Review Article The Impact of Intravenous Lidocaine on ICP in ...Review Article The Impact of...
13
Review Article The Impact of Intravenous Lidocaine on ICP in Neurological Illness: A Systematic Review F. A. Zeiler, 1 N. Sader, 2 and C. J. Kazina 1 1 Section of Neurosurgery, Department of Surgery, University of Manitoba, GB1-820 Sherbrook Street, Winnipeg, MB, Canada R3A 1R9 2 University of Manitoba, GB1-820 Sherbrook Street, Winnipeg, MB, Canada R3A 1R9 Correspondence should be addressed to F. A. Zeiler; [email protected] Received 30 May 2015; Revised 17 August 2015; Accepted 25 August 2015 Academic Editor: Robert Boots Copyright © 2015 F. A. Zeiler et al. is is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. Background. e goal of our study was to perform a systematic review of the literature to determine the effect that intravenous (IV) lidocaine had on ICP in patients with neurological illness. Methods. All articles are from MEDLINE, BIOSIS, EMBASE, Global Health, Scopus, Cochrane Library, the International Clinical Trials Registry Platform (inception to March 2015). e strength of evidence was adjudicated using both the Oxford and GRADE methodology. Results. Ten original articles were considered for the final review. ere were 189 patients studied. Seven studies focused on prophylactic pretreatment with IV lidocaine to determine if there would be an attenuation of ICP spikes during stimulation, with 4 displaying an attenuation of ICP. ree studies focused on a therapeutic administration of IV lidocaine in order to determine ICP reduction effects. All therapeutic studies displayed a reduction in ICP. Conclusions. We cannot make a strong definitive recommendation on the effectiveness of IV lidocaine on the attenuation of ICP spikes during stimulation. ere currently exists both Oxford 2b and GRADE B literature to support and refute the attenuation of ICP spikes with IV lidocaine during stimulation. ere currently exists Oxford 2b, GRADE B evidence to support ICP reduction with lidocaine when used as a therapeutic agent. 1. Introduction Numerous medical therapies have been utilized in the treat- ment of elevated intracranial pressure (ICP) [1]. e majority of ICP therapies are directed at reducing cerebral blood volume, attenuation of edema, cerebrospinal fluid (CSF) diversion, and decreasing metabolic demands of the neural tissue, with the goal of maintaining adequate cerebral blood flow (CBF) and cellular preservation. Specific concerns of ICP elevations occur during the peri- intubation period, due to the significant stimulation that occurs during definitive airway management. Lidocaine use, both intravenous (IV) and laryngotracheal (LT), has been reported to blunt the ICP elevations during intubation [2]. ough one would assume that the ICP mediated effects of lidocaine stem from its local anesthetic effect, there are other proposed mechanisms of ICP reduction via the IV route. Lidocaine injected IV has been shown in models to induce cerebral vasoconstriction leading to a decrease in cerebral blood volume and thus ICP [2, 3]. Furthermore, IV lidocaine leads to sodium channel inhibition and thus a reduction in cerebral activity and metabolic demands [3, 4], as well as excitotoxicity [5], leading to a potential ICP reduction effect. To date few studies have documented the ICP effect of IV lidocaine in humans with neurological illness [6–16]. e goal of our study is to perform a systematic review of the literature on the use of intravenous lidocaine and its effects on ICP in patients with neurological illness. 2. Methods A systematic review using the methodology outlined in the Cochrane Handbook for Systematic Reviewers [17] was conducted. e data was reported following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) [18]. e review question and search strategy were decided upon by the primary author (F. A. Zeiler) and supervisor (C. J. Kazina). 2.1. Search Question, Population, and Inclusion and Exclusion Criteria. e question posed for systematic review was the following: What is the effect of IV lidocaine on ICP in Hindawi Publishing Corporation Critical Care Research and Practice Volume 2015, Article ID 485802, 12 pages http://dx.doi.org/10.1155/2015/485802
Transcript of Review Article The Impact of Intravenous Lidocaine on ICP in ...Review Article The Impact of...

Review ArticleThe Impact of Intravenous Lidocaine on ICP inNeurological Illness: A Systematic Review
F. A. Zeiler,1 N. Sader,2 and C. J. Kazina1
1Section of Neurosurgery, Department of Surgery, University of Manitoba, GB1-820 Sherbrook Street, Winnipeg, MB, Canada R3A 1R92University of Manitoba, GB1-820 Sherbrook Street, Winnipeg, MB, Canada R3A 1R9
Correspondence should be addressed to F. A. Zeiler; [email protected]
Received 30 May 2015; Revised 17 August 2015; Accepted 25 August 2015
Academic Editor: Robert Boots
Copyright © 2015 F. A. Zeiler et al. This is an open access article distributed under the Creative Commons Attribution License,which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Background. The goal of our study was to perform a systematic review of the literature to determine the effect that intravenous (IV)lidocaine had on ICP in patients with neurological illness. Methods. All articles are from MEDLINE, BIOSIS, EMBASE, GlobalHealth, Scopus, Cochrane Library, the International Clinical Trials Registry Platform (inception to March 2015). The strength ofevidence was adjudicated using both the Oxford and GRADE methodology. Results. Ten original articles were considered for thefinal review. There were 189 patients studied. Seven studies focused on prophylactic pretreatment with IV lidocaine to determineif there would be an attenuation of ICP spikes during stimulation, with 4 displaying an attenuation of ICP. Three studies focusedon a therapeutic administration of IV lidocaine in order to determine ICP reduction effects. All therapeutic studies displayed areduction in ICP. Conclusions. We cannot make a strong definitive recommendation on the effectiveness of IV lidocaine on theattenuation of ICP spikes during stimulation. There currently exists both Oxford 2b and GRADE B literature to support and refutethe attenuation of ICP spikes with IV lidocaine during stimulation.There currently exists Oxford 2b, GRADEB evidence to supportICP reduction with lidocaine when used as a therapeutic agent.
1. Introduction
Numerous medical therapies have been utilized in the treat-ment of elevated intracranial pressure (ICP) [1].Themajorityof ICP therapies are directed at reducing cerebral bloodvolume, attenuation of edema, cerebrospinal fluid (CSF)diversion, and decreasing metabolic demands of the neuraltissue, with the goal of maintaining adequate cerebral bloodflow (CBF) and cellular preservation.
Specific concerns of ICP elevations occur during the peri-intubation period, due to the significant stimulation thatoccurs during definitive airway management. Lidocaine use,both intravenous (IV) and laryngotracheal (LT), has beenreported to blunt the ICP elevations during intubation [2].Though one would assume that the ICP mediated effects oflidocaine stem from its local anesthetic effect, there are otherproposed mechanisms of ICP reduction via the IV route.Lidocaine injected IV has been shown in models to inducecerebral vasoconstriction leading to a decrease in cerebralblood volume and thus ICP [2, 3]. Furthermore, IV lidocaineleads to sodium channel inhibition and thus a reduction in
cerebral activity and metabolic demands [3, 4], as well asexcitotoxicity [5], leading to a potential ICP reduction effect.
