RESPECT PROTECT - Australian Nursing & Midwifery .../media/files/anmf/ohs/10pointplan-gui… · But...
24
RESPECT AND PROTECT OUR VICTORIAN HEALTHCARE WORKERS anmfvic.asn.au/ovaguide
Transcript of RESPECT PROTECT - Australian Nursing & Midwifery .../media/files/anmf/ohs/10pointplan-gui… · But...

RESPECT AND PROTECT OUR VICTORIAN HEALTHCARE WORKERS
anmfvic.asn.au/ovaguide

CONTENTS
Message from Victorian Health Minister Jill Hennessey page 1
Message from ANMF (Vic Branch) Secretary Lisa Fitzpatrick page 1
Introduction page 2
• Pre-conditions
• Scope
• Terminology
• Instructionsforuse
1. Improvesecurity page 4
2. Identifyrisktostaffandothers page 6
3. Includefamilyinthedevelopmentofpatientcareplans* page 9
4. Report,investigateandact page 10
5. Preventviolencethroughworkplacedesign page 11
6. Provideeducationandtrainingtohealthcarestaff page 12
7. Integratelegislation,policiesandprocedures page 14
8. Providepost-incidentsupport page 16
9. Applyanti-violenceapproachacrossallhealthdisciplines page 17
10. Empowerstafftoexpectasafeworkplace page 18
*ANMFNote:ReferraltoPatientCarePlanincludesallassociateddocumentse.g.BehaviouralManagementPlan.
First edition published in 2017. This edition was revised and printed in October 2018.

© This work is copyright. Apart from any use permitted under the Copyright Act 1968, no part may be reproduced by any process, nor may any other exclusive right be exercised, without the permission of The Secretary, Australian Nursing & Midwifery Federation (Victorian Branch), Melbourne, 2017. PAGE 1
MESSAGE FROM THE HON JILL HENNESSY MP Minister for Health, Minister for Ambulance Services
Nursesandmidwiveshavetherighttobesafe–andfeelsafe –atwork.Youcareforusatourmostvulnerableanddeservetheutmostrespectfortheworkyoudo.
You–andeverybodywhoworksinthehealthcaresystem–deservestogohomesafelytotheirfamilyaftereachshift.Violenceandaggressionjustshouldn’tbepartofthejob.
Yetitoftenis.
It’ssomethingourGovernmentisdeterminedtoaddress.
Wewon’ttolerateoccupationalviolenceandaggressionagainstnurses,midwivesandotherhealthcareworkersandwewillcontinuetowork withyoutomakeyourworkplacessafer.
IwanttothanktheANMFforitsleadershipindevelopingthis10 Point Plan to End Violence and Aggression: A Guide for Health Services.Thisisanimportanttool–whichalongsidearangeofresources–outlinestheactionshealthcareorganisationscantaketoendviolenceandaggressioninourworkplaces.
Saferworkplacesarevitalsothatnursesandmidwivescanconcentrate onwhatyoudobest–takingcareofthecommunity.
MESSAGE FROM LISA FITZPATRICKBranch Secretary, ANMF (Vic Branch)
Nursesandmidwives,andotherhealthworkers,areexperiencing frequentandfrighteningseriousphysicalandpsychologicalinjuriesatwork. Manyarerightlysayingenoughisenough.
Butweneedmorethanwordstoensurethepeoplewhoworkinourhealthcaresystemgohomesafelytotheirfamiliesandfriendsaftereachshift.
Tostoptheunacceptablenumberofassaults,theAustralianNursingandMidwiferyFederation(VictorianBranch)developedandreleasedthe10pointplantoendviolenceandaggressionin2014.We’vebeenworkingsincetotreatviolenceasanoccupationalhealthandsafetyrisk.
Theknowledge,informationandactionsnecessarytoendpreventableviolenceatworkareinthisguide.Thisiswhatasuccessfulorganisationalresponsetothepreventionofviolenceandaggressionshouldlooklike.
ThisguidewillonlyworkifchiefexecutiveofficersandhospitalboardsdrivethesechangessothatasaferwayofdoingthingsisabsorbedintotheDNAofeverylevel ofmanagement.
Nomorefragmentation.Toberunningahospitaloperatinginthegreensafezoneof thisguide,theworkofclinicalmanagersmustintersectwiththeoccupationalhealth andsafetyandthehumanresourcesmanagers.
Thedataismounting.Thespecificsofviolentincidentsandthehumancostareconfronting.Weknowthereisaproblem.Herearethesolutions.
Thiswilltakeleadershipandwholeofcommunityapproach–government,hospitalmanagementandthepublic.
Thisguideoutlinestheactionshospitalscancontrol.Let’sworktogethertooperateinthegreenzonesowecanstoptheunacceptablelevelsofviolenceinourhealthcarefacilities.

© This work is copyright. Apart from any use permitted under the Copyright Act 1968, no part may be reproduced by any process, nor may any other exclusive right be exercised, without the permission of The Secretary, Australian Nursing & Midwifery Federation (Victorian Branch), Melbourne, 2017. PAGE 2
INTRODUCTION
HEALTH CARE WORKERS
PREVENTION OF OVA
DepartmentofHealth andHumanServices
OHSRegulatorWorkSafe
Hospital OHS SystemHospital Management Systems
Public Health Care System
Public Service
Public
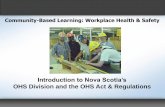
Diagram: Ending violence and aggression requires changes to all levels of systems
Endingviolenceandaggressionrequireschangestoalllevelsofsystems,asdemonstratedintheadjacentdiagram.ThisGuideisatooltoenablehealthcareorganisationstoreviewtheirmanagementandoccupationalhealthandsafetysystems,andensurethatoccupationalviolenceandaggressionisappropriatelyrecognised,representedandincludedasarisk,andactionstakentopreventincidents.

© This work is copyright. Apart from any use permitted under the Copyright Act 1968, no part may be reproduced by any process, nor may any other exclusive right be exercised, without the permission of The Secretary, Australian Nursing & Midwifery Federation (Victorian Branch), Melbourne, 2017. PAGE 3
Pre-conditionsCommitment: theGuidewillonlybesuccessfulifimplementedinanorganisation(andsystem)whichhasacommitmenttothepreventionofoccupationalviolencewhichisrealandirrefutable.Thiscommitmentneedstocomefromnotjust themiddlemanagementofafacility,butisrequiredfrom thosewiththeultimatepowerinthehealthsystem.
Thiscommitmenthasbeendemonstratedbythoseinchargeandincontrol,fromtheVictorianPremierandHealthMinister,throughtotheDepartmentofHealthandHumanServices.ThisGuideisintendedtoassistthoseatthehealthservicesindividually.Validationofthecommitmentcomesinmanyforms,nottheleastofwhichistherecognitionoftheproblemtobeginwith,andthededicationofresourcestoimplementstrategiestopreventandaddressthesystemicissues.
Thiscommitmentmustmanifestatthechiefexecutiveofficerandboardofdirectorlevel,withagain,theacknowledgment ofthefailingsofthesysteminitscurrentform,andapledge toaddresstheshortcomings.Suchademonstrationshouldalsoincludeareportingstructurewhichmeansthateachboardofdirectorsisprovidedwithanin-depthreportateachmeeting ofthenumberofassaultsthathaveoccurredwithintheirhospitalnetwork,thedetailsofeachassault,theinjuriessufferedbythestaff,andthecorrectiveactionswhichhave beenputinplacetoreducetheriskofrecurrence.
Communication,consultationandcollaboration:another pre-conditiontotheframeworkisacommitmentbythoserunningthehealthservicetoundertakethe‘ThreeCs’–communication,consultationandcollaboration,inrelation tooccupationalviolenceandaggression,butmorebroadly asamanagementimperative.
WhilsttheOccupational Health and Safety Act 2004mandateshealthservicestoundertakeconsultationinrelationtomatterswhichaffect(ormayaffect)thehealthandsafetyofstaff,experienceshowsthatthisisrarelyundertakeninthemanner inwhichitisdescribed.Again,thismustbedemonstratedfromdecisionmakers,inordertoaffectchangeatalocallevel. Suchcommunication,consultationandcollaborationmustinvolverepresentativesofallstakeholders,includinghealthservices,unions,workers,healthandsafetyrepresentatives andconsumers.
Moreover,thepresenceandinputatbothastrategicandlocallevelintosuchstrategieswillallowmorerobustsystemstobedevelopedandimplemented,whichwillleadtowideracceptance,andincreasedownership.
ScopeTheprinciplesandcontentoftheANMF(VicBranch) 10pointplanisapplicabletoallhealthserviceand hospitalfacilities,includingmentalhealth,acute, emergencydepartments,agedcare,communitycare andlocationsexternaltoapurposebuiltworkplace e.g.visitinghealthservices.
TerminologyClinicalstaff–includesnurses,midwives,doctors,allied healthandotherclinicalstaff
HSRs –healthandsafetyrepresentatives
OVA–occupationalviolenceandaggression,whichis definedbyWorkSafeVictoria(‘Preventionandmanagement ofviolenceandaggressioninhealthservices’,June2017) asanincident‘inwhichapersonisabused,threatened orassaultedincircumstancesrelatedtotheirwork… OVAincludesabroadrangeofactionsandbehaviours thatcancreaterisktohealthandsafetyofemployees. Itincludesbehaviouroftendescribedasactingout, challengingbehaviourandbehavioursofconcern.
OVAcanresultinanemployeesustainingphysicaland/orpsychologicalinjuries,andcansometimesbefatal.EmployeescanbeexposedtoOVAfromarangeofsourcesincludingclients,consumers,patients,residents,visitorsandmembers ofthepublic.ExamplesofOVAinclude,butarenotlimitedto:
• biting,spitting,scratching,hitting,kicking
• pushing,shoving,tripping,grabbing
• throwingobjects,damagingproperty
• verbalabuseandthreats
• usingorthreateningtouseaweapon
• sexualharassmentorassault.’
PatientCarePlan-documentse.g.BehaviouralManagementPlan,admissiondocumentation,riskassessmentsetc.
Patients–wherepatientsarereferredto,thismayalsobereadtoincludeclients,residentsandconsumersasappropriate.
NB:atallstepsoftheprocess,itiscriticalthatfrontlinestaffandHSRsareinvolvedinconsultation.
InstructionsforuseThetrafficlightapproachsupportshealthservicesintheirmovementfromasituationwithhighriskfactorstothelowerrisksolutions,steppingalongtheway.TheGuidecanalsobeusedasan‘audit-type’tool,wherebyhealthservicesareabletoself-assessagainstthecriteriaintheguide,andidentifytheirareasforimprovement.
TheGuideprovidesastartingpointforhealthservicestoworktowardsinrelationtoimplementationofanorganisationalapproachtothepreventionofoccupationalviolenceandaggression.Ithasidentifiedkeyfactorsthatcompriseeachofthe10Points,andthatdemonstrateorindicatecompliancewiththefactors,andprovidesexamplesofhigh,mediumandlowrisksolutionstoeachofthefactors.
Itisexpectedthatfacilitieswouldbeworkingtowardsthelowestrisksolutionsinordertoensurethattheirstaffareprovidedanenvironmentthatisassafeaspossible.Giventheongoingdevelopmentsoccurringwithinpreventionofoccupationalviolenceandaggression,thisguideprovidesastartingpoint,howeveracommitmenttocontinuousimprovement,andongoingreviewandrevisionofcontrols inthisareaisrequired.

