RESPIRATOR AND VENTILATOR BASICS - albany.edu · Silvercrest – Respirator and Ventilator Basics...
20
Silvercrest – Respirator and Ventilator Basics UAlbany – 01/28/2011 NYS DOH Surveyor Training RESPIRATOR AND VENTILATOR BASICS STATE UNIVERSITY OF NEW YORK UNIVERSITY OF ALBANY NEW YORK STATE DEPARTMENT OF HEALTH SURVEYOR TRAINING – WEBINAR #1 Friday • January 28 th , 2011 • 10:00AM Agenda Welcome Who Needs Respiratory / Ventilator Care Respiratory Diseases Neurological Diseases Post-Cardiac Surgery & Other Indications Indications for Mechanical Ventilation What is Mechanical Ventilation Life Expectancy / Outcomes Common Comorbidities and Related Clinical Issues Documentation and Care Planning Webinar #1 – Respiratory and Ventilator Basics Welcome Format of Webinars The Silvercrest Center Speakers Robert Fleming, MD FCCP Mustafa Salehmohamed, DO Daniel Russo, MD CMD Denise Lawson, RN Webinar #1 – Respiratory and Ventilator Basics
Transcript of RESPIRATOR AND VENTILATOR BASICS - albany.edu · Silvercrest – Respirator and Ventilator Basics...

Silvercrest – Respirator and Ventilator Basics UAlbany – 01/28/2011
NYS DOH Surveyor Training
RESPIRATOR AND VENTILATOR BASICSSTATE UNIVERSITY OF NEW YORK
UNIVERSITY OF ALBANY
NEW YORK STATE DEPARTMENT OF HEALTHSURVEYOR TRAINING – WEBINAR #1
Friday • January 28th, 2011 • 10:00AM
Agenda
Welcome
Who Needs Respiratory / Ventilator Care Respiratory Diseases
Neurological Diseases
Post-Cardiac Surgery & Other Indications
Indications for Mechanical Ventilation
What is Mechanical Ventilation
Life Expectancy / Outcomes
Common Comorbidities and Related Clinical Issues
Documentation and Care Planning
Webinar #1 – Respiratory and Ventilator Basics
Welcome
Format of Webinars
The Silvercrest Center
Speakers
Robert Fleming, MD FCCP
Mustafa Salehmohamed, DO
Daniel Russo, MD CMD
Denise Lawson, RN
Webinar #1 – Respiratory and Ventilator Basics

Silvercrest – Respirator and Ventilator Basics UAlbany – 01/28/2011
NYS DOH Surveyor Training
Welcome
Webinars
Respiratory / Ventilator Basics 01/28/11
Ventilator / Tracheostomy Mechanics 02/25/11
Vent Weaning & Best Practices 03/25/11
Each webinar is 2 hours in length
10:00am to 12:00pm
1 ½ hour presentation & ½ hour for Q & A
Webinar #1 – Respiratory and Ventilator Basics
Welcome
The Silvercrest Center 320 Skilled Nursing Facility in Queens, NY
Case Mix Index 1.23 Full House
1.64 Vents
Largest SNF Vent Program in NY State Ventilator Program Started in 1992
48 Certified Ventilator Dependent Beds in Discrete Unit
ADC 70 Vents (Private Pay and Commercial Insurance)
Member of the NewYork-Presbyterian Healthcare Systemand an Affiliate of Weill Medical Cornell College
Webinar #1 – Respiratory and Ventilator Basics
Welcome
Speakers Robert Fleming, MD FCCP Director of the Ventilator Unit at The Silvercrest Center for Nursing
and Rehabilitation and Director for the Respiratory DiseaseManagement Unit at New York Hospital Queens
Mustafa Salehmohamed, DO Pulmonologist at The Silvercrest Center for Nursing and
Rehabilitation and New York Hospital Queens
Daniel Russo, MD CMD Vice President of Services and Medical Director at The Silvercrest
Center for Nursing and Rehabilitation
Denise Lawson, RN Director for Performance Improvement at The Silvercrest Center
for Nursing and Rehabilitation
Webinar #1 – Respiratory and Ventilator Basics

