Review Article Paclitaxel and Its Evolving Role in the...
22
Review Article Paclitaxel and Its Evolving Role in the Management of Ovarian Cancer Nirmala Chandralega Kampan, 1,2 Mutsa Tatenda Madondo, 1 Orla M. McNally, 2,3 Michael Quinn, 2,3 and Magdalena Plebanski 1 1 Department of Immunology, Monash University, Level 6, e Alfred, Commercial Road, Melbourne, VIC 3181, Australia 2 Gynaeoncology Unit, Royal Women’s Hospital, 20 Flemington Road, Parkville, Melbourne, VIC 3052, Australia 3 Department of Obstetrics and Gynaecology, University of Melbourne, Melbourne, VIC 3052, Australia Correspondence should be addressed to Nirmala Chandralega Kampan; nirmala [email protected] and Magdalena Plebanski; [email protected] Received 20 February 2015; Accepted 7 April 2015 Academic Editor: Rohit S. Mulik Copyright © 2015 Nirmala Chandralega Kampan et al. is is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. Paclitaxel, a class of taxane with microtubule stabilising ability, has remained with platinum based therapy, the standard care for primary ovarian cancer management. A deeper understanding of the immunological basis and other potential mechanisms of action together with new dosing schedules and/or routes of administration may potentiate its clinical benefit. Newer forms of taxanes, with better safety profiles and higher intratumoural cytotoxicity, have yet to demonstrate clinical superiority over the parent compound. 1. Introduction Epithelial ovarian cancer is one of the leading causes of cancer death. One woman in 70 will develop ovarian cancer in her lifetime and the majority of these women will die from the disease. Although the prognosis for women with ovarian cancer is relatively poor due to its late presentation and the lack of scientifically validated screening tools, the 5- year survival rate increased significantly from 33% in 1982– 1987 to 40% in 2000–2006 [1]. e standard of care in advanced epithelial ovarian cancer encompasses surgical staging and resection followed by administration of paclitaxel-platinum based chemother- apy. Maximal effort cytoreductive surgery, either initial or interval, with the aim of debulking to the point of no visible residual disease is associated with improved patient out- comes, with every 10% increase in the optimal cytoreduction rate leading to a 5.5% increase in median survival [2, 3]. Based on level-1 evidence, paclitaxel (175 mg/m 2 ) in com- bination with carboplatin (AUC 5–7.5) every 3 weeks for 6 cycles, administered intravenously was accepted as the standard of care for first line chemotherapy by the GCIG Consensus Meeting in 2005 [4–8]. Approximately two- thirds of patients will respond to this combined surgery- chemotherapy approach, but tumour recurrence occurs in almost all these patients at a median of 15 months from initial diagnosis [9] and subsequent chemotherapy treatments are increasingly linked to chemoresistance. Response rates in this setting are proportional to the treatment-free interval. For instance, there is a 75% response when the treatment-free interval is at least two years but with a treatment-free interval of only six to nine months, the second line response is only 35% [10]. Other than its contribution as one of the first line agent in a combined therapy, paclitaxel has been promising, as early as 1990, as a second line agent in relapsed platinum- refractory epithelial ovarian cancer. e clinical therapeutic effect of paclitaxel is promising with modulation of dose and route of administration for use in advanced ovarian cancer, either in primary or recurrent setting. ere is thus still a strong need for novel, highly effective therapies for the treatment of advanced epithelial ovarian cancer. However, maximising the potential of paclitaxel is also a reasonable approach. is review will focus on how such new therapeutic strategies such as dose-dense paclitaxel Hindawi Publishing Corporation BioMed Research International Volume 2015, Article ID 413076, 21 pages http://dx.doi.org/10.1155/2015/413076
Transcript of Review Article Paclitaxel and Its Evolving Role in the...

Review ArticlePaclitaxel and Its Evolving Role in the Management ofOvarian Cancer
Nirmala Chandralega Kampan12 Mutsa Tatenda Madondo1 Orla M McNally23
Michael Quinn23 and Magdalena Plebanski1
1Department of Immunology Monash University Level 6 The Alfred Commercial Road Melbourne VIC 3181 Australia2Gynaeoncology Unit Royal Womenrsquos Hospital 20 Flemington Road Parkville Melbourne VIC 3052 Australia3Department of Obstetrics and Gynaecology University of Melbourne Melbourne VIC 3052 Australia
Correspondence should be addressed to Nirmala Chandralega Kampan nirmala khotmailcomand Magdalena Plebanski magdalenaplebanskimonashedu
Received 20 February 2015 Accepted 7 April 2015
Academic Editor Rohit S Mulik
Copyright copy 2015 Nirmala Chandralega Kampan et al This is an open access article distributed under the Creative CommonsAttribution License which permits unrestricted use distribution and reproduction in any medium provided the original work isproperly cited
Paclitaxel a class of taxane with microtubule stabilising ability has remained with platinum based therapy the standard care forprimary ovarian cancermanagement Adeeper understanding of the immunological basis and other potentialmechanisms of actiontogether with new dosing schedules andor routes of administrationmay potentiate its clinical benefit Newer forms of taxanes withbetter safety profiles and higher intratumoural cytotoxicity have yet to demonstrate clinical superiority over the parent compound
1 Introduction
Epithelial ovarian cancer is one of the leading causes ofcancer death One woman in 70 will develop ovarian cancerin her lifetime and the majority of these women will diefrom the disease Although the prognosis for women withovarian cancer is relatively poor due to its late presentationand the lack of scientifically validated screening tools the 5-year survival rate increased significantly from 33 in 1982ndash1987 to 40 in 2000ndash2006 [1]
The standard of care in advanced epithelial ovariancancer encompasses surgical staging and resection followedby administration of paclitaxel-platinum based chemother-apy Maximal effort cytoreductive surgery either initial orinterval with the aim of debulking to the point of no visibleresidual disease is associated with improved patient out-comes with every 10 increase in the optimal cytoreductionrate leading to a 55 increase in median survival [2 3]
Based on level-1 evidence paclitaxel (175mgm2) in com-bination with carboplatin (AUC 5ndash75) every 3 weeks for6 cycles administered intravenously was accepted as thestandard of care for first line chemotherapy by the GCIG
Consensus Meeting in 2005 [4ndash8] Approximately two-thirds of patients will respond to this combined surgery-chemotherapy approach but tumour recurrence occurs inalmost all these patients at a median of 15 months from initialdiagnosis [9] and subsequent chemotherapy treatments areincreasingly linked to chemoresistance Response rates in thissetting are proportional to the treatment-free interval Forinstance there is a 75 response when the treatment-freeinterval is at least two years but with a treatment-free intervalof only six to nine months the second line response is only35 [10] Other than its contribution as one of the first lineagent in a combined therapy paclitaxel has been promisingas early as 1990 as a second line agent in relapsed platinum-refractory epithelial ovarian cancer The clinical therapeuticeffect of paclitaxel is promising with modulation of dose androute of administration for use in advanced ovarian cancereither in primary or recurrent setting
There is thus still a strong need for novel highly effectivetherapies for the treatment of advanced epithelial ovariancancer However maximising the potential of paclitaxel isalso a reasonable approach This review will focus on howsuch new therapeutic strategies such as dose-dense paclitaxel
Hindawi Publishing CorporationBioMed Research InternationalVolume 2015 Article ID 413076 21 pageshttpdxdoiorg1011552015413076
2 BioMed Research International
National cancer institute (NCI) and US department of agriculture (USDA) colloborated on plant screening programme forfinding new and effective anticancer agents 15000 plants were collected and 115000 extracts were tested
Crude extracts of the yewrsquosbark were repetitively fractionated by Monroe Wall and MansukhWanifrom natural products laboratory and identified the active ingredient that was responsible for cytotoxicity activity and named it Taxol
Samples of the Pacific yewrsquos bark Taxus brevifolia were collected by a team of botanists headed by Arthur Barclay in Gifford Pinchot National Forest Washington
Taxol was found to have excellent spectrum of activity in vitro and in vivo butlack of supply and poor aqueous solubility deterred further preclinical development
Dr Susan Horwitz received a grant from NCI to study Taxolrsquos mechanism of action and found that Taxol was unique as it wasable to bind to microtubule inhibit depolymerization ofmicrotubule leading to cell arrest at mitosis and subsequent apoptosis
Paclitaxel was able to regress mammary tumours in a
model
Semisynthetic Taxol discovered
Solubility problem resolved with Cremophor EL
Taxol entered phase I clinical trials and found to have partial or complete response in 30 patients with advanced ovarian cancer
FDA approved Taxol for treatment against ovarian cancer and two years later for treatment of advanced breast cancer
xenograft
1960 1962 1965 1977 1978 1979 1984 1992ndash1994
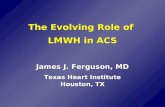
Figure 1 History of paclitaxel development The search for the natural resources began in 1960 headed by NCI and USDA which ledto discovery of Pacific yewrsquos bark The active ingredient was isolated by Monroe Wall and Mansukh Wani and was named Taxol Taxoldemonstrated both in vivo and in vitro antineoplastic activity as well in xenograft models with breast tumours The mechanism of actionwhich was unique was identified and subsequently after 22 years Taxol entered clinical trials and demonstrated good cytotoxicity activityand was finally approved by FDA for treatment against ovarian and breast cancers
chemotherapy IP paclitaxel treatment and newer forms ofpaclitaxel may add to the clinical benefit in patients with thismalignancy
2 The Evolution of Paclitaxel
Paclitaxel was not a chance discovery but the result of acollaborative effort of the National Cancer Institute (NCI)and the US Department of Agriculture (USDA) using aplant-screening programme in search of new and effectiveanticancer agents [26] The history of paclitaxel developmentis summarised in Figure 1
The NCI Plant Programme headed by Jonathan Hartwella natural product chemist liaised with Robert Perdue aUSDA botanist and analysed over 15000 natural plantsworldwide as well as testing 115000 extracts for anticanceractivity over the period from 1960 to 1981 When the NCIscreening programme concluded in 1981 paclitaxel was theonly compound entered into clinical trials [27]
In August 1962 paclitaxel was isolated from the barkof the Pacific yew tree Taxus brevifolia Nutt (Taxaceae)shipped in from Gifford Pinchot National Forest to USDAheadquarters in Maryland by a 32-year-old USDA botanistArthur S Barclay [26 28 29] Although the cytotoxic activityof the bark of the samples soon became evident by September1964 as it was found to be able to inhibit the in vitro growthin 9KB cell cultures containing human oral epidermoid
carcinoma [30 31] it took MansukhWani and Monroe Wallworking under contractwith theNCI at theResearchTriangleInstitute (Research Triangle Park NC) till 1967 to isolate andidentify the extractrsquos most active ingredient and named itpaclitaxel [26]
Paclitaxel was reported to have a broad spectrum ofantitumour activity following in vivo screens in tumoursimplanted in laboratory mice [27] With grant aid fromNCI Dr Susan Horwitz from the Albert Einstein College ofMedicine further enhanced the interest in paclitaxel with thenovel discovery of its unique mechanism of action Anotherbreakthrough came in November 1978 with the ability ofpaclitaxel to cause tumour regression in a mammary tumourxenograft [26]
Although clinical trials to study the effect of paclitaxelon various cancers mushroomed not many were able tocommence as planned due to scarcity in the supply the onlysource being the extremely slow-growing Pacific yew Hart-well soon realized that for every 13 kilograms of dried bark hewas producing just half a gram of purified paclitaxel extractIn 1990 a petition to include the severely depletedT brevifoliaon the list of endangered species concluded in the Pacific YewAct being passed in 1992 to protect the tree [32]
Despite the scarcity paclitaxel entered clinical trials after22 years from its discovery in 1984 Wiernik and colleaguesreported a phase 1 trial in 1987 [33] Paclitaxel was found tohave cytotoxic activity of clinical significance when a study
BioMed Research International 3
Empirical formula C47H51NO14
Molecular weight 8539 gmol
Average mass 8539Da
Systemic name (2120572 5120573 7120573 10120573 13120572)-
(benzoylamino)-2-hydroxy-3-
phenylpropanoyl]oxy-17-
dihydroxy-9-oxo-520-epoxytax-11-
en-2-yl benzoate
410-Diacetoxy-13-[(2R 3S)-3-
O
O
O
O
O
O O
O
O
NHH3C
H3998400 CH3
CH3
CH3
CH345
OH
HO
OH
OH
13
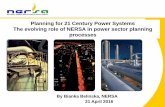
Figure 2 Chemical structure of paclitaxel Paclitaxel consist of taxane ring with a four-membered oxetane side ring at positions C4 and C5and an active homochiral ester side chain at C13 that binds tomicrotubules in a guanosine triphosphate (GTP) independentmanner to inducecytotoxicity activity
on ovarian cancer concluded that 30 of patients withplatinum-resistant ovarian cancer responded to paclitaxeltherapy either completely or partially [34] Another issue wasthe insolubility of the paclitaxel in water but these problemswere eventually overcome with a formulation in ethanoland Cremophor EL Cremophor EL is a polyethoxylatedcastor oil which was used as a vehicle for solubilisation ofhydrophobic drug like paclitaxel [35] However the mostserious side effect observed following use of Cremophor asthe drug vehicle was that of hypersensitivity reactions whichwere unpredictable and led to two deaths and this almosthalted any further clinical trials A longer and slower infusiontaking 24 hours reduced this severe adverse effect [33]
In December 1992 paclitaxel was registered as chemo-therapy for the treatment for ovarian cancer To meetincreasing demand a commercially viable semisynthetic wasdeveloped by Robert Holton and colleagues [31] Researchersalso tested the effectiveness of paclitaxel as a treatment foradvanced breast cancer Subsequent clinical trials found thatthe drug was effective against this disease and in 1994 theFDA approved paclitaxel for use against breast cancer Pacli-taxel is now used (either as a single agent or in combinationwith other drugs such as cisplatin or carboplatin) for thetreatment of ovarian cancer [36] breast cancer [5] and non-small-cell lung cancer [37]
3 Chemical Structure
Paclitaxel a class of taxane drugs is a diterpenoid pseudoal-kaloid with the empirical formula C
47H51NO14
(Figure 2)and has a corresponding molecular weight of 8539 gmolPaclitaxel consist of two molecules a taxane ring with a four-membered oxetane side ring at positions C4 and C5 and ahomochiral ester side chain at C13 The side chain at C13plays a crucial role as this is the active portion that binds tomicrotubules stabilises the tubulin bundles and stimulatesdisassembly of microtubules in a guanosine triphosphate(GTP)-independent manner As a result cell proliferation isinhibited by halting the cell cycle at the metaphaseanaphase
boundary and by formation of an incomplete metaphaseplate of chromosomes induced by the stabilization of themicrotubule dynamics Extensive research has concluded thatan intact taxane ring and an ester side-chainwere essential forcytotoxic activity [38 39]
4 Mechanism of Action
Paclitaxel is an anticancer drug that targets microtubulesMicrotubules consist of cylindrical hollow bodies of about25ndash30 nm in diameter composed of polymers of tubulin indynamic equilibrium with tubulin heterodimers (consistingof alpha and beta protein subunits) [40 41] The principalfunction of microtubules is the formation of the mitoticspindle during cell division In addition they are required forthe maintenance of cell structure motility and cytoplasmicmovement within the cell The synthesis of tubulin and theassembly of microtubules occur during the G2 phase and theprophase of mitosis Microtubules are in a state of dynamicequilibrium with their subunit tubulins 120572 and 120573 arrangedin a head to tail fashion with preferential faster growth(plus ends) at one end and slower growth (minus ends) atthe other end Under steady-state conditions the length ofthe microtubule is unchanged as the net tubulin assemblyrate equals the net disassembly rate The minus ends part ofmicrotubule are usually anchored mainly at the centrosome[42] while the plus ends explore the cytoplasm and interactwith cellular structures [43 44]
Dr Horwitz discovered that paclitaxel unlike vincaalkaloids which prevent microtubule assembly prevents celldivision by promoting the assembly of stable microtubulesespecially from 120573-tubulin heterodimers and inhibits theirdepolymerisation hence exposed cells are arrested in theG2M-phase of the cell cycle [45] and eventually undergoapoptosis [46] thereby inhibiting cell replication [40 47]Paclitaxel binds specifically in a reversible manner to theN-terminal 31 amino acids of the beta-tubulin subunit inthe microtubules rather than to tubulin dimers [47 48]Paclitaxel also has the unique ability to promote microtubule
4 BioMed Research International
formation in vitro even at cold temperatures (4∘C) and in theabsence of GTP [46]
Further research into understanding themolecularmech-anisms of microtubule formation has discovered that pacli-taxel may have other mechanism that allows cells to escapedrug toxicity which then develops into resistance and failurein chemotherapy [44] Ganguly and his colleagues found thatmicrotubule dynamics suppression was not related to celldivision Treatment of mutant cell lines Tax 11-6 (mutation in120572-tubulin) and Tax 18 (mutation in 120573-tubulin) at concentra-tion of 50 to 100 nmolL that should hypothetically increasemicrotubule assembly to more normal levels and allow thecells to proliferate normally further suppress microtubuledynamics rather than restoring behaviour to normal [44]Low concentrations of paclitaxel that suppressed dynamicshence they did not affect the rate ofmicrotubule detachmentbut the higher drug concentrations that allowed normalcell division strongly inhibited detachment in the mutantcell lines and returned the rate to near normal levels Thisaction seems to be related to ability of paclitaxel to inhibitmicrotubule fragmentation rather than its ability to suppressmicrotubule dynamics which was further confirmed by livecell imaging that demonstrated that microtubule detach-ment from centrosomes might be responsible for generat-ing microtubule fragments a process that was reversed bypaclitaxel [44] Recent studies have also found that at lowconcentrations (less than nanomolar concentrations) pacli-taxel inhibits the depolymerisation of microtubules whereasat high-dose paclitaxel increase the number and mass ofmicrotubules hence increasing stability of microtubules andalso render them nonfunctional by blocking the detachmentof microtubule minus ends from centrosomes rather thanplus ends [44 49]
The proposed mechanism of action of weekly paclitaxeladministration may be based on its apoptotic effects Theinduction of apoptotic modulator genes by paclitaxel appearsto be independent of microtubule stabilization It may be dueto modulation of the transcription of different genes suchas DNA-damage response proteins cytokines or proteinsinvolved in the control of cellular proliferation apoptosis andinflammation The apoptotic effect of paclitaxel is dependenton the concentration and duration of exposure With con-centration amounts of at least 10 nM and exposure of at least12 hours apoptosis may be induced in the S phase withoutmitotic arrest Two different mechanisms of apoptosis havebeen proposed depending on the dose concentration ofpaclitaxel At concentration of ge9 nM paclitaxel induces Raf-1 activation which is responsible for apoptotic control Atle9 nM there is absence of Raf-1 kinase involvement butapoptosis induction still occurs under the influence of p53and p21 [50 51] With the same concentration at 24-hourexposure in addition to apoptotic arrest paclitaxel producesan irreversible mitotic arrest [52] p53 is a major tumoursuppressor regulating proliferation and apoptosis and itsmutation occurs in more than 50 of human cancers Innormal cells DNA damage increases p53 levels which thenactivates a G1 cell-cycle arrest mediated by p21 to promoteeither the DNA damage repair mechanisms or apoptosis andnaturally limiting proliferation of genetically transformed cell
clones A functional p53 signaling pathway is necessary tosensitise cancer cells to DNA-damaging chemotherapeuticagents to reduce chemo resistance Currently paclitaxelactivity is considered to be independent of p53 status whichis an important aspect as the presence of silent ormutated p53does not modify the sensitivity of cancer cells to taxane thusreducing chemoresistance [53ndash56]
Paclitaxel also exerts its mechanism of action by activa-tion of multiple signal-transduction pathways which maybe associated with proapoptotic signaling The pathwaysassociated with paclitaxel are TLR-4 dependent pathway(either via MyD88 dependent or independent pathway) c-Jun N-terminal kinase (JNK) P38 Mitogen activated protein(MAP)Kinase nuclear factor kappa B (NF-120581B) Janus kinase-(JAK-) signal transducer and activator of transcription factor(STAT) pathway One of the pathways for induction ofapoptosis is via mitogen-activated protein kinase (MAPK)pathway resulting in dephosphorylation of the proapoptoticprotein Bad and Bax phosphorylation of Bcl2 and inductionof apoptosis Bad and Bax (promote apoptosis) and Bcl2 (sup-press apoptosis) are regulatory proteins which are membersof the Bcl2 family and are involved in programmed cell deathInduction of cytokines and pro-inflammatory proteins willlead to immunomodulatory effect of paclitaxel at low-doseconcentration and cell death at higher dose Changes thatoccur in these pathways are also responsible for developmentof resistance to paclitaxel [57ndash60]
Weekly paclitaxel also exhibits strong angiogenic inhibi-tory activity [61 62] In murine studies paclitaxel was ableto reduce new vessel formation at low noncytotoxic doses(03 and 6mgkg per day in mice) by suppressing VEGFexpression [63 64] Low dose weekly paclitaxel has beentested in patients with advanced ovarian cancer metastaticmelanoma and advanced head and neck cancer resulting instable disease [65ndash67] This additional mechanism of actionof paclitaxel by rescheduling the duration of administrationmay be helpful in cancers which have become resistant to thesame drug given on a 3-weekly conventional schedule [11 13]
Paclitaxel had also been reported to induce reactiveoxygen species (ROS) generation and increase hydroperoxideproduction by enhancing the activity of nicotinamide ade-nine dinucleotide phosphate (NADPH) oxidase which con-tributes to oxidative stress and may play a role in the potencyof the anticancer activity of paclitaxel [68 69] The combi-nation of paclitaxel with inhibitors of glucose (ie 2-deoxy-D-glucose 2DG) and hydroperoxide (ie L-buthionine-S R-sulfoximine BSO) metabolism has been found to selectivelyenhance breast cancer cell killing via hydrogen peroxide-induced metabolic oxidative stress which may be effectivelyutilised to treat breast cancers [69] However the relationshipof oxidative stress to the overall cytotoxicity mechanism ofpaclitaxel is not well established The mechanism of action ofpaclitaxel is summarised in Figure 3
5 Mechanism of Drug Resistance
Themechanism of paclitaxel resistance is complex involvingmultistep and multiple genes and not yet fully elucidated
BioMed Research International 5
Microtubules(MT)
MyD88 dependent
MyD88 independent
S
G2G1
M
PTX
Cell cycle arrest
N-terminal amino acids of beta
tubulin subunit
Inhibit depolymerisation ofmicrotubules
and suppress MT dynamics
Increase number and mass of microtubules increase
stability and block detachment
Apoptosis induced in G1S phase (absence mitotic
arrest)
Raf-1
p21
STAT 3
G0
JAK
MEK
MAPK
Bax Bcl2Bad
IRAK
TRAF
TKR
TRIF TRAM
ROS
Mitotic arrest at G2M phase
PI3KAKTApoptosis regulator
protein
p53
VEGFR
Angiogenesis
Apoptosis
TLR4
High concentrationLow concentration
NF-120581B
PTXle 9nM12hr
PTXge 9nM12hr
PTXle 9nM24hr
I120581B
Figure 3 Mechanism of action of paclitaxel Paclitaxel targets microtubules At high concentration PTX causes mitotic arrest at G2M phasewhereas at low concentration apoptosis is induced at G0 and G1S phase either via Raf-1 kinase activation or p53p21 depending on the doseconcentration Even at lower dose but with exposure beyond 24 hours paclitaxel can cause mitotic arrest Paclitaxel also activates multiplesignaling pathway to exert proapoptotic activity as well as immunomodulatory effect Paclitaxel also develops resistance via these signalingpathways PTX Paclitaxel TLR4 Toll-like receptor 4 G0 resting phase G1 cells enlarge andmake new protein S phase DNA replication G2preparation for division M phase cell divisionmitosis Raf-1 Raf kinase family MEKMAPK mitogen activated protein kinase IRAK IL-1receptor associated kinase TRAF TNFR associated factor NF-120581B nuclear factor kappa B TRIFTRAM TIR-domain-containing adapter-inducing interferon-120573 TKR tyrosine kinase receptor VEGFR vascular endothelial growth receptor PI3K phosphoinositide 3-kinase JAKjanus kinase STAT signal transducer and activator of transcription factor
Development of drug resistance leading to aggressive diseasethat is refractory to treatment is responsible for 90 ofthe deaths among patients with advanced ovarian cancer[70] Multidrug resistance (MDR) is a phenomenon definedby the ability of cancer cell to overcome either structurallyor functionally unrelated cytotoxic drugs Mechanism ofMDR can be broadly divided into three types (a) externalmechanism involving changes in pharmacokinetics of drugor (b) within tumour microenvironment which includeshypoxia leading to clonal selection pressure or (c) at cellu-lar level [71] MDR can be intrinsic or acquired IntrinsicMDR or also known as inherent occurs when cancer cellsdevelop resistant to any chemotherapy and this is most likelyattributed by tumour microenvironment Acquired MDRdevelops following exposure to chemotherapeutic agents andmay occur as a result of the pharmacokinetic of drug itself orsecondary to changes within the tumour cells [71]
Paclitaxel-derived resistance is mainly attributed bychanges involving mRNA and protein (such as multiple
ribosomal genes and translation factors) synthesis oxidativestress (UGT1A6 MAOA and CYBA) glycolysis (ADH1AHK1 and ENO3) glutathione metabolism and leukocytetransendothelial migration pathways [71] A study on geneexpression changes on a series of drug resistant ovariancancer cell lines following exposure to paclitaxel cisplatinor doxorubicin revealed that among 845 genes analysed atotal of 337 genes were significantly altered in cells resistantto paclitaxel [70] Changes in genes expression may createinterpatient variation in drug effect alteration in tumourmicroenvironment and changes within cellular structuresmetabolism and functions that promotes towards drug resis-tance
Tumour cells grow rapidly with formation of numerousnew vessels attributing to irregular blood flow and increasedoxygen demand which lead to development areas devoidof adequate oxygenation within ovarian cancer tissues [72]In response to chronic hypoxia (oxygen depletion) tumourmicroenvironment adapts processes to keep cells alive in
6 BioMed Research International
hypoxic and acidic state This hypoxic adaptation promotestumour proliferation dissemination and progression of dis-ease [73] and also reduces chemosensitivity [74]
Hypoxia-induced chemoresistance occurs due to geno-mic instability Oxygen depletion induces proteomic andgenomic changes that activates the level of p53 inhibits apop-tosis promotes angiogenesis (angiogenic molecules such asvascular endothelial growth factor [VEGF] and angiogenin)upregulates growth factors (platelet-derived growth factor[PDGF] transforming growth factor-beta and insulin-likegrowth factor [IGF]) and induces anaerobic metabolism andglycolysis (glycolytic enzymes glucose transporters) leadingto reduction in potential for cell cycle arrest and cellulardifferentiationwhich prevent tumour cell death [74]Hypoxiacan induce either p-53-dependent (involving Apaf-1 andcaspase-9 effector pathways) or p53-independent (involvinghypoxic-inducible factor 1 [HIF-1] and Bcl-2 family genespathways) apoptosis in both normal and tumour cells HIF-1 is a common transcription factor consisting of HIF-1120572 and HIF-1120573 subunits which controls hypoxic-induciblegenes and the concentration of HIF-1 protein increasedexponentially in the presence of hypoxic environment Lossof apoptotic potential of tumour cells mediated by hypoxicenvironment and HIF-1 which arrest cell cycle at G0G1reduces chemosensitivity to chemotherapeutic agents includ-ing paclitaxel [70 75]
Other transcriptional factors which are activated byhypoxia are nuclear factor kappa B (NF-120581B) and STAT3 also known as proinflammatory transcriptional factorsNF-120581B and STAT 3 regulate multiple gene products whichare involved in inflammation angiogenesis cell survivalproliferation and metastasis Paclitaxel which mediates itscytotoxic action via NF-120581B pathway is vulnerable to developresistance in the presence of hypoxic tumour microen-vironment with activation of NF-120581B transcription factorwhich induces serine phosphorylation and also regulatesBCL-2 an antiapoptotic protein preventing cell death andpromoting tumorigenesis [76] Inhibition of activated STAT3 found overexpressed in most paclitaxel-resistant ovariancancer cells has resulted in reduction in paclitaxel resistanceHowever further research is required to determine the exactmechanism [77]
Intracellular drug concentration is important for effectivecytotoxic activity of paclitaxel Drug resistance may beattributed to either reduced accumulation of drug withinovarian tumours or increased efflux of drug from tumourcells [78] Alteration in pharmacokinetic of paclitaxel eitherattributed by the drug itself such as lower concentration ofdrug administered shorter duration of drug exposure highfirst pass metabolism increased hepatic or renal clearanceinadequate binding to tubulinsmicrotubules or othermacro-molecules or presence of higher tumour density or vascular-ity may result in reduced accumulation of intratumoral drugconcentration [71]
Drug efflux is the most common mechanism for chemo-resistance observed in paclitaxel-treated cancer cells Drugefflux from cancer cells is mediated by ATP-binding cassette(ABC) transporters such as P-glycoprotein (P-gp) P-gp alsoknown as ABCB1 or multidrug-resistance associated-protein
(MRP) a transmembrane protein encoded by MDR1 geneplays a role as an efflux pump which is crucial for occurrenceof many cellular processes that require transfer of substratesacross cellularmembranes P-gp hence can affect intracellulardrug concentration andhave been shown to correlate in vitroto chemosensitivity to paclitaxel [59] However evidence fortheir role in clinical drug resistance in ovarian cancer hasemerged with P-gp found to be overexpressed in ovariancancer cells in vitro and also on paclitaxel-resistant celllines [70] P-gp and MDR1 expression levels were higherin chemoresistant ovarian cancer patients as compared withtheir chemosensitive counterpart Overall survival time wasalso statistically higher in patientswith low expression of P-gpandMDR1 in their tumor tissuesHence P-gp andMDR1mayhave a predictive role in determining the outcome of patientswith advanced ovarian cancer [58 79ndash82] Mechanism ofpaclitaxel resistance is complicated and specifically inhibitingABC transporters have given mixed results [59 83]
Another major mechanism of paclitaxel resistance ismediated by either a reduction in total intracellular tubulinconcentrations point mutation at prominently expressedtubulin genes or by selective alterations in expression oftubulin isotypes such as Class III 120573-tubulin [52 84 85]Microtubule dynamic stability was significantly impairedin the paclitaxel-resistant cells [86] Microtubule dynamicsdisruption caused by paclitaxel result in cell cycle arrestapoptosis and drug resistance
Other mechanism responsible for development of pacli-taxel resistant are inhibition of apoptosis activation ofmitogen-activated protein kinase Raf-1 kinase or intra-cellular signalling pathway PIK3 (phosphatidylinositol-45-bisphosphate 3-kinase) changes in apoptotic regulatory pro-teins such as Bcl-2 increase in expression of proinflammatorycytokines such as TNF-120572 IL-6 and IL-8 and activation oflipopolysaccharide-inducible genes and tumour suppressionprotein p53 [57 83 86 87]
In summary paclitaxel resistance is multifactorial inc-luding changes in signaling pathways upregulation of P-glycoprotein (P-gp) [80 88 89] alteration in tubulin dyna-mic mutations in 120573-tubulin gene or expression of 120573-tubulinisotypes [52 84 85] and changes in apoptotic mechanismIdentification of mechanism of resistance could help topotentially develop novel agents to improve chemosensitivityof patients with advanced ovarian cancer
6 Pharmacokinetics
Paclitaxel is a white to off-white crystalline powder highlylipophilic and is insoluble in water and so difficult to formu-late into solution It has a melting point of 216-217∘C [90 91]More than 90 of the drug binds rapidly and extensively toplasma proteins [33 40] whereas binding onto red blood cellsis approximately 50 The presence of premedication drugs(before chemotherapy) such as ranitidine dexamethasone ordiphenhydramine did not affect protein binding of paclitaxelPaclitaxel has a large volume of distribution of about 55 Lm2but this is reduced in the females [33]
BioMed Research International 7
AUC (area under the plasma concentration)
Cmax (maximum concentration)
Pacli
taxe
l con
cent
ratio
n (120583
M)
0 10 20 30 40
Time (hr)
0
1
2
3
4
5
Figure 4 Plasma pharmacokinetics of paclitaxel The pharmacoki-netics generally were linear for 6 or 24 hour infusions but becomenonlinear for infusions of shorter durations due to variation inthe elimination clearance with the dose administered An increasein plasma concentration of paclitaxel results in disproportionatelarger increase in 119862max (maximum plasma concentration) and AUC(area under plasma concentration) followed by decrease in drugelimination from body tissues
The disappearance of paclitaxel from plasma is tradition-ally believed to be biphasic [33] The initial rapid declinerepresents distribution to the peripheral compartment andelimination of the drug The later phase is due in part tothe slow efflux of paclitaxel from the peripheral compartment[92] In the presence of more sensitive assay methods andlater sampling times a three-compartment model seems tobe more accurate [40 93] Paclitaxel has been shown tohave a nonlinear pattern of pharmacokinetics (Figure 4)Thepharmacokinetics were generally linear for 6- or 24-hourinfusions but become nonlinear for infusions of shorterdurations because the elimination clearance varies with thedose administered With increasing plasma concentrationof paclitaxel there is a disproportionately larger increasein 119862max (maximum plasma concentration) and AUC (areaunder plasma concentration) accompanied by decrease indrug elimination from body tissues The clinical importanceof this nonlinear pattern is that dose escalationmay result in adisproportionate increase in toxicity whereas dose reductionmay affect its efficacy [33 90 91 94]
The pharmacokinetics of paclitaxel has been evaluatedover a wide range of doses up to 300mgm2 and withinfusion schedules ranging from 3 to 24 hours Maximumplasma concentrations are dose-related In patients treatedwith single dose infusion of 135 and 175mgm2 given as3- and 24-hour infusions mean steady state volume ofdistribution has ranged from 198 to 688 Lm2 indicatingextensive extravascular distribution andor tissue bindingTerminal half-life has ranged from 13 to 86 hours (mean 5hours) [40 93] and total body clearance has ranged from116 to 240 Lhrm2 Preclinical results in animals have shown
high levels in most tissues Being highly protein-boundpaclitaxel has a high affinity for distribution in specific tissuesincluding kidney lung spleen and extracellular fluids likeascites and pleural fluids [40 95] but the uptake of the drugin the brain is minimal [96 97] Exposure to paclitaxel isrelatively high in tumour tissue compared with other tissuesand in addition to slow elimination from tumour tissue theAUC in tumour tissue is about five-fold higher than that inplasma [97]
There is no evidence of accumulation of paclitaxel withmultiple treatment courses as the variability in systemicpaclitaxel exposure as measured by AUC (0ndashinfin) (area underplasma concentration-time curve from time 0 to infinity)for successive treatment courses are minimal [98] Paclitaxelclearance is however sequence dependent Patients receiv-ing a platinum-based agent prior to paclitaxel have lowerclearance and greater clinical toxicity than patients receivingpaclitaxel before cisplatin [93]
The drug administered intravenously undergoes anextensive P-450mediated hepaticmetabolism by cytochromeenzymes (CYP3A andCYP2C8) with 70ndash80being excretedinto bile by adenosine triphosphate- (ATP-) binding cassettemultidrug transporters such as P-glycoprotein (P-gp) andmultidrug resistance protein 2 (MRP-2) either asmetabolitesor as the parent drug Variation in MRP-2 activity hasbeen found to have direct effect on the effective exposureto paclitaxel [99] The bioavailability is poor following oraladministration due to enterocyte expression of P-gp and first-pass metabolism in the liver Most of the drug is eliminatedin feces Less than 10 drug in the unchanged form isexcreted in the urine indicating extensive nonrenal clearance[96] Combinations of inhibitors of CYP3A and P-gp mightpossibly improve the oral bioavailability of the taxanes [8997 100]
7 Paclitaxel and the Immune System
The immune system consists of two different but interactingmechanisms which are innate and adaptivemechanismsTheinnate mechanism is the first line of defense and consists of agroup of cells which includes mainly macrophages dendriticcells (DCs) and natural killer (NK) cells while the adaptiveimmunemechanism is represented by T-lymphocytes All thecomponents of innate and adaptive mechanism are involvedin antitumour immunity which includes tumour recognitioncontrol and elimination However cancer cells are able toevade immune detection and actively suppress antitumourimmunity
Paclitaxel has a wide range of dose dependent immuno-modulatory effects described in Figure 5 At standard dosepaclitaxel is broadly immunosuppressive and this is becauseit inhibits a number of cell types involved in tumour rejectionsuch asmacrophages effector T cells andNK cells [101] How-ever at lower doses than typically used for chemotherapypaclitaxel has an important immunogenic role promotingantitumour immunity [101 102] Hence understanding theimmunological basis of paclitaxel may help to maximise themanipulation of the immunomodulatory effects of paclitaxel
8 BioMed Research International
Immunomodulatory effect of
paclitaxel
Stimulate direct cytotoxic activity by
macrophage
Induce activation maturation and priming of DCs
Stimulate NK-dependent antitumour immunity
Activation of tumour-specificCTL Expansion of memory T cells
Secretion of proinflammatory cytokine
Shift from Th2 to Th1 type ofresponse
Depletion of Tregs andmodulation of MDSC
Downregulates the expression of VEGFR-2
and inhibits angiogenesis
IL-6 IL-12 TNF-120572 and i-NOS
Figure 5 Immunomodulatory effect of paclitaxel Paclitaxel a toll-like receptor 4 (TLR4) ligand binds to TLR4 receptor and triggers TLR4signaling via MyD88 dependent and independent pathway Paclitaxel then promotes anticancer immune response directly by stimulatingmacrophages to kill cancer cells or indirectly by secretion of proinflammatory cytokines which upregulates activation of DCs NK andtumour specific CTL Paclitaxel promotes effective CTL response by upregulation of mannose-6-phosphate which facilitate permeabilityto granzyme B and cytokine patterns of T helper type 1 Paclitaxel modulates MDSC and ablates Tregs Memory T cells (CD4+CD45RO+and CD8+CD45RO+) increased significantly while regulatory T cells (Tregs) decreased around 2 weeks creating an opportunity window fordose-dense therapy and immunomodulatory agents to achieve clinical benefit Dose-dense and low dose paclitaxel also blocks new vesselformation by downregulating VEGF-receptor 2 reduces resistance by alternative mechanism of action
to develop better therapeutic options in the management ofadvanced ovarian cancer
Paclitaxel is a ligand to toll-like receptor 4 (TLR4) whichis expressed on innate immune cells including macrophagesThe binding of paclitaxel to TLR4 on macrophages trig-gers the MyD88 mitogen-activated protein kinase (MAPK)and transcription of nuclear factor NF-kappa B (NF-120581B)pathways (Figure 3) resulting in their activation and releaseof immunostimulatory cytokines such as tumour necrosisfactor-120572 (TNF-120572) interleukin-1 (IL-1) interleukin-6 (IL-6)and interleukin-8 (IL-8) [103ndash105] Activated macrophagescan either cause direct tumour cell lysis via release oflysosomal enzymes and nitric oxide (NO) or indirectly byactivating NK cells DCs and tumour-specific cytotoxic T-lymphocytes (CTLs) [101]
NK cells are also innate immune cells capable of killingtumour cells particularly those cells that have reduced classI MHC expression and therefore can escape killing by CTLsPaclitaxel can enhance NK cell function by inducing mRNAand protein production of perforin an effector moleculeinvolved inNKcell-mediated cytotoxicity [106]However theeffect of low dose paclitaxel on NK cells is controversial Inanother study it was found that treatment of human NK cellswith paclitaxel effectively inhibits NK cell-mediated killing ofK562 (human erythroleukemia) target cells in vitro withoutaffecting the viability of NK cells [107] However weeklypaclitaxel therapy for non-small cell lung cancer patients was
only able to reduce the NK cell function up to completion ofthe first cycle but thereafter it gradually recovered [108]
Dendritic cells also express TLR4 and can be directlyactivated by paclitaxel The binding of paclitaxel to TLR onimmature DCs promotes DC maturation by upregulatingantigen-processing machinery gene components costimu-latory molecules and IL-12p70 [102] This enhances theability of DCs to prime T cells which facilitate antitumourimmunity [109] Paclitaxel can also promote cytotoxic T-cell function by upregulating mannose-6-phosphate whichfacilitates permeability to granzyme B and also inducescytokine production patterns typical of the T helper type 1phenotype via IL-2 (CD4 T cell) and IFN-120574 (CD8 T cell)secretion [104 110] Activated CD8+ T cells can differentiateinto CTL type 1 (Tc1) cells producingmainly IFN-120574 and CTLtype 2 (Tc2) cells producing mostly IL-4 IL-5 and IL-10 Tc1cells are potent CTL involved in the defense against cancerTc1 cells are able to recognise tumour antigens in the contextof MHC class I and mediate tumour cell lysis The role of Tc2cells in the immune response is not clearly known althoughtheir presence has been associated with disease progression[111]
CD4+ CD25+ regulatory T-cells (Tregs) constitutingapproximately 5ndash10 of peripheral CD4+ T cells [112 113]play an important role in tumour immune evasion [114]There is growing evidence that supports the existence ofelevated numbers of Tregs in tumours [115ndash117] which may
BioMed Research International 9
suppress immune responses of other CD4+ and CD8+ cells[118ndash120] and promote tumour progression In murine stud-ies paclitaxel exhibits the ability to reduce the number andsize of Treg cells thereby enhancing antitumour immunity[119 121] Similar findingswere seenwith a selective reductionin the size and number of Treg populations in peripheralblood samples from non-small cell lung cancer (NSCLC)patients [122]
Paclitaxel also decreased the expression of the anti-apoptotic molecule Bcl-2 in Treg cells while increasing thecorresponding proapoptoticmember Bax which contributedto the apoptotic sensitivity of Treg to paclitaxel [87]This wasseen in a study using the 3LL Lewis tumour model whichdemonstrated that Treg cells exposed to paclitaxel displayeddown regulation of Bcl-2 and upregulation of Bax and uponblocking the Bcl-2 pathway the ability of paclitaxel to ablateTreg cells compared toT effectorswas impaired and bothTregand T effectors were affected These results may suggest thatpaclitaxel targets Bcl-2 rather than tubulin to contribute tothe distinctive effect on Treg cells [119] It has recently beenshown in vitro that paclitaxel could target Bcl-2 and thereforelead to apoptosis Bcl-2 family proteins are key regulators ofapoptosis and play an important role in tumourigenesis andmulti-drug resistance by blocking apoptosis [119 123]
Few studies have also shown effect of paclitaxel onmyeloid-derived suppressor cells (MDSCs) a heterogeneouspopulation of immature myeloid cells immunosuppressivein nature are recruited by cancer cells and are found inincreased amount in advanced epithelial ovarian cancer [124]In a murine study using C57BL6 mice administration ofpaclitaxel at ultralow dose modulates MDSCs to differentiateinto DCs in a TLR4 independent manner [110] Hencepaclitaxel in ultralow noncytotoxic doses together with itsangiogenesis blocking ability may potentially enhance theefficacy of immunotherapy by ablation of immunosuppres-sive populations such as Tregs and MDSCs in tumour-bearing hosts [50 102]
In immunocompromised patients with advanced ovariancancer with increased Tregs and decreased levels of CD4+T cell CD8+ T cell and NK subsets after a single courseof combined carboplatin and paclitaxel chemotherapy theimmunosuppression is reversed around 12 to 14 days later butnot before one week or after three to four weeks Not only areTregs decreased but also the proportions of IFN-120574 secretingCD8+ T cells T helper-1 Tc1 and NKT cells The ratio of Tc1to Tc2 cells increases significantly [111 120 125]
Following chemotherapy both CD4+CD45RO+ andCD8+CD45RO+ memory T cells increased significantly andpeaked around 2 weeks The increase of memory T cellsin ovarian cancer patients following chemotherapy prob-ably opens the door of opportunity to develop long-termimmunological memory which could prevent recurrenceand metastases [120] Administration of dose-dense therapygiven weekly may hence be beneficial immunologically tomount an adequate immune response compared to standard3-week therapy In addition administration of immunother-apy agentsmay also be ideal during the period of 2weeks afterchemotherapy where temporary immune system reconstitu-tion takes place
8 Clinical Studies
In the past two decades paclitaxel had been administered indoses ranging from 60 to 250mgm2 over 1ndash96 hours andfrom 1 to 3 weekly intervals Prolonged exposure up to 96hours was believed to be effective as demonstrated with pre-clinical data but later refuted in large prospective studies [14126 127] A 24-hour infusion of paclitaxel was subsequentlyadministered to reduce the risk of hypersensitivity reactionshowever it was shown to increase mucosal and bone marrowtoxicity without improved efficacy [127 128] Development ofeffective premedication has led to administration of shorterinfusions (lt3 hours) which are better tolerated in particularfrom a haematologic perspective but patients remain at riskof myalgia and neuropathy at higher doses Weekly one-hourlow dose paclitaxel also known as dose-dense therapy hasrecently emerged as another possible strategy to improveoutcomes
9 Dose-Dense Therapy
Dose-dense treatment is defined by delivery of a maintainedper-cycle dose or overall dose with administration of drugat shorter time intervals than is standard This differs fromdose intensity which refers to dose (per unit weight or bodysurface area) delivered per unit time Hence either escalationof dose per cycle or reducing the time in between cycles maymodify dose intensity [129 130]
The rationale for the dose-dense approach of weeklypaclitaxel is that more frequent delivery of moderate dosesmay achieve greater efficacy by allowing sustained exposureof dividing tumour cells to paclitaxelrsquos cytotoxic and antian-giogenic effects hence reducing resistance delaying relapseand increasing the possibility of cancer remission Three 1-hour infusions of paclitaxel given at a week interval achievedgreater dose-density as well as dose-intensity than a singleadministration every 3 weeksThe initial tissue concentration(gt50 nM) for 1-hour infusion is similar to that of 3-hourinfusion but the concentration in the plasma instead oflasting for 8 hours in a 3-hour infusion rapidly falls below50 nM in less than 75 minutes for 1-hour infusion and hencereduces the risk of neutropenia However the rate of fallexperienced in tissue concentration of the drug is slowerthan plasma concentration of the drug hence efficacy ismaintained [131 132] A shorter infusion time allows bettercontrol of toxicities improved patient comfort and reducedhospitalisation hours
Several studies have used dose-dense paclitaxel in thetreatment of advanced ovarian cancer and are summarizedin Table 1 Based on phase 1 studies the recommendeddose for weekly paclitaxel ranges between 80 and 90mgm2compared with 45mgm2 per week with 3-weekly paclitaxeland is given over 1-hour duration Weekly scheduling hasdemonstrated consistent activities in ovarian cancer studies[11ndash13] Response rates were in the 20ndash50 range whereusually less than 10 would be expected Grade-4 doselimiting toxicities in particular neutropenia were not evidentat any dose below 100mgm2week [11 133]
10 BioMed Research International
Table1Ph
ases
Iand
IIstu
dies
onintravenou
sdose-densep
aclitaxel
Stud
yRe
gimen
119899()
PI(m
)RR
()
CR(119899)
MedianPF
S(m
)Median
OS
(m)
Adversee
ffects
Com
ments
Paclitaxel
dose
(mgm
2 )Ca
rbop
latin
dose
(mgm
2 )Ph
aseIsinglea
gent
Lofflerre
tal1996
[11]
40ndash9
0week
1-hou
rinfusionfor
6weeks
5040
5NA
NA
(i)Hem
atologictoxicity-m
ild(ii)N
ograde3
or4
haem
atologicaltoxicity
neurologicalor
cardiotoxicityup
to90
mgm
2 wk
(iii)Nohypersensitivity
reactio
ns(patientsreceivedprem
edication)
(i)100
priorc
hemotherapy
(ii)M
ediando
seintensity
was
410m
gm
2 6w
k(range200
to540m
gm
2 6w
k)
Fenn
ellyetal
1997
[12]
40ndash100w
eek
1830
NA
NA
NA
(i)Nomucositiso
rgrade
III
neurop
athy
was
seen
(ii)A
lopeciao
ccurredin
one
(i)100
priorc
hemotherapy
(2ndash5
priorregim
ens)
(ii)P
artia
lrespo
nses
weres
eenin
four
of13
assessablepatients
(30
)(iii)Dose-lim
iting
toxicitywas
reachedat100m
gm
2 (iv
)2-3
patie
ntse
xperience
treatmentd
elay
(v)M
axim
um-to
lerateddo
seof
80mgm
2 Ab
u-Ru
stum
etal
1997
[13]
60ndash100
over
1ho
urw
eek
45289
NA
NA
NA
(i)Nopatie
nthadfebrile
neutropenia
(i)100
priorc
hemotherapy
(1ndash8
priorregim
ens)
PhaseIISing
leagent
Markm
anetal
2001
[14]
80over
1ho
urw
eek
53(52)
25NA
NA
NA
Therapydiscon
tinuedin
(i)4patie
ntsw
hohadperip
heral
neurop
athy
(ii)1
patie
ntdu
etopainful
fingernailbeds
(i)100
platinum
andpaclita
xel
resistant
(ii)Th
erapywas
discon
tinuedin
5patie
ntsb
ecause
oftoxicity
(iii)Only13
(1)w
erem
odified
(doser
eductio
nor
treatment
delay)
becauseo
fsidee
ffects
PhaseIICom
binedwith
platinum
agent
Kiku
chietal
2005
[15]
80over
1ho
urw
eek
AUC2week
27gt6
818
483
NA
(i)Neutro
penia(
17)
thrombo
cytopenia(
51
)(ii)N
ocaseso
fperipheral
neurop
athy
(grades3
and4)
inweeklycombinedT-C
Cadron
etal2007
[16]
90over
1ho
urw
eek
AUC4week
24 9gt6le6
73 38NR
8105
675
(i)Grade
34neutropenia(
34)
andneutropenicfever
in2
(ii)N
auseaa
ndvomiting
and
fatig
uewerethe
mostfrequ
ent
nonh
ematologicalsid
eeffects
(i)Doser
eductio
nwas
necessary
in25of
patie
nts
Pign
atae
tal2008
[17]
60over
1ho
urw
eek
AUC2week
24(13)lowastlowast
1stline
385
2320
136
(i)Notoxicd
eath
was
recorded
(ii)G
rade
2anaemiawas
repo
rted
insevenpatie
nts(27)
(iii)Nofebrile
neutropeniaw
asob
served
(iv)G
rade
3and4neutropenia
was
recorded
infive(19)a
ndon
e(4
)patients
(v)G
rade
3thrombo
cytopenia
occurred
inon
epatient
(4)
BioMed Research International 11
Table1Con
tinued
Stud
yRe
gimen
119899()
PI(m
)RR
()
CR(119899)
MedianPF
S(m
)Median
OS
(m)
Adversee
ffects
Com
ments
Paclitaxel
dose
(mgm
2 )Ca
rbop
latin
dose
(mgm
2 )
Safrae
tal2014
[18]
80over
1ho
urw
eek
AUC2week
133
1stline
864
645
274
(i)Highera
naem
ia(grade
III+
IV68vs53)+
IVneutropenia(
144vs69)
decreasedgradeIIa
lopecia(
235
vs981
)and
thrombo
cytopenia
(grade
III+
IV0
vs23)
Havrilesky
etal
2003
[19]
80over
1ho
urw
eek
AUC2weekD1
D8D15
until
progressionCR
+8courses
29 21 8
Total
grou
pgt6lt6
83 100
38
16 15 1114
115
137
32
(i)Hem
atologictoxicitywas
common
(grade
3neutropenia
32n
ograde4
neutropenia
grade3
or4thrombo
cytopenia
142)
(i)To
xicitymanaged
bytre
atment
delaydo
seredu
ctionof
paclitaxel
ordiscon
tinuatio
nof
carbop
latin
vanderB
urgetal
2014
[20]
90over
1ho
urw
eek
AUC4weekD1
D8D15
D29
D36
D49
+6x
TCq3w
108
65 43
Total
grou
pgt6lt6
76 5816 42
26 158 13
(i)Neutro
penia3
0
thrombo
cytopenia8
febrile
neutropenia0
5
(ii)N
onhaem
atologictoxicitywas
low
(i)Treatm
entw
asdelayedin
16
anddo
seredu
cedin
2of
cycle
s
119899num
bero
fpatientsassessableforrespo
nsemm
onthsPIplatinum
treatmentfreeintervalRR
respo
nser
ateCR
com
pleterem
issionT
paclitaxelC
carbop
latin
PFS
progressio
nfre
esurvivalOSoverall
survivalN
An
otavailableinpapero
rabstractandNR
notyetreached
lowastlowastElderly
popu
lation
patient
agedge70
years
12 BioMed Research International
Numerous phase II studies have explored the tolerabilityand the activity of weekly paclitaxel either as a single agent orin combination with several other drugs or biological agents(Table 1) A number of regimens combining weekly paclitaxelwith carboplatin have been used as first-line treatment inovarian cancer Carboplatin has been administered weeklyat AUC of 2 with dose escalation in some studies whilepaclitaxel had been infused at 60ndash80mgm2week Thiscombined regimen was well tolerated with a low incidence ofbone marrow suppression Overall response rates have beenhigh in the range of 60ndash80 in most studies even in heavilypretreated patients with platinum-resistant disease (diseaserecurrence or progression within 6 months of the last lineof platinum-based therapy) [15ndash20 134] The promising datafrom these phase II trials then led to the evolution of largerphase III trials
Three phase III studies Japanese Gynecologic OncologyGroup- (JGOG-) Trial 3016 [21ndash23] Multicentre Italian Trialin Ovarian Cancer-Trial 7 (MITO-7) [25] and GynecologicOncology Group GOG-262 Trial [24] have explored dosedense therapy The results of these trials are summarised inTable 2
The Japanese Gynecologic Oncology Group (JGOG)conducted a randomized phase 3 trial of dose-dense weeklypaclitaxel 80mgm2week in combination with 3-weeklycarboplatin compared to standard 3-weekly carboplatin andpaclitaxel 180mgm2 in patients with advanced epithelialovarian peritoneal or fallopian tube cancer (JGOG 3016NOVEL trial) In both arms carboplatin was given at AUC6 and the median number of cycles was six In this largestudy (119899 = 637) with a median follow up of 77 months therewas an 11-month improvement in themedian progression freesurvival (PFS) in the dose-dense treatment group comparedwith the standard treatment arm (282 versus 175 monthsHR 076 95 CI 062ndash091 119901 = 00037) Median OS wasalso higher in the dose-dense treatment arm (1005 versus622 months HR 079 95 CI 063ndash099 119901 = 0039)On subgroup analysis suboptimally debulked patients withresidual disease of gt1 cm (119899 = 342) had a significantlyhigher median overall survival in the dose dense arm (512versus 335 months HR-075 95 CI 057ndash097 119901 = 0027)There was no significant advantage to dose-dense treatmentfor patients with optimally cytoreduced disease Dose-densetherapy survival benefits were also not seen in patients withclear cell or mucinous histology type unlike serous typeHowever patient treated with dose dense therapy had asignificantly higher frequency of hematologic toxicity thanwith the standard arm (212 versus 94) which resultedin lower treatment completion rates (63 versus 48) withfrequent episodes of delay (76 versus 67) and dosereductions (48versus 35) [21 22]Therewas no significantdifference in terms of overall quality of life between the twoarms (119901 = 046) [23]
Using a similar regimen as in JGOG-3016 a GynecologicOncology Group (GOG)-262 Trial was conducted in theUnited States In this group most patients had stage IIIdisease (66ndash70) and two-thirds had suboptimal debulkingwith residual disease of gt1 cm This was a randomized phase
III trial of 3 weekly paclitaxel versus dose-dense weeklypaclitaxel in combination with carboplatin in patients withadvanced epithelial ovarian peritoneal or fallopian tubecancer Though optional concurrent and maintenance beva-cizumab were received by the majority of patients in botharms (835 versus 841 resp) There was no significantdifference in PFS in the patients who received the dosedense paclitaxelcarboplatin regimen compared to those whoreceived the standard paclitaxelcarboplatin regimen (148versus 143 months HR 097 95 CI 079ndash118) Howeverin a subgroup analysis there was a significant difference inPFS in the dose dense paclitaxel arm who did not receivebevacizumab 119899 = 112 (142 versus 103 months HR 059 95CI 037ndash096 119901 = 0003) Overall survival data is still imma-ture There was higher frequency of grade 3 anaemia (408versus 157 119901 lt 0001) and grade 2 sensory neuropathy(259 versus 178 119901 = 0012) but a lower incidence ofneutropenia (72 versus 83 119901 lt 0001) [24]
In 2008 the Multicentre Italian Trials in Ovarian Cancer(MITO-7) randomised 810 women in a phase 3 trial toreceive either standard carboplatin (AUC = 6) and paclitaxel175mgm2 every 3 weeks or a weekly schedule of paclitaxel(60mgm2) with carboplatin (AUC = 2) The majority ofpatients in both arms (83ndash90) received six cycles of therapyMost patients (58ndash63) had stage II1 disease 23 of themwere suboptimally debulked Median PFS did not differsignificantly (173 months and 183 months 119901 = 066)between the standard and dose-dense arms respectivelyThere was no significant difference in response rate betweenthe two arms nor the estimated 2-year overall survivalSubgroup analysis did not identify any subgroup that mayhave benefited from the dose-dense regimen Unlike theJGOG-3016 trial the incidence of grade 3-4 neutropenia wassignificantly lower in the dose-dense group compared to the3-weekly regimen (42 versus 50) A similar pattern wasseen for the incidence of febrile neutropenia (lt1 versus 3119901 = 002) thrombocytopenia (1 versus 7 119901 lt 0001)and other nonhaematological toxicities such as alopeciavomiting renal dysfunction and neuropathy Quality of lifewas reported to be significantly better in the dose-dense arm(119901 lt 00001) which was discordant with the JGOG-3016quality of life data [25]
In summary there was significant improvement inmedian PFS and overall survival in studies using paclitaxelat 80mgm2week dose-dense therapy [21 24] but withhigher haematological toxicity whereas MITO-7 [25] whichwas using paclitaxel at 60mgm2week was only equivalentlyeffective but less toxicThis does not conclude that the higherpaclitaxel dose is more clinically beneficial as there are manyother confounding factors in all three studies
In a multivariate analysis the JGOG-3016 study [21]reported that a lower dose intensity of paclitaxel (lt80) wasassociated with poorer overall survival (hazard ratio = 14295 confidence interval 112ndash181 119901 = 0004) however itmust be highlighted that the investigational arm carboplatinschedules were not standardised in these studies The JGOGand GOG trials delivered a 3-weekly carboplatin (AUC =6) arm whereas in the MITO-7 study the carboplatin was
BioMed Research International 13
Table2Ph
aseIIIstu
dies
onintravenou
sdose-densep
aclitaxel
Stud
yRe
gimen
119899
MedianPF
S(m
)
Median
OS
(m)
Adversee
ffects
Com
ments
Katsu
matae
tal2009
[21]
Katsu
matae
tal2013
[22]
Haranoetal2014
[23]
JGOG3016
631
(i)Haematologicaltoxicityhigh
erin
dose
dense-211versus
94
Lower
treatmentcom
pletionin
dose-dense
63versus
48
Frequent
episo
deso
fdelay
indo
se-dense
76versus
67
Doser
eductio
nsin
dose-dense
48versus
35
Nosig
nificantd
ifference
inoverallQ
OL
betweenbo
thgrou
ps(119901=046)
Paclitaxel80m
gm
2D18
15+carbop
latin
AUC63
weeklyversus
Paclitaxel180
mgm
2+
carbop
latin
AUC63
weekly
312
282
1005
Both
givenfor6
ndash9cycle
s319
175
622
Chan
etal2013
[24]
GOG-262
(i)Higherfrequ
ency
ofgrade3
anaemia
(408versus
157119901lt0001)
grade2
sensoryneurop
athy
(259versus
178
119901=0012)b
utlower
incidenceo
fneutropenia(
72versus
83119901lt0001)
Paclitaxel80m
gm
2D18
15+carbop
latin
AUC63
weeklyversus
Paclitaxel175
mgm
2+
carbop
latin
AUC63
weekly
346
148
NR
Both
givenfor6
cycle
s346
143
NR
Bevacizumab
given
optio
nally
112
(did
not
receive
bevazicumab)
142vs
103
Pign
atae
tal2014
[25]
MITO-7
810
(i)Lo
wer
incidenceo
fgrade
3-4
neutropenia(
42versus
50)febrile
neutropenia(lt1v
ersus3
119901=002)
thrombo
cytopenia(
1versus7
119901lt0001)andothern
onhaem
atological
toxicitie
ssuchas
alop
eciavom
iting
renald
ysfunctio
nandneurop
athy
Qualityof
lifeb
etterindo
sedensea
rm(119901lt00001)
Paclitaxel60m
gm
2 weekly+carbop
latin
AUC
2weeklyversus
Paclitaxel175
mgm
2+
carbop
latin
AUC63
weekly
406
404
183 173
77lowast
79lowast
119899num
bero
fpatientsmm
onthsDday
PFSprogressionfre
esurvivalOSoverallsurvivalNAnot
availableinpapero
rabstractandNR
notyetreached
lowastSurvivalrateat2years
14 BioMed Research International
dose-dense (AUC 2 weekly) Although it is possible that thedose scheduling for the platinum-based agent is not essentialfor a survival benefit as shown by previous studies usingdose-dense cisplatin direct cross-trial comparison cannot bemade Unlike paclitaxel carboplatin probably requires peakdose for optimal therapeutic benefit hence this may accountfor the inferior survival outcome in MITO-7 trial Anotherconfounding factor may be difference in ethnicity All threestudies used different ethnic populations and Asian patientsin JGOG-3016 appear to have better survival outcomes thanthe MITO-7 Western population Ethnicity with possibleunderlying genetic causes may be responsible for the variableresponses to chemotherapy across individuals [135] This wasexplored by Millward et al who studied 68 Caucasian andAsian lung cancer patients treated with a combination ofpaclitaxel and carboplatin and found that the incidence offebrile neutropenia was 50 of an initially treated cohortof Asians and when carboplatin was subsequently dosereduced in all Asian patients the overall incidence of febrileneutropenia was also reduced to 26 [136]
Although early clinical data from phase I and phaseII dose-dense paclitaxel trials in advanced ovarian cancerwere promising the results from phase III studies in havebeen inconsistent as a result of differences in paclitaxel dosecarboplatin AUC and schedule addition of bevacizumabas well as different ethnic populations The results of arecently completed randomised three arms GynaecologicCancer InterGroup (GCIG) phase II trial ICON 8 mayfurther inform the clinical benefit of dose dense paclitaxeltherapy
This multicentre trial involving 111 centres in the UKSouth Korea Mexico Ireland Australia and New Zealandwith a target population of 1485 patients with stage IC-IV epithelial ovarian cancer or peritoneal or fallopian tubecancer compared two dose-dense arms (i) JGOG-like armcarboplatin AUC 5 plus weekly 80mgm2 paclitaxel and (ii)MITO-7-like arm weekly carboplatin AUC 167 plus weekly80mgm2 paclitaxel to the standard 3-weekly treatment(carboplatin AUC 5 plus 175mgm2 paclitaxel) for stage IC toIV epithelial ovarian cancer The dose-dense arms of MITO-7 and JGOG-3016 as well as the ethnic heterogeneity will befurther addressed
10 Intraperitoneal (IP) Chemotherapy
In addition to dose and scheduling the route of adminis-tration of chemotherapy agents plays an important role inoutcome Intraperitoneal spread is common and likely anearly event in epithelial ovarian cancer hence the deliveryof chemotherapy intraperitoneally in theory would exposethe microcirculation of tumour to higher doses of drug thansystemic administration while limiting systemic toxicityTheideal drug for IP chemotherapy is one that is systemicallyeffective penetrates deep into the inner core of tumour tissueand remains within the peritoneal cavity for a prolongedperiod of time [137ndash139]
Early clinical studies confirmed that indeed the peritonealcavity could be exposed to 10 to 20-fold higher (cisplatin
and carboplatin) drug concentration than when using theintravenous approach and since 1978 this route had beenadopted as a form of therapeutic intervention [137 139]A subsequent phase I trial showed that IP paclitaxel haddose-limiting toxicity in the form of abdominal pain [140]Another phase 1 GOG pilot study administered weekly IPpaclitaxel at an initial dose of 20mgm2 for 16 weeks to33 patients and found that IP paclitaxel at this dose wasfeasible and well tolerated At dose levels 60 to 65mgm2there were significant levels of paclitaxel for a week afterdrug administration suggesting very slow clearance andcontinuous exposure of the peritoneal cavity to active drugconcentrations [132]
Hence this initiated a phase II study [141] that used pacli-taxel intraperitoneally at a dose of 60ndash65mgm2week In thisphase II GOG study 76 patients with small-volume resid-ual disease carcinoma (05 cm or less) involving the ovaryperitoneal or fallopian tube were treated with paclitaxel60mgm2week intraperitoneally for 16 weeks followed bysurgical evaluation in patients without disease progressionThe Gynaecologic Oncology group (GOG) currently definesno visible disease as microscopic disease being the idealsurgical outcome 75 of patients had received prior systemictherapy and 70 received all 16 courses that were planned Of28 patients with microscopic disease at the start of therapy61 achieved a surgically defined complete response whereasonly 1 out of 31 patients with macroscopic disease achieved acomplete response The median time-to-recurrence was 167months with an estimated survival rate at 2 years being 58Treatment was generally well tolerated [141]
Another study looked into the effect of IP paclitaxel asconsolidation therapy in advanced ovarian cancer Twenty-eight patients who had initial residual macroscopic disease(lt1 cm) after primary surgery or interval debulking but hadcomplete pathological response following standard treatmentwith at least 6 cycles of platinum-based chemotherapy regi-men received paclitaxel 60mgm2week intraperitoneally for12ndash16 weeks as consolidation therapy The median time torecurrence was 25 months but overall survival did not differsignificantly when compared with control group submittedto observation only Treatment-related toxicity was mild andtechnical difficulties were observed in 11 of patients [142]
Multicenter randomised phase 3 trials as well as meta-analysis of IP chemotherapy have been performed anddemonstrated that chemotherapy drugs administered intra-peritoneally are superior to intravenous standard regimensin patient with optimally debulked epithelial ovarian cancerThe most impressive data comes from GOG 114 [14] and172 trial [143] In GOG 114 patients received either sixcycles of intravenous paclitaxel 135mgm2 and cisplatin75mgm2 every 3 weeks or intravenous carboplatin (AUC= 9) every 28 days for two cycles followed by six 3-weeklycycles of intravenous paclitaxel 135mgm2 and IP cisplatin100mgm2 [14] whereas in GOG 172 patients received eitherintravenous paclitaxel 135mgm2 followed by intravenouscisplatin 75mgm2 or intravenous paclitaxel 135mgm2 fol-lowed by IP combination of cisplatin 100mgm2 and pacli-taxel 60mgm2 on day 8 Both trials had a combined total
BioMed Research International 15
of 876 women with stage III epithelial ovarian carcinomaoptimally debulked to le1 cm residual tumour [143] Themedian follow-up for GOG 114 [14] was 138 years with GOG172 [143] was 97 years The primary results of the individualtrials reported up to 6-month improvement in median PFSfollowing IP therapy In the combined analysis of the datafrom both trials the data continued to show a 5-monthdifference in favour of IP therapy (25 versus 20 months)which translates into 16 reduction in the hazard ratio forprogression (119901 = 003) In GOG 114 [14] reported in 2001there was only borderline improvement in overall survivalassociated with this regimen (median 63 versus 52 monthsrelative risk 081 119901 = 005)
However in combined analysis in 2013 which was pre-sented at the Society of Gynecologic Oncology AnnualMeeting [144] the overall survival showed an 11-monthimprovement in favour of IP therapy in GOG 114 whereasGOG 172 reported a 16-month survival advantage Amongpatients treated with IP therapy the 5-year survival rateincreased from 18 following completion of 1-2 cycles to 59for patients who completed 5-6 cycles of treatment Howeverthere was increased toxicity observed in the IP arm grade 3-4 leukopenia thrombocytopenia and abdominal pain Only42 of patients in the GOG172 trial [143] completed all sixcycles of planned treatment in the IP arm while 18 ofpatients in GOG 114 trial [14] received fewer than two coursesof IP chemotherapy
Another randomised phase III trial involving patientswith stages II-III epithelial ovarian carcinoma is the GOG252 study with three arms Arm 1-dose-dense intravenouscarboplatin and paclitaxel Arm 2-dose-dense intravenouspaclitaxel and IP carboplatin and Arm 3 consists of 3-weeklyintravenous paclitaxel (day 1) followed by IP cisplatin (day 2)and IP paclitaxel (day 3) regimen All three arms also incor-porate the combination and maintenance of bevacizumabGOG 252 has completed accrual and results are awaited [139]
11 Newer Forms of Paclitaxel
Development of next-generation taxanes has taken place overthe past 40 years aimed at eliminating toxicity improvingefficacy and ease of administration Abraxane is a novelcompound which incorporates paclitaxel into an albuminnanoparticle soluble in saline hence eliminating the needfor Cremophor EL which is responsible for hypersensitivityreactions experienced during paclitaxel infusion [145] Thenanoparticle albumin in nab-paclitaxel is able to bind toglycoprotein gp60 receptor an albumin receptor and activatecaveolin-1 a protein that in human is encoded byCAV-1 geneleading to formation of caveoli hence allowing nab-paclitaxelto migrate across the endothelial cell membrane into theinterstitial space leading to higher intratumoural drug con-centration In addition Abraxane exhibits linear pharma-cokinetics and can therefore be given at a relatively higherdose than standard intravenous paclitaxel leading to a highertherapeutic ratio and heightened efficacy in solid tumoursmainlymetastatic breast cancer [146 147] Nab-paclitaxel hadFDA approval in 2005 for treatment of breast cancer [148]
Nab-paclitaxel has been studied in recurrent ovariancancer As a single agent in phase II 44 patients withrecurrent ovarian cancer were treated with Nab-paclitaxel260mgm2 intravenously for 30 minutes every 3 weeks for6 cycles Ninety-two percent of patients were platinum-sensitive while 89 had had previous exposure to standardtaxane The objective response rate was 64 with 15 patientsachieving complete response and 13 of them had partialresponse Estimated median PFS was 85 months No hyper-sensitivity reactions were observed and there were infrequentcases of grade 4 neutropenia (11) and grade 2-3 neuropathy(13) [149]
Another phase II study by GOG enrolled 51 patients withplatinum- and taxane-resistant recurrent ovarian cancer outof which 47 were evaluable The objective response rate was38 with one patient achieving a complete response and 10patients a partial response The median PFS was 45 monthswhile overall survival rate was 174 months Severe haema-tological and nonhaematological toxicities including neuro-toxicity were uncommon These results are quite impressivegiven the treatment population consisted of patients withvery poor prognosis with a median platinum and taxane freeinterval of 21 days and 70 had their recurrence within 3months of completion of primary treatment [150] Severalother trials of this formulation are in progress
Paclitaxel poliglumex (PPX) also known as Xyotax isanother prodrug a novel conjugate of paclitaxel and 120572-poly-L-glutamic acid which accumulates within tumour tissuedue to increased permeability of the tumour vessels and lackof lymphatic drainage [148 151 152] Paclitaxel poliglumexenhances solubility of paclitaxel allows direct delivery tothe intratumoural microenvironment and allows prolongedexposure to the active drug while minimising systemictoxicities [151] In Phase I dose escalation studies as a singleagent the recommended dose of PPX was 235mgm2 over 10minutes every 3 weeks or 70mgm2 weekly [153] In a PhaseII GOG study of relapsed ovarian cancer a response rate of16 was seen with infrequent serious adverse events grade3 and 4 neutropenia (24 and 20) and grade 3 neuropathy(24) [154] A phase III trial (GOG-0212) on the use of PPXas consolidation ormaintenance therapy in advanced ovariancancer is in progress
DHA-paclitaxel also known as Taxoprexin is a prodrugwhere paclitaxel is covalently conjugated with the naturallyoccurring omega-3 fatty acid docosahexaenoic acid (DHA)a fatty acid that is easily taken up by tumour cells henceincreasing intratumoural concentration of paclitaxel leadingtumour cell apoptosis [155 156] DHA-paclitaxel exhibitslinear pharmacokinetics and lower toxicity and also ease ofadministration when compared to conventional paclitaxeland has demonstrated antineoplastic activity in animal mod-els of cancer as well as in a phase III trial involving metastaticmelanoma [156ndash160] In a recent study on human ovariancancer cells it was found that DHA could reverse paclitaxelresistance by inhibiting P-gp as well as downregulatingthe expression of multidrug resistance associated proteins(MRP) and inhibiting the activity of NF-120581B and p38 MAPKsignalling pathways [161]
16 BioMed Research International
12 Future Directions
A plateau has been reached regarding the benefits associatedwith standard 3-weekly intravenous administration of cyto-toxic chemotherapy in advanced epithelial ovarian cancerThe ongoing battle for a better treatment regimen to delayrelapse promote remission and most importantly improvethe quality of life of patients with advanced epithelial ovariancancer need not to go further than the ability to relook at thechemotherapy agents that are already available in a differentapproach
Novel compounds to date have not yet shown clinicalsuperiority and parent compounds such as paclitaxel con-tinue to surprise us with their feasibility effectiveness andmanageable toxicity profiles Intraperitoneal paclitaxel willrequire further evaluation Better effort in understanding themechanism of action of drugs including the role of dosescheduling and the effect on the immune systemmay providea more cost-effective route to better clinical outcomes
Conflict of Interests
The authors declare no conflict of interests in this work
Acknowledgments
The authors would like to thank the many researchers whohave contributed to our current knowledge of paclitaxelNirmala Kampan is supported by Australian Monash Uni-versity Institute of Graduate Research Scholarship as wellas Universiti Kebangsaan Malaysia Postgraduate ScholarshipAward Mutsa Madondo has received Postgraduate Pub-lication Award from Monash University and MagdalenaPlebanski has been awarded Senior NHMRC Fellowship
References
[1] Australian Institute of Health and Welfare and National Breastand Ovarian Cancer Centre (Australia) Ovarian Cancer inAustralia AnOverview 2010 Cancer Series Australian Instituteof Health and Welfare Canberra Australia 2010
[2] R E Bristow R S Tomacruz D K Armstrong E L Trimbleand F J Montz ldquoSurvival effect of maximal cytoreductivesurgery for advanced ovarian carcinoma during the platinumera a meta-analysisrdquo Journal of Clinical Oncology vol 20 no 5pp 1248ndash1259 2002
[3] ZKempand JA Ledermann ldquoUpdate onfirst-line treatment ofadvanced ovarian carcinomardquo International Journal of WomenrsquosHealth vol 5 no 1 pp 45ndash51 2013
[4] A du Bois H-J Luck W Meier et al ldquoA randomized clinicaltrial of cisplatinpaclitaxel versus carboplatinpaclitaxel as first-line treatment of ovarian cancerrdquo Journal of the National CancerInstitute vol 95 no 17 pp 1320ndash1330 2003
[5] R F Ozols B N Bundy B E Greer et al ldquoPhase III trialof carboplatin and paclitaxel compared with cisplatin andpaclitaxel in patients with optimally resected stage III ovariancancer A Gynecologic Oncology Group studyrdquo Journal ofClinical Oncology vol 21 no 17 pp 3194ndash3200 2003
[6] W P McGuire W J Hoskins M F Brady et al ldquoCyclophos-phamide and cisplatin compared with paclitaxel and cisplatin
in patients with stage III and stage IV ovarian cancerrdquoThe NewEngland Journal of Medicine vol 334 no 1 pp 1ndash6 1996
[7] W P McGuire W J Hoskins M F Brady et al ldquoCyclophos-phamide and cisplatin versus paclitaxel and cisplatin a phase IIIrandomized trial in patients with suboptimal stage IIIIV ovar-ian cancer (from the gynecologic oncology group)rdquo Seminars inOncology vol 23 no 5 supplement 12 pp 40ndash47 1996
[8] M J Piccart K Bertelsen K James et al ldquoRandomized inter-group trial of cisplatin-paclitaxel versus cisplatin-cyclophosph-amide inwomenwith advanced epithelial ovarian cancer three-year resultsrdquo Journal of the National Cancer Institute vol 92 no9 pp 699ndash708 2000
[9] P A Vasey G C Jayson A Gordon et al ldquoPhase III random-ized trial of docetaxel-carboplatin versus paclitaxel-carboplatinas first-line chemotherpy for ovarian carcinomardquo Journal of theNational Cancer Institute vol 96 no 22 pp 1682ndash1691 2004
[10] B Gronlund C Hogdall H H Hansen and S A EngelholmldquoResults of reinduction therapy with paclitaxel and carboplatinin recurrent epithelial ovarian cancerrdquo Gynecologic Oncologyvol 83 no 1 pp 128ndash134 2001
[11] T M Loffler W Freund J Lipke and T-U HausamenldquoSchedule- and dose-intensified paclitaxel as weekly 1-hourinfusion in pretreated solid tumors results of a phase III trialrdquoSeminars in Oncology vol 23 no 6 supplement 16 pp 32ndash341996
[12] D Fennelly C Aghajanian F Shapiro et al ldquoPhase I and phar-macologic study of paclitaxel administered weekly in patientswith relapsed ovarian cancerrdquo Journal of Clinical Oncology vol15 no 1 pp 187ndash192 1997
[13] N R Abu-Rustum C Aghajanian R R Barakat D Fennelly FShapiro and D Spriggs ldquoSalvage weekly paclitaxel in recurrentovarian cancerrdquo Seminars inOncology vol 24 no 5 supplement15 pp S15-62ndashS15-67 1997
[14] M Markman B N Bundy D S Alberts et al ldquoPhase III trialof standard-dose intravenous cisplatin plus paclitaxel versusmoderately high-dose carboplatin followed by intravenouspaclitaxel and intraperitoneal cisplatin in small-volume stageIII ovarian carcinoma an intergroup study of the gynecologiconcology group Southwestern Oncology Group and EasternCooperativeOncologyGrouprdquo Journal of Clinical Oncology vol19 no 4 pp 1001ndash1007 2001
[15] A Kikuchi H Sakamoto and T Yamamoto ldquoWeekly car-boplatin and paclitaxel is safe active and well tolerated inrecurrent ovarian cancer cases of Japanese women previouslytreated with cisplatin-containing multidrug chemotherapyrdquoInternational Journal of Gynecological Cancer vol 15 no 1 pp45ndash49 2005
[16] I Cadron K Leunen F Amant T van Gorp P Nevenand I Vergote ldquoThe lsquoLeuvenrsquo dose-dense paclitaxelcarboplatinregimen in patients with recurrent ovarian cancerrdquo GynecologicOncology vol 106 no 2 pp 354ndash361 2007
[17] S Pignata E Breda G Scambia et al ldquoA phase II studyof weekly carboplatin and paclitaxel as first-line treatment ofelderly patients with advanced ovarian cancer A Multicen-tre Italian Trial in Ovarian cancer (MITO-5) studyrdquo CriticalReviews in OncologyHematology vol 66 no 3 pp 229ndash2362008
[18] T Safra S Shamai J Greenberg et al ldquoWeekly carboplatinwith paclitaxel compared to standard three-weekly treatment inadvanced epithelial ovarian carcinomamdasha retrospective studyrdquoGynecologic Oncology vol 132 no 1 pp 18ndash22 2014
BioMed Research International 17
[19] L J Havrilesky A A Alvarez R A Sayer et al ldquoWeekly low-dose carboplatin and paclitaxel in the treatment of recurrentovarian and peritoneal cancerrdquo Gynecologic Oncology vol 88no 1 pp 51ndash57 2003
[20] M van der BurgW Onstenk I Boere et al ldquoLong-term resultsof a randomised phase III trial of weekly versus three-weeklypaclitaxelplatinum induction therapy followed by standardor extended three-weekly paclitaxelplatinum in Europeanpatients with advanced epithelial ovarian cancerrdquo EuropeanJournal of Cancer vol 50 no 15 pp 2592ndash2601 2014
[21] N Katsumata M Yasuda F Takahashi et al ldquoDose-densepaclitaxel once a week in combination with carboplatin every3 weeks for advanced ovarian cancer a phase 3 open-labelrandomised controlled trialrdquoThe Lancet vol 374 no 9698 pp1331ndash1338 2009
[22] N Katsumata M Yasuda S Isonishi et al ldquoLong-term resultsof dose-dense paclitaxel and carboplatin versus conventionalpaclitaxel and carboplatin for treatment of advanced epithelialovarian fallopian tube or primary peritoneal cancer (JGOG3016) a randomised controlled open-label trialrdquo The LancetOncology vol 14 no 10 pp 1020ndash1026 2013
[23] K Harano F Terauchi N Katsumata et al ldquoQuality-of-lifeoutcomes from a randomized phase III trial of dose-denseweekly paclitaxel and carboplatin compared with conventionalpaclitaxel and carboplatin as a first-line treatment for stage II-IV ovarian cancer Japanese Gynecologic OncologyGroup Trial(JGOG3016)rdquo Annals of Oncology vol 25 no 1 pp 251ndash2572014
[24] J Chan M F Brady R Penson et al ldquoPhase III trial ofevery-3-weeks paclitaxel vs dose dense weekly paclitaxel withcarboplatin +minus bevacizumab in epithelial ovarian peritonealfallopian tube cancer GOG 262 (NCT01167712)rdquo InternationalJournal of Gynecological Cancer vol 23 no 8 supplement 1 pp9ndash10 2013
[25] S Pignata G Scambia D Katsaros et al ldquoCarboplatin pluspaclitaxel once a week versus every 3 weeks in patients withadvanced ovarian cancer (MITO-7) a randomisedmulticentreopen-label phase 3 trialrdquoThe Lancet Oncology vol 15 no 4 pp396ndash405 2014
[26] V Walsh and J Goodman ldquoFrom taxol to Taxol the changingidentities and ownership of an anti-cancer drugrdquo MedicalAnthropology vol 21 no 3-4 pp 307ndash336 2002
[27] R Renneberg ldquoBiotech History yew trees paclitaxel synthesisand fungirdquo Biotechnology Journal vol 2 no 10 pp 1207ndash12092007
[28] J E Liebmann J A Cook C Lipschultz D Teague J Fisherand J B Mitchell ldquoCytotoxic studies of paclitaxel (Taxol) inhuman tumour cell linesrdquo British Journal of Cancer vol 68 no6 pp 1104ndash1109 1993
[29] J J Manfredi and S B Horwitz ldquoTaxol an antimitotic agentwith a newmechanism of actionrdquo Pharmacology andTherapeu-tics vol 25 no 1 pp 83ndash125 1984
[30] D G I Kingston ldquoRecent advances in the chemistry of taxolrdquoJournal of Natural Products vol 63 no 5 pp 726ndash734 2000
[31] D G I Kingston ldquoThe shape of things to come structural andsynthetic studies of taxol and related compoundsrdquo Phytochem-istry vol 68 no 14 pp 1844ndash1854 2007
[32] V Walsh and J Goodman ldquoCancer chemotherapy biodiversitypublic and private property the case of the anti-cancer drugTaxolrdquo Social Science amp Medicine vol 49 no 9 pp 1215ndash12251999
[33] P H Wiernik E L Schwartz J J Strauman J P Dutcher RB Lipton and E Paietta ldquoPhase I clinical and pharmacokineticstudy of taxolrdquo Cancer Research vol 47 no 9 pp 2486ndash24931987
[34] W P McGuire E K Rowinsky N B Rosenhein et alldquoTaxol a unique antineoplastic agent with significant activityin advanced ovarian epithelial neoplasmsrdquo Annals of InternalMedicine vol 111 no 4 pp 273ndash279 1989
[35] ldquoDiscovery and development of taxolrdquo in Taxol Science andApplications M W M E Suffness Ed pp 3ndash25 CRC PressBoca Raton Fla USA 1995
[36] M J Piccart and F Cardoso ldquoProgress in systemic therapy forbreast cancer an overview and perspectivesrdquo European Journalof Cancer Supplement vol 1 no 2 pp 56ndash69 2003
[37] P Bonomi K B Kim and J Kugler ldquoComparison of survival forstage IIIB versus stage IV non-small cell lung cancer (NSCLC)patients with etoposide-cisplatin versus taxol-cisplatin an East-ern Cooperative Oncology Group (ECOG) trialrdquo in Proceedingsof the American Society of Clinical Oncology vol 16 p 454a1997
[38] D Guenard F Gueritte-Voegelein J Dubois and P PotierldquoStructure-activity relationships of Taxol and Taxotere ana-loguesrdquo Journal of the National Cancer Institute Monographsno 15 pp 79ndash82 1993
[39] D G I Kingston ldquoTaxol the chemistry and structure-activityrelationships of a novel anticancer agentrdquo Trends in Biotechnol-ogy vol 12 no 6 pp 222ndash227 1994
[40] E K Rowinsky and R C Donehower ldquoPaclitaxel (taxol)rdquo TheNew England Journal of Medicine vol 332 no 15 pp 1004ndash10141995
[41] J Parness and S B Horwitz ldquoTaxol binds to polymerizedtubulin in vitrordquo Journal of Cell Biology vol 91 no 2 pp 479ndash487 1981
[42] A Dammermann A Desai and K Oegema ldquoTheminus end insightrdquo Current Biology vol 13 no 15 pp R614ndashR624 2003
[43] CWiese and Y Zheng ldquoMicrotubule nucleation 120574-tubulin andbeyondrdquo Journal of Cell Science vol 119 no 20 pp 4143ndash41532006
[44] A Ganguly H Yang and F Cabral ldquoPaclitaxel-dependent celllines reveal a novel drug activityrdquo Molecular Cancer Therapeu-tics vol 9 no 11 pp 2914ndash2923 2010
[45] P B Schiff and S B Horwitz ldquoTaxol stabilizes microtubules inmouse fibroblast cellsrdquo Proceedings of the National Academy ofSciences of the United States of America vol 77 no 3 pp 1561ndash1565 1980
[46] P B Schiff J Fant and S B Horwitz ldquoPromotion of micro-tubule assembly in vitro by Taxolrdquo Nature vol 277 no 5698pp 665ndash667 1979
[47] D Zhang R Yang S Wang and Z Dong ldquoPaclitaxel new usesfor an old drugrdquoDrug Design Development andTherapy vol 8pp 279ndash284 2014
[48] S Rao G A Orr A G Chaudhary D G I Kingston and SB Horwitz ldquoCharacterization of the taxol binding site on themicrotubule 2-(m-Azidobenzoyl)taxol photolabels a peptide(amino acids 217-231) of beta-tubulinrdquoThe Journal of BiologicalChemistry vol 270 no 35 pp 20235ndash20238 1995
[49] F Wang Y Cao W Zhao H Liu Z Fu and R Han ldquoTaxolinhibits melanoma metastases through apoptosis inductionangiogenesis inhibition and restoration of E-cadherin andnm23 expressionrdquo Journal of Pharmacological Sciences vol 93no 2 pp 197ndash203 2003
18 BioMed Research International
[50] A Sevko V Kremer C Falk et al ldquoApplication of paclitaxel inlow non-cytotoxic doses supports vaccination with melanomaantigens in normal micerdquo Journal of Immunotoxicology vol 9no 3 pp 275ndash281 2012
[51] T Kreis and R Vale Guidebook to the Cytoskeletal and MotorProteins Oxford University Press Oxford UK 2nd edition1999
[52] P Giannakakou D L Sackett Y-K Kang et al ldquoPaclitaxel-resistant human ovarian cancer cells have mutant 120573-tubulinsthat exhibit impaired paclitaxel-driven polymerizationrdquo TheJournal of Biological Chemistry vol 272 no 27 pp 17118ndash171251997
[53] E Rakovitch W Mellado E J Hall T K Pandita S Sawantand C R Geard ldquoPaclitaxel sensitivity correlates with p53status and DNA fragmentation but not G2M accumulationrdquoInternational Journal of Radiation Oncology Biology Physics vol44 no 5 pp 1119ndash1124 1999
[54] S W Lowe S Bodis A McClatchey et al ldquop53 status and theefficacy of cancer therapy in vivordquo Science vol 266 no 5186 pp807ndash810 1994
[55] C C Zhang J-M Yang E White M Murphy A Levine andW N Hait ldquoThe role of MAP4 expression in the sensitivity topaclitaxel and resistance to vinca alkaloids in p53 mutant cellsrdquoOncogene vol 16 no 12 pp 1617ndash1624 1998
[56] K Fukasawa T Choi R Kuriyama S Rulong and G F VandeWoude ldquoAbnormal centrosome amplification in the absence ofp53rdquo Science vol 271 no 5256 pp 1744ndash1747 1996
[57] T-H Wang Y-H Chan C-W Chen et al ldquoPaclitaxel (Taxol)upregulates expression of functional interleukin-6 in humanovarian cancer cells through multiple signaling pathwaysrdquoOncogene vol 25 no 35 pp 4857ndash4866 2006
[58] E Yakirevich E Sabo I Naroditsky Y Sova O Lavie andM B Resnick ldquoMultidrug resistance-related phenotype andapoptosis-related protein expression in ovarian serous carcino-masrdquo Gynecologic Oncology vol 100 no 1 pp 152ndash159 2006
[59] G Szakacs J K Paterson J A Ludwig C Booth-Genthe andM M Gottesman ldquoTargeting multidrug resistance in cancerrdquoNature Reviews Drug Discovery vol 5 no 3 pp 219ndash234 2006
[60] L W Pfannenstiel S S K Lam L A Emens E M Jaffeeand T D Armstrong ldquoPaclitaxel enhances early dendritic cellmaturation and function through TLR4 signaling in micerdquoCellular Immunology vol 263 no 1 pp 79ndash87 2010
[61] N Klauber S Parangi E Flynn E Hamel and R J DrsquoAmatoldquoInhibition of angiogenesis and breast cancer in mice by themicrotubule inhibitors 2-methoxyestradiol and Taxolrdquo CancerResearch vol 57 no 1 pp 81ndash86 1997
[62] D Belotti V Vergani T Drudis et al ldquoThe microtubule-affecting drug paclitaxel has antiangiogenic activityrdquo ClinicalCancer Research vol 2 no 11 pp 1843ndash1849 1996
[63] D H Lau L Xue L J Young P A Burke and A T CheungldquoPaclitaxel (Taxol) an inhibitor of angiogenesis in a highlyvascularized transgenic breast cancerrdquo Cancer Biotherapy andRadiopharmaceuticals vol 14 no 1 pp 31ndash36 1999
[64] X Jiang ldquoHarnessing the immune system for the treatment ofbreast cancerrdquo Journal of Zhejiang University Science B vol 15no 1 pp 1ndash15 2014
[65] A Gadducci D Katsaros P Zola et al ldquoWeekly low-dosepaclitaxel as maintenance treatment in patients with advancedovarian cancer who had microscopic residual disease atsecond-look surgery after 6 cycles of paclitaxelplatinum-basedchemotherapy Results of an open noncomparative phase 2
multicenter italian study (after-6 protocol 2)rdquo InternationalJournal of Gynecological Cancer vol 19 no 4 pp 615ndash619 2009
[66] R S Bhatt J Merchan R Parker et al ldquoA phase 2 pilot trial oflow-dose continuous infusion or lsquometronomicrsquo paclitaxel andoral celecoxib in patients with metastatic melanomardquo Cancervol 116 no 7 pp 1751ndash1756 2010
[67] M Caballero J J Grau J L Blanch et al ldquoSerum vascularendothelial growth factor as a predictive factor in metronomic(weekly) paclitaxel treatment for advanced head and neckcancerrdquo Archives of OtolaryngologymdashHead and Neck Surgeryvol 133 no 11 pp 1143ndash1148 2007
[68] J Alexandre Y Hu W Lu H Pelicano and P Huang ldquoNovelaction of paclitaxel against cancer cells bystander effect medi-ated by reactive oxygen speciesrdquo Cancer Research vol 67 no 8pp 3512ndash3517 2007
[69] T Hadzic N Aykin-Burns Y Zhu et al ldquoPaclitaxel combinedwith inhibitors of glucose and hydroperoxide metabolismenhances breast cancer cell killing viaH
2O2-mediated oxidative
stressrdquo Free Radical Biology and Medicine vol 48 no 8 pp1024ndash1033 2010
[70] C A Sherman-Baust K G Becker W H Wood III Y Zhangand P J Morin ldquoGene expression and pathway analysis of ovar-ian cancer cells selected for resistance to cisplatin paclitaxel ordoxorubicinrdquo Journal of Ovarian Research vol 4 no 1 article21 2011
[71] R Agarwal and S B Kaye ldquoOvarian cancer strategies for over-coming resistance to chemotherapyrdquo Nature Reviews Cancervol 3 no 7 pp 502ndash516 2003
[72] T Acker and K H Plate ldquoRole of hypoxia in tumorangiogenesismdashmolecular and cellular angiogenic crosstalkrdquoCell and Tissue Research vol 314 no 1 pp 145ndash155 2003
[73] M Hockel and P Vaupel ldquoBiological consequences of tumorhypoxiardquo Seminars in Oncology vol 28 supplement 8 no 2 pp36ndash41 2001
[74] L Huang Q-H Zhang Q-L Ao H Xing Y-P Lu and DMa ldquoEffect of hypoxia on the chemotherapeutic sensitivity ofhuman ovarian cancer cells to paclitaxel and its mechanismrdquoZhonghua Zhong Liu Za Zhi vol 29 no 2 pp 96ndash100 2007
[75] N Rohwer and T Cramer ldquoHypoxia-mediated drug resistancenovel insights on the functional interaction of HIFs and celldeath pathwaysrdquoDrug Resistance Updates vol 14 no 3 pp 191ndash201 2011
[76] B B Aggarwal R V Vijayalekshmi and B Sung ldquoTargetinginflammatory pathways for prevention and therapy of cancershort-term friend long-term foerdquo Clinical Cancer Research vol15 no 2 pp 425ndash430 2009
[77] Z Duan R Foster D A Bell et al ldquoSignal transducersand activators of transcription 3 pathway activation in drug-resistant ovarian cancerrdquo Clinical Cancer Research vol 12 no17 pp 5055ndash5063 2006
[78] H-J Kuh S H Jang M G Wientjes J R Weaver and J L-SAu ldquoDeterminants of paclitaxel penetration and accumulationin human solid tumorrdquo Journal of Pharmacology and Experi-mental Therapeutics vol 290 no 2 pp 871ndash880 1999
[79] S Arao H Suwa M Mandai et al ldquoHypoxia-mediated drugresistance novel insights on the functional interaction of HIFsand cell death pathwaysrdquo Cancer Research vol 54 no 5 pp1355ndash1359 1994
[80] S E Johnatty J Beesley B Gao et al ldquoABCB1 (MDR1)polymorphisms and ovarian cancer progression and survivala comprehensive analysis from the Ovarian Cancer Association
BioMed Research International 19
Consortium and the Cancer GenomeAtlasrdquoGynecologic Oncol-ogy vol 131 no 1 pp 8ndash14 2013
[81] X Yang A K Iyer A Singh et al ldquoCluster of differentiation44 targeted hyaluronic acid based nanoparticles for MDR1siRNA delivery to overcome drug resistance in ovarian cancerrdquoPharmaceutical Research 2014
[82] D A Zajchowski B Y Karlan and L K Shawver ldquoTreatment-related protein biomarker expression differs between primaryand recurrent ovarian carcinomasrdquoMolecular CancerTherapeu-tics vol 11 no 2 pp 492ndash502 2012
[83] MM Gottesman J Ludwig D Xia and G Szakacs ldquoDefeatingdrug resistance in cancerrdquoDiscovery Medicine vol 6 no 31 pp18ndash23 2006
[84] S Mozzetti C Ferlini P Concolino et al ldquoClass III 120573-tubulin overexpression is a prominent mechanism of paclitaxelresistance in ovarian cancer patientsrdquo Clinical Cancer Researchvol 11 no 1 pp 298ndash305 2005
[85] M Kavallaris D Y S Kuo C A Burkhart et al ldquoTaxol-resistant epithelial ovarian tumors are associated with alteredexpression of specific beta-tubulin isotypesrdquo Journal of ClinicalInvestigation vol 100 no 5 pp 1282ndash1293 1997
[86] G A Orr P Verdier-Pinard H McDaid and S B HorwitzldquoMechanisms of Taxol resistance related to microtubulesrdquoOncogene vol 22 no 47 pp 7280ndash7295 2003
[87] C Ferlini L Cicchillitti G Raspaglio et al ldquoPaclitaxel directlybinds to Bcl-2 and functionally mimics activity of Nur77rdquoCancer Research vol 69 no 17 pp 6906ndash6914 2009
[88] E Mechetner A Kyshtoobayeva S Zonis et al ldquoLevels ofmultidrug resistance (MDR1) P-glycoprotein expression byhuman breast cancer correlate with in vitro resistance to taxoland doxorubicinrdquo Clinical Cancer Research vol 4 no 2 pp389ndash398 1998
[89] J S Lagas C W N Damen R A B VanWaterschoot D IusufJ H Beijnen and A H Schinkel ldquoP-glycoprotein multidrug-resistance associated protein 2 Cyp3a and carboxylesteraseaffect the oral availability and metabolism of vinorelbinerdquoMolecular Pharmacology vol 82 no 4 pp 636ndash644 2012
[90] M T Huizing J B Vermorken H Rosing et al ldquoPharmacoki-netics of paclitaxel and three major metabolites in patients withadvanced breast carcinoma refractory to anthracycline therapytreated with a 3-hour paclitaxel infusion a European CancerCentre (ECC) trialrdquo Annals of Oncology vol 6 no 7 pp 699ndash704 1995
[91] R Panchagnula ldquoPharmaceutical aspects of paclitaxelrdquo Interna-tional Journal of Pharmaceutics vol 172 no 1-2 pp 1ndash15 1998
[92] S H Jang M G Wientjes and J L-S Au ldquoDeterminants ofpaclitaxel uptake accumulation and retention in solid tumorsrdquoInvestigational New Drugs vol 19 no 2 pp 113ndash123 2001
[93] D S Sonnichsen andM V Relling ldquoClinical pharmacokineticsof paclitaxelrdquo Clinical Pharmacokinetics vol 27 no 4 pp 256ndash269 1994
[94] T Ohtsu Y Sasaki T Tamura et al ldquoClinical pharmacokineticsand pharmacodynamics of paclitaxel a 3-hour infusion versusa 24-hour infusionrdquo Clinical Cancer Research vol 1 no 6 pp599ndash606 1995
[95] M Czejka J Schueller H Schnait B Springer and I EderldquoClinical pharmacokinetics andmetabolism of paclitaxel after athree-hour infusion comparison of two preparationsrdquo Journalof Oncology Pharmacy Practice vol 9 no 4 pp 129ndash136 2003
[96] J Rizzo C Riley D VonHoff J Kuhn J Phillips and T BrownldquoAnalysis of anticancer drugs in biological fluids determination
of taxol with application to clinical pharmacokineticsrdquo Journalof Pharmaceutical and Biomedical Analysis vol 8 no 2 pp 159ndash164 1990
[97] V A de Weger J H Beijnen and J H M Schellens ldquoCel-lular and clinical pharmacology of the taxanes docetaxel andpaclitaxelmdasha reviewrdquoAnti-Cancer Drugs vol 25 no 5 pp 488ndash494 2014
[98] S Kumar H Mahdi C Bryant J P Shah G Garg andA Munkarah ldquoClinical trials and progress with paclitaxel inovarian cancerrdquo International Journal of Womenrsquos Health vol 2no 1 pp 411ndash427 2010
[99] B Huang J Zhao J C Unkeless Z H Feng and H XiongldquoTLR signaling by tumor and immune cells a double-edgedswordrdquo Oncogene vol 27 no 2 pp 218ndash224 2008
[100] R A Jibodh J S Lagas B Nuijen J H Beijnen and J HM Schellens ldquoTaxanes old drugs new oral formulationsrdquoEuropean Journal of Pharmacology vol 717 no 1ndash3 pp 40ndash462013
[101] A Javeed M Ashraf A Riaz A Ghafoor S Afzal and M MMukhtar ldquoPaclitaxel and immune systemrdquo European Journal ofPharmaceutical Sciences vol 38 no 4 pp 283ndash290 2009
[102] L Bracci G Schiavoni A Sistigu and F Belardelli ldquoImmune-based mechanisms of cytotoxic chemotherapy implications forthe design of novel and rationale-based combined treatmentsagainst cancerrdquo Cell Death and Differentiation vol 21 no 1 pp15ndash25 2014
[103] C A Byrd-Leifer E F Block K Takeda S Akira and A DingldquoThe role of MyD88 and TLR4 in the LPS-mimetic activity ofTaxolrdquo European Journal of Immunology vol 31 no 8 pp 2448ndash2457 2001
[104] A-C Wang Y-B Ma F-X Wu et al ldquoTLR4 induces tumorgrowth and inhibits paclitaxel activity in MyD88-positivehuman ovarian carcinoma in vitrordquo Oncology Letters vol 7 no3 pp 871ndash877 2014
[105] Y Zhu N Liu S D Xiong Y J Zheng and Y W ChuldquoCD4+Foxp3+ regulatory T-cell impairment by paclitaxel isindependent of toll-like receptor 4rdquo Scandinavian Journal ofImmunology vol 73 no 4 pp 301ndash308 2011
[106] M Kubo T Morisaki K Matsumoto et al ldquoPaclitaxel probablyenhances cytotoxicity of natural killer cells against breastcarcinoma cells by increasing perforin productionrdquo CancerImmunology Immunotherapy vol 54 no 5 pp 468ndash476 2005
[107] L Markasz G Stuber B Vanherberghen et al ldquoEffect of fre-quently used chemotherapeutic drugs on the cytotoxic activityof human natural killer cellsrdquo Molecular Cancer Therapeuticsvol 6 no 2 pp 644ndash654 2007
[108] T Sako N Burioka K Yasuda et al ldquoCellular immune profile inpatients with non-small cell lung cancer after weekly paclitaxeltherapyrdquo Acta Oncologica vol 43 no 1 pp 15ndash19 2004
[109] R Kaneno G V Shurin I L Tourkova and M R ShurinldquoChemomodulation of human dendritic cell function by anti-neoplastic agents in low noncytotoxic concentrationsrdquo Journalof Translational Medicine vol 7 article 58 2009
[110] TMichels G V ShurinHNaiditch A Sevko VUmansky andM R Shurin ldquoPaclitaxel promotes differentiation of myeloid-derived suppressor cells into dendritic cells in vitro in a TLR4-independent mannerrdquo Journal of Immunotoxicology vol 9 no3 pp 292ndash300 2012
[111] R A Kemp and F Ronchese ldquoTumor-specific Tc1 but not Tc2cells deliver protective antitumor immunityrdquo The Journal ofImmunology vol 167 no 11 pp 6497ndash6502 2001
20 BioMed Research International
[112] A Y Rudensky ldquoRegulatory T cells and Foxp3rdquo ImmunologicalReviews vol 241 no 1 pp 260ndash268 2011
[113] EM Shevach ldquoCD4+CD25+ suppressor T cellsmore questionsthan answersrdquo Nature Reviews Immunology vol 2 no 6 pp389ndash400 2002
[114] S Sakaguchi T Yamaguchi T Nomura and M Ono ldquoRegu-latory T cells and immune tolerancerdquo Cell vol 133 no 5 pp775ndash787 2008
[115] H Nishikawa and S Sakaguchi ldquoRegulatory T cells in tumorimmunityrdquo International Journal of Cancer vol 127 no 4 pp759ndash767 2010
[116] W Zou ldquoRegulatory T cells tumour immunity and immuno-therapyrdquoNature Reviews Immunology vol 6 no 4 pp 295ndash3072006
[117] A Fialova S Partlova L Sojka et al ldquoDynamics of T-cell infil-tration during the course of ovarian cancer The gradual shiftfrom aTh17 effector cell response to a predominant infiltrationby regulatory T-cellsrdquo International Journal of Cancer vol 132no 5 pp 1070ndash1079 2013
[118] A E Albers R L Ferris G G Kim K Chikamatsu A BDeLeo and T L Whiteside ldquoImmune responses to p53 inpatients with cancer enrichment in tetramer+ p53 peptide-specific T cells and regulatory T cells at tumor sitesrdquo CancerImmunology Immunotherapy vol 54 no 11 pp 1072ndash10812005
[119] N Liu Y Zheng Y Zhu S Xiong andYChu ldquoSelective impair-ment of CD4 + CD25 + Foxp3 + regulatory T cells by paclitaxelis explained by Bcl-2Bax mediated apoptosisrdquo InternationalImmunopharmacology vol 11 no 2 pp 212ndash219 2011
[120] X Wu Q-M Feng Y Wang J Shi H-L Ge and W DildquoThe immunologic aspects in advanced ovarian cancer patientstreated with paclitaxel and carboplatin chemotherapyrdquo CancerImmunology Immunotherapy vol 59 no 2 pp 279ndash291 2010
[121] A P Vicari R Luu N Zhang et al ldquoPaclitaxel reducesregulatoryT cell numbers and inhibitory function and enhancesthe anti-tumor effects of the TLR9 agonist PF-3512676 in themouserdquo Cancer Immunology Immunotherapy vol 58 no 4 pp615ndash628 2009
[122] L Zhang K Dermawan M Jin et al ldquoDifferential impairmentof regulatory T cells rather than effector T cells by paclitaxel-based chemotherapyrdquo Clinical Immunology vol 129 no 2 pp219ndash229 2008
[123] Y Tabuchi J Matsuoka M Gunduz et al ldquoResistance topaclitaxel therapy is related with Bcl-2 expression through anestrogen receptor mediated pathway in breast cancerrdquo Interna-tional Journal of Oncology vol 34 no 2 pp 313ndash319 2009
[124] N Obermajer R Muthuswamy K Odunsi R P Edwards andP Kalinski ldquoPGE
2-induced CXCL12 production and CXCR4
expression controls the accumulation of human MDSCs inovarian cancer environmentrdquo Cancer Research vol 71 no 24pp 7463ndash7470 2011
[125] Q M Feng W Di and X Wu ldquoImmune reconstitution inadvanced ovarian cancer patients undergoing first line chemo-therapyrdquo Xi Bao Yu Fen Zi Mian Yi Xue Za Zhi vol 25 no 11pp 1023ndash1025 2009
[126] A D Seidman D Hochhauser M Gollub et al ldquoNinety-six-hour paclitaxel infusion after progression during short taxaneexposure a phase II pharmacokinetic and pharmacodynamicstudy in metastatic breast cancerrdquo Journal of Clinical Oncologyvol 14 no 6 pp 1877ndash1884 1996
[127] D R Spriggs M F Brady L Vaccarello et al ldquoPhase IIIrandomized trial of intravenous cisplatin plus a 24- or 96-hour
infusion of paclitaxel in epithelial ovarian cancer a gynecologiconcology group studyrdquo Journal of Clinical Oncology vol 25 no28 pp 4466ndash4471 2007
[128] G A Omura M F Brady K Y Look et al ldquoPhase III trial ofpaclitaxel at two dose levels the higher dose accompanied byfilgrastim at two dose levels in platinum-pretreated epithelialovarian cancer an intergroup studyrdquo Journal of Clinical Oncol-ogy vol 21 no 15 pp 2843ndash2848 2003
[129] R Simon and L Norton ldquoThe Norton-Simon hypothesisdesigning more effective and less toxic chemotherapeutic reg-imensrdquoNature Clinical Practice Oncology vol 3 no 8 pp 406ndash407 2006
[130] A Kumar P Hoskins and A Tinker ldquoDose-dense paclitaxel inadvanced ovarian cancerrdquo Clinical Oncology vol 27 no 1 pp40ndash47 2015
[131] P Marchetti S Urien G A Cappellini G Ronzino and CFicorella ldquoWeekly administration of paclitaxel theoretical andclinical basisrdquoCritical Reviews in OncologyHematology vol 44supplement pp S3ndashS13 2002
[132] P Francis E Rowinsky J Schneider T Hakes W Hoskinsand M Markman ldquoPhase I feasibility and pharmacologic studyof weekly intraperitoneal paclitaxel A Gynecologic OncologyGroup pilot studyrdquo Journal of Clinical Oncology vol 13 no 12pp 2961ndash2967 1995
[133] H Thomas and P Rosenberg ldquoRole of weekly paclitaxel inthe treatment of advanced ovarian cancerrdquo Critical Reviews inOncologyHematology vol 44 supplement pp S43ndashS51 2002
[134] M Markman J Markman K Webster et al ldquoDuration ofresponse to second-line platinum-based chemotherapy forovarian cancer implications for patient management and clini-cal trial designrdquo Journal of Clinical Oncology vol 22 no 15 pp3120ndash3125 2004
[135] P H OrsquoDonnell M Eileen Dolan E Gamazon et al ldquoPopu-lation differences in platinum toxicity as a means to identifynovel genetic susceptibility variantsrdquo Pharmacogenetics andGenomics vol 20 no 5 pp 327ndash337 2010
[136] M J Millward M J Boyer M Lehnert et al ldquoDocetaxel andcarboplatin is an active regimen in advanced non-small-celllung cancer a phase II study in Caucasian and Asian patientsrdquoAnnals of Oncology vol 14 no 3 pp 449ndash454 2003
[137] M Markman ldquoIntraperitoneal therapy of ovarian cancerrdquoOncologist vol 1 no 1-2 pp 18ndash21 1996
[138] M Markman and J L Walker ldquoIntraperitoneal chemotherapyof ovarian cancer a review with a focus on practical aspects oftreatmentrdquo Journal of Clinical Oncology vol 24 no 6 pp 988ndash994 2006
[139] K Fujiwara S Nagao E Aotani and K Hasegawa ldquoPrincipleand evolving role of intraperitoneal chemotherapy in ovariancancerrdquo Expert Opinion on Pharmacotherapy vol 14 no 13 pp1797ndash1806 2013
[140] M Markman E Rowinsky T Hakes et al ldquoPhase I trialof intraperitoneal taxol a gynecoloic oncology group studyrdquoJournal of Clinical Oncology vol 10 no 9 pp 1485ndash1491 1992
[141] M Markman M F Brady N M Spirtos P Hanjani and S CRubin ldquoPhase II trial of intraperitoneal paclitaxel in carcinomaof the ovary tube and peritoneum a gynecologic oncologygroup studyrdquo Journal of Clinical Oncology vol 16 no 8 pp2620ndash2624 1998
[142] P B Panici I Palaia M Graziano F Bellati N Manci and RAngioli ldquoIntraperitoneal paclitaxel as consolidation treatmentin ovarian cancer patients a case control studyrdquo Oncology vol78 no 1 pp 20ndash25 2010
BioMed Research International 21
[143] D K Armstrong B Bundy L Wenzel et al ldquoIntraperitonealcisplatin and paclitaxel in ovarian cancerrdquo The New EnglandJournal of Medicine vol 354 no 1 pp 34ndash43 2006
[144] D Tewari J Java and R Salani ldquoLong-term survival advantageof intraperitoneal chemotherapy treatment in advanced ovariancancer an analysis of a Gynecologic Oncology Group ancillarydata studyrdquo in Proceedings of the 2013 Society of GynecologicOncology Annual Meeting on Womenrsquos Cancer (GOG114172Abstract) Los Angeles Calif USA 2013
[145] D A Yardley ldquonab-paclitaxel mechanisms of action and deliv-eryrdquo Journal of Controlled Release vol 170 no 3 pp 365ndash3722013
[146] M Ando K Yonemori N Katsumata et al ldquoPhase I and phar-macokinetic study of nab-paclitaxel nanoparticle albumin-bound paclitaxel administeredweekly to Japanese patients withsolid tumors and metastatic breast cancerrdquo Cancer Chemother-apy and Pharmacology vol 69 no 2 pp 457ndash465 2012
[147] N Desai V Trieu Z Yao et al ldquoIncreased antitumor activityintratumor paclitaxel concentrations and endothelial cell trans-port of cremophor-free albumin-bound paclitaxel ABI-007compared with cremophor-based paclitaxelrdquo Clinical CancerResearch vol 12 no 4 pp 1317ndash1324 2006
[148] J A Yared and K H R Tkaczuk ldquoUpdate on taxane devel-opment new analogs and new formulationsrdquo Drug DesignDevelopment andTherapy vol 6 pp 371ndash384 2012
[149] M G Teneriello P C Tseng M Crozier et al ldquoPhase IIevaluation of nanoparticle albumin-bound paclitaxel in plati-num-sensitive patients with recurrent ovarian peritoneal orfallopian tube cancerrdquo Journal of Clinical Oncology vol 27 no9 pp 1426ndash1431 2009
[150] R L Coleman W E Brady D S McMeekin et al ldquoA phase IIevaluation of nanoparticle albumin-bound (nab) paclitaxel inthe treatment of recurrent or persistent platinum-resistant ovar-ian fallopian tube or primary peritoneal cancer a GynecologicOncology Group Studyrdquo Gynecologic Oncology vol 122 no 1pp 111ndash115 2011
[151] J W Singer ldquoPaclitaxel poliglumex (XYOTAX CT-2103) amacromolecular taxanerdquo Journal of Controlled Release vol 109no 1ndash3 pp 120ndash126 2005
[152] C Li D-F Yu R A Newman et al ldquoComplete regressionof well-established tumors using a novel water-soluble poly(L-glutamic acid)-paclitaxel conjugaterdquo Cancer Research vol 58no 11 pp 2404ndash2409 1998
[153] M Mita A Mita J Sarantopoulos et al ldquoPhase I study ofpaclitaxel poliglumex administered weekly for patients withadvanced solid malignanciesrdquo Cancer Chemotherapy and Phar-macology vol 64 no 2 pp 287ndash295 2009
[154] P Sabbatini M W Sill D OrsquoMalley L Adler and A ASecord ldquoA phase II trial of paclitaxel poliglumex in recurrentor persistent ovarian or primary peritoneal cancer (EOC) agynecologic oncology group studyrdquo Gynecologic Oncology vol111 no 3 pp 455ndash460 2008
[155] M O Bradley C S Swindell F H Anthony et al ldquoTumortargeting by conjugation of DHA to paclitaxelrdquo Journal ofControlled Release vol 74 no 1ndash3 pp 233ndash236 2001
[156] M O Bradley N L Webb F H Anthony et al ldquoTumortargeting by covalent conjugation of a natural fatty acid topaclitaxelrdquo Clinical Cancer Research vol 7 no 10 pp 3229ndash3238 2001
[157] A C Wolff R C Donehower M K Carducci et al ldquoPhaseI study of docosahexaenoic acid-paclitaxel a taxane-fatty acid
conjugate with a unique pharmacology and toxicity profilerdquoClinical Cancer Research vol 9 no 10 part 1 pp 3589ndash35972003
[158] A Sparreboom A C Wolff J Verweij et al ldquoDispositionof docosahexaenoic acid-paclitaxel a novel taxane in bloodin vitro and clinical pharmacokinetic studiesrdquo Clinical CancerResearch vol 9 no 1 pp 151ndash159 2003
[159] P M Fracasso J Picus J D Wildi et al ldquoPhase 1 and phar-macokinetic study of weekly docosahexaenoic acid-paclitaxelTaxoprexin in resistant solid tumor malignanciesrdquo CancerChemotherapy and Pharmacology vol 63 no 3 pp 451ndash4582009
[160] A Y Bedikian R C DeConti R Conry et al ldquoPhase 3 study ofdocosahexaenoic acid-paclitaxel versus dacarbazine in patientswith metastatic malignant melanomardquo Annals of Oncology vol22 no 4 pp 787ndash793 2011
[161] Y-N Wu S-L Wang Y-C Wang et al ldquoReversal effect ofdocosahexaenoic acid on taxol resistance in human ovarian car-cinoma A2780T cellsrdquo Obstetrics amp Gynecology InternationalJournal vol 1 no 3 Article ID 00018 2014
Submit your manuscripts athttpwwwhindawicom
PainResearch and TreatmentHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom
Volume 2014
ToxinsJournal of
VaccinesJournal of
Hindawi Publishing Corporation httpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
AntibioticsInternational Journal of
ToxicologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
StrokeResearch and TreatmentHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Drug DeliveryJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Advances in Pharmacological Sciences
Tropical MedicineJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Medicinal ChemistryInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
AddictionJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
Emergency Medicine InternationalHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Autoimmune Diseases
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Anesthesiology Research and Practice
ScientificaHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Pharmaceutics
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of

2 BioMed Research International
National cancer institute (NCI) and US department of agriculture (USDA) colloborated on plant screening programme forfinding new and effective anticancer agents 15000 plants were collected and 115000 extracts were tested
Crude extracts of the yewrsquosbark were repetitively fractionated by Monroe Wall and MansukhWanifrom natural products laboratory and identified the active ingredient that was responsible for cytotoxicity activity and named it Taxol
Samples of the Pacific yewrsquos bark Taxus brevifolia were collected by a team of botanists headed by Arthur Barclay in Gifford Pinchot National Forest Washington
Taxol was found to have excellent spectrum of activity in vitro and in vivo butlack of supply and poor aqueous solubility deterred further preclinical development
Dr Susan Horwitz received a grant from NCI to study Taxolrsquos mechanism of action and found that Taxol was unique as it wasable to bind to microtubule inhibit depolymerization ofmicrotubule leading to cell arrest at mitosis and subsequent apoptosis
Paclitaxel was able to regress mammary tumours in a
model
Semisynthetic Taxol discovered
Solubility problem resolved with Cremophor EL
Taxol entered phase I clinical trials and found to have partial or complete response in 30 patients with advanced ovarian cancer
FDA approved Taxol for treatment against ovarian cancer and two years later for treatment of advanced breast cancer
xenograft
1960 1962 1965 1977 1978 1979 1984 1992ndash1994
Figure 1 History of paclitaxel development The search for the natural resources began in 1960 headed by NCI and USDA which ledto discovery of Pacific yewrsquos bark The active ingredient was isolated by Monroe Wall and Mansukh Wani and was named Taxol Taxoldemonstrated both in vivo and in vitro antineoplastic activity as well in xenograft models with breast tumours The mechanism of actionwhich was unique was identified and subsequently after 22 years Taxol entered clinical trials and demonstrated good cytotoxicity activityand was finally approved by FDA for treatment against ovarian and breast cancers
chemotherapy IP paclitaxel treatment and newer forms ofpaclitaxel may add to the clinical benefit in patients with thismalignancy
2 The Evolution of Paclitaxel
Paclitaxel was not a chance discovery but the result of acollaborative effort of the National Cancer Institute (NCI)and the US Department of Agriculture (USDA) using aplant-screening programme in search of new and effectiveanticancer agents [26] The history of paclitaxel developmentis summarised in Figure 1
The NCI Plant Programme headed by Jonathan Hartwella natural product chemist liaised with Robert Perdue aUSDA botanist and analysed over 15000 natural plantsworldwide as well as testing 115000 extracts for anticanceractivity over the period from 1960 to 1981 When the NCIscreening programme concluded in 1981 paclitaxel was theonly compound entered into clinical trials [27]
In August 1962 paclitaxel was isolated from the barkof the Pacific yew tree Taxus brevifolia Nutt (Taxaceae)shipped in from Gifford Pinchot National Forest to USDAheadquarters in Maryland by a 32-year-old USDA botanistArthur S Barclay [26 28 29] Although the cytotoxic activityof the bark of the samples soon became evident by September1964 as it was found to be able to inhibit the in vitro growthin 9KB cell cultures containing human oral epidermoid
carcinoma [30 31] it took MansukhWani and Monroe Wallworking under contractwith theNCI at theResearchTriangleInstitute (Research Triangle Park NC) till 1967 to isolate andidentify the extractrsquos most active ingredient and named itpaclitaxel [26]
Paclitaxel was reported to have a broad spectrum ofantitumour activity following in vivo screens in tumoursimplanted in laboratory mice [27] With grant aid fromNCI Dr Susan Horwitz from the Albert Einstein College ofMedicine further enhanced the interest in paclitaxel with thenovel discovery of its unique mechanism of action Anotherbreakthrough came in November 1978 with the ability ofpaclitaxel to cause tumour regression in a mammary tumourxenograft [26]
Although clinical trials to study the effect of paclitaxelon various cancers mushroomed not many were able tocommence as planned due to scarcity in the supply the onlysource being the extremely slow-growing Pacific yew Hart-well soon realized that for every 13 kilograms of dried bark hewas producing just half a gram of purified paclitaxel extractIn 1990 a petition to include the severely depletedT brevifoliaon the list of endangered species concluded in the Pacific YewAct being passed in 1992 to protect the tree [32]
Despite the scarcity paclitaxel entered clinical trials after22 years from its discovery in 1984 Wiernik and colleaguesreported a phase 1 trial in 1987 [33] Paclitaxel was found tohave cytotoxic activity of clinical significance when a study
BioMed Research International 3
Empirical formula C47H51NO14
Molecular weight 8539 gmol
Average mass 8539Da
Systemic name (2120572 5120573 7120573 10120573 13120572)-
(benzoylamino)-2-hydroxy-3-
phenylpropanoyl]oxy-17-
dihydroxy-9-oxo-520-epoxytax-11-
en-2-yl benzoate
410-Diacetoxy-13-[(2R 3S)-3-
O
O
O
O
O
O O
O
O
NHH3C
H3998400 CH3
CH3
CH3
CH345
OH
HO
OH
OH
13
Figure 2 Chemical structure of paclitaxel Paclitaxel consist of taxane ring with a four-membered oxetane side ring at positions C4 and C5and an active homochiral ester side chain at C13 that binds tomicrotubules in a guanosine triphosphate (GTP) independentmanner to inducecytotoxicity activity
on ovarian cancer concluded that 30 of patients withplatinum-resistant ovarian cancer responded to paclitaxeltherapy either completely or partially [34] Another issue wasthe insolubility of the paclitaxel in water but these problemswere eventually overcome with a formulation in ethanoland Cremophor EL Cremophor EL is a polyethoxylatedcastor oil which was used as a vehicle for solubilisation ofhydrophobic drug like paclitaxel [35] However the mostserious side effect observed following use of Cremophor asthe drug vehicle was that of hypersensitivity reactions whichwere unpredictable and led to two deaths and this almosthalted any further clinical trials A longer and slower infusiontaking 24 hours reduced this severe adverse effect [33]
In December 1992 paclitaxel was registered as chemo-therapy for the treatment for ovarian cancer To meetincreasing demand a commercially viable semisynthetic wasdeveloped by Robert Holton and colleagues [31] Researchersalso tested the effectiveness of paclitaxel as a treatment foradvanced breast cancer Subsequent clinical trials found thatthe drug was effective against this disease and in 1994 theFDA approved paclitaxel for use against breast cancer Pacli-taxel is now used (either as a single agent or in combinationwith other drugs such as cisplatin or carboplatin) for thetreatment of ovarian cancer [36] breast cancer [5] and non-small-cell lung cancer [37]
3 Chemical Structure
Paclitaxel a class of taxane drugs is a diterpenoid pseudoal-kaloid with the empirical formula C
47H51NO14
(Figure 2)and has a corresponding molecular weight of 8539 gmolPaclitaxel consist of two molecules a taxane ring with a four-membered oxetane side ring at positions C4 and C5 and ahomochiral ester side chain at C13 The side chain at C13plays a crucial role as this is the active portion that binds tomicrotubules stabilises the tubulin bundles and stimulatesdisassembly of microtubules in a guanosine triphosphate(GTP)-independent manner As a result cell proliferation isinhibited by halting the cell cycle at the metaphaseanaphase
boundary and by formation of an incomplete metaphaseplate of chromosomes induced by the stabilization of themicrotubule dynamics Extensive research has concluded thatan intact taxane ring and an ester side-chainwere essential forcytotoxic activity [38 39]
4 Mechanism of Action
Paclitaxel is an anticancer drug that targets microtubulesMicrotubules consist of cylindrical hollow bodies of about25ndash30 nm in diameter composed of polymers of tubulin indynamic equilibrium with tubulin heterodimers (consistingof alpha and beta protein subunits) [40 41] The principalfunction of microtubules is the formation of the mitoticspindle during cell division In addition they are required forthe maintenance of cell structure motility and cytoplasmicmovement within the cell The synthesis of tubulin and theassembly of microtubules occur during the G2 phase and theprophase of mitosis Microtubules are in a state of dynamicequilibrium with their subunit tubulins 120572 and 120573 arrangedin a head to tail fashion with preferential faster growth(plus ends) at one end and slower growth (minus ends) atthe other end Under steady-state conditions the length ofthe microtubule is unchanged as the net tubulin assemblyrate equals the net disassembly rate The minus ends part ofmicrotubule are usually anchored mainly at the centrosome[42] while the plus ends explore the cytoplasm and interactwith cellular structures [43 44]
Dr Horwitz discovered that paclitaxel unlike vincaalkaloids which prevent microtubule assembly prevents celldivision by promoting the assembly of stable microtubulesespecially from 120573-tubulin heterodimers and inhibits theirdepolymerisation hence exposed cells are arrested in theG2M-phase of the cell cycle [45] and eventually undergoapoptosis [46] thereby inhibiting cell replication [40 47]Paclitaxel binds specifically in a reversible manner to theN-terminal 31 amino acids of the beta-tubulin subunit inthe microtubules rather than to tubulin dimers [47 48]Paclitaxel also has the unique ability to promote microtubule
4 BioMed Research International
formation in vitro even at cold temperatures (4∘C) and in theabsence of GTP [46]
Further research into understanding themolecularmech-anisms of microtubule formation has discovered that pacli-taxel may have other mechanism that allows cells to escapedrug toxicity which then develops into resistance and failurein chemotherapy [44] Ganguly and his colleagues found thatmicrotubule dynamics suppression was not related to celldivision Treatment of mutant cell lines Tax 11-6 (mutation in120572-tubulin) and Tax 18 (mutation in 120573-tubulin) at concentra-tion of 50 to 100 nmolL that should hypothetically increasemicrotubule assembly to more normal levels and allow thecells to proliferate normally further suppress microtubuledynamics rather than restoring behaviour to normal [44]Low concentrations of paclitaxel that suppressed dynamicshence they did not affect the rate ofmicrotubule detachmentbut the higher drug concentrations that allowed normalcell division strongly inhibited detachment in the mutantcell lines and returned the rate to near normal levels Thisaction seems to be related to ability of paclitaxel to inhibitmicrotubule fragmentation rather than its ability to suppressmicrotubule dynamics which was further confirmed by livecell imaging that demonstrated that microtubule detach-ment from centrosomes might be responsible for generat-ing microtubule fragments a process that was reversed bypaclitaxel [44] Recent studies have also found that at lowconcentrations (less than nanomolar concentrations) pacli-taxel inhibits the depolymerisation of microtubules whereasat high-dose paclitaxel increase the number and mass ofmicrotubules hence increasing stability of microtubules andalso render them nonfunctional by blocking the detachmentof microtubule minus ends from centrosomes rather thanplus ends [44 49]
The proposed mechanism of action of weekly paclitaxeladministration may be based on its apoptotic effects Theinduction of apoptotic modulator genes by paclitaxel appearsto be independent of microtubule stabilization It may be dueto modulation of the transcription of different genes suchas DNA-damage response proteins cytokines or proteinsinvolved in the control of cellular proliferation apoptosis andinflammation The apoptotic effect of paclitaxel is dependenton the concentration and duration of exposure With con-centration amounts of at least 10 nM and exposure of at least12 hours apoptosis may be induced in the S phase withoutmitotic arrest Two different mechanisms of apoptosis havebeen proposed depending on the dose concentration ofpaclitaxel At concentration of ge9 nM paclitaxel induces Raf-1 activation which is responsible for apoptotic control Atle9 nM there is absence of Raf-1 kinase involvement butapoptosis induction still occurs under the influence of p53and p21 [50 51] With the same concentration at 24-hourexposure in addition to apoptotic arrest paclitaxel producesan irreversible mitotic arrest [52] p53 is a major tumoursuppressor regulating proliferation and apoptosis and itsmutation occurs in more than 50 of human cancers Innormal cells DNA damage increases p53 levels which thenactivates a G1 cell-cycle arrest mediated by p21 to promoteeither the DNA damage repair mechanisms or apoptosis andnaturally limiting proliferation of genetically transformed cell
clones A functional p53 signaling pathway is necessary tosensitise cancer cells to DNA-damaging chemotherapeuticagents to reduce chemo resistance Currently paclitaxelactivity is considered to be independent of p53 status whichis an important aspect as the presence of silent ormutated p53does not modify the sensitivity of cancer cells to taxane thusreducing chemoresistance [53ndash56]
Paclitaxel also exerts its mechanism of action by activa-tion of multiple signal-transduction pathways which maybe associated with proapoptotic signaling The pathwaysassociated with paclitaxel are TLR-4 dependent pathway(either via MyD88 dependent or independent pathway) c-Jun N-terminal kinase (JNK) P38 Mitogen activated protein(MAP)Kinase nuclear factor kappa B (NF-120581B) Janus kinase-(JAK-) signal transducer and activator of transcription factor(STAT) pathway One of the pathways for induction ofapoptosis is via mitogen-activated protein kinase (MAPK)pathway resulting in dephosphorylation of the proapoptoticprotein Bad and Bax phosphorylation of Bcl2 and inductionof apoptosis Bad and Bax (promote apoptosis) and Bcl2 (sup-press apoptosis) are regulatory proteins which are membersof the Bcl2 family and are involved in programmed cell deathInduction of cytokines and pro-inflammatory proteins willlead to immunomodulatory effect of paclitaxel at low-doseconcentration and cell death at higher dose Changes thatoccur in these pathways are also responsible for developmentof resistance to paclitaxel [57ndash60]
Weekly paclitaxel also exhibits strong angiogenic inhibi-tory activity [61 62] In murine studies paclitaxel was ableto reduce new vessel formation at low noncytotoxic doses(03 and 6mgkg per day in mice) by suppressing VEGFexpression [63 64] Low dose weekly paclitaxel has beentested in patients with advanced ovarian cancer metastaticmelanoma and advanced head and neck cancer resulting instable disease [65ndash67] This additional mechanism of actionof paclitaxel by rescheduling the duration of administrationmay be helpful in cancers which have become resistant to thesame drug given on a 3-weekly conventional schedule [11 13]
Paclitaxel had also been reported to induce reactiveoxygen species (ROS) generation and increase hydroperoxideproduction by enhancing the activity of nicotinamide ade-nine dinucleotide phosphate (NADPH) oxidase which con-tributes to oxidative stress and may play a role in the potencyof the anticancer activity of paclitaxel [68 69] The combi-nation of paclitaxel with inhibitors of glucose (ie 2-deoxy-D-glucose 2DG) and hydroperoxide (ie L-buthionine-S R-sulfoximine BSO) metabolism has been found to selectivelyenhance breast cancer cell killing via hydrogen peroxide-induced metabolic oxidative stress which may be effectivelyutilised to treat breast cancers [69] However the relationshipof oxidative stress to the overall cytotoxicity mechanism ofpaclitaxel is not well established The mechanism of action ofpaclitaxel is summarised in Figure 3
5 Mechanism of Drug Resistance
Themechanism of paclitaxel resistance is complex involvingmultistep and multiple genes and not yet fully elucidated
BioMed Research International 5
Microtubules(MT)
MyD88 dependent
MyD88 independent
S
G2G1
M
PTX
Cell cycle arrest
N-terminal amino acids of beta
tubulin subunit
Inhibit depolymerisation ofmicrotubules
and suppress MT dynamics
Increase number and mass of microtubules increase
stability and block detachment
Apoptosis induced in G1S phase (absence mitotic
arrest)
Raf-1
p21
STAT 3
G0
JAK
MEK
MAPK
Bax Bcl2Bad
IRAK
TRAF
TKR
TRIF TRAM
ROS
Mitotic arrest at G2M phase
PI3KAKTApoptosis regulator
protein
p53
VEGFR
Angiogenesis
Apoptosis
TLR4
High concentrationLow concentration
NF-120581B
PTXle 9nM12hr
PTXge 9nM12hr
PTXle 9nM24hr
I120581B
Figure 3 Mechanism of action of paclitaxel Paclitaxel targets microtubules At high concentration PTX causes mitotic arrest at G2M phasewhereas at low concentration apoptosis is induced at G0 and G1S phase either via Raf-1 kinase activation or p53p21 depending on the doseconcentration Even at lower dose but with exposure beyond 24 hours paclitaxel can cause mitotic arrest Paclitaxel also activates multiplesignaling pathway to exert proapoptotic activity as well as immunomodulatory effect Paclitaxel also develops resistance via these signalingpathways PTX Paclitaxel TLR4 Toll-like receptor 4 G0 resting phase G1 cells enlarge andmake new protein S phase DNA replication G2preparation for division M phase cell divisionmitosis Raf-1 Raf kinase family MEKMAPK mitogen activated protein kinase IRAK IL-1receptor associated kinase TRAF TNFR associated factor NF-120581B nuclear factor kappa B TRIFTRAM TIR-domain-containing adapter-inducing interferon-120573 TKR tyrosine kinase receptor VEGFR vascular endothelial growth receptor PI3K phosphoinositide 3-kinase JAKjanus kinase STAT signal transducer and activator of transcription factor
Development of drug resistance leading to aggressive diseasethat is refractory to treatment is responsible for 90 ofthe deaths among patients with advanced ovarian cancer[70] Multidrug resistance (MDR) is a phenomenon definedby the ability of cancer cell to overcome either structurallyor functionally unrelated cytotoxic drugs Mechanism ofMDR can be broadly divided into three types (a) externalmechanism involving changes in pharmacokinetics of drugor (b) within tumour microenvironment which includeshypoxia leading to clonal selection pressure or (c) at cellu-lar level [71] MDR can be intrinsic or acquired IntrinsicMDR or also known as inherent occurs when cancer cellsdevelop resistant to any chemotherapy and this is most likelyattributed by tumour microenvironment Acquired MDRdevelops following exposure to chemotherapeutic agents andmay occur as a result of the pharmacokinetic of drug itself orsecondary to changes within the tumour cells [71]
Paclitaxel-derived resistance is mainly attributed bychanges involving mRNA and protein (such as multiple
ribosomal genes and translation factors) synthesis oxidativestress (UGT1A6 MAOA and CYBA) glycolysis (ADH1AHK1 and ENO3) glutathione metabolism and leukocytetransendothelial migration pathways [71] A study on geneexpression changes on a series of drug resistant ovariancancer cell lines following exposure to paclitaxel cisplatinor doxorubicin revealed that among 845 genes analysed atotal of 337 genes were significantly altered in cells resistantto paclitaxel [70] Changes in genes expression may createinterpatient variation in drug effect alteration in tumourmicroenvironment and changes within cellular structuresmetabolism and functions that promotes towards drug resis-tance
Tumour cells grow rapidly with formation of numerousnew vessels attributing to irregular blood flow and increasedoxygen demand which lead to development areas devoidof adequate oxygenation within ovarian cancer tissues [72]In response to chronic hypoxia (oxygen depletion) tumourmicroenvironment adapts processes to keep cells alive in
6 BioMed Research International
hypoxic and acidic state This hypoxic adaptation promotestumour proliferation dissemination and progression of dis-ease [73] and also reduces chemosensitivity [74]
Hypoxia-induced chemoresistance occurs due to geno-mic instability Oxygen depletion induces proteomic andgenomic changes that activates the level of p53 inhibits apop-tosis promotes angiogenesis (angiogenic molecules such asvascular endothelial growth factor [VEGF] and angiogenin)upregulates growth factors (platelet-derived growth factor[PDGF] transforming growth factor-beta and insulin-likegrowth factor [IGF]) and induces anaerobic metabolism andglycolysis (glycolytic enzymes glucose transporters) leadingto reduction in potential for cell cycle arrest and cellulardifferentiationwhich prevent tumour cell death [74]Hypoxiacan induce either p-53-dependent (involving Apaf-1 andcaspase-9 effector pathways) or p53-independent (involvinghypoxic-inducible factor 1 [HIF-1] and Bcl-2 family genespathways) apoptosis in both normal and tumour cells HIF-1 is a common transcription factor consisting of HIF-1120572 and HIF-1120573 subunits which controls hypoxic-induciblegenes and the concentration of HIF-1 protein increasedexponentially in the presence of hypoxic environment Lossof apoptotic potential of tumour cells mediated by hypoxicenvironment and HIF-1 which arrest cell cycle at G0G1reduces chemosensitivity to chemotherapeutic agents includ-ing paclitaxel [70 75]
Other transcriptional factors which are activated byhypoxia are nuclear factor kappa B (NF-120581B) and STAT3 also known as proinflammatory transcriptional factorsNF-120581B and STAT 3 regulate multiple gene products whichare involved in inflammation angiogenesis cell survivalproliferation and metastasis Paclitaxel which mediates itscytotoxic action via NF-120581B pathway is vulnerable to developresistance in the presence of hypoxic tumour microen-vironment with activation of NF-120581B transcription factorwhich induces serine phosphorylation and also regulatesBCL-2 an antiapoptotic protein preventing cell death andpromoting tumorigenesis [76] Inhibition of activated STAT3 found overexpressed in most paclitaxel-resistant ovariancancer cells has resulted in reduction in paclitaxel resistanceHowever further research is required to determine the exactmechanism [77]
Intracellular drug concentration is important for effectivecytotoxic activity of paclitaxel Drug resistance may beattributed to either reduced accumulation of drug withinovarian tumours or increased efflux of drug from tumourcells [78] Alteration in pharmacokinetic of paclitaxel eitherattributed by the drug itself such as lower concentration ofdrug administered shorter duration of drug exposure highfirst pass metabolism increased hepatic or renal clearanceinadequate binding to tubulinsmicrotubules or othermacro-molecules or presence of higher tumour density or vascular-ity may result in reduced accumulation of intratumoral drugconcentration [71]
Drug efflux is the most common mechanism for chemo-resistance observed in paclitaxel-treated cancer cells Drugefflux from cancer cells is mediated by ATP-binding cassette(ABC) transporters such as P-glycoprotein (P-gp) P-gp alsoknown as ABCB1 or multidrug-resistance associated-protein
(MRP) a transmembrane protein encoded by MDR1 geneplays a role as an efflux pump which is crucial for occurrenceof many cellular processes that require transfer of substratesacross cellularmembranes P-gp hence can affect intracellulardrug concentration andhave been shown to correlate in vitroto chemosensitivity to paclitaxel [59] However evidence fortheir role in clinical drug resistance in ovarian cancer hasemerged with P-gp found to be overexpressed in ovariancancer cells in vitro and also on paclitaxel-resistant celllines [70] P-gp and MDR1 expression levels were higherin chemoresistant ovarian cancer patients as compared withtheir chemosensitive counterpart Overall survival time wasalso statistically higher in patientswith low expression of P-gpandMDR1 in their tumor tissuesHence P-gp andMDR1mayhave a predictive role in determining the outcome of patientswith advanced ovarian cancer [58 79ndash82] Mechanism ofpaclitaxel resistance is complicated and specifically inhibitingABC transporters have given mixed results [59 83]
Another major mechanism of paclitaxel resistance ismediated by either a reduction in total intracellular tubulinconcentrations point mutation at prominently expressedtubulin genes or by selective alterations in expression oftubulin isotypes such as Class III 120573-tubulin [52 84 85]Microtubule dynamic stability was significantly impairedin the paclitaxel-resistant cells [86] Microtubule dynamicsdisruption caused by paclitaxel result in cell cycle arrestapoptosis and drug resistance
Other mechanism responsible for development of pacli-taxel resistant are inhibition of apoptosis activation ofmitogen-activated protein kinase Raf-1 kinase or intra-cellular signalling pathway PIK3 (phosphatidylinositol-45-bisphosphate 3-kinase) changes in apoptotic regulatory pro-teins such as Bcl-2 increase in expression of proinflammatorycytokines such as TNF-120572 IL-6 and IL-8 and activation oflipopolysaccharide-inducible genes and tumour suppressionprotein p53 [57 83 86 87]
In summary paclitaxel resistance is multifactorial inc-luding changes in signaling pathways upregulation of P-glycoprotein (P-gp) [80 88 89] alteration in tubulin dyna-mic mutations in 120573-tubulin gene or expression of 120573-tubulinisotypes [52 84 85] and changes in apoptotic mechanismIdentification of mechanism of resistance could help topotentially develop novel agents to improve chemosensitivityof patients with advanced ovarian cancer
6 Pharmacokinetics
Paclitaxel is a white to off-white crystalline powder highlylipophilic and is insoluble in water and so difficult to formu-late into solution It has a melting point of 216-217∘C [90 91]More than 90 of the drug binds rapidly and extensively toplasma proteins [33 40] whereas binding onto red blood cellsis approximately 50 The presence of premedication drugs(before chemotherapy) such as ranitidine dexamethasone ordiphenhydramine did not affect protein binding of paclitaxelPaclitaxel has a large volume of distribution of about 55 Lm2but this is reduced in the females [33]
BioMed Research International 7
AUC (area under the plasma concentration)
Cmax (maximum concentration)
Pacli
taxe
l con
cent
ratio
n (120583
M)
0 10 20 30 40
Time (hr)
0
1
2
3
4
5
Figure 4 Plasma pharmacokinetics of paclitaxel The pharmacoki-netics generally were linear for 6 or 24 hour infusions but becomenonlinear for infusions of shorter durations due to variation inthe elimination clearance with the dose administered An increasein plasma concentration of paclitaxel results in disproportionatelarger increase in 119862max (maximum plasma concentration) and AUC(area under plasma concentration) followed by decrease in drugelimination from body tissues
The disappearance of paclitaxel from plasma is tradition-ally believed to be biphasic [33] The initial rapid declinerepresents distribution to the peripheral compartment andelimination of the drug The later phase is due in part tothe slow efflux of paclitaxel from the peripheral compartment[92] In the presence of more sensitive assay methods andlater sampling times a three-compartment model seems tobe more accurate [40 93] Paclitaxel has been shown tohave a nonlinear pattern of pharmacokinetics (Figure 4)Thepharmacokinetics were generally linear for 6- or 24-hourinfusions but become nonlinear for infusions of shorterdurations because the elimination clearance varies with thedose administered With increasing plasma concentrationof paclitaxel there is a disproportionately larger increasein 119862max (maximum plasma concentration) and AUC (areaunder plasma concentration) accompanied by decrease indrug elimination from body tissues The clinical importanceof this nonlinear pattern is that dose escalationmay result in adisproportionate increase in toxicity whereas dose reductionmay affect its efficacy [33 90 91 94]
The pharmacokinetics of paclitaxel has been evaluatedover a wide range of doses up to 300mgm2 and withinfusion schedules ranging from 3 to 24 hours Maximumplasma concentrations are dose-related In patients treatedwith single dose infusion of 135 and 175mgm2 given as3- and 24-hour infusions mean steady state volume ofdistribution has ranged from 198 to 688 Lm2 indicatingextensive extravascular distribution andor tissue bindingTerminal half-life has ranged from 13 to 86 hours (mean 5hours) [40 93] and total body clearance has ranged from116 to 240 Lhrm2 Preclinical results in animals have shown
high levels in most tissues Being highly protein-boundpaclitaxel has a high affinity for distribution in specific tissuesincluding kidney lung spleen and extracellular fluids likeascites and pleural fluids [40 95] but the uptake of the drugin the brain is minimal [96 97] Exposure to paclitaxel isrelatively high in tumour tissue compared with other tissuesand in addition to slow elimination from tumour tissue theAUC in tumour tissue is about five-fold higher than that inplasma [97]
There is no evidence of accumulation of paclitaxel withmultiple treatment courses as the variability in systemicpaclitaxel exposure as measured by AUC (0ndashinfin) (area underplasma concentration-time curve from time 0 to infinity)for successive treatment courses are minimal [98] Paclitaxelclearance is however sequence dependent Patients receiv-ing a platinum-based agent prior to paclitaxel have lowerclearance and greater clinical toxicity than patients receivingpaclitaxel before cisplatin [93]
The drug administered intravenously undergoes anextensive P-450mediated hepaticmetabolism by cytochromeenzymes (CYP3A andCYP2C8) with 70ndash80being excretedinto bile by adenosine triphosphate- (ATP-) binding cassettemultidrug transporters such as P-glycoprotein (P-gp) andmultidrug resistance protein 2 (MRP-2) either asmetabolitesor as the parent drug Variation in MRP-2 activity hasbeen found to have direct effect on the effective exposureto paclitaxel [99] The bioavailability is poor following oraladministration due to enterocyte expression of P-gp and first-pass metabolism in the liver Most of the drug is eliminatedin feces Less than 10 drug in the unchanged form isexcreted in the urine indicating extensive nonrenal clearance[96] Combinations of inhibitors of CYP3A and P-gp mightpossibly improve the oral bioavailability of the taxanes [8997 100]
7 Paclitaxel and the Immune System
The immune system consists of two different but interactingmechanisms which are innate and adaptivemechanismsTheinnate mechanism is the first line of defense and consists of agroup of cells which includes mainly macrophages dendriticcells (DCs) and natural killer (NK) cells while the adaptiveimmunemechanism is represented by T-lymphocytes All thecomponents of innate and adaptive mechanism are involvedin antitumour immunity which includes tumour recognitioncontrol and elimination However cancer cells are able toevade immune detection and actively suppress antitumourimmunity
Paclitaxel has a wide range of dose dependent immuno-modulatory effects described in Figure 5 At standard dosepaclitaxel is broadly immunosuppressive and this is becauseit inhibits a number of cell types involved in tumour rejectionsuch asmacrophages effector T cells andNK cells [101] How-ever at lower doses than typically used for chemotherapypaclitaxel has an important immunogenic role promotingantitumour immunity [101 102] Hence understanding theimmunological basis of paclitaxel may help to maximise themanipulation of the immunomodulatory effects of paclitaxel
8 BioMed Research International
Immunomodulatory effect of
paclitaxel
Stimulate direct cytotoxic activity by
macrophage
Induce activation maturation and priming of DCs
Stimulate NK-dependent antitumour immunity
Activation of tumour-specificCTL Expansion of memory T cells
Secretion of proinflammatory cytokine
Shift from Th2 to Th1 type ofresponse
Depletion of Tregs andmodulation of MDSC
Downregulates the expression of VEGFR-2
and inhibits angiogenesis
IL-6 IL-12 TNF-120572 and i-NOS
Figure 5 Immunomodulatory effect of paclitaxel Paclitaxel a toll-like receptor 4 (TLR4) ligand binds to TLR4 receptor and triggers TLR4signaling via MyD88 dependent and independent pathway Paclitaxel then promotes anticancer immune response directly by stimulatingmacrophages to kill cancer cells or indirectly by secretion of proinflammatory cytokines which upregulates activation of DCs NK andtumour specific CTL Paclitaxel promotes effective CTL response by upregulation of mannose-6-phosphate which facilitate permeabilityto granzyme B and cytokine patterns of T helper type 1 Paclitaxel modulates MDSC and ablates Tregs Memory T cells (CD4+CD45RO+and CD8+CD45RO+) increased significantly while regulatory T cells (Tregs) decreased around 2 weeks creating an opportunity window fordose-dense therapy and immunomodulatory agents to achieve clinical benefit Dose-dense and low dose paclitaxel also blocks new vesselformation by downregulating VEGF-receptor 2 reduces resistance by alternative mechanism of action
to develop better therapeutic options in the management ofadvanced ovarian cancer
Paclitaxel is a ligand to toll-like receptor 4 (TLR4) whichis expressed on innate immune cells including macrophagesThe binding of paclitaxel to TLR4 on macrophages trig-gers the MyD88 mitogen-activated protein kinase (MAPK)and transcription of nuclear factor NF-kappa B (NF-120581B)pathways (Figure 3) resulting in their activation and releaseof immunostimulatory cytokines such as tumour necrosisfactor-120572 (TNF-120572) interleukin-1 (IL-1) interleukin-6 (IL-6)and interleukin-8 (IL-8) [103ndash105] Activated macrophagescan either cause direct tumour cell lysis via release oflysosomal enzymes and nitric oxide (NO) or indirectly byactivating NK cells DCs and tumour-specific cytotoxic T-lymphocytes (CTLs) [101]
NK cells are also innate immune cells capable of killingtumour cells particularly those cells that have reduced classI MHC expression and therefore can escape killing by CTLsPaclitaxel can enhance NK cell function by inducing mRNAand protein production of perforin an effector moleculeinvolved inNKcell-mediated cytotoxicity [106]However theeffect of low dose paclitaxel on NK cells is controversial Inanother study it was found that treatment of human NK cellswith paclitaxel effectively inhibits NK cell-mediated killing ofK562 (human erythroleukemia) target cells in vitro withoutaffecting the viability of NK cells [107] However weeklypaclitaxel therapy for non-small cell lung cancer patients was
only able to reduce the NK cell function up to completion ofthe first cycle but thereafter it gradually recovered [108]
Dendritic cells also express TLR4 and can be directlyactivated by paclitaxel The binding of paclitaxel to TLR onimmature DCs promotes DC maturation by upregulatingantigen-processing machinery gene components costimu-latory molecules and IL-12p70 [102] This enhances theability of DCs to prime T cells which facilitate antitumourimmunity [109] Paclitaxel can also promote cytotoxic T-cell function by upregulating mannose-6-phosphate whichfacilitates permeability to granzyme B and also inducescytokine production patterns typical of the T helper type 1phenotype via IL-2 (CD4 T cell) and IFN-120574 (CD8 T cell)secretion [104 110] Activated CD8+ T cells can differentiateinto CTL type 1 (Tc1) cells producingmainly IFN-120574 and CTLtype 2 (Tc2) cells producing mostly IL-4 IL-5 and IL-10 Tc1cells are potent CTL involved in the defense against cancerTc1 cells are able to recognise tumour antigens in the contextof MHC class I and mediate tumour cell lysis The role of Tc2cells in the immune response is not clearly known althoughtheir presence has been associated with disease progression[111]
CD4+ CD25+ regulatory T-cells (Tregs) constitutingapproximately 5ndash10 of peripheral CD4+ T cells [112 113]play an important role in tumour immune evasion [114]There is growing evidence that supports the existence ofelevated numbers of Tregs in tumours [115ndash117] which may
BioMed Research International 9
suppress immune responses of other CD4+ and CD8+ cells[118ndash120] and promote tumour progression In murine stud-ies paclitaxel exhibits the ability to reduce the number andsize of Treg cells thereby enhancing antitumour immunity[119 121] Similar findingswere seenwith a selective reductionin the size and number of Treg populations in peripheralblood samples from non-small cell lung cancer (NSCLC)patients [122]
Paclitaxel also decreased the expression of the anti-apoptotic molecule Bcl-2 in Treg cells while increasing thecorresponding proapoptoticmember Bax which contributedto the apoptotic sensitivity of Treg to paclitaxel [87]This wasseen in a study using the 3LL Lewis tumour model whichdemonstrated that Treg cells exposed to paclitaxel displayeddown regulation of Bcl-2 and upregulation of Bax and uponblocking the Bcl-2 pathway the ability of paclitaxel to ablateTreg cells compared toT effectorswas impaired and bothTregand T effectors were affected These results may suggest thatpaclitaxel targets Bcl-2 rather than tubulin to contribute tothe distinctive effect on Treg cells [119] It has recently beenshown in vitro that paclitaxel could target Bcl-2 and thereforelead to apoptosis Bcl-2 family proteins are key regulators ofapoptosis and play an important role in tumourigenesis andmulti-drug resistance by blocking apoptosis [119 123]
Few studies have also shown effect of paclitaxel onmyeloid-derived suppressor cells (MDSCs) a heterogeneouspopulation of immature myeloid cells immunosuppressivein nature are recruited by cancer cells and are found inincreased amount in advanced epithelial ovarian cancer [124]In a murine study using C57BL6 mice administration ofpaclitaxel at ultralow dose modulates MDSCs to differentiateinto DCs in a TLR4 independent manner [110] Hencepaclitaxel in ultralow noncytotoxic doses together with itsangiogenesis blocking ability may potentially enhance theefficacy of immunotherapy by ablation of immunosuppres-sive populations such as Tregs and MDSCs in tumour-bearing hosts [50 102]
In immunocompromised patients with advanced ovariancancer with increased Tregs and decreased levels of CD4+T cell CD8+ T cell and NK subsets after a single courseof combined carboplatin and paclitaxel chemotherapy theimmunosuppression is reversed around 12 to 14 days later butnot before one week or after three to four weeks Not only areTregs decreased but also the proportions of IFN-120574 secretingCD8+ T cells T helper-1 Tc1 and NKT cells The ratio of Tc1to Tc2 cells increases significantly [111 120 125]
Following chemotherapy both CD4+CD45RO+ andCD8+CD45RO+ memory T cells increased significantly andpeaked around 2 weeks The increase of memory T cellsin ovarian cancer patients following chemotherapy prob-ably opens the door of opportunity to develop long-termimmunological memory which could prevent recurrenceand metastases [120] Administration of dose-dense therapygiven weekly may hence be beneficial immunologically tomount an adequate immune response compared to standard3-week therapy In addition administration of immunother-apy agentsmay also be ideal during the period of 2weeks afterchemotherapy where temporary immune system reconstitu-tion takes place
8 Clinical Studies
In the past two decades paclitaxel had been administered indoses ranging from 60 to 250mgm2 over 1ndash96 hours andfrom 1 to 3 weekly intervals Prolonged exposure up to 96hours was believed to be effective as demonstrated with pre-clinical data but later refuted in large prospective studies [14126 127] A 24-hour infusion of paclitaxel was subsequentlyadministered to reduce the risk of hypersensitivity reactionshowever it was shown to increase mucosal and bone marrowtoxicity without improved efficacy [127 128] Development ofeffective premedication has led to administration of shorterinfusions (lt3 hours) which are better tolerated in particularfrom a haematologic perspective but patients remain at riskof myalgia and neuropathy at higher doses Weekly one-hourlow dose paclitaxel also known as dose-dense therapy hasrecently emerged as another possible strategy to improveoutcomes
9 Dose-Dense Therapy
Dose-dense treatment is defined by delivery of a maintainedper-cycle dose or overall dose with administration of drugat shorter time intervals than is standard This differs fromdose intensity which refers to dose (per unit weight or bodysurface area) delivered per unit time Hence either escalationof dose per cycle or reducing the time in between cycles maymodify dose intensity [129 130]
The rationale for the dose-dense approach of weeklypaclitaxel is that more frequent delivery of moderate dosesmay achieve greater efficacy by allowing sustained exposureof dividing tumour cells to paclitaxelrsquos cytotoxic and antian-giogenic effects hence reducing resistance delaying relapseand increasing the possibility of cancer remission Three 1-hour infusions of paclitaxel given at a week interval achievedgreater dose-density as well as dose-intensity than a singleadministration every 3 weeksThe initial tissue concentration(gt50 nM) for 1-hour infusion is similar to that of 3-hourinfusion but the concentration in the plasma instead oflasting for 8 hours in a 3-hour infusion rapidly falls below50 nM in less than 75 minutes for 1-hour infusion and hencereduces the risk of neutropenia However the rate of fallexperienced in tissue concentration of the drug is slowerthan plasma concentration of the drug hence efficacy ismaintained [131 132] A shorter infusion time allows bettercontrol of toxicities improved patient comfort and reducedhospitalisation hours
Several studies have used dose-dense paclitaxel in thetreatment of advanced ovarian cancer and are summarizedin Table 1 Based on phase 1 studies the recommendeddose for weekly paclitaxel ranges between 80 and 90mgm2compared with 45mgm2 per week with 3-weekly paclitaxeland is given over 1-hour duration Weekly scheduling hasdemonstrated consistent activities in ovarian cancer studies[11ndash13] Response rates were in the 20ndash50 range whereusually less than 10 would be expected Grade-4 doselimiting toxicities in particular neutropenia were not evidentat any dose below 100mgm2week [11 133]
10 BioMed Research International
Table1Ph
ases
Iand
IIstu
dies
onintravenou
sdose-densep
aclitaxel
Stud
yRe
gimen
119899()
PI(m
)RR
()
CR(119899)
MedianPF
S(m
)Median
OS
(m)
Adversee
ffects
Com
ments
Paclitaxel
dose
(mgm
2 )Ca
rbop
latin
dose
(mgm
2 )Ph
aseIsinglea
gent
Lofflerre
tal1996
[11]
40ndash9
0week
1-hou
rinfusionfor
6weeks
5040
5NA
NA
(i)Hem
atologictoxicity-m
ild(ii)N
ograde3
or4
haem
atologicaltoxicity
neurologicalor
cardiotoxicityup
to90
mgm
2 wk
(iii)Nohypersensitivity
reactio
ns(patientsreceivedprem
edication)
(i)100
priorc
hemotherapy
(ii)M
ediando
seintensity
was
410m
gm
2 6w
k(range200
to540m
gm
2 6w
k)
Fenn
ellyetal
1997
[12]
40ndash100w
eek
1830
NA
NA
NA
(i)Nomucositiso
rgrade
III
neurop
athy
was
seen
(ii)A
lopeciao
ccurredin
one
(i)100
priorc
hemotherapy
(2ndash5
priorregim
ens)
(ii)P
artia
lrespo
nses
weres
eenin
four
of13
assessablepatients
(30
)(iii)Dose-lim
iting
toxicitywas
reachedat100m
gm
2 (iv
)2-3
patie
ntse
xperience
treatmentd
elay
(v)M
axim
um-to
lerateddo
seof
80mgm
2 Ab
u-Ru
stum
etal
1997
[13]
60ndash100
over
1ho
urw
eek
45289
NA
NA
NA
(i)Nopatie
nthadfebrile
neutropenia
(i)100
priorc
hemotherapy
(1ndash8
priorregim
ens)
PhaseIISing
leagent
Markm
anetal
2001
[14]
80over
1ho
urw
eek
53(52)
25NA
NA
NA
Therapydiscon
tinuedin
(i)4patie
ntsw
hohadperip
heral
neurop
athy
(ii)1
patie
ntdu
etopainful
fingernailbeds
(i)100
platinum
andpaclita
xel
resistant
(ii)Th
erapywas
discon
tinuedin
5patie
ntsb
ecause
oftoxicity
(iii)Only13
(1)w
erem
odified
(doser
eductio
nor
treatment
delay)
becauseo
fsidee
ffects
PhaseIICom
binedwith
platinum
agent
Kiku
chietal
2005
[15]
80over
1ho
urw
eek
AUC2week
27gt6
818
483
NA
(i)Neutro
penia(
17)
thrombo
cytopenia(
51
)(ii)N
ocaseso
fperipheral
neurop
athy
(grades3
and4)
inweeklycombinedT-C
Cadron
etal2007
[16]
90over
1ho
urw
eek
AUC4week
24 9gt6le6
73 38NR
8105
675
(i)Grade
34neutropenia(
34)
andneutropenicfever
in2
(ii)N
auseaa
ndvomiting
and
fatig
uewerethe
mostfrequ
ent
nonh
ematologicalsid
eeffects
(i)Doser
eductio
nwas
necessary
in25of
patie
nts
Pign
atae
tal2008
[17]
60over
1ho
urw
eek
AUC2week
24(13)lowastlowast
1stline
385
2320
136
(i)Notoxicd
eath
was
recorded
(ii)G
rade
2anaemiawas
repo
rted
insevenpatie
nts(27)
(iii)Nofebrile
neutropeniaw
asob
served
(iv)G
rade
3and4neutropenia
was
recorded
infive(19)a
ndon
e(4
)patients
(v)G
rade
3thrombo
cytopenia
occurred
inon
epatient
(4)
BioMed Research International 11
Table1Con
tinued
Stud
yRe
gimen
119899()
PI(m
)RR
()
CR(119899)
MedianPF
S(m
)Median
OS
(m)
Adversee
ffects
Com
ments
Paclitaxel
dose
(mgm
2 )Ca
rbop
latin
dose
(mgm
2 )
Safrae
tal2014
[18]
80over
1ho
urw
eek
AUC2week
133
1stline
864
645
274
(i)Highera
naem
ia(grade
III+
IV68vs53)+
IVneutropenia(
144vs69)
decreasedgradeIIa
lopecia(
235
vs981
)and
thrombo
cytopenia
(grade
III+
IV0
vs23)
Havrilesky
etal
2003
[19]
80over
1ho
urw
eek
AUC2weekD1
D8D15
until
progressionCR
+8courses
29 21 8
Total
grou
pgt6lt6
83 100
38
16 15 1114
115
137
32
(i)Hem
atologictoxicitywas
common
(grade
3neutropenia
32n
ograde4
neutropenia
grade3
or4thrombo
cytopenia
142)
(i)To
xicitymanaged
bytre
atment
delaydo
seredu
ctionof
paclitaxel
ordiscon
tinuatio
nof
carbop
latin
vanderB
urgetal
2014
[20]
90over
1ho
urw
eek
AUC4weekD1
D8D15
D29
D36
D49
+6x
TCq3w
108
65 43
Total
grou
pgt6lt6
76 5816 42
26 158 13
(i)Neutro
penia3
0
thrombo
cytopenia8
febrile
neutropenia0
5
(ii)N
onhaem
atologictoxicitywas
low
(i)Treatm
entw
asdelayedin
16
anddo
seredu
cedin
2of
cycle
s
119899num
bero
fpatientsassessableforrespo
nsemm
onthsPIplatinum
treatmentfreeintervalRR
respo
nser
ateCR
com
pleterem
issionT
paclitaxelC
carbop
latin
PFS
progressio
nfre
esurvivalOSoverall
survivalN
An
otavailableinpapero
rabstractandNR
notyetreached
lowastlowastElderly
popu
lation
patient
agedge70
years
12 BioMed Research International
Numerous phase II studies have explored the tolerabilityand the activity of weekly paclitaxel either as a single agent orin combination with several other drugs or biological agents(Table 1) A number of regimens combining weekly paclitaxelwith carboplatin have been used as first-line treatment inovarian cancer Carboplatin has been administered weeklyat AUC of 2 with dose escalation in some studies whilepaclitaxel had been infused at 60ndash80mgm2week Thiscombined regimen was well tolerated with a low incidence ofbone marrow suppression Overall response rates have beenhigh in the range of 60ndash80 in most studies even in heavilypretreated patients with platinum-resistant disease (diseaserecurrence or progression within 6 months of the last lineof platinum-based therapy) [15ndash20 134] The promising datafrom these phase II trials then led to the evolution of largerphase III trials
Three phase III studies Japanese Gynecologic OncologyGroup- (JGOG-) Trial 3016 [21ndash23] Multicentre Italian Trialin Ovarian Cancer-Trial 7 (MITO-7) [25] and GynecologicOncology Group GOG-262 Trial [24] have explored dosedense therapy The results of these trials are summarised inTable 2
The Japanese Gynecologic Oncology Group (JGOG)conducted a randomized phase 3 trial of dose-dense weeklypaclitaxel 80mgm2week in combination with 3-weeklycarboplatin compared to standard 3-weekly carboplatin andpaclitaxel 180mgm2 in patients with advanced epithelialovarian peritoneal or fallopian tube cancer (JGOG 3016NOVEL trial) In both arms carboplatin was given at AUC6 and the median number of cycles was six In this largestudy (119899 = 637) with a median follow up of 77 months therewas an 11-month improvement in themedian progression freesurvival (PFS) in the dose-dense treatment group comparedwith the standard treatment arm (282 versus 175 monthsHR 076 95 CI 062ndash091 119901 = 00037) Median OS wasalso higher in the dose-dense treatment arm (1005 versus622 months HR 079 95 CI 063ndash099 119901 = 0039)On subgroup analysis suboptimally debulked patients withresidual disease of gt1 cm (119899 = 342) had a significantlyhigher median overall survival in the dose dense arm (512versus 335 months HR-075 95 CI 057ndash097 119901 = 0027)There was no significant advantage to dose-dense treatmentfor patients with optimally cytoreduced disease Dose-densetherapy survival benefits were also not seen in patients withclear cell or mucinous histology type unlike serous typeHowever patient treated with dose dense therapy had asignificantly higher frequency of hematologic toxicity thanwith the standard arm (212 versus 94) which resultedin lower treatment completion rates (63 versus 48) withfrequent episodes of delay (76 versus 67) and dosereductions (48versus 35) [21 22]Therewas no significantdifference in terms of overall quality of life between the twoarms (119901 = 046) [23]
Using a similar regimen as in JGOG-3016 a GynecologicOncology Group (GOG)-262 Trial was conducted in theUnited States In this group most patients had stage IIIdisease (66ndash70) and two-thirds had suboptimal debulkingwith residual disease of gt1 cm This was a randomized phase
III trial of 3 weekly paclitaxel versus dose-dense weeklypaclitaxel in combination with carboplatin in patients withadvanced epithelial ovarian peritoneal or fallopian tubecancer Though optional concurrent and maintenance beva-cizumab were received by the majority of patients in botharms (835 versus 841 resp) There was no significantdifference in PFS in the patients who received the dosedense paclitaxelcarboplatin regimen compared to those whoreceived the standard paclitaxelcarboplatin regimen (148versus 143 months HR 097 95 CI 079ndash118) Howeverin a subgroup analysis there was a significant difference inPFS in the dose dense paclitaxel arm who did not receivebevacizumab 119899 = 112 (142 versus 103 months HR 059 95CI 037ndash096 119901 = 0003) Overall survival data is still imma-ture There was higher frequency of grade 3 anaemia (408versus 157 119901 lt 0001) and grade 2 sensory neuropathy(259 versus 178 119901 = 0012) but a lower incidence ofneutropenia (72 versus 83 119901 lt 0001) [24]
In 2008 the Multicentre Italian Trials in Ovarian Cancer(MITO-7) randomised 810 women in a phase 3 trial toreceive either standard carboplatin (AUC = 6) and paclitaxel175mgm2 every 3 weeks or a weekly schedule of paclitaxel(60mgm2) with carboplatin (AUC = 2) The majority ofpatients in both arms (83ndash90) received six cycles of therapyMost patients (58ndash63) had stage II1 disease 23 of themwere suboptimally debulked Median PFS did not differsignificantly (173 months and 183 months 119901 = 066)between the standard and dose-dense arms respectivelyThere was no significant difference in response rate betweenthe two arms nor the estimated 2-year overall survivalSubgroup analysis did not identify any subgroup that mayhave benefited from the dose-dense regimen Unlike theJGOG-3016 trial the incidence of grade 3-4 neutropenia wassignificantly lower in the dose-dense group compared to the3-weekly regimen (42 versus 50) A similar pattern wasseen for the incidence of febrile neutropenia (lt1 versus 3119901 = 002) thrombocytopenia (1 versus 7 119901 lt 0001)and other nonhaematological toxicities such as alopeciavomiting renal dysfunction and neuropathy Quality of lifewas reported to be significantly better in the dose-dense arm(119901 lt 00001) which was discordant with the JGOG-3016quality of life data [25]
In summary there was significant improvement inmedian PFS and overall survival in studies using paclitaxelat 80mgm2week dose-dense therapy [21 24] but withhigher haematological toxicity whereas MITO-7 [25] whichwas using paclitaxel at 60mgm2week was only equivalentlyeffective but less toxicThis does not conclude that the higherpaclitaxel dose is more clinically beneficial as there are manyother confounding factors in all three studies
In a multivariate analysis the JGOG-3016 study [21]reported that a lower dose intensity of paclitaxel (lt80) wasassociated with poorer overall survival (hazard ratio = 14295 confidence interval 112ndash181 119901 = 0004) however itmust be highlighted that the investigational arm carboplatinschedules were not standardised in these studies The JGOGand GOG trials delivered a 3-weekly carboplatin (AUC =6) arm whereas in the MITO-7 study the carboplatin was
BioMed Research International 13
Table2Ph
aseIIIstu
dies
onintravenou
sdose-densep
aclitaxel
Stud
yRe
gimen
119899
MedianPF
S(m
)
Median
OS
(m)
Adversee
ffects
Com
ments
Katsu
matae
tal2009
[21]
Katsu
matae
tal2013
[22]
Haranoetal2014
[23]
JGOG3016
631
(i)Haematologicaltoxicityhigh
erin
dose
dense-211versus
94
Lower
treatmentcom
pletionin
dose-dense
63versus
48
Frequent
episo
deso
fdelay
indo
se-dense
76versus
67
Doser
eductio
nsin
dose-dense
48versus
35
Nosig
nificantd
ifference
inoverallQ
OL
betweenbo
thgrou
ps(119901=046)
Paclitaxel80m
gm
2D18
15+carbop
latin
AUC63
weeklyversus
Paclitaxel180
mgm
2+
carbop
latin
AUC63
weekly
312
282
1005
Both
givenfor6
ndash9cycle
s319
175
622
Chan
etal2013
[24]
GOG-262
(i)Higherfrequ
ency
ofgrade3
anaemia
(408versus
157119901lt0001)
grade2
sensoryneurop
athy
(259versus
178
119901=0012)b
utlower
incidenceo
fneutropenia(
72versus
83119901lt0001)
Paclitaxel80m
gm
2D18
15+carbop
latin
AUC63
weeklyversus
Paclitaxel175
mgm
2+
carbop
latin
AUC63
weekly
346
148
NR
Both
givenfor6
cycle
s346
143
NR
Bevacizumab
given
optio
nally
112
(did
not
receive
bevazicumab)
142vs
103
Pign
atae
tal2014
[25]
MITO-7
810
(i)Lo
wer
incidenceo
fgrade
3-4
neutropenia(
42versus
50)febrile
neutropenia(lt1v
ersus3
119901=002)
thrombo
cytopenia(
1versus7
119901lt0001)andothern
onhaem
atological
toxicitie
ssuchas
alop
eciavom
iting
renald
ysfunctio
nandneurop
athy
Qualityof
lifeb
etterindo
sedensea
rm(119901lt00001)
Paclitaxel60m
gm
2 weekly+carbop
latin
AUC
2weeklyversus
Paclitaxel175
mgm
2+
carbop
latin
AUC63
weekly
406
404
183 173
77lowast
79lowast
119899num
bero
fpatientsmm
onthsDday
PFSprogressionfre
esurvivalOSoverallsurvivalNAnot
availableinpapero
rabstractandNR
notyetreached
lowastSurvivalrateat2years
14 BioMed Research International
dose-dense (AUC 2 weekly) Although it is possible that thedose scheduling for the platinum-based agent is not essentialfor a survival benefit as shown by previous studies usingdose-dense cisplatin direct cross-trial comparison cannot bemade Unlike paclitaxel carboplatin probably requires peakdose for optimal therapeutic benefit hence this may accountfor the inferior survival outcome in MITO-7 trial Anotherconfounding factor may be difference in ethnicity All threestudies used different ethnic populations and Asian patientsin JGOG-3016 appear to have better survival outcomes thanthe MITO-7 Western population Ethnicity with possibleunderlying genetic causes may be responsible for the variableresponses to chemotherapy across individuals [135] This wasexplored by Millward et al who studied 68 Caucasian andAsian lung cancer patients treated with a combination ofpaclitaxel and carboplatin and found that the incidence offebrile neutropenia was 50 of an initially treated cohortof Asians and when carboplatin was subsequently dosereduced in all Asian patients the overall incidence of febrileneutropenia was also reduced to 26 [136]
Although early clinical data from phase I and phaseII dose-dense paclitaxel trials in advanced ovarian cancerwere promising the results from phase III studies in havebeen inconsistent as a result of differences in paclitaxel dosecarboplatin AUC and schedule addition of bevacizumabas well as different ethnic populations The results of arecently completed randomised three arms GynaecologicCancer InterGroup (GCIG) phase II trial ICON 8 mayfurther inform the clinical benefit of dose dense paclitaxeltherapy
This multicentre trial involving 111 centres in the UKSouth Korea Mexico Ireland Australia and New Zealandwith a target population of 1485 patients with stage IC-IV epithelial ovarian cancer or peritoneal or fallopian tubecancer compared two dose-dense arms (i) JGOG-like armcarboplatin AUC 5 plus weekly 80mgm2 paclitaxel and (ii)MITO-7-like arm weekly carboplatin AUC 167 plus weekly80mgm2 paclitaxel to the standard 3-weekly treatment(carboplatin AUC 5 plus 175mgm2 paclitaxel) for stage IC toIV epithelial ovarian cancer The dose-dense arms of MITO-7 and JGOG-3016 as well as the ethnic heterogeneity will befurther addressed
10 Intraperitoneal (IP) Chemotherapy
In addition to dose and scheduling the route of adminis-tration of chemotherapy agents plays an important role inoutcome Intraperitoneal spread is common and likely anearly event in epithelial ovarian cancer hence the deliveryof chemotherapy intraperitoneally in theory would exposethe microcirculation of tumour to higher doses of drug thansystemic administration while limiting systemic toxicityTheideal drug for IP chemotherapy is one that is systemicallyeffective penetrates deep into the inner core of tumour tissueand remains within the peritoneal cavity for a prolongedperiod of time [137ndash139]
Early clinical studies confirmed that indeed the peritonealcavity could be exposed to 10 to 20-fold higher (cisplatin
and carboplatin) drug concentration than when using theintravenous approach and since 1978 this route had beenadopted as a form of therapeutic intervention [137 139]A subsequent phase I trial showed that IP paclitaxel haddose-limiting toxicity in the form of abdominal pain [140]Another phase 1 GOG pilot study administered weekly IPpaclitaxel at an initial dose of 20mgm2 for 16 weeks to33 patients and found that IP paclitaxel at this dose wasfeasible and well tolerated At dose levels 60 to 65mgm2there were significant levels of paclitaxel for a week afterdrug administration suggesting very slow clearance andcontinuous exposure of the peritoneal cavity to active drugconcentrations [132]
Hence this initiated a phase II study [141] that used pacli-taxel intraperitoneally at a dose of 60ndash65mgm2week In thisphase II GOG study 76 patients with small-volume resid-ual disease carcinoma (05 cm or less) involving the ovaryperitoneal or fallopian tube were treated with paclitaxel60mgm2week intraperitoneally for 16 weeks followed bysurgical evaluation in patients without disease progressionThe Gynaecologic Oncology group (GOG) currently definesno visible disease as microscopic disease being the idealsurgical outcome 75 of patients had received prior systemictherapy and 70 received all 16 courses that were planned Of28 patients with microscopic disease at the start of therapy61 achieved a surgically defined complete response whereasonly 1 out of 31 patients with macroscopic disease achieved acomplete response The median time-to-recurrence was 167months with an estimated survival rate at 2 years being 58Treatment was generally well tolerated [141]
Another study looked into the effect of IP paclitaxel asconsolidation therapy in advanced ovarian cancer Twenty-eight patients who had initial residual macroscopic disease(lt1 cm) after primary surgery or interval debulking but hadcomplete pathological response following standard treatmentwith at least 6 cycles of platinum-based chemotherapy regi-men received paclitaxel 60mgm2week intraperitoneally for12ndash16 weeks as consolidation therapy The median time torecurrence was 25 months but overall survival did not differsignificantly when compared with control group submittedto observation only Treatment-related toxicity was mild andtechnical difficulties were observed in 11 of patients [142]
Multicenter randomised phase 3 trials as well as meta-analysis of IP chemotherapy have been performed anddemonstrated that chemotherapy drugs administered intra-peritoneally are superior to intravenous standard regimensin patient with optimally debulked epithelial ovarian cancerThe most impressive data comes from GOG 114 [14] and172 trial [143] In GOG 114 patients received either sixcycles of intravenous paclitaxel 135mgm2 and cisplatin75mgm2 every 3 weeks or intravenous carboplatin (AUC= 9) every 28 days for two cycles followed by six 3-weeklycycles of intravenous paclitaxel 135mgm2 and IP cisplatin100mgm2 [14] whereas in GOG 172 patients received eitherintravenous paclitaxel 135mgm2 followed by intravenouscisplatin 75mgm2 or intravenous paclitaxel 135mgm2 fol-lowed by IP combination of cisplatin 100mgm2 and pacli-taxel 60mgm2 on day 8 Both trials had a combined total
BioMed Research International 15
of 876 women with stage III epithelial ovarian carcinomaoptimally debulked to le1 cm residual tumour [143] Themedian follow-up for GOG 114 [14] was 138 years with GOG172 [143] was 97 years The primary results of the individualtrials reported up to 6-month improvement in median PFSfollowing IP therapy In the combined analysis of the datafrom both trials the data continued to show a 5-monthdifference in favour of IP therapy (25 versus 20 months)which translates into 16 reduction in the hazard ratio forprogression (119901 = 003) In GOG 114 [14] reported in 2001there was only borderline improvement in overall survivalassociated with this regimen (median 63 versus 52 monthsrelative risk 081 119901 = 005)
However in combined analysis in 2013 which was pre-sented at the Society of Gynecologic Oncology AnnualMeeting [144] the overall survival showed an 11-monthimprovement in favour of IP therapy in GOG 114 whereasGOG 172 reported a 16-month survival advantage Amongpatients treated with IP therapy the 5-year survival rateincreased from 18 following completion of 1-2 cycles to 59for patients who completed 5-6 cycles of treatment Howeverthere was increased toxicity observed in the IP arm grade 3-4 leukopenia thrombocytopenia and abdominal pain Only42 of patients in the GOG172 trial [143] completed all sixcycles of planned treatment in the IP arm while 18 ofpatients in GOG 114 trial [14] received fewer than two coursesof IP chemotherapy
Another randomised phase III trial involving patientswith stages II-III epithelial ovarian carcinoma is the GOG252 study with three arms Arm 1-dose-dense intravenouscarboplatin and paclitaxel Arm 2-dose-dense intravenouspaclitaxel and IP carboplatin and Arm 3 consists of 3-weeklyintravenous paclitaxel (day 1) followed by IP cisplatin (day 2)and IP paclitaxel (day 3) regimen All three arms also incor-porate the combination and maintenance of bevacizumabGOG 252 has completed accrual and results are awaited [139]
11 Newer Forms of Paclitaxel
Development of next-generation taxanes has taken place overthe past 40 years aimed at eliminating toxicity improvingefficacy and ease of administration Abraxane is a novelcompound which incorporates paclitaxel into an albuminnanoparticle soluble in saline hence eliminating the needfor Cremophor EL which is responsible for hypersensitivityreactions experienced during paclitaxel infusion [145] Thenanoparticle albumin in nab-paclitaxel is able to bind toglycoprotein gp60 receptor an albumin receptor and activatecaveolin-1 a protein that in human is encoded byCAV-1 geneleading to formation of caveoli hence allowing nab-paclitaxelto migrate across the endothelial cell membrane into theinterstitial space leading to higher intratumoural drug con-centration In addition Abraxane exhibits linear pharma-cokinetics and can therefore be given at a relatively higherdose than standard intravenous paclitaxel leading to a highertherapeutic ratio and heightened efficacy in solid tumoursmainlymetastatic breast cancer [146 147] Nab-paclitaxel hadFDA approval in 2005 for treatment of breast cancer [148]
Nab-paclitaxel has been studied in recurrent ovariancancer As a single agent in phase II 44 patients withrecurrent ovarian cancer were treated with Nab-paclitaxel260mgm2 intravenously for 30 minutes every 3 weeks for6 cycles Ninety-two percent of patients were platinum-sensitive while 89 had had previous exposure to standardtaxane The objective response rate was 64 with 15 patientsachieving complete response and 13 of them had partialresponse Estimated median PFS was 85 months No hyper-sensitivity reactions were observed and there were infrequentcases of grade 4 neutropenia (11) and grade 2-3 neuropathy(13) [149]
Another phase II study by GOG enrolled 51 patients withplatinum- and taxane-resistant recurrent ovarian cancer outof which 47 were evaluable The objective response rate was38 with one patient achieving a complete response and 10patients a partial response The median PFS was 45 monthswhile overall survival rate was 174 months Severe haema-tological and nonhaematological toxicities including neuro-toxicity were uncommon These results are quite impressivegiven the treatment population consisted of patients withvery poor prognosis with a median platinum and taxane freeinterval of 21 days and 70 had their recurrence within 3months of completion of primary treatment [150] Severalother trials of this formulation are in progress
Paclitaxel poliglumex (PPX) also known as Xyotax isanother prodrug a novel conjugate of paclitaxel and 120572-poly-L-glutamic acid which accumulates within tumour tissuedue to increased permeability of the tumour vessels and lackof lymphatic drainage [148 151 152] Paclitaxel poliglumexenhances solubility of paclitaxel allows direct delivery tothe intratumoural microenvironment and allows prolongedexposure to the active drug while minimising systemictoxicities [151] In Phase I dose escalation studies as a singleagent the recommended dose of PPX was 235mgm2 over 10minutes every 3 weeks or 70mgm2 weekly [153] In a PhaseII GOG study of relapsed ovarian cancer a response rate of16 was seen with infrequent serious adverse events grade3 and 4 neutropenia (24 and 20) and grade 3 neuropathy(24) [154] A phase III trial (GOG-0212) on the use of PPXas consolidation ormaintenance therapy in advanced ovariancancer is in progress
DHA-paclitaxel also known as Taxoprexin is a prodrugwhere paclitaxel is covalently conjugated with the naturallyoccurring omega-3 fatty acid docosahexaenoic acid (DHA)a fatty acid that is easily taken up by tumour cells henceincreasing intratumoural concentration of paclitaxel leadingtumour cell apoptosis [155 156] DHA-paclitaxel exhibitslinear pharmacokinetics and lower toxicity and also ease ofadministration when compared to conventional paclitaxeland has demonstrated antineoplastic activity in animal mod-els of cancer as well as in a phase III trial involving metastaticmelanoma [156ndash160] In a recent study on human ovariancancer cells it was found that DHA could reverse paclitaxelresistance by inhibiting P-gp as well as downregulatingthe expression of multidrug resistance associated proteins(MRP) and inhibiting the activity of NF-120581B and p38 MAPKsignalling pathways [161]
16 BioMed Research International
12 Future Directions
A plateau has been reached regarding the benefits associatedwith standard 3-weekly intravenous administration of cyto-toxic chemotherapy in advanced epithelial ovarian cancerThe ongoing battle for a better treatment regimen to delayrelapse promote remission and most importantly improvethe quality of life of patients with advanced epithelial ovariancancer need not to go further than the ability to relook at thechemotherapy agents that are already available in a differentapproach
Novel compounds to date have not yet shown clinicalsuperiority and parent compounds such as paclitaxel con-tinue to surprise us with their feasibility effectiveness andmanageable toxicity profiles Intraperitoneal paclitaxel willrequire further evaluation Better effort in understanding themechanism of action of drugs including the role of dosescheduling and the effect on the immune systemmay providea more cost-effective route to better clinical outcomes
Conflict of Interests
The authors declare no conflict of interests in this work
Acknowledgments
The authors would like to thank the many researchers whohave contributed to our current knowledge of paclitaxelNirmala Kampan is supported by Australian Monash Uni-versity Institute of Graduate Research Scholarship as wellas Universiti Kebangsaan Malaysia Postgraduate ScholarshipAward Mutsa Madondo has received Postgraduate Pub-lication Award from Monash University and MagdalenaPlebanski has been awarded Senior NHMRC Fellowship
References
[1] Australian Institute of Health and Welfare and National Breastand Ovarian Cancer Centre (Australia) Ovarian Cancer inAustralia AnOverview 2010 Cancer Series Australian Instituteof Health and Welfare Canberra Australia 2010
[2] R E Bristow R S Tomacruz D K Armstrong E L Trimbleand F J Montz ldquoSurvival effect of maximal cytoreductivesurgery for advanced ovarian carcinoma during the platinumera a meta-analysisrdquo Journal of Clinical Oncology vol 20 no 5pp 1248ndash1259 2002
[3] ZKempand JA Ledermann ldquoUpdate onfirst-line treatment ofadvanced ovarian carcinomardquo International Journal of WomenrsquosHealth vol 5 no 1 pp 45ndash51 2013
[4] A du Bois H-J Luck W Meier et al ldquoA randomized clinicaltrial of cisplatinpaclitaxel versus carboplatinpaclitaxel as first-line treatment of ovarian cancerrdquo Journal of the National CancerInstitute vol 95 no 17 pp 1320ndash1330 2003
[5] R F Ozols B N Bundy B E Greer et al ldquoPhase III trialof carboplatin and paclitaxel compared with cisplatin andpaclitaxel in patients with optimally resected stage III ovariancancer A Gynecologic Oncology Group studyrdquo Journal ofClinical Oncology vol 21 no 17 pp 3194ndash3200 2003
[6] W P McGuire W J Hoskins M F Brady et al ldquoCyclophos-phamide and cisplatin compared with paclitaxel and cisplatin
in patients with stage III and stage IV ovarian cancerrdquoThe NewEngland Journal of Medicine vol 334 no 1 pp 1ndash6 1996
[7] W P McGuire W J Hoskins M F Brady et al ldquoCyclophos-phamide and cisplatin versus paclitaxel and cisplatin a phase IIIrandomized trial in patients with suboptimal stage IIIIV ovar-ian cancer (from the gynecologic oncology group)rdquo Seminars inOncology vol 23 no 5 supplement 12 pp 40ndash47 1996
[8] M J Piccart K Bertelsen K James et al ldquoRandomized inter-group trial of cisplatin-paclitaxel versus cisplatin-cyclophosph-amide inwomenwith advanced epithelial ovarian cancer three-year resultsrdquo Journal of the National Cancer Institute vol 92 no9 pp 699ndash708 2000
[9] P A Vasey G C Jayson A Gordon et al ldquoPhase III random-ized trial of docetaxel-carboplatin versus paclitaxel-carboplatinas first-line chemotherpy for ovarian carcinomardquo Journal of theNational Cancer Institute vol 96 no 22 pp 1682ndash1691 2004
[10] B Gronlund C Hogdall H H Hansen and S A EngelholmldquoResults of reinduction therapy with paclitaxel and carboplatinin recurrent epithelial ovarian cancerrdquo Gynecologic Oncologyvol 83 no 1 pp 128ndash134 2001
[11] T M Loffler W Freund J Lipke and T-U HausamenldquoSchedule- and dose-intensified paclitaxel as weekly 1-hourinfusion in pretreated solid tumors results of a phase III trialrdquoSeminars in Oncology vol 23 no 6 supplement 16 pp 32ndash341996
[12] D Fennelly C Aghajanian F Shapiro et al ldquoPhase I and phar-macologic study of paclitaxel administered weekly in patientswith relapsed ovarian cancerrdquo Journal of Clinical Oncology vol15 no 1 pp 187ndash192 1997
[13] N R Abu-Rustum C Aghajanian R R Barakat D Fennelly FShapiro and D Spriggs ldquoSalvage weekly paclitaxel in recurrentovarian cancerrdquo Seminars inOncology vol 24 no 5 supplement15 pp S15-62ndashS15-67 1997
[14] M Markman B N Bundy D S Alberts et al ldquoPhase III trialof standard-dose intravenous cisplatin plus paclitaxel versusmoderately high-dose carboplatin followed by intravenouspaclitaxel and intraperitoneal cisplatin in small-volume stageIII ovarian carcinoma an intergroup study of the gynecologiconcology group Southwestern Oncology Group and EasternCooperativeOncologyGrouprdquo Journal of Clinical Oncology vol19 no 4 pp 1001ndash1007 2001
[15] A Kikuchi H Sakamoto and T Yamamoto ldquoWeekly car-boplatin and paclitaxel is safe active and well tolerated inrecurrent ovarian cancer cases of Japanese women previouslytreated with cisplatin-containing multidrug chemotherapyrdquoInternational Journal of Gynecological Cancer vol 15 no 1 pp45ndash49 2005
[16] I Cadron K Leunen F Amant T van Gorp P Nevenand I Vergote ldquoThe lsquoLeuvenrsquo dose-dense paclitaxelcarboplatinregimen in patients with recurrent ovarian cancerrdquo GynecologicOncology vol 106 no 2 pp 354ndash361 2007
[17] S Pignata E Breda G Scambia et al ldquoA phase II studyof weekly carboplatin and paclitaxel as first-line treatment ofelderly patients with advanced ovarian cancer A Multicen-tre Italian Trial in Ovarian cancer (MITO-5) studyrdquo CriticalReviews in OncologyHematology vol 66 no 3 pp 229ndash2362008
[18] T Safra S Shamai J Greenberg et al ldquoWeekly carboplatinwith paclitaxel compared to standard three-weekly treatment inadvanced epithelial ovarian carcinomamdasha retrospective studyrdquoGynecologic Oncology vol 132 no 1 pp 18ndash22 2014
BioMed Research International 17
[19] L J Havrilesky A A Alvarez R A Sayer et al ldquoWeekly low-dose carboplatin and paclitaxel in the treatment of recurrentovarian and peritoneal cancerrdquo Gynecologic Oncology vol 88no 1 pp 51ndash57 2003
[20] M van der BurgW Onstenk I Boere et al ldquoLong-term resultsof a randomised phase III trial of weekly versus three-weeklypaclitaxelplatinum induction therapy followed by standardor extended three-weekly paclitaxelplatinum in Europeanpatients with advanced epithelial ovarian cancerrdquo EuropeanJournal of Cancer vol 50 no 15 pp 2592ndash2601 2014
[21] N Katsumata M Yasuda F Takahashi et al ldquoDose-densepaclitaxel once a week in combination with carboplatin every3 weeks for advanced ovarian cancer a phase 3 open-labelrandomised controlled trialrdquoThe Lancet vol 374 no 9698 pp1331ndash1338 2009
[22] N Katsumata M Yasuda S Isonishi et al ldquoLong-term resultsof dose-dense paclitaxel and carboplatin versus conventionalpaclitaxel and carboplatin for treatment of advanced epithelialovarian fallopian tube or primary peritoneal cancer (JGOG3016) a randomised controlled open-label trialrdquo The LancetOncology vol 14 no 10 pp 1020ndash1026 2013
[23] K Harano F Terauchi N Katsumata et al ldquoQuality-of-lifeoutcomes from a randomized phase III trial of dose-denseweekly paclitaxel and carboplatin compared with conventionalpaclitaxel and carboplatin as a first-line treatment for stage II-IV ovarian cancer Japanese Gynecologic OncologyGroup Trial(JGOG3016)rdquo Annals of Oncology vol 25 no 1 pp 251ndash2572014
[24] J Chan M F Brady R Penson et al ldquoPhase III trial ofevery-3-weeks paclitaxel vs dose dense weekly paclitaxel withcarboplatin +minus bevacizumab in epithelial ovarian peritonealfallopian tube cancer GOG 262 (NCT01167712)rdquo InternationalJournal of Gynecological Cancer vol 23 no 8 supplement 1 pp9ndash10 2013
[25] S Pignata G Scambia D Katsaros et al ldquoCarboplatin pluspaclitaxel once a week versus every 3 weeks in patients withadvanced ovarian cancer (MITO-7) a randomisedmulticentreopen-label phase 3 trialrdquoThe Lancet Oncology vol 15 no 4 pp396ndash405 2014
[26] V Walsh and J Goodman ldquoFrom taxol to Taxol the changingidentities and ownership of an anti-cancer drugrdquo MedicalAnthropology vol 21 no 3-4 pp 307ndash336 2002
[27] R Renneberg ldquoBiotech History yew trees paclitaxel synthesisand fungirdquo Biotechnology Journal vol 2 no 10 pp 1207ndash12092007
[28] J E Liebmann J A Cook C Lipschultz D Teague J Fisherand J B Mitchell ldquoCytotoxic studies of paclitaxel (Taxol) inhuman tumour cell linesrdquo British Journal of Cancer vol 68 no6 pp 1104ndash1109 1993
[29] J J Manfredi and S B Horwitz ldquoTaxol an antimitotic agentwith a newmechanism of actionrdquo Pharmacology andTherapeu-tics vol 25 no 1 pp 83ndash125 1984
[30] D G I Kingston ldquoRecent advances in the chemistry of taxolrdquoJournal of Natural Products vol 63 no 5 pp 726ndash734 2000
[31] D G I Kingston ldquoThe shape of things to come structural andsynthetic studies of taxol and related compoundsrdquo Phytochem-istry vol 68 no 14 pp 1844ndash1854 2007
[32] V Walsh and J Goodman ldquoCancer chemotherapy biodiversitypublic and private property the case of the anti-cancer drugTaxolrdquo Social Science amp Medicine vol 49 no 9 pp 1215ndash12251999
[33] P H Wiernik E L Schwartz J J Strauman J P Dutcher RB Lipton and E Paietta ldquoPhase I clinical and pharmacokineticstudy of taxolrdquo Cancer Research vol 47 no 9 pp 2486ndash24931987
[34] W P McGuire E K Rowinsky N B Rosenhein et alldquoTaxol a unique antineoplastic agent with significant activityin advanced ovarian epithelial neoplasmsrdquo Annals of InternalMedicine vol 111 no 4 pp 273ndash279 1989
[35] ldquoDiscovery and development of taxolrdquo in Taxol Science andApplications M W M E Suffness Ed pp 3ndash25 CRC PressBoca Raton Fla USA 1995
[36] M J Piccart and F Cardoso ldquoProgress in systemic therapy forbreast cancer an overview and perspectivesrdquo European Journalof Cancer Supplement vol 1 no 2 pp 56ndash69 2003
[37] P Bonomi K B Kim and J Kugler ldquoComparison of survival forstage IIIB versus stage IV non-small cell lung cancer (NSCLC)patients with etoposide-cisplatin versus taxol-cisplatin an East-ern Cooperative Oncology Group (ECOG) trialrdquo in Proceedingsof the American Society of Clinical Oncology vol 16 p 454a1997
[38] D Guenard F Gueritte-Voegelein J Dubois and P PotierldquoStructure-activity relationships of Taxol and Taxotere ana-loguesrdquo Journal of the National Cancer Institute Monographsno 15 pp 79ndash82 1993
[39] D G I Kingston ldquoTaxol the chemistry and structure-activityrelationships of a novel anticancer agentrdquo Trends in Biotechnol-ogy vol 12 no 6 pp 222ndash227 1994
[40] E K Rowinsky and R C Donehower ldquoPaclitaxel (taxol)rdquo TheNew England Journal of Medicine vol 332 no 15 pp 1004ndash10141995
[41] J Parness and S B Horwitz ldquoTaxol binds to polymerizedtubulin in vitrordquo Journal of Cell Biology vol 91 no 2 pp 479ndash487 1981
[42] A Dammermann A Desai and K Oegema ldquoTheminus end insightrdquo Current Biology vol 13 no 15 pp R614ndashR624 2003
[43] CWiese and Y Zheng ldquoMicrotubule nucleation 120574-tubulin andbeyondrdquo Journal of Cell Science vol 119 no 20 pp 4143ndash41532006
[44] A Ganguly H Yang and F Cabral ldquoPaclitaxel-dependent celllines reveal a novel drug activityrdquo Molecular Cancer Therapeu-tics vol 9 no 11 pp 2914ndash2923 2010
[45] P B Schiff and S B Horwitz ldquoTaxol stabilizes microtubules inmouse fibroblast cellsrdquo Proceedings of the National Academy ofSciences of the United States of America vol 77 no 3 pp 1561ndash1565 1980
[46] P B Schiff J Fant and S B Horwitz ldquoPromotion of micro-tubule assembly in vitro by Taxolrdquo Nature vol 277 no 5698pp 665ndash667 1979
[47] D Zhang R Yang S Wang and Z Dong ldquoPaclitaxel new usesfor an old drugrdquoDrug Design Development andTherapy vol 8pp 279ndash284 2014
[48] S Rao G A Orr A G Chaudhary D G I Kingston and SB Horwitz ldquoCharacterization of the taxol binding site on themicrotubule 2-(m-Azidobenzoyl)taxol photolabels a peptide(amino acids 217-231) of beta-tubulinrdquoThe Journal of BiologicalChemistry vol 270 no 35 pp 20235ndash20238 1995
[49] F Wang Y Cao W Zhao H Liu Z Fu and R Han ldquoTaxolinhibits melanoma metastases through apoptosis inductionangiogenesis inhibition and restoration of E-cadherin andnm23 expressionrdquo Journal of Pharmacological Sciences vol 93no 2 pp 197ndash203 2003
18 BioMed Research International
[50] A Sevko V Kremer C Falk et al ldquoApplication of paclitaxel inlow non-cytotoxic doses supports vaccination with melanomaantigens in normal micerdquo Journal of Immunotoxicology vol 9no 3 pp 275ndash281 2012
[51] T Kreis and R Vale Guidebook to the Cytoskeletal and MotorProteins Oxford University Press Oxford UK 2nd edition1999
[52] P Giannakakou D L Sackett Y-K Kang et al ldquoPaclitaxel-resistant human ovarian cancer cells have mutant 120573-tubulinsthat exhibit impaired paclitaxel-driven polymerizationrdquo TheJournal of Biological Chemistry vol 272 no 27 pp 17118ndash171251997
[53] E Rakovitch W Mellado E J Hall T K Pandita S Sawantand C R Geard ldquoPaclitaxel sensitivity correlates with p53status and DNA fragmentation but not G2M accumulationrdquoInternational Journal of Radiation Oncology Biology Physics vol44 no 5 pp 1119ndash1124 1999
[54] S W Lowe S Bodis A McClatchey et al ldquop53 status and theefficacy of cancer therapy in vivordquo Science vol 266 no 5186 pp807ndash810 1994
[55] C C Zhang J-M Yang E White M Murphy A Levine andW N Hait ldquoThe role of MAP4 expression in the sensitivity topaclitaxel and resistance to vinca alkaloids in p53 mutant cellsrdquoOncogene vol 16 no 12 pp 1617ndash1624 1998
[56] K Fukasawa T Choi R Kuriyama S Rulong and G F VandeWoude ldquoAbnormal centrosome amplification in the absence ofp53rdquo Science vol 271 no 5256 pp 1744ndash1747 1996
[57] T-H Wang Y-H Chan C-W Chen et al ldquoPaclitaxel (Taxol)upregulates expression of functional interleukin-6 in humanovarian cancer cells through multiple signaling pathwaysrdquoOncogene vol 25 no 35 pp 4857ndash4866 2006
[58] E Yakirevich E Sabo I Naroditsky Y Sova O Lavie andM B Resnick ldquoMultidrug resistance-related phenotype andapoptosis-related protein expression in ovarian serous carcino-masrdquo Gynecologic Oncology vol 100 no 1 pp 152ndash159 2006
[59] G Szakacs J K Paterson J A Ludwig C Booth-Genthe andM M Gottesman ldquoTargeting multidrug resistance in cancerrdquoNature Reviews Drug Discovery vol 5 no 3 pp 219ndash234 2006
[60] L W Pfannenstiel S S K Lam L A Emens E M Jaffeeand T D Armstrong ldquoPaclitaxel enhances early dendritic cellmaturation and function through TLR4 signaling in micerdquoCellular Immunology vol 263 no 1 pp 79ndash87 2010
[61] N Klauber S Parangi E Flynn E Hamel and R J DrsquoAmatoldquoInhibition of angiogenesis and breast cancer in mice by themicrotubule inhibitors 2-methoxyestradiol and Taxolrdquo CancerResearch vol 57 no 1 pp 81ndash86 1997
[62] D Belotti V Vergani T Drudis et al ldquoThe microtubule-affecting drug paclitaxel has antiangiogenic activityrdquo ClinicalCancer Research vol 2 no 11 pp 1843ndash1849 1996
[63] D H Lau L Xue L J Young P A Burke and A T CheungldquoPaclitaxel (Taxol) an inhibitor of angiogenesis in a highlyvascularized transgenic breast cancerrdquo Cancer Biotherapy andRadiopharmaceuticals vol 14 no 1 pp 31ndash36 1999
[64] X Jiang ldquoHarnessing the immune system for the treatment ofbreast cancerrdquo Journal of Zhejiang University Science B vol 15no 1 pp 1ndash15 2014
[65] A Gadducci D Katsaros P Zola et al ldquoWeekly low-dosepaclitaxel as maintenance treatment in patients with advancedovarian cancer who had microscopic residual disease atsecond-look surgery after 6 cycles of paclitaxelplatinum-basedchemotherapy Results of an open noncomparative phase 2
multicenter italian study (after-6 protocol 2)rdquo InternationalJournal of Gynecological Cancer vol 19 no 4 pp 615ndash619 2009
[66] R S Bhatt J Merchan R Parker et al ldquoA phase 2 pilot trial oflow-dose continuous infusion or lsquometronomicrsquo paclitaxel andoral celecoxib in patients with metastatic melanomardquo Cancervol 116 no 7 pp 1751ndash1756 2010
[67] M Caballero J J Grau J L Blanch et al ldquoSerum vascularendothelial growth factor as a predictive factor in metronomic(weekly) paclitaxel treatment for advanced head and neckcancerrdquo Archives of OtolaryngologymdashHead and Neck Surgeryvol 133 no 11 pp 1143ndash1148 2007
[68] J Alexandre Y Hu W Lu H Pelicano and P Huang ldquoNovelaction of paclitaxel against cancer cells bystander effect medi-ated by reactive oxygen speciesrdquo Cancer Research vol 67 no 8pp 3512ndash3517 2007
[69] T Hadzic N Aykin-Burns Y Zhu et al ldquoPaclitaxel combinedwith inhibitors of glucose and hydroperoxide metabolismenhances breast cancer cell killing viaH
2O2-mediated oxidative
stressrdquo Free Radical Biology and Medicine vol 48 no 8 pp1024ndash1033 2010
[70] C A Sherman-Baust K G Becker W H Wood III Y Zhangand P J Morin ldquoGene expression and pathway analysis of ovar-ian cancer cells selected for resistance to cisplatin paclitaxel ordoxorubicinrdquo Journal of Ovarian Research vol 4 no 1 article21 2011
[71] R Agarwal and S B Kaye ldquoOvarian cancer strategies for over-coming resistance to chemotherapyrdquo Nature Reviews Cancervol 3 no 7 pp 502ndash516 2003
[72] T Acker and K H Plate ldquoRole of hypoxia in tumorangiogenesismdashmolecular and cellular angiogenic crosstalkrdquoCell and Tissue Research vol 314 no 1 pp 145ndash155 2003
[73] M Hockel and P Vaupel ldquoBiological consequences of tumorhypoxiardquo Seminars in Oncology vol 28 supplement 8 no 2 pp36ndash41 2001
[74] L Huang Q-H Zhang Q-L Ao H Xing Y-P Lu and DMa ldquoEffect of hypoxia on the chemotherapeutic sensitivity ofhuman ovarian cancer cells to paclitaxel and its mechanismrdquoZhonghua Zhong Liu Za Zhi vol 29 no 2 pp 96ndash100 2007
[75] N Rohwer and T Cramer ldquoHypoxia-mediated drug resistancenovel insights on the functional interaction of HIFs and celldeath pathwaysrdquoDrug Resistance Updates vol 14 no 3 pp 191ndash201 2011
[76] B B Aggarwal R V Vijayalekshmi and B Sung ldquoTargetinginflammatory pathways for prevention and therapy of cancershort-term friend long-term foerdquo Clinical Cancer Research vol15 no 2 pp 425ndash430 2009
[77] Z Duan R Foster D A Bell et al ldquoSignal transducersand activators of transcription 3 pathway activation in drug-resistant ovarian cancerrdquo Clinical Cancer Research vol 12 no17 pp 5055ndash5063 2006
[78] H-J Kuh S H Jang M G Wientjes J R Weaver and J L-SAu ldquoDeterminants of paclitaxel penetration and accumulationin human solid tumorrdquo Journal of Pharmacology and Experi-mental Therapeutics vol 290 no 2 pp 871ndash880 1999
[79] S Arao H Suwa M Mandai et al ldquoHypoxia-mediated drugresistance novel insights on the functional interaction of HIFsand cell death pathwaysrdquo Cancer Research vol 54 no 5 pp1355ndash1359 1994
[80] S E Johnatty J Beesley B Gao et al ldquoABCB1 (MDR1)polymorphisms and ovarian cancer progression and survivala comprehensive analysis from the Ovarian Cancer Association
BioMed Research International 19
Consortium and the Cancer GenomeAtlasrdquoGynecologic Oncol-ogy vol 131 no 1 pp 8ndash14 2013
[81] X Yang A K Iyer A Singh et al ldquoCluster of differentiation44 targeted hyaluronic acid based nanoparticles for MDR1siRNA delivery to overcome drug resistance in ovarian cancerrdquoPharmaceutical Research 2014
[82] D A Zajchowski B Y Karlan and L K Shawver ldquoTreatment-related protein biomarker expression differs between primaryand recurrent ovarian carcinomasrdquoMolecular CancerTherapeu-tics vol 11 no 2 pp 492ndash502 2012
[83] MM Gottesman J Ludwig D Xia and G Szakacs ldquoDefeatingdrug resistance in cancerrdquoDiscovery Medicine vol 6 no 31 pp18ndash23 2006
[84] S Mozzetti C Ferlini P Concolino et al ldquoClass III 120573-tubulin overexpression is a prominent mechanism of paclitaxelresistance in ovarian cancer patientsrdquo Clinical Cancer Researchvol 11 no 1 pp 298ndash305 2005
[85] M Kavallaris D Y S Kuo C A Burkhart et al ldquoTaxol-resistant epithelial ovarian tumors are associated with alteredexpression of specific beta-tubulin isotypesrdquo Journal of ClinicalInvestigation vol 100 no 5 pp 1282ndash1293 1997
[86] G A Orr P Verdier-Pinard H McDaid and S B HorwitzldquoMechanisms of Taxol resistance related to microtubulesrdquoOncogene vol 22 no 47 pp 7280ndash7295 2003
[87] C Ferlini L Cicchillitti G Raspaglio et al ldquoPaclitaxel directlybinds to Bcl-2 and functionally mimics activity of Nur77rdquoCancer Research vol 69 no 17 pp 6906ndash6914 2009
[88] E Mechetner A Kyshtoobayeva S Zonis et al ldquoLevels ofmultidrug resistance (MDR1) P-glycoprotein expression byhuman breast cancer correlate with in vitro resistance to taxoland doxorubicinrdquo Clinical Cancer Research vol 4 no 2 pp389ndash398 1998
[89] J S Lagas C W N Damen R A B VanWaterschoot D IusufJ H Beijnen and A H Schinkel ldquoP-glycoprotein multidrug-resistance associated protein 2 Cyp3a and carboxylesteraseaffect the oral availability and metabolism of vinorelbinerdquoMolecular Pharmacology vol 82 no 4 pp 636ndash644 2012
[90] M T Huizing J B Vermorken H Rosing et al ldquoPharmacoki-netics of paclitaxel and three major metabolites in patients withadvanced breast carcinoma refractory to anthracycline therapytreated with a 3-hour paclitaxel infusion a European CancerCentre (ECC) trialrdquo Annals of Oncology vol 6 no 7 pp 699ndash704 1995
[91] R Panchagnula ldquoPharmaceutical aspects of paclitaxelrdquo Interna-tional Journal of Pharmaceutics vol 172 no 1-2 pp 1ndash15 1998
[92] S H Jang M G Wientjes and J L-S Au ldquoDeterminants ofpaclitaxel uptake accumulation and retention in solid tumorsrdquoInvestigational New Drugs vol 19 no 2 pp 113ndash123 2001
[93] D S Sonnichsen andM V Relling ldquoClinical pharmacokineticsof paclitaxelrdquo Clinical Pharmacokinetics vol 27 no 4 pp 256ndash269 1994
[94] T Ohtsu Y Sasaki T Tamura et al ldquoClinical pharmacokineticsand pharmacodynamics of paclitaxel a 3-hour infusion versusa 24-hour infusionrdquo Clinical Cancer Research vol 1 no 6 pp599ndash606 1995
[95] M Czejka J Schueller H Schnait B Springer and I EderldquoClinical pharmacokinetics andmetabolism of paclitaxel after athree-hour infusion comparison of two preparationsrdquo Journalof Oncology Pharmacy Practice vol 9 no 4 pp 129ndash136 2003
[96] J Rizzo C Riley D VonHoff J Kuhn J Phillips and T BrownldquoAnalysis of anticancer drugs in biological fluids determination
of taxol with application to clinical pharmacokineticsrdquo Journalof Pharmaceutical and Biomedical Analysis vol 8 no 2 pp 159ndash164 1990
[97] V A de Weger J H Beijnen and J H M Schellens ldquoCel-lular and clinical pharmacology of the taxanes docetaxel andpaclitaxelmdasha reviewrdquoAnti-Cancer Drugs vol 25 no 5 pp 488ndash494 2014
[98] S Kumar H Mahdi C Bryant J P Shah G Garg andA Munkarah ldquoClinical trials and progress with paclitaxel inovarian cancerrdquo International Journal of Womenrsquos Health vol 2no 1 pp 411ndash427 2010
[99] B Huang J Zhao J C Unkeless Z H Feng and H XiongldquoTLR signaling by tumor and immune cells a double-edgedswordrdquo Oncogene vol 27 no 2 pp 218ndash224 2008
[100] R A Jibodh J S Lagas B Nuijen J H Beijnen and J HM Schellens ldquoTaxanes old drugs new oral formulationsrdquoEuropean Journal of Pharmacology vol 717 no 1ndash3 pp 40ndash462013
[101] A Javeed M Ashraf A Riaz A Ghafoor S Afzal and M MMukhtar ldquoPaclitaxel and immune systemrdquo European Journal ofPharmaceutical Sciences vol 38 no 4 pp 283ndash290 2009
[102] L Bracci G Schiavoni A Sistigu and F Belardelli ldquoImmune-based mechanisms of cytotoxic chemotherapy implications forthe design of novel and rationale-based combined treatmentsagainst cancerrdquo Cell Death and Differentiation vol 21 no 1 pp15ndash25 2014
[103] C A Byrd-Leifer E F Block K Takeda S Akira and A DingldquoThe role of MyD88 and TLR4 in the LPS-mimetic activity ofTaxolrdquo European Journal of Immunology vol 31 no 8 pp 2448ndash2457 2001
[104] A-C Wang Y-B Ma F-X Wu et al ldquoTLR4 induces tumorgrowth and inhibits paclitaxel activity in MyD88-positivehuman ovarian carcinoma in vitrordquo Oncology Letters vol 7 no3 pp 871ndash877 2014
[105] Y Zhu N Liu S D Xiong Y J Zheng and Y W ChuldquoCD4+Foxp3+ regulatory T-cell impairment by paclitaxel isindependent of toll-like receptor 4rdquo Scandinavian Journal ofImmunology vol 73 no 4 pp 301ndash308 2011
[106] M Kubo T Morisaki K Matsumoto et al ldquoPaclitaxel probablyenhances cytotoxicity of natural killer cells against breastcarcinoma cells by increasing perforin productionrdquo CancerImmunology Immunotherapy vol 54 no 5 pp 468ndash476 2005
[107] L Markasz G Stuber B Vanherberghen et al ldquoEffect of fre-quently used chemotherapeutic drugs on the cytotoxic activityof human natural killer cellsrdquo Molecular Cancer Therapeuticsvol 6 no 2 pp 644ndash654 2007
[108] T Sako N Burioka K Yasuda et al ldquoCellular immune profile inpatients with non-small cell lung cancer after weekly paclitaxeltherapyrdquo Acta Oncologica vol 43 no 1 pp 15ndash19 2004
[109] R Kaneno G V Shurin I L Tourkova and M R ShurinldquoChemomodulation of human dendritic cell function by anti-neoplastic agents in low noncytotoxic concentrationsrdquo Journalof Translational Medicine vol 7 article 58 2009
[110] TMichels G V ShurinHNaiditch A Sevko VUmansky andM R Shurin ldquoPaclitaxel promotes differentiation of myeloid-derived suppressor cells into dendritic cells in vitro in a TLR4-independent mannerrdquo Journal of Immunotoxicology vol 9 no3 pp 292ndash300 2012
[111] R A Kemp and F Ronchese ldquoTumor-specific Tc1 but not Tc2cells deliver protective antitumor immunityrdquo The Journal ofImmunology vol 167 no 11 pp 6497ndash6502 2001
20 BioMed Research International
[112] A Y Rudensky ldquoRegulatory T cells and Foxp3rdquo ImmunologicalReviews vol 241 no 1 pp 260ndash268 2011
[113] EM Shevach ldquoCD4+CD25+ suppressor T cellsmore questionsthan answersrdquo Nature Reviews Immunology vol 2 no 6 pp389ndash400 2002
[114] S Sakaguchi T Yamaguchi T Nomura and M Ono ldquoRegu-latory T cells and immune tolerancerdquo Cell vol 133 no 5 pp775ndash787 2008
[115] H Nishikawa and S Sakaguchi ldquoRegulatory T cells in tumorimmunityrdquo International Journal of Cancer vol 127 no 4 pp759ndash767 2010
[116] W Zou ldquoRegulatory T cells tumour immunity and immuno-therapyrdquoNature Reviews Immunology vol 6 no 4 pp 295ndash3072006
[117] A Fialova S Partlova L Sojka et al ldquoDynamics of T-cell infil-tration during the course of ovarian cancer The gradual shiftfrom aTh17 effector cell response to a predominant infiltrationby regulatory T-cellsrdquo International Journal of Cancer vol 132no 5 pp 1070ndash1079 2013
[118] A E Albers R L Ferris G G Kim K Chikamatsu A BDeLeo and T L Whiteside ldquoImmune responses to p53 inpatients with cancer enrichment in tetramer+ p53 peptide-specific T cells and regulatory T cells at tumor sitesrdquo CancerImmunology Immunotherapy vol 54 no 11 pp 1072ndash10812005
[119] N Liu Y Zheng Y Zhu S Xiong andYChu ldquoSelective impair-ment of CD4 + CD25 + Foxp3 + regulatory T cells by paclitaxelis explained by Bcl-2Bax mediated apoptosisrdquo InternationalImmunopharmacology vol 11 no 2 pp 212ndash219 2011
[120] X Wu Q-M Feng Y Wang J Shi H-L Ge and W DildquoThe immunologic aspects in advanced ovarian cancer patientstreated with paclitaxel and carboplatin chemotherapyrdquo CancerImmunology Immunotherapy vol 59 no 2 pp 279ndash291 2010
[121] A P Vicari R Luu N Zhang et al ldquoPaclitaxel reducesregulatoryT cell numbers and inhibitory function and enhancesthe anti-tumor effects of the TLR9 agonist PF-3512676 in themouserdquo Cancer Immunology Immunotherapy vol 58 no 4 pp615ndash628 2009
[122] L Zhang K Dermawan M Jin et al ldquoDifferential impairmentof regulatory T cells rather than effector T cells by paclitaxel-based chemotherapyrdquo Clinical Immunology vol 129 no 2 pp219ndash229 2008
[123] Y Tabuchi J Matsuoka M Gunduz et al ldquoResistance topaclitaxel therapy is related with Bcl-2 expression through anestrogen receptor mediated pathway in breast cancerrdquo Interna-tional Journal of Oncology vol 34 no 2 pp 313ndash319 2009
[124] N Obermajer R Muthuswamy K Odunsi R P Edwards andP Kalinski ldquoPGE
2-induced CXCL12 production and CXCR4
expression controls the accumulation of human MDSCs inovarian cancer environmentrdquo Cancer Research vol 71 no 24pp 7463ndash7470 2011
[125] Q M Feng W Di and X Wu ldquoImmune reconstitution inadvanced ovarian cancer patients undergoing first line chemo-therapyrdquo Xi Bao Yu Fen Zi Mian Yi Xue Za Zhi vol 25 no 11pp 1023ndash1025 2009
[126] A D Seidman D Hochhauser M Gollub et al ldquoNinety-six-hour paclitaxel infusion after progression during short taxaneexposure a phase II pharmacokinetic and pharmacodynamicstudy in metastatic breast cancerrdquo Journal of Clinical Oncologyvol 14 no 6 pp 1877ndash1884 1996
[127] D R Spriggs M F Brady L Vaccarello et al ldquoPhase IIIrandomized trial of intravenous cisplatin plus a 24- or 96-hour
infusion of paclitaxel in epithelial ovarian cancer a gynecologiconcology group studyrdquo Journal of Clinical Oncology vol 25 no28 pp 4466ndash4471 2007
[128] G A Omura M F Brady K Y Look et al ldquoPhase III trial ofpaclitaxel at two dose levels the higher dose accompanied byfilgrastim at two dose levels in platinum-pretreated epithelialovarian cancer an intergroup studyrdquo Journal of Clinical Oncol-ogy vol 21 no 15 pp 2843ndash2848 2003
[129] R Simon and L Norton ldquoThe Norton-Simon hypothesisdesigning more effective and less toxic chemotherapeutic reg-imensrdquoNature Clinical Practice Oncology vol 3 no 8 pp 406ndash407 2006
[130] A Kumar P Hoskins and A Tinker ldquoDose-dense paclitaxel inadvanced ovarian cancerrdquo Clinical Oncology vol 27 no 1 pp40ndash47 2015
[131] P Marchetti S Urien G A Cappellini G Ronzino and CFicorella ldquoWeekly administration of paclitaxel theoretical andclinical basisrdquoCritical Reviews in OncologyHematology vol 44supplement pp S3ndashS13 2002
[132] P Francis E Rowinsky J Schneider T Hakes W Hoskinsand M Markman ldquoPhase I feasibility and pharmacologic studyof weekly intraperitoneal paclitaxel A Gynecologic OncologyGroup pilot studyrdquo Journal of Clinical Oncology vol 13 no 12pp 2961ndash2967 1995
[133] H Thomas and P Rosenberg ldquoRole of weekly paclitaxel inthe treatment of advanced ovarian cancerrdquo Critical Reviews inOncologyHematology vol 44 supplement pp S43ndashS51 2002
[134] M Markman J Markman K Webster et al ldquoDuration ofresponse to second-line platinum-based chemotherapy forovarian cancer implications for patient management and clini-cal trial designrdquo Journal of Clinical Oncology vol 22 no 15 pp3120ndash3125 2004
[135] P H OrsquoDonnell M Eileen Dolan E Gamazon et al ldquoPopu-lation differences in platinum toxicity as a means to identifynovel genetic susceptibility variantsrdquo Pharmacogenetics andGenomics vol 20 no 5 pp 327ndash337 2010
[136] M J Millward M J Boyer M Lehnert et al ldquoDocetaxel andcarboplatin is an active regimen in advanced non-small-celllung cancer a phase II study in Caucasian and Asian patientsrdquoAnnals of Oncology vol 14 no 3 pp 449ndash454 2003
[137] M Markman ldquoIntraperitoneal therapy of ovarian cancerrdquoOncologist vol 1 no 1-2 pp 18ndash21 1996
[138] M Markman and J L Walker ldquoIntraperitoneal chemotherapyof ovarian cancer a review with a focus on practical aspects oftreatmentrdquo Journal of Clinical Oncology vol 24 no 6 pp 988ndash994 2006
[139] K Fujiwara S Nagao E Aotani and K Hasegawa ldquoPrincipleand evolving role of intraperitoneal chemotherapy in ovariancancerrdquo Expert Opinion on Pharmacotherapy vol 14 no 13 pp1797ndash1806 2013
[140] M Markman E Rowinsky T Hakes et al ldquoPhase I trialof intraperitoneal taxol a gynecoloic oncology group studyrdquoJournal of Clinical Oncology vol 10 no 9 pp 1485ndash1491 1992
[141] M Markman M F Brady N M Spirtos P Hanjani and S CRubin ldquoPhase II trial of intraperitoneal paclitaxel in carcinomaof the ovary tube and peritoneum a gynecologic oncologygroup studyrdquo Journal of Clinical Oncology vol 16 no 8 pp2620ndash2624 1998
[142] P B Panici I Palaia M Graziano F Bellati N Manci and RAngioli ldquoIntraperitoneal paclitaxel as consolidation treatmentin ovarian cancer patients a case control studyrdquo Oncology vol78 no 1 pp 20ndash25 2010
BioMed Research International 21
[143] D K Armstrong B Bundy L Wenzel et al ldquoIntraperitonealcisplatin and paclitaxel in ovarian cancerrdquo The New EnglandJournal of Medicine vol 354 no 1 pp 34ndash43 2006
[144] D Tewari J Java and R Salani ldquoLong-term survival advantageof intraperitoneal chemotherapy treatment in advanced ovariancancer an analysis of a Gynecologic Oncology Group ancillarydata studyrdquo in Proceedings of the 2013 Society of GynecologicOncology Annual Meeting on Womenrsquos Cancer (GOG114172Abstract) Los Angeles Calif USA 2013
[145] D A Yardley ldquonab-paclitaxel mechanisms of action and deliv-eryrdquo Journal of Controlled Release vol 170 no 3 pp 365ndash3722013
[146] M Ando K Yonemori N Katsumata et al ldquoPhase I and phar-macokinetic study of nab-paclitaxel nanoparticle albumin-bound paclitaxel administeredweekly to Japanese patients withsolid tumors and metastatic breast cancerrdquo Cancer Chemother-apy and Pharmacology vol 69 no 2 pp 457ndash465 2012
[147] N Desai V Trieu Z Yao et al ldquoIncreased antitumor activityintratumor paclitaxel concentrations and endothelial cell trans-port of cremophor-free albumin-bound paclitaxel ABI-007compared with cremophor-based paclitaxelrdquo Clinical CancerResearch vol 12 no 4 pp 1317ndash1324 2006
[148] J A Yared and K H R Tkaczuk ldquoUpdate on taxane devel-opment new analogs and new formulationsrdquo Drug DesignDevelopment andTherapy vol 6 pp 371ndash384 2012
[149] M G Teneriello P C Tseng M Crozier et al ldquoPhase IIevaluation of nanoparticle albumin-bound paclitaxel in plati-num-sensitive patients with recurrent ovarian peritoneal orfallopian tube cancerrdquo Journal of Clinical Oncology vol 27 no9 pp 1426ndash1431 2009
[150] R L Coleman W E Brady D S McMeekin et al ldquoA phase IIevaluation of nanoparticle albumin-bound (nab) paclitaxel inthe treatment of recurrent or persistent platinum-resistant ovar-ian fallopian tube or primary peritoneal cancer a GynecologicOncology Group Studyrdquo Gynecologic Oncology vol 122 no 1pp 111ndash115 2011
[151] J W Singer ldquoPaclitaxel poliglumex (XYOTAX CT-2103) amacromolecular taxanerdquo Journal of Controlled Release vol 109no 1ndash3 pp 120ndash126 2005
[152] C Li D-F Yu R A Newman et al ldquoComplete regressionof well-established tumors using a novel water-soluble poly(L-glutamic acid)-paclitaxel conjugaterdquo Cancer Research vol 58no 11 pp 2404ndash2409 1998
[153] M Mita A Mita J Sarantopoulos et al ldquoPhase I study ofpaclitaxel poliglumex administered weekly for patients withadvanced solid malignanciesrdquo Cancer Chemotherapy and Phar-macology vol 64 no 2 pp 287ndash295 2009
[154] P Sabbatini M W Sill D OrsquoMalley L Adler and A ASecord ldquoA phase II trial of paclitaxel poliglumex in recurrentor persistent ovarian or primary peritoneal cancer (EOC) agynecologic oncology group studyrdquo Gynecologic Oncology vol111 no 3 pp 455ndash460 2008
[155] M O Bradley C S Swindell F H Anthony et al ldquoTumortargeting by conjugation of DHA to paclitaxelrdquo Journal ofControlled Release vol 74 no 1ndash3 pp 233ndash236 2001
[156] M O Bradley N L Webb F H Anthony et al ldquoTumortargeting by covalent conjugation of a natural fatty acid topaclitaxelrdquo Clinical Cancer Research vol 7 no 10 pp 3229ndash3238 2001
[157] A C Wolff R C Donehower M K Carducci et al ldquoPhaseI study of docosahexaenoic acid-paclitaxel a taxane-fatty acid
conjugate with a unique pharmacology and toxicity profilerdquoClinical Cancer Research vol 9 no 10 part 1 pp 3589ndash35972003
[158] A Sparreboom A C Wolff J Verweij et al ldquoDispositionof docosahexaenoic acid-paclitaxel a novel taxane in bloodin vitro and clinical pharmacokinetic studiesrdquo Clinical CancerResearch vol 9 no 1 pp 151ndash159 2003
[159] P M Fracasso J Picus J D Wildi et al ldquoPhase 1 and phar-macokinetic study of weekly docosahexaenoic acid-paclitaxelTaxoprexin in resistant solid tumor malignanciesrdquo CancerChemotherapy and Pharmacology vol 63 no 3 pp 451ndash4582009
[160] A Y Bedikian R C DeConti R Conry et al ldquoPhase 3 study ofdocosahexaenoic acid-paclitaxel versus dacarbazine in patientswith metastatic malignant melanomardquo Annals of Oncology vol22 no 4 pp 787ndash793 2011
[161] Y-N Wu S-L Wang Y-C Wang et al ldquoReversal effect ofdocosahexaenoic acid on taxol resistance in human ovarian car-cinoma A2780T cellsrdquo Obstetrics amp Gynecology InternationalJournal vol 1 no 3 Article ID 00018 2014
Submit your manuscripts athttpwwwhindawicom
PainResearch and TreatmentHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom
Volume 2014
ToxinsJournal of
VaccinesJournal of
Hindawi Publishing Corporation httpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
AntibioticsInternational Journal of
ToxicologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
StrokeResearch and TreatmentHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Drug DeliveryJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Advances in Pharmacological Sciences
Tropical MedicineJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Medicinal ChemistryInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
AddictionJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
Emergency Medicine InternationalHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Autoimmune Diseases
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Anesthesiology Research and Practice
ScientificaHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Pharmaceutics
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of

