Reversible Focal Ischemic Injury Demonstrated by...
8
1304 Reversible Focal Ischemic Injury Demonstrated by Diffusion-Weighted Magnetic Resonance Imaging in Rats Kazuo Minematsu, MD; Limin Li, PhD; Christopher H. Sotak, PhD; Michael A. Davis, MD, ScD; and Marc Fisher, MD Background and Purpose: Diffusion-weighted magnetic resonance imaging (DWI) can quantitatively display focal brain abnormalities within minutes after the onset of ischemia. We performed the present study to determine the effects of 1 and 2 hours of temporary ischemia on DWI. Methods: We examined DWI and T2-weighted magnetic resonance images (T2WI) during and after 1 and 2 hours of temporary middle cerebral artery occlusion in rats (n=10 for each group). In a subgroup of four animals from each group, we employed perfusion magnetic resonance imaging to monitor cerebral perfusion. Neurological outcome and infarct size after survival for 24 hours were compared between the groups and correlated with DWI and T2WI studies. Results: Perfusion studies qualitatively documented hypoperfusion and reperfusion during and after temporary occlusion. Lesion size on DWI during reperfusion was significantly less than that during ischemia for 1 (55% decline, p<0.02) but not 2 hours of occlusion. The DWI signal intensity ratio (intensity compared with that in the contralateral homologous area) just before withdrawal of the occluder was significantly less in regions where the hyperintensity disappeared after withdrawal than in regions with persistent hyperintensity (p<0.002). The T2WI studies revealed few or no abnormalities, except after 2 hours of occlusion. The neurological outcome was significantly better in the 1-hour than in the 2-hour group (p<0.05). Postmortem infarct volume was significantly smaller in the 1-hour group than in the 2-hour group (p<0.05). The postwithdrawal DWI accurately predicted infarct size («=0.96,/><0.0001). Conclusions: The present study indicates that DWI can rapidly display not only irreversible but also reversible ischemic brain damage and enhances the importance of DWI as a diagnostic modality for stroke. (Stroke 1992;23:1304-1311) KEY WORDS • cerebral ischemia • magnetic resonance imaging • reperfusion • rats T he development of infarction depends primarily on the severity and duration of ischemia. 1 - 2 Ischemic brain injury may recover if blood flow is restored after a brief period of ischemia. 1 - 3 - 7 This concept has led to several therapeutic attempts to restore blood flow in animal stroke models and in human stroke by using thrombolytic therapy. 8 - 9 How- ever, if irreversible ischemic injury has already oc- curred, reperfusion of the ischemic tissue will not be useful and may be hazardous because reperfusion could exacerbate brain edema or promote hemorrhagic transformation. 3 - 9 - 1 ' From the Department of Neurology (K.M., M.F.), The Medical Center of Central Massachusetts, the Department of Biomedical Engineering (L.L., C.H.S.), Worcester Polytechnic Institute, and the Departments of Radiology (C.H.S., M.A.D., M.F.) and Neu- rology (M.F.), University of Massachusetts Medical School, Worcester, Mass. Supported in part by the Harrington Neurological Research Fund and the University of Massachusetts, Department of Radi- ology Research Support Fund. Address for reprints: Dr. Kazuo Minematsu, Neurology, The Medical Center of Central Massachusetts-Memorial, 119 Belmont Street, Worcester, MA 01605. Received February 19, 1992; final revision received April 10, 1992; accepted April 29, 1992. Efforts to distinguish reversible from irreversible brain damage in experimental and clinical stroke have led to the concept of the ischemic penumbra. 1213 How- ever, it has been difficult to differentiate salvageable tissue from irreversibly damaged tissue. Positron emis- sion tomography may provide useful information con- cerning tissue viability, 14 but this technique has several disadvantages, including cost, manpower, examination time, and invasiveness. X-ray computed tomography and standard magnetic resonance imaging (MRI) with See Editorial Comment, p 1310 Tl- and T2-weighted images (T2WI) cannot detect ischemic lesions for hours after the onset of isch- emia. 1516 Diffusion-weighted MRI (DWI) can display regions of ischemic injury within minutes after on- set. 17 - 19 Differences in the apparent diffusion coefficient (ADC) of water protons, reflecting molecular transla- tional movement (Brownian motion) of water mole- cules, generate contrast in DWI. 20 - 22 Regions of re- duced water molecule motion appear hyperintense. In ischemic lesions, a rapid failure of energy metabolism and associated ion pumps leads to the accumulation of sodium ions (Na + ) and water within ischemic cells (cytotoxic edema). 23 - 25 Hyperintense areas displayed on DWI soon after an ischemic insult may represent cyto- by guest on July 15, 2018 http://stroke.ahajournals.org/ Downloaded from
Transcript of Reversible Focal Ischemic Injury Demonstrated by...

1304
Reversible Focal Ischemic Injury Demonstratedby Diffusion-Weighted Magnetic Resonance
Imaging in Rats
Kazuo Minematsu, MD; Limin Li, PhD; Christopher H. Sotak, PhD;Michael A. Davis, MD, ScD; and Marc Fisher, MD
Background and Purpose: Diffusion-weighted magnetic resonance imaging (DWI) can quantitativelydisplay focal brain abnormalities within minutes after the onset of ischemia. We performed the presentstudy to determine the effects of 1 and 2 hours of temporary ischemia on DWI.
Methods: We examined DWI and T2-weighted magnetic resonance images (T2WI) during and after 1and 2 hours of temporary middle cerebral artery occlusion in rats (n=10 for each group). In a subgroupof four animals from each group, we employed perfusion magnetic resonance imaging to monitor cerebralperfusion. Neurological outcome and infarct size after survival for 24 hours were compared between thegroups and correlated with DWI and T2WI studies.
Results: Perfusion studies qualitatively documented hypoperfusion and reperfusion during and aftertemporary occlusion. Lesion size on DWI during reperfusion was significantly less than that duringischemia for 1 (55% decline, p<0.02) but not 2 hours of occlusion. The DWI signal intensity ratio(intensity compared with that in the contralateral homologous area) just before withdrawal of the occluderwas significantly less in regions where the hyperintensity disappeared after withdrawal than in regionswith persistent hyperintensity (p<0.002). The T2WI studies revealed few or no abnormalities, except after2 hours of occlusion. The neurological outcome was significantly better in the 1-hour than in the 2-hourgroup (p<0.05). Postmortem infarct volume was significantly smaller in the 1-hour group than in the2-hour group (p<0.05). The postwithdrawal DWI accurately predicted infarct size («=0.96,/><0.0001).