Silvercrest – Respirator and Ventilator Basics UAlbany – 01/28/2011
NYS DOH Surveyor Training
Who Needs Respiratory / Ventilator Care
Respiratory Diseases
Neurological Diseases
Post-Cardiac Surgery and Other Indications
Indications for Mechanical Ventilation
What is Mechanical Ventilation?
Presenter: Dr. Robert Fleming
Director of the Ventilator Unit at The Silvercrest Center forNursing and Rehabilitation and Director for the RespiratoryDisease Management Unit at New York Hospital Queens
Webinar #1 – Respiratory and Ventilator Basics
Who Needs Respiratory / Ventilator Care
Respiratory Diseases
Chronic diseases of the airways & other structures ofthe lung. Most common examples:
Asthma
Chronic Obstructive Pulmonary Disease (COPD) Chronic Bronchitis
Emphysema
Respiratory Allergies
Occupational Lung Disease
Pulmonary Hypertension
Webinar #1 – Respiratory and Ventilator Basics
Who Needs Respiratory / Ventilator Care
Respiratory Diseases
Important Risk Factors for chronic respiratory disease:
Occupational Risks and Vulnerability
Indoor and Outdoor Air Pollution
Allergens
Smoking
Webinar #1 – Respiratory and Ventilator Basics

Silvercrest – Respirator and Ventilator Basics UAlbany – 01/28/2011
NYS DOH Surveyor Training
Who Needs Respiratory / Ventilator Care
Respiratory Diseases
2007 World Health Organization estimates:
300 million with asthma
210 million with COPD
2009 NYS Asthma Surveillance Report
1 in 11 children and adults in NYS has asthma
1.3 million New Yorkers had self reported currentdiagnosed asthma
17.2 per 100,000 mortality rate in 2007
Webinar #1 – Respiratory and Ventilator Basics
Who Needs Respiratory / Ventilator Care
Respiratory Diseases COPD 4th leading cause of death
in America, 120,970 in 20061
85%-90% of COPD deathscaused by smoking2
12.1 million U.S. adults wereestimated to have COPD3
672,000 hospital discharges in2006; a discharge rate of 22.5per 100,000 population. 4
Approximately 64% ofdischarges were in the 65 yearsand older population in 2006. 5
Webinar #1 – Respiratory and Ventilator Basics
Normal Damage+Cholinergic tone
Bronchi and COPD
Who Needs Respiratory / Ventilator Care
Respiratory Diseases COPD Age-Adjusted Death Rates Based on the 1940
and 2000 Standard Populations, 1979-2006
Webinar #1 – Respiratory and Ventilator Basics

Silvercrest – Respirator and Ventilator Basics UAlbany – 01/28/2011
NYS DOH Surveyor Training
Who Needs Respiratory / Ventilator Care
First-Listed Hospital Discharge Rates per 10,000 Population by Age, 1979-2006
Webinar #1 – Respiratory and Ventilator Basics
Who Needs Respiratory / Ventilator Care
Neurological Diseases
Amyotrophic Lateral Sclerosis (ALS or Lou Gehrig’s Disease)
Motor neurons in lungs affected affecting strength of respiratorymuscles
Maybe gradual or sudden
Spinal Cord Injuries (SCI)
Pulmonary failure and related complications are the most commoncauses of death in SCI patients
At 5 years after injury, 33% of ventilator dependent SCI patientsremain alive
Guillian-Barre (GB)
Webinar #1 – Respiratory and Ventilator Basics
Who Needs Respiratory / Ventilator Care
Post-Cardiac Surgery and Other Indications
Post Operatively
Over sedation
Paralytics
Pain control
Webinar #1 – Respiratory and Ventilator Basics

