Reversing HF: LVAD & clenbuterol LVAD with biological therapies for the reversal of HF. Myth or...
52
Reversing HF: LVAD & clenbuterol LVAD with biological therapies for the reversal of HF. Myth or reality? Sir Magdi Yacoub, FRS Imperial College London Harefield Heart Science Centre 5th STEM CELL THERAPY Madrid 2008
-
Upload
victor-stobbs -
Category
Documents
-
view
215 -
download
1
Transcript of Reversing HF: LVAD & clenbuterol LVAD with biological therapies for the reversal of HF. Myth or...
Reversing HF: LVAD & clenbuterol
LVAD with biological therapies for the reversal of HF.
Myth or reality?
Sir Magdi Yacoub, FRSImperial College London
Harefield Heart Science Centre
5th STEM CELL THERAPYMadrid 2008
Reversing HF: LVAD & clenbuterol• Chronology
– Beneficial and harmful effects of LVAD unloading
– ? optimal length of time for LVAD-induced functional recovery
– ? link between structural and functional reverse remodelling
– The role of clenbuterol
– Translational research (Harefield protocol)
– Clinical results
Reversing HF: LVAD & clenbuterol• Benefits of unloading
– Experimental (heterotopic Tx in murine models of HF)• Whole heart function• Cellular• Molecular• ECM
– Clinical• Bridge to Tx• Bridge to recovery
Reversing HF: LVAD & clenbuterol• Benefits of unloading
– Experimental (heterotopic Tx in murine models of HF)• Whole heart function
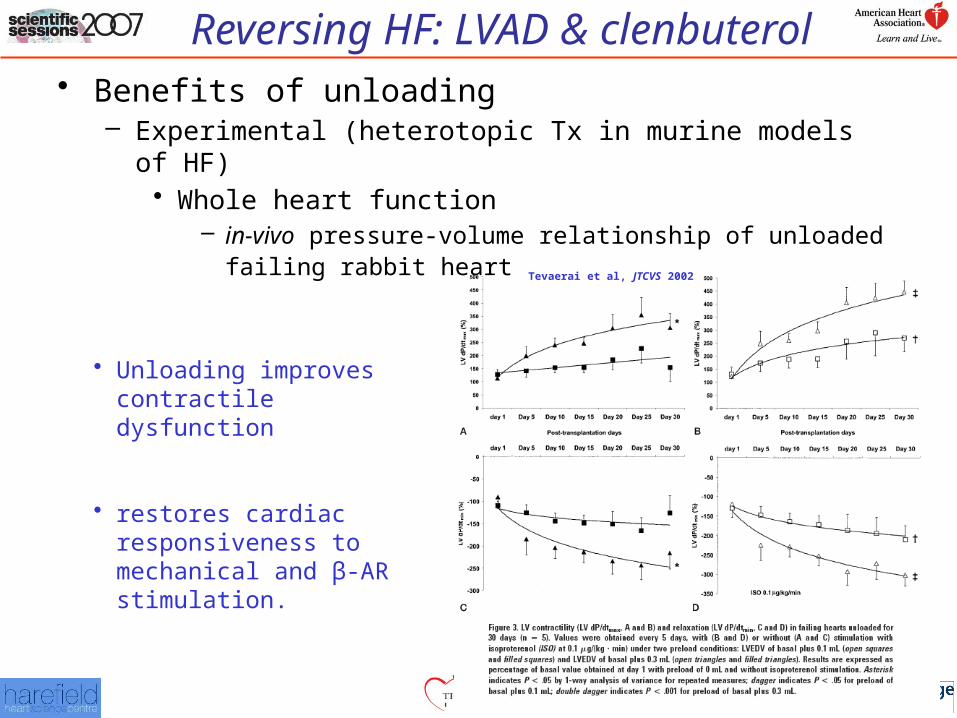
– in-vivo pressure-volume relationship of unloaded failing rabbit heart Tevaerai et al, JTCVS 2002
• Unloading improves contractile dysfunction
• restores cardiac responsiveness to mechanical and β-AR stimulation.
Reversing HF: LVAD & clenbuterol• Benefits of unloading
– Experimental (heterotopic Tx in murine models of HF)• Whole heart function
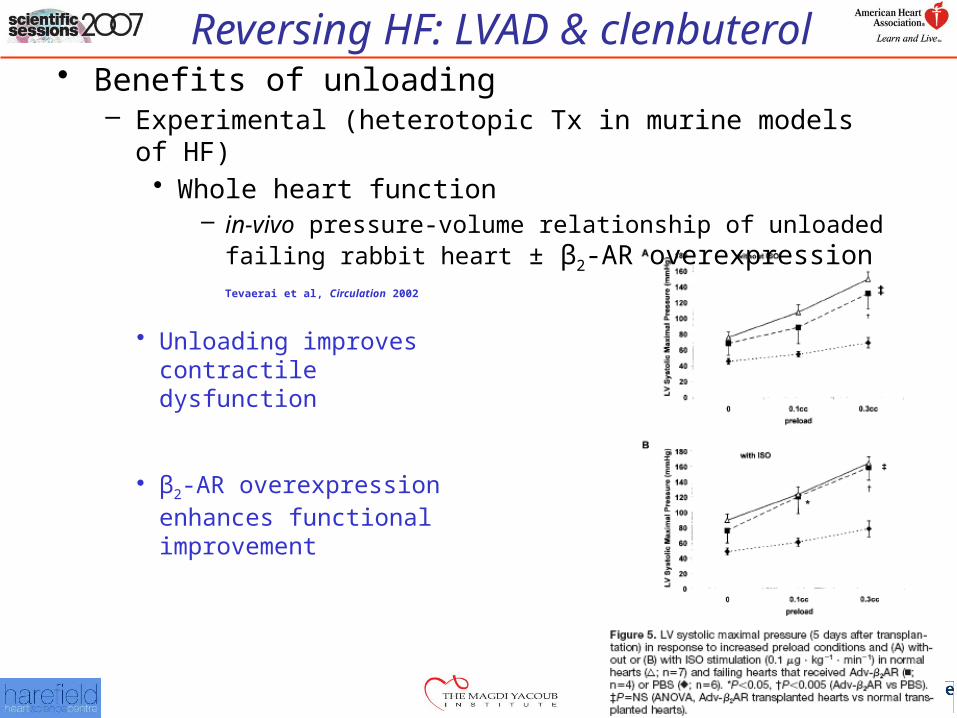
– in-vivo pressure-volume relationship of unloaded failing rabbit heart ± β2-AR overexpression Tevaerai et al, Circulation 2002
• Unloading improves contractile dysfunction
• β2-AR overexpression enhances functional improvement
Reversing HF: LVAD & clenbuterol• Benefits of unloading
– Experimental (heterotopic Tx in murine models of HF)• Whole heart function
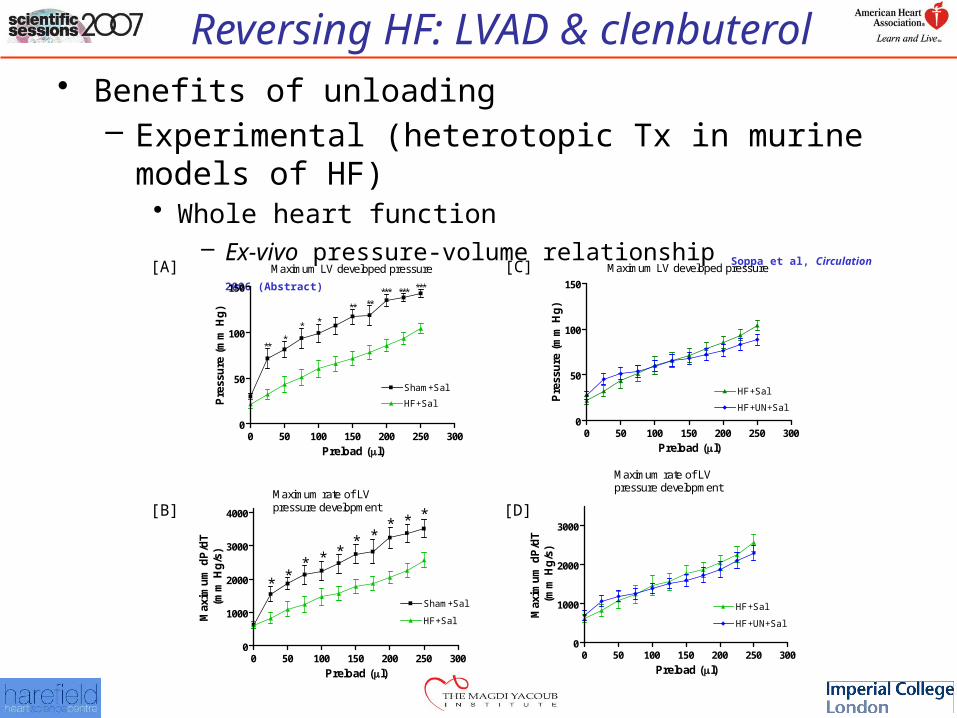
– Ex-vivo pressure-volume relationship Soppa et al, Circulation 2006 (Abstract)
Maximum LV developed pressure
0 50 100 150 200 250 3000
50
100
150
Sham+Sal
HF+Sal
*
***
**
* *
** ***** ***
Preload (l)
Pre
ssu
re (
mm
Hg
)
0 50 100 150 200 250 3000
1000
2000
3000
4000
Sham+Sal
*** *
**
HF+Sal
**
*
*Maximum rate of LVpressure development
Preload (l)
Max
imu
m d
P/d
T(m
m H
g/s
)
Maximum LV developed pressure
0 50 100 150 200 250 3000
50
100
150
HF+Sal
HF+UN+Sal
Preload (l)
Pre
ssu
re (
mm
Hg
)
0 50 100 150 200 250 3000
1000
2000
3000
HF+Sal
HF+UN+Sal
Maximum rate of LVpressure development
Preload (l)
Max
imu
m d
P/d
T(m
m H
g/s
)
[A]
[B]
[C]
[D]
Reversing HF: LVAD & clenbuterol• Benefits of unloading
– Experimental (heterotopic Tx in murine models of HF)• Whole heart function• Cellular
– Cardiomyocyte size – Contractility– Ca2+ transient kinetics
• Molecular• ECM

Reversing HF: LVAD & clenbuterol• Benefits of unloading
– Experimental (heterotopic Tx in murine models of HF)• Whole heart function• Cellular
