Retrograde Approaches in tic Therapy

of 12
-
Upload
florin-ionescu -
Category
Documents
-
view
226 -
download
0
Transcript of Retrograde Approaches in tic Therapy
-
8/3/2019 Retrograde Approaches in tic Therapy
1/12
-
8/3/2019 Retrograde Approaches in tic Therapy
2/12
-
8/3/2019 Retrograde Approaches in tic Therapy
3/12
Re t ro g ra d e e n d o d o n t ic t re a tme n100 76.3
1Hirs
7
Fema9
|111 00CDJOro oPoz
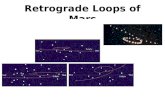
I n t r a s u r g i c a l r o o tc a n a l t r e a t m e n t P r e v i o u s r o o tc a n a l tr e a t m e n t Equal use ofb o t h t e c h n i q u e sFig. L Graphic representation of the success rate of apical surgery as reported in 36 studies. The prognosis is related to the surgicaand endodontic technique, and the studies are grouped accordingly. The mean success rate of each group is presented above thcolumns. Studies in which orthograde endodontic treatment was performed in conjunction with surgery demonstrate the highessuccess rate.
composite resins to dentin improves their sealingability (27, 28), which may be advantageous to theapplication of composite resins as retrograde fillingmaterials. However, the efficacy of the dentin bond-ing systems for composite resins is reduced by ex-posure of the prepared dentin surface to moisture(29). Depending on the type of material used, com-posite resins may be applied as retrograde fillingsby a plastic instrum ent or by a syringe. Light-curedcomposite resins offer the advantage that their set-ting can be controlled (30).
.^inc oxide eug enol cement The man ipu la t ion o fzinc oxide eugenol cement is simple, making it aconvenient retrograde filling material which "re-quires considerably less skill in handling and controlthan does amalgam" (5). Plain zinc oxide eugenolcement m ay be used as a retrograd e filling ma terial,but it is absorbable by vital tissue (1). Consequently,the use of reinforced zinc oxide eugenol cement hasbeen suggested as an alternative (30-36). Zinc oxideeugenol reinforced with methyl methacrylate poly-mer, e.g. IR M (Cau lk, Milford, DE ) is being usedas a retrograde filling material (31-33), but it maystill be resorbable (30, 34). EBA cement, a compo-sition of zinc oxide and aluminum oxide mixed with
tissue (34) and it is capable of adhering to dentin(34). The setting time of EBA cement cannot becontrolled predictably (32), and voids may formduring placement ofthe material (35).Glass ionomer cement - Theoretically, the advanof using glass ionomer cement as a retrograde fillingmaterial is its chemical bond with dentin, whichallegedly results in a superior seal (39 -41 ). Ho wever, the setting reaction of glass ionomer cement iadversely affected by hydration and dehydration(42), both of which are difficult to control clinicallyAs a result, the suitability of glass ionomer cemenas a retrograde filling material is questioned (39)Glass ionomer cements of the latest generation arless affected by moisture (43), and may be bettesuited for clinical use as retrograde filling materialthan former glass ionomer cements. Glass ionomecement is sticky, and its application as a retrogradefilling is difficult (44). Ap plica tion is usua lly facilitated by use of a syringe.
Polycarboxylate cement - Zinc polycarboxylatement consists of zinc oxide, magnesium oxide andpossibly aluminum oxide, mixed with a water solution of polyacrylic acid. It is used in dental procedures both as a luting cement and a restorative
-
8/3/2019 Retrograde Approaches in tic Therapy
4/12
S h i m o n F r i e d m a n(45-47). However, the adherence of polycarboxylatecement to dentin is lesser than to enamel (38). Fur-thermore, the bond to dentin is adversely affectedby moisture and protein contamination, such ascontact with blood or saliva (38). Polycarboxylatecement is hard ly soluble in water (38), adding to itstheoretical advantages as a retrograde filling ma-terial (46). In a vital tissue, however, it may bepartly absorbed (38). The application of polycar-bo xyla te cem ent is difficult as a result of its viscosity,and because ofth e a cceleration of its setting reac tionin a warm environment (38).
Cavit - Cavit (Premier Dental Products, Norris-town, PA) is a synthetic, zinc oxide-based tem pora ryfilling material. Over the years it has been con-sidered for use as a retrograde filling material pri-marily because of its easy application, which doesnot require any manipulation or mixing (48-50).Cavit is a hygroscopic material which expands lin-earily as a result of water absorption during setting( 5 1 ) . Consequently, its adaptation to the cavitywalls is expected to be good, but possibly a mini-mum thickness of the material is required for anoptimal seal to be obtained (52). Inasmuch as thesetting of Cavit is enhanced by tissue fiuids, in vivoit is soluble and may be quickly disintegrated (51).Other materials - Gold foil (53), Tefion (31), poly-Hem a and Hyd ron (54), zinc-phosphate cement( 4 7 ) , and cyanoacrylate cement (55, 56), have allbeen mentioned as potential retrograde filling ma-terials. Each one of these materials is suggested tohave advantages that would merit its clinical use inthis capacity, but their mention in the literature inrelation to retrograde filling is sporadic. Conse-quently, these materials cannot be compared con-clusively with the formerly listed retrograde fillingmaterials. Some reports indicate that other materialsmay have to be considered as retrograde filling ma-terials in the future. These materials are the innertand non-corrosive titanium screws (57), and bioma-terials which may be fused to dentin by laser, suchas enamel and dentin chips (58) or syntered hy-droxyapati te (59).