© This work is copyright. Apart from any use permitted under the Copyright Act 1968, no part may be reproduced by any process, nor may any other exclusive right be exercised, without the permission of The Secretary, Australian Nursing & Midwifery Federation (Victorian Branch), Melbourne, 2017. PAGE 4
1 IMPROVE SECURITY
CRITERIA HIGH RISK REDUCED RISK SOLUTION LOW RISK SOLUTION
1.1 The Department of Health and Human Services must develop adequate baseline standards for security and fund public health services to comply, whilst private organisationsmustdedicatefunding.
Thehealthservicedoesnotapplyforfundingopportunities,noristherefundingforsecurity.
Thehealthserviceappliesforallfundingopportunities, andrespondstosecurityfundingneeds.
Thehealthserviceappliesforallfundingopportunitiesandsubmissionsarebasedonpriorityareasevidencedfromriskassessmentfindings.Further,dedicatedongoingsecurityfundingisidentifiedinbudgets.
1.2 Specificallytrainedsecuritypersonnel(seealso6–Provideeducationandtrainingtohealthcarestaff).
Noareasorpartialareasandsiteshaveon-sitesecuritypersonnelavailable.
Someon-sitesecuritypersonnelareavailableforsomeareasandsiteswheneveroperational.
On-sitesecuritypersonnelareavailableinadequatesafenumbersforallareasandsitesduringalloperationalhours.
Thetrainingandexperienceofsecuritypersonnelisnotcheckedtoidentifywhethertheyhavehealthcarespecifictrainingandexperience.
Thetrainingandexperienceofsecuritypersonnelisinconsistentlyreviewed,againstanundocumentedsetofrequirements.
Allsecuritypersonnelhavehadhealthcareandorganisation-specifictrainingintheirrole,whichischeckedpriortoengagementagainstadocumentedsetofcriteria,andisregularlyreviewedandupdated.
1.3 Access to secure areas and safe zones.
Thefacilityhasnostaffsecureareas,safezonesand lock-downareaorprocedures.
Therearesomeestablishedstaffsecureareas,safezones,lockdownareasandproceduresbuttherearenosystemsinplace.
Asecurityauditofallestablishedstaffsecureareas, safezonesandlockdownareasandprocedureshas beenconductedandimprovementrecommendations havebeenimplemented.
Asecurityriskassessmentofallareasinthefacilityhas notbeenconducted.
Asecurityriskassessmentofallareasinthefacilityhasbeenconductedtoidentifyhighriskareas,secureareas,safezonesandlockdownareasincludingprocedures.
Asecurityriskassessmentofallareasinthefacilityhasbeenconductedtoidentifyhighriskareas,secureareas,safezonesandlockdownareasincludingprocedures andrecommendationshavebeenfullyimplemented andreviewed.
1.4 Security cameras. CCTVisnotinstalledon-site. CCTVisinstalledinspotsacrossareasandsitesincludingcarparkswithinconsistentmonitoringoffootage/feed.
Asecurityriskassessmenthasbeenconductedtoensure:• CCTVisinstalledinkeyareasacrossallareasand
sitesincludingcarparkswithaccompanyingCCTVwarningsignagealsodisplayedinkeyareasfor patientsandvisitors
• CCTVisusedforevidenceinhospitaland/orpoliceinvestigationswhereappropriate
• identificationofwaysinwhichCCTVcouldbeused inapreventativemanneroccurregularly e.g.trainingreviews
• proceduresareinplacetoensurefootageismonitoredaccordingtoidentifiedhighriskareas.
ThehealthservicedoesnothaveproceduresforaccessingCCTVfootage.
ThehealthservicehasproceduresforaccessingCCTVfootage.

© This work is copyright. Apart from any use permitted under the Copyright Act 1968, no part may be reproduced by any process, nor may any other exclusive right be exercised, without the permission of The Secretary, Australian Nursing & Midwifery Federation (Victorian Branch), Melbourne, 2017. PAGE 5
CRITERIA HIGH RISK REDUCED RISK SOLUTION LOW RISK SOLUTION
1.5 Personal duress alarms. Ariskassessmentofallareasinthehealthservicehas notbeenconductedtoidentifyanyneedforpersonalduressalarms.
Ariskassessmentofallareasinthehealthservicehasbeenconductedtoidentifyhighriskareasforstaffneedingwallmountedandpersonalduressalarms,includinglocationidentification.
AriskassessmentofallareasinthehealthservicehasbeenconductedinconsultationwithHSRsandstafftoidentifyhighriskareasforstaffneedingwallmountedandpersonalduressalarmsincludinglocationidentification,andrecommendationshavebeenimplemented.
Personalandwallmountedduresssystemisnottested. Personalandwallmountedduresssystemisregularlytested.
Thefacilityhasaduressalarmsystemprocedureandtestingschedule.Personalandwallmountedduress systemisregularlytestedandresultsdocumented.
Thereisnotrainingofstaffintheuseofduressalarms. Inconsistentandunregulatedtrainingofstaffintheuse ofduressalarms.
Regular,consistenttrainingofstaffintheuseof duressalarms,governedbyprocedure,includingtrialingthealarms.
1.6 Searching or personal belongings.
Seealso2–Identifyrisktostaffandothersand6–Provideeducationandtrainingtohealthcarestaff.
Noproceduresinplaceregardingsearchingpatientandvisitorsuponadmissionandduringapatient’sstay.
Limitedproceduresareinplaceregardingsearchingpatientandvisitorsuponadmissionandduringapatient’sstay.
Thefacilityhasclearproceduresaroundperformingpatientandvisitorsearchestoensureaconsistentapproach.
1.7 Regular security audits of health services, including maintaining security equipment.
Thefacilitydoesnothaveadocumentedsecurityaudit andriskassessmentprocess.
Thefacilityhasadocumentedsecurityauditandriskassessmentprocess.
Thefacilityhasadocumentedsecurityauditandriskassessmentprocesswithregularschedulingandimplementationandreviewofidentifiedrisks.
Thefacilityhasnotreviewedthesecurityauditandriskassessmenttool.
Thefacilityhasreviewedthesecurityauditandriskassessmenttool.
ThefacilityhasreviewedthesecurityauditandriskassessmenttoolandhasadocumentedongoingreviewschedulewithresultsreportedtotheOHS/OVAgovernancecommitteeforoversight.
1.8 Monitoring systems for community clinics.
Asecurityriskassessmentofthecommunityclinicsincludingmonitoringsystemshasnotbeenconducted.
Asecurityriskassessmentofthecommunityclinicsincludingmonitoringsystemshasbeenconducted.
Asecurityriskassessmentofthecommunityclinicsincludingmonitoringsystemshavebeenconducted andrecommendationshavebeenimplemented.
1 IMPROVE SECURITY CONTINUED