Conclusions: The present study indicates that DWI can rapidly display not only irreversible but alsoreversible ischemic brain damage and enhances the importance of DWI as a diagnostic modality forstroke. (Stroke 1992;23:1304-1311)
KEY WORDS • cerebral ischemia • magnetic resonance imaging • reperfusion • rats
The development of infarction depends primarilyon the severity and duration of ischemia.1-2
Ischemic brain injury may recover if blood flowis restored after a brief period of ischemia.1-3-7 Thisconcept has led to several therapeutic attempts torestore blood flow in animal stroke models and inhuman stroke by using thrombolytic therapy.8-9 How-ever, if irreversible ischemic injury has already oc-curred, reperfusion of the ischemic tissue will not beuseful and may be hazardous because reperfusion couldexacerbate brain edema or promote hemorrhagictransformation.3-9-1'
From the Department of Neurology (K.M., M.F.), The MedicalCenter of Central Massachusetts, the Department of BiomedicalEngineering (L.L., C.H.S.), Worcester Polytechnic Institute, andthe Departments of Radiology (C.H.S., M.A.D., M.F.) and Neu-rology (M.F.), University of Massachusetts Medical School,Worcester, Mass.
Supported in part by the Harrington Neurological ResearchFund and the University of Massachusetts, Department of Radi-ology Research Support Fund.
Address for reprints: Dr. Kazuo Minematsu, Neurology, TheMedical Center of Central Massachusetts-Memorial, 119 BelmontStreet, Worcester, MA 01605.
Received February 19, 1992; final revision received April 10,1992; accepted April 29, 1992.
Efforts to distinguish reversible from irreversiblebrain damage in experimental and clinical stroke haveled to the concept of the ischemic penumbra.1213 How-ever, it has been difficult to differentiate salvageabletissue from irreversibly damaged tissue. Positron emis-sion tomography may provide useful information con-cerning tissue viability,14 but this technique has severaldisadvantages, including cost, manpower, examinationtime, and invasiveness. X-ray computed tomographyand standard magnetic resonance imaging (MRI) with
See Editorial Comment, p 1310Tl- and T2-weighted images (T2WI) cannot detectischemic lesions for hours after the onset of isch-emia.1516 Diffusion-weighted MRI (DWI) can displayregions of ischemic injury within minutes after on-set.17-19 Differences in the apparent diffusion coefficient(ADC) of water protons, reflecting molecular transla-tional movement (Brownian motion) of water mole-cules, generate contrast in DWI.20-22 Regions of re-duced water molecule motion appear hyperintense. Inischemic lesions, a rapid failure of energy metabolismand associated ion pumps leads to the accumulation ofsodium ions (Na+) and water within ischemic cells(cytotoxic edema).23-25 Hyperintense areas displayed onDWI soon after an ischemic insult may represent cyto-
by guest on July 15, 2018http://stroke.ahajournals.org/
Dow
nloaded from
Minematsu et al Reperfusion and Diffusion-Weighted Images 1305
toxic edema formation in ischemic tissue.17 Our previ-ous study demonstrated that DWI displays hyperintenseareas, encompassing most of the middle cerebral artery(MCA) territory, 30 minutes after suture MCA occlu-sion in rats and that the size of the hyperintense area ishighly correlated with that of infarction demonstratedwith 2,3,5 -triphenyltetrazolium chloride (TTC) stainingafter survival for 24 hours.19 In a similar MCA occlusionmodel in rats, regions of DWI hyperintensity revert tonormal if the occluder is removed from the intracranialartery 33 minutes after occlusion.18 These observationsindicate that DWI studies soon after arterial occlusionaccurately predict the ultimate area of infarction, butearly DWI abnormalities in part represent reversiblydamaged tissue that may improve with appropriateintervention.
Dynamic contrast-enhanced perfusion MRI, usingmultiple, repetitive, ultrafast imagings combined withthe intravenous injection of a paramagnetic or super-paramagnetic contrast agent, can monitor a transientdecrease in T2*-weighted signal intensity caused by astrong contrast agent-induced field gradient betweenthe capillary space and surrounding tissue and canevaluate the cerebral perfusion state.2627 We performedthe present study using a rat intraluminal suture MCAocclusion model to determine the effects of 1 and 2hours of temporary MCA occlusion on serial changes inearly DWI and T2WI, perfusion MRI, neurologicaloutcome, and postmortem infarct size at 24 hours.
Materials and MethodsWe studied 20 adult male Sprague-Dawley rats
weighing 280-370 g. Our procedures were approved bythe Animal Research Committee of the University ofMassachusetts Medical School (ARC Protocol #A-643). Two groups of 10 rats each were randomly as-signed to temporary occlusion of the MCA for 1 or 2hours. Animals were anesthetized with 400 mg/kg bodywt i.p. chloral hydrate. Polyethylene catheters wereintroduced into the left femoral artery and into the venacava through the left femoral vein. The rat's bodytemperature was maintained close to 37.0°C with a heatlamp during the operation.
We used a modified intraluminal suture MCA occlu-sion model described in detail previously.19 Briefly, anintraluminal occluder, 4-0 monofilament nylon suturewith its tip rounded by flame heating, was introducedthrough the right common carotid artery (CCA) intothe internal carotid artery, then advanced intracraniallyapproximately 17 mm from the CCA bifurcation. Withthis procedure, the intraluminal suture occludes theorigin of the MCA.1928"30 Restoration of perfusion tothe ischemic tissue was accomplished by pulling theoccluder back to the CCA.
Four rats in each group were subjected to experimentA, perfusion MRI and DWI studies. DWI and perfusionMRI studies were performed 30 and 15 minutes beforewithdrawing the occluder, respectively. Perfusion MRIstudies were repeated 15 minutes after withdrawing theoccluder and were followed by DWI and T2WI studies30 minutes after withdrawal. The other six rats in eachgroup were examined only with serial DWI and T2WIstudies to analyze sequential changes in the area anddegree of hyperintensities (experiment B). Initial DWIand T2WI studies were performed at 30 minutes in the
1-hour group. In the 2-hour group, MRI studies wereobtained 30, 60, and 90 minutes after arterial occlusion.After withdrawal of the occluder, DWI and T2WIstudies were repeated at 30-minute intervals for 120(1-hour group) or 90 (2-hour group) minutes.
Each rat was placed in the prone position, fixed to abird-cage radiofrequency coil, and anesthetized with0.5-1.0% isoflurane during the imaging protocol. Bodytemperature was kept close to 37.0°C with a water-circulating heating pad (K-module model K-20, Amer-ican Pharmaseal, Valencia, Calif.).19 Arterial bloodpressure was monitored continuously, and a 0.5-mlaliquot of arterial blood was collected for measuringblood gases at baseline, before MCA occlusion, and 20and 180 minutes after MCA occlusion.
