Research criteria for the diagnosis of prodromal dementia ... · The prodromal phase of dementia...
14
VIEWS & REVIEWS OPEN ACCESS Research criteria for the diagnosis of prodromal dementia with Lewy bodies Ian G. McKeith, F Med Sci, MD, Tanis J. Ferman, PhD, Alan J. Thomas, PhD, Fr´ ed´ eric Blanc, MD, Bradley F. Boeve, MD, Hiroshige Fujishiro, MD, Kejal Kantarci, MD, MS, Cristina Muscio, PhD, John T. O’Brien, F Med Sci, DM, Ronald B. Postuma, MD, MSc, Dag Aarsland, PhD, Clive Ballard, MD, Laura Bonanni, MD, PhD, Paul Donaghy, PhD, Murat Emre, MD, James E. Galvin, MD, MPH, Douglas Galasko, MD, Jennifer G. Goldman, MD, MS, Stephen N. Gomperts, MD, PhD, Lawrence S. Honig, MD, PhD, Manabu Ikeda, MD, PhD, James B. Leverenz, MD, Simon J.G. Lewis, MD, Karen S. Marder, MD, MPH, Mario Masellis, MD, PhD, David P. Salmon, PhD, John Paul Taylor, MB, BS, PhD, Debby W. Tsuang, MD, Zuzana Walker, MD, and Pietro Tiraboschi, MD, for the prodromal DLB Diagnostic Study Group Neurology ® 2020;94:743-755. doi:10.1212/WNL.0000000000009323 Correspondence Dr. McKeith [email protected] Abstract The prodromal phase of dementia with Lewy bodies (DLB) includes (1) mild cognitive impairment (MCI), (2) delirium-onset, and (3) psychiatric-onset presentations. The purpose of our review is to determine whether there is sufficient information yet available to justify development of diagnostic criteria for each of these. Our goal is to achieve evidence-based recommendations for the recognition of DLB at a predementia, symptomatic stage. We pro- pose operationalized diagnostic criteria for probable and possible mild cognitive impairment with Lewy bodies, which are intended for use in research settings pending validation for use in clinical practice. They are compatible with current criteria for other prodromal neurodegen- erative disorders including Alzheimer and Parkinson disease. Although there is still insufficient evidence to propose formal criteria for delirium-onset and psychiatric-onset presentations of DLB, we feel that it is important to characterize them, raising the index of diagnostic suspicion and prioritizing them for further investigation. Introduction Dementia with Lewy bodies (DLB) accounts for 7·5% or more of all dementias in older people. 1 It is characterized by dementia together with varying combinations of the core clinical features of parkinsonism, REM sleep behavior disorder (RBD), fluctuating cognition/alertness, and visual hallucinations. 2 There is a variable progression of α-synuclein aggregation many years before the full DLB syndrome develops, e1 which likely determines the pattern of early clinical changes. Prodromal DLB refers to a predementia stage with signs or symptoms indicating that DLB will subsequently develop and encompasses not only cognitive deficits but also a variable mixture of noncognitive clinical features including motor symptoms and signs, sleep disorders, autonomic dysfunction, and neuropsychiatric disturbance. 3 Because these first clinical mani- festations can occur 15 years or more before dementia onset, precise early diagnosis of DLB presents particular challenges, individuals being extremely difficult to distinguish from those with the first manifestations of Parkinson disease (PD) or multiple system atrophy (MSA), which are also α-synuclein–related syndromes, 4 or of other dementing disorders, particularly Alzheimer disease (AD). From the Newcastle University (I.G.M., A.J.T., P.D., J.P.T.); Mayo Clinic (T.J.F.), Jacksonville; University of Strasbourg (F.B.); Mayo Clinic (B.F.B., K.K.), Rochester; Nagoya University (H.F.), Kawasaki Memorial Hospital; Istituto Neurologico “Carlo Besta” (C.M., P.T.), Milan; Cambridge University (F.M.S.); McGill University (R.B.P.); King’s College London and Stavanger University Hospital (D.A.); University of Exeter (C.B.); University of Chieti-Pescara (L.B.); Istanbul Faculty of Medicine (M.E.); University of Miami Miller School of Medicine (J.E.G.); University of California (D.G., D.P.S.), San Diego; Feinberg School of Medicine (J.G.G.); Massachusetts General Hospital (S.N.G.); Columbia University Irving Medical Center (L.S.H., K.S.M.); Osaka University (M.I.); Lou Ruvo Center of Brain Health (J.B.L.), Cleveland Clinic; University of Sydney (S.J.G.L.); Sunnybrook Health Sciences Centre (M.M.), University of Toronto; VA Puget Sound & University of Washington (D.W.T.); University College London (Z.W.). Go to Neurology.org/N for full disclosures. Funding information and disclosures deemed relevant by the authors, if any, are provided at the end of the article. The Article Processing Charge was funded by the NIHR Newcastle Biomedical Research Centre. This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial-NoDerivatives License 4.0 (CC BY-NC-ND), which permits downloading and sharing the work provided it is properly cited. The work cannot be changed in any way or used commercially without permission from the journal. Copyright © 2020 The Author(s). Published by Wolters Kluwer Health, Inc. on behalf of the American Academy of Neurology. 743
Transcript of Research criteria for the diagnosis of prodromal dementia ... · The prodromal phase of dementia...

VIEWS amp REVIEWS OPEN ACCESS
Research criteria for the diagnosis of prodromaldementia with Lewy bodiesIan G McKeith F Med Sci MD Tanis J Ferman PhD Alan J Thomas PhD Frederic Blanc MD
Bradley F Boeve MD Hiroshige Fujishiro MD Kejal Kantarci MD MS Cristina Muscio PhD
John T OrsquoBrien F Med Sci DM Ronald B Postuma MD MSc Dag Aarsland PhD Clive Ballard MD
Laura BonanniMD PhD Paul Donaghy PhDMurat EmreMD James EGalvinMDMPH DouglasGalaskoMD
Jennifer G Goldman MD MS Stephen N Gomperts MD PhD Lawrence S Honig MD PhD
Manabu Ikeda MD PhD James B Leverenz MD Simon JG Lewis MD Karen S Marder MD MPH
Mario Masellis MD PhD David P Salmon PhD John Paul Taylor MB BS PhD Debby W Tsuang MD
Zuzana Walker MD and Pietro Tiraboschi MD for the prodromal DLB Diagnostic Study Group
Neurologyreg 202094743-755 doi101212WNL0000000000009323
Correspondence
Dr McKeith
igmckeithnclacuk
AbstractThe prodromal phase of dementia with Lewy bodies (DLB) includes (1) mild cognitiveimpairment (MCI) (2) delirium-onset and (3) psychiatric-onset presentations The purposeof our review is to determine whether there is sufficient information yet available to justifydevelopment of diagnostic criteria for each of these Our goal is to achieve evidence-basedrecommendations for the recognition of DLB at a predementia symptomatic stage We pro-pose operationalized diagnostic criteria for probable and possible mild cognitive impairmentwith Lewy bodies which are intended for use in research settings pending validation for use inclinical practice They are compatible with current criteria for other prodromal neurodegen-erative disorders including Alzheimer and Parkinson disease Although there is still insufficientevidence to propose formal criteria for delirium-onset and psychiatric-onset presentations ofDLB we feel that it is important to characterize them raising the index of diagnostic suspicionand prioritizing them for further investigation
IntroductionDementia with Lewy bodies (DLB) accounts for 7middot5 or more of all dementias in olderpeople1 It is characterized by dementia together with varying combinations of the core clinicalfeatures of parkinsonism REM sleep behavior disorder (RBD) fluctuating cognitionalertnessand visual hallucinations2 There is a variable progression of α-synuclein aggregationmany yearsbefore the full DLB syndrome developse1 which likely determines the pattern of early clinicalchanges Prodromal DLB refers to a predementia stage with signs or symptoms indicating thatDLB will subsequently develop and encompasses not only cognitive deficits but also a variablemixture of noncognitive clinical features including motor symptoms and signs sleep disordersautonomic dysfunction and neuropsychiatric disturbance3 Because these first clinical mani-festations can occur 15 years or more before dementia onset precise early diagnosis of DLBpresents particular challenges individuals being extremely difficult to distinguish from thosewith the first manifestations of Parkinson disease (PD) or multiple system atrophy (MSA)which are also α-synucleinndashrelated syndromes4 or of other dementing disorders particularlyAlzheimer disease (AD)
From the Newcastle University (IGM AJT PD JPT) Mayo Clinic (TJF) Jacksonville University of Strasbourg (FB) Mayo Clinic (BFB KK) Rochester Nagoya University (HF)Kawasaki Memorial Hospital Istituto Neurologico ldquoCarlo Bestardquo (CM PT) Milan Cambridge University (FMS) McGill University (RBP) Kingrsquos College London and StavangerUniversity Hospital (DA) University of Exeter (CB) University of Chieti-Pescara (LB) Istanbul Faculty of Medicine (ME) University of Miami Miller School of Medicine (JEG)University of California (DG DPS) San Diego Feinberg School of Medicine (JGG) Massachusetts General Hospital (SNG) Columbia University Irving Medical Center (LSHKSM) Osaka University (MI) Lou Ruvo Center of Brain Health (JBL) Cleveland Clinic University of Sydney (SJGL) Sunnybrook Health Sciences Centre (MM) University ofToronto VA Puget Sound amp University of Washington (DWT) University College London (ZW)
Go to NeurologyorgN for full disclosures Funding information and disclosures deemed relevant by the authors if any are provided at the end of the article
The Article Processing Charge was funded by the NIHR Newcastle Biomedical Research Centre
This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial-NoDerivatives License 40 (CC BY-NC-ND) which permits downloadingand sharing the work provided it is properly cited The work cannot be changed in any way or used commercially without permission from the journal
Copyright copy 2020 The Author(s) Published by Wolters Kluwer Health Inc on behalf of the American Academy of Neurology 743
Reliable identification of prodromal DLB would enable earlyintervention while pathologic burden is circumscribed andbefore clinical symptoms become debilitating It would assistclinicians to streamline care anticipate treatment optionsknown to be effective in DLBe2 and to avoid or minimizeiatrogenic adverse events with the goal of fewer office andemergency department visitse3 Importantly early diagnosiswould help patients and families to plan and to implementearly nonpharmacologic interventions (eg exercise andbehavioral strategies) It would also facilitate selection fortrials of targeted therapies as these become available
MethodsWe performed electronic searches of MEDLINE PubMedand EMBASE databases using the combination of a number ofmedical subject headings Emtree subject headings and free-text terms (ldquodementia with Lewy bodiesrdquo ldquoLewy body de-mentiardquo ldquoLewy body diseaserdquo ldquoprodromalrdquo ldquodeliriumrdquoldquopsychosisrdquo ldquomild cognitive impairmentrdquo ldquorapid eye move-ment sleep behavior disorderrdquo for clinical categories andldquoneuropsychological testrdquo ldquodopamine transporter imagingrdquoldquopositron emission tomographyrdquo ldquometa-iodobenzylguanidinemyocardial scintigraphyrdquo ldquonuclear magnetic resonance im-agingrdquo ldquoelectroencephalographyrdquo ldquocerebrospinal fluidrdquoldquorapid eye movement sleep without atoniardquo for biomarkers)All relevant articles were retrieved placing restrictions onfields (free-text terms searched exclusively in the title orabstract of the articles) and date (last 5 years) Except forbook chapters all publication types (original articlesreviews editorials and letters) were considered Because thefocus of this review was on prodromal DLB studies on thebroader less specific category of Lewy body disease (whichcomprises both DLB and PD) were also considered Wethen used Refworks to remove duplicates and share theresulting 3570 records among the lead authors Of all full-text articles assessed for eligibility after the abstract screen-ing phase those eventually included either as listed or ase-references were selected based on their relevance (dataavailable from Dryad e-references doi105061dryad1c59zw3rv) Seminal papers on the topic were included re-gardless of publication date The preliminary findings andrecommendations were presented for discussion and feed-back at a session of the International Lewy Body DementiaConference in Las Vegas NV USA in June 2019 followingwhich further revision and review took place
How does prodromal DLB usually presentOne or more of the core clinical features characteristic of fullydeveloped DLB may develop before dementia and are usuallyaccompanied by mild cognitive complaints5 Spontaneousparkinsonism often develops within the predementia stagebut is not present in all patients36 RBD is a parasomnia thattypically occurs years and even decades before the onset ofdementia or parkinsonism and may presage any of theα-synucleinopathies47e4 In patients with mild cognitive def-icits who later develop dementia both parkinsonism and RBDstrongly predict a later transition to DLB rather than to AD orother dementia types68 Delirium can occur during the pre-dementia stage of DLB9 as can fluctuations of cognition andarousal3 that may give rise to a diagnosis of delirium Visualhallucinations (VHs) either spontaneous or provoked by ill-ness or medication are more likely to occur compared withnormal controls or prodromal AD1011 There are also casereports of delusions hallucinations depression and anxiety aspresenting features of DLB12 Based on such observations 3prototypic prodromal DLB syndromes have been proposed13
as (1) mild cognitive impairment (MCI) (2) delirium-onsetor (3) psychiatric-onset
MCI with Lewy bodiesThe National Institute on Aging and Alzheimerrsquos Associationcriteria for MCI14 e5 provide a standardized approach to di-agnosis and form the basis for our proposed MCI with Lewybody (MCI-LB) criteria They require a cognitive complaint fromthe patient or from an informant or clinician who knows themand has observed a decline Also required are deficits in one ormore cognitive domains that are greater than would be expectedfrom normal aging do not represent lifelong patterns of lowercognitive function and are not associated with acute medical orneurologic insults Although people with MCI may be less effi-cient or less capable at performing tasks they have performedpreviously their cognitive deficits should not be sufficient tointerfere with their typical daily functioning In other words thereshould be an overall preservation of their prior level of in-dependence with minimal interference in day-to-day functionalabilities which by definition does not constitute a dementia
Objective cognitive impairment is optimally based on stan-dardized assessment with scores on neuropsychologicalmeasures that are typically 1 to 1middot5 SDs below the mean fortheir age and education matched peers on culturally appro-priate normative data (ie for the impaired domain(s) whenavailable) It is emphasized that these ranges are guidelines
GlossaryAD = Alzheimer disease DAT = dopamine transporter DLB = dementia with Lewy bodies FTD = frontotemporal dementiaMCI = mild cognitive impairment MCI-LB = MCI with Lewy bodies MIBG = meta-iodobenzylguanidine MSA = multiplesystem atrophy NCD = neurocognitive disorder PD = Parkinson disease PSG = polysomnography QEEEG = QuantitativeEEG RBD = REM sleep behavior disorder RSWA = REM sleep without atonia VH = visual hallucination VRH = ventilatoryresponse to hypercapnia
744 Neurology | Volume 94 Number 17 | April 28 2020 NeurologyorgN
and not cutoff scores14 Impairment on neuropsychologicaltests may also be demonstrated by significant decline dem-onstrated on serial testing or significant decline from esti-mated premorbid abilitiese5 Cognitive impairment mayadditionally be categorized as single or multiple domain andas amnestic or nonamnestic which may help to classify po-tential subgroups as they relate (1) to biomarkers and path-ologic correlates and (2) to differences in the rate of declineand progression to dementia each of which may be importantin the conduct of clinical trials A further refinement to de-scribe the cognitive profile of MCI-LB may be provided byusing the MDS level II criteria for PD-MCI15e6e7
The cognitive presentation of MCI-LBThe cognitive pattern ofMCI-LB is similar toDLB and typicallyincludes disproportionate attentionexecutive and visual pro-cessing deficits and relatively preserved memory and objectnaming16e8e9 Impairment on tasks of attention processingspeed and verbal fluency typically constitute the attentionexecutive deficits and tasks of visual discrimination assemblyand figure drawing typically constitute the visual perceptual andspatial deficits5617ndash19
Diagnostic criteria for DLB emphasize that prominent or per-sistent memory impairment may not necessarily occur in theearly stages2 but patients and carers frequently offer memorycomplaints as a presenting symptom20Of 49 patients withMCIwho progressed to DLB 27 had multidomain amnestic MCIbut only 6 had single-domain amnestic MCI3 similar to otherreports1921 When patients with MCI-LB have memory im-pairment attention andor visual processing deficits also tend tobe present3 and may precede the memory difficulties Patientswith RBD who later developed DLB had attentionexecutivedeficits up to 6 years before the diagnosis of dementia andmemory deficits up to 2 years before the diagnosis22 The basisfor verbal memory impairment in DLB or MCI-LB may berelated to slowed processing speed and deficits in workingmemory and retrieval that characterize the attention and exec-utive deficitse10 consistent with hippocampal preservation inMCI-LB compared with MCI-AD23e11 However impairedmemory in DLB may also be related to the extent of coexistingAD-related pathologye9 characterized by greater hippocampalatrophy on imaging e12 and greater CA1 hippocampal subfieldpathology on autopsye13 Similar to other subtypes of MCIa proportion of patients may revert to being cognitively normalalthough they remain at a greater risk of the eventual de-velopment of dementiae14 Some instability of an MCI-LB di-agnosis is to be expected given inherent fluctuating cognitionworsening with neuroleptics or anticholinergics or improve-ment with levodopa-carbidopa or cholinesterase inhibitors
In summary the performance pattern of MCI-LB is bestcharacterized as single- or multidomain nonamnestic MCI oras multidomain amnestic MCI whereas single-domainamnestic MCI is more likely to represent MCI-AD TheMCI-LB cognitive pattern is often seen in patients with 1 ormore core DLB features5 although these may develop
later318 Nonamnestic MCI seldom develops into AD but isassociated with a greater risk of transition to DLB1021 witha ten-fold risk compared with amnestic MCI3 Becausea substantial subset of patients with DLB have coexisting AD-related pathology that may influence their cognitive profileMCI-LB still should be considered an important part of thedifferential diagnosis in amnestic subjects
Operationalization of MCI-LBThe scheme suggested in table 1 for the identification ofMCI-LBallows a diagnosis of either possible or probable MCI-LB basedon the number of qualifying clinical features or biomarkers Theterms possible and probable refer to the likelihood of underlyingLB disease and not to the MCI syndrome Structured diagnosticinstruments may assist identification of the core clinical featuresof DLB that precede coincide with or follow the onset of cog-nitive difficulties24ndash26 Cognitive fluctuations may be of lesseramplitude or frequency than in more severe disease Passage andsense of presence hallucinatory phenomena may precede thedevelopment of recurrent well-formed and detailed VH Clinicalfeatures supportive of DLBmay occur secondary to other causesreducing their diagnostic specificity but they can be usefulindicators of underlying LBdisease particularly when they persistover time or occur in combination
Use of the possible MCI-LB category may raise diagnosticsuspicion prompting further clinical and biomarker in-vestigation Some possible MCI-LB combinations will likelyprove better predictors than others for example multidomainnonamnestic MCI plus clinically well-defined RBD is antici-pated to be more predictive of progression to DLB thansingle-domain amnestic MCI plus a history of cognitivefluctuation The utility of different combinations of clinicalfeatures and biomarkers remains to be established
MCI-LB and PD-MCIUncertainty may occur in deciding how patients exhibitingboth MCI and parkinsonism are best categorized PD-MCIwill usually be the most appropriate diagnosis when PD isdiagnosed before significant cognitive decline occurs Theadoption of a 1-year rule similar to that used to separate DLBand PD dementia may be helpful to distinguish someMCI-LBand PD-MCI cases if the onset and order of mild symptoms ofparkinsonism and cognitive decline can be clearly establishedIf not an initial diagnosis of prodromal LB disease may bepreferable recognizing that this will require revision as the fullclinical picture evolves Individuals with poor global cognitivetest performance identified in community samples have beenreported to be at a greater risk of developing PD over sub-sequent yearse15e16 but poor cognitive test scores are notequivalent to MCI and this increased risk was no longerstatistically significant when individuals with subtle motorsigns at baseline were excludede15 There are data to suggestthat patients with MCI-LB may have greater cognitive im-pairment than those with PD-MCI27 but this is not easilyoperationalized to differentiate individual subjects The cog-nitive deficits of PD-MCI can be heterogeneouse17 with
NeurologyorgN Neurology | Volume 94 Number 17 | April 28 2020 745
disproportionately affected attentionexecutive function22
visuospatial skillse18 and memory28 Similar toMCI-LB thereis evidence that nonamnestic MCI is more common thanamnestic MCI and that multidomain amnestic MCI is morecommon than single-domain amnestic MCI29
Biomarkers for prodromal DLBDirect measures of α-synuclein pathology would offer de-finitive diagnosis at an early stage several are under de-velopment but none is yet validated or available for useantemortem Surrogate biomarkers of LB disease must
Table 1 Research criteria for the clinical diagnosis of probable and possible MCI-LB
Essential for a diagnosis of MCI-LB is MCI defined by the presence of each of the following
Concern by the patient informant or clinician regarding cognitive decline
Objective evidence of impairment in 1 or more cognitive domains The cognitive impairment may include any domain but is more likely to be associatedwith attention-executive andor visual processing deficits
Preserved or minimally affected performance of previously attained independence in functional abilities which do not meet the criteria for dementia
Core clinical features
Fluctuating cognition with variations in attention and alertness
Recurrent visual hallucinations
RBD
One or more spontaneous cardinal features of parkinsonism these are bradykinesia (defined as slowness of movement and decrement in amplitude orspeed) rest tremor or rigidity
Proposed biomarkers
Reduced dopamine transporter uptake in basal ganglia demonstrated by SPECT or PET
Polysomnographic confirmation of REM sleep without atonia
Reduced meta-iodobenzylguanidine (MIBG) uptake on myocardial scintigraphy
Probable MCI-LB can be diagnosed if
Two or more core clinical features of DLB are present with or without the presence of a proposed biomarker or
Only 1 core clinical feature is present but with 1 or more proposed biomarkers
Probable MCI-LB should not be diagnosed based on biomarkers alone
Possible MCI-LB can be diagnosed if
Only 1 core clinical feature of DLB is present with no proposed biomarkers or
One or more of the proposed biomarkers is present but there are no core clinical features
Supportive clinical features
Severe sensitivity to antipsychotic agents postural instability repeated falls syncope or other transient episodes of unresponsiveness prolonged orrecurrent delirium autonomic dysfunction eg constipation orthostatic hypotension urinary incontinence hypersomnia hyposmia hallucinations inother modalities including passage and sense of presence phenomena systematized delusions apathy anxiety and depression
Potential biomarkers of MCI-LB
Quantitative EEG showing slowing and dominant frequency variability
Relative preservation of medial temporal lobe structures on structural imaging
Insular thinning and gray matter volume loss on MRI
Low occipital uptake on perfusionmetabolism scan
MCI plus supportive clinical features or potential biomarkers are insufficient to diagnose MCI-LB but may raise suspicion of it and prompt biomarkerinvestigation and may add weight to an existing MCI-LB diagnosis
MCI-LB is less likely in the presence of any other physical illness or brain disease including cerebrovascular disease sufficient to account in part or in total forthe clinical picture although these do not exclude anMCI-LB diagnosis andmay serve to indicatemixed ormultiple pathologies contributing to the clinicalpresentation
Abbreviations DLB = dementia with Lewy bodies MCI = mild cognitive impairment MCI-LB = MCI with Lewy bodiesThese should be used in conjunction with the corresponding article text which gives further information about core and supportive clinical features and theuse of biomarkers as they apply to MCI-LB
746 Neurology | Volume 94 Number 17 | April 28 2020 NeurologyorgN
therefore be used as is the case for the diagnosis of DLBitself2 We propose biomarkers for the diagnosis of prodromalDLB where there is either sufficient good quality publishedevidence of adequate diagnostic specificity in prodromal DLBor this can be reasonably extrapolated from fully developedDLB or related disorders We categorize biomarkers for whichonly limited data are available as potential biomarkers rec-ognizing that such distinctions are likely to require revision asnew data become available
Proposed biomarkers
Reduced dopamine transporter (DAT) uptake in basalganglia demonstrated by SPECT or PETThe utility of DAT imaging in discriminating DLB from ADis already well established2 and its sensitivity in dis-tinguishing MCI with LB (MCI-LB) fromMCI with AD was54 and specificity 8930 whenMCI-LB was defined by thepresence of 1 core clinical feature of DLB in patients withMCI A higher sensitivity of 61 was achieved when 2 coreclinical symptoms were present30 Reduced striatal DATuptake therefore seems suggestive of prodromal DLB ina person with MCI but normal striatal DAT uptake does notexclude it
Polysomnographic confirmation of REM sleep withoutatoniaThe association between RBD and synucleinopathy is highlyspecific (eg a multicenter autopsy study found that of 80subjects with polysomnography [PSG]-confirmed RBD anda coexisting neurodegenerative disorder only 2 had a diseaseunrelated to α-synuclein deposition)e4 These data imply thata patient presenting with MCI and having PSG-confirmedRBD that is a history of probable RBD plus clear docu-mentation of REM sleep without atonia (RSWA) on PSGalso has a high probability of an underlying prodromal syn-ucleinopathy Because around a quarter of patients with DLBdo not report symptoms of RBD andor have normal REMsleep atonia on PSG a normal PSG does not exclude a pro-dromal DLB diagnosis31
Reduced meta-iodobenzylguanidine uptake onmyocardial scintigraphyReduced meta-iodobenzylguanidine (MIBG) uptake is anindicative biomarker for DLB2 and has also been reported tooccur in a small series of patients with late-onset psychiatricdisorder and PSG-confirmed RBD32 reinforcing its associa-tion with underlying α-synucleinopathy Of 2 patients withamnestic MCI with low MIBG uptake one developed DLBafter 2 years the other had no clinical follow-up reportede19
VHs andor RBD were reported among 7 of 13 patients withMCI with reduced MIBG uptake the majority of whom alsohad autonomic symptoms suggestive of LB disease but theywere not followed to determine conversion to DLBe20 De-spite a paucity of longitudinal datae21 there seems to be suf-ficient evidence that abnormal MIBGmyocardial scintigraphyin a patient with MCI supports a prodromal DLB diagnosisbut further studies are required
Potential biomarkersThese are biomarkers consistent with underlying LB diseasewhich may help the diagnostic evaluation but for which thereis still insufficient evidence of diagnostic sensitivity andspecificity in early disease This will change as new evidenceemerges at which point these or other candidates may be-come considered as indicative of prodromal DLB
Quantitative EEG showing slowing and dominantfrequency variabilityEEG slowing has been reported as predictive of dementia inboth PDe22 and RBDe23 posterior slow wave activity withperiodic fluctuations in the pre-alpha range being supportiveof DLB2 Quantitative EEG (QEEG) methods show thata dominant frequency lt8 Hz and dominant frequency vari-ability gt1middot5 Hz is typical of DLB and in a 3-year follow-upstudy 83 of subjects with MCI with this pattern at pre-sentation converted to DLB If these findings are replicatedQEEG may represent a powerful predictor of progressionfrom MCI to DLB33
Relative preservation of medial temporal lobestructures on structural imagingAbsent or minimal medial temporal lobe atrophy is consistentwith DLB but not sufficiently specific to differentiate it fromAD2 Lewy body disease with RBD is characterized by pre-served hippocampal volumes34 and hippocampal preserva-tion in patients with MCI supports progression to DLBinstead of AD dementia with a sensitivity of 85 and a spec-ificity of 6123 Suboptimal specificity may be due to thevariability of hippocampal atrophy in AD35 and contributionof other pathologic processes such as TAR DNA bindingprotein 43 (TDP43)e24
Insular thinning and gray matter volume lossInsular cortical thinning occurs in prodromal DLB relative tohealthy controls using MRI T1 sequences with gray matteratrophy predominantly affecting the anterior cingulum andmedial frontal structures This contrasts with more extensiveloss of gray matter in the temporal frontal and parietalregions of subjects with prodromal AD Insular corticalthinning may therefore differentiate patients with prodromalDLB not only from healthy controls but also from theirprodromal AD counterparts36 No group differences in insularvolumes are seen between DLB and AD at the dementia stageso longitudinal studies are required to determine its precisevalue as an early diagnostic marker of DLB37 Insula is alsoinvolved early in frontotemporal dementia (FTD) being thefirst cortical area to show atrophy in presymptomatic GRNMAPT or C9ORF72 mutation carrierse25 and unlikelytherefore to be helpful in differentiating DLB from FTD
Low occipital uptake on perfusionmetabolism scanOccipital hypometabolism on FDG-PET is associated withDLB38 and together with relative preservation of posteriorcingulate metabolism (the cingulate island sign)e26 is a sup-portive biomarker of DLB2 How frequently the cingulate
NeurologyorgN Neurology | Volume 94 Number 17 | April 28 2020 747
island sign is seen in prodromal DLB remains to be estab-lished significantly reduced posterior cingulate metabolismmay be a useful indication of the concurrence of additionalneurofibrillary tangle pathologye27
Other biomarkersThere is currently no α-synuclein radioligand with sufficientevidence supporting its utility for imaging DLB or any otherα-synucleinopathy nor have any diagnostically applicablebiofluid peripheral tissue or genotypic biomarkers beenestablished2 CSF measures cannot reliably discriminate be-tween DLB and AD39 although the measurement of CSFα-synuclein aggregates using seeding aggregation assays suchas protein misfolding cyclic amplification and real-timequaking-induced conversion is providing encouraging pre-liminary results and may be extended to more accessiblebiofluids including saliva plasma serum or urinee28 Com-bining CSF markers may be useful for example addition ofCSF phospho-tau to α-synuclein significantly improved thedifferential diagnosis between MCI-LB and MCI-AD in-creasing sensitivity and specificity both gt than 95e29 Otherdirect or indirect biomarker candidates that may occur earlyinclude identification of phosphorylated α-synuclein depositsin peripheral nervous tissue from skin biopsy40 gait ana-lysise30 and abnormalities in color vision discrimination4142
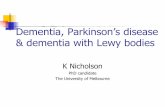
The figure shows a framework for considering a wider range ofbiomarkers in the setting of prodromal DLB determining theextent to which AD-related pathology is contributing to thedementia syndrome and influencing clinical trajectories inthese patients4344e31e32 Aβ42 declines earlier in AD thanDLB whereas Aβ40 levels increase alone in AD A low
Aβ42Aβ40 ratio may therefore differentiate patients withprodromal AD from patients with prodromal DLB better thanindividual measures43 There is also evidence showing dif-ferent frequencies and topographies of abnormal uptake onamyloid and tau PET imaging in DLB vs AD45
Delirium-onset DLBCognitive fluctuations or pronounced variations in alertnessand arousal are a core feature of DLB apparent as markedfluctuations in cognitive ability or function detectable byobservation or informant report and measurable using sen-sitive cognitive and electrophysiologic measurese33 The oc-currence of delirium (sometimes referred to as acuteconfusional state) as an early presenting feature of DLB hasbeen described in numerous case reports and seriese34 in-cluding in those with no apparent previous history of cogni-tive impairment46e35 Whether this represents a greatervulnerability to delirium in subjects with DLB or the mis-diagnosis of severe fluctuations with clouding of conscious-ness as delirium or a combination of both is unclear
Recognition that DLB may first present as delirium is im-portant because most guidelines for behavioral disturbancesin delirium recommend antipsychotics as first-line pharma-cologic treatment Delirium or marked fluctuations in con-sciousness were reported by 43 of caregivers before DLBdiagnosis47 and previous episodes of delirium were muchmore frequent in patients with DLB compared with patientswith AD (25 vs 7) with 1 in 4 of those with DLB havingrepeated delirium11 In the majority of these potential pro-voking causes were present A similarly higher incidence ofdelirium was found for subjects with DLB compared with
Figure Multimodal biomarkers for prodromal DLB
Reduced dopamine transporter uptake in basal gan-glia demonstrated by SPECT or PET PSG-confirmedREM sleep without atonia and MIBG myocardial scin-tigraphy are proposed as biomarkers of prodromalDLB Multimodality biomarkers are also important incharacterizing patients with prodromal DLB in whomthe pathologic mechanisms of cognitive impairmentinclude both LB and AD pathologies and who mayhave abnormalities associated with both Medialtemporal lobe uptake on tau PET medial temporallobe atrophy on MRI and high levels of uptake onamyloid PET and positive CSF biomarkers of AD-re-lated pathology may characterize patients with pro-dromal DLB with significant AD pathology It isexpected that biomarker abnormalities detected inthe earliest stages will remain abnormal as diseaseprogresses with additional biomarkers showingchanges later during the progression from pro-dromal to dementia phase DLB DLB = dementia withLewy bodies MIBG = meta-iodobenzylguanidine
748 Neurology | Volume 94 Number 17 | April 28 2020 NeurologyorgN
subjects with AD in the year before diagnosis (17middot6 v 3middot2100person-years)9 and admissions for delirium were morecommon in those already diagnosed with DLB than for otherdementias Prolonged delirium may also raise the index ofsuspicion for DLBe36 In an FDG-PET imaging study ofprolonged delirium 32 of subjects were found to havea DLB like pattern a high proportion in regard both to theknown prevalence of the disease and to that of their matchedcognitively impaired control group (4)e37
The similarities between the marked fluctuations in DLB anddisturbances of attention and consciousness in delirium havebeen noted and reviewed46 but there is as yet little un-derstanding of a shared neurobiological basis There havebeen few pathologic studies and although in anepidemiologic-based autopsy cohort there was no link be-tween delirium and LB pathology at autopsye38 a significantlyincreased risk of postoperative delirium in those with pe-ripheral α-synuclein pathology has been described48 Deliriumhas been suggested to bemore common in those subjects withDLB with later age at onsete39 but further evidence is needed
In summary (table 2) it is clear that DLB can present withdelirium and in patients diagnosed with delirium a carefulsearch for other DLB features should be made with a lowthreshold for undertaking DLB biomarker examinations es-pecially in those with recurrent unexplained or prolongeddelirium The extent to which delirium presentations of DLBhave the biomarker abnormalities associated with establishedDLB or other prodromal DLB presentations is unclear
although the PET imaging study cited above supports thise37
as does a report of reduced DAT uptake in a patient withacute unexplained delirium49 The link between delirium andDLB is an important area for future research to clarify therelationship between the 2 and to establish which factorsassociated with delirium should raise the index of suspicionfor underlying prodromal DLB
Psychiatric-onset DLBEarly clinicopathologic studies suggested that DLB maypresent as a primary psychiatric disorder5051 but subsequentfocus on the cognitive and motor aspects of DLB has limitedthe documentation of such cases outside of a fewcenters123252ndash54e36 Late-onset major depressive disorderand late-onset psychosis are the most frequently reportedpresentations differing markedly from the construct of mildbehavioral impairmente40 and sometimes sufficiently severe torequire hospitalization Symptoms include hallucinations invisual and in other modalities and systematized delusionsincluding Capgras syndrome55 apathy anxiety and de-pression Psychiatric-onset DLB cases are not easily differ-entiated from non-LB late-onset psychosis cases on the basisof primary psychiatric phenomenology or neuropsychologicalprofile alone54 Psychomotor retardation such as slowedspeech thinking and body movements can resemble thebradykinesia of parkinsonism The occurrence of rest tremoror rigidity is more helpful than bradykinesia to suspect pro-dromal DLB in patients with depressive disorder53 butpsychotropic-induced parkinsonism may complicate di-agnosis Atypical clinical features may prove valuable pointers
Table 2 Summary of key features of delirium-onset DLB
Patients with DLB are more susceptible to delirium than people with Alzheimer disease and this delirium may occur as their presenting complaint beforedementia develops
Such episodes may be provoked by multiple factors including surgery infectionssepsis fever or other systemic illness or secondary to use or suddenwithdrawal of alcohol or psychoactive drugs
Prodromal DLB should be particularly suspected in patients
bull in whom adequate provoking factors for the delirium are not found
bull with prolonged or recurrent delirium
bull who later develop progressive cognitive decline or subsequent dementia
Core clinical features of DLB are likely to be of more limited diagnostic weight in a patient with delirium because
bull cognitive fluctuation and clouding of consciousness can also occur in non-DLB delirium ie are not diagnostically specific for DLB in this situation
bull visual hallucinations may occur in non-DLB delirium particularly drug-induced or provoked by alcohol abstinence
bull motor parkinsonism present may be due to antipsychotic medications used to treat delirium
bull the diagnostic significance of a history of RBD in a person with delirium is not yet established
Identification of delirium-onset DLB
bull may be assisted by use of MCI-LB biomarkers but further research evidence of this is required
bull is important to inform the management plan including the avoidance or minimization of antipsychotic and anticholinergic agents
Abbreviations DLB = dementia with Lewy bodies MCI = mild cognitive impairment MCI-LB = MCI with Lewy bodies RBD = REM sleep behavior disorder
NeurologyorgN Neurology | Volume 94 Number 17 | April 28 2020 749
to underlying LB pathology particularly the presence of re-current VH12 when these occur before cognitive impairmentbecomes evident As with all α-synucleinopathies RBD maybe a useful indicator although a relationship between anti-depressant usage and subsequent RBD onset is a potentialconfoundere41 Although the primary psychiatric manifes-tations are often accompanied by mild cognitive deficits54
cognitive evaluation and interpretation of performance can bedifficult when psychiatric symptoms are prominent The fre-quency of cognitive fluctuations in psychiatric-onset LB caseshas not been determined
Initial reports suggest that 123I-MIBG scintigraphy may behelpful in psychiatric-onset DLB525356 Eighteen of 35patients with a first onset of major depressive disorder gt50years and with bradykinesia developed a clinical diagnosis ofDLB after 6 years of follow-up All 18 had an abnormal ven-tilatory response to hypercapnia (VRH) indicative of severeautonomic dysfunction whereas none of the 17 patients witha normal VRH converted to DLB within the study period Forthe converters the most common presentation was withpsychotic and melancholic features simultaneously The fre-quency of hypersensitivity to antipsychotics antidepressantsand antianxiety drugs was higher in converters than in non-converters53 Further studies need to confirm these findingsand to determine the value of other DLB biomarkers inpsychiatric-onset cases325256
In summary it is not yet clear how to identify patients withprominent late-onset psychiatric symptoms who may haveunderlying LB disease and subsequently progress to DLB It is
premature to try to construct formal criteria for psychiatric-onset DLB but clinicians in mental health and other settingsneed to be aware that this possibility exists not least becauseof the risk of severe antipsychotic sensitivity reactions withincreased morbidity and mortality The small available liter-ature including reports such as those cited above does providesome useful guidance summarized in table 3 but requiresreplication and further investigation
Idiopathic REM sleep behavior disorderRBD is characterized by abnormal dream enactment behaviorduring REM sleep accompanied by loss of muscle atonia duringREM sleep (REM sleep without atonia or RSWA) on PSG Forthe purpose of a prodromal DLB diagnosis a clinical history ofRBD is obtained in the same way as for DLB2 that is a clearcomplaint of dream enactment by a bedpartner or other witnesswith no evidence of sleep disorders that may mimic RBD onclinical interview Conditions known to mimic or masquerade asRBD include non-REM parasomnias (sleep walking sleep talk-ing or other behaviors that emerge fromnon-REM sleep stages)obstructive sleep apnea confusional arousals or nocturnal seiz-ures In the absence of PSG the risk of a false-positive clinicaldiagnosis of RBD is reduced by using optimized sleep ques-tionnaires which can have sensitivity and specificity over 90e42
RBDmay be considered as idiopathic until it is associated withanother ongoing neurologic condition the most frequentbeing an α-synucleinopathy (PD DLB or MSA) In a recentlarge study 735 of patients with RBD converted to an overtneurodegenerative syndrome after 12-year follow-up 565developing parkinsonism and 435 dementia as their first
Table 3 Summary of key features of psychiatric-onset DLB
Is characterized by predominant psychiatric symptoms that typically correspond to late-onset major depressive disorder or late-onset psychosis which mayfeature hallucinations in visual and in other modalities and systematized delusions including Capgras syndrome
bull may also present with apathy anxiety and depression
bull may be sufficiently severe to require hospitalization
bull the frequency of LB disease as a cause of late-onset psychiatric disorder is not known
When assessing for core clinical features of DLB in a patient with a primary psychiatric presentation
bull bradykinesia may be mimicked by psychomotor retardation which is commonly seen in depressive disorders
bull parkinsonism may be induced by antipsychotic medications used to treat psychiatric disorder
bull RBD (and REM sleep without atonia) may be induced by antidepressant medications
bull mild cognitive disturbance may be present but is not predominant and may fluctuate
bull formal neuropsychological testing may be confounded by the psychiatric mental state
bull the frequency and character of cognitive fluctuations is unknown
Identification of psychiatric-onset DLB
bull may be assisted by use of MCI-LB biomarkers but further research evidence of this is required
bull is important to inform the management plan including the avoidance or minimization of antipsychotic and anticholinergic agents
Abbreviations DLB = dementia with Lewy bodies MCI = mild cognitive impairment
750 Neurology | Volume 94 Number 17 | April 28 2020 NeurologyorgN
disease manifestation Among many predictive markerstested only the cognitive variables differed at baseline be-tween those converting to primary dementia vs parkinson-ism7 Other multicenter studies confirm that the only clinicalfeature that predicts dementia vs parkinsonism first is neu-ropsychological performance those with RBD who exhibitcognitive changes are more likely to evolve first into MCI orDLB22e4 Thus although RBD may be regarded an earlymanifestation of α-synucleinopathy it is not possible to clearlydistinguish whether an individual presenting with RBD willdevelop dementia first that is evolve into a primary DLBdiagnosis or parkinsonism first that is a primary PDMSAdiagnosis Any MCI subtype associated with PSG-confirmedRBD is highly likely to represent underlying LB disease Al-though idiopathic RBD is a useful model to study the earlystages of LB disease progression it is not necessarily repre-sentative of the whole spectrum of patients with PD and DLBa significant minority of whom do not have RBD42
Autonomic dysfunctionanosmia and othernonspecific prodromal LB disease symptomsPatients with DLB frequently report a history of autonomicdysfunction at first clinic attendance with 25ndash50 com-plaining of one of more among constipation orthostatic diz-ziness urinary incontinence erectile dysfunction increasedsweating or increased saliva5657 In a cohort of patients withpure autonomic failure 34 converted to an overt α-synu-cleinopathy over 6 years of follow-up this was to DLB (52)PD (24) orMSA (24)58 However because there are manyother causes for autonomic dysfunction in older people thesesymptoms either alone or in combination have low positivepredictive value59 The situation is similar for hyposmia whichalso frequently occurs early in prodromal DLB and PD42 butwhich can have many other causes in this age group
Conclusions and future directionDiagnosis of DLB at the dementia stage depends on identifyingfully expressed core clinical features which may be mild orabsent at the prodromal stage when biomarker evidence mayalso be weaker and may even differ from that found at thedementia stage Several new biomarker candidates direct andindirect are in development and we will continue to reviewthese to update our recommendations as soon as sufficientevidence accumulates We recognize that the clinical pheno-type of neurodegenerative disorders reflects interaction be-tween several rather than a single brain pathology and it istherefore likely that multiple biomarkers of individual pathol-ogies (eg α-synuclein β-amyloid and tau) or of disease sur-rogates (eg metabolic imagingEEG) will be required
Although we have described the 3 prodromal DLB syndromesseparately they are unlikely to be mutually exclusive andthere may be substantial overlap We propose operationalizedcriteria only for MCI-LB because the evidence base from oursystematic review albeit relatively limited is sufficient to
support recommendations that are immediately applicableand testable Our recommendations should be used alongsideguidance about the prodromal manifestations of PD1559
MSA60 and AD14 with which there is overlap Notwith-standing the potential benefits of early diagnosis we are alsomindful of the importance of avoiding incorrect (false-positive) diagnosis of prodromal DLB and the potentialnegative consequences this could have for an individual Wesuggest that the predictive validity of different categories andcombinations of our proposed criteria should be clarified byprospective studies before they are adopted for widespreadclinical use and that they will enable standardization for in-clusion in research studies and clinical trials
Some published guidance about the early clinical diagnosis ofDLB does already exist DSM5 recommends a diagnosis ofmild neurocognitive disorder (NCD) with LB ldquofor individualswho present with the core or suggestive features at a stagewhen cognitive or functional impairments are not of sufficientseverity to fulfill criteria for major NCDrdquoe43 This is basedhowever on the 2005 version of DLB guidelines and requiresupdating ICD-11 takes a similar approach toward diagnosingmild NCD at a syndromic level and lists both Lewy bodydisease and PD as possible causese44
The diagnostic position for other prodromal manifestations ofDLB that is delirium-onset and psychiatric-onset is less clearthan for MCI Operationalization of specific criteria for thesesyndromes is not yet justified and the reliable differentiationof the minority of delirious and psychiatrically ill patients whohave underlying LB pathology from the majority who do notwill probably only be achieved when routinely applicablebiomarkers are developed LB disease is seldom if ever cur-rently considered as part of the differential diagnosis of de-lirium or late-onset psychiatric disorder and we hope that theinformation we provide in the text and accompanying boxeswill raise cliniciansrsquo awareness of that possibility
Study fundingNo targeted funding reported
DisclosureI McKeith receives support from the NIHR Biomedical Re-search Centre awarded to the Newcastle upon Tyne HospitalsNHS Foundation Trust and Newcastle University and hasconsulted for GE Healthcare Sanofi Eisai Sumitomo Dai-nippon Pharma and Axovant T Ferman receives support fromNIH P50-AG16574 P30-AG062677 U01-NS100620 and theMangurian Foundation for Lewy body disease research AThomas receives support from the NIHR Biomedical ResearchCentre awarded to the Newcastle upon Tyne Hospitals NHSFoundation Trust and Newcastle University and has receivedgrants from GE Healthcare F Blanc has served as nationalclinical trial coordinator for Eisai and Axovant B Boevereceives support from NIH P50-AG16574 P30-AG062677U01-NS100620 and the Mangurian Foundation for Lewybody disease research has consulted for the Scientific Advisory
NeurologyorgN Neurology | Volume 94 Number 17 | April 28 2020 751
BoardmdashTau Consortium and received grants from Biogenthe NIH theMangurian Foundation Alector the Little FamilyFoundation and the Turner Family H Fujishiro has receivedsupport from Fujifilm RI Pharma Co Ltd K Kantarci receivessupport from NIH P50-AG16574 P30-AG062677 U01-NS100620 and the Mangurian Foundation for Lewy bodydisease research and has received grants from Avid Radio-pharmaceuticals and acted on a Data Safety Monitoring Boardfor Takeda Global Research C Muscio acknowledges thesupport of the Italian Ministry of Health GRANT NET-2011-02346784 J OrsquoBrien is supported by the NIHR CambridgeBiomedical Research Centre Dementia and Neuro-degeneration and Mental Health Themes and the CambridgeCentre for Parkinsonrsquos Plus Disorders has consulted forTauRx Axon GE Healthcare Eisai and AvidLilly and re-ceived grants fromAvidLilly andAllianceMedical R Postumahas received grants from and consulted for Fonds de laRecherche en Sante received grants from the Canadian Insti-tutes of Health Research the Parkinson Society of Canada theWeston-Garfield Foundation The Michael J Fox Foundationand the Webster Foundation and consulted for TakedaRocheProthena Teva Neurosciences Novartis Canada Bio-gen Boehringer Ingelheim Theranexus GE Healthcare JazzPharmaceuticals AbbVie Jannsen Otsuko PhytopharmicsInception Sciences and Parkinson Canada D Aarsland isa Royal Society Wolfson Research Merit Award Holder andwould like to thank the Wolfson Foundation and the RoyalSociety for their support He has received research supportandor honoraria from AstraZeneca H Lundbeck NovartisPharmaceuticals and GE Health and served as paid consultantfor H Lundbeck Eisai Heptares Sanofi and Mentis Cura CBallard reports unrelated current grant funding from MRCWellcome Trust European Union Gillings FoundationNIHR Alzheimerrsquos Society Alzheimerrsquos Research UK Par-kinsonrsquos Society and Lewy Body Society during the conduct ofthe study and personal fees from Acadia pharmaceutical com-pany Lundbeck Roche Otsuka Eli Lilly and AARP outsidethe submitted work L Bonanni is a member of the steeringcommittee of the E-DLB consortium and program chair of theLBD-PIA (ISTAART) and is funded for research on DLB bythe Italian Ministry of Health P Donaghy receives supportfrom the NIHR Biomedical Research Centre awarded to theNewcastle upon Tyne Hospitals NHS Foundation Trust andNewcastle UniversityM Emre served on the scientific advisoryboard for AC Immune J Galvin receives support from NIHgrants (R01 AG040211 R01 NS101482 R01 AG057681 andU01 NS100610) and the Lewy Body Dementia AssociationResearch Center of Excellence reports research support fromthe NIH the Lewy Body Dementia Association The Harry TMangurian Foundation and Albert Charitable Trust directsclinical trials for Biogen and Novartis receives licensing feesfrom Biogen Roche Eli Lilly Quintiles Roobrik ContinuumClinical and Langland and receives consulting fees fromBiogen Eisai Bracket and Medavante D Galasko receivessupport from NIA grant AGO5131 and the Michael J FoxFoundation and has acted as consultant for vTv Pharmaceut-icals Inc Esai Inc and for Fujirebio Inc been a member of
a DSMB for Probiodrug and paid editor for Alzheimerrsquos Re-search amp Therapy J Goldman receives grantsupport fromTheMichael J Fox Foundation and Parkinsonrsquos Foundation andhas received consulting feeshonoraria from Acadia AptinyxSunovion and Worldwide Med S Gomperts receives supportfrom NIH grants R01 AG054551 P30AG062421 R01AG062208 P50 AG005134 R21 NS109833 DODCDMRPW81XW1810516 the Farmer Family ParkinsonrsquosInitiative and the Lewy Body Dementia Association and hasserved on advisory boards for Acadia Pharmaceuticals andSanofi L Honig acknowledges research grant support fromNYS CEAD grant C031425 LBDA RCOE and NIHgrants U01NS100600 P50AG008702 R21AG058020R21MH111596 U01AG051412 U01AG045390U01AG016976 U01AG023749 U19063893 andU19AG024904 He receives research funding support fromAbbVie Alector Biogen Eisai Genentech Roche and Wash-ington University and has received income for consulting forCortexyme and Eisai M Ikeda reports departmental grants andhonoraria fees from Sumitomo Dainippon Pharma Eisai andNiho Medicine-Physics J Leverenz acknowledges supportfrom the National Institutes of Health P30 AG053762 UO1NS100610 and R13NS111954 and Jane and Lee Seidman andDouglas Herthel DVMMemorial Funds and reports consultingfees from Aptinyx Acadia Biogen Eisai GE HealthcareGenzymeSanofi and Takeda Pharmaceuticals and grant sup-port from Alzheimerrsquos Drug Discovery Foundation De-partment of Defense GE Healthcare GenzymeSanofi TheMichael J Fox Foundation and the NIH (NIA andNINDS) SLewis is supported by NHMRC-ARC Dementia Fellows KMarder is funded by the NIH R01NS100600 NS107168UL1TR001873 andNS073671 with research support from theLBDA Parkinson Foundation Michael J Fox HDSA andCHDI and has acted as site investigator for Vaccinex andGenentech member of Springer editorial board and scientificadvisory board Voyager Therapeutics M Masellis was sup-ported by a Canadian Institutes of Health Research grant(MOP13129) and an Early Researcher Award from the Min-istry of Research Innovation and Science (MRIS ON) andreports personal fees for ad hoc consultancy from ArkudaTherapeutics Ionis Pharmaceuticals and Alector Pharmaceut-icals royalties fromHenry Stewart Talks Ltd and grants to theinstitution from Roche Novartis Washington University andAxovant Sciences D Salmon acknowledges support from NIHP30AG062429 and is a paid consultant for Takeda Inc Apti-nyx Inc and Biogen Inc J-P Taylor receives support from theNIHR Biomedical Research Centre awarded to the Newcastleupon Tyne Hospitals NHS Foundation Trust and NewcastleUniversity and reports grants from the UKNational Institute ofHealth Research (NIHR) travel award from Axovant researchsupport costs from Sonsei-Heptares and personal fees fromGEHealthcare D Tsuang acknowledges support from NIHR21AG064271 R03 NS103950 and U01 NS100610 ZWalker has been supported by ESRC NIHR (co-app) ARUK(co-app) EU IMI 2 (co-app) and Dunhill Medical Trust Shehas received consultancy fees travel expenses and researchsupport from GE Healthcare and research support from Life
752 Neurology | Volume 94 Number 17 | April 28 2020 NeurologyorgN
Molecular Imaging P Tiraboschi acknowledges the support ofthe Italian Ministry of Health GRANT NET-2011-02346784Go to NeurologyorgN for full disclosures
Publication historyReceived by Neurology October 30 2019 Accepted in final formFebruary 25 2020
Appendix Authors
Name Location Contribution
Ian GMcKeith FMed Sci MD
Newcastle University Design and conceptualizationof the study acquisition ofdata analysis andinterpretation of the data anddrafting and revising themanuscript for intellectualcontent
Tanis JFermanPhD
Mayo ClinicJacksonville
Design and conceptualizationof the study acquisition ofdata analysis andinterpretation of the data anddrafting and revising themanuscript for intellectualcontent
Alan JThomasPhD
Newcastle University Design and conceptualizationof the study acquisition ofdata analysis andinterpretation of the data anddrafting and revising themanuscript for intellectualcontent
FredericBlanc MD
University ofStrasbourg
Design and conceptualizationof the study acquisition ofdata analysis andinterpretation of the data anddrafting and revising themanuscript for intellectualcontent
Bradley FBoeve MD
Mayo Clinic Rochester Design and conceptualizationof the study acquisition ofdata analysis andinterpretation of the data anddrafting and revising themanuscript for intellectualcontent
HiroshigeFujishiroMD
Nagoya UniversityKawasaki MemorialHospital
Design and conceptualizationof the study acquisition ofdata analysis andinterpretation of the data anddrafting and revising themanuscript for intellectualcontent
KejalKantarciMD MS
Mayo Clinic Rochester Design and conceptualizationof the study acquisition ofdata analysis andinterpretation of the data anddrafting and revising themanuscript for intellectualcontent
CristinaMuscio PhD
Istituto NeurologicoldquoCarlo Bestardquo Milan
Design and conceptualizationof the study acquisition ofdata analysis andinterpretation of the data anddrafting and revising themanuscript for intellectualcontent
Appendix (continued)
Name Location Contribution
John TOrsquoBrien FMed Sci DM
Cambridge University Design and conceptualizationof the study acquisition ofdata analysis andinterpretation of the data anddrafting and revising themanuscript for intellectualcontent
Ronald BPostumaMD MSc
McGill University Design and conceptualizationof the study acquisition ofdata analysis andinterpretation of the data anddrafting and revising themanuscript for intellectualcontent
DagAarslandPhD
Kingrsquos College Londonand StavangerUniversityHospital
Revising the manuscript forintellectual content
CliveBallard MD
University of Exeter Revising the manuscript forintellectual content
LauraBonanniMD PhD
University of Chieti-Pescara
Revising the manuscript forintellectual content
PaulDonaghyPhD
Newcastle University Revising the manuscript forintellectual content
Murat EmreMD
Istanbul Faculty ofMedicine
Revising the manuscript forintellectual content
James EGalvin MDMPH
University of MiamiMiller School ofMedicine
Revising the manuscript forintellectual content
DouglasGalasko MD
University of CaliforniaSan Diego
Revising the manuscript forintellectual content
Jennifer GGoldmanMD MS
Feinberg School ofMedicine
Revising the manuscript forintellectual content
Stephen NGompertsMD PhD
Massachusetts GeneralHospital
Revising the manuscript forintellectual content
Lawrence SHonig MDPhD
Columbia UniversityIrving Medical Center
Revising the manuscript forintellectual content
ManabuIkeda MDPhD
Osaka University Revising the manuscript forintellectual content
James BLeverenzMD
Lou Ruvo Center ofBrain Health ClevelandClinic
Revising the manuscript forintellectual content
Simon JGLewis MD
University of Sydney Revising the manuscript forintellectual content
Karen SMarder MDMPH
Columbia UniversityIrving Medical Center
Revising the manuscript forintellectual content
MarioMasellisMD PhD
Sunnybrook HealthSciences CentreUniversity of Toronto
Revising the manuscript forintellectual content
David PSalmon PhD
University of CaliforniaSan Diego
Revising the manuscript forintellectual content
Continued
NeurologyorgN Neurology | Volume 94 Number 17 | April 28 2020 753
References1 Walker Z Possin KL Boeve BF Aarsland D Lewy body dementias Lancet 2015386
1683ndash16972 McKeith IG Boeve BF Dickson DW et al Diagnosis and management of dementia
with Lewy bodies fourth consensus report of the DLB consortium Neurology 20178988ndash100
3 Ferman TJ Smith GE Kantarci K et al Nonamnestic mild cognitive impairmentprogresses to dementia with Lewy bodies Neurology 2013812032ndash2038
4 Savica R Bradley BF Mielke MM When do alpha-synucleinopathies start An epi-demiological timeline A review JAMA Neurol 201875503ndash509
5 Donaghy PC Taylor JP OrsquoBrien JT et al Neuropsychiatric symptoms and cognitiveprofile in mild cognitive impairment with Lewy bodies Psychol Med 2018482384ndash2390
6 Cagnin A Bussse C Gardini S et al Clinical and cognitive phenotype of mildcognitive impairment evolving to dementia with Lewy bodies Dement Geriatr CognDis Extra 20155442ndash449
7 Postuma RB Iranzo A HuM et al Risk and predictors of dementia and parkinsonismin idiopathic REM sleep behaviour disorder a multicentre study Brain 2019142744ndash759
8 Sadiq D Whitfield T Lee L Stevens T Costafreda S Walker Z Prodromal dementiawith Lewy bodies and prodromal Alzheimerrsquos disease a comparison of the cognitiveand clinical profiles J Alzheimers Dis 201758463ndash470
9 FitzGerald JM Perera G Chang-Tave A et al The incidence of recorded de-lirium episodes before and after dementia diagnosis differences between de-mentia with Lewy bodies and Alzheimerrsquos disease J Am Med Dir Assoc 201920604ndash609
10 Jicha GA Schmitt FA Abner E et al Prodromal clinical manifestations of neu-ropathologically confirmed Lewy body disease Neurobiol Aging 2010311805ndash1813
11 Vardy E Holt R Gerhard A Richardson A Snowden J Neary D History of a sus-pected delirium is more common in dementia with Lewy bodies than Alzheimerrsquosdisease a retrospective study Int J Geriatr Psychiatry 201429178ndash181
12 Fujishiro H Nakamura S Sato K Iseki E Prodromal dementia with Lewy bodiesGeriatr Gerontol Int 201515817ndash826
13 McKeith I Taylor JP Thomas A Donaghy P Kane J Revisiting DLB diagnosisa consideration of prodromal DLB and of the diagnostic overlap with Alzheimerdisease J Geriatr Psychiatry Neurol 201629249ndash253
14 Albert MS DeKosky ST Dickson D et al The diagnosis of mild cognitive impairmentdue to Alzheimerrsquos disease recommendations from the National Institute on Aging-Alzheimerrsquos Association workgroups on diagnostic guidelines for Alzheimerrsquos diseaseAlzheimers Dement 20117270ndash279
15 Litvan I Goldman JG Troster AI et al Diagnostic criteria for mild cognitive im-pairment in Parkinsonrsquos disease Movement Disorder Society Task Force guidelinesMov Disord 201227349ndash356
16 Ferman TJ Smith GE Boeve BF et al Neuropsychological differentiation of de-mentia with Lewy bodies from normal aging and Alzheimerrsquos disease Clin Neuro-psychol 200620623ndash636
17 Cagnin A Busse C Jelcic N Gnoato F Mitolo M Caffarra P High specificity ofMMSE pentagon scoring for diagnosis of prodromal dementia with Lewy bodiesParkinsonism Relat Disord 201521303ndash305
18 Yoon JH Kim M Moon SY Yong SW Hong JM Olfactory function and neuro-psychological profile to differentiate dementia with Lewy bodies from Alzheimerrsquosdisease in patients with mild cognitive impairment a 5-year follow-up study J NeurolSci 2015355174ndash179
19 Kemp J Philippi N Phillipps C et al Cognitive profile in prodromal dementia withLewy bodies Alzheimers Res Ther 2017919
20 Auning E Rongve A Fladby T et al Early and presenting symptoms of dementia withLewy bodies Dement Geriatr Cogn Disord 201132202ndash208
21 Kondo D Ota K Kasanuki K et al Characteristics of mild cognitive impairmenttending to convert into Alzheimerrsquos disease or dementia with Lewy bodies a follow-upstudy in a memory clinic J Neurol Sci 2016369102ndash108