– Cardiomyocyte size » 1 week - ↓21% in cell area Soppa et al, Circulation 2006 (Abstract)
» 2weeks – ↓23% in myocyte diameter Tsuneyoshi et al, ASAIO 2005
» 2 weeks – ↓27%, 4 weeks – ↓41%, 8 weeks – ↓56% in myocyte diameter Oriyanhan et al, JHLT 2007
– Contractility– Ca2+ transient kinetics
• Molecular• ECM
Reversing HF: LVAD & clenbuterol• Benefits of unloading
– Experimental (heterotopic Tx in murine models of HF)• Whole heart function• Cellular
– Cardiomyocyte size – Contractility
» Time-dependent improvement followed by deterioration of papillary function and contractile reserve Oriyanhan et al, JHLT 2007
» Improved myocyte contractility after 2 weeks Takaseya et al, JACC 2004
» Unchanged myocyte contractility after 1 week Soppa et al, Circulation 2006 (Abstract)
– Ca2+ transient kinetics
• Molecular• ECM
Reversing HF: LVAD & clenbuterol• Benefits of unloading
– Experimental (heterotopic Tx in murine models of HF)• Whole heart function• Cellular
– Cardiomyocyte size – Contractility– Ca2+ transient kinetics
» Normalization of deranged Ca2+ transient kinetics after 2 weeks unloading Takaseya et al, JACC 2004
» Unaffected deranged Ca2+ transient kinetics after 1 week unloading Soppa et al, Circulation 2006 (Abstract)
• Molecular• ECM
Reversing HF: LVAD & clenbuterol• Benefits of unloading
– Experimental (heterotopic Tx in murine models of HF)• Whole heart function• Cellular
– Cardiomyocyte size – Contractility– Ca2+ transient kinetics
• Molecular– Gene and protein expression
» ↑SERCA2a Tsuneyoshi et al, ASAIO 2005; Takaseya et al, JACC 2004
» normalization of ↑BNP Tsuneyoshi et al, ASAIO 2005
» ↑β2-AR Tsuneyoshi et al, ASAIO 2005
• ECM
Reversing HF: LVAD & clenbuterol• Benefits of unloading
– Experimental (heterotopic Tx in murine models of HF)• Whole heart function• Cellular• Molecular• ECM
– ↑fibrosis Oriyanhan et al, JHLT 2007
Reversing HF: LVAD & clenbuterolHarmful effects of unloading
– Experimental (heterotopic Tx in murine models of HF)• Whole heart function – unchanged at 1 week
Soppa et al, Circulation 2006 (Abstract)
• Cellular– Contractility
» Unchanged at 1 week Soppa et al, Circulation 2006 (Abstract)
» Time dependent reduction in contractile function and contractile reserve Oriyanhan et al, JHLT 2007
– Ca2+ transient kinetics» Unchanged at 1 week Soppa et al, Circulation 2006 (Abstract)
• Molecular – not known• ECM
– ↑fibrosis Oriyanhan et al, JHLT 2007
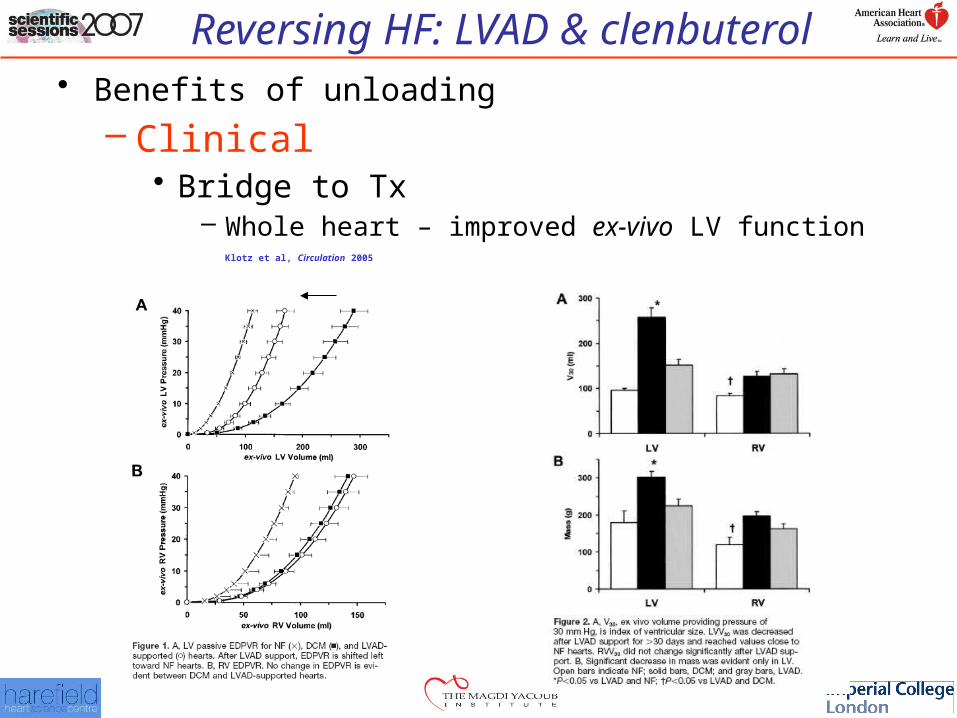
Reversing HF: LVAD & clenbuterol• Benefits of unloading
– Clinical• Bridge to Tx
– Whole heart – improved ex-vivo LV function Klotz et al, Circulation 2005
Reversing HF: LVAD & clenbuterol• Benefits of unloading
– Clinical• Bridge to Tx
– Whole heart» Improved LVEF, off-pump Frazier et al, ATS 1996; Muller et al, Circulation 1997
» Low incidence of myocardial functional recovery (4-24%) Frazier et al, ATS 1999; Mancini et al, Circulation 1998; Dandel et al, Circulation 2005
– Cellular» Reduction in cell size Zafeiridis et al, Circulation 1998; Bruckner et al, JHLT 2001
» Improved EC coupling
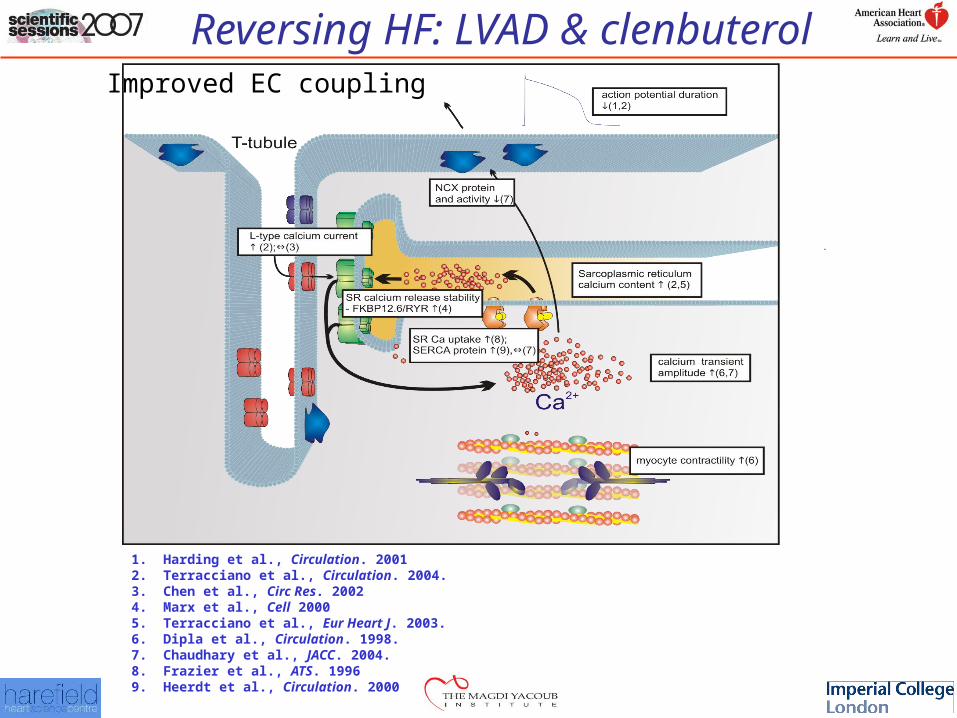
Reversing HF: LVAD & clenbuterol