The MRI studies were performed in a General Elec-tric CSI-II 2.0-T/45-cm imaging spectrometer (GE Co.,Fremont, Calif.) equipped with self-shielded gradientcoils capable of producing a maximum field strength of±20 G/cm. Before the formal MRI studies, previewspin/echo images were obtained to determine exact sliceplanes. Dynamic contrast-enhanced perfusion MRIstudies were performed at a coronal slice with a thick-ness of 2 mm, involving the optic chiasm (chiasmaticslice), using echo-planar imaging (EPI).31 EPIs wereacquired at 1-second intervals over 16 seconds immedi-ately after a bolus injection of 0.3 ml physiological salinecontaining 0.05 mmol superparamagnetic iron oxideparticles/kg iron (AquaMag 100 magnetic fluid, catalogNo. 4180, Advanced Magnetics, Inc., Cambridge, Mass.)via an intravenous catheter over 1 second.2732 The EPIswere acquired using an incarnation of the EPI sequencein which the whole k-space is scanned in a "sawtooth"pattern.31 A set of imaging data was acquired in 65.5msec, with a repetition time (TR) of 1 second. DWI andT2WI were also obtained at the same slice position. Inexperiment B, MRI signals were recorded from fourslices, and the chiasmatic slice was selected for furtheranalysis. DWIs were collected over 8 minutes with a TRof 1,800 msec, an echo time (TE) of 45 msec, andhalf-sine-shaped diffusion-sensitive gradient pulseswith a duration of 10 msec, a pulse separation of 20msec, and strength of 15 G/cm, yielding a b value of1,142 sec/mm2. T2WIs with a TR of 2,200 msec and a TEof 90 msec were obtained over 10 minutes.19
After the MRI protocols, the rats were permitted torecover from the anesthesia. Neurological evaluationwas performed 24 hours after the induction of ischemiaand scored on the following six-point scale, which wasmodified from the scale proposed by Zea Longa et al28:0, no neurological deficit; 1, failure to extend leftforepaw fully; 2, circling to the left; 3, falling to the left;4, no spontaneous walking with a depressed level ofconsciousness; and 5, dead. Then the animals wereanesthetized with 300 mg/kg i.p. chloral hydrate anddecapitated. The brains were quickly removed, sec-tioned coronally at 2-mm intervals, stained with a 2%TTC solution at 37°C for 30 minutes,33 and fixed byimmersion in a 10% phosphate-buffered formalin solu-tion. The six brain sections per animal stained with TTCwere photographed with a 35-mm camera mounted on asurgical microscope after 48 hours of formalin fixation.
Data from perfusion MRI, DWI, T2WI, and TTCstudies were blindly analyzed by an observer unaware ofthe group and of the study time point. The perfusion
by guest on July 15, 2018http://stroke.ahajournals.org/
Dow
nloaded from
1306 Stroke Vol 23, No 9 September 1992
state in the MCA territory as determined with perfusionMRI studies was qualitatively graded (perfusion scale)as 0, no difference from the contralateral MCA terri-tory; 1, delayed transit of the contrast agent as evi-denced by slower decline and recovery in signal inten-sity than in the contralateral MCA territory; 2, part ofthe MCA territory had an incomplete decline in signalintensity; 3, the entire MCA territory had an incom-plete decline in signal intensity; and 4, no decline insignal intensity in the entire MCA territory. Imagesfrom DWI and T2WI studies were photographed aftermodifying window levels to contrast the hyperintenseareas with background normal tissues. The enlargedphotographs were evaluated with a computer-assisteddigitizer (Sigma-Scan V3.10, Jandel Scientific, CorteMadera, Calif., and Numonics 2200, Numonics Corp.,Montgomeryville, Pa.). The border of the hyperintensearea was visually judged and traced. The area of thehyperintense region was divided by the area of theipsilateral hemisphere to obtain the percent hemi-spheric lesion area (%HLA). Photographs of TTC-stained sections were similarly evaluated using thedigitizer to determine %HLA. Areas not stained redwere considered as infarcted. The infarct volume (incubic millimeters) was calculated by using numericalintegration of the lesion areas for all TTC sections perrat and the distances between them. Only in animals forexperiment B, the degree of DWI hyperintensity wasevaluated using the signal intensity ratio (SIR), theaverage signal intensity within the region of interest(ROI) (1.0x1.0x2.0 mm3) divided by that in the con-tralateral, nonischemic, homologous region. SIR wascalculated in three ROIs (eaudoputamen, frontopari-etal cortex, and temporal cortex) for each rat. ROIswith DWI hyperintense areas demonstrated only duringocclusion were defined as reversible and those withareas of persistent hyperintensity as irreversible. SIRvalues were compared between reversible and irrevers-ible ROIs for each DWI study time point. Animals inexperiment A were not used for analyzing SIR becauseof the potential decrease in signal intensity caused byiron particles circulating in the blood.
For comparison of parametric variables, analysis ofvariance was used. Wilcoxon and Mann-Whitney testswere applied for comparison of paired and unpairednonparametric data sets, respectively. Because distribu-tions of observed values for %HLA and infarct volumediffered from a normal distribution, these values werealso analyzed with the nonparametric methods. Forcomparison of the observed frequencies in multiplecategories, contingency table analysis was used. Linearregression analysis was used for correlating parametricdata sets. For assessing correlation of the nonparamet-ric graded scales with other variables, Spearman's rankcorrelation coefficient analysis was applied. All valuespresented are mean±SEM. A two-tailed probabilityvalue of less than 0.05 was considered significant.
ResultsNo significant differences between the groups were
observed in any physiological measurement (data notshown) except Pco2, which declined after the onset ofocclusion in both groups (p=0.0076). All rats exceptone in each group survived for 24 hours after MCAocclusion. The animals that died just before 24 hours
were scored as 5 on the neurological grading scale, thentheir brains were immediately subjected to TTC stain-ing. The neurological scale score at 24 hours was1.0±0.6 in the 1-hour group, significantly better than thevalue in the 2-hour group (2.7±0.5,/?<0.05).