22 Marchand DG Postuma RB Escudier F et al How does dementia with Lewy bodiesstart prodromal cognitive changes in REM sleep behavior disorder Ann Neurol2018831016ndash1026
23 Kantarci K Lesnick T Ferman TJ et al Hippocampal volumes predict risk of de-mentia with Lewy bodies in mild cognitive impairment Neurology 2016872317ndash2323
24 Thomas AJ Taylor JP McKeith I et al Revision of assessment toolkits for improvingthe diagnosis of Lewy body dementia the DIAMOND Lewy study Int J GeriatrPsychiatry 2018331293ndash1304
25 Galvin JE Improving the clinical detection of Lewy body dementia with the Lewybody composite risk score Alzheimerrsquos Demen (Amsterdam Netherlands) 20151316ndash324
26 Belden CM Kahlon V Malek-Ahmadi M Tsai A Sabbagh MN Clinical character-ization of mild cognitive impairment as a prodrome to dementia with Lewy bodiesAm J Alzheimers Dis Other Demen 201530173ndash177
27 Yoon JH Lee JE Yong SW Moon SY Lee PH The mild cognitive impairment stageof dementia with Lewy bodies and Parkinson disease A comparison of cognitiveprofiles Alzheimer Dis Assoc Disord 201428151ndash155
28 Fengler S Liepelt-Scarfone I Brockmann K Schaffer E Berg D Kalbe E Cognitivechanges in prodromal Parkinsonrsquos disease a review Mov Disord 2017321655ndash1666
29 Kalbe E Rehberg SP Heber I et al Subtypes of mild cognitive impairment in patientswith Parkinsonrsquos disease evidence from the LANDSCAPE study J Neurol NeurosurgPsychiatry 2016871099ndash1105
30 Thomas AJ Donaghy P Roberts G et al Diagnostic accuracy of dopaminergic im-aging in prodromal dementia with Lewy bodies Psychol Med 20181ndash7
31 Ferman TJ Boeve BF Smith GE et al Inclusion of RBD improves the diagnosticclassification of dementia with Lewy bodies Neurology 201177875ndash882
32 Fujishiro H Okuda M Iwamoto K et al Early diagnosis of Lewy body disease inpatients with late-onset psychiatric disorders using clinical history of rapid eyemovement sleep behavior disorder and I-123 -metaiodobenzylguanidine cardiacscintigraphy Psychiatry Clin Neurosci 201872423ndash434
33 Bonanni L Perfetti B Bifolchetti S et al Quantitative electroencephalogram utility inpredicting conversion of mild cognitive impairment to dementia with Lewy bodiesNeurobiol Aging 201536434ndash445
34 Murray ME Ferman TJ Boeve BF et al MRI and pathology of REM sleep behaviordisorder in dementia with Lewy bodies Neurology 2013811681ndash1689
35 Murray ME Graff-Radford NR Ross OA Petersen RC Duara R Dickson DWNeuropathologically defined subtypes of Alzheimerrsquos disease with distinct clinicalcharacteristics a retrospective study Lancet Neurol 201110785ndash796
36 Blanc F Colloby SJ Cretin B et al Grey matter atrophy in prodromal stage ofdementia with Lewy bodies and Alzheimerrsquos disease Alzheimers Res Ther 2016831
37 Blanc F Colloby SJ Philippi N et al Cortical thickness in dementia with Lewy bodiesand Alzheimerrsquos disease a comparison of prodromal and dementia stages Plos One201510e0127396
38 Surendranathan A OrsquoBrien JT Clinical imaging in dementia with Lewy bodies EvidBased Ment Health 20182161ndash65
39 Outeiro TF Koss DJ Erskine D et al Dementia with Lewy bodies an update andoutlook Mol Neurodegener 2019145
40 Donadio V Incensi A Rizzo G et al A new potential biomarker for dementiawith Lewy bodies Skin nerve alpha-synuclein deposits Neurology 201789318ndash326
41 Flanigan PM Khosravi MA Leverenz JB Tousi B Color vision impairment differ-entiates Alzheimer dementia from dementia with Lewy bodies J Geriatr PsychiatryNeurol 20183197ndash102
42 Fereshtehnejad SM Yao C Pelletier A Montplaisir JY Gagnon JF Postuma RBEvolution of prodromal Parkinsonrsquos disease and dementia with Lewy bodies a pro-spective study Brain 20191422051ndash2067
43 Bousiges O Bombois S Schraen S et al Cerebrospinal fluid Alzheimer biomarkerscan be useful for discriminating dementia with Lewy bodies from Alzheimerrsquos diseaseat the prodromal stage J Neurol Neurosurg Psychiatry 201889467ndash475
44 Kantarci K Lowe VJ Boeve BF et al Multimodality imaging characteristics of de-mentia with Lewy bodies Neurobiol Aging 2012332091ndash2105
45 Kantarci K Lowe VJ Boeve BF et al AV-1451 tau and beta-amyloid positronemission tomography imaging in dementia with Lewy bodies Ann Neurol 20178158ndash67
46 Gore RL Vardy E OrsquoBrien JT Delirium and dementia with Lewy bodies distinctdiagnoses or part of the same spectrum J Neurol Neurosurg Psychiatry 20158650ndash59
47 Aarsland DS Auning E The pre-dementia stage of dementia with Lewy bodies Eur JNeurol 20111869
48 Sunwoo MK Hong JY Choi J Park HJ Kim SH Lee PH alpha-Synuclein pathologyis related to postoperative delirium in patients undergoing gastrectomy Neurology201380810ndash813
49 Akintade O Pierres F Acute presentation of dementia with Lewy bodies Clin Med201919327ndash330
50 Kosaka K Diffuse Lewy body disease in Japan J Neurol 1990237197ndash20451 Birkett DP Desouky A Han L Kaufman M Lewy bodies in psychiatric patients Int J
Geriatr Psychiatry 19927235ndash240
Appendix (continued)
Name Location Contribution
John PaulTaylor MBBS PhD
Newcastle University Revising the manuscript forintellectual content
Debby WTsuang MD
VA Puget Sound ampUniversity ofWashington
Revising the manuscript forintellectual content
ZuzanaWalker MD
University CollegeLondon
Revising the manuscript forintellectual content
PietroTiraboschiMD
Istituto NeurologicoldquoCarlo Bestardquo Milan
Design and conceptualizationof the study acquisition ofdata analysis andinterpretation of the data anddrafting and revising themanuscript for intellectualcontent
754 Neurology | Volume 94 Number 17 | April 28 2020 NeurologyorgN
52 Kobayashi K Nakano H Akiyama N Maeda T Yamamori S Pure psychiatric pre-sentation of the Lewy body disease is depressionmdashan analysis of 60 cases verified withmyocardial meta-iodobenzylguanidine study Int J Geriatr Psychiatry 201530663ndash668
53 Takahashi S Mizukami K Arai T et al Ventilatory response to hypercapnia predictsdementia with Lewy bodies in late-onset major depressive disorder J Alzheimers Dis201650751ndash758
54 Van Assche L Van Aubel E Van de Ven L Bouckaert F Luyten P Vandenbulcke MThe neuropsychological profile and phenomenology of late onset psychosis a cross-sectional study on the differential diagnosis of very-late-onset Schizophrenia-likepsychosis dementia with Lewy bodies and Alzheimerrsquos type dementia with psychosisArch Clin Neuropsychol 201934183ndash199
55 Thaipisuttikul P Lobach I Zweig Y Gurnani A Galvin JE Capgras syndrome indementia with Lewy bodies Int Psychogeriatr 201325843ndash849
56 Fujishiro H Iseki E Nakamura S et al Dementia with Lewy bodies early diagnosticchallenges Psychogeriatrics 201313128ndash138
57 Chiba Y Fujishiro H Iseki E et al Retrospective survey of prodromal symptoms indementia with Lewy bodies comparison with Alzheimerrsquos disease Dement GeriatrCogn Disord 201233273ndash281
58 Kaufmann H Norcliffe-Kaufmann L Palma JA et al Natural history of pure auto-nomic failure a United States prospective cohort Ann Neurol 201781287ndash297
59 Heinzel S Berg D Gasser T et al Update of the MDS research criteria for prodromalParkinsonrsquos disease Mov Disord 2019341464ndash1470
60 Palma JA Norcliffe-Kaufmann L Kaufmann H Diagnosis of multiple system atrophyAuton Neurosci 201821115ndash25Data available fromDryad (Additional References References e1ndashe44) doi105061dryad1c59zw3rv
Subspecialty Alerts by E-mail
Customize your online journal experience by signing up for e-mail alerts related to your subspecialty or area of interest Accessthis free service by clicking on the ldquoMy Alertsrdquo link on the home page An extensive list of subspecialties methods and studydesign choices will be available for you to choose frommdashallowing you priority alerts to cutting-edge research in your field
COVID-19 and Neurologic Disease Call for Papers
The editors of Neurology are interested in papers that address the neurological aspects of COVID-19infection and challenges to the management of patients with chronic neurological conditions whohave or are at risk for the infection Relevant papers that pass initial internal review will undergoexpedited peer review and online publication We will consider papers posted in preprint servers
Submit observational studies and clinical trials as Articles and case series and case reports underthe ClinicalScientific Notes category to httpssubmitneurologyorg today
Visit the Neurologyreg Website at NeurologyorgN More article-based content on home pages Streamlined menus and navigation Enhanced blog sections for specialty areas Same experience on desktop tablet and mobile devices Improved article reading experience links more evident (pdf analytics social media) Neurologyreg Clinical Practice initiative ldquoPractice Currentrdquo global surveys will be accessible across sites
Find Neurologyreg on Facebook httptinyurlcomneurologyfan
Follow Neurologyreg on Twitter httpstwittercomGreenJournal
NeurologyorgN Neurology | Volume 94 Number 17 | April 28 2020 755
DOI 101212WNL0000000000009323202094743-755 Published Online before print April 2 2020Neurology
Ian G McKeith Tanis J Ferman Alan J Thomas et al Research criteria for the diagnosis of prodromal dementia with Lewy bodies
This information is current as of April 2 2020
ServicesUpdated Information amp
httpnneurologyorgcontent9417743fullincluding high resolution figures can be found at
References httpnneurologyorgcontent9417743fullref-list-1
This article cites 59 articles 12 of which you can access for free at
Subspecialty Collections
httpnneurologyorgcgicollectionpsychosisPsychosis a
httpnneurologyorgcgicollectionparkinsons_disease_with_dementiParkinsons disease with dementia
httpnneurologyorgcgicollectionmci_mild_cognitive_impairmentMCI (mild cognitive impairment)
httpnneurologyorgcgicollectiondementia_with_lewy_bodiesDementia with Lewy bodies
httpnneurologyorgcgicollectiondeliriumDeliriumfollowing collection(s) This article along with others on similar topics appears in the
Permissions amp Licensing
httpwwwneurologyorgaboutabout_the_journalpermissionsits entirety can be found online atInformation about reproducing this article in parts (figurestables) or in
Reprints
httpnneurologyorgsubscribersadvertiseInformation about ordering reprints can be found online
ISSN 0028-3878 Online ISSN 1526-632XWolters Kluwer Health Inc on behalf of the American Academy of Neurology All rights reserved Print1951 it is now a weekly with 48 issues per year Copyright Copyright copy 2020 The Author(s) Published by
reg is the official journal of the American Academy of Neurology Published continuously sinceNeurology

Reliable identification of prodromal DLB would enable earlyintervention while pathologic burden is circumscribed andbefore clinical symptoms become debilitating It would assistclinicians to streamline care anticipate treatment optionsknown to be effective in DLBe2 and to avoid or minimizeiatrogenic adverse events with the goal of fewer office andemergency department visitse3 Importantly early diagnosiswould help patients and families to plan and to implementearly nonpharmacologic interventions (eg exercise andbehavioral strategies) It would also facilitate selection fortrials of targeted therapies as these become available
MethodsWe performed electronic searches of MEDLINE PubMedand EMBASE databases using the combination of a number ofmedical subject headings Emtree subject headings and free-text terms (ldquodementia with Lewy bodiesrdquo ldquoLewy body de-mentiardquo ldquoLewy body diseaserdquo ldquoprodromalrdquo ldquodeliriumrdquoldquopsychosisrdquo ldquomild cognitive impairmentrdquo ldquorapid eye move-ment sleep behavior disorderrdquo for clinical categories andldquoneuropsychological testrdquo ldquodopamine transporter imagingrdquoldquopositron emission tomographyrdquo ldquometa-iodobenzylguanidinemyocardial scintigraphyrdquo ldquonuclear magnetic resonance im-agingrdquo ldquoelectroencephalographyrdquo ldquocerebrospinal fluidrdquoldquorapid eye movement sleep without atoniardquo for biomarkers)All relevant articles were retrieved placing restrictions onfields (free-text terms searched exclusively in the title orabstract of the articles) and date (last 5 years) Except forbook chapters all publication types (original articlesreviews editorials and letters) were considered Because thefocus of this review was on prodromal DLB studies on thebroader less specific category of Lewy body disease (whichcomprises both DLB and PD) were also considered Wethen used Refworks to remove duplicates and share theresulting 3570 records among the lead authors Of all full-text articles assessed for eligibility after the abstract screen-ing phase those eventually included either as listed or ase-references were selected based on their relevance (dataavailable from Dryad e-references doi105061dryad1c59zw3rv) Seminal papers on the topic were included re-gardless of publication date The preliminary findings andrecommendations were presented for discussion and feed-back at a session of the International Lewy Body DementiaConference in Las Vegas NV USA in June 2019 followingwhich further revision and review took place
How does prodromal DLB usually presentOne or more of the core clinical features characteristic of fullydeveloped DLB may develop before dementia and are usuallyaccompanied by mild cognitive complaints5 Spontaneousparkinsonism often develops within the predementia stagebut is not present in all patients36 RBD is a parasomnia thattypically occurs years and even decades before the onset ofdementia or parkinsonism and may presage any of theα-synucleinopathies47e4 In patients with mild cognitive def-icits who later develop dementia both parkinsonism and RBDstrongly predict a later transition to DLB rather than to AD orother dementia types68 Delirium can occur during the pre-dementia stage of DLB9 as can fluctuations of cognition andarousal3 that may give rise to a diagnosis of delirium Visualhallucinations (VHs) either spontaneous or provoked by ill-ness or medication are more likely to occur compared withnormal controls or prodromal AD1011 There are also casereports of delusions hallucinations depression and anxiety aspresenting features of DLB12 Based on such observations 3prototypic prodromal DLB syndromes have been proposed13
as (1) mild cognitive impairment (MCI) (2) delirium-onsetor (3) psychiatric-onset
MCI with Lewy bodiesThe National Institute on Aging and Alzheimerrsquos Associationcriteria for MCI14 e5 provide a standardized approach to di-agnosis and form the basis for our proposed MCI with Lewybody (MCI-LB) criteria They require a cognitive complaint fromthe patient or from an informant or clinician who knows themand has observed a decline Also required are deficits in one ormore cognitive domains that are greater than would be expectedfrom normal aging do not represent lifelong patterns of lowercognitive function and are not associated with acute medical orneurologic insults Although people with MCI may be less effi-cient or less capable at performing tasks they have performedpreviously their cognitive deficits should not be sufficient tointerfere with their typical daily functioning In other words thereshould be an overall preservation of their prior level of in-dependence with minimal interference in day-to-day functionalabilities which by definition does not constitute a dementia
Objective cognitive impairment is optimally based on stan-dardized assessment with scores on neuropsychologicalmeasures that are typically 1 to 1middot5 SDs below the mean fortheir age and education matched peers on culturally appro-priate normative data (ie for the impaired domain(s) whenavailable) It is emphasized that these ranges are guidelines
GlossaryAD = Alzheimer disease DAT = dopamine transporter DLB = dementia with Lewy bodies FTD = frontotemporal dementiaMCI = mild cognitive impairment MCI-LB = MCI with Lewy bodies MIBG = meta-iodobenzylguanidine MSA = multiplesystem atrophy NCD = neurocognitive disorder PD = Parkinson disease PSG = polysomnography QEEEG = QuantitativeEEG RBD = REM sleep behavior disorder RSWA = REM sleep without atonia VH = visual hallucination VRH = ventilatoryresponse to hypercapnia
744 Neurology | Volume 94 Number 17 | April 28 2020 NeurologyorgN
and not cutoff scores14 Impairment on neuropsychologicaltests may also be demonstrated by significant decline dem-onstrated on serial testing or significant decline from esti-mated premorbid abilitiese5 Cognitive impairment mayadditionally be categorized as single or multiple domain andas amnestic or nonamnestic which may help to classify po-tential subgroups as they relate (1) to biomarkers and path-ologic correlates and (2) to differences in the rate of declineand progression to dementia each of which may be importantin the conduct of clinical trials A further refinement to de-scribe the cognitive profile of MCI-LB may be provided byusing the MDS level II criteria for PD-MCI15e6e7
The cognitive presentation of MCI-LBThe cognitive pattern ofMCI-LB is similar toDLB and typicallyincludes disproportionate attentionexecutive and visual pro-cessing deficits and relatively preserved memory and objectnaming16e8e9 Impairment on tasks of attention processingspeed and verbal fluency typically constitute the attentionexecutive deficits and tasks of visual discrimination assemblyand figure drawing typically constitute the visual perceptual andspatial deficits5617ndash19
Diagnostic criteria for DLB emphasize that prominent or per-sistent memory impairment may not necessarily occur in theearly stages2 but patients and carers frequently offer memorycomplaints as a presenting symptom20Of 49 patients withMCIwho progressed to DLB 27 had multidomain amnestic MCIbut only 6 had single-domain amnestic MCI3 similar to otherreports1921 When patients with MCI-LB have memory im-pairment attention andor visual processing deficits also tend tobe present3 and may precede the memory difficulties Patientswith RBD who later developed DLB had attentionexecutivedeficits up to 6 years before the diagnosis of dementia andmemory deficits up to 2 years before the diagnosis22 The basisfor verbal memory impairment in DLB or MCI-LB may berelated to slowed processing speed and deficits in workingmemory and retrieval that characterize the attention and exec-utive deficitse10 consistent with hippocampal preservation inMCI-LB compared with MCI-AD23e11 However impairedmemory in DLB may also be related to the extent of coexistingAD-related pathologye9 characterized by greater hippocampalatrophy on imaging e12 and greater CA1 hippocampal subfieldpathology on autopsye13 Similar to other subtypes of MCIa proportion of patients may revert to being cognitively normalalthough they remain at a greater risk of the eventual de-velopment of dementiae14 Some instability of an MCI-LB di-agnosis is to be expected given inherent fluctuating cognitionworsening with neuroleptics or anticholinergics or improve-ment with levodopa-carbidopa or cholinesterase inhibitors
In summary the performance pattern of MCI-LB is bestcharacterized as single- or multidomain nonamnestic MCI oras multidomain amnestic MCI whereas single-domainamnestic MCI is more likely to represent MCI-AD TheMCI-LB cognitive pattern is often seen in patients with 1 ormore core DLB features5 although these may develop
later318 Nonamnestic MCI seldom develops into AD but isassociated with a greater risk of transition to DLB1021 witha ten-fold risk compared with amnestic MCI3 Becausea substantial subset of patients with DLB have coexisting AD-related pathology that may influence their cognitive profileMCI-LB still should be considered an important part of thedifferential diagnosis in amnestic subjects
Operationalization of MCI-LBThe scheme suggested in table 1 for the identification ofMCI-LBallows a diagnosis of either possible or probable MCI-LB basedon the number of qualifying clinical features or biomarkers Theterms possible and probable refer to the likelihood of underlyingLB disease and not to the MCI syndrome Structured diagnosticinstruments may assist identification of the core clinical featuresof DLB that precede coincide with or follow the onset of cog-nitive difficulties24ndash26 Cognitive fluctuations may be of lesseramplitude or frequency than in more severe disease Passage andsense of presence hallucinatory phenomena may precede thedevelopment of recurrent well-formed and detailed VH Clinicalfeatures supportive of DLBmay occur secondary to other causesreducing their diagnostic specificity but they can be usefulindicators of underlying LBdisease particularly when they persistover time or occur in combination
Use of the possible MCI-LB category may raise diagnosticsuspicion prompting further clinical and biomarker in-vestigation Some possible MCI-LB combinations will likelyprove better predictors than others for example multidomainnonamnestic MCI plus clinically well-defined RBD is antici-pated to be more predictive of progression to DLB thansingle-domain amnestic MCI plus a history of cognitivefluctuation The utility of different combinations of clinicalfeatures and biomarkers remains to be established
MCI-LB and PD-MCIUncertainty may occur in deciding how patients exhibitingboth MCI and parkinsonism are best categorized PD-MCIwill usually be the most appropriate diagnosis when PD isdiagnosed before significant cognitive decline occurs Theadoption of a 1-year rule similar to that used to separate DLBand PD dementia may be helpful to distinguish someMCI-LBand PD-MCI cases if the onset and order of mild symptoms ofparkinsonism and cognitive decline can be clearly establishedIf not an initial diagnosis of prodromal LB disease may bepreferable recognizing that this will require revision as the fullclinical picture evolves Individuals with poor global cognitivetest performance identified in community samples have beenreported to be at a greater risk of developing PD over sub-sequent yearse15e16 but poor cognitive test scores are notequivalent to MCI and this increased risk was no longerstatistically significant when individuals with subtle motorsigns at baseline were excludede15 There are data to suggestthat patients with MCI-LB may have greater cognitive im-pairment than those with PD-MCI27 but this is not easilyoperationalized to differentiate individual subjects The cog-nitive deficits of PD-MCI can be heterogeneouse17 with
NeurologyorgN Neurology | Volume 94 Number 17 | April 28 2020 745
disproportionately affected attentionexecutive function22
visuospatial skillse18 and memory28 Similar toMCI-LB thereis evidence that nonamnestic MCI is more common thanamnestic MCI and that multidomain amnestic MCI is morecommon than single-domain amnestic MCI29
Biomarkers for prodromal DLBDirect measures of α-synuclein pathology would offer de-finitive diagnosis at an early stage several are under de-velopment but none is yet validated or available for useantemortem Surrogate biomarkers of LB disease must
Table 1 Research criteria for the clinical diagnosis of probable and possible MCI-LB
Essential for a diagnosis of MCI-LB is MCI defined by the presence of each of the following
Concern by the patient informant or clinician regarding cognitive decline
Objective evidence of impairment in 1 or more cognitive domains The cognitive impairment may include any domain but is more likely to be associatedwith attention-executive andor visual processing deficits
Preserved or minimally affected performance of previously attained independence in functional abilities which do not meet the criteria for dementia
Core clinical features
Fluctuating cognition with variations in attention and alertness
Recurrent visual hallucinations
RBD
One or more spontaneous cardinal features of parkinsonism these are bradykinesia (defined as slowness of movement and decrement in amplitude orspeed) rest tremor or rigidity
Proposed biomarkers
Reduced dopamine transporter uptake in basal ganglia demonstrated by SPECT or PET
Polysomnographic confirmation of REM sleep without atonia
Reduced meta-iodobenzylguanidine (MIBG) uptake on myocardial scintigraphy
Probable MCI-LB can be diagnosed if
Two or more core clinical features of DLB are present with or without the presence of a proposed biomarker or
Only 1 core clinical feature is present but with 1 or more proposed biomarkers
Probable MCI-LB should not be diagnosed based on biomarkers alone
Possible MCI-LB can be diagnosed if
Only 1 core clinical feature of DLB is present with no proposed biomarkers or
One or more of the proposed biomarkers is present but there are no core clinical features
Supportive clinical features
Severe sensitivity to antipsychotic agents postural instability repeated falls syncope or other transient episodes of unresponsiveness prolonged orrecurrent delirium autonomic dysfunction eg constipation orthostatic hypotension urinary incontinence hypersomnia hyposmia hallucinations inother modalities including passage and sense of presence phenomena systematized delusions apathy anxiety and depression
Potential biomarkers of MCI-LB
Quantitative EEG showing slowing and dominant frequency variability
Relative preservation of medial temporal lobe structures on structural imaging
Insular thinning and gray matter volume loss on MRI
Low occipital uptake on perfusionmetabolism scan
MCI plus supportive clinical features or potential biomarkers are insufficient to diagnose MCI-LB but may raise suspicion of it and prompt biomarkerinvestigation and may add weight to an existing MCI-LB diagnosis
MCI-LB is less likely in the presence of any other physical illness or brain disease including cerebrovascular disease sufficient to account in part or in total forthe clinical picture although these do not exclude anMCI-LB diagnosis andmay serve to indicatemixed ormultiple pathologies contributing to the clinicalpresentation
Abbreviations DLB = dementia with Lewy bodies MCI = mild cognitive impairment MCI-LB = MCI with Lewy bodiesThese should be used in conjunction with the corresponding article text which gives further information about core and supportive clinical features and theuse of biomarkers as they apply to MCI-LB
746 Neurology | Volume 94 Number 17 | April 28 2020 NeurologyorgN
therefore be used as is the case for the diagnosis of DLBitself2 We propose biomarkers for the diagnosis of prodromalDLB where there is either sufficient good quality publishedevidence of adequate diagnostic specificity in prodromal DLBor this can be reasonably extrapolated from fully developedDLB or related disorders We categorize biomarkers for whichonly limited data are available as potential biomarkers rec-ognizing that such distinctions are likely to require revision asnew data become available
Proposed biomarkers
Reduced dopamine transporter (DAT) uptake in basalganglia demonstrated by SPECT or PETThe utility of DAT imaging in discriminating DLB from ADis already well established2 and its sensitivity in dis-tinguishing MCI with LB (MCI-LB) fromMCI with AD was54 and specificity 8930 whenMCI-LB was defined by thepresence of 1 core clinical feature of DLB in patients withMCI A higher sensitivity of 61 was achieved when 2 coreclinical symptoms were present30 Reduced striatal DATuptake therefore seems suggestive of prodromal DLB ina person with MCI but normal striatal DAT uptake does notexclude it
Polysomnographic confirmation of REM sleep withoutatoniaThe association between RBD and synucleinopathy is highlyspecific (eg a multicenter autopsy study found that of 80subjects with polysomnography [PSG]-confirmed RBD anda coexisting neurodegenerative disorder only 2 had a diseaseunrelated to α-synuclein deposition)e4 These data imply thata patient presenting with MCI and having PSG-confirmedRBD that is a history of probable RBD plus clear docu-mentation of REM sleep without atonia (RSWA) on PSGalso has a high probability of an underlying prodromal syn-ucleinopathy Because around a quarter of patients with DLBdo not report symptoms of RBD andor have normal REMsleep atonia on PSG a normal PSG does not exclude a pro-dromal DLB diagnosis31
Reduced meta-iodobenzylguanidine uptake onmyocardial scintigraphyReduced meta-iodobenzylguanidine (MIBG) uptake is anindicative biomarker for DLB2 and has also been reported tooccur in a small series of patients with late-onset psychiatricdisorder and PSG-confirmed RBD32 reinforcing its associa-tion with underlying α-synucleinopathy Of 2 patients withamnestic MCI with low MIBG uptake one developed DLBafter 2 years the other had no clinical follow-up reportede19
VHs andor RBD were reported among 7 of 13 patients withMCI with reduced MIBG uptake the majority of whom alsohad autonomic symptoms suggestive of LB disease but theywere not followed to determine conversion to DLBe20 De-spite a paucity of longitudinal datae21 there seems to be suf-ficient evidence that abnormal MIBGmyocardial scintigraphyin a patient with MCI supports a prodromal DLB diagnosisbut further studies are required
Potential biomarkersThese are biomarkers consistent with underlying LB diseasewhich may help the diagnostic evaluation but for which thereis still insufficient evidence of diagnostic sensitivity andspecificity in early disease This will change as new evidenceemerges at which point these or other candidates may be-come considered as indicative of prodromal DLB
Quantitative EEG showing slowing and dominantfrequency variabilityEEG slowing has been reported as predictive of dementia inboth PDe22 and RBDe23 posterior slow wave activity withperiodic fluctuations in the pre-alpha range being supportiveof DLB2 Quantitative EEG (QEEG) methods show thata dominant frequency lt8 Hz and dominant frequency vari-ability gt1middot5 Hz is typical of DLB and in a 3-year follow-upstudy 83 of subjects with MCI with this pattern at pre-sentation converted to DLB If these findings are replicatedQEEG may represent a powerful predictor of progressionfrom MCI to DLB33
Relative preservation of medial temporal lobestructures on structural imagingAbsent or minimal medial temporal lobe atrophy is consistentwith DLB but not sufficiently specific to differentiate it fromAD2 Lewy body disease with RBD is characterized by pre-served hippocampal volumes34 and hippocampal preserva-tion in patients with MCI supports progression to DLBinstead of AD dementia with a sensitivity of 85 and a spec-ificity of 6123 Suboptimal specificity may be due to thevariability of hippocampal atrophy in AD35 and contributionof other pathologic processes such as TAR DNA bindingprotein 43 (TDP43)e24
Insular thinning and gray matter volume lossInsular cortical thinning occurs in prodromal DLB relative tohealthy controls using MRI T1 sequences with gray matteratrophy predominantly affecting the anterior cingulum andmedial frontal structures This contrasts with more extensiveloss of gray matter in the temporal frontal and parietalregions of subjects with prodromal AD Insular corticalthinning may therefore differentiate patients with prodromalDLB not only from healthy controls but also from theirprodromal AD counterparts36 No group differences in insularvolumes are seen between DLB and AD at the dementia stageso longitudinal studies are required to determine its precisevalue as an early diagnostic marker of DLB37 Insula is alsoinvolved early in frontotemporal dementia (FTD) being thefirst cortical area to show atrophy in presymptomatic GRNMAPT or C9ORF72 mutation carrierse25 and unlikelytherefore to be helpful in differentiating DLB from FTD
Low occipital uptake on perfusionmetabolism scanOccipital hypometabolism on FDG-PET is associated withDLB38 and together with relative preservation of posteriorcingulate metabolism (the cingulate island sign)e26 is a sup-portive biomarker of DLB2 How frequently the cingulate
NeurologyorgN Neurology | Volume 94 Number 17 | April 28 2020 747
island sign is seen in prodromal DLB remains to be estab-lished significantly reduced posterior cingulate metabolismmay be a useful indication of the concurrence of additionalneurofibrillary tangle pathologye27
Other biomarkersThere is currently no α-synuclein radioligand with sufficientevidence supporting its utility for imaging DLB or any otherα-synucleinopathy nor have any diagnostically applicablebiofluid peripheral tissue or genotypic biomarkers beenestablished2 CSF measures cannot reliably discriminate be-tween DLB and AD39 although the measurement of CSFα-synuclein aggregates using seeding aggregation assays suchas protein misfolding cyclic amplification and real-timequaking-induced conversion is providing encouraging pre-liminary results and may be extended to more accessiblebiofluids including saliva plasma serum or urinee28 Com-bining CSF markers may be useful for example addition ofCSF phospho-tau to α-synuclein significantly improved thedifferential diagnosis between MCI-LB and MCI-AD in-creasing sensitivity and specificity both gt than 95e29 Otherdirect or indirect biomarker candidates that may occur earlyinclude identification of phosphorylated α-synuclein depositsin peripheral nervous tissue from skin biopsy40 gait ana-lysise30 and abnormalities in color vision discrimination4142
The figure shows a framework for considering a wider range ofbiomarkers in the setting of prodromal DLB determining theextent to which AD-related pathology is contributing to thedementia syndrome and influencing clinical trajectories inthese patients4344e31e32 Aβ42 declines earlier in AD thanDLB whereas Aβ40 levels increase alone in AD A low
Aβ42Aβ40 ratio may therefore differentiate patients withprodromal AD from patients with prodromal DLB better thanindividual measures43 There is also evidence showing dif-ferent frequencies and topographies of abnormal uptake onamyloid and tau PET imaging in DLB vs AD45
Delirium-onset DLBCognitive fluctuations or pronounced variations in alertnessand arousal are a core feature of DLB apparent as markedfluctuations in cognitive ability or function detectable byobservation or informant report and measurable using sen-sitive cognitive and electrophysiologic measurese33 The oc-currence of delirium (sometimes referred to as acuteconfusional state) as an early presenting feature of DLB hasbeen described in numerous case reports and seriese34 in-cluding in those with no apparent previous history of cogni-tive impairment46e35 Whether this represents a greatervulnerability to delirium in subjects with DLB or the mis-diagnosis of severe fluctuations with clouding of conscious-ness as delirium or a combination of both is unclear
Recognition that DLB may first present as delirium is im-portant because most guidelines for behavioral disturbancesin delirium recommend antipsychotics as first-line pharma-cologic treatment Delirium or marked fluctuations in con-sciousness were reported by 43 of caregivers before DLBdiagnosis47 and previous episodes of delirium were muchmore frequent in patients with DLB compared with patientswith AD (25 vs 7) with 1 in 4 of those with DLB havingrepeated delirium11 In the majority of these potential pro-voking causes were present A similarly higher incidence ofdelirium was found for subjects with DLB compared with
Figure Multimodal biomarkers for prodromal DLB
Reduced dopamine transporter uptake in basal gan-glia demonstrated by SPECT or PET PSG-confirmedREM sleep without atonia and MIBG myocardial scin-tigraphy are proposed as biomarkers of prodromalDLB Multimodality biomarkers are also important incharacterizing patients with prodromal DLB in whomthe pathologic mechanisms of cognitive impairmentinclude both LB and AD pathologies and who mayhave abnormalities associated with both Medialtemporal lobe uptake on tau PET medial temporallobe atrophy on MRI and high levels of uptake onamyloid PET and positive CSF biomarkers of AD-re-lated pathology may characterize patients with pro-dromal DLB with significant AD pathology It isexpected that biomarker abnormalities detected inthe earliest stages will remain abnormal as diseaseprogresses with additional biomarkers showingchanges later during the progression from pro-dromal to dementia phase DLB DLB = dementia withLewy bodies MIBG = meta-iodobenzylguanidine
748 Neurology | Volume 94 Number 17 | April 28 2020 NeurologyorgN
subjects with AD in the year before diagnosis (17middot6 v 3middot2100person-years)9 and admissions for delirium were morecommon in those already diagnosed with DLB than for otherdementias Prolonged delirium may also raise the index ofsuspicion for DLBe36 In an FDG-PET imaging study ofprolonged delirium 32 of subjects were found to havea DLB like pattern a high proportion in regard both to theknown prevalence of the disease and to that of their matchedcognitively impaired control group (4)e37
The similarities between the marked fluctuations in DLB anddisturbances of attention and consciousness in delirium havebeen noted and reviewed46 but there is as yet little un-derstanding of a shared neurobiological basis There havebeen few pathologic studies and although in anepidemiologic-based autopsy cohort there was no link be-tween delirium and LB pathology at autopsye38 a significantlyincreased risk of postoperative delirium in those with pe-ripheral α-synuclein pathology has been described48 Deliriumhas been suggested to bemore common in those subjects withDLB with later age at onsete39 but further evidence is needed
In summary (table 2) it is clear that DLB can present withdelirium and in patients diagnosed with delirium a carefulsearch for other DLB features should be made with a lowthreshold for undertaking DLB biomarker examinations es-pecially in those with recurrent unexplained or prolongeddelirium The extent to which delirium presentations of DLBhave the biomarker abnormalities associated with establishedDLB or other prodromal DLB presentations is unclear
although the PET imaging study cited above supports thise37
as does a report of reduced DAT uptake in a patient withacute unexplained delirium49 The link between delirium andDLB is an important area for future research to clarify therelationship between the 2 and to establish which factorsassociated with delirium should raise the index of suspicionfor underlying prodromal DLB
Psychiatric-onset DLBEarly clinicopathologic studies suggested that DLB maypresent as a primary psychiatric disorder5051 but subsequentfocus on the cognitive and motor aspects of DLB has limitedthe documentation of such cases outside of a fewcenters123252ndash54e36 Late-onset major depressive disorderand late-onset psychosis are the most frequently reportedpresentations differing markedly from the construct of mildbehavioral impairmente40 and sometimes sufficiently severe torequire hospitalization Symptoms include hallucinations invisual and in other modalities and systematized delusionsincluding Capgras syndrome55 apathy anxiety and de-pression Psychiatric-onset DLB cases are not easily differ-entiated from non-LB late-onset psychosis cases on the basisof primary psychiatric phenomenology or neuropsychologicalprofile alone54 Psychomotor retardation such as slowedspeech thinking and body movements can resemble thebradykinesia of parkinsonism The occurrence of rest tremoror rigidity is more helpful than bradykinesia to suspect pro-dromal DLB in patients with depressive disorder53 butpsychotropic-induced parkinsonism may complicate di-agnosis Atypical clinical features may prove valuable pointers
Table 2 Summary of key features of delirium-onset DLB
Patients with DLB are more susceptible to delirium than people with Alzheimer disease and this delirium may occur as their presenting complaint beforedementia develops
Such episodes may be provoked by multiple factors including surgery infectionssepsis fever or other systemic illness or secondary to use or suddenwithdrawal of alcohol or psychoactive drugs
Prodromal DLB should be particularly suspected in patients
bull in whom adequate provoking factors for the delirium are not found
bull with prolonged or recurrent delirium
bull who later develop progressive cognitive decline or subsequent dementia
Core clinical features of DLB are likely to be of more limited diagnostic weight in a patient with delirium because
bull cognitive fluctuation and clouding of consciousness can also occur in non-DLB delirium ie are not diagnostically specific for DLB in this situation
bull visual hallucinations may occur in non-DLB delirium particularly drug-induced or provoked by alcohol abstinence
bull motor parkinsonism present may be due to antipsychotic medications used to treat delirium
bull the diagnostic significance of a history of RBD in a person with delirium is not yet established
Identification of delirium-onset DLB
bull may be assisted by use of MCI-LB biomarkers but further research evidence of this is required
bull is important to inform the management plan including the avoidance or minimization of antipsychotic and anticholinergic agents
Abbreviations DLB = dementia with Lewy bodies MCI = mild cognitive impairment MCI-LB = MCI with Lewy bodies RBD = REM sleep behavior disorder
NeurologyorgN Neurology | Volume 94 Number 17 | April 28 2020 749
to underlying LB pathology particularly the presence of re-current VH12 when these occur before cognitive impairmentbecomes evident As with all α-synucleinopathies RBD maybe a useful indicator although a relationship between anti-depressant usage and subsequent RBD onset is a potentialconfoundere41 Although the primary psychiatric manifes-tations are often accompanied by mild cognitive deficits54
cognitive evaluation and interpretation of performance can bedifficult when psychiatric symptoms are prominent The fre-quency of cognitive fluctuations in psychiatric-onset LB caseshas not been determined
Initial reports suggest that 123I-MIBG scintigraphy may behelpful in psychiatric-onset DLB525356 Eighteen of 35patients with a first onset of major depressive disorder gt50years and with bradykinesia developed a clinical diagnosis ofDLB after 6 years of follow-up All 18 had an abnormal ven-tilatory response to hypercapnia (VRH) indicative of severeautonomic dysfunction whereas none of the 17 patients witha normal VRH converted to DLB within the study period Forthe converters the most common presentation was withpsychotic and melancholic features simultaneously The fre-quency of hypersensitivity to antipsychotics antidepressantsand antianxiety drugs was higher in converters than in non-converters53 Further studies need to confirm these findingsand to determine the value of other DLB biomarkers inpsychiatric-onset cases325256
In summary it is not yet clear how to identify patients withprominent late-onset psychiatric symptoms who may haveunderlying LB disease and subsequently progress to DLB It is
premature to try to construct formal criteria for psychiatric-onset DLB but clinicians in mental health and other settingsneed to be aware that this possibility exists not least becauseof the risk of severe antipsychotic sensitivity reactions withincreased morbidity and mortality The small available liter-ature including reports such as those cited above does providesome useful guidance summarized in table 3 but requiresreplication and further investigation
Idiopathic REM sleep behavior disorderRBD is characterized by abnormal dream enactment behaviorduring REM sleep accompanied by loss of muscle atonia duringREM sleep (REM sleep without atonia or RSWA) on PSG Forthe purpose of a prodromal DLB diagnosis a clinical history ofRBD is obtained in the same way as for DLB2 that is a clearcomplaint of dream enactment by a bedpartner or other witnesswith no evidence of sleep disorders that may mimic RBD onclinical interview Conditions known to mimic or masquerade asRBD include non-REM parasomnias (sleep walking sleep talk-ing or other behaviors that emerge fromnon-REM sleep stages)obstructive sleep apnea confusional arousals or nocturnal seiz-ures In the absence of PSG the risk of a false-positive clinicaldiagnosis of RBD is reduced by using optimized sleep ques-tionnaires which can have sensitivity and specificity over 90e42
RBDmay be considered as idiopathic until it is associated withanother ongoing neurologic condition the most frequentbeing an α-synucleinopathy (PD DLB or MSA) In a recentlarge study 735 of patients with RBD converted to an overtneurodegenerative syndrome after 12-year follow-up 565developing parkinsonism and 435 dementia as their first
Table 3 Summary of key features of psychiatric-onset DLB
Is characterized by predominant psychiatric symptoms that typically correspond to late-onset major depressive disorder or late-onset psychosis which mayfeature hallucinations in visual and in other modalities and systematized delusions including Capgras syndrome
bull may also present with apathy anxiety and depression
bull may be sufficiently severe to require hospitalization
bull the frequency of LB disease as a cause of late-onset psychiatric disorder is not known
When assessing for core clinical features of DLB in a patient with a primary psychiatric presentation
bull bradykinesia may be mimicked by psychomotor retardation which is commonly seen in depressive disorders
bull parkinsonism may be induced by antipsychotic medications used to treat psychiatric disorder
bull RBD (and REM sleep without atonia) may be induced by antidepressant medications
bull mild cognitive disturbance may be present but is not predominant and may fluctuate
bull formal neuropsychological testing may be confounded by the psychiatric mental state
bull the frequency and character of cognitive fluctuations is unknown
Identification of psychiatric-onset DLB
bull may be assisted by use of MCI-LB biomarkers but further research evidence of this is required
bull is important to inform the management plan including the avoidance or minimization of antipsychotic and anticholinergic agents
Abbreviations DLB = dementia with Lewy bodies MCI = mild cognitive impairment
750 Neurology | Volume 94 Number 17 | April 28 2020 NeurologyorgN
disease manifestation Among many predictive markerstested only the cognitive variables differed at baseline be-tween those converting to primary dementia vs parkinson-ism7 Other multicenter studies confirm that the only clinicalfeature that predicts dementia vs parkinsonism first is neu-ropsychological performance those with RBD who exhibitcognitive changes are more likely to evolve first into MCI orDLB22e4 Thus although RBD may be regarded an earlymanifestation of α-synucleinopathy it is not possible to clearlydistinguish whether an individual presenting with RBD willdevelop dementia first that is evolve into a primary DLBdiagnosis or parkinsonism first that is a primary PDMSAdiagnosis Any MCI subtype associated with PSG-confirmedRBD is highly likely to represent underlying LB disease Al-though idiopathic RBD is a useful model to study the earlystages of LB disease progression it is not necessarily repre-sentative of the whole spectrum of patients with PD and DLBa significant minority of whom do not have RBD42
Autonomic dysfunctionanosmia and othernonspecific prodromal LB disease symptomsPatients with DLB frequently report a history of autonomicdysfunction at first clinic attendance with 25ndash50 com-plaining of one of more among constipation orthostatic diz-ziness urinary incontinence erectile dysfunction increasedsweating or increased saliva5657 In a cohort of patients withpure autonomic failure 34 converted to an overt α-synu-cleinopathy over 6 years of follow-up this was to DLB (52)PD (24) orMSA (24)58 However because there are manyother causes for autonomic dysfunction in older people thesesymptoms either alone or in combination have low positivepredictive value59 The situation is similar for hyposmia whichalso frequently occurs early in prodromal DLB and PD42 butwhich can have many other causes in this age group
Conclusions and future directionDiagnosis of DLB at the dementia stage depends on identifyingfully expressed core clinical features which may be mild orabsent at the prodromal stage when biomarker evidence mayalso be weaker and may even differ from that found at thedementia stage Several new biomarker candidates direct andindirect are in development and we will continue to reviewthese to update our recommendations as soon as sufficientevidence accumulates We recognize that the clinical pheno-type of neurodegenerative disorders reflects interaction be-tween several rather than a single brain pathology and it istherefore likely that multiple biomarkers of individual pathol-ogies (eg α-synuclein β-amyloid and tau) or of disease sur-rogates (eg metabolic imagingEEG) will be required
Although we have described the 3 prodromal DLB syndromesseparately they are unlikely to be mutually exclusive andthere may be substantial overlap We propose operationalizedcriteria only for MCI-LB because the evidence base from oursystematic review albeit relatively limited is sufficient to
support recommendations that are immediately applicableand testable Our recommendations should be used alongsideguidance about the prodromal manifestations of PD1559
MSA60 and AD14 with which there is overlap Notwith-standing the potential benefits of early diagnosis we are alsomindful of the importance of avoiding incorrect (false-positive) diagnosis of prodromal DLB and the potentialnegative consequences this could have for an individual Wesuggest that the predictive validity of different categories andcombinations of our proposed criteria should be clarified byprospective studies before they are adopted for widespreadclinical use and that they will enable standardization for in-clusion in research studies and clinical trials
Some published guidance about the early clinical diagnosis ofDLB does already exist DSM5 recommends a diagnosis ofmild neurocognitive disorder (NCD) with LB ldquofor individualswho present with the core or suggestive features at a stagewhen cognitive or functional impairments are not of sufficientseverity to fulfill criteria for major NCDrdquoe43 This is basedhowever on the 2005 version of DLB guidelines and requiresupdating ICD-11 takes a similar approach toward diagnosingmild NCD at a syndromic level and lists both Lewy bodydisease and PD as possible causese44
The diagnostic position for other prodromal manifestations ofDLB that is delirium-onset and psychiatric-onset is less clearthan for MCI Operationalization of specific criteria for thesesyndromes is not yet justified and the reliable differentiationof the minority of delirious and psychiatrically ill patients whohave underlying LB pathology from the majority who do notwill probably only be achieved when routinely applicablebiomarkers are developed LB disease is seldom if ever cur-rently considered as part of the differential diagnosis of de-lirium or late-onset psychiatric disorder and we hope that theinformation we provide in the text and accompanying boxeswill raise cliniciansrsquo awareness of that possibility
Study fundingNo targeted funding reported
DisclosureI McKeith receives support from the NIHR Biomedical Re-search Centre awarded to the Newcastle upon Tyne HospitalsNHS Foundation Trust and Newcastle University and hasconsulted for GE Healthcare Sanofi Eisai Sumitomo Dai-nippon Pharma and Axovant T Ferman receives support fromNIH P50-AG16574 P30-AG062677 U01-NS100620 and theMangurian Foundation for Lewy body disease research AThomas receives support from the NIHR Biomedical ResearchCentre awarded to the Newcastle upon Tyne Hospitals NHSFoundation Trust and Newcastle University and has receivedgrants from GE Healthcare F Blanc has served as nationalclinical trial coordinator for Eisai and Axovant B Boevereceives support from NIH P50-AG16574 P30-AG062677U01-NS100620 and the Mangurian Foundation for Lewybody disease research has consulted for the Scientific Advisory
NeurologyorgN Neurology | Volume 94 Number 17 | April 28 2020 751
BoardmdashTau Consortium and received grants from Biogenthe NIH theMangurian Foundation Alector the Little FamilyFoundation and the Turner Family H Fujishiro has receivedsupport from Fujifilm RI Pharma Co Ltd K Kantarci receivessupport from NIH P50-AG16574 P30-AG062677 U01-NS100620 and the Mangurian Foundation for Lewy bodydisease research and has received grants from Avid Radio-pharmaceuticals and acted on a Data Safety Monitoring Boardfor Takeda Global Research C Muscio acknowledges thesupport of the Italian Ministry of Health GRANT NET-2011-02346784 J OrsquoBrien is supported by the NIHR CambridgeBiomedical Research Centre Dementia and Neuro-degeneration and Mental Health Themes and the CambridgeCentre for Parkinsonrsquos Plus Disorders has consulted forTauRx Axon GE Healthcare Eisai and AvidLilly and re-ceived grants fromAvidLilly andAllianceMedical R Postumahas received grants from and consulted for Fonds de laRecherche en Sante received grants from the Canadian Insti-tutes of Health Research the Parkinson Society of Canada theWeston-Garfield Foundation The Michael J Fox Foundationand the Webster Foundation and consulted for TakedaRocheProthena Teva Neurosciences Novartis Canada Bio-gen Boehringer Ingelheim Theranexus GE Healthcare JazzPharmaceuticals AbbVie Jannsen Otsuko PhytopharmicsInception Sciences and Parkinson Canada D Aarsland isa Royal Society Wolfson Research Merit Award Holder andwould like to thank the Wolfson Foundation and the RoyalSociety for their support He has received research supportandor honoraria from AstraZeneca H Lundbeck NovartisPharmaceuticals and GE Health and served as paid consultantfor H Lundbeck Eisai Heptares Sanofi and Mentis Cura CBallard reports unrelated current grant funding from MRCWellcome Trust European Union Gillings FoundationNIHR Alzheimerrsquos Society Alzheimerrsquos Research UK Par-kinsonrsquos Society and Lewy Body Society during the conduct ofthe study and personal fees from Acadia pharmaceutical com-pany Lundbeck Roche Otsuka Eli Lilly and AARP outsidethe submitted work L Bonanni is a member of the steeringcommittee of the E-DLB consortium and program chair of theLBD-PIA (ISTAART) and is funded for research on DLB bythe Italian Ministry of Health P Donaghy receives supportfrom the NIHR Biomedical Research Centre awarded to theNewcastle upon Tyne Hospitals NHS Foundation Trust andNewcastle UniversityM Emre served on the scientific advisoryboard for AC Immune J Galvin receives support from NIHgrants (R01 AG040211 R01 NS101482 R01 AG057681 andU01 NS100610) and the Lewy Body Dementia AssociationResearch Center of Excellence reports research support fromthe NIH the Lewy Body Dementia Association The Harry TMangurian Foundation and Albert Charitable Trust directsclinical trials for Biogen and Novartis receives licensing feesfrom Biogen Roche Eli Lilly Quintiles Roobrik ContinuumClinical and Langland and receives consulting fees fromBiogen Eisai Bracket and Medavante D Galasko receivessupport from NIA grant AGO5131 and the Michael J FoxFoundation and has acted as consultant for vTv Pharmaceut-icals Inc Esai Inc and for Fujirebio Inc been a member of
a DSMB for Probiodrug and paid editor for Alzheimerrsquos Re-search amp Therapy J Goldman receives grantsupport fromTheMichael J Fox Foundation and Parkinsonrsquos Foundation andhas received consulting feeshonoraria from Acadia AptinyxSunovion and Worldwide Med S Gomperts receives supportfrom NIH grants R01 AG054551 P30AG062421 R01AG062208 P50 AG005134 R21 NS109833 DODCDMRPW81XW1810516 the Farmer Family ParkinsonrsquosInitiative and the Lewy Body Dementia Association and hasserved on advisory boards for Acadia Pharmaceuticals andSanofi L Honig acknowledges research grant support fromNYS CEAD grant C031425 LBDA RCOE and NIHgrants U01NS100600 P50AG008702 R21AG058020R21MH111596 U01AG051412 U01AG045390U01AG016976 U01AG023749 U19063893 andU19AG024904 He receives research funding support fromAbbVie Alector Biogen Eisai Genentech Roche and Wash-ington University and has received income for consulting forCortexyme and Eisai M Ikeda reports departmental grants andhonoraria fees from Sumitomo Dainippon Pharma Eisai andNiho Medicine-Physics J Leverenz acknowledges supportfrom the National Institutes of Health P30 AG053762 UO1NS100610 and R13NS111954 and Jane and Lee Seidman andDouglas Herthel DVMMemorial Funds and reports consultingfees from Aptinyx Acadia Biogen Eisai GE HealthcareGenzymeSanofi and Takeda Pharmaceuticals and grant sup-port from Alzheimerrsquos Drug Discovery Foundation De-partment of Defense GE Healthcare GenzymeSanofi TheMichael J Fox Foundation and the NIH (NIA andNINDS) SLewis is supported by NHMRC-ARC Dementia Fellows KMarder is funded by the NIH R01NS100600 NS107168UL1TR001873 andNS073671 with research support from theLBDA Parkinson Foundation Michael J Fox HDSA andCHDI and has acted as site investigator for Vaccinex andGenentech member of Springer editorial board and scientificadvisory board Voyager Therapeutics M Masellis was sup-ported by a Canadian Institutes of Health Research grant(MOP13129) and an Early Researcher Award from the Min-istry of Research Innovation and Science (MRIS ON) andreports personal fees for ad hoc consultancy from ArkudaTherapeutics Ionis Pharmaceuticals and Alector Pharmaceut-icals royalties fromHenry Stewart Talks Ltd and grants to theinstitution from Roche Novartis Washington University andAxovant Sciences D Salmon acknowledges support from NIHP30AG062429 and is a paid consultant for Takeda Inc Apti-nyx Inc and Biogen Inc J-P Taylor receives support from theNIHR Biomedical Research Centre awarded to the Newcastleupon Tyne Hospitals NHS Foundation Trust and NewcastleUniversity and reports grants from the UKNational Institute ofHealth Research (NIHR) travel award from Axovant researchsupport costs from Sonsei-Heptares and personal fees fromGEHealthcare D Tsuang acknowledges support from NIHR21AG064271 R03 NS103950 and U01 NS100610 ZWalker has been supported by ESRC NIHR (co-app) ARUK(co-app) EU IMI 2 (co-app) and Dunhill Medical Trust Shehas received consultancy fees travel expenses and researchsupport from GE Healthcare and research support from Life
752 Neurology | Volume 94 Number 17 | April 28 2020 NeurologyorgN
Molecular Imaging P Tiraboschi acknowledges the support ofthe Italian Ministry of Health GRANT NET-2011-02346784Go to NeurologyorgN for full disclosures
Publication historyReceived by Neurology October 30 2019 Accepted in final formFebruary 25 2020
Appendix Authors
Name Location Contribution
Ian GMcKeith FMed Sci MD
Newcastle University Design and conceptualizationof the study acquisition ofdata analysis andinterpretation of the data anddrafting and revising themanuscript for intellectualcontent
Tanis JFermanPhD
Mayo ClinicJacksonville
Design and conceptualizationof the study acquisition ofdata analysis andinterpretation of the data anddrafting and revising themanuscript for intellectualcontent
Alan JThomasPhD
Newcastle University Design and conceptualizationof the study acquisition ofdata analysis andinterpretation of the data anddrafting and revising themanuscript for intellectualcontent
FredericBlanc MD
University ofStrasbourg
Design and conceptualizationof the study acquisition ofdata analysis andinterpretation of the data anddrafting and revising themanuscript for intellectualcontent
Bradley FBoeve MD
Mayo Clinic Rochester Design and conceptualizationof the study acquisition ofdata analysis andinterpretation of the data anddrafting and revising themanuscript for intellectualcontent
HiroshigeFujishiroMD
Nagoya UniversityKawasaki MemorialHospital
Design and conceptualizationof the study acquisition ofdata analysis andinterpretation of the data anddrafting and revising themanuscript for intellectualcontent
KejalKantarciMD MS
Mayo Clinic Rochester Design and conceptualizationof the study acquisition ofdata analysis andinterpretation of the data anddrafting and revising themanuscript for intellectualcontent
CristinaMuscio PhD
Istituto NeurologicoldquoCarlo Bestardquo Milan
Design and conceptualizationof the study acquisition ofdata analysis andinterpretation of the data anddrafting and revising themanuscript for intellectualcontent
Appendix (continued)
Name Location Contribution
John TOrsquoBrien FMed Sci DM
Cambridge University Design and conceptualizationof the study acquisition ofdata analysis andinterpretation of the data anddrafting and revising themanuscript for intellectualcontent
Ronald BPostumaMD MSc
McGill University Design and conceptualizationof the study acquisition ofdata analysis andinterpretation of the data anddrafting and revising themanuscript for intellectualcontent
DagAarslandPhD
Kingrsquos College Londonand StavangerUniversityHospital
Revising the manuscript forintellectual content
CliveBallard MD
University of Exeter Revising the manuscript forintellectual content
LauraBonanniMD PhD
University of Chieti-Pescara
Revising the manuscript forintellectual content
PaulDonaghyPhD
Newcastle University Revising the manuscript forintellectual content
Murat EmreMD
Istanbul Faculty ofMedicine
Revising the manuscript forintellectual content
James EGalvin MDMPH
University of MiamiMiller School ofMedicine
Revising the manuscript forintellectual content
DouglasGalasko MD
University of CaliforniaSan Diego
Revising the manuscript forintellectual content
Jennifer GGoldmanMD MS
Feinberg School ofMedicine
Revising the manuscript forintellectual content
Stephen NGompertsMD PhD
Massachusetts GeneralHospital
Revising the manuscript forintellectual content
Lawrence SHonig MDPhD
Columbia UniversityIrving Medical Center
Revising the manuscript forintellectual content
ManabuIkeda MDPhD
Osaka University Revising the manuscript forintellectual content
James BLeverenzMD
Lou Ruvo Center ofBrain Health ClevelandClinic
Revising the manuscript forintellectual content
Simon JGLewis MD
University of Sydney Revising the manuscript forintellectual content
Karen SMarder MDMPH
Columbia UniversityIrving Medical Center
Revising the manuscript forintellectual content
MarioMasellisMD PhD
Sunnybrook HealthSciences CentreUniversity of Toronto
Revising the manuscript forintellectual content
David PSalmon PhD
University of CaliforniaSan Diego
Revising the manuscript forintellectual content
Continued
NeurologyorgN Neurology | Volume 94 Number 17 | April 28 2020 753
References1 Walker Z Possin KL Boeve BF Aarsland D Lewy body dementias Lancet 2015386
1683ndash16972 McKeith IG Boeve BF Dickson DW et al Diagnosis and management of dementia
with Lewy bodies fourth consensus report of the DLB consortium Neurology 20178988ndash100
3 Ferman TJ Smith GE Kantarci K et al Nonamnestic mild cognitive impairmentprogresses to dementia with Lewy bodies Neurology 2013812032ndash2038
4 Savica R Bradley BF Mielke MM When do alpha-synucleinopathies start An epi-demiological timeline A review JAMA Neurol 201875503ndash509
5 Donaghy PC Taylor JP OrsquoBrien JT et al Neuropsychiatric symptoms and cognitiveprofile in mild cognitive impairment with Lewy bodies Psychol Med 2018482384ndash2390
6 Cagnin A Bussse C Gardini S et al Clinical and cognitive phenotype of mildcognitive impairment evolving to dementia with Lewy bodies Dement Geriatr CognDis Extra 20155442ndash449
7 Postuma RB Iranzo A HuM et al Risk and predictors of dementia and parkinsonismin idiopathic REM sleep behaviour disorder a multicentre study Brain 2019142744ndash759
8 Sadiq D Whitfield T Lee L Stevens T Costafreda S Walker Z Prodromal dementiawith Lewy bodies and prodromal Alzheimerrsquos disease a comparison of the cognitiveand clinical profiles J Alzheimers Dis 201758463ndash470
9 FitzGerald JM Perera G Chang-Tave A et al The incidence of recorded de-lirium episodes before and after dementia diagnosis differences between de-mentia with Lewy bodies and Alzheimerrsquos disease J Am Med Dir Assoc 201920604ndash609
10 Jicha GA Schmitt FA Abner E et al Prodromal clinical manifestations of neu-ropathologically confirmed Lewy body disease Neurobiol Aging 2010311805ndash1813
11 Vardy E Holt R Gerhard A Richardson A Snowden J Neary D History of a sus-pected delirium is more common in dementia with Lewy bodies than Alzheimerrsquosdisease a retrospective study Int J Geriatr Psychiatry 201429178ndash181
12 Fujishiro H Nakamura S Sato K Iseki E Prodromal dementia with Lewy bodiesGeriatr Gerontol Int 201515817ndash826
13 McKeith I Taylor JP Thomas A Donaghy P Kane J Revisiting DLB diagnosisa consideration of prodromal DLB and of the diagnostic overlap with Alzheimerdisease J Geriatr Psychiatry Neurol 201629249ndash253
14 Albert MS DeKosky ST Dickson D et al The diagnosis of mild cognitive impairmentdue to Alzheimerrsquos disease recommendations from the National Institute on Aging-Alzheimerrsquos Association workgroups on diagnostic guidelines for Alzheimerrsquos diseaseAlzheimers Dement 20117270ndash279
15 Litvan I Goldman JG Troster AI et al Diagnostic criteria for mild cognitive im-pairment in Parkinsonrsquos disease Movement Disorder Society Task Force guidelinesMov Disord 201227349ndash356
16 Ferman TJ Smith GE Boeve BF et al Neuropsychological differentiation of de-mentia with Lewy bodies from normal aging and Alzheimerrsquos disease Clin Neuro-psychol 200620623ndash636
17 Cagnin A Busse C Jelcic N Gnoato F Mitolo M Caffarra P High specificity ofMMSE pentagon scoring for diagnosis of prodromal dementia with Lewy bodiesParkinsonism Relat Disord 201521303ndash305