1. Harding et al., Circulation. 20012. Terracciano et al., Circulation. 2004.3. Chen et al., Circ Res. 20024. Marx et al., Cell 20005. Terracciano et al., Eur Heart J. 2003.6. Dipla et al., Circulation. 1998.7. Chaudhary et al., JACC. 2004.8. Frazier et al., ATS. 19969. Heerdt et al., Circulation. 2000
Improved EC coupling
Reversing HF: LVAD & clenbuterol• Benefits of unloading
– Clinical• Bridge to Tx
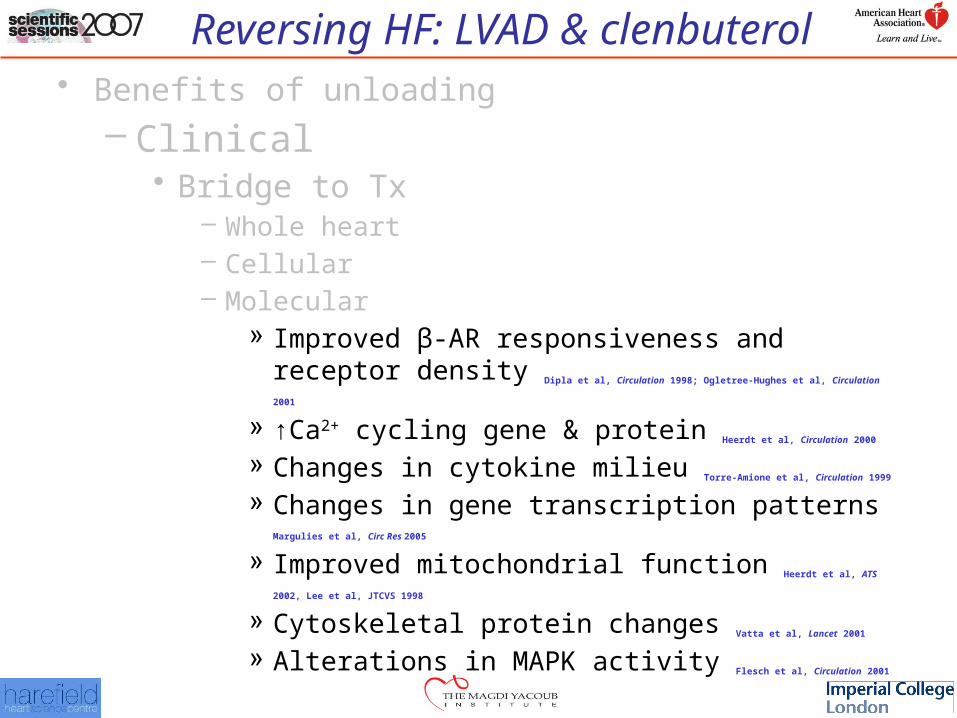
– Whole heart– Cellular– Molecular
» Improved β-AR responsiveness and receptor density Dipla et al, Circulation 1998; Ogletree-Hughes et al, Circulation 2001
» ↑Ca2+ cycling gene & protein Heerdt et al, Circulation 2000
» Changes in cytokine milieu Torre-Amione et al, Circulation 1999
» Changes in gene transcription patterns Margulies et al, Circ Res 2005
» Improved mitochondrial function Heerdt et al, ATS 2002, Lee et al, JTCVS 1998
» Cytoskeletal protein changes Vatta et al, Lancet 2001 » Alterations in MAPK activity Flesch et al, Circulation 2001
Reversing HF: LVAD & clenbuterol• Benefits of unloading
– Clinical• Bridge to Tx
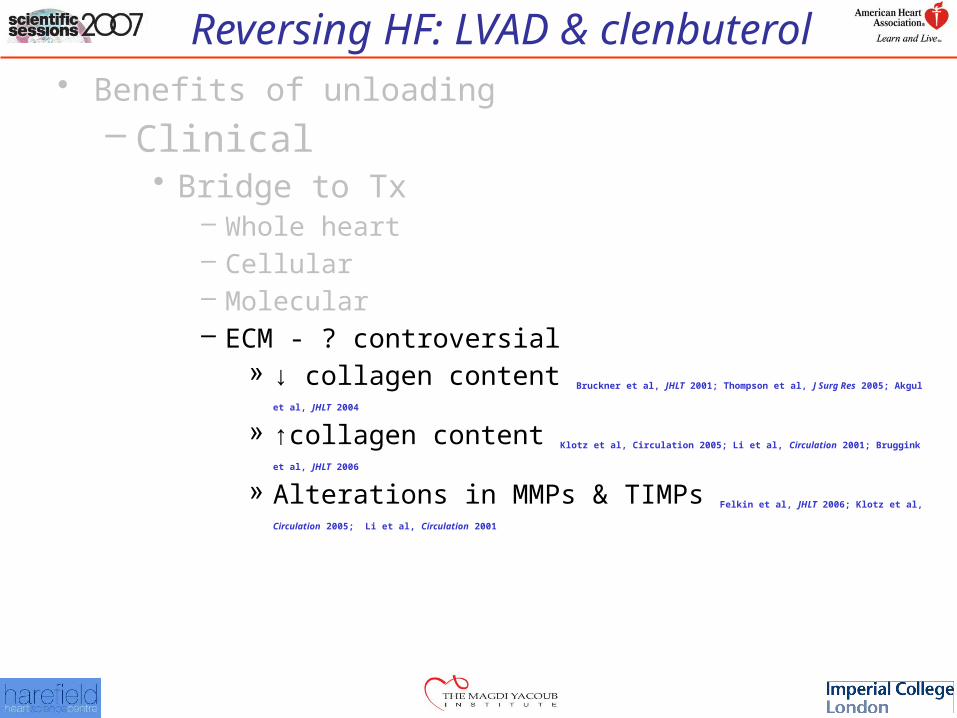
– Whole heart– Cellular– Molecular– ECM - ? controversial
» ↓ collagen content Bruckner et al, JHLT 2001; Thompson et al, J Surg Res 2005; Akgul et al, JHLT 2004
» ↑collagen content Klotz et al, Circulation 2005; Li et al, Circulation 2001; Bruggink et al, JHLT 2006
» Alterations in MMPs & TIMPs Felkin et al, JHLT 2006; Klotz et al, Circulation 2005; Li et al,
Circulation 2001
Reversing HF: LVAD & clenbuterol• Chronology
– Beneficial and harmful effects of LVAD unloading
– ? optimal length of time for LVAD-induced functional recovery
– ? link between structural and functional reverse remodelling
– The role of clenbuterol
– Translational research (Harefield protocol)
– Clinical results
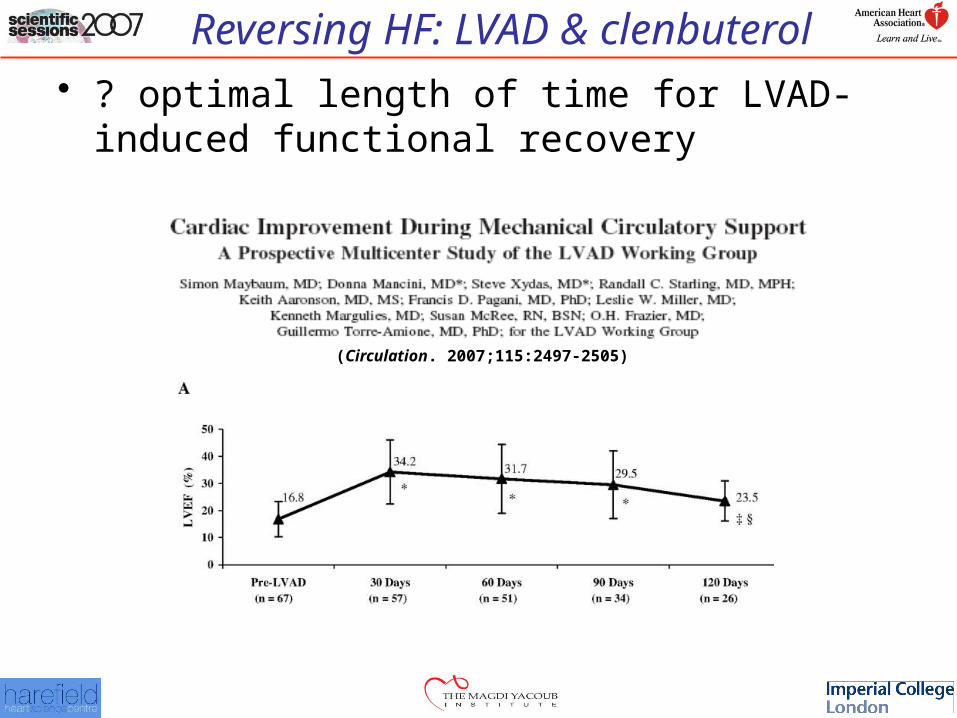
Reversing HF: LVAD & clenbuterol• ? optimal length of time for LVAD-induced
functional recovery
(Circulation. 2007;115:2497-2505)
Reversing HF: LVAD & clenbuterol
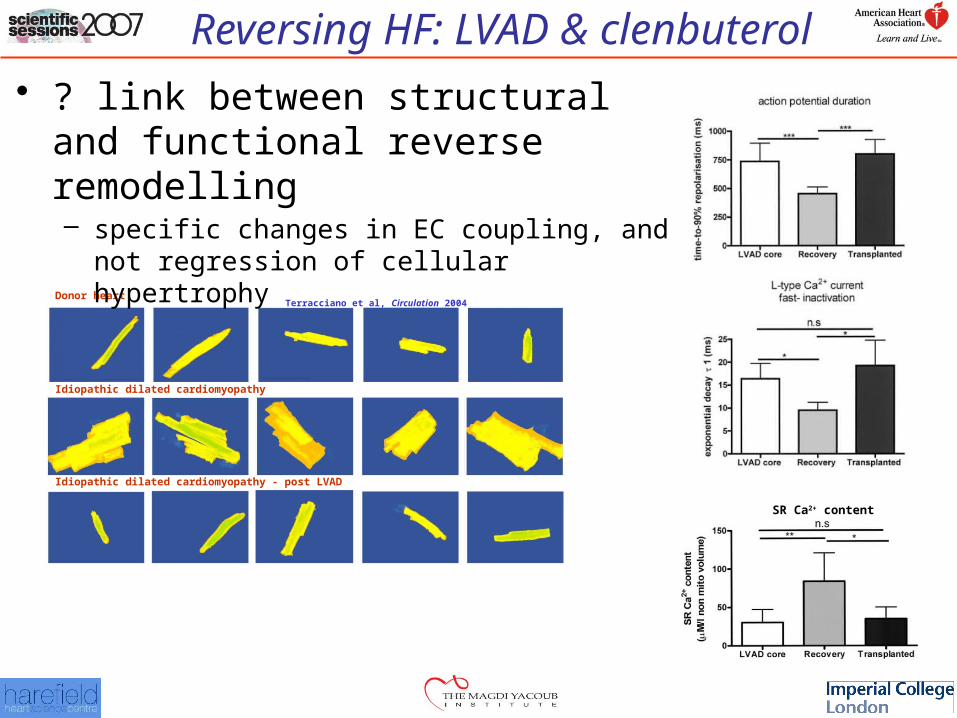
SR Ca2+ content
Donor heart
Idiopathic dilated cardiomyopathy
Idiopathic dilated cardiomyopathy - post LVAD
• ? link between structural and functional reverse remodelling– specific changes in EC coupling, and not
regression of cellular hypertrophy Terracciano et al, Circulation 2004

Reversing HF: LVAD & clenbuterol
Translational research (Harefield protocol)
“…. on its own, unloading appears to be inadequate. We therefore evolved a strategy of combination therapy, aiming at inducing maximal regression of pathological hypertrophy, followed by induction of physiological hypertrophy of both cardiac and skeletal muscle (using clenbuterol).”
Evolution of a concept
MH Yacoub
Reversing HF: LVAD & clenbuterol
Translational research (Harefield protocol)
• Pharmacological therapy– Phase 1: intended to enhance reverse remodeling
• Digoxin
• ACE inhibition – SAVE, SOLVD, HOPE (Lisinopril)
• Angiotensin II inhibition - RESOLVD (Losartan)
• Aldosterone receptor blockade - RALES (Spironolactone)
• β-blockade (Carvedilol)
Reversing HF: LVAD & clenbuterol
Translational research (Harefield protocol)
• Pharmacological therapy– Phase 2: intended to limit unloading-induced atrophy.