To date few studies have documented the ICP effect of IVlidocaine in humanswith neurological illness [6–16].The goalof our study is to perform a systematic review of the literatureon the use of intravenous lidocaine and its effects on ICP inpatients with neurological illness.
2. Methods
A systematic review using the methodology outlined inthe Cochrane Handbook for Systematic Reviewers [17] wasconducted. The data was reported following the PreferredReporting Items for Systematic Reviews and Meta-Analyses(PRISMA) [18]. The review question and search strategywere decided upon by the primary author (F. A. Zeiler) andsupervisor (C. J. Kazina).
2.1. Search Question, Population, and Inclusion and ExclusionCriteria. The question posed for systematic review was thefollowing: What is the effect of IV lidocaine on ICP in
Hindawi Publishing CorporationCritical Care Research and PracticeVolume 2015, Article ID 485802, 12 pageshttp://dx.doi.org/10.1155/2015/485802

2 Critical Care Research and Practice
patients with neurological illness? We posed this broadquestion so as to include all eligible studies with objective ICPdocumentation during IV lidocaine administration, since wesuspected the literature to be scarce.
All studies, prospective and retrospective, were included.Studies of any language were included, with relevantmanuscripts translated in order to ensure that they metthe predefined inclusion/exclusion criteria. The reason foran all-inclusive search was based on the small number ofstudies of any type identified by the primary author duringa preliminary search of MEDLINE.
The primary outcome measure was documented effectof IV lidocaine on ICP. Secondary outcome measures werepatient outcomes and adverse effects of lidocaine therapy.
Inclusion criteria were all studies including human sub-jects with neurological illness, prospective or retrospectivestudies of any size, any age category, any language, the use ofIV lidocaine, and documentation of ICP response. Exclusioncriteria were animal studies, those studies not documentingthe ICP response, and the use of LT lidocaine only.
2.2. Search Strategy. MEDLINE, BIOSIS, EMBASE, GlobalHealth, SCOPUS, and Cochrane Library from inceptionto March 2015 were searched using individualized searchstrategies for each database. The search strategy for MED-LINE can be seen in Appendix A of the supplementarymaterial (see Supplementary Material available online athttp://dx.doi.org/10.1155/2015/485802), with a similar searchstrategy utilized for the other databases. In addition, theWorld Health Organization’s International Clinical Tri-als Registry Platform and https://clinicaltrials.gov/ weresearched looking for studies planned or underway.
In addition, meeting proceedings for the last 5 yearslooking for ongoing and unpublished work based on lido-caine therapy in neurological patientswere examined by handsearching the published proceedings for individual meet-ings. Both electronic and paper publications were searchedwhen available. The meeting proceedings of the followingprofessional societies were searched: Canadian Neurologi-cal Sciences Federation (CNSF), American Association ofNeurological Surgeons (AANS), Congress of NeurologicalSurgeons (CNS), European Neurosurgical Society (ENSS),World Federation of Neurological Surgeons (WFNS), Amer-ican Neurology Association (ANA), American Academy ofNeurology (AAN), European Federation of NeurologicalScience (EFNS),World Congress of Neurology (WCN), Soci-ety of Critical Care Medicine (SCCM), Neurocritical CareSociety (NCS), World Federation of Societies of Intensiveand Critical Care Medicine (WFSICCM), American Societyfor Anesthesiologists (ASA), World Federation of Societiesof Anesthesiologist (WFSA), Australian Society of Anesthe-siologists, International Anesthesia Research Society (IARS),Society of Neurosurgical Anesthesiology and Critical Care(SNACC), Society for Neuroscience in Anesthesiology andCritical Care, and the Japanese Society of Neuroanesthesiaand Critical Care (JSNCC).
Finally, reference lists of any review articles or systematicreviews on IV lidocaine, or ICP control, in neurologically illpatients were reviewed for relevant studies.
2.3. Study Selection. Utilizing two reviewers (F. A. Zeilerand N. Sader), a two-step review of all articles returnedby our search strategies was performed. First, the reviewersindependently screened all titles and abstracts of the returnedarticles to decide if they met the inclusion criteria. Second,full text of the chosen articles was then assessed to confirm ifthey met the inclusion criteria and that the primary outcomeof ICP response was reported in the study. Any discrepanciesbetween the two reviewers were resolved by discussion and athird party (C. J. Kazina) if necessary.
2.4. Data Collection. Data was extracted from the selectedarticles and stored in an electronic database. Data fieldsincluded patient demographics, type of study (prospectiveor retrospective), number of patients, dose of lidocaine,duration of therapy, effect on ICP, adverse effects, and patientoutcome.
2.5. Quality of Evidence Assessment. Assessment of the levelof evidence for each included study was conducted by twoindependent reviewers (F. A. Zeiler andC. J. Kazina), utilizingthe Oxford criteria [19] and the Grading of RecommendationAssessment Development and Education (GRADE) criteria[20–25] for level of evidence. We elected on utilizing twodifferent systems to grade level of evidence given the factthat these two systems are amongst the most commonly usedsystems. We believe this would allow a larger audience tofollow our systematic approach in the setting of unfamiliaritywith a particular grading system.
TheOxford criteria consist of a 5-level grading system forliterature. Level 1 is split into subcategories 1a, 1b, and 1cwhichrepresent a systematic review of randomized control trials(RCT) with homogeneity, individual RCTwith narrow confi-dence interval, and all or none studies, respectively. Oxfordlevel 2 is split into 2a, 2b, and 2c representing systematicreview of cohort studies with homogeneity of data, individualcohort study or low quality RCT, and outcomes research,respectively. Oxford level 3 is split into 3a and 3b representingsystematic review of case-control studies with homogeneityof data and individual case-control study, respectively.Oxfordlevel 4 represents case-series and poor cohort studies. Finally,Oxford level 5 represents expert opinion.
The GRADE level of evidence is split into 4 levels: A,B, C, and D. GRADE level A represents high evidencewith multiple high quality studies having consistent results.GRADE level B represents moderate evidence with one highquality study, or multiple low quality studies. GRADE level Cevidence represents low evidence with one or more studieswith severe limitations. Finally, GRADE level D representsvery low evidence based on either expert opinion or fewstudies with severe limitations.
Any discrepancies between the grading of the two review-ers were resolved via discussion and a third reviewer whenrequired.
2.6. Statistical Analysis. A meta-analysis was not performedin this study due to the heterogeneity of data and study designwithin the articles identified.

Critical Care Research and Practice 3
Total number of articles fromdatabase and other sources
470
Articles from database search
466
Articles from search of other sources
4
Articles after duplicate removal
414
Articles after application of inclusion/exclusion criteria to
title and abstract (1stscreening):
39
Articles after application of inclusion/exclusion criteria to full text (2nd screening):11 articles (10 original articles, with 1 companion pub.)
Duplicates removed 56
375 removed because of thefollowing:(i) 49 non-English studies that
were nonrelevant(ii) 22 animal studies
(iii) 304 nonrelevant
29 removed because of thefollowing:
(i) 11 review articles(ii) 3 LT lidocaine only
(iii) 1 no mention of IV lidocaine effect on ICP after treatment
(iv) 1 animal study(v) 13 nonrelevant
1 added from reference sections
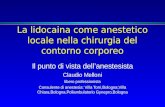
Figure 1: Flow diagram of search results.
