Review Heterotopic ossi cation: a systematic review · the skeletal system to continuously adapt to...
7
Heterotopic ossification: a systematic review Dafydd S Edwards, 1 J C Clasper 2 1 Centre for Blast Injury Studies, Imperial College London, London, UK 2 Defence Professor of Trauma & Orthopaedics, Academic Department of Military Surgery and Trauma, RCDM Birmingham, UK Correspondence to Maj Dafydd S Edwards, Centre for Blast Injury Studies, Imperial College London, South Kensington, London SW7 2AZ, UK; [email protected] Received 27 March 2014 Revised 25 May 2014 Accepted 10 June 2014 Published Online First 11 July 2014 To cite: Edwards DS, Clasper JC. J R Army Med Corps 2015;161:315–321. ABSTRACT Heterotopic ossification (HO) is the formation of mature lamellar bone in extraskeletal soft tissues. It was first described 1000 years ago in the healing of fractures, and in relation to military wounds, texts from the American Civil War and World War I refer to HO specific- ally. It continues to cause problems to injured service personnel; the consequences of wound and soft tissue complications in traumatic amputations pose particular problems to rehabilitation and prosthetic use. While HO is seen in rare genetic conditions, it is most prevalent after joint replacement surgery and trauma. In the civil- ian setting HO has been commonly described in patients after traumatic brain injuries, spinal cord injuries and burns. Militarily, as a consequence of recent operations, and the characteristic injury of blast-related amputations, a renewed interest in HO has emerged due to an increased incidence seen in casualties. The heteroge- neous nature of a blast related amputation makes it diffi- cult for a single aetiological event to be identified, although it is now accepted that blast, amputation through the zone of injury, increased injury severity and associated brain injuries are significant risk factors in HO formation. The exact cellular event leading to HO has yet to be identified, and as a consequence its prevention is restricted to the use of anti-inflammatory medication and radiation, which is often contraindicated in the acute complex military casualty. A systematic review in PubMed and the Cochrane Database identified research articles related to HO to illustrate the military problem of HO and its management, current research concepts and experimental theories regarding HO. This also served as a gap analysis providing the researchers detail of any knowledge deficit in this field, in particular to the mili- tary aspects of HO; 637 out of 7891 articles initially identified that referenced HO were relevant to this review. INTRODUCTION Heterotopic ossification (HO) (Figure 1) is the for- mation of mature lamellar bone in extraskeletal soft tissues. It was first described in the literature nearly 1000 years ago in the healing of fractures, 1 and in relation to military wounds, and complications of amputations, texts from the American Civil War and World War I make specific reference to it. 2 To date HO continues to cause problems to the injured service personnel 34 with its consequences posing particular difficulties to rehabilitation 56 and long-term prosthetic use. 3 It can be classified into congenital or acquired; the latter usually being associated with trauma. In the military and the civilian settings traumatic brain injury (TBI) and traumatic amputations are recog- nised risk factors for HO 7–9 ; despite these associa- tions the exact pathogenic mechanism remains elusive. The prevalence of HO in the military setting is reported to be increasing. 10 This is thought to be due to increased survivorship of casualties with more severe extremity injuries seen in recent opera- tions. 11 In addition the characteristic mechanism of injury seen in operations in Afghanistan, and the latter stages in Iraq, has been blast from improvised explosive devices (IEDs). Many studies have tried to identify causal factors from the mechanism of injury, management of wounds and complications and the subsequent formation of HO. 49 However with so many variables involved in the formation and treatment of a complex military wound, it is difficult to isolate a single aetiological event. Due to the injury severity of the casualty, and the complexity and highly contaminated wounds, primary prevention is unlikely to be possible; there- fore the military surgeon is left with little in his armoury apart from surgical excision, after the for- mation of HO. Case series of individual depart- ment experiences in the management of HO are seen in the literature 10 12 but there is no consistent management consensus. Until recently research and evidence concerning HO has been led by civilian academic departments, however the increased prevalence and functional compromise has driven the military requirement for further workon its aetiology, structure, biology, prevention and treatment. To identify scientific needs and future research directions, a systematic review of literature related to HO was performed. METHODS We employed ‘PRISMA ’ systematic review guide- lines; searching the PubMed database for references using the search terms ‘heterotopic’ and ‘ossifica- tion’ as keywords, and limiting our search to the last 100 years. Primary and secondary exclusion cri- teria were then used to filter the results (Table 1) after a secondary filter, further filtering, or the use of additional keywords, was found to over-refine our search and significant articles excluded. Therefore it was felt that further searches should be done manually. Manual strategies employed to establish relevance, in order of hierarchical import- ance, were (1) Title review, (2) MeSH term review, (3) Abstract review and finally (4) Full article review. A flow chart of the search is demonstrated in Figure 2. Relevant articles were subsequently grouped into related subjects (Table 2). RESULTS Initially 7891 articles related to HO (Figure 3) were identified which was reduced to 637 after refining the search using the primary, secondary and manual exclusion strategies. The number of articles published in the last 10 years increased from 54 to 88, between 2003 and 2013. Three Review Edwards DS, Clasper JC. J R Army Med Corps 2015;161:315–321. doi:10.1136/jramc-2014-000277 315 copyright. on November 11, 2020 by guest. Protected by http://militaryhealth.bmj.com/ J R Army Med Corps: first published as 10.1136/jramc-2014-000277 on 11 July 2014. Downloaded from
Transcript of Review Heterotopic ossi cation: a systematic review · the skeletal system to continuously adapt to...