• β2 stimulation (Clenbuterol)
Reversing HF: LVAD & clenbuterol
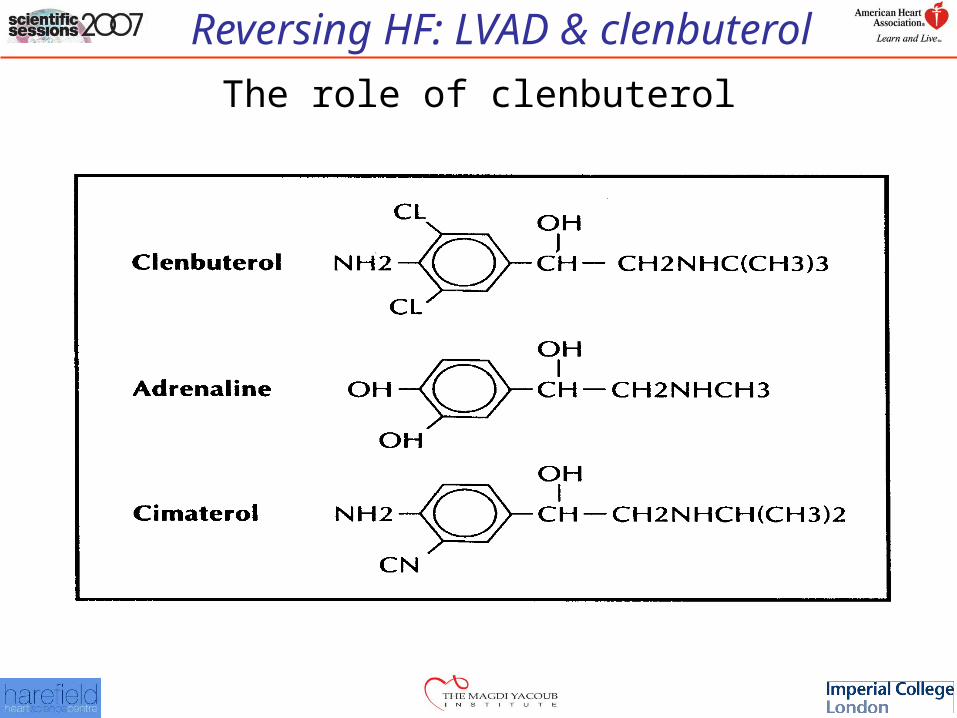
The role of clenbuterol
Reversing HF: LVAD & clenbuterol
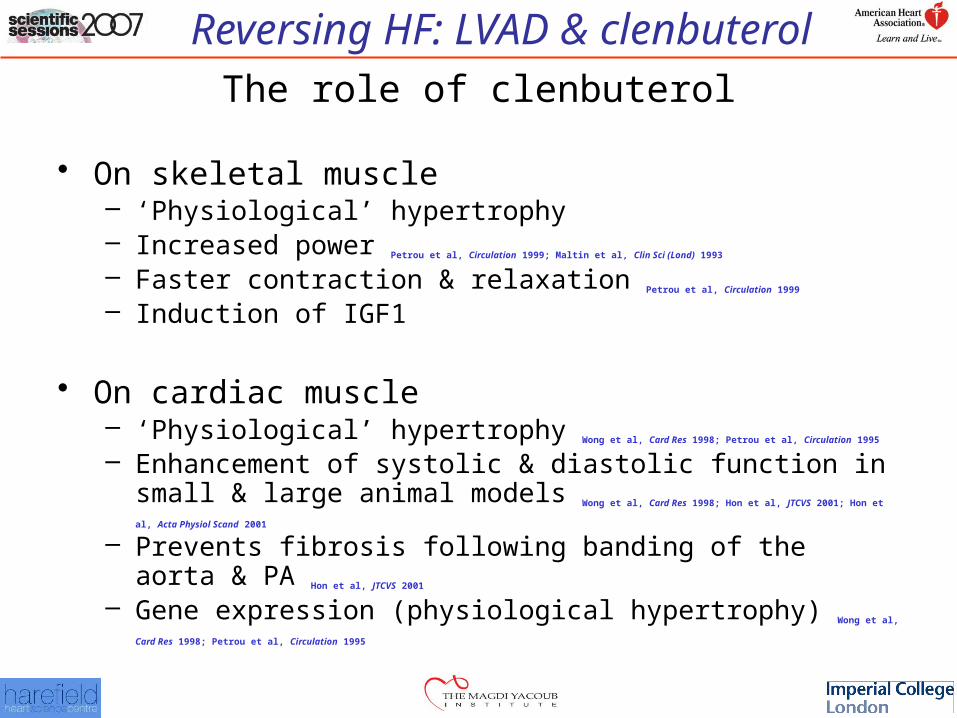
Reversing HF: LVAD & clenbuterolThe role of clenbuterol
• On skeletal muscle– ‘Physiological’ hypertrophy– Increased power Petrou et al, Circulation 1999; Maltin et al, Clin Sci (Lond) 1993
– Faster contraction & relaxation Petrou et al, Circulation 1999
– Induction of IGF1
• On cardiac muscle– ‘Physiological’ hypertrophy Wong et al, Card Res 1998; Petrou et al, Circulation 1995
– Enhancement of systolic & diastolic function in small & large animal models Wong et al, Card Res 1998; Hon et al, JTCVS 2001; Hon et al, Acta Physiol Scand 2001
– Prevents fibrosis following banding of the aorta & PA Hon et al, JTCVS 2001
– Gene expression (physiological hypertrophy) Wong et al, Card Res 1998; Petrou et al, Circulation
1995
Reversing HF: LVAD & clenbuterol
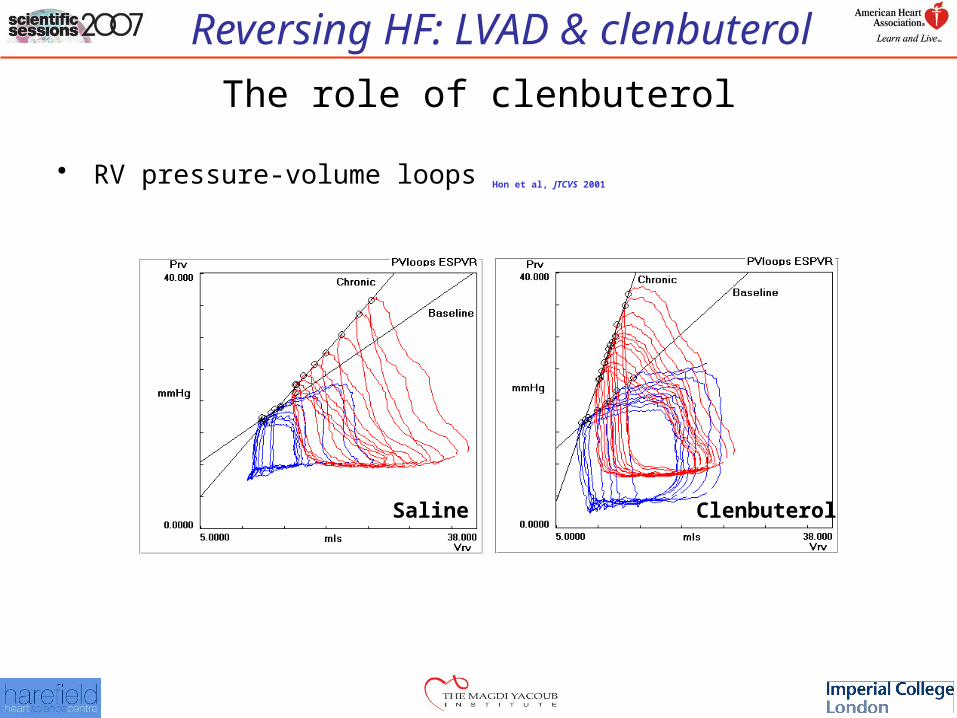
The role of clenbuterol
• RV pressure-volume loops Hon et al, JTCVS 2001
Saline Clenbuterol
Reversing HF: LVAD & clenbuterol
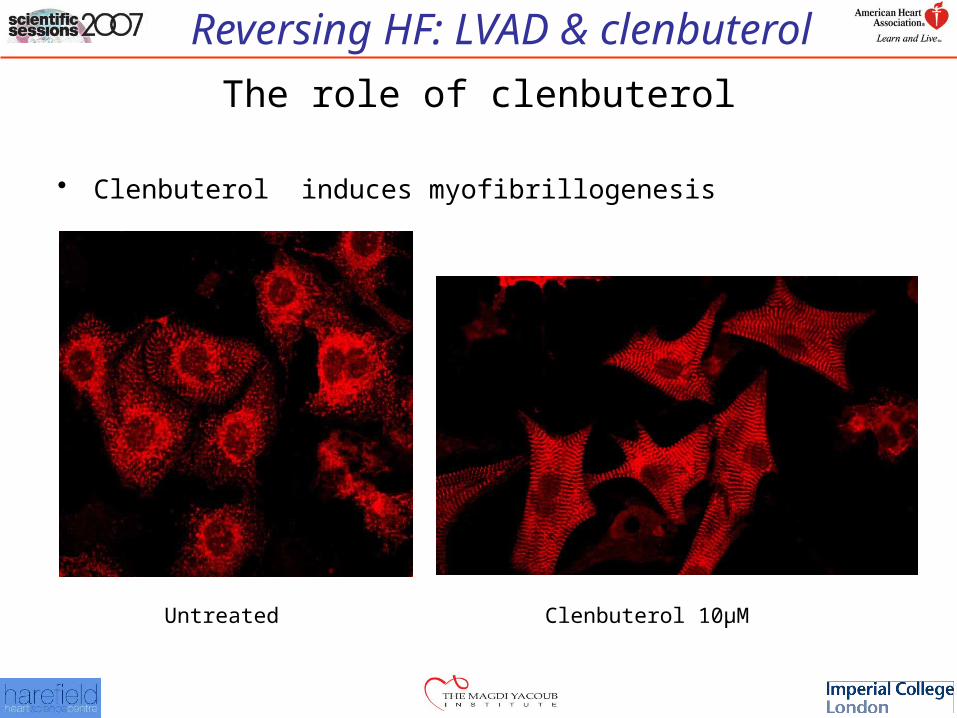
The role of clenbuterol
• Clenbuterol induces myofibrillogenesis
Clenbuterol 10µMUntreated
Reversing HF: LVAD & clenbuterol
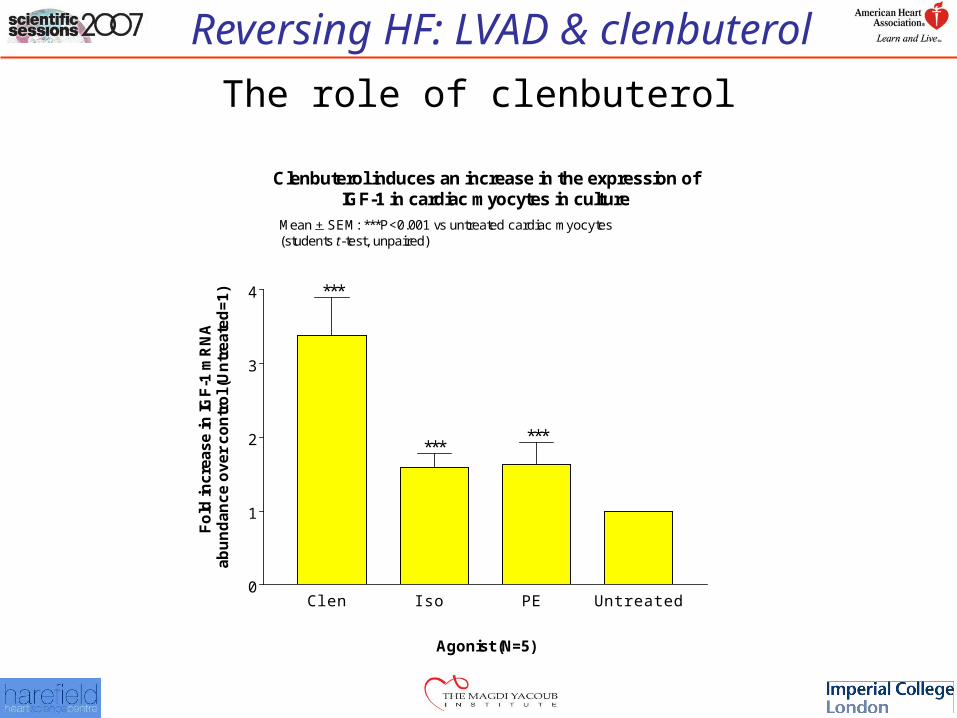
Clenbuterol induces an increase in the expression ofIGF-1 in cardiac myocytes in culture
Clen Iso PE Untreated0
1
2
3
4 ***