BioMed Research International 3
Empirical formula C47H51NO14
Molecular weight 8539 gmol
Average mass 8539Da
Systemic name (2120572 5120573 7120573 10120573 13120572)-
(benzoylamino)-2-hydroxy-3-
phenylpropanoyl]oxy-17-
dihydroxy-9-oxo-520-epoxytax-11-
en-2-yl benzoate
410-Diacetoxy-13-[(2R 3S)-3-
O
O
O
O
O
O O
O
O
NHH3C
H3998400 CH3
CH3
CH3
CH345
OH
HO
OH
OH
13
Figure 2 Chemical structure of paclitaxel Paclitaxel consist of taxane ring with a four-membered oxetane side ring at positions C4 and C5and an active homochiral ester side chain at C13 that binds tomicrotubules in a guanosine triphosphate (GTP) independentmanner to inducecytotoxicity activity
on ovarian cancer concluded that 30 of patients withplatinum-resistant ovarian cancer responded to paclitaxeltherapy either completely or partially [34] Another issue wasthe insolubility of the paclitaxel in water but these problemswere eventually overcome with a formulation in ethanoland Cremophor EL Cremophor EL is a polyethoxylatedcastor oil which was used as a vehicle for solubilisation ofhydrophobic drug like paclitaxel [35] However the mostserious side effect observed following use of Cremophor asthe drug vehicle was that of hypersensitivity reactions whichwere unpredictable and led to two deaths and this almosthalted any further clinical trials A longer and slower infusiontaking 24 hours reduced this severe adverse effect [33]
In December 1992 paclitaxel was registered as chemo-therapy for the treatment for ovarian cancer To meetincreasing demand a commercially viable semisynthetic wasdeveloped by Robert Holton and colleagues [31] Researchersalso tested the effectiveness of paclitaxel as a treatment foradvanced breast cancer Subsequent clinical trials found thatthe drug was effective against this disease and in 1994 theFDA approved paclitaxel for use against breast cancer Pacli-taxel is now used (either as a single agent or in combinationwith other drugs such as cisplatin or carboplatin) for thetreatment of ovarian cancer [36] breast cancer [5] and non-small-cell lung cancer [37]
3 Chemical Structure
Paclitaxel a class of taxane drugs is a diterpenoid pseudoal-kaloid with the empirical formula C
47H51NO14
(Figure 2)and has a corresponding molecular weight of 8539 gmolPaclitaxel consist of two molecules a taxane ring with a four-membered oxetane side ring at positions C4 and C5 and ahomochiral ester side chain at C13 The side chain at C13plays a crucial role as this is the active portion that binds tomicrotubules stabilises the tubulin bundles and stimulatesdisassembly of microtubules in a guanosine triphosphate(GTP)-independent manner As a result cell proliferation isinhibited by halting the cell cycle at the metaphaseanaphase
boundary and by formation of an incomplete metaphaseplate of chromosomes induced by the stabilization of themicrotubule dynamics Extensive research has concluded thatan intact taxane ring and an ester side-chainwere essential forcytotoxic activity [38 39]
4 Mechanism of Action
Paclitaxel is an anticancer drug that targets microtubulesMicrotubules consist of cylindrical hollow bodies of about25ndash30 nm in diameter composed of polymers of tubulin indynamic equilibrium with tubulin heterodimers (consistingof alpha and beta protein subunits) [40 41] The principalfunction of microtubules is the formation of the mitoticspindle during cell division In addition they are required forthe maintenance of cell structure motility and cytoplasmicmovement within the cell The synthesis of tubulin and theassembly of microtubules occur during the G2 phase and theprophase of mitosis Microtubules are in a state of dynamicequilibrium with their subunit tubulins 120572 and 120573 arrangedin a head to tail fashion with preferential faster growth(plus ends) at one end and slower growth (minus ends) atthe other end Under steady-state conditions the length ofthe microtubule is unchanged as the net tubulin assemblyrate equals the net disassembly rate The minus ends part ofmicrotubule are usually anchored mainly at the centrosome[42] while the plus ends explore the cytoplasm and interactwith cellular structures [43 44]
Dr Horwitz discovered that paclitaxel unlike vincaalkaloids which prevent microtubule assembly prevents celldivision by promoting the assembly of stable microtubulesespecially from 120573-tubulin heterodimers and inhibits theirdepolymerisation hence exposed cells are arrested in theG2M-phase of the cell cycle [45] and eventually undergoapoptosis [46] thereby inhibiting cell replication [40 47]Paclitaxel binds specifically in a reversible manner to theN-terminal 31 amino acids of the beta-tubulin subunit inthe microtubules rather than to tubulin dimers [47 48]Paclitaxel also has the unique ability to promote microtubule
4 BioMed Research International
formation in vitro even at cold temperatures (4∘C) and in theabsence of GTP [46]
Further research into understanding themolecularmech-anisms of microtubule formation has discovered that pacli-taxel may have other mechanism that allows cells to escapedrug toxicity which then develops into resistance and failurein chemotherapy [44] Ganguly and his colleagues found thatmicrotubule dynamics suppression was not related to celldivision Treatment of mutant cell lines Tax 11-6 (mutation in120572-tubulin) and Tax 18 (mutation in 120573-tubulin) at concentra-tion of 50 to 100 nmolL that should hypothetically increasemicrotubule assembly to more normal levels and allow thecells to proliferate normally further suppress microtubuledynamics rather than restoring behaviour to normal [44]Low concentrations of paclitaxel that suppressed dynamicshence they did not affect the rate ofmicrotubule detachmentbut the higher drug concentrations that allowed normalcell division strongly inhibited detachment in the mutantcell lines and returned the rate to near normal levels Thisaction seems to be related to ability of paclitaxel to inhibitmicrotubule fragmentation rather than its ability to suppressmicrotubule dynamics which was further confirmed by livecell imaging that demonstrated that microtubule detach-ment from centrosomes might be responsible for generat-ing microtubule fragments a process that was reversed bypaclitaxel [44] Recent studies have also found that at lowconcentrations (less than nanomolar concentrations) pacli-taxel inhibits the depolymerisation of microtubules whereasat high-dose paclitaxel increase the number and mass ofmicrotubules hence increasing stability of microtubules andalso render them nonfunctional by blocking the detachmentof microtubule minus ends from centrosomes rather thanplus ends [44 49]
The proposed mechanism of action of weekly paclitaxeladministration may be based on its apoptotic effects Theinduction of apoptotic modulator genes by paclitaxel appearsto be independent of microtubule stabilization It may be dueto modulation of the transcription of different genes suchas DNA-damage response proteins cytokines or proteinsinvolved in the control of cellular proliferation apoptosis andinflammation The apoptotic effect of paclitaxel is dependenton the concentration and duration of exposure With con-centration amounts of at least 10 nM and exposure of at least12 hours apoptosis may be induced in the S phase withoutmitotic arrest Two different mechanisms of apoptosis havebeen proposed depending on the dose concentration ofpaclitaxel At concentration of ge9 nM paclitaxel induces Raf-1 activation which is responsible for apoptotic control Atle9 nM there is absence of Raf-1 kinase involvement butapoptosis induction still occurs under the influence of p53and p21 [50 51] With the same concentration at 24-hourexposure in addition to apoptotic arrest paclitaxel producesan irreversible mitotic arrest [52] p53 is a major tumoursuppressor regulating proliferation and apoptosis and itsmutation occurs in more than 50 of human cancers Innormal cells DNA damage increases p53 levels which thenactivates a G1 cell-cycle arrest mediated by p21 to promoteeither the DNA damage repair mechanisms or apoptosis andnaturally limiting proliferation of genetically transformed cell
clones A functional p53 signaling pathway is necessary tosensitise cancer cells to DNA-damaging chemotherapeuticagents to reduce chemo resistance Currently paclitaxelactivity is considered to be independent of p53 status whichis an important aspect as the presence of silent ormutated p53does not modify the sensitivity of cancer cells to taxane thusreducing chemoresistance [53ndash56]
Paclitaxel also exerts its mechanism of action by activa-tion of multiple signal-transduction pathways which maybe associated with proapoptotic signaling The pathwaysassociated with paclitaxel are TLR-4 dependent pathway(either via MyD88 dependent or independent pathway) c-Jun N-terminal kinase (JNK) P38 Mitogen activated protein(MAP)Kinase nuclear factor kappa B (NF-120581B) Janus kinase-(JAK-) signal transducer and activator of transcription factor(STAT) pathway One of the pathways for induction ofapoptosis is via mitogen-activated protein kinase (MAPK)pathway resulting in dephosphorylation of the proapoptoticprotein Bad and Bax phosphorylation of Bcl2 and inductionof apoptosis Bad and Bax (promote apoptosis) and Bcl2 (sup-press apoptosis) are regulatory proteins which are membersof the Bcl2 family and are involved in programmed cell deathInduction of cytokines and pro-inflammatory proteins willlead to immunomodulatory effect of paclitaxel at low-doseconcentration and cell death at higher dose Changes thatoccur in these pathways are also responsible for developmentof resistance to paclitaxel [57ndash60]
Weekly paclitaxel also exhibits strong angiogenic inhibi-tory activity [61 62] In murine studies paclitaxel was ableto reduce new vessel formation at low noncytotoxic doses(03 and 6mgkg per day in mice) by suppressing VEGFexpression [63 64] Low dose weekly paclitaxel has beentested in patients with advanced ovarian cancer metastaticmelanoma and advanced head and neck cancer resulting instable disease [65ndash67] This additional mechanism of actionof paclitaxel by rescheduling the duration of administrationmay be helpful in cancers which have become resistant to thesame drug given on a 3-weekly conventional schedule [11 13]
Paclitaxel had also been reported to induce reactiveoxygen species (ROS) generation and increase hydroperoxideproduction by enhancing the activity of nicotinamide ade-nine dinucleotide phosphate (NADPH) oxidase which con-tributes to oxidative stress and may play a role in the potencyof the anticancer activity of paclitaxel [68 69] The combi-nation of paclitaxel with inhibitors of glucose (ie 2-deoxy-D-glucose 2DG) and hydroperoxide (ie L-buthionine-S R-sulfoximine BSO) metabolism has been found to selectivelyenhance breast cancer cell killing via hydrogen peroxide-induced metabolic oxidative stress which may be effectivelyutilised to treat breast cancers [69] However the relationshipof oxidative stress to the overall cytotoxicity mechanism ofpaclitaxel is not well established The mechanism of action ofpaclitaxel is summarised in Figure 3
5 Mechanism of Drug Resistance
Themechanism of paclitaxel resistance is complex involvingmultistep and multiple genes and not yet fully elucidated
BioMed Research International 5
Microtubules(MT)
MyD88 dependent
MyD88 independent
S
G2G1
M
PTX
Cell cycle arrest
N-terminal amino acids of beta
tubulin subunit
Inhibit depolymerisation ofmicrotubules
and suppress MT dynamics
Increase number and mass of microtubules increase
stability and block detachment
Apoptosis induced in G1S phase (absence mitotic
arrest)
Raf-1
p21
STAT 3
G0
JAK
MEK
MAPK
Bax Bcl2Bad
IRAK
TRAF
TKR
TRIF TRAM
ROS
Mitotic arrest at G2M phase
PI3KAKTApoptosis regulator
protein
p53
VEGFR
Angiogenesis
Apoptosis
TLR4
High concentrationLow concentration
NF-120581B
PTXle 9nM12hr
PTXge 9nM12hr
PTXle 9nM24hr
I120581B
Figure 3 Mechanism of action of paclitaxel Paclitaxel targets microtubules At high concentration PTX causes mitotic arrest at G2M phasewhereas at low concentration apoptosis is induced at G0 and G1S phase either via Raf-1 kinase activation or p53p21 depending on the doseconcentration Even at lower dose but with exposure beyond 24 hours paclitaxel can cause mitotic arrest Paclitaxel also activates multiplesignaling pathway to exert proapoptotic activity as well as immunomodulatory effect Paclitaxel also develops resistance via these signalingpathways PTX Paclitaxel TLR4 Toll-like receptor 4 G0 resting phase G1 cells enlarge andmake new protein S phase DNA replication G2preparation for division M phase cell divisionmitosis Raf-1 Raf kinase family MEKMAPK mitogen activated protein kinase IRAK IL-1receptor associated kinase TRAF TNFR associated factor NF-120581B nuclear factor kappa B TRIFTRAM TIR-domain-containing adapter-inducing interferon-120573 TKR tyrosine kinase receptor VEGFR vascular endothelial growth receptor PI3K phosphoinositide 3-kinase JAKjanus kinase STAT signal transducer and activator of transcription factor
Development of drug resistance leading to aggressive diseasethat is refractory to treatment is responsible for 90 ofthe deaths among patients with advanced ovarian cancer[70] Multidrug resistance (MDR) is a phenomenon definedby the ability of cancer cell to overcome either structurallyor functionally unrelated cytotoxic drugs Mechanism ofMDR can be broadly divided into three types (a) externalmechanism involving changes in pharmacokinetics of drugor (b) within tumour microenvironment which includeshypoxia leading to clonal selection pressure or (c) at cellu-lar level [71] MDR can be intrinsic or acquired IntrinsicMDR or also known as inherent occurs when cancer cellsdevelop resistant to any chemotherapy and this is most likelyattributed by tumour microenvironment Acquired MDRdevelops following exposure to chemotherapeutic agents andmay occur as a result of the pharmacokinetic of drug itself orsecondary to changes within the tumour cells [71]
Paclitaxel-derived resistance is mainly attributed bychanges involving mRNA and protein (such as multiple
ribosomal genes and translation factors) synthesis oxidativestress (UGT1A6 MAOA and CYBA) glycolysis (ADH1AHK1 and ENO3) glutathione metabolism and leukocytetransendothelial migration pathways [71] A study on geneexpression changes on a series of drug resistant ovariancancer cell lines following exposure to paclitaxel cisplatinor doxorubicin revealed that among 845 genes analysed atotal of 337 genes were significantly altered in cells resistantto paclitaxel [70] Changes in genes expression may createinterpatient variation in drug effect alteration in tumourmicroenvironment and changes within cellular structuresmetabolism and functions that promotes towards drug resis-tance
Tumour cells grow rapidly with formation of numerousnew vessels attributing to irregular blood flow and increasedoxygen demand which lead to development areas devoidof adequate oxygenation within ovarian cancer tissues [72]In response to chronic hypoxia (oxygen depletion) tumourmicroenvironment adapts processes to keep cells alive in
6 BioMed Research International
hypoxic and acidic state This hypoxic adaptation promotestumour proliferation dissemination and progression of dis-ease [73] and also reduces chemosensitivity [74]
Hypoxia-induced chemoresistance occurs due to geno-mic instability Oxygen depletion induces proteomic andgenomic changes that activates the level of p53 inhibits apop-tosis promotes angiogenesis (angiogenic molecules such asvascular endothelial growth factor [VEGF] and angiogenin)upregulates growth factors (platelet-derived growth factor[PDGF] transforming growth factor-beta and insulin-likegrowth factor [IGF]) and induces anaerobic metabolism andglycolysis (glycolytic enzymes glucose transporters) leadingto reduction in potential for cell cycle arrest and cellulardifferentiationwhich prevent tumour cell death [74]Hypoxiacan induce either p-53-dependent (involving Apaf-1 andcaspase-9 effector pathways) or p53-independent (involvinghypoxic-inducible factor 1 [HIF-1] and Bcl-2 family genespathways) apoptosis in both normal and tumour cells HIF-1 is a common transcription factor consisting of HIF-1120572 and HIF-1120573 subunits which controls hypoxic-induciblegenes and the concentration of HIF-1 protein increasedexponentially in the presence of hypoxic environment Lossof apoptotic potential of tumour cells mediated by hypoxicenvironment and HIF-1 which arrest cell cycle at G0G1reduces chemosensitivity to chemotherapeutic agents includ-ing paclitaxel [70 75]
Other transcriptional factors which are activated byhypoxia are nuclear factor kappa B (NF-120581B) and STAT3 also known as proinflammatory transcriptional factorsNF-120581B and STAT 3 regulate multiple gene products whichare involved in inflammation angiogenesis cell survivalproliferation and metastasis Paclitaxel which mediates itscytotoxic action via NF-120581B pathway is vulnerable to developresistance in the presence of hypoxic tumour microen-vironment with activation of NF-120581B transcription factorwhich induces serine phosphorylation and also regulatesBCL-2 an antiapoptotic protein preventing cell death andpromoting tumorigenesis [76] Inhibition of activated STAT3 found overexpressed in most paclitaxel-resistant ovariancancer cells has resulted in reduction in paclitaxel resistanceHowever further research is required to determine the exactmechanism [77]
Intracellular drug concentration is important for effectivecytotoxic activity of paclitaxel Drug resistance may beattributed to either reduced accumulation of drug withinovarian tumours or increased efflux of drug from tumourcells [78] Alteration in pharmacokinetic of paclitaxel eitherattributed by the drug itself such as lower concentration ofdrug administered shorter duration of drug exposure highfirst pass metabolism increased hepatic or renal clearanceinadequate binding to tubulinsmicrotubules or othermacro-molecules or presence of higher tumour density or vascular-ity may result in reduced accumulation of intratumoral drugconcentration [71]
Drug efflux is the most common mechanism for chemo-resistance observed in paclitaxel-treated cancer cells Drugefflux from cancer cells is mediated by ATP-binding cassette(ABC) transporters such as P-glycoprotein (P-gp) P-gp alsoknown as ABCB1 or multidrug-resistance associated-protein
(MRP) a transmembrane protein encoded by MDR1 geneplays a role as an efflux pump which is crucial for occurrenceof many cellular processes that require transfer of substratesacross cellularmembranes P-gp hence can affect intracellulardrug concentration andhave been shown to correlate in vitroto chemosensitivity to paclitaxel [59] However evidence fortheir role in clinical drug resistance in ovarian cancer hasemerged with P-gp found to be overexpressed in ovariancancer cells in vitro and also on paclitaxel-resistant celllines [70] P-gp and MDR1 expression levels were higherin chemoresistant ovarian cancer patients as compared withtheir chemosensitive counterpart Overall survival time wasalso statistically higher in patientswith low expression of P-gpandMDR1 in their tumor tissuesHence P-gp andMDR1mayhave a predictive role in determining the outcome of patientswith advanced ovarian cancer [58 79ndash82] Mechanism ofpaclitaxel resistance is complicated and specifically inhibitingABC transporters have given mixed results [59 83]
Another major mechanism of paclitaxel resistance ismediated by either a reduction in total intracellular tubulinconcentrations point mutation at prominently expressedtubulin genes or by selective alterations in expression oftubulin isotypes such as Class III 120573-tubulin [52 84 85]Microtubule dynamic stability was significantly impairedin the paclitaxel-resistant cells [86] Microtubule dynamicsdisruption caused by paclitaxel result in cell cycle arrestapoptosis and drug resistance
Other mechanism responsible for development of pacli-taxel resistant are inhibition of apoptosis activation ofmitogen-activated protein kinase Raf-1 kinase or intra-cellular signalling pathway PIK3 (phosphatidylinositol-45-bisphosphate 3-kinase) changes in apoptotic regulatory pro-teins such as Bcl-2 increase in expression of proinflammatorycytokines such as TNF-120572 IL-6 and IL-8 and activation oflipopolysaccharide-inducible genes and tumour suppressionprotein p53 [57 83 86 87]
In summary paclitaxel resistance is multifactorial inc-luding changes in signaling pathways upregulation of P-glycoprotein (P-gp) [80 88 89] alteration in tubulin dyna-mic mutations in 120573-tubulin gene or expression of 120573-tubulinisotypes [52 84 85] and changes in apoptotic mechanismIdentification of mechanism of resistance could help topotentially develop novel agents to improve chemosensitivityof patients with advanced ovarian cancer
6 Pharmacokinetics
Paclitaxel is a white to off-white crystalline powder highlylipophilic and is insoluble in water and so difficult to formu-late into solution It has a melting point of 216-217∘C [90 91]More than 90 of the drug binds rapidly and extensively toplasma proteins [33 40] whereas binding onto red blood cellsis approximately 50 The presence of premedication drugs(before chemotherapy) such as ranitidine dexamethasone ordiphenhydramine did not affect protein binding of paclitaxelPaclitaxel has a large volume of distribution of about 55 Lm2but this is reduced in the females [33]
BioMed Research International 7
AUC (area under the plasma concentration)
Cmax (maximum concentration)
Pacli
taxe
l con
cent
ratio
n (120583
M)
0 10 20 30 40
Time (hr)
0
1
2
3
4
5
Figure 4 Plasma pharmacokinetics of paclitaxel The pharmacoki-netics generally were linear for 6 or 24 hour infusions but becomenonlinear for infusions of shorter durations due to variation inthe elimination clearance with the dose administered An increasein plasma concentration of paclitaxel results in disproportionatelarger increase in 119862max (maximum plasma concentration) and AUC(area under plasma concentration) followed by decrease in drugelimination from body tissues
The disappearance of paclitaxel from plasma is tradition-ally believed to be biphasic [33] The initial rapid declinerepresents distribution to the peripheral compartment andelimination of the drug The later phase is due in part tothe slow efflux of paclitaxel from the peripheral compartment[92] In the presence of more sensitive assay methods andlater sampling times a three-compartment model seems tobe more accurate [40 93] Paclitaxel has been shown tohave a nonlinear pattern of pharmacokinetics (Figure 4)Thepharmacokinetics were generally linear for 6- or 24-hourinfusions but become nonlinear for infusions of shorterdurations because the elimination clearance varies with thedose administered With increasing plasma concentrationof paclitaxel there is a disproportionately larger increasein 119862max (maximum plasma concentration) and AUC (areaunder plasma concentration) accompanied by decrease indrug elimination from body tissues The clinical importanceof this nonlinear pattern is that dose escalationmay result in adisproportionate increase in toxicity whereas dose reductionmay affect its efficacy [33 90 91 94]
The pharmacokinetics of paclitaxel has been evaluatedover a wide range of doses up to 300mgm2 and withinfusion schedules ranging from 3 to 24 hours Maximumplasma concentrations are dose-related In patients treatedwith single dose infusion of 135 and 175mgm2 given as3- and 24-hour infusions mean steady state volume ofdistribution has ranged from 198 to 688 Lm2 indicatingextensive extravascular distribution andor tissue bindingTerminal half-life has ranged from 13 to 86 hours (mean 5hours) [40 93] and total body clearance has ranged from116 to 240 Lhrm2 Preclinical results in animals have shown
high levels in most tissues Being highly protein-boundpaclitaxel has a high affinity for distribution in specific tissuesincluding kidney lung spleen and extracellular fluids likeascites and pleural fluids [40 95] but the uptake of the drugin the brain is minimal [96 97] Exposure to paclitaxel isrelatively high in tumour tissue compared with other tissuesand in addition to slow elimination from tumour tissue theAUC in tumour tissue is about five-fold higher than that inplasma [97]
There is no evidence of accumulation of paclitaxel withmultiple treatment courses as the variability in systemicpaclitaxel exposure as measured by AUC (0ndashinfin) (area underplasma concentration-time curve from time 0 to infinity)for successive treatment courses are minimal [98] Paclitaxelclearance is however sequence dependent Patients receiv-ing a platinum-based agent prior to paclitaxel have lowerclearance and greater clinical toxicity than patients receivingpaclitaxel before cisplatin [93]
The drug administered intravenously undergoes anextensive P-450mediated hepaticmetabolism by cytochromeenzymes (CYP3A andCYP2C8) with 70ndash80being excretedinto bile by adenosine triphosphate- (ATP-) binding cassettemultidrug transporters such as P-glycoprotein (P-gp) andmultidrug resistance protein 2 (MRP-2) either asmetabolitesor as the parent drug Variation in MRP-2 activity hasbeen found to have direct effect on the effective exposureto paclitaxel [99] The bioavailability is poor following oraladministration due to enterocyte expression of P-gp and first-pass metabolism in the liver Most of the drug is eliminatedin feces Less than 10 drug in the unchanged form isexcreted in the urine indicating extensive nonrenal clearance[96] Combinations of inhibitors of CYP3A and P-gp mightpossibly improve the oral bioavailability of the taxanes [8997 100]
7 Paclitaxel and the Immune System
The immune system consists of two different but interactingmechanisms which are innate and adaptivemechanismsTheinnate mechanism is the first line of defense and consists of agroup of cells which includes mainly macrophages dendriticcells (DCs) and natural killer (NK) cells while the adaptiveimmunemechanism is represented by T-lymphocytes All thecomponents of innate and adaptive mechanism are involvedin antitumour immunity which includes tumour recognitioncontrol and elimination However cancer cells are able toevade immune detection and actively suppress antitumourimmunity
Paclitaxel has a wide range of dose dependent immuno-modulatory effects described in Figure 5 At standard dosepaclitaxel is broadly immunosuppressive and this is becauseit inhibits a number of cell types involved in tumour rejectionsuch asmacrophages effector T cells andNK cells [101] How-ever at lower doses than typically used for chemotherapypaclitaxel has an important immunogenic role promotingantitumour immunity [101 102] Hence understanding theimmunological basis of paclitaxel may help to maximise themanipulation of the immunomodulatory effects of paclitaxel
8 BioMed Research International
Immunomodulatory effect of
paclitaxel
Stimulate direct cytotoxic activity by
macrophage
Induce activation maturation and priming of DCs
Stimulate NK-dependent antitumour immunity
Activation of tumour-specificCTL Expansion of memory T cells
Secretion of proinflammatory cytokine
Shift from Th2 to Th1 type ofresponse
Depletion of Tregs andmodulation of MDSC
Downregulates the expression of VEGFR-2
and inhibits angiogenesis
IL-6 IL-12 TNF-120572 and i-NOS
Figure 5 Immunomodulatory effect of paclitaxel Paclitaxel a toll-like receptor 4 (TLR4) ligand binds to TLR4 receptor and triggers TLR4signaling via MyD88 dependent and independent pathway Paclitaxel then promotes anticancer immune response directly by stimulatingmacrophages to kill cancer cells or indirectly by secretion of proinflammatory cytokines which upregulates activation of DCs NK andtumour specific CTL Paclitaxel promotes effective CTL response by upregulation of mannose-6-phosphate which facilitate permeabilityto granzyme B and cytokine patterns of T helper type 1 Paclitaxel modulates MDSC and ablates Tregs Memory T cells (CD4+CD45RO+and CD8+CD45RO+) increased significantly while regulatory T cells (Tregs) decreased around 2 weeks creating an opportunity window fordose-dense therapy and immunomodulatory agents to achieve clinical benefit Dose-dense and low dose paclitaxel also blocks new vesselformation by downregulating VEGF-receptor 2 reduces resistance by alternative mechanism of action
to develop better therapeutic options in the management ofadvanced ovarian cancer
Paclitaxel is a ligand to toll-like receptor 4 (TLR4) whichis expressed on innate immune cells including macrophagesThe binding of paclitaxel to TLR4 on macrophages trig-gers the MyD88 mitogen-activated protein kinase (MAPK)and transcription of nuclear factor NF-kappa B (NF-120581B)pathways (Figure 3) resulting in their activation and releaseof immunostimulatory cytokines such as tumour necrosisfactor-120572 (TNF-120572) interleukin-1 (IL-1) interleukin-6 (IL-6)and interleukin-8 (IL-8) [103ndash105] Activated macrophagescan either cause direct tumour cell lysis via release oflysosomal enzymes and nitric oxide (NO) or indirectly byactivating NK cells DCs and tumour-specific cytotoxic T-lymphocytes (CTLs) [101]
NK cells are also innate immune cells capable of killingtumour cells particularly those cells that have reduced classI MHC expression and therefore can escape killing by CTLsPaclitaxel can enhance NK cell function by inducing mRNAand protein production of perforin an effector moleculeinvolved inNKcell-mediated cytotoxicity [106]However theeffect of low dose paclitaxel on NK cells is controversial Inanother study it was found that treatment of human NK cellswith paclitaxel effectively inhibits NK cell-mediated killing ofK562 (human erythroleukemia) target cells in vitro withoutaffecting the viability of NK cells [107] However weeklypaclitaxel therapy for non-small cell lung cancer patients was
only able to reduce the NK cell function up to completion ofthe first cycle but thereafter it gradually recovered [108]
Dendritic cells also express TLR4 and can be directlyactivated by paclitaxel The binding of paclitaxel to TLR onimmature DCs promotes DC maturation by upregulatingantigen-processing machinery gene components costimu-latory molecules and IL-12p70 [102] This enhances theability of DCs to prime T cells which facilitate antitumourimmunity [109] Paclitaxel can also promote cytotoxic T-cell function by upregulating mannose-6-phosphate whichfacilitates permeability to granzyme B and also inducescytokine production patterns typical of the T helper type 1phenotype via IL-2 (CD4 T cell) and IFN-120574 (CD8 T cell)secretion [104 110] Activated CD8+ T cells can differentiateinto CTL type 1 (Tc1) cells producingmainly IFN-120574 and CTLtype 2 (Tc2) cells producing mostly IL-4 IL-5 and IL-10 Tc1cells are potent CTL involved in the defense against cancerTc1 cells are able to recognise tumour antigens in the contextof MHC class I and mediate tumour cell lysis The role of Tc2cells in the immune response is not clearly known althoughtheir presence has been associated with disease progression[111]
CD4+ CD25+ regulatory T-cells (Tregs) constitutingapproximately 5ndash10 of peripheral CD4+ T cells [112 113]play an important role in tumour immune evasion [114]There is growing evidence that supports the existence ofelevated numbers of Tregs in tumours [115ndash117] which may
BioMed Research International 9
suppress immune responses of other CD4+ and CD8+ cells[118ndash120] and promote tumour progression In murine stud-ies paclitaxel exhibits the ability to reduce the number andsize of Treg cells thereby enhancing antitumour immunity[119 121] Similar findingswere seenwith a selective reductionin the size and number of Treg populations in peripheralblood samples from non-small cell lung cancer (NSCLC)patients [122]
Paclitaxel also decreased the expression of the anti-apoptotic molecule Bcl-2 in Treg cells while increasing thecorresponding proapoptoticmember Bax which contributedto the apoptotic sensitivity of Treg to paclitaxel [87]This wasseen in a study using the 3LL Lewis tumour model whichdemonstrated that Treg cells exposed to paclitaxel displayeddown regulation of Bcl-2 and upregulation of Bax and uponblocking the Bcl-2 pathway the ability of paclitaxel to ablateTreg cells compared toT effectorswas impaired and bothTregand T effectors were affected These results may suggest thatpaclitaxel targets Bcl-2 rather than tubulin to contribute tothe distinctive effect on Treg cells [119] It has recently beenshown in vitro that paclitaxel could target Bcl-2 and thereforelead to apoptosis Bcl-2 family proteins are key regulators ofapoptosis and play an important role in tumourigenesis andmulti-drug resistance by blocking apoptosis [119 123]
Few studies have also shown effect of paclitaxel onmyeloid-derived suppressor cells (MDSCs) a heterogeneouspopulation of immature myeloid cells immunosuppressivein nature are recruited by cancer cells and are found inincreased amount in advanced epithelial ovarian cancer [124]In a murine study using C57BL6 mice administration ofpaclitaxel at ultralow dose modulates MDSCs to differentiateinto DCs in a TLR4 independent manner [110] Hencepaclitaxel in ultralow noncytotoxic doses together with itsangiogenesis blocking ability may potentially enhance theefficacy of immunotherapy by ablation of immunosuppres-sive populations such as Tregs and MDSCs in tumour-bearing hosts [50 102]
In immunocompromised patients with advanced ovariancancer with increased Tregs and decreased levels of CD4+T cell CD8+ T cell and NK subsets after a single courseof combined carboplatin and paclitaxel chemotherapy theimmunosuppression is reversed around 12 to 14 days later butnot before one week or after three to four weeks Not only areTregs decreased but also the proportions of IFN-120574 secretingCD8+ T cells T helper-1 Tc1 and NKT cells The ratio of Tc1to Tc2 cells increases significantly [111 120 125]
Following chemotherapy both CD4+CD45RO+ andCD8+CD45RO+ memory T cells increased significantly andpeaked around 2 weeks The increase of memory T cellsin ovarian cancer patients following chemotherapy prob-ably opens the door of opportunity to develop long-termimmunological memory which could prevent recurrenceand metastases [120] Administration of dose-dense therapygiven weekly may hence be beneficial immunologically tomount an adequate immune response compared to standard3-week therapy In addition administration of immunother-apy agentsmay also be ideal during the period of 2weeks afterchemotherapy where temporary immune system reconstitu-tion takes place
8 Clinical Studies
In the past two decades paclitaxel had been administered indoses ranging from 60 to 250mgm2 over 1ndash96 hours andfrom 1 to 3 weekly intervals Prolonged exposure up to 96hours was believed to be effective as demonstrated with pre-clinical data but later refuted in large prospective studies [14126 127] A 24-hour infusion of paclitaxel was subsequentlyadministered to reduce the risk of hypersensitivity reactionshowever it was shown to increase mucosal and bone marrowtoxicity without improved efficacy [127 128] Development ofeffective premedication has led to administration of shorterinfusions (lt3 hours) which are better tolerated in particularfrom a haematologic perspective but patients remain at riskof myalgia and neuropathy at higher doses Weekly one-hourlow dose paclitaxel also known as dose-dense therapy hasrecently emerged as another possible strategy to improveoutcomes
9 Dose-Dense Therapy
Dose-dense treatment is defined by delivery of a maintainedper-cycle dose or overall dose with administration of drugat shorter time intervals than is standard This differs fromdose intensity which refers to dose (per unit weight or bodysurface area) delivered per unit time Hence either escalationof dose per cycle or reducing the time in between cycles maymodify dose intensity [129 130]
The rationale for the dose-dense approach of weeklypaclitaxel is that more frequent delivery of moderate dosesmay achieve greater efficacy by allowing sustained exposureof dividing tumour cells to paclitaxelrsquos cytotoxic and antian-giogenic effects hence reducing resistance delaying relapseand increasing the possibility of cancer remission Three 1-hour infusions of paclitaxel given at a week interval achievedgreater dose-density as well as dose-intensity than a singleadministration every 3 weeksThe initial tissue concentration(gt50 nM) for 1-hour infusion is similar to that of 3-hourinfusion but the concentration in the plasma instead oflasting for 8 hours in a 3-hour infusion rapidly falls below50 nM in less than 75 minutes for 1-hour infusion and hencereduces the risk of neutropenia However the rate of fallexperienced in tissue concentration of the drug is slowerthan plasma concentration of the drug hence efficacy ismaintained [131 132] A shorter infusion time allows bettercontrol of toxicities improved patient comfort and reducedhospitalisation hours
Several studies have used dose-dense paclitaxel in thetreatment of advanced ovarian cancer and are summarizedin Table 1 Based on phase 1 studies the recommendeddose for weekly paclitaxel ranges between 80 and 90mgm2compared with 45mgm2 per week with 3-weekly paclitaxeland is given over 1-hour duration Weekly scheduling hasdemonstrated consistent activities in ovarian cancer studies[11ndash13] Response rates were in the 20ndash50 range whereusually less than 10 would be expected Grade-4 doselimiting toxicities in particular neutropenia were not evidentat any dose below 100mgm2week [11 133]
10 BioMed Research International
Table1Ph
ases
Iand
IIstu
dies
onintravenou
sdose-densep
aclitaxel
Stud
yRe
gimen
119899()
PI(m
)RR
()
CR(119899)
MedianPF
S(m
)Median
OS
(m)
Adversee
ffects
Com
ments
Paclitaxel
dose
(mgm
2 )Ca
rbop
latin
dose
(mgm
2 )Ph
aseIsinglea
gent
Lofflerre
tal1996
[11]
40ndash9
0week
1-hou
rinfusionfor
6weeks
5040
5NA
NA
(i)Hem
atologictoxicity-m
ild(ii)N
ograde3
or4
haem
atologicaltoxicity
neurologicalor
cardiotoxicityup
to90
mgm
2 wk
(iii)Nohypersensitivity
reactio
ns(patientsreceivedprem
edication)
(i)100
priorc
hemotherapy
(ii)M
ediando
seintensity
was
410m
gm
2 6w
k(range200
to540m
gm
2 6w
k)
Fenn
ellyetal
1997
[12]
40ndash100w
eek
1830
NA
NA
NA
(i)Nomucositiso
rgrade
III
neurop
athy
was
seen
(ii)A
lopeciao
ccurredin
one
(i)100
priorc
hemotherapy
(2ndash5
priorregim
ens)
(ii)P
artia
lrespo
nses
weres
eenin
four
of13
assessablepatients
(30
)(iii)Dose-lim
iting
toxicitywas
reachedat100m
gm
2 (iv
)2-3
patie
ntse
xperience
treatmentd
elay
(v)M
axim
um-to
lerateddo
seof
80mgm
2 Ab
u-Ru
stum
etal
1997
[13]
60ndash100
over
1ho
urw
eek
45289
NA
NA
NA
(i)Nopatie
nthadfebrile
neutropenia
(i)100
priorc
hemotherapy
(1ndash8
priorregim
ens)
PhaseIISing
leagent
Markm
anetal
2001
[14]
80over
1ho
urw
eek
53(52)
25NA
NA
NA
Therapydiscon
tinuedin
(i)4patie
ntsw
hohadperip
heral
neurop
athy
(ii)1
patie
ntdu
etopainful
fingernailbeds
(i)100
platinum
andpaclita
xel
resistant
(ii)Th
erapywas
discon
tinuedin
5patie
ntsb
ecause
oftoxicity
(iii)Only13
(1)w
erem
odified
(doser
eductio
nor
treatment
delay)
becauseo
fsidee
ffects
PhaseIICom
binedwith
platinum
agent
Kiku
chietal
2005
[15]
80over
1ho
urw
eek
AUC2week
27gt6
818
483
NA
(i)Neutro
penia(
17)
thrombo
cytopenia(
51
)(ii)N
ocaseso
fperipheral
neurop
athy
(grades3
and4)
inweeklycombinedT-C
Cadron
etal2007
[16]
90over
1ho
urw
eek
AUC4week
24 9gt6le6
73 38NR
8105
675
(i)Grade
34neutropenia(
34)
andneutropenicfever
in2
(ii)N
auseaa
ndvomiting
and
fatig
uewerethe
mostfrequ
ent
nonh
ematologicalsid
eeffects
(i)Doser
eductio
nwas
necessary
in25of
patie
nts
Pign
atae
tal2008
[17]
60over
1ho
urw
eek
AUC2week
24(13)lowastlowast
1stline
385
2320
136
(i)Notoxicd
eath
was
recorded
(ii)G
rade
2anaemiawas
repo
rted
insevenpatie
nts(27)
(iii)Nofebrile
neutropeniaw
asob
served
(iv)G
rade
3and4neutropenia
was
recorded
infive(19)a
ndon
e(4
)patients
(v)G
rade
3thrombo
cytopenia
occurred
inon
epatient
(4)
BioMed Research International 11
Table1Con
tinued
Stud
yRe
gimen
119899()
PI(m
)RR
()
CR(119899)
MedianPF
S(m
)Median
OS
(m)
Adversee
ffects
Com
ments
Paclitaxel
dose
(mgm
2 )Ca
rbop
latin
dose
(mgm
2 )
Safrae
tal2014
[18]
80over
1ho
urw
eek
AUC2week
133
1stline
864
645
274
(i)Highera
naem
ia(grade
III+
IV68vs53)+
IVneutropenia(
144vs69)
decreasedgradeIIa
lopecia(
235
vs981
)and
thrombo
cytopenia
(grade
III+
IV0
vs23)
Havrilesky
etal
2003
[19]
80over
1ho
urw
eek
AUC2weekD1
D8D15
until
progressionCR
+8courses
29 21 8
Total
grou
pgt6lt6
83 100
38
16 15 1114
115
137
32
(i)Hem
atologictoxicitywas
common
(grade
3neutropenia
32n
ograde4
neutropenia
grade3
or4thrombo
cytopenia
142)
(i)To
xicitymanaged
bytre
atment
delaydo
seredu
ctionof
paclitaxel
ordiscon
tinuatio
nof
carbop
latin
vanderB
urgetal
2014
[20]
90over
1ho
urw
eek
AUC4weekD1
D8D15
D29
D36
D49
+6x
TCq3w
108
65 43
Total
grou
pgt6lt6
76 5816 42
26 158 13
(i)Neutro
penia3
0
thrombo
cytopenia8
febrile
neutropenia0
5
(ii)N
onhaem
atologictoxicitywas
low
(i)Treatm
entw
asdelayedin
16
anddo
seredu
cedin
2of
cycle
s
119899num
bero
fpatientsassessableforrespo
nsemm
onthsPIplatinum
treatmentfreeintervalRR
respo
nser
ateCR
com
pleterem
issionT
paclitaxelC
carbop
latin
PFS
progressio
nfre
esurvivalOSoverall
survivalN
An
otavailableinpapero
rabstractandNR
notyetreached
lowastlowastElderly
popu
lation
patient
agedge70
years
12 BioMed Research International
Numerous phase II studies have explored the tolerabilityand the activity of weekly paclitaxel either as a single agent orin combination with several other drugs or biological agents(Table 1) A number of regimens combining weekly paclitaxelwith carboplatin have been used as first-line treatment inovarian cancer Carboplatin has been administered weeklyat AUC of 2 with dose escalation in some studies whilepaclitaxel had been infused at 60ndash80mgm2week Thiscombined regimen was well tolerated with a low incidence ofbone marrow suppression Overall response rates have beenhigh in the range of 60ndash80 in most studies even in heavilypretreated patients with platinum-resistant disease (diseaserecurrence or progression within 6 months of the last lineof platinum-based therapy) [15ndash20 134] The promising datafrom these phase II trials then led to the evolution of largerphase III trials
Three phase III studies Japanese Gynecologic OncologyGroup- (JGOG-) Trial 3016 [21ndash23] Multicentre Italian Trialin Ovarian Cancer-Trial 7 (MITO-7) [25] and GynecologicOncology Group GOG-262 Trial [24] have explored dosedense therapy The results of these trials are summarised inTable 2
The Japanese Gynecologic Oncology Group (JGOG)conducted a randomized phase 3 trial of dose-dense weeklypaclitaxel 80mgm2week in combination with 3-weeklycarboplatin compared to standard 3-weekly carboplatin andpaclitaxel 180mgm2 in patients with advanced epithelialovarian peritoneal or fallopian tube cancer (JGOG 3016NOVEL trial) In both arms carboplatin was given at AUC6 and the median number of cycles was six In this largestudy (119899 = 637) with a median follow up of 77 months therewas an 11-month improvement in themedian progression freesurvival (PFS) in the dose-dense treatment group comparedwith the standard treatment arm (282 versus 175 monthsHR 076 95 CI 062ndash091 119901 = 00037) Median OS wasalso higher in the dose-dense treatment arm (1005 versus622 months HR 079 95 CI 063ndash099 119901 = 0039)On subgroup analysis suboptimally debulked patients withresidual disease of gt1 cm (119899 = 342) had a significantlyhigher median overall survival in the dose dense arm (512versus 335 months HR-075 95 CI 057ndash097 119901 = 0027)There was no significant advantage to dose-dense treatmentfor patients with optimally cytoreduced disease Dose-densetherapy survival benefits were also not seen in patients withclear cell or mucinous histology type unlike serous typeHowever patient treated with dose dense therapy had asignificantly higher frequency of hematologic toxicity thanwith the standard arm (212 versus 94) which resultedin lower treatment completion rates (63 versus 48) withfrequent episodes of delay (76 versus 67) and dosereductions (48versus 35) [21 22]Therewas no significantdifference in terms of overall quality of life between the twoarms (119901 = 046) [23]
Using a similar regimen as in JGOG-3016 a GynecologicOncology Group (GOG)-262 Trial was conducted in theUnited States In this group most patients had stage IIIdisease (66ndash70) and two-thirds had suboptimal debulkingwith residual disease of gt1 cm This was a randomized phase
III trial of 3 weekly paclitaxel versus dose-dense weeklypaclitaxel in combination with carboplatin in patients withadvanced epithelial ovarian peritoneal or fallopian tubecancer Though optional concurrent and maintenance beva-cizumab were received by the majority of patients in botharms (835 versus 841 resp) There was no significantdifference in PFS in the patients who received the dosedense paclitaxelcarboplatin regimen compared to those whoreceived the standard paclitaxelcarboplatin regimen (148versus 143 months HR 097 95 CI 079ndash118) Howeverin a subgroup analysis there was a significant difference inPFS in the dose dense paclitaxel arm who did not receivebevacizumab 119899 = 112 (142 versus 103 months HR 059 95CI 037ndash096 119901 = 0003) Overall survival data is still imma-ture There was higher frequency of grade 3 anaemia (408versus 157 119901 lt 0001) and grade 2 sensory neuropathy(259 versus 178 119901 = 0012) but a lower incidence ofneutropenia (72 versus 83 119901 lt 0001) [24]
In 2008 the Multicentre Italian Trials in Ovarian Cancer(MITO-7) randomised 810 women in a phase 3 trial toreceive either standard carboplatin (AUC = 6) and paclitaxel175mgm2 every 3 weeks or a weekly schedule of paclitaxel(60mgm2) with carboplatin (AUC = 2) The majority ofpatients in both arms (83ndash90) received six cycles of therapyMost patients (58ndash63) had stage II1 disease 23 of themwere suboptimally debulked Median PFS did not differsignificantly (173 months and 183 months 119901 = 066)between the standard and dose-dense arms respectivelyThere was no significant difference in response rate betweenthe two arms nor the estimated 2-year overall survivalSubgroup analysis did not identify any subgroup that mayhave benefited from the dose-dense regimen Unlike theJGOG-3016 trial the incidence of grade 3-4 neutropenia wassignificantly lower in the dose-dense group compared to the3-weekly regimen (42 versus 50) A similar pattern wasseen for the incidence of febrile neutropenia (lt1 versus 3119901 = 002) thrombocytopenia (1 versus 7 119901 lt 0001)and other nonhaematological toxicities such as alopeciavomiting renal dysfunction and neuropathy Quality of lifewas reported to be significantly better in the dose-dense arm(119901 lt 00001) which was discordant with the JGOG-3016quality of life data [25]
In summary there was significant improvement inmedian PFS and overall survival in studies using paclitaxelat 80mgm2week dose-dense therapy [21 24] but withhigher haematological toxicity whereas MITO-7 [25] whichwas using paclitaxel at 60mgm2week was only equivalentlyeffective but less toxicThis does not conclude that the higherpaclitaxel dose is more clinically beneficial as there are manyother confounding factors in all three studies
In a multivariate analysis the JGOG-3016 study [21]reported that a lower dose intensity of paclitaxel (lt80) wasassociated with poorer overall survival (hazard ratio = 14295 confidence interval 112ndash181 119901 = 0004) however itmust be highlighted that the investigational arm carboplatinschedules were not standardised in these studies The JGOGand GOG trials delivered a 3-weekly carboplatin (AUC =6) arm whereas in the MITO-7 study the carboplatin was
BioMed Research International 13
Table2Ph
aseIIIstu
dies
onintravenou
sdose-densep
aclitaxel
Stud
yRe
gimen
119899
MedianPF
S(m
)
Median
OS
(m)
Adversee
ffects
Com
ments
Katsu
matae
tal2009
[21]
Katsu
matae
tal2013
[22]
Haranoetal2014
[23]
JGOG3016
631
(i)Haematologicaltoxicityhigh
erin
dose
dense-211versus
94
Lower
treatmentcom
pletionin
dose-dense
63versus
48
Frequent
episo
deso
fdelay
indo
se-dense
76versus
67
Doser
eductio
nsin
dose-dense
48versus
35
Nosig
nificantd
ifference
inoverallQ
OL
betweenbo
thgrou
ps(119901=046)
Paclitaxel80m
gm
2D18
15+carbop
latin
AUC63
weeklyversus
Paclitaxel180
mgm
2+
carbop
latin
AUC63
weekly
312
282
1005
Both
givenfor6
ndash9cycle
s319
175
622
Chan
etal2013
[24]
GOG-262
(i)Higherfrequ
ency
ofgrade3
anaemia
(408versus
157119901lt0001)
grade2
sensoryneurop
athy
(259versus
178
119901=0012)b
utlower
incidenceo
fneutropenia(
72versus
83119901lt0001)
Paclitaxel80m
gm
2D18
15+carbop
latin
AUC63
weeklyversus
Paclitaxel175
mgm
2+
carbop
latin
AUC63
weekly
346
148
NR
Both
givenfor6
cycle
s346
143
NR
Bevacizumab
given
optio
nally
112
(did
not
receive
bevazicumab)
142vs
103
Pign
atae
tal2014
[25]
MITO-7
810
(i)Lo
wer
incidenceo
fgrade
3-4
neutropenia(
42versus
50)febrile
neutropenia(lt1v
ersus3
119901=002)
thrombo
cytopenia(
1versus7
119901lt0001)andothern
onhaem
atological
toxicitie
ssuchas
alop
eciavom
iting
renald
ysfunctio
nandneurop
athy
Qualityof
lifeb
etterindo
sedensea
rm(119901lt00001)
Paclitaxel60m
gm
2 weekly+carbop
latin
AUC
2weeklyversus
Paclitaxel175
mgm
2+
carbop
latin
AUC63
weekly
406
404
183 173
77lowast
79lowast
119899num
bero
fpatientsmm
onthsDday
PFSprogressionfre
esurvivalOSoverallsurvivalNAnot
availableinpapero
rabstractandNR
notyetreached
lowastSurvivalrateat2years
14 BioMed Research International
dose-dense (AUC 2 weekly) Although it is possible that thedose scheduling for the platinum-based agent is not essentialfor a survival benefit as shown by previous studies usingdose-dense cisplatin direct cross-trial comparison cannot bemade Unlike paclitaxel carboplatin probably requires peakdose for optimal therapeutic benefit hence this may accountfor the inferior survival outcome in MITO-7 trial Anotherconfounding factor may be difference in ethnicity All threestudies used different ethnic populations and Asian patientsin JGOG-3016 appear to have better survival outcomes thanthe MITO-7 Western population Ethnicity with possibleunderlying genetic causes may be responsible for the variableresponses to chemotherapy across individuals [135] This wasexplored by Millward et al who studied 68 Caucasian andAsian lung cancer patients treated with a combination ofpaclitaxel and carboplatin and found that the incidence offebrile neutropenia was 50 of an initially treated cohortof Asians and when carboplatin was subsequently dosereduced in all Asian patients the overall incidence of febrileneutropenia was also reduced to 26 [136]
Although early clinical data from phase I and phaseII dose-dense paclitaxel trials in advanced ovarian cancerwere promising the results from phase III studies in havebeen inconsistent as a result of differences in paclitaxel dosecarboplatin AUC and schedule addition of bevacizumabas well as different ethnic populations The results of arecently completed randomised three arms GynaecologicCancer InterGroup (GCIG) phase II trial ICON 8 mayfurther inform the clinical benefit of dose dense paclitaxeltherapy
This multicentre trial involving 111 centres in the UKSouth Korea Mexico Ireland Australia and New Zealandwith a target population of 1485 patients with stage IC-IV epithelial ovarian cancer or peritoneal or fallopian tubecancer compared two dose-dense arms (i) JGOG-like armcarboplatin AUC 5 plus weekly 80mgm2 paclitaxel and (ii)MITO-7-like arm weekly carboplatin AUC 167 plus weekly80mgm2 paclitaxel to the standard 3-weekly treatment(carboplatin AUC 5 plus 175mgm2 paclitaxel) for stage IC toIV epithelial ovarian cancer The dose-dense arms of MITO-7 and JGOG-3016 as well as the ethnic heterogeneity will befurther addressed
10 Intraperitoneal (IP) Chemotherapy
In addition to dose and scheduling the route of adminis-tration of chemotherapy agents plays an important role inoutcome Intraperitoneal spread is common and likely anearly event in epithelial ovarian cancer hence the deliveryof chemotherapy intraperitoneally in theory would exposethe microcirculation of tumour to higher doses of drug thansystemic administration while limiting systemic toxicityTheideal drug for IP chemotherapy is one that is systemicallyeffective penetrates deep into the inner core of tumour tissueand remains within the peritoneal cavity for a prolongedperiod of time [137ndash139]
Early clinical studies confirmed that indeed the peritonealcavity could be exposed to 10 to 20-fold higher (cisplatin
and carboplatin) drug concentration than when using theintravenous approach and since 1978 this route had beenadopted as a form of therapeutic intervention [137 139]A subsequent phase I trial showed that IP paclitaxel haddose-limiting toxicity in the form of abdominal pain [140]Another phase 1 GOG pilot study administered weekly IPpaclitaxel at an initial dose of 20mgm2 for 16 weeks to33 patients and found that IP paclitaxel at this dose wasfeasible and well tolerated At dose levels 60 to 65mgm2there were significant levels of paclitaxel for a week afterdrug administration suggesting very slow clearance andcontinuous exposure of the peritoneal cavity to active drugconcentrations [132]
Hence this initiated a phase II study [141] that used pacli-taxel intraperitoneally at a dose of 60ndash65mgm2week In thisphase II GOG study 76 patients with small-volume resid-ual disease carcinoma (05 cm or less) involving the ovaryperitoneal or fallopian tube were treated with paclitaxel60mgm2week intraperitoneally for 16 weeks followed bysurgical evaluation in patients without disease progressionThe Gynaecologic Oncology group (GOG) currently definesno visible disease as microscopic disease being the idealsurgical outcome 75 of patients had received prior systemictherapy and 70 received all 16 courses that were planned Of28 patients with microscopic disease at the start of therapy61 achieved a surgically defined complete response whereasonly 1 out of 31 patients with macroscopic disease achieved acomplete response The median time-to-recurrence was 167months with an estimated survival rate at 2 years being 58Treatment was generally well tolerated [141]
Another study looked into the effect of IP paclitaxel asconsolidation therapy in advanced ovarian cancer Twenty-eight patients who had initial residual macroscopic disease(lt1 cm) after primary surgery or interval debulking but hadcomplete pathological response following standard treatmentwith at least 6 cycles of platinum-based chemotherapy regi-men received paclitaxel 60mgm2week intraperitoneally for12ndash16 weeks as consolidation therapy The median time torecurrence was 25 months but overall survival did not differsignificantly when compared with control group submittedto observation only Treatment-related toxicity was mild andtechnical difficulties were observed in 11 of patients [142]
Multicenter randomised phase 3 trials as well as meta-analysis of IP chemotherapy have been performed anddemonstrated that chemotherapy drugs administered intra-peritoneally are superior to intravenous standard regimensin patient with optimally debulked epithelial ovarian cancerThe most impressive data comes from GOG 114 [14] and172 trial [143] In GOG 114 patients received either sixcycles of intravenous paclitaxel 135mgm2 and cisplatin75mgm2 every 3 weeks or intravenous carboplatin (AUC= 9) every 28 days for two cycles followed by six 3-weeklycycles of intravenous paclitaxel 135mgm2 and IP cisplatin100mgm2 [14] whereas in GOG 172 patients received eitherintravenous paclitaxel 135mgm2 followed by intravenouscisplatin 75mgm2 or intravenous paclitaxel 135mgm2 fol-lowed by IP combination of cisplatin 100mgm2 and pacli-taxel 60mgm2 on day 8 Both trials had a combined total
BioMed Research International 15
of 876 women with stage III epithelial ovarian carcinomaoptimally debulked to le1 cm residual tumour [143] Themedian follow-up for GOG 114 [14] was 138 years with GOG172 [143] was 97 years The primary results of the individualtrials reported up to 6-month improvement in median PFSfollowing IP therapy In the combined analysis of the datafrom both trials the data continued to show a 5-monthdifference in favour of IP therapy (25 versus 20 months)which translates into 16 reduction in the hazard ratio forprogression (119901 = 003) In GOG 114 [14] reported in 2001there was only borderline improvement in overall survivalassociated with this regimen (median 63 versus 52 monthsrelative risk 081 119901 = 005)
However in combined analysis in 2013 which was pre-sented at the Society of Gynecologic Oncology AnnualMeeting [144] the overall survival showed an 11-monthimprovement in favour of IP therapy in GOG 114 whereasGOG 172 reported a 16-month survival advantage Amongpatients treated with IP therapy the 5-year survival rateincreased from 18 following completion of 1-2 cycles to 59for patients who completed 5-6 cycles of treatment Howeverthere was increased toxicity observed in the IP arm grade 3-4 leukopenia thrombocytopenia and abdominal pain Only42 of patients in the GOG172 trial [143] completed all sixcycles of planned treatment in the IP arm while 18 ofpatients in GOG 114 trial [14] received fewer than two coursesof IP chemotherapy
Another randomised phase III trial involving patientswith stages II-III epithelial ovarian carcinoma is the GOG252 study with three arms Arm 1-dose-dense intravenouscarboplatin and paclitaxel Arm 2-dose-dense intravenouspaclitaxel and IP carboplatin and Arm 3 consists of 3-weeklyintravenous paclitaxel (day 1) followed by IP cisplatin (day 2)and IP paclitaxel (day 3) regimen All three arms also incor-porate the combination and maintenance of bevacizumabGOG 252 has completed accrual and results are awaited [139]
11 Newer Forms of Paclitaxel
Development of next-generation taxanes has taken place overthe past 40 years aimed at eliminating toxicity improvingefficacy and ease of administration Abraxane is a novelcompound which incorporates paclitaxel into an albuminnanoparticle soluble in saline hence eliminating the needfor Cremophor EL which is responsible for hypersensitivityreactions experienced during paclitaxel infusion [145] Thenanoparticle albumin in nab-paclitaxel is able to bind toglycoprotein gp60 receptor an albumin receptor and activatecaveolin-1 a protein that in human is encoded byCAV-1 geneleading to formation of caveoli hence allowing nab-paclitaxelto migrate across the endothelial cell membrane into theinterstitial space leading to higher intratumoural drug con-centration In addition Abraxane exhibits linear pharma-cokinetics and can therefore be given at a relatively higherdose than standard intravenous paclitaxel leading to a highertherapeutic ratio and heightened efficacy in solid tumoursmainlymetastatic breast cancer [146 147] Nab-paclitaxel hadFDA approval in 2005 for treatment of breast cancer [148]
Nab-paclitaxel has been studied in recurrent ovariancancer As a single agent in phase II 44 patients withrecurrent ovarian cancer were treated with Nab-paclitaxel260mgm2 intravenously for 30 minutes every 3 weeks for6 cycles Ninety-two percent of patients were platinum-sensitive while 89 had had previous exposure to standardtaxane The objective response rate was 64 with 15 patientsachieving complete response and 13 of them had partialresponse Estimated median PFS was 85 months No hyper-sensitivity reactions were observed and there were infrequentcases of grade 4 neutropenia (11) and grade 2-3 neuropathy(13) [149]
Another phase II study by GOG enrolled 51 patients withplatinum- and taxane-resistant recurrent ovarian cancer outof which 47 were evaluable The objective response rate was38 with one patient achieving a complete response and 10patients a partial response The median PFS was 45 monthswhile overall survival rate was 174 months Severe haema-tological and nonhaematological toxicities including neuro-toxicity were uncommon These results are quite impressivegiven the treatment population consisted of patients withvery poor prognosis with a median platinum and taxane freeinterval of 21 days and 70 had their recurrence within 3months of completion of primary treatment [150] Severalother trials of this formulation are in progress
Paclitaxel poliglumex (PPX) also known as Xyotax isanother prodrug a novel conjugate of paclitaxel and 120572-poly-L-glutamic acid which accumulates within tumour tissuedue to increased permeability of the tumour vessels and lackof lymphatic drainage [148 151 152] Paclitaxel poliglumexenhances solubility of paclitaxel allows direct delivery tothe intratumoural microenvironment and allows prolongedexposure to the active drug while minimising systemictoxicities [151] In Phase I dose escalation studies as a singleagent the recommended dose of PPX was 235mgm2 over 10minutes every 3 weeks or 70mgm2 weekly [153] In a PhaseII GOG study of relapsed ovarian cancer a response rate of16 was seen with infrequent serious adverse events grade3 and 4 neutropenia (24 and 20) and grade 3 neuropathy(24) [154] A phase III trial (GOG-0212) on the use of PPXas consolidation ormaintenance therapy in advanced ovariancancer is in progress
DHA-paclitaxel also known as Taxoprexin is a prodrugwhere paclitaxel is covalently conjugated with the naturallyoccurring omega-3 fatty acid docosahexaenoic acid (DHA)a fatty acid that is easily taken up by tumour cells henceincreasing intratumoural concentration of paclitaxel leadingtumour cell apoptosis [155 156] DHA-paclitaxel exhibitslinear pharmacokinetics and lower toxicity and also ease ofadministration when compared to conventional paclitaxeland has demonstrated antineoplastic activity in animal mod-els of cancer as well as in a phase III trial involving metastaticmelanoma [156ndash160] In a recent study on human ovariancancer cells it was found that DHA could reverse paclitaxelresistance by inhibiting P-gp as well as downregulatingthe expression of multidrug resistance associated proteins(MRP) and inhibiting the activity of NF-120581B and p38 MAPKsignalling pathways [161]
16 BioMed Research International
12 Future Directions
A plateau has been reached regarding the benefits associatedwith standard 3-weekly intravenous administration of cyto-toxic chemotherapy in advanced epithelial ovarian cancerThe ongoing battle for a better treatment regimen to delayrelapse promote remission and most importantly improvethe quality of life of patients with advanced epithelial ovariancancer need not to go further than the ability to relook at thechemotherapy agents that are already available in a differentapproach
Novel compounds to date have not yet shown clinicalsuperiority and parent compounds such as paclitaxel con-tinue to surprise us with their feasibility effectiveness andmanageable toxicity profiles Intraperitoneal paclitaxel willrequire further evaluation Better effort in understanding themechanism of action of drugs including the role of dosescheduling and the effect on the immune systemmay providea more cost-effective route to better clinical outcomes
Conflict of Interests
The authors declare no conflict of interests in this work
Acknowledgments
The authors would like to thank the many researchers whohave contributed to our current knowledge of paclitaxelNirmala Kampan is supported by Australian Monash Uni-versity Institute of Graduate Research Scholarship as wellas Universiti Kebangsaan Malaysia Postgraduate ScholarshipAward Mutsa Madondo has received Postgraduate Pub-lication Award from Monash University and MagdalenaPlebanski has been awarded Senior NHMRC Fellowship
References
[1] Australian Institute of Health and Welfare and National Breastand Ovarian Cancer Centre (Australia) Ovarian Cancer inAustralia AnOverview 2010 Cancer Series Australian Instituteof Health and Welfare Canberra Australia 2010
[2] R E Bristow R S Tomacruz D K Armstrong E L Trimbleand F J Montz ldquoSurvival effect of maximal cytoreductivesurgery for advanced ovarian carcinoma during the platinumera a meta-analysisrdquo Journal of Clinical Oncology vol 20 no 5pp 1248ndash1259 2002
[3] ZKempand JA Ledermann ldquoUpdate onfirst-line treatment ofadvanced ovarian carcinomardquo International Journal of WomenrsquosHealth vol 5 no 1 pp 45ndash51 2013
[4] A du Bois H-J Luck W Meier et al ldquoA randomized clinicaltrial of cisplatinpaclitaxel versus carboplatinpaclitaxel as first-line treatment of ovarian cancerrdquo Journal of the National CancerInstitute vol 95 no 17 pp 1320ndash1330 2003
[5] R F Ozols B N Bundy B E Greer et al ldquoPhase III trialof carboplatin and paclitaxel compared with cisplatin andpaclitaxel in patients with optimally resected stage III ovariancancer A Gynecologic Oncology Group studyrdquo Journal ofClinical Oncology vol 21 no 17 pp 3194ndash3200 2003
[6] W P McGuire W J Hoskins M F Brady et al ldquoCyclophos-phamide and cisplatin compared with paclitaxel and cisplatin
in patients with stage III and stage IV ovarian cancerrdquoThe NewEngland Journal of Medicine vol 334 no 1 pp 1ndash6 1996
[7] W P McGuire W J Hoskins M F Brady et al ldquoCyclophos-phamide and cisplatin versus paclitaxel and cisplatin a phase IIIrandomized trial in patients with suboptimal stage IIIIV ovar-ian cancer (from the gynecologic oncology group)rdquo Seminars inOncology vol 23 no 5 supplement 12 pp 40ndash47 1996
[8] M J Piccart K Bertelsen K James et al ldquoRandomized inter-group trial of cisplatin-paclitaxel versus cisplatin-cyclophosph-amide inwomenwith advanced epithelial ovarian cancer three-year resultsrdquo Journal of the National Cancer Institute vol 92 no9 pp 699ndash708 2000
[9] P A Vasey G C Jayson A Gordon et al ldquoPhase III random-ized trial of docetaxel-carboplatin versus paclitaxel-carboplatinas first-line chemotherpy for ovarian carcinomardquo Journal of theNational Cancer Institute vol 96 no 22 pp 1682ndash1691 2004
[10] B Gronlund C Hogdall H H Hansen and S A EngelholmldquoResults of reinduction therapy with paclitaxel and carboplatinin recurrent epithelial ovarian cancerrdquo Gynecologic Oncologyvol 83 no 1 pp 128ndash134 2001
[11] T M Loffler W Freund J Lipke and T-U HausamenldquoSchedule- and dose-intensified paclitaxel as weekly 1-hourinfusion in pretreated solid tumors results of a phase III trialrdquoSeminars in Oncology vol 23 no 6 supplement 16 pp 32ndash341996
[12] D Fennelly C Aghajanian F Shapiro et al ldquoPhase I and phar-macologic study of paclitaxel administered weekly in patientswith relapsed ovarian cancerrdquo Journal of Clinical Oncology vol15 no 1 pp 187ndash192 1997
[13] N R Abu-Rustum C Aghajanian R R Barakat D Fennelly FShapiro and D Spriggs ldquoSalvage weekly paclitaxel in recurrentovarian cancerrdquo Seminars inOncology vol 24 no 5 supplement15 pp S15-62ndashS15-67 1997
[14] M Markman B N Bundy D S Alberts et al ldquoPhase III trialof standard-dose intravenous cisplatin plus paclitaxel versusmoderately high-dose carboplatin followed by intravenouspaclitaxel and intraperitoneal cisplatin in small-volume stageIII ovarian carcinoma an intergroup study of the gynecologiconcology group Southwestern Oncology Group and EasternCooperativeOncologyGrouprdquo Journal of Clinical Oncology vol19 no 4 pp 1001ndash1007 2001
[15] A Kikuchi H Sakamoto and T Yamamoto ldquoWeekly car-boplatin and paclitaxel is safe active and well tolerated inrecurrent ovarian cancer cases of Japanese women previouslytreated with cisplatin-containing multidrug chemotherapyrdquoInternational Journal of Gynecological Cancer vol 15 no 1 pp45ndash49 2005
[16] I Cadron K Leunen F Amant T van Gorp P Nevenand I Vergote ldquoThe lsquoLeuvenrsquo dose-dense paclitaxelcarboplatinregimen in patients with recurrent ovarian cancerrdquo GynecologicOncology vol 106 no 2 pp 354ndash361 2007
[17] S Pignata E Breda G Scambia et al ldquoA phase II studyof weekly carboplatin and paclitaxel as first-line treatment ofelderly patients with advanced ovarian cancer A Multicen-tre Italian Trial in Ovarian cancer (MITO-5) studyrdquo CriticalReviews in OncologyHematology vol 66 no 3 pp 229ndash2362008
[18] T Safra S Shamai J Greenberg et al ldquoWeekly carboplatinwith paclitaxel compared to standard three-weekly treatment inadvanced epithelial ovarian carcinomamdasha retrospective studyrdquoGynecologic Oncology vol 132 no 1 pp 18ndash22 2014
BioMed Research International 17
[19] L J Havrilesky A A Alvarez R A Sayer et al ldquoWeekly low-dose carboplatin and paclitaxel in the treatment of recurrentovarian and peritoneal cancerrdquo Gynecologic Oncology vol 88no 1 pp 51ndash57 2003
[20] M van der BurgW Onstenk I Boere et al ldquoLong-term resultsof a randomised phase III trial of weekly versus three-weeklypaclitaxelplatinum induction therapy followed by standardor extended three-weekly paclitaxelplatinum in Europeanpatients with advanced epithelial ovarian cancerrdquo EuropeanJournal of Cancer vol 50 no 15 pp 2592ndash2601 2014
[21] N Katsumata M Yasuda F Takahashi et al ldquoDose-densepaclitaxel once a week in combination with carboplatin every3 weeks for advanced ovarian cancer a phase 3 open-labelrandomised controlled trialrdquoThe Lancet vol 374 no 9698 pp1331ndash1338 2009
[22] N Katsumata M Yasuda S Isonishi et al ldquoLong-term resultsof dose-dense paclitaxel and carboplatin versus conventionalpaclitaxel and carboplatin for treatment of advanced epithelialovarian fallopian tube or primary peritoneal cancer (JGOG3016) a randomised controlled open-label trialrdquo The LancetOncology vol 14 no 10 pp 1020ndash1026 2013
[23] K Harano F Terauchi N Katsumata et al ldquoQuality-of-lifeoutcomes from a randomized phase III trial of dose-denseweekly paclitaxel and carboplatin compared with conventionalpaclitaxel and carboplatin as a first-line treatment for stage II-IV ovarian cancer Japanese Gynecologic OncologyGroup Trial(JGOG3016)rdquo Annals of Oncology vol 25 no 1 pp 251ndash2572014
[24] J Chan M F Brady R Penson et al ldquoPhase III trial ofevery-3-weeks paclitaxel vs dose dense weekly paclitaxel withcarboplatin +minus bevacizumab in epithelial ovarian peritonealfallopian tube cancer GOG 262 (NCT01167712)rdquo InternationalJournal of Gynecological Cancer vol 23 no 8 supplement 1 pp9ndash10 2013
[25] S Pignata G Scambia D Katsaros et al ldquoCarboplatin pluspaclitaxel once a week versus every 3 weeks in patients withadvanced ovarian cancer (MITO-7) a randomisedmulticentreopen-label phase 3 trialrdquoThe Lancet Oncology vol 15 no 4 pp396ndash405 2014
[26] V Walsh and J Goodman ldquoFrom taxol to Taxol the changingidentities and ownership of an anti-cancer drugrdquo MedicalAnthropology vol 21 no 3-4 pp 307ndash336 2002
[27] R Renneberg ldquoBiotech History yew trees paclitaxel synthesisand fungirdquo Biotechnology Journal vol 2 no 10 pp 1207ndash12092007
[28] J E Liebmann J A Cook C Lipschultz D Teague J Fisherand J B Mitchell ldquoCytotoxic studies of paclitaxel (Taxol) inhuman tumour cell linesrdquo British Journal of Cancer vol 68 no6 pp 1104ndash1109 1993
[29] J J Manfredi and S B Horwitz ldquoTaxol an antimitotic agentwith a newmechanism of actionrdquo Pharmacology andTherapeu-tics vol 25 no 1 pp 83ndash125 1984
[30] D G I Kingston ldquoRecent advances in the chemistry of taxolrdquoJournal of Natural Products vol 63 no 5 pp 726ndash734 2000
[31] D G I Kingston ldquoThe shape of things to come structural andsynthetic studies of taxol and related compoundsrdquo Phytochem-istry vol 68 no 14 pp 1844ndash1854 2007
[32] V Walsh and J Goodman ldquoCancer chemotherapy biodiversitypublic and private property the case of the anti-cancer drugTaxolrdquo Social Science amp Medicine vol 49 no 9 pp 1215ndash12251999
[33] P H Wiernik E L Schwartz J J Strauman J P Dutcher RB Lipton and E Paietta ldquoPhase I clinical and pharmacokineticstudy of taxolrdquo Cancer Research vol 47 no 9 pp 2486ndash24931987
[34] W P McGuire E K Rowinsky N B Rosenhein et alldquoTaxol a unique antineoplastic agent with significant activityin advanced ovarian epithelial neoplasmsrdquo Annals of InternalMedicine vol 111 no 4 pp 273ndash279 1989
[35] ldquoDiscovery and development of taxolrdquo in Taxol Science andApplications M W M E Suffness Ed pp 3ndash25 CRC PressBoca Raton Fla USA 1995
[36] M J Piccart and F Cardoso ldquoProgress in systemic therapy forbreast cancer an overview and perspectivesrdquo European Journalof Cancer Supplement vol 1 no 2 pp 56ndash69 2003
[37] P Bonomi K B Kim and J Kugler ldquoComparison of survival forstage IIIB versus stage IV non-small cell lung cancer (NSCLC)patients with etoposide-cisplatin versus taxol-cisplatin an East-ern Cooperative Oncology Group (ECOG) trialrdquo in Proceedingsof the American Society of Clinical Oncology vol 16 p 454a1997
[38] D Guenard F Gueritte-Voegelein J Dubois and P PotierldquoStructure-activity relationships of Taxol and Taxotere ana-loguesrdquo Journal of the National Cancer Institute Monographsno 15 pp 79ndash82 1993
[39] D G I Kingston ldquoTaxol the chemistry and structure-activityrelationships of a novel anticancer agentrdquo Trends in Biotechnol-ogy vol 12 no 6 pp 222ndash227 1994
[40] E K Rowinsky and R C Donehower ldquoPaclitaxel (taxol)rdquo TheNew England Journal of Medicine vol 332 no 15 pp 1004ndash10141995
[41] J Parness and S B Horwitz ldquoTaxol binds to polymerizedtubulin in vitrordquo Journal of Cell Biology vol 91 no 2 pp 479ndash487 1981
[42] A Dammermann A Desai and K Oegema ldquoTheminus end insightrdquo Current Biology vol 13 no 15 pp R614ndashR624 2003
[43] CWiese and Y Zheng ldquoMicrotubule nucleation 120574-tubulin andbeyondrdquo Journal of Cell Science vol 119 no 20 pp 4143ndash41532006
[44] A Ganguly H Yang and F Cabral ldquoPaclitaxel-dependent celllines reveal a novel drug activityrdquo Molecular Cancer Therapeu-tics vol 9 no 11 pp 2914ndash2923 2010
[45] P B Schiff and S B Horwitz ldquoTaxol stabilizes microtubules inmouse fibroblast cellsrdquo Proceedings of the National Academy ofSciences of the United States of America vol 77 no 3 pp 1561ndash1565 1980
[46] P B Schiff J Fant and S B Horwitz ldquoPromotion of micro-tubule assembly in vitro by Taxolrdquo Nature vol 277 no 5698pp 665ndash667 1979
[47] D Zhang R Yang S Wang and Z Dong ldquoPaclitaxel new usesfor an old drugrdquoDrug Design Development andTherapy vol 8pp 279ndash284 2014
[48] S Rao G A Orr A G Chaudhary D G I Kingston and SB Horwitz ldquoCharacterization of the taxol binding site on themicrotubule 2-(m-Azidobenzoyl)taxol photolabels a peptide(amino acids 217-231) of beta-tubulinrdquoThe Journal of BiologicalChemistry vol 270 no 35 pp 20235ndash20238 1995
[49] F Wang Y Cao W Zhao H Liu Z Fu and R Han ldquoTaxolinhibits melanoma metastases through apoptosis inductionangiogenesis inhibition and restoration of E-cadherin andnm23 expressionrdquo Journal of Pharmacological Sciences vol 93no 2 pp 197ndash203 2003
18 BioMed Research International
[50] A Sevko V Kremer C Falk et al ldquoApplication of paclitaxel inlow non-cytotoxic doses supports vaccination with melanomaantigens in normal micerdquo Journal of Immunotoxicology vol 9no 3 pp 275ndash281 2012
[51] T Kreis and R Vale Guidebook to the Cytoskeletal and MotorProteins Oxford University Press Oxford UK 2nd edition1999
[52] P Giannakakou D L Sackett Y-K Kang et al ldquoPaclitaxel-resistant human ovarian cancer cells have mutant 120573-tubulinsthat exhibit impaired paclitaxel-driven polymerizationrdquo TheJournal of Biological Chemistry vol 272 no 27 pp 17118ndash171251997
[53] E Rakovitch W Mellado E J Hall T K Pandita S Sawantand C R Geard ldquoPaclitaxel sensitivity correlates with p53status and DNA fragmentation but not G2M accumulationrdquoInternational Journal of Radiation Oncology Biology Physics vol44 no 5 pp 1119ndash1124 1999
[54] S W Lowe S Bodis A McClatchey et al ldquop53 status and theefficacy of cancer therapy in vivordquo Science vol 266 no 5186 pp807ndash810 1994
[55] C C Zhang J-M Yang E White M Murphy A Levine andW N Hait ldquoThe role of MAP4 expression in the sensitivity topaclitaxel and resistance to vinca alkaloids in p53 mutant cellsrdquoOncogene vol 16 no 12 pp 1617ndash1624 1998
[56] K Fukasawa T Choi R Kuriyama S Rulong and G F VandeWoude ldquoAbnormal centrosome amplification in the absence ofp53rdquo Science vol 271 no 5256 pp 1744ndash1747 1996
[57] T-H Wang Y-H Chan C-W Chen et al ldquoPaclitaxel (Taxol)upregulates expression of functional interleukin-6 in humanovarian cancer cells through multiple signaling pathwaysrdquoOncogene vol 25 no 35 pp 4857ndash4866 2006
[58] E Yakirevich E Sabo I Naroditsky Y Sova O Lavie andM B Resnick ldquoMultidrug resistance-related phenotype andapoptosis-related protein expression in ovarian serous carcino-masrdquo Gynecologic Oncology vol 100 no 1 pp 152ndash159 2006
[59] G Szakacs J K Paterson J A Ludwig C Booth-Genthe andM M Gottesman ldquoTargeting multidrug resistance in cancerrdquoNature Reviews Drug Discovery vol 5 no 3 pp 219ndash234 2006
[60] L W Pfannenstiel S S K Lam L A Emens E M Jaffeeand T D Armstrong ldquoPaclitaxel enhances early dendritic cellmaturation and function through TLR4 signaling in micerdquoCellular Immunology vol 263 no 1 pp 79ndash87 2010
[61] N Klauber S Parangi E Flynn E Hamel and R J DrsquoAmatoldquoInhibition of angiogenesis and breast cancer in mice by themicrotubule inhibitors 2-methoxyestradiol and Taxolrdquo CancerResearch vol 57 no 1 pp 81ndash86 1997
[62] D Belotti V Vergani T Drudis et al ldquoThe microtubule-affecting drug paclitaxel has antiangiogenic activityrdquo ClinicalCancer Research vol 2 no 11 pp 1843ndash1849 1996
[63] D H Lau L Xue L J Young P A Burke and A T CheungldquoPaclitaxel (Taxol) an inhibitor of angiogenesis in a highlyvascularized transgenic breast cancerrdquo Cancer Biotherapy andRadiopharmaceuticals vol 14 no 1 pp 31ndash36 1999
[64] X Jiang ldquoHarnessing the immune system for the treatment ofbreast cancerrdquo Journal of Zhejiang University Science B vol 15no 1 pp 1ndash15 2014
[65] A Gadducci D Katsaros P Zola et al ldquoWeekly low-dosepaclitaxel as maintenance treatment in patients with advancedovarian cancer who had microscopic residual disease atsecond-look surgery after 6 cycles of paclitaxelplatinum-basedchemotherapy Results of an open noncomparative phase 2
multicenter italian study (after-6 protocol 2)rdquo InternationalJournal of Gynecological Cancer vol 19 no 4 pp 615ndash619 2009
[66] R S Bhatt J Merchan R Parker et al ldquoA phase 2 pilot trial oflow-dose continuous infusion or lsquometronomicrsquo paclitaxel andoral celecoxib in patients with metastatic melanomardquo Cancervol 116 no 7 pp 1751ndash1756 2010
[67] M Caballero J J Grau J L Blanch et al ldquoSerum vascularendothelial growth factor as a predictive factor in metronomic(weekly) paclitaxel treatment for advanced head and neckcancerrdquo Archives of OtolaryngologymdashHead and Neck Surgeryvol 133 no 11 pp 1143ndash1148 2007
[68] J Alexandre Y Hu W Lu H Pelicano and P Huang ldquoNovelaction of paclitaxel against cancer cells bystander effect medi-ated by reactive oxygen speciesrdquo Cancer Research vol 67 no 8pp 3512ndash3517 2007
[69] T Hadzic N Aykin-Burns Y Zhu et al ldquoPaclitaxel combinedwith inhibitors of glucose and hydroperoxide metabolismenhances breast cancer cell killing viaH
2O2-mediated oxidative
stressrdquo Free Radical Biology and Medicine vol 48 no 8 pp1024ndash1033 2010
[70] C A Sherman-Baust K G Becker W H Wood III Y Zhangand P J Morin ldquoGene expression and pathway analysis of ovar-ian cancer cells selected for resistance to cisplatin paclitaxel ordoxorubicinrdquo Journal of Ovarian Research vol 4 no 1 article21 2011
[71] R Agarwal and S B Kaye ldquoOvarian cancer strategies for over-coming resistance to chemotherapyrdquo Nature Reviews Cancervol 3 no 7 pp 502ndash516 2003
[72] T Acker and K H Plate ldquoRole of hypoxia in tumorangiogenesismdashmolecular and cellular angiogenic crosstalkrdquoCell and Tissue Research vol 314 no 1 pp 145ndash155 2003
[73] M Hockel and P Vaupel ldquoBiological consequences of tumorhypoxiardquo Seminars in Oncology vol 28 supplement 8 no 2 pp36ndash41 2001
[74] L Huang Q-H Zhang Q-L Ao H Xing Y-P Lu and DMa ldquoEffect of hypoxia on the chemotherapeutic sensitivity ofhuman ovarian cancer cells to paclitaxel and its mechanismrdquoZhonghua Zhong Liu Za Zhi vol 29 no 2 pp 96ndash100 2007
[75] N Rohwer and T Cramer ldquoHypoxia-mediated drug resistancenovel insights on the functional interaction of HIFs and celldeath pathwaysrdquoDrug Resistance Updates vol 14 no 3 pp 191ndash201 2011
[76] B B Aggarwal R V Vijayalekshmi and B Sung ldquoTargetinginflammatory pathways for prevention and therapy of cancershort-term friend long-term foerdquo Clinical Cancer Research vol15 no 2 pp 425ndash430 2009
[77] Z Duan R Foster D A Bell et al ldquoSignal transducersand activators of transcription 3 pathway activation in drug-resistant ovarian cancerrdquo Clinical Cancer Research vol 12 no17 pp 5055ndash5063 2006
[78] H-J Kuh S H Jang M G Wientjes J R Weaver and J L-SAu ldquoDeterminants of paclitaxel penetration and accumulationin human solid tumorrdquo Journal of Pharmacology and Experi-mental Therapeutics vol 290 no 2 pp 871ndash880 1999
[79] S Arao H Suwa M Mandai et al ldquoHypoxia-mediated drugresistance novel insights on the functional interaction of HIFsand cell death pathwaysrdquo Cancer Research vol 54 no 5 pp1355ndash1359 1994
[80] S E Johnatty J Beesley B Gao et al ldquoABCB1 (MDR1)polymorphisms and ovarian cancer progression and survivala comprehensive analysis from the Ovarian Cancer Association
BioMed Research International 19
Consortium and the Cancer GenomeAtlasrdquoGynecologic Oncol-ogy vol 131 no 1 pp 8ndash14 2013
[81] X Yang A K Iyer A Singh et al ldquoCluster of differentiation44 targeted hyaluronic acid based nanoparticles for MDR1siRNA delivery to overcome drug resistance in ovarian cancerrdquoPharmaceutical Research 2014
[82] D A Zajchowski B Y Karlan and L K Shawver ldquoTreatment-related protein biomarker expression differs between primaryand recurrent ovarian carcinomasrdquoMolecular CancerTherapeu-tics vol 11 no 2 pp 492ndash502 2012
[83] MM Gottesman J Ludwig D Xia and G Szakacs ldquoDefeatingdrug resistance in cancerrdquoDiscovery Medicine vol 6 no 31 pp18ndash23 2006
[84] S Mozzetti C Ferlini P Concolino et al ldquoClass III 120573-tubulin overexpression is a prominent mechanism of paclitaxelresistance in ovarian cancer patientsrdquo Clinical Cancer Researchvol 11 no 1 pp 298ndash305 2005
[85] M Kavallaris D Y S Kuo C A Burkhart et al ldquoTaxol-resistant epithelial ovarian tumors are associated with alteredexpression of specific beta-tubulin isotypesrdquo Journal of ClinicalInvestigation vol 100 no 5 pp 1282ndash1293 1997
[86] G A Orr P Verdier-Pinard H McDaid and S B HorwitzldquoMechanisms of Taxol resistance related to microtubulesrdquoOncogene vol 22 no 47 pp 7280ndash7295 2003
[87] C Ferlini L Cicchillitti G Raspaglio et al ldquoPaclitaxel directlybinds to Bcl-2 and functionally mimics activity of Nur77rdquoCancer Research vol 69 no 17 pp 6906ndash6914 2009
[88] E Mechetner A Kyshtoobayeva S Zonis et al ldquoLevels ofmultidrug resistance (MDR1) P-glycoprotein expression byhuman breast cancer correlate with in vitro resistance to taxoland doxorubicinrdquo Clinical Cancer Research vol 4 no 2 pp389ndash398 1998
[89] J S Lagas C W N Damen R A B VanWaterschoot D IusufJ H Beijnen and A H Schinkel ldquoP-glycoprotein multidrug-resistance associated protein 2 Cyp3a and carboxylesteraseaffect the oral availability and metabolism of vinorelbinerdquoMolecular Pharmacology vol 82 no 4 pp 636ndash644 2012
[90] M T Huizing J B Vermorken H Rosing et al ldquoPharmacoki-netics of paclitaxel and three major metabolites in patients withadvanced breast carcinoma refractory to anthracycline therapytreated with a 3-hour paclitaxel infusion a European CancerCentre (ECC) trialrdquo Annals of Oncology vol 6 no 7 pp 699ndash704 1995
[91] R Panchagnula ldquoPharmaceutical aspects of paclitaxelrdquo Interna-tional Journal of Pharmaceutics vol 172 no 1-2 pp 1ndash15 1998
[92] S H Jang M G Wientjes and J L-S Au ldquoDeterminants ofpaclitaxel uptake accumulation and retention in solid tumorsrdquoInvestigational New Drugs vol 19 no 2 pp 113ndash123 2001
[93] D S Sonnichsen andM V Relling ldquoClinical pharmacokineticsof paclitaxelrdquo Clinical Pharmacokinetics vol 27 no 4 pp 256ndash269 1994
[94] T Ohtsu Y Sasaki T Tamura et al ldquoClinical pharmacokineticsand pharmacodynamics of paclitaxel a 3-hour infusion versusa 24-hour infusionrdquo Clinical Cancer Research vol 1 no 6 pp599ndash606 1995
[95] M Czejka J Schueller H Schnait B Springer and I EderldquoClinical pharmacokinetics andmetabolism of paclitaxel after athree-hour infusion comparison of two preparationsrdquo Journalof Oncology Pharmacy Practice vol 9 no 4 pp 129ndash136 2003
[96] J Rizzo C Riley D VonHoff J Kuhn J Phillips and T BrownldquoAnalysis of anticancer drugs in biological fluids determination
of taxol with application to clinical pharmacokineticsrdquo Journalof Pharmaceutical and Biomedical Analysis vol 8 no 2 pp 159ndash164 1990
[97] V A de Weger J H Beijnen and J H M Schellens ldquoCel-lular and clinical pharmacology of the taxanes docetaxel andpaclitaxelmdasha reviewrdquoAnti-Cancer Drugs vol 25 no 5 pp 488ndash494 2014
[98] S Kumar H Mahdi C Bryant J P Shah G Garg andA Munkarah ldquoClinical trials and progress with paclitaxel inovarian cancerrdquo International Journal of Womenrsquos Health vol 2no 1 pp 411ndash427 2010
[99] B Huang J Zhao J C Unkeless Z H Feng and H XiongldquoTLR signaling by tumor and immune cells a double-edgedswordrdquo Oncogene vol 27 no 2 pp 218ndash224 2008
[100] R A Jibodh J S Lagas B Nuijen J H Beijnen and J HM Schellens ldquoTaxanes old drugs new oral formulationsrdquoEuropean Journal of Pharmacology vol 717 no 1ndash3 pp 40ndash462013
[101] A Javeed M Ashraf A Riaz A Ghafoor S Afzal and M MMukhtar ldquoPaclitaxel and immune systemrdquo European Journal ofPharmaceutical Sciences vol 38 no 4 pp 283ndash290 2009
[102] L Bracci G Schiavoni A Sistigu and F Belardelli ldquoImmune-based mechanisms of cytotoxic chemotherapy implications forthe design of novel and rationale-based combined treatmentsagainst cancerrdquo Cell Death and Differentiation vol 21 no 1 pp15ndash25 2014
[103] C A Byrd-Leifer E F Block K Takeda S Akira and A DingldquoThe role of MyD88 and TLR4 in the LPS-mimetic activity ofTaxolrdquo European Journal of Immunology vol 31 no 8 pp 2448ndash2457 2001
[104] A-C Wang Y-B Ma F-X Wu et al ldquoTLR4 induces tumorgrowth and inhibits paclitaxel activity in MyD88-positivehuman ovarian carcinoma in vitrordquo Oncology Letters vol 7 no3 pp 871ndash877 2014
[105] Y Zhu N Liu S D Xiong Y J Zheng and Y W ChuldquoCD4+Foxp3+ regulatory T-cell impairment by paclitaxel isindependent of toll-like receptor 4rdquo Scandinavian Journal ofImmunology vol 73 no 4 pp 301ndash308 2011
[106] M Kubo T Morisaki K Matsumoto et al ldquoPaclitaxel probablyenhances cytotoxicity of natural killer cells against breastcarcinoma cells by increasing perforin productionrdquo CancerImmunology Immunotherapy vol 54 no 5 pp 468ndash476 2005
[107] L Markasz G Stuber B Vanherberghen et al ldquoEffect of fre-quently used chemotherapeutic drugs on the cytotoxic activityof human natural killer cellsrdquo Molecular Cancer Therapeuticsvol 6 no 2 pp 644ndash654 2007
[108] T Sako N Burioka K Yasuda et al ldquoCellular immune profile inpatients with non-small cell lung cancer after weekly paclitaxeltherapyrdquo Acta Oncologica vol 43 no 1 pp 15ndash19 2004
[109] R Kaneno G V Shurin I L Tourkova and M R ShurinldquoChemomodulation of human dendritic cell function by anti-neoplastic agents in low noncytotoxic concentrationsrdquo Journalof Translational Medicine vol 7 article 58 2009
[110] TMichels G V ShurinHNaiditch A Sevko VUmansky andM R Shurin ldquoPaclitaxel promotes differentiation of myeloid-derived suppressor cells into dendritic cells in vitro in a TLR4-independent mannerrdquo Journal of Immunotoxicology vol 9 no3 pp 292ndash300 2012
[111] R A Kemp and F Ronchese ldquoTumor-specific Tc1 but not Tc2cells deliver protective antitumor immunityrdquo The Journal ofImmunology vol 167 no 11 pp 6497ndash6502 2001
20 BioMed Research International
[112] A Y Rudensky ldquoRegulatory T cells and Foxp3rdquo ImmunologicalReviews vol 241 no 1 pp 260ndash268 2011
[113] EM Shevach ldquoCD4+CD25+ suppressor T cellsmore questionsthan answersrdquo Nature Reviews Immunology vol 2 no 6 pp389ndash400 2002
[114] S Sakaguchi T Yamaguchi T Nomura and M Ono ldquoRegu-latory T cells and immune tolerancerdquo Cell vol 133 no 5 pp775ndash787 2008
[115] H Nishikawa and S Sakaguchi ldquoRegulatory T cells in tumorimmunityrdquo International Journal of Cancer vol 127 no 4 pp759ndash767 2010
[116] W Zou ldquoRegulatory T cells tumour immunity and immuno-therapyrdquoNature Reviews Immunology vol 6 no 4 pp 295ndash3072006
[117] A Fialova S Partlova L Sojka et al ldquoDynamics of T-cell infil-tration during the course of ovarian cancer The gradual shiftfrom aTh17 effector cell response to a predominant infiltrationby regulatory T-cellsrdquo International Journal of Cancer vol 132no 5 pp 1070ndash1079 2013
[118] A E Albers R L Ferris G G Kim K Chikamatsu A BDeLeo and T L Whiteside ldquoImmune responses to p53 inpatients with cancer enrichment in tetramer+ p53 peptide-specific T cells and regulatory T cells at tumor sitesrdquo CancerImmunology Immunotherapy vol 54 no 11 pp 1072ndash10812005
[119] N Liu Y Zheng Y Zhu S Xiong andYChu ldquoSelective impair-ment of CD4 + CD25 + Foxp3 + regulatory T cells by paclitaxelis explained by Bcl-2Bax mediated apoptosisrdquo InternationalImmunopharmacology vol 11 no 2 pp 212ndash219 2011
[120] X Wu Q-M Feng Y Wang J Shi H-L Ge and W DildquoThe immunologic aspects in advanced ovarian cancer patientstreated with paclitaxel and carboplatin chemotherapyrdquo CancerImmunology Immunotherapy vol 59 no 2 pp 279ndash291 2010
[121] A P Vicari R Luu N Zhang et al ldquoPaclitaxel reducesregulatoryT cell numbers and inhibitory function and enhancesthe anti-tumor effects of the TLR9 agonist PF-3512676 in themouserdquo Cancer Immunology Immunotherapy vol 58 no 4 pp615ndash628 2009
[122] L Zhang K Dermawan M Jin et al ldquoDifferential impairmentof regulatory T cells rather than effector T cells by paclitaxel-based chemotherapyrdquo Clinical Immunology vol 129 no 2 pp219ndash229 2008
[123] Y Tabuchi J Matsuoka M Gunduz et al ldquoResistance topaclitaxel therapy is related with Bcl-2 expression through anestrogen receptor mediated pathway in breast cancerrdquo Interna-tional Journal of Oncology vol 34 no 2 pp 313ndash319 2009
[124] N Obermajer R Muthuswamy K Odunsi R P Edwards andP Kalinski ldquoPGE
2-induced CXCL12 production and CXCR4
expression controls the accumulation of human MDSCs inovarian cancer environmentrdquo Cancer Research vol 71 no 24pp 7463ndash7470 2011
[125] Q M Feng W Di and X Wu ldquoImmune reconstitution inadvanced ovarian cancer patients undergoing first line chemo-therapyrdquo Xi Bao Yu Fen Zi Mian Yi Xue Za Zhi vol 25 no 11pp 1023ndash1025 2009
[126] A D Seidman D Hochhauser M Gollub et al ldquoNinety-six-hour paclitaxel infusion after progression during short taxaneexposure a phase II pharmacokinetic and pharmacodynamicstudy in metastatic breast cancerrdquo Journal of Clinical Oncologyvol 14 no 6 pp 1877ndash1884 1996
[127] D R Spriggs M F Brady L Vaccarello et al ldquoPhase IIIrandomized trial of intravenous cisplatin plus a 24- or 96-hour
infusion of paclitaxel in epithelial ovarian cancer a gynecologiconcology group studyrdquo Journal of Clinical Oncology vol 25 no28 pp 4466ndash4471 2007
[128] G A Omura M F Brady K Y Look et al ldquoPhase III trial ofpaclitaxel at two dose levels the higher dose accompanied byfilgrastim at two dose levels in platinum-pretreated epithelialovarian cancer an intergroup studyrdquo Journal of Clinical Oncol-ogy vol 21 no 15 pp 2843ndash2848 2003
[129] R Simon and L Norton ldquoThe Norton-Simon hypothesisdesigning more effective and less toxic chemotherapeutic reg-imensrdquoNature Clinical Practice Oncology vol 3 no 8 pp 406ndash407 2006
[130] A Kumar P Hoskins and A Tinker ldquoDose-dense paclitaxel inadvanced ovarian cancerrdquo Clinical Oncology vol 27 no 1 pp40ndash47 2015
[131] P Marchetti S Urien G A Cappellini G Ronzino and CFicorella ldquoWeekly administration of paclitaxel theoretical andclinical basisrdquoCritical Reviews in OncologyHematology vol 44supplement pp S3ndashS13 2002
[132] P Francis E Rowinsky J Schneider T Hakes W Hoskinsand M Markman ldquoPhase I feasibility and pharmacologic studyof weekly intraperitoneal paclitaxel A Gynecologic OncologyGroup pilot studyrdquo Journal of Clinical Oncology vol 13 no 12pp 2961ndash2967 1995
[133] H Thomas and P Rosenberg ldquoRole of weekly paclitaxel inthe treatment of advanced ovarian cancerrdquo Critical Reviews inOncologyHematology vol 44 supplement pp S43ndashS51 2002
[134] M Markman J Markman K Webster et al ldquoDuration ofresponse to second-line platinum-based chemotherapy forovarian cancer implications for patient management and clini-cal trial designrdquo Journal of Clinical Oncology vol 22 no 15 pp3120ndash3125 2004
[135] P H OrsquoDonnell M Eileen Dolan E Gamazon et al ldquoPopu-lation differences in platinum toxicity as a means to identifynovel genetic susceptibility variantsrdquo Pharmacogenetics andGenomics vol 20 no 5 pp 327ndash337 2010
[136] M J Millward M J Boyer M Lehnert et al ldquoDocetaxel andcarboplatin is an active regimen in advanced non-small-celllung cancer a phase II study in Caucasian and Asian patientsrdquoAnnals of Oncology vol 14 no 3 pp 449ndash454 2003
[137] M Markman ldquoIntraperitoneal therapy of ovarian cancerrdquoOncologist vol 1 no 1-2 pp 18ndash21 1996
[138] M Markman and J L Walker ldquoIntraperitoneal chemotherapyof ovarian cancer a review with a focus on practical aspects oftreatmentrdquo Journal of Clinical Oncology vol 24 no 6 pp 988ndash994 2006
[139] K Fujiwara S Nagao E Aotani and K Hasegawa ldquoPrincipleand evolving role of intraperitoneal chemotherapy in ovariancancerrdquo Expert Opinion on Pharmacotherapy vol 14 no 13 pp1797ndash1806 2013
[140] M Markman E Rowinsky T Hakes et al ldquoPhase I trialof intraperitoneal taxol a gynecoloic oncology group studyrdquoJournal of Clinical Oncology vol 10 no 9 pp 1485ndash1491 1992
[141] M Markman M F Brady N M Spirtos P Hanjani and S CRubin ldquoPhase II trial of intraperitoneal paclitaxel in carcinomaof the ovary tube and peritoneum a gynecologic oncologygroup studyrdquo Journal of Clinical Oncology vol 16 no 8 pp2620ndash2624 1998
[142] P B Panici I Palaia M Graziano F Bellati N Manci and RAngioli ldquoIntraperitoneal paclitaxel as consolidation treatmentin ovarian cancer patients a case control studyrdquo Oncology vol78 no 1 pp 20ndash25 2010
BioMed Research International 21
[143] D K Armstrong B Bundy L Wenzel et al ldquoIntraperitonealcisplatin and paclitaxel in ovarian cancerrdquo The New EnglandJournal of Medicine vol 354 no 1 pp 34ndash43 2006
[144] D Tewari J Java and R Salani ldquoLong-term survival advantageof intraperitoneal chemotherapy treatment in advanced ovariancancer an analysis of a Gynecologic Oncology Group ancillarydata studyrdquo in Proceedings of the 2013 Society of GynecologicOncology Annual Meeting on Womenrsquos Cancer (GOG114172Abstract) Los Angeles Calif USA 2013
[145] D A Yardley ldquonab-paclitaxel mechanisms of action and deliv-eryrdquo Journal of Controlled Release vol 170 no 3 pp 365ndash3722013
[146] M Ando K Yonemori N Katsumata et al ldquoPhase I and phar-macokinetic study of nab-paclitaxel nanoparticle albumin-bound paclitaxel administeredweekly to Japanese patients withsolid tumors and metastatic breast cancerrdquo Cancer Chemother-apy and Pharmacology vol 69 no 2 pp 457ndash465 2012
[147] N Desai V Trieu Z Yao et al ldquoIncreased antitumor activityintratumor paclitaxel concentrations and endothelial cell trans-port of cremophor-free albumin-bound paclitaxel ABI-007compared with cremophor-based paclitaxelrdquo Clinical CancerResearch vol 12 no 4 pp 1317ndash1324 2006
[148] J A Yared and K H R Tkaczuk ldquoUpdate on taxane devel-opment new analogs and new formulationsrdquo Drug DesignDevelopment andTherapy vol 6 pp 371ndash384 2012
[149] M G Teneriello P C Tseng M Crozier et al ldquoPhase IIevaluation of nanoparticle albumin-bound paclitaxel in plati-num-sensitive patients with recurrent ovarian peritoneal orfallopian tube cancerrdquo Journal of Clinical Oncology vol 27 no9 pp 1426ndash1431 2009
[150] R L Coleman W E Brady D S McMeekin et al ldquoA phase IIevaluation of nanoparticle albumin-bound (nab) paclitaxel inthe treatment of recurrent or persistent platinum-resistant ovar-ian fallopian tube or primary peritoneal cancer a GynecologicOncology Group Studyrdquo Gynecologic Oncology vol 122 no 1pp 111ndash115 2011
[151] J W Singer ldquoPaclitaxel poliglumex (XYOTAX CT-2103) amacromolecular taxanerdquo Journal of Controlled Release vol 109no 1ndash3 pp 120ndash126 2005
[152] C Li D-F Yu R A Newman et al ldquoComplete regressionof well-established tumors using a novel water-soluble poly(L-glutamic acid)-paclitaxel conjugaterdquo Cancer Research vol 58no 11 pp 2404ndash2409 1998
[153] M Mita A Mita J Sarantopoulos et al ldquoPhase I study ofpaclitaxel poliglumex administered weekly for patients withadvanced solid malignanciesrdquo Cancer Chemotherapy and Phar-macology vol 64 no 2 pp 287ndash295 2009
[154] P Sabbatini M W Sill D OrsquoMalley L Adler and A ASecord ldquoA phase II trial of paclitaxel poliglumex in recurrentor persistent ovarian or primary peritoneal cancer (EOC) agynecologic oncology group studyrdquo Gynecologic Oncology vol111 no 3 pp 455ndash460 2008
[155] M O Bradley C S Swindell F H Anthony et al ldquoTumortargeting by conjugation of DHA to paclitaxelrdquo Journal ofControlled Release vol 74 no 1ndash3 pp 233ndash236 2001
[156] M O Bradley N L Webb F H Anthony et al ldquoTumortargeting by covalent conjugation of a natural fatty acid topaclitaxelrdquo Clinical Cancer Research vol 7 no 10 pp 3229ndash3238 2001
[157] A C Wolff R C Donehower M K Carducci et al ldquoPhaseI study of docosahexaenoic acid-paclitaxel a taxane-fatty acid
conjugate with a unique pharmacology and toxicity profilerdquoClinical Cancer Research vol 9 no 10 part 1 pp 3589ndash35972003
[158] A Sparreboom A C Wolff J Verweij et al ldquoDispositionof docosahexaenoic acid-paclitaxel a novel taxane in bloodin vitro and clinical pharmacokinetic studiesrdquo Clinical CancerResearch vol 9 no 1 pp 151ndash159 2003
[159] P M Fracasso J Picus J D Wildi et al ldquoPhase 1 and phar-macokinetic study of weekly docosahexaenoic acid-paclitaxelTaxoprexin in resistant solid tumor malignanciesrdquo CancerChemotherapy and Pharmacology vol 63 no 3 pp 451ndash4582009
[160] A Y Bedikian R C DeConti R Conry et al ldquoPhase 3 study ofdocosahexaenoic acid-paclitaxel versus dacarbazine in patientswith metastatic malignant melanomardquo Annals of Oncology vol22 no 4 pp 787ndash793 2011
[161] Y-N Wu S-L Wang Y-C Wang et al ldquoReversal effect ofdocosahexaenoic acid on taxol resistance in human ovarian car-cinoma A2780T cellsrdquo Obstetrics amp Gynecology InternationalJournal vol 1 no 3 Article ID 00018 2014
Submit your manuscripts athttpwwwhindawicom
PainResearch and TreatmentHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom
Volume 2014
ToxinsJournal of
VaccinesJournal of
Hindawi Publishing Corporation httpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
AntibioticsInternational Journal of
ToxicologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
StrokeResearch and TreatmentHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Drug DeliveryJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Advances in Pharmacological Sciences
Tropical MedicineJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Medicinal ChemistryInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
AddictionJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
Emergency Medicine InternationalHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Autoimmune Diseases
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Anesthesiology Research and Practice
ScientificaHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Pharmaceutics
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of

