
Response to TNF-I Therapy: PTPRC gene
1,115 UK RA patients on TNF-I therapy
29 SNPs established as RA susceptibility variants
PTPRC rs10919563 SNP associated with improved
treatment response; no association with other loci seen
“meta-analysis combining these data with results from
previous study strengthened the evidence (p=5.13 X 10-5)”
* P 0.04; Plant D, et al. Arthritis Rheum 2012;64:665-70
Genotype Baseline DAS28 Change in DAS28
1/1 6.66 ± 0.95 -2.53 ± 1.51
1/2 6.73 ± 0.99 - 2.32 ± 1.46*
2/2 6.75 ± 1.00 - 2.35 ± 1.43*
Personalized medicine: KRAS and other
mutations in colorectal and NSCLC
*Van Cutsem E et al. N Engl J Med 2009;360:1408-17
FDA approves Therascreen KRAS PCR Kit (Qiagen). www.cancer.gov July 6,
2012. New test for 280 (Foundation Medicine) different genetic mutations
($5,800); ‘~ 70% cases mutation targeted by an approved or in-trial drug’
Oncogene
(prevalence)
Rx Response,
NSCLC pts
EGFR (40%
Asian,10% Cau
erlotinib: ~ 82%
geftinib: ~ 72%
KRAS a-EGFR ~0-5%
ALK crizotinib ~55%
*

Personalized Medicine
Chen R, et al. Cell
2012;148:1293-1307.
“integrated personal omics
profile”; included genomics,
transcriptomics, proteomics,
metabolomics, and
autoantibody profiles.
Correlated with “health and
disease” including development
of type II DM
>3 X 109 measurements, 20
time points over 14 months,
single pt (Michael Snyder, PI)
Clinical Responses to TNF Inhibitors
28 Swollen Joint Count
Co
un
t
50
40
30
20
10
0 -20 -15 -10 -5 0 5 10 15 20 25
Co
un
t
50
40
30
20
10 5
0 -20 -15 -10 -5 0 5 10 15 20 25
28 Tender Joint Count
30
100
ESR
Co
un
t
50
40
30
20
10
0 -40 -20 0 20 40 60 80
60 70
60
50
40
30
20
10
0 -2.5 2.0 -1.5 -.5 0 .5 1 1.5 2.0 2.5 -1.0
HAQ Score
Co
un
t
Van Vollenhoven RF, Klareskog L. Clinical responses to TNF antagonists do not
show a bimodal distribution. Arthritis Rheum 2003;48:1500–1503.
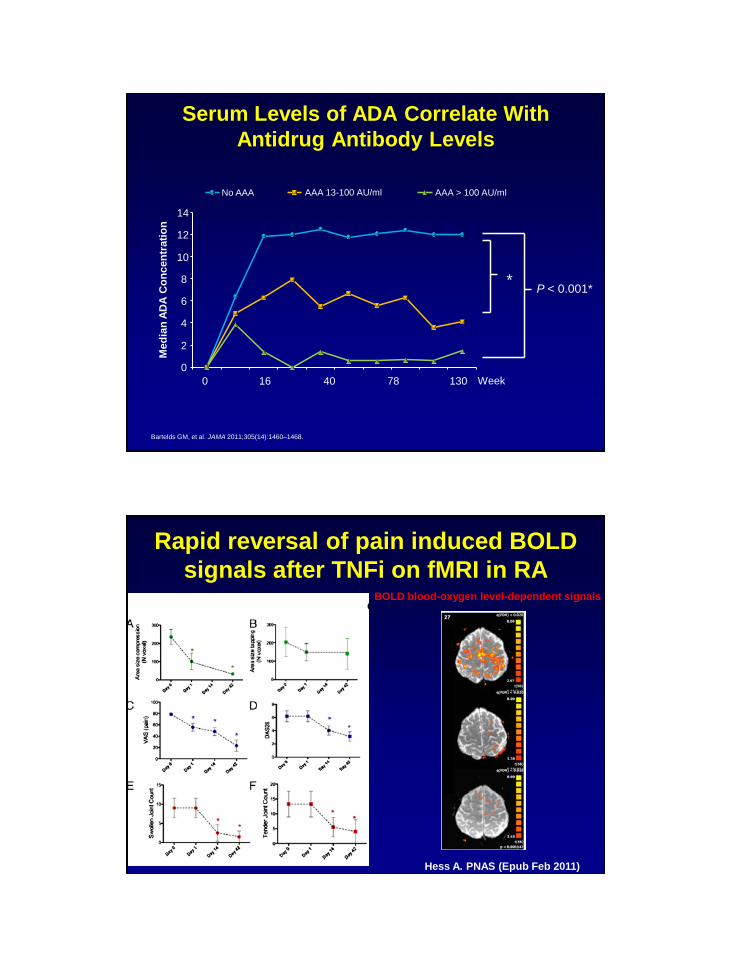
Med
ian
AD
A C
on
cen
trati
on
0
2
4
6
8
10
12
14
0 16 40 78 130
No AAA AAA 13-100 AU/ml AAA > 100 AU/ml
P < 0.001* *
Serum Levels of ADA Correlate With
Antidrug Antibody Levels
Bartelds GM, et al. JAMA 2011;305(14):1460–1468.
