REPORT OF THE - Radiological Council · QUALIFICATIONS AND TRAINING OF RADIATION USERS 5 CHANGES TO...
46
Transcript of REPORT OF THE - Radiological Council · QUALIFICATIONS AND TRAINING OF RADIATION USERS 5 CHANGES TO...


REPORT OF THE
RADIOLOGICAL COUNCIL
for the year ended
31 December 2007

TABLE OF CONTENTS
CHAIRMAN’S REVIEW I
RADIATION SAFETY ACT 1975 – 2004 3
STATUTORY RESPONSIBILITIES OF THE COUNCIL 3
MEMBERSHIP OF THE COUNCIL 3
ADVISORY COMMITTEES 4
ADMINISTRATIVE SUPPORT 4
STATE ELECTORAL ACT 5
STATE RECORDS ACT 5
THE RADIOLOGICAL COUNCIL WEBSITE 5
REGISTRATIONS, LICENCES AND TEMPORARY PERMITS 5
QUALIFICATIONS AND TRAINING OF RADIATION USERS 5
CHANGES TO LEGISLATION 5
RADIATION INCIDENTS 6
PROSECUTIONS 17
MEDICAL AND RELATED RADIATION MATTERS 18
Compliance Testing 18
Compliance Testing Working Group 18
Licensing of Medical Radiation Technologists 19
Approvals for Exposure to Radiation for Human Subjects in Medical Research 20

Radiological Council 2007 Annual Report
INDUSTRIAL, ENVIRONMENTAL AND MINING RADIATION 21
Industrial Compliance Testing 21
Standards for Council Examinations 21
MISCELLANEOUS 21
Solaria 21
Radiation Health Committee 21
National Directory for Radiation Protection 22
Personal Radiation Monitoring Services 22
APPENDIX 1: REGISTRATION AND LICENSING 24
APPENDIX 2: LICENCE PREREQUISITES 26
ATTACHMENT 1: RADIOLOGICAL COUNCIL 27
ATTACHMENT 2: LEGISLATION AMENDMENTS 28
ATTACHMENT 3: COMPLIANCE TESTING 29
ATTACHMENT 4: INDUSTRIAL RADIATION SAFETY EXAMINATIONS 30
ATTACHMENT 5: REGISTERED IRRADIATING APPARATUS, ELECTRONIC PRODUCTS AND RADIOACTIVE SUBSTANCES (SEALED SOURCES) 31
ATTACHMENT 6: LICENCES AND REGISTRATIONS 33
ABBREVIATIONS 37

CHAIRMAN’S REVIEW
This is the 8th Annual report that I have had the pleasure of presenting since my appointment as Chairman of the Radiological Council in June 2000. This year, as in previous years, the Council has dealt with a number of very important issues which are described more fully in the body of this report. Amongst these was the introduction of licensing under the Radiation Safety Act (1975) for Medical Radiation Technologists. This was brought about by the promulgation of the Medical
Radiation Technologists Act (2006) which introduced a number of consequential amendments to the Radiation Safety Act. 836 new licences were issued in the second half of 2007 to technologists performing Medical Imaging, Radiation Therapy or Diagnostic Nuclear Medicine. The volume of work entailed in the issue of such licences within a short period of time strained the resources of the Radiation Health Branch, the branch of the Department of Health which provides administrative and scientific support to the Council. The use of solaria by the public, and recognition that use of such solaria increases the risk of skin cancer, has prompted the Council to reconsider the regulation of these premises and their equipment in Western Australia. Other Australian jurisdictions are similarly committed. The Council became actively involved in formulation of a national approach to this matter and it is anticipated that this will lead eventually to more stringent control of these premises within Australia in an effort to protect public health. In the medical field, the Council has strongly supported and contributed to the development of a national medical code of practice to cover radiation safety standards in medical imaging, radiotherapy and nuclear medicine. Introduction of the Code, expected in 2008, will require all public and private practices to develop and submit radiation management plans to the Council.

Radiological Council 2007 Annual Report
The number of radiation incidents reported to the Council in 2007 has increased from those reported in previous years. This increase may indeed be a reflection of the readiness with which such incidents are now being reported rather than an actual steep increase in incidents. It is, of course, to be expected that with an increase in the number of radiological apparata, radioactive substances and users the occurrence of incidents will also increase. While the majority of incidents reported have been relatively minor, the Council continues to monitor incidents to ensure that public safety is not compromised and expresses appropriate concern as necessary. In this regard, the Council keeps itself informed of best international practice in radiation safety and has reviewed a range of reports dealing with regulatory developments.
The trend in loss of staff of the Radiation Health Branch observed in the previous few years continued in 2007 and remains to be of concern to the Council. Western Australia has experienced significant growth over several years in the number and complexity of irradiating apparata and radioactive substances used and regulated under the Act. This relentless growth coupled with the loss of experienced and trained staff seeking better career prospects elsewhere and emerging regulatory considerations, place considerable pressure on the remaining officers of the Branch. I once again wish to thank them for their professionalism and dedication to their work, sometimes under adverse conditions in guarding the safety of people of Western Australia from the detrimental effects of ionising radiation if these apparata and substances were not adequately controlled.
Finally I wish to thank all members of the Council for their support, continued contributions, in and out of sessions, and sheer hard work during 2007. Their individual strengths and expertise, together with the assistance of officers of the Radiation Health Branch, permit the Council to fulfil its statutory function smoothly.
Dr P Psaila-Savona CHAIRMAN
20 March 2008
Radiological Council 2007 Annual Report
Page 3
RADIATION SAFETY ACT 1975 – 2004 STATUTORY RESPONSIBILITIES OF THE COUNCIL
The Radiological Council is appointed under section 13 of the Radiation Safety Act to assist the Minister to protect public health and to maintain safe practices in the use of radiation.
In its position as an independent regulatory authority, the Council is required to administer the Act and to —
implement the scheme of licensing and registration;
conduct inquiries into alleged contraventions of the Act and, where necessary, to suspend or cancel licences and registrations;
advise the Minister and make recommendations with respect to the technical aspects of radiation safety requirements, the methods that may be used to prevent or minimise the dangers arising from the use of radioactive substances, irradiating apparatus and electronic products, including the preparation of regulations;
investigate and prosecute offences.
The Council is also required to keep under review manufactured or assembled devices which emit radiation to determine if control of these devices is necessary under the Act.
Section 10 requires the Minister at all times to have regard to the expressed views of the Council.
MEMBERSHIP OF THE COUNCIL
The Council comprises —
a medical practitioner appointed by the Governor on the recommendation of the Executive Director Public Health;
a medical practitioner who is a specialist in radiology or radiotherapy;
a physician specialising in nuclear medicine;
a person who possesses relevant qualifications or experience as a physicist;
a person who possesses relevant qualifications or experience as a radiation engineer or electronic engineer;
Radiological Council 2007 Annual Report
Page 4
a representative of the interests of tertiary educational institutions.
Two other persons with special expertise in radiation protection may be nominated by the Minister on the advice of the other members of the Council.
The present members, approved by the Governor, are listed in attachment 1.
The Council met seven times in 2007.
ADVISORY COMMITTEES
The Council may appoint committees under section 19 of the Act to investigate and advise on any aspect of its functions, or to carry out any function other than those relating to licences and registrations. The present policy is to create, when necessary, short-term working parties which address a specific issue and report back to the Council.
The only exception is Council’s Chiropractic Advisory Committee which is appointed to supervise the radiation safety examination for chiropractors who wish to apply for licences to operate diagnostic x-ray equipment. The committee, which also advises Council on other chiropractic matters, met twice in 2007.
ADMINISTRATIVE SUPPORT
Section 10(4) of the Act provides for the administration of the Act to be paid out of moneys appropriated by Parliament for the purpose. However, the Council is not funded directly and relies on the Department of Health’s Radiation Health Branch for administrative and scientific support. While the greater part of the Branch’s duties are directly concerned with supporting the Council’s needs, and many of the staff are appointed authorised officers under section 4(1) of the Act for this purpose, the Branch also provides separate advice to the Department on a range of radiation issues.
The Radiation Health Branch also provides the Secretary of the Council. The position has been held by Ms H Upton (Managing Health Physicist) since February 2002, with Mr L Dahlskog (Senior Health Physicist) and Mrs M Aerts (Health Physicist) performing these duties in Ms Upton’s absence.