Silvercrest – Respirator and Ventilator Basics UAlbany – 01/28/2011
NYS DOH Surveyor Training
Who Needs Respiratory / Ventilator Care
Indications for Mechanical Ventilation
Impending Respiratory Failure
Acute Respiratory Failure / Arrest
Airway Establishment and Control
Webinar #1 – Respiratory and Ventilator Basics
Who Needs Respiratory / Ventilator Care
Indications for Mechanical Ventilation
Impending Respiratory Failure
Progressively worsening clinical appearance
Worsening chest x-ray (CXR)
Hypoxemic respiratory failure Too little oxygen (O2) in the blood
Examples: CHF and Pneumonia
Hypercapnic respiratory failure
Too much carbon dioxide (CO2) in the blood
Examples: ALS and COPD
Webinar #1 – Respiratory and Ventilator Basics
Who Needs Respiratory / Ventilator Care
Indications for Mechanical Ventilation
Acute Respiratory Failure / Arrest
Acute change in arterial blood gas (ABG) / pulse oximeterresults
Respiratory arrest / Status post CPR
Acute epiglottitis / anaphylaxis Swelling of the epiglottis, a flap of tissue that covers the
windpipe during swallowing to protect against choking. Swellingof the epiglottis is a potentially life-threatening breathingobstruction
Webinar #1 – Respiratory and Ventilator Basics

Silvercrest – Respirator and Ventilator Basics UAlbany – 01/28/2011
NYS DOH Surveyor Training
Who Needs Respiratory / Ventilator Care
Indications for Mechanical Ventilation
Airway Establishment and Control
Clearing the upper airway
Maintaining an open air passage with amechanical device
Assisting with respirations
Webinar #1 – Respiratory and Ventilator Basics
Endotracheal - Acute
Tracheostomy – Post Acute
Situations Requiring Airway ControlEmergencies Urgencies
• Cardiac arrest• Respiratory arrest or
apnea (eg, due to CNSdisease, drugs, or hypoxia)
• Deep coma, when thetongue relaxes to occludethe glottis
• Acute laryngeal edema• Laryngospasm• Foreign body at the larynx
(eg, “cafe coronary”)• Drowning• Upper airway trauma• Head or high spinal cord
injuries
• Respiratory failure• Need for ventilatory support (eg, in acute respiratory distress
syndrome, smoke or toxic inhalation, respiratory burns,gastric aspiration, exacerbations of COPD or asthma, diffuseinfectious or other parenchymal lung problems,neuromuscular diseases, respiratory center depression, orextreme respiratory muscle fatigue)
• Need to relieve the work of breathing in patients in shock orwith low cardiac output or myocardial stress that must bedecreased
• Before gastric lavage in patients with an oral drug overdoseand altered consciousness
• Before esophagogastroscopy in patients with upper GI bleeding• Before bronchoscopy in patients with marginal respiratory status• Before radiologic procedures in patients with altered sensorium,
particularly if sedation is required
Webinar #1 – Respiratory and Ventilator Basics
What is Mechanical Ventilation?
The simplest way to look at mechanical ventilation is as a way tokeep the blood gases normal.
Mechanical ventilation is a life support treatment.
A mechanical ventilator is a machine that helps people breathewhen they are not able to breathe enough on their own.
The mechanical ventilator is also called a ventilator, respirator, orbreathing machine.
Most patients who need support from a ventilator because of asevere illness are cared for in a hospital’s intensive care unit (ICU).
People who need a ventilator for a longer time may be in a regularunit of a hospital, a rehabilitation facility, or cared for at home.
Webinar #1 – Respiratory and Ventilator Basics

Silvercrest – Respirator and Ventilator Basics UAlbany – 01/28/2011
NYS DOH Surveyor Training
What is Mechanical Ventilation?
Why are ventilators used? To get oxygen into the lungs and body
To help the lungs get rid of carbon dioxide
To ease the work of breathing—Some people can breathebut it is very hard. They feel short of breath anduncomfortable.
To breathe for a patient who is not breathing because ofbrain damage or injury (like a coma) or high spinal cordinjury or very weak muscles. If a person has had a seriousinjury or illness that causes breathing effort to stop, aventilator can be used to help the lungs breathe until theperson recovers.
Webinar #1 – Respiratory and Ventilator Basics
What is Mechanical Ventilation?
Key Terms in Mechanical Ventilation:
Inspiration = Act of breathing in; inhalation
Expiration = Process of expelling air from the lungs;exhalation
Ventilation = Breathing, or more specifically, the act ofmoving air into and out of the lungs
Respiration = Transport and exchange of gasesbetween the atmosphere and the cells via the lungs andblood vessels
Webinar #1 – Respiratory and Ventilator Basics
What is Mechanical Ventilation?
Webinar #1 – Respiratory and Ventilator Basics
Physiology of Breathing