18 Yoon JH Kim M Moon SY Yong SW Hong JM Olfactory function and neuro-psychological profile to differentiate dementia with Lewy bodies from Alzheimerrsquosdisease in patients with mild cognitive impairment a 5-year follow-up study J NeurolSci 2015355174ndash179
19 Kemp J Philippi N Phillipps C et al Cognitive profile in prodromal dementia withLewy bodies Alzheimers Res Ther 2017919
20 Auning E Rongve A Fladby T et al Early and presenting symptoms of dementia withLewy bodies Dement Geriatr Cogn Disord 201132202ndash208
21 Kondo D Ota K Kasanuki K et al Characteristics of mild cognitive impairmenttending to convert into Alzheimerrsquos disease or dementia with Lewy bodies a follow-upstudy in a memory clinic J Neurol Sci 2016369102ndash108
22 Marchand DG Postuma RB Escudier F et al How does dementia with Lewy bodiesstart prodromal cognitive changes in REM sleep behavior disorder Ann Neurol2018831016ndash1026
23 Kantarci K Lesnick T Ferman TJ et al Hippocampal volumes predict risk of de-mentia with Lewy bodies in mild cognitive impairment Neurology 2016872317ndash2323
24 Thomas AJ Taylor JP McKeith I et al Revision of assessment toolkits for improvingthe diagnosis of Lewy body dementia the DIAMOND Lewy study Int J GeriatrPsychiatry 2018331293ndash1304
25 Galvin JE Improving the clinical detection of Lewy body dementia with the Lewybody composite risk score Alzheimerrsquos Demen (Amsterdam Netherlands) 20151316ndash324
26 Belden CM Kahlon V Malek-Ahmadi M Tsai A Sabbagh MN Clinical character-ization of mild cognitive impairment as a prodrome to dementia with Lewy bodiesAm J Alzheimers Dis Other Demen 201530173ndash177
27 Yoon JH Lee JE Yong SW Moon SY Lee PH The mild cognitive impairment stageof dementia with Lewy bodies and Parkinson disease A comparison of cognitiveprofiles Alzheimer Dis Assoc Disord 201428151ndash155
28 Fengler S Liepelt-Scarfone I Brockmann K Schaffer E Berg D Kalbe E Cognitivechanges in prodromal Parkinsonrsquos disease a review Mov Disord 2017321655ndash1666
29 Kalbe E Rehberg SP Heber I et al Subtypes of mild cognitive impairment in patientswith Parkinsonrsquos disease evidence from the LANDSCAPE study J Neurol NeurosurgPsychiatry 2016871099ndash1105
30 Thomas AJ Donaghy P Roberts G et al Diagnostic accuracy of dopaminergic im-aging in prodromal dementia with Lewy bodies Psychol Med 20181ndash7
31 Ferman TJ Boeve BF Smith GE et al Inclusion of RBD improves the diagnosticclassification of dementia with Lewy bodies Neurology 201177875ndash882
32 Fujishiro H Okuda M Iwamoto K et al Early diagnosis of Lewy body disease inpatients with late-onset psychiatric disorders using clinical history of rapid eyemovement sleep behavior disorder and I-123 -metaiodobenzylguanidine cardiacscintigraphy Psychiatry Clin Neurosci 201872423ndash434
33 Bonanni L Perfetti B Bifolchetti S et al Quantitative electroencephalogram utility inpredicting conversion of mild cognitive impairment to dementia with Lewy bodiesNeurobiol Aging 201536434ndash445
34 Murray ME Ferman TJ Boeve BF et al MRI and pathology of REM sleep behaviordisorder in dementia with Lewy bodies Neurology 2013811681ndash1689
35 Murray ME Graff-Radford NR Ross OA Petersen RC Duara R Dickson DWNeuropathologically defined subtypes of Alzheimerrsquos disease with distinct clinicalcharacteristics a retrospective study Lancet Neurol 201110785ndash796
36 Blanc F Colloby SJ Cretin B et al Grey matter atrophy in prodromal stage ofdementia with Lewy bodies and Alzheimerrsquos disease Alzheimers Res Ther 2016831
37 Blanc F Colloby SJ Philippi N et al Cortical thickness in dementia with Lewy bodiesand Alzheimerrsquos disease a comparison of prodromal and dementia stages Plos One201510e0127396
38 Surendranathan A OrsquoBrien JT Clinical imaging in dementia with Lewy bodies EvidBased Ment Health 20182161ndash65
39 Outeiro TF Koss DJ Erskine D et al Dementia with Lewy bodies an update andoutlook Mol Neurodegener 2019145
40 Donadio V Incensi A Rizzo G et al A new potential biomarker for dementiawith Lewy bodies Skin nerve alpha-synuclein deposits Neurology 201789318ndash326
41 Flanigan PM Khosravi MA Leverenz JB Tousi B Color vision impairment differ-entiates Alzheimer dementia from dementia with Lewy bodies J Geriatr PsychiatryNeurol 20183197ndash102
42 Fereshtehnejad SM Yao C Pelletier A Montplaisir JY Gagnon JF Postuma RBEvolution of prodromal Parkinsonrsquos disease and dementia with Lewy bodies a pro-spective study Brain 20191422051ndash2067
43 Bousiges O Bombois S Schraen S et al Cerebrospinal fluid Alzheimer biomarkerscan be useful for discriminating dementia with Lewy bodies from Alzheimerrsquos diseaseat the prodromal stage J Neurol Neurosurg Psychiatry 201889467ndash475
44 Kantarci K Lowe VJ Boeve BF et al Multimodality imaging characteristics of de-mentia with Lewy bodies Neurobiol Aging 2012332091ndash2105
45 Kantarci K Lowe VJ Boeve BF et al AV-1451 tau and beta-amyloid positronemission tomography imaging in dementia with Lewy bodies Ann Neurol 20178158ndash67
46 Gore RL Vardy E OrsquoBrien JT Delirium and dementia with Lewy bodies distinctdiagnoses or part of the same spectrum J Neurol Neurosurg Psychiatry 20158650ndash59
47 Aarsland DS Auning E The pre-dementia stage of dementia with Lewy bodies Eur JNeurol 20111869
48 Sunwoo MK Hong JY Choi J Park HJ Kim SH Lee PH alpha-Synuclein pathologyis related to postoperative delirium in patients undergoing gastrectomy Neurology201380810ndash813
49 Akintade O Pierres F Acute presentation of dementia with Lewy bodies Clin Med201919327ndash330
50 Kosaka K Diffuse Lewy body disease in Japan J Neurol 1990237197ndash20451 Birkett DP Desouky A Han L Kaufman M Lewy bodies in psychiatric patients Int J
Geriatr Psychiatry 19927235ndash240
Appendix (continued)
Name Location Contribution
John PaulTaylor MBBS PhD
Newcastle University Revising the manuscript forintellectual content
Debby WTsuang MD
VA Puget Sound ampUniversity ofWashington
Revising the manuscript forintellectual content
ZuzanaWalker MD
University CollegeLondon
Revising the manuscript forintellectual content
PietroTiraboschiMD
Istituto NeurologicoldquoCarlo Bestardquo Milan
Design and conceptualizationof the study acquisition ofdata analysis andinterpretation of the data anddrafting and revising themanuscript for intellectualcontent
754 Neurology | Volume 94 Number 17 | April 28 2020 NeurologyorgN
52 Kobayashi K Nakano H Akiyama N Maeda T Yamamori S Pure psychiatric pre-sentation of the Lewy body disease is depressionmdashan analysis of 60 cases verified withmyocardial meta-iodobenzylguanidine study Int J Geriatr Psychiatry 201530663ndash668
53 Takahashi S Mizukami K Arai T et al Ventilatory response to hypercapnia predictsdementia with Lewy bodies in late-onset major depressive disorder J Alzheimers Dis201650751ndash758
54 Van Assche L Van Aubel E Van de Ven L Bouckaert F Luyten P Vandenbulcke MThe neuropsychological profile and phenomenology of late onset psychosis a cross-sectional study on the differential diagnosis of very-late-onset Schizophrenia-likepsychosis dementia with Lewy bodies and Alzheimerrsquos type dementia with psychosisArch Clin Neuropsychol 201934183ndash199
55 Thaipisuttikul P Lobach I Zweig Y Gurnani A Galvin JE Capgras syndrome indementia with Lewy bodies Int Psychogeriatr 201325843ndash849
56 Fujishiro H Iseki E Nakamura S et al Dementia with Lewy bodies early diagnosticchallenges Psychogeriatrics 201313128ndash138
57 Chiba Y Fujishiro H Iseki E et al Retrospective survey of prodromal symptoms indementia with Lewy bodies comparison with Alzheimerrsquos disease Dement GeriatrCogn Disord 201233273ndash281
58 Kaufmann H Norcliffe-Kaufmann L Palma JA et al Natural history of pure auto-nomic failure a United States prospective cohort Ann Neurol 201781287ndash297
59 Heinzel S Berg D Gasser T et al Update of the MDS research criteria for prodromalParkinsonrsquos disease Mov Disord 2019341464ndash1470
60 Palma JA Norcliffe-Kaufmann L Kaufmann H Diagnosis of multiple system atrophyAuton Neurosci 201821115ndash25Data available fromDryad (Additional References References e1ndashe44) doi105061dryad1c59zw3rv
Subspecialty Alerts by E-mail
Customize your online journal experience by signing up for e-mail alerts related to your subspecialty or area of interest Accessthis free service by clicking on the ldquoMy Alertsrdquo link on the home page An extensive list of subspecialties methods and studydesign choices will be available for you to choose frommdashallowing you priority alerts to cutting-edge research in your field
COVID-19 and Neurologic Disease Call for Papers
The editors of Neurology are interested in papers that address the neurological aspects of COVID-19infection and challenges to the management of patients with chronic neurological conditions whohave or are at risk for the infection Relevant papers that pass initial internal review will undergoexpedited peer review and online publication We will consider papers posted in preprint servers
Submit observational studies and clinical trials as Articles and case series and case reports underthe ClinicalScientific Notes category to httpssubmitneurologyorg today
Visit the Neurologyreg Website at NeurologyorgN More article-based content on home pages Streamlined menus and navigation Enhanced blog sections for specialty areas Same experience on desktop tablet and mobile devices Improved article reading experience links more evident (pdf analytics social media) Neurologyreg Clinical Practice initiative ldquoPractice Currentrdquo global surveys will be accessible across sites
Find Neurologyreg on Facebook httptinyurlcomneurologyfan
Follow Neurologyreg on Twitter httpstwittercomGreenJournal
NeurologyorgN Neurology | Volume 94 Number 17 | April 28 2020 755
DOI 101212WNL0000000000009323202094743-755 Published Online before print April 2 2020Neurology
Ian G McKeith Tanis J Ferman Alan J Thomas et al Research criteria for the diagnosis of prodromal dementia with Lewy bodies
This information is current as of April 2 2020
ServicesUpdated Information amp
httpnneurologyorgcontent9417743fullincluding high resolution figures can be found at
References httpnneurologyorgcontent9417743fullref-list-1
This article cites 59 articles 12 of which you can access for free at
Subspecialty Collections
httpnneurologyorgcgicollectionpsychosisPsychosis a
httpnneurologyorgcgicollectionparkinsons_disease_with_dementiParkinsons disease with dementia
httpnneurologyorgcgicollectionmci_mild_cognitive_impairmentMCI (mild cognitive impairment)
httpnneurologyorgcgicollectiondementia_with_lewy_bodiesDementia with Lewy bodies
httpnneurologyorgcgicollectiondeliriumDeliriumfollowing collection(s) This article along with others on similar topics appears in the
Permissions amp Licensing
httpwwwneurologyorgaboutabout_the_journalpermissionsits entirety can be found online atInformation about reproducing this article in parts (figurestables) or in
Reprints
httpnneurologyorgsubscribersadvertiseInformation about ordering reprints can be found online
ISSN 0028-3878 Online ISSN 1526-632XWolters Kluwer Health Inc on behalf of the American Academy of Neurology All rights reserved Print1951 it is now a weekly with 48 issues per year Copyright Copyright copy 2020 The Author(s) Published by
reg is the official journal of the American Academy of Neurology Published continuously sinceNeurology

and not cutoff scores14 Impairment on neuropsychologicaltests may also be demonstrated by significant decline dem-onstrated on serial testing or significant decline from esti-mated premorbid abilitiese5 Cognitive impairment mayadditionally be categorized as single or multiple domain andas amnestic or nonamnestic which may help to classify po-tential subgroups as they relate (1) to biomarkers and path-ologic correlates and (2) to differences in the rate of declineand progression to dementia each of which may be importantin the conduct of clinical trials A further refinement to de-scribe the cognitive profile of MCI-LB may be provided byusing the MDS level II criteria for PD-MCI15e6e7
The cognitive presentation of MCI-LBThe cognitive pattern ofMCI-LB is similar toDLB and typicallyincludes disproportionate attentionexecutive and visual pro-cessing deficits and relatively preserved memory and objectnaming16e8e9 Impairment on tasks of attention processingspeed and verbal fluency typically constitute the attentionexecutive deficits and tasks of visual discrimination assemblyand figure drawing typically constitute the visual perceptual andspatial deficits5617ndash19
Diagnostic criteria for DLB emphasize that prominent or per-sistent memory impairment may not necessarily occur in theearly stages2 but patients and carers frequently offer memorycomplaints as a presenting symptom20Of 49 patients withMCIwho progressed to DLB 27 had multidomain amnestic MCIbut only 6 had single-domain amnestic MCI3 similar to otherreports1921 When patients with MCI-LB have memory im-pairment attention andor visual processing deficits also tend tobe present3 and may precede the memory difficulties Patientswith RBD who later developed DLB had attentionexecutivedeficits up to 6 years before the diagnosis of dementia andmemory deficits up to 2 years before the diagnosis22 The basisfor verbal memory impairment in DLB or MCI-LB may berelated to slowed processing speed and deficits in workingmemory and retrieval that characterize the attention and exec-utive deficitse10 consistent with hippocampal preservation inMCI-LB compared with MCI-AD23e11 However impairedmemory in DLB may also be related to the extent of coexistingAD-related pathologye9 characterized by greater hippocampalatrophy on imaging e12 and greater CA1 hippocampal subfieldpathology on autopsye13 Similar to other subtypes of MCIa proportion of patients may revert to being cognitively normalalthough they remain at a greater risk of the eventual de-velopment of dementiae14 Some instability of an MCI-LB di-agnosis is to be expected given inherent fluctuating cognitionworsening with neuroleptics or anticholinergics or improve-ment with levodopa-carbidopa or cholinesterase inhibitors
In summary the performance pattern of MCI-LB is bestcharacterized as single- or multidomain nonamnestic MCI oras multidomain amnestic MCI whereas single-domainamnestic MCI is more likely to represent MCI-AD TheMCI-LB cognitive pattern is often seen in patients with 1 ormore core DLB features5 although these may develop
later318 Nonamnestic MCI seldom develops into AD but isassociated with a greater risk of transition to DLB1021 witha ten-fold risk compared with amnestic MCI3 Becausea substantial subset of patients with DLB have coexisting AD-related pathology that may influence their cognitive profileMCI-LB still should be considered an important part of thedifferential diagnosis in amnestic subjects
Operationalization of MCI-LBThe scheme suggested in table 1 for the identification ofMCI-LBallows a diagnosis of either possible or probable MCI-LB basedon the number of qualifying clinical features or biomarkers Theterms possible and probable refer to the likelihood of underlyingLB disease and not to the MCI syndrome Structured diagnosticinstruments may assist identification of the core clinical featuresof DLB that precede coincide with or follow the onset of cog-nitive difficulties24ndash26 Cognitive fluctuations may be of lesseramplitude or frequency than in more severe disease Passage andsense of presence hallucinatory phenomena may precede thedevelopment of recurrent well-formed and detailed VH Clinicalfeatures supportive of DLBmay occur secondary to other causesreducing their diagnostic specificity but they can be usefulindicators of underlying LBdisease particularly when they persistover time or occur in combination
Use of the possible MCI-LB category may raise diagnosticsuspicion prompting further clinical and biomarker in-vestigation Some possible MCI-LB combinations will likelyprove better predictors than others for example multidomainnonamnestic MCI plus clinically well-defined RBD is antici-pated to be more predictive of progression to DLB thansingle-domain amnestic MCI plus a history of cognitivefluctuation The utility of different combinations of clinicalfeatures and biomarkers remains to be established
MCI-LB and PD-MCIUncertainty may occur in deciding how patients exhibitingboth MCI and parkinsonism are best categorized PD-MCIwill usually be the most appropriate diagnosis when PD isdiagnosed before significant cognitive decline occurs Theadoption of a 1-year rule similar to that used to separate DLBand PD dementia may be helpful to distinguish someMCI-LBand PD-MCI cases if the onset and order of mild symptoms ofparkinsonism and cognitive decline can be clearly establishedIf not an initial diagnosis of prodromal LB disease may bepreferable recognizing that this will require revision as the fullclinical picture evolves Individuals with poor global cognitivetest performance identified in community samples have beenreported to be at a greater risk of developing PD over sub-sequent yearse15e16 but poor cognitive test scores are notequivalent to MCI and this increased risk was no longerstatistically significant when individuals with subtle motorsigns at baseline were excludede15 There are data to suggestthat patients with MCI-LB may have greater cognitive im-pairment than those with PD-MCI27 but this is not easilyoperationalized to differentiate individual subjects The cog-nitive deficits of PD-MCI can be heterogeneouse17 with
NeurologyorgN Neurology | Volume 94 Number 17 | April 28 2020 745
disproportionately affected attentionexecutive function22
visuospatial skillse18 and memory28 Similar toMCI-LB thereis evidence that nonamnestic MCI is more common thanamnestic MCI and that multidomain amnestic MCI is morecommon than single-domain amnestic MCI29
Biomarkers for prodromal DLBDirect measures of α-synuclein pathology would offer de-finitive diagnosis at an early stage several are under de-velopment but none is yet validated or available for useantemortem Surrogate biomarkers of LB disease must
Table 1 Research criteria for the clinical diagnosis of probable and possible MCI-LB
Essential for a diagnosis of MCI-LB is MCI defined by the presence of each of the following
Concern by the patient informant or clinician regarding cognitive decline
Objective evidence of impairment in 1 or more cognitive domains The cognitive impairment may include any domain but is more likely to be associatedwith attention-executive andor visual processing deficits
Preserved or minimally affected performance of previously attained independence in functional abilities which do not meet the criteria for dementia
Core clinical features
Fluctuating cognition with variations in attention and alertness
Recurrent visual hallucinations
RBD
One or more spontaneous cardinal features of parkinsonism these are bradykinesia (defined as slowness of movement and decrement in amplitude orspeed) rest tremor or rigidity
Proposed biomarkers
Reduced dopamine transporter uptake in basal ganglia demonstrated by SPECT or PET
Polysomnographic confirmation of REM sleep without atonia
Reduced meta-iodobenzylguanidine (MIBG) uptake on myocardial scintigraphy
Probable MCI-LB can be diagnosed if
Two or more core clinical features of DLB are present with or without the presence of a proposed biomarker or
Only 1 core clinical feature is present but with 1 or more proposed biomarkers
Probable MCI-LB should not be diagnosed based on biomarkers alone
Possible MCI-LB can be diagnosed if
Only 1 core clinical feature of DLB is present with no proposed biomarkers or
One or more of the proposed biomarkers is present but there are no core clinical features
Supportive clinical features
Severe sensitivity to antipsychotic agents postural instability repeated falls syncope or other transient episodes of unresponsiveness prolonged orrecurrent delirium autonomic dysfunction eg constipation orthostatic hypotension urinary incontinence hypersomnia hyposmia hallucinations inother modalities including passage and sense of presence phenomena systematized delusions apathy anxiety and depression
Potential biomarkers of MCI-LB
Quantitative EEG showing slowing and dominant frequency variability
Relative preservation of medial temporal lobe structures on structural imaging
Insular thinning and gray matter volume loss on MRI
Low occipital uptake on perfusionmetabolism scan
MCI plus supportive clinical features or potential biomarkers are insufficient to diagnose MCI-LB but may raise suspicion of it and prompt biomarkerinvestigation and may add weight to an existing MCI-LB diagnosis
MCI-LB is less likely in the presence of any other physical illness or brain disease including cerebrovascular disease sufficient to account in part or in total forthe clinical picture although these do not exclude anMCI-LB diagnosis andmay serve to indicatemixed ormultiple pathologies contributing to the clinicalpresentation
Abbreviations DLB = dementia with Lewy bodies MCI = mild cognitive impairment MCI-LB = MCI with Lewy bodiesThese should be used in conjunction with the corresponding article text which gives further information about core and supportive clinical features and theuse of biomarkers as they apply to MCI-LB
746 Neurology | Volume 94 Number 17 | April 28 2020 NeurologyorgN
therefore be used as is the case for the diagnosis of DLBitself2 We propose biomarkers for the diagnosis of prodromalDLB where there is either sufficient good quality publishedevidence of adequate diagnostic specificity in prodromal DLBor this can be reasonably extrapolated from fully developedDLB or related disorders We categorize biomarkers for whichonly limited data are available as potential biomarkers rec-ognizing that such distinctions are likely to require revision asnew data become available
Proposed biomarkers
Reduced dopamine transporter (DAT) uptake in basalganglia demonstrated by SPECT or PETThe utility of DAT imaging in discriminating DLB from ADis already well established2 and its sensitivity in dis-tinguishing MCI with LB (MCI-LB) fromMCI with AD was54 and specificity 8930 whenMCI-LB was defined by thepresence of 1 core clinical feature of DLB in patients withMCI A higher sensitivity of 61 was achieved when 2 coreclinical symptoms were present30 Reduced striatal DATuptake therefore seems suggestive of prodromal DLB ina person with MCI but normal striatal DAT uptake does notexclude it
Polysomnographic confirmation of REM sleep withoutatoniaThe association between RBD and synucleinopathy is highlyspecific (eg a multicenter autopsy study found that of 80subjects with polysomnography [PSG]-confirmed RBD anda coexisting neurodegenerative disorder only 2 had a diseaseunrelated to α-synuclein deposition)e4 These data imply thata patient presenting with MCI and having PSG-confirmedRBD that is a history of probable RBD plus clear docu-mentation of REM sleep without atonia (RSWA) on PSGalso has a high probability of an underlying prodromal syn-ucleinopathy Because around a quarter of patients with DLBdo not report symptoms of RBD andor have normal REMsleep atonia on PSG a normal PSG does not exclude a pro-dromal DLB diagnosis31
Reduced meta-iodobenzylguanidine uptake onmyocardial scintigraphyReduced meta-iodobenzylguanidine (MIBG) uptake is anindicative biomarker for DLB2 and has also been reported tooccur in a small series of patients with late-onset psychiatricdisorder and PSG-confirmed RBD32 reinforcing its associa-tion with underlying α-synucleinopathy Of 2 patients withamnestic MCI with low MIBG uptake one developed DLBafter 2 years the other had no clinical follow-up reportede19
VHs andor RBD were reported among 7 of 13 patients withMCI with reduced MIBG uptake the majority of whom alsohad autonomic symptoms suggestive of LB disease but theywere not followed to determine conversion to DLBe20 De-spite a paucity of longitudinal datae21 there seems to be suf-ficient evidence that abnormal MIBGmyocardial scintigraphyin a patient with MCI supports a prodromal DLB diagnosisbut further studies are required
Potential biomarkersThese are biomarkers consistent with underlying LB diseasewhich may help the diagnostic evaluation but for which thereis still insufficient evidence of diagnostic sensitivity andspecificity in early disease This will change as new evidenceemerges at which point these or other candidates may be-come considered as indicative of prodromal DLB
Quantitative EEG showing slowing and dominantfrequency variabilityEEG slowing has been reported as predictive of dementia inboth PDe22 and RBDe23 posterior slow wave activity withperiodic fluctuations in the pre-alpha range being supportiveof DLB2 Quantitative EEG (QEEG) methods show thata dominant frequency lt8 Hz and dominant frequency vari-ability gt1middot5 Hz is typical of DLB and in a 3-year follow-upstudy 83 of subjects with MCI with this pattern at pre-sentation converted to DLB If these findings are replicatedQEEG may represent a powerful predictor of progressionfrom MCI to DLB33
Relative preservation of medial temporal lobestructures on structural imagingAbsent or minimal medial temporal lobe atrophy is consistentwith DLB but not sufficiently specific to differentiate it fromAD2 Lewy body disease with RBD is characterized by pre-served hippocampal volumes34 and hippocampal preserva-tion in patients with MCI supports progression to DLBinstead of AD dementia with a sensitivity of 85 and a spec-ificity of 6123 Suboptimal specificity may be due to thevariability of hippocampal atrophy in AD35 and contributionof other pathologic processes such as TAR DNA bindingprotein 43 (TDP43)e24
Insular thinning and gray matter volume lossInsular cortical thinning occurs in prodromal DLB relative tohealthy controls using MRI T1 sequences with gray matteratrophy predominantly affecting the anterior cingulum andmedial frontal structures This contrasts with more extensiveloss of gray matter in the temporal frontal and parietalregions of subjects with prodromal AD Insular corticalthinning may therefore differentiate patients with prodromalDLB not only from healthy controls but also from theirprodromal AD counterparts36 No group differences in insularvolumes are seen between DLB and AD at the dementia stageso longitudinal studies are required to determine its precisevalue as an early diagnostic marker of DLB37 Insula is alsoinvolved early in frontotemporal dementia (FTD) being thefirst cortical area to show atrophy in presymptomatic GRNMAPT or C9ORF72 mutation carrierse25 and unlikelytherefore to be helpful in differentiating DLB from FTD
Low occipital uptake on perfusionmetabolism scanOccipital hypometabolism on FDG-PET is associated withDLB38 and together with relative preservation of posteriorcingulate metabolism (the cingulate island sign)e26 is a sup-portive biomarker of DLB2 How frequently the cingulate
NeurologyorgN Neurology | Volume 94 Number 17 | April 28 2020 747
island sign is seen in prodromal DLB remains to be estab-lished significantly reduced posterior cingulate metabolismmay be a useful indication of the concurrence of additionalneurofibrillary tangle pathologye27
Other biomarkersThere is currently no α-synuclein radioligand with sufficientevidence supporting its utility for imaging DLB or any otherα-synucleinopathy nor have any diagnostically applicablebiofluid peripheral tissue or genotypic biomarkers beenestablished2 CSF measures cannot reliably discriminate be-tween DLB and AD39 although the measurement of CSFα-synuclein aggregates using seeding aggregation assays suchas protein misfolding cyclic amplification and real-timequaking-induced conversion is providing encouraging pre-liminary results and may be extended to more accessiblebiofluids including saliva plasma serum or urinee28 Com-bining CSF markers may be useful for example addition ofCSF phospho-tau to α-synuclein significantly improved thedifferential diagnosis between MCI-LB and MCI-AD in-creasing sensitivity and specificity both gt than 95e29 Otherdirect or indirect biomarker candidates that may occur earlyinclude identification of phosphorylated α-synuclein depositsin peripheral nervous tissue from skin biopsy40 gait ana-lysise30 and abnormalities in color vision discrimination4142
The figure shows a framework for considering a wider range ofbiomarkers in the setting of prodromal DLB determining theextent to which AD-related pathology is contributing to thedementia syndrome and influencing clinical trajectories inthese patients4344e31e32 Aβ42 declines earlier in AD thanDLB whereas Aβ40 levels increase alone in AD A low
Aβ42Aβ40 ratio may therefore differentiate patients withprodromal AD from patients with prodromal DLB better thanindividual measures43 There is also evidence showing dif-ferent frequencies and topographies of abnormal uptake onamyloid and tau PET imaging in DLB vs AD45
Delirium-onset DLBCognitive fluctuations or pronounced variations in alertnessand arousal are a core feature of DLB apparent as markedfluctuations in cognitive ability or function detectable byobservation or informant report and measurable using sen-sitive cognitive and electrophysiologic measurese33 The oc-currence of delirium (sometimes referred to as acuteconfusional state) as an early presenting feature of DLB hasbeen described in numerous case reports and seriese34 in-cluding in those with no apparent previous history of cogni-tive impairment46e35 Whether this represents a greatervulnerability to delirium in subjects with DLB or the mis-diagnosis of severe fluctuations with clouding of conscious-ness as delirium or a combination of both is unclear
Recognition that DLB may first present as delirium is im-portant because most guidelines for behavioral disturbancesin delirium recommend antipsychotics as first-line pharma-cologic treatment Delirium or marked fluctuations in con-sciousness were reported by 43 of caregivers before DLBdiagnosis47 and previous episodes of delirium were muchmore frequent in patients with DLB compared with patientswith AD (25 vs 7) with 1 in 4 of those with DLB havingrepeated delirium11 In the majority of these potential pro-voking causes were present A similarly higher incidence ofdelirium was found for subjects with DLB compared with
Figure Multimodal biomarkers for prodromal DLB
Reduced dopamine transporter uptake in basal gan-glia demonstrated by SPECT or PET PSG-confirmedREM sleep without atonia and MIBG myocardial scin-tigraphy are proposed as biomarkers of prodromalDLB Multimodality biomarkers are also important incharacterizing patients with prodromal DLB in whomthe pathologic mechanisms of cognitive impairmentinclude both LB and AD pathologies and who mayhave abnormalities associated with both Medialtemporal lobe uptake on tau PET medial temporallobe atrophy on MRI and high levels of uptake onamyloid PET and positive CSF biomarkers of AD-re-lated pathology may characterize patients with pro-dromal DLB with significant AD pathology It isexpected that biomarker abnormalities detected inthe earliest stages will remain abnormal as diseaseprogresses with additional biomarkers showingchanges later during the progression from pro-dromal to dementia phase DLB DLB = dementia withLewy bodies MIBG = meta-iodobenzylguanidine
748 Neurology | Volume 94 Number 17 | April 28 2020 NeurologyorgN
subjects with AD in the year before diagnosis (17middot6 v 3middot2100person-years)9 and admissions for delirium were morecommon in those already diagnosed with DLB than for otherdementias Prolonged delirium may also raise the index ofsuspicion for DLBe36 In an FDG-PET imaging study ofprolonged delirium 32 of subjects were found to havea DLB like pattern a high proportion in regard both to theknown prevalence of the disease and to that of their matchedcognitively impaired control group (4)e37
The similarities between the marked fluctuations in DLB anddisturbances of attention and consciousness in delirium havebeen noted and reviewed46 but there is as yet little un-derstanding of a shared neurobiological basis There havebeen few pathologic studies and although in anepidemiologic-based autopsy cohort there was no link be-tween delirium and LB pathology at autopsye38 a significantlyincreased risk of postoperative delirium in those with pe-ripheral α-synuclein pathology has been described48 Deliriumhas been suggested to bemore common in those subjects withDLB with later age at onsete39 but further evidence is needed
In summary (table 2) it is clear that DLB can present withdelirium and in patients diagnosed with delirium a carefulsearch for other DLB features should be made with a lowthreshold for undertaking DLB biomarker examinations es-pecially in those with recurrent unexplained or prolongeddelirium The extent to which delirium presentations of DLBhave the biomarker abnormalities associated with establishedDLB or other prodromal DLB presentations is unclear
although the PET imaging study cited above supports thise37
as does a report of reduced DAT uptake in a patient withacute unexplained delirium49 The link between delirium andDLB is an important area for future research to clarify therelationship between the 2 and to establish which factorsassociated with delirium should raise the index of suspicionfor underlying prodromal DLB
Psychiatric-onset DLBEarly clinicopathologic studies suggested that DLB maypresent as a primary psychiatric disorder5051 but subsequentfocus on the cognitive and motor aspects of DLB has limitedthe documentation of such cases outside of a fewcenters123252ndash54e36 Late-onset major depressive disorderand late-onset psychosis are the most frequently reportedpresentations differing markedly from the construct of mildbehavioral impairmente40 and sometimes sufficiently severe torequire hospitalization Symptoms include hallucinations invisual and in other modalities and systematized delusionsincluding Capgras syndrome55 apathy anxiety and de-pression Psychiatric-onset DLB cases are not easily differ-entiated from non-LB late-onset psychosis cases on the basisof primary psychiatric phenomenology or neuropsychologicalprofile alone54 Psychomotor retardation such as slowedspeech thinking and body movements can resemble thebradykinesia of parkinsonism The occurrence of rest tremoror rigidity is more helpful than bradykinesia to suspect pro-dromal DLB in patients with depressive disorder53 butpsychotropic-induced parkinsonism may complicate di-agnosis Atypical clinical features may prove valuable pointers
Table 2 Summary of key features of delirium-onset DLB
Patients with DLB are more susceptible to delirium than people with Alzheimer disease and this delirium may occur as their presenting complaint beforedementia develops
Such episodes may be provoked by multiple factors including surgery infectionssepsis fever or other systemic illness or secondary to use or suddenwithdrawal of alcohol or psychoactive drugs
Prodromal DLB should be particularly suspected in patients
bull in whom adequate provoking factors for the delirium are not found
bull with prolonged or recurrent delirium
bull who later develop progressive cognitive decline or subsequent dementia
Core clinical features of DLB are likely to be of more limited diagnostic weight in a patient with delirium because
bull cognitive fluctuation and clouding of consciousness can also occur in non-DLB delirium ie are not diagnostically specific for DLB in this situation
bull visual hallucinations may occur in non-DLB delirium particularly drug-induced or provoked by alcohol abstinence
bull motor parkinsonism present may be due to antipsychotic medications used to treat delirium
bull the diagnostic significance of a history of RBD in a person with delirium is not yet established
Identification of delirium-onset DLB
bull may be assisted by use of MCI-LB biomarkers but further research evidence of this is required
bull is important to inform the management plan including the avoidance or minimization of antipsychotic and anticholinergic agents
Abbreviations DLB = dementia with Lewy bodies MCI = mild cognitive impairment MCI-LB = MCI with Lewy bodies RBD = REM sleep behavior disorder
NeurologyorgN Neurology | Volume 94 Number 17 | April 28 2020 749
to underlying LB pathology particularly the presence of re-current VH12 when these occur before cognitive impairmentbecomes evident As with all α-synucleinopathies RBD maybe a useful indicator although a relationship between anti-depressant usage and subsequent RBD onset is a potentialconfoundere41 Although the primary psychiatric manifes-tations are often accompanied by mild cognitive deficits54
cognitive evaluation and interpretation of performance can bedifficult when psychiatric symptoms are prominent The fre-quency of cognitive fluctuations in psychiatric-onset LB caseshas not been determined
Initial reports suggest that 123I-MIBG scintigraphy may behelpful in psychiatric-onset DLB525356 Eighteen of 35patients with a first onset of major depressive disorder gt50years and with bradykinesia developed a clinical diagnosis ofDLB after 6 years of follow-up All 18 had an abnormal ven-tilatory response to hypercapnia (VRH) indicative of severeautonomic dysfunction whereas none of the 17 patients witha normal VRH converted to DLB within the study period Forthe converters the most common presentation was withpsychotic and melancholic features simultaneously The fre-quency of hypersensitivity to antipsychotics antidepressantsand antianxiety drugs was higher in converters than in non-converters53 Further studies need to confirm these findingsand to determine the value of other DLB biomarkers inpsychiatric-onset cases325256
In summary it is not yet clear how to identify patients withprominent late-onset psychiatric symptoms who may haveunderlying LB disease and subsequently progress to DLB It is
premature to try to construct formal criteria for psychiatric-onset DLB but clinicians in mental health and other settingsneed to be aware that this possibility exists not least becauseof the risk of severe antipsychotic sensitivity reactions withincreased morbidity and mortality The small available liter-ature including reports such as those cited above does providesome useful guidance summarized in table 3 but requiresreplication and further investigation
Idiopathic REM sleep behavior disorderRBD is characterized by abnormal dream enactment behaviorduring REM sleep accompanied by loss of muscle atonia duringREM sleep (REM sleep without atonia or RSWA) on PSG Forthe purpose of a prodromal DLB diagnosis a clinical history ofRBD is obtained in the same way as for DLB2 that is a clearcomplaint of dream enactment by a bedpartner or other witnesswith no evidence of sleep disorders that may mimic RBD onclinical interview Conditions known to mimic or masquerade asRBD include non-REM parasomnias (sleep walking sleep talk-ing or other behaviors that emerge fromnon-REM sleep stages)obstructive sleep apnea confusional arousals or nocturnal seiz-ures In the absence of PSG the risk of a false-positive clinicaldiagnosis of RBD is reduced by using optimized sleep ques-tionnaires which can have sensitivity and specificity over 90e42
RBDmay be considered as idiopathic until it is associated withanother ongoing neurologic condition the most frequentbeing an α-synucleinopathy (PD DLB or MSA) In a recentlarge study 735 of patients with RBD converted to an overtneurodegenerative syndrome after 12-year follow-up 565developing parkinsonism and 435 dementia as their first
Table 3 Summary of key features of psychiatric-onset DLB
Is characterized by predominant psychiatric symptoms that typically correspond to late-onset major depressive disorder or late-onset psychosis which mayfeature hallucinations in visual and in other modalities and systematized delusions including Capgras syndrome
bull may also present with apathy anxiety and depression
bull may be sufficiently severe to require hospitalization
bull the frequency of LB disease as a cause of late-onset psychiatric disorder is not known
When assessing for core clinical features of DLB in a patient with a primary psychiatric presentation
bull bradykinesia may be mimicked by psychomotor retardation which is commonly seen in depressive disorders
bull parkinsonism may be induced by antipsychotic medications used to treat psychiatric disorder
bull RBD (and REM sleep without atonia) may be induced by antidepressant medications
bull mild cognitive disturbance may be present but is not predominant and may fluctuate
bull formal neuropsychological testing may be confounded by the psychiatric mental state
bull the frequency and character of cognitive fluctuations is unknown
Identification of psychiatric-onset DLB
bull may be assisted by use of MCI-LB biomarkers but further research evidence of this is required
bull is important to inform the management plan including the avoidance or minimization of antipsychotic and anticholinergic agents
Abbreviations DLB = dementia with Lewy bodies MCI = mild cognitive impairment
750 Neurology | Volume 94 Number 17 | April 28 2020 NeurologyorgN
disease manifestation Among many predictive markerstested only the cognitive variables differed at baseline be-tween those converting to primary dementia vs parkinson-ism7 Other multicenter studies confirm that the only clinicalfeature that predicts dementia vs parkinsonism first is neu-ropsychological performance those with RBD who exhibitcognitive changes are more likely to evolve first into MCI orDLB22e4 Thus although RBD may be regarded an earlymanifestation of α-synucleinopathy it is not possible to clearlydistinguish whether an individual presenting with RBD willdevelop dementia first that is evolve into a primary DLBdiagnosis or parkinsonism first that is a primary PDMSAdiagnosis Any MCI subtype associated with PSG-confirmedRBD is highly likely to represent underlying LB disease Al-though idiopathic RBD is a useful model to study the earlystages of LB disease progression it is not necessarily repre-sentative of the whole spectrum of patients with PD and DLBa significant minority of whom do not have RBD42
Autonomic dysfunctionanosmia and othernonspecific prodromal LB disease symptomsPatients with DLB frequently report a history of autonomicdysfunction at first clinic attendance with 25ndash50 com-plaining of one of more among constipation orthostatic diz-ziness urinary incontinence erectile dysfunction increasedsweating or increased saliva5657 In a cohort of patients withpure autonomic failure 34 converted to an overt α-synu-cleinopathy over 6 years of follow-up this was to DLB (52)PD (24) orMSA (24)58 However because there are manyother causes for autonomic dysfunction in older people thesesymptoms either alone or in combination have low positivepredictive value59 The situation is similar for hyposmia whichalso frequently occurs early in prodromal DLB and PD42 butwhich can have many other causes in this age group
Conclusions and future directionDiagnosis of DLB at the dementia stage depends on identifyingfully expressed core clinical features which may be mild orabsent at the prodromal stage when biomarker evidence mayalso be weaker and may even differ from that found at thedementia stage Several new biomarker candidates direct andindirect are in development and we will continue to reviewthese to update our recommendations as soon as sufficientevidence accumulates We recognize that the clinical pheno-type of neurodegenerative disorders reflects interaction be-tween several rather than a single brain pathology and it istherefore likely that multiple biomarkers of individual pathol-ogies (eg α-synuclein β-amyloid and tau) or of disease sur-rogates (eg metabolic imagingEEG) will be required
Although we have described the 3 prodromal DLB syndromesseparately they are unlikely to be mutually exclusive andthere may be substantial overlap We propose operationalizedcriteria only for MCI-LB because the evidence base from oursystematic review albeit relatively limited is sufficient to
support recommendations that are immediately applicableand testable Our recommendations should be used alongsideguidance about the prodromal manifestations of PD1559
MSA60 and AD14 with which there is overlap Notwith-standing the potential benefits of early diagnosis we are alsomindful of the importance of avoiding incorrect (false-positive) diagnosis of prodromal DLB and the potentialnegative consequences this could have for an individual Wesuggest that the predictive validity of different categories andcombinations of our proposed criteria should be clarified byprospective studies before they are adopted for widespreadclinical use and that they will enable standardization for in-clusion in research studies and clinical trials
Some published guidance about the early clinical diagnosis ofDLB does already exist DSM5 recommends a diagnosis ofmild neurocognitive disorder (NCD) with LB ldquofor individualswho present with the core or suggestive features at a stagewhen cognitive or functional impairments are not of sufficientseverity to fulfill criteria for major NCDrdquoe43 This is basedhowever on the 2005 version of DLB guidelines and requiresupdating ICD-11 takes a similar approach toward diagnosingmild NCD at a syndromic level and lists both Lewy bodydisease and PD as possible causese44
The diagnostic position for other prodromal manifestations ofDLB that is delirium-onset and psychiatric-onset is less clearthan for MCI Operationalization of specific criteria for thesesyndromes is not yet justified and the reliable differentiationof the minority of delirious and psychiatrically ill patients whohave underlying LB pathology from the majority who do notwill probably only be achieved when routinely applicablebiomarkers are developed LB disease is seldom if ever cur-rently considered as part of the differential diagnosis of de-lirium or late-onset psychiatric disorder and we hope that theinformation we provide in the text and accompanying boxeswill raise cliniciansrsquo awareness of that possibility
Study fundingNo targeted funding reported
DisclosureI McKeith receives support from the NIHR Biomedical Re-search Centre awarded to the Newcastle upon Tyne HospitalsNHS Foundation Trust and Newcastle University and hasconsulted for GE Healthcare Sanofi Eisai Sumitomo Dai-nippon Pharma and Axovant T Ferman receives support fromNIH P50-AG16574 P30-AG062677 U01-NS100620 and theMangurian Foundation for Lewy body disease research AThomas receives support from the NIHR Biomedical ResearchCentre awarded to the Newcastle upon Tyne Hospitals NHSFoundation Trust and Newcastle University and has receivedgrants from GE Healthcare F Blanc has served as nationalclinical trial coordinator for Eisai and Axovant B Boevereceives support from NIH P50-AG16574 P30-AG062677U01-NS100620 and the Mangurian Foundation for Lewybody disease research has consulted for the Scientific Advisory
NeurologyorgN Neurology | Volume 94 Number 17 | April 28 2020 751
BoardmdashTau Consortium and received grants from Biogenthe NIH theMangurian Foundation Alector the Little FamilyFoundation and the Turner Family H Fujishiro has receivedsupport from Fujifilm RI Pharma Co Ltd K Kantarci receivessupport from NIH P50-AG16574 P30-AG062677 U01-NS100620 and the Mangurian Foundation for Lewy bodydisease research and has received grants from Avid Radio-pharmaceuticals and acted on a Data Safety Monitoring Boardfor Takeda Global Research C Muscio acknowledges thesupport of the Italian Ministry of Health GRANT NET-2011-02346784 J OrsquoBrien is supported by the NIHR CambridgeBiomedical Research Centre Dementia and Neuro-degeneration and Mental Health Themes and the CambridgeCentre for Parkinsonrsquos Plus Disorders has consulted forTauRx Axon GE Healthcare Eisai and AvidLilly and re-ceived grants fromAvidLilly andAllianceMedical R Postumahas received grants from and consulted for Fonds de laRecherche en Sante received grants from the Canadian Insti-tutes of Health Research the Parkinson Society of Canada theWeston-Garfield Foundation The Michael J Fox Foundationand the Webster Foundation and consulted for TakedaRocheProthena Teva Neurosciences Novartis Canada Bio-gen Boehringer Ingelheim Theranexus GE Healthcare JazzPharmaceuticals AbbVie Jannsen Otsuko PhytopharmicsInception Sciences and Parkinson Canada D Aarsland isa Royal Society Wolfson Research Merit Award Holder andwould like to thank the Wolfson Foundation and the RoyalSociety for their support He has received research supportandor honoraria from AstraZeneca H Lundbeck NovartisPharmaceuticals and GE Health and served as paid consultantfor H Lundbeck Eisai Heptares Sanofi and Mentis Cura CBallard reports unrelated current grant funding from MRCWellcome Trust European Union Gillings FoundationNIHR Alzheimerrsquos Society Alzheimerrsquos Research UK Par-kinsonrsquos Society and Lewy Body Society during the conduct ofthe study and personal fees from Acadia pharmaceutical com-pany Lundbeck Roche Otsuka Eli Lilly and AARP outsidethe submitted work L Bonanni is a member of the steeringcommittee of the E-DLB consortium and program chair of theLBD-PIA (ISTAART) and is funded for research on DLB bythe Italian Ministry of Health P Donaghy receives supportfrom the NIHR Biomedical Research Centre awarded to theNewcastle upon Tyne Hospitals NHS Foundation Trust andNewcastle UniversityM Emre served on the scientific advisoryboard for AC Immune J Galvin receives support from NIHgrants (R01 AG040211 R01 NS101482 R01 AG057681 andU01 NS100610) and the Lewy Body Dementia AssociationResearch Center of Excellence reports research support fromthe NIH the Lewy Body Dementia Association The Harry TMangurian Foundation and Albert Charitable Trust directsclinical trials for Biogen and Novartis receives licensing feesfrom Biogen Roche Eli Lilly Quintiles Roobrik ContinuumClinical and Langland and receives consulting fees fromBiogen Eisai Bracket and Medavante D Galasko receivessupport from NIA grant AGO5131 and the Michael J FoxFoundation and has acted as consultant for vTv Pharmaceut-icals Inc Esai Inc and for Fujirebio Inc been a member of
a DSMB for Probiodrug and paid editor for Alzheimerrsquos Re-search amp Therapy J Goldman receives grantsupport fromTheMichael J Fox Foundation and Parkinsonrsquos Foundation andhas received consulting feeshonoraria from Acadia AptinyxSunovion and Worldwide Med S Gomperts receives supportfrom NIH grants R01 AG054551 P30AG062421 R01AG062208 P50 AG005134 R21 NS109833 DODCDMRPW81XW1810516 the Farmer Family ParkinsonrsquosInitiative and the Lewy Body Dementia Association and hasserved on advisory boards for Acadia Pharmaceuticals andSanofi L Honig acknowledges research grant support fromNYS CEAD grant C031425 LBDA RCOE and NIHgrants U01NS100600 P50AG008702 R21AG058020R21MH111596 U01AG051412 U01AG045390U01AG016976 U01AG023749 U19063893 andU19AG024904 He receives research funding support fromAbbVie Alector Biogen Eisai Genentech Roche and Wash-ington University and has received income for consulting forCortexyme and Eisai M Ikeda reports departmental grants andhonoraria fees from Sumitomo Dainippon Pharma Eisai andNiho Medicine-Physics J Leverenz acknowledges supportfrom the National Institutes of Health P30 AG053762 UO1NS100610 and R13NS111954 and Jane and Lee Seidman andDouglas Herthel DVMMemorial Funds and reports consultingfees from Aptinyx Acadia Biogen Eisai GE HealthcareGenzymeSanofi and Takeda Pharmaceuticals and grant sup-port from Alzheimerrsquos Drug Discovery Foundation De-partment of Defense GE Healthcare GenzymeSanofi TheMichael J Fox Foundation and the NIH (NIA andNINDS) SLewis is supported by NHMRC-ARC Dementia Fellows KMarder is funded by the NIH R01NS100600 NS107168UL1TR001873 andNS073671 with research support from theLBDA Parkinson Foundation Michael J Fox HDSA andCHDI and has acted as site investigator for Vaccinex andGenentech member of Springer editorial board and scientificadvisory board Voyager Therapeutics M Masellis was sup-ported by a Canadian Institutes of Health Research grant(MOP13129) and an Early Researcher Award from the Min-istry of Research Innovation and Science (MRIS ON) andreports personal fees for ad hoc consultancy from ArkudaTherapeutics Ionis Pharmaceuticals and Alector Pharmaceut-icals royalties fromHenry Stewart Talks Ltd and grants to theinstitution from Roche Novartis Washington University andAxovant Sciences D Salmon acknowledges support from NIHP30AG062429 and is a paid consultant for Takeda Inc Apti-nyx Inc and Biogen Inc J-P Taylor receives support from theNIHR Biomedical Research Centre awarded to the Newcastleupon Tyne Hospitals NHS Foundation Trust and NewcastleUniversity and reports grants from the UKNational Institute ofHealth Research (NIHR) travel award from Axovant researchsupport costs from Sonsei-Heptares and personal fees fromGEHealthcare D Tsuang acknowledges support from NIHR21AG064271 R03 NS103950 and U01 NS100610 ZWalker has been supported by ESRC NIHR (co-app) ARUK(co-app) EU IMI 2 (co-app) and Dunhill Medical Trust Shehas received consultancy fees travel expenses and researchsupport from GE Healthcare and research support from Life
752 Neurology | Volume 94 Number 17 | April 28 2020 NeurologyorgN
Molecular Imaging P Tiraboschi acknowledges the support ofthe Italian Ministry of Health GRANT NET-2011-02346784Go to NeurologyorgN for full disclosures
Publication historyReceived by Neurology October 30 2019 Accepted in final formFebruary 25 2020
Appendix Authors
Name Location Contribution
Ian GMcKeith FMed Sci MD
Newcastle University Design and conceptualizationof the study acquisition ofdata analysis andinterpretation of the data anddrafting and revising themanuscript for intellectualcontent
Tanis JFermanPhD
Mayo ClinicJacksonville
Design and conceptualizationof the study acquisition ofdata analysis andinterpretation of the data anddrafting and revising themanuscript for intellectualcontent
Alan JThomasPhD
Newcastle University Design and conceptualizationof the study acquisition ofdata analysis andinterpretation of the data anddrafting and revising themanuscript for intellectualcontent
FredericBlanc MD
University ofStrasbourg
Design and conceptualizationof the study acquisition ofdata analysis andinterpretation of the data anddrafting and revising themanuscript for intellectualcontent
Bradley FBoeve MD
Mayo Clinic Rochester Design and conceptualizationof the study acquisition ofdata analysis andinterpretation of the data anddrafting and revising themanuscript for intellectualcontent
HiroshigeFujishiroMD
Nagoya UniversityKawasaki MemorialHospital
Design and conceptualizationof the study acquisition ofdata analysis andinterpretation of the data anddrafting and revising themanuscript for intellectualcontent
KejalKantarciMD MS
Mayo Clinic Rochester Design and conceptualizationof the study acquisition ofdata analysis andinterpretation of the data anddrafting and revising themanuscript for intellectualcontent
CristinaMuscio PhD
Istituto NeurologicoldquoCarlo Bestardquo Milan
Design and conceptualizationof the study acquisition ofdata analysis andinterpretation of the data anddrafting and revising themanuscript for intellectualcontent
Appendix (continued)
Name Location Contribution
John TOrsquoBrien FMed Sci DM
Cambridge University Design and conceptualizationof the study acquisition ofdata analysis andinterpretation of the data anddrafting and revising themanuscript for intellectualcontent
Ronald BPostumaMD MSc
McGill University Design and conceptualizationof the study acquisition ofdata analysis andinterpretation of the data anddrafting and revising themanuscript for intellectualcontent
DagAarslandPhD
Kingrsquos College Londonand StavangerUniversityHospital
Revising the manuscript forintellectual content
CliveBallard MD
University of Exeter Revising the manuscript forintellectual content
LauraBonanniMD PhD
University of Chieti-Pescara
Revising the manuscript forintellectual content
PaulDonaghyPhD
Newcastle University Revising the manuscript forintellectual content
Murat EmreMD
Istanbul Faculty ofMedicine
Revising the manuscript forintellectual content
James EGalvin MDMPH
University of MiamiMiller School ofMedicine
Revising the manuscript forintellectual content
DouglasGalasko MD
University of CaliforniaSan Diego
Revising the manuscript forintellectual content
Jennifer GGoldmanMD MS
Feinberg School ofMedicine
Revising the manuscript forintellectual content
Stephen NGompertsMD PhD
Massachusetts GeneralHospital
Revising the manuscript forintellectual content
Lawrence SHonig MDPhD
Columbia UniversityIrving Medical Center
Revising the manuscript forintellectual content
ManabuIkeda MDPhD
Osaka University Revising the manuscript forintellectual content
James BLeverenzMD
Lou Ruvo Center ofBrain Health ClevelandClinic
Revising the manuscript forintellectual content
Simon JGLewis MD
University of Sydney Revising the manuscript forintellectual content
Karen SMarder MDMPH
Columbia UniversityIrving Medical Center
Revising the manuscript forintellectual content
MarioMasellisMD PhD
Sunnybrook HealthSciences CentreUniversity of Toronto
Revising the manuscript forintellectual content
David PSalmon PhD
University of CaliforniaSan Diego
Revising the manuscript forintellectual content
Continued
NeurologyorgN Neurology | Volume 94 Number 17 | April 28 2020 753
References1 Walker Z Possin KL Boeve BF Aarsland D Lewy body dementias Lancet 2015386
1683ndash16972 McKeith IG Boeve BF Dickson DW et al Diagnosis and management of dementia
with Lewy bodies fourth consensus report of the DLB consortium Neurology 20178988ndash100
3 Ferman TJ Smith GE Kantarci K et al Nonamnestic mild cognitive impairmentprogresses to dementia with Lewy bodies Neurology 2013812032ndash2038
4 Savica R Bradley BF Mielke MM When do alpha-synucleinopathies start An epi-demiological timeline A review JAMA Neurol 201875503ndash509
5 Donaghy PC Taylor JP OrsquoBrien JT et al Neuropsychiatric symptoms and cognitiveprofile in mild cognitive impairment with Lewy bodies Psychol Med 2018482384ndash2390
6 Cagnin A Bussse C Gardini S et al Clinical and cognitive phenotype of mildcognitive impairment evolving to dementia with Lewy bodies Dement Geriatr CognDis Extra 20155442ndash449
7 Postuma RB Iranzo A HuM et al Risk and predictors of dementia and parkinsonismin idiopathic REM sleep behaviour disorder a multicentre study Brain 2019142744ndash759
8 Sadiq D Whitfield T Lee L Stevens T Costafreda S Walker Z Prodromal dementiawith Lewy bodies and prodromal Alzheimerrsquos disease a comparison of the cognitiveand clinical profiles J Alzheimers Dis 201758463ndash470
9 FitzGerald JM Perera G Chang-Tave A et al The incidence of recorded de-lirium episodes before and after dementia diagnosis differences between de-mentia with Lewy bodies and Alzheimerrsquos disease J Am Med Dir Assoc 201920604ndash609
10 Jicha GA Schmitt FA Abner E et al Prodromal clinical manifestations of neu-ropathologically confirmed Lewy body disease Neurobiol Aging 2010311805ndash1813
11 Vardy E Holt R Gerhard A Richardson A Snowden J Neary D History of a sus-pected delirium is more common in dementia with Lewy bodies than Alzheimerrsquosdisease a retrospective study Int J Geriatr Psychiatry 201429178ndash181
12 Fujishiro H Nakamura S Sato K Iseki E Prodromal dementia with Lewy bodiesGeriatr Gerontol Int 201515817ndash826
13 McKeith I Taylor JP Thomas A Donaghy P Kane J Revisiting DLB diagnosisa consideration of prodromal DLB and of the diagnostic overlap with Alzheimerdisease J Geriatr Psychiatry Neurol 201629249ndash253
14 Albert MS DeKosky ST Dickson D et al The diagnosis of mild cognitive impairmentdue to Alzheimerrsquos disease recommendations from the National Institute on Aging-Alzheimerrsquos Association workgroups on diagnostic guidelines for Alzheimerrsquos diseaseAlzheimers Dement 20117270ndash279
15 Litvan I Goldman JG Troster AI et al Diagnostic criteria for mild cognitive im-pairment in Parkinsonrsquos disease Movement Disorder Society Task Force guidelinesMov Disord 201227349ndash356
16 Ferman TJ Smith GE Boeve BF et al Neuropsychological differentiation of de-mentia with Lewy bodies from normal aging and Alzheimerrsquos disease Clin Neuro-psychol 200620623ndash636
17 Cagnin A Busse C Jelcic N Gnoato F Mitolo M Caffarra P High specificity ofMMSE pentagon scoring for diagnosis of prodromal dementia with Lewy bodiesParkinsonism Relat Disord 201521303ndash305
18 Yoon JH Kim M Moon SY Yong SW Hong JM Olfactory function and neuro-psychological profile to differentiate dementia with Lewy bodies from Alzheimerrsquosdisease in patients with mild cognitive impairment a 5-year follow-up study J NeurolSci 2015355174ndash179
19 Kemp J Philippi N Phillipps C et al Cognitive profile in prodromal dementia withLewy bodies Alzheimers Res Ther 2017919
20 Auning E Rongve A Fladby T et al Early and presenting symptoms of dementia withLewy bodies Dement Geriatr Cogn Disord 201132202ndash208
21 Kondo D Ota K Kasanuki K et al Characteristics of mild cognitive impairmenttending to convert into Alzheimerrsquos disease or dementia with Lewy bodies a follow-upstudy in a memory clinic J Neurol Sci 2016369102ndash108
22 Marchand DG Postuma RB Escudier F et al How does dementia with Lewy bodiesstart prodromal cognitive changes in REM sleep behavior disorder Ann Neurol2018831016ndash1026
23 Kantarci K Lesnick T Ferman TJ et al Hippocampal volumes predict risk of de-mentia with Lewy bodies in mild cognitive impairment Neurology 2016872317ndash2323
24 Thomas AJ Taylor JP McKeith I et al Revision of assessment toolkits for improvingthe diagnosis of Lewy body dementia the DIAMOND Lewy study Int J GeriatrPsychiatry 2018331293ndash1304
25 Galvin JE Improving the clinical detection of Lewy body dementia with the Lewybody composite risk score Alzheimerrsquos Demen (Amsterdam Netherlands) 20151316ndash324
26 Belden CM Kahlon V Malek-Ahmadi M Tsai A Sabbagh MN Clinical character-ization of mild cognitive impairment as a prodrome to dementia with Lewy bodiesAm J Alzheimers Dis Other Demen 201530173ndash177
27 Yoon JH Lee JE Yong SW Moon SY Lee PH The mild cognitive impairment stageof dementia with Lewy bodies and Parkinson disease A comparison of cognitiveprofiles Alzheimer Dis Assoc Disord 201428151ndash155
28 Fengler S Liepelt-Scarfone I Brockmann K Schaffer E Berg D Kalbe E Cognitivechanges in prodromal Parkinsonrsquos disease a review Mov Disord 2017321655ndash1666
29 Kalbe E Rehberg SP Heber I et al Subtypes of mild cognitive impairment in patientswith Parkinsonrsquos disease evidence from the LANDSCAPE study J Neurol NeurosurgPsychiatry 2016871099ndash1105
30 Thomas AJ Donaghy P Roberts G et al Diagnostic accuracy of dopaminergic im-aging in prodromal dementia with Lewy bodies Psychol Med 20181ndash7
31 Ferman TJ Boeve BF Smith GE et al Inclusion of RBD improves the diagnosticclassification of dementia with Lewy bodies Neurology 201177875ndash882
32 Fujishiro H Okuda M Iwamoto K et al Early diagnosis of Lewy body disease inpatients with late-onset psychiatric disorders using clinical history of rapid eyemovement sleep behavior disorder and I-123 -metaiodobenzylguanidine cardiacscintigraphy Psychiatry Clin Neurosci 201872423ndash434
33 Bonanni L Perfetti B Bifolchetti S et al Quantitative electroencephalogram utility inpredicting conversion of mild cognitive impairment to dementia with Lewy bodiesNeurobiol Aging 201536434ndash445
34 Murray ME Ferman TJ Boeve BF et al MRI and pathology of REM sleep behaviordisorder in dementia with Lewy bodies Neurology 2013811681ndash1689
35 Murray ME Graff-Radford NR Ross OA Petersen RC Duara R Dickson DWNeuropathologically defined subtypes of Alzheimerrsquos disease with distinct clinicalcharacteristics a retrospective study Lancet Neurol 201110785ndash796
36 Blanc F Colloby SJ Cretin B et al Grey matter atrophy in prodromal stage ofdementia with Lewy bodies and Alzheimerrsquos disease Alzheimers Res Ther 2016831
37 Blanc F Colloby SJ Philippi N et al Cortical thickness in dementia with Lewy bodiesand Alzheimerrsquos disease a comparison of prodromal and dementia stages Plos One201510e0127396
38 Surendranathan A OrsquoBrien JT Clinical imaging in dementia with Lewy bodies EvidBased Ment Health 20182161ndash65
39 Outeiro TF Koss DJ Erskine D et al Dementia with Lewy bodies an update andoutlook Mol Neurodegener 2019145
40 Donadio V Incensi A Rizzo G et al A new potential biomarker for dementiawith Lewy bodies Skin nerve alpha-synuclein deposits Neurology 201789318ndash326
41 Flanigan PM Khosravi MA Leverenz JB Tousi B Color vision impairment differ-entiates Alzheimer dementia from dementia with Lewy bodies J Geriatr PsychiatryNeurol 20183197ndash102
42 Fereshtehnejad SM Yao C Pelletier A Montplaisir JY Gagnon JF Postuma RBEvolution of prodromal Parkinsonrsquos disease and dementia with Lewy bodies a pro-spective study Brain 20191422051ndash2067
43 Bousiges O Bombois S Schraen S et al Cerebrospinal fluid Alzheimer biomarkerscan be useful for discriminating dementia with Lewy bodies from Alzheimerrsquos diseaseat the prodromal stage J Neurol Neurosurg Psychiatry 201889467ndash475
44 Kantarci K Lowe VJ Boeve BF et al Multimodality imaging characteristics of de-mentia with Lewy bodies Neurobiol Aging 2012332091ndash2105
45 Kantarci K Lowe VJ Boeve BF et al AV-1451 tau and beta-amyloid positronemission tomography imaging in dementia with Lewy bodies Ann Neurol 20178158ndash67