3. Results
The results of the search strategy across all databases andother sources are summarized in Figure 1. Overall a totalof 470 articles were identified, with 466 from the databasesearch and 4 from the search of published meeting pro-ceedings. A total of 56 were removed due to duplicationof reference, leaving 414 to review. By applying the inclu-sion/exclusion criteria to the title and abstract of these arti-cles, we identified 39 articles that fit these criteria. An addi-tional 1 article was added from reference sections of pertinentreview articles, leaving a total of 40 fullmanuscripts to review.Of the 40 identified, 36 were from the database search and4 were from published meeting proceedings. Applying theinclusion/exclusion criteria to the full text documents, only11 articles were eligible for inclusion in the systematic review,with 8 fromdatabase and 3 frommeeting proceeding sources.The 29 articles thatwere excludedwere done so because eitherthey did not report details around IV lidocaine administra-tion, there was no documentation of ICP, they were reviewarticles, or they were nonrelevant basic science articles.
Of the 11 articles identified, one article was a companionabstract publication [9] to a formal manuscript publication[8]. The data from this companion abstract [9] was includedin the tables for completeness only and was not included inthe data synthesis in order to prevent duplication of patient
data. Thus, 10 original articles were included in the datareview and data analysis. Two of the manuscripts were non-English papers requiring translation [13, 14], with one beingFrench [14] and the other Italian [13].
Of the 10 original articles included in the review [6–8, 10–16], all were prospective studies. There were 4 prospectiveRCT [7, 10, 11, 14], 2 prospective nonrandomized trials [6, 12],and 4 prospective cohort studies [8, 13, 15, 16].
Four of the articles [8, 13, 15, 16] focused on achievingthe ICP response to IV lidocaine in severe traumatic braininjury (TBI) patient populations, while 3 articles describedmalignant elective brain tumor patients [6, 7, 11], and 1 studymentioned hydrocephalus patients with elevated ICP10. Twostudies failed to detail the patient populations and statedthey were “post-operative neurosurgical patients” or “electiveoperative neurosurgical patients” and also failed to indicate ifthe patients had elevated ICP prior to lidocaine administra-tion [12, 14]. The ICP was recorded via cranial monitoring inall but 1 study, which utilized lumbar cisternal pressure [14].
Overall, there were 189 patients across the 10 stud-ies included in the review, with 133 given IV lidocaineand 56 serving as controls. The control patients wereadministered the following: esmolol (11), LT lidocaine(11), thiopental (10), placebo (10), steroid/glycerin (7), andsteroids/glycerin/nitroglycerin (7).

4 Critical Care Research and Practice
There were 54 severe TBI patients, 62 elective tumorpatients, and 30 hydrocephalus patients undergoing ven-triculoperitoneal shunt (VPS) placement, and 43 patientswere listed as “post-operative neurosurgical patients” [12] or“elective operative neurosurgical patients” [14].
The average age across all studies was 34.6 to 55 years.Five studies failed to document patient age [8, 10–12, 15].Study demographics and patient characteristics can be seenin Table 1, while treatment characteristics and effect on ICPand adverse events are reported in Table 2.
3.1. IV Lidocaine Treatment Characteristics. Within the 10studies identified [6–8, 10–16], 4 were prospective RCT [7, 10,11, 14]. The first study [7] compared IV lidocaine (𝑛 = 10)versus saline placebo (𝑛 = 10) pretreatment, in elective tumorpatients undergoing surgery, to determine the effect on ICPcontrol during laryngoscopy. The dose of lidocaine used wasa single 1.5mg/kg IV bolus. The second study [10] compared3 different IV lidocaine doses, in patients with hydrocephalusand elevated ICP, in order to determine the effect on ICPonce the patient was under a general anesthetic. The doses oflidocaine studied were 1mg/kg IV (𝑛 = 10), 1.5mg/kg IV (𝑛 =10), and 2mg/kg IV (𝑛 = 10). The third study [11] comparedIV lidocaine (𝑛 = 11) to LT lidocaine (𝑛 = 11), in electivetumor patients, in order to determine the effect on ICPduringlaryngoscopy. The doses of lidocaine used were 1.5mg/kgIV bolus and 4mL of 4% lidocaine instilled directly. Thefourth study [14] compared pretreatment with IV lidocaine(𝑛 = 10) versus IV esmolol (𝑛 = 10), in elective operativeneurosurgical patients, in order to determine the effect onICP (measured via lumbar drain) during laryngoscopy. Thedoses of the medication used were lidocaine 1.5mg/kg IVsingle dose and esmolol 1.5mg/kg IV single dose.
There were 2 prospective nonrandomized studies [6,12]. The first study [6] compared IV lidocaine (𝑛 = 10)versus thiopental (𝑛 = 10), in elective tumor operationswith sustained ICP elevations after induction, in order todetermine the impact on ICP control. The doses of medi-cation studied were lidocaine 1.5mg/kg IV single dose andthiopental 3mg/kg IV single dose. The second study [12]compared steroids/glycerin/IV lidocaine (𝑛 = 7) versussteroids/glycerin (𝑛 = 7) and steroids/glycerin/nitroglycerin(𝑛 = 7), in postoperative neurosurgical patients, inorder to determine the impact on ICP control. All patientsreceived dexamethasone 5–10mg three times daily andglycerin 200 gm/day. The doses of lidocaine and nitroglyc-erin were 1.5–3mg/kg/min IV continuous infusion and 3–7mcg/kg/min continuous infusion, respectively. The dura-tion of the continuous infusions was not specified.
Four prospective cohort studies [8, 13, 15, 16] evaluatedthe effects of IV lidocaine on ICP control. The first study [8]prospectively followed 10 severe TBI patients with refractoryICP issues.This study documented the effects of pretreatmentwith 1.5mg/kg single bolus IV lidocaine and saline boluses inevery patient, in order to determine the impact on ICP duringsuctioning. The second study [13] prospectively followed 20severe TBI patients with refractory ICP and compared theeffect of no lidocaine, IV lidocaine, and LT lidocaine beforetreatment on ICP during suctioning in all patients.The doses
of lidocaine used were 1.5mg/kg IV single dose and 2 mLof 5% lidocaine instilled directly via the endotracheal tube.The third study [15] prospectively followed 15 severe TBIpatients with refractory ICP and compared the effects ofa variety of pretreatments (saline, fentanyl, thiopental, IVlidocaine/succinylcholine, and LT lidocaine) on ICP controlduring suctioning. The dose of lidocaine used was 1.5mg/kgIV single bolus and LT 1.5mg/kg instilled directly. Thefinal study [16] prospectively followed 9 severe TBI patientsto determine the effects of pretreatment with IV and LTlidocaine impacted ICP control during suctioning. Both IVand LT were administered in all patients during separateperiods. The dose of lidocaine used was 1.5mg/kg IV singledose and 2 mL of 4% lidocaine single direct instillation.The lidocaine was administered at different intervals prior tosuctioning: 1, 3, 5, 10, and 15 minutes.