© This work is copyright. Apart from any use permitted under the Copyright Act 1968, no part may be reproduced by any process, nor may any other exclusive right be exercised, without the permission of The Secretary, Australian Nursing & Midwifery Federation (Victorian Branch), Melbourne, 2017. PAGE 6
2 IDENTIFY RISK TO STAFF AND OTHERS
CRITERIA HIGH RISK REDUCED RISK SOLUTION LOW RISK SOLUTION
2.1 Identifyingtheriskofapatientorothers (e.g. visitors or family) being aggressiveorviolenttowardsstaffmust be part of clinical pre-admission (prior to decision to admit).
Thefacilitydoesnotperformclinicalpre-admissionOVAriskassessmentsofpatients.
Thefacilityperformsclinicalpre-admissionriskassessmentsbutthecriteriatoassessandidentifythe riskofthepatient/othersbeingaggressiveorviolent islimited.
Thefacilityperformsclinicalpre-admissionriskassessmentsincludingappropriatecriteriatoassessandidentifytheriskofthepatient/othersbeingaggressive orviolent.Thisalsoconsidersthepatientmedicalrecordfrompreviousadmissionsandispartofthehandoverforambulanceandpolice.
Iftheclinicalpre-admissionriskassessmentidentifies riskofthepatient/othersbeingaggressiveorviolent,thereisnosystemtoensureimplementationofpreventativecontrols.
Iftheclinicalpre-admissionriskassessmentidentifies riskofthepatient/othersbeingaggressiveorviolent,thereisanadhocsystemofimplementationofpreventativecontrols.
Whentheclinicalpre-admissionriskassessmentidentifiesriskofthepatient/othersbeingaggressiveorviolent,thereisasystemtoensureappropriatepreventativemeasuresareimplementedandmonitoredthroughoutthepatientstay.
Thefacilityhasnotdevelopedaguidancelistofpreventivemeasuresavailableforuseatclinicalpre-admission.
Thefacilityhasdevelopedalimitedguidancelistofpreventativemeasuresavailableforuseattheclinical pre-admissionstage.
Thefacilityhasdevelopedarobustguidancelistofpreventativemeasuresavailableforuseattheclinicalpre-admissionstagee.g.speciallingpatients,nursinginpairs,placingthepatientinahighlyvisiblearea,sourcingmoreappropriatefacilityforadmission,ensuringappropriatelyqualifiedandexperiencedstaffareallocatedforcare,notificationofsecuritypersonnel.
Clinicalpre-admissiondoesnotincludereviewoftheappropriatesetting(environmentandmodelofcare) fortheindividualpatient.
Clinicalpre-admissionincludesreviewoftheappropriatesetting(environmentandmodelofcare)fortheindividualpatient.
Clinicalpre-admissionincludesreviewoftheappropriatesetting(environmentandmodelofcare)fortheindividualpatientandrecommendedpreventativemeasuresareimplementedpriortoadmission.
Thefacility/unithasnopatientadmission/exclusioncriteria.
Thefacilityorunithaspatientadmissioncriteriabuttheinclusionandexclusioncriteriarelatingtostaffandpatientsafetyarenotconsistentlycompliedwithorsupported, orarelimited.
Thefacilityorunithaspatientadmissioncriteriawithclearinclusionandexclusioncriteriarelatingtostaffandpatientsafetyanditisusedduringtheclinicalpre-admissionassessment.Complianceisconsistentanddecisionsmadeusingthecriteriaaresupportedbymanagement.
2.2 Identifyingtheriskofapatientorother being aggressive or violent towardsstaffmustbepartofadmission procedures (at admission).
ThefacilitydoesnotperformclinicaladmissionOVA riskassessmentsofpatients.
Thefacilityperformsclinicaladmissionriskassessmentsbutthecriteriatoassessandidentifytheriskofthepatient/othersbeingaggressiveorviolentislimited.
Thefacilityperformsclinicaladmissionriskassessmentsincludingappropriatecriteriatoassessandidentifythe riskofthepatient/othersbeingaggressiveorviolent. Thisalsoconsidersthepatientmedicalrecordfrompreviousadmissionsandispartofthehandoverforambulanceandpolice.
Iftheclinicaladmissionriskassessmentidentifiesriskofthepatient/othersbeingaggressiveorviolent,thereisnosystemtoensureimplementationofpreventativecontrols.
Iftheclinicalpre-admissionriskassessmentidentifies riskofthepatient/othersbeingaggressiveorviolent,thereisanadhocsystemofimplementationofpreventativecontrols.
Whentheclinicaladmissionriskassessmentidentifiesriskofthepatient/othersbeingaggressiveorviolent,thereisasystemtoensurepreventativemeasuresareimplementedandmonitoredthroughoutthepatientstay.

© This work is copyright. Apart from any use permitted under the Copyright Act 1968, no part may be reproduced by any process, nor may any other exclusive right be exercised, without the permission of The Secretary, Australian Nursing & Midwifery Federation (Victorian Branch), Melbourne, 2017. PAGE 7
CRITERIA HIGH RISK REDUCED RISK SOLUTION LOW RISK SOLUTION
2.2 Continued. Thefacilityhasnotdevelopedaguidancelistofpreventivemeasuresavailableforuseatclinicaladmission.
Thefacilityhasdevelopedalimitedguidancelistofpreventativemeasuresavailableforuseattheclinicaladmissionstage.
Thefacilityhasdevelopedarobustguidancelistofpreventativemeasuresavailableforuseattheclinicaladmissionstagee.g.speciallingpatients,nursinginpairs,placingthepatientinahighlyvisiblearea,sourcingmoreappropriatefacilityforadmission,ensuringappropriatelyqualifiedandexperiencedstaffareallocatedforcareetc.
Thefacility/unithasnopatientadmission/exclusioncriteria.
Thefacilityorunithaspatientadmissioncriteriabutinclusionandexclusioncriteriarelatingtostaffandpatientsafetyarenotconsistentlycompliedwithorsupported, orarelimited.
Thefacilityorunithaspatientadmissioncriteriawithclearinclusionandexclusioncriteriarelatingtostaffandpatientsafetyanditisusedduringtheclinicaladmissionassessment.Complianceisconsistentanddecisionsmadeusingthecriteriaaresupportedbymanagement.
Clinicaladmissiondoesnotincludereviewoftheappropriatesetting(environmentandmodelofcare)fortheindividualpatient.
Clinicaladmissionincludesreviewoftheappropriatesetting(environmentandmodelofcare)forthe individualpatient.
Clinicaladmissionincludesreviewoftheappropriatesetting(environmentandmodelofcare)forthe individualpatientandrecommendedpreventativemeasuresareimplemented.
TransferofpatientOVAriskinformationdoesnotoccurfromdischargingunit/healthservicetotheadmittingunit/healthservice.
Transferofinformationisrequestedbyadmittingorganisation/ward/unitorprovidedbydischargingorganisation/ward/unitbuttheinformationislimitedormissingandtheprocessisadhoc.
Transferofinformationisactivelyrequestedbyadmittingorganisation/ward/unitandprovidedbydischargingorganisation/ward/unitsincludingand/orpolice. Followupsystemsareinplacetoensurethisinformation isavailableandactedupon.
2.3 Identifyingtheriskofapatientorother being aggressive or violent throughoutthepatient’sstay.
Clinicaldocumentationdoesnotincludeprovisiontoidentifyandassessapatient/othersbeingaggressive orviolent.
Clinicaldocumentation(includingclinicalhandoverandclinicalassessment)acrossallwards,areasandsiteshaveprovisionforidentifyingtheriskofapatient/othersbeingaggressiveorviolent.
Allclinicaldocumentation(includingclinicalhandoverandclinicalassessment)acrossallwards,areasandsiteshaveprovisiontoidentify,reviewandupdatetheriskof apatient/othersbeingaggressiveorviolentandthere areclearprocedurestoimplementcontrolswhererisk isidentified.Thisalsoconsidersthepatientmedicalrecordfrompreviousadmissionsandispartofthehandoverforambulanceandpolice.
2.4 Whenapatientisadmittedwithoutnoticetoahealthcarefacility–forexampletoanemergencydepartment – a violence risk assessmentmustbeinitiated assoonaspracticable.
OVAriskassessmentsarenotcompletedassoon aspracticableoratallwhenapatientisadmitted withoutnotice.
OVAriskassessmentsaresometimescompletedassoonaspracticablewhenapatientisadmittedwithoutnotice.
OVAriskassessmentsarecompletedassoonaspracticablewhenapatientisadmittedwithoutnoticeandappropriatepreventativeactionsareimplemented.
2 IDENTIFY RISK TO STAFF AND OTHERS CONTINUED

© This work is copyright. Apart from any use permitted under the Copyright Act 1968, no part may be reproduced by any process, nor may any other exclusive right be exercised, without the permission of The Secretary, Australian Nursing & Midwifery Federation (Victorian Branch), Melbourne, 2017. PAGE 8
CRITERIA HIGH RISK REDUCED RISK SOLUTION LOW RISK SOLUTION
2.5 Staffarealertedassoonaspracticabletotheriskofapatient or other being violent or aggressive.
Currentbehaviouralcontractsarenotdisseminatedwithinandacrosssites.
Behaviouralcontractsaredevelopedbutarenotdistributed.Staffcaringforpatientsarenotawareofthem.
Currentbehaviouralcontractsaredisseminatedwithinandacrosssites,andflaggedoncomputersystems.
Therearenocommunicationprocessestoadvisestaffoftheriskofapatientorotherbeingviolentoraggressive.
Communicationprocessestoadvisestaffoftheriskofapatientorotherbeingviolentoraggressivearenotimmediate.
Communicationprocessestoadvisestaffoftheriskofapatientorotherbeingviolentoraggressiveareimmediateincludingdisseminationofbehaviouralmanagementplansandassociatedinformationwithinandacrosssites.
ClinicaldocumentationhasnoprovisiontoreviewandupdateOVAriskandrequirementswithinandacrosssites.
Clinicaldocumentationincludingassessmentand handoverhavelimitedprovisiontoreviewandupdate OVArequirementswithinandacrosssites.
Allclinicaldocumentationincludingassessment,careplansandhandoverdocumentationhaveprovisiontoreviewandupdateOVArequirementswithinandacrosssites.
2.6 Staffarealertedassoonaspossibletotheriskofarelative/visitor being violent or aggressive.
Currentbehaviouralcontractsregardingrelatives/visitorsarenotdisseminatedwithinandacrosssites.
Currentbehaviouralcontractsregardingrelatives/visitorsaredisseminatedamongstthehealthservice’sexecutivemanagementonly,orotherwiselimitedin theirdistribution.
Currentbehaviouralcontractsregardingrelatives/visitorsaredisseminatedwithinandacrosssites,andflaggedoncomputersystems.
Therearenocommunicationprocessestoadvisestaffoftheriskofarelative/visitorbeingviolentoraggressive.
Communicationprocessestoadvisestaffoftheriskofarelative/visitorbeingviolentoraggressivearenotimmediatewithinandacrosssites.
Communicationprocessestoadvisestaffofortheriskofarelative/visitorbeingviolentoraggressiveareimmediateincludingdisseminationofbehaviouralmanagementplansandassociatedinformationwithinandacrosssites.
Noviolentandaggressivevisitor/relativealertsystemisavailable.
Someareasandsiteshaveaviolentandaggressiverelative/visitoralertsystem.
Allareasandsiteshaveaviolentandaggressiverelative/visitoralertsystemwithclearprocessestoflagand manageidentifiedrelatives/visitors.
2.7 Healthservicesmustensurepatientalert systems, including violent or aggressive behaviour, are part ofadmissionandpatientstayprocedures.
Noviolentandaggressivepatientalertsystemisavailable. Someareasandsiteshaveaviolentandaggressivepatientalertsystem.
Allareasandsiteshaveaviolentandaggressivepatientalertsystemwithclearprocessestoflagandmanageidentifiedpatients.
Theviolentandaggressivepatientalertssystemisnotintegratedintotheadmissionandpatientstayprocess.
Theviolentandaggressivepatientalertssystemissomewhatintegratedintotheadmissionandpatient stayprocess.
Theviolentandaggressivepatientalertssystemis fullyintegratedintotheadmissionandpatientstay processtoensurehighriskpatientsareidentifiedandappropriatelymanaged.
Theviolentandaggressivepatientalertsystemisnotcompatibleacrossthenetworksystems.
Theviolentandaggressivepatientalertsystemhas limiteduniformityacrossthenetwork.
Theviolentandaggressivepatientalertsystemisuniformacrossthenetworkandiscompatiblewithallpatientinformationsystems.
ThepatientalertsystemdoesnotprovideinformationinrelationtopreviousOVAriskfactorsandincidentsspecifictothepatient.
ThepatientalertsystemprovideslimitedinformationinrelationtopreviousOVAriskfactorsandincidentsspecifictothepatient,butisusedinconsistentlyandonanadhocbasis,withtheinformationunreliable.
Thepatientalertsystemprovidesinformationinrelation toOVAriskfactorsandincidentsspecifictothepatient, isusedconsistentlyandtheinformationisreliable.
2 IDENTIFY RISK TO STAFF AND OTHERS CONTINUED