Heterotopic ossification: a systematic reviewDafydd S Edwards,1 J C Clasper2
1Centre for Blast Injury Studies,Imperial College London,London, UK2Defence Professor of Trauma& Orthopaedics, AcademicDepartment of Military Surgeryand Trauma, RCDMBirmingham, UK
Correspondence toMaj Dafydd S Edwards,Centre for Blast Injury Studies,Imperial College London,South Kensington, LondonSW7 2AZ, UK;[email protected]
Received 27 March 2014Revised 25 May 2014Accepted 10 June 2014Published Online First11 July 2014
To cite: Edwards DS,Clasper JC. J R Army MedCorps 2015;161:315–321.
ABSTRACTHeterotopic ossification (HO) is the formation of maturelamellar bone in extraskeletal soft tissues. It was firstdescribed 1000 years ago in the healing of fractures,and in relation to military wounds, texts from theAmerican Civil War and World War I refer to HO specific-ally. It continues to cause problems to injured servicepersonnel; the consequences of wound and soft tissuecomplications in traumatic amputations pose particularproblems to rehabilitation and prosthetic use. While HOis seen in rare genetic conditions, it is most prevalentafter joint replacement surgery and trauma. In the civil-ian setting HO has been commonly described in patientsafter traumatic brain injuries, spinal cord injuries andburns. Militarily, as a consequence of recent operations,and the characteristic injury of blast-related amputations,a renewed interest in HO has emerged due to anincreased incidence seen in casualties. The heteroge-neous nature of a blast related amputation makes it diffi-cult for a single aetiological event to be identified,although it is now accepted that blast, amputationthrough the zone of injury, increased injury severity andassociated brain injuries are significant risk factors in HOformation. The exact cellular event leading to HO has yetto be identified, and as a consequence its prevention isrestricted to the use of anti-inflammatory medication andradiation, which is often contraindicated in the acutecomplex military casualty. A systematic review inPubMed and the Cochrane Database identified researcharticles related to HO to illustrate the military problem ofHO and its management, current research concepts andexperimental theories regarding HO. This also served asa gap analysis providing the researchers detail of anyknowledge deficit in this field, in particular to the mili-tary aspects of HO; 637 out of 7891 articles initiallyidentified that referenced HO were relevant to thisreview.
INTRODUCTIONHeterotopic ossification (HO) (Figure 1) is the for-mation of mature lamellar bone in extraskeletal softtissues. It was first described in the literature nearly1000 years ago in the healing of fractures,1 and inrelation to military wounds, and complications ofamputations, texts from the American Civil Warand World War I make specific reference to it.2 Todate HO continues to cause problems to theinjured service personnel3 4 with its consequencesposing particular difficulties to rehabilitation5 6 andlong-term prosthetic use.3
It can be classified into congenital or acquired;the latter usually being associated with trauma. Inthe military and the civilian settings traumatic braininjury (TBI) and traumatic amputations are recog-nised risk factors for HO7–9; despite these associa-tions the exact pathogenic mechanism remainselusive.
The prevalence of HO in the military setting isreported to be increasing.10 This is thought to bedue to increased survivorship of casualties withmore severe extremity injuries seen in recent opera-tions.11 In addition the characteristic mechanism ofinjury seen in operations in Afghanistan, and thelatter stages in Iraq, has been blast from improvisedexplosive devices (IEDs). Many studies have triedto identify causal factors from the mechanism ofinjury, management of wounds and complicationsand the subsequent formation of HO.4 9 Howeverwith so many variables involved in the formationand treatment of a complex military wound, it isdifficult to isolate a single aetiological event.Due to the injury severity of the casualty, and the
complexity and highly contaminated wounds,primary prevention is unlikely to be possible; there-fore the military surgeon is left with little in hisarmoury apart from surgical excision, after the for-mation of HO. Case series of individual depart-ment experiences in the management of HO areseen in the literature10 12 but there is no consistentmanagement consensus.Until recently research and evidence concerning
HO has been led by civilian academic departments,however the increased prevalence and functionalcompromise has driven the military requirementfor further work on its aetiology, structure, biology,prevention and treatment. To identify scientificneeds and future research directions, a systematicreview of literature related to HO was performed.
METHODSWe employed ‘PRISMA’ systematic review guide-lines; searching the PubMed database for referencesusing the search terms ‘heterotopic’ and ‘ossifica-tion’ as keywords, and limiting our search to thelast 100 years. Primary and secondary exclusion cri-teria were then used to filter the results (Table 1)after a secondary filter, further filtering, or the useof additional keywords, was found to over-refineour search and significant articles excluded.Therefore it was felt that further searches shouldbe done manually. Manual strategies employed toestablish relevance, in order of hierarchical import-ance, were (1) Title review, (2) MeSH term review,(3) Abstract review and finally (4) Full articlereview. A flow chart of the search is demonstratedin Figure 2. Relevant articles were subsequentlygrouped into related subjects (Table 2).