4 BioMed Research International
formation in vitro even at cold temperatures (4∘C) and in theabsence of GTP [46]
Further research into understanding themolecularmech-anisms of microtubule formation has discovered that pacli-taxel may have other mechanism that allows cells to escapedrug toxicity which then develops into resistance and failurein chemotherapy [44] Ganguly and his colleagues found thatmicrotubule dynamics suppression was not related to celldivision Treatment of mutant cell lines Tax 11-6 (mutation in120572-tubulin) and Tax 18 (mutation in 120573-tubulin) at concentra-tion of 50 to 100 nmolL that should hypothetically increasemicrotubule assembly to more normal levels and allow thecells to proliferate normally further suppress microtubuledynamics rather than restoring behaviour to normal [44]Low concentrations of paclitaxel that suppressed dynamicshence they did not affect the rate ofmicrotubule detachmentbut the higher drug concentrations that allowed normalcell division strongly inhibited detachment in the mutantcell lines and returned the rate to near normal levels Thisaction seems to be related to ability of paclitaxel to inhibitmicrotubule fragmentation rather than its ability to suppressmicrotubule dynamics which was further confirmed by livecell imaging that demonstrated that microtubule detach-ment from centrosomes might be responsible for generat-ing microtubule fragments a process that was reversed bypaclitaxel [44] Recent studies have also found that at lowconcentrations (less than nanomolar concentrations) pacli-taxel inhibits the depolymerisation of microtubules whereasat high-dose paclitaxel increase the number and mass ofmicrotubules hence increasing stability of microtubules andalso render them nonfunctional by blocking the detachmentof microtubule minus ends from centrosomes rather thanplus ends [44 49]
The proposed mechanism of action of weekly paclitaxeladministration may be based on its apoptotic effects Theinduction of apoptotic modulator genes by paclitaxel appearsto be independent of microtubule stabilization It may be dueto modulation of the transcription of different genes suchas DNA-damage response proteins cytokines or proteinsinvolved in the control of cellular proliferation apoptosis andinflammation The apoptotic effect of paclitaxel is dependenton the concentration and duration of exposure With con-centration amounts of at least 10 nM and exposure of at least12 hours apoptosis may be induced in the S phase withoutmitotic arrest Two different mechanisms of apoptosis havebeen proposed depending on the dose concentration ofpaclitaxel At concentration of ge9 nM paclitaxel induces Raf-1 activation which is responsible for apoptotic control Atle9 nM there is absence of Raf-1 kinase involvement butapoptosis induction still occurs under the influence of p53and p21 [50 51] With the same concentration at 24-hourexposure in addition to apoptotic arrest paclitaxel producesan irreversible mitotic arrest [52] p53 is a major tumoursuppressor regulating proliferation and apoptosis and itsmutation occurs in more than 50 of human cancers Innormal cells DNA damage increases p53 levels which thenactivates a G1 cell-cycle arrest mediated by p21 to promoteeither the DNA damage repair mechanisms or apoptosis andnaturally limiting proliferation of genetically transformed cell
clones A functional p53 signaling pathway is necessary tosensitise cancer cells to DNA-damaging chemotherapeuticagents to reduce chemo resistance Currently paclitaxelactivity is considered to be independent of p53 status whichis an important aspect as the presence of silent ormutated p53does not modify the sensitivity of cancer cells to taxane thusreducing chemoresistance [53ndash56]
Paclitaxel also exerts its mechanism of action by activa-tion of multiple signal-transduction pathways which maybe associated with proapoptotic signaling The pathwaysassociated with paclitaxel are TLR-4 dependent pathway(either via MyD88 dependent or independent pathway) c-Jun N-terminal kinase (JNK) P38 Mitogen activated protein(MAP)Kinase nuclear factor kappa B (NF-120581B) Janus kinase-(JAK-) signal transducer and activator of transcription factor(STAT) pathway One of the pathways for induction ofapoptosis is via mitogen-activated protein kinase (MAPK)pathway resulting in dephosphorylation of the proapoptoticprotein Bad and Bax phosphorylation of Bcl2 and inductionof apoptosis Bad and Bax (promote apoptosis) and Bcl2 (sup-press apoptosis) are regulatory proteins which are membersof the Bcl2 family and are involved in programmed cell deathInduction of cytokines and pro-inflammatory proteins willlead to immunomodulatory effect of paclitaxel at low-doseconcentration and cell death at higher dose Changes thatoccur in these pathways are also responsible for developmentof resistance to paclitaxel [57ndash60]
Weekly paclitaxel also exhibits strong angiogenic inhibi-tory activity [61 62] In murine studies paclitaxel was ableto reduce new vessel formation at low noncytotoxic doses(03 and 6mgkg per day in mice) by suppressing VEGFexpression [63 64] Low dose weekly paclitaxel has beentested in patients with advanced ovarian cancer metastaticmelanoma and advanced head and neck cancer resulting instable disease [65ndash67] This additional mechanism of actionof paclitaxel by rescheduling the duration of administrationmay be helpful in cancers which have become resistant to thesame drug given on a 3-weekly conventional schedule [11 13]
Paclitaxel had also been reported to induce reactiveoxygen species (ROS) generation and increase hydroperoxideproduction by enhancing the activity of nicotinamide ade-nine dinucleotide phosphate (NADPH) oxidase which con-tributes to oxidative stress and may play a role in the potencyof the anticancer activity of paclitaxel [68 69] The combi-nation of paclitaxel with inhibitors of glucose (ie 2-deoxy-D-glucose 2DG) and hydroperoxide (ie L-buthionine-S R-sulfoximine BSO) metabolism has been found to selectivelyenhance breast cancer cell killing via hydrogen peroxide-induced metabolic oxidative stress which may be effectivelyutilised to treat breast cancers [69] However the relationshipof oxidative stress to the overall cytotoxicity mechanism ofpaclitaxel is not well established The mechanism of action ofpaclitaxel is summarised in Figure 3
5 Mechanism of Drug Resistance
Themechanism of paclitaxel resistance is complex involvingmultistep and multiple genes and not yet fully elucidated
BioMed Research International 5
Microtubules(MT)
MyD88 dependent
MyD88 independent
S
G2G1
M
PTX
Cell cycle arrest
N-terminal amino acids of beta
tubulin subunit
Inhibit depolymerisation ofmicrotubules
and suppress MT dynamics
Increase number and mass of microtubules increase
stability and block detachment
Apoptosis induced in G1S phase (absence mitotic
arrest)
Raf-1
p21
STAT 3
G0
JAK
MEK
MAPK
Bax Bcl2Bad
IRAK
TRAF
TKR
TRIF TRAM
ROS
Mitotic arrest at G2M phase
PI3KAKTApoptosis regulator
protein
p53
VEGFR
Angiogenesis
Apoptosis
TLR4
High concentrationLow concentration
NF-120581B
PTXle 9nM12hr
PTXge 9nM12hr
PTXle 9nM24hr
I120581B
Figure 3 Mechanism of action of paclitaxel Paclitaxel targets microtubules At high concentration PTX causes mitotic arrest at G2M phasewhereas at low concentration apoptosis is induced at G0 and G1S phase either via Raf-1 kinase activation or p53p21 depending on the doseconcentration Even at lower dose but with exposure beyond 24 hours paclitaxel can cause mitotic arrest Paclitaxel also activates multiplesignaling pathway to exert proapoptotic activity as well as immunomodulatory effect Paclitaxel also develops resistance via these signalingpathways PTX Paclitaxel TLR4 Toll-like receptor 4 G0 resting phase G1 cells enlarge andmake new protein S phase DNA replication G2preparation for division M phase cell divisionmitosis Raf-1 Raf kinase family MEKMAPK mitogen activated protein kinase IRAK IL-1receptor associated kinase TRAF TNFR associated factor NF-120581B nuclear factor kappa B TRIFTRAM TIR-domain-containing adapter-inducing interferon-120573 TKR tyrosine kinase receptor VEGFR vascular endothelial growth receptor PI3K phosphoinositide 3-kinase JAKjanus kinase STAT signal transducer and activator of transcription factor
Development of drug resistance leading to aggressive diseasethat is refractory to treatment is responsible for 90 ofthe deaths among patients with advanced ovarian cancer[70] Multidrug resistance (MDR) is a phenomenon definedby the ability of cancer cell to overcome either structurallyor functionally unrelated cytotoxic drugs Mechanism ofMDR can be broadly divided into three types (a) externalmechanism involving changes in pharmacokinetics of drugor (b) within tumour microenvironment which includeshypoxia leading to clonal selection pressure or (c) at cellu-lar level [71] MDR can be intrinsic or acquired IntrinsicMDR or also known as inherent occurs when cancer cellsdevelop resistant to any chemotherapy and this is most likelyattributed by tumour microenvironment Acquired MDRdevelops following exposure to chemotherapeutic agents andmay occur as a result of the pharmacokinetic of drug itself orsecondary to changes within the tumour cells [71]
Paclitaxel-derived resistance is mainly attributed bychanges involving mRNA and protein (such as multiple
ribosomal genes and translation factors) synthesis oxidativestress (UGT1A6 MAOA and CYBA) glycolysis (ADH1AHK1 and ENO3) glutathione metabolism and leukocytetransendothelial migration pathways [71] A study on geneexpression changes on a series of drug resistant ovariancancer cell lines following exposure to paclitaxel cisplatinor doxorubicin revealed that among 845 genes analysed atotal of 337 genes were significantly altered in cells resistantto paclitaxel [70] Changes in genes expression may createinterpatient variation in drug effect alteration in tumourmicroenvironment and changes within cellular structuresmetabolism and functions that promotes towards drug resis-tance
Tumour cells grow rapidly with formation of numerousnew vessels attributing to irregular blood flow and increasedoxygen demand which lead to development areas devoidof adequate oxygenation within ovarian cancer tissues [72]In response to chronic hypoxia (oxygen depletion) tumourmicroenvironment adapts processes to keep cells alive in
6 BioMed Research International
hypoxic and acidic state This hypoxic adaptation promotestumour proliferation dissemination and progression of dis-ease [73] and also reduces chemosensitivity [74]
Hypoxia-induced chemoresistance occurs due to geno-mic instability Oxygen depletion induces proteomic andgenomic changes that activates the level of p53 inhibits apop-tosis promotes angiogenesis (angiogenic molecules such asvascular endothelial growth factor [VEGF] and angiogenin)upregulates growth factors (platelet-derived growth factor[PDGF] transforming growth factor-beta and insulin-likegrowth factor [IGF]) and induces anaerobic metabolism andglycolysis (glycolytic enzymes glucose transporters) leadingto reduction in potential for cell cycle arrest and cellulardifferentiationwhich prevent tumour cell death [74]Hypoxiacan induce either p-53-dependent (involving Apaf-1 andcaspase-9 effector pathways) or p53-independent (involvinghypoxic-inducible factor 1 [HIF-1] and Bcl-2 family genespathways) apoptosis in both normal and tumour cells HIF-1 is a common transcription factor consisting of HIF-1120572 and HIF-1120573 subunits which controls hypoxic-induciblegenes and the concentration of HIF-1 protein increasedexponentially in the presence of hypoxic environment Lossof apoptotic potential of tumour cells mediated by hypoxicenvironment and HIF-1 which arrest cell cycle at G0G1reduces chemosensitivity to chemotherapeutic agents includ-ing paclitaxel [70 75]
Other transcriptional factors which are activated byhypoxia are nuclear factor kappa B (NF-120581B) and STAT3 also known as proinflammatory transcriptional factorsNF-120581B and STAT 3 regulate multiple gene products whichare involved in inflammation angiogenesis cell survivalproliferation and metastasis Paclitaxel which mediates itscytotoxic action via NF-120581B pathway is vulnerable to developresistance in the presence of hypoxic tumour microen-vironment with activation of NF-120581B transcription factorwhich induces serine phosphorylation and also regulatesBCL-2 an antiapoptotic protein preventing cell death andpromoting tumorigenesis [76] Inhibition of activated STAT3 found overexpressed in most paclitaxel-resistant ovariancancer cells has resulted in reduction in paclitaxel resistanceHowever further research is required to determine the exactmechanism [77]
Intracellular drug concentration is important for effectivecytotoxic activity of paclitaxel Drug resistance may beattributed to either reduced accumulation of drug withinovarian tumours or increased efflux of drug from tumourcells [78] Alteration in pharmacokinetic of paclitaxel eitherattributed by the drug itself such as lower concentration ofdrug administered shorter duration of drug exposure highfirst pass metabolism increased hepatic or renal clearanceinadequate binding to tubulinsmicrotubules or othermacro-molecules or presence of higher tumour density or vascular-ity may result in reduced accumulation of intratumoral drugconcentration [71]
Drug efflux is the most common mechanism for chemo-resistance observed in paclitaxel-treated cancer cells Drugefflux from cancer cells is mediated by ATP-binding cassette(ABC) transporters such as P-glycoprotein (P-gp) P-gp alsoknown as ABCB1 or multidrug-resistance associated-protein
(MRP) a transmembrane protein encoded by MDR1 geneplays a role as an efflux pump which is crucial for occurrenceof many cellular processes that require transfer of substratesacross cellularmembranes P-gp hence can affect intracellulardrug concentration andhave been shown to correlate in vitroto chemosensitivity to paclitaxel [59] However evidence fortheir role in clinical drug resistance in ovarian cancer hasemerged with P-gp found to be overexpressed in ovariancancer cells in vitro and also on paclitaxel-resistant celllines [70] P-gp and MDR1 expression levels were higherin chemoresistant ovarian cancer patients as compared withtheir chemosensitive counterpart Overall survival time wasalso statistically higher in patientswith low expression of P-gpandMDR1 in their tumor tissuesHence P-gp andMDR1mayhave a predictive role in determining the outcome of patientswith advanced ovarian cancer [58 79ndash82] Mechanism ofpaclitaxel resistance is complicated and specifically inhibitingABC transporters have given mixed results [59 83]
Another major mechanism of paclitaxel resistance ismediated by either a reduction in total intracellular tubulinconcentrations point mutation at prominently expressedtubulin genes or by selective alterations in expression oftubulin isotypes such as Class III 120573-tubulin [52 84 85]Microtubule dynamic stability was significantly impairedin the paclitaxel-resistant cells [86] Microtubule dynamicsdisruption caused by paclitaxel result in cell cycle arrestapoptosis and drug resistance
Other mechanism responsible for development of pacli-taxel resistant are inhibition of apoptosis activation ofmitogen-activated protein kinase Raf-1 kinase or intra-cellular signalling pathway PIK3 (phosphatidylinositol-45-bisphosphate 3-kinase) changes in apoptotic regulatory pro-teins such as Bcl-2 increase in expression of proinflammatorycytokines such as TNF-120572 IL-6 and IL-8 and activation oflipopolysaccharide-inducible genes and tumour suppressionprotein p53 [57 83 86 87]
In summary paclitaxel resistance is multifactorial inc-luding changes in signaling pathways upregulation of P-glycoprotein (P-gp) [80 88 89] alteration in tubulin dyna-mic mutations in 120573-tubulin gene or expression of 120573-tubulinisotypes [52 84 85] and changes in apoptotic mechanismIdentification of mechanism of resistance could help topotentially develop novel agents to improve chemosensitivityof patients with advanced ovarian cancer
6 Pharmacokinetics
Paclitaxel is a white to off-white crystalline powder highlylipophilic and is insoluble in water and so difficult to formu-late into solution It has a melting point of 216-217∘C [90 91]More than 90 of the drug binds rapidly and extensively toplasma proteins [33 40] whereas binding onto red blood cellsis approximately 50 The presence of premedication drugs(before chemotherapy) such as ranitidine dexamethasone ordiphenhydramine did not affect protein binding of paclitaxelPaclitaxel has a large volume of distribution of about 55 Lm2but this is reduced in the females [33]
BioMed Research International 7
AUC (area under the plasma concentration)
Cmax (maximum concentration)
Pacli
taxe
l con
cent
ratio
n (120583
M)
0 10 20 30 40
Time (hr)
0
1
2
3
4
5
Figure 4 Plasma pharmacokinetics of paclitaxel The pharmacoki-netics generally were linear for 6 or 24 hour infusions but becomenonlinear for infusions of shorter durations due to variation inthe elimination clearance with the dose administered An increasein plasma concentration of paclitaxel results in disproportionatelarger increase in 119862max (maximum plasma concentration) and AUC(area under plasma concentration) followed by decrease in drugelimination from body tissues
The disappearance of paclitaxel from plasma is tradition-ally believed to be biphasic [33] The initial rapid declinerepresents distribution to the peripheral compartment andelimination of the drug The later phase is due in part tothe slow efflux of paclitaxel from the peripheral compartment[92] In the presence of more sensitive assay methods andlater sampling times a three-compartment model seems tobe more accurate [40 93] Paclitaxel has been shown tohave a nonlinear pattern of pharmacokinetics (Figure 4)Thepharmacokinetics were generally linear for 6- or 24-hourinfusions but become nonlinear for infusions of shorterdurations because the elimination clearance varies with thedose administered With increasing plasma concentrationof paclitaxel there is a disproportionately larger increasein 119862max (maximum plasma concentration) and AUC (areaunder plasma concentration) accompanied by decrease indrug elimination from body tissues The clinical importanceof this nonlinear pattern is that dose escalationmay result in adisproportionate increase in toxicity whereas dose reductionmay affect its efficacy [33 90 91 94]
The pharmacokinetics of paclitaxel has been evaluatedover a wide range of doses up to 300mgm2 and withinfusion schedules ranging from 3 to 24 hours Maximumplasma concentrations are dose-related In patients treatedwith single dose infusion of 135 and 175mgm2 given as3- and 24-hour infusions mean steady state volume ofdistribution has ranged from 198 to 688 Lm2 indicatingextensive extravascular distribution andor tissue bindingTerminal half-life has ranged from 13 to 86 hours (mean 5hours) [40 93] and total body clearance has ranged from116 to 240 Lhrm2 Preclinical results in animals have shown
high levels in most tissues Being highly protein-boundpaclitaxel has a high affinity for distribution in specific tissuesincluding kidney lung spleen and extracellular fluids likeascites and pleural fluids [40 95] but the uptake of the drugin the brain is minimal [96 97] Exposure to paclitaxel isrelatively high in tumour tissue compared with other tissuesand in addition to slow elimination from tumour tissue theAUC in tumour tissue is about five-fold higher than that inplasma [97]
There is no evidence of accumulation of paclitaxel withmultiple treatment courses as the variability in systemicpaclitaxel exposure as measured by AUC (0ndashinfin) (area underplasma concentration-time curve from time 0 to infinity)for successive treatment courses are minimal [98] Paclitaxelclearance is however sequence dependent Patients receiv-ing a platinum-based agent prior to paclitaxel have lowerclearance and greater clinical toxicity than patients receivingpaclitaxel before cisplatin [93]
The drug administered intravenously undergoes anextensive P-450mediated hepaticmetabolism by cytochromeenzymes (CYP3A andCYP2C8) with 70ndash80being excretedinto bile by adenosine triphosphate- (ATP-) binding cassettemultidrug transporters such as P-glycoprotein (P-gp) andmultidrug resistance protein 2 (MRP-2) either asmetabolitesor as the parent drug Variation in MRP-2 activity hasbeen found to have direct effect on the effective exposureto paclitaxel [99] The bioavailability is poor following oraladministration due to enterocyte expression of P-gp and first-pass metabolism in the liver Most of the drug is eliminatedin feces Less than 10 drug in the unchanged form isexcreted in the urine indicating extensive nonrenal clearance[96] Combinations of inhibitors of CYP3A and P-gp mightpossibly improve the oral bioavailability of the taxanes [8997 100]
7 Paclitaxel and the Immune System
The immune system consists of two different but interactingmechanisms which are innate and adaptivemechanismsTheinnate mechanism is the first line of defense and consists of agroup of cells which includes mainly macrophages dendriticcells (DCs) and natural killer (NK) cells while the adaptiveimmunemechanism is represented by T-lymphocytes All thecomponents of innate and adaptive mechanism are involvedin antitumour immunity which includes tumour recognitioncontrol and elimination However cancer cells are able toevade immune detection and actively suppress antitumourimmunity
Paclitaxel has a wide range of dose dependent immuno-modulatory effects described in Figure 5 At standard dosepaclitaxel is broadly immunosuppressive and this is becauseit inhibits a number of cell types involved in tumour rejectionsuch asmacrophages effector T cells andNK cells [101] How-ever at lower doses than typically used for chemotherapypaclitaxel has an important immunogenic role promotingantitumour immunity [101 102] Hence understanding theimmunological basis of paclitaxel may help to maximise themanipulation of the immunomodulatory effects of paclitaxel
8 BioMed Research International
Immunomodulatory effect of
paclitaxel
Stimulate direct cytotoxic activity by
macrophage
Induce activation maturation and priming of DCs
Stimulate NK-dependent antitumour immunity
Activation of tumour-specificCTL Expansion of memory T cells
Secretion of proinflammatory cytokine
Shift from Th2 to Th1 type ofresponse
Depletion of Tregs andmodulation of MDSC
Downregulates the expression of VEGFR-2
and inhibits angiogenesis
IL-6 IL-12 TNF-120572 and i-NOS
Figure 5 Immunomodulatory effect of paclitaxel Paclitaxel a toll-like receptor 4 (TLR4) ligand binds to TLR4 receptor and triggers TLR4signaling via MyD88 dependent and independent pathway Paclitaxel then promotes anticancer immune response directly by stimulatingmacrophages to kill cancer cells or indirectly by secretion of proinflammatory cytokines which upregulates activation of DCs NK andtumour specific CTL Paclitaxel promotes effective CTL response by upregulation of mannose-6-phosphate which facilitate permeabilityto granzyme B and cytokine patterns of T helper type 1 Paclitaxel modulates MDSC and ablates Tregs Memory T cells (CD4+CD45RO+and CD8+CD45RO+) increased significantly while regulatory T cells (Tregs) decreased around 2 weeks creating an opportunity window fordose-dense therapy and immunomodulatory agents to achieve clinical benefit Dose-dense and low dose paclitaxel also blocks new vesselformation by downregulating VEGF-receptor 2 reduces resistance by alternative mechanism of action
to develop better therapeutic options in the management ofadvanced ovarian cancer
Paclitaxel is a ligand to toll-like receptor 4 (TLR4) whichis expressed on innate immune cells including macrophagesThe binding of paclitaxel to TLR4 on macrophages trig-gers the MyD88 mitogen-activated protein kinase (MAPK)and transcription of nuclear factor NF-kappa B (NF-120581B)pathways (Figure 3) resulting in their activation and releaseof immunostimulatory cytokines such as tumour necrosisfactor-120572 (TNF-120572) interleukin-1 (IL-1) interleukin-6 (IL-6)and interleukin-8 (IL-8) [103ndash105] Activated macrophagescan either cause direct tumour cell lysis via release oflysosomal enzymes and nitric oxide (NO) or indirectly byactivating NK cells DCs and tumour-specific cytotoxic T-lymphocytes (CTLs) [101]
NK cells are also innate immune cells capable of killingtumour cells particularly those cells that have reduced classI MHC expression and therefore can escape killing by CTLsPaclitaxel can enhance NK cell function by inducing mRNAand protein production of perforin an effector moleculeinvolved inNKcell-mediated cytotoxicity [106]However theeffect of low dose paclitaxel on NK cells is controversial Inanother study it was found that treatment of human NK cellswith paclitaxel effectively inhibits NK cell-mediated killing ofK562 (human erythroleukemia) target cells in vitro withoutaffecting the viability of NK cells [107] However weeklypaclitaxel therapy for non-small cell lung cancer patients was
only able to reduce the NK cell function up to completion ofthe first cycle but thereafter it gradually recovered [108]
Dendritic cells also express TLR4 and can be directlyactivated by paclitaxel The binding of paclitaxel to TLR onimmature DCs promotes DC maturation by upregulatingantigen-processing machinery gene components costimu-latory molecules and IL-12p70 [102] This enhances theability of DCs to prime T cells which facilitate antitumourimmunity [109] Paclitaxel can also promote cytotoxic T-cell function by upregulating mannose-6-phosphate whichfacilitates permeability to granzyme B and also inducescytokine production patterns typical of the T helper type 1phenotype via IL-2 (CD4 T cell) and IFN-120574 (CD8 T cell)secretion [104 110] Activated CD8+ T cells can differentiateinto CTL type 1 (Tc1) cells producingmainly IFN-120574 and CTLtype 2 (Tc2) cells producing mostly IL-4 IL-5 and IL-10 Tc1cells are potent CTL involved in the defense against cancerTc1 cells are able to recognise tumour antigens in the contextof MHC class I and mediate tumour cell lysis The role of Tc2cells in the immune response is not clearly known althoughtheir presence has been associated with disease progression[111]
CD4+ CD25+ regulatory T-cells (Tregs) constitutingapproximately 5ndash10 of peripheral CD4+ T cells [112 113]play an important role in tumour immune evasion [114]There is growing evidence that supports the existence ofelevated numbers of Tregs in tumours [115ndash117] which may
BioMed Research International 9
suppress immune responses of other CD4+ and CD8+ cells[118ndash120] and promote tumour progression In murine stud-ies paclitaxel exhibits the ability to reduce the number andsize of Treg cells thereby enhancing antitumour immunity[119 121] Similar findingswere seenwith a selective reductionin the size and number of Treg populations in peripheralblood samples from non-small cell lung cancer (NSCLC)patients [122]
Paclitaxel also decreased the expression of the anti-apoptotic molecule Bcl-2 in Treg cells while increasing thecorresponding proapoptoticmember Bax which contributedto the apoptotic sensitivity of Treg to paclitaxel [87]This wasseen in a study using the 3LL Lewis tumour model whichdemonstrated that Treg cells exposed to paclitaxel displayeddown regulation of Bcl-2 and upregulation of Bax and uponblocking the Bcl-2 pathway the ability of paclitaxel to ablateTreg cells compared toT effectorswas impaired and bothTregand T effectors were affected These results may suggest thatpaclitaxel targets Bcl-2 rather than tubulin to contribute tothe distinctive effect on Treg cells [119] It has recently beenshown in vitro that paclitaxel could target Bcl-2 and thereforelead to apoptosis Bcl-2 family proteins are key regulators ofapoptosis and play an important role in tumourigenesis andmulti-drug resistance by blocking apoptosis [119 123]
Few studies have also shown effect of paclitaxel onmyeloid-derived suppressor cells (MDSCs) a heterogeneouspopulation of immature myeloid cells immunosuppressivein nature are recruited by cancer cells and are found inincreased amount in advanced epithelial ovarian cancer [124]In a murine study using C57BL6 mice administration ofpaclitaxel at ultralow dose modulates MDSCs to differentiateinto DCs in a TLR4 independent manner [110] Hencepaclitaxel in ultralow noncytotoxic doses together with itsangiogenesis blocking ability may potentially enhance theefficacy of immunotherapy by ablation of immunosuppres-sive populations such as Tregs and MDSCs in tumour-bearing hosts [50 102]
In immunocompromised patients with advanced ovariancancer with increased Tregs and decreased levels of CD4+T cell CD8+ T cell and NK subsets after a single courseof combined carboplatin and paclitaxel chemotherapy theimmunosuppression is reversed around 12 to 14 days later butnot before one week or after three to four weeks Not only areTregs decreased but also the proportions of IFN-120574 secretingCD8+ T cells T helper-1 Tc1 and NKT cells The ratio of Tc1to Tc2 cells increases significantly [111 120 125]
Following chemotherapy both CD4+CD45RO+ andCD8+CD45RO+ memory T cells increased significantly andpeaked around 2 weeks The increase of memory T cellsin ovarian cancer patients following chemotherapy prob-ably opens the door of opportunity to develop long-termimmunological memory which could prevent recurrenceand metastases [120] Administration of dose-dense therapygiven weekly may hence be beneficial immunologically tomount an adequate immune response compared to standard3-week therapy In addition administration of immunother-apy agentsmay also be ideal during the period of 2weeks afterchemotherapy where temporary immune system reconstitu-tion takes place
8 Clinical Studies
In the past two decades paclitaxel had been administered indoses ranging from 60 to 250mgm2 over 1ndash96 hours andfrom 1 to 3 weekly intervals Prolonged exposure up to 96hours was believed to be effective as demonstrated with pre-clinical data but later refuted in large prospective studies [14126 127] A 24-hour infusion of paclitaxel was subsequentlyadministered to reduce the risk of hypersensitivity reactionshowever it was shown to increase mucosal and bone marrowtoxicity without improved efficacy [127 128] Development ofeffective premedication has led to administration of shorterinfusions (lt3 hours) which are better tolerated in particularfrom a haematologic perspective but patients remain at riskof myalgia and neuropathy at higher doses Weekly one-hourlow dose paclitaxel also known as dose-dense therapy hasrecently emerged as another possible strategy to improveoutcomes
9 Dose-Dense Therapy
Dose-dense treatment is defined by delivery of a maintainedper-cycle dose or overall dose with administration of drugat shorter time intervals than is standard This differs fromdose intensity which refers to dose (per unit weight or bodysurface area) delivered per unit time Hence either escalationof dose per cycle or reducing the time in between cycles maymodify dose intensity [129 130]
The rationale for the dose-dense approach of weeklypaclitaxel is that more frequent delivery of moderate dosesmay achieve greater efficacy by allowing sustained exposureof dividing tumour cells to paclitaxelrsquos cytotoxic and antian-giogenic effects hence reducing resistance delaying relapseand increasing the possibility of cancer remission Three 1-hour infusions of paclitaxel given at a week interval achievedgreater dose-density as well as dose-intensity than a singleadministration every 3 weeksThe initial tissue concentration(gt50 nM) for 1-hour infusion is similar to that of 3-hourinfusion but the concentration in the plasma instead oflasting for 8 hours in a 3-hour infusion rapidly falls below50 nM in less than 75 minutes for 1-hour infusion and hencereduces the risk of neutropenia However the rate of fallexperienced in tissue concentration of the drug is slowerthan plasma concentration of the drug hence efficacy ismaintained [131 132] A shorter infusion time allows bettercontrol of toxicities improved patient comfort and reducedhospitalisation hours
Several studies have used dose-dense paclitaxel in thetreatment of advanced ovarian cancer and are summarizedin Table 1 Based on phase 1 studies the recommendeddose for weekly paclitaxel ranges between 80 and 90mgm2compared with 45mgm2 per week with 3-weekly paclitaxeland is given over 1-hour duration Weekly scheduling hasdemonstrated consistent activities in ovarian cancer studies[11ndash13] Response rates were in the 20ndash50 range whereusually less than 10 would be expected Grade-4 doselimiting toxicities in particular neutropenia were not evidentat any dose below 100mgm2week [11 133]
10 BioMed Research International
Table1Ph
ases
Iand
IIstu
dies
onintravenou
sdose-densep
aclitaxel
Stud
yRe
gimen
119899()
PI(m
)RR
()
CR(119899)
MedianPF
S(m
)Median
OS
(m)
Adversee
ffects
Com
ments
Paclitaxel
dose
(mgm
2 )Ca
rbop
latin
dose
(mgm
2 )Ph
aseIsinglea
gent
Lofflerre
tal1996
[11]
40ndash9
0week
1-hou
rinfusionfor
6weeks
5040
5NA
NA
(i)Hem
atologictoxicity-m
ild(ii)N
ograde3
or4
haem
atologicaltoxicity
neurologicalor
cardiotoxicityup
to90
mgm
2 wk
(iii)Nohypersensitivity
reactio
ns(patientsreceivedprem
edication)
(i)100
priorc
hemotherapy
(ii)M
ediando
seintensity
was
410m
gm
2 6w
k(range200
to540m
gm
2 6w
k)
Fenn
ellyetal
1997
[12]
40ndash100w
eek
1830
NA
NA
NA
(i)Nomucositiso
rgrade
III
neurop
athy
was
seen
(ii)A
lopeciao
ccurredin
one
(i)100
priorc
hemotherapy
(2ndash5
priorregim
ens)
(ii)P
artia
lrespo
nses
weres
eenin
four
of13
assessablepatients
(30
)(iii)Dose-lim
iting
toxicitywas
reachedat100m
gm
2 (iv
)2-3
patie
ntse
xperience
treatmentd
elay
(v)M
axim
um-to
lerateddo
seof
80mgm
2 Ab
u-Ru
stum
etal
1997
[13]
60ndash100
over
1ho
urw
eek
45289
NA
NA
NA
(i)Nopatie
nthadfebrile
neutropenia
(i)100
priorc
hemotherapy
(1ndash8
priorregim
ens)
PhaseIISing
leagent
Markm
anetal
2001
[14]
80over
1ho
urw
eek
53(52)
25NA
NA
NA
Therapydiscon
tinuedin
(i)4patie
ntsw
hohadperip
heral
neurop
athy
(ii)1
patie
ntdu
etopainful
fingernailbeds
(i)100
platinum
andpaclita
xel
resistant
(ii)Th
erapywas
discon
tinuedin
5patie
ntsb
ecause
oftoxicity
(iii)Only13
(1)w
erem
odified
(doser
eductio
nor
treatment
delay)
becauseo
fsidee
ffects
PhaseIICom
binedwith
platinum
agent
Kiku
chietal
2005
[15]
80over
1ho
urw
eek
AUC2week
27gt6
818
483
NA
(i)Neutro
penia(
17)
thrombo
cytopenia(
51
)(ii)N
ocaseso
fperipheral
neurop
athy
(grades3
and4)
inweeklycombinedT-C
Cadron
etal2007
[16]
90over
1ho
urw
eek
AUC4week
24 9gt6le6
73 38NR
8105
675
(i)Grade
34neutropenia(
34)
andneutropenicfever
in2
(ii)N
auseaa
ndvomiting
and
fatig
uewerethe
mostfrequ
ent
nonh
ematologicalsid
eeffects
(i)Doser
eductio
nwas
necessary
in25of
patie
nts
Pign
atae
tal2008
[17]
60over
1ho
urw
eek
AUC2week
24(13)lowastlowast
1stline
385
2320
136
(i)Notoxicd
eath
was
recorded
(ii)G
rade
2anaemiawas
repo
rted
insevenpatie
nts(27)
(iii)Nofebrile
neutropeniaw
asob
served
(iv)G
rade
3and4neutropenia
was
recorded
infive(19)a
ndon
e(4
)patients
(v)G
rade
3thrombo
cytopenia
occurred
inon
epatient
(4)
BioMed Research International 11
Table1Con
tinued
Stud
yRe
gimen
119899()
PI(m
)RR
()
CR(119899)
MedianPF
S(m
)Median
OS
(m)
Adversee
ffects
Com
ments
Paclitaxel
dose
(mgm
2 )Ca
rbop
latin
dose
(mgm
2 )
Safrae
tal2014
[18]
80over
1ho
urw
eek
AUC2week
133
1stline
864
645
274
(i)Highera
naem
ia(grade
III+
IV68vs53)+
IVneutropenia(
144vs69)
decreasedgradeIIa
lopecia(
235
vs981
)and
thrombo
cytopenia
(grade
III+
IV0
vs23)
Havrilesky
etal
2003
[19]
80over
1ho
urw
eek
AUC2weekD1
D8D15
until
progressionCR
+8courses
29 21 8
Total
grou
pgt6lt6
83 100
38
16 15 1114
115
137
32
(i)Hem
atologictoxicitywas
common
(grade
3neutropenia
32n
ograde4
neutropenia
grade3
or4thrombo
cytopenia
142)
(i)To
xicitymanaged
bytre
atment
delaydo
seredu
ctionof
paclitaxel
ordiscon
tinuatio
nof
carbop
latin
vanderB
urgetal
2014
[20]
90over
1ho
urw
eek
AUC4weekD1
D8D15
D29
D36
D49
+6x
TCq3w
108
65 43
Total
grou
pgt6lt6
76 5816 42
26 158 13
(i)Neutro
penia3
0
thrombo
cytopenia8
febrile
neutropenia0
5
(ii)N
onhaem
atologictoxicitywas
low
(i)Treatm
entw
asdelayedin
16
anddo
seredu
cedin
2of
cycle
s
119899num
bero
fpatientsassessableforrespo
nsemm
onthsPIplatinum
treatmentfreeintervalRR
respo
nser
ateCR
com
pleterem
issionT
paclitaxelC
carbop
latin
PFS
progressio
nfre
esurvivalOSoverall
survivalN
An
otavailableinpapero
rabstractandNR
notyetreached
lowastlowastElderly
popu
lation
patient
agedge70
years
12 BioMed Research International
Numerous phase II studies have explored the tolerabilityand the activity of weekly paclitaxel either as a single agent orin combination with several other drugs or biological agents(Table 1) A number of regimens combining weekly paclitaxelwith carboplatin have been used as first-line treatment inovarian cancer Carboplatin has been administered weeklyat AUC of 2 with dose escalation in some studies whilepaclitaxel had been infused at 60ndash80mgm2week Thiscombined regimen was well tolerated with a low incidence ofbone marrow suppression Overall response rates have beenhigh in the range of 60ndash80 in most studies even in heavilypretreated patients with platinum-resistant disease (diseaserecurrence or progression within 6 months of the last lineof platinum-based therapy) [15ndash20 134] The promising datafrom these phase II trials then led to the evolution of largerphase III trials
Three phase III studies Japanese Gynecologic OncologyGroup- (JGOG-) Trial 3016 [21ndash23] Multicentre Italian Trialin Ovarian Cancer-Trial 7 (MITO-7) [25] and GynecologicOncology Group GOG-262 Trial [24] have explored dosedense therapy The results of these trials are summarised inTable 2
The Japanese Gynecologic Oncology Group (JGOG)conducted a randomized phase 3 trial of dose-dense weeklypaclitaxel 80mgm2week in combination with 3-weeklycarboplatin compared to standard 3-weekly carboplatin andpaclitaxel 180mgm2 in patients with advanced epithelialovarian peritoneal or fallopian tube cancer (JGOG 3016NOVEL trial) In both arms carboplatin was given at AUC6 and the median number of cycles was six In this largestudy (119899 = 637) with a median follow up of 77 months therewas an 11-month improvement in themedian progression freesurvival (PFS) in the dose-dense treatment group comparedwith the standard treatment arm (282 versus 175 monthsHR 076 95 CI 062ndash091 119901 = 00037) Median OS wasalso higher in the dose-dense treatment arm (1005 versus622 months HR 079 95 CI 063ndash099 119901 = 0039)On subgroup analysis suboptimally debulked patients withresidual disease of gt1 cm (119899 = 342) had a significantlyhigher median overall survival in the dose dense arm (512versus 335 months HR-075 95 CI 057ndash097 119901 = 0027)There was no significant advantage to dose-dense treatmentfor patients with optimally cytoreduced disease Dose-densetherapy survival benefits were also not seen in patients withclear cell or mucinous histology type unlike serous typeHowever patient treated with dose dense therapy had asignificantly higher frequency of hematologic toxicity thanwith the standard arm (212 versus 94) which resultedin lower treatment completion rates (63 versus 48) withfrequent episodes of delay (76 versus 67) and dosereductions (48versus 35) [21 22]Therewas no significantdifference in terms of overall quality of life between the twoarms (119901 = 046) [23]
Using a similar regimen as in JGOG-3016 a GynecologicOncology Group (GOG)-262 Trial was conducted in theUnited States In this group most patients had stage IIIdisease (66ndash70) and two-thirds had suboptimal debulkingwith residual disease of gt1 cm This was a randomized phase
III trial of 3 weekly paclitaxel versus dose-dense weeklypaclitaxel in combination with carboplatin in patients withadvanced epithelial ovarian peritoneal or fallopian tubecancer Though optional concurrent and maintenance beva-cizumab were received by the majority of patients in botharms (835 versus 841 resp) There was no significantdifference in PFS in the patients who received the dosedense paclitaxelcarboplatin regimen compared to those whoreceived the standard paclitaxelcarboplatin regimen (148versus 143 months HR 097 95 CI 079ndash118) Howeverin a subgroup analysis there was a significant difference inPFS in the dose dense paclitaxel arm who did not receivebevacizumab 119899 = 112 (142 versus 103 months HR 059 95CI 037ndash096 119901 = 0003) Overall survival data is still imma-ture There was higher frequency of grade 3 anaemia (408versus 157 119901 lt 0001) and grade 2 sensory neuropathy(259 versus 178 119901 = 0012) but a lower incidence ofneutropenia (72 versus 83 119901 lt 0001) [24]
In 2008 the Multicentre Italian Trials in Ovarian Cancer(MITO-7) randomised 810 women in a phase 3 trial toreceive either standard carboplatin (AUC = 6) and paclitaxel175mgm2 every 3 weeks or a weekly schedule of paclitaxel(60mgm2) with carboplatin (AUC = 2) The majority ofpatients in both arms (83ndash90) received six cycles of therapyMost patients (58ndash63) had stage II1 disease 23 of themwere suboptimally debulked Median PFS did not differsignificantly (173 months and 183 months 119901 = 066)between the standard and dose-dense arms respectivelyThere was no significant difference in response rate betweenthe two arms nor the estimated 2-year overall survivalSubgroup analysis did not identify any subgroup that mayhave benefited from the dose-dense regimen Unlike theJGOG-3016 trial the incidence of grade 3-4 neutropenia wassignificantly lower in the dose-dense group compared to the3-weekly regimen (42 versus 50) A similar pattern wasseen for the incidence of febrile neutropenia (lt1 versus 3119901 = 002) thrombocytopenia (1 versus 7 119901 lt 0001)and other nonhaematological toxicities such as alopeciavomiting renal dysfunction and neuropathy Quality of lifewas reported to be significantly better in the dose-dense arm(119901 lt 00001) which was discordant with the JGOG-3016quality of life data [25]
In summary there was significant improvement inmedian PFS and overall survival in studies using paclitaxelat 80mgm2week dose-dense therapy [21 24] but withhigher haematological toxicity whereas MITO-7 [25] whichwas using paclitaxel at 60mgm2week was only equivalentlyeffective but less toxicThis does not conclude that the higherpaclitaxel dose is more clinically beneficial as there are manyother confounding factors in all three studies
In a multivariate analysis the JGOG-3016 study [21]reported that a lower dose intensity of paclitaxel (lt80) wasassociated with poorer overall survival (hazard ratio = 14295 confidence interval 112ndash181 119901 = 0004) however itmust be highlighted that the investigational arm carboplatinschedules were not standardised in these studies The JGOGand GOG trials delivered a 3-weekly carboplatin (AUC =6) arm whereas in the MITO-7 study the carboplatin was
BioMed Research International 13
Table2Ph
aseIIIstu
dies
onintravenou
sdose-densep
aclitaxel
Stud
yRe
gimen
119899
MedianPF
S(m
)
Median
OS
(m)
Adversee
ffects
Com
ments
Katsu
matae
tal2009
[21]
Katsu
matae
tal2013
[22]
Haranoetal2014
[23]
JGOG3016
631
(i)Haematologicaltoxicityhigh
erin
dose
dense-211versus
94
Lower
treatmentcom
pletionin
dose-dense
63versus
48
Frequent
episo
deso
fdelay
indo
se-dense
76versus
67
Doser
eductio
nsin
dose-dense
48versus
35
Nosig
nificantd
ifference
inoverallQ
OL
betweenbo
thgrou
ps(119901=046)
Paclitaxel80m
gm
2D18
15+carbop
latin
AUC63
weeklyversus
Paclitaxel180
mgm
2+
carbop
latin
AUC63
weekly
312
282
1005
Both
givenfor6
ndash9cycle
s319
175
622
Chan
etal2013
[24]
GOG-262
(i)Higherfrequ
ency
ofgrade3
anaemia
(408versus
157119901lt0001)
grade2
sensoryneurop
athy
(259versus
178
119901=0012)b
utlower
incidenceo
fneutropenia(
72versus
83119901lt0001)
Paclitaxel80m
gm
2D18
15+carbop
latin
AUC63
weeklyversus
Paclitaxel175
mgm
2+
carbop
latin
AUC63
weekly
346
148
NR
Both
givenfor6
cycle
s346
143
NR
Bevacizumab
given
optio
nally
112
(did
not
receive
bevazicumab)
142vs
103
Pign
atae
tal2014
[25]
MITO-7
810
(i)Lo
wer
incidenceo
fgrade
3-4
neutropenia(
42versus
50)febrile
neutropenia(lt1v
ersus3
119901=002)
thrombo
cytopenia(
1versus7
119901lt0001)andothern
onhaem
atological
toxicitie
ssuchas
alop
eciavom
iting
renald
ysfunctio
nandneurop
athy
Qualityof
lifeb
etterindo
sedensea
rm(119901lt00001)
Paclitaxel60m
gm
2 weekly+carbop
latin
AUC
2weeklyversus
Paclitaxel175
mgm
2+
carbop
latin
AUC63
weekly
406
404
183 173
77lowast
79lowast
119899num
bero
fpatientsmm
onthsDday
PFSprogressionfre
esurvivalOSoverallsurvivalNAnot
availableinpapero
rabstractandNR
notyetreached
lowastSurvivalrateat2years
14 BioMed Research International
dose-dense (AUC 2 weekly) Although it is possible that thedose scheduling for the platinum-based agent is not essentialfor a survival benefit as shown by previous studies usingdose-dense cisplatin direct cross-trial comparison cannot bemade Unlike paclitaxel carboplatin probably requires peakdose for optimal therapeutic benefit hence this may accountfor the inferior survival outcome in MITO-7 trial Anotherconfounding factor may be difference in ethnicity All threestudies used different ethnic populations and Asian patientsin JGOG-3016 appear to have better survival outcomes thanthe MITO-7 Western population Ethnicity with possibleunderlying genetic causes may be responsible for the variableresponses to chemotherapy across individuals [135] This wasexplored by Millward et al who studied 68 Caucasian andAsian lung cancer patients treated with a combination ofpaclitaxel and carboplatin and found that the incidence offebrile neutropenia was 50 of an initially treated cohortof Asians and when carboplatin was subsequently dosereduced in all Asian patients the overall incidence of febrileneutropenia was also reduced to 26 [136]
Although early clinical data from phase I and phaseII dose-dense paclitaxel trials in advanced ovarian cancerwere promising the results from phase III studies in havebeen inconsistent as a result of differences in paclitaxel dosecarboplatin AUC and schedule addition of bevacizumabas well as different ethnic populations The results of arecently completed randomised three arms GynaecologicCancer InterGroup (GCIG) phase II trial ICON 8 mayfurther inform the clinical benefit of dose dense paclitaxeltherapy
This multicentre trial involving 111 centres in the UKSouth Korea Mexico Ireland Australia and New Zealandwith a target population of 1485 patients with stage IC-IV epithelial ovarian cancer or peritoneal or fallopian tubecancer compared two dose-dense arms (i) JGOG-like armcarboplatin AUC 5 plus weekly 80mgm2 paclitaxel and (ii)MITO-7-like arm weekly carboplatin AUC 167 plus weekly80mgm2 paclitaxel to the standard 3-weekly treatment(carboplatin AUC 5 plus 175mgm2 paclitaxel) for stage IC toIV epithelial ovarian cancer The dose-dense arms of MITO-7 and JGOG-3016 as well as the ethnic heterogeneity will befurther addressed
10 Intraperitoneal (IP) Chemotherapy
In addition to dose and scheduling the route of adminis-tration of chemotherapy agents plays an important role inoutcome Intraperitoneal spread is common and likely anearly event in epithelial ovarian cancer hence the deliveryof chemotherapy intraperitoneally in theory would exposethe microcirculation of tumour to higher doses of drug thansystemic administration while limiting systemic toxicityTheideal drug for IP chemotherapy is one that is systemicallyeffective penetrates deep into the inner core of tumour tissueand remains within the peritoneal cavity for a prolongedperiod of time [137ndash139]
Early clinical studies confirmed that indeed the peritonealcavity could be exposed to 10 to 20-fold higher (cisplatin
and carboplatin) drug concentration than when using theintravenous approach and since 1978 this route had beenadopted as a form of therapeutic intervention [137 139]A subsequent phase I trial showed that IP paclitaxel haddose-limiting toxicity in the form of abdominal pain [140]Another phase 1 GOG pilot study administered weekly IPpaclitaxel at an initial dose of 20mgm2 for 16 weeks to33 patients and found that IP paclitaxel at this dose wasfeasible and well tolerated At dose levels 60 to 65mgm2there were significant levels of paclitaxel for a week afterdrug administration suggesting very slow clearance andcontinuous exposure of the peritoneal cavity to active drugconcentrations [132]
Hence this initiated a phase II study [141] that used pacli-taxel intraperitoneally at a dose of 60ndash65mgm2week In thisphase II GOG study 76 patients with small-volume resid-ual disease carcinoma (05 cm or less) involving the ovaryperitoneal or fallopian tube were treated with paclitaxel60mgm2week intraperitoneally for 16 weeks followed bysurgical evaluation in patients without disease progressionThe Gynaecologic Oncology group (GOG) currently definesno visible disease as microscopic disease being the idealsurgical outcome 75 of patients had received prior systemictherapy and 70 received all 16 courses that were planned Of28 patients with microscopic disease at the start of therapy61 achieved a surgically defined complete response whereasonly 1 out of 31 patients with macroscopic disease achieved acomplete response The median time-to-recurrence was 167months with an estimated survival rate at 2 years being 58Treatment was generally well tolerated [141]
Another study looked into the effect of IP paclitaxel asconsolidation therapy in advanced ovarian cancer Twenty-eight patients who had initial residual macroscopic disease(lt1 cm) after primary surgery or interval debulking but hadcomplete pathological response following standard treatmentwith at least 6 cycles of platinum-based chemotherapy regi-men received paclitaxel 60mgm2week intraperitoneally for12ndash16 weeks as consolidation therapy The median time torecurrence was 25 months but overall survival did not differsignificantly when compared with control group submittedto observation only Treatment-related toxicity was mild andtechnical difficulties were observed in 11 of patients [142]
Multicenter randomised phase 3 trials as well as meta-analysis of IP chemotherapy have been performed anddemonstrated that chemotherapy drugs administered intra-peritoneally are superior to intravenous standard regimensin patient with optimally debulked epithelial ovarian cancerThe most impressive data comes from GOG 114 [14] and172 trial [143] In GOG 114 patients received either sixcycles of intravenous paclitaxel 135mgm2 and cisplatin75mgm2 every 3 weeks or intravenous carboplatin (AUC= 9) every 28 days for two cycles followed by six 3-weeklycycles of intravenous paclitaxel 135mgm2 and IP cisplatin100mgm2 [14] whereas in GOG 172 patients received eitherintravenous paclitaxel 135mgm2 followed by intravenouscisplatin 75mgm2 or intravenous paclitaxel 135mgm2 fol-lowed by IP combination of cisplatin 100mgm2 and pacli-taxel 60mgm2 on day 8 Both trials had a combined total
BioMed Research International 15
of 876 women with stage III epithelial ovarian carcinomaoptimally debulked to le1 cm residual tumour [143] Themedian follow-up for GOG 114 [14] was 138 years with GOG172 [143] was 97 years The primary results of the individualtrials reported up to 6-month improvement in median PFSfollowing IP therapy In the combined analysis of the datafrom both trials the data continued to show a 5-monthdifference in favour of IP therapy (25 versus 20 months)which translates into 16 reduction in the hazard ratio forprogression (119901 = 003) In GOG 114 [14] reported in 2001there was only borderline improvement in overall survivalassociated with this regimen (median 63 versus 52 monthsrelative risk 081 119901 = 005)
However in combined analysis in 2013 which was pre-sented at the Society of Gynecologic Oncology AnnualMeeting [144] the overall survival showed an 11-monthimprovement in favour of IP therapy in GOG 114 whereasGOG 172 reported a 16-month survival advantage Amongpatients treated with IP therapy the 5-year survival rateincreased from 18 following completion of 1-2 cycles to 59for patients who completed 5-6 cycles of treatment Howeverthere was increased toxicity observed in the IP arm grade 3-4 leukopenia thrombocytopenia and abdominal pain Only42 of patients in the GOG172 trial [143] completed all sixcycles of planned treatment in the IP arm while 18 ofpatients in GOG 114 trial [14] received fewer than two coursesof IP chemotherapy
Another randomised phase III trial involving patientswith stages II-III epithelial ovarian carcinoma is the GOG252 study with three arms Arm 1-dose-dense intravenouscarboplatin and paclitaxel Arm 2-dose-dense intravenouspaclitaxel and IP carboplatin and Arm 3 consists of 3-weeklyintravenous paclitaxel (day 1) followed by IP cisplatin (day 2)and IP paclitaxel (day 3) regimen All three arms also incor-porate the combination and maintenance of bevacizumabGOG 252 has completed accrual and results are awaited [139]
11 Newer Forms of Paclitaxel
Development of next-generation taxanes has taken place overthe past 40 years aimed at eliminating toxicity improvingefficacy and ease of administration Abraxane is a novelcompound which incorporates paclitaxel into an albuminnanoparticle soluble in saline hence eliminating the needfor Cremophor EL which is responsible for hypersensitivityreactions experienced during paclitaxel infusion [145] Thenanoparticle albumin in nab-paclitaxel is able to bind toglycoprotein gp60 receptor an albumin receptor and activatecaveolin-1 a protein that in human is encoded byCAV-1 geneleading to formation of caveoli hence allowing nab-paclitaxelto migrate across the endothelial cell membrane into theinterstitial space leading to higher intratumoural drug con-centration In addition Abraxane exhibits linear pharma-cokinetics and can therefore be given at a relatively higherdose than standard intravenous paclitaxel leading to a highertherapeutic ratio and heightened efficacy in solid tumoursmainlymetastatic breast cancer [146 147] Nab-paclitaxel hadFDA approval in 2005 for treatment of breast cancer [148]
Nab-paclitaxel has been studied in recurrent ovariancancer As a single agent in phase II 44 patients withrecurrent ovarian cancer were treated with Nab-paclitaxel260mgm2 intravenously for 30 minutes every 3 weeks for6 cycles Ninety-two percent of patients were platinum-sensitive while 89 had had previous exposure to standardtaxane The objective response rate was 64 with 15 patientsachieving complete response and 13 of them had partialresponse Estimated median PFS was 85 months No hyper-sensitivity reactions were observed and there were infrequentcases of grade 4 neutropenia (11) and grade 2-3 neuropathy(13) [149]
Another phase II study by GOG enrolled 51 patients withplatinum- and taxane-resistant recurrent ovarian cancer outof which 47 were evaluable The objective response rate was38 with one patient achieving a complete response and 10patients a partial response The median PFS was 45 monthswhile overall survival rate was 174 months Severe haema-tological and nonhaematological toxicities including neuro-toxicity were uncommon These results are quite impressivegiven the treatment population consisted of patients withvery poor prognosis with a median platinum and taxane freeinterval of 21 days and 70 had their recurrence within 3months of completion of primary treatment [150] Severalother trials of this formulation are in progress
Paclitaxel poliglumex (PPX) also known as Xyotax isanother prodrug a novel conjugate of paclitaxel and 120572-poly-L-glutamic acid which accumulates within tumour tissuedue to increased permeability of the tumour vessels and lackof lymphatic drainage [148 151 152] Paclitaxel poliglumexenhances solubility of paclitaxel allows direct delivery tothe intratumoural microenvironment and allows prolongedexposure to the active drug while minimising systemictoxicities [151] In Phase I dose escalation studies as a singleagent the recommended dose of PPX was 235mgm2 over 10minutes every 3 weeks or 70mgm2 weekly [153] In a PhaseII GOG study of relapsed ovarian cancer a response rate of16 was seen with infrequent serious adverse events grade3 and 4 neutropenia (24 and 20) and grade 3 neuropathy(24) [154] A phase III trial (GOG-0212) on the use of PPXas consolidation ormaintenance therapy in advanced ovariancancer is in progress
DHA-paclitaxel also known as Taxoprexin is a prodrugwhere paclitaxel is covalently conjugated with the naturallyoccurring omega-3 fatty acid docosahexaenoic acid (DHA)a fatty acid that is easily taken up by tumour cells henceincreasing intratumoural concentration of paclitaxel leadingtumour cell apoptosis [155 156] DHA-paclitaxel exhibitslinear pharmacokinetics and lower toxicity and also ease ofadministration when compared to conventional paclitaxeland has demonstrated antineoplastic activity in animal mod-els of cancer as well as in a phase III trial involving metastaticmelanoma [156ndash160] In a recent study on human ovariancancer cells it was found that DHA could reverse paclitaxelresistance by inhibiting P-gp as well as downregulatingthe expression of multidrug resistance associated proteins(MRP) and inhibiting the activity of NF-120581B and p38 MAPKsignalling pathways [161]
16 BioMed Research International
12 Future Directions
A plateau has been reached regarding the benefits associatedwith standard 3-weekly intravenous administration of cyto-toxic chemotherapy in advanced epithelial ovarian cancerThe ongoing battle for a better treatment regimen to delayrelapse promote remission and most importantly improvethe quality of life of patients with advanced epithelial ovariancancer need not to go further than the ability to relook at thechemotherapy agents that are already available in a differentapproach
Novel compounds to date have not yet shown clinicalsuperiority and parent compounds such as paclitaxel con-tinue to surprise us with their feasibility effectiveness andmanageable toxicity profiles Intraperitoneal paclitaxel willrequire further evaluation Better effort in understanding themechanism of action of drugs including the role of dosescheduling and the effect on the immune systemmay providea more cost-effective route to better clinical outcomes
Conflict of Interests
The authors declare no conflict of interests in this work
Acknowledgments
The authors would like to thank the many researchers whohave contributed to our current knowledge of paclitaxelNirmala Kampan is supported by Australian Monash Uni-versity Institute of Graduate Research Scholarship as wellas Universiti Kebangsaan Malaysia Postgraduate ScholarshipAward Mutsa Madondo has received Postgraduate Pub-lication Award from Monash University and MagdalenaPlebanski has been awarded Senior NHMRC Fellowship
References
[1] Australian Institute of Health and Welfare and National Breastand Ovarian Cancer Centre (Australia) Ovarian Cancer inAustralia AnOverview 2010 Cancer Series Australian Instituteof Health and Welfare Canberra Australia 2010
[2] R E Bristow R S Tomacruz D K Armstrong E L Trimbleand F J Montz ldquoSurvival effect of maximal cytoreductivesurgery for advanced ovarian carcinoma during the platinumera a meta-analysisrdquo Journal of Clinical Oncology vol 20 no 5pp 1248ndash1259 2002
[3] ZKempand JA Ledermann ldquoUpdate onfirst-line treatment ofadvanced ovarian carcinomardquo International Journal of WomenrsquosHealth vol 5 no 1 pp 45ndash51 2013
[4] A du Bois H-J Luck W Meier et al ldquoA randomized clinicaltrial of cisplatinpaclitaxel versus carboplatinpaclitaxel as first-line treatment of ovarian cancerrdquo Journal of the National CancerInstitute vol 95 no 17 pp 1320ndash1330 2003
[5] R F Ozols B N Bundy B E Greer et al ldquoPhase III trialof carboplatin and paclitaxel compared with cisplatin andpaclitaxel in patients with optimally resected stage III ovariancancer A Gynecologic Oncology Group studyrdquo Journal ofClinical Oncology vol 21 no 17 pp 3194ndash3200 2003
[6] W P McGuire W J Hoskins M F Brady et al ldquoCyclophos-phamide and cisplatin compared with paclitaxel and cisplatin
in patients with stage III and stage IV ovarian cancerrdquoThe NewEngland Journal of Medicine vol 334 no 1 pp 1ndash6 1996
[7] W P McGuire W J Hoskins M F Brady et al ldquoCyclophos-phamide and cisplatin versus paclitaxel and cisplatin a phase IIIrandomized trial in patients with suboptimal stage IIIIV ovar-ian cancer (from the gynecologic oncology group)rdquo Seminars inOncology vol 23 no 5 supplement 12 pp 40ndash47 1996
[8] M J Piccart K Bertelsen K James et al ldquoRandomized inter-group trial of cisplatin-paclitaxel versus cisplatin-cyclophosph-amide inwomenwith advanced epithelial ovarian cancer three-year resultsrdquo Journal of the National Cancer Institute vol 92 no9 pp 699ndash708 2000
[9] P A Vasey G C Jayson A Gordon et al ldquoPhase III random-ized trial of docetaxel-carboplatin versus paclitaxel-carboplatinas first-line chemotherpy for ovarian carcinomardquo Journal of theNational Cancer Institute vol 96 no 22 pp 1682ndash1691 2004
[10] B Gronlund C Hogdall H H Hansen and S A EngelholmldquoResults of reinduction therapy with paclitaxel and carboplatinin recurrent epithelial ovarian cancerrdquo Gynecologic Oncologyvol 83 no 1 pp 128ndash134 2001
[11] T M Loffler W Freund J Lipke and T-U HausamenldquoSchedule- and dose-intensified paclitaxel as weekly 1-hourinfusion in pretreated solid tumors results of a phase III trialrdquoSeminars in Oncology vol 23 no 6 supplement 16 pp 32ndash341996
[12] D Fennelly C Aghajanian F Shapiro et al ldquoPhase I and phar-macologic study of paclitaxel administered weekly in patientswith relapsed ovarian cancerrdquo Journal of Clinical Oncology vol15 no 1 pp 187ndash192 1997
[13] N R Abu-Rustum C Aghajanian R R Barakat D Fennelly FShapiro and D Spriggs ldquoSalvage weekly paclitaxel in recurrentovarian cancerrdquo Seminars inOncology vol 24 no 5 supplement15 pp S15-62ndashS15-67 1997
[14] M Markman B N Bundy D S Alberts et al ldquoPhase III trialof standard-dose intravenous cisplatin plus paclitaxel versusmoderately high-dose carboplatin followed by intravenouspaclitaxel and intraperitoneal cisplatin in small-volume stageIII ovarian carcinoma an intergroup study of the gynecologiconcology group Southwestern Oncology Group and EasternCooperativeOncologyGrouprdquo Journal of Clinical Oncology vol19 no 4 pp 1001ndash1007 2001
[15] A Kikuchi H Sakamoto and T Yamamoto ldquoWeekly car-boplatin and paclitaxel is safe active and well tolerated inrecurrent ovarian cancer cases of Japanese women previouslytreated with cisplatin-containing multidrug chemotherapyrdquoInternational Journal of Gynecological Cancer vol 15 no 1 pp45ndash49 2005
[16] I Cadron K Leunen F Amant T van Gorp P Nevenand I Vergote ldquoThe lsquoLeuvenrsquo dose-dense paclitaxelcarboplatinregimen in patients with recurrent ovarian cancerrdquo GynecologicOncology vol 106 no 2 pp 354ndash361 2007
[17] S Pignata E Breda G Scambia et al ldquoA phase II studyof weekly carboplatin and paclitaxel as first-line treatment ofelderly patients with advanced ovarian cancer A Multicen-tre Italian Trial in Ovarian cancer (MITO-5) studyrdquo CriticalReviews in OncologyHematology vol 66 no 3 pp 229ndash2362008
[18] T Safra S Shamai J Greenberg et al ldquoWeekly carboplatinwith paclitaxel compared to standard three-weekly treatment inadvanced epithelial ovarian carcinomamdasha retrospective studyrdquoGynecologic Oncology vol 132 no 1 pp 18ndash22 2014
BioMed Research International 17
[19] L J Havrilesky A A Alvarez R A Sayer et al ldquoWeekly low-dose carboplatin and paclitaxel in the treatment of recurrentovarian and peritoneal cancerrdquo Gynecologic Oncology vol 88no 1 pp 51ndash57 2003
[20] M van der BurgW Onstenk I Boere et al ldquoLong-term resultsof a randomised phase III trial of weekly versus three-weeklypaclitaxelplatinum induction therapy followed by standardor extended three-weekly paclitaxelplatinum in Europeanpatients with advanced epithelial ovarian cancerrdquo EuropeanJournal of Cancer vol 50 no 15 pp 2592ndash2601 2014
[21] N Katsumata M Yasuda F Takahashi et al ldquoDose-densepaclitaxel once a week in combination with carboplatin every3 weeks for advanced ovarian cancer a phase 3 open-labelrandomised controlled trialrdquoThe Lancet vol 374 no 9698 pp1331ndash1338 2009
[22] N Katsumata M Yasuda S Isonishi et al ldquoLong-term resultsof dose-dense paclitaxel and carboplatin versus conventionalpaclitaxel and carboplatin for treatment of advanced epithelialovarian fallopian tube or primary peritoneal cancer (JGOG3016) a randomised controlled open-label trialrdquo The LancetOncology vol 14 no 10 pp 1020ndash1026 2013
[23] K Harano F Terauchi N Katsumata et al ldquoQuality-of-lifeoutcomes from a randomized phase III trial of dose-denseweekly paclitaxel and carboplatin compared with conventionalpaclitaxel and carboplatin as a first-line treatment for stage II-IV ovarian cancer Japanese Gynecologic OncologyGroup Trial(JGOG3016)rdquo Annals of Oncology vol 25 no 1 pp 251ndash2572014
[24] J Chan M F Brady R Penson et al ldquoPhase III trial ofevery-3-weeks paclitaxel vs dose dense weekly paclitaxel withcarboplatin +minus bevacizumab in epithelial ovarian peritonealfallopian tube cancer GOG 262 (NCT01167712)rdquo InternationalJournal of Gynecological Cancer vol 23 no 8 supplement 1 pp9ndash10 2013
[25] S Pignata G Scambia D Katsaros et al ldquoCarboplatin pluspaclitaxel once a week versus every 3 weeks in patients withadvanced ovarian cancer (MITO-7) a randomisedmulticentreopen-label phase 3 trialrdquoThe Lancet Oncology vol 15 no 4 pp396ndash405 2014
[26] V Walsh and J Goodman ldquoFrom taxol to Taxol the changingidentities and ownership of an anti-cancer drugrdquo MedicalAnthropology vol 21 no 3-4 pp 307ndash336 2002
[27] R Renneberg ldquoBiotech History yew trees paclitaxel synthesisand fungirdquo Biotechnology Journal vol 2 no 10 pp 1207ndash12092007
[28] J E Liebmann J A Cook C Lipschultz D Teague J Fisherand J B Mitchell ldquoCytotoxic studies of paclitaxel (Taxol) inhuman tumour cell linesrdquo British Journal of Cancer vol 68 no6 pp 1104ndash1109 1993
[29] J J Manfredi and S B Horwitz ldquoTaxol an antimitotic agentwith a newmechanism of actionrdquo Pharmacology andTherapeu-tics vol 25 no 1 pp 83ndash125 1984
[30] D G I Kingston ldquoRecent advances in the chemistry of taxolrdquoJournal of Natural Products vol 63 no 5 pp 726ndash734 2000
[31] D G I Kingston ldquoThe shape of things to come structural andsynthetic studies of taxol and related compoundsrdquo Phytochem-istry vol 68 no 14 pp 1844ndash1854 2007
[32] V Walsh and J Goodman ldquoCancer chemotherapy biodiversitypublic and private property the case of the anti-cancer drugTaxolrdquo Social Science amp Medicine vol 49 no 9 pp 1215ndash12251999
[33] P H Wiernik E L Schwartz J J Strauman J P Dutcher RB Lipton and E Paietta ldquoPhase I clinical and pharmacokineticstudy of taxolrdquo Cancer Research vol 47 no 9 pp 2486ndash24931987
[34] W P McGuire E K Rowinsky N B Rosenhein et alldquoTaxol a unique antineoplastic agent with significant activityin advanced ovarian epithelial neoplasmsrdquo Annals of InternalMedicine vol 111 no 4 pp 273ndash279 1989
[35] ldquoDiscovery and development of taxolrdquo in Taxol Science andApplications M W M E Suffness Ed pp 3ndash25 CRC PressBoca Raton Fla USA 1995
[36] M J Piccart and F Cardoso ldquoProgress in systemic therapy forbreast cancer an overview and perspectivesrdquo European Journalof Cancer Supplement vol 1 no 2 pp 56ndash69 2003
[37] P Bonomi K B Kim and J Kugler ldquoComparison of survival forstage IIIB versus stage IV non-small cell lung cancer (NSCLC)patients with etoposide-cisplatin versus taxol-cisplatin an East-ern Cooperative Oncology Group (ECOG) trialrdquo in Proceedingsof the American Society of Clinical Oncology vol 16 p 454a1997
[38] D Guenard F Gueritte-Voegelein J Dubois and P PotierldquoStructure-activity relationships of Taxol and Taxotere ana-loguesrdquo Journal of the National Cancer Institute Monographsno 15 pp 79ndash82 1993
[39] D G I Kingston ldquoTaxol the chemistry and structure-activityrelationships of a novel anticancer agentrdquo Trends in Biotechnol-ogy vol 12 no 6 pp 222ndash227 1994
[40] E K Rowinsky and R C Donehower ldquoPaclitaxel (taxol)rdquo TheNew England Journal of Medicine vol 332 no 15 pp 1004ndash10141995
[41] J Parness and S B Horwitz ldquoTaxol binds to polymerizedtubulin in vitrordquo Journal of Cell Biology vol 91 no 2 pp 479ndash487 1981
[42] A Dammermann A Desai and K Oegema ldquoTheminus end insightrdquo Current Biology vol 13 no 15 pp R614ndashR624 2003
[43] CWiese and Y Zheng ldquoMicrotubule nucleation 120574-tubulin andbeyondrdquo Journal of Cell Science vol 119 no 20 pp 4143ndash41532006
[44] A Ganguly H Yang and F Cabral ldquoPaclitaxel-dependent celllines reveal a novel drug activityrdquo Molecular Cancer Therapeu-tics vol 9 no 11 pp 2914ndash2923 2010
[45] P B Schiff and S B Horwitz ldquoTaxol stabilizes microtubules inmouse fibroblast cellsrdquo Proceedings of the National Academy ofSciences of the United States of America vol 77 no 3 pp 1561ndash1565 1980
[46] P B Schiff J Fant and S B Horwitz ldquoPromotion of micro-tubule assembly in vitro by Taxolrdquo Nature vol 277 no 5698pp 665ndash667 1979
[47] D Zhang R Yang S Wang and Z Dong ldquoPaclitaxel new usesfor an old drugrdquoDrug Design Development andTherapy vol 8pp 279ndash284 2014
[48] S Rao G A Orr A G Chaudhary D G I Kingston and SB Horwitz ldquoCharacterization of the taxol binding site on themicrotubule 2-(m-Azidobenzoyl)taxol photolabels a peptide(amino acids 217-231) of beta-tubulinrdquoThe Journal of BiologicalChemistry vol 270 no 35 pp 20235ndash20238 1995
[49] F Wang Y Cao W Zhao H Liu Z Fu and R Han ldquoTaxolinhibits melanoma metastases through apoptosis inductionangiogenesis inhibition and restoration of E-cadherin andnm23 expressionrdquo Journal of Pharmacological Sciences vol 93no 2 pp 197ndash203 2003
18 BioMed Research International
[50] A Sevko V Kremer C Falk et al ldquoApplication of paclitaxel inlow non-cytotoxic doses supports vaccination with melanomaantigens in normal micerdquo Journal of Immunotoxicology vol 9no 3 pp 275ndash281 2012
[51] T Kreis and R Vale Guidebook to the Cytoskeletal and MotorProteins Oxford University Press Oxford UK 2nd edition1999
[52] P Giannakakou D L Sackett Y-K Kang et al ldquoPaclitaxel-resistant human ovarian cancer cells have mutant 120573-tubulinsthat exhibit impaired paclitaxel-driven polymerizationrdquo TheJournal of Biological Chemistry vol 272 no 27 pp 17118ndash171251997
[53] E Rakovitch W Mellado E J Hall T K Pandita S Sawantand C R Geard ldquoPaclitaxel sensitivity correlates with p53status and DNA fragmentation but not G2M accumulationrdquoInternational Journal of Radiation Oncology Biology Physics vol44 no 5 pp 1119ndash1124 1999
[54] S W Lowe S Bodis A McClatchey et al ldquop53 status and theefficacy of cancer therapy in vivordquo Science vol 266 no 5186 pp807ndash810 1994
[55] C C Zhang J-M Yang E White M Murphy A Levine andW N Hait ldquoThe role of MAP4 expression in the sensitivity topaclitaxel and resistance to vinca alkaloids in p53 mutant cellsrdquoOncogene vol 16 no 12 pp 1617ndash1624 1998
[56] K Fukasawa T Choi R Kuriyama S Rulong and G F VandeWoude ldquoAbnormal centrosome amplification in the absence ofp53rdquo Science vol 271 no 5256 pp 1744ndash1747 1996
[57] T-H Wang Y-H Chan C-W Chen et al ldquoPaclitaxel (Taxol)upregulates expression of functional interleukin-6 in humanovarian cancer cells through multiple signaling pathwaysrdquoOncogene vol 25 no 35 pp 4857ndash4866 2006
[58] E Yakirevich E Sabo I Naroditsky Y Sova O Lavie andM B Resnick ldquoMultidrug resistance-related phenotype andapoptosis-related protein expression in ovarian serous carcino-masrdquo Gynecologic Oncology vol 100 no 1 pp 152ndash159 2006
[59] G Szakacs J K Paterson J A Ludwig C Booth-Genthe andM M Gottesman ldquoTargeting multidrug resistance in cancerrdquoNature Reviews Drug Discovery vol 5 no 3 pp 219ndash234 2006
[60] L W Pfannenstiel S S K Lam L A Emens E M Jaffeeand T D Armstrong ldquoPaclitaxel enhances early dendritic cellmaturation and function through TLR4 signaling in micerdquoCellular Immunology vol 263 no 1 pp 79ndash87 2010
[61] N Klauber S Parangi E Flynn E Hamel and R J DrsquoAmatoldquoInhibition of angiogenesis and breast cancer in mice by themicrotubule inhibitors 2-methoxyestradiol and Taxolrdquo CancerResearch vol 57 no 1 pp 81ndash86 1997
[62] D Belotti V Vergani T Drudis et al ldquoThe microtubule-affecting drug paclitaxel has antiangiogenic activityrdquo ClinicalCancer Research vol 2 no 11 pp 1843ndash1849 1996
[63] D H Lau L Xue L J Young P A Burke and A T CheungldquoPaclitaxel (Taxol) an inhibitor of angiogenesis in a highlyvascularized transgenic breast cancerrdquo Cancer Biotherapy andRadiopharmaceuticals vol 14 no 1 pp 31ndash36 1999
[64] X Jiang ldquoHarnessing the immune system for the treatment ofbreast cancerrdquo Journal of Zhejiang University Science B vol 15no 1 pp 1ndash15 2014
[65] A Gadducci D Katsaros P Zola et al ldquoWeekly low-dosepaclitaxel as maintenance treatment in patients with advancedovarian cancer who had microscopic residual disease atsecond-look surgery after 6 cycles of paclitaxelplatinum-basedchemotherapy Results of an open noncomparative phase 2
multicenter italian study (after-6 protocol 2)rdquo InternationalJournal of Gynecological Cancer vol 19 no 4 pp 615ndash619 2009
[66] R S Bhatt J Merchan R Parker et al ldquoA phase 2 pilot trial oflow-dose continuous infusion or lsquometronomicrsquo paclitaxel andoral celecoxib in patients with metastatic melanomardquo Cancervol 116 no 7 pp 1751ndash1756 2010
[67] M Caballero J J Grau J L Blanch et al ldquoSerum vascularendothelial growth factor as a predictive factor in metronomic(weekly) paclitaxel treatment for advanced head and neckcancerrdquo Archives of OtolaryngologymdashHead and Neck Surgeryvol 133 no 11 pp 1143ndash1148 2007
[68] J Alexandre Y Hu W Lu H Pelicano and P Huang ldquoNovelaction of paclitaxel against cancer cells bystander effect medi-ated by reactive oxygen speciesrdquo Cancer Research vol 67 no 8pp 3512ndash3517 2007
[69] T Hadzic N Aykin-Burns Y Zhu et al ldquoPaclitaxel combinedwith inhibitors of glucose and hydroperoxide metabolismenhances breast cancer cell killing viaH
2O2-mediated oxidative
stressrdquo Free Radical Biology and Medicine vol 48 no 8 pp1024ndash1033 2010
[70] C A Sherman-Baust K G Becker W H Wood III Y Zhangand P J Morin ldquoGene expression and pathway analysis of ovar-ian cancer cells selected for resistance to cisplatin paclitaxel ordoxorubicinrdquo Journal of Ovarian Research vol 4 no 1 article21 2011
[71] R Agarwal and S B Kaye ldquoOvarian cancer strategies for over-coming resistance to chemotherapyrdquo Nature Reviews Cancervol 3 no 7 pp 502ndash516 2003
[72] T Acker and K H Plate ldquoRole of hypoxia in tumorangiogenesismdashmolecular and cellular angiogenic crosstalkrdquoCell and Tissue Research vol 314 no 1 pp 145ndash155 2003
[73] M Hockel and P Vaupel ldquoBiological consequences of tumorhypoxiardquo Seminars in Oncology vol 28 supplement 8 no 2 pp36ndash41 2001
[74] L Huang Q-H Zhang Q-L Ao H Xing Y-P Lu and DMa ldquoEffect of hypoxia on the chemotherapeutic sensitivity ofhuman ovarian cancer cells to paclitaxel and its mechanismrdquoZhonghua Zhong Liu Za Zhi vol 29 no 2 pp 96ndash100 2007
[75] N Rohwer and T Cramer ldquoHypoxia-mediated drug resistancenovel insights on the functional interaction of HIFs and celldeath pathwaysrdquoDrug Resistance Updates vol 14 no 3 pp 191ndash201 2011
[76] B B Aggarwal R V Vijayalekshmi and B Sung ldquoTargetinginflammatory pathways for prevention and therapy of cancershort-term friend long-term foerdquo Clinical Cancer Research vol15 no 2 pp 425ndash430 2009
[77] Z Duan R Foster D A Bell et al ldquoSignal transducersand activators of transcription 3 pathway activation in drug-resistant ovarian cancerrdquo Clinical Cancer Research vol 12 no17 pp 5055ndash5063 2006
[78] H-J Kuh S H Jang M G Wientjes J R Weaver and J L-SAu ldquoDeterminants of paclitaxel penetration and accumulationin human solid tumorrdquo Journal of Pharmacology and Experi-mental Therapeutics vol 290 no 2 pp 871ndash880 1999
[79] S Arao H Suwa M Mandai et al ldquoHypoxia-mediated drugresistance novel insights on the functional interaction of HIFsand cell death pathwaysrdquo Cancer Research vol 54 no 5 pp1355ndash1359 1994
[80] S E Johnatty J Beesley B Gao et al ldquoABCB1 (MDR1)polymorphisms and ovarian cancer progression and survivala comprehensive analysis from the Ovarian Cancer Association
BioMed Research International 19
Consortium and the Cancer GenomeAtlasrdquoGynecologic Oncol-ogy vol 131 no 1 pp 8ndash14 2013
[81] X Yang A K Iyer A Singh et al ldquoCluster of differentiation44 targeted hyaluronic acid based nanoparticles for MDR1siRNA delivery to overcome drug resistance in ovarian cancerrdquoPharmaceutical Research 2014
[82] D A Zajchowski B Y Karlan and L K Shawver ldquoTreatment-related protein biomarker expression differs between primaryand recurrent ovarian carcinomasrdquoMolecular CancerTherapeu-tics vol 11 no 2 pp 492ndash502 2012
[83] MM Gottesman J Ludwig D Xia and G Szakacs ldquoDefeatingdrug resistance in cancerrdquoDiscovery Medicine vol 6 no 31 pp18ndash23 2006
[84] S Mozzetti C Ferlini P Concolino et al ldquoClass III 120573-tubulin overexpression is a prominent mechanism of paclitaxelresistance in ovarian cancer patientsrdquo Clinical Cancer Researchvol 11 no 1 pp 298ndash305 2005
[85] M Kavallaris D Y S Kuo C A Burkhart et al ldquoTaxol-resistant epithelial ovarian tumors are associated with alteredexpression of specific beta-tubulin isotypesrdquo Journal of ClinicalInvestigation vol 100 no 5 pp 1282ndash1293 1997
[86] G A Orr P Verdier-Pinard H McDaid and S B HorwitzldquoMechanisms of Taxol resistance related to microtubulesrdquoOncogene vol 22 no 47 pp 7280ndash7295 2003
[87] C Ferlini L Cicchillitti G Raspaglio et al ldquoPaclitaxel directlybinds to Bcl-2 and functionally mimics activity of Nur77rdquoCancer Research vol 69 no 17 pp 6906ndash6914 2009
[88] E Mechetner A Kyshtoobayeva S Zonis et al ldquoLevels ofmultidrug resistance (MDR1) P-glycoprotein expression byhuman breast cancer correlate with in vitro resistance to taxoland doxorubicinrdquo Clinical Cancer Research vol 4 no 2 pp389ndash398 1998
[89] J S Lagas C W N Damen R A B VanWaterschoot D IusufJ H Beijnen and A H Schinkel ldquoP-glycoprotein multidrug-resistance associated protein 2 Cyp3a and carboxylesteraseaffect the oral availability and metabolism of vinorelbinerdquoMolecular Pharmacology vol 82 no 4 pp 636ndash644 2012
[90] M T Huizing J B Vermorken H Rosing et al ldquoPharmacoki-netics of paclitaxel and three major metabolites in patients withadvanced breast carcinoma refractory to anthracycline therapytreated with a 3-hour paclitaxel infusion a European CancerCentre (ECC) trialrdquo Annals of Oncology vol 6 no 7 pp 699ndash704 1995
[91] R Panchagnula ldquoPharmaceutical aspects of paclitaxelrdquo Interna-tional Journal of Pharmaceutics vol 172 no 1-2 pp 1ndash15 1998
[92] S H Jang M G Wientjes and J L-S Au ldquoDeterminants ofpaclitaxel uptake accumulation and retention in solid tumorsrdquoInvestigational New Drugs vol 19 no 2 pp 113ndash123 2001
[93] D S Sonnichsen andM V Relling ldquoClinical pharmacokineticsof paclitaxelrdquo Clinical Pharmacokinetics vol 27 no 4 pp 256ndash269 1994
[94] T Ohtsu Y Sasaki T Tamura et al ldquoClinical pharmacokineticsand pharmacodynamics of paclitaxel a 3-hour infusion versusa 24-hour infusionrdquo Clinical Cancer Research vol 1 no 6 pp599ndash606 1995
[95] M Czejka J Schueller H Schnait B Springer and I EderldquoClinical pharmacokinetics andmetabolism of paclitaxel after athree-hour infusion comparison of two preparationsrdquo Journalof Oncology Pharmacy Practice vol 9 no 4 pp 129ndash136 2003
[96] J Rizzo C Riley D VonHoff J Kuhn J Phillips and T BrownldquoAnalysis of anticancer drugs in biological fluids determination
of taxol with application to clinical pharmacokineticsrdquo Journalof Pharmaceutical and Biomedical Analysis vol 8 no 2 pp 159ndash164 1990
[97] V A de Weger J H Beijnen and J H M Schellens ldquoCel-lular and clinical pharmacology of the taxanes docetaxel andpaclitaxelmdasha reviewrdquoAnti-Cancer Drugs vol 25 no 5 pp 488ndash494 2014
[98] S Kumar H Mahdi C Bryant J P Shah G Garg andA Munkarah ldquoClinical trials and progress with paclitaxel inovarian cancerrdquo International Journal of Womenrsquos Health vol 2no 1 pp 411ndash427 2010
[99] B Huang J Zhao J C Unkeless Z H Feng and H XiongldquoTLR signaling by tumor and immune cells a double-edgedswordrdquo Oncogene vol 27 no 2 pp 218ndash224 2008
[100] R A Jibodh J S Lagas B Nuijen J H Beijnen and J HM Schellens ldquoTaxanes old drugs new oral formulationsrdquoEuropean Journal of Pharmacology vol 717 no 1ndash3 pp 40ndash462013
[101] A Javeed M Ashraf A Riaz A Ghafoor S Afzal and M MMukhtar ldquoPaclitaxel and immune systemrdquo European Journal ofPharmaceutical Sciences vol 38 no 4 pp 283ndash290 2009
[102] L Bracci G Schiavoni A Sistigu and F Belardelli ldquoImmune-based mechanisms of cytotoxic chemotherapy implications forthe design of novel and rationale-based combined treatmentsagainst cancerrdquo Cell Death and Differentiation vol 21 no 1 pp15ndash25 2014
[103] C A Byrd-Leifer E F Block K Takeda S Akira and A DingldquoThe role of MyD88 and TLR4 in the LPS-mimetic activity ofTaxolrdquo European Journal of Immunology vol 31 no 8 pp 2448ndash2457 2001
[104] A-C Wang Y-B Ma F-X Wu et al ldquoTLR4 induces tumorgrowth and inhibits paclitaxel activity in MyD88-positivehuman ovarian carcinoma in vitrordquo Oncology Letters vol 7 no3 pp 871ndash877 2014
[105] Y Zhu N Liu S D Xiong Y J Zheng and Y W ChuldquoCD4+Foxp3+ regulatory T-cell impairment by paclitaxel isindependent of toll-like receptor 4rdquo Scandinavian Journal ofImmunology vol 73 no 4 pp 301ndash308 2011
[106] M Kubo T Morisaki K Matsumoto et al ldquoPaclitaxel probablyenhances cytotoxicity of natural killer cells against breastcarcinoma cells by increasing perforin productionrdquo CancerImmunology Immunotherapy vol 54 no 5 pp 468ndash476 2005
[107] L Markasz G Stuber B Vanherberghen et al ldquoEffect of fre-quently used chemotherapeutic drugs on the cytotoxic activityof human natural killer cellsrdquo Molecular Cancer Therapeuticsvol 6 no 2 pp 644ndash654 2007
[108] T Sako N Burioka K Yasuda et al ldquoCellular immune profile inpatients with non-small cell lung cancer after weekly paclitaxeltherapyrdquo Acta Oncologica vol 43 no 1 pp 15ndash19 2004
[109] R Kaneno G V Shurin I L Tourkova and M R ShurinldquoChemomodulation of human dendritic cell function by anti-neoplastic agents in low noncytotoxic concentrationsrdquo Journalof Translational Medicine vol 7 article 58 2009
[110] TMichels G V ShurinHNaiditch A Sevko VUmansky andM R Shurin ldquoPaclitaxel promotes differentiation of myeloid-derived suppressor cells into dendritic cells in vitro in a TLR4-independent mannerrdquo Journal of Immunotoxicology vol 9 no3 pp 292ndash300 2012
[111] R A Kemp and F Ronchese ldquoTumor-specific Tc1 but not Tc2cells deliver protective antitumor immunityrdquo The Journal ofImmunology vol 167 no 11 pp 6497ndash6502 2001
20 BioMed Research International
[112] A Y Rudensky ldquoRegulatory T cells and Foxp3rdquo ImmunologicalReviews vol 241 no 1 pp 260ndash268 2011
[113] EM Shevach ldquoCD4+CD25+ suppressor T cellsmore questionsthan answersrdquo Nature Reviews Immunology vol 2 no 6 pp389ndash400 2002
[114] S Sakaguchi T Yamaguchi T Nomura and M Ono ldquoRegu-latory T cells and immune tolerancerdquo Cell vol 133 no 5 pp775ndash787 2008
[115] H Nishikawa and S Sakaguchi ldquoRegulatory T cells in tumorimmunityrdquo International Journal of Cancer vol 127 no 4 pp759ndash767 2010
[116] W Zou ldquoRegulatory T cells tumour immunity and immuno-therapyrdquoNature Reviews Immunology vol 6 no 4 pp 295ndash3072006
[117] A Fialova S Partlova L Sojka et al ldquoDynamics of T-cell infil-tration during the course of ovarian cancer The gradual shiftfrom aTh17 effector cell response to a predominant infiltrationby regulatory T-cellsrdquo International Journal of Cancer vol 132no 5 pp 1070ndash1079 2013
[118] A E Albers R L Ferris G G Kim K Chikamatsu A BDeLeo and T L Whiteside ldquoImmune responses to p53 inpatients with cancer enrichment in tetramer+ p53 peptide-specific T cells and regulatory T cells at tumor sitesrdquo CancerImmunology Immunotherapy vol 54 no 11 pp 1072ndash10812005
[119] N Liu Y Zheng Y Zhu S Xiong andYChu ldquoSelective impair-ment of CD4 + CD25 + Foxp3 + regulatory T cells by paclitaxelis explained by Bcl-2Bax mediated apoptosisrdquo InternationalImmunopharmacology vol 11 no 2 pp 212ndash219 2011
[120] X Wu Q-M Feng Y Wang J Shi H-L Ge and W DildquoThe immunologic aspects in advanced ovarian cancer patientstreated with paclitaxel and carboplatin chemotherapyrdquo CancerImmunology Immunotherapy vol 59 no 2 pp 279ndash291 2010
[121] A P Vicari R Luu N Zhang et al ldquoPaclitaxel reducesregulatoryT cell numbers and inhibitory function and enhancesthe anti-tumor effects of the TLR9 agonist PF-3512676 in themouserdquo Cancer Immunology Immunotherapy vol 58 no 4 pp615ndash628 2009
[122] L Zhang K Dermawan M Jin et al ldquoDifferential impairmentof regulatory T cells rather than effector T cells by paclitaxel-based chemotherapyrdquo Clinical Immunology vol 129 no 2 pp219ndash229 2008
[123] Y Tabuchi J Matsuoka M Gunduz et al ldquoResistance topaclitaxel therapy is related with Bcl-2 expression through anestrogen receptor mediated pathway in breast cancerrdquo Interna-tional Journal of Oncology vol 34 no 2 pp 313ndash319 2009
[124] N Obermajer R Muthuswamy K Odunsi R P Edwards andP Kalinski ldquoPGE
2-induced CXCL12 production and CXCR4
expression controls the accumulation of human MDSCs inovarian cancer environmentrdquo Cancer Research vol 71 no 24pp 7463ndash7470 2011
[125] Q M Feng W Di and X Wu ldquoImmune reconstitution inadvanced ovarian cancer patients undergoing first line chemo-therapyrdquo Xi Bao Yu Fen Zi Mian Yi Xue Za Zhi vol 25 no 11pp 1023ndash1025 2009
[126] A D Seidman D Hochhauser M Gollub et al ldquoNinety-six-hour paclitaxel infusion after progression during short taxaneexposure a phase II pharmacokinetic and pharmacodynamicstudy in metastatic breast cancerrdquo Journal of Clinical Oncologyvol 14 no 6 pp 1877ndash1884 1996
[127] D R Spriggs M F Brady L Vaccarello et al ldquoPhase IIIrandomized trial of intravenous cisplatin plus a 24- or 96-hour
infusion of paclitaxel in epithelial ovarian cancer a gynecologiconcology group studyrdquo Journal of Clinical Oncology vol 25 no28 pp 4466ndash4471 2007
[128] G A Omura M F Brady K Y Look et al ldquoPhase III trial ofpaclitaxel at two dose levels the higher dose accompanied byfilgrastim at two dose levels in platinum-pretreated epithelialovarian cancer an intergroup studyrdquo Journal of Clinical Oncol-ogy vol 21 no 15 pp 2843ndash2848 2003
[129] R Simon and L Norton ldquoThe Norton-Simon hypothesisdesigning more effective and less toxic chemotherapeutic reg-imensrdquoNature Clinical Practice Oncology vol 3 no 8 pp 406ndash407 2006
[130] A Kumar P Hoskins and A Tinker ldquoDose-dense paclitaxel inadvanced ovarian cancerrdquo Clinical Oncology vol 27 no 1 pp40ndash47 2015
[131] P Marchetti S Urien G A Cappellini G Ronzino and CFicorella ldquoWeekly administration of paclitaxel theoretical andclinical basisrdquoCritical Reviews in OncologyHematology vol 44supplement pp S3ndashS13 2002
[132] P Francis E Rowinsky J Schneider T Hakes W Hoskinsand M Markman ldquoPhase I feasibility and pharmacologic studyof weekly intraperitoneal paclitaxel A Gynecologic OncologyGroup pilot studyrdquo Journal of Clinical Oncology vol 13 no 12pp 2961ndash2967 1995
[133] H Thomas and P Rosenberg ldquoRole of weekly paclitaxel inthe treatment of advanced ovarian cancerrdquo Critical Reviews inOncologyHematology vol 44 supplement pp S43ndashS51 2002
[134] M Markman J Markman K Webster et al ldquoDuration ofresponse to second-line platinum-based chemotherapy forovarian cancer implications for patient management and clini-cal trial designrdquo Journal of Clinical Oncology vol 22 no 15 pp3120ndash3125 2004
[135] P H OrsquoDonnell M Eileen Dolan E Gamazon et al ldquoPopu-lation differences in platinum toxicity as a means to identifynovel genetic susceptibility variantsrdquo Pharmacogenetics andGenomics vol 20 no 5 pp 327ndash337 2010
[136] M J Millward M J Boyer M Lehnert et al ldquoDocetaxel andcarboplatin is an active regimen in advanced non-small-celllung cancer a phase II study in Caucasian and Asian patientsrdquoAnnals of Oncology vol 14 no 3 pp 449ndash454 2003
[137] M Markman ldquoIntraperitoneal therapy of ovarian cancerrdquoOncologist vol 1 no 1-2 pp 18ndash21 1996
[138] M Markman and J L Walker ldquoIntraperitoneal chemotherapyof ovarian cancer a review with a focus on practical aspects oftreatmentrdquo Journal of Clinical Oncology vol 24 no 6 pp 988ndash994 2006
[139] K Fujiwara S Nagao E Aotani and K Hasegawa ldquoPrincipleand evolving role of intraperitoneal chemotherapy in ovariancancerrdquo Expert Opinion on Pharmacotherapy vol 14 no 13 pp1797ndash1806 2013
[140] M Markman E Rowinsky T Hakes et al ldquoPhase I trialof intraperitoneal taxol a gynecoloic oncology group studyrdquoJournal of Clinical Oncology vol 10 no 9 pp 1485ndash1491 1992
[141] M Markman M F Brady N M Spirtos P Hanjani and S CRubin ldquoPhase II trial of intraperitoneal paclitaxel in carcinomaof the ovary tube and peritoneum a gynecologic oncologygroup studyrdquo Journal of Clinical Oncology vol 16 no 8 pp2620ndash2624 1998
[142] P B Panici I Palaia M Graziano F Bellati N Manci and RAngioli ldquoIntraperitoneal paclitaxel as consolidation treatmentin ovarian cancer patients a case control studyrdquo Oncology vol78 no 1 pp 20ndash25 2010
BioMed Research International 21
[143] D K Armstrong B Bundy L Wenzel et al ldquoIntraperitonealcisplatin and paclitaxel in ovarian cancerrdquo The New EnglandJournal of Medicine vol 354 no 1 pp 34ndash43 2006
[144] D Tewari J Java and R Salani ldquoLong-term survival advantageof intraperitoneal chemotherapy treatment in advanced ovariancancer an analysis of a Gynecologic Oncology Group ancillarydata studyrdquo in Proceedings of the 2013 Society of GynecologicOncology Annual Meeting on Womenrsquos Cancer (GOG114172Abstract) Los Angeles Calif USA 2013
[145] D A Yardley ldquonab-paclitaxel mechanisms of action and deliv-eryrdquo Journal of Controlled Release vol 170 no 3 pp 365ndash3722013
[146] M Ando K Yonemori N Katsumata et al ldquoPhase I and phar-macokinetic study of nab-paclitaxel nanoparticle albumin-bound paclitaxel administeredweekly to Japanese patients withsolid tumors and metastatic breast cancerrdquo Cancer Chemother-apy and Pharmacology vol 69 no 2 pp 457ndash465 2012
[147] N Desai V Trieu Z Yao et al ldquoIncreased antitumor activityintratumor paclitaxel concentrations and endothelial cell trans-port of cremophor-free albumin-bound paclitaxel ABI-007compared with cremophor-based paclitaxelrdquo Clinical CancerResearch vol 12 no 4 pp 1317ndash1324 2006
[148] J A Yared and K H R Tkaczuk ldquoUpdate on taxane devel-opment new analogs and new formulationsrdquo Drug DesignDevelopment andTherapy vol 6 pp 371ndash384 2012
[149] M G Teneriello P C Tseng M Crozier et al ldquoPhase IIevaluation of nanoparticle albumin-bound paclitaxel in plati-num-sensitive patients with recurrent ovarian peritoneal orfallopian tube cancerrdquo Journal of Clinical Oncology vol 27 no9 pp 1426ndash1431 2009
[150] R L Coleman W E Brady D S McMeekin et al ldquoA phase IIevaluation of nanoparticle albumin-bound (nab) paclitaxel inthe treatment of recurrent or persistent platinum-resistant ovar-ian fallopian tube or primary peritoneal cancer a GynecologicOncology Group Studyrdquo Gynecologic Oncology vol 122 no 1pp 111ndash115 2011
[151] J W Singer ldquoPaclitaxel poliglumex (XYOTAX CT-2103) amacromolecular taxanerdquo Journal of Controlled Release vol 109no 1ndash3 pp 120ndash126 2005
[152] C Li D-F Yu R A Newman et al ldquoComplete regressionof well-established tumors using a novel water-soluble poly(L-glutamic acid)-paclitaxel conjugaterdquo Cancer Research vol 58no 11 pp 2404ndash2409 1998
[153] M Mita A Mita J Sarantopoulos et al ldquoPhase I study ofpaclitaxel poliglumex administered weekly for patients withadvanced solid malignanciesrdquo Cancer Chemotherapy and Phar-macology vol 64 no 2 pp 287ndash295 2009
[154] P Sabbatini M W Sill D OrsquoMalley L Adler and A ASecord ldquoA phase II trial of paclitaxel poliglumex in recurrentor persistent ovarian or primary peritoneal cancer (EOC) agynecologic oncology group studyrdquo Gynecologic Oncology vol111 no 3 pp 455ndash460 2008
[155] M O Bradley C S Swindell F H Anthony et al ldquoTumortargeting by conjugation of DHA to paclitaxelrdquo Journal ofControlled Release vol 74 no 1ndash3 pp 233ndash236 2001
[156] M O Bradley N L Webb F H Anthony et al ldquoTumortargeting by covalent conjugation of a natural fatty acid topaclitaxelrdquo Clinical Cancer Research vol 7 no 10 pp 3229ndash3238 2001
[157] A C Wolff R C Donehower M K Carducci et al ldquoPhaseI study of docosahexaenoic acid-paclitaxel a taxane-fatty acid
conjugate with a unique pharmacology and toxicity profilerdquoClinical Cancer Research vol 9 no 10 part 1 pp 3589ndash35972003
[158] A Sparreboom A C Wolff J Verweij et al ldquoDispositionof docosahexaenoic acid-paclitaxel a novel taxane in bloodin vitro and clinical pharmacokinetic studiesrdquo Clinical CancerResearch vol 9 no 1 pp 151ndash159 2003
[159] P M Fracasso J Picus J D Wildi et al ldquoPhase 1 and phar-macokinetic study of weekly docosahexaenoic acid-paclitaxelTaxoprexin in resistant solid tumor malignanciesrdquo CancerChemotherapy and Pharmacology vol 63 no 3 pp 451ndash4582009
[160] A Y Bedikian R C DeConti R Conry et al ldquoPhase 3 study ofdocosahexaenoic acid-paclitaxel versus dacarbazine in patientswith metastatic malignant melanomardquo Annals of Oncology vol22 no 4 pp 787ndash793 2011
[161] Y-N Wu S-L Wang Y-C Wang et al ldquoReversal effect ofdocosahexaenoic acid on taxol resistance in human ovarian car-cinoma A2780T cellsrdquo Obstetrics amp Gynecology InternationalJournal vol 1 no 3 Article ID 00018 2014
Submit your manuscripts athttpwwwhindawicom
PainResearch and TreatmentHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom
Volume 2014
ToxinsJournal of
VaccinesJournal of
Hindawi Publishing Corporation httpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
AntibioticsInternational Journal of
ToxicologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
StrokeResearch and TreatmentHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Drug DeliveryJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Advances in Pharmacological Sciences
Tropical MedicineJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Medicinal ChemistryInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
AddictionJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
Emergency Medicine InternationalHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Autoimmune Diseases
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Anesthesiology Research and Practice
ScientificaHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Pharmaceutics
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of

BioMed Research International 5
Microtubules(MT)
MyD88 dependent
MyD88 independent
S
G2G1
M
PTX
Cell cycle arrest
N-terminal amino acids of beta
tubulin subunit
Inhibit depolymerisation ofmicrotubules
and suppress MT dynamics
Increase number and mass of microtubules increase
stability and block detachment
Apoptosis induced in G1S phase (absence mitotic
arrest)
Raf-1
p21
STAT 3
G0
JAK
MEK
MAPK
Bax Bcl2Bad
IRAK
TRAF
TKR
TRIF TRAM
ROS
Mitotic arrest at G2M phase
PI3KAKTApoptosis regulator
protein
p53
VEGFR
Angiogenesis
Apoptosis
TLR4
High concentrationLow concentration
NF-120581B
PTXle 9nM12hr
PTXge 9nM12hr
PTXle 9nM24hr
I120581B
Figure 3 Mechanism of action of paclitaxel Paclitaxel targets microtubules At high concentration PTX causes mitotic arrest at G2M phasewhereas at low concentration apoptosis is induced at G0 and G1S phase either via Raf-1 kinase activation or p53p21 depending on the doseconcentration Even at lower dose but with exposure beyond 24 hours paclitaxel can cause mitotic arrest Paclitaxel also activates multiplesignaling pathway to exert proapoptotic activity as well as immunomodulatory effect Paclitaxel also develops resistance via these signalingpathways PTX Paclitaxel TLR4 Toll-like receptor 4 G0 resting phase G1 cells enlarge andmake new protein S phase DNA replication G2preparation for division M phase cell divisionmitosis Raf-1 Raf kinase family MEKMAPK mitogen activated protein kinase IRAK IL-1receptor associated kinase TRAF TNFR associated factor NF-120581B nuclear factor kappa B TRIFTRAM TIR-domain-containing adapter-inducing interferon-120573 TKR tyrosine kinase receptor VEGFR vascular endothelial growth receptor PI3K phosphoinositide 3-kinase JAKjanus kinase STAT signal transducer and activator of transcription factor
Development of drug resistance leading to aggressive diseasethat is refractory to treatment is responsible for 90 ofthe deaths among patients with advanced ovarian cancer[70] Multidrug resistance (MDR) is a phenomenon definedby the ability of cancer cell to overcome either structurallyor functionally unrelated cytotoxic drugs Mechanism ofMDR can be broadly divided into three types (a) externalmechanism involving changes in pharmacokinetics of drugor (b) within tumour microenvironment which includeshypoxia leading to clonal selection pressure or (c) at cellu-lar level [71] MDR can be intrinsic or acquired IntrinsicMDR or also known as inherent occurs when cancer cellsdevelop resistant to any chemotherapy and this is most likelyattributed by tumour microenvironment Acquired MDRdevelops following exposure to chemotherapeutic agents andmay occur as a result of the pharmacokinetic of drug itself orsecondary to changes within the tumour cells [71]
Paclitaxel-derived resistance is mainly attributed bychanges involving mRNA and protein (such as multiple
ribosomal genes and translation factors) synthesis oxidativestress (UGT1A6 MAOA and CYBA) glycolysis (ADH1AHK1 and ENO3) glutathione metabolism and leukocytetransendothelial migration pathways [71] A study on geneexpression changes on a series of drug resistant ovariancancer cell lines following exposure to paclitaxel cisplatinor doxorubicin revealed that among 845 genes analysed atotal of 337 genes were significantly altered in cells resistantto paclitaxel [70] Changes in genes expression may createinterpatient variation in drug effect alteration in tumourmicroenvironment and changes within cellular structuresmetabolism and functions that promotes towards drug resis-tance
Tumour cells grow rapidly with formation of numerousnew vessels attributing to irregular blood flow and increasedoxygen demand which lead to development areas devoidof adequate oxygenation within ovarian cancer tissues [72]In response to chronic hypoxia (oxygen depletion) tumourmicroenvironment adapts processes to keep cells alive in
6 BioMed Research International
hypoxic and acidic state This hypoxic adaptation promotestumour proliferation dissemination and progression of dis-ease [73] and also reduces chemosensitivity [74]
Hypoxia-induced chemoresistance occurs due to geno-mic instability Oxygen depletion induces proteomic andgenomic changes that activates the level of p53 inhibits apop-tosis promotes angiogenesis (angiogenic molecules such asvascular endothelial growth factor [VEGF] and angiogenin)upregulates growth factors (platelet-derived growth factor[PDGF] transforming growth factor-beta and insulin-likegrowth factor [IGF]) and induces anaerobic metabolism andglycolysis (glycolytic enzymes glucose transporters) leadingto reduction in potential for cell cycle arrest and cellulardifferentiationwhich prevent tumour cell death [74]Hypoxiacan induce either p-53-dependent (involving Apaf-1 andcaspase-9 effector pathways) or p53-independent (involvinghypoxic-inducible factor 1 [HIF-1] and Bcl-2 family genespathways) apoptosis in both normal and tumour cells HIF-1 is a common transcription factor consisting of HIF-1120572 and HIF-1120573 subunits which controls hypoxic-induciblegenes and the concentration of HIF-1 protein increasedexponentially in the presence of hypoxic environment Lossof apoptotic potential of tumour cells mediated by hypoxicenvironment and HIF-1 which arrest cell cycle at G0G1reduces chemosensitivity to chemotherapeutic agents includ-ing paclitaxel [70 75]
Other transcriptional factors which are activated byhypoxia are nuclear factor kappa B (NF-120581B) and STAT3 also known as proinflammatory transcriptional factorsNF-120581B and STAT 3 regulate multiple gene products whichare involved in inflammation angiogenesis cell survivalproliferation and metastasis Paclitaxel which mediates itscytotoxic action via NF-120581B pathway is vulnerable to developresistance in the presence of hypoxic tumour microen-vironment with activation of NF-120581B transcription factorwhich induces serine phosphorylation and also regulatesBCL-2 an antiapoptotic protein preventing cell death andpromoting tumorigenesis [76] Inhibition of activated STAT3 found overexpressed in most paclitaxel-resistant ovariancancer cells has resulted in reduction in paclitaxel resistanceHowever further research is required to determine the exactmechanism [77]
Intracellular drug concentration is important for effectivecytotoxic activity of paclitaxel Drug resistance may beattributed to either reduced accumulation of drug withinovarian tumours or increased efflux of drug from tumourcells [78] Alteration in pharmacokinetic of paclitaxel eitherattributed by the drug itself such as lower concentration ofdrug administered shorter duration of drug exposure highfirst pass metabolism increased hepatic or renal clearanceinadequate binding to tubulinsmicrotubules or othermacro-molecules or presence of higher tumour density or vascular-ity may result in reduced accumulation of intratumoral drugconcentration [71]
Drug efflux is the most common mechanism for chemo-resistance observed in paclitaxel-treated cancer cells Drugefflux from cancer cells is mediated by ATP-binding cassette(ABC) transporters such as P-glycoprotein (P-gp) P-gp alsoknown as ABCB1 or multidrug-resistance associated-protein
(MRP) a transmembrane protein encoded by MDR1 geneplays a role as an efflux pump which is crucial for occurrenceof many cellular processes that require transfer of substratesacross cellularmembranes P-gp hence can affect intracellulardrug concentration andhave been shown to correlate in vitroto chemosensitivity to paclitaxel [59] However evidence fortheir role in clinical drug resistance in ovarian cancer hasemerged with P-gp found to be overexpressed in ovariancancer cells in vitro and also on paclitaxel-resistant celllines [70] P-gp and MDR1 expression levels were higherin chemoresistant ovarian cancer patients as compared withtheir chemosensitive counterpart Overall survival time wasalso statistically higher in patientswith low expression of P-gpandMDR1 in their tumor tissuesHence P-gp andMDR1mayhave a predictive role in determining the outcome of patientswith advanced ovarian cancer [58 79ndash82] Mechanism ofpaclitaxel resistance is complicated and specifically inhibitingABC transporters have given mixed results [59 83]
Another major mechanism of paclitaxel resistance ismediated by either a reduction in total intracellular tubulinconcentrations point mutation at prominently expressedtubulin genes or by selective alterations in expression oftubulin isotypes such as Class III 120573-tubulin [52 84 85]Microtubule dynamic stability was significantly impairedin the paclitaxel-resistant cells [86] Microtubule dynamicsdisruption caused by paclitaxel result in cell cycle arrestapoptosis and drug resistance
Other mechanism responsible for development of pacli-taxel resistant are inhibition of apoptosis activation ofmitogen-activated protein kinase Raf-1 kinase or intra-cellular signalling pathway PIK3 (phosphatidylinositol-45-bisphosphate 3-kinase) changes in apoptotic regulatory pro-teins such as Bcl-2 increase in expression of proinflammatorycytokines such as TNF-120572 IL-6 and IL-8 and activation oflipopolysaccharide-inducible genes and tumour suppressionprotein p53 [57 83 86 87]
In summary paclitaxel resistance is multifactorial inc-luding changes in signaling pathways upregulation of P-glycoprotein (P-gp) [80 88 89] alteration in tubulin dyna-mic mutations in 120573-tubulin gene or expression of 120573-tubulinisotypes [52 84 85] and changes in apoptotic mechanismIdentification of mechanism of resistance could help topotentially develop novel agents to improve chemosensitivityof patients with advanced ovarian cancer
6 Pharmacokinetics
Paclitaxel is a white to off-white crystalline powder highlylipophilic and is insoluble in water and so difficult to formu-late into solution It has a melting point of 216-217∘C [90 91]More than 90 of the drug binds rapidly and extensively toplasma proteins [33 40] whereas binding onto red blood cellsis approximately 50 The presence of premedication drugs(before chemotherapy) such as ranitidine dexamethasone ordiphenhydramine did not affect protein binding of paclitaxelPaclitaxel has a large volume of distribution of about 55 Lm2but this is reduced in the females [33]
BioMed Research International 7
AUC (area under the plasma concentration)
Cmax (maximum concentration)
Pacli
taxe
l con
cent
ratio
n (120583
M)
0 10 20 30 40
Time (hr)
0
1
2
3
4
5
Figure 4 Plasma pharmacokinetics of paclitaxel The pharmacoki-netics generally were linear for 6 or 24 hour infusions but becomenonlinear for infusions of shorter durations due to variation inthe elimination clearance with the dose administered An increasein plasma concentration of paclitaxel results in disproportionatelarger increase in 119862max (maximum plasma concentration) and AUC(area under plasma concentration) followed by decrease in drugelimination from body tissues
The disappearance of paclitaxel from plasma is tradition-ally believed to be biphasic [33] The initial rapid declinerepresents distribution to the peripheral compartment andelimination of the drug The later phase is due in part tothe slow efflux of paclitaxel from the peripheral compartment[92] In the presence of more sensitive assay methods andlater sampling times a three-compartment model seems tobe more accurate [40 93] Paclitaxel has been shown tohave a nonlinear pattern of pharmacokinetics (Figure 4)Thepharmacokinetics were generally linear for 6- or 24-hourinfusions but become nonlinear for infusions of shorterdurations because the elimination clearance varies with thedose administered With increasing plasma concentrationof paclitaxel there is a disproportionately larger increasein 119862max (maximum plasma concentration) and AUC (areaunder plasma concentration) accompanied by decrease indrug elimination from body tissues The clinical importanceof this nonlinear pattern is that dose escalationmay result in adisproportionate increase in toxicity whereas dose reductionmay affect its efficacy [33 90 91 94]
The pharmacokinetics of paclitaxel has been evaluatedover a wide range of doses up to 300mgm2 and withinfusion schedules ranging from 3 to 24 hours Maximumplasma concentrations are dose-related In patients treatedwith single dose infusion of 135 and 175mgm2 given as3- and 24-hour infusions mean steady state volume ofdistribution has ranged from 198 to 688 Lm2 indicatingextensive extravascular distribution andor tissue bindingTerminal half-life has ranged from 13 to 86 hours (mean 5hours) [40 93] and total body clearance has ranged from116 to 240 Lhrm2 Preclinical results in animals have shown
high levels in most tissues Being highly protein-boundpaclitaxel has a high affinity for distribution in specific tissuesincluding kidney lung spleen and extracellular fluids likeascites and pleural fluids [40 95] but the uptake of the drugin the brain is minimal [96 97] Exposure to paclitaxel isrelatively high in tumour tissue compared with other tissuesand in addition to slow elimination from tumour tissue theAUC in tumour tissue is about five-fold higher than that inplasma [97]
There is no evidence of accumulation of paclitaxel withmultiple treatment courses as the variability in systemicpaclitaxel exposure as measured by AUC (0ndashinfin) (area underplasma concentration-time curve from time 0 to infinity)for successive treatment courses are minimal [98] Paclitaxelclearance is however sequence dependent Patients receiv-ing a platinum-based agent prior to paclitaxel have lowerclearance and greater clinical toxicity than patients receivingpaclitaxel before cisplatin [93]
The drug administered intravenously undergoes anextensive P-450mediated hepaticmetabolism by cytochromeenzymes (CYP3A andCYP2C8) with 70ndash80being excretedinto bile by adenosine triphosphate- (ATP-) binding cassettemultidrug transporters such as P-glycoprotein (P-gp) andmultidrug resistance protein 2 (MRP-2) either asmetabolitesor as the parent drug Variation in MRP-2 activity hasbeen found to have direct effect on the effective exposureto paclitaxel [99] The bioavailability is poor following oraladministration due to enterocyte expression of P-gp and first-pass metabolism in the liver Most of the drug is eliminatedin feces Less than 10 drug in the unchanged form isexcreted in the urine indicating extensive nonrenal clearance[96] Combinations of inhibitors of CYP3A and P-gp mightpossibly improve the oral bioavailability of the taxanes [8997 100]
7 Paclitaxel and the Immune System
The immune system consists of two different but interactingmechanisms which are innate and adaptivemechanismsTheinnate mechanism is the first line of defense and consists of agroup of cells which includes mainly macrophages dendriticcells (DCs) and natural killer (NK) cells while the adaptiveimmunemechanism is represented by T-lymphocytes All thecomponents of innate and adaptive mechanism are involvedin antitumour immunity which includes tumour recognitioncontrol and elimination However cancer cells are able toevade immune detection and actively suppress antitumourimmunity
Paclitaxel has a wide range of dose dependent immuno-modulatory effects described in Figure 5 At standard dosepaclitaxel is broadly immunosuppressive and this is becauseit inhibits a number of cell types involved in tumour rejectionsuch asmacrophages effector T cells andNK cells [101] How-ever at lower doses than typically used for chemotherapypaclitaxel has an important immunogenic role promotingantitumour immunity [101 102] Hence understanding theimmunological basis of paclitaxel may help to maximise themanipulation of the immunomodulatory effects of paclitaxel
8 BioMed Research International
Immunomodulatory effect of
paclitaxel
Stimulate direct cytotoxic activity by
macrophage
Induce activation maturation and priming of DCs
Stimulate NK-dependent antitumour immunity
Activation of tumour-specificCTL Expansion of memory T cells
Secretion of proinflammatory cytokine
Shift from Th2 to Th1 type ofresponse
Depletion of Tregs andmodulation of MDSC
Downregulates the expression of VEGFR-2
and inhibits angiogenesis
IL-6 IL-12 TNF-120572 and i-NOS
Figure 5 Immunomodulatory effect of paclitaxel Paclitaxel a toll-like receptor 4 (TLR4) ligand binds to TLR4 receptor and triggers TLR4signaling via MyD88 dependent and independent pathway Paclitaxel then promotes anticancer immune response directly by stimulatingmacrophages to kill cancer cells or indirectly by secretion of proinflammatory cytokines which upregulates activation of DCs NK andtumour specific CTL Paclitaxel promotes effective CTL response by upregulation of mannose-6-phosphate which facilitate permeabilityto granzyme B and cytokine patterns of T helper type 1 Paclitaxel modulates MDSC and ablates Tregs Memory T cells (CD4+CD45RO+and CD8+CD45RO+) increased significantly while regulatory T cells (Tregs) decreased around 2 weeks creating an opportunity window fordose-dense therapy and immunomodulatory agents to achieve clinical benefit Dose-dense and low dose paclitaxel also blocks new vesselformation by downregulating VEGF-receptor 2 reduces resistance by alternative mechanism of action
to develop better therapeutic options in the management ofadvanced ovarian cancer
Paclitaxel is a ligand to toll-like receptor 4 (TLR4) whichis expressed on innate immune cells including macrophagesThe binding of paclitaxel to TLR4 on macrophages trig-gers the MyD88 mitogen-activated protein kinase (MAPK)and transcription of nuclear factor NF-kappa B (NF-120581B)pathways (Figure 3) resulting in their activation and releaseof immunostimulatory cytokines such as tumour necrosisfactor-120572 (TNF-120572) interleukin-1 (IL-1) interleukin-6 (IL-6)and interleukin-8 (IL-8) [103ndash105] Activated macrophagescan either cause direct tumour cell lysis via release oflysosomal enzymes and nitric oxide (NO) or indirectly byactivating NK cells DCs and tumour-specific cytotoxic T-lymphocytes (CTLs) [101]
NK cells are also innate immune cells capable of killingtumour cells particularly those cells that have reduced classI MHC expression and therefore can escape killing by CTLsPaclitaxel can enhance NK cell function by inducing mRNAand protein production of perforin an effector moleculeinvolved inNKcell-mediated cytotoxicity [106]However theeffect of low dose paclitaxel on NK cells is controversial Inanother study it was found that treatment of human NK cellswith paclitaxel effectively inhibits NK cell-mediated killing ofK562 (human erythroleukemia) target cells in vitro withoutaffecting the viability of NK cells [107] However weeklypaclitaxel therapy for non-small cell lung cancer patients was
only able to reduce the NK cell function up to completion ofthe first cycle but thereafter it gradually recovered [108]
Dendritic cells also express TLR4 and can be directlyactivated by paclitaxel The binding of paclitaxel to TLR onimmature DCs promotes DC maturation by upregulatingantigen-processing machinery gene components costimu-latory molecules and IL-12p70 [102] This enhances theability of DCs to prime T cells which facilitate antitumourimmunity [109] Paclitaxel can also promote cytotoxic T-cell function by upregulating mannose-6-phosphate whichfacilitates permeability to granzyme B and also inducescytokine production patterns typical of the T helper type 1phenotype via IL-2 (CD4 T cell) and IFN-120574 (CD8 T cell)secretion [104 110] Activated CD8+ T cells can differentiateinto CTL type 1 (Tc1) cells producingmainly IFN-120574 and CTLtype 2 (Tc2) cells producing mostly IL-4 IL-5 and IL-10 Tc1cells are potent CTL involved in the defense against cancerTc1 cells are able to recognise tumour antigens in the contextof MHC class I and mediate tumour cell lysis The role of Tc2cells in the immune response is not clearly known althoughtheir presence has been associated with disease progression[111]
CD4+ CD25+ regulatory T-cells (Tregs) constitutingapproximately 5ndash10 of peripheral CD4+ T cells [112 113]play an important role in tumour immune evasion [114]There is growing evidence that supports the existence ofelevated numbers of Tregs in tumours [115ndash117] which may
BioMed Research International 9
suppress immune responses of other CD4+ and CD8+ cells[118ndash120] and promote tumour progression In murine stud-ies paclitaxel exhibits the ability to reduce the number andsize of Treg cells thereby enhancing antitumour immunity[119 121] Similar findingswere seenwith a selective reductionin the size and number of Treg populations in peripheralblood samples from non-small cell lung cancer (NSCLC)patients [122]
Paclitaxel also decreased the expression of the anti-apoptotic molecule Bcl-2 in Treg cells while increasing thecorresponding proapoptoticmember Bax which contributedto the apoptotic sensitivity of Treg to paclitaxel [87]This wasseen in a study using the 3LL Lewis tumour model whichdemonstrated that Treg cells exposed to paclitaxel displayeddown regulation of Bcl-2 and upregulation of Bax and uponblocking the Bcl-2 pathway the ability of paclitaxel to ablateTreg cells compared toT effectorswas impaired and bothTregand T effectors were affected These results may suggest thatpaclitaxel targets Bcl-2 rather than tubulin to contribute tothe distinctive effect on Treg cells [119] It has recently beenshown in vitro that paclitaxel could target Bcl-2 and thereforelead to apoptosis Bcl-2 family proteins are key regulators ofapoptosis and play an important role in tumourigenesis andmulti-drug resistance by blocking apoptosis [119 123]
Few studies have also shown effect of paclitaxel onmyeloid-derived suppressor cells (MDSCs) a heterogeneouspopulation of immature myeloid cells immunosuppressivein nature are recruited by cancer cells and are found inincreased amount in advanced epithelial ovarian cancer [124]In a murine study using C57BL6 mice administration ofpaclitaxel at ultralow dose modulates MDSCs to differentiateinto DCs in a TLR4 independent manner [110] Hencepaclitaxel in ultralow noncytotoxic doses together with itsangiogenesis blocking ability may potentially enhance theefficacy of immunotherapy by ablation of immunosuppres-sive populations such as Tregs and MDSCs in tumour-bearing hosts [50 102]
In immunocompromised patients with advanced ovariancancer with increased Tregs and decreased levels of CD4+T cell CD8+ T cell and NK subsets after a single courseof combined carboplatin and paclitaxel chemotherapy theimmunosuppression is reversed around 12 to 14 days later butnot before one week or after three to four weeks Not only areTregs decreased but also the proportions of IFN-120574 secretingCD8+ T cells T helper-1 Tc1 and NKT cells The ratio of Tc1to Tc2 cells increases significantly [111 120 125]
Following chemotherapy both CD4+CD45RO+ andCD8+CD45RO+ memory T cells increased significantly andpeaked around 2 weeks The increase of memory T cellsin ovarian cancer patients following chemotherapy prob-ably opens the door of opportunity to develop long-termimmunological memory which could prevent recurrenceand metastases [120] Administration of dose-dense therapygiven weekly may hence be beneficial immunologically tomount an adequate immune response compared to standard3-week therapy In addition administration of immunother-apy agentsmay also be ideal during the period of 2weeks afterchemotherapy where temporary immune system reconstitu-tion takes place
8 Clinical Studies
In the past two decades paclitaxel had been administered indoses ranging from 60 to 250mgm2 over 1ndash96 hours andfrom 1 to 3 weekly intervals Prolonged exposure up to 96hours was believed to be effective as demonstrated with pre-clinical data but later refuted in large prospective studies [14126 127] A 24-hour infusion of paclitaxel was subsequentlyadministered to reduce the risk of hypersensitivity reactionshowever it was shown to increase mucosal and bone marrowtoxicity without improved efficacy [127 128] Development ofeffective premedication has led to administration of shorterinfusions (lt3 hours) which are better tolerated in particularfrom a haematologic perspective but patients remain at riskof myalgia and neuropathy at higher doses Weekly one-hourlow dose paclitaxel also known as dose-dense therapy hasrecently emerged as another possible strategy to improveoutcomes
9 Dose-Dense Therapy
Dose-dense treatment is defined by delivery of a maintainedper-cycle dose or overall dose with administration of drugat shorter time intervals than is standard This differs fromdose intensity which refers to dose (per unit weight or bodysurface area) delivered per unit time Hence either escalationof dose per cycle or reducing the time in between cycles maymodify dose intensity [129 130]
The rationale for the dose-dense approach of weeklypaclitaxel is that more frequent delivery of moderate dosesmay achieve greater efficacy by allowing sustained exposureof dividing tumour cells to paclitaxelrsquos cytotoxic and antian-giogenic effects hence reducing resistance delaying relapseand increasing the possibility of cancer remission Three 1-hour infusions of paclitaxel given at a week interval achievedgreater dose-density as well as dose-intensity than a singleadministration every 3 weeksThe initial tissue concentration(gt50 nM) for 1-hour infusion is similar to that of 3-hourinfusion but the concentration in the plasma instead oflasting for 8 hours in a 3-hour infusion rapidly falls below50 nM in less than 75 minutes for 1-hour infusion and hencereduces the risk of neutropenia However the rate of fallexperienced in tissue concentration of the drug is slowerthan plasma concentration of the drug hence efficacy ismaintained [131 132] A shorter infusion time allows bettercontrol of toxicities improved patient comfort and reducedhospitalisation hours
Several studies have used dose-dense paclitaxel in thetreatment of advanced ovarian cancer and are summarizedin Table 1 Based on phase 1 studies the recommendeddose for weekly paclitaxel ranges between 80 and 90mgm2compared with 45mgm2 per week with 3-weekly paclitaxeland is given over 1-hour duration Weekly scheduling hasdemonstrated consistent activities in ovarian cancer studies[11ndash13] Response rates were in the 20ndash50 range whereusually less than 10 would be expected Grade-4 doselimiting toxicities in particular neutropenia were not evidentat any dose below 100mgm2week [11 133]
10 BioMed Research International
Table1Ph
ases
Iand
IIstu
dies
onintravenou
sdose-densep
aclitaxel
Stud
yRe
gimen
119899()
PI(m
)RR
()
CR(119899)
MedianPF
S(m
)Median
OS
(m)
Adversee
ffects
Com
ments
Paclitaxel
dose
(mgm
2 )Ca
rbop
latin
dose
(mgm
2 )Ph
aseIsinglea
gent
Lofflerre
tal1996
[11]
40ndash9
0week
1-hou
rinfusionfor
6weeks
5040
5NA
NA
(i)Hem
atologictoxicity-m
ild(ii)N
ograde3
or4
haem
atologicaltoxicity
neurologicalor
cardiotoxicityup
to90
mgm
2 wk
(iii)Nohypersensitivity
reactio
ns(patientsreceivedprem
edication)
(i)100
priorc
hemotherapy
(ii)M
ediando
seintensity
was
410m
gm
2 6w
k(range200
to540m
gm
2 6w
k)
Fenn
ellyetal
1997
[12]
40ndash100w
eek
1830
NA
NA
NA
(i)Nomucositiso
rgrade
III
neurop
athy
was
seen
(ii)A
lopeciao
ccurredin
one
(i)100
priorc
hemotherapy
(2ndash5
priorregim
ens)
(ii)P
artia
lrespo
nses
weres
eenin
four
of13
assessablepatients
(30
)(iii)Dose-lim
iting
toxicitywas
reachedat100m
gm
2 (iv
)2-3
patie
ntse
xperience
treatmentd
elay
(v)M
axim
um-to
lerateddo
seof
80mgm
2 Ab
u-Ru
stum
etal
1997
[13]
60ndash100
over
1ho
urw
eek
45289
NA
NA
NA
(i)Nopatie
nthadfebrile
neutropenia
(i)100
priorc
hemotherapy
(1ndash8
priorregim
ens)
PhaseIISing
leagent
Markm
anetal
2001
[14]
80over
1ho
urw
eek
53(52)
25NA
NA
NA
Therapydiscon
tinuedin
(i)4patie
ntsw
hohadperip
heral
neurop
athy
(ii)1
patie
ntdu
etopainful
fingernailbeds
(i)100
platinum
andpaclita
xel
resistant
(ii)Th
erapywas
discon
tinuedin
5patie
ntsb
ecause
oftoxicity
(iii)Only13
(1)w
erem
odified
(doser
eductio
nor
treatment
delay)
becauseo
fsidee
ffects
PhaseIICom
binedwith
platinum
agent
Kiku
chietal
2005
[15]
80over
1ho
urw
eek
AUC2week
27gt6
818
483
NA
(i)Neutro
penia(
17)
thrombo
cytopenia(
51
)(ii)N
ocaseso
fperipheral
neurop
athy
(grades3
and4)
inweeklycombinedT-C
Cadron
etal2007
[16]
90over
1ho
urw
eek
AUC4week
24 9gt6le6
73 38NR
8105
675
(i)Grade
34neutropenia(
34)
andneutropenicfever
in2
(ii)N
auseaa
ndvomiting
and
fatig
uewerethe
mostfrequ
ent
nonh
ematologicalsid
eeffects
(i)Doser
eductio
nwas
necessary
in25of
patie
nts
Pign
atae
tal2008
[17]
60over
1ho
urw
eek
AUC2week
24(13)lowastlowast
1stline
385
2320
136
(i)Notoxicd
eath
was
recorded
(ii)G
rade
2anaemiawas
repo
rted
insevenpatie
nts(27)
(iii)Nofebrile
neutropeniaw
asob
served
(iv)G
rade
3and4neutropenia
was
recorded
infive(19)a
ndon
e(4
)patients
(v)G
rade
3thrombo
cytopenia
occurred
inon
epatient
(4)
BioMed Research International 11
Table1Con
tinued
Stud
yRe
gimen
119899()
PI(m
)RR
()
CR(119899)
MedianPF
S(m
)Median
OS
(m)
Adversee
ffects
Com
ments
Paclitaxel
dose
(mgm
2 )Ca
rbop
latin
dose
(mgm
2 )
Safrae
tal2014
[18]
80over
1ho
urw
eek
AUC2week
133
1stline
864
645
274
(i)Highera
naem
ia(grade
III+
IV68vs53)+
IVneutropenia(
144vs69)
decreasedgradeIIa
lopecia(
235
vs981
)and
thrombo
cytopenia
(grade
III+
IV0
vs23)
Havrilesky
etal
2003
[19]
80over
1ho
urw
eek
AUC2weekD1
D8D15
until
progressionCR
+8courses
29 21 8
Total
grou
pgt6lt6
83 100
38
16 15 1114
115
137
32
(i)Hem
atologictoxicitywas
common
(grade
3neutropenia
32n
ograde4
neutropenia
grade3
or4thrombo
cytopenia
142)
(i)To
xicitymanaged
bytre
atment
delaydo
seredu
ctionof
paclitaxel
ordiscon
tinuatio
nof
carbop
latin
vanderB
urgetal
2014
[20]
90over
1ho
urw
eek
AUC4weekD1
D8D15
D29
D36
D49
+6x
TCq3w
108
65 43
Total
grou
pgt6lt6
76 5816 42
26 158 13
(i)Neutro
penia3
0
thrombo
cytopenia8
febrile
neutropenia0
5
(ii)N
onhaem
atologictoxicitywas
low
(i)Treatm
entw
asdelayedin
16
anddo
seredu
cedin
2of
cycle
s
119899num
bero
fpatientsassessableforrespo
nsemm
onthsPIplatinum
treatmentfreeintervalRR
respo
nser
ateCR
com
pleterem
issionT
paclitaxelC
carbop
latin
PFS
progressio
nfre
esurvivalOSoverall
survivalN
An
otavailableinpapero
rabstractandNR
notyetreached
lowastlowastElderly
popu
lation
patient
agedge70
years
12 BioMed Research International
Numerous phase II studies have explored the tolerabilityand the activity of weekly paclitaxel either as a single agent orin combination with several other drugs or biological agents(Table 1) A number of regimens combining weekly paclitaxelwith carboplatin have been used as first-line treatment inovarian cancer Carboplatin has been administered weeklyat AUC of 2 with dose escalation in some studies whilepaclitaxel had been infused at 60ndash80mgm2week Thiscombined regimen was well tolerated with a low incidence ofbone marrow suppression Overall response rates have beenhigh in the range of 60ndash80 in most studies even in heavilypretreated patients with platinum-resistant disease (diseaserecurrence or progression within 6 months of the last lineof platinum-based therapy) [15ndash20 134] The promising datafrom these phase II trials then led to the evolution of largerphase III trials
Three phase III studies Japanese Gynecologic OncologyGroup- (JGOG-) Trial 3016 [21ndash23] Multicentre Italian Trialin Ovarian Cancer-Trial 7 (MITO-7) [25] and GynecologicOncology Group GOG-262 Trial [24] have explored dosedense therapy The results of these trials are summarised inTable 2
The Japanese Gynecologic Oncology Group (JGOG)conducted a randomized phase 3 trial of dose-dense weeklypaclitaxel 80mgm2week in combination with 3-weeklycarboplatin compared to standard 3-weekly carboplatin andpaclitaxel 180mgm2 in patients with advanced epithelialovarian peritoneal or fallopian tube cancer (JGOG 3016NOVEL trial) In both arms carboplatin was given at AUC6 and the median number of cycles was six In this largestudy (119899 = 637) with a median follow up of 77 months therewas an 11-month improvement in themedian progression freesurvival (PFS) in the dose-dense treatment group comparedwith the standard treatment arm (282 versus 175 monthsHR 076 95 CI 062ndash091 119901 = 00037) Median OS wasalso higher in the dose-dense treatment arm (1005 versus622 months HR 079 95 CI 063ndash099 119901 = 0039)On subgroup analysis suboptimally debulked patients withresidual disease of gt1 cm (119899 = 342) had a significantlyhigher median overall survival in the dose dense arm (512versus 335 months HR-075 95 CI 057ndash097 119901 = 0027)There was no significant advantage to dose-dense treatmentfor patients with optimally cytoreduced disease Dose-densetherapy survival benefits were also not seen in patients withclear cell or mucinous histology type unlike serous typeHowever patient treated with dose dense therapy had asignificantly higher frequency of hematologic toxicity thanwith the standard arm (212 versus 94) which resultedin lower treatment completion rates (63 versus 48) withfrequent episodes of delay (76 versus 67) and dosereductions (48versus 35) [21 22]Therewas no significantdifference in terms of overall quality of life between the twoarms (119901 = 046) [23]
Using a similar regimen as in JGOG-3016 a GynecologicOncology Group (GOG)-262 Trial was conducted in theUnited States In this group most patients had stage IIIdisease (66ndash70) and two-thirds had suboptimal debulkingwith residual disease of gt1 cm This was a randomized phase
III trial of 3 weekly paclitaxel versus dose-dense weeklypaclitaxel in combination with carboplatin in patients withadvanced epithelial ovarian peritoneal or fallopian tubecancer Though optional concurrent and maintenance beva-cizumab were received by the majority of patients in botharms (835 versus 841 resp) There was no significantdifference in PFS in the patients who received the dosedense paclitaxelcarboplatin regimen compared to those whoreceived the standard paclitaxelcarboplatin regimen (148versus 143 months HR 097 95 CI 079ndash118) Howeverin a subgroup analysis there was a significant difference inPFS in the dose dense paclitaxel arm who did not receivebevacizumab 119899 = 112 (142 versus 103 months HR 059 95CI 037ndash096 119901 = 0003) Overall survival data is still imma-ture There was higher frequency of grade 3 anaemia (408versus 157 119901 lt 0001) and grade 2 sensory neuropathy(259 versus 178 119901 = 0012) but a lower incidence ofneutropenia (72 versus 83 119901 lt 0001) [24]
In 2008 the Multicentre Italian Trials in Ovarian Cancer(MITO-7) randomised 810 women in a phase 3 trial toreceive either standard carboplatin (AUC = 6) and paclitaxel175mgm2 every 3 weeks or a weekly schedule of paclitaxel(60mgm2) with carboplatin (AUC = 2) The majority ofpatients in both arms (83ndash90) received six cycles of therapyMost patients (58ndash63) had stage II1 disease 23 of themwere suboptimally debulked Median PFS did not differsignificantly (173 months and 183 months 119901 = 066)between the standard and dose-dense arms respectivelyThere was no significant difference in response rate betweenthe two arms nor the estimated 2-year overall survivalSubgroup analysis did not identify any subgroup that mayhave benefited from the dose-dense regimen Unlike theJGOG-3016 trial the incidence of grade 3-4 neutropenia wassignificantly lower in the dose-dense group compared to the3-weekly regimen (42 versus 50) A similar pattern wasseen for the incidence of febrile neutropenia (lt1 versus 3119901 = 002) thrombocytopenia (1 versus 7 119901 lt 0001)and other nonhaematological toxicities such as alopeciavomiting renal dysfunction and neuropathy Quality of lifewas reported to be significantly better in the dose-dense arm(119901 lt 00001) which was discordant with the JGOG-3016quality of life data [25]
In summary there was significant improvement inmedian PFS and overall survival in studies using paclitaxelat 80mgm2week dose-dense therapy [21 24] but withhigher haematological toxicity whereas MITO-7 [25] whichwas using paclitaxel at 60mgm2week was only equivalentlyeffective but less toxicThis does not conclude that the higherpaclitaxel dose is more clinically beneficial as there are manyother confounding factors in all three studies
In a multivariate analysis the JGOG-3016 study [21]reported that a lower dose intensity of paclitaxel (lt80) wasassociated with poorer overall survival (hazard ratio = 14295 confidence interval 112ndash181 119901 = 0004) however itmust be highlighted that the investigational arm carboplatinschedules were not standardised in these studies The JGOGand GOG trials delivered a 3-weekly carboplatin (AUC =6) arm whereas in the MITO-7 study the carboplatin was
BioMed Research International 13
Table2Ph
aseIIIstu
dies
onintravenou
sdose-densep
aclitaxel
Stud
yRe
gimen
119899
MedianPF
S(m
)
Median
OS
(m)
Adversee
ffects
Com
ments
Katsu
matae
tal2009
[21]
Katsu
matae
tal2013
[22]
Haranoetal2014
[23]
JGOG3016
631
(i)Haematologicaltoxicityhigh
erin
dose
dense-211versus
94
Lower
treatmentcom
pletionin
dose-dense
63versus
48
Frequent
episo
deso
fdelay
indo
se-dense
76versus
67
Doser
eductio
nsin
dose-dense
48versus
35
Nosig
nificantd
ifference
inoverallQ
OL
betweenbo
thgrou
ps(119901=046)
Paclitaxel80m
gm
2D18
15+carbop
latin
AUC63
weeklyversus
Paclitaxel180
mgm
2+
carbop
latin
AUC63
weekly
312
282
1005
Both
givenfor6
ndash9cycle
s319
175
622
Chan
etal2013
[24]
GOG-262
(i)Higherfrequ
ency
ofgrade3
anaemia
(408versus
157119901lt0001)
grade2
sensoryneurop
athy
(259versus
178
119901=0012)b
utlower
incidenceo
fneutropenia(
72versus
83119901lt0001)
Paclitaxel80m
gm
2D18
15+carbop
latin
AUC63
weeklyversus
Paclitaxel175
mgm
2+
carbop
latin
AUC63
weekly
346
148
NR
Both
givenfor6
cycle
s346
143
NR
Bevacizumab
given
optio
nally
112
(did
not
receive
bevazicumab)
142vs
103
Pign
atae
tal2014
[25]
MITO-7
810
(i)Lo
wer
incidenceo
fgrade
3-4
neutropenia(
42versus
50)febrile
neutropenia(lt1v
ersus3
119901=002)
thrombo
cytopenia(
1versus7
119901lt0001)andothern
onhaem
atological
toxicitie
ssuchas
alop
eciavom
iting
renald
ysfunctio
nandneurop
athy
Qualityof
lifeb
etterindo
sedensea
rm(119901lt00001)
Paclitaxel60m
gm
2 weekly+carbop
latin
AUC
2weeklyversus
Paclitaxel175
mgm
2+
carbop
latin
AUC63
weekly
406
404
183 173
77lowast
79lowast
119899num
bero
fpatientsmm
onthsDday
PFSprogressionfre
esurvivalOSoverallsurvivalNAnot
availableinpapero
rabstractandNR
notyetreached
lowastSurvivalrateat2years
14 BioMed Research International
dose-dense (AUC 2 weekly) Although it is possible that thedose scheduling for the platinum-based agent is not essentialfor a survival benefit as shown by previous studies usingdose-dense cisplatin direct cross-trial comparison cannot bemade Unlike paclitaxel carboplatin probably requires peakdose for optimal therapeutic benefit hence this may accountfor the inferior survival outcome in MITO-7 trial Anotherconfounding factor may be difference in ethnicity All threestudies used different ethnic populations and Asian patientsin JGOG-3016 appear to have better survival outcomes thanthe MITO-7 Western population Ethnicity with possibleunderlying genetic causes may be responsible for the variableresponses to chemotherapy across individuals [135] This wasexplored by Millward et al who studied 68 Caucasian andAsian lung cancer patients treated with a combination ofpaclitaxel and carboplatin and found that the incidence offebrile neutropenia was 50 of an initially treated cohortof Asians and when carboplatin was subsequently dosereduced in all Asian patients the overall incidence of febrileneutropenia was also reduced to 26 [136]
Although early clinical data from phase I and phaseII dose-dense paclitaxel trials in advanced ovarian cancerwere promising the results from phase III studies in havebeen inconsistent as a result of differences in paclitaxel dosecarboplatin AUC and schedule addition of bevacizumabas well as different ethnic populations The results of arecently completed randomised three arms GynaecologicCancer InterGroup (GCIG) phase II trial ICON 8 mayfurther inform the clinical benefit of dose dense paclitaxeltherapy
This multicentre trial involving 111 centres in the UKSouth Korea Mexico Ireland Australia and New Zealandwith a target population of 1485 patients with stage IC-IV epithelial ovarian cancer or peritoneal or fallopian tubecancer compared two dose-dense arms (i) JGOG-like armcarboplatin AUC 5 plus weekly 80mgm2 paclitaxel and (ii)MITO-7-like arm weekly carboplatin AUC 167 plus weekly80mgm2 paclitaxel to the standard 3-weekly treatment(carboplatin AUC 5 plus 175mgm2 paclitaxel) for stage IC toIV epithelial ovarian cancer The dose-dense arms of MITO-7 and JGOG-3016 as well as the ethnic heterogeneity will befurther addressed
10 Intraperitoneal (IP) Chemotherapy
In addition to dose and scheduling the route of adminis-tration of chemotherapy agents plays an important role inoutcome Intraperitoneal spread is common and likely anearly event in epithelial ovarian cancer hence the deliveryof chemotherapy intraperitoneally in theory would exposethe microcirculation of tumour to higher doses of drug thansystemic administration while limiting systemic toxicityTheideal drug for IP chemotherapy is one that is systemicallyeffective penetrates deep into the inner core of tumour tissueand remains within the peritoneal cavity for a prolongedperiod of time [137ndash139]
Early clinical studies confirmed that indeed the peritonealcavity could be exposed to 10 to 20-fold higher (cisplatin
and carboplatin) drug concentration than when using theintravenous approach and since 1978 this route had beenadopted as a form of therapeutic intervention [137 139]A subsequent phase I trial showed that IP paclitaxel haddose-limiting toxicity in the form of abdominal pain [140]Another phase 1 GOG pilot study administered weekly IPpaclitaxel at an initial dose of 20mgm2 for 16 weeks to33 patients and found that IP paclitaxel at this dose wasfeasible and well tolerated At dose levels 60 to 65mgm2there were significant levels of paclitaxel for a week afterdrug administration suggesting very slow clearance andcontinuous exposure of the peritoneal cavity to active drugconcentrations [132]
Hence this initiated a phase II study [141] that used pacli-taxel intraperitoneally at a dose of 60ndash65mgm2week In thisphase II GOG study 76 patients with small-volume resid-ual disease carcinoma (05 cm or less) involving the ovaryperitoneal or fallopian tube were treated with paclitaxel60mgm2week intraperitoneally for 16 weeks followed bysurgical evaluation in patients without disease progressionThe Gynaecologic Oncology group (GOG) currently definesno visible disease as microscopic disease being the idealsurgical outcome 75 of patients had received prior systemictherapy and 70 received all 16 courses that were planned Of28 patients with microscopic disease at the start of therapy61 achieved a surgically defined complete response whereasonly 1 out of 31 patients with macroscopic disease achieved acomplete response The median time-to-recurrence was 167months with an estimated survival rate at 2 years being 58Treatment was generally well tolerated [141]
Another study looked into the effect of IP paclitaxel asconsolidation therapy in advanced ovarian cancer Twenty-eight patients who had initial residual macroscopic disease(lt1 cm) after primary surgery or interval debulking but hadcomplete pathological response following standard treatmentwith at least 6 cycles of platinum-based chemotherapy regi-men received paclitaxel 60mgm2week intraperitoneally for12ndash16 weeks as consolidation therapy The median time torecurrence was 25 months but overall survival did not differsignificantly when compared with control group submittedto observation only Treatment-related toxicity was mild andtechnical difficulties were observed in 11 of patients [142]
Multicenter randomised phase 3 trials as well as meta-analysis of IP chemotherapy have been performed anddemonstrated that chemotherapy drugs administered intra-peritoneally are superior to intravenous standard regimensin patient with optimally debulked epithelial ovarian cancerThe most impressive data comes from GOG 114 [14] and172 trial [143] In GOG 114 patients received either sixcycles of intravenous paclitaxel 135mgm2 and cisplatin75mgm2 every 3 weeks or intravenous carboplatin (AUC= 9) every 28 days for two cycles followed by six 3-weeklycycles of intravenous paclitaxel 135mgm2 and IP cisplatin100mgm2 [14] whereas in GOG 172 patients received eitherintravenous paclitaxel 135mgm2 followed by intravenouscisplatin 75mgm2 or intravenous paclitaxel 135mgm2 fol-lowed by IP combination of cisplatin 100mgm2 and pacli-taxel 60mgm2 on day 8 Both trials had a combined total
BioMed Research International 15
of 876 women with stage III epithelial ovarian carcinomaoptimally debulked to le1 cm residual tumour [143] Themedian follow-up for GOG 114 [14] was 138 years with GOG172 [143] was 97 years The primary results of the individualtrials reported up to 6-month improvement in median PFSfollowing IP therapy In the combined analysis of the datafrom both trials the data continued to show a 5-monthdifference in favour of IP therapy (25 versus 20 months)which translates into 16 reduction in the hazard ratio forprogression (119901 = 003) In GOG 114 [14] reported in 2001there was only borderline improvement in overall survivalassociated with this regimen (median 63 versus 52 monthsrelative risk 081 119901 = 005)
However in combined analysis in 2013 which was pre-sented at the Society of Gynecologic Oncology AnnualMeeting [144] the overall survival showed an 11-monthimprovement in favour of IP therapy in GOG 114 whereasGOG 172 reported a 16-month survival advantage Amongpatients treated with IP therapy the 5-year survival rateincreased from 18 following completion of 1-2 cycles to 59for patients who completed 5-6 cycles of treatment Howeverthere was increased toxicity observed in the IP arm grade 3-4 leukopenia thrombocytopenia and abdominal pain Only42 of patients in the GOG172 trial [143] completed all sixcycles of planned treatment in the IP arm while 18 ofpatients in GOG 114 trial [14] received fewer than two coursesof IP chemotherapy
Another randomised phase III trial involving patientswith stages II-III epithelial ovarian carcinoma is the GOG252 study with three arms Arm 1-dose-dense intravenouscarboplatin and paclitaxel Arm 2-dose-dense intravenouspaclitaxel and IP carboplatin and Arm 3 consists of 3-weeklyintravenous paclitaxel (day 1) followed by IP cisplatin (day 2)and IP paclitaxel (day 3) regimen All three arms also incor-porate the combination and maintenance of bevacizumabGOG 252 has completed accrual and results are awaited [139]
11 Newer Forms of Paclitaxel
Development of next-generation taxanes has taken place overthe past 40 years aimed at eliminating toxicity improvingefficacy and ease of administration Abraxane is a novelcompound which incorporates paclitaxel into an albuminnanoparticle soluble in saline hence eliminating the needfor Cremophor EL which is responsible for hypersensitivityreactions experienced during paclitaxel infusion [145] Thenanoparticle albumin in nab-paclitaxel is able to bind toglycoprotein gp60 receptor an albumin receptor and activatecaveolin-1 a protein that in human is encoded byCAV-1 geneleading to formation of caveoli hence allowing nab-paclitaxelto migrate across the endothelial cell membrane into theinterstitial space leading to higher intratumoural drug con-centration In addition Abraxane exhibits linear pharma-cokinetics and can therefore be given at a relatively higherdose than standard intravenous paclitaxel leading to a highertherapeutic ratio and heightened efficacy in solid tumoursmainlymetastatic breast cancer [146 147] Nab-paclitaxel hadFDA approval in 2005 for treatment of breast cancer [148]
Nab-paclitaxel has been studied in recurrent ovariancancer As a single agent in phase II 44 patients withrecurrent ovarian cancer were treated with Nab-paclitaxel260mgm2 intravenously for 30 minutes every 3 weeks for6 cycles Ninety-two percent of patients were platinum-sensitive while 89 had had previous exposure to standardtaxane The objective response rate was 64 with 15 patientsachieving complete response and 13 of them had partialresponse Estimated median PFS was 85 months No hyper-sensitivity reactions were observed and there were infrequentcases of grade 4 neutropenia (11) and grade 2-3 neuropathy(13) [149]
Another phase II study by GOG enrolled 51 patients withplatinum- and taxane-resistant recurrent ovarian cancer outof which 47 were evaluable The objective response rate was38 with one patient achieving a complete response and 10patients a partial response The median PFS was 45 monthswhile overall survival rate was 174 months Severe haema-tological and nonhaematological toxicities including neuro-toxicity were uncommon These results are quite impressivegiven the treatment population consisted of patients withvery poor prognosis with a median platinum and taxane freeinterval of 21 days and 70 had their recurrence within 3months of completion of primary treatment [150] Severalother trials of this formulation are in progress
Paclitaxel poliglumex (PPX) also known as Xyotax isanother prodrug a novel conjugate of paclitaxel and 120572-poly-L-glutamic acid which accumulates within tumour tissuedue to increased permeability of the tumour vessels and lackof lymphatic drainage [148 151 152] Paclitaxel poliglumexenhances solubility of paclitaxel allows direct delivery tothe intratumoural microenvironment and allows prolongedexposure to the active drug while minimising systemictoxicities [151] In Phase I dose escalation studies as a singleagent the recommended dose of PPX was 235mgm2 over 10minutes every 3 weeks or 70mgm2 weekly [153] In a PhaseII GOG study of relapsed ovarian cancer a response rate of16 was seen with infrequent serious adverse events grade3 and 4 neutropenia (24 and 20) and grade 3 neuropathy(24) [154] A phase III trial (GOG-0212) on the use of PPXas consolidation ormaintenance therapy in advanced ovariancancer is in progress
DHA-paclitaxel also known as Taxoprexin is a prodrugwhere paclitaxel is covalently conjugated with the naturallyoccurring omega-3 fatty acid docosahexaenoic acid (DHA)a fatty acid that is easily taken up by tumour cells henceincreasing intratumoural concentration of paclitaxel leadingtumour cell apoptosis [155 156] DHA-paclitaxel exhibitslinear pharmacokinetics and lower toxicity and also ease ofadministration when compared to conventional paclitaxeland has demonstrated antineoplastic activity in animal mod-els of cancer as well as in a phase III trial involving metastaticmelanoma [156ndash160] In a recent study on human ovariancancer cells it was found that DHA could reverse paclitaxelresistance by inhibiting P-gp as well as downregulatingthe expression of multidrug resistance associated proteins(MRP) and inhibiting the activity of NF-120581B and p38 MAPKsignalling pathways [161]
16 BioMed Research International
12 Future Directions
A plateau has been reached regarding the benefits associatedwith standard 3-weekly intravenous administration of cyto-toxic chemotherapy in advanced epithelial ovarian cancerThe ongoing battle for a better treatment regimen to delayrelapse promote remission and most importantly improvethe quality of life of patients with advanced epithelial ovariancancer need not to go further than the ability to relook at thechemotherapy agents that are already available in a differentapproach
Novel compounds to date have not yet shown clinicalsuperiority and parent compounds such as paclitaxel con-tinue to surprise us with their feasibility effectiveness andmanageable toxicity profiles Intraperitoneal paclitaxel willrequire further evaluation Better effort in understanding themechanism of action of drugs including the role of dosescheduling and the effect on the immune systemmay providea more cost-effective route to better clinical outcomes
Conflict of Interests
The authors declare no conflict of interests in this work
Acknowledgments
The authors would like to thank the many researchers whohave contributed to our current knowledge of paclitaxelNirmala Kampan is supported by Australian Monash Uni-versity Institute of Graduate Research Scholarship as wellas Universiti Kebangsaan Malaysia Postgraduate ScholarshipAward Mutsa Madondo has received Postgraduate Pub-lication Award from Monash University and MagdalenaPlebanski has been awarded Senior NHMRC Fellowship
References
[1] Australian Institute of Health and Welfare and National Breastand Ovarian Cancer Centre (Australia) Ovarian Cancer inAustralia AnOverview 2010 Cancer Series Australian Instituteof Health and Welfare Canberra Australia 2010
[2] R E Bristow R S Tomacruz D K Armstrong E L Trimbleand F J Montz ldquoSurvival effect of maximal cytoreductivesurgery for advanced ovarian carcinoma during the platinumera a meta-analysisrdquo Journal of Clinical Oncology vol 20 no 5pp 1248ndash1259 2002
[3] ZKempand JA Ledermann ldquoUpdate onfirst-line treatment ofadvanced ovarian carcinomardquo International Journal of WomenrsquosHealth vol 5 no 1 pp 45ndash51 2013
[4] A du Bois H-J Luck W Meier et al ldquoA randomized clinicaltrial of cisplatinpaclitaxel versus carboplatinpaclitaxel as first-line treatment of ovarian cancerrdquo Journal of the National CancerInstitute vol 95 no 17 pp 1320ndash1330 2003
[5] R F Ozols B N Bundy B E Greer et al ldquoPhase III trialof carboplatin and paclitaxel compared with cisplatin andpaclitaxel in patients with optimally resected stage III ovariancancer A Gynecologic Oncology Group studyrdquo Journal ofClinical Oncology vol 21 no 17 pp 3194ndash3200 2003
[6] W P McGuire W J Hoskins M F Brady et al ldquoCyclophos-phamide and cisplatin compared with paclitaxel and cisplatin
in patients with stage III and stage IV ovarian cancerrdquoThe NewEngland Journal of Medicine vol 334 no 1 pp 1ndash6 1996
[7] W P McGuire W J Hoskins M F Brady et al ldquoCyclophos-phamide and cisplatin versus paclitaxel and cisplatin a phase IIIrandomized trial in patients with suboptimal stage IIIIV ovar-ian cancer (from the gynecologic oncology group)rdquo Seminars inOncology vol 23 no 5 supplement 12 pp 40ndash47 1996
[8] M J Piccart K Bertelsen K James et al ldquoRandomized inter-group trial of cisplatin-paclitaxel versus cisplatin-cyclophosph-amide inwomenwith advanced epithelial ovarian cancer three-year resultsrdquo Journal of the National Cancer Institute vol 92 no9 pp 699ndash708 2000
[9] P A Vasey G C Jayson A Gordon et al ldquoPhase III random-ized trial of docetaxel-carboplatin versus paclitaxel-carboplatinas first-line chemotherpy for ovarian carcinomardquo Journal of theNational Cancer Institute vol 96 no 22 pp 1682ndash1691 2004
[10] B Gronlund C Hogdall H H Hansen and S A EngelholmldquoResults of reinduction therapy with paclitaxel and carboplatinin recurrent epithelial ovarian cancerrdquo Gynecologic Oncologyvol 83 no 1 pp 128ndash134 2001
[11] T M Loffler W Freund J Lipke and T-U HausamenldquoSchedule- and dose-intensified paclitaxel as weekly 1-hourinfusion in pretreated solid tumors results of a phase III trialrdquoSeminars in Oncology vol 23 no 6 supplement 16 pp 32ndash341996
[12] D Fennelly C Aghajanian F Shapiro et al ldquoPhase I and phar-macologic study of paclitaxel administered weekly in patientswith relapsed ovarian cancerrdquo Journal of Clinical Oncology vol15 no 1 pp 187ndash192 1997
[13] N R Abu-Rustum C Aghajanian R R Barakat D Fennelly FShapiro and D Spriggs ldquoSalvage weekly paclitaxel in recurrentovarian cancerrdquo Seminars inOncology vol 24 no 5 supplement15 pp S15-62ndashS15-67 1997
[14] M Markman B N Bundy D S Alberts et al ldquoPhase III trialof standard-dose intravenous cisplatin plus paclitaxel versusmoderately high-dose carboplatin followed by intravenouspaclitaxel and intraperitoneal cisplatin in small-volume stageIII ovarian carcinoma an intergroup study of the gynecologiconcology group Southwestern Oncology Group and EasternCooperativeOncologyGrouprdquo Journal of Clinical Oncology vol19 no 4 pp 1001ndash1007 2001
[15] A Kikuchi H Sakamoto and T Yamamoto ldquoWeekly car-boplatin and paclitaxel is safe active and well tolerated inrecurrent ovarian cancer cases of Japanese women previouslytreated with cisplatin-containing multidrug chemotherapyrdquoInternational Journal of Gynecological Cancer vol 15 no 1 pp45ndash49 2005
[16] I Cadron K Leunen F Amant T van Gorp P Nevenand I Vergote ldquoThe lsquoLeuvenrsquo dose-dense paclitaxelcarboplatinregimen in patients with recurrent ovarian cancerrdquo GynecologicOncology vol 106 no 2 pp 354ndash361 2007
[17] S Pignata E Breda G Scambia et al ldquoA phase II studyof weekly carboplatin and paclitaxel as first-line treatment ofelderly patients with advanced ovarian cancer A Multicen-tre Italian Trial in Ovarian cancer (MITO-5) studyrdquo CriticalReviews in OncologyHematology vol 66 no 3 pp 229ndash2362008
[18] T Safra S Shamai J Greenberg et al ldquoWeekly carboplatinwith paclitaxel compared to standard three-weekly treatment inadvanced epithelial ovarian carcinomamdasha retrospective studyrdquoGynecologic Oncology vol 132 no 1 pp 18ndash22 2014
BioMed Research International 17
[19] L J Havrilesky A A Alvarez R A Sayer et al ldquoWeekly low-dose carboplatin and paclitaxel in the treatment of recurrentovarian and peritoneal cancerrdquo Gynecologic Oncology vol 88no 1 pp 51ndash57 2003
[20] M van der BurgW Onstenk I Boere et al ldquoLong-term resultsof a randomised phase III trial of weekly versus three-weeklypaclitaxelplatinum induction therapy followed by standardor extended three-weekly paclitaxelplatinum in Europeanpatients with advanced epithelial ovarian cancerrdquo EuropeanJournal of Cancer vol 50 no 15 pp 2592ndash2601 2014
[21] N Katsumata M Yasuda F Takahashi et al ldquoDose-densepaclitaxel once a week in combination with carboplatin every3 weeks for advanced ovarian cancer a phase 3 open-labelrandomised controlled trialrdquoThe Lancet vol 374 no 9698 pp1331ndash1338 2009
[22] N Katsumata M Yasuda S Isonishi et al ldquoLong-term resultsof dose-dense paclitaxel and carboplatin versus conventionalpaclitaxel and carboplatin for treatment of advanced epithelialovarian fallopian tube or primary peritoneal cancer (JGOG3016) a randomised controlled open-label trialrdquo The LancetOncology vol 14 no 10 pp 1020ndash1026 2013
[23] K Harano F Terauchi N Katsumata et al ldquoQuality-of-lifeoutcomes from a randomized phase III trial of dose-denseweekly paclitaxel and carboplatin compared with conventionalpaclitaxel and carboplatin as a first-line treatment for stage II-IV ovarian cancer Japanese Gynecologic OncologyGroup Trial(JGOG3016)rdquo Annals of Oncology vol 25 no 1 pp 251ndash2572014
[24] J Chan M F Brady R Penson et al ldquoPhase III trial ofevery-3-weeks paclitaxel vs dose dense weekly paclitaxel withcarboplatin +minus bevacizumab in epithelial ovarian peritonealfallopian tube cancer GOG 262 (NCT01167712)rdquo InternationalJournal of Gynecological Cancer vol 23 no 8 supplement 1 pp9ndash10 2013
[25] S Pignata G Scambia D Katsaros et al ldquoCarboplatin pluspaclitaxel once a week versus every 3 weeks in patients withadvanced ovarian cancer (MITO-7) a randomisedmulticentreopen-label phase 3 trialrdquoThe Lancet Oncology vol 15 no 4 pp396ndash405 2014
[26] V Walsh and J Goodman ldquoFrom taxol to Taxol the changingidentities and ownership of an anti-cancer drugrdquo MedicalAnthropology vol 21 no 3-4 pp 307ndash336 2002
[27] R Renneberg ldquoBiotech History yew trees paclitaxel synthesisand fungirdquo Biotechnology Journal vol 2 no 10 pp 1207ndash12092007
[28] J E Liebmann J A Cook C Lipschultz D Teague J Fisherand J B Mitchell ldquoCytotoxic studies of paclitaxel (Taxol) inhuman tumour cell linesrdquo British Journal of Cancer vol 68 no6 pp 1104ndash1109 1993
[29] J J Manfredi and S B Horwitz ldquoTaxol an antimitotic agentwith a newmechanism of actionrdquo Pharmacology andTherapeu-tics vol 25 no 1 pp 83ndash125 1984
[30] D G I Kingston ldquoRecent advances in the chemistry of taxolrdquoJournal of Natural Products vol 63 no 5 pp 726ndash734 2000
[31] D G I Kingston ldquoThe shape of things to come structural andsynthetic studies of taxol and related compoundsrdquo Phytochem-istry vol 68 no 14 pp 1844ndash1854 2007
[32] V Walsh and J Goodman ldquoCancer chemotherapy biodiversitypublic and private property the case of the anti-cancer drugTaxolrdquo Social Science amp Medicine vol 49 no 9 pp 1215ndash12251999
[33] P H Wiernik E L Schwartz J J Strauman J P Dutcher RB Lipton and E Paietta ldquoPhase I clinical and pharmacokineticstudy of taxolrdquo Cancer Research vol 47 no 9 pp 2486ndash24931987
[34] W P McGuire E K Rowinsky N B Rosenhein et alldquoTaxol a unique antineoplastic agent with significant activityin advanced ovarian epithelial neoplasmsrdquo Annals of InternalMedicine vol 111 no 4 pp 273ndash279 1989
[35] ldquoDiscovery and development of taxolrdquo in Taxol Science andApplications M W M E Suffness Ed pp 3ndash25 CRC PressBoca Raton Fla USA 1995
[36] M J Piccart and F Cardoso ldquoProgress in systemic therapy forbreast cancer an overview and perspectivesrdquo European Journalof Cancer Supplement vol 1 no 2 pp 56ndash69 2003
[37] P Bonomi K B Kim and J Kugler ldquoComparison of survival forstage IIIB versus stage IV non-small cell lung cancer (NSCLC)patients with etoposide-cisplatin versus taxol-cisplatin an East-ern Cooperative Oncology Group (ECOG) trialrdquo in Proceedingsof the American Society of Clinical Oncology vol 16 p 454a1997
[38] D Guenard F Gueritte-Voegelein J Dubois and P PotierldquoStructure-activity relationships of Taxol and Taxotere ana-loguesrdquo Journal of the National Cancer Institute Monographsno 15 pp 79ndash82 1993
[39] D G I Kingston ldquoTaxol the chemistry and structure-activityrelationships of a novel anticancer agentrdquo Trends in Biotechnol-ogy vol 12 no 6 pp 222ndash227 1994
[40] E K Rowinsky and R C Donehower ldquoPaclitaxel (taxol)rdquo TheNew England Journal of Medicine vol 332 no 15 pp 1004ndash10141995
[41] J Parness and S B Horwitz ldquoTaxol binds to polymerizedtubulin in vitrordquo Journal of Cell Biology vol 91 no 2 pp 479ndash487 1981
[42] A Dammermann A Desai and K Oegema ldquoTheminus end insightrdquo Current Biology vol 13 no 15 pp R614ndashR624 2003
[43] CWiese and Y Zheng ldquoMicrotubule nucleation 120574-tubulin andbeyondrdquo Journal of Cell Science vol 119 no 20 pp 4143ndash41532006
[44] A Ganguly H Yang and F Cabral ldquoPaclitaxel-dependent celllines reveal a novel drug activityrdquo Molecular Cancer Therapeu-tics vol 9 no 11 pp 2914ndash2923 2010
[45] P B Schiff and S B Horwitz ldquoTaxol stabilizes microtubules inmouse fibroblast cellsrdquo Proceedings of the National Academy ofSciences of the United States of America vol 77 no 3 pp 1561ndash1565 1980
[46] P B Schiff J Fant and S B Horwitz ldquoPromotion of micro-tubule assembly in vitro by Taxolrdquo Nature vol 277 no 5698pp 665ndash667 1979
[47] D Zhang R Yang S Wang and Z Dong ldquoPaclitaxel new usesfor an old drugrdquoDrug Design Development andTherapy vol 8pp 279ndash284 2014
[48] S Rao G A Orr A G Chaudhary D G I Kingston and SB Horwitz ldquoCharacterization of the taxol binding site on themicrotubule 2-(m-Azidobenzoyl)taxol photolabels a peptide(amino acids 217-231) of beta-tubulinrdquoThe Journal of BiologicalChemistry vol 270 no 35 pp 20235ndash20238 1995
[49] F Wang Y Cao W Zhao H Liu Z Fu and R Han ldquoTaxolinhibits melanoma metastases through apoptosis inductionangiogenesis inhibition and restoration of E-cadherin andnm23 expressionrdquo Journal of Pharmacological Sciences vol 93no 2 pp 197ndash203 2003
18 BioMed Research International
[50] A Sevko V Kremer C Falk et al ldquoApplication of paclitaxel inlow non-cytotoxic doses supports vaccination with melanomaantigens in normal micerdquo Journal of Immunotoxicology vol 9no 3 pp 275ndash281 2012
[51] T Kreis and R Vale Guidebook to the Cytoskeletal and MotorProteins Oxford University Press Oxford UK 2nd edition1999
[52] P Giannakakou D L Sackett Y-K Kang et al ldquoPaclitaxel-resistant human ovarian cancer cells have mutant 120573-tubulinsthat exhibit impaired paclitaxel-driven polymerizationrdquo TheJournal of Biological Chemistry vol 272 no 27 pp 17118ndash171251997
[53] E Rakovitch W Mellado E J Hall T K Pandita S Sawantand C R Geard ldquoPaclitaxel sensitivity correlates with p53status and DNA fragmentation but not G2M accumulationrdquoInternational Journal of Radiation Oncology Biology Physics vol44 no 5 pp 1119ndash1124 1999
[54] S W Lowe S Bodis A McClatchey et al ldquop53 status and theefficacy of cancer therapy in vivordquo Science vol 266 no 5186 pp807ndash810 1994
[55] C C Zhang J-M Yang E White M Murphy A Levine andW N Hait ldquoThe role of MAP4 expression in the sensitivity topaclitaxel and resistance to vinca alkaloids in p53 mutant cellsrdquoOncogene vol 16 no 12 pp 1617ndash1624 1998
[56] K Fukasawa T Choi R Kuriyama S Rulong and G F VandeWoude ldquoAbnormal centrosome amplification in the absence ofp53rdquo Science vol 271 no 5256 pp 1744ndash1747 1996
[57] T-H Wang Y-H Chan C-W Chen et al ldquoPaclitaxel (Taxol)upregulates expression of functional interleukin-6 in humanovarian cancer cells through multiple signaling pathwaysrdquoOncogene vol 25 no 35 pp 4857ndash4866 2006
[58] E Yakirevich E Sabo I Naroditsky Y Sova O Lavie andM B Resnick ldquoMultidrug resistance-related phenotype andapoptosis-related protein expression in ovarian serous carcino-masrdquo Gynecologic Oncology vol 100 no 1 pp 152ndash159 2006
[59] G Szakacs J K Paterson J A Ludwig C Booth-Genthe andM M Gottesman ldquoTargeting multidrug resistance in cancerrdquoNature Reviews Drug Discovery vol 5 no 3 pp 219ndash234 2006
[60] L W Pfannenstiel S S K Lam L A Emens E M Jaffeeand T D Armstrong ldquoPaclitaxel enhances early dendritic cellmaturation and function through TLR4 signaling in micerdquoCellular Immunology vol 263 no 1 pp 79ndash87 2010
[61] N Klauber S Parangi E Flynn E Hamel and R J DrsquoAmatoldquoInhibition of angiogenesis and breast cancer in mice by themicrotubule inhibitors 2-methoxyestradiol and Taxolrdquo CancerResearch vol 57 no 1 pp 81ndash86 1997
[62] D Belotti V Vergani T Drudis et al ldquoThe microtubule-affecting drug paclitaxel has antiangiogenic activityrdquo ClinicalCancer Research vol 2 no 11 pp 1843ndash1849 1996
[63] D H Lau L Xue L J Young P A Burke and A T CheungldquoPaclitaxel (Taxol) an inhibitor of angiogenesis in a highlyvascularized transgenic breast cancerrdquo Cancer Biotherapy andRadiopharmaceuticals vol 14 no 1 pp 31ndash36 1999
[64] X Jiang ldquoHarnessing the immune system for the treatment ofbreast cancerrdquo Journal of Zhejiang University Science B vol 15no 1 pp 1ndash15 2014
[65] A Gadducci D Katsaros P Zola et al ldquoWeekly low-dosepaclitaxel as maintenance treatment in patients with advancedovarian cancer who had microscopic residual disease atsecond-look surgery after 6 cycles of paclitaxelplatinum-basedchemotherapy Results of an open noncomparative phase 2
multicenter italian study (after-6 protocol 2)rdquo InternationalJournal of Gynecological Cancer vol 19 no 4 pp 615ndash619 2009
[66] R S Bhatt J Merchan R Parker et al ldquoA phase 2 pilot trial oflow-dose continuous infusion or lsquometronomicrsquo paclitaxel andoral celecoxib in patients with metastatic melanomardquo Cancervol 116 no 7 pp 1751ndash1756 2010
[67] M Caballero J J Grau J L Blanch et al ldquoSerum vascularendothelial growth factor as a predictive factor in metronomic(weekly) paclitaxel treatment for advanced head and neckcancerrdquo Archives of OtolaryngologymdashHead and Neck Surgeryvol 133 no 11 pp 1143ndash1148 2007
[68] J Alexandre Y Hu W Lu H Pelicano and P Huang ldquoNovelaction of paclitaxel against cancer cells bystander effect medi-ated by reactive oxygen speciesrdquo Cancer Research vol 67 no 8pp 3512ndash3517 2007
[69] T Hadzic N Aykin-Burns Y Zhu et al ldquoPaclitaxel combinedwith inhibitors of glucose and hydroperoxide metabolismenhances breast cancer cell killing viaH
2O2-mediated oxidative
stressrdquo Free Radical Biology and Medicine vol 48 no 8 pp1024ndash1033 2010
[70] C A Sherman-Baust K G Becker W H Wood III Y Zhangand P J Morin ldquoGene expression and pathway analysis of ovar-ian cancer cells selected for resistance to cisplatin paclitaxel ordoxorubicinrdquo Journal of Ovarian Research vol 4 no 1 article21 2011
[71] R Agarwal and S B Kaye ldquoOvarian cancer strategies for over-coming resistance to chemotherapyrdquo Nature Reviews Cancervol 3 no 7 pp 502ndash516 2003
[72] T Acker and K H Plate ldquoRole of hypoxia in tumorangiogenesismdashmolecular and cellular angiogenic crosstalkrdquoCell and Tissue Research vol 314 no 1 pp 145ndash155 2003
[73] M Hockel and P Vaupel ldquoBiological consequences of tumorhypoxiardquo Seminars in Oncology vol 28 supplement 8 no 2 pp36ndash41 2001
[74] L Huang Q-H Zhang Q-L Ao H Xing Y-P Lu and DMa ldquoEffect of hypoxia on the chemotherapeutic sensitivity ofhuman ovarian cancer cells to paclitaxel and its mechanismrdquoZhonghua Zhong Liu Za Zhi vol 29 no 2 pp 96ndash100 2007
[75] N Rohwer and T Cramer ldquoHypoxia-mediated drug resistancenovel insights on the functional interaction of HIFs and celldeath pathwaysrdquoDrug Resistance Updates vol 14 no 3 pp 191ndash201 2011
[76] B B Aggarwal R V Vijayalekshmi and B Sung ldquoTargetinginflammatory pathways for prevention and therapy of cancershort-term friend long-term foerdquo Clinical Cancer Research vol15 no 2 pp 425ndash430 2009
[77] Z Duan R Foster D A Bell et al ldquoSignal transducersand activators of transcription 3 pathway activation in drug-resistant ovarian cancerrdquo Clinical Cancer Research vol 12 no17 pp 5055ndash5063 2006
[78] H-J Kuh S H Jang M G Wientjes J R Weaver and J L-SAu ldquoDeterminants of paclitaxel penetration and accumulationin human solid tumorrdquo Journal of Pharmacology and Experi-mental Therapeutics vol 290 no 2 pp 871ndash880 1999
[79] S Arao H Suwa M Mandai et al ldquoHypoxia-mediated drugresistance novel insights on the functional interaction of HIFsand cell death pathwaysrdquo Cancer Research vol 54 no 5 pp1355ndash1359 1994
[80] S E Johnatty J Beesley B Gao et al ldquoABCB1 (MDR1)polymorphisms and ovarian cancer progression and survivala comprehensive analysis from the Ovarian Cancer Association
BioMed Research International 19
Consortium and the Cancer GenomeAtlasrdquoGynecologic Oncol-ogy vol 131 no 1 pp 8ndash14 2013
[81] X Yang A K Iyer A Singh et al ldquoCluster of differentiation44 targeted hyaluronic acid based nanoparticles for MDR1siRNA delivery to overcome drug resistance in ovarian cancerrdquoPharmaceutical Research 2014
[82] D A Zajchowski B Y Karlan and L K Shawver ldquoTreatment-related protein biomarker expression differs between primaryand recurrent ovarian carcinomasrdquoMolecular CancerTherapeu-tics vol 11 no 2 pp 492ndash502 2012
[83] MM Gottesman J Ludwig D Xia and G Szakacs ldquoDefeatingdrug resistance in cancerrdquoDiscovery Medicine vol 6 no 31 pp18ndash23 2006
[84] S Mozzetti C Ferlini P Concolino et al ldquoClass III 120573-tubulin overexpression is a prominent mechanism of paclitaxelresistance in ovarian cancer patientsrdquo Clinical Cancer Researchvol 11 no 1 pp 298ndash305 2005
[85] M Kavallaris D Y S Kuo C A Burkhart et al ldquoTaxol-resistant epithelial ovarian tumors are associated with alteredexpression of specific beta-tubulin isotypesrdquo Journal of ClinicalInvestigation vol 100 no 5 pp 1282ndash1293 1997
[86] G A Orr P Verdier-Pinard H McDaid and S B HorwitzldquoMechanisms of Taxol resistance related to microtubulesrdquoOncogene vol 22 no 47 pp 7280ndash7295 2003
[87] C Ferlini L Cicchillitti G Raspaglio et al ldquoPaclitaxel directlybinds to Bcl-2 and functionally mimics activity of Nur77rdquoCancer Research vol 69 no 17 pp 6906ndash6914 2009
[88] E Mechetner A Kyshtoobayeva S Zonis et al ldquoLevels ofmultidrug resistance (MDR1) P-glycoprotein expression byhuman breast cancer correlate with in vitro resistance to taxoland doxorubicinrdquo Clinical Cancer Research vol 4 no 2 pp389ndash398 1998
[89] J S Lagas C W N Damen R A B VanWaterschoot D IusufJ H Beijnen and A H Schinkel ldquoP-glycoprotein multidrug-resistance associated protein 2 Cyp3a and carboxylesteraseaffect the oral availability and metabolism of vinorelbinerdquoMolecular Pharmacology vol 82 no 4 pp 636ndash644 2012
[90] M T Huizing J B Vermorken H Rosing et al ldquoPharmacoki-netics of paclitaxel and three major metabolites in patients withadvanced breast carcinoma refractory to anthracycline therapytreated with a 3-hour paclitaxel infusion a European CancerCentre (ECC) trialrdquo Annals of Oncology vol 6 no 7 pp 699ndash704 1995
[91] R Panchagnula ldquoPharmaceutical aspects of paclitaxelrdquo Interna-tional Journal of Pharmaceutics vol 172 no 1-2 pp 1ndash15 1998
[92] S H Jang M G Wientjes and J L-S Au ldquoDeterminants ofpaclitaxel uptake accumulation and retention in solid tumorsrdquoInvestigational New Drugs vol 19 no 2 pp 113ndash123 2001
[93] D S Sonnichsen andM V Relling ldquoClinical pharmacokineticsof paclitaxelrdquo Clinical Pharmacokinetics vol 27 no 4 pp 256ndash269 1994
[94] T Ohtsu Y Sasaki T Tamura et al ldquoClinical pharmacokineticsand pharmacodynamics of paclitaxel a 3-hour infusion versusa 24-hour infusionrdquo Clinical Cancer Research vol 1 no 6 pp599ndash606 1995
[95] M Czejka J Schueller H Schnait B Springer and I EderldquoClinical pharmacokinetics andmetabolism of paclitaxel after athree-hour infusion comparison of two preparationsrdquo Journalof Oncology Pharmacy Practice vol 9 no 4 pp 129ndash136 2003
[96] J Rizzo C Riley D VonHoff J Kuhn J Phillips and T BrownldquoAnalysis of anticancer drugs in biological fluids determination
of taxol with application to clinical pharmacokineticsrdquo Journalof Pharmaceutical and Biomedical Analysis vol 8 no 2 pp 159ndash164 1990
[97] V A de Weger J H Beijnen and J H M Schellens ldquoCel-lular and clinical pharmacology of the taxanes docetaxel andpaclitaxelmdasha reviewrdquoAnti-Cancer Drugs vol 25 no 5 pp 488ndash494 2014
[98] S Kumar H Mahdi C Bryant J P Shah G Garg andA Munkarah ldquoClinical trials and progress with paclitaxel inovarian cancerrdquo International Journal of Womenrsquos Health vol 2no 1 pp 411ndash427 2010
[99] B Huang J Zhao J C Unkeless Z H Feng and H XiongldquoTLR signaling by tumor and immune cells a double-edgedswordrdquo Oncogene vol 27 no 2 pp 218ndash224 2008
[100] R A Jibodh J S Lagas B Nuijen J H Beijnen and J HM Schellens ldquoTaxanes old drugs new oral formulationsrdquoEuropean Journal of Pharmacology vol 717 no 1ndash3 pp 40ndash462013
[101] A Javeed M Ashraf A Riaz A Ghafoor S Afzal and M MMukhtar ldquoPaclitaxel and immune systemrdquo European Journal ofPharmaceutical Sciences vol 38 no 4 pp 283ndash290 2009
[102] L Bracci G Schiavoni A Sistigu and F Belardelli ldquoImmune-based mechanisms of cytotoxic chemotherapy implications forthe design of novel and rationale-based combined treatmentsagainst cancerrdquo Cell Death and Differentiation vol 21 no 1 pp15ndash25 2014
[103] C A Byrd-Leifer E F Block K Takeda S Akira and A DingldquoThe role of MyD88 and TLR4 in the LPS-mimetic activity ofTaxolrdquo European Journal of Immunology vol 31 no 8 pp 2448ndash2457 2001
[104] A-C Wang Y-B Ma F-X Wu et al ldquoTLR4 induces tumorgrowth and inhibits paclitaxel activity in MyD88-positivehuman ovarian carcinoma in vitrordquo Oncology Letters vol 7 no3 pp 871ndash877 2014
[105] Y Zhu N Liu S D Xiong Y J Zheng and Y W ChuldquoCD4+Foxp3+ regulatory T-cell impairment by paclitaxel isindependent of toll-like receptor 4rdquo Scandinavian Journal ofImmunology vol 73 no 4 pp 301ndash308 2011
[106] M Kubo T Morisaki K Matsumoto et al ldquoPaclitaxel probablyenhances cytotoxicity of natural killer cells against breastcarcinoma cells by increasing perforin productionrdquo CancerImmunology Immunotherapy vol 54 no 5 pp 468ndash476 2005
[107] L Markasz G Stuber B Vanherberghen et al ldquoEffect of fre-quently used chemotherapeutic drugs on the cytotoxic activityof human natural killer cellsrdquo Molecular Cancer Therapeuticsvol 6 no 2 pp 644ndash654 2007
[108] T Sako N Burioka K Yasuda et al ldquoCellular immune profile inpatients with non-small cell lung cancer after weekly paclitaxeltherapyrdquo Acta Oncologica vol 43 no 1 pp 15ndash19 2004
[109] R Kaneno G V Shurin I L Tourkova and M R ShurinldquoChemomodulation of human dendritic cell function by anti-neoplastic agents in low noncytotoxic concentrationsrdquo Journalof Translational Medicine vol 7 article 58 2009
[110] TMichels G V ShurinHNaiditch A Sevko VUmansky andM R Shurin ldquoPaclitaxel promotes differentiation of myeloid-derived suppressor cells into dendritic cells in vitro in a TLR4-independent mannerrdquo Journal of Immunotoxicology vol 9 no3 pp 292ndash300 2012
[111] R A Kemp and F Ronchese ldquoTumor-specific Tc1 but not Tc2cells deliver protective antitumor immunityrdquo The Journal ofImmunology vol 167 no 11 pp 6497ndash6502 2001
20 BioMed Research International
[112] A Y Rudensky ldquoRegulatory T cells and Foxp3rdquo ImmunologicalReviews vol 241 no 1 pp 260ndash268 2011
[113] EM Shevach ldquoCD4+CD25+ suppressor T cellsmore questionsthan answersrdquo Nature Reviews Immunology vol 2 no 6 pp389ndash400 2002
[114] S Sakaguchi T Yamaguchi T Nomura and M Ono ldquoRegu-latory T cells and immune tolerancerdquo Cell vol 133 no 5 pp775ndash787 2008
[115] H Nishikawa and S Sakaguchi ldquoRegulatory T cells in tumorimmunityrdquo International Journal of Cancer vol 127 no 4 pp759ndash767 2010
[116] W Zou ldquoRegulatory T cells tumour immunity and immuno-therapyrdquoNature Reviews Immunology vol 6 no 4 pp 295ndash3072006
[117] A Fialova S Partlova L Sojka et al ldquoDynamics of T-cell infil-tration during the course of ovarian cancer The gradual shiftfrom aTh17 effector cell response to a predominant infiltrationby regulatory T-cellsrdquo International Journal of Cancer vol 132no 5 pp 1070ndash1079 2013
[118] A E Albers R L Ferris G G Kim K Chikamatsu A BDeLeo and T L Whiteside ldquoImmune responses to p53 inpatients with cancer enrichment in tetramer+ p53 peptide-specific T cells and regulatory T cells at tumor sitesrdquo CancerImmunology Immunotherapy vol 54 no 11 pp 1072ndash10812005
[119] N Liu Y Zheng Y Zhu S Xiong andYChu ldquoSelective impair-ment of CD4 + CD25 + Foxp3 + regulatory T cells by paclitaxelis explained by Bcl-2Bax mediated apoptosisrdquo InternationalImmunopharmacology vol 11 no 2 pp 212ndash219 2011
[120] X Wu Q-M Feng Y Wang J Shi H-L Ge and W DildquoThe immunologic aspects in advanced ovarian cancer patientstreated with paclitaxel and carboplatin chemotherapyrdquo CancerImmunology Immunotherapy vol 59 no 2 pp 279ndash291 2010
[121] A P Vicari R Luu N Zhang et al ldquoPaclitaxel reducesregulatoryT cell numbers and inhibitory function and enhancesthe anti-tumor effects of the TLR9 agonist PF-3512676 in themouserdquo Cancer Immunology Immunotherapy vol 58 no 4 pp615ndash628 2009
[122] L Zhang K Dermawan M Jin et al ldquoDifferential impairmentof regulatory T cells rather than effector T cells by paclitaxel-based chemotherapyrdquo Clinical Immunology vol 129 no 2 pp219ndash229 2008
[123] Y Tabuchi J Matsuoka M Gunduz et al ldquoResistance topaclitaxel therapy is related with Bcl-2 expression through anestrogen receptor mediated pathway in breast cancerrdquo Interna-tional Journal of Oncology vol 34 no 2 pp 313ndash319 2009
[124] N Obermajer R Muthuswamy K Odunsi R P Edwards andP Kalinski ldquoPGE
2-induced CXCL12 production and CXCR4
expression controls the accumulation of human MDSCs inovarian cancer environmentrdquo Cancer Research vol 71 no 24pp 7463ndash7470 2011
[125] Q M Feng W Di and X Wu ldquoImmune reconstitution inadvanced ovarian cancer patients undergoing first line chemo-therapyrdquo Xi Bao Yu Fen Zi Mian Yi Xue Za Zhi vol 25 no 11pp 1023ndash1025 2009
[126] A D Seidman D Hochhauser M Gollub et al ldquoNinety-six-hour paclitaxel infusion after progression during short taxaneexposure a phase II pharmacokinetic and pharmacodynamicstudy in metastatic breast cancerrdquo Journal of Clinical Oncologyvol 14 no 6 pp 1877ndash1884 1996
[127] D R Spriggs M F Brady L Vaccarello et al ldquoPhase IIIrandomized trial of intravenous cisplatin plus a 24- or 96-hour
infusion of paclitaxel in epithelial ovarian cancer a gynecologiconcology group studyrdquo Journal of Clinical Oncology vol 25 no28 pp 4466ndash4471 2007
[128] G A Omura M F Brady K Y Look et al ldquoPhase III trial ofpaclitaxel at two dose levels the higher dose accompanied byfilgrastim at two dose levels in platinum-pretreated epithelialovarian cancer an intergroup studyrdquo Journal of Clinical Oncol-ogy vol 21 no 15 pp 2843ndash2848 2003
[129] R Simon and L Norton ldquoThe Norton-Simon hypothesisdesigning more effective and less toxic chemotherapeutic reg-imensrdquoNature Clinical Practice Oncology vol 3 no 8 pp 406ndash407 2006
[130] A Kumar P Hoskins and A Tinker ldquoDose-dense paclitaxel inadvanced ovarian cancerrdquo Clinical Oncology vol 27 no 1 pp40ndash47 2015
[131] P Marchetti S Urien G A Cappellini G Ronzino and CFicorella ldquoWeekly administration of paclitaxel theoretical andclinical basisrdquoCritical Reviews in OncologyHematology vol 44supplement pp S3ndashS13 2002
[132] P Francis E Rowinsky J Schneider T Hakes W Hoskinsand M Markman ldquoPhase I feasibility and pharmacologic studyof weekly intraperitoneal paclitaxel A Gynecologic OncologyGroup pilot studyrdquo Journal of Clinical Oncology vol 13 no 12pp 2961ndash2967 1995
[133] H Thomas and P Rosenberg ldquoRole of weekly paclitaxel inthe treatment of advanced ovarian cancerrdquo Critical Reviews inOncologyHematology vol 44 supplement pp S43ndashS51 2002
[134] M Markman J Markman K Webster et al ldquoDuration ofresponse to second-line platinum-based chemotherapy forovarian cancer implications for patient management and clini-cal trial designrdquo Journal of Clinical Oncology vol 22 no 15 pp3120ndash3125 2004
[135] P H OrsquoDonnell M Eileen Dolan E Gamazon et al ldquoPopu-lation differences in platinum toxicity as a means to identifynovel genetic susceptibility variantsrdquo Pharmacogenetics andGenomics vol 20 no 5 pp 327ndash337 2010
[136] M J Millward M J Boyer M Lehnert et al ldquoDocetaxel andcarboplatin is an active regimen in advanced non-small-celllung cancer a phase II study in Caucasian and Asian patientsrdquoAnnals of Oncology vol 14 no 3 pp 449ndash454 2003
[137] M Markman ldquoIntraperitoneal therapy of ovarian cancerrdquoOncologist vol 1 no 1-2 pp 18ndash21 1996
[138] M Markman and J L Walker ldquoIntraperitoneal chemotherapyof ovarian cancer a review with a focus on practical aspects oftreatmentrdquo Journal of Clinical Oncology vol 24 no 6 pp 988ndash994 2006
[139] K Fujiwara S Nagao E Aotani and K Hasegawa ldquoPrincipleand evolving role of intraperitoneal chemotherapy in ovariancancerrdquo Expert Opinion on Pharmacotherapy vol 14 no 13 pp1797ndash1806 2013
[140] M Markman E Rowinsky T Hakes et al ldquoPhase I trialof intraperitoneal taxol a gynecoloic oncology group studyrdquoJournal of Clinical Oncology vol 10 no 9 pp 1485ndash1491 1992
[141] M Markman M F Brady N M Spirtos P Hanjani and S CRubin ldquoPhase II trial of intraperitoneal paclitaxel in carcinomaof the ovary tube and peritoneum a gynecologic oncologygroup studyrdquo Journal of Clinical Oncology vol 16 no 8 pp2620ndash2624 1998
[142] P B Panici I Palaia M Graziano F Bellati N Manci and RAngioli ldquoIntraperitoneal paclitaxel as consolidation treatmentin ovarian cancer patients a case control studyrdquo Oncology vol78 no 1 pp 20ndash25 2010
BioMed Research International 21
[143] D K Armstrong B Bundy L Wenzel et al ldquoIntraperitonealcisplatin and paclitaxel in ovarian cancerrdquo The New EnglandJournal of Medicine vol 354 no 1 pp 34ndash43 2006
[144] D Tewari J Java and R Salani ldquoLong-term survival advantageof intraperitoneal chemotherapy treatment in advanced ovariancancer an analysis of a Gynecologic Oncology Group ancillarydata studyrdquo in Proceedings of the 2013 Society of GynecologicOncology Annual Meeting on Womenrsquos Cancer (GOG114172Abstract) Los Angeles Calif USA 2013
[145] D A Yardley ldquonab-paclitaxel mechanisms of action and deliv-eryrdquo Journal of Controlled Release vol 170 no 3 pp 365ndash3722013
[146] M Ando K Yonemori N Katsumata et al ldquoPhase I and phar-macokinetic study of nab-paclitaxel nanoparticle albumin-bound paclitaxel administeredweekly to Japanese patients withsolid tumors and metastatic breast cancerrdquo Cancer Chemother-apy and Pharmacology vol 69 no 2 pp 457ndash465 2012
[147] N Desai V Trieu Z Yao et al ldquoIncreased antitumor activityintratumor paclitaxel concentrations and endothelial cell trans-port of cremophor-free albumin-bound paclitaxel ABI-007compared with cremophor-based paclitaxelrdquo Clinical CancerResearch vol 12 no 4 pp 1317ndash1324 2006
[148] J A Yared and K H R Tkaczuk ldquoUpdate on taxane devel-opment new analogs and new formulationsrdquo Drug DesignDevelopment andTherapy vol 6 pp 371ndash384 2012
[149] M G Teneriello P C Tseng M Crozier et al ldquoPhase IIevaluation of nanoparticle albumin-bound paclitaxel in plati-num-sensitive patients with recurrent ovarian peritoneal orfallopian tube cancerrdquo Journal of Clinical Oncology vol 27 no9 pp 1426ndash1431 2009
[150] R L Coleman W E Brady D S McMeekin et al ldquoA phase IIevaluation of nanoparticle albumin-bound (nab) paclitaxel inthe treatment of recurrent or persistent platinum-resistant ovar-ian fallopian tube or primary peritoneal cancer a GynecologicOncology Group Studyrdquo Gynecologic Oncology vol 122 no 1pp 111ndash115 2011
[151] J W Singer ldquoPaclitaxel poliglumex (XYOTAX CT-2103) amacromolecular taxanerdquo Journal of Controlled Release vol 109no 1ndash3 pp 120ndash126 2005
[152] C Li D-F Yu R A Newman et al ldquoComplete regressionof well-established tumors using a novel water-soluble poly(L-glutamic acid)-paclitaxel conjugaterdquo Cancer Research vol 58no 11 pp 2404ndash2409 1998
[153] M Mita A Mita J Sarantopoulos et al ldquoPhase I study ofpaclitaxel poliglumex administered weekly for patients withadvanced solid malignanciesrdquo Cancer Chemotherapy and Phar-macology vol 64 no 2 pp 287ndash295 2009
[154] P Sabbatini M W Sill D OrsquoMalley L Adler and A ASecord ldquoA phase II trial of paclitaxel poliglumex in recurrentor persistent ovarian or primary peritoneal cancer (EOC) agynecologic oncology group studyrdquo Gynecologic Oncology vol111 no 3 pp 455ndash460 2008
[155] M O Bradley C S Swindell F H Anthony et al ldquoTumortargeting by conjugation of DHA to paclitaxelrdquo Journal ofControlled Release vol 74 no 1ndash3 pp 233ndash236 2001
[156] M O Bradley N L Webb F H Anthony et al ldquoTumortargeting by covalent conjugation of a natural fatty acid topaclitaxelrdquo Clinical Cancer Research vol 7 no 10 pp 3229ndash3238 2001
[157] A C Wolff R C Donehower M K Carducci et al ldquoPhaseI study of docosahexaenoic acid-paclitaxel a taxane-fatty acid
conjugate with a unique pharmacology and toxicity profilerdquoClinical Cancer Research vol 9 no 10 part 1 pp 3589ndash35972003
[158] A Sparreboom A C Wolff J Verweij et al ldquoDispositionof docosahexaenoic acid-paclitaxel a novel taxane in bloodin vitro and clinical pharmacokinetic studiesrdquo Clinical CancerResearch vol 9 no 1 pp 151ndash159 2003
[159] P M Fracasso J Picus J D Wildi et al ldquoPhase 1 and phar-macokinetic study of weekly docosahexaenoic acid-paclitaxelTaxoprexin in resistant solid tumor malignanciesrdquo CancerChemotherapy and Pharmacology vol 63 no 3 pp 451ndash4582009
[160] A Y Bedikian R C DeConti R Conry et al ldquoPhase 3 study ofdocosahexaenoic acid-paclitaxel versus dacarbazine in patientswith metastatic malignant melanomardquo Annals of Oncology vol22 no 4 pp 787ndash793 2011
[161] Y-N Wu S-L Wang Y-C Wang et al ldquoReversal effect ofdocosahexaenoic acid on taxol resistance in human ovarian car-cinoma A2780T cellsrdquo Obstetrics amp Gynecology InternationalJournal vol 1 no 3 Article ID 00018 2014
Submit your manuscripts athttpwwwhindawicom
PainResearch and TreatmentHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom
Volume 2014
ToxinsJournal of
VaccinesJournal of
Hindawi Publishing Corporation httpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
AntibioticsInternational Journal of
ToxicologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
StrokeResearch and TreatmentHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Drug DeliveryJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Advances in Pharmacological Sciences
Tropical MedicineJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Medicinal ChemistryInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
AddictionJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
Emergency Medicine InternationalHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Autoimmune Diseases
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Anesthesiology Research and Practice
ScientificaHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Pharmaceutics
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of