46 Gore RL Vardy E OrsquoBrien JT Delirium and dementia with Lewy bodies distinctdiagnoses or part of the same spectrum J Neurol Neurosurg Psychiatry 20158650ndash59
47 Aarsland DS Auning E The pre-dementia stage of dementia with Lewy bodies Eur JNeurol 20111869
48 Sunwoo MK Hong JY Choi J Park HJ Kim SH Lee PH alpha-Synuclein pathologyis related to postoperative delirium in patients undergoing gastrectomy Neurology201380810ndash813
49 Akintade O Pierres F Acute presentation of dementia with Lewy bodies Clin Med201919327ndash330
50 Kosaka K Diffuse Lewy body disease in Japan J Neurol 1990237197ndash20451 Birkett DP Desouky A Han L Kaufman M Lewy bodies in psychiatric patients Int J
Geriatr Psychiatry 19927235ndash240
Appendix (continued)
Name Location Contribution
John PaulTaylor MBBS PhD
Newcastle University Revising the manuscript forintellectual content
Debby WTsuang MD
VA Puget Sound ampUniversity ofWashington
Revising the manuscript forintellectual content
ZuzanaWalker MD
University CollegeLondon
Revising the manuscript forintellectual content
PietroTiraboschiMD
Istituto NeurologicoldquoCarlo Bestardquo Milan
Design and conceptualizationof the study acquisition ofdata analysis andinterpretation of the data anddrafting and revising themanuscript for intellectualcontent
754 Neurology | Volume 94 Number 17 | April 28 2020 NeurologyorgN
52 Kobayashi K Nakano H Akiyama N Maeda T Yamamori S Pure psychiatric pre-sentation of the Lewy body disease is depressionmdashan analysis of 60 cases verified withmyocardial meta-iodobenzylguanidine study Int J Geriatr Psychiatry 201530663ndash668
53 Takahashi S Mizukami K Arai T et al Ventilatory response to hypercapnia predictsdementia with Lewy bodies in late-onset major depressive disorder J Alzheimers Dis201650751ndash758
54 Van Assche L Van Aubel E Van de Ven L Bouckaert F Luyten P Vandenbulcke MThe neuropsychological profile and phenomenology of late onset psychosis a cross-sectional study on the differential diagnosis of very-late-onset Schizophrenia-likepsychosis dementia with Lewy bodies and Alzheimerrsquos type dementia with psychosisArch Clin Neuropsychol 201934183ndash199
55 Thaipisuttikul P Lobach I Zweig Y Gurnani A Galvin JE Capgras syndrome indementia with Lewy bodies Int Psychogeriatr 201325843ndash849
56 Fujishiro H Iseki E Nakamura S et al Dementia with Lewy bodies early diagnosticchallenges Psychogeriatrics 201313128ndash138
57 Chiba Y Fujishiro H Iseki E et al Retrospective survey of prodromal symptoms indementia with Lewy bodies comparison with Alzheimerrsquos disease Dement GeriatrCogn Disord 201233273ndash281
58 Kaufmann H Norcliffe-Kaufmann L Palma JA et al Natural history of pure auto-nomic failure a United States prospective cohort Ann Neurol 201781287ndash297
59 Heinzel S Berg D Gasser T et al Update of the MDS research criteria for prodromalParkinsonrsquos disease Mov Disord 2019341464ndash1470
60 Palma JA Norcliffe-Kaufmann L Kaufmann H Diagnosis of multiple system atrophyAuton Neurosci 201821115ndash25Data available fromDryad (Additional References References e1ndashe44) doi105061dryad1c59zw3rv
Subspecialty Alerts by E-mail
Customize your online journal experience by signing up for e-mail alerts related to your subspecialty or area of interest Accessthis free service by clicking on the ldquoMy Alertsrdquo link on the home page An extensive list of subspecialties methods and studydesign choices will be available for you to choose frommdashallowing you priority alerts to cutting-edge research in your field
COVID-19 and Neurologic Disease Call for Papers
The editors of Neurology are interested in papers that address the neurological aspects of COVID-19infection and challenges to the management of patients with chronic neurological conditions whohave or are at risk for the infection Relevant papers that pass initial internal review will undergoexpedited peer review and online publication We will consider papers posted in preprint servers
Submit observational studies and clinical trials as Articles and case series and case reports underthe ClinicalScientific Notes category to httpssubmitneurologyorg today
Visit the Neurologyreg Website at NeurologyorgN More article-based content on home pages Streamlined menus and navigation Enhanced blog sections for specialty areas Same experience on desktop tablet and mobile devices Improved article reading experience links more evident (pdf analytics social media) Neurologyreg Clinical Practice initiative ldquoPractice Currentrdquo global surveys will be accessible across sites
Find Neurologyreg on Facebook httptinyurlcomneurologyfan
Follow Neurologyreg on Twitter httpstwittercomGreenJournal
NeurologyorgN Neurology | Volume 94 Number 17 | April 28 2020 755
DOI 101212WNL0000000000009323202094743-755 Published Online before print April 2 2020Neurology
Ian G McKeith Tanis J Ferman Alan J Thomas et al Research criteria for the diagnosis of prodromal dementia with Lewy bodies
This information is current as of April 2 2020
ServicesUpdated Information amp
httpnneurologyorgcontent9417743fullincluding high resolution figures can be found at
References httpnneurologyorgcontent9417743fullref-list-1
This article cites 59 articles 12 of which you can access for free at
Subspecialty Collections
httpnneurologyorgcgicollectionpsychosisPsychosis a
httpnneurologyorgcgicollectionparkinsons_disease_with_dementiParkinsons disease with dementia
httpnneurologyorgcgicollectionmci_mild_cognitive_impairmentMCI (mild cognitive impairment)
httpnneurologyorgcgicollectiondementia_with_lewy_bodiesDementia with Lewy bodies
httpnneurologyorgcgicollectiondeliriumDeliriumfollowing collection(s) This article along with others on similar topics appears in the
Permissions amp Licensing
httpwwwneurologyorgaboutabout_the_journalpermissionsits entirety can be found online atInformation about reproducing this article in parts (figurestables) or in
Reprints
httpnneurologyorgsubscribersadvertiseInformation about ordering reprints can be found online
ISSN 0028-3878 Online ISSN 1526-632XWolters Kluwer Health Inc on behalf of the American Academy of Neurology All rights reserved Print1951 it is now a weekly with 48 issues per year Copyright Copyright copy 2020 The Author(s) Published by
reg is the official journal of the American Academy of Neurology Published continuously sinceNeurology

disproportionately affected attentionexecutive function22
visuospatial skillse18 and memory28 Similar toMCI-LB thereis evidence that nonamnestic MCI is more common thanamnestic MCI and that multidomain amnestic MCI is morecommon than single-domain amnestic MCI29
Biomarkers for prodromal DLBDirect measures of α-synuclein pathology would offer de-finitive diagnosis at an early stage several are under de-velopment but none is yet validated or available for useantemortem Surrogate biomarkers of LB disease must
Table 1 Research criteria for the clinical diagnosis of probable and possible MCI-LB
Essential for a diagnosis of MCI-LB is MCI defined by the presence of each of the following
Concern by the patient informant or clinician regarding cognitive decline
Objective evidence of impairment in 1 or more cognitive domains The cognitive impairment may include any domain but is more likely to be associatedwith attention-executive andor visual processing deficits
Preserved or minimally affected performance of previously attained independence in functional abilities which do not meet the criteria for dementia
Core clinical features
Fluctuating cognition with variations in attention and alertness
Recurrent visual hallucinations
RBD
One or more spontaneous cardinal features of parkinsonism these are bradykinesia (defined as slowness of movement and decrement in amplitude orspeed) rest tremor or rigidity
Proposed biomarkers
Reduced dopamine transporter uptake in basal ganglia demonstrated by SPECT or PET
Polysomnographic confirmation of REM sleep without atonia
Reduced meta-iodobenzylguanidine (MIBG) uptake on myocardial scintigraphy
Probable MCI-LB can be diagnosed if
Two or more core clinical features of DLB are present with or without the presence of a proposed biomarker or
Only 1 core clinical feature is present but with 1 or more proposed biomarkers
Probable MCI-LB should not be diagnosed based on biomarkers alone
Possible MCI-LB can be diagnosed if
Only 1 core clinical feature of DLB is present with no proposed biomarkers or
One or more of the proposed biomarkers is present but there are no core clinical features
Supportive clinical features
Severe sensitivity to antipsychotic agents postural instability repeated falls syncope or other transient episodes of unresponsiveness prolonged orrecurrent delirium autonomic dysfunction eg constipation orthostatic hypotension urinary incontinence hypersomnia hyposmia hallucinations inother modalities including passage and sense of presence phenomena systematized delusions apathy anxiety and depression
Potential biomarkers of MCI-LB
Quantitative EEG showing slowing and dominant frequency variability
Relative preservation of medial temporal lobe structures on structural imaging
Insular thinning and gray matter volume loss on MRI
Low occipital uptake on perfusionmetabolism scan
MCI plus supportive clinical features or potential biomarkers are insufficient to diagnose MCI-LB but may raise suspicion of it and prompt biomarkerinvestigation and may add weight to an existing MCI-LB diagnosis
MCI-LB is less likely in the presence of any other physical illness or brain disease including cerebrovascular disease sufficient to account in part or in total forthe clinical picture although these do not exclude anMCI-LB diagnosis andmay serve to indicatemixed ormultiple pathologies contributing to the clinicalpresentation
Abbreviations DLB = dementia with Lewy bodies MCI = mild cognitive impairment MCI-LB = MCI with Lewy bodiesThese should be used in conjunction with the corresponding article text which gives further information about core and supportive clinical features and theuse of biomarkers as they apply to MCI-LB
746 Neurology | Volume 94 Number 17 | April 28 2020 NeurologyorgN
therefore be used as is the case for the diagnosis of DLBitself2 We propose biomarkers for the diagnosis of prodromalDLB where there is either sufficient good quality publishedevidence of adequate diagnostic specificity in prodromal DLBor this can be reasonably extrapolated from fully developedDLB or related disorders We categorize biomarkers for whichonly limited data are available as potential biomarkers rec-ognizing that such distinctions are likely to require revision asnew data become available
Proposed biomarkers
Reduced dopamine transporter (DAT) uptake in basalganglia demonstrated by SPECT or PETThe utility of DAT imaging in discriminating DLB from ADis already well established2 and its sensitivity in dis-tinguishing MCI with LB (MCI-LB) fromMCI with AD was54 and specificity 8930 whenMCI-LB was defined by thepresence of 1 core clinical feature of DLB in patients withMCI A higher sensitivity of 61 was achieved when 2 coreclinical symptoms were present30 Reduced striatal DATuptake therefore seems suggestive of prodromal DLB ina person with MCI but normal striatal DAT uptake does notexclude it
Polysomnographic confirmation of REM sleep withoutatoniaThe association between RBD and synucleinopathy is highlyspecific (eg a multicenter autopsy study found that of 80subjects with polysomnography [PSG]-confirmed RBD anda coexisting neurodegenerative disorder only 2 had a diseaseunrelated to α-synuclein deposition)e4 These data imply thata patient presenting with MCI and having PSG-confirmedRBD that is a history of probable RBD plus clear docu-mentation of REM sleep without atonia (RSWA) on PSGalso has a high probability of an underlying prodromal syn-ucleinopathy Because around a quarter of patients with DLBdo not report symptoms of RBD andor have normal REMsleep atonia on PSG a normal PSG does not exclude a pro-dromal DLB diagnosis31
Reduced meta-iodobenzylguanidine uptake onmyocardial scintigraphyReduced meta-iodobenzylguanidine (MIBG) uptake is anindicative biomarker for DLB2 and has also been reported tooccur in a small series of patients with late-onset psychiatricdisorder and PSG-confirmed RBD32 reinforcing its associa-tion with underlying α-synucleinopathy Of 2 patients withamnestic MCI with low MIBG uptake one developed DLBafter 2 years the other had no clinical follow-up reportede19
VHs andor RBD were reported among 7 of 13 patients withMCI with reduced MIBG uptake the majority of whom alsohad autonomic symptoms suggestive of LB disease but theywere not followed to determine conversion to DLBe20 De-spite a paucity of longitudinal datae21 there seems to be suf-ficient evidence that abnormal MIBGmyocardial scintigraphyin a patient with MCI supports a prodromal DLB diagnosisbut further studies are required
Potential biomarkersThese are biomarkers consistent with underlying LB diseasewhich may help the diagnostic evaluation but for which thereis still insufficient evidence of diagnostic sensitivity andspecificity in early disease This will change as new evidenceemerges at which point these or other candidates may be-come considered as indicative of prodromal DLB
Quantitative EEG showing slowing and dominantfrequency variabilityEEG slowing has been reported as predictive of dementia inboth PDe22 and RBDe23 posterior slow wave activity withperiodic fluctuations in the pre-alpha range being supportiveof DLB2 Quantitative EEG (QEEG) methods show thata dominant frequency lt8 Hz and dominant frequency vari-ability gt1middot5 Hz is typical of DLB and in a 3-year follow-upstudy 83 of subjects with MCI with this pattern at pre-sentation converted to DLB If these findings are replicatedQEEG may represent a powerful predictor of progressionfrom MCI to DLB33
Relative preservation of medial temporal lobestructures on structural imagingAbsent or minimal medial temporal lobe atrophy is consistentwith DLB but not sufficiently specific to differentiate it fromAD2 Lewy body disease with RBD is characterized by pre-served hippocampal volumes34 and hippocampal preserva-tion in patients with MCI supports progression to DLBinstead of AD dementia with a sensitivity of 85 and a spec-ificity of 6123 Suboptimal specificity may be due to thevariability of hippocampal atrophy in AD35 and contributionof other pathologic processes such as TAR DNA bindingprotein 43 (TDP43)e24
Insular thinning and gray matter volume lossInsular cortical thinning occurs in prodromal DLB relative tohealthy controls using MRI T1 sequences with gray matteratrophy predominantly affecting the anterior cingulum andmedial frontal structures This contrasts with more extensiveloss of gray matter in the temporal frontal and parietalregions of subjects with prodromal AD Insular corticalthinning may therefore differentiate patients with prodromalDLB not only from healthy controls but also from theirprodromal AD counterparts36 No group differences in insularvolumes are seen between DLB and AD at the dementia stageso longitudinal studies are required to determine its precisevalue as an early diagnostic marker of DLB37 Insula is alsoinvolved early in frontotemporal dementia (FTD) being thefirst cortical area to show atrophy in presymptomatic GRNMAPT or C9ORF72 mutation carrierse25 and unlikelytherefore to be helpful in differentiating DLB from FTD
Low occipital uptake on perfusionmetabolism scanOccipital hypometabolism on FDG-PET is associated withDLB38 and together with relative preservation of posteriorcingulate metabolism (the cingulate island sign)e26 is a sup-portive biomarker of DLB2 How frequently the cingulate
NeurologyorgN Neurology | Volume 94 Number 17 | April 28 2020 747
island sign is seen in prodromal DLB remains to be estab-lished significantly reduced posterior cingulate metabolismmay be a useful indication of the concurrence of additionalneurofibrillary tangle pathologye27
Other biomarkersThere is currently no α-synuclein radioligand with sufficientevidence supporting its utility for imaging DLB or any otherα-synucleinopathy nor have any diagnostically applicablebiofluid peripheral tissue or genotypic biomarkers beenestablished2 CSF measures cannot reliably discriminate be-tween DLB and AD39 although the measurement of CSFα-synuclein aggregates using seeding aggregation assays suchas protein misfolding cyclic amplification and real-timequaking-induced conversion is providing encouraging pre-liminary results and may be extended to more accessiblebiofluids including saliva plasma serum or urinee28 Com-bining CSF markers may be useful for example addition ofCSF phospho-tau to α-synuclein significantly improved thedifferential diagnosis between MCI-LB and MCI-AD in-creasing sensitivity and specificity both gt than 95e29 Otherdirect or indirect biomarker candidates that may occur earlyinclude identification of phosphorylated α-synuclein depositsin peripheral nervous tissue from skin biopsy40 gait ana-lysise30 and abnormalities in color vision discrimination4142
The figure shows a framework for considering a wider range ofbiomarkers in the setting of prodromal DLB determining theextent to which AD-related pathology is contributing to thedementia syndrome and influencing clinical trajectories inthese patients4344e31e32 Aβ42 declines earlier in AD thanDLB whereas Aβ40 levels increase alone in AD A low
Aβ42Aβ40 ratio may therefore differentiate patients withprodromal AD from patients with prodromal DLB better thanindividual measures43 There is also evidence showing dif-ferent frequencies and topographies of abnormal uptake onamyloid and tau PET imaging in DLB vs AD45
Delirium-onset DLBCognitive fluctuations or pronounced variations in alertnessand arousal are a core feature of DLB apparent as markedfluctuations in cognitive ability or function detectable byobservation or informant report and measurable using sen-sitive cognitive and electrophysiologic measurese33 The oc-currence of delirium (sometimes referred to as acuteconfusional state) as an early presenting feature of DLB hasbeen described in numerous case reports and seriese34 in-cluding in those with no apparent previous history of cogni-tive impairment46e35 Whether this represents a greatervulnerability to delirium in subjects with DLB or the mis-diagnosis of severe fluctuations with clouding of conscious-ness as delirium or a combination of both is unclear
Recognition that DLB may first present as delirium is im-portant because most guidelines for behavioral disturbancesin delirium recommend antipsychotics as first-line pharma-cologic treatment Delirium or marked fluctuations in con-sciousness were reported by 43 of caregivers before DLBdiagnosis47 and previous episodes of delirium were muchmore frequent in patients with DLB compared with patientswith AD (25 vs 7) with 1 in 4 of those with DLB havingrepeated delirium11 In the majority of these potential pro-voking causes were present A similarly higher incidence ofdelirium was found for subjects with DLB compared with
Figure Multimodal biomarkers for prodromal DLB
Reduced dopamine transporter uptake in basal gan-glia demonstrated by SPECT or PET PSG-confirmedREM sleep without atonia and MIBG myocardial scin-tigraphy are proposed as biomarkers of prodromalDLB Multimodality biomarkers are also important incharacterizing patients with prodromal DLB in whomthe pathologic mechanisms of cognitive impairmentinclude both LB and AD pathologies and who mayhave abnormalities associated with both Medialtemporal lobe uptake on tau PET medial temporallobe atrophy on MRI and high levels of uptake onamyloid PET and positive CSF biomarkers of AD-re-lated pathology may characterize patients with pro-dromal DLB with significant AD pathology It isexpected that biomarker abnormalities detected inthe earliest stages will remain abnormal as diseaseprogresses with additional biomarkers showingchanges later during the progression from pro-dromal to dementia phase DLB DLB = dementia withLewy bodies MIBG = meta-iodobenzylguanidine
748 Neurology | Volume 94 Number 17 | April 28 2020 NeurologyorgN
subjects with AD in the year before diagnosis (17middot6 v 3middot2100person-years)9 and admissions for delirium were morecommon in those already diagnosed with DLB than for otherdementias Prolonged delirium may also raise the index ofsuspicion for DLBe36 In an FDG-PET imaging study ofprolonged delirium 32 of subjects were found to havea DLB like pattern a high proportion in regard both to theknown prevalence of the disease and to that of their matchedcognitively impaired control group (4)e37
The similarities between the marked fluctuations in DLB anddisturbances of attention and consciousness in delirium havebeen noted and reviewed46 but there is as yet little un-derstanding of a shared neurobiological basis There havebeen few pathologic studies and although in anepidemiologic-based autopsy cohort there was no link be-tween delirium and LB pathology at autopsye38 a significantlyincreased risk of postoperative delirium in those with pe-ripheral α-synuclein pathology has been described48 Deliriumhas been suggested to bemore common in those subjects withDLB with later age at onsete39 but further evidence is needed
In summary (table 2) it is clear that DLB can present withdelirium and in patients diagnosed with delirium a carefulsearch for other DLB features should be made with a lowthreshold for undertaking DLB biomarker examinations es-pecially in those with recurrent unexplained or prolongeddelirium The extent to which delirium presentations of DLBhave the biomarker abnormalities associated with establishedDLB or other prodromal DLB presentations is unclear
although the PET imaging study cited above supports thise37
as does a report of reduced DAT uptake in a patient withacute unexplained delirium49 The link between delirium andDLB is an important area for future research to clarify therelationship between the 2 and to establish which factorsassociated with delirium should raise the index of suspicionfor underlying prodromal DLB
Psychiatric-onset DLBEarly clinicopathologic studies suggested that DLB maypresent as a primary psychiatric disorder5051 but subsequentfocus on the cognitive and motor aspects of DLB has limitedthe documentation of such cases outside of a fewcenters123252ndash54e36 Late-onset major depressive disorderand late-onset psychosis are the most frequently reportedpresentations differing markedly from the construct of mildbehavioral impairmente40 and sometimes sufficiently severe torequire hospitalization Symptoms include hallucinations invisual and in other modalities and systematized delusionsincluding Capgras syndrome55 apathy anxiety and de-pression Psychiatric-onset DLB cases are not easily differ-entiated from non-LB late-onset psychosis cases on the basisof primary psychiatric phenomenology or neuropsychologicalprofile alone54 Psychomotor retardation such as slowedspeech thinking and body movements can resemble thebradykinesia of parkinsonism The occurrence of rest tremoror rigidity is more helpful than bradykinesia to suspect pro-dromal DLB in patients with depressive disorder53 butpsychotropic-induced parkinsonism may complicate di-agnosis Atypical clinical features may prove valuable pointers
Table 2 Summary of key features of delirium-onset DLB
Patients with DLB are more susceptible to delirium than people with Alzheimer disease and this delirium may occur as their presenting complaint beforedementia develops
Such episodes may be provoked by multiple factors including surgery infectionssepsis fever or other systemic illness or secondary to use or suddenwithdrawal of alcohol or psychoactive drugs
Prodromal DLB should be particularly suspected in patients
bull in whom adequate provoking factors for the delirium are not found
bull with prolonged or recurrent delirium
bull who later develop progressive cognitive decline or subsequent dementia
Core clinical features of DLB are likely to be of more limited diagnostic weight in a patient with delirium because
bull cognitive fluctuation and clouding of consciousness can also occur in non-DLB delirium ie are not diagnostically specific for DLB in this situation
bull visual hallucinations may occur in non-DLB delirium particularly drug-induced or provoked by alcohol abstinence
bull motor parkinsonism present may be due to antipsychotic medications used to treat delirium
bull the diagnostic significance of a history of RBD in a person with delirium is not yet established
Identification of delirium-onset DLB
bull may be assisted by use of MCI-LB biomarkers but further research evidence of this is required
bull is important to inform the management plan including the avoidance or minimization of antipsychotic and anticholinergic agents
Abbreviations DLB = dementia with Lewy bodies MCI = mild cognitive impairment MCI-LB = MCI with Lewy bodies RBD = REM sleep behavior disorder
NeurologyorgN Neurology | Volume 94 Number 17 | April 28 2020 749
to underlying LB pathology particularly the presence of re-current VH12 when these occur before cognitive impairmentbecomes evident As with all α-synucleinopathies RBD maybe a useful indicator although a relationship between anti-depressant usage and subsequent RBD onset is a potentialconfoundere41 Although the primary psychiatric manifes-tations are often accompanied by mild cognitive deficits54
cognitive evaluation and interpretation of performance can bedifficult when psychiatric symptoms are prominent The fre-quency of cognitive fluctuations in psychiatric-onset LB caseshas not been determined
Initial reports suggest that 123I-MIBG scintigraphy may behelpful in psychiatric-onset DLB525356 Eighteen of 35patients with a first onset of major depressive disorder gt50years and with bradykinesia developed a clinical diagnosis ofDLB after 6 years of follow-up All 18 had an abnormal ven-tilatory response to hypercapnia (VRH) indicative of severeautonomic dysfunction whereas none of the 17 patients witha normal VRH converted to DLB within the study period Forthe converters the most common presentation was withpsychotic and melancholic features simultaneously The fre-quency of hypersensitivity to antipsychotics antidepressantsand antianxiety drugs was higher in converters than in non-converters53 Further studies need to confirm these findingsand to determine the value of other DLB biomarkers inpsychiatric-onset cases325256
In summary it is not yet clear how to identify patients withprominent late-onset psychiatric symptoms who may haveunderlying LB disease and subsequently progress to DLB It is
premature to try to construct formal criteria for psychiatric-onset DLB but clinicians in mental health and other settingsneed to be aware that this possibility exists not least becauseof the risk of severe antipsychotic sensitivity reactions withincreased morbidity and mortality The small available liter-ature including reports such as those cited above does providesome useful guidance summarized in table 3 but requiresreplication and further investigation
Idiopathic REM sleep behavior disorderRBD is characterized by abnormal dream enactment behaviorduring REM sleep accompanied by loss of muscle atonia duringREM sleep (REM sleep without atonia or RSWA) on PSG Forthe purpose of a prodromal DLB diagnosis a clinical history ofRBD is obtained in the same way as for DLB2 that is a clearcomplaint of dream enactment by a bedpartner or other witnesswith no evidence of sleep disorders that may mimic RBD onclinical interview Conditions known to mimic or masquerade asRBD include non-REM parasomnias (sleep walking sleep talk-ing or other behaviors that emerge fromnon-REM sleep stages)obstructive sleep apnea confusional arousals or nocturnal seiz-ures In the absence of PSG the risk of a false-positive clinicaldiagnosis of RBD is reduced by using optimized sleep ques-tionnaires which can have sensitivity and specificity over 90e42
RBDmay be considered as idiopathic until it is associated withanother ongoing neurologic condition the most frequentbeing an α-synucleinopathy (PD DLB or MSA) In a recentlarge study 735 of patients with RBD converted to an overtneurodegenerative syndrome after 12-year follow-up 565developing parkinsonism and 435 dementia as their first
Table 3 Summary of key features of psychiatric-onset DLB
Is characterized by predominant psychiatric symptoms that typically correspond to late-onset major depressive disorder or late-onset psychosis which mayfeature hallucinations in visual and in other modalities and systematized delusions including Capgras syndrome
bull may also present with apathy anxiety and depression
bull may be sufficiently severe to require hospitalization
bull the frequency of LB disease as a cause of late-onset psychiatric disorder is not known
When assessing for core clinical features of DLB in a patient with a primary psychiatric presentation
bull bradykinesia may be mimicked by psychomotor retardation which is commonly seen in depressive disorders
bull parkinsonism may be induced by antipsychotic medications used to treat psychiatric disorder
bull RBD (and REM sleep without atonia) may be induced by antidepressant medications
bull mild cognitive disturbance may be present but is not predominant and may fluctuate
bull formal neuropsychological testing may be confounded by the psychiatric mental state
bull the frequency and character of cognitive fluctuations is unknown
Identification of psychiatric-onset DLB
bull may be assisted by use of MCI-LB biomarkers but further research evidence of this is required
bull is important to inform the management plan including the avoidance or minimization of antipsychotic and anticholinergic agents
Abbreviations DLB = dementia with Lewy bodies MCI = mild cognitive impairment
750 Neurology | Volume 94 Number 17 | April 28 2020 NeurologyorgN
disease manifestation Among many predictive markerstested only the cognitive variables differed at baseline be-tween those converting to primary dementia vs parkinson-ism7 Other multicenter studies confirm that the only clinicalfeature that predicts dementia vs parkinsonism first is neu-ropsychological performance those with RBD who exhibitcognitive changes are more likely to evolve first into MCI orDLB22e4 Thus although RBD may be regarded an earlymanifestation of α-synucleinopathy it is not possible to clearlydistinguish whether an individual presenting with RBD willdevelop dementia first that is evolve into a primary DLBdiagnosis or parkinsonism first that is a primary PDMSAdiagnosis Any MCI subtype associated with PSG-confirmedRBD is highly likely to represent underlying LB disease Al-though idiopathic RBD is a useful model to study the earlystages of LB disease progression it is not necessarily repre-sentative of the whole spectrum of patients with PD and DLBa significant minority of whom do not have RBD42
Autonomic dysfunctionanosmia and othernonspecific prodromal LB disease symptomsPatients with DLB frequently report a history of autonomicdysfunction at first clinic attendance with 25ndash50 com-plaining of one of more among constipation orthostatic diz-ziness urinary incontinence erectile dysfunction increasedsweating or increased saliva5657 In a cohort of patients withpure autonomic failure 34 converted to an overt α-synu-cleinopathy over 6 years of follow-up this was to DLB (52)PD (24) orMSA (24)58 However because there are manyother causes for autonomic dysfunction in older people thesesymptoms either alone or in combination have low positivepredictive value59 The situation is similar for hyposmia whichalso frequently occurs early in prodromal DLB and PD42 butwhich can have many other causes in this age group
Conclusions and future directionDiagnosis of DLB at the dementia stage depends on identifyingfully expressed core clinical features which may be mild orabsent at the prodromal stage when biomarker evidence mayalso be weaker and may even differ from that found at thedementia stage Several new biomarker candidates direct andindirect are in development and we will continue to reviewthese to update our recommendations as soon as sufficientevidence accumulates We recognize that the clinical pheno-type of neurodegenerative disorders reflects interaction be-tween several rather than a single brain pathology and it istherefore likely that multiple biomarkers of individual pathol-ogies (eg α-synuclein β-amyloid and tau) or of disease sur-rogates (eg metabolic imagingEEG) will be required
Although we have described the 3 prodromal DLB syndromesseparately they are unlikely to be mutually exclusive andthere may be substantial overlap We propose operationalizedcriteria only for MCI-LB because the evidence base from oursystematic review albeit relatively limited is sufficient to
support recommendations that are immediately applicableand testable Our recommendations should be used alongsideguidance about the prodromal manifestations of PD1559
MSA60 and AD14 with which there is overlap Notwith-standing the potential benefits of early diagnosis we are alsomindful of the importance of avoiding incorrect (false-positive) diagnosis of prodromal DLB and the potentialnegative consequences this could have for an individual Wesuggest that the predictive validity of different categories andcombinations of our proposed criteria should be clarified byprospective studies before they are adopted for widespreadclinical use and that they will enable standardization for in-clusion in research studies and clinical trials
Some published guidance about the early clinical diagnosis ofDLB does already exist DSM5 recommends a diagnosis ofmild neurocognitive disorder (NCD) with LB ldquofor individualswho present with the core or suggestive features at a stagewhen cognitive or functional impairments are not of sufficientseverity to fulfill criteria for major NCDrdquoe43 This is basedhowever on the 2005 version of DLB guidelines and requiresupdating ICD-11 takes a similar approach toward diagnosingmild NCD at a syndromic level and lists both Lewy bodydisease and PD as possible causese44
The diagnostic position for other prodromal manifestations ofDLB that is delirium-onset and psychiatric-onset is less clearthan for MCI Operationalization of specific criteria for thesesyndromes is not yet justified and the reliable differentiationof the minority of delirious and psychiatrically ill patients whohave underlying LB pathology from the majority who do notwill probably only be achieved when routinely applicablebiomarkers are developed LB disease is seldom if ever cur-rently considered as part of the differential diagnosis of de-lirium or late-onset psychiatric disorder and we hope that theinformation we provide in the text and accompanying boxeswill raise cliniciansrsquo awareness of that possibility
Study fundingNo targeted funding reported
DisclosureI McKeith receives support from the NIHR Biomedical Re-search Centre awarded to the Newcastle upon Tyne HospitalsNHS Foundation Trust and Newcastle University and hasconsulted for GE Healthcare Sanofi Eisai Sumitomo Dai-nippon Pharma and Axovant T Ferman receives support fromNIH P50-AG16574 P30-AG062677 U01-NS100620 and theMangurian Foundation for Lewy body disease research AThomas receives support from the NIHR Biomedical ResearchCentre awarded to the Newcastle upon Tyne Hospitals NHSFoundation Trust and Newcastle University and has receivedgrants from GE Healthcare F Blanc has served as nationalclinical trial coordinator for Eisai and Axovant B Boevereceives support from NIH P50-AG16574 P30-AG062677U01-NS100620 and the Mangurian Foundation for Lewybody disease research has consulted for the Scientific Advisory
NeurologyorgN Neurology | Volume 94 Number 17 | April 28 2020 751
BoardmdashTau Consortium and received grants from Biogenthe NIH theMangurian Foundation Alector the Little FamilyFoundation and the Turner Family H Fujishiro has receivedsupport from Fujifilm RI Pharma Co Ltd K Kantarci receivessupport from NIH P50-AG16574 P30-AG062677 U01-NS100620 and the Mangurian Foundation for Lewy bodydisease research and has received grants from Avid Radio-pharmaceuticals and acted on a Data Safety Monitoring Boardfor Takeda Global Research C Muscio acknowledges thesupport of the Italian Ministry of Health GRANT NET-2011-02346784 J OrsquoBrien is supported by the NIHR CambridgeBiomedical Research Centre Dementia and Neuro-degeneration and Mental Health Themes and the CambridgeCentre for Parkinsonrsquos Plus Disorders has consulted forTauRx Axon GE Healthcare Eisai and AvidLilly and re-ceived grants fromAvidLilly andAllianceMedical R Postumahas received grants from and consulted for Fonds de laRecherche en Sante received grants from the Canadian Insti-tutes of Health Research the Parkinson Society of Canada theWeston-Garfield Foundation The Michael J Fox Foundationand the Webster Foundation and consulted for TakedaRocheProthena Teva Neurosciences Novartis Canada Bio-gen Boehringer Ingelheim Theranexus GE Healthcare JazzPharmaceuticals AbbVie Jannsen Otsuko PhytopharmicsInception Sciences and Parkinson Canada D Aarsland isa Royal Society Wolfson Research Merit Award Holder andwould like to thank the Wolfson Foundation and the RoyalSociety for their support He has received research supportandor honoraria from AstraZeneca H Lundbeck NovartisPharmaceuticals and GE Health and served as paid consultantfor H Lundbeck Eisai Heptares Sanofi and Mentis Cura CBallard reports unrelated current grant funding from MRCWellcome Trust European Union Gillings FoundationNIHR Alzheimerrsquos Society Alzheimerrsquos Research UK Par-kinsonrsquos Society and Lewy Body Society during the conduct ofthe study and personal fees from Acadia pharmaceutical com-pany Lundbeck Roche Otsuka Eli Lilly and AARP outsidethe submitted work L Bonanni is a member of the steeringcommittee of the E-DLB consortium and program chair of theLBD-PIA (ISTAART) and is funded for research on DLB bythe Italian Ministry of Health P Donaghy receives supportfrom the NIHR Biomedical Research Centre awarded to theNewcastle upon Tyne Hospitals NHS Foundation Trust andNewcastle UniversityM Emre served on the scientific advisoryboard for AC Immune J Galvin receives support from NIHgrants (R01 AG040211 R01 NS101482 R01 AG057681 andU01 NS100610) and the Lewy Body Dementia AssociationResearch Center of Excellence reports research support fromthe NIH the Lewy Body Dementia Association The Harry TMangurian Foundation and Albert Charitable Trust directsclinical trials for Biogen and Novartis receives licensing feesfrom Biogen Roche Eli Lilly Quintiles Roobrik ContinuumClinical and Langland and receives consulting fees fromBiogen Eisai Bracket and Medavante D Galasko receivessupport from NIA grant AGO5131 and the Michael J FoxFoundation and has acted as consultant for vTv Pharmaceut-icals Inc Esai Inc and for Fujirebio Inc been a member of
a DSMB for Probiodrug and paid editor for Alzheimerrsquos Re-search amp Therapy J Goldman receives grantsupport fromTheMichael J Fox Foundation and Parkinsonrsquos Foundation andhas received consulting feeshonoraria from Acadia AptinyxSunovion and Worldwide Med S Gomperts receives supportfrom NIH grants R01 AG054551 P30AG062421 R01AG062208 P50 AG005134 R21 NS109833 DODCDMRPW81XW1810516 the Farmer Family ParkinsonrsquosInitiative and the Lewy Body Dementia Association and hasserved on advisory boards for Acadia Pharmaceuticals andSanofi L Honig acknowledges research grant support fromNYS CEAD grant C031425 LBDA RCOE and NIHgrants U01NS100600 P50AG008702 R21AG058020R21MH111596 U01AG051412 U01AG045390U01AG016976 U01AG023749 U19063893 andU19AG024904 He receives research funding support fromAbbVie Alector Biogen Eisai Genentech Roche and Wash-ington University and has received income for consulting forCortexyme and Eisai M Ikeda reports departmental grants andhonoraria fees from Sumitomo Dainippon Pharma Eisai andNiho Medicine-Physics J Leverenz acknowledges supportfrom the National Institutes of Health P30 AG053762 UO1NS100610 and R13NS111954 and Jane and Lee Seidman andDouglas Herthel DVMMemorial Funds and reports consultingfees from Aptinyx Acadia Biogen Eisai GE HealthcareGenzymeSanofi and Takeda Pharmaceuticals and grant sup-port from Alzheimerrsquos Drug Discovery Foundation De-partment of Defense GE Healthcare GenzymeSanofi TheMichael J Fox Foundation and the NIH (NIA andNINDS) SLewis is supported by NHMRC-ARC Dementia Fellows KMarder is funded by the NIH R01NS100600 NS107168UL1TR001873 andNS073671 with research support from theLBDA Parkinson Foundation Michael J Fox HDSA andCHDI and has acted as site investigator for Vaccinex andGenentech member of Springer editorial board and scientificadvisory board Voyager Therapeutics M Masellis was sup-ported by a Canadian Institutes of Health Research grant(MOP13129) and an Early Researcher Award from the Min-istry of Research Innovation and Science (MRIS ON) andreports personal fees for ad hoc consultancy from ArkudaTherapeutics Ionis Pharmaceuticals and Alector Pharmaceut-icals royalties fromHenry Stewart Talks Ltd and grants to theinstitution from Roche Novartis Washington University andAxovant Sciences D Salmon acknowledges support from NIHP30AG062429 and is a paid consultant for Takeda Inc Apti-nyx Inc and Biogen Inc J-P Taylor receives support from theNIHR Biomedical Research Centre awarded to the Newcastleupon Tyne Hospitals NHS Foundation Trust and NewcastleUniversity and reports grants from the UKNational Institute ofHealth Research (NIHR) travel award from Axovant researchsupport costs from Sonsei-Heptares and personal fees fromGEHealthcare D Tsuang acknowledges support from NIHR21AG064271 R03 NS103950 and U01 NS100610 ZWalker has been supported by ESRC NIHR (co-app) ARUK(co-app) EU IMI 2 (co-app) and Dunhill Medical Trust Shehas received consultancy fees travel expenses and researchsupport from GE Healthcare and research support from Life
752 Neurology | Volume 94 Number 17 | April 28 2020 NeurologyorgN
Molecular Imaging P Tiraboschi acknowledges the support ofthe Italian Ministry of Health GRANT NET-2011-02346784Go to NeurologyorgN for full disclosures
Publication historyReceived by Neurology October 30 2019 Accepted in final formFebruary 25 2020
Appendix Authors
Name Location Contribution
Ian GMcKeith FMed Sci MD
Newcastle University Design and conceptualizationof the study acquisition ofdata analysis andinterpretation of the data anddrafting and revising themanuscript for intellectualcontent
Tanis JFermanPhD
Mayo ClinicJacksonville
Design and conceptualizationof the study acquisition ofdata analysis andinterpretation of the data anddrafting and revising themanuscript for intellectualcontent
Alan JThomasPhD
Newcastle University Design and conceptualizationof the study acquisition ofdata analysis andinterpretation of the data anddrafting and revising themanuscript for intellectualcontent
FredericBlanc MD
University ofStrasbourg
Design and conceptualizationof the study acquisition ofdata analysis andinterpretation of the data anddrafting and revising themanuscript for intellectualcontent
Bradley FBoeve MD
Mayo Clinic Rochester Design and conceptualizationof the study acquisition ofdata analysis andinterpretation of the data anddrafting and revising themanuscript for intellectualcontent
HiroshigeFujishiroMD
Nagoya UniversityKawasaki MemorialHospital
Design and conceptualizationof the study acquisition ofdata analysis andinterpretation of the data anddrafting and revising themanuscript for intellectualcontent
KejalKantarciMD MS
Mayo Clinic Rochester Design and conceptualizationof the study acquisition ofdata analysis andinterpretation of the data anddrafting and revising themanuscript for intellectualcontent
CristinaMuscio PhD
Istituto NeurologicoldquoCarlo Bestardquo Milan
Design and conceptualizationof the study acquisition ofdata analysis andinterpretation of the data anddrafting and revising themanuscript for intellectualcontent
Appendix (continued)
Name Location Contribution
John TOrsquoBrien FMed Sci DM
Cambridge University Design and conceptualizationof the study acquisition ofdata analysis andinterpretation of the data anddrafting and revising themanuscript for intellectualcontent
Ronald BPostumaMD MSc
McGill University Design and conceptualizationof the study acquisition ofdata analysis andinterpretation of the data anddrafting and revising themanuscript for intellectualcontent
DagAarslandPhD
Kingrsquos College Londonand StavangerUniversityHospital
Revising the manuscript forintellectual content
CliveBallard MD
University of Exeter Revising the manuscript forintellectual content
LauraBonanniMD PhD
University of Chieti-Pescara
Revising the manuscript forintellectual content
PaulDonaghyPhD
Newcastle University Revising the manuscript forintellectual content
Murat EmreMD
Istanbul Faculty ofMedicine
Revising the manuscript forintellectual content
James EGalvin MDMPH
University of MiamiMiller School ofMedicine
Revising the manuscript forintellectual content
DouglasGalasko MD
University of CaliforniaSan Diego
Revising the manuscript forintellectual content
Jennifer GGoldmanMD MS
Feinberg School ofMedicine
Revising the manuscript forintellectual content
Stephen NGompertsMD PhD
Massachusetts GeneralHospital
Revising the manuscript forintellectual content
Lawrence SHonig MDPhD
Columbia UniversityIrving Medical Center
Revising the manuscript forintellectual content
ManabuIkeda MDPhD
Osaka University Revising the manuscript forintellectual content
James BLeverenzMD
Lou Ruvo Center ofBrain Health ClevelandClinic
Revising the manuscript forintellectual content
Simon JGLewis MD
University of Sydney Revising the manuscript forintellectual content
Karen SMarder MDMPH
Columbia UniversityIrving Medical Center
Revising the manuscript forintellectual content
MarioMasellisMD PhD
Sunnybrook HealthSciences CentreUniversity of Toronto
Revising the manuscript forintellectual content
David PSalmon PhD
University of CaliforniaSan Diego
Revising the manuscript forintellectual content
Continued
NeurologyorgN Neurology | Volume 94 Number 17 | April 28 2020 753
References1 Walker Z Possin KL Boeve BF Aarsland D Lewy body dementias Lancet 2015386
1683ndash16972 McKeith IG Boeve BF Dickson DW et al Diagnosis and management of dementia
with Lewy bodies fourth consensus report of the DLB consortium Neurology 20178988ndash100
3 Ferman TJ Smith GE Kantarci K et al Nonamnestic mild cognitive impairmentprogresses to dementia with Lewy bodies Neurology 2013812032ndash2038
4 Savica R Bradley BF Mielke MM When do alpha-synucleinopathies start An epi-demiological timeline A review JAMA Neurol 201875503ndash509
5 Donaghy PC Taylor JP OrsquoBrien JT et al Neuropsychiatric symptoms and cognitiveprofile in mild cognitive impairment with Lewy bodies Psychol Med 2018482384ndash2390
6 Cagnin A Bussse C Gardini S et al Clinical and cognitive phenotype of mildcognitive impairment evolving to dementia with Lewy bodies Dement Geriatr CognDis Extra 20155442ndash449
7 Postuma RB Iranzo A HuM et al Risk and predictors of dementia and parkinsonismin idiopathic REM sleep behaviour disorder a multicentre study Brain 2019142744ndash759
8 Sadiq D Whitfield T Lee L Stevens T Costafreda S Walker Z Prodromal dementiawith Lewy bodies and prodromal Alzheimerrsquos disease a comparison of the cognitiveand clinical profiles J Alzheimers Dis 201758463ndash470
9 FitzGerald JM Perera G Chang-Tave A et al The incidence of recorded de-lirium episodes before and after dementia diagnosis differences between de-mentia with Lewy bodies and Alzheimerrsquos disease J Am Med Dir Assoc 201920604ndash609
10 Jicha GA Schmitt FA Abner E et al Prodromal clinical manifestations of neu-ropathologically confirmed Lewy body disease Neurobiol Aging 2010311805ndash1813
11 Vardy E Holt R Gerhard A Richardson A Snowden J Neary D History of a sus-pected delirium is more common in dementia with Lewy bodies than Alzheimerrsquosdisease a retrospective study Int J Geriatr Psychiatry 201429178ndash181
12 Fujishiro H Nakamura S Sato K Iseki E Prodromal dementia with Lewy bodiesGeriatr Gerontol Int 201515817ndash826
13 McKeith I Taylor JP Thomas A Donaghy P Kane J Revisiting DLB diagnosisa consideration of prodromal DLB and of the diagnostic overlap with Alzheimerdisease J Geriatr Psychiatry Neurol 201629249ndash253
14 Albert MS DeKosky ST Dickson D et al The diagnosis of mild cognitive impairmentdue to Alzheimerrsquos disease recommendations from the National Institute on Aging-Alzheimerrsquos Association workgroups on diagnostic guidelines for Alzheimerrsquos diseaseAlzheimers Dement 20117270ndash279
15 Litvan I Goldman JG Troster AI et al Diagnostic criteria for mild cognitive im-pairment in Parkinsonrsquos disease Movement Disorder Society Task Force guidelinesMov Disord 201227349ndash356
16 Ferman TJ Smith GE Boeve BF et al Neuropsychological differentiation of de-mentia with Lewy bodies from normal aging and Alzheimerrsquos disease Clin Neuro-psychol 200620623ndash636
17 Cagnin A Busse C Jelcic N Gnoato F Mitolo M Caffarra P High specificity ofMMSE pentagon scoring for diagnosis of prodromal dementia with Lewy bodiesParkinsonism Relat Disord 201521303ndash305
18 Yoon JH Kim M Moon SY Yong SW Hong JM Olfactory function and neuro-psychological profile to differentiate dementia with Lewy bodies from Alzheimerrsquosdisease in patients with mild cognitive impairment a 5-year follow-up study J NeurolSci 2015355174ndash179
19 Kemp J Philippi N Phillipps C et al Cognitive profile in prodromal dementia withLewy bodies Alzheimers Res Ther 2017919
20 Auning E Rongve A Fladby T et al Early and presenting symptoms of dementia withLewy bodies Dement Geriatr Cogn Disord 201132202ndash208
21 Kondo D Ota K Kasanuki K et al Characteristics of mild cognitive impairmenttending to convert into Alzheimerrsquos disease or dementia with Lewy bodies a follow-upstudy in a memory clinic J Neurol Sci 2016369102ndash108
22 Marchand DG Postuma RB Escudier F et al How does dementia with Lewy bodiesstart prodromal cognitive changes in REM sleep behavior disorder Ann Neurol2018831016ndash1026
23 Kantarci K Lesnick T Ferman TJ et al Hippocampal volumes predict risk of de-mentia with Lewy bodies in mild cognitive impairment Neurology 2016872317ndash2323
24 Thomas AJ Taylor JP McKeith I et al Revision of assessment toolkits for improvingthe diagnosis of Lewy body dementia the DIAMOND Lewy study Int J GeriatrPsychiatry 2018331293ndash1304
25 Galvin JE Improving the clinical detection of Lewy body dementia with the Lewybody composite risk score Alzheimerrsquos Demen (Amsterdam Netherlands) 20151316ndash324
26 Belden CM Kahlon V Malek-Ahmadi M Tsai A Sabbagh MN Clinical character-ization of mild cognitive impairment as a prodrome to dementia with Lewy bodiesAm J Alzheimers Dis Other Demen 201530173ndash177
27 Yoon JH Lee JE Yong SW Moon SY Lee PH The mild cognitive impairment stageof dementia with Lewy bodies and Parkinson disease A comparison of cognitiveprofiles Alzheimer Dis Assoc Disord 201428151ndash155
28 Fengler S Liepelt-Scarfone I Brockmann K Schaffer E Berg D Kalbe E Cognitivechanges in prodromal Parkinsonrsquos disease a review Mov Disord 2017321655ndash1666
29 Kalbe E Rehberg SP Heber I et al Subtypes of mild cognitive impairment in patientswith Parkinsonrsquos disease evidence from the LANDSCAPE study J Neurol NeurosurgPsychiatry 2016871099ndash1105
30 Thomas AJ Donaghy P Roberts G et al Diagnostic accuracy of dopaminergic im-aging in prodromal dementia with Lewy bodies Psychol Med 20181ndash7
31 Ferman TJ Boeve BF Smith GE et al Inclusion of RBD improves the diagnosticclassification of dementia with Lewy bodies Neurology 201177875ndash882
32 Fujishiro H Okuda M Iwamoto K et al Early diagnosis of Lewy body disease inpatients with late-onset psychiatric disorders using clinical history of rapid eyemovement sleep behavior disorder and I-123 -metaiodobenzylguanidine cardiacscintigraphy Psychiatry Clin Neurosci 201872423ndash434
33 Bonanni L Perfetti B Bifolchetti S et al Quantitative electroencephalogram utility inpredicting conversion of mild cognitive impairment to dementia with Lewy bodiesNeurobiol Aging 201536434ndash445
34 Murray ME Ferman TJ Boeve BF et al MRI and pathology of REM sleep behaviordisorder in dementia with Lewy bodies Neurology 2013811681ndash1689
35 Murray ME Graff-Radford NR Ross OA Petersen RC Duara R Dickson DWNeuropathologically defined subtypes of Alzheimerrsquos disease with distinct clinicalcharacteristics a retrospective study Lancet Neurol 201110785ndash796
36 Blanc F Colloby SJ Cretin B et al Grey matter atrophy in prodromal stage ofdementia with Lewy bodies and Alzheimerrsquos disease Alzheimers Res Ther 2016831
37 Blanc F Colloby SJ Philippi N et al Cortical thickness in dementia with Lewy bodiesand Alzheimerrsquos disease a comparison of prodromal and dementia stages Plos One201510e0127396
38 Surendranathan A OrsquoBrien JT Clinical imaging in dementia with Lewy bodies EvidBased Ment Health 20182161ndash65
39 Outeiro TF Koss DJ Erskine D et al Dementia with Lewy bodies an update andoutlook Mol Neurodegener 2019145
40 Donadio V Incensi A Rizzo G et al A new potential biomarker for dementiawith Lewy bodies Skin nerve alpha-synuclein deposits Neurology 201789318ndash326
41 Flanigan PM Khosravi MA Leverenz JB Tousi B Color vision impairment differ-entiates Alzheimer dementia from dementia with Lewy bodies J Geriatr PsychiatryNeurol 20183197ndash102
42 Fereshtehnejad SM Yao C Pelletier A Montplaisir JY Gagnon JF Postuma RBEvolution of prodromal Parkinsonrsquos disease and dementia with Lewy bodies a pro-spective study Brain 20191422051ndash2067
43 Bousiges O Bombois S Schraen S et al Cerebrospinal fluid Alzheimer biomarkerscan be useful for discriminating dementia with Lewy bodies from Alzheimerrsquos diseaseat the prodromal stage J Neurol Neurosurg Psychiatry 201889467ndash475
44 Kantarci K Lowe VJ Boeve BF et al Multimodality imaging characteristics of de-mentia with Lewy bodies Neurobiol Aging 2012332091ndash2105
45 Kantarci K Lowe VJ Boeve BF et al AV-1451 tau and beta-amyloid positronemission tomography imaging in dementia with Lewy bodies Ann Neurol 20178158ndash67
46 Gore RL Vardy E OrsquoBrien JT Delirium and dementia with Lewy bodies distinctdiagnoses or part of the same spectrum J Neurol Neurosurg Psychiatry 20158650ndash59
47 Aarsland DS Auning E The pre-dementia stage of dementia with Lewy bodies Eur JNeurol 20111869
48 Sunwoo MK Hong JY Choi J Park HJ Kim SH Lee PH alpha-Synuclein pathologyis related to postoperative delirium in patients undergoing gastrectomy Neurology201380810ndash813
49 Akintade O Pierres F Acute presentation of dementia with Lewy bodies Clin Med201919327ndash330
50 Kosaka K Diffuse Lewy body disease in Japan J Neurol 1990237197ndash20451 Birkett DP Desouky A Han L Kaufman M Lewy bodies in psychiatric patients Int J
Geriatr Psychiatry 19927235ndash240
Appendix (continued)
Name Location Contribution
John PaulTaylor MBBS PhD
Newcastle University Revising the manuscript forintellectual content
Debby WTsuang MD
VA Puget Sound ampUniversity ofWashington
Revising the manuscript forintellectual content
ZuzanaWalker MD
University CollegeLondon
Revising the manuscript forintellectual content
PietroTiraboschiMD
Istituto NeurologicoldquoCarlo Bestardquo Milan
Design and conceptualizationof the study acquisition ofdata analysis andinterpretation of the data anddrafting and revising themanuscript for intellectualcontent
754 Neurology | Volume 94 Number 17 | April 28 2020 NeurologyorgN
52 Kobayashi K Nakano H Akiyama N Maeda T Yamamori S Pure psychiatric pre-sentation of the Lewy body disease is depressionmdashan analysis of 60 cases verified withmyocardial meta-iodobenzylguanidine study Int J Geriatr Psychiatry 201530663ndash668
53 Takahashi S Mizukami K Arai T et al Ventilatory response to hypercapnia predictsdementia with Lewy bodies in late-onset major depressive disorder J Alzheimers Dis201650751ndash758
54 Van Assche L Van Aubel E Van de Ven L Bouckaert F Luyten P Vandenbulcke MThe neuropsychological profile and phenomenology of late onset psychosis a cross-sectional study on the differential diagnosis of very-late-onset Schizophrenia-likepsychosis dementia with Lewy bodies and Alzheimerrsquos type dementia with psychosisArch Clin Neuropsychol 201934183ndash199
55 Thaipisuttikul P Lobach I Zweig Y Gurnani A Galvin JE Capgras syndrome indementia with Lewy bodies Int Psychogeriatr 201325843ndash849
56 Fujishiro H Iseki E Nakamura S et al Dementia with Lewy bodies early diagnosticchallenges Psychogeriatrics 201313128ndash138
57 Chiba Y Fujishiro H Iseki E et al Retrospective survey of prodromal symptoms indementia with Lewy bodies comparison with Alzheimerrsquos disease Dement GeriatrCogn Disord 201233273ndash281
58 Kaufmann H Norcliffe-Kaufmann L Palma JA et al Natural history of pure auto-nomic failure a United States prospective cohort Ann Neurol 201781287ndash297
59 Heinzel S Berg D Gasser T et al Update of the MDS research criteria for prodromalParkinsonrsquos disease Mov Disord 2019341464ndash1470
60 Palma JA Norcliffe-Kaufmann L Kaufmann H Diagnosis of multiple system atrophyAuton Neurosci 201821115ndash25Data available fromDryad (Additional References References e1ndashe44) doi105061dryad1c59zw3rv
Subspecialty Alerts by E-mail
Customize your online journal experience by signing up for e-mail alerts related to your subspecialty or area of interest Accessthis free service by clicking on the ldquoMy Alertsrdquo link on the home page An extensive list of subspecialties methods and studydesign choices will be available for you to choose frommdashallowing you priority alerts to cutting-edge research in your field
COVID-19 and Neurologic Disease Call for Papers
The editors of Neurology are interested in papers that address the neurological aspects of COVID-19infection and challenges to the management of patients with chronic neurological conditions whohave or are at risk for the infection Relevant papers that pass initial internal review will undergoexpedited peer review and online publication We will consider papers posted in preprint servers
Submit observational studies and clinical trials as Articles and case series and case reports underthe ClinicalScientific Notes category to httpssubmitneurologyorg today
Visit the Neurologyreg Website at NeurologyorgN More article-based content on home pages Streamlined menus and navigation Enhanced blog sections for specialty areas Same experience on desktop tablet and mobile devices Improved article reading experience links more evident (pdf analytics social media) Neurologyreg Clinical Practice initiative ldquoPractice Currentrdquo global surveys will be accessible across sites
Find Neurologyreg on Facebook httptinyurlcomneurologyfan
Follow Neurologyreg on Twitter httpstwittercomGreenJournal
NeurologyorgN Neurology | Volume 94 Number 17 | April 28 2020 755
DOI 101212WNL0000000000009323202094743-755 Published Online before print April 2 2020Neurology
Ian G McKeith Tanis J Ferman Alan J Thomas et al Research criteria for the diagnosis of prodromal dementia with Lewy bodies
This information is current as of April 2 2020
ServicesUpdated Information amp
httpnneurologyorgcontent9417743fullincluding high resolution figures can be found at
References httpnneurologyorgcontent9417743fullref-list-1
This article cites 59 articles 12 of which you can access for free at
Subspecialty Collections
httpnneurologyorgcgicollectionpsychosisPsychosis a
httpnneurologyorgcgicollectionparkinsons_disease_with_dementiParkinsons disease with dementia
httpnneurologyorgcgicollectionmci_mild_cognitive_impairmentMCI (mild cognitive impairment)
httpnneurologyorgcgicollectiondementia_with_lewy_bodiesDementia with Lewy bodies
httpnneurologyorgcgicollectiondeliriumDeliriumfollowing collection(s) This article along with others on similar topics appears in the
Permissions amp Licensing
httpwwwneurologyorgaboutabout_the_journalpermissionsits entirety can be found online atInformation about reproducing this article in parts (figurestables) or in
Reprints
httpnneurologyorgsubscribersadvertiseInformation about ordering reprints can be found online
ISSN 0028-3878 Online ISSN 1526-632XWolters Kluwer Health Inc on behalf of the American Academy of Neurology All rights reserved Print1951 it is now a weekly with 48 issues per year Copyright Copyright copy 2020 The Author(s) Published by
reg is the official journal of the American Academy of Neurology Published continuously sinceNeurology

therefore be used as is the case for the diagnosis of DLBitself2 We propose biomarkers for the diagnosis of prodromalDLB where there is either sufficient good quality publishedevidence of adequate diagnostic specificity in prodromal DLBor this can be reasonably extrapolated from fully developedDLB or related disorders We categorize biomarkers for whichonly limited data are available as potential biomarkers rec-ognizing that such distinctions are likely to require revision asnew data become available
Proposed biomarkers
Reduced dopamine transporter (DAT) uptake in basalganglia demonstrated by SPECT or PETThe utility of DAT imaging in discriminating DLB from ADis already well established2 and its sensitivity in dis-tinguishing MCI with LB (MCI-LB) fromMCI with AD was54 and specificity 8930 whenMCI-LB was defined by thepresence of 1 core clinical feature of DLB in patients withMCI A higher sensitivity of 61 was achieved when 2 coreclinical symptoms were present30 Reduced striatal DATuptake therefore seems suggestive of prodromal DLB ina person with MCI but normal striatal DAT uptake does notexclude it
Polysomnographic confirmation of REM sleep withoutatoniaThe association between RBD and synucleinopathy is highlyspecific (eg a multicenter autopsy study found that of 80subjects with polysomnography [PSG]-confirmed RBD anda coexisting neurodegenerative disorder only 2 had a diseaseunrelated to α-synuclein deposition)e4 These data imply thata patient presenting with MCI and having PSG-confirmedRBD that is a history of probable RBD plus clear docu-mentation of REM sleep without atonia (RSWA) on PSGalso has a high probability of an underlying prodromal syn-ucleinopathy Because around a quarter of patients with DLBdo not report symptoms of RBD andor have normal REMsleep atonia on PSG a normal PSG does not exclude a pro-dromal DLB diagnosis31
Reduced meta-iodobenzylguanidine uptake onmyocardial scintigraphyReduced meta-iodobenzylguanidine (MIBG) uptake is anindicative biomarker for DLB2 and has also been reported tooccur in a small series of patients with late-onset psychiatricdisorder and PSG-confirmed RBD32 reinforcing its associa-tion with underlying α-synucleinopathy Of 2 patients withamnestic MCI with low MIBG uptake one developed DLBafter 2 years the other had no clinical follow-up reportede19
VHs andor RBD were reported among 7 of 13 patients withMCI with reduced MIBG uptake the majority of whom alsohad autonomic symptoms suggestive of LB disease but theywere not followed to determine conversion to DLBe20 De-spite a paucity of longitudinal datae21 there seems to be suf-ficient evidence that abnormal MIBGmyocardial scintigraphyin a patient with MCI supports a prodromal DLB diagnosisbut further studies are required
Potential biomarkersThese are biomarkers consistent with underlying LB diseasewhich may help the diagnostic evaluation but for which thereis still insufficient evidence of diagnostic sensitivity andspecificity in early disease This will change as new evidenceemerges at which point these or other candidates may be-come considered as indicative of prodromal DLB
Quantitative EEG showing slowing and dominantfrequency variabilityEEG slowing has been reported as predictive of dementia inboth PDe22 and RBDe23 posterior slow wave activity withperiodic fluctuations in the pre-alpha range being supportiveof DLB2 Quantitative EEG (QEEG) methods show thata dominant frequency lt8 Hz and dominant frequency vari-ability gt1middot5 Hz is typical of DLB and in a 3-year follow-upstudy 83 of subjects with MCI with this pattern at pre-sentation converted to DLB If these findings are replicatedQEEG may represent a powerful predictor of progressionfrom MCI to DLB33
Relative preservation of medial temporal lobestructures on structural imagingAbsent or minimal medial temporal lobe atrophy is consistentwith DLB but not sufficiently specific to differentiate it fromAD2 Lewy body disease with RBD is characterized by pre-served hippocampal volumes34 and hippocampal preserva-tion in patients with MCI supports progression to DLBinstead of AD dementia with a sensitivity of 85 and a spec-ificity of 6123 Suboptimal specificity may be due to thevariability of hippocampal atrophy in AD35 and contributionof other pathologic processes such as TAR DNA bindingprotein 43 (TDP43)e24
Insular thinning and gray matter volume lossInsular cortical thinning occurs in prodromal DLB relative tohealthy controls using MRI T1 sequences with gray matteratrophy predominantly affecting the anterior cingulum andmedial frontal structures This contrasts with more extensiveloss of gray matter in the temporal frontal and parietalregions of subjects with prodromal AD Insular corticalthinning may therefore differentiate patients with prodromalDLB not only from healthy controls but also from theirprodromal AD counterparts36 No group differences in insularvolumes are seen between DLB and AD at the dementia stageso longitudinal studies are required to determine its precisevalue as an early diagnostic marker of DLB37 Insula is alsoinvolved early in frontotemporal dementia (FTD) being thefirst cortical area to show atrophy in presymptomatic GRNMAPT or C9ORF72 mutation carrierse25 and unlikelytherefore to be helpful in differentiating DLB from FTD