Week
Rapid reversal of pain induced BOLD
signals after TNFi on fMRI in RA
Hess A. PNAS (Epub Feb 2011)
BOLD blood-oxygen level-dependent signals

Biosimilar (CT-P13) vs IFX in MTX-IR RA
and in AS: Two studies
• 606 RA patients – 1:1 IFX (n=304) vs CT-P13 (n=302)
– 3 mg/kg + MTX at Weeks 0, 2, 6,
14, 22, 30
– 1º outcome ACR20 at Week 30
CT-P13 has efficacy, safety and PK similar to IFX in MTX-IR
RA patients and in AS patients
CT-P13 IFX
AE (%) 35.2% 35.9%
Infection AE (%) 15.3% 16.9%
Infusion Rx (%) 5% 6%
TB (n) 3 1
ACR responder rates at Week 30
Yoo DH, et al. EULAR 2012, Berlin, #FRI0143;
Park W, et al bid OP0167
• 250 AS patients:
– 5 mg/kg at wks 0, 2, 6, 14, 22, 30
– 1º outcome: PK (AUC/Cmax) similar
– ASAS20: 70.5% vs 72.4% IFX
– ASAS40: 51.8% vs 47.4% IFX
adalimumab
biosimilar
launch US
RA – emerging and future therapies
2010 2020 2011 2012 2013 2014 2019 2018 2017 2016 2015
rituximab
biosimilar
launch EU
etanercept
/Infliximab
biosimilar
launch EU
abatacept
biosimilar
launch EU adalimumab
biosimilar
launch EU
rituximab
biosimilar
launch US
Etanercept/IFX
biosimilar
launch US
2009
B-Cell Inhibitors
New small molecules
T-Cell Inhibitors
Anti-TNF
Anti-IL6
Simponi iv
Actemra sc
Olokizumab
Sirukumab (CNTO136)
ALD-518
Ofatumumab sc
Simponi sc
Cimzia
Actemra iv
tofacitinib Fostamatinib INCB 28050
Orencia sc
Sarilumab (REGN-88)
abatacept
biosimilar
launch US
tocilizumab
biosimilar
launch EU
Anti-IL17
Secukinumab

Fibroblast Lymphoid Myeloid
Early Synovial Histopathology
Macrophage
Dendritic cell