RESULTSInitially 7891 articles related to HO (Figure 3)were identified which was reduced to 637 afterrefining the search using the primary, secondaryand manual exclusion strategies. The number ofarticles published in the last 10 years increasedfrom 54 to 88, between 2003 and 2013. Three
Review
Edwards DS, Clasper JC. J R Army Med Corps 2015;161:315–321. doi:10.1136/jramc-2014-000277 315
copyright. on N
ovember 11, 2020 by guest. P
rotected byhttp://m
ilitaryhealth.bmj.com
/J R
Arm
y Med C
orps: first published as 10.1136/jramc-2014-000277 on 11 July 2014. D
ownloaded from

distinct groups of research were evident, elective surgery,trauma surgery and scientific basis of disease, representing 54%,25% and 21%, respectively, of the articles published. The mostcommon publication subject was that of HO related to hiparthroplasty (n=218, 34.2%). Only 26 articles were foundreferring to HO in the military trauma setting.
One limitation encountered in the systematic review was achange in nomenclature of HO. Terms such as ectopic bone for-mation, myositis ossificans and heterotopic ossification wereused interchangeably in history.
Normal bone formationPrerequisites for bone formation are inductive signalling path-ways, consisting of chemical mediators (chemokines and cyto-kines), including bone morphogenetic protein (BMP), plateletderived growth factors, fibroblast growth factors, prostaglandins(PGs) and interleukins, all of which trigger bone formation;inducible osteoprogenitor cells which are cells capable of beingdifferentiated into bone forming osteoblasts and finally an envir-onment conducive to osteogenesis (a scaffold for the deposition
of new bone).7 10 (Figure 4) In the normal physiological statethese prerequistes exist, together with osteoclast resorption, toallow a slow metabolic turnover of normal bone. This enablesthe skeletal system to continuously adapt to changes in normalphysiological loads, such as growth or increased physical activity
Scientific basis of diseaseGeneticsHO can be divided into congenital (or genetic) and acquired.Acquired causes are by far the most common; however, geneticcauses provide evidence of the genetic basis for the formationof HO. Two congenital conditions exist specifically related tothe formation of ectopic bone. Fibrodysplasia ossificans progres-siva (FOP) and progressive osseous hyperplasia are rare geneticconditions which result in severe disability secondary to exten-sive bone formation in all soft tissues.13 In FOP the exactmutated gene has yet to be identified and is usually a spontan-eous occurrence, but where familial tendency exists it seems toconfer an autosomal dominant pattern.14 In the early stages ofthe disease a lymphocyte-associated mechanism has been identi-fied thereby inferring an inflammatory pathogenic process.15
Geneticists have demonstrated that the expression of BMP-4, aninflammatory mediator, is significantly increased in cases ofFOP.16 The downregulation of Noggin, a BMP-4 antagonist hasalso been shown in FOP.17
An autosomal inheritance pattern is seen in progressiveosseous hyperplasia with the heterozygous inactivation of theGNAS1 gene exclusively inherited from the father.18 Thisresults in decreased expression of the stimulatory G protein ofadenylyl cyclase, another inflammatory mediator. BMP-4 andstimulatory G protein are associated with bone formation.
Pathological bone formationThe relevance of normal bone formation to pathological boneformation is summarised by Kirsch who states that the molecu-lar mechanisms that are normally found regulating physiologicalbone formation and turnover are present in pathological condi-tions of ectopic bone formation in the skeletal system, andextraosseous soft tissues such as cartilage, blood vessels andmuscles.19 How this is achieved in the soft tissues of blastrelated patients is unknown. However, with the release of cyto-kines and chemokines seen in blast related tissues,20 which arecapable of the stimulation of osteogenesis and the recruitmentof bone forming units, an inflammatory mediated cellular mech-anism is likely. Proinflammatory mediators, platelet derivedgrowth factors,21 fibroblast growth factors,22 transforminggrowth factor-β,23 insulin-like growth factor I24 and insulin-likegrowth factor–II,25 epidermal growth factors,26 and PGs27 haveall been implicated in osteoblast DNA synthesis and are presentin bone matrix. Analysis of wounds further details that certaininflammatory cytokines and chemokines were upregulated as aconsequence of high energy penetrating extremity wounds.Serum factors identified were IL-6, IL-10 and human monocytechemotactic protein-1. Wound effluent proteins upregulatedwere macrophage inflammatory protein-1α andinterferon-γ-inducible protein-10.28 This biochemical evidencesuggests that the formation of HO is associated with a systemicand localised hyperinflammatory response to the index injury.Laboratory manipulation of local and systemic cytokines havebeen proven to influence stem cell differentiation. Progenitorcells from muscle, periosteum and capillaries are capable of dif-ferentiation into osteoprogenitor cells thereby providing osteo-blast precursors in the generetaion of new bone.29 Furthermodulation of local stem cells is possible by the intrinsic nature
Table 1 Filter levels and elements
Filter Filter elements
Primary exclusions Audio-visualNewspaperLecturesBooksBiographies
Secondary exclusions LettersRetracted articlesCommentsEditorialsConference articles
Manual search/exclusions Anomalous articlesDuplicated articlesFOP/POHOPLL/DISH
DISH, diffuse idiopathic skeletal hyperostosis; FOP, fibrodysplasia ossificansprogressiva; OPLL, ossification of the posterior longitudinal ligament; POH,progressive osseous hyperplasia.