Seven studies evaluated IV lidocaine in a prophylacticmanner prior to stimulation [7, 8, 11, 13–16], in order todetermine the drugs ability to attenuate ICP elevations.Threestudies evaluated IV lidocaine in a therapeutic manner, inorder to determine the potential ICP reduction effects of thedrug [6, 10, 12].The lidocaine treatment characteristics can beseen in Table 2.
3.2. ICP Response
3.2.1. Pretreatment Regimens. Among the 4 RCT [7, 10, 11, 14]manuscripts identified, 3 studies focused on pretreatmentwith IV lidocaine prior to laryngoscopy or suctioning [7, 11,14]. The first study [7], comparing lidocaine to placebo, dis-played an attenuation of ICP elevation favoring IV lidocaine.The lidocaine group displayed a max mean ICP elevationof 6mmHg, versus 16mmHg in the placebo group. Thesecond study [11] comparing IV versus LT lidocaine displayeda significant reduction in baseline ICP in the IV group andattenuation of ICP elevation during laryngoscopy in the IVgroup.The LT lidocaine group displayed no effect on ICP.Thethird study [14] compared IV lidocaine versus esmolol andfailed to display a difference in either group on ICP control.Both lidocaine and esmolol pretreatment failed to attenuateICP elevations with intubation.
Within the 4 prospective cohort studies identified [8, 13,15, 16], all focused on pretreatment with IV lidocaine priorto endotracheal suctioning. Two displayed a suppression ofICP elevations with IV lidocaine [8, 16], while the other 2failed to demonstrate an attenuation of this response with IVlidocaine [13, 15]. However, one study which failed to displayan attenuation of ICP during suctioning, did show a baselinereduction in ICP by 4–6mmHg prior to stimulation [15].
3.2.2. Therapeutic Regimens. One RCT study was identifiedwhich studied the therapeutic effect of IV lidocaine on ICP[10]. This study compared different doses of lidocaine inhydrocephalus patients and displayed a significant reductionin ICP from baseline in all groups studied. The study alsodisplayed a dose-dependent ICP reduction effect with thelowest dose (1.0mg/kg) and the highest dose (2mg/kg)displaying a 17.5% and 37.5% reduction, respectively.

Critical Care Research and Practice 5
Table1:Stud
ycharacteris
ticsa
ndpatie
ntdemograph
ics.
Reference
Num
bero
fpatients
Stud
ytype
Article
locatio
nMeanage(years)
Patie
ntcharacteris
tics
Prim
aryandsecond
arygoalof
study
Bedford
etal.[6]
20Lidocaine(𝑛=10)
Thiopental(𝑛=10)
Prospective
nonrando
mized
ManuscriptLidocaine=
51.1±4.4
Thiopental=47.5±5.0
Braintumorsu
ndergoingele
ctiver
esectio
nhaving
susta
ined
ICPele
vatio
nsfor>
30sec
after
indu
ction
Anesthetic:
thiopental,n
itrou
soxide/O2,
andmorph
ine
Prim
ary:to
determ
inethe
effecto
fIV
lidocaine
versus
thiopentalon
ICP
controlfor
sustainedICPele
vatio
nsSecond
ary:no
nesta
ted
Bedford
etal.[7]
20Lidocaine(𝑛=10)
Placebo(𝑛=10)
Prospective
rand
omized
controltria
l
Meetin
gabstr
act
Lidocaine=
49±6
Placebo=55±6
Braintumorsu
ndergoingele
ctiver
esectio
nAn
esthetic:
thiopental,n
itrou
soxide/O2,
andmorph
ine
Prim
ary:to
determ
inethe
effecto
fIV
lidocaine
versus
salin
e(atindu
ction)
onICPdu
ringlaryngoscopy
Second
ary:no
nesta
ted
Don
egan
and
Bedford
[8]
10Prospective
coho
rtManuscript
Unk
nown
Severe
TBIw
ithICP>20
mmHgdu
ring
suctioning
Concurrent
ICPtherapy:hyperventilation
(pCO2goal30
mmHg),m
annitol,
dexamethasone,and
pentob
arbital(𝑛=5)
Prim
ary:to
determ
inethe
effecto
fIV
lidocaine
versus
salin
eonICPdu
ring
suctioning
Second
ary:no
tstated
∗Don
egan
etal.[9]
9Prospective
coho
rtMeetin
gabstr
act
Unk
nown
Severe
TBIw
ithICP>20
mmHgdu
ring
suctioning
Concurrent
ICPtherapy:hyperventilation
(pCO2goal30
mmHg),m
annitol,
dexamethasone,and
pentob
arbital(𝑛=5)
Prim
ary:to
determ
inethe
effecto
fIV
lidocaine
versus
salin
eonICPdu
ring
suctioning
Second
ary:no
tstated
Grover
etal.[10]
30Prospective
rand
omized
trial
Manuscript
Age>5years
Clinicallyraise
dICPandun
dergoing
VPS
surgery
Anesthetic:
thiopentalindu
ctionwith
suxametho
nium
NMBA
Maintenance
with
66%nitro
usoxide/oxygen
mix,pancuronium
,and
morph
ine
Prim
ary:to
determ
inethe
effecto
fdifferent
IVlid
ocaine
doseso
nICP
Second
ary:no
tstated
Ham
illetal.[11]
22LT
Lidocaine(𝑛=11)
IVLidocaine(𝑛=11)
Prospective
rand
omized
trial
Manuscript
Unk
nown
Braintumorsu
ndergoingele
ctiver
esectio
nAn
esthetic:
thiopental,succinylch
oline,and
50%nitro
usoxide/oxygen
mix
Prim
ary:to
determ
inee
ffectof
LTversus
IVlid
ocaine
onICPdu
ringlaryngoscopy
Second
ary:HRandMABP
Hira
yama
etal.[12]
21patie
nts
Steroid/gly
cerin
(𝑛=7)
Steroid/gly
cerin
/lidocaine(𝑛=7)
Steroid/gly
cerin
/nitroglyc
erin
(𝑛=7)
Prospective
nonrando
mized
Meetin
gabstr
act
Unk
nown
“Postoperativ
e”neurosurgery
patie
nts
Concurrent
ICPtherapy:dexamethasone
5–10mgTID,glycerin
200g
m/day
Prim
ary:to
determ
inethe
effectsof
IVlid
ocaine
versus
nitro
glycerin
onICP
Second
ary:no
tstated

6 Critical Care Research and Practice
Table1:Con
tinued.