Silvercrest – Respirator and Ventilator Basics UAlbany – 01/28/2011
NYS DOH Surveyor Training
What is Mechanical Ventilation?
Origins of MechanicalVentilation
Negative-pressureventilators (“iron lungs”)
Air is sucked into the lungs
Non-invasive ventilationfirst used in BostonChildren’s Hospital in 1928
Used extensively duringpolio outbreaks in 1940s –1950s
Webinar #1 – Respiratory and Ventilator Basics
The iron lung created negative pressure in abdomen aswell as the chest, decreasing cardiac output.
Iron lung polio ward at Rancho Los Amigos Hospital in 1953.
What is Mechanical Ventilation?
Origins of MechanicalVentilation
Positive-pressureventilators
Air is forced into the lungs
Invasive ventilation firstused at MassachusettsGeneral Hospital in 1955
Now the modern standardof mechanical ventilation
Webinar #1 – Respiratory and Ventilator Basics
Massachusetts General 1955
Portable ventilators in various settings
What is Mechanical Ventilation?
Future of Mechanical Ventilation
Portable, negative and positive pressure ventilator with infinite powerand oxygen sources
Webinar #1 – Respiratory and Ventilator Basics

Silvercrest – Respirator and Ventilator Basics UAlbany – 01/28/2011
NYS DOH Surveyor Training
Life Expectancy / Outcomes
Webinar #1 – Respiratory and Ventilator Basics
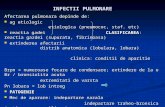
Life Expectancy / Outcomes
Webinar #1 – Respiratory and Ventilator Basics
Figure 2. Survival among low-risk patients (.70%probability of surviving 2 months), medium-riskpatients (51% to 70%), high-risk patients(≤50%), and patients in whom ventilator supportwas withheld in anticipation of death.
Agenda
Common Comorbidities and Related ClinicalIssues Presenter: Mustafa Salehmohamed, DO
Pulmonologist at The Silvercrest Center for Nursing andRehabilitation and New York Hospital Queens
Webinar #1 – Respiratory and Ventilator Basics

Silvercrest – Respirator and Ventilator Basics UAlbany – 01/28/2011
NYS DOH Surveyor Training
Common Comorbidities and Related Clinical IssuesLife Expectancy / Outcomes
Webinar #1 – Respiratory and Ventilator Basics
Infections
Ventilator Associated Pneumonia (VAP)
MRSA
C Diff
Sepsis
Pressure Ulcers and Other Skin Conditions
Common Comorbidities and Related Clinical IssuesLife Expectancy / Outcomes
Webinar #1 – Respiratory and Ventilator Basics
Decannulation and Trach Tube Dislodgements Restraints
Feeding and Hydration Incontinence
PEG Tubes
Speech Disorders and Dysphasia Communication
Paralysis and Quadriplegia
Quality of Life
Common Comorbidities and Related Clinical IssuesLife Expectancy / Outcomes
Webinar #1 – Respiratory and Ventilator Basics
Tracheostomy vs. Oral Intubation
Dysphagia requiring PEG tube
SNFs in general do not accept nasogastric tubes
Ventilator associated pneumonia (VAP)
Multidrug Resistant Organisms (MDRO)
MRSA, VRE, C Diff, etc