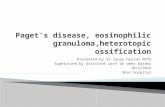
Figure 1 Heterotopic ossification in a transfemoral amputee.
Review
316 Edwards DS, Clasper JC. J R Army Med Corps 2015;161:315–321. doi:10.1136/jramc-2014-000277
copyright. on N
ovember 11, 2020 by guest. P
rotected byhttp://m
ilitaryhealth.bmj.com
/J R
Arm
y Med C
orps: first published as 10.1136/jramc-2014-000277 on 11 July 2014. D
ownloaded from

of the local tissue. It has been recently reported that a strictacidic environment is capable of reprogramming pluripotentcells from one cell lineage to another, thereby demonstratingbidirectional manipulation.30 31
Experimental models of heterotopic ossificationUrist reported an experimental model of new bone formationafter trauma in the 1930s.32 Prior to that Blessig published theossification of the kidney in response to ischaemia caused by
ligation of the renal artery in rabbits. Subsequently the identifi-cation, and isolation, of BMPs have allowed controlled osteoin-duction within animal soft tissue models.
Broadly speaking three basic models of HO formation arenow described33: Trauma-induced animal models; animalosteoinductive models (the interaction of native undifferentiatedcells and implanted BMPs) and osteogenetic cell transplantationmodels.
With the recognition that the formation of HO is related to ablast injury and amputation through the zone of injury, labora-tory experiments, including cellular and animal models, havebeen designed.34–36 A physiological model aims to combine allthree basic models of HO formation where the blast wavecauses localised injury and ischaemia, amputation results inrelease of mesenchymal stem cells residing in the bone canaland subsequent inflammation causing the release of inflamma-tory mediators, including BMPs. The heterogeneous events sur-rounding HO formation lead to experimental difficulties.Tannous reported good results from a Sprague-Dawley ratanimal model, however concerns lay in the delivery of the blast(water column) and relatively low survival rate.36
Elective surgery related heterotopic ossificationHip arthroplastyOver the last 50 years, total hip arthroplasty (THA) has becomeincreasingly common in the management of hip arthritis. The for-mation of HO post surgery is frequently noted20 and its incidencehas been reported to range from 8%37 to 90%.38 However,
Figure 2 A flow chart of the reviewprocess.
Table 2 Relevant article grouping
Relevant articles by group Filter elements
Elective surgery HipSpineShoulderElbow
Trauma surgery CivilianMilitaryBurnsTBI/SCIAmputations
Scientific basis of disease CellularAnimalHuman
TBI, traumatic brain injury.
Review
Edwards DS, Clasper JC. J R Army Med Corps 2015;161:315–321. doi:10.1136/jramc-2014-000277 317
copyright. on N
ovember 11, 2020 by guest. P
rotected byhttp://m
ilitaryhealth.bmj.com
/J R
Arm
y Med C
orps: first published as 10.1136/jramc-2014-000277 on 11 July 2014. D
ownloaded from

Brooker et al report the incidence of HO resulting in significantdisability is limited to those with high grades of HO and demon-strate, using their classification, that it is the final stage of ankylosis(Grade 4) that is most problematic for the patient.39 In the civiliansetting the principles of management of HO is that of primary pre-vention in higher risk patients. The recognised methods of preven-tion are the use of non-steroidal anti-inflammatory drugs, orcyclo-oxygenase-2 (COX-2) selective non-steroidal anti-inflammatory drug, and radiation therapy.40
Heterotopic ossification prophylaxisA Cochrane Review, which included 16 Level 1 trials, demon-strated the benefit of regular indomethacin use during THAreporting a 59% reduction in the incidence of HO.40–42 Themechanism of action is via a combined effect of inhibition of
mesenchymal stem cells and the suppression of inflammation bythe inhibition of PG.43 However it was noted in these articlesthat the side effects of gastrointestinal ulcers and increased riskof postoperative bleeding were not benign. This has led to apreference for COX-2 inhibitors.
The inhibition of bone growth by radiation was establishedover 50 years ago.44 Doses in excess of 20 Grays resulted in thesuppression of vertebral growth in children. This has beenexploited in orthopaedics during THA.45 Preoperative or earlypostoperative local exposure of 7–8 Grays has been demon-strated to prevent the formation of HO45–47; however thetiming is relevant. By the 3rd postoperative day the mesenchy-mal stem cells have already differentiated, and treatment afterthis time is ineffective.48
Trauma related heterotopic ossificationCivilianPost-traumatic HO, traumatic myositis ossificans and myositis ossifi-cans circumspecta are all terms that have been used to define thesame problem—that of bone formation outside the skeletal systemfollowing trauma. In general the trauma in which HO is formedranges from muscle sprains and contusions through to open frac-tures of long bone.49 HO is seen in civilian, as well as military prac-tice; its formation is often subclinical and noted incidentally onradiographs. However, in particular during major trauma, the for-mation of HO may compromise rehabilitation if formed aroundlarge joints or dependent limbs. In the trauma environment, the lit-erature demonstrates that plastic surgeons have referenced, andinvestigated, that in patients with TBI and spinal cord injury (SCI),HO is a well-recognised phenomenon and its incidence ranges from10% to 20% of patients suffering a TBI and 20% to 30% ofpatients with SCI.50–52 Neurogenic HO (NHO) has been demon-strated to have a genetic element; the injury dictating the temporalrelation to its formation while the presence of HLA B27 identifyingthe population at risk of HO.53 The absence of HLA B27 does notpreclude the formation of NHO.53 HLA B27 is associated withinflammatory arthropathies such as ankylosing spondylitis and sero-negative spondyloarthropathies such as Reiter’s disease.54 Despitethe fact that a genetic predisposition is present, centrally released
Figure 3 Numbers of published articles on heterotopic ossification by year.