Reference
Num
bero
fpatients
Stud
ytype
Article
locatio
nMeanage(years)
Patie
ntcharacteris
tics
Prim
aryandsecond
arygoalof
study
Mon
tarry
etal.[13]
20Prospective
coho
rtManuscript
32
Severe
TBI
Concurrent
ICPtherapy:
thiopental,m
aintainednegativ
efluid
balance,pC
O2goal28
mmHg
Prim
ary:to
determ
inethe
effectsof
IVversus
LTlid
ocaine
onICPcontrol
durin
gendo
trachealsuctioning
Second
ary:cerebralperfusionpressure
Samaha
etal.[14]
22Esmolol(𝑛=11)
Lidocaine(𝑛=11)
Prospective
rand
omized
trial
Manuscript
Esmolol:50±13
Lidocaine:47±16
Electiv
eneurosurgicalpatie
nts(tumors
andaneurysm
clipp
ings)
∗ICPmeasuredviaLD
Anesthetic:
thiopentalindu
ction,
sevoflu
rane,
maintenance,pCO2goal33–35m
mHg
Prim
ary:to
determ
inethe
effecto
fesmololversus
lidocaine
IVbo
lus(130s
ecbefore
intubatio
n)on
lumbarc
istern
pressuresd
uringlaryngoscopy
(ICP
measuredbefore,during,and2and5m
inaft
erintubatio
n)Second
ary:MABP
,CPP
White
etal.[15]
15Prospective
coho
rtManuscript
Unk
nown
Severe
TBIw
ithele
vatio
nsof
ICP>
20mmHgdu
ringor
immediatelyaft
ersuctioning
Concurrent
ICPtherapy:sedatio
nwith
diazepam
andmorph
ine,hyperventilation
(pCO225–30m
mHg)
Prim
ary:to
determ
inethe
effectsof
different
pretreatment(salin
e,fentanyl,
thiopental,lidocaine,and
succinylcholine)on
ICPdu
ring
suctioning
Second
ary:MABP
Yano
etal.
[16]
9Prospective
coho
rtManuscript
34.6(range:16to
71)
Severe
TBI
Concurrent
ICPtherapy:no
tspecific,
hyperventilated
topC
O2goalof
25to
30mmHg
Prim
ary:to
determ
inethe
effecto
fIVand
LTlid
ocaine
onICPdu
ringsuctioning
Second
ary:no
tstated
𝑛=nu
mbero
fpatients,HR=heartrate,MABP
=meanarteria
lblood
pressure,ICP
=intracranialpressure,C
PP=cerebralperfusionpressure,C
SF=cerebrospinalfl
uid,
mmHg=millim
eterso
fmercury,IV=
intra
veno
us,LT=laryngotracheal,TB
I=traumaticbraininjury,L
D=lumbard
rain,and
sec=second
.∗Don
egan
andBe
dford[8]a
ndDon
egan
etal.[9]
arecompanion
publications,w
ithDon
egan
etal.[9]
representin
gthem
eetin
gabstr
actp
ublishedpriortothefullm
anuscript[8].Th
edatafrom
Don
egan
etal.[9]
isno
tincludedin
thes
ynthesisof
dataandison
lyinclu
dedin
thetablesfor
completeness.

Critical Care Research and Practice 7
Table2:Lido
cainetreatmentcharacteristicsa
ndICPrespon
se.
Reference
Lido
cained
ose
Meandu
ratio
nof
lidocaine
administratio
n(days)
ICPrespon
seOther
prim
ary/second
ary
outcom
es
Adverse
effectsto
lidocaine
Con
clusio
ns
Bedford
etal.[6]
1.5mg/kg
IVbo
lusx
1(𝑛=10)
Thiopentaldose(𝑛=10)=
3mg/kg
IVx1
Sing
lebo
lus
dose
Lidocaine:decrease
inmeanICP
from
28mmHgto
13mmHg,with
nadirreached
atam
ean66±10sec
Thiopental:decreaseinmeanICP
from
33mmHgto
14mmHg,with
anadirreached
atam
ean48±9s
ec
MeanMABP
decrease
of26
mm
Hgwith
thiopental
NoMABP
changesw
ithlid
ocaine
Non
edescrib
ed
Lido
cainea
ndthiopental
aree
quallyan
effectin
redu
ctionof
ICPviaI
Vbo
lus,with
lidocaine
preserving
syste
mic
hemod
ynam
ics
Bedford
etal.[7]
1.5mg/kg
IVbo
lusx
1(𝑛=10)
Salin
e(𝑛=10)=
samev
olum
eSing
lebo
lus
dose
Pretreatmentw
ithIV
lidocaine
ledto
amaxim
ummeanICPincrease
of6m
mHgand4m
mHgat30
and
60sec
Salin
eplacebo
meanincrease
inICP
of16mmHgand13mmHgat30
and
60sec
MABP
increase
was
less
with
lidocaine
compared
toplacebo
Non
edescrib
ed
IVlid
ocaine
durin
glaryngoscopy
leadstoan
attenu
ationofICPele
vatio
ncomparedto
salin
e.
Don
egan
and
Bedford
[8]
1.5mg/kg
IVbo
lusx
1Salin
ewas
givenin
thesam
evolum
eas
lidocaine
Patientsreceiv
edboth
therapies
Sing
lebo
lus
dose
Lido
cainep
resuctionledto
amean
increase
inICPof
3.4±6.2m
mHg
and1.8±2.6m
mHgin
thoseo
nand
offbarbitu
ratesd
uringsuctioning
Salin
eplacebo
presuctio
nledto
ameanincrease
inICP19±4.7m
mHg
and5.7±3.2m
mHgin
thoseo
nand
offbarbitu
ratesd
uringsuctioning
Nosig
nificantd
ifference
inMABP
changes
durin
gsuctioning
Non
edescrib
ed
Lido
cainep
resuctioning
leadstoan
attenu
ationof
ICPele
vatio
nscomparedto
salin
e
∗Don
egan
etal.[9]
1.5mg/kg
IVbo
lusx
1Salin
ewas
givenin
thesam
evolum
eas
lidocaine
Patientsreceiv
edboth
therapies
Sing
lebo
lus
dose
Lido
cainep
retre
atmentled
toa
significantatte
nuationin
ICP
elevationwith
suctioning
Not
stated
Non
edescrib
ed
Lido
cainep
resuctioning
leadstoan
attenu
ationof
ICPele
vatio
nscomparedto
salin
e
Grover
etal.[10]
Threeg
roup
s:Group
1(𝑛=10):1m
g/kg
IVbo
lusx
1Group
2(𝑛=10):1.5
mg/kg
bolusx
1Group
3(𝑛=10):2m
g/kg
bolusx
1
Sing
lebo
lus
dose
Allgrou
psdisplayedas
ignificant
decrease
inICPwith
in2m
inof
lidocaine
administratio
nGroup
3display
eda3
7.5%redu
ction
inmeanICP,andGroup
1disp
layeda
17.5%
meanredu
ction
Group
3was
theo
nly
grou
pto
display
significantd
ropin
SBP
SBP
decreased
with
2mg/kg
IVbo
lus
dose
IVlid
ocaine
bolusleads
tosig
nificantreductio
nsin
ICPHighlid
ocaine
dosin
gmay
lead
todrop
sinSB
P
Ham
illetal.[11]
LT(𝑛=11):4m
L4%
lidocaine
endo
tracheal
IV(𝑛=11):1.5
mg/kg
IVbo
lusx
1Sing
ledo
se
IVlid
ocaine
ledto
asignificant
decrease
inbaselin
eICP
with
noele
vatio
nsdu
ringlaryngoscopy
LTlid
ocaine
failedto
decrease
ICP
andallp
atientsh
adas
ignificant
elevationin
ICPdu
ringintubatio
n
Sign
ificant
HRand
MABP
increase
inLT
grou
p
Non
edescrib
ed
IVlid
ocaine
ledto
decrease
inbaselin
eICP
and
attenu
ated
ICPele
vatio
nsdu
ringlaryngoscopy

8 Critical Care Research and Practice
Table2:Con
tinued.