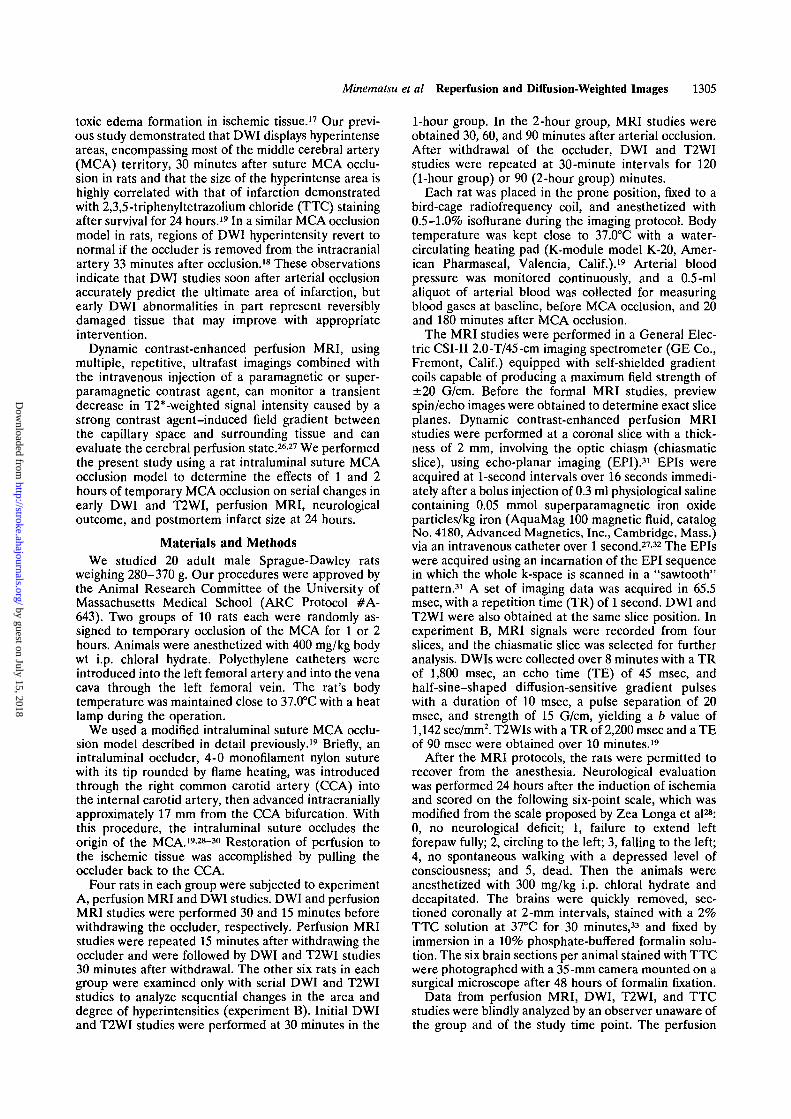
In all rats in experiment A, perfusion MRI studiesduring occlusion demonstrated hypoperfusion in theright MCA territory (perfusion scale grade of3.50±0.27; Figure 1, top). The perfusion scale grade wassignificantly correlated with prewithdrawal DWI%HLA (i?Spearroan=0.866, p<0.025). The perfusion ab-normalities improved after withdrawal of the occluderin all animals (perfusion scale grade 0.88±0.35,/?<0.02;Figure 1, bottom). Perfusion scale grades before andafter withdrawal of the occluder in the 1-hour group(data not shown) were not different from those in the2-hour group.
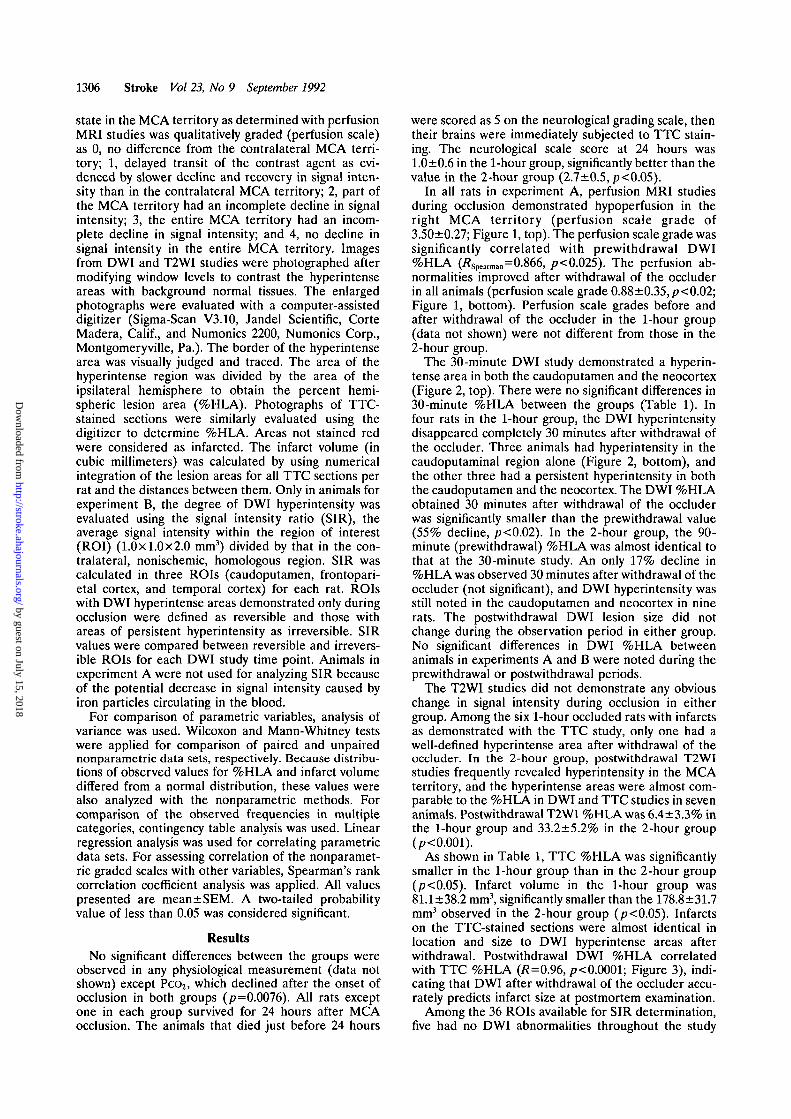
The 30-minute DWI study demonstrated a hyperin-tense area in both the eaudoputamen and the neocortex(Figure 2, top). There were no significant differences in30-minute %HLA between the groups (Table 1). Infour rats in the 1-hour group, the DWI hyperintensitydisappeared completely 30 minutes after withdrawal ofthe occluder. Three animals had hyperintensity in thecaudoputaminal region alone (Figure 2, bottom), andthe other three had a persistent hyperintensity in boththe eaudoputamen and the neocortex. The DWI %HLAobtained 30 minutes after withdrawal of the occluderwas significantly smaller than the prewithdrawal value(55% decline, /?<0.02). In the 2-hour group, the 90-minute (prewithdrawal) %HLA was almost identical tothat at the 30-minute study. An only 17% decline in%HLA was observed 30 minutes after withdrawal of theoccluder (not significant), and DWI hyperintensity wasstill noted in the eaudoputamen and neocortex in ninerats. The postwithdrawal DWI lesion size did notchange during the observation period in either group.No significant differences in DWI %HLA betweenanimals in experiments A and B were noted during theprewithdrawal or postwithdrawal periods.