Gutta-percha - Gutta-percha is the material ofchoice when retrograde endodontic treatment is per-formed (1). As a retrogra de filling, gutta-p erch a isused in conjunction with chloropercha (11), or in athermoplasticized form (60, 61), so that the retro-grade filling may be adapted to the cavity walls.However, i t is the orthograde gutta-percha rootcana l ob tura tion that is frequently associated w ithapical surgery by being burnished after apicoectomywith either a hot or cold burnisher. This procedure
with that of retrograde filling with some of thementioned materials (62-69).E v a i u a t ie n o f r e t r o g r a d e f i i i i n g m a t e r i a isThe evaluation of the suitability of potential rgrade filling materials for their intended usebeen the purpose of numerous studies. The invgated aspects of the materials are mainly their ing ability, marginal adaptation, and biocombility, as well as their clinical efficacy.S e a l a b i l i t yComparing the sealing ability of retrograde fimaterials by testing leakage has been a comevaluation method, utilizing such tracers as ( 2 2 , 24, 28, 30-32, 35, 39, 44, 45, 56, 57, 669-72) , radionu cfides (23, 36, 46, 47), pressuliquid (73), electrolytes (25, 74), and bacteria5 7 ) . The results ofthe studies utilizing those valeakage techniques are not comparable (74, 7Most leakage studies were performed in without exposing the retrograde filling materiathe infiuence of tissue and tissue fiuids. The leabehavior of retrograde fillings performed with ous materials differs in a dry and a wet environ( 7 2 , 76). Polycarboxylate cement, Tefion, EBA cement (72) and glass ionomer cement all sealed better when tested "dry" than when t"wet". Conversely, amalgam sealed better "wet" experiment than in a "dry" one (72). Tresults demonstrate the distortion that is introdby comparing these particular retrograde fillingterials in a dry environment, as was the casm any sealability studies (24, 31, 32, 35, 36, 47,Another limitation of in vitro sealability studithe short time span in which they are usually formed. The margins of amalgam fillings are gressively sealed by corrosion products (77), reing in a gradually improved seal (23, 46). In term exp erim ents this is no t effected (46, 77),neither is the possible deterioration of materialsCavit ( 48-5 0), polycarbox ylate cement (38, zinc oxide eugenol or glass ionomer cement.
Clearly, the main limitation of in vitro leastudies is their inadequate simulation of operrestrictions and of the clinical environment. methodology of sealability studies has beenproved by subcutaneously implanting rootswhich retrograde fillings had been placed extraly (23 ). To further im prove the methodo logy seresearchers performed retrograde fillings in an
-
8/3/2019 Retrograde Approaches in tic Therapy
5/12
R e t r o g r a d e e n d o d o n t i c t r e a t m e n(46) the leakage of retrograde fillings performedwith various materials was compared under theseexperimental conditions, and also in a 48-hour invitro experim ent. T he leakage of the retro grade fill-ings performed in vivo varied from the leakage ofthe retrograde fillings performed in vitro with thesame materials (46). This demo nstrated discrepancyfurther undermines the validity of the in vitro leak-age investigations.In addition to the limitation of sealability studiesin simulating the clinical aspects of retrograde fill-ing, also the methodology of testing leakage is dis-puted. Some researchers conclude that to obtainreliable results in dye leakage studies the air mustbe evacuated from the specimens before leakage istested (78, 79). This technique, however, is notcommonly applied in sealability studies of retro-grade filling materials. Another disputed issue isthe molecular size of the tracers used for recordingleakage. Small tracers are often used as the worstpossible test (47) so as to demonstrate minute differ-ences in leakage. But, being smaller than the irri-tants they are supposed to simulate, the validity oftoo small trac ers is dou btful (80). In this respect it is
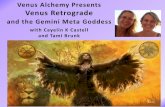
suggested that the only clinically significant leakagemay be that of large molecules, comparable in sizeto bacteria or to bacterial toxins (80). For examplethe widely utilized tracer methylene blue dye is osmall molecular weight, and it was shown to readilypenetrate into gaps that are impenetrable to bacteria-sized molecules (80).The frequent contradictions in the results of thesealability studies are demonstrated in Table 1, accentuating their limitations. However, when the information in all the studies is considered on anaccumulative basis it appears that some materialseal better than others (Fig. 2). These materials areamalgam used in conjunction with cavity varnishcomposite resin used with or without dentin bonding, and glass ionomer cement. Based upon thestudies in which the sealability of these materialswas tested in vivo, the following conclusions emergeAmalgam retrograde fillings, placed without cavityvarnish, permitted less leakage than retrograde fillings performed of polycarboxylate cement or Cavitboth of which suffered m argin al disintegration (46)Retrograde fillings performed with zinc-free amalgam demonstrated less leakage after 22 months than
Table 1. The summarized results of sealability studies. The comparison results are coded as the following: 2 - best, 1 - mediocre, 0 - worst.Author year A M * AM GI CR GP IRM EBA PCC CAV otherIn vitro studiesBarryDelivanisKosAbdalDalaiSzeremeta-BrowarShaniMattisonL u o m a n e nVertucciSmeeMcDonaldBeltesZetterqvistNegmBarkhordarSchwartzTuggteBarkhordarShawBondraThirawatMcDonaldFournierI n v i v o s t u d i e sDelivanisBramwellTronstad
197619781982198219831984198419851985198619871987198819881988198819881989198919891989198919901990
197819861983
2
202
2102120001
2
21102000100020101
1
220
21
12
22
2
22
2
22
0
22
0101
000010000
0
2
1
2
0
2
2
1
202
00
12 T S2 T F
2CA
-
8/3/2019 Retrograde Approaches in tic Therapy
6/12
S h i m o n F r i e d m a n2.0-1 Amalgam
Amalgam and varnishGutta-percha, hot
Gutta-percha, cold Composite resin
Glass ionomerEBA cement
1 Cavit0 IRM
23 15 10 9 8 7 5 4 3Number of summarized studies
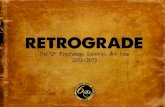
Fig. 2. Graphic summary of the combined results of 29 sealability studies of retrograde fillihg materials. The materials were giscores according to how they compared in each study; the best scored 2, the mediocre scored 1, and the worst scored 0. The tscores, presented on top of the columns, were obtained by summing the scores of all the studies in which each of the materialscompared. The figures at the bottom indicate the number of studies evaluating each material. The columns represent the ratio betwthe total score and the number of relevant studies, indicating the overall performance of the materials in the studies.