Reference
Lido
cained
ose
Meandu
ratio
nof
lidocaine
administratio
n(days)
ICPrespon
seOther
prim
ary/second
ary
outcom
es
Adverse
effectsto
lidocaine
Con
clusio
ns
Hira
yama
etal.[12]
Allhaddexamethasone
andglycerin,
with𝑛=7thistherapyin
isolatio
n.Lido
caine(𝑛=7):10%lid
ocaine
continuo
usinfusio
nat1.5
–3mg/min
Nitroglycerin
e(𝑛=7):
3–7m
cg/kg/min
Con
tinuo
usinfusio
n
Thea
ddition
oflid
ocaine
toglycerin
therapyledto
areductio
nin
ICP
spikes,w
itham
eanredu
ctionin
ICP
of8.9m
mHgover
24ho
urs
Thea
ddition
ofnitro
glycerin
toglycerin
ledto
ameanredu
ctionof
ICPof
7.4mmHgover
24ho
urs
Not
stated
Non
edescrib
ed
Both
IVlid
ocaine
and
nitro
glycerin
inthe
presence
ofglycerin
therapylead
toICP
redu
ctions
at24
hours
Mon
tarry
etal.[13]
Allpatie
ntsu
nderwentsuctio
ning
with
outlidocaine,thenwith
IV,and
finallywith
LTLidocaineIV:
1.5mg/kg
of2%
lidocaine
bolusx
1Lidocaine
LT:5%
lidocaine
Sing
ledo
se
NodifferenceintheICP
over
6min
forn
olid
ocaine,ore
ither
ofthe
lidocaine
routes,duringsuctioning
.10
patie
ntsh
addo
cumentedICP>
20mmHgandhadthes
ame
lidocaine
treatment
LidocaineIVled
toamild
redu
ction
inICPover6m
inby
approx.2
mmHg
LTlid
ocaine
didnoth
avea
nysig
nificanteffectcomparedtobaselin
e
NodifferenceinCP
PNot
describ
ed
Lido
caineIVor
LTdidno
tlead
toas
uppressio
nof
ICP
durin
gsuctioning
Lido
caineIVbo
lusd
uring
acuteICP
elevations
may
lead
tomild
redu
ctionin
ICP.
Samaha
etal.[14]
Lidocaine:1.5
mg/kg
IVx1
Esmolol:1.5mg/kg
IVx1
Sing
ledo
se
Postintubatio
nICProse
significantly
inbo
thgrou
psEsmolol:increased
from
11±
6mmHgto
17±10mmHg
Lidocaine:increasedfro
m10±
6mmHgto
16±9m
mHg
Sign
ificant
decrease
inCP
Pin
both
grou
psdu
ringintubatio
nEsmololdecreasedfro
ma
meanof92
to62
mmHg
Lidocained
ecreased
from
ameanof96
to68
mmHg
Afterintubatio
nCP
Pincreasedto99±
23mmHga
nd99±
17mmHginthee
smolol
andlid
ocaine
groups
Not
describ
ed
Both
lidocaine
andesmolol
failedto
attenu
atethe
elevatio
nin
CPPandICP
after
intubatio
n
White
etal.[15]
Everypatie
ntreceived
alltreatments
durin
gindividu
alsuctioning
episo
des
Salin
e=2m
LFentanyl=1m
cg/kg
Thiopental=3m
g/kg
Lido
caine=
1.5mg/kg
+succinylcholine=
1.5mg/kg
Lido
caineL
Talon
e=1.5
mg/kg
Sing
lebo
lus
dose
Lido
caine/succinylcholineIVand
thiopentallead
toam
eandecrease
inICPby
4–6m
mHgbu
thad
noeffect
ontheICP
durin
gsuctioning
LTlid
ocaine
hadmoree
ffectat
attenu
atingcoug
handICPele
vatio
nsdu
ringsuctioning
.How
ever,during
instillationitinitiated
coug
hing
and
ledto
ICPspikes
Fentanylhadno
effecto
nICP
MABP
notaffected
byanyregimen
Non
edescrib
ed
Lido
caineIVleadstoICP
redu
ctionbu
tnot
attenu
ationof
coug
hmediatedICPspikes
LTlid
ocaine
may
besuperio
rinpreventin
gcoug
hing
related
ICPspikes

Critical Care Research and Practice 9
Table2:Con
tinued.
Reference
Lido
cained
ose
Meandu
ratio
nof
lidocaine
administratio
n(days)
ICPrespon
seOther
prim
ary/second
ary
outcom
es
Adverse
effectsto
lidocaine
Con
clusio
ns
Yano
etal.
[16]
1.5mg/kg
IVbo
lusd
osea
tthe
follo
wingintervalsp
riorto
suctioning
:1,3,5,10,and15min
LTlid
ocaine
=2m
Lof
4%lid
ocaine
acrossthes
ameintervals
Sing
lebo
lus
doses
Neither
IVof
LTlid
ocaine
lowered
baselin
eICP
,but
both
supp
ressed
ICPele
vatio
nswith
suctioning
LTlid
ocaine
ledto
alow
erpeak
ICP
comparedto
IV
Not
stated
Non
edescrib
ed
Both
IVandLT
lidocaine
supp
ressICPele
vatio
nsdu
ringsuctioning
𝑁=nu
mbero
fpatients,mg=milligram,m
cg=microgram
,mL=milliliters,w
t=weight,kg
=kilogram
,hr=
hour,m
in=minute,HR=heartrate,MABP
=meanarteria
lblood
pressure,ICP
=intracranial
pressure,C
PP=cerebralperfusionpressure,C
SF=cerebrospinalfluid,mmHg=
millim
eterso
fmercury,IV=intravenou
s,LT
=laryngotracheal,T
BI=traumaticbraininjury,LD=lumbard
rain,and
sec=
second
.∗Don
egan
andBe
dford[8]and
Don
egan
etal.[9]
arec
ompanion
publications,w
ithDon
egan
etal.[9]
representin
gthem
eetin
gabstr
actp
ublishedpriortothefullm
anuscript[8].Th
edatafrom
Don
egan
etal.[9]
isno
tincludedin
thes
ynthesisof
dataandison
lyinclu
dedin
thetables
forc
ompleteness.

10 Critical Care Research and Practice
Table 3: Oxford and GRADE level of evidence.
Reference Study type Oxford level of evidence GRADE level of evidenceBedford et al. [6] Prospective nonrandomized 2b BBedford et al. [7] Prospective randomized trial 2b BDonegan and Bedford [8] Prospective cohort 2b C∗Donegan et al. [9] Prospective cohort 2b CGrover et al. [10] Prospective randomized trial 2b BHamill et al. [11] Prospective randomized trial 2b BHirayama et al. [12] Prospective nonrandomized 2b CMontarry et al. [13] Prospective cohort 2b CSamaha et al. [14] Prospective randomized trial 2b BWhite et al. [15] Prospective cohort 2b CYano et al. [16] Prospective cohort 2b C∗Donegan and Bedford [8] and Donegan et al. [9] are companion publications, with Donegan et al. [9] representing the meeting abstract published prior tothe full manuscript [8]. The data from Donegan et al. [9] is not included in the synthesis of data and is only included in the tables for completeness.