******
Mean + SEM: ***P<0.001 vs untreated cardiac myocytes(students t-test, unpaired)
Agonist (N=5)
Fo
ld in
cre
as
e in
IGF
-1 m
RN
Aa
bu
nd
an
ce
ov
er
co
ntr
ol (
Un
tre
ate
d=
1)
The role of clenbuterol
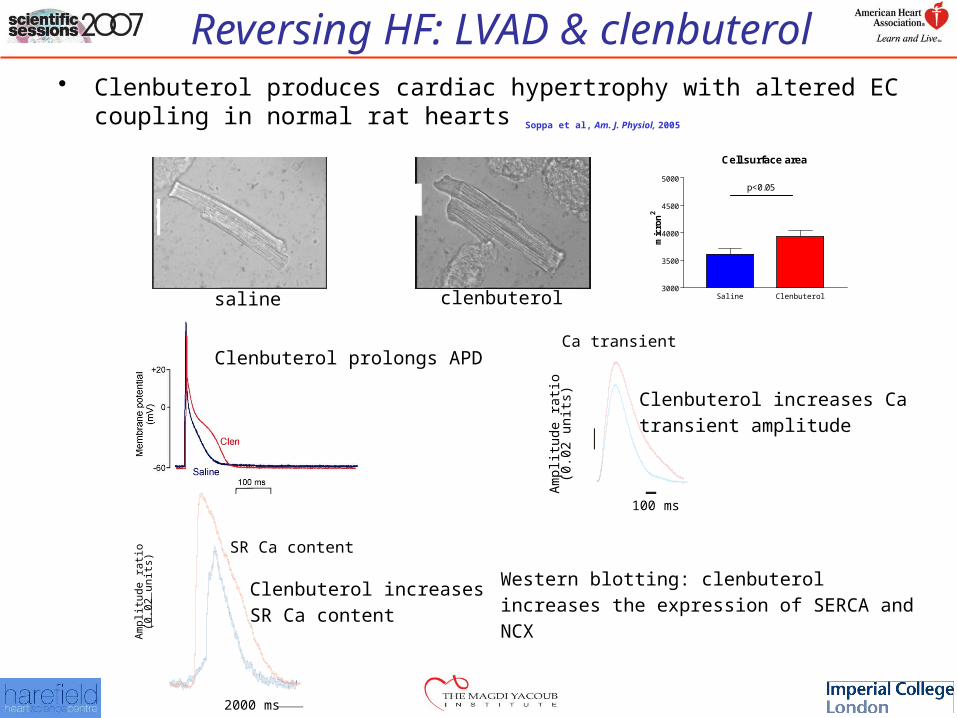
Reversing HF: LVAD & clenbuterol• Clenbuterol produces cardiac hypertrophy with altered EC coupling in
normal rat hearts Soppa et al, Am. J. Physiol, 2005
Cell surface area
Saline Clenbuterol3000
3500
4000
4500
5000p<0.05
mic
ron
2
saline clenbuterol
Clenbuterol prolongs APD
Am
plitu
de r
atio
(0.0
2 un
its)
Ca transient
Clenbuterol increases Ca
transient amplitude
100 ms
2000 ms
SR Ca content
Am
plitu
de r
atio
(0.0
2 un
its)
Clenbuterol increases
SR Ca content
Western blotting: clenbuterol
increases the expression of SERCA and
NCX
Reversing HF: LVAD & clenbuterol
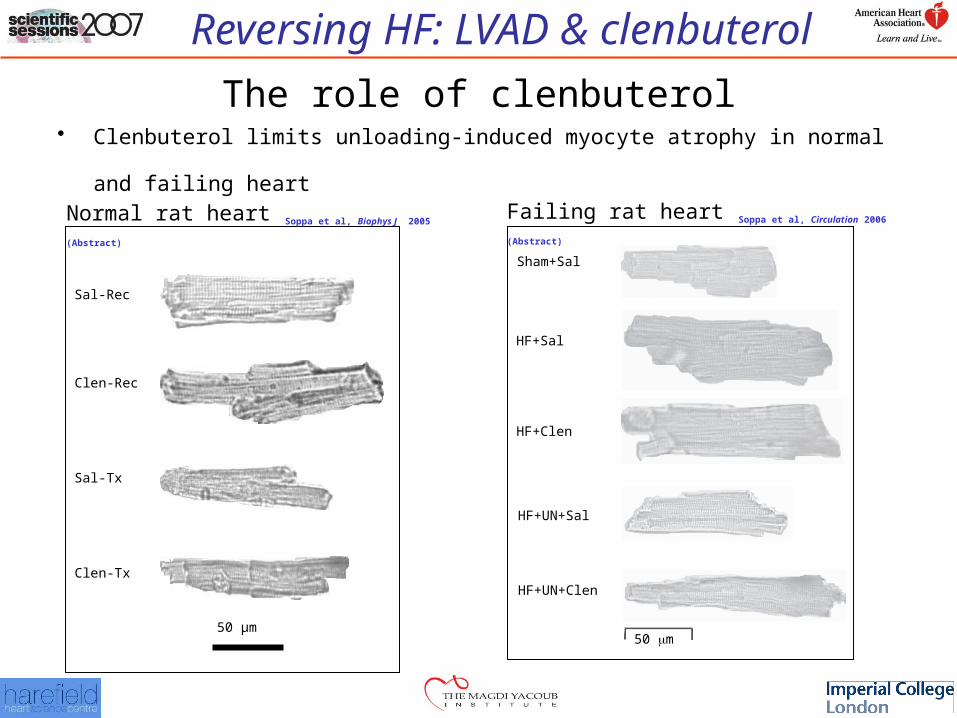
The role of clenbuterol•
Clenbuterol limits unloading-induced myocyte atrophy in normal and failing heart
Clen-Tx
Sal-Tx
Clen-Rec
Sal-Rec
50 µm50 m
Sham+Sal
HF+Sal
HF+Clen
HF+UN+Sal
HF+UN+Clen
Normal rat heart Soppa et al, Biophys J 2005 (Abstract)Failing rat heart Soppa et al, Circulation 2006 (Abstract)
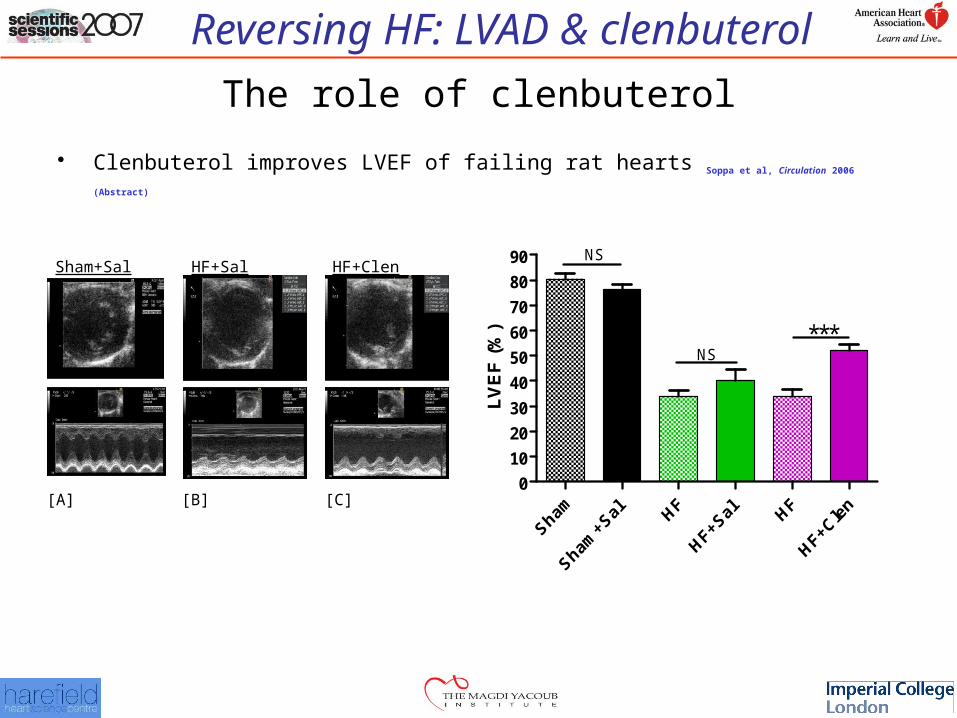
Reversing HF: LVAD & clenbuterol
Representative 2D and M-mode recordings showing development of LV dysfunction [A, B and C]. Graph [D] showing the effect of treatment with Sal or Clen on LVEF assessed by 2D short-axis views at the mid-papillary level.