Figure 4 Biological prerequisites for heterotopic ossification.
Review
318 Edwards DS, Clasper JC. J R Army Med Corps 2015;161:315–321. doi:10.1136/jramc-2014-000277
copyright. on N
ovember 11, 2020 by guest. P
rotected byhttp://m
ilitaryhealth.bmj.com
/J R
Arm
y Med C
orps: first published as 10.1136/jramc-2014-000277 on 11 July 2014. D
ownloaded from

humoral factors previously described continue to be shown to drivebone formation.55
MilitaryHO has been described in history for over a 1000 years56; observedin amputees from the American Civil war,51 World War I2 and therecent conflicts in Iraq and Afghanistan.4 28 57–59 Contemporarymilitary operations have demonstrated an increased prevalenceof HO in military wounds, when compared with civiliancounterparts.4 51 52 The increase in its incidence from veteransserving in the US forces during Operation Iraqi Freedom andOperation Enduring Freedom has resulted in a renewed interestin HO and its extent documented in American and British mili-tary literature.4 9 The increased prevalence in recent conflictsmay be due to increased survivor rates due to enhanced bodyarmour, rapid medical care to the severely injured solider andsubsequent increased survivorship, as well as the mechanism ofinjury, particularly the IED. Specific wound related factors thatcorrelated with the development of HO included impairedhealing and bacterial colonisation.28 Disturbance of local micro-vasculature renders the soft tissues susceptible to HO formation.Localised changes in the arterial supply and reduced oxygentension render the soft tissues hypoxic and acidic. This favoursmineralisation and bone formation as the oxygen tension isrecovered through surgery or ventilation.60 61 The acidicenvironment may also be capable of modulating the cell lineagein soft tissues.30 31
In recent operations, the incidence of HO has been reported as60–64%.4 58 Box 1 details the factors that, demonstrated in a com-parative paper between the UK and USA, place the military casualtyat risk for the development of HO.4 It is likely that systematic andlocal factors come into play in the formation of HO (Figure 5).
Current and potential future military issuesWith amputees seen from operations in Afghanistan11 and a highrate of HO, rehabilitation may be compromised in this casualtygroup to a greater extent than previously seen. Significant disabil-ity has been reported in casualties from Vietnam with unilateraltransfemoral amputations and the majority of bilateral transfe-moral amputees in the Vietnam cohort abandoned their prosthe-tics and rely on a wheelchair for mobility; it was prosthetic relatedissues that led the patient abandoning a prosthetic.3 62
The current management of HO is restricted to operativeexcision in symptomatic patients who have failed non-operativemanagement such as rest, adjustment of pain medication,selected injections, and nerve ablation of neuromas, socketmodification and physiotherapy.10 63 Separately publishedBritish and American military experience in surgical excisionappears similar.58 63 Multiple centres in the UK and the USA
report the necessity of primary excision of symptomatic HOwithin the 1st year after injury, combined with indomethacin orCOX-2 use. Good functional outcome and no significant recur-rence at 12 months after surgery with this approach are seen.59
Additionally, British Plastic and Reconstructive surgeons at theRoyal Centre of Defence Medicine described a technique ofserial operations to elevate, protect or excise overlying skin andsoft tissues to improve the weight bearing surface.63
REQUIRED RESEARCHAnimal heterotopic ossification modelHO formation in rodents has been achieved but included cyto-kine modulation of the animal.35 The model produced byTannous et al used local blast to the lower limb and thereforesystemic causes of blast related HO were not taken intoaccount.36 However, Alfieri et al describe ongoing work atWalter Reed National Military Medical Center, of a reliablereproducible systemic blast model with open fractures, woundischaemia, a large zone of injury, an appropriate bioburden andamputations through the zone of injury.58 The required experi-mental animal model for HO formation is a complex one.However, a reliable small animal model requires validation andto be expanded to larger species. Once established, individualvariables, such as blast magnitude and morphology, infection,
Figure 5 Interaction of local and systemic factors in the formation ofheterotopic ossification.
Box 1 Casualty factors leading to increased risk ofheterotopic ossification (HO)4
▸ Age▸ Blast mechanism of injury (MOI)▸ Zone of injury (ZOI) and subsequent amputation▸ Injury severity score >16▸ Topical negative pressure (TNP) dressings▸ Traumatic brain injury (TBI)▸ Multiple extremity injuries▸ Number of debridements before closure
Review
Edwards DS, Clasper JC. J R Army Med Corps 2015;161:315–321. doi:10.1136/jramc-2014-000277 319
copyright. on N
ovember 11, 2020 by guest. P
rotected byhttp://m
ilitaryhealth.bmj.com
/J R
Arm
y Med C
orps: first published as 10.1136/jramc-2014-000277 on 11 July 2014. D
ownloaded from

surgical debridement zones and local biomechanics, can bemanipulated to help in the prevention and management of HO.