Two nonrandomized trials studied the therapeutic effectof ICP lidocaine on ICP [6, 12]. The first displayed a meandecrease in ICP of 15mmHg, with a mean time to nadir of66 ± 10 seconds [6]. This was equivalent to the thiopentalcomparison group. The second trial studied IV lidocaine(with steroids and glycerine) versus steroids/glycerine andsteroids/glycerin/nitroglycerin [12]. The lidocaine group dis-played a mean ICP reduction of 8.9mmHg over 24 hoursof continuous infusion. The nitroglycerine group displayedsimilar results.
3.3. Adverse Effects of Lidocaine Therapy. Two studiesrecorded adverse events related to IV lidocaine therapy [10,14]. The first displayed a dose related decrease in systolicblood pressure, with this effect documented at a dose of2mg/kg [10].The second study displayed a trend to significantreductions in cerebral perfusion pressure during lidocaineadministration [14].
The remaining studies included in the review [6–8, 11–13, 15, 16] failed to document any events or clearly state that“there were no adverse events.”
3.4. FunctionalOutcome. Patient functional outcomewas notreported in any study, as the focus of the manuscripts was todetermine the ICP effects of lidocaine.
3.5. Level of Evidence. Based on two independent reviewers(F. A. Zeiler and C. J. Kazina), there were a total of 10studies reviewed. The question “What is the effect of IVlidocaine on ICP in patients with neurological illness?” wasevaluated based on the Oxford and GRADE criteria for levelof evidence.
3.5.1. Oxford Level of Evidence: Pretreatment Regimens. Fourstudies were Oxford level 2b [7, 8, 11, 16] evidence supportingan attenuation of ICP elevation with IV lidocaine pretreat-ment prior to stimulation.Three studies were Oxford level 2b[13–15] evidence against the attenuation of ICP elevation withIV lidocaine pretreatment.
3.5.2. Oxford Level of Evidence: Therapeutic Regimens. Threestudies were Oxford level 2b [6, 10, 12] evidence supporting adecrease in ICP when IV lidocaine is utilized in a therapeuticmanner.
3.5.3. GRADE Level of Evidence: Pretreatment Regimens. Twostudies were GRADE B [7, 11] and 2 were GRADE C [8, 16]evidence supporting an attenuation of ICP elevation with IVlidocaine pretreatment prior to stimulation. One study wasGRADEB [14] and twowereGRADEC [13, 15] evidence. Onestudy was GRADE level B [10] and 2 were GRADE level C[5, 7] evidence against the attenuation of ICP elevation withIV lidocaine pretreatment.
3.5.4. GRADE Level of Evidence: Therapeutic Regimens. Twostudies were GRADE B [6, 10] and 1 was GRADE C [12]evidence supporting a decrease in ICP when IV lidocaine isutilized in a therapeutic manner.
A summary of all levels of evidence for individual articlescan be seen in Table 3.
4. Discussion
Some important aspects of IV lidocaine therapy in theneurological population have been emphasized during thisreview. First, there lacks convincing evidence to suggest thatIV lidocaine, when utilized as a pretreatment for stimulation(laryngoscopy/suctioning), has any impact on the attenuationof ICP spikes. There exists evidence to both support andrefute this. Second, there exists evidence, though limited,to suggest an ICP reduction effect of IV lidocaine whenused as a therapeutic measure. This ICP reduction effect wasdisplayed in both patients with and without elevated ICP.However, there lacks objective evidence to suggest that eithera reduction in cerebral metabolism, or cerebral vasoconstric-tion, are mechanisms leading to this ICP reduction. Third,comments on the ICP reduction effect of IV lidocaine whenutilized therapeutically can only be made for bolus dosingalone. Only 1 study was identified using continuous infusions

Critical Care Research and Practice 11
of lidocaine. Fourth, hypotension seems common with IVlidocaine therapy when utilized in both a pretreatmentand therapeutic fashion. This hypotensive effect seems dosedependent [10]. Finally, patient outcome secondary to IVlidocaine therapy cannot be made at this time.
Several important limitations exist to this study. First,there were a small number of studies, making the con-clusions of this review difficult to generalize to all neuro-logical patients. Furthermore, the 43 patients had unclearneuropathology identified within the studies thus making ithard to determine if there was a pathology specific benefitto lidocaine therapy. Third, the use of other ICP directedmedical therapies during lidocaine administration makesinterpreting the data on ICP response difficult. The majorityof the studies did not detail the other therapies that werebeing administered. Fourth, given the absence of outcomedata reported, we cannot make any comments on the impactof IV lidocaine on functional outcome. Fifth, the degree oftherapies applied to the TBI, hydrocephalus, and brain tumorpatient populations were likely dramatically different. A fulloutline of ICP therapies was not present in the majorityof studies, and this suspected variation between separatepathologies limits our ability to generalize the results forall patients with neurological illness. Finally, there is likelya significant publication bias with only those studies withpositive results making it to publication within the literature.
Through this review, the ICP response to IV lidocainehas been thoroughly outlined. The current literature doesnot strongly support a “protective effect” of IV lidocaineduring laryngoscopy/suctioning.Thepotential ICP reductioneffect of IV lidocaine when used as a therapeutic measureseems to exist, though the exact mechanism is unclear.Further prospective trials need to be conducted to confirmthe efficacy of IV lidocaine in both the pretreatment andtherapeutic settings.
Future study should focus on the severe TBI popula-tion with lidocaine use both as a bolus dose based ICPreduction agent and in the context of a continuous infusion.The potential benefit of bolus based regimens could beassessed via comparing IV lidocaine bolus to either sedationbolus or hypertonic/hyperosmotic solutions bolus. Similarly,the continuous infusion dosing regimen for ICP reductioncould be assessed in a prospective randomized fashion withimplementation during crisis. One could also foresee thepotential for early implementation of continuous IV lidocaineas a prophylactic measure for ICP reduction, in an attemptto reduce the sedation and hypertonic/hyperosmotic agentrequirements.
Final Recommendations. Overall, we cannot make a strongdefinitive recommendation on the effectiveness of pretreat-ment IV lidocaine for the attenuation of ICP elevationsduring stimulation.There isOxford 2b,GRADEB level of evi-dence supporting both the attenuation of ICP increases, andno impact on ICP control, with pretreatment IV lidocaine.
Therapeutic use of IV lidocaine for ICP reduction cur-rently displays Oxford 2b, GRADE B evidence supportingICP reduction with lidocaine administration.
5. Conclusions
There lacks strong literature to support the effectivenessof pretreatment IV lidocaine for the attenuation of ICPelevations during stimulation. There is Oxford 2b, GRADEB level of evidence supporting both the attenuation of ICPincreases, and no impact on ICP control, with pretreat-ment IV lidocaine. Therapeutic use of IV lidocaine for ICPreduction currently displays Oxford 2b, GRADE B evidencesupporting ICP reduction with lidocaine administration.
Conflict of Interests
The authors have no conflict of interests.
