Expedition: Improving Safety and Reliability for Surgical ...

Research ArticleImproving Surgical Access in Rural Africa througha Surgical Camp Model
M Galukande1 O Kituuka1 E Elobu1 J Jombwe2 J Sekabira2
Elissa Butler3 and J Faulal2
1Department of Surgery College of Health Sciences Makerere University Kampala Uganda2Department of Surgery Mulago National Referral Hospital Kampala Uganda3University of Minnesota Medical School Minneapolis MN 55455 USA
Correspondence should be addressed to M Galukande mosesgimgcoug
Received 11 January 2016 Revised 18 May 2016 Accepted 18 May 2016
Academic Editor Gasparini Giulio
Copyright copy 2016 M Galukande et al This is an open access article distributed under the Creative Commons Attribution Licensewhich permits unrestricted use distribution and reproduction in any medium provided the original work is properly cited
Introduction Surgical camps are preplanned activities where volunteer surgical teams congregate at specified place(s) and performa wide range of mostly elective procedures for a limited period of time This is usually at no cost to the patients who belongto vulnerable (poor and hard to reach) communities We describe a surgical camp model and its challenges as a means ofimproving access to surgical servicesMethods A cross-sectional descriptive study Data from a recent Association of Surgeons ofUganda surgical camp were collected and analyzed for demographics costs procedure types and rates and in addition challengesencountered and solutions Personnel that participated in this exercise included specialist surgeons surgical residents medicalofficers clinical officers anesthetists and theater nurses (a total of 121 staff)Results In total 551 procedures were performed duringa four-day-long camp Mean age was 35 years (SD 23) M F ratio was 2 1 Herniorrhaphy skin lump excision hydrocelectomyand thyroidectomy formed 81 of all the procedures Average cost per procedure was $73 USD Conclusion Surgical camps offerincreased access to surgical services to vulnerable populations Hernias and goiters were most common Surgical camps shouldbecome an integral part of the Health Service delivery in low-resourced environments
1 Introduction
Surgical conditions are neglected in healthcare systems inSub-Saharan Africa [1 2] There is limited access to surgicalservices and accordingly low surgical output compared toricher nations [3 4] The reasons for limited access tosurgical services are numerous including but not limitedto inadequate Human Resources for Health (HRH) limitedsurgical supplies and lack of transportation to get to thedistant health facilities that can offer the appropriate surgicalservices [5 6]
In response to these realities the Association of Surgeonsof Uganda (ASOU) piloted the first surgical camp in 2001 innorthernUganda a 6-hour drive from the capital city ofKam-pala Due to the success of this first camp general surgeonscontinue to offer annual camps Additionally subspecialtycamps occur regularly such as for open heart surgery andplastic-cleft lip repairs [7 8] On average 1 to 2 surgical
ASOU endorsed camps are carried out every year in differentregions of the country each time
Surgical camps are preplanned activities were volunteersurgical teams congregate at a specified place and performa wide range of mostly elective procedures for a limitedand specified period of time normally a week or little moreusually at no cost to the patient Several fundraising activitiesprecede the camp to cover direct costs such as transportationfood and water at the venues The sources of funds arefrom the business private sector individuals and Ministry ofHealthThere is normally no monetary compensation for thepersonnel services are offered pro bono
The purpose of this study therefore was to describe thissurgical camp model as an approach to improving access tosurgical services for vulnerable communities and estimatethe unmet burden of surgical disease in the areas where thecamps took place
Hindawi Publishing CorporationSurgery Research and PracticeVolume 2016 Article ID 9021945 6 pageshttpdxdoiorg10115520169021945
2 Surgery Research and Practice
2 Materials and Methods
21 Study Design This is a cross-sectional descriptive studyusing both quantitative and qualitative data collection meth-ods
22 Study Settings The study took place in NortheasternUganda at 8 rural sites including 3 district hospitals 4 healthcenter level IVs and 1 regional hospital in the month of July2013
All sites had operating rooms postoperative recoveryareas and the admission space for those who required itThe teams at the sites included specialist general surgeonsnursesmedical officers andmedical students Patient follow-up was conducted by the resident health worker at the hostsites following routine standard protocols
23 Data Collection Before the camp mobilization activitiestook place to recruit patients including but not limited toradio announcements announcements at special gatheringssuch as church services advertisements at health facilitiesand house-to-house visits by the village health teams and thelocal council committee
Aday or twoprior to commencement of surgeries clinicalscreening was conducted and those eligible for surgerywere selected Clinicianrsquos judgment based on history andphysical exam determined fitness for surgery and anesthesiaas laboratory and imaging capacity was limited Personnelthat participated in the camp included 20 specialist surgeons6 surgical residents 6 medical officers 7 clinical officers 17anesthetists and 55 theater nurses (a total of 121 staff in all)
Operating logs were filled during the camp whichincluded the date of procedure patient age and genderclinical diagnosis operation performed and type of anes-thesia Data were extracted from the operating logs Campsummary reports were submitted which included challengesencountered and solutions undertaken Direct expendituredetails were obtained from the finance secretary of theAssociationcamp
24 Data Analysis Data were entered in Excel from paperoperating logs and analyzed Variables considered were agegender diagnosis procedure done direct cost per patientand type of anesthesia Data from the summary reports andinterviews were collected into themes and presented in atable
25 Ethical Issues All patients gave their informed writtenconsent for the procedures done
3 Results
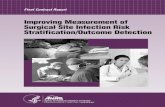
31 Patient Demographics A total of 536 patients wereoperated on and 551 procedureswere performedover a periodof 4 days across 8 sites Mean age was 35 years (SD 23) andgender ratio was 2 1 (male female)The age distribution hada bimodal trend as shown in Figure 1 However for herniarepair and hydrocelectomy the age distribution was constant(see Table 3)
90
80
70
60
50
40
30
20
10
0
Num
ber o
f pat
ient
s
lt5
5ndash9
10
ndash18
19
ndash29
30
ndash39
40
ndash49
50
ndash59
60
ndash69
70
ndash79
gt80
Age (years)
Age distribution
5954
4844
80 77
68
4338
12
Mean age 352 (SD 234)Median age 36 (IQR 13ndash53)Age unknown for 13 patients
Figure 1 Age distribution of patients receiving surgery at thesurgical camp Uganda 2013
32 Clinical Diagnoses and Surgical Procedures Of the 551procedures the most common diagnoses were inguinalhernia hydrocele lipoma epidermoid cyst and goiter con-tributing to 70 of all diagnoses (see Table 1) The four mostcommon procedures were herniorrhaphy skin lump exci-sions hydrocelectomy and thyroidectomy accounting for81 of all procedures (see Table 2) Immediate postoperativemortality was zero (1ndash4 days) In total 70 were done underlocal or spinal anesthesia
33 Challenges Several logistical challenges were encoun-tered including power outages inadequate sterilization andanesthetic equipment lack of running water and inadequatesurgical sets Others included an overwhelming number ofpatients inadequate nursing personnel to cover the recoverybays and limited laboratory and imaging investigative capa-bility (see Table 4)
34 Expenses The gross expenditure on direct costs was100000000 Uganda Shillings ($40000) This converts to187000 Uganda Shillings (or $75) per patient and 182000Uganda Shillings (or $73) per procedure
35 Types of Anesthesia Used at the Surgical Camp in UgandaThere were three types of anesthesia as follows
General anesthesia 109 (30)Locoregional anesthesia 206 (57)Spinal anesthesia 97 (13)
4 Discussion
The surgical camp model for providing surgical services tovulnerable or underserved populations in Africa is not newand in the case of Uganda and ASOU this has been done forthe past decade [7] However data on patient demographicsand the scope of surgical procedures have not been previouslydocumented in the literature
Surgery Research and Practice 3
Table 1 Surgical procedures at a campsite in Uganda 2013
Amuriadagger Kaberamaidodagger Soroti998771 Ngoralowast Katakwidagger Kumilowast Atururlowast Sereredagger TotalHerniorrhaphy 13 26 20 26 13 4 21 55 178Skin excisions 12 10 16 12 18 8 26 29 131Hydrocelectomy 26 19 6 6 24 3 11 10 105Thyroidectomy 0 0 15 10 0 9 0 1 35Gluteal fibrosis release 0 0 0 0 0 17 1 0 18Anorectal procedures1 0 2 7 1 1 0 6 0 17Wound-related procedure2 2 1 7 0 1 0 4 1 16Laparotomy 0 0 3 0 0 4 1 2 10Obstetric3 conditions 6 0 0 0 0 0 1 1 8Hysterectomy 0 0 0 1 0 0 5 1 7Orchiopexy 0 5 0 0 0 0 1 1 7Orthopedic procedures 0 1 3 0 1 0 0 0 5Appendectomy 0 0 1 0 0 1 0 2 4Other procedures 0 0 2 5 0 1 2 0 10Total 59 64 80 61 58 47 79 103 5511Hemorrhoidectomy parasagittal anorectoplasty lateral internal sphincterotomy and manual anal dilation2Incision and drainage debridement and surgical toilet3Cesarian section and uterine evacuationlowastDistrict hospitals with a 100-bed capacity all state owned public hospitalsdaggerHealth center IVs outpatient facilities with 20-bed in-patient facilities998771A regional referral hospital 250 beds with some specialist services
Table 2 Showing diagnosis by age campsite in Uganda 2013
Procedure Age groups Unknown age Totallt5 5ndash18 19ndash39 40ndash59 ge60