Radiological Council 2007 Annual Report
Page 5
STATE ELECTORAL ACT
For the purposes of section 175ZE of the State Electoral Act, the Radiological Council has no expenditure to report. Council’s functions are supported from within the budget assigned by the Department of Health to the Radiation Health Branch. The Council does not have a budget in its own right.
STATE RECORDS ACT
The Radiological Council’s record keeping systems are managed by the Radiation Health Branch of the Department of Health, and thus the Council’s compliance with the State Records Commission Standard 2, Principle 6 is linked to compliance by the Department of Health.
THE RADIOLOGICAL COUNCIL WEBSITE
In 2004 the first version of the Radiological Council Website was finalised and was made available for access by the public at the address www.radiologicalcouncil.wa.gov.au. There were no amendments made to the website during 2007.
REGISTRATIONS, LICENCES AND TEMPORARY PERMITS
Registration and licensing are the principal means by which the use of radiation is regulated. A summary of the legislative system for registration and licensing in Western Australia is included in appendix 1.
QUALIFICATIONS AND TRAINING OF RADIATION USERS
A summary of the legislative scheme for ensuring the appropriate qualifications and competence of persons applying for licences is included in appendix 2.
CHANGES TO LEGISLATION
The consequential amendments made to the Radiation Safety Act in 2006, as a result of the Medical Radiation Technologists Act 2006, commenced on 1 July 2007.

Radiological Council 2007 Annual Report
Page 6
There were no other changes to the legislation administered by the Council during 2007.
RADIATION INCIDENTS
Reported incidents involving radiation rarely pose a major health risk to the individuals exposed. Regulation 19A of the Radiation Safety (General) Regulations requires registrants to notify the Council in writing and as soon as practicable should any of the abnormal or unplanned radiation exposures specified in that regulation occur.
Although there is no certainty that all incidents are reported, Council encourages reporting and rigorous investigation of the cause as this provides a forum for improving work practices and minimising the recurrence of such incidents
The Council was notified of 18 incidents during 2007:
Medical Incidents
A report was received regarding a spill of 450 MBq of 99mTc within a hospital Nuclear Medicine Department.
The incident was caused when a plastic shield usually placed around the plunger of the radiopharmaceutical container to prevent it being accidentally pushed in was omitted. During transportation from the dispensing area to the injection room about half of the original 900 MBq within the syringe was released into the ward injection box. The spill was noticed by the nuclear medicine technologist immediately on opening the injection box. The box was closed and kept shielded within the department’s isotope laboratory until the contamination had decayed to acceptable levels.
The nuclear medicine technician involved was cautioned and a more suitable carrying arrangement was put into place to prevent similar incidents from occurring in the future. Council noted that the incident appeared to have been due to human error and agreed that no further action was necessary. Council received a report from a hospital’s Radiation Safety Officer regarding a spill of 15 GBq 99mTc within the dispensing laboratory of the Nuclear Medicine Department.
A Nuclear Medicine Technologist failed to release the positive pressure from a vial prior to attempting to inject the 99mTc into the vial. The pressure was sufficient to blow 99mTc out of the syringe and

Radiological Council 2007 Annual Report
Page 7
into the dispensing area. The Technologist and the supervisor, with the help of the Senior Physicist, acted immediately to decontaminate the site.
The Technologist was subsequently counselled and given instruction to work with less haste and more caution to avoid similar incidents in the future.
Council noted the report and agreed that no further action was necessary.
Council was advised of an incident involving the spill of 900 MBq 99mTc within a hospital nuclear medicine department.
The incident occurred during a myocardial stress test while the patient was exercising on a treadmill. Extension tubing which connects the cannula in the patient to the radiopharmaceutical came loose during the exercise. The particular device was relatively new to the Hospital and is understood to have been used because it was less expensive, even though clinical staff had noted it might not be suitable for the procedures being carried out. The difficulties experienced did not occur with previously used devices.
Contamination from the 99mTc was limited to the ECG table, cables, computer keyboard and the floor of the stress testing room.
A recommendation was made by the departmental Radiation Safety Officer that suitable extension tubing be used and that prepared radiopharmaceuticals should not be placed on the ECG table.
The Radiation Safety Officer at a university advised that a medical imaging technology student had recorded a radiation dose of 57.12 mSv over a three month period, the pro-rata dose limit for the period being 5 mSv. The university reported that the student had left his radiation monitoring device attached to his laboratory coat in the fluoroscopy x-ray room for a week while on clinical placement and on a second occasion had deliberately imaged his bag with the device inside it.
Council agreed that the recorded dose should remain on the student’s personal dose history and agreed to remind the student of his responsibilities with respect to the use of personal monitoring devices.
Council was advised that a doctor working in a hospital cardiology department had successive reportable radiation doses for three

Radiological Council 2007 Annual Report
Page 8
months in 2007. In May the doctor recorded 22mSv on his collar badge and 2 mSv on his trunk badge. In June 2007 he recorded 19 mSv on his collar badge and 1.8 mSv on his trunk badge and in July, 21 mSv on his collar badge and 2 mSv on his trunk badge. Council noted that using established dose assessment procedures, this gave the doctor a total combined effective radiation dose of 4.45 mSv for the period May-June 2007.
The hospital’s Radiation Safety Officer (RSO) advised that in both months the doctor had been required to attend to a cardiac arrest during fluoroscopic x-ray procedures, requiring him to step out from behind a protective screen to maintain the patient’s airway until an anaesthetist arrived. The RSO advised that he had observed the doctor’s usual working practices and could find no other obvious reason for these readings.
The Council was concerned at the doctor’s work practices and questioned why the fluoroscopic x-ray exposure should continue when a cardiac arrest occurs. Council agreed to seek further information concerning the supervision of the doctor.
Council received a letter from the Director of Medical Services at a hospital regarding a reportable dose recorded for a consultant cardiovascular surgeon. For a one month period the surgeon had received a radiation dose of 0.21 mSv to his collar dosimeter and a dose of 2.9 mSv to his trunk dosimeter. As the doses were inappropriate to their location on the body, the circumstances were investigated by the hospital which found that the surgeon had inadvertently swapped his collar and trunk badges.
The hospital’s Radiation Safety Officer made a notation in the surgeon’s dose records and requested the monitoring service provider to do the same.
Council agreed that the actions taken appeared appropriate.
A report was received from a hospital’s Radiation Safety Officer regarding a dose of 14.86 mSv recorded for a radiation therapist.
Personal radiation monitoring devices are worn by radiation therapists for a period of 3 months and under Regulation 15 2(a) a report must be made in writing to the Council within 7 days of notification of the recorded dose.
The report stated that the radiation therapist’s badge had fallen off his person and slipped between a patient and the bed immediately