T-cell
B-cell
Synoviocyte
BONE & CARTILAGE
Cytokine
Interplay IL-2, IL-4, IL-7 IL-
9, IL-10, IL-12 IL-
13 IL-15, IL-21, IL-
23, IL-27, IFNg,
TGFb
IL-1, TNF
IL-6
IL-11, IL-10, IL-
12 IL-27, IL-32,
OSM GM-CSF,
M-CSF, IFNg,
PDGF, RANKL,
TGFb
IL-1, TNF
IL-6
OSM, IL-11, IL-
17, IL-18, IFNg,
IL-19, IL-20, IL-
22 TGFb
IL-1, TNF
IL-6 (sIL-6R)
Choy E, Kavanaugh A, Jones S. Nat Rev Rheumatol 2013;9:154-63
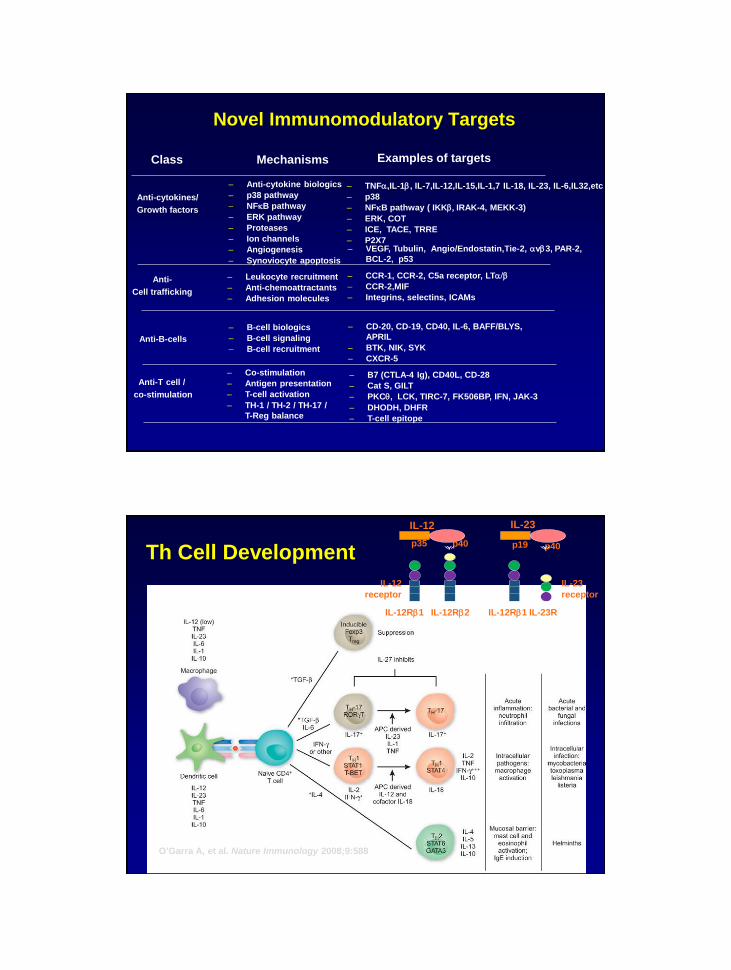
Novel Immunomodulatory Targets
– Anti-cytokine biologics
– p38 pathway
– NFkB pathway
– ERK pathway
– Proteases
– Ion channels
– Angiogenesis
– Synoviocyte apoptosis
Mechanisms Examples of targets Class
Anti-cytokines/
Growth factors
Anti-B-cells
– TNF,IL-1b, IL-7,IL-12,IL-15,IL-1,7 IL-18, IL-23, IL-6,IL32,etc
– p38
– NFkB pathway ( IKKb, IRAK-4, MEKK-3)
– ERK, COT
– ICE, TACE, TRRE
– P2X7
– B-cell biologics
– B-cell signaling
– B-cell recruitment
– CD-20, CD-19, CD40, IL-6, BAFF/BLYS,
APRIL
– BTK, NIK, SYK
– CXCR-5
Anti-
Cell trafficking
– Leukocyte recruitment
– Anti-chemoattractants
– Adhesion molecules
– CCR-1, CCR-2, C5a receptor, LT/b
– CCR-2,MIF
– Integrins, selectins, ICAMs
Anti-T cell /
co-stimulation
– Co-stimulation
– Antigen presentation
– T-cell activation
– TH-1 / TH-2 / TH-17 /
T-Reg balance
– B7 (CTLA-4 Ig), CD40L, CD-28
– Cat S, GILT
– PKC, LCK, TIRC-7, FK506BP, IFN, JAK-3
– DHODH, DHFR
– T-cell epitope
– VEGF, Tubulin, Angio/Endostatin,Tie-2, vb3, PAR-2,
BCL-2, p53
Th Cell Development
O’Garra A, et al. Nature Immunology 2008;9:588.