0
10
20
30
40
50
60
70
80
90
***NS
NS
LV
EF
(%
)
HF+SalSham+Sal HF+Clen
[A] [B] [C]
The role of clenbuterol
• Clenbuterol improves LVEF of failing rat hearts Soppa et al, Circulation 2006 (Abstract)
Reversing HF: LVAD & clenbuterol
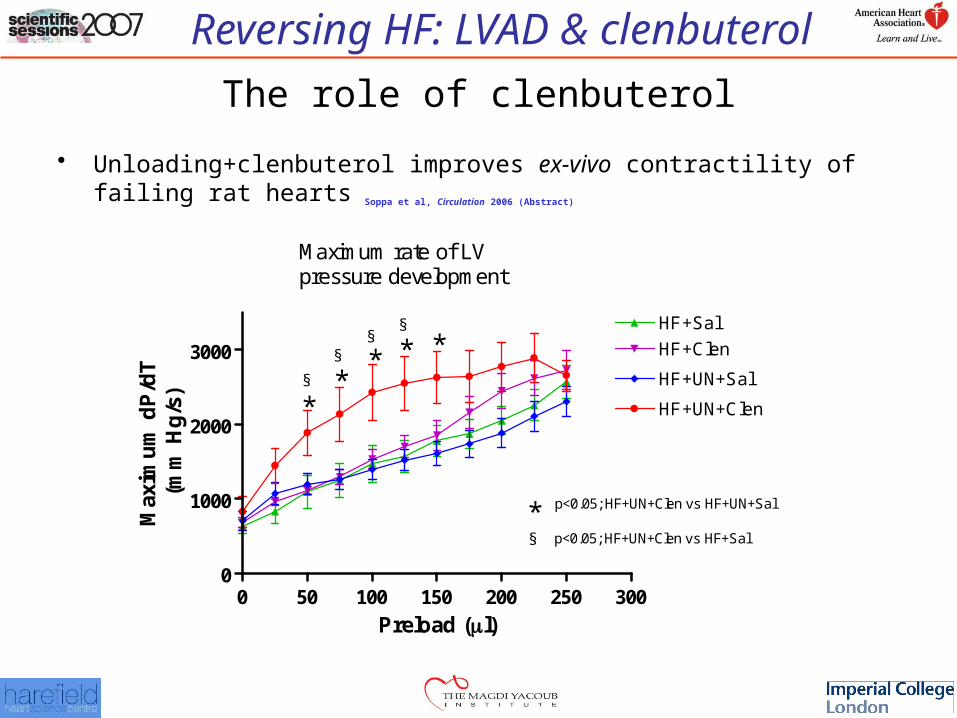
0 50 100 150 200 250 3000
1000
2000
3000HF+Sal
HF+Clen
HF+UN+Sal
HF+UN+Clen*
* **
*§
§§
§
p<0.05; HF+UN+Clen vs HF+UN+Sal*§ p<0.05; HF+UN+Clen vs HF+Sal
Maximum rate of LVpressure development
Preload (l)
Max
imu
m d
P/d
T(m
m H
g/s
)
The role of clenbuterol
• Unloading+clenbuterol improves ex-vivo contractility of failing rat hearts Soppa et
al, Circulation 2006 (Abstract)
Reversing HF: LVAD & clenbuterol
0.0 0.2 0.4 0.6 0.8 1.00.30
0.35
0.40
0.45
0.50
0.55
0.0 0.2 0.4 0.6 0.8 1.01.48
1.53
1.58
1.63
1.68
0.0
5 ra
tio u
nits
0.0
5 µ
m
200 ms
HF+Sal
HF+UN+Clen
0.0 0.2 0.4 0.6 0.8 1.00.30
0.35
0.40
0.45
0.50
0.55
0.0 0.2 0.4 0.6 0.8 1.01.48
1.53
1.58
1.63
1.68
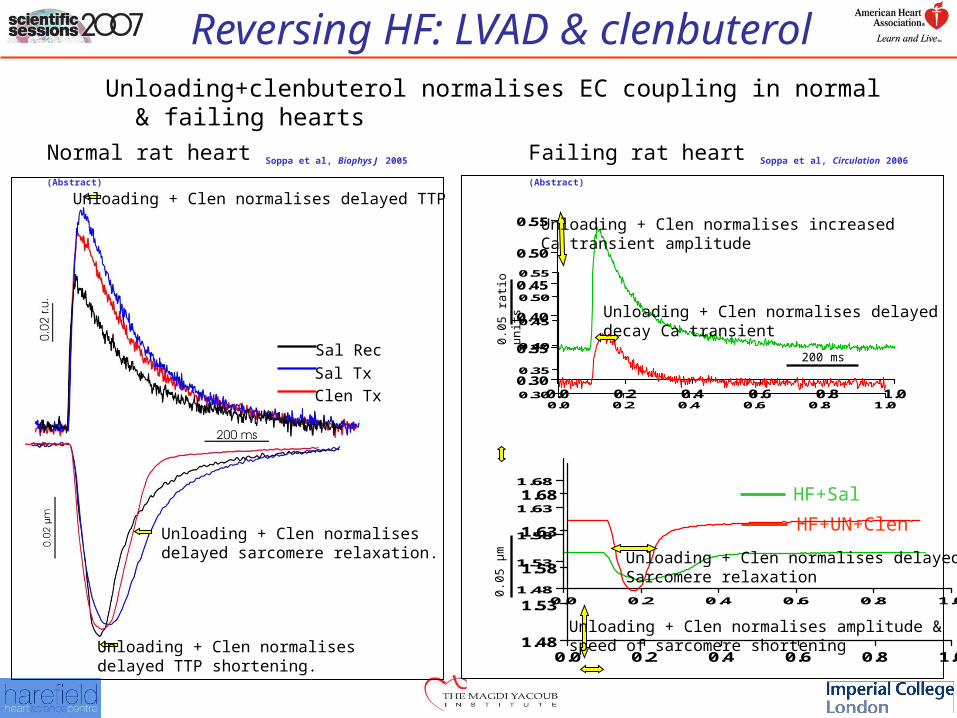
Unloading+clenbuterol normalises EC coupling in normal & failing hearts
Unloading + Clen normalises delayed TTP shortening.
Sal Tx
Sal Rec
Clen Tx
Unloading + Clen normalises delayed sarcomere relaxation.
Unloading + Clen normalises delayed TTP
Normal rat heart Soppa et al, Biophys J 2005 (Abstract)
Unloading + Clen normalises increased Ca transient amplitude
Unloading + Clen normalises delayed decay Ca transient
Unloading + Clen normalises amplitude & speed of sarcomere shortening
Unloading + Clen normalises delayed Sarcomere relaxation
Failing rat heart Soppa et al, Circulation 2006 (Abstract)
Reversing HF: LVAD & clenbuterol
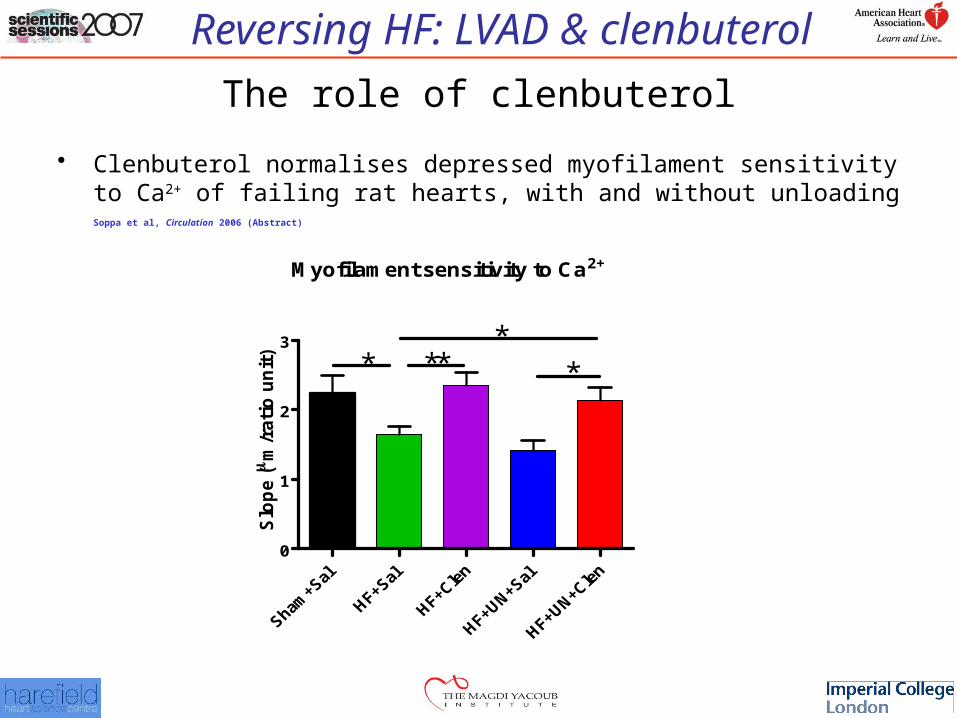
The role of clenbuterol
• Clenbuterol normalises depressed myofilament sensitivity to Ca2+ of failing rat hearts, with and without unloading Soppa et al, Circulation 2006 (Abstract)
Myofilament sensitivity to Ca2+
0
1
2
3
* ****
Slo
pe (
m/r
ati
o u
nit
)
Reversing HF: LVAD & clenbuterol
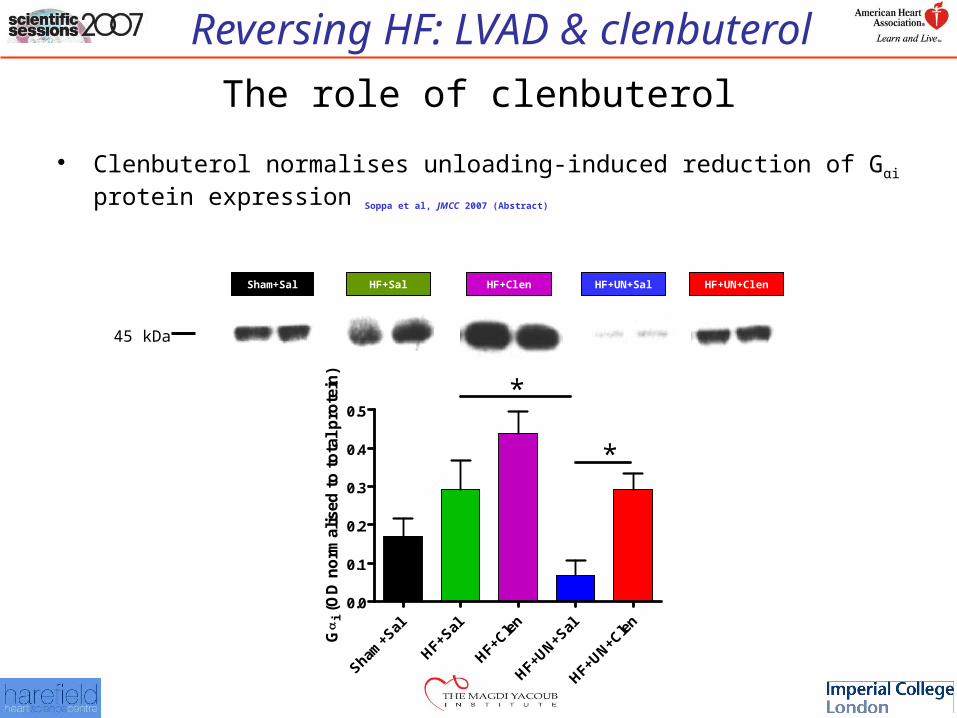
The role of clenbuterol
• Clenbuterol normalises unloading-induced reduction of Gαi protein expression Soppa et al, JMCC 2007 (Abstract)
Sham+Sal HF+Sal HF+Clen HF+UN+Sal HF+UN+Clen
45 kDa
Sham+S
al
HF+Sal
HF+Cle
n
HF+UN+Sal
HF+UN+Cle
n
0.0
0.1
0.2
0.3
0.4
0.5*
*
G
i (O
D n
orm
alis
ed t
o t
ota
l p
rote
in)
Reversing HF: LVAD & clenbuterol
The role of clenbuterol
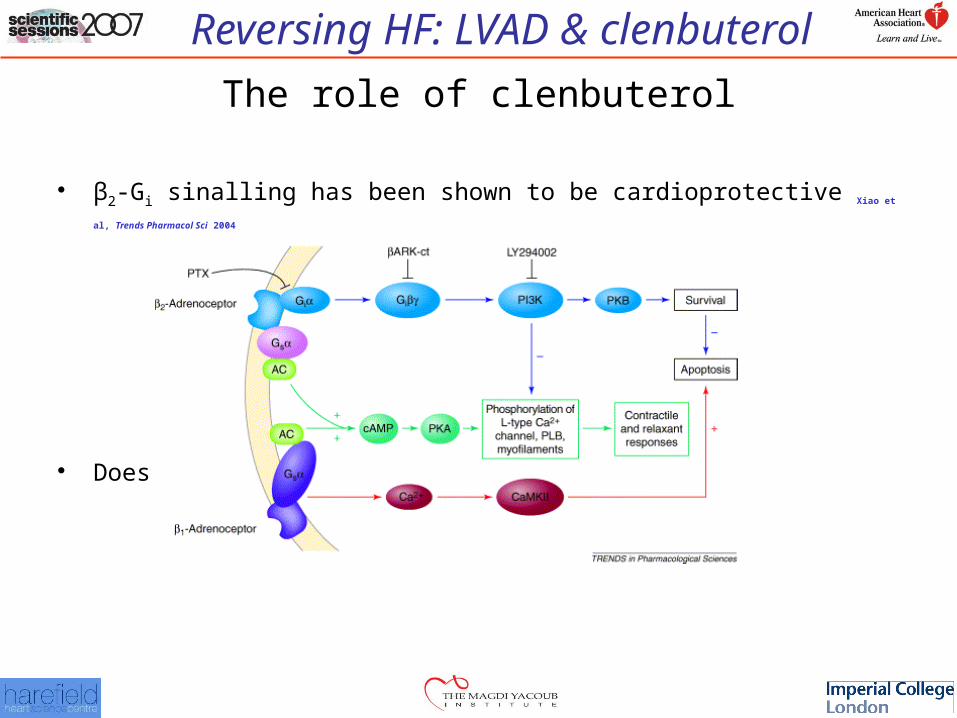
• β2-Gi sinalling has been shown to be cardioprotective Xiao et al, Trends Pharmacol Sci 2004
• Does clenbuterol activate the β2-Gi pathway?
