Retroperitoneal Anatomy
13
Chapter #1 – Anatomy of Retroperitoneum, Adrenals, Kidneys, and Ureters THE RETROPERITONEUM Posterior Abdominal Wall Describe the lumbodorsal fascia - surrounds sacrospinalis & quadratus lumborum muscles, making posterior abdominal wall - originates from spinous processes of lumbar vertebrae & extends anteriorly and cranially - separates into 3 layers: 1) posterior posterior covering of sacrospinalis & origin of latissimus dorsi 2) middle b/w sacrospinalis posteriorly & quadratus lumborum anteriorly 3) anterior anterior covering of quadratus lumborum and forms posterior margin of retroperitoneum - 3 layers connect laterally with transversus abdominis muscle What is the significance of the dorsal lumbotomy incision? - vertical incision lateral to border of sacrospinalis & quadratus lumborum } Petit’s triangle sacrospinalis is middle layer - allows entrance to retroperitoneum without violation of musculature } no muscles are cut What are the muscles of the lateral flank? - External oblique from lower ribs, moving lateral to medial going caudally attaches to iliac crest caudally and rectus sheath anteriorly - Internal oblique from lower ribs, moving medial to lateral going caudally attaches to iliac crest caudally and lumbodorsal fascia posteriorly - Transversus abdominis from lumbodorsal fascia, running directly transversely attaches anteriorly and medially to rectus sheath - transversalis fascia lies directly beneath transversus abdominis m. and above retroperitoneum Describe the Psoas and Iliacus muscles - Psoas originates from T12 to L5 and is covered by the psoas fascia 50% have psoas minor, which sits medial to psoas major - Iliacus attaches to the inner aspect of the iliac wing (lateral to psoas) - psoas & iliacus join caudally to form iliopsoas muscle, which inserts into lesser trochanter What are the limits of the pleura? - anteriorly 8 th rib - midaxillary line 10 th rib - posteriorly 12 th rib
-
Upload
drsonosy1976 -
Category
Documents
-
view
66 -
download
3
description
anatomy of the retroperitoneum for urologists
Transcript of Retroperitoneal Anatomy

Chapter #1 – Anatomy of Retroperitoneum, Adrenals, Kidneys, and Ureters
THE RETROPERITONEUM Posterior Abdominal Wall Describe the lumbodorsal fascia - surrounds sacrospinalis & quadratus lumborum muscles, making posterior abdominal wall - originates from spinous processes of lumbar vertebrae & extends anteriorly and cranially - separates into 3 layers: 1) posterior posterior covering of sacrospinalis & origin of latissimus dorsi 2) middle b/w sacrospinalis posteriorly & quadratus lumborum anteriorly 3) anterior anterior covering of quadratus lumborum and forms posterior margin of
retroperitoneum - 3 layers connect laterally with transversus abdominis muscle What is the significance of the dorsal lumbotomy incision? - vertical incision lateral to border of sacrospinalis & quadratus lumborum } Petit’s triangle sacrospinalis is middle layer - allows entrance to retroperitoneum without violation of musculature } no muscles are cut What are the muscles of the lateral flank? - External oblique from lower ribs, moving lateral to medial going caudally attaches to iliac crest caudally and rectus sheath anteriorly - Internal oblique from lower ribs, moving medial to lateral going caudally attaches to iliac crest caudally and lumbodorsal fascia posteriorly - Transversus abdominis from lumbodorsal fascia, running directly transversely attaches anteriorly and medially to rectus sheath - transversalis fascia lies directly beneath transversus abdominis m. and above retroperitoneum Describe the Psoas and Iliacus muscles - Psoas originates from T12 to L5 and is covered by the psoas fascia 50% have psoas minor, which sits medial to psoas major
- Iliacus attaches to the inner aspect of the iliac wing (lateral to psoas) - psoas & iliacus join caudally to form iliopsoas muscle, which inserts into lesser trochanter What are the limits of the pleura? - anteriorly 8th rib
- midaxillary line 10th rib - posteriorly 12th rib