© This work is copyright. Apart from any use permitted under the Copyright Act 1968, no part may be reproduced by any process, nor may any other exclusive right be exercised, without the permission of The Secretary, Australian Nursing & Midwifery Federation (Victorian Branch), Melbourne, 2017. PAGE 9
3 INCLUDE FAMILY IN THE DEVELOPMENT OF PATIENT CARE PLANS*
CRITERIA HIGH RISK REDUCED RISK SOLUTION LOW RISK SOLUTION
3.1 PatientCarePlansdonotonlytakeinto account the clinical component ofcaringforapatientbutalsohowcaringforthepatientmayimpactonthehealthandorsafetyofstafforothers.
TheprocessofdevelopingthePatientCarePlanonlyconsiderstheclinicalcomponentofcaringforapatient.
ThedocumentedprocessofdevelopingthePatientCarePlanconsiderssomefactorswhichmayimpactonthehealthand/orsafetyofstaffandothers,butdoesnotidentifypreventativemeasures.
ThedocumentedprocessofdevelopingthePatientCarePlannotonlyconsiderstheclinicalcomponentofcaring forapatientbutalsoconsidershowcaringforthepatientmayimpactonthehealthand/orsafetyofstafforothersandrequiresidentificationandimplementation ofpreventativeactions.
Theidentifiedpotentialimpactstothehealthand/orsafetyofstafforothersarenotformallydocumentedwithinthePatientCarePlanwhendevelopingaPatientCarePlan.
Theidentifiedpotentialimpactstothehealthand/orsafetyofstafforothersareformallydocumentedwithinthePatientCarePlanwhendevelopingaPatientCarePlan.
Theidentifiedpotentialimpactstothehealthand/orsafetyofstafforothersandpreventativemeasuresareformallydocumentedwithinthePatientCarePlanwhendevelopingaPatientCarePlan.
Clinicalstaff(doctors,nurses,midwives,alliedhealthandothers)involvedinthedevelopmentofaPatientCarePlandonotconsiderhowaPatientCarePlanmayimpacton thehealthand/orsafetyofstafforothers.
Someclinicalstaff(doctors,nurses,midwives,alliedhealthandothers)involvedinthedevelopmentofaPatientCarePlanconsiderhowaPatientCarePlanmayimpactonthehealthand/orsafetyofstafforothers.
Allclinicalstaff(doctors,nurses,midwives,alliedhealthandothers)involvedinthedevelopmentofaPatientCarePlanconsiderhowaPatientCarePlanmayimpactonthehealthand/orsafetyofstafforothers.
3.2 Thepatient’shistory,presentationand risk factors, and those of their visitorsandrelatives,aretakenintoaccount in the development ofPatientCarePlans.
Thepatient’shistory,presentationandriskfactors,andthoseoftheirvisitorsandrelatives,arenottakenintoaccountinthedevelopmentofPatientCarePlans.
Thepatient’spresentationonlyistakenintoaccountwhendevelopingPatientCarePlansandconsideringhowthecaremayaffectthehealthandsafetyofstafforothers.
Thepatient’shistory,presentationandriskfactors,andthoseoftheirvisitorsandrelatives,aretakenintoaccountwhendevelopingPatientCarePlansandconsideringhowthecaremayaffectthehealthandsafetyofstafforothers.
3.3 Wherepossible,PatientCarePlansshould involve family members to ensure clear standards of behavior are set and healthcare professionals can provide a consistent approach.
PatientCarePlansarenotdevelopedinconjunction withthepatientandfamily/carer.
PatientCarePlansaredevelopedinconjunctionwiththepatientandfamily/carer.
PatientCarePlansaredevelopedinconjunctionwiththepatientandfamily/carer,andclearstandardsofbehaviortowardsstaffaresetanddocumented.
PatientCarePlansarenotdevelopedinconjunction withthepatientandfamily/carer.
PatientCarePlansdevelopedinconjunctionwithpatientandfamily/carersdonotseekobservations,insights,informationandadviceonstrategiesthatmayincreaseand/orreducetheriskofaggressiveorviolentpatientbehaviourandproactiveearlyinterventionstrategiesthatmayreducetheriskthattheviolentoraggressivebehaviorwillescalatefurther.
PatientCarePlansdevelopedinconjunctionwiththepatientandfamily/carerseekobservations,insights,informationandadviceonstrategiesthatmayincreaseand/orreducetheriskofaggressiveorviolentpatientbehaviourandproactiveearlyinterventionstrategiesthatmayreducetheriskthattheviolentoraggressivebehaviorwillescalatefurther.ThisinformationisthenusedinthedevelopmentoftheCarePlan.
Thefacilityhasnobehavioralcontractpolicyandprocedure.
Thefacilityhasabehavioralcontractpolicybutitisinconsistentlyapplied.
Thefacilityhasabehaviouralcontractpolicyandprocedurewithsupportingtoolsthatareconsistentlyapplied,andsupportisprovidedbymanagementforthis.
*ANMFNote:ReferraltoPatientCarePlanincludesallassociateddocumentse.g.BehaviouralManagementPlan.

© This work is copyright. Apart from any use permitted under the Copyright Act 1968, no part may be reproduced by any process, nor may any other exclusive right be exercised, without the permission of The Secretary, Australian Nursing & Midwifery Federation (Victorian Branch), Melbourne, 2017. PAGE 10
4 REPORT, INVESTIGATE AND ACT
CRITERIA HIGH RISK REDUCED RISK SOLUTION LOW RISK SOLUTION
4.1 Health services must build trust byinvestigatingincidentsinaconsultativeandcollaborativemanner.
Healthandsafetyincidentinvestigationsdonotcommenceorarenotcompletedinatimelymanner.
Healthandsafetyincidentinvestigationsarecommencedandcompletedinatimelymanner.
Healthandsafetyrootcauseincidentinvestigationsarecommencedandcompletedinacollaborative,timelymanner(includingwithANMFinvolvementasrequested),andthisisdocumentedintheincidentinvestigationprocedure.
Staff/HSRsarenotconsultedduringOVAincidentinvestigations.
Limitedconsultationwithstaff/HSRsoccursduring OVAincidentinvestigations.
Staff/HSRsareconsultedduringOVAincidentinvestigations.
FollowinganOVAincident,thecommencementofan OVAincidentinvestigationisnotcommunicatedtostaff.
FollowinganOVAincident,thecommencementofan OVAincidentinvestigationiscommunicatedtoinjured stafformanagementonly.
FollowinganOVAincident,thecommencementofan OVAincidentinvestigationiscommunicatedtoallstafflocatedwithintheworkareae.g.onaward,allshifts wouldbeadvised.
FollowinganOVAincidentInvestigation,systemlearningsarenotdisseminatedbacktostaff.
FollowinganOVAincidentinvestigation,systemlearningsaredisseminatedtoaffectedstaffonly.
FollowinganOVAincidentinvestigation,systemlearningsaredisseminatedtoallstafflocatedwithintheworkareaandorganisationallywhereappropriate.
OVAincidentinvestigationsarenotundertaken. OVAincidentinvestigationstakeintoaccountonlyclinicalorOHScontributingfactors,and/orfocusonidentifyingindividualcontributions,ratherthansystemfactors.
OVAincidentinvestigationstakeintoaccountallrelevantcontributingfactors,witha‘noblame’focus.
4.2 Health services must build trust bytakingclearandrelevantactionover incidents.
PreventativeactionsarenotidentifiednorimplementedafteranyOVAincidentsornearmisses.
PreventativeactionsareidentifiedandimplementedafteronlymultipleorhighriskOVAincidentsbutarenotidentifiedforlesscriticalOVAincidents.
PreventativeactionsareidentifiedandimplementedafterallOVAincidentsandnearmisses,andtrendsanalysedtoidentifyanypatterns.
Nomonitoringandreviewsystemisinplacetocollateandreviewtrends,incidentreportsandinvestigationstoestablishifclearandrelevantactionsaretakenandprocessesfollowed.
Aformalmonitoringandreviewsystemisinplacetocollateandreviewtrends,incidentreportsandinvestigationstoestablishifclearandrelevantactionsaretakenandprocessesfollowed,butisimplementedonanadhocbasis.
Formalcollating,monitoringandreviewofincidentinvestigationsandreportsareundertakentoestablishtrendsasperthemonitoringandreviewprocess.Thisissubjecttoformalreportingmeasuresinthehealthservice.
OVAincidentsarenotinvestigated. OVAincidentsareinvestigatedasasilo(i.e.thecurrentincidentonly).
OVAincidentinvestigationsaresystematicandincludeareviewofthepatientOVAhistoryacrossadmissions/timeandreviewofanypreviousimplementedpreventativemeasures,aswellasthecurrentincident.Investigationswillalsoconsiderthehistoryofincidentsintheunit/wardtoidentifysystemicfactorsand/orenvironmentalcontributingfactors.
- InvestigationofthecurrentOVAincidentdoesnotreviewtheleadupacrosstimetotheOVAincident(e.g.pre-admissionprocedure,admissionprocedure,preincidentstrategies,proactiveearlyinterventionstrategiesetc.)
InvestigationofthecurrentOVAincidentreviewstheleadupacrosstimetotheOVAincident(e.g.pre-admissionprocedure,admissionprocedure,preincidentstrategies,proactiveearlyinterventionstrategiesetc.)