Silvercrest – Respirator and Ventilator Basics UAlbany – 01/28/2011
NYS DOH Surveyor Training
Common Comorbidities and Related Clinical IssuesLife Expectancy / Outcomes
Webinar #1 – Respiratory and Ventilator Basics
Infections Ventilator Associated Pneumonia (VAP)
MRSA
C Diff
Sepsis
Pressure Ulcers and Other Skin Conditions
Decannulation and Trach Tube Dislodgements Restraints
Feeding and Hydration Incontinence
PEG Tubes
Speech Disorders and Dysphasia
Paralysis and Quadriplegia
Quality of Life
Communication
Common Comorbidities and Related Clinical IssuesCase Study
Webinar #1 – Respiratory and Ventilator Basics
PHYSICIAN'S MONTHLY ASSESSMENT
PROGRESS NOTE: 71 y.o. man with Resp. failure on vent support, s/p hospitalization at NYHQ12/23/10 – 12/30/10 for Hematemesis, GI bleed, Anemia, s/p Blood trabsfusion, VAP, s/pEGD on EGD on 12/27/10, found with Hiatus hernia, GERD with esophagitis, deformedgastric antrum, scarring of duodenal bulb; suggested PPI`s & Reglan. S/p PICC line placementon 12/30/10. . Since re-admission:- completed ABT for Pneumonia (IV Zosyn & Flagyl) on 1/5/10;- s/p GI cons done on 1/6/10, sug to r/o Celiac disease, w/u done, neg;-Dx with Vitamin D deficiency, started vit D 1000 IU via GT daily;-observed with diarrhea, Leukocytosis, elevated ESR thought due to C.Diff Colitis; orderedStool for C.Diff x 3, started Flagyl 500 mg via GT q 8 h on 1/12/11; Stool C.Diff neg x 3,completed Flagyl course today;-D/C-ed foley cath on 1/12/11, no SxS of urinary retention noted;- decrease FSBG monitoring to BIW (Mo & Thu);-s/p Pulmonary f/u on 1/10/11, pt was entered into the weaning protocol;-Today – no fever, mild lethargy, still with diarrhea.
Common Comorbidities and Related Clinical IssuesCase Study – Continued
Webinar #1 – Respiratory and Ventilator Basics
PAST MEDICAL HISTORY: DM, CAD, HTN, s/p CABG, s/p PPM (ventricular), Hyperlipidemia, PVD,s/p R 1st & 2nd toes amputation, GERD, Cataracts, s/p CVA w L HP, Seizure d/o, Resp.Failure, s/p Trach(8/30/10), s/p PEG (9/2/10), s/p Pneumonia (8/10), UTIECHO (8/15/10): EF 50-55%. Mild LVH.ECHO (11/3/10): normal LVEF 65-70%, hypokinesis basal anteroseptal wall, mild AI.Carotid Doppler (8/16/10): moderate stenosis RECA & RICA; L ECA&ICA wnl.Hospitalizations:-8/14/10 – 9/10/10 – Flushing Medical Center for CVA w L HP, Seizure d/o, RESP. FAILURE,s/p TRACH (8/30/10), s/p PEG (9/2/10), s/p Pneumonia (8/10), UTI.-10/30/10 – 11/05/10 – NYHQ, for Hematemesis, H/H remained stable, stool guaiac pos,s/p GI eval., no endoscopic procedure done; Dx with VRE UTI, Candiduria, started ABT; PPMinterrogated (11/4/10).-12/23/10 – 12/30/10 – NYHQ for Hematemesis, GI bleed, Anemia, s/p Blood trabsfusion,VAP, s/p EGD on EGD on 12/27/10, found with Hiatus hernia, GERD with esophagitis,deformed gastric antrum, scarring of duodenal bulb; suggested PPI`s & Reglan. S/p PICC lineplacement on 12/30/10.
CONSULTATIONS (this month): Pulmonary (1/10/11), Wound care specialist, Wound NP
REVIEW OF SYSTEMS: no fever, no cough, no SOB, no edema, no abdominal distension, +diarrhea, no constipation, no vomiting, no melena, no bruising, no dysuria, no hematuria, noagitation.