Inguinal hernia 29 29 23 29 27 6 143Hydrocele 10 19 12 36 33 2 112Lipoma 2 7 14 19 14 1 57Goiter 0 0 16 15 3 1 35Epidermoid cyst 2 5 11 8 5 1 32Other hernias 0 1 8 9 8 1 27Congenital conditions 13 5 2 1 0 0 21Gluteal fibrosis 0 18 0 0 0 0 18Anorectal 0 1 10 5 1 0 17Infection 1 4 3 6 2 0 16Tumor 2 3 6 3 1 1 16Gynecologic 0 1 6 6 0 0 13Intra-abdominal masses 0 3 3 4 1 0 11Ganglion cyst 0 2 2 1 2 0 7Obstructed labor 0 2 4 0 0 0 6Trauma 0 1 3 2 0 0 6Other procedures 0 6 4 3 1 0 14Total 59 107 127 147 98 13 551
Persons with surgical disease are young and form thebulk of the Ugandan productive work force The bimodaldistribution of age showed that the paediatric (below 18 years)population and those between 30 and 60 years representthe bulk of the surgical burden of disease This emphasizesthe need for paediatric surgical skills in surgical training formedical officers
Males were overrepresented likely due to the high burdenof inguinal hernias and hydroceles Although the procedureper population rate was estimated at 125 100000 in thisreview at some sites it was as high as 146 100000 close towhat was estimated by Nordberg [9] in 1984 three decadesago Inguinal hernia and hydrocele occurrence were in equalproportions throughout age distribution
4 Surgery Research and Practice
Table 3 Procedure per population rates campsite in Uganda 2013
Site Catchment population (201011 estimates)Category and number of
procedures Procedure per 100000 of populationProcedure Number
Amuria 315900Hernia 13 1 41
Hydrocele 26 1 82Goiter 0 mdash
Kaberamaido 195400Hernia 18 1 92
Hydrocele 25 1 128Goiter 0 mdash
Katakwi 153600Hernia 10 1 65
Hydrocele 24 1 156Goiter 8 1 52
Serere 176500lowastHernia 45 1 255
Hydrocele 10 1 57Goiter 13 1 74
Ngora 101900lowastHernia 18 1 177
Hydrocele 6 1 59Goiter 10 1 98
Kumi and Aturur 13000Hernia 19 1 146
Hydrocele 15 1 115Goiter 9 1 69
Soroti 241200Hernia 20 1 83
Hydrocele 6 1 25Goiter 15 1 99
Overall 1197500Hernia 147 1 125
Hydrocele 112 1 10Goiter 35 1 29
lowast2002 population census estimates
The most common conditions seen in our study werehernia hydrocele and goiter These procedures are withinthe realm of competence of a medical officer (nonspecialistphysician) if properly trained and supported [10] What isalso true is that surgical camps environment is a platformfor apprenticeship the less experienced surgeons or traineeswork with more experienced colleagues to learn more in apractical setting handling high volumes of surgical cases in ashort period of time
Locoregional anesthesia was used in 70 of cases Thisaligns with recommendations made previously on the basisof cost of care and safety
This study also allowed us to estimate procedure perpopulation rate for the less common surgical conditions Theprevalence of correctable surgical congenital anomalies inUganda is not known In total 4 of all procedures donewerefor congenital anomalies Gluteal fibrosis or gluteal musclecontracture caused by repeated intramuscular quinine injec-tions accounted for 3 of surgical diagnoses It accountedfor 3 of surgical diagnoses GMC first reported by Valder-rama is a clinical syndrome pathologically characterized by
degeneration necrosis and fibrosis of the glutealmuscles andfascia leading to serious limitation of hip movements [11 12]Malaria is endemic in Uganda and in some places injectablequinine is used indiscriminately
Several challenges were encountered screening forcomorbidities such as NIDDM (non-insulin dependent dia-betes mellitus) and cardiorespiratory diseases was limited toclinical assessmentwithout lab and imaging formost patientsyet we know there is a significant burden of prediabetic anddiabetic states amongUgandans [11]The consequences of notscreening are not known in this context
Whereas these populations have close geographical accessto health centers they likely delay in access to appropriatecare due to a number of reasons including lack of skilledmanpower at the health centers drug stock-outs for anesthet-ics and health centers prioritizing resources for emergencyprocedures like Cesarean sections [13] During the campseveral logistical challenges were faced ranging from poweroutages inadequate sterilization capacity limited surgicalinstruments limited operating room space and intermittentsupply of running water These are not new [2 5 14]
Surgery Research and Practice 5
Table 4 Challenges reported solutions and future plans
Domain Challenges Solutions
Water andelectricity
Lack of running water at some sitesProlonged power outages at two sites
Patients andor their attendants to provide 20 litres ofwater eachUsing a generator (consider standby generators infuture surgical camps)
Inadequate number of anesthetistsNo anesthetic machine
Predetermining personnel needs and secure personnel(anesthetists) beforehand
Sterilization andsupplies
Limited capacity to sterilize (due to inadequate numberof autoclaves) power outages and inadequate linensuppliesDrugs and surgical sundries were in short supply
Better projections and resource mobilization for futurecampsConsidering hiring autoclavesContact nearby hospitals to participate and share
Equipment andinstruments
Equipment and instruments were limited (surgical setsanesthesia equipment)There was a concurrent ophthalmology camp going onWe had only one oxygen source
Doing better projections hiring equipment andinstrumentsConsidering portable oxygen supply
Human resource
Several patients with gynecological conditions came yetwe had no gynecologistsOperating theater condition some were very olddilapidatedFew staff in the theater to help in coordination andpatient flowInadequate postoperative nursing manpowerOne of the team members fell sick
Including gynecologists in future campsInstituting quality assurance and safety guidelines andagreeing on the minimum standardsGetting required personnel to commit before the campbegins
Demand forservice
Overwhelming number of casesSome pediatric cases could not be worked on
Planning triage days before the camp begins andgenerating manageable operating lists
Technicaloperativedifficulties
Giant hydroceles and hernias that had stayed for over 10years were a challenge with no intensive care unit(ICU) facilities
Triage and referral to better facilitated centersAllocating ldquodifficultyrdquo cases to the experiencedsurgeonsPriority was given to children the elderly and thosewhose conditions greatly affecting the quality of lifeMainly cases which need minimal postoperativenursing care were done
Others
Only a handful presented for preoperative screeningDue to limited working space privacy could not beobserved all the timeInadequate linen
Encouraging preoperative screening in future campsProcuring tents as a way of availing more working spaceGetting more linen
they impede access to surgical services even for stop-gapapproaches like surgical camps Documenting these chal-lenges is part of advocacy to mobilize resources and engagethose that have the power to prioritize available resources forservice
What has also been highlighted here (albeit crudely) is thecost of surgical interventionThe cost of surgical interventionwas $7250 per procedure This cost however was furthersubsidized by the infrastructure that already exists
What is clear from this study is that the scope ofconditions that were seen over ten years ago is still thesame However a population-based estimate of the burdenof surgical disease [3] and regular documentation of thecampsrsquo outcomes have not been done Estimates indicatethat surgery can address 7 of DALYs (disability-adjustedlife years) that occur in Africa [15] and this burden is mostprobably increasing rapidly [14]
Organizing a camp successfully requires a clear objectivea group of individuals or organization(s) finance(s) andan appropriate target population (beneficiary group) In
addition there was an agreedwork planwith the involvementof all stakeholders including local leaders hosting healthcenters sponsors Ministries of Health and the personnelthat carry out the procedures Publicity of these activities isencouraged in order to promote the service gain support andensure sustainability on the long term
5 Study Limitations
The data for screened patients that did not qualify for surgerywere unavailable The catchment population is an estimatethere may be overlap of health facility catchment areasand previously done procedures in the areacatchment werenot known No postoperation data was collected to assesspostoperative complicationswhichmay inform future camps
6 Conclusion
Surgical camps improve access of surgical services to vulner-able populations Inguinal hernias formed the bulk surgical
6 Surgery Research and Practice
disease encountered Hydroceles and thyroid disease alsocontribute significantly to the burden of disease in Sub-Saharan Africa Surgical camps should become an integralpart of health service delivery in rural Africa
Abbreviations
ASOU Association of Surgeons of UgandaGMC Gluteal muscle contractureHRH Human Resources for Health
Additional Points
The economic and social implications of unrepaired hernianeed to be investigated For future camps postoperativemorbidity data should be collected and the total number ofscreened patients Mostly importantly we consider surgicalcamps as an integral part of surgical service delivery byhospitals medical schools and Ministries of Health
Competing Interests
The authors declare no competing interests
Authorsrsquo Contributions
M Galukande wrote the first draft Elissa Butler E Elobuand M Galukande analyzed data O Kituuka J Jombwe JSekabira J Faulal performed critical reviews for intellectualcontent All authors authorized submission of this work forpublication and agreed to content
Acknowledgments
All staff of participatory sites all the patients local leadershipand volunteers
References
[1] D Ozgediz and R Riviello ldquoThe lsquootherrsquo neglected diseases inglobal public health surgical conditions in sub-SaharanAfricardquoPLoS Medicine vol 5 no 6 article e121 2008
[2] M Galukande J von Schreeb A Wladis et al ldquoEssentialsurgery at the district hospital a retrospective descriptiveanalysis in three African countriesrdquo PLoS Medicine vol 7 no3 Article ID e1000243 2010