Low occipital uptake on perfusionmetabolism scanOccipital hypometabolism on FDG-PET is associated withDLB38 and together with relative preservation of posteriorcingulate metabolism (the cingulate island sign)e26 is a sup-portive biomarker of DLB2 How frequently the cingulate
NeurologyorgN Neurology | Volume 94 Number 17 | April 28 2020 747
island sign is seen in prodromal DLB remains to be estab-lished significantly reduced posterior cingulate metabolismmay be a useful indication of the concurrence of additionalneurofibrillary tangle pathologye27
Other biomarkersThere is currently no α-synuclein radioligand with sufficientevidence supporting its utility for imaging DLB or any otherα-synucleinopathy nor have any diagnostically applicablebiofluid peripheral tissue or genotypic biomarkers beenestablished2 CSF measures cannot reliably discriminate be-tween DLB and AD39 although the measurement of CSFα-synuclein aggregates using seeding aggregation assays suchas protein misfolding cyclic amplification and real-timequaking-induced conversion is providing encouraging pre-liminary results and may be extended to more accessiblebiofluids including saliva plasma serum or urinee28 Com-bining CSF markers may be useful for example addition ofCSF phospho-tau to α-synuclein significantly improved thedifferential diagnosis between MCI-LB and MCI-AD in-creasing sensitivity and specificity both gt than 95e29 Otherdirect or indirect biomarker candidates that may occur earlyinclude identification of phosphorylated α-synuclein depositsin peripheral nervous tissue from skin biopsy40 gait ana-lysise30 and abnormalities in color vision discrimination4142
The figure shows a framework for considering a wider range ofbiomarkers in the setting of prodromal DLB determining theextent to which AD-related pathology is contributing to thedementia syndrome and influencing clinical trajectories inthese patients4344e31e32 Aβ42 declines earlier in AD thanDLB whereas Aβ40 levels increase alone in AD A low
Aβ42Aβ40 ratio may therefore differentiate patients withprodromal AD from patients with prodromal DLB better thanindividual measures43 There is also evidence showing dif-ferent frequencies and topographies of abnormal uptake onamyloid and tau PET imaging in DLB vs AD45
Delirium-onset DLBCognitive fluctuations or pronounced variations in alertnessand arousal are a core feature of DLB apparent as markedfluctuations in cognitive ability or function detectable byobservation or informant report and measurable using sen-sitive cognitive and electrophysiologic measurese33 The oc-currence of delirium (sometimes referred to as acuteconfusional state) as an early presenting feature of DLB hasbeen described in numerous case reports and seriese34 in-cluding in those with no apparent previous history of cogni-tive impairment46e35 Whether this represents a greatervulnerability to delirium in subjects with DLB or the mis-diagnosis of severe fluctuations with clouding of conscious-ness as delirium or a combination of both is unclear
Recognition that DLB may first present as delirium is im-portant because most guidelines for behavioral disturbancesin delirium recommend antipsychotics as first-line pharma-cologic treatment Delirium or marked fluctuations in con-sciousness were reported by 43 of caregivers before DLBdiagnosis47 and previous episodes of delirium were muchmore frequent in patients with DLB compared with patientswith AD (25 vs 7) with 1 in 4 of those with DLB havingrepeated delirium11 In the majority of these potential pro-voking causes were present A similarly higher incidence ofdelirium was found for subjects with DLB compared with
Figure Multimodal biomarkers for prodromal DLB
Reduced dopamine transporter uptake in basal gan-glia demonstrated by SPECT or PET PSG-confirmedREM sleep without atonia and MIBG myocardial scin-tigraphy are proposed as biomarkers of prodromalDLB Multimodality biomarkers are also important incharacterizing patients with prodromal DLB in whomthe pathologic mechanisms of cognitive impairmentinclude both LB and AD pathologies and who mayhave abnormalities associated with both Medialtemporal lobe uptake on tau PET medial temporallobe atrophy on MRI and high levels of uptake onamyloid PET and positive CSF biomarkers of AD-re-lated pathology may characterize patients with pro-dromal DLB with significant AD pathology It isexpected that biomarker abnormalities detected inthe earliest stages will remain abnormal as diseaseprogresses with additional biomarkers showingchanges later during the progression from pro-dromal to dementia phase DLB DLB = dementia withLewy bodies MIBG = meta-iodobenzylguanidine
748 Neurology | Volume 94 Number 17 | April 28 2020 NeurologyorgN
subjects with AD in the year before diagnosis (17middot6 v 3middot2100person-years)9 and admissions for delirium were morecommon in those already diagnosed with DLB than for otherdementias Prolonged delirium may also raise the index ofsuspicion for DLBe36 In an FDG-PET imaging study ofprolonged delirium 32 of subjects were found to havea DLB like pattern a high proportion in regard both to theknown prevalence of the disease and to that of their matchedcognitively impaired control group (4)e37
The similarities between the marked fluctuations in DLB anddisturbances of attention and consciousness in delirium havebeen noted and reviewed46 but there is as yet little un-derstanding of a shared neurobiological basis There havebeen few pathologic studies and although in anepidemiologic-based autopsy cohort there was no link be-tween delirium and LB pathology at autopsye38 a significantlyincreased risk of postoperative delirium in those with pe-ripheral α-synuclein pathology has been described48 Deliriumhas been suggested to bemore common in those subjects withDLB with later age at onsete39 but further evidence is needed
In summary (table 2) it is clear that DLB can present withdelirium and in patients diagnosed with delirium a carefulsearch for other DLB features should be made with a lowthreshold for undertaking DLB biomarker examinations es-pecially in those with recurrent unexplained or prolongeddelirium The extent to which delirium presentations of DLBhave the biomarker abnormalities associated with establishedDLB or other prodromal DLB presentations is unclear
although the PET imaging study cited above supports thise37
as does a report of reduced DAT uptake in a patient withacute unexplained delirium49 The link between delirium andDLB is an important area for future research to clarify therelationship between the 2 and to establish which factorsassociated with delirium should raise the index of suspicionfor underlying prodromal DLB
Psychiatric-onset DLBEarly clinicopathologic studies suggested that DLB maypresent as a primary psychiatric disorder5051 but subsequentfocus on the cognitive and motor aspects of DLB has limitedthe documentation of such cases outside of a fewcenters123252ndash54e36 Late-onset major depressive disorderand late-onset psychosis are the most frequently reportedpresentations differing markedly from the construct of mildbehavioral impairmente40 and sometimes sufficiently severe torequire hospitalization Symptoms include hallucinations invisual and in other modalities and systematized delusionsincluding Capgras syndrome55 apathy anxiety and de-pression Psychiatric-onset DLB cases are not easily differ-entiated from non-LB late-onset psychosis cases on the basisof primary psychiatric phenomenology or neuropsychologicalprofile alone54 Psychomotor retardation such as slowedspeech thinking and body movements can resemble thebradykinesia of parkinsonism The occurrence of rest tremoror rigidity is more helpful than bradykinesia to suspect pro-dromal DLB in patients with depressive disorder53 butpsychotropic-induced parkinsonism may complicate di-agnosis Atypical clinical features may prove valuable pointers
Table 2 Summary of key features of delirium-onset DLB
Patients with DLB are more susceptible to delirium than people with Alzheimer disease and this delirium may occur as their presenting complaint beforedementia develops
Such episodes may be provoked by multiple factors including surgery infectionssepsis fever or other systemic illness or secondary to use or suddenwithdrawal of alcohol or psychoactive drugs
Prodromal DLB should be particularly suspected in patients
bull in whom adequate provoking factors for the delirium are not found
bull with prolonged or recurrent delirium
bull who later develop progressive cognitive decline or subsequent dementia
Core clinical features of DLB are likely to be of more limited diagnostic weight in a patient with delirium because
bull cognitive fluctuation and clouding of consciousness can also occur in non-DLB delirium ie are not diagnostically specific for DLB in this situation
bull visual hallucinations may occur in non-DLB delirium particularly drug-induced or provoked by alcohol abstinence
bull motor parkinsonism present may be due to antipsychotic medications used to treat delirium
bull the diagnostic significance of a history of RBD in a person with delirium is not yet established
Identification of delirium-onset DLB
bull may be assisted by use of MCI-LB biomarkers but further research evidence of this is required
bull is important to inform the management plan including the avoidance or minimization of antipsychotic and anticholinergic agents
Abbreviations DLB = dementia with Lewy bodies MCI = mild cognitive impairment MCI-LB = MCI with Lewy bodies RBD = REM sleep behavior disorder
NeurologyorgN Neurology | Volume 94 Number 17 | April 28 2020 749
to underlying LB pathology particularly the presence of re-current VH12 when these occur before cognitive impairmentbecomes evident As with all α-synucleinopathies RBD maybe a useful indicator although a relationship between anti-depressant usage and subsequent RBD onset is a potentialconfoundere41 Although the primary psychiatric manifes-tations are often accompanied by mild cognitive deficits54
cognitive evaluation and interpretation of performance can bedifficult when psychiatric symptoms are prominent The fre-quency of cognitive fluctuations in psychiatric-onset LB caseshas not been determined
Initial reports suggest that 123I-MIBG scintigraphy may behelpful in psychiatric-onset DLB525356 Eighteen of 35patients with a first onset of major depressive disorder gt50years and with bradykinesia developed a clinical diagnosis ofDLB after 6 years of follow-up All 18 had an abnormal ven-tilatory response to hypercapnia (VRH) indicative of severeautonomic dysfunction whereas none of the 17 patients witha normal VRH converted to DLB within the study period Forthe converters the most common presentation was withpsychotic and melancholic features simultaneously The fre-quency of hypersensitivity to antipsychotics antidepressantsand antianxiety drugs was higher in converters than in non-converters53 Further studies need to confirm these findingsand to determine the value of other DLB biomarkers inpsychiatric-onset cases325256
In summary it is not yet clear how to identify patients withprominent late-onset psychiatric symptoms who may haveunderlying LB disease and subsequently progress to DLB It is
premature to try to construct formal criteria for psychiatric-onset DLB but clinicians in mental health and other settingsneed to be aware that this possibility exists not least becauseof the risk of severe antipsychotic sensitivity reactions withincreased morbidity and mortality The small available liter-ature including reports such as those cited above does providesome useful guidance summarized in table 3 but requiresreplication and further investigation
Idiopathic REM sleep behavior disorderRBD is characterized by abnormal dream enactment behaviorduring REM sleep accompanied by loss of muscle atonia duringREM sleep (REM sleep without atonia or RSWA) on PSG Forthe purpose of a prodromal DLB diagnosis a clinical history ofRBD is obtained in the same way as for DLB2 that is a clearcomplaint of dream enactment by a bedpartner or other witnesswith no evidence of sleep disorders that may mimic RBD onclinical interview Conditions known to mimic or masquerade asRBD include non-REM parasomnias (sleep walking sleep talk-ing or other behaviors that emerge fromnon-REM sleep stages)obstructive sleep apnea confusional arousals or nocturnal seiz-ures In the absence of PSG the risk of a false-positive clinicaldiagnosis of RBD is reduced by using optimized sleep ques-tionnaires which can have sensitivity and specificity over 90e42
RBDmay be considered as idiopathic until it is associated withanother ongoing neurologic condition the most frequentbeing an α-synucleinopathy (PD DLB or MSA) In a recentlarge study 735 of patients with RBD converted to an overtneurodegenerative syndrome after 12-year follow-up 565developing parkinsonism and 435 dementia as their first
Table 3 Summary of key features of psychiatric-onset DLB
Is characterized by predominant psychiatric symptoms that typically correspond to late-onset major depressive disorder or late-onset psychosis which mayfeature hallucinations in visual and in other modalities and systematized delusions including Capgras syndrome
bull may also present with apathy anxiety and depression
bull may be sufficiently severe to require hospitalization
bull the frequency of LB disease as a cause of late-onset psychiatric disorder is not known
When assessing for core clinical features of DLB in a patient with a primary psychiatric presentation
bull bradykinesia may be mimicked by psychomotor retardation which is commonly seen in depressive disorders
bull parkinsonism may be induced by antipsychotic medications used to treat psychiatric disorder
bull RBD (and REM sleep without atonia) may be induced by antidepressant medications
bull mild cognitive disturbance may be present but is not predominant and may fluctuate
bull formal neuropsychological testing may be confounded by the psychiatric mental state
bull the frequency and character of cognitive fluctuations is unknown
Identification of psychiatric-onset DLB
bull may be assisted by use of MCI-LB biomarkers but further research evidence of this is required
bull is important to inform the management plan including the avoidance or minimization of antipsychotic and anticholinergic agents
Abbreviations DLB = dementia with Lewy bodies MCI = mild cognitive impairment
750 Neurology | Volume 94 Number 17 | April 28 2020 NeurologyorgN
disease manifestation Among many predictive markerstested only the cognitive variables differed at baseline be-tween those converting to primary dementia vs parkinson-ism7 Other multicenter studies confirm that the only clinicalfeature that predicts dementia vs parkinsonism first is neu-ropsychological performance those with RBD who exhibitcognitive changes are more likely to evolve first into MCI orDLB22e4 Thus although RBD may be regarded an earlymanifestation of α-synucleinopathy it is not possible to clearlydistinguish whether an individual presenting with RBD willdevelop dementia first that is evolve into a primary DLBdiagnosis or parkinsonism first that is a primary PDMSAdiagnosis Any MCI subtype associated with PSG-confirmedRBD is highly likely to represent underlying LB disease Al-though idiopathic RBD is a useful model to study the earlystages of LB disease progression it is not necessarily repre-sentative of the whole spectrum of patients with PD and DLBa significant minority of whom do not have RBD42
Autonomic dysfunctionanosmia and othernonspecific prodromal LB disease symptomsPatients with DLB frequently report a history of autonomicdysfunction at first clinic attendance with 25ndash50 com-plaining of one of more among constipation orthostatic diz-ziness urinary incontinence erectile dysfunction increasedsweating or increased saliva5657 In a cohort of patients withpure autonomic failure 34 converted to an overt α-synu-cleinopathy over 6 years of follow-up this was to DLB (52)PD (24) orMSA (24)58 However because there are manyother causes for autonomic dysfunction in older people thesesymptoms either alone or in combination have low positivepredictive value59 The situation is similar for hyposmia whichalso frequently occurs early in prodromal DLB and PD42 butwhich can have many other causes in this age group
Conclusions and future directionDiagnosis of DLB at the dementia stage depends on identifyingfully expressed core clinical features which may be mild orabsent at the prodromal stage when biomarker evidence mayalso be weaker and may even differ from that found at thedementia stage Several new biomarker candidates direct andindirect are in development and we will continue to reviewthese to update our recommendations as soon as sufficientevidence accumulates We recognize that the clinical pheno-type of neurodegenerative disorders reflects interaction be-tween several rather than a single brain pathology and it istherefore likely that multiple biomarkers of individual pathol-ogies (eg α-synuclein β-amyloid and tau) or of disease sur-rogates (eg metabolic imagingEEG) will be required
Although we have described the 3 prodromal DLB syndromesseparately they are unlikely to be mutually exclusive andthere may be substantial overlap We propose operationalizedcriteria only for MCI-LB because the evidence base from oursystematic review albeit relatively limited is sufficient to
support recommendations that are immediately applicableand testable Our recommendations should be used alongsideguidance about the prodromal manifestations of PD1559
MSA60 and AD14 with which there is overlap Notwith-standing the potential benefits of early diagnosis we are alsomindful of the importance of avoiding incorrect (false-positive) diagnosis of prodromal DLB and the potentialnegative consequences this could have for an individual Wesuggest that the predictive validity of different categories andcombinations of our proposed criteria should be clarified byprospective studies before they are adopted for widespreadclinical use and that they will enable standardization for in-clusion in research studies and clinical trials
Some published guidance about the early clinical diagnosis ofDLB does already exist DSM5 recommends a diagnosis ofmild neurocognitive disorder (NCD) with LB ldquofor individualswho present with the core or suggestive features at a stagewhen cognitive or functional impairments are not of sufficientseverity to fulfill criteria for major NCDrdquoe43 This is basedhowever on the 2005 version of DLB guidelines and requiresupdating ICD-11 takes a similar approach toward diagnosingmild NCD at a syndromic level and lists both Lewy bodydisease and PD as possible causese44
The diagnostic position for other prodromal manifestations ofDLB that is delirium-onset and psychiatric-onset is less clearthan for MCI Operationalization of specific criteria for thesesyndromes is not yet justified and the reliable differentiationof the minority of delirious and psychiatrically ill patients whohave underlying LB pathology from the majority who do notwill probably only be achieved when routinely applicablebiomarkers are developed LB disease is seldom if ever cur-rently considered as part of the differential diagnosis of de-lirium or late-onset psychiatric disorder and we hope that theinformation we provide in the text and accompanying boxeswill raise cliniciansrsquo awareness of that possibility
Study fundingNo targeted funding reported
DisclosureI McKeith receives support from the NIHR Biomedical Re-search Centre awarded to the Newcastle upon Tyne HospitalsNHS Foundation Trust and Newcastle University and hasconsulted for GE Healthcare Sanofi Eisai Sumitomo Dai-nippon Pharma and Axovant T Ferman receives support fromNIH P50-AG16574 P30-AG062677 U01-NS100620 and theMangurian Foundation for Lewy body disease research AThomas receives support from the NIHR Biomedical ResearchCentre awarded to the Newcastle upon Tyne Hospitals NHSFoundation Trust and Newcastle University and has receivedgrants from GE Healthcare F Blanc has served as nationalclinical trial coordinator for Eisai and Axovant B Boevereceives support from NIH P50-AG16574 P30-AG062677U01-NS100620 and the Mangurian Foundation for Lewybody disease research has consulted for the Scientific Advisory
NeurologyorgN Neurology | Volume 94 Number 17 | April 28 2020 751
BoardmdashTau Consortium and received grants from Biogenthe NIH theMangurian Foundation Alector the Little FamilyFoundation and the Turner Family H Fujishiro has receivedsupport from Fujifilm RI Pharma Co Ltd K Kantarci receivessupport from NIH P50-AG16574 P30-AG062677 U01-NS100620 and the Mangurian Foundation for Lewy bodydisease research and has received grants from Avid Radio-pharmaceuticals and acted on a Data Safety Monitoring Boardfor Takeda Global Research C Muscio acknowledges thesupport of the Italian Ministry of Health GRANT NET-2011-02346784 J OrsquoBrien is supported by the NIHR CambridgeBiomedical Research Centre Dementia and Neuro-degeneration and Mental Health Themes and the CambridgeCentre for Parkinsonrsquos Plus Disorders has consulted forTauRx Axon GE Healthcare Eisai and AvidLilly and re-ceived grants fromAvidLilly andAllianceMedical R Postumahas received grants from and consulted for Fonds de laRecherche en Sante received grants from the Canadian Insti-tutes of Health Research the Parkinson Society of Canada theWeston-Garfield Foundation The Michael J Fox Foundationand the Webster Foundation and consulted for TakedaRocheProthena Teva Neurosciences Novartis Canada Bio-gen Boehringer Ingelheim Theranexus GE Healthcare JazzPharmaceuticals AbbVie Jannsen Otsuko PhytopharmicsInception Sciences and Parkinson Canada D Aarsland isa Royal Society Wolfson Research Merit Award Holder andwould like to thank the Wolfson Foundation and the RoyalSociety for their support He has received research supportandor honoraria from AstraZeneca H Lundbeck NovartisPharmaceuticals and GE Health and served as paid consultantfor H Lundbeck Eisai Heptares Sanofi and Mentis Cura CBallard reports unrelated current grant funding from MRCWellcome Trust European Union Gillings FoundationNIHR Alzheimerrsquos Society Alzheimerrsquos Research UK Par-kinsonrsquos Society and Lewy Body Society during the conduct ofthe study and personal fees from Acadia pharmaceutical com-pany Lundbeck Roche Otsuka Eli Lilly and AARP outsidethe submitted work L Bonanni is a member of the steeringcommittee of the E-DLB consortium and program chair of theLBD-PIA (ISTAART) and is funded for research on DLB bythe Italian Ministry of Health P Donaghy receives supportfrom the NIHR Biomedical Research Centre awarded to theNewcastle upon Tyne Hospitals NHS Foundation Trust andNewcastle UniversityM Emre served on the scientific advisoryboard for AC Immune J Galvin receives support from NIHgrants (R01 AG040211 R01 NS101482 R01 AG057681 andU01 NS100610) and the Lewy Body Dementia AssociationResearch Center of Excellence reports research support fromthe NIH the Lewy Body Dementia Association The Harry TMangurian Foundation and Albert Charitable Trust directsclinical trials for Biogen and Novartis receives licensing feesfrom Biogen Roche Eli Lilly Quintiles Roobrik ContinuumClinical and Langland and receives consulting fees fromBiogen Eisai Bracket and Medavante D Galasko receivessupport from NIA grant AGO5131 and the Michael J FoxFoundation and has acted as consultant for vTv Pharmaceut-icals Inc Esai Inc and for Fujirebio Inc been a member of
a DSMB for Probiodrug and paid editor for Alzheimerrsquos Re-search amp Therapy J Goldman receives grantsupport fromTheMichael J Fox Foundation and Parkinsonrsquos Foundation andhas received consulting feeshonoraria from Acadia AptinyxSunovion and Worldwide Med S Gomperts receives supportfrom NIH grants R01 AG054551 P30AG062421 R01AG062208 P50 AG005134 R21 NS109833 DODCDMRPW81XW1810516 the Farmer Family ParkinsonrsquosInitiative and the Lewy Body Dementia Association and hasserved on advisory boards for Acadia Pharmaceuticals andSanofi L Honig acknowledges research grant support fromNYS CEAD grant C031425 LBDA RCOE and NIHgrants U01NS100600 P50AG008702 R21AG058020R21MH111596 U01AG051412 U01AG045390U01AG016976 U01AG023749 U19063893 andU19AG024904 He receives research funding support fromAbbVie Alector Biogen Eisai Genentech Roche and Wash-ington University and has received income for consulting forCortexyme and Eisai M Ikeda reports departmental grants andhonoraria fees from Sumitomo Dainippon Pharma Eisai andNiho Medicine-Physics J Leverenz acknowledges supportfrom the National Institutes of Health P30 AG053762 UO1NS100610 and R13NS111954 and Jane and Lee Seidman andDouglas Herthel DVMMemorial Funds and reports consultingfees from Aptinyx Acadia Biogen Eisai GE HealthcareGenzymeSanofi and Takeda Pharmaceuticals and grant sup-port from Alzheimerrsquos Drug Discovery Foundation De-partment of Defense GE Healthcare GenzymeSanofi TheMichael J Fox Foundation and the NIH (NIA andNINDS) SLewis is supported by NHMRC-ARC Dementia Fellows KMarder is funded by the NIH R01NS100600 NS107168UL1TR001873 andNS073671 with research support from theLBDA Parkinson Foundation Michael J Fox HDSA andCHDI and has acted as site investigator for Vaccinex andGenentech member of Springer editorial board and scientificadvisory board Voyager Therapeutics M Masellis was sup-ported by a Canadian Institutes of Health Research grant(MOP13129) and an Early Researcher Award from the Min-istry of Research Innovation and Science (MRIS ON) andreports personal fees for ad hoc consultancy from ArkudaTherapeutics Ionis Pharmaceuticals and Alector Pharmaceut-icals royalties fromHenry Stewart Talks Ltd and grants to theinstitution from Roche Novartis Washington University andAxovant Sciences D Salmon acknowledges support from NIHP30AG062429 and is a paid consultant for Takeda Inc Apti-nyx Inc and Biogen Inc J-P Taylor receives support from theNIHR Biomedical Research Centre awarded to the Newcastleupon Tyne Hospitals NHS Foundation Trust and NewcastleUniversity and reports grants from the UKNational Institute ofHealth Research (NIHR) travel award from Axovant researchsupport costs from Sonsei-Heptares and personal fees fromGEHealthcare D Tsuang acknowledges support from NIHR21AG064271 R03 NS103950 and U01 NS100610 ZWalker has been supported by ESRC NIHR (co-app) ARUK(co-app) EU IMI 2 (co-app) and Dunhill Medical Trust Shehas received consultancy fees travel expenses and researchsupport from GE Healthcare and research support from Life
752 Neurology | Volume 94 Number 17 | April 28 2020 NeurologyorgN
Molecular Imaging P Tiraboschi acknowledges the support ofthe Italian Ministry of Health GRANT NET-2011-02346784Go to NeurologyorgN for full disclosures
Publication historyReceived by Neurology October 30 2019 Accepted in final formFebruary 25 2020
Appendix Authors
Name Location Contribution
Ian GMcKeith FMed Sci MD
Newcastle University Design and conceptualizationof the study acquisition ofdata analysis andinterpretation of the data anddrafting and revising themanuscript for intellectualcontent
Tanis JFermanPhD
Mayo ClinicJacksonville
Design and conceptualizationof the study acquisition ofdata analysis andinterpretation of the data anddrafting and revising themanuscript for intellectualcontent
Alan JThomasPhD
Newcastle University Design and conceptualizationof the study acquisition ofdata analysis andinterpretation of the data anddrafting and revising themanuscript for intellectualcontent
FredericBlanc MD
University ofStrasbourg
Design and conceptualizationof the study acquisition ofdata analysis andinterpretation of the data anddrafting and revising themanuscript for intellectualcontent
Bradley FBoeve MD
Mayo Clinic Rochester Design and conceptualizationof the study acquisition ofdata analysis andinterpretation of the data anddrafting and revising themanuscript for intellectualcontent
HiroshigeFujishiroMD
Nagoya UniversityKawasaki MemorialHospital
Design and conceptualizationof the study acquisition ofdata analysis andinterpretation of the data anddrafting and revising themanuscript for intellectualcontent
KejalKantarciMD MS
Mayo Clinic Rochester Design and conceptualizationof the study acquisition ofdata analysis andinterpretation of the data anddrafting and revising themanuscript for intellectualcontent
CristinaMuscio PhD
Istituto NeurologicoldquoCarlo Bestardquo Milan
Design and conceptualizationof the study acquisition ofdata analysis andinterpretation of the data anddrafting and revising themanuscript for intellectualcontent
Appendix (continued)
Name Location Contribution
John TOrsquoBrien FMed Sci DM
Cambridge University Design and conceptualizationof the study acquisition ofdata analysis andinterpretation of the data anddrafting and revising themanuscript for intellectualcontent
Ronald BPostumaMD MSc
McGill University Design and conceptualizationof the study acquisition ofdata analysis andinterpretation of the data anddrafting and revising themanuscript for intellectualcontent
DagAarslandPhD
Kingrsquos College Londonand StavangerUniversityHospital
Revising the manuscript forintellectual content
CliveBallard MD
University of Exeter Revising the manuscript forintellectual content
LauraBonanniMD PhD
University of Chieti-Pescara
Revising the manuscript forintellectual content
PaulDonaghyPhD
Newcastle University Revising the manuscript forintellectual content
Murat EmreMD
Istanbul Faculty ofMedicine
Revising the manuscript forintellectual content
James EGalvin MDMPH
University of MiamiMiller School ofMedicine
Revising the manuscript forintellectual content
DouglasGalasko MD
University of CaliforniaSan Diego
Revising the manuscript forintellectual content
Jennifer GGoldmanMD MS
Feinberg School ofMedicine
Revising the manuscript forintellectual content
Stephen NGompertsMD PhD
Massachusetts GeneralHospital
Revising the manuscript forintellectual content
Lawrence SHonig MDPhD
Columbia UniversityIrving Medical Center
Revising the manuscript forintellectual content
ManabuIkeda MDPhD
Osaka University Revising the manuscript forintellectual content
James BLeverenzMD
Lou Ruvo Center ofBrain Health ClevelandClinic
Revising the manuscript forintellectual content
Simon JGLewis MD
University of Sydney Revising the manuscript forintellectual content
Karen SMarder MDMPH
Columbia UniversityIrving Medical Center
Revising the manuscript forintellectual content
MarioMasellisMD PhD
Sunnybrook HealthSciences CentreUniversity of Toronto
Revising the manuscript forintellectual content
David PSalmon PhD
University of CaliforniaSan Diego
Revising the manuscript forintellectual content
Continued
NeurologyorgN Neurology | Volume 94 Number 17 | April 28 2020 753
References1 Walker Z Possin KL Boeve BF Aarsland D Lewy body dementias Lancet 2015386
1683ndash16972 McKeith IG Boeve BF Dickson DW et al Diagnosis and management of dementia
with Lewy bodies fourth consensus report of the DLB consortium Neurology 20178988ndash100
3 Ferman TJ Smith GE Kantarci K et al Nonamnestic mild cognitive impairmentprogresses to dementia with Lewy bodies Neurology 2013812032ndash2038
4 Savica R Bradley BF Mielke MM When do alpha-synucleinopathies start An epi-demiological timeline A review JAMA Neurol 201875503ndash509
5 Donaghy PC Taylor JP OrsquoBrien JT et al Neuropsychiatric symptoms and cognitiveprofile in mild cognitive impairment with Lewy bodies Psychol Med 2018482384ndash2390
6 Cagnin A Bussse C Gardini S et al Clinical and cognitive phenotype of mildcognitive impairment evolving to dementia with Lewy bodies Dement Geriatr CognDis Extra 20155442ndash449
7 Postuma RB Iranzo A HuM et al Risk and predictors of dementia and parkinsonismin idiopathic REM sleep behaviour disorder a multicentre study Brain 2019142744ndash759
8 Sadiq D Whitfield T Lee L Stevens T Costafreda S Walker Z Prodromal dementiawith Lewy bodies and prodromal Alzheimerrsquos disease a comparison of the cognitiveand clinical profiles J Alzheimers Dis 201758463ndash470
9 FitzGerald JM Perera G Chang-Tave A et al The incidence of recorded de-lirium episodes before and after dementia diagnosis differences between de-mentia with Lewy bodies and Alzheimerrsquos disease J Am Med Dir Assoc 201920604ndash609
10 Jicha GA Schmitt FA Abner E et al Prodromal clinical manifestations of neu-ropathologically confirmed Lewy body disease Neurobiol Aging 2010311805ndash1813
11 Vardy E Holt R Gerhard A Richardson A Snowden J Neary D History of a sus-pected delirium is more common in dementia with Lewy bodies than Alzheimerrsquosdisease a retrospective study Int J Geriatr Psychiatry 201429178ndash181
12 Fujishiro H Nakamura S Sato K Iseki E Prodromal dementia with Lewy bodiesGeriatr Gerontol Int 201515817ndash826
13 McKeith I Taylor JP Thomas A Donaghy P Kane J Revisiting DLB diagnosisa consideration of prodromal DLB and of the diagnostic overlap with Alzheimerdisease J Geriatr Psychiatry Neurol 201629249ndash253
14 Albert MS DeKosky ST Dickson D et al The diagnosis of mild cognitive impairmentdue to Alzheimerrsquos disease recommendations from the National Institute on Aging-Alzheimerrsquos Association workgroups on diagnostic guidelines for Alzheimerrsquos diseaseAlzheimers Dement 20117270ndash279
15 Litvan I Goldman JG Troster AI et al Diagnostic criteria for mild cognitive im-pairment in Parkinsonrsquos disease Movement Disorder Society Task Force guidelinesMov Disord 201227349ndash356
16 Ferman TJ Smith GE Boeve BF et al Neuropsychological differentiation of de-mentia with Lewy bodies from normal aging and Alzheimerrsquos disease Clin Neuro-psychol 200620623ndash636
17 Cagnin A Busse C Jelcic N Gnoato F Mitolo M Caffarra P High specificity ofMMSE pentagon scoring for diagnosis of prodromal dementia with Lewy bodiesParkinsonism Relat Disord 201521303ndash305
18 Yoon JH Kim M Moon SY Yong SW Hong JM Olfactory function and neuro-psychological profile to differentiate dementia with Lewy bodies from Alzheimerrsquosdisease in patients with mild cognitive impairment a 5-year follow-up study J NeurolSci 2015355174ndash179
19 Kemp J Philippi N Phillipps C et al Cognitive profile in prodromal dementia withLewy bodies Alzheimers Res Ther 2017919
20 Auning E Rongve A Fladby T et al Early and presenting symptoms of dementia withLewy bodies Dement Geriatr Cogn Disord 201132202ndash208
21 Kondo D Ota K Kasanuki K et al Characteristics of mild cognitive impairmenttending to convert into Alzheimerrsquos disease or dementia with Lewy bodies a follow-upstudy in a memory clinic J Neurol Sci 2016369102ndash108
22 Marchand DG Postuma RB Escudier F et al How does dementia with Lewy bodiesstart prodromal cognitive changes in REM sleep behavior disorder Ann Neurol2018831016ndash1026
23 Kantarci K Lesnick T Ferman TJ et al Hippocampal volumes predict risk of de-mentia with Lewy bodies in mild cognitive impairment Neurology 2016872317ndash2323
24 Thomas AJ Taylor JP McKeith I et al Revision of assessment toolkits for improvingthe diagnosis of Lewy body dementia the DIAMOND Lewy study Int J GeriatrPsychiatry 2018331293ndash1304
25 Galvin JE Improving the clinical detection of Lewy body dementia with the Lewybody composite risk score Alzheimerrsquos Demen (Amsterdam Netherlands) 20151316ndash324
26 Belden CM Kahlon V Malek-Ahmadi M Tsai A Sabbagh MN Clinical character-ization of mild cognitive impairment as a prodrome to dementia with Lewy bodiesAm J Alzheimers Dis Other Demen 201530173ndash177
27 Yoon JH Lee JE Yong SW Moon SY Lee PH The mild cognitive impairment stageof dementia with Lewy bodies and Parkinson disease A comparison of cognitiveprofiles Alzheimer Dis Assoc Disord 201428151ndash155
28 Fengler S Liepelt-Scarfone I Brockmann K Schaffer E Berg D Kalbe E Cognitivechanges in prodromal Parkinsonrsquos disease a review Mov Disord 2017321655ndash1666
29 Kalbe E Rehberg SP Heber I et al Subtypes of mild cognitive impairment in patientswith Parkinsonrsquos disease evidence from the LANDSCAPE study J Neurol NeurosurgPsychiatry 2016871099ndash1105
30 Thomas AJ Donaghy P Roberts G et al Diagnostic accuracy of dopaminergic im-aging in prodromal dementia with Lewy bodies Psychol Med 20181ndash7
31 Ferman TJ Boeve BF Smith GE et al Inclusion of RBD improves the diagnosticclassification of dementia with Lewy bodies Neurology 201177875ndash882
32 Fujishiro H Okuda M Iwamoto K et al Early diagnosis of Lewy body disease inpatients with late-onset psychiatric disorders using clinical history of rapid eyemovement sleep behavior disorder and I-123 -metaiodobenzylguanidine cardiacscintigraphy Psychiatry Clin Neurosci 201872423ndash434
33 Bonanni L Perfetti B Bifolchetti S et al Quantitative electroencephalogram utility inpredicting conversion of mild cognitive impairment to dementia with Lewy bodiesNeurobiol Aging 201536434ndash445
34 Murray ME Ferman TJ Boeve BF et al MRI and pathology of REM sleep behaviordisorder in dementia with Lewy bodies Neurology 2013811681ndash1689
35 Murray ME Graff-Radford NR Ross OA Petersen RC Duara R Dickson DWNeuropathologically defined subtypes of Alzheimerrsquos disease with distinct clinicalcharacteristics a retrospective study Lancet Neurol 201110785ndash796
36 Blanc F Colloby SJ Cretin B et al Grey matter atrophy in prodromal stage ofdementia with Lewy bodies and Alzheimerrsquos disease Alzheimers Res Ther 2016831
37 Blanc F Colloby SJ Philippi N et al Cortical thickness in dementia with Lewy bodiesand Alzheimerrsquos disease a comparison of prodromal and dementia stages Plos One201510e0127396
38 Surendranathan A OrsquoBrien JT Clinical imaging in dementia with Lewy bodies EvidBased Ment Health 20182161ndash65
39 Outeiro TF Koss DJ Erskine D et al Dementia with Lewy bodies an update andoutlook Mol Neurodegener 2019145
40 Donadio V Incensi A Rizzo G et al A new potential biomarker for dementiawith Lewy bodies Skin nerve alpha-synuclein deposits Neurology 201789318ndash326
41 Flanigan PM Khosravi MA Leverenz JB Tousi B Color vision impairment differ-entiates Alzheimer dementia from dementia with Lewy bodies J Geriatr PsychiatryNeurol 20183197ndash102
42 Fereshtehnejad SM Yao C Pelletier A Montplaisir JY Gagnon JF Postuma RBEvolution of prodromal Parkinsonrsquos disease and dementia with Lewy bodies a pro-spective study Brain 20191422051ndash2067
43 Bousiges O Bombois S Schraen S et al Cerebrospinal fluid Alzheimer biomarkerscan be useful for discriminating dementia with Lewy bodies from Alzheimerrsquos diseaseat the prodromal stage J Neurol Neurosurg Psychiatry 201889467ndash475
44 Kantarci K Lowe VJ Boeve BF et al Multimodality imaging characteristics of de-mentia with Lewy bodies Neurobiol Aging 2012332091ndash2105
45 Kantarci K Lowe VJ Boeve BF et al AV-1451 tau and beta-amyloid positronemission tomography imaging in dementia with Lewy bodies Ann Neurol 20178158ndash67
46 Gore RL Vardy E OrsquoBrien JT Delirium and dementia with Lewy bodies distinctdiagnoses or part of the same spectrum J Neurol Neurosurg Psychiatry 20158650ndash59
47 Aarsland DS Auning E The pre-dementia stage of dementia with Lewy bodies Eur JNeurol 20111869
48 Sunwoo MK Hong JY Choi J Park HJ Kim SH Lee PH alpha-Synuclein pathologyis related to postoperative delirium in patients undergoing gastrectomy Neurology201380810ndash813
49 Akintade O Pierres F Acute presentation of dementia with Lewy bodies Clin Med201919327ndash330
50 Kosaka K Diffuse Lewy body disease in Japan J Neurol 1990237197ndash20451 Birkett DP Desouky A Han L Kaufman M Lewy bodies in psychiatric patients Int J
Geriatr Psychiatry 19927235ndash240
Appendix (continued)
Name Location Contribution
John PaulTaylor MBBS PhD
Newcastle University Revising the manuscript forintellectual content
Debby WTsuang MD
VA Puget Sound ampUniversity ofWashington
Revising the manuscript forintellectual content
ZuzanaWalker MD
University CollegeLondon
Revising the manuscript forintellectual content
PietroTiraboschiMD
Istituto NeurologicoldquoCarlo Bestardquo Milan
Design and conceptualizationof the study acquisition ofdata analysis andinterpretation of the data anddrafting and revising themanuscript for intellectualcontent
754 Neurology | Volume 94 Number 17 | April 28 2020 NeurologyorgN
52 Kobayashi K Nakano H Akiyama N Maeda T Yamamori S Pure psychiatric pre-sentation of the Lewy body disease is depressionmdashan analysis of 60 cases verified withmyocardial meta-iodobenzylguanidine study Int J Geriatr Psychiatry 201530663ndash668
53 Takahashi S Mizukami K Arai T et al Ventilatory response to hypercapnia predictsdementia with Lewy bodies in late-onset major depressive disorder J Alzheimers Dis201650751ndash758
54 Van Assche L Van Aubel E Van de Ven L Bouckaert F Luyten P Vandenbulcke MThe neuropsychological profile and phenomenology of late onset psychosis a cross-sectional study on the differential diagnosis of very-late-onset Schizophrenia-likepsychosis dementia with Lewy bodies and Alzheimerrsquos type dementia with psychosisArch Clin Neuropsychol 201934183ndash199
55 Thaipisuttikul P Lobach I Zweig Y Gurnani A Galvin JE Capgras syndrome indementia with Lewy bodies Int Psychogeriatr 201325843ndash849
56 Fujishiro H Iseki E Nakamura S et al Dementia with Lewy bodies early diagnosticchallenges Psychogeriatrics 201313128ndash138
57 Chiba Y Fujishiro H Iseki E et al Retrospective survey of prodromal symptoms indementia with Lewy bodies comparison with Alzheimerrsquos disease Dement GeriatrCogn Disord 201233273ndash281
58 Kaufmann H Norcliffe-Kaufmann L Palma JA et al Natural history of pure auto-nomic failure a United States prospective cohort Ann Neurol 201781287ndash297
59 Heinzel S Berg D Gasser T et al Update of the MDS research criteria for prodromalParkinsonrsquos disease Mov Disord 2019341464ndash1470
60 Palma JA Norcliffe-Kaufmann L Kaufmann H Diagnosis of multiple system atrophyAuton Neurosci 201821115ndash25Data available fromDryad (Additional References References e1ndashe44) doi105061dryad1c59zw3rv
Subspecialty Alerts by E-mail
Customize your online journal experience by signing up for e-mail alerts related to your subspecialty or area of interest Accessthis free service by clicking on the ldquoMy Alertsrdquo link on the home page An extensive list of subspecialties methods and studydesign choices will be available for you to choose frommdashallowing you priority alerts to cutting-edge research in your field
COVID-19 and Neurologic Disease Call for Papers
The editors of Neurology are interested in papers that address the neurological aspects of COVID-19infection and challenges to the management of patients with chronic neurological conditions whohave or are at risk for the infection Relevant papers that pass initial internal review will undergoexpedited peer review and online publication We will consider papers posted in preprint servers
Submit observational studies and clinical trials as Articles and case series and case reports underthe ClinicalScientific Notes category to httpssubmitneurologyorg today
Visit the Neurologyreg Website at NeurologyorgN More article-based content on home pages Streamlined menus and navigation Enhanced blog sections for specialty areas Same experience on desktop tablet and mobile devices Improved article reading experience links more evident (pdf analytics social media) Neurologyreg Clinical Practice initiative ldquoPractice Currentrdquo global surveys will be accessible across sites
Find Neurologyreg on Facebook httptinyurlcomneurologyfan
Follow Neurologyreg on Twitter httpstwittercomGreenJournal
NeurologyorgN Neurology | Volume 94 Number 17 | April 28 2020 755
DOI 101212WNL0000000000009323202094743-755 Published Online before print April 2 2020Neurology
Ian G McKeith Tanis J Ferman Alan J Thomas et al Research criteria for the diagnosis of prodromal dementia with Lewy bodies
This information is current as of April 2 2020
ServicesUpdated Information amp
httpnneurologyorgcontent9417743fullincluding high resolution figures can be found at
References httpnneurologyorgcontent9417743fullref-list-1
This article cites 59 articles 12 of which you can access for free at
Subspecialty Collections
httpnneurologyorgcgicollectionpsychosisPsychosis a
httpnneurologyorgcgicollectionparkinsons_disease_with_dementiParkinsons disease with dementia
httpnneurologyorgcgicollectionmci_mild_cognitive_impairmentMCI (mild cognitive impairment)
httpnneurologyorgcgicollectiondementia_with_lewy_bodiesDementia with Lewy bodies
httpnneurologyorgcgicollectiondeliriumDeliriumfollowing collection(s) This article along with others on similar topics appears in the
Permissions amp Licensing
httpwwwneurologyorgaboutabout_the_journalpermissionsits entirety can be found online atInformation about reproducing this article in parts (figurestables) or in
Reprints
httpnneurologyorgsubscribersadvertiseInformation about ordering reprints can be found online
ISSN 0028-3878 Online ISSN 1526-632XWolters Kluwer Health Inc on behalf of the American Academy of Neurology All rights reserved Print1951 it is now a weekly with 48 issues per year Copyright Copyright copy 2020 The Author(s) Published by
reg is the official journal of the American Academy of Neurology Published continuously sinceNeurology

island sign is seen in prodromal DLB remains to be estab-lished significantly reduced posterior cingulate metabolismmay be a useful indication of the concurrence of additionalneurofibrillary tangle pathologye27
Other biomarkersThere is currently no α-synuclein radioligand with sufficientevidence supporting its utility for imaging DLB or any otherα-synucleinopathy nor have any diagnostically applicablebiofluid peripheral tissue or genotypic biomarkers beenestablished2 CSF measures cannot reliably discriminate be-tween DLB and AD39 although the measurement of CSFα-synuclein aggregates using seeding aggregation assays suchas protein misfolding cyclic amplification and real-timequaking-induced conversion is providing encouraging pre-liminary results and may be extended to more accessiblebiofluids including saliva plasma serum or urinee28 Com-bining CSF markers may be useful for example addition ofCSF phospho-tau to α-synuclein significantly improved thedifferential diagnosis between MCI-LB and MCI-AD in-creasing sensitivity and specificity both gt than 95e29 Otherdirect or indirect biomarker candidates that may occur earlyinclude identification of phosphorylated α-synuclein depositsin peripheral nervous tissue from skin biopsy40 gait ana-lysise30 and abnormalities in color vision discrimination4142
The figure shows a framework for considering a wider range ofbiomarkers in the setting of prodromal DLB determining theextent to which AD-related pathology is contributing to thedementia syndrome and influencing clinical trajectories inthese patients4344e31e32 Aβ42 declines earlier in AD thanDLB whereas Aβ40 levels increase alone in AD A low
Aβ42Aβ40 ratio may therefore differentiate patients withprodromal AD from patients with prodromal DLB better thanindividual measures43 There is also evidence showing dif-ferent frequencies and topographies of abnormal uptake onamyloid and tau PET imaging in DLB vs AD45
Delirium-onset DLBCognitive fluctuations or pronounced variations in alertnessand arousal are a core feature of DLB apparent as markedfluctuations in cognitive ability or function detectable byobservation or informant report and measurable using sen-sitive cognitive and electrophysiologic measurese33 The oc-currence of delirium (sometimes referred to as acuteconfusional state) as an early presenting feature of DLB hasbeen described in numerous case reports and seriese34 in-cluding in those with no apparent previous history of cogni-tive impairment46e35 Whether this represents a greatervulnerability to delirium in subjects with DLB or the mis-diagnosis of severe fluctuations with clouding of conscious-ness as delirium or a combination of both is unclear
Recognition that DLB may first present as delirium is im-portant because most guidelines for behavioral disturbancesin delirium recommend antipsychotics as first-line pharma-cologic treatment Delirium or marked fluctuations in con-sciousness were reported by 43 of caregivers before DLBdiagnosis47 and previous episodes of delirium were muchmore frequent in patients with DLB compared with patientswith AD (25 vs 7) with 1 in 4 of those with DLB havingrepeated delirium11 In the majority of these potential pro-voking causes were present A similarly higher incidence ofdelirium was found for subjects with DLB compared with
Figure Multimodal biomarkers for prodromal DLB
Reduced dopamine transporter uptake in basal gan-glia demonstrated by SPECT or PET PSG-confirmedREM sleep without atonia and MIBG myocardial scin-tigraphy are proposed as biomarkers of prodromalDLB Multimodality biomarkers are also important incharacterizing patients with prodromal DLB in whomthe pathologic mechanisms of cognitive impairmentinclude both LB and AD pathologies and who mayhave abnormalities associated with both Medialtemporal lobe uptake on tau PET medial temporallobe atrophy on MRI and high levels of uptake onamyloid PET and positive CSF biomarkers of AD-re-lated pathology may characterize patients with pro-dromal DLB with significant AD pathology It isexpected that biomarker abnormalities detected inthe earliest stages will remain abnormal as diseaseprogresses with additional biomarkers showingchanges later during the progression from pro-dromal to dementia phase DLB DLB = dementia withLewy bodies MIBG = meta-iodobenzylguanidine
748 Neurology | Volume 94 Number 17 | April 28 2020 NeurologyorgN
subjects with AD in the year before diagnosis (17middot6 v 3middot2100person-years)9 and admissions for delirium were morecommon in those already diagnosed with DLB than for otherdementias Prolonged delirium may also raise the index ofsuspicion for DLBe36 In an FDG-PET imaging study ofprolonged delirium 32 of subjects were found to havea DLB like pattern a high proportion in regard both to theknown prevalence of the disease and to that of their matchedcognitively impaired control group (4)e37
The similarities between the marked fluctuations in DLB anddisturbances of attention and consciousness in delirium havebeen noted and reviewed46 but there is as yet little un-derstanding of a shared neurobiological basis There havebeen few pathologic studies and although in anepidemiologic-based autopsy cohort there was no link be-tween delirium and LB pathology at autopsye38 a significantlyincreased risk of postoperative delirium in those with pe-ripheral α-synuclein pathology has been described48 Deliriumhas been suggested to bemore common in those subjects withDLB with later age at onsete39 but further evidence is needed
In summary (table 2) it is clear that DLB can present withdelirium and in patients diagnosed with delirium a carefulsearch for other DLB features should be made with a lowthreshold for undertaking DLB biomarker examinations es-pecially in those with recurrent unexplained or prolongeddelirium The extent to which delirium presentations of DLBhave the biomarker abnormalities associated with establishedDLB or other prodromal DLB presentations is unclear
although the PET imaging study cited above supports thise37
as does a report of reduced DAT uptake in a patient withacute unexplained delirium49 The link between delirium andDLB is an important area for future research to clarify therelationship between the 2 and to establish which factorsassociated with delirium should raise the index of suspicionfor underlying prodromal DLB
Psychiatric-onset DLBEarly clinicopathologic studies suggested that DLB maypresent as a primary psychiatric disorder5051 but subsequentfocus on the cognitive and motor aspects of DLB has limitedthe documentation of such cases outside of a fewcenters123252ndash54e36 Late-onset major depressive disorderand late-onset psychosis are the most frequently reportedpresentations differing markedly from the construct of mildbehavioral impairmente40 and sometimes sufficiently severe torequire hospitalization Symptoms include hallucinations invisual and in other modalities and systematized delusionsincluding Capgras syndrome55 apathy anxiety and de-pression Psychiatric-onset DLB cases are not easily differ-entiated from non-LB late-onset psychosis cases on the basisof primary psychiatric phenomenology or neuropsychologicalprofile alone54 Psychomotor retardation such as slowedspeech thinking and body movements can resemble thebradykinesia of parkinsonism The occurrence of rest tremoror rigidity is more helpful than bradykinesia to suspect pro-dromal DLB in patients with depressive disorder53 butpsychotropic-induced parkinsonism may complicate di-agnosis Atypical clinical features may prove valuable pointers
Table 2 Summary of key features of delirium-onset DLB
Patients with DLB are more susceptible to delirium than people with Alzheimer disease and this delirium may occur as their presenting complaint beforedementia develops
Such episodes may be provoked by multiple factors including surgery infectionssepsis fever or other systemic illness or secondary to use or suddenwithdrawal of alcohol or psychoactive drugs
Prodromal DLB should be particularly suspected in patients
bull in whom adequate provoking factors for the delirium are not found
bull with prolonged or recurrent delirium
bull who later develop progressive cognitive decline or subsequent dementia
Core clinical features of DLB are likely to be of more limited diagnostic weight in a patient with delirium because
bull cognitive fluctuation and clouding of consciousness can also occur in non-DLB delirium ie are not diagnostically specific for DLB in this situation
bull visual hallucinations may occur in non-DLB delirium particularly drug-induced or provoked by alcohol abstinence
bull motor parkinsonism present may be due to antipsychotic medications used to treat delirium
bull the diagnostic significance of a history of RBD in a person with delirium is not yet established
Identification of delirium-onset DLB
bull may be assisted by use of MCI-LB biomarkers but further research evidence of this is required
bull is important to inform the management plan including the avoidance or minimization of antipsychotic and anticholinergic agents
Abbreviations DLB = dementia with Lewy bodies MCI = mild cognitive impairment MCI-LB = MCI with Lewy bodies RBD = REM sleep behavior disorder
NeurologyorgN Neurology | Volume 94 Number 17 | April 28 2020 749
to underlying LB pathology particularly the presence of re-current VH12 when these occur before cognitive impairmentbecomes evident As with all α-synucleinopathies RBD maybe a useful indicator although a relationship between anti-depressant usage and subsequent RBD onset is a potentialconfoundere41 Although the primary psychiatric manifes-tations are often accompanied by mild cognitive deficits54
cognitive evaluation and interpretation of performance can bedifficult when psychiatric symptoms are prominent The fre-quency of cognitive fluctuations in psychiatric-onset LB caseshas not been determined
Initial reports suggest that 123I-MIBG scintigraphy may behelpful in psychiatric-onset DLB525356 Eighteen of 35patients with a first onset of major depressive disorder gt50years and with bradykinesia developed a clinical diagnosis ofDLB after 6 years of follow-up All 18 had an abnormal ven-tilatory response to hypercapnia (VRH) indicative of severeautonomic dysfunction whereas none of the 17 patients witha normal VRH converted to DLB within the study period Forthe converters the most common presentation was withpsychotic and melancholic features simultaneously The fre-quency of hypersensitivity to antipsychotics antidepressantsand antianxiety drugs was higher in converters than in non-converters53 Further studies need to confirm these findingsand to determine the value of other DLB biomarkers inpsychiatric-onset cases325256
In summary it is not yet clear how to identify patients withprominent late-onset psychiatric symptoms who may haveunderlying LB disease and subsequently progress to DLB It is
premature to try to construct formal criteria for psychiatric-onset DLB but clinicians in mental health and other settingsneed to be aware that this possibility exists not least becauseof the risk of severe antipsychotic sensitivity reactions withincreased morbidity and mortality The small available liter-ature including reports such as those cited above does providesome useful guidance summarized in table 3 but requiresreplication and further investigation
Idiopathic REM sleep behavior disorderRBD is characterized by abnormal dream enactment behaviorduring REM sleep accompanied by loss of muscle atonia duringREM sleep (REM sleep without atonia or RSWA) on PSG Forthe purpose of a prodromal DLB diagnosis a clinical history ofRBD is obtained in the same way as for DLB2 that is a clearcomplaint of dream enactment by a bedpartner or other witnesswith no evidence of sleep disorders that may mimic RBD onclinical interview Conditions known to mimic or masquerade asRBD include non-REM parasomnias (sleep walking sleep talk-ing or other behaviors that emerge fromnon-REM sleep stages)obstructive sleep apnea confusional arousals or nocturnal seiz-ures In the absence of PSG the risk of a false-positive clinicaldiagnosis of RBD is reduced by using optimized sleep ques-tionnaires which can have sensitivity and specificity over 90e42
RBDmay be considered as idiopathic until it is associated withanother ongoing neurologic condition the most frequentbeing an α-synucleinopathy (PD DLB or MSA) In a recentlarge study 735 of patients with RBD converted to an overtneurodegenerative syndrome after 12-year follow-up 565developing parkinsonism and 435 dementia as their first
Table 3 Summary of key features of psychiatric-onset DLB
Is characterized by predominant psychiatric symptoms that typically correspond to late-onset major depressive disorder or late-onset psychosis which mayfeature hallucinations in visual and in other modalities and systematized delusions including Capgras syndrome
bull may also present with apathy anxiety and depression
bull may be sufficiently severe to require hospitalization
bull the frequency of LB disease as a cause of late-onset psychiatric disorder is not known
When assessing for core clinical features of DLB in a patient with a primary psychiatric presentation
bull bradykinesia may be mimicked by psychomotor retardation which is commonly seen in depressive disorders
bull parkinsonism may be induced by antipsychotic medications used to treat psychiatric disorder
bull RBD (and REM sleep without atonia) may be induced by antidepressant medications
bull mild cognitive disturbance may be present but is not predominant and may fluctuate
bull formal neuropsychological testing may be confounded by the psychiatric mental state
bull the frequency and character of cognitive fluctuations is unknown
Identification of psychiatric-onset DLB
bull may be assisted by use of MCI-LB biomarkers but further research evidence of this is required
bull is important to inform the management plan including the avoidance or minimization of antipsychotic and anticholinergic agents
Abbreviations DLB = dementia with Lewy bodies MCI = mild cognitive impairment
750 Neurology | Volume 94 Number 17 | April 28 2020 NeurologyorgN
disease manifestation Among many predictive markerstested only the cognitive variables differed at baseline be-tween those converting to primary dementia vs parkinson-ism7 Other multicenter studies confirm that the only clinicalfeature that predicts dementia vs parkinsonism first is neu-ropsychological performance those with RBD who exhibitcognitive changes are more likely to evolve first into MCI orDLB22e4 Thus although RBD may be regarded an earlymanifestation of α-synucleinopathy it is not possible to clearlydistinguish whether an individual presenting with RBD willdevelop dementia first that is evolve into a primary DLBdiagnosis or parkinsonism first that is a primary PDMSAdiagnosis Any MCI subtype associated with PSG-confirmedRBD is highly likely to represent underlying LB disease Al-though idiopathic RBD is a useful model to study the earlystages of LB disease progression it is not necessarily repre-sentative of the whole spectrum of patients with PD and DLBa significant minority of whom do not have RBD42
Autonomic dysfunctionanosmia and othernonspecific prodromal LB disease symptomsPatients with DLB frequently report a history of autonomicdysfunction at first clinic attendance with 25ndash50 com-plaining of one of more among constipation orthostatic diz-ziness urinary incontinence erectile dysfunction increasedsweating or increased saliva5657 In a cohort of patients withpure autonomic failure 34 converted to an overt α-synu-cleinopathy over 6 years of follow-up this was to DLB (52)PD (24) orMSA (24)58 However because there are manyother causes for autonomic dysfunction in older people thesesymptoms either alone or in combination have low positivepredictive value59 The situation is similar for hyposmia whichalso frequently occurs early in prodromal DLB and PD42 butwhich can have many other causes in this age group
Conclusions and future directionDiagnosis of DLB at the dementia stage depends on identifyingfully expressed core clinical features which may be mild orabsent at the prodromal stage when biomarker evidence mayalso be weaker and may even differ from that found at thedementia stage Several new biomarker candidates direct andindirect are in development and we will continue to reviewthese to update our recommendations as soon as sufficientevidence accumulates We recognize that the clinical pheno-type of neurodegenerative disorders reflects interaction be-tween several rather than a single brain pathology and it istherefore likely that multiple biomarkers of individual pathol-ogies (eg α-synuclein β-amyloid and tau) or of disease sur-rogates (eg metabolic imagingEEG) will be required
Although we have described the 3 prodromal DLB syndromesseparately they are unlikely to be mutually exclusive andthere may be substantial overlap We propose operationalizedcriteria only for MCI-LB because the evidence base from oursystematic review albeit relatively limited is sufficient to
support recommendations that are immediately applicableand testable Our recommendations should be used alongsideguidance about the prodromal manifestations of PD1559
MSA60 and AD14 with which there is overlap Notwith-standing the potential benefits of early diagnosis we are alsomindful of the importance of avoiding incorrect (false-positive) diagnosis of prodromal DLB and the potentialnegative consequences this could have for an individual Wesuggest that the predictive validity of different categories andcombinations of our proposed criteria should be clarified byprospective studies before they are adopted for widespreadclinical use and that they will enable standardization for in-clusion in research studies and clinical trials
Some published guidance about the early clinical diagnosis ofDLB does already exist DSM5 recommends a diagnosis ofmild neurocognitive disorder (NCD) with LB ldquofor individualswho present with the core or suggestive features at a stagewhen cognitive or functional impairments are not of sufficientseverity to fulfill criteria for major NCDrdquoe43 This is basedhowever on the 2005 version of DLB guidelines and requiresupdating ICD-11 takes a similar approach toward diagnosingmild NCD at a syndromic level and lists both Lewy bodydisease and PD as possible causese44
The diagnostic position for other prodromal manifestations ofDLB that is delirium-onset and psychiatric-onset is less clearthan for MCI Operationalization of specific criteria for thesesyndromes is not yet justified and the reliable differentiationof the minority of delirious and psychiatrically ill patients whohave underlying LB pathology from the majority who do notwill probably only be achieved when routinely applicablebiomarkers are developed LB disease is seldom if ever cur-rently considered as part of the differential diagnosis of de-lirium or late-onset psychiatric disorder and we hope that theinformation we provide in the text and accompanying boxeswill raise cliniciansrsquo awareness of that possibility
Study fundingNo targeted funding reported
DisclosureI McKeith receives support from the NIHR Biomedical Re-search Centre awarded to the Newcastle upon Tyne HospitalsNHS Foundation Trust and Newcastle University and hasconsulted for GE Healthcare Sanofi Eisai Sumitomo Dai-nippon Pharma and Axovant T Ferman receives support fromNIH P50-AG16574 P30-AG062677 U01-NS100620 and theMangurian Foundation for Lewy body disease research AThomas receives support from the NIHR Biomedical ResearchCentre awarded to the Newcastle upon Tyne Hospitals NHSFoundation Trust and Newcastle University and has receivedgrants from GE Healthcare F Blanc has served as nationalclinical trial coordinator for Eisai and Axovant B Boevereceives support from NIH P50-AG16574 P30-AG062677U01-NS100620 and the Mangurian Foundation for Lewybody disease research has consulted for the Scientific Advisory