Silvercrest – Respirator and Ventilator Basics UAlbany – 01/28/2011
NYS DOH Surveyor Training
Common Comorbidities and Related Clinical IssuesCase Study – Continued
Webinar #1 – Respiratory and Ventilator Basics
PHYSICAL EXAMINATIONVS T 97.6 Pulse 79 R 14 BP 124/67WEIGHT: 154.6 lbs [ ]Stable [x]Weight change – -2.8 lbs (Re-adm. Wt 151.8 lbs)O: MENTAL STATUS: Drowsy, arousable, in NAD.HEENT: PEERL, no eye discharge, no ear discharge.ORAL CAVITY: moist, no ulcers.NECK: supple, no JVD, trach in place, no carotid murmur.CHEST: no local tenderness, no deformityBREASTS: normal maleLUNGS: b/l AE, b/l scat rhonchi, no rales, no wheezing.C.V.: S1S2 RRR, no S3.ABDOMEN: soft, non tender, BS +. PEG site with min sero-sanguineous oozing.RECTAL: loose brown stool, no BRBPRGU: normal male.EXTREMITIES: no leg edema, no clubbing, diminished peripheral pulses, LUE contacted in elbow & swollen.Amputated R 1st & 2nd toes.CONTRACTURES: LUENEURO: MS as above, L HPHEMIPLEGIA/HEMIPARESIS: L HPPSYCH/BEHAVIOR: no agitationSKIN: Full thickness arterial wound dorsal bordering lateral and medial aspects right 3rd toe
Common Comorbidities and Related Clinical IssuesCase Study – Continued
Webinar #1 – Respiratory and Ventilator Basics
SPECIAL PROBLEMSFeeding Tube: [ ]Not Applicable [ x ]Yes Reason: DysphagiaIf YES, type: [ ]NG [ x ]GT [ ]JT[ x ]Continue [ ]Discontinue
Catheter[x ]Not Applicable [ ]YesReason: [ ]Indwelling [ ]Cystostomy [ ]Texas[ ]Continue [ ]Discontinue
Tracheostomy[ ]Not Applicable [ x ]YesIndication: Respiratory failure
Oxygen:[ ]Not Applicable [ x ]Yes[ ]PRN for:[ x ]Continuously For: Respiratory failure
Common Comorbidities and Related Clinical IssuesCase Study – Continued
Webinar #1 – Respiratory and Ventilator Basics
Antipsychotic Meds[ ]Not Applicable[x ]YesDrugs: Seroquel 25 mg via GT BID, Clonazepam 0.25 mg via GT q 12 hReason - Target behavior(s): anxiety, agitationis it effective?: YesSide Effects: [ ]T.D. [ ]Other: none
Restraints[ ] Not applicable [x] YesIf YES, type: Right hand "peek-a boo" mittensMedical Symptom(s)/Reason: to prevent self decanulationAlternatives tried: [ ] Yes [ ] No NAIf YES, Type:Reduction attempted: [ ] Yes [ ] NoIf YES, Successful? [ ] Yes [ ] No[ x ] Continue Restraint [ ] Discontinue Restraint
Pain Evaluation:[ ] No Pain [ X ] Pain presentPlan (if applicable): Tylenol 650 mg via GT 1 h prior to dressing change

Silvercrest – Respirator and Ventilator Basics UAlbany – 01/28/2011
NYS DOH Surveyor Training
Common Comorbidities and Related Clinical IssuesCase Study – Continued
Webinar #1 – Respiratory and Ventilator Basics
DIAGNOSIS/PROBLEMS / PLAN OF CARE:
- RESPIRATORY FAILURE – in the weaning protocol, tolerating CPAP well. P: continuebronchodilators, weaning as per Pulmonary.
-S/p VAP – resolved clinically. P: observe off ABx.
-Diarrhea – no evidence of C.Diff colitis; completed 2 week course of Flagyl today. P: repeatstool for C.Diff, Stool for O&P, no more ABx for now, hydration via GT, labs next week.
-CAD, HTN, s/p CABG, s/p PPM – continue Plavix 75 mg via GT daily, Metoprolol 25 mg viaGT q 12 h, Isosorbide 20 mg via GT TID, monitor P&BP q shift, monitor SxS of CHF, off ASA inview of recurrent hematemesis. Pacemaker check q month. Last Pacemaker interrogation duringhospitalization (11/4/10 - see copy of report in chart).
Common Comorbidities and Related Clinical IssuesCase Study – Continued
Webinar #1 – Respiratory and Ventilator Basics
DIAGNOSIS/PROBLEMS / PLAN OF CARE:
-DM – HgbA1C 6% on 12/14/10. FSBG 96 - 109. P: off meds, FSBG BIW TID AC, f/uHgbA1C in 3/10.
-Anemia – prob. ACD + Iron deficiency, s/p blood transfusion during hospitalization on12/27/10. P: continue Iron supplement, monitor CBC prn.
-GERD/ Recurrent vomiting/ Hematemesis / GI PROPHYLAXIS – Omeprazole 20 mg via GTdaily, Reglan 10 mg via GT TID AC.
-S/P CVA w L HP, Dysphagia, s/p PEG – continue Plavix 75 mg via GT daily for CVAprophylaxis, off ASA in view of recurrent hematemesis, supportive care, GT feeds.
-Seizure d/o – Trileptal 300 mg via GT BID, seizure precautions.
Common Comorbidities and Related Clinical IssuesCase Study – Continued
Webinar #1 – Respiratory and Ventilator Basics
DIAGNOSIS/PROBLEMS / PLAN OF CARE:
-Vascular Dementia with delusions/psychosis – s/p Psych cons 9/30/10. Plan: continue Clonazepam 0.25mg via GT q 12 h, Seroquel 25 mg BID. Monitor for behavioral disturbances and behavior modificationmanagement. Psych f/u.
-BPH – s/p D/C foley cath on 1/12/11, no SxS of urinary retention. P: off foley cath, Flomax 0.8 mg viaGT qhs.
-DVT PROPHYLAXIS – Heparin 5000 units SQ q 12 h.
-Ulcer R 3rd toe – continue local Tx as per order, vit C to promote wound healing.
-Dermatitis scrotum – Zn oxide oint top q shift
-Vitamin D deficiency – vit D 1000 IU via GT daily, f/u level in 1-2 mo.
-Multiple full thickness wounds b/LE – top Tx as per order, pressure relief as much as possible, nutrition asper dietary), Wound NP f/u.
DNR Conditions Met? [ ]Not Applicable [ x ]YesDNR Ordered? [ ]Not Applicable [ x ]YesResident Plan of Care Discussed? [ ]Yes [ x ]No Reason: Patient unable to comprehend due to Dementia.