filfings with zinc-co ntaining am algam (22). In thatstudy, both amalgam types were used without appli-cation of cavity varnish. A copper-containingspherical amalgam was superior to silver amalgamand dispersed phase amalgam (23). Regardless ofthe type of amalgam used, less leakage occurredwhen varnish was applied to the retrograde cavitywalls before placement ofthe retrograde filling (23).Finally, when the seaiability of retrograde fillingsperformed in vivo with either amalgam with cavityvarnish, dentin-bonded composite resin or glass ion-omer cement were compared by dye leakage, amal-gam with varnish demonstrated the better seal, al-though the differences were not statistically signifi-cant (71).M a r g i n a l a d a p t a t i o nThe marginal adaptation of retrograde fillings, ob-served with the scanning electron microscope, as-sumedly reflects their sealing potential (66). Thecorrelation between these two parameters was dem-onstrated in retrograde filfings in vitro (26), butrecently it was challenged (73). Generally, the useof the scanning electron microscope in these studies
gra de filfings, which may be interpreted as margigaps. To avoid such artifacts replicas of the spemens' surfaces are prepared, and actually observunder the microscope instead of the original spemens (26). Furthermore , the marginal adaptatiof a retro gra de filling may not be uniform all arouits circumference, and it differs between the inncoronal, and the outer, apical, surfaces of the fill(26). Because only one surface is observed in scning electron microscopy, it is possible that the mginal gaps observed on that surface are not represtative of the marginal adaptation elsewhere arouthe retrograde filling. Despite these limitations, thappears to be a consensus that amalgam retrografillings have the largest marginal gaps of all retgrade fining materials, ranging from 10-150 |(26, 66, 73). These gaps are believed to be sealinitially by the cavity varnish, and later by corrosiproducts (23, 77). Other retrograde filling materdemonstrated marginal adaptation of comparabquafity, with the exception of composite resiwhich demonstrate minimal marginal gaps, meaured in one study to be 1 |im wide (26).
-
8/3/2019 Retrograde Approaches in tic Therapy
7/12
ing other dental materials, as summarized by theFDI Commission on Dental Materials (81). Fre-quently performed studies include in vitro cytotox-icity tests in cell or tissue cultures (82-87) and sub-cutaneous or bone implant tests (88-92). The in-terpretation and correlation of results obtained insuch studies is problematic (93). Usage tests (22, 40,6 7 , 68) observe histologically the specific interactionbetween retrograde fillings and the periapicaltissues, and they are therefore clinically relevant.Despite their limitations, however, all the biocom-patibility screening tests are a simple and essentialway to indicate which materials to discard andwhich to test further (82).
In summary ofthe information regarding the bio-compatibility of retrograde filling materials most ofthe commonly discussed materials have been con-firmed to the biocompatible, including various zincoxide eugenol formulations (34, 85), glass ionomercement (40, 68, 87, 89 -9 1), polycarboxylate cement(92) and gutta-percha (67, 68). In contrast, thebiocom patibility of a composite resin (Restodent;Lee Pharmaceuticals , South El Monte, CA) hasbeen questioned (83, 84). Methyl cyanoacrylate ce-ment (55) is not bioco m patible, whereas the biocom-patibility of isobutyl cyan oacrylate cemen t is accept-able (56). Results of studies on the toxicity of Cavitare confiicting, with observations of both high tox-icity (85, 88) and no toxicity (83). Amalgam cor-rosion products were also found to be toxic (86),but the good biocompatibility of the currently usedamalgam types has been confirmed in several usagetests (22, 40, 67).