© This work is copyright. Apart from any use permitted under the Copyright Act 1968, no part may be reproduced by any process, nor may any other exclusive right be exercised, without the permission of The Secretary, Australian Nursing & Midwifery Federation (Victorian Branch), Melbourne, 2017. PAGE 11
CRITERIA HIGH RISK REDUCED RISK SOLUTION LOW RISK SOLUTION
4.3 Health services must build trust by communicatingactionstakenasaresult of incident reports.
Actionstakenasaresultofincidentreportsarenotcommunicatedtothepersonsreporting.
Actionstakenasaresultofincidentreportsarecommunicatedtothepersonsreportingviaawritten entryintotheincidentreportingsystemonly.
Actionstakenasaresultofanincidentreportareverballycommunicatedtothepersonsreporting,aswellasviawrittenentryintotheincidentreportingsystem.
- - Actionstakenasaresultofanincidentreportarecommunicatedtoallstafflocatedwithintheworkarea.
4.4 Health services must meet their governance and funding requirements by ensuring boards are provided with details of violent incidents,notjuststatistics,sotheyunderstandtheeffectsofviolence on healthcare workers.
Thefacility’sboardandCEOdonotreceiveOVA reportdata.
Thefacility’sboardandCEOreceiveOVAstatisticalinformationonly.
Thefacility’sboardandCEOreceivedetailsaboutviolentandaggressiveincidentsandeffectsonhealthcareworkers,aswellasOVAstatisticaldata,andinformationaroundpreventativeactionstaken.
4.5 Health services must build trust by working with police to enable prosecutionofoffenders.
Healthservicesdonothaveacollaborativerelationshipwithlocalpolice.
Thehealthservicehasasporadic,adhocrelationshipwithlocalpolice.
ThehealthservicehasacollaborativerelationshipwithlocalpolicethatassistsstafftopursuetheirrighttoprosecutionofoffendersofOVAinasupportivemanner.
4 REPORT, INVESTIGATE AND ACT CONTINUED
5 PREVENT VIOLENCE THROUGH WORKPLACE DESIGN
CRITERIA HIGH RISK REDUCED RISK SOLUTION LOW RISK SOLUTION
5.1 Theprinciplesofcrimepreventionthrough environmental design should be mandatory in designing, refurbishing,renovatingandretrofittingworkplacesto prevent and minimise violence.
Theprinciplesofcrimepreventionthroughenvironmentaldesign(CPTED)arenotconsideredduringthedesignprocess(design,briefpreparation,feasibility,contractdocumentation,construction,pre-occupancyandpost-occupancyevaluation).
Thehealthservicehasadesignpolicythatprovidesmandatorycommitmenttoconsidertheprinciplesof crimepreventionthroughenvironmentaldesign(CPTED)duringallstagesofthedesignprocess.
Thehealthservicehasadesignpolicythatprovidesamandatorycommitmenttoconsiderandimplementtheprinciplesofcrimepreventionthroughenvironmentaldesign(CPTED)duringallstagesofthedesignprocess.
Thehealthservicehasnotundertakenanenvironmentalandworkplacedesignriskassessment.
ThehealthservicehasundertakenanenvironmentalandworkplacedesignriskassessmentacrosssomeareasandsitesreviewingandidentifyinginfrastructureandprocessimprovementsinaccordancewithCPTEDprinciples.
Thehealthservicehasundertakenenvironmentalandworkplacedesignriskassessmentsacrossallareasandsites,reviewingandidentifyinginfrastructureandprocessimprovementsinaccordancewithCPTEDprinciples,andrecommendationshavebeenimplemented,orwherenotyetimplemented,budgetedforandprioritisedsuchimprovementsaccordingtolevelofrisk.

© This work is copyright. Apart from any use permitted under the Copyright Act 1968, no part may be reproduced by any process, nor may any other exclusive right be exercised, without the permission of The Secretary, Australian Nursing & Midwifery Federation (Victorian Branch), Melbourne, 2017. PAGE 12
CRITERIA HIGH RISK REDUCED RISK SOLUTION LOW RISK SOLUTION
6.1 Educationabouthowtoprevent and respond to aggression and violence should begin at the undergraduate level.
Thehealthservicedoesnotmonitororreviewtheeducationprovidedtonewlyqualifiednursesand midwivesabouthowtopreventandrespondto aggressionandviolence.
Thehealthservicemonitorseducationprovidedonanadhocbasis,buthasnoorganisationalpoliciestoensureconsistentminimumeducationonhowtorespondandpreventOVAisprovided.
Thehealthservicemonitorsandreviewseducationprovidedtonewlyqualifiednursesandmidwives,andhasaprocessinplacetoensureconsistentminimumeducationisprovidedonhowtosystematicallypreventandrespondtoOVA.
Studentnursesdonotreceiveemployerspecifictraining onhowtopreventandrespondtoOVA.
Thehealthserviceprovidesemployer-specifictraining toallstudentnursesonhowtopreventandrespond toOVAfromanindividualperspectiveaspartoftheirclinicalplacements.
Thehealthserviceprovidesemployer-specifictrainingtoallstudentnursesontheirroleinhowtheorganisationwillsystematicallypreventandrespondtoOVAaspartoftheirclinicalplacements,atthestartoftheirplacement.
GraduatenursesdonotreceiveemployerspecifictrainingonhowtopreventandrespondtoOVA.
Thehealthserviceprovidesemployer-specifictraining toallgraduatenursesonhowtopreventandrespondtoOVAfromanindividualperspectiveaspartoftheirgraduateyear.
Thehealthserviceprovidesemployer-specifictrainingto allgraduatenursesontheirroleinhowtheorganisationwillsystematicallypreventandrespondtoOVAaspartoftheirgraduateyearasaninductionitemi.e.atthebeginningoftheyear.
6.2 Educationabouthowtoconductincidentinvestigations,preventandrespond to aggression and violence shouldcontinuethroughoutahealthworker’scareer.
Thehealthservice’snewstaffinduction/orientationprogramdoesnotincludeemployerspecifictraining abouthowtopreventandrespondtoOVA.
Allnewstaffreceiveemployer-specifictrainingonhowtopreventandrespondtoOVAfromanindividualperspectiveaspartofthehealthservice’sinduction/orientationprogram.
Allnewclinical(doctors,nurses,midwives,alliedhealthandothers)andnon-clinicalstaffreceiveemployer-specific,multi-disciplinarytrainingonhowtheorganisationwillsystematicallypreventandrespondtoOVAaspartofthehealthservice’sinduction/orientationprogram.Thisincludesvisiting(VMOs),consultantsandGPs.
Healthworkersdonotreceiveeducationabouthowtopreventandrespondtoaggressionandviolencethroughouttheircareerwhichisrelevanttotheirknowledge,roleandexperience.
Healthworkershavegenericrefreshertrainingabouthowtopreventandrespondtoaggressionandviolenceavailableonanelectivebasis.
Healthworkersreceivemandatory,regularrefreshertrainingandeducationabouthowtopreventandrespondtoaggressionandviolencethroughouttheircareerwhichisrelevanttotheirknowledge,roleandexperience,whichincludesafacetofacecomponent.Thiswouldincluderecognitionofearlywarningsignsforagitationandpre-coderesponses,developmentofskillstoreduceconflict,implementationofemployerprocessesthatconsistentlyidentifyandrecordrisksoforactualviolenceandsafetymanagementplans.
Staffreceivenoeducationandtrainingaboutthe functionsandpowersofsecuritystaffandVictoriaPolice.
StaffreceivelimitedgenericeducationaboutthefunctionsandpowersofsecuritystaffandVictoriaPoliceincludinghowandwhytolodgeapolicereport.
Allclinical(doctors,nurses,midwives,alliedhealthandothers)andnon-clinicalstaffreceivemandatory,multidisciplinarytrainingandeducationaboutthefunctionsandpowersofsecuritystaffandVictoriaPoliceincludingtheirroleinOVApreventionandmanagement,andhowandwhytolodgeapolicereport.Thisincludesvisiting(VMOs),consultantsandGPs.
6 PROVIDE EDUCATION AND TRAINING TO HEALTHCARE STAFF