Radiological Council 2007 Annual Report
Page 9
before a radiotherapy treatment. The badge was recovered after the treatment and handed to the officer responsible for personal radiation monitoring in the Radiation Oncology Department who replaced it with a new badge. The replacement badge received less than the detectable limit for the remainder of the monitoring period and it is this result that has been used on the radiation therapist’s dose record.
Council agreed that the higher dose should not be included in the therapist’s personal dose record.
However, no record had been kept of the incident by the radiation oncology department or the hospital apparently in the belief that the matter was not significant. The Council informed the hospital that its response in relation to the matter had been inappropriate
Council was advised of an incident at a hospital involving the misadministration of part of a radiopharmaceutical dose of 40 MBq 99mTc to a 51 year old male patient.
The radiopharmaceutical, administered by a nuclear medicine technologist 9 months into her professional development year training, was 99mTc MAG 3 instead of 80 MBq 99mTc MAA.
The effective radiation dose estimate to the patient from the misadministration was 0.28 mSv.
The hospital advised the Council that the nuclear medicine technologist was retrained in the correct procedures for confirming patient identity and the prescribed radiopharmaceutical to prevent similar incidents from occurring in future. Departmental guidelines were also updated to ensure the correct procedures are clearly documented. Council agreed with the actions taken.
Council was advised of an incident at a hospital involving the misadministration of 900 MBq 99mTc MDP instead of the prescribed 900MBq 99mTc MIBI. The radiopharmaceutical had been incorrectly labelled. The patient received an estimated effective radiation dose of approximately 5.1mSv.
The hospital’s Radiation Safety Officer and the manager of the dispensing laboratory also reported their concern with the competence of the technologist involved. Council noted the report and the apparent failure of the technologist to follow established protocols.
Radiological Council 2007 Annual Report
Page 10
Industrial
The Radiation Safety Officer (RSO) for an industrial radiography company notified the Council of two related incidents which occurred where an industrial radiography source holder (also known as a pigtail) had detached from a wind-out cable during a radiographic exposure.
An industrial radiography licensee and his approved assistant were performing radiography at a field site in Kwinana when the pigtail disconnected from the radiography projector’s wind-out cable leaving it in the collimator (a device used to restrict the size and shape of the radiation beam). The pigtail was recovered and placed in a shielded recovery pot.
The RSO later reloaded the pigtail into the radiography projector at the company’s workshop and, after checking the mechanical tolerances of the pigtail and wind-out cable connector, determined that except for a slightly dirty spring, which was cleaned and checked, the device was in good working order. The RSO believed that the incident had been caused by the user incorrectly connecting the pigtail to the wind-out cable.
The projector was put back into operation the following day but the pigtail again disconnected. The projector was taken out of service and returned to the supplier for maintenance. A later report confirmed that the reason for both incidents was a faulty source holder connection.
Council wrote to the industrial radiography company and reminded it of its obligations under the Act to ensure that equipment is properly maintained.
The Radiation Safety Officer (RSO) for a mining company notified the Council of an incident involving a radioactive in-stream analysis gauge containing 1.11 GBq 241Am. Maintenance personnel had been working on the electronic components of the gauge with shielding for the radioactive source incorrectly positioned. The RSO estimated a maximum radiation dose to one worker of 350 µSv.
The risk from the estimated dose was insignificant but Council reviewed the company’s written working rules for servicing the device. The review indicated that the rules had been followed but the cause
Radiological Council 2007 Annual Report
Page 11
of the exposure was a shielding plate which had been incorrectly positioned allowing a small radiation beam to pass through a screw hole in the shield.
Council wrote to users of this type of gauge outlining the incident and directing them to ensure that their working rules stipulate when and how radiation survey meters are to be used during servicing and maintenance procedures. The gauge manufacturer was also advised of the incident.
Council was informed of an incident involving two employees of an industrial radiography company at a field site in the North West of the State where the radioactive source holder became detached from the wind-out cable.
The employees were aware that the radioactive source had failed to return to its shielded container through the high radiation dose rate on the survey meter and their personal audible alarms. Recovery operations were undertaken successfully and the source holder was reconnected to the wind-out cable. The incident apparently was due to operator error whereby the assistant had connected the guide tube to the source container but had forgotten to connect the radioactive source holder to the wind-out cable.
Council noted that the source projector was designed before the current version of ISO 3999 Apparatus for Industrial Gamma Radiography which is referenced in the Code of Practice for the Safe Use of Industrial Radiography Equipment. That standard requires industrial radiography containers to be failsafe such that the radioactive source can not be released from the safe position unless secure attachment has been made between the control cable and the source assembly, between the control cable sheath and the container, and between the guide tube and the container.
Council required the particular industrial radiography projector to be withdrawn from service. The company was also required to amend its working rules to ensure that the integrity of connections is verified prior to the use of industrial radiography equipment and that the equipment is regularly inspected for compliance with the manufacturer’s specifications.
Council was advised that a vehicle transporting a moisture/density gauge had rolled over approximately 10 km south of Kalbarri. Moisture density gauges contain the radioactive sources 137Cs and 241Am/Be.

Radiological Council 2007 Annual Report
Page 12
A licensee for the company attended the crash scene and found that the moisture/density gauge had a cracked case but otherwise was intact within its steel cage. Radiation levels around the gauge did not suggest any damage to the source shielding. Wipe tests, used to establish whether any radioactive material has leaked from its encapsulation, were free of contamination. The gauge owner later advised that the gauge would be returned to the manufacturer.
Investigations by Council Officers found that the gauge was being transported in compliance with the Radiation Safety (Transport of Radioactive Substances) Regulations and within the conditions imposed on the licence.
Council agreed that the incident had been managed in a responsible manner.
Council was notified that a portable radioactive moisture/density gauge had been run over and crushed by a front-end loader on a road works site.
The front-end loader operator was preparing a test site approximately 20-25 m from the vehicle of the gauge operator. After giving the all clear to the front-end loader operator the licensee went back to his vehicle to complete his paperwork, leaving the gauge on the ground approximately 5 m behind his vehicle. The front-end loader operator did not see the gauge and drove over it. Although flashing lights and radiation “keep clear” signs were present on top of the vehicle, none were on the ground next to the gauge.
An exclusion zone was set up around the gauge until a survey meter was used to check dose rates. The pieces of the gauge were placed in plastic bags and returned to the owner’s premises. Wipe tests and soil samples taken from the scene were analysed by the Radiation Health Branch. No evidence of contamination was detected.
Council’s Officer reported the gauge’s electronics were damaged but the radioactive source holders had remained intact.
A review of the incident did not establish any breaches of the Act.
Council was notified of two incidents where a well logging company had abandoned radioactive sources in bore-holes offshore in the North West of Western Australia.
In early August, the company was working on an offshore well when logging tools fitted with 137Cs and 241Am-Be radioactive sources
Radiological Council 2007 Annual Report
Page 13
became stuck at a depth of around 3300 m. Source recovery operations were unsuccessful and the tools were deemed unrecoverable.
Later that month the company was working on another well when the logging tools fitted with 137Cs and 241Am-Be radioactive sources became stuck at a depth of around 3200 m. Source recovery operations were again unsuccessful and these tools also were deemed unrecoverable.
The conditions of the company’s registration require that where a radioactive source is irretrievably lost in a bore-hole written notification is given to the owner and/or operator of the bore-hole that the source is to be cemented in situ, the location of the source is documented for the owner’s records and no further drilling is permitted in the immediate vicinity of the source that risks intersecting with the source. In compliance with the conditions of registration, the registrant took the specified actions to cement the source in place.
Council also notified the National Offshore Petroleum Safety Authority and the Petroleum Division of the Department of Industry and Resources.
Council received a report concerning two mine employees who had worked near a 370 MBq 137Cs level gauge without first ensuring that the gauge was locked off.
The company Radiation Safety Officer (RSO) advised that the two workers may have accidently exposed parts of their bodies to the unshielded radiation beam but that the worst case scenario would have resulted in a radiation dose of approximately 1 mSv (the annual dose limit for members of the public).
A warning sign for the gauge was in position but the gauge had only recently been installed and at the time of the incident was still undergoing commissioning.
The RSO later reported that rules for the vessel containing the newly installed gauge had not been updated to include requirements for isolating the gauge before entry. This was an error in the company’s change management process and would be addressed.
No further action was necessary.
Notification was received from a well logging company that two logging sources (74 GBq 137Cs and 703 GBq 241Am-Be) had been abandoned in a bore-hole offshore in the north west of the State.