Silvercrest – Respirator and Ventilator Basics UAlbany – 01/28/2011
NYS DOH Surveyor Training
Documentation and Care Planning
Assessments
Orders
Plans of Care
Evaluation of Progress
Presenter: Denise Lawson, RN
Director for Performance Improvement at TheSilvercrest Center for Nursing and Rehabilitation
Webinar #1 – Respiratory and Ventilator Basics
Documentation and Care Planning
Assessments Basic
Enhanced
Medical/Pulmonary
Nursing
Respiratory
Dietary
Rehabilitation
Social Services
Therapeutic Recreation / Activities
Webinar #1 – Respiratory and Ventilator Basics
Documentation and Care Planning
Documentation for ventilator dependent residents must meet thestandard for all residents in a Skilled Nursing Facility however thefollowing F Tags are the most significant to this population: F221
F248 F278
F279
F280
F281
F309
F314
F328
F329
Webinar #1 – Respiratory and Ventilator Basics

Silvercrest – Respirator and Ventilator Basics UAlbany – 01/28/2011
NYS DOH Surveyor Training
Documentation and Care Planning
Assessments
Medical/Pulmonary
Co-morbidities acute or chronic such as COPD, CHF, Post Cardiac surgery,
Diabetes, pressure ulcers, neurological (ALS, Guillian-Barre, etc.)
Current respiratory status, history including underlyingcardio-pulmonary conditions/diagnoses
Overall stability of conditions and wean potential
Webinar #1 – Respiratory and Ventilator Basics
Documentation and Care Planning
Assessments
Nursing
System, symptom and diagnosis specific for example;FLACC tool for non-verbal pain assessment
Skilled needs for example IV hydration
Safety issues for example preventing unplanneddecannulation
Education; importance adhering to aspirationprecautions
Webinar #1 – Respiratory and Ventilator Basics
Documentation and Care Planning
Assessments
Respiratory
Respiratory pattern for example normal or labored
Breath sounds
Secretions, i.e., amount, viscosity and color
Ventilator settings, including tidal volume, rate andoxygen
Equipment, including tracheostomy tube type(specialty versus standard) and size
Webinar #1 – Respiratory and Ventilator Basics