IL-12
p35 p40
IL-23
p19 p40
IL-12Rb1 IL-12Rb2 IL-12Rb1 IL-23R
IL-23
receptor
IL-12
receptor
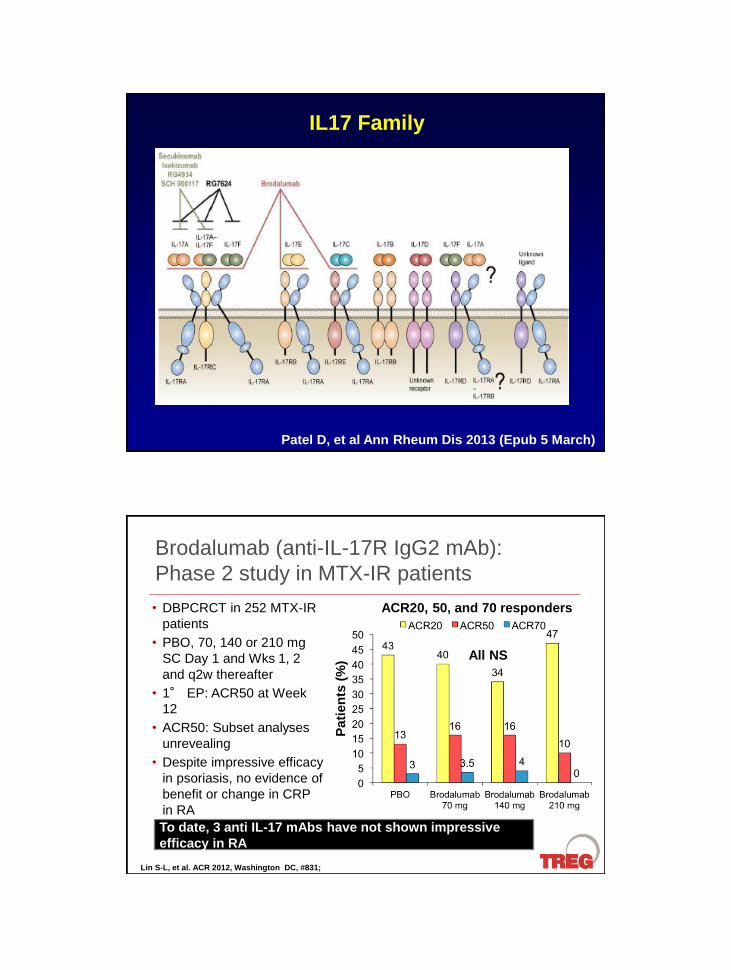
IL17 Family
Patel D, et al Ann Rheum Dis 2013 (Epub 5 March)
Brodalumab (anti-IL-17R IgG2 mAb):
Phase 2 study in MTX-IR patients
• DBPCRCT in 252 MTX-IR
patients
• PBO, 70, 140 or 210 mg
SC Day 1 and Wks 1, 2
and q2w thereafter
• 1° EP: ACR50 at Week
12
• ACR50: Subset analyses
unrevealing
• Despite impressive efficacy
in psoriasis, no evidence of
benefit or change in CRP
in RA
Lin S-L, et al. ACR 2012, Washington DC, #831;
To date, 3 anti IL-17 mAbs have not shown impressive
efficacy in RA
All NS
ACR20, 50, and 70 responders
Pati
en
ts (
%)
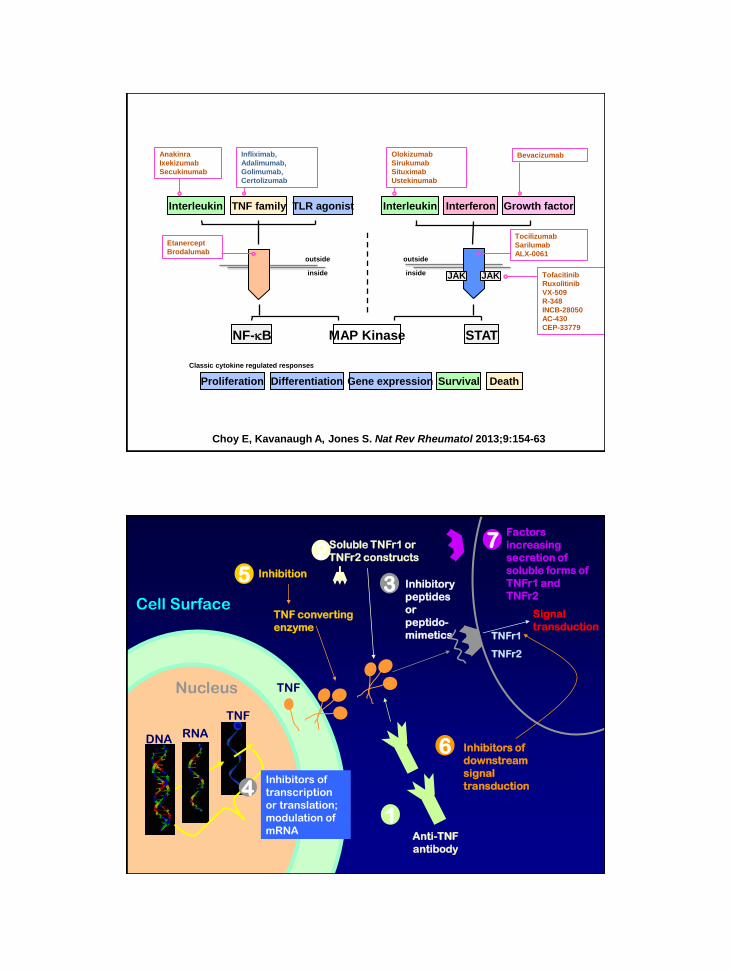
Interleukin TLR agonist
NF-kB MAP Kinase
Interleukin Interferon Growth factor TNF family
STAT
JAK JAK
outside
inside
outside
inside
Survival Proliferation Death
Classic cytokine regulated responses
Differentiation Gene expression
Tofacitinib
Ruxolitinib
VX-509
R-348
INCB-28050
AC-430