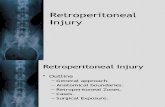
LUMBODORSAL INCISION } no muscles cut
Great Vessels What are the branches of the aorta? enters at T12 via aortic hiatus and bifurcates at level of L4 1) paired inferior phrenics inferior diaphragm & superior portion of adrenal 2) celiac trunk stomach, liver, spleen, GB, duodenum
common hepatic, L gastric, & splenic arteries - gastroduodenal a. comes off common hepatic, then gives off R gastroepiploic a.
- L gastroepiploic a. comes off splenic artery 3) paired adrenals 4) SMA entire small bowel & majority of colon communicates with celiac trunk vasculature via pancreaticoduodenal artery
- this can supply liver retrogradely if celiac trunk tied off (trauma) 5) paired renals overlie L2
6) paired gonadals can be ligated due to collaterals (deferential & cremasteric; uterine) 7) IMA distal end of transverse colon, descending, sigmoid, & rectum can be ligated due to collaterals (SMA, middle hemorrhoidal, inferior hemorrhoidal) 8) 4 paired lumbars posterior body wall & spine 9) middle sacral posterior branch just before bifurcation
supplies rectum & anterior sacrum
What is the course of the gonadal artery? - male crosses anterior to IVC on right crosses over ureter and exits retroperitoneum at internal inguinal ring - female crosses anterior to IVC on right crosses over ureter moving laterally then crosses back over external iliacs into pelvis, where it proceeds via suspensory ligament to ovary

What are the tributaries to the IVC?
from the confluence of the common iliacs at L5, which lies posterior and to the right of the aortic bifurcation
1) middle sacral posterior tributary at jxn of common iliac veins 2) paired lumbars generally parallel to lumbar arteries also connects IVC to azygous on R and hemiazygous on L, providing alternate
venous drainage of retroperitoneum 3) gonadal veins course similar to gonadal arteries but different once close to IVC drains into IVC on R, into left renal vein on L runs lateral to ureter 4) paired renal veins generally directly anterior to renal arteries
R is short (2-4cm), L is long (6-10cm) small minority will have R gonadal or lumbar entering R renal vein posteriorly L renal vein gets gonadal inferiorly, lumbar posteriorly, & adrenal superiorly
before crossing anterior to the aorta, just under SMA L renal vein can be retroaortic on occasion 5) adrenal R adrenal goes directly into IVC but posteriorly, making dissection difficult
L adrenal drains into L renal vein 6) short hepatic 7) inferior phrenic R drains into IVC on posterolateral aspect, L drains into L renal 8) hepatic veins 3 large trunks from liver

Nervous System What autonomic nerves lie within the retroperitoneum? - sympathetic
preganglionic fibers originate from T and L spine (T1-L3) enter retroperitoneum via paired sympathetic chains & lumbar spinal nerves from sympathetic chain, preganglionic fibers have 3 different courses;
1) travels into autonomic plexuses (splanchnic nerves) where they synapse with postganglionic fibers these proceed to the abdo viscera
2) synapses within sympathetic chain, where postganglionic fibers are sent to body wall & lower extremities
3) travels directly to adrenal medulla, controlling release of catecholamines - parasympathetics
preganglionic fibers originate from C and S spine also get input from vagus nerve travel into aortic autonomic plexuses, where they synapse with postganglionic fibers that
are distributed to the viscera and organs What are the major autonomic nerve plexuses? 1) celiac } largest plexus; innervates kidney, adrenal, renal pelvis, and ureter 2) superior hypogastric } innervates pelvic urinary and genital tract
} lies on aorta anterior to bifurcation, extending down on anterior surface of L5 3) inferior hypogastric } contiguous with superior hypogastric plexus and extends into pelvis
What somatic nerves lie within the retroperitoneum? arises from the lumbosacral plexus (T12-L5) superior branches form within and pierce the psoas inferior branches pass medial to the psoas - Subcostal (T12) extends laterally beneath 12th rib - Iliohypogastric (L1) motor to internal oblique & transversus
sensory to posterolateral gluteal skin - Ilioinguinal (L1) motor to internal oblique & transversus sensory to upper medial thigh & base of penis/anterior scrotum/mons pubis
- Lateral Cutaneous nerve of thigh (L2-L3) sensory to anterior and lateral thigh to knee - Genitofemoral (L1-L2) lies directly atop and parallels psoas
motor to cremaster & dartos muscles in scrotum (genital branch only) sensory to scrotum/mons/labia majora & skin of upper thigh
(genital & femoral branches) - Femoral (L2-L4) hidden by psoas until it exits abdomen just lateral to femoral artery
motor to psoas, iliacus, and large muscles of anterior thigh (quads) sensory to anterior thigh & medial leg
can be injured by retractor placed on inguinal ligament (can’t extend knee, numb on anterior thigh)
- Obturator (L2-L4) motor to adductor muscles of thigh (longus, brevis, gracilis, pectineus) sensory to medial thigh
can be injured during RP pelvic LN dissection (can’t adduct leg) - Sciatic (L4-S3) body’s largest nerve
motor & sensory to legs (common peroneal + tibial) - Pudendal (S2-S4) branches include inferior rectal, perineal, dorsal penile nerves