NeurologyorgN Neurology | Volume 94 Number 17 | April 28 2020 751
BoardmdashTau Consortium and received grants from Biogenthe NIH theMangurian Foundation Alector the Little FamilyFoundation and the Turner Family H Fujishiro has receivedsupport from Fujifilm RI Pharma Co Ltd K Kantarci receivessupport from NIH P50-AG16574 P30-AG062677 U01-NS100620 and the Mangurian Foundation for Lewy bodydisease research and has received grants from Avid Radio-pharmaceuticals and acted on a Data Safety Monitoring Boardfor Takeda Global Research C Muscio acknowledges thesupport of the Italian Ministry of Health GRANT NET-2011-02346784 J OrsquoBrien is supported by the NIHR CambridgeBiomedical Research Centre Dementia and Neuro-degeneration and Mental Health Themes and the CambridgeCentre for Parkinsonrsquos Plus Disorders has consulted forTauRx Axon GE Healthcare Eisai and AvidLilly and re-ceived grants fromAvidLilly andAllianceMedical R Postumahas received grants from and consulted for Fonds de laRecherche en Sante received grants from the Canadian Insti-tutes of Health Research the Parkinson Society of Canada theWeston-Garfield Foundation The Michael J Fox Foundationand the Webster Foundation and consulted for TakedaRocheProthena Teva Neurosciences Novartis Canada Bio-gen Boehringer Ingelheim Theranexus GE Healthcare JazzPharmaceuticals AbbVie Jannsen Otsuko PhytopharmicsInception Sciences and Parkinson Canada D Aarsland isa Royal Society Wolfson Research Merit Award Holder andwould like to thank the Wolfson Foundation and the RoyalSociety for their support He has received research supportandor honoraria from AstraZeneca H Lundbeck NovartisPharmaceuticals and GE Health and served as paid consultantfor H Lundbeck Eisai Heptares Sanofi and Mentis Cura CBallard reports unrelated current grant funding from MRCWellcome Trust European Union Gillings FoundationNIHR Alzheimerrsquos Society Alzheimerrsquos Research UK Par-kinsonrsquos Society and Lewy Body Society during the conduct ofthe study and personal fees from Acadia pharmaceutical com-pany Lundbeck Roche Otsuka Eli Lilly and AARP outsidethe submitted work L Bonanni is a member of the steeringcommittee of the E-DLB consortium and program chair of theLBD-PIA (ISTAART) and is funded for research on DLB bythe Italian Ministry of Health P Donaghy receives supportfrom the NIHR Biomedical Research Centre awarded to theNewcastle upon Tyne Hospitals NHS Foundation Trust andNewcastle UniversityM Emre served on the scientific advisoryboard for AC Immune J Galvin receives support from NIHgrants (R01 AG040211 R01 NS101482 R01 AG057681 andU01 NS100610) and the Lewy Body Dementia AssociationResearch Center of Excellence reports research support fromthe NIH the Lewy Body Dementia Association The Harry TMangurian Foundation and Albert Charitable Trust directsclinical trials for Biogen and Novartis receives licensing feesfrom Biogen Roche Eli Lilly Quintiles Roobrik ContinuumClinical and Langland and receives consulting fees fromBiogen Eisai Bracket and Medavante D Galasko receivessupport from NIA grant AGO5131 and the Michael J FoxFoundation and has acted as consultant for vTv Pharmaceut-icals Inc Esai Inc and for Fujirebio Inc been a member of
a DSMB for Probiodrug and paid editor for Alzheimerrsquos Re-search amp Therapy J Goldman receives grantsupport fromTheMichael J Fox Foundation and Parkinsonrsquos Foundation andhas received consulting feeshonoraria from Acadia AptinyxSunovion and Worldwide Med S Gomperts receives supportfrom NIH grants R01 AG054551 P30AG062421 R01AG062208 P50 AG005134 R21 NS109833 DODCDMRPW81XW1810516 the Farmer Family ParkinsonrsquosInitiative and the Lewy Body Dementia Association and hasserved on advisory boards for Acadia Pharmaceuticals andSanofi L Honig acknowledges research grant support fromNYS CEAD grant C031425 LBDA RCOE and NIHgrants U01NS100600 P50AG008702 R21AG058020R21MH111596 U01AG051412 U01AG045390U01AG016976 U01AG023749 U19063893 andU19AG024904 He receives research funding support fromAbbVie Alector Biogen Eisai Genentech Roche and Wash-ington University and has received income for consulting forCortexyme and Eisai M Ikeda reports departmental grants andhonoraria fees from Sumitomo Dainippon Pharma Eisai andNiho Medicine-Physics J Leverenz acknowledges supportfrom the National Institutes of Health P30 AG053762 UO1NS100610 and R13NS111954 and Jane and Lee Seidman andDouglas Herthel DVMMemorial Funds and reports consultingfees from Aptinyx Acadia Biogen Eisai GE HealthcareGenzymeSanofi and Takeda Pharmaceuticals and grant sup-port from Alzheimerrsquos Drug Discovery Foundation De-partment of Defense GE Healthcare GenzymeSanofi TheMichael J Fox Foundation and the NIH (NIA andNINDS) SLewis is supported by NHMRC-ARC Dementia Fellows KMarder is funded by the NIH R01NS100600 NS107168UL1TR001873 andNS073671 with research support from theLBDA Parkinson Foundation Michael J Fox HDSA andCHDI and has acted as site investigator for Vaccinex andGenentech member of Springer editorial board and scientificadvisory board Voyager Therapeutics M Masellis was sup-ported by a Canadian Institutes of Health Research grant(MOP13129) and an Early Researcher Award from the Min-istry of Research Innovation and Science (MRIS ON) andreports personal fees for ad hoc consultancy from ArkudaTherapeutics Ionis Pharmaceuticals and Alector Pharmaceut-icals royalties fromHenry Stewart Talks Ltd and grants to theinstitution from Roche Novartis Washington University andAxovant Sciences D Salmon acknowledges support from NIHP30AG062429 and is a paid consultant for Takeda Inc Apti-nyx Inc and Biogen Inc J-P Taylor receives support from theNIHR Biomedical Research Centre awarded to the Newcastleupon Tyne Hospitals NHS Foundation Trust and NewcastleUniversity and reports grants from the UKNational Institute ofHealth Research (NIHR) travel award from Axovant researchsupport costs from Sonsei-Heptares and personal fees fromGEHealthcare D Tsuang acknowledges support from NIHR21AG064271 R03 NS103950 and U01 NS100610 ZWalker has been supported by ESRC NIHR (co-app) ARUK(co-app) EU IMI 2 (co-app) and Dunhill Medical Trust Shehas received consultancy fees travel expenses and researchsupport from GE Healthcare and research support from Life
752 Neurology | Volume 94 Number 17 | April 28 2020 NeurologyorgN
Molecular Imaging P Tiraboschi acknowledges the support ofthe Italian Ministry of Health GRANT NET-2011-02346784Go to NeurologyorgN for full disclosures
Publication historyReceived by Neurology October 30 2019 Accepted in final formFebruary 25 2020
Appendix Authors
Name Location Contribution
Ian GMcKeith FMed Sci MD
Newcastle University Design and conceptualizationof the study acquisition ofdata analysis andinterpretation of the data anddrafting and revising themanuscript for intellectualcontent
Tanis JFermanPhD
Mayo ClinicJacksonville
Design and conceptualizationof the study acquisition ofdata analysis andinterpretation of the data anddrafting and revising themanuscript for intellectualcontent
Alan JThomasPhD
Newcastle University Design and conceptualizationof the study acquisition ofdata analysis andinterpretation of the data anddrafting and revising themanuscript for intellectualcontent
FredericBlanc MD
University ofStrasbourg
Design and conceptualizationof the study acquisition ofdata analysis andinterpretation of the data anddrafting and revising themanuscript for intellectualcontent
Bradley FBoeve MD
Mayo Clinic Rochester Design and conceptualizationof the study acquisition ofdata analysis andinterpretation of the data anddrafting and revising themanuscript for intellectualcontent
HiroshigeFujishiroMD
Nagoya UniversityKawasaki MemorialHospital
Design and conceptualizationof the study acquisition ofdata analysis andinterpretation of the data anddrafting and revising themanuscript for intellectualcontent
KejalKantarciMD MS
Mayo Clinic Rochester Design and conceptualizationof the study acquisition ofdata analysis andinterpretation of the data anddrafting and revising themanuscript for intellectualcontent
CristinaMuscio PhD
Istituto NeurologicoldquoCarlo Bestardquo Milan
Design and conceptualizationof the study acquisition ofdata analysis andinterpretation of the data anddrafting and revising themanuscript for intellectualcontent
Appendix (continued)
Name Location Contribution
John TOrsquoBrien FMed Sci DM
Cambridge University Design and conceptualizationof the study acquisition ofdata analysis andinterpretation of the data anddrafting and revising themanuscript for intellectualcontent
Ronald BPostumaMD MSc
McGill University Design and conceptualizationof the study acquisition ofdata analysis andinterpretation of the data anddrafting and revising themanuscript for intellectualcontent
DagAarslandPhD
Kingrsquos College Londonand StavangerUniversityHospital
Revising the manuscript forintellectual content
CliveBallard MD
University of Exeter Revising the manuscript forintellectual content
LauraBonanniMD PhD
University of Chieti-Pescara
Revising the manuscript forintellectual content
PaulDonaghyPhD
Newcastle University Revising the manuscript forintellectual content
Murat EmreMD
Istanbul Faculty ofMedicine
Revising the manuscript forintellectual content
James EGalvin MDMPH
University of MiamiMiller School ofMedicine
Revising the manuscript forintellectual content
DouglasGalasko MD
University of CaliforniaSan Diego
Revising the manuscript forintellectual content
Jennifer GGoldmanMD MS
Feinberg School ofMedicine
Revising the manuscript forintellectual content
Stephen NGompertsMD PhD
Massachusetts GeneralHospital
Revising the manuscript forintellectual content
Lawrence SHonig MDPhD
Columbia UniversityIrving Medical Center
Revising the manuscript forintellectual content
ManabuIkeda MDPhD
Osaka University Revising the manuscript forintellectual content
James BLeverenzMD
Lou Ruvo Center ofBrain Health ClevelandClinic
Revising the manuscript forintellectual content
Simon JGLewis MD
University of Sydney Revising the manuscript forintellectual content
Karen SMarder MDMPH
Columbia UniversityIrving Medical Center
Revising the manuscript forintellectual content
MarioMasellisMD PhD
Sunnybrook HealthSciences CentreUniversity of Toronto
Revising the manuscript forintellectual content
David PSalmon PhD
University of CaliforniaSan Diego
Revising the manuscript forintellectual content
Continued
NeurologyorgN Neurology | Volume 94 Number 17 | April 28 2020 753
References1 Walker Z Possin KL Boeve BF Aarsland D Lewy body dementias Lancet 2015386
1683ndash16972 McKeith IG Boeve BF Dickson DW et al Diagnosis and management of dementia
with Lewy bodies fourth consensus report of the DLB consortium Neurology 20178988ndash100
3 Ferman TJ Smith GE Kantarci K et al Nonamnestic mild cognitive impairmentprogresses to dementia with Lewy bodies Neurology 2013812032ndash2038
4 Savica R Bradley BF Mielke MM When do alpha-synucleinopathies start An epi-demiological timeline A review JAMA Neurol 201875503ndash509
5 Donaghy PC Taylor JP OrsquoBrien JT et al Neuropsychiatric symptoms and cognitiveprofile in mild cognitive impairment with Lewy bodies Psychol Med 2018482384ndash2390
6 Cagnin A Bussse C Gardini S et al Clinical and cognitive phenotype of mildcognitive impairment evolving to dementia with Lewy bodies Dement Geriatr CognDis Extra 20155442ndash449
7 Postuma RB Iranzo A HuM et al Risk and predictors of dementia and parkinsonismin idiopathic REM sleep behaviour disorder a multicentre study Brain 2019142744ndash759
8 Sadiq D Whitfield T Lee L Stevens T Costafreda S Walker Z Prodromal dementiawith Lewy bodies and prodromal Alzheimerrsquos disease a comparison of the cognitiveand clinical profiles J Alzheimers Dis 201758463ndash470
9 FitzGerald JM Perera G Chang-Tave A et al The incidence of recorded de-lirium episodes before and after dementia diagnosis differences between de-mentia with Lewy bodies and Alzheimerrsquos disease J Am Med Dir Assoc 201920604ndash609
10 Jicha GA Schmitt FA Abner E et al Prodromal clinical manifestations of neu-ropathologically confirmed Lewy body disease Neurobiol Aging 2010311805ndash1813
11 Vardy E Holt R Gerhard A Richardson A Snowden J Neary D History of a sus-pected delirium is more common in dementia with Lewy bodies than Alzheimerrsquosdisease a retrospective study Int J Geriatr Psychiatry 201429178ndash181
12 Fujishiro H Nakamura S Sato K Iseki E Prodromal dementia with Lewy bodiesGeriatr Gerontol Int 201515817ndash826
13 McKeith I Taylor JP Thomas A Donaghy P Kane J Revisiting DLB diagnosisa consideration of prodromal DLB and of the diagnostic overlap with Alzheimerdisease J Geriatr Psychiatry Neurol 201629249ndash253
14 Albert MS DeKosky ST Dickson D et al The diagnosis of mild cognitive impairmentdue to Alzheimerrsquos disease recommendations from the National Institute on Aging-Alzheimerrsquos Association workgroups on diagnostic guidelines for Alzheimerrsquos diseaseAlzheimers Dement 20117270ndash279
15 Litvan I Goldman JG Troster AI et al Diagnostic criteria for mild cognitive im-pairment in Parkinsonrsquos disease Movement Disorder Society Task Force guidelinesMov Disord 201227349ndash356
16 Ferman TJ Smith GE Boeve BF et al Neuropsychological differentiation of de-mentia with Lewy bodies from normal aging and Alzheimerrsquos disease Clin Neuro-psychol 200620623ndash636
17 Cagnin A Busse C Jelcic N Gnoato F Mitolo M Caffarra P High specificity ofMMSE pentagon scoring for diagnosis of prodromal dementia with Lewy bodiesParkinsonism Relat Disord 201521303ndash305
18 Yoon JH Kim M Moon SY Yong SW Hong JM Olfactory function and neuro-psychological profile to differentiate dementia with Lewy bodies from Alzheimerrsquosdisease in patients with mild cognitive impairment a 5-year follow-up study J NeurolSci 2015355174ndash179
19 Kemp J Philippi N Phillipps C et al Cognitive profile in prodromal dementia withLewy bodies Alzheimers Res Ther 2017919
20 Auning E Rongve A Fladby T et al Early and presenting symptoms of dementia withLewy bodies Dement Geriatr Cogn Disord 201132202ndash208
21 Kondo D Ota K Kasanuki K et al Characteristics of mild cognitive impairmenttending to convert into Alzheimerrsquos disease or dementia with Lewy bodies a follow-upstudy in a memory clinic J Neurol Sci 2016369102ndash108
22 Marchand DG Postuma RB Escudier F et al How does dementia with Lewy bodiesstart prodromal cognitive changes in REM sleep behavior disorder Ann Neurol2018831016ndash1026
23 Kantarci K Lesnick T Ferman TJ et al Hippocampal volumes predict risk of de-mentia with Lewy bodies in mild cognitive impairment Neurology 2016872317ndash2323
24 Thomas AJ Taylor JP McKeith I et al Revision of assessment toolkits for improvingthe diagnosis of Lewy body dementia the DIAMOND Lewy study Int J GeriatrPsychiatry 2018331293ndash1304
25 Galvin JE Improving the clinical detection of Lewy body dementia with the Lewybody composite risk score Alzheimerrsquos Demen (Amsterdam Netherlands) 20151316ndash324
26 Belden CM Kahlon V Malek-Ahmadi M Tsai A Sabbagh MN Clinical character-ization of mild cognitive impairment as a prodrome to dementia with Lewy bodiesAm J Alzheimers Dis Other Demen 201530173ndash177
27 Yoon JH Lee JE Yong SW Moon SY Lee PH The mild cognitive impairment stageof dementia with Lewy bodies and Parkinson disease A comparison of cognitiveprofiles Alzheimer Dis Assoc Disord 201428151ndash155
28 Fengler S Liepelt-Scarfone I Brockmann K Schaffer E Berg D Kalbe E Cognitivechanges in prodromal Parkinsonrsquos disease a review Mov Disord 2017321655ndash1666
29 Kalbe E Rehberg SP Heber I et al Subtypes of mild cognitive impairment in patientswith Parkinsonrsquos disease evidence from the LANDSCAPE study J Neurol NeurosurgPsychiatry 2016871099ndash1105
30 Thomas AJ Donaghy P Roberts G et al Diagnostic accuracy of dopaminergic im-aging in prodromal dementia with Lewy bodies Psychol Med 20181ndash7
31 Ferman TJ Boeve BF Smith GE et al Inclusion of RBD improves the diagnosticclassification of dementia with Lewy bodies Neurology 201177875ndash882
32 Fujishiro H Okuda M Iwamoto K et al Early diagnosis of Lewy body disease inpatients with late-onset psychiatric disorders using clinical history of rapid eyemovement sleep behavior disorder and I-123 -metaiodobenzylguanidine cardiacscintigraphy Psychiatry Clin Neurosci 201872423ndash434
33 Bonanni L Perfetti B Bifolchetti S et al Quantitative electroencephalogram utility inpredicting conversion of mild cognitive impairment to dementia with Lewy bodiesNeurobiol Aging 201536434ndash445
34 Murray ME Ferman TJ Boeve BF et al MRI and pathology of REM sleep behaviordisorder in dementia with Lewy bodies Neurology 2013811681ndash1689
35 Murray ME Graff-Radford NR Ross OA Petersen RC Duara R Dickson DWNeuropathologically defined subtypes of Alzheimerrsquos disease with distinct clinicalcharacteristics a retrospective study Lancet Neurol 201110785ndash796
36 Blanc F Colloby SJ Cretin B et al Grey matter atrophy in prodromal stage ofdementia with Lewy bodies and Alzheimerrsquos disease Alzheimers Res Ther 2016831
37 Blanc F Colloby SJ Philippi N et al Cortical thickness in dementia with Lewy bodiesand Alzheimerrsquos disease a comparison of prodromal and dementia stages Plos One201510e0127396
38 Surendranathan A OrsquoBrien JT Clinical imaging in dementia with Lewy bodies EvidBased Ment Health 20182161ndash65
39 Outeiro TF Koss DJ Erskine D et al Dementia with Lewy bodies an update andoutlook Mol Neurodegener 2019145
40 Donadio V Incensi A Rizzo G et al A new potential biomarker for dementiawith Lewy bodies Skin nerve alpha-synuclein deposits Neurology 201789318ndash326
41 Flanigan PM Khosravi MA Leverenz JB Tousi B Color vision impairment differ-entiates Alzheimer dementia from dementia with Lewy bodies J Geriatr PsychiatryNeurol 20183197ndash102
42 Fereshtehnejad SM Yao C Pelletier A Montplaisir JY Gagnon JF Postuma RBEvolution of prodromal Parkinsonrsquos disease and dementia with Lewy bodies a pro-spective study Brain 20191422051ndash2067
43 Bousiges O Bombois S Schraen S et al Cerebrospinal fluid Alzheimer biomarkerscan be useful for discriminating dementia with Lewy bodies from Alzheimerrsquos diseaseat the prodromal stage J Neurol Neurosurg Psychiatry 201889467ndash475
44 Kantarci K Lowe VJ Boeve BF et al Multimodality imaging characteristics of de-mentia with Lewy bodies Neurobiol Aging 2012332091ndash2105
45 Kantarci K Lowe VJ Boeve BF et al AV-1451 tau and beta-amyloid positronemission tomography imaging in dementia with Lewy bodies Ann Neurol 20178158ndash67
46 Gore RL Vardy E OrsquoBrien JT Delirium and dementia with Lewy bodies distinctdiagnoses or part of the same spectrum J Neurol Neurosurg Psychiatry 20158650ndash59
47 Aarsland DS Auning E The pre-dementia stage of dementia with Lewy bodies Eur JNeurol 20111869
48 Sunwoo MK Hong JY Choi J Park HJ Kim SH Lee PH alpha-Synuclein pathologyis related to postoperative delirium in patients undergoing gastrectomy Neurology201380810ndash813
49 Akintade O Pierres F Acute presentation of dementia with Lewy bodies Clin Med201919327ndash330
50 Kosaka K Diffuse Lewy body disease in Japan J Neurol 1990237197ndash20451 Birkett DP Desouky A Han L Kaufman M Lewy bodies in psychiatric patients Int J
Geriatr Psychiatry 19927235ndash240
Appendix (continued)
Name Location Contribution
John PaulTaylor MBBS PhD
Newcastle University Revising the manuscript forintellectual content
Debby WTsuang MD
VA Puget Sound ampUniversity ofWashington
Revising the manuscript forintellectual content
ZuzanaWalker MD
University CollegeLondon
Revising the manuscript forintellectual content
PietroTiraboschiMD
Istituto NeurologicoldquoCarlo Bestardquo Milan
Design and conceptualizationof the study acquisition ofdata analysis andinterpretation of the data anddrafting and revising themanuscript for intellectualcontent
754 Neurology | Volume 94 Number 17 | April 28 2020 NeurologyorgN
52 Kobayashi K Nakano H Akiyama N Maeda T Yamamori S Pure psychiatric pre-sentation of the Lewy body disease is depressionmdashan analysis of 60 cases verified withmyocardial meta-iodobenzylguanidine study Int J Geriatr Psychiatry 201530663ndash668
53 Takahashi S Mizukami K Arai T et al Ventilatory response to hypercapnia predictsdementia with Lewy bodies in late-onset major depressive disorder J Alzheimers Dis201650751ndash758
54 Van Assche L Van Aubel E Van de Ven L Bouckaert F Luyten P Vandenbulcke MThe neuropsychological profile and phenomenology of late onset psychosis a cross-sectional study on the differential diagnosis of very-late-onset Schizophrenia-likepsychosis dementia with Lewy bodies and Alzheimerrsquos type dementia with psychosisArch Clin Neuropsychol 201934183ndash199
55 Thaipisuttikul P Lobach I Zweig Y Gurnani A Galvin JE Capgras syndrome indementia with Lewy bodies Int Psychogeriatr 201325843ndash849
56 Fujishiro H Iseki E Nakamura S et al Dementia with Lewy bodies early diagnosticchallenges Psychogeriatrics 201313128ndash138
57 Chiba Y Fujishiro H Iseki E et al Retrospective survey of prodromal symptoms indementia with Lewy bodies comparison with Alzheimerrsquos disease Dement GeriatrCogn Disord 201233273ndash281
58 Kaufmann H Norcliffe-Kaufmann L Palma JA et al Natural history of pure auto-nomic failure a United States prospective cohort Ann Neurol 201781287ndash297
59 Heinzel S Berg D Gasser T et al Update of the MDS research criteria for prodromalParkinsonrsquos disease Mov Disord 2019341464ndash1470
60 Palma JA Norcliffe-Kaufmann L Kaufmann H Diagnosis of multiple system atrophyAuton Neurosci 201821115ndash25Data available fromDryad (Additional References References e1ndashe44) doi105061dryad1c59zw3rv
Subspecialty Alerts by E-mail
Customize your online journal experience by signing up for e-mail alerts related to your subspecialty or area of interest Accessthis free service by clicking on the ldquoMy Alertsrdquo link on the home page An extensive list of subspecialties methods and studydesign choices will be available for you to choose frommdashallowing you priority alerts to cutting-edge research in your field
COVID-19 and Neurologic Disease Call for Papers
The editors of Neurology are interested in papers that address the neurological aspects of COVID-19infection and challenges to the management of patients with chronic neurological conditions whohave or are at risk for the infection Relevant papers that pass initial internal review will undergoexpedited peer review and online publication We will consider papers posted in preprint servers
Submit observational studies and clinical trials as Articles and case series and case reports underthe ClinicalScientific Notes category to httpssubmitneurologyorg today
Visit the Neurologyreg Website at NeurologyorgN More article-based content on home pages Streamlined menus and navigation Enhanced blog sections for specialty areas Same experience on desktop tablet and mobile devices Improved article reading experience links more evident (pdf analytics social media) Neurologyreg Clinical Practice initiative ldquoPractice Currentrdquo global surveys will be accessible across sites
Find Neurologyreg on Facebook httptinyurlcomneurologyfan
Follow Neurologyreg on Twitter httpstwittercomGreenJournal
NeurologyorgN Neurology | Volume 94 Number 17 | April 28 2020 755
DOI 101212WNL0000000000009323202094743-755 Published Online before print April 2 2020Neurology
Ian G McKeith Tanis J Ferman Alan J Thomas et al Research criteria for the diagnosis of prodromal dementia with Lewy bodies
This information is current as of April 2 2020
ServicesUpdated Information amp
httpnneurologyorgcontent9417743fullincluding high resolution figures can be found at
References httpnneurologyorgcontent9417743fullref-list-1
This article cites 59 articles 12 of which you can access for free at
Subspecialty Collections
httpnneurologyorgcgicollectionpsychosisPsychosis a
httpnneurologyorgcgicollectionparkinsons_disease_with_dementiParkinsons disease with dementia
httpnneurologyorgcgicollectionmci_mild_cognitive_impairmentMCI (mild cognitive impairment)
httpnneurologyorgcgicollectiondementia_with_lewy_bodiesDementia with Lewy bodies
httpnneurologyorgcgicollectiondeliriumDeliriumfollowing collection(s) This article along with others on similar topics appears in the
Permissions amp Licensing
httpwwwneurologyorgaboutabout_the_journalpermissionsits entirety can be found online atInformation about reproducing this article in parts (figurestables) or in
Reprints
httpnneurologyorgsubscribersadvertiseInformation about ordering reprints can be found online
ISSN 0028-3878 Online ISSN 1526-632XWolters Kluwer Health Inc on behalf of the American Academy of Neurology All rights reserved Print1951 it is now a weekly with 48 issues per year Copyright Copyright copy 2020 The Author(s) Published by
reg is the official journal of the American Academy of Neurology Published continuously sinceNeurology

subjects with AD in the year before diagnosis (17middot6 v 3middot2100person-years)9 and admissions for delirium were morecommon in those already diagnosed with DLB than for otherdementias Prolonged delirium may also raise the index ofsuspicion for DLBe36 In an FDG-PET imaging study ofprolonged delirium 32 of subjects were found to havea DLB like pattern a high proportion in regard both to theknown prevalence of the disease and to that of their matchedcognitively impaired control group (4)e37
The similarities between the marked fluctuations in DLB anddisturbances of attention and consciousness in delirium havebeen noted and reviewed46 but there is as yet little un-derstanding of a shared neurobiological basis There havebeen few pathologic studies and although in anepidemiologic-based autopsy cohort there was no link be-tween delirium and LB pathology at autopsye38 a significantlyincreased risk of postoperative delirium in those with pe-ripheral α-synuclein pathology has been described48 Deliriumhas been suggested to bemore common in those subjects withDLB with later age at onsete39 but further evidence is needed
In summary (table 2) it is clear that DLB can present withdelirium and in patients diagnosed with delirium a carefulsearch for other DLB features should be made with a lowthreshold for undertaking DLB biomarker examinations es-pecially in those with recurrent unexplained or prolongeddelirium The extent to which delirium presentations of DLBhave the biomarker abnormalities associated with establishedDLB or other prodromal DLB presentations is unclear
although the PET imaging study cited above supports thise37
as does a report of reduced DAT uptake in a patient withacute unexplained delirium49 The link between delirium andDLB is an important area for future research to clarify therelationship between the 2 and to establish which factorsassociated with delirium should raise the index of suspicionfor underlying prodromal DLB
Psychiatric-onset DLBEarly clinicopathologic studies suggested that DLB maypresent as a primary psychiatric disorder5051 but subsequentfocus on the cognitive and motor aspects of DLB has limitedthe documentation of such cases outside of a fewcenters123252ndash54e36 Late-onset major depressive disorderand late-onset psychosis are the most frequently reportedpresentations differing markedly from the construct of mildbehavioral impairmente40 and sometimes sufficiently severe torequire hospitalization Symptoms include hallucinations invisual and in other modalities and systematized delusionsincluding Capgras syndrome55 apathy anxiety and de-pression Psychiatric-onset DLB cases are not easily differ-entiated from non-LB late-onset psychosis cases on the basisof primary psychiatric phenomenology or neuropsychologicalprofile alone54 Psychomotor retardation such as slowedspeech thinking and body movements can resemble thebradykinesia of parkinsonism The occurrence of rest tremoror rigidity is more helpful than bradykinesia to suspect pro-dromal DLB in patients with depressive disorder53 butpsychotropic-induced parkinsonism may complicate di-agnosis Atypical clinical features may prove valuable pointers
Table 2 Summary of key features of delirium-onset DLB
Patients with DLB are more susceptible to delirium than people with Alzheimer disease and this delirium may occur as their presenting complaint beforedementia develops
Such episodes may be provoked by multiple factors including surgery infectionssepsis fever or other systemic illness or secondary to use or suddenwithdrawal of alcohol or psychoactive drugs
Prodromal DLB should be particularly suspected in patients
bull in whom adequate provoking factors for the delirium are not found
bull with prolonged or recurrent delirium
bull who later develop progressive cognitive decline or subsequent dementia
Core clinical features of DLB are likely to be of more limited diagnostic weight in a patient with delirium because
bull cognitive fluctuation and clouding of consciousness can also occur in non-DLB delirium ie are not diagnostically specific for DLB in this situation
bull visual hallucinations may occur in non-DLB delirium particularly drug-induced or provoked by alcohol abstinence
bull motor parkinsonism present may be due to antipsychotic medications used to treat delirium
bull the diagnostic significance of a history of RBD in a person with delirium is not yet established
Identification of delirium-onset DLB
bull may be assisted by use of MCI-LB biomarkers but further research evidence of this is required
bull is important to inform the management plan including the avoidance or minimization of antipsychotic and anticholinergic agents
Abbreviations DLB = dementia with Lewy bodies MCI = mild cognitive impairment MCI-LB = MCI with Lewy bodies RBD = REM sleep behavior disorder
NeurologyorgN Neurology | Volume 94 Number 17 | April 28 2020 749
to underlying LB pathology particularly the presence of re-current VH12 when these occur before cognitive impairmentbecomes evident As with all α-synucleinopathies RBD maybe a useful indicator although a relationship between anti-depressant usage and subsequent RBD onset is a potentialconfoundere41 Although the primary psychiatric manifes-tations are often accompanied by mild cognitive deficits54
cognitive evaluation and interpretation of performance can bedifficult when psychiatric symptoms are prominent The fre-quency of cognitive fluctuations in psychiatric-onset LB caseshas not been determined
Initial reports suggest that 123I-MIBG scintigraphy may behelpful in psychiatric-onset DLB525356 Eighteen of 35patients with a first onset of major depressive disorder gt50years and with bradykinesia developed a clinical diagnosis ofDLB after 6 years of follow-up All 18 had an abnormal ven-tilatory response to hypercapnia (VRH) indicative of severeautonomic dysfunction whereas none of the 17 patients witha normal VRH converted to DLB within the study period Forthe converters the most common presentation was withpsychotic and melancholic features simultaneously The fre-quency of hypersensitivity to antipsychotics antidepressantsand antianxiety drugs was higher in converters than in non-converters53 Further studies need to confirm these findingsand to determine the value of other DLB biomarkers inpsychiatric-onset cases325256
In summary it is not yet clear how to identify patients withprominent late-onset psychiatric symptoms who may haveunderlying LB disease and subsequently progress to DLB It is
premature to try to construct formal criteria for psychiatric-onset DLB but clinicians in mental health and other settingsneed to be aware that this possibility exists not least becauseof the risk of severe antipsychotic sensitivity reactions withincreased morbidity and mortality The small available liter-ature including reports such as those cited above does providesome useful guidance summarized in table 3 but requiresreplication and further investigation
Idiopathic REM sleep behavior disorderRBD is characterized by abnormal dream enactment behaviorduring REM sleep accompanied by loss of muscle atonia duringREM sleep (REM sleep without atonia or RSWA) on PSG Forthe purpose of a prodromal DLB diagnosis a clinical history ofRBD is obtained in the same way as for DLB2 that is a clearcomplaint of dream enactment by a bedpartner or other witnesswith no evidence of sleep disorders that may mimic RBD onclinical interview Conditions known to mimic or masquerade asRBD include non-REM parasomnias (sleep walking sleep talk-ing or other behaviors that emerge fromnon-REM sleep stages)obstructive sleep apnea confusional arousals or nocturnal seiz-ures In the absence of PSG the risk of a false-positive clinicaldiagnosis of RBD is reduced by using optimized sleep ques-tionnaires which can have sensitivity and specificity over 90e42
RBDmay be considered as idiopathic until it is associated withanother ongoing neurologic condition the most frequentbeing an α-synucleinopathy (PD DLB or MSA) In a recentlarge study 735 of patients with RBD converted to an overtneurodegenerative syndrome after 12-year follow-up 565developing parkinsonism and 435 dementia as their first
Table 3 Summary of key features of psychiatric-onset DLB
Is characterized by predominant psychiatric symptoms that typically correspond to late-onset major depressive disorder or late-onset psychosis which mayfeature hallucinations in visual and in other modalities and systematized delusions including Capgras syndrome
bull may also present with apathy anxiety and depression
bull may be sufficiently severe to require hospitalization
bull the frequency of LB disease as a cause of late-onset psychiatric disorder is not known
When assessing for core clinical features of DLB in a patient with a primary psychiatric presentation
bull bradykinesia may be mimicked by psychomotor retardation which is commonly seen in depressive disorders
bull parkinsonism may be induced by antipsychotic medications used to treat psychiatric disorder
bull RBD (and REM sleep without atonia) may be induced by antidepressant medications
bull mild cognitive disturbance may be present but is not predominant and may fluctuate
bull formal neuropsychological testing may be confounded by the psychiatric mental state
bull the frequency and character of cognitive fluctuations is unknown
Identification of psychiatric-onset DLB
bull may be assisted by use of MCI-LB biomarkers but further research evidence of this is required
bull is important to inform the management plan including the avoidance or minimization of antipsychotic and anticholinergic agents
Abbreviations DLB = dementia with Lewy bodies MCI = mild cognitive impairment
750 Neurology | Volume 94 Number 17 | April 28 2020 NeurologyorgN
disease manifestation Among many predictive markerstested only the cognitive variables differed at baseline be-tween those converting to primary dementia vs parkinson-ism7 Other multicenter studies confirm that the only clinicalfeature that predicts dementia vs parkinsonism first is neu-ropsychological performance those with RBD who exhibitcognitive changes are more likely to evolve first into MCI orDLB22e4 Thus although RBD may be regarded an earlymanifestation of α-synucleinopathy it is not possible to clearlydistinguish whether an individual presenting with RBD willdevelop dementia first that is evolve into a primary DLBdiagnosis or parkinsonism first that is a primary PDMSAdiagnosis Any MCI subtype associated with PSG-confirmedRBD is highly likely to represent underlying LB disease Al-though idiopathic RBD is a useful model to study the earlystages of LB disease progression it is not necessarily repre-sentative of the whole spectrum of patients with PD and DLBa significant minority of whom do not have RBD42
Autonomic dysfunctionanosmia and othernonspecific prodromal LB disease symptomsPatients with DLB frequently report a history of autonomicdysfunction at first clinic attendance with 25ndash50 com-plaining of one of more among constipation orthostatic diz-ziness urinary incontinence erectile dysfunction increasedsweating or increased saliva5657 In a cohort of patients withpure autonomic failure 34 converted to an overt α-synu-cleinopathy over 6 years of follow-up this was to DLB (52)PD (24) orMSA (24)58 However because there are manyother causes for autonomic dysfunction in older people thesesymptoms either alone or in combination have low positivepredictive value59 The situation is similar for hyposmia whichalso frequently occurs early in prodromal DLB and PD42 butwhich can have many other causes in this age group
Conclusions and future directionDiagnosis of DLB at the dementia stage depends on identifyingfully expressed core clinical features which may be mild orabsent at the prodromal stage when biomarker evidence mayalso be weaker and may even differ from that found at thedementia stage Several new biomarker candidates direct andindirect are in development and we will continue to reviewthese to update our recommendations as soon as sufficientevidence accumulates We recognize that the clinical pheno-type of neurodegenerative disorders reflects interaction be-tween several rather than a single brain pathology and it istherefore likely that multiple biomarkers of individual pathol-ogies (eg α-synuclein β-amyloid and tau) or of disease sur-rogates (eg metabolic imagingEEG) will be required
Although we have described the 3 prodromal DLB syndromesseparately they are unlikely to be mutually exclusive andthere may be substantial overlap We propose operationalizedcriteria only for MCI-LB because the evidence base from oursystematic review albeit relatively limited is sufficient to
support recommendations that are immediately applicableand testable Our recommendations should be used alongsideguidance about the prodromal manifestations of PD1559
MSA60 and AD14 with which there is overlap Notwith-standing the potential benefits of early diagnosis we are alsomindful of the importance of avoiding incorrect (false-positive) diagnosis of prodromal DLB and the potentialnegative consequences this could have for an individual Wesuggest that the predictive validity of different categories andcombinations of our proposed criteria should be clarified byprospective studies before they are adopted for widespreadclinical use and that they will enable standardization for in-clusion in research studies and clinical trials
Some published guidance about the early clinical diagnosis ofDLB does already exist DSM5 recommends a diagnosis ofmild neurocognitive disorder (NCD) with LB ldquofor individualswho present with the core or suggestive features at a stagewhen cognitive or functional impairments are not of sufficientseverity to fulfill criteria for major NCDrdquoe43 This is basedhowever on the 2005 version of DLB guidelines and requiresupdating ICD-11 takes a similar approach toward diagnosingmild NCD at a syndromic level and lists both Lewy bodydisease and PD as possible causese44
The diagnostic position for other prodromal manifestations ofDLB that is delirium-onset and psychiatric-onset is less clearthan for MCI Operationalization of specific criteria for thesesyndromes is not yet justified and the reliable differentiationof the minority of delirious and psychiatrically ill patients whohave underlying LB pathology from the majority who do notwill probably only be achieved when routinely applicablebiomarkers are developed LB disease is seldom if ever cur-rently considered as part of the differential diagnosis of de-lirium or late-onset psychiatric disorder and we hope that theinformation we provide in the text and accompanying boxeswill raise cliniciansrsquo awareness of that possibility
Study fundingNo targeted funding reported
DisclosureI McKeith receives support from the NIHR Biomedical Re-search Centre awarded to the Newcastle upon Tyne HospitalsNHS Foundation Trust and Newcastle University and hasconsulted for GE Healthcare Sanofi Eisai Sumitomo Dai-nippon Pharma and Axovant T Ferman receives support fromNIH P50-AG16574 P30-AG062677 U01-NS100620 and theMangurian Foundation for Lewy body disease research AThomas receives support from the NIHR Biomedical ResearchCentre awarded to the Newcastle upon Tyne Hospitals NHSFoundation Trust and Newcastle University and has receivedgrants from GE Healthcare F Blanc has served as nationalclinical trial coordinator for Eisai and Axovant B Boevereceives support from NIH P50-AG16574 P30-AG062677U01-NS100620 and the Mangurian Foundation for Lewybody disease research has consulted for the Scientific Advisory
NeurologyorgN Neurology | Volume 94 Number 17 | April 28 2020 751
BoardmdashTau Consortium and received grants from Biogenthe NIH theMangurian Foundation Alector the Little FamilyFoundation and the Turner Family H Fujishiro has receivedsupport from Fujifilm RI Pharma Co Ltd K Kantarci receivessupport from NIH P50-AG16574 P30-AG062677 U01-NS100620 and the Mangurian Foundation for Lewy bodydisease research and has received grants from Avid Radio-pharmaceuticals and acted on a Data Safety Monitoring Boardfor Takeda Global Research C Muscio acknowledges thesupport of the Italian Ministry of Health GRANT NET-2011-02346784 J OrsquoBrien is supported by the NIHR CambridgeBiomedical Research Centre Dementia and Neuro-degeneration and Mental Health Themes and the CambridgeCentre for Parkinsonrsquos Plus Disorders has consulted forTauRx Axon GE Healthcare Eisai and AvidLilly and re-ceived grants fromAvidLilly andAllianceMedical R Postumahas received grants from and consulted for Fonds de laRecherche en Sante received grants from the Canadian Insti-tutes of Health Research the Parkinson Society of Canada theWeston-Garfield Foundation The Michael J Fox Foundationand the Webster Foundation and consulted for TakedaRocheProthena Teva Neurosciences Novartis Canada Bio-gen Boehringer Ingelheim Theranexus GE Healthcare JazzPharmaceuticals AbbVie Jannsen Otsuko PhytopharmicsInception Sciences and Parkinson Canada D Aarsland isa Royal Society Wolfson Research Merit Award Holder andwould like to thank the Wolfson Foundation and the RoyalSociety for their support He has received research supportandor honoraria from AstraZeneca H Lundbeck NovartisPharmaceuticals and GE Health and served as paid consultantfor H Lundbeck Eisai Heptares Sanofi and Mentis Cura CBallard reports unrelated current grant funding from MRCWellcome Trust European Union Gillings FoundationNIHR Alzheimerrsquos Society Alzheimerrsquos Research UK Par-kinsonrsquos Society and Lewy Body Society during the conduct ofthe study and personal fees from Acadia pharmaceutical com-pany Lundbeck Roche Otsuka Eli Lilly and AARP outsidethe submitted work L Bonanni is a member of the steeringcommittee of the E-DLB consortium and program chair of theLBD-PIA (ISTAART) and is funded for research on DLB bythe Italian Ministry of Health P Donaghy receives supportfrom the NIHR Biomedical Research Centre awarded to theNewcastle upon Tyne Hospitals NHS Foundation Trust andNewcastle UniversityM Emre served on the scientific advisoryboard for AC Immune J Galvin receives support from NIHgrants (R01 AG040211 R01 NS101482 R01 AG057681 andU01 NS100610) and the Lewy Body Dementia AssociationResearch Center of Excellence reports research support fromthe NIH the Lewy Body Dementia Association The Harry TMangurian Foundation and Albert Charitable Trust directsclinical trials for Biogen and Novartis receives licensing feesfrom Biogen Roche Eli Lilly Quintiles Roobrik ContinuumClinical and Langland and receives consulting fees fromBiogen Eisai Bracket and Medavante D Galasko receivessupport from NIA grant AGO5131 and the Michael J FoxFoundation and has acted as consultant for vTv Pharmaceut-icals Inc Esai Inc and for Fujirebio Inc been a member of
a DSMB for Probiodrug and paid editor for Alzheimerrsquos Re-search amp Therapy J Goldman receives grantsupport fromTheMichael J Fox Foundation and Parkinsonrsquos Foundation andhas received consulting feeshonoraria from Acadia AptinyxSunovion and Worldwide Med S Gomperts receives supportfrom NIH grants R01 AG054551 P30AG062421 R01AG062208 P50 AG005134 R21 NS109833 DODCDMRPW81XW1810516 the Farmer Family ParkinsonrsquosInitiative and the Lewy Body Dementia Association and hasserved on advisory boards for Acadia Pharmaceuticals andSanofi L Honig acknowledges research grant support fromNYS CEAD grant C031425 LBDA RCOE and NIHgrants U01NS100600 P50AG008702 R21AG058020R21MH111596 U01AG051412 U01AG045390U01AG016976 U01AG023749 U19063893 andU19AG024904 He receives research funding support fromAbbVie Alector Biogen Eisai Genentech Roche and Wash-ington University and has received income for consulting forCortexyme and Eisai M Ikeda reports departmental grants andhonoraria fees from Sumitomo Dainippon Pharma Eisai andNiho Medicine-Physics J Leverenz acknowledges supportfrom the National Institutes of Health P30 AG053762 UO1NS100610 and R13NS111954 and Jane and Lee Seidman andDouglas Herthel DVMMemorial Funds and reports consultingfees from Aptinyx Acadia Biogen Eisai GE HealthcareGenzymeSanofi and Takeda Pharmaceuticals and grant sup-port from Alzheimerrsquos Drug Discovery Foundation De-partment of Defense GE Healthcare GenzymeSanofi TheMichael J Fox Foundation and the NIH (NIA andNINDS) SLewis is supported by NHMRC-ARC Dementia Fellows KMarder is funded by the NIH R01NS100600 NS107168UL1TR001873 andNS073671 with research support from theLBDA Parkinson Foundation Michael J Fox HDSA andCHDI and has acted as site investigator for Vaccinex andGenentech member of Springer editorial board and scientificadvisory board Voyager Therapeutics M Masellis was sup-ported by a Canadian Institutes of Health Research grant(MOP13129) and an Early Researcher Award from the Min-istry of Research Innovation and Science (MRIS ON) andreports personal fees for ad hoc consultancy from ArkudaTherapeutics Ionis Pharmaceuticals and Alector Pharmaceut-icals royalties fromHenry Stewart Talks Ltd and grants to theinstitution from Roche Novartis Washington University andAxovant Sciences D Salmon acknowledges support from NIHP30AG062429 and is a paid consultant for Takeda Inc Apti-nyx Inc and Biogen Inc J-P Taylor receives support from theNIHR Biomedical Research Centre awarded to the Newcastleupon Tyne Hospitals NHS Foundation Trust and NewcastleUniversity and reports grants from the UKNational Institute ofHealth Research (NIHR) travel award from Axovant researchsupport costs from Sonsei-Heptares and personal fees fromGEHealthcare D Tsuang acknowledges support from NIHR21AG064271 R03 NS103950 and U01 NS100610 ZWalker has been supported by ESRC NIHR (co-app) ARUK(co-app) EU IMI 2 (co-app) and Dunhill Medical Trust Shehas received consultancy fees travel expenses and researchsupport from GE Healthcare and research support from Life
752 Neurology | Volume 94 Number 17 | April 28 2020 NeurologyorgN
Molecular Imaging P Tiraboschi acknowledges the support ofthe Italian Ministry of Health GRANT NET-2011-02346784Go to NeurologyorgN for full disclosures
Publication historyReceived by Neurology October 30 2019 Accepted in final formFebruary 25 2020
Appendix Authors
Name Location Contribution
Ian GMcKeith FMed Sci MD
Newcastle University Design and conceptualizationof the study acquisition ofdata analysis andinterpretation of the data anddrafting and revising themanuscript for intellectualcontent
Tanis JFermanPhD
Mayo ClinicJacksonville
Design and conceptualizationof the study acquisition ofdata analysis andinterpretation of the data anddrafting and revising themanuscript for intellectualcontent
Alan JThomasPhD
Newcastle University Design and conceptualizationof the study acquisition ofdata analysis andinterpretation of the data anddrafting and revising themanuscript for intellectualcontent
FredericBlanc MD
University ofStrasbourg
Design and conceptualizationof the study acquisition ofdata analysis andinterpretation of the data anddrafting and revising themanuscript for intellectualcontent
Bradley FBoeve MD
Mayo Clinic Rochester Design and conceptualizationof the study acquisition ofdata analysis andinterpretation of the data anddrafting and revising themanuscript for intellectualcontent
HiroshigeFujishiroMD
Nagoya UniversityKawasaki MemorialHospital
Design and conceptualizationof the study acquisition ofdata analysis andinterpretation of the data anddrafting and revising themanuscript for intellectualcontent
KejalKantarciMD MS
Mayo Clinic Rochester Design and conceptualizationof the study acquisition ofdata analysis andinterpretation of the data anddrafting and revising themanuscript for intellectualcontent
CristinaMuscio PhD
Istituto NeurologicoldquoCarlo Bestardquo Milan
Design and conceptualizationof the study acquisition ofdata analysis andinterpretation of the data anddrafting and revising themanuscript for intellectualcontent
Appendix (continued)
Name Location Contribution
John TOrsquoBrien FMed Sci DM
Cambridge University Design and conceptualizationof the study acquisition ofdata analysis andinterpretation of the data anddrafting and revising themanuscript for intellectualcontent
Ronald BPostumaMD MSc
McGill University Design and conceptualizationof the study acquisition ofdata analysis andinterpretation of the data anddrafting and revising themanuscript for intellectualcontent
DagAarslandPhD
Kingrsquos College Londonand StavangerUniversityHospital
Revising the manuscript forintellectual content
CliveBallard MD
University of Exeter Revising the manuscript forintellectual content
LauraBonanniMD PhD
University of Chieti-Pescara
Revising the manuscript forintellectual content
PaulDonaghyPhD
Newcastle University Revising the manuscript forintellectual content
Murat EmreMD
Istanbul Faculty ofMedicine
Revising the manuscript forintellectual content
James EGalvin MDMPH
University of MiamiMiller School ofMedicine
Revising the manuscript forintellectual content
DouglasGalasko MD
University of CaliforniaSan Diego
Revising the manuscript forintellectual content
Jennifer GGoldmanMD MS
Feinberg School ofMedicine
Revising the manuscript forintellectual content
Stephen NGompertsMD PhD
Massachusetts GeneralHospital
Revising the manuscript forintellectual content
Lawrence SHonig MDPhD
Columbia UniversityIrving Medical Center
Revising the manuscript forintellectual content
ManabuIkeda MDPhD
Osaka University Revising the manuscript forintellectual content
James BLeverenzMD
Lou Ruvo Center ofBrain Health ClevelandClinic
Revising the manuscript forintellectual content
Simon JGLewis MD
University of Sydney Revising the manuscript forintellectual content
Karen SMarder MDMPH
Columbia UniversityIrving Medical Center
Revising the manuscript forintellectual content
MarioMasellisMD PhD
Sunnybrook HealthSciences CentreUniversity of Toronto
Revising the manuscript forintellectual content
David PSalmon PhD
University of CaliforniaSan Diego
Revising the manuscript forintellectual content
Continued
NeurologyorgN Neurology | Volume 94 Number 17 | April 28 2020 753
References1 Walker Z Possin KL Boeve BF Aarsland D Lewy body dementias Lancet 2015386
1683ndash16972 McKeith IG Boeve BF Dickson DW et al Diagnosis and management of dementia
with Lewy bodies fourth consensus report of the DLB consortium Neurology 20178988ndash100
3 Ferman TJ Smith GE Kantarci K et al Nonamnestic mild cognitive impairmentprogresses to dementia with Lewy bodies Neurology 2013812032ndash2038
4 Savica R Bradley BF Mielke MM When do alpha-synucleinopathies start An epi-demiological timeline A review JAMA Neurol 201875503ndash509
5 Donaghy PC Taylor JP OrsquoBrien JT et al Neuropsychiatric symptoms and cognitiveprofile in mild cognitive impairment with Lewy bodies Psychol Med 2018482384ndash2390
6 Cagnin A Bussse C Gardini S et al Clinical and cognitive phenotype of mildcognitive impairment evolving to dementia with Lewy bodies Dement Geriatr CognDis Extra 20155442ndash449
7 Postuma RB Iranzo A HuM et al Risk and predictors of dementia and parkinsonismin idiopathic REM sleep behaviour disorder a multicentre study Brain 2019142744ndash759
8 Sadiq D Whitfield T Lee L Stevens T Costafreda S Walker Z Prodromal dementiawith Lewy bodies and prodromal Alzheimerrsquos disease a comparison of the cognitiveand clinical profiles J Alzheimers Dis 201758463ndash470
9 FitzGerald JM Perera G Chang-Tave A et al The incidence of recorded de-lirium episodes before and after dementia diagnosis differences between de-mentia with Lewy bodies and Alzheimerrsquos disease J Am Med Dir Assoc 201920604ndash609
10 Jicha GA Schmitt FA Abner E et al Prodromal clinical manifestations of neu-ropathologically confirmed Lewy body disease Neurobiol Aging 2010311805ndash1813
11 Vardy E Holt R Gerhard A Richardson A Snowden J Neary D History of a sus-pected delirium is more common in dementia with Lewy bodies than Alzheimerrsquosdisease a retrospective study Int J Geriatr Psychiatry 201429178ndash181
12 Fujishiro H Nakamura S Sato K Iseki E Prodromal dementia with Lewy bodiesGeriatr Gerontol Int 201515817ndash826
13 McKeith I Taylor JP Thomas A Donaghy P Kane J Revisiting DLB diagnosisa consideration of prodromal DLB and of the diagnostic overlap with Alzheimerdisease J Geriatr Psychiatry Neurol 201629249ndash253
14 Albert MS DeKosky ST Dickson D et al The diagnosis of mild cognitive impairmentdue to Alzheimerrsquos disease recommendations from the National Institute on Aging-Alzheimerrsquos Association workgroups on diagnostic guidelines for Alzheimerrsquos diseaseAlzheimers Dement 20117270ndash279
15 Litvan I Goldman JG Troster AI et al Diagnostic criteria for mild cognitive im-pairment in Parkinsonrsquos disease Movement Disorder Society Task Force guidelinesMov Disord 201227349ndash356
16 Ferman TJ Smith GE Boeve BF et al Neuropsychological differentiation of de-mentia with Lewy bodies from normal aging and Alzheimerrsquos disease Clin Neuro-psychol 200620623ndash636
17 Cagnin A Busse C Jelcic N Gnoato F Mitolo M Caffarra P High specificity ofMMSE pentagon scoring for diagnosis of prodromal dementia with Lewy bodiesParkinsonism Relat Disord 201521303ndash305
18 Yoon JH Kim M Moon SY Yong SW Hong JM Olfactory function and neuro-psychological profile to differentiate dementia with Lewy bodies from Alzheimerrsquosdisease in patients with mild cognitive impairment a 5-year follow-up study J NeurolSci 2015355174ndash179
19 Kemp J Philippi N Phillipps C et al Cognitive profile in prodromal dementia withLewy bodies Alzheimers Res Ther 2017919
20 Auning E Rongve A Fladby T et al Early and presenting symptoms of dementia withLewy bodies Dement Geriatr Cogn Disord 201132202ndash208
21 Kondo D Ota K Kasanuki K et al Characteristics of mild cognitive impairmenttending to convert into Alzheimerrsquos disease or dementia with Lewy bodies a follow-upstudy in a memory clinic J Neurol Sci 2016369102ndash108
22 Marchand DG Postuma RB Escudier F et al How does dementia with Lewy bodiesstart prodromal cognitive changes in REM sleep behavior disorder Ann Neurol2018831016ndash1026
23 Kantarci K Lesnick T Ferman TJ et al Hippocampal volumes predict risk of de-mentia with Lewy bodies in mild cognitive impairment Neurology 2016872317ndash2323
24 Thomas AJ Taylor JP McKeith I et al Revision of assessment toolkits for improvingthe diagnosis of Lewy body dementia the DIAMOND Lewy study Int J GeriatrPsychiatry 2018331293ndash1304
25 Galvin JE Improving the clinical detection of Lewy body dementia with the Lewybody composite risk score Alzheimerrsquos Demen (Amsterdam Netherlands) 20151316ndash324
26 Belden CM Kahlon V Malek-Ahmadi M Tsai A Sabbagh MN Clinical character-ization of mild cognitive impairment as a prodrome to dementia with Lewy bodiesAm J Alzheimers Dis Other Demen 201530173ndash177
27 Yoon JH Lee JE Yong SW Moon SY Lee PH The mild cognitive impairment stageof dementia with Lewy bodies and Parkinson disease A comparison of cognitiveprofiles Alzheimer Dis Assoc Disord 201428151ndash155
28 Fengler S Liepelt-Scarfone I Brockmann K Schaffer E Berg D Kalbe E Cognitivechanges in prodromal Parkinsonrsquos disease a review Mov Disord 2017321655ndash1666
29 Kalbe E Rehberg SP Heber I et al Subtypes of mild cognitive impairment in patientswith Parkinsonrsquos disease evidence from the LANDSCAPE study J Neurol NeurosurgPsychiatry 2016871099ndash1105
30 Thomas AJ Donaghy P Roberts G et al Diagnostic accuracy of dopaminergic im-aging in prodromal dementia with Lewy bodies Psychol Med 20181ndash7
31 Ferman TJ Boeve BF Smith GE et al Inclusion of RBD improves the diagnosticclassification of dementia with Lewy bodies Neurology 201177875ndash882
32 Fujishiro H Okuda M Iwamoto K et al Early diagnosis of Lewy body disease inpatients with late-onset psychiatric disorders using clinical history of rapid eyemovement sleep behavior disorder and I-123 -metaiodobenzylguanidine cardiacscintigraphy Psychiatry Clin Neurosci 201872423ndash434
33 Bonanni L Perfetti B Bifolchetti S et al Quantitative electroencephalogram utility inpredicting conversion of mild cognitive impairment to dementia with Lewy bodiesNeurobiol Aging 201536434ndash445
34 Murray ME Ferman TJ Boeve BF et al MRI and pathology of REM sleep behaviordisorder in dementia with Lewy bodies Neurology 2013811681ndash1689
35 Murray ME Graff-Radford NR Ross OA Petersen RC Duara R Dickson DWNeuropathologically defined subtypes of Alzheimerrsquos disease with distinct clinicalcharacteristics a retrospective study Lancet Neurol 201110785ndash796
36 Blanc F Colloby SJ Cretin B et al Grey matter atrophy in prodromal stage ofdementia with Lewy bodies and Alzheimerrsquos disease Alzheimers Res Ther 2016831
37 Blanc F Colloby SJ Philippi N et al Cortical thickness in dementia with Lewy bodiesand Alzheimerrsquos disease a comparison of prodromal and dementia stages Plos One201510e0127396
38 Surendranathan A OrsquoBrien JT Clinical imaging in dementia with Lewy bodies EvidBased Ment Health 20182161ndash65
39 Outeiro TF Koss DJ Erskine D et al Dementia with Lewy bodies an update andoutlook Mol Neurodegener 2019145
40 Donadio V Incensi A Rizzo G et al A new potential biomarker for dementiawith Lewy bodies Skin nerve alpha-synuclein deposits Neurology 201789318ndash326
41 Flanigan PM Khosravi MA Leverenz JB Tousi B Color vision impairment differ-entiates Alzheimer dementia from dementia with Lewy bodies J Geriatr PsychiatryNeurol 20183197ndash102
42 Fereshtehnejad SM Yao C Pelletier A Montplaisir JY Gagnon JF Postuma RBEvolution of prodromal Parkinsonrsquos disease and dementia with Lewy bodies a pro-spective study Brain 20191422051ndash2067
43 Bousiges O Bombois S Schraen S et al Cerebrospinal fluid Alzheimer biomarkerscan be useful for discriminating dementia with Lewy bodies from Alzheimerrsquos diseaseat the prodromal stage J Neurol Neurosurg Psychiatry 201889467ndash475
44 Kantarci K Lowe VJ Boeve BF et al Multimodality imaging characteristics of de-mentia with Lewy bodies Neurobiol Aging 2012332091ndash2105
45 Kantarci K Lowe VJ Boeve BF et al AV-1451 tau and beta-amyloid positronemission tomography imaging in dementia with Lewy bodies Ann Neurol 20178158ndash67
46 Gore RL Vardy E OrsquoBrien JT Delirium and dementia with Lewy bodies distinctdiagnoses or part of the same spectrum J Neurol Neurosurg Psychiatry 20158650ndash59
47 Aarsland DS Auning E The pre-dementia stage of dementia with Lewy bodies Eur JNeurol 20111869
48 Sunwoo MK Hong JY Choi J Park HJ Kim SH Lee PH alpha-Synuclein pathologyis related to postoperative delirium in patients undergoing gastrectomy Neurology201380810ndash813
49 Akintade O Pierres F Acute presentation of dementia with Lewy bodies Clin Med201919327ndash330
50 Kosaka K Diffuse Lewy body disease in Japan J Neurol 1990237197ndash20451 Birkett DP Desouky A Han L Kaufman M Lewy bodies in psychiatric patients Int J
Geriatr Psychiatry 19927235ndash240
Appendix (continued)
Name Location Contribution
John PaulTaylor MBBS PhD
Newcastle University Revising the manuscript forintellectual content
Debby WTsuang MD
VA Puget Sound ampUniversity ofWashington
Revising the manuscript forintellectual content
ZuzanaWalker MD
University CollegeLondon
Revising the manuscript forintellectual content
PietroTiraboschiMD
Istituto NeurologicoldquoCarlo Bestardquo Milan
Design and conceptualizationof the study acquisition ofdata analysis andinterpretation of the data anddrafting and revising themanuscript for intellectualcontent
754 Neurology | Volume 94 Number 17 | April 28 2020 NeurologyorgN
52 Kobayashi K Nakano H Akiyama N Maeda T Yamamori S Pure psychiatric pre-sentation of the Lewy body disease is depressionmdashan analysis of 60 cases verified withmyocardial meta-iodobenzylguanidine study Int J Geriatr Psychiatry 201530663ndash668
53 Takahashi S Mizukami K Arai T et al Ventilatory response to hypercapnia predictsdementia with Lewy bodies in late-onset major depressive disorder J Alzheimers Dis201650751ndash758
54 Van Assche L Van Aubel E Van de Ven L Bouckaert F Luyten P Vandenbulcke MThe neuropsychological profile and phenomenology of late onset psychosis a cross-sectional study on the differential diagnosis of very-late-onset Schizophrenia-likepsychosis dementia with Lewy bodies and Alzheimerrsquos type dementia with psychosisArch Clin Neuropsychol 201934183ndash199
55 Thaipisuttikul P Lobach I Zweig Y Gurnani A Galvin JE Capgras syndrome indementia with Lewy bodies Int Psychogeriatr 201325843ndash849
56 Fujishiro H Iseki E Nakamura S et al Dementia with Lewy bodies early diagnosticchallenges Psychogeriatrics 201313128ndash138
57 Chiba Y Fujishiro H Iseki E et al Retrospective survey of prodromal symptoms indementia with Lewy bodies comparison with Alzheimerrsquos disease Dement GeriatrCogn Disord 201233273ndash281
58 Kaufmann H Norcliffe-Kaufmann L Palma JA et al Natural history of pure auto-nomic failure a United States prospective cohort Ann Neurol 201781287ndash297
59 Heinzel S Berg D Gasser T et al Update of the MDS research criteria for prodromalParkinsonrsquos disease Mov Disord 2019341464ndash1470
60 Palma JA Norcliffe-Kaufmann L Kaufmann H Diagnosis of multiple system atrophyAuton Neurosci 201821115ndash25Data available fromDryad (Additional References References e1ndashe44) doi105061dryad1c59zw3rv
Subspecialty Alerts by E-mail
Customize your online journal experience by signing up for e-mail alerts related to your subspecialty or area of interest Accessthis free service by clicking on the ldquoMy Alertsrdquo link on the home page An extensive list of subspecialties methods and studydesign choices will be available for you to choose frommdashallowing you priority alerts to cutting-edge research in your field
COVID-19 and Neurologic Disease Call for Papers
The editors of Neurology are interested in papers that address the neurological aspects of COVID-19infection and challenges to the management of patients with chronic neurological conditions whohave or are at risk for the infection Relevant papers that pass initial internal review will undergoexpedited peer review and online publication We will consider papers posted in preprint servers
Submit observational studies and clinical trials as Articles and case series and case reports underthe ClinicalScientific Notes category to httpssubmitneurologyorg today
Visit the Neurologyreg Website at NeurologyorgN More article-based content on home pages Streamlined menus and navigation Enhanced blog sections for specialty areas Same experience on desktop tablet and mobile devices Improved article reading experience links more evident (pdf analytics social media) Neurologyreg Clinical Practice initiative ldquoPractice Currentrdquo global surveys will be accessible across sites
Find Neurologyreg on Facebook httptinyurlcomneurologyfan
Follow Neurologyreg on Twitter httpstwittercomGreenJournal
NeurologyorgN Neurology | Volume 94 Number 17 | April 28 2020 755
DOI 101212WNL0000000000009323202094743-755 Published Online before print April 2 2020Neurology
Ian G McKeith Tanis J Ferman Alan J Thomas et al Research criteria for the diagnosis of prodromal dementia with Lewy bodies
This information is current as of April 2 2020
ServicesUpdated Information amp
httpnneurologyorgcontent9417743fullincluding high resolution figures can be found at
References httpnneurologyorgcontent9417743fullref-list-1
This article cites 59 articles 12 of which you can access for free at
Subspecialty Collections
httpnneurologyorgcgicollectionpsychosisPsychosis a
httpnneurologyorgcgicollectionparkinsons_disease_with_dementiParkinsons disease with dementia
httpnneurologyorgcgicollectionmci_mild_cognitive_impairmentMCI (mild cognitive impairment)
httpnneurologyorgcgicollectiondementia_with_lewy_bodiesDementia with Lewy bodies
httpnneurologyorgcgicollectiondeliriumDeliriumfollowing collection(s) This article along with others on similar topics appears in the
Permissions amp Licensing
httpwwwneurologyorgaboutabout_the_journalpermissionsits entirety can be found online atInformation about reproducing this article in parts (figurestables) or in
Reprints
httpnneurologyorgsubscribersadvertiseInformation about ordering reprints can be found online
ISSN 0028-3878 Online ISSN 1526-632XWolters Kluwer Health Inc on behalf of the American Academy of Neurology All rights reserved Print1951 it is now a weekly with 48 issues per year Copyright Copyright copy 2020 The Author(s) Published by