Cellular levelTo date a reliable cellular model of HO formation secondary toblast has yet to be published. Detailed structural evaluation isstill lacking in the literature. Limited imaging techniques aredescribed, however, detailed structure of the cortex and lamellarconfiguration of HO, in comparison with normal bone, is yet tobe seen. This would also provide control data to samplesretrieved from experimental models.
Military aetiological factorsThe comparative study by Brown et al showed significant simi-larities between the UK and US experiences of wounds and sub-sequent HO formation in Iraq and the early years inAfghanistan.4 However, the UK data set only included casualtiesup to 2008. It is well recognised that the modus operandi of theTaliban and insurgents changed at this time to the use of IEDsof greater magnitude.
Muscle ischaemia and necrosis are believed to be related toHO formation.64 Therefore tourniquet related data requirescomparison in these subjects and larger subject numbers arerequired to further evaluate the link to topical negative dressingsand HO, that was noted previously.4
Management of HO in military populationMilitary amputees requiring surgery for wound and residuumrelated problems during rehabilitation, such as those seen inlimbs complicated by HO, are referred from their rehabilitationcentre to secondary care specialists for surgical managementthroughout the UK. This provides an opportunity for data ana-lysis on protocols used and complication/recurrence rates afterHO surgery at different centres. Ideally a prospective cohortstudy in the use of medical and surgical strategies in manage-ment of HO should be considered. However, a retrospectivecomparative multiarm case series would give direction to futureresearch. The timing of HO excision may be the key; as detailedpreviously, surgery is contemplated when rehabilitation is com-promised. However, once risk stratification is analysed, andwhen HO can be clinically recognised early in its development,surgery may be expedited to prevent rehabilitation delays.
CONCLUSIONIt is likely that HO will continue to compromise the rehabilita-tion and long-term outcome of the cohort of traumatic ampu-tees from operations in Afghanistan, the magnitude of which,while at present is unknown, is likely to reflect the experience inIraq and the early stages of Afghanistan. As noted, there remainsignificant gaps in the understanding of this condition. Work isrequired in this field to fully understand its pathogenesis fromthe triggering traumatic event, cellular inception to primary pre-vention. Understanding the key to unlocking its formation islikely to help its prevention and/or subsequent management.
Contributors DSE: main researcher and author. JCC: research supervisor andguarantor.
Competing interests None.
Provenance and peer review Not commissioned; externally peer reviewed.
REFERENCES1 Abū’l-Qāsim Halaf b.’Abbās az-Zahrāwī. Albucasis: on surgery and instruments.
Translated by Spink MS and Lewis GL. Berkeley: University of California Press,1973.
2 Dejerne A, Ceillier A. Para-osteo-arthropathies des paraplegiques par lesionmedullaire; etude clinique et radiographique. Ann Med 1918;5:497.
3 Dougherty PJ, McFarland LV, Smith DG, et al. Multiple traumatic limb loss: acomparison of Vietnam veterans to OIF/OEF servicemembers. J Rehabil Res Dev2010;47:333–48.
4 Brown KV, Dharm-Datta S, Potter BK, et al. Comparison of development ofheterotopic ossification in injured US and UK Armed Services personnel withcombat-related amputations: preliminary findings and hypotheses regardingcausality. J Trauma 2010;69:S116–22.
5 Masini BD, Waterman SM, Wenke JC, et al. Resource utilization and disabilityoutcome assessment of combat casualties from Operation Iraqi Freedom andOperation Enduring Freedom. J Orthop Trauma 2009;23:261–6.
6 Gajewski D, Granville R. The United States Armed Forces Amputee Patient CareProgram. J Am Acad Orthop Surg 2006;14(10 Spec No.):S183–7.
7 Chalmers J, Gray DH, Rush J. Observations on the induction of bone in soft tissues.J Bone Joint Surg Br 1975;57:36–45.
8 Cipriano CA, Pill SG, Keenan MA. Heterotopic ossification following traumatic braininjury and spinal cord injury. J Am Acad Orthop Surg 2009;17:689–97.
9 Potter BK, Burns TC, Lacap AP, et al. Heterotopic ossification in the residual limbsof traumatic and combat-related amputees. J Am Acad Orthop Surg 2006;14(10Spec No.):S191–7.
10 Potter BK, Burns TC, Lacap AP, et al. Heterotopic ossification following traumaticand combat-related amputations. Prevalence, risk factors, and preliminary results ofexcision. J Bone Joint Surg Am 2007;89:476–86.
11 Brown KV, Clasper JC. The changing pattern of amputations. J R Army Med Corps2013;159:300–3.
12 Ramasamy A, Harrisson SE, Clasper JC, et al. Injuries from roadside improvisedexplosive devices. J Trauma 2008;65:910–14.