6 BioMed Research International
hypoxic and acidic state This hypoxic adaptation promotestumour proliferation dissemination and progression of dis-ease [73] and also reduces chemosensitivity [74]
Hypoxia-induced chemoresistance occurs due to geno-mic instability Oxygen depletion induces proteomic andgenomic changes that activates the level of p53 inhibits apop-tosis promotes angiogenesis (angiogenic molecules such asvascular endothelial growth factor [VEGF] and angiogenin)upregulates growth factors (platelet-derived growth factor[PDGF] transforming growth factor-beta and insulin-likegrowth factor [IGF]) and induces anaerobic metabolism andglycolysis (glycolytic enzymes glucose transporters) leadingto reduction in potential for cell cycle arrest and cellulardifferentiationwhich prevent tumour cell death [74]Hypoxiacan induce either p-53-dependent (involving Apaf-1 andcaspase-9 effector pathways) or p53-independent (involvinghypoxic-inducible factor 1 [HIF-1] and Bcl-2 family genespathways) apoptosis in both normal and tumour cells HIF-1 is a common transcription factor consisting of HIF-1120572 and HIF-1120573 subunits which controls hypoxic-induciblegenes and the concentration of HIF-1 protein increasedexponentially in the presence of hypoxic environment Lossof apoptotic potential of tumour cells mediated by hypoxicenvironment and HIF-1 which arrest cell cycle at G0G1reduces chemosensitivity to chemotherapeutic agents includ-ing paclitaxel [70 75]
Other transcriptional factors which are activated byhypoxia are nuclear factor kappa B (NF-120581B) and STAT3 also known as proinflammatory transcriptional factorsNF-120581B and STAT 3 regulate multiple gene products whichare involved in inflammation angiogenesis cell survivalproliferation and metastasis Paclitaxel which mediates itscytotoxic action via NF-120581B pathway is vulnerable to developresistance in the presence of hypoxic tumour microen-vironment with activation of NF-120581B transcription factorwhich induces serine phosphorylation and also regulatesBCL-2 an antiapoptotic protein preventing cell death andpromoting tumorigenesis [76] Inhibition of activated STAT3 found overexpressed in most paclitaxel-resistant ovariancancer cells has resulted in reduction in paclitaxel resistanceHowever further research is required to determine the exactmechanism [77]
Intracellular drug concentration is important for effectivecytotoxic activity of paclitaxel Drug resistance may beattributed to either reduced accumulation of drug withinovarian tumours or increased efflux of drug from tumourcells [78] Alteration in pharmacokinetic of paclitaxel eitherattributed by the drug itself such as lower concentration ofdrug administered shorter duration of drug exposure highfirst pass metabolism increased hepatic or renal clearanceinadequate binding to tubulinsmicrotubules or othermacro-molecules or presence of higher tumour density or vascular-ity may result in reduced accumulation of intratumoral drugconcentration [71]
Drug efflux is the most common mechanism for chemo-resistance observed in paclitaxel-treated cancer cells Drugefflux from cancer cells is mediated by ATP-binding cassette(ABC) transporters such as P-glycoprotein (P-gp) P-gp alsoknown as ABCB1 or multidrug-resistance associated-protein
(MRP) a transmembrane protein encoded by MDR1 geneplays a role as an efflux pump which is crucial for occurrenceof many cellular processes that require transfer of substratesacross cellularmembranes P-gp hence can affect intracellulardrug concentration andhave been shown to correlate in vitroto chemosensitivity to paclitaxel [59] However evidence fortheir role in clinical drug resistance in ovarian cancer hasemerged with P-gp found to be overexpressed in ovariancancer cells in vitro and also on paclitaxel-resistant celllines [70] P-gp and MDR1 expression levels were higherin chemoresistant ovarian cancer patients as compared withtheir chemosensitive counterpart Overall survival time wasalso statistically higher in patientswith low expression of P-gpandMDR1 in their tumor tissuesHence P-gp andMDR1mayhave a predictive role in determining the outcome of patientswith advanced ovarian cancer [58 79ndash82] Mechanism ofpaclitaxel resistance is complicated and specifically inhibitingABC transporters have given mixed results [59 83]
Another major mechanism of paclitaxel resistance ismediated by either a reduction in total intracellular tubulinconcentrations point mutation at prominently expressedtubulin genes or by selective alterations in expression oftubulin isotypes such as Class III 120573-tubulin [52 84 85]Microtubule dynamic stability was significantly impairedin the paclitaxel-resistant cells [86] Microtubule dynamicsdisruption caused by paclitaxel result in cell cycle arrestapoptosis and drug resistance
Other mechanism responsible for development of pacli-taxel resistant are inhibition of apoptosis activation ofmitogen-activated protein kinase Raf-1 kinase or intra-cellular signalling pathway PIK3 (phosphatidylinositol-45-bisphosphate 3-kinase) changes in apoptotic regulatory pro-teins such as Bcl-2 increase in expression of proinflammatorycytokines such as TNF-120572 IL-6 and IL-8 and activation oflipopolysaccharide-inducible genes and tumour suppressionprotein p53 [57 83 86 87]
In summary paclitaxel resistance is multifactorial inc-luding changes in signaling pathways upregulation of P-glycoprotein (P-gp) [80 88 89] alteration in tubulin dyna-mic mutations in 120573-tubulin gene or expression of 120573-tubulinisotypes [52 84 85] and changes in apoptotic mechanismIdentification of mechanism of resistance could help topotentially develop novel agents to improve chemosensitivityof patients with advanced ovarian cancer
6 Pharmacokinetics
Paclitaxel is a white to off-white crystalline powder highlylipophilic and is insoluble in water and so difficult to formu-late into solution It has a melting point of 216-217∘C [90 91]More than 90 of the drug binds rapidly and extensively toplasma proteins [33 40] whereas binding onto red blood cellsis approximately 50 The presence of premedication drugs(before chemotherapy) such as ranitidine dexamethasone ordiphenhydramine did not affect protein binding of paclitaxelPaclitaxel has a large volume of distribution of about 55 Lm2but this is reduced in the females [33]
BioMed Research International 7
AUC (area under the plasma concentration)
Cmax (maximum concentration)
Pacli
taxe
l con
cent
ratio
n (120583
M)
0 10 20 30 40
Time (hr)
0
1
2
3
4
5
Figure 4 Plasma pharmacokinetics of paclitaxel The pharmacoki-netics generally were linear for 6 or 24 hour infusions but becomenonlinear for infusions of shorter durations due to variation inthe elimination clearance with the dose administered An increasein plasma concentration of paclitaxel results in disproportionatelarger increase in 119862max (maximum plasma concentration) and AUC(area under plasma concentration) followed by decrease in drugelimination from body tissues
The disappearance of paclitaxel from plasma is tradition-ally believed to be biphasic [33] The initial rapid declinerepresents distribution to the peripheral compartment andelimination of the drug The later phase is due in part tothe slow efflux of paclitaxel from the peripheral compartment[92] In the presence of more sensitive assay methods andlater sampling times a three-compartment model seems tobe more accurate [40 93] Paclitaxel has been shown tohave a nonlinear pattern of pharmacokinetics (Figure 4)Thepharmacokinetics were generally linear for 6- or 24-hourinfusions but become nonlinear for infusions of shorterdurations because the elimination clearance varies with thedose administered With increasing plasma concentrationof paclitaxel there is a disproportionately larger increasein 119862max (maximum plasma concentration) and AUC (areaunder plasma concentration) accompanied by decrease indrug elimination from body tissues The clinical importanceof this nonlinear pattern is that dose escalationmay result in adisproportionate increase in toxicity whereas dose reductionmay affect its efficacy [33 90 91 94]
The pharmacokinetics of paclitaxel has been evaluatedover a wide range of doses up to 300mgm2 and withinfusion schedules ranging from 3 to 24 hours Maximumplasma concentrations are dose-related In patients treatedwith single dose infusion of 135 and 175mgm2 given as3- and 24-hour infusions mean steady state volume ofdistribution has ranged from 198 to 688 Lm2 indicatingextensive extravascular distribution andor tissue bindingTerminal half-life has ranged from 13 to 86 hours (mean 5hours) [40 93] and total body clearance has ranged from116 to 240 Lhrm2 Preclinical results in animals have shown
high levels in most tissues Being highly protein-boundpaclitaxel has a high affinity for distribution in specific tissuesincluding kidney lung spleen and extracellular fluids likeascites and pleural fluids [40 95] but the uptake of the drugin the brain is minimal [96 97] Exposure to paclitaxel isrelatively high in tumour tissue compared with other tissuesand in addition to slow elimination from tumour tissue theAUC in tumour tissue is about five-fold higher than that inplasma [97]
There is no evidence of accumulation of paclitaxel withmultiple treatment courses as the variability in systemicpaclitaxel exposure as measured by AUC (0ndashinfin) (area underplasma concentration-time curve from time 0 to infinity)for successive treatment courses are minimal [98] Paclitaxelclearance is however sequence dependent Patients receiv-ing a platinum-based agent prior to paclitaxel have lowerclearance and greater clinical toxicity than patients receivingpaclitaxel before cisplatin [93]
The drug administered intravenously undergoes anextensive P-450mediated hepaticmetabolism by cytochromeenzymes (CYP3A andCYP2C8) with 70ndash80being excretedinto bile by adenosine triphosphate- (ATP-) binding cassettemultidrug transporters such as P-glycoprotein (P-gp) andmultidrug resistance protein 2 (MRP-2) either asmetabolitesor as the parent drug Variation in MRP-2 activity hasbeen found to have direct effect on the effective exposureto paclitaxel [99] The bioavailability is poor following oraladministration due to enterocyte expression of P-gp and first-pass metabolism in the liver Most of the drug is eliminatedin feces Less than 10 drug in the unchanged form isexcreted in the urine indicating extensive nonrenal clearance[96] Combinations of inhibitors of CYP3A and P-gp mightpossibly improve the oral bioavailability of the taxanes [8997 100]
7 Paclitaxel and the Immune System
The immune system consists of two different but interactingmechanisms which are innate and adaptivemechanismsTheinnate mechanism is the first line of defense and consists of agroup of cells which includes mainly macrophages dendriticcells (DCs) and natural killer (NK) cells while the adaptiveimmunemechanism is represented by T-lymphocytes All thecomponents of innate and adaptive mechanism are involvedin antitumour immunity which includes tumour recognitioncontrol and elimination However cancer cells are able toevade immune detection and actively suppress antitumourimmunity
Paclitaxel has a wide range of dose dependent immuno-modulatory effects described in Figure 5 At standard dosepaclitaxel is broadly immunosuppressive and this is becauseit inhibits a number of cell types involved in tumour rejectionsuch asmacrophages effector T cells andNK cells [101] How-ever at lower doses than typically used for chemotherapypaclitaxel has an important immunogenic role promotingantitumour immunity [101 102] Hence understanding theimmunological basis of paclitaxel may help to maximise themanipulation of the immunomodulatory effects of paclitaxel
8 BioMed Research International
Immunomodulatory effect of
paclitaxel
Stimulate direct cytotoxic activity by
macrophage
Induce activation maturation and priming of DCs
Stimulate NK-dependent antitumour immunity
Activation of tumour-specificCTL Expansion of memory T cells
Secretion of proinflammatory cytokine
Shift from Th2 to Th1 type ofresponse
Depletion of Tregs andmodulation of MDSC
Downregulates the expression of VEGFR-2
and inhibits angiogenesis
IL-6 IL-12 TNF-120572 and i-NOS
Figure 5 Immunomodulatory effect of paclitaxel Paclitaxel a toll-like receptor 4 (TLR4) ligand binds to TLR4 receptor and triggers TLR4signaling via MyD88 dependent and independent pathway Paclitaxel then promotes anticancer immune response directly by stimulatingmacrophages to kill cancer cells or indirectly by secretion of proinflammatory cytokines which upregulates activation of DCs NK andtumour specific CTL Paclitaxel promotes effective CTL response by upregulation of mannose-6-phosphate which facilitate permeabilityto granzyme B and cytokine patterns of T helper type 1 Paclitaxel modulates MDSC and ablates Tregs Memory T cells (CD4+CD45RO+and CD8+CD45RO+) increased significantly while regulatory T cells (Tregs) decreased around 2 weeks creating an opportunity window fordose-dense therapy and immunomodulatory agents to achieve clinical benefit Dose-dense and low dose paclitaxel also blocks new vesselformation by downregulating VEGF-receptor 2 reduces resistance by alternative mechanism of action
to develop better therapeutic options in the management ofadvanced ovarian cancer
Paclitaxel is a ligand to toll-like receptor 4 (TLR4) whichis expressed on innate immune cells including macrophagesThe binding of paclitaxel to TLR4 on macrophages trig-gers the MyD88 mitogen-activated protein kinase (MAPK)and transcription of nuclear factor NF-kappa B (NF-120581B)pathways (Figure 3) resulting in their activation and releaseof immunostimulatory cytokines such as tumour necrosisfactor-120572 (TNF-120572) interleukin-1 (IL-1) interleukin-6 (IL-6)and interleukin-8 (IL-8) [103ndash105] Activated macrophagescan either cause direct tumour cell lysis via release oflysosomal enzymes and nitric oxide (NO) or indirectly byactivating NK cells DCs and tumour-specific cytotoxic T-lymphocytes (CTLs) [101]
NK cells are also innate immune cells capable of killingtumour cells particularly those cells that have reduced classI MHC expression and therefore can escape killing by CTLsPaclitaxel can enhance NK cell function by inducing mRNAand protein production of perforin an effector moleculeinvolved inNKcell-mediated cytotoxicity [106]However theeffect of low dose paclitaxel on NK cells is controversial Inanother study it was found that treatment of human NK cellswith paclitaxel effectively inhibits NK cell-mediated killing ofK562 (human erythroleukemia) target cells in vitro withoutaffecting the viability of NK cells [107] However weeklypaclitaxel therapy for non-small cell lung cancer patients was
only able to reduce the NK cell function up to completion ofthe first cycle but thereafter it gradually recovered [108]
Dendritic cells also express TLR4 and can be directlyactivated by paclitaxel The binding of paclitaxel to TLR onimmature DCs promotes DC maturation by upregulatingantigen-processing machinery gene components costimu-latory molecules and IL-12p70 [102] This enhances theability of DCs to prime T cells which facilitate antitumourimmunity [109] Paclitaxel can also promote cytotoxic T-cell function by upregulating mannose-6-phosphate whichfacilitates permeability to granzyme B and also inducescytokine production patterns typical of the T helper type 1phenotype via IL-2 (CD4 T cell) and IFN-120574 (CD8 T cell)secretion [104 110] Activated CD8+ T cells can differentiateinto CTL type 1 (Tc1) cells producingmainly IFN-120574 and CTLtype 2 (Tc2) cells producing mostly IL-4 IL-5 and IL-10 Tc1cells are potent CTL involved in the defense against cancerTc1 cells are able to recognise tumour antigens in the contextof MHC class I and mediate tumour cell lysis The role of Tc2cells in the immune response is not clearly known althoughtheir presence has been associated with disease progression[111]
CD4+ CD25+ regulatory T-cells (Tregs) constitutingapproximately 5ndash10 of peripheral CD4+ T cells [112 113]play an important role in tumour immune evasion [114]There is growing evidence that supports the existence ofelevated numbers of Tregs in tumours [115ndash117] which may
BioMed Research International 9
suppress immune responses of other CD4+ and CD8+ cells[118ndash120] and promote tumour progression In murine stud-ies paclitaxel exhibits the ability to reduce the number andsize of Treg cells thereby enhancing antitumour immunity[119 121] Similar findingswere seenwith a selective reductionin the size and number of Treg populations in peripheralblood samples from non-small cell lung cancer (NSCLC)patients [122]
Paclitaxel also decreased the expression of the anti-apoptotic molecule Bcl-2 in Treg cells while increasing thecorresponding proapoptoticmember Bax which contributedto the apoptotic sensitivity of Treg to paclitaxel [87]This wasseen in a study using the 3LL Lewis tumour model whichdemonstrated that Treg cells exposed to paclitaxel displayeddown regulation of Bcl-2 and upregulation of Bax and uponblocking the Bcl-2 pathway the ability of paclitaxel to ablateTreg cells compared toT effectorswas impaired and bothTregand T effectors were affected These results may suggest thatpaclitaxel targets Bcl-2 rather than tubulin to contribute tothe distinctive effect on Treg cells [119] It has recently beenshown in vitro that paclitaxel could target Bcl-2 and thereforelead to apoptosis Bcl-2 family proteins are key regulators ofapoptosis and play an important role in tumourigenesis andmulti-drug resistance by blocking apoptosis [119 123]
Few studies have also shown effect of paclitaxel onmyeloid-derived suppressor cells (MDSCs) a heterogeneouspopulation of immature myeloid cells immunosuppressivein nature are recruited by cancer cells and are found inincreased amount in advanced epithelial ovarian cancer [124]In a murine study using C57BL6 mice administration ofpaclitaxel at ultralow dose modulates MDSCs to differentiateinto DCs in a TLR4 independent manner [110] Hencepaclitaxel in ultralow noncytotoxic doses together with itsangiogenesis blocking ability may potentially enhance theefficacy of immunotherapy by ablation of immunosuppres-sive populations such as Tregs and MDSCs in tumour-bearing hosts [50 102]
In immunocompromised patients with advanced ovariancancer with increased Tregs and decreased levels of CD4+T cell CD8+ T cell and NK subsets after a single courseof combined carboplatin and paclitaxel chemotherapy theimmunosuppression is reversed around 12 to 14 days later butnot before one week or after three to four weeks Not only areTregs decreased but also the proportions of IFN-120574 secretingCD8+ T cells T helper-1 Tc1 and NKT cells The ratio of Tc1to Tc2 cells increases significantly [111 120 125]
Following chemotherapy both CD4+CD45RO+ andCD8+CD45RO+ memory T cells increased significantly andpeaked around 2 weeks The increase of memory T cellsin ovarian cancer patients following chemotherapy prob-ably opens the door of opportunity to develop long-termimmunological memory which could prevent recurrenceand metastases [120] Administration of dose-dense therapygiven weekly may hence be beneficial immunologically tomount an adequate immune response compared to standard3-week therapy In addition administration of immunother-apy agentsmay also be ideal during the period of 2weeks afterchemotherapy where temporary immune system reconstitu-tion takes place
8 Clinical Studies
In the past two decades paclitaxel had been administered indoses ranging from 60 to 250mgm2 over 1ndash96 hours andfrom 1 to 3 weekly intervals Prolonged exposure up to 96hours was believed to be effective as demonstrated with pre-clinical data but later refuted in large prospective studies [14126 127] A 24-hour infusion of paclitaxel was subsequentlyadministered to reduce the risk of hypersensitivity reactionshowever it was shown to increase mucosal and bone marrowtoxicity without improved efficacy [127 128] Development ofeffective premedication has led to administration of shorterinfusions (lt3 hours) which are better tolerated in particularfrom a haematologic perspective but patients remain at riskof myalgia and neuropathy at higher doses Weekly one-hourlow dose paclitaxel also known as dose-dense therapy hasrecently emerged as another possible strategy to improveoutcomes
9 Dose-Dense Therapy
Dose-dense treatment is defined by delivery of a maintainedper-cycle dose or overall dose with administration of drugat shorter time intervals than is standard This differs fromdose intensity which refers to dose (per unit weight or bodysurface area) delivered per unit time Hence either escalationof dose per cycle or reducing the time in between cycles maymodify dose intensity [129 130]
The rationale for the dose-dense approach of weeklypaclitaxel is that more frequent delivery of moderate dosesmay achieve greater efficacy by allowing sustained exposureof dividing tumour cells to paclitaxelrsquos cytotoxic and antian-giogenic effects hence reducing resistance delaying relapseand increasing the possibility of cancer remission Three 1-hour infusions of paclitaxel given at a week interval achievedgreater dose-density as well as dose-intensity than a singleadministration every 3 weeksThe initial tissue concentration(gt50 nM) for 1-hour infusion is similar to that of 3-hourinfusion but the concentration in the plasma instead oflasting for 8 hours in a 3-hour infusion rapidly falls below50 nM in less than 75 minutes for 1-hour infusion and hencereduces the risk of neutropenia However the rate of fallexperienced in tissue concentration of the drug is slowerthan plasma concentration of the drug hence efficacy ismaintained [131 132] A shorter infusion time allows bettercontrol of toxicities improved patient comfort and reducedhospitalisation hours
Several studies have used dose-dense paclitaxel in thetreatment of advanced ovarian cancer and are summarizedin Table 1 Based on phase 1 studies the recommendeddose for weekly paclitaxel ranges between 80 and 90mgm2compared with 45mgm2 per week with 3-weekly paclitaxeland is given over 1-hour duration Weekly scheduling hasdemonstrated consistent activities in ovarian cancer studies[11ndash13] Response rates were in the 20ndash50 range whereusually less than 10 would be expected Grade-4 doselimiting toxicities in particular neutropenia were not evidentat any dose below 100mgm2week [11 133]
10 BioMed Research International
Table1Ph
ases
Iand
IIstu
dies
onintravenou
sdose-densep
aclitaxel
Stud
yRe
gimen
119899()
PI(m
)RR
()
CR(119899)
MedianPF
S(m
)Median
OS
(m)
Adversee
ffects
Com
ments
Paclitaxel
dose
(mgm
2 )Ca
rbop
latin
dose
(mgm
2 )Ph
aseIsinglea
gent
Lofflerre
tal1996
[11]
40ndash9
0week
1-hou
rinfusionfor
6weeks
5040
5NA
NA
(i)Hem
atologictoxicity-m
ild(ii)N
ograde3
or4
haem
atologicaltoxicity
neurologicalor
cardiotoxicityup
to90
mgm
2 wk
(iii)Nohypersensitivity
reactio
ns(patientsreceivedprem
edication)
(i)100
priorc
hemotherapy
(ii)M
ediando
seintensity
was
410m
gm
2 6w
k(range200
to540m
gm
2 6w
k)
Fenn
ellyetal
1997
[12]
40ndash100w
eek
1830
NA
NA
NA
(i)Nomucositiso
rgrade
III
neurop
athy
was
seen
(ii)A
lopeciao
ccurredin
one
(i)100
priorc
hemotherapy
(2ndash5
priorregim
ens)
(ii)P
artia
lrespo
nses
weres
eenin
four
of13
assessablepatients
(30
)(iii)Dose-lim
iting
toxicitywas
reachedat100m
gm
2 (iv
)2-3
patie
ntse
xperience
treatmentd
elay
(v)M
axim
um-to
lerateddo
seof
80mgm
2 Ab
u-Ru
stum
etal
1997
[13]
60ndash100
over
1ho
urw
eek
45289
NA
NA
NA
(i)Nopatie
nthadfebrile
neutropenia
(i)100
priorc
hemotherapy
(1ndash8
priorregim
ens)
PhaseIISing
leagent
Markm
anetal
2001
[14]
80over
1ho
urw
eek
53(52)
25NA
NA
NA
Therapydiscon
tinuedin
(i)4patie
ntsw
hohadperip
heral
neurop
athy
(ii)1
patie
ntdu
etopainful
fingernailbeds
(i)100
platinum
andpaclita
xel
resistant
(ii)Th
erapywas
discon
tinuedin
5patie
ntsb
ecause
oftoxicity
(iii)Only13
(1)w
erem
odified
(doser
eductio
nor
treatment
delay)
becauseo
fsidee
ffects
PhaseIICom
binedwith
platinum
agent
Kiku
chietal
2005
[15]
80over
1ho
urw
eek
AUC2week
27gt6
818
483
NA
(i)Neutro
penia(
17)
thrombo
cytopenia(
51
)(ii)N
ocaseso
fperipheral
neurop
athy
(grades3
and4)
inweeklycombinedT-C
Cadron
etal2007
[16]
90over
1ho
urw
eek
AUC4week
24 9gt6le6
73 38NR
8105
675
(i)Grade
34neutropenia(
34)
andneutropenicfever
in2
(ii)N
auseaa
ndvomiting
and
fatig
uewerethe
mostfrequ
ent
nonh
ematologicalsid
eeffects
(i)Doser
eductio
nwas
necessary
in25of
patie
nts
Pign
atae
tal2008
[17]
60over
1ho
urw
eek
AUC2week
24(13)lowastlowast
1stline
385
2320
136
(i)Notoxicd
eath
was
recorded
(ii)G
rade
2anaemiawas
repo
rted
insevenpatie
nts(27)
(iii)Nofebrile
neutropeniaw
asob
served
(iv)G
rade
3and4neutropenia
was
recorded
infive(19)a
ndon
e(4
)patients
(v)G
rade
3thrombo
cytopenia
occurred
inon
epatient
(4)
BioMed Research International 11
Table1Con
tinued
Stud
yRe
gimen
119899()
PI(m
)RR
()
CR(119899)
MedianPF
S(m
)Median
OS
(m)
Adversee
ffects
Com
ments
Paclitaxel
dose
(mgm
2 )Ca
rbop
latin
dose
(mgm
2 )
Safrae
tal2014
[18]
80over
1ho
urw
eek
AUC2week
133
1stline
864
645
274
(i)Highera
naem
ia(grade
III+
IV68vs53)+
IVneutropenia(
144vs69)
decreasedgradeIIa
lopecia(
235
vs981
)and
thrombo
cytopenia
(grade
III+
IV0
vs23)
Havrilesky
etal
2003
[19]
80over
1ho
urw
eek
AUC2weekD1
D8D15
until
progressionCR
+8courses
29 21 8
Total
grou
pgt6lt6
83 100
38
16 15 1114
115
137
32
(i)Hem
atologictoxicitywas
common
(grade
3neutropenia
32n
ograde4
neutropenia
grade3
or4thrombo
cytopenia
142)
(i)To
xicitymanaged
bytre
atment
delaydo
seredu
ctionof
paclitaxel
ordiscon
tinuatio
nof
carbop
latin
vanderB
urgetal
2014
[20]
90over
1ho
urw
eek
AUC4weekD1
D8D15
D29
D36
D49
+6x
TCq3w
108
65 43
Total
grou
pgt6lt6
76 5816 42
26 158 13
(i)Neutro
penia3
0
thrombo
cytopenia8
febrile
neutropenia0
5
(ii)N
onhaem
atologictoxicitywas
low
(i)Treatm
entw
asdelayedin
16
anddo
seredu
cedin
2of
cycle
s
119899num
bero
fpatientsassessableforrespo
nsemm
onthsPIplatinum
treatmentfreeintervalRR
respo
nser
ateCR
com
pleterem
issionT
paclitaxelC
carbop
latin
PFS
progressio
nfre
esurvivalOSoverall
survivalN
An
otavailableinpapero
rabstractandNR
notyetreached
lowastlowastElderly
popu
lation
patient
agedge70
years
12 BioMed Research International
Numerous phase II studies have explored the tolerabilityand the activity of weekly paclitaxel either as a single agent orin combination with several other drugs or biological agents(Table 1) A number of regimens combining weekly paclitaxelwith carboplatin have been used as first-line treatment inovarian cancer Carboplatin has been administered weeklyat AUC of 2 with dose escalation in some studies whilepaclitaxel had been infused at 60ndash80mgm2week Thiscombined regimen was well tolerated with a low incidence ofbone marrow suppression Overall response rates have beenhigh in the range of 60ndash80 in most studies even in heavilypretreated patients with platinum-resistant disease (diseaserecurrence or progression within 6 months of the last lineof platinum-based therapy) [15ndash20 134] The promising datafrom these phase II trials then led to the evolution of largerphase III trials
Three phase III studies Japanese Gynecologic OncologyGroup- (JGOG-) Trial 3016 [21ndash23] Multicentre Italian Trialin Ovarian Cancer-Trial 7 (MITO-7) [25] and GynecologicOncology Group GOG-262 Trial [24] have explored dosedense therapy The results of these trials are summarised inTable 2
The Japanese Gynecologic Oncology Group (JGOG)conducted a randomized phase 3 trial of dose-dense weeklypaclitaxel 80mgm2week in combination with 3-weeklycarboplatin compared to standard 3-weekly carboplatin andpaclitaxel 180mgm2 in patients with advanced epithelialovarian peritoneal or fallopian tube cancer (JGOG 3016NOVEL trial) In both arms carboplatin was given at AUC6 and the median number of cycles was six In this largestudy (119899 = 637) with a median follow up of 77 months therewas an 11-month improvement in themedian progression freesurvival (PFS) in the dose-dense treatment group comparedwith the standard treatment arm (282 versus 175 monthsHR 076 95 CI 062ndash091 119901 = 00037) Median OS wasalso higher in the dose-dense treatment arm (1005 versus622 months HR 079 95 CI 063ndash099 119901 = 0039)On subgroup analysis suboptimally debulked patients withresidual disease of gt1 cm (119899 = 342) had a significantlyhigher median overall survival in the dose dense arm (512versus 335 months HR-075 95 CI 057ndash097 119901 = 0027)There was no significant advantage to dose-dense treatmentfor patients with optimally cytoreduced disease Dose-densetherapy survival benefits were also not seen in patients withclear cell or mucinous histology type unlike serous typeHowever patient treated with dose dense therapy had asignificantly higher frequency of hematologic toxicity thanwith the standard arm (212 versus 94) which resultedin lower treatment completion rates (63 versus 48) withfrequent episodes of delay (76 versus 67) and dosereductions (48versus 35) [21 22]Therewas no significantdifference in terms of overall quality of life between the twoarms (119901 = 046) [23]
Using a similar regimen as in JGOG-3016 a GynecologicOncology Group (GOG)-262 Trial was conducted in theUnited States In this group most patients had stage IIIdisease (66ndash70) and two-thirds had suboptimal debulkingwith residual disease of gt1 cm This was a randomized phase
III trial of 3 weekly paclitaxel versus dose-dense weeklypaclitaxel in combination with carboplatin in patients withadvanced epithelial ovarian peritoneal or fallopian tubecancer Though optional concurrent and maintenance beva-cizumab were received by the majority of patients in botharms (835 versus 841 resp) There was no significantdifference in PFS in the patients who received the dosedense paclitaxelcarboplatin regimen compared to those whoreceived the standard paclitaxelcarboplatin regimen (148versus 143 months HR 097 95 CI 079ndash118) Howeverin a subgroup analysis there was a significant difference inPFS in the dose dense paclitaxel arm who did not receivebevacizumab 119899 = 112 (142 versus 103 months HR 059 95CI 037ndash096 119901 = 0003) Overall survival data is still imma-ture There was higher frequency of grade 3 anaemia (408versus 157 119901 lt 0001) and grade 2 sensory neuropathy(259 versus 178 119901 = 0012) but a lower incidence ofneutropenia (72 versus 83 119901 lt 0001) [24]
In 2008 the Multicentre Italian Trials in Ovarian Cancer(MITO-7) randomised 810 women in a phase 3 trial toreceive either standard carboplatin (AUC = 6) and paclitaxel175mgm2 every 3 weeks or a weekly schedule of paclitaxel(60mgm2) with carboplatin (AUC = 2) The majority ofpatients in both arms (83ndash90) received six cycles of therapyMost patients (58ndash63) had stage II1 disease 23 of themwere suboptimally debulked Median PFS did not differsignificantly (173 months and 183 months 119901 = 066)between the standard and dose-dense arms respectivelyThere was no significant difference in response rate betweenthe two arms nor the estimated 2-year overall survivalSubgroup analysis did not identify any subgroup that mayhave benefited from the dose-dense regimen Unlike theJGOG-3016 trial the incidence of grade 3-4 neutropenia wassignificantly lower in the dose-dense group compared to the3-weekly regimen (42 versus 50) A similar pattern wasseen for the incidence of febrile neutropenia (lt1 versus 3119901 = 002) thrombocytopenia (1 versus 7 119901 lt 0001)and other nonhaematological toxicities such as alopeciavomiting renal dysfunction and neuropathy Quality of lifewas reported to be significantly better in the dose-dense arm(119901 lt 00001) which was discordant with the JGOG-3016quality of life data [25]
In summary there was significant improvement inmedian PFS and overall survival in studies using paclitaxelat 80mgm2week dose-dense therapy [21 24] but withhigher haematological toxicity whereas MITO-7 [25] whichwas using paclitaxel at 60mgm2week was only equivalentlyeffective but less toxicThis does not conclude that the higherpaclitaxel dose is more clinically beneficial as there are manyother confounding factors in all three studies
In a multivariate analysis the JGOG-3016 study [21]reported that a lower dose intensity of paclitaxel (lt80) wasassociated with poorer overall survival (hazard ratio = 14295 confidence interval 112ndash181 119901 = 0004) however itmust be highlighted that the investigational arm carboplatinschedules were not standardised in these studies The JGOGand GOG trials delivered a 3-weekly carboplatin (AUC =6) arm whereas in the MITO-7 study the carboplatin was
BioMed Research International 13
Table2Ph
aseIIIstu
dies
onintravenou
sdose-densep
aclitaxel
Stud
yRe
gimen
119899
MedianPF
S(m
)
Median
OS
(m)
Adversee
ffects
Com
ments
Katsu
matae
tal2009
[21]
Katsu
matae
tal2013
[22]
Haranoetal2014
[23]
JGOG3016
631
(i)Haematologicaltoxicityhigh
erin
dose
dense-211versus
94
Lower
treatmentcom
pletionin
dose-dense
63versus
48
Frequent
episo
deso
fdelay
indo
se-dense
76versus
67
Doser
eductio
nsin
dose-dense
48versus
35
Nosig
nificantd
ifference
inoverallQ
OL
betweenbo
thgrou
ps(119901=046)
Paclitaxel80m
gm
2D18
15+carbop
latin
AUC63
weeklyversus
Paclitaxel180
mgm
2+
carbop
latin
AUC63
weekly
312
282
1005
Both
givenfor6
ndash9cycle
s319
175
622
Chan
etal2013
[24]
GOG-262
(i)Higherfrequ
ency
ofgrade3
anaemia
(408versus
157119901lt0001)
grade2
sensoryneurop
athy
(259versus
178
119901=0012)b
utlower
incidenceo
fneutropenia(
72versus
83119901lt0001)
Paclitaxel80m
gm
2D18
15+carbop
latin
AUC63
weeklyversus
Paclitaxel175
mgm
2+
carbop
latin
AUC63
weekly
346
148
NR
Both
givenfor6
cycle
s346
143
NR
Bevacizumab
given
optio
nally
112
(did
not
receive
bevazicumab)
142vs
103
Pign
atae
tal2014
[25]
MITO-7
810
(i)Lo
wer
incidenceo
fgrade
3-4
neutropenia(
42versus
50)febrile
neutropenia(lt1v
ersus3
119901=002)
thrombo
cytopenia(
1versus7
119901lt0001)andothern
onhaem
atological
toxicitie
ssuchas
alop
eciavom
iting
renald
ysfunctio
nandneurop
athy
Qualityof
lifeb
etterindo
sedensea
rm(119901lt00001)
Paclitaxel60m
gm
2 weekly+carbop
latin
AUC
2weeklyversus
Paclitaxel175
mgm
2+
carbop
latin
AUC63
weekly
406
404
183 173
77lowast
79lowast
119899num
bero
fpatientsmm
onthsDday
PFSprogressionfre
esurvivalOSoverallsurvivalNAnot
availableinpapero
rabstractandNR
notyetreached
lowastSurvivalrateat2years
14 BioMed Research International
dose-dense (AUC 2 weekly) Although it is possible that thedose scheduling for the platinum-based agent is not essentialfor a survival benefit as shown by previous studies usingdose-dense cisplatin direct cross-trial comparison cannot bemade Unlike paclitaxel carboplatin probably requires peakdose for optimal therapeutic benefit hence this may accountfor the inferior survival outcome in MITO-7 trial Anotherconfounding factor may be difference in ethnicity All threestudies used different ethnic populations and Asian patientsin JGOG-3016 appear to have better survival outcomes thanthe MITO-7 Western population Ethnicity with possibleunderlying genetic causes may be responsible for the variableresponses to chemotherapy across individuals [135] This wasexplored by Millward et al who studied 68 Caucasian andAsian lung cancer patients treated with a combination ofpaclitaxel and carboplatin and found that the incidence offebrile neutropenia was 50 of an initially treated cohortof Asians and when carboplatin was subsequently dosereduced in all Asian patients the overall incidence of febrileneutropenia was also reduced to 26 [136]
Although early clinical data from phase I and phaseII dose-dense paclitaxel trials in advanced ovarian cancerwere promising the results from phase III studies in havebeen inconsistent as a result of differences in paclitaxel dosecarboplatin AUC and schedule addition of bevacizumabas well as different ethnic populations The results of arecently completed randomised three arms GynaecologicCancer InterGroup (GCIG) phase II trial ICON 8 mayfurther inform the clinical benefit of dose dense paclitaxeltherapy
This multicentre trial involving 111 centres in the UKSouth Korea Mexico Ireland Australia and New Zealandwith a target population of 1485 patients with stage IC-IV epithelial ovarian cancer or peritoneal or fallopian tubecancer compared two dose-dense arms (i) JGOG-like armcarboplatin AUC 5 plus weekly 80mgm2 paclitaxel and (ii)MITO-7-like arm weekly carboplatin AUC 167 plus weekly80mgm2 paclitaxel to the standard 3-weekly treatment(carboplatin AUC 5 plus 175mgm2 paclitaxel) for stage IC toIV epithelial ovarian cancer The dose-dense arms of MITO-7 and JGOG-3016 as well as the ethnic heterogeneity will befurther addressed
10 Intraperitoneal (IP) Chemotherapy
In addition to dose and scheduling the route of adminis-tration of chemotherapy agents plays an important role inoutcome Intraperitoneal spread is common and likely anearly event in epithelial ovarian cancer hence the deliveryof chemotherapy intraperitoneally in theory would exposethe microcirculation of tumour to higher doses of drug thansystemic administration while limiting systemic toxicityTheideal drug for IP chemotherapy is one that is systemicallyeffective penetrates deep into the inner core of tumour tissueand remains within the peritoneal cavity for a prolongedperiod of time [137ndash139]
Early clinical studies confirmed that indeed the peritonealcavity could be exposed to 10 to 20-fold higher (cisplatin
and carboplatin) drug concentration than when using theintravenous approach and since 1978 this route had beenadopted as a form of therapeutic intervention [137 139]A subsequent phase I trial showed that IP paclitaxel haddose-limiting toxicity in the form of abdominal pain [140]Another phase 1 GOG pilot study administered weekly IPpaclitaxel at an initial dose of 20mgm2 for 16 weeks to33 patients and found that IP paclitaxel at this dose wasfeasible and well tolerated At dose levels 60 to 65mgm2there were significant levels of paclitaxel for a week afterdrug administration suggesting very slow clearance andcontinuous exposure of the peritoneal cavity to active drugconcentrations [132]
Hence this initiated a phase II study [141] that used pacli-taxel intraperitoneally at a dose of 60ndash65mgm2week In thisphase II GOG study 76 patients with small-volume resid-ual disease carcinoma (05 cm or less) involving the ovaryperitoneal or fallopian tube were treated with paclitaxel60mgm2week intraperitoneally for 16 weeks followed bysurgical evaluation in patients without disease progressionThe Gynaecologic Oncology group (GOG) currently definesno visible disease as microscopic disease being the idealsurgical outcome 75 of patients had received prior systemictherapy and 70 received all 16 courses that were planned Of28 patients with microscopic disease at the start of therapy61 achieved a surgically defined complete response whereasonly 1 out of 31 patients with macroscopic disease achieved acomplete response The median time-to-recurrence was 167months with an estimated survival rate at 2 years being 58Treatment was generally well tolerated [141]
Another study looked into the effect of IP paclitaxel asconsolidation therapy in advanced ovarian cancer Twenty-eight patients who had initial residual macroscopic disease(lt1 cm) after primary surgery or interval debulking but hadcomplete pathological response following standard treatmentwith at least 6 cycles of platinum-based chemotherapy regi-men received paclitaxel 60mgm2week intraperitoneally for12ndash16 weeks as consolidation therapy The median time torecurrence was 25 months but overall survival did not differsignificantly when compared with control group submittedto observation only Treatment-related toxicity was mild andtechnical difficulties were observed in 11 of patients [142]
Multicenter randomised phase 3 trials as well as meta-analysis of IP chemotherapy have been performed anddemonstrated that chemotherapy drugs administered intra-peritoneally are superior to intravenous standard regimensin patient with optimally debulked epithelial ovarian cancerThe most impressive data comes from GOG 114 [14] and172 trial [143] In GOG 114 patients received either sixcycles of intravenous paclitaxel 135mgm2 and cisplatin75mgm2 every 3 weeks or intravenous carboplatin (AUC= 9) every 28 days for two cycles followed by six 3-weeklycycles of intravenous paclitaxel 135mgm2 and IP cisplatin100mgm2 [14] whereas in GOG 172 patients received eitherintravenous paclitaxel 135mgm2 followed by intravenouscisplatin 75mgm2 or intravenous paclitaxel 135mgm2 fol-lowed by IP combination of cisplatin 100mgm2 and pacli-taxel 60mgm2 on day 8 Both trials had a combined total
BioMed Research International 15
of 876 women with stage III epithelial ovarian carcinomaoptimally debulked to le1 cm residual tumour [143] Themedian follow-up for GOG 114 [14] was 138 years with GOG172 [143] was 97 years The primary results of the individualtrials reported up to 6-month improvement in median PFSfollowing IP therapy In the combined analysis of the datafrom both trials the data continued to show a 5-monthdifference in favour of IP therapy (25 versus 20 months)which translates into 16 reduction in the hazard ratio forprogression (119901 = 003) In GOG 114 [14] reported in 2001there was only borderline improvement in overall survivalassociated with this regimen (median 63 versus 52 monthsrelative risk 081 119901 = 005)
However in combined analysis in 2013 which was pre-sented at the Society of Gynecologic Oncology AnnualMeeting [144] the overall survival showed an 11-monthimprovement in favour of IP therapy in GOG 114 whereasGOG 172 reported a 16-month survival advantage Amongpatients treated with IP therapy the 5-year survival rateincreased from 18 following completion of 1-2 cycles to 59for patients who completed 5-6 cycles of treatment Howeverthere was increased toxicity observed in the IP arm grade 3-4 leukopenia thrombocytopenia and abdominal pain Only42 of patients in the GOG172 trial [143] completed all sixcycles of planned treatment in the IP arm while 18 ofpatients in GOG 114 trial [14] received fewer than two coursesof IP chemotherapy
Another randomised phase III trial involving patientswith stages II-III epithelial ovarian carcinoma is the GOG252 study with three arms Arm 1-dose-dense intravenouscarboplatin and paclitaxel Arm 2-dose-dense intravenouspaclitaxel and IP carboplatin and Arm 3 consists of 3-weeklyintravenous paclitaxel (day 1) followed by IP cisplatin (day 2)and IP paclitaxel (day 3) regimen All three arms also incor-porate the combination and maintenance of bevacizumabGOG 252 has completed accrual and results are awaited [139]
11 Newer Forms of Paclitaxel
Development of next-generation taxanes has taken place overthe past 40 years aimed at eliminating toxicity improvingefficacy and ease of administration Abraxane is a novelcompound which incorporates paclitaxel into an albuminnanoparticle soluble in saline hence eliminating the needfor Cremophor EL which is responsible for hypersensitivityreactions experienced during paclitaxel infusion [145] Thenanoparticle albumin in nab-paclitaxel is able to bind toglycoprotein gp60 receptor an albumin receptor and activatecaveolin-1 a protein that in human is encoded byCAV-1 geneleading to formation of caveoli hence allowing nab-paclitaxelto migrate across the endothelial cell membrane into theinterstitial space leading to higher intratumoural drug con-centration In addition Abraxane exhibits linear pharma-cokinetics and can therefore be given at a relatively higherdose than standard intravenous paclitaxel leading to a highertherapeutic ratio and heightened efficacy in solid tumoursmainlymetastatic breast cancer [146 147] Nab-paclitaxel hadFDA approval in 2005 for treatment of breast cancer [148]
Nab-paclitaxel has been studied in recurrent ovariancancer As a single agent in phase II 44 patients withrecurrent ovarian cancer were treated with Nab-paclitaxel260mgm2 intravenously for 30 minutes every 3 weeks for6 cycles Ninety-two percent of patients were platinum-sensitive while 89 had had previous exposure to standardtaxane The objective response rate was 64 with 15 patientsachieving complete response and 13 of them had partialresponse Estimated median PFS was 85 months No hyper-sensitivity reactions were observed and there were infrequentcases of grade 4 neutropenia (11) and grade 2-3 neuropathy(13) [149]
Another phase II study by GOG enrolled 51 patients withplatinum- and taxane-resistant recurrent ovarian cancer outof which 47 were evaluable The objective response rate was38 with one patient achieving a complete response and 10patients a partial response The median PFS was 45 monthswhile overall survival rate was 174 months Severe haema-tological and nonhaematological toxicities including neuro-toxicity were uncommon These results are quite impressivegiven the treatment population consisted of patients withvery poor prognosis with a median platinum and taxane freeinterval of 21 days and 70 had their recurrence within 3months of completion of primary treatment [150] Severalother trials of this formulation are in progress
Paclitaxel poliglumex (PPX) also known as Xyotax isanother prodrug a novel conjugate of paclitaxel and 120572-poly-L-glutamic acid which accumulates within tumour tissuedue to increased permeability of the tumour vessels and lackof lymphatic drainage [148 151 152] Paclitaxel poliglumexenhances solubility of paclitaxel allows direct delivery tothe intratumoural microenvironment and allows prolongedexposure to the active drug while minimising systemictoxicities [151] In Phase I dose escalation studies as a singleagent the recommended dose of PPX was 235mgm2 over 10minutes every 3 weeks or 70mgm2 weekly [153] In a PhaseII GOG study of relapsed ovarian cancer a response rate of16 was seen with infrequent serious adverse events grade3 and 4 neutropenia (24 and 20) and grade 3 neuropathy(24) [154] A phase III trial (GOG-0212) on the use of PPXas consolidation ormaintenance therapy in advanced ovariancancer is in progress
DHA-paclitaxel also known as Taxoprexin is a prodrugwhere paclitaxel is covalently conjugated with the naturallyoccurring omega-3 fatty acid docosahexaenoic acid (DHA)a fatty acid that is easily taken up by tumour cells henceincreasing intratumoural concentration of paclitaxel leadingtumour cell apoptosis [155 156] DHA-paclitaxel exhibitslinear pharmacokinetics and lower toxicity and also ease ofadministration when compared to conventional paclitaxeland has demonstrated antineoplastic activity in animal mod-els of cancer as well as in a phase III trial involving metastaticmelanoma [156ndash160] In a recent study on human ovariancancer cells it was found that DHA could reverse paclitaxelresistance by inhibiting P-gp as well as downregulatingthe expression of multidrug resistance associated proteins(MRP) and inhibiting the activity of NF-120581B and p38 MAPKsignalling pathways [161]
16 BioMed Research International
12 Future Directions
A plateau has been reached regarding the benefits associatedwith standard 3-weekly intravenous administration of cyto-toxic chemotherapy in advanced epithelial ovarian cancerThe ongoing battle for a better treatment regimen to delayrelapse promote remission and most importantly improvethe quality of life of patients with advanced epithelial ovariancancer need not to go further than the ability to relook at thechemotherapy agents that are already available in a differentapproach
Novel compounds to date have not yet shown clinicalsuperiority and parent compounds such as paclitaxel con-tinue to surprise us with their feasibility effectiveness andmanageable toxicity profiles Intraperitoneal paclitaxel willrequire further evaluation Better effort in understanding themechanism of action of drugs including the role of dosescheduling and the effect on the immune systemmay providea more cost-effective route to better clinical outcomes
Conflict of Interests
The authors declare no conflict of interests in this work
Acknowledgments
The authors would like to thank the many researchers whohave contributed to our current knowledge of paclitaxelNirmala Kampan is supported by Australian Monash Uni-versity Institute of Graduate Research Scholarship as wellas Universiti Kebangsaan Malaysia Postgraduate ScholarshipAward Mutsa Madondo has received Postgraduate Pub-lication Award from Monash University and MagdalenaPlebanski has been awarded Senior NHMRC Fellowship
References
[1] Australian Institute of Health and Welfare and National Breastand Ovarian Cancer Centre (Australia) Ovarian Cancer inAustralia AnOverview 2010 Cancer Series Australian Instituteof Health and Welfare Canberra Australia 2010
[2] R E Bristow R S Tomacruz D K Armstrong E L Trimbleand F J Montz ldquoSurvival effect of maximal cytoreductivesurgery for advanced ovarian carcinoma during the platinumera a meta-analysisrdquo Journal of Clinical Oncology vol 20 no 5pp 1248ndash1259 2002
[3] ZKempand JA Ledermann ldquoUpdate onfirst-line treatment ofadvanced ovarian carcinomardquo International Journal of WomenrsquosHealth vol 5 no 1 pp 45ndash51 2013
[4] A du Bois H-J Luck W Meier et al ldquoA randomized clinicaltrial of cisplatinpaclitaxel versus carboplatinpaclitaxel as first-line treatment of ovarian cancerrdquo Journal of the National CancerInstitute vol 95 no 17 pp 1320ndash1330 2003
[5] R F Ozols B N Bundy B E Greer et al ldquoPhase III trialof carboplatin and paclitaxel compared with cisplatin andpaclitaxel in patients with optimally resected stage III ovariancancer A Gynecologic Oncology Group studyrdquo Journal ofClinical Oncology vol 21 no 17 pp 3194ndash3200 2003
[6] W P McGuire W J Hoskins M F Brady et al ldquoCyclophos-phamide and cisplatin compared with paclitaxel and cisplatin
in patients with stage III and stage IV ovarian cancerrdquoThe NewEngland Journal of Medicine vol 334 no 1 pp 1ndash6 1996
[7] W P McGuire W J Hoskins M F Brady et al ldquoCyclophos-phamide and cisplatin versus paclitaxel and cisplatin a phase IIIrandomized trial in patients with suboptimal stage IIIIV ovar-ian cancer (from the gynecologic oncology group)rdquo Seminars inOncology vol 23 no 5 supplement 12 pp 40ndash47 1996
[8] M J Piccart K Bertelsen K James et al ldquoRandomized inter-group trial of cisplatin-paclitaxel versus cisplatin-cyclophosph-amide inwomenwith advanced epithelial ovarian cancer three-year resultsrdquo Journal of the National Cancer Institute vol 92 no9 pp 699ndash708 2000
[9] P A Vasey G C Jayson A Gordon et al ldquoPhase III random-ized trial of docetaxel-carboplatin versus paclitaxel-carboplatinas first-line chemotherpy for ovarian carcinomardquo Journal of theNational Cancer Institute vol 96 no 22 pp 1682ndash1691 2004
[10] B Gronlund C Hogdall H H Hansen and S A EngelholmldquoResults of reinduction therapy with paclitaxel and carboplatinin recurrent epithelial ovarian cancerrdquo Gynecologic Oncologyvol 83 no 1 pp 128ndash134 2001
[11] T M Loffler W Freund J Lipke and T-U HausamenldquoSchedule- and dose-intensified paclitaxel as weekly 1-hourinfusion in pretreated solid tumors results of a phase III trialrdquoSeminars in Oncology vol 23 no 6 supplement 16 pp 32ndash341996
[12] D Fennelly C Aghajanian F Shapiro et al ldquoPhase I and phar-macologic study of paclitaxel administered weekly in patientswith relapsed ovarian cancerrdquo Journal of Clinical Oncology vol15 no 1 pp 187ndash192 1997
[13] N R Abu-Rustum C Aghajanian R R Barakat D Fennelly FShapiro and D Spriggs ldquoSalvage weekly paclitaxel in recurrentovarian cancerrdquo Seminars inOncology vol 24 no 5 supplement15 pp S15-62ndashS15-67 1997
[14] M Markman B N Bundy D S Alberts et al ldquoPhase III trialof standard-dose intravenous cisplatin plus paclitaxel versusmoderately high-dose carboplatin followed by intravenouspaclitaxel and intraperitoneal cisplatin in small-volume stageIII ovarian carcinoma an intergroup study of the gynecologiconcology group Southwestern Oncology Group and EasternCooperativeOncologyGrouprdquo Journal of Clinical Oncology vol19 no 4 pp 1001ndash1007 2001
[15] A Kikuchi H Sakamoto and T Yamamoto ldquoWeekly car-boplatin and paclitaxel is safe active and well tolerated inrecurrent ovarian cancer cases of Japanese women previouslytreated with cisplatin-containing multidrug chemotherapyrdquoInternational Journal of Gynecological Cancer vol 15 no 1 pp45ndash49 2005
[16] I Cadron K Leunen F Amant T van Gorp P Nevenand I Vergote ldquoThe lsquoLeuvenrsquo dose-dense paclitaxelcarboplatinregimen in patients with recurrent ovarian cancerrdquo GynecologicOncology vol 106 no 2 pp 354ndash361 2007
[17] S Pignata E Breda G Scambia et al ldquoA phase II studyof weekly carboplatin and paclitaxel as first-line treatment ofelderly patients with advanced ovarian cancer A Multicen-tre Italian Trial in Ovarian cancer (MITO-5) studyrdquo CriticalReviews in OncologyHematology vol 66 no 3 pp 229ndash2362008
[18] T Safra S Shamai J Greenberg et al ldquoWeekly carboplatinwith paclitaxel compared to standard three-weekly treatment inadvanced epithelial ovarian carcinomamdasha retrospective studyrdquoGynecologic Oncology vol 132 no 1 pp 18ndash22 2014
BioMed Research International 17
[19] L J Havrilesky A A Alvarez R A Sayer et al ldquoWeekly low-dose carboplatin and paclitaxel in the treatment of recurrentovarian and peritoneal cancerrdquo Gynecologic Oncology vol 88no 1 pp 51ndash57 2003
[20] M van der BurgW Onstenk I Boere et al ldquoLong-term resultsof a randomised phase III trial of weekly versus three-weeklypaclitaxelplatinum induction therapy followed by standardor extended three-weekly paclitaxelplatinum in Europeanpatients with advanced epithelial ovarian cancerrdquo EuropeanJournal of Cancer vol 50 no 15 pp 2592ndash2601 2014
[21] N Katsumata M Yasuda F Takahashi et al ldquoDose-densepaclitaxel once a week in combination with carboplatin every3 weeks for advanced ovarian cancer a phase 3 open-labelrandomised controlled trialrdquoThe Lancet vol 374 no 9698 pp1331ndash1338 2009
[22] N Katsumata M Yasuda S Isonishi et al ldquoLong-term resultsof dose-dense paclitaxel and carboplatin versus conventionalpaclitaxel and carboplatin for treatment of advanced epithelialovarian fallopian tube or primary peritoneal cancer (JGOG3016) a randomised controlled open-label trialrdquo The LancetOncology vol 14 no 10 pp 1020ndash1026 2013
[23] K Harano F Terauchi N Katsumata et al ldquoQuality-of-lifeoutcomes from a randomized phase III trial of dose-denseweekly paclitaxel and carboplatin compared with conventionalpaclitaxel and carboplatin as a first-line treatment for stage II-IV ovarian cancer Japanese Gynecologic OncologyGroup Trial(JGOG3016)rdquo Annals of Oncology vol 25 no 1 pp 251ndash2572014
[24] J Chan M F Brady R Penson et al ldquoPhase III trial ofevery-3-weeks paclitaxel vs dose dense weekly paclitaxel withcarboplatin +minus bevacizumab in epithelial ovarian peritonealfallopian tube cancer GOG 262 (NCT01167712)rdquo InternationalJournal of Gynecological Cancer vol 23 no 8 supplement 1 pp9ndash10 2013
[25] S Pignata G Scambia D Katsaros et al ldquoCarboplatin pluspaclitaxel once a week versus every 3 weeks in patients withadvanced ovarian cancer (MITO-7) a randomisedmulticentreopen-label phase 3 trialrdquoThe Lancet Oncology vol 15 no 4 pp396ndash405 2014
[26] V Walsh and J Goodman ldquoFrom taxol to Taxol the changingidentities and ownership of an anti-cancer drugrdquo MedicalAnthropology vol 21 no 3-4 pp 307ndash336 2002
[27] R Renneberg ldquoBiotech History yew trees paclitaxel synthesisand fungirdquo Biotechnology Journal vol 2 no 10 pp 1207ndash12092007
[28] J E Liebmann J A Cook C Lipschultz D Teague J Fisherand J B Mitchell ldquoCytotoxic studies of paclitaxel (Taxol) inhuman tumour cell linesrdquo British Journal of Cancer vol 68 no6 pp 1104ndash1109 1993
[29] J J Manfredi and S B Horwitz ldquoTaxol an antimitotic agentwith a newmechanism of actionrdquo Pharmacology andTherapeu-tics vol 25 no 1 pp 83ndash125 1984
[30] D G I Kingston ldquoRecent advances in the chemistry of taxolrdquoJournal of Natural Products vol 63 no 5 pp 726ndash734 2000
[31] D G I Kingston ldquoThe shape of things to come structural andsynthetic studies of taxol and related compoundsrdquo Phytochem-istry vol 68 no 14 pp 1844ndash1854 2007
[32] V Walsh and J Goodman ldquoCancer chemotherapy biodiversitypublic and private property the case of the anti-cancer drugTaxolrdquo Social Science amp Medicine vol 49 no 9 pp 1215ndash12251999
[33] P H Wiernik E L Schwartz J J Strauman J P Dutcher RB Lipton and E Paietta ldquoPhase I clinical and pharmacokineticstudy of taxolrdquo Cancer Research vol 47 no 9 pp 2486ndash24931987
[34] W P McGuire E K Rowinsky N B Rosenhein et alldquoTaxol a unique antineoplastic agent with significant activityin advanced ovarian epithelial neoplasmsrdquo Annals of InternalMedicine vol 111 no 4 pp 273ndash279 1989
[35] ldquoDiscovery and development of taxolrdquo in Taxol Science andApplications M W M E Suffness Ed pp 3ndash25 CRC PressBoca Raton Fla USA 1995
[36] M J Piccart and F Cardoso ldquoProgress in systemic therapy forbreast cancer an overview and perspectivesrdquo European Journalof Cancer Supplement vol 1 no 2 pp 56ndash69 2003
[37] P Bonomi K B Kim and J Kugler ldquoComparison of survival forstage IIIB versus stage IV non-small cell lung cancer (NSCLC)patients with etoposide-cisplatin versus taxol-cisplatin an East-ern Cooperative Oncology Group (ECOG) trialrdquo in Proceedingsof the American Society of Clinical Oncology vol 16 p 454a1997
[38] D Guenard F Gueritte-Voegelein J Dubois and P PotierldquoStructure-activity relationships of Taxol and Taxotere ana-loguesrdquo Journal of the National Cancer Institute Monographsno 15 pp 79ndash82 1993
[39] D G I Kingston ldquoTaxol the chemistry and structure-activityrelationships of a novel anticancer agentrdquo Trends in Biotechnol-ogy vol 12 no 6 pp 222ndash227 1994
[40] E K Rowinsky and R C Donehower ldquoPaclitaxel (taxol)rdquo TheNew England Journal of Medicine vol 332 no 15 pp 1004ndash10141995
[41] J Parness and S B Horwitz ldquoTaxol binds to polymerizedtubulin in vitrordquo Journal of Cell Biology vol 91 no 2 pp 479ndash487 1981
[42] A Dammermann A Desai and K Oegema ldquoTheminus end insightrdquo Current Biology vol 13 no 15 pp R614ndashR624 2003
[43] CWiese and Y Zheng ldquoMicrotubule nucleation 120574-tubulin andbeyondrdquo Journal of Cell Science vol 119 no 20 pp 4143ndash41532006
[44] A Ganguly H Yang and F Cabral ldquoPaclitaxel-dependent celllines reveal a novel drug activityrdquo Molecular Cancer Therapeu-tics vol 9 no 11 pp 2914ndash2923 2010
[45] P B Schiff and S B Horwitz ldquoTaxol stabilizes microtubules inmouse fibroblast cellsrdquo Proceedings of the National Academy ofSciences of the United States of America vol 77 no 3 pp 1561ndash1565 1980
[46] P B Schiff J Fant and S B Horwitz ldquoPromotion of micro-tubule assembly in vitro by Taxolrdquo Nature vol 277 no 5698pp 665ndash667 1979
[47] D Zhang R Yang S Wang and Z Dong ldquoPaclitaxel new usesfor an old drugrdquoDrug Design Development andTherapy vol 8pp 279ndash284 2014
[48] S Rao G A Orr A G Chaudhary D G I Kingston and SB Horwitz ldquoCharacterization of the taxol binding site on themicrotubule 2-(m-Azidobenzoyl)taxol photolabels a peptide(amino acids 217-231) of beta-tubulinrdquoThe Journal of BiologicalChemistry vol 270 no 35 pp 20235ndash20238 1995
[49] F Wang Y Cao W Zhao H Liu Z Fu and R Han ldquoTaxolinhibits melanoma metastases through apoptosis inductionangiogenesis inhibition and restoration of E-cadherin andnm23 expressionrdquo Journal of Pharmacological Sciences vol 93no 2 pp 197ndash203 2003
18 BioMed Research International
[50] A Sevko V Kremer C Falk et al ldquoApplication of paclitaxel inlow non-cytotoxic doses supports vaccination with melanomaantigens in normal micerdquo Journal of Immunotoxicology vol 9no 3 pp 275ndash281 2012
[51] T Kreis and R Vale Guidebook to the Cytoskeletal and MotorProteins Oxford University Press Oxford UK 2nd edition1999
[52] P Giannakakou D L Sackett Y-K Kang et al ldquoPaclitaxel-resistant human ovarian cancer cells have mutant 120573-tubulinsthat exhibit impaired paclitaxel-driven polymerizationrdquo TheJournal of Biological Chemistry vol 272 no 27 pp 17118ndash171251997
[53] E Rakovitch W Mellado E J Hall T K Pandita S Sawantand C R Geard ldquoPaclitaxel sensitivity correlates with p53status and DNA fragmentation but not G2M accumulationrdquoInternational Journal of Radiation Oncology Biology Physics vol44 no 5 pp 1119ndash1124 1999
[54] S W Lowe S Bodis A McClatchey et al ldquop53 status and theefficacy of cancer therapy in vivordquo Science vol 266 no 5186 pp807ndash810 1994
[55] C C Zhang J-M Yang E White M Murphy A Levine andW N Hait ldquoThe role of MAP4 expression in the sensitivity topaclitaxel and resistance to vinca alkaloids in p53 mutant cellsrdquoOncogene vol 16 no 12 pp 1617ndash1624 1998
[56] K Fukasawa T Choi R Kuriyama S Rulong and G F VandeWoude ldquoAbnormal centrosome amplification in the absence ofp53rdquo Science vol 271 no 5256 pp 1744ndash1747 1996
[57] T-H Wang Y-H Chan C-W Chen et al ldquoPaclitaxel (Taxol)upregulates expression of functional interleukin-6 in humanovarian cancer cells through multiple signaling pathwaysrdquoOncogene vol 25 no 35 pp 4857ndash4866 2006
[58] E Yakirevich E Sabo I Naroditsky Y Sova O Lavie andM B Resnick ldquoMultidrug resistance-related phenotype andapoptosis-related protein expression in ovarian serous carcino-masrdquo Gynecologic Oncology vol 100 no 1 pp 152ndash159 2006
[59] G Szakacs J K Paterson J A Ludwig C Booth-Genthe andM M Gottesman ldquoTargeting multidrug resistance in cancerrdquoNature Reviews Drug Discovery vol 5 no 3 pp 219ndash234 2006
[60] L W Pfannenstiel S S K Lam L A Emens E M Jaffeeand T D Armstrong ldquoPaclitaxel enhances early dendritic cellmaturation and function through TLR4 signaling in micerdquoCellular Immunology vol 263 no 1 pp 79ndash87 2010
[61] N Klauber S Parangi E Flynn E Hamel and R J DrsquoAmatoldquoInhibition of angiogenesis and breast cancer in mice by themicrotubule inhibitors 2-methoxyestradiol and Taxolrdquo CancerResearch vol 57 no 1 pp 81ndash86 1997
[62] D Belotti V Vergani T Drudis et al ldquoThe microtubule-affecting drug paclitaxel has antiangiogenic activityrdquo ClinicalCancer Research vol 2 no 11 pp 1843ndash1849 1996
[63] D H Lau L Xue L J Young P A Burke and A T CheungldquoPaclitaxel (Taxol) an inhibitor of angiogenesis in a highlyvascularized transgenic breast cancerrdquo Cancer Biotherapy andRadiopharmaceuticals vol 14 no 1 pp 31ndash36 1999
[64] X Jiang ldquoHarnessing the immune system for the treatment ofbreast cancerrdquo Journal of Zhejiang University Science B vol 15no 1 pp 1ndash15 2014
[65] A Gadducci D Katsaros P Zola et al ldquoWeekly low-dosepaclitaxel as maintenance treatment in patients with advancedovarian cancer who had microscopic residual disease atsecond-look surgery after 6 cycles of paclitaxelplatinum-basedchemotherapy Results of an open noncomparative phase 2
multicenter italian study (after-6 protocol 2)rdquo InternationalJournal of Gynecological Cancer vol 19 no 4 pp 615ndash619 2009
[66] R S Bhatt J Merchan R Parker et al ldquoA phase 2 pilot trial oflow-dose continuous infusion or lsquometronomicrsquo paclitaxel andoral celecoxib in patients with metastatic melanomardquo Cancervol 116 no 7 pp 1751ndash1756 2010
[67] M Caballero J J Grau J L Blanch et al ldquoSerum vascularendothelial growth factor as a predictive factor in metronomic(weekly) paclitaxel treatment for advanced head and neckcancerrdquo Archives of OtolaryngologymdashHead and Neck Surgeryvol 133 no 11 pp 1143ndash1148 2007
[68] J Alexandre Y Hu W Lu H Pelicano and P Huang ldquoNovelaction of paclitaxel against cancer cells bystander effect medi-ated by reactive oxygen speciesrdquo Cancer Research vol 67 no 8pp 3512ndash3517 2007
[69] T Hadzic N Aykin-Burns Y Zhu et al ldquoPaclitaxel combinedwith inhibitors of glucose and hydroperoxide metabolismenhances breast cancer cell killing viaH
2O2-mediated oxidative
stressrdquo Free Radical Biology and Medicine vol 48 no 8 pp1024ndash1033 2010
[70] C A Sherman-Baust K G Becker W H Wood III Y Zhangand P J Morin ldquoGene expression and pathway analysis of ovar-ian cancer cells selected for resistance to cisplatin paclitaxel ordoxorubicinrdquo Journal of Ovarian Research vol 4 no 1 article21 2011
[71] R Agarwal and S B Kaye ldquoOvarian cancer strategies for over-coming resistance to chemotherapyrdquo Nature Reviews Cancervol 3 no 7 pp 502ndash516 2003
[72] T Acker and K H Plate ldquoRole of hypoxia in tumorangiogenesismdashmolecular and cellular angiogenic crosstalkrdquoCell and Tissue Research vol 314 no 1 pp 145ndash155 2003
[73] M Hockel and P Vaupel ldquoBiological consequences of tumorhypoxiardquo Seminars in Oncology vol 28 supplement 8 no 2 pp36ndash41 2001
[74] L Huang Q-H Zhang Q-L Ao H Xing Y-P Lu and DMa ldquoEffect of hypoxia on the chemotherapeutic sensitivity ofhuman ovarian cancer cells to paclitaxel and its mechanismrdquoZhonghua Zhong Liu Za Zhi vol 29 no 2 pp 96ndash100 2007
[75] N Rohwer and T Cramer ldquoHypoxia-mediated drug resistancenovel insights on the functional interaction of HIFs and celldeath pathwaysrdquoDrug Resistance Updates vol 14 no 3 pp 191ndash201 2011
[76] B B Aggarwal R V Vijayalekshmi and B Sung ldquoTargetinginflammatory pathways for prevention and therapy of cancershort-term friend long-term foerdquo Clinical Cancer Research vol15 no 2 pp 425ndash430 2009
[77] Z Duan R Foster D A Bell et al ldquoSignal transducersand activators of transcription 3 pathway activation in drug-resistant ovarian cancerrdquo Clinical Cancer Research vol 12 no17 pp 5055ndash5063 2006
[78] H-J Kuh S H Jang M G Wientjes J R Weaver and J L-SAu ldquoDeterminants of paclitaxel penetration and accumulationin human solid tumorrdquo Journal of Pharmacology and Experi-mental Therapeutics vol 290 no 2 pp 871ndash880 1999
[79] S Arao H Suwa M Mandai et al ldquoHypoxia-mediated drugresistance novel insights on the functional interaction of HIFsand cell death pathwaysrdquo Cancer Research vol 54 no 5 pp1355ndash1359 1994
[80] S E Johnatty J Beesley B Gao et al ldquoABCB1 (MDR1)polymorphisms and ovarian cancer progression and survivala comprehensive analysis from the Ovarian Cancer Association
BioMed Research International 19
Consortium and the Cancer GenomeAtlasrdquoGynecologic Oncol-ogy vol 131 no 1 pp 8ndash14 2013
[81] X Yang A K Iyer A Singh et al ldquoCluster of differentiation44 targeted hyaluronic acid based nanoparticles for MDR1siRNA delivery to overcome drug resistance in ovarian cancerrdquoPharmaceutical Research 2014
[82] D A Zajchowski B Y Karlan and L K Shawver ldquoTreatment-related protein biomarker expression differs between primaryand recurrent ovarian carcinomasrdquoMolecular CancerTherapeu-tics vol 11 no 2 pp 492ndash502 2012
[83] MM Gottesman J Ludwig D Xia and G Szakacs ldquoDefeatingdrug resistance in cancerrdquoDiscovery Medicine vol 6 no 31 pp18ndash23 2006
[84] S Mozzetti C Ferlini P Concolino et al ldquoClass III 120573-tubulin overexpression is a prominent mechanism of paclitaxelresistance in ovarian cancer patientsrdquo Clinical Cancer Researchvol 11 no 1 pp 298ndash305 2005
[85] M Kavallaris D Y S Kuo C A Burkhart et al ldquoTaxol-resistant epithelial ovarian tumors are associated with alteredexpression of specific beta-tubulin isotypesrdquo Journal of ClinicalInvestigation vol 100 no 5 pp 1282ndash1293 1997
[86] G A Orr P Verdier-Pinard H McDaid and S B HorwitzldquoMechanisms of Taxol resistance related to microtubulesrdquoOncogene vol 22 no 47 pp 7280ndash7295 2003
[87] C Ferlini L Cicchillitti G Raspaglio et al ldquoPaclitaxel directlybinds to Bcl-2 and functionally mimics activity of Nur77rdquoCancer Research vol 69 no 17 pp 6906ndash6914 2009
[88] E Mechetner A Kyshtoobayeva S Zonis et al ldquoLevels ofmultidrug resistance (MDR1) P-glycoprotein expression byhuman breast cancer correlate with in vitro resistance to taxoland doxorubicinrdquo Clinical Cancer Research vol 4 no 2 pp389ndash398 1998
[89] J S Lagas C W N Damen R A B VanWaterschoot D IusufJ H Beijnen and A H Schinkel ldquoP-glycoprotein multidrug-resistance associated protein 2 Cyp3a and carboxylesteraseaffect the oral availability and metabolism of vinorelbinerdquoMolecular Pharmacology vol 82 no 4 pp 636ndash644 2012
[90] M T Huizing J B Vermorken H Rosing et al ldquoPharmacoki-netics of paclitaxel and three major metabolites in patients withadvanced breast carcinoma refractory to anthracycline therapytreated with a 3-hour paclitaxel infusion a European CancerCentre (ECC) trialrdquo Annals of Oncology vol 6 no 7 pp 699ndash704 1995
[91] R Panchagnula ldquoPharmaceutical aspects of paclitaxelrdquo Interna-tional Journal of Pharmaceutics vol 172 no 1-2 pp 1ndash15 1998
[92] S H Jang M G Wientjes and J L-S Au ldquoDeterminants ofpaclitaxel uptake accumulation and retention in solid tumorsrdquoInvestigational New Drugs vol 19 no 2 pp 113ndash123 2001
[93] D S Sonnichsen andM V Relling ldquoClinical pharmacokineticsof paclitaxelrdquo Clinical Pharmacokinetics vol 27 no 4 pp 256ndash269 1994
[94] T Ohtsu Y Sasaki T Tamura et al ldquoClinical pharmacokineticsand pharmacodynamics of paclitaxel a 3-hour infusion versusa 24-hour infusionrdquo Clinical Cancer Research vol 1 no 6 pp599ndash606 1995
[95] M Czejka J Schueller H Schnait B Springer and I EderldquoClinical pharmacokinetics andmetabolism of paclitaxel after athree-hour infusion comparison of two preparationsrdquo Journalof Oncology Pharmacy Practice vol 9 no 4 pp 129ndash136 2003
[96] J Rizzo C Riley D VonHoff J Kuhn J Phillips and T BrownldquoAnalysis of anticancer drugs in biological fluids determination
of taxol with application to clinical pharmacokineticsrdquo Journalof Pharmaceutical and Biomedical Analysis vol 8 no 2 pp 159ndash164 1990
[97] V A de Weger J H Beijnen and J H M Schellens ldquoCel-lular and clinical pharmacology of the taxanes docetaxel andpaclitaxelmdasha reviewrdquoAnti-Cancer Drugs vol 25 no 5 pp 488ndash494 2014
[98] S Kumar H Mahdi C Bryant J P Shah G Garg andA Munkarah ldquoClinical trials and progress with paclitaxel inovarian cancerrdquo International Journal of Womenrsquos Health vol 2no 1 pp 411ndash427 2010
[99] B Huang J Zhao J C Unkeless Z H Feng and H XiongldquoTLR signaling by tumor and immune cells a double-edgedswordrdquo Oncogene vol 27 no 2 pp 218ndash224 2008
[100] R A Jibodh J S Lagas B Nuijen J H Beijnen and J HM Schellens ldquoTaxanes old drugs new oral formulationsrdquoEuropean Journal of Pharmacology vol 717 no 1ndash3 pp 40ndash462013
[101] A Javeed M Ashraf A Riaz A Ghafoor S Afzal and M MMukhtar ldquoPaclitaxel and immune systemrdquo European Journal ofPharmaceutical Sciences vol 38 no 4 pp 283ndash290 2009
[102] L Bracci G Schiavoni A Sistigu and F Belardelli ldquoImmune-based mechanisms of cytotoxic chemotherapy implications forthe design of novel and rationale-based combined treatmentsagainst cancerrdquo Cell Death and Differentiation vol 21 no 1 pp15ndash25 2014
[103] C A Byrd-Leifer E F Block K Takeda S Akira and A DingldquoThe role of MyD88 and TLR4 in the LPS-mimetic activity ofTaxolrdquo European Journal of Immunology vol 31 no 8 pp 2448ndash2457 2001
[104] A-C Wang Y-B Ma F-X Wu et al ldquoTLR4 induces tumorgrowth and inhibits paclitaxel activity in MyD88-positivehuman ovarian carcinoma in vitrordquo Oncology Letters vol 7 no3 pp 871ndash877 2014
[105] Y Zhu N Liu S D Xiong Y J Zheng and Y W ChuldquoCD4+Foxp3+ regulatory T-cell impairment by paclitaxel isindependent of toll-like receptor 4rdquo Scandinavian Journal ofImmunology vol 73 no 4 pp 301ndash308 2011
[106] M Kubo T Morisaki K Matsumoto et al ldquoPaclitaxel probablyenhances cytotoxicity of natural killer cells against breastcarcinoma cells by increasing perforin productionrdquo CancerImmunology Immunotherapy vol 54 no 5 pp 468ndash476 2005
[107] L Markasz G Stuber B Vanherberghen et al ldquoEffect of fre-quently used chemotherapeutic drugs on the cytotoxic activityof human natural killer cellsrdquo Molecular Cancer Therapeuticsvol 6 no 2 pp 644ndash654 2007
[108] T Sako N Burioka K Yasuda et al ldquoCellular immune profile inpatients with non-small cell lung cancer after weekly paclitaxeltherapyrdquo Acta Oncologica vol 43 no 1 pp 15ndash19 2004
[109] R Kaneno G V Shurin I L Tourkova and M R ShurinldquoChemomodulation of human dendritic cell function by anti-neoplastic agents in low noncytotoxic concentrationsrdquo Journalof Translational Medicine vol 7 article 58 2009
[110] TMichels G V ShurinHNaiditch A Sevko VUmansky andM R Shurin ldquoPaclitaxel promotes differentiation of myeloid-derived suppressor cells into dendritic cells in vitro in a TLR4-independent mannerrdquo Journal of Immunotoxicology vol 9 no3 pp 292ndash300 2012
[111] R A Kemp and F Ronchese ldquoTumor-specific Tc1 but not Tc2cells deliver protective antitumor immunityrdquo The Journal ofImmunology vol 167 no 11 pp 6497ndash6502 2001
20 BioMed Research International
[112] A Y Rudensky ldquoRegulatory T cells and Foxp3rdquo ImmunologicalReviews vol 241 no 1 pp 260ndash268 2011
[113] EM Shevach ldquoCD4+CD25+ suppressor T cellsmore questionsthan answersrdquo Nature Reviews Immunology vol 2 no 6 pp389ndash400 2002
[114] S Sakaguchi T Yamaguchi T Nomura and M Ono ldquoRegu-latory T cells and immune tolerancerdquo Cell vol 133 no 5 pp775ndash787 2008
[115] H Nishikawa and S Sakaguchi ldquoRegulatory T cells in tumorimmunityrdquo International Journal of Cancer vol 127 no 4 pp759ndash767 2010
[116] W Zou ldquoRegulatory T cells tumour immunity and immuno-therapyrdquoNature Reviews Immunology vol 6 no 4 pp 295ndash3072006
[117] A Fialova S Partlova L Sojka et al ldquoDynamics of T-cell infil-tration during the course of ovarian cancer The gradual shiftfrom aTh17 effector cell response to a predominant infiltrationby regulatory T-cellsrdquo International Journal of Cancer vol 132no 5 pp 1070ndash1079 2013
[118] A E Albers R L Ferris G G Kim K Chikamatsu A BDeLeo and T L Whiteside ldquoImmune responses to p53 inpatients with cancer enrichment in tetramer+ p53 peptide-specific T cells and regulatory T cells at tumor sitesrdquo CancerImmunology Immunotherapy vol 54 no 11 pp 1072ndash10812005
[119] N Liu Y Zheng Y Zhu S Xiong andYChu ldquoSelective impair-ment of CD4 + CD25 + Foxp3 + regulatory T cells by paclitaxelis explained by Bcl-2Bax mediated apoptosisrdquo InternationalImmunopharmacology vol 11 no 2 pp 212ndash219 2011
[120] X Wu Q-M Feng Y Wang J Shi H-L Ge and W DildquoThe immunologic aspects in advanced ovarian cancer patientstreated with paclitaxel and carboplatin chemotherapyrdquo CancerImmunology Immunotherapy vol 59 no 2 pp 279ndash291 2010
[121] A P Vicari R Luu N Zhang et al ldquoPaclitaxel reducesregulatoryT cell numbers and inhibitory function and enhancesthe anti-tumor effects of the TLR9 agonist PF-3512676 in themouserdquo Cancer Immunology Immunotherapy vol 58 no 4 pp615ndash628 2009
[122] L Zhang K Dermawan M Jin et al ldquoDifferential impairmentof regulatory T cells rather than effector T cells by paclitaxel-based chemotherapyrdquo Clinical Immunology vol 129 no 2 pp219ndash229 2008
[123] Y Tabuchi J Matsuoka M Gunduz et al ldquoResistance topaclitaxel therapy is related with Bcl-2 expression through anestrogen receptor mediated pathway in breast cancerrdquo Interna-tional Journal of Oncology vol 34 no 2 pp 313ndash319 2009
[124] N Obermajer R Muthuswamy K Odunsi R P Edwards andP Kalinski ldquoPGE
2-induced CXCL12 production and CXCR4
expression controls the accumulation of human MDSCs inovarian cancer environmentrdquo Cancer Research vol 71 no 24pp 7463ndash7470 2011
[125] Q M Feng W Di and X Wu ldquoImmune reconstitution inadvanced ovarian cancer patients undergoing first line chemo-therapyrdquo Xi Bao Yu Fen Zi Mian Yi Xue Za Zhi vol 25 no 11pp 1023ndash1025 2009
[126] A D Seidman D Hochhauser M Gollub et al ldquoNinety-six-hour paclitaxel infusion after progression during short taxaneexposure a phase II pharmacokinetic and pharmacodynamicstudy in metastatic breast cancerrdquo Journal of Clinical Oncologyvol 14 no 6 pp 1877ndash1884 1996
[127] D R Spriggs M F Brady L Vaccarello et al ldquoPhase IIIrandomized trial of intravenous cisplatin plus a 24- or 96-hour
infusion of paclitaxel in epithelial ovarian cancer a gynecologiconcology group studyrdquo Journal of Clinical Oncology vol 25 no28 pp 4466ndash4471 2007
[128] G A Omura M F Brady K Y Look et al ldquoPhase III trial ofpaclitaxel at two dose levels the higher dose accompanied byfilgrastim at two dose levels in platinum-pretreated epithelialovarian cancer an intergroup studyrdquo Journal of Clinical Oncol-ogy vol 21 no 15 pp 2843ndash2848 2003
[129] R Simon and L Norton ldquoThe Norton-Simon hypothesisdesigning more effective and less toxic chemotherapeutic reg-imensrdquoNature Clinical Practice Oncology vol 3 no 8 pp 406ndash407 2006
[130] A Kumar P Hoskins and A Tinker ldquoDose-dense paclitaxel inadvanced ovarian cancerrdquo Clinical Oncology vol 27 no 1 pp40ndash47 2015
[131] P Marchetti S Urien G A Cappellini G Ronzino and CFicorella ldquoWeekly administration of paclitaxel theoretical andclinical basisrdquoCritical Reviews in OncologyHematology vol 44supplement pp S3ndashS13 2002
[132] P Francis E Rowinsky J Schneider T Hakes W Hoskinsand M Markman ldquoPhase I feasibility and pharmacologic studyof weekly intraperitoneal paclitaxel A Gynecologic OncologyGroup pilot studyrdquo Journal of Clinical Oncology vol 13 no 12pp 2961ndash2967 1995
[133] H Thomas and P Rosenberg ldquoRole of weekly paclitaxel inthe treatment of advanced ovarian cancerrdquo Critical Reviews inOncologyHematology vol 44 supplement pp S43ndashS51 2002
[134] M Markman J Markman K Webster et al ldquoDuration ofresponse to second-line platinum-based chemotherapy forovarian cancer implications for patient management and clini-cal trial designrdquo Journal of Clinical Oncology vol 22 no 15 pp3120ndash3125 2004
[135] P H OrsquoDonnell M Eileen Dolan E Gamazon et al ldquoPopu-lation differences in platinum toxicity as a means to identifynovel genetic susceptibility variantsrdquo Pharmacogenetics andGenomics vol 20 no 5 pp 327ndash337 2010
[136] M J Millward M J Boyer M Lehnert et al ldquoDocetaxel andcarboplatin is an active regimen in advanced non-small-celllung cancer a phase II study in Caucasian and Asian patientsrdquoAnnals of Oncology vol 14 no 3 pp 449ndash454 2003
[137] M Markman ldquoIntraperitoneal therapy of ovarian cancerrdquoOncologist vol 1 no 1-2 pp 18ndash21 1996
[138] M Markman and J L Walker ldquoIntraperitoneal chemotherapyof ovarian cancer a review with a focus on practical aspects oftreatmentrdquo Journal of Clinical Oncology vol 24 no 6 pp 988ndash994 2006
[139] K Fujiwara S Nagao E Aotani and K Hasegawa ldquoPrincipleand evolving role of intraperitoneal chemotherapy in ovariancancerrdquo Expert Opinion on Pharmacotherapy vol 14 no 13 pp1797ndash1806 2013
[140] M Markman E Rowinsky T Hakes et al ldquoPhase I trialof intraperitoneal taxol a gynecoloic oncology group studyrdquoJournal of Clinical Oncology vol 10 no 9 pp 1485ndash1491 1992
[141] M Markman M F Brady N M Spirtos P Hanjani and S CRubin ldquoPhase II trial of intraperitoneal paclitaxel in carcinomaof the ovary tube and peritoneum a gynecologic oncologygroup studyrdquo Journal of Clinical Oncology vol 16 no 8 pp2620ndash2624 1998
[142] P B Panici I Palaia M Graziano F Bellati N Manci and RAngioli ldquoIntraperitoneal paclitaxel as consolidation treatmentin ovarian cancer patients a case control studyrdquo Oncology vol78 no 1 pp 20ndash25 2010
BioMed Research International 21
[143] D K Armstrong B Bundy L Wenzel et al ldquoIntraperitonealcisplatin and paclitaxel in ovarian cancerrdquo The New EnglandJournal of Medicine vol 354 no 1 pp 34ndash43 2006
[144] D Tewari J Java and R Salani ldquoLong-term survival advantageof intraperitoneal chemotherapy treatment in advanced ovariancancer an analysis of a Gynecologic Oncology Group ancillarydata studyrdquo in Proceedings of the 2013 Society of GynecologicOncology Annual Meeting on Womenrsquos Cancer (GOG114172Abstract) Los Angeles Calif USA 2013
[145] D A Yardley ldquonab-paclitaxel mechanisms of action and deliv-eryrdquo Journal of Controlled Release vol 170 no 3 pp 365ndash3722013
[146] M Ando K Yonemori N Katsumata et al ldquoPhase I and phar-macokinetic study of nab-paclitaxel nanoparticle albumin-bound paclitaxel administeredweekly to Japanese patients withsolid tumors and metastatic breast cancerrdquo Cancer Chemother-apy and Pharmacology vol 69 no 2 pp 457ndash465 2012
[147] N Desai V Trieu Z Yao et al ldquoIncreased antitumor activityintratumor paclitaxel concentrations and endothelial cell trans-port of cremophor-free albumin-bound paclitaxel ABI-007compared with cremophor-based paclitaxelrdquo Clinical CancerResearch vol 12 no 4 pp 1317ndash1324 2006
[148] J A Yared and K H R Tkaczuk ldquoUpdate on taxane devel-opment new analogs and new formulationsrdquo Drug DesignDevelopment andTherapy vol 6 pp 371ndash384 2012
[149] M G Teneriello P C Tseng M Crozier et al ldquoPhase IIevaluation of nanoparticle albumin-bound paclitaxel in plati-num-sensitive patients with recurrent ovarian peritoneal orfallopian tube cancerrdquo Journal of Clinical Oncology vol 27 no9 pp 1426ndash1431 2009
[150] R L Coleman W E Brady D S McMeekin et al ldquoA phase IIevaluation of nanoparticle albumin-bound (nab) paclitaxel inthe treatment of recurrent or persistent platinum-resistant ovar-ian fallopian tube or primary peritoneal cancer a GynecologicOncology Group Studyrdquo Gynecologic Oncology vol 122 no 1pp 111ndash115 2011
[151] J W Singer ldquoPaclitaxel poliglumex (XYOTAX CT-2103) amacromolecular taxanerdquo Journal of Controlled Release vol 109no 1ndash3 pp 120ndash126 2005
[152] C Li D-F Yu R A Newman et al ldquoComplete regressionof well-established tumors using a novel water-soluble poly(L-glutamic acid)-paclitaxel conjugaterdquo Cancer Research vol 58no 11 pp 2404ndash2409 1998
[153] M Mita A Mita J Sarantopoulos et al ldquoPhase I study ofpaclitaxel poliglumex administered weekly for patients withadvanced solid malignanciesrdquo Cancer Chemotherapy and Phar-macology vol 64 no 2 pp 287ndash295 2009
[154] P Sabbatini M W Sill D OrsquoMalley L Adler and A ASecord ldquoA phase II trial of paclitaxel poliglumex in recurrentor persistent ovarian or primary peritoneal cancer (EOC) agynecologic oncology group studyrdquo Gynecologic Oncology vol111 no 3 pp 455ndash460 2008
[155] M O Bradley C S Swindell F H Anthony et al ldquoTumortargeting by conjugation of DHA to paclitaxelrdquo Journal ofControlled Release vol 74 no 1ndash3 pp 233ndash236 2001
[156] M O Bradley N L Webb F H Anthony et al ldquoTumortargeting by covalent conjugation of a natural fatty acid topaclitaxelrdquo Clinical Cancer Research vol 7 no 10 pp 3229ndash3238 2001
[157] A C Wolff R C Donehower M K Carducci et al ldquoPhaseI study of docosahexaenoic acid-paclitaxel a taxane-fatty acid
conjugate with a unique pharmacology and toxicity profilerdquoClinical Cancer Research vol 9 no 10 part 1 pp 3589ndash35972003
[158] A Sparreboom A C Wolff J Verweij et al ldquoDispositionof docosahexaenoic acid-paclitaxel a novel taxane in bloodin vitro and clinical pharmacokinetic studiesrdquo Clinical CancerResearch vol 9 no 1 pp 151ndash159 2003
[159] P M Fracasso J Picus J D Wildi et al ldquoPhase 1 and phar-macokinetic study of weekly docosahexaenoic acid-paclitaxelTaxoprexin in resistant solid tumor malignanciesrdquo CancerChemotherapy and Pharmacology vol 63 no 3 pp 451ndash4582009
[160] A Y Bedikian R C DeConti R Conry et al ldquoPhase 3 study ofdocosahexaenoic acid-paclitaxel versus dacarbazine in patientswith metastatic malignant melanomardquo Annals of Oncology vol22 no 4 pp 787ndash793 2011
[161] Y-N Wu S-L Wang Y-C Wang et al ldquoReversal effect ofdocosahexaenoic acid on taxol resistance in human ovarian car-cinoma A2780T cellsrdquo Obstetrics amp Gynecology InternationalJournal vol 1 no 3 Article ID 00018 2014
Submit your manuscripts athttpwwwhindawicom
PainResearch and TreatmentHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom
Volume 2014
ToxinsJournal of
VaccinesJournal of
Hindawi Publishing Corporation httpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
AntibioticsInternational Journal of
ToxicologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
StrokeResearch and TreatmentHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Drug DeliveryJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Advances in Pharmacological Sciences
Tropical MedicineJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Medicinal ChemistryInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
AddictionJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
Emergency Medicine InternationalHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Autoimmune Diseases
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Anesthesiology Research and Practice
ScientificaHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Pharmaceutics
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of

BioMed Research International 7
AUC (area under the plasma concentration)
Cmax (maximum concentration)
Pacli
taxe
l con
cent
ratio
n (120583
M)
0 10 20 30 40
Time (hr)
0
1
2
3
4
5
Figure 4 Plasma pharmacokinetics of paclitaxel The pharmacoki-netics generally were linear for 6 or 24 hour infusions but becomenonlinear for infusions of shorter durations due to variation inthe elimination clearance with the dose administered An increasein plasma concentration of paclitaxel results in disproportionatelarger increase in 119862max (maximum plasma concentration) and AUC(area under plasma concentration) followed by decrease in drugelimination from body tissues
The disappearance of paclitaxel from plasma is tradition-ally believed to be biphasic [33] The initial rapid declinerepresents distribution to the peripheral compartment andelimination of the drug The later phase is due in part tothe slow efflux of paclitaxel from the peripheral compartment[92] In the presence of more sensitive assay methods andlater sampling times a three-compartment model seems tobe more accurate [40 93] Paclitaxel has been shown tohave a nonlinear pattern of pharmacokinetics (Figure 4)Thepharmacokinetics were generally linear for 6- or 24-hourinfusions but become nonlinear for infusions of shorterdurations because the elimination clearance varies with thedose administered With increasing plasma concentrationof paclitaxel there is a disproportionately larger increasein 119862max (maximum plasma concentration) and AUC (areaunder plasma concentration) accompanied by decrease indrug elimination from body tissues The clinical importanceof this nonlinear pattern is that dose escalationmay result in adisproportionate increase in toxicity whereas dose reductionmay affect its efficacy [33 90 91 94]
The pharmacokinetics of paclitaxel has been evaluatedover a wide range of doses up to 300mgm2 and withinfusion schedules ranging from 3 to 24 hours Maximumplasma concentrations are dose-related In patients treatedwith single dose infusion of 135 and 175mgm2 given as3- and 24-hour infusions mean steady state volume ofdistribution has ranged from 198 to 688 Lm2 indicatingextensive extravascular distribution andor tissue bindingTerminal half-life has ranged from 13 to 86 hours (mean 5hours) [40 93] and total body clearance has ranged from116 to 240 Lhrm2 Preclinical results in animals have shown
high levels in most tissues Being highly protein-boundpaclitaxel has a high affinity for distribution in specific tissuesincluding kidney lung spleen and extracellular fluids likeascites and pleural fluids [40 95] but the uptake of the drugin the brain is minimal [96 97] Exposure to paclitaxel isrelatively high in tumour tissue compared with other tissuesand in addition to slow elimination from tumour tissue theAUC in tumour tissue is about five-fold higher than that inplasma [97]
There is no evidence of accumulation of paclitaxel withmultiple treatment courses as the variability in systemicpaclitaxel exposure as measured by AUC (0ndashinfin) (area underplasma concentration-time curve from time 0 to infinity)for successive treatment courses are minimal [98] Paclitaxelclearance is however sequence dependent Patients receiv-ing a platinum-based agent prior to paclitaxel have lowerclearance and greater clinical toxicity than patients receivingpaclitaxel before cisplatin [93]
The drug administered intravenously undergoes anextensive P-450mediated hepaticmetabolism by cytochromeenzymes (CYP3A andCYP2C8) with 70ndash80being excretedinto bile by adenosine triphosphate- (ATP-) binding cassettemultidrug transporters such as P-glycoprotein (P-gp) andmultidrug resistance protein 2 (MRP-2) either asmetabolitesor as the parent drug Variation in MRP-2 activity hasbeen found to have direct effect on the effective exposureto paclitaxel [99] The bioavailability is poor following oraladministration due to enterocyte expression of P-gp and first-pass metabolism in the liver Most of the drug is eliminatedin feces Less than 10 drug in the unchanged form isexcreted in the urine indicating extensive nonrenal clearance[96] Combinations of inhibitors of CYP3A and P-gp mightpossibly improve the oral bioavailability of the taxanes [8997 100]
7 Paclitaxel and the Immune System
The immune system consists of two different but interactingmechanisms which are innate and adaptivemechanismsTheinnate mechanism is the first line of defense and consists of agroup of cells which includes mainly macrophages dendriticcells (DCs) and natural killer (NK) cells while the adaptiveimmunemechanism is represented by T-lymphocytes All thecomponents of innate and adaptive mechanism are involvedin antitumour immunity which includes tumour recognitioncontrol and elimination However cancer cells are able toevade immune detection and actively suppress antitumourimmunity
Paclitaxel has a wide range of dose dependent immuno-modulatory effects described in Figure 5 At standard dosepaclitaxel is broadly immunosuppressive and this is becauseit inhibits a number of cell types involved in tumour rejectionsuch asmacrophages effector T cells andNK cells [101] How-ever at lower doses than typically used for chemotherapypaclitaxel has an important immunogenic role promotingantitumour immunity [101 102] Hence understanding theimmunological basis of paclitaxel may help to maximise themanipulation of the immunomodulatory effects of paclitaxel
8 BioMed Research International
Immunomodulatory effect of
paclitaxel
Stimulate direct cytotoxic activity by
macrophage
Induce activation maturation and priming of DCs
Stimulate NK-dependent antitumour immunity
Activation of tumour-specificCTL Expansion of memory T cells
Secretion of proinflammatory cytokine
Shift from Th2 to Th1 type ofresponse
Depletion of Tregs andmodulation of MDSC
Downregulates the expression of VEGFR-2
and inhibits angiogenesis
IL-6 IL-12 TNF-120572 and i-NOS
Figure 5 Immunomodulatory effect of paclitaxel Paclitaxel a toll-like receptor 4 (TLR4) ligand binds to TLR4 receptor and triggers TLR4signaling via MyD88 dependent and independent pathway Paclitaxel then promotes anticancer immune response directly by stimulatingmacrophages to kill cancer cells or indirectly by secretion of proinflammatory cytokines which upregulates activation of DCs NK andtumour specific CTL Paclitaxel promotes effective CTL response by upregulation of mannose-6-phosphate which facilitate permeabilityto granzyme B and cytokine patterns of T helper type 1 Paclitaxel modulates MDSC and ablates Tregs Memory T cells (CD4+CD45RO+and CD8+CD45RO+) increased significantly while regulatory T cells (Tregs) decreased around 2 weeks creating an opportunity window fordose-dense therapy and immunomodulatory agents to achieve clinical benefit Dose-dense and low dose paclitaxel also blocks new vesselformation by downregulating VEGF-receptor 2 reduces resistance by alternative mechanism of action
to develop better therapeutic options in the management ofadvanced ovarian cancer
Paclitaxel is a ligand to toll-like receptor 4 (TLR4) whichis expressed on innate immune cells including macrophagesThe binding of paclitaxel to TLR4 on macrophages trig-gers the MyD88 mitogen-activated protein kinase (MAPK)and transcription of nuclear factor NF-kappa B (NF-120581B)pathways (Figure 3) resulting in their activation and releaseof immunostimulatory cytokines such as tumour necrosisfactor-120572 (TNF-120572) interleukin-1 (IL-1) interleukin-6 (IL-6)and interleukin-8 (IL-8) [103ndash105] Activated macrophagescan either cause direct tumour cell lysis via release oflysosomal enzymes and nitric oxide (NO) or indirectly byactivating NK cells DCs and tumour-specific cytotoxic T-lymphocytes (CTLs) [101]
NK cells are also innate immune cells capable of killingtumour cells particularly those cells that have reduced classI MHC expression and therefore can escape killing by CTLsPaclitaxel can enhance NK cell function by inducing mRNAand protein production of perforin an effector moleculeinvolved inNKcell-mediated cytotoxicity [106]However theeffect of low dose paclitaxel on NK cells is controversial Inanother study it was found that treatment of human NK cellswith paclitaxel effectively inhibits NK cell-mediated killing ofK562 (human erythroleukemia) target cells in vitro withoutaffecting the viability of NK cells [107] However weeklypaclitaxel therapy for non-small cell lung cancer patients was
only able to reduce the NK cell function up to completion ofthe first cycle but thereafter it gradually recovered [108]
Dendritic cells also express TLR4 and can be directlyactivated by paclitaxel The binding of paclitaxel to TLR onimmature DCs promotes DC maturation by upregulatingantigen-processing machinery gene components costimu-latory molecules and IL-12p70 [102] This enhances theability of DCs to prime T cells which facilitate antitumourimmunity [109] Paclitaxel can also promote cytotoxic T-cell function by upregulating mannose-6-phosphate whichfacilitates permeability to granzyme B and also inducescytokine production patterns typical of the T helper type 1phenotype via IL-2 (CD4 T cell) and IFN-120574 (CD8 T cell)secretion [104 110] Activated CD8+ T cells can differentiateinto CTL type 1 (Tc1) cells producingmainly IFN-120574 and CTLtype 2 (Tc2) cells producing mostly IL-4 IL-5 and IL-10 Tc1cells are potent CTL involved in the defense against cancerTc1 cells are able to recognise tumour antigens in the contextof MHC class I and mediate tumour cell lysis The role of Tc2cells in the immune response is not clearly known althoughtheir presence has been associated with disease progression[111]
CD4+ CD25+ regulatory T-cells (Tregs) constitutingapproximately 5ndash10 of peripheral CD4+ T cells [112 113]play an important role in tumour immune evasion [114]There is growing evidence that supports the existence ofelevated numbers of Tregs in tumours [115ndash117] which may
BioMed Research International 9
suppress immune responses of other CD4+ and CD8+ cells[118ndash120] and promote tumour progression In murine stud-ies paclitaxel exhibits the ability to reduce the number andsize of Treg cells thereby enhancing antitumour immunity[119 121] Similar findingswere seenwith a selective reductionin the size and number of Treg populations in peripheralblood samples from non-small cell lung cancer (NSCLC)patients [122]
Paclitaxel also decreased the expression of the anti-apoptotic molecule Bcl-2 in Treg cells while increasing thecorresponding proapoptoticmember Bax which contributedto the apoptotic sensitivity of Treg to paclitaxel [87]This wasseen in a study using the 3LL Lewis tumour model whichdemonstrated that Treg cells exposed to paclitaxel displayeddown regulation of Bcl-2 and upregulation of Bax and uponblocking the Bcl-2 pathway the ability of paclitaxel to ablateTreg cells compared toT effectorswas impaired and bothTregand T effectors were affected These results may suggest thatpaclitaxel targets Bcl-2 rather than tubulin to contribute tothe distinctive effect on Treg cells [119] It has recently beenshown in vitro that paclitaxel could target Bcl-2 and thereforelead to apoptosis Bcl-2 family proteins are key regulators ofapoptosis and play an important role in tumourigenesis andmulti-drug resistance by blocking apoptosis [119 123]
Few studies have also shown effect of paclitaxel onmyeloid-derived suppressor cells (MDSCs) a heterogeneouspopulation of immature myeloid cells immunosuppressivein nature are recruited by cancer cells and are found inincreased amount in advanced epithelial ovarian cancer [124]In a murine study using C57BL6 mice administration ofpaclitaxel at ultralow dose modulates MDSCs to differentiateinto DCs in a TLR4 independent manner [110] Hencepaclitaxel in ultralow noncytotoxic doses together with itsangiogenesis blocking ability may potentially enhance theefficacy of immunotherapy by ablation of immunosuppres-sive populations such as Tregs and MDSCs in tumour-bearing hosts [50 102]
In immunocompromised patients with advanced ovariancancer with increased Tregs and decreased levels of CD4+T cell CD8+ T cell and NK subsets after a single courseof combined carboplatin and paclitaxel chemotherapy theimmunosuppression is reversed around 12 to 14 days later butnot before one week or after three to four weeks Not only areTregs decreased but also the proportions of IFN-120574 secretingCD8+ T cells T helper-1 Tc1 and NKT cells The ratio of Tc1to Tc2 cells increases significantly [111 120 125]
Following chemotherapy both CD4+CD45RO+ andCD8+CD45RO+ memory T cells increased significantly andpeaked around 2 weeks The increase of memory T cellsin ovarian cancer patients following chemotherapy prob-ably opens the door of opportunity to develop long-termimmunological memory which could prevent recurrenceand metastases [120] Administration of dose-dense therapygiven weekly may hence be beneficial immunologically tomount an adequate immune response compared to standard3-week therapy In addition administration of immunother-apy agentsmay also be ideal during the period of 2weeks afterchemotherapy where temporary immune system reconstitu-tion takes place
8 Clinical Studies
In the past two decades paclitaxel had been administered indoses ranging from 60 to 250mgm2 over 1ndash96 hours andfrom 1 to 3 weekly intervals Prolonged exposure up to 96hours was believed to be effective as demonstrated with pre-clinical data but later refuted in large prospective studies [14126 127] A 24-hour infusion of paclitaxel was subsequentlyadministered to reduce the risk of hypersensitivity reactionshowever it was shown to increase mucosal and bone marrowtoxicity without improved efficacy [127 128] Development ofeffective premedication has led to administration of shorterinfusions (lt3 hours) which are better tolerated in particularfrom a haematologic perspective but patients remain at riskof myalgia and neuropathy at higher doses Weekly one-hourlow dose paclitaxel also known as dose-dense therapy hasrecently emerged as another possible strategy to improveoutcomes
9 Dose-Dense Therapy
Dose-dense treatment is defined by delivery of a maintainedper-cycle dose or overall dose with administration of drugat shorter time intervals than is standard This differs fromdose intensity which refers to dose (per unit weight or bodysurface area) delivered per unit time Hence either escalationof dose per cycle or reducing the time in between cycles maymodify dose intensity [129 130]
The rationale for the dose-dense approach of weeklypaclitaxel is that more frequent delivery of moderate dosesmay achieve greater efficacy by allowing sustained exposureof dividing tumour cells to paclitaxelrsquos cytotoxic and antian-giogenic effects hence reducing resistance delaying relapseand increasing the possibility of cancer remission Three 1-hour infusions of paclitaxel given at a week interval achievedgreater dose-density as well as dose-intensity than a singleadministration every 3 weeksThe initial tissue concentration(gt50 nM) for 1-hour infusion is similar to that of 3-hourinfusion but the concentration in the plasma instead oflasting for 8 hours in a 3-hour infusion rapidly falls below50 nM in less than 75 minutes for 1-hour infusion and hencereduces the risk of neutropenia However the rate of fallexperienced in tissue concentration of the drug is slowerthan plasma concentration of the drug hence efficacy ismaintained [131 132] A shorter infusion time allows bettercontrol of toxicities improved patient comfort and reducedhospitalisation hours
Several studies have used dose-dense paclitaxel in thetreatment of advanced ovarian cancer and are summarizedin Table 1 Based on phase 1 studies the recommendeddose for weekly paclitaxel ranges between 80 and 90mgm2compared with 45mgm2 per week with 3-weekly paclitaxeland is given over 1-hour duration Weekly scheduling hasdemonstrated consistent activities in ovarian cancer studies[11ndash13] Response rates were in the 20ndash50 range whereusually less than 10 would be expected Grade-4 doselimiting toxicities in particular neutropenia were not evidentat any dose below 100mgm2week [11 133]
10 BioMed Research International
Table1Ph
ases
Iand
IIstu
dies
onintravenou
sdose-densep
aclitaxel
Stud
yRe
gimen
119899()
PI(m
)RR
()
CR(119899)
MedianPF
S(m
)Median
OS
(m)
Adversee
ffects
Com
ments
Paclitaxel
dose
(mgm
2 )Ca
rbop
latin
dose
(mgm
2 )Ph
aseIsinglea
gent
Lofflerre
tal1996
[11]
40ndash9
0week
1-hou
rinfusionfor
6weeks
5040
5NA
NA
(i)Hem
atologictoxicity-m
ild(ii)N
ograde3
or4
haem
atologicaltoxicity
neurologicalor
cardiotoxicityup
to90
mgm
2 wk
(iii)Nohypersensitivity
reactio
ns(patientsreceivedprem
edication)
(i)100
priorc
hemotherapy
(ii)M
ediando
seintensity
was
410m
gm
2 6w
k(range200
to540m
gm
2 6w
k)
Fenn
ellyetal
1997
[12]
40ndash100w
eek
1830
NA
NA
NA
(i)Nomucositiso
rgrade
III
neurop
athy
was
seen
(ii)A
lopeciao
ccurredin
one
(i)100
priorc
hemotherapy
(2ndash5
priorregim
ens)
(ii)P
artia
lrespo
nses
weres
eenin
four
of13
assessablepatients
(30
)(iii)Dose-lim
iting
toxicitywas
reachedat100m
gm
2 (iv
)2-3
patie
ntse
xperience
treatmentd
elay
(v)M
axim
um-to
lerateddo
seof
80mgm
2 Ab
u-Ru
stum
etal
1997
[13]
60ndash100
over
1ho
urw
eek
45289
NA
NA
NA
(i)Nopatie
nthadfebrile
neutropenia
(i)100
priorc
hemotherapy
(1ndash8
priorregim
ens)
PhaseIISing
leagent
Markm
anetal
2001
[14]
80over
1ho
urw
eek
53(52)
25NA
NA
NA
Therapydiscon
tinuedin
(i)4patie
ntsw
hohadperip
heral
neurop
athy
(ii)1
patie
ntdu
etopainful
fingernailbeds
(i)100
platinum
andpaclita
xel
resistant
(ii)Th
erapywas
discon
tinuedin
5patie
ntsb
ecause
oftoxicity
(iii)Only13
(1)w
erem
odified
(doser
eductio
nor
treatment
delay)
becauseo
fsidee
ffects
PhaseIICom
binedwith
platinum
agent
Kiku
chietal
2005
[15]
80over
1ho
urw
eek
AUC2week
27gt6
818
483
NA
(i)Neutro
penia(
17)
thrombo
cytopenia(
51
)(ii)N
ocaseso
fperipheral
neurop
athy
(grades3
and4)
inweeklycombinedT-C
Cadron
etal2007
[16]
90over
1ho
urw
eek
AUC4week
24 9gt6le6
73 38NR
8105
675
(i)Grade
34neutropenia(
34)
andneutropenicfever
in2
(ii)N
auseaa
ndvomiting
and
fatig
uewerethe
mostfrequ
ent
nonh
ematologicalsid
eeffects
(i)Doser
eductio
nwas
necessary
in25of
patie
nts
Pign
atae
tal2008
[17]
60over
1ho
urw
eek
AUC2week
24(13)lowastlowast
1stline
385
2320
136
(i)Notoxicd
eath
was
recorded
(ii)G
rade
2anaemiawas
repo
rted
insevenpatie
nts(27)
(iii)Nofebrile
neutropeniaw
asob
served
(iv)G
rade
3and4neutropenia
was
recorded
infive(19)a
ndon
e(4
)patients
(v)G
rade
3thrombo
cytopenia
occurred
inon
epatient
(4)
BioMed Research International 11
Table1Con
tinued
Stud
yRe
gimen
119899()
PI(m
)RR
()
CR(119899)
MedianPF
S(m
)Median
OS
(m)
Adversee
ffects
Com
ments
Paclitaxel
dose
(mgm
2 )Ca
rbop
latin
dose
(mgm
2 )
Safrae
tal2014
[18]
80over
1ho
urw
eek
AUC2week
133
1stline
864
645
274
(i)Highera
naem
ia(grade
III+
IV68vs53)+
IVneutropenia(
144vs69)
decreasedgradeIIa
lopecia(
235
vs981
)and
thrombo
cytopenia
(grade
III+
IV0
vs23)
Havrilesky
etal
2003
[19]
80over
1ho
urw
eek
AUC2weekD1
D8D15
until
progressionCR
+8courses
29 21 8
Total
grou
pgt6lt6
83 100
38
16 15 1114
115
137
32
(i)Hem
atologictoxicitywas
common
(grade
3neutropenia
32n
ograde4
neutropenia
grade3
or4thrombo
cytopenia
142)
(i)To
xicitymanaged
bytre
atment
delaydo
seredu
ctionof
paclitaxel
ordiscon
tinuatio
nof
carbop
latin
vanderB
urgetal
2014
[20]
90over
1ho
urw
eek
AUC4weekD1
D8D15
D29
D36
D49
+6x
TCq3w
108
65 43
Total
grou
pgt6lt6
76 5816 42
26 158 13
(i)Neutro
penia3
0
thrombo
cytopenia8
febrile
neutropenia0
5
(ii)N
onhaem
atologictoxicitywas
low
(i)Treatm
entw
asdelayedin
16
anddo
seredu
cedin
2of
cycle
s
119899num
bero
fpatientsassessableforrespo
nsemm
onthsPIplatinum
treatmentfreeintervalRR
respo
nser
ateCR
com
pleterem
issionT
paclitaxelC
carbop
latin
PFS
progressio
nfre
esurvivalOSoverall
survivalN
An
otavailableinpapero
rabstractandNR
notyetreached
lowastlowastElderly
popu
lation
patient
agedge70
years
12 BioMed Research International
Numerous phase II studies have explored the tolerabilityand the activity of weekly paclitaxel either as a single agent orin combination with several other drugs or biological agents(Table 1) A number of regimens combining weekly paclitaxelwith carboplatin have been used as first-line treatment inovarian cancer Carboplatin has been administered weeklyat AUC of 2 with dose escalation in some studies whilepaclitaxel had been infused at 60ndash80mgm2week Thiscombined regimen was well tolerated with a low incidence ofbone marrow suppression Overall response rates have beenhigh in the range of 60ndash80 in most studies even in heavilypretreated patients with platinum-resistant disease (diseaserecurrence or progression within 6 months of the last lineof platinum-based therapy) [15ndash20 134] The promising datafrom these phase II trials then led to the evolution of largerphase III trials
Three phase III studies Japanese Gynecologic OncologyGroup- (JGOG-) Trial 3016 [21ndash23] Multicentre Italian Trialin Ovarian Cancer-Trial 7 (MITO-7) [25] and GynecologicOncology Group GOG-262 Trial [24] have explored dosedense therapy The results of these trials are summarised inTable 2
The Japanese Gynecologic Oncology Group (JGOG)conducted a randomized phase 3 trial of dose-dense weeklypaclitaxel 80mgm2week in combination with 3-weeklycarboplatin compared to standard 3-weekly carboplatin andpaclitaxel 180mgm2 in patients with advanced epithelialovarian peritoneal or fallopian tube cancer (JGOG 3016NOVEL trial) In both arms carboplatin was given at AUC6 and the median number of cycles was six In this largestudy (119899 = 637) with a median follow up of 77 months therewas an 11-month improvement in themedian progression freesurvival (PFS) in the dose-dense treatment group comparedwith the standard treatment arm (282 versus 175 monthsHR 076 95 CI 062ndash091 119901 = 00037) Median OS wasalso higher in the dose-dense treatment arm (1005 versus622 months HR 079 95 CI 063ndash099 119901 = 0039)On subgroup analysis suboptimally debulked patients withresidual disease of gt1 cm (119899 = 342) had a significantlyhigher median overall survival in the dose dense arm (512versus 335 months HR-075 95 CI 057ndash097 119901 = 0027)There was no significant advantage to dose-dense treatmentfor patients with optimally cytoreduced disease Dose-densetherapy survival benefits were also not seen in patients withclear cell or mucinous histology type unlike serous typeHowever patient treated with dose dense therapy had asignificantly higher frequency of hematologic toxicity thanwith the standard arm (212 versus 94) which resultedin lower treatment completion rates (63 versus 48) withfrequent episodes of delay (76 versus 67) and dosereductions (48versus 35) [21 22]Therewas no significantdifference in terms of overall quality of life between the twoarms (119901 = 046) [23]
Using a similar regimen as in JGOG-3016 a GynecologicOncology Group (GOG)-262 Trial was conducted in theUnited States In this group most patients had stage IIIdisease (66ndash70) and two-thirds had suboptimal debulkingwith residual disease of gt1 cm This was a randomized phase
III trial of 3 weekly paclitaxel versus dose-dense weeklypaclitaxel in combination with carboplatin in patients withadvanced epithelial ovarian peritoneal or fallopian tubecancer Though optional concurrent and maintenance beva-cizumab were received by the majority of patients in botharms (835 versus 841 resp) There was no significantdifference in PFS in the patients who received the dosedense paclitaxelcarboplatin regimen compared to those whoreceived the standard paclitaxelcarboplatin regimen (148versus 143 months HR 097 95 CI 079ndash118) Howeverin a subgroup analysis there was a significant difference inPFS in the dose dense paclitaxel arm who did not receivebevacizumab 119899 = 112 (142 versus 103 months HR 059 95CI 037ndash096 119901 = 0003) Overall survival data is still imma-ture There was higher frequency of grade 3 anaemia (408versus 157 119901 lt 0001) and grade 2 sensory neuropathy(259 versus 178 119901 = 0012) but a lower incidence ofneutropenia (72 versus 83 119901 lt 0001) [24]
In 2008 the Multicentre Italian Trials in Ovarian Cancer(MITO-7) randomised 810 women in a phase 3 trial toreceive either standard carboplatin (AUC = 6) and paclitaxel175mgm2 every 3 weeks or a weekly schedule of paclitaxel(60mgm2) with carboplatin (AUC = 2) The majority ofpatients in both arms (83ndash90) received six cycles of therapyMost patients (58ndash63) had stage II1 disease 23 of themwere suboptimally debulked Median PFS did not differsignificantly (173 months and 183 months 119901 = 066)between the standard and dose-dense arms respectivelyThere was no significant difference in response rate betweenthe two arms nor the estimated 2-year overall survivalSubgroup analysis did not identify any subgroup that mayhave benefited from the dose-dense regimen Unlike theJGOG-3016 trial the incidence of grade 3-4 neutropenia wassignificantly lower in the dose-dense group compared to the3-weekly regimen (42 versus 50) A similar pattern wasseen for the incidence of febrile neutropenia (lt1 versus 3119901 = 002) thrombocytopenia (1 versus 7 119901 lt 0001)and other nonhaematological toxicities such as alopeciavomiting renal dysfunction and neuropathy Quality of lifewas reported to be significantly better in the dose-dense arm(119901 lt 00001) which was discordant with the JGOG-3016quality of life data [25]
In summary there was significant improvement inmedian PFS and overall survival in studies using paclitaxelat 80mgm2week dose-dense therapy [21 24] but withhigher haematological toxicity whereas MITO-7 [25] whichwas using paclitaxel at 60mgm2week was only equivalentlyeffective but less toxicThis does not conclude that the higherpaclitaxel dose is more clinically beneficial as there are manyother confounding factors in all three studies
In a multivariate analysis the JGOG-3016 study [21]reported that a lower dose intensity of paclitaxel (lt80) wasassociated with poorer overall survival (hazard ratio = 14295 confidence interval 112ndash181 119901 = 0004) however itmust be highlighted that the investigational arm carboplatinschedules were not standardised in these studies The JGOGand GOG trials delivered a 3-weekly carboplatin (AUC =6) arm whereas in the MITO-7 study the carboplatin was
BioMed Research International 13
Table2Ph
aseIIIstu
dies
onintravenou
sdose-densep
aclitaxel
Stud
yRe
gimen
119899
MedianPF
S(m
)
Median
OS
(m)
Adversee
ffects
Com
ments
Katsu
matae
tal2009
[21]
Katsu
matae
tal2013
[22]
Haranoetal2014
[23]
JGOG3016
631
(i)Haematologicaltoxicityhigh
erin
dose
dense-211versus
94
Lower
treatmentcom
pletionin
dose-dense
63versus
48
Frequent
episo
deso
fdelay
indo
se-dense
76versus
67
Doser
eductio
nsin
dose-dense
48versus
35
Nosig
nificantd
ifference
inoverallQ
OL
betweenbo
thgrou
ps(119901=046)
Paclitaxel80m
gm
2D18
15+carbop
latin
AUC63
weeklyversus
Paclitaxel180
mgm
2+
carbop
latin
AUC63
weekly
312
282
1005
Both
givenfor6
ndash9cycle
s319
175
622
Chan
etal2013
[24]
GOG-262
(i)Higherfrequ
ency
ofgrade3
anaemia
(408versus
157119901lt0001)
grade2
sensoryneurop
athy
(259versus
178
119901=0012)b
utlower
incidenceo
fneutropenia(
72versus
83119901lt0001)
Paclitaxel80m
gm
2D18
15+carbop
latin
AUC63
weeklyversus
Paclitaxel175
mgm
2+
carbop
latin
AUC63
weekly
346
148
NR
Both
givenfor6
cycle
s346
143
NR
Bevacizumab
given
optio
nally
112
(did
not
receive
bevazicumab)
142vs
103
Pign
atae
tal2014
[25]
MITO-7
810
(i)Lo
wer
incidenceo
fgrade
3-4
neutropenia(
42versus
50)febrile
neutropenia(lt1v
ersus3
119901=002)
thrombo
cytopenia(
1versus7
119901lt0001)andothern
onhaem
atological
toxicitie
ssuchas
alop
eciavom
iting
renald
ysfunctio
nandneurop
athy
Qualityof
lifeb
etterindo
sedensea
rm(119901lt00001)
Paclitaxel60m
gm
2 weekly+carbop
latin
AUC
2weeklyversus
Paclitaxel175
mgm
2+
carbop
latin
AUC63
weekly
406
404
183 173
77lowast
79lowast
119899num
bero
fpatientsmm
onthsDday
PFSprogressionfre
esurvivalOSoverallsurvivalNAnot
availableinpapero
rabstractandNR
notyetreached
lowastSurvivalrateat2years
14 BioMed Research International
dose-dense (AUC 2 weekly) Although it is possible that thedose scheduling for the platinum-based agent is not essentialfor a survival benefit as shown by previous studies usingdose-dense cisplatin direct cross-trial comparison cannot bemade Unlike paclitaxel carboplatin probably requires peakdose for optimal therapeutic benefit hence this may accountfor the inferior survival outcome in MITO-7 trial Anotherconfounding factor may be difference in ethnicity All threestudies used different ethnic populations and Asian patientsin JGOG-3016 appear to have better survival outcomes thanthe MITO-7 Western population Ethnicity with possibleunderlying genetic causes may be responsible for the variableresponses to chemotherapy across individuals [135] This wasexplored by Millward et al who studied 68 Caucasian andAsian lung cancer patients treated with a combination ofpaclitaxel and carboplatin and found that the incidence offebrile neutropenia was 50 of an initially treated cohortof Asians and when carboplatin was subsequently dosereduced in all Asian patients the overall incidence of febrileneutropenia was also reduced to 26 [136]
Although early clinical data from phase I and phaseII dose-dense paclitaxel trials in advanced ovarian cancerwere promising the results from phase III studies in havebeen inconsistent as a result of differences in paclitaxel dosecarboplatin AUC and schedule addition of bevacizumabas well as different ethnic populations The results of arecently completed randomised three arms GynaecologicCancer InterGroup (GCIG) phase II trial ICON 8 mayfurther inform the clinical benefit of dose dense paclitaxeltherapy
This multicentre trial involving 111 centres in the UKSouth Korea Mexico Ireland Australia and New Zealandwith a target population of 1485 patients with stage IC-IV epithelial ovarian cancer or peritoneal or fallopian tubecancer compared two dose-dense arms (i) JGOG-like armcarboplatin AUC 5 plus weekly 80mgm2 paclitaxel and (ii)MITO-7-like arm weekly carboplatin AUC 167 plus weekly80mgm2 paclitaxel to the standard 3-weekly treatment(carboplatin AUC 5 plus 175mgm2 paclitaxel) for stage IC toIV epithelial ovarian cancer The dose-dense arms of MITO-7 and JGOG-3016 as well as the ethnic heterogeneity will befurther addressed
10 Intraperitoneal (IP) Chemotherapy
In addition to dose and scheduling the route of adminis-tration of chemotherapy agents plays an important role inoutcome Intraperitoneal spread is common and likely anearly event in epithelial ovarian cancer hence the deliveryof chemotherapy intraperitoneally in theory would exposethe microcirculation of tumour to higher doses of drug thansystemic administration while limiting systemic toxicityTheideal drug for IP chemotherapy is one that is systemicallyeffective penetrates deep into the inner core of tumour tissueand remains within the peritoneal cavity for a prolongedperiod of time [137ndash139]
Early clinical studies confirmed that indeed the peritonealcavity could be exposed to 10 to 20-fold higher (cisplatin
and carboplatin) drug concentration than when using theintravenous approach and since 1978 this route had beenadopted as a form of therapeutic intervention [137 139]A subsequent phase I trial showed that IP paclitaxel haddose-limiting toxicity in the form of abdominal pain [140]Another phase 1 GOG pilot study administered weekly IPpaclitaxel at an initial dose of 20mgm2 for 16 weeks to33 patients and found that IP paclitaxel at this dose wasfeasible and well tolerated At dose levels 60 to 65mgm2there were significant levels of paclitaxel for a week afterdrug administration suggesting very slow clearance andcontinuous exposure of the peritoneal cavity to active drugconcentrations [132]
Hence this initiated a phase II study [141] that used pacli-taxel intraperitoneally at a dose of 60ndash65mgm2week In thisphase II GOG study 76 patients with small-volume resid-ual disease carcinoma (05 cm or less) involving the ovaryperitoneal or fallopian tube were treated with paclitaxel60mgm2week intraperitoneally for 16 weeks followed bysurgical evaluation in patients without disease progressionThe Gynaecologic Oncology group (GOG) currently definesno visible disease as microscopic disease being the idealsurgical outcome 75 of patients had received prior systemictherapy and 70 received all 16 courses that were planned Of28 patients with microscopic disease at the start of therapy61 achieved a surgically defined complete response whereasonly 1 out of 31 patients with macroscopic disease achieved acomplete response The median time-to-recurrence was 167months with an estimated survival rate at 2 years being 58Treatment was generally well tolerated [141]
Another study looked into the effect of IP paclitaxel asconsolidation therapy in advanced ovarian cancer Twenty-eight patients who had initial residual macroscopic disease(lt1 cm) after primary surgery or interval debulking but hadcomplete pathological response following standard treatmentwith at least 6 cycles of platinum-based chemotherapy regi-men received paclitaxel 60mgm2week intraperitoneally for12ndash16 weeks as consolidation therapy The median time torecurrence was 25 months but overall survival did not differsignificantly when compared with control group submittedto observation only Treatment-related toxicity was mild andtechnical difficulties were observed in 11 of patients [142]
Multicenter randomised phase 3 trials as well as meta-analysis of IP chemotherapy have been performed anddemonstrated that chemotherapy drugs administered intra-peritoneally are superior to intravenous standard regimensin patient with optimally debulked epithelial ovarian cancerThe most impressive data comes from GOG 114 [14] and172 trial [143] In GOG 114 patients received either sixcycles of intravenous paclitaxel 135mgm2 and cisplatin75mgm2 every 3 weeks or intravenous carboplatin (AUC= 9) every 28 days for two cycles followed by six 3-weeklycycles of intravenous paclitaxel 135mgm2 and IP cisplatin100mgm2 [14] whereas in GOG 172 patients received eitherintravenous paclitaxel 135mgm2 followed by intravenouscisplatin 75mgm2 or intravenous paclitaxel 135mgm2 fol-lowed by IP combination of cisplatin 100mgm2 and pacli-taxel 60mgm2 on day 8 Both trials had a combined total
BioMed Research International 15
of 876 women with stage III epithelial ovarian carcinomaoptimally debulked to le1 cm residual tumour [143] Themedian follow-up for GOG 114 [14] was 138 years with GOG172 [143] was 97 years The primary results of the individualtrials reported up to 6-month improvement in median PFSfollowing IP therapy In the combined analysis of the datafrom both trials the data continued to show a 5-monthdifference in favour of IP therapy (25 versus 20 months)which translates into 16 reduction in the hazard ratio forprogression (119901 = 003) In GOG 114 [14] reported in 2001there was only borderline improvement in overall survivalassociated with this regimen (median 63 versus 52 monthsrelative risk 081 119901 = 005)
However in combined analysis in 2013 which was pre-sented at the Society of Gynecologic Oncology AnnualMeeting [144] the overall survival showed an 11-monthimprovement in favour of IP therapy in GOG 114 whereasGOG 172 reported a 16-month survival advantage Amongpatients treated with IP therapy the 5-year survival rateincreased from 18 following completion of 1-2 cycles to 59for patients who completed 5-6 cycles of treatment Howeverthere was increased toxicity observed in the IP arm grade 3-4 leukopenia thrombocytopenia and abdominal pain Only42 of patients in the GOG172 trial [143] completed all sixcycles of planned treatment in the IP arm while 18 ofpatients in GOG 114 trial [14] received fewer than two coursesof IP chemotherapy
Another randomised phase III trial involving patientswith stages II-III epithelial ovarian carcinoma is the GOG252 study with three arms Arm 1-dose-dense intravenouscarboplatin and paclitaxel Arm 2-dose-dense intravenouspaclitaxel and IP carboplatin and Arm 3 consists of 3-weeklyintravenous paclitaxel (day 1) followed by IP cisplatin (day 2)and IP paclitaxel (day 3) regimen All three arms also incor-porate the combination and maintenance of bevacizumabGOG 252 has completed accrual and results are awaited [139]
11 Newer Forms of Paclitaxel
Development of next-generation taxanes has taken place overthe past 40 years aimed at eliminating toxicity improvingefficacy and ease of administration Abraxane is a novelcompound which incorporates paclitaxel into an albuminnanoparticle soluble in saline hence eliminating the needfor Cremophor EL which is responsible for hypersensitivityreactions experienced during paclitaxel infusion [145] Thenanoparticle albumin in nab-paclitaxel is able to bind toglycoprotein gp60 receptor an albumin receptor and activatecaveolin-1 a protein that in human is encoded byCAV-1 geneleading to formation of caveoli hence allowing nab-paclitaxelto migrate across the endothelial cell membrane into theinterstitial space leading to higher intratumoural drug con-centration In addition Abraxane exhibits linear pharma-cokinetics and can therefore be given at a relatively higherdose than standard intravenous paclitaxel leading to a highertherapeutic ratio and heightened efficacy in solid tumoursmainlymetastatic breast cancer [146 147] Nab-paclitaxel hadFDA approval in 2005 for treatment of breast cancer [148]
Nab-paclitaxel has been studied in recurrent ovariancancer As a single agent in phase II 44 patients withrecurrent ovarian cancer were treated with Nab-paclitaxel260mgm2 intravenously for 30 minutes every 3 weeks for6 cycles Ninety-two percent of patients were platinum-sensitive while 89 had had previous exposure to standardtaxane The objective response rate was 64 with 15 patientsachieving complete response and 13 of them had partialresponse Estimated median PFS was 85 months No hyper-sensitivity reactions were observed and there were infrequentcases of grade 4 neutropenia (11) and grade 2-3 neuropathy(13) [149]
Another phase II study by GOG enrolled 51 patients withplatinum- and taxane-resistant recurrent ovarian cancer outof which 47 were evaluable The objective response rate was38 with one patient achieving a complete response and 10patients a partial response The median PFS was 45 monthswhile overall survival rate was 174 months Severe haema-tological and nonhaematological toxicities including neuro-toxicity were uncommon These results are quite impressivegiven the treatment population consisted of patients withvery poor prognosis with a median platinum and taxane freeinterval of 21 days and 70 had their recurrence within 3months of completion of primary treatment [150] Severalother trials of this formulation are in progress
Paclitaxel poliglumex (PPX) also known as Xyotax isanother prodrug a novel conjugate of paclitaxel and 120572-poly-L-glutamic acid which accumulates within tumour tissuedue to increased permeability of the tumour vessels and lackof lymphatic drainage [148 151 152] Paclitaxel poliglumexenhances solubility of paclitaxel allows direct delivery tothe intratumoural microenvironment and allows prolongedexposure to the active drug while minimising systemictoxicities [151] In Phase I dose escalation studies as a singleagent the recommended dose of PPX was 235mgm2 over 10minutes every 3 weeks or 70mgm2 weekly [153] In a PhaseII GOG study of relapsed ovarian cancer a response rate of16 was seen with infrequent serious adverse events grade3 and 4 neutropenia (24 and 20) and grade 3 neuropathy(24) [154] A phase III trial (GOG-0212) on the use of PPXas consolidation ormaintenance therapy in advanced ovariancancer is in progress
DHA-paclitaxel also known as Taxoprexin is a prodrugwhere paclitaxel is covalently conjugated with the naturallyoccurring omega-3 fatty acid docosahexaenoic acid (DHA)a fatty acid that is easily taken up by tumour cells henceincreasing intratumoural concentration of paclitaxel leadingtumour cell apoptosis [155 156] DHA-paclitaxel exhibitslinear pharmacokinetics and lower toxicity and also ease ofadministration when compared to conventional paclitaxeland has demonstrated antineoplastic activity in animal mod-els of cancer as well as in a phase III trial involving metastaticmelanoma [156ndash160] In a recent study on human ovariancancer cells it was found that DHA could reverse paclitaxelresistance by inhibiting P-gp as well as downregulatingthe expression of multidrug resistance associated proteins(MRP) and inhibiting the activity of NF-120581B and p38 MAPKsignalling pathways [161]
16 BioMed Research International
12 Future Directions
A plateau has been reached regarding the benefits associatedwith standard 3-weekly intravenous administration of cyto-toxic chemotherapy in advanced epithelial ovarian cancerThe ongoing battle for a better treatment regimen to delayrelapse promote remission and most importantly improvethe quality of life of patients with advanced epithelial ovariancancer need not to go further than the ability to relook at thechemotherapy agents that are already available in a differentapproach
Novel compounds to date have not yet shown clinicalsuperiority and parent compounds such as paclitaxel con-tinue to surprise us with their feasibility effectiveness andmanageable toxicity profiles Intraperitoneal paclitaxel willrequire further evaluation Better effort in understanding themechanism of action of drugs including the role of dosescheduling and the effect on the immune systemmay providea more cost-effective route to better clinical outcomes
Conflict of Interests
The authors declare no conflict of interests in this work
Acknowledgments
The authors would like to thank the many researchers whohave contributed to our current knowledge of paclitaxelNirmala Kampan is supported by Australian Monash Uni-versity Institute of Graduate Research Scholarship as wellas Universiti Kebangsaan Malaysia Postgraduate ScholarshipAward Mutsa Madondo has received Postgraduate Pub-lication Award from Monash University and MagdalenaPlebanski has been awarded Senior NHMRC Fellowship
References
[1] Australian Institute of Health and Welfare and National Breastand Ovarian Cancer Centre (Australia) Ovarian Cancer inAustralia AnOverview 2010 Cancer Series Australian Instituteof Health and Welfare Canberra Australia 2010
[2] R E Bristow R S Tomacruz D K Armstrong E L Trimbleand F J Montz ldquoSurvival effect of maximal cytoreductivesurgery for advanced ovarian carcinoma during the platinumera a meta-analysisrdquo Journal of Clinical Oncology vol 20 no 5pp 1248ndash1259 2002
[3] ZKempand JA Ledermann ldquoUpdate onfirst-line treatment ofadvanced ovarian carcinomardquo International Journal of WomenrsquosHealth vol 5 no 1 pp 45ndash51 2013
[4] A du Bois H-J Luck W Meier et al ldquoA randomized clinicaltrial of cisplatinpaclitaxel versus carboplatinpaclitaxel as first-line treatment of ovarian cancerrdquo Journal of the National CancerInstitute vol 95 no 17 pp 1320ndash1330 2003
[5] R F Ozols B N Bundy B E Greer et al ldquoPhase III trialof carboplatin and paclitaxel compared with cisplatin andpaclitaxel in patients with optimally resected stage III ovariancancer A Gynecologic Oncology Group studyrdquo Journal ofClinical Oncology vol 21 no 17 pp 3194ndash3200 2003
[6] W P McGuire W J Hoskins M F Brady et al ldquoCyclophos-phamide and cisplatin compared with paclitaxel and cisplatin
in patients with stage III and stage IV ovarian cancerrdquoThe NewEngland Journal of Medicine vol 334 no 1 pp 1ndash6 1996
[7] W P McGuire W J Hoskins M F Brady et al ldquoCyclophos-phamide and cisplatin versus paclitaxel and cisplatin a phase IIIrandomized trial in patients with suboptimal stage IIIIV ovar-ian cancer (from the gynecologic oncology group)rdquo Seminars inOncology vol 23 no 5 supplement 12 pp 40ndash47 1996
[8] M J Piccart K Bertelsen K James et al ldquoRandomized inter-group trial of cisplatin-paclitaxel versus cisplatin-cyclophosph-amide inwomenwith advanced epithelial ovarian cancer three-year resultsrdquo Journal of the National Cancer Institute vol 92 no9 pp 699ndash708 2000
[9] P A Vasey G C Jayson A Gordon et al ldquoPhase III random-ized trial of docetaxel-carboplatin versus paclitaxel-carboplatinas first-line chemotherpy for ovarian carcinomardquo Journal of theNational Cancer Institute vol 96 no 22 pp 1682ndash1691 2004
[10] B Gronlund C Hogdall H H Hansen and S A EngelholmldquoResults of reinduction therapy with paclitaxel and carboplatinin recurrent epithelial ovarian cancerrdquo Gynecologic Oncologyvol 83 no 1 pp 128ndash134 2001
[11] T M Loffler W Freund J Lipke and T-U HausamenldquoSchedule- and dose-intensified paclitaxel as weekly 1-hourinfusion in pretreated solid tumors results of a phase III trialrdquoSeminars in Oncology vol 23 no 6 supplement 16 pp 32ndash341996
[12] D Fennelly C Aghajanian F Shapiro et al ldquoPhase I and phar-macologic study of paclitaxel administered weekly in patientswith relapsed ovarian cancerrdquo Journal of Clinical Oncology vol15 no 1 pp 187ndash192 1997
[13] N R Abu-Rustum C Aghajanian R R Barakat D Fennelly FShapiro and D Spriggs ldquoSalvage weekly paclitaxel in recurrentovarian cancerrdquo Seminars inOncology vol 24 no 5 supplement15 pp S15-62ndashS15-67 1997
[14] M Markman B N Bundy D S Alberts et al ldquoPhase III trialof standard-dose intravenous cisplatin plus paclitaxel versusmoderately high-dose carboplatin followed by intravenouspaclitaxel and intraperitoneal cisplatin in small-volume stageIII ovarian carcinoma an intergroup study of the gynecologiconcology group Southwestern Oncology Group and EasternCooperativeOncologyGrouprdquo Journal of Clinical Oncology vol19 no 4 pp 1001ndash1007 2001
[15] A Kikuchi H Sakamoto and T Yamamoto ldquoWeekly car-boplatin and paclitaxel is safe active and well tolerated inrecurrent ovarian cancer cases of Japanese women previouslytreated with cisplatin-containing multidrug chemotherapyrdquoInternational Journal of Gynecological Cancer vol 15 no 1 pp45ndash49 2005
[16] I Cadron K Leunen F Amant T van Gorp P Nevenand I Vergote ldquoThe lsquoLeuvenrsquo dose-dense paclitaxelcarboplatinregimen in patients with recurrent ovarian cancerrdquo GynecologicOncology vol 106 no 2 pp 354ndash361 2007
[17] S Pignata E Breda G Scambia et al ldquoA phase II studyof weekly carboplatin and paclitaxel as first-line treatment ofelderly patients with advanced ovarian cancer A Multicen-tre Italian Trial in Ovarian cancer (MITO-5) studyrdquo CriticalReviews in OncologyHematology vol 66 no 3 pp 229ndash2362008
[18] T Safra S Shamai J Greenberg et al ldquoWeekly carboplatinwith paclitaxel compared to standard three-weekly treatment inadvanced epithelial ovarian carcinomamdasha retrospective studyrdquoGynecologic Oncology vol 132 no 1 pp 18ndash22 2014
BioMed Research International 17
[19] L J Havrilesky A A Alvarez R A Sayer et al ldquoWeekly low-dose carboplatin and paclitaxel in the treatment of recurrentovarian and peritoneal cancerrdquo Gynecologic Oncology vol 88no 1 pp 51ndash57 2003
[20] M van der BurgW Onstenk I Boere et al ldquoLong-term resultsof a randomised phase III trial of weekly versus three-weeklypaclitaxelplatinum induction therapy followed by standardor extended three-weekly paclitaxelplatinum in Europeanpatients with advanced epithelial ovarian cancerrdquo EuropeanJournal of Cancer vol 50 no 15 pp 2592ndash2601 2014
[21] N Katsumata M Yasuda F Takahashi et al ldquoDose-densepaclitaxel once a week in combination with carboplatin every3 weeks for advanced ovarian cancer a phase 3 open-labelrandomised controlled trialrdquoThe Lancet vol 374 no 9698 pp1331ndash1338 2009
[22] N Katsumata M Yasuda S Isonishi et al ldquoLong-term resultsof dose-dense paclitaxel and carboplatin versus conventionalpaclitaxel and carboplatin for treatment of advanced epithelialovarian fallopian tube or primary peritoneal cancer (JGOG3016) a randomised controlled open-label trialrdquo The LancetOncology vol 14 no 10 pp 1020ndash1026 2013
[23] K Harano F Terauchi N Katsumata et al ldquoQuality-of-lifeoutcomes from a randomized phase III trial of dose-denseweekly paclitaxel and carboplatin compared with conventionalpaclitaxel and carboplatin as a first-line treatment for stage II-IV ovarian cancer Japanese Gynecologic OncologyGroup Trial(JGOG3016)rdquo Annals of Oncology vol 25 no 1 pp 251ndash2572014
[24] J Chan M F Brady R Penson et al ldquoPhase III trial ofevery-3-weeks paclitaxel vs dose dense weekly paclitaxel withcarboplatin +minus bevacizumab in epithelial ovarian peritonealfallopian tube cancer GOG 262 (NCT01167712)rdquo InternationalJournal of Gynecological Cancer vol 23 no 8 supplement 1 pp9ndash10 2013
[25] S Pignata G Scambia D Katsaros et al ldquoCarboplatin pluspaclitaxel once a week versus every 3 weeks in patients withadvanced ovarian cancer (MITO-7) a randomisedmulticentreopen-label phase 3 trialrdquoThe Lancet Oncology vol 15 no 4 pp396ndash405 2014
[26] V Walsh and J Goodman ldquoFrom taxol to Taxol the changingidentities and ownership of an anti-cancer drugrdquo MedicalAnthropology vol 21 no 3-4 pp 307ndash336 2002
[27] R Renneberg ldquoBiotech History yew trees paclitaxel synthesisand fungirdquo Biotechnology Journal vol 2 no 10 pp 1207ndash12092007
[28] J E Liebmann J A Cook C Lipschultz D Teague J Fisherand J B Mitchell ldquoCytotoxic studies of paclitaxel (Taxol) inhuman tumour cell linesrdquo British Journal of Cancer vol 68 no6 pp 1104ndash1109 1993
[29] J J Manfredi and S B Horwitz ldquoTaxol an antimitotic agentwith a newmechanism of actionrdquo Pharmacology andTherapeu-tics vol 25 no 1 pp 83ndash125 1984
[30] D G I Kingston ldquoRecent advances in the chemistry of taxolrdquoJournal of Natural Products vol 63 no 5 pp 726ndash734 2000
[31] D G I Kingston ldquoThe shape of things to come structural andsynthetic studies of taxol and related compoundsrdquo Phytochem-istry vol 68 no 14 pp 1844ndash1854 2007
[32] V Walsh and J Goodman ldquoCancer chemotherapy biodiversitypublic and private property the case of the anti-cancer drugTaxolrdquo Social Science amp Medicine vol 49 no 9 pp 1215ndash12251999
[33] P H Wiernik E L Schwartz J J Strauman J P Dutcher RB Lipton and E Paietta ldquoPhase I clinical and pharmacokineticstudy of taxolrdquo Cancer Research vol 47 no 9 pp 2486ndash24931987
[34] W P McGuire E K Rowinsky N B Rosenhein et alldquoTaxol a unique antineoplastic agent with significant activityin advanced ovarian epithelial neoplasmsrdquo Annals of InternalMedicine vol 111 no 4 pp 273ndash279 1989
[35] ldquoDiscovery and development of taxolrdquo in Taxol Science andApplications M W M E Suffness Ed pp 3ndash25 CRC PressBoca Raton Fla USA 1995
[36] M J Piccart and F Cardoso ldquoProgress in systemic therapy forbreast cancer an overview and perspectivesrdquo European Journalof Cancer Supplement vol 1 no 2 pp 56ndash69 2003
[37] P Bonomi K B Kim and J Kugler ldquoComparison of survival forstage IIIB versus stage IV non-small cell lung cancer (NSCLC)patients with etoposide-cisplatin versus taxol-cisplatin an East-ern Cooperative Oncology Group (ECOG) trialrdquo in Proceedingsof the American Society of Clinical Oncology vol 16 p 454a1997
[38] D Guenard F Gueritte-Voegelein J Dubois and P PotierldquoStructure-activity relationships of Taxol and Taxotere ana-loguesrdquo Journal of the National Cancer Institute Monographsno 15 pp 79ndash82 1993
[39] D G I Kingston ldquoTaxol the chemistry and structure-activityrelationships of a novel anticancer agentrdquo Trends in Biotechnol-ogy vol 12 no 6 pp 222ndash227 1994
[40] E K Rowinsky and R C Donehower ldquoPaclitaxel (taxol)rdquo TheNew England Journal of Medicine vol 332 no 15 pp 1004ndash10141995
[41] J Parness and S B Horwitz ldquoTaxol binds to polymerizedtubulin in vitrordquo Journal of Cell Biology vol 91 no 2 pp 479ndash487 1981
[42] A Dammermann A Desai and K Oegema ldquoTheminus end insightrdquo Current Biology vol 13 no 15 pp R614ndashR624 2003
[43] CWiese and Y Zheng ldquoMicrotubule nucleation 120574-tubulin andbeyondrdquo Journal of Cell Science vol 119 no 20 pp 4143ndash41532006
[44] A Ganguly H Yang and F Cabral ldquoPaclitaxel-dependent celllines reveal a novel drug activityrdquo Molecular Cancer Therapeu-tics vol 9 no 11 pp 2914ndash2923 2010
[45] P B Schiff and S B Horwitz ldquoTaxol stabilizes microtubules inmouse fibroblast cellsrdquo Proceedings of the National Academy ofSciences of the United States of America vol 77 no 3 pp 1561ndash1565 1980
[46] P B Schiff J Fant and S B Horwitz ldquoPromotion of micro-tubule assembly in vitro by Taxolrdquo Nature vol 277 no 5698pp 665ndash667 1979
[47] D Zhang R Yang S Wang and Z Dong ldquoPaclitaxel new usesfor an old drugrdquoDrug Design Development andTherapy vol 8pp 279ndash284 2014
[48] S Rao G A Orr A G Chaudhary D G I Kingston and SB Horwitz ldquoCharacterization of the taxol binding site on themicrotubule 2-(m-Azidobenzoyl)taxol photolabels a peptide(amino acids 217-231) of beta-tubulinrdquoThe Journal of BiologicalChemistry vol 270 no 35 pp 20235ndash20238 1995
[49] F Wang Y Cao W Zhao H Liu Z Fu and R Han ldquoTaxolinhibits melanoma metastases through apoptosis inductionangiogenesis inhibition and restoration of E-cadherin andnm23 expressionrdquo Journal of Pharmacological Sciences vol 93no 2 pp 197ndash203 2003
18 BioMed Research International
[50] A Sevko V Kremer C Falk et al ldquoApplication of paclitaxel inlow non-cytotoxic doses supports vaccination with melanomaantigens in normal micerdquo Journal of Immunotoxicology vol 9no 3 pp 275ndash281 2012
[51] T Kreis and R Vale Guidebook to the Cytoskeletal and MotorProteins Oxford University Press Oxford UK 2nd edition1999
[52] P Giannakakou D L Sackett Y-K Kang et al ldquoPaclitaxel-resistant human ovarian cancer cells have mutant 120573-tubulinsthat exhibit impaired paclitaxel-driven polymerizationrdquo TheJournal of Biological Chemistry vol 272 no 27 pp 17118ndash171251997
[53] E Rakovitch W Mellado E J Hall T K Pandita S Sawantand C R Geard ldquoPaclitaxel sensitivity correlates with p53status and DNA fragmentation but not G2M accumulationrdquoInternational Journal of Radiation Oncology Biology Physics vol44 no 5 pp 1119ndash1124 1999
[54] S W Lowe S Bodis A McClatchey et al ldquop53 status and theefficacy of cancer therapy in vivordquo Science vol 266 no 5186 pp807ndash810 1994
[55] C C Zhang J-M Yang E White M Murphy A Levine andW N Hait ldquoThe role of MAP4 expression in the sensitivity topaclitaxel and resistance to vinca alkaloids in p53 mutant cellsrdquoOncogene vol 16 no 12 pp 1617ndash1624 1998
[56] K Fukasawa T Choi R Kuriyama S Rulong and G F VandeWoude ldquoAbnormal centrosome amplification in the absence ofp53rdquo Science vol 271 no 5256 pp 1744ndash1747 1996
[57] T-H Wang Y-H Chan C-W Chen et al ldquoPaclitaxel (Taxol)upregulates expression of functional interleukin-6 in humanovarian cancer cells through multiple signaling pathwaysrdquoOncogene vol 25 no 35 pp 4857ndash4866 2006
[58] E Yakirevich E Sabo I Naroditsky Y Sova O Lavie andM B Resnick ldquoMultidrug resistance-related phenotype andapoptosis-related protein expression in ovarian serous carcino-masrdquo Gynecologic Oncology vol 100 no 1 pp 152ndash159 2006
[59] G Szakacs J K Paterson J A Ludwig C Booth-Genthe andM M Gottesman ldquoTargeting multidrug resistance in cancerrdquoNature Reviews Drug Discovery vol 5 no 3 pp 219ndash234 2006
[60] L W Pfannenstiel S S K Lam L A Emens E M Jaffeeand T D Armstrong ldquoPaclitaxel enhances early dendritic cellmaturation and function through TLR4 signaling in micerdquoCellular Immunology vol 263 no 1 pp 79ndash87 2010
[61] N Klauber S Parangi E Flynn E Hamel and R J DrsquoAmatoldquoInhibition of angiogenesis and breast cancer in mice by themicrotubule inhibitors 2-methoxyestradiol and Taxolrdquo CancerResearch vol 57 no 1 pp 81ndash86 1997
[62] D Belotti V Vergani T Drudis et al ldquoThe microtubule-affecting drug paclitaxel has antiangiogenic activityrdquo ClinicalCancer Research vol 2 no 11 pp 1843ndash1849 1996
[63] D H Lau L Xue L J Young P A Burke and A T CheungldquoPaclitaxel (Taxol) an inhibitor of angiogenesis in a highlyvascularized transgenic breast cancerrdquo Cancer Biotherapy andRadiopharmaceuticals vol 14 no 1 pp 31ndash36 1999
[64] X Jiang ldquoHarnessing the immune system for the treatment ofbreast cancerrdquo Journal of Zhejiang University Science B vol 15no 1 pp 1ndash15 2014
[65] A Gadducci D Katsaros P Zola et al ldquoWeekly low-dosepaclitaxel as maintenance treatment in patients with advancedovarian cancer who had microscopic residual disease atsecond-look surgery after 6 cycles of paclitaxelplatinum-basedchemotherapy Results of an open noncomparative phase 2
multicenter italian study (after-6 protocol 2)rdquo InternationalJournal of Gynecological Cancer vol 19 no 4 pp 615ndash619 2009
[66] R S Bhatt J Merchan R Parker et al ldquoA phase 2 pilot trial oflow-dose continuous infusion or lsquometronomicrsquo paclitaxel andoral celecoxib in patients with metastatic melanomardquo Cancervol 116 no 7 pp 1751ndash1756 2010
[67] M Caballero J J Grau J L Blanch et al ldquoSerum vascularendothelial growth factor as a predictive factor in metronomic(weekly) paclitaxel treatment for advanced head and neckcancerrdquo Archives of OtolaryngologymdashHead and Neck Surgeryvol 133 no 11 pp 1143ndash1148 2007
[68] J Alexandre Y Hu W Lu H Pelicano and P Huang ldquoNovelaction of paclitaxel against cancer cells bystander effect medi-ated by reactive oxygen speciesrdquo Cancer Research vol 67 no 8pp 3512ndash3517 2007
[69] T Hadzic N Aykin-Burns Y Zhu et al ldquoPaclitaxel combinedwith inhibitors of glucose and hydroperoxide metabolismenhances breast cancer cell killing viaH
2O2-mediated oxidative
stressrdquo Free Radical Biology and Medicine vol 48 no 8 pp1024ndash1033 2010
[70] C A Sherman-Baust K G Becker W H Wood III Y Zhangand P J Morin ldquoGene expression and pathway analysis of ovar-ian cancer cells selected for resistance to cisplatin paclitaxel ordoxorubicinrdquo Journal of Ovarian Research vol 4 no 1 article21 2011
[71] R Agarwal and S B Kaye ldquoOvarian cancer strategies for over-coming resistance to chemotherapyrdquo Nature Reviews Cancervol 3 no 7 pp 502ndash516 2003
[72] T Acker and K H Plate ldquoRole of hypoxia in tumorangiogenesismdashmolecular and cellular angiogenic crosstalkrdquoCell and Tissue Research vol 314 no 1 pp 145ndash155 2003
[73] M Hockel and P Vaupel ldquoBiological consequences of tumorhypoxiardquo Seminars in Oncology vol 28 supplement 8 no 2 pp36ndash41 2001
[74] L Huang Q-H Zhang Q-L Ao H Xing Y-P Lu and DMa ldquoEffect of hypoxia on the chemotherapeutic sensitivity ofhuman ovarian cancer cells to paclitaxel and its mechanismrdquoZhonghua Zhong Liu Za Zhi vol 29 no 2 pp 96ndash100 2007
[75] N Rohwer and T Cramer ldquoHypoxia-mediated drug resistancenovel insights on the functional interaction of HIFs and celldeath pathwaysrdquoDrug Resistance Updates vol 14 no 3 pp 191ndash201 2011
[76] B B Aggarwal R V Vijayalekshmi and B Sung ldquoTargetinginflammatory pathways for prevention and therapy of cancershort-term friend long-term foerdquo Clinical Cancer Research vol15 no 2 pp 425ndash430 2009
[77] Z Duan R Foster D A Bell et al ldquoSignal transducersand activators of transcription 3 pathway activation in drug-resistant ovarian cancerrdquo Clinical Cancer Research vol 12 no17 pp 5055ndash5063 2006
[78] H-J Kuh S H Jang M G Wientjes J R Weaver and J L-SAu ldquoDeterminants of paclitaxel penetration and accumulationin human solid tumorrdquo Journal of Pharmacology and Experi-mental Therapeutics vol 290 no 2 pp 871ndash880 1999
[79] S Arao H Suwa M Mandai et al ldquoHypoxia-mediated drugresistance novel insights on the functional interaction of HIFsand cell death pathwaysrdquo Cancer Research vol 54 no 5 pp1355ndash1359 1994
[80] S E Johnatty J Beesley B Gao et al ldquoABCB1 (MDR1)polymorphisms and ovarian cancer progression and survivala comprehensive analysis from the Ovarian Cancer Association
BioMed Research International 19
Consortium and the Cancer GenomeAtlasrdquoGynecologic Oncol-ogy vol 131 no 1 pp 8ndash14 2013
[81] X Yang A K Iyer A Singh et al ldquoCluster of differentiation44 targeted hyaluronic acid based nanoparticles for MDR1siRNA delivery to overcome drug resistance in ovarian cancerrdquoPharmaceutical Research 2014
[82] D A Zajchowski B Y Karlan and L K Shawver ldquoTreatment-related protein biomarker expression differs between primaryand recurrent ovarian carcinomasrdquoMolecular CancerTherapeu-tics vol 11 no 2 pp 492ndash502 2012
[83] MM Gottesman J Ludwig D Xia and G Szakacs ldquoDefeatingdrug resistance in cancerrdquoDiscovery Medicine vol 6 no 31 pp18ndash23 2006
[84] S Mozzetti C Ferlini P Concolino et al ldquoClass III 120573-tubulin overexpression is a prominent mechanism of paclitaxelresistance in ovarian cancer patientsrdquo Clinical Cancer Researchvol 11 no 1 pp 298ndash305 2005
[85] M Kavallaris D Y S Kuo C A Burkhart et al ldquoTaxol-resistant epithelial ovarian tumors are associated with alteredexpression of specific beta-tubulin isotypesrdquo Journal of ClinicalInvestigation vol 100 no 5 pp 1282ndash1293 1997
[86] G A Orr P Verdier-Pinard H McDaid and S B HorwitzldquoMechanisms of Taxol resistance related to microtubulesrdquoOncogene vol 22 no 47 pp 7280ndash7295 2003
[87] C Ferlini L Cicchillitti G Raspaglio et al ldquoPaclitaxel directlybinds to Bcl-2 and functionally mimics activity of Nur77rdquoCancer Research vol 69 no 17 pp 6906ndash6914 2009
[88] E Mechetner A Kyshtoobayeva S Zonis et al ldquoLevels ofmultidrug resistance (MDR1) P-glycoprotein expression byhuman breast cancer correlate with in vitro resistance to taxoland doxorubicinrdquo Clinical Cancer Research vol 4 no 2 pp389ndash398 1998
[89] J S Lagas C W N Damen R A B VanWaterschoot D IusufJ H Beijnen and A H Schinkel ldquoP-glycoprotein multidrug-resistance associated protein 2 Cyp3a and carboxylesteraseaffect the oral availability and metabolism of vinorelbinerdquoMolecular Pharmacology vol 82 no 4 pp 636ndash644 2012
[90] M T Huizing J B Vermorken H Rosing et al ldquoPharmacoki-netics of paclitaxel and three major metabolites in patients withadvanced breast carcinoma refractory to anthracycline therapytreated with a 3-hour paclitaxel infusion a European CancerCentre (ECC) trialrdquo Annals of Oncology vol 6 no 7 pp 699ndash704 1995
[91] R Panchagnula ldquoPharmaceutical aspects of paclitaxelrdquo Interna-tional Journal of Pharmaceutics vol 172 no 1-2 pp 1ndash15 1998
[92] S H Jang M G Wientjes and J L-S Au ldquoDeterminants ofpaclitaxel uptake accumulation and retention in solid tumorsrdquoInvestigational New Drugs vol 19 no 2 pp 113ndash123 2001
[93] D S Sonnichsen andM V Relling ldquoClinical pharmacokineticsof paclitaxelrdquo Clinical Pharmacokinetics vol 27 no 4 pp 256ndash269 1994
[94] T Ohtsu Y Sasaki T Tamura et al ldquoClinical pharmacokineticsand pharmacodynamics of paclitaxel a 3-hour infusion versusa 24-hour infusionrdquo Clinical Cancer Research vol 1 no 6 pp599ndash606 1995
[95] M Czejka J Schueller H Schnait B Springer and I EderldquoClinical pharmacokinetics andmetabolism of paclitaxel after athree-hour infusion comparison of two preparationsrdquo Journalof Oncology Pharmacy Practice vol 9 no 4 pp 129ndash136 2003
[96] J Rizzo C Riley D VonHoff J Kuhn J Phillips and T BrownldquoAnalysis of anticancer drugs in biological fluids determination
of taxol with application to clinical pharmacokineticsrdquo Journalof Pharmaceutical and Biomedical Analysis vol 8 no 2 pp 159ndash164 1990
[97] V A de Weger J H Beijnen and J H M Schellens ldquoCel-lular and clinical pharmacology of the taxanes docetaxel andpaclitaxelmdasha reviewrdquoAnti-Cancer Drugs vol 25 no 5 pp 488ndash494 2014
[98] S Kumar H Mahdi C Bryant J P Shah G Garg andA Munkarah ldquoClinical trials and progress with paclitaxel inovarian cancerrdquo International Journal of Womenrsquos Health vol 2no 1 pp 411ndash427 2010
[99] B Huang J Zhao J C Unkeless Z H Feng and H XiongldquoTLR signaling by tumor and immune cells a double-edgedswordrdquo Oncogene vol 27 no 2 pp 218ndash224 2008
[100] R A Jibodh J S Lagas B Nuijen J H Beijnen and J HM Schellens ldquoTaxanes old drugs new oral formulationsrdquoEuropean Journal of Pharmacology vol 717 no 1ndash3 pp 40ndash462013
[101] A Javeed M Ashraf A Riaz A Ghafoor S Afzal and M MMukhtar ldquoPaclitaxel and immune systemrdquo European Journal ofPharmaceutical Sciences vol 38 no 4 pp 283ndash290 2009
[102] L Bracci G Schiavoni A Sistigu and F Belardelli ldquoImmune-based mechanisms of cytotoxic chemotherapy implications forthe design of novel and rationale-based combined treatmentsagainst cancerrdquo Cell Death and Differentiation vol 21 no 1 pp15ndash25 2014
[103] C A Byrd-Leifer E F Block K Takeda S Akira and A DingldquoThe role of MyD88 and TLR4 in the LPS-mimetic activity ofTaxolrdquo European Journal of Immunology vol 31 no 8 pp 2448ndash2457 2001
[104] A-C Wang Y-B Ma F-X Wu et al ldquoTLR4 induces tumorgrowth and inhibits paclitaxel activity in MyD88-positivehuman ovarian carcinoma in vitrordquo Oncology Letters vol 7 no3 pp 871ndash877 2014
[105] Y Zhu N Liu S D Xiong Y J Zheng and Y W ChuldquoCD4+Foxp3+ regulatory T-cell impairment by paclitaxel isindependent of toll-like receptor 4rdquo Scandinavian Journal ofImmunology vol 73 no 4 pp 301ndash308 2011
[106] M Kubo T Morisaki K Matsumoto et al ldquoPaclitaxel probablyenhances cytotoxicity of natural killer cells against breastcarcinoma cells by increasing perforin productionrdquo CancerImmunology Immunotherapy vol 54 no 5 pp 468ndash476 2005
[107] L Markasz G Stuber B Vanherberghen et al ldquoEffect of fre-quently used chemotherapeutic drugs on the cytotoxic activityof human natural killer cellsrdquo Molecular Cancer Therapeuticsvol 6 no 2 pp 644ndash654 2007
[108] T Sako N Burioka K Yasuda et al ldquoCellular immune profile inpatients with non-small cell lung cancer after weekly paclitaxeltherapyrdquo Acta Oncologica vol 43 no 1 pp 15ndash19 2004
[109] R Kaneno G V Shurin I L Tourkova and M R ShurinldquoChemomodulation of human dendritic cell function by anti-neoplastic agents in low noncytotoxic concentrationsrdquo Journalof Translational Medicine vol 7 article 58 2009
[110] TMichels G V ShurinHNaiditch A Sevko VUmansky andM R Shurin ldquoPaclitaxel promotes differentiation of myeloid-derived suppressor cells into dendritic cells in vitro in a TLR4-independent mannerrdquo Journal of Immunotoxicology vol 9 no3 pp 292ndash300 2012
[111] R A Kemp and F Ronchese ldquoTumor-specific Tc1 but not Tc2cells deliver protective antitumor immunityrdquo The Journal ofImmunology vol 167 no 11 pp 6497ndash6502 2001
20 BioMed Research International
[112] A Y Rudensky ldquoRegulatory T cells and Foxp3rdquo ImmunologicalReviews vol 241 no 1 pp 260ndash268 2011
[113] EM Shevach ldquoCD4+CD25+ suppressor T cellsmore questionsthan answersrdquo Nature Reviews Immunology vol 2 no 6 pp389ndash400 2002
[114] S Sakaguchi T Yamaguchi T Nomura and M Ono ldquoRegu-latory T cells and immune tolerancerdquo Cell vol 133 no 5 pp775ndash787 2008
[115] H Nishikawa and S Sakaguchi ldquoRegulatory T cells in tumorimmunityrdquo International Journal of Cancer vol 127 no 4 pp759ndash767 2010
[116] W Zou ldquoRegulatory T cells tumour immunity and immuno-therapyrdquoNature Reviews Immunology vol 6 no 4 pp 295ndash3072006
[117] A Fialova S Partlova L Sojka et al ldquoDynamics of T-cell infil-tration during the course of ovarian cancer The gradual shiftfrom aTh17 effector cell response to a predominant infiltrationby regulatory T-cellsrdquo International Journal of Cancer vol 132no 5 pp 1070ndash1079 2013
[118] A E Albers R L Ferris G G Kim K Chikamatsu A BDeLeo and T L Whiteside ldquoImmune responses to p53 inpatients with cancer enrichment in tetramer+ p53 peptide-specific T cells and regulatory T cells at tumor sitesrdquo CancerImmunology Immunotherapy vol 54 no 11 pp 1072ndash10812005
[119] N Liu Y Zheng Y Zhu S Xiong andYChu ldquoSelective impair-ment of CD4 + CD25 + Foxp3 + regulatory T cells by paclitaxelis explained by Bcl-2Bax mediated apoptosisrdquo InternationalImmunopharmacology vol 11 no 2 pp 212ndash219 2011
[120] X Wu Q-M Feng Y Wang J Shi H-L Ge and W DildquoThe immunologic aspects in advanced ovarian cancer patientstreated with paclitaxel and carboplatin chemotherapyrdquo CancerImmunology Immunotherapy vol 59 no 2 pp 279ndash291 2010
[121] A P Vicari R Luu N Zhang et al ldquoPaclitaxel reducesregulatoryT cell numbers and inhibitory function and enhancesthe anti-tumor effects of the TLR9 agonist PF-3512676 in themouserdquo Cancer Immunology Immunotherapy vol 58 no 4 pp615ndash628 2009
[122] L Zhang K Dermawan M Jin et al ldquoDifferential impairmentof regulatory T cells rather than effector T cells by paclitaxel-based chemotherapyrdquo Clinical Immunology vol 129 no 2 pp219ndash229 2008
[123] Y Tabuchi J Matsuoka M Gunduz et al ldquoResistance topaclitaxel therapy is related with Bcl-2 expression through anestrogen receptor mediated pathway in breast cancerrdquo Interna-tional Journal of Oncology vol 34 no 2 pp 313ndash319 2009
[124] N Obermajer R Muthuswamy K Odunsi R P Edwards andP Kalinski ldquoPGE
2-induced CXCL12 production and CXCR4
expression controls the accumulation of human MDSCs inovarian cancer environmentrdquo Cancer Research vol 71 no 24pp 7463ndash7470 2011
[125] Q M Feng W Di and X Wu ldquoImmune reconstitution inadvanced ovarian cancer patients undergoing first line chemo-therapyrdquo Xi Bao Yu Fen Zi Mian Yi Xue Za Zhi vol 25 no 11pp 1023ndash1025 2009
[126] A D Seidman D Hochhauser M Gollub et al ldquoNinety-six-hour paclitaxel infusion after progression during short taxaneexposure a phase II pharmacokinetic and pharmacodynamicstudy in metastatic breast cancerrdquo Journal of Clinical Oncologyvol 14 no 6 pp 1877ndash1884 1996
[127] D R Spriggs M F Brady L Vaccarello et al ldquoPhase IIIrandomized trial of intravenous cisplatin plus a 24- or 96-hour
infusion of paclitaxel in epithelial ovarian cancer a gynecologiconcology group studyrdquo Journal of Clinical Oncology vol 25 no28 pp 4466ndash4471 2007
[128] G A Omura M F Brady K Y Look et al ldquoPhase III trial ofpaclitaxel at two dose levels the higher dose accompanied byfilgrastim at two dose levels in platinum-pretreated epithelialovarian cancer an intergroup studyrdquo Journal of Clinical Oncol-ogy vol 21 no 15 pp 2843ndash2848 2003
[129] R Simon and L Norton ldquoThe Norton-Simon hypothesisdesigning more effective and less toxic chemotherapeutic reg-imensrdquoNature Clinical Practice Oncology vol 3 no 8 pp 406ndash407 2006
[130] A Kumar P Hoskins and A Tinker ldquoDose-dense paclitaxel inadvanced ovarian cancerrdquo Clinical Oncology vol 27 no 1 pp40ndash47 2015
[131] P Marchetti S Urien G A Cappellini G Ronzino and CFicorella ldquoWeekly administration of paclitaxel theoretical andclinical basisrdquoCritical Reviews in OncologyHematology vol 44supplement pp S3ndashS13 2002
[132] P Francis E Rowinsky J Schneider T Hakes W Hoskinsand M Markman ldquoPhase I feasibility and pharmacologic studyof weekly intraperitoneal paclitaxel A Gynecologic OncologyGroup pilot studyrdquo Journal of Clinical Oncology vol 13 no 12pp 2961ndash2967 1995
[133] H Thomas and P Rosenberg ldquoRole of weekly paclitaxel inthe treatment of advanced ovarian cancerrdquo Critical Reviews inOncologyHematology vol 44 supplement pp S43ndashS51 2002
[134] M Markman J Markman K Webster et al ldquoDuration ofresponse to second-line platinum-based chemotherapy forovarian cancer implications for patient management and clini-cal trial designrdquo Journal of Clinical Oncology vol 22 no 15 pp3120ndash3125 2004
[135] P H OrsquoDonnell M Eileen Dolan E Gamazon et al ldquoPopu-lation differences in platinum toxicity as a means to identifynovel genetic susceptibility variantsrdquo Pharmacogenetics andGenomics vol 20 no 5 pp 327ndash337 2010
[136] M J Millward M J Boyer M Lehnert et al ldquoDocetaxel andcarboplatin is an active regimen in advanced non-small-celllung cancer a phase II study in Caucasian and Asian patientsrdquoAnnals of Oncology vol 14 no 3 pp 449ndash454 2003
[137] M Markman ldquoIntraperitoneal therapy of ovarian cancerrdquoOncologist vol 1 no 1-2 pp 18ndash21 1996
[138] M Markman and J L Walker ldquoIntraperitoneal chemotherapyof ovarian cancer a review with a focus on practical aspects oftreatmentrdquo Journal of Clinical Oncology vol 24 no 6 pp 988ndash994 2006
[139] K Fujiwara S Nagao E Aotani and K Hasegawa ldquoPrincipleand evolving role of intraperitoneal chemotherapy in ovariancancerrdquo Expert Opinion on Pharmacotherapy vol 14 no 13 pp1797ndash1806 2013
[140] M Markman E Rowinsky T Hakes et al ldquoPhase I trialof intraperitoneal taxol a gynecoloic oncology group studyrdquoJournal of Clinical Oncology vol 10 no 9 pp 1485ndash1491 1992
[141] M Markman M F Brady N M Spirtos P Hanjani and S CRubin ldquoPhase II trial of intraperitoneal paclitaxel in carcinomaof the ovary tube and peritoneum a gynecologic oncologygroup studyrdquo Journal of Clinical Oncology vol 16 no 8 pp2620ndash2624 1998
[142] P B Panici I Palaia M Graziano F Bellati N Manci and RAngioli ldquoIntraperitoneal paclitaxel as consolidation treatmentin ovarian cancer patients a case control studyrdquo Oncology vol78 no 1 pp 20ndash25 2010
BioMed Research International 21
[143] D K Armstrong B Bundy L Wenzel et al ldquoIntraperitonealcisplatin and paclitaxel in ovarian cancerrdquo The New EnglandJournal of Medicine vol 354 no 1 pp 34ndash43 2006
[144] D Tewari J Java and R Salani ldquoLong-term survival advantageof intraperitoneal chemotherapy treatment in advanced ovariancancer an analysis of a Gynecologic Oncology Group ancillarydata studyrdquo in Proceedings of the 2013 Society of GynecologicOncology Annual Meeting on Womenrsquos Cancer (GOG114172Abstract) Los Angeles Calif USA 2013
[145] D A Yardley ldquonab-paclitaxel mechanisms of action and deliv-eryrdquo Journal of Controlled Release vol 170 no 3 pp 365ndash3722013
[146] M Ando K Yonemori N Katsumata et al ldquoPhase I and phar-macokinetic study of nab-paclitaxel nanoparticle albumin-bound paclitaxel administeredweekly to Japanese patients withsolid tumors and metastatic breast cancerrdquo Cancer Chemother-apy and Pharmacology vol 69 no 2 pp 457ndash465 2012
[147] N Desai V Trieu Z Yao et al ldquoIncreased antitumor activityintratumor paclitaxel concentrations and endothelial cell trans-port of cremophor-free albumin-bound paclitaxel ABI-007compared with cremophor-based paclitaxelrdquo Clinical CancerResearch vol 12 no 4 pp 1317ndash1324 2006
[148] J A Yared and K H R Tkaczuk ldquoUpdate on taxane devel-opment new analogs and new formulationsrdquo Drug DesignDevelopment andTherapy vol 6 pp 371ndash384 2012
[149] M G Teneriello P C Tseng M Crozier et al ldquoPhase IIevaluation of nanoparticle albumin-bound paclitaxel in plati-num-sensitive patients with recurrent ovarian peritoneal orfallopian tube cancerrdquo Journal of Clinical Oncology vol 27 no9 pp 1426ndash1431 2009
[150] R L Coleman W E Brady D S McMeekin et al ldquoA phase IIevaluation of nanoparticle albumin-bound (nab) paclitaxel inthe treatment of recurrent or persistent platinum-resistant ovar-ian fallopian tube or primary peritoneal cancer a GynecologicOncology Group Studyrdquo Gynecologic Oncology vol 122 no 1pp 111ndash115 2011
[151] J W Singer ldquoPaclitaxel poliglumex (XYOTAX CT-2103) amacromolecular taxanerdquo Journal of Controlled Release vol 109no 1ndash3 pp 120ndash126 2005
[152] C Li D-F Yu R A Newman et al ldquoComplete regressionof well-established tumors using a novel water-soluble poly(L-glutamic acid)-paclitaxel conjugaterdquo Cancer Research vol 58no 11 pp 2404ndash2409 1998
[153] M Mita A Mita J Sarantopoulos et al ldquoPhase I study ofpaclitaxel poliglumex administered weekly for patients withadvanced solid malignanciesrdquo Cancer Chemotherapy and Phar-macology vol 64 no 2 pp 287ndash295 2009
[154] P Sabbatini M W Sill D OrsquoMalley L Adler and A ASecord ldquoA phase II trial of paclitaxel poliglumex in recurrentor persistent ovarian or primary peritoneal cancer (EOC) agynecologic oncology group studyrdquo Gynecologic Oncology vol111 no 3 pp 455ndash460 2008
[155] M O Bradley C S Swindell F H Anthony et al ldquoTumortargeting by conjugation of DHA to paclitaxelrdquo Journal ofControlled Release vol 74 no 1ndash3 pp 233ndash236 2001
[156] M O Bradley N L Webb F H Anthony et al ldquoTumortargeting by covalent conjugation of a natural fatty acid topaclitaxelrdquo Clinical Cancer Research vol 7 no 10 pp 3229ndash3238 2001
[157] A C Wolff R C Donehower M K Carducci et al ldquoPhaseI study of docosahexaenoic acid-paclitaxel a taxane-fatty acid
conjugate with a unique pharmacology and toxicity profilerdquoClinical Cancer Research vol 9 no 10 part 1 pp 3589ndash35972003
[158] A Sparreboom A C Wolff J Verweij et al ldquoDispositionof docosahexaenoic acid-paclitaxel a novel taxane in bloodin vitro and clinical pharmacokinetic studiesrdquo Clinical CancerResearch vol 9 no 1 pp 151ndash159 2003
[159] P M Fracasso J Picus J D Wildi et al ldquoPhase 1 and phar-macokinetic study of weekly docosahexaenoic acid-paclitaxelTaxoprexin in resistant solid tumor malignanciesrdquo CancerChemotherapy and Pharmacology vol 63 no 3 pp 451ndash4582009
[160] A Y Bedikian R C DeConti R Conry et al ldquoPhase 3 study ofdocosahexaenoic acid-paclitaxel versus dacarbazine in patientswith metastatic malignant melanomardquo Annals of Oncology vol22 no 4 pp 787ndash793 2011
[161] Y-N Wu S-L Wang Y-C Wang et al ldquoReversal effect ofdocosahexaenoic acid on taxol resistance in human ovarian car-cinoma A2780T cellsrdquo Obstetrics amp Gynecology InternationalJournal vol 1 no 3 Article ID 00018 2014
Submit your manuscripts athttpwwwhindawicom
PainResearch and TreatmentHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom
Volume 2014
ToxinsJournal of
VaccinesJournal of
Hindawi Publishing Corporation httpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
AntibioticsInternational Journal of
ToxicologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
StrokeResearch and TreatmentHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Drug DeliveryJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Advances in Pharmacological Sciences
Tropical MedicineJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Medicinal ChemistryInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
AddictionJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
Emergency Medicine InternationalHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Autoimmune Diseases
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Anesthesiology Research and Practice
ScientificaHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Pharmaceutics
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of