The T2WI studies did not demonstrate any obviouschange in signal intensity during occlusion in eithergroup. Among the six 1-hour occluded rats with infarctsas demonstrated with the TTC study, only one had awell-defined hyperintense area after withdrawal of theoccluder. In the 2-hour group, postwithdrawal T2WIstudies frequently revealed hyperintensity in the MCAterritory, and the hyperintense areas were almost com-parable to the %HLA in DWI and TTC studies in sevenanimals. Postwithdrawal T2WI %HLA was 6.4±3.3% inthe 1-hour group and 33.2±5.2% in the 2-hour group(p<0.001).
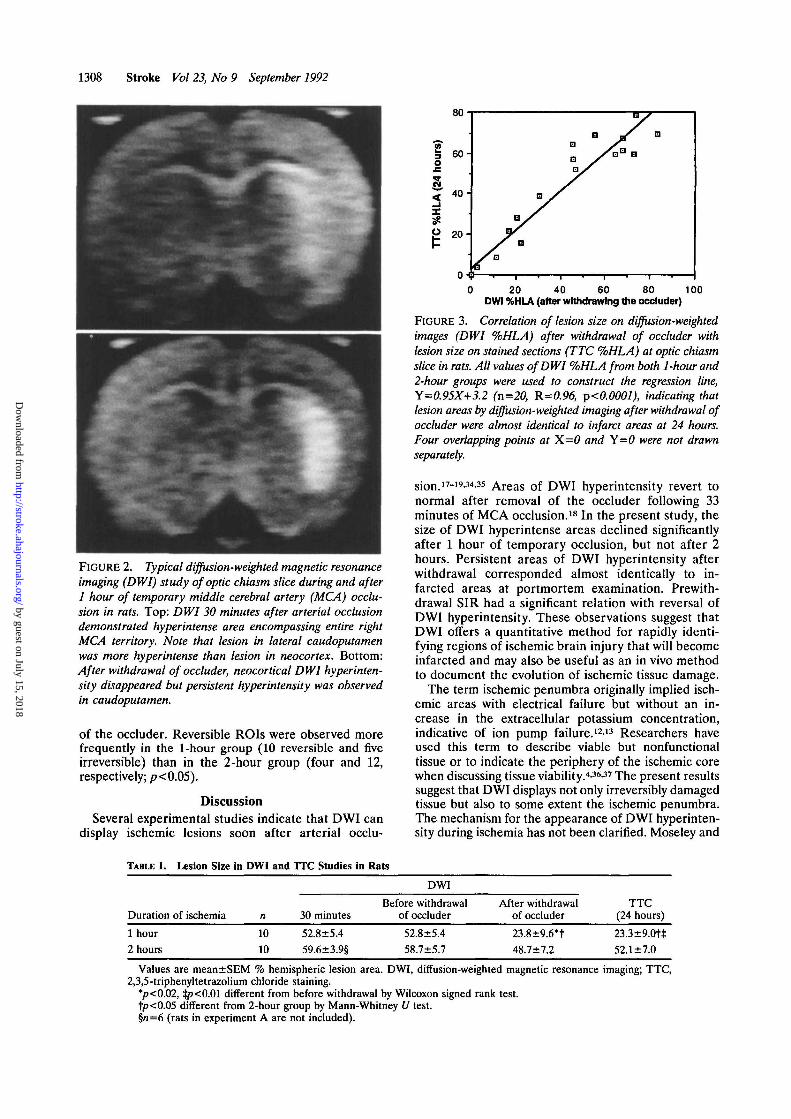
As shown in Table 1, TTC %HLA was significantlysmaller in the 1-hour group than in the 2-hour group(p<0.05). Infarct volume in the 1-hour group was81.1±38.2 mm3, significantly smaller than the 178.8±31.7mm3 observed in the 2-hour group (p<0.05). Infarctson the TTC-stained sections were almost identical inlocation and size to DWI hyperintense areas afterwithdrawal. Postwithdrawal DWI %HLA correlatedwith TTC %HLA (R=0.96, p<0.0001; Figure 3), indi-cating that DWI after withdrawal of the occluder accu-rately predicts infarct size at postmortem examination.
Among the 36 ROIs available for SIR determination,five had no DWI abnormalities throughout the study
by guest on July 15, 2018http://stroke.ahajournals.org/
Dow
nloaded from

Minematsu et al Reperfusion and Diffusion-Weighted Images 1307
F I G U R E 1. Per fusion mag-netic resonance imaging studiesduring and after 2 hours of tem-porary middle cerebral artery(MCA) occlusion in rats. Coro-nal, echo-planar T2-weightedimages at chiasmatic slice wereobtained at 1-second intervalsimmediately after bolus injectionof superparamagnetic contrastagent. Left upper, right upper,left lower, and right lower im-ages were obtained 0, 1, 2, and 3seconds after injection, respec-tively. Top: During arterial oc-clusion, rapid and significantdecline in signal intensity wasobserved in all areas except rightMCA territory. In almost theentire territory of the occludedMCA signal intensity did notnoticeably decline (perfusionscale grade of 3), indicatingmoderate hypoperfusion. Bot-tom: Immediately after with-drawal of occluder, signal wasattenuated from entire brain, in-cluding previously hyperintenseright MCA territory (perfusionscale grade ofO), indicating nor-mal perfusion in previously oc-cluded MCA territory.
period. Among the other 31 ROIs, 14 were reversibleand the remaining were irreversible. SIR just beforewithdrawal of the occluder was 1.186±0.027 in the
reversible ROIs, significantly less than the value in theirreversible ROIs (1.397±0.052, p<0.002). SIR in theirreversible ROIs increased over time after withdrawal
by guest on July 15, 2018http://stroke.ahajournals.org/
Dow
nloaded from
1308 Stroke Vol 23, No 9 September 1992
FIGURE 2. Typical diffusion-weighted magnetic resonanceimaging (DWI) study of optic chiasm slice during and after1 hour of temporary middle cerebral artery (MCA) occlu-sion in rats. Top: DWI 30 minutes after arterial occlusiondemonstrated hyperintense area encompassing entire rightMCA territory. Note that lesion in lateral caudoputamenwas more hyperintense than lesion in neocortex. Bottom:After withdrawal of occluder, neocortical DWI hyperinten-sity disappeared but persistent hyperintensity was observedin caudoputamen.
of the occluder. Reversible ROIs were observed morefrequently in the 1-hour group (10 reversible and fiveirreversible) than in the 2-hour group (four and 12,respectively; p<0.05).