[3] M Ohene-Yeboah and F A Abantanga ldquoInguinal hernia dis-ease in Africa a common but neglected surgical conditionrdquoWest African Journal of Medicine vol 30 no 2 pp 77ndash83 2011
[4] S Luboga S B Macfarlane J von Schreeb et al ldquoIncreasingaccess to surgical services in sub-saharan Africa prioritiesfor national and international agencies recommended by theBellagio Essential Surgery Grouprdquo PLoSMedicine vol 6 no 12Article ID e1000200 2009
[5] A F Linden F S Sekidde M Galukande L M Knowlton SChackungal and K A K McQueen ldquoChallenges of surgery indeveloping countries a survey of surgical and anesthesia capac-ity in ugandarsquos public hospitalsrdquo World Journal of Surgery vol36 no 5 pp 1056ndash1065 2012
[6] R Y Hsia N A Mbembati S Macfarlane and M E KrukldquoAccess to emergency and surgical care in sub-Saharan Africathe infrastructure gaprdquo Health Policy and Planning vol 27 no3 pp 234ndash244 2012
[7] I Kakande W W Obote and K Sebbaale Surgical camps TheUganda experience ECAJS 2007 httpwwwbiolineorgbrjs
[8] H Jaques ldquoSurgical innovation abroad and at homerdquo BMJCareers 2013 httpcareersbmjcomcareersadvicSurgicalinnovation abroad and at home
[9] E M Nordberg ldquoIncidence and estimated need of caesareansection inguinal hernia repair and operation for strangulatedhernia in rural Africardquo British Medical Journal vol 289 no6437 pp 92ndash93 1984
[10] M Galukande S Kaggwa P Sekimpi et al ldquoUse of surgicaltask shifting to scale up essential surgical services a feasibilityanalysis at facility level in Ugandardquo BMC Health ServicesResearch vol 13 no 1 article 292 2013
[11] J A F Valderrama ldquoA cause of limited flexion and adduction ofthe hip in childrenrdquoThe Journal of Bone amp Joint Surgery vol 52article 179 1970
[12] C-G Zhao X-J He B Lu H-P Li D Wang and Z-ZZhu ldquoClassification of gluteal muscle contracture in childrenand outcome of different treatmentsrdquo BMC MusculoskeletalDisorders vol 10 article 34 2009
[13] C E Grimes K G Bowman CM Dodgion and C B D LavyldquoSystematic review of barriers to surgical care in low-incomeandmiddle-income countriesrdquoWorld Journal of Surgery vol 35no 5 pp 941ndash950 2011
[14] D Ozgediz D Jamison M Cherian and K McQueen ldquoTheburden of surgical conditions and access to surgical care inlowmdashand middle-income countriesrdquo Bulletin of the WorldHealth Organization vol 86 no 8 pp 646ndash647 2008
[15] H TDebas R Gosselin CMcCord andAThind ldquoSurgeryrdquo inDiseaseControl Priorities inDevelopingCountries D T JamisonJ G Breman A R Measham et al Eds pp 1245ndash1259 WorldBank Washington DC USA Oxford University Press NewYork NY USA 2nd edition 2006
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

2 Surgery Research and Practice
2 Materials and Methods
21 Study Design This is a cross-sectional descriptive studyusing both quantitative and qualitative data collection meth-ods
22 Study Settings The study took place in NortheasternUganda at 8 rural sites including 3 district hospitals 4 healthcenter level IVs and 1 regional hospital in the month of July2013
All sites had operating rooms postoperative recoveryareas and the admission space for those who required itThe teams at the sites included specialist general surgeonsnursesmedical officers andmedical students Patient follow-up was conducted by the resident health worker at the hostsites following routine standard protocols
23 Data Collection Before the camp mobilization activitiestook place to recruit patients including but not limited toradio announcements announcements at special gatheringssuch as church services advertisements at health facilitiesand house-to-house visits by the village health teams and thelocal council committee
Aday or twoprior to commencement of surgeries clinicalscreening was conducted and those eligible for surgerywere selected Clinicianrsquos judgment based on history andphysical exam determined fitness for surgery and anesthesiaas laboratory and imaging capacity was limited Personnelthat participated in the camp included 20 specialist surgeons6 surgical residents 6 medical officers 7 clinical officers 17anesthetists and 55 theater nurses (a total of 121 staff in all)
Operating logs were filled during the camp whichincluded the date of procedure patient age and genderclinical diagnosis operation performed and type of anes-thesia Data were extracted from the operating logs Campsummary reports were submitted which included challengesencountered and solutions undertaken Direct expendituredetails were obtained from the finance secretary of theAssociationcamp
24 Data Analysis Data were entered in Excel from paperoperating logs and analyzed Variables considered were agegender diagnosis procedure done direct cost per patientand type of anesthesia Data from the summary reports andinterviews were collected into themes and presented in atable
25 Ethical Issues All patients gave their informed writtenconsent for the procedures done
3 Results
31 Patient Demographics A total of 536 patients wereoperated on and 551 procedureswere performedover a periodof 4 days across 8 sites Mean age was 35 years (SD 23) andgender ratio was 2 1 (male female)The age distribution hada bimodal trend as shown in Figure 1 However for herniarepair and hydrocelectomy the age distribution was constant(see Table 3)
90
80
70
60
50
40
30
20
10
0
Num
ber o
f pat
ient
s
lt5
5ndash9
10
ndash18
19
ndash29
30
ndash39
40
ndash49
50
ndash59
60
ndash69
70
ndash79
gt80
Age (years)
Age distribution
5954
4844
80 77
68
4338
12
Mean age 352 (SD 234)Median age 36 (IQR 13ndash53)Age unknown for 13 patients
Figure 1 Age distribution of patients receiving surgery at thesurgical camp Uganda 2013
32 Clinical Diagnoses and Surgical Procedures Of the 551procedures the most common diagnoses were inguinalhernia hydrocele lipoma epidermoid cyst and goiter con-tributing to 70 of all diagnoses (see Table 1) The four mostcommon procedures were herniorrhaphy skin lump exci-sions hydrocelectomy and thyroidectomy accounting for81 of all procedures (see Table 2) Immediate postoperativemortality was zero (1ndash4 days) In total 70 were done underlocal or spinal anesthesia
33 Challenges Several logistical challenges were encoun-tered including power outages inadequate sterilization andanesthetic equipment lack of running water and inadequatesurgical sets Others included an overwhelming number ofpatients inadequate nursing personnel to cover the recoverybays and limited laboratory and imaging investigative capa-bility (see Table 4)
34 Expenses The gross expenditure on direct costs was100000000 Uganda Shillings ($40000) This converts to187000 Uganda Shillings (or $75) per patient and 182000Uganda Shillings (or $73) per procedure
35 Types of Anesthesia Used at the Surgical Camp in UgandaThere were three types of anesthesia as follows
General anesthesia 109 (30)Locoregional anesthesia 206 (57)Spinal anesthesia 97 (13)
4 Discussion
The surgical camp model for providing surgical services tovulnerable or underserved populations in Africa is not newand in the case of Uganda and ASOU this has been done forthe past decade [7] However data on patient demographicsand the scope of surgical procedures have not been previouslydocumented in the literature
Surgery Research and Practice 3
Table 1 Surgical procedures at a campsite in Uganda 2013
Amuriadagger Kaberamaidodagger Soroti998771 Ngoralowast Katakwidagger Kumilowast Atururlowast Sereredagger TotalHerniorrhaphy 13 26 20 26 13 4 21 55 178Skin excisions 12 10 16 12 18 8 26 29 131Hydrocelectomy 26 19 6 6 24 3 11 10 105Thyroidectomy 0 0 15 10 0 9 0 1 35Gluteal fibrosis release 0 0 0 0 0 17 1 0 18Anorectal procedures1 0 2 7 1 1 0 6 0 17Wound-related procedure2 2 1 7 0 1 0 4 1 16Laparotomy 0 0 3 0 0 4 1 2 10Obstetric3 conditions 6 0 0 0 0 0 1 1 8Hysterectomy 0 0 0 1 0 0 5 1 7Orchiopexy 0 5 0 0 0 0 1 1 7Orthopedic procedures 0 1 3 0 1 0 0 0 5Appendectomy 0 0 1 0 0 1 0 2 4Other procedures 0 0 2 5 0 1 2 0 10Total 59 64 80 61 58 47 79 103 5511Hemorrhoidectomy parasagittal anorectoplasty lateral internal sphincterotomy and manual anal dilation2Incision and drainage debridement and surgical toilet3Cesarian section and uterine evacuationlowastDistrict hospitals with a 100-bed capacity all state owned public hospitalsdaggerHealth center IVs outpatient facilities with 20-bed in-patient facilities998771A regional referral hospital 250 beds with some specialist services
Table 2 Showing diagnosis by age campsite in Uganda 2013
Procedure Age groups Unknown age Totallt5 5ndash18 19ndash39 40ndash59 ge60
Inguinal hernia 29 29 23 29 27 6 143Hydrocele 10 19 12 36 33 2 112Lipoma 2 7 14 19 14 1 57Goiter 0 0 16 15 3 1 35Epidermoid cyst 2 5 11 8 5 1 32Other hernias 0 1 8 9 8 1 27Congenital conditions 13 5 2 1 0 0 21Gluteal fibrosis 0 18 0 0 0 0 18Anorectal 0 1 10 5 1 0 17Infection 1 4 3 6 2 0 16Tumor 2 3 6 3 1 1 16Gynecologic 0 1 6 6 0 0 13Intra-abdominal masses 0 3 3 4 1 0 11Ganglion cyst 0 2 2 1 2 0 7Obstructed labor 0 2 4 0 0 0 6Trauma 0 1 3 2 0 0 6Other procedures 0 6 4 3 1 0 14Total 59 107 127 147 98 13 551
Persons with surgical disease are young and form thebulk of the Ugandan productive work force The bimodaldistribution of age showed that the paediatric (below 18 years)population and those between 30 and 60 years representthe bulk of the surgical burden of disease This emphasizesthe need for paediatric surgical skills in surgical training formedical officers
Males were overrepresented likely due to the high burdenof inguinal hernias and hydroceles Although the procedureper population rate was estimated at 125 100000 in thisreview at some sites it was as high as 146 100000 close towhat was estimated by Nordberg [9] in 1984 three decadesago Inguinal hernia and hydrocele occurrence were in equalproportions throughout age distribution
4 Surgery Research and Practice
Table 3 Procedure per population rates campsite in Uganda 2013
Site Catchment population (201011 estimates)Category and number of