8 BioMed Research International
Immunomodulatory effect of
paclitaxel
Stimulate direct cytotoxic activity by
macrophage
Induce activation maturation and priming of DCs
Stimulate NK-dependent antitumour immunity
Activation of tumour-specificCTL Expansion of memory T cells
Secretion of proinflammatory cytokine
Shift from Th2 to Th1 type ofresponse
Depletion of Tregs andmodulation of MDSC
Downregulates the expression of VEGFR-2
and inhibits angiogenesis
IL-6 IL-12 TNF-120572 and i-NOS
Figure 5 Immunomodulatory effect of paclitaxel Paclitaxel a toll-like receptor 4 (TLR4) ligand binds to TLR4 receptor and triggers TLR4signaling via MyD88 dependent and independent pathway Paclitaxel then promotes anticancer immune response directly by stimulatingmacrophages to kill cancer cells or indirectly by secretion of proinflammatory cytokines which upregulates activation of DCs NK andtumour specific CTL Paclitaxel promotes effective CTL response by upregulation of mannose-6-phosphate which facilitate permeabilityto granzyme B and cytokine patterns of T helper type 1 Paclitaxel modulates MDSC and ablates Tregs Memory T cells (CD4+CD45RO+and CD8+CD45RO+) increased significantly while regulatory T cells (Tregs) decreased around 2 weeks creating an opportunity window fordose-dense therapy and immunomodulatory agents to achieve clinical benefit Dose-dense and low dose paclitaxel also blocks new vesselformation by downregulating VEGF-receptor 2 reduces resistance by alternative mechanism of action
to develop better therapeutic options in the management ofadvanced ovarian cancer
Paclitaxel is a ligand to toll-like receptor 4 (TLR4) whichis expressed on innate immune cells including macrophagesThe binding of paclitaxel to TLR4 on macrophages trig-gers the MyD88 mitogen-activated protein kinase (MAPK)and transcription of nuclear factor NF-kappa B (NF-120581B)pathways (Figure 3) resulting in their activation and releaseof immunostimulatory cytokines such as tumour necrosisfactor-120572 (TNF-120572) interleukin-1 (IL-1) interleukin-6 (IL-6)and interleukin-8 (IL-8) [103ndash105] Activated macrophagescan either cause direct tumour cell lysis via release oflysosomal enzymes and nitric oxide (NO) or indirectly byactivating NK cells DCs and tumour-specific cytotoxic T-lymphocytes (CTLs) [101]
NK cells are also innate immune cells capable of killingtumour cells particularly those cells that have reduced classI MHC expression and therefore can escape killing by CTLsPaclitaxel can enhance NK cell function by inducing mRNAand protein production of perforin an effector moleculeinvolved inNKcell-mediated cytotoxicity [106]However theeffect of low dose paclitaxel on NK cells is controversial Inanother study it was found that treatment of human NK cellswith paclitaxel effectively inhibits NK cell-mediated killing ofK562 (human erythroleukemia) target cells in vitro withoutaffecting the viability of NK cells [107] However weeklypaclitaxel therapy for non-small cell lung cancer patients was
only able to reduce the NK cell function up to completion ofthe first cycle but thereafter it gradually recovered [108]
Dendritic cells also express TLR4 and can be directlyactivated by paclitaxel The binding of paclitaxel to TLR onimmature DCs promotes DC maturation by upregulatingantigen-processing machinery gene components costimu-latory molecules and IL-12p70 [102] This enhances theability of DCs to prime T cells which facilitate antitumourimmunity [109] Paclitaxel can also promote cytotoxic T-cell function by upregulating mannose-6-phosphate whichfacilitates permeability to granzyme B and also inducescytokine production patterns typical of the T helper type 1phenotype via IL-2 (CD4 T cell) and IFN-120574 (CD8 T cell)secretion [104 110] Activated CD8+ T cells can differentiateinto CTL type 1 (Tc1) cells producingmainly IFN-120574 and CTLtype 2 (Tc2) cells producing mostly IL-4 IL-5 and IL-10 Tc1cells are potent CTL involved in the defense against cancerTc1 cells are able to recognise tumour antigens in the contextof MHC class I and mediate tumour cell lysis The role of Tc2cells in the immune response is not clearly known althoughtheir presence has been associated with disease progression[111]
CD4+ CD25+ regulatory T-cells (Tregs) constitutingapproximately 5ndash10 of peripheral CD4+ T cells [112 113]play an important role in tumour immune evasion [114]There is growing evidence that supports the existence ofelevated numbers of Tregs in tumours [115ndash117] which may
BioMed Research International 9
suppress immune responses of other CD4+ and CD8+ cells[118ndash120] and promote tumour progression In murine stud-ies paclitaxel exhibits the ability to reduce the number andsize of Treg cells thereby enhancing antitumour immunity[119 121] Similar findingswere seenwith a selective reductionin the size and number of Treg populations in peripheralblood samples from non-small cell lung cancer (NSCLC)patients [122]
Paclitaxel also decreased the expression of the anti-apoptotic molecule Bcl-2 in Treg cells while increasing thecorresponding proapoptoticmember Bax which contributedto the apoptotic sensitivity of Treg to paclitaxel [87]This wasseen in a study using the 3LL Lewis tumour model whichdemonstrated that Treg cells exposed to paclitaxel displayeddown regulation of Bcl-2 and upregulation of Bax and uponblocking the Bcl-2 pathway the ability of paclitaxel to ablateTreg cells compared toT effectorswas impaired and bothTregand T effectors were affected These results may suggest thatpaclitaxel targets Bcl-2 rather than tubulin to contribute tothe distinctive effect on Treg cells [119] It has recently beenshown in vitro that paclitaxel could target Bcl-2 and thereforelead to apoptosis Bcl-2 family proteins are key regulators ofapoptosis and play an important role in tumourigenesis andmulti-drug resistance by blocking apoptosis [119 123]
Few studies have also shown effect of paclitaxel onmyeloid-derived suppressor cells (MDSCs) a heterogeneouspopulation of immature myeloid cells immunosuppressivein nature are recruited by cancer cells and are found inincreased amount in advanced epithelial ovarian cancer [124]In a murine study using C57BL6 mice administration ofpaclitaxel at ultralow dose modulates MDSCs to differentiateinto DCs in a TLR4 independent manner [110] Hencepaclitaxel in ultralow noncytotoxic doses together with itsangiogenesis blocking ability may potentially enhance theefficacy of immunotherapy by ablation of immunosuppres-sive populations such as Tregs and MDSCs in tumour-bearing hosts [50 102]
In immunocompromised patients with advanced ovariancancer with increased Tregs and decreased levels of CD4+T cell CD8+ T cell and NK subsets after a single courseof combined carboplatin and paclitaxel chemotherapy theimmunosuppression is reversed around 12 to 14 days later butnot before one week or after three to four weeks Not only areTregs decreased but also the proportions of IFN-120574 secretingCD8+ T cells T helper-1 Tc1 and NKT cells The ratio of Tc1to Tc2 cells increases significantly [111 120 125]
Following chemotherapy both CD4+CD45RO+ andCD8+CD45RO+ memory T cells increased significantly andpeaked around 2 weeks The increase of memory T cellsin ovarian cancer patients following chemotherapy prob-ably opens the door of opportunity to develop long-termimmunological memory which could prevent recurrenceand metastases [120] Administration of dose-dense therapygiven weekly may hence be beneficial immunologically tomount an adequate immune response compared to standard3-week therapy In addition administration of immunother-apy agentsmay also be ideal during the period of 2weeks afterchemotherapy where temporary immune system reconstitu-tion takes place
8 Clinical Studies
In the past two decades paclitaxel had been administered indoses ranging from 60 to 250mgm2 over 1ndash96 hours andfrom 1 to 3 weekly intervals Prolonged exposure up to 96hours was believed to be effective as demonstrated with pre-clinical data but later refuted in large prospective studies [14126 127] A 24-hour infusion of paclitaxel was subsequentlyadministered to reduce the risk of hypersensitivity reactionshowever it was shown to increase mucosal and bone marrowtoxicity without improved efficacy [127 128] Development ofeffective premedication has led to administration of shorterinfusions (lt3 hours) which are better tolerated in particularfrom a haematologic perspective but patients remain at riskof myalgia and neuropathy at higher doses Weekly one-hourlow dose paclitaxel also known as dose-dense therapy hasrecently emerged as another possible strategy to improveoutcomes
9 Dose-Dense Therapy
Dose-dense treatment is defined by delivery of a maintainedper-cycle dose or overall dose with administration of drugat shorter time intervals than is standard This differs fromdose intensity which refers to dose (per unit weight or bodysurface area) delivered per unit time Hence either escalationof dose per cycle or reducing the time in between cycles maymodify dose intensity [129 130]
The rationale for the dose-dense approach of weeklypaclitaxel is that more frequent delivery of moderate dosesmay achieve greater efficacy by allowing sustained exposureof dividing tumour cells to paclitaxelrsquos cytotoxic and antian-giogenic effects hence reducing resistance delaying relapseand increasing the possibility of cancer remission Three 1-hour infusions of paclitaxel given at a week interval achievedgreater dose-density as well as dose-intensity than a singleadministration every 3 weeksThe initial tissue concentration(gt50 nM) for 1-hour infusion is similar to that of 3-hourinfusion but the concentration in the plasma instead oflasting for 8 hours in a 3-hour infusion rapidly falls below50 nM in less than 75 minutes for 1-hour infusion and hencereduces the risk of neutropenia However the rate of fallexperienced in tissue concentration of the drug is slowerthan plasma concentration of the drug hence efficacy ismaintained [131 132] A shorter infusion time allows bettercontrol of toxicities improved patient comfort and reducedhospitalisation hours
Several studies have used dose-dense paclitaxel in thetreatment of advanced ovarian cancer and are summarizedin Table 1 Based on phase 1 studies the recommendeddose for weekly paclitaxel ranges between 80 and 90mgm2compared with 45mgm2 per week with 3-weekly paclitaxeland is given over 1-hour duration Weekly scheduling hasdemonstrated consistent activities in ovarian cancer studies[11ndash13] Response rates were in the 20ndash50 range whereusually less than 10 would be expected Grade-4 doselimiting toxicities in particular neutropenia were not evidentat any dose below 100mgm2week [11 133]
10 BioMed Research International
Table1Ph
ases
Iand
IIstu
dies
onintravenou
sdose-densep
aclitaxel
Stud
yRe
gimen
119899()
PI(m
)RR
()
CR(119899)
MedianPF
S(m
)Median
OS
(m)
Adversee
ffects
Com
ments
Paclitaxel
dose
(mgm
2 )Ca
rbop
latin
dose
(mgm
2 )Ph
aseIsinglea
gent
Lofflerre
tal1996
[11]
40ndash9
0week
1-hou
rinfusionfor
6weeks
5040
5NA
NA
(i)Hem
atologictoxicity-m
ild(ii)N
ograde3
or4
haem
atologicaltoxicity
neurologicalor
cardiotoxicityup
to90
mgm
2 wk
(iii)Nohypersensitivity
reactio
ns(patientsreceivedprem
edication)
(i)100
priorc
hemotherapy
(ii)M
ediando
seintensity
was
410m
gm
2 6w
k(range200
to540m
gm
2 6w
k)
Fenn
ellyetal
1997
[12]
40ndash100w
eek
1830
NA
NA
NA
(i)Nomucositiso
rgrade
III
neurop
athy
was
seen
(ii)A
lopeciao
ccurredin
one
(i)100
priorc
hemotherapy
(2ndash5
priorregim
ens)
(ii)P
artia
lrespo
nses
weres
eenin
four
of13
assessablepatients
(30
)(iii)Dose-lim
iting
toxicitywas
reachedat100m
gm
2 (iv
)2-3
patie
ntse
xperience
treatmentd
elay
(v)M
axim
um-to
lerateddo
seof
80mgm
2 Ab
u-Ru
stum
etal
1997
[13]
60ndash100
over
1ho
urw
eek
45289
NA
NA
NA
(i)Nopatie
nthadfebrile
neutropenia
(i)100
priorc
hemotherapy
(1ndash8
priorregim
ens)
PhaseIISing
leagent
Markm
anetal
2001
[14]
80over
1ho
urw
eek
53(52)
25NA
NA
NA
Therapydiscon
tinuedin
(i)4patie
ntsw
hohadperip
heral
neurop
athy
(ii)1
patie
ntdu
etopainful
fingernailbeds
(i)100
platinum
andpaclita
xel
resistant
(ii)Th
erapywas
discon
tinuedin
5patie
ntsb
ecause
oftoxicity
(iii)Only13
(1)w
erem
odified
(doser
eductio
nor
treatment
delay)
becauseo
fsidee
ffects
PhaseIICom
binedwith
platinum
agent
Kiku
chietal
2005
[15]
80over
1ho
urw
eek
AUC2week
27gt6
818
483
NA
(i)Neutro
penia(
17)
thrombo
cytopenia(
51
)(ii)N
ocaseso
fperipheral
neurop
athy
(grades3
and4)
inweeklycombinedT-C
Cadron
etal2007
[16]
90over
1ho
urw
eek
AUC4week
24 9gt6le6
73 38NR
8105
675
(i)Grade
34neutropenia(
34)
andneutropenicfever
in2
(ii)N
auseaa
ndvomiting
and
fatig
uewerethe
mostfrequ
ent
nonh
ematologicalsid
eeffects
(i)Doser
eductio
nwas
necessary
in25of
patie
nts
Pign
atae
tal2008
[17]
60over
1ho
urw
eek
AUC2week
24(13)lowastlowast
1stline
385
2320
136
(i)Notoxicd
eath
was
recorded
(ii)G
rade
2anaemiawas
repo
rted
insevenpatie
nts(27)
(iii)Nofebrile
neutropeniaw
asob
served
(iv)G
rade
3and4neutropenia
was
recorded
infive(19)a
ndon
e(4
)patients
(v)G
rade
3thrombo
cytopenia
occurred
inon
epatient
(4)
BioMed Research International 11
Table1Con
tinued
Stud
yRe
gimen
119899()
PI(m
)RR
()
CR(119899)
MedianPF
S(m
)Median
OS
(m)
Adversee
ffects
Com
ments
Paclitaxel
dose
(mgm
2 )Ca
rbop
latin
dose
(mgm
2 )
Safrae
tal2014
[18]
80over
1ho
urw
eek
AUC2week
133
1stline
864
645
274
(i)Highera
naem
ia(grade
III+
IV68vs53)+
IVneutropenia(
144vs69)
decreasedgradeIIa
lopecia(
235
vs981
)and
thrombo
cytopenia
(grade
III+
IV0
vs23)
Havrilesky
etal
2003
[19]
80over
1ho
urw
eek
AUC2weekD1
D8D15
until
progressionCR
+8courses
29 21 8
Total
grou
pgt6lt6
83 100
38
16 15 1114
115
137
32
(i)Hem
atologictoxicitywas
common
(grade
3neutropenia
32n
ograde4
neutropenia
grade3
or4thrombo
cytopenia
142)
(i)To
xicitymanaged
bytre
atment
delaydo
seredu
ctionof
paclitaxel
ordiscon
tinuatio
nof
carbop
latin
vanderB
urgetal
2014
[20]
90over
1ho
urw
eek
AUC4weekD1
D8D15
D29
D36
D49
+6x
TCq3w
108
65 43
Total
grou
pgt6lt6
76 5816 42
26 158 13
(i)Neutro
penia3
0
thrombo
cytopenia8
febrile
neutropenia0
5
(ii)N
onhaem
atologictoxicitywas
low
(i)Treatm
entw
asdelayedin
16
anddo
seredu
cedin
2of
cycle
s
119899num
bero
fpatientsassessableforrespo
nsemm
onthsPIplatinum
treatmentfreeintervalRR
respo
nser
ateCR
com
pleterem
issionT
paclitaxelC
carbop
latin
PFS
progressio
nfre
esurvivalOSoverall
survivalN
An
otavailableinpapero
rabstractandNR
notyetreached
lowastlowastElderly
popu
lation
patient
agedge70
years
12 BioMed Research International
Numerous phase II studies have explored the tolerabilityand the activity of weekly paclitaxel either as a single agent orin combination with several other drugs or biological agents(Table 1) A number of regimens combining weekly paclitaxelwith carboplatin have been used as first-line treatment inovarian cancer Carboplatin has been administered weeklyat AUC of 2 with dose escalation in some studies whilepaclitaxel had been infused at 60ndash80mgm2week Thiscombined regimen was well tolerated with a low incidence ofbone marrow suppression Overall response rates have beenhigh in the range of 60ndash80 in most studies even in heavilypretreated patients with platinum-resistant disease (diseaserecurrence or progression within 6 months of the last lineof platinum-based therapy) [15ndash20 134] The promising datafrom these phase II trials then led to the evolution of largerphase III trials
Three phase III studies Japanese Gynecologic OncologyGroup- (JGOG-) Trial 3016 [21ndash23] Multicentre Italian Trialin Ovarian Cancer-Trial 7 (MITO-7) [25] and GynecologicOncology Group GOG-262 Trial [24] have explored dosedense therapy The results of these trials are summarised inTable 2
The Japanese Gynecologic Oncology Group (JGOG)conducted a randomized phase 3 trial of dose-dense weeklypaclitaxel 80mgm2week in combination with 3-weeklycarboplatin compared to standard 3-weekly carboplatin andpaclitaxel 180mgm2 in patients with advanced epithelialovarian peritoneal or fallopian tube cancer (JGOG 3016NOVEL trial) In both arms carboplatin was given at AUC6 and the median number of cycles was six In this largestudy (119899 = 637) with a median follow up of 77 months therewas an 11-month improvement in themedian progression freesurvival (PFS) in the dose-dense treatment group comparedwith the standard treatment arm (282 versus 175 monthsHR 076 95 CI 062ndash091 119901 = 00037) Median OS wasalso higher in the dose-dense treatment arm (1005 versus622 months HR 079 95 CI 063ndash099 119901 = 0039)On subgroup analysis suboptimally debulked patients withresidual disease of gt1 cm (119899 = 342) had a significantlyhigher median overall survival in the dose dense arm (512versus 335 months HR-075 95 CI 057ndash097 119901 = 0027)There was no significant advantage to dose-dense treatmentfor patients with optimally cytoreduced disease Dose-densetherapy survival benefits were also not seen in patients withclear cell or mucinous histology type unlike serous typeHowever patient treated with dose dense therapy had asignificantly higher frequency of hematologic toxicity thanwith the standard arm (212 versus 94) which resultedin lower treatment completion rates (63 versus 48) withfrequent episodes of delay (76 versus 67) and dosereductions (48versus 35) [21 22]Therewas no significantdifference in terms of overall quality of life between the twoarms (119901 = 046) [23]
Using a similar regimen as in JGOG-3016 a GynecologicOncology Group (GOG)-262 Trial was conducted in theUnited States In this group most patients had stage IIIdisease (66ndash70) and two-thirds had suboptimal debulkingwith residual disease of gt1 cm This was a randomized phase
III trial of 3 weekly paclitaxel versus dose-dense weeklypaclitaxel in combination with carboplatin in patients withadvanced epithelial ovarian peritoneal or fallopian tubecancer Though optional concurrent and maintenance beva-cizumab were received by the majority of patients in botharms (835 versus 841 resp) There was no significantdifference in PFS in the patients who received the dosedense paclitaxelcarboplatin regimen compared to those whoreceived the standard paclitaxelcarboplatin regimen (148versus 143 months HR 097 95 CI 079ndash118) Howeverin a subgroup analysis there was a significant difference inPFS in the dose dense paclitaxel arm who did not receivebevacizumab 119899 = 112 (142 versus 103 months HR 059 95CI 037ndash096 119901 = 0003) Overall survival data is still imma-ture There was higher frequency of grade 3 anaemia (408versus 157 119901 lt 0001) and grade 2 sensory neuropathy(259 versus 178 119901 = 0012) but a lower incidence ofneutropenia (72 versus 83 119901 lt 0001) [24]
In 2008 the Multicentre Italian Trials in Ovarian Cancer(MITO-7) randomised 810 women in a phase 3 trial toreceive either standard carboplatin (AUC = 6) and paclitaxel175mgm2 every 3 weeks or a weekly schedule of paclitaxel(60mgm2) with carboplatin (AUC = 2) The majority ofpatients in both arms (83ndash90) received six cycles of therapyMost patients (58ndash63) had stage II1 disease 23 of themwere suboptimally debulked Median PFS did not differsignificantly (173 months and 183 months 119901 = 066)between the standard and dose-dense arms respectivelyThere was no significant difference in response rate betweenthe two arms nor the estimated 2-year overall survivalSubgroup analysis did not identify any subgroup that mayhave benefited from the dose-dense regimen Unlike theJGOG-3016 trial the incidence of grade 3-4 neutropenia wassignificantly lower in the dose-dense group compared to the3-weekly regimen (42 versus 50) A similar pattern wasseen for the incidence of febrile neutropenia (lt1 versus 3119901 = 002) thrombocytopenia (1 versus 7 119901 lt 0001)and other nonhaematological toxicities such as alopeciavomiting renal dysfunction and neuropathy Quality of lifewas reported to be significantly better in the dose-dense arm(119901 lt 00001) which was discordant with the JGOG-3016quality of life data [25]
In summary there was significant improvement inmedian PFS and overall survival in studies using paclitaxelat 80mgm2week dose-dense therapy [21 24] but withhigher haematological toxicity whereas MITO-7 [25] whichwas using paclitaxel at 60mgm2week was only equivalentlyeffective but less toxicThis does not conclude that the higherpaclitaxel dose is more clinically beneficial as there are manyother confounding factors in all three studies
In a multivariate analysis the JGOG-3016 study [21]reported that a lower dose intensity of paclitaxel (lt80) wasassociated with poorer overall survival (hazard ratio = 14295 confidence interval 112ndash181 119901 = 0004) however itmust be highlighted that the investigational arm carboplatinschedules were not standardised in these studies The JGOGand GOG trials delivered a 3-weekly carboplatin (AUC =6) arm whereas in the MITO-7 study the carboplatin was
BioMed Research International 13
Table2Ph
aseIIIstu
dies
onintravenou
sdose-densep
aclitaxel
Stud
yRe
gimen
119899
MedianPF
S(m
)
Median
OS
(m)
Adversee
ffects
Com
ments
Katsu
matae
tal2009
[21]
Katsu
matae
tal2013
[22]
Haranoetal2014
[23]
JGOG3016
631
(i)Haematologicaltoxicityhigh
erin
dose
dense-211versus
94
Lower
treatmentcom
pletionin
dose-dense
63versus
48
Frequent
episo
deso
fdelay
indo
se-dense
76versus
67
Doser
eductio
nsin
dose-dense
48versus
35
Nosig
nificantd
ifference
inoverallQ
OL
betweenbo
thgrou
ps(119901=046)
Paclitaxel80m
gm
2D18
15+carbop
latin
AUC63
weeklyversus
Paclitaxel180
mgm
2+
carbop
latin
AUC63
weekly
312
282
1005
Both
givenfor6
ndash9cycle
s319
175
622
Chan
etal2013
[24]
GOG-262
(i)Higherfrequ
ency
ofgrade3
anaemia
(408versus
157119901lt0001)
grade2
sensoryneurop
athy
(259versus
178
119901=0012)b
utlower
incidenceo
fneutropenia(
72versus
83119901lt0001)
Paclitaxel80m
gm
2D18
15+carbop
latin
AUC63
weeklyversus
Paclitaxel175
mgm
2+
carbop
latin
AUC63
weekly
346
148
NR
Both
givenfor6
cycle
s346
143
NR
Bevacizumab
given
optio
nally
112
(did
not
receive
bevazicumab)
142vs
103
Pign
atae
tal2014
[25]
MITO-7
810
(i)Lo
wer
incidenceo
fgrade
3-4
neutropenia(
42versus
50)febrile
neutropenia(lt1v
ersus3
119901=002)
thrombo
cytopenia(
1versus7
119901lt0001)andothern
onhaem
atological
toxicitie
ssuchas
alop
eciavom
iting
renald
ysfunctio
nandneurop
athy
Qualityof
lifeb
etterindo
sedensea
rm(119901lt00001)
Paclitaxel60m
gm
2 weekly+carbop
latin
AUC
2weeklyversus
Paclitaxel175
mgm
2+
carbop
latin
AUC63
weekly
406
404
183 173
77lowast
79lowast
119899num
bero
fpatientsmm
onthsDday
PFSprogressionfre
esurvivalOSoverallsurvivalNAnot
availableinpapero
rabstractandNR
notyetreached
lowastSurvivalrateat2years
14 BioMed Research International
dose-dense (AUC 2 weekly) Although it is possible that thedose scheduling for the platinum-based agent is not essentialfor a survival benefit as shown by previous studies usingdose-dense cisplatin direct cross-trial comparison cannot bemade Unlike paclitaxel carboplatin probably requires peakdose for optimal therapeutic benefit hence this may accountfor the inferior survival outcome in MITO-7 trial Anotherconfounding factor may be difference in ethnicity All threestudies used different ethnic populations and Asian patientsin JGOG-3016 appear to have better survival outcomes thanthe MITO-7 Western population Ethnicity with possibleunderlying genetic causes may be responsible for the variableresponses to chemotherapy across individuals [135] This wasexplored by Millward et al who studied 68 Caucasian andAsian lung cancer patients treated with a combination ofpaclitaxel and carboplatin and found that the incidence offebrile neutropenia was 50 of an initially treated cohortof Asians and when carboplatin was subsequently dosereduced in all Asian patients the overall incidence of febrileneutropenia was also reduced to 26 [136]
Although early clinical data from phase I and phaseII dose-dense paclitaxel trials in advanced ovarian cancerwere promising the results from phase III studies in havebeen inconsistent as a result of differences in paclitaxel dosecarboplatin AUC and schedule addition of bevacizumabas well as different ethnic populations The results of arecently completed randomised three arms GynaecologicCancer InterGroup (GCIG) phase II trial ICON 8 mayfurther inform the clinical benefit of dose dense paclitaxeltherapy
This multicentre trial involving 111 centres in the UKSouth Korea Mexico Ireland Australia and New Zealandwith a target population of 1485 patients with stage IC-IV epithelial ovarian cancer or peritoneal or fallopian tubecancer compared two dose-dense arms (i) JGOG-like armcarboplatin AUC 5 plus weekly 80mgm2 paclitaxel and (ii)MITO-7-like arm weekly carboplatin AUC 167 plus weekly80mgm2 paclitaxel to the standard 3-weekly treatment(carboplatin AUC 5 plus 175mgm2 paclitaxel) for stage IC toIV epithelial ovarian cancer The dose-dense arms of MITO-7 and JGOG-3016 as well as the ethnic heterogeneity will befurther addressed
10 Intraperitoneal (IP) Chemotherapy
In addition to dose and scheduling the route of adminis-tration of chemotherapy agents plays an important role inoutcome Intraperitoneal spread is common and likely anearly event in epithelial ovarian cancer hence the deliveryof chemotherapy intraperitoneally in theory would exposethe microcirculation of tumour to higher doses of drug thansystemic administration while limiting systemic toxicityTheideal drug for IP chemotherapy is one that is systemicallyeffective penetrates deep into the inner core of tumour tissueand remains within the peritoneal cavity for a prolongedperiod of time [137ndash139]
Early clinical studies confirmed that indeed the peritonealcavity could be exposed to 10 to 20-fold higher (cisplatin
and carboplatin) drug concentration than when using theintravenous approach and since 1978 this route had beenadopted as a form of therapeutic intervention [137 139]A subsequent phase I trial showed that IP paclitaxel haddose-limiting toxicity in the form of abdominal pain [140]Another phase 1 GOG pilot study administered weekly IPpaclitaxel at an initial dose of 20mgm2 for 16 weeks to33 patients and found that IP paclitaxel at this dose wasfeasible and well tolerated At dose levels 60 to 65mgm2there were significant levels of paclitaxel for a week afterdrug administration suggesting very slow clearance andcontinuous exposure of the peritoneal cavity to active drugconcentrations [132]
Hence this initiated a phase II study [141] that used pacli-taxel intraperitoneally at a dose of 60ndash65mgm2week In thisphase II GOG study 76 patients with small-volume resid-ual disease carcinoma (05 cm or less) involving the ovaryperitoneal or fallopian tube were treated with paclitaxel60mgm2week intraperitoneally for 16 weeks followed bysurgical evaluation in patients without disease progressionThe Gynaecologic Oncology group (GOG) currently definesno visible disease as microscopic disease being the idealsurgical outcome 75 of patients had received prior systemictherapy and 70 received all 16 courses that were planned Of28 patients with microscopic disease at the start of therapy61 achieved a surgically defined complete response whereasonly 1 out of 31 patients with macroscopic disease achieved acomplete response The median time-to-recurrence was 167months with an estimated survival rate at 2 years being 58Treatment was generally well tolerated [141]
Another study looked into the effect of IP paclitaxel asconsolidation therapy in advanced ovarian cancer Twenty-eight patients who had initial residual macroscopic disease(lt1 cm) after primary surgery or interval debulking but hadcomplete pathological response following standard treatmentwith at least 6 cycles of platinum-based chemotherapy regi-men received paclitaxel 60mgm2week intraperitoneally for12ndash16 weeks as consolidation therapy The median time torecurrence was 25 months but overall survival did not differsignificantly when compared with control group submittedto observation only Treatment-related toxicity was mild andtechnical difficulties were observed in 11 of patients [142]
Multicenter randomised phase 3 trials as well as meta-analysis of IP chemotherapy have been performed anddemonstrated that chemotherapy drugs administered intra-peritoneally are superior to intravenous standard regimensin patient with optimally debulked epithelial ovarian cancerThe most impressive data comes from GOG 114 [14] and172 trial [143] In GOG 114 patients received either sixcycles of intravenous paclitaxel 135mgm2 and cisplatin75mgm2 every 3 weeks or intravenous carboplatin (AUC= 9) every 28 days for two cycles followed by six 3-weeklycycles of intravenous paclitaxel 135mgm2 and IP cisplatin100mgm2 [14] whereas in GOG 172 patients received eitherintravenous paclitaxel 135mgm2 followed by intravenouscisplatin 75mgm2 or intravenous paclitaxel 135mgm2 fol-lowed by IP combination of cisplatin 100mgm2 and pacli-taxel 60mgm2 on day 8 Both trials had a combined total
BioMed Research International 15
of 876 women with stage III epithelial ovarian carcinomaoptimally debulked to le1 cm residual tumour [143] Themedian follow-up for GOG 114 [14] was 138 years with GOG172 [143] was 97 years The primary results of the individualtrials reported up to 6-month improvement in median PFSfollowing IP therapy In the combined analysis of the datafrom both trials the data continued to show a 5-monthdifference in favour of IP therapy (25 versus 20 months)which translates into 16 reduction in the hazard ratio forprogression (119901 = 003) In GOG 114 [14] reported in 2001there was only borderline improvement in overall survivalassociated with this regimen (median 63 versus 52 monthsrelative risk 081 119901 = 005)
However in combined analysis in 2013 which was pre-sented at the Society of Gynecologic Oncology AnnualMeeting [144] the overall survival showed an 11-monthimprovement in favour of IP therapy in GOG 114 whereasGOG 172 reported a 16-month survival advantage Amongpatients treated with IP therapy the 5-year survival rateincreased from 18 following completion of 1-2 cycles to 59for patients who completed 5-6 cycles of treatment Howeverthere was increased toxicity observed in the IP arm grade 3-4 leukopenia thrombocytopenia and abdominal pain Only42 of patients in the GOG172 trial [143] completed all sixcycles of planned treatment in the IP arm while 18 ofpatients in GOG 114 trial [14] received fewer than two coursesof IP chemotherapy
Another randomised phase III trial involving patientswith stages II-III epithelial ovarian carcinoma is the GOG252 study with three arms Arm 1-dose-dense intravenouscarboplatin and paclitaxel Arm 2-dose-dense intravenouspaclitaxel and IP carboplatin and Arm 3 consists of 3-weeklyintravenous paclitaxel (day 1) followed by IP cisplatin (day 2)and IP paclitaxel (day 3) regimen All three arms also incor-porate the combination and maintenance of bevacizumabGOG 252 has completed accrual and results are awaited [139]
11 Newer Forms of Paclitaxel
Development of next-generation taxanes has taken place overthe past 40 years aimed at eliminating toxicity improvingefficacy and ease of administration Abraxane is a novelcompound which incorporates paclitaxel into an albuminnanoparticle soluble in saline hence eliminating the needfor Cremophor EL which is responsible for hypersensitivityreactions experienced during paclitaxel infusion [145] Thenanoparticle albumin in nab-paclitaxel is able to bind toglycoprotein gp60 receptor an albumin receptor and activatecaveolin-1 a protein that in human is encoded byCAV-1 geneleading to formation of caveoli hence allowing nab-paclitaxelto migrate across the endothelial cell membrane into theinterstitial space leading to higher intratumoural drug con-centration In addition Abraxane exhibits linear pharma-cokinetics and can therefore be given at a relatively higherdose than standard intravenous paclitaxel leading to a highertherapeutic ratio and heightened efficacy in solid tumoursmainlymetastatic breast cancer [146 147] Nab-paclitaxel hadFDA approval in 2005 for treatment of breast cancer [148]
Nab-paclitaxel has been studied in recurrent ovariancancer As a single agent in phase II 44 patients withrecurrent ovarian cancer were treated with Nab-paclitaxel260mgm2 intravenously for 30 minutes every 3 weeks for6 cycles Ninety-two percent of patients were platinum-sensitive while 89 had had previous exposure to standardtaxane The objective response rate was 64 with 15 patientsachieving complete response and 13 of them had partialresponse Estimated median PFS was 85 months No hyper-sensitivity reactions were observed and there were infrequentcases of grade 4 neutropenia (11) and grade 2-3 neuropathy(13) [149]
Another phase II study by GOG enrolled 51 patients withplatinum- and taxane-resistant recurrent ovarian cancer outof which 47 were evaluable The objective response rate was38 with one patient achieving a complete response and 10patients a partial response The median PFS was 45 monthswhile overall survival rate was 174 months Severe haema-tological and nonhaematological toxicities including neuro-toxicity were uncommon These results are quite impressivegiven the treatment population consisted of patients withvery poor prognosis with a median platinum and taxane freeinterval of 21 days and 70 had their recurrence within 3months of completion of primary treatment [150] Severalother trials of this formulation are in progress
Paclitaxel poliglumex (PPX) also known as Xyotax isanother prodrug a novel conjugate of paclitaxel and 120572-poly-L-glutamic acid which accumulates within tumour tissuedue to increased permeability of the tumour vessels and lackof lymphatic drainage [148 151 152] Paclitaxel poliglumexenhances solubility of paclitaxel allows direct delivery tothe intratumoural microenvironment and allows prolongedexposure to the active drug while minimising systemictoxicities [151] In Phase I dose escalation studies as a singleagent the recommended dose of PPX was 235mgm2 over 10minutes every 3 weeks or 70mgm2 weekly [153] In a PhaseII GOG study of relapsed ovarian cancer a response rate of16 was seen with infrequent serious adverse events grade3 and 4 neutropenia (24 and 20) and grade 3 neuropathy(24) [154] A phase III trial (GOG-0212) on the use of PPXas consolidation ormaintenance therapy in advanced ovariancancer is in progress
DHA-paclitaxel also known as Taxoprexin is a prodrugwhere paclitaxel is covalently conjugated with the naturallyoccurring omega-3 fatty acid docosahexaenoic acid (DHA)a fatty acid that is easily taken up by tumour cells henceincreasing intratumoural concentration of paclitaxel leadingtumour cell apoptosis [155 156] DHA-paclitaxel exhibitslinear pharmacokinetics and lower toxicity and also ease ofadministration when compared to conventional paclitaxeland has demonstrated antineoplastic activity in animal mod-els of cancer as well as in a phase III trial involving metastaticmelanoma [156ndash160] In a recent study on human ovariancancer cells it was found that DHA could reverse paclitaxelresistance by inhibiting P-gp as well as downregulatingthe expression of multidrug resistance associated proteins(MRP) and inhibiting the activity of NF-120581B and p38 MAPKsignalling pathways [161]
16 BioMed Research International
12 Future Directions
A plateau has been reached regarding the benefits associatedwith standard 3-weekly intravenous administration of cyto-toxic chemotherapy in advanced epithelial ovarian cancerThe ongoing battle for a better treatment regimen to delayrelapse promote remission and most importantly improvethe quality of life of patients with advanced epithelial ovariancancer need not to go further than the ability to relook at thechemotherapy agents that are already available in a differentapproach
Novel compounds to date have not yet shown clinicalsuperiority and parent compounds such as paclitaxel con-tinue to surprise us with their feasibility effectiveness andmanageable toxicity profiles Intraperitoneal paclitaxel willrequire further evaluation Better effort in understanding themechanism of action of drugs including the role of dosescheduling and the effect on the immune systemmay providea more cost-effective route to better clinical outcomes
Conflict of Interests
The authors declare no conflict of interests in this work
Acknowledgments
The authors would like to thank the many researchers whohave contributed to our current knowledge of paclitaxelNirmala Kampan is supported by Australian Monash Uni-versity Institute of Graduate Research Scholarship as wellas Universiti Kebangsaan Malaysia Postgraduate ScholarshipAward Mutsa Madondo has received Postgraduate Pub-lication Award from Monash University and MagdalenaPlebanski has been awarded Senior NHMRC Fellowship
References
[1] Australian Institute of Health and Welfare and National Breastand Ovarian Cancer Centre (Australia) Ovarian Cancer inAustralia AnOverview 2010 Cancer Series Australian Instituteof Health and Welfare Canberra Australia 2010
[2] R E Bristow R S Tomacruz D K Armstrong E L Trimbleand F J Montz ldquoSurvival effect of maximal cytoreductivesurgery for advanced ovarian carcinoma during the platinumera a meta-analysisrdquo Journal of Clinical Oncology vol 20 no 5pp 1248ndash1259 2002
[3] ZKempand JA Ledermann ldquoUpdate onfirst-line treatment ofadvanced ovarian carcinomardquo International Journal of WomenrsquosHealth vol 5 no 1 pp 45ndash51 2013
[4] A du Bois H-J Luck W Meier et al ldquoA randomized clinicaltrial of cisplatinpaclitaxel versus carboplatinpaclitaxel as first-line treatment of ovarian cancerrdquo Journal of the National CancerInstitute vol 95 no 17 pp 1320ndash1330 2003
[5] R F Ozols B N Bundy B E Greer et al ldquoPhase III trialof carboplatin and paclitaxel compared with cisplatin andpaclitaxel in patients with optimally resected stage III ovariancancer A Gynecologic Oncology Group studyrdquo Journal ofClinical Oncology vol 21 no 17 pp 3194ndash3200 2003
[6] W P McGuire W J Hoskins M F Brady et al ldquoCyclophos-phamide and cisplatin compared with paclitaxel and cisplatin
in patients with stage III and stage IV ovarian cancerrdquoThe NewEngland Journal of Medicine vol 334 no 1 pp 1ndash6 1996
[7] W P McGuire W J Hoskins M F Brady et al ldquoCyclophos-phamide and cisplatin versus paclitaxel and cisplatin a phase IIIrandomized trial in patients with suboptimal stage IIIIV ovar-ian cancer (from the gynecologic oncology group)rdquo Seminars inOncology vol 23 no 5 supplement 12 pp 40ndash47 1996
[8] M J Piccart K Bertelsen K James et al ldquoRandomized inter-group trial of cisplatin-paclitaxel versus cisplatin-cyclophosph-amide inwomenwith advanced epithelial ovarian cancer three-year resultsrdquo Journal of the National Cancer Institute vol 92 no9 pp 699ndash708 2000
[9] P A Vasey G C Jayson A Gordon et al ldquoPhase III random-ized trial of docetaxel-carboplatin versus paclitaxel-carboplatinas first-line chemotherpy for ovarian carcinomardquo Journal of theNational Cancer Institute vol 96 no 22 pp 1682ndash1691 2004
[10] B Gronlund C Hogdall H H Hansen and S A EngelholmldquoResults of reinduction therapy with paclitaxel and carboplatinin recurrent epithelial ovarian cancerrdquo Gynecologic Oncologyvol 83 no 1 pp 128ndash134 2001
[11] T M Loffler W Freund J Lipke and T-U HausamenldquoSchedule- and dose-intensified paclitaxel as weekly 1-hourinfusion in pretreated solid tumors results of a phase III trialrdquoSeminars in Oncology vol 23 no 6 supplement 16 pp 32ndash341996
[12] D Fennelly C Aghajanian F Shapiro et al ldquoPhase I and phar-macologic study of paclitaxel administered weekly in patientswith relapsed ovarian cancerrdquo Journal of Clinical Oncology vol15 no 1 pp 187ndash192 1997
[13] N R Abu-Rustum C Aghajanian R R Barakat D Fennelly FShapiro and D Spriggs ldquoSalvage weekly paclitaxel in recurrentovarian cancerrdquo Seminars inOncology vol 24 no 5 supplement15 pp S15-62ndashS15-67 1997
[14] M Markman B N Bundy D S Alberts et al ldquoPhase III trialof standard-dose intravenous cisplatin plus paclitaxel versusmoderately high-dose carboplatin followed by intravenouspaclitaxel and intraperitoneal cisplatin in small-volume stageIII ovarian carcinoma an intergroup study of the gynecologiconcology group Southwestern Oncology Group and EasternCooperativeOncologyGrouprdquo Journal of Clinical Oncology vol19 no 4 pp 1001ndash1007 2001
[15] A Kikuchi H Sakamoto and T Yamamoto ldquoWeekly car-boplatin and paclitaxel is safe active and well tolerated inrecurrent ovarian cancer cases of Japanese women previouslytreated with cisplatin-containing multidrug chemotherapyrdquoInternational Journal of Gynecological Cancer vol 15 no 1 pp45ndash49 2005
[16] I Cadron K Leunen F Amant T van Gorp P Nevenand I Vergote ldquoThe lsquoLeuvenrsquo dose-dense paclitaxelcarboplatinregimen in patients with recurrent ovarian cancerrdquo GynecologicOncology vol 106 no 2 pp 354ndash361 2007
[17] S Pignata E Breda G Scambia et al ldquoA phase II studyof weekly carboplatin and paclitaxel as first-line treatment ofelderly patients with advanced ovarian cancer A Multicen-tre Italian Trial in Ovarian cancer (MITO-5) studyrdquo CriticalReviews in OncologyHematology vol 66 no 3 pp 229ndash2362008
[18] T Safra S Shamai J Greenberg et al ldquoWeekly carboplatinwith paclitaxel compared to standard three-weekly treatment inadvanced epithelial ovarian carcinomamdasha retrospective studyrdquoGynecologic Oncology vol 132 no 1 pp 18ndash22 2014
BioMed Research International 17
[19] L J Havrilesky A A Alvarez R A Sayer et al ldquoWeekly low-dose carboplatin and paclitaxel in the treatment of recurrentovarian and peritoneal cancerrdquo Gynecologic Oncology vol 88no 1 pp 51ndash57 2003
[20] M van der BurgW Onstenk I Boere et al ldquoLong-term resultsof a randomised phase III trial of weekly versus three-weeklypaclitaxelplatinum induction therapy followed by standardor extended three-weekly paclitaxelplatinum in Europeanpatients with advanced epithelial ovarian cancerrdquo EuropeanJournal of Cancer vol 50 no 15 pp 2592ndash2601 2014
[21] N Katsumata M Yasuda F Takahashi et al ldquoDose-densepaclitaxel once a week in combination with carboplatin every3 weeks for advanced ovarian cancer a phase 3 open-labelrandomised controlled trialrdquoThe Lancet vol 374 no 9698 pp1331ndash1338 2009
[22] N Katsumata M Yasuda S Isonishi et al ldquoLong-term resultsof dose-dense paclitaxel and carboplatin versus conventionalpaclitaxel and carboplatin for treatment of advanced epithelialovarian fallopian tube or primary peritoneal cancer (JGOG3016) a randomised controlled open-label trialrdquo The LancetOncology vol 14 no 10 pp 1020ndash1026 2013
[23] K Harano F Terauchi N Katsumata et al ldquoQuality-of-lifeoutcomes from a randomized phase III trial of dose-denseweekly paclitaxel and carboplatin compared with conventionalpaclitaxel and carboplatin as a first-line treatment for stage II-IV ovarian cancer Japanese Gynecologic OncologyGroup Trial(JGOG3016)rdquo Annals of Oncology vol 25 no 1 pp 251ndash2572014
[24] J Chan M F Brady R Penson et al ldquoPhase III trial ofevery-3-weeks paclitaxel vs dose dense weekly paclitaxel withcarboplatin +minus bevacizumab in epithelial ovarian peritonealfallopian tube cancer GOG 262 (NCT01167712)rdquo InternationalJournal of Gynecological Cancer vol 23 no 8 supplement 1 pp9ndash10 2013
[25] S Pignata G Scambia D Katsaros et al ldquoCarboplatin pluspaclitaxel once a week versus every 3 weeks in patients withadvanced ovarian cancer (MITO-7) a randomisedmulticentreopen-label phase 3 trialrdquoThe Lancet Oncology vol 15 no 4 pp396ndash405 2014
[26] V Walsh and J Goodman ldquoFrom taxol to Taxol the changingidentities and ownership of an anti-cancer drugrdquo MedicalAnthropology vol 21 no 3-4 pp 307ndash336 2002
[27] R Renneberg ldquoBiotech History yew trees paclitaxel synthesisand fungirdquo Biotechnology Journal vol 2 no 10 pp 1207ndash12092007
[28] J E Liebmann J A Cook C Lipschultz D Teague J Fisherand J B Mitchell ldquoCytotoxic studies of paclitaxel (Taxol) inhuman tumour cell linesrdquo British Journal of Cancer vol 68 no6 pp 1104ndash1109 1993
[29] J J Manfredi and S B Horwitz ldquoTaxol an antimitotic agentwith a newmechanism of actionrdquo Pharmacology andTherapeu-tics vol 25 no 1 pp 83ndash125 1984
[30] D G I Kingston ldquoRecent advances in the chemistry of taxolrdquoJournal of Natural Products vol 63 no 5 pp 726ndash734 2000
[31] D G I Kingston ldquoThe shape of things to come structural andsynthetic studies of taxol and related compoundsrdquo Phytochem-istry vol 68 no 14 pp 1844ndash1854 2007
[32] V Walsh and J Goodman ldquoCancer chemotherapy biodiversitypublic and private property the case of the anti-cancer drugTaxolrdquo Social Science amp Medicine vol 49 no 9 pp 1215ndash12251999
[33] P H Wiernik E L Schwartz J J Strauman J P Dutcher RB Lipton and E Paietta ldquoPhase I clinical and pharmacokineticstudy of taxolrdquo Cancer Research vol 47 no 9 pp 2486ndash24931987
[34] W P McGuire E K Rowinsky N B Rosenhein et alldquoTaxol a unique antineoplastic agent with significant activityin advanced ovarian epithelial neoplasmsrdquo Annals of InternalMedicine vol 111 no 4 pp 273ndash279 1989
[35] ldquoDiscovery and development of taxolrdquo in Taxol Science andApplications M W M E Suffness Ed pp 3ndash25 CRC PressBoca Raton Fla USA 1995
[36] M J Piccart and F Cardoso ldquoProgress in systemic therapy forbreast cancer an overview and perspectivesrdquo European Journalof Cancer Supplement vol 1 no 2 pp 56ndash69 2003
[37] P Bonomi K B Kim and J Kugler ldquoComparison of survival forstage IIIB versus stage IV non-small cell lung cancer (NSCLC)patients with etoposide-cisplatin versus taxol-cisplatin an East-ern Cooperative Oncology Group (ECOG) trialrdquo in Proceedingsof the American Society of Clinical Oncology vol 16 p 454a1997
[38] D Guenard F Gueritte-Voegelein J Dubois and P PotierldquoStructure-activity relationships of Taxol and Taxotere ana-loguesrdquo Journal of the National Cancer Institute Monographsno 15 pp 79ndash82 1993
[39] D G I Kingston ldquoTaxol the chemistry and structure-activityrelationships of a novel anticancer agentrdquo Trends in Biotechnol-ogy vol 12 no 6 pp 222ndash227 1994
[40] E K Rowinsky and R C Donehower ldquoPaclitaxel (taxol)rdquo TheNew England Journal of Medicine vol 332 no 15 pp 1004ndash10141995
[41] J Parness and S B Horwitz ldquoTaxol binds to polymerizedtubulin in vitrordquo Journal of Cell Biology vol 91 no 2 pp 479ndash487 1981
[42] A Dammermann A Desai and K Oegema ldquoTheminus end insightrdquo Current Biology vol 13 no 15 pp R614ndashR624 2003
[43] CWiese and Y Zheng ldquoMicrotubule nucleation 120574-tubulin andbeyondrdquo Journal of Cell Science vol 119 no 20 pp 4143ndash41532006
[44] A Ganguly H Yang and F Cabral ldquoPaclitaxel-dependent celllines reveal a novel drug activityrdquo Molecular Cancer Therapeu-tics vol 9 no 11 pp 2914ndash2923 2010
[45] P B Schiff and S B Horwitz ldquoTaxol stabilizes microtubules inmouse fibroblast cellsrdquo Proceedings of the National Academy ofSciences of the United States of America vol 77 no 3 pp 1561ndash1565 1980
[46] P B Schiff J Fant and S B Horwitz ldquoPromotion of micro-tubule assembly in vitro by Taxolrdquo Nature vol 277 no 5698pp 665ndash667 1979
[47] D Zhang R Yang S Wang and Z Dong ldquoPaclitaxel new usesfor an old drugrdquoDrug Design Development andTherapy vol 8pp 279ndash284 2014
[48] S Rao G A Orr A G Chaudhary D G I Kingston and SB Horwitz ldquoCharacterization of the taxol binding site on themicrotubule 2-(m-Azidobenzoyl)taxol photolabels a peptide(amino acids 217-231) of beta-tubulinrdquoThe Journal of BiologicalChemistry vol 270 no 35 pp 20235ndash20238 1995
[49] F Wang Y Cao W Zhao H Liu Z Fu and R Han ldquoTaxolinhibits melanoma metastases through apoptosis inductionangiogenesis inhibition and restoration of E-cadherin andnm23 expressionrdquo Journal of Pharmacological Sciences vol 93no 2 pp 197ndash203 2003
18 BioMed Research International
[50] A Sevko V Kremer C Falk et al ldquoApplication of paclitaxel inlow non-cytotoxic doses supports vaccination with melanomaantigens in normal micerdquo Journal of Immunotoxicology vol 9no 3 pp 275ndash281 2012
[51] T Kreis and R Vale Guidebook to the Cytoskeletal and MotorProteins Oxford University Press Oxford UK 2nd edition1999
[52] P Giannakakou D L Sackett Y-K Kang et al ldquoPaclitaxel-resistant human ovarian cancer cells have mutant 120573-tubulinsthat exhibit impaired paclitaxel-driven polymerizationrdquo TheJournal of Biological Chemistry vol 272 no 27 pp 17118ndash171251997
[53] E Rakovitch W Mellado E J Hall T K Pandita S Sawantand C R Geard ldquoPaclitaxel sensitivity correlates with p53status and DNA fragmentation but not G2M accumulationrdquoInternational Journal of Radiation Oncology Biology Physics vol44 no 5 pp 1119ndash1124 1999
[54] S W Lowe S Bodis A McClatchey et al ldquop53 status and theefficacy of cancer therapy in vivordquo Science vol 266 no 5186 pp807ndash810 1994
[55] C C Zhang J-M Yang E White M Murphy A Levine andW N Hait ldquoThe role of MAP4 expression in the sensitivity topaclitaxel and resistance to vinca alkaloids in p53 mutant cellsrdquoOncogene vol 16 no 12 pp 1617ndash1624 1998
[56] K Fukasawa T Choi R Kuriyama S Rulong and G F VandeWoude ldquoAbnormal centrosome amplification in the absence ofp53rdquo Science vol 271 no 5256 pp 1744ndash1747 1996
[57] T-H Wang Y-H Chan C-W Chen et al ldquoPaclitaxel (Taxol)upregulates expression of functional interleukin-6 in humanovarian cancer cells through multiple signaling pathwaysrdquoOncogene vol 25 no 35 pp 4857ndash4866 2006
[58] E Yakirevich E Sabo I Naroditsky Y Sova O Lavie andM B Resnick ldquoMultidrug resistance-related phenotype andapoptosis-related protein expression in ovarian serous carcino-masrdquo Gynecologic Oncology vol 100 no 1 pp 152ndash159 2006
[59] G Szakacs J K Paterson J A Ludwig C Booth-Genthe andM M Gottesman ldquoTargeting multidrug resistance in cancerrdquoNature Reviews Drug Discovery vol 5 no 3 pp 219ndash234 2006
[60] L W Pfannenstiel S S K Lam L A Emens E M Jaffeeand T D Armstrong ldquoPaclitaxel enhances early dendritic cellmaturation and function through TLR4 signaling in micerdquoCellular Immunology vol 263 no 1 pp 79ndash87 2010
[61] N Klauber S Parangi E Flynn E Hamel and R J DrsquoAmatoldquoInhibition of angiogenesis and breast cancer in mice by themicrotubule inhibitors 2-methoxyestradiol and Taxolrdquo CancerResearch vol 57 no 1 pp 81ndash86 1997
[62] D Belotti V Vergani T Drudis et al ldquoThe microtubule-affecting drug paclitaxel has antiangiogenic activityrdquo ClinicalCancer Research vol 2 no 11 pp 1843ndash1849 1996
[63] D H Lau L Xue L J Young P A Burke and A T CheungldquoPaclitaxel (Taxol) an inhibitor of angiogenesis in a highlyvascularized transgenic breast cancerrdquo Cancer Biotherapy andRadiopharmaceuticals vol 14 no 1 pp 31ndash36 1999
[64] X Jiang ldquoHarnessing the immune system for the treatment ofbreast cancerrdquo Journal of Zhejiang University Science B vol 15no 1 pp 1ndash15 2014
[65] A Gadducci D Katsaros P Zola et al ldquoWeekly low-dosepaclitaxel as maintenance treatment in patients with advancedovarian cancer who had microscopic residual disease atsecond-look surgery after 6 cycles of paclitaxelplatinum-basedchemotherapy Results of an open noncomparative phase 2
multicenter italian study (after-6 protocol 2)rdquo InternationalJournal of Gynecological Cancer vol 19 no 4 pp 615ndash619 2009
[66] R S Bhatt J Merchan R Parker et al ldquoA phase 2 pilot trial oflow-dose continuous infusion or lsquometronomicrsquo paclitaxel andoral celecoxib in patients with metastatic melanomardquo Cancervol 116 no 7 pp 1751ndash1756 2010
[67] M Caballero J J Grau J L Blanch et al ldquoSerum vascularendothelial growth factor as a predictive factor in metronomic(weekly) paclitaxel treatment for advanced head and neckcancerrdquo Archives of OtolaryngologymdashHead and Neck Surgeryvol 133 no 11 pp 1143ndash1148 2007
[68] J Alexandre Y Hu W Lu H Pelicano and P Huang ldquoNovelaction of paclitaxel against cancer cells bystander effect medi-ated by reactive oxygen speciesrdquo Cancer Research vol 67 no 8pp 3512ndash3517 2007
[69] T Hadzic N Aykin-Burns Y Zhu et al ldquoPaclitaxel combinedwith inhibitors of glucose and hydroperoxide metabolismenhances breast cancer cell killing viaH
2O2-mediated oxidative
stressrdquo Free Radical Biology and Medicine vol 48 no 8 pp1024ndash1033 2010
[70] C A Sherman-Baust K G Becker W H Wood III Y Zhangand P J Morin ldquoGene expression and pathway analysis of ovar-ian cancer cells selected for resistance to cisplatin paclitaxel ordoxorubicinrdquo Journal of Ovarian Research vol 4 no 1 article21 2011
[71] R Agarwal and S B Kaye ldquoOvarian cancer strategies for over-coming resistance to chemotherapyrdquo Nature Reviews Cancervol 3 no 7 pp 502ndash516 2003
[72] T Acker and K H Plate ldquoRole of hypoxia in tumorangiogenesismdashmolecular and cellular angiogenic crosstalkrdquoCell and Tissue Research vol 314 no 1 pp 145ndash155 2003
[73] M Hockel and P Vaupel ldquoBiological consequences of tumorhypoxiardquo Seminars in Oncology vol 28 supplement 8 no 2 pp36ndash41 2001
[74] L Huang Q-H Zhang Q-L Ao H Xing Y-P Lu and DMa ldquoEffect of hypoxia on the chemotherapeutic sensitivity ofhuman ovarian cancer cells to paclitaxel and its mechanismrdquoZhonghua Zhong Liu Za Zhi vol 29 no 2 pp 96ndash100 2007
[75] N Rohwer and T Cramer ldquoHypoxia-mediated drug resistancenovel insights on the functional interaction of HIFs and celldeath pathwaysrdquoDrug Resistance Updates vol 14 no 3 pp 191ndash201 2011
[76] B B Aggarwal R V Vijayalekshmi and B Sung ldquoTargetinginflammatory pathways for prevention and therapy of cancershort-term friend long-term foerdquo Clinical Cancer Research vol15 no 2 pp 425ndash430 2009
[77] Z Duan R Foster D A Bell et al ldquoSignal transducersand activators of transcription 3 pathway activation in drug-resistant ovarian cancerrdquo Clinical Cancer Research vol 12 no17 pp 5055ndash5063 2006
[78] H-J Kuh S H Jang M G Wientjes J R Weaver and J L-SAu ldquoDeterminants of paclitaxel penetration and accumulationin human solid tumorrdquo Journal of Pharmacology and Experi-mental Therapeutics vol 290 no 2 pp 871ndash880 1999
[79] S Arao H Suwa M Mandai et al ldquoHypoxia-mediated drugresistance novel insights on the functional interaction of HIFsand cell death pathwaysrdquo Cancer Research vol 54 no 5 pp1355ndash1359 1994
[80] S E Johnatty J Beesley B Gao et al ldquoABCB1 (MDR1)polymorphisms and ovarian cancer progression and survivala comprehensive analysis from the Ovarian Cancer Association
BioMed Research International 19
Consortium and the Cancer GenomeAtlasrdquoGynecologic Oncol-ogy vol 131 no 1 pp 8ndash14 2013
[81] X Yang A K Iyer A Singh et al ldquoCluster of differentiation44 targeted hyaluronic acid based nanoparticles for MDR1siRNA delivery to overcome drug resistance in ovarian cancerrdquoPharmaceutical Research 2014
[82] D A Zajchowski B Y Karlan and L K Shawver ldquoTreatment-related protein biomarker expression differs between primaryand recurrent ovarian carcinomasrdquoMolecular CancerTherapeu-tics vol 11 no 2 pp 492ndash502 2012
[83] MM Gottesman J Ludwig D Xia and G Szakacs ldquoDefeatingdrug resistance in cancerrdquoDiscovery Medicine vol 6 no 31 pp18ndash23 2006
[84] S Mozzetti C Ferlini P Concolino et al ldquoClass III 120573-tubulin overexpression is a prominent mechanism of paclitaxelresistance in ovarian cancer patientsrdquo Clinical Cancer Researchvol 11 no 1 pp 298ndash305 2005
[85] M Kavallaris D Y S Kuo C A Burkhart et al ldquoTaxol-resistant epithelial ovarian tumors are associated with alteredexpression of specific beta-tubulin isotypesrdquo Journal of ClinicalInvestigation vol 100 no 5 pp 1282ndash1293 1997
[86] G A Orr P Verdier-Pinard H McDaid and S B HorwitzldquoMechanisms of Taxol resistance related to microtubulesrdquoOncogene vol 22 no 47 pp 7280ndash7295 2003
[87] C Ferlini L Cicchillitti G Raspaglio et al ldquoPaclitaxel directlybinds to Bcl-2 and functionally mimics activity of Nur77rdquoCancer Research vol 69 no 17 pp 6906ndash6914 2009
[88] E Mechetner A Kyshtoobayeva S Zonis et al ldquoLevels ofmultidrug resistance (MDR1) P-glycoprotein expression byhuman breast cancer correlate with in vitro resistance to taxoland doxorubicinrdquo Clinical Cancer Research vol 4 no 2 pp389ndash398 1998
[89] J S Lagas C W N Damen R A B VanWaterschoot D IusufJ H Beijnen and A H Schinkel ldquoP-glycoprotein multidrug-resistance associated protein 2 Cyp3a and carboxylesteraseaffect the oral availability and metabolism of vinorelbinerdquoMolecular Pharmacology vol 82 no 4 pp 636ndash644 2012
[90] M T Huizing J B Vermorken H Rosing et al ldquoPharmacoki-netics of paclitaxel and three major metabolites in patients withadvanced breast carcinoma refractory to anthracycline therapytreated with a 3-hour paclitaxel infusion a European CancerCentre (ECC) trialrdquo Annals of Oncology vol 6 no 7 pp 699ndash704 1995
[91] R Panchagnula ldquoPharmaceutical aspects of paclitaxelrdquo Interna-tional Journal of Pharmaceutics vol 172 no 1-2 pp 1ndash15 1998
[92] S H Jang M G Wientjes and J L-S Au ldquoDeterminants ofpaclitaxel uptake accumulation and retention in solid tumorsrdquoInvestigational New Drugs vol 19 no 2 pp 113ndash123 2001
[93] D S Sonnichsen andM V Relling ldquoClinical pharmacokineticsof paclitaxelrdquo Clinical Pharmacokinetics vol 27 no 4 pp 256ndash269 1994
[94] T Ohtsu Y Sasaki T Tamura et al ldquoClinical pharmacokineticsand pharmacodynamics of paclitaxel a 3-hour infusion versusa 24-hour infusionrdquo Clinical Cancer Research vol 1 no 6 pp599ndash606 1995
[95] M Czejka J Schueller H Schnait B Springer and I EderldquoClinical pharmacokinetics andmetabolism of paclitaxel after athree-hour infusion comparison of two preparationsrdquo Journalof Oncology Pharmacy Practice vol 9 no 4 pp 129ndash136 2003
[96] J Rizzo C Riley D VonHoff J Kuhn J Phillips and T BrownldquoAnalysis of anticancer drugs in biological fluids determination
of taxol with application to clinical pharmacokineticsrdquo Journalof Pharmaceutical and Biomedical Analysis vol 8 no 2 pp 159ndash164 1990
[97] V A de Weger J H Beijnen and J H M Schellens ldquoCel-lular and clinical pharmacology of the taxanes docetaxel andpaclitaxelmdasha reviewrdquoAnti-Cancer Drugs vol 25 no 5 pp 488ndash494 2014
[98] S Kumar H Mahdi C Bryant J P Shah G Garg andA Munkarah ldquoClinical trials and progress with paclitaxel inovarian cancerrdquo International Journal of Womenrsquos Health vol 2no 1 pp 411ndash427 2010
[99] B Huang J Zhao J C Unkeless Z H Feng and H XiongldquoTLR signaling by tumor and immune cells a double-edgedswordrdquo Oncogene vol 27 no 2 pp 218ndash224 2008
[100] R A Jibodh J S Lagas B Nuijen J H Beijnen and J HM Schellens ldquoTaxanes old drugs new oral formulationsrdquoEuropean Journal of Pharmacology vol 717 no 1ndash3 pp 40ndash462013
[101] A Javeed M Ashraf A Riaz A Ghafoor S Afzal and M MMukhtar ldquoPaclitaxel and immune systemrdquo European Journal ofPharmaceutical Sciences vol 38 no 4 pp 283ndash290 2009
[102] L Bracci G Schiavoni A Sistigu and F Belardelli ldquoImmune-based mechanisms of cytotoxic chemotherapy implications forthe design of novel and rationale-based combined treatmentsagainst cancerrdquo Cell Death and Differentiation vol 21 no 1 pp15ndash25 2014
[103] C A Byrd-Leifer E F Block K Takeda S Akira and A DingldquoThe role of MyD88 and TLR4 in the LPS-mimetic activity ofTaxolrdquo European Journal of Immunology vol 31 no 8 pp 2448ndash2457 2001
[104] A-C Wang Y-B Ma F-X Wu et al ldquoTLR4 induces tumorgrowth and inhibits paclitaxel activity in MyD88-positivehuman ovarian carcinoma in vitrordquo Oncology Letters vol 7 no3 pp 871ndash877 2014
[105] Y Zhu N Liu S D Xiong Y J Zheng and Y W ChuldquoCD4+Foxp3+ regulatory T-cell impairment by paclitaxel isindependent of toll-like receptor 4rdquo Scandinavian Journal ofImmunology vol 73 no 4 pp 301ndash308 2011
[106] M Kubo T Morisaki K Matsumoto et al ldquoPaclitaxel probablyenhances cytotoxicity of natural killer cells against breastcarcinoma cells by increasing perforin productionrdquo CancerImmunology Immunotherapy vol 54 no 5 pp 468ndash476 2005
[107] L Markasz G Stuber B Vanherberghen et al ldquoEffect of fre-quently used chemotherapeutic drugs on the cytotoxic activityof human natural killer cellsrdquo Molecular Cancer Therapeuticsvol 6 no 2 pp 644ndash654 2007
[108] T Sako N Burioka K Yasuda et al ldquoCellular immune profile inpatients with non-small cell lung cancer after weekly paclitaxeltherapyrdquo Acta Oncologica vol 43 no 1 pp 15ndash19 2004
[109] R Kaneno G V Shurin I L Tourkova and M R ShurinldquoChemomodulation of human dendritic cell function by anti-neoplastic agents in low noncytotoxic concentrationsrdquo Journalof Translational Medicine vol 7 article 58 2009
[110] TMichels G V ShurinHNaiditch A Sevko VUmansky andM R Shurin ldquoPaclitaxel promotes differentiation of myeloid-derived suppressor cells into dendritic cells in vitro in a TLR4-independent mannerrdquo Journal of Immunotoxicology vol 9 no3 pp 292ndash300 2012
[111] R A Kemp and F Ronchese ldquoTumor-specific Tc1 but not Tc2cells deliver protective antitumor immunityrdquo The Journal ofImmunology vol 167 no 11 pp 6497ndash6502 2001
20 BioMed Research International
[112] A Y Rudensky ldquoRegulatory T cells and Foxp3rdquo ImmunologicalReviews vol 241 no 1 pp 260ndash268 2011
[113] EM Shevach ldquoCD4+CD25+ suppressor T cellsmore questionsthan answersrdquo Nature Reviews Immunology vol 2 no 6 pp389ndash400 2002
[114] S Sakaguchi T Yamaguchi T Nomura and M Ono ldquoRegu-latory T cells and immune tolerancerdquo Cell vol 133 no 5 pp775ndash787 2008
[115] H Nishikawa and S Sakaguchi ldquoRegulatory T cells in tumorimmunityrdquo International Journal of Cancer vol 127 no 4 pp759ndash767 2010
[116] W Zou ldquoRegulatory T cells tumour immunity and immuno-therapyrdquoNature Reviews Immunology vol 6 no 4 pp 295ndash3072006
[117] A Fialova S Partlova L Sojka et al ldquoDynamics of T-cell infil-tration during the course of ovarian cancer The gradual shiftfrom aTh17 effector cell response to a predominant infiltrationby regulatory T-cellsrdquo International Journal of Cancer vol 132no 5 pp 1070ndash1079 2013
[118] A E Albers R L Ferris G G Kim K Chikamatsu A BDeLeo and T L Whiteside ldquoImmune responses to p53 inpatients with cancer enrichment in tetramer+ p53 peptide-specific T cells and regulatory T cells at tumor sitesrdquo CancerImmunology Immunotherapy vol 54 no 11 pp 1072ndash10812005
[119] N Liu Y Zheng Y Zhu S Xiong andYChu ldquoSelective impair-ment of CD4 + CD25 + Foxp3 + regulatory T cells by paclitaxelis explained by Bcl-2Bax mediated apoptosisrdquo InternationalImmunopharmacology vol 11 no 2 pp 212ndash219 2011
[120] X Wu Q-M Feng Y Wang J Shi H-L Ge and W DildquoThe immunologic aspects in advanced ovarian cancer patientstreated with paclitaxel and carboplatin chemotherapyrdquo CancerImmunology Immunotherapy vol 59 no 2 pp 279ndash291 2010
[121] A P Vicari R Luu N Zhang et al ldquoPaclitaxel reducesregulatoryT cell numbers and inhibitory function and enhancesthe anti-tumor effects of the TLR9 agonist PF-3512676 in themouserdquo Cancer Immunology Immunotherapy vol 58 no 4 pp615ndash628 2009
[122] L Zhang K Dermawan M Jin et al ldquoDifferential impairmentof regulatory T cells rather than effector T cells by paclitaxel-based chemotherapyrdquo Clinical Immunology vol 129 no 2 pp219ndash229 2008
[123] Y Tabuchi J Matsuoka M Gunduz et al ldquoResistance topaclitaxel therapy is related with Bcl-2 expression through anestrogen receptor mediated pathway in breast cancerrdquo Interna-tional Journal of Oncology vol 34 no 2 pp 313ndash319 2009
[124] N Obermajer R Muthuswamy K Odunsi R P Edwards andP Kalinski ldquoPGE
2-induced CXCL12 production and CXCR4
expression controls the accumulation of human MDSCs inovarian cancer environmentrdquo Cancer Research vol 71 no 24pp 7463ndash7470 2011
[125] Q M Feng W Di and X Wu ldquoImmune reconstitution inadvanced ovarian cancer patients undergoing first line chemo-therapyrdquo Xi Bao Yu Fen Zi Mian Yi Xue Za Zhi vol 25 no 11pp 1023ndash1025 2009
[126] A D Seidman D Hochhauser M Gollub et al ldquoNinety-six-hour paclitaxel infusion after progression during short taxaneexposure a phase II pharmacokinetic and pharmacodynamicstudy in metastatic breast cancerrdquo Journal of Clinical Oncologyvol 14 no 6 pp 1877ndash1884 1996
[127] D R Spriggs M F Brady L Vaccarello et al ldquoPhase IIIrandomized trial of intravenous cisplatin plus a 24- or 96-hour
infusion of paclitaxel in epithelial ovarian cancer a gynecologiconcology group studyrdquo Journal of Clinical Oncology vol 25 no28 pp 4466ndash4471 2007
[128] G A Omura M F Brady K Y Look et al ldquoPhase III trial ofpaclitaxel at two dose levels the higher dose accompanied byfilgrastim at two dose levels in platinum-pretreated epithelialovarian cancer an intergroup studyrdquo Journal of Clinical Oncol-ogy vol 21 no 15 pp 2843ndash2848 2003
[129] R Simon and L Norton ldquoThe Norton-Simon hypothesisdesigning more effective and less toxic chemotherapeutic reg-imensrdquoNature Clinical Practice Oncology vol 3 no 8 pp 406ndash407 2006
[130] A Kumar P Hoskins and A Tinker ldquoDose-dense paclitaxel inadvanced ovarian cancerrdquo Clinical Oncology vol 27 no 1 pp40ndash47 2015
[131] P Marchetti S Urien G A Cappellini G Ronzino and CFicorella ldquoWeekly administration of paclitaxel theoretical andclinical basisrdquoCritical Reviews in OncologyHematology vol 44supplement pp S3ndashS13 2002
[132] P Francis E Rowinsky J Schneider T Hakes W Hoskinsand M Markman ldquoPhase I feasibility and pharmacologic studyof weekly intraperitoneal paclitaxel A Gynecologic OncologyGroup pilot studyrdquo Journal of Clinical Oncology vol 13 no 12pp 2961ndash2967 1995
[133] H Thomas and P Rosenberg ldquoRole of weekly paclitaxel inthe treatment of advanced ovarian cancerrdquo Critical Reviews inOncologyHematology vol 44 supplement pp S43ndashS51 2002
[134] M Markman J Markman K Webster et al ldquoDuration ofresponse to second-line platinum-based chemotherapy forovarian cancer implications for patient management and clini-cal trial designrdquo Journal of Clinical Oncology vol 22 no 15 pp3120ndash3125 2004
[135] P H OrsquoDonnell M Eileen Dolan E Gamazon et al ldquoPopu-lation differences in platinum toxicity as a means to identifynovel genetic susceptibility variantsrdquo Pharmacogenetics andGenomics vol 20 no 5 pp 327ndash337 2010
[136] M J Millward M J Boyer M Lehnert et al ldquoDocetaxel andcarboplatin is an active regimen in advanced non-small-celllung cancer a phase II study in Caucasian and Asian patientsrdquoAnnals of Oncology vol 14 no 3 pp 449ndash454 2003
[137] M Markman ldquoIntraperitoneal therapy of ovarian cancerrdquoOncologist vol 1 no 1-2 pp 18ndash21 1996
[138] M Markman and J L Walker ldquoIntraperitoneal chemotherapyof ovarian cancer a review with a focus on practical aspects oftreatmentrdquo Journal of Clinical Oncology vol 24 no 6 pp 988ndash994 2006
[139] K Fujiwara S Nagao E Aotani and K Hasegawa ldquoPrincipleand evolving role of intraperitoneal chemotherapy in ovariancancerrdquo Expert Opinion on Pharmacotherapy vol 14 no 13 pp1797ndash1806 2013
[140] M Markman E Rowinsky T Hakes et al ldquoPhase I trialof intraperitoneal taxol a gynecoloic oncology group studyrdquoJournal of Clinical Oncology vol 10 no 9 pp 1485ndash1491 1992
[141] M Markman M F Brady N M Spirtos P Hanjani and S CRubin ldquoPhase II trial of intraperitoneal paclitaxel in carcinomaof the ovary tube and peritoneum a gynecologic oncologygroup studyrdquo Journal of Clinical Oncology vol 16 no 8 pp2620ndash2624 1998
[142] P B Panici I Palaia M Graziano F Bellati N Manci and RAngioli ldquoIntraperitoneal paclitaxel as consolidation treatmentin ovarian cancer patients a case control studyrdquo Oncology vol78 no 1 pp 20ndash25 2010
BioMed Research International 21
[143] D K Armstrong B Bundy L Wenzel et al ldquoIntraperitonealcisplatin and paclitaxel in ovarian cancerrdquo The New EnglandJournal of Medicine vol 354 no 1 pp 34ndash43 2006
[144] D Tewari J Java and R Salani ldquoLong-term survival advantageof intraperitoneal chemotherapy treatment in advanced ovariancancer an analysis of a Gynecologic Oncology Group ancillarydata studyrdquo in Proceedings of the 2013 Society of GynecologicOncology Annual Meeting on Womenrsquos Cancer (GOG114172Abstract) Los Angeles Calif USA 2013
[145] D A Yardley ldquonab-paclitaxel mechanisms of action and deliv-eryrdquo Journal of Controlled Release vol 170 no 3 pp 365ndash3722013
[146] M Ando K Yonemori N Katsumata et al ldquoPhase I and phar-macokinetic study of nab-paclitaxel nanoparticle albumin-bound paclitaxel administeredweekly to Japanese patients withsolid tumors and metastatic breast cancerrdquo Cancer Chemother-apy and Pharmacology vol 69 no 2 pp 457ndash465 2012
[147] N Desai V Trieu Z Yao et al ldquoIncreased antitumor activityintratumor paclitaxel concentrations and endothelial cell trans-port of cremophor-free albumin-bound paclitaxel ABI-007compared with cremophor-based paclitaxelrdquo Clinical CancerResearch vol 12 no 4 pp 1317ndash1324 2006
[148] J A Yared and K H R Tkaczuk ldquoUpdate on taxane devel-opment new analogs and new formulationsrdquo Drug DesignDevelopment andTherapy vol 6 pp 371ndash384 2012
[149] M G Teneriello P C Tseng M Crozier et al ldquoPhase IIevaluation of nanoparticle albumin-bound paclitaxel in plati-num-sensitive patients with recurrent ovarian peritoneal orfallopian tube cancerrdquo Journal of Clinical Oncology vol 27 no9 pp 1426ndash1431 2009
[150] R L Coleman W E Brady D S McMeekin et al ldquoA phase IIevaluation of nanoparticle albumin-bound (nab) paclitaxel inthe treatment of recurrent or persistent platinum-resistant ovar-ian fallopian tube or primary peritoneal cancer a GynecologicOncology Group Studyrdquo Gynecologic Oncology vol 122 no 1pp 111ndash115 2011
[151] J W Singer ldquoPaclitaxel poliglumex (XYOTAX CT-2103) amacromolecular taxanerdquo Journal of Controlled Release vol 109no 1ndash3 pp 120ndash126 2005
[152] C Li D-F Yu R A Newman et al ldquoComplete regressionof well-established tumors using a novel water-soluble poly(L-glutamic acid)-paclitaxel conjugaterdquo Cancer Research vol 58no 11 pp 2404ndash2409 1998
[153] M Mita A Mita J Sarantopoulos et al ldquoPhase I study ofpaclitaxel poliglumex administered weekly for patients withadvanced solid malignanciesrdquo Cancer Chemotherapy and Phar-macology vol 64 no 2 pp 287ndash295 2009
[154] P Sabbatini M W Sill D OrsquoMalley L Adler and A ASecord ldquoA phase II trial of paclitaxel poliglumex in recurrentor persistent ovarian or primary peritoneal cancer (EOC) agynecologic oncology group studyrdquo Gynecologic Oncology vol111 no 3 pp 455ndash460 2008
[155] M O Bradley C S Swindell F H Anthony et al ldquoTumortargeting by conjugation of DHA to paclitaxelrdquo Journal ofControlled Release vol 74 no 1ndash3 pp 233ndash236 2001
[156] M O Bradley N L Webb F H Anthony et al ldquoTumortargeting by covalent conjugation of a natural fatty acid topaclitaxelrdquo Clinical Cancer Research vol 7 no 10 pp 3229ndash3238 2001
[157] A C Wolff R C Donehower M K Carducci et al ldquoPhaseI study of docosahexaenoic acid-paclitaxel a taxane-fatty acid
conjugate with a unique pharmacology and toxicity profilerdquoClinical Cancer Research vol 9 no 10 part 1 pp 3589ndash35972003
[158] A Sparreboom A C Wolff J Verweij et al ldquoDispositionof docosahexaenoic acid-paclitaxel a novel taxane in bloodin vitro and clinical pharmacokinetic studiesrdquo Clinical CancerResearch vol 9 no 1 pp 151ndash159 2003
[159] P M Fracasso J Picus J D Wildi et al ldquoPhase 1 and phar-macokinetic study of weekly docosahexaenoic acid-paclitaxelTaxoprexin in resistant solid tumor malignanciesrdquo CancerChemotherapy and Pharmacology vol 63 no 3 pp 451ndash4582009
[160] A Y Bedikian R C DeConti R Conry et al ldquoPhase 3 study ofdocosahexaenoic acid-paclitaxel versus dacarbazine in patientswith metastatic malignant melanomardquo Annals of Oncology vol22 no 4 pp 787ndash793 2011
[161] Y-N Wu S-L Wang Y-C Wang et al ldquoReversal effect ofdocosahexaenoic acid on taxol resistance in human ovarian car-cinoma A2780T cellsrdquo Obstetrics amp Gynecology InternationalJournal vol 1 no 3 Article ID 00018 2014
Submit your manuscripts athttpwwwhindawicom
PainResearch and TreatmentHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom
Volume 2014
ToxinsJournal of
VaccinesJournal of
Hindawi Publishing Corporation httpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
AntibioticsInternational Journal of
ToxicologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
StrokeResearch and TreatmentHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Drug DeliveryJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Advances in Pharmacological Sciences
Tropical MedicineJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Medicinal ChemistryInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
AddictionJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
Emergency Medicine InternationalHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Autoimmune Diseases
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Anesthesiology Research and Practice
ScientificaHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Pharmaceutics
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of

BioMed Research International 9
suppress immune responses of other CD4+ and CD8+ cells[118ndash120] and promote tumour progression In murine stud-ies paclitaxel exhibits the ability to reduce the number andsize of Treg cells thereby enhancing antitumour immunity[119 121] Similar findingswere seenwith a selective reductionin the size and number of Treg populations in peripheralblood samples from non-small cell lung cancer (NSCLC)patients [122]
Paclitaxel also decreased the expression of the anti-apoptotic molecule Bcl-2 in Treg cells while increasing thecorresponding proapoptoticmember Bax which contributedto the apoptotic sensitivity of Treg to paclitaxel [87]This wasseen in a study using the 3LL Lewis tumour model whichdemonstrated that Treg cells exposed to paclitaxel displayeddown regulation of Bcl-2 and upregulation of Bax and uponblocking the Bcl-2 pathway the ability of paclitaxel to ablateTreg cells compared toT effectorswas impaired and bothTregand T effectors were affected These results may suggest thatpaclitaxel targets Bcl-2 rather than tubulin to contribute tothe distinctive effect on Treg cells [119] It has recently beenshown in vitro that paclitaxel could target Bcl-2 and thereforelead to apoptosis Bcl-2 family proteins are key regulators ofapoptosis and play an important role in tumourigenesis andmulti-drug resistance by blocking apoptosis [119 123]
Few studies have also shown effect of paclitaxel onmyeloid-derived suppressor cells (MDSCs) a heterogeneouspopulation of immature myeloid cells immunosuppressivein nature are recruited by cancer cells and are found inincreased amount in advanced epithelial ovarian cancer [124]In a murine study using C57BL6 mice administration ofpaclitaxel at ultralow dose modulates MDSCs to differentiateinto DCs in a TLR4 independent manner [110] Hencepaclitaxel in ultralow noncytotoxic doses together with itsangiogenesis blocking ability may potentially enhance theefficacy of immunotherapy by ablation of immunosuppres-sive populations such as Tregs and MDSCs in tumour-bearing hosts [50 102]
In immunocompromised patients with advanced ovariancancer with increased Tregs and decreased levels of CD4+T cell CD8+ T cell and NK subsets after a single courseof combined carboplatin and paclitaxel chemotherapy theimmunosuppression is reversed around 12 to 14 days later butnot before one week or after three to four weeks Not only areTregs decreased but also the proportions of IFN-120574 secretingCD8+ T cells T helper-1 Tc1 and NKT cells The ratio of Tc1to Tc2 cells increases significantly [111 120 125]
Following chemotherapy both CD4+CD45RO+ andCD8+CD45RO+ memory T cells increased significantly andpeaked around 2 weeks The increase of memory T cellsin ovarian cancer patients following chemotherapy prob-ably opens the door of opportunity to develop long-termimmunological memory which could prevent recurrenceand metastases [120] Administration of dose-dense therapygiven weekly may hence be beneficial immunologically tomount an adequate immune response compared to standard3-week therapy In addition administration of immunother-apy agentsmay also be ideal during the period of 2weeks afterchemotherapy where temporary immune system reconstitu-tion takes place
8 Clinical Studies
In the past two decades paclitaxel had been administered indoses ranging from 60 to 250mgm2 over 1ndash96 hours andfrom 1 to 3 weekly intervals Prolonged exposure up to 96hours was believed to be effective as demonstrated with pre-clinical data but later refuted in large prospective studies [14126 127] A 24-hour infusion of paclitaxel was subsequentlyadministered to reduce the risk of hypersensitivity reactionshowever it was shown to increase mucosal and bone marrowtoxicity without improved efficacy [127 128] Development ofeffective premedication has led to administration of shorterinfusions (lt3 hours) which are better tolerated in particularfrom a haematologic perspective but patients remain at riskof myalgia and neuropathy at higher doses Weekly one-hourlow dose paclitaxel also known as dose-dense therapy hasrecently emerged as another possible strategy to improveoutcomes
9 Dose-Dense Therapy
Dose-dense treatment is defined by delivery of a maintainedper-cycle dose or overall dose with administration of drugat shorter time intervals than is standard This differs fromdose intensity which refers to dose (per unit weight or bodysurface area) delivered per unit time Hence either escalationof dose per cycle or reducing the time in between cycles maymodify dose intensity [129 130]
The rationale for the dose-dense approach of weeklypaclitaxel is that more frequent delivery of moderate dosesmay achieve greater efficacy by allowing sustained exposureof dividing tumour cells to paclitaxelrsquos cytotoxic and antian-giogenic effects hence reducing resistance delaying relapseand increasing the possibility of cancer remission Three 1-hour infusions of paclitaxel given at a week interval achievedgreater dose-density as well as dose-intensity than a singleadministration every 3 weeksThe initial tissue concentration(gt50 nM) for 1-hour infusion is similar to that of 3-hourinfusion but the concentration in the plasma instead oflasting for 8 hours in a 3-hour infusion rapidly falls below50 nM in less than 75 minutes for 1-hour infusion and hencereduces the risk of neutropenia However the rate of fallexperienced in tissue concentration of the drug is slowerthan plasma concentration of the drug hence efficacy ismaintained [131 132] A shorter infusion time allows bettercontrol of toxicities improved patient comfort and reducedhospitalisation hours
Several studies have used dose-dense paclitaxel in thetreatment of advanced ovarian cancer and are summarizedin Table 1 Based on phase 1 studies the recommendeddose for weekly paclitaxel ranges between 80 and 90mgm2compared with 45mgm2 per week with 3-weekly paclitaxeland is given over 1-hour duration Weekly scheduling hasdemonstrated consistent activities in ovarian cancer studies[11ndash13] Response rates were in the 20ndash50 range whereusually less than 10 would be expected Grade-4 doselimiting toxicities in particular neutropenia were not evidentat any dose below 100mgm2week [11 133]
10 BioMed Research International
Table1Ph
ases
Iand
IIstu
dies
onintravenou
sdose-densep
aclitaxel
Stud
yRe
gimen
119899()
PI(m
)RR
()
CR(119899)
MedianPF
S(m
)Median
OS
(m)
Adversee
ffects
Com
ments
Paclitaxel
dose
(mgm
2 )Ca
rbop
latin
dose
(mgm
2 )Ph
aseIsinglea
gent
Lofflerre
tal1996
[11]
40ndash9
0week
1-hou
rinfusionfor
6weeks
5040
5NA
NA
(i)Hem
atologictoxicity-m
ild(ii)N
ograde3
or4
haem
atologicaltoxicity
neurologicalor
cardiotoxicityup
to90
mgm
2 wk
(iii)Nohypersensitivity
reactio
ns(patientsreceivedprem
edication)
(i)100
priorc
hemotherapy
(ii)M
ediando
seintensity
was
410m
gm
2 6w
k(range200
to540m
gm
2 6w
k)
Fenn
ellyetal
1997
[12]
40ndash100w
eek
1830
NA
NA
NA
(i)Nomucositiso
rgrade
III
neurop
athy
was
seen
(ii)A
lopeciao
ccurredin
one
(i)100
priorc
hemotherapy
(2ndash5
priorregim
ens)
(ii)P
artia
lrespo
nses
weres
eenin
four
of13
assessablepatients
(30
)(iii)Dose-lim
iting
toxicitywas
reachedat100m
gm
2 (iv
)2-3
patie
ntse
xperience
treatmentd
elay
(v)M
axim
um-to
lerateddo
seof
80mgm
2 Ab
u-Ru
stum
etal
1997
[13]
60ndash100
over
1ho
urw
eek
45289
NA
NA
NA
(i)Nopatie
nthadfebrile
neutropenia
(i)100
priorc
hemotherapy
(1ndash8
priorregim
ens)
PhaseIISing
leagent
Markm
anetal
2001
[14]
80over
1ho
urw
eek
53(52)
25NA
NA
NA
Therapydiscon
tinuedin
(i)4patie
ntsw
hohadperip
heral
neurop
athy
(ii)1
patie
ntdu
etopainful
fingernailbeds
(i)100
platinum
andpaclita
xel
resistant
(ii)Th
erapywas
discon
tinuedin
5patie
ntsb
ecause
oftoxicity
(iii)Only13
(1)w
erem
odified
(doser
eductio
nor
treatment
delay)
becauseo
fsidee
ffects
PhaseIICom
binedwith
platinum
agent
Kiku
chietal
2005
[15]
80over
1ho
urw
eek
AUC2week
27gt6
818
483
NA
(i)Neutro
penia(
17)
thrombo
cytopenia(
51
)(ii)N
ocaseso
fperipheral
neurop
athy
(grades3
and4)
inweeklycombinedT-C
Cadron
etal2007
[16]
90over
1ho
urw
eek
AUC4week
24 9gt6le6
73 38NR
8105
675
(i)Grade
34neutropenia(
34)
andneutropenicfever
in2
(ii)N
auseaa
ndvomiting
and
fatig
uewerethe
mostfrequ
ent
nonh
ematologicalsid
eeffects
(i)Doser
eductio
nwas
necessary
in25of
patie
nts
Pign
atae
tal2008
[17]
60over
1ho
urw
eek
AUC2week
24(13)lowastlowast
1stline
385
2320
136
(i)Notoxicd
eath
was
recorded
(ii)G
rade
2anaemiawas
repo
rted
insevenpatie
nts(27)
(iii)Nofebrile
neutropeniaw
asob
served
(iv)G
rade
3and4neutropenia
was
recorded
infive(19)a
ndon
e(4
)patients
(v)G
rade
3thrombo
cytopenia
occurred
inon
epatient
(4)
BioMed Research International 11
Table1Con
tinued
Stud
yRe
gimen
119899()
PI(m
)RR
()
CR(119899)
MedianPF
S(m
)Median
OS
(m)
Adversee
ffects
Com
ments
Paclitaxel
dose
(mgm
2 )Ca
rbop
latin
dose
(mgm
2 )
Safrae
tal2014
[18]
80over
1ho
urw
eek
AUC2week
133
1stline
864
645
274
(i)Highera
naem
ia(grade
III+
IV68vs53)+
IVneutropenia(
144vs69)
decreasedgradeIIa
lopecia(
235
vs981
)and
thrombo
cytopenia
(grade
III+
IV0
vs23)
Havrilesky
etal
2003
[19]
80over
1ho
urw
eek
AUC2weekD1
D8D15
until
progressionCR
+8courses
29 21 8
Total
grou
pgt6lt6
83 100
38
16 15 1114
115
137
32
(i)Hem
atologictoxicitywas
common
(grade
3neutropenia
32n
ograde4
neutropenia
grade3
or4thrombo
cytopenia
142)
(i)To
xicitymanaged
bytre
atment
delaydo
seredu
ctionof
paclitaxel
ordiscon
tinuatio
nof
carbop
latin
vanderB
urgetal
2014
[20]
90over
1ho
urw
eek
AUC4weekD1
D8D15
D29
D36
D49
+6x
TCq3w
108
65 43
Total
grou
pgt6lt6
76 5816 42
26 158 13
(i)Neutro
penia3
0
thrombo
cytopenia8
febrile
neutropenia0
5
(ii)N
onhaem
atologictoxicitywas
low
(i)Treatm
entw
asdelayedin
16
anddo
seredu
cedin
2of
cycle
s
119899num
bero
fpatientsassessableforrespo
nsemm
onthsPIplatinum
treatmentfreeintervalRR
respo
nser
ateCR
com
pleterem
issionT
paclitaxelC
carbop
latin
PFS
progressio
nfre
esurvivalOSoverall
survivalN
An
otavailableinpapero
rabstractandNR
notyetreached
lowastlowastElderly
popu
lation
patient
agedge70
years
12 BioMed Research International
Numerous phase II studies have explored the tolerabilityand the activity of weekly paclitaxel either as a single agent orin combination with several other drugs or biological agents(Table 1) A number of regimens combining weekly paclitaxelwith carboplatin have been used as first-line treatment inovarian cancer Carboplatin has been administered weeklyat AUC of 2 with dose escalation in some studies whilepaclitaxel had been infused at 60ndash80mgm2week Thiscombined regimen was well tolerated with a low incidence ofbone marrow suppression Overall response rates have beenhigh in the range of 60ndash80 in most studies even in heavilypretreated patients with platinum-resistant disease (diseaserecurrence or progression within 6 months of the last lineof platinum-based therapy) [15ndash20 134] The promising datafrom these phase II trials then led to the evolution of largerphase III trials
Three phase III studies Japanese Gynecologic OncologyGroup- (JGOG-) Trial 3016 [21ndash23] Multicentre Italian Trialin Ovarian Cancer-Trial 7 (MITO-7) [25] and GynecologicOncology Group GOG-262 Trial [24] have explored dosedense therapy The results of these trials are summarised inTable 2
The Japanese Gynecologic Oncology Group (JGOG)conducted a randomized phase 3 trial of dose-dense weeklypaclitaxel 80mgm2week in combination with 3-weeklycarboplatin compared to standard 3-weekly carboplatin andpaclitaxel 180mgm2 in patients with advanced epithelialovarian peritoneal or fallopian tube cancer (JGOG 3016NOVEL trial) In both arms carboplatin was given at AUC6 and the median number of cycles was six In this largestudy (119899 = 637) with a median follow up of 77 months therewas an 11-month improvement in themedian progression freesurvival (PFS) in the dose-dense treatment group comparedwith the standard treatment arm (282 versus 175 monthsHR 076 95 CI 062ndash091 119901 = 00037) Median OS wasalso higher in the dose-dense treatment arm (1005 versus622 months HR 079 95 CI 063ndash099 119901 = 0039)On subgroup analysis suboptimally debulked patients withresidual disease of gt1 cm (119899 = 342) had a significantlyhigher median overall survival in the dose dense arm (512versus 335 months HR-075 95 CI 057ndash097 119901 = 0027)There was no significant advantage to dose-dense treatmentfor patients with optimally cytoreduced disease Dose-densetherapy survival benefits were also not seen in patients withclear cell or mucinous histology type unlike serous typeHowever patient treated with dose dense therapy had asignificantly higher frequency of hematologic toxicity thanwith the standard arm (212 versus 94) which resultedin lower treatment completion rates (63 versus 48) withfrequent episodes of delay (76 versus 67) and dosereductions (48versus 35) [21 22]Therewas no significantdifference in terms of overall quality of life between the twoarms (119901 = 046) [23]
Using a similar regimen as in JGOG-3016 a GynecologicOncology Group (GOG)-262 Trial was conducted in theUnited States In this group most patients had stage IIIdisease (66ndash70) and two-thirds had suboptimal debulkingwith residual disease of gt1 cm This was a randomized phase
III trial of 3 weekly paclitaxel versus dose-dense weeklypaclitaxel in combination with carboplatin in patients withadvanced epithelial ovarian peritoneal or fallopian tubecancer Though optional concurrent and maintenance beva-cizumab were received by the majority of patients in botharms (835 versus 841 resp) There was no significantdifference in PFS in the patients who received the dosedense paclitaxelcarboplatin regimen compared to those whoreceived the standard paclitaxelcarboplatin regimen (148versus 143 months HR 097 95 CI 079ndash118) Howeverin a subgroup analysis there was a significant difference inPFS in the dose dense paclitaxel arm who did not receivebevacizumab 119899 = 112 (142 versus 103 months HR 059 95CI 037ndash096 119901 = 0003) Overall survival data is still imma-ture There was higher frequency of grade 3 anaemia (408versus 157 119901 lt 0001) and grade 2 sensory neuropathy(259 versus 178 119901 = 0012) but a lower incidence ofneutropenia (72 versus 83 119901 lt 0001) [24]
In 2008 the Multicentre Italian Trials in Ovarian Cancer(MITO-7) randomised 810 women in a phase 3 trial toreceive either standard carboplatin (AUC = 6) and paclitaxel175mgm2 every 3 weeks or a weekly schedule of paclitaxel(60mgm2) with carboplatin (AUC = 2) The majority ofpatients in both arms (83ndash90) received six cycles of therapyMost patients (58ndash63) had stage II1 disease 23 of themwere suboptimally debulked Median PFS did not differsignificantly (173 months and 183 months 119901 = 066)between the standard and dose-dense arms respectivelyThere was no significant difference in response rate betweenthe two arms nor the estimated 2-year overall survivalSubgroup analysis did not identify any subgroup that mayhave benefited from the dose-dense regimen Unlike theJGOG-3016 trial the incidence of grade 3-4 neutropenia wassignificantly lower in the dose-dense group compared to the3-weekly regimen (42 versus 50) A similar pattern wasseen for the incidence of febrile neutropenia (lt1 versus 3119901 = 002) thrombocytopenia (1 versus 7 119901 lt 0001)and other nonhaematological toxicities such as alopeciavomiting renal dysfunction and neuropathy Quality of lifewas reported to be significantly better in the dose-dense arm(119901 lt 00001) which was discordant with the JGOG-3016quality of life data [25]
In summary there was significant improvement inmedian PFS and overall survival in studies using paclitaxelat 80mgm2week dose-dense therapy [21 24] but withhigher haematological toxicity whereas MITO-7 [25] whichwas using paclitaxel at 60mgm2week was only equivalentlyeffective but less toxicThis does not conclude that the higherpaclitaxel dose is more clinically beneficial as there are manyother confounding factors in all three studies
In a multivariate analysis the JGOG-3016 study [21]reported that a lower dose intensity of paclitaxel (lt80) wasassociated with poorer overall survival (hazard ratio = 14295 confidence interval 112ndash181 119901 = 0004) however itmust be highlighted that the investigational arm carboplatinschedules were not standardised in these studies The JGOGand GOG trials delivered a 3-weekly carboplatin (AUC =6) arm whereas in the MITO-7 study the carboplatin was
BioMed Research International 13
Table2Ph
aseIIIstu
dies
onintravenou
sdose-densep
aclitaxel
Stud
yRe
gimen
119899
MedianPF
S(m
)
Median
OS
(m)
Adversee
ffects
Com
ments
Katsu
matae
tal2009
[21]
Katsu
matae
tal2013
[22]
Haranoetal2014
[23]
JGOG3016
631
(i)Haematologicaltoxicityhigh
erin
dose
dense-211versus
94
Lower
treatmentcom
pletionin
dose-dense
63versus
48
Frequent
episo
deso
fdelay
indo
se-dense
76versus
67
Doser
eductio
nsin
dose-dense
48versus
35
Nosig
nificantd
ifference
inoverallQ
OL
betweenbo
thgrou
ps(119901=046)
Paclitaxel80m
gm
2D18
15+carbop
latin
AUC63
weeklyversus
Paclitaxel180
mgm
2+
carbop
latin
AUC63
weekly
312
282
1005
Both
givenfor6
ndash9cycle
s319
175
622
Chan
etal2013
[24]
GOG-262
(i)Higherfrequ
ency
ofgrade3
anaemia
(408versus
157119901lt0001)
grade2
sensoryneurop
athy
(259versus
178
119901=0012)b
utlower
incidenceo
fneutropenia(
72versus
83119901lt0001)
Paclitaxel80m
gm
2D18
15+carbop
latin
AUC63
weeklyversus
Paclitaxel175
mgm
2+
carbop
latin
AUC63
weekly
346
148
NR
Both
givenfor6
cycle
s346
143
NR
Bevacizumab
given
optio
nally
112
(did
not
receive
bevazicumab)
142vs
103
Pign
atae
tal2014
[25]
MITO-7
810
(i)Lo
wer
incidenceo
fgrade
3-4
neutropenia(
42versus
50)febrile
neutropenia(lt1v
ersus3
119901=002)
thrombo
cytopenia(
1versus7
119901lt0001)andothern
onhaem
atological
toxicitie
ssuchas
alop
eciavom
iting
renald
ysfunctio
nandneurop
athy
Qualityof
lifeb
etterindo
sedensea
rm(119901lt00001)
Paclitaxel60m
gm
2 weekly+carbop
latin
AUC
2weeklyversus
Paclitaxel175
mgm
2+
carbop
latin
AUC63
weekly
406
404
183 173
77lowast
79lowast
119899num
bero
fpatientsmm
onthsDday
PFSprogressionfre
esurvivalOSoverallsurvivalNAnot
availableinpapero
rabstractandNR
notyetreached
lowastSurvivalrateat2years
14 BioMed Research International
dose-dense (AUC 2 weekly) Although it is possible that thedose scheduling for the platinum-based agent is not essentialfor a survival benefit as shown by previous studies usingdose-dense cisplatin direct cross-trial comparison cannot bemade Unlike paclitaxel carboplatin probably requires peakdose for optimal therapeutic benefit hence this may accountfor the inferior survival outcome in MITO-7 trial Anotherconfounding factor may be difference in ethnicity All threestudies used different ethnic populations and Asian patientsin JGOG-3016 appear to have better survival outcomes thanthe MITO-7 Western population Ethnicity with possibleunderlying genetic causes may be responsible for the variableresponses to chemotherapy across individuals [135] This wasexplored by Millward et al who studied 68 Caucasian andAsian lung cancer patients treated with a combination ofpaclitaxel and carboplatin and found that the incidence offebrile neutropenia was 50 of an initially treated cohortof Asians and when carboplatin was subsequently dosereduced in all Asian patients the overall incidence of febrileneutropenia was also reduced to 26 [136]
Although early clinical data from phase I and phaseII dose-dense paclitaxel trials in advanced ovarian cancerwere promising the results from phase III studies in havebeen inconsistent as a result of differences in paclitaxel dosecarboplatin AUC and schedule addition of bevacizumabas well as different ethnic populations The results of arecently completed randomised three arms GynaecologicCancer InterGroup (GCIG) phase II trial ICON 8 mayfurther inform the clinical benefit of dose dense paclitaxeltherapy
This multicentre trial involving 111 centres in the UKSouth Korea Mexico Ireland Australia and New Zealandwith a target population of 1485 patients with stage IC-IV epithelial ovarian cancer or peritoneal or fallopian tubecancer compared two dose-dense arms (i) JGOG-like armcarboplatin AUC 5 plus weekly 80mgm2 paclitaxel and (ii)MITO-7-like arm weekly carboplatin AUC 167 plus weekly80mgm2 paclitaxel to the standard 3-weekly treatment(carboplatin AUC 5 plus 175mgm2 paclitaxel) for stage IC toIV epithelial ovarian cancer The dose-dense arms of MITO-7 and JGOG-3016 as well as the ethnic heterogeneity will befurther addressed
10 Intraperitoneal (IP) Chemotherapy
In addition to dose and scheduling the route of adminis-tration of chemotherapy agents plays an important role inoutcome Intraperitoneal spread is common and likely anearly event in epithelial ovarian cancer hence the deliveryof chemotherapy intraperitoneally in theory would exposethe microcirculation of tumour to higher doses of drug thansystemic administration while limiting systemic toxicityTheideal drug for IP chemotherapy is one that is systemicallyeffective penetrates deep into the inner core of tumour tissueand remains within the peritoneal cavity for a prolongedperiod of time [137ndash139]
Early clinical studies confirmed that indeed the peritonealcavity could be exposed to 10 to 20-fold higher (cisplatin
and carboplatin) drug concentration than when using theintravenous approach and since 1978 this route had beenadopted as a form of therapeutic intervention [137 139]A subsequent phase I trial showed that IP paclitaxel haddose-limiting toxicity in the form of abdominal pain [140]Another phase 1 GOG pilot study administered weekly IPpaclitaxel at an initial dose of 20mgm2 for 16 weeks to33 patients and found that IP paclitaxel at this dose wasfeasible and well tolerated At dose levels 60 to 65mgm2there were significant levels of paclitaxel for a week afterdrug administration suggesting very slow clearance andcontinuous exposure of the peritoneal cavity to active drugconcentrations [132]
Hence this initiated a phase II study [141] that used pacli-taxel intraperitoneally at a dose of 60ndash65mgm2week In thisphase II GOG study 76 patients with small-volume resid-ual disease carcinoma (05 cm or less) involving the ovaryperitoneal or fallopian tube were treated with paclitaxel60mgm2week intraperitoneally for 16 weeks followed bysurgical evaluation in patients without disease progressionThe Gynaecologic Oncology group (GOG) currently definesno visible disease as microscopic disease being the idealsurgical outcome 75 of patients had received prior systemictherapy and 70 received all 16 courses that were planned Of28 patients with microscopic disease at the start of therapy61 achieved a surgically defined complete response whereasonly 1 out of 31 patients with macroscopic disease achieved acomplete response The median time-to-recurrence was 167months with an estimated survival rate at 2 years being 58Treatment was generally well tolerated [141]
Another study looked into the effect of IP paclitaxel asconsolidation therapy in advanced ovarian cancer Twenty-eight patients who had initial residual macroscopic disease(lt1 cm) after primary surgery or interval debulking but hadcomplete pathological response following standard treatmentwith at least 6 cycles of platinum-based chemotherapy regi-men received paclitaxel 60mgm2week intraperitoneally for12ndash16 weeks as consolidation therapy The median time torecurrence was 25 months but overall survival did not differsignificantly when compared with control group submittedto observation only Treatment-related toxicity was mild andtechnical difficulties were observed in 11 of patients [142]
Multicenter randomised phase 3 trials as well as meta-analysis of IP chemotherapy have been performed anddemonstrated that chemotherapy drugs administered intra-peritoneally are superior to intravenous standard regimensin patient with optimally debulked epithelial ovarian cancerThe most impressive data comes from GOG 114 [14] and172 trial [143] In GOG 114 patients received either sixcycles of intravenous paclitaxel 135mgm2 and cisplatin75mgm2 every 3 weeks or intravenous carboplatin (AUC= 9) every 28 days for two cycles followed by six 3-weeklycycles of intravenous paclitaxel 135mgm2 and IP cisplatin100mgm2 [14] whereas in GOG 172 patients received eitherintravenous paclitaxel 135mgm2 followed by intravenouscisplatin 75mgm2 or intravenous paclitaxel 135mgm2 fol-lowed by IP combination of cisplatin 100mgm2 and pacli-taxel 60mgm2 on day 8 Both trials had a combined total
BioMed Research International 15
of 876 women with stage III epithelial ovarian carcinomaoptimally debulked to le1 cm residual tumour [143] Themedian follow-up for GOG 114 [14] was 138 years with GOG172 [143] was 97 years The primary results of the individualtrials reported up to 6-month improvement in median PFSfollowing IP therapy In the combined analysis of the datafrom both trials the data continued to show a 5-monthdifference in favour of IP therapy (25 versus 20 months)which translates into 16 reduction in the hazard ratio forprogression (119901 = 003) In GOG 114 [14] reported in 2001there was only borderline improvement in overall survivalassociated with this regimen (median 63 versus 52 monthsrelative risk 081 119901 = 005)
However in combined analysis in 2013 which was pre-sented at the Society of Gynecologic Oncology AnnualMeeting [144] the overall survival showed an 11-monthimprovement in favour of IP therapy in GOG 114 whereasGOG 172 reported a 16-month survival advantage Amongpatients treated with IP therapy the 5-year survival rateincreased from 18 following completion of 1-2 cycles to 59for patients who completed 5-6 cycles of treatment Howeverthere was increased toxicity observed in the IP arm grade 3-4 leukopenia thrombocytopenia and abdominal pain Only42 of patients in the GOG172 trial [143] completed all sixcycles of planned treatment in the IP arm while 18 ofpatients in GOG 114 trial [14] received fewer than two coursesof IP chemotherapy
Another randomised phase III trial involving patientswith stages II-III epithelial ovarian carcinoma is the GOG252 study with three arms Arm 1-dose-dense intravenouscarboplatin and paclitaxel Arm 2-dose-dense intravenouspaclitaxel and IP carboplatin and Arm 3 consists of 3-weeklyintravenous paclitaxel (day 1) followed by IP cisplatin (day 2)and IP paclitaxel (day 3) regimen All three arms also incor-porate the combination and maintenance of bevacizumabGOG 252 has completed accrual and results are awaited [139]
11 Newer Forms of Paclitaxel
Development of next-generation taxanes has taken place overthe past 40 years aimed at eliminating toxicity improvingefficacy and ease of administration Abraxane is a novelcompound which incorporates paclitaxel into an albuminnanoparticle soluble in saline hence eliminating the needfor Cremophor EL which is responsible for hypersensitivityreactions experienced during paclitaxel infusion [145] Thenanoparticle albumin in nab-paclitaxel is able to bind toglycoprotein gp60 receptor an albumin receptor and activatecaveolin-1 a protein that in human is encoded byCAV-1 geneleading to formation of caveoli hence allowing nab-paclitaxelto migrate across the endothelial cell membrane into theinterstitial space leading to higher intratumoural drug con-centration In addition Abraxane exhibits linear pharma-cokinetics and can therefore be given at a relatively higherdose than standard intravenous paclitaxel leading to a highertherapeutic ratio and heightened efficacy in solid tumoursmainlymetastatic breast cancer [146 147] Nab-paclitaxel hadFDA approval in 2005 for treatment of breast cancer [148]
Nab-paclitaxel has been studied in recurrent ovariancancer As a single agent in phase II 44 patients withrecurrent ovarian cancer were treated with Nab-paclitaxel260mgm2 intravenously for 30 minutes every 3 weeks for6 cycles Ninety-two percent of patients were platinum-sensitive while 89 had had previous exposure to standardtaxane The objective response rate was 64 with 15 patientsachieving complete response and 13 of them had partialresponse Estimated median PFS was 85 months No hyper-sensitivity reactions were observed and there were infrequentcases of grade 4 neutropenia (11) and grade 2-3 neuropathy(13) [149]
Another phase II study by GOG enrolled 51 patients withplatinum- and taxane-resistant recurrent ovarian cancer outof which 47 were evaluable The objective response rate was38 with one patient achieving a complete response and 10patients a partial response The median PFS was 45 monthswhile overall survival rate was 174 months Severe haema-tological and nonhaematological toxicities including neuro-toxicity were uncommon These results are quite impressivegiven the treatment population consisted of patients withvery poor prognosis with a median platinum and taxane freeinterval of 21 days and 70 had their recurrence within 3months of completion of primary treatment [150] Severalother trials of this formulation are in progress
Paclitaxel poliglumex (PPX) also known as Xyotax isanother prodrug a novel conjugate of paclitaxel and 120572-poly-L-glutamic acid which accumulates within tumour tissuedue to increased permeability of the tumour vessels and lackof lymphatic drainage [148 151 152] Paclitaxel poliglumexenhances solubility of paclitaxel allows direct delivery tothe intratumoural microenvironment and allows prolongedexposure to the active drug while minimising systemictoxicities [151] In Phase I dose escalation studies as a singleagent the recommended dose of PPX was 235mgm2 over 10minutes every 3 weeks or 70mgm2 weekly [153] In a PhaseII GOG study of relapsed ovarian cancer a response rate of16 was seen with infrequent serious adverse events grade3 and 4 neutropenia (24 and 20) and grade 3 neuropathy(24) [154] A phase III trial (GOG-0212) on the use of PPXas consolidation ormaintenance therapy in advanced ovariancancer is in progress
DHA-paclitaxel also known as Taxoprexin is a prodrugwhere paclitaxel is covalently conjugated with the naturallyoccurring omega-3 fatty acid docosahexaenoic acid (DHA)a fatty acid that is easily taken up by tumour cells henceincreasing intratumoural concentration of paclitaxel leadingtumour cell apoptosis [155 156] DHA-paclitaxel exhibitslinear pharmacokinetics and lower toxicity and also ease ofadministration when compared to conventional paclitaxeland has demonstrated antineoplastic activity in animal mod-els of cancer as well as in a phase III trial involving metastaticmelanoma [156ndash160] In a recent study on human ovariancancer cells it was found that DHA could reverse paclitaxelresistance by inhibiting P-gp as well as downregulatingthe expression of multidrug resistance associated proteins(MRP) and inhibiting the activity of NF-120581B and p38 MAPKsignalling pathways [161]
16 BioMed Research International
12 Future Directions
A plateau has been reached regarding the benefits associatedwith standard 3-weekly intravenous administration of cyto-toxic chemotherapy in advanced epithelial ovarian cancerThe ongoing battle for a better treatment regimen to delayrelapse promote remission and most importantly improvethe quality of life of patients with advanced epithelial ovariancancer need not to go further than the ability to relook at thechemotherapy agents that are already available in a differentapproach
Novel compounds to date have not yet shown clinicalsuperiority and parent compounds such as paclitaxel con-tinue to surprise us with their feasibility effectiveness andmanageable toxicity profiles Intraperitoneal paclitaxel willrequire further evaluation Better effort in understanding themechanism of action of drugs including the role of dosescheduling and the effect on the immune systemmay providea more cost-effective route to better clinical outcomes
Conflict of Interests
The authors declare no conflict of interests in this work
Acknowledgments
The authors would like to thank the many researchers whohave contributed to our current knowledge of paclitaxelNirmala Kampan is supported by Australian Monash Uni-versity Institute of Graduate Research Scholarship as wellas Universiti Kebangsaan Malaysia Postgraduate ScholarshipAward Mutsa Madondo has received Postgraduate Pub-lication Award from Monash University and MagdalenaPlebanski has been awarded Senior NHMRC Fellowship
References
[1] Australian Institute of Health and Welfare and National Breastand Ovarian Cancer Centre (Australia) Ovarian Cancer inAustralia AnOverview 2010 Cancer Series Australian Instituteof Health and Welfare Canberra Australia 2010
[2] R E Bristow R S Tomacruz D K Armstrong E L Trimbleand F J Montz ldquoSurvival effect of maximal cytoreductivesurgery for advanced ovarian carcinoma during the platinumera a meta-analysisrdquo Journal of Clinical Oncology vol 20 no 5pp 1248ndash1259 2002
[3] ZKempand JA Ledermann ldquoUpdate onfirst-line treatment ofadvanced ovarian carcinomardquo International Journal of WomenrsquosHealth vol 5 no 1 pp 45ndash51 2013
[4] A du Bois H-J Luck W Meier et al ldquoA randomized clinicaltrial of cisplatinpaclitaxel versus carboplatinpaclitaxel as first-line treatment of ovarian cancerrdquo Journal of the National CancerInstitute vol 95 no 17 pp 1320ndash1330 2003
[5] R F Ozols B N Bundy B E Greer et al ldquoPhase III trialof carboplatin and paclitaxel compared with cisplatin andpaclitaxel in patients with optimally resected stage III ovariancancer A Gynecologic Oncology Group studyrdquo Journal ofClinical Oncology vol 21 no 17 pp 3194ndash3200 2003
[6] W P McGuire W J Hoskins M F Brady et al ldquoCyclophos-phamide and cisplatin compared with paclitaxel and cisplatin
in patients with stage III and stage IV ovarian cancerrdquoThe NewEngland Journal of Medicine vol 334 no 1 pp 1ndash6 1996
[7] W P McGuire W J Hoskins M F Brady et al ldquoCyclophos-phamide and cisplatin versus paclitaxel and cisplatin a phase IIIrandomized trial in patients with suboptimal stage IIIIV ovar-ian cancer (from the gynecologic oncology group)rdquo Seminars inOncology vol 23 no 5 supplement 12 pp 40ndash47 1996
[8] M J Piccart K Bertelsen K James et al ldquoRandomized inter-group trial of cisplatin-paclitaxel versus cisplatin-cyclophosph-amide inwomenwith advanced epithelial ovarian cancer three-year resultsrdquo Journal of the National Cancer Institute vol 92 no9 pp 699ndash708 2000
[9] P A Vasey G C Jayson A Gordon et al ldquoPhase III random-ized trial of docetaxel-carboplatin versus paclitaxel-carboplatinas first-line chemotherpy for ovarian carcinomardquo Journal of theNational Cancer Institute vol 96 no 22 pp 1682ndash1691 2004
[10] B Gronlund C Hogdall H H Hansen and S A EngelholmldquoResults of reinduction therapy with paclitaxel and carboplatinin recurrent epithelial ovarian cancerrdquo Gynecologic Oncologyvol 83 no 1 pp 128ndash134 2001
[11] T M Loffler W Freund J Lipke and T-U HausamenldquoSchedule- and dose-intensified paclitaxel as weekly 1-hourinfusion in pretreated solid tumors results of a phase III trialrdquoSeminars in Oncology vol 23 no 6 supplement 16 pp 32ndash341996
[12] D Fennelly C Aghajanian F Shapiro et al ldquoPhase I and phar-macologic study of paclitaxel administered weekly in patientswith relapsed ovarian cancerrdquo Journal of Clinical Oncology vol15 no 1 pp 187ndash192 1997
[13] N R Abu-Rustum C Aghajanian R R Barakat D Fennelly FShapiro and D Spriggs ldquoSalvage weekly paclitaxel in recurrentovarian cancerrdquo Seminars inOncology vol 24 no 5 supplement15 pp S15-62ndashS15-67 1997
[14] M Markman B N Bundy D S Alberts et al ldquoPhase III trialof standard-dose intravenous cisplatin plus paclitaxel versusmoderately high-dose carboplatin followed by intravenouspaclitaxel and intraperitoneal cisplatin in small-volume stageIII ovarian carcinoma an intergroup study of the gynecologiconcology group Southwestern Oncology Group and EasternCooperativeOncologyGrouprdquo Journal of Clinical Oncology vol19 no 4 pp 1001ndash1007 2001
[15] A Kikuchi H Sakamoto and T Yamamoto ldquoWeekly car-boplatin and paclitaxel is safe active and well tolerated inrecurrent ovarian cancer cases of Japanese women previouslytreated with cisplatin-containing multidrug chemotherapyrdquoInternational Journal of Gynecological Cancer vol 15 no 1 pp45ndash49 2005
[16] I Cadron K Leunen F Amant T van Gorp P Nevenand I Vergote ldquoThe lsquoLeuvenrsquo dose-dense paclitaxelcarboplatinregimen in patients with recurrent ovarian cancerrdquo GynecologicOncology vol 106 no 2 pp 354ndash361 2007
[17] S Pignata E Breda G Scambia et al ldquoA phase II studyof weekly carboplatin and paclitaxel as first-line treatment ofelderly patients with advanced ovarian cancer A Multicen-tre Italian Trial in Ovarian cancer (MITO-5) studyrdquo CriticalReviews in OncologyHematology vol 66 no 3 pp 229ndash2362008
[18] T Safra S Shamai J Greenberg et al ldquoWeekly carboplatinwith paclitaxel compared to standard three-weekly treatment inadvanced epithelial ovarian carcinomamdasha retrospective studyrdquoGynecologic Oncology vol 132 no 1 pp 18ndash22 2014
BioMed Research International 17
[19] L J Havrilesky A A Alvarez R A Sayer et al ldquoWeekly low-dose carboplatin and paclitaxel in the treatment of recurrentovarian and peritoneal cancerrdquo Gynecologic Oncology vol 88no 1 pp 51ndash57 2003
[20] M van der BurgW Onstenk I Boere et al ldquoLong-term resultsof a randomised phase III trial of weekly versus three-weeklypaclitaxelplatinum induction therapy followed by standardor extended three-weekly paclitaxelplatinum in Europeanpatients with advanced epithelial ovarian cancerrdquo EuropeanJournal of Cancer vol 50 no 15 pp 2592ndash2601 2014
[21] N Katsumata M Yasuda F Takahashi et al ldquoDose-densepaclitaxel once a week in combination with carboplatin every3 weeks for advanced ovarian cancer a phase 3 open-labelrandomised controlled trialrdquoThe Lancet vol 374 no 9698 pp1331ndash1338 2009
[22] N Katsumata M Yasuda S Isonishi et al ldquoLong-term resultsof dose-dense paclitaxel and carboplatin versus conventionalpaclitaxel and carboplatin for treatment of advanced epithelialovarian fallopian tube or primary peritoneal cancer (JGOG3016) a randomised controlled open-label trialrdquo The LancetOncology vol 14 no 10 pp 1020ndash1026 2013
[23] K Harano F Terauchi N Katsumata et al ldquoQuality-of-lifeoutcomes from a randomized phase III trial of dose-denseweekly paclitaxel and carboplatin compared with conventionalpaclitaxel and carboplatin as a first-line treatment for stage II-IV ovarian cancer Japanese Gynecologic OncologyGroup Trial(JGOG3016)rdquo Annals of Oncology vol 25 no 1 pp 251ndash2572014
[24] J Chan M F Brady R Penson et al ldquoPhase III trial ofevery-3-weeks paclitaxel vs dose dense weekly paclitaxel withcarboplatin +minus bevacizumab in epithelial ovarian peritonealfallopian tube cancer GOG 262 (NCT01167712)rdquo InternationalJournal of Gynecological Cancer vol 23 no 8 supplement 1 pp9ndash10 2013
[25] S Pignata G Scambia D Katsaros et al ldquoCarboplatin pluspaclitaxel once a week versus every 3 weeks in patients withadvanced ovarian cancer (MITO-7) a randomisedmulticentreopen-label phase 3 trialrdquoThe Lancet Oncology vol 15 no 4 pp396ndash405 2014
[26] V Walsh and J Goodman ldquoFrom taxol to Taxol the changingidentities and ownership of an anti-cancer drugrdquo MedicalAnthropology vol 21 no 3-4 pp 307ndash336 2002
[27] R Renneberg ldquoBiotech History yew trees paclitaxel synthesisand fungirdquo Biotechnology Journal vol 2 no 10 pp 1207ndash12092007
[28] J E Liebmann J A Cook C Lipschultz D Teague J Fisherand J B Mitchell ldquoCytotoxic studies of paclitaxel (Taxol) inhuman tumour cell linesrdquo British Journal of Cancer vol 68 no6 pp 1104ndash1109 1993
[29] J J Manfredi and S B Horwitz ldquoTaxol an antimitotic agentwith a newmechanism of actionrdquo Pharmacology andTherapeu-tics vol 25 no 1 pp 83ndash125 1984
[30] D G I Kingston ldquoRecent advances in the chemistry of taxolrdquoJournal of Natural Products vol 63 no 5 pp 726ndash734 2000
[31] D G I Kingston ldquoThe shape of things to come structural andsynthetic studies of taxol and related compoundsrdquo Phytochem-istry vol 68 no 14 pp 1844ndash1854 2007
[32] V Walsh and J Goodman ldquoCancer chemotherapy biodiversitypublic and private property the case of the anti-cancer drugTaxolrdquo Social Science amp Medicine vol 49 no 9 pp 1215ndash12251999
[33] P H Wiernik E L Schwartz J J Strauman J P Dutcher RB Lipton and E Paietta ldquoPhase I clinical and pharmacokineticstudy of taxolrdquo Cancer Research vol 47 no 9 pp 2486ndash24931987
[34] W P McGuire E K Rowinsky N B Rosenhein et alldquoTaxol a unique antineoplastic agent with significant activityin advanced ovarian epithelial neoplasmsrdquo Annals of InternalMedicine vol 111 no 4 pp 273ndash279 1989
[35] ldquoDiscovery and development of taxolrdquo in Taxol Science andApplications M W M E Suffness Ed pp 3ndash25 CRC PressBoca Raton Fla USA 1995
[36] M J Piccart and F Cardoso ldquoProgress in systemic therapy forbreast cancer an overview and perspectivesrdquo European Journalof Cancer Supplement vol 1 no 2 pp 56ndash69 2003
[37] P Bonomi K B Kim and J Kugler ldquoComparison of survival forstage IIIB versus stage IV non-small cell lung cancer (NSCLC)patients with etoposide-cisplatin versus taxol-cisplatin an East-ern Cooperative Oncology Group (ECOG) trialrdquo in Proceedingsof the American Society of Clinical Oncology vol 16 p 454a1997
[38] D Guenard F Gueritte-Voegelein J Dubois and P PotierldquoStructure-activity relationships of Taxol and Taxotere ana-loguesrdquo Journal of the National Cancer Institute Monographsno 15 pp 79ndash82 1993
[39] D G I Kingston ldquoTaxol the chemistry and structure-activityrelationships of a novel anticancer agentrdquo Trends in Biotechnol-ogy vol 12 no 6 pp 222ndash227 1994
[40] E K Rowinsky and R C Donehower ldquoPaclitaxel (taxol)rdquo TheNew England Journal of Medicine vol 332 no 15 pp 1004ndash10141995
[41] J Parness and S B Horwitz ldquoTaxol binds to polymerizedtubulin in vitrordquo Journal of Cell Biology vol 91 no 2 pp 479ndash487 1981
[42] A Dammermann A Desai and K Oegema ldquoTheminus end insightrdquo Current Biology vol 13 no 15 pp R614ndashR624 2003
[43] CWiese and Y Zheng ldquoMicrotubule nucleation 120574-tubulin andbeyondrdquo Journal of Cell Science vol 119 no 20 pp 4143ndash41532006
[44] A Ganguly H Yang and F Cabral ldquoPaclitaxel-dependent celllines reveal a novel drug activityrdquo Molecular Cancer Therapeu-tics vol 9 no 11 pp 2914ndash2923 2010
[45] P B Schiff and S B Horwitz ldquoTaxol stabilizes microtubules inmouse fibroblast cellsrdquo Proceedings of the National Academy ofSciences of the United States of America vol 77 no 3 pp 1561ndash1565 1980
[46] P B Schiff J Fant and S B Horwitz ldquoPromotion of micro-tubule assembly in vitro by Taxolrdquo Nature vol 277 no 5698pp 665ndash667 1979
[47] D Zhang R Yang S Wang and Z Dong ldquoPaclitaxel new usesfor an old drugrdquoDrug Design Development andTherapy vol 8pp 279ndash284 2014
[48] S Rao G A Orr A G Chaudhary D G I Kingston and SB Horwitz ldquoCharacterization of the taxol binding site on themicrotubule 2-(m-Azidobenzoyl)taxol photolabels a peptide(amino acids 217-231) of beta-tubulinrdquoThe Journal of BiologicalChemistry vol 270 no 35 pp 20235ndash20238 1995
[49] F Wang Y Cao W Zhao H Liu Z Fu and R Han ldquoTaxolinhibits melanoma metastases through apoptosis inductionangiogenesis inhibition and restoration of E-cadherin andnm23 expressionrdquo Journal of Pharmacological Sciences vol 93no 2 pp 197ndash203 2003
18 BioMed Research International
[50] A Sevko V Kremer C Falk et al ldquoApplication of paclitaxel inlow non-cytotoxic doses supports vaccination with melanomaantigens in normal micerdquo Journal of Immunotoxicology vol 9no 3 pp 275ndash281 2012
[51] T Kreis and R Vale Guidebook to the Cytoskeletal and MotorProteins Oxford University Press Oxford UK 2nd edition1999
[52] P Giannakakou D L Sackett Y-K Kang et al ldquoPaclitaxel-resistant human ovarian cancer cells have mutant 120573-tubulinsthat exhibit impaired paclitaxel-driven polymerizationrdquo TheJournal of Biological Chemistry vol 272 no 27 pp 17118ndash171251997
[53] E Rakovitch W Mellado E J Hall T K Pandita S Sawantand C R Geard ldquoPaclitaxel sensitivity correlates with p53status and DNA fragmentation but not G2M accumulationrdquoInternational Journal of Radiation Oncology Biology Physics vol44 no 5 pp 1119ndash1124 1999
[54] S W Lowe S Bodis A McClatchey et al ldquop53 status and theefficacy of cancer therapy in vivordquo Science vol 266 no 5186 pp807ndash810 1994
[55] C C Zhang J-M Yang E White M Murphy A Levine andW N Hait ldquoThe role of MAP4 expression in the sensitivity topaclitaxel and resistance to vinca alkaloids in p53 mutant cellsrdquoOncogene vol 16 no 12 pp 1617ndash1624 1998
[56] K Fukasawa T Choi R Kuriyama S Rulong and G F VandeWoude ldquoAbnormal centrosome amplification in the absence ofp53rdquo Science vol 271 no 5256 pp 1744ndash1747 1996
[57] T-H Wang Y-H Chan C-W Chen et al ldquoPaclitaxel (Taxol)upregulates expression of functional interleukin-6 in humanovarian cancer cells through multiple signaling pathwaysrdquoOncogene vol 25 no 35 pp 4857ndash4866 2006
[58] E Yakirevich E Sabo I Naroditsky Y Sova O Lavie andM B Resnick ldquoMultidrug resistance-related phenotype andapoptosis-related protein expression in ovarian serous carcino-masrdquo Gynecologic Oncology vol 100 no 1 pp 152ndash159 2006
[59] G Szakacs J K Paterson J A Ludwig C Booth-Genthe andM M Gottesman ldquoTargeting multidrug resistance in cancerrdquoNature Reviews Drug Discovery vol 5 no 3 pp 219ndash234 2006
[60] L W Pfannenstiel S S K Lam L A Emens E M Jaffeeand T D Armstrong ldquoPaclitaxel enhances early dendritic cellmaturation and function through TLR4 signaling in micerdquoCellular Immunology vol 263 no 1 pp 79ndash87 2010
[61] N Klauber S Parangi E Flynn E Hamel and R J DrsquoAmatoldquoInhibition of angiogenesis and breast cancer in mice by themicrotubule inhibitors 2-methoxyestradiol and Taxolrdquo CancerResearch vol 57 no 1 pp 81ndash86 1997
[62] D Belotti V Vergani T Drudis et al ldquoThe microtubule-affecting drug paclitaxel has antiangiogenic activityrdquo ClinicalCancer Research vol 2 no 11 pp 1843ndash1849 1996
[63] D H Lau L Xue L J Young P A Burke and A T CheungldquoPaclitaxel (Taxol) an inhibitor of angiogenesis in a highlyvascularized transgenic breast cancerrdquo Cancer Biotherapy andRadiopharmaceuticals vol 14 no 1 pp 31ndash36 1999
[64] X Jiang ldquoHarnessing the immune system for the treatment ofbreast cancerrdquo Journal of Zhejiang University Science B vol 15no 1 pp 1ndash15 2014
[65] A Gadducci D Katsaros P Zola et al ldquoWeekly low-dosepaclitaxel as maintenance treatment in patients with advancedovarian cancer who had microscopic residual disease atsecond-look surgery after 6 cycles of paclitaxelplatinum-basedchemotherapy Results of an open noncomparative phase 2
multicenter italian study (after-6 protocol 2)rdquo InternationalJournal of Gynecological Cancer vol 19 no 4 pp 615ndash619 2009
[66] R S Bhatt J Merchan R Parker et al ldquoA phase 2 pilot trial oflow-dose continuous infusion or lsquometronomicrsquo paclitaxel andoral celecoxib in patients with metastatic melanomardquo Cancervol 116 no 7 pp 1751ndash1756 2010
[67] M Caballero J J Grau J L Blanch et al ldquoSerum vascularendothelial growth factor as a predictive factor in metronomic(weekly) paclitaxel treatment for advanced head and neckcancerrdquo Archives of OtolaryngologymdashHead and Neck Surgeryvol 133 no 11 pp 1143ndash1148 2007
[68] J Alexandre Y Hu W Lu H Pelicano and P Huang ldquoNovelaction of paclitaxel against cancer cells bystander effect medi-ated by reactive oxygen speciesrdquo Cancer Research vol 67 no 8pp 3512ndash3517 2007
[69] T Hadzic N Aykin-Burns Y Zhu et al ldquoPaclitaxel combinedwith inhibitors of glucose and hydroperoxide metabolismenhances breast cancer cell killing viaH
2O2-mediated oxidative
stressrdquo Free Radical Biology and Medicine vol 48 no 8 pp1024ndash1033 2010
[70] C A Sherman-Baust K G Becker W H Wood III Y Zhangand P J Morin ldquoGene expression and pathway analysis of ovar-ian cancer cells selected for resistance to cisplatin paclitaxel ordoxorubicinrdquo Journal of Ovarian Research vol 4 no 1 article21 2011
[71] R Agarwal and S B Kaye ldquoOvarian cancer strategies for over-coming resistance to chemotherapyrdquo Nature Reviews Cancervol 3 no 7 pp 502ndash516 2003
[72] T Acker and K H Plate ldquoRole of hypoxia in tumorangiogenesismdashmolecular and cellular angiogenic crosstalkrdquoCell and Tissue Research vol 314 no 1 pp 145ndash155 2003
[73] M Hockel and P Vaupel ldquoBiological consequences of tumorhypoxiardquo Seminars in Oncology vol 28 supplement 8 no 2 pp36ndash41 2001
[74] L Huang Q-H Zhang Q-L Ao H Xing Y-P Lu and DMa ldquoEffect of hypoxia on the chemotherapeutic sensitivity ofhuman ovarian cancer cells to paclitaxel and its mechanismrdquoZhonghua Zhong Liu Za Zhi vol 29 no 2 pp 96ndash100 2007
[75] N Rohwer and T Cramer ldquoHypoxia-mediated drug resistancenovel insights on the functional interaction of HIFs and celldeath pathwaysrdquoDrug Resistance Updates vol 14 no 3 pp 191ndash201 2011
[76] B B Aggarwal R V Vijayalekshmi and B Sung ldquoTargetinginflammatory pathways for prevention and therapy of cancershort-term friend long-term foerdquo Clinical Cancer Research vol15 no 2 pp 425ndash430 2009
[77] Z Duan R Foster D A Bell et al ldquoSignal transducersand activators of transcription 3 pathway activation in drug-resistant ovarian cancerrdquo Clinical Cancer Research vol 12 no17 pp 5055ndash5063 2006
[78] H-J Kuh S H Jang M G Wientjes J R Weaver and J L-SAu ldquoDeterminants of paclitaxel penetration and accumulationin human solid tumorrdquo Journal of Pharmacology and Experi-mental Therapeutics vol 290 no 2 pp 871ndash880 1999
[79] S Arao H Suwa M Mandai et al ldquoHypoxia-mediated drugresistance novel insights on the functional interaction of HIFsand cell death pathwaysrdquo Cancer Research vol 54 no 5 pp1355ndash1359 1994
[80] S E Johnatty J Beesley B Gao et al ldquoABCB1 (MDR1)polymorphisms and ovarian cancer progression and survivala comprehensive analysis from the Ovarian Cancer Association
BioMed Research International 19
Consortium and the Cancer GenomeAtlasrdquoGynecologic Oncol-ogy vol 131 no 1 pp 8ndash14 2013
[81] X Yang A K Iyer A Singh et al ldquoCluster of differentiation44 targeted hyaluronic acid based nanoparticles for MDR1siRNA delivery to overcome drug resistance in ovarian cancerrdquoPharmaceutical Research 2014
[82] D A Zajchowski B Y Karlan and L K Shawver ldquoTreatment-related protein biomarker expression differs between primaryand recurrent ovarian carcinomasrdquoMolecular CancerTherapeu-tics vol 11 no 2 pp 492ndash502 2012
[83] MM Gottesman J Ludwig D Xia and G Szakacs ldquoDefeatingdrug resistance in cancerrdquoDiscovery Medicine vol 6 no 31 pp18ndash23 2006
[84] S Mozzetti C Ferlini P Concolino et al ldquoClass III 120573-tubulin overexpression is a prominent mechanism of paclitaxelresistance in ovarian cancer patientsrdquo Clinical Cancer Researchvol 11 no 1 pp 298ndash305 2005
[85] M Kavallaris D Y S Kuo C A Burkhart et al ldquoTaxol-resistant epithelial ovarian tumors are associated with alteredexpression of specific beta-tubulin isotypesrdquo Journal of ClinicalInvestigation vol 100 no 5 pp 1282ndash1293 1997
[86] G A Orr P Verdier-Pinard H McDaid and S B HorwitzldquoMechanisms of Taxol resistance related to microtubulesrdquoOncogene vol 22 no 47 pp 7280ndash7295 2003
[87] C Ferlini L Cicchillitti G Raspaglio et al ldquoPaclitaxel directlybinds to Bcl-2 and functionally mimics activity of Nur77rdquoCancer Research vol 69 no 17 pp 6906ndash6914 2009
[88] E Mechetner A Kyshtoobayeva S Zonis et al ldquoLevels ofmultidrug resistance (MDR1) P-glycoprotein expression byhuman breast cancer correlate with in vitro resistance to taxoland doxorubicinrdquo Clinical Cancer Research vol 4 no 2 pp389ndash398 1998
[89] J S Lagas C W N Damen R A B VanWaterschoot D IusufJ H Beijnen and A H Schinkel ldquoP-glycoprotein multidrug-resistance associated protein 2 Cyp3a and carboxylesteraseaffect the oral availability and metabolism of vinorelbinerdquoMolecular Pharmacology vol 82 no 4 pp 636ndash644 2012
[90] M T Huizing J B Vermorken H Rosing et al ldquoPharmacoki-netics of paclitaxel and three major metabolites in patients withadvanced breast carcinoma refractory to anthracycline therapytreated with a 3-hour paclitaxel infusion a European CancerCentre (ECC) trialrdquo Annals of Oncology vol 6 no 7 pp 699ndash704 1995
[91] R Panchagnula ldquoPharmaceutical aspects of paclitaxelrdquo Interna-tional Journal of Pharmaceutics vol 172 no 1-2 pp 1ndash15 1998
[92] S H Jang M G Wientjes and J L-S Au ldquoDeterminants ofpaclitaxel uptake accumulation and retention in solid tumorsrdquoInvestigational New Drugs vol 19 no 2 pp 113ndash123 2001
[93] D S Sonnichsen andM V Relling ldquoClinical pharmacokineticsof paclitaxelrdquo Clinical Pharmacokinetics vol 27 no 4 pp 256ndash269 1994
[94] T Ohtsu Y Sasaki T Tamura et al ldquoClinical pharmacokineticsand pharmacodynamics of paclitaxel a 3-hour infusion versusa 24-hour infusionrdquo Clinical Cancer Research vol 1 no 6 pp599ndash606 1995
[95] M Czejka J Schueller H Schnait B Springer and I EderldquoClinical pharmacokinetics andmetabolism of paclitaxel after athree-hour infusion comparison of two preparationsrdquo Journalof Oncology Pharmacy Practice vol 9 no 4 pp 129ndash136 2003
[96] J Rizzo C Riley D VonHoff J Kuhn J Phillips and T BrownldquoAnalysis of anticancer drugs in biological fluids determination
of taxol with application to clinical pharmacokineticsrdquo Journalof Pharmaceutical and Biomedical Analysis vol 8 no 2 pp 159ndash164 1990
[97] V A de Weger J H Beijnen and J H M Schellens ldquoCel-lular and clinical pharmacology of the taxanes docetaxel andpaclitaxelmdasha reviewrdquoAnti-Cancer Drugs vol 25 no 5 pp 488ndash494 2014
[98] S Kumar H Mahdi C Bryant J P Shah G Garg andA Munkarah ldquoClinical trials and progress with paclitaxel inovarian cancerrdquo International Journal of Womenrsquos Health vol 2no 1 pp 411ndash427 2010
[99] B Huang J Zhao J C Unkeless Z H Feng and H XiongldquoTLR signaling by tumor and immune cells a double-edgedswordrdquo Oncogene vol 27 no 2 pp 218ndash224 2008
[100] R A Jibodh J S Lagas B Nuijen J H Beijnen and J HM Schellens ldquoTaxanes old drugs new oral formulationsrdquoEuropean Journal of Pharmacology vol 717 no 1ndash3 pp 40ndash462013
[101] A Javeed M Ashraf A Riaz A Ghafoor S Afzal and M MMukhtar ldquoPaclitaxel and immune systemrdquo European Journal ofPharmaceutical Sciences vol 38 no 4 pp 283ndash290 2009
[102] L Bracci G Schiavoni A Sistigu and F Belardelli ldquoImmune-based mechanisms of cytotoxic chemotherapy implications forthe design of novel and rationale-based combined treatmentsagainst cancerrdquo Cell Death and Differentiation vol 21 no 1 pp15ndash25 2014
[103] C A Byrd-Leifer E F Block K Takeda S Akira and A DingldquoThe role of MyD88 and TLR4 in the LPS-mimetic activity ofTaxolrdquo European Journal of Immunology vol 31 no 8 pp 2448ndash2457 2001
[104] A-C Wang Y-B Ma F-X Wu et al ldquoTLR4 induces tumorgrowth and inhibits paclitaxel activity in MyD88-positivehuman ovarian carcinoma in vitrordquo Oncology Letters vol 7 no3 pp 871ndash877 2014
[105] Y Zhu N Liu S D Xiong Y J Zheng and Y W ChuldquoCD4+Foxp3+ regulatory T-cell impairment by paclitaxel isindependent of toll-like receptor 4rdquo Scandinavian Journal ofImmunology vol 73 no 4 pp 301ndash308 2011
[106] M Kubo T Morisaki K Matsumoto et al ldquoPaclitaxel probablyenhances cytotoxicity of natural killer cells against breastcarcinoma cells by increasing perforin productionrdquo CancerImmunology Immunotherapy vol 54 no 5 pp 468ndash476 2005
[107] L Markasz G Stuber B Vanherberghen et al ldquoEffect of fre-quently used chemotherapeutic drugs on the cytotoxic activityof human natural killer cellsrdquo Molecular Cancer Therapeuticsvol 6 no 2 pp 644ndash654 2007
[108] T Sako N Burioka K Yasuda et al ldquoCellular immune profile inpatients with non-small cell lung cancer after weekly paclitaxeltherapyrdquo Acta Oncologica vol 43 no 1 pp 15ndash19 2004
[109] R Kaneno G V Shurin I L Tourkova and M R ShurinldquoChemomodulation of human dendritic cell function by anti-neoplastic agents in low noncytotoxic concentrationsrdquo Journalof Translational Medicine vol 7 article 58 2009
[110] TMichels G V ShurinHNaiditch A Sevko VUmansky andM R Shurin ldquoPaclitaxel promotes differentiation of myeloid-derived suppressor cells into dendritic cells in vitro in a TLR4-independent mannerrdquo Journal of Immunotoxicology vol 9 no3 pp 292ndash300 2012
[111] R A Kemp and F Ronchese ldquoTumor-specific Tc1 but not Tc2cells deliver protective antitumor immunityrdquo The Journal ofImmunology vol 167 no 11 pp 6497ndash6502 2001
20 BioMed Research International
[112] A Y Rudensky ldquoRegulatory T cells and Foxp3rdquo ImmunologicalReviews vol 241 no 1 pp 260ndash268 2011
[113] EM Shevach ldquoCD4+CD25+ suppressor T cellsmore questionsthan answersrdquo Nature Reviews Immunology vol 2 no 6 pp389ndash400 2002
[114] S Sakaguchi T Yamaguchi T Nomura and M Ono ldquoRegu-latory T cells and immune tolerancerdquo Cell vol 133 no 5 pp775ndash787 2008
[115] H Nishikawa and S Sakaguchi ldquoRegulatory T cells in tumorimmunityrdquo International Journal of Cancer vol 127 no 4 pp759ndash767 2010
[116] W Zou ldquoRegulatory T cells tumour immunity and immuno-therapyrdquoNature Reviews Immunology vol 6 no 4 pp 295ndash3072006
[117] A Fialova S Partlova L Sojka et al ldquoDynamics of T-cell infil-tration during the course of ovarian cancer The gradual shiftfrom aTh17 effector cell response to a predominant infiltrationby regulatory T-cellsrdquo International Journal of Cancer vol 132no 5 pp 1070ndash1079 2013
[118] A E Albers R L Ferris G G Kim K Chikamatsu A BDeLeo and T L Whiteside ldquoImmune responses to p53 inpatients with cancer enrichment in tetramer+ p53 peptide-specific T cells and regulatory T cells at tumor sitesrdquo CancerImmunology Immunotherapy vol 54 no 11 pp 1072ndash10812005
[119] N Liu Y Zheng Y Zhu S Xiong andYChu ldquoSelective impair-ment of CD4 + CD25 + Foxp3 + regulatory T cells by paclitaxelis explained by Bcl-2Bax mediated apoptosisrdquo InternationalImmunopharmacology vol 11 no 2 pp 212ndash219 2011
[120] X Wu Q-M Feng Y Wang J Shi H-L Ge and W DildquoThe immunologic aspects in advanced ovarian cancer patientstreated with paclitaxel and carboplatin chemotherapyrdquo CancerImmunology Immunotherapy vol 59 no 2 pp 279ndash291 2010
[121] A P Vicari R Luu N Zhang et al ldquoPaclitaxel reducesregulatoryT cell numbers and inhibitory function and enhancesthe anti-tumor effects of the TLR9 agonist PF-3512676 in themouserdquo Cancer Immunology Immunotherapy vol 58 no 4 pp615ndash628 2009
[122] L Zhang K Dermawan M Jin et al ldquoDifferential impairmentof regulatory T cells rather than effector T cells by paclitaxel-based chemotherapyrdquo Clinical Immunology vol 129 no 2 pp219ndash229 2008
[123] Y Tabuchi J Matsuoka M Gunduz et al ldquoResistance topaclitaxel therapy is related with Bcl-2 expression through anestrogen receptor mediated pathway in breast cancerrdquo Interna-tional Journal of Oncology vol 34 no 2 pp 313ndash319 2009
[124] N Obermajer R Muthuswamy K Odunsi R P Edwards andP Kalinski ldquoPGE
2-induced CXCL12 production and CXCR4
expression controls the accumulation of human MDSCs inovarian cancer environmentrdquo Cancer Research vol 71 no 24pp 7463ndash7470 2011
[125] Q M Feng W Di and X Wu ldquoImmune reconstitution inadvanced ovarian cancer patients undergoing first line chemo-therapyrdquo Xi Bao Yu Fen Zi Mian Yi Xue Za Zhi vol 25 no 11pp 1023ndash1025 2009
[126] A D Seidman D Hochhauser M Gollub et al ldquoNinety-six-hour paclitaxel infusion after progression during short taxaneexposure a phase II pharmacokinetic and pharmacodynamicstudy in metastatic breast cancerrdquo Journal of Clinical Oncologyvol 14 no 6 pp 1877ndash1884 1996
[127] D R Spriggs M F Brady L Vaccarello et al ldquoPhase IIIrandomized trial of intravenous cisplatin plus a 24- or 96-hour
infusion of paclitaxel in epithelial ovarian cancer a gynecologiconcology group studyrdquo Journal of Clinical Oncology vol 25 no28 pp 4466ndash4471 2007
[128] G A Omura M F Brady K Y Look et al ldquoPhase III trial ofpaclitaxel at two dose levels the higher dose accompanied byfilgrastim at two dose levels in platinum-pretreated epithelialovarian cancer an intergroup studyrdquo Journal of Clinical Oncol-ogy vol 21 no 15 pp 2843ndash2848 2003
[129] R Simon and L Norton ldquoThe Norton-Simon hypothesisdesigning more effective and less toxic chemotherapeutic reg-imensrdquoNature Clinical Practice Oncology vol 3 no 8 pp 406ndash407 2006
[130] A Kumar P Hoskins and A Tinker ldquoDose-dense paclitaxel inadvanced ovarian cancerrdquo Clinical Oncology vol 27 no 1 pp40ndash47 2015
[131] P Marchetti S Urien G A Cappellini G Ronzino and CFicorella ldquoWeekly administration of paclitaxel theoretical andclinical basisrdquoCritical Reviews in OncologyHematology vol 44supplement pp S3ndashS13 2002
[132] P Francis E Rowinsky J Schneider T Hakes W Hoskinsand M Markman ldquoPhase I feasibility and pharmacologic studyof weekly intraperitoneal paclitaxel A Gynecologic OncologyGroup pilot studyrdquo Journal of Clinical Oncology vol 13 no 12pp 2961ndash2967 1995
[133] H Thomas and P Rosenberg ldquoRole of weekly paclitaxel inthe treatment of advanced ovarian cancerrdquo Critical Reviews inOncologyHematology vol 44 supplement pp S43ndashS51 2002
[134] M Markman J Markman K Webster et al ldquoDuration ofresponse to second-line platinum-based chemotherapy forovarian cancer implications for patient management and clini-cal trial designrdquo Journal of Clinical Oncology vol 22 no 15 pp3120ndash3125 2004
[135] P H OrsquoDonnell M Eileen Dolan E Gamazon et al ldquoPopu-lation differences in platinum toxicity as a means to identifynovel genetic susceptibility variantsrdquo Pharmacogenetics andGenomics vol 20 no 5 pp 327ndash337 2010
[136] M J Millward M J Boyer M Lehnert et al ldquoDocetaxel andcarboplatin is an active regimen in advanced non-small-celllung cancer a phase II study in Caucasian and Asian patientsrdquoAnnals of Oncology vol 14 no 3 pp 449ndash454 2003
[137] M Markman ldquoIntraperitoneal therapy of ovarian cancerrdquoOncologist vol 1 no 1-2 pp 18ndash21 1996
[138] M Markman and J L Walker ldquoIntraperitoneal chemotherapyof ovarian cancer a review with a focus on practical aspects oftreatmentrdquo Journal of Clinical Oncology vol 24 no 6 pp 988ndash994 2006
[139] K Fujiwara S Nagao E Aotani and K Hasegawa ldquoPrincipleand evolving role of intraperitoneal chemotherapy in ovariancancerrdquo Expert Opinion on Pharmacotherapy vol 14 no 13 pp1797ndash1806 2013
[140] M Markman E Rowinsky T Hakes et al ldquoPhase I trialof intraperitoneal taxol a gynecoloic oncology group studyrdquoJournal of Clinical Oncology vol 10 no 9 pp 1485ndash1491 1992
[141] M Markman M F Brady N M Spirtos P Hanjani and S CRubin ldquoPhase II trial of intraperitoneal paclitaxel in carcinomaof the ovary tube and peritoneum a gynecologic oncologygroup studyrdquo Journal of Clinical Oncology vol 16 no 8 pp2620ndash2624 1998
[142] P B Panici I Palaia M Graziano F Bellati N Manci and RAngioli ldquoIntraperitoneal paclitaxel as consolidation treatmentin ovarian cancer patients a case control studyrdquo Oncology vol78 no 1 pp 20ndash25 2010
BioMed Research International 21
[143] D K Armstrong B Bundy L Wenzel et al ldquoIntraperitonealcisplatin and paclitaxel in ovarian cancerrdquo The New EnglandJournal of Medicine vol 354 no 1 pp 34ndash43 2006
[144] D Tewari J Java and R Salani ldquoLong-term survival advantageof intraperitoneal chemotherapy treatment in advanced ovariancancer an analysis of a Gynecologic Oncology Group ancillarydata studyrdquo in Proceedings of the 2013 Society of GynecologicOncology Annual Meeting on Womenrsquos Cancer (GOG114172Abstract) Los Angeles Calif USA 2013
[145] D A Yardley ldquonab-paclitaxel mechanisms of action and deliv-eryrdquo Journal of Controlled Release vol 170 no 3 pp 365ndash3722013
[146] M Ando K Yonemori N Katsumata et al ldquoPhase I and phar-macokinetic study of nab-paclitaxel nanoparticle albumin-bound paclitaxel administeredweekly to Japanese patients withsolid tumors and metastatic breast cancerrdquo Cancer Chemother-apy and Pharmacology vol 69 no 2 pp 457ndash465 2012
[147] N Desai V Trieu Z Yao et al ldquoIncreased antitumor activityintratumor paclitaxel concentrations and endothelial cell trans-port of cremophor-free albumin-bound paclitaxel ABI-007compared with cremophor-based paclitaxelrdquo Clinical CancerResearch vol 12 no 4 pp 1317ndash1324 2006
[148] J A Yared and K H R Tkaczuk ldquoUpdate on taxane devel-opment new analogs and new formulationsrdquo Drug DesignDevelopment andTherapy vol 6 pp 371ndash384 2012
[149] M G Teneriello P C Tseng M Crozier et al ldquoPhase IIevaluation of nanoparticle albumin-bound paclitaxel in plati-num-sensitive patients with recurrent ovarian peritoneal orfallopian tube cancerrdquo Journal of Clinical Oncology vol 27 no9 pp 1426ndash1431 2009
[150] R L Coleman W E Brady D S McMeekin et al ldquoA phase IIevaluation of nanoparticle albumin-bound (nab) paclitaxel inthe treatment of recurrent or persistent platinum-resistant ovar-ian fallopian tube or primary peritoneal cancer a GynecologicOncology Group Studyrdquo Gynecologic Oncology vol 122 no 1pp 111ndash115 2011
[151] J W Singer ldquoPaclitaxel poliglumex (XYOTAX CT-2103) amacromolecular taxanerdquo Journal of Controlled Release vol 109no 1ndash3 pp 120ndash126 2005
[152] C Li D-F Yu R A Newman et al ldquoComplete regressionof well-established tumors using a novel water-soluble poly(L-glutamic acid)-paclitaxel conjugaterdquo Cancer Research vol 58no 11 pp 2404ndash2409 1998
[153] M Mita A Mita J Sarantopoulos et al ldquoPhase I study ofpaclitaxel poliglumex administered weekly for patients withadvanced solid malignanciesrdquo Cancer Chemotherapy and Phar-macology vol 64 no 2 pp 287ndash295 2009
[154] P Sabbatini M W Sill D OrsquoMalley L Adler and A ASecord ldquoA phase II trial of paclitaxel poliglumex in recurrentor persistent ovarian or primary peritoneal cancer (EOC) agynecologic oncology group studyrdquo Gynecologic Oncology vol111 no 3 pp 455ndash460 2008
[155] M O Bradley C S Swindell F H Anthony et al ldquoTumortargeting by conjugation of DHA to paclitaxelrdquo Journal ofControlled Release vol 74 no 1ndash3 pp 233ndash236 2001
[156] M O Bradley N L Webb F H Anthony et al ldquoTumortargeting by covalent conjugation of a natural fatty acid topaclitaxelrdquo Clinical Cancer Research vol 7 no 10 pp 3229ndash3238 2001
[157] A C Wolff R C Donehower M K Carducci et al ldquoPhaseI study of docosahexaenoic acid-paclitaxel a taxane-fatty acid
conjugate with a unique pharmacology and toxicity profilerdquoClinical Cancer Research vol 9 no 10 part 1 pp 3589ndash35972003
[158] A Sparreboom A C Wolff J Verweij et al ldquoDispositionof docosahexaenoic acid-paclitaxel a novel taxane in bloodin vitro and clinical pharmacokinetic studiesrdquo Clinical CancerResearch vol 9 no 1 pp 151ndash159 2003
[159] P M Fracasso J Picus J D Wildi et al ldquoPhase 1 and phar-macokinetic study of weekly docosahexaenoic acid-paclitaxelTaxoprexin in resistant solid tumor malignanciesrdquo CancerChemotherapy and Pharmacology vol 63 no 3 pp 451ndash4582009
[160] A Y Bedikian R C DeConti R Conry et al ldquoPhase 3 study ofdocosahexaenoic acid-paclitaxel versus dacarbazine in patientswith metastatic malignant melanomardquo Annals of Oncology vol22 no 4 pp 787ndash793 2011
[161] Y-N Wu S-L Wang Y-C Wang et al ldquoReversal effect ofdocosahexaenoic acid on taxol resistance in human ovarian car-cinoma A2780T cellsrdquo Obstetrics amp Gynecology InternationalJournal vol 1 no 3 Article ID 00018 2014
Submit your manuscripts athttpwwwhindawicom
PainResearch and TreatmentHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom
Volume 2014
ToxinsJournal of
VaccinesJournal of
Hindawi Publishing Corporation httpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
AntibioticsInternational Journal of
ToxicologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
StrokeResearch and TreatmentHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Drug DeliveryJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Advances in Pharmacological Sciences
Tropical MedicineJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Medicinal ChemistryInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
AddictionJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
Emergency Medicine InternationalHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Autoimmune Diseases
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Anesthesiology Research and Practice
ScientificaHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Pharmaceutics
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of