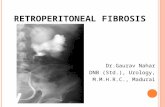
LUMBOSACRAL NERVOUS PLEXUS

LUMBAR PLEXUS IN POSTERIOR ABDOMINAL REGION
Lymphatics What is the lymphatic drainage of the lower extremities, perineum and external genitalia? - external iliac nodes common iliac nodes vertical lumbar lymphatic chains - lumbar lymphatics are important as the primary drainage from the kidneys & testes
- flow is cranial and also R L - GI lymphatics follow the vasculature (IMA, SMA, celiac) - eventually these lymphatics join posterior to aorta, between aorta and IVC, at level of L1 or L2 to form
cisterna chyli (R side of aorta), which becomes the thoracic duct cisternal chyli is a retrocrural structure - thoracic duct turns toward left thorax at level of T4 to join venous system at jxn of left jugular
and subclavian veins What is the lymphatic drainage of the testes? - right right inter-aortocaval nodes & paracaval small amount of drainage to left para-aortic nodes
- left left para-aortic nodes

Duodenum, Pancreas, Colon What are the 4 sections of the duodenum? 1) ascending 5cm and is closely related to GB 2) descending lies immediately anterior to R renal hilum & pelvis and surrounds head of pancreas
(also receives common bile duct) often Kocherized to access R kidney, R renal pelvis & upper abdo structures 3) horizontal crosses anterior to the IVC 4) distal ascending cross anterior to aorta to transition into jejunum Where is the pancreas situated? - head lies on medial aspect of 2nd portion of duodenum, close to R renal hilum/pelvis - tail lies close to L adrenal gland and upper pole of L kidney - splenic artery & vein travel laterally from the celiac along the posterior aspect of the pancreas Which aspects of the colon are retroperitoneal? - ascending & descending colon - hepatic & splenic flexure overlie the ipsilateral kidney - hepatocolic and splenocolic ligaments tether the liver and spleen to the colon
THE ADRENALS Describe the gross anatomy of the adrenal glands - 3-5cm in adults, weighing about 5g and yellow-gold in colour - enclosed within Gerota’s fascia and separated from the UP of the kidney by a layer of connective tissue - R more superior & pyramidal in shape; often has a retrocaval wing - L more inferior & crescentic; lies more medial to upper pole What is the composition of the adrenal gland? - embryologically distinct from kidney - adrenal cortex makes up 90% of adrenal mass and is of mesodermal origin - zona glomerulosa mineralocorticoids (eg aldosterone) - zona fasciculate glucocorticoids (eg cortisol) & sex steroids - zona reticularis sex steroids (eg androgens) - adrenal medulla is made up of chromaffin cells derived from neural crest origin - innervated directly by preganglionic sympathetic fibers - catecholamine release is controlled by sympathetics What is the blood supply to the adrenals? - arterial branches from inferior phrenic artery, aorta and renal artery - venous single vein that exits anteromedially into aorta on R and renal vein on L
What is the lymphatic drainage of the adrenals? - follows the adrenal vein and empties into the para-aortic nodes