C l i n i c a l s t u d i e sAfter the biocompatibihty of retrograde filling ma-terials is ascertained, a clinical comparison appearsto be the most valid method for evaluating theirefficacy. Nordenram (55) studied the success rate in31 teeth in which re trog rad e fillings were performedwith Biobond, a methyl cyanoacrylate based ma-terial. Radiographic and clinical criteria were usedduring a 6-24 month observation period. The suc-cess rate with Biobond was similar to that observedin 35 teeth in which gutta-percha was used as theretrograde filling material. The success rate in bothgroups was lower than that found in 34 teeth inwhich no retrograde fillings were placed. In a pro-spective study Persson et al. (49) and Finne et al.(50) have examined 220 teeth in which retrogradefillings had been performed with amalgam and Cav-it, one and three years after surgery, respectively.Based on radiographic and clinical criteria, they
R e t r o g r a d e e n d o d o n t ic t r e a tm e n tretrograde fillings with Cavit have been consider-ably dissolved (50). Dalai and Gohil (69) comparedthe results of apical surgery in 40 teeth, six monthsafter retrograde filling had been performed witheither amalgam, glass ionomer cement or gutta-percha. Using radiographic and clinical criteria forthe evaluation they claim that performing retro-grade fillings with amalgam has been significantlymore successful than using glass ionomer cementor gutta-percha (69). Rud et al . (94) comparedradiographically the success rate of apical surgeryusing Retroplast, a dentin-bonded composite resin,and amalgam as retrograde fillings. In their studythe composite resin had been used as a dentin-bonded coating over the resected root surface, whichwas scooped to contain the material without prepa-ration of a retrograde cavity (94). After an obser-vation period of six to twelve months, the successrate using the com posite resin in 388 roots was 74%Comparing that result with the success rate theyfound som e 15 years earlier using am alg am foretrograde filling, these authors conclude that thecompo site resin is superior to am alga m (9 4). Despitthe encouraging results, the authors caution againsthe toxicity ofthe composite resin if not used strictlydry, and they mention that in two patients severosteitis evolved after using Retroplast (94). Recently, Dorn and Gartner (33) reported on a retrospective clinical comparison of am algam , I R M andEBA cement used as retrograde filling materialsBased on a six-month radiographic observationthey compared the success rate in 294 teeth retrograde-filled with amalgam, with that of 129 teethand 65 teeth in which IRM and EBA cement hadbeen used, respectively. The clinical procedures hadbeen performed by several operators in each one otwo different clinics. They conclude that both EBAcement and IRM significantly improve the succesrate as compared to amalgam when used as retrograde fillings in apical surgery (33). In all thosstudies amalgam was used without cavity varnishThese clinical studies refiect the operative diffculties associated with retrograde filling, as well athe long term behavior of the retrograde filling materials in the periapical environment. However, because the prognosis of apical surgery is affected bnumerous clinical factors (9, 12, 16), the influencof factors other than the efficacy of the retrogradfillings on the results of these studies may not bdisregarded. Consequently, the differences in thsuccess rate observed in clinical comparisons mabe related reliably to differences in the efficacy othe retrograde fillings compared only by using largpopulations, firm evaluation criteria, and sufficien
-
8/3/2019 Retrograde Approaches in tic Therapy
8/12
S h i m o n F r i e d m a nevaluating the forementioned clinical comparisonsof retrograde filling materials it is concluded thatall these studies, except that of Persson et al. (49)and Finne et al. (50), are compromised by method-ological shortcomings which render the clinicalvalue of their conclusions questionable. Also, be-cause of the use in all these studies of amalgamwithout cavity varnish, their results cannot be ex-trapolated to indicate the clinical efficacy of retro-grade filling using amalgam in conjunction withcavity varnish.In an attempt to overcome some of the require-ments and limitations of comparing retrograde fill-ing materials in patients, Friedman et al. (95) per-formed such a comparison in dogs. After infectingthe teeth, they performed apical surgery and retro-grade filling with either amalgam with cavity var-nish, dentin-bonded composite resin or glass iono-mer cement. Based on a six-month radiographicobservation of healing, a significantly higher successrate was reported after retrograde filling with amal-gam and varnish than after using the compositeresin. The glass ionomer cement was inferior to theamalgam and superior to the composite resin, butin both comparisons the differences were not statisti-cally significant (95).
In summary of the clinical studies, they are toofew and diverse to be conclusive when all are con-sidered together. It appears that all of amalgamwith varnish, glass ionomer cement, dentin-bondedcomposite resin, IRM and EBA cement may beused successfully as retrograde filling materials.Therefore, future clinical studies will have to focuson comparing these materials with each other.iW e c iia n i ca l a s p e c t s o f r e t r o g r a d e f ii ii n gHav ing chosen the retrograd e filling material it mustbe remembered that also the retrograde cavity de-sign is important for successful retrograde filling.Com mon ly, a simple cavity is prep ared by enlargingthe canal orifice, often referred to as a Class I prepa-ration, which may be elongated to include two canalorifices and a connecting isthmus (20). The prepara-tion should be extended as far coronallv as it isclinically feasible, to improve the seal (25). In ad-dition, by extending the retrograde cavity coronally,dentinal tubuli which may communicate betweenthe root canal and the bevelled root surface areblocked from within (63, 9 6). With a restricted a c-cess an alternative, slot type, cavity is prepared fromthe buccal aspect ofthe root tip, into the buccal andthe bevelled root surfaces (20). Th e disadv antage s ofthis design are the increased dependence on the
The retrog rade cavity should include prep araof retention form if the retrograde filling matto be used does not adhere to dentin. Retrogfilling materials capable of adhering to dentin require less machanical retention than other terials (34, 68). Furthermore, in two recent stucomposite resins were used as retrograde fillingterials being bonded onto the bevelled root surwithout cavity preparation (29, 94). In both tstudies the results obtain ed with this tech nique cpared favourably with the results obtained conventional retrograde filling techniques.R e t r o g r a d e e n d o d o n t i c t r e a t m e n tEven when performed under the best conditionswith suitable materials, retrograde filling ofthe canal cannot be considered a substitute fothorough treatment of the entire root canal. cause success in nonsurgical endodontics is basethe principles of thorough debridement and cplete obturation ofthe root canal system, it is lognot to ignore or compromise these principlesteeth requiring endodontic surgery" (97). Thfore, when the coronal access to the root canaobstructed, it is appropriate to attempt treatmenthe root canal through the apical access rather just place a retrograde filling (1). Cleansing shaping of the root canal is performed with edontic instruments, which are modified so apermit their entry into the root canal throughrestrictive, surgical access (1, 9 7-9 9 ). After the canal is prepared, it is obturated with gutta-pe( 1 , 9 7-9 9 ). Various clinicians used different nato describe this procedure, such as "surgical edontic retreatment" and "retrograde root ctreatm ent" (9 8), "retrograd e instrumentat ion obturat ion" (97), or "retrograde gutta-percha filling" ( 9 9 ) , but i t appears that "retrograde edontic t reatment" is a sui table name.