Radiological Council 2007 Annual Report
Page 14
The company was working on an offshore well when the logging tools fitted with the radioactive sources became stuck at a depth of around 2400 m. Source recovery operations were unsuccessful and the tools were deemed unrecoverable.
The conditions of the company’s registration require that where a source is irretrievably lost in a bore-hole written notification is given to the owner and/or operator of the bore-hole that the source is to be cemented in situ, the location of the source is documented for the owner’s records and that no further drilling is permitted in the immediate vicinity of the source that risks intersecting with the source. In compliance with the conditions of registration, the registrant took the specified actions to cement the source in place.
Council notified the National Offshore Petroleum Safety Authority and the Petroleum Division of the Department of Industry and Resources.
Council received advice that a brewery had recently ceased operations and was transferring a small number of radioactive level gauges containing 241Am (mostly 3.7 GBq) to a brewery in Tasmania. It was reported that one of the gauges had been sent in a sea container without the required documentation and not in compliance with the Radiation Safety (Transport of Radioactive Substances) Regulations. This was not discovered this until the truck was in Ceduna, near the Western Australian and South Australian border.
As the freight was due to stop at a depot in Victoria before heading to Tasmania, Council’s officers advised the regulatory authorities in both Victoria and Tasmania. Upon arrival in Victoria officers from that State’s Department of Human Services inspected the source, ensuring it was secured for transport and that the required documentation was completed before on-forwarding to Tasmania.
Council officers wrote to the brewing company reminding them of their obligations under the Act and requested an explanation of the circumstances that led to the apparent breach of the Radiation Safety (Transport of Radioactive Substances) Regulations.
Incidents reported to Council prior to 2007 but which were finalised in 2007.
In December 2006 Council was notified by a well logging company that a 592 GBq 241Am-Be radioactive source used during oil and gas exploration was missing. The source had been ordered from the

Radiological Council 2007 Annual Report
Page 15
United States of America and while records traced its movements to Australia and within Western Australia, the owner did not realise the source was missing until it failed to arrive at its intended location.
Council’s officers led the search and successful recovery operation in conjunction with WA Police, the Fire and Emergency Services, the owner of the source and the company responsible for transportation of the source. The source was recovered intact in January 2007 and, following verification that it had not been damaged, was finally transported to its owner.
In 2006 Council was advised that a personal radiation monitoring device assigned to a licensee who uses portable moisture/density gauges had received a reportable dose over a three-month monitoring period of 8.11 mSv. The monitoring report estimated that the energy of the radiation giving rise to the dose was 60 keV.
In his report, the company’s Radiation Safety Officer suggested that the dose was not work related because the licensee had been in Bulgaria. Although he had taken the personal monitoring device with him he had not been working with radioactive substances during the dose monitoring period. The reports suggested that the dose may have been the result of security x-ray scanning during the round trip to Bulgaria.
Council noted that background radiation levels in Bulgaria ranged from 0.1 – 0.3 µSv/h with an average of 0.2 µSv/h. However, the estimate of the energy of the radiation causing the dose was more consistent with the average energy emitted by x-ray baggage screening machines. Some airport security cabinet x-ray scanners (for checked-in baggage) appear to be capable of giving doses in the order of 20-30 mSv.
Council agreed that the dose should not remain on the personal record of the licensee.
Council was informed in 2006 of an incident in which two employees of a well logging company received radiation doses. A 1.6 GBq 60Cologging source had become detached from the source holder inside the logging tool and was then carried in the passenger section of the work vehicle. The two workers, unaware that the radioactive source was in the vehicle with them, received doses of 2.71 mSv and 1.27 mSv respectively.
The source holder and tool were sent to a consultant to determine how the source became detached from the holder. It had been
Radiological Council 2007 Annual Report
Page 16
concluded that a grub screw used to hold two sections of the source holder together unfastened due to the thread in the drill hole not being tapped deep enough. In addition, an adhesive compound had not been used to further secure the grub screw.
Council officers concluded that the incident occurred as a result of the following circumstances:
• the source holder manufacturer had not tapped the thread in the drill hole in the ‘bull plug’ deep enough to adequately secure the grub screw;
• the person who had loaded the source into the source holder did not notice that the grub screw was not completely screwed in nor did he use an adhesive compound normally used to further secure the screw; and
• the two employees, although in possession of a radiation survey meter, did not use the meter to confirm that the radioactive source had been properly returned to its shielded source container.
Council was also advised that the conditions applied to well logging licences did not require licensees to use a survey meter after each procedure to confirm that the source was in place and properly shielded. Council amended the licence conditions to address this shortcoming and notified logging companies and their licensees of these changes.

Radiological Council 2007 Annual Report
Page 17
PROSECUTIONS
The following matters were initiated in 2007 but not finalised in the year.
Council initiated prosecution of a company under section 52 (2) of the Act for the alleged continuing offence of failing to register a cabinet x-ray unit.
Section 52(2) of the Act requires that a person who, when required to do so under this Act, fails to furnish within a reasonable time thereafter any information which the Council or an authorized officer has asked for in relation to any matter, or furnishes false of misleading information, commits an offence.
Council considered the loss in transit of a 592 GBq 241Am-Be logging source between 18 November 2006 and 16 January 2007 (see Incidents). The location in which the source was later recovered strongly suggests that the consignment was improperly secured during transportation.
The Council initiated prosecution of the transporting company in relation to regulations 6(1) and 6(2) of the Radiation Safety (Transport of Radioactive Substances) Regulations for failure to comply with the requirements of the Code of Practice for the Safe Transport of Radioactive Materials.

Radiological Council 2007 Annual Report
Page 18
MEDICAL AND RELATED RADIATION MATTERS
Compliance Testing
Council’s compliance testing program, which commenced in 1997, applies to all diagnostic x-ray equipment used on living humans for medical radiography and fluoroscopy, chiropractic and dental radiography, and computed tomography.
No x-ray equipment may be used for human diagnostic purposes unless it has a current certificate of compliance, a certificate of conditional compliance, or an exemption from compliance.
Through conditions imposed on the registration under Section 36 of the Act, the registrant (the owner) is legally responsible for satisfying the requirements of the compliance testing program.
The number of compliance tests of diagnostic x-ray equipment assessed by Council in 2007 increased by 6% from 2006 to a total of 1128. A summary of the statistics for the compliance program per type of diagnostic medical imaging equipment is included in attachment 3.
Compliance Testing Working Group
The Council’s Compliance Testing Working Group developed a set of workbooks for digital radiographic equipment testing which were approved by the Council at its October 2007 meeting.
The five digital workbooks, developed with the extensive pro bono publico assistance of a former Radiation Health Branch Officer, Mr Peter Henson, apply to Mobile Digital Radiographic, Digital Mammographic, Major Digital Radiographic, Digital Fluoroscopic and Dental Digital Radiographic Equipment.
The workbooks compliment the existing six workbooks previously developed by the Compliance Testing Working Group. The Working Group has now developed 11 workbooks that comprehensively describe the tests to be undertaken for each category of equipment as well as the approved test protocols to ensure that the full range of diagnostic x-ray equipment can be periodically tested for compliance with the State’s Radiation Safety (General) Regulations and any additional criteria that the Council may apply to the equipment under test.