THE KIDNEYS
Gross and Microscopic Anatomy What are the 8 main functions of the kidney? }} “WEB DECAF” 1) Waste excretion
2) Electrolyte regulation 3) BP control 4) Drug metabolism 5) Epo production 6) Ca and PO4 metabolism (1,25-dihydroxyVit D) 7) Acid-base regulation 8) Fluid homeostasis
What do the kidneys look like grossly? - 150g in M, 135g in F
- 10-12cm vertically, 5-7cm transversely, and 3cm in AP - R tends to be shorter & wider, and sits 1-2cm lower - in kids, relatively larger with more prominent fetal lobations - can find a Dromedary Hump focal bulge in parenchyma along lateral contour (normal) - renal sinus lies at medial aspect of kidney and is filled with renal sinus fat and contains vascular structures and collecting system before exiting the kidney - composed of cortex (peripheral, lighter in colour) & medulla (distinct renal pyramids, darker in colour) - apex of renal medulla is papilla each papilla is cupped by a minor calyx
Describe the rotational axes of the kidney - 30° anterior rotation, medial tilt of upper poles, anterior displacement of lower pole What are the columns of Bertin? - extensions of renal cortex found between the renal medullary pyramids - contain renal vessels perforating to periphery from renal sinus (interlobar arteries) avoided during PCNL to decrease blood loss puncture into collecting system through renal medullary pyramid into calyx

Relations and Investing Fascia Where are the kidneys located in relation to the spinal column? - L body of T12 to top of L3 - R top of L1 to bottom of L3 What are the structures surrounding the kidney? - posteriorly (upper 1/3rd) diaphragm - medially (lower 2/3rds) psoas - laterally quadratus lumborum and aponeurosis of transversus abdominis muscle - right kidney } hepatorenal ligament extension of parietal peritoneum } upper pole adrenal } medial of right (upper 1/3rd) duodenum } anteriorly hepatic flexure of colon - left kidney } splenorenal ligament attaches to splenic capsule } upper pole adrenal (slightly medial), spleen, tail of pancreas, and splenic vessels } anteriorly splenic flexure of colon
Describe Gerota’s fascia - extension off transversalis fascia (intermediate stratum)
Toldt’s leaf (anterior), Zuckerkandl’s leaf (posterior) - encloses kidney & perinephric fat } surrounded by paranephric fat - closed superiorly & laterally } fuses with other side medially, extending across midline } open potential space inferiorly What are the boundaries of Petit’s triangle? - inferiorly crest of ilium \ - laterally external oblique muscle \ can drain psoas/retroperitoneal abscess - medially latissimus dorsi muscle / via Petit’s triangle - floor internal oblique muscle /
Renal Vasculature Describe the renal pedicle - at level of L2 vertebra } vein anterior, artery posterior, renal pelvis and ureter most posterior (VAP) Describe the arterial blood supply of the kidney *** no collaterals end arteries *** - renal artery } gives off branches (adrenal, renal pelvis, ureter) - segmental most commonly;
1 posterior (branches before entering hilum, so posterior to renal pelvis) *** can cause UPJO if crosses anterior to ureter ***
4 anterior (apical, upper, middle, lower/basilar variability) - lobar - interlobar (run through columns of Bertin) - arcuate (run along corticomedullary jxn) - interlobular - afferent (to glomerulus) efferent to vasa recta
Describe the venous drainage of the kidney *** ++ collaterals *** - efferent arteriole to vasa recta - interlobular (communicate freely via subcapsular plexus) - arcuate - interlobar - lobar - segmental (parallels segmental arteries } due to collaterals, can be sacrificed)
- renal vein