Clearly, the advan tage of retrograde endodotreatment over retrograde filling is the debrideofthe root canal (97, 98), and its prognosis shbe expected to be better than that of retrogfilling. Clinical reports of retrograde endodotreatment have been encouraging, report ing hisuccess rates than most studies in which retrogfining was performed (9 8, 9 9 ). Technically, hever, retrograde endodontic treatment is criticdependent on accessibility, and it requires spearm am enta rium (9 7-9 9 ) . Because of these techdifficulties retrograde endodontic treatment ispracticed widely despite of its obvious advantaIt appears that the universal acceptance of r
-
8/3/2019 Retrograde Approaches in tic Therapy
9/12
R e t r o g r a d e e n d o d o n t i c t r e a t m e nclinical advantages over retrograde filling in com-parative studies.S u m m a ry a n d c o n c i u s i o n sProperly performed, with suitable materials, retro-grade filling is a clinically valuable procedure pro-moting the prognosis of apical surgery, particularlywhen orthogr ade o bturation is not performed inconjunction with surgery. Despite its cfinical value,retrograde filling should be considered second alter-nat ive to retrograde endodontic t reatment . Thechoice of retrograde filling material is based on ex-perimental data. Clinical evaluation and experi-ments performed in vivo are more relevant thanstudies performed in vitro. The most valid evalu-ations would appear to be long term prospectiveclinical studies of large populations. Such evalu-ations, however, are too few to be conclusive. Ani-mal studies are a valuable adjunct to the clinicalevaluation of retrograde filling materials. Consider-ing all the reviewed information it is concludedthat at present amalgam, used in conjunction withvarnish, is the retrograde filling material of choice.Nevertheless, in some countries the use of amalgamis prohibited and efforts must continue to selectappropriate alternatives for amalgam as a retro-grade filling material.
R e f e r e n c e s1. NYGAARD- OS TBY B. Introduction to endodontics. Oslo, Uni-versitetsforlaget; 1971.2 . GARVI N MH. Root resection. J Can Dent Assoc 1942; 8:126-9 .3 . S ELTZER S . Endodontology. Biologic considerations in endo-dontic procedures. Philadelphia: Lea & Febiger, 1988.4 . HARRISON JW , TODD MJ. The effect of root resection on thesealing property of root canal obturations. Oral Surg 1980;50 : 264-72 .5 . NicHOLLS E. Retrograde filling of the root canal. Oral Surg
1 9 6 2 ; 15 : 463-^73.6. TRONSTAD L , BARNETT F, RISO K , SLOTS J. Extraradicularendodontic infections. Endod Dent Traumatol 1987; 3: 8 6 - 9 0 .7 . TRONSTAD L, BARNETT F, CERVONE F. Periapical bacterialplaque in teeth refractory to endodontic treatment. FndodDent Traumatol 1990; 6: 1?>-^1.8 . H A PP O N E N R - P , S O D ER L IN G E , V IA N D E R M , L I N K O - K E T T U -NEN L, PELLINIEMI LJ. Immunocytochemical demonstra tionof Actynomyces species and Arachnia propionica in peri-apical infections. J Oral Fathol 1985; 1 4 : 405 13.9 . H I R SC H J - M , A H LS TR O M U , H E N R IK S ON P - A , H E Y D E N G ,
P E T E R S O N L - E . Periapical surgery. Int J Oral Surg 1979; 8:173-85.1 0 . MlKKO"NEN M , KuLLAA-MlKKONEN A , KoTILAINEN R . Glin -ical and radiologic re-examination of apicoectomized teeth.Oral Surg 1983; 55 : 302-6.