procedures Procedure per 100000 of populationProcedure Number
Amuria 315900Hernia 13 1 41
Hydrocele 26 1 82Goiter 0 mdash
Kaberamaido 195400Hernia 18 1 92
Hydrocele 25 1 128Goiter 0 mdash
Katakwi 153600Hernia 10 1 65
Hydrocele 24 1 156Goiter 8 1 52
Serere 176500lowastHernia 45 1 255
Hydrocele 10 1 57Goiter 13 1 74
Ngora 101900lowastHernia 18 1 177
Hydrocele 6 1 59Goiter 10 1 98
Kumi and Aturur 13000Hernia 19 1 146
Hydrocele 15 1 115Goiter 9 1 69
Soroti 241200Hernia 20 1 83
Hydrocele 6 1 25Goiter 15 1 99
Overall 1197500Hernia 147 1 125
Hydrocele 112 1 10Goiter 35 1 29
lowast2002 population census estimates
The most common conditions seen in our study werehernia hydrocele and goiter These procedures are withinthe realm of competence of a medical officer (nonspecialistphysician) if properly trained and supported [10] What isalso true is that surgical camps environment is a platformfor apprenticeship the less experienced surgeons or traineeswork with more experienced colleagues to learn more in apractical setting handling high volumes of surgical cases in ashort period of time
Locoregional anesthesia was used in 70 of cases Thisaligns with recommendations made previously on the basisof cost of care and safety
This study also allowed us to estimate procedure perpopulation rate for the less common surgical conditions Theprevalence of correctable surgical congenital anomalies inUganda is not known In total 4 of all procedures donewerefor congenital anomalies Gluteal fibrosis or gluteal musclecontracture caused by repeated intramuscular quinine injec-tions accounted for 3 of surgical diagnoses It accountedfor 3 of surgical diagnoses GMC first reported by Valder-rama is a clinical syndrome pathologically characterized by
degeneration necrosis and fibrosis of the glutealmuscles andfascia leading to serious limitation of hip movements [11 12]Malaria is endemic in Uganda and in some places injectablequinine is used indiscriminately
Several challenges were encountered screening forcomorbidities such as NIDDM (non-insulin dependent dia-betes mellitus) and cardiorespiratory diseases was limited toclinical assessmentwithout lab and imaging formost patientsyet we know there is a significant burden of prediabetic anddiabetic states amongUgandans [11]The consequences of notscreening are not known in this context
Whereas these populations have close geographical accessto health centers they likely delay in access to appropriatecare due to a number of reasons including lack of skilledmanpower at the health centers drug stock-outs for anesthet-ics and health centers prioritizing resources for emergencyprocedures like Cesarean sections [13] During the campseveral logistical challenges were faced ranging from poweroutages inadequate sterilization capacity limited surgicalinstruments limited operating room space and intermittentsupply of running water These are not new [2 5 14]
Surgery Research and Practice 5
Table 4 Challenges reported solutions and future plans
Domain Challenges Solutions
Water andelectricity
Lack of running water at some sitesProlonged power outages at two sites
Patients andor their attendants to provide 20 litres ofwater eachUsing a generator (consider standby generators infuture surgical camps)
Inadequate number of anesthetistsNo anesthetic machine
Predetermining personnel needs and secure personnel(anesthetists) beforehand
Sterilization andsupplies
Limited capacity to sterilize (due to inadequate numberof autoclaves) power outages and inadequate linensuppliesDrugs and surgical sundries were in short supply
Better projections and resource mobilization for futurecampsConsidering hiring autoclavesContact nearby hospitals to participate and share
Equipment andinstruments
Equipment and instruments were limited (surgical setsanesthesia equipment)There was a concurrent ophthalmology camp going onWe had only one oxygen source
Doing better projections hiring equipment andinstrumentsConsidering portable oxygen supply
Human resource
Several patients with gynecological conditions came yetwe had no gynecologistsOperating theater condition some were very olddilapidatedFew staff in the theater to help in coordination andpatient flowInadequate postoperative nursing manpowerOne of the team members fell sick
Including gynecologists in future campsInstituting quality assurance and safety guidelines andagreeing on the minimum standardsGetting required personnel to commit before the campbegins
Demand forservice
Overwhelming number of casesSome pediatric cases could not be worked on
Planning triage days before the camp begins andgenerating manageable operating lists
Technicaloperativedifficulties
Giant hydroceles and hernias that had stayed for over 10years were a challenge with no intensive care unit(ICU) facilities
Triage and referral to better facilitated centersAllocating ldquodifficultyrdquo cases to the experiencedsurgeonsPriority was given to children the elderly and thosewhose conditions greatly affecting the quality of lifeMainly cases which need minimal postoperativenursing care were done
Others
Only a handful presented for preoperative screeningDue to limited working space privacy could not beobserved all the timeInadequate linen
Encouraging preoperative screening in future campsProcuring tents as a way of availing more working spaceGetting more linen
they impede access to surgical services even for stop-gapapproaches like surgical camps Documenting these chal-lenges is part of advocacy to mobilize resources and engagethose that have the power to prioritize available resources forservice
What has also been highlighted here (albeit crudely) is thecost of surgical interventionThe cost of surgical interventionwas $7250 per procedure This cost however was furthersubsidized by the infrastructure that already exists
What is clear from this study is that the scope ofconditions that were seen over ten years ago is still thesame However a population-based estimate of the burdenof surgical disease [3] and regular documentation of thecampsrsquo outcomes have not been done Estimates indicatethat surgery can address 7 of DALYs (disability-adjustedlife years) that occur in Africa [15] and this burden is mostprobably increasing rapidly [14]
Organizing a camp successfully requires a clear objectivea group of individuals or organization(s) finance(s) andan appropriate target population (beneficiary group) In
addition there was an agreedwork planwith the involvementof all stakeholders including local leaders hosting healthcenters sponsors Ministries of Health and the personnelthat carry out the procedures Publicity of these activities isencouraged in order to promote the service gain support andensure sustainability on the long term
5 Study Limitations
The data for screened patients that did not qualify for surgerywere unavailable The catchment population is an estimatethere may be overlap of health facility catchment areasand previously done procedures in the areacatchment werenot known No postoperation data was collected to assesspostoperative complicationswhichmay inform future camps
6 Conclusion
Surgical camps improve access of surgical services to vulner-able populations Inguinal hernias formed the bulk surgical
6 Surgery Research and Practice
disease encountered Hydroceles and thyroid disease alsocontribute significantly to the burden of disease in Sub-Saharan Africa Surgical camps should become an integralpart of health service delivery in rural Africa
Abbreviations
ASOU Association of Surgeons of UgandaGMC Gluteal muscle contractureHRH Human Resources for Health
Additional Points
The economic and social implications of unrepaired hernianeed to be investigated For future camps postoperativemorbidity data should be collected and the total number ofscreened patients Mostly importantly we consider surgicalcamps as an integral part of surgical service delivery byhospitals medical schools and Ministries of Health
Competing Interests
The authors declare no competing interests
Authorsrsquo Contributions
M Galukande wrote the first draft Elissa Butler E Elobuand M Galukande analyzed data O Kituuka J Jombwe JSekabira J Faulal performed critical reviews for intellectualcontent All authors authorized submission of this work forpublication and agreed to content
Acknowledgments
All staff of participatory sites all the patients local leadershipand volunteers
References
[1] D Ozgediz and R Riviello ldquoThe lsquootherrsquo neglected diseases inglobal public health surgical conditions in sub-SaharanAfricardquoPLoS Medicine vol 5 no 6 article e121 2008
[2] M Galukande J von Schreeb A Wladis et al ldquoEssentialsurgery at the district hospital a retrospective descriptiveanalysis in three African countriesrdquo PLoS Medicine vol 7 no3 Article ID e1000243 2010
[3] M Ohene-Yeboah and F A Abantanga ldquoInguinal hernia dis-ease in Africa a common but neglected surgical conditionrdquoWest African Journal of Medicine vol 30 no 2 pp 77ndash83 2011
[4] S Luboga S B Macfarlane J von Schreeb et al ldquoIncreasingaccess to surgical services in sub-saharan Africa prioritiesfor national and international agencies recommended by theBellagio Essential Surgery Grouprdquo PLoSMedicine vol 6 no 12Article ID e1000200 2009
[5] A F Linden F S Sekidde M Galukande L M Knowlton SChackungal and K A K McQueen ldquoChallenges of surgery indeveloping countries a survey of surgical and anesthesia capac-ity in ugandarsquos public hospitalsrdquo World Journal of Surgery vol36 no 5 pp 1056ndash1065 2012
[6] R Y Hsia N A Mbembati S Macfarlane and M E KrukldquoAccess to emergency and surgical care in sub-Saharan Africathe infrastructure gaprdquo Health Policy and Planning vol 27 no3 pp 234ndash244 2012
[7] I Kakande W W Obote and K Sebbaale Surgical camps TheUganda experience ECAJS 2007 httpwwwbiolineorgbrjs
[8] H Jaques ldquoSurgical innovation abroad and at homerdquo BMJCareers 2013 httpcareersbmjcomcareersadvicSurgicalinnovation abroad and at home