13 Connor JM, Evans DA. Fibrodysplasia ossificans progressiva. The clinical featuresand natural history of 34 patients. J Bone Joint Surg Br 1982;64:76–83.
14 Kaplan FS, McCluskey W, Hahn G, et al. Genetic transmission of fibrodysplasiaossificans progressiva. Report of a family. J Bone Joint Surg Am 1993;75:1214–20.
15 Gannon FH, Valentine BA, Shore EM, et al. Acute lymphocytic infiltration in anextremely early lesion of fibrodysplasia ossificans progressiva. Clin Orthop Relat Res1998(346):19–25.
16 Shafritz AB, Shore EM, Gannon FH, et al. Overexpression of an osteogenicmorphogen in fibrodysplasia ossificans progressiva. N Engl J Med1996;335:555–61.
17 Ahn J, Serrano de la Pena L, Shore EM, et al. Paresis of a bone morphogeneticprotein-antagonist response in a genetic disorder of heterotopic skeletogenesis.J Bone Joint Surg Am 2003;85-A:667–74.
18 Shore EM, Ahn J, Jan de Beur S, et al. Paternally inherited inactivating mutationsof the GNAS1 gene in progressive osseous heteroplasia. N Engl J Med2002;346:99–106.
19 Kirsch T. Determinants of pathological mineralization. Curr Opin Rheumatol2006;18:174–80.
20 Kaplan FS, Glaser DL, Hebela N, et al. Heterotopic ossification. J Am Acad OrthopSurg 2004;12:116–25.
21 Canalis E. Effect of platelet-derived growth factor on DNA and protein synthesis incultured rat calvaria. Metabolism 1981;30:970–5.
22 Rodan SB, Wesolowski G, Thomas K, et al. Growth stimulation of rat calvariaosteoblastic cells by acidic fibroblast growth factor. Endocrinology1987;121:1917–23.
23 Centrella M, McCarthy TL, Canalis E. Transforming growth factor beta is abifunctional regulator of replication and collagen synthesis in osteoblast-enrichedcell cultures from fetal rat bone. J Biol Chem 1987;262:2869–74.
24 Hock JM, Centrella M, Canalis E. Insulin-like growth factor I has independenteffects on bone matrix formation and cell replication. Endocrinology1988;122:254–60.
25 Mohan S, Jennings JC, Linkhart TA, et al. Primary structure of human skeletalgrowth factor: homology with human insulin-like growth factor-II. Biochim BiophysActa 1988;966:44–55.
26 Canalis E, Raisz LG. Effect of epidermal growth factor on bone formation in vitro.Endocrinology 1979;104:862–9.
27 Nauth A, Giles E, Potter BK, et al. Heterotopic ossification in orthopaedic trauma.J Orthop Trauma 2012;26:684–8.
28 Evans KN, Forsberg JA, Potter BK, et al. Inflammatory cytokine and chemokineexpression is associated with heterotopic ossification in high-energy penetrating warinjuries. J Orthop Trauma 2012;26:e204–13.
29 Davis TA, O’Brien FP, Anam K, et al. Heterotopic ossification in complexorthopaedic combat wounds: quantification and characterization of osteogenicprecursor cell activity in traumatized muscle. J Bone Joint Surg Am2011;93:1122–31.
30 Obokata H, Sasai Y, Niwa H, et al. Bidirectional developmental potential inreprogrammed cells with acquired pluripotency. Nature 2014;505:676–80.
31 Obokata H, Wakayama T, Sasai Y, et al. Stimulus-triggered fate conversionof somatic cells into pluripotency. Nature 2014;505:641–7.
32 Urist MR. Bone: formation by autoinduction. Science 1965;150:893–9.
Review
320 Edwards DS, Clasper JC. J R Army Med Corps 2015;161:315–321. doi:10.1136/jramc-2014-000277
copyright. on N
ovember 11, 2020 by guest. P
rotected byhttp://m
ilitaryhealth.bmj.com
/J R
Arm
y Med C
orps: first published as 10.1136/jramc-2014-000277 on 11 July 2014. D
ownloaded from

33 Ekelund A, Brosjo O, Nilsson OS. Experimental induction of heterotopic bone. ClinOrthop Relat Res 1991(263):102–12.
34 Liu X, Kang H, Shahnazari M, et al. A novel mouse model of trauma inducedheterotopic ossification. J Orthop Res 2014;32:183–8.
35 Zotz TG, Paula JB, Moser AD. Experimental model of heterotopic ossification inWistar rats. Braz J Med Biol Res 2012;45:497–501.
36 Tannous O, Griffith C, O’Toole RV, et al. Heterotopic ossification after extremity blastamputation in a Sprague-Dawley rat animal model. J Orthop Trauma 2011;25:506–10.
37 Amstutz HC. Complications of total hip replacement. Clin Orthop Relat Res1970;72:123–37.
38 Rosendahl S, Christoffersen JK, Norgaard M. Para-articular ossification following hipreplacement. 70 arthroplasties ad modum Moore using McFarland’s approach. ActaOrthop Scand 1977;48:400–4.
39 Brooker AF, Bowerman JW, Robinson RA, et al. Ectopic ossification following totalhip replacement. Incidence and a method of classification. J Bone Joint Surg Am1973;55:1629–32.