Reversing HF: LVAD & clenbuterol
Flu
o-4
flu
ore
sc
en
ce (
F/F
0)(r
.u.
0.2
) 500 ms
control 3x10-5 M 10-4 M wash out
clenbuterol
Sar
co
me
re l
eng
th (m
m)
wash out3 x10-5 M 10-4 M
1.9
1.8
##
#
The role of clenbuterol
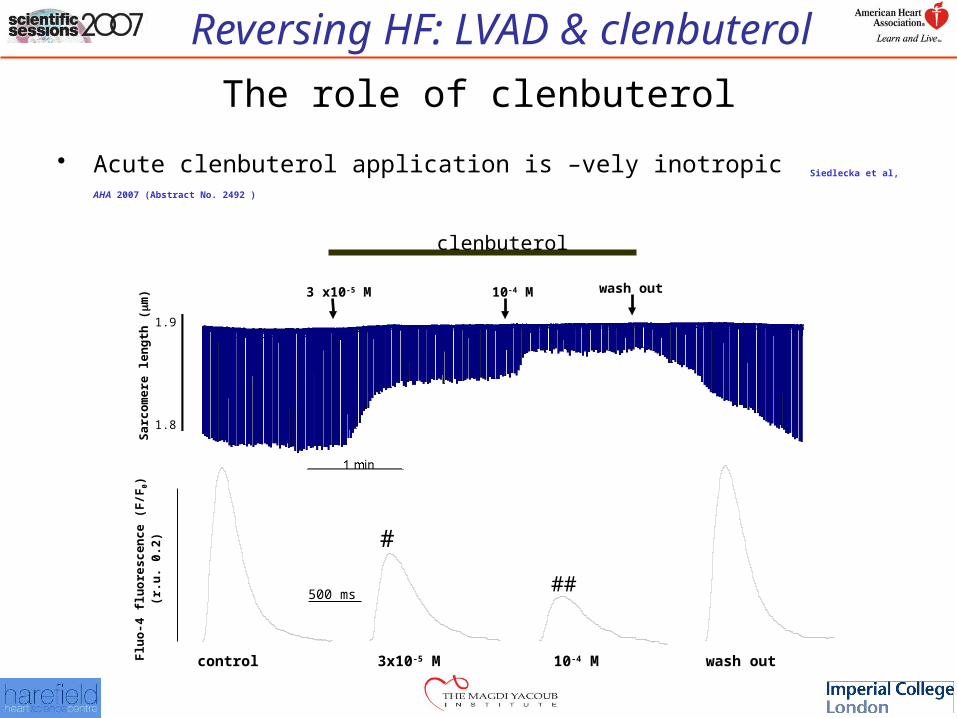
• Acute clenbuterol application is –vely inotropic Siedlecka et al, AHA 2007 (Abstract No. 2492 )
Reversing HF: LVAD & clenbuterol
-8 -7 -6 -5 -4control0
50
100
150
200
250 clenbuterol (n=6)
salbutamol (n=9)
fenoterol (n=9)
washout
**
***
##
## ###
###
###***
***
***
log [ 2-agonist] [M]
Co
ntr
acti
on
Am
pli
tud
e[%
of
con
tro
l]
-6 -5 -4control0
50
100
CLEN + CGP 20712A 300 nM (n=10)
CLEN + CGP 20712A 300 nM + ICI 118551 50 nM (n=10)
washout
# ##
###
###
###
CLEN (n=13)
**
#
######
######
###
log [clenbuterol] [M]
Co
ntr
acti
on
Am
pli
tud
e[%
of
con
tro
l]
-4.5 -4.0control0
50
100
150
CLEN + CGP 20712 nM (n=7)
washout
* ***
CLEN + CGP 20712 nM + PTX 2 g/ml (n=6)
###
###
log [clenbuterol] [M]
Co
ntr
acti
on
Am
pli
tud
e[%
of
con
tro
l]
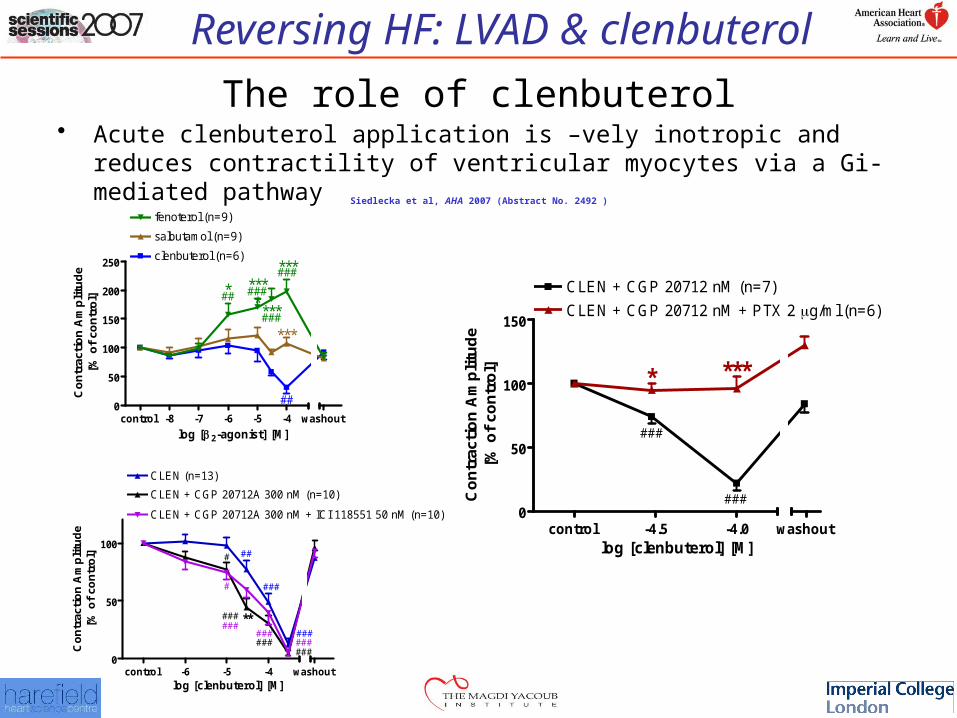
The role of clenbuterol• Acute clenbuterol application is –vely inotropic and reduces contractility of
ventricular myocytes via a Gi-mediated pathway Siedlecka et al, AHA 2007 (Abstract No. 2492 )
Reversing HF: LVAD & clenbuterol
Reversing HF: LVAD & clenbuterol
Translational research (Harefield protocol)
• Explantation criteria
– LV dimensions with device off EDD <60mm, ESD <50 mm,
– EF >45%
– LVEDP <12 mmHg
– Resting CI >2.8 L/min/m2
– mVO2 >20 ml/kg/min & VE/VCO2 slope <34
Reversing HF: LVAD & clenbuterol
Drug Therapy For Myocardial Recovery
Reversing HF: LVAD & clenbuterol
Imperial CollegeOF SCIENCE TECHNOLOGY AND MEDICINE
Harefield HospitalRoyal Brompton & Harefield NHS Trust
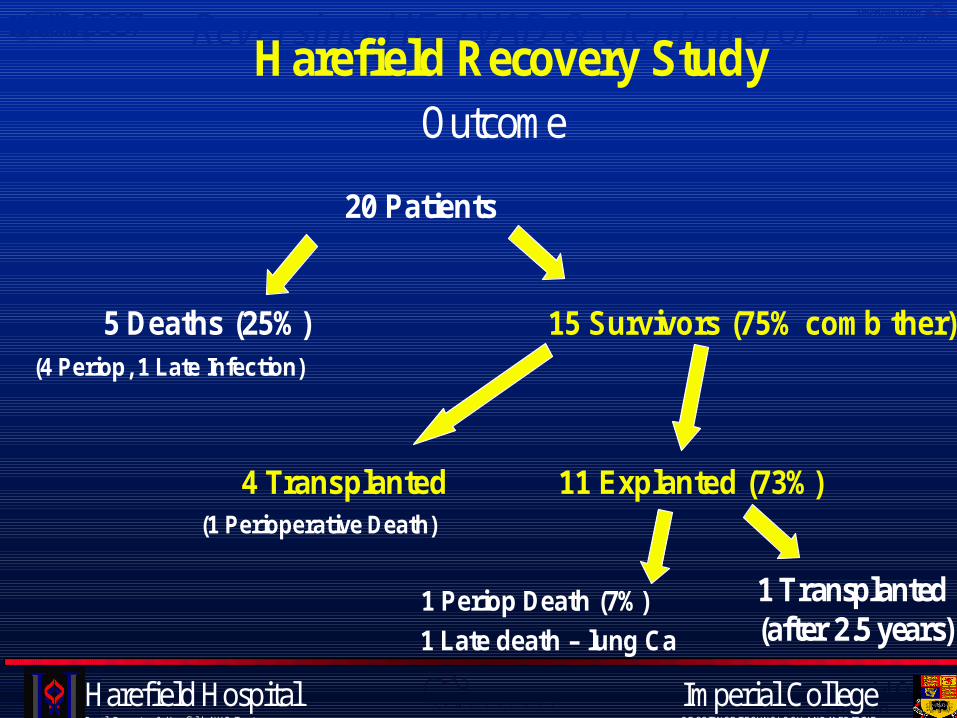
20 Patients
5 Deaths (25%) 15 Survivors (75% comb ther)(4 Periop, 1 Late Infection)
4 Transplanted 11 Explanted (73%)(1 Perioperative Death)
1 Periop Death (7%)
1 Late death – lung Ca
Harefield Recovery StudyOutcome
1 Transplanted(after 2.5 years)
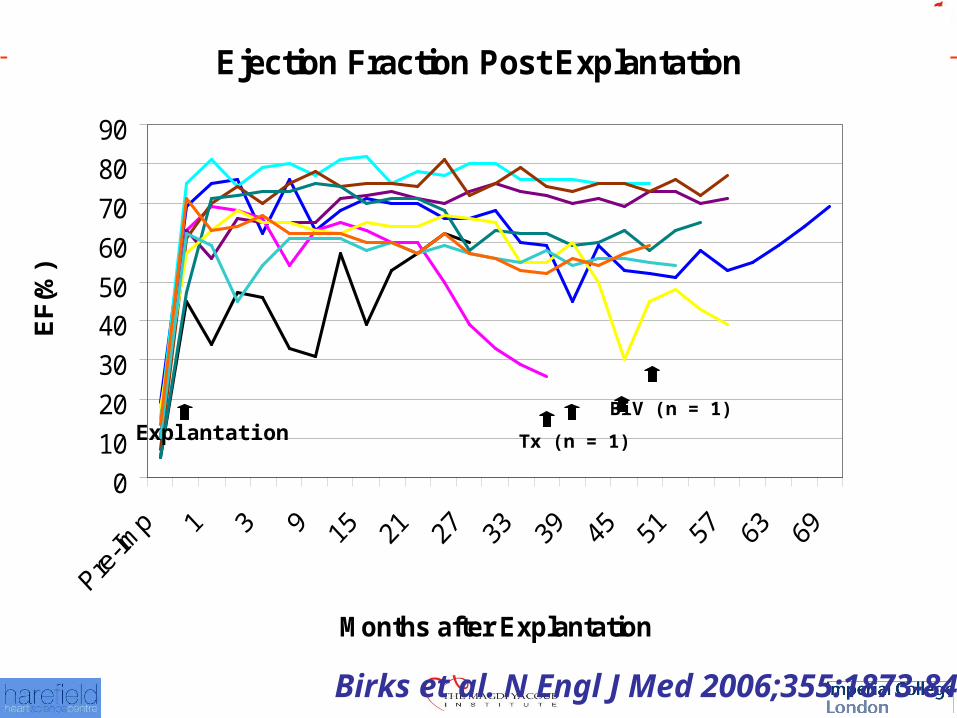
Reversing HF: LVAD & clenbuterolEjection Fraction Post Explantation
0
10
20
30
40
50
60
70
80
90
Months after Explantation
EF
(%)
Tx (n = 1)ExplantationBiV (n = 1)