Radiological Council 2007 Annual Report
Page 19
Licensing of Medical Radiation Technologists
The Medical Radiation Technologists Act 2006 amended the Radiation Safety Act 1975 to provide for the licensing of Medical Radiation Technologists (MRTs). The amendments to the Radiation Safety Act commenced on 1 July 2007.
As a consequence to the amendments, MRTs are required to hold individual licences for medical imaging, nuclear medicine or radiation therapy.
Licensing of MRTs commenced on 1 July 2007 and by 31 December 2007 all MRTs were expected to hold a licence relevant to their profession. During the 6 month period to 31 December 2007, 836 licences where issued by the Council for the three areas covering MRTs.
Radiological Council 2007 Annual Report
Page 20
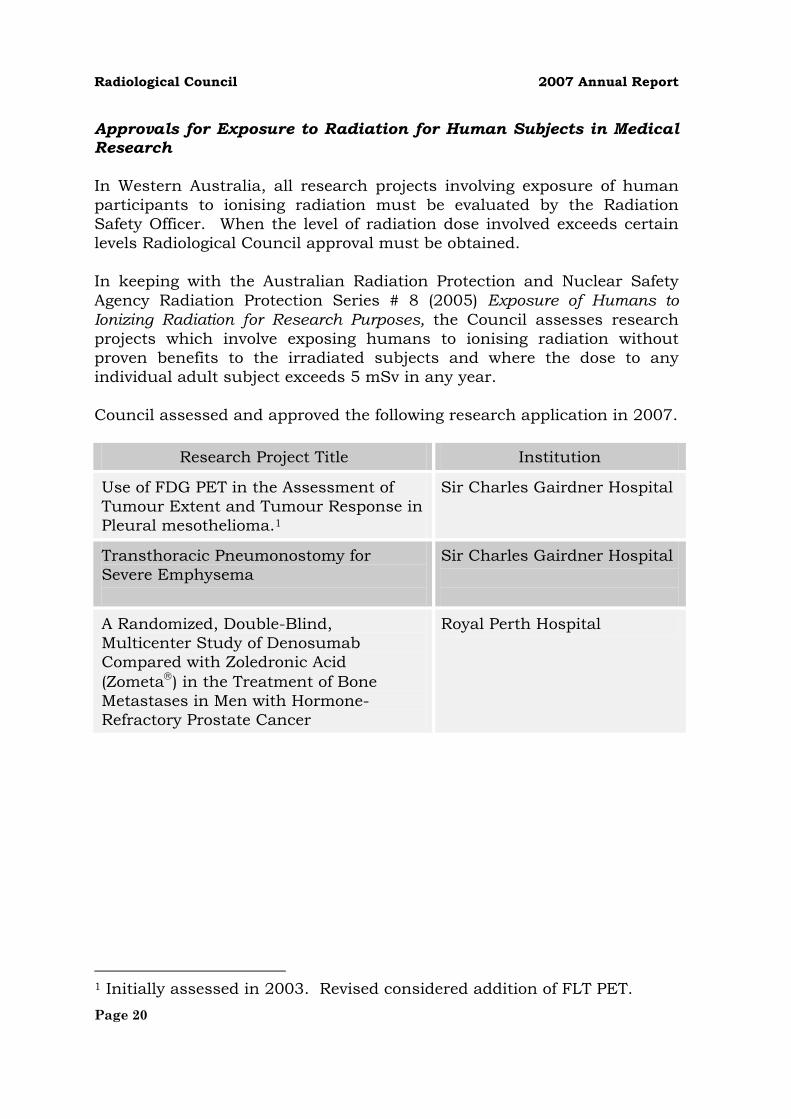
Approvals for Exposure to Radiation for Human Subjects in Medical Research
In Western Australia, all research projects involving exposure of human participants to ionising radiation must be evaluated by the Radiation Safety Officer. When the level of radiation dose involved exceeds certain levels Radiological Council approval must be obtained.
In keeping with the Australian Radiation Protection and Nuclear Safety Agency Radiation Protection Series # 8 (2005) Exposure of Humans to Ionizing Radiation for Research Purposes, the Council assesses research projects which involve exposing humans to ionising radiation without proven benefits to the irradiated subjects and where the dose to any individual adult subject exceeds 5 mSv in any year.
Council assessed and approved the following research application in 2007.
Research Project Title Institution
Use of FDG PET in the Assessment of Tumour Extent and Tumour Response in Pleural mesothelioma.1
Sir Charles Gairdner Hospital
Transthoracic Pneumonostomy for Severe Emphysema
Sir Charles Gairdner Hospital
A Randomized, Double-Blind, Multicenter Study of Denosumab Compared with Zoledronic Acid (Zometa ) in the Treatment of Bone Metastases in Men with Hormone-Refractory Prostate Cancer
Royal Perth Hospital
1 Initially assessed in 2003. Revised considered addition of FLT PET.

Radiological Council 2007 Annual Report
Page 21
INDUSTRIAL, ENVIRONMENTAL and MINING RADIATION
Industrial Compliance Testing
The Council’s compliance testing program for fixed radiation gauges commenced in 1999. The program requires that gauges are not used unless they have a current certificate of compliance. The number of compliance tests received by the Council in 2007 for the industrial compliance testing program increased by 37% compared to 2006 to a total of 712. A summary of compliance tests assessed in 2007 is included in attachment 3.
Standards for Council Examinations
Council had previously agreed that improved control over industrial radiation safety examination standards was necessary and had decided that while course providers may continue to invigilate examinations, all industrial papers would be returned to Council’s officers for marking. The program commenced during the last quarter of 2002. In 2007, Council officers marked 409 industrial examination papers. The number of exams marked in each category is listed in attachment 4.
MISCELLANEOUS
Solaria
In late 2007 the Minister sought advice from the Council on options available under the Act for the regulation of solaria.
Council responded to the Minister with a number of options and the public health outcomes that could be achieved.
Discussions with the Minister are continuing.
Radiation Health Committee
The Radiation Health Committee is a body established to advise the Chief Executive Officer of the Australian Radiation Protection and Nuclear Safety Agency and its Radiation Health & Safety Advisory Council on matters relating to radiation protection, formulating draft national policies, codes and standards for consideration by the Commonwealth, States and Territories.

Radiological Council 2007 Annual Report
Page 22
Western Australia has representation on the Radiation Health Committee through the Secretary of the Radiological Council who attends the committee meetings tri-monthly.
Council officers and staff of the Radiation Health Branch participate as members of working groups formulated by the committee to develop codes and polices. Council considered and provided comment to the Committee during 2007 for the development of:
regulation of solaria Code of Practice: Radiation Protection in the Medical Applications of Ionising Radiation Safety Guide for Radiation Protection in Radiotherapy.
National Directory for Radiation Protection
At the Australian Health Ministers’ Conference (AHMC) held in June 2004, the Ministers endorsed the adoption of the National Directory for Radiation Protection, Edition 1, as the Framework for National Uniformity in Radiation Protection. The Ministers also agreed that the first edition of the Directory would not be applied to the mining and mineral processing industries until further work regarding exemption criteria has been undertaken.
Further development of Edition 2 of the National Directory continued in 2007 through the national Radiation Health Committee.
Council continued its participation in the development of the National Directory and provided comment to the Radiation Health Committee.
Although Edition 2 of the National Directory was anticipated for Council’s final consideration during 2007, Council was advised the document would not be released for public comment during 2007.
Personal Radiation Monitoring Services
Council currently recognises five organisations for the provision of a personal radiation monitoring service in accordance with the Regulations:
• ARPANSA (Australian Radiation Protection and Nuclear Safety Agency), the Commonwealth Government’s radiation safety agency in Victoria
• New Zealand National Radiation Laboratory, the New Zealand national radiation safety organisation (Australian agent: Australia Radiation Services Pty Ltd, Victoria)

Radiological Council 2007 Annual Report
Page 23
• Australia Radiation Services Pty Ltd, a company based in Victoria
• Landauer Inc (USA) for the Luxel based system.(Agent: Landauer Australasia Pty Ltd.)
• Global Dosimetry Solutions, a company based in USA.