Where is the avascular plane of the kidney? - between the posterior segmental & anterior segmentals } Brodel’s line - usually posterior to lateral margin } can inject dye into posterior branch to identify How common are anatomic variations in renal vasculature? - occurs in 25-40% of people - most common variation is supernumerary renal arteries (more often on L) more common to UP than LP
- less common to have supernumerary renal veins (usually on right) - may have retroaortic left renal vein can also have circum-aortic renal vein - variations more common in ectopic kidneys, horseshoe kidneys
Renal Lymphatics Describe the lymphatic drainage of the kidney - lymphatics drain through columns of Bertin into renal sinus, then exit vial hilum - branches from renal capsule, pelvis, upper ureter, perinephric tissues drain into LNs near renal vein - the drainage then varies according to side (NO left to right); right paracaval and right interaortocaval nodes (from common iliacs to diaphragm) can also go to retrocrural nodes or the para-aortic nodes left para-aortic nodes (from IMA to diaphragm) can also go to retrocrural nodes or directly into thoracic duct above diaphragm Renal Collecting System Describe the microscopic anatomy of the collecting system - renal corpuscle
in renal cortex } glomerulus (covered by podocytes) and Bowman’s capsule - PCT - loop of Henle extends variable lengths into medulla (descending and ascending limbs) - DCT - collecting tubules - collecting duct empties into apex of medulla, the renal papilla Describe the gross anatomy of the collecting system 1) renal papilla
- usually 7-9 per kidney } anterior (lateral) & posterior (posterior) rows - drains into minor calyces
2) minor calyces - have intrinsic pacemaker cells that are responsible for ureteral peristalsis
- compound calyces more common at upper & lower poles (more prone to scarring) 3) infundibulum variable diameters
4) major calyces upper, middle, lower pole 5) renal pelvis variable size from small intrarenal to large extrarenal 6) UPJ Renal Innervation
What is the innervation of the kidney? - autonomic vasomotor control (although not essential eg Tx) - sympathetics T8 to L1 celiac & aorticorenal ganglia via autonomic plexus along renal artery - parasympathetics vagus nerve travel with sympathetics

THE URETERS Describe the 3 layers of the ureter - generally 22-30cm, ~5mm in diameter 1) inner layer transitional epithelium overlying lamina propria 2) muscle layer smooth muscle layer contiguous with muscle covering renal calyces & renal pelvis consists of inner longitudinal & outer circular layer; provides peristalsis 3rd outer smooth muscle layer exists in distal ureter 3) outer layer adventitial layer that encompasses blood vessels & lymphatics that travel along ureter Describe the course of the ureters? - begins at UPJ, which lies posterior to renal artery - travels inferiorly along anterior surface of psoas muscle - 1/3 of way to bladder, the ureter crosses under the gonadal vessels then crosses over the iliac vessels,
generally marking the bifurcation of common iliacs into internal & external - in F pelvis, the ureter is crossed anteriorly by the uterine artery & is closely related to cervix common locations for ureteric injury during gyne OR - head toward bladder underneath obliterated umbilical artery (branch of internal iliac) List structures that cross over the ureter in the female - gonadal vein - round ligament - obliterated umbilical artery - uterine artery - superior vesical artery - inferior vesical artery What are the 3 narrowest parts of the ureter? 1) UPJ 2) crossing over the iliac vessels 3) UVJ narrowest part Describe the ureteral segments 1) abdominal ureter (UPJ to iliacs) and pelvic ureter (iliacs to UVJ) 2) upper (UPJ to upper border of sacrum), middle (upper to lower border of sacrum) & lower (lower
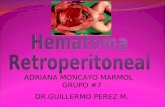
border of sacrum to bladder) What is the blood supply to the ureters? - arterial supply from multiple branches along its course (venous follows arterial) - MEDIAL supply to abdominal ureter & LATERAL supply to pelvic ureter - upper renal artery, gonadal artery, aorta, common iliac artery - lower internal iliac artery or its branches (vesical, uterine, middle rectal, vaginal arteries) - ureteric arterial vessels travel longitudinally within periureteral adventitia What is the lymphatic drainage of the ureters? - abdominal para-aortic for L ureter; right paracaval & inter-aortocaval nodes for R - pelvic internal, external & common iliac nodes - upper & renal pelvis joins renal lymphatics

What is the innervation of the ureter? - peristalsis doesn’t need outside autonomic input - peristalsis originates & propagates from intrinsic smooth muscle pacemaker sites in minor calyces - ureter does get some autonomic input (likely a modulating effect) put the role is unclear; - sympathetics } some preganglionic fibers from T10-L2 } some postganglionic fibers from ganglia in aorticorenal, superior & inferior
hypogastric autonomic plexuses - parasympathetics } S2-S4 Why does renal colic occur? - renal pain fibers stimulated by distention in renal capsule, renal collecting system, or ureter mediated by PGs } role of NSAIDs in management of renal colic
- direct mucosal irritation may also stimulate nociceptors - signals travel with the sympathetics and result in a visceral-type pain
can get N/V
ARTERIAL BLOOD SUPPLY TO THE URETER