reg is the official journal of the American Academy of Neurology Published continuously sinceNeurology

to underlying LB pathology particularly the presence of re-current VH12 when these occur before cognitive impairmentbecomes evident As with all α-synucleinopathies RBD maybe a useful indicator although a relationship between anti-depressant usage and subsequent RBD onset is a potentialconfoundere41 Although the primary psychiatric manifes-tations are often accompanied by mild cognitive deficits54
cognitive evaluation and interpretation of performance can bedifficult when psychiatric symptoms are prominent The fre-quency of cognitive fluctuations in psychiatric-onset LB caseshas not been determined
Initial reports suggest that 123I-MIBG scintigraphy may behelpful in psychiatric-onset DLB525356 Eighteen of 35patients with a first onset of major depressive disorder gt50years and with bradykinesia developed a clinical diagnosis ofDLB after 6 years of follow-up All 18 had an abnormal ven-tilatory response to hypercapnia (VRH) indicative of severeautonomic dysfunction whereas none of the 17 patients witha normal VRH converted to DLB within the study period Forthe converters the most common presentation was withpsychotic and melancholic features simultaneously The fre-quency of hypersensitivity to antipsychotics antidepressantsand antianxiety drugs was higher in converters than in non-converters53 Further studies need to confirm these findingsand to determine the value of other DLB biomarkers inpsychiatric-onset cases325256
In summary it is not yet clear how to identify patients withprominent late-onset psychiatric symptoms who may haveunderlying LB disease and subsequently progress to DLB It is
premature to try to construct formal criteria for psychiatric-onset DLB but clinicians in mental health and other settingsneed to be aware that this possibility exists not least becauseof the risk of severe antipsychotic sensitivity reactions withincreased morbidity and mortality The small available liter-ature including reports such as those cited above does providesome useful guidance summarized in table 3 but requiresreplication and further investigation
Idiopathic REM sleep behavior disorderRBD is characterized by abnormal dream enactment behaviorduring REM sleep accompanied by loss of muscle atonia duringREM sleep (REM sleep without atonia or RSWA) on PSG Forthe purpose of a prodromal DLB diagnosis a clinical history ofRBD is obtained in the same way as for DLB2 that is a clearcomplaint of dream enactment by a bedpartner or other witnesswith no evidence of sleep disorders that may mimic RBD onclinical interview Conditions known to mimic or masquerade asRBD include non-REM parasomnias (sleep walking sleep talk-ing or other behaviors that emerge fromnon-REM sleep stages)obstructive sleep apnea confusional arousals or nocturnal seiz-ures In the absence of PSG the risk of a false-positive clinicaldiagnosis of RBD is reduced by using optimized sleep ques-tionnaires which can have sensitivity and specificity over 90e42
RBDmay be considered as idiopathic until it is associated withanother ongoing neurologic condition the most frequentbeing an α-synucleinopathy (PD DLB or MSA) In a recentlarge study 735 of patients with RBD converted to an overtneurodegenerative syndrome after 12-year follow-up 565developing parkinsonism and 435 dementia as their first
Table 3 Summary of key features of psychiatric-onset DLB
Is characterized by predominant psychiatric symptoms that typically correspond to late-onset major depressive disorder or late-onset psychosis which mayfeature hallucinations in visual and in other modalities and systematized delusions including Capgras syndrome
bull may also present with apathy anxiety and depression
bull may be sufficiently severe to require hospitalization
bull the frequency of LB disease as a cause of late-onset psychiatric disorder is not known
When assessing for core clinical features of DLB in a patient with a primary psychiatric presentation
bull bradykinesia may be mimicked by psychomotor retardation which is commonly seen in depressive disorders
bull parkinsonism may be induced by antipsychotic medications used to treat psychiatric disorder
bull RBD (and REM sleep without atonia) may be induced by antidepressant medications
bull mild cognitive disturbance may be present but is not predominant and may fluctuate
bull formal neuropsychological testing may be confounded by the psychiatric mental state
bull the frequency and character of cognitive fluctuations is unknown
Identification of psychiatric-onset DLB
bull may be assisted by use of MCI-LB biomarkers but further research evidence of this is required
bull is important to inform the management plan including the avoidance or minimization of antipsychotic and anticholinergic agents
Abbreviations DLB = dementia with Lewy bodies MCI = mild cognitive impairment
750 Neurology | Volume 94 Number 17 | April 28 2020 NeurologyorgN
disease manifestation Among many predictive markerstested only the cognitive variables differed at baseline be-tween those converting to primary dementia vs parkinson-ism7 Other multicenter studies confirm that the only clinicalfeature that predicts dementia vs parkinsonism first is neu-ropsychological performance those with RBD who exhibitcognitive changes are more likely to evolve first into MCI orDLB22e4 Thus although RBD may be regarded an earlymanifestation of α-synucleinopathy it is not possible to clearlydistinguish whether an individual presenting with RBD willdevelop dementia first that is evolve into a primary DLBdiagnosis or parkinsonism first that is a primary PDMSAdiagnosis Any MCI subtype associated with PSG-confirmedRBD is highly likely to represent underlying LB disease Al-though idiopathic RBD is a useful model to study the earlystages of LB disease progression it is not necessarily repre-sentative of the whole spectrum of patients with PD and DLBa significant minority of whom do not have RBD42
Autonomic dysfunctionanosmia and othernonspecific prodromal LB disease symptomsPatients with DLB frequently report a history of autonomicdysfunction at first clinic attendance with 25ndash50 com-plaining of one of more among constipation orthostatic diz-ziness urinary incontinence erectile dysfunction increasedsweating or increased saliva5657 In a cohort of patients withpure autonomic failure 34 converted to an overt α-synu-cleinopathy over 6 years of follow-up this was to DLB (52)PD (24) orMSA (24)58 However because there are manyother causes for autonomic dysfunction in older people thesesymptoms either alone or in combination have low positivepredictive value59 The situation is similar for hyposmia whichalso frequently occurs early in prodromal DLB and PD42 butwhich can have many other causes in this age group
Conclusions and future directionDiagnosis of DLB at the dementia stage depends on identifyingfully expressed core clinical features which may be mild orabsent at the prodromal stage when biomarker evidence mayalso be weaker and may even differ from that found at thedementia stage Several new biomarker candidates direct andindirect are in development and we will continue to reviewthese to update our recommendations as soon as sufficientevidence accumulates We recognize that the clinical pheno-type of neurodegenerative disorders reflects interaction be-tween several rather than a single brain pathology and it istherefore likely that multiple biomarkers of individual pathol-ogies (eg α-synuclein β-amyloid and tau) or of disease sur-rogates (eg metabolic imagingEEG) will be required
Although we have described the 3 prodromal DLB syndromesseparately they are unlikely to be mutually exclusive andthere may be substantial overlap We propose operationalizedcriteria only for MCI-LB because the evidence base from oursystematic review albeit relatively limited is sufficient to
support recommendations that are immediately applicableand testable Our recommendations should be used alongsideguidance about the prodromal manifestations of PD1559
MSA60 and AD14 with which there is overlap Notwith-standing the potential benefits of early diagnosis we are alsomindful of the importance of avoiding incorrect (false-positive) diagnosis of prodromal DLB and the potentialnegative consequences this could have for an individual Wesuggest that the predictive validity of different categories andcombinations of our proposed criteria should be clarified byprospective studies before they are adopted for widespreadclinical use and that they will enable standardization for in-clusion in research studies and clinical trials
Some published guidance about the early clinical diagnosis ofDLB does already exist DSM5 recommends a diagnosis ofmild neurocognitive disorder (NCD) with LB ldquofor individualswho present with the core or suggestive features at a stagewhen cognitive or functional impairments are not of sufficientseverity to fulfill criteria for major NCDrdquoe43 This is basedhowever on the 2005 version of DLB guidelines and requiresupdating ICD-11 takes a similar approach toward diagnosingmild NCD at a syndromic level and lists both Lewy bodydisease and PD as possible causese44
The diagnostic position for other prodromal manifestations ofDLB that is delirium-onset and psychiatric-onset is less clearthan for MCI Operationalization of specific criteria for thesesyndromes is not yet justified and the reliable differentiationof the minority of delirious and psychiatrically ill patients whohave underlying LB pathology from the majority who do notwill probably only be achieved when routinely applicablebiomarkers are developed LB disease is seldom if ever cur-rently considered as part of the differential diagnosis of de-lirium or late-onset psychiatric disorder and we hope that theinformation we provide in the text and accompanying boxeswill raise cliniciansrsquo awareness of that possibility
Study fundingNo targeted funding reported
DisclosureI McKeith receives support from the NIHR Biomedical Re-search Centre awarded to the Newcastle upon Tyne HospitalsNHS Foundation Trust and Newcastle University and hasconsulted for GE Healthcare Sanofi Eisai Sumitomo Dai-nippon Pharma and Axovant T Ferman receives support fromNIH P50-AG16574 P30-AG062677 U01-NS100620 and theMangurian Foundation for Lewy body disease research AThomas receives support from the NIHR Biomedical ResearchCentre awarded to the Newcastle upon Tyne Hospitals NHSFoundation Trust and Newcastle University and has receivedgrants from GE Healthcare F Blanc has served as nationalclinical trial coordinator for Eisai and Axovant B Boevereceives support from NIH P50-AG16574 P30-AG062677U01-NS100620 and the Mangurian Foundation for Lewybody disease research has consulted for the Scientific Advisory
NeurologyorgN Neurology | Volume 94 Number 17 | April 28 2020 751
BoardmdashTau Consortium and received grants from Biogenthe NIH theMangurian Foundation Alector the Little FamilyFoundation and the Turner Family H Fujishiro has receivedsupport from Fujifilm RI Pharma Co Ltd K Kantarci receivessupport from NIH P50-AG16574 P30-AG062677 U01-NS100620 and the Mangurian Foundation for Lewy bodydisease research and has received grants from Avid Radio-pharmaceuticals and acted on a Data Safety Monitoring Boardfor Takeda Global Research C Muscio acknowledges thesupport of the Italian Ministry of Health GRANT NET-2011-02346784 J OrsquoBrien is supported by the NIHR CambridgeBiomedical Research Centre Dementia and Neuro-degeneration and Mental Health Themes and the CambridgeCentre for Parkinsonrsquos Plus Disorders has consulted forTauRx Axon GE Healthcare Eisai and AvidLilly and re-ceived grants fromAvidLilly andAllianceMedical R Postumahas received grants from and consulted for Fonds de laRecherche en Sante received grants from the Canadian Insti-tutes of Health Research the Parkinson Society of Canada theWeston-Garfield Foundation The Michael J Fox Foundationand the Webster Foundation and consulted for TakedaRocheProthena Teva Neurosciences Novartis Canada Bio-gen Boehringer Ingelheim Theranexus GE Healthcare JazzPharmaceuticals AbbVie Jannsen Otsuko PhytopharmicsInception Sciences and Parkinson Canada D Aarsland isa Royal Society Wolfson Research Merit Award Holder andwould like to thank the Wolfson Foundation and the RoyalSociety for their support He has received research supportandor honoraria from AstraZeneca H Lundbeck NovartisPharmaceuticals and GE Health and served as paid consultantfor H Lundbeck Eisai Heptares Sanofi and Mentis Cura CBallard reports unrelated current grant funding from MRCWellcome Trust European Union Gillings FoundationNIHR Alzheimerrsquos Society Alzheimerrsquos Research UK Par-kinsonrsquos Society and Lewy Body Society during the conduct ofthe study and personal fees from Acadia pharmaceutical com-pany Lundbeck Roche Otsuka Eli Lilly and AARP outsidethe submitted work L Bonanni is a member of the steeringcommittee of the E-DLB consortium and program chair of theLBD-PIA (ISTAART) and is funded for research on DLB bythe Italian Ministry of Health P Donaghy receives supportfrom the NIHR Biomedical Research Centre awarded to theNewcastle upon Tyne Hospitals NHS Foundation Trust andNewcastle UniversityM Emre served on the scientific advisoryboard for AC Immune J Galvin receives support from NIHgrants (R01 AG040211 R01 NS101482 R01 AG057681 andU01 NS100610) and the Lewy Body Dementia AssociationResearch Center of Excellence reports research support fromthe NIH the Lewy Body Dementia Association The Harry TMangurian Foundation and Albert Charitable Trust directsclinical trials for Biogen and Novartis receives licensing feesfrom Biogen Roche Eli Lilly Quintiles Roobrik ContinuumClinical and Langland and receives consulting fees fromBiogen Eisai Bracket and Medavante D Galasko receivessupport from NIA grant AGO5131 and the Michael J FoxFoundation and has acted as consultant for vTv Pharmaceut-icals Inc Esai Inc and for Fujirebio Inc been a member of
a DSMB for Probiodrug and paid editor for Alzheimerrsquos Re-search amp Therapy J Goldman receives grantsupport fromTheMichael J Fox Foundation and Parkinsonrsquos Foundation andhas received consulting feeshonoraria from Acadia AptinyxSunovion and Worldwide Med S Gomperts receives supportfrom NIH grants R01 AG054551 P30AG062421 R01AG062208 P50 AG005134 R21 NS109833 DODCDMRPW81XW1810516 the Farmer Family ParkinsonrsquosInitiative and the Lewy Body Dementia Association and hasserved on advisory boards for Acadia Pharmaceuticals andSanofi L Honig acknowledges research grant support fromNYS CEAD grant C031425 LBDA RCOE and NIHgrants U01NS100600 P50AG008702 R21AG058020R21MH111596 U01AG051412 U01AG045390U01AG016976 U01AG023749 U19063893 andU19AG024904 He receives research funding support fromAbbVie Alector Biogen Eisai Genentech Roche and Wash-ington University and has received income for consulting forCortexyme and Eisai M Ikeda reports departmental grants andhonoraria fees from Sumitomo Dainippon Pharma Eisai andNiho Medicine-Physics J Leverenz acknowledges supportfrom the National Institutes of Health P30 AG053762 UO1NS100610 and R13NS111954 and Jane and Lee Seidman andDouglas Herthel DVMMemorial Funds and reports consultingfees from Aptinyx Acadia Biogen Eisai GE HealthcareGenzymeSanofi and Takeda Pharmaceuticals and grant sup-port from Alzheimerrsquos Drug Discovery Foundation De-partment of Defense GE Healthcare GenzymeSanofi TheMichael J Fox Foundation and the NIH (NIA andNINDS) SLewis is supported by NHMRC-ARC Dementia Fellows KMarder is funded by the NIH R01NS100600 NS107168UL1TR001873 andNS073671 with research support from theLBDA Parkinson Foundation Michael J Fox HDSA andCHDI and has acted as site investigator for Vaccinex andGenentech member of Springer editorial board and scientificadvisory board Voyager Therapeutics M Masellis was sup-ported by a Canadian Institutes of Health Research grant(MOP13129) and an Early Researcher Award from the Min-istry of Research Innovation and Science (MRIS ON) andreports personal fees for ad hoc consultancy from ArkudaTherapeutics Ionis Pharmaceuticals and Alector Pharmaceut-icals royalties fromHenry Stewart Talks Ltd and grants to theinstitution from Roche Novartis Washington University andAxovant Sciences D Salmon acknowledges support from NIHP30AG062429 and is a paid consultant for Takeda Inc Apti-nyx Inc and Biogen Inc J-P Taylor receives support from theNIHR Biomedical Research Centre awarded to the Newcastleupon Tyne Hospitals NHS Foundation Trust and NewcastleUniversity and reports grants from the UKNational Institute ofHealth Research (NIHR) travel award from Axovant researchsupport costs from Sonsei-Heptares and personal fees fromGEHealthcare D Tsuang acknowledges support from NIHR21AG064271 R03 NS103950 and U01 NS100610 ZWalker has been supported by ESRC NIHR (co-app) ARUK(co-app) EU IMI 2 (co-app) and Dunhill Medical Trust Shehas received consultancy fees travel expenses and researchsupport from GE Healthcare and research support from Life
752 Neurology | Volume 94 Number 17 | April 28 2020 NeurologyorgN
Molecular Imaging P Tiraboschi acknowledges the support ofthe Italian Ministry of Health GRANT NET-2011-02346784Go to NeurologyorgN for full disclosures
Publication historyReceived by Neurology October 30 2019 Accepted in final formFebruary 25 2020
Appendix Authors
Name Location Contribution
Ian GMcKeith FMed Sci MD
Newcastle University Design and conceptualizationof the study acquisition ofdata analysis andinterpretation of the data anddrafting and revising themanuscript for intellectualcontent
Tanis JFermanPhD
Mayo ClinicJacksonville
Design and conceptualizationof the study acquisition ofdata analysis andinterpretation of the data anddrafting and revising themanuscript for intellectualcontent
Alan JThomasPhD
Newcastle University Design and conceptualizationof the study acquisition ofdata analysis andinterpretation of the data anddrafting and revising themanuscript for intellectualcontent
FredericBlanc MD
University ofStrasbourg
Design and conceptualizationof the study acquisition ofdata analysis andinterpretation of the data anddrafting and revising themanuscript for intellectualcontent
Bradley FBoeve MD
Mayo Clinic Rochester Design and conceptualizationof the study acquisition ofdata analysis andinterpretation of the data anddrafting and revising themanuscript for intellectualcontent
HiroshigeFujishiroMD
Nagoya UniversityKawasaki MemorialHospital
Design and conceptualizationof the study acquisition ofdata analysis andinterpretation of the data anddrafting and revising themanuscript for intellectualcontent
KejalKantarciMD MS
Mayo Clinic Rochester Design and conceptualizationof the study acquisition ofdata analysis andinterpretation of the data anddrafting and revising themanuscript for intellectualcontent
CristinaMuscio PhD
Istituto NeurologicoldquoCarlo Bestardquo Milan
Design and conceptualizationof the study acquisition ofdata analysis andinterpretation of the data anddrafting and revising themanuscript for intellectualcontent
Appendix (continued)
Name Location Contribution
John TOrsquoBrien FMed Sci DM
Cambridge University Design and conceptualizationof the study acquisition ofdata analysis andinterpretation of the data anddrafting and revising themanuscript for intellectualcontent
Ronald BPostumaMD MSc
McGill University Design and conceptualizationof the study acquisition ofdata analysis andinterpretation of the data anddrafting and revising themanuscript for intellectualcontent
DagAarslandPhD
Kingrsquos College Londonand StavangerUniversityHospital
Revising the manuscript forintellectual content
CliveBallard MD
University of Exeter Revising the manuscript forintellectual content
LauraBonanniMD PhD
University of Chieti-Pescara
Revising the manuscript forintellectual content
PaulDonaghyPhD
Newcastle University Revising the manuscript forintellectual content
Murat EmreMD
Istanbul Faculty ofMedicine
Revising the manuscript forintellectual content
James EGalvin MDMPH
University of MiamiMiller School ofMedicine
Revising the manuscript forintellectual content
DouglasGalasko MD
University of CaliforniaSan Diego
Revising the manuscript forintellectual content
Jennifer GGoldmanMD MS
Feinberg School ofMedicine
Revising the manuscript forintellectual content
Stephen NGompertsMD PhD
Massachusetts GeneralHospital
Revising the manuscript forintellectual content
Lawrence SHonig MDPhD
Columbia UniversityIrving Medical Center
Revising the manuscript forintellectual content
ManabuIkeda MDPhD
Osaka University Revising the manuscript forintellectual content
James BLeverenzMD
Lou Ruvo Center ofBrain Health ClevelandClinic
Revising the manuscript forintellectual content
Simon JGLewis MD
University of Sydney Revising the manuscript forintellectual content
Karen SMarder MDMPH
Columbia UniversityIrving Medical Center
Revising the manuscript forintellectual content
MarioMasellisMD PhD
Sunnybrook HealthSciences CentreUniversity of Toronto
Revising the manuscript forintellectual content
David PSalmon PhD
University of CaliforniaSan Diego
Revising the manuscript forintellectual content
Continued
NeurologyorgN Neurology | Volume 94 Number 17 | April 28 2020 753
References1 Walker Z Possin KL Boeve BF Aarsland D Lewy body dementias Lancet 2015386
1683ndash16972 McKeith IG Boeve BF Dickson DW et al Diagnosis and management of dementia
with Lewy bodies fourth consensus report of the DLB consortium Neurology 20178988ndash100
3 Ferman TJ Smith GE Kantarci K et al Nonamnestic mild cognitive impairmentprogresses to dementia with Lewy bodies Neurology 2013812032ndash2038
4 Savica R Bradley BF Mielke MM When do alpha-synucleinopathies start An epi-demiological timeline A review JAMA Neurol 201875503ndash509
5 Donaghy PC Taylor JP OrsquoBrien JT et al Neuropsychiatric symptoms and cognitiveprofile in mild cognitive impairment with Lewy bodies Psychol Med 2018482384ndash2390
6 Cagnin A Bussse C Gardini S et al Clinical and cognitive phenotype of mildcognitive impairment evolving to dementia with Lewy bodies Dement Geriatr CognDis Extra 20155442ndash449
7 Postuma RB Iranzo A HuM et al Risk and predictors of dementia and parkinsonismin idiopathic REM sleep behaviour disorder a multicentre study Brain 2019142744ndash759
8 Sadiq D Whitfield T Lee L Stevens T Costafreda S Walker Z Prodromal dementiawith Lewy bodies and prodromal Alzheimerrsquos disease a comparison of the cognitiveand clinical profiles J Alzheimers Dis 201758463ndash470
9 FitzGerald JM Perera G Chang-Tave A et al The incidence of recorded de-lirium episodes before and after dementia diagnosis differences between de-mentia with Lewy bodies and Alzheimerrsquos disease J Am Med Dir Assoc 201920604ndash609
10 Jicha GA Schmitt FA Abner E et al Prodromal clinical manifestations of neu-ropathologically confirmed Lewy body disease Neurobiol Aging 2010311805ndash1813
11 Vardy E Holt R Gerhard A Richardson A Snowden J Neary D History of a sus-pected delirium is more common in dementia with Lewy bodies than Alzheimerrsquosdisease a retrospective study Int J Geriatr Psychiatry 201429178ndash181
12 Fujishiro H Nakamura S Sato K Iseki E Prodromal dementia with Lewy bodiesGeriatr Gerontol Int 201515817ndash826
13 McKeith I Taylor JP Thomas A Donaghy P Kane J Revisiting DLB diagnosisa consideration of prodromal DLB and of the diagnostic overlap with Alzheimerdisease J Geriatr Psychiatry Neurol 201629249ndash253
14 Albert MS DeKosky ST Dickson D et al The diagnosis of mild cognitive impairmentdue to Alzheimerrsquos disease recommendations from the National Institute on Aging-Alzheimerrsquos Association workgroups on diagnostic guidelines for Alzheimerrsquos diseaseAlzheimers Dement 20117270ndash279
15 Litvan I Goldman JG Troster AI et al Diagnostic criteria for mild cognitive im-pairment in Parkinsonrsquos disease Movement Disorder Society Task Force guidelinesMov Disord 201227349ndash356
16 Ferman TJ Smith GE Boeve BF et al Neuropsychological differentiation of de-mentia with Lewy bodies from normal aging and Alzheimerrsquos disease Clin Neuro-psychol 200620623ndash636
17 Cagnin A Busse C Jelcic N Gnoato F Mitolo M Caffarra P High specificity ofMMSE pentagon scoring for diagnosis of prodromal dementia with Lewy bodiesParkinsonism Relat Disord 201521303ndash305
18 Yoon JH Kim M Moon SY Yong SW Hong JM Olfactory function and neuro-psychological profile to differentiate dementia with Lewy bodies from Alzheimerrsquosdisease in patients with mild cognitive impairment a 5-year follow-up study J NeurolSci 2015355174ndash179
19 Kemp J Philippi N Phillipps C et al Cognitive profile in prodromal dementia withLewy bodies Alzheimers Res Ther 2017919
20 Auning E Rongve A Fladby T et al Early and presenting symptoms of dementia withLewy bodies Dement Geriatr Cogn Disord 201132202ndash208
21 Kondo D Ota K Kasanuki K et al Characteristics of mild cognitive impairmenttending to convert into Alzheimerrsquos disease or dementia with Lewy bodies a follow-upstudy in a memory clinic J Neurol Sci 2016369102ndash108
22 Marchand DG Postuma RB Escudier F et al How does dementia with Lewy bodiesstart prodromal cognitive changes in REM sleep behavior disorder Ann Neurol2018831016ndash1026
23 Kantarci K Lesnick T Ferman TJ et al Hippocampal volumes predict risk of de-mentia with Lewy bodies in mild cognitive impairment Neurology 2016872317ndash2323
24 Thomas AJ Taylor JP McKeith I et al Revision of assessment toolkits for improvingthe diagnosis of Lewy body dementia the DIAMOND Lewy study Int J GeriatrPsychiatry 2018331293ndash1304
25 Galvin JE Improving the clinical detection of Lewy body dementia with the Lewybody composite risk score Alzheimerrsquos Demen (Amsterdam Netherlands) 20151316ndash324
26 Belden CM Kahlon V Malek-Ahmadi M Tsai A Sabbagh MN Clinical character-ization of mild cognitive impairment as a prodrome to dementia with Lewy bodiesAm J Alzheimers Dis Other Demen 201530173ndash177
27 Yoon JH Lee JE Yong SW Moon SY Lee PH The mild cognitive impairment stageof dementia with Lewy bodies and Parkinson disease A comparison of cognitiveprofiles Alzheimer Dis Assoc Disord 201428151ndash155
28 Fengler S Liepelt-Scarfone I Brockmann K Schaffer E Berg D Kalbe E Cognitivechanges in prodromal Parkinsonrsquos disease a review Mov Disord 2017321655ndash1666
29 Kalbe E Rehberg SP Heber I et al Subtypes of mild cognitive impairment in patientswith Parkinsonrsquos disease evidence from the LANDSCAPE study J Neurol NeurosurgPsychiatry 2016871099ndash1105
30 Thomas AJ Donaghy P Roberts G et al Diagnostic accuracy of dopaminergic im-aging in prodromal dementia with Lewy bodies Psychol Med 20181ndash7
31 Ferman TJ Boeve BF Smith GE et al Inclusion of RBD improves the diagnosticclassification of dementia with Lewy bodies Neurology 201177875ndash882
32 Fujishiro H Okuda M Iwamoto K et al Early diagnosis of Lewy body disease inpatients with late-onset psychiatric disorders using clinical history of rapid eyemovement sleep behavior disorder and I-123 -metaiodobenzylguanidine cardiacscintigraphy Psychiatry Clin Neurosci 201872423ndash434
33 Bonanni L Perfetti B Bifolchetti S et al Quantitative electroencephalogram utility inpredicting conversion of mild cognitive impairment to dementia with Lewy bodiesNeurobiol Aging 201536434ndash445
34 Murray ME Ferman TJ Boeve BF et al MRI and pathology of REM sleep behaviordisorder in dementia with Lewy bodies Neurology 2013811681ndash1689
35 Murray ME Graff-Radford NR Ross OA Petersen RC Duara R Dickson DWNeuropathologically defined subtypes of Alzheimerrsquos disease with distinct clinicalcharacteristics a retrospective study Lancet Neurol 201110785ndash796
36 Blanc F Colloby SJ Cretin B et al Grey matter atrophy in prodromal stage ofdementia with Lewy bodies and Alzheimerrsquos disease Alzheimers Res Ther 2016831
37 Blanc F Colloby SJ Philippi N et al Cortical thickness in dementia with Lewy bodiesand Alzheimerrsquos disease a comparison of prodromal and dementia stages Plos One201510e0127396
38 Surendranathan A OrsquoBrien JT Clinical imaging in dementia with Lewy bodies EvidBased Ment Health 20182161ndash65
39 Outeiro TF Koss DJ Erskine D et al Dementia with Lewy bodies an update andoutlook Mol Neurodegener 2019145
40 Donadio V Incensi A Rizzo G et al A new potential biomarker for dementiawith Lewy bodies Skin nerve alpha-synuclein deposits Neurology 201789318ndash326
41 Flanigan PM Khosravi MA Leverenz JB Tousi B Color vision impairment differ-entiates Alzheimer dementia from dementia with Lewy bodies J Geriatr PsychiatryNeurol 20183197ndash102
42 Fereshtehnejad SM Yao C Pelletier A Montplaisir JY Gagnon JF Postuma RBEvolution of prodromal Parkinsonrsquos disease and dementia with Lewy bodies a pro-spective study Brain 20191422051ndash2067
43 Bousiges O Bombois S Schraen S et al Cerebrospinal fluid Alzheimer biomarkerscan be useful for discriminating dementia with Lewy bodies from Alzheimerrsquos diseaseat the prodromal stage J Neurol Neurosurg Psychiatry 201889467ndash475
44 Kantarci K Lowe VJ Boeve BF et al Multimodality imaging characteristics of de-mentia with Lewy bodies Neurobiol Aging 2012332091ndash2105
45 Kantarci K Lowe VJ Boeve BF et al AV-1451 tau and beta-amyloid positronemission tomography imaging in dementia with Lewy bodies Ann Neurol 20178158ndash67
46 Gore RL Vardy E OrsquoBrien JT Delirium and dementia with Lewy bodies distinctdiagnoses or part of the same spectrum J Neurol Neurosurg Psychiatry 20158650ndash59
47 Aarsland DS Auning E The pre-dementia stage of dementia with Lewy bodies Eur JNeurol 20111869
48 Sunwoo MK Hong JY Choi J Park HJ Kim SH Lee PH alpha-Synuclein pathologyis related to postoperative delirium in patients undergoing gastrectomy Neurology201380810ndash813
49 Akintade O Pierres F Acute presentation of dementia with Lewy bodies Clin Med201919327ndash330
50 Kosaka K Diffuse Lewy body disease in Japan J Neurol 1990237197ndash20451 Birkett DP Desouky A Han L Kaufman M Lewy bodies in psychiatric patients Int J
Geriatr Psychiatry 19927235ndash240
Appendix (continued)
Name Location Contribution
John PaulTaylor MBBS PhD
Newcastle University Revising the manuscript forintellectual content
Debby WTsuang MD
VA Puget Sound ampUniversity ofWashington
Revising the manuscript forintellectual content
ZuzanaWalker MD
University CollegeLondon
Revising the manuscript forintellectual content
PietroTiraboschiMD
Istituto NeurologicoldquoCarlo Bestardquo Milan
Design and conceptualizationof the study acquisition ofdata analysis andinterpretation of the data anddrafting and revising themanuscript for intellectualcontent
754 Neurology | Volume 94 Number 17 | April 28 2020 NeurologyorgN
52 Kobayashi K Nakano H Akiyama N Maeda T Yamamori S Pure psychiatric pre-sentation of the Lewy body disease is depressionmdashan analysis of 60 cases verified withmyocardial meta-iodobenzylguanidine study Int J Geriatr Psychiatry 201530663ndash668
53 Takahashi S Mizukami K Arai T et al Ventilatory response to hypercapnia predictsdementia with Lewy bodies in late-onset major depressive disorder J Alzheimers Dis201650751ndash758
54 Van Assche L Van Aubel E Van de Ven L Bouckaert F Luyten P Vandenbulcke MThe neuropsychological profile and phenomenology of late onset psychosis a cross-sectional study on the differential diagnosis of very-late-onset Schizophrenia-likepsychosis dementia with Lewy bodies and Alzheimerrsquos type dementia with psychosisArch Clin Neuropsychol 201934183ndash199
55 Thaipisuttikul P Lobach I Zweig Y Gurnani A Galvin JE Capgras syndrome indementia with Lewy bodies Int Psychogeriatr 201325843ndash849
56 Fujishiro H Iseki E Nakamura S et al Dementia with Lewy bodies early diagnosticchallenges Psychogeriatrics 201313128ndash138
57 Chiba Y Fujishiro H Iseki E et al Retrospective survey of prodromal symptoms indementia with Lewy bodies comparison with Alzheimerrsquos disease Dement GeriatrCogn Disord 201233273ndash281
58 Kaufmann H Norcliffe-Kaufmann L Palma JA et al Natural history of pure auto-nomic failure a United States prospective cohort Ann Neurol 201781287ndash297
59 Heinzel S Berg D Gasser T et al Update of the MDS research criteria for prodromalParkinsonrsquos disease Mov Disord 2019341464ndash1470
60 Palma JA Norcliffe-Kaufmann L Kaufmann H Diagnosis of multiple system atrophyAuton Neurosci 201821115ndash25Data available fromDryad (Additional References References e1ndashe44) doi105061dryad1c59zw3rv
Subspecialty Alerts by E-mail
Customize your online journal experience by signing up for e-mail alerts related to your subspecialty or area of interest Accessthis free service by clicking on the ldquoMy Alertsrdquo link on the home page An extensive list of subspecialties methods and studydesign choices will be available for you to choose frommdashallowing you priority alerts to cutting-edge research in your field
COVID-19 and Neurologic Disease Call for Papers
The editors of Neurology are interested in papers that address the neurological aspects of COVID-19infection and challenges to the management of patients with chronic neurological conditions whohave or are at risk for the infection Relevant papers that pass initial internal review will undergoexpedited peer review and online publication We will consider papers posted in preprint servers
Submit observational studies and clinical trials as Articles and case series and case reports underthe ClinicalScientific Notes category to httpssubmitneurologyorg today
Visit the Neurologyreg Website at NeurologyorgN More article-based content on home pages Streamlined menus and navigation Enhanced blog sections for specialty areas Same experience on desktop tablet and mobile devices Improved article reading experience links more evident (pdf analytics social media) Neurologyreg Clinical Practice initiative ldquoPractice Currentrdquo global surveys will be accessible across sites
Find Neurologyreg on Facebook httptinyurlcomneurologyfan
Follow Neurologyreg on Twitter httpstwittercomGreenJournal
NeurologyorgN Neurology | Volume 94 Number 17 | April 28 2020 755
DOI 101212WNL0000000000009323202094743-755 Published Online before print April 2 2020Neurology
Ian G McKeith Tanis J Ferman Alan J Thomas et al Research criteria for the diagnosis of prodromal dementia with Lewy bodies
This information is current as of April 2 2020
ServicesUpdated Information amp
httpnneurologyorgcontent9417743fullincluding high resolution figures can be found at
References httpnneurologyorgcontent9417743fullref-list-1
This article cites 59 articles 12 of which you can access for free at
Subspecialty Collections
httpnneurologyorgcgicollectionpsychosisPsychosis a
httpnneurologyorgcgicollectionparkinsons_disease_with_dementiParkinsons disease with dementia
httpnneurologyorgcgicollectionmci_mild_cognitive_impairmentMCI (mild cognitive impairment)
httpnneurologyorgcgicollectiondementia_with_lewy_bodiesDementia with Lewy bodies
httpnneurologyorgcgicollectiondeliriumDeliriumfollowing collection(s) This article along with others on similar topics appears in the
Permissions amp Licensing
httpwwwneurologyorgaboutabout_the_journalpermissionsits entirety can be found online atInformation about reproducing this article in parts (figurestables) or in
Reprints
httpnneurologyorgsubscribersadvertiseInformation about ordering reprints can be found online
ISSN 0028-3878 Online ISSN 1526-632XWolters Kluwer Health Inc on behalf of the American Academy of Neurology All rights reserved Print1951 it is now a weekly with 48 issues per year Copyright Copyright copy 2020 The Author(s) Published by
reg is the official journal of the American Academy of Neurology Published continuously sinceNeurology

disease manifestation Among many predictive markerstested only the cognitive variables differed at baseline be-tween those converting to primary dementia vs parkinson-ism7 Other multicenter studies confirm that the only clinicalfeature that predicts dementia vs parkinsonism first is neu-ropsychological performance those with RBD who exhibitcognitive changes are more likely to evolve first into MCI orDLB22e4 Thus although RBD may be regarded an earlymanifestation of α-synucleinopathy it is not possible to clearlydistinguish whether an individual presenting with RBD willdevelop dementia first that is evolve into a primary DLBdiagnosis or parkinsonism first that is a primary PDMSAdiagnosis Any MCI subtype associated with PSG-confirmedRBD is highly likely to represent underlying LB disease Al-though idiopathic RBD is a useful model to study the earlystages of LB disease progression it is not necessarily repre-sentative of the whole spectrum of patients with PD and DLBa significant minority of whom do not have RBD42
Autonomic dysfunctionanosmia and othernonspecific prodromal LB disease symptomsPatients with DLB frequently report a history of autonomicdysfunction at first clinic attendance with 25ndash50 com-plaining of one of more among constipation orthostatic diz-ziness urinary incontinence erectile dysfunction increasedsweating or increased saliva5657 In a cohort of patients withpure autonomic failure 34 converted to an overt α-synu-cleinopathy over 6 years of follow-up this was to DLB (52)PD (24) orMSA (24)58 However because there are manyother causes for autonomic dysfunction in older people thesesymptoms either alone or in combination have low positivepredictive value59 The situation is similar for hyposmia whichalso frequently occurs early in prodromal DLB and PD42 butwhich can have many other causes in this age group
Conclusions and future directionDiagnosis of DLB at the dementia stage depends on identifyingfully expressed core clinical features which may be mild orabsent at the prodromal stage when biomarker evidence mayalso be weaker and may even differ from that found at thedementia stage Several new biomarker candidates direct andindirect are in development and we will continue to reviewthese to update our recommendations as soon as sufficientevidence accumulates We recognize that the clinical pheno-type of neurodegenerative disorders reflects interaction be-tween several rather than a single brain pathology and it istherefore likely that multiple biomarkers of individual pathol-ogies (eg α-synuclein β-amyloid and tau) or of disease sur-rogates (eg metabolic imagingEEG) will be required
Although we have described the 3 prodromal DLB syndromesseparately they are unlikely to be mutually exclusive andthere may be substantial overlap We propose operationalizedcriteria only for MCI-LB because the evidence base from oursystematic review albeit relatively limited is sufficient to
support recommendations that are immediately applicableand testable Our recommendations should be used alongsideguidance about the prodromal manifestations of PD1559
MSA60 and AD14 with which there is overlap Notwith-standing the potential benefits of early diagnosis we are alsomindful of the importance of avoiding incorrect (false-positive) diagnosis of prodromal DLB and the potentialnegative consequences this could have for an individual Wesuggest that the predictive validity of different categories andcombinations of our proposed criteria should be clarified byprospective studies before they are adopted for widespreadclinical use and that they will enable standardization for in-clusion in research studies and clinical trials
Some published guidance about the early clinical diagnosis ofDLB does already exist DSM5 recommends a diagnosis ofmild neurocognitive disorder (NCD) with LB ldquofor individualswho present with the core or suggestive features at a stagewhen cognitive or functional impairments are not of sufficientseverity to fulfill criteria for major NCDrdquoe43 This is basedhowever on the 2005 version of DLB guidelines and requiresupdating ICD-11 takes a similar approach toward diagnosingmild NCD at a syndromic level and lists both Lewy bodydisease and PD as possible causese44
The diagnostic position for other prodromal manifestations ofDLB that is delirium-onset and psychiatric-onset is less clearthan for MCI Operationalization of specific criteria for thesesyndromes is not yet justified and the reliable differentiationof the minority of delirious and psychiatrically ill patients whohave underlying LB pathology from the majority who do notwill probably only be achieved when routinely applicablebiomarkers are developed LB disease is seldom if ever cur-rently considered as part of the differential diagnosis of de-lirium or late-onset psychiatric disorder and we hope that theinformation we provide in the text and accompanying boxeswill raise cliniciansrsquo awareness of that possibility
Study fundingNo targeted funding reported
DisclosureI McKeith receives support from the NIHR Biomedical Re-search Centre awarded to the Newcastle upon Tyne HospitalsNHS Foundation Trust and Newcastle University and hasconsulted for GE Healthcare Sanofi Eisai Sumitomo Dai-nippon Pharma and Axovant T Ferman receives support fromNIH P50-AG16574 P30-AG062677 U01-NS100620 and theMangurian Foundation for Lewy body disease research AThomas receives support from the NIHR Biomedical ResearchCentre awarded to the Newcastle upon Tyne Hospitals NHSFoundation Trust and Newcastle University and has receivedgrants from GE Healthcare F Blanc has served as nationalclinical trial coordinator for Eisai and Axovant B Boevereceives support from NIH P50-AG16574 P30-AG062677U01-NS100620 and the Mangurian Foundation for Lewybody disease research has consulted for the Scientific Advisory
NeurologyorgN Neurology | Volume 94 Number 17 | April 28 2020 751
BoardmdashTau Consortium and received grants from Biogenthe NIH theMangurian Foundation Alector the Little FamilyFoundation and the Turner Family H Fujishiro has receivedsupport from Fujifilm RI Pharma Co Ltd K Kantarci receivessupport from NIH P50-AG16574 P30-AG062677 U01-NS100620 and the Mangurian Foundation for Lewy bodydisease research and has received grants from Avid Radio-pharmaceuticals and acted on a Data Safety Monitoring Boardfor Takeda Global Research C Muscio acknowledges thesupport of the Italian Ministry of Health GRANT NET-2011-02346784 J OrsquoBrien is supported by the NIHR CambridgeBiomedical Research Centre Dementia and Neuro-degeneration and Mental Health Themes and the CambridgeCentre for Parkinsonrsquos Plus Disorders has consulted forTauRx Axon GE Healthcare Eisai and AvidLilly and re-ceived grants fromAvidLilly andAllianceMedical R Postumahas received grants from and consulted for Fonds de laRecherche en Sante received grants from the Canadian Insti-tutes of Health Research the Parkinson Society of Canada theWeston-Garfield Foundation The Michael J Fox Foundationand the Webster Foundation and consulted for TakedaRocheProthena Teva Neurosciences Novartis Canada Bio-gen Boehringer Ingelheim Theranexus GE Healthcare JazzPharmaceuticals AbbVie Jannsen Otsuko PhytopharmicsInception Sciences and Parkinson Canada D Aarsland isa Royal Society Wolfson Research Merit Award Holder andwould like to thank the Wolfson Foundation and the RoyalSociety for their support He has received research supportandor honoraria from AstraZeneca H Lundbeck NovartisPharmaceuticals and GE Health and served as paid consultantfor H Lundbeck Eisai Heptares Sanofi and Mentis Cura CBallard reports unrelated current grant funding from MRCWellcome Trust European Union Gillings FoundationNIHR Alzheimerrsquos Society Alzheimerrsquos Research UK Par-kinsonrsquos Society and Lewy Body Society during the conduct ofthe study and personal fees from Acadia pharmaceutical com-pany Lundbeck Roche Otsuka Eli Lilly and AARP outsidethe submitted work L Bonanni is a member of the steeringcommittee of the E-DLB consortium and program chair of theLBD-PIA (ISTAART) and is funded for research on DLB bythe Italian Ministry of Health P Donaghy receives supportfrom the NIHR Biomedical Research Centre awarded to theNewcastle upon Tyne Hospitals NHS Foundation Trust andNewcastle UniversityM Emre served on the scientific advisoryboard for AC Immune J Galvin receives support from NIHgrants (R01 AG040211 R01 NS101482 R01 AG057681 andU01 NS100610) and the Lewy Body Dementia AssociationResearch Center of Excellence reports research support fromthe NIH the Lewy Body Dementia Association The Harry TMangurian Foundation and Albert Charitable Trust directsclinical trials for Biogen and Novartis receives licensing feesfrom Biogen Roche Eli Lilly Quintiles Roobrik ContinuumClinical and Langland and receives consulting fees fromBiogen Eisai Bracket and Medavante D Galasko receivessupport from NIA grant AGO5131 and the Michael J FoxFoundation and has acted as consultant for vTv Pharmaceut-icals Inc Esai Inc and for Fujirebio Inc been a member of
a DSMB for Probiodrug and paid editor for Alzheimerrsquos Re-search amp Therapy J Goldman receives grantsupport fromTheMichael J Fox Foundation and Parkinsonrsquos Foundation andhas received consulting feeshonoraria from Acadia AptinyxSunovion and Worldwide Med S Gomperts receives supportfrom NIH grants R01 AG054551 P30AG062421 R01AG062208 P50 AG005134 R21 NS109833 DODCDMRPW81XW1810516 the Farmer Family ParkinsonrsquosInitiative and the Lewy Body Dementia Association and hasserved on advisory boards for Acadia Pharmaceuticals andSanofi L Honig acknowledges research grant support fromNYS CEAD grant C031425 LBDA RCOE and NIHgrants U01NS100600 P50AG008702 R21AG058020R21MH111596 U01AG051412 U01AG045390U01AG016976 U01AG023749 U19063893 andU19AG024904 He receives research funding support fromAbbVie Alector Biogen Eisai Genentech Roche and Wash-ington University and has received income for consulting forCortexyme and Eisai M Ikeda reports departmental grants andhonoraria fees from Sumitomo Dainippon Pharma Eisai andNiho Medicine-Physics J Leverenz acknowledges supportfrom the National Institutes of Health P30 AG053762 UO1NS100610 and R13NS111954 and Jane and Lee Seidman andDouglas Herthel DVMMemorial Funds and reports consultingfees from Aptinyx Acadia Biogen Eisai GE HealthcareGenzymeSanofi and Takeda Pharmaceuticals and grant sup-port from Alzheimerrsquos Drug Discovery Foundation De-partment of Defense GE Healthcare GenzymeSanofi TheMichael J Fox Foundation and the NIH (NIA andNINDS) SLewis is supported by NHMRC-ARC Dementia Fellows KMarder is funded by the NIH R01NS100600 NS107168UL1TR001873 andNS073671 with research support from theLBDA Parkinson Foundation Michael J Fox HDSA andCHDI and has acted as site investigator for Vaccinex andGenentech member of Springer editorial board and scientificadvisory board Voyager Therapeutics M Masellis was sup-ported by a Canadian Institutes of Health Research grant(MOP13129) and an Early Researcher Award from the Min-istry of Research Innovation and Science (MRIS ON) andreports personal fees for ad hoc consultancy from ArkudaTherapeutics Ionis Pharmaceuticals and Alector Pharmaceut-icals royalties fromHenry Stewart Talks Ltd and grants to theinstitution from Roche Novartis Washington University andAxovant Sciences D Salmon acknowledges support from NIHP30AG062429 and is a paid consultant for Takeda Inc Apti-nyx Inc and Biogen Inc J-P Taylor receives support from theNIHR Biomedical Research Centre awarded to the Newcastleupon Tyne Hospitals NHS Foundation Trust and NewcastleUniversity and reports grants from the UKNational Institute ofHealth Research (NIHR) travel award from Axovant researchsupport costs from Sonsei-Heptares and personal fees fromGEHealthcare D Tsuang acknowledges support from NIHR21AG064271 R03 NS103950 and U01 NS100610 ZWalker has been supported by ESRC NIHR (co-app) ARUK(co-app) EU IMI 2 (co-app) and Dunhill Medical Trust Shehas received consultancy fees travel expenses and researchsupport from GE Healthcare and research support from Life
752 Neurology | Volume 94 Number 17 | April 28 2020 NeurologyorgN
Molecular Imaging P Tiraboschi acknowledges the support ofthe Italian Ministry of Health GRANT NET-2011-02346784Go to NeurologyorgN for full disclosures
Publication historyReceived by Neurology October 30 2019 Accepted in final formFebruary 25 2020
Appendix Authors
Name Location Contribution
Ian GMcKeith FMed Sci MD
Newcastle University Design and conceptualizationof the study acquisition ofdata analysis andinterpretation of the data anddrafting and revising themanuscript for intellectualcontent
Tanis JFermanPhD
Mayo ClinicJacksonville
Design and conceptualizationof the study acquisition ofdata analysis andinterpretation of the data anddrafting and revising themanuscript for intellectualcontent
Alan JThomasPhD
Newcastle University Design and conceptualizationof the study acquisition ofdata analysis andinterpretation of the data anddrafting and revising themanuscript for intellectualcontent
FredericBlanc MD
University ofStrasbourg
Design and conceptualizationof the study acquisition ofdata analysis andinterpretation of the data anddrafting and revising themanuscript for intellectualcontent
Bradley FBoeve MD
Mayo Clinic Rochester Design and conceptualizationof the study acquisition ofdata analysis andinterpretation of the data anddrafting and revising themanuscript for intellectualcontent
HiroshigeFujishiroMD
Nagoya UniversityKawasaki MemorialHospital
Design and conceptualizationof the study acquisition ofdata analysis andinterpretation of the data anddrafting and revising themanuscript for intellectualcontent
KejalKantarciMD MS
Mayo Clinic Rochester Design and conceptualizationof the study acquisition ofdata analysis andinterpretation of the data anddrafting and revising themanuscript for intellectualcontent
CristinaMuscio PhD
Istituto NeurologicoldquoCarlo Bestardquo Milan
Design and conceptualizationof the study acquisition ofdata analysis andinterpretation of the data anddrafting and revising themanuscript for intellectualcontent
Appendix (continued)
Name Location Contribution
John TOrsquoBrien FMed Sci DM
Cambridge University Design and conceptualizationof the study acquisition ofdata analysis andinterpretation of the data anddrafting and revising themanuscript for intellectualcontent
Ronald BPostumaMD MSc
McGill University Design and conceptualizationof the study acquisition ofdata analysis andinterpretation of the data anddrafting and revising themanuscript for intellectualcontent
DagAarslandPhD
Kingrsquos College Londonand StavangerUniversityHospital
Revising the manuscript forintellectual content
CliveBallard MD
University of Exeter Revising the manuscript forintellectual content
LauraBonanniMD PhD
University of Chieti-Pescara
Revising the manuscript forintellectual content
PaulDonaghyPhD
Newcastle University Revising the manuscript forintellectual content
Murat EmreMD
Istanbul Faculty ofMedicine
Revising the manuscript forintellectual content
James EGalvin MDMPH
University of MiamiMiller School ofMedicine
Revising the manuscript forintellectual content
DouglasGalasko MD
University of CaliforniaSan Diego
Revising the manuscript forintellectual content
Jennifer GGoldmanMD MS
Feinberg School ofMedicine
Revising the manuscript forintellectual content
Stephen NGompertsMD PhD
Massachusetts GeneralHospital
Revising the manuscript forintellectual content
Lawrence SHonig MDPhD
Columbia UniversityIrving Medical Center
Revising the manuscript forintellectual content
ManabuIkeda MDPhD
Osaka University Revising the manuscript forintellectual content
James BLeverenzMD
Lou Ruvo Center ofBrain Health ClevelandClinic
Revising the manuscript forintellectual content
Simon JGLewis MD
University of Sydney Revising the manuscript forintellectual content
Karen SMarder MDMPH
Columbia UniversityIrving Medical Center
Revising the manuscript forintellectual content
MarioMasellisMD PhD
Sunnybrook HealthSciences CentreUniversity of Toronto
Revising the manuscript forintellectual content
David PSalmon PhD
University of CaliforniaSan Diego
Revising the manuscript forintellectual content
Continued
NeurologyorgN Neurology | Volume 94 Number 17 | April 28 2020 753
References1 Walker Z Possin KL Boeve BF Aarsland D Lewy body dementias Lancet 2015386
1683ndash16972 McKeith IG Boeve BF Dickson DW et al Diagnosis and management of dementia
with Lewy bodies fourth consensus report of the DLB consortium Neurology 20178988ndash100
3 Ferman TJ Smith GE Kantarci K et al Nonamnestic mild cognitive impairmentprogresses to dementia with Lewy bodies Neurology 2013812032ndash2038
4 Savica R Bradley BF Mielke MM When do alpha-synucleinopathies start An epi-demiological timeline A review JAMA Neurol 201875503ndash509
5 Donaghy PC Taylor JP OrsquoBrien JT et al Neuropsychiatric symptoms and cognitiveprofile in mild cognitive impairment with Lewy bodies Psychol Med 2018482384ndash2390
6 Cagnin A Bussse C Gardini S et al Clinical and cognitive phenotype of mildcognitive impairment evolving to dementia with Lewy bodies Dement Geriatr CognDis Extra 20155442ndash449
7 Postuma RB Iranzo A HuM et al Risk and predictors of dementia and parkinsonismin idiopathic REM sleep behaviour disorder a multicentre study Brain 2019142744ndash759
8 Sadiq D Whitfield T Lee L Stevens T Costafreda S Walker Z Prodromal dementiawith Lewy bodies and prodromal Alzheimerrsquos disease a comparison of the cognitiveand clinical profiles J Alzheimers Dis 201758463ndash470
9 FitzGerald JM Perera G Chang-Tave A et al The incidence of recorded de-lirium episodes before and after dementia diagnosis differences between de-mentia with Lewy bodies and Alzheimerrsquos disease J Am Med Dir Assoc 201920604ndash609
10 Jicha GA Schmitt FA Abner E et al Prodromal clinical manifestations of neu-ropathologically confirmed Lewy body disease Neurobiol Aging 2010311805ndash1813
11 Vardy E Holt R Gerhard A Richardson A Snowden J Neary D History of a sus-pected delirium is more common in dementia with Lewy bodies than Alzheimerrsquosdisease a retrospective study Int J Geriatr Psychiatry 201429178ndash181
12 Fujishiro H Nakamura S Sato K Iseki E Prodromal dementia with Lewy bodiesGeriatr Gerontol Int 201515817ndash826
13 McKeith I Taylor JP Thomas A Donaghy P Kane J Revisiting DLB diagnosisa consideration of prodromal DLB and of the diagnostic overlap with Alzheimerdisease J Geriatr Psychiatry Neurol 201629249ndash253
14 Albert MS DeKosky ST Dickson D et al The diagnosis of mild cognitive impairmentdue to Alzheimerrsquos disease recommendations from the National Institute on Aging-Alzheimerrsquos Association workgroups on diagnostic guidelines for Alzheimerrsquos diseaseAlzheimers Dement 20117270ndash279
15 Litvan I Goldman JG Troster AI et al Diagnostic criteria for mild cognitive im-pairment in Parkinsonrsquos disease Movement Disorder Society Task Force guidelinesMov Disord 201227349ndash356
16 Ferman TJ Smith GE Boeve BF et al Neuropsychological differentiation of de-mentia with Lewy bodies from normal aging and Alzheimerrsquos disease Clin Neuro-psychol 200620623ndash636
17 Cagnin A Busse C Jelcic N Gnoato F Mitolo M Caffarra P High specificity ofMMSE pentagon scoring for diagnosis of prodromal dementia with Lewy bodiesParkinsonism Relat Disord 201521303ndash305
18 Yoon JH Kim M Moon SY Yong SW Hong JM Olfactory function and neuro-psychological profile to differentiate dementia with Lewy bodies from Alzheimerrsquosdisease in patients with mild cognitive impairment a 5-year follow-up study J NeurolSci 2015355174ndash179
19 Kemp J Philippi N Phillipps C et al Cognitive profile in prodromal dementia withLewy bodies Alzheimers Res Ther 2017919
20 Auning E Rongve A Fladby T et al Early and presenting symptoms of dementia withLewy bodies Dement Geriatr Cogn Disord 201132202ndash208
21 Kondo D Ota K Kasanuki K et al Characteristics of mild cognitive impairmenttending to convert into Alzheimerrsquos disease or dementia with Lewy bodies a follow-upstudy in a memory clinic J Neurol Sci 2016369102ndash108
22 Marchand DG Postuma RB Escudier F et al How does dementia with Lewy bodiesstart prodromal cognitive changes in REM sleep behavior disorder Ann Neurol2018831016ndash1026
23 Kantarci K Lesnick T Ferman TJ et al Hippocampal volumes predict risk of de-mentia with Lewy bodies in mild cognitive impairment Neurology 2016872317ndash2323
24 Thomas AJ Taylor JP McKeith I et al Revision of assessment toolkits for improvingthe diagnosis of Lewy body dementia the DIAMOND Lewy study Int J GeriatrPsychiatry 2018331293ndash1304
25 Galvin JE Improving the clinical detection of Lewy body dementia with the Lewybody composite risk score Alzheimerrsquos Demen (Amsterdam Netherlands) 20151316ndash324
26 Belden CM Kahlon V Malek-Ahmadi M Tsai A Sabbagh MN Clinical character-ization of mild cognitive impairment as a prodrome to dementia with Lewy bodiesAm J Alzheimers Dis Other Demen 201530173ndash177
27 Yoon JH Lee JE Yong SW Moon SY Lee PH The mild cognitive impairment stageof dementia with Lewy bodies and Parkinson disease A comparison of cognitiveprofiles Alzheimer Dis Assoc Disord 201428151ndash155
28 Fengler S Liepelt-Scarfone I Brockmann K Schaffer E Berg D Kalbe E Cognitivechanges in prodromal Parkinsonrsquos disease a review Mov Disord 2017321655ndash1666
29 Kalbe E Rehberg SP Heber I et al Subtypes of mild cognitive impairment in patientswith Parkinsonrsquos disease evidence from the LANDSCAPE study J Neurol NeurosurgPsychiatry 2016871099ndash1105
30 Thomas AJ Donaghy P Roberts G et al Diagnostic accuracy of dopaminergic im-aging in prodromal dementia with Lewy bodies Psychol Med 20181ndash7
31 Ferman TJ Boeve BF Smith GE et al Inclusion of RBD improves the diagnosticclassification of dementia with Lewy bodies Neurology 201177875ndash882
32 Fujishiro H Okuda M Iwamoto K et al Early diagnosis of Lewy body disease inpatients with late-onset psychiatric disorders using clinical history of rapid eyemovement sleep behavior disorder and I-123 -metaiodobenzylguanidine cardiacscintigraphy Psychiatry Clin Neurosci 201872423ndash434
33 Bonanni L Perfetti B Bifolchetti S et al Quantitative electroencephalogram utility inpredicting conversion of mild cognitive impairment to dementia with Lewy bodiesNeurobiol Aging 201536434ndash445
34 Murray ME Ferman TJ Boeve BF et al MRI and pathology of REM sleep behaviordisorder in dementia with Lewy bodies Neurology 2013811681ndash1689
35 Murray ME Graff-Radford NR Ross OA Petersen RC Duara R Dickson DWNeuropathologically defined subtypes of Alzheimerrsquos disease with distinct clinicalcharacteristics a retrospective study Lancet Neurol 201110785ndash796
36 Blanc F Colloby SJ Cretin B et al Grey matter atrophy in prodromal stage ofdementia with Lewy bodies and Alzheimerrsquos disease Alzheimers Res Ther 2016831
37 Blanc F Colloby SJ Philippi N et al Cortical thickness in dementia with Lewy bodiesand Alzheimerrsquos disease a comparison of prodromal and dementia stages Plos One201510e0127396
38 Surendranathan A OrsquoBrien JT Clinical imaging in dementia with Lewy bodies EvidBased Ment Health 20182161ndash65
39 Outeiro TF Koss DJ Erskine D et al Dementia with Lewy bodies an update andoutlook Mol Neurodegener 2019145
40 Donadio V Incensi A Rizzo G et al A new potential biomarker for dementiawith Lewy bodies Skin nerve alpha-synuclein deposits Neurology 201789318ndash326
41 Flanigan PM Khosravi MA Leverenz JB Tousi B Color vision impairment differ-entiates Alzheimer dementia from dementia with Lewy bodies J Geriatr PsychiatryNeurol 20183197ndash102
42 Fereshtehnejad SM Yao C Pelletier A Montplaisir JY Gagnon JF Postuma RBEvolution of prodromal Parkinsonrsquos disease and dementia with Lewy bodies a pro-spective study Brain 20191422051ndash2067
43 Bousiges O Bombois S Schraen S et al Cerebrospinal fluid Alzheimer biomarkerscan be useful for discriminating dementia with Lewy bodies from Alzheimerrsquos diseaseat the prodromal stage J Neurol Neurosurg Psychiatry 201889467ndash475
44 Kantarci K Lowe VJ Boeve BF et al Multimodality imaging characteristics of de-mentia with Lewy bodies Neurobiol Aging 2012332091ndash2105
45 Kantarci K Lowe VJ Boeve BF et al AV-1451 tau and beta-amyloid positronemission tomography imaging in dementia with Lewy bodies Ann Neurol 20178158ndash67
46 Gore RL Vardy E OrsquoBrien JT Delirium and dementia with Lewy bodies distinctdiagnoses or part of the same spectrum J Neurol Neurosurg Psychiatry 20158650ndash59
47 Aarsland DS Auning E The pre-dementia stage of dementia with Lewy bodies Eur JNeurol 20111869
48 Sunwoo MK Hong JY Choi J Park HJ Kim SH Lee PH alpha-Synuclein pathologyis related to postoperative delirium in patients undergoing gastrectomy Neurology201380810ndash813
49 Akintade O Pierres F Acute presentation of dementia with Lewy bodies Clin Med201919327ndash330
50 Kosaka K Diffuse Lewy body disease in Japan J Neurol 1990237197ndash20451 Birkett DP Desouky A Han L Kaufman M Lewy bodies in psychiatric patients Int J
Geriatr Psychiatry 19927235ndash240
Appendix (continued)
Name Location Contribution
John PaulTaylor MBBS PhD
Newcastle University Revising the manuscript forintellectual content
Debby WTsuang MD
VA Puget Sound ampUniversity ofWashington
Revising the manuscript forintellectual content
ZuzanaWalker MD
University CollegeLondon
Revising the manuscript forintellectual content
PietroTiraboschiMD
Istituto NeurologicoldquoCarlo Bestardquo Milan
Design and conceptualizationof the study acquisition ofdata analysis andinterpretation of the data anddrafting and revising themanuscript for intellectualcontent
754 Neurology | Volume 94 Number 17 | April 28 2020 NeurologyorgN
52 Kobayashi K Nakano H Akiyama N Maeda T Yamamori S Pure psychiatric pre-sentation of the Lewy body disease is depressionmdashan analysis of 60 cases verified withmyocardial meta-iodobenzylguanidine study Int J Geriatr Psychiatry 201530663ndash668
53 Takahashi S Mizukami K Arai T et al Ventilatory response to hypercapnia predictsdementia with Lewy bodies in late-onset major depressive disorder J Alzheimers Dis201650751ndash758
54 Van Assche L Van Aubel E Van de Ven L Bouckaert F Luyten P Vandenbulcke MThe neuropsychological profile and phenomenology of late onset psychosis a cross-sectional study on the differential diagnosis of very-late-onset Schizophrenia-likepsychosis dementia with Lewy bodies and Alzheimerrsquos type dementia with psychosisArch Clin Neuropsychol 201934183ndash199
55 Thaipisuttikul P Lobach I Zweig Y Gurnani A Galvin JE Capgras syndrome indementia with Lewy bodies Int Psychogeriatr 201325843ndash849
56 Fujishiro H Iseki E Nakamura S et al Dementia with Lewy bodies early diagnosticchallenges Psychogeriatrics 201313128ndash138
57 Chiba Y Fujishiro H Iseki E et al Retrospective survey of prodromal symptoms indementia with Lewy bodies comparison with Alzheimerrsquos disease Dement GeriatrCogn Disord 201233273ndash281
58 Kaufmann H Norcliffe-Kaufmann L Palma JA et al Natural history of pure auto-nomic failure a United States prospective cohort Ann Neurol 201781287ndash297
59 Heinzel S Berg D Gasser T et al Update of the MDS research criteria for prodromalParkinsonrsquos disease Mov Disord 2019341464ndash1470
60 Palma JA Norcliffe-Kaufmann L Kaufmann H Diagnosis of multiple system atrophyAuton Neurosci 201821115ndash25Data available fromDryad (Additional References References e1ndashe44) doi105061dryad1c59zw3rv
Subspecialty Alerts by E-mail
Customize your online journal experience by signing up for e-mail alerts related to your subspecialty or area of interest Accessthis free service by clicking on the ldquoMy Alertsrdquo link on the home page An extensive list of subspecialties methods and studydesign choices will be available for you to choose frommdashallowing you priority alerts to cutting-edge research in your field
COVID-19 and Neurologic Disease Call for Papers
The editors of Neurology are interested in papers that address the neurological aspects of COVID-19infection and challenges to the management of patients with chronic neurological conditions whohave or are at risk for the infection Relevant papers that pass initial internal review will undergoexpedited peer review and online publication We will consider papers posted in preprint servers
Submit observational studies and clinical trials as Articles and case series and case reports underthe ClinicalScientific Notes category to httpssubmitneurologyorg today
Visit the Neurologyreg Website at NeurologyorgN More article-based content on home pages Streamlined menus and navigation Enhanced blog sections for specialty areas Same experience on desktop tablet and mobile devices Improved article reading experience links more evident (pdf analytics social media) Neurologyreg Clinical Practice initiative ldquoPractice Currentrdquo global surveys will be accessible across sites
Find Neurologyreg on Facebook httptinyurlcomneurologyfan
Follow Neurologyreg on Twitter httpstwittercomGreenJournal
NeurologyorgN Neurology | Volume 94 Number 17 | April 28 2020 755
DOI 101212WNL0000000000009323202094743-755 Published Online before print April 2 2020Neurology
Ian G McKeith Tanis J Ferman Alan J Thomas et al Research criteria for the diagnosis of prodromal dementia with Lewy bodies
This information is current as of April 2 2020
ServicesUpdated Information amp
httpnneurologyorgcontent9417743fullincluding high resolution figures can be found at
References httpnneurologyorgcontent9417743fullref-list-1
This article cites 59 articles 12 of which you can access for free at
Subspecialty Collections
httpnneurologyorgcgicollectionpsychosisPsychosis a