DiscussionSeveral experimental studies indicate that DWI can
display ischemic lesions soon after arterial occlu-
0 20 40 60 80 100DWI %HLA (after withdrawing the occluder)
FIGURE 3. Correlation of lesion size on diffusion-weightedimages (DWI %HLA) after withdrawal of occluder withlesion size on stained sections (TTC %HLA) at optic chiasmslice in rats. All values of DWI %HLA from both 1-hour and2-hour groups were used to construct the regression line,Y=0.95X+3.2 (n=20, R=0.96, p<0.0001), indicating thatlesion areas by diffusion-weighted imaging after withdrawal ofoccluder were almost identical to infarct areas at 24 hours.Four overlapping points at X=0 and Y=0 were not drawnseparately.
sion.17~19-34-35 Areas of DWI hyperintensity revert tonormal after removal of the occluder following 33minutes of MCA occlusion.18 In the present study, thesize of DWI hyperintense areas declined significantlyafter 1 hour of temporary occlusion, but not after 2hours. Persistent areas of DWI hyperintensity afterwithdrawal corresponded almost identically to in-farcted areas at portmortem examination. Prewith-drawal SIR had a significant relation with reversal ofDWI hyperintensity. These observations suggest thatDWI offers a quantitative method for rapidly identi-fying regions of ischemic brain injury that will becomeinfarcted and may also be useful as an in vivo methodto document the evolution of ischemic tissue damage.
The term ischemic penumbra originally implied isch-emic areas with electrical failure but without an in-crease in the extracellular potassium concentration,indicative of ion pump failure.12-13 Researchers haveused this term to describe viable but nonfunctionaltissue or to indicate the periphery of the ischemic corewhen discussing tissue viability.4-36-37 The present resultssuggest that DWI displays not only irreversibly damagedtissue but also to some extent the ischemic penumbra.The mechanism for the appearance of DWI hyperinten-sity during ischemia has not been clarified. Moseley and
TABLE 1.
Duration
1 hour2 hours
Lesion Size
of ischemia
in DWI
n
1010
and I'lC Studies
30 minutes
52.8±5.459.6±3.9§
in RatsDWI
Before withdrawalof occluder
52.8±5.458.7±5.7
After withdrawalof occluder
23.8±9.6*t48.7 ±7.2
TTC(24 hours)
23.3±9.0tt52.1±7.0
Values are mean±SEM % hemispheric lesion area. DWI, diffusion-weighted magnetic resonance imaging; TTC,2,3,5-triphenyltetrazolium chloride staining.
•p<0.02, :jp<0.01 different from before withdrawal by Wilcoxon signed rank test.1p<0.05 different from 2-hour group by Mann-Whitney U test.§/i=6 (rats in experiment A are not included).
by guest on July 15, 2018http://stroke.ahajournals.org/
Dow
nloaded from

Minematsu et al Reperfusion and Diffusion-Weighted Images 1309
colleagues1718 speculated that the drop in ADC result-ing in DWI hyperintensity is related to cytotoxic edema.Acute energy and ionic failure, which results in cyto-toxic edema, does not per se indicate irreversible dam-age and may in part recover even after prolongedischemia.l2-13-38 Local hypothermic effects, changes intissue osmolarity, and the lack of pulsatile flow inoccluded vessels are other possible, but less likely,factors affecting the ADC of water protons soon afterthe onset of ischemia.39 We cannot exclude the contri-bution of these factors in the appearance and reversal ofDWI hyperintensity.
The present study suggests that the potential forreversal of DWI hyperintensity after withdrawal of theoccluder can partly be predicted by prewithdrawal SIR.This result may imply less reduction in water diffusion inreversible lesions because ADC is the most importantdeterminant of DWI signal intensity. SIR assessmentsof DWI reversibility, however, may be complicated bychanges in other MRI parameters such as Tl, T2, andproton density. These parameters do not account forDWI signal intensity during the early ischemia-reperfu-sion period,18'35 but this may not be true later. Increasesin proton density and T2 prolongation probably contrib-uted to T2WI hyperintensity after withdrawal in the2-hour group and possibly to further increases in SIR onDWI in the irreversible ROIs. DWI signal intensity isvulnerable to motion artifact and varies depending onthe gradient b value. The acquisition of ultrafast diffu-sion studies allows for the rapid calculation of ADC ateach pixel, which should provide a better indicator forreversibility of ischemic tissue injury than SIR.40
In rat MCA occlusion models, reestablishing bloodflow into ischemic regions is difficult and can reliably bedone in only a few models.6-736 Selman et al6 reportedthat a significant recovery in energy metabolism wasnoted in a 1-hour temporary occlusion group but not ina 2-hour group. Kaplan et al7 investigated the effects ofvarious durations of temporary arterial occlusion inspontaneously hypertensive rats on the neocortical in-farct volume at 24 hours. These authors found that focalischemia for 1 hour caused little or no infarction, whileischemic intervals of 2 and 3 hours produced largervolumes of infarcted tissue. In a study using a ratintraluminal suture MCA occlusion model, infarcts in-volved mainly the caudoputamen after 60 minutes oftemporary occlusion but encompassed the whole cau-doputamen and large parts of the neocortex, resemblingthe lesions observed with permanent occlusion, after180 minutes of occlusion.37 Based on these observationsand our data, it appears that in rat temporary MCAocclusion models, 1 hour of ischemia is reproduciblyassociated with ischemic lesion reversibility, particularlyin neocortical regions.
In similar rat suture MCA occlusion models, bloodflow in the MCA territory drops to 2-30% of baselinelevels during arterial occlusion but recovers to approx-imately 70% 2 hours after withdrawal of the oc-cluder.3041 We performed the perfusion MRI studies toqualitatively document lack of tissue perfusion duringarterial occlusion and restoration of tissue perfusionafter withdrawing the occluder because this method wasreadily adaptable to the present study, which used ratsnot subjected to craniectomy, examined in a strongmagnetic field, and permitted to survive for 24 hours. A
recent study confirmed the reliability of the perfusionMRI technique for detecting ischemic regions.27 Thesignificant correlation of perfusion scale grade withDWI %HLA during ischemia in the present studysupports this observation. The perfusion MRI studiesqualitatively demonstrated recovery of perfusion afterwithdrawal of the occluder but did not always shownormal perfusion, probably related to perfusion distur-bances during recirculation previously observed afterglobal42-43 and focal10-36 brain ischemia in animals.