© This work is copyright. Apart from any use permitted under the Copyright Act 1968, no part may be reproduced by any process, nor may any other exclusive right be exercised, without the permission of The Secretary, Australian Nursing & Midwifery Federation (Victorian Branch), Melbourne, 2017. PAGE 13
CRITERIA HIGH RISK REDUCED RISK SOLUTION LOW RISK SOLUTION
6.2 Continued. OHSincidentinvestigationandpost-incidentsupporttrainingformiddlemanagement(i.e.NUMs,ANUMs,MUMs,AMUMsetc.)isnotprovided.
OHSincidentinvestigationandpost-incidentsupporttrainingisavailableonanelectivebasis.
AllmiddlemanagementreceivemandatoryOHSincidentinvestigationandpost-incidentsupporttraining.
6.3 Employer-specifictrainingandeducationforbothhealthworkersandsecuritystaffshouldbeprovided.
Emergencyproceduretrainingdrills(includingCodeGreyandBlack)arenotundertaken.
Emergencyproceduretrainingdrillsareinfrequentlyundertaken.
Emergencyproceduretrainingdrills(includingCodeGreyandBlack)arescheduledregularly,aremandatoryandattendedbyallmembersoftheemergencyteams,suchasCodeGreyandBlack.Debriefsareconductedaftereachtoidentifylearningsandimprovements.
Employeesarenottrainedinproceduresforsearchingpatientandvisitors.
Employeesreceivelimitedtraininginproceduresforsearchingpatientandvisitors.
Employeesreceiveregular,mandatorytraininginproceduresforsearchingpatientandvisitorsthatarecompliantwithlegislativeprovisionsandrelatedpolicies.Thisincludesvisiting(VMOs),consultantsandGPs.
Notrainingisprovidedinrelationtobehaviouralcontracts,nordutyofcareobligations/withdrawalofservicefollowingaggressiveincidents.
Trainingisavailabletostaffinrelationtobehaviouralcontractsonanelectivebasis.
Employeesincludingcorporaterepresentativesreceiveeducationtoassistallstafftounderstandandenactbehavioralcontracts.Clearguidelinesareprovidedinrelationtowithdrawalofservice.
OVA-relatedtraininghasnotbeendevelopedinconsultationwithstaff.
OVA-relatedtraininghasbeendevelopedinconsultationwithsomeclinicalstaff.
AllOVA-relatedtraininghasbeendevelopedinconsultationwithstafffromallclinicalandnon-clinicalareas,andisregularlyreviewedforappropriateness.
6.4 Standardised training for both health workersandsecuritystaffshouldoccur.
ThehealthservicehasnotbenchmarkedOVAtrainingprogramsagainstsimilarhealthservicesnorDepartment ofHealthandHumanServicesstandardsforconsistencyandquality.
ThehealthservicehasstartedtobenchmarkOVAtrainingprogramsagainstsimilarhealthservicesandDepartmentofHealthandHumanServicesstandardsforconsistencyandquality,buthasnotimplementedchangestoaddressgaps.
ThehealthservicehasbenchmarkedallOVAtrainingprogramsagainstsimilarhealthservicesandDepartmentofHealthandHumanServicesstandardsforconsistencyandquality,andhasaddressedidentifiedgaps.
6.5 Regular,multidisciplinaryrefreshertraining for health workers and securitystaff.
ThefacilitydoesnotofferOVArefreshertrainingtoallclinical(doctors,nurses,midwives,alliedhealthandothers)andnon-clinicalstaff.
Allclinical(doctors,nurses,midwives,alliedhealth andothers)andnon-clinicalstaffcanaccessOVA refreshertraining.
Allclinical(doctors,nurses,midwives,alliedhealthandother)andnon-clinicalstaffreceiveregular,mandatory OVArefreshertraining,includingafacetoface componentatleastannually.Trainingiscollectiveandmulti-disciplinary,involvingworkersfromclinicaland non-clinicaldepartments.Thisincludesvisiting(VMOs),consultantsandGPs.
6 PROVIDE EDUCATION AND TRAINING TO HEALTHCARE STAFF CONTINUED

© This work is copyright. Apart from any use permitted under the Copyright Act 1968, no part may be reproduced by any process, nor may any other exclusive right be exercised, without the permission of The Secretary, Australian Nursing & Midwifery Federation (Victorian Branch), Melbourne, 2017. PAGE 14
CRITERIA HIGH RISK REDUCED RISK SOLUTION LOW RISK SOLUTION
7.1 Healthservices’responsestoaggression and violence such as Code Grey and Code Black must be consistent with state-wide guidance, and apply to all situationsofoccupational violence and aggression.
ThefacilitydoesnothaveaCodeGreyprocedure. ThefacilityhasaCodeGreyprocedurebutitisnotinlinewithDepartmentofHealthandHumanServicesguidelinesorisnotfullyimplemented.
ThefacilityhasaneffectiveCodeGreyprocedureinlinewithDepartmentofHealthandHumanServicesguidelinesthatisimplemented,regularlytrialedandusedbystaff.
NoclearprocessexistsforwhenmultipleconcurrentCodeGreys/Blacksarecalled.
- AclearprocessandresponseplanexistsforwhenmultipleconcurrentCodeGreys/Blacksareactivated,whichisimplementedandtrialled.
- Forhealthserviceswhodonothaveacapacitytoperform5personCodeGreyresponse,othermeansofaddressingthisissuemustbedevelopedandimplemented.
-
ThefacilitydoesnothaveaCodeBlackprocedure. ThefacilityhasaCodeBlackprocedureinlinewithAustralianStandards(AS4083).
ThefacilityhasaCodeBlackprocedureinlinewithAustralianStandards(AS4083),whichisimplemented,regularlytrialledandisusedbystaff.
- TheOVApreventionandresponsesystem,policyandproceduresdonotcoverallidentifiedsituationsatriskofoccupationalviolenceandaggression.
TheOVApreventionandresponsesystem,policyandprocedureshavebeenimplementedandreviewed,andcoverallidentifiedsituationsatriskofoccupationalviolenceandaggression,andstaffhavebeenprovided witheducationaboutanyupdates.
7.2 Workplaces should integrate their violencepreventionpolicieswithother policies such as clinical assessment,de-escalation,escalation,postincidentsupport,trainingandeducationand security policies.
OVApreventionandresponsesystem,policyandproceduresarenotintegrated.
OVApreventionandresponsesystem,policyandprocedureshavebeenreviewedandhavelimitedintegration.
OVApreventionandresponsesystem,policyandprocedures(inclusiveofeducationandtrainingforallstaff)areimplementedandregularlyreviewedforconsistency,andareintegratedintothehealthservice’sbroadersystems,suchas:• securitypolicies• equipmente.g.personalduressandfixedalarms,
CCTV,patientsearchesandstorageofbelongings(includingweapons),storageofdangerousgoods,mandatorytraining.
OVApreventionandresponsesystem,policyandprocedureshavenotbeenreviewedandintegratedwithsecuritypolicies.
OVApreventionandresponsesystem,policyandprocedureshavebeenreviewedwithsecuritypoliciesandinconsistencieshavebeenidentified.
OVApreventionandresponsesystem,policyandproceduresareimplementedandregularlyreviewedwithsecuritypoliciesforconsistency,andareintegrated.
OVApreventionandresponsesystem,policyandprocedureshavenotbeenreviewedandintegrated withclinicalandnon-clinicalOVA-relatedtrainingandeducationpolicies.
OVApreventionandresponsesystem,policyandprocedureshavebeenreviewedwithclinicalandnon-clinicalOVA-relatedtrainingandeducationpoliciesandinconsistencieshavebeenidentified.
OVApreventionandresponsesystem,policyandproceduresareregularlyreviewedwithclinicalandnon-clinicalOVA-relatedtrainingandeducationpoliciesforconsistencyandareintegrated.
7 INTEGRATE LEGISLATION, POLICIES AND PROCEDURES

© This work is copyright. Apart from any use permitted under the Copyright Act 1968, no part may be reproduced by any process, nor may any other exclusive right be exercised, without the permission of The Secretary, Australian Nursing & Midwifery Federation (Victorian Branch), Melbourne, 2017. PAGE 15
CRITERIA HIGH RISK REDUCED RISK SOLUTION LOW RISK SOLUTION
7.2 Continued. Clinicalandnon-clinicalOVA-relatedtraininghasnotbeenupdatedtoensurebestpracticeandcurrentinformation.
Clinicalandnon-clinicalOVA-relatedtraininghasbeenpartiallyupdatedtoensurebestpracticeandcurrentinformation.
Allclinicalandnon-clinicalOVA-relatedtrainingisregularlyreviewedtoensureitcoversallaspectsofOVA,hascurrencywithOVAindustryknowledge,changesinthehealthservice’ssystemduetotheOVAactionplan, keyOHSculturalapproachesandconsistencyofOVA/ OHSmessaging.
Localareaprocessesforpreventingandrespondingtoviolencehavenotbeenreviewedandarenotconsistentwithorganisationalpolicies.
Localareaprocessesforpreventingandresponding toviolencehavebeenreviewedinlinewith organisationalpoliciesbutarenotfullyconsistent withorganisationalpolicies.
Localareaprocessesforpreventingandrespondingtoviolencehavebeenreviewedatregularintervalsand areconsistentwithorganisationalpolicies.
NoconsultationwithemployeesisundertakenregardingdevelopmentandreviewofOVA-relatedpoliciesandprocedures.
LimitedconsultationisundertakenwithemployeesregardingdevelopmentandreviewofOVA-relatedpoliciesandprocedures.
StaffareregularlyconsultedinthedevelopmentandreviewofallOVA-relatedpoliciesandprocedures.
7.3 Systemic policy changes and decisionsaboutapatient’scareshouldtakeintoconsideration anypotentialforthechangetoincrease the incidence of aggression and violence.
SystemicpolicychangesdonotconsiderthepotentialtoincreasetheprevalenceofOVAincidents.
SystemicpolicychangesconsiderthepotentialtoincreasetheprevalenceofOVAincidentsbutthisprocessisnotintegratedwithinthehealthservice’ssystemtopreventandminimiseimpacts.
Systemicpolicychangesconsiderthepotentialto increasetheprevalenceofOVAincidentsandthis processisformallyintegratedwithinthehealthservice’ssystemtopreventandminimisetheimpacts.
Decisionsaboutapatient’scaredonotconsiderthepotentialtoincreasetheprevalenceofOVAincidents.
Decisionsaboutapatient’scareconsiderthepotentialtoincreasetheprevalenceofOVAincidentsbutthisprocessisnotformallyintegratedwithinthehealthservice’ssystem,noristhereaprocesstopreventandminimisetheimpacts.
Decisionsaboutapatient’scareconsiderthepotential toincreasetheprevalenceofOVAincidentsandthisprocessisformallyintegratedwithinthehealthservice’ssystem,withactionsimplementedtopreventand minimisetheimpacts.
7 INTEGRATE LEGISLATION, POLICIES AND PROCEDURES CONTINUED