surgery. J Endodon, in press.1 3 . LEHTI NEN R, AI TAS ALO K . Comparison ofthe clinical anroentgenological state at the re-examination of root resections. Froc Finn Dent S o c 1972; 68 : 2 0 9 -1 1 .1 4 . M A T T I L A K , A L T O N EN M . A clinical and roentgenologicastudy of apicoectomized teeth. Odontol Tidskr 1968; 76389-407 .1 5 . A L T O N EN M , M A T T I L A K . Follow-up study of apicoectomzed molars. Int J Oral Surg 1976; 5: 33-40 .1 6 . R U D J , ANDREASEN J O , J EN SE N M J E . A multivariate analysof the influence of various factors upon healing after endodontic surgery. In t J Oral Surg 1972; /; 258-71.1 7 . MALMSTROM M , PERKKI K, LINDQVIST K . Apicectomy. retrospective study. Froc Finn Dent S o c 1982; 78 : 26-31.1 8 . G R U N G B , M O L V E N O , H A L S E A. Periapical surgery in No rweg ian cou nty h ospital: follow-up fmdings of 477 teethJ Endodon 1990; 16 : 411-7 .1 9 . LiNDEMANN U, Kopp S, HoFFMEisTER B. Die ergebnisse depraoperativen und intraoperativen wurzelfuUung bei dewurtelspitzenresektion im vergleich. Dtsch ^ahnarzU Z 1987
4 2 : 245-7 .2 0 . ARENS D E , ADAMS W R , D E C A S T R O RA. Endodontic surgerPhiladelphia: Harper & Row; 1981.2 1 . JoRGENSEN KD, S AI TO T. Structure and corrosion of dentaamalgams. Acta Odont Scand 1970; 28 : 129-42.2 2 . KiMURA JT . A com para tive analysis of zinc and non-zinalloys used in retrog rade endod ontic surgery. Part 1: Apicseal and tissue reaction. J Endodon 1982; 8: 3 5 9 - 6 3 .2 3 . TRONSTAD L, TRO P E M , DOERI NG A, HASSELGREN G . Sealinability of dental amalg ams as retrograde fillings in endod ontic therapy. J Endodon 1983; 9: 551-3 .2 4 . ABDAL A K , R E T I E F D H , J AM I SO N H C . The apical seal vithe retrosurgical approach. H. An evaluation of retrofillinmaterials. Oral Surg 1982; 54 : 213-8 .25 . MATTI S ON G D , VON F RAUNHOF ER A, DELI VANIS P D , ANDE R
SO N AN. Microleakage of re trograde amalgams. J Endodo1 9 8 5 ; 11 : 340-5 .
2 6 . STABHOLZ A , SHANI J , FRIEDMAN S, ABED J . Marg ina l adaptation of retrograde fillings and its correlation with sealabilty. J Endodon 1985; 11 : 218-23 .2 7 . DuMSHA T BiRON G. In hib ition of ma rgin al leakage with dentin bonding agent. J Dent Res 1984; 63 : 1247-55.2 8 . M C D O N A L D N J, DUMSHA TC . A comparative retrofill leakagstudy utilizing a dentin bonding material. J Endodon 19
1 3 : 224-7 .2 9 . M C D O N A L D N J, DUMSHA TC. An evaluation of the retrograde apical seal using dentine bonding materials. In t EndJ 1990; 23 : 156-62.3 0 . T H I R A W A T J , EDMUNDS DH. The sealing ability of materiaused as retrograde root fillings in endodontic surgery. InEndod J 1989; 22: 295-8.31. SMEE G , BOLANOS OR , MO RSE DR, FURST ML , YESILSOY CA comparative leakage study of P-30 resin bonded ceramicTeflon, amalg am , and I R M as retrofilling. J Endodon 198
1 3 : 117-21.32 . BONDRA DL, HART WEL L GR, MACP HER S ON MG, P ORTELFR. Leakage in vitro with IRM, high copper amalgam, anEBA cement as retrofilling materials. J Endodon 1989; 1157-60.3 3 . D O R N SO , G A R T N E R AH. Retrograde filling materials: retrospective success-failure study of amalgam, EBA, anI R M . J Endodon 1990; 16 : 3 91 -3 .3 4 . OYNI CK J , OYNI CK T. A study of a new material for retrograde fillings. J Endodon 1978; 4: 203-6 .
-
8/3/2019 Retrograde Approaches in tic Therapy
10/12
S h i m o n F r i e d m a nniques: An autoradiographic study. Oral Surg 1985; 59: 82-1.