40 Fransen M, Neal B. Non-steroidal anti-inflammatory drugs for preventingheterotopic bone formation after hip arthroplasty. Cochrane Database Syst Rev2004;(3):CD001160.
41 Matta JM, Siebenrock KA. Does indomethacin reduce heterotopic bone formationafter operations for acetabular fractures? A prospective randomised study. J BoneJoint Surg Br 1997;79:959–63.
42 Haran M, Bhuta T, Lee B. Pharmacological interventions for treating acuteheterotopic ossification. Cochrane Database Syst Rev 2004;(4):CD003321.
43 Sell S, Willms R, Jany R, et al. The suppression of heterotopic ossifications: radiationversus NSAID therapy--a prospective study. J Arthroplasty 1998;13:854–9.
44 Neuhauser EB, Wittenborg MH, Berman CZ, et al. Irradiation effects of roentgentherapy on the growing spine. Radiology 1952;59:637–50.
45 Coventry MB, Scanlon PW. The use of radiation to discourage ectopic bone. Anine-year study in surgery about the hip. J Bone Joint Surg Am 1981;63:201–8.
46 Anthony P, Keys H, Evarts CM, et al. Prevention of heterotopic bone formation withearly post operative irradiation in high risk patients undergoing total hiparthroplasty: comparison of 10.00 Gy vs 20.00 Gy schedules. Int J Radiat OncolBiol Phys 1987;13:365–9.
47 Healy WL, Lo TC, DeSimone AA, et al. Single-dose irradiation for the preventionof heterotopic ossification after total hip arthroplasty. A comparison of doses of fivehundred and fifty and seven hundred centigray. J Bone Joint Surg Am1995;77:590–5.
48 Lo TC, Healy WL, Covall DJ, et al. Heterotopic bone formation after hip surgery:prevention with single-dose postoperative hip irradiation. Radiology1988;168:851–4.
49 Garland DE. A clinical perspective on common forms of acquired heterotopicossification. Clin Orthop Relat Res 1991(263):13–29.
50 Garland DE, Blum CE, Waters RL. Periarticular heterotopic ossification inhead-injured adults. Incidence and location. J Bone Joint Surg Am1980;62:1143–6.
51 Garland DE. Clinical observations on fractures and heterotopic ossification in thespinal cord and traumatic brain injured populations. Clin Orthop Relat Res1988:86–101.
52 Wittenberg RH, Peschke U, Botel U. Heterotopic ossification after spinal cord injury.Epidemiology and risk factors. J Bone Joint Surg Br 1992;74:215–18.
53 Larson JM, Michalski JP, Collacott EA, et al. Increased prevalence of HLA-B27 inpatients with ectopic ossification following traumatic spinal cord injury. RheumatolRehabil 1981;20:193–7.
54 Moll JM, Haslock I, Macrae IF, et al. Associations between ankylosing spondylitis,psoriatic arthritis, Reiter’s disease, the intestinal arthropathies, and Behcet’ssyndrome. Medicine (Baltimore) 1974;53:343–64.
55 Toffoli AM, Gautschi OP, Frey SP, et al. From brain to bone: evidence for therelease of osteogenic humoral factors after traumatic brain injury. Brain Inj2008;22:511–18.
56 Chao ST, Joyce MJ, Suh JH. Treatment of heterotopic ossification. Orthopedics2007;30:457–64; quiz 65–6.
57 Melcer T, Belnap B, Walker GJ, et al. Heterotopic ossification in combat amputeesfrom Afghanistan and Iraq wars: five case histories and results from a small seriesof patients. J Rehabil Res Dev 2011;48:1–12.
58 Alfieri KA, Forsberg JA, Potter BK. Blast injuries and heterotopic ossification. BoneJoint Res 2012;1:192–7.
59 Forsberg JA, Pepek JM, Wagner S, et al. Heterotopic ossification in high-energywartime extremity injuries: prevalence and risk factors. J Bone Joint Surg Am2009;91:1084–91.
60 Pape HC, Marsh S, Morley JR, et al. Current concepts in the development ofheterotopic ossification. J Bone Joint Surg Br 2004;86:783–7.
61 Hewitt MS, Garland DE, Ayyoub Z. Heterotopic ossification complicating prolongedintubation: case report and review of the literature. J Spinal Cord Med2002;25:46–9.
62 Dougherty PJ. Armored vehicle crew casualties. Mil Med 1990;155:417–20.63 Evriviades D, Jeffery S, Cubison T, et al. Shaping the military wound: issues
surrounding the reconstruction of injured servicemen at the Royal Centre forDefence Medicine. Philos Trans R Soc B Biol Sci 2011;366:219–30.
64 Stein DA, Patel R, Egol KA, et al. Prevention of heterotopic ossification at theelbow following trauma using radiation therapy. Bull Hosp Jt Dis 2003;61:151–4.
Review
Edwards DS, Clasper JC. J R Army Med Corps 2015;161:315–321. doi:10.1136/jramc-2014-000277 321
copyright. on N
ovember 11, 2020 by guest. P
rotected byhttp://m
ilitaryhealth.bmj.com
/J R
Arm
y Med C
orps: first published as 10.1136/jramc-2014-000277 on 11 July 2014. D
ownloaded from