Silvercrest – Respirator and Ventilator Basics UAlbany – 01/28/2011
NYS DOH Surveyor Training
Documentation and Care Planning
Assessments Dietary Nutritional needs, for example caloric requirement, protein,
supplements, hydration Modified diet based on swallowing ability Therapeutic diet based on diagnosis for example diabetic and renal Preferences and culturally sensitive choices
Rehabilitation Restorative or maintenance PT/OT/SLP or unit based program
(PROM) Need for splints, adaptive or other devices Swallowing ability and secretion management Communication needs, vocal or non-vocal
Webinar #1 – Respiratory and Ventilator Basics
Documentation and Care Planning
Assessments Social Services Psychosocial needs
Advance Directives
End of life care
Family support
Expressions of sadness or hopelessness
Discharge potential
Therapeutic Recreation Spiritual needs
Leisure interests/recreational needs
Potential for isolation
Webinar #1 – Respiratory and Ventilator Basics
Documentation and Care Planning
Orders
Basic
Enhanced
Respiratory
Dietary
Advanced Directives
Webinar #1 – Respiratory and Ventilator Basics

Silvercrest – Respirator and Ventilator Basics UAlbany – 01/28/2011
NYS DOH Surveyor Training
Documentation and Care Planning
Orders Enhanced
Respiratory Ventilator settings for example ventilator mode (ventilator gives all breaths or
resident participates in taking/triggering a breath) Weaning protocol or modified weaning protocol (gradual decrease in ventilator
support and oxygen percentage based on specific parameters and individualtolerance)
Tracheostomy tube type and size Tracheostomy care
Tracheostomy tube change/frequency Inner cannula tube change/frequency
Ventilator tubing change/frequency Suctioning frequency Respiratory treatments/medications Other specialty areas
Speaking valve use Cuff deflation
Webinar #1 – Respiratory and Ventilator Basics
Documentation and Care Planning
Orders Enhanced Diet
Regular/Modified
Tube Feeding
Pleasurable
Adaptive device
Advance Directives DNR
DNI
Hospice
Palliative Care
Webinar #1 – Respiratory and Ventilator Basics
Documentation and Care Planning
Plan of Care
Basic
Enhanced
Medical/Pulmonary
Nursing
Respiratory
Dietary
Rehabilitation
Social Services
Therapeutic Recreation / Activities
Webinar #1 – Respiratory and Ventilator Basics

Silvercrest – Respirator and Ventilator Basics UAlbany – 01/28/2011
NYS DOH Surveyor Training
Documentation and Care Planning
Plan of Care
Enhanced
Medical/Pulmonary
Co-morbidities
Respiratory medications and treatments
Respiratory care including suctioning, tracheostomy tubecare, maintaining ventilator settings
Weaning
Webinar #1 – Respiratory and Ventilator Basics
Documentation and Care Planning
Plan of Care Enhanced
Nursing Diagnosis specific for example diabetes High-Risk/Population specific
Pressure ulcer prevention and management Infections for example UTI, Sepsis and Ventilator Associated Pneumonia Tube feeding; gastrostomy and jejunostomy Hydration including IV fluids PICC line management Urinary catheters Restraints Polypharmacy Pain Safety for example unplanned decannulation Resident/family education for example Weaning Protocol
Webinar #1 – Respiratory and Ventilator Basics
Documentation and Care Planning
Plan of Care Enhanced Respiratory
Ventilator support
Weaning
Capping and Decannulation
Treatments
Equipment, including specialty equipment
Dietary Nutritional status
Diet type and supplements
Weight loss/gain
Webinar #1 – Respiratory and Ventilator Basics

Silvercrest – Respirator and Ventilator Basics UAlbany – 01/28/2011
NYS DOH Surveyor Training
Documentation and Care Planning
Plan of Care Enhanced Rehabilitation
Restorative or maintenance PT/OT/SLP or unit based program
Swallowing and/or secretion management
Communication, vocal or non-vocal
Social Services Psychosocial/isolation/depression
Advance Directives
Therapeutic Recreation Spiritual
Leisure/recreational activities
Webinar #1 – Respiratory and Ventilator Basics
Documentation and Care Planning
Evaluation of Progress
Care plan meetings
Ventilator Rounds
Respiratory/Ventilator checks
As indicated
Webinar #1 – Respiratory and Ventilator Basics
RESPIRATOR AND VENTILATOR BASICS
ANY QUESTIONS?
FOR ADDITIONAL INFO VISIT US AT:WWW.SILVERCREST.ORGOR CALL 718-480-4026
Friday • January 28th, 2011 • 10:00AM