10 BioMed Research International
Table1Ph
ases
Iand
IIstu
dies
onintravenou
sdose-densep
aclitaxel
Stud
yRe
gimen
119899()
PI(m
)RR
()
CR(119899)
MedianPF
S(m
)Median
OS
(m)
Adversee
ffects
Com
ments
Paclitaxel
dose
(mgm
2 )Ca
rbop
latin
dose
(mgm
2 )Ph
aseIsinglea
gent
Lofflerre
tal1996
[11]
40ndash9
0week
1-hou
rinfusionfor
6weeks
5040
5NA
NA
(i)Hem
atologictoxicity-m
ild(ii)N
ograde3
or4
haem
atologicaltoxicity
neurologicalor
cardiotoxicityup
to90
mgm
2 wk
(iii)Nohypersensitivity
reactio
ns(patientsreceivedprem
edication)
(i)100
priorc
hemotherapy
(ii)M
ediando
seintensity
was
410m
gm
2 6w
k(range200
to540m
gm
2 6w
k)
Fenn
ellyetal
1997
[12]
40ndash100w
eek
1830
NA
NA
NA
(i)Nomucositiso
rgrade
III
neurop
athy
was
seen
(ii)A
lopeciao
ccurredin
one
(i)100
priorc
hemotherapy
(2ndash5
priorregim
ens)
(ii)P
artia
lrespo
nses
weres
eenin
four
of13
assessablepatients
(30
)(iii)Dose-lim
iting
toxicitywas
reachedat100m
gm
2 (iv
)2-3
patie
ntse
xperience
treatmentd
elay
(v)M
axim
um-to
lerateddo
seof
80mgm
2 Ab
u-Ru
stum
etal
1997
[13]
60ndash100
over
1ho
urw
eek
45289
NA
NA
NA
(i)Nopatie
nthadfebrile
neutropenia
(i)100
priorc
hemotherapy
(1ndash8
priorregim
ens)
PhaseIISing
leagent
Markm
anetal
2001
[14]
80over
1ho
urw
eek
53(52)
25NA
NA
NA
Therapydiscon
tinuedin
(i)4patie
ntsw
hohadperip
heral
neurop
athy
(ii)1
patie
ntdu
etopainful
fingernailbeds
(i)100
platinum
andpaclita
xel
resistant
(ii)Th
erapywas
discon
tinuedin
5patie
ntsb
ecause
oftoxicity
(iii)Only13
(1)w
erem
odified
(doser
eductio
nor
treatment
delay)
becauseo
fsidee
ffects
PhaseIICom
binedwith
platinum
agent
Kiku
chietal
2005
[15]
80over
1ho
urw
eek
AUC2week
27gt6
818
483
NA
(i)Neutro
penia(
17)
thrombo
cytopenia(
51
)(ii)N
ocaseso
fperipheral
neurop
athy
(grades3
and4)
inweeklycombinedT-C
Cadron
etal2007
[16]
90over
1ho
urw
eek
AUC4week
24 9gt6le6
73 38NR
8105
675
(i)Grade
34neutropenia(
34)
andneutropenicfever
in2
(ii)N
auseaa
ndvomiting
and
fatig
uewerethe
mostfrequ
ent
nonh
ematologicalsid
eeffects
(i)Doser
eductio
nwas
necessary
in25of
patie
nts
Pign
atae
tal2008
[17]
60over
1ho
urw
eek
AUC2week
24(13)lowastlowast
1stline
385
2320
136
(i)Notoxicd
eath
was
recorded
(ii)G
rade
2anaemiawas
repo
rted
insevenpatie
nts(27)
(iii)Nofebrile
neutropeniaw
asob
served
(iv)G
rade
3and4neutropenia
was
recorded
infive(19)a
ndon
e(4
)patients
(v)G
rade
3thrombo
cytopenia
occurred
inon
epatient
(4)
BioMed Research International 11
Table1Con
tinued
Stud
yRe
gimen
119899()
PI(m
)RR
()
CR(119899)
MedianPF
S(m
)Median
OS
(m)
Adversee
ffects
Com
ments
Paclitaxel
dose
(mgm
2 )Ca
rbop
latin
dose
(mgm
2 )
Safrae
tal2014
[18]
80over
1ho
urw
eek
AUC2week
133
1stline
864
645
274
(i)Highera
naem
ia(grade
III+
IV68vs53)+
IVneutropenia(
144vs69)
decreasedgradeIIa
lopecia(
235
vs981
)and
thrombo
cytopenia
(grade
III+
IV0
vs23)
Havrilesky
etal
2003
[19]
80over
1ho
urw
eek
AUC2weekD1
D8D15
until
progressionCR
+8courses
29 21 8
Total
grou
pgt6lt6
83 100
38
16 15 1114
115
137
32
(i)Hem
atologictoxicitywas
common
(grade
3neutropenia
32n
ograde4
neutropenia
grade3
or4thrombo
cytopenia
142)
(i)To
xicitymanaged
bytre
atment
delaydo
seredu
ctionof
paclitaxel
ordiscon
tinuatio
nof
carbop
latin
vanderB
urgetal
2014
[20]
90over
1ho
urw
eek
AUC4weekD1
D8D15
D29
D36
D49
+6x
TCq3w
108
65 43
Total
grou
pgt6lt6
76 5816 42
26 158 13
(i)Neutro
penia3
0
thrombo
cytopenia8
febrile
neutropenia0
5
(ii)N
onhaem
atologictoxicitywas
low
(i)Treatm
entw
asdelayedin
16
anddo
seredu
cedin
2of
cycle
s
119899num
bero
fpatientsassessableforrespo
nsemm
onthsPIplatinum
treatmentfreeintervalRR
respo
nser
ateCR
com
pleterem
issionT
paclitaxelC
carbop
latin
PFS
progressio
nfre
esurvivalOSoverall
survivalN
An
otavailableinpapero
rabstractandNR
notyetreached
lowastlowastElderly
popu
lation
patient
agedge70
years
12 BioMed Research International
Numerous phase II studies have explored the tolerabilityand the activity of weekly paclitaxel either as a single agent orin combination with several other drugs or biological agents(Table 1) A number of regimens combining weekly paclitaxelwith carboplatin have been used as first-line treatment inovarian cancer Carboplatin has been administered weeklyat AUC of 2 with dose escalation in some studies whilepaclitaxel had been infused at 60ndash80mgm2week Thiscombined regimen was well tolerated with a low incidence ofbone marrow suppression Overall response rates have beenhigh in the range of 60ndash80 in most studies even in heavilypretreated patients with platinum-resistant disease (diseaserecurrence or progression within 6 months of the last lineof platinum-based therapy) [15ndash20 134] The promising datafrom these phase II trials then led to the evolution of largerphase III trials
Three phase III studies Japanese Gynecologic OncologyGroup- (JGOG-) Trial 3016 [21ndash23] Multicentre Italian Trialin Ovarian Cancer-Trial 7 (MITO-7) [25] and GynecologicOncology Group GOG-262 Trial [24] have explored dosedense therapy The results of these trials are summarised inTable 2
The Japanese Gynecologic Oncology Group (JGOG)conducted a randomized phase 3 trial of dose-dense weeklypaclitaxel 80mgm2week in combination with 3-weeklycarboplatin compared to standard 3-weekly carboplatin andpaclitaxel 180mgm2 in patients with advanced epithelialovarian peritoneal or fallopian tube cancer (JGOG 3016NOVEL trial) In both arms carboplatin was given at AUC6 and the median number of cycles was six In this largestudy (119899 = 637) with a median follow up of 77 months therewas an 11-month improvement in themedian progression freesurvival (PFS) in the dose-dense treatment group comparedwith the standard treatment arm (282 versus 175 monthsHR 076 95 CI 062ndash091 119901 = 00037) Median OS wasalso higher in the dose-dense treatment arm (1005 versus622 months HR 079 95 CI 063ndash099 119901 = 0039)On subgroup analysis suboptimally debulked patients withresidual disease of gt1 cm (119899 = 342) had a significantlyhigher median overall survival in the dose dense arm (512versus 335 months HR-075 95 CI 057ndash097 119901 = 0027)There was no significant advantage to dose-dense treatmentfor patients with optimally cytoreduced disease Dose-densetherapy survival benefits were also not seen in patients withclear cell or mucinous histology type unlike serous typeHowever patient treated with dose dense therapy had asignificantly higher frequency of hematologic toxicity thanwith the standard arm (212 versus 94) which resultedin lower treatment completion rates (63 versus 48) withfrequent episodes of delay (76 versus 67) and dosereductions (48versus 35) [21 22]Therewas no significantdifference in terms of overall quality of life between the twoarms (119901 = 046) [23]
Using a similar regimen as in JGOG-3016 a GynecologicOncology Group (GOG)-262 Trial was conducted in theUnited States In this group most patients had stage IIIdisease (66ndash70) and two-thirds had suboptimal debulkingwith residual disease of gt1 cm This was a randomized phase
III trial of 3 weekly paclitaxel versus dose-dense weeklypaclitaxel in combination with carboplatin in patients withadvanced epithelial ovarian peritoneal or fallopian tubecancer Though optional concurrent and maintenance beva-cizumab were received by the majority of patients in botharms (835 versus 841 resp) There was no significantdifference in PFS in the patients who received the dosedense paclitaxelcarboplatin regimen compared to those whoreceived the standard paclitaxelcarboplatin regimen (148versus 143 months HR 097 95 CI 079ndash118) Howeverin a subgroup analysis there was a significant difference inPFS in the dose dense paclitaxel arm who did not receivebevacizumab 119899 = 112 (142 versus 103 months HR 059 95CI 037ndash096 119901 = 0003) Overall survival data is still imma-ture There was higher frequency of grade 3 anaemia (408versus 157 119901 lt 0001) and grade 2 sensory neuropathy(259 versus 178 119901 = 0012) but a lower incidence ofneutropenia (72 versus 83 119901 lt 0001) [24]
In 2008 the Multicentre Italian Trials in Ovarian Cancer(MITO-7) randomised 810 women in a phase 3 trial toreceive either standard carboplatin (AUC = 6) and paclitaxel175mgm2 every 3 weeks or a weekly schedule of paclitaxel(60mgm2) with carboplatin (AUC = 2) The majority ofpatients in both arms (83ndash90) received six cycles of therapyMost patients (58ndash63) had stage II1 disease 23 of themwere suboptimally debulked Median PFS did not differsignificantly (173 months and 183 months 119901 = 066)between the standard and dose-dense arms respectivelyThere was no significant difference in response rate betweenthe two arms nor the estimated 2-year overall survivalSubgroup analysis did not identify any subgroup that mayhave benefited from the dose-dense regimen Unlike theJGOG-3016 trial the incidence of grade 3-4 neutropenia wassignificantly lower in the dose-dense group compared to the3-weekly regimen (42 versus 50) A similar pattern wasseen for the incidence of febrile neutropenia (lt1 versus 3119901 = 002) thrombocytopenia (1 versus 7 119901 lt 0001)and other nonhaematological toxicities such as alopeciavomiting renal dysfunction and neuropathy Quality of lifewas reported to be significantly better in the dose-dense arm(119901 lt 00001) which was discordant with the JGOG-3016quality of life data [25]
In summary there was significant improvement inmedian PFS and overall survival in studies using paclitaxelat 80mgm2week dose-dense therapy [21 24] but withhigher haematological toxicity whereas MITO-7 [25] whichwas using paclitaxel at 60mgm2week was only equivalentlyeffective but less toxicThis does not conclude that the higherpaclitaxel dose is more clinically beneficial as there are manyother confounding factors in all three studies
In a multivariate analysis the JGOG-3016 study [21]reported that a lower dose intensity of paclitaxel (lt80) wasassociated with poorer overall survival (hazard ratio = 14295 confidence interval 112ndash181 119901 = 0004) however itmust be highlighted that the investigational arm carboplatinschedules were not standardised in these studies The JGOGand GOG trials delivered a 3-weekly carboplatin (AUC =6) arm whereas in the MITO-7 study the carboplatin was
BioMed Research International 13
Table2Ph
aseIIIstu
dies
onintravenou
sdose-densep
aclitaxel
Stud
yRe
gimen
119899
MedianPF
S(m
)
Median
OS
(m)
Adversee
ffects
Com
ments
Katsu
matae
tal2009
[21]
Katsu
matae
tal2013
[22]
Haranoetal2014
[23]
JGOG3016
631
(i)Haematologicaltoxicityhigh
erin
dose
dense-211versus
94
Lower
treatmentcom
pletionin
dose-dense
63versus
48
Frequent
episo
deso
fdelay
indo
se-dense
76versus
67
Doser
eductio
nsin
dose-dense
48versus
35
Nosig
nificantd
ifference
inoverallQ
OL
betweenbo
thgrou
ps(119901=046)
Paclitaxel80m
gm
2D18
15+carbop
latin
AUC63
weeklyversus
Paclitaxel180
mgm
2+
carbop
latin
AUC63
weekly
312
282
1005
Both
givenfor6
ndash9cycle
s319
175
622
Chan
etal2013
[24]
GOG-262
(i)Higherfrequ
ency
ofgrade3
anaemia
(408versus
157119901lt0001)
grade2
sensoryneurop
athy
(259versus
178
119901=0012)b
utlower
incidenceo
fneutropenia(
72versus
83119901lt0001)
Paclitaxel80m
gm
2D18
15+carbop
latin
AUC63
weeklyversus
Paclitaxel175
mgm
2+
carbop
latin
AUC63
weekly
346
148
NR
Both
givenfor6
cycle
s346
143
NR
Bevacizumab
given
optio
nally
112
(did
not
receive
bevazicumab)
142vs
103
Pign
atae
tal2014
[25]
MITO-7
810
(i)Lo
wer
incidenceo
fgrade
3-4
neutropenia(
42versus
50)febrile
neutropenia(lt1v
ersus3
119901=002)
thrombo
cytopenia(
1versus7
119901lt0001)andothern
onhaem
atological
toxicitie
ssuchas
alop
eciavom
iting
renald
ysfunctio
nandneurop
athy
Qualityof
lifeb
etterindo
sedensea
rm(119901lt00001)
Paclitaxel60m
gm
2 weekly+carbop
latin
AUC
2weeklyversus
Paclitaxel175
mgm
2+
carbop
latin
AUC63
weekly
406
404
183 173
77lowast
79lowast
119899num
bero
fpatientsmm
onthsDday
PFSprogressionfre
esurvivalOSoverallsurvivalNAnot
availableinpapero
rabstractandNR
notyetreached
lowastSurvivalrateat2years
14 BioMed Research International
dose-dense (AUC 2 weekly) Although it is possible that thedose scheduling for the platinum-based agent is not essentialfor a survival benefit as shown by previous studies usingdose-dense cisplatin direct cross-trial comparison cannot bemade Unlike paclitaxel carboplatin probably requires peakdose for optimal therapeutic benefit hence this may accountfor the inferior survival outcome in MITO-7 trial Anotherconfounding factor may be difference in ethnicity All threestudies used different ethnic populations and Asian patientsin JGOG-3016 appear to have better survival outcomes thanthe MITO-7 Western population Ethnicity with possibleunderlying genetic causes may be responsible for the variableresponses to chemotherapy across individuals [135] This wasexplored by Millward et al who studied 68 Caucasian andAsian lung cancer patients treated with a combination ofpaclitaxel and carboplatin and found that the incidence offebrile neutropenia was 50 of an initially treated cohortof Asians and when carboplatin was subsequently dosereduced in all Asian patients the overall incidence of febrileneutropenia was also reduced to 26 [136]
Although early clinical data from phase I and phaseII dose-dense paclitaxel trials in advanced ovarian cancerwere promising the results from phase III studies in havebeen inconsistent as a result of differences in paclitaxel dosecarboplatin AUC and schedule addition of bevacizumabas well as different ethnic populations The results of arecently completed randomised three arms GynaecologicCancer InterGroup (GCIG) phase II trial ICON 8 mayfurther inform the clinical benefit of dose dense paclitaxeltherapy
This multicentre trial involving 111 centres in the UKSouth Korea Mexico Ireland Australia and New Zealandwith a target population of 1485 patients with stage IC-IV epithelial ovarian cancer or peritoneal or fallopian tubecancer compared two dose-dense arms (i) JGOG-like armcarboplatin AUC 5 plus weekly 80mgm2 paclitaxel and (ii)MITO-7-like arm weekly carboplatin AUC 167 plus weekly80mgm2 paclitaxel to the standard 3-weekly treatment(carboplatin AUC 5 plus 175mgm2 paclitaxel) for stage IC toIV epithelial ovarian cancer The dose-dense arms of MITO-7 and JGOG-3016 as well as the ethnic heterogeneity will befurther addressed
10 Intraperitoneal (IP) Chemotherapy
In addition to dose and scheduling the route of adminis-tration of chemotherapy agents plays an important role inoutcome Intraperitoneal spread is common and likely anearly event in epithelial ovarian cancer hence the deliveryof chemotherapy intraperitoneally in theory would exposethe microcirculation of tumour to higher doses of drug thansystemic administration while limiting systemic toxicityTheideal drug for IP chemotherapy is one that is systemicallyeffective penetrates deep into the inner core of tumour tissueand remains within the peritoneal cavity for a prolongedperiod of time [137ndash139]
Early clinical studies confirmed that indeed the peritonealcavity could be exposed to 10 to 20-fold higher (cisplatin
and carboplatin) drug concentration than when using theintravenous approach and since 1978 this route had beenadopted as a form of therapeutic intervention [137 139]A subsequent phase I trial showed that IP paclitaxel haddose-limiting toxicity in the form of abdominal pain [140]Another phase 1 GOG pilot study administered weekly IPpaclitaxel at an initial dose of 20mgm2 for 16 weeks to33 patients and found that IP paclitaxel at this dose wasfeasible and well tolerated At dose levels 60 to 65mgm2there were significant levels of paclitaxel for a week afterdrug administration suggesting very slow clearance andcontinuous exposure of the peritoneal cavity to active drugconcentrations [132]
Hence this initiated a phase II study [141] that used pacli-taxel intraperitoneally at a dose of 60ndash65mgm2week In thisphase II GOG study 76 patients with small-volume resid-ual disease carcinoma (05 cm or less) involving the ovaryperitoneal or fallopian tube were treated with paclitaxel60mgm2week intraperitoneally for 16 weeks followed bysurgical evaluation in patients without disease progressionThe Gynaecologic Oncology group (GOG) currently definesno visible disease as microscopic disease being the idealsurgical outcome 75 of patients had received prior systemictherapy and 70 received all 16 courses that were planned Of28 patients with microscopic disease at the start of therapy61 achieved a surgically defined complete response whereasonly 1 out of 31 patients with macroscopic disease achieved acomplete response The median time-to-recurrence was 167months with an estimated survival rate at 2 years being 58Treatment was generally well tolerated [141]
Another study looked into the effect of IP paclitaxel asconsolidation therapy in advanced ovarian cancer Twenty-eight patients who had initial residual macroscopic disease(lt1 cm) after primary surgery or interval debulking but hadcomplete pathological response following standard treatmentwith at least 6 cycles of platinum-based chemotherapy regi-men received paclitaxel 60mgm2week intraperitoneally for12ndash16 weeks as consolidation therapy The median time torecurrence was 25 months but overall survival did not differsignificantly when compared with control group submittedto observation only Treatment-related toxicity was mild andtechnical difficulties were observed in 11 of patients [142]
Multicenter randomised phase 3 trials as well as meta-analysis of IP chemotherapy have been performed anddemonstrated that chemotherapy drugs administered intra-peritoneally are superior to intravenous standard regimensin patient with optimally debulked epithelial ovarian cancerThe most impressive data comes from GOG 114 [14] and172 trial [143] In GOG 114 patients received either sixcycles of intravenous paclitaxel 135mgm2 and cisplatin75mgm2 every 3 weeks or intravenous carboplatin (AUC= 9) every 28 days for two cycles followed by six 3-weeklycycles of intravenous paclitaxel 135mgm2 and IP cisplatin100mgm2 [14] whereas in GOG 172 patients received eitherintravenous paclitaxel 135mgm2 followed by intravenouscisplatin 75mgm2 or intravenous paclitaxel 135mgm2 fol-lowed by IP combination of cisplatin 100mgm2 and pacli-taxel 60mgm2 on day 8 Both trials had a combined total
BioMed Research International 15
of 876 women with stage III epithelial ovarian carcinomaoptimally debulked to le1 cm residual tumour [143] Themedian follow-up for GOG 114 [14] was 138 years with GOG172 [143] was 97 years The primary results of the individualtrials reported up to 6-month improvement in median PFSfollowing IP therapy In the combined analysis of the datafrom both trials the data continued to show a 5-monthdifference in favour of IP therapy (25 versus 20 months)which translates into 16 reduction in the hazard ratio forprogression (119901 = 003) In GOG 114 [14] reported in 2001there was only borderline improvement in overall survivalassociated with this regimen (median 63 versus 52 monthsrelative risk 081 119901 = 005)
However in combined analysis in 2013 which was pre-sented at the Society of Gynecologic Oncology AnnualMeeting [144] the overall survival showed an 11-monthimprovement in favour of IP therapy in GOG 114 whereasGOG 172 reported a 16-month survival advantage Amongpatients treated with IP therapy the 5-year survival rateincreased from 18 following completion of 1-2 cycles to 59for patients who completed 5-6 cycles of treatment Howeverthere was increased toxicity observed in the IP arm grade 3-4 leukopenia thrombocytopenia and abdominal pain Only42 of patients in the GOG172 trial [143] completed all sixcycles of planned treatment in the IP arm while 18 ofpatients in GOG 114 trial [14] received fewer than two coursesof IP chemotherapy
Another randomised phase III trial involving patientswith stages II-III epithelial ovarian carcinoma is the GOG252 study with three arms Arm 1-dose-dense intravenouscarboplatin and paclitaxel Arm 2-dose-dense intravenouspaclitaxel and IP carboplatin and Arm 3 consists of 3-weeklyintravenous paclitaxel (day 1) followed by IP cisplatin (day 2)and IP paclitaxel (day 3) regimen All three arms also incor-porate the combination and maintenance of bevacizumabGOG 252 has completed accrual and results are awaited [139]
11 Newer Forms of Paclitaxel
Development of next-generation taxanes has taken place overthe past 40 years aimed at eliminating toxicity improvingefficacy and ease of administration Abraxane is a novelcompound which incorporates paclitaxel into an albuminnanoparticle soluble in saline hence eliminating the needfor Cremophor EL which is responsible for hypersensitivityreactions experienced during paclitaxel infusion [145] Thenanoparticle albumin in nab-paclitaxel is able to bind toglycoprotein gp60 receptor an albumin receptor and activatecaveolin-1 a protein that in human is encoded byCAV-1 geneleading to formation of caveoli hence allowing nab-paclitaxelto migrate across the endothelial cell membrane into theinterstitial space leading to higher intratumoural drug con-centration In addition Abraxane exhibits linear pharma-cokinetics and can therefore be given at a relatively higherdose than standard intravenous paclitaxel leading to a highertherapeutic ratio and heightened efficacy in solid tumoursmainlymetastatic breast cancer [146 147] Nab-paclitaxel hadFDA approval in 2005 for treatment of breast cancer [148]
Nab-paclitaxel has been studied in recurrent ovariancancer As a single agent in phase II 44 patients withrecurrent ovarian cancer were treated with Nab-paclitaxel260mgm2 intravenously for 30 minutes every 3 weeks for6 cycles Ninety-two percent of patients were platinum-sensitive while 89 had had previous exposure to standardtaxane The objective response rate was 64 with 15 patientsachieving complete response and 13 of them had partialresponse Estimated median PFS was 85 months No hyper-sensitivity reactions were observed and there were infrequentcases of grade 4 neutropenia (11) and grade 2-3 neuropathy(13) [149]
Another phase II study by GOG enrolled 51 patients withplatinum- and taxane-resistant recurrent ovarian cancer outof which 47 were evaluable The objective response rate was38 with one patient achieving a complete response and 10patients a partial response The median PFS was 45 monthswhile overall survival rate was 174 months Severe haema-tological and nonhaematological toxicities including neuro-toxicity were uncommon These results are quite impressivegiven the treatment population consisted of patients withvery poor prognosis with a median platinum and taxane freeinterval of 21 days and 70 had their recurrence within 3months of completion of primary treatment [150] Severalother trials of this formulation are in progress
Paclitaxel poliglumex (PPX) also known as Xyotax isanother prodrug a novel conjugate of paclitaxel and 120572-poly-L-glutamic acid which accumulates within tumour tissuedue to increased permeability of the tumour vessels and lackof lymphatic drainage [148 151 152] Paclitaxel poliglumexenhances solubility of paclitaxel allows direct delivery tothe intratumoural microenvironment and allows prolongedexposure to the active drug while minimising systemictoxicities [151] In Phase I dose escalation studies as a singleagent the recommended dose of PPX was 235mgm2 over 10minutes every 3 weeks or 70mgm2 weekly [153] In a PhaseII GOG study of relapsed ovarian cancer a response rate of16 was seen with infrequent serious adverse events grade3 and 4 neutropenia (24 and 20) and grade 3 neuropathy(24) [154] A phase III trial (GOG-0212) on the use of PPXas consolidation ormaintenance therapy in advanced ovariancancer is in progress
DHA-paclitaxel also known as Taxoprexin is a prodrugwhere paclitaxel is covalently conjugated with the naturallyoccurring omega-3 fatty acid docosahexaenoic acid (DHA)a fatty acid that is easily taken up by tumour cells henceincreasing intratumoural concentration of paclitaxel leadingtumour cell apoptosis [155 156] DHA-paclitaxel exhibitslinear pharmacokinetics and lower toxicity and also ease ofadministration when compared to conventional paclitaxeland has demonstrated antineoplastic activity in animal mod-els of cancer as well as in a phase III trial involving metastaticmelanoma [156ndash160] In a recent study on human ovariancancer cells it was found that DHA could reverse paclitaxelresistance by inhibiting P-gp as well as downregulatingthe expression of multidrug resistance associated proteins(MRP) and inhibiting the activity of NF-120581B and p38 MAPKsignalling pathways [161]
16 BioMed Research International
12 Future Directions
A plateau has been reached regarding the benefits associatedwith standard 3-weekly intravenous administration of cyto-toxic chemotherapy in advanced epithelial ovarian cancerThe ongoing battle for a better treatment regimen to delayrelapse promote remission and most importantly improvethe quality of life of patients with advanced epithelial ovariancancer need not to go further than the ability to relook at thechemotherapy agents that are already available in a differentapproach
Novel compounds to date have not yet shown clinicalsuperiority and parent compounds such as paclitaxel con-tinue to surprise us with their feasibility effectiveness andmanageable toxicity profiles Intraperitoneal paclitaxel willrequire further evaluation Better effort in understanding themechanism of action of drugs including the role of dosescheduling and the effect on the immune systemmay providea more cost-effective route to better clinical outcomes
Conflict of Interests
The authors declare no conflict of interests in this work
Acknowledgments
The authors would like to thank the many researchers whohave contributed to our current knowledge of paclitaxelNirmala Kampan is supported by Australian Monash Uni-versity Institute of Graduate Research Scholarship as wellas Universiti Kebangsaan Malaysia Postgraduate ScholarshipAward Mutsa Madondo has received Postgraduate Pub-lication Award from Monash University and MagdalenaPlebanski has been awarded Senior NHMRC Fellowship
References
[1] Australian Institute of Health and Welfare and National Breastand Ovarian Cancer Centre (Australia) Ovarian Cancer inAustralia AnOverview 2010 Cancer Series Australian Instituteof Health and Welfare Canberra Australia 2010
[2] R E Bristow R S Tomacruz D K Armstrong E L Trimbleand F J Montz ldquoSurvival effect of maximal cytoreductivesurgery for advanced ovarian carcinoma during the platinumera a meta-analysisrdquo Journal of Clinical Oncology vol 20 no 5pp 1248ndash1259 2002
[3] ZKempand JA Ledermann ldquoUpdate onfirst-line treatment ofadvanced ovarian carcinomardquo International Journal of WomenrsquosHealth vol 5 no 1 pp 45ndash51 2013
[4] A du Bois H-J Luck W Meier et al ldquoA randomized clinicaltrial of cisplatinpaclitaxel versus carboplatinpaclitaxel as first-line treatment of ovarian cancerrdquo Journal of the National CancerInstitute vol 95 no 17 pp 1320ndash1330 2003
[5] R F Ozols B N Bundy B E Greer et al ldquoPhase III trialof carboplatin and paclitaxel compared with cisplatin andpaclitaxel in patients with optimally resected stage III ovariancancer A Gynecologic Oncology Group studyrdquo Journal ofClinical Oncology vol 21 no 17 pp 3194ndash3200 2003
[6] W P McGuire W J Hoskins M F Brady et al ldquoCyclophos-phamide and cisplatin compared with paclitaxel and cisplatin
in patients with stage III and stage IV ovarian cancerrdquoThe NewEngland Journal of Medicine vol 334 no 1 pp 1ndash6 1996
[7] W P McGuire W J Hoskins M F Brady et al ldquoCyclophos-phamide and cisplatin versus paclitaxel and cisplatin a phase IIIrandomized trial in patients with suboptimal stage IIIIV ovar-ian cancer (from the gynecologic oncology group)rdquo Seminars inOncology vol 23 no 5 supplement 12 pp 40ndash47 1996
[8] M J Piccart K Bertelsen K James et al ldquoRandomized inter-group trial of cisplatin-paclitaxel versus cisplatin-cyclophosph-amide inwomenwith advanced epithelial ovarian cancer three-year resultsrdquo Journal of the National Cancer Institute vol 92 no9 pp 699ndash708 2000
[9] P A Vasey G C Jayson A Gordon et al ldquoPhase III random-ized trial of docetaxel-carboplatin versus paclitaxel-carboplatinas first-line chemotherpy for ovarian carcinomardquo Journal of theNational Cancer Institute vol 96 no 22 pp 1682ndash1691 2004
[10] B Gronlund C Hogdall H H Hansen and S A EngelholmldquoResults of reinduction therapy with paclitaxel and carboplatinin recurrent epithelial ovarian cancerrdquo Gynecologic Oncologyvol 83 no 1 pp 128ndash134 2001
[11] T M Loffler W Freund J Lipke and T-U HausamenldquoSchedule- and dose-intensified paclitaxel as weekly 1-hourinfusion in pretreated solid tumors results of a phase III trialrdquoSeminars in Oncology vol 23 no 6 supplement 16 pp 32ndash341996
[12] D Fennelly C Aghajanian F Shapiro et al ldquoPhase I and phar-macologic study of paclitaxel administered weekly in patientswith relapsed ovarian cancerrdquo Journal of Clinical Oncology vol15 no 1 pp 187ndash192 1997
[13] N R Abu-Rustum C Aghajanian R R Barakat D Fennelly FShapiro and D Spriggs ldquoSalvage weekly paclitaxel in recurrentovarian cancerrdquo Seminars inOncology vol 24 no 5 supplement15 pp S15-62ndashS15-67 1997
[14] M Markman B N Bundy D S Alberts et al ldquoPhase III trialof standard-dose intravenous cisplatin plus paclitaxel versusmoderately high-dose carboplatin followed by intravenouspaclitaxel and intraperitoneal cisplatin in small-volume stageIII ovarian carcinoma an intergroup study of the gynecologiconcology group Southwestern Oncology Group and EasternCooperativeOncologyGrouprdquo Journal of Clinical Oncology vol19 no 4 pp 1001ndash1007 2001
[15] A Kikuchi H Sakamoto and T Yamamoto ldquoWeekly car-boplatin and paclitaxel is safe active and well tolerated inrecurrent ovarian cancer cases of Japanese women previouslytreated with cisplatin-containing multidrug chemotherapyrdquoInternational Journal of Gynecological Cancer vol 15 no 1 pp45ndash49 2005
[16] I Cadron K Leunen F Amant T van Gorp P Nevenand I Vergote ldquoThe lsquoLeuvenrsquo dose-dense paclitaxelcarboplatinregimen in patients with recurrent ovarian cancerrdquo GynecologicOncology vol 106 no 2 pp 354ndash361 2007
[17] S Pignata E Breda G Scambia et al ldquoA phase II studyof weekly carboplatin and paclitaxel as first-line treatment ofelderly patients with advanced ovarian cancer A Multicen-tre Italian Trial in Ovarian cancer (MITO-5) studyrdquo CriticalReviews in OncologyHematology vol 66 no 3 pp 229ndash2362008
[18] T Safra S Shamai J Greenberg et al ldquoWeekly carboplatinwith paclitaxel compared to standard three-weekly treatment inadvanced epithelial ovarian carcinomamdasha retrospective studyrdquoGynecologic Oncology vol 132 no 1 pp 18ndash22 2014
BioMed Research International 17
[19] L J Havrilesky A A Alvarez R A Sayer et al ldquoWeekly low-dose carboplatin and paclitaxel in the treatment of recurrentovarian and peritoneal cancerrdquo Gynecologic Oncology vol 88no 1 pp 51ndash57 2003
[20] M van der BurgW Onstenk I Boere et al ldquoLong-term resultsof a randomised phase III trial of weekly versus three-weeklypaclitaxelplatinum induction therapy followed by standardor extended three-weekly paclitaxelplatinum in Europeanpatients with advanced epithelial ovarian cancerrdquo EuropeanJournal of Cancer vol 50 no 15 pp 2592ndash2601 2014
[21] N Katsumata M Yasuda F Takahashi et al ldquoDose-densepaclitaxel once a week in combination with carboplatin every3 weeks for advanced ovarian cancer a phase 3 open-labelrandomised controlled trialrdquoThe Lancet vol 374 no 9698 pp1331ndash1338 2009
[22] N Katsumata M Yasuda S Isonishi et al ldquoLong-term resultsof dose-dense paclitaxel and carboplatin versus conventionalpaclitaxel and carboplatin for treatment of advanced epithelialovarian fallopian tube or primary peritoneal cancer (JGOG3016) a randomised controlled open-label trialrdquo The LancetOncology vol 14 no 10 pp 1020ndash1026 2013
[23] K Harano F Terauchi N Katsumata et al ldquoQuality-of-lifeoutcomes from a randomized phase III trial of dose-denseweekly paclitaxel and carboplatin compared with conventionalpaclitaxel and carboplatin as a first-line treatment for stage II-IV ovarian cancer Japanese Gynecologic OncologyGroup Trial(JGOG3016)rdquo Annals of Oncology vol 25 no 1 pp 251ndash2572014
[24] J Chan M F Brady R Penson et al ldquoPhase III trial ofevery-3-weeks paclitaxel vs dose dense weekly paclitaxel withcarboplatin +minus bevacizumab in epithelial ovarian peritonealfallopian tube cancer GOG 262 (NCT01167712)rdquo InternationalJournal of Gynecological Cancer vol 23 no 8 supplement 1 pp9ndash10 2013
[25] S Pignata G Scambia D Katsaros et al ldquoCarboplatin pluspaclitaxel once a week versus every 3 weeks in patients withadvanced ovarian cancer (MITO-7) a randomisedmulticentreopen-label phase 3 trialrdquoThe Lancet Oncology vol 15 no 4 pp396ndash405 2014
[26] V Walsh and J Goodman ldquoFrom taxol to Taxol the changingidentities and ownership of an anti-cancer drugrdquo MedicalAnthropology vol 21 no 3-4 pp 307ndash336 2002
[27] R Renneberg ldquoBiotech History yew trees paclitaxel synthesisand fungirdquo Biotechnology Journal vol 2 no 10 pp 1207ndash12092007
[28] J E Liebmann J A Cook C Lipschultz D Teague J Fisherand J B Mitchell ldquoCytotoxic studies of paclitaxel (Taxol) inhuman tumour cell linesrdquo British Journal of Cancer vol 68 no6 pp 1104ndash1109 1993
[29] J J Manfredi and S B Horwitz ldquoTaxol an antimitotic agentwith a newmechanism of actionrdquo Pharmacology andTherapeu-tics vol 25 no 1 pp 83ndash125 1984
[30] D G I Kingston ldquoRecent advances in the chemistry of taxolrdquoJournal of Natural Products vol 63 no 5 pp 726ndash734 2000
[31] D G I Kingston ldquoThe shape of things to come structural andsynthetic studies of taxol and related compoundsrdquo Phytochem-istry vol 68 no 14 pp 1844ndash1854 2007
[32] V Walsh and J Goodman ldquoCancer chemotherapy biodiversitypublic and private property the case of the anti-cancer drugTaxolrdquo Social Science amp Medicine vol 49 no 9 pp 1215ndash12251999
[33] P H Wiernik E L Schwartz J J Strauman J P Dutcher RB Lipton and E Paietta ldquoPhase I clinical and pharmacokineticstudy of taxolrdquo Cancer Research vol 47 no 9 pp 2486ndash24931987
[34] W P McGuire E K Rowinsky N B Rosenhein et alldquoTaxol a unique antineoplastic agent with significant activityin advanced ovarian epithelial neoplasmsrdquo Annals of InternalMedicine vol 111 no 4 pp 273ndash279 1989
[35] ldquoDiscovery and development of taxolrdquo in Taxol Science andApplications M W M E Suffness Ed pp 3ndash25 CRC PressBoca Raton Fla USA 1995
[36] M J Piccart and F Cardoso ldquoProgress in systemic therapy forbreast cancer an overview and perspectivesrdquo European Journalof Cancer Supplement vol 1 no 2 pp 56ndash69 2003
[37] P Bonomi K B Kim and J Kugler ldquoComparison of survival forstage IIIB versus stage IV non-small cell lung cancer (NSCLC)patients with etoposide-cisplatin versus taxol-cisplatin an East-ern Cooperative Oncology Group (ECOG) trialrdquo in Proceedingsof the American Society of Clinical Oncology vol 16 p 454a1997
[38] D Guenard F Gueritte-Voegelein J Dubois and P PotierldquoStructure-activity relationships of Taxol and Taxotere ana-loguesrdquo Journal of the National Cancer Institute Monographsno 15 pp 79ndash82 1993
[39] D G I Kingston ldquoTaxol the chemistry and structure-activityrelationships of a novel anticancer agentrdquo Trends in Biotechnol-ogy vol 12 no 6 pp 222ndash227 1994
[40] E K Rowinsky and R C Donehower ldquoPaclitaxel (taxol)rdquo TheNew England Journal of Medicine vol 332 no 15 pp 1004ndash10141995
[41] J Parness and S B Horwitz ldquoTaxol binds to polymerizedtubulin in vitrordquo Journal of Cell Biology vol 91 no 2 pp 479ndash487 1981
[42] A Dammermann A Desai and K Oegema ldquoTheminus end insightrdquo Current Biology vol 13 no 15 pp R614ndashR624 2003
[43] CWiese and Y Zheng ldquoMicrotubule nucleation 120574-tubulin andbeyondrdquo Journal of Cell Science vol 119 no 20 pp 4143ndash41532006
[44] A Ganguly H Yang and F Cabral ldquoPaclitaxel-dependent celllines reveal a novel drug activityrdquo Molecular Cancer Therapeu-tics vol 9 no 11 pp 2914ndash2923 2010
[45] P B Schiff and S B Horwitz ldquoTaxol stabilizes microtubules inmouse fibroblast cellsrdquo Proceedings of the National Academy ofSciences of the United States of America vol 77 no 3 pp 1561ndash1565 1980
[46] P B Schiff J Fant and S B Horwitz ldquoPromotion of micro-tubule assembly in vitro by Taxolrdquo Nature vol 277 no 5698pp 665ndash667 1979
[47] D Zhang R Yang S Wang and Z Dong ldquoPaclitaxel new usesfor an old drugrdquoDrug Design Development andTherapy vol 8pp 279ndash284 2014
[48] S Rao G A Orr A G Chaudhary D G I Kingston and SB Horwitz ldquoCharacterization of the taxol binding site on themicrotubule 2-(m-Azidobenzoyl)taxol photolabels a peptide(amino acids 217-231) of beta-tubulinrdquoThe Journal of BiologicalChemistry vol 270 no 35 pp 20235ndash20238 1995
[49] F Wang Y Cao W Zhao H Liu Z Fu and R Han ldquoTaxolinhibits melanoma metastases through apoptosis inductionangiogenesis inhibition and restoration of E-cadherin andnm23 expressionrdquo Journal of Pharmacological Sciences vol 93no 2 pp 197ndash203 2003
18 BioMed Research International
[50] A Sevko V Kremer C Falk et al ldquoApplication of paclitaxel inlow non-cytotoxic doses supports vaccination with melanomaantigens in normal micerdquo Journal of Immunotoxicology vol 9no 3 pp 275ndash281 2012
[51] T Kreis and R Vale Guidebook to the Cytoskeletal and MotorProteins Oxford University Press Oxford UK 2nd edition1999
[52] P Giannakakou D L Sackett Y-K Kang et al ldquoPaclitaxel-resistant human ovarian cancer cells have mutant 120573-tubulinsthat exhibit impaired paclitaxel-driven polymerizationrdquo TheJournal of Biological Chemistry vol 272 no 27 pp 17118ndash171251997
[53] E Rakovitch W Mellado E J Hall T K Pandita S Sawantand C R Geard ldquoPaclitaxel sensitivity correlates with p53status and DNA fragmentation but not G2M accumulationrdquoInternational Journal of Radiation Oncology Biology Physics vol44 no 5 pp 1119ndash1124 1999
[54] S W Lowe S Bodis A McClatchey et al ldquop53 status and theefficacy of cancer therapy in vivordquo Science vol 266 no 5186 pp807ndash810 1994
[55] C C Zhang J-M Yang E White M Murphy A Levine andW N Hait ldquoThe role of MAP4 expression in the sensitivity topaclitaxel and resistance to vinca alkaloids in p53 mutant cellsrdquoOncogene vol 16 no 12 pp 1617ndash1624 1998
[56] K Fukasawa T Choi R Kuriyama S Rulong and G F VandeWoude ldquoAbnormal centrosome amplification in the absence ofp53rdquo Science vol 271 no 5256 pp 1744ndash1747 1996
[57] T-H Wang Y-H Chan C-W Chen et al ldquoPaclitaxel (Taxol)upregulates expression of functional interleukin-6 in humanovarian cancer cells through multiple signaling pathwaysrdquoOncogene vol 25 no 35 pp 4857ndash4866 2006
[58] E Yakirevich E Sabo I Naroditsky Y Sova O Lavie andM B Resnick ldquoMultidrug resistance-related phenotype andapoptosis-related protein expression in ovarian serous carcino-masrdquo Gynecologic Oncology vol 100 no 1 pp 152ndash159 2006
[59] G Szakacs J K Paterson J A Ludwig C Booth-Genthe andM M Gottesman ldquoTargeting multidrug resistance in cancerrdquoNature Reviews Drug Discovery vol 5 no 3 pp 219ndash234 2006
[60] L W Pfannenstiel S S K Lam L A Emens E M Jaffeeand T D Armstrong ldquoPaclitaxel enhances early dendritic cellmaturation and function through TLR4 signaling in micerdquoCellular Immunology vol 263 no 1 pp 79ndash87 2010
[61] N Klauber S Parangi E Flynn E Hamel and R J DrsquoAmatoldquoInhibition of angiogenesis and breast cancer in mice by themicrotubule inhibitors 2-methoxyestradiol and Taxolrdquo CancerResearch vol 57 no 1 pp 81ndash86 1997
[62] D Belotti V Vergani T Drudis et al ldquoThe microtubule-affecting drug paclitaxel has antiangiogenic activityrdquo ClinicalCancer Research vol 2 no 11 pp 1843ndash1849 1996
[63] D H Lau L Xue L J Young P A Burke and A T CheungldquoPaclitaxel (Taxol) an inhibitor of angiogenesis in a highlyvascularized transgenic breast cancerrdquo Cancer Biotherapy andRadiopharmaceuticals vol 14 no 1 pp 31ndash36 1999
[64] X Jiang ldquoHarnessing the immune system for the treatment ofbreast cancerrdquo Journal of Zhejiang University Science B vol 15no 1 pp 1ndash15 2014
[65] A Gadducci D Katsaros P Zola et al ldquoWeekly low-dosepaclitaxel as maintenance treatment in patients with advancedovarian cancer who had microscopic residual disease atsecond-look surgery after 6 cycles of paclitaxelplatinum-basedchemotherapy Results of an open noncomparative phase 2
multicenter italian study (after-6 protocol 2)rdquo InternationalJournal of Gynecological Cancer vol 19 no 4 pp 615ndash619 2009
[66] R S Bhatt J Merchan R Parker et al ldquoA phase 2 pilot trial oflow-dose continuous infusion or lsquometronomicrsquo paclitaxel andoral celecoxib in patients with metastatic melanomardquo Cancervol 116 no 7 pp 1751ndash1756 2010
[67] M Caballero J J Grau J L Blanch et al ldquoSerum vascularendothelial growth factor as a predictive factor in metronomic(weekly) paclitaxel treatment for advanced head and neckcancerrdquo Archives of OtolaryngologymdashHead and Neck Surgeryvol 133 no 11 pp 1143ndash1148 2007
[68] J Alexandre Y Hu W Lu H Pelicano and P Huang ldquoNovelaction of paclitaxel against cancer cells bystander effect medi-ated by reactive oxygen speciesrdquo Cancer Research vol 67 no 8pp 3512ndash3517 2007
[69] T Hadzic N Aykin-Burns Y Zhu et al ldquoPaclitaxel combinedwith inhibitors of glucose and hydroperoxide metabolismenhances breast cancer cell killing viaH
2O2-mediated oxidative
stressrdquo Free Radical Biology and Medicine vol 48 no 8 pp1024ndash1033 2010
[70] C A Sherman-Baust K G Becker W H Wood III Y Zhangand P J Morin ldquoGene expression and pathway analysis of ovar-ian cancer cells selected for resistance to cisplatin paclitaxel ordoxorubicinrdquo Journal of Ovarian Research vol 4 no 1 article21 2011
[71] R Agarwal and S B Kaye ldquoOvarian cancer strategies for over-coming resistance to chemotherapyrdquo Nature Reviews Cancervol 3 no 7 pp 502ndash516 2003
[72] T Acker and K H Plate ldquoRole of hypoxia in tumorangiogenesismdashmolecular and cellular angiogenic crosstalkrdquoCell and Tissue Research vol 314 no 1 pp 145ndash155 2003
[73] M Hockel and P Vaupel ldquoBiological consequences of tumorhypoxiardquo Seminars in Oncology vol 28 supplement 8 no 2 pp36ndash41 2001
[74] L Huang Q-H Zhang Q-L Ao H Xing Y-P Lu and DMa ldquoEffect of hypoxia on the chemotherapeutic sensitivity ofhuman ovarian cancer cells to paclitaxel and its mechanismrdquoZhonghua Zhong Liu Za Zhi vol 29 no 2 pp 96ndash100 2007
[75] N Rohwer and T Cramer ldquoHypoxia-mediated drug resistancenovel insights on the functional interaction of HIFs and celldeath pathwaysrdquoDrug Resistance Updates vol 14 no 3 pp 191ndash201 2011
[76] B B Aggarwal R V Vijayalekshmi and B Sung ldquoTargetinginflammatory pathways for prevention and therapy of cancershort-term friend long-term foerdquo Clinical Cancer Research vol15 no 2 pp 425ndash430 2009
[77] Z Duan R Foster D A Bell et al ldquoSignal transducersand activators of transcription 3 pathway activation in drug-resistant ovarian cancerrdquo Clinical Cancer Research vol 12 no17 pp 5055ndash5063 2006
[78] H-J Kuh S H Jang M G Wientjes J R Weaver and J L-SAu ldquoDeterminants of paclitaxel penetration and accumulationin human solid tumorrdquo Journal of Pharmacology and Experi-mental Therapeutics vol 290 no 2 pp 871ndash880 1999
[79] S Arao H Suwa M Mandai et al ldquoHypoxia-mediated drugresistance novel insights on the functional interaction of HIFsand cell death pathwaysrdquo Cancer Research vol 54 no 5 pp1355ndash1359 1994
[80] S E Johnatty J Beesley B Gao et al ldquoABCB1 (MDR1)polymorphisms and ovarian cancer progression and survivala comprehensive analysis from the Ovarian Cancer Association
BioMed Research International 19
Consortium and the Cancer GenomeAtlasrdquoGynecologic Oncol-ogy vol 131 no 1 pp 8ndash14 2013
[81] X Yang A K Iyer A Singh et al ldquoCluster of differentiation44 targeted hyaluronic acid based nanoparticles for MDR1siRNA delivery to overcome drug resistance in ovarian cancerrdquoPharmaceutical Research 2014
[82] D A Zajchowski B Y Karlan and L K Shawver ldquoTreatment-related protein biomarker expression differs between primaryand recurrent ovarian carcinomasrdquoMolecular CancerTherapeu-tics vol 11 no 2 pp 492ndash502 2012
[83] MM Gottesman J Ludwig D Xia and G Szakacs ldquoDefeatingdrug resistance in cancerrdquoDiscovery Medicine vol 6 no 31 pp18ndash23 2006
[84] S Mozzetti C Ferlini P Concolino et al ldquoClass III 120573-tubulin overexpression is a prominent mechanism of paclitaxelresistance in ovarian cancer patientsrdquo Clinical Cancer Researchvol 11 no 1 pp 298ndash305 2005
[85] M Kavallaris D Y S Kuo C A Burkhart et al ldquoTaxol-resistant epithelial ovarian tumors are associated with alteredexpression of specific beta-tubulin isotypesrdquo Journal of ClinicalInvestigation vol 100 no 5 pp 1282ndash1293 1997
[86] G A Orr P Verdier-Pinard H McDaid and S B HorwitzldquoMechanisms of Taxol resistance related to microtubulesrdquoOncogene vol 22 no 47 pp 7280ndash7295 2003
[87] C Ferlini L Cicchillitti G Raspaglio et al ldquoPaclitaxel directlybinds to Bcl-2 and functionally mimics activity of Nur77rdquoCancer Research vol 69 no 17 pp 6906ndash6914 2009
[88] E Mechetner A Kyshtoobayeva S Zonis et al ldquoLevels ofmultidrug resistance (MDR1) P-glycoprotein expression byhuman breast cancer correlate with in vitro resistance to taxoland doxorubicinrdquo Clinical Cancer Research vol 4 no 2 pp389ndash398 1998
[89] J S Lagas C W N Damen R A B VanWaterschoot D IusufJ H Beijnen and A H Schinkel ldquoP-glycoprotein multidrug-resistance associated protein 2 Cyp3a and carboxylesteraseaffect the oral availability and metabolism of vinorelbinerdquoMolecular Pharmacology vol 82 no 4 pp 636ndash644 2012
[90] M T Huizing J B Vermorken H Rosing et al ldquoPharmacoki-netics of paclitaxel and three major metabolites in patients withadvanced breast carcinoma refractory to anthracycline therapytreated with a 3-hour paclitaxel infusion a European CancerCentre (ECC) trialrdquo Annals of Oncology vol 6 no 7 pp 699ndash704 1995
[91] R Panchagnula ldquoPharmaceutical aspects of paclitaxelrdquo Interna-tional Journal of Pharmaceutics vol 172 no 1-2 pp 1ndash15 1998
[92] S H Jang M G Wientjes and J L-S Au ldquoDeterminants ofpaclitaxel uptake accumulation and retention in solid tumorsrdquoInvestigational New Drugs vol 19 no 2 pp 113ndash123 2001
[93] D S Sonnichsen andM V Relling ldquoClinical pharmacokineticsof paclitaxelrdquo Clinical Pharmacokinetics vol 27 no 4 pp 256ndash269 1994
[94] T Ohtsu Y Sasaki T Tamura et al ldquoClinical pharmacokineticsand pharmacodynamics of paclitaxel a 3-hour infusion versusa 24-hour infusionrdquo Clinical Cancer Research vol 1 no 6 pp599ndash606 1995
[95] M Czejka J Schueller H Schnait B Springer and I EderldquoClinical pharmacokinetics andmetabolism of paclitaxel after athree-hour infusion comparison of two preparationsrdquo Journalof Oncology Pharmacy Practice vol 9 no 4 pp 129ndash136 2003
[96] J Rizzo C Riley D VonHoff J Kuhn J Phillips and T BrownldquoAnalysis of anticancer drugs in biological fluids determination
of taxol with application to clinical pharmacokineticsrdquo Journalof Pharmaceutical and Biomedical Analysis vol 8 no 2 pp 159ndash164 1990
[97] V A de Weger J H Beijnen and J H M Schellens ldquoCel-lular and clinical pharmacology of the taxanes docetaxel andpaclitaxelmdasha reviewrdquoAnti-Cancer Drugs vol 25 no 5 pp 488ndash494 2014
[98] S Kumar H Mahdi C Bryant J P Shah G Garg andA Munkarah ldquoClinical trials and progress with paclitaxel inovarian cancerrdquo International Journal of Womenrsquos Health vol 2no 1 pp 411ndash427 2010
[99] B Huang J Zhao J C Unkeless Z H Feng and H XiongldquoTLR signaling by tumor and immune cells a double-edgedswordrdquo Oncogene vol 27 no 2 pp 218ndash224 2008
[100] R A Jibodh J S Lagas B Nuijen J H Beijnen and J HM Schellens ldquoTaxanes old drugs new oral formulationsrdquoEuropean Journal of Pharmacology vol 717 no 1ndash3 pp 40ndash462013
[101] A Javeed M Ashraf A Riaz A Ghafoor S Afzal and M MMukhtar ldquoPaclitaxel and immune systemrdquo European Journal ofPharmaceutical Sciences vol 38 no 4 pp 283ndash290 2009
[102] L Bracci G Schiavoni A Sistigu and F Belardelli ldquoImmune-based mechanisms of cytotoxic chemotherapy implications forthe design of novel and rationale-based combined treatmentsagainst cancerrdquo Cell Death and Differentiation vol 21 no 1 pp15ndash25 2014
[103] C A Byrd-Leifer E F Block K Takeda S Akira and A DingldquoThe role of MyD88 and TLR4 in the LPS-mimetic activity ofTaxolrdquo European Journal of Immunology vol 31 no 8 pp 2448ndash2457 2001
[104] A-C Wang Y-B Ma F-X Wu et al ldquoTLR4 induces tumorgrowth and inhibits paclitaxel activity in MyD88-positivehuman ovarian carcinoma in vitrordquo Oncology Letters vol 7 no3 pp 871ndash877 2014
[105] Y Zhu N Liu S D Xiong Y J Zheng and Y W ChuldquoCD4+Foxp3+ regulatory T-cell impairment by paclitaxel isindependent of toll-like receptor 4rdquo Scandinavian Journal ofImmunology vol 73 no 4 pp 301ndash308 2011
[106] M Kubo T Morisaki K Matsumoto et al ldquoPaclitaxel probablyenhances cytotoxicity of natural killer cells against breastcarcinoma cells by increasing perforin productionrdquo CancerImmunology Immunotherapy vol 54 no 5 pp 468ndash476 2005
[107] L Markasz G Stuber B Vanherberghen et al ldquoEffect of fre-quently used chemotherapeutic drugs on the cytotoxic activityof human natural killer cellsrdquo Molecular Cancer Therapeuticsvol 6 no 2 pp 644ndash654 2007
[108] T Sako N Burioka K Yasuda et al ldquoCellular immune profile inpatients with non-small cell lung cancer after weekly paclitaxeltherapyrdquo Acta Oncologica vol 43 no 1 pp 15ndash19 2004
[109] R Kaneno G V Shurin I L Tourkova and M R ShurinldquoChemomodulation of human dendritic cell function by anti-neoplastic agents in low noncytotoxic concentrationsrdquo Journalof Translational Medicine vol 7 article 58 2009
[110] TMichels G V ShurinHNaiditch A Sevko VUmansky andM R Shurin ldquoPaclitaxel promotes differentiation of myeloid-derived suppressor cells into dendritic cells in vitro in a TLR4-independent mannerrdquo Journal of Immunotoxicology vol 9 no3 pp 292ndash300 2012
[111] R A Kemp and F Ronchese ldquoTumor-specific Tc1 but not Tc2cells deliver protective antitumor immunityrdquo The Journal ofImmunology vol 167 no 11 pp 6497ndash6502 2001
20 BioMed Research International
[112] A Y Rudensky ldquoRegulatory T cells and Foxp3rdquo ImmunologicalReviews vol 241 no 1 pp 260ndash268 2011
[113] EM Shevach ldquoCD4+CD25+ suppressor T cellsmore questionsthan answersrdquo Nature Reviews Immunology vol 2 no 6 pp389ndash400 2002
[114] S Sakaguchi T Yamaguchi T Nomura and M Ono ldquoRegu-latory T cells and immune tolerancerdquo Cell vol 133 no 5 pp775ndash787 2008
[115] H Nishikawa and S Sakaguchi ldquoRegulatory T cells in tumorimmunityrdquo International Journal of Cancer vol 127 no 4 pp759ndash767 2010
[116] W Zou ldquoRegulatory T cells tumour immunity and immuno-therapyrdquoNature Reviews Immunology vol 6 no 4 pp 295ndash3072006
[117] A Fialova S Partlova L Sojka et al ldquoDynamics of T-cell infil-tration during the course of ovarian cancer The gradual shiftfrom aTh17 effector cell response to a predominant infiltrationby regulatory T-cellsrdquo International Journal of Cancer vol 132no 5 pp 1070ndash1079 2013
[118] A E Albers R L Ferris G G Kim K Chikamatsu A BDeLeo and T L Whiteside ldquoImmune responses to p53 inpatients with cancer enrichment in tetramer+ p53 peptide-specific T cells and regulatory T cells at tumor sitesrdquo CancerImmunology Immunotherapy vol 54 no 11 pp 1072ndash10812005
[119] N Liu Y Zheng Y Zhu S Xiong andYChu ldquoSelective impair-ment of CD4 + CD25 + Foxp3 + regulatory T cells by paclitaxelis explained by Bcl-2Bax mediated apoptosisrdquo InternationalImmunopharmacology vol 11 no 2 pp 212ndash219 2011
[120] X Wu Q-M Feng Y Wang J Shi H-L Ge and W DildquoThe immunologic aspects in advanced ovarian cancer patientstreated with paclitaxel and carboplatin chemotherapyrdquo CancerImmunology Immunotherapy vol 59 no 2 pp 279ndash291 2010
[121] A P Vicari R Luu N Zhang et al ldquoPaclitaxel reducesregulatoryT cell numbers and inhibitory function and enhancesthe anti-tumor effects of the TLR9 agonist PF-3512676 in themouserdquo Cancer Immunology Immunotherapy vol 58 no 4 pp615ndash628 2009
[122] L Zhang K Dermawan M Jin et al ldquoDifferential impairmentof regulatory T cells rather than effector T cells by paclitaxel-based chemotherapyrdquo Clinical Immunology vol 129 no 2 pp219ndash229 2008
[123] Y Tabuchi J Matsuoka M Gunduz et al ldquoResistance topaclitaxel therapy is related with Bcl-2 expression through anestrogen receptor mediated pathway in breast cancerrdquo Interna-tional Journal of Oncology vol 34 no 2 pp 313ndash319 2009
[124] N Obermajer R Muthuswamy K Odunsi R P Edwards andP Kalinski ldquoPGE
2-induced CXCL12 production and CXCR4
expression controls the accumulation of human MDSCs inovarian cancer environmentrdquo Cancer Research vol 71 no 24pp 7463ndash7470 2011
[125] Q M Feng W Di and X Wu ldquoImmune reconstitution inadvanced ovarian cancer patients undergoing first line chemo-therapyrdquo Xi Bao Yu Fen Zi Mian Yi Xue Za Zhi vol 25 no 11pp 1023ndash1025 2009
[126] A D Seidman D Hochhauser M Gollub et al ldquoNinety-six-hour paclitaxel infusion after progression during short taxaneexposure a phase II pharmacokinetic and pharmacodynamicstudy in metastatic breast cancerrdquo Journal of Clinical Oncologyvol 14 no 6 pp 1877ndash1884 1996
[127] D R Spriggs M F Brady L Vaccarello et al ldquoPhase IIIrandomized trial of intravenous cisplatin plus a 24- or 96-hour
infusion of paclitaxel in epithelial ovarian cancer a gynecologiconcology group studyrdquo Journal of Clinical Oncology vol 25 no28 pp 4466ndash4471 2007
[128] G A Omura M F Brady K Y Look et al ldquoPhase III trial ofpaclitaxel at two dose levels the higher dose accompanied byfilgrastim at two dose levels in platinum-pretreated epithelialovarian cancer an intergroup studyrdquo Journal of Clinical Oncol-ogy vol 21 no 15 pp 2843ndash2848 2003
[129] R Simon and L Norton ldquoThe Norton-Simon hypothesisdesigning more effective and less toxic chemotherapeutic reg-imensrdquoNature Clinical Practice Oncology vol 3 no 8 pp 406ndash407 2006
[130] A Kumar P Hoskins and A Tinker ldquoDose-dense paclitaxel inadvanced ovarian cancerrdquo Clinical Oncology vol 27 no 1 pp40ndash47 2015
[131] P Marchetti S Urien G A Cappellini G Ronzino and CFicorella ldquoWeekly administration of paclitaxel theoretical andclinical basisrdquoCritical Reviews in OncologyHematology vol 44supplement pp S3ndashS13 2002
[132] P Francis E Rowinsky J Schneider T Hakes W Hoskinsand M Markman ldquoPhase I feasibility and pharmacologic studyof weekly intraperitoneal paclitaxel A Gynecologic OncologyGroup pilot studyrdquo Journal of Clinical Oncology vol 13 no 12pp 2961ndash2967 1995
[133] H Thomas and P Rosenberg ldquoRole of weekly paclitaxel inthe treatment of advanced ovarian cancerrdquo Critical Reviews inOncologyHematology vol 44 supplement pp S43ndashS51 2002
[134] M Markman J Markman K Webster et al ldquoDuration ofresponse to second-line platinum-based chemotherapy forovarian cancer implications for patient management and clini-cal trial designrdquo Journal of Clinical Oncology vol 22 no 15 pp3120ndash3125 2004
[135] P H OrsquoDonnell M Eileen Dolan E Gamazon et al ldquoPopu-lation differences in platinum toxicity as a means to identifynovel genetic susceptibility variantsrdquo Pharmacogenetics andGenomics vol 20 no 5 pp 327ndash337 2010
[136] M J Millward M J Boyer M Lehnert et al ldquoDocetaxel andcarboplatin is an active regimen in advanced non-small-celllung cancer a phase II study in Caucasian and Asian patientsrdquoAnnals of Oncology vol 14 no 3 pp 449ndash454 2003
[137] M Markman ldquoIntraperitoneal therapy of ovarian cancerrdquoOncologist vol 1 no 1-2 pp 18ndash21 1996
[138] M Markman and J L Walker ldquoIntraperitoneal chemotherapyof ovarian cancer a review with a focus on practical aspects oftreatmentrdquo Journal of Clinical Oncology vol 24 no 6 pp 988ndash994 2006
[139] K Fujiwara S Nagao E Aotani and K Hasegawa ldquoPrincipleand evolving role of intraperitoneal chemotherapy in ovariancancerrdquo Expert Opinion on Pharmacotherapy vol 14 no 13 pp1797ndash1806 2013
[140] M Markman E Rowinsky T Hakes et al ldquoPhase I trialof intraperitoneal taxol a gynecoloic oncology group studyrdquoJournal of Clinical Oncology vol 10 no 9 pp 1485ndash1491 1992
[141] M Markman M F Brady N M Spirtos P Hanjani and S CRubin ldquoPhase II trial of intraperitoneal paclitaxel in carcinomaof the ovary tube and peritoneum a gynecologic oncologygroup studyrdquo Journal of Clinical Oncology vol 16 no 8 pp2620ndash2624 1998
[142] P B Panici I Palaia M Graziano F Bellati N Manci and RAngioli ldquoIntraperitoneal paclitaxel as consolidation treatmentin ovarian cancer patients a case control studyrdquo Oncology vol78 no 1 pp 20ndash25 2010
BioMed Research International 21
[143] D K Armstrong B Bundy L Wenzel et al ldquoIntraperitonealcisplatin and paclitaxel in ovarian cancerrdquo The New EnglandJournal of Medicine vol 354 no 1 pp 34ndash43 2006
[144] D Tewari J Java and R Salani ldquoLong-term survival advantageof intraperitoneal chemotherapy treatment in advanced ovariancancer an analysis of a Gynecologic Oncology Group ancillarydata studyrdquo in Proceedings of the 2013 Society of GynecologicOncology Annual Meeting on Womenrsquos Cancer (GOG114172Abstract) Los Angeles Calif USA 2013
[145] D A Yardley ldquonab-paclitaxel mechanisms of action and deliv-eryrdquo Journal of Controlled Release vol 170 no 3 pp 365ndash3722013
[146] M Ando K Yonemori N Katsumata et al ldquoPhase I and phar-macokinetic study of nab-paclitaxel nanoparticle albumin-bound paclitaxel administeredweekly to Japanese patients withsolid tumors and metastatic breast cancerrdquo Cancer Chemother-apy and Pharmacology vol 69 no 2 pp 457ndash465 2012
[147] N Desai V Trieu Z Yao et al ldquoIncreased antitumor activityintratumor paclitaxel concentrations and endothelial cell trans-port of cremophor-free albumin-bound paclitaxel ABI-007compared with cremophor-based paclitaxelrdquo Clinical CancerResearch vol 12 no 4 pp 1317ndash1324 2006
[148] J A Yared and K H R Tkaczuk ldquoUpdate on taxane devel-opment new analogs and new formulationsrdquo Drug DesignDevelopment andTherapy vol 6 pp 371ndash384 2012
[149] M G Teneriello P C Tseng M Crozier et al ldquoPhase IIevaluation of nanoparticle albumin-bound paclitaxel in plati-num-sensitive patients with recurrent ovarian peritoneal orfallopian tube cancerrdquo Journal of Clinical Oncology vol 27 no9 pp 1426ndash1431 2009
[150] R L Coleman W E Brady D S McMeekin et al ldquoA phase IIevaluation of nanoparticle albumin-bound (nab) paclitaxel inthe treatment of recurrent or persistent platinum-resistant ovar-ian fallopian tube or primary peritoneal cancer a GynecologicOncology Group Studyrdquo Gynecologic Oncology vol 122 no 1pp 111ndash115 2011
[151] J W Singer ldquoPaclitaxel poliglumex (XYOTAX CT-2103) amacromolecular taxanerdquo Journal of Controlled Release vol 109no 1ndash3 pp 120ndash126 2005
[152] C Li D-F Yu R A Newman et al ldquoComplete regressionof well-established tumors using a novel water-soluble poly(L-glutamic acid)-paclitaxel conjugaterdquo Cancer Research vol 58no 11 pp 2404ndash2409 1998
[153] M Mita A Mita J Sarantopoulos et al ldquoPhase I study ofpaclitaxel poliglumex administered weekly for patients withadvanced solid malignanciesrdquo Cancer Chemotherapy and Phar-macology vol 64 no 2 pp 287ndash295 2009
[154] P Sabbatini M W Sill D OrsquoMalley L Adler and A ASecord ldquoA phase II trial of paclitaxel poliglumex in recurrentor persistent ovarian or primary peritoneal cancer (EOC) agynecologic oncology group studyrdquo Gynecologic Oncology vol111 no 3 pp 455ndash460 2008
[155] M O Bradley C S Swindell F H Anthony et al ldquoTumortargeting by conjugation of DHA to paclitaxelrdquo Journal ofControlled Release vol 74 no 1ndash3 pp 233ndash236 2001
[156] M O Bradley N L Webb F H Anthony et al ldquoTumortargeting by covalent conjugation of a natural fatty acid topaclitaxelrdquo Clinical Cancer Research vol 7 no 10 pp 3229ndash3238 2001
[157] A C Wolff R C Donehower M K Carducci et al ldquoPhaseI study of docosahexaenoic acid-paclitaxel a taxane-fatty acid
conjugate with a unique pharmacology and toxicity profilerdquoClinical Cancer Research vol 9 no 10 part 1 pp 3589ndash35972003
[158] A Sparreboom A C Wolff J Verweij et al ldquoDispositionof docosahexaenoic acid-paclitaxel a novel taxane in bloodin vitro and clinical pharmacokinetic studiesrdquo Clinical CancerResearch vol 9 no 1 pp 151ndash159 2003
[159] P M Fracasso J Picus J D Wildi et al ldquoPhase 1 and phar-macokinetic study of weekly docosahexaenoic acid-paclitaxelTaxoprexin in resistant solid tumor malignanciesrdquo CancerChemotherapy and Pharmacology vol 63 no 3 pp 451ndash4582009
[160] A Y Bedikian R C DeConti R Conry et al ldquoPhase 3 study ofdocosahexaenoic acid-paclitaxel versus dacarbazine in patientswith metastatic malignant melanomardquo Annals of Oncology vol22 no 4 pp 787ndash793 2011
[161] Y-N Wu S-L Wang Y-C Wang et al ldquoReversal effect ofdocosahexaenoic acid on taxol resistance in human ovarian car-cinoma A2780T cellsrdquo Obstetrics amp Gynecology InternationalJournal vol 1 no 3 Article ID 00018 2014
Submit your manuscripts athttpwwwhindawicom
PainResearch and TreatmentHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom
Volume 2014
ToxinsJournal of
VaccinesJournal of
Hindawi Publishing Corporation httpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
AntibioticsInternational Journal of
ToxicologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
StrokeResearch and TreatmentHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Drug DeliveryJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Advances in Pharmacological Sciences
Tropical MedicineJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Medicinal ChemistryInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
AddictionJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
Emergency Medicine InternationalHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Autoimmune Diseases
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Anesthesiology Research and Practice
ScientificaHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Pharmaceutics
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of

BioMed Research International 11
Table1Con
tinued
Stud
yRe
gimen
119899()
PI(m
)RR
()
CR(119899)
MedianPF
S(m
)Median
OS
(m)
Adversee
ffects
Com
ments
Paclitaxel
dose
(mgm
2 )Ca
rbop
latin
dose
(mgm
2 )
Safrae
tal2014
[18]
80over
1ho
urw
eek
AUC2week
133
1stline
864
645
274
(i)Highera
naem
ia(grade
III+
IV68vs53)+
IVneutropenia(
144vs69)
decreasedgradeIIa
lopecia(
235
vs981
)and
thrombo
cytopenia
(grade
III+
IV0
vs23)
Havrilesky
etal
2003
[19]
80over
1ho
urw
eek
AUC2weekD1
D8D15
until
progressionCR
+8courses
29 21 8
Total
grou
pgt6lt6
83 100
38
16 15 1114
115
137
32
(i)Hem
atologictoxicitywas
common
(grade
3neutropenia
32n
ograde4
neutropenia
grade3
or4thrombo
cytopenia
142)
(i)To
xicitymanaged
bytre
atment
delaydo
seredu
ctionof
paclitaxel
ordiscon
tinuatio
nof
carbop
latin
vanderB
urgetal
2014
[20]
90over
1ho
urw
eek
AUC4weekD1
D8D15
D29
D36
D49
+6x
TCq3w
108
65 43
Total
grou
pgt6lt6
76 5816 42
26 158 13
(i)Neutro
penia3
0
thrombo
cytopenia8
febrile
neutropenia0
5
(ii)N
onhaem
atologictoxicitywas
low
(i)Treatm
entw
asdelayedin
16
anddo
seredu
cedin
2of
cycle
s
119899num
bero
fpatientsassessableforrespo
nsemm
onthsPIplatinum
treatmentfreeintervalRR
respo
nser
ateCR
com
pleterem
issionT
paclitaxelC
carbop
latin
PFS
progressio
nfre
esurvivalOSoverall
survivalN
An
otavailableinpapero
rabstractandNR
notyetreached
lowastlowastElderly
popu
lation
patient
agedge70
years
12 BioMed Research International
Numerous phase II studies have explored the tolerabilityand the activity of weekly paclitaxel either as a single agent orin combination with several other drugs or biological agents(Table 1) A number of regimens combining weekly paclitaxelwith carboplatin have been used as first-line treatment inovarian cancer Carboplatin has been administered weeklyat AUC of 2 with dose escalation in some studies whilepaclitaxel had been infused at 60ndash80mgm2week Thiscombined regimen was well tolerated with a low incidence ofbone marrow suppression Overall response rates have beenhigh in the range of 60ndash80 in most studies even in heavilypretreated patients with platinum-resistant disease (diseaserecurrence or progression within 6 months of the last lineof platinum-based therapy) [15ndash20 134] The promising datafrom these phase II trials then led to the evolution of largerphase III trials
Three phase III studies Japanese Gynecologic OncologyGroup- (JGOG-) Trial 3016 [21ndash23] Multicentre Italian Trialin Ovarian Cancer-Trial 7 (MITO-7) [25] and GynecologicOncology Group GOG-262 Trial [24] have explored dosedense therapy The results of these trials are summarised inTable 2
The Japanese Gynecologic Oncology Group (JGOG)conducted a randomized phase 3 trial of dose-dense weeklypaclitaxel 80mgm2week in combination with 3-weeklycarboplatin compared to standard 3-weekly carboplatin andpaclitaxel 180mgm2 in patients with advanced epithelialovarian peritoneal or fallopian tube cancer (JGOG 3016NOVEL trial) In both arms carboplatin was given at AUC6 and the median number of cycles was six In this largestudy (119899 = 637) with a median follow up of 77 months therewas an 11-month improvement in themedian progression freesurvival (PFS) in the dose-dense treatment group comparedwith the standard treatment arm (282 versus 175 monthsHR 076 95 CI 062ndash091 119901 = 00037) Median OS wasalso higher in the dose-dense treatment arm (1005 versus622 months HR 079 95 CI 063ndash099 119901 = 0039)On subgroup analysis suboptimally debulked patients withresidual disease of gt1 cm (119899 = 342) had a significantlyhigher median overall survival in the dose dense arm (512versus 335 months HR-075 95 CI 057ndash097 119901 = 0027)There was no significant advantage to dose-dense treatmentfor patients with optimally cytoreduced disease Dose-densetherapy survival benefits were also not seen in patients withclear cell or mucinous histology type unlike serous typeHowever patient treated with dose dense therapy had asignificantly higher frequency of hematologic toxicity thanwith the standard arm (212 versus 94) which resultedin lower treatment completion rates (63 versus 48) withfrequent episodes of delay (76 versus 67) and dosereductions (48versus 35) [21 22]Therewas no significantdifference in terms of overall quality of life between the twoarms (119901 = 046) [23]
Using a similar regimen as in JGOG-3016 a GynecologicOncology Group (GOG)-262 Trial was conducted in theUnited States In this group most patients had stage IIIdisease (66ndash70) and two-thirds had suboptimal debulkingwith residual disease of gt1 cm This was a randomized phase
III trial of 3 weekly paclitaxel versus dose-dense weeklypaclitaxel in combination with carboplatin in patients withadvanced epithelial ovarian peritoneal or fallopian tubecancer Though optional concurrent and maintenance beva-cizumab were received by the majority of patients in botharms (835 versus 841 resp) There was no significantdifference in PFS in the patients who received the dosedense paclitaxelcarboplatin regimen compared to those whoreceived the standard paclitaxelcarboplatin regimen (148versus 143 months HR 097 95 CI 079ndash118) Howeverin a subgroup analysis there was a significant difference inPFS in the dose dense paclitaxel arm who did not receivebevacizumab 119899 = 112 (142 versus 103 months HR 059 95CI 037ndash096 119901 = 0003) Overall survival data is still imma-ture There was higher frequency of grade 3 anaemia (408versus 157 119901 lt 0001) and grade 2 sensory neuropathy(259 versus 178 119901 = 0012) but a lower incidence ofneutropenia (72 versus 83 119901 lt 0001) [24]
In 2008 the Multicentre Italian Trials in Ovarian Cancer(MITO-7) randomised 810 women in a phase 3 trial toreceive either standard carboplatin (AUC = 6) and paclitaxel175mgm2 every 3 weeks or a weekly schedule of paclitaxel(60mgm2) with carboplatin (AUC = 2) The majority ofpatients in both arms (83ndash90) received six cycles of therapyMost patients (58ndash63) had stage II1 disease 23 of themwere suboptimally debulked Median PFS did not differsignificantly (173 months and 183 months 119901 = 066)between the standard and dose-dense arms respectivelyThere was no significant difference in response rate betweenthe two arms nor the estimated 2-year overall survivalSubgroup analysis did not identify any subgroup that mayhave benefited from the dose-dense regimen Unlike theJGOG-3016 trial the incidence of grade 3-4 neutropenia wassignificantly lower in the dose-dense group compared to the3-weekly regimen (42 versus 50) A similar pattern wasseen for the incidence of febrile neutropenia (lt1 versus 3119901 = 002) thrombocytopenia (1 versus 7 119901 lt 0001)and other nonhaematological toxicities such as alopeciavomiting renal dysfunction and neuropathy Quality of lifewas reported to be significantly better in the dose-dense arm(119901 lt 00001) which was discordant with the JGOG-3016quality of life data [25]
In summary there was significant improvement inmedian PFS and overall survival in studies using paclitaxelat 80mgm2week dose-dense therapy [21 24] but withhigher haematological toxicity whereas MITO-7 [25] whichwas using paclitaxel at 60mgm2week was only equivalentlyeffective but less toxicThis does not conclude that the higherpaclitaxel dose is more clinically beneficial as there are manyother confounding factors in all three studies
In a multivariate analysis the JGOG-3016 study [21]reported that a lower dose intensity of paclitaxel (lt80) wasassociated with poorer overall survival (hazard ratio = 14295 confidence interval 112ndash181 119901 = 0004) however itmust be highlighted that the investigational arm carboplatinschedules were not standardised in these studies The JGOGand GOG trials delivered a 3-weekly carboplatin (AUC =6) arm whereas in the MITO-7 study the carboplatin was
BioMed Research International 13
Table2Ph
aseIIIstu
dies
onintravenou
sdose-densep
aclitaxel
Stud
yRe
gimen
119899
MedianPF
S(m
)
Median
OS
(m)
Adversee
ffects
Com
ments
Katsu
matae
tal2009
[21]
Katsu
matae
tal2013
[22]
Haranoetal2014
[23]
JGOG3016
631
(i)Haematologicaltoxicityhigh
erin
dose
dense-211versus
94
Lower
treatmentcom
pletionin
dose-dense
63versus
48
Frequent
episo
deso
fdelay
indo
se-dense
76versus
67
Doser
eductio
nsin
dose-dense
48versus
35
Nosig
nificantd
ifference
inoverallQ
OL
betweenbo
thgrou
ps(119901=046)
Paclitaxel80m
gm
2D18
15+carbop
latin
AUC63
weeklyversus
Paclitaxel180
mgm
2+
carbop
latin
AUC63
weekly
312
282
1005
Both
givenfor6
ndash9cycle
s319
175
622
Chan
etal2013
[24]
GOG-262
(i)Higherfrequ
ency
ofgrade3
anaemia
(408versus
157119901lt0001)
grade2
sensoryneurop
athy
(259versus
178
119901=0012)b
utlower
incidenceo
fneutropenia(
72versus
83119901lt0001)
Paclitaxel80m
gm
2D18
15+carbop
latin
AUC63
weeklyversus
Paclitaxel175
mgm
2+
carbop
latin
AUC63
weekly
346
148
NR
Both
givenfor6
cycle
s346
143
NR
Bevacizumab
given
optio
nally
112
(did
not
receive
bevazicumab)
142vs
103
Pign
atae
tal2014
[25]
MITO-7
810
(i)Lo
wer
incidenceo
fgrade
3-4
neutropenia(
42versus
50)febrile
neutropenia(lt1v
ersus3
119901=002)
thrombo
cytopenia(
1versus7
119901lt0001)andothern
onhaem
atological
toxicitie
ssuchas
alop
eciavom
iting
renald
ysfunctio
nandneurop
athy
Qualityof
lifeb
etterindo
sedensea
rm(119901lt00001)
Paclitaxel60m
gm
2 weekly+carbop
latin
AUC
2weeklyversus
Paclitaxel175
mgm
2+
carbop
latin
AUC63
weekly
406
404
183 173
77lowast
79lowast
119899num
bero
fpatientsmm
onthsDday
PFSprogressionfre
esurvivalOSoverallsurvivalNAnot
availableinpapero
rabstractandNR
notyetreached
lowastSurvivalrateat2years
14 BioMed Research International
dose-dense (AUC 2 weekly) Although it is possible that thedose scheduling for the platinum-based agent is not essentialfor a survival benefit as shown by previous studies usingdose-dense cisplatin direct cross-trial comparison cannot bemade Unlike paclitaxel carboplatin probably requires peakdose for optimal therapeutic benefit hence this may accountfor the inferior survival outcome in MITO-7 trial Anotherconfounding factor may be difference in ethnicity All threestudies used different ethnic populations and Asian patientsin JGOG-3016 appear to have better survival outcomes thanthe MITO-7 Western population Ethnicity with possibleunderlying genetic causes may be responsible for the variableresponses to chemotherapy across individuals [135] This wasexplored by Millward et al who studied 68 Caucasian andAsian lung cancer patients treated with a combination ofpaclitaxel and carboplatin and found that the incidence offebrile neutropenia was 50 of an initially treated cohortof Asians and when carboplatin was subsequently dosereduced in all Asian patients the overall incidence of febrileneutropenia was also reduced to 26 [136]
Although early clinical data from phase I and phaseII dose-dense paclitaxel trials in advanced ovarian cancerwere promising the results from phase III studies in havebeen inconsistent as a result of differences in paclitaxel dosecarboplatin AUC and schedule addition of bevacizumabas well as different ethnic populations The results of arecently completed randomised three arms GynaecologicCancer InterGroup (GCIG) phase II trial ICON 8 mayfurther inform the clinical benefit of dose dense paclitaxeltherapy
This multicentre trial involving 111 centres in the UKSouth Korea Mexico Ireland Australia and New Zealandwith a target population of 1485 patients with stage IC-IV epithelial ovarian cancer or peritoneal or fallopian tubecancer compared two dose-dense arms (i) JGOG-like armcarboplatin AUC 5 plus weekly 80mgm2 paclitaxel and (ii)MITO-7-like arm weekly carboplatin AUC 167 plus weekly80mgm2 paclitaxel to the standard 3-weekly treatment(carboplatin AUC 5 plus 175mgm2 paclitaxel) for stage IC toIV epithelial ovarian cancer The dose-dense arms of MITO-7 and JGOG-3016 as well as the ethnic heterogeneity will befurther addressed
10 Intraperitoneal (IP) Chemotherapy
In addition to dose and scheduling the route of adminis-tration of chemotherapy agents plays an important role inoutcome Intraperitoneal spread is common and likely anearly event in epithelial ovarian cancer hence the deliveryof chemotherapy intraperitoneally in theory would exposethe microcirculation of tumour to higher doses of drug thansystemic administration while limiting systemic toxicityTheideal drug for IP chemotherapy is one that is systemicallyeffective penetrates deep into the inner core of tumour tissueand remains within the peritoneal cavity for a prolongedperiod of time [137ndash139]
Early clinical studies confirmed that indeed the peritonealcavity could be exposed to 10 to 20-fold higher (cisplatin
and carboplatin) drug concentration than when using theintravenous approach and since 1978 this route had beenadopted as a form of therapeutic intervention [137 139]A subsequent phase I trial showed that IP paclitaxel haddose-limiting toxicity in the form of abdominal pain [140]Another phase 1 GOG pilot study administered weekly IPpaclitaxel at an initial dose of 20mgm2 for 16 weeks to33 patients and found that IP paclitaxel at this dose wasfeasible and well tolerated At dose levels 60 to 65mgm2there were significant levels of paclitaxel for a week afterdrug administration suggesting very slow clearance andcontinuous exposure of the peritoneal cavity to active drugconcentrations [132]
Hence this initiated a phase II study [141] that used pacli-taxel intraperitoneally at a dose of 60ndash65mgm2week In thisphase II GOG study 76 patients with small-volume resid-ual disease carcinoma (05 cm or less) involving the ovaryperitoneal or fallopian tube were treated with paclitaxel60mgm2week intraperitoneally for 16 weeks followed bysurgical evaluation in patients without disease progressionThe Gynaecologic Oncology group (GOG) currently definesno visible disease as microscopic disease being the idealsurgical outcome 75 of patients had received prior systemictherapy and 70 received all 16 courses that were planned Of28 patients with microscopic disease at the start of therapy61 achieved a surgically defined complete response whereasonly 1 out of 31 patients with macroscopic disease achieved acomplete response The median time-to-recurrence was 167months with an estimated survival rate at 2 years being 58Treatment was generally well tolerated [141]
Another study looked into the effect of IP paclitaxel asconsolidation therapy in advanced ovarian cancer Twenty-eight patients who had initial residual macroscopic disease(lt1 cm) after primary surgery or interval debulking but hadcomplete pathological response following standard treatmentwith at least 6 cycles of platinum-based chemotherapy regi-men received paclitaxel 60mgm2week intraperitoneally for12ndash16 weeks as consolidation therapy The median time torecurrence was 25 months but overall survival did not differsignificantly when compared with control group submittedto observation only Treatment-related toxicity was mild andtechnical difficulties were observed in 11 of patients [142]
Multicenter randomised phase 3 trials as well as meta-analysis of IP chemotherapy have been performed anddemonstrated that chemotherapy drugs administered intra-peritoneally are superior to intravenous standard regimensin patient with optimally debulked epithelial ovarian cancerThe most impressive data comes from GOG 114 [14] and172 trial [143] In GOG 114 patients received either sixcycles of intravenous paclitaxel 135mgm2 and cisplatin75mgm2 every 3 weeks or intravenous carboplatin (AUC= 9) every 28 days for two cycles followed by six 3-weeklycycles of intravenous paclitaxel 135mgm2 and IP cisplatin100mgm2 [14] whereas in GOG 172 patients received eitherintravenous paclitaxel 135mgm2 followed by intravenouscisplatin 75mgm2 or intravenous paclitaxel 135mgm2 fol-lowed by IP combination of cisplatin 100mgm2 and pacli-taxel 60mgm2 on day 8 Both trials had a combined total
BioMed Research International 15
of 876 women with stage III epithelial ovarian carcinomaoptimally debulked to le1 cm residual tumour [143] Themedian follow-up for GOG 114 [14] was 138 years with GOG172 [143] was 97 years The primary results of the individualtrials reported up to 6-month improvement in median PFSfollowing IP therapy In the combined analysis of the datafrom both trials the data continued to show a 5-monthdifference in favour of IP therapy (25 versus 20 months)which translates into 16 reduction in the hazard ratio forprogression (119901 = 003) In GOG 114 [14] reported in 2001there was only borderline improvement in overall survivalassociated with this regimen (median 63 versus 52 monthsrelative risk 081 119901 = 005)
However in combined analysis in 2013 which was pre-sented at the Society of Gynecologic Oncology AnnualMeeting [144] the overall survival showed an 11-monthimprovement in favour of IP therapy in GOG 114 whereasGOG 172 reported a 16-month survival advantage Amongpatients treated with IP therapy the 5-year survival rateincreased from 18 following completion of 1-2 cycles to 59for patients who completed 5-6 cycles of treatment Howeverthere was increased toxicity observed in the IP arm grade 3-4 leukopenia thrombocytopenia and abdominal pain Only42 of patients in the GOG172 trial [143] completed all sixcycles of planned treatment in the IP arm while 18 ofpatients in GOG 114 trial [14] received fewer than two coursesof IP chemotherapy
Another randomised phase III trial involving patientswith stages II-III epithelial ovarian carcinoma is the GOG252 study with three arms Arm 1-dose-dense intravenouscarboplatin and paclitaxel Arm 2-dose-dense intravenouspaclitaxel and IP carboplatin and Arm 3 consists of 3-weeklyintravenous paclitaxel (day 1) followed by IP cisplatin (day 2)and IP paclitaxel (day 3) regimen All three arms also incor-porate the combination and maintenance of bevacizumabGOG 252 has completed accrual and results are awaited [139]
11 Newer Forms of Paclitaxel
Development of next-generation taxanes has taken place overthe past 40 years aimed at eliminating toxicity improvingefficacy and ease of administration Abraxane is a novelcompound which incorporates paclitaxel into an albuminnanoparticle soluble in saline hence eliminating the needfor Cremophor EL which is responsible for hypersensitivityreactions experienced during paclitaxel infusion [145] Thenanoparticle albumin in nab-paclitaxel is able to bind toglycoprotein gp60 receptor an albumin receptor and activatecaveolin-1 a protein that in human is encoded byCAV-1 geneleading to formation of caveoli hence allowing nab-paclitaxelto migrate across the endothelial cell membrane into theinterstitial space leading to higher intratumoural drug con-centration In addition Abraxane exhibits linear pharma-cokinetics and can therefore be given at a relatively higherdose than standard intravenous paclitaxel leading to a highertherapeutic ratio and heightened efficacy in solid tumoursmainlymetastatic breast cancer [146 147] Nab-paclitaxel hadFDA approval in 2005 for treatment of breast cancer [148]
Nab-paclitaxel has been studied in recurrent ovariancancer As a single agent in phase II 44 patients withrecurrent ovarian cancer were treated with Nab-paclitaxel260mgm2 intravenously for 30 minutes every 3 weeks for6 cycles Ninety-two percent of patients were platinum-sensitive while 89 had had previous exposure to standardtaxane The objective response rate was 64 with 15 patientsachieving complete response and 13 of them had partialresponse Estimated median PFS was 85 months No hyper-sensitivity reactions were observed and there were infrequentcases of grade 4 neutropenia (11) and grade 2-3 neuropathy(13) [149]
Another phase II study by GOG enrolled 51 patients withplatinum- and taxane-resistant recurrent ovarian cancer outof which 47 were evaluable The objective response rate was38 with one patient achieving a complete response and 10patients a partial response The median PFS was 45 monthswhile overall survival rate was 174 months Severe haema-tological and nonhaematological toxicities including neuro-toxicity were uncommon These results are quite impressivegiven the treatment population consisted of patients withvery poor prognosis with a median platinum and taxane freeinterval of 21 days and 70 had their recurrence within 3months of completion of primary treatment [150] Severalother trials of this formulation are in progress
Paclitaxel poliglumex (PPX) also known as Xyotax isanother prodrug a novel conjugate of paclitaxel and 120572-poly-L-glutamic acid which accumulates within tumour tissuedue to increased permeability of the tumour vessels and lackof lymphatic drainage [148 151 152] Paclitaxel poliglumexenhances solubility of paclitaxel allows direct delivery tothe intratumoural microenvironment and allows prolongedexposure to the active drug while minimising systemictoxicities [151] In Phase I dose escalation studies as a singleagent the recommended dose of PPX was 235mgm2 over 10minutes every 3 weeks or 70mgm2 weekly [153] In a PhaseII GOG study of relapsed ovarian cancer a response rate of16 was seen with infrequent serious adverse events grade3 and 4 neutropenia (24 and 20) and grade 3 neuropathy(24) [154] A phase III trial (GOG-0212) on the use of PPXas consolidation ormaintenance therapy in advanced ovariancancer is in progress
DHA-paclitaxel also known as Taxoprexin is a prodrugwhere paclitaxel is covalently conjugated with the naturallyoccurring omega-3 fatty acid docosahexaenoic acid (DHA)a fatty acid that is easily taken up by tumour cells henceincreasing intratumoural concentration of paclitaxel leadingtumour cell apoptosis [155 156] DHA-paclitaxel exhibitslinear pharmacokinetics and lower toxicity and also ease ofadministration when compared to conventional paclitaxeland has demonstrated antineoplastic activity in animal mod-els of cancer as well as in a phase III trial involving metastaticmelanoma [156ndash160] In a recent study on human ovariancancer cells it was found that DHA could reverse paclitaxelresistance by inhibiting P-gp as well as downregulatingthe expression of multidrug resistance associated proteins(MRP) and inhibiting the activity of NF-120581B and p38 MAPKsignalling pathways [161]
16 BioMed Research International
12 Future Directions
A plateau has been reached regarding the benefits associatedwith standard 3-weekly intravenous administration of cyto-toxic chemotherapy in advanced epithelial ovarian cancerThe ongoing battle for a better treatment regimen to delayrelapse promote remission and most importantly improvethe quality of life of patients with advanced epithelial ovariancancer need not to go further than the ability to relook at thechemotherapy agents that are already available in a differentapproach
Novel compounds to date have not yet shown clinicalsuperiority and parent compounds such as paclitaxel con-tinue to surprise us with their feasibility effectiveness andmanageable toxicity profiles Intraperitoneal paclitaxel willrequire further evaluation Better effort in understanding themechanism of action of drugs including the role of dosescheduling and the effect on the immune systemmay providea more cost-effective route to better clinical outcomes
Conflict of Interests
The authors declare no conflict of interests in this work
Acknowledgments
The authors would like to thank the many researchers whohave contributed to our current knowledge of paclitaxelNirmala Kampan is supported by Australian Monash Uni-versity Institute of Graduate Research Scholarship as wellas Universiti Kebangsaan Malaysia Postgraduate ScholarshipAward Mutsa Madondo has received Postgraduate Pub-lication Award from Monash University and MagdalenaPlebanski has been awarded Senior NHMRC Fellowship
References
[1] Australian Institute of Health and Welfare and National Breastand Ovarian Cancer Centre (Australia) Ovarian Cancer inAustralia AnOverview 2010 Cancer Series Australian Instituteof Health and Welfare Canberra Australia 2010
[2] R E Bristow R S Tomacruz D K Armstrong E L Trimbleand F J Montz ldquoSurvival effect of maximal cytoreductivesurgery for advanced ovarian carcinoma during the platinumera a meta-analysisrdquo Journal of Clinical Oncology vol 20 no 5pp 1248ndash1259 2002
[3] ZKempand JA Ledermann ldquoUpdate onfirst-line treatment ofadvanced ovarian carcinomardquo International Journal of WomenrsquosHealth vol 5 no 1 pp 45ndash51 2013
[4] A du Bois H-J Luck W Meier et al ldquoA randomized clinicaltrial of cisplatinpaclitaxel versus carboplatinpaclitaxel as first-line treatment of ovarian cancerrdquo Journal of the National CancerInstitute vol 95 no 17 pp 1320ndash1330 2003
[5] R F Ozols B N Bundy B E Greer et al ldquoPhase III trialof carboplatin and paclitaxel compared with cisplatin andpaclitaxel in patients with optimally resected stage III ovariancancer A Gynecologic Oncology Group studyrdquo Journal ofClinical Oncology vol 21 no 17 pp 3194ndash3200 2003
[6] W P McGuire W J Hoskins M F Brady et al ldquoCyclophos-phamide and cisplatin compared with paclitaxel and cisplatin
in patients with stage III and stage IV ovarian cancerrdquoThe NewEngland Journal of Medicine vol 334 no 1 pp 1ndash6 1996
[7] W P McGuire W J Hoskins M F Brady et al ldquoCyclophos-phamide and cisplatin versus paclitaxel and cisplatin a phase IIIrandomized trial in patients with suboptimal stage IIIIV ovar-ian cancer (from the gynecologic oncology group)rdquo Seminars inOncology vol 23 no 5 supplement 12 pp 40ndash47 1996
[8] M J Piccart K Bertelsen K James et al ldquoRandomized inter-group trial of cisplatin-paclitaxel versus cisplatin-cyclophosph-amide inwomenwith advanced epithelial ovarian cancer three-year resultsrdquo Journal of the National Cancer Institute vol 92 no9 pp 699ndash708 2000
[9] P A Vasey G C Jayson A Gordon et al ldquoPhase III random-ized trial of docetaxel-carboplatin versus paclitaxel-carboplatinas first-line chemotherpy for ovarian carcinomardquo Journal of theNational Cancer Institute vol 96 no 22 pp 1682ndash1691 2004
[10] B Gronlund C Hogdall H H Hansen and S A EngelholmldquoResults of reinduction therapy with paclitaxel and carboplatinin recurrent epithelial ovarian cancerrdquo Gynecologic Oncologyvol 83 no 1 pp 128ndash134 2001
[11] T M Loffler W Freund J Lipke and T-U HausamenldquoSchedule- and dose-intensified paclitaxel as weekly 1-hourinfusion in pretreated solid tumors results of a phase III trialrdquoSeminars in Oncology vol 23 no 6 supplement 16 pp 32ndash341996
[12] D Fennelly C Aghajanian F Shapiro et al ldquoPhase I and phar-macologic study of paclitaxel administered weekly in patientswith relapsed ovarian cancerrdquo Journal of Clinical Oncology vol15 no 1 pp 187ndash192 1997
[13] N R Abu-Rustum C Aghajanian R R Barakat D Fennelly FShapiro and D Spriggs ldquoSalvage weekly paclitaxel in recurrentovarian cancerrdquo Seminars inOncology vol 24 no 5 supplement15 pp S15-62ndashS15-67 1997
[14] M Markman B N Bundy D S Alberts et al ldquoPhase III trialof standard-dose intravenous cisplatin plus paclitaxel versusmoderately high-dose carboplatin followed by intravenouspaclitaxel and intraperitoneal cisplatin in small-volume stageIII ovarian carcinoma an intergroup study of the gynecologiconcology group Southwestern Oncology Group and EasternCooperativeOncologyGrouprdquo Journal of Clinical Oncology vol19 no 4 pp 1001ndash1007 2001
[15] A Kikuchi H Sakamoto and T Yamamoto ldquoWeekly car-boplatin and paclitaxel is safe active and well tolerated inrecurrent ovarian cancer cases of Japanese women previouslytreated with cisplatin-containing multidrug chemotherapyrdquoInternational Journal of Gynecological Cancer vol 15 no 1 pp45ndash49 2005
[16] I Cadron K Leunen F Amant T van Gorp P Nevenand I Vergote ldquoThe lsquoLeuvenrsquo dose-dense paclitaxelcarboplatinregimen in patients with recurrent ovarian cancerrdquo GynecologicOncology vol 106 no 2 pp 354ndash361 2007
[17] S Pignata E Breda G Scambia et al ldquoA phase II studyof weekly carboplatin and paclitaxel as first-line treatment ofelderly patients with advanced ovarian cancer A Multicen-tre Italian Trial in Ovarian cancer (MITO-5) studyrdquo CriticalReviews in OncologyHematology vol 66 no 3 pp 229ndash2362008
[18] T Safra S Shamai J Greenberg et al ldquoWeekly carboplatinwith paclitaxel compared to standard three-weekly treatment inadvanced epithelial ovarian carcinomamdasha retrospective studyrdquoGynecologic Oncology vol 132 no 1 pp 18ndash22 2014
BioMed Research International 17
[19] L J Havrilesky A A Alvarez R A Sayer et al ldquoWeekly low-dose carboplatin and paclitaxel in the treatment of recurrentovarian and peritoneal cancerrdquo Gynecologic Oncology vol 88no 1 pp 51ndash57 2003
[20] M van der BurgW Onstenk I Boere et al ldquoLong-term resultsof a randomised phase III trial of weekly versus three-weeklypaclitaxelplatinum induction therapy followed by standardor extended three-weekly paclitaxelplatinum in Europeanpatients with advanced epithelial ovarian cancerrdquo EuropeanJournal of Cancer vol 50 no 15 pp 2592ndash2601 2014
[21] N Katsumata M Yasuda F Takahashi et al ldquoDose-densepaclitaxel once a week in combination with carboplatin every3 weeks for advanced ovarian cancer a phase 3 open-labelrandomised controlled trialrdquoThe Lancet vol 374 no 9698 pp1331ndash1338 2009
[22] N Katsumata M Yasuda S Isonishi et al ldquoLong-term resultsof dose-dense paclitaxel and carboplatin versus conventionalpaclitaxel and carboplatin for treatment of advanced epithelialovarian fallopian tube or primary peritoneal cancer (JGOG3016) a randomised controlled open-label trialrdquo The LancetOncology vol 14 no 10 pp 1020ndash1026 2013
[23] K Harano F Terauchi N Katsumata et al ldquoQuality-of-lifeoutcomes from a randomized phase III trial of dose-denseweekly paclitaxel and carboplatin compared with conventionalpaclitaxel and carboplatin as a first-line treatment for stage II-IV ovarian cancer Japanese Gynecologic OncologyGroup Trial(JGOG3016)rdquo Annals of Oncology vol 25 no 1 pp 251ndash2572014
[24] J Chan M F Brady R Penson et al ldquoPhase III trial ofevery-3-weeks paclitaxel vs dose dense weekly paclitaxel withcarboplatin +minus bevacizumab in epithelial ovarian peritonealfallopian tube cancer GOG 262 (NCT01167712)rdquo InternationalJournal of Gynecological Cancer vol 23 no 8 supplement 1 pp9ndash10 2013
[25] S Pignata G Scambia D Katsaros et al ldquoCarboplatin pluspaclitaxel once a week versus every 3 weeks in patients withadvanced ovarian cancer (MITO-7) a randomisedmulticentreopen-label phase 3 trialrdquoThe Lancet Oncology vol 15 no 4 pp396ndash405 2014
[26] V Walsh and J Goodman ldquoFrom taxol to Taxol the changingidentities and ownership of an anti-cancer drugrdquo MedicalAnthropology vol 21 no 3-4 pp 307ndash336 2002
[27] R Renneberg ldquoBiotech History yew trees paclitaxel synthesisand fungirdquo Biotechnology Journal vol 2 no 10 pp 1207ndash12092007
[28] J E Liebmann J A Cook C Lipschultz D Teague J Fisherand J B Mitchell ldquoCytotoxic studies of paclitaxel (Taxol) inhuman tumour cell linesrdquo British Journal of Cancer vol 68 no6 pp 1104ndash1109 1993
[29] J J Manfredi and S B Horwitz ldquoTaxol an antimitotic agentwith a newmechanism of actionrdquo Pharmacology andTherapeu-tics vol 25 no 1 pp 83ndash125 1984
[30] D G I Kingston ldquoRecent advances in the chemistry of taxolrdquoJournal of Natural Products vol 63 no 5 pp 726ndash734 2000
[31] D G I Kingston ldquoThe shape of things to come structural andsynthetic studies of taxol and related compoundsrdquo Phytochem-istry vol 68 no 14 pp 1844ndash1854 2007
[32] V Walsh and J Goodman ldquoCancer chemotherapy biodiversitypublic and private property the case of the anti-cancer drugTaxolrdquo Social Science amp Medicine vol 49 no 9 pp 1215ndash12251999
[33] P H Wiernik E L Schwartz J J Strauman J P Dutcher RB Lipton and E Paietta ldquoPhase I clinical and pharmacokineticstudy of taxolrdquo Cancer Research vol 47 no 9 pp 2486ndash24931987
[34] W P McGuire E K Rowinsky N B Rosenhein et alldquoTaxol a unique antineoplastic agent with significant activityin advanced ovarian epithelial neoplasmsrdquo Annals of InternalMedicine vol 111 no 4 pp 273ndash279 1989
[35] ldquoDiscovery and development of taxolrdquo in Taxol Science andApplications M W M E Suffness Ed pp 3ndash25 CRC PressBoca Raton Fla USA 1995
[36] M J Piccart and F Cardoso ldquoProgress in systemic therapy forbreast cancer an overview and perspectivesrdquo European Journalof Cancer Supplement vol 1 no 2 pp 56ndash69 2003
[37] P Bonomi K B Kim and J Kugler ldquoComparison of survival forstage IIIB versus stage IV non-small cell lung cancer (NSCLC)patients with etoposide-cisplatin versus taxol-cisplatin an East-ern Cooperative Oncology Group (ECOG) trialrdquo in Proceedingsof the American Society of Clinical Oncology vol 16 p 454a1997
[38] D Guenard F Gueritte-Voegelein J Dubois and P PotierldquoStructure-activity relationships of Taxol and Taxotere ana-loguesrdquo Journal of the National Cancer Institute Monographsno 15 pp 79ndash82 1993
[39] D G I Kingston ldquoTaxol the chemistry and structure-activityrelationships of a novel anticancer agentrdquo Trends in Biotechnol-ogy vol 12 no 6 pp 222ndash227 1994
[40] E K Rowinsky and R C Donehower ldquoPaclitaxel (taxol)rdquo TheNew England Journal of Medicine vol 332 no 15 pp 1004ndash10141995
[41] J Parness and S B Horwitz ldquoTaxol binds to polymerizedtubulin in vitrordquo Journal of Cell Biology vol 91 no 2 pp 479ndash487 1981
[42] A Dammermann A Desai and K Oegema ldquoTheminus end insightrdquo Current Biology vol 13 no 15 pp R614ndashR624 2003
[43] CWiese and Y Zheng ldquoMicrotubule nucleation 120574-tubulin andbeyondrdquo Journal of Cell Science vol 119 no 20 pp 4143ndash41532006
[44] A Ganguly H Yang and F Cabral ldquoPaclitaxel-dependent celllines reveal a novel drug activityrdquo Molecular Cancer Therapeu-tics vol 9 no 11 pp 2914ndash2923 2010
[45] P B Schiff and S B Horwitz ldquoTaxol stabilizes microtubules inmouse fibroblast cellsrdquo Proceedings of the National Academy ofSciences of the United States of America vol 77 no 3 pp 1561ndash1565 1980
[46] P B Schiff J Fant and S B Horwitz ldquoPromotion of micro-tubule assembly in vitro by Taxolrdquo Nature vol 277 no 5698pp 665ndash667 1979
[47] D Zhang R Yang S Wang and Z Dong ldquoPaclitaxel new usesfor an old drugrdquoDrug Design Development andTherapy vol 8pp 279ndash284 2014
[48] S Rao G A Orr A G Chaudhary D G I Kingston and SB Horwitz ldquoCharacterization of the taxol binding site on themicrotubule 2-(m-Azidobenzoyl)taxol photolabels a peptide(amino acids 217-231) of beta-tubulinrdquoThe Journal of BiologicalChemistry vol 270 no 35 pp 20235ndash20238 1995
[49] F Wang Y Cao W Zhao H Liu Z Fu and R Han ldquoTaxolinhibits melanoma metastases through apoptosis inductionangiogenesis inhibition and restoration of E-cadherin andnm23 expressionrdquo Journal of Pharmacological Sciences vol 93no 2 pp 197ndash203 2003
18 BioMed Research International
[50] A Sevko V Kremer C Falk et al ldquoApplication of paclitaxel inlow non-cytotoxic doses supports vaccination with melanomaantigens in normal micerdquo Journal of Immunotoxicology vol 9no 3 pp 275ndash281 2012
[51] T Kreis and R Vale Guidebook to the Cytoskeletal and MotorProteins Oxford University Press Oxford UK 2nd edition1999
[52] P Giannakakou D L Sackett Y-K Kang et al ldquoPaclitaxel-resistant human ovarian cancer cells have mutant 120573-tubulinsthat exhibit impaired paclitaxel-driven polymerizationrdquo TheJournal of Biological Chemistry vol 272 no 27 pp 17118ndash171251997
[53] E Rakovitch W Mellado E J Hall T K Pandita S Sawantand C R Geard ldquoPaclitaxel sensitivity correlates with p53status and DNA fragmentation but not G2M accumulationrdquoInternational Journal of Radiation Oncology Biology Physics vol44 no 5 pp 1119ndash1124 1999
[54] S W Lowe S Bodis A McClatchey et al ldquop53 status and theefficacy of cancer therapy in vivordquo Science vol 266 no 5186 pp807ndash810 1994
[55] C C Zhang J-M Yang E White M Murphy A Levine andW N Hait ldquoThe role of MAP4 expression in the sensitivity topaclitaxel and resistance to vinca alkaloids in p53 mutant cellsrdquoOncogene vol 16 no 12 pp 1617ndash1624 1998
[56] K Fukasawa T Choi R Kuriyama S Rulong and G F VandeWoude ldquoAbnormal centrosome amplification in the absence ofp53rdquo Science vol 271 no 5256 pp 1744ndash1747 1996
[57] T-H Wang Y-H Chan C-W Chen et al ldquoPaclitaxel (Taxol)upregulates expression of functional interleukin-6 in humanovarian cancer cells through multiple signaling pathwaysrdquoOncogene vol 25 no 35 pp 4857ndash4866 2006
[58] E Yakirevich E Sabo I Naroditsky Y Sova O Lavie andM B Resnick ldquoMultidrug resistance-related phenotype andapoptosis-related protein expression in ovarian serous carcino-masrdquo Gynecologic Oncology vol 100 no 1 pp 152ndash159 2006
[59] G Szakacs J K Paterson J A Ludwig C Booth-Genthe andM M Gottesman ldquoTargeting multidrug resistance in cancerrdquoNature Reviews Drug Discovery vol 5 no 3 pp 219ndash234 2006
[60] L W Pfannenstiel S S K Lam L A Emens E M Jaffeeand T D Armstrong ldquoPaclitaxel enhances early dendritic cellmaturation and function through TLR4 signaling in micerdquoCellular Immunology vol 263 no 1 pp 79ndash87 2010
[61] N Klauber S Parangi E Flynn E Hamel and R J DrsquoAmatoldquoInhibition of angiogenesis and breast cancer in mice by themicrotubule inhibitors 2-methoxyestradiol and Taxolrdquo CancerResearch vol 57 no 1 pp 81ndash86 1997
[62] D Belotti V Vergani T Drudis et al ldquoThe microtubule-affecting drug paclitaxel has antiangiogenic activityrdquo ClinicalCancer Research vol 2 no 11 pp 1843ndash1849 1996
[63] D H Lau L Xue L J Young P A Burke and A T CheungldquoPaclitaxel (Taxol) an inhibitor of angiogenesis in a highlyvascularized transgenic breast cancerrdquo Cancer Biotherapy andRadiopharmaceuticals vol 14 no 1 pp 31ndash36 1999
[64] X Jiang ldquoHarnessing the immune system for the treatment ofbreast cancerrdquo Journal of Zhejiang University Science B vol 15no 1 pp 1ndash15 2014
[65] A Gadducci D Katsaros P Zola et al ldquoWeekly low-dosepaclitaxel as maintenance treatment in patients with advancedovarian cancer who had microscopic residual disease atsecond-look surgery after 6 cycles of paclitaxelplatinum-basedchemotherapy Results of an open noncomparative phase 2
multicenter italian study (after-6 protocol 2)rdquo InternationalJournal of Gynecological Cancer vol 19 no 4 pp 615ndash619 2009
[66] R S Bhatt J Merchan R Parker et al ldquoA phase 2 pilot trial oflow-dose continuous infusion or lsquometronomicrsquo paclitaxel andoral celecoxib in patients with metastatic melanomardquo Cancervol 116 no 7 pp 1751ndash1756 2010
[67] M Caballero J J Grau J L Blanch et al ldquoSerum vascularendothelial growth factor as a predictive factor in metronomic(weekly) paclitaxel treatment for advanced head and neckcancerrdquo Archives of OtolaryngologymdashHead and Neck Surgeryvol 133 no 11 pp 1143ndash1148 2007
[68] J Alexandre Y Hu W Lu H Pelicano and P Huang ldquoNovelaction of paclitaxel against cancer cells bystander effect medi-ated by reactive oxygen speciesrdquo Cancer Research vol 67 no 8pp 3512ndash3517 2007
[69] T Hadzic N Aykin-Burns Y Zhu et al ldquoPaclitaxel combinedwith inhibitors of glucose and hydroperoxide metabolismenhances breast cancer cell killing viaH
2O2-mediated oxidative
stressrdquo Free Radical Biology and Medicine vol 48 no 8 pp1024ndash1033 2010
[70] C A Sherman-Baust K G Becker W H Wood III Y Zhangand P J Morin ldquoGene expression and pathway analysis of ovar-ian cancer cells selected for resistance to cisplatin paclitaxel ordoxorubicinrdquo Journal of Ovarian Research vol 4 no 1 article21 2011
[71] R Agarwal and S B Kaye ldquoOvarian cancer strategies for over-coming resistance to chemotherapyrdquo Nature Reviews Cancervol 3 no 7 pp 502ndash516 2003
[72] T Acker and K H Plate ldquoRole of hypoxia in tumorangiogenesismdashmolecular and cellular angiogenic crosstalkrdquoCell and Tissue Research vol 314 no 1 pp 145ndash155 2003
[73] M Hockel and P Vaupel ldquoBiological consequences of tumorhypoxiardquo Seminars in Oncology vol 28 supplement 8 no 2 pp36ndash41 2001
[74] L Huang Q-H Zhang Q-L Ao H Xing Y-P Lu and DMa ldquoEffect of hypoxia on the chemotherapeutic sensitivity ofhuman ovarian cancer cells to paclitaxel and its mechanismrdquoZhonghua Zhong Liu Za Zhi vol 29 no 2 pp 96ndash100 2007
[75] N Rohwer and T Cramer ldquoHypoxia-mediated drug resistancenovel insights on the functional interaction of HIFs and celldeath pathwaysrdquoDrug Resistance Updates vol 14 no 3 pp 191ndash201 2011
[76] B B Aggarwal R V Vijayalekshmi and B Sung ldquoTargetinginflammatory pathways for prevention and therapy of cancershort-term friend long-term foerdquo Clinical Cancer Research vol15 no 2 pp 425ndash430 2009
[77] Z Duan R Foster D A Bell et al ldquoSignal transducersand activators of transcription 3 pathway activation in drug-resistant ovarian cancerrdquo Clinical Cancer Research vol 12 no17 pp 5055ndash5063 2006
[78] H-J Kuh S H Jang M G Wientjes J R Weaver and J L-SAu ldquoDeterminants of paclitaxel penetration and accumulationin human solid tumorrdquo Journal of Pharmacology and Experi-mental Therapeutics vol 290 no 2 pp 871ndash880 1999
[79] S Arao H Suwa M Mandai et al ldquoHypoxia-mediated drugresistance novel insights on the functional interaction of HIFsand cell death pathwaysrdquo Cancer Research vol 54 no 5 pp1355ndash1359 1994
[80] S E Johnatty J Beesley B Gao et al ldquoABCB1 (MDR1)polymorphisms and ovarian cancer progression and survivala comprehensive analysis from the Ovarian Cancer Association
BioMed Research International 19
Consortium and the Cancer GenomeAtlasrdquoGynecologic Oncol-ogy vol 131 no 1 pp 8ndash14 2013
[81] X Yang A K Iyer A Singh et al ldquoCluster of differentiation44 targeted hyaluronic acid based nanoparticles for MDR1siRNA delivery to overcome drug resistance in ovarian cancerrdquoPharmaceutical Research 2014
[82] D A Zajchowski B Y Karlan and L K Shawver ldquoTreatment-related protein biomarker expression differs between primaryand recurrent ovarian carcinomasrdquoMolecular CancerTherapeu-tics vol 11 no 2 pp 492ndash502 2012
[83] MM Gottesman J Ludwig D Xia and G Szakacs ldquoDefeatingdrug resistance in cancerrdquoDiscovery Medicine vol 6 no 31 pp18ndash23 2006
[84] S Mozzetti C Ferlini P Concolino et al ldquoClass III 120573-tubulin overexpression is a prominent mechanism of paclitaxelresistance in ovarian cancer patientsrdquo Clinical Cancer Researchvol 11 no 1 pp 298ndash305 2005
[85] M Kavallaris D Y S Kuo C A Burkhart et al ldquoTaxol-resistant epithelial ovarian tumors are associated with alteredexpression of specific beta-tubulin isotypesrdquo Journal of ClinicalInvestigation vol 100 no 5 pp 1282ndash1293 1997
[86] G A Orr P Verdier-Pinard H McDaid and S B HorwitzldquoMechanisms of Taxol resistance related to microtubulesrdquoOncogene vol 22 no 47 pp 7280ndash7295 2003
[87] C Ferlini L Cicchillitti G Raspaglio et al ldquoPaclitaxel directlybinds to Bcl-2 and functionally mimics activity of Nur77rdquoCancer Research vol 69 no 17 pp 6906ndash6914 2009
[88] E Mechetner A Kyshtoobayeva S Zonis et al ldquoLevels ofmultidrug resistance (MDR1) P-glycoprotein expression byhuman breast cancer correlate with in vitro resistance to taxoland doxorubicinrdquo Clinical Cancer Research vol 4 no 2 pp389ndash398 1998
[89] J S Lagas C W N Damen R A B VanWaterschoot D IusufJ H Beijnen and A H Schinkel ldquoP-glycoprotein multidrug-resistance associated protein 2 Cyp3a and carboxylesteraseaffect the oral availability and metabolism of vinorelbinerdquoMolecular Pharmacology vol 82 no 4 pp 636ndash644 2012
[90] M T Huizing J B Vermorken H Rosing et al ldquoPharmacoki-netics of paclitaxel and three major metabolites in patients withadvanced breast carcinoma refractory to anthracycline therapytreated with a 3-hour paclitaxel infusion a European CancerCentre (ECC) trialrdquo Annals of Oncology vol 6 no 7 pp 699ndash704 1995
[91] R Panchagnula ldquoPharmaceutical aspects of paclitaxelrdquo Interna-tional Journal of Pharmaceutics vol 172 no 1-2 pp 1ndash15 1998
[92] S H Jang M G Wientjes and J L-S Au ldquoDeterminants ofpaclitaxel uptake accumulation and retention in solid tumorsrdquoInvestigational New Drugs vol 19 no 2 pp 113ndash123 2001
[93] D S Sonnichsen andM V Relling ldquoClinical pharmacokineticsof paclitaxelrdquo Clinical Pharmacokinetics vol 27 no 4 pp 256ndash269 1994
[94] T Ohtsu Y Sasaki T Tamura et al ldquoClinical pharmacokineticsand pharmacodynamics of paclitaxel a 3-hour infusion versusa 24-hour infusionrdquo Clinical Cancer Research vol 1 no 6 pp599ndash606 1995
[95] M Czejka J Schueller H Schnait B Springer and I EderldquoClinical pharmacokinetics andmetabolism of paclitaxel after athree-hour infusion comparison of two preparationsrdquo Journalof Oncology Pharmacy Practice vol 9 no 4 pp 129ndash136 2003
[96] J Rizzo C Riley D VonHoff J Kuhn J Phillips and T BrownldquoAnalysis of anticancer drugs in biological fluids determination
of taxol with application to clinical pharmacokineticsrdquo Journalof Pharmaceutical and Biomedical Analysis vol 8 no 2 pp 159ndash164 1990
[97] V A de Weger J H Beijnen and J H M Schellens ldquoCel-lular and clinical pharmacology of the taxanes docetaxel andpaclitaxelmdasha reviewrdquoAnti-Cancer Drugs vol 25 no 5 pp 488ndash494 2014
[98] S Kumar H Mahdi C Bryant J P Shah G Garg andA Munkarah ldquoClinical trials and progress with paclitaxel inovarian cancerrdquo International Journal of Womenrsquos Health vol 2no 1 pp 411ndash427 2010
[99] B Huang J Zhao J C Unkeless Z H Feng and H XiongldquoTLR signaling by tumor and immune cells a double-edgedswordrdquo Oncogene vol 27 no 2 pp 218ndash224 2008
[100] R A Jibodh J S Lagas B Nuijen J H Beijnen and J HM Schellens ldquoTaxanes old drugs new oral formulationsrdquoEuropean Journal of Pharmacology vol 717 no 1ndash3 pp 40ndash462013
[101] A Javeed M Ashraf A Riaz A Ghafoor S Afzal and M MMukhtar ldquoPaclitaxel and immune systemrdquo European Journal ofPharmaceutical Sciences vol 38 no 4 pp 283ndash290 2009
[102] L Bracci G Schiavoni A Sistigu and F Belardelli ldquoImmune-based mechanisms of cytotoxic chemotherapy implications forthe design of novel and rationale-based combined treatmentsagainst cancerrdquo Cell Death and Differentiation vol 21 no 1 pp15ndash25 2014
[103] C A Byrd-Leifer E F Block K Takeda S Akira and A DingldquoThe role of MyD88 and TLR4 in the LPS-mimetic activity ofTaxolrdquo European Journal of Immunology vol 31 no 8 pp 2448ndash2457 2001
[104] A-C Wang Y-B Ma F-X Wu et al ldquoTLR4 induces tumorgrowth and inhibits paclitaxel activity in MyD88-positivehuman ovarian carcinoma in vitrordquo Oncology Letters vol 7 no3 pp 871ndash877 2014
[105] Y Zhu N Liu S D Xiong Y J Zheng and Y W ChuldquoCD4+Foxp3+ regulatory T-cell impairment by paclitaxel isindependent of toll-like receptor 4rdquo Scandinavian Journal ofImmunology vol 73 no 4 pp 301ndash308 2011
[106] M Kubo T Morisaki K Matsumoto et al ldquoPaclitaxel probablyenhances cytotoxicity of natural killer cells against breastcarcinoma cells by increasing perforin productionrdquo CancerImmunology Immunotherapy vol 54 no 5 pp 468ndash476 2005
[107] L Markasz G Stuber B Vanherberghen et al ldquoEffect of fre-quently used chemotherapeutic drugs on the cytotoxic activityof human natural killer cellsrdquo Molecular Cancer Therapeuticsvol 6 no 2 pp 644ndash654 2007
[108] T Sako N Burioka K Yasuda et al ldquoCellular immune profile inpatients with non-small cell lung cancer after weekly paclitaxeltherapyrdquo Acta Oncologica vol 43 no 1 pp 15ndash19 2004
[109] R Kaneno G V Shurin I L Tourkova and M R ShurinldquoChemomodulation of human dendritic cell function by anti-neoplastic agents in low noncytotoxic concentrationsrdquo Journalof Translational Medicine vol 7 article 58 2009
[110] TMichels G V ShurinHNaiditch A Sevko VUmansky andM R Shurin ldquoPaclitaxel promotes differentiation of myeloid-derived suppressor cells into dendritic cells in vitro in a TLR4-independent mannerrdquo Journal of Immunotoxicology vol 9 no3 pp 292ndash300 2012
[111] R A Kemp and F Ronchese ldquoTumor-specific Tc1 but not Tc2cells deliver protective antitumor immunityrdquo The Journal ofImmunology vol 167 no 11 pp 6497ndash6502 2001
20 BioMed Research International
[112] A Y Rudensky ldquoRegulatory T cells and Foxp3rdquo ImmunologicalReviews vol 241 no 1 pp 260ndash268 2011
[113] EM Shevach ldquoCD4+CD25+ suppressor T cellsmore questionsthan answersrdquo Nature Reviews Immunology vol 2 no 6 pp389ndash400 2002
[114] S Sakaguchi T Yamaguchi T Nomura and M Ono ldquoRegu-latory T cells and immune tolerancerdquo Cell vol 133 no 5 pp775ndash787 2008
[115] H Nishikawa and S Sakaguchi ldquoRegulatory T cells in tumorimmunityrdquo International Journal of Cancer vol 127 no 4 pp759ndash767 2010
[116] W Zou ldquoRegulatory T cells tumour immunity and immuno-therapyrdquoNature Reviews Immunology vol 6 no 4 pp 295ndash3072006
[117] A Fialova S Partlova L Sojka et al ldquoDynamics of T-cell infil-tration during the course of ovarian cancer The gradual shiftfrom aTh17 effector cell response to a predominant infiltrationby regulatory T-cellsrdquo International Journal of Cancer vol 132no 5 pp 1070ndash1079 2013
[118] A E Albers R L Ferris G G Kim K Chikamatsu A BDeLeo and T L Whiteside ldquoImmune responses to p53 inpatients with cancer enrichment in tetramer+ p53 peptide-specific T cells and regulatory T cells at tumor sitesrdquo CancerImmunology Immunotherapy vol 54 no 11 pp 1072ndash10812005
[119] N Liu Y Zheng Y Zhu S Xiong andYChu ldquoSelective impair-ment of CD4 + CD25 + Foxp3 + regulatory T cells by paclitaxelis explained by Bcl-2Bax mediated apoptosisrdquo InternationalImmunopharmacology vol 11 no 2 pp 212ndash219 2011
[120] X Wu Q-M Feng Y Wang J Shi H-L Ge and W DildquoThe immunologic aspects in advanced ovarian cancer patientstreated with paclitaxel and carboplatin chemotherapyrdquo CancerImmunology Immunotherapy vol 59 no 2 pp 279ndash291 2010
[121] A P Vicari R Luu N Zhang et al ldquoPaclitaxel reducesregulatoryT cell numbers and inhibitory function and enhancesthe anti-tumor effects of the TLR9 agonist PF-3512676 in themouserdquo Cancer Immunology Immunotherapy vol 58 no 4 pp615ndash628 2009
[122] L Zhang K Dermawan M Jin et al ldquoDifferential impairmentof regulatory T cells rather than effector T cells by paclitaxel-based chemotherapyrdquo Clinical Immunology vol 129 no 2 pp219ndash229 2008
[123] Y Tabuchi J Matsuoka M Gunduz et al ldquoResistance topaclitaxel therapy is related with Bcl-2 expression through anestrogen receptor mediated pathway in breast cancerrdquo Interna-tional Journal of Oncology vol 34 no 2 pp 313ndash319 2009
[124] N Obermajer R Muthuswamy K Odunsi R P Edwards andP Kalinski ldquoPGE
2-induced CXCL12 production and CXCR4
expression controls the accumulation of human MDSCs inovarian cancer environmentrdquo Cancer Research vol 71 no 24pp 7463ndash7470 2011
[125] Q M Feng W Di and X Wu ldquoImmune reconstitution inadvanced ovarian cancer patients undergoing first line chemo-therapyrdquo Xi Bao Yu Fen Zi Mian Yi Xue Za Zhi vol 25 no 11pp 1023ndash1025 2009
[126] A D Seidman D Hochhauser M Gollub et al ldquoNinety-six-hour paclitaxel infusion after progression during short taxaneexposure a phase II pharmacokinetic and pharmacodynamicstudy in metastatic breast cancerrdquo Journal of Clinical Oncologyvol 14 no 6 pp 1877ndash1884 1996
[127] D R Spriggs M F Brady L Vaccarello et al ldquoPhase IIIrandomized trial of intravenous cisplatin plus a 24- or 96-hour
infusion of paclitaxel in epithelial ovarian cancer a gynecologiconcology group studyrdquo Journal of Clinical Oncology vol 25 no28 pp 4466ndash4471 2007
[128] G A Omura M F Brady K Y Look et al ldquoPhase III trial ofpaclitaxel at two dose levels the higher dose accompanied byfilgrastim at two dose levels in platinum-pretreated epithelialovarian cancer an intergroup studyrdquo Journal of Clinical Oncol-ogy vol 21 no 15 pp 2843ndash2848 2003
[129] R Simon and L Norton ldquoThe Norton-Simon hypothesisdesigning more effective and less toxic chemotherapeutic reg-imensrdquoNature Clinical Practice Oncology vol 3 no 8 pp 406ndash407 2006
[130] A Kumar P Hoskins and A Tinker ldquoDose-dense paclitaxel inadvanced ovarian cancerrdquo Clinical Oncology vol 27 no 1 pp40ndash47 2015
[131] P Marchetti S Urien G A Cappellini G Ronzino and CFicorella ldquoWeekly administration of paclitaxel theoretical andclinical basisrdquoCritical Reviews in OncologyHematology vol 44supplement pp S3ndashS13 2002
[132] P Francis E Rowinsky J Schneider T Hakes W Hoskinsand M Markman ldquoPhase I feasibility and pharmacologic studyof weekly intraperitoneal paclitaxel A Gynecologic OncologyGroup pilot studyrdquo Journal of Clinical Oncology vol 13 no 12pp 2961ndash2967 1995
[133] H Thomas and P Rosenberg ldquoRole of weekly paclitaxel inthe treatment of advanced ovarian cancerrdquo Critical Reviews inOncologyHematology vol 44 supplement pp S43ndashS51 2002
[134] M Markman J Markman K Webster et al ldquoDuration ofresponse to second-line platinum-based chemotherapy forovarian cancer implications for patient management and clini-cal trial designrdquo Journal of Clinical Oncology vol 22 no 15 pp3120ndash3125 2004
[135] P H OrsquoDonnell M Eileen Dolan E Gamazon et al ldquoPopu-lation differences in platinum toxicity as a means to identifynovel genetic susceptibility variantsrdquo Pharmacogenetics andGenomics vol 20 no 5 pp 327ndash337 2010
[136] M J Millward M J Boyer M Lehnert et al ldquoDocetaxel andcarboplatin is an active regimen in advanced non-small-celllung cancer a phase II study in Caucasian and Asian patientsrdquoAnnals of Oncology vol 14 no 3 pp 449ndash454 2003
[137] M Markman ldquoIntraperitoneal therapy of ovarian cancerrdquoOncologist vol 1 no 1-2 pp 18ndash21 1996
[138] M Markman and J L Walker ldquoIntraperitoneal chemotherapyof ovarian cancer a review with a focus on practical aspects oftreatmentrdquo Journal of Clinical Oncology vol 24 no 6 pp 988ndash994 2006
[139] K Fujiwara S Nagao E Aotani and K Hasegawa ldquoPrincipleand evolving role of intraperitoneal chemotherapy in ovariancancerrdquo Expert Opinion on Pharmacotherapy vol 14 no 13 pp1797ndash1806 2013
[140] M Markman E Rowinsky T Hakes et al ldquoPhase I trialof intraperitoneal taxol a gynecoloic oncology group studyrdquoJournal of Clinical Oncology vol 10 no 9 pp 1485ndash1491 1992
[141] M Markman M F Brady N M Spirtos P Hanjani and S CRubin ldquoPhase II trial of intraperitoneal paclitaxel in carcinomaof the ovary tube and peritoneum a gynecologic oncologygroup studyrdquo Journal of Clinical Oncology vol 16 no 8 pp2620ndash2624 1998
[142] P B Panici I Palaia M Graziano F Bellati N Manci and RAngioli ldquoIntraperitoneal paclitaxel as consolidation treatmentin ovarian cancer patients a case control studyrdquo Oncology vol78 no 1 pp 20ndash25 2010
BioMed Research International 21
[143] D K Armstrong B Bundy L Wenzel et al ldquoIntraperitonealcisplatin and paclitaxel in ovarian cancerrdquo The New EnglandJournal of Medicine vol 354 no 1 pp 34ndash43 2006
[144] D Tewari J Java and R Salani ldquoLong-term survival advantageof intraperitoneal chemotherapy treatment in advanced ovariancancer an analysis of a Gynecologic Oncology Group ancillarydata studyrdquo in Proceedings of the 2013 Society of GynecologicOncology Annual Meeting on Womenrsquos Cancer (GOG114172Abstract) Los Angeles Calif USA 2013
[145] D A Yardley ldquonab-paclitaxel mechanisms of action and deliv-eryrdquo Journal of Controlled Release vol 170 no 3 pp 365ndash3722013
[146] M Ando K Yonemori N Katsumata et al ldquoPhase I and phar-macokinetic study of nab-paclitaxel nanoparticle albumin-bound paclitaxel administeredweekly to Japanese patients withsolid tumors and metastatic breast cancerrdquo Cancer Chemother-apy and Pharmacology vol 69 no 2 pp 457ndash465 2012
[147] N Desai V Trieu Z Yao et al ldquoIncreased antitumor activityintratumor paclitaxel concentrations and endothelial cell trans-port of cremophor-free albumin-bound paclitaxel ABI-007compared with cremophor-based paclitaxelrdquo Clinical CancerResearch vol 12 no 4 pp 1317ndash1324 2006
[148] J A Yared and K H R Tkaczuk ldquoUpdate on taxane devel-opment new analogs and new formulationsrdquo Drug DesignDevelopment andTherapy vol 6 pp 371ndash384 2012
[149] M G Teneriello P C Tseng M Crozier et al ldquoPhase IIevaluation of nanoparticle albumin-bound paclitaxel in plati-num-sensitive patients with recurrent ovarian peritoneal orfallopian tube cancerrdquo Journal of Clinical Oncology vol 27 no9 pp 1426ndash1431 2009
[150] R L Coleman W E Brady D S McMeekin et al ldquoA phase IIevaluation of nanoparticle albumin-bound (nab) paclitaxel inthe treatment of recurrent or persistent platinum-resistant ovar-ian fallopian tube or primary peritoneal cancer a GynecologicOncology Group Studyrdquo Gynecologic Oncology vol 122 no 1pp 111ndash115 2011
[151] J W Singer ldquoPaclitaxel poliglumex (XYOTAX CT-2103) amacromolecular taxanerdquo Journal of Controlled Release vol 109no 1ndash3 pp 120ndash126 2005
[152] C Li D-F Yu R A Newman et al ldquoComplete regressionof well-established tumors using a novel water-soluble poly(L-glutamic acid)-paclitaxel conjugaterdquo Cancer Research vol 58no 11 pp 2404ndash2409 1998
[153] M Mita A Mita J Sarantopoulos et al ldquoPhase I study ofpaclitaxel poliglumex administered weekly for patients withadvanced solid malignanciesrdquo Cancer Chemotherapy and Phar-macology vol 64 no 2 pp 287ndash295 2009
[154] P Sabbatini M W Sill D OrsquoMalley L Adler and A ASecord ldquoA phase II trial of paclitaxel poliglumex in recurrentor persistent ovarian or primary peritoneal cancer (EOC) agynecologic oncology group studyrdquo Gynecologic Oncology vol111 no 3 pp 455ndash460 2008
[155] M O Bradley C S Swindell F H Anthony et al ldquoTumortargeting by conjugation of DHA to paclitaxelrdquo Journal ofControlled Release vol 74 no 1ndash3 pp 233ndash236 2001
[156] M O Bradley N L Webb F H Anthony et al ldquoTumortargeting by covalent conjugation of a natural fatty acid topaclitaxelrdquo Clinical Cancer Research vol 7 no 10 pp 3229ndash3238 2001
[157] A C Wolff R C Donehower M K Carducci et al ldquoPhaseI study of docosahexaenoic acid-paclitaxel a taxane-fatty acid
conjugate with a unique pharmacology and toxicity profilerdquoClinical Cancer Research vol 9 no 10 part 1 pp 3589ndash35972003
[158] A Sparreboom A C Wolff J Verweij et al ldquoDispositionof docosahexaenoic acid-paclitaxel a novel taxane in bloodin vitro and clinical pharmacokinetic studiesrdquo Clinical CancerResearch vol 9 no 1 pp 151ndash159 2003
[159] P M Fracasso J Picus J D Wildi et al ldquoPhase 1 and phar-macokinetic study of weekly docosahexaenoic acid-paclitaxelTaxoprexin in resistant solid tumor malignanciesrdquo CancerChemotherapy and Pharmacology vol 63 no 3 pp 451ndash4582009
[160] A Y Bedikian R C DeConti R Conry et al ldquoPhase 3 study ofdocosahexaenoic acid-paclitaxel versus dacarbazine in patientswith metastatic malignant melanomardquo Annals of Oncology vol22 no 4 pp 787ndash793 2011
[161] Y-N Wu S-L Wang Y-C Wang et al ldquoReversal effect ofdocosahexaenoic acid on taxol resistance in human ovarian car-cinoma A2780T cellsrdquo Obstetrics amp Gynecology InternationalJournal vol 1 no 3 Article ID 00018 2014
Submit your manuscripts athttpwwwhindawicom
PainResearch and TreatmentHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom
Volume 2014
ToxinsJournal of
VaccinesJournal of
Hindawi Publishing Corporation httpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
AntibioticsInternational Journal of
ToxicologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
StrokeResearch and TreatmentHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Drug DeliveryJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Advances in Pharmacological Sciences
Tropical MedicineJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Medicinal ChemistryInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
AddictionJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
Emergency Medicine InternationalHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Autoimmune Diseases
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Anesthesiology Research and Practice
ScientificaHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Pharmaceutics
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of

12 BioMed Research International
Numerous phase II studies have explored the tolerabilityand the activity of weekly paclitaxel either as a single agent orin combination with several other drugs or biological agents(Table 1) A number of regimens combining weekly paclitaxelwith carboplatin have been used as first-line treatment inovarian cancer Carboplatin has been administered weeklyat AUC of 2 with dose escalation in some studies whilepaclitaxel had been infused at 60ndash80mgm2week Thiscombined regimen was well tolerated with a low incidence ofbone marrow suppression Overall response rates have beenhigh in the range of 60ndash80 in most studies even in heavilypretreated patients with platinum-resistant disease (diseaserecurrence or progression within 6 months of the last lineof platinum-based therapy) [15ndash20 134] The promising datafrom these phase II trials then led to the evolution of largerphase III trials
Three phase III studies Japanese Gynecologic OncologyGroup- (JGOG-) Trial 3016 [21ndash23] Multicentre Italian Trialin Ovarian Cancer-Trial 7 (MITO-7) [25] and GynecologicOncology Group GOG-262 Trial [24] have explored dosedense therapy The results of these trials are summarised inTable 2
The Japanese Gynecologic Oncology Group (JGOG)conducted a randomized phase 3 trial of dose-dense weeklypaclitaxel 80mgm2week in combination with 3-weeklycarboplatin compared to standard 3-weekly carboplatin andpaclitaxel 180mgm2 in patients with advanced epithelialovarian peritoneal or fallopian tube cancer (JGOG 3016NOVEL trial) In both arms carboplatin was given at AUC6 and the median number of cycles was six In this largestudy (119899 = 637) with a median follow up of 77 months therewas an 11-month improvement in themedian progression freesurvival (PFS) in the dose-dense treatment group comparedwith the standard treatment arm (282 versus 175 monthsHR 076 95 CI 062ndash091 119901 = 00037) Median OS wasalso higher in the dose-dense treatment arm (1005 versus622 months HR 079 95 CI 063ndash099 119901 = 0039)On subgroup analysis suboptimally debulked patients withresidual disease of gt1 cm (119899 = 342) had a significantlyhigher median overall survival in the dose dense arm (512versus 335 months HR-075 95 CI 057ndash097 119901 = 0027)There was no significant advantage to dose-dense treatmentfor patients with optimally cytoreduced disease Dose-densetherapy survival benefits were also not seen in patients withclear cell or mucinous histology type unlike serous typeHowever patient treated with dose dense therapy had asignificantly higher frequency of hematologic toxicity thanwith the standard arm (212 versus 94) which resultedin lower treatment completion rates (63 versus 48) withfrequent episodes of delay (76 versus 67) and dosereductions (48versus 35) [21 22]Therewas no significantdifference in terms of overall quality of life between the twoarms (119901 = 046) [23]
Using a similar regimen as in JGOG-3016 a GynecologicOncology Group (GOG)-262 Trial was conducted in theUnited States In this group most patients had stage IIIdisease (66ndash70) and two-thirds had suboptimal debulkingwith residual disease of gt1 cm This was a randomized phase
III trial of 3 weekly paclitaxel versus dose-dense weeklypaclitaxel in combination with carboplatin in patients withadvanced epithelial ovarian peritoneal or fallopian tubecancer Though optional concurrent and maintenance beva-cizumab were received by the majority of patients in botharms (835 versus 841 resp) There was no significantdifference in PFS in the patients who received the dosedense paclitaxelcarboplatin regimen compared to those whoreceived the standard paclitaxelcarboplatin regimen (148versus 143 months HR 097 95 CI 079ndash118) Howeverin a subgroup analysis there was a significant difference inPFS in the dose dense paclitaxel arm who did not receivebevacizumab 119899 = 112 (142 versus 103 months HR 059 95CI 037ndash096 119901 = 0003) Overall survival data is still imma-ture There was higher frequency of grade 3 anaemia (408versus 157 119901 lt 0001) and grade 2 sensory neuropathy(259 versus 178 119901 = 0012) but a lower incidence ofneutropenia (72 versus 83 119901 lt 0001) [24]
In 2008 the Multicentre Italian Trials in Ovarian Cancer(MITO-7) randomised 810 women in a phase 3 trial toreceive either standard carboplatin (AUC = 6) and paclitaxel175mgm2 every 3 weeks or a weekly schedule of paclitaxel(60mgm2) with carboplatin (AUC = 2) The majority ofpatients in both arms (83ndash90) received six cycles of therapyMost patients (58ndash63) had stage II1 disease 23 of themwere suboptimally debulked Median PFS did not differsignificantly (173 months and 183 months 119901 = 066)between the standard and dose-dense arms respectivelyThere was no significant difference in response rate betweenthe two arms nor the estimated 2-year overall survivalSubgroup analysis did not identify any subgroup that mayhave benefited from the dose-dense regimen Unlike theJGOG-3016 trial the incidence of grade 3-4 neutropenia wassignificantly lower in the dose-dense group compared to the3-weekly regimen (42 versus 50) A similar pattern wasseen for the incidence of febrile neutropenia (lt1 versus 3119901 = 002) thrombocytopenia (1 versus 7 119901 lt 0001)and other nonhaematological toxicities such as alopeciavomiting renal dysfunction and neuropathy Quality of lifewas reported to be significantly better in the dose-dense arm(119901 lt 00001) which was discordant with the JGOG-3016quality of life data [25]
In summary there was significant improvement inmedian PFS and overall survival in studies using paclitaxelat 80mgm2week dose-dense therapy [21 24] but withhigher haematological toxicity whereas MITO-7 [25] whichwas using paclitaxel at 60mgm2week was only equivalentlyeffective but less toxicThis does not conclude that the higherpaclitaxel dose is more clinically beneficial as there are manyother confounding factors in all three studies
In a multivariate analysis the JGOG-3016 study [21]reported that a lower dose intensity of paclitaxel (lt80) wasassociated with poorer overall survival (hazard ratio = 14295 confidence interval 112ndash181 119901 = 0004) however itmust be highlighted that the investigational arm carboplatinschedules were not standardised in these studies The JGOGand GOG trials delivered a 3-weekly carboplatin (AUC =6) arm whereas in the MITO-7 study the carboplatin was
BioMed Research International 13
Table2Ph
aseIIIstu
dies
onintravenou
sdose-densep
aclitaxel
Stud
yRe
gimen
119899
MedianPF
S(m
)
Median
OS
(m)
Adversee
ffects
Com
ments
Katsu
matae
tal2009
[21]
Katsu
matae
tal2013
[22]
Haranoetal2014
[23]
JGOG3016
631
(i)Haematologicaltoxicityhigh
erin
dose
dense-211versus
94
Lower
treatmentcom
pletionin
dose-dense
63versus
48
Frequent
episo
deso
fdelay
indo
se-dense
76versus
67
Doser
eductio
nsin
dose-dense
48versus
35
Nosig
nificantd
ifference
inoverallQ
OL
betweenbo
thgrou
ps(119901=046)
Paclitaxel80m
gm
2D18
15+carbop
latin
AUC63
weeklyversus
Paclitaxel180
mgm
2+
carbop
latin
AUC63
weekly
312
282
1005
Both
givenfor6
ndash9cycle
s319
175
622
Chan
etal2013
[24]
GOG-262
(i)Higherfrequ
ency
ofgrade3
anaemia
(408versus
157119901lt0001)
grade2
sensoryneurop
athy
(259versus
178
119901=0012)b
utlower
incidenceo
fneutropenia(
72versus
83119901lt0001)
Paclitaxel80m
gm
2D18
15+carbop
latin
AUC63
weeklyversus
Paclitaxel175
mgm
2+
carbop
latin
AUC63
weekly
346
148
NR
Both
givenfor6
cycle
s346
143
NR
Bevacizumab
given
optio
nally
112
(did
not
receive
bevazicumab)
142vs
103
Pign
atae
tal2014
[25]
MITO-7
810
(i)Lo
wer
incidenceo
fgrade
3-4
neutropenia(
42versus
50)febrile
neutropenia(lt1v
ersus3
119901=002)
thrombo
cytopenia(
1versus7
119901lt0001)andothern
onhaem
atological
toxicitie
ssuchas
alop
eciavom
iting
renald
ysfunctio
nandneurop
athy
Qualityof
lifeb
etterindo
sedensea
rm(119901lt00001)
Paclitaxel60m
gm
2 weekly+carbop
latin
AUC
2weeklyversus
Paclitaxel175
mgm
2+
carbop
latin
AUC63
weekly
406
404
183 173
77lowast
79lowast
119899num
bero
fpatientsmm
onthsDday
PFSprogressionfre
esurvivalOSoverallsurvivalNAnot
availableinpapero
rabstractandNR
notyetreached
lowastSurvivalrateat2years
14 BioMed Research International
dose-dense (AUC 2 weekly) Although it is possible that thedose scheduling for the platinum-based agent is not essentialfor a survival benefit as shown by previous studies usingdose-dense cisplatin direct cross-trial comparison cannot bemade Unlike paclitaxel carboplatin probably requires peakdose for optimal therapeutic benefit hence this may accountfor the inferior survival outcome in MITO-7 trial Anotherconfounding factor may be difference in ethnicity All threestudies used different ethnic populations and Asian patientsin JGOG-3016 appear to have better survival outcomes thanthe MITO-7 Western population Ethnicity with possibleunderlying genetic causes may be responsible for the variableresponses to chemotherapy across individuals [135] This wasexplored by Millward et al who studied 68 Caucasian andAsian lung cancer patients treated with a combination ofpaclitaxel and carboplatin and found that the incidence offebrile neutropenia was 50 of an initially treated cohortof Asians and when carboplatin was subsequently dosereduced in all Asian patients the overall incidence of febrileneutropenia was also reduced to 26 [136]
Although early clinical data from phase I and phaseII dose-dense paclitaxel trials in advanced ovarian cancerwere promising the results from phase III studies in havebeen inconsistent as a result of differences in paclitaxel dosecarboplatin AUC and schedule addition of bevacizumabas well as different ethnic populations The results of arecently completed randomised three arms GynaecologicCancer InterGroup (GCIG) phase II trial ICON 8 mayfurther inform the clinical benefit of dose dense paclitaxeltherapy
This multicentre trial involving 111 centres in the UKSouth Korea Mexico Ireland Australia and New Zealandwith a target population of 1485 patients with stage IC-IV epithelial ovarian cancer or peritoneal or fallopian tubecancer compared two dose-dense arms (i) JGOG-like armcarboplatin AUC 5 plus weekly 80mgm2 paclitaxel and (ii)MITO-7-like arm weekly carboplatin AUC 167 plus weekly80mgm2 paclitaxel to the standard 3-weekly treatment(carboplatin AUC 5 plus 175mgm2 paclitaxel) for stage IC toIV epithelial ovarian cancer The dose-dense arms of MITO-7 and JGOG-3016 as well as the ethnic heterogeneity will befurther addressed
10 Intraperitoneal (IP) Chemotherapy
In addition to dose and scheduling the route of adminis-tration of chemotherapy agents plays an important role inoutcome Intraperitoneal spread is common and likely anearly event in epithelial ovarian cancer hence the deliveryof chemotherapy intraperitoneally in theory would exposethe microcirculation of tumour to higher doses of drug thansystemic administration while limiting systemic toxicityTheideal drug for IP chemotherapy is one that is systemicallyeffective penetrates deep into the inner core of tumour tissueand remains within the peritoneal cavity for a prolongedperiod of time [137ndash139]
Early clinical studies confirmed that indeed the peritonealcavity could be exposed to 10 to 20-fold higher (cisplatin
and carboplatin) drug concentration than when using theintravenous approach and since 1978 this route had beenadopted as a form of therapeutic intervention [137 139]A subsequent phase I trial showed that IP paclitaxel haddose-limiting toxicity in the form of abdominal pain [140]Another phase 1 GOG pilot study administered weekly IPpaclitaxel at an initial dose of 20mgm2 for 16 weeks to33 patients and found that IP paclitaxel at this dose wasfeasible and well tolerated At dose levels 60 to 65mgm2there were significant levels of paclitaxel for a week afterdrug administration suggesting very slow clearance andcontinuous exposure of the peritoneal cavity to active drugconcentrations [132]
Hence this initiated a phase II study [141] that used pacli-taxel intraperitoneally at a dose of 60ndash65mgm2week In thisphase II GOG study 76 patients with small-volume resid-ual disease carcinoma (05 cm or less) involving the ovaryperitoneal or fallopian tube were treated with paclitaxel60mgm2week intraperitoneally for 16 weeks followed bysurgical evaluation in patients without disease progressionThe Gynaecologic Oncology group (GOG) currently definesno visible disease as microscopic disease being the idealsurgical outcome 75 of patients had received prior systemictherapy and 70 received all 16 courses that were planned Of28 patients with microscopic disease at the start of therapy61 achieved a surgically defined complete response whereasonly 1 out of 31 patients with macroscopic disease achieved acomplete response The median time-to-recurrence was 167months with an estimated survival rate at 2 years being 58Treatment was generally well tolerated [141]
Another study looked into the effect of IP paclitaxel asconsolidation therapy in advanced ovarian cancer Twenty-eight patients who had initial residual macroscopic disease(lt1 cm) after primary surgery or interval debulking but hadcomplete pathological response following standard treatmentwith at least 6 cycles of platinum-based chemotherapy regi-men received paclitaxel 60mgm2week intraperitoneally for12ndash16 weeks as consolidation therapy The median time torecurrence was 25 months but overall survival did not differsignificantly when compared with control group submittedto observation only Treatment-related toxicity was mild andtechnical difficulties were observed in 11 of patients [142]
Multicenter randomised phase 3 trials as well as meta-analysis of IP chemotherapy have been performed anddemonstrated that chemotherapy drugs administered intra-peritoneally are superior to intravenous standard regimensin patient with optimally debulked epithelial ovarian cancerThe most impressive data comes from GOG 114 [14] and172 trial [143] In GOG 114 patients received either sixcycles of intravenous paclitaxel 135mgm2 and cisplatin75mgm2 every 3 weeks or intravenous carboplatin (AUC= 9) every 28 days for two cycles followed by six 3-weeklycycles of intravenous paclitaxel 135mgm2 and IP cisplatin100mgm2 [14] whereas in GOG 172 patients received eitherintravenous paclitaxel 135mgm2 followed by intravenouscisplatin 75mgm2 or intravenous paclitaxel 135mgm2 fol-lowed by IP combination of cisplatin 100mgm2 and pacli-taxel 60mgm2 on day 8 Both trials had a combined total
BioMed Research International 15
of 876 women with stage III epithelial ovarian carcinomaoptimally debulked to le1 cm residual tumour [143] Themedian follow-up for GOG 114 [14] was 138 years with GOG172 [143] was 97 years The primary results of the individualtrials reported up to 6-month improvement in median PFSfollowing IP therapy In the combined analysis of the datafrom both trials the data continued to show a 5-monthdifference in favour of IP therapy (25 versus 20 months)which translates into 16 reduction in the hazard ratio forprogression (119901 = 003) In GOG 114 [14] reported in 2001there was only borderline improvement in overall survivalassociated with this regimen (median 63 versus 52 monthsrelative risk 081 119901 = 005)
However in combined analysis in 2013 which was pre-sented at the Society of Gynecologic Oncology AnnualMeeting [144] the overall survival showed an 11-monthimprovement in favour of IP therapy in GOG 114 whereasGOG 172 reported a 16-month survival advantage Amongpatients treated with IP therapy the 5-year survival rateincreased from 18 following completion of 1-2 cycles to 59for patients who completed 5-6 cycles of treatment Howeverthere was increased toxicity observed in the IP arm grade 3-4 leukopenia thrombocytopenia and abdominal pain Only42 of patients in the GOG172 trial [143] completed all sixcycles of planned treatment in the IP arm while 18 ofpatients in GOG 114 trial [14] received fewer than two coursesof IP chemotherapy
Another randomised phase III trial involving patientswith stages II-III epithelial ovarian carcinoma is the GOG252 study with three arms Arm 1-dose-dense intravenouscarboplatin and paclitaxel Arm 2-dose-dense intravenouspaclitaxel and IP carboplatin and Arm 3 consists of 3-weeklyintravenous paclitaxel (day 1) followed by IP cisplatin (day 2)and IP paclitaxel (day 3) regimen All three arms also incor-porate the combination and maintenance of bevacizumabGOG 252 has completed accrual and results are awaited [139]
11 Newer Forms of Paclitaxel
Development of next-generation taxanes has taken place overthe past 40 years aimed at eliminating toxicity improvingefficacy and ease of administration Abraxane is a novelcompound which incorporates paclitaxel into an albuminnanoparticle soluble in saline hence eliminating the needfor Cremophor EL which is responsible for hypersensitivityreactions experienced during paclitaxel infusion [145] Thenanoparticle albumin in nab-paclitaxel is able to bind toglycoprotein gp60 receptor an albumin receptor and activatecaveolin-1 a protein that in human is encoded byCAV-1 geneleading to formation of caveoli hence allowing nab-paclitaxelto migrate across the endothelial cell membrane into theinterstitial space leading to higher intratumoural drug con-centration In addition Abraxane exhibits linear pharma-cokinetics and can therefore be given at a relatively higherdose than standard intravenous paclitaxel leading to a highertherapeutic ratio and heightened efficacy in solid tumoursmainlymetastatic breast cancer [146 147] Nab-paclitaxel hadFDA approval in 2005 for treatment of breast cancer [148]
Nab-paclitaxel has been studied in recurrent ovariancancer As a single agent in phase II 44 patients withrecurrent ovarian cancer were treated with Nab-paclitaxel260mgm2 intravenously for 30 minutes every 3 weeks for6 cycles Ninety-two percent of patients were platinum-sensitive while 89 had had previous exposure to standardtaxane The objective response rate was 64 with 15 patientsachieving complete response and 13 of them had partialresponse Estimated median PFS was 85 months No hyper-sensitivity reactions were observed and there were infrequentcases of grade 4 neutropenia (11) and grade 2-3 neuropathy(13) [149]
Another phase II study by GOG enrolled 51 patients withplatinum- and taxane-resistant recurrent ovarian cancer outof which 47 were evaluable The objective response rate was38 with one patient achieving a complete response and 10patients a partial response The median PFS was 45 monthswhile overall survival rate was 174 months Severe haema-tological and nonhaematological toxicities including neuro-toxicity were uncommon These results are quite impressivegiven the treatment population consisted of patients withvery poor prognosis with a median platinum and taxane freeinterval of 21 days and 70 had their recurrence within 3months of completion of primary treatment [150] Severalother trials of this formulation are in progress
Paclitaxel poliglumex (PPX) also known as Xyotax isanother prodrug a novel conjugate of paclitaxel and 120572-poly-L-glutamic acid which accumulates within tumour tissuedue to increased permeability of the tumour vessels and lackof lymphatic drainage [148 151 152] Paclitaxel poliglumexenhances solubility of paclitaxel allows direct delivery tothe intratumoural microenvironment and allows prolongedexposure to the active drug while minimising systemictoxicities [151] In Phase I dose escalation studies as a singleagent the recommended dose of PPX was 235mgm2 over 10minutes every 3 weeks or 70mgm2 weekly [153] In a PhaseII GOG study of relapsed ovarian cancer a response rate of16 was seen with infrequent serious adverse events grade3 and 4 neutropenia (24 and 20) and grade 3 neuropathy(24) [154] A phase III trial (GOG-0212) on the use of PPXas consolidation ormaintenance therapy in advanced ovariancancer is in progress
DHA-paclitaxel also known as Taxoprexin is a prodrugwhere paclitaxel is covalently conjugated with the naturallyoccurring omega-3 fatty acid docosahexaenoic acid (DHA)a fatty acid that is easily taken up by tumour cells henceincreasing intratumoural concentration of paclitaxel leadingtumour cell apoptosis [155 156] DHA-paclitaxel exhibitslinear pharmacokinetics and lower toxicity and also ease ofadministration when compared to conventional paclitaxeland has demonstrated antineoplastic activity in animal mod-els of cancer as well as in a phase III trial involving metastaticmelanoma [156ndash160] In a recent study on human ovariancancer cells it was found that DHA could reverse paclitaxelresistance by inhibiting P-gp as well as downregulatingthe expression of multidrug resistance associated proteins(MRP) and inhibiting the activity of NF-120581B and p38 MAPKsignalling pathways [161]
16 BioMed Research International
12 Future Directions
A plateau has been reached regarding the benefits associatedwith standard 3-weekly intravenous administration of cyto-toxic chemotherapy in advanced epithelial ovarian cancerThe ongoing battle for a better treatment regimen to delayrelapse promote remission and most importantly improvethe quality of life of patients with advanced epithelial ovariancancer need not to go further than the ability to relook at thechemotherapy agents that are already available in a differentapproach
Novel compounds to date have not yet shown clinicalsuperiority and parent compounds such as paclitaxel con-tinue to surprise us with their feasibility effectiveness andmanageable toxicity profiles Intraperitoneal paclitaxel willrequire further evaluation Better effort in understanding themechanism of action of drugs including the role of dosescheduling and the effect on the immune systemmay providea more cost-effective route to better clinical outcomes
Conflict of Interests
The authors declare no conflict of interests in this work
Acknowledgments
The authors would like to thank the many researchers whohave contributed to our current knowledge of paclitaxelNirmala Kampan is supported by Australian Monash Uni-versity Institute of Graduate Research Scholarship as wellas Universiti Kebangsaan Malaysia Postgraduate ScholarshipAward Mutsa Madondo has received Postgraduate Pub-lication Award from Monash University and MagdalenaPlebanski has been awarded Senior NHMRC Fellowship
References
[1] Australian Institute of Health and Welfare and National Breastand Ovarian Cancer Centre (Australia) Ovarian Cancer inAustralia AnOverview 2010 Cancer Series Australian Instituteof Health and Welfare Canberra Australia 2010
[2] R E Bristow R S Tomacruz D K Armstrong E L Trimbleand F J Montz ldquoSurvival effect of maximal cytoreductivesurgery for advanced ovarian carcinoma during the platinumera a meta-analysisrdquo Journal of Clinical Oncology vol 20 no 5pp 1248ndash1259 2002
[3] ZKempand JA Ledermann ldquoUpdate onfirst-line treatment ofadvanced ovarian carcinomardquo International Journal of WomenrsquosHealth vol 5 no 1 pp 45ndash51 2013
[4] A du Bois H-J Luck W Meier et al ldquoA randomized clinicaltrial of cisplatinpaclitaxel versus carboplatinpaclitaxel as first-line treatment of ovarian cancerrdquo Journal of the National CancerInstitute vol 95 no 17 pp 1320ndash1330 2003
[5] R F Ozols B N Bundy B E Greer et al ldquoPhase III trialof carboplatin and paclitaxel compared with cisplatin andpaclitaxel in patients with optimally resected stage III ovariancancer A Gynecologic Oncology Group studyrdquo Journal ofClinical Oncology vol 21 no 17 pp 3194ndash3200 2003
[6] W P McGuire W J Hoskins M F Brady et al ldquoCyclophos-phamide and cisplatin compared with paclitaxel and cisplatin
in patients with stage III and stage IV ovarian cancerrdquoThe NewEngland Journal of Medicine vol 334 no 1 pp 1ndash6 1996
[7] W P McGuire W J Hoskins M F Brady et al ldquoCyclophos-phamide and cisplatin versus paclitaxel and cisplatin a phase IIIrandomized trial in patients with suboptimal stage IIIIV ovar-ian cancer (from the gynecologic oncology group)rdquo Seminars inOncology vol 23 no 5 supplement 12 pp 40ndash47 1996
[8] M J Piccart K Bertelsen K James et al ldquoRandomized inter-group trial of cisplatin-paclitaxel versus cisplatin-cyclophosph-amide inwomenwith advanced epithelial ovarian cancer three-year resultsrdquo Journal of the National Cancer Institute vol 92 no9 pp 699ndash708 2000
[9] P A Vasey G C Jayson A Gordon et al ldquoPhase III random-ized trial of docetaxel-carboplatin versus paclitaxel-carboplatinas first-line chemotherpy for ovarian carcinomardquo Journal of theNational Cancer Institute vol 96 no 22 pp 1682ndash1691 2004
[10] B Gronlund C Hogdall H H Hansen and S A EngelholmldquoResults of reinduction therapy with paclitaxel and carboplatinin recurrent epithelial ovarian cancerrdquo Gynecologic Oncologyvol 83 no 1 pp 128ndash134 2001
[11] T M Loffler W Freund J Lipke and T-U HausamenldquoSchedule- and dose-intensified paclitaxel as weekly 1-hourinfusion in pretreated solid tumors results of a phase III trialrdquoSeminars in Oncology vol 23 no 6 supplement 16 pp 32ndash341996
[12] D Fennelly C Aghajanian F Shapiro et al ldquoPhase I and phar-macologic study of paclitaxel administered weekly in patientswith relapsed ovarian cancerrdquo Journal of Clinical Oncology vol15 no 1 pp 187ndash192 1997
[13] N R Abu-Rustum C Aghajanian R R Barakat D Fennelly FShapiro and D Spriggs ldquoSalvage weekly paclitaxel in recurrentovarian cancerrdquo Seminars inOncology vol 24 no 5 supplement15 pp S15-62ndashS15-67 1997
[14] M Markman B N Bundy D S Alberts et al ldquoPhase III trialof standard-dose intravenous cisplatin plus paclitaxel versusmoderately high-dose carboplatin followed by intravenouspaclitaxel and intraperitoneal cisplatin in small-volume stageIII ovarian carcinoma an intergroup study of the gynecologiconcology group Southwestern Oncology Group and EasternCooperativeOncologyGrouprdquo Journal of Clinical Oncology vol19 no 4 pp 1001ndash1007 2001
[15] A Kikuchi H Sakamoto and T Yamamoto ldquoWeekly car-boplatin and paclitaxel is safe active and well tolerated inrecurrent ovarian cancer cases of Japanese women previouslytreated with cisplatin-containing multidrug chemotherapyrdquoInternational Journal of Gynecological Cancer vol 15 no 1 pp45ndash49 2005
[16] I Cadron K Leunen F Amant T van Gorp P Nevenand I Vergote ldquoThe lsquoLeuvenrsquo dose-dense paclitaxelcarboplatinregimen in patients with recurrent ovarian cancerrdquo GynecologicOncology vol 106 no 2 pp 354ndash361 2007
[17] S Pignata E Breda G Scambia et al ldquoA phase II studyof weekly carboplatin and paclitaxel as first-line treatment ofelderly patients with advanced ovarian cancer A Multicen-tre Italian Trial in Ovarian cancer (MITO-5) studyrdquo CriticalReviews in OncologyHematology vol 66 no 3 pp 229ndash2362008
[18] T Safra S Shamai J Greenberg et al ldquoWeekly carboplatinwith paclitaxel compared to standard three-weekly treatment inadvanced epithelial ovarian carcinomamdasha retrospective studyrdquoGynecologic Oncology vol 132 no 1 pp 18ndash22 2014
BioMed Research International 17
[19] L J Havrilesky A A Alvarez R A Sayer et al ldquoWeekly low-dose carboplatin and paclitaxel in the treatment of recurrentovarian and peritoneal cancerrdquo Gynecologic Oncology vol 88no 1 pp 51ndash57 2003
[20] M van der BurgW Onstenk I Boere et al ldquoLong-term resultsof a randomised phase III trial of weekly versus three-weeklypaclitaxelplatinum induction therapy followed by standardor extended three-weekly paclitaxelplatinum in Europeanpatients with advanced epithelial ovarian cancerrdquo EuropeanJournal of Cancer vol 50 no 15 pp 2592ndash2601 2014
[21] N Katsumata M Yasuda F Takahashi et al ldquoDose-densepaclitaxel once a week in combination with carboplatin every3 weeks for advanced ovarian cancer a phase 3 open-labelrandomised controlled trialrdquoThe Lancet vol 374 no 9698 pp1331ndash1338 2009
[22] N Katsumata M Yasuda S Isonishi et al ldquoLong-term resultsof dose-dense paclitaxel and carboplatin versus conventionalpaclitaxel and carboplatin for treatment of advanced epithelialovarian fallopian tube or primary peritoneal cancer (JGOG3016) a randomised controlled open-label trialrdquo The LancetOncology vol 14 no 10 pp 1020ndash1026 2013
[23] K Harano F Terauchi N Katsumata et al ldquoQuality-of-lifeoutcomes from a randomized phase III trial of dose-denseweekly paclitaxel and carboplatin compared with conventionalpaclitaxel and carboplatin as a first-line treatment for stage II-IV ovarian cancer Japanese Gynecologic OncologyGroup Trial(JGOG3016)rdquo Annals of Oncology vol 25 no 1 pp 251ndash2572014
[24] J Chan M F Brady R Penson et al ldquoPhase III trial ofevery-3-weeks paclitaxel vs dose dense weekly paclitaxel withcarboplatin +minus bevacizumab in epithelial ovarian peritonealfallopian tube cancer GOG 262 (NCT01167712)rdquo InternationalJournal of Gynecological Cancer vol 23 no 8 supplement 1 pp9ndash10 2013
[25] S Pignata G Scambia D Katsaros et al ldquoCarboplatin pluspaclitaxel once a week versus every 3 weeks in patients withadvanced ovarian cancer (MITO-7) a randomisedmulticentreopen-label phase 3 trialrdquoThe Lancet Oncology vol 15 no 4 pp396ndash405 2014
[26] V Walsh and J Goodman ldquoFrom taxol to Taxol the changingidentities and ownership of an anti-cancer drugrdquo MedicalAnthropology vol 21 no 3-4 pp 307ndash336 2002
[27] R Renneberg ldquoBiotech History yew trees paclitaxel synthesisand fungirdquo Biotechnology Journal vol 2 no 10 pp 1207ndash12092007
[28] J E Liebmann J A Cook C Lipschultz D Teague J Fisherand J B Mitchell ldquoCytotoxic studies of paclitaxel (Taxol) inhuman tumour cell linesrdquo British Journal of Cancer vol 68 no6 pp 1104ndash1109 1993
[29] J J Manfredi and S B Horwitz ldquoTaxol an antimitotic agentwith a newmechanism of actionrdquo Pharmacology andTherapeu-tics vol 25 no 1 pp 83ndash125 1984
[30] D G I Kingston ldquoRecent advances in the chemistry of taxolrdquoJournal of Natural Products vol 63 no 5 pp 726ndash734 2000
[31] D G I Kingston ldquoThe shape of things to come structural andsynthetic studies of taxol and related compoundsrdquo Phytochem-istry vol 68 no 14 pp 1844ndash1854 2007
[32] V Walsh and J Goodman ldquoCancer chemotherapy biodiversitypublic and private property the case of the anti-cancer drugTaxolrdquo Social Science amp Medicine vol 49 no 9 pp 1215ndash12251999
[33] P H Wiernik E L Schwartz J J Strauman J P Dutcher RB Lipton and E Paietta ldquoPhase I clinical and pharmacokineticstudy of taxolrdquo Cancer Research vol 47 no 9 pp 2486ndash24931987
[34] W P McGuire E K Rowinsky N B Rosenhein et alldquoTaxol a unique antineoplastic agent with significant activityin advanced ovarian epithelial neoplasmsrdquo Annals of InternalMedicine vol 111 no 4 pp 273ndash279 1989
[35] ldquoDiscovery and development of taxolrdquo in Taxol Science andApplications M W M E Suffness Ed pp 3ndash25 CRC PressBoca Raton Fla USA 1995
[36] M J Piccart and F Cardoso ldquoProgress in systemic therapy forbreast cancer an overview and perspectivesrdquo European Journalof Cancer Supplement vol 1 no 2 pp 56ndash69 2003
[37] P Bonomi K B Kim and J Kugler ldquoComparison of survival forstage IIIB versus stage IV non-small cell lung cancer (NSCLC)patients with etoposide-cisplatin versus taxol-cisplatin an East-ern Cooperative Oncology Group (ECOG) trialrdquo in Proceedingsof the American Society of Clinical Oncology vol 16 p 454a1997
[38] D Guenard F Gueritte-Voegelein J Dubois and P PotierldquoStructure-activity relationships of Taxol and Taxotere ana-loguesrdquo Journal of the National Cancer Institute Monographsno 15 pp 79ndash82 1993
[39] D G I Kingston ldquoTaxol the chemistry and structure-activityrelationships of a novel anticancer agentrdquo Trends in Biotechnol-ogy vol 12 no 6 pp 222ndash227 1994
[40] E K Rowinsky and R C Donehower ldquoPaclitaxel (taxol)rdquo TheNew England Journal of Medicine vol 332 no 15 pp 1004ndash10141995
[41] J Parness and S B Horwitz ldquoTaxol binds to polymerizedtubulin in vitrordquo Journal of Cell Biology vol 91 no 2 pp 479ndash487 1981
[42] A Dammermann A Desai and K Oegema ldquoTheminus end insightrdquo Current Biology vol 13 no 15 pp R614ndashR624 2003
[43] CWiese and Y Zheng ldquoMicrotubule nucleation 120574-tubulin andbeyondrdquo Journal of Cell Science vol 119 no 20 pp 4143ndash41532006
[44] A Ganguly H Yang and F Cabral ldquoPaclitaxel-dependent celllines reveal a novel drug activityrdquo Molecular Cancer Therapeu-tics vol 9 no 11 pp 2914ndash2923 2010
[45] P B Schiff and S B Horwitz ldquoTaxol stabilizes microtubules inmouse fibroblast cellsrdquo Proceedings of the National Academy ofSciences of the United States of America vol 77 no 3 pp 1561ndash1565 1980
[46] P B Schiff J Fant and S B Horwitz ldquoPromotion of micro-tubule assembly in vitro by Taxolrdquo Nature vol 277 no 5698pp 665ndash667 1979
[47] D Zhang R Yang S Wang and Z Dong ldquoPaclitaxel new usesfor an old drugrdquoDrug Design Development andTherapy vol 8pp 279ndash284 2014
[48] S Rao G A Orr A G Chaudhary D G I Kingston and SB Horwitz ldquoCharacterization of the taxol binding site on themicrotubule 2-(m-Azidobenzoyl)taxol photolabels a peptide(amino acids 217-231) of beta-tubulinrdquoThe Journal of BiologicalChemistry vol 270 no 35 pp 20235ndash20238 1995
[49] F Wang Y Cao W Zhao H Liu Z Fu and R Han ldquoTaxolinhibits melanoma metastases through apoptosis inductionangiogenesis inhibition and restoration of E-cadherin andnm23 expressionrdquo Journal of Pharmacological Sciences vol 93no 2 pp 197ndash203 2003
18 BioMed Research International
[50] A Sevko V Kremer C Falk et al ldquoApplication of paclitaxel inlow non-cytotoxic doses supports vaccination with melanomaantigens in normal micerdquo Journal of Immunotoxicology vol 9no 3 pp 275ndash281 2012
[51] T Kreis and R Vale Guidebook to the Cytoskeletal and MotorProteins Oxford University Press Oxford UK 2nd edition1999
[52] P Giannakakou D L Sackett Y-K Kang et al ldquoPaclitaxel-resistant human ovarian cancer cells have mutant 120573-tubulinsthat exhibit impaired paclitaxel-driven polymerizationrdquo TheJournal of Biological Chemistry vol 272 no 27 pp 17118ndash171251997
[53] E Rakovitch W Mellado E J Hall T K Pandita S Sawantand C R Geard ldquoPaclitaxel sensitivity correlates with p53status and DNA fragmentation but not G2M accumulationrdquoInternational Journal of Radiation Oncology Biology Physics vol44 no 5 pp 1119ndash1124 1999
[54] S W Lowe S Bodis A McClatchey et al ldquop53 status and theefficacy of cancer therapy in vivordquo Science vol 266 no 5186 pp807ndash810 1994
[55] C C Zhang J-M Yang E White M Murphy A Levine andW N Hait ldquoThe role of MAP4 expression in the sensitivity topaclitaxel and resistance to vinca alkaloids in p53 mutant cellsrdquoOncogene vol 16 no 12 pp 1617ndash1624 1998
[56] K Fukasawa T Choi R Kuriyama S Rulong and G F VandeWoude ldquoAbnormal centrosome amplification in the absence ofp53rdquo Science vol 271 no 5256 pp 1744ndash1747 1996
[57] T-H Wang Y-H Chan C-W Chen et al ldquoPaclitaxel (Taxol)upregulates expression of functional interleukin-6 in humanovarian cancer cells through multiple signaling pathwaysrdquoOncogene vol 25 no 35 pp 4857ndash4866 2006
[58] E Yakirevich E Sabo I Naroditsky Y Sova O Lavie andM B Resnick ldquoMultidrug resistance-related phenotype andapoptosis-related protein expression in ovarian serous carcino-masrdquo Gynecologic Oncology vol 100 no 1 pp 152ndash159 2006
[59] G Szakacs J K Paterson J A Ludwig C Booth-Genthe andM M Gottesman ldquoTargeting multidrug resistance in cancerrdquoNature Reviews Drug Discovery vol 5 no 3 pp 219ndash234 2006
[60] L W Pfannenstiel S S K Lam L A Emens E M Jaffeeand T D Armstrong ldquoPaclitaxel enhances early dendritic cellmaturation and function through TLR4 signaling in micerdquoCellular Immunology vol 263 no 1 pp 79ndash87 2010
[61] N Klauber S Parangi E Flynn E Hamel and R J DrsquoAmatoldquoInhibition of angiogenesis and breast cancer in mice by themicrotubule inhibitors 2-methoxyestradiol and Taxolrdquo CancerResearch vol 57 no 1 pp 81ndash86 1997
[62] D Belotti V Vergani T Drudis et al ldquoThe microtubule-affecting drug paclitaxel has antiangiogenic activityrdquo ClinicalCancer Research vol 2 no 11 pp 1843ndash1849 1996
[63] D H Lau L Xue L J Young P A Burke and A T CheungldquoPaclitaxel (Taxol) an inhibitor of angiogenesis in a highlyvascularized transgenic breast cancerrdquo Cancer Biotherapy andRadiopharmaceuticals vol 14 no 1 pp 31ndash36 1999
[64] X Jiang ldquoHarnessing the immune system for the treatment ofbreast cancerrdquo Journal of Zhejiang University Science B vol 15no 1 pp 1ndash15 2014
[65] A Gadducci D Katsaros P Zola et al ldquoWeekly low-dosepaclitaxel as maintenance treatment in patients with advancedovarian cancer who had microscopic residual disease atsecond-look surgery after 6 cycles of paclitaxelplatinum-basedchemotherapy Results of an open noncomparative phase 2
multicenter italian study (after-6 protocol 2)rdquo InternationalJournal of Gynecological Cancer vol 19 no 4 pp 615ndash619 2009
[66] R S Bhatt J Merchan R Parker et al ldquoA phase 2 pilot trial oflow-dose continuous infusion or lsquometronomicrsquo paclitaxel andoral celecoxib in patients with metastatic melanomardquo Cancervol 116 no 7 pp 1751ndash1756 2010
[67] M Caballero J J Grau J L Blanch et al ldquoSerum vascularendothelial growth factor as a predictive factor in metronomic(weekly) paclitaxel treatment for advanced head and neckcancerrdquo Archives of OtolaryngologymdashHead and Neck Surgeryvol 133 no 11 pp 1143ndash1148 2007
[68] J Alexandre Y Hu W Lu H Pelicano and P Huang ldquoNovelaction of paclitaxel against cancer cells bystander effect medi-ated by reactive oxygen speciesrdquo Cancer Research vol 67 no 8pp 3512ndash3517 2007
[69] T Hadzic N Aykin-Burns Y Zhu et al ldquoPaclitaxel combinedwith inhibitors of glucose and hydroperoxide metabolismenhances breast cancer cell killing viaH
2O2-mediated oxidative
stressrdquo Free Radical Biology and Medicine vol 48 no 8 pp1024ndash1033 2010
[70] C A Sherman-Baust K G Becker W H Wood III Y Zhangand P J Morin ldquoGene expression and pathway analysis of ovar-ian cancer cells selected for resistance to cisplatin paclitaxel ordoxorubicinrdquo Journal of Ovarian Research vol 4 no 1 article21 2011
[71] R Agarwal and S B Kaye ldquoOvarian cancer strategies for over-coming resistance to chemotherapyrdquo Nature Reviews Cancervol 3 no 7 pp 502ndash516 2003
[72] T Acker and K H Plate ldquoRole of hypoxia in tumorangiogenesismdashmolecular and cellular angiogenic crosstalkrdquoCell and Tissue Research vol 314 no 1 pp 145ndash155 2003
[73] M Hockel and P Vaupel ldquoBiological consequences of tumorhypoxiardquo Seminars in Oncology vol 28 supplement 8 no 2 pp36ndash41 2001
[74] L Huang Q-H Zhang Q-L Ao H Xing Y-P Lu and DMa ldquoEffect of hypoxia on the chemotherapeutic sensitivity ofhuman ovarian cancer cells to paclitaxel and its mechanismrdquoZhonghua Zhong Liu Za Zhi vol 29 no 2 pp 96ndash100 2007
[75] N Rohwer and T Cramer ldquoHypoxia-mediated drug resistancenovel insights on the functional interaction of HIFs and celldeath pathwaysrdquoDrug Resistance Updates vol 14 no 3 pp 191ndash201 2011
[76] B B Aggarwal R V Vijayalekshmi and B Sung ldquoTargetinginflammatory pathways for prevention and therapy of cancershort-term friend long-term foerdquo Clinical Cancer Research vol15 no 2 pp 425ndash430 2009
[77] Z Duan R Foster D A Bell et al ldquoSignal transducersand activators of transcription 3 pathway activation in drug-resistant ovarian cancerrdquo Clinical Cancer Research vol 12 no17 pp 5055ndash5063 2006
[78] H-J Kuh S H Jang M G Wientjes J R Weaver and J L-SAu ldquoDeterminants of paclitaxel penetration and accumulationin human solid tumorrdquo Journal of Pharmacology and Experi-mental Therapeutics vol 290 no 2 pp 871ndash880 1999
[79] S Arao H Suwa M Mandai et al ldquoHypoxia-mediated drugresistance novel insights on the functional interaction of HIFsand cell death pathwaysrdquo Cancer Research vol 54 no 5 pp1355ndash1359 1994
[80] S E Johnatty J Beesley B Gao et al ldquoABCB1 (MDR1)polymorphisms and ovarian cancer progression and survivala comprehensive analysis from the Ovarian Cancer Association
BioMed Research International 19
Consortium and the Cancer GenomeAtlasrdquoGynecologic Oncol-ogy vol 131 no 1 pp 8ndash14 2013
[81] X Yang A K Iyer A Singh et al ldquoCluster of differentiation44 targeted hyaluronic acid based nanoparticles for MDR1siRNA delivery to overcome drug resistance in ovarian cancerrdquoPharmaceutical Research 2014
[82] D A Zajchowski B Y Karlan and L K Shawver ldquoTreatment-related protein biomarker expression differs between primaryand recurrent ovarian carcinomasrdquoMolecular CancerTherapeu-tics vol 11 no 2 pp 492ndash502 2012
[83] MM Gottesman J Ludwig D Xia and G Szakacs ldquoDefeatingdrug resistance in cancerrdquoDiscovery Medicine vol 6 no 31 pp18ndash23 2006
[84] S Mozzetti C Ferlini P Concolino et al ldquoClass III 120573-tubulin overexpression is a prominent mechanism of paclitaxelresistance in ovarian cancer patientsrdquo Clinical Cancer Researchvol 11 no 1 pp 298ndash305 2005
[85] M Kavallaris D Y S Kuo C A Burkhart et al ldquoTaxol-resistant epithelial ovarian tumors are associated with alteredexpression of specific beta-tubulin isotypesrdquo Journal of ClinicalInvestigation vol 100 no 5 pp 1282ndash1293 1997
[86] G A Orr P Verdier-Pinard H McDaid and S B HorwitzldquoMechanisms of Taxol resistance related to microtubulesrdquoOncogene vol 22 no 47 pp 7280ndash7295 2003
[87] C Ferlini L Cicchillitti G Raspaglio et al ldquoPaclitaxel directlybinds to Bcl-2 and functionally mimics activity of Nur77rdquoCancer Research vol 69 no 17 pp 6906ndash6914 2009
[88] E Mechetner A Kyshtoobayeva S Zonis et al ldquoLevels ofmultidrug resistance (MDR1) P-glycoprotein expression byhuman breast cancer correlate with in vitro resistance to taxoland doxorubicinrdquo Clinical Cancer Research vol 4 no 2 pp389ndash398 1998
[89] J S Lagas C W N Damen R A B VanWaterschoot D IusufJ H Beijnen and A H Schinkel ldquoP-glycoprotein multidrug-resistance associated protein 2 Cyp3a and carboxylesteraseaffect the oral availability and metabolism of vinorelbinerdquoMolecular Pharmacology vol 82 no 4 pp 636ndash644 2012
[90] M T Huizing J B Vermorken H Rosing et al ldquoPharmacoki-netics of paclitaxel and three major metabolites in patients withadvanced breast carcinoma refractory to anthracycline therapytreated with a 3-hour paclitaxel infusion a European CancerCentre (ECC) trialrdquo Annals of Oncology vol 6 no 7 pp 699ndash704 1995
[91] R Panchagnula ldquoPharmaceutical aspects of paclitaxelrdquo Interna-tional Journal of Pharmaceutics vol 172 no 1-2 pp 1ndash15 1998
[92] S H Jang M G Wientjes and J L-S Au ldquoDeterminants ofpaclitaxel uptake accumulation and retention in solid tumorsrdquoInvestigational New Drugs vol 19 no 2 pp 113ndash123 2001
[93] D S Sonnichsen andM V Relling ldquoClinical pharmacokineticsof paclitaxelrdquo Clinical Pharmacokinetics vol 27 no 4 pp 256ndash269 1994
[94] T Ohtsu Y Sasaki T Tamura et al ldquoClinical pharmacokineticsand pharmacodynamics of paclitaxel a 3-hour infusion versusa 24-hour infusionrdquo Clinical Cancer Research vol 1 no 6 pp599ndash606 1995
[95] M Czejka J Schueller H Schnait B Springer and I EderldquoClinical pharmacokinetics andmetabolism of paclitaxel after athree-hour infusion comparison of two preparationsrdquo Journalof Oncology Pharmacy Practice vol 9 no 4 pp 129ndash136 2003
[96] J Rizzo C Riley D VonHoff J Kuhn J Phillips and T BrownldquoAnalysis of anticancer drugs in biological fluids determination
of taxol with application to clinical pharmacokineticsrdquo Journalof Pharmaceutical and Biomedical Analysis vol 8 no 2 pp 159ndash164 1990
[97] V A de Weger J H Beijnen and J H M Schellens ldquoCel-lular and clinical pharmacology of the taxanes docetaxel andpaclitaxelmdasha reviewrdquoAnti-Cancer Drugs vol 25 no 5 pp 488ndash494 2014
[98] S Kumar H Mahdi C Bryant J P Shah G Garg andA Munkarah ldquoClinical trials and progress with paclitaxel inovarian cancerrdquo International Journal of Womenrsquos Health vol 2no 1 pp 411ndash427 2010
[99] B Huang J Zhao J C Unkeless Z H Feng and H XiongldquoTLR signaling by tumor and immune cells a double-edgedswordrdquo Oncogene vol 27 no 2 pp 218ndash224 2008
[100] R A Jibodh J S Lagas B Nuijen J H Beijnen and J HM Schellens ldquoTaxanes old drugs new oral formulationsrdquoEuropean Journal of Pharmacology vol 717 no 1ndash3 pp 40ndash462013
[101] A Javeed M Ashraf A Riaz A Ghafoor S Afzal and M MMukhtar ldquoPaclitaxel and immune systemrdquo European Journal ofPharmaceutical Sciences vol 38 no 4 pp 283ndash290 2009
[102] L Bracci G Schiavoni A Sistigu and F Belardelli ldquoImmune-based mechanisms of cytotoxic chemotherapy implications forthe design of novel and rationale-based combined treatmentsagainst cancerrdquo Cell Death and Differentiation vol 21 no 1 pp15ndash25 2014
[103] C A Byrd-Leifer E F Block K Takeda S Akira and A DingldquoThe role of MyD88 and TLR4 in the LPS-mimetic activity ofTaxolrdquo European Journal of Immunology vol 31 no 8 pp 2448ndash2457 2001
[104] A-C Wang Y-B Ma F-X Wu et al ldquoTLR4 induces tumorgrowth and inhibits paclitaxel activity in MyD88-positivehuman ovarian carcinoma in vitrordquo Oncology Letters vol 7 no3 pp 871ndash877 2014
[105] Y Zhu N Liu S D Xiong Y J Zheng and Y W ChuldquoCD4+Foxp3+ regulatory T-cell impairment by paclitaxel isindependent of toll-like receptor 4rdquo Scandinavian Journal ofImmunology vol 73 no 4 pp 301ndash308 2011
[106] M Kubo T Morisaki K Matsumoto et al ldquoPaclitaxel probablyenhances cytotoxicity of natural killer cells against breastcarcinoma cells by increasing perforin productionrdquo CancerImmunology Immunotherapy vol 54 no 5 pp 468ndash476 2005
[107] L Markasz G Stuber B Vanherberghen et al ldquoEffect of fre-quently used chemotherapeutic drugs on the cytotoxic activityof human natural killer cellsrdquo Molecular Cancer Therapeuticsvol 6 no 2 pp 644ndash654 2007
[108] T Sako N Burioka K Yasuda et al ldquoCellular immune profile inpatients with non-small cell lung cancer after weekly paclitaxeltherapyrdquo Acta Oncologica vol 43 no 1 pp 15ndash19 2004
[109] R Kaneno G V Shurin I L Tourkova and M R ShurinldquoChemomodulation of human dendritic cell function by anti-neoplastic agents in low noncytotoxic concentrationsrdquo Journalof Translational Medicine vol 7 article 58 2009
[110] TMichels G V ShurinHNaiditch A Sevko VUmansky andM R Shurin ldquoPaclitaxel promotes differentiation of myeloid-derived suppressor cells into dendritic cells in vitro in a TLR4-independent mannerrdquo Journal of Immunotoxicology vol 9 no3 pp 292ndash300 2012
[111] R A Kemp and F Ronchese ldquoTumor-specific Tc1 but not Tc2cells deliver protective antitumor immunityrdquo The Journal ofImmunology vol 167 no 11 pp 6497ndash6502 2001
20 BioMed Research International
[112] A Y Rudensky ldquoRegulatory T cells and Foxp3rdquo ImmunologicalReviews vol 241 no 1 pp 260ndash268 2011
[113] EM Shevach ldquoCD4+CD25+ suppressor T cellsmore questionsthan answersrdquo Nature Reviews Immunology vol 2 no 6 pp389ndash400 2002
[114] S Sakaguchi T Yamaguchi T Nomura and M Ono ldquoRegu-latory T cells and immune tolerancerdquo Cell vol 133 no 5 pp775ndash787 2008
[115] H Nishikawa and S Sakaguchi ldquoRegulatory T cells in tumorimmunityrdquo International Journal of Cancer vol 127 no 4 pp759ndash767 2010
[116] W Zou ldquoRegulatory T cells tumour immunity and immuno-therapyrdquoNature Reviews Immunology vol 6 no 4 pp 295ndash3072006
[117] A Fialova S Partlova L Sojka et al ldquoDynamics of T-cell infil-tration during the course of ovarian cancer The gradual shiftfrom aTh17 effector cell response to a predominant infiltrationby regulatory T-cellsrdquo International Journal of Cancer vol 132no 5 pp 1070ndash1079 2013
[118] A E Albers R L Ferris G G Kim K Chikamatsu A BDeLeo and T L Whiteside ldquoImmune responses to p53 inpatients with cancer enrichment in tetramer+ p53 peptide-specific T cells and regulatory T cells at tumor sitesrdquo CancerImmunology Immunotherapy vol 54 no 11 pp 1072ndash10812005
[119] N Liu Y Zheng Y Zhu S Xiong andYChu ldquoSelective impair-ment of CD4 + CD25 + Foxp3 + regulatory T cells by paclitaxelis explained by Bcl-2Bax mediated apoptosisrdquo InternationalImmunopharmacology vol 11 no 2 pp 212ndash219 2011
[120] X Wu Q-M Feng Y Wang J Shi H-L Ge and W DildquoThe immunologic aspects in advanced ovarian cancer patientstreated with paclitaxel and carboplatin chemotherapyrdquo CancerImmunology Immunotherapy vol 59 no 2 pp 279ndash291 2010
[121] A P Vicari R Luu N Zhang et al ldquoPaclitaxel reducesregulatoryT cell numbers and inhibitory function and enhancesthe anti-tumor effects of the TLR9 agonist PF-3512676 in themouserdquo Cancer Immunology Immunotherapy vol 58 no 4 pp615ndash628 2009
[122] L Zhang K Dermawan M Jin et al ldquoDifferential impairmentof regulatory T cells rather than effector T cells by paclitaxel-based chemotherapyrdquo Clinical Immunology vol 129 no 2 pp219ndash229 2008
[123] Y Tabuchi J Matsuoka M Gunduz et al ldquoResistance topaclitaxel therapy is related with Bcl-2 expression through anestrogen receptor mediated pathway in breast cancerrdquo Interna-tional Journal of Oncology vol 34 no 2 pp 313ndash319 2009
[124] N Obermajer R Muthuswamy K Odunsi R P Edwards andP Kalinski ldquoPGE
2-induced CXCL12 production and CXCR4
expression controls the accumulation of human MDSCs inovarian cancer environmentrdquo Cancer Research vol 71 no 24pp 7463ndash7470 2011
[125] Q M Feng W Di and X Wu ldquoImmune reconstitution inadvanced ovarian cancer patients undergoing first line chemo-therapyrdquo Xi Bao Yu Fen Zi Mian Yi Xue Za Zhi vol 25 no 11pp 1023ndash1025 2009
[126] A D Seidman D Hochhauser M Gollub et al ldquoNinety-six-hour paclitaxel infusion after progression during short taxaneexposure a phase II pharmacokinetic and pharmacodynamicstudy in metastatic breast cancerrdquo Journal of Clinical Oncologyvol 14 no 6 pp 1877ndash1884 1996
[127] D R Spriggs M F Brady L Vaccarello et al ldquoPhase IIIrandomized trial of intravenous cisplatin plus a 24- or 96-hour
infusion of paclitaxel in epithelial ovarian cancer a gynecologiconcology group studyrdquo Journal of Clinical Oncology vol 25 no28 pp 4466ndash4471 2007
[128] G A Omura M F Brady K Y Look et al ldquoPhase III trial ofpaclitaxel at two dose levels the higher dose accompanied byfilgrastim at two dose levels in platinum-pretreated epithelialovarian cancer an intergroup studyrdquo Journal of Clinical Oncol-ogy vol 21 no 15 pp 2843ndash2848 2003
[129] R Simon and L Norton ldquoThe Norton-Simon hypothesisdesigning more effective and less toxic chemotherapeutic reg-imensrdquoNature Clinical Practice Oncology vol 3 no 8 pp 406ndash407 2006
[130] A Kumar P Hoskins and A Tinker ldquoDose-dense paclitaxel inadvanced ovarian cancerrdquo Clinical Oncology vol 27 no 1 pp40ndash47 2015
[131] P Marchetti S Urien G A Cappellini G Ronzino and CFicorella ldquoWeekly administration of paclitaxel theoretical andclinical basisrdquoCritical Reviews in OncologyHematology vol 44supplement pp S3ndashS13 2002
[132] P Francis E Rowinsky J Schneider T Hakes W Hoskinsand M Markman ldquoPhase I feasibility and pharmacologic studyof weekly intraperitoneal paclitaxel A Gynecologic OncologyGroup pilot studyrdquo Journal of Clinical Oncology vol 13 no 12pp 2961ndash2967 1995
[133] H Thomas and P Rosenberg ldquoRole of weekly paclitaxel inthe treatment of advanced ovarian cancerrdquo Critical Reviews inOncologyHematology vol 44 supplement pp S43ndashS51 2002
[134] M Markman J Markman K Webster et al ldquoDuration ofresponse to second-line platinum-based chemotherapy forovarian cancer implications for patient management and clini-cal trial designrdquo Journal of Clinical Oncology vol 22 no 15 pp3120ndash3125 2004
[135] P H OrsquoDonnell M Eileen Dolan E Gamazon et al ldquoPopu-lation differences in platinum toxicity as a means to identifynovel genetic susceptibility variantsrdquo Pharmacogenetics andGenomics vol 20 no 5 pp 327ndash337 2010
[136] M J Millward M J Boyer M Lehnert et al ldquoDocetaxel andcarboplatin is an active regimen in advanced non-small-celllung cancer a phase II study in Caucasian and Asian patientsrdquoAnnals of Oncology vol 14 no 3 pp 449ndash454 2003
[137] M Markman ldquoIntraperitoneal therapy of ovarian cancerrdquoOncologist vol 1 no 1-2 pp 18ndash21 1996
[138] M Markman and J L Walker ldquoIntraperitoneal chemotherapyof ovarian cancer a review with a focus on practical aspects oftreatmentrdquo Journal of Clinical Oncology vol 24 no 6 pp 988ndash994 2006
[139] K Fujiwara S Nagao E Aotani and K Hasegawa ldquoPrincipleand evolving role of intraperitoneal chemotherapy in ovariancancerrdquo Expert Opinion on Pharmacotherapy vol 14 no 13 pp1797ndash1806 2013
[140] M Markman E Rowinsky T Hakes et al ldquoPhase I trialof intraperitoneal taxol a gynecoloic oncology group studyrdquoJournal of Clinical Oncology vol 10 no 9 pp 1485ndash1491 1992
[141] M Markman M F Brady N M Spirtos P Hanjani and S CRubin ldquoPhase II trial of intraperitoneal paclitaxel in carcinomaof the ovary tube and peritoneum a gynecologic oncologygroup studyrdquo Journal of Clinical Oncology vol 16 no 8 pp2620ndash2624 1998
[142] P B Panici I Palaia M Graziano F Bellati N Manci and RAngioli ldquoIntraperitoneal paclitaxel as consolidation treatmentin ovarian cancer patients a case control studyrdquo Oncology vol78 no 1 pp 20ndash25 2010
BioMed Research International 21
[143] D K Armstrong B Bundy L Wenzel et al ldquoIntraperitonealcisplatin and paclitaxel in ovarian cancerrdquo The New EnglandJournal of Medicine vol 354 no 1 pp 34ndash43 2006
[144] D Tewari J Java and R Salani ldquoLong-term survival advantageof intraperitoneal chemotherapy treatment in advanced ovariancancer an analysis of a Gynecologic Oncology Group ancillarydata studyrdquo in Proceedings of the 2013 Society of GynecologicOncology Annual Meeting on Womenrsquos Cancer (GOG114172Abstract) Los Angeles Calif USA 2013
[145] D A Yardley ldquonab-paclitaxel mechanisms of action and deliv-eryrdquo Journal of Controlled Release vol 170 no 3 pp 365ndash3722013
[146] M Ando K Yonemori N Katsumata et al ldquoPhase I and phar-macokinetic study of nab-paclitaxel nanoparticle albumin-bound paclitaxel administeredweekly to Japanese patients withsolid tumors and metastatic breast cancerrdquo Cancer Chemother-apy and Pharmacology vol 69 no 2 pp 457ndash465 2012
[147] N Desai V Trieu Z Yao et al ldquoIncreased antitumor activityintratumor paclitaxel concentrations and endothelial cell trans-port of cremophor-free albumin-bound paclitaxel ABI-007compared with cremophor-based paclitaxelrdquo Clinical CancerResearch vol 12 no 4 pp 1317ndash1324 2006
[148] J A Yared and K H R Tkaczuk ldquoUpdate on taxane devel-opment new analogs and new formulationsrdquo Drug DesignDevelopment andTherapy vol 6 pp 371ndash384 2012
[149] M G Teneriello P C Tseng M Crozier et al ldquoPhase IIevaluation of nanoparticle albumin-bound paclitaxel in plati-num-sensitive patients with recurrent ovarian peritoneal orfallopian tube cancerrdquo Journal of Clinical Oncology vol 27 no9 pp 1426ndash1431 2009
[150] R L Coleman W E Brady D S McMeekin et al ldquoA phase IIevaluation of nanoparticle albumin-bound (nab) paclitaxel inthe treatment of recurrent or persistent platinum-resistant ovar-ian fallopian tube or primary peritoneal cancer a GynecologicOncology Group Studyrdquo Gynecologic Oncology vol 122 no 1pp 111ndash115 2011
[151] J W Singer ldquoPaclitaxel poliglumex (XYOTAX CT-2103) amacromolecular taxanerdquo Journal of Controlled Release vol 109no 1ndash3 pp 120ndash126 2005
[152] C Li D-F Yu R A Newman et al ldquoComplete regressionof well-established tumors using a novel water-soluble poly(L-glutamic acid)-paclitaxel conjugaterdquo Cancer Research vol 58no 11 pp 2404ndash2409 1998
[153] M Mita A Mita J Sarantopoulos et al ldquoPhase I study ofpaclitaxel poliglumex administered weekly for patients withadvanced solid malignanciesrdquo Cancer Chemotherapy and Phar-macology vol 64 no 2 pp 287ndash295 2009
[154] P Sabbatini M W Sill D OrsquoMalley L Adler and A ASecord ldquoA phase II trial of paclitaxel poliglumex in recurrentor persistent ovarian or primary peritoneal cancer (EOC) agynecologic oncology group studyrdquo Gynecologic Oncology vol111 no 3 pp 455ndash460 2008
[155] M O Bradley C S Swindell F H Anthony et al ldquoTumortargeting by conjugation of DHA to paclitaxelrdquo Journal ofControlled Release vol 74 no 1ndash3 pp 233ndash236 2001
[156] M O Bradley N L Webb F H Anthony et al ldquoTumortargeting by covalent conjugation of a natural fatty acid topaclitaxelrdquo Clinical Cancer Research vol 7 no 10 pp 3229ndash3238 2001
[157] A C Wolff R C Donehower M K Carducci et al ldquoPhaseI study of docosahexaenoic acid-paclitaxel a taxane-fatty acid
conjugate with a unique pharmacology and toxicity profilerdquoClinical Cancer Research vol 9 no 10 part 1 pp 3589ndash35972003
[158] A Sparreboom A C Wolff J Verweij et al ldquoDispositionof docosahexaenoic acid-paclitaxel a novel taxane in bloodin vitro and clinical pharmacokinetic studiesrdquo Clinical CancerResearch vol 9 no 1 pp 151ndash159 2003
[159] P M Fracasso J Picus J D Wildi et al ldquoPhase 1 and phar-macokinetic study of weekly docosahexaenoic acid-paclitaxelTaxoprexin in resistant solid tumor malignanciesrdquo CancerChemotherapy and Pharmacology vol 63 no 3 pp 451ndash4582009
[160] A Y Bedikian R C DeConti R Conry et al ldquoPhase 3 study ofdocosahexaenoic acid-paclitaxel versus dacarbazine in patientswith metastatic malignant melanomardquo Annals of Oncology vol22 no 4 pp 787ndash793 2011
[161] Y-N Wu S-L Wang Y-C Wang et al ldquoReversal effect ofdocosahexaenoic acid on taxol resistance in human ovarian car-cinoma A2780T cellsrdquo Obstetrics amp Gynecology InternationalJournal vol 1 no 3 Article ID 00018 2014
Submit your manuscripts athttpwwwhindawicom
PainResearch and TreatmentHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom
Volume 2014
ToxinsJournal of
VaccinesJournal of
Hindawi Publishing Corporation httpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
AntibioticsInternational Journal of
ToxicologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
StrokeResearch and TreatmentHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Drug DeliveryJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Advances in Pharmacological Sciences
Tropical MedicineJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Medicinal ChemistryInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
AddictionJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
Emergency Medicine InternationalHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Autoimmune Diseases
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Anesthesiology Research and Practice
ScientificaHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Pharmaceutics
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of