DWI offers a novel method for rapidly identifyingregions of ischemic injury in vivo and could potentiallyhelp to determine which tissue damage is reversible.Warach et al44 have demonstrated that DWI can showan infarct during the first few hours after stroke onset inhumans, in agreement with previous animal studies.This method might be adaptable to treatment trials ofhuman stroke because it offers the capability to monitorthe evolution of ischemic tissue damage, as shown in thepresent study. Further investigations are necessary toobtain more accurate indicators for tissue damage re-versibility in ischemic regions and to apply this technol-ogy as an in vivo assessment of therapeutic interventionfor animal and human ischemic stroke.
AcknowledgmentsThe authors are grateful to Drs. Robert Turner (Laboratory
of Cardiac Energetics, National Institutes of Health) andMichael E. Moseley (Department of Radiology, University ofCalifornia, San Francisco) for the echo-planar imaging pulsesequences and helpful discussions regarding their use. Wewould like to thank Vanessa Brown and Mary-Ellen Meadowsfor their technical assistance.
References1. Jones TH, Morawetz RB, Crowell RM, Marcoux FW, FitzGibbon
SJ, DeGirolami U, Ojemann RG: Thresholds of focal cerebralischemia in awake monkeys. J Neurosurg 1981;54:773-782
2. Heiss W-D, Rosner G: Functional recovery of cortical neurons asrelated to degree and duration of ischemia. Ann Neurol 1983;14:294-301
3. Sundt TM Jr, Grant WC, Garcia JH: Restoration of middle cere-bral artery flow in experimental infarction. J Neurosurg 1969;31:311-322
4. Olsen TS, Larsen B, Herning M, Skriver EB, Lassen NA: Bloodflow and vascular reactivity in collaterally perfused brain tissue:Evidence of an ischemic penumbra in patients with acute stroke.Stroke 1983;14:332-341
5. Weinstein PR, Anderson GG, Telles DA: Neurological deficit andcerebral infarction after temporary middle cerebral artery occlu-sion in unanesthetized cats. Stroke 1986;17:318-324
6. Selman WR, Crumrine RC, Ricci AJ, LaManna JC, RatchesonRA, Lust WD: Impairment of metabolic recovery with increasingperiods of middle cerebral artery occlusion in rats. Stroke 1990;21:467-471
7. Kaplan B, Brint S, Tanabe J, Jacewicz M, Wang X-J, Pulsinelli W:Temporal thresholds for neocortical infarction in rats subjected toreversible focal cerebral ischemia. Stroke 1991;22:1032-1039
8. Zivin J, Fisher M, DeGirolami U, Hemenway CC, Stashak JA:Tissue plasminogen activator reduces neurological damage aftercerebral embolism. Science 1985;230:1289-1292
9. Del Zoppo GJ, Zeumer H, Harker LA: Thrombolytic therapy instroke: Possibilities and hazards. Stroke 1986;17:595-607
10. Tamura A, Asano T, Sano K: Correlation between rCBF andhistological changes following temporary middle cerebral arteryocclusion. Stroke 1980;ll:487-493
11. Koizumi J, Yoshida Y, Nishigaya K, Kanai H, Ooneda G: Exper-imental studies of ischemic brain edema: Effect of recirculation ofthe blood flow after ischemia on post-ischemic brain edema. Jpn JStroke 1989;11:11-17
by guest on July 15, 2018http://stroke.ahajournals.org/
Dow
nloaded from

1310 Stroke Vol 23, No 9 September 1992
12. Astrup J, Symon L, Branston NM, Lassen NA: Cortical evokedpotential and extracellular K* and H+ at critical levels of brainischemia. Stroke 1977;8:51-57
13. Astrup J, Siesjo BK, Symon L: Thresholds in cerebral ischemia:The ischemic penumbra. Stroke 1981;6:723-725
14. Powers WJ: Cerebral hemodynamics in ischemic cerebrovasculardisease. Ann Neurol 1991 ;29:231-240
15. Brant-Zawadzki M, Pereira B, Weinstein P, Moore S, KucharczykW, Berry I, McNamara M, Derugin N: MR imaging of acuteexperimental ischemia in cats. AJNR 1986;7:7-11
16. Yuh WTC, Crain MR, Loes DJ, Greene GM, Ryals TJ, Sato Y:MR imaging of cerebral ischemia: Findings in the first 24 hours.AJNR 1991;12:621-629
17. Moseley ME, Cohen Y, Mintorovitch J, Chileuitt L, Shimizu H,Kucharczyk J, Wendland MF, Weinstein PR: Early detection ofregional cerebral ischemia in cats: Comparison of diffusion- andT2-weighted MRI and spectroscopy. Magn Reson Med 1990;14:330-346
18. Mintorovitch J, Moseley ME, Chileuitt L, Shimizu H, Cohen Y,Weinstein PR: Comparison of diffusion- and T2-weighted MRI forthe early detection of cerebral ischemia and reperfusion in rats.Magn Reson Med 1991;18:39-50
19. Minematsu K, Li L, Fisher M, Sotak CH, Davis MA, Fiandaca MS:Diffusion-weighted magnetic resonance imaging: Rapid and quan-titative detection of focal brain ischemia. Neurology 1992;42:235-240
20. Stejskal EO, Tanner JE: Spin diffusion measurements: Spin echoesin the presence of a time-dependent field gradient. J Chem Phys1965;42:288-292
21. Le Bihan D, Breton E, Lallemand D, Grenier P, Cabanis E,Laval-Jeantet M: MR imaging of intravoxel incoherent motions:Application to diffusion and perfusion in neurologic disorders.Radiology 1986;161:401-407
22. Le Bihan D, Breton E, Lallemand D, Aubin ML, Vignaud J,Laval-Jeantet M: Separation of diffusion and perfusion in intra-voxel incoherent motion (IVIM) MR imaging. Radiology 1988;168:497-505
23. Schuier FJ, Hossmann K-A: Experimental brain infarcts in cats: II.Ischemic brain edema. Stroke 1980;l 1:593-601
24. Klatzo I: Pathophysiological aspects of brain edema. Ada Neuro-pathol (Berl) 1987;72:236-239
25. Auer RN, Siesjo BK: Biological differences between ischemia,hypoglycemia and epilepsy. Ann Neurol 1988;24:699-707
26. Rosen BR, Belliveau JW, Vevea JM, Brady TJ: Perfusion imagingwith NMR contrast agents. Magn Reson Med 1990;14:249-265
27. Wendland MF, White DL, Aicher KP, Tzika AA, Moseley ME:Detection with echo-planar MR imaging of transit of susceptibilitycontrast medium in a rat model of regional brain ischemia. JMRI1991;l:285-292