[9] E M Nordberg ldquoIncidence and estimated need of caesareansection inguinal hernia repair and operation for strangulatedhernia in rural Africardquo British Medical Journal vol 289 no6437 pp 92ndash93 1984
[10] M Galukande S Kaggwa P Sekimpi et al ldquoUse of surgicaltask shifting to scale up essential surgical services a feasibilityanalysis at facility level in Ugandardquo BMC Health ServicesResearch vol 13 no 1 article 292 2013
[11] J A F Valderrama ldquoA cause of limited flexion and adduction ofthe hip in childrenrdquoThe Journal of Bone amp Joint Surgery vol 52article 179 1970
[12] C-G Zhao X-J He B Lu H-P Li D Wang and Z-ZZhu ldquoClassification of gluteal muscle contracture in childrenand outcome of different treatmentsrdquo BMC MusculoskeletalDisorders vol 10 article 34 2009
[13] C E Grimes K G Bowman CM Dodgion and C B D LavyldquoSystematic review of barriers to surgical care in low-incomeandmiddle-income countriesrdquoWorld Journal of Surgery vol 35no 5 pp 941ndash950 2011
[14] D Ozgediz D Jamison M Cherian and K McQueen ldquoTheburden of surgical conditions and access to surgical care inlowmdashand middle-income countriesrdquo Bulletin of the WorldHealth Organization vol 86 no 8 pp 646ndash647 2008
[15] H TDebas R Gosselin CMcCord andAThind ldquoSurgeryrdquo inDiseaseControl Priorities inDevelopingCountries D T JamisonJ G Breman A R Measham et al Eds pp 1245ndash1259 WorldBank Washington DC USA Oxford University Press NewYork NY USA 2nd edition 2006
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

Surgery Research and Practice 3
Table 1 Surgical procedures at a campsite in Uganda 2013
Amuriadagger Kaberamaidodagger Soroti998771 Ngoralowast Katakwidagger Kumilowast Atururlowast Sereredagger TotalHerniorrhaphy 13 26 20 26 13 4 21 55 178Skin excisions 12 10 16 12 18 8 26 29 131Hydrocelectomy 26 19 6 6 24 3 11 10 105Thyroidectomy 0 0 15 10 0 9 0 1 35Gluteal fibrosis release 0 0 0 0 0 17 1 0 18Anorectal procedures1 0 2 7 1 1 0 6 0 17Wound-related procedure2 2 1 7 0 1 0 4 1 16Laparotomy 0 0 3 0 0 4 1 2 10Obstetric3 conditions 6 0 0 0 0 0 1 1 8Hysterectomy 0 0 0 1 0 0 5 1 7Orchiopexy 0 5 0 0 0 0 1 1 7Orthopedic procedures 0 1 3 0 1 0 0 0 5Appendectomy 0 0 1 0 0 1 0 2 4Other procedures 0 0 2 5 0 1 2 0 10Total 59 64 80 61 58 47 79 103 5511Hemorrhoidectomy parasagittal anorectoplasty lateral internal sphincterotomy and manual anal dilation2Incision and drainage debridement and surgical toilet3Cesarian section and uterine evacuationlowastDistrict hospitals with a 100-bed capacity all state owned public hospitalsdaggerHealth center IVs outpatient facilities with 20-bed in-patient facilities998771A regional referral hospital 250 beds with some specialist services
Table 2 Showing diagnosis by age campsite in Uganda 2013
Procedure Age groups Unknown age Totallt5 5ndash18 19ndash39 40ndash59 ge60
Inguinal hernia 29 29 23 29 27 6 143Hydrocele 10 19 12 36 33 2 112Lipoma 2 7 14 19 14 1 57Goiter 0 0 16 15 3 1 35Epidermoid cyst 2 5 11 8 5 1 32Other hernias 0 1 8 9 8 1 27Congenital conditions 13 5 2 1 0 0 21Gluteal fibrosis 0 18 0 0 0 0 18Anorectal 0 1 10 5 1 0 17Infection 1 4 3 6 2 0 16Tumor 2 3 6 3 1 1 16Gynecologic 0 1 6 6 0 0 13Intra-abdominal masses 0 3 3 4 1 0 11Ganglion cyst 0 2 2 1 2 0 7Obstructed labor 0 2 4 0 0 0 6Trauma 0 1 3 2 0 0 6Other procedures 0 6 4 3 1 0 14Total 59 107 127 147 98 13 551
Persons with surgical disease are young and form thebulk of the Ugandan productive work force The bimodaldistribution of age showed that the paediatric (below 18 years)population and those between 30 and 60 years representthe bulk of the surgical burden of disease This emphasizesthe need for paediatric surgical skills in surgical training formedical officers
Males were overrepresented likely due to the high burdenof inguinal hernias and hydroceles Although the procedureper population rate was estimated at 125 100000 in thisreview at some sites it was as high as 146 100000 close towhat was estimated by Nordberg [9] in 1984 three decadesago Inguinal hernia and hydrocele occurrence were in equalproportions throughout age distribution
4 Surgery Research and Practice
Table 3 Procedure per population rates campsite in Uganda 2013
Site Catchment population (201011 estimates)Category and number of
procedures Procedure per 100000 of populationProcedure Number
Amuria 315900Hernia 13 1 41
Hydrocele 26 1 82Goiter 0 mdash
Kaberamaido 195400Hernia 18 1 92
Hydrocele 25 1 128Goiter 0 mdash
Katakwi 153600Hernia 10 1 65
Hydrocele 24 1 156Goiter 8 1 52
Serere 176500lowastHernia 45 1 255
Hydrocele 10 1 57Goiter 13 1 74
Ngora 101900lowastHernia 18 1 177
Hydrocele 6 1 59Goiter 10 1 98
Kumi and Aturur 13000Hernia 19 1 146
Hydrocele 15 1 115Goiter 9 1 69
Soroti 241200Hernia 20 1 83
Hydrocele 6 1 25Goiter 15 1 99
Overall 1197500Hernia 147 1 125
Hydrocele 112 1 10Goiter 35 1 29
lowast2002 population census estimates
The most common conditions seen in our study werehernia hydrocele and goiter These procedures are withinthe realm of competence of a medical officer (nonspecialistphysician) if properly trained and supported [10] What isalso true is that surgical camps environment is a platformfor apprenticeship the less experienced surgeons or traineeswork with more experienced colleagues to learn more in apractical setting handling high volumes of surgical cases in ashort period of time
Locoregional anesthesia was used in 70 of cases Thisaligns with recommendations made previously on the basisof cost of care and safety
This study also allowed us to estimate procedure perpopulation rate for the less common surgical conditions Theprevalence of correctable surgical congenital anomalies inUganda is not known In total 4 of all procedures donewerefor congenital anomalies Gluteal fibrosis or gluteal musclecontracture caused by repeated intramuscular quinine injec-tions accounted for 3 of surgical diagnoses It accountedfor 3 of surgical diagnoses GMC first reported by Valder-rama is a clinical syndrome pathologically characterized by
degeneration necrosis and fibrosis of the glutealmuscles andfascia leading to serious limitation of hip movements [11 12]Malaria is endemic in Uganda and in some places injectablequinine is used indiscriminately
Several challenges were encountered screening forcomorbidities such as NIDDM (non-insulin dependent dia-betes mellitus) and cardiorespiratory diseases was limited toclinical assessmentwithout lab and imaging formost patientsyet we know there is a significant burden of prediabetic anddiabetic states amongUgandans [11]The consequences of notscreening are not known in this context
Whereas these populations have close geographical accessto health centers they likely delay in access to appropriatecare due to a number of reasons including lack of skilledmanpower at the health centers drug stock-outs for anesthet-ics and health centers prioritizing resources for emergencyprocedures like Cesarean sections [13] During the campseveral logistical challenges were faced ranging from poweroutages inadequate sterilization capacity limited surgicalinstruments limited operating room space and intermittentsupply of running water These are not new [2 5 14]
Surgery Research and Practice 5
Table 4 Challenges reported solutions and future plans
Domain Challenges Solutions
Water andelectricity
Lack of running water at some sitesProlonged power outages at two sites
Patients andor their attendants to provide 20 litres ofwater eachUsing a generator (consider standby generators infuture surgical camps)
Inadequate number of anesthetistsNo anesthetic machine
Predetermining personnel needs and secure personnel(anesthetists) beforehand
Sterilization andsupplies
Limited capacity to sterilize (due to inadequate numberof autoclaves) power outages and inadequate linensuppliesDrugs and surgical sundries were in short supply
Better projections and resource mobilization for futurecampsConsidering hiring autoclavesContact nearby hospitals to participate and share
Equipment andinstruments
Equipment and instruments were limited (surgical setsanesthesia equipment)There was a concurrent ophthalmology camp going onWe had only one oxygen source
Doing better projections hiring equipment andinstrumentsConsidering portable oxygen supply
Human resource
Several patients with gynecological conditions came yetwe had no gynecologistsOperating theater condition some were very olddilapidatedFew staff in the theater to help in coordination andpatient flowInadequate postoperative nursing manpowerOne of the team members fell sick
Including gynecologists in future campsInstituting quality assurance and safety guidelines andagreeing on the minimum standardsGetting required personnel to commit before the campbegins
Demand forservice
Overwhelming number of casesSome pediatric cases could not be worked on
Planning triage days before the camp begins andgenerating manageable operating lists
Technicaloperativedifficulties
Giant hydroceles and hernias that had stayed for over 10years were a challenge with no intensive care unit(ICU) facilities
Triage and referral to better facilitated centersAllocating ldquodifficultyrdquo cases to the experiencedsurgeonsPriority was given to children the elderly and thosewhose conditions greatly affecting the quality of lifeMainly cases which need minimal postoperativenursing care were done
Others
Only a handful presented for preoperative screeningDue to limited working space privacy could not beobserved all the timeInadequate linen
Encouraging preoperative screening in future campsProcuring tents as a way of availing more working spaceGetting more linen
they impede access to surgical services even for stop-gapapproaches like surgical camps Documenting these chal-lenges is part of advocacy to mobilize resources and engagethose that have the power to prioritize available resources forservice
What has also been highlighted here (albeit crudely) is thecost of surgical interventionThe cost of surgical interventionwas $7250 per procedure This cost however was furthersubsidized by the infrastructure that already exists