3 7 . CivjAN S, B R AU ER G M . Physical properties of cements,based on zinc oxide, hydrogenated resin, o-ethoxybenzoicacid, and eugenol. J Dent Res 1964; 43 : 2 8 1 - 9 9 .3 8 . SMITH DC . A review of the zinc polycarboxylate cements. J
C a n Dent Assoc 1971; 37 : 2 2 - 9 .3 9 . ZETTERQVIST L, ANNEROTH G, DANIN J , RO D IN G K . Micro-leakage of retrograde fillings - a comparative investigationbetween amalgam and glass ionomer cement in vitro. In tEndod J 1988; 21 : 1-8.4 0 . ZETTERQVIST L, ANNEROTH G, NORDENRAM A. Glass ionomercement as retrograde fil ling material. An exp erimental inves-tigation in monkeys. Int J Oral Maxillofac Surg 1987; 16 :459-64 .4 1 . BARKHORDAR R A , PELZN ER RB , STA RK MM. Use of glassionomers as retrofilling materials. Oral Surg 1989; 67 : 7349.4 2 . M O U N T G J, MAKINSOS OF. Glass-ionomer restorative ce-ments: Clinical implications ofthe setting reaction. Oper Dent
1 9 8 2 ; 7; 134-41.4 3 . ATKINSON AS, PEARSON GJ. The evolution of glass-ionomercements. Br Dent J 1985; 1 5 9 : 335-7.4 4 . BELTES P, ZERVAS P, LAMBRIANIDIS T, MOLYVDAS I. In vitrostudy of the sealing ability of four retrogr ade filling materials.Endod Dent Traumatol 1988; 4: 82-4.4 5 . B A RR Y G N , S E LB ST A G , D ' A N T O N E W , M A D DE N R M . Seal-ing quality of polycarboxylate cements when compared toamalgam as retrofilling material. Oral Surg 1976; 42 : 109-16.4 6 . DELIVANIS P, TABIBI A. A comparative sealability study ofdifferent retrofilling materials. Oral Surg 1978; 45 : 273-81.4 7 . SHANI J , FRIEDMAN S, STABHOLZ A, ABED J. A radionuclidicmodel for evaluating sealability of retrograde filling ma-terials. Int J .Nucl Med Biol 1984; //. 46-52.4 8 . NoRD PG. Retrograde rootfilling with Cavit: A clinical androentgenological study. Svensk Tandlak T 1970; 63 : 261-73 .4 9 . PERSSON G, LENNARTSON B , LUNDSTROM I. Results of retro-grade root-filling with special reference to amalgam andCavit as root-filling materials. Svensk Tandlak T 1974; 68 :123-33.5 0 . FINNE K , NORD PG , PERSSON G, LENNARTSSON B. Retrograderoot filling with amalgam and Cavit. Oral Surg 1977; 43 :621-6.5 1 . WiDERMAN F H , EAMES W B, S E R E N E T P . The physical andbiological properties of Cavit. J Am Dent Assoc 19 71; 52.-378-82.5 2 . WEBER R T, DEL RIO C E, BRADY J M , SEGALL RO. Sealingquality of a temporary filling material. Oral Surg 1978; 46 :123-30.5 3 . WAIKAKUL A, PUNWUTIKORN J. Gold leaf as an alternative
retrograde filling material. Oral Surg 1989; 67 : 746-9 .5 4 . Kos WL, AuLOZZi DP, GERSTEIN H . A comparative bacterialmicroleakage study of retrofilling materials. J Endodon 1982;8: 355-8.5 5 . NORDENRAM A. Biobond for retrograde root filling in apico-ectomy. Scand J Dent Res 1970; 78 : 251-5 .56. BARKHORDAR RA, JAV ID B, ABBASI J , WATANABE LG . Cy-anoacrylate as a retrofilling material. Oral Surg 1988; 65 :468-73 .5 7 . LU OMA N EN M , TU O MPO H . Study of titanium screws as retro-grade fillings using bacteria and dye. Scand J Dent Res 1985;
9 3 : 5 5 5 - 9 .5 8 . ZAKARIASEN K L , D E D E R IC H D N , T U L I P J. Lasers in dentistry."Star wars", dreaming or a future reality? J C a n Dent Assoc
1 9 8 8 ; 54 : 27-30 .5 9 . S T E W A RT L , P O W E L L G L , W R I G H T S . Hydroxyapatite at-
61. MA CPH ERSO N MG , H A RTW ELL G R, BO N DRA D L, WERN. Leakage in vitro with high-temperature thermopcized gutta-percha, high copper amalgam, and warm percha when used as retrofilling materials. J Endodon1 5 : 212-5 .
6 2 . BRAMWELL J D , HICKS ML. Sealing ability of four retroftechniques. J Endodon 1986; 12 : 9 5 - 1 0 0 .6 3 . VERTUCCI FJ , BEATTY RG. Apical leakage associatedretrofilling techniques: A dye study. J Endodon 198331-6.6 4 . S H A W C S , B E G O L E EA , JACOBSEN EL. The apical sefficacy of two reverse filling techniques versus cold-shed gutta percha. J Endodon 1989; 15 : 350-4.6 5 . NEGM M M . The effect of varnish a nd p it and fissure seon the sealing capacity of retrofilling techniques. Ora
1 9 8 8 ; 66 : 483-8 .6 6 . TANZILLI JP , RA PH A EL D , MO O D N IK RM. A comparisthe margina l adap tation of retrogra de techniques: a scaelectron microscopic study. Oral Surg 1980; 50 : 7480.6 7 . MA RCO TTE L R , DOWSON J , R O W E NH. Apical healingretrofill ing materials amalgam and gutta-percha. J En
1 9 7 5 ; /. 63-5.6 8 . CALLIS PD , SANTINI A. Tissue response to retrogradefillings in the ferret canine: A comparison of a glass ioncement and gutta-percha with sealer. Oral Surg 198475-9 .6 9 . D A LA L M B , G O H I L KS . Comp arison of silver amalg amionomer cement and gutta percha as retrofill ing matean in vivo and an in vitro study. J Indian Dent Assoc
5 5 : 153-8.7 0 . SCH WA RTZ SA , ALEXANDER JB. A comparison of lebetween silver-glass ionomer cement and amalgam fiHings. J Endodon 1988; 14 : 3 8 5 - 9 1 .7 1 . FRIEDMAN S, ROTSTEIN I, K O R E N L , T R O P E M . Dye lein retrofilled dog teeth and its correlation with radiogrhealing. J Endodon., in press.72. FOURNIER MJ, SZEREMETA-BROWAR T, OSETEK E, HEUE
LANDENSCHLAGER E. Leakage of different retrograde fmaterials in wet and dry environments (abstract 1Endodon 1990; 16 : 189.7 3 . YosHiMURA M , MA RSH A LL FJ, TIN K LE JS. In vitro quacation of the apical sealing ability of retrograde amafillings. J Endodon 1990; 16 : 9 - 1 1 .7 4 . DELIVANIS PD , C H AP M A N K A . Comparison and reliabiltechniques for measuring leakage and marginal penetraOral Surg 1982; 53 : 410-6.7 5 . MA TLO FF IR , J EN SEN J R . SIN G ER L , TA BIBI A. A compaof methods used in root canal sealability studies. Ora
1 9 8 2 ; 53 : 203-8 .7 6 . M A C N E I L K , B E A T T Y R . Ketac Silver and Fuji II as refillings: a dye study (abstract 1520). J Dent Res 19872 9 7 .