Authors’ Contribution
F. A. Zeiler contributed in the study design, data acquisition,data analysis, and paper composition. N. Sader contributedin data acquisition and data analysis. C. J. Kazina contributedin data analysis and paper composition.
References
[1] N. Stocchetti and A. I. R. Maas, “Traumatic intracranial hyper-tension,”The New England Journal of Medicine, vol. 370, no. 22,pp. 2121–2130, 2014.
[2] J. J. Brucia, D. C. Owen, and E. B. Rudy, “The effects of lidocaineon intracranial hypertension,” The Journal of NeuroscienceNursing, vol. 24, no. 4, pp. 205–214, 1992.
[3] P. Scheinberg, H. W. Jayne, L. I. Blackburn, and M. Rich,“Studies of cerebral circulatory functions following intravenousadministration of procaine hydrochloride,” Archives of Neurol-ogy and Psychiatry, vol. 68, no. 6, pp. 815–818, 1952.
[4] T. Sakabe, T. Maekawa, T. Ishikawa, and H. Takeshita, “Theeffects of lidocaine on canine cerebral metabolism and circu-lation related to the electroencephalogram,”Anesthesiology, vol.40, no. 5, pp. 433–441, 1974.
[5] T.-Y. Lin, C.-Y. Chung, C.-W. Lu, S.-K. Huang, J.-S. Shieh, andS.-J. Wang, “Local anesthetics inhibit glutamate release from ratcerebral cortex synaptosomes,” Synapse, vol. 67, no. 9, pp. 568–579, 2013.
[6] R. F. Bedford, J. A. Persing, L. Pobereskin, and A. Butler,“Lidocaine or thiopental for rapid control of intracranial hyper-tension?” Anesthesia and Analgesia, vol. 59, no. 6, pp. 435–437,1980.
[7] R. F. Bedford, H. R. Winn, G. Tyson, T. S. Park, and J. A. Jane,“Lidocaine prevents increased ICP after endotracheal intuba-tion,” in Intracranial Pressure IV, K. Shulman, A. Marmarou, J.D. Miller, D. P. Becker, G. M. Hochwald, and M. Brock, Eds., p.595, Springer, Berlin, Germany, 1980.
[8] M. F. Donegan and R. F. Bedford, “Intravenously administeredlidocaine prevents intracranial hypertension during endotra-cheal suctioning,” Anesthesiology, vol. 52, no. 6, pp. 516–518,1980.
[9] M. Donegan, R. F. Bedford, and R. Dacey, “IV lidocaine forprevention of intracranial hypertension,”Anesthesiology, vol. 51,no. 3, article S201, 1979.
[10] V. K. Grover, G. M. S. R. Reddy, V. K. Kak, and S. Singh,“Intracranial pressure changeswith different doses of lignocaine

12 Critical Care Research and Practice
under general anaesthesia,” Neurology India, vol. 47, no. 2, pp.118–121, 1999.
[11] J. F. Hamill, R. F. Bedford, D. C. Weaver, and A. R. Colo-han, “Lidocaine before endotracheal intubation: intravenous orlaryngotracheal?” Anesthesiology, vol. 55, no. 5, pp. 578–581,1981.
[12] A. Hirayama, S. Yamasaki, and K. Miyata, “A pilot study onpostoperative ICP control by glycerin combined with lidocaineor nitroglycerin,” in Intracranial Pressure VIII, C. J. J. Avezaat, J.H. M. van Eijndhoven, A. I. R. Maas, and J. T. J. Tans, Eds., pp.609–611, Springer, Berlin, Germany, 1993.
[13] M. Montarry, J. F. Poussel, F. Artru, and R. Chacornac, “Lido-caine protection of the pressure of cerebral perfusion in trachealstimulation,” Minerva Anestesiologica, vol. 51, no. 7-8, pp. 405–410, 1985.
[14] T. Samaha, P. Ravussin, C. Claquin, and C. Ecoffey, “Preventionde l’augmentation de la pression arterielle et de la pres-sion intracranienne lors de l’intubation endotracheale enneurochirurgie: esmolol versus lidocaıne,” Annales Francaisesd’Anesthesie et de Reanimation, vol. 15, no. 1, pp. 36–40, 1996.
[15] P. F. White, R. M. Schlobohm, L. H. Pitts, and J. M. Lindauer, “Arandomized study of drugs for preventing increases in intracra-nial pressure during endotracheal suctioning,” Anesthesiology,vol. 57, no. 3, pp. 242–244, 1982.
[16] M. Yano, H. Nishiyama, H. Yokota, K. Kato, Y. Yamamoto, andT. Otsuka, “Effect of lidocaine on ICP response to endotrachealsuctioning,” Anesthesiology, vol. 64, no. 5, pp. 651–653, 1986.
[17] J. P. T. Higgins and S. Green, Eds., Cochrane Handbookfor Systematic Reviews of Interventions Version 5.1.0, 2013,http://handbook.cochrane.org.
[18] D. Moher, A. Liberati, J. Tetzlaff, and D. G. Altman, “Preferredreporting items for systematic reviews and meta-analysis: thePRISMA statement,” Annals of Internal Medicine, vol. 151, no. 4,pp. 264–269, 2009.
[19] B. Phillips, C. Ball, D. Sackett, S. Straus, B. Haynes, and M.Dawes, “Oxford Centre for Evidence-Based Medicine Levels ofEvidence,” 2009, http://www.cebm.net/?o=1025.
[20] G. H. Guyatt, A. D. Oxman, G. E. Vist et al., “GRADE: anemerging consensus on rating quality of evidence and strengthof recommendations,” British Medical Journal, vol. 336, no.7650, pp. 924–926, 2008.
[21] G. H. Guyatt, A. D. Oxman, R. Kunz, G. E. Vist, Y. Falck-Ytter,andH. J. Schunemann, “Rating quality of evidence and strengthof recommendations: what is ‘quality of evidence’ and why is itimportant to clinicians?” British Medical Journal, vol. 336, no.7651, pp. 995–998, 2008.
[22] H. J. Schunemann, A. D. Oxman, J. Brozek et al., “GRADE:Grading quality of evidence and strength of recommendationsfor diagnostic tests and strategies,” British Medical Journal, vol.336, no. 7653, pp. 1106–1110, 2008.
[23] G. H. Guyatt, A. D. Oxman, R. Kunz et al., “Rating quality ofevidence and strength of recommendations: incorporating con-siderations of resources use into grading recommendations,”The British Medical Journal, vol. 336, no. 7654, pp. 1170–1173,2008.
[24] G. H. Guyatt, A. D. Oxman, R. Kunz et al., “Rating qualityof evidence and strength of recommendations: going fromevidence to recommendations,”TheBritishMedical Journal, vol.336, no. 7652, pp. 1049–1051, 2008.
[25] R. Jaeschke, G. H. Guyatt, P. Dellinger et al., “Use of GRADEgrid to reach decisions on clinical practice guidelines whenconsensus is elusive,” BMJ, vol. 337, article a744, 2008.

Submit your manuscripts athttp://www.hindawi.com
Stem CellsInternational
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Disease Markers
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation http://www.hindawi.com Volume 2014
Immunology ResearchHindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Parkinson’s Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttp://www.hindawi.com