What is clear from this study is that the scope ofconditions that were seen over ten years ago is still thesame However a population-based estimate of the burdenof surgical disease [3] and regular documentation of thecampsrsquo outcomes have not been done Estimates indicatethat surgery can address 7 of DALYs (disability-adjustedlife years) that occur in Africa [15] and this burden is mostprobably increasing rapidly [14]
Organizing a camp successfully requires a clear objectivea group of individuals or organization(s) finance(s) andan appropriate target population (beneficiary group) In
addition there was an agreedwork planwith the involvementof all stakeholders including local leaders hosting healthcenters sponsors Ministries of Health and the personnelthat carry out the procedures Publicity of these activities isencouraged in order to promote the service gain support andensure sustainability on the long term
5 Study Limitations
The data for screened patients that did not qualify for surgerywere unavailable The catchment population is an estimatethere may be overlap of health facility catchment areasand previously done procedures in the areacatchment werenot known No postoperation data was collected to assesspostoperative complicationswhichmay inform future camps
6 Conclusion
Surgical camps improve access of surgical services to vulner-able populations Inguinal hernias formed the bulk surgical
6 Surgery Research and Practice
disease encountered Hydroceles and thyroid disease alsocontribute significantly to the burden of disease in Sub-Saharan Africa Surgical camps should become an integralpart of health service delivery in rural Africa
Abbreviations
ASOU Association of Surgeons of UgandaGMC Gluteal muscle contractureHRH Human Resources for Health
Additional Points
The economic and social implications of unrepaired hernianeed to be investigated For future camps postoperativemorbidity data should be collected and the total number ofscreened patients Mostly importantly we consider surgicalcamps as an integral part of surgical service delivery byhospitals medical schools and Ministries of Health
Competing Interests
The authors declare no competing interests
Authorsrsquo Contributions
M Galukande wrote the first draft Elissa Butler E Elobuand M Galukande analyzed data O Kituuka J Jombwe JSekabira J Faulal performed critical reviews for intellectualcontent All authors authorized submission of this work forpublication and agreed to content
Acknowledgments
All staff of participatory sites all the patients local leadershipand volunteers
References
[1] D Ozgediz and R Riviello ldquoThe lsquootherrsquo neglected diseases inglobal public health surgical conditions in sub-SaharanAfricardquoPLoS Medicine vol 5 no 6 article e121 2008
[2] M Galukande J von Schreeb A Wladis et al ldquoEssentialsurgery at the district hospital a retrospective descriptiveanalysis in three African countriesrdquo PLoS Medicine vol 7 no3 Article ID e1000243 2010
[3] M Ohene-Yeboah and F A Abantanga ldquoInguinal hernia dis-ease in Africa a common but neglected surgical conditionrdquoWest African Journal of Medicine vol 30 no 2 pp 77ndash83 2011
[4] S Luboga S B Macfarlane J von Schreeb et al ldquoIncreasingaccess to surgical services in sub-saharan Africa prioritiesfor national and international agencies recommended by theBellagio Essential Surgery Grouprdquo PLoSMedicine vol 6 no 12Article ID e1000200 2009
[5] A F Linden F S Sekidde M Galukande L M Knowlton SChackungal and K A K McQueen ldquoChallenges of surgery indeveloping countries a survey of surgical and anesthesia capac-ity in ugandarsquos public hospitalsrdquo World Journal of Surgery vol36 no 5 pp 1056ndash1065 2012
[6] R Y Hsia N A Mbembati S Macfarlane and M E KrukldquoAccess to emergency and surgical care in sub-Saharan Africathe infrastructure gaprdquo Health Policy and Planning vol 27 no3 pp 234ndash244 2012
[7] I Kakande W W Obote and K Sebbaale Surgical camps TheUganda experience ECAJS 2007 httpwwwbiolineorgbrjs
[8] H Jaques ldquoSurgical innovation abroad and at homerdquo BMJCareers 2013 httpcareersbmjcomcareersadvicSurgicalinnovation abroad and at home
[9] E M Nordberg ldquoIncidence and estimated need of caesareansection inguinal hernia repair and operation for strangulatedhernia in rural Africardquo British Medical Journal vol 289 no6437 pp 92ndash93 1984
[10] M Galukande S Kaggwa P Sekimpi et al ldquoUse of surgicaltask shifting to scale up essential surgical services a feasibilityanalysis at facility level in Ugandardquo BMC Health ServicesResearch vol 13 no 1 article 292 2013
[11] J A F Valderrama ldquoA cause of limited flexion and adduction ofthe hip in childrenrdquoThe Journal of Bone amp Joint Surgery vol 52article 179 1970
[12] C-G Zhao X-J He B Lu H-P Li D Wang and Z-ZZhu ldquoClassification of gluteal muscle contracture in childrenand outcome of different treatmentsrdquo BMC MusculoskeletalDisorders vol 10 article 34 2009
[13] C E Grimes K G Bowman CM Dodgion and C B D LavyldquoSystematic review of barriers to surgical care in low-incomeandmiddle-income countriesrdquoWorld Journal of Surgery vol 35no 5 pp 941ndash950 2011
[14] D Ozgediz D Jamison M Cherian and K McQueen ldquoTheburden of surgical conditions and access to surgical care inlowmdashand middle-income countriesrdquo Bulletin of the WorldHealth Organization vol 86 no 8 pp 646ndash647 2008
[15] H TDebas R Gosselin CMcCord andAThind ldquoSurgeryrdquo inDiseaseControl Priorities inDevelopingCountries D T JamisonJ G Breman A R Measham et al Eds pp 1245ndash1259 WorldBank Washington DC USA Oxford University Press NewYork NY USA 2nd edition 2006
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

4 Surgery Research and Practice
Table 3 Procedure per population rates campsite in Uganda 2013
Site Catchment population (201011 estimates)Category and number of
procedures Procedure per 100000 of populationProcedure Number
Amuria 315900Hernia 13 1 41
Hydrocele 26 1 82Goiter 0 mdash
Kaberamaido 195400Hernia 18 1 92
Hydrocele 25 1 128Goiter 0 mdash
Katakwi 153600Hernia 10 1 65
Hydrocele 24 1 156Goiter 8 1 52
Serere 176500lowastHernia 45 1 255
Hydrocele 10 1 57Goiter 13 1 74
Ngora 101900lowastHernia 18 1 177
Hydrocele 6 1 59Goiter 10 1 98
Kumi and Aturur 13000Hernia 19 1 146
Hydrocele 15 1 115Goiter 9 1 69
Soroti 241200Hernia 20 1 83
Hydrocele 6 1 25Goiter 15 1 99
Overall 1197500Hernia 147 1 125
Hydrocele 112 1 10Goiter 35 1 29
lowast2002 population census estimates
The most common conditions seen in our study werehernia hydrocele and goiter These procedures are withinthe realm of competence of a medical officer (nonspecialistphysician) if properly trained and supported [10] What isalso true is that surgical camps environment is a platformfor apprenticeship the less experienced surgeons or traineeswork with more experienced colleagues to learn more in apractical setting handling high volumes of surgical cases in ashort period of time
Locoregional anesthesia was used in 70 of cases Thisaligns with recommendations made previously on the basisof cost of care and safety
This study also allowed us to estimate procedure perpopulation rate for the less common surgical conditions Theprevalence of correctable surgical congenital anomalies inUganda is not known In total 4 of all procedures donewerefor congenital anomalies Gluteal fibrosis or gluteal musclecontracture caused by repeated intramuscular quinine injec-tions accounted for 3 of surgical diagnoses It accountedfor 3 of surgical diagnoses GMC first reported by Valder-rama is a clinical syndrome pathologically characterized by
degeneration necrosis and fibrosis of the glutealmuscles andfascia leading to serious limitation of hip movements [11 12]Malaria is endemic in Uganda and in some places injectablequinine is used indiscriminately
Several challenges were encountered screening forcomorbidities such as NIDDM (non-insulin dependent dia-betes mellitus) and cardiorespiratory diseases was limited toclinical assessmentwithout lab and imaging formost patientsyet we know there is a significant burden of prediabetic anddiabetic states amongUgandans [11]The consequences of notscreening are not known in this context
Whereas these populations have close geographical accessto health centers they likely delay in access to appropriatecare due to a number of reasons including lack of skilledmanpower at the health centers drug stock-outs for anesthet-ics and health centers prioritizing resources for emergencyprocedures like Cesarean sections [13] During the campseveral logistical challenges were faced ranging from poweroutages inadequate sterilization capacity limited surgicalinstruments limited operating room space and intermittentsupply of running water These are not new [2 5 14]
Surgery Research and Practice 5
Table 4 Challenges reported solutions and future plans
Domain Challenges Solutions
Water andelectricity
Lack of running water at some sitesProlonged power outages at two sites
Patients andor their attendants to provide 20 litres ofwater eachUsing a generator (consider standby generators infuture surgical camps)
Inadequate number of anesthetistsNo anesthetic machine
Predetermining personnel needs and secure personnel(anesthetists) beforehand
Sterilization andsupplies
Limited capacity to sterilize (due to inadequate numberof autoclaves) power outages and inadequate linensuppliesDrugs and surgical sundries were in short supply
Better projections and resource mobilization for futurecampsConsidering hiring autoclavesContact nearby hospitals to participate and share
Equipment andinstruments
Equipment and instruments were limited (surgical setsanesthesia equipment)There was a concurrent ophthalmology camp going onWe had only one oxygen source
Doing better projections hiring equipment andinstrumentsConsidering portable oxygen supply
Human resource
Several patients with gynecological conditions came yetwe had no gynecologistsOperating theater condition some were very olddilapidatedFew staff in the theater to help in coordination andpatient flowInadequate postoperative nursing manpowerOne of the team members fell sick