Radiological Council 2007 Annual Report
Page 24
Appendix 1: Registration and Licensing
Registrations
Section 28 of the Act requires prescribed radioactive substances, x-ray equipment and electronic products, together with the associated premises, to be registered. Registrants may include individuals, companies, organisations or institutions.
All x-ray equipment is prescribed while prescribed electronic products include lasers, transilluminators and microwave ovens.
Radioactive substances that exceed the exempt quantities prescribed in the regulations are subject to registration. A small number of devices containing radioactive substances in excess of the exempt limits, but which pose a minimal hazard to users, have been exempted by regulation from control under the Act.
The numbers of devices and sealed radiation sources registered as at 31 December 2007 are included in attachment 5.
Licences
Section 25 of the Act requires persons who manufacture, store, transport, sell, possess, install, service, maintain, repair, use, operate or otherwise deal with prescribed radioactive substances, x-ray equipment or electronic products to be licensed or, where permitted, work under the direction and supervision of a licensee.
Section 29 of the Act also creates an offence for a person to sell any prescribed substances or devices unless they require the purchaser to produce evidence that they hold a relevant licence or are otherwise exempted by the Act or regulations. Sales also must be notified in writing to the Council, without delay, identifying the purchaser and the particulars of the relevant licence or exemption.
Exemptions from Licence
A licence is not required where a general exemption is provided by the regulations or where a person has been granted an individual exemption from licence. Although exempt from licensing, the regulations nevertheless specify the minimum qualifications or training required for these radiation workers.

Radiological Council 2007 Annual Report
Page 25
Temporary Permits
The shortest period for which a licence or registration can be granted is 12 months. However, for shorter periods an application may be made for a Temporary Permit. Permits cannot exceed a duration of 3 months. Thirteen Temporary Permits were current as at 31 December 2007.
Conditions, Restrictions and Limitations
A range of performance and safety requirements for radioactive substances, x-ray equipment and the prescribed electronic products are specified in the regulations. However, additional safety measures may be applied by the Council under section 36 of the Act through conditions, restrictions and limitations applied to registrations, licences, temporary permits and exemptions.
Failure to comply with a condition is an offence.
Attachment 6 shows the types and numbers of licences and registrations (or individual exemptions) granted or renewed in 2007.
Commonwealth Government Agencies and Contractors
The Radiation Safety Act does not apply to Commonwealth agencies or to their employees (or contractors) who might use radiation in Western Australia. Those agencies are regulated by the Australian Radiation Protection and Nuclear Safety Agency (ARPANSA) under the Commonwealth Government’s Australian Radiation Protection and Nuclear Safety Act 1999.

Radiological Council 2007 Annual Report
Page 26
Appendix 2: Licence Prerequisites
Before a licence may be granted, the Council has an obligation to ensure that an applicant has appropriate qualifications, competence and experience (section 33).
Protocols have been developed which prescribe the prerequisite qualifications and experience necessary for a wide range of radiation uses. Some qualifications are recognised by the Council because an appropriate degree of radiation safety training is inherent in gaining those qualifications. However, other applicants may be required to attend a recognised radiation safety course and pass an examination. The Council has authority to impose examinations under the Radiation Safety (Qualifications) Regulations.
Persons who are not required to hold a licence themselves but who must work under the direction and supervision of a licensee may also be required to hold certain qualifications or to have undergone additional radiation safety training. These requirements may be imposed by regulation or through conditions, restrictions and limitations imposed under section 36. The registrant for the premises where the individual works is primarily responsible for ensuring compliance with these criteria.
Courses in various aspects of radiation safety are offered by both the government and private sectors, for example:
Bone Densitometry Compliance Testing of Diagnostic X-ray Equipment Fluoroscopy – Medical Fixed Radioactive Gauges Industrial Radiography Lasers – Medical and Industrial Portable Radioactive Gauges Transport of Radioactive Substances Unsealed Radioisotope Handling Well (Borehole) Logging X-ray Operator

Radiological Council 2007 Annual Report
Page 27
Attachment 1: Radiological Council
MEMBERS OF THE 11TH RADIOLOGICAL COUNCIL
Members Qualification or Designation Deputy
Appointment under sections 13(2)(a) and 13(3) of the Act
Dr P Psaila-Savona (Chairman)
Medical Practitioner Dr G Groom
Appointment under sections 13(2)(b), 15(1) and 17 (1) of the Act
Dr E Wylie Radiologist Dr M Bynevelt
Dr G Groom Nuclear Medicine Physician Dr G Bower
Dr R Fox Physicist Dr R Price
Mr J Hunter Electronic Engineer Vacant
Professor C Atkins2 Tertiary Institutions representative Vacant
Mr N Tsurikov Expert in Mining Radiation Hazards Mr G Fee
Mr N Hicks Expert in Medical Imaging Mr B Stock
Mr B Cobb Co-opted member not applicable
2007 MEETING ATTENDANCE
19 Jan 8 Feb 19 Apr 14 Jun 9 Aug
11Oct 13 Dec
Dr P Psaila-Savona
Professor C Atkins NA NA NA NA NA
Dr R Fox
Dr G Groom A D
Mr N Hicks D A D
Mr J Hunter A
Dr E Wylie A
Mr B Cobb
Mr N Tsurikov
2 Appointed by the Governor on 14 August 2007 for the period ending 29 February 2008
attended A apology D deputy NA not appointed at the time

Radiological Council 2007 Annual Report
Page 28
Attachment 2: Legislation Amendments
RADIATION SAFETY ACT
None
RADIATION SAFETY (GENERAL) REGULATIONS
None
RADIATION SAFETY (TRANSPORT OF RADIOACTIVE SUBSTANCES) REGULATIONS
None
RADIATION SAFETY (QUALIFICATIONS) AMENDMENT REGULATIONS
None

Radiological Council 2007 Annual Report
Page 29
Attachment 3: Compliance Testing
Medical
A CompliantB Conditionally compliantC Non-compliant3
Category A B C TotalCT 38 - 5 43Dental – intraoral 522 5 43 570Dental – panoramic and/or cephalometric 62 - 1 63Fluoroscopic – fixed 32 5 24 61Fluoroscopic – fixed C or U arm 24 1 4 29Fluoroscopic – mobile 72 2 13 87Mammography 53 2 5 60Radiographic – fixed 89 - 34 123Radiographic – mobile 84 - 8 92
Total 976 15 137 1128
Industrial – Fixed Gauges
A CompliantB Non-compliant4
Category A B TotalDensity 540 31 571In-stream analysis 77 - 77Level 63 - 63Thickness 1 - 1
Total 681 31 712
3 Equipment deemed to be non-compliant may continue to be used for a further three months while the problem is being addressed provided that the reason for non-compliance does not significantly increase the radiation dose to the patient. A re-test is then required. Of the 127 re-tests conducted during 2007, 98% resulted in the equipment being granted either a compliance or conditional compliance certificate. 4 Equipment that has been assessed as non-compliant cannot be used until it has been re-tested and issued with a certificate of compliance.

Radiological Council 2007 Annual Report
Page 30
Attachment 4: Industrial Radiation Safety Examinations
Current at 31 December 2007
Category 2007 2006 2005 2004Borehole Logging 46 23 28 45Fixed Gauges 78 82 57 105Industrial Radiography 40 35 26 22Industrial Radiography (Advanced) 0 0 0 2Industrial Radiography (Assistant) 65 85 64 33Portable Gauges 96 61 61 45Portable Gauges (WA Requirements) 4 2 0 9Transport 28 11 13 16Service – Cabinet X-ray 1 5 2 1Service – Industrial Radiography (X-ray) 1 0 0 0Service – Linear Accelerators (Industrial) 0 0 0 1Service – X-ray Analysis 0 0 0 3X-ray Analysis – Use 0 5 9 8X-ray Analysis – Use and Restricted Service 50 43 27 42
Total 409 352 287 332

Radiological Council 2007 Annual Report
Page 31
Attachment 5: Registered Irradiating Apparatus, Electronic Products and Radioactive Substances (sealed sources)
Current at 31 December 2007
A Irradiating apparatus and electronic productsB Radioactive substances (sealed sources only)
Category A BBone densitometry 43 -Cabinet x-ray equipment 106 -Calibration 2 316CT 128 -CT/SPECT 4 -Dental – intraoral 1863 -Dental – panoramic and/or cephalometric 235 -Education and research 16 856Fluoroscopic – fixed5 150 -Fluoroscopic – mobile 119 -Gauges – density/level 7 1862Gauges – in stream analysis - 111Gauges – logging 19 231Gauges – neutron moisture/density portable - 273Gauges – other - 71Irradiator - 47Isotope Production 1 -Laser – entertainment 39 -Laser – industrial 52 -Laser – medical 174 -Laser – other medical 125 -Laser – research 82 -Linear accelerator 12 -Mammography 105 -Non-destructive testing 67 62Non-destructive testing – crawler control - 4Portable mineral analyser - 20Radiographic – fixed 435 -Radiographic – mobile 523 -Sealed Sources – other - 90Simulator 2 -
5 Includes equipment used in DSA/Cardiac Cath Lab