CEP-33779
Tocilizumab
Sarilumab
ALX-0061
Olokizumab
Sirukumab
Situximab
Ustekinumab
Bevacizumab Anakinra
Ixekizumab
Secukinumab
Etanercept
Brodalumab
Infliximab,
Adalimumab,
Golimumab,
Certolizumab
Choy E, Kavanaugh A, Jones S. Nat Rev Rheumatol 2013;9:154-63
Nucleus
DNA RNA
TNF
Inhibitors of
transcription
or translation;
modulation of
mRNA
TNF
Cell Surface TNF converting
enzyme
4
5 Inhibition
2 Soluble TNFr1 or
TNFr2 constructs
3 Inhibitory
peptides
or
peptido-
mimetics
1 Anti-TNF
antibody
6 Inhibitors of
downstream
signal
transduction
Signal
transduction TNFr1
TNFr2
7 Factors
increasing
secretion of
soluble forms of
TNFr1 and
TNFr2

Intracellular Signaling Pathways / Molecules
MAPK Syk
P13K cAMP/PKA
JAK
Kinases
ERK
PI3K
Lipid
messengers
cAMP
STAT
STAT
STAT
STAT
Syk PI3K
AC Gas
JAK JAK
Gene transcription
Nucleus
Kinases
p38
JNK
PKA
Second
messengers
PKC
Second
messengers
PKA
NF-κB
IKK
PDE4
NF-κB
Tas SW, et al. Curr Pharm Design. 2005;11:581-611; Schafer P. Biochem Pharmacol. 2012;83: 1583–1590.