BioMed Research International 13
Table2Ph
aseIIIstu
dies
onintravenou
sdose-densep
aclitaxel
Stud
yRe
gimen
119899
MedianPF
S(m
)
Median
OS
(m)
Adversee
ffects
Com
ments
Katsu
matae
tal2009
[21]
Katsu
matae
tal2013
[22]
Haranoetal2014
[23]
JGOG3016
631
(i)Haematologicaltoxicityhigh
erin
dose
dense-211versus
94
Lower
treatmentcom
pletionin
dose-dense
63versus
48
Frequent
episo
deso
fdelay
indo
se-dense
76versus
67
Doser
eductio
nsin
dose-dense
48versus
35
Nosig
nificantd
ifference
inoverallQ
OL
betweenbo
thgrou
ps(119901=046)
Paclitaxel80m
gm
2D18
15+carbop
latin
AUC63
weeklyversus
Paclitaxel180
mgm
2+
carbop
latin
AUC63
weekly
312
282
1005
Both
givenfor6
ndash9cycle
s319
175
622
Chan
etal2013
[24]
GOG-262
(i)Higherfrequ
ency
ofgrade3
anaemia
(408versus
157119901lt0001)
grade2
sensoryneurop
athy
(259versus
178
119901=0012)b
utlower
incidenceo
fneutropenia(
72versus
83119901lt0001)
Paclitaxel80m
gm
2D18
15+carbop
latin
AUC63
weeklyversus
Paclitaxel175
mgm
2+
carbop
latin
AUC63
weekly
346
148
NR
Both
givenfor6
cycle
s346
143
NR
Bevacizumab
given
optio
nally
112
(did
not
receive
bevazicumab)
142vs
103
Pign
atae
tal2014
[25]
MITO-7
810
(i)Lo
wer
incidenceo
fgrade
3-4
neutropenia(
42versus
50)febrile
neutropenia(lt1v
ersus3
119901=002)
thrombo
cytopenia(
1versus7
119901lt0001)andothern
onhaem
atological
toxicitie
ssuchas
alop
eciavom
iting
renald
ysfunctio
nandneurop
athy
Qualityof
lifeb
etterindo
sedensea
rm(119901lt00001)
Paclitaxel60m
gm
2 weekly+carbop
latin
AUC
2weeklyversus
Paclitaxel175
mgm
2+
carbop
latin
AUC63
weekly
406
404
183 173
77lowast
79lowast
119899num
bero
fpatientsmm
onthsDday
PFSprogressionfre
esurvivalOSoverallsurvivalNAnot
availableinpapero
rabstractandNR
notyetreached
lowastSurvivalrateat2years
14 BioMed Research International
dose-dense (AUC 2 weekly) Although it is possible that thedose scheduling for the platinum-based agent is not essentialfor a survival benefit as shown by previous studies usingdose-dense cisplatin direct cross-trial comparison cannot bemade Unlike paclitaxel carboplatin probably requires peakdose for optimal therapeutic benefit hence this may accountfor the inferior survival outcome in MITO-7 trial Anotherconfounding factor may be difference in ethnicity All threestudies used different ethnic populations and Asian patientsin JGOG-3016 appear to have better survival outcomes thanthe MITO-7 Western population Ethnicity with possibleunderlying genetic causes may be responsible for the variableresponses to chemotherapy across individuals [135] This wasexplored by Millward et al who studied 68 Caucasian andAsian lung cancer patients treated with a combination ofpaclitaxel and carboplatin and found that the incidence offebrile neutropenia was 50 of an initially treated cohortof Asians and when carboplatin was subsequently dosereduced in all Asian patients the overall incidence of febrileneutropenia was also reduced to 26 [136]
Although early clinical data from phase I and phaseII dose-dense paclitaxel trials in advanced ovarian cancerwere promising the results from phase III studies in havebeen inconsistent as a result of differences in paclitaxel dosecarboplatin AUC and schedule addition of bevacizumabas well as different ethnic populations The results of arecently completed randomised three arms GynaecologicCancer InterGroup (GCIG) phase II trial ICON 8 mayfurther inform the clinical benefit of dose dense paclitaxeltherapy
This multicentre trial involving 111 centres in the UKSouth Korea Mexico Ireland Australia and New Zealandwith a target population of 1485 patients with stage IC-IV epithelial ovarian cancer or peritoneal or fallopian tubecancer compared two dose-dense arms (i) JGOG-like armcarboplatin AUC 5 plus weekly 80mgm2 paclitaxel and (ii)MITO-7-like arm weekly carboplatin AUC 167 plus weekly80mgm2 paclitaxel to the standard 3-weekly treatment(carboplatin AUC 5 plus 175mgm2 paclitaxel) for stage IC toIV epithelial ovarian cancer The dose-dense arms of MITO-7 and JGOG-3016 as well as the ethnic heterogeneity will befurther addressed
10 Intraperitoneal (IP) Chemotherapy
In addition to dose and scheduling the route of adminis-tration of chemotherapy agents plays an important role inoutcome Intraperitoneal spread is common and likely anearly event in epithelial ovarian cancer hence the deliveryof chemotherapy intraperitoneally in theory would exposethe microcirculation of tumour to higher doses of drug thansystemic administration while limiting systemic toxicityTheideal drug for IP chemotherapy is one that is systemicallyeffective penetrates deep into the inner core of tumour tissueand remains within the peritoneal cavity for a prolongedperiod of time [137ndash139]
Early clinical studies confirmed that indeed the peritonealcavity could be exposed to 10 to 20-fold higher (cisplatin
and carboplatin) drug concentration than when using theintravenous approach and since 1978 this route had beenadopted as a form of therapeutic intervention [137 139]A subsequent phase I trial showed that IP paclitaxel haddose-limiting toxicity in the form of abdominal pain [140]Another phase 1 GOG pilot study administered weekly IPpaclitaxel at an initial dose of 20mgm2 for 16 weeks to33 patients and found that IP paclitaxel at this dose wasfeasible and well tolerated At dose levels 60 to 65mgm2there were significant levels of paclitaxel for a week afterdrug administration suggesting very slow clearance andcontinuous exposure of the peritoneal cavity to active drugconcentrations [132]
Hence this initiated a phase II study [141] that used pacli-taxel intraperitoneally at a dose of 60ndash65mgm2week In thisphase II GOG study 76 patients with small-volume resid-ual disease carcinoma (05 cm or less) involving the ovaryperitoneal or fallopian tube were treated with paclitaxel60mgm2week intraperitoneally for 16 weeks followed bysurgical evaluation in patients without disease progressionThe Gynaecologic Oncology group (GOG) currently definesno visible disease as microscopic disease being the idealsurgical outcome 75 of patients had received prior systemictherapy and 70 received all 16 courses that were planned Of28 patients with microscopic disease at the start of therapy61 achieved a surgically defined complete response whereasonly 1 out of 31 patients with macroscopic disease achieved acomplete response The median time-to-recurrence was 167months with an estimated survival rate at 2 years being 58Treatment was generally well tolerated [141]
Another study looked into the effect of IP paclitaxel asconsolidation therapy in advanced ovarian cancer Twenty-eight patients who had initial residual macroscopic disease(lt1 cm) after primary surgery or interval debulking but hadcomplete pathological response following standard treatmentwith at least 6 cycles of platinum-based chemotherapy regi-men received paclitaxel 60mgm2week intraperitoneally for12ndash16 weeks as consolidation therapy The median time torecurrence was 25 months but overall survival did not differsignificantly when compared with control group submittedto observation only Treatment-related toxicity was mild andtechnical difficulties were observed in 11 of patients [142]
Multicenter randomised phase 3 trials as well as meta-analysis of IP chemotherapy have been performed anddemonstrated that chemotherapy drugs administered intra-peritoneally are superior to intravenous standard regimensin patient with optimally debulked epithelial ovarian cancerThe most impressive data comes from GOG 114 [14] and172 trial [143] In GOG 114 patients received either sixcycles of intravenous paclitaxel 135mgm2 and cisplatin75mgm2 every 3 weeks or intravenous carboplatin (AUC= 9) every 28 days for two cycles followed by six 3-weeklycycles of intravenous paclitaxel 135mgm2 and IP cisplatin100mgm2 [14] whereas in GOG 172 patients received eitherintravenous paclitaxel 135mgm2 followed by intravenouscisplatin 75mgm2 or intravenous paclitaxel 135mgm2 fol-lowed by IP combination of cisplatin 100mgm2 and pacli-taxel 60mgm2 on day 8 Both trials had a combined total
BioMed Research International 15
of 876 women with stage III epithelial ovarian carcinomaoptimally debulked to le1 cm residual tumour [143] Themedian follow-up for GOG 114 [14] was 138 years with GOG172 [143] was 97 years The primary results of the individualtrials reported up to 6-month improvement in median PFSfollowing IP therapy In the combined analysis of the datafrom both trials the data continued to show a 5-monthdifference in favour of IP therapy (25 versus 20 months)which translates into 16 reduction in the hazard ratio forprogression (119901 = 003) In GOG 114 [14] reported in 2001there was only borderline improvement in overall survivalassociated with this regimen (median 63 versus 52 monthsrelative risk 081 119901 = 005)
However in combined analysis in 2013 which was pre-sented at the Society of Gynecologic Oncology AnnualMeeting [144] the overall survival showed an 11-monthimprovement in favour of IP therapy in GOG 114 whereasGOG 172 reported a 16-month survival advantage Amongpatients treated with IP therapy the 5-year survival rateincreased from 18 following completion of 1-2 cycles to 59for patients who completed 5-6 cycles of treatment Howeverthere was increased toxicity observed in the IP arm grade 3-4 leukopenia thrombocytopenia and abdominal pain Only42 of patients in the GOG172 trial [143] completed all sixcycles of planned treatment in the IP arm while 18 ofpatients in GOG 114 trial [14] received fewer than two coursesof IP chemotherapy
Another randomised phase III trial involving patientswith stages II-III epithelial ovarian carcinoma is the GOG252 study with three arms Arm 1-dose-dense intravenouscarboplatin and paclitaxel Arm 2-dose-dense intravenouspaclitaxel and IP carboplatin and Arm 3 consists of 3-weeklyintravenous paclitaxel (day 1) followed by IP cisplatin (day 2)and IP paclitaxel (day 3) regimen All three arms also incor-porate the combination and maintenance of bevacizumabGOG 252 has completed accrual and results are awaited [139]
11 Newer Forms of Paclitaxel
Development of next-generation taxanes has taken place overthe past 40 years aimed at eliminating toxicity improvingefficacy and ease of administration Abraxane is a novelcompound which incorporates paclitaxel into an albuminnanoparticle soluble in saline hence eliminating the needfor Cremophor EL which is responsible for hypersensitivityreactions experienced during paclitaxel infusion [145] Thenanoparticle albumin in nab-paclitaxel is able to bind toglycoprotein gp60 receptor an albumin receptor and activatecaveolin-1 a protein that in human is encoded byCAV-1 geneleading to formation of caveoli hence allowing nab-paclitaxelto migrate across the endothelial cell membrane into theinterstitial space leading to higher intratumoural drug con-centration In addition Abraxane exhibits linear pharma-cokinetics and can therefore be given at a relatively higherdose than standard intravenous paclitaxel leading to a highertherapeutic ratio and heightened efficacy in solid tumoursmainlymetastatic breast cancer [146 147] Nab-paclitaxel hadFDA approval in 2005 for treatment of breast cancer [148]
Nab-paclitaxel has been studied in recurrent ovariancancer As a single agent in phase II 44 patients withrecurrent ovarian cancer were treated with Nab-paclitaxel260mgm2 intravenously for 30 minutes every 3 weeks for6 cycles Ninety-two percent of patients were platinum-sensitive while 89 had had previous exposure to standardtaxane The objective response rate was 64 with 15 patientsachieving complete response and 13 of them had partialresponse Estimated median PFS was 85 months No hyper-sensitivity reactions were observed and there were infrequentcases of grade 4 neutropenia (11) and grade 2-3 neuropathy(13) [149]
Another phase II study by GOG enrolled 51 patients withplatinum- and taxane-resistant recurrent ovarian cancer outof which 47 were evaluable The objective response rate was38 with one patient achieving a complete response and 10patients a partial response The median PFS was 45 monthswhile overall survival rate was 174 months Severe haema-tological and nonhaematological toxicities including neuro-toxicity were uncommon These results are quite impressivegiven the treatment population consisted of patients withvery poor prognosis with a median platinum and taxane freeinterval of 21 days and 70 had their recurrence within 3months of completion of primary treatment [150] Severalother trials of this formulation are in progress
Paclitaxel poliglumex (PPX) also known as Xyotax isanother prodrug a novel conjugate of paclitaxel and 120572-poly-L-glutamic acid which accumulates within tumour tissuedue to increased permeability of the tumour vessels and lackof lymphatic drainage [148 151 152] Paclitaxel poliglumexenhances solubility of paclitaxel allows direct delivery tothe intratumoural microenvironment and allows prolongedexposure to the active drug while minimising systemictoxicities [151] In Phase I dose escalation studies as a singleagent the recommended dose of PPX was 235mgm2 over 10minutes every 3 weeks or 70mgm2 weekly [153] In a PhaseII GOG study of relapsed ovarian cancer a response rate of16 was seen with infrequent serious adverse events grade3 and 4 neutropenia (24 and 20) and grade 3 neuropathy(24) [154] A phase III trial (GOG-0212) on the use of PPXas consolidation ormaintenance therapy in advanced ovariancancer is in progress
DHA-paclitaxel also known as Taxoprexin is a prodrugwhere paclitaxel is covalently conjugated with the naturallyoccurring omega-3 fatty acid docosahexaenoic acid (DHA)a fatty acid that is easily taken up by tumour cells henceincreasing intratumoural concentration of paclitaxel leadingtumour cell apoptosis [155 156] DHA-paclitaxel exhibitslinear pharmacokinetics and lower toxicity and also ease ofadministration when compared to conventional paclitaxeland has demonstrated antineoplastic activity in animal mod-els of cancer as well as in a phase III trial involving metastaticmelanoma [156ndash160] In a recent study on human ovariancancer cells it was found that DHA could reverse paclitaxelresistance by inhibiting P-gp as well as downregulatingthe expression of multidrug resistance associated proteins(MRP) and inhibiting the activity of NF-120581B and p38 MAPKsignalling pathways [161]
16 BioMed Research International
12 Future Directions
A plateau has been reached regarding the benefits associatedwith standard 3-weekly intravenous administration of cyto-toxic chemotherapy in advanced epithelial ovarian cancerThe ongoing battle for a better treatment regimen to delayrelapse promote remission and most importantly improvethe quality of life of patients with advanced epithelial ovariancancer need not to go further than the ability to relook at thechemotherapy agents that are already available in a differentapproach
Novel compounds to date have not yet shown clinicalsuperiority and parent compounds such as paclitaxel con-tinue to surprise us with their feasibility effectiveness andmanageable toxicity profiles Intraperitoneal paclitaxel willrequire further evaluation Better effort in understanding themechanism of action of drugs including the role of dosescheduling and the effect on the immune systemmay providea more cost-effective route to better clinical outcomes
Conflict of Interests
The authors declare no conflict of interests in this work
Acknowledgments
The authors would like to thank the many researchers whohave contributed to our current knowledge of paclitaxelNirmala Kampan is supported by Australian Monash Uni-versity Institute of Graduate Research Scholarship as wellas Universiti Kebangsaan Malaysia Postgraduate ScholarshipAward Mutsa Madondo has received Postgraduate Pub-lication Award from Monash University and MagdalenaPlebanski has been awarded Senior NHMRC Fellowship
References
[1] Australian Institute of Health and Welfare and National Breastand Ovarian Cancer Centre (Australia) Ovarian Cancer inAustralia AnOverview 2010 Cancer Series Australian Instituteof Health and Welfare Canberra Australia 2010
[2] R E Bristow R S Tomacruz D K Armstrong E L Trimbleand F J Montz ldquoSurvival effect of maximal cytoreductivesurgery for advanced ovarian carcinoma during the platinumera a meta-analysisrdquo Journal of Clinical Oncology vol 20 no 5pp 1248ndash1259 2002
[3] ZKempand JA Ledermann ldquoUpdate onfirst-line treatment ofadvanced ovarian carcinomardquo International Journal of WomenrsquosHealth vol 5 no 1 pp 45ndash51 2013
[4] A du Bois H-J Luck W Meier et al ldquoA randomized clinicaltrial of cisplatinpaclitaxel versus carboplatinpaclitaxel as first-line treatment of ovarian cancerrdquo Journal of the National CancerInstitute vol 95 no 17 pp 1320ndash1330 2003
[5] R F Ozols B N Bundy B E Greer et al ldquoPhase III trialof carboplatin and paclitaxel compared with cisplatin andpaclitaxel in patients with optimally resected stage III ovariancancer A Gynecologic Oncology Group studyrdquo Journal ofClinical Oncology vol 21 no 17 pp 3194ndash3200 2003
[6] W P McGuire W J Hoskins M F Brady et al ldquoCyclophos-phamide and cisplatin compared with paclitaxel and cisplatin
in patients with stage III and stage IV ovarian cancerrdquoThe NewEngland Journal of Medicine vol 334 no 1 pp 1ndash6 1996
[7] W P McGuire W J Hoskins M F Brady et al ldquoCyclophos-phamide and cisplatin versus paclitaxel and cisplatin a phase IIIrandomized trial in patients with suboptimal stage IIIIV ovar-ian cancer (from the gynecologic oncology group)rdquo Seminars inOncology vol 23 no 5 supplement 12 pp 40ndash47 1996
[8] M J Piccart K Bertelsen K James et al ldquoRandomized inter-group trial of cisplatin-paclitaxel versus cisplatin-cyclophosph-amide inwomenwith advanced epithelial ovarian cancer three-year resultsrdquo Journal of the National Cancer Institute vol 92 no9 pp 699ndash708 2000
[9] P A Vasey G C Jayson A Gordon et al ldquoPhase III random-ized trial of docetaxel-carboplatin versus paclitaxel-carboplatinas first-line chemotherpy for ovarian carcinomardquo Journal of theNational Cancer Institute vol 96 no 22 pp 1682ndash1691 2004
[10] B Gronlund C Hogdall H H Hansen and S A EngelholmldquoResults of reinduction therapy with paclitaxel and carboplatinin recurrent epithelial ovarian cancerrdquo Gynecologic Oncologyvol 83 no 1 pp 128ndash134 2001
[11] T M Loffler W Freund J Lipke and T-U HausamenldquoSchedule- and dose-intensified paclitaxel as weekly 1-hourinfusion in pretreated solid tumors results of a phase III trialrdquoSeminars in Oncology vol 23 no 6 supplement 16 pp 32ndash341996
[12] D Fennelly C Aghajanian F Shapiro et al ldquoPhase I and phar-macologic study of paclitaxel administered weekly in patientswith relapsed ovarian cancerrdquo Journal of Clinical Oncology vol15 no 1 pp 187ndash192 1997
[13] N R Abu-Rustum C Aghajanian R R Barakat D Fennelly FShapiro and D Spriggs ldquoSalvage weekly paclitaxel in recurrentovarian cancerrdquo Seminars inOncology vol 24 no 5 supplement15 pp S15-62ndashS15-67 1997
[14] M Markman B N Bundy D S Alberts et al ldquoPhase III trialof standard-dose intravenous cisplatin plus paclitaxel versusmoderately high-dose carboplatin followed by intravenouspaclitaxel and intraperitoneal cisplatin in small-volume stageIII ovarian carcinoma an intergroup study of the gynecologiconcology group Southwestern Oncology Group and EasternCooperativeOncologyGrouprdquo Journal of Clinical Oncology vol19 no 4 pp 1001ndash1007 2001
[15] A Kikuchi H Sakamoto and T Yamamoto ldquoWeekly car-boplatin and paclitaxel is safe active and well tolerated inrecurrent ovarian cancer cases of Japanese women previouslytreated with cisplatin-containing multidrug chemotherapyrdquoInternational Journal of Gynecological Cancer vol 15 no 1 pp45ndash49 2005
[16] I Cadron K Leunen F Amant T van Gorp P Nevenand I Vergote ldquoThe lsquoLeuvenrsquo dose-dense paclitaxelcarboplatinregimen in patients with recurrent ovarian cancerrdquo GynecologicOncology vol 106 no 2 pp 354ndash361 2007
[17] S Pignata E Breda G Scambia et al ldquoA phase II studyof weekly carboplatin and paclitaxel as first-line treatment ofelderly patients with advanced ovarian cancer A Multicen-tre Italian Trial in Ovarian cancer (MITO-5) studyrdquo CriticalReviews in OncologyHematology vol 66 no 3 pp 229ndash2362008
[18] T Safra S Shamai J Greenberg et al ldquoWeekly carboplatinwith paclitaxel compared to standard three-weekly treatment inadvanced epithelial ovarian carcinomamdasha retrospective studyrdquoGynecologic Oncology vol 132 no 1 pp 18ndash22 2014
BioMed Research International 17
[19] L J Havrilesky A A Alvarez R A Sayer et al ldquoWeekly low-dose carboplatin and paclitaxel in the treatment of recurrentovarian and peritoneal cancerrdquo Gynecologic Oncology vol 88no 1 pp 51ndash57 2003
[20] M van der BurgW Onstenk I Boere et al ldquoLong-term resultsof a randomised phase III trial of weekly versus three-weeklypaclitaxelplatinum induction therapy followed by standardor extended three-weekly paclitaxelplatinum in Europeanpatients with advanced epithelial ovarian cancerrdquo EuropeanJournal of Cancer vol 50 no 15 pp 2592ndash2601 2014
[21] N Katsumata M Yasuda F Takahashi et al ldquoDose-densepaclitaxel once a week in combination with carboplatin every3 weeks for advanced ovarian cancer a phase 3 open-labelrandomised controlled trialrdquoThe Lancet vol 374 no 9698 pp1331ndash1338 2009
[22] N Katsumata M Yasuda S Isonishi et al ldquoLong-term resultsof dose-dense paclitaxel and carboplatin versus conventionalpaclitaxel and carboplatin for treatment of advanced epithelialovarian fallopian tube or primary peritoneal cancer (JGOG3016) a randomised controlled open-label trialrdquo The LancetOncology vol 14 no 10 pp 1020ndash1026 2013
[23] K Harano F Terauchi N Katsumata et al ldquoQuality-of-lifeoutcomes from a randomized phase III trial of dose-denseweekly paclitaxel and carboplatin compared with conventionalpaclitaxel and carboplatin as a first-line treatment for stage II-IV ovarian cancer Japanese Gynecologic OncologyGroup Trial(JGOG3016)rdquo Annals of Oncology vol 25 no 1 pp 251ndash2572014
[24] J Chan M F Brady R Penson et al ldquoPhase III trial ofevery-3-weeks paclitaxel vs dose dense weekly paclitaxel withcarboplatin +minus bevacizumab in epithelial ovarian peritonealfallopian tube cancer GOG 262 (NCT01167712)rdquo InternationalJournal of Gynecological Cancer vol 23 no 8 supplement 1 pp9ndash10 2013
[25] S Pignata G Scambia D Katsaros et al ldquoCarboplatin pluspaclitaxel once a week versus every 3 weeks in patients withadvanced ovarian cancer (MITO-7) a randomisedmulticentreopen-label phase 3 trialrdquoThe Lancet Oncology vol 15 no 4 pp396ndash405 2014
[26] V Walsh and J Goodman ldquoFrom taxol to Taxol the changingidentities and ownership of an anti-cancer drugrdquo MedicalAnthropology vol 21 no 3-4 pp 307ndash336 2002
[27] R Renneberg ldquoBiotech History yew trees paclitaxel synthesisand fungirdquo Biotechnology Journal vol 2 no 10 pp 1207ndash12092007
[28] J E Liebmann J A Cook C Lipschultz D Teague J Fisherand J B Mitchell ldquoCytotoxic studies of paclitaxel (Taxol) inhuman tumour cell linesrdquo British Journal of Cancer vol 68 no6 pp 1104ndash1109 1993
[29] J J Manfredi and S B Horwitz ldquoTaxol an antimitotic agentwith a newmechanism of actionrdquo Pharmacology andTherapeu-tics vol 25 no 1 pp 83ndash125 1984
[30] D G I Kingston ldquoRecent advances in the chemistry of taxolrdquoJournal of Natural Products vol 63 no 5 pp 726ndash734 2000
[31] D G I Kingston ldquoThe shape of things to come structural andsynthetic studies of taxol and related compoundsrdquo Phytochem-istry vol 68 no 14 pp 1844ndash1854 2007
[32] V Walsh and J Goodman ldquoCancer chemotherapy biodiversitypublic and private property the case of the anti-cancer drugTaxolrdquo Social Science amp Medicine vol 49 no 9 pp 1215ndash12251999
[33] P H Wiernik E L Schwartz J J Strauman J P Dutcher RB Lipton and E Paietta ldquoPhase I clinical and pharmacokineticstudy of taxolrdquo Cancer Research vol 47 no 9 pp 2486ndash24931987
[34] W P McGuire E K Rowinsky N B Rosenhein et alldquoTaxol a unique antineoplastic agent with significant activityin advanced ovarian epithelial neoplasmsrdquo Annals of InternalMedicine vol 111 no 4 pp 273ndash279 1989
[35] ldquoDiscovery and development of taxolrdquo in Taxol Science andApplications M W M E Suffness Ed pp 3ndash25 CRC PressBoca Raton Fla USA 1995
[36] M J Piccart and F Cardoso ldquoProgress in systemic therapy forbreast cancer an overview and perspectivesrdquo European Journalof Cancer Supplement vol 1 no 2 pp 56ndash69 2003
[37] P Bonomi K B Kim and J Kugler ldquoComparison of survival forstage IIIB versus stage IV non-small cell lung cancer (NSCLC)patients with etoposide-cisplatin versus taxol-cisplatin an East-ern Cooperative Oncology Group (ECOG) trialrdquo in Proceedingsof the American Society of Clinical Oncology vol 16 p 454a1997
[38] D Guenard F Gueritte-Voegelein J Dubois and P PotierldquoStructure-activity relationships of Taxol and Taxotere ana-loguesrdquo Journal of the National Cancer Institute Monographsno 15 pp 79ndash82 1993
[39] D G I Kingston ldquoTaxol the chemistry and structure-activityrelationships of a novel anticancer agentrdquo Trends in Biotechnol-ogy vol 12 no 6 pp 222ndash227 1994
[40] E K Rowinsky and R C Donehower ldquoPaclitaxel (taxol)rdquo TheNew England Journal of Medicine vol 332 no 15 pp 1004ndash10141995
[41] J Parness and S B Horwitz ldquoTaxol binds to polymerizedtubulin in vitrordquo Journal of Cell Biology vol 91 no 2 pp 479ndash487 1981
[42] A Dammermann A Desai and K Oegema ldquoTheminus end insightrdquo Current Biology vol 13 no 15 pp R614ndashR624 2003
[43] CWiese and Y Zheng ldquoMicrotubule nucleation 120574-tubulin andbeyondrdquo Journal of Cell Science vol 119 no 20 pp 4143ndash41532006
[44] A Ganguly H Yang and F Cabral ldquoPaclitaxel-dependent celllines reveal a novel drug activityrdquo Molecular Cancer Therapeu-tics vol 9 no 11 pp 2914ndash2923 2010
[45] P B Schiff and S B Horwitz ldquoTaxol stabilizes microtubules inmouse fibroblast cellsrdquo Proceedings of the National Academy ofSciences of the United States of America vol 77 no 3 pp 1561ndash1565 1980
[46] P B Schiff J Fant and S B Horwitz ldquoPromotion of micro-tubule assembly in vitro by Taxolrdquo Nature vol 277 no 5698pp 665ndash667 1979
[47] D Zhang R Yang S Wang and Z Dong ldquoPaclitaxel new usesfor an old drugrdquoDrug Design Development andTherapy vol 8pp 279ndash284 2014
[48] S Rao G A Orr A G Chaudhary D G I Kingston and SB Horwitz ldquoCharacterization of the taxol binding site on themicrotubule 2-(m-Azidobenzoyl)taxol photolabels a peptide(amino acids 217-231) of beta-tubulinrdquoThe Journal of BiologicalChemistry vol 270 no 35 pp 20235ndash20238 1995
[49] F Wang Y Cao W Zhao H Liu Z Fu and R Han ldquoTaxolinhibits melanoma metastases through apoptosis inductionangiogenesis inhibition and restoration of E-cadherin andnm23 expressionrdquo Journal of Pharmacological Sciences vol 93no 2 pp 197ndash203 2003
18 BioMed Research International
[50] A Sevko V Kremer C Falk et al ldquoApplication of paclitaxel inlow non-cytotoxic doses supports vaccination with melanomaantigens in normal micerdquo Journal of Immunotoxicology vol 9no 3 pp 275ndash281 2012
[51] T Kreis and R Vale Guidebook to the Cytoskeletal and MotorProteins Oxford University Press Oxford UK 2nd edition1999
[52] P Giannakakou D L Sackett Y-K Kang et al ldquoPaclitaxel-resistant human ovarian cancer cells have mutant 120573-tubulinsthat exhibit impaired paclitaxel-driven polymerizationrdquo TheJournal of Biological Chemistry vol 272 no 27 pp 17118ndash171251997
[53] E Rakovitch W Mellado E J Hall T K Pandita S Sawantand C R Geard ldquoPaclitaxel sensitivity correlates with p53status and DNA fragmentation but not G2M accumulationrdquoInternational Journal of Radiation Oncology Biology Physics vol44 no 5 pp 1119ndash1124 1999
[54] S W Lowe S Bodis A McClatchey et al ldquop53 status and theefficacy of cancer therapy in vivordquo Science vol 266 no 5186 pp807ndash810 1994
[55] C C Zhang J-M Yang E White M Murphy A Levine andW N Hait ldquoThe role of MAP4 expression in the sensitivity topaclitaxel and resistance to vinca alkaloids in p53 mutant cellsrdquoOncogene vol 16 no 12 pp 1617ndash1624 1998
[56] K Fukasawa T Choi R Kuriyama S Rulong and G F VandeWoude ldquoAbnormal centrosome amplification in the absence ofp53rdquo Science vol 271 no 5256 pp 1744ndash1747 1996
[57] T-H Wang Y-H Chan C-W Chen et al ldquoPaclitaxel (Taxol)upregulates expression of functional interleukin-6 in humanovarian cancer cells through multiple signaling pathwaysrdquoOncogene vol 25 no 35 pp 4857ndash4866 2006
[58] E Yakirevich E Sabo I Naroditsky Y Sova O Lavie andM B Resnick ldquoMultidrug resistance-related phenotype andapoptosis-related protein expression in ovarian serous carcino-masrdquo Gynecologic Oncology vol 100 no 1 pp 152ndash159 2006
[59] G Szakacs J K Paterson J A Ludwig C Booth-Genthe andM M Gottesman ldquoTargeting multidrug resistance in cancerrdquoNature Reviews Drug Discovery vol 5 no 3 pp 219ndash234 2006
[60] L W Pfannenstiel S S K Lam L A Emens E M Jaffeeand T D Armstrong ldquoPaclitaxel enhances early dendritic cellmaturation and function through TLR4 signaling in micerdquoCellular Immunology vol 263 no 1 pp 79ndash87 2010
[61] N Klauber S Parangi E Flynn E Hamel and R J DrsquoAmatoldquoInhibition of angiogenesis and breast cancer in mice by themicrotubule inhibitors 2-methoxyestradiol and Taxolrdquo CancerResearch vol 57 no 1 pp 81ndash86 1997
[62] D Belotti V Vergani T Drudis et al ldquoThe microtubule-affecting drug paclitaxel has antiangiogenic activityrdquo ClinicalCancer Research vol 2 no 11 pp 1843ndash1849 1996
[63] D H Lau L Xue L J Young P A Burke and A T CheungldquoPaclitaxel (Taxol) an inhibitor of angiogenesis in a highlyvascularized transgenic breast cancerrdquo Cancer Biotherapy andRadiopharmaceuticals vol 14 no 1 pp 31ndash36 1999
[64] X Jiang ldquoHarnessing the immune system for the treatment ofbreast cancerrdquo Journal of Zhejiang University Science B vol 15no 1 pp 1ndash15 2014
[65] A Gadducci D Katsaros P Zola et al ldquoWeekly low-dosepaclitaxel as maintenance treatment in patients with advancedovarian cancer who had microscopic residual disease atsecond-look surgery after 6 cycles of paclitaxelplatinum-basedchemotherapy Results of an open noncomparative phase 2
multicenter italian study (after-6 protocol 2)rdquo InternationalJournal of Gynecological Cancer vol 19 no 4 pp 615ndash619 2009
[66] R S Bhatt J Merchan R Parker et al ldquoA phase 2 pilot trial oflow-dose continuous infusion or lsquometronomicrsquo paclitaxel andoral celecoxib in patients with metastatic melanomardquo Cancervol 116 no 7 pp 1751ndash1756 2010
[67] M Caballero J J Grau J L Blanch et al ldquoSerum vascularendothelial growth factor as a predictive factor in metronomic(weekly) paclitaxel treatment for advanced head and neckcancerrdquo Archives of OtolaryngologymdashHead and Neck Surgeryvol 133 no 11 pp 1143ndash1148 2007
[68] J Alexandre Y Hu W Lu H Pelicano and P Huang ldquoNovelaction of paclitaxel against cancer cells bystander effect medi-ated by reactive oxygen speciesrdquo Cancer Research vol 67 no 8pp 3512ndash3517 2007
[69] T Hadzic N Aykin-Burns Y Zhu et al ldquoPaclitaxel combinedwith inhibitors of glucose and hydroperoxide metabolismenhances breast cancer cell killing viaH
2O2-mediated oxidative
stressrdquo Free Radical Biology and Medicine vol 48 no 8 pp1024ndash1033 2010
[70] C A Sherman-Baust K G Becker W H Wood III Y Zhangand P J Morin ldquoGene expression and pathway analysis of ovar-ian cancer cells selected for resistance to cisplatin paclitaxel ordoxorubicinrdquo Journal of Ovarian Research vol 4 no 1 article21 2011
[71] R Agarwal and S B Kaye ldquoOvarian cancer strategies for over-coming resistance to chemotherapyrdquo Nature Reviews Cancervol 3 no 7 pp 502ndash516 2003
[72] T Acker and K H Plate ldquoRole of hypoxia in tumorangiogenesismdashmolecular and cellular angiogenic crosstalkrdquoCell and Tissue Research vol 314 no 1 pp 145ndash155 2003
[73] M Hockel and P Vaupel ldquoBiological consequences of tumorhypoxiardquo Seminars in Oncology vol 28 supplement 8 no 2 pp36ndash41 2001
[74] L Huang Q-H Zhang Q-L Ao H Xing Y-P Lu and DMa ldquoEffect of hypoxia on the chemotherapeutic sensitivity ofhuman ovarian cancer cells to paclitaxel and its mechanismrdquoZhonghua Zhong Liu Za Zhi vol 29 no 2 pp 96ndash100 2007
[75] N Rohwer and T Cramer ldquoHypoxia-mediated drug resistancenovel insights on the functional interaction of HIFs and celldeath pathwaysrdquoDrug Resistance Updates vol 14 no 3 pp 191ndash201 2011
[76] B B Aggarwal R V Vijayalekshmi and B Sung ldquoTargetinginflammatory pathways for prevention and therapy of cancershort-term friend long-term foerdquo Clinical Cancer Research vol15 no 2 pp 425ndash430 2009
[77] Z Duan R Foster D A Bell et al ldquoSignal transducersand activators of transcription 3 pathway activation in drug-resistant ovarian cancerrdquo Clinical Cancer Research vol 12 no17 pp 5055ndash5063 2006
[78] H-J Kuh S H Jang M G Wientjes J R Weaver and J L-SAu ldquoDeterminants of paclitaxel penetration and accumulationin human solid tumorrdquo Journal of Pharmacology and Experi-mental Therapeutics vol 290 no 2 pp 871ndash880 1999
[79] S Arao H Suwa M Mandai et al ldquoHypoxia-mediated drugresistance novel insights on the functional interaction of HIFsand cell death pathwaysrdquo Cancer Research vol 54 no 5 pp1355ndash1359 1994
[80] S E Johnatty J Beesley B Gao et al ldquoABCB1 (MDR1)polymorphisms and ovarian cancer progression and survivala comprehensive analysis from the Ovarian Cancer Association
BioMed Research International 19
Consortium and the Cancer GenomeAtlasrdquoGynecologic Oncol-ogy vol 131 no 1 pp 8ndash14 2013
[81] X Yang A K Iyer A Singh et al ldquoCluster of differentiation44 targeted hyaluronic acid based nanoparticles for MDR1siRNA delivery to overcome drug resistance in ovarian cancerrdquoPharmaceutical Research 2014
[82] D A Zajchowski B Y Karlan and L K Shawver ldquoTreatment-related protein biomarker expression differs between primaryand recurrent ovarian carcinomasrdquoMolecular CancerTherapeu-tics vol 11 no 2 pp 492ndash502 2012
[83] MM Gottesman J Ludwig D Xia and G Szakacs ldquoDefeatingdrug resistance in cancerrdquoDiscovery Medicine vol 6 no 31 pp18ndash23 2006
[84] S Mozzetti C Ferlini P Concolino et al ldquoClass III 120573-tubulin overexpression is a prominent mechanism of paclitaxelresistance in ovarian cancer patientsrdquo Clinical Cancer Researchvol 11 no 1 pp 298ndash305 2005
[85] M Kavallaris D Y S Kuo C A Burkhart et al ldquoTaxol-resistant epithelial ovarian tumors are associated with alteredexpression of specific beta-tubulin isotypesrdquo Journal of ClinicalInvestigation vol 100 no 5 pp 1282ndash1293 1997
[86] G A Orr P Verdier-Pinard H McDaid and S B HorwitzldquoMechanisms of Taxol resistance related to microtubulesrdquoOncogene vol 22 no 47 pp 7280ndash7295 2003
[87] C Ferlini L Cicchillitti G Raspaglio et al ldquoPaclitaxel directlybinds to Bcl-2 and functionally mimics activity of Nur77rdquoCancer Research vol 69 no 17 pp 6906ndash6914 2009
[88] E Mechetner A Kyshtoobayeva S Zonis et al ldquoLevels ofmultidrug resistance (MDR1) P-glycoprotein expression byhuman breast cancer correlate with in vitro resistance to taxoland doxorubicinrdquo Clinical Cancer Research vol 4 no 2 pp389ndash398 1998
[89] J S Lagas C W N Damen R A B VanWaterschoot D IusufJ H Beijnen and A H Schinkel ldquoP-glycoprotein multidrug-resistance associated protein 2 Cyp3a and carboxylesteraseaffect the oral availability and metabolism of vinorelbinerdquoMolecular Pharmacology vol 82 no 4 pp 636ndash644 2012
[90] M T Huizing J B Vermorken H Rosing et al ldquoPharmacoki-netics of paclitaxel and three major metabolites in patients withadvanced breast carcinoma refractory to anthracycline therapytreated with a 3-hour paclitaxel infusion a European CancerCentre (ECC) trialrdquo Annals of Oncology vol 6 no 7 pp 699ndash704 1995
[91] R Panchagnula ldquoPharmaceutical aspects of paclitaxelrdquo Interna-tional Journal of Pharmaceutics vol 172 no 1-2 pp 1ndash15 1998
[92] S H Jang M G Wientjes and J L-S Au ldquoDeterminants ofpaclitaxel uptake accumulation and retention in solid tumorsrdquoInvestigational New Drugs vol 19 no 2 pp 113ndash123 2001
[93] D S Sonnichsen andM V Relling ldquoClinical pharmacokineticsof paclitaxelrdquo Clinical Pharmacokinetics vol 27 no 4 pp 256ndash269 1994
[94] T Ohtsu Y Sasaki T Tamura et al ldquoClinical pharmacokineticsand pharmacodynamics of paclitaxel a 3-hour infusion versusa 24-hour infusionrdquo Clinical Cancer Research vol 1 no 6 pp599ndash606 1995
[95] M Czejka J Schueller H Schnait B Springer and I EderldquoClinical pharmacokinetics andmetabolism of paclitaxel after athree-hour infusion comparison of two preparationsrdquo Journalof Oncology Pharmacy Practice vol 9 no 4 pp 129ndash136 2003
[96] J Rizzo C Riley D VonHoff J Kuhn J Phillips and T BrownldquoAnalysis of anticancer drugs in biological fluids determination
of taxol with application to clinical pharmacokineticsrdquo Journalof Pharmaceutical and Biomedical Analysis vol 8 no 2 pp 159ndash164 1990
[97] V A de Weger J H Beijnen and J H M Schellens ldquoCel-lular and clinical pharmacology of the taxanes docetaxel andpaclitaxelmdasha reviewrdquoAnti-Cancer Drugs vol 25 no 5 pp 488ndash494 2014
[98] S Kumar H Mahdi C Bryant J P Shah G Garg andA Munkarah ldquoClinical trials and progress with paclitaxel inovarian cancerrdquo International Journal of Womenrsquos Health vol 2no 1 pp 411ndash427 2010
[99] B Huang J Zhao J C Unkeless Z H Feng and H XiongldquoTLR signaling by tumor and immune cells a double-edgedswordrdquo Oncogene vol 27 no 2 pp 218ndash224 2008
[100] R A Jibodh J S Lagas B Nuijen J H Beijnen and J HM Schellens ldquoTaxanes old drugs new oral formulationsrdquoEuropean Journal of Pharmacology vol 717 no 1ndash3 pp 40ndash462013
[101] A Javeed M Ashraf A Riaz A Ghafoor S Afzal and M MMukhtar ldquoPaclitaxel and immune systemrdquo European Journal ofPharmaceutical Sciences vol 38 no 4 pp 283ndash290 2009
[102] L Bracci G Schiavoni A Sistigu and F Belardelli ldquoImmune-based mechanisms of cytotoxic chemotherapy implications forthe design of novel and rationale-based combined treatmentsagainst cancerrdquo Cell Death and Differentiation vol 21 no 1 pp15ndash25 2014
[103] C A Byrd-Leifer E F Block K Takeda S Akira and A DingldquoThe role of MyD88 and TLR4 in the LPS-mimetic activity ofTaxolrdquo European Journal of Immunology vol 31 no 8 pp 2448ndash2457 2001
[104] A-C Wang Y-B Ma F-X Wu et al ldquoTLR4 induces tumorgrowth and inhibits paclitaxel activity in MyD88-positivehuman ovarian carcinoma in vitrordquo Oncology Letters vol 7 no3 pp 871ndash877 2014
[105] Y Zhu N Liu S D Xiong Y J Zheng and Y W ChuldquoCD4+Foxp3+ regulatory T-cell impairment by paclitaxel isindependent of toll-like receptor 4rdquo Scandinavian Journal ofImmunology vol 73 no 4 pp 301ndash308 2011
[106] M Kubo T Morisaki K Matsumoto et al ldquoPaclitaxel probablyenhances cytotoxicity of natural killer cells against breastcarcinoma cells by increasing perforin productionrdquo CancerImmunology Immunotherapy vol 54 no 5 pp 468ndash476 2005
[107] L Markasz G Stuber B Vanherberghen et al ldquoEffect of fre-quently used chemotherapeutic drugs on the cytotoxic activityof human natural killer cellsrdquo Molecular Cancer Therapeuticsvol 6 no 2 pp 644ndash654 2007
[108] T Sako N Burioka K Yasuda et al ldquoCellular immune profile inpatients with non-small cell lung cancer after weekly paclitaxeltherapyrdquo Acta Oncologica vol 43 no 1 pp 15ndash19 2004
[109] R Kaneno G V Shurin I L Tourkova and M R ShurinldquoChemomodulation of human dendritic cell function by anti-neoplastic agents in low noncytotoxic concentrationsrdquo Journalof Translational Medicine vol 7 article 58 2009
[110] TMichels G V ShurinHNaiditch A Sevko VUmansky andM R Shurin ldquoPaclitaxel promotes differentiation of myeloid-derived suppressor cells into dendritic cells in vitro in a TLR4-independent mannerrdquo Journal of Immunotoxicology vol 9 no3 pp 292ndash300 2012
[111] R A Kemp and F Ronchese ldquoTumor-specific Tc1 but not Tc2cells deliver protective antitumor immunityrdquo The Journal ofImmunology vol 167 no 11 pp 6497ndash6502 2001
20 BioMed Research International
[112] A Y Rudensky ldquoRegulatory T cells and Foxp3rdquo ImmunologicalReviews vol 241 no 1 pp 260ndash268 2011
[113] EM Shevach ldquoCD4+CD25+ suppressor T cellsmore questionsthan answersrdquo Nature Reviews Immunology vol 2 no 6 pp389ndash400 2002
[114] S Sakaguchi T Yamaguchi T Nomura and M Ono ldquoRegu-latory T cells and immune tolerancerdquo Cell vol 133 no 5 pp775ndash787 2008
[115] H Nishikawa and S Sakaguchi ldquoRegulatory T cells in tumorimmunityrdquo International Journal of Cancer vol 127 no 4 pp759ndash767 2010
[116] W Zou ldquoRegulatory T cells tumour immunity and immuno-therapyrdquoNature Reviews Immunology vol 6 no 4 pp 295ndash3072006
[117] A Fialova S Partlova L Sojka et al ldquoDynamics of T-cell infil-tration during the course of ovarian cancer The gradual shiftfrom aTh17 effector cell response to a predominant infiltrationby regulatory T-cellsrdquo International Journal of Cancer vol 132no 5 pp 1070ndash1079 2013
[118] A E Albers R L Ferris G G Kim K Chikamatsu A BDeLeo and T L Whiteside ldquoImmune responses to p53 inpatients with cancer enrichment in tetramer+ p53 peptide-specific T cells and regulatory T cells at tumor sitesrdquo CancerImmunology Immunotherapy vol 54 no 11 pp 1072ndash10812005
[119] N Liu Y Zheng Y Zhu S Xiong andYChu ldquoSelective impair-ment of CD4 + CD25 + Foxp3 + regulatory T cells by paclitaxelis explained by Bcl-2Bax mediated apoptosisrdquo InternationalImmunopharmacology vol 11 no 2 pp 212ndash219 2011
[120] X Wu Q-M Feng Y Wang J Shi H-L Ge and W DildquoThe immunologic aspects in advanced ovarian cancer patientstreated with paclitaxel and carboplatin chemotherapyrdquo CancerImmunology Immunotherapy vol 59 no 2 pp 279ndash291 2010
[121] A P Vicari R Luu N Zhang et al ldquoPaclitaxel reducesregulatoryT cell numbers and inhibitory function and enhancesthe anti-tumor effects of the TLR9 agonist PF-3512676 in themouserdquo Cancer Immunology Immunotherapy vol 58 no 4 pp615ndash628 2009
[122] L Zhang K Dermawan M Jin et al ldquoDifferential impairmentof regulatory T cells rather than effector T cells by paclitaxel-based chemotherapyrdquo Clinical Immunology vol 129 no 2 pp219ndash229 2008
[123] Y Tabuchi J Matsuoka M Gunduz et al ldquoResistance topaclitaxel therapy is related with Bcl-2 expression through anestrogen receptor mediated pathway in breast cancerrdquo Interna-tional Journal of Oncology vol 34 no 2 pp 313ndash319 2009
[124] N Obermajer R Muthuswamy K Odunsi R P Edwards andP Kalinski ldquoPGE
2-induced CXCL12 production and CXCR4
expression controls the accumulation of human MDSCs inovarian cancer environmentrdquo Cancer Research vol 71 no 24pp 7463ndash7470 2011
[125] Q M Feng W Di and X Wu ldquoImmune reconstitution inadvanced ovarian cancer patients undergoing first line chemo-therapyrdquo Xi Bao Yu Fen Zi Mian Yi Xue Za Zhi vol 25 no 11pp 1023ndash1025 2009
[126] A D Seidman D Hochhauser M Gollub et al ldquoNinety-six-hour paclitaxel infusion after progression during short taxaneexposure a phase II pharmacokinetic and pharmacodynamicstudy in metastatic breast cancerrdquo Journal of Clinical Oncologyvol 14 no 6 pp 1877ndash1884 1996
[127] D R Spriggs M F Brady L Vaccarello et al ldquoPhase IIIrandomized trial of intravenous cisplatin plus a 24- or 96-hour
infusion of paclitaxel in epithelial ovarian cancer a gynecologiconcology group studyrdquo Journal of Clinical Oncology vol 25 no28 pp 4466ndash4471 2007
[128] G A Omura M F Brady K Y Look et al ldquoPhase III trial ofpaclitaxel at two dose levels the higher dose accompanied byfilgrastim at two dose levels in platinum-pretreated epithelialovarian cancer an intergroup studyrdquo Journal of Clinical Oncol-ogy vol 21 no 15 pp 2843ndash2848 2003
[129] R Simon and L Norton ldquoThe Norton-Simon hypothesisdesigning more effective and less toxic chemotherapeutic reg-imensrdquoNature Clinical Practice Oncology vol 3 no 8 pp 406ndash407 2006
[130] A Kumar P Hoskins and A Tinker ldquoDose-dense paclitaxel inadvanced ovarian cancerrdquo Clinical Oncology vol 27 no 1 pp40ndash47 2015
[131] P Marchetti S Urien G A Cappellini G Ronzino and CFicorella ldquoWeekly administration of paclitaxel theoretical andclinical basisrdquoCritical Reviews in OncologyHematology vol 44supplement pp S3ndashS13 2002
[132] P Francis E Rowinsky J Schneider T Hakes W Hoskinsand M Markman ldquoPhase I feasibility and pharmacologic studyof weekly intraperitoneal paclitaxel A Gynecologic OncologyGroup pilot studyrdquo Journal of Clinical Oncology vol 13 no 12pp 2961ndash2967 1995
[133] H Thomas and P Rosenberg ldquoRole of weekly paclitaxel inthe treatment of advanced ovarian cancerrdquo Critical Reviews inOncologyHematology vol 44 supplement pp S43ndashS51 2002
[134] M Markman J Markman K Webster et al ldquoDuration ofresponse to second-line platinum-based chemotherapy forovarian cancer implications for patient management and clini-cal trial designrdquo Journal of Clinical Oncology vol 22 no 15 pp3120ndash3125 2004
[135] P H OrsquoDonnell M Eileen Dolan E Gamazon et al ldquoPopu-lation differences in platinum toxicity as a means to identifynovel genetic susceptibility variantsrdquo Pharmacogenetics andGenomics vol 20 no 5 pp 327ndash337 2010
[136] M J Millward M J Boyer M Lehnert et al ldquoDocetaxel andcarboplatin is an active regimen in advanced non-small-celllung cancer a phase II study in Caucasian and Asian patientsrdquoAnnals of Oncology vol 14 no 3 pp 449ndash454 2003
[137] M Markman ldquoIntraperitoneal therapy of ovarian cancerrdquoOncologist vol 1 no 1-2 pp 18ndash21 1996
[138] M Markman and J L Walker ldquoIntraperitoneal chemotherapyof ovarian cancer a review with a focus on practical aspects oftreatmentrdquo Journal of Clinical Oncology vol 24 no 6 pp 988ndash994 2006
[139] K Fujiwara S Nagao E Aotani and K Hasegawa ldquoPrincipleand evolving role of intraperitoneal chemotherapy in ovariancancerrdquo Expert Opinion on Pharmacotherapy vol 14 no 13 pp1797ndash1806 2013
[140] M Markman E Rowinsky T Hakes et al ldquoPhase I trialof intraperitoneal taxol a gynecoloic oncology group studyrdquoJournal of Clinical Oncology vol 10 no 9 pp 1485ndash1491 1992
[141] M Markman M F Brady N M Spirtos P Hanjani and S CRubin ldquoPhase II trial of intraperitoneal paclitaxel in carcinomaof the ovary tube and peritoneum a gynecologic oncologygroup studyrdquo Journal of Clinical Oncology vol 16 no 8 pp2620ndash2624 1998
[142] P B Panici I Palaia M Graziano F Bellati N Manci and RAngioli ldquoIntraperitoneal paclitaxel as consolidation treatmentin ovarian cancer patients a case control studyrdquo Oncology vol78 no 1 pp 20ndash25 2010
BioMed Research International 21
[143] D K Armstrong B Bundy L Wenzel et al ldquoIntraperitonealcisplatin and paclitaxel in ovarian cancerrdquo The New EnglandJournal of Medicine vol 354 no 1 pp 34ndash43 2006
[144] D Tewari J Java and R Salani ldquoLong-term survival advantageof intraperitoneal chemotherapy treatment in advanced ovariancancer an analysis of a Gynecologic Oncology Group ancillarydata studyrdquo in Proceedings of the 2013 Society of GynecologicOncology Annual Meeting on Womenrsquos Cancer (GOG114172Abstract) Los Angeles Calif USA 2013
[145] D A Yardley ldquonab-paclitaxel mechanisms of action and deliv-eryrdquo Journal of Controlled Release vol 170 no 3 pp 365ndash3722013
[146] M Ando K Yonemori N Katsumata et al ldquoPhase I and phar-macokinetic study of nab-paclitaxel nanoparticle albumin-bound paclitaxel administeredweekly to Japanese patients withsolid tumors and metastatic breast cancerrdquo Cancer Chemother-apy and Pharmacology vol 69 no 2 pp 457ndash465 2012
[147] N Desai V Trieu Z Yao et al ldquoIncreased antitumor activityintratumor paclitaxel concentrations and endothelial cell trans-port of cremophor-free albumin-bound paclitaxel ABI-007compared with cremophor-based paclitaxelrdquo Clinical CancerResearch vol 12 no 4 pp 1317ndash1324 2006
[148] J A Yared and K H R Tkaczuk ldquoUpdate on taxane devel-opment new analogs and new formulationsrdquo Drug DesignDevelopment andTherapy vol 6 pp 371ndash384 2012
[149] M G Teneriello P C Tseng M Crozier et al ldquoPhase IIevaluation of nanoparticle albumin-bound paclitaxel in plati-num-sensitive patients with recurrent ovarian peritoneal orfallopian tube cancerrdquo Journal of Clinical Oncology vol 27 no9 pp 1426ndash1431 2009
[150] R L Coleman W E Brady D S McMeekin et al ldquoA phase IIevaluation of nanoparticle albumin-bound (nab) paclitaxel inthe treatment of recurrent or persistent platinum-resistant ovar-ian fallopian tube or primary peritoneal cancer a GynecologicOncology Group Studyrdquo Gynecologic Oncology vol 122 no 1pp 111ndash115 2011
[151] J W Singer ldquoPaclitaxel poliglumex (XYOTAX CT-2103) amacromolecular taxanerdquo Journal of Controlled Release vol 109no 1ndash3 pp 120ndash126 2005
[152] C Li D-F Yu R A Newman et al ldquoComplete regressionof well-established tumors using a novel water-soluble poly(L-glutamic acid)-paclitaxel conjugaterdquo Cancer Research vol 58no 11 pp 2404ndash2409 1998
[153] M Mita A Mita J Sarantopoulos et al ldquoPhase I study ofpaclitaxel poliglumex administered weekly for patients withadvanced solid malignanciesrdquo Cancer Chemotherapy and Phar-macology vol 64 no 2 pp 287ndash295 2009
[154] P Sabbatini M W Sill D OrsquoMalley L Adler and A ASecord ldquoA phase II trial of paclitaxel poliglumex in recurrentor persistent ovarian or primary peritoneal cancer (EOC) agynecologic oncology group studyrdquo Gynecologic Oncology vol111 no 3 pp 455ndash460 2008
[155] M O Bradley C S Swindell F H Anthony et al ldquoTumortargeting by conjugation of DHA to paclitaxelrdquo Journal ofControlled Release vol 74 no 1ndash3 pp 233ndash236 2001
[156] M O Bradley N L Webb F H Anthony et al ldquoTumortargeting by covalent conjugation of a natural fatty acid topaclitaxelrdquo Clinical Cancer Research vol 7 no 10 pp 3229ndash3238 2001
[157] A C Wolff R C Donehower M K Carducci et al ldquoPhaseI study of docosahexaenoic acid-paclitaxel a taxane-fatty acid
conjugate with a unique pharmacology and toxicity profilerdquoClinical Cancer Research vol 9 no 10 part 1 pp 3589ndash35972003
[158] A Sparreboom A C Wolff J Verweij et al ldquoDispositionof docosahexaenoic acid-paclitaxel a novel taxane in bloodin vitro and clinical pharmacokinetic studiesrdquo Clinical CancerResearch vol 9 no 1 pp 151ndash159 2003
[159] P M Fracasso J Picus J D Wildi et al ldquoPhase 1 and phar-macokinetic study of weekly docosahexaenoic acid-paclitaxelTaxoprexin in resistant solid tumor malignanciesrdquo CancerChemotherapy and Pharmacology vol 63 no 3 pp 451ndash4582009
[160] A Y Bedikian R C DeConti R Conry et al ldquoPhase 3 study ofdocosahexaenoic acid-paclitaxel versus dacarbazine in patientswith metastatic malignant melanomardquo Annals of Oncology vol22 no 4 pp 787ndash793 2011
[161] Y-N Wu S-L Wang Y-C Wang et al ldquoReversal effect ofdocosahexaenoic acid on taxol resistance in human ovarian car-cinoma A2780T cellsrdquo Obstetrics amp Gynecology InternationalJournal vol 1 no 3 Article ID 00018 2014
Submit your manuscripts athttpwwwhindawicom
PainResearch and TreatmentHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom
Volume 2014
ToxinsJournal of
VaccinesJournal of
Hindawi Publishing Corporation httpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
AntibioticsInternational Journal of
ToxicologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
StrokeResearch and TreatmentHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Drug DeliveryJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Advances in Pharmacological Sciences
Tropical MedicineJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Medicinal ChemistryInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
AddictionJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
Emergency Medicine InternationalHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Autoimmune Diseases
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Anesthesiology Research and Practice
ScientificaHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Pharmaceutics
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of

14 BioMed Research International
dose-dense (AUC 2 weekly) Although it is possible that thedose scheduling for the platinum-based agent is not essentialfor a survival benefit as shown by previous studies usingdose-dense cisplatin direct cross-trial comparison cannot bemade Unlike paclitaxel carboplatin probably requires peakdose for optimal therapeutic benefit hence this may accountfor the inferior survival outcome in MITO-7 trial Anotherconfounding factor may be difference in ethnicity All threestudies used different ethnic populations and Asian patientsin JGOG-3016 appear to have better survival outcomes thanthe MITO-7 Western population Ethnicity with possibleunderlying genetic causes may be responsible for the variableresponses to chemotherapy across individuals [135] This wasexplored by Millward et al who studied 68 Caucasian andAsian lung cancer patients treated with a combination ofpaclitaxel and carboplatin and found that the incidence offebrile neutropenia was 50 of an initially treated cohortof Asians and when carboplatin was subsequently dosereduced in all Asian patients the overall incidence of febrileneutropenia was also reduced to 26 [136]
Although early clinical data from phase I and phaseII dose-dense paclitaxel trials in advanced ovarian cancerwere promising the results from phase III studies in havebeen inconsistent as a result of differences in paclitaxel dosecarboplatin AUC and schedule addition of bevacizumabas well as different ethnic populations The results of arecently completed randomised three arms GynaecologicCancer InterGroup (GCIG) phase II trial ICON 8 mayfurther inform the clinical benefit of dose dense paclitaxeltherapy
This multicentre trial involving 111 centres in the UKSouth Korea Mexico Ireland Australia and New Zealandwith a target population of 1485 patients with stage IC-IV epithelial ovarian cancer or peritoneal or fallopian tubecancer compared two dose-dense arms (i) JGOG-like armcarboplatin AUC 5 plus weekly 80mgm2 paclitaxel and (ii)MITO-7-like arm weekly carboplatin AUC 167 plus weekly80mgm2 paclitaxel to the standard 3-weekly treatment(carboplatin AUC 5 plus 175mgm2 paclitaxel) for stage IC toIV epithelial ovarian cancer The dose-dense arms of MITO-7 and JGOG-3016 as well as the ethnic heterogeneity will befurther addressed
10 Intraperitoneal (IP) Chemotherapy
In addition to dose and scheduling the route of adminis-tration of chemotherapy agents plays an important role inoutcome Intraperitoneal spread is common and likely anearly event in epithelial ovarian cancer hence the deliveryof chemotherapy intraperitoneally in theory would exposethe microcirculation of tumour to higher doses of drug thansystemic administration while limiting systemic toxicityTheideal drug for IP chemotherapy is one that is systemicallyeffective penetrates deep into the inner core of tumour tissueand remains within the peritoneal cavity for a prolongedperiod of time [137ndash139]
Early clinical studies confirmed that indeed the peritonealcavity could be exposed to 10 to 20-fold higher (cisplatin
and carboplatin) drug concentration than when using theintravenous approach and since 1978 this route had beenadopted as a form of therapeutic intervention [137 139]A subsequent phase I trial showed that IP paclitaxel haddose-limiting toxicity in the form of abdominal pain [140]Another phase 1 GOG pilot study administered weekly IPpaclitaxel at an initial dose of 20mgm2 for 16 weeks to33 patients and found that IP paclitaxel at this dose wasfeasible and well tolerated At dose levels 60 to 65mgm2there were significant levels of paclitaxel for a week afterdrug administration suggesting very slow clearance andcontinuous exposure of the peritoneal cavity to active drugconcentrations [132]
Hence this initiated a phase II study [141] that used pacli-taxel intraperitoneally at a dose of 60ndash65mgm2week In thisphase II GOG study 76 patients with small-volume resid-ual disease carcinoma (05 cm or less) involving the ovaryperitoneal or fallopian tube were treated with paclitaxel60mgm2week intraperitoneally for 16 weeks followed bysurgical evaluation in patients without disease progressionThe Gynaecologic Oncology group (GOG) currently definesno visible disease as microscopic disease being the idealsurgical outcome 75 of patients had received prior systemictherapy and 70 received all 16 courses that were planned Of28 patients with microscopic disease at the start of therapy61 achieved a surgically defined complete response whereasonly 1 out of 31 patients with macroscopic disease achieved acomplete response The median time-to-recurrence was 167months with an estimated survival rate at 2 years being 58Treatment was generally well tolerated [141]
Another study looked into the effect of IP paclitaxel asconsolidation therapy in advanced ovarian cancer Twenty-eight patients who had initial residual macroscopic disease(lt1 cm) after primary surgery or interval debulking but hadcomplete pathological response following standard treatmentwith at least 6 cycles of platinum-based chemotherapy regi-men received paclitaxel 60mgm2week intraperitoneally for12ndash16 weeks as consolidation therapy The median time torecurrence was 25 months but overall survival did not differsignificantly when compared with control group submittedto observation only Treatment-related toxicity was mild andtechnical difficulties were observed in 11 of patients [142]
Multicenter randomised phase 3 trials as well as meta-analysis of IP chemotherapy have been performed anddemonstrated that chemotherapy drugs administered intra-peritoneally are superior to intravenous standard regimensin patient with optimally debulked epithelial ovarian cancerThe most impressive data comes from GOG 114 [14] and172 trial [143] In GOG 114 patients received either sixcycles of intravenous paclitaxel 135mgm2 and cisplatin75mgm2 every 3 weeks or intravenous carboplatin (AUC= 9) every 28 days for two cycles followed by six 3-weeklycycles of intravenous paclitaxel 135mgm2 and IP cisplatin100mgm2 [14] whereas in GOG 172 patients received eitherintravenous paclitaxel 135mgm2 followed by intravenouscisplatin 75mgm2 or intravenous paclitaxel 135mgm2 fol-lowed by IP combination of cisplatin 100mgm2 and pacli-taxel 60mgm2 on day 8 Both trials had a combined total
BioMed Research International 15
of 876 women with stage III epithelial ovarian carcinomaoptimally debulked to le1 cm residual tumour [143] Themedian follow-up for GOG 114 [14] was 138 years with GOG172 [143] was 97 years The primary results of the individualtrials reported up to 6-month improvement in median PFSfollowing IP therapy In the combined analysis of the datafrom both trials the data continued to show a 5-monthdifference in favour of IP therapy (25 versus 20 months)which translates into 16 reduction in the hazard ratio forprogression (119901 = 003) In GOG 114 [14] reported in 2001there was only borderline improvement in overall survivalassociated with this regimen (median 63 versus 52 monthsrelative risk 081 119901 = 005)
However in combined analysis in 2013 which was pre-sented at the Society of Gynecologic Oncology AnnualMeeting [144] the overall survival showed an 11-monthimprovement in favour of IP therapy in GOG 114 whereasGOG 172 reported a 16-month survival advantage Amongpatients treated with IP therapy the 5-year survival rateincreased from 18 following completion of 1-2 cycles to 59for patients who completed 5-6 cycles of treatment Howeverthere was increased toxicity observed in the IP arm grade 3-4 leukopenia thrombocytopenia and abdominal pain Only42 of patients in the GOG172 trial [143] completed all sixcycles of planned treatment in the IP arm while 18 ofpatients in GOG 114 trial [14] received fewer than two coursesof IP chemotherapy
Another randomised phase III trial involving patientswith stages II-III epithelial ovarian carcinoma is the GOG252 study with three arms Arm 1-dose-dense intravenouscarboplatin and paclitaxel Arm 2-dose-dense intravenouspaclitaxel and IP carboplatin and Arm 3 consists of 3-weeklyintravenous paclitaxel (day 1) followed by IP cisplatin (day 2)and IP paclitaxel (day 3) regimen All three arms also incor-porate the combination and maintenance of bevacizumabGOG 252 has completed accrual and results are awaited [139]
11 Newer Forms of Paclitaxel
Development of next-generation taxanes has taken place overthe past 40 years aimed at eliminating toxicity improvingefficacy and ease of administration Abraxane is a novelcompound which incorporates paclitaxel into an albuminnanoparticle soluble in saline hence eliminating the needfor Cremophor EL which is responsible for hypersensitivityreactions experienced during paclitaxel infusion [145] Thenanoparticle albumin in nab-paclitaxel is able to bind toglycoprotein gp60 receptor an albumin receptor and activatecaveolin-1 a protein that in human is encoded byCAV-1 geneleading to formation of caveoli hence allowing nab-paclitaxelto migrate across the endothelial cell membrane into theinterstitial space leading to higher intratumoural drug con-centration In addition Abraxane exhibits linear pharma-cokinetics and can therefore be given at a relatively higherdose than standard intravenous paclitaxel leading to a highertherapeutic ratio and heightened efficacy in solid tumoursmainlymetastatic breast cancer [146 147] Nab-paclitaxel hadFDA approval in 2005 for treatment of breast cancer [148]
Nab-paclitaxel has been studied in recurrent ovariancancer As a single agent in phase II 44 patients withrecurrent ovarian cancer were treated with Nab-paclitaxel260mgm2 intravenously for 30 minutes every 3 weeks for6 cycles Ninety-two percent of patients were platinum-sensitive while 89 had had previous exposure to standardtaxane The objective response rate was 64 with 15 patientsachieving complete response and 13 of them had partialresponse Estimated median PFS was 85 months No hyper-sensitivity reactions were observed and there were infrequentcases of grade 4 neutropenia (11) and grade 2-3 neuropathy(13) [149]
Another phase II study by GOG enrolled 51 patients withplatinum- and taxane-resistant recurrent ovarian cancer outof which 47 were evaluable The objective response rate was38 with one patient achieving a complete response and 10patients a partial response The median PFS was 45 monthswhile overall survival rate was 174 months Severe haema-tological and nonhaematological toxicities including neuro-toxicity were uncommon These results are quite impressivegiven the treatment population consisted of patients withvery poor prognosis with a median platinum and taxane freeinterval of 21 days and 70 had their recurrence within 3months of completion of primary treatment [150] Severalother trials of this formulation are in progress
Paclitaxel poliglumex (PPX) also known as Xyotax isanother prodrug a novel conjugate of paclitaxel and 120572-poly-L-glutamic acid which accumulates within tumour tissuedue to increased permeability of the tumour vessels and lackof lymphatic drainage [148 151 152] Paclitaxel poliglumexenhances solubility of paclitaxel allows direct delivery tothe intratumoural microenvironment and allows prolongedexposure to the active drug while minimising systemictoxicities [151] In Phase I dose escalation studies as a singleagent the recommended dose of PPX was 235mgm2 over 10minutes every 3 weeks or 70mgm2 weekly [153] In a PhaseII GOG study of relapsed ovarian cancer a response rate of16 was seen with infrequent serious adverse events grade3 and 4 neutropenia (24 and 20) and grade 3 neuropathy(24) [154] A phase III trial (GOG-0212) on the use of PPXas consolidation ormaintenance therapy in advanced ovariancancer is in progress
DHA-paclitaxel also known as Taxoprexin is a prodrugwhere paclitaxel is covalently conjugated with the naturallyoccurring omega-3 fatty acid docosahexaenoic acid (DHA)a fatty acid that is easily taken up by tumour cells henceincreasing intratumoural concentration of paclitaxel leadingtumour cell apoptosis [155 156] DHA-paclitaxel exhibitslinear pharmacokinetics and lower toxicity and also ease ofadministration when compared to conventional paclitaxeland has demonstrated antineoplastic activity in animal mod-els of cancer as well as in a phase III trial involving metastaticmelanoma [156ndash160] In a recent study on human ovariancancer cells it was found that DHA could reverse paclitaxelresistance by inhibiting P-gp as well as downregulatingthe expression of multidrug resistance associated proteins(MRP) and inhibiting the activity of NF-120581B and p38 MAPKsignalling pathways [161]
16 BioMed Research International
12 Future Directions
A plateau has been reached regarding the benefits associatedwith standard 3-weekly intravenous administration of cyto-toxic chemotherapy in advanced epithelial ovarian cancerThe ongoing battle for a better treatment regimen to delayrelapse promote remission and most importantly improvethe quality of life of patients with advanced epithelial ovariancancer need not to go further than the ability to relook at thechemotherapy agents that are already available in a differentapproach
Novel compounds to date have not yet shown clinicalsuperiority and parent compounds such as paclitaxel con-tinue to surprise us with their feasibility effectiveness andmanageable toxicity profiles Intraperitoneal paclitaxel willrequire further evaluation Better effort in understanding themechanism of action of drugs including the role of dosescheduling and the effect on the immune systemmay providea more cost-effective route to better clinical outcomes
Conflict of Interests
The authors declare no conflict of interests in this work
Acknowledgments
The authors would like to thank the many researchers whohave contributed to our current knowledge of paclitaxelNirmala Kampan is supported by Australian Monash Uni-versity Institute of Graduate Research Scholarship as wellas Universiti Kebangsaan Malaysia Postgraduate ScholarshipAward Mutsa Madondo has received Postgraduate Pub-lication Award from Monash University and MagdalenaPlebanski has been awarded Senior NHMRC Fellowship
References
[1] Australian Institute of Health and Welfare and National Breastand Ovarian Cancer Centre (Australia) Ovarian Cancer inAustralia AnOverview 2010 Cancer Series Australian Instituteof Health and Welfare Canberra Australia 2010
[2] R E Bristow R S Tomacruz D K Armstrong E L Trimbleand F J Montz ldquoSurvival effect of maximal cytoreductivesurgery for advanced ovarian carcinoma during the platinumera a meta-analysisrdquo Journal of Clinical Oncology vol 20 no 5pp 1248ndash1259 2002
[3] ZKempand JA Ledermann ldquoUpdate onfirst-line treatment ofadvanced ovarian carcinomardquo International Journal of WomenrsquosHealth vol 5 no 1 pp 45ndash51 2013
[4] A du Bois H-J Luck W Meier et al ldquoA randomized clinicaltrial of cisplatinpaclitaxel versus carboplatinpaclitaxel as first-line treatment of ovarian cancerrdquo Journal of the National CancerInstitute vol 95 no 17 pp 1320ndash1330 2003
[5] R F Ozols B N Bundy B E Greer et al ldquoPhase III trialof carboplatin and paclitaxel compared with cisplatin andpaclitaxel in patients with optimally resected stage III ovariancancer A Gynecologic Oncology Group studyrdquo Journal ofClinical Oncology vol 21 no 17 pp 3194ndash3200 2003
[6] W P McGuire W J Hoskins M F Brady et al ldquoCyclophos-phamide and cisplatin compared with paclitaxel and cisplatin
in patients with stage III and stage IV ovarian cancerrdquoThe NewEngland Journal of Medicine vol 334 no 1 pp 1ndash6 1996
[7] W P McGuire W J Hoskins M F Brady et al ldquoCyclophos-phamide and cisplatin versus paclitaxel and cisplatin a phase IIIrandomized trial in patients with suboptimal stage IIIIV ovar-ian cancer (from the gynecologic oncology group)rdquo Seminars inOncology vol 23 no 5 supplement 12 pp 40ndash47 1996
[8] M J Piccart K Bertelsen K James et al ldquoRandomized inter-group trial of cisplatin-paclitaxel versus cisplatin-cyclophosph-amide inwomenwith advanced epithelial ovarian cancer three-year resultsrdquo Journal of the National Cancer Institute vol 92 no9 pp 699ndash708 2000
[9] P A Vasey G C Jayson A Gordon et al ldquoPhase III random-ized trial of docetaxel-carboplatin versus paclitaxel-carboplatinas first-line chemotherpy for ovarian carcinomardquo Journal of theNational Cancer Institute vol 96 no 22 pp 1682ndash1691 2004
[10] B Gronlund C Hogdall H H Hansen and S A EngelholmldquoResults of reinduction therapy with paclitaxel and carboplatinin recurrent epithelial ovarian cancerrdquo Gynecologic Oncologyvol 83 no 1 pp 128ndash134 2001
[11] T M Loffler W Freund J Lipke and T-U HausamenldquoSchedule- and dose-intensified paclitaxel as weekly 1-hourinfusion in pretreated solid tumors results of a phase III trialrdquoSeminars in Oncology vol 23 no 6 supplement 16 pp 32ndash341996
[12] D Fennelly C Aghajanian F Shapiro et al ldquoPhase I and phar-macologic study of paclitaxel administered weekly in patientswith relapsed ovarian cancerrdquo Journal of Clinical Oncology vol15 no 1 pp 187ndash192 1997
[13] N R Abu-Rustum C Aghajanian R R Barakat D Fennelly FShapiro and D Spriggs ldquoSalvage weekly paclitaxel in recurrentovarian cancerrdquo Seminars inOncology vol 24 no 5 supplement15 pp S15-62ndashS15-67 1997
[14] M Markman B N Bundy D S Alberts et al ldquoPhase III trialof standard-dose intravenous cisplatin plus paclitaxel versusmoderately high-dose carboplatin followed by intravenouspaclitaxel and intraperitoneal cisplatin in small-volume stageIII ovarian carcinoma an intergroup study of the gynecologiconcology group Southwestern Oncology Group and EasternCooperativeOncologyGrouprdquo Journal of Clinical Oncology vol19 no 4 pp 1001ndash1007 2001
[15] A Kikuchi H Sakamoto and T Yamamoto ldquoWeekly car-boplatin and paclitaxel is safe active and well tolerated inrecurrent ovarian cancer cases of Japanese women previouslytreated with cisplatin-containing multidrug chemotherapyrdquoInternational Journal of Gynecological Cancer vol 15 no 1 pp45ndash49 2005
[16] I Cadron K Leunen F Amant T van Gorp P Nevenand I Vergote ldquoThe lsquoLeuvenrsquo dose-dense paclitaxelcarboplatinregimen in patients with recurrent ovarian cancerrdquo GynecologicOncology vol 106 no 2 pp 354ndash361 2007
[17] S Pignata E Breda G Scambia et al ldquoA phase II studyof weekly carboplatin and paclitaxel as first-line treatment ofelderly patients with advanced ovarian cancer A Multicen-tre Italian Trial in Ovarian cancer (MITO-5) studyrdquo CriticalReviews in OncologyHematology vol 66 no 3 pp 229ndash2362008
[18] T Safra S Shamai J Greenberg et al ldquoWeekly carboplatinwith paclitaxel compared to standard three-weekly treatment inadvanced epithelial ovarian carcinomamdasha retrospective studyrdquoGynecologic Oncology vol 132 no 1 pp 18ndash22 2014
BioMed Research International 17
[19] L J Havrilesky A A Alvarez R A Sayer et al ldquoWeekly low-dose carboplatin and paclitaxel in the treatment of recurrentovarian and peritoneal cancerrdquo Gynecologic Oncology vol 88no 1 pp 51ndash57 2003
[20] M van der BurgW Onstenk I Boere et al ldquoLong-term resultsof a randomised phase III trial of weekly versus three-weeklypaclitaxelplatinum induction therapy followed by standardor extended three-weekly paclitaxelplatinum in Europeanpatients with advanced epithelial ovarian cancerrdquo EuropeanJournal of Cancer vol 50 no 15 pp 2592ndash2601 2014
[21] N Katsumata M Yasuda F Takahashi et al ldquoDose-densepaclitaxel once a week in combination with carboplatin every3 weeks for advanced ovarian cancer a phase 3 open-labelrandomised controlled trialrdquoThe Lancet vol 374 no 9698 pp1331ndash1338 2009
[22] N Katsumata M Yasuda S Isonishi et al ldquoLong-term resultsof dose-dense paclitaxel and carboplatin versus conventionalpaclitaxel and carboplatin for treatment of advanced epithelialovarian fallopian tube or primary peritoneal cancer (JGOG3016) a randomised controlled open-label trialrdquo The LancetOncology vol 14 no 10 pp 1020ndash1026 2013
[23] K Harano F Terauchi N Katsumata et al ldquoQuality-of-lifeoutcomes from a randomized phase III trial of dose-denseweekly paclitaxel and carboplatin compared with conventionalpaclitaxel and carboplatin as a first-line treatment for stage II-IV ovarian cancer Japanese Gynecologic OncologyGroup Trial(JGOG3016)rdquo Annals of Oncology vol 25 no 1 pp 251ndash2572014
[24] J Chan M F Brady R Penson et al ldquoPhase III trial ofevery-3-weeks paclitaxel vs dose dense weekly paclitaxel withcarboplatin +minus bevacizumab in epithelial ovarian peritonealfallopian tube cancer GOG 262 (NCT01167712)rdquo InternationalJournal of Gynecological Cancer vol 23 no 8 supplement 1 pp9ndash10 2013
[25] S Pignata G Scambia D Katsaros et al ldquoCarboplatin pluspaclitaxel once a week versus every 3 weeks in patients withadvanced ovarian cancer (MITO-7) a randomisedmulticentreopen-label phase 3 trialrdquoThe Lancet Oncology vol 15 no 4 pp396ndash405 2014
[26] V Walsh and J Goodman ldquoFrom taxol to Taxol the changingidentities and ownership of an anti-cancer drugrdquo MedicalAnthropology vol 21 no 3-4 pp 307ndash336 2002
[27] R Renneberg ldquoBiotech History yew trees paclitaxel synthesisand fungirdquo Biotechnology Journal vol 2 no 10 pp 1207ndash12092007
[28] J E Liebmann J A Cook C Lipschultz D Teague J Fisherand J B Mitchell ldquoCytotoxic studies of paclitaxel (Taxol) inhuman tumour cell linesrdquo British Journal of Cancer vol 68 no6 pp 1104ndash1109 1993
[29] J J Manfredi and S B Horwitz ldquoTaxol an antimitotic agentwith a newmechanism of actionrdquo Pharmacology andTherapeu-tics vol 25 no 1 pp 83ndash125 1984
[30] D G I Kingston ldquoRecent advances in the chemistry of taxolrdquoJournal of Natural Products vol 63 no 5 pp 726ndash734 2000
[31] D G I Kingston ldquoThe shape of things to come structural andsynthetic studies of taxol and related compoundsrdquo Phytochem-istry vol 68 no 14 pp 1844ndash1854 2007
[32] V Walsh and J Goodman ldquoCancer chemotherapy biodiversitypublic and private property the case of the anti-cancer drugTaxolrdquo Social Science amp Medicine vol 49 no 9 pp 1215ndash12251999
[33] P H Wiernik E L Schwartz J J Strauman J P Dutcher RB Lipton and E Paietta ldquoPhase I clinical and pharmacokineticstudy of taxolrdquo Cancer Research vol 47 no 9 pp 2486ndash24931987
[34] W P McGuire E K Rowinsky N B Rosenhein et alldquoTaxol a unique antineoplastic agent with significant activityin advanced ovarian epithelial neoplasmsrdquo Annals of InternalMedicine vol 111 no 4 pp 273ndash279 1989
[35] ldquoDiscovery and development of taxolrdquo in Taxol Science andApplications M W M E Suffness Ed pp 3ndash25 CRC PressBoca Raton Fla USA 1995
[36] M J Piccart and F Cardoso ldquoProgress in systemic therapy forbreast cancer an overview and perspectivesrdquo European Journalof Cancer Supplement vol 1 no 2 pp 56ndash69 2003
[37] P Bonomi K B Kim and J Kugler ldquoComparison of survival forstage IIIB versus stage IV non-small cell lung cancer (NSCLC)patients with etoposide-cisplatin versus taxol-cisplatin an East-ern Cooperative Oncology Group (ECOG) trialrdquo in Proceedingsof the American Society of Clinical Oncology vol 16 p 454a1997
[38] D Guenard F Gueritte-Voegelein J Dubois and P PotierldquoStructure-activity relationships of Taxol and Taxotere ana-loguesrdquo Journal of the National Cancer Institute Monographsno 15 pp 79ndash82 1993
[39] D G I Kingston ldquoTaxol the chemistry and structure-activityrelationships of a novel anticancer agentrdquo Trends in Biotechnol-ogy vol 12 no 6 pp 222ndash227 1994
[40] E K Rowinsky and R C Donehower ldquoPaclitaxel (taxol)rdquo TheNew England Journal of Medicine vol 332 no 15 pp 1004ndash10141995
[41] J Parness and S B Horwitz ldquoTaxol binds to polymerizedtubulin in vitrordquo Journal of Cell Biology vol 91 no 2 pp 479ndash487 1981
[42] A Dammermann A Desai and K Oegema ldquoTheminus end insightrdquo Current Biology vol 13 no 15 pp R614ndashR624 2003
[43] CWiese and Y Zheng ldquoMicrotubule nucleation 120574-tubulin andbeyondrdquo Journal of Cell Science vol 119 no 20 pp 4143ndash41532006
[44] A Ganguly H Yang and F Cabral ldquoPaclitaxel-dependent celllines reveal a novel drug activityrdquo Molecular Cancer Therapeu-tics vol 9 no 11 pp 2914ndash2923 2010
[45] P B Schiff and S B Horwitz ldquoTaxol stabilizes microtubules inmouse fibroblast cellsrdquo Proceedings of the National Academy ofSciences of the United States of America vol 77 no 3 pp 1561ndash1565 1980
[46] P B Schiff J Fant and S B Horwitz ldquoPromotion of micro-tubule assembly in vitro by Taxolrdquo Nature vol 277 no 5698pp 665ndash667 1979
[47] D Zhang R Yang S Wang and Z Dong ldquoPaclitaxel new usesfor an old drugrdquoDrug Design Development andTherapy vol 8pp 279ndash284 2014
[48] S Rao G A Orr A G Chaudhary D G I Kingston and SB Horwitz ldquoCharacterization of the taxol binding site on themicrotubule 2-(m-Azidobenzoyl)taxol photolabels a peptide(amino acids 217-231) of beta-tubulinrdquoThe Journal of BiologicalChemistry vol 270 no 35 pp 20235ndash20238 1995
[49] F Wang Y Cao W Zhao H Liu Z Fu and R Han ldquoTaxolinhibits melanoma metastases through apoptosis inductionangiogenesis inhibition and restoration of E-cadherin andnm23 expressionrdquo Journal of Pharmacological Sciences vol 93no 2 pp 197ndash203 2003
18 BioMed Research International
[50] A Sevko V Kremer C Falk et al ldquoApplication of paclitaxel inlow non-cytotoxic doses supports vaccination with melanomaantigens in normal micerdquo Journal of Immunotoxicology vol 9no 3 pp 275ndash281 2012
[51] T Kreis and R Vale Guidebook to the Cytoskeletal and MotorProteins Oxford University Press Oxford UK 2nd edition1999
[52] P Giannakakou D L Sackett Y-K Kang et al ldquoPaclitaxel-resistant human ovarian cancer cells have mutant 120573-tubulinsthat exhibit impaired paclitaxel-driven polymerizationrdquo TheJournal of Biological Chemistry vol 272 no 27 pp 17118ndash171251997
[53] E Rakovitch W Mellado E J Hall T K Pandita S Sawantand C R Geard ldquoPaclitaxel sensitivity correlates with p53status and DNA fragmentation but not G2M accumulationrdquoInternational Journal of Radiation Oncology Biology Physics vol44 no 5 pp 1119ndash1124 1999
[54] S W Lowe S Bodis A McClatchey et al ldquop53 status and theefficacy of cancer therapy in vivordquo Science vol 266 no 5186 pp807ndash810 1994
[55] C C Zhang J-M Yang E White M Murphy A Levine andW N Hait ldquoThe role of MAP4 expression in the sensitivity topaclitaxel and resistance to vinca alkaloids in p53 mutant cellsrdquoOncogene vol 16 no 12 pp 1617ndash1624 1998
[56] K Fukasawa T Choi R Kuriyama S Rulong and G F VandeWoude ldquoAbnormal centrosome amplification in the absence ofp53rdquo Science vol 271 no 5256 pp 1744ndash1747 1996
[57] T-H Wang Y-H Chan C-W Chen et al ldquoPaclitaxel (Taxol)upregulates expression of functional interleukin-6 in humanovarian cancer cells through multiple signaling pathwaysrdquoOncogene vol 25 no 35 pp 4857ndash4866 2006
[58] E Yakirevich E Sabo I Naroditsky Y Sova O Lavie andM B Resnick ldquoMultidrug resistance-related phenotype andapoptosis-related protein expression in ovarian serous carcino-masrdquo Gynecologic Oncology vol 100 no 1 pp 152ndash159 2006
[59] G Szakacs J K Paterson J A Ludwig C Booth-Genthe andM M Gottesman ldquoTargeting multidrug resistance in cancerrdquoNature Reviews Drug Discovery vol 5 no 3 pp 219ndash234 2006
[60] L W Pfannenstiel S S K Lam L A Emens E M Jaffeeand T D Armstrong ldquoPaclitaxel enhances early dendritic cellmaturation and function through TLR4 signaling in micerdquoCellular Immunology vol 263 no 1 pp 79ndash87 2010
[61] N Klauber S Parangi E Flynn E Hamel and R J DrsquoAmatoldquoInhibition of angiogenesis and breast cancer in mice by themicrotubule inhibitors 2-methoxyestradiol and Taxolrdquo CancerResearch vol 57 no 1 pp 81ndash86 1997
[62] D Belotti V Vergani T Drudis et al ldquoThe microtubule-affecting drug paclitaxel has antiangiogenic activityrdquo ClinicalCancer Research vol 2 no 11 pp 1843ndash1849 1996
[63] D H Lau L Xue L J Young P A Burke and A T CheungldquoPaclitaxel (Taxol) an inhibitor of angiogenesis in a highlyvascularized transgenic breast cancerrdquo Cancer Biotherapy andRadiopharmaceuticals vol 14 no 1 pp 31ndash36 1999
[64] X Jiang ldquoHarnessing the immune system for the treatment ofbreast cancerrdquo Journal of Zhejiang University Science B vol 15no 1 pp 1ndash15 2014
[65] A Gadducci D Katsaros P Zola et al ldquoWeekly low-dosepaclitaxel as maintenance treatment in patients with advancedovarian cancer who had microscopic residual disease atsecond-look surgery after 6 cycles of paclitaxelplatinum-basedchemotherapy Results of an open noncomparative phase 2
multicenter italian study (after-6 protocol 2)rdquo InternationalJournal of Gynecological Cancer vol 19 no 4 pp 615ndash619 2009
[66] R S Bhatt J Merchan R Parker et al ldquoA phase 2 pilot trial oflow-dose continuous infusion or lsquometronomicrsquo paclitaxel andoral celecoxib in patients with metastatic melanomardquo Cancervol 116 no 7 pp 1751ndash1756 2010
[67] M Caballero J J Grau J L Blanch et al ldquoSerum vascularendothelial growth factor as a predictive factor in metronomic(weekly) paclitaxel treatment for advanced head and neckcancerrdquo Archives of OtolaryngologymdashHead and Neck Surgeryvol 133 no 11 pp 1143ndash1148 2007
[68] J Alexandre Y Hu W Lu H Pelicano and P Huang ldquoNovelaction of paclitaxel against cancer cells bystander effect medi-ated by reactive oxygen speciesrdquo Cancer Research vol 67 no 8pp 3512ndash3517 2007
[69] T Hadzic N Aykin-Burns Y Zhu et al ldquoPaclitaxel combinedwith inhibitors of glucose and hydroperoxide metabolismenhances breast cancer cell killing viaH
2O2-mediated oxidative
stressrdquo Free Radical Biology and Medicine vol 48 no 8 pp1024ndash1033 2010
[70] C A Sherman-Baust K G Becker W H Wood III Y Zhangand P J Morin ldquoGene expression and pathway analysis of ovar-ian cancer cells selected for resistance to cisplatin paclitaxel ordoxorubicinrdquo Journal of Ovarian Research vol 4 no 1 article21 2011
[71] R Agarwal and S B Kaye ldquoOvarian cancer strategies for over-coming resistance to chemotherapyrdquo Nature Reviews Cancervol 3 no 7 pp 502ndash516 2003
[72] T Acker and K H Plate ldquoRole of hypoxia in tumorangiogenesismdashmolecular and cellular angiogenic crosstalkrdquoCell and Tissue Research vol 314 no 1 pp 145ndash155 2003
[73] M Hockel and P Vaupel ldquoBiological consequences of tumorhypoxiardquo Seminars in Oncology vol 28 supplement 8 no 2 pp36ndash41 2001
[74] L Huang Q-H Zhang Q-L Ao H Xing Y-P Lu and DMa ldquoEffect of hypoxia on the chemotherapeutic sensitivity ofhuman ovarian cancer cells to paclitaxel and its mechanismrdquoZhonghua Zhong Liu Za Zhi vol 29 no 2 pp 96ndash100 2007
[75] N Rohwer and T Cramer ldquoHypoxia-mediated drug resistancenovel insights on the functional interaction of HIFs and celldeath pathwaysrdquoDrug Resistance Updates vol 14 no 3 pp 191ndash201 2011
[76] B B Aggarwal R V Vijayalekshmi and B Sung ldquoTargetinginflammatory pathways for prevention and therapy of cancershort-term friend long-term foerdquo Clinical Cancer Research vol15 no 2 pp 425ndash430 2009
[77] Z Duan R Foster D A Bell et al ldquoSignal transducersand activators of transcription 3 pathway activation in drug-resistant ovarian cancerrdquo Clinical Cancer Research vol 12 no17 pp 5055ndash5063 2006
[78] H-J Kuh S H Jang M G Wientjes J R Weaver and J L-SAu ldquoDeterminants of paclitaxel penetration and accumulationin human solid tumorrdquo Journal of Pharmacology and Experi-mental Therapeutics vol 290 no 2 pp 871ndash880 1999
[79] S Arao H Suwa M Mandai et al ldquoHypoxia-mediated drugresistance novel insights on the functional interaction of HIFsand cell death pathwaysrdquo Cancer Research vol 54 no 5 pp1355ndash1359 1994
[80] S E Johnatty J Beesley B Gao et al ldquoABCB1 (MDR1)polymorphisms and ovarian cancer progression and survivala comprehensive analysis from the Ovarian Cancer Association
BioMed Research International 19
Consortium and the Cancer GenomeAtlasrdquoGynecologic Oncol-ogy vol 131 no 1 pp 8ndash14 2013
[81] X Yang A K Iyer A Singh et al ldquoCluster of differentiation44 targeted hyaluronic acid based nanoparticles for MDR1siRNA delivery to overcome drug resistance in ovarian cancerrdquoPharmaceutical Research 2014
[82] D A Zajchowski B Y Karlan and L K Shawver ldquoTreatment-related protein biomarker expression differs between primaryand recurrent ovarian carcinomasrdquoMolecular CancerTherapeu-tics vol 11 no 2 pp 492ndash502 2012
[83] MM Gottesman J Ludwig D Xia and G Szakacs ldquoDefeatingdrug resistance in cancerrdquoDiscovery Medicine vol 6 no 31 pp18ndash23 2006
[84] S Mozzetti C Ferlini P Concolino et al ldquoClass III 120573-tubulin overexpression is a prominent mechanism of paclitaxelresistance in ovarian cancer patientsrdquo Clinical Cancer Researchvol 11 no 1 pp 298ndash305 2005
[85] M Kavallaris D Y S Kuo C A Burkhart et al ldquoTaxol-resistant epithelial ovarian tumors are associated with alteredexpression of specific beta-tubulin isotypesrdquo Journal of ClinicalInvestigation vol 100 no 5 pp 1282ndash1293 1997
[86] G A Orr P Verdier-Pinard H McDaid and S B HorwitzldquoMechanisms of Taxol resistance related to microtubulesrdquoOncogene vol 22 no 47 pp 7280ndash7295 2003
[87] C Ferlini L Cicchillitti G Raspaglio et al ldquoPaclitaxel directlybinds to Bcl-2 and functionally mimics activity of Nur77rdquoCancer Research vol 69 no 17 pp 6906ndash6914 2009
[88] E Mechetner A Kyshtoobayeva S Zonis et al ldquoLevels ofmultidrug resistance (MDR1) P-glycoprotein expression byhuman breast cancer correlate with in vitro resistance to taxoland doxorubicinrdquo Clinical Cancer Research vol 4 no 2 pp389ndash398 1998
[89] J S Lagas C W N Damen R A B VanWaterschoot D IusufJ H Beijnen and A H Schinkel ldquoP-glycoprotein multidrug-resistance associated protein 2 Cyp3a and carboxylesteraseaffect the oral availability and metabolism of vinorelbinerdquoMolecular Pharmacology vol 82 no 4 pp 636ndash644 2012
[90] M T Huizing J B Vermorken H Rosing et al ldquoPharmacoki-netics of paclitaxel and three major metabolites in patients withadvanced breast carcinoma refractory to anthracycline therapytreated with a 3-hour paclitaxel infusion a European CancerCentre (ECC) trialrdquo Annals of Oncology vol 6 no 7 pp 699ndash704 1995
[91] R Panchagnula ldquoPharmaceutical aspects of paclitaxelrdquo Interna-tional Journal of Pharmaceutics vol 172 no 1-2 pp 1ndash15 1998
[92] S H Jang M G Wientjes and J L-S Au ldquoDeterminants ofpaclitaxel uptake accumulation and retention in solid tumorsrdquoInvestigational New Drugs vol 19 no 2 pp 113ndash123 2001
[93] D S Sonnichsen andM V Relling ldquoClinical pharmacokineticsof paclitaxelrdquo Clinical Pharmacokinetics vol 27 no 4 pp 256ndash269 1994
[94] T Ohtsu Y Sasaki T Tamura et al ldquoClinical pharmacokineticsand pharmacodynamics of paclitaxel a 3-hour infusion versusa 24-hour infusionrdquo Clinical Cancer Research vol 1 no 6 pp599ndash606 1995
[95] M Czejka J Schueller H Schnait B Springer and I EderldquoClinical pharmacokinetics andmetabolism of paclitaxel after athree-hour infusion comparison of two preparationsrdquo Journalof Oncology Pharmacy Practice vol 9 no 4 pp 129ndash136 2003
[96] J Rizzo C Riley D VonHoff J Kuhn J Phillips and T BrownldquoAnalysis of anticancer drugs in biological fluids determination
of taxol with application to clinical pharmacokineticsrdquo Journalof Pharmaceutical and Biomedical Analysis vol 8 no 2 pp 159ndash164 1990
[97] V A de Weger J H Beijnen and J H M Schellens ldquoCel-lular and clinical pharmacology of the taxanes docetaxel andpaclitaxelmdasha reviewrdquoAnti-Cancer Drugs vol 25 no 5 pp 488ndash494 2014
[98] S Kumar H Mahdi C Bryant J P Shah G Garg andA Munkarah ldquoClinical trials and progress with paclitaxel inovarian cancerrdquo International Journal of Womenrsquos Health vol 2no 1 pp 411ndash427 2010
[99] B Huang J Zhao J C Unkeless Z H Feng and H XiongldquoTLR signaling by tumor and immune cells a double-edgedswordrdquo Oncogene vol 27 no 2 pp 218ndash224 2008
[100] R A Jibodh J S Lagas B Nuijen J H Beijnen and J HM Schellens ldquoTaxanes old drugs new oral formulationsrdquoEuropean Journal of Pharmacology vol 717 no 1ndash3 pp 40ndash462013
[101] A Javeed M Ashraf A Riaz A Ghafoor S Afzal and M MMukhtar ldquoPaclitaxel and immune systemrdquo European Journal ofPharmaceutical Sciences vol 38 no 4 pp 283ndash290 2009
[102] L Bracci G Schiavoni A Sistigu and F Belardelli ldquoImmune-based mechanisms of cytotoxic chemotherapy implications forthe design of novel and rationale-based combined treatmentsagainst cancerrdquo Cell Death and Differentiation vol 21 no 1 pp15ndash25 2014
[103] C A Byrd-Leifer E F Block K Takeda S Akira and A DingldquoThe role of MyD88 and TLR4 in the LPS-mimetic activity ofTaxolrdquo European Journal of Immunology vol 31 no 8 pp 2448ndash2457 2001
[104] A-C Wang Y-B Ma F-X Wu et al ldquoTLR4 induces tumorgrowth and inhibits paclitaxel activity in MyD88-positivehuman ovarian carcinoma in vitrordquo Oncology Letters vol 7 no3 pp 871ndash877 2014
[105] Y Zhu N Liu S D Xiong Y J Zheng and Y W ChuldquoCD4+Foxp3+ regulatory T-cell impairment by paclitaxel isindependent of toll-like receptor 4rdquo Scandinavian Journal ofImmunology vol 73 no 4 pp 301ndash308 2011
[106] M Kubo T Morisaki K Matsumoto et al ldquoPaclitaxel probablyenhances cytotoxicity of natural killer cells against breastcarcinoma cells by increasing perforin productionrdquo CancerImmunology Immunotherapy vol 54 no 5 pp 468ndash476 2005
[107] L Markasz G Stuber B Vanherberghen et al ldquoEffect of fre-quently used chemotherapeutic drugs on the cytotoxic activityof human natural killer cellsrdquo Molecular Cancer Therapeuticsvol 6 no 2 pp 644ndash654 2007
[108] T Sako N Burioka K Yasuda et al ldquoCellular immune profile inpatients with non-small cell lung cancer after weekly paclitaxeltherapyrdquo Acta Oncologica vol 43 no 1 pp 15ndash19 2004
[109] R Kaneno G V Shurin I L Tourkova and M R ShurinldquoChemomodulation of human dendritic cell function by anti-neoplastic agents in low noncytotoxic concentrationsrdquo Journalof Translational Medicine vol 7 article 58 2009
[110] TMichels G V ShurinHNaiditch A Sevko VUmansky andM R Shurin ldquoPaclitaxel promotes differentiation of myeloid-derived suppressor cells into dendritic cells in vitro in a TLR4-independent mannerrdquo Journal of Immunotoxicology vol 9 no3 pp 292ndash300 2012
[111] R A Kemp and F Ronchese ldquoTumor-specific Tc1 but not Tc2cells deliver protective antitumor immunityrdquo The Journal ofImmunology vol 167 no 11 pp 6497ndash6502 2001
20 BioMed Research International
[112] A Y Rudensky ldquoRegulatory T cells and Foxp3rdquo ImmunologicalReviews vol 241 no 1 pp 260ndash268 2011
[113] EM Shevach ldquoCD4+CD25+ suppressor T cellsmore questionsthan answersrdquo Nature Reviews Immunology vol 2 no 6 pp389ndash400 2002
[114] S Sakaguchi T Yamaguchi T Nomura and M Ono ldquoRegu-latory T cells and immune tolerancerdquo Cell vol 133 no 5 pp775ndash787 2008
[115] H Nishikawa and S Sakaguchi ldquoRegulatory T cells in tumorimmunityrdquo International Journal of Cancer vol 127 no 4 pp759ndash767 2010
[116] W Zou ldquoRegulatory T cells tumour immunity and immuno-therapyrdquoNature Reviews Immunology vol 6 no 4 pp 295ndash3072006
[117] A Fialova S Partlova L Sojka et al ldquoDynamics of T-cell infil-tration during the course of ovarian cancer The gradual shiftfrom aTh17 effector cell response to a predominant infiltrationby regulatory T-cellsrdquo International Journal of Cancer vol 132no 5 pp 1070ndash1079 2013
[118] A E Albers R L Ferris G G Kim K Chikamatsu A BDeLeo and T L Whiteside ldquoImmune responses to p53 inpatients with cancer enrichment in tetramer+ p53 peptide-specific T cells and regulatory T cells at tumor sitesrdquo CancerImmunology Immunotherapy vol 54 no 11 pp 1072ndash10812005
[119] N Liu Y Zheng Y Zhu S Xiong andYChu ldquoSelective impair-ment of CD4 + CD25 + Foxp3 + regulatory T cells by paclitaxelis explained by Bcl-2Bax mediated apoptosisrdquo InternationalImmunopharmacology vol 11 no 2 pp 212ndash219 2011
[120] X Wu Q-M Feng Y Wang J Shi H-L Ge and W DildquoThe immunologic aspects in advanced ovarian cancer patientstreated with paclitaxel and carboplatin chemotherapyrdquo CancerImmunology Immunotherapy vol 59 no 2 pp 279ndash291 2010
[121] A P Vicari R Luu N Zhang et al ldquoPaclitaxel reducesregulatoryT cell numbers and inhibitory function and enhancesthe anti-tumor effects of the TLR9 agonist PF-3512676 in themouserdquo Cancer Immunology Immunotherapy vol 58 no 4 pp615ndash628 2009
[122] L Zhang K Dermawan M Jin et al ldquoDifferential impairmentof regulatory T cells rather than effector T cells by paclitaxel-based chemotherapyrdquo Clinical Immunology vol 129 no 2 pp219ndash229 2008
[123] Y Tabuchi J Matsuoka M Gunduz et al ldquoResistance topaclitaxel therapy is related with Bcl-2 expression through anestrogen receptor mediated pathway in breast cancerrdquo Interna-tional Journal of Oncology vol 34 no 2 pp 313ndash319 2009
[124] N Obermajer R Muthuswamy K Odunsi R P Edwards andP Kalinski ldquoPGE
2-induced CXCL12 production and CXCR4
expression controls the accumulation of human MDSCs inovarian cancer environmentrdquo Cancer Research vol 71 no 24pp 7463ndash7470 2011
[125] Q M Feng W Di and X Wu ldquoImmune reconstitution inadvanced ovarian cancer patients undergoing first line chemo-therapyrdquo Xi Bao Yu Fen Zi Mian Yi Xue Za Zhi vol 25 no 11pp 1023ndash1025 2009
[126] A D Seidman D Hochhauser M Gollub et al ldquoNinety-six-hour paclitaxel infusion after progression during short taxaneexposure a phase II pharmacokinetic and pharmacodynamicstudy in metastatic breast cancerrdquo Journal of Clinical Oncologyvol 14 no 6 pp 1877ndash1884 1996
[127] D R Spriggs M F Brady L Vaccarello et al ldquoPhase IIIrandomized trial of intravenous cisplatin plus a 24- or 96-hour
infusion of paclitaxel in epithelial ovarian cancer a gynecologiconcology group studyrdquo Journal of Clinical Oncology vol 25 no28 pp 4466ndash4471 2007
[128] G A Omura M F Brady K Y Look et al ldquoPhase III trial ofpaclitaxel at two dose levels the higher dose accompanied byfilgrastim at two dose levels in platinum-pretreated epithelialovarian cancer an intergroup studyrdquo Journal of Clinical Oncol-ogy vol 21 no 15 pp 2843ndash2848 2003
[129] R Simon and L Norton ldquoThe Norton-Simon hypothesisdesigning more effective and less toxic chemotherapeutic reg-imensrdquoNature Clinical Practice Oncology vol 3 no 8 pp 406ndash407 2006
[130] A Kumar P Hoskins and A Tinker ldquoDose-dense paclitaxel inadvanced ovarian cancerrdquo Clinical Oncology vol 27 no 1 pp40ndash47 2015
[131] P Marchetti S Urien G A Cappellini G Ronzino and CFicorella ldquoWeekly administration of paclitaxel theoretical andclinical basisrdquoCritical Reviews in OncologyHematology vol 44supplement pp S3ndashS13 2002
[132] P Francis E Rowinsky J Schneider T Hakes W Hoskinsand M Markman ldquoPhase I feasibility and pharmacologic studyof weekly intraperitoneal paclitaxel A Gynecologic OncologyGroup pilot studyrdquo Journal of Clinical Oncology vol 13 no 12pp 2961ndash2967 1995
[133] H Thomas and P Rosenberg ldquoRole of weekly paclitaxel inthe treatment of advanced ovarian cancerrdquo Critical Reviews inOncologyHematology vol 44 supplement pp S43ndashS51 2002
[134] M Markman J Markman K Webster et al ldquoDuration ofresponse to second-line platinum-based chemotherapy forovarian cancer implications for patient management and clini-cal trial designrdquo Journal of Clinical Oncology vol 22 no 15 pp3120ndash3125 2004
[135] P H OrsquoDonnell M Eileen Dolan E Gamazon et al ldquoPopu-lation differences in platinum toxicity as a means to identifynovel genetic susceptibility variantsrdquo Pharmacogenetics andGenomics vol 20 no 5 pp 327ndash337 2010
[136] M J Millward M J Boyer M Lehnert et al ldquoDocetaxel andcarboplatin is an active regimen in advanced non-small-celllung cancer a phase II study in Caucasian and Asian patientsrdquoAnnals of Oncology vol 14 no 3 pp 449ndash454 2003
[137] M Markman ldquoIntraperitoneal therapy of ovarian cancerrdquoOncologist vol 1 no 1-2 pp 18ndash21 1996
[138] M Markman and J L Walker ldquoIntraperitoneal chemotherapyof ovarian cancer a review with a focus on practical aspects oftreatmentrdquo Journal of Clinical Oncology vol 24 no 6 pp 988ndash994 2006
[139] K Fujiwara S Nagao E Aotani and K Hasegawa ldquoPrincipleand evolving role of intraperitoneal chemotherapy in ovariancancerrdquo Expert Opinion on Pharmacotherapy vol 14 no 13 pp1797ndash1806 2013
[140] M Markman E Rowinsky T Hakes et al ldquoPhase I trialof intraperitoneal taxol a gynecoloic oncology group studyrdquoJournal of Clinical Oncology vol 10 no 9 pp 1485ndash1491 1992
[141] M Markman M F Brady N M Spirtos P Hanjani and S CRubin ldquoPhase II trial of intraperitoneal paclitaxel in carcinomaof the ovary tube and peritoneum a gynecologic oncologygroup studyrdquo Journal of Clinical Oncology vol 16 no 8 pp2620ndash2624 1998
[142] P B Panici I Palaia M Graziano F Bellati N Manci and RAngioli ldquoIntraperitoneal paclitaxel as consolidation treatmentin ovarian cancer patients a case control studyrdquo Oncology vol78 no 1 pp 20ndash25 2010
BioMed Research International 21
[143] D K Armstrong B Bundy L Wenzel et al ldquoIntraperitonealcisplatin and paclitaxel in ovarian cancerrdquo The New EnglandJournal of Medicine vol 354 no 1 pp 34ndash43 2006
[144] D Tewari J Java and R Salani ldquoLong-term survival advantageof intraperitoneal chemotherapy treatment in advanced ovariancancer an analysis of a Gynecologic Oncology Group ancillarydata studyrdquo in Proceedings of the 2013 Society of GynecologicOncology Annual Meeting on Womenrsquos Cancer (GOG114172Abstract) Los Angeles Calif USA 2013
[145] D A Yardley ldquonab-paclitaxel mechanisms of action and deliv-eryrdquo Journal of Controlled Release vol 170 no 3 pp 365ndash3722013
[146] M Ando K Yonemori N Katsumata et al ldquoPhase I and phar-macokinetic study of nab-paclitaxel nanoparticle albumin-bound paclitaxel administeredweekly to Japanese patients withsolid tumors and metastatic breast cancerrdquo Cancer Chemother-apy and Pharmacology vol 69 no 2 pp 457ndash465 2012
[147] N Desai V Trieu Z Yao et al ldquoIncreased antitumor activityintratumor paclitaxel concentrations and endothelial cell trans-port of cremophor-free albumin-bound paclitaxel ABI-007compared with cremophor-based paclitaxelrdquo Clinical CancerResearch vol 12 no 4 pp 1317ndash1324 2006
[148] J A Yared and K H R Tkaczuk ldquoUpdate on taxane devel-opment new analogs and new formulationsrdquo Drug DesignDevelopment andTherapy vol 6 pp 371ndash384 2012
[149] M G Teneriello P C Tseng M Crozier et al ldquoPhase IIevaluation of nanoparticle albumin-bound paclitaxel in plati-num-sensitive patients with recurrent ovarian peritoneal orfallopian tube cancerrdquo Journal of Clinical Oncology vol 27 no9 pp 1426ndash1431 2009
[150] R L Coleman W E Brady D S McMeekin et al ldquoA phase IIevaluation of nanoparticle albumin-bound (nab) paclitaxel inthe treatment of recurrent or persistent platinum-resistant ovar-ian fallopian tube or primary peritoneal cancer a GynecologicOncology Group Studyrdquo Gynecologic Oncology vol 122 no 1pp 111ndash115 2011
[151] J W Singer ldquoPaclitaxel poliglumex (XYOTAX CT-2103) amacromolecular taxanerdquo Journal of Controlled Release vol 109no 1ndash3 pp 120ndash126 2005
[152] C Li D-F Yu R A Newman et al ldquoComplete regressionof well-established tumors using a novel water-soluble poly(L-glutamic acid)-paclitaxel conjugaterdquo Cancer Research vol 58no 11 pp 2404ndash2409 1998
[153] M Mita A Mita J Sarantopoulos et al ldquoPhase I study ofpaclitaxel poliglumex administered weekly for patients withadvanced solid malignanciesrdquo Cancer Chemotherapy and Phar-macology vol 64 no 2 pp 287ndash295 2009
[154] P Sabbatini M W Sill D OrsquoMalley L Adler and A ASecord ldquoA phase II trial of paclitaxel poliglumex in recurrentor persistent ovarian or primary peritoneal cancer (EOC) agynecologic oncology group studyrdquo Gynecologic Oncology vol111 no 3 pp 455ndash460 2008
[155] M O Bradley C S Swindell F H Anthony et al ldquoTumortargeting by conjugation of DHA to paclitaxelrdquo Journal ofControlled Release vol 74 no 1ndash3 pp 233ndash236 2001
[156] M O Bradley N L Webb F H Anthony et al ldquoTumortargeting by covalent conjugation of a natural fatty acid topaclitaxelrdquo Clinical Cancer Research vol 7 no 10 pp 3229ndash3238 2001
[157] A C Wolff R C Donehower M K Carducci et al ldquoPhaseI study of docosahexaenoic acid-paclitaxel a taxane-fatty acid
conjugate with a unique pharmacology and toxicity profilerdquoClinical Cancer Research vol 9 no 10 part 1 pp 3589ndash35972003
[158] A Sparreboom A C Wolff J Verweij et al ldquoDispositionof docosahexaenoic acid-paclitaxel a novel taxane in bloodin vitro and clinical pharmacokinetic studiesrdquo Clinical CancerResearch vol 9 no 1 pp 151ndash159 2003
[159] P M Fracasso J Picus J D Wildi et al ldquoPhase 1 and phar-macokinetic study of weekly docosahexaenoic acid-paclitaxelTaxoprexin in resistant solid tumor malignanciesrdquo CancerChemotherapy and Pharmacology vol 63 no 3 pp 451ndash4582009
[160] A Y Bedikian R C DeConti R Conry et al ldquoPhase 3 study ofdocosahexaenoic acid-paclitaxel versus dacarbazine in patientswith metastatic malignant melanomardquo Annals of Oncology vol22 no 4 pp 787ndash793 2011
[161] Y-N Wu S-L Wang Y-C Wang et al ldquoReversal effect ofdocosahexaenoic acid on taxol resistance in human ovarian car-cinoma A2780T cellsrdquo Obstetrics amp Gynecology InternationalJournal vol 1 no 3 Article ID 00018 2014
Submit your manuscripts athttpwwwhindawicom
PainResearch and TreatmentHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom
Volume 2014
ToxinsJournal of
VaccinesJournal of
Hindawi Publishing Corporation httpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
AntibioticsInternational Journal of
ToxicologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
StrokeResearch and TreatmentHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Drug DeliveryJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Advances in Pharmacological Sciences
Tropical MedicineJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Medicinal ChemistryInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
AddictionJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
Emergency Medicine InternationalHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Autoimmune Diseases
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Anesthesiology Research and Practice
ScientificaHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Pharmaceutics
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of

BioMed Research International 15
of 876 women with stage III epithelial ovarian carcinomaoptimally debulked to le1 cm residual tumour [143] Themedian follow-up for GOG 114 [14] was 138 years with GOG172 [143] was 97 years The primary results of the individualtrials reported up to 6-month improvement in median PFSfollowing IP therapy In the combined analysis of the datafrom both trials the data continued to show a 5-monthdifference in favour of IP therapy (25 versus 20 months)which translates into 16 reduction in the hazard ratio forprogression (119901 = 003) In GOG 114 [14] reported in 2001there was only borderline improvement in overall survivalassociated with this regimen (median 63 versus 52 monthsrelative risk 081 119901 = 005)
However in combined analysis in 2013 which was pre-sented at the Society of Gynecologic Oncology AnnualMeeting [144] the overall survival showed an 11-monthimprovement in favour of IP therapy in GOG 114 whereasGOG 172 reported a 16-month survival advantage Amongpatients treated with IP therapy the 5-year survival rateincreased from 18 following completion of 1-2 cycles to 59for patients who completed 5-6 cycles of treatment Howeverthere was increased toxicity observed in the IP arm grade 3-4 leukopenia thrombocytopenia and abdominal pain Only42 of patients in the GOG172 trial [143] completed all sixcycles of planned treatment in the IP arm while 18 ofpatients in GOG 114 trial [14] received fewer than two coursesof IP chemotherapy
Another randomised phase III trial involving patientswith stages II-III epithelial ovarian carcinoma is the GOG252 study with three arms Arm 1-dose-dense intravenouscarboplatin and paclitaxel Arm 2-dose-dense intravenouspaclitaxel and IP carboplatin and Arm 3 consists of 3-weeklyintravenous paclitaxel (day 1) followed by IP cisplatin (day 2)and IP paclitaxel (day 3) regimen All three arms also incor-porate the combination and maintenance of bevacizumabGOG 252 has completed accrual and results are awaited [139]
11 Newer Forms of Paclitaxel
Development of next-generation taxanes has taken place overthe past 40 years aimed at eliminating toxicity improvingefficacy and ease of administration Abraxane is a novelcompound which incorporates paclitaxel into an albuminnanoparticle soluble in saline hence eliminating the needfor Cremophor EL which is responsible for hypersensitivityreactions experienced during paclitaxel infusion [145] Thenanoparticle albumin in nab-paclitaxel is able to bind toglycoprotein gp60 receptor an albumin receptor and activatecaveolin-1 a protein that in human is encoded byCAV-1 geneleading to formation of caveoli hence allowing nab-paclitaxelto migrate across the endothelial cell membrane into theinterstitial space leading to higher intratumoural drug con-centration In addition Abraxane exhibits linear pharma-cokinetics and can therefore be given at a relatively higherdose than standard intravenous paclitaxel leading to a highertherapeutic ratio and heightened efficacy in solid tumoursmainlymetastatic breast cancer [146 147] Nab-paclitaxel hadFDA approval in 2005 for treatment of breast cancer [148]
Nab-paclitaxel has been studied in recurrent ovariancancer As a single agent in phase II 44 patients withrecurrent ovarian cancer were treated with Nab-paclitaxel260mgm2 intravenously for 30 minutes every 3 weeks for6 cycles Ninety-two percent of patients were platinum-sensitive while 89 had had previous exposure to standardtaxane The objective response rate was 64 with 15 patientsachieving complete response and 13 of them had partialresponse Estimated median PFS was 85 months No hyper-sensitivity reactions were observed and there were infrequentcases of grade 4 neutropenia (11) and grade 2-3 neuropathy(13) [149]
Another phase II study by GOG enrolled 51 patients withplatinum- and taxane-resistant recurrent ovarian cancer outof which 47 were evaluable The objective response rate was38 with one patient achieving a complete response and 10patients a partial response The median PFS was 45 monthswhile overall survival rate was 174 months Severe haema-tological and nonhaematological toxicities including neuro-toxicity were uncommon These results are quite impressivegiven the treatment population consisted of patients withvery poor prognosis with a median platinum and taxane freeinterval of 21 days and 70 had their recurrence within 3months of completion of primary treatment [150] Severalother trials of this formulation are in progress
Paclitaxel poliglumex (PPX) also known as Xyotax isanother prodrug a novel conjugate of paclitaxel and 120572-poly-L-glutamic acid which accumulates within tumour tissuedue to increased permeability of the tumour vessels and lackof lymphatic drainage [148 151 152] Paclitaxel poliglumexenhances solubility of paclitaxel allows direct delivery tothe intratumoural microenvironment and allows prolongedexposure to the active drug while minimising systemictoxicities [151] In Phase I dose escalation studies as a singleagent the recommended dose of PPX was 235mgm2 over 10minutes every 3 weeks or 70mgm2 weekly [153] In a PhaseII GOG study of relapsed ovarian cancer a response rate of16 was seen with infrequent serious adverse events grade3 and 4 neutropenia (24 and 20) and grade 3 neuropathy(24) [154] A phase III trial (GOG-0212) on the use of PPXas consolidation ormaintenance therapy in advanced ovariancancer is in progress
DHA-paclitaxel also known as Taxoprexin is a prodrugwhere paclitaxel is covalently conjugated with the naturallyoccurring omega-3 fatty acid docosahexaenoic acid (DHA)a fatty acid that is easily taken up by tumour cells henceincreasing intratumoural concentration of paclitaxel leadingtumour cell apoptosis [155 156] DHA-paclitaxel exhibitslinear pharmacokinetics and lower toxicity and also ease ofadministration when compared to conventional paclitaxeland has demonstrated antineoplastic activity in animal mod-els of cancer as well as in a phase III trial involving metastaticmelanoma [156ndash160] In a recent study on human ovariancancer cells it was found that DHA could reverse paclitaxelresistance by inhibiting P-gp as well as downregulatingthe expression of multidrug resistance associated proteins(MRP) and inhibiting the activity of NF-120581B and p38 MAPKsignalling pathways [161]
16 BioMed Research International
12 Future Directions
A plateau has been reached regarding the benefits associatedwith standard 3-weekly intravenous administration of cyto-toxic chemotherapy in advanced epithelial ovarian cancerThe ongoing battle for a better treatment regimen to delayrelapse promote remission and most importantly improvethe quality of life of patients with advanced epithelial ovariancancer need not to go further than the ability to relook at thechemotherapy agents that are already available in a differentapproach
Novel compounds to date have not yet shown clinicalsuperiority and parent compounds such as paclitaxel con-tinue to surprise us with their feasibility effectiveness andmanageable toxicity profiles Intraperitoneal paclitaxel willrequire further evaluation Better effort in understanding themechanism of action of drugs including the role of dosescheduling and the effect on the immune systemmay providea more cost-effective route to better clinical outcomes
Conflict of Interests
The authors declare no conflict of interests in this work
Acknowledgments
The authors would like to thank the many researchers whohave contributed to our current knowledge of paclitaxelNirmala Kampan is supported by Australian Monash Uni-versity Institute of Graduate Research Scholarship as wellas Universiti Kebangsaan Malaysia Postgraduate ScholarshipAward Mutsa Madondo has received Postgraduate Pub-lication Award from Monash University and MagdalenaPlebanski has been awarded Senior NHMRC Fellowship
References
[1] Australian Institute of Health and Welfare and National Breastand Ovarian Cancer Centre (Australia) Ovarian Cancer inAustralia AnOverview 2010 Cancer Series Australian Instituteof Health and Welfare Canberra Australia 2010
[2] R E Bristow R S Tomacruz D K Armstrong E L Trimbleand F J Montz ldquoSurvival effect of maximal cytoreductivesurgery for advanced ovarian carcinoma during the platinumera a meta-analysisrdquo Journal of Clinical Oncology vol 20 no 5pp 1248ndash1259 2002
[3] ZKempand JA Ledermann ldquoUpdate onfirst-line treatment ofadvanced ovarian carcinomardquo International Journal of WomenrsquosHealth vol 5 no 1 pp 45ndash51 2013
[4] A du Bois H-J Luck W Meier et al ldquoA randomized clinicaltrial of cisplatinpaclitaxel versus carboplatinpaclitaxel as first-line treatment of ovarian cancerrdquo Journal of the National CancerInstitute vol 95 no 17 pp 1320ndash1330 2003
[5] R F Ozols B N Bundy B E Greer et al ldquoPhase III trialof carboplatin and paclitaxel compared with cisplatin andpaclitaxel in patients with optimally resected stage III ovariancancer A Gynecologic Oncology Group studyrdquo Journal ofClinical Oncology vol 21 no 17 pp 3194ndash3200 2003
[6] W P McGuire W J Hoskins M F Brady et al ldquoCyclophos-phamide and cisplatin compared with paclitaxel and cisplatin
in patients with stage III and stage IV ovarian cancerrdquoThe NewEngland Journal of Medicine vol 334 no 1 pp 1ndash6 1996
[7] W P McGuire W J Hoskins M F Brady et al ldquoCyclophos-phamide and cisplatin versus paclitaxel and cisplatin a phase IIIrandomized trial in patients with suboptimal stage IIIIV ovar-ian cancer (from the gynecologic oncology group)rdquo Seminars inOncology vol 23 no 5 supplement 12 pp 40ndash47 1996
[8] M J Piccart K Bertelsen K James et al ldquoRandomized inter-group trial of cisplatin-paclitaxel versus cisplatin-cyclophosph-amide inwomenwith advanced epithelial ovarian cancer three-year resultsrdquo Journal of the National Cancer Institute vol 92 no9 pp 699ndash708 2000
[9] P A Vasey G C Jayson A Gordon et al ldquoPhase III random-ized trial of docetaxel-carboplatin versus paclitaxel-carboplatinas first-line chemotherpy for ovarian carcinomardquo Journal of theNational Cancer Institute vol 96 no 22 pp 1682ndash1691 2004
[10] B Gronlund C Hogdall H H Hansen and S A EngelholmldquoResults of reinduction therapy with paclitaxel and carboplatinin recurrent epithelial ovarian cancerrdquo Gynecologic Oncologyvol 83 no 1 pp 128ndash134 2001
[11] T M Loffler W Freund J Lipke and T-U HausamenldquoSchedule- and dose-intensified paclitaxel as weekly 1-hourinfusion in pretreated solid tumors results of a phase III trialrdquoSeminars in Oncology vol 23 no 6 supplement 16 pp 32ndash341996
[12] D Fennelly C Aghajanian F Shapiro et al ldquoPhase I and phar-macologic study of paclitaxel administered weekly in patientswith relapsed ovarian cancerrdquo Journal of Clinical Oncology vol15 no 1 pp 187ndash192 1997
[13] N R Abu-Rustum C Aghajanian R R Barakat D Fennelly FShapiro and D Spriggs ldquoSalvage weekly paclitaxel in recurrentovarian cancerrdquo Seminars inOncology vol 24 no 5 supplement15 pp S15-62ndashS15-67 1997
[14] M Markman B N Bundy D S Alberts et al ldquoPhase III trialof standard-dose intravenous cisplatin plus paclitaxel versusmoderately high-dose carboplatin followed by intravenouspaclitaxel and intraperitoneal cisplatin in small-volume stageIII ovarian carcinoma an intergroup study of the gynecologiconcology group Southwestern Oncology Group and EasternCooperativeOncologyGrouprdquo Journal of Clinical Oncology vol19 no 4 pp 1001ndash1007 2001
[15] A Kikuchi H Sakamoto and T Yamamoto ldquoWeekly car-boplatin and paclitaxel is safe active and well tolerated inrecurrent ovarian cancer cases of Japanese women previouslytreated with cisplatin-containing multidrug chemotherapyrdquoInternational Journal of Gynecological Cancer vol 15 no 1 pp45ndash49 2005
[16] I Cadron K Leunen F Amant T van Gorp P Nevenand I Vergote ldquoThe lsquoLeuvenrsquo dose-dense paclitaxelcarboplatinregimen in patients with recurrent ovarian cancerrdquo GynecologicOncology vol 106 no 2 pp 354ndash361 2007
[17] S Pignata E Breda G Scambia et al ldquoA phase II studyof weekly carboplatin and paclitaxel as first-line treatment ofelderly patients with advanced ovarian cancer A Multicen-tre Italian Trial in Ovarian cancer (MITO-5) studyrdquo CriticalReviews in OncologyHematology vol 66 no 3 pp 229ndash2362008
[18] T Safra S Shamai J Greenberg et al ldquoWeekly carboplatinwith paclitaxel compared to standard three-weekly treatment inadvanced epithelial ovarian carcinomamdasha retrospective studyrdquoGynecologic Oncology vol 132 no 1 pp 18ndash22 2014
BioMed Research International 17
[19] L J Havrilesky A A Alvarez R A Sayer et al ldquoWeekly low-dose carboplatin and paclitaxel in the treatment of recurrentovarian and peritoneal cancerrdquo Gynecologic Oncology vol 88no 1 pp 51ndash57 2003
[20] M van der BurgW Onstenk I Boere et al ldquoLong-term resultsof a randomised phase III trial of weekly versus three-weeklypaclitaxelplatinum induction therapy followed by standardor extended three-weekly paclitaxelplatinum in Europeanpatients with advanced epithelial ovarian cancerrdquo EuropeanJournal of Cancer vol 50 no 15 pp 2592ndash2601 2014
[21] N Katsumata M Yasuda F Takahashi et al ldquoDose-densepaclitaxel once a week in combination with carboplatin every3 weeks for advanced ovarian cancer a phase 3 open-labelrandomised controlled trialrdquoThe Lancet vol 374 no 9698 pp1331ndash1338 2009
[22] N Katsumata M Yasuda S Isonishi et al ldquoLong-term resultsof dose-dense paclitaxel and carboplatin versus conventionalpaclitaxel and carboplatin for treatment of advanced epithelialovarian fallopian tube or primary peritoneal cancer (JGOG3016) a randomised controlled open-label trialrdquo The LancetOncology vol 14 no 10 pp 1020ndash1026 2013
[23] K Harano F Terauchi N Katsumata et al ldquoQuality-of-lifeoutcomes from a randomized phase III trial of dose-denseweekly paclitaxel and carboplatin compared with conventionalpaclitaxel and carboplatin as a first-line treatment for stage II-IV ovarian cancer Japanese Gynecologic OncologyGroup Trial(JGOG3016)rdquo Annals of Oncology vol 25 no 1 pp 251ndash2572014
[24] J Chan M F Brady R Penson et al ldquoPhase III trial ofevery-3-weeks paclitaxel vs dose dense weekly paclitaxel withcarboplatin +minus bevacizumab in epithelial ovarian peritonealfallopian tube cancer GOG 262 (NCT01167712)rdquo InternationalJournal of Gynecological Cancer vol 23 no 8 supplement 1 pp9ndash10 2013
[25] S Pignata G Scambia D Katsaros et al ldquoCarboplatin pluspaclitaxel once a week versus every 3 weeks in patients withadvanced ovarian cancer (MITO-7) a randomisedmulticentreopen-label phase 3 trialrdquoThe Lancet Oncology vol 15 no 4 pp396ndash405 2014
[26] V Walsh and J Goodman ldquoFrom taxol to Taxol the changingidentities and ownership of an anti-cancer drugrdquo MedicalAnthropology vol 21 no 3-4 pp 307ndash336 2002
[27] R Renneberg ldquoBiotech History yew trees paclitaxel synthesisand fungirdquo Biotechnology Journal vol 2 no 10 pp 1207ndash12092007
[28] J E Liebmann J A Cook C Lipschultz D Teague J Fisherand J B Mitchell ldquoCytotoxic studies of paclitaxel (Taxol) inhuman tumour cell linesrdquo British Journal of Cancer vol 68 no6 pp 1104ndash1109 1993
[29] J J Manfredi and S B Horwitz ldquoTaxol an antimitotic agentwith a newmechanism of actionrdquo Pharmacology andTherapeu-tics vol 25 no 1 pp 83ndash125 1984
[30] D G I Kingston ldquoRecent advances in the chemistry of taxolrdquoJournal of Natural Products vol 63 no 5 pp 726ndash734 2000
[31] D G I Kingston ldquoThe shape of things to come structural andsynthetic studies of taxol and related compoundsrdquo Phytochem-istry vol 68 no 14 pp 1844ndash1854 2007
[32] V Walsh and J Goodman ldquoCancer chemotherapy biodiversitypublic and private property the case of the anti-cancer drugTaxolrdquo Social Science amp Medicine vol 49 no 9 pp 1215ndash12251999
[33] P H Wiernik E L Schwartz J J Strauman J P Dutcher RB Lipton and E Paietta ldquoPhase I clinical and pharmacokineticstudy of taxolrdquo Cancer Research vol 47 no 9 pp 2486ndash24931987
[34] W P McGuire E K Rowinsky N B Rosenhein et alldquoTaxol a unique antineoplastic agent with significant activityin advanced ovarian epithelial neoplasmsrdquo Annals of InternalMedicine vol 111 no 4 pp 273ndash279 1989
[35] ldquoDiscovery and development of taxolrdquo in Taxol Science andApplications M W M E Suffness Ed pp 3ndash25 CRC PressBoca Raton Fla USA 1995
[36] M J Piccart and F Cardoso ldquoProgress in systemic therapy forbreast cancer an overview and perspectivesrdquo European Journalof Cancer Supplement vol 1 no 2 pp 56ndash69 2003
[37] P Bonomi K B Kim and J Kugler ldquoComparison of survival forstage IIIB versus stage IV non-small cell lung cancer (NSCLC)patients with etoposide-cisplatin versus taxol-cisplatin an East-ern Cooperative Oncology Group (ECOG) trialrdquo in Proceedingsof the American Society of Clinical Oncology vol 16 p 454a1997
[38] D Guenard F Gueritte-Voegelein J Dubois and P PotierldquoStructure-activity relationships of Taxol and Taxotere ana-loguesrdquo Journal of the National Cancer Institute Monographsno 15 pp 79ndash82 1993
[39] D G I Kingston ldquoTaxol the chemistry and structure-activityrelationships of a novel anticancer agentrdquo Trends in Biotechnol-ogy vol 12 no 6 pp 222ndash227 1994
[40] E K Rowinsky and R C Donehower ldquoPaclitaxel (taxol)rdquo TheNew England Journal of Medicine vol 332 no 15 pp 1004ndash10141995
[41] J Parness and S B Horwitz ldquoTaxol binds to polymerizedtubulin in vitrordquo Journal of Cell Biology vol 91 no 2 pp 479ndash487 1981
[42] A Dammermann A Desai and K Oegema ldquoTheminus end insightrdquo Current Biology vol 13 no 15 pp R614ndashR624 2003
[43] CWiese and Y Zheng ldquoMicrotubule nucleation 120574-tubulin andbeyondrdquo Journal of Cell Science vol 119 no 20 pp 4143ndash41532006
[44] A Ganguly H Yang and F Cabral ldquoPaclitaxel-dependent celllines reveal a novel drug activityrdquo Molecular Cancer Therapeu-tics vol 9 no 11 pp 2914ndash2923 2010
[45] P B Schiff and S B Horwitz ldquoTaxol stabilizes microtubules inmouse fibroblast cellsrdquo Proceedings of the National Academy ofSciences of the United States of America vol 77 no 3 pp 1561ndash1565 1980
[46] P B Schiff J Fant and S B Horwitz ldquoPromotion of micro-tubule assembly in vitro by Taxolrdquo Nature vol 277 no 5698pp 665ndash667 1979
[47] D Zhang R Yang S Wang and Z Dong ldquoPaclitaxel new usesfor an old drugrdquoDrug Design Development andTherapy vol 8pp 279ndash284 2014
[48] S Rao G A Orr A G Chaudhary D G I Kingston and SB Horwitz ldquoCharacterization of the taxol binding site on themicrotubule 2-(m-Azidobenzoyl)taxol photolabels a peptide(amino acids 217-231) of beta-tubulinrdquoThe Journal of BiologicalChemistry vol 270 no 35 pp 20235ndash20238 1995
[49] F Wang Y Cao W Zhao H Liu Z Fu and R Han ldquoTaxolinhibits melanoma metastases through apoptosis inductionangiogenesis inhibition and restoration of E-cadherin andnm23 expressionrdquo Journal of Pharmacological Sciences vol 93no 2 pp 197ndash203 2003
18 BioMed Research International
[50] A Sevko V Kremer C Falk et al ldquoApplication of paclitaxel inlow non-cytotoxic doses supports vaccination with melanomaantigens in normal micerdquo Journal of Immunotoxicology vol 9no 3 pp 275ndash281 2012
[51] T Kreis and R Vale Guidebook to the Cytoskeletal and MotorProteins Oxford University Press Oxford UK 2nd edition1999
[52] P Giannakakou D L Sackett Y-K Kang et al ldquoPaclitaxel-resistant human ovarian cancer cells have mutant 120573-tubulinsthat exhibit impaired paclitaxel-driven polymerizationrdquo TheJournal of Biological Chemistry vol 272 no 27 pp 17118ndash171251997
[53] E Rakovitch W Mellado E J Hall T K Pandita S Sawantand C R Geard ldquoPaclitaxel sensitivity correlates with p53status and DNA fragmentation but not G2M accumulationrdquoInternational Journal of Radiation Oncology Biology Physics vol44 no 5 pp 1119ndash1124 1999
[54] S W Lowe S Bodis A McClatchey et al ldquop53 status and theefficacy of cancer therapy in vivordquo Science vol 266 no 5186 pp807ndash810 1994
[55] C C Zhang J-M Yang E White M Murphy A Levine andW N Hait ldquoThe role of MAP4 expression in the sensitivity topaclitaxel and resistance to vinca alkaloids in p53 mutant cellsrdquoOncogene vol 16 no 12 pp 1617ndash1624 1998
[56] K Fukasawa T Choi R Kuriyama S Rulong and G F VandeWoude ldquoAbnormal centrosome amplification in the absence ofp53rdquo Science vol 271 no 5256 pp 1744ndash1747 1996
[57] T-H Wang Y-H Chan C-W Chen et al ldquoPaclitaxel (Taxol)upregulates expression of functional interleukin-6 in humanovarian cancer cells through multiple signaling pathwaysrdquoOncogene vol 25 no 35 pp 4857ndash4866 2006
[58] E Yakirevich E Sabo I Naroditsky Y Sova O Lavie andM B Resnick ldquoMultidrug resistance-related phenotype andapoptosis-related protein expression in ovarian serous carcino-masrdquo Gynecologic Oncology vol 100 no 1 pp 152ndash159 2006
[59] G Szakacs J K Paterson J A Ludwig C Booth-Genthe andM M Gottesman ldquoTargeting multidrug resistance in cancerrdquoNature Reviews Drug Discovery vol 5 no 3 pp 219ndash234 2006
[60] L W Pfannenstiel S S K Lam L A Emens E M Jaffeeand T D Armstrong ldquoPaclitaxel enhances early dendritic cellmaturation and function through TLR4 signaling in micerdquoCellular Immunology vol 263 no 1 pp 79ndash87 2010
[61] N Klauber S Parangi E Flynn E Hamel and R J DrsquoAmatoldquoInhibition of angiogenesis and breast cancer in mice by themicrotubule inhibitors 2-methoxyestradiol and Taxolrdquo CancerResearch vol 57 no 1 pp 81ndash86 1997
[62] D Belotti V Vergani T Drudis et al ldquoThe microtubule-affecting drug paclitaxel has antiangiogenic activityrdquo ClinicalCancer Research vol 2 no 11 pp 1843ndash1849 1996
[63] D H Lau L Xue L J Young P A Burke and A T CheungldquoPaclitaxel (Taxol) an inhibitor of angiogenesis in a highlyvascularized transgenic breast cancerrdquo Cancer Biotherapy andRadiopharmaceuticals vol 14 no 1 pp 31ndash36 1999
[64] X Jiang ldquoHarnessing the immune system for the treatment ofbreast cancerrdquo Journal of Zhejiang University Science B vol 15no 1 pp 1ndash15 2014
[65] A Gadducci D Katsaros P Zola et al ldquoWeekly low-dosepaclitaxel as maintenance treatment in patients with advancedovarian cancer who had microscopic residual disease atsecond-look surgery after 6 cycles of paclitaxelplatinum-basedchemotherapy Results of an open noncomparative phase 2
multicenter italian study (after-6 protocol 2)rdquo InternationalJournal of Gynecological Cancer vol 19 no 4 pp 615ndash619 2009
[66] R S Bhatt J Merchan R Parker et al ldquoA phase 2 pilot trial oflow-dose continuous infusion or lsquometronomicrsquo paclitaxel andoral celecoxib in patients with metastatic melanomardquo Cancervol 116 no 7 pp 1751ndash1756 2010
[67] M Caballero J J Grau J L Blanch et al ldquoSerum vascularendothelial growth factor as a predictive factor in metronomic(weekly) paclitaxel treatment for advanced head and neckcancerrdquo Archives of OtolaryngologymdashHead and Neck Surgeryvol 133 no 11 pp 1143ndash1148 2007
[68] J Alexandre Y Hu W Lu H Pelicano and P Huang ldquoNovelaction of paclitaxel against cancer cells bystander effect medi-ated by reactive oxygen speciesrdquo Cancer Research vol 67 no 8pp 3512ndash3517 2007
[69] T Hadzic N Aykin-Burns Y Zhu et al ldquoPaclitaxel combinedwith inhibitors of glucose and hydroperoxide metabolismenhances breast cancer cell killing viaH
2O2-mediated oxidative
stressrdquo Free Radical Biology and Medicine vol 48 no 8 pp1024ndash1033 2010
[70] C A Sherman-Baust K G Becker W H Wood III Y Zhangand P J Morin ldquoGene expression and pathway analysis of ovar-ian cancer cells selected for resistance to cisplatin paclitaxel ordoxorubicinrdquo Journal of Ovarian Research vol 4 no 1 article21 2011
[71] R Agarwal and S B Kaye ldquoOvarian cancer strategies for over-coming resistance to chemotherapyrdquo Nature Reviews Cancervol 3 no 7 pp 502ndash516 2003
[72] T Acker and K H Plate ldquoRole of hypoxia in tumorangiogenesismdashmolecular and cellular angiogenic crosstalkrdquoCell and Tissue Research vol 314 no 1 pp 145ndash155 2003
[73] M Hockel and P Vaupel ldquoBiological consequences of tumorhypoxiardquo Seminars in Oncology vol 28 supplement 8 no 2 pp36ndash41 2001
[74] L Huang Q-H Zhang Q-L Ao H Xing Y-P Lu and DMa ldquoEffect of hypoxia on the chemotherapeutic sensitivity ofhuman ovarian cancer cells to paclitaxel and its mechanismrdquoZhonghua Zhong Liu Za Zhi vol 29 no 2 pp 96ndash100 2007
[75] N Rohwer and T Cramer ldquoHypoxia-mediated drug resistancenovel insights on the functional interaction of HIFs and celldeath pathwaysrdquoDrug Resistance Updates vol 14 no 3 pp 191ndash201 2011
[76] B B Aggarwal R V Vijayalekshmi and B Sung ldquoTargetinginflammatory pathways for prevention and therapy of cancershort-term friend long-term foerdquo Clinical Cancer Research vol15 no 2 pp 425ndash430 2009
[77] Z Duan R Foster D A Bell et al ldquoSignal transducersand activators of transcription 3 pathway activation in drug-resistant ovarian cancerrdquo Clinical Cancer Research vol 12 no17 pp 5055ndash5063 2006
[78] H-J Kuh S H Jang M G Wientjes J R Weaver and J L-SAu ldquoDeterminants of paclitaxel penetration and accumulationin human solid tumorrdquo Journal of Pharmacology and Experi-mental Therapeutics vol 290 no 2 pp 871ndash880 1999
[79] S Arao H Suwa M Mandai et al ldquoHypoxia-mediated drugresistance novel insights on the functional interaction of HIFsand cell death pathwaysrdquo Cancer Research vol 54 no 5 pp1355ndash1359 1994
[80] S E Johnatty J Beesley B Gao et al ldquoABCB1 (MDR1)polymorphisms and ovarian cancer progression and survivala comprehensive analysis from the Ovarian Cancer Association
BioMed Research International 19
Consortium and the Cancer GenomeAtlasrdquoGynecologic Oncol-ogy vol 131 no 1 pp 8ndash14 2013
[81] X Yang A K Iyer A Singh et al ldquoCluster of differentiation44 targeted hyaluronic acid based nanoparticles for MDR1siRNA delivery to overcome drug resistance in ovarian cancerrdquoPharmaceutical Research 2014
[82] D A Zajchowski B Y Karlan and L K Shawver ldquoTreatment-related protein biomarker expression differs between primaryand recurrent ovarian carcinomasrdquoMolecular CancerTherapeu-tics vol 11 no 2 pp 492ndash502 2012
[83] MM Gottesman J Ludwig D Xia and G Szakacs ldquoDefeatingdrug resistance in cancerrdquoDiscovery Medicine vol 6 no 31 pp18ndash23 2006
[84] S Mozzetti C Ferlini P Concolino et al ldquoClass III 120573-tubulin overexpression is a prominent mechanism of paclitaxelresistance in ovarian cancer patientsrdquo Clinical Cancer Researchvol 11 no 1 pp 298ndash305 2005
[85] M Kavallaris D Y S Kuo C A Burkhart et al ldquoTaxol-resistant epithelial ovarian tumors are associated with alteredexpression of specific beta-tubulin isotypesrdquo Journal of ClinicalInvestigation vol 100 no 5 pp 1282ndash1293 1997
[86] G A Orr P Verdier-Pinard H McDaid and S B HorwitzldquoMechanisms of Taxol resistance related to microtubulesrdquoOncogene vol 22 no 47 pp 7280ndash7295 2003
[87] C Ferlini L Cicchillitti G Raspaglio et al ldquoPaclitaxel directlybinds to Bcl-2 and functionally mimics activity of Nur77rdquoCancer Research vol 69 no 17 pp 6906ndash6914 2009
[88] E Mechetner A Kyshtoobayeva S Zonis et al ldquoLevels ofmultidrug resistance (MDR1) P-glycoprotein expression byhuman breast cancer correlate with in vitro resistance to taxoland doxorubicinrdquo Clinical Cancer Research vol 4 no 2 pp389ndash398 1998
[89] J S Lagas C W N Damen R A B VanWaterschoot D IusufJ H Beijnen and A H Schinkel ldquoP-glycoprotein multidrug-resistance associated protein 2 Cyp3a and carboxylesteraseaffect the oral availability and metabolism of vinorelbinerdquoMolecular Pharmacology vol 82 no 4 pp 636ndash644 2012
[90] M T Huizing J B Vermorken H Rosing et al ldquoPharmacoki-netics of paclitaxel and three major metabolites in patients withadvanced breast carcinoma refractory to anthracycline therapytreated with a 3-hour paclitaxel infusion a European CancerCentre (ECC) trialrdquo Annals of Oncology vol 6 no 7 pp 699ndash704 1995
[91] R Panchagnula ldquoPharmaceutical aspects of paclitaxelrdquo Interna-tional Journal of Pharmaceutics vol 172 no 1-2 pp 1ndash15 1998
[92] S H Jang M G Wientjes and J L-S Au ldquoDeterminants ofpaclitaxel uptake accumulation and retention in solid tumorsrdquoInvestigational New Drugs vol 19 no 2 pp 113ndash123 2001
[93] D S Sonnichsen andM V Relling ldquoClinical pharmacokineticsof paclitaxelrdquo Clinical Pharmacokinetics vol 27 no 4 pp 256ndash269 1994
[94] T Ohtsu Y Sasaki T Tamura et al ldquoClinical pharmacokineticsand pharmacodynamics of paclitaxel a 3-hour infusion versusa 24-hour infusionrdquo Clinical Cancer Research vol 1 no 6 pp599ndash606 1995
[95] M Czejka J Schueller H Schnait B Springer and I EderldquoClinical pharmacokinetics andmetabolism of paclitaxel after athree-hour infusion comparison of two preparationsrdquo Journalof Oncology Pharmacy Practice vol 9 no 4 pp 129ndash136 2003
[96] J Rizzo C Riley D VonHoff J Kuhn J Phillips and T BrownldquoAnalysis of anticancer drugs in biological fluids determination
of taxol with application to clinical pharmacokineticsrdquo Journalof Pharmaceutical and Biomedical Analysis vol 8 no 2 pp 159ndash164 1990
[97] V A de Weger J H Beijnen and J H M Schellens ldquoCel-lular and clinical pharmacology of the taxanes docetaxel andpaclitaxelmdasha reviewrdquoAnti-Cancer Drugs vol 25 no 5 pp 488ndash494 2014
[98] S Kumar H Mahdi C Bryant J P Shah G Garg andA Munkarah ldquoClinical trials and progress with paclitaxel inovarian cancerrdquo International Journal of Womenrsquos Health vol 2no 1 pp 411ndash427 2010
[99] B Huang J Zhao J C Unkeless Z H Feng and H XiongldquoTLR signaling by tumor and immune cells a double-edgedswordrdquo Oncogene vol 27 no 2 pp 218ndash224 2008
[100] R A Jibodh J S Lagas B Nuijen J H Beijnen and J HM Schellens ldquoTaxanes old drugs new oral formulationsrdquoEuropean Journal of Pharmacology vol 717 no 1ndash3 pp 40ndash462013
[101] A Javeed M Ashraf A Riaz A Ghafoor S Afzal and M MMukhtar ldquoPaclitaxel and immune systemrdquo European Journal ofPharmaceutical Sciences vol 38 no 4 pp 283ndash290 2009
[102] L Bracci G Schiavoni A Sistigu and F Belardelli ldquoImmune-based mechanisms of cytotoxic chemotherapy implications forthe design of novel and rationale-based combined treatmentsagainst cancerrdquo Cell Death and Differentiation vol 21 no 1 pp15ndash25 2014
[103] C A Byrd-Leifer E F Block K Takeda S Akira and A DingldquoThe role of MyD88 and TLR4 in the LPS-mimetic activity ofTaxolrdquo European Journal of Immunology vol 31 no 8 pp 2448ndash2457 2001
[104] A-C Wang Y-B Ma F-X Wu et al ldquoTLR4 induces tumorgrowth and inhibits paclitaxel activity in MyD88-positivehuman ovarian carcinoma in vitrordquo Oncology Letters vol 7 no3 pp 871ndash877 2014
[105] Y Zhu N Liu S D Xiong Y J Zheng and Y W ChuldquoCD4+Foxp3+ regulatory T-cell impairment by paclitaxel isindependent of toll-like receptor 4rdquo Scandinavian Journal ofImmunology vol 73 no 4 pp 301ndash308 2011
[106] M Kubo T Morisaki K Matsumoto et al ldquoPaclitaxel probablyenhances cytotoxicity of natural killer cells against breastcarcinoma cells by increasing perforin productionrdquo CancerImmunology Immunotherapy vol 54 no 5 pp 468ndash476 2005
[107] L Markasz G Stuber B Vanherberghen et al ldquoEffect of fre-quently used chemotherapeutic drugs on the cytotoxic activityof human natural killer cellsrdquo Molecular Cancer Therapeuticsvol 6 no 2 pp 644ndash654 2007
[108] T Sako N Burioka K Yasuda et al ldquoCellular immune profile inpatients with non-small cell lung cancer after weekly paclitaxeltherapyrdquo Acta Oncologica vol 43 no 1 pp 15ndash19 2004
[109] R Kaneno G V Shurin I L Tourkova and M R ShurinldquoChemomodulation of human dendritic cell function by anti-neoplastic agents in low noncytotoxic concentrationsrdquo Journalof Translational Medicine vol 7 article 58 2009
[110] TMichels G V ShurinHNaiditch A Sevko VUmansky andM R Shurin ldquoPaclitaxel promotes differentiation of myeloid-derived suppressor cells into dendritic cells in vitro in a TLR4-independent mannerrdquo Journal of Immunotoxicology vol 9 no3 pp 292ndash300 2012
[111] R A Kemp and F Ronchese ldquoTumor-specific Tc1 but not Tc2cells deliver protective antitumor immunityrdquo The Journal ofImmunology vol 167 no 11 pp 6497ndash6502 2001
20 BioMed Research International
[112] A Y Rudensky ldquoRegulatory T cells and Foxp3rdquo ImmunologicalReviews vol 241 no 1 pp 260ndash268 2011
[113] EM Shevach ldquoCD4+CD25+ suppressor T cellsmore questionsthan answersrdquo Nature Reviews Immunology vol 2 no 6 pp389ndash400 2002
[114] S Sakaguchi T Yamaguchi T Nomura and M Ono ldquoRegu-latory T cells and immune tolerancerdquo Cell vol 133 no 5 pp775ndash787 2008
[115] H Nishikawa and S Sakaguchi ldquoRegulatory T cells in tumorimmunityrdquo International Journal of Cancer vol 127 no 4 pp759ndash767 2010
[116] W Zou ldquoRegulatory T cells tumour immunity and immuno-therapyrdquoNature Reviews Immunology vol 6 no 4 pp 295ndash3072006
[117] A Fialova S Partlova L Sojka et al ldquoDynamics of T-cell infil-tration during the course of ovarian cancer The gradual shiftfrom aTh17 effector cell response to a predominant infiltrationby regulatory T-cellsrdquo International Journal of Cancer vol 132no 5 pp 1070ndash1079 2013
[118] A E Albers R L Ferris G G Kim K Chikamatsu A BDeLeo and T L Whiteside ldquoImmune responses to p53 inpatients with cancer enrichment in tetramer+ p53 peptide-specific T cells and regulatory T cells at tumor sitesrdquo CancerImmunology Immunotherapy vol 54 no 11 pp 1072ndash10812005
[119] N Liu Y Zheng Y Zhu S Xiong andYChu ldquoSelective impair-ment of CD4 + CD25 + Foxp3 + regulatory T cells by paclitaxelis explained by Bcl-2Bax mediated apoptosisrdquo InternationalImmunopharmacology vol 11 no 2 pp 212ndash219 2011
[120] X Wu Q-M Feng Y Wang J Shi H-L Ge and W DildquoThe immunologic aspects in advanced ovarian cancer patientstreated with paclitaxel and carboplatin chemotherapyrdquo CancerImmunology Immunotherapy vol 59 no 2 pp 279ndash291 2010
[121] A P Vicari R Luu N Zhang et al ldquoPaclitaxel reducesregulatoryT cell numbers and inhibitory function and enhancesthe anti-tumor effects of the TLR9 agonist PF-3512676 in themouserdquo Cancer Immunology Immunotherapy vol 58 no 4 pp615ndash628 2009
[122] L Zhang K Dermawan M Jin et al ldquoDifferential impairmentof regulatory T cells rather than effector T cells by paclitaxel-based chemotherapyrdquo Clinical Immunology vol 129 no 2 pp219ndash229 2008
[123] Y Tabuchi J Matsuoka M Gunduz et al ldquoResistance topaclitaxel therapy is related with Bcl-2 expression through anestrogen receptor mediated pathway in breast cancerrdquo Interna-tional Journal of Oncology vol 34 no 2 pp 313ndash319 2009
[124] N Obermajer R Muthuswamy K Odunsi R P Edwards andP Kalinski ldquoPGE
2-induced CXCL12 production and CXCR4
expression controls the accumulation of human MDSCs inovarian cancer environmentrdquo Cancer Research vol 71 no 24pp 7463ndash7470 2011
[125] Q M Feng W Di and X Wu ldquoImmune reconstitution inadvanced ovarian cancer patients undergoing first line chemo-therapyrdquo Xi Bao Yu Fen Zi Mian Yi Xue Za Zhi vol 25 no 11pp 1023ndash1025 2009
[126] A D Seidman D Hochhauser M Gollub et al ldquoNinety-six-hour paclitaxel infusion after progression during short taxaneexposure a phase II pharmacokinetic and pharmacodynamicstudy in metastatic breast cancerrdquo Journal of Clinical Oncologyvol 14 no 6 pp 1877ndash1884 1996
[127] D R Spriggs M F Brady L Vaccarello et al ldquoPhase IIIrandomized trial of intravenous cisplatin plus a 24- or 96-hour
infusion of paclitaxel in epithelial ovarian cancer a gynecologiconcology group studyrdquo Journal of Clinical Oncology vol 25 no28 pp 4466ndash4471 2007
[128] G A Omura M F Brady K Y Look et al ldquoPhase III trial ofpaclitaxel at two dose levels the higher dose accompanied byfilgrastim at two dose levels in platinum-pretreated epithelialovarian cancer an intergroup studyrdquo Journal of Clinical Oncol-ogy vol 21 no 15 pp 2843ndash2848 2003
[129] R Simon and L Norton ldquoThe Norton-Simon hypothesisdesigning more effective and less toxic chemotherapeutic reg-imensrdquoNature Clinical Practice Oncology vol 3 no 8 pp 406ndash407 2006
[130] A Kumar P Hoskins and A Tinker ldquoDose-dense paclitaxel inadvanced ovarian cancerrdquo Clinical Oncology vol 27 no 1 pp40ndash47 2015
[131] P Marchetti S Urien G A Cappellini G Ronzino and CFicorella ldquoWeekly administration of paclitaxel theoretical andclinical basisrdquoCritical Reviews in OncologyHematology vol 44supplement pp S3ndashS13 2002
[132] P Francis E Rowinsky J Schneider T Hakes W Hoskinsand M Markman ldquoPhase I feasibility and pharmacologic studyof weekly intraperitoneal paclitaxel A Gynecologic OncologyGroup pilot studyrdquo Journal of Clinical Oncology vol 13 no 12pp 2961ndash2967 1995
[133] H Thomas and P Rosenberg ldquoRole of weekly paclitaxel inthe treatment of advanced ovarian cancerrdquo Critical Reviews inOncologyHematology vol 44 supplement pp S43ndashS51 2002
[134] M Markman J Markman K Webster et al ldquoDuration ofresponse to second-line platinum-based chemotherapy forovarian cancer implications for patient management and clini-cal trial designrdquo Journal of Clinical Oncology vol 22 no 15 pp3120ndash3125 2004
[135] P H OrsquoDonnell M Eileen Dolan E Gamazon et al ldquoPopu-lation differences in platinum toxicity as a means to identifynovel genetic susceptibility variantsrdquo Pharmacogenetics andGenomics vol 20 no 5 pp 327ndash337 2010
[136] M J Millward M J Boyer M Lehnert et al ldquoDocetaxel andcarboplatin is an active regimen in advanced non-small-celllung cancer a phase II study in Caucasian and Asian patientsrdquoAnnals of Oncology vol 14 no 3 pp 449ndash454 2003
[137] M Markman ldquoIntraperitoneal therapy of ovarian cancerrdquoOncologist vol 1 no 1-2 pp 18ndash21 1996
[138] M Markman and J L Walker ldquoIntraperitoneal chemotherapyof ovarian cancer a review with a focus on practical aspects oftreatmentrdquo Journal of Clinical Oncology vol 24 no 6 pp 988ndash994 2006
[139] K Fujiwara S Nagao E Aotani and K Hasegawa ldquoPrincipleand evolving role of intraperitoneal chemotherapy in ovariancancerrdquo Expert Opinion on Pharmacotherapy vol 14 no 13 pp1797ndash1806 2013
[140] M Markman E Rowinsky T Hakes et al ldquoPhase I trialof intraperitoneal taxol a gynecoloic oncology group studyrdquoJournal of Clinical Oncology vol 10 no 9 pp 1485ndash1491 1992
[141] M Markman M F Brady N M Spirtos P Hanjani and S CRubin ldquoPhase II trial of intraperitoneal paclitaxel in carcinomaof the ovary tube and peritoneum a gynecologic oncologygroup studyrdquo Journal of Clinical Oncology vol 16 no 8 pp2620ndash2624 1998
[142] P B Panici I Palaia M Graziano F Bellati N Manci and RAngioli ldquoIntraperitoneal paclitaxel as consolidation treatmentin ovarian cancer patients a case control studyrdquo Oncology vol78 no 1 pp 20ndash25 2010
BioMed Research International 21
[143] D K Armstrong B Bundy L Wenzel et al ldquoIntraperitonealcisplatin and paclitaxel in ovarian cancerrdquo The New EnglandJournal of Medicine vol 354 no 1 pp 34ndash43 2006
[144] D Tewari J Java and R Salani ldquoLong-term survival advantageof intraperitoneal chemotherapy treatment in advanced ovariancancer an analysis of a Gynecologic Oncology Group ancillarydata studyrdquo in Proceedings of the 2013 Society of GynecologicOncology Annual Meeting on Womenrsquos Cancer (GOG114172Abstract) Los Angeles Calif USA 2013
[145] D A Yardley ldquonab-paclitaxel mechanisms of action and deliv-eryrdquo Journal of Controlled Release vol 170 no 3 pp 365ndash3722013
[146] M Ando K Yonemori N Katsumata et al ldquoPhase I and phar-macokinetic study of nab-paclitaxel nanoparticle albumin-bound paclitaxel administeredweekly to Japanese patients withsolid tumors and metastatic breast cancerrdquo Cancer Chemother-apy and Pharmacology vol 69 no 2 pp 457ndash465 2012
[147] N Desai V Trieu Z Yao et al ldquoIncreased antitumor activityintratumor paclitaxel concentrations and endothelial cell trans-port of cremophor-free albumin-bound paclitaxel ABI-007compared with cremophor-based paclitaxelrdquo Clinical CancerResearch vol 12 no 4 pp 1317ndash1324 2006
[148] J A Yared and K H R Tkaczuk ldquoUpdate on taxane devel-opment new analogs and new formulationsrdquo Drug DesignDevelopment andTherapy vol 6 pp 371ndash384 2012
[149] M G Teneriello P C Tseng M Crozier et al ldquoPhase IIevaluation of nanoparticle albumin-bound paclitaxel in plati-num-sensitive patients with recurrent ovarian peritoneal orfallopian tube cancerrdquo Journal of Clinical Oncology vol 27 no9 pp 1426ndash1431 2009
[150] R L Coleman W E Brady D S McMeekin et al ldquoA phase IIevaluation of nanoparticle albumin-bound (nab) paclitaxel inthe treatment of recurrent or persistent platinum-resistant ovar-ian fallopian tube or primary peritoneal cancer a GynecologicOncology Group Studyrdquo Gynecologic Oncology vol 122 no 1pp 111ndash115 2011
[151] J W Singer ldquoPaclitaxel poliglumex (XYOTAX CT-2103) amacromolecular taxanerdquo Journal of Controlled Release vol 109no 1ndash3 pp 120ndash126 2005
[152] C Li D-F Yu R A Newman et al ldquoComplete regressionof well-established tumors using a novel water-soluble poly(L-glutamic acid)-paclitaxel conjugaterdquo Cancer Research vol 58no 11 pp 2404ndash2409 1998
[153] M Mita A Mita J Sarantopoulos et al ldquoPhase I study ofpaclitaxel poliglumex administered weekly for patients withadvanced solid malignanciesrdquo Cancer Chemotherapy and Phar-macology vol 64 no 2 pp 287ndash295 2009
[154] P Sabbatini M W Sill D OrsquoMalley L Adler and A ASecord ldquoA phase II trial of paclitaxel poliglumex in recurrentor persistent ovarian or primary peritoneal cancer (EOC) agynecologic oncology group studyrdquo Gynecologic Oncology vol111 no 3 pp 455ndash460 2008
[155] M O Bradley C S Swindell F H Anthony et al ldquoTumortargeting by conjugation of DHA to paclitaxelrdquo Journal ofControlled Release vol 74 no 1ndash3 pp 233ndash236 2001
[156] M O Bradley N L Webb F H Anthony et al ldquoTumortargeting by covalent conjugation of a natural fatty acid topaclitaxelrdquo Clinical Cancer Research vol 7 no 10 pp 3229ndash3238 2001
[157] A C Wolff R C Donehower M K Carducci et al ldquoPhaseI study of docosahexaenoic acid-paclitaxel a taxane-fatty acid
conjugate with a unique pharmacology and toxicity profilerdquoClinical Cancer Research vol 9 no 10 part 1 pp 3589ndash35972003
[158] A Sparreboom A C Wolff J Verweij et al ldquoDispositionof docosahexaenoic acid-paclitaxel a novel taxane in bloodin vitro and clinical pharmacokinetic studiesrdquo Clinical CancerResearch vol 9 no 1 pp 151ndash159 2003
[159] P M Fracasso J Picus J D Wildi et al ldquoPhase 1 and phar-macokinetic study of weekly docosahexaenoic acid-paclitaxelTaxoprexin in resistant solid tumor malignanciesrdquo CancerChemotherapy and Pharmacology vol 63 no 3 pp 451ndash4582009
[160] A Y Bedikian R C DeConti R Conry et al ldquoPhase 3 study ofdocosahexaenoic acid-paclitaxel versus dacarbazine in patientswith metastatic malignant melanomardquo Annals of Oncology vol22 no 4 pp 787ndash793 2011
[161] Y-N Wu S-L Wang Y-C Wang et al ldquoReversal effect ofdocosahexaenoic acid on taxol resistance in human ovarian car-cinoma A2780T cellsrdquo Obstetrics amp Gynecology InternationalJournal vol 1 no 3 Article ID 00018 2014
Submit your manuscripts athttpwwwhindawicom
PainResearch and TreatmentHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom
Volume 2014
ToxinsJournal of
VaccinesJournal of
Hindawi Publishing Corporation httpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
AntibioticsInternational Journal of
ToxicologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
StrokeResearch and TreatmentHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Drug DeliveryJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Advances in Pharmacological Sciences
Tropical MedicineJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Medicinal ChemistryInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
AddictionJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
Emergency Medicine InternationalHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Autoimmune Diseases
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Anesthesiology Research and Practice
ScientificaHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Pharmaceutics
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of