28. Zea Longa E, Weinstein PR, Carlson S, Cummins R: Reversiblemiddle cerebral artery occlusion without craniectomy in rats.Stroke 1989;20:84-91
29. Koizumi J, Yoshida Y, Nakazawa T, Ooneda G: Experimentalstudies of ischemic brain edema: 1. A new experimental model ofcerebral embolism in rats in which recirculation can be introducedin the ischemic area. Jpn J Stroke 1986;8:l-8
30. Nagasawa H, Kogure K: Correlation between cerebral blood flowand histologic changes in a new rat model of middle cerebral arteryocclusion. Stroke 1989;20:1037-1043
31. Mansfield P: Multiplanar image formation using NMR spin-echoes. J Phys Chem Solid State Phys 1977;10:L55-L58
32. Stehling MK, Turner R, Mansfield P: Echo-planar imaging: Mag-netic resonance imaging in a fraction of a second. Science 1991;254:43-50
33. Bederson JB, Pitts LH, Germano SM, Nishimura MC, Davis RL,Bartkowski HM: Evaluation of 2, 3, 5-triphenyltetrazolium chlo-ride as a stain for detection and quantification of experimentalcerebral infarction in rats. Stroke 1986;17:1304-1308
34. Moseley ME, Kucharczyk J, Mintorovitch J, Cohen Y,Kurhanewicz J, Derugin N, Asgari H, Norman D: Diffusion-weighted MR imaging of acute stroke: Correlation withT2-weighted and magnetic susceptibility-enhanced MR imaging incats. AJNR 1990;l 1:423-429
35. Knight RA, Ordidge RJ, Helpern JA, Chopp M, Rodolosi LC,Peck D: Temporal evolution of ischemic damage in rat brain mea-sured by proton nuclear magnetic resonance imaging. Stroke 1991;22:802-808
36. Shigeno T, Teasdale GM, McCulloch J, Graham DI: Recirculationmodel following MCA occlusion in rats: Cerebral blood flow, cere-brovascular permeability, and brain edema. J Neurosurg 1985;63:272-277
37. Memezawa H, Smith M-L, Terashi A, Siesjo BK: Ischemic pen-umbra in a model of middle cerebral artery occlusion in the rat.(abstract) J Cereb Blood Flow Metab 1991; 11 (suppl 2):S550
38. Hossmann K-A, Sakaki S, Zimmermann V: Cation activities inreversible ischemia of the cat brain. Stroke 1977;8:77-81
39. Le Bihan D: Molecular diffusion nuclear magnetic resonanceimaging. Magn Reson Q 1991;7:l-30
40. Fisher M, Sotak CH, Minematsu K, Li L: Innovative magneticresonance technologies for evaluating cerebrovascular disease.Ann Neurol (in press)
41. Nishigaya K, Yoshida Y, Sasuga M, Nukui H, Ooneda G: Effect ofrecirculation on exacerbation of ischemic vascular lesions in ratbrain. Stroke 1991;22:635-642
42. Ames A III, Wright RL, Kowada M, Thurston JM, Majno G:Cerebral ischemia: II. The no-reflow phenomenon. Am J Pathol1968;52:437-453
43. Ginsberg MD, Budd WW, Welsh FA: Diffuse cerebral ischemia inthe cat: I. Local blood flow during severe ischemia and recircula-tion. Ann Neurol 1978;3:482-492
44. Warach S, Chien D, Li W, Ronthal M, Edelman RR: Fast mag-netic resonance diffusion-weighted imaging of acute human stroke.Neurology (in press)
Editorial Comment
Water molecules in tissue undergo semirandom trans-lational movement, known as restricted diffusion. Theassociated coefficient of diffusion is exquisitely sensitiveto the viscosity of the tissue and the presence andintegrity of cellular structures. With the imposition ofpulsed magnetic field gradients onto spin/echo magneticresonance imaging (MRI),1 changes of restricted diffu-sion of water protons in intact and damaged tissues canbe presented in an image format and highlighted.2 Thetechnique of generating image contrast based on differ-ences of restricted diffusion coefficients of water protonsin tissue is known as diffusion-weighted MRI (DWI).
In a major step forward in the application of DWI tothe investigation of cerebral ischemia, Minematsu et alreport that DWI performed within 30 minutes after
transient occlusion of the middle cerebral artery in ratsaccurately predicts tissue destined for infarction andmay discriminate between reversibly and irreversiblydamaged tissue.
DWI is emerging as an effective and sensitive imagingmodality for studies of experimental cerebral ischemia.DWI allows recognition of focal ischemic injury withinminutes after an ischemic insult, far faster and withgreater sensitivity than techniques employing T2-weighted MRI.3-5 The evolution of the restricted diffu-sion coefficient in the lesion, and thereby the progressionof ischemic cell damage, can be monitored,6 and incombination with T2-weighted imaging DWI may dis-cern the pathophysiology of developing lesions.7 Move-ment of water is essential to cell viability, and alterations
by guest on July 15, 2018http://stroke.ahajournals.org/
Dow
nloaded from

K Minematsu, L Li, C H Sotak, M A Davis and M Fisherimaging in rats.
Reversible focal ischemic injury demonstrated by diffusion-weighted magnetic resonance
Print ISSN: 0039-2499. Online ISSN: 1524-4628 Copyright © 1992 American Heart Association, Inc. All rights reserved.
is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231Stroke doi: 10.1161/01.STR.23.9.1304
1992;23:1304-1310Stroke.
http://stroke.ahajournals.org/content/23/9/1304World Wide Web at:
The online version of this article, along with updated information and services, is located on the
http://stroke.ahajournals.org//subscriptions/
is online at: Stroke Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document. Permissions and Rights Question and Answer available in the
Permissions in the middle column of the Web page under Services. Further information about this process isOnce the online version of the published article for which permission is being requested is located, click Request
can be obtained via RightsLink, a service of the Copyright Clearance Center, not the Editorial Office.Stroke Requests for permissions to reproduce figures, tables, or portions of articles originally published inPermissions:
by guest on July 15, 2018http://stroke.ahajournals.org/
Dow
nloaded from