Including gynecologists in future campsInstituting quality assurance and safety guidelines andagreeing on the minimum standardsGetting required personnel to commit before the campbegins
Demand forservice
Overwhelming number of casesSome pediatric cases could not be worked on
Planning triage days before the camp begins andgenerating manageable operating lists
Technicaloperativedifficulties
Giant hydroceles and hernias that had stayed for over 10years were a challenge with no intensive care unit(ICU) facilities
Triage and referral to better facilitated centersAllocating ldquodifficultyrdquo cases to the experiencedsurgeonsPriority was given to children the elderly and thosewhose conditions greatly affecting the quality of lifeMainly cases which need minimal postoperativenursing care were done
Others
Only a handful presented for preoperative screeningDue to limited working space privacy could not beobserved all the timeInadequate linen
Encouraging preoperative screening in future campsProcuring tents as a way of availing more working spaceGetting more linen
they impede access to surgical services even for stop-gapapproaches like surgical camps Documenting these chal-lenges is part of advocacy to mobilize resources and engagethose that have the power to prioritize available resources forservice
What has also been highlighted here (albeit crudely) is thecost of surgical interventionThe cost of surgical interventionwas $7250 per procedure This cost however was furthersubsidized by the infrastructure that already exists
What is clear from this study is that the scope ofconditions that were seen over ten years ago is still thesame However a population-based estimate of the burdenof surgical disease [3] and regular documentation of thecampsrsquo outcomes have not been done Estimates indicatethat surgery can address 7 of DALYs (disability-adjustedlife years) that occur in Africa [15] and this burden is mostprobably increasing rapidly [14]
Organizing a camp successfully requires a clear objectivea group of individuals or organization(s) finance(s) andan appropriate target population (beneficiary group) In
addition there was an agreedwork planwith the involvementof all stakeholders including local leaders hosting healthcenters sponsors Ministries of Health and the personnelthat carry out the procedures Publicity of these activities isencouraged in order to promote the service gain support andensure sustainability on the long term
5 Study Limitations
The data for screened patients that did not qualify for surgerywere unavailable The catchment population is an estimatethere may be overlap of health facility catchment areasand previously done procedures in the areacatchment werenot known No postoperation data was collected to assesspostoperative complicationswhichmay inform future camps
6 Conclusion
Surgical camps improve access of surgical services to vulner-able populations Inguinal hernias formed the bulk surgical
6 Surgery Research and Practice
disease encountered Hydroceles and thyroid disease alsocontribute significantly to the burden of disease in Sub-Saharan Africa Surgical camps should become an integralpart of health service delivery in rural Africa
Abbreviations
ASOU Association of Surgeons of UgandaGMC Gluteal muscle contractureHRH Human Resources for Health
Additional Points
The economic and social implications of unrepaired hernianeed to be investigated For future camps postoperativemorbidity data should be collected and the total number ofscreened patients Mostly importantly we consider surgicalcamps as an integral part of surgical service delivery byhospitals medical schools and Ministries of Health
Competing Interests
The authors declare no competing interests
Authorsrsquo Contributions
M Galukande wrote the first draft Elissa Butler E Elobuand M Galukande analyzed data O Kituuka J Jombwe JSekabira J Faulal performed critical reviews for intellectualcontent All authors authorized submission of this work forpublication and agreed to content
Acknowledgments
All staff of participatory sites all the patients local leadershipand volunteers
References
[1] D Ozgediz and R Riviello ldquoThe lsquootherrsquo neglected diseases inglobal public health surgical conditions in sub-SaharanAfricardquoPLoS Medicine vol 5 no 6 article e121 2008
[2] M Galukande J von Schreeb A Wladis et al ldquoEssentialsurgery at the district hospital a retrospective descriptiveanalysis in three African countriesrdquo PLoS Medicine vol 7 no3 Article ID e1000243 2010
[3] M Ohene-Yeboah and F A Abantanga ldquoInguinal hernia dis-ease in Africa a common but neglected surgical conditionrdquoWest African Journal of Medicine vol 30 no 2 pp 77ndash83 2011
[4] S Luboga S B Macfarlane J von Schreeb et al ldquoIncreasingaccess to surgical services in sub-saharan Africa prioritiesfor national and international agencies recommended by theBellagio Essential Surgery Grouprdquo PLoSMedicine vol 6 no 12Article ID e1000200 2009
[5] A F Linden F S Sekidde M Galukande L M Knowlton SChackungal and K A K McQueen ldquoChallenges of surgery indeveloping countries a survey of surgical and anesthesia capac-ity in ugandarsquos public hospitalsrdquo World Journal of Surgery vol36 no 5 pp 1056ndash1065 2012
[6] R Y Hsia N A Mbembati S Macfarlane and M E KrukldquoAccess to emergency and surgical care in sub-Saharan Africathe infrastructure gaprdquo Health Policy and Planning vol 27 no3 pp 234ndash244 2012
[7] I Kakande W W Obote and K Sebbaale Surgical camps TheUganda experience ECAJS 2007 httpwwwbiolineorgbrjs
[8] H Jaques ldquoSurgical innovation abroad and at homerdquo BMJCareers 2013 httpcareersbmjcomcareersadvicSurgicalinnovation abroad and at home
[9] E M Nordberg ldquoIncidence and estimated need of caesareansection inguinal hernia repair and operation for strangulatedhernia in rural Africardquo British Medical Journal vol 289 no6437 pp 92ndash93 1984
[10] M Galukande S Kaggwa P Sekimpi et al ldquoUse of surgicaltask shifting to scale up essential surgical services a feasibilityanalysis at facility level in Ugandardquo BMC Health ServicesResearch vol 13 no 1 article 292 2013
[11] J A F Valderrama ldquoA cause of limited flexion and adduction ofthe hip in childrenrdquoThe Journal of Bone amp Joint Surgery vol 52article 179 1970
[12] C-G Zhao X-J He B Lu H-P Li D Wang and Z-ZZhu ldquoClassification of gluteal muscle contracture in childrenand outcome of different treatmentsrdquo BMC MusculoskeletalDisorders vol 10 article 34 2009
[13] C E Grimes K G Bowman CM Dodgion and C B D LavyldquoSystematic review of barriers to surgical care in low-incomeandmiddle-income countriesrdquoWorld Journal of Surgery vol 35no 5 pp 941ndash950 2011
[14] D Ozgediz D Jamison M Cherian and K McQueen ldquoTheburden of surgical conditions and access to surgical care inlowmdashand middle-income countriesrdquo Bulletin of the WorldHealth Organization vol 86 no 8 pp 646ndash647 2008
[15] H TDebas R Gosselin CMcCord andAThind ldquoSurgeryrdquo inDiseaseControl Priorities inDevelopingCountries D T JamisonJ G Breman A R Measham et al Eds pp 1245ndash1259 WorldBank Washington DC USA Oxford University Press NewYork NY USA 2nd edition 2006
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

Surgery Research and Practice 5
Table 4 Challenges reported solutions and future plans
Domain Challenges Solutions
Water andelectricity
Lack of running water at some sitesProlonged power outages at two sites
Patients andor their attendants to provide 20 litres ofwater eachUsing a generator (consider standby generators infuture surgical camps)
Inadequate number of anesthetistsNo anesthetic machine
Predetermining personnel needs and secure personnel(anesthetists) beforehand
Sterilization andsupplies
Limited capacity to sterilize (due to inadequate numberof autoclaves) power outages and inadequate linensuppliesDrugs and surgical sundries were in short supply
Better projections and resource mobilization for futurecampsConsidering hiring autoclavesContact nearby hospitals to participate and share
Equipment andinstruments
Equipment and instruments were limited (surgical setsanesthesia equipment)There was a concurrent ophthalmology camp going onWe had only one oxygen source
Doing better projections hiring equipment andinstrumentsConsidering portable oxygen supply
Human resource
Several patients with gynecological conditions came yetwe had no gynecologistsOperating theater condition some were very olddilapidatedFew staff in the theater to help in coordination andpatient flowInadequate postoperative nursing manpowerOne of the team members fell sick
Including gynecologists in future campsInstituting quality assurance and safety guidelines andagreeing on the minimum standardsGetting required personnel to commit before the campbegins
Demand forservice
Overwhelming number of casesSome pediatric cases could not be worked on
Planning triage days before the camp begins andgenerating manageable operating lists
Technicaloperativedifficulties
Giant hydroceles and hernias that had stayed for over 10years were a challenge with no intensive care unit(ICU) facilities
Triage and referral to better facilitated centersAllocating ldquodifficultyrdquo cases to the experiencedsurgeonsPriority was given to children the elderly and thosewhose conditions greatly affecting the quality of lifeMainly cases which need minimal postoperativenursing care were done
Others
Only a handful presented for preoperative screeningDue to limited working space privacy could not beobserved all the timeInadequate linen
Encouraging preoperative screening in future campsProcuring tents as a way of availing more working spaceGetting more linen
they impede access to surgical services even for stop-gapapproaches like surgical camps Documenting these chal-lenges is part of advocacy to mobilize resources and engagethose that have the power to prioritize available resources forservice
What has also been highlighted here (albeit crudely) is thecost of surgical interventionThe cost of surgical interventionwas $7250 per procedure This cost however was furthersubsidized by the infrastructure that already exists