Birks et al. N Engl J Med 2006;355:1873-84
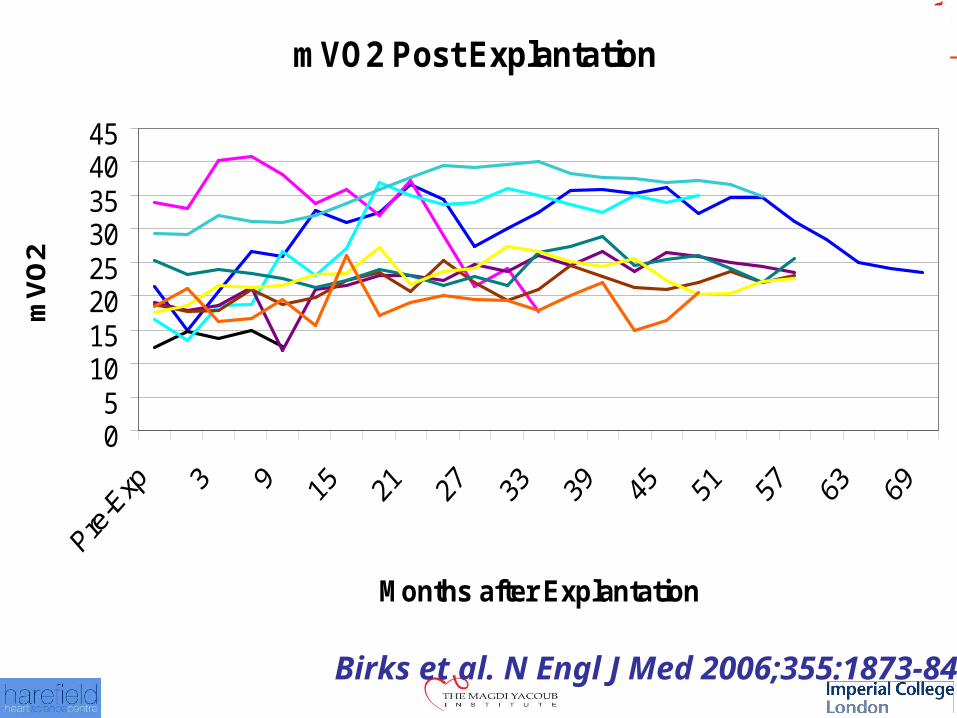
Reversing HF: LVAD & clenbuterolmVO2 Post Explantation
05
1015202530354045
Months after Explantation
mV
O2
Birks et al. N Engl J Med 2006;355:1873-84
Reversing HF: LVAD & clenbuterol• Benefits of unloading+clenbuterol
– Clinical• Bridge to Recovery
– Whole heart» ↑LVEF and CI Birks et al NEJM 2006; Dandel et al, Circulation 2005; Frazier et al, ATS 1999
– Cellular» ↓size & normalised EC coupling Terracciano et al, Circulation 2004; Terracciano et al, EHJ 2003
– Molecular» Specific changes in cytoskeletal genes and proteins Latif et al, JHLT
2007; Birks et al, Circulation 2005 » Specific changes EPAC2, Integrin signalling pathway Hall et al, EHJ
2007
» AGAT – creatine synthesis Cullen et al, Circulation 2006
» ↑IGF-1 expression Barton et al, Circulation 2005
» ↑Apelin receptor expression Farkasfalvi et al, Circulation 2006 (Abstract)
– ECM – not known
Reversing HF: LVAD & clenbuterolConclusions
• Reversal of HF using LVAD + Clen in non-ischemic DCM has given encouraging results (single centre)
• The molecular & cellular mechanisms responsible have been partially studied experimentally & clinically
• A multicentre study of the ‘Harefield protocol’ (HARPS) is on the way
• Need to evaluate the combination therapy in – Ischemic DCM
– With continuous flow pumps
Reversing HF: LVAD & clenbuterol
HARPS Investigator’s Meeting
Boston, MA April 10, 2008
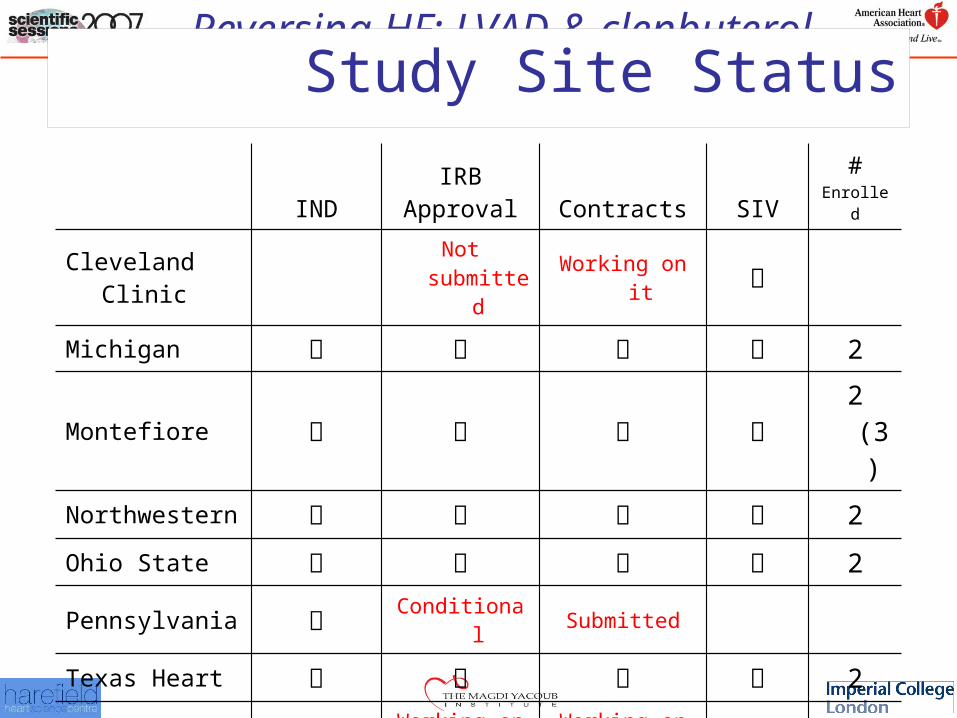
Reversing HF: LVAD & clenbuterolStudy Site Status
INDIRB
Approval Contracts SIV#
Enrolled
Cleveland Clinic Not submitted Working on it
Michigan 2
Montefiore 2 (3)
Northwestern 2
Ohio State 2
Pennsylvania Conditional Submitted
Texas Heart 2
UAB ? Working on it Working on it
Washington 1
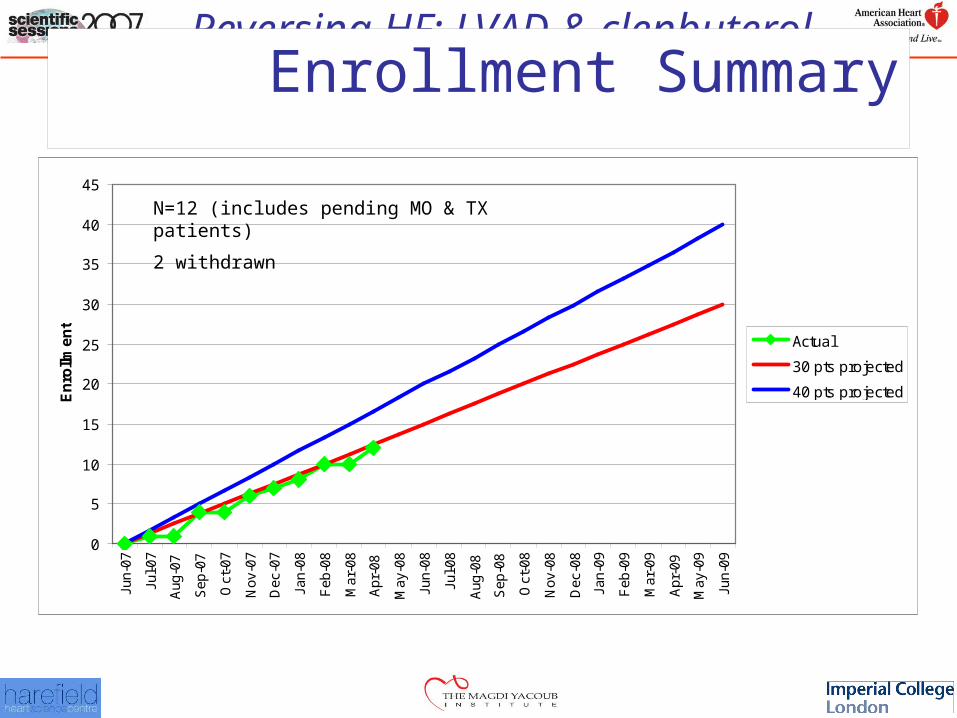
Reversing HF: LVAD & clenbuterolEnrollment Summary
0
5
10
15
20
25
30
35
40
45
Jun-
07
Jul-0
7
Aug
-07
Sep
-07
Oct
-07
Nov
-07
Dec
-07
Jan-
08
Feb
-08
Mar
-08
Apr
-08
May
-08
Jun-
08
Jul-0
8
Aug
-08
Sep
-08
Oct
-08
Nov
-08
Dec
-08
Jan-
09
Feb
-09
Mar
-09
Apr
-09
May
-09
Jun-
09
En
rollm
en
t
Actual
30 pts projected
40 pts projected
N=12 (includes pending MO & TX patients)
2 withdrawn
Reversing HF: LVAD & clenbuterol