Radiological Council 2007 Annual Report
Page 32
Category A BSpecial purpose x-ray 64 -Static detection/measurement - 3Static elimination - 4Storage - 188Superficial radiotherapy 5 -Test source 5 -Therapy 1 43Therapy – HDR brachytherapy - 2Transilluminator 109 -X-ray analysis 216 -
Total 4709 4183
Radiological Council 2007 Annual Report
Page 33
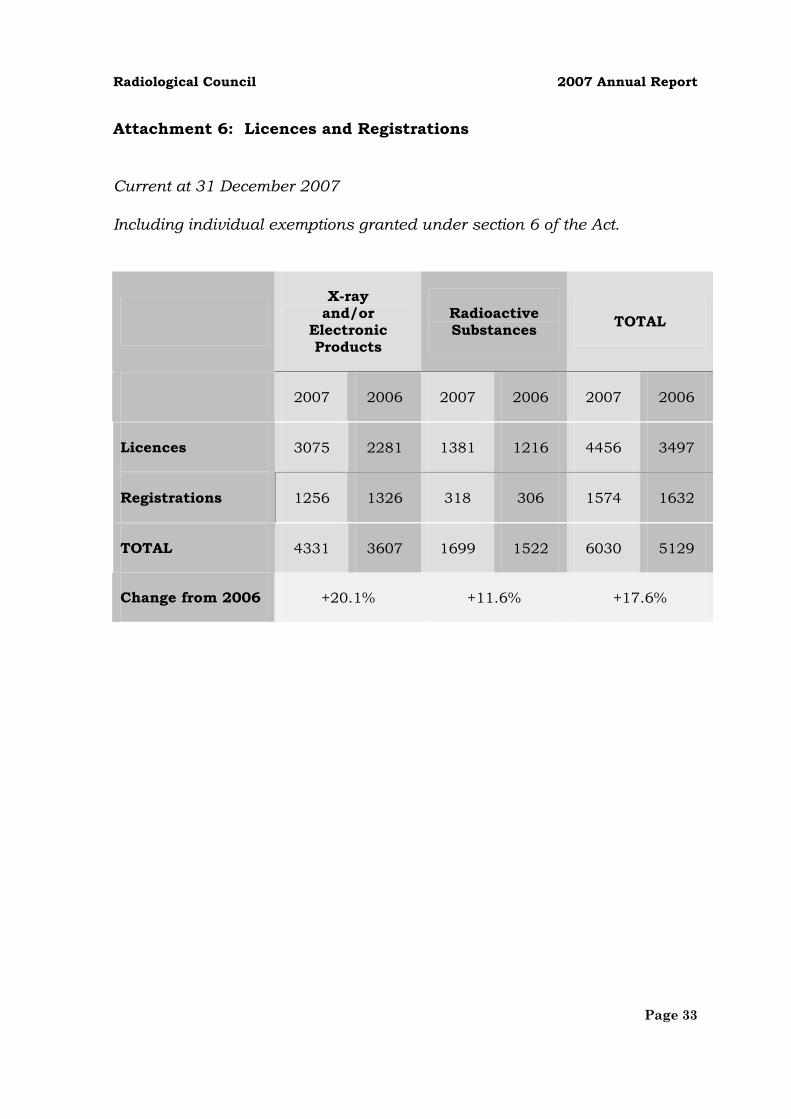
Attachment 6: Licences and Registrations
Current at 31 December 2007
Including individual exemptions granted under section 6 of the Act.
X-rayand/or
ElectronicProducts
RadioactiveSubstances TOTAL
2007 2006 2007 2006 2007 2006
Licences 3075 2281 1381 1216 4456 3497
Registrations 1256 1326 318 306 1574 1632
TOTAL 4331 3607 1699 1522 6030 5129
Change from 2006 +20.1% +11.6% +17.6%

Radiological Council 2007 Annual Report
Page 34
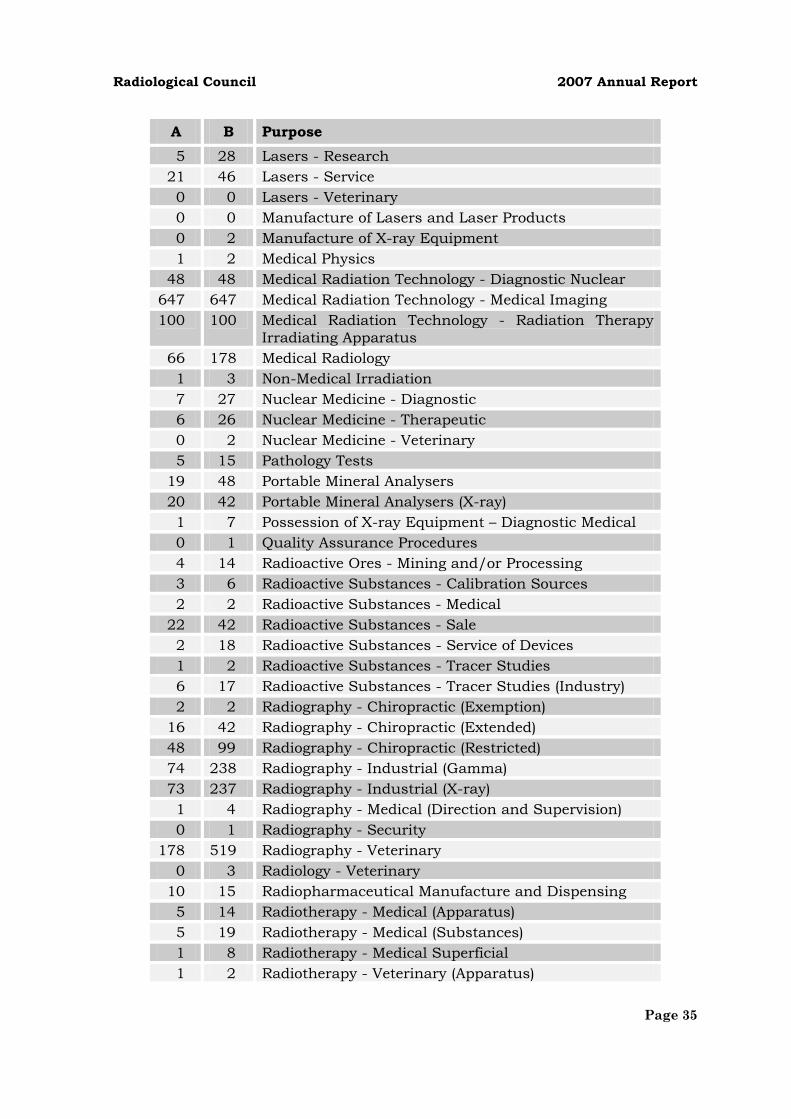
Attachment 6 (cont)
Purposes for Licences and Exemptions from Licence
Note: A single licence may be granted for one or more purposes.
A Granted or renewed in 2007B Total current
A B Purpose2 3 Bone Densitometry 4 4 Bone Densitometry (Exemption)
32 65 Cabinet X-ray Equipment 0 2 Cobalt Teletherapy Maintenance
15 47 Compliance Testing - Diagnostic X-ray Equipment 32 82 Compliance Testing - Radioactive Gauges 2 3 Cyclotron Operation 4 6 Cyclotron Servicing 0 5 Education (Apparatus)
12 43 Education (Substances) 71 164 Fluoroscopy - Medical 41 173 Fluoroscopy - Medical (Exemption) 0 2 Fluoroscopy - Medical (Non-Specialist Exemption) 0 0 Fluoroscopy - Research 0 1 Fluoroscopy - Veterinary 1 2 Gamma Irradiator - Use
96 245 Gauges - Industrial 4 13 Gauges - Industrial (Installation) 2 3 Gauges - Level (CO2)
114 220 Gauges - Logging 167 349 Gauges - Moisture and/or Density (Portable)
3 6 Gauges - Other (Apparatus) 5 21 Gauges - Other (Substances) 0 1 Installation of X-ray Equipment 2 6 Installation of X-ray Equipment - Dental 3 14 Lasers - Acupuncture 0 7 Lasers - Chiropractic
14 41 Lasers - Dental 4 9 Lasers - Educational 4 9 Lasers - Entertainment
20 48 Lasers - Industrial 61 208 Lasers - Medical 22 64 Lasers - Physiotherapy
Radiological Council 2007 Annual Report
Page 35
A B Purpose5 28 Lasers - Research
21 46 Lasers - Service 0 0 Lasers - Veterinary 0 0 Manufacture of Lasers and Laser Products 0 2 Manufacture of X-ray Equipment 1 2 Medical Physics
48 48 Medical Radiation Technology - Diagnostic Nuclear 647 647 Medical Radiation Technology - Medical Imaging 100 100 Medical Radiation Technology - Radiation Therapy
Irradiating Apparatus 66 178 Medical Radiology 1 3 Non-Medical Irradiation 7 27 Nuclear Medicine - Diagnostic 6 26 Nuclear Medicine - Therapeutic 0 2 Nuclear Medicine - Veterinary 5 15 Pathology Tests
19 48 Portable Mineral Analysers 20 42 Portable Mineral Analysers (X-ray) 1 7 Possession of X-ray Equipment – Diagnostic Medical 0 1 Quality Assurance Procedures 4 14 Radioactive Ores - Mining and/or Processing 3 6 Radioactive Substances - Calibration Sources 2 2 Radioactive Substances - Medical
22 42 Radioactive Substances - Sale 2 18 Radioactive Substances - Service of Devices 1 2 Radioactive Substances - Tracer Studies 6 17 Radioactive Substances - Tracer Studies (Industry) 2 2 Radiography - Chiropractic (Exemption)
16 42 Radiography - Chiropractic (Extended) 48 99 Radiography - Chiropractic (Restricted) 74 238 Radiography - Industrial (Gamma) 73 237 Radiography - Industrial (X-ray) 1 4 Radiography - Medical (Direction and Supervision) 0 1 Radiography - Security
178 519 Radiography - Veterinary 0 3 Radiology - Veterinary
10 15 Radiopharmaceutical Manufacture and Dispensing 5 14 Radiotherapy - Medical (Apparatus) 5 19 Radiotherapy - Medical (Substances) 1 8 Radiotherapy - Medical Superficial 1 2 Radiotherapy - Veterinary (Apparatus)