© This work is copyright. Apart from any use permitted under the Copyright Act 1968, no part may be reproduced by any process, nor may any other exclusive right be exercised, without the permission of The Secretary, Australian Nursing & Midwifery Federation (Victorian Branch), Melbourne, 2017. PAGE 16
CRITERIA HIGH RISK REDUCED RISK SOLUTION LOW RISK SOLUTION
8.1 In the event of aggressive or violent incidents,staffmembersshouldreceiveextensiveandappropriatefollow up, support and care, including informationabout,andaccessto,theworkers’compensationsystemandthepolicereportingsystemprocess.
Nodocumentedpostincidentreportingprocedureexists. Apostincidentreportingprocedureexiststhatdoesnotincorporateallminimumstandards,orisimplementedonanadhocbasis.
Thehealthservicehasadocumented,implementedpostincidentreportingprocedurewhichcovers:• postincidentfollowuptimelinesandprocessesfor
contactinginvolvedworkers• protocolsthatensureevidenceisundisturbed(where
applicable)• supportandcareoptionsforallstaff/patientsinvolved• information,accesstoandprocessesforworkers’
compensationsystem• documentedreviewofthepatientcareplaninclusiveof
implementingmechanismstoprovideasafeworkplace• responsibilityforarrangingrepairsetcwithoutdelay• information,accesstoandprocessesforpolicereporting
systemwithoutlossofpay.
- Thehealthservice’spostincidentreportingprocedure,processesandtoolsareimplementedandreviewedforimprovement.
Thehealthservice’spostincidentreportingprocedure,processesandtoolsareimplementedandregularlyreviewedforimprovementandrecommendationsimplemented.
Thehealthservicedoesnotprovideinformation,supportoraccompanystaffduringthepolicereportingprocess.
Thehealthserviceprovideslimitedsupporttostafftopursuepolicereporting.
Thehealthserviceprovidesworkerswithinformationandsupportandoptionforaccompanyingstaffduringthepolicereportingandprosecutionprocessasrequested.
Thehealthservicedoesnothaveapoliceliaison. Thehealthservicehasanidentifiedpoliceliaison. Thehealthservicehasapoliceliaisonandappropriateemployerrepresentative(s)conductregularcontactmeetings.AregularreportonthesemeetingsisprovidedtotheOHScommittee,andinformation/updatesare alsodistributedtostaff.
Criticalincident,generalandoperationaldebriefsarenotconductedfollowingincidents.
Criticalincident,generaland/oroperationaldebriefsaresometimesconductedfollowingincidents.
Clearprocesses,requirementsandappropriatelytrainedstaffareavailabletoconductcriticalincident,generalandoperationaldebriefsfollowingincidents.
8.2 Incidentinvestigationand actionstakenasaresultmust also be reported.
Actionstakenasaresultofanincidentarenotcommunicatedtotheworkersinvolved.
Actionstakenasaresultofanincidentarerecordedandareavailabletothoseinvolved.
Actionstakenasaresultofanincidentarecommunicateddirectlytotheinvolvedworkers,andothersintheservicewhoarepotentiallyaffected,withoutemployeeprivacybeingbreached.
8 PROVIDE POST-INCIDENT SUPPORT

© This work is copyright. Apart from any use permitted under the Copyright Act 1968, no part may be reproduced by any process, nor may any other exclusive right be exercised, without the permission of The Secretary, Australian Nursing & Midwifery Federation (Victorian Branch), Melbourne, 2017. PAGE 17
9 APPLY ANTI-VIOLENCE APPROACH ACROSS ALL HEALTH DISCIPLINES
CRITERIA HIGH RISK REDUCED RISK SOLUTION LOW RISK SOLUTION
9.1 All healthcare workers and other workers who come into contact withpatients(andtheirfamiliesandvisitors) have consistent knowledge aroundthepreventionandresponsestoviolence,andthehealthservice’sproceduresandexpectations.
Seealso6–Provideeducationandtrainingtohealthcarestaff
NoOVAtrainingisavailableorthereareonlylimitedplacesforstafftoattend.
Somecategoriesofclinicalstaffreceiveandattend OVAtraining.
Allclinical(doctors,nurses,midwives,alliedhealthandothers)andnon-clinicalstaffreceiveandattendmultidisciplinary,mandatoryOVAtrainingatorientationandthenatregularintervals.
Thereisnomessagingforpatients,familyandvisitors inrelationtoacceptablebehaviouralstandardsinthehealthservice.
Thereissomemessagingaroundbehaviouralexpectationswhichisnotproactivelyprovidedtoallpatients,family andvisitorspre-admission/onarrival/admissiontothehealthservice.
Clearmessagingisprovidedtoallpatients,familyandvisitorspre-admission/onarrival/admissiontothehealthservicesettingoutappropriatebehaviour,andthepossibleconsequencesoffailingtocomplywiththeseexpectations.
TheOVAworkingpartydoesnothaverepresentationofallworkgroups.
Thereislimitedrepresentationofclinicalandnon-clinicalworkersontheOVAworkingparty,withlittleopportunityforconsiderationoftheirviewsandexperiences.
Allclinicalandnon-clinicalworkersandANMF(asrequested)arerepresentedontheOVAworkingparty andtheirviewsandexperiencesconsideredinthedevelopmentandimplementationoftheOVAactionplan.
9.2 Allworkersinhealthcaresettingsshouldhavetheexpectationthatthey will not encounter violence or aggression at their workplace.
See10-Empowerstafftoexpectasafe workplace
Workersdonotreceivemessagingfrommanagement thattheyshouldnotacceptviolenceoraggressionin theirworkplace.
Allworkersreceiveinformalmessagingfrommanagementthattheyshouldnotacceptviolenceoraggressionin theirworkplace.
Allworkersinthehealthservicereceiveconsistentandsupportivemodellingfrommanagementthattheyshouldnotacceptviolenceoraggressionintheirworkplace e.g.formalcomponentoftraining,policies,messaging,policies,followupetcandputintoaction.
Noreviewofclinicaltraining,practices,policiesandproceduresaroundbehaviorsofconcernhasoccurred toensurealignmentwithOVAmessaging,policies andprocedures.
Limitedreviewofclinicaltraining,practices,policiesandproceduresaroundbehaviorsofconcernhasoccurredtoalignwithOVAmessaging,policiesandprocedures.
Allclinicaltraining,practices,policiesandproceduresaroundbehaviorsofconcernareregularlyreviewedto alignwithOVAmessaging,policiesandprocedures.
9.3 Allworkers’reportsaboutaggressiveorviolentbehaviorfromapatientor their visitors should be taken intoconsiderationwhenmakingdecisionsaboutthepatient’scareand management.
OVAincidentreports,includingCodeGreyandCodeBlackreports,andinclinicalnotes,aboutthepatientorvisitorarenotreflectedinthepatientcareplanortakenintoconsiderationwhenmakingdecisionsaboutthepatient’scareandmanagement.
OVAincidentreports,includingCodeGreyandCodeBlackreports,andinclinicalnotes,aboutthepatientorvisitoraretakenintoconsiderationwhenmakingdecisionsaboutthepatient’scareandmanagementbutthereisnoclearstandardiseddocumentedprocess.
AclearprocessexistsandisimplementedtoensureOVAincidentreports,includingCodeGreyandCodeBlackincidents,inclinicalnotes,andanyotherknownformsofviolenceoraggressioninrelationtothepatientorvisitor(s)arerecordedinthemedicalrecords,andthatthepatientcareplanreflectstheidentifiedhazard.
Noweightisgiventoreportsbynursesandmidwivesofaggressiveorviolentpatientbehaviourbythosemakingdecisionsaboutapatient’scareplan.
Littleweightisgiventoreportsbynursesandmidwivesofaggressiveorviolentpatientbehaviourbythosemakingdecisionsaboutapatient’scareplan.
ConsiderationisgiventothepotentialOVArisksasidentifiedbyalldisciplinesatalltimes,andactionsimplementedtoreflectconcernsandprevent/ minimiseimpacts.
9.4 In making decisions, it is important to communicate, consult and collaboratewithallstaffinvolvedinthepatient’smanagementandcare.
Collaborativemulti-disciplinarycaseconferencesforpatientswithchallengingbehaviordonotoccur.
Noclearmodelorprocessexistsforregularcollaborativemulti-disciplinarycaseconferencesforpatientswithchallengingbehavior.
Aclearmodelandprocessexistsandisimplementedforregularcollaborativemulti-disciplinarycaseconferencesforpatientswithchallengingbehavior,withOVAasaspecificconsideration.Whereappropriate,thisinvolvesfamilymembers,carersand/ornominatedpersons.