16 BioMed Research International
12 Future Directions
A plateau has been reached regarding the benefits associatedwith standard 3-weekly intravenous administration of cyto-toxic chemotherapy in advanced epithelial ovarian cancerThe ongoing battle for a better treatment regimen to delayrelapse promote remission and most importantly improvethe quality of life of patients with advanced epithelial ovariancancer need not to go further than the ability to relook at thechemotherapy agents that are already available in a differentapproach
Novel compounds to date have not yet shown clinicalsuperiority and parent compounds such as paclitaxel con-tinue to surprise us with their feasibility effectiveness andmanageable toxicity profiles Intraperitoneal paclitaxel willrequire further evaluation Better effort in understanding themechanism of action of drugs including the role of dosescheduling and the effect on the immune systemmay providea more cost-effective route to better clinical outcomes
Conflict of Interests
The authors declare no conflict of interests in this work
Acknowledgments
The authors would like to thank the many researchers whohave contributed to our current knowledge of paclitaxelNirmala Kampan is supported by Australian Monash Uni-versity Institute of Graduate Research Scholarship as wellas Universiti Kebangsaan Malaysia Postgraduate ScholarshipAward Mutsa Madondo has received Postgraduate Pub-lication Award from Monash University and MagdalenaPlebanski has been awarded Senior NHMRC Fellowship
References
[1] Australian Institute of Health and Welfare and National Breastand Ovarian Cancer Centre (Australia) Ovarian Cancer inAustralia AnOverview 2010 Cancer Series Australian Instituteof Health and Welfare Canberra Australia 2010
[2] R E Bristow R S Tomacruz D K Armstrong E L Trimbleand F J Montz ldquoSurvival effect of maximal cytoreductivesurgery for advanced ovarian carcinoma during the platinumera a meta-analysisrdquo Journal of Clinical Oncology vol 20 no 5pp 1248ndash1259 2002
[3] ZKempand JA Ledermann ldquoUpdate onfirst-line treatment ofadvanced ovarian carcinomardquo International Journal of WomenrsquosHealth vol 5 no 1 pp 45ndash51 2013
[4] A du Bois H-J Luck W Meier et al ldquoA randomized clinicaltrial of cisplatinpaclitaxel versus carboplatinpaclitaxel as first-line treatment of ovarian cancerrdquo Journal of the National CancerInstitute vol 95 no 17 pp 1320ndash1330 2003
[5] R F Ozols B N Bundy B E Greer et al ldquoPhase III trialof carboplatin and paclitaxel compared with cisplatin andpaclitaxel in patients with optimally resected stage III ovariancancer A Gynecologic Oncology Group studyrdquo Journal ofClinical Oncology vol 21 no 17 pp 3194ndash3200 2003
[6] W P McGuire W J Hoskins M F Brady et al ldquoCyclophos-phamide and cisplatin compared with paclitaxel and cisplatin
in patients with stage III and stage IV ovarian cancerrdquoThe NewEngland Journal of Medicine vol 334 no 1 pp 1ndash6 1996
[7] W P McGuire W J Hoskins M F Brady et al ldquoCyclophos-phamide and cisplatin versus paclitaxel and cisplatin a phase IIIrandomized trial in patients with suboptimal stage IIIIV ovar-ian cancer (from the gynecologic oncology group)rdquo Seminars inOncology vol 23 no 5 supplement 12 pp 40ndash47 1996
[8] M J Piccart K Bertelsen K James et al ldquoRandomized inter-group trial of cisplatin-paclitaxel versus cisplatin-cyclophosph-amide inwomenwith advanced epithelial ovarian cancer three-year resultsrdquo Journal of the National Cancer Institute vol 92 no9 pp 699ndash708 2000
[9] P A Vasey G C Jayson A Gordon et al ldquoPhase III random-ized trial of docetaxel-carboplatin versus paclitaxel-carboplatinas first-line chemotherpy for ovarian carcinomardquo Journal of theNational Cancer Institute vol 96 no 22 pp 1682ndash1691 2004
[10] B Gronlund C Hogdall H H Hansen and S A EngelholmldquoResults of reinduction therapy with paclitaxel and carboplatinin recurrent epithelial ovarian cancerrdquo Gynecologic Oncologyvol 83 no 1 pp 128ndash134 2001
[11] T M Loffler W Freund J Lipke and T-U HausamenldquoSchedule- and dose-intensified paclitaxel as weekly 1-hourinfusion in pretreated solid tumors results of a phase III trialrdquoSeminars in Oncology vol 23 no 6 supplement 16 pp 32ndash341996
[12] D Fennelly C Aghajanian F Shapiro et al ldquoPhase I and phar-macologic study of paclitaxel administered weekly in patientswith relapsed ovarian cancerrdquo Journal of Clinical Oncology vol15 no 1 pp 187ndash192 1997
[13] N R Abu-Rustum C Aghajanian R R Barakat D Fennelly FShapiro and D Spriggs ldquoSalvage weekly paclitaxel in recurrentovarian cancerrdquo Seminars inOncology vol 24 no 5 supplement15 pp S15-62ndashS15-67 1997
[14] M Markman B N Bundy D S Alberts et al ldquoPhase III trialof standard-dose intravenous cisplatin plus paclitaxel versusmoderately high-dose carboplatin followed by intravenouspaclitaxel and intraperitoneal cisplatin in small-volume stageIII ovarian carcinoma an intergroup study of the gynecologiconcology group Southwestern Oncology Group and EasternCooperativeOncologyGrouprdquo Journal of Clinical Oncology vol19 no 4 pp 1001ndash1007 2001
[15] A Kikuchi H Sakamoto and T Yamamoto ldquoWeekly car-boplatin and paclitaxel is safe active and well tolerated inrecurrent ovarian cancer cases of Japanese women previouslytreated with cisplatin-containing multidrug chemotherapyrdquoInternational Journal of Gynecological Cancer vol 15 no 1 pp45ndash49 2005
[16] I Cadron K Leunen F Amant T van Gorp P Nevenand I Vergote ldquoThe lsquoLeuvenrsquo dose-dense paclitaxelcarboplatinregimen in patients with recurrent ovarian cancerrdquo GynecologicOncology vol 106 no 2 pp 354ndash361 2007
[17] S Pignata E Breda G Scambia et al ldquoA phase II studyof weekly carboplatin and paclitaxel as first-line treatment ofelderly patients with advanced ovarian cancer A Multicen-tre Italian Trial in Ovarian cancer (MITO-5) studyrdquo CriticalReviews in OncologyHematology vol 66 no 3 pp 229ndash2362008
[18] T Safra S Shamai J Greenberg et al ldquoWeekly carboplatinwith paclitaxel compared to standard three-weekly treatment inadvanced epithelial ovarian carcinomamdasha retrospective studyrdquoGynecologic Oncology vol 132 no 1 pp 18ndash22 2014
BioMed Research International 17
[19] L J Havrilesky A A Alvarez R A Sayer et al ldquoWeekly low-dose carboplatin and paclitaxel in the treatment of recurrentovarian and peritoneal cancerrdquo Gynecologic Oncology vol 88no 1 pp 51ndash57 2003
[20] M van der BurgW Onstenk I Boere et al ldquoLong-term resultsof a randomised phase III trial of weekly versus three-weeklypaclitaxelplatinum induction therapy followed by standardor extended three-weekly paclitaxelplatinum in Europeanpatients with advanced epithelial ovarian cancerrdquo EuropeanJournal of Cancer vol 50 no 15 pp 2592ndash2601 2014
[21] N Katsumata M Yasuda F Takahashi et al ldquoDose-densepaclitaxel once a week in combination with carboplatin every3 weeks for advanced ovarian cancer a phase 3 open-labelrandomised controlled trialrdquoThe Lancet vol 374 no 9698 pp1331ndash1338 2009
[22] N Katsumata M Yasuda S Isonishi et al ldquoLong-term resultsof dose-dense paclitaxel and carboplatin versus conventionalpaclitaxel and carboplatin for treatment of advanced epithelialovarian fallopian tube or primary peritoneal cancer (JGOG3016) a randomised controlled open-label trialrdquo The LancetOncology vol 14 no 10 pp 1020ndash1026 2013
[23] K Harano F Terauchi N Katsumata et al ldquoQuality-of-lifeoutcomes from a randomized phase III trial of dose-denseweekly paclitaxel and carboplatin compared with conventionalpaclitaxel and carboplatin as a first-line treatment for stage II-IV ovarian cancer Japanese Gynecologic OncologyGroup Trial(JGOG3016)rdquo Annals of Oncology vol 25 no 1 pp 251ndash2572014
[24] J Chan M F Brady R Penson et al ldquoPhase III trial ofevery-3-weeks paclitaxel vs dose dense weekly paclitaxel withcarboplatin +minus bevacizumab in epithelial ovarian peritonealfallopian tube cancer GOG 262 (NCT01167712)rdquo InternationalJournal of Gynecological Cancer vol 23 no 8 supplement 1 pp9ndash10 2013
[25] S Pignata G Scambia D Katsaros et al ldquoCarboplatin pluspaclitaxel once a week versus every 3 weeks in patients withadvanced ovarian cancer (MITO-7) a randomisedmulticentreopen-label phase 3 trialrdquoThe Lancet Oncology vol 15 no 4 pp396ndash405 2014
[26] V Walsh and J Goodman ldquoFrom taxol to Taxol the changingidentities and ownership of an anti-cancer drugrdquo MedicalAnthropology vol 21 no 3-4 pp 307ndash336 2002
[27] R Renneberg ldquoBiotech History yew trees paclitaxel synthesisand fungirdquo Biotechnology Journal vol 2 no 10 pp 1207ndash12092007
[28] J E Liebmann J A Cook C Lipschultz D Teague J Fisherand J B Mitchell ldquoCytotoxic studies of paclitaxel (Taxol) inhuman tumour cell linesrdquo British Journal of Cancer vol 68 no6 pp 1104ndash1109 1993
[29] J J Manfredi and S B Horwitz ldquoTaxol an antimitotic agentwith a newmechanism of actionrdquo Pharmacology andTherapeu-tics vol 25 no 1 pp 83ndash125 1984
[30] D G I Kingston ldquoRecent advances in the chemistry of taxolrdquoJournal of Natural Products vol 63 no 5 pp 726ndash734 2000
[31] D G I Kingston ldquoThe shape of things to come structural andsynthetic studies of taxol and related compoundsrdquo Phytochem-istry vol 68 no 14 pp 1844ndash1854 2007
[32] V Walsh and J Goodman ldquoCancer chemotherapy biodiversitypublic and private property the case of the anti-cancer drugTaxolrdquo Social Science amp Medicine vol 49 no 9 pp 1215ndash12251999
[33] P H Wiernik E L Schwartz J J Strauman J P Dutcher RB Lipton and E Paietta ldquoPhase I clinical and pharmacokineticstudy of taxolrdquo Cancer Research vol 47 no 9 pp 2486ndash24931987
[34] W P McGuire E K Rowinsky N B Rosenhein et alldquoTaxol a unique antineoplastic agent with significant activityin advanced ovarian epithelial neoplasmsrdquo Annals of InternalMedicine vol 111 no 4 pp 273ndash279 1989
[35] ldquoDiscovery and development of taxolrdquo in Taxol Science andApplications M W M E Suffness Ed pp 3ndash25 CRC PressBoca Raton Fla USA 1995
[36] M J Piccart and F Cardoso ldquoProgress in systemic therapy forbreast cancer an overview and perspectivesrdquo European Journalof Cancer Supplement vol 1 no 2 pp 56ndash69 2003
[37] P Bonomi K B Kim and J Kugler ldquoComparison of survival forstage IIIB versus stage IV non-small cell lung cancer (NSCLC)patients with etoposide-cisplatin versus taxol-cisplatin an East-ern Cooperative Oncology Group (ECOG) trialrdquo in Proceedingsof the American Society of Clinical Oncology vol 16 p 454a1997
[38] D Guenard F Gueritte-Voegelein J Dubois and P PotierldquoStructure-activity relationships of Taxol and Taxotere ana-loguesrdquo Journal of the National Cancer Institute Monographsno 15 pp 79ndash82 1993
[39] D G I Kingston ldquoTaxol the chemistry and structure-activityrelationships of a novel anticancer agentrdquo Trends in Biotechnol-ogy vol 12 no 6 pp 222ndash227 1994
[40] E K Rowinsky and R C Donehower ldquoPaclitaxel (taxol)rdquo TheNew England Journal of Medicine vol 332 no 15 pp 1004ndash10141995
[41] J Parness and S B Horwitz ldquoTaxol binds to polymerizedtubulin in vitrordquo Journal of Cell Biology vol 91 no 2 pp 479ndash487 1981
[42] A Dammermann A Desai and K Oegema ldquoTheminus end insightrdquo Current Biology vol 13 no 15 pp R614ndashR624 2003
[43] CWiese and Y Zheng ldquoMicrotubule nucleation 120574-tubulin andbeyondrdquo Journal of Cell Science vol 119 no 20 pp 4143ndash41532006
[44] A Ganguly H Yang and F Cabral ldquoPaclitaxel-dependent celllines reveal a novel drug activityrdquo Molecular Cancer Therapeu-tics vol 9 no 11 pp 2914ndash2923 2010
[45] P B Schiff and S B Horwitz ldquoTaxol stabilizes microtubules inmouse fibroblast cellsrdquo Proceedings of the National Academy ofSciences of the United States of America vol 77 no 3 pp 1561ndash1565 1980
[46] P B Schiff J Fant and S B Horwitz ldquoPromotion of micro-tubule assembly in vitro by Taxolrdquo Nature vol 277 no 5698pp 665ndash667 1979
[47] D Zhang R Yang S Wang and Z Dong ldquoPaclitaxel new usesfor an old drugrdquoDrug Design Development andTherapy vol 8pp 279ndash284 2014
[48] S Rao G A Orr A G Chaudhary D G I Kingston and SB Horwitz ldquoCharacterization of the taxol binding site on themicrotubule 2-(m-Azidobenzoyl)taxol photolabels a peptide(amino acids 217-231) of beta-tubulinrdquoThe Journal of BiologicalChemistry vol 270 no 35 pp 20235ndash20238 1995
[49] F Wang Y Cao W Zhao H Liu Z Fu and R Han ldquoTaxolinhibits melanoma metastases through apoptosis inductionangiogenesis inhibition and restoration of E-cadherin andnm23 expressionrdquo Journal of Pharmacological Sciences vol 93no 2 pp 197ndash203 2003
18 BioMed Research International
[50] A Sevko V Kremer C Falk et al ldquoApplication of paclitaxel inlow non-cytotoxic doses supports vaccination with melanomaantigens in normal micerdquo Journal of Immunotoxicology vol 9no 3 pp 275ndash281 2012
[51] T Kreis and R Vale Guidebook to the Cytoskeletal and MotorProteins Oxford University Press Oxford UK 2nd edition1999
[52] P Giannakakou D L Sackett Y-K Kang et al ldquoPaclitaxel-resistant human ovarian cancer cells have mutant 120573-tubulinsthat exhibit impaired paclitaxel-driven polymerizationrdquo TheJournal of Biological Chemistry vol 272 no 27 pp 17118ndash171251997
[53] E Rakovitch W Mellado E J Hall T K Pandita S Sawantand C R Geard ldquoPaclitaxel sensitivity correlates with p53status and DNA fragmentation but not G2M accumulationrdquoInternational Journal of Radiation Oncology Biology Physics vol44 no 5 pp 1119ndash1124 1999
[54] S W Lowe S Bodis A McClatchey et al ldquop53 status and theefficacy of cancer therapy in vivordquo Science vol 266 no 5186 pp807ndash810 1994
[55] C C Zhang J-M Yang E White M Murphy A Levine andW N Hait ldquoThe role of MAP4 expression in the sensitivity topaclitaxel and resistance to vinca alkaloids in p53 mutant cellsrdquoOncogene vol 16 no 12 pp 1617ndash1624 1998
[56] K Fukasawa T Choi R Kuriyama S Rulong and G F VandeWoude ldquoAbnormal centrosome amplification in the absence ofp53rdquo Science vol 271 no 5256 pp 1744ndash1747 1996
[57] T-H Wang Y-H Chan C-W Chen et al ldquoPaclitaxel (Taxol)upregulates expression of functional interleukin-6 in humanovarian cancer cells through multiple signaling pathwaysrdquoOncogene vol 25 no 35 pp 4857ndash4866 2006
[58] E Yakirevich E Sabo I Naroditsky Y Sova O Lavie andM B Resnick ldquoMultidrug resistance-related phenotype andapoptosis-related protein expression in ovarian serous carcino-masrdquo Gynecologic Oncology vol 100 no 1 pp 152ndash159 2006
[59] G Szakacs J K Paterson J A Ludwig C Booth-Genthe andM M Gottesman ldquoTargeting multidrug resistance in cancerrdquoNature Reviews Drug Discovery vol 5 no 3 pp 219ndash234 2006
[60] L W Pfannenstiel S S K Lam L A Emens E M Jaffeeand T D Armstrong ldquoPaclitaxel enhances early dendritic cellmaturation and function through TLR4 signaling in micerdquoCellular Immunology vol 263 no 1 pp 79ndash87 2010
[61] N Klauber S Parangi E Flynn E Hamel and R J DrsquoAmatoldquoInhibition of angiogenesis and breast cancer in mice by themicrotubule inhibitors 2-methoxyestradiol and Taxolrdquo CancerResearch vol 57 no 1 pp 81ndash86 1997
[62] D Belotti V Vergani T Drudis et al ldquoThe microtubule-affecting drug paclitaxel has antiangiogenic activityrdquo ClinicalCancer Research vol 2 no 11 pp 1843ndash1849 1996
[63] D H Lau L Xue L J Young P A Burke and A T CheungldquoPaclitaxel (Taxol) an inhibitor of angiogenesis in a highlyvascularized transgenic breast cancerrdquo Cancer Biotherapy andRadiopharmaceuticals vol 14 no 1 pp 31ndash36 1999
[64] X Jiang ldquoHarnessing the immune system for the treatment ofbreast cancerrdquo Journal of Zhejiang University Science B vol 15no 1 pp 1ndash15 2014
[65] A Gadducci D Katsaros P Zola et al ldquoWeekly low-dosepaclitaxel as maintenance treatment in patients with advancedovarian cancer who had microscopic residual disease atsecond-look surgery after 6 cycles of paclitaxelplatinum-basedchemotherapy Results of an open noncomparative phase 2
multicenter italian study (after-6 protocol 2)rdquo InternationalJournal of Gynecological Cancer vol 19 no 4 pp 615ndash619 2009
[66] R S Bhatt J Merchan R Parker et al ldquoA phase 2 pilot trial oflow-dose continuous infusion or lsquometronomicrsquo paclitaxel andoral celecoxib in patients with metastatic melanomardquo Cancervol 116 no 7 pp 1751ndash1756 2010
[67] M Caballero J J Grau J L Blanch et al ldquoSerum vascularendothelial growth factor as a predictive factor in metronomic(weekly) paclitaxel treatment for advanced head and neckcancerrdquo Archives of OtolaryngologymdashHead and Neck Surgeryvol 133 no 11 pp 1143ndash1148 2007
[68] J Alexandre Y Hu W Lu H Pelicano and P Huang ldquoNovelaction of paclitaxel against cancer cells bystander effect medi-ated by reactive oxygen speciesrdquo Cancer Research vol 67 no 8pp 3512ndash3517 2007
[69] T Hadzic N Aykin-Burns Y Zhu et al ldquoPaclitaxel combinedwith inhibitors of glucose and hydroperoxide metabolismenhances breast cancer cell killing viaH
2O2-mediated oxidative
stressrdquo Free Radical Biology and Medicine vol 48 no 8 pp1024ndash1033 2010
[70] C A Sherman-Baust K G Becker W H Wood III Y Zhangand P J Morin ldquoGene expression and pathway analysis of ovar-ian cancer cells selected for resistance to cisplatin paclitaxel ordoxorubicinrdquo Journal of Ovarian Research vol 4 no 1 article21 2011
[71] R Agarwal and S B Kaye ldquoOvarian cancer strategies for over-coming resistance to chemotherapyrdquo Nature Reviews Cancervol 3 no 7 pp 502ndash516 2003
[72] T Acker and K H Plate ldquoRole of hypoxia in tumorangiogenesismdashmolecular and cellular angiogenic crosstalkrdquoCell and Tissue Research vol 314 no 1 pp 145ndash155 2003
[73] M Hockel and P Vaupel ldquoBiological consequences of tumorhypoxiardquo Seminars in Oncology vol 28 supplement 8 no 2 pp36ndash41 2001
[74] L Huang Q-H Zhang Q-L Ao H Xing Y-P Lu and DMa ldquoEffect of hypoxia on the chemotherapeutic sensitivity ofhuman ovarian cancer cells to paclitaxel and its mechanismrdquoZhonghua Zhong Liu Za Zhi vol 29 no 2 pp 96ndash100 2007
[75] N Rohwer and T Cramer ldquoHypoxia-mediated drug resistancenovel insights on the functional interaction of HIFs and celldeath pathwaysrdquoDrug Resistance Updates vol 14 no 3 pp 191ndash201 2011
[76] B B Aggarwal R V Vijayalekshmi and B Sung ldquoTargetinginflammatory pathways for prevention and therapy of cancershort-term friend long-term foerdquo Clinical Cancer Research vol15 no 2 pp 425ndash430 2009
[77] Z Duan R Foster D A Bell et al ldquoSignal transducersand activators of transcription 3 pathway activation in drug-resistant ovarian cancerrdquo Clinical Cancer Research vol 12 no17 pp 5055ndash5063 2006
[78] H-J Kuh S H Jang M G Wientjes J R Weaver and J L-SAu ldquoDeterminants of paclitaxel penetration and accumulationin human solid tumorrdquo Journal of Pharmacology and Experi-mental Therapeutics vol 290 no 2 pp 871ndash880 1999
[79] S Arao H Suwa M Mandai et al ldquoHypoxia-mediated drugresistance novel insights on the functional interaction of HIFsand cell death pathwaysrdquo Cancer Research vol 54 no 5 pp1355ndash1359 1994
[80] S E Johnatty J Beesley B Gao et al ldquoABCB1 (MDR1)polymorphisms and ovarian cancer progression and survivala comprehensive analysis from the Ovarian Cancer Association
BioMed Research International 19
Consortium and the Cancer GenomeAtlasrdquoGynecologic Oncol-ogy vol 131 no 1 pp 8ndash14 2013
[81] X Yang A K Iyer A Singh et al ldquoCluster of differentiation44 targeted hyaluronic acid based nanoparticles for MDR1siRNA delivery to overcome drug resistance in ovarian cancerrdquoPharmaceutical Research 2014
[82] D A Zajchowski B Y Karlan and L K Shawver ldquoTreatment-related protein biomarker expression differs between primaryand recurrent ovarian carcinomasrdquoMolecular CancerTherapeu-tics vol 11 no 2 pp 492ndash502 2012
[83] MM Gottesman J Ludwig D Xia and G Szakacs ldquoDefeatingdrug resistance in cancerrdquoDiscovery Medicine vol 6 no 31 pp18ndash23 2006
[84] S Mozzetti C Ferlini P Concolino et al ldquoClass III 120573-tubulin overexpression is a prominent mechanism of paclitaxelresistance in ovarian cancer patientsrdquo Clinical Cancer Researchvol 11 no 1 pp 298ndash305 2005
[85] M Kavallaris D Y S Kuo C A Burkhart et al ldquoTaxol-resistant epithelial ovarian tumors are associated with alteredexpression of specific beta-tubulin isotypesrdquo Journal of ClinicalInvestigation vol 100 no 5 pp 1282ndash1293 1997
[86] G A Orr P Verdier-Pinard H McDaid and S B HorwitzldquoMechanisms of Taxol resistance related to microtubulesrdquoOncogene vol 22 no 47 pp 7280ndash7295 2003
[87] C Ferlini L Cicchillitti G Raspaglio et al ldquoPaclitaxel directlybinds to Bcl-2 and functionally mimics activity of Nur77rdquoCancer Research vol 69 no 17 pp 6906ndash6914 2009
[88] E Mechetner A Kyshtoobayeva S Zonis et al ldquoLevels ofmultidrug resistance (MDR1) P-glycoprotein expression byhuman breast cancer correlate with in vitro resistance to taxoland doxorubicinrdquo Clinical Cancer Research vol 4 no 2 pp389ndash398 1998
[89] J S Lagas C W N Damen R A B VanWaterschoot D IusufJ H Beijnen and A H Schinkel ldquoP-glycoprotein multidrug-resistance associated protein 2 Cyp3a and carboxylesteraseaffect the oral availability and metabolism of vinorelbinerdquoMolecular Pharmacology vol 82 no 4 pp 636ndash644 2012
[90] M T Huizing J B Vermorken H Rosing et al ldquoPharmacoki-netics of paclitaxel and three major metabolites in patients withadvanced breast carcinoma refractory to anthracycline therapytreated with a 3-hour paclitaxel infusion a European CancerCentre (ECC) trialrdquo Annals of Oncology vol 6 no 7 pp 699ndash704 1995
[91] R Panchagnula ldquoPharmaceutical aspects of paclitaxelrdquo Interna-tional Journal of Pharmaceutics vol 172 no 1-2 pp 1ndash15 1998
[92] S H Jang M G Wientjes and J L-S Au ldquoDeterminants ofpaclitaxel uptake accumulation and retention in solid tumorsrdquoInvestigational New Drugs vol 19 no 2 pp 113ndash123 2001
[93] D S Sonnichsen andM V Relling ldquoClinical pharmacokineticsof paclitaxelrdquo Clinical Pharmacokinetics vol 27 no 4 pp 256ndash269 1994
[94] T Ohtsu Y Sasaki T Tamura et al ldquoClinical pharmacokineticsand pharmacodynamics of paclitaxel a 3-hour infusion versusa 24-hour infusionrdquo Clinical Cancer Research vol 1 no 6 pp599ndash606 1995
[95] M Czejka J Schueller H Schnait B Springer and I EderldquoClinical pharmacokinetics andmetabolism of paclitaxel after athree-hour infusion comparison of two preparationsrdquo Journalof Oncology Pharmacy Practice vol 9 no 4 pp 129ndash136 2003
[96] J Rizzo C Riley D VonHoff J Kuhn J Phillips and T BrownldquoAnalysis of anticancer drugs in biological fluids determination
of taxol with application to clinical pharmacokineticsrdquo Journalof Pharmaceutical and Biomedical Analysis vol 8 no 2 pp 159ndash164 1990
[97] V A de Weger J H Beijnen and J H M Schellens ldquoCel-lular and clinical pharmacology of the taxanes docetaxel andpaclitaxelmdasha reviewrdquoAnti-Cancer Drugs vol 25 no 5 pp 488ndash494 2014
[98] S Kumar H Mahdi C Bryant J P Shah G Garg andA Munkarah ldquoClinical trials and progress with paclitaxel inovarian cancerrdquo International Journal of Womenrsquos Health vol 2no 1 pp 411ndash427 2010
[99] B Huang J Zhao J C Unkeless Z H Feng and H XiongldquoTLR signaling by tumor and immune cells a double-edgedswordrdquo Oncogene vol 27 no 2 pp 218ndash224 2008
[100] R A Jibodh J S Lagas B Nuijen J H Beijnen and J HM Schellens ldquoTaxanes old drugs new oral formulationsrdquoEuropean Journal of Pharmacology vol 717 no 1ndash3 pp 40ndash462013
[101] A Javeed M Ashraf A Riaz A Ghafoor S Afzal and M MMukhtar ldquoPaclitaxel and immune systemrdquo European Journal ofPharmaceutical Sciences vol 38 no 4 pp 283ndash290 2009
[102] L Bracci G Schiavoni A Sistigu and F Belardelli ldquoImmune-based mechanisms of cytotoxic chemotherapy implications forthe design of novel and rationale-based combined treatmentsagainst cancerrdquo Cell Death and Differentiation vol 21 no 1 pp15ndash25 2014
[103] C A Byrd-Leifer E F Block K Takeda S Akira and A DingldquoThe role of MyD88 and TLR4 in the LPS-mimetic activity ofTaxolrdquo European Journal of Immunology vol 31 no 8 pp 2448ndash2457 2001
[104] A-C Wang Y-B Ma F-X Wu et al ldquoTLR4 induces tumorgrowth and inhibits paclitaxel activity in MyD88-positivehuman ovarian carcinoma in vitrordquo Oncology Letters vol 7 no3 pp 871ndash877 2014
[105] Y Zhu N Liu S D Xiong Y J Zheng and Y W ChuldquoCD4+Foxp3+ regulatory T-cell impairment by paclitaxel isindependent of toll-like receptor 4rdquo Scandinavian Journal ofImmunology vol 73 no 4 pp 301ndash308 2011
[106] M Kubo T Morisaki K Matsumoto et al ldquoPaclitaxel probablyenhances cytotoxicity of natural killer cells against breastcarcinoma cells by increasing perforin productionrdquo CancerImmunology Immunotherapy vol 54 no 5 pp 468ndash476 2005
[107] L Markasz G Stuber B Vanherberghen et al ldquoEffect of fre-quently used chemotherapeutic drugs on the cytotoxic activityof human natural killer cellsrdquo Molecular Cancer Therapeuticsvol 6 no 2 pp 644ndash654 2007
[108] T Sako N Burioka K Yasuda et al ldquoCellular immune profile inpatients with non-small cell lung cancer after weekly paclitaxeltherapyrdquo Acta Oncologica vol 43 no 1 pp 15ndash19 2004
[109] R Kaneno G V Shurin I L Tourkova and M R ShurinldquoChemomodulation of human dendritic cell function by anti-neoplastic agents in low noncytotoxic concentrationsrdquo Journalof Translational Medicine vol 7 article 58 2009
[110] TMichels G V ShurinHNaiditch A Sevko VUmansky andM R Shurin ldquoPaclitaxel promotes differentiation of myeloid-derived suppressor cells into dendritic cells in vitro in a TLR4-independent mannerrdquo Journal of Immunotoxicology vol 9 no3 pp 292ndash300 2012
[111] R A Kemp and F Ronchese ldquoTumor-specific Tc1 but not Tc2cells deliver protective antitumor immunityrdquo The Journal ofImmunology vol 167 no 11 pp 6497ndash6502 2001
20 BioMed Research International
[112] A Y Rudensky ldquoRegulatory T cells and Foxp3rdquo ImmunologicalReviews vol 241 no 1 pp 260ndash268 2011
[113] EM Shevach ldquoCD4+CD25+ suppressor T cellsmore questionsthan answersrdquo Nature Reviews Immunology vol 2 no 6 pp389ndash400 2002
[114] S Sakaguchi T Yamaguchi T Nomura and M Ono ldquoRegu-latory T cells and immune tolerancerdquo Cell vol 133 no 5 pp775ndash787 2008
[115] H Nishikawa and S Sakaguchi ldquoRegulatory T cells in tumorimmunityrdquo International Journal of Cancer vol 127 no 4 pp759ndash767 2010
[116] W Zou ldquoRegulatory T cells tumour immunity and immuno-therapyrdquoNature Reviews Immunology vol 6 no 4 pp 295ndash3072006
[117] A Fialova S Partlova L Sojka et al ldquoDynamics of T-cell infil-tration during the course of ovarian cancer The gradual shiftfrom aTh17 effector cell response to a predominant infiltrationby regulatory T-cellsrdquo International Journal of Cancer vol 132no 5 pp 1070ndash1079 2013
[118] A E Albers R L Ferris G G Kim K Chikamatsu A BDeLeo and T L Whiteside ldquoImmune responses to p53 inpatients with cancer enrichment in tetramer+ p53 peptide-specific T cells and regulatory T cells at tumor sitesrdquo CancerImmunology Immunotherapy vol 54 no 11 pp 1072ndash10812005
[119] N Liu Y Zheng Y Zhu S Xiong andYChu ldquoSelective impair-ment of CD4 + CD25 + Foxp3 + regulatory T cells by paclitaxelis explained by Bcl-2Bax mediated apoptosisrdquo InternationalImmunopharmacology vol 11 no 2 pp 212ndash219 2011
[120] X Wu Q-M Feng Y Wang J Shi H-L Ge and W DildquoThe immunologic aspects in advanced ovarian cancer patientstreated with paclitaxel and carboplatin chemotherapyrdquo CancerImmunology Immunotherapy vol 59 no 2 pp 279ndash291 2010
[121] A P Vicari R Luu N Zhang et al ldquoPaclitaxel reducesregulatoryT cell numbers and inhibitory function and enhancesthe anti-tumor effects of the TLR9 agonist PF-3512676 in themouserdquo Cancer Immunology Immunotherapy vol 58 no 4 pp615ndash628 2009
[122] L Zhang K Dermawan M Jin et al ldquoDifferential impairmentof regulatory T cells rather than effector T cells by paclitaxel-based chemotherapyrdquo Clinical Immunology vol 129 no 2 pp219ndash229 2008
[123] Y Tabuchi J Matsuoka M Gunduz et al ldquoResistance topaclitaxel therapy is related with Bcl-2 expression through anestrogen receptor mediated pathway in breast cancerrdquo Interna-tional Journal of Oncology vol 34 no 2 pp 313ndash319 2009
[124] N Obermajer R Muthuswamy K Odunsi R P Edwards andP Kalinski ldquoPGE
2-induced CXCL12 production and CXCR4
expression controls the accumulation of human MDSCs inovarian cancer environmentrdquo Cancer Research vol 71 no 24pp 7463ndash7470 2011
[125] Q M Feng W Di and X Wu ldquoImmune reconstitution inadvanced ovarian cancer patients undergoing first line chemo-therapyrdquo Xi Bao Yu Fen Zi Mian Yi Xue Za Zhi vol 25 no 11pp 1023ndash1025 2009
[126] A D Seidman D Hochhauser M Gollub et al ldquoNinety-six-hour paclitaxel infusion after progression during short taxaneexposure a phase II pharmacokinetic and pharmacodynamicstudy in metastatic breast cancerrdquo Journal of Clinical Oncologyvol 14 no 6 pp 1877ndash1884 1996
[127] D R Spriggs M F Brady L Vaccarello et al ldquoPhase IIIrandomized trial of intravenous cisplatin plus a 24- or 96-hour
infusion of paclitaxel in epithelial ovarian cancer a gynecologiconcology group studyrdquo Journal of Clinical Oncology vol 25 no28 pp 4466ndash4471 2007
[128] G A Omura M F Brady K Y Look et al ldquoPhase III trial ofpaclitaxel at two dose levels the higher dose accompanied byfilgrastim at two dose levels in platinum-pretreated epithelialovarian cancer an intergroup studyrdquo Journal of Clinical Oncol-ogy vol 21 no 15 pp 2843ndash2848 2003
[129] R Simon and L Norton ldquoThe Norton-Simon hypothesisdesigning more effective and less toxic chemotherapeutic reg-imensrdquoNature Clinical Practice Oncology vol 3 no 8 pp 406ndash407 2006
[130] A Kumar P Hoskins and A Tinker ldquoDose-dense paclitaxel inadvanced ovarian cancerrdquo Clinical Oncology vol 27 no 1 pp40ndash47 2015
[131] P Marchetti S Urien G A Cappellini G Ronzino and CFicorella ldquoWeekly administration of paclitaxel theoretical andclinical basisrdquoCritical Reviews in OncologyHematology vol 44supplement pp S3ndashS13 2002
[132] P Francis E Rowinsky J Schneider T Hakes W Hoskinsand M Markman ldquoPhase I feasibility and pharmacologic studyof weekly intraperitoneal paclitaxel A Gynecologic OncologyGroup pilot studyrdquo Journal of Clinical Oncology vol 13 no 12pp 2961ndash2967 1995
[133] H Thomas and P Rosenberg ldquoRole of weekly paclitaxel inthe treatment of advanced ovarian cancerrdquo Critical Reviews inOncologyHematology vol 44 supplement pp S43ndashS51 2002
[134] M Markman J Markman K Webster et al ldquoDuration ofresponse to second-line platinum-based chemotherapy forovarian cancer implications for patient management and clini-cal trial designrdquo Journal of Clinical Oncology vol 22 no 15 pp3120ndash3125 2004
[135] P H OrsquoDonnell M Eileen Dolan E Gamazon et al ldquoPopu-lation differences in platinum toxicity as a means to identifynovel genetic susceptibility variantsrdquo Pharmacogenetics andGenomics vol 20 no 5 pp 327ndash337 2010
[136] M J Millward M J Boyer M Lehnert et al ldquoDocetaxel andcarboplatin is an active regimen in advanced non-small-celllung cancer a phase II study in Caucasian and Asian patientsrdquoAnnals of Oncology vol 14 no 3 pp 449ndash454 2003
[137] M Markman ldquoIntraperitoneal therapy of ovarian cancerrdquoOncologist vol 1 no 1-2 pp 18ndash21 1996
[138] M Markman and J L Walker ldquoIntraperitoneal chemotherapyof ovarian cancer a review with a focus on practical aspects oftreatmentrdquo Journal of Clinical Oncology vol 24 no 6 pp 988ndash994 2006
[139] K Fujiwara S Nagao E Aotani and K Hasegawa ldquoPrincipleand evolving role of intraperitoneal chemotherapy in ovariancancerrdquo Expert Opinion on Pharmacotherapy vol 14 no 13 pp1797ndash1806 2013
[140] M Markman E Rowinsky T Hakes et al ldquoPhase I trialof intraperitoneal taxol a gynecoloic oncology group studyrdquoJournal of Clinical Oncology vol 10 no 9 pp 1485ndash1491 1992
[141] M Markman M F Brady N M Spirtos P Hanjani and S CRubin ldquoPhase II trial of intraperitoneal paclitaxel in carcinomaof the ovary tube and peritoneum a gynecologic oncologygroup studyrdquo Journal of Clinical Oncology vol 16 no 8 pp2620ndash2624 1998
[142] P B Panici I Palaia M Graziano F Bellati N Manci and RAngioli ldquoIntraperitoneal paclitaxel as consolidation treatmentin ovarian cancer patients a case control studyrdquo Oncology vol78 no 1 pp 20ndash25 2010
BioMed Research International 21
[143] D K Armstrong B Bundy L Wenzel et al ldquoIntraperitonealcisplatin and paclitaxel in ovarian cancerrdquo The New EnglandJournal of Medicine vol 354 no 1 pp 34ndash43 2006
[144] D Tewari J Java and R Salani ldquoLong-term survival advantageof intraperitoneal chemotherapy treatment in advanced ovariancancer an analysis of a Gynecologic Oncology Group ancillarydata studyrdquo in Proceedings of the 2013 Society of GynecologicOncology Annual Meeting on Womenrsquos Cancer (GOG114172Abstract) Los Angeles Calif USA 2013
[145] D A Yardley ldquonab-paclitaxel mechanisms of action and deliv-eryrdquo Journal of Controlled Release vol 170 no 3 pp 365ndash3722013
[146] M Ando K Yonemori N Katsumata et al ldquoPhase I and phar-macokinetic study of nab-paclitaxel nanoparticle albumin-bound paclitaxel administeredweekly to Japanese patients withsolid tumors and metastatic breast cancerrdquo Cancer Chemother-apy and Pharmacology vol 69 no 2 pp 457ndash465 2012
[147] N Desai V Trieu Z Yao et al ldquoIncreased antitumor activityintratumor paclitaxel concentrations and endothelial cell trans-port of cremophor-free albumin-bound paclitaxel ABI-007compared with cremophor-based paclitaxelrdquo Clinical CancerResearch vol 12 no 4 pp 1317ndash1324 2006
[148] J A Yared and K H R Tkaczuk ldquoUpdate on taxane devel-opment new analogs and new formulationsrdquo Drug DesignDevelopment andTherapy vol 6 pp 371ndash384 2012
[149] M G Teneriello P C Tseng M Crozier et al ldquoPhase IIevaluation of nanoparticle albumin-bound paclitaxel in plati-num-sensitive patients with recurrent ovarian peritoneal orfallopian tube cancerrdquo Journal of Clinical Oncology vol 27 no9 pp 1426ndash1431 2009
[150] R L Coleman W E Brady D S McMeekin et al ldquoA phase IIevaluation of nanoparticle albumin-bound (nab) paclitaxel inthe treatment of recurrent or persistent platinum-resistant ovar-ian fallopian tube or primary peritoneal cancer a GynecologicOncology Group Studyrdquo Gynecologic Oncology vol 122 no 1pp 111ndash115 2011
[151] J W Singer ldquoPaclitaxel poliglumex (XYOTAX CT-2103) amacromolecular taxanerdquo Journal of Controlled Release vol 109no 1ndash3 pp 120ndash126 2005
[152] C Li D-F Yu R A Newman et al ldquoComplete regressionof well-established tumors using a novel water-soluble poly(L-glutamic acid)-paclitaxel conjugaterdquo Cancer Research vol 58no 11 pp 2404ndash2409 1998
[153] M Mita A Mita J Sarantopoulos et al ldquoPhase I study ofpaclitaxel poliglumex administered weekly for patients withadvanced solid malignanciesrdquo Cancer Chemotherapy and Phar-macology vol 64 no 2 pp 287ndash295 2009
[154] P Sabbatini M W Sill D OrsquoMalley L Adler and A ASecord ldquoA phase II trial of paclitaxel poliglumex in recurrentor persistent ovarian or primary peritoneal cancer (EOC) agynecologic oncology group studyrdquo Gynecologic Oncology vol111 no 3 pp 455ndash460 2008
[155] M O Bradley C S Swindell F H Anthony et al ldquoTumortargeting by conjugation of DHA to paclitaxelrdquo Journal ofControlled Release vol 74 no 1ndash3 pp 233ndash236 2001
[156] M O Bradley N L Webb F H Anthony et al ldquoTumortargeting by covalent conjugation of a natural fatty acid topaclitaxelrdquo Clinical Cancer Research vol 7 no 10 pp 3229ndash3238 2001
[157] A C Wolff R C Donehower M K Carducci et al ldquoPhaseI study of docosahexaenoic acid-paclitaxel a taxane-fatty acid
conjugate with a unique pharmacology and toxicity profilerdquoClinical Cancer Research vol 9 no 10 part 1 pp 3589ndash35972003
[158] A Sparreboom A C Wolff J Verweij et al ldquoDispositionof docosahexaenoic acid-paclitaxel a novel taxane in bloodin vitro and clinical pharmacokinetic studiesrdquo Clinical CancerResearch vol 9 no 1 pp 151ndash159 2003
[159] P M Fracasso J Picus J D Wildi et al ldquoPhase 1 and phar-macokinetic study of weekly docosahexaenoic acid-paclitaxelTaxoprexin in resistant solid tumor malignanciesrdquo CancerChemotherapy and Pharmacology vol 63 no 3 pp 451ndash4582009
[160] A Y Bedikian R C DeConti R Conry et al ldquoPhase 3 study ofdocosahexaenoic acid-paclitaxel versus dacarbazine in patientswith metastatic malignant melanomardquo Annals of Oncology vol22 no 4 pp 787ndash793 2011
[161] Y-N Wu S-L Wang Y-C Wang et al ldquoReversal effect ofdocosahexaenoic acid on taxol resistance in human ovarian car-cinoma A2780T cellsrdquo Obstetrics amp Gynecology InternationalJournal vol 1 no 3 Article ID 00018 2014
Submit your manuscripts athttpwwwhindawicom
PainResearch and TreatmentHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom
Volume 2014
ToxinsJournal of
VaccinesJournal of
Hindawi Publishing Corporation httpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
AntibioticsInternational Journal of
ToxicologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
StrokeResearch and TreatmentHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Drug DeliveryJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Advances in Pharmacological Sciences
Tropical MedicineJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Medicinal ChemistryInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
AddictionJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
Emergency Medicine InternationalHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Autoimmune Diseases
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Anesthesiology Research and Practice
ScientificaHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Pharmaceutics
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of

BioMed Research International 17
[19] L J Havrilesky A A Alvarez R A Sayer et al ldquoWeekly low-dose carboplatin and paclitaxel in the treatment of recurrentovarian and peritoneal cancerrdquo Gynecologic Oncology vol 88no 1 pp 51ndash57 2003
[20] M van der BurgW Onstenk I Boere et al ldquoLong-term resultsof a randomised phase III trial of weekly versus three-weeklypaclitaxelplatinum induction therapy followed by standardor extended three-weekly paclitaxelplatinum in Europeanpatients with advanced epithelial ovarian cancerrdquo EuropeanJournal of Cancer vol 50 no 15 pp 2592ndash2601 2014
[21] N Katsumata M Yasuda F Takahashi et al ldquoDose-densepaclitaxel once a week in combination with carboplatin every3 weeks for advanced ovarian cancer a phase 3 open-labelrandomised controlled trialrdquoThe Lancet vol 374 no 9698 pp1331ndash1338 2009
[22] N Katsumata M Yasuda S Isonishi et al ldquoLong-term resultsof dose-dense paclitaxel and carboplatin versus conventionalpaclitaxel and carboplatin for treatment of advanced epithelialovarian fallopian tube or primary peritoneal cancer (JGOG3016) a randomised controlled open-label trialrdquo The LancetOncology vol 14 no 10 pp 1020ndash1026 2013
[23] K Harano F Terauchi N Katsumata et al ldquoQuality-of-lifeoutcomes from a randomized phase III trial of dose-denseweekly paclitaxel and carboplatin compared with conventionalpaclitaxel and carboplatin as a first-line treatment for stage II-IV ovarian cancer Japanese Gynecologic OncologyGroup Trial(JGOG3016)rdquo Annals of Oncology vol 25 no 1 pp 251ndash2572014
[24] J Chan M F Brady R Penson et al ldquoPhase III trial ofevery-3-weeks paclitaxel vs dose dense weekly paclitaxel withcarboplatin +minus bevacizumab in epithelial ovarian peritonealfallopian tube cancer GOG 262 (NCT01167712)rdquo InternationalJournal of Gynecological Cancer vol 23 no 8 supplement 1 pp9ndash10 2013
[25] S Pignata G Scambia D Katsaros et al ldquoCarboplatin pluspaclitaxel once a week versus every 3 weeks in patients withadvanced ovarian cancer (MITO-7) a randomisedmulticentreopen-label phase 3 trialrdquoThe Lancet Oncology vol 15 no 4 pp396ndash405 2014
[26] V Walsh and J Goodman ldquoFrom taxol to Taxol the changingidentities and ownership of an anti-cancer drugrdquo MedicalAnthropology vol 21 no 3-4 pp 307ndash336 2002
[27] R Renneberg ldquoBiotech History yew trees paclitaxel synthesisand fungirdquo Biotechnology Journal vol 2 no 10 pp 1207ndash12092007
[28] J E Liebmann J A Cook C Lipschultz D Teague J Fisherand J B Mitchell ldquoCytotoxic studies of paclitaxel (Taxol) inhuman tumour cell linesrdquo British Journal of Cancer vol 68 no6 pp 1104ndash1109 1993
[29] J J Manfredi and S B Horwitz ldquoTaxol an antimitotic agentwith a newmechanism of actionrdquo Pharmacology andTherapeu-tics vol 25 no 1 pp 83ndash125 1984
[30] D G I Kingston ldquoRecent advances in the chemistry of taxolrdquoJournal of Natural Products vol 63 no 5 pp 726ndash734 2000
[31] D G I Kingston ldquoThe shape of things to come structural andsynthetic studies of taxol and related compoundsrdquo Phytochem-istry vol 68 no 14 pp 1844ndash1854 2007
[32] V Walsh and J Goodman ldquoCancer chemotherapy biodiversitypublic and private property the case of the anti-cancer drugTaxolrdquo Social Science amp Medicine vol 49 no 9 pp 1215ndash12251999
[33] P H Wiernik E L Schwartz J J Strauman J P Dutcher RB Lipton and E Paietta ldquoPhase I clinical and pharmacokineticstudy of taxolrdquo Cancer Research vol 47 no 9 pp 2486ndash24931987
[34] W P McGuire E K Rowinsky N B Rosenhein et alldquoTaxol a unique antineoplastic agent with significant activityin advanced ovarian epithelial neoplasmsrdquo Annals of InternalMedicine vol 111 no 4 pp 273ndash279 1989
[35] ldquoDiscovery and development of taxolrdquo in Taxol Science andApplications M W M E Suffness Ed pp 3ndash25 CRC PressBoca Raton Fla USA 1995
[36] M J Piccart and F Cardoso ldquoProgress in systemic therapy forbreast cancer an overview and perspectivesrdquo European Journalof Cancer Supplement vol 1 no 2 pp 56ndash69 2003
[37] P Bonomi K B Kim and J Kugler ldquoComparison of survival forstage IIIB versus stage IV non-small cell lung cancer (NSCLC)patients with etoposide-cisplatin versus taxol-cisplatin an East-ern Cooperative Oncology Group (ECOG) trialrdquo in Proceedingsof the American Society of Clinical Oncology vol 16 p 454a1997
[38] D Guenard F Gueritte-Voegelein J Dubois and P PotierldquoStructure-activity relationships of Taxol and Taxotere ana-loguesrdquo Journal of the National Cancer Institute Monographsno 15 pp 79ndash82 1993
[39] D G I Kingston ldquoTaxol the chemistry and structure-activityrelationships of a novel anticancer agentrdquo Trends in Biotechnol-ogy vol 12 no 6 pp 222ndash227 1994
[40] E K Rowinsky and R C Donehower ldquoPaclitaxel (taxol)rdquo TheNew England Journal of Medicine vol 332 no 15 pp 1004ndash10141995
[41] J Parness and S B Horwitz ldquoTaxol binds to polymerizedtubulin in vitrordquo Journal of Cell Biology vol 91 no 2 pp 479ndash487 1981
[42] A Dammermann A Desai and K Oegema ldquoTheminus end insightrdquo Current Biology vol 13 no 15 pp R614ndashR624 2003
[43] CWiese and Y Zheng ldquoMicrotubule nucleation 120574-tubulin andbeyondrdquo Journal of Cell Science vol 119 no 20 pp 4143ndash41532006
[44] A Ganguly H Yang and F Cabral ldquoPaclitaxel-dependent celllines reveal a novel drug activityrdquo Molecular Cancer Therapeu-tics vol 9 no 11 pp 2914ndash2923 2010
[45] P B Schiff and S B Horwitz ldquoTaxol stabilizes microtubules inmouse fibroblast cellsrdquo Proceedings of the National Academy ofSciences of the United States of America vol 77 no 3 pp 1561ndash1565 1980
[46] P B Schiff J Fant and S B Horwitz ldquoPromotion of micro-tubule assembly in vitro by Taxolrdquo Nature vol 277 no 5698pp 665ndash667 1979
[47] D Zhang R Yang S Wang and Z Dong ldquoPaclitaxel new usesfor an old drugrdquoDrug Design Development andTherapy vol 8pp 279ndash284 2014
[48] S Rao G A Orr A G Chaudhary D G I Kingston and SB Horwitz ldquoCharacterization of the taxol binding site on themicrotubule 2-(m-Azidobenzoyl)taxol photolabels a peptide(amino acids 217-231) of beta-tubulinrdquoThe Journal of BiologicalChemistry vol 270 no 35 pp 20235ndash20238 1995
[49] F Wang Y Cao W Zhao H Liu Z Fu and R Han ldquoTaxolinhibits melanoma metastases through apoptosis inductionangiogenesis inhibition and restoration of E-cadherin andnm23 expressionrdquo Journal of Pharmacological Sciences vol 93no 2 pp 197ndash203 2003
18 BioMed Research International
[50] A Sevko V Kremer C Falk et al ldquoApplication of paclitaxel inlow non-cytotoxic doses supports vaccination with melanomaantigens in normal micerdquo Journal of Immunotoxicology vol 9no 3 pp 275ndash281 2012
[51] T Kreis and R Vale Guidebook to the Cytoskeletal and MotorProteins Oxford University Press Oxford UK 2nd edition1999
[52] P Giannakakou D L Sackett Y-K Kang et al ldquoPaclitaxel-resistant human ovarian cancer cells have mutant 120573-tubulinsthat exhibit impaired paclitaxel-driven polymerizationrdquo TheJournal of Biological Chemistry vol 272 no 27 pp 17118ndash171251997
[53] E Rakovitch W Mellado E J Hall T K Pandita S Sawantand C R Geard ldquoPaclitaxel sensitivity correlates with p53status and DNA fragmentation but not G2M accumulationrdquoInternational Journal of Radiation Oncology Biology Physics vol44 no 5 pp 1119ndash1124 1999
[54] S W Lowe S Bodis A McClatchey et al ldquop53 status and theefficacy of cancer therapy in vivordquo Science vol 266 no 5186 pp807ndash810 1994
[55] C C Zhang J-M Yang E White M Murphy A Levine andW N Hait ldquoThe role of MAP4 expression in the sensitivity topaclitaxel and resistance to vinca alkaloids in p53 mutant cellsrdquoOncogene vol 16 no 12 pp 1617ndash1624 1998
[56] K Fukasawa T Choi R Kuriyama S Rulong and G F VandeWoude ldquoAbnormal centrosome amplification in the absence ofp53rdquo Science vol 271 no 5256 pp 1744ndash1747 1996
[57] T-H Wang Y-H Chan C-W Chen et al ldquoPaclitaxel (Taxol)upregulates expression of functional interleukin-6 in humanovarian cancer cells through multiple signaling pathwaysrdquoOncogene vol 25 no 35 pp 4857ndash4866 2006
[58] E Yakirevich E Sabo I Naroditsky Y Sova O Lavie andM B Resnick ldquoMultidrug resistance-related phenotype andapoptosis-related protein expression in ovarian serous carcino-masrdquo Gynecologic Oncology vol 100 no 1 pp 152ndash159 2006
[59] G Szakacs J K Paterson J A Ludwig C Booth-Genthe andM M Gottesman ldquoTargeting multidrug resistance in cancerrdquoNature Reviews Drug Discovery vol 5 no 3 pp 219ndash234 2006
[60] L W Pfannenstiel S S K Lam L A Emens E M Jaffeeand T D Armstrong ldquoPaclitaxel enhances early dendritic cellmaturation and function through TLR4 signaling in micerdquoCellular Immunology vol 263 no 1 pp 79ndash87 2010
[61] N Klauber S Parangi E Flynn E Hamel and R J DrsquoAmatoldquoInhibition of angiogenesis and breast cancer in mice by themicrotubule inhibitors 2-methoxyestradiol and Taxolrdquo CancerResearch vol 57 no 1 pp 81ndash86 1997
[62] D Belotti V Vergani T Drudis et al ldquoThe microtubule-affecting drug paclitaxel has antiangiogenic activityrdquo ClinicalCancer Research vol 2 no 11 pp 1843ndash1849 1996
[63] D H Lau L Xue L J Young P A Burke and A T CheungldquoPaclitaxel (Taxol) an inhibitor of angiogenesis in a highlyvascularized transgenic breast cancerrdquo Cancer Biotherapy andRadiopharmaceuticals vol 14 no 1 pp 31ndash36 1999
[64] X Jiang ldquoHarnessing the immune system for the treatment ofbreast cancerrdquo Journal of Zhejiang University Science B vol 15no 1 pp 1ndash15 2014
[65] A Gadducci D Katsaros P Zola et al ldquoWeekly low-dosepaclitaxel as maintenance treatment in patients with advancedovarian cancer who had microscopic residual disease atsecond-look surgery after 6 cycles of paclitaxelplatinum-basedchemotherapy Results of an open noncomparative phase 2
multicenter italian study (after-6 protocol 2)rdquo InternationalJournal of Gynecological Cancer vol 19 no 4 pp 615ndash619 2009
[66] R S Bhatt J Merchan R Parker et al ldquoA phase 2 pilot trial oflow-dose continuous infusion or lsquometronomicrsquo paclitaxel andoral celecoxib in patients with metastatic melanomardquo Cancervol 116 no 7 pp 1751ndash1756 2010
[67] M Caballero J J Grau J L Blanch et al ldquoSerum vascularendothelial growth factor as a predictive factor in metronomic(weekly) paclitaxel treatment for advanced head and neckcancerrdquo Archives of OtolaryngologymdashHead and Neck Surgeryvol 133 no 11 pp 1143ndash1148 2007
[68] J Alexandre Y Hu W Lu H Pelicano and P Huang ldquoNovelaction of paclitaxel against cancer cells bystander effect medi-ated by reactive oxygen speciesrdquo Cancer Research vol 67 no 8pp 3512ndash3517 2007
[69] T Hadzic N Aykin-Burns Y Zhu et al ldquoPaclitaxel combinedwith inhibitors of glucose and hydroperoxide metabolismenhances breast cancer cell killing viaH
2O2-mediated oxidative
stressrdquo Free Radical Biology and Medicine vol 48 no 8 pp1024ndash1033 2010
[70] C A Sherman-Baust K G Becker W H Wood III Y Zhangand P J Morin ldquoGene expression and pathway analysis of ovar-ian cancer cells selected for resistance to cisplatin paclitaxel ordoxorubicinrdquo Journal of Ovarian Research vol 4 no 1 article21 2011
[71] R Agarwal and S B Kaye ldquoOvarian cancer strategies for over-coming resistance to chemotherapyrdquo Nature Reviews Cancervol 3 no 7 pp 502ndash516 2003
[72] T Acker and K H Plate ldquoRole of hypoxia in tumorangiogenesismdashmolecular and cellular angiogenic crosstalkrdquoCell and Tissue Research vol 314 no 1 pp 145ndash155 2003
[73] M Hockel and P Vaupel ldquoBiological consequences of tumorhypoxiardquo Seminars in Oncology vol 28 supplement 8 no 2 pp36ndash41 2001
[74] L Huang Q-H Zhang Q-L Ao H Xing Y-P Lu and DMa ldquoEffect of hypoxia on the chemotherapeutic sensitivity ofhuman ovarian cancer cells to paclitaxel and its mechanismrdquoZhonghua Zhong Liu Za Zhi vol 29 no 2 pp 96ndash100 2007
[75] N Rohwer and T Cramer ldquoHypoxia-mediated drug resistancenovel insights on the functional interaction of HIFs and celldeath pathwaysrdquoDrug Resistance Updates vol 14 no 3 pp 191ndash201 2011
[76] B B Aggarwal R V Vijayalekshmi and B Sung ldquoTargetinginflammatory pathways for prevention and therapy of cancershort-term friend long-term foerdquo Clinical Cancer Research vol15 no 2 pp 425ndash430 2009
[77] Z Duan R Foster D A Bell et al ldquoSignal transducersand activators of transcription 3 pathway activation in drug-resistant ovarian cancerrdquo Clinical Cancer Research vol 12 no17 pp 5055ndash5063 2006
[78] H-J Kuh S H Jang M G Wientjes J R Weaver and J L-SAu ldquoDeterminants of paclitaxel penetration and accumulationin human solid tumorrdquo Journal of Pharmacology and Experi-mental Therapeutics vol 290 no 2 pp 871ndash880 1999
[79] S Arao H Suwa M Mandai et al ldquoHypoxia-mediated drugresistance novel insights on the functional interaction of HIFsand cell death pathwaysrdquo Cancer Research vol 54 no 5 pp1355ndash1359 1994
[80] S E Johnatty J Beesley B Gao et al ldquoABCB1 (MDR1)polymorphisms and ovarian cancer progression and survivala comprehensive analysis from the Ovarian Cancer Association
BioMed Research International 19
Consortium and the Cancer GenomeAtlasrdquoGynecologic Oncol-ogy vol 131 no 1 pp 8ndash14 2013
[81] X Yang A K Iyer A Singh et al ldquoCluster of differentiation44 targeted hyaluronic acid based nanoparticles for MDR1siRNA delivery to overcome drug resistance in ovarian cancerrdquoPharmaceutical Research 2014
[82] D A Zajchowski B Y Karlan and L K Shawver ldquoTreatment-related protein biomarker expression differs between primaryand recurrent ovarian carcinomasrdquoMolecular CancerTherapeu-tics vol 11 no 2 pp 492ndash502 2012
[83] MM Gottesman J Ludwig D Xia and G Szakacs ldquoDefeatingdrug resistance in cancerrdquoDiscovery Medicine vol 6 no 31 pp18ndash23 2006
[84] S Mozzetti C Ferlini P Concolino et al ldquoClass III 120573-tubulin overexpression is a prominent mechanism of paclitaxelresistance in ovarian cancer patientsrdquo Clinical Cancer Researchvol 11 no 1 pp 298ndash305 2005
[85] M Kavallaris D Y S Kuo C A Burkhart et al ldquoTaxol-resistant epithelial ovarian tumors are associated with alteredexpression of specific beta-tubulin isotypesrdquo Journal of ClinicalInvestigation vol 100 no 5 pp 1282ndash1293 1997
[86] G A Orr P Verdier-Pinard H McDaid and S B HorwitzldquoMechanisms of Taxol resistance related to microtubulesrdquoOncogene vol 22 no 47 pp 7280ndash7295 2003
[87] C Ferlini L Cicchillitti G Raspaglio et al ldquoPaclitaxel directlybinds to Bcl-2 and functionally mimics activity of Nur77rdquoCancer Research vol 69 no 17 pp 6906ndash6914 2009
[88] E Mechetner A Kyshtoobayeva S Zonis et al ldquoLevels ofmultidrug resistance (MDR1) P-glycoprotein expression byhuman breast cancer correlate with in vitro resistance to taxoland doxorubicinrdquo Clinical Cancer Research vol 4 no 2 pp389ndash398 1998
[89] J S Lagas C W N Damen R A B VanWaterschoot D IusufJ H Beijnen and A H Schinkel ldquoP-glycoprotein multidrug-resistance associated protein 2 Cyp3a and carboxylesteraseaffect the oral availability and metabolism of vinorelbinerdquoMolecular Pharmacology vol 82 no 4 pp 636ndash644 2012
[90] M T Huizing J B Vermorken H Rosing et al ldquoPharmacoki-netics of paclitaxel and three major metabolites in patients withadvanced breast carcinoma refractory to anthracycline therapytreated with a 3-hour paclitaxel infusion a European CancerCentre (ECC) trialrdquo Annals of Oncology vol 6 no 7 pp 699ndash704 1995
[91] R Panchagnula ldquoPharmaceutical aspects of paclitaxelrdquo Interna-tional Journal of Pharmaceutics vol 172 no 1-2 pp 1ndash15 1998
[92] S H Jang M G Wientjes and J L-S Au ldquoDeterminants ofpaclitaxel uptake accumulation and retention in solid tumorsrdquoInvestigational New Drugs vol 19 no 2 pp 113ndash123 2001
[93] D S Sonnichsen andM V Relling ldquoClinical pharmacokineticsof paclitaxelrdquo Clinical Pharmacokinetics vol 27 no 4 pp 256ndash269 1994
[94] T Ohtsu Y Sasaki T Tamura et al ldquoClinical pharmacokineticsand pharmacodynamics of paclitaxel a 3-hour infusion versusa 24-hour infusionrdquo Clinical Cancer Research vol 1 no 6 pp599ndash606 1995
[95] M Czejka J Schueller H Schnait B Springer and I EderldquoClinical pharmacokinetics andmetabolism of paclitaxel after athree-hour infusion comparison of two preparationsrdquo Journalof Oncology Pharmacy Practice vol 9 no 4 pp 129ndash136 2003
[96] J Rizzo C Riley D VonHoff J Kuhn J Phillips and T BrownldquoAnalysis of anticancer drugs in biological fluids determination
of taxol with application to clinical pharmacokineticsrdquo Journalof Pharmaceutical and Biomedical Analysis vol 8 no 2 pp 159ndash164 1990
[97] V A de Weger J H Beijnen and J H M Schellens ldquoCel-lular and clinical pharmacology of the taxanes docetaxel andpaclitaxelmdasha reviewrdquoAnti-Cancer Drugs vol 25 no 5 pp 488ndash494 2014
[98] S Kumar H Mahdi C Bryant J P Shah G Garg andA Munkarah ldquoClinical trials and progress with paclitaxel inovarian cancerrdquo International Journal of Womenrsquos Health vol 2no 1 pp 411ndash427 2010
[99] B Huang J Zhao J C Unkeless Z H Feng and H XiongldquoTLR signaling by tumor and immune cells a double-edgedswordrdquo Oncogene vol 27 no 2 pp 218ndash224 2008
[100] R A Jibodh J S Lagas B Nuijen J H Beijnen and J HM Schellens ldquoTaxanes old drugs new oral formulationsrdquoEuropean Journal of Pharmacology vol 717 no 1ndash3 pp 40ndash462013
[101] A Javeed M Ashraf A Riaz A Ghafoor S Afzal and M MMukhtar ldquoPaclitaxel and immune systemrdquo European Journal ofPharmaceutical Sciences vol 38 no 4 pp 283ndash290 2009
[102] L Bracci G Schiavoni A Sistigu and F Belardelli ldquoImmune-based mechanisms of cytotoxic chemotherapy implications forthe design of novel and rationale-based combined treatmentsagainst cancerrdquo Cell Death and Differentiation vol 21 no 1 pp15ndash25 2014
[103] C A Byrd-Leifer E F Block K Takeda S Akira and A DingldquoThe role of MyD88 and TLR4 in the LPS-mimetic activity ofTaxolrdquo European Journal of Immunology vol 31 no 8 pp 2448ndash2457 2001
[104] A-C Wang Y-B Ma F-X Wu et al ldquoTLR4 induces tumorgrowth and inhibits paclitaxel activity in MyD88-positivehuman ovarian carcinoma in vitrordquo Oncology Letters vol 7 no3 pp 871ndash877 2014
[105] Y Zhu N Liu S D Xiong Y J Zheng and Y W ChuldquoCD4+Foxp3+ regulatory T-cell impairment by paclitaxel isindependent of toll-like receptor 4rdquo Scandinavian Journal ofImmunology vol 73 no 4 pp 301ndash308 2011
[106] M Kubo T Morisaki K Matsumoto et al ldquoPaclitaxel probablyenhances cytotoxicity of natural killer cells against breastcarcinoma cells by increasing perforin productionrdquo CancerImmunology Immunotherapy vol 54 no 5 pp 468ndash476 2005
[107] L Markasz G Stuber B Vanherberghen et al ldquoEffect of fre-quently used chemotherapeutic drugs on the cytotoxic activityof human natural killer cellsrdquo Molecular Cancer Therapeuticsvol 6 no 2 pp 644ndash654 2007
[108] T Sako N Burioka K Yasuda et al ldquoCellular immune profile inpatients with non-small cell lung cancer after weekly paclitaxeltherapyrdquo Acta Oncologica vol 43 no 1 pp 15ndash19 2004
[109] R Kaneno G V Shurin I L Tourkova and M R ShurinldquoChemomodulation of human dendritic cell function by anti-neoplastic agents in low noncytotoxic concentrationsrdquo Journalof Translational Medicine vol 7 article 58 2009
[110] TMichels G V ShurinHNaiditch A Sevko VUmansky andM R Shurin ldquoPaclitaxel promotes differentiation of myeloid-derived suppressor cells into dendritic cells in vitro in a TLR4-independent mannerrdquo Journal of Immunotoxicology vol 9 no3 pp 292ndash300 2012
[111] R A Kemp and F Ronchese ldquoTumor-specific Tc1 but not Tc2cells deliver protective antitumor immunityrdquo The Journal ofImmunology vol 167 no 11 pp 6497ndash6502 2001
20 BioMed Research International
[112] A Y Rudensky ldquoRegulatory T cells and Foxp3rdquo ImmunologicalReviews vol 241 no 1 pp 260ndash268 2011
[113] EM Shevach ldquoCD4+CD25+ suppressor T cellsmore questionsthan answersrdquo Nature Reviews Immunology vol 2 no 6 pp389ndash400 2002
[114] S Sakaguchi T Yamaguchi T Nomura and M Ono ldquoRegu-latory T cells and immune tolerancerdquo Cell vol 133 no 5 pp775ndash787 2008
[115] H Nishikawa and S Sakaguchi ldquoRegulatory T cells in tumorimmunityrdquo International Journal of Cancer vol 127 no 4 pp759ndash767 2010
[116] W Zou ldquoRegulatory T cells tumour immunity and immuno-therapyrdquoNature Reviews Immunology vol 6 no 4 pp 295ndash3072006
[117] A Fialova S Partlova L Sojka et al ldquoDynamics of T-cell infil-tration during the course of ovarian cancer The gradual shiftfrom aTh17 effector cell response to a predominant infiltrationby regulatory T-cellsrdquo International Journal of Cancer vol 132no 5 pp 1070ndash1079 2013
[118] A E Albers R L Ferris G G Kim K Chikamatsu A BDeLeo and T L Whiteside ldquoImmune responses to p53 inpatients with cancer enrichment in tetramer+ p53 peptide-specific T cells and regulatory T cells at tumor sitesrdquo CancerImmunology Immunotherapy vol 54 no 11 pp 1072ndash10812005
[119] N Liu Y Zheng Y Zhu S Xiong andYChu ldquoSelective impair-ment of CD4 + CD25 + Foxp3 + regulatory T cells by paclitaxelis explained by Bcl-2Bax mediated apoptosisrdquo InternationalImmunopharmacology vol 11 no 2 pp 212ndash219 2011
[120] X Wu Q-M Feng Y Wang J Shi H-L Ge and W DildquoThe immunologic aspects in advanced ovarian cancer patientstreated with paclitaxel and carboplatin chemotherapyrdquo CancerImmunology Immunotherapy vol 59 no 2 pp 279ndash291 2010
[121] A P Vicari R Luu N Zhang et al ldquoPaclitaxel reducesregulatoryT cell numbers and inhibitory function and enhancesthe anti-tumor effects of the TLR9 agonist PF-3512676 in themouserdquo Cancer Immunology Immunotherapy vol 58 no 4 pp615ndash628 2009
[122] L Zhang K Dermawan M Jin et al ldquoDifferential impairmentof regulatory T cells rather than effector T cells by paclitaxel-based chemotherapyrdquo Clinical Immunology vol 129 no 2 pp219ndash229 2008
[123] Y Tabuchi J Matsuoka M Gunduz et al ldquoResistance topaclitaxel therapy is related with Bcl-2 expression through anestrogen receptor mediated pathway in breast cancerrdquo Interna-tional Journal of Oncology vol 34 no 2 pp 313ndash319 2009
[124] N Obermajer R Muthuswamy K Odunsi R P Edwards andP Kalinski ldquoPGE
2-induced CXCL12 production and CXCR4
expression controls the accumulation of human MDSCs inovarian cancer environmentrdquo Cancer Research vol 71 no 24pp 7463ndash7470 2011
[125] Q M Feng W Di and X Wu ldquoImmune reconstitution inadvanced ovarian cancer patients undergoing first line chemo-therapyrdquo Xi Bao Yu Fen Zi Mian Yi Xue Za Zhi vol 25 no 11pp 1023ndash1025 2009
[126] A D Seidman D Hochhauser M Gollub et al ldquoNinety-six-hour paclitaxel infusion after progression during short taxaneexposure a phase II pharmacokinetic and pharmacodynamicstudy in metastatic breast cancerrdquo Journal of Clinical Oncologyvol 14 no 6 pp 1877ndash1884 1996
[127] D R Spriggs M F Brady L Vaccarello et al ldquoPhase IIIrandomized trial of intravenous cisplatin plus a 24- or 96-hour
infusion of paclitaxel in epithelial ovarian cancer a gynecologiconcology group studyrdquo Journal of Clinical Oncology vol 25 no28 pp 4466ndash4471 2007
[128] G A Omura M F Brady K Y Look et al ldquoPhase III trial ofpaclitaxel at two dose levels the higher dose accompanied byfilgrastim at two dose levels in platinum-pretreated epithelialovarian cancer an intergroup studyrdquo Journal of Clinical Oncol-ogy vol 21 no 15 pp 2843ndash2848 2003
[129] R Simon and L Norton ldquoThe Norton-Simon hypothesisdesigning more effective and less toxic chemotherapeutic reg-imensrdquoNature Clinical Practice Oncology vol 3 no 8 pp 406ndash407 2006
[130] A Kumar P Hoskins and A Tinker ldquoDose-dense paclitaxel inadvanced ovarian cancerrdquo Clinical Oncology vol 27 no 1 pp40ndash47 2015
[131] P Marchetti S Urien G A Cappellini G Ronzino and CFicorella ldquoWeekly administration of paclitaxel theoretical andclinical basisrdquoCritical Reviews in OncologyHematology vol 44supplement pp S3ndashS13 2002
[132] P Francis E Rowinsky J Schneider T Hakes W Hoskinsand M Markman ldquoPhase I feasibility and pharmacologic studyof weekly intraperitoneal paclitaxel A Gynecologic OncologyGroup pilot studyrdquo Journal of Clinical Oncology vol 13 no 12pp 2961ndash2967 1995
[133] H Thomas and P Rosenberg ldquoRole of weekly paclitaxel inthe treatment of advanced ovarian cancerrdquo Critical Reviews inOncologyHematology vol 44 supplement pp S43ndashS51 2002
[134] M Markman J Markman K Webster et al ldquoDuration ofresponse to second-line platinum-based chemotherapy forovarian cancer implications for patient management and clini-cal trial designrdquo Journal of Clinical Oncology vol 22 no 15 pp3120ndash3125 2004
[135] P H OrsquoDonnell M Eileen Dolan E Gamazon et al ldquoPopu-lation differences in platinum toxicity as a means to identifynovel genetic susceptibility variantsrdquo Pharmacogenetics andGenomics vol 20 no 5 pp 327ndash337 2010
[136] M J Millward M J Boyer M Lehnert et al ldquoDocetaxel andcarboplatin is an active regimen in advanced non-small-celllung cancer a phase II study in Caucasian and Asian patientsrdquoAnnals of Oncology vol 14 no 3 pp 449ndash454 2003
[137] M Markman ldquoIntraperitoneal therapy of ovarian cancerrdquoOncologist vol 1 no 1-2 pp 18ndash21 1996
[138] M Markman and J L Walker ldquoIntraperitoneal chemotherapyof ovarian cancer a review with a focus on practical aspects oftreatmentrdquo Journal of Clinical Oncology vol 24 no 6 pp 988ndash994 2006
[139] K Fujiwara S Nagao E Aotani and K Hasegawa ldquoPrincipleand evolving role of intraperitoneal chemotherapy in ovariancancerrdquo Expert Opinion on Pharmacotherapy vol 14 no 13 pp1797ndash1806 2013
[140] M Markman E Rowinsky T Hakes et al ldquoPhase I trialof intraperitoneal taxol a gynecoloic oncology group studyrdquoJournal of Clinical Oncology vol 10 no 9 pp 1485ndash1491 1992
[141] M Markman M F Brady N M Spirtos P Hanjani and S CRubin ldquoPhase II trial of intraperitoneal paclitaxel in carcinomaof the ovary tube and peritoneum a gynecologic oncologygroup studyrdquo Journal of Clinical Oncology vol 16 no 8 pp2620ndash2624 1998
[142] P B Panici I Palaia M Graziano F Bellati N Manci and RAngioli ldquoIntraperitoneal paclitaxel as consolidation treatmentin ovarian cancer patients a case control studyrdquo Oncology vol78 no 1 pp 20ndash25 2010
BioMed Research International 21
[143] D K Armstrong B Bundy L Wenzel et al ldquoIntraperitonealcisplatin and paclitaxel in ovarian cancerrdquo The New EnglandJournal of Medicine vol 354 no 1 pp 34ndash43 2006
[144] D Tewari J Java and R Salani ldquoLong-term survival advantageof intraperitoneal chemotherapy treatment in advanced ovariancancer an analysis of a Gynecologic Oncology Group ancillarydata studyrdquo in Proceedings of the 2013 Society of GynecologicOncology Annual Meeting on Womenrsquos Cancer (GOG114172Abstract) Los Angeles Calif USA 2013
[145] D A Yardley ldquonab-paclitaxel mechanisms of action and deliv-eryrdquo Journal of Controlled Release vol 170 no 3 pp 365ndash3722013
[146] M Ando K Yonemori N Katsumata et al ldquoPhase I and phar-macokinetic study of nab-paclitaxel nanoparticle albumin-bound paclitaxel administeredweekly to Japanese patients withsolid tumors and metastatic breast cancerrdquo Cancer Chemother-apy and Pharmacology vol 69 no 2 pp 457ndash465 2012
[147] N Desai V Trieu Z Yao et al ldquoIncreased antitumor activityintratumor paclitaxel concentrations and endothelial cell trans-port of cremophor-free albumin-bound paclitaxel ABI-007compared with cremophor-based paclitaxelrdquo Clinical CancerResearch vol 12 no 4 pp 1317ndash1324 2006
[148] J A Yared and K H R Tkaczuk ldquoUpdate on taxane devel-opment new analogs and new formulationsrdquo Drug DesignDevelopment andTherapy vol 6 pp 371ndash384 2012
[149] M G Teneriello P C Tseng M Crozier et al ldquoPhase IIevaluation of nanoparticle albumin-bound paclitaxel in plati-num-sensitive patients with recurrent ovarian peritoneal orfallopian tube cancerrdquo Journal of Clinical Oncology vol 27 no9 pp 1426ndash1431 2009
[150] R L Coleman W E Brady D S McMeekin et al ldquoA phase IIevaluation of nanoparticle albumin-bound (nab) paclitaxel inthe treatment of recurrent or persistent platinum-resistant ovar-ian fallopian tube or primary peritoneal cancer a GynecologicOncology Group Studyrdquo Gynecologic Oncology vol 122 no 1pp 111ndash115 2011
[151] J W Singer ldquoPaclitaxel poliglumex (XYOTAX CT-2103) amacromolecular taxanerdquo Journal of Controlled Release vol 109no 1ndash3 pp 120ndash126 2005
[152] C Li D-F Yu R A Newman et al ldquoComplete regressionof well-established tumors using a novel water-soluble poly(L-glutamic acid)-paclitaxel conjugaterdquo Cancer Research vol 58no 11 pp 2404ndash2409 1998
[153] M Mita A Mita J Sarantopoulos et al ldquoPhase I study ofpaclitaxel poliglumex administered weekly for patients withadvanced solid malignanciesrdquo Cancer Chemotherapy and Phar-macology vol 64 no 2 pp 287ndash295 2009
[154] P Sabbatini M W Sill D OrsquoMalley L Adler and A ASecord ldquoA phase II trial of paclitaxel poliglumex in recurrentor persistent ovarian or primary peritoneal cancer (EOC) agynecologic oncology group studyrdquo Gynecologic Oncology vol111 no 3 pp 455ndash460 2008
[155] M O Bradley C S Swindell F H Anthony et al ldquoTumortargeting by conjugation of DHA to paclitaxelrdquo Journal ofControlled Release vol 74 no 1ndash3 pp 233ndash236 2001
[156] M O Bradley N L Webb F H Anthony et al ldquoTumortargeting by covalent conjugation of a natural fatty acid topaclitaxelrdquo Clinical Cancer Research vol 7 no 10 pp 3229ndash3238 2001
[157] A C Wolff R C Donehower M K Carducci et al ldquoPhaseI study of docosahexaenoic acid-paclitaxel a taxane-fatty acid
conjugate with a unique pharmacology and toxicity profilerdquoClinical Cancer Research vol 9 no 10 part 1 pp 3589ndash35972003
[158] A Sparreboom A C Wolff J Verweij et al ldquoDispositionof docosahexaenoic acid-paclitaxel a novel taxane in bloodin vitro and clinical pharmacokinetic studiesrdquo Clinical CancerResearch vol 9 no 1 pp 151ndash159 2003
[159] P M Fracasso J Picus J D Wildi et al ldquoPhase 1 and phar-macokinetic study of weekly docosahexaenoic acid-paclitaxelTaxoprexin in resistant solid tumor malignanciesrdquo CancerChemotherapy and Pharmacology vol 63 no 3 pp 451ndash4582009
[160] A Y Bedikian R C DeConti R Conry et al ldquoPhase 3 study ofdocosahexaenoic acid-paclitaxel versus dacarbazine in patientswith metastatic malignant melanomardquo Annals of Oncology vol22 no 4 pp 787ndash793 2011
[161] Y-N Wu S-L Wang Y-C Wang et al ldquoReversal effect ofdocosahexaenoic acid on taxol resistance in human ovarian car-cinoma A2780T cellsrdquo Obstetrics amp Gynecology InternationalJournal vol 1 no 3 Article ID 00018 2014
Submit your manuscripts athttpwwwhindawicom
PainResearch and TreatmentHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom
Volume 2014
ToxinsJournal of
VaccinesJournal of
Hindawi Publishing Corporation httpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
AntibioticsInternational Journal of
ToxicologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
StrokeResearch and TreatmentHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Drug DeliveryJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Advances in Pharmacological Sciences
Tropical MedicineJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Medicinal ChemistryInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
AddictionJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
Emergency Medicine InternationalHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Autoimmune Diseases
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Anesthesiology Research and Practice
ScientificaHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Pharmaceutics
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of

18 BioMed Research International
[50] A Sevko V Kremer C Falk et al ldquoApplication of paclitaxel inlow non-cytotoxic doses supports vaccination with melanomaantigens in normal micerdquo Journal of Immunotoxicology vol 9no 3 pp 275ndash281 2012
[51] T Kreis and R Vale Guidebook to the Cytoskeletal and MotorProteins Oxford University Press Oxford UK 2nd edition1999
[52] P Giannakakou D L Sackett Y-K Kang et al ldquoPaclitaxel-resistant human ovarian cancer cells have mutant 120573-tubulinsthat exhibit impaired paclitaxel-driven polymerizationrdquo TheJournal of Biological Chemistry vol 272 no 27 pp 17118ndash171251997
[53] E Rakovitch W Mellado E J Hall T K Pandita S Sawantand C R Geard ldquoPaclitaxel sensitivity correlates with p53status and DNA fragmentation but not G2M accumulationrdquoInternational Journal of Radiation Oncology Biology Physics vol44 no 5 pp 1119ndash1124 1999
[54] S W Lowe S Bodis A McClatchey et al ldquop53 status and theefficacy of cancer therapy in vivordquo Science vol 266 no 5186 pp807ndash810 1994
[55] C C Zhang J-M Yang E White M Murphy A Levine andW N Hait ldquoThe role of MAP4 expression in the sensitivity topaclitaxel and resistance to vinca alkaloids in p53 mutant cellsrdquoOncogene vol 16 no 12 pp 1617ndash1624 1998
[56] K Fukasawa T Choi R Kuriyama S Rulong and G F VandeWoude ldquoAbnormal centrosome amplification in the absence ofp53rdquo Science vol 271 no 5256 pp 1744ndash1747 1996
[57] T-H Wang Y-H Chan C-W Chen et al ldquoPaclitaxel (Taxol)upregulates expression of functional interleukin-6 in humanovarian cancer cells through multiple signaling pathwaysrdquoOncogene vol 25 no 35 pp 4857ndash4866 2006
[58] E Yakirevich E Sabo I Naroditsky Y Sova O Lavie andM B Resnick ldquoMultidrug resistance-related phenotype andapoptosis-related protein expression in ovarian serous carcino-masrdquo Gynecologic Oncology vol 100 no 1 pp 152ndash159 2006
[59] G Szakacs J K Paterson J A Ludwig C Booth-Genthe andM M Gottesman ldquoTargeting multidrug resistance in cancerrdquoNature Reviews Drug Discovery vol 5 no 3 pp 219ndash234 2006
[60] L W Pfannenstiel S S K Lam L A Emens E M Jaffeeand T D Armstrong ldquoPaclitaxel enhances early dendritic cellmaturation and function through TLR4 signaling in micerdquoCellular Immunology vol 263 no 1 pp 79ndash87 2010
[61] N Klauber S Parangi E Flynn E Hamel and R J DrsquoAmatoldquoInhibition of angiogenesis and breast cancer in mice by themicrotubule inhibitors 2-methoxyestradiol and Taxolrdquo CancerResearch vol 57 no 1 pp 81ndash86 1997
[62] D Belotti V Vergani T Drudis et al ldquoThe microtubule-affecting drug paclitaxel has antiangiogenic activityrdquo ClinicalCancer Research vol 2 no 11 pp 1843ndash1849 1996
[63] D H Lau L Xue L J Young P A Burke and A T CheungldquoPaclitaxel (Taxol) an inhibitor of angiogenesis in a highlyvascularized transgenic breast cancerrdquo Cancer Biotherapy andRadiopharmaceuticals vol 14 no 1 pp 31ndash36 1999
[64] X Jiang ldquoHarnessing the immune system for the treatment ofbreast cancerrdquo Journal of Zhejiang University Science B vol 15no 1 pp 1ndash15 2014
[65] A Gadducci D Katsaros P Zola et al ldquoWeekly low-dosepaclitaxel as maintenance treatment in patients with advancedovarian cancer who had microscopic residual disease atsecond-look surgery after 6 cycles of paclitaxelplatinum-basedchemotherapy Results of an open noncomparative phase 2
multicenter italian study (after-6 protocol 2)rdquo InternationalJournal of Gynecological Cancer vol 19 no 4 pp 615ndash619 2009
[66] R S Bhatt J Merchan R Parker et al ldquoA phase 2 pilot trial oflow-dose continuous infusion or lsquometronomicrsquo paclitaxel andoral celecoxib in patients with metastatic melanomardquo Cancervol 116 no 7 pp 1751ndash1756 2010
[67] M Caballero J J Grau J L Blanch et al ldquoSerum vascularendothelial growth factor as a predictive factor in metronomic(weekly) paclitaxel treatment for advanced head and neckcancerrdquo Archives of OtolaryngologymdashHead and Neck Surgeryvol 133 no 11 pp 1143ndash1148 2007
[68] J Alexandre Y Hu W Lu H Pelicano and P Huang ldquoNovelaction of paclitaxel against cancer cells bystander effect medi-ated by reactive oxygen speciesrdquo Cancer Research vol 67 no 8pp 3512ndash3517 2007
[69] T Hadzic N Aykin-Burns Y Zhu et al ldquoPaclitaxel combinedwith inhibitors of glucose and hydroperoxide metabolismenhances breast cancer cell killing viaH
2O2-mediated oxidative
stressrdquo Free Radical Biology and Medicine vol 48 no 8 pp1024ndash1033 2010
[70] C A Sherman-Baust K G Becker W H Wood III Y Zhangand P J Morin ldquoGene expression and pathway analysis of ovar-ian cancer cells selected for resistance to cisplatin paclitaxel ordoxorubicinrdquo Journal of Ovarian Research vol 4 no 1 article21 2011
[71] R Agarwal and S B Kaye ldquoOvarian cancer strategies for over-coming resistance to chemotherapyrdquo Nature Reviews Cancervol 3 no 7 pp 502ndash516 2003
[72] T Acker and K H Plate ldquoRole of hypoxia in tumorangiogenesismdashmolecular and cellular angiogenic crosstalkrdquoCell and Tissue Research vol 314 no 1 pp 145ndash155 2003
[73] M Hockel and P Vaupel ldquoBiological consequences of tumorhypoxiardquo Seminars in Oncology vol 28 supplement 8 no 2 pp36ndash41 2001
[74] L Huang Q-H Zhang Q-L Ao H Xing Y-P Lu and DMa ldquoEffect of hypoxia on the chemotherapeutic sensitivity ofhuman ovarian cancer cells to paclitaxel and its mechanismrdquoZhonghua Zhong Liu Za Zhi vol 29 no 2 pp 96ndash100 2007
[75] N Rohwer and T Cramer ldquoHypoxia-mediated drug resistancenovel insights on the functional interaction of HIFs and celldeath pathwaysrdquoDrug Resistance Updates vol 14 no 3 pp 191ndash201 2011
[76] B B Aggarwal R V Vijayalekshmi and B Sung ldquoTargetinginflammatory pathways for prevention and therapy of cancershort-term friend long-term foerdquo Clinical Cancer Research vol15 no 2 pp 425ndash430 2009
[77] Z Duan R Foster D A Bell et al ldquoSignal transducersand activators of transcription 3 pathway activation in drug-resistant ovarian cancerrdquo Clinical Cancer Research vol 12 no17 pp 5055ndash5063 2006
[78] H-J Kuh S H Jang M G Wientjes J R Weaver and J L-SAu ldquoDeterminants of paclitaxel penetration and accumulationin human solid tumorrdquo Journal of Pharmacology and Experi-mental Therapeutics vol 290 no 2 pp 871ndash880 1999
[79] S Arao H Suwa M Mandai et al ldquoHypoxia-mediated drugresistance novel insights on the functional interaction of HIFsand cell death pathwaysrdquo Cancer Research vol 54 no 5 pp1355ndash1359 1994
[80] S E Johnatty J Beesley B Gao et al ldquoABCB1 (MDR1)polymorphisms and ovarian cancer progression and survivala comprehensive analysis from the Ovarian Cancer Association
BioMed Research International 19
Consortium and the Cancer GenomeAtlasrdquoGynecologic Oncol-ogy vol 131 no 1 pp 8ndash14 2013
[81] X Yang A K Iyer A Singh et al ldquoCluster of differentiation44 targeted hyaluronic acid based nanoparticles for MDR1siRNA delivery to overcome drug resistance in ovarian cancerrdquoPharmaceutical Research 2014
[82] D A Zajchowski B Y Karlan and L K Shawver ldquoTreatment-related protein biomarker expression differs between primaryand recurrent ovarian carcinomasrdquoMolecular CancerTherapeu-tics vol 11 no 2 pp 492ndash502 2012
[83] MM Gottesman J Ludwig D Xia and G Szakacs ldquoDefeatingdrug resistance in cancerrdquoDiscovery Medicine vol 6 no 31 pp18ndash23 2006
[84] S Mozzetti C Ferlini P Concolino et al ldquoClass III 120573-tubulin overexpression is a prominent mechanism of paclitaxelresistance in ovarian cancer patientsrdquo Clinical Cancer Researchvol 11 no 1 pp 298ndash305 2005
[85] M Kavallaris D Y S Kuo C A Burkhart et al ldquoTaxol-resistant epithelial ovarian tumors are associated with alteredexpression of specific beta-tubulin isotypesrdquo Journal of ClinicalInvestigation vol 100 no 5 pp 1282ndash1293 1997
[86] G A Orr P Verdier-Pinard H McDaid and S B HorwitzldquoMechanisms of Taxol resistance related to microtubulesrdquoOncogene vol 22 no 47 pp 7280ndash7295 2003
[87] C Ferlini L Cicchillitti G Raspaglio et al ldquoPaclitaxel directlybinds to Bcl-2 and functionally mimics activity of Nur77rdquoCancer Research vol 69 no 17 pp 6906ndash6914 2009
[88] E Mechetner A Kyshtoobayeva S Zonis et al ldquoLevels ofmultidrug resistance (MDR1) P-glycoprotein expression byhuman breast cancer correlate with in vitro resistance to taxoland doxorubicinrdquo Clinical Cancer Research vol 4 no 2 pp389ndash398 1998
[89] J S Lagas C W N Damen R A B VanWaterschoot D IusufJ H Beijnen and A H Schinkel ldquoP-glycoprotein multidrug-resistance associated protein 2 Cyp3a and carboxylesteraseaffect the oral availability and metabolism of vinorelbinerdquoMolecular Pharmacology vol 82 no 4 pp 636ndash644 2012
[90] M T Huizing J B Vermorken H Rosing et al ldquoPharmacoki-netics of paclitaxel and three major metabolites in patients withadvanced breast carcinoma refractory to anthracycline therapytreated with a 3-hour paclitaxel infusion a European CancerCentre (ECC) trialrdquo Annals of Oncology vol 6 no 7 pp 699ndash704 1995
[91] R Panchagnula ldquoPharmaceutical aspects of paclitaxelrdquo Interna-tional Journal of Pharmaceutics vol 172 no 1-2 pp 1ndash15 1998
[92] S H Jang M G Wientjes and J L-S Au ldquoDeterminants ofpaclitaxel uptake accumulation and retention in solid tumorsrdquoInvestigational New Drugs vol 19 no 2 pp 113ndash123 2001
[93] D S Sonnichsen andM V Relling ldquoClinical pharmacokineticsof paclitaxelrdquo Clinical Pharmacokinetics vol 27 no 4 pp 256ndash269 1994
[94] T Ohtsu Y Sasaki T Tamura et al ldquoClinical pharmacokineticsand pharmacodynamics of paclitaxel a 3-hour infusion versusa 24-hour infusionrdquo Clinical Cancer Research vol 1 no 6 pp599ndash606 1995
[95] M Czejka J Schueller H Schnait B Springer and I EderldquoClinical pharmacokinetics andmetabolism of paclitaxel after athree-hour infusion comparison of two preparationsrdquo Journalof Oncology Pharmacy Practice vol 9 no 4 pp 129ndash136 2003
[96] J Rizzo C Riley D VonHoff J Kuhn J Phillips and T BrownldquoAnalysis of anticancer drugs in biological fluids determination
of taxol with application to clinical pharmacokineticsrdquo Journalof Pharmaceutical and Biomedical Analysis vol 8 no 2 pp 159ndash164 1990
[97] V A de Weger J H Beijnen and J H M Schellens ldquoCel-lular and clinical pharmacology of the taxanes docetaxel andpaclitaxelmdasha reviewrdquoAnti-Cancer Drugs vol 25 no 5 pp 488ndash494 2014
[98] S Kumar H Mahdi C Bryant J P Shah G Garg andA Munkarah ldquoClinical trials and progress with paclitaxel inovarian cancerrdquo International Journal of Womenrsquos Health vol 2no 1 pp 411ndash427 2010
[99] B Huang J Zhao J C Unkeless Z H Feng and H XiongldquoTLR signaling by tumor and immune cells a double-edgedswordrdquo Oncogene vol 27 no 2 pp 218ndash224 2008
[100] R A Jibodh J S Lagas B Nuijen J H Beijnen and J HM Schellens ldquoTaxanes old drugs new oral formulationsrdquoEuropean Journal of Pharmacology vol 717 no 1ndash3 pp 40ndash462013
[101] A Javeed M Ashraf A Riaz A Ghafoor S Afzal and M MMukhtar ldquoPaclitaxel and immune systemrdquo European Journal ofPharmaceutical Sciences vol 38 no 4 pp 283ndash290 2009
[102] L Bracci G Schiavoni A Sistigu and F Belardelli ldquoImmune-based mechanisms of cytotoxic chemotherapy implications forthe design of novel and rationale-based combined treatmentsagainst cancerrdquo Cell Death and Differentiation vol 21 no 1 pp15ndash25 2014
[103] C A Byrd-Leifer E F Block K Takeda S Akira and A DingldquoThe role of MyD88 and TLR4 in the LPS-mimetic activity ofTaxolrdquo European Journal of Immunology vol 31 no 8 pp 2448ndash2457 2001
[104] A-C Wang Y-B Ma F-X Wu et al ldquoTLR4 induces tumorgrowth and inhibits paclitaxel activity in MyD88-positivehuman ovarian carcinoma in vitrordquo Oncology Letters vol 7 no3 pp 871ndash877 2014
[105] Y Zhu N Liu S D Xiong Y J Zheng and Y W ChuldquoCD4+Foxp3+ regulatory T-cell impairment by paclitaxel isindependent of toll-like receptor 4rdquo Scandinavian Journal ofImmunology vol 73 no 4 pp 301ndash308 2011
[106] M Kubo T Morisaki K Matsumoto et al ldquoPaclitaxel probablyenhances cytotoxicity of natural killer cells against breastcarcinoma cells by increasing perforin productionrdquo CancerImmunology Immunotherapy vol 54 no 5 pp 468ndash476 2005
[107] L Markasz G Stuber B Vanherberghen et al ldquoEffect of fre-quently used chemotherapeutic drugs on the cytotoxic activityof human natural killer cellsrdquo Molecular Cancer Therapeuticsvol 6 no 2 pp 644ndash654 2007
[108] T Sako N Burioka K Yasuda et al ldquoCellular immune profile inpatients with non-small cell lung cancer after weekly paclitaxeltherapyrdquo Acta Oncologica vol 43 no 1 pp 15ndash19 2004
[109] R Kaneno G V Shurin I L Tourkova and M R ShurinldquoChemomodulation of human dendritic cell function by anti-neoplastic agents in low noncytotoxic concentrationsrdquo Journalof Translational Medicine vol 7 article 58 2009
[110] TMichels G V ShurinHNaiditch A Sevko VUmansky andM R Shurin ldquoPaclitaxel promotes differentiation of myeloid-derived suppressor cells into dendritic cells in vitro in a TLR4-independent mannerrdquo Journal of Immunotoxicology vol 9 no3 pp 292ndash300 2012
[111] R A Kemp and F Ronchese ldquoTumor-specific Tc1 but not Tc2cells deliver protective antitumor immunityrdquo The Journal ofImmunology vol 167 no 11 pp 6497ndash6502 2001
20 BioMed Research International
[112] A Y Rudensky ldquoRegulatory T cells and Foxp3rdquo ImmunologicalReviews vol 241 no 1 pp 260ndash268 2011
[113] EM Shevach ldquoCD4+CD25+ suppressor T cellsmore questionsthan answersrdquo Nature Reviews Immunology vol 2 no 6 pp389ndash400 2002
[114] S Sakaguchi T Yamaguchi T Nomura and M Ono ldquoRegu-latory T cells and immune tolerancerdquo Cell vol 133 no 5 pp775ndash787 2008
[115] H Nishikawa and S Sakaguchi ldquoRegulatory T cells in tumorimmunityrdquo International Journal of Cancer vol 127 no 4 pp759ndash767 2010
[116] W Zou ldquoRegulatory T cells tumour immunity and immuno-therapyrdquoNature Reviews Immunology vol 6 no 4 pp 295ndash3072006
[117] A Fialova S Partlova L Sojka et al ldquoDynamics of T-cell infil-tration during the course of ovarian cancer The gradual shiftfrom aTh17 effector cell response to a predominant infiltrationby regulatory T-cellsrdquo International Journal of Cancer vol 132no 5 pp 1070ndash1079 2013
[118] A E Albers R L Ferris G G Kim K Chikamatsu A BDeLeo and T L Whiteside ldquoImmune responses to p53 inpatients with cancer enrichment in tetramer+ p53 peptide-specific T cells and regulatory T cells at tumor sitesrdquo CancerImmunology Immunotherapy vol 54 no 11 pp 1072ndash10812005
[119] N Liu Y Zheng Y Zhu S Xiong andYChu ldquoSelective impair-ment of CD4 + CD25 + Foxp3 + regulatory T cells by paclitaxelis explained by Bcl-2Bax mediated apoptosisrdquo InternationalImmunopharmacology vol 11 no 2 pp 212ndash219 2011
[120] X Wu Q-M Feng Y Wang J Shi H-L Ge and W DildquoThe immunologic aspects in advanced ovarian cancer patientstreated with paclitaxel and carboplatin chemotherapyrdquo CancerImmunology Immunotherapy vol 59 no 2 pp 279ndash291 2010
[121] A P Vicari R Luu N Zhang et al ldquoPaclitaxel reducesregulatoryT cell numbers and inhibitory function and enhancesthe anti-tumor effects of the TLR9 agonist PF-3512676 in themouserdquo Cancer Immunology Immunotherapy vol 58 no 4 pp615ndash628 2009
[122] L Zhang K Dermawan M Jin et al ldquoDifferential impairmentof regulatory T cells rather than effector T cells by paclitaxel-based chemotherapyrdquo Clinical Immunology vol 129 no 2 pp219ndash229 2008
[123] Y Tabuchi J Matsuoka M Gunduz et al ldquoResistance topaclitaxel therapy is related with Bcl-2 expression through anestrogen receptor mediated pathway in breast cancerrdquo Interna-tional Journal of Oncology vol 34 no 2 pp 313ndash319 2009
[124] N Obermajer R Muthuswamy K Odunsi R P Edwards andP Kalinski ldquoPGE
2-induced CXCL12 production and CXCR4
expression controls the accumulation of human MDSCs inovarian cancer environmentrdquo Cancer Research vol 71 no 24pp 7463ndash7470 2011
[125] Q M Feng W Di and X Wu ldquoImmune reconstitution inadvanced ovarian cancer patients undergoing first line chemo-therapyrdquo Xi Bao Yu Fen Zi Mian Yi Xue Za Zhi vol 25 no 11pp 1023ndash1025 2009
[126] A D Seidman D Hochhauser M Gollub et al ldquoNinety-six-hour paclitaxel infusion after progression during short taxaneexposure a phase II pharmacokinetic and pharmacodynamicstudy in metastatic breast cancerrdquo Journal of Clinical Oncologyvol 14 no 6 pp 1877ndash1884 1996
[127] D R Spriggs M F Brady L Vaccarello et al ldquoPhase IIIrandomized trial of intravenous cisplatin plus a 24- or 96-hour
infusion of paclitaxel in epithelial ovarian cancer a gynecologiconcology group studyrdquo Journal of Clinical Oncology vol 25 no28 pp 4466ndash4471 2007
[128] G A Omura M F Brady K Y Look et al ldquoPhase III trial ofpaclitaxel at two dose levels the higher dose accompanied byfilgrastim at two dose levels in platinum-pretreated epithelialovarian cancer an intergroup studyrdquo Journal of Clinical Oncol-ogy vol 21 no 15 pp 2843ndash2848 2003
[129] R Simon and L Norton ldquoThe Norton-Simon hypothesisdesigning more effective and less toxic chemotherapeutic reg-imensrdquoNature Clinical Practice Oncology vol 3 no 8 pp 406ndash407 2006
[130] A Kumar P Hoskins and A Tinker ldquoDose-dense paclitaxel inadvanced ovarian cancerrdquo Clinical Oncology vol 27 no 1 pp40ndash47 2015
[131] P Marchetti S Urien G A Cappellini G Ronzino and CFicorella ldquoWeekly administration of paclitaxel theoretical andclinical basisrdquoCritical Reviews in OncologyHematology vol 44supplement pp S3ndashS13 2002
[132] P Francis E Rowinsky J Schneider T Hakes W Hoskinsand M Markman ldquoPhase I feasibility and pharmacologic studyof weekly intraperitoneal paclitaxel A Gynecologic OncologyGroup pilot studyrdquo Journal of Clinical Oncology vol 13 no 12pp 2961ndash2967 1995
[133] H Thomas and P Rosenberg ldquoRole of weekly paclitaxel inthe treatment of advanced ovarian cancerrdquo Critical Reviews inOncologyHematology vol 44 supplement pp S43ndashS51 2002
[134] M Markman J Markman K Webster et al ldquoDuration ofresponse to second-line platinum-based chemotherapy forovarian cancer implications for patient management and clini-cal trial designrdquo Journal of Clinical Oncology vol 22 no 15 pp3120ndash3125 2004
[135] P H OrsquoDonnell M Eileen Dolan E Gamazon et al ldquoPopu-lation differences in platinum toxicity as a means to identifynovel genetic susceptibility variantsrdquo Pharmacogenetics andGenomics vol 20 no 5 pp 327ndash337 2010
[136] M J Millward M J Boyer M Lehnert et al ldquoDocetaxel andcarboplatin is an active regimen in advanced non-small-celllung cancer a phase II study in Caucasian and Asian patientsrdquoAnnals of Oncology vol 14 no 3 pp 449ndash454 2003
[137] M Markman ldquoIntraperitoneal therapy of ovarian cancerrdquoOncologist vol 1 no 1-2 pp 18ndash21 1996
[138] M Markman and J L Walker ldquoIntraperitoneal chemotherapyof ovarian cancer a review with a focus on practical aspects oftreatmentrdquo Journal of Clinical Oncology vol 24 no 6 pp 988ndash994 2006
[139] K Fujiwara S Nagao E Aotani and K Hasegawa ldquoPrincipleand evolving role of intraperitoneal chemotherapy in ovariancancerrdquo Expert Opinion on Pharmacotherapy vol 14 no 13 pp1797ndash1806 2013
[140] M Markman E Rowinsky T Hakes et al ldquoPhase I trialof intraperitoneal taxol a gynecoloic oncology group studyrdquoJournal of Clinical Oncology vol 10 no 9 pp 1485ndash1491 1992
[141] M Markman M F Brady N M Spirtos P Hanjani and S CRubin ldquoPhase II trial of intraperitoneal paclitaxel in carcinomaof the ovary tube and peritoneum a gynecologic oncologygroup studyrdquo Journal of Clinical Oncology vol 16 no 8 pp2620ndash2624 1998
[142] P B Panici I Palaia M Graziano F Bellati N Manci and RAngioli ldquoIntraperitoneal paclitaxel as consolidation treatmentin ovarian cancer patients a case control studyrdquo Oncology vol78 no 1 pp 20ndash25 2010
BioMed Research International 21
[143] D K Armstrong B Bundy L Wenzel et al ldquoIntraperitonealcisplatin and paclitaxel in ovarian cancerrdquo The New EnglandJournal of Medicine vol 354 no 1 pp 34ndash43 2006
[144] D Tewari J Java and R Salani ldquoLong-term survival advantageof intraperitoneal chemotherapy treatment in advanced ovariancancer an analysis of a Gynecologic Oncology Group ancillarydata studyrdquo in Proceedings of the 2013 Society of GynecologicOncology Annual Meeting on Womenrsquos Cancer (GOG114172Abstract) Los Angeles Calif USA 2013
[145] D A Yardley ldquonab-paclitaxel mechanisms of action and deliv-eryrdquo Journal of Controlled Release vol 170 no 3 pp 365ndash3722013
[146] M Ando K Yonemori N Katsumata et al ldquoPhase I and phar-macokinetic study of nab-paclitaxel nanoparticle albumin-bound paclitaxel administeredweekly to Japanese patients withsolid tumors and metastatic breast cancerrdquo Cancer Chemother-apy and Pharmacology vol 69 no 2 pp 457ndash465 2012
[147] N Desai V Trieu Z Yao et al ldquoIncreased antitumor activityintratumor paclitaxel concentrations and endothelial cell trans-port of cremophor-free albumin-bound paclitaxel ABI-007compared with cremophor-based paclitaxelrdquo Clinical CancerResearch vol 12 no 4 pp 1317ndash1324 2006
[148] J A Yared and K H R Tkaczuk ldquoUpdate on taxane devel-opment new analogs and new formulationsrdquo Drug DesignDevelopment andTherapy vol 6 pp 371ndash384 2012
[149] M G Teneriello P C Tseng M Crozier et al ldquoPhase IIevaluation of nanoparticle albumin-bound paclitaxel in plati-num-sensitive patients with recurrent ovarian peritoneal orfallopian tube cancerrdquo Journal of Clinical Oncology vol 27 no9 pp 1426ndash1431 2009
[150] R L Coleman W E Brady D S McMeekin et al ldquoA phase IIevaluation of nanoparticle albumin-bound (nab) paclitaxel inthe treatment of recurrent or persistent platinum-resistant ovar-ian fallopian tube or primary peritoneal cancer a GynecologicOncology Group Studyrdquo Gynecologic Oncology vol 122 no 1pp 111ndash115 2011
[151] J W Singer ldquoPaclitaxel poliglumex (XYOTAX CT-2103) amacromolecular taxanerdquo Journal of Controlled Release vol 109no 1ndash3 pp 120ndash126 2005
[152] C Li D-F Yu R A Newman et al ldquoComplete regressionof well-established tumors using a novel water-soluble poly(L-glutamic acid)-paclitaxel conjugaterdquo Cancer Research vol 58no 11 pp 2404ndash2409 1998
[153] M Mita A Mita J Sarantopoulos et al ldquoPhase I study ofpaclitaxel poliglumex administered weekly for patients withadvanced solid malignanciesrdquo Cancer Chemotherapy and Phar-macology vol 64 no 2 pp 287ndash295 2009
[154] P Sabbatini M W Sill D OrsquoMalley L Adler and A ASecord ldquoA phase II trial of paclitaxel poliglumex in recurrentor persistent ovarian or primary peritoneal cancer (EOC) agynecologic oncology group studyrdquo Gynecologic Oncology vol111 no 3 pp 455ndash460 2008
[155] M O Bradley C S Swindell F H Anthony et al ldquoTumortargeting by conjugation of DHA to paclitaxelrdquo Journal ofControlled Release vol 74 no 1ndash3 pp 233ndash236 2001
[156] M O Bradley N L Webb F H Anthony et al ldquoTumortargeting by covalent conjugation of a natural fatty acid topaclitaxelrdquo Clinical Cancer Research vol 7 no 10 pp 3229ndash3238 2001
[157] A C Wolff R C Donehower M K Carducci et al ldquoPhaseI study of docosahexaenoic acid-paclitaxel a taxane-fatty acid
conjugate with a unique pharmacology and toxicity profilerdquoClinical Cancer Research vol 9 no 10 part 1 pp 3589ndash35972003
[158] A Sparreboom A C Wolff J Verweij et al ldquoDispositionof docosahexaenoic acid-paclitaxel a novel taxane in bloodin vitro and clinical pharmacokinetic studiesrdquo Clinical CancerResearch vol 9 no 1 pp 151ndash159 2003
[159] P M Fracasso J Picus J D Wildi et al ldquoPhase 1 and phar-macokinetic study of weekly docosahexaenoic acid-paclitaxelTaxoprexin in resistant solid tumor malignanciesrdquo CancerChemotherapy and Pharmacology vol 63 no 3 pp 451ndash4582009
[160] A Y Bedikian R C DeConti R Conry et al ldquoPhase 3 study ofdocosahexaenoic acid-paclitaxel versus dacarbazine in patientswith metastatic malignant melanomardquo Annals of Oncology vol22 no 4 pp 787ndash793 2011
[161] Y-N Wu S-L Wang Y-C Wang et al ldquoReversal effect ofdocosahexaenoic acid on taxol resistance in human ovarian car-cinoma A2780T cellsrdquo Obstetrics amp Gynecology InternationalJournal vol 1 no 3 Article ID 00018 2014
Submit your manuscripts athttpwwwhindawicom
PainResearch and TreatmentHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom
Volume 2014
ToxinsJournal of
VaccinesJournal of
Hindawi Publishing Corporation httpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
AntibioticsInternational Journal of
ToxicologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
StrokeResearch and TreatmentHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Drug DeliveryJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Advances in Pharmacological Sciences
Tropical MedicineJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Medicinal ChemistryInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
AddictionJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
Emergency Medicine InternationalHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Autoimmune Diseases
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Anesthesiology Research and Practice
ScientificaHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Pharmaceutics
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of

BioMed Research International 19
Consortium and the Cancer GenomeAtlasrdquoGynecologic Oncol-ogy vol 131 no 1 pp 8ndash14 2013
[81] X Yang A K Iyer A Singh et al ldquoCluster of differentiation44 targeted hyaluronic acid based nanoparticles for MDR1siRNA delivery to overcome drug resistance in ovarian cancerrdquoPharmaceutical Research 2014
[82] D A Zajchowski B Y Karlan and L K Shawver ldquoTreatment-related protein biomarker expression differs between primaryand recurrent ovarian carcinomasrdquoMolecular CancerTherapeu-tics vol 11 no 2 pp 492ndash502 2012
[83] MM Gottesman J Ludwig D Xia and G Szakacs ldquoDefeatingdrug resistance in cancerrdquoDiscovery Medicine vol 6 no 31 pp18ndash23 2006
[84] S Mozzetti C Ferlini P Concolino et al ldquoClass III 120573-tubulin overexpression is a prominent mechanism of paclitaxelresistance in ovarian cancer patientsrdquo Clinical Cancer Researchvol 11 no 1 pp 298ndash305 2005
[85] M Kavallaris D Y S Kuo C A Burkhart et al ldquoTaxol-resistant epithelial ovarian tumors are associated with alteredexpression of specific beta-tubulin isotypesrdquo Journal of ClinicalInvestigation vol 100 no 5 pp 1282ndash1293 1997
[86] G A Orr P Verdier-Pinard H McDaid and S B HorwitzldquoMechanisms of Taxol resistance related to microtubulesrdquoOncogene vol 22 no 47 pp 7280ndash7295 2003
[87] C Ferlini L Cicchillitti G Raspaglio et al ldquoPaclitaxel directlybinds to Bcl-2 and functionally mimics activity of Nur77rdquoCancer Research vol 69 no 17 pp 6906ndash6914 2009
[88] E Mechetner A Kyshtoobayeva S Zonis et al ldquoLevels ofmultidrug resistance (MDR1) P-glycoprotein expression byhuman breast cancer correlate with in vitro resistance to taxoland doxorubicinrdquo Clinical Cancer Research vol 4 no 2 pp389ndash398 1998
[89] J S Lagas C W N Damen R A B VanWaterschoot D IusufJ H Beijnen and A H Schinkel ldquoP-glycoprotein multidrug-resistance associated protein 2 Cyp3a and carboxylesteraseaffect the oral availability and metabolism of vinorelbinerdquoMolecular Pharmacology vol 82 no 4 pp 636ndash644 2012
[90] M T Huizing J B Vermorken H Rosing et al ldquoPharmacoki-netics of paclitaxel and three major metabolites in patients withadvanced breast carcinoma refractory to anthracycline therapytreated with a 3-hour paclitaxel infusion a European CancerCentre (ECC) trialrdquo Annals of Oncology vol 6 no 7 pp 699ndash704 1995
[91] R Panchagnula ldquoPharmaceutical aspects of paclitaxelrdquo Interna-tional Journal of Pharmaceutics vol 172 no 1-2 pp 1ndash15 1998
[92] S H Jang M G Wientjes and J L-S Au ldquoDeterminants ofpaclitaxel uptake accumulation and retention in solid tumorsrdquoInvestigational New Drugs vol 19 no 2 pp 113ndash123 2001
[93] D S Sonnichsen andM V Relling ldquoClinical pharmacokineticsof paclitaxelrdquo Clinical Pharmacokinetics vol 27 no 4 pp 256ndash269 1994
[94] T Ohtsu Y Sasaki T Tamura et al ldquoClinical pharmacokineticsand pharmacodynamics of paclitaxel a 3-hour infusion versusa 24-hour infusionrdquo Clinical Cancer Research vol 1 no 6 pp599ndash606 1995
[95] M Czejka J Schueller H Schnait B Springer and I EderldquoClinical pharmacokinetics andmetabolism of paclitaxel after athree-hour infusion comparison of two preparationsrdquo Journalof Oncology Pharmacy Practice vol 9 no 4 pp 129ndash136 2003
[96] J Rizzo C Riley D VonHoff J Kuhn J Phillips and T BrownldquoAnalysis of anticancer drugs in biological fluids determination
of taxol with application to clinical pharmacokineticsrdquo Journalof Pharmaceutical and Biomedical Analysis vol 8 no 2 pp 159ndash164 1990
[97] V A de Weger J H Beijnen and J H M Schellens ldquoCel-lular and clinical pharmacology of the taxanes docetaxel andpaclitaxelmdasha reviewrdquoAnti-Cancer Drugs vol 25 no 5 pp 488ndash494 2014
[98] S Kumar H Mahdi C Bryant J P Shah G Garg andA Munkarah ldquoClinical trials and progress with paclitaxel inovarian cancerrdquo International Journal of Womenrsquos Health vol 2no 1 pp 411ndash427 2010
[99] B Huang J Zhao J C Unkeless Z H Feng and H XiongldquoTLR signaling by tumor and immune cells a double-edgedswordrdquo Oncogene vol 27 no 2 pp 218ndash224 2008
[100] R A Jibodh J S Lagas B Nuijen J H Beijnen and J HM Schellens ldquoTaxanes old drugs new oral formulationsrdquoEuropean Journal of Pharmacology vol 717 no 1ndash3 pp 40ndash462013
[101] A Javeed M Ashraf A Riaz A Ghafoor S Afzal and M MMukhtar ldquoPaclitaxel and immune systemrdquo European Journal ofPharmaceutical Sciences vol 38 no 4 pp 283ndash290 2009
[102] L Bracci G Schiavoni A Sistigu and F Belardelli ldquoImmune-based mechanisms of cytotoxic chemotherapy implications forthe design of novel and rationale-based combined treatmentsagainst cancerrdquo Cell Death and Differentiation vol 21 no 1 pp15ndash25 2014
[103] C A Byrd-Leifer E F Block K Takeda S Akira and A DingldquoThe role of MyD88 and TLR4 in the LPS-mimetic activity ofTaxolrdquo European Journal of Immunology vol 31 no 8 pp 2448ndash2457 2001
[104] A-C Wang Y-B Ma F-X Wu et al ldquoTLR4 induces tumorgrowth and inhibits paclitaxel activity in MyD88-positivehuman ovarian carcinoma in vitrordquo Oncology Letters vol 7 no3 pp 871ndash877 2014
[105] Y Zhu N Liu S D Xiong Y J Zheng and Y W ChuldquoCD4+Foxp3+ regulatory T-cell impairment by paclitaxel isindependent of toll-like receptor 4rdquo Scandinavian Journal ofImmunology vol 73 no 4 pp 301ndash308 2011
[106] M Kubo T Morisaki K Matsumoto et al ldquoPaclitaxel probablyenhances cytotoxicity of natural killer cells against breastcarcinoma cells by increasing perforin productionrdquo CancerImmunology Immunotherapy vol 54 no 5 pp 468ndash476 2005
[107] L Markasz G Stuber B Vanherberghen et al ldquoEffect of fre-quently used chemotherapeutic drugs on the cytotoxic activityof human natural killer cellsrdquo Molecular Cancer Therapeuticsvol 6 no 2 pp 644ndash654 2007
[108] T Sako N Burioka K Yasuda et al ldquoCellular immune profile inpatients with non-small cell lung cancer after weekly paclitaxeltherapyrdquo Acta Oncologica vol 43 no 1 pp 15ndash19 2004
[109] R Kaneno G V Shurin I L Tourkova and M R ShurinldquoChemomodulation of human dendritic cell function by anti-neoplastic agents in low noncytotoxic concentrationsrdquo Journalof Translational Medicine vol 7 article 58 2009
[110] TMichels G V ShurinHNaiditch A Sevko VUmansky andM R Shurin ldquoPaclitaxel promotes differentiation of myeloid-derived suppressor cells into dendritic cells in vitro in a TLR4-independent mannerrdquo Journal of Immunotoxicology vol 9 no3 pp 292ndash300 2012
[111] R A Kemp and F Ronchese ldquoTumor-specific Tc1 but not Tc2cells deliver protective antitumor immunityrdquo The Journal ofImmunology vol 167 no 11 pp 6497ndash6502 2001
20 BioMed Research International
[112] A Y Rudensky ldquoRegulatory T cells and Foxp3rdquo ImmunologicalReviews vol 241 no 1 pp 260ndash268 2011
[113] EM Shevach ldquoCD4+CD25+ suppressor T cellsmore questionsthan answersrdquo Nature Reviews Immunology vol 2 no 6 pp389ndash400 2002
[114] S Sakaguchi T Yamaguchi T Nomura and M Ono ldquoRegu-latory T cells and immune tolerancerdquo Cell vol 133 no 5 pp775ndash787 2008
[115] H Nishikawa and S Sakaguchi ldquoRegulatory T cells in tumorimmunityrdquo International Journal of Cancer vol 127 no 4 pp759ndash767 2010
[116] W Zou ldquoRegulatory T cells tumour immunity and immuno-therapyrdquoNature Reviews Immunology vol 6 no 4 pp 295ndash3072006
[117] A Fialova S Partlova L Sojka et al ldquoDynamics of T-cell infil-tration during the course of ovarian cancer The gradual shiftfrom aTh17 effector cell response to a predominant infiltrationby regulatory T-cellsrdquo International Journal of Cancer vol 132no 5 pp 1070ndash1079 2013
[118] A E Albers R L Ferris G G Kim K Chikamatsu A BDeLeo and T L Whiteside ldquoImmune responses to p53 inpatients with cancer enrichment in tetramer+ p53 peptide-specific T cells and regulatory T cells at tumor sitesrdquo CancerImmunology Immunotherapy vol 54 no 11 pp 1072ndash10812005
[119] N Liu Y Zheng Y Zhu S Xiong andYChu ldquoSelective impair-ment of CD4 + CD25 + Foxp3 + regulatory T cells by paclitaxelis explained by Bcl-2Bax mediated apoptosisrdquo InternationalImmunopharmacology vol 11 no 2 pp 212ndash219 2011
[120] X Wu Q-M Feng Y Wang J Shi H-L Ge and W DildquoThe immunologic aspects in advanced ovarian cancer patientstreated with paclitaxel and carboplatin chemotherapyrdquo CancerImmunology Immunotherapy vol 59 no 2 pp 279ndash291 2010
[121] A P Vicari R Luu N Zhang et al ldquoPaclitaxel reducesregulatoryT cell numbers and inhibitory function and enhancesthe anti-tumor effects of the TLR9 agonist PF-3512676 in themouserdquo Cancer Immunology Immunotherapy vol 58 no 4 pp615ndash628 2009
[122] L Zhang K Dermawan M Jin et al ldquoDifferential impairmentof regulatory T cells rather than effector T cells by paclitaxel-based chemotherapyrdquo Clinical Immunology vol 129 no 2 pp219ndash229 2008
[123] Y Tabuchi J Matsuoka M Gunduz et al ldquoResistance topaclitaxel therapy is related with Bcl-2 expression through anestrogen receptor mediated pathway in breast cancerrdquo Interna-tional Journal of Oncology vol 34 no 2 pp 313ndash319 2009
[124] N Obermajer R Muthuswamy K Odunsi R P Edwards andP Kalinski ldquoPGE
2-induced CXCL12 production and CXCR4
expression controls the accumulation of human MDSCs inovarian cancer environmentrdquo Cancer Research vol 71 no 24pp 7463ndash7470 2011
[125] Q M Feng W Di and X Wu ldquoImmune reconstitution inadvanced ovarian cancer patients undergoing first line chemo-therapyrdquo Xi Bao Yu Fen Zi Mian Yi Xue Za Zhi vol 25 no 11pp 1023ndash1025 2009
[126] A D Seidman D Hochhauser M Gollub et al ldquoNinety-six-hour paclitaxel infusion after progression during short taxaneexposure a phase II pharmacokinetic and pharmacodynamicstudy in metastatic breast cancerrdquo Journal of Clinical Oncologyvol 14 no 6 pp 1877ndash1884 1996
[127] D R Spriggs M F Brady L Vaccarello et al ldquoPhase IIIrandomized trial of intravenous cisplatin plus a 24- or 96-hour
infusion of paclitaxel in epithelial ovarian cancer a gynecologiconcology group studyrdquo Journal of Clinical Oncology vol 25 no28 pp 4466ndash4471 2007
[128] G A Omura M F Brady K Y Look et al ldquoPhase III trial ofpaclitaxel at two dose levels the higher dose accompanied byfilgrastim at two dose levels in platinum-pretreated epithelialovarian cancer an intergroup studyrdquo Journal of Clinical Oncol-ogy vol 21 no 15 pp 2843ndash2848 2003
[129] R Simon and L Norton ldquoThe Norton-Simon hypothesisdesigning more effective and less toxic chemotherapeutic reg-imensrdquoNature Clinical Practice Oncology vol 3 no 8 pp 406ndash407 2006
[130] A Kumar P Hoskins and A Tinker ldquoDose-dense paclitaxel inadvanced ovarian cancerrdquo Clinical Oncology vol 27 no 1 pp40ndash47 2015
[131] P Marchetti S Urien G A Cappellini G Ronzino and CFicorella ldquoWeekly administration of paclitaxel theoretical andclinical basisrdquoCritical Reviews in OncologyHematology vol 44supplement pp S3ndashS13 2002
[132] P Francis E Rowinsky J Schneider T Hakes W Hoskinsand M Markman ldquoPhase I feasibility and pharmacologic studyof weekly intraperitoneal paclitaxel A Gynecologic OncologyGroup pilot studyrdquo Journal of Clinical Oncology vol 13 no 12pp 2961ndash2967 1995
[133] H Thomas and P Rosenberg ldquoRole of weekly paclitaxel inthe treatment of advanced ovarian cancerrdquo Critical Reviews inOncologyHematology vol 44 supplement pp S43ndashS51 2002
[134] M Markman J Markman K Webster et al ldquoDuration ofresponse to second-line platinum-based chemotherapy forovarian cancer implications for patient management and clini-cal trial designrdquo Journal of Clinical Oncology vol 22 no 15 pp3120ndash3125 2004
[135] P H OrsquoDonnell M Eileen Dolan E Gamazon et al ldquoPopu-lation differences in platinum toxicity as a means to identifynovel genetic susceptibility variantsrdquo Pharmacogenetics andGenomics vol 20 no 5 pp 327ndash337 2010
[136] M J Millward M J Boyer M Lehnert et al ldquoDocetaxel andcarboplatin is an active regimen in advanced non-small-celllung cancer a phase II study in Caucasian and Asian patientsrdquoAnnals of Oncology vol 14 no 3 pp 449ndash454 2003
[137] M Markman ldquoIntraperitoneal therapy of ovarian cancerrdquoOncologist vol 1 no 1-2 pp 18ndash21 1996
[138] M Markman and J L Walker ldquoIntraperitoneal chemotherapyof ovarian cancer a review with a focus on practical aspects oftreatmentrdquo Journal of Clinical Oncology vol 24 no 6 pp 988ndash994 2006
[139] K Fujiwara S Nagao E Aotani and K Hasegawa ldquoPrincipleand evolving role of intraperitoneal chemotherapy in ovariancancerrdquo Expert Opinion on Pharmacotherapy vol 14 no 13 pp1797ndash1806 2013
[140] M Markman E Rowinsky T Hakes et al ldquoPhase I trialof intraperitoneal taxol a gynecoloic oncology group studyrdquoJournal of Clinical Oncology vol 10 no 9 pp 1485ndash1491 1992
[141] M Markman M F Brady N M Spirtos P Hanjani and S CRubin ldquoPhase II trial of intraperitoneal paclitaxel in carcinomaof the ovary tube and peritoneum a gynecologic oncologygroup studyrdquo Journal of Clinical Oncology vol 16 no 8 pp2620ndash2624 1998
[142] P B Panici I Palaia M Graziano F Bellati N Manci and RAngioli ldquoIntraperitoneal paclitaxel as consolidation treatmentin ovarian cancer patients a case control studyrdquo Oncology vol78 no 1 pp 20ndash25 2010
BioMed Research International 21
[143] D K Armstrong B Bundy L Wenzel et al ldquoIntraperitonealcisplatin and paclitaxel in ovarian cancerrdquo The New EnglandJournal of Medicine vol 354 no 1 pp 34ndash43 2006
[144] D Tewari J Java and R Salani ldquoLong-term survival advantageof intraperitoneal chemotherapy treatment in advanced ovariancancer an analysis of a Gynecologic Oncology Group ancillarydata studyrdquo in Proceedings of the 2013 Society of GynecologicOncology Annual Meeting on Womenrsquos Cancer (GOG114172Abstract) Los Angeles Calif USA 2013
[145] D A Yardley ldquonab-paclitaxel mechanisms of action and deliv-eryrdquo Journal of Controlled Release vol 170 no 3 pp 365ndash3722013
[146] M Ando K Yonemori N Katsumata et al ldquoPhase I and phar-macokinetic study of nab-paclitaxel nanoparticle albumin-bound paclitaxel administeredweekly to Japanese patients withsolid tumors and metastatic breast cancerrdquo Cancer Chemother-apy and Pharmacology vol 69 no 2 pp 457ndash465 2012
[147] N Desai V Trieu Z Yao et al ldquoIncreased antitumor activityintratumor paclitaxel concentrations and endothelial cell trans-port of cremophor-free albumin-bound paclitaxel ABI-007compared with cremophor-based paclitaxelrdquo Clinical CancerResearch vol 12 no 4 pp 1317ndash1324 2006
[148] J A Yared and K H R Tkaczuk ldquoUpdate on taxane devel-opment new analogs and new formulationsrdquo Drug DesignDevelopment andTherapy vol 6 pp 371ndash384 2012
[149] M G Teneriello P C Tseng M Crozier et al ldquoPhase IIevaluation of nanoparticle albumin-bound paclitaxel in plati-num-sensitive patients with recurrent ovarian peritoneal orfallopian tube cancerrdquo Journal of Clinical Oncology vol 27 no9 pp 1426ndash1431 2009
[150] R L Coleman W E Brady D S McMeekin et al ldquoA phase IIevaluation of nanoparticle albumin-bound (nab) paclitaxel inthe treatment of recurrent or persistent platinum-resistant ovar-ian fallopian tube or primary peritoneal cancer a GynecologicOncology Group Studyrdquo Gynecologic Oncology vol 122 no 1pp 111ndash115 2011
[151] J W Singer ldquoPaclitaxel poliglumex (XYOTAX CT-2103) amacromolecular taxanerdquo Journal of Controlled Release vol 109no 1ndash3 pp 120ndash126 2005
[152] C Li D-F Yu R A Newman et al ldquoComplete regressionof well-established tumors using a novel water-soluble poly(L-glutamic acid)-paclitaxel conjugaterdquo Cancer Research vol 58no 11 pp 2404ndash2409 1998
[153] M Mita A Mita J Sarantopoulos et al ldquoPhase I study ofpaclitaxel poliglumex administered weekly for patients withadvanced solid malignanciesrdquo Cancer Chemotherapy and Phar-macology vol 64 no 2 pp 287ndash295 2009
[154] P Sabbatini M W Sill D OrsquoMalley L Adler and A ASecord ldquoA phase II trial of paclitaxel poliglumex in recurrentor persistent ovarian or primary peritoneal cancer (EOC) agynecologic oncology group studyrdquo Gynecologic Oncology vol111 no 3 pp 455ndash460 2008
[155] M O Bradley C S Swindell F H Anthony et al ldquoTumortargeting by conjugation of DHA to paclitaxelrdquo Journal ofControlled Release vol 74 no 1ndash3 pp 233ndash236 2001
[156] M O Bradley N L Webb F H Anthony et al ldquoTumortargeting by covalent conjugation of a natural fatty acid topaclitaxelrdquo Clinical Cancer Research vol 7 no 10 pp 3229ndash3238 2001
[157] A C Wolff R C Donehower M K Carducci et al ldquoPhaseI study of docosahexaenoic acid-paclitaxel a taxane-fatty acid
conjugate with a unique pharmacology and toxicity profilerdquoClinical Cancer Research vol 9 no 10 part 1 pp 3589ndash35972003
[158] A Sparreboom A C Wolff J Verweij et al ldquoDispositionof docosahexaenoic acid-paclitaxel a novel taxane in bloodin vitro and clinical pharmacokinetic studiesrdquo Clinical CancerResearch vol 9 no 1 pp 151ndash159 2003
[159] P M Fracasso J Picus J D Wildi et al ldquoPhase 1 and phar-macokinetic study of weekly docosahexaenoic acid-paclitaxelTaxoprexin in resistant solid tumor malignanciesrdquo CancerChemotherapy and Pharmacology vol 63 no 3 pp 451ndash4582009
[160] A Y Bedikian R C DeConti R Conry et al ldquoPhase 3 study ofdocosahexaenoic acid-paclitaxel versus dacarbazine in patientswith metastatic malignant melanomardquo Annals of Oncology vol22 no 4 pp 787ndash793 2011
[161] Y-N Wu S-L Wang Y-C Wang et al ldquoReversal effect ofdocosahexaenoic acid on taxol resistance in human ovarian car-cinoma A2780T cellsrdquo Obstetrics amp Gynecology InternationalJournal vol 1 no 3 Article ID 00018 2014
Submit your manuscripts athttpwwwhindawicom
PainResearch and TreatmentHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom
Volume 2014
ToxinsJournal of
VaccinesJournal of
Hindawi Publishing Corporation httpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
AntibioticsInternational Journal of
ToxicologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
StrokeResearch and TreatmentHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Drug DeliveryJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Advances in Pharmacological Sciences
Tropical MedicineJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Medicinal ChemistryInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
AddictionJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
Emergency Medicine InternationalHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Autoimmune Diseases
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Anesthesiology Research and Practice
ScientificaHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Pharmaceutics
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of

20 BioMed Research International
[112] A Y Rudensky ldquoRegulatory T cells and Foxp3rdquo ImmunologicalReviews vol 241 no 1 pp 260ndash268 2011
[113] EM Shevach ldquoCD4+CD25+ suppressor T cellsmore questionsthan answersrdquo Nature Reviews Immunology vol 2 no 6 pp389ndash400 2002
[114] S Sakaguchi T Yamaguchi T Nomura and M Ono ldquoRegu-latory T cells and immune tolerancerdquo Cell vol 133 no 5 pp775ndash787 2008
[115] H Nishikawa and S Sakaguchi ldquoRegulatory T cells in tumorimmunityrdquo International Journal of Cancer vol 127 no 4 pp759ndash767 2010
[116] W Zou ldquoRegulatory T cells tumour immunity and immuno-therapyrdquoNature Reviews Immunology vol 6 no 4 pp 295ndash3072006
[117] A Fialova S Partlova L Sojka et al ldquoDynamics of T-cell infil-tration during the course of ovarian cancer The gradual shiftfrom aTh17 effector cell response to a predominant infiltrationby regulatory T-cellsrdquo International Journal of Cancer vol 132no 5 pp 1070ndash1079 2013
[118] A E Albers R L Ferris G G Kim K Chikamatsu A BDeLeo and T L Whiteside ldquoImmune responses to p53 inpatients with cancer enrichment in tetramer+ p53 peptide-specific T cells and regulatory T cells at tumor sitesrdquo CancerImmunology Immunotherapy vol 54 no 11 pp 1072ndash10812005
[119] N Liu Y Zheng Y Zhu S Xiong andYChu ldquoSelective impair-ment of CD4 + CD25 + Foxp3 + regulatory T cells by paclitaxelis explained by Bcl-2Bax mediated apoptosisrdquo InternationalImmunopharmacology vol 11 no 2 pp 212ndash219 2011
[120] X Wu Q-M Feng Y Wang J Shi H-L Ge and W DildquoThe immunologic aspects in advanced ovarian cancer patientstreated with paclitaxel and carboplatin chemotherapyrdquo CancerImmunology Immunotherapy vol 59 no 2 pp 279ndash291 2010
[121] A P Vicari R Luu N Zhang et al ldquoPaclitaxel reducesregulatoryT cell numbers and inhibitory function and enhancesthe anti-tumor effects of the TLR9 agonist PF-3512676 in themouserdquo Cancer Immunology Immunotherapy vol 58 no 4 pp615ndash628 2009
[122] L Zhang K Dermawan M Jin et al ldquoDifferential impairmentof regulatory T cells rather than effector T cells by paclitaxel-based chemotherapyrdquo Clinical Immunology vol 129 no 2 pp219ndash229 2008
[123] Y Tabuchi J Matsuoka M Gunduz et al ldquoResistance topaclitaxel therapy is related with Bcl-2 expression through anestrogen receptor mediated pathway in breast cancerrdquo Interna-tional Journal of Oncology vol 34 no 2 pp 313ndash319 2009
[124] N Obermajer R Muthuswamy K Odunsi R P Edwards andP Kalinski ldquoPGE
2-induced CXCL12 production and CXCR4
expression controls the accumulation of human MDSCs inovarian cancer environmentrdquo Cancer Research vol 71 no 24pp 7463ndash7470 2011
[125] Q M Feng W Di and X Wu ldquoImmune reconstitution inadvanced ovarian cancer patients undergoing first line chemo-therapyrdquo Xi Bao Yu Fen Zi Mian Yi Xue Za Zhi vol 25 no 11pp 1023ndash1025 2009
[126] A D Seidman D Hochhauser M Gollub et al ldquoNinety-six-hour paclitaxel infusion after progression during short taxaneexposure a phase II pharmacokinetic and pharmacodynamicstudy in metastatic breast cancerrdquo Journal of Clinical Oncologyvol 14 no 6 pp 1877ndash1884 1996
[127] D R Spriggs M F Brady L Vaccarello et al ldquoPhase IIIrandomized trial of intravenous cisplatin plus a 24- or 96-hour
infusion of paclitaxel in epithelial ovarian cancer a gynecologiconcology group studyrdquo Journal of Clinical Oncology vol 25 no28 pp 4466ndash4471 2007
[128] G A Omura M F Brady K Y Look et al ldquoPhase III trial ofpaclitaxel at two dose levels the higher dose accompanied byfilgrastim at two dose levels in platinum-pretreated epithelialovarian cancer an intergroup studyrdquo Journal of Clinical Oncol-ogy vol 21 no 15 pp 2843ndash2848 2003
[129] R Simon and L Norton ldquoThe Norton-Simon hypothesisdesigning more effective and less toxic chemotherapeutic reg-imensrdquoNature Clinical Practice Oncology vol 3 no 8 pp 406ndash407 2006
[130] A Kumar P Hoskins and A Tinker ldquoDose-dense paclitaxel inadvanced ovarian cancerrdquo Clinical Oncology vol 27 no 1 pp40ndash47 2015
[131] P Marchetti S Urien G A Cappellini G Ronzino and CFicorella ldquoWeekly administration of paclitaxel theoretical andclinical basisrdquoCritical Reviews in OncologyHematology vol 44supplement pp S3ndashS13 2002
[132] P Francis E Rowinsky J Schneider T Hakes W Hoskinsand M Markman ldquoPhase I feasibility and pharmacologic studyof weekly intraperitoneal paclitaxel A Gynecologic OncologyGroup pilot studyrdquo Journal of Clinical Oncology vol 13 no 12pp 2961ndash2967 1995
[133] H Thomas and P Rosenberg ldquoRole of weekly paclitaxel inthe treatment of advanced ovarian cancerrdquo Critical Reviews inOncologyHematology vol 44 supplement pp S43ndashS51 2002
[134] M Markman J Markman K Webster et al ldquoDuration ofresponse to second-line platinum-based chemotherapy forovarian cancer implications for patient management and clini-cal trial designrdquo Journal of Clinical Oncology vol 22 no 15 pp3120ndash3125 2004
[135] P H OrsquoDonnell M Eileen Dolan E Gamazon et al ldquoPopu-lation differences in platinum toxicity as a means to identifynovel genetic susceptibility variantsrdquo Pharmacogenetics andGenomics vol 20 no 5 pp 327ndash337 2010
[136] M J Millward M J Boyer M Lehnert et al ldquoDocetaxel andcarboplatin is an active regimen in advanced non-small-celllung cancer a phase II study in Caucasian and Asian patientsrdquoAnnals of Oncology vol 14 no 3 pp 449ndash454 2003
[137] M Markman ldquoIntraperitoneal therapy of ovarian cancerrdquoOncologist vol 1 no 1-2 pp 18ndash21 1996
[138] M Markman and J L Walker ldquoIntraperitoneal chemotherapyof ovarian cancer a review with a focus on practical aspects oftreatmentrdquo Journal of Clinical Oncology vol 24 no 6 pp 988ndash994 2006
[139] K Fujiwara S Nagao E Aotani and K Hasegawa ldquoPrincipleand evolving role of intraperitoneal chemotherapy in ovariancancerrdquo Expert Opinion on Pharmacotherapy vol 14 no 13 pp1797ndash1806 2013
[140] M Markman E Rowinsky T Hakes et al ldquoPhase I trialof intraperitoneal taxol a gynecoloic oncology group studyrdquoJournal of Clinical Oncology vol 10 no 9 pp 1485ndash1491 1992
[141] M Markman M F Brady N M Spirtos P Hanjani and S CRubin ldquoPhase II trial of intraperitoneal paclitaxel in carcinomaof the ovary tube and peritoneum a gynecologic oncologygroup studyrdquo Journal of Clinical Oncology vol 16 no 8 pp2620ndash2624 1998
[142] P B Panici I Palaia M Graziano F Bellati N Manci and RAngioli ldquoIntraperitoneal paclitaxel as consolidation treatmentin ovarian cancer patients a case control studyrdquo Oncology vol78 no 1 pp 20ndash25 2010
BioMed Research International 21
[143] D K Armstrong B Bundy L Wenzel et al ldquoIntraperitonealcisplatin and paclitaxel in ovarian cancerrdquo The New EnglandJournal of Medicine vol 354 no 1 pp 34ndash43 2006
[144] D Tewari J Java and R Salani ldquoLong-term survival advantageof intraperitoneal chemotherapy treatment in advanced ovariancancer an analysis of a Gynecologic Oncology Group ancillarydata studyrdquo in Proceedings of the 2013 Society of GynecologicOncology Annual Meeting on Womenrsquos Cancer (GOG114172Abstract) Los Angeles Calif USA 2013
[145] D A Yardley ldquonab-paclitaxel mechanisms of action and deliv-eryrdquo Journal of Controlled Release vol 170 no 3 pp 365ndash3722013
[146] M Ando K Yonemori N Katsumata et al ldquoPhase I and phar-macokinetic study of nab-paclitaxel nanoparticle albumin-bound paclitaxel administeredweekly to Japanese patients withsolid tumors and metastatic breast cancerrdquo Cancer Chemother-apy and Pharmacology vol 69 no 2 pp 457ndash465 2012
[147] N Desai V Trieu Z Yao et al ldquoIncreased antitumor activityintratumor paclitaxel concentrations and endothelial cell trans-port of cremophor-free albumin-bound paclitaxel ABI-007compared with cremophor-based paclitaxelrdquo Clinical CancerResearch vol 12 no 4 pp 1317ndash1324 2006
[148] J A Yared and K H R Tkaczuk ldquoUpdate on taxane devel-opment new analogs and new formulationsrdquo Drug DesignDevelopment andTherapy vol 6 pp 371ndash384 2012
[149] M G Teneriello P C Tseng M Crozier et al ldquoPhase IIevaluation of nanoparticle albumin-bound paclitaxel in plati-num-sensitive patients with recurrent ovarian peritoneal orfallopian tube cancerrdquo Journal of Clinical Oncology vol 27 no9 pp 1426ndash1431 2009
[150] R L Coleman W E Brady D S McMeekin et al ldquoA phase IIevaluation of nanoparticle albumin-bound (nab) paclitaxel inthe treatment of recurrent or persistent platinum-resistant ovar-ian fallopian tube or primary peritoneal cancer a GynecologicOncology Group Studyrdquo Gynecologic Oncology vol 122 no 1pp 111ndash115 2011
[151] J W Singer ldquoPaclitaxel poliglumex (XYOTAX CT-2103) amacromolecular taxanerdquo Journal of Controlled Release vol 109no 1ndash3 pp 120ndash126 2005
[152] C Li D-F Yu R A Newman et al ldquoComplete regressionof well-established tumors using a novel water-soluble poly(L-glutamic acid)-paclitaxel conjugaterdquo Cancer Research vol 58no 11 pp 2404ndash2409 1998
[153] M Mita A Mita J Sarantopoulos et al ldquoPhase I study ofpaclitaxel poliglumex administered weekly for patients withadvanced solid malignanciesrdquo Cancer Chemotherapy and Phar-macology vol 64 no 2 pp 287ndash295 2009
[154] P Sabbatini M W Sill D OrsquoMalley L Adler and A ASecord ldquoA phase II trial of paclitaxel poliglumex in recurrentor persistent ovarian or primary peritoneal cancer (EOC) agynecologic oncology group studyrdquo Gynecologic Oncology vol111 no 3 pp 455ndash460 2008
[155] M O Bradley C S Swindell F H Anthony et al ldquoTumortargeting by conjugation of DHA to paclitaxelrdquo Journal ofControlled Release vol 74 no 1ndash3 pp 233ndash236 2001
[156] M O Bradley N L Webb F H Anthony et al ldquoTumortargeting by covalent conjugation of a natural fatty acid topaclitaxelrdquo Clinical Cancer Research vol 7 no 10 pp 3229ndash3238 2001
[157] A C Wolff R C Donehower M K Carducci et al ldquoPhaseI study of docosahexaenoic acid-paclitaxel a taxane-fatty acid
conjugate with a unique pharmacology and toxicity profilerdquoClinical Cancer Research vol 9 no 10 part 1 pp 3589ndash35972003
[158] A Sparreboom A C Wolff J Verweij et al ldquoDispositionof docosahexaenoic acid-paclitaxel a novel taxane in bloodin vitro and clinical pharmacokinetic studiesrdquo Clinical CancerResearch vol 9 no 1 pp 151ndash159 2003
[159] P M Fracasso J Picus J D Wildi et al ldquoPhase 1 and phar-macokinetic study of weekly docosahexaenoic acid-paclitaxelTaxoprexin in resistant solid tumor malignanciesrdquo CancerChemotherapy and Pharmacology vol 63 no 3 pp 451ndash4582009
[160] A Y Bedikian R C DeConti R Conry et al ldquoPhase 3 study ofdocosahexaenoic acid-paclitaxel versus dacarbazine in patientswith metastatic malignant melanomardquo Annals of Oncology vol22 no 4 pp 787ndash793 2011
[161] Y-N Wu S-L Wang Y-C Wang et al ldquoReversal effect ofdocosahexaenoic acid on taxol resistance in human ovarian car-cinoma A2780T cellsrdquo Obstetrics amp Gynecology InternationalJournal vol 1 no 3 Article ID 00018 2014
Submit your manuscripts athttpwwwhindawicom
PainResearch and TreatmentHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom
Volume 2014
ToxinsJournal of
VaccinesJournal of
Hindawi Publishing Corporation httpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
AntibioticsInternational Journal of
ToxicologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
StrokeResearch and TreatmentHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Drug DeliveryJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Advances in Pharmacological Sciences
Tropical MedicineJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Medicinal ChemistryInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
AddictionJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
Emergency Medicine InternationalHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Autoimmune Diseases
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Anesthesiology Research and Practice
ScientificaHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Pharmaceutics
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of

BioMed Research International 21
[143] D K Armstrong B Bundy L Wenzel et al ldquoIntraperitonealcisplatin and paclitaxel in ovarian cancerrdquo The New EnglandJournal of Medicine vol 354 no 1 pp 34ndash43 2006
[144] D Tewari J Java and R Salani ldquoLong-term survival advantageof intraperitoneal chemotherapy treatment in advanced ovariancancer an analysis of a Gynecologic Oncology Group ancillarydata studyrdquo in Proceedings of the 2013 Society of GynecologicOncology Annual Meeting on Womenrsquos Cancer (GOG114172Abstract) Los Angeles Calif USA 2013
[145] D A Yardley ldquonab-paclitaxel mechanisms of action and deliv-eryrdquo Journal of Controlled Release vol 170 no 3 pp 365ndash3722013
[146] M Ando K Yonemori N Katsumata et al ldquoPhase I and phar-macokinetic study of nab-paclitaxel nanoparticle albumin-bound paclitaxel administeredweekly to Japanese patients withsolid tumors and metastatic breast cancerrdquo Cancer Chemother-apy and Pharmacology vol 69 no 2 pp 457ndash465 2012
[147] N Desai V Trieu Z Yao et al ldquoIncreased antitumor activityintratumor paclitaxel concentrations and endothelial cell trans-port of cremophor-free albumin-bound paclitaxel ABI-007compared with cremophor-based paclitaxelrdquo Clinical CancerResearch vol 12 no 4 pp 1317ndash1324 2006
[148] J A Yared and K H R Tkaczuk ldquoUpdate on taxane devel-opment new analogs and new formulationsrdquo Drug DesignDevelopment andTherapy vol 6 pp 371ndash384 2012
[149] M G Teneriello P C Tseng M Crozier et al ldquoPhase IIevaluation of nanoparticle albumin-bound paclitaxel in plati-num-sensitive patients with recurrent ovarian peritoneal orfallopian tube cancerrdquo Journal of Clinical Oncology vol 27 no9 pp 1426ndash1431 2009
[150] R L Coleman W E Brady D S McMeekin et al ldquoA phase IIevaluation of nanoparticle albumin-bound (nab) paclitaxel inthe treatment of recurrent or persistent platinum-resistant ovar-ian fallopian tube or primary peritoneal cancer a GynecologicOncology Group Studyrdquo Gynecologic Oncology vol 122 no 1pp 111ndash115 2011
[151] J W Singer ldquoPaclitaxel poliglumex (XYOTAX CT-2103) amacromolecular taxanerdquo Journal of Controlled Release vol 109no 1ndash3 pp 120ndash126 2005
[152] C Li D-F Yu R A Newman et al ldquoComplete regressionof well-established tumors using a novel water-soluble poly(L-glutamic acid)-paclitaxel conjugaterdquo Cancer Research vol 58no 11 pp 2404ndash2409 1998
[153] M Mita A Mita J Sarantopoulos et al ldquoPhase I study ofpaclitaxel poliglumex administered weekly for patients withadvanced solid malignanciesrdquo Cancer Chemotherapy and Phar-macology vol 64 no 2 pp 287ndash295 2009
[154] P Sabbatini M W Sill D OrsquoMalley L Adler and A ASecord ldquoA phase II trial of paclitaxel poliglumex in recurrentor persistent ovarian or primary peritoneal cancer (EOC) agynecologic oncology group studyrdquo Gynecologic Oncology vol111 no 3 pp 455ndash460 2008
[155] M O Bradley C S Swindell F H Anthony et al ldquoTumortargeting by conjugation of DHA to paclitaxelrdquo Journal ofControlled Release vol 74 no 1ndash3 pp 233ndash236 2001
[156] M O Bradley N L Webb F H Anthony et al ldquoTumortargeting by covalent conjugation of a natural fatty acid topaclitaxelrdquo Clinical Cancer Research vol 7 no 10 pp 3229ndash3238 2001
[157] A C Wolff R C Donehower M K Carducci et al ldquoPhaseI study of docosahexaenoic acid-paclitaxel a taxane-fatty acid
conjugate with a unique pharmacology and toxicity profilerdquoClinical Cancer Research vol 9 no 10 part 1 pp 3589ndash35972003
[158] A Sparreboom A C Wolff J Verweij et al ldquoDispositionof docosahexaenoic acid-paclitaxel a novel taxane in bloodin vitro and clinical pharmacokinetic studiesrdquo Clinical CancerResearch vol 9 no 1 pp 151ndash159 2003
[159] P M Fracasso J Picus J D Wildi et al ldquoPhase 1 and phar-macokinetic study of weekly docosahexaenoic acid-paclitaxelTaxoprexin in resistant solid tumor malignanciesrdquo CancerChemotherapy and Pharmacology vol 63 no 3 pp 451ndash4582009
[160] A Y Bedikian R C DeConti R Conry et al ldquoPhase 3 study ofdocosahexaenoic acid-paclitaxel versus dacarbazine in patientswith metastatic malignant melanomardquo Annals of Oncology vol22 no 4 pp 787ndash793 2011
[161] Y-N Wu S-L Wang Y-C Wang et al ldquoReversal effect ofdocosahexaenoic acid on taxol resistance in human ovarian car-cinoma A2780T cellsrdquo Obstetrics amp Gynecology InternationalJournal vol 1 no 3 Article ID 00018 2014
Submit your manuscripts athttpwwwhindawicom
PainResearch and TreatmentHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom
Volume 2014
ToxinsJournal of
VaccinesJournal of
Hindawi Publishing Corporation httpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
AntibioticsInternational Journal of
ToxicologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
StrokeResearch and TreatmentHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Drug DeliveryJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Advances in Pharmacological Sciences
Tropical MedicineJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Medicinal ChemistryInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
AddictionJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
Emergency Medicine InternationalHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Autoimmune Diseases
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Anesthesiology Research and Practice
ScientificaHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Pharmaceutics
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of

Submit your manuscripts athttpwwwhindawicom
PainResearch and TreatmentHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom
Volume 2014
ToxinsJournal of
VaccinesJournal of
Hindawi Publishing Corporation httpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
AntibioticsInternational Journal of
ToxicologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
StrokeResearch and TreatmentHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Drug DeliveryJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Advances in Pharmacological Sciences
Tropical MedicineJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Medicinal ChemistryInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
AddictionJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
Emergency Medicine InternationalHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Autoimmune Diseases
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Anesthesiology Research and Practice
ScientificaHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Pharmaceutics
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of