Janus Kinases (JAK) family

JAK Family Cytokine Small Molecule inhibitor
JAK-1 IL-2, IL-4 IL-7, IL-9, IL-13 IL-15, IL-21
IL-6, IL-11, IL-27, LIF, OSM, CNTF, CT1, Leptin
IL-10, IL-19, IL-20, IL-22, (IL-24, IL-26)
IFN, IFNb, IFNg, IL-28, IL-29, IL-30 (type-III IFN)
Tofacitinib
Ruxolitinib
INCB-28050
GLPG-0634
JAK-2 IL-3, IL-5, GM-CSF
IL-6, IL-11, IL-27, LIF, OSM, CNTF, CT1, CLC
IL-12, IL-23
EPO, GH, PRL, Leptin
Tofacitinib
Ruxolitinib
INCB-28050
AC-430
JAK-3 IL-2, IL-4 IL-7, IL-9, IL-13 IL-15, IL-21 Tofacitinib
VX-509
R-348
TYK-2 IL-6, IL-11, IL-27, LIF, OSM, CNTF, CT1, CLC
IL-12, IL-23
IFN, IFNb, IFNg, IL-28, IL-29, IL-30 (type-III IFN)
Leptin
--
Cytokine regulation of JAK family members and small
molecule targeted interventions
Baricitinib, Oral JAK 1/2 inhibitor: 12-week Phase 2b
dose-ranging study in MTX-IR (Lilly/Incyte)
Keystone E, et al. EULAR 2012, Berlin, #LB0005;
Genovese M, et al. ACR 2012 Wash DC, #2487
Statistical significance w/ 1, 4, 8 mg by 1° EP at Wk 12;
Clinical benefit at 12 weeks sustained with further improvement
at 24 weeks
41
10 2
57*
31*
12*
54
17
8
75*
35*
23*
78*
40*
20*
0
20
40
60
80
100
ACR20 ACR50 ACR70
Placebo 1 mg QD 2 mg QD
4 mg QD 8 mg QD
ACR Responses at Week 12
*1, 4 and 8 mg all p<0.001
vs PBO
Pati
en
ts (
%)
ACR Responses at Week 24

Treat to target algorithm
Smolen JS et al. Ann Rheum Dis. 2010;69:631-637
Active RA Sustained Remission
Sustained Low Disease
Activity
Assess disease activity about every 3 to 6
months
Use a composite measure of
disease activity every 1 to 3
months
Adapt therapy according to
disease activity
Adapt therapy according to
disease activity
Adapt therapy if state is lost
Adapt therapy if state is lost
Low Disease Activity
Alternative target
Remission
Main target
PRESERVE: Established RA, can TNFi be
lowered or discontinued?
• 604 RA pts w/ moderate RA (DAS28 3.2–5.1) on ETN/MTX x 9 mos LDAS
• DBRCT: 1) Continue E50/MTX; 2) Reduce E25/MTX; 3) Placebo/MTX
•
• No differences in SAE: 2 deaths in E50/M
• SIE = 6; Malignancies = 7; TB = 0
After 9 mo induction of LDAS with MTX/ETN, pts can safely continue or ↓
ETN dosing; maintenance on MTX alone insufficient to maintain LDAS
Time to loss of LDAS & DAS >0.6