httpnneurologyorgcgicollectionparkinsons_disease_with_dementiParkinsons disease with dementia
httpnneurologyorgcgicollectionmci_mild_cognitive_impairmentMCI (mild cognitive impairment)
httpnneurologyorgcgicollectiondementia_with_lewy_bodiesDementia with Lewy bodies
httpnneurologyorgcgicollectiondeliriumDeliriumfollowing collection(s) This article along with others on similar topics appears in the
Permissions amp Licensing
httpwwwneurologyorgaboutabout_the_journalpermissionsits entirety can be found online atInformation about reproducing this article in parts (figurestables) or in
Reprints
httpnneurologyorgsubscribersadvertiseInformation about ordering reprints can be found online
ISSN 0028-3878 Online ISSN 1526-632XWolters Kluwer Health Inc on behalf of the American Academy of Neurology All rights reserved Print1951 it is now a weekly with 48 issues per year Copyright Copyright copy 2020 The Author(s) Published by
reg is the official journal of the American Academy of Neurology Published continuously sinceNeurology

BoardmdashTau Consortium and received grants from Biogenthe NIH theMangurian Foundation Alector the Little FamilyFoundation and the Turner Family H Fujishiro has receivedsupport from Fujifilm RI Pharma Co Ltd K Kantarci receivessupport from NIH P50-AG16574 P30-AG062677 U01-NS100620 and the Mangurian Foundation for Lewy bodydisease research and has received grants from Avid Radio-pharmaceuticals and acted on a Data Safety Monitoring Boardfor Takeda Global Research C Muscio acknowledges thesupport of the Italian Ministry of Health GRANT NET-2011-02346784 J OrsquoBrien is supported by the NIHR CambridgeBiomedical Research Centre Dementia and Neuro-degeneration and Mental Health Themes and the CambridgeCentre for Parkinsonrsquos Plus Disorders has consulted forTauRx Axon GE Healthcare Eisai and AvidLilly and re-ceived grants fromAvidLilly andAllianceMedical R Postumahas received grants from and consulted for Fonds de laRecherche en Sante received grants from the Canadian Insti-tutes of Health Research the Parkinson Society of Canada theWeston-Garfield Foundation The Michael J Fox Foundationand the Webster Foundation and consulted for TakedaRocheProthena Teva Neurosciences Novartis Canada Bio-gen Boehringer Ingelheim Theranexus GE Healthcare JazzPharmaceuticals AbbVie Jannsen Otsuko PhytopharmicsInception Sciences and Parkinson Canada D Aarsland isa Royal Society Wolfson Research Merit Award Holder andwould like to thank the Wolfson Foundation and the RoyalSociety for their support He has received research supportandor honoraria from AstraZeneca H Lundbeck NovartisPharmaceuticals and GE Health and served as paid consultantfor H Lundbeck Eisai Heptares Sanofi and Mentis Cura CBallard reports unrelated current grant funding from MRCWellcome Trust European Union Gillings FoundationNIHR Alzheimerrsquos Society Alzheimerrsquos Research UK Par-kinsonrsquos Society and Lewy Body Society during the conduct ofthe study and personal fees from Acadia pharmaceutical com-pany Lundbeck Roche Otsuka Eli Lilly and AARP outsidethe submitted work L Bonanni is a member of the steeringcommittee of the E-DLB consortium and program chair of theLBD-PIA (ISTAART) and is funded for research on DLB bythe Italian Ministry of Health P Donaghy receives supportfrom the NIHR Biomedical Research Centre awarded to theNewcastle upon Tyne Hospitals NHS Foundation Trust andNewcastle UniversityM Emre served on the scientific advisoryboard for AC Immune J Galvin receives support from NIHgrants (R01 AG040211 R01 NS101482 R01 AG057681 andU01 NS100610) and the Lewy Body Dementia AssociationResearch Center of Excellence reports research support fromthe NIH the Lewy Body Dementia Association The Harry TMangurian Foundation and Albert Charitable Trust directsclinical trials for Biogen and Novartis receives licensing feesfrom Biogen Roche Eli Lilly Quintiles Roobrik ContinuumClinical and Langland and receives consulting fees fromBiogen Eisai Bracket and Medavante D Galasko receivessupport from NIA grant AGO5131 and the Michael J FoxFoundation and has acted as consultant for vTv Pharmaceut-icals Inc Esai Inc and for Fujirebio Inc been a member of
a DSMB for Probiodrug and paid editor for Alzheimerrsquos Re-search amp Therapy J Goldman receives grantsupport fromTheMichael J Fox Foundation and Parkinsonrsquos Foundation andhas received consulting feeshonoraria from Acadia AptinyxSunovion and Worldwide Med S Gomperts receives supportfrom NIH grants R01 AG054551 P30AG062421 R01AG062208 P50 AG005134 R21 NS109833 DODCDMRPW81XW1810516 the Farmer Family ParkinsonrsquosInitiative and the Lewy Body Dementia Association and hasserved on advisory boards for Acadia Pharmaceuticals andSanofi L Honig acknowledges research grant support fromNYS CEAD grant C031425 LBDA RCOE and NIHgrants U01NS100600 P50AG008702 R21AG058020R21MH111596 U01AG051412 U01AG045390U01AG016976 U01AG023749 U19063893 andU19AG024904 He receives research funding support fromAbbVie Alector Biogen Eisai Genentech Roche and Wash-ington University and has received income for consulting forCortexyme and Eisai M Ikeda reports departmental grants andhonoraria fees from Sumitomo Dainippon Pharma Eisai andNiho Medicine-Physics J Leverenz acknowledges supportfrom the National Institutes of Health P30 AG053762 UO1NS100610 and R13NS111954 and Jane and Lee Seidman andDouglas Herthel DVMMemorial Funds and reports consultingfees from Aptinyx Acadia Biogen Eisai GE HealthcareGenzymeSanofi and Takeda Pharmaceuticals and grant sup-port from Alzheimerrsquos Drug Discovery Foundation De-partment of Defense GE Healthcare GenzymeSanofi TheMichael J Fox Foundation and the NIH (NIA andNINDS) SLewis is supported by NHMRC-ARC Dementia Fellows KMarder is funded by the NIH R01NS100600 NS107168UL1TR001873 andNS073671 with research support from theLBDA Parkinson Foundation Michael J Fox HDSA andCHDI and has acted as site investigator for Vaccinex andGenentech member of Springer editorial board and scientificadvisory board Voyager Therapeutics M Masellis was sup-ported by a Canadian Institutes of Health Research grant(MOP13129) and an Early Researcher Award from the Min-istry of Research Innovation and Science (MRIS ON) andreports personal fees for ad hoc consultancy from ArkudaTherapeutics Ionis Pharmaceuticals and Alector Pharmaceut-icals royalties fromHenry Stewart Talks Ltd and grants to theinstitution from Roche Novartis Washington University andAxovant Sciences D Salmon acknowledges support from NIHP30AG062429 and is a paid consultant for Takeda Inc Apti-nyx Inc and Biogen Inc J-P Taylor receives support from theNIHR Biomedical Research Centre awarded to the Newcastleupon Tyne Hospitals NHS Foundation Trust and NewcastleUniversity and reports grants from the UKNational Institute ofHealth Research (NIHR) travel award from Axovant researchsupport costs from Sonsei-Heptares and personal fees fromGEHealthcare D Tsuang acknowledges support from NIHR21AG064271 R03 NS103950 and U01 NS100610 ZWalker has been supported by ESRC NIHR (co-app) ARUK(co-app) EU IMI 2 (co-app) and Dunhill Medical Trust Shehas received consultancy fees travel expenses and researchsupport from GE Healthcare and research support from Life
752 Neurology | Volume 94 Number 17 | April 28 2020 NeurologyorgN
Molecular Imaging P Tiraboschi acknowledges the support ofthe Italian Ministry of Health GRANT NET-2011-02346784Go to NeurologyorgN for full disclosures
Publication historyReceived by Neurology October 30 2019 Accepted in final formFebruary 25 2020
Appendix Authors
Name Location Contribution
Ian GMcKeith FMed Sci MD
Newcastle University Design and conceptualizationof the study acquisition ofdata analysis andinterpretation of the data anddrafting and revising themanuscript for intellectualcontent
Tanis JFermanPhD
Mayo ClinicJacksonville
Design and conceptualizationof the study acquisition ofdata analysis andinterpretation of the data anddrafting and revising themanuscript for intellectualcontent
Alan JThomasPhD
Newcastle University Design and conceptualizationof the study acquisition ofdata analysis andinterpretation of the data anddrafting and revising themanuscript for intellectualcontent
FredericBlanc MD
University ofStrasbourg
Design and conceptualizationof the study acquisition ofdata analysis andinterpretation of the data anddrafting and revising themanuscript for intellectualcontent
Bradley FBoeve MD
Mayo Clinic Rochester Design and conceptualizationof the study acquisition ofdata analysis andinterpretation of the data anddrafting and revising themanuscript for intellectualcontent
HiroshigeFujishiroMD
Nagoya UniversityKawasaki MemorialHospital
Design and conceptualizationof the study acquisition ofdata analysis andinterpretation of the data anddrafting and revising themanuscript for intellectualcontent
KejalKantarciMD MS
Mayo Clinic Rochester Design and conceptualizationof the study acquisition ofdata analysis andinterpretation of the data anddrafting and revising themanuscript for intellectualcontent
CristinaMuscio PhD
Istituto NeurologicoldquoCarlo Bestardquo Milan
Design and conceptualizationof the study acquisition ofdata analysis andinterpretation of the data anddrafting and revising themanuscript for intellectualcontent
Appendix (continued)
Name Location Contribution
John TOrsquoBrien FMed Sci DM
Cambridge University Design and conceptualizationof the study acquisition ofdata analysis andinterpretation of the data anddrafting and revising themanuscript for intellectualcontent
Ronald BPostumaMD MSc
McGill University Design and conceptualizationof the study acquisition ofdata analysis andinterpretation of the data anddrafting and revising themanuscript for intellectualcontent
DagAarslandPhD
Kingrsquos College Londonand StavangerUniversityHospital
Revising the manuscript forintellectual content
CliveBallard MD
University of Exeter Revising the manuscript forintellectual content
LauraBonanniMD PhD
University of Chieti-Pescara
Revising the manuscript forintellectual content
PaulDonaghyPhD
Newcastle University Revising the manuscript forintellectual content
Murat EmreMD
Istanbul Faculty ofMedicine
Revising the manuscript forintellectual content
James EGalvin MDMPH
University of MiamiMiller School ofMedicine
Revising the manuscript forintellectual content
DouglasGalasko MD
University of CaliforniaSan Diego
Revising the manuscript forintellectual content
Jennifer GGoldmanMD MS
Feinberg School ofMedicine
Revising the manuscript forintellectual content
Stephen NGompertsMD PhD
Massachusetts GeneralHospital
Revising the manuscript forintellectual content
Lawrence SHonig MDPhD
Columbia UniversityIrving Medical Center
Revising the manuscript forintellectual content
ManabuIkeda MDPhD
Osaka University Revising the manuscript forintellectual content
James BLeverenzMD
Lou Ruvo Center ofBrain Health ClevelandClinic
Revising the manuscript forintellectual content
Simon JGLewis MD
University of Sydney Revising the manuscript forintellectual content
Karen SMarder MDMPH
Columbia UniversityIrving Medical Center
Revising the manuscript forintellectual content
MarioMasellisMD PhD
Sunnybrook HealthSciences CentreUniversity of Toronto
Revising the manuscript forintellectual content
David PSalmon PhD
University of CaliforniaSan Diego
Revising the manuscript forintellectual content
Continued
NeurologyorgN Neurology | Volume 94 Number 17 | April 28 2020 753
References1 Walker Z Possin KL Boeve BF Aarsland D Lewy body dementias Lancet 2015386
1683ndash16972 McKeith IG Boeve BF Dickson DW et al Diagnosis and management of dementia
with Lewy bodies fourth consensus report of the DLB consortium Neurology 20178988ndash100
3 Ferman TJ Smith GE Kantarci K et al Nonamnestic mild cognitive impairmentprogresses to dementia with Lewy bodies Neurology 2013812032ndash2038
4 Savica R Bradley BF Mielke MM When do alpha-synucleinopathies start An epi-demiological timeline A review JAMA Neurol 201875503ndash509
5 Donaghy PC Taylor JP OrsquoBrien JT et al Neuropsychiatric symptoms and cognitiveprofile in mild cognitive impairment with Lewy bodies Psychol Med 2018482384ndash2390
6 Cagnin A Bussse C Gardini S et al Clinical and cognitive phenotype of mildcognitive impairment evolving to dementia with Lewy bodies Dement Geriatr CognDis Extra 20155442ndash449
7 Postuma RB Iranzo A HuM et al Risk and predictors of dementia and parkinsonismin idiopathic REM sleep behaviour disorder a multicentre study Brain 2019142744ndash759
8 Sadiq D Whitfield T Lee L Stevens T Costafreda S Walker Z Prodromal dementiawith Lewy bodies and prodromal Alzheimerrsquos disease a comparison of the cognitiveand clinical profiles J Alzheimers Dis 201758463ndash470
9 FitzGerald JM Perera G Chang-Tave A et al The incidence of recorded de-lirium episodes before and after dementia diagnosis differences between de-mentia with Lewy bodies and Alzheimerrsquos disease J Am Med Dir Assoc 201920604ndash609
10 Jicha GA Schmitt FA Abner E et al Prodromal clinical manifestations of neu-ropathologically confirmed Lewy body disease Neurobiol Aging 2010311805ndash1813
11 Vardy E Holt R Gerhard A Richardson A Snowden J Neary D History of a sus-pected delirium is more common in dementia with Lewy bodies than Alzheimerrsquosdisease a retrospective study Int J Geriatr Psychiatry 201429178ndash181
12 Fujishiro H Nakamura S Sato K Iseki E Prodromal dementia with Lewy bodiesGeriatr Gerontol Int 201515817ndash826
13 McKeith I Taylor JP Thomas A Donaghy P Kane J Revisiting DLB diagnosisa consideration of prodromal DLB and of the diagnostic overlap with Alzheimerdisease J Geriatr Psychiatry Neurol 201629249ndash253
14 Albert MS DeKosky ST Dickson D et al The diagnosis of mild cognitive impairmentdue to Alzheimerrsquos disease recommendations from the National Institute on Aging-Alzheimerrsquos Association workgroups on diagnostic guidelines for Alzheimerrsquos diseaseAlzheimers Dement 20117270ndash279
15 Litvan I Goldman JG Troster AI et al Diagnostic criteria for mild cognitive im-pairment in Parkinsonrsquos disease Movement Disorder Society Task Force guidelinesMov Disord 201227349ndash356
16 Ferman TJ Smith GE Boeve BF et al Neuropsychological differentiation of de-mentia with Lewy bodies from normal aging and Alzheimerrsquos disease Clin Neuro-psychol 200620623ndash636
17 Cagnin A Busse C Jelcic N Gnoato F Mitolo M Caffarra P High specificity ofMMSE pentagon scoring for diagnosis of prodromal dementia with Lewy bodiesParkinsonism Relat Disord 201521303ndash305
18 Yoon JH Kim M Moon SY Yong SW Hong JM Olfactory function and neuro-psychological profile to differentiate dementia with Lewy bodies from Alzheimerrsquosdisease in patients with mild cognitive impairment a 5-year follow-up study J NeurolSci 2015355174ndash179
19 Kemp J Philippi N Phillipps C et al Cognitive profile in prodromal dementia withLewy bodies Alzheimers Res Ther 2017919
20 Auning E Rongve A Fladby T et al Early and presenting symptoms of dementia withLewy bodies Dement Geriatr Cogn Disord 201132202ndash208
21 Kondo D Ota K Kasanuki K et al Characteristics of mild cognitive impairmenttending to convert into Alzheimerrsquos disease or dementia with Lewy bodies a follow-upstudy in a memory clinic J Neurol Sci 2016369102ndash108
22 Marchand DG Postuma RB Escudier F et al How does dementia with Lewy bodiesstart prodromal cognitive changes in REM sleep behavior disorder Ann Neurol2018831016ndash1026
23 Kantarci K Lesnick T Ferman TJ et al Hippocampal volumes predict risk of de-mentia with Lewy bodies in mild cognitive impairment Neurology 2016872317ndash2323
24 Thomas AJ Taylor JP McKeith I et al Revision of assessment toolkits for improvingthe diagnosis of Lewy body dementia the DIAMOND Lewy study Int J GeriatrPsychiatry 2018331293ndash1304
25 Galvin JE Improving the clinical detection of Lewy body dementia with the Lewybody composite risk score Alzheimerrsquos Demen (Amsterdam Netherlands) 20151316ndash324
26 Belden CM Kahlon V Malek-Ahmadi M Tsai A Sabbagh MN Clinical character-ization of mild cognitive impairment as a prodrome to dementia with Lewy bodiesAm J Alzheimers Dis Other Demen 201530173ndash177
27 Yoon JH Lee JE Yong SW Moon SY Lee PH The mild cognitive impairment stageof dementia with Lewy bodies and Parkinson disease A comparison of cognitiveprofiles Alzheimer Dis Assoc Disord 201428151ndash155
28 Fengler S Liepelt-Scarfone I Brockmann K Schaffer E Berg D Kalbe E Cognitivechanges in prodromal Parkinsonrsquos disease a review Mov Disord 2017321655ndash1666
29 Kalbe E Rehberg SP Heber I et al Subtypes of mild cognitive impairment in patientswith Parkinsonrsquos disease evidence from the LANDSCAPE study J Neurol NeurosurgPsychiatry 2016871099ndash1105
30 Thomas AJ Donaghy P Roberts G et al Diagnostic accuracy of dopaminergic im-aging in prodromal dementia with Lewy bodies Psychol Med 20181ndash7
31 Ferman TJ Boeve BF Smith GE et al Inclusion of RBD improves the diagnosticclassification of dementia with Lewy bodies Neurology 201177875ndash882
32 Fujishiro H Okuda M Iwamoto K et al Early diagnosis of Lewy body disease inpatients with late-onset psychiatric disorders using clinical history of rapid eyemovement sleep behavior disorder and I-123 -metaiodobenzylguanidine cardiacscintigraphy Psychiatry Clin Neurosci 201872423ndash434
33 Bonanni L Perfetti B Bifolchetti S et al Quantitative electroencephalogram utility inpredicting conversion of mild cognitive impairment to dementia with Lewy bodiesNeurobiol Aging 201536434ndash445
34 Murray ME Ferman TJ Boeve BF et al MRI and pathology of REM sleep behaviordisorder in dementia with Lewy bodies Neurology 2013811681ndash1689
35 Murray ME Graff-Radford NR Ross OA Petersen RC Duara R Dickson DWNeuropathologically defined subtypes of Alzheimerrsquos disease with distinct clinicalcharacteristics a retrospective study Lancet Neurol 201110785ndash796
36 Blanc F Colloby SJ Cretin B et al Grey matter atrophy in prodromal stage ofdementia with Lewy bodies and Alzheimerrsquos disease Alzheimers Res Ther 2016831
37 Blanc F Colloby SJ Philippi N et al Cortical thickness in dementia with Lewy bodiesand Alzheimerrsquos disease a comparison of prodromal and dementia stages Plos One201510e0127396
38 Surendranathan A OrsquoBrien JT Clinical imaging in dementia with Lewy bodies EvidBased Ment Health 20182161ndash65
39 Outeiro TF Koss DJ Erskine D et al Dementia with Lewy bodies an update andoutlook Mol Neurodegener 2019145
40 Donadio V Incensi A Rizzo G et al A new potential biomarker for dementiawith Lewy bodies Skin nerve alpha-synuclein deposits Neurology 201789318ndash326
41 Flanigan PM Khosravi MA Leverenz JB Tousi B Color vision impairment differ-entiates Alzheimer dementia from dementia with Lewy bodies J Geriatr PsychiatryNeurol 20183197ndash102
42 Fereshtehnejad SM Yao C Pelletier A Montplaisir JY Gagnon JF Postuma RBEvolution of prodromal Parkinsonrsquos disease and dementia with Lewy bodies a pro-spective study Brain 20191422051ndash2067
43 Bousiges O Bombois S Schraen S et al Cerebrospinal fluid Alzheimer biomarkerscan be useful for discriminating dementia with Lewy bodies from Alzheimerrsquos diseaseat the prodromal stage J Neurol Neurosurg Psychiatry 201889467ndash475
44 Kantarci K Lowe VJ Boeve BF et al Multimodality imaging characteristics of de-mentia with Lewy bodies Neurobiol Aging 2012332091ndash2105
45 Kantarci K Lowe VJ Boeve BF et al AV-1451 tau and beta-amyloid positronemission tomography imaging in dementia with Lewy bodies Ann Neurol 20178158ndash67
46 Gore RL Vardy E OrsquoBrien JT Delirium and dementia with Lewy bodies distinctdiagnoses or part of the same spectrum J Neurol Neurosurg Psychiatry 20158650ndash59
47 Aarsland DS Auning E The pre-dementia stage of dementia with Lewy bodies Eur JNeurol 20111869
48 Sunwoo MK Hong JY Choi J Park HJ Kim SH Lee PH alpha-Synuclein pathologyis related to postoperative delirium in patients undergoing gastrectomy Neurology201380810ndash813
49 Akintade O Pierres F Acute presentation of dementia with Lewy bodies Clin Med201919327ndash330
50 Kosaka K Diffuse Lewy body disease in Japan J Neurol 1990237197ndash20451 Birkett DP Desouky A Han L Kaufman M Lewy bodies in psychiatric patients Int J
Geriatr Psychiatry 19927235ndash240
Appendix (continued)
Name Location Contribution
John PaulTaylor MBBS PhD
Newcastle University Revising the manuscript forintellectual content
Debby WTsuang MD
VA Puget Sound ampUniversity ofWashington
Revising the manuscript forintellectual content
ZuzanaWalker MD
University CollegeLondon
Revising the manuscript forintellectual content
PietroTiraboschiMD
Istituto NeurologicoldquoCarlo Bestardquo Milan
Design and conceptualizationof the study acquisition ofdata analysis andinterpretation of the data anddrafting and revising themanuscript for intellectualcontent
754 Neurology | Volume 94 Number 17 | April 28 2020 NeurologyorgN
52 Kobayashi K Nakano H Akiyama N Maeda T Yamamori S Pure psychiatric pre-sentation of the Lewy body disease is depressionmdashan analysis of 60 cases verified withmyocardial meta-iodobenzylguanidine study Int J Geriatr Psychiatry 201530663ndash668
53 Takahashi S Mizukami K Arai T et al Ventilatory response to hypercapnia predictsdementia with Lewy bodies in late-onset major depressive disorder J Alzheimers Dis201650751ndash758
54 Van Assche L Van Aubel E Van de Ven L Bouckaert F Luyten P Vandenbulcke MThe neuropsychological profile and phenomenology of late onset psychosis a cross-sectional study on the differential diagnosis of very-late-onset Schizophrenia-likepsychosis dementia with Lewy bodies and Alzheimerrsquos type dementia with psychosisArch Clin Neuropsychol 201934183ndash199
55 Thaipisuttikul P Lobach I Zweig Y Gurnani A Galvin JE Capgras syndrome indementia with Lewy bodies Int Psychogeriatr 201325843ndash849
56 Fujishiro H Iseki E Nakamura S et al Dementia with Lewy bodies early diagnosticchallenges Psychogeriatrics 201313128ndash138
57 Chiba Y Fujishiro H Iseki E et al Retrospective survey of prodromal symptoms indementia with Lewy bodies comparison with Alzheimerrsquos disease Dement GeriatrCogn Disord 201233273ndash281
58 Kaufmann H Norcliffe-Kaufmann L Palma JA et al Natural history of pure auto-nomic failure a United States prospective cohort Ann Neurol 201781287ndash297
59 Heinzel S Berg D Gasser T et al Update of the MDS research criteria for prodromalParkinsonrsquos disease Mov Disord 2019341464ndash1470
60 Palma JA Norcliffe-Kaufmann L Kaufmann H Diagnosis of multiple system atrophyAuton Neurosci 201821115ndash25Data available fromDryad (Additional References References e1ndashe44) doi105061dryad1c59zw3rv
Subspecialty Alerts by E-mail
Customize your online journal experience by signing up for e-mail alerts related to your subspecialty or area of interest Accessthis free service by clicking on the ldquoMy Alertsrdquo link on the home page An extensive list of subspecialties methods and studydesign choices will be available for you to choose frommdashallowing you priority alerts to cutting-edge research in your field
COVID-19 and Neurologic Disease Call for Papers
The editors of Neurology are interested in papers that address the neurological aspects of COVID-19infection and challenges to the management of patients with chronic neurological conditions whohave or are at risk for the infection Relevant papers that pass initial internal review will undergoexpedited peer review and online publication We will consider papers posted in preprint servers
Submit observational studies and clinical trials as Articles and case series and case reports underthe ClinicalScientific Notes category to httpssubmitneurologyorg today
Visit the Neurologyreg Website at NeurologyorgN More article-based content on home pages Streamlined menus and navigation Enhanced blog sections for specialty areas Same experience on desktop tablet and mobile devices Improved article reading experience links more evident (pdf analytics social media) Neurologyreg Clinical Practice initiative ldquoPractice Currentrdquo global surveys will be accessible across sites
Find Neurologyreg on Facebook httptinyurlcomneurologyfan
Follow Neurologyreg on Twitter httpstwittercomGreenJournal
NeurologyorgN Neurology | Volume 94 Number 17 | April 28 2020 755
DOI 101212WNL0000000000009323202094743-755 Published Online before print April 2 2020Neurology
Ian G McKeith Tanis J Ferman Alan J Thomas et al Research criteria for the diagnosis of prodromal dementia with Lewy bodies
This information is current as of April 2 2020
ServicesUpdated Information amp
httpnneurologyorgcontent9417743fullincluding high resolution figures can be found at
References httpnneurologyorgcontent9417743fullref-list-1
This article cites 59 articles 12 of which you can access for free at
Subspecialty Collections
httpnneurologyorgcgicollectionpsychosisPsychosis a
httpnneurologyorgcgicollectionparkinsons_disease_with_dementiParkinsons disease with dementia
httpnneurologyorgcgicollectionmci_mild_cognitive_impairmentMCI (mild cognitive impairment)
httpnneurologyorgcgicollectiondementia_with_lewy_bodiesDementia with Lewy bodies
httpnneurologyorgcgicollectiondeliriumDeliriumfollowing collection(s) This article along with others on similar topics appears in the
Permissions amp Licensing
httpwwwneurologyorgaboutabout_the_journalpermissionsits entirety can be found online atInformation about reproducing this article in parts (figurestables) or in
Reprints
httpnneurologyorgsubscribersadvertiseInformation about ordering reprints can be found online
ISSN 0028-3878 Online ISSN 1526-632XWolters Kluwer Health Inc on behalf of the American Academy of Neurology All rights reserved Print1951 it is now a weekly with 48 issues per year Copyright Copyright copy 2020 The Author(s) Published by
reg is the official journal of the American Academy of Neurology Published continuously sinceNeurology

Molecular Imaging P Tiraboschi acknowledges the support ofthe Italian Ministry of Health GRANT NET-2011-02346784Go to NeurologyorgN for full disclosures
Publication historyReceived by Neurology October 30 2019 Accepted in final formFebruary 25 2020
Appendix Authors
Name Location Contribution
Ian GMcKeith FMed Sci MD
Newcastle University Design and conceptualizationof the study acquisition ofdata analysis andinterpretation of the data anddrafting and revising themanuscript for intellectualcontent
Tanis JFermanPhD
Mayo ClinicJacksonville
Design and conceptualizationof the study acquisition ofdata analysis andinterpretation of the data anddrafting and revising themanuscript for intellectualcontent
Alan JThomasPhD
Newcastle University Design and conceptualizationof the study acquisition ofdata analysis andinterpretation of the data anddrafting and revising themanuscript for intellectualcontent
FredericBlanc MD
University ofStrasbourg
Design and conceptualizationof the study acquisition ofdata analysis andinterpretation of the data anddrafting and revising themanuscript for intellectualcontent
Bradley FBoeve MD
Mayo Clinic Rochester Design and conceptualizationof the study acquisition ofdata analysis andinterpretation of the data anddrafting and revising themanuscript for intellectualcontent
HiroshigeFujishiroMD
Nagoya UniversityKawasaki MemorialHospital
Design and conceptualizationof the study acquisition ofdata analysis andinterpretation of the data anddrafting and revising themanuscript for intellectualcontent
KejalKantarciMD MS
Mayo Clinic Rochester Design and conceptualizationof the study acquisition ofdata analysis andinterpretation of the data anddrafting and revising themanuscript for intellectualcontent
CristinaMuscio PhD
Istituto NeurologicoldquoCarlo Bestardquo Milan
Design and conceptualizationof the study acquisition ofdata analysis andinterpretation of the data anddrafting and revising themanuscript for intellectualcontent
Appendix (continued)
Name Location Contribution
John TOrsquoBrien FMed Sci DM
Cambridge University Design and conceptualizationof the study acquisition ofdata analysis andinterpretation of the data anddrafting and revising themanuscript for intellectualcontent
Ronald BPostumaMD MSc
McGill University Design and conceptualizationof the study acquisition ofdata analysis andinterpretation of the data anddrafting and revising themanuscript for intellectualcontent
DagAarslandPhD
Kingrsquos College Londonand StavangerUniversityHospital
Revising the manuscript forintellectual content
CliveBallard MD
University of Exeter Revising the manuscript forintellectual content
LauraBonanniMD PhD
University of Chieti-Pescara
Revising the manuscript forintellectual content
PaulDonaghyPhD
Newcastle University Revising the manuscript forintellectual content
Murat EmreMD
Istanbul Faculty ofMedicine
Revising the manuscript forintellectual content
James EGalvin MDMPH
University of MiamiMiller School ofMedicine
Revising the manuscript forintellectual content
DouglasGalasko MD
University of CaliforniaSan Diego
Revising the manuscript forintellectual content
Jennifer GGoldmanMD MS
Feinberg School ofMedicine
Revising the manuscript forintellectual content
Stephen NGompertsMD PhD
Massachusetts GeneralHospital
Revising the manuscript forintellectual content
Lawrence SHonig MDPhD
Columbia UniversityIrving Medical Center
Revising the manuscript forintellectual content
ManabuIkeda MDPhD
Osaka University Revising the manuscript forintellectual content
James BLeverenzMD
Lou Ruvo Center ofBrain Health ClevelandClinic
Revising the manuscript forintellectual content
Simon JGLewis MD
University of Sydney Revising the manuscript forintellectual content
Karen SMarder MDMPH
Columbia UniversityIrving Medical Center
Revising the manuscript forintellectual content
MarioMasellisMD PhD
Sunnybrook HealthSciences CentreUniversity of Toronto
Revising the manuscript forintellectual content
David PSalmon PhD
University of CaliforniaSan Diego
Revising the manuscript forintellectual content
Continued
NeurologyorgN Neurology | Volume 94 Number 17 | April 28 2020 753
References1 Walker Z Possin KL Boeve BF Aarsland D Lewy body dementias Lancet 2015386
1683ndash16972 McKeith IG Boeve BF Dickson DW et al Diagnosis and management of dementia
with Lewy bodies fourth consensus report of the DLB consortium Neurology 20178988ndash100
3 Ferman TJ Smith GE Kantarci K et al Nonamnestic mild cognitive impairmentprogresses to dementia with Lewy bodies Neurology 2013812032ndash2038
4 Savica R Bradley BF Mielke MM When do alpha-synucleinopathies start An epi-demiological timeline A review JAMA Neurol 201875503ndash509
5 Donaghy PC Taylor JP OrsquoBrien JT et al Neuropsychiatric symptoms and cognitiveprofile in mild cognitive impairment with Lewy bodies Psychol Med 2018482384ndash2390
6 Cagnin A Bussse C Gardini S et al Clinical and cognitive phenotype of mildcognitive impairment evolving to dementia with Lewy bodies Dement Geriatr CognDis Extra 20155442ndash449
7 Postuma RB Iranzo A HuM et al Risk and predictors of dementia and parkinsonismin idiopathic REM sleep behaviour disorder a multicentre study Brain 2019142744ndash759
8 Sadiq D Whitfield T Lee L Stevens T Costafreda S Walker Z Prodromal dementiawith Lewy bodies and prodromal Alzheimerrsquos disease a comparison of the cognitiveand clinical profiles J Alzheimers Dis 201758463ndash470
9 FitzGerald JM Perera G Chang-Tave A et al The incidence of recorded de-lirium episodes before and after dementia diagnosis differences between de-mentia with Lewy bodies and Alzheimerrsquos disease J Am Med Dir Assoc 201920604ndash609
10 Jicha GA Schmitt FA Abner E et al Prodromal clinical manifestations of neu-ropathologically confirmed Lewy body disease Neurobiol Aging 2010311805ndash1813
11 Vardy E Holt R Gerhard A Richardson A Snowden J Neary D History of a sus-pected delirium is more common in dementia with Lewy bodies than Alzheimerrsquosdisease a retrospective study Int J Geriatr Psychiatry 201429178ndash181
12 Fujishiro H Nakamura S Sato K Iseki E Prodromal dementia with Lewy bodiesGeriatr Gerontol Int 201515817ndash826
13 McKeith I Taylor JP Thomas A Donaghy P Kane J Revisiting DLB diagnosisa consideration of prodromal DLB and of the diagnostic overlap with Alzheimerdisease J Geriatr Psychiatry Neurol 201629249ndash253
14 Albert MS DeKosky ST Dickson D et al The diagnosis of mild cognitive impairmentdue to Alzheimerrsquos disease recommendations from the National Institute on Aging-Alzheimerrsquos Association workgroups on diagnostic guidelines for Alzheimerrsquos diseaseAlzheimers Dement 20117270ndash279
15 Litvan I Goldman JG Troster AI et al Diagnostic criteria for mild cognitive im-pairment in Parkinsonrsquos disease Movement Disorder Society Task Force guidelinesMov Disord 201227349ndash356
16 Ferman TJ Smith GE Boeve BF et al Neuropsychological differentiation of de-mentia with Lewy bodies from normal aging and Alzheimerrsquos disease Clin Neuro-psychol 200620623ndash636
17 Cagnin A Busse C Jelcic N Gnoato F Mitolo M Caffarra P High specificity ofMMSE pentagon scoring for diagnosis of prodromal dementia with Lewy bodiesParkinsonism Relat Disord 201521303ndash305
18 Yoon JH Kim M Moon SY Yong SW Hong JM Olfactory function and neuro-psychological profile to differentiate dementia with Lewy bodies from Alzheimerrsquosdisease in patients with mild cognitive impairment a 5-year follow-up study J NeurolSci 2015355174ndash179
19 Kemp J Philippi N Phillipps C et al Cognitive profile in prodromal dementia withLewy bodies Alzheimers Res Ther 2017919
20 Auning E Rongve A Fladby T et al Early and presenting symptoms of dementia withLewy bodies Dement Geriatr Cogn Disord 201132202ndash208
21 Kondo D Ota K Kasanuki K et al Characteristics of mild cognitive impairmenttending to convert into Alzheimerrsquos disease or dementia with Lewy bodies a follow-upstudy in a memory clinic J Neurol Sci 2016369102ndash108
22 Marchand DG Postuma RB Escudier F et al How does dementia with Lewy bodiesstart prodromal cognitive changes in REM sleep behavior disorder Ann Neurol2018831016ndash1026
23 Kantarci K Lesnick T Ferman TJ et al Hippocampal volumes predict risk of de-mentia with Lewy bodies in mild cognitive impairment Neurology 2016872317ndash2323
24 Thomas AJ Taylor JP McKeith I et al Revision of assessment toolkits for improvingthe diagnosis of Lewy body dementia the DIAMOND Lewy study Int J GeriatrPsychiatry 2018331293ndash1304
25 Galvin JE Improving the clinical detection of Lewy body dementia with the Lewybody composite risk score Alzheimerrsquos Demen (Amsterdam Netherlands) 20151316ndash324
26 Belden CM Kahlon V Malek-Ahmadi M Tsai A Sabbagh MN Clinical character-ization of mild cognitive impairment as a prodrome to dementia with Lewy bodiesAm J Alzheimers Dis Other Demen 201530173ndash177
27 Yoon JH Lee JE Yong SW Moon SY Lee PH The mild cognitive impairment stageof dementia with Lewy bodies and Parkinson disease A comparison of cognitiveprofiles Alzheimer Dis Assoc Disord 201428151ndash155
28 Fengler S Liepelt-Scarfone I Brockmann K Schaffer E Berg D Kalbe E Cognitivechanges in prodromal Parkinsonrsquos disease a review Mov Disord 2017321655ndash1666
29 Kalbe E Rehberg SP Heber I et al Subtypes of mild cognitive impairment in patientswith Parkinsonrsquos disease evidence from the LANDSCAPE study J Neurol NeurosurgPsychiatry 2016871099ndash1105
30 Thomas AJ Donaghy P Roberts G et al Diagnostic accuracy of dopaminergic im-aging in prodromal dementia with Lewy bodies Psychol Med 20181ndash7
31 Ferman TJ Boeve BF Smith GE et al Inclusion of RBD improves the diagnosticclassification of dementia with Lewy bodies Neurology 201177875ndash882
32 Fujishiro H Okuda M Iwamoto K et al Early diagnosis of Lewy body disease inpatients with late-onset psychiatric disorders using clinical history of rapid eyemovement sleep behavior disorder and I-123 -metaiodobenzylguanidine cardiacscintigraphy Psychiatry Clin Neurosci 201872423ndash434
33 Bonanni L Perfetti B Bifolchetti S et al Quantitative electroencephalogram utility inpredicting conversion of mild cognitive impairment to dementia with Lewy bodiesNeurobiol Aging 201536434ndash445
34 Murray ME Ferman TJ Boeve BF et al MRI and pathology of REM sleep behaviordisorder in dementia with Lewy bodies Neurology 2013811681ndash1689
35 Murray ME Graff-Radford NR Ross OA Petersen RC Duara R Dickson DWNeuropathologically defined subtypes of Alzheimerrsquos disease with distinct clinicalcharacteristics a retrospective study Lancet Neurol 201110785ndash796
36 Blanc F Colloby SJ Cretin B et al Grey matter atrophy in prodromal stage ofdementia with Lewy bodies and Alzheimerrsquos disease Alzheimers Res Ther 2016831
37 Blanc F Colloby SJ Philippi N et al Cortical thickness in dementia with Lewy bodiesand Alzheimerrsquos disease a comparison of prodromal and dementia stages Plos One201510e0127396
38 Surendranathan A OrsquoBrien JT Clinical imaging in dementia with Lewy bodies EvidBased Ment Health 20182161ndash65
39 Outeiro TF Koss DJ Erskine D et al Dementia with Lewy bodies an update andoutlook Mol Neurodegener 2019145
40 Donadio V Incensi A Rizzo G et al A new potential biomarker for dementiawith Lewy bodies Skin nerve alpha-synuclein deposits Neurology 201789318ndash326
41 Flanigan PM Khosravi MA Leverenz JB Tousi B Color vision impairment differ-entiates Alzheimer dementia from dementia with Lewy bodies J Geriatr PsychiatryNeurol 20183197ndash102
42 Fereshtehnejad SM Yao C Pelletier A Montplaisir JY Gagnon JF Postuma RBEvolution of prodromal Parkinsonrsquos disease and dementia with Lewy bodies a pro-spective study Brain 20191422051ndash2067
43 Bousiges O Bombois S Schraen S et al Cerebrospinal fluid Alzheimer biomarkerscan be useful for discriminating dementia with Lewy bodies from Alzheimerrsquos diseaseat the prodromal stage J Neurol Neurosurg Psychiatry 201889467ndash475
44 Kantarci K Lowe VJ Boeve BF et al Multimodality imaging characteristics of de-mentia with Lewy bodies Neurobiol Aging 2012332091ndash2105
45 Kantarci K Lowe VJ Boeve BF et al AV-1451 tau and beta-amyloid positronemission tomography imaging in dementia with Lewy bodies Ann Neurol 20178158ndash67
46 Gore RL Vardy E OrsquoBrien JT Delirium and dementia with Lewy bodies distinctdiagnoses or part of the same spectrum J Neurol Neurosurg Psychiatry 20158650ndash59
47 Aarsland DS Auning E The pre-dementia stage of dementia with Lewy bodies Eur JNeurol 20111869
48 Sunwoo MK Hong JY Choi J Park HJ Kim SH Lee PH alpha-Synuclein pathologyis related to postoperative delirium in patients undergoing gastrectomy Neurology201380810ndash813
49 Akintade O Pierres F Acute presentation of dementia with Lewy bodies Clin Med201919327ndash330
50 Kosaka K Diffuse Lewy body disease in Japan J Neurol 1990237197ndash20451 Birkett DP Desouky A Han L Kaufman M Lewy bodies in psychiatric patients Int J
Geriatr Psychiatry 19927235ndash240
Appendix (continued)
Name Location Contribution
John PaulTaylor MBBS PhD
Newcastle University Revising the manuscript forintellectual content
Debby WTsuang MD
VA Puget Sound ampUniversity ofWashington
Revising the manuscript forintellectual content
ZuzanaWalker MD
University CollegeLondon
Revising the manuscript forintellectual content
PietroTiraboschiMD
Istituto NeurologicoldquoCarlo Bestardquo Milan
Design and conceptualizationof the study acquisition ofdata analysis andinterpretation of the data anddrafting and revising themanuscript for intellectualcontent
754 Neurology | Volume 94 Number 17 | April 28 2020 NeurologyorgN
52 Kobayashi K Nakano H Akiyama N Maeda T Yamamori S Pure psychiatric pre-sentation of the Lewy body disease is depressionmdashan analysis of 60 cases verified withmyocardial meta-iodobenzylguanidine study Int J Geriatr Psychiatry 201530663ndash668
53 Takahashi S Mizukami K Arai T et al Ventilatory response to hypercapnia predictsdementia with Lewy bodies in late-onset major depressive disorder J Alzheimers Dis201650751ndash758
54 Van Assche L Van Aubel E Van de Ven L Bouckaert F Luyten P Vandenbulcke MThe neuropsychological profile and phenomenology of late onset psychosis a cross-sectional study on the differential diagnosis of very-late-onset Schizophrenia-likepsychosis dementia with Lewy bodies and Alzheimerrsquos type dementia with psychosisArch Clin Neuropsychol 201934183ndash199
55 Thaipisuttikul P Lobach I Zweig Y Gurnani A Galvin JE Capgras syndrome indementia with Lewy bodies Int Psychogeriatr 201325843ndash849
56 Fujishiro H Iseki E Nakamura S et al Dementia with Lewy bodies early diagnosticchallenges Psychogeriatrics 201313128ndash138
57 Chiba Y Fujishiro H Iseki E et al Retrospective survey of prodromal symptoms indementia with Lewy bodies comparison with Alzheimerrsquos disease Dement GeriatrCogn Disord 201233273ndash281
58 Kaufmann H Norcliffe-Kaufmann L Palma JA et al Natural history of pure auto-nomic failure a United States prospective cohort Ann Neurol 201781287ndash297
59 Heinzel S Berg D Gasser T et al Update of the MDS research criteria for prodromalParkinsonrsquos disease Mov Disord 2019341464ndash1470
60 Palma JA Norcliffe-Kaufmann L Kaufmann H Diagnosis of multiple system atrophyAuton Neurosci 201821115ndash25Data available fromDryad (Additional References References e1ndashe44) doi105061dryad1c59zw3rv
Subspecialty Alerts by E-mail
Customize your online journal experience by signing up for e-mail alerts related to your subspecialty or area of interest Accessthis free service by clicking on the ldquoMy Alertsrdquo link on the home page An extensive list of subspecialties methods and studydesign choices will be available for you to choose frommdashallowing you priority alerts to cutting-edge research in your field
COVID-19 and Neurologic Disease Call for Papers
The editors of Neurology are interested in papers that address the neurological aspects of COVID-19infection and challenges to the management of patients with chronic neurological conditions whohave or are at risk for the infection Relevant papers that pass initial internal review will undergoexpedited peer review and online publication We will consider papers posted in preprint servers
Submit observational studies and clinical trials as Articles and case series and case reports underthe ClinicalScientific Notes category to httpssubmitneurologyorg today
Visit the Neurologyreg Website at NeurologyorgN More article-based content on home pages Streamlined menus and navigation Enhanced blog sections for specialty areas Same experience on desktop tablet and mobile devices Improved article reading experience links more evident (pdf analytics social media) Neurologyreg Clinical Practice initiative ldquoPractice Currentrdquo global surveys will be accessible across sites
Find Neurologyreg on Facebook httptinyurlcomneurologyfan
Follow Neurologyreg on Twitter httpstwittercomGreenJournal
NeurologyorgN Neurology | Volume 94 Number 17 | April 28 2020 755
DOI 101212WNL0000000000009323202094743-755 Published Online before print April 2 2020Neurology
Ian G McKeith Tanis J Ferman Alan J Thomas et al Research criteria for the diagnosis of prodromal dementia with Lewy bodies
This information is current as of April 2 2020
ServicesUpdated Information amp
httpnneurologyorgcontent9417743fullincluding high resolution figures can be found at
References httpnneurologyorgcontent9417743fullref-list-1
This article cites 59 articles 12 of which you can access for free at
Subspecialty Collections
httpnneurologyorgcgicollectionpsychosisPsychosis a
httpnneurologyorgcgicollectionparkinsons_disease_with_dementiParkinsons disease with dementia
httpnneurologyorgcgicollectionmci_mild_cognitive_impairmentMCI (mild cognitive impairment)
httpnneurologyorgcgicollectiondementia_with_lewy_bodiesDementia with Lewy bodies
httpnneurologyorgcgicollectiondeliriumDeliriumfollowing collection(s) This article along with others on similar topics appears in the
Permissions amp Licensing
httpwwwneurologyorgaboutabout_the_journalpermissionsits entirety can be found online atInformation about reproducing this article in parts (figurestables) or in
Reprints
httpnneurologyorgsubscribersadvertiseInformation about ordering reprints can be found online
ISSN 0028-3878 Online ISSN 1526-632XWolters Kluwer Health Inc on behalf of the American Academy of Neurology All rights reserved Print1951 it is now a weekly with 48 issues per year Copyright Copyright copy 2020 The Author(s) Published by
reg is the official journal of the American Academy of Neurology Published continuously sinceNeurology

References1 Walker Z Possin KL Boeve BF Aarsland D Lewy body dementias Lancet 2015386
1683ndash16972 McKeith IG Boeve BF Dickson DW et al Diagnosis and management of dementia
with Lewy bodies fourth consensus report of the DLB consortium Neurology 20178988ndash100
3 Ferman TJ Smith GE Kantarci K et al Nonamnestic mild cognitive impairmentprogresses to dementia with Lewy bodies Neurology 2013812032ndash2038
4 Savica R Bradley BF Mielke MM When do alpha-synucleinopathies start An epi-demiological timeline A review JAMA Neurol 201875503ndash509
5 Donaghy PC Taylor JP OrsquoBrien JT et al Neuropsychiatric symptoms and cognitiveprofile in mild cognitive impairment with Lewy bodies Psychol Med 2018482384ndash2390
6 Cagnin A Bussse C Gardini S et al Clinical and cognitive phenotype of mildcognitive impairment evolving to dementia with Lewy bodies Dement Geriatr CognDis Extra 20155442ndash449
7 Postuma RB Iranzo A HuM et al Risk and predictors of dementia and parkinsonismin idiopathic REM sleep behaviour disorder a multicentre study Brain 2019142744ndash759
8 Sadiq D Whitfield T Lee L Stevens T Costafreda S Walker Z Prodromal dementiawith Lewy bodies and prodromal Alzheimerrsquos disease a comparison of the cognitiveand clinical profiles J Alzheimers Dis 201758463ndash470
9 FitzGerald JM Perera G Chang-Tave A et al The incidence of recorded de-lirium episodes before and after dementia diagnosis differences between de-mentia with Lewy bodies and Alzheimerrsquos disease J Am Med Dir Assoc 201920604ndash609
10 Jicha GA Schmitt FA Abner E et al Prodromal clinical manifestations of neu-ropathologically confirmed Lewy body disease Neurobiol Aging 2010311805ndash1813
11 Vardy E Holt R Gerhard A Richardson A Snowden J Neary D History of a sus-pected delirium is more common in dementia with Lewy bodies than Alzheimerrsquosdisease a retrospective study Int J Geriatr Psychiatry 201429178ndash181
12 Fujishiro H Nakamura S Sato K Iseki E Prodromal dementia with Lewy bodiesGeriatr Gerontol Int 201515817ndash826
13 McKeith I Taylor JP Thomas A Donaghy P Kane J Revisiting DLB diagnosisa consideration of prodromal DLB and of the diagnostic overlap with Alzheimerdisease J Geriatr Psychiatry Neurol 201629249ndash253
14 Albert MS DeKosky ST Dickson D et al The diagnosis of mild cognitive impairmentdue to Alzheimerrsquos disease recommendations from the National Institute on Aging-Alzheimerrsquos Association workgroups on diagnostic guidelines for Alzheimerrsquos diseaseAlzheimers Dement 20117270ndash279
15 Litvan I Goldman JG Troster AI et al Diagnostic criteria for mild cognitive im-pairment in Parkinsonrsquos disease Movement Disorder Society Task Force guidelinesMov Disord 201227349ndash356
16 Ferman TJ Smith GE Boeve BF et al Neuropsychological differentiation of de-mentia with Lewy bodies from normal aging and Alzheimerrsquos disease Clin Neuro-psychol 200620623ndash636
17 Cagnin A Busse C Jelcic N Gnoato F Mitolo M Caffarra P High specificity ofMMSE pentagon scoring for diagnosis of prodromal dementia with Lewy bodiesParkinsonism Relat Disord 201521303ndash305
18 Yoon JH Kim M Moon SY Yong SW Hong JM Olfactory function and neuro-psychological profile to differentiate dementia with Lewy bodies from Alzheimerrsquosdisease in patients with mild cognitive impairment a 5-year follow-up study J NeurolSci 2015355174ndash179
19 Kemp J Philippi N Phillipps C et al Cognitive profile in prodromal dementia withLewy bodies Alzheimers Res Ther 2017919
20 Auning E Rongve A Fladby T et al Early and presenting symptoms of dementia withLewy bodies Dement Geriatr Cogn Disord 201132202ndash208
21 Kondo D Ota K Kasanuki K et al Characteristics of mild cognitive impairmenttending to convert into Alzheimerrsquos disease or dementia with Lewy bodies a follow-upstudy in a memory clinic J Neurol Sci 2016369102ndash108
22 Marchand DG Postuma RB Escudier F et al How does dementia with Lewy bodiesstart prodromal cognitive changes in REM sleep behavior disorder Ann Neurol2018831016ndash1026
23 Kantarci K Lesnick T Ferman TJ et al Hippocampal volumes predict risk of de-mentia with Lewy bodies in mild cognitive impairment Neurology 2016872317ndash2323
24 Thomas AJ Taylor JP McKeith I et al Revision of assessment toolkits for improvingthe diagnosis of Lewy body dementia the DIAMOND Lewy study Int J GeriatrPsychiatry 2018331293ndash1304
25 Galvin JE Improving the clinical detection of Lewy body dementia with the Lewybody composite risk score Alzheimerrsquos Demen (Amsterdam Netherlands) 20151316ndash324
26 Belden CM Kahlon V Malek-Ahmadi M Tsai A Sabbagh MN Clinical character-ization of mild cognitive impairment as a prodrome to dementia with Lewy bodiesAm J Alzheimers Dis Other Demen 201530173ndash177
27 Yoon JH Lee JE Yong SW Moon SY Lee PH The mild cognitive impairment stageof dementia with Lewy bodies and Parkinson disease A comparison of cognitiveprofiles Alzheimer Dis Assoc Disord 201428151ndash155
28 Fengler S Liepelt-Scarfone I Brockmann K Schaffer E Berg D Kalbe E Cognitivechanges in prodromal Parkinsonrsquos disease a review Mov Disord 2017321655ndash1666
29 Kalbe E Rehberg SP Heber I et al Subtypes of mild cognitive impairment in patientswith Parkinsonrsquos disease evidence from the LANDSCAPE study J Neurol NeurosurgPsychiatry 2016871099ndash1105
30 Thomas AJ Donaghy P Roberts G et al Diagnostic accuracy of dopaminergic im-aging in prodromal dementia with Lewy bodies Psychol Med 20181ndash7
31 Ferman TJ Boeve BF Smith GE et al Inclusion of RBD improves the diagnosticclassification of dementia with Lewy bodies Neurology 201177875ndash882
32 Fujishiro H Okuda M Iwamoto K et al Early diagnosis of Lewy body disease inpatients with late-onset psychiatric disorders using clinical history of rapid eyemovement sleep behavior disorder and I-123 -metaiodobenzylguanidine cardiacscintigraphy Psychiatry Clin Neurosci 201872423ndash434
33 Bonanni L Perfetti B Bifolchetti S et al Quantitative electroencephalogram utility inpredicting conversion of mild cognitive impairment to dementia with Lewy bodiesNeurobiol Aging 201536434ndash445
34 Murray ME Ferman TJ Boeve BF et al MRI and pathology of REM sleep behaviordisorder in dementia with Lewy bodies Neurology 2013811681ndash1689
35 Murray ME Graff-Radford NR Ross OA Petersen RC Duara R Dickson DWNeuropathologically defined subtypes of Alzheimerrsquos disease with distinct clinicalcharacteristics a retrospective study Lancet Neurol 201110785ndash796
36 Blanc F Colloby SJ Cretin B et al Grey matter atrophy in prodromal stage ofdementia with Lewy bodies and Alzheimerrsquos disease Alzheimers Res Ther 2016831
37 Blanc F Colloby SJ Philippi N et al Cortical thickness in dementia with Lewy bodiesand Alzheimerrsquos disease a comparison of prodromal and dementia stages Plos One201510e0127396
38 Surendranathan A OrsquoBrien JT Clinical imaging in dementia with Lewy bodies EvidBased Ment Health 20182161ndash65
39 Outeiro TF Koss DJ Erskine D et al Dementia with Lewy bodies an update andoutlook Mol Neurodegener 2019145
40 Donadio V Incensi A Rizzo G et al A new potential biomarker for dementiawith Lewy bodies Skin nerve alpha-synuclein deposits Neurology 201789318ndash326
41 Flanigan PM Khosravi MA Leverenz JB Tousi B Color vision impairment differ-entiates Alzheimer dementia from dementia with Lewy bodies J Geriatr PsychiatryNeurol 20183197ndash102
42 Fereshtehnejad SM Yao C Pelletier A Montplaisir JY Gagnon JF Postuma RBEvolution of prodromal Parkinsonrsquos disease and dementia with Lewy bodies a pro-spective study Brain 20191422051ndash2067
43 Bousiges O Bombois S Schraen S et al Cerebrospinal fluid Alzheimer biomarkerscan be useful for discriminating dementia with Lewy bodies from Alzheimerrsquos diseaseat the prodromal stage J Neurol Neurosurg Psychiatry 201889467ndash475
44 Kantarci K Lowe VJ Boeve BF et al Multimodality imaging characteristics of de-mentia with Lewy bodies Neurobiol Aging 2012332091ndash2105
45 Kantarci K Lowe VJ Boeve BF et al AV-1451 tau and beta-amyloid positronemission tomography imaging in dementia with Lewy bodies Ann Neurol 20178158ndash67
46 Gore RL Vardy E OrsquoBrien JT Delirium and dementia with Lewy bodies distinctdiagnoses or part of the same spectrum J Neurol Neurosurg Psychiatry 20158650ndash59
47 Aarsland DS Auning E The pre-dementia stage of dementia with Lewy bodies Eur JNeurol 20111869
48 Sunwoo MK Hong JY Choi J Park HJ Kim SH Lee PH alpha-Synuclein pathologyis related to postoperative delirium in patients undergoing gastrectomy Neurology201380810ndash813
49 Akintade O Pierres F Acute presentation of dementia with Lewy bodies Clin Med201919327ndash330
50 Kosaka K Diffuse Lewy body disease in Japan J Neurol 1990237197ndash20451 Birkett DP Desouky A Han L Kaufman M Lewy bodies in psychiatric patients Int J
Geriatr Psychiatry 19927235ndash240
Appendix (continued)
Name Location Contribution
John PaulTaylor MBBS PhD
Newcastle University Revising the manuscript forintellectual content
Debby WTsuang MD
VA Puget Sound ampUniversity ofWashington
Revising the manuscript forintellectual content
ZuzanaWalker MD
University CollegeLondon
Revising the manuscript forintellectual content
PietroTiraboschiMD
Istituto NeurologicoldquoCarlo Bestardquo Milan
Design and conceptualizationof the study acquisition ofdata analysis andinterpretation of the data anddrafting and revising themanuscript for intellectualcontent
754 Neurology | Volume 94 Number 17 | April 28 2020 NeurologyorgN
52 Kobayashi K Nakano H Akiyama N Maeda T Yamamori S Pure psychiatric pre-sentation of the Lewy body disease is depressionmdashan analysis of 60 cases verified withmyocardial meta-iodobenzylguanidine study Int J Geriatr Psychiatry 201530663ndash668
53 Takahashi S Mizukami K Arai T et al Ventilatory response to hypercapnia predictsdementia with Lewy bodies in late-onset major depressive disorder J Alzheimers Dis201650751ndash758
54 Van Assche L Van Aubel E Van de Ven L Bouckaert F Luyten P Vandenbulcke MThe neuropsychological profile and phenomenology of late onset psychosis a cross-sectional study on the differential diagnosis of very-late-onset Schizophrenia-likepsychosis dementia with Lewy bodies and Alzheimerrsquos type dementia with psychosisArch Clin Neuropsychol 201934183ndash199
55 Thaipisuttikul P Lobach I Zweig Y Gurnani A Galvin JE Capgras syndrome indementia with Lewy bodies Int Psychogeriatr 201325843ndash849
56 Fujishiro H Iseki E Nakamura S et al Dementia with Lewy bodies early diagnosticchallenges Psychogeriatrics 201313128ndash138
57 Chiba Y Fujishiro H Iseki E et al Retrospective survey of prodromal symptoms indementia with Lewy bodies comparison with Alzheimerrsquos disease Dement GeriatrCogn Disord 201233273ndash281
58 Kaufmann H Norcliffe-Kaufmann L Palma JA et al Natural history of pure auto-nomic failure a United States prospective cohort Ann Neurol 201781287ndash297
59 Heinzel S Berg D Gasser T et al Update of the MDS research criteria for prodromalParkinsonrsquos disease Mov Disord 2019341464ndash1470
60 Palma JA Norcliffe-Kaufmann L Kaufmann H Diagnosis of multiple system atrophyAuton Neurosci 201821115ndash25Data available fromDryad (Additional References References e1ndashe44) doi105061dryad1c59zw3rv
Subspecialty Alerts by E-mail
Customize your online journal experience by signing up for e-mail alerts related to your subspecialty or area of interest Accessthis free service by clicking on the ldquoMy Alertsrdquo link on the home page An extensive list of subspecialties methods and studydesign choices will be available for you to choose frommdashallowing you priority alerts to cutting-edge research in your field
COVID-19 and Neurologic Disease Call for Papers
The editors of Neurology are interested in papers that address the neurological aspects of COVID-19infection and challenges to the management of patients with chronic neurological conditions whohave or are at risk for the infection Relevant papers that pass initial internal review will undergoexpedited peer review and online publication We will consider papers posted in preprint servers
Submit observational studies and clinical trials as Articles and case series and case reports underthe ClinicalScientific Notes category to httpssubmitneurologyorg today
Visit the Neurologyreg Website at NeurologyorgN More article-based content on home pages Streamlined menus and navigation Enhanced blog sections for specialty areas Same experience on desktop tablet and mobile devices Improved article reading experience links more evident (pdf analytics social media) Neurologyreg Clinical Practice initiative ldquoPractice Currentrdquo global surveys will be accessible across sites
Find Neurologyreg on Facebook httptinyurlcomneurologyfan
Follow Neurologyreg on Twitter httpstwittercomGreenJournal
NeurologyorgN Neurology | Volume 94 Number 17 | April 28 2020 755
DOI 101212WNL0000000000009323202094743-755 Published Online before print April 2 2020Neurology
Ian G McKeith Tanis J Ferman Alan J Thomas et al Research criteria for the diagnosis of prodromal dementia with Lewy bodies
This information is current as of April 2 2020
ServicesUpdated Information amp
httpnneurologyorgcontent9417743fullincluding high resolution figures can be found at
References httpnneurologyorgcontent9417743fullref-list-1
This article cites 59 articles 12 of which you can access for free at
Subspecialty Collections
httpnneurologyorgcgicollectionpsychosisPsychosis a
httpnneurologyorgcgicollectionparkinsons_disease_with_dementiParkinsons disease with dementia
httpnneurologyorgcgicollectionmci_mild_cognitive_impairmentMCI (mild cognitive impairment)
httpnneurologyorgcgicollectiondementia_with_lewy_bodiesDementia with Lewy bodies
httpnneurologyorgcgicollectiondeliriumDeliriumfollowing collection(s) This article along with others on similar topics appears in the
Permissions amp Licensing
httpwwwneurologyorgaboutabout_the_journalpermissionsits entirety can be found online atInformation about reproducing this article in parts (figurestables) or in
Reprints
httpnneurologyorgsubscribersadvertiseInformation about ordering reprints can be found online
ISSN 0028-3878 Online ISSN 1526-632XWolters Kluwer Health Inc on behalf of the American Academy of Neurology All rights reserved Print1951 it is now a weekly with 48 issues per year Copyright Copyright copy 2020 The Author(s) Published by
reg is the official journal of the American Academy of Neurology Published continuously sinceNeurology

52 Kobayashi K Nakano H Akiyama N Maeda T Yamamori S Pure psychiatric pre-sentation of the Lewy body disease is depressionmdashan analysis of 60 cases verified withmyocardial meta-iodobenzylguanidine study Int J Geriatr Psychiatry 201530663ndash668
53 Takahashi S Mizukami K Arai T et al Ventilatory response to hypercapnia predictsdementia with Lewy bodies in late-onset major depressive disorder J Alzheimers Dis201650751ndash758
54 Van Assche L Van Aubel E Van de Ven L Bouckaert F Luyten P Vandenbulcke MThe neuropsychological profile and phenomenology of late onset psychosis a cross-sectional study on the differential diagnosis of very-late-onset Schizophrenia-likepsychosis dementia with Lewy bodies and Alzheimerrsquos type dementia with psychosisArch Clin Neuropsychol 201934183ndash199
55 Thaipisuttikul P Lobach I Zweig Y Gurnani A Galvin JE Capgras syndrome indementia with Lewy bodies Int Psychogeriatr 201325843ndash849
56 Fujishiro H Iseki E Nakamura S et al Dementia with Lewy bodies early diagnosticchallenges Psychogeriatrics 201313128ndash138
57 Chiba Y Fujishiro H Iseki E et al Retrospective survey of prodromal symptoms indementia with Lewy bodies comparison with Alzheimerrsquos disease Dement GeriatrCogn Disord 201233273ndash281
58 Kaufmann H Norcliffe-Kaufmann L Palma JA et al Natural history of pure auto-nomic failure a United States prospective cohort Ann Neurol 201781287ndash297
59 Heinzel S Berg D Gasser T et al Update of the MDS research criteria for prodromalParkinsonrsquos disease Mov Disord 2019341464ndash1470
60 Palma JA Norcliffe-Kaufmann L Kaufmann H Diagnosis of multiple system atrophyAuton Neurosci 201821115ndash25Data available fromDryad (Additional References References e1ndashe44) doi105061dryad1c59zw3rv
Subspecialty Alerts by E-mail
Customize your online journal experience by signing up for e-mail alerts related to your subspecialty or area of interest Accessthis free service by clicking on the ldquoMy Alertsrdquo link on the home page An extensive list of subspecialties methods and studydesign choices will be available for you to choose frommdashallowing you priority alerts to cutting-edge research in your field
COVID-19 and Neurologic Disease Call for Papers
The editors of Neurology are interested in papers that address the neurological aspects of COVID-19infection and challenges to the management of patients with chronic neurological conditions whohave or are at risk for the infection Relevant papers that pass initial internal review will undergoexpedited peer review and online publication We will consider papers posted in preprint servers
Submit observational studies and clinical trials as Articles and case series and case reports underthe ClinicalScientific Notes category to httpssubmitneurologyorg today
Visit the Neurologyreg Website at NeurologyorgN More article-based content on home pages Streamlined menus and navigation Enhanced blog sections for specialty areas Same experience on desktop tablet and mobile devices Improved article reading experience links more evident (pdf analytics social media) Neurologyreg Clinical Practice initiative ldquoPractice Currentrdquo global surveys will be accessible across sites
Find Neurologyreg on Facebook httptinyurlcomneurologyfan
Follow Neurologyreg on Twitter httpstwittercomGreenJournal
NeurologyorgN Neurology | Volume 94 Number 17 | April 28 2020 755
DOI 101212WNL0000000000009323202094743-755 Published Online before print April 2 2020Neurology
Ian G McKeith Tanis J Ferman Alan J Thomas et al Research criteria for the diagnosis of prodromal dementia with Lewy bodies
This information is current as of April 2 2020
ServicesUpdated Information amp
httpnneurologyorgcontent9417743fullincluding high resolution figures can be found at
References httpnneurologyorgcontent9417743fullref-list-1
This article cites 59 articles 12 of which you can access for free at
Subspecialty Collections
httpnneurologyorgcgicollectionpsychosisPsychosis a
httpnneurologyorgcgicollectionparkinsons_disease_with_dementiParkinsons disease with dementia
httpnneurologyorgcgicollectionmci_mild_cognitive_impairmentMCI (mild cognitive impairment)
httpnneurologyorgcgicollectiondementia_with_lewy_bodiesDementia with Lewy bodies
httpnneurologyorgcgicollectiondeliriumDeliriumfollowing collection(s) This article along with others on similar topics appears in the
Permissions amp Licensing
httpwwwneurologyorgaboutabout_the_journalpermissionsits entirety can be found online atInformation about reproducing this article in parts (figurestables) or in
Reprints
httpnneurologyorgsubscribersadvertiseInformation about ordering reprints can be found online
ISSN 0028-3878 Online ISSN 1526-632XWolters Kluwer Health Inc on behalf of the American Academy of Neurology All rights reserved Print1951 it is now a weekly with 48 issues per year Copyright Copyright copy 2020 The Author(s) Published by
reg is the official journal of the American Academy of Neurology Published continuously sinceNeurology

DOI 101212WNL0000000000009323202094743-755 Published Online before print April 2 2020Neurology
Ian G McKeith Tanis J Ferman Alan J Thomas et al Research criteria for the diagnosis of prodromal dementia with Lewy bodies
This information is current as of April 2 2020
ServicesUpdated Information amp
httpnneurologyorgcontent9417743fullincluding high resolution figures can be found at
References httpnneurologyorgcontent9417743fullref-list-1
This article cites 59 articles 12 of which you can access for free at
Subspecialty Collections
httpnneurologyorgcgicollectionpsychosisPsychosis a
httpnneurologyorgcgicollectionparkinsons_disease_with_dementiParkinsons disease with dementia
httpnneurologyorgcgicollectionmci_mild_cognitive_impairmentMCI (mild cognitive impairment)
httpnneurologyorgcgicollectiondementia_with_lewy_bodiesDementia with Lewy bodies
httpnneurologyorgcgicollectiondeliriumDeliriumfollowing collection(s) This article along with others on similar topics appears in the
Permissions amp Licensing
httpwwwneurologyorgaboutabout_the_journalpermissionsits entirety can be found online atInformation about reproducing this article in parts (figurestables) or in
Reprints
httpnneurologyorgsubscribersadvertiseInformation about ordering reprints can be found online
ISSN 0028-3878 Online ISSN 1526-632XWolters Kluwer Health Inc on behalf of the American Academy of Neurology All rights reserved Print1951 it is now a weekly with 48 issues per year Copyright Copyright copy 2020 The Author(s) Published by
reg is the official journal of the American Academy of Neurology Published continuously sinceNeurology