Renal haemangioma presenting as an abdominal mass in a neonate
2
British Journal of Urology (1998), 82, 763–764 CASE REPORT Renal haemangioma presenting as an abdominal mass in a neonate S.Z. ZAIDI, Y. MOR, I. SCHEIMBERG*, G.F. QUIMBY andP.D.E. MOURIQUAND Department of Urology and *Histopathology, Great Ormond Street Hospital For Children, London, UK Case report A 1-day-old male infant was admitted with a right renal mass after an uneventful pregnancy and normal delivery. Ultrasonography of the fetus at 14 and 28 weeks showed no abnormality; on admission he was normotensive. Preoperative investigations included ultrasonography, showing a solid mass in the right kidney, and normal urinary levels of homovanillic and vanillyl mandelic acid. On day 3 the child underwent a right nephrectomy and made an uneventful recovery. The kidney specimen weighed 129.4 g (expected weight 24 g) and on sectioning (Fig. 1) most of the kidney was replaced by a smooth, haem- orrhagic, multilobulated tumour. Microscopy showed a highly cellular tumour composed of oval cells and a Fig. 2. Immunocytochemical stain for vascular markers (JC70) prominent vascular pattern with marked haemorrhage; highlights both branching small blood vessels and endothelial cells there were normal mitoses. Entrapped mature tubules were with a central lumen. ×200. seen within the tumour. Immunocytochemical stains for vascular markers (Fig. 2), Ulex europeaus agglutinin and multicystic dysplastic kidney, when the mass is cystic, JC70, were extensively positive [1]. or renal vein thrombosis, infantile polycystic kidney or tumour when ultrasonography shows a solid structure. Comment Renal tumours are extremely rare in this age group and include congenital mesoblastic nephroma, Wilms’ A renal mass in a neonate usually represents a benign tumour, neuroblastoma and teratoma [2]. Renal hae- lesion. Possible aetiologies include hydronephrosis or mangiomas may be part of a congenital disorder, as in Klippel-Trenuanay Syndrome, characterized by soft tissue and bony hypertrophy, varicose veins and port- wine haemangiomas. Ultrasonography can help in diagnosing renal involvement in such cases. However, they are generally seen as isolated lesions, usually soli- tary and unilateral and seldom clinically manifest before 20 years of age. The age range for patients with this entity is 4 months to 78 years [3]. To our knowledge, there is no reported case of a renal haemangioma in a newborn and this diagnosis should be considered when faced with a renal mass in a neonate. References 1 Parums DV, Cordell JL, Micklem K et al. JC70: A new monoclonal antibody that detects vascular endothelium associated antigen on routinely processed tissue. J Clin Pathol Fig. 1. Macroscopic section of the kidney showing almost complete replacement by a smooth haemorrhagic multilobulated tumour. 1990; 43: 752–7 763 © 1998 British Journal of Urology
Transcript of Renal haemangioma presenting as an abdominal mass in a neonate

British Journal of Urology (1998), 82, 763–764
CASE RE PORT
Renal haemangioma presenting as an abdominal massin a neonateS.Z. Z AIDI , Y. MOR, I. S CHEIMBERG*, G.F. QUIMBY and P.D.E. MOURIQUANDDepartment of Urology and *Histopathology, Great Ormond Street Hospital For Children, London, UK
Case report
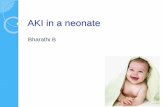
A 1-day-old male infant was admitted with a right renalmass after an uneventful pregnancy and normal delivery.Ultrasonography of the fetus at 14 and 28 weeks showedno abnormality; on admission he was normotensive.Preoperative investigations included ultrasonography,showing a solid mass in the right kidney, and normalurinary levels of homovanillic and vanillyl mandelic acid.On day 3 the child underwent a right nephrectomy andmade an uneventful recovery. The kidney specimenweighed 129.4 g (expected weight 24 g) and on sectioning(Fig. 1) most of the kidney was replaced by a smooth, haem-orrhagic, multilobulated tumour. Microscopy showed ahighly cellular tumour composed of oval cells and a
Fig. 2. Immunocytochemical stain for vascular markers (JC70)prominent vascular pattern with marked haemorrhage; highlights both branching small blood vessels and endothelial cellsthere were normal mitoses. Entrapped mature tubules were with a central lumen. ×200.seen within the tumour. Immunocytochemical stains forvascular markers (Fig. 2), Ulex europeaus agglutinin and
multicystic dysplastic kidney, when the mass is cystic,JC70, were extensively positive [1].
or renal vein thrombosis, infantile polycystic kidney ortumour when ultrasonography shows a solid structure.
Comment Renal tumours are extremely rare in this age group andinclude congenital mesoblastic nephroma, Wilms’
A renal mass in a neonate usually represents a benigntumour, neuroblastoma and teratoma [2]. Renal hae-
lesion. Possible aetiologies include hydronephrosis ormangiomas may be part of a congenital disorder, as inKlippel-Trenuanay Syndrome, characterized by softtissue and bony hypertrophy, varicose veins and port-wine haemangiomas. Ultrasonography can help indiagnosing renal involvement in such cases. However,they are generally seen as isolated lesions, usually soli-tary and unilateral and seldom clinically manifest before20 years of age. The age range for patients with thisentity is 4 months to 78 years [3]. To our knowledge,there is no reported case of a renal haemangioma in anewborn and this diagnosis should be considered whenfaced with a renal mass in a neonate.
References
1 Parums DV, Cordell JL, Micklem K et al. JC70: A newmonoclonal antibody that detects vascular endotheliumassociated antigen on routinely processed tissue. J Clin PatholFig. 1. Macroscopic section of the kidney showing almost complete
replacement by a smooth haemorrhagic multilobulated tumour. 1990; 43: 752–7
763© 1998 British Journal of Urology

764 CASE REPORTS
2 Woodard JR, Gosalbez R. Neonatal and perinatal emerg- Authorsencies. In Walsh PC, Retik AB, Stamey TA, Vaughan ED, S.Z. Zaidi, FRCS, Senior Registrar.eds, Campbell’s Urology, 6th edn, Vol. II. Philadelphia: Y. Mor, MD, Senior Registrar.Saunders, 1992: 1595–99 I. Scheimberg, MD, MRCPath, Senior Registrar.
3 Jahn H, Nissen HM. Haemangioma of the urinary tract: G.F. Quimby, MD, Senior Registrar.review of the literature. Br J Urol 1991; 68: 113–7 P.D.E. Mouriquand, MD, FEBU, Consultant.
Correspondence: Mr S.Z. Zaidi,Consultant Urologist, The Kidney Centre, 197/9 RafiquiShaheed Road, Karachi 75530, Pakistan.
© 1998 British Journal of Urology 82, 763–764