Smolen J, et al. Lancet 2013
Week 88 outcomes
Period 2 Arm LDAS Rem mTSS
E50/M (continue) 82.6 66.7 –0.06*
E25/M (Reduce) 79.1 60.2 +0.5
P/M (MTX w/d) 42.6 29.4 +0.6*
**P<0.001 vs P/M; *P<0.05 vs P/M
Kap
lan
-Meie
r su
rviv
al
esti
mate
s (
%)
20
40
60
80
100
100 0 200 300 400
Days relative to first double-blind dose
0
ETN 50 mg + MTX
ETN 25 mg + MTX
PBO + MTX
In P2; mITT, observed cases. P<0.0001, ETN 50 mg/
25 mg + MTX vs PBO +MTX, from log rank test
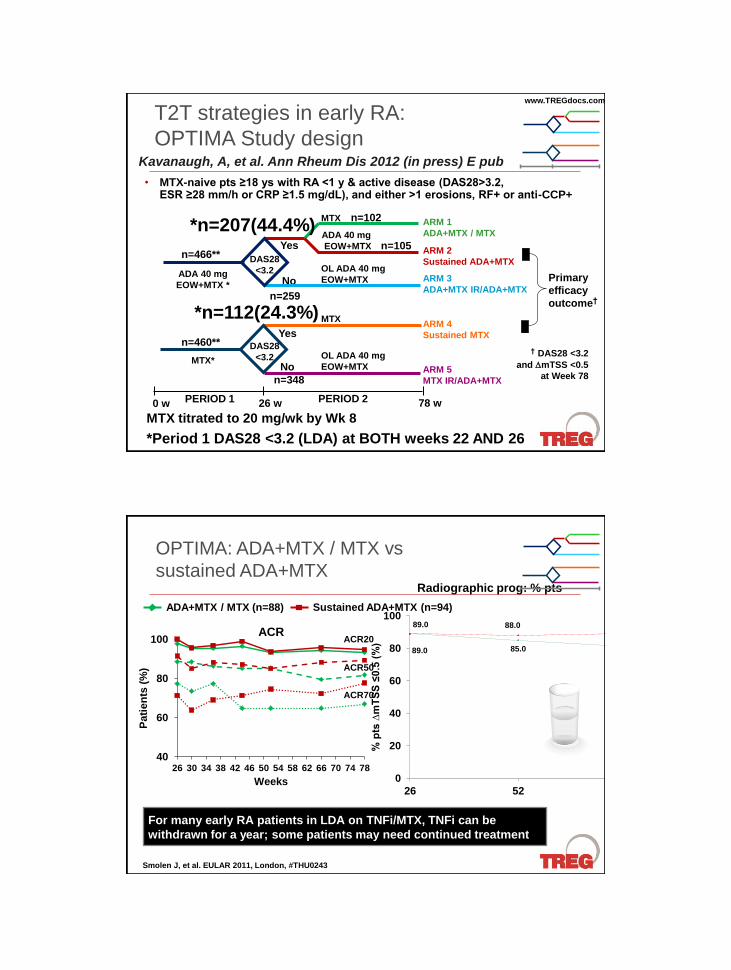
T2T strategies in early RA:
OPTIMA Study design
MTX titrated to 20 mg/wk by Wk 8
*Period 1 DAS28 <3.2 (LDA) at BOTH weeks 22 AND 26
MTX
Yes ADA 40 mg
EOW+MTX
OL ADA 40 mg
EOW+MTX No
No OL ADA 40 mg
EOW+MTX
Yes
MTX
ADA 40 mg
EOW+MTX *
DAS28
<3.2
MTX*
ARM 1
ADA+MTX / MTX
ARM 2
Sustained ADA+MTX
ARM 3
ADA+MTX IR/ADA+MTX
ARM 4
Sustained MTX
ARM 5
MTX IR/ADA+MTX
PERIOD 1 PERIOD 2 0 w 26 w 78 w
Primary
efficacy
outcome†
† DAS28 <3.2
and mTSS <0.5
at Week 78
n=466**
n=460**
*n=112(24.3%)
n=348
n=259
*n=207(44.4%) n=102
n=105
DAS28
<3.2
• MTX-naive pts ≥18 ys with RA <1 y & active disease (DAS28>3.2, ESR ≥28 mm/h or CRP ≥1.5 mg/dL), and either >1 erosions, RF+ or anti-CCP+
www.TREGdocs.com
Kavanaugh, A, et al. Ann Rheum Dis 2012 (in press) E pub
OPTIMA: ADA+MTX / MTX vs
sustained ADA+MTX
89.0 85.0 81.0
89.0 88.0 89.0
0
20
40
60
80
100
26 52 78
% p
ts ∆
mT
SS
≤0.5
(%
)
Weeks
Radiographic prog: % pts
ADA+MTX / MTX (n=88) Sustained ADA+MTX (n=94)
For many early RA patients in LDA on TNFi/MTX, TNFi can be
withdrawn for a year; some patients may need continued treatment
Smolen J, et al. EULAR 2011, London, #THU0243
40
60
80
100
26 30 34 38 42 46 50 54 58 62 66 70 74 78
Pati
en
ts (
%)
Weeks
ACR ACR20
ACR50
ACR70

The Benefit / Risk Balance
Benefit Risk
Infection
Malignancy
Other adverse events
Cost
Signs / symptoms
Quality of life / function
Prevent X-ray damage
Work / home productivity
Cost-efficacy
Patient demographics
Comorbidity
Disease characteristics
Other medications
Rheumatoid Arthritis: New and
Emerging Agents and Trends
Arthur Kavanaugh, MD
Director, Center for Innovative Therapy
Professor of Medicine
Division of Rheumatology, Allergy, and Immunology
University of California San Diego
San Diego, CA