7 7 . S M IT H G A , W I L SO N N H F , C O M BE EC. Microleakage ofventional and ternary amalgam restorations in vitro. BrJ 1978; 144: 6 9 - 7 3 .7 8 . GOLDMAN M , SIMMONDS S, RUS H R . The usefulness of penetration studies reexamined. Oral Surg 1989 ; 67 : 327 9 . SPAN G BERG L SW , A CIERN O T G , Y ON GBUM CH A B . Influof entrapped air on the accuracy of leakage studies udye penetration methods. J Endodon 1989; 15 : 548-518 0 . K E R ST E N H W , M O O R E R WR. Particles and molecule
endodontic leakage. In t Endod J 1989 ; 22 : 118-24.8 1 . F. D. I. Commission on Dental Materials, InstrumEquipment and Therapeut ics . Stanford JW, Chairman.
-
8/3/2019 Retrograde Approaches in tic Therapy
11/12
of the toxicity of a composite resin, silver amalgam, andCavit. J Endodon 1988; 14 : 236-8 .84. S AFAVI K E , S P ANGBERG L, S APOULAS G , MACAL I S TER T J .In vitro evaluation of biocompatibility and m arginal a dap -tation of root retrofilling materials. J Endodon 1988; 14 :538-42.8 5 . WENNBERG A, HASSELGREN G. Cytotoxicity evaluation of
temporary filling materials. Int Endod J 1981; 14 : 121-4.8 6 . MiLLEDiNG P, WENNBERG A, HASSELGREN G. Cytotoxicity ofcorroded and non-corroded dental silver amalgam. Scand JDent Res 1985; 93 : 76-83.8 7 . KAWAH ARA H , IMANISHI Y, OSHIMA H. Biological evaluationon glass ionomer cement. J Dent Res 1979; 58 : 1080-6.8 8 . FLANDERS D H , JAMES GA, BURCH B, DOCKUM N . Compara -tive histopatho logic study of zinc free am alga m and Cav itin connective tissue ofthe rat. J Endodon 1975; /.- 65-8.8 9 . BLACKMAN R, GROSS M , SELTZ ER S. An evaluation of thebiocompatibility of a glass ionomer-silver cement in rat con-nective tissue. J Endodon 1989; 15 : 7 6 - 9 .9 0 . LEHTI NEN R. Tissue reaction lo glass ionomer cement anddental amalgam in the rat. Froc Finn Dent Soc 1986; 82 :144--7.9 1 . ZMENER O . Tissue response to a glass ionomer used as an
R e t r o g r a d e e n d o d o n t i c t r e a t m e n tendodontic cement. A preliminary study in dogs. Oral Surg1 9 8 3 ; 56 : 198-205.
9 2 . ZARTNER R J, JAMES GA, B U R C H B S . Bone tissue response tozinc polycarboxylate cement a nd zinc free am algam . J Endo-do n 1976; 2: 203-8.9 3 . MjOR IA. A comparison of in vivo and in vitro methods fortoxicity testing of dental materials. Int Endod J 1980; 13 :
139-42.9 4 . R U D J , ANDREASEN J O , R U D V. Retrog rad rodfyldning medplast og dentinbinder: helingsfrekvens sammenlignet medretrograd amalgam. Tandlaegebladet 1989; 93 : 267-73 .9 5 . FRIEDMAN S, ROTSTEIN I, MAHAMID A. In vivo efficacy ofvarious retrofills and of CO2 laser in apical surgery. EndodDent Traumatol 1991 ; 7: 19-25.9 6 . TiDMARSH BG, ARROWSMITH MG. Dentinal tubules at theroot ends of apicected teeth: A scanning electron microscopicstudy. In t Endod J 1989; 22 : 184-9 .9 7 . F L A T H R K , H I CK S ML. Retrograde instrumentation andobturation with new devices. J Endodon 1987; 13 : 546-9 .9 8 . REI T C , HI RS CH J. Surgical endodontic retreatment. Int En-
d o d J 1986; 19 : 107-112.9 9 . AMAGASA T, NAGASE M , SATO T, SHIODA S. Apicoectomywith retrograde gutta-percha root filling. Oral Surg 1989; 68339-42 .
-
8/3/2019 Retrograde Approaches in tic Therapy
12/12