Radiological Council 2007 Annual Report
Page 36
A B Purpose2 3 Radiotherapy - Veterinary (Substances) 5 20 Research
31 87 Research - Unsealed Radioactive Substances 2 8 Research - X-ray 2 15 Sale of Electronic Products
18 59 Sale of X-ray Equipment 6 17 Service of X-ray Equipment - Analytical 2 12 Service of X-ray Equipment - Dental
30 71 Service of X-ray Equipment - Diagnostic 9 19 Service of X-ray Equipment - Diagnostic (Extended) 0 1 Service of X-ray Equipment - High Energy Therapeutic 1 7 Service of X-ray Equipment - Industrial NDT 2 2 Service of X-ray Equipment - Intraoral 9 12 Service of X-ray Equipment - Linear Accelerators 7 20 Service of X-ray Equipment - Other
Smoke Detectors - Sale 2 11 Special Purpose Enclosed X-ray Equipment 0 1 Static Detection 0 1 Static Electricity Measurement 0 1 Static Elimination 2 4 Storage9 22 Transilluminators
23 69 Transport 1 2 X-ray Analysis 0 1 X-ray Analysis (Research)
22 53 X-ray Analysis - Use 36 125 X-ray Analysis - Use and Service (Restricted)
Radiological Council 2007 Annual Report
Page 37
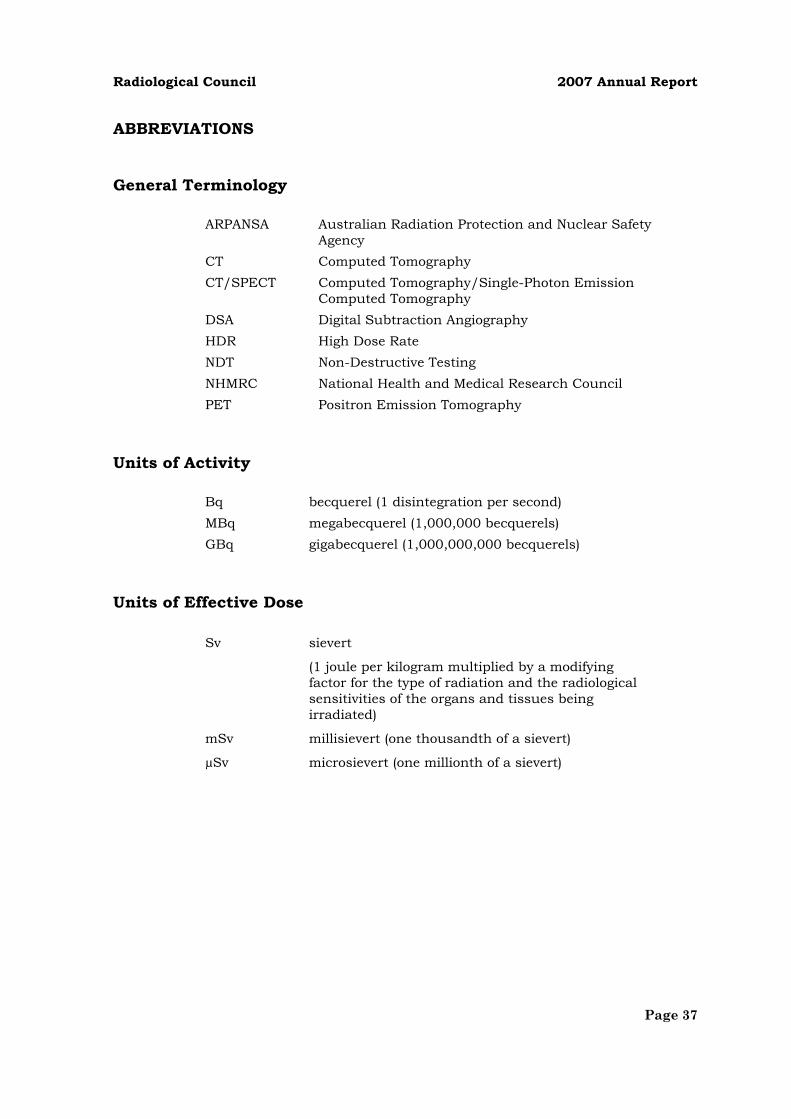
ABBREVIATIONS
General Terminology
ARPANSA Australian Radiation Protection and Nuclear Safety Agency
CT Computed Tomography CT/SPECT Computed Tomography/Single-Photon Emission
Computed Tomography DSA Digital Subtraction Angiography HDR High Dose Rate NDT Non-Destructive Testing NHMRC National Health and Medical Research Council PET Positron Emission Tomography
Units of Activity
Bq becquerel (1 disintegration per second) MBq megabecquerel (1,000,000 becquerels) GBq gigabecquerel (1,000,000,000 becquerels)
Units of Effective Dose
Sv sievert
(1 joule per kilogram multiplied by a modifying factor for the type of radiation and the radiological sensitivities of the organs and tissues being irradiated)
mSv millisievert (one thousandth of a sievert)
µSv microsievert (one millionth of a sievert)