© This work is copyright. Apart from any use permitted under the Copyright Act 1968, no part may be reproduced by any process, nor may any other exclusive right be exercised, without the permission of The Secretary, Australian Nursing & Midwifery Federation (Victorian Branch), Melbourne, 2017. PAGE 18
10 EMPOWER STAFF TO EXPECT A SAFE WORKPLACE
CRITERIA HIGH RISK REDUCED RISK SOLUTION LOW RISK SOLUTION
10.1 Management must demonstrate commitment to changing the culture ofhealthcareworkplacestoreflectno acceptance of aggression or violence in health services.
In workplaces where there is no acceptance of aggression orviolence,staffwillbecomeempowered to report incidents, andimplementpreventative actions,andbelieveintheir right to a safe workplace.
ThereisnoOVAworkingparty,norOVAoversightcommitteewithoversightofimplementationofactions inrelationtoOVA.
ThereisanOVAworkingpartydoingworkinrelationtopreventionofviolenceandaggression,butthereisnooverarchingstrategy,oritdoesnothavereportingresponsibilitytoahigherlevelOVAoversightcommittee.
Ahigh-levelOVAcommitteeisdesignatedtohaveoversightofallOVAwork,andafurtherOVAworkingpartyhasdevelopedanOVAstrategyandactionplantoimplementanorganisational,riskmanagementapproachtopreventionofviolenceandaggression.ANMFisrepresentedontheOVAoversightcommitteeandOVAworkingpartyuponrequest.
NoexecutivemanagementrepresentativesareactivemembersoftheOVAworkingparty.
SomeexecutivemanagementrepresentativesareactivemembersoftheOVAworkingparty
Thehealthservice’sCEOandexecutivemanagement areactivemembersoftheOVAworkingparty.
ExecutivemanagementdonotreceiveanysafetycultureandOVA-specifictraining.
ExecutivemanagementincludingtheCEOreceivelimitedsafetycultureandOVA-specifictraining.
Allmanagementroles(includingtheCEO,boardandexecutive)receivesafetycultureandOVA-specifictraining.
Thehealthservicedoesnothaveapreventionof OVApolicy.
ThehealthservicehasapreventionofOVApolicy. Thehealthservicehasacollaboratively-developedpreventionofOVApolicythatisfullyendorsed(signed) bytheCEOandchairoftheboard.
Thehealthservice’sincidentreportingandinvestigationpoliciesdonotpromoteanoblameculture.
Thehealthservice’spoliciesrefertoanoblameculture,butthisisnotactivelysupportedintoolsetc,orisnot fullyandactivelyimplemented.
Thehealthservice’sincidentreportingandinvestigationpoliciespromoteanoblameculturewithatleast90%ofstaffreportingthattheno-blamecultureisactivelyimplemented.Further,managersareprovidedwitheducationandtraining,andhaveaccesstoincidentreportingandinvestigationtools.
OVAtrainingdoesnotexistordoesnotpromoteanon-acceptanceofaggressionorviolenceintheworkplace.
OVAtrainingdoesnotactivelypromoteanon-acceptanceofaggressionorviolenceintheworkplace,orisnotbasedonappropriatepolicy.
OVAtrainingactivelypromotesnon-acceptanceofaggressionorviolenceintheworkplaceandincludesworkers’rightsforsafeworkplaceandprovisionsifthis isbreached.
Useoflanguagebyseniorandmiddlemanagementaroundnon-acceptanceofOVAdoesnotdemonstratepositivesafetyculturee.g.languageisusedwhichsuggeststhatviolenceisaninevitablepartofhealthcareworkplaces.
Useoflanguagebyseniorandmiddlemanagementaroundnon-acceptanceofOVAsporadicallyand/orinconsistentlydemonstratespositivesafetyculturee.g.languageissometimes/inconsistentlyusedwhichsuggeststhatviolenceisnotokay,butsometimesisusedsuggestingviolenceisaninevitablepartofhealthcareworkplaces.
Positivesafetycultureisdemonstratedthroughconsistentuseoflanguagewhichpromotesnon-acceptanceofOVA byallstaff,includingseniorandmiddlemanagement e.g.languageisalwaysusedwhichpromotesthemessagethatviolenceisneverokay,andstepswillbetakentoinvestigateandreducetheriskintothefuture.
TherearenoOVAstrategicprogramsnoractionplans inplace.
ThereareeitherOVAstrategicprogramsoractionplansinplace,whichhavenotbeendevelopedwithstakeholders,orarenotmonitoredbyanoversightcommittee.Theboarddoesnotreceiveprogressreports.
OVAstrategicprogramsandactionplanshavebeendevelopedinconsultationwithstakeholdersincludingANMF,andaremonitoredbyanOVAoversightcommittee,withregularreportsonprogresspresentedtotheboard.
NoextraresourcingisprovidedtoachievingOVAactionplanandOVAstrategicoutcomes.
LimitedresourcingisallocatedtoachievingOVAactionplanandOVAstrategicoutcomes.
ExtraresourcingisallocatedtoachievingOVAaction planandOVAstrategicoutcomes.

© This work is copyright. Apart from any use permitted under the Copyright Act 1968, no part may be reproduced by any process, nor may any other exclusive right be exercised, without the permission of The Secretary, Australian Nursing & Midwifery Federation (Victorian Branch), Melbourne, 2017. PAGE 19
CRITERIA HIGH RISK REDUCED RISK SOLUTION LOW RISK SOLUTION
10.1 Continued. ThehealthservicedoesnotinvitenorrecogniseemployeeOVAachievements(e.g.OVAsafetysuggestionsbyemployees,actionstakenbyemployeestoidentify OVAhazardsandimprovesafety).
EmployeeOVAachievementsareinvitedandrecognisedinalimitedcapacityatanorganisationalwideandlocallevel(withintheunits).
EmployeeOVAachievementsandsuggestionsareactivelyinvitedandrecognisedbothatanorganisationalwideandlocallevel(withinunits).Improvementsaremadeasaresultwithappropriateacknowledgement.
Noclarityaroundemployee’scontrolordecisionmakingabilityisprovidedtopreventorminimiseOVA.
Thefacilityhasanescalationpolicybutitdoesnotprovideclearboundaries.
Thefacilityhasaclearescalationpolicythatcreates clarityaboutemployee,manager(NUM/ANUM)andexecutivemanagementescalationpointsanddecisionmakingability,andisimplementedwithdecisionsfor extraresourcessupported.
Organisationalvaluesplaceprimeandsolefocusonpatientsafetyandexperience,withoutregardforstaffsafety.
Organisationalvaluesrecognizestaffsafety,butitisconsideredsecondarytopatientsafety.
Safetycultureforbothpatientsandstaffareincludedandrepresentedasofequalimportanceinorganisationalvaluesandrepresentedinallbranding.
10.2 Allactionplansaroundpreventionand management of violent and aggressive incidents should be developedinconsultationwithstaff.
ThereisnoOVAworkingparty,norOVAoversightcommitteewithoversightofimplementationofactions inrelationtoOVA.
ThereisanOVAworkingpartydoingworkinrelationtopreventionofviolenceandaggression,butthereisnooverarchingstrategy,oritdoesnothavereportingresponsibilitytoahigher-levelOVAoversightcommittee.
AhighlevelOVAcommitteeisdesignatedtohaveoversightofallOVAwork,andafurtherOVAworkingpartyhasdevelopedanOVAstrategyandactionplantoimplementanorganisational,riskmanagementapproachtopreventionofviolenceandaggression.ANMFisrepresentedontheOVAoversightcommitteeandOVAworkingpartyuponrequest.
Norepresentativesfromclinical(doctors,nursing,midwives,alliedhealthandothers)andnon-clinicalareasontheOVAworkingparty.
ThefacilitydemonstratesalimitedcommitmenttoanintegratedapproachtoOVApreventionbyrepresentativesofsomeclinical(doctors,nursing,midwives,alliedhealthandothers)andnon-clinicalareasbeingactivemembers oftheOVAworkingparty.
ThefacilityhasanintegratedapproachtoOVApreventionandmanagementbyactivelyincludingrepresentativesofallclinical(doctors,nursing,midwives,alliedhealthandothers)andnon-clinicalareas/departmentsandANMF (asrequested)asbeingactivemembersoftheOVAworkingparty,withmeetingsscheduledattimesthatenablestafftoattend.
NoHSRsaremembersoftheOVAworkingparty. HSRsareinvited(butnotactivelyencouraged)tobemembersoftheOVAworkingpartyand/ormeetingsarenotscheduledtofacilitateattendance.
AppropriatenumberofHSRsareactivemembersoftheOVAworkingparty,andareencouragedandfacilitatedtoattendinpaidtime.
HSRsandemployeesarenotconsultedintheformulationofthehealthservice’sOVAstrategyandactionplan.
LimitedconsultationwithHSRsandemployeeshasoccurredinregardtothedevelopmentandproject workofthehealthservice’sOVAstrategyandaction planwithlessthan85%awarenessoftheOVAaction planamongststaff.
HSRs,employeesandANMFhavebeenandareregularly consultedinthedevelopmentandprojectworkofthehealthservice’sOVAstrategyandactionplan,andthereisgreaterthan85%awarenessoftheOVAactionplanamongststaff.
10 EMPOWER STAFF TO EXPECT A SAFE WORKPLACE CONTINUED

© This work is copyright. Apart from any use permitted under the Copyright Act 1968, no part may be reproduced by any process, nor may any other exclusive right be exercised, without the permission of The Secretary, Australian Nursing & Midwifery Federation (Victorian Branch), Melbourne, 2017. PAGE 20


anmfvic.asn.au