What is clear from this study is that the scope ofconditions that were seen over ten years ago is still thesame However a population-based estimate of the burdenof surgical disease [3] and regular documentation of thecampsrsquo outcomes have not been done Estimates indicatethat surgery can address 7 of DALYs (disability-adjustedlife years) that occur in Africa [15] and this burden is mostprobably increasing rapidly [14]
Organizing a camp successfully requires a clear objectivea group of individuals or organization(s) finance(s) andan appropriate target population (beneficiary group) In
addition there was an agreedwork planwith the involvementof all stakeholders including local leaders hosting healthcenters sponsors Ministries of Health and the personnelthat carry out the procedures Publicity of these activities isencouraged in order to promote the service gain support andensure sustainability on the long term
5 Study Limitations
The data for screened patients that did not qualify for surgerywere unavailable The catchment population is an estimatethere may be overlap of health facility catchment areasand previously done procedures in the areacatchment werenot known No postoperation data was collected to assesspostoperative complicationswhichmay inform future camps
6 Conclusion
Surgical camps improve access of surgical services to vulner-able populations Inguinal hernias formed the bulk surgical
6 Surgery Research and Practice
disease encountered Hydroceles and thyroid disease alsocontribute significantly to the burden of disease in Sub-Saharan Africa Surgical camps should become an integralpart of health service delivery in rural Africa
Abbreviations
ASOU Association of Surgeons of UgandaGMC Gluteal muscle contractureHRH Human Resources for Health
Additional Points
The economic and social implications of unrepaired hernianeed to be investigated For future camps postoperativemorbidity data should be collected and the total number ofscreened patients Mostly importantly we consider surgicalcamps as an integral part of surgical service delivery byhospitals medical schools and Ministries of Health
Competing Interests
The authors declare no competing interests
Authorsrsquo Contributions
M Galukande wrote the first draft Elissa Butler E Elobuand M Galukande analyzed data O Kituuka J Jombwe JSekabira J Faulal performed critical reviews for intellectualcontent All authors authorized submission of this work forpublication and agreed to content
Acknowledgments
All staff of participatory sites all the patients local leadershipand volunteers
References
[1] D Ozgediz and R Riviello ldquoThe lsquootherrsquo neglected diseases inglobal public health surgical conditions in sub-SaharanAfricardquoPLoS Medicine vol 5 no 6 article e121 2008
[2] M Galukande J von Schreeb A Wladis et al ldquoEssentialsurgery at the district hospital a retrospective descriptiveanalysis in three African countriesrdquo PLoS Medicine vol 7 no3 Article ID e1000243 2010
[3] M Ohene-Yeboah and F A Abantanga ldquoInguinal hernia dis-ease in Africa a common but neglected surgical conditionrdquoWest African Journal of Medicine vol 30 no 2 pp 77ndash83 2011
[4] S Luboga S B Macfarlane J von Schreeb et al ldquoIncreasingaccess to surgical services in sub-saharan Africa prioritiesfor national and international agencies recommended by theBellagio Essential Surgery Grouprdquo PLoSMedicine vol 6 no 12Article ID e1000200 2009
[5] A F Linden F S Sekidde M Galukande L M Knowlton SChackungal and K A K McQueen ldquoChallenges of surgery indeveloping countries a survey of surgical and anesthesia capac-ity in ugandarsquos public hospitalsrdquo World Journal of Surgery vol36 no 5 pp 1056ndash1065 2012
[6] R Y Hsia N A Mbembati S Macfarlane and M E KrukldquoAccess to emergency and surgical care in sub-Saharan Africathe infrastructure gaprdquo Health Policy and Planning vol 27 no3 pp 234ndash244 2012
[7] I Kakande W W Obote and K Sebbaale Surgical camps TheUganda experience ECAJS 2007 httpwwwbiolineorgbrjs
[8] H Jaques ldquoSurgical innovation abroad and at homerdquo BMJCareers 2013 httpcareersbmjcomcareersadvicSurgicalinnovation abroad and at home
[9] E M Nordberg ldquoIncidence and estimated need of caesareansection inguinal hernia repair and operation for strangulatedhernia in rural Africardquo British Medical Journal vol 289 no6437 pp 92ndash93 1984
[10] M Galukande S Kaggwa P Sekimpi et al ldquoUse of surgicaltask shifting to scale up essential surgical services a feasibilityanalysis at facility level in Ugandardquo BMC Health ServicesResearch vol 13 no 1 article 292 2013
[11] J A F Valderrama ldquoA cause of limited flexion and adduction ofthe hip in childrenrdquoThe Journal of Bone amp Joint Surgery vol 52article 179 1970
[12] C-G Zhao X-J He B Lu H-P Li D Wang and Z-ZZhu ldquoClassification of gluteal muscle contracture in childrenand outcome of different treatmentsrdquo BMC MusculoskeletalDisorders vol 10 article 34 2009
[13] C E Grimes K G Bowman CM Dodgion and C B D LavyldquoSystematic review of barriers to surgical care in low-incomeandmiddle-income countriesrdquoWorld Journal of Surgery vol 35no 5 pp 941ndash950 2011
[14] D Ozgediz D Jamison M Cherian and K McQueen ldquoTheburden of surgical conditions and access to surgical care inlowmdashand middle-income countriesrdquo Bulletin of the WorldHealth Organization vol 86 no 8 pp 646ndash647 2008
[15] H TDebas R Gosselin CMcCord andAThind ldquoSurgeryrdquo inDiseaseControl Priorities inDevelopingCountries D T JamisonJ G Breman A R Measham et al Eds pp 1245ndash1259 WorldBank Washington DC USA Oxford University Press NewYork NY USA 2nd edition 2006
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

6 Surgery Research and Practice
disease encountered Hydroceles and thyroid disease alsocontribute significantly to the burden of disease in Sub-Saharan Africa Surgical camps should become an integralpart of health service delivery in rural Africa
Abbreviations
ASOU Association of Surgeons of UgandaGMC Gluteal muscle contractureHRH Human Resources for Health
Additional Points
The economic and social implications of unrepaired hernianeed to be investigated For future camps postoperativemorbidity data should be collected and the total number ofscreened patients Mostly importantly we consider surgicalcamps as an integral part of surgical service delivery byhospitals medical schools and Ministries of Health
Competing Interests
The authors declare no competing interests
Authorsrsquo Contributions
M Galukande wrote the first draft Elissa Butler E Elobuand M Galukande analyzed data O Kituuka J Jombwe JSekabira J Faulal performed critical reviews for intellectualcontent All authors authorized submission of this work forpublication and agreed to content
Acknowledgments
All staff of participatory sites all the patients local leadershipand volunteers
References
[1] D Ozgediz and R Riviello ldquoThe lsquootherrsquo neglected diseases inglobal public health surgical conditions in sub-SaharanAfricardquoPLoS Medicine vol 5 no 6 article e121 2008
[2] M Galukande J von Schreeb A Wladis et al ldquoEssentialsurgery at the district hospital a retrospective descriptiveanalysis in three African countriesrdquo PLoS Medicine vol 7 no3 Article ID e1000243 2010
[3] M Ohene-Yeboah and F A Abantanga ldquoInguinal hernia dis-ease in Africa a common but neglected surgical conditionrdquoWest African Journal of Medicine vol 30 no 2 pp 77ndash83 2011
[4] S Luboga S B Macfarlane J von Schreeb et al ldquoIncreasingaccess to surgical services in sub-saharan Africa prioritiesfor national and international agencies recommended by theBellagio Essential Surgery Grouprdquo PLoSMedicine vol 6 no 12Article ID e1000200 2009
[5] A F Linden F S Sekidde M Galukande L M Knowlton SChackungal and K A K McQueen ldquoChallenges of surgery indeveloping countries a survey of surgical and anesthesia capac-ity in ugandarsquos public hospitalsrdquo World Journal of Surgery vol36 no 5 pp 1056ndash1065 2012
[6] R Y Hsia N A Mbembati S Macfarlane and M E KrukldquoAccess to emergency and surgical care in sub-Saharan Africathe infrastructure gaprdquo Health Policy and Planning vol 27 no3 pp 234ndash244 2012
[7] I Kakande W W Obote and K Sebbaale Surgical camps TheUganda experience ECAJS 2007 httpwwwbiolineorgbrjs
[8] H Jaques ldquoSurgical innovation abroad and at homerdquo BMJCareers 2013 httpcareersbmjcomcareersadvicSurgicalinnovation abroad and at home
[9] E M Nordberg ldquoIncidence and estimated need of caesareansection inguinal hernia repair and operation for strangulatedhernia in rural Africardquo British Medical Journal vol 289 no6437 pp 92ndash93 1984
[10] M Galukande S Kaggwa P Sekimpi et al ldquoUse of surgicaltask shifting to scale up essential surgical services a feasibilityanalysis at facility level in Ugandardquo BMC Health ServicesResearch vol 13 no 1 article 292 2013
[11] J A F Valderrama ldquoA cause of limited flexion and adduction ofthe hip in childrenrdquoThe Journal of Bone amp Joint Surgery vol 52article 179 1970
[12] C-G Zhao X-J He B Lu H-P Li D Wang and Z-ZZhu ldquoClassification of gluteal muscle contracture in childrenand outcome of different treatmentsrdquo BMC MusculoskeletalDisorders vol 10 article 34 2009
[13] C E Grimes K G Bowman CM Dodgion and C B D LavyldquoSystematic review of barriers to surgical care in low-incomeandmiddle-income countriesrdquoWorld Journal of Surgery vol 35no 5 pp 941ndash950 2011
[14] D Ozgediz D Jamison M Cherian and K McQueen ldquoTheburden of surgical conditions and access to surgical care inlowmdashand middle-income countriesrdquo Bulletin of the WorldHealth Organization vol 86 no 8 pp 646ndash647 2008
[15] H TDebas R Gosselin CMcCord andAThind ldquoSurgeryrdquo inDiseaseControl Priorities inDevelopingCountries D T JamisonJ G Breman A R Measham et al Eds pp 1245ndash1259 WorldBank Washington DC USA Oxford University Press NewYork NY USA